AHA Consensus Statement CIR.0b013e31829d8654.full
User Manual: Pdf AHA consensus statement جÙدة اÙØ¥Ùعاش اÙÙÙب٠اÙرئÙÙ - Ùار٠٠ÙÙ Ùس
Open the PDF directly: View PDF ![]() .
.
Page Count: 20
AHA Consensus Statement
1
Worldwide, there are >135 million cardiovascular deaths
each year, and the prevalence of coronary heart dis-
ease is increasing.1 Globally, the incidence of out-of-hospi-
tal cardiac arrest ranges from 20 to 140 per 100 000 people,
and survival ranges from 2% to 11%.2 In the United States,
>500 000 children and adults experience a cardiac arrest, and
<15% survive.3–5 This establishes cardiac arrest as one of
the most lethal public health problems in the United States,
© 2013 American Heart Association, Inc.
Circulation is available at http://circ.ahajournals.org DOI: 10.1161/CIR.0b013e31829d8654
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship
or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete
and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This statement was approved by the American Heart Association Science Advisory and Coordinating Committee on May 7, 2013. A copy of the
document is available at http://my.americanheart.org/statements by selecting either the “By Topic” link or the “By Publication Date” link. To purchase
additional reprints, call 843-216-2533 or e-mail kelle.ramsay@wolterskluwer.com.
The American Heart Association requests that this document be cited as follows: Meaney PA, Bobrow BJ, Mancini ME, Christenson J, de Caen AR, Bhanji
F, Abella BS, Kleinman ME, Edelson DP, Berg RA, Aufderheide TP, Menon V, Leary M; on behalf of the CPR Quality Summit Investigators, the American
Heart Association Emergency Cardiovascular Care Committee, and the Council on Cardiopulmonary, Critical Care, Perioperative and Resuscitation.
CPR quality: improving cardiac resuscitation outcomes both inside and outside the hospital: a consensus statement from the American Heart Association.
Circulation. 2013;128:XXX–XXX.
Expert peer review of AHA Scientific Statements is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines
development, visit http://my.americanheart.org/statements and select the “Policies and Development” link.
Permissions: Multiple copies, modification, alteration, enhancement, and/or distribution of this document are not permitted without the express
permission of the American Heart Association. Instructions for obtaining permission are located at http://www.heart.org/HEARTORG/General/Copyright-
Permission-Guidelines_UCM_300404_Article.jsp. A link to the “Copyright Permissions Request Form” appears on the right side of the page.
23
July
2013
Abstract—The "2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency
Cardiovascular Care" increased the focus on methods to ensure that high-quality cardiopulmonary resuscitation (CPR) is
performed in all resuscitation attempts. There are 5 critical components of high-quality CPR: minimize interruptions in
chest compressions, provide compressions of adequate rate and depth, avoid leaning between compressions, and avoid
excessive ventilation. Although it is clear that high-quality CPR is the primary component in influencing survival from
cardiac arrest, there is considerable variation in monitoring, implementation, and quality improvement. As such, CPR
quality varies widely between systems and locations. Victims often do not receive high-quality CPR because of provider
ambiguity in prioritization of resuscitative efforts during an arrest. This ambiguity also impedes the development of
optimal systems of care to increase survival from cardiac arrest. This consensus statement addresses the following key
areas of CPR quality for the trained rescuer: metrics of CPR performance; monitoring, feedback, and integration of
the patient’s response to CPR; team-level logistics to ensure performance of high-quality CPR; and continuous quality
improvement on provider, team, and systems levels. Clear definitions of metrics and methods to consistently deliver and
improve the quality of CPR will narrow the gap between resuscitation science and the victims, both in and out of the
hospital, and lay the foundation for further improvements in the future. (Circulation. 2013;128:00-00.)
Key Words: AHA Scientific Statements ◼ cardiac arrest ◼ CPR ◼ CPR quality ◼ outcomes ◼ resuscitation
CPR Quality: Improving Cardiac Resuscitation
Outcomes Both Inside and Outside the Hospital
A Consensus Statement From the American Heart Association
Endorsed by the American College of Emergency Physicians
Peter A. Meaney, MD, MPH, Chair; Bentley J. Bobrow, MD, FAHA, Co-Chair;
Mary E. Mancini, RN, PhD, NE-BC, FAHA; Jim Christenson, MD; Allan R. de Caen, MD;
Farhan Bhanji, MD, MSc, FAHA; Benjamin S. Abella, MD, MPhil, FAHA;
Monica E. Kleinman, MD; Dana P. Edelson, MD, MS, FAHA; Robert A. Berg, MD, FAHA;
Tom P. Aufderheide, MD, FAHA; Venu Menon, MD, FAHA; Marion Leary, MSN, RN;
on behalf of the CPR Quality Summit Investigators, the American Heart Association Emergency
Cardiovascular Care Committee, and the Council on Cardiopulmonary, Critical Care,
Perioperative and Resuscitation
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

2 Circulation July 23, 2013
claiming more lives than colorectal cancer, breast cancer,
prostate cancer, influenza, pneumonia, auto accidents, HIV,
firearms, and house fires combined.6 In many cases, as Claude
Beck noted, cardiac arrest victims have “hearts too good to
die.”7 In these cases, prompt intervention can result in suc-
cessful resuscitation. Yet overall survival rates remain low.
Why? An increasing body of evidence indicates that even
after controlling for patient and event characteristics, there is
significant variability in survival rates both across and within
prehospital and in-hospital settings. Examples include the
following:
• In the prehospital setting, among participating centers in
the Resuscitation Outcomes Consortium (ROC) Epistry,
survival from out-of-hospital arrest ranged from 3.0% to
16.3%.3 In the United Kingdom, survival-to-discharge
rates within the National Health Service ambulance sys-
tem ranged from 2% to 12%.8
• In the hospital setting, among participating centers in
the Get With The Guidelines-Resuscitation quality-
improvement program, the median hospital survival rate
from adult cardiac arrest is 18% (interquartile range,
12%–22%) and from pediatric cardiac arrest, it is 36%
(interquartile range, 33%–49%).
• In a hospital setting, survival is >20% if the arrest occurs
between the hours of 7 am and 11 pm but only 15% if the
arrest occurs between 11 pm and 7 am.9 There is signifi-
cant variability with regard to location, with 9% survival
at night in unmonitored settings compared with nearly
37% survival in operating room/postanesthesia care unit
locations during the day.9
• Patient survival is linked to quality of cardiopulmonary
resuscitation (CPR). When rescuers compress at a depth of
<38 mm, survival-to-discharge rates after out-of-hospital
arrest are reduced by 30%.10 Similarly, when rescuers com-
press too slowly, return of spontaneous circulation (ROSC)
after in-hospital cardiac arrest falls from 72% to 42%.11
The variations in performance and survival described in these
studies provide the resuscitation community with an incen-
tive to improve outcomes. To maximize survival from cardiac
arrest, the time has come to focus efforts on optimizing the
quality of CPR specifically, as well as the performance of
resuscitation processes in general.
CPR is a lifesaving intervention and the cornerstone of
resuscitation from cardiac arrest.12–14 Survival from cardiac
arrest depends on early recognition of the event and immediate
activation of the emergency response system, but equally criti-
cal is the quality of CPR delivered. Both animal and clinical
studies demonstrate that the quality of CPR during resuscita-
tion has a significant impact on survival and contributes to the
wide variability of survival noted between and within systems
of care.3,15 CPR is inherently inefficient; it provides only 10%
to 30% of normal blood flow to the heart and 30% to 40%
of normal blood flow to the brain16–19 even when delivered
according to guidelines. This inefficiency highlights the need
for trained rescuers to deliver the highest-quality CPR possible.
Poor-quality CPR should be considered a preventable
harm. In healthcare environments, variability in clinician
performance has affected the ability to reduce healthcare-
associated complications,20 and a standardized approach has
been advocated to improve outcomes and reduce prevent-
able harms.21 The use of a systematic continuous quality
improvement (CQI) approach has been shown to optimize
outcomes in a number of urgent healthcare conditions.22–24
Despite this evidence, few healthcare organizations apply
these techniques to cardiac arrest by consistently monitor-
ing CPR quality and outcomes. As a result, there remains an
unacceptable disparity in the quality of resuscitation care
delivered, as well as the presence of significant opportuni-
ties to save more lives.
Today, a large gap exists between current knowledge of
CPR quality and its optimal implementation, which leads to
preventable deaths attributable to cardiac arrest. Resuscitative
efforts must be tailored to each patient. Cardiac arrest
occurs in diverse settings with varying epidemiology and
resources, yet effective solutions exist to improve CPR qual-
ity in each of these settings. The purpose of the present con-
sensus statement is to stimulate transformative change on a
large scale by providing healthcare practitioners and health-
care systems a tangible framework with which to maximize
the quality of CPR and save more lives. The intent is to fill
the gap between the existing scientific evidence surround-
ing resuscitation (as presented in the "2010 American Heart
Association Guidelines for Cardiopulmonary Resuscitation
and Emergency Cardiovascular Care" [2010 AHA Guidelines
for CPR and ECC]) and the translation of the guidelines into
routine clinical practice. The approach taken is the use of
expert opinion and interpretation of existing studies to pro-
vide a practical hands-on approach to implementing the 2010
AHA Guidelines for CPR and ECC. Although there are many
factors—population (eg, neonatal), chain of survival (eg,
bystander CPR, postresuscitation care), CPR mechanics (hand
position, duty cycle, airway adjuncts), and education (adult
learning principles, feedback devices during training)—that
impact patient survival, this consensus statement is focused
on the critical parameters of CPR that can be enhanced to help
trained providers optimize performance during cardiac arrest
in an adult or a child.
Four areas related to CPR quality will be addressed:
• Metrics of CPR performance by the provider team
• Monitoring and feedback: options and techniques for
monitoring patient response to resuscitation, as well as
team performance
• Team-level logistics: how to ensure high-quality CPR in
complex settings
• CQI for CPR
In addition, gaps in existing knowledge and technologies
will be reviewed and prioritized and recommendations for
optimal resuscitation practice made.
Methods
The contributors to this statement were selected for their
expertise in the disciplines relevant to adult and pediatric car-
diac resuscitation and CPR quality. Selection of participants
and contributors was restricted to North America, and other
international groups were not represented. After a series of
telephone conferences and webinars between the chair and
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 3
program planning committee, members of the writing group
were selected and writing teams formed to generate the content
of each section. Selection of the writing group was performed
in accordance with the AHA’s conflict of interest management
policy. The chair of the writing group assigned individual con-
tributors to work on 1 or more writing teams that generally
reflected their area of expertise. Articles and abstracts presented
at scientific meetings relevant to CPR quality and systems
improvement were identified through the International Liaison
Committee on Resuscitation’s "2010 International Consensus
on CPR and ECC Science With Treatment Recommendations"
statement and the 2010 International Liaison Committee on
Resuscitation worksheets, PubMed, Embase, and an AHA
master resuscitation reference library. This was supplemented
by manual searches of key articles and abstracts. Statements
generated from literature review were drafted by the writing
group and presented to leaders in CPR quality at a CPR Quality
Summit held May 20–21, 2012, in Irving, TX. Participants
evaluated each statement, and suggested modifications were
incorporated into the draft. Drafts of each section were written
and agreed on by members of the writing team and then sent to
the chair for editing and incorporation into a single document.
The first draft of the complete document was circulated among
writing team leaders for initial comments and editing. A revised
version of the document was circulated among all contributors,
and consensus was achieved. This revised consensus statement
was submitted for independent peer review and endorsed by
several major professional organizations (see endorsements).
The AHA Emergency Cardiovascular Care Committee and
Science Advisory and Coordinating Committee approved the
final version for publication.
Metrics of CPR Performance
by the Provider Team
Oxygen and substrate delivery to vital tissues is the central goal
of CPR during the period of cardiac arrest. To deliver oxygen
and substrate, adequate blood flow must be generated by effec-
tive chest compressions during a majority of the total cardiac
arrest time. ROSC after CPR is dependent on adequate myocar-
dial oxygen delivery and myocardial blood flow during CPR.16–18
Coronary perfusion pressure (CPP, the difference between aor-
tic diastolic and right atrial diastolic pressure during the relax-
ation phase of chest compressions) is the primary determinant
of myocardial blood flow during CPR.25–27 Therefore, maximiz-
ing CPP during CPR is the primary physiological goal. Because
CPP cannot be measured easily in most patients, rescuers should
focus on the specific components of CPR that have evidence to
support either better hemodynamics or human survival.
Five main components of high-performance CPR have
been identified: chest compression fraction (CCF), chest
compression rate, chest compression depth, chest recoil
(residual leaning), and ventilation. These CPR components
were identified because of their contribution to blood flow
and outcome. Understanding the importance of these compo-
nents and their relative relationships is essential for providers
to improve outcomes for individual patients, for educators to
improve the quality of resuscitation training, for administra-
tors to monitor performance to ensure high quality within the
healthcare system, and for vendors to develop the necessary
equipment needed to optimize CPR quality for providers,
educators, and administrators.
Minimize Interruptions: CCF >80%
For adequate tissue oxygenation, it is essential that healthcare
providers minimize interruptions in chest compressions and
therefore maximize the amount of time chest compressions
generate blood flow.12,28 CCF is the proportion of time that
chest compressions are performed during a cardiac arrest. The
duration of arrest is defined as the time cardiac arrest is first
identified until time of first return of sustained circulation. To
maximize perfusion, the 2010 AHA Guidelines for CPR and
ECC recommend minimizing pauses in chest compressions.
Expert consensus is that a CCF of 80% is achievable in a vari-
ety of settings. Data on out-of-hospital cardiac arrest indicate
that lower CCF is associated with decreased ROSC and sur-
vival to hospital discharge.29,30 One method to increase CCF
that has improved survival is through reduction in preshock
pause31; other techniques are discussed later in “Team-Level
Logistics.”
