Calcaneus Fractures
2014-02-04
: Pdf Calcaneus Fractures Calcaneus_Fractures 2 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 120 [warning: Documents this large are best viewed by clicking the View PDF Link!]
2/4/2014
1
Fractures of the Calcaneus
R.J. Claridge MD
Mayo Clinic
Scottsdale Arizona
Fractures of the Calcaneus
R.J. Claridge MD
Mayo Clinic
Scottsdale Arizona
Evaluation & Indications
Fractures of the Calcaneus
Disclosures
•No disclosures pertinent to this
presentation
2/4/2014
2
Fractures of the Calcaneus
Evaluation
•History and Physical:
Mechanism of injury
Concomitant injuries
Diabetes, neuropathy
Smoking history, vascular disease
Soft tissue damage
Bone quality
Fractures of the Calcaneus
Evaluation
Fractures of the Calcaneus
Evaluation
2/4/2014
3
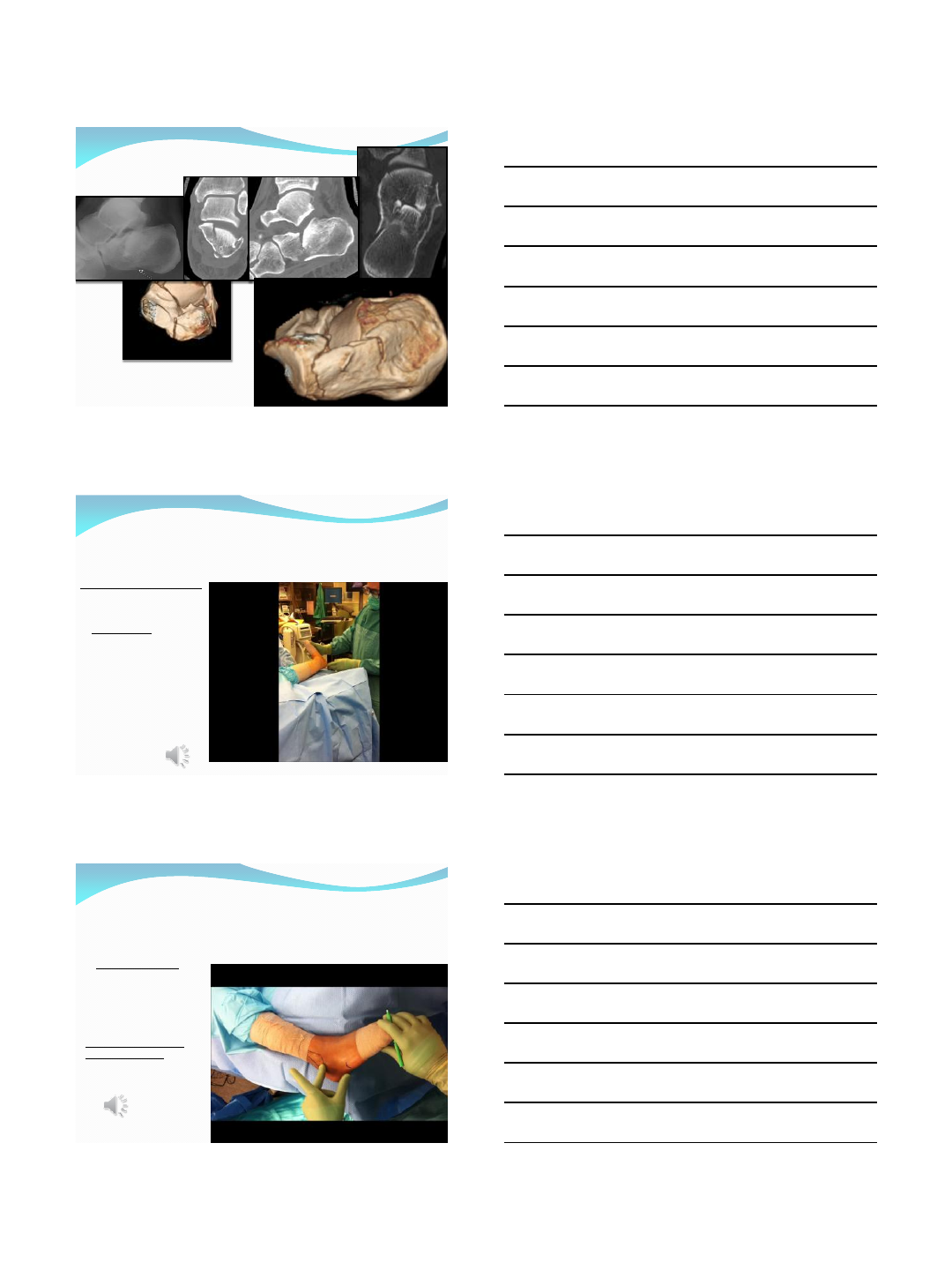
Fractures of the Calcaneus
Evaluation
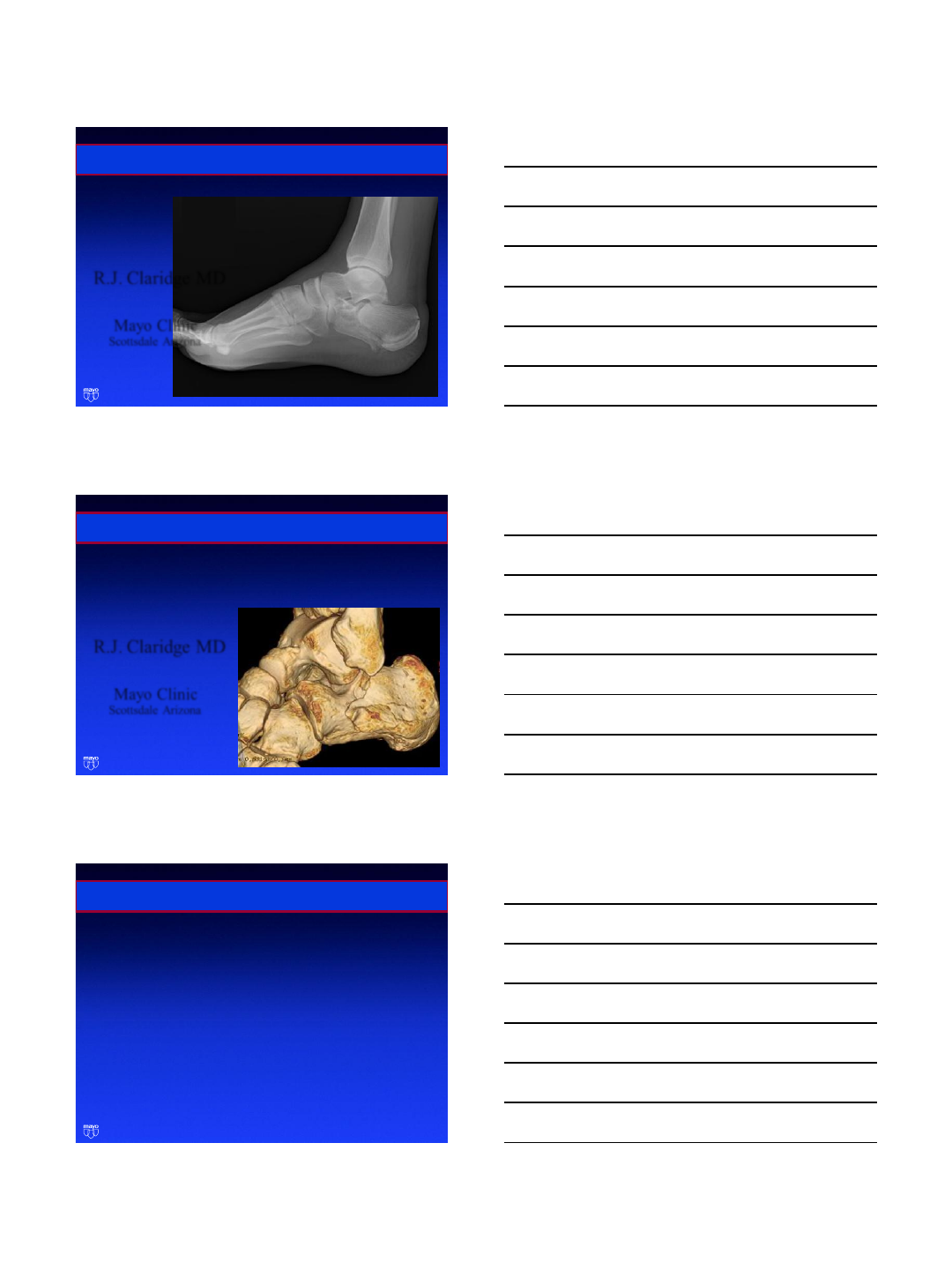
•Radiographs:
Foot, 3 views
AP ankle
Harris view