Chest Compression Rate of 100 to 120/min
The 2010 AHA Guidelines for CPR and ECC recommend a
chest compression rate of ≥100/min.28 As chest compression
rates fall, a significant drop-off in ROSC occurs, and higher
rates may reduce coronary blood flow11,32 and decrease the
percentage of compressions that achieve target depth.10,33 Data
from the ROC Epistry provide the best evidence of associa-
tion between compression rate and survival and suggest an
optimum target of between 100 and 120 compressions per
minute.34 Consistent rates above or below that range appear to
reduce survival to discharge.
Chest Compression Depth of ≥50 mm in Adults
and at Least One Third the Anterior-Posterior
Dimension of the Chest in Infants and Children
Compressions generate critical blood flow and oxygen
and energy delivery to the heart and brain. The 2010 AHA
Guidelines for CPR and ECC recommend a single minimum
depth for compressions of ≥2 inches (50 mm) in adults. Less
information is available for children, but it is reasonable to
aim for a compression depth of at least one third of the ante-
rior-posterior dimension of the chest in infants and children
(≈1½ inches, or 4 cm, in infants and ≈2 inches, or 5 cm, in
children).35,36
Although a recent study suggested that a depth of ≥44 mm
in adults may be adequate to ensure optimal outcomes,37 the
preponderance of literature suggests that rescuers often do
not compress the chest deeply enough despite recommenda-
tions.10,37–39 Earlier studies suggested that compressions at a
depth >50 mm may improve defibrillation success and ROSC
in adults.40–43 A recent study examined chest compression
depth and survival in out-of-hospital cardiac arrest in adults
and concluded that a depth of <38 mm was associated with
a decrease in ROSC and rates of survival.10 Confusion may
result when a range of depths is recommended and training
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

4 Circulation July 23, 2013
targets differ from operational performance targets. Optimal
depth may depend on factors such as patient size, compres-
sion rate, and environmental features (such as the presence
of a supporting mattress). Outcome studies to date have been
limited by the use of mean compression depth of CPR, the
impact of the variability of chest compression depth, and the
change in chest compliance over time.
Full Chest Recoil: No Residual Leaning
Incomplete chest wall release occurs when the chest com-
pressor does not allow the chest to fully recoil on comple-
tion of the compression.44,45 This can occur when a rescuer
leans over the patient’s chest, impeding full chest expansion.
Leaning is known to decrease the blood flow throughout the
heart and can decrease venous return and cardiac output.46
Although data are sparse regarding outcomes related to lean-
ing, animal studies have shown that leaning increases right
atrial pressure and decreases cerebral and coronary perfu-
sion pressure, cardiac index, and left ventricular myocardial
flow.46–48 Human studies show that a majority of rescuers
often lean during CPR and do not allow the chest to recoil
fully.49,50 Therefore, the expert panel agrees that leaning
should be minimized.
Avoid Excessive Ventilation: Rate <12 Breaths per
Minute, Minimal Chest Rise
Although oxygen delivery is essential during CPR, the
appropriate timeframe for interventions to supplement exist-
ing oxygen in the blood is unclear and likely varies with the
type of arrest (arrhythmic versus asphyxial). The metabolic
demands for oxygen are also substantially reduced in the
patient in arrest even during chest compressions. When sud-
den arrhythmic arrest is present, oxygen content is initially
sufficient, and high-quality chest compressions can circulate
oxygenated blood throughout the body. Studies in animals and
humans suggest that compressions without ventilations may
be adequate early in nonasphyxial arrests.51–54 When asphyxia
is the cause of the arrest, the combination of assisted ventila-
tion and high-quality chest compressions is critical to ensure
sufficient oxygen delivery. Animal and human studies of
asphyxial arrests have found improved outcomes when both
assisted ventilations and high-quality chest compressions are
delivered.55,56
Providing sufficient oxygen to the blood without imped-
ing perfusion is the goal of assisted ventilation during CPR.
Positive-pressure ventilation reduces CPP during CPR,57 and
synchronous ventilation (recommended in the absence of
an advanced airway)35 requires interruptions, which reduces
CCF. Excessive ventilation, either by rate or tidal volume, is
common in resuscitation environments.38,57–60 Although chest
compression−only CPR by bystanders has yielded similar
survival outcomes from out-of-hospital arrest as standard
CPR,38,51,52 there is presently not enough evidence to define
when or if ventilation should be withheld by experienced pro-
viders, and more data will be required.
Rate <12 Breaths per Minute
Current guideline recommendations for ventilation rate
(breaths per minute) are dependent on the presence of an
advanced airway (8 to 10 breaths per minute), as well as the
patient’s age and the number of rescuers present (compres-
sion-to-ventilation ratio of 15:2 versus 30:2). When other rec-
ommended goals are achieved (ie, compression rate of 100
to 120/min, inflation time of 1 second for each breath), these
ratios lead to ventilation rates of between 6 and 12 breaths
per minute. Animal studies have yielded mixed results regard-
ing harm with high ventilation rates,57,61 but there are no data
showing that ventilating a patient at a higher rate is beneficial.
Currently recommended compression-ventilation ratios are
designed as a memory aid to optimize myocardial blood flow
while adequately maintaining oxygenation and CO2 clear-
ance of the blood. The expert panel supports the 2010 AHA
Guidelines for CPR and ECC and recommends a ventilation
rate of <12 breaths per minute to minimize the impact of pos-
itive-pressure ventilation on blood flow.
Minimal Chest Rise: Optimal Ventilation Pressure and
Volume
Ventilation volume should produce no more than visible
chest rise. Positive-pressure ventilation significantly lowers
cardiac output in both spontaneous circulation and during
CPR.57,62–65 Use of lower tidal volumes during prolonged
cardiac arrest was not associated with significant differences
in Pao2
66 and is currently recommended.67 Additionally,
positive-pressure ventilation in an unprotected airway may
cause gastric insufflation and aspiration of gastric contents.
Lung compliance is affected by compressions during car-
diac arrest,68 and the optimal inflation pressure is not known.
Although the conceptual relevance of ventilation pressure
and volume monitoring during CPR is well established, cur-
rent monitoring equipment and training equipment do not
readily or reliably measure these parameters, and clinical
studies supporting the optimal titration of these parameters
during CPR are lacking.
Monitoring and Feedback: Options
and Techniques for Monitoring
Patient Response to Resuscitation
The adage, “if you don’t measure it, you can’t improve it”
applies directly to monitoring CPR quality. Monitoring the
quality and performance of CPR by rescuers at the scene of
cardiac arrest has been transformative to resuscitation sci-
ence and clinical practice. Studies have demonstrated that
trained rescuers often had poor CCF ratios, depth of compres-
sions, and compression-ventilation rates,39,57,58,69 which were
associated with worse outcomes.11,34 With monitoring, there
is increased clarity about optimal preshock pause, CCF, and
chest compression depth.10,29,31 With newer technology capa-
ble of monitoring CPR parameters during resuscitation, inves-
tigators and clinicians are now able to monitor the quality of
CPR in real time. Given the insights into clinical performance
and discoveries in optimal practice, monitoring of CPR qual-
ity is arguably one of the most significant advances in resus-
citation practice in the past 20 years and one that should be
incorporated into every resuscitation and every professional
rescuer program.
The types of monitoring for CPR quality can be classified
(and prioritized) into physiological (how the patient is doing)
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 5
and CPR performance (how the rescuers are doing) metrics.
Both types of monitoring can provide both real-time feed-
back to rescuers and retrospective system-wide feedback. It
is important to emphasize that types of CPR quality monitor-
ing are not mutually exclusive and that several types can (and
should) be used simultaneously.
How the Patient Is Doing: Monitoring the Patient’s
Physiological Response to Resuscitative Efforts
Physiological data during CPR that are pertinent for monitor-
ing include invasive hemodynamic data (arterial and central
venous pressures when available) and end-tidal carbon dioxide
concentrations (etco2). Abundant experimental literature has
established that (1) survival after CPR is dependent on ade-
quate myocardial oxygen delivery and myocardial blood flow
during CPR, and (2) CPP during the relaxation phase of chest
compressions is the primary determinant of myocardial blood
flow during CPR.17,18,25,26,70,71 CPP during cardiac arrest is the
difference between aortic diastolic pressure and right atrial
diastolic pressure but may be best conceptualized as diastolic
blood pressure–central venous pressure. Although the concep-
tual relevance of hemodynamic and etco2 monitoring during
CPR is well established, clinical studies supporting the optimal
titration of these parameters during human CPR are lacking.
Nevertheless, the opinions and clinical experience of experts
at the CPR Quality Summit strongly support prioritizing use of
hemodynamic and etco2 concentrations to adjust compression
technique during CPR when available. Furthermore, the expert
panel recommends a hierarchal and situational contextualiza-
tion of physiological monitoring based on the available data
most closely related to myocardial blood flow:
1. Invasive Monitoring: CPP >20 mm Hg
Successful adult resuscitation is more likely when CPP is
>20 mm Hg and when diastolic blood pressure is >25 to
30 mm Hg.16,17,25–27,72–77 Although optimal CPP has not been
established, the expert panel agrees with the 2010 AHA
Guidelines for CPR and ECC that monitoring and titration
of CPP during CPR is reasonable.13 Moreover, the expert
panel recommends that this physiological target be the pri-
mary end point when arterial and central venous catheters
are in place at the time of the cardiac arrest and CPR. Data
are insufficient to make a recommendation for CPP goals
for infants and children.
2. Arterial Line Only: Arterial Diastolic Pressure
>25 mm Hg
Consistent with these experimental data, limited published
clinical studies indicate that the provision of successful adult
resuscitation depends on maintaining diastolic blood pressure
at >25 mm Hg.26,75,76 The expert panel recommends that this
physiological target be the primary end point when an arterial
catheter is in place without a central venous catheter at the
time of the cardiac arrest and CPR. The 2010 AHA Guidelines
for CPR and ECC recommend “trying to improve quality of
CPR by optimizing chest compression parameters or giv-
ing vasopressors or both” if diastolic blood pressure is <20
mm Hg.13 The expert panel recommends that rescuers titrate
to a diastolic blood pressure >25 mm Hg for adult victims of
cardiac arrest.
3. Capnography Only: etco2 >20 mm Hg
etco2 concentrations during CPR are primarily dependent
on pulmonary blood flow and therefore reflect cardiac out-
put.78,79 Failure to maintain etco2 at >10 mm Hg during
adult CPR reflects poor cardiac output and strongly predicts
unsuccessful resuscitation.80–82 The 2010 AHA Guidelines
for CPR and ECC recommend monitoring etco2 during CPR
to assess blood flow in 2 ways: to improve chest compression
performance if etco2 is <10 mm Hg during CPR and to con-
sider an abrupt sustained increase to a normal value (35 to
40 mm Hg) as an indicator of ROSC.13 The expert panel rec-
ommends that when available, etco2 should be the primary
physiological metric when neither an arterial nor a central
venous catheter is in place at the time of the cardiac arrest
and CPR. On the basis of limited animal data and personal
experience, the expert panel recommends titrating CPR per-
formance to a goal etco2 of >20 mm Hg while not exces-
sively ventilating the patient (rate <12 breaths per minute,
with only minimal chest rise).
How the Rescuers Are Doing: Monitoring
CPR Performance
Monitors to measure CPR performance are now widely avail-
able. They provide rescuers with invaluable real-time feed-
back on the quality of CPR delivered during resuscitative
efforts, data for debriefing after resuscitation, and retrospec-
tive information for system-wide CPR CQI programs. Without
CPR measurement and subsequent understanding of CPR per-
formance, improvement and optimized performance cannot
occur. Providing CPR without monitoring performance can be
likened to flying an airplane without an altimeter.
Routinely available feedback on CPR performance char-
acteristics includes chest compression rate, depth, and recoil.
Currently, certain important parameters (CCF and preshock,
perishock, and postshock pauses) can be reviewed only retro-
spectively, whereas others (ventilation rate, airway pressure,
tidal volume, and inflation duration) cannot be assessed ade-
quately by current technology. Additionally, accelerometers
are insensitive to mattress compression, and current devices
often prioritize the order of feedback by use of a rigid algo-
rithm in a manner that may not be optimal or realistic (eg,
an accelerometer cannot measure depth if there is too much
leaning, so the device will prioritize feedback to correct lean-
ing before correcting depth). Although some software (auto-
mated algorithms) and hardware solutions currently exist
(smart backboard, dual accelerometers, reference markers,
and others), continued development of optimal and widely
available CPR monitoring is a key component to improved
performance.
Human Supervision and Direction of CPR
Visual observation provides qualitative information about
depth and rate of chest compressions, as well as rate and
tidal volume of ventilations. Although invasive hemodynamic
monitoring (via intra-arterial and central venous catheters)
provides superior quantitative data about patients’ physiol-
ogy, direct observation can reveal important artifacts (eg, pads
were not selected on the monitor/defibrillator, “flat” arterial
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

6 Circulation July 23, 2013
pressure waveform from a turned stopcock obstructed the arte-
rial line tubing), as well as the recognized limitations of feed-
back technology of CPR performance described above. More
rigorous, semiquantitative determination of chest compres-
sion depth and rate can be developed by rescuers with increas-
ing experience, especially after effective feedback. Healthcare
providers may be accustomed to feel for a pulse as an indica-
tion of the adequacy of chest compression, but pulse palpa-
tion during CPR is fraught with potential problems83–85 and is
therefore not recommended as a reliable means of monitoring
the effectiveness of CPR.28,35 Observers can quickly identify
rescuer-patient mismatch (eg, a 40-kg rescuer versus a 120-kg
patient), as well as recommend switching chest compressors if
a rescuer manifests early signs of fatigue. In addition, observ-
ers can integrate the physiological factors (CPP, arterial relax-
ation pressure, or etco2) with quantitative feedback of CPR
quality parameters (depth, rate, leaning) to best achieve opti-
mal CPR delivery.86
New methods and technology that accurately monitor both
team performance and a patient’s physiology during cardiac
arrest should be developed. These may include additional
markers of perfusion such as ventricular fibrillation waveform
analysis, cerebral oximetry, impedance, and near-infrared
spectroscopy. We challenge both researchers and industry to
provide rescuers with robust solutions to monitor patient and
provider performance.
Team-Level Logistics: How to Ensure
High-Quality CPR in the Complex
Setting of Cardiac Resuscitation
Basic life support skills are generally taught and practiced
individually or in pairs.87 In actual practice, CPR is frequently
performed as part of a full resuscitative effort that includes
multiple rescuers and advanced equipment. These additional
resources allow tasks to be performed in parallel so that CPR
can be optimized while the team determines and treats the
underlying cause of the arrest. However, the performance of
secondary tasks frequently consumes large portions of time
and can detract from CPR quality if not managed carefully.88
Resuscitation team composition varies widely, depending
on location (in hospital versus out of hospital), setting (field,
emergency department, hospital ward), and circumstances.
Little is known about the optimal number and background of
professional rescuers.89 Examples of high-functioning resus-
citation teams for both prehospital and in-hospital cardiac
arrest are presented at http://www.heart.org/cprquality. These
examples are meant to be descriptive of how to maintain high-
quality CPR with varying team size and environment rather
than prescriptive if-then rules.
There are, however, data to suggest that resuscitation team
leadership training and demonstration of leadership behaviors
(eg, setting clear expectations, being decisive, and taking a
hands-off approach) are associated with improved CPR per-
formance, especially an increase in CCF.90–92 As such, it is the
recommendation of the expert panel that every resuscitation
event should have a designated team leader who directs and
coordinates all components of the resuscitation with a cen-
tral focus on delivering high-quality CPR. The team leader’s
responsibility is to organize a team of experts into an expert
team by directing and prioritizing the essential activities.
Interactions of CPR Performance Characteristics
There are no clear data on the interactions between com-
pression fraction, rate or depth of compressions, leaning
while performing compressions, and ventilation. All play a
vital role in the transport of substrate to the vital organs
during arrest. For instance, characteristics of chest compres-
sions may be interrelated (eg, higher rate may be associated
with lower depth, and greater depth may lead to increased
leaning), and in practice, the rescuer may need to alter one
component at a time, holding the others constant so as not
to correct one component at the expense of another. The
expert panel proposes that if the patient is not responding
to resuscitative efforts (ie, etco2 <20 mm Hg), team leaders
should prioritize the optimization of individual components
of chest compression delivery in the following order: (1)
compression fraction, (2) compression rate, (3) compres-
sion depth, (4) leaning, and (5) avoidance of excessive ven-
tilation. This order is recommended in part because of the
strength of the science as discussed in the prior sections (eg,
there is stronger evidence for compression fraction, rate,
and depth than leaning) but also for the sake of feasibility,
as discussed below.
Maximization of CCF
Prompt initiation of compressions is the first step toward maxi-
mizing CCF. However, to achieve a target CCF >80%, careful
management of interruptions is critical. The following strate-
gies minimize both the frequency and duration of interruptions.
Choreograph Team Activities
Any tasks that can be effectively accomplished during ongo-
ing chest compressions should be performed without introduc-
ing a pause (Table 1). Additional tasks for which a pause in
compressions is needed should be coordinated and performed
simultaneously in a “pit crew” fashion. The team leader should
communicate clearly with team members about impending
pauses in compression to enable multiple rescuers to anticipate
and then use the same brief pause to achieve multiple tasks.
Table 1. Compression Pause Requirements for Resuscitation
Tasks
Pause Requirement Task
Generally required Defibrillation
Rhythm analysis
Rotation of compressors
Backboard placement
Transition to mechanical CPR or ECMO
Sometimes required Complicated advanced airway placement in
patients who cannot be ventilated effectively
by bag-valve-mask
Assessment for return of spontaneous
circulation
Generally not required Application of defibrillator pads
Uncomplicated advanced airway placement
IV/IO placement
CPR indicates cardiopulmonary resuscitation; ECMO, extracorporeal
membrane oxygenation; and IV/IO, intravenous/intraosseous.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 7
Minimize Interruptions for Airway Placement
The optimal time for insertion of an advanced airway dur-
ing management of cardiac arrest has not been established.
An important consideration is that endotracheal intubation
often accounts for long pauses in performance of chest com-
pressions.93 Supraglottic airways can be used as an alter-
native to invasive airways, although a recent large study
showed worse outcomes when supraglottic airways were
compared with endotracheal intubation.94 Patients who can
be ventilated adequately by a bag-mask device may not
need an advanced airway at all.95 If endotracheal intuba-
tion is performed, the experienced provider should first
attempt laryngoscopy during ongoing chest compressions.
If a pause is required, it should be kept as short as possible,
ideally <10 seconds. If a surgical airway is required, a lon-
ger pause may be necessary. However, in all such cases,
the expert panel recommends performing any portion of the
procedure that can be done during ongoing compressions to
minimize the pause.
Avoid Unnecessary Pulse Checks
Manual palpation for a pulse can result in unnecessarily long
pauses and is often unreliable.83,85,96–100 These pauses can often
be avoided when available monitoring (such as an arterial
line or capnography) indicates a level of cardiac output or a
rhythm (such as ventricular fibrillation) that is incompatible
with organ perfusion.
Minimize Perishock Pauses
The preshock phase may be particularly vulnerable to inter-
ruption of chest compressions because of the need to provide
a safe environment for the rescuer. It is important to mini-
mize preshock pauses, because outcomes are improved with
decreasing duration of pauses before shock delivery, possibly
as short as 9 seconds.31,41,101 A strategy of applying the pads
and charging the defibrillator during ongoing chest compres-
sions results in shorter perishock pauses, and this practice is
recommended.33,102 Development of technology that mini-
mizes all interruptions (eg, compression artifact waveform
filters that enable rhythm analysis during ongoing chest com-
pressions)103 in blood flow, particularly around defibrillation,
is encouraged. Chest compressions should be restarted with-
out delay after delivery of the shock. In one study, elimination
of stacked shocks and extension of the duration of CPR from
1 to 2 minutes before postshock rhythm analyses increased
CCF from 48% to 69% and was associated with increased
survival.104
Tight Regulation of Compression Rate
Once chest compressions have begun, achievement of the tar-
get rate is often the easiest parameter to adjust and maintain.
Real-time CPR feedback devices, as well as low-cost solu-
tions such as metronomes and music, are known to decrease
variability and result in compression rates closer to the tar-
get rate of 100 to 120/min.58,105,106 It is essential to continue to
monitor and adjust for degradation in compression rate over
time and after modifications to other parameters.
Maximizing Compression Depth
With CCF optimized and compressions ongoing at a rate of
100 to 120/min, focus should turn to ensuring that compression
depth is ≥50 mm. This parameter is one of the most difficult to
achieve because of the physical force required. However, the
following are some strategies to help ensure adequate depth:
1. Ensure a Firm, Hard Surface
The 2010 AHA Guidelines for CPR and ECC recommend
performing CPR on a firm, hard surface. Backboards are com-
monly used to achieve target depths107–109 and reduce rescuer
exertion,110 but their placement interrupts CPR.111 For this rea-
son, the expert panel recommends placement of a backboard
or firm, hard surface as soon as possible and in coordination
with other mandatory pauses in compressions to minimize
interruption time.
2. Optimize Provider Mechanics of Compressions
Compression mechanics often degrade over time,112 and res-
cuers often do not perceive fatigue before skill deteriora-
tion.113–115 Although the 2010 AHA Guidelines for CPR and
ECC recommend rotating chest compressors every 2 min-
utes,12 large interindividual differences in chest compression
quality exist.114,116 Some can perform good-quality compres-
sions for up to 10 minutes, whereas inadequate chest com-
pression depths have been observed after only 1 minute of
continuous chest compressions114,116 or even at the initiation
of CPR.114,116 Others have demonstrated that a switch at 2
minutes may be trading optimal compressions for significant
leaning after the switch86 and decreased CCF caused by the
frequency of switching.117 The use of feedback devices, espe-
cially visual, can counteract degradation of CPR mechanics
to some degree.118,119 The expert panel recommends that the
team leader monitor compressors for signs of fatigue. If there
is evidence of inadequate compressions being performed by a
rescuer that cannot be corrected with feedback or adjustments
in positioning, responsibility for chest compressions should
be transferred to another team member as quickly as possible,
even if 2 minutes has not passed. With proper communica-
tion and preparation for the handoff, the switch can be accom-
plished in <3 seconds.86
Compression mechanics are affected by rescuer position-
ing, but there is no consensus on the optimal rescuer position
for chest compressions. Although there may be no degradation
in compression quality over a short duration,111,120,121 rescuer
work appears to increase in the standing position compared
with use of a step stool or when kneeling.122,123 In addition,
step stools have been shown to increase compression depth,
especially for rescuers of short stature.124 The expert panel rec-
ommends adjustable-height surface (such as a hospital bed),
that the height of the surface be lowered, or that a step stool be
used to enable rescuers to achieve optimal depth during CPR.
Avoid Leaning
Increasing compression depth is often accompanied by
increased leaning. Leaning is a bigger concern for taller res-
cuers and those using a step stool.124 The expert panel recom-
mends that as modifications are made to achieve the target
depth, rescuers should monitor for leaning and adjust posi-
tioning as necessary to ensure adequate depth without residual
pressure on the patient’s chest between compressions.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from
8 Circulation July 23, 2013
Avoid Excessive Ventilation
Unlike the compression characteristics, which have effects
that are intertwined, ventilation is a stand-alone skill that can
be optimized in parallel with chest compressions. Methods to
decrease ventilation rate, such as use of metronomes, are well
established,106,125 whereas methods to limit excessive tidal vol-
ume and inspiratory pressure are less well developed but may
include the use of smaller resuscitation bags, manometers, and
direct observation.66,67,126–128
Additional Logistic Considerations
Incorporation of Mechanical CPR
Trials of mechanical CPR devices to date have failed to
demonstrate a consistent benefit in patient outcomes com-
pared with manual CPR.129–133 The most likely explanation is
that inexperienced rescuers underestimate the time required
to apply the device,134 which leads to a significant decrease
in CCF during the first 5 minutes of an arrest135–137 despite
increases in CCF later in the resuscitation.138 There is evi-
dence that pre-event “pit crew” team training can reduce
the pause required to apply the device.139 Three large-scale
implementation studies (Circulation Improving Resuscitation
Care [CIRC],140 Prehospital Randomized Assessment
of a Mechanical Compression Device in Cardiac Arrest
[PARAMEDIC],141 and LUCAS in Cardiac Arrest [LINC])142
may provide clarity about the optimal timing and environ-
ment for mechanical CPR. In the absence of published evi-
dence demonstrating benefit, the decision to use mechanical
CPR may be influenced by system considerations such as in
rural settings with limited numbers of providers and/or long
transport times.
Patient Transport
Performing chest compressions in a mobile environment has
additional challenges and almost uniformly requires that the
rescuer be unsecured, thus posing an additional safety concern
for providers. Manual chest compressions provided in a mov-
ing ambulance are affected by factors such as vehicle move-
ment, acceleration/deceleration, and rotational forces and can
compromise compression fraction, rate, and depth.143,144 There
is no consensus on the ideal ambulance speed to address these
concerns.145,146 Studies of mechanical versus manual CPR in
a moving ambulance show less effect on CPR quality when a
mechanical device is used.130,147
CPR and Systematic CQI
Systematic CQI has optimized outcomes in a number of
healthcare conditions,22–24 increases safety, and reduces
harm.21 Review of the quality and performance of CPR by
professional rescuers after cardiac arrest has been shown to be
feasible and improves outcomes.40,137,148 Despite this evidence,
few healthcare organizations apply these techniques to cardiac
arrest by consistently monitoring CPR quality and outcomes.
As a result, there remains an unacceptable variability in the
quality of resuscitation care delivered.
Debriefing
An effective approach to improving resuscitation quality on
an ongoing basis is the use of debriefing after arrest events.
In this context, debriefing refers to a focused discussion
after a cardiac arrest event in which individual actions and
team performance are reviewed. This technique can be very
effective for achieving improved performance; CPR quality
is reviewed while the resuscitation is fresh in the rescuer’s
mind. This approach, easily adaptable for either out-of-
hospital or in-hospital cardiac arrest, can take a number
of forms. One simple approach is represented by a “group
huddle” among providers after a resuscitation attempt to
briefly discuss their opinions about quality of care and what
could have been improved. Similar discussions among pro-
viders who actually gave care can be performed on a regu-
larly scheduled basis, and such an approach using weekly
debriefing sessions has been shown to improve both CPR
performance and ROSC after in-hospital cardiac arrest.40
Preexisting structures in hospitals and emergency medical
services (EMS) systems can be efficiently adapted to debrief
A
B
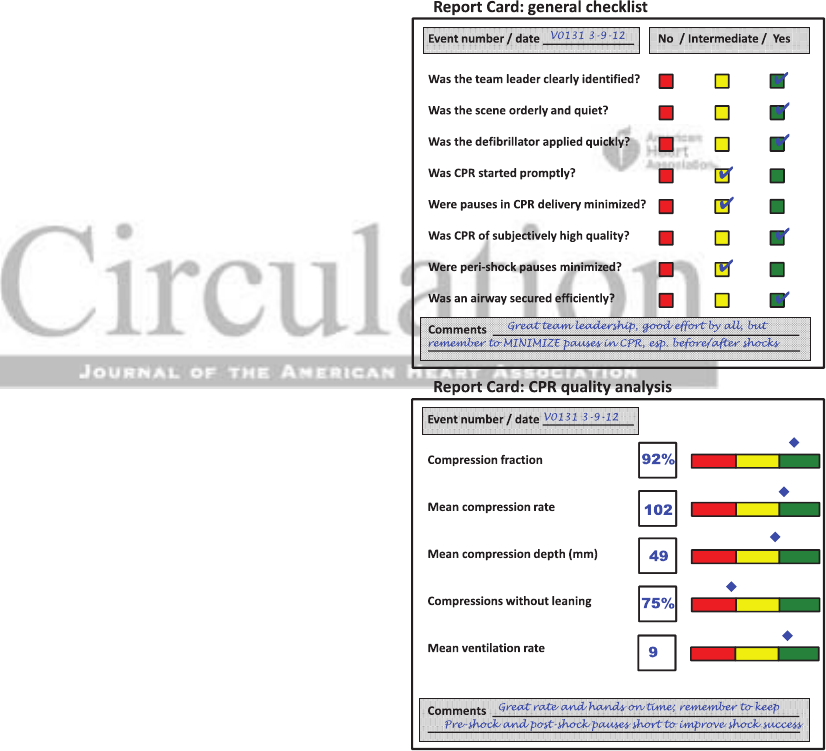
Figure 1. Illustration of proposed resuscitation “report cards.”
Routine use of a brief tool to document resuscitation quality
would assist debriefing efforts and quality improvement efforts
for hospital and emergency medical services systems. A, General
checklist. Example of a general checklist report card that could
be completed by a trained observer to a resuscitation event.
B, CPR quality analysis. Example of a report card that relies on
objective recording of CPR metrics. Ideally, both observational
(A) and objective (B) reports could be used together in a
combined report. CPR indicates cardiopulmonary resuscitation.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from
Meaney et al Improving CPR Quality 9
arrest events. This has also been confirmed by a number
of simulation studies among rescuers of both pediatric and
adult victims of cardiac arrest.149,150 If this approach is taken,
it is crucial that the actual care providers be present for the
discussion.
Use of Checklists
Debriefing can be greatly enhanced by structuring the discus-
sion; that is, basing it on a quality checklist prompted by a
short set of questions on quality metrics. Short CPR check-
lists can provide invaluable feedback directly from multiple
sources. Systems should develop or adapt CPR quality check-
lists as CQI tools. These postevent checklists can be as simple
as a short debriefing checklist (Figure 1 [“report card”]) on
specific quality metrics that can be easily filled out after arrest
events.
Use of Monitoring Data
Inclusion of monitoring data (physiological response of the
patient to resuscitative efforts, performance of CPR by the
provider) can provide an excellent data set for debriefing,
because it allows a more objective approach that avoids per-
ceptions of judgmental feedback. Every EMS system, hospi-
tal, and other professional rescuer program should strongly
consider acquiring technology to capture CPR quality data for
all cardiac arrests. Equipment that measures metrics of CPR
performance must be able to provide resuscitation teams with
the information necessary to implement immediate review
sessions.
Integration With Existing Education
Quality-improvement strategies to improve CPR should
include education to ensure optimal resuscitation team per-
formance. Training in basic or advanced life support provides
foundational knowledge and skills that can be lifesaving and
improve outcomes.151–153 Unfortunately, skills acquired during
these infrequent training programs deteriorate rapidly (within
6–12 months) if not used frequently.154–160 Recent evidence
suggests that frequent short-duration “refreshing” of CPR
skills prevents that decay and improves acquisition and reten-
tion of skills.150,161,162 Therefore, there is increasing interest in
using this as the foundation for maintenance of competence/
certification. Although the various continuous training strat-
egies differ in their advantages, disadvantages, and resource
intensiveness, the expert panel recommends that some form
of continuous training should be a minimum standard for all
CPR CQI programs.
Improved individual healthcare provider and resuscitation
team performance can also be achieved through the use of
simulated resuscitation exercises, or “mock codes.” Use of
these kinds of team-training exercises also helps reinforce
the importance of human factors in resuscitation team func-
tion163 and may prove to be an important systematic program
to improve survival from cardiac arrest.164 Resuscitation train-
ing and education should not be considered a course or a sin-
gle “event” but rather a long-term progression in the ongoing
quest to optimize CPR quality.
Systems Review/Quality Improvement
Every EMS system, hospital, and other professional rescuer
program should have an ongoing CPR CQI program that pro-
vides feedback to the director, managers, and providers. CPR
CQI programs can and should implement systems to acquire
and centrally store metrics of CPR performance. System-wide
performance (which is optimally linked with survival rate)
should be reviewed intermittently, deficiencies identified, and
corrective action implemented. Routinely scheduled hospital
cardiac arrest committee meetings, departmental “morbidity
and mortality” meetings, and EMS quality review meetings
can serve as platforms to discuss selected cases of arrest care
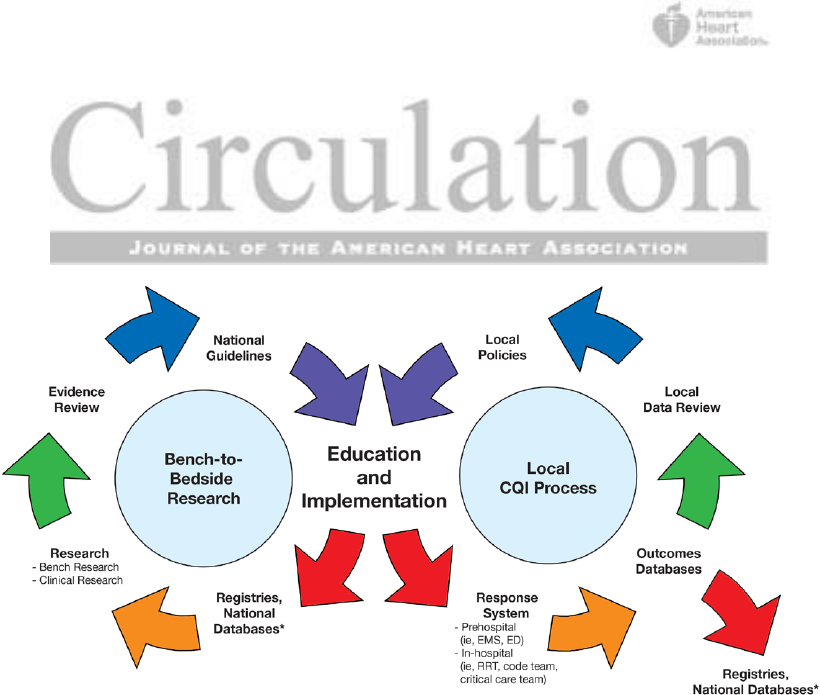
Figure 2. A continuous process evaluates and improves clinical care and generates new guidelines and therapy. Outcome data from
cardiac arrest and periarrest periods are reviewed in a continuous quality-improvement (CQI) process. Research and clinical initiatives
are reviewed periodically in an evidence-based process. Experts then evaluate new therapy and make clinical and educational
recommendations for patient care. The process is repeated, and continual progress and care improvements are generated. ED indicates
emergency department; EMS, emergency medical services; and RRT, rapid response team. *This is an overlap point in the cycle. That is,
data come from outcomes databases (shown on the right) and go into registries and national databases (shown on the left).
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

10 Circulation July 23, 2013
in detail and provide opportunities for feedback and reinforce-
ment of quality goals. For example, time to first defibrillation
attempt and CCF have both been shown to directly relate to
clinical outcomes and are discrete metrics with clear mean-
ing and opportunities for tracking over months or years. Over
time, lessons learned from both a system-wide evaluation
of performance and individual performance of teams from
debriefing can provide invaluable objective feedback to sys-
tems to pinpoint opportunities for targeted training. The deliv-
ery of these messages needs to be consistent with the culture
of the organization.
A number of large data collection initiatives have enriched
clinical resuscitation science and represent opportunities
to improve CQI processes. Similarly, the integration of
local CQI processes, policies, and education through reg-
istries and national databases helps determine and drive
regional, national, and global agendas (Figure 2). Get With
The Guidelines-Resuscitation is an AHA-sponsored registry
representing >250 000 in-hospital cardiac arrest events. The
Cardiac Arrest Registry to Enhance Survival (CARES), estab-
lished by the Centers for Disease Control and Prevention, col-
lects national data on out-of-hospital cardiac arrest. The ROC
has developed Epistry, a large database of out-of-hospital car-
diac arrest events, which includes granular CPR quality met-
rics. A consortium of the European Resuscitation Council has
created EuReCa (European Cardiac Arrest Registry), a mul-
tinational, multicultural database for out-of-hospital cardiac
arrest. The value of these registries has been demonstrated
by numerous research studies using registry data to identify
variability in survival, development of standardized mortality
ratios for comparing healthcare settings, and specific resusci-
tation quality deficiencies. In addition, a recent study has sug-
gested that longer participation by hospitals in Get With The
Guidelines-Resuscitation is associated with improvements in
rates of survival from in-hospital cardiac arrest over time.165
Hospitals and EMS systems are strongly encouraged to par-
ticipate in these collaborative registry programs. The costs of
participation are modest and the potential benefits large. Not
taking advantage of these mechanisms for data collection and
benchmarking means that improved quality of care and sur-
vival will remain elusive.
Many existing obstacles to a systematic improvement in
CPR quality are related to ease of data capture from monitor-
ing systems for systematic review. Currently, most monitors
capable of measuring mechanical parameters of CPR provide
feedback to optimize performance during cardiac arrest, and
some may provide for event review immediately afterward,
but none readily lend themselves to systems review. In cur-
rent practice, for example, most CPR-recording defibrillators
require a manual downloading process. A number of chal-
lenges remain for CQI tools that are not limited to integration
of these data into workflow and processing. Although many
devices now exist to capture CPR quality metrics, robust wire-
less methods to transmit these data need to be less expensive
and more widespread. To make CPR quality data collection
routine, these processes need to be much more effortless. We
Table 2. Final Recommendations
1. High-quality CPR should be recognized as the foundation on which all other resuscitative efforts are built. Target CPR performance metrics include
a. CCF >80%
b. Compression rate of 100 to 120/min
c. Compression depth of ≥50 mm in adults with no residual leaning
i. (At least one third the anterior-posterior dimension of the chest in infants and children)
d. Avoid excessive ventilation
i. (Only minimal chest rise and a rate of <12 breaths/min)
2. At every cardiac arrest attended by professional rescuers
a. Use at least 1 modality of monitoring the team’s CPR performance
b. Depending on available resources, use at least 1 modality of monitoring the patient’s physiological response to resuscitative efforts
c. Continually adjust resuscitative efforts based on the patient’s physiological response
3. Resuscitation teams should coordinate efforts to optimize CPR during cardiac arrest by
a. Starting compressions rapidly and optimizing CPR performance early
b. Making sure that a team leader oversees the effort and delegates effectively to ensure rapid and optimal CPR performance
c. Maintaining optimal CPR delivery while integrating advanced care and transport
4. Systems of care (EMS system, hospital, and other professional rescuer programs) should
a. Determine a coordinated code team response with specific role responsibilities to ensure that high-quality CPR is delivered during the entire event
b. Capture CPR performance data in every cardiac arrest and use an ongoing CPR CQI program to optimize future resuscitative efforts
c. Implement strategies for continuous improvement in CPR quality and incorporate education, maintenance of competency, and review of arrest characteristics
that include available CPR quality metrics
5. A national system for standardized reporting of CPR quality metrics should be developed:
a. CPR quality metrics should be included and collected in national registries and databases for reviewing, reporting, and conducting research on resuscitation
b. The AHA, appropriate government agencies, and device manufacturers should develop industry standards for interoperable raw data downloads and reporting
from electronic data collected during resuscitation for both quality improvement and research
AHA indicates American Heart Association; CCF, chest compression fraction; CPR, cardiopulmonary resuscitation; CQI, continuous quality improvement;
EMS, emergency medical services.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 11
encourage manufacturers to work with systems to develop
seamless means of collecting, transmitting, and compiling
resuscitation quality data and linking them to registries to
improve future training and survival from cardiac arrest.
Conclusions
As the science of CPR evolves, we have a tremendous oppor-
tunity to improve CPR performance during resuscitation
events both inside and outside the hospital. Through better
measurement, training, and systems-improvement processes
of CPR quality, we can have a significant impact on survival
from cardiac arrest and eliminate the gap between current and
optimal outcomes. To achieve this goal, the expert panel pro-
poses 5 recommendations (Table 2), as well as future direc-
tions to close existing gaps in knowledge.
Future Directions
The expert panel expressed full consensus that there is a sig-
nificant need to improve the monitoring and quality of CPR
in all settings. Although there is a much better understanding
of CPR, several critical knowledge gaps currently impede the
implementation and widespread dissemination of high-quality
CPR (Table 3). Research focused on these knowledge gaps
will provide the information necessary to advance the delivery
of optimal CPR and ultimately save more lives. Additionally,
we encourage key stakeholders such as professional societ-
ies, manufacturers, and appropriate government agencies to
work with systems to develop seamless means of collecting
and compiling resuscitation quality data and to link them to
registries to improve future training and rates of survival from
cardiac arrest.
Acknowledgments
We thank the following individuals for their collaborations on the state
of knowledge summary development and summit participation. Along
with the writing group, the CPR Quality Summit investigators include
Lance B. Becker, M. Allen McCullough, Robert M. Sutton, Dana E.
Niles, Mark Venuti, Mary Fran Hazinski, Jose G. Cabanas, Thomas
Rea, Andrew Travers, Elizabeth A. Hunt, Graham Nichol, Michael A.
Rosen, Kathy Duncan, Vinay M. Nadkarni, and Michael R. Sayre.
Sources of Funding
Unrestricted funding for the CPR Quality Summit was provided by
the CPR Improvement Working Group (Laerdal Medical, Philips
Healthcare, and ZOLL Medical Corporation).
Table 3. Future Directions Needed to Improve CPR Quality: Research and Development
Research
• To determine the optimal targets for CPR characteristics (CCF, compression rate and depth, lean, and ventilation), as well as their relative importance to patient
outcome
• To determine the effect of a victim’s age and cause of arrest on optimal CPR characteristics (especially initiation and method of ventilation)
• To further characterize the relationships between individual CPR characteristics
• To further characterize which CPR characteristics and relationships between them are time dependent
• To determine the impact of the variability during the arrest of CPR characteristics (especially CCF and depth) on patient outcome
• To clarify whether ventilation characteristics (time-, pressure-, volume-based parameters) during CPR impact patient outcome
• To determine optimal titration of hemodynamic and etco2 monitoring during human CPR
• To determine whether etco2 monitoring of a noninvasive airway is a reliable and useful monitor of CPR quality
• To determine optimal relationship between preshock CPR characteristics (ie, depth, pause) and ROSC/survival
• To determine the optimal number of rescuers and the effect of rescuer characteristics on CPR quality and patient outcome
• To further characterize the impact of provider fatigue and recovery on patient outcome
• To determine the impact of work environment, training environment, and provider characteristics on CPR performance and patient survival
• To clarify methods of integration of CPR training into advanced courses and continuing maintenance of competency
• To determine the method of education, as well as its timing and location, at a system level to ensure optimal CPR performance and patient outcome
• To develop a global CPR metric that can be used to measure and optimize educational and systems improvement processes
Development
• To standardize the reporting of CPR quality and the integration of these data with existing systems improvement processes and registries
• To develop a device with the ability to measure and monitor CPR quality during training and delivered in real events and integrate it with existing quality
improvement and registries
• To develop optimal CPR systems improvement processes that provide reliable, automated reporting of CPR quality parameters with the capacity for continuous
CPR quality monitoring in all healthcare systems
• To develop feedback technology that prioritizes feedback in an optimal manner (eg, correct weighting and prioritization of the CPR characteristics themselves)
• To develop a more reliable, inexpensive, noninvasive physiological monitor that will increase our ability to optimize CPR for individual victims of cardiac arrest
• To develop training equipment that provides rescuers with robust skills to readily and reliably provide quality CPR
• To develop improved mechanical systems of monitoring CPR, including consistent and reliable capture of ventilation rate, tidal volume, inspiratory pressure, and
duration, as well as complete chest recoil
CCF indicates chest compression fraction; CPR, cardiopulmonary resuscitation; and ROSC, return of spontaneous circulation.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from
12 Circulation July 23, 2013
Writing Group Disclosures
Writing
Group
Member Employment Research Grant
Other Research
Support
Speakers’ Bureau/
Honoraria Ownership Interest
Consultant/
Advisory Board Other
Peter A.
Meaney
The University of
Pennsylvania
None None None None None Expert witness:
Serve as medical
expert reviewer
for medical issues
not pertaining to
CPR*
Bentley J.
Bobrow
University of
Arizona; Arizona
Department of
Health Services;
Maricopa Medical
Center
Principal Investigator for
institutional grant to the
University of Arizona from
Medtronic Foundation for
implementing statewide
system of cardiac care†;
NIH funding to study
traumatic brain injury:
1R01NS071049-01A1
(Adults)
3R01NS071049-S1
(EPIC4Kids)†
None None None None None
Benjamin S.
Abella
University of
Pennsylvania
Medtronic Foundation:
project on cardiac arrest
outcomes; payment to
institution†; Doris Duke
Foundation: project on
postresuscitation injury;
payment to institution†;
NIH NHLBI R18: project on
CPR training of lay public;
payment to institution†;
Philips Healthcare: project
on CPR hemodynamics
and quality; payment
to institution†; Stryker
Medical: postarrest care;
payment to institution†
None Medivance: honoraria
for lectures pertaining to
hypothermia after arrest*
Resuscor, a
company focused
on healthcare
provider education
in resuscitation
science: ownership
stake*
HeartSine
Corp: advisory
board role to
evaluate AED
development*;
Velomedix Corp:
postarrest care*
None
Tom P.
Aufderheide
Medical College of
Wisconsin
NHLBI: Resuscitation
Outcomes Consortium;
money comes to institution,
not to me directly†;
NHLBI: Immediate
Trial; money comes
to institution†; NHLBI:
ResQTrial; money comes
to institution†; NINDS:
Neurological Emergency
Treatment Trials (NETT)
Network; money comes to
institution†
Zoll Medical:
software provided
directly from
Zoll Medical
to Milwaukee
County
Emergency
Medical Services
to complete
research trials for
the Resuscitation
Outcomes
Consortium and
Immediate Trials†
None None President,
Citizen CPR
Foundation
(volunteer)*;
Secretary, Take
Heart America
(volunteer)*;
Medtronic paid
consultant;
consultant on an
acute MI trial;
money went to
my institution;
discontinued
consultant
position
November
2010*
National American
Heart Association
volunteer on
Basic Life Support
Subcommittee
and Research
Working Group*;
As a member of
the Institute of
Medicine (IOM)
and a member of
the AHA Research
Working Group,
works with both
institutions to
generate funding
for an IOM report
on cardiac arrest
(volunteer)*
(Continued)
Disclosures
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 13
Writing Group Disclosures, Continued
Writing
Group
Member Employment Research Grant
Other Research
Support
Speakers’ Bureau/
Honoraria Ownership Interest
Consultant/
Advisory Board Other
Robert A.
Berg
University of
Pennsylvania
Perelman School
of Medicine
None None Society of Critical Care
Medicine’s 2012 Asmund
S. Laerdal Memorial
Lecture Award for
outstanding career as a
resuscitation scientist*
None None None
Farhan
Bhanji
Montreal Children’s
Hospital,
McGill University
None None None None None None
Jim
Christenson
University of British
Columbia, Faculty
of Medicine
Resuscitation Outcomes
Consortium group grant
funded until 2016 on CPR
quality; has published
a paper on chest
compression fraction and
its relationship to survival
and is coauthor on several
papers evaluating various
potential aspects of CPR
quality†
None None None None None
Allan R. de
Caen
Self-employed None None None None None None
Dana P.
Edelson
University of
Chicago
Philips Healthcare: funds
paid to institution for
projects on CPR quality and
hemodynamics;
Laerdal Medical: funds paid
to institution for piloting
new Basic Life Support
training†; NIH NHLBI:
funds paid to institution for
strategies to prevent and
predict in-hospital cardiac
arrests†
None None Quant HC: Develops
products for risk
stratification
of hospitalized
patients†
CARES Advisory
Council:
Member*;
Sudden
Cardiac Arrest
Foundation
Board of
Directors:
Member*;
FIERCE
Certification
Advisory
Council:
Member*
Monica E.
Kleinman
Children’s Hospital
Anesthesia
Foundation
None None None None None Expert witness:
Review of
medical-legal
cases on behalf of
defendants*
Marion
Leary
University of
Pennsylvania
None None Speaking honoraria a few
years ago from Philips
Healthcare*
None Have reviewed
devices
for Philips
Healthcare
and Laerdal
surrounding CPR
quality devices,
neither for any
money*
Philips Healthcare
has given
research group
QCPR devices to
use for research*
(Continued)
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

14 Circulation July 23, 2013
Writing Group Disclosures, Continued
Writing
Group
Member Employment Research Grant
Other Research
Support
Speakers’ Bureau/
Honoraria Ownership Interest
Consultant/
Advisory Board Other
Mary E.
Mancini
The University of
Texas at Arlington
None None Received honoraria for
keynote speeches at
national professional
meetings such as
National League for
Nursing Education
Summit on Nursing
education. Topics
included the importance
of maintenance of
competency and
simulation; no long-term
agreements to provide
services related to a
speakers’ bureau.*
No personal financial
interest but named
on a patent for CPR
device. University
will receive the
royalty if and
when the device is
commercialized.*
Serves on an
advisory board
for an LWW
nursing product
in development
that will support
nursing students
in developing
critical thinking
skills; one
situation to be
covered is care
of the patient
with a cardiac
arrest.*
None
Venu Menon Cleveland Clinic None None None None None None
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the
Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (1) the person
receives $10 000 or more during any 12-month period, or 5% or more of the person’s gross income; or (2) the person owns 5% or more of the voting stock or share of
the entity, or owns $10 000 or more of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding
definition.
*Modest.
†Significant.
Reviewer Disclosures
Reviewer Employment
Research
Grant
Other Research
Support
Speakers’
Bureau/Honoraria
Expert
Witness
Ownership
Interest
Consultant/
Advisory Board Other
Sheldon
Cheskes
Sunnybrook Center for
Prehospital Medicine, Canada
None COPI Toronto site
(Resuscitation
Outcomes
Consortium)†
None None None None None
Gavin
Perkins
Warwick Medical School
and Heart of England NHS
Foundation Trust, United
Kingdom
NIH (money
paid to
institution)†
None None None None None None
Elizabeth H.
Sinz
Penn State Hershey Medical
Center
None None None None None None AHA, Associate
Science Editor
(money paid to
institution)†
Kjetil Sunde University of Oslo, Norway None None None None None None None
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure
Questionnaire, which all reviewers are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives $10 000 or more during
any 12-month period, or 5% or more of the person’s gross income; or (2) the person owns 5% or more of the voting stock or share of the entity, or owns $10 000 or more
of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
†Significant.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 15
References
1. Ahern RM, Lozano R, Naghavi M, Foreman K, Gakidou E, Murray CJ.
Improving the public health utility of global cardiovascular mortality data:
the rise of ischemic heart disease. Popul Health Metr. 2011;9:8.
2. Berdowski J, Berg RA, Tijssen JG, Koster RW. Global incidences of out-
of-hospital cardiac arrest and survival rates: systematic review of 67 pro-
spective studies. Resuscitation. 2010;81:1479–1487.
3. Nichol G, Thomas E, Callaway CW, Hedges J, Powell JL, Aufderheide TP,
Rea T, Lowe R, Brown T, Dreyer J, Davis D, Idris A, Stiell I; Resuscitation
Outcomes Consortium Investigators. Regional variation in out-of-hospital
cardiac arrest incidence and outcome [published correction appears in
JAMA. 2008;300:1763]. JAMA. 2008;300:1423–1431.
4. Go AS, Mozaffarian D, Roger VL, Benjamin EJ, Berry JD, Borden WB,
Bravata DM, Dai S, Ford ES, Fox CS, Franco S, Fullerton HJ, Gillespie C,
Hailpern SM, Heit JA, Howard VJ, Huffman MD, Kissela BM, Kittner SJ,
Lackland DT, Lichtman JH, Lisabeth LD, Magid D, Marcus GM, Marelli
A, Matchar DB, McGuire DK, Mohler ER, Moy CS, Mussolino ME,
Nichol G, Paynter NP, Schreiner PJ, Sorlie PD, Stein J, Turan TN, Virani
SS, Wong ND, Woo D, Turner MB; American Heart Association Statistics
Committee and Stroke Statistics Subcommittee. Heart disease and stroke
statistics–2013 update: a report from the American Heart Association
[published correction appears in Circulation. 2013;127:doi:10.1161/
CIR.0b013e31828124ad]. Circulation. 2013;127:e6–e245.
5. Merchant RM, Yang L, Becker LB, Berg RA, Nadkarni V, Nichol G,
Carr BG, Mitra N, Bradley SM, Abella BS, Groeneveld PW; American
Heart Association Get With The Guidelines-Resuscitation Investigators.
Incidence of treated cardiac arrest in hospitalized patients in the United
States. Crit Care Med. 2011;39:2401–2406.
6. Centers for Disease Control and Prevention. National Vital Statistics
Reports, December 29, 2011. http://www.cdc.gov/nchs/data/nvsr/nvsr60/
nvsr60_03.pdf. Accessed October 31, 2012.
7. Beck CS, Leighninger DS. Death after a clean bill of health: so-called
“fatal” heart attacks and treatment with resuscitation techniques. JAMA.
1960;174:133–135.
8. Perkins GD, Cooke MW. Variability in cardiac arrest survival: the NHS
Ambulance Service Quality Indicators. Emerg Med J. 2012;29:3–5.
9. Peberdy MA, Ornato JP, Larkin GL, Braithwaite RS, Kashner TM,
Carey SM, Meaney PA, Cen L, Nadkarni VM, Praestgaard AH, Berg
RA; National Registry of Cardiopulmonary Resuscitation Investigators.
Survival from in-hospital cardiac arrest during nights and weekends.
JAMA. 2008;299:785–792.
10. Stiell IG, Brown SP, Christenson J, Cheskes S, Nichol G, Powell J, Bigham
B, Morrison LJ, Larsen J, Hess E, Vaillancourt C, Davis DP, Callaway
CW; Resuscitation Outcomes Consortium (ROC) Investigators. What is
the role of chest compression depth during out-of-hospital cardiac arrest
resuscitation? Crit Care Med. 2012;40:1192–1198.
11. Abella BS, Sandbo N, Vassilatos P, Alvarado JP, O’Hearn N, Wigder HN,
Hoffman P, Tynus K, Vanden Hoek TL, Becker LB. Chest compression
rates during cardiopulmonary resuscitation are suboptimal: a prospective
study during in-hospital cardiac arrest. Circulation. 2005;111:428–434.
12. Travers AH, Rea TD, Bobrow BJ, Edelson DP, Berg RA, Sayre MR,
Berg MD, Chameides L, O’Connor RE, Swor RA. Part 4: CPR over-
view: 2010 American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Circulation.
2010;122(suppl 3):S676–S684.
13. Neumar RW, Otto CW, Link MS, Kronick SL, Shuster M, Callaway CW,
Kudenchuk PJ, Ornato JP, McNally B, Silvers SM, Passman RS, White
RD, Hess EP, Tang W, Davis D, Sinz E, Morrison LJ. Part 8: adult advanced
cardiovascular life support: 2010 American Heart Association Guidelines
for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care
[published correction appears in Circulation. 2011;123:e236]. Circulation.
2010;122(suppl 3):S729–S767.
14. Kleinman ME, Chameides L, Schexnayder SM, Samson RA, Hazinski
MF, Atkins DL, Berg MD, de Caen AR, Fink EL, Freid EB, Hickey RW,
Marino BS, Nadkarni VM, Proctor LT, Qureshi FA, Sartorelli K, Topjian
A, van der Jagt EW, Zaritsky AL. Part 14: pediatric advanced life sup-
port: 2010 American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Circulation.
2010;122(suppl 3):S876–S908.
15. Nichol G, Aufderheide TP, Eigel B, Neumar RW, Lurie KG, Bufalino
VJ, Callaway CW, Menon V, Bass RR, Abella BS, Sayre M, Dougherty
CM, Racht EM, Kleinman ME, O’Connor RE, Reilly JP, Ossmann EW,
Peterson E; American Heart Association Emergency Cardiovascular
Care Committee; Council on Arteriosclerosis, Thrombosis, and Vascular
Biology; Council on Cardiopulmonary, Critical Care, Perioperative and
Resuscitation; Council on Cardiovascular Nursing; Council on Clinical
Cardiology; Advocacy Committee; Council on Quality of Care and
Outcomes Research. Regional systems of care for out-of-hospital cardiac
arrest: a policy statement from the American Heart Association [pub-
lished correction appears in Circulation. 2010;122:e439]. Circulation.
2010;121:709–729.
16. Ralston SH, Voorhees WD, Babbs CF. Intrapulmonary epinephrine during
prolonged cardiopulmonary resuscitation: improved regional blood flow
and resuscitation in dogs. Ann Emerg Med. 1984;13:79–86.
17. Michael JR, Guerci AD, Koehler RC, Shi AY, Tsitlik J, Chandra N,
Niedermeyer E, Rogers MC, Traystman RJ, Weisfeldt ML. Mechanisms
by which epinephrine augments cerebral and myocardial perfusion during
cardiopulmonary resuscitation in dogs. Circulation. 1984;69:822–835.
18. Halperin HR, Tsitlik JE, Guerci AD, Mellits ED, Levin HR, Shi
AY, Chandra N, Weisfeldt ML. Determinants of blood flow to vital
organs during cardiopulmonary resuscitation in dogs. Circulation.
1986;73:539–550.
19. Rubertsson S, Karlsten R. Increased cortical cerebral blood flow with
LUCAS, a new device for mechanical chest compressions compared to
standard external compressions during experimental cardiopulmonary
resuscitation. Resuscitation. 2005;65:357–363.
20. Gurses AP, Seidl KL, Vaidya V, Bochicchio G, Harris AD, Hebden
J, Xiao Y. Systems ambiguity and guideline compliance: a qualita-
tive study of how intensive care units follow evidence-based guide-
lines to reduce healthcare-associated infections. Qual Saf Health Care.
2008;17:351–359.
21. Pronovost PJ, Bo-Linn GW. Preventing patient harms through systems of
care. JAMA. 2012;308:769–770.
22. Jollis JG, Granger CB, Henry TD, Antman EM, Berger PB, Moyer PH,
Pratt FD, Rokos IC, Acuña AR, Roettig ML, Jacobs AK. Systems of
care for ST-segment-elevation myocardial infarction: a report from the
American Heart Association’s Mission: Lifeline. Circ Cardiovasc Qual
Outcomes. 2012;5:423–428.
23. Nestler DM, Noheria A, Haro LH, Stead LG, Decker WW, Scanlan-
Hanson LN, Lennon RJ, Lim CC, Holmes DR Jr, Rihal CS, Bell MR, Ting
HH. Sustaining improvement in door-to-balloon time over 4 years: the
Mayo Clinic ST-elevation myocardial infarction protocol. Circ Cardiovasc
Qual Outcomes. 2009;2:508–513.
24. Santana MJ, Stelfox HT. Quality indicators used by trauma centers for per-
formance measurement. J Trauma Acute Care Surg. 2012;72:1298–1302.
25. Niemann JT, Rosborough JP, Ung S, Criley JM. Coronary perfusion pres-
sure during experimental cardiopulmonary resuscitation. Ann Emerg Med.
1982;11:127–131.
26. Paradis NA, Martin GB, Rivers EP, Goetting MG, Appleton TJ, Feingold
M, Nowak RM. Coronary perfusion pressure and the return of sponta-
neous circulation in human cardiopulmonary resuscitation. JAMA.
1990;263:1106–1113.
27. Sanders AB, Ogle M, Ewy GA. Coronary perfusion pressure during car-
diopulmonary resuscitation. Am J Emerg Med. 1985;3:11–14.
28. Berg RA, Hemphill R, Abella BS, Aufderheide TP, Cave DM, Hazinski
MF, Lerner EB, Rea TD, Sayre MR, Swor RA. Part 5: adult basic life sup-
port: 2010 American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care [published correction
appears in Circulation. 2011;124:e402]. Circulation. 2010;122(suppl
3):S685–S705.
29. Christenson J, Andrusiek D, Everson-Stewart S, Kudenchuk P, Hostler D,
Powell J, Callaway CW, Bishop D, Vaillancourt C, Davis D, Aufderheide
TP, Idris A, Stouffer JA, Stiell I, Berg R; Resuscitation Outcomes
Consortium Investigators. Chest compression fraction determines sur-
vival in patients with out-of-hospital ventricular fibrillation. Circulation.
2009;120:1241–1247.
30. Vaillancourt C, Everson-Stewart S, Christenson J, Andrusiek D, Powell
J, Nichol G, Cheskes S, Aufderheide TP, Berg R, Stiell IG; Resuscitation
Outcomes Consortium Investigators. The impact of increased chest com-
pression fraction on return of spontaneous circulation for out-of-hospital
cardiac arrest patients not in ventricular fibrillation. Resuscitation.
2011;82:1501–1507.
31. Cheskes S, Schmicker RH, Christenson J, Salcido DD, Rea T, Powell J,
Edelson DP, Sell R, May S, Menegazzi JJ, Van Ottingham L, Olsufka M,
Pennington S, Simonini J, Berg RA, Stiell I, Idris A, Bigham B, Morrison
L; Resuscitation Outcomes Consortium (ROC) Investigators. Perishock
pause: an independent predictor of survival from out-of-hospital shock-
able cardiac arrest. Circulation. 2011;124:58–66.
32. Wolfe JA, Maier GW, Newton JR Jr, Glower DD, Tyson GS Jr, Spratt
JA, Rankin JS, Olsen CO. Physiologic determinants of coronary blood
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

16 Circulation July 23, 2013
flow during external cardiac massage. J Thorac Cardiovasc Surg.
1988;95:523–532.
33. Monsieurs KG, De Regge M, Vansteelandt K, De Smet J, Annaert E,
Lemoyne S, Kalmar AF, Calle PA. Excessive chest compression rate is
associated with insufficient compression depth in prehospital cardiac
arrest. Resuscitation. 2012;83:1319–1323.
34. Idris AH, Guffey D, Aufderheide TP, Brown S, Morrison LJ, Nichols
P, Powell J, Daya M, Bigham BL, Atkins DL, Berg R, Davis D, Stiell
I, Sopko G, Nichol G; Resuscitation Outcomes Consortium (ROC)
Investigators. Relationship between chest compression rates and outcomes
from cardiac arrest. Circulation. 2012;125:3004–3012.
35. Berg MD, Schexnayder SM, Chameides L, Terry M, Donoghue A, Hickey
RW, Berg RA, Sutton RM, Hazinski MF. Part 13: pediatric basic life sup-
port: 2010 American Heart Association Guidelines for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Circulation.
2010;122(suppl 3):S862–S875.
36. Sutton RM, French B, Nishisaki A, Niles DE, Maltese MR, Boyle L,
Stavland M, Eilevstjønn J, Arbogast KB, Berg RA, Nadkarni VM.
American Heart Association cardiopulmonary resuscitation quality targets
are associated with improved arterial blood pressure during pediatric car-
diac arrest. Resuscitation. 2013;84:168–172.
37. Stiell IG, Brown S, Calloway CW, Aufderheide TP, Cheskes S,
Vaillancourt C, Hostler D, Davis DP, Idris A, Christenson J, Morrison
M, Stouffer J, Free C, Nichol G; Resuscitation Outcomes Consortium
Investigators. What is the optimal chest compression depth during resus-
citation from out-of-hospital cardiac arrest in adult patients? Circulation.
2012;126:A287. Abstract.
38. Abella BS, Alvarado JP, Myklebust H, Edelson DP, Barry A, O’Hearn N,
Vanden Hoek TL, Becker LB. Quality of cardiopulmonary resuscitation
during in-hospital cardiac arrest. JAMA. 2005;293:305–310.
39. Wik L, Kramer-Johansen J, Myklebust H, Sørebø H, Svensson L, Fellows B,
Steen PA. Quality of cardiopulmonary resuscitation during out-of-hospital
cardiac arrest. JAMA. 2005;293:299–304.
40. Edelson DP, Litzinger B, Arora V, Walsh D, Kim S, Lauderdale DS,
Vanden Hoek TL, Becker LB, Abella BS. Improving in-hospital cardiac
arrest process and outcomes with performance debriefing. Arch Intern
Med. 2008;168:1063–1069.
41. Edelson DP, Abella BS, Kramer-Johansen J, Wik L, Myklebust H, Barry
AM, Merchant RM, Hoek TL, Steen PA, Becker LB. Effects of compres-
sion depth and pre-shock pauses predict defibrillation failure during car-
diac arrest. Resuscitation. 2006;71:137–145.
42. Kramer-Johansen J, Myklebust H, Wik L, Fellows B, Svensson L, Sørebø
H, Steen PA. Quality of out-of-hospital cardiopulmonary resuscitation
with real time automated feedback: a prospective interventional study.
Resuscitation. 2006;71:283–292.
43. Babbs CF, Kemeny AE, Quan W, Freeman G. A new paradigm for
human resuscitation research using intelligent devices. Resuscitation.
2008;77:306–315.
44. Aufderheide TP, Pirrallo RG, Yannopoulos D, Klein JP, von Briesen C,
Sparks CW, Deja KA, Conrad CJ, Kitscha DJ, Provo TA, Lurie KG.
Incomplete chest wall decompression: a clinical evaluation of CPR per-
formance by EMS personnel and assessment of alternative manual chest
compression-decompression techniques. Resuscitation. 2005;64:353–362.
45. Yannopoulos D, McKnite S, Aufderheide TP, Sigurdsson G, Pirrallo
RG, Benditt D, Lurie KG. Effects of incomplete chest wall decompres-
sion during cardiopulmonary resuscitation on coronary and cerebral
perfusion pressures in a porcine model of cardiac arrest. Resuscitation.
2005;64:363–372.
46. Zuercher M, Hilwig RW, Ranger-Moore J, Nysaether J, Nadkarni VM,
Berg MD, Kern KB, Sutton R, Berg RA. Leaning during chest compres-
sions impairs cardiac output and left ventricular myocardial blood flow in
piglet cardiac arrest. Crit Care Med. 2010;38:1141–1146.
47. Sutton RM, Niles D, Nysaether J, Stavland M, Thomas M, Ferry S,
Bishnoi R, Litman R, Allen J, Srinivasan V, Berg RA, Nadkarni VM.
Effect of residual leaning force on intrathoracic pressure during mechani-
cal ventilation in children. Resuscitation. 2010;81:857–860.
48. Niles DE, Sutton RM, Nadkarni VM, Glatz A, Zuercher M, Maltese MR,
Eilevstjønn J, Abella BS, Becker LB, Berg RA. Prevalence and hemo-
dynamic effects of leaning during CPR. Resuscitation. 2011;82(suppl
2):S23–S26.
49. Fried DA, Leary M, Smith DA, Sutton RM, Niles D, Herzberg DL, Becker
LB, Abella BS. The prevalence of chest compression leaning during in-hos-
pital cardiopulmonary resuscitation. Resuscitation. 2011;82:1019–1024.
50. Niles D, Nysaether J, Sutton R, Nishisaki A, Abella BS, Arbogast K,
Maltese MR, Berg RA, Helfaer M, Nadkarni V. Leaning is common
during in-hospital pediatric CPR, and decreased with automated correc-
tive feedback. Resuscitation. 2009;80:553–557.
51. Hallstrom A, Cobb L, Johnson E, Copass M. Cardiopulmonary resuscita-
tion by chest compression alone or with mouth-to-mouth ventilation. N
Engl J Med. 2000;342:1546–1553.
52. Van Hoeyweghen RJ, Bossaert LL, Mullie A, Calle P, Martens P, Buylaert
WA, Delooz H. Quality and efficiency of bystander CPR: Belgian Cerebral
Resuscitation Study Group. Resuscitation. 1993;26:47–52.
53. Bobrow BJ, Clark LL, Ewy GA, Chikani V, Sanders AB, Berg RA,
Richman PB, Kern KB. Minimally interrupted cardiac resuscitation by
emergency medical services for out-of-hospital cardiac arrest. JAMA.
2008;299:1158–1165.
54. Dorph E, Wik L, Strømme TA, Eriksen M, Steen PA. Oxygen delivery
and return of spontaneous circulation with ventilation:compression
ratio 2:30 versus chest compressions only CPR in pigs. Resuscitation.
2004;60:309–318.
55. Kitamura T, Iwami T, Kawamura T, Nagao K, Tanaka H, Nadkarni VM,
Berg RA, Hiraide A; Implementation Working Group for All-Japan Utstein
Registry of the Fire and Disaster Management Agency. Conventional
and chest-compression-only cardiopulmonary resuscitation by bystand-
ers for children who have out-of-hospital cardiac arrests: a prospec-
tive, nationwide, population-based cohort study. Lancet. 2010;375:
1347–1354.
56. Berg RA, Hilwig RW, Kern KB, Babar I, Ewy GA. Simulated mouth-
to-mouth ventilation and chest compressions (bystander cardiopulmonary
resuscitation) improves outcome in a swine model of prehospital pediatric
asphyxial cardiac arrest. Crit Care Med. 1999;27:1893–1899.
57. Aufderheide TP, Sigurdsson G, Pirrallo RG, Yannopoulos D, McKnite
S, von Briesen C, Sparks CW, Conrad CJ, Provo TA, Lurie KG.
Hyperventilation-induced hypotension during cardiopulmonary resuscita-
tion. Circulation. 2004;109:1960–1965.
58. Milander MM, Hiscok PS, Sanders AB, Kern KB, Berg RA, Ewy
GA. Chest compression and ventilation rates during cardiopulmonary
resuscitation: the effects of audible tone guidance. Acad Emerg Med.
1995;2:708–713.
59. O’Neill JF, Deakin CD. Do we hyperventilate cardiac arrest patients?
Resuscitation. 2007;73:82–85.
60. McInnes AD, Sutton RM, Orioles A, Nishisaki A, Niles D, Abella BS,
Maltese MR, Berg RA, Nadkarni V. The first quantitative report of ventila-
tion rate during in-hospital resuscitation of older children and adolescents.
Resuscitation. 2011;82:1025–1029.
61. Gazmuri RJ, Ayoub IM, Radhakrishnan J, Motl J, Upadhyaya MP.
Clinically plausible hyperventilation does not exert adverse hemodynamic
effects during CPR but markedly reduces end-tidal PCO2. Resuscitation.
2012;83:259–264.
62. Woda RP, Dzwonczyk R, Bernacki BL, Cannon M, Lynn L. The ventila-
tory effects of auto-positive end-expiratory pressure development during
cardiopulmonary resuscitation. Crit Care Med. 1999;27:2212–2217.
63. Pepe PE, Marini JJ. Occult positive end-expiratory pressure in mechani-
cally ventilated patients with airflow obstruction: the auto-PEEP effect.
Am Rev Respir Dis. 1982;126:166–170.
64. Cournand A, Motley HL. Physiological studies of the effects of intermit-
tent positive pressure breathing on cardiac output in man. Am J Physiol.
1948;152:162–174.
65. Sykes MK, Adams AP, Finlay WE, McCormick PW, Economides A. The
effects of variations in end-expiratory inflation pressure on cardiorespi-
ratory function in normo-, hypo-and hypervolaemic dogs. Br J Anaesth.
1970;42:669–677.
66. Langhelle A, Sunde K, Wik L, Steen PA. Arterial blood-gases with 500-
versus 1000-ml tidal volumes during out-of-hospital CPR. Resuscitation.
2000;45:27–33.
67. Wenzel V, Keller C, Idris AH, Dörges V, Lindner KH, Brimacombe JR.
Effects of smaller tidal volumes during basic life support ventilation in
patients with respiratory arrest: good ventilation, less risk? Resuscitation.
1999;43:25–29.
68. Fuerst R, Idris A, Banner M, Wenzel V, Orban D. Changes in respira-
tory system compliance during cardiopulmonary arrest with and without
closed chest compressions. Ann Emerg Med. 1993;22:931.
69. Valenzuela TD, Kern KB, Clark LL, Berg RA, Berg MD, Berg DD,
Hilwig RW, Otto CW, Newburn D, Ewy GA. Interruptions of chest com-
pressions during emergency medical systems resuscitation. Circulation.
2005;112:1259–1265.
70. Crile G, Dolley DH. An experimental research into the resuscitation of
dogs killed by anesthetics and asphyxia. J Exp Med. 1906;8:713–725.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 17
71. Berg RA, Kern KB, Hilwig RW, Ewy GA. Assisted ventilation during
“bystander” CPR in a swine acute myocardial infarction model does not
improve outcome. Circulation. 1997;96:4364–4371.
72. Redding JS, Pearson JW. Resuscitation from ventricular fibrillation: drug
therapy. JAMA. 1968;203:255–260.
73. Kern KB, Ewy GA, Voorhees WD, Babbs CF, Tacker WA. Myocardial
perfusion pressure: a predictor of 24-hour survival during prolonged car-
diac arrest in dogs. Resuscitation. 1988;16:241–250.
74. Lindner KH, Prengel AW, Pfenninger EG, Lindner IM, Strohmenger HU,
Georgieff M, Lurie KG. Vasopressin improves vital organ blood flow
during closed-chest cardiopulmonary resuscitation in pigs. Circulation.
1995;91:215–221.
75. Martin GB, Carden DL, Nowak RM, Lewinter JR, Johnston W,
Tomlanovich MC. Aortic and right atrial pressures during standard and
simultaneous compression and ventilation CPR in human beings. Ann
Emerg Med. 1986;15:125–130.
76. Timerman S, Cardoso LF, Ramires JA, Halperin H. Improved hemody-
namic performance with a novel chest compression device during treat-
ment of in-hospital cardiac arrest. Resuscitation. 2004;61:273–280.
77. Pearson JW, Redding JS. Peripheral vascular tone on cardiac resuscitation.
Anesth Analg. 1965;44:746–752.
78. Ornato JP, Garnett AR, Glauser FL. Relationship between cardiac
output and the end-tidal carbon dioxide tension. Ann Emerg Med.
1990;19:1104–1106.
79. Weil MH, Bisera J, Trevino RP, Rackow EC. Cardiac output and end-tidal
carbon dioxide. Crit Care Med. 1985;13:907–909.
80. Levine RL, Wayne MA, Miller CC. End-tidal carbon dioxide and outcome
of out-of-hospital cardiac arrest. N Engl J Med. 1997;337:301–306.
81. Sanders AB, Kern KB, Otto CW, Milander MM, Ewy GA. End-tidal car-
bon dioxide monitoring during cardiopulmonary resuscitation: a prognos-
tic indicator for survival. JAMA. 1989;262:1347–1351.
82. Cantineau JP, Lambert Y, Merckx P, Reynaud P, Porte F, Bertrand C,
Duvaldestin P. End-tidal carbon dioxide during cardiopulmonary resusci-
tation in humans presenting mostly with asystole: a predictor of outcome.
Crit Care Med. 1996;24:791–796.
83. Eberle B, Dick WF, Schneider T, Wisser G, Doetsch S, Tzanova I.
Checking the carotid pulse check: diagnostic accuracy of first respond-
ers in patients with and without a pulse. Resuscitation. 1996;33:
107–116.
84. Tibballs J, Russell P. Reliability of pulse palpation by healthcare personnel
to diagnose paediatric cardiac arrest. Resuscitation. 2009;80:61–64.
85. Lapostolle F, Le Toumelin P, Agostinucci JM, Catineau J, Adnet F.
Basic cardiac life support providers checking the carotid pulse: perfor-
mance, degree of conviction, and influencing factors. Acad Emerg Med.
2004;11:878–880.
86. Sutton RM, Maltese MR, Niles D, French B, Nishisaki A, Arbogast KB,
Donoghue A, Berg RA, Helfaer MA, Nadkarni V. Quantitative analysis of
chest compression interruptions during in-hospital resuscitation of older
children and adolescents. Resuscitation. 2009;80:1259–1263.
87. Hazinski MF, ed. BLS for Healthcare Providers Student Manual. Dallas,
TX: American Heart Association; 2011.
88. Tschan F, Vetterli M, Semmer NK, Hunziker S, Marsch SC. Activities
during interruptions in cardiopulmonary resuscitation: a simulator study.
Resuscitation. 2011;82:1419–1423.
89. Eschmann NM, Pirrallo RG, Aufderheide TP, Lerner EB. The association
between emergency medical services staffing patterns and out-of-hospital
cardiac arrest survival. Prehosp Emerg Care. 2010;14:71–77.
90. Yeung JH, Ong GJ, Davies RP, Gao F, Perkins GD. Factors affecting team
leadership skills and their relationship with quality of cardiopulmonary
resuscitation. Crit Care Med. 2012;40:2617–2621.
91. Hunziker S, Bühlmann C, Tschan F, Balestra G, Legeret C, Schumacher
C, Semmer NK, Hunziker P, Marsch S. Brief leadership instructions
improve cardiopulmonary resuscitation in a high-fidelity simulation: a
randomized controlled trial [published correction appears in Crit Care
Med. 2010;38:1510]. Crit Care Med. 2010;38:1086–1091.
92. Cooper S, Wakelam A. Leadership of resuscitation teams: “Lighthouse
Leadership.” Resuscitation. 1999;42:27–45.
93. Wang HE, Simeone SJ, Weaver MD, Callaway CW. Interruptions in car-
diopulmonary resuscitation from paramedic endotracheal intubation. Ann
Emerg Med. 2009;54:645–652.e1.
94. Wang HE, Szydlo D, Stouffer JA, Lin S, Carlson JN, Vaillancourt C,
Sears G, Verbeek RP, Fowler R, Idris AH, Koenig K, Christenson J,
Minokadeh A, Brandt J, Rea T; ROC Investigators. Endotracheal intuba-
tion versus supraglottic airway insertion in out-of-hospital cardiac arrest.
Resuscitation. 2012;83:1061–1066.
95. Hanif MA, Kaji AH, Niemann JT. Advanced airway management does
not improve outcome of out-of-hospital cardiac arrest. Acad Emerg Med.
2010;17:926–931.
96. Bahr J, Klingler H, Panzer W, Rode H, Kettler D. Skills of lay people in
checking the carotid pulse. Resuscitation. 1997;35:23–26.
97. Moule P. Checking the carotid pulse: diagnostic accuracy in students of
the healthcare professions. Resuscitation. 2000;44:195–201.
98. Nyman J, Sihvonen M. Cardiopulmonary resuscitation skills in nurses
and nursing students. Resuscitation. 2000;47:179–184.
99. Ochoa FJ, Ramalle-Gómara E, Carpintero JM, García A, Saralegui
I. Competence of health professionals to check the carotid pulse.
Resuscitation. 1998;37:173–175.
100. Mather C, O’Kelly S. The palpation of pulses. Anaesthesia.
1996;51:189–191.
101. Sell RE, Sarno R, Lawrence B, Castillo EM, Fisher R, Brainard C,
Dunford JV, Davis DP. Minimizing pre- and post-defibrillation pauses
increases the likelihood of return of spontaneous circulation (ROSC).
Resuscitation. 2010;81:822–825.
102. Perkins GD, Davies RP, Soar J, Thickett DR. The impact of manual defi-
brillation technique on no-flow time during simulated cardiopulmonary
resuscitation. Resuscitation. 2007;73:109–114.
103. Li Y, Bisera J, Weil MH, Tang W. An algorithm used for ventricular
fibrillation detection without interrupting chest compression. IEEE Trans
Biomed Eng. 2012;59:78–86.
104. Rea TD, Helbock M, Perry S, Garcia M, Cloyd D, Becker L, Eisenberg
M. Increasing use of cardiopulmonary resuscitation during out-of-hos-
pital ventricular fibrillation arrest: survival implications of guideline
changes. Circulation. 2006;114:2760–2765.
105. Chung TN, Bae J, Kim EC, Cho YK, You JS, Choi SW, Kim OJ. Induction
of a shorter compression phase is correlated with a deeper chest compres-
sion during metronome-guided cardiopulmonary resuscitation: a manikin
study. Emerg Med J. July 25, 2012. doi:10.1136/emermed-2012-201534.
http://emj.bmj.com/content/early/2012/07/24/emermed-2012-201534.
long. Accessed June 11, 2013.
106. Kern KB, Stickney RE, Gallison L, Smith RE. Metronome improves
compression and ventilation rates during CPR on a manikin in a random-
ized trial. Resuscitation. 2010;81:206–210.
107. Sato H, Komasawa N, Ueki R, Yamamoto N, Fujii A, Nishi S, Kaminoh
Y. Backboard insertion in the operating table increases chest compres-
sion depth: a manikin study. J Anesth. 2011;25:770–772.
108. Nishisaki A, Maltese MR, Niles DE, Sutton RM, Urbano J, Berg RA,
Nadkarni VM. Backboards are important when chest compressions are
provided on a soft mattress. Resuscitation. 2012;83:1013–1020.
109. Andersen LØ, Isbye DL, Rasmussen LS. Increasing compression depth
during manikin CPR using a simple backboard. Acta Anaesthesiol Scand.
2007;51:747–750.
110. Noordergraaf GJ, Paulussen IW, Venema A, van Berkom PF, Woerlee
PH, Scheffer GJ, Noordergraaf A. The impact of compliant surfaces
on in-hospital chest compressions: effects of common mattresses and a
backboard. Resuscitation. 2009;80:546–552.
111. Perkins GD, Smith CM, Augre C, Allan M, Rogers H, Stephenson B,
Thickett DR. Effects of a backboard, bed height, and operator position on
compression depth during simulated resuscitation. Intensive Care Med.
2006;32:1632–1635.
112. Sugerman NT, Edelson DP, Leary M, Weidman EK, Herzberg DL,
Vanden Hoek TL, Becker LB, Abella BS. Rescuer fatigue during actual
in-hospital cardiopulmonary resuscitation with audiovisual feedback: a
prospective multicenter study. Resuscitation. 2009;80:981–984.
113. Ochoa FJ, Ramalle-Gómara E, Lisa V, Saralegui I. The effect of res-
cuer fatigue on the quality of chest compressions. Resuscitation.
1998;37:149–152.
114. Ashton A, McCluskey A, Gwinnutt CL, Keenan AM. Effect of rescuer
fatigue on performance of continuous external chest compressions over 3
min. Resuscitation. 2002;55:151–155.
115. Hightower D, Thomas SH, Stone CK, Dunn K, March JA. Decay in
quality of closed-chest compressions over time. Ann Emerg Med.
1995;26:300–303.
116. Bjørshol CA, Sunde K, Myklebust H, Assmus J, Søreide E. Decay in
chest compression quality due to fatigue is rare during prolonged
advanced life support in a manikin model. Scand J Trauma Resusc Emerg
Med. 2011;19:46.
117. Manders S, Geijsel FE. Alternating providers during continuous chest
compressions for cardiac arrest: every minute or every two minutes?
Resuscitation. 2009;80:1015–1018.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

18 Circulation July 23, 2013
118. Cason CL, Trowbridge C, Baxley SM, Ricard MD. A counterbalanced
cross-over study of the effects of visual, auditory and no feedback on per-
formance measures in a simulated cardiopulmonary resuscitation. BMC
Nurs. 2011;10:15.
119. Pozner CN, Almozlino A, Elmer J, Poole S, McNamara D, Barash D.
Cardiopulmonary resuscitation feedback improves the quality of chest
compression provided by hospital health care professionals. Am J Emerg
Med. 2011;29:618–625.
120. Chi CH, Tsou JY, Su FC. Effects of rescuer position on the kinematics
of cardiopulmonary resuscitation (CPR) and the force of delivered com-
pressions. Resuscitation. 2008;76:69–75.
121. Jäntti H, Silfvast T, Turpeinen A, Kiviniemi V, Uusaro A. Quality of car-
diopulmonary resuscitation on manikins: on the floor and in the bed. Acta
Anaesthesiol Scand. 2009;53:1131–1137.
122. Foo NP, Chang JH, Lin HJ, Guo HR. Rescuer fatigue and cardiopul-
monary resuscitation positions: a randomized controlled crossover trial.
Resuscitation. 2010;81:579–584.
123. Jones AY, Lee RY. Rescuer’s position and energy consumption, spinal
kinetics, and effectiveness of simulated cardiac compression. Am J Crit
Care. 2008;17:417–425.
124. Edelson DP, Call SL, Yuen TC, Vanden Hoek TL. The impact of a step
stool on cardiopulmonary resuscitation: a cross-over mannequin study.
Resuscitation. 2012;83:874–878.
125. Lim JS, Cho YC, Kwon OY, Chung SP, Yu K, Kim SW. Precise minute
ventilation delivery using a bag-valve mask and audible feedback. Am J
Emerg Med. 2012;30:1068–1071.
126. Sherren PB, Lewinsohn A, Jovaisa T, Wijayatilake DS. Comparison of
the Mapleson C system and adult and paediatric self-inflating bags for
delivering guideline-consistent ventilation during simulated adult cardio-
pulmonary resuscitation. Anaesthesia. 2011;66:563–567.
127. Nehme Z, Boyle MJ. Smaller self-inflating bags produce greater guide-
line consistent ventilation in simulated cardiopulmonary resuscitation.
BMC Emerg Med. 2009;9:4.
128. Terndrup TE, Rhee J. Available ventilation monitoring methods
during pre-hospital cardiopulmonary resuscitation. Resuscitation.
2006;71:10–18.
129. Dickinson ET, Verdile VP, Schneider RM, Salluzzo RF. Effectiveness of
mechanical versus manual chest compressions in out-of-hospital cardiac
arrest resuscitation: a pilot study. Am J Emerg Med. 1998;16:289–292.
130. Hallstrom A, Rea TD, Sayre MR, Christenson J, Anton AR, Mosesso
VN Jr, Van Ottingham L, Olsufka M, Pennington S, White LJ, Yahn
S, Husar J, Morris MF, Cobb LA. Manual chest compression vs use
of an automated chest compression device during resuscitation follow-
ing out-of-hospital cardiac arrest: a randomized trial. JAMA. 2006;295:
2620–2628.
131. Smekal D, Johansson J, Huzevka T, Rubertsson S. A pilot study of
mechanical chest compressions with the LUCAS™ device in cardiopul-
monary resuscitation. Resuscitation. 2011;82:702–706.
132. Axelsson C, Nestin J, Svensson L, Axelsson AB, Herlitz J. Clinical con-
sequences of the introduction of mechanical chest compression in the
EMS system for treatment of out-of-hospital cardiac arrest: a pilot study.
Resuscitation. 2006;71:47–55.
133. Rubertsson S, Silfverstolpe J, Rehn L, Nyman T, Lichtveld R, Boomars
R, Bruins W, Ahlstedt B, Puggioli H, Lindgren E, Smekal D, Skoog G,
Kastberg R, Lindblad A, Halliwell D, Box M, Arnwald F, Hardig BM,
Chamberlain D, Herlitz J, Karlsten R. The study protocol for the LINC
(LUCAS in cardiac arrest) study: a study comparing conventional adult
out-of-hospital cardiopulmonary resuscitation with a concept with
mechanical chest compressions and simultaneous defibrillation. Scand J
Trauma Resusc Emerg Med. 2013;21:5.
134. Yost D, Phillips RH, Gonzales L, Lick CJ, Satterlee P, Levy M, Barger J,
Dodson P, Poggi S, Wojcik K, Niskanen RA, Chapman FW. Assessment
of CPR interruptions from transthoracic impedance during use of
the LUCAS™ mechanical chest compression system. Resuscitation.
2012;83:961–965.
135. Ong ME, Annathurai A, Shahidah A, Leong BS, Ong VY, Tiah L, Ang
SH, Yong KL, Sultana P. Cardiopulmonary resuscitation interruptions
with use of a load-distributing band device during emergency department
cardiac arrest. Ann Emerg Med. 2010;56:233–241.
136. Fischer H, Neuhold S, Zapletal B, Hochbrugger E, Koinig H, Steinlechner
B, Frantal S, Stumpf D, Greif R. A manually powered mechanical resus-
citation device used by a single rescuer: a randomised controlled manikin
study. Resuscitation. 2011;82:913–919.
137. Fischer H, Neuhold S, Hochbrugger E, Steinlechner B, Koinig H,
Milosevic L, Havel C, Frantal S, Greif R. Quality of resuscitation: flight
attendants in an airplane simulator use a new mechanical resuscitation
device: a randomized simulation study. Resuscitation. 2011;82:459–463.
138. Tomte O, Sunde K, Lorem T, Auestad B, Souders C, Jensen J, Wik L.
Advanced life support performance with manual and mechanical chest
compressions in a randomized, multicentre manikin study. Resuscitation.
2009;80:1152–1157.
139. Ong ME, Quah JL, Annathurai A, Noor NM, Koh ZX, Tan KB,
Pothiawala S, Poh AH, Loy CK, Fook-Chong S. Improving the quality of
cardiopulmonary resuscitation by training dedicated cardiac arrest teams
incorporating a mechanical load-distributing device at the emergency
department. Resuscitation. 2013;84:508–514.
140. Circulation Improving Resuscitation Care (CIRC Study). ClinicalTrials.
gov Web site. http://clinicaltrials.gov/ct2/show/record/nct00597207.
Accessed February 28, 2013.
141. Perkins GD, Woollard M, Cooke MW, Deakin C, Horton J, Lall R, Lamb
SE, McCabe C, Quinn T, Slowther A, Gates S; PARAMEDIC Trial
Collaborators. Prehospital randomised assessment of a mechanical com-
pression device in cardiac arrest (PaRAMeDIC) trial protocol. Scand J
Trauma Resusc Emerg Med. 2010;18:58.
142. A Comparison of Conventional Adult Out-of-hospital Cardiopulmonary
Resuscitation Against a Concept With Mechanical Chest Compressions
and Simultaneous Defibrillation (LINC Study). ClinicalTrials.gov Web
site. http://clinicaltrials.gov/ct2/show/nct00609778?term=linc&rank=1.
Accessed February 28, 2013.
143. Havel C, Schreiber W, Riedmuller E, Haugk M, Richling N, Trimmel H,
Malzer R, Sterz F, Herkner H. Quality of closed chest compression in
ambulance vehicles, flying helicopters and at the scene. Resuscitation.
2007;73:264–270.
144. Olasveengen TM, Wik L, Steen PA. Quality of cardiopulmonary resus-
citation before and during transport in out-of-hospital cardiac arrest.
Resuscitation. 2008;76:185–190.
145. Chung TN, Kim SW, Cho YS, Chung SP, Park I, Kim SH. Effect of vehi-
cle speed on the quality of closed-chest compression during ambulance
transport. Resuscitation. 2010;81:841–847.
146. Kurz MC, Dante SA, Puckett BJ. Estimating the impact of off-balancing
forces upon cardiopulmonary resuscitation during ambulance transport.
Resuscitation. 2012;83:1085–1089.
147. Sunde K, Wik L, Steen PA. Quality of mechanical, manual standard and
active compression-decompression CPR on the arrest site and during
transport in a manikin model. Resuscitation. 1997;34:235–242.
148. Zebuhr C, Sutton RM, Morrison W, Niles D, Boyle L, Nishisaki
A, Meaney P, Leffelman J, Berg RA, Nadkarni VM. Evaluation of
quantitative debriefing after pediatric cardiac arrest. Resuscitation.
2012;83:1124–1128.
149. Dine CJ, Gersh RE, Leary M, Riegel BJ, Bellini LM, Abella BS.
Improving cardiopulmonary resuscitation quality and resuscitation train-
ing by combining audiovisual feedback and debriefing. Crit Care Med.
2008;36:2817–2822.
150. Sutton RM, Niles D, Meaney PA, Aplenc R, French B, Abella BS,
Lengetti EL, Berg RA, Helfaer MA, Nadkarni V. Low-dose, high-fre-
quency CPR training improves skill retention of in-hospital pediatric
providers. Pediatrics. 2011;128:e145–e151.
151. Dane FC, Russell-Lindgren KS, Parish DC, Durham MD, Brown TD.
In-hospital resuscitation: association between ACLS training and sur-
vival to discharge. Resuscitation. 2000;47:83–87.
152. Moretti MA, Cesar LA, Nusbacher A, Kern KB, Timerman S,
Ramires JA. Advanced cardiac life support training improves long-
term survival from in-hospital cardiac arrest. Resuscitation. 2007;72:
458–465.
153. Bobrow BJ, Vadeboncoeur TF, Stolz U, Silver AE, Tobin JM, Crawford
SA, Mason TK, Schirmer J, Smith GA, Spaite DW. The influence of
scenario-based training and real-time audiovisual feedback on out-of-
hospital cardiopulmonary resuscitation quality and survival from out-of-
hospital cardiac arrest. Ann Emerg Med. March 7, 2013. doi:10.1016/j.
annemergmed.2012.12.010. http://www.annemergmed.com/article/S0196-
0644(12)01853-7/abstract. Accessed June 11, 2013.
154. Yang CW, Yen ZS, McGowan JE, Chen HC, Chiang WC, Mancini ME,
Soar J, Lai MS, Ma MH. A systematic review of retention of adult
advanced life support knowledge and skills in healthcare providers.
Resuscitation. 2012;83:1055–1060.
155. Roppolo LP, Pepe PE, Campbell L, Ohman K, Kulkarni H, Miller R,
Idris A, Bean L, Bettes TN, Idris AH. Prospective, randomized trial of the
effectiveness and retention of 30-min layperson training for cardiopul-
monary resuscitation and automated external defibrillators: the American
Airlines Study. Resuscitation. 2007;74:276–285.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from

Meaney et al Improving CPR Quality 19
156. Einspruch EL, Lynch B, Aufderheide TP, Nichol G, Becker L. Retention
of CPR skills learned in a traditional AHA Heartsaver course versus
30-min video self-training: a controlled randomized study. Resuscitation.
2007;74:476–486.
157. Wik L, Myklebust H, Auestad BH, Steen PA. Retention of basic life
support skills 6 months after training with an automated voice advisory
manikin system without instructor involvement. Resuscitation. 2002;52:
273–279.
158. Wik L, Myklebust H, Auestad BH, Steen PA. Twelve-month retention
of CPR skills with automatic correcting verbal feedback. Resuscitation.
2005;66:27–30.
159. Smith KK, Gilcreast D, Pierce K. Evaluation of staff’s retention of ACLS
and BLS skills. Resuscitation. 2008;78:59–65.
160. Meaney PA, Sutton RM, Tsima B, Steenhoff AP, Shilkofski N, Boulet
JR, Davis A, Kestler AM, Church KK, Niles DE, Irving SY, Mazhani
L, Nadkarni VM. Training hospital providers in basic CPR skills in
Botswana: acquisition, retention and impact of novel training techniques.
Resuscitation. 2012;83:1484–1490.
161. Niles D, Sutton RM, Donoghue A, Kalsi MS, Roberts K, Boyle L,
Nishisaki A, Arbogast KB, Helfaer M, Nadkarni V. “Rolling Refreshers”:
a novel approach to maintain CPR psychomotor skill competence.
Resuscitation. 2009;80:909–912.
162. Oermann MH, Kardong-Edgren SE, Odom-Maryon T. Effects of
monthly practice on nursing students’ CPR psychomotor skill perfor-
mance. Resuscitation. 2011;82:447–453.
163. Hunziker S, Johansson AC, Tschan F, Semmer NK, Rock L, Howell MD,
Marsch S. Teamwork and leadership in cardiopulmonary resuscitation. J
Am Coll Cardiol. 2011;57:2381–2388.
164. Andreatta P, Saxton E, Thompson M, Annich G. Simulation-based
mock codes significantly correlate with improved pediatric patient car-
diopulmonary arrest survival rates. Pediatr Crit Care Med. 2011;12:
33–38.
165. Bradley SM, Huszti E, Warren SA, Merchant RM, Sayre MR, Nichol
G. Duration of hospital participation in Get With the Guidelines-
Resuscitation and survival of in-hospital cardiac arrest. Resuscitation.
2012;83:1349–1357.
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from
Tom P. Aufderheide, Venu Menon and Marion Leary
Farhan Bhanji, Benjamin S. Abella, Monica E. Kleinman, Dana P. Edelson, Robert A. Berg,
Peter A. Meaney, Bentley J. Bobrow, Mary E. Mancini, Jim Christenson, Allan R. de Caen,
Hospital: A Consensus Statement From the American Heart Association
CPR Quality: Improving Cardiac Resuscitation Outcomes Both Inside and Outside the
Print ISSN: 0009-7322. Online ISSN: 1524-4539
Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation published online June 25, 2013;Circulation.
http://circ.ahajournals.org/content/early/2013/06/25/CIR.0b013e31829d8654
World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circ.ahajournals.org//subscriptions/ is online at: Circulation Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer this process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information about
Office. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the EditorialCirculationin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on January 16, 2018http://circ.ahajournals.org/Downloaded from
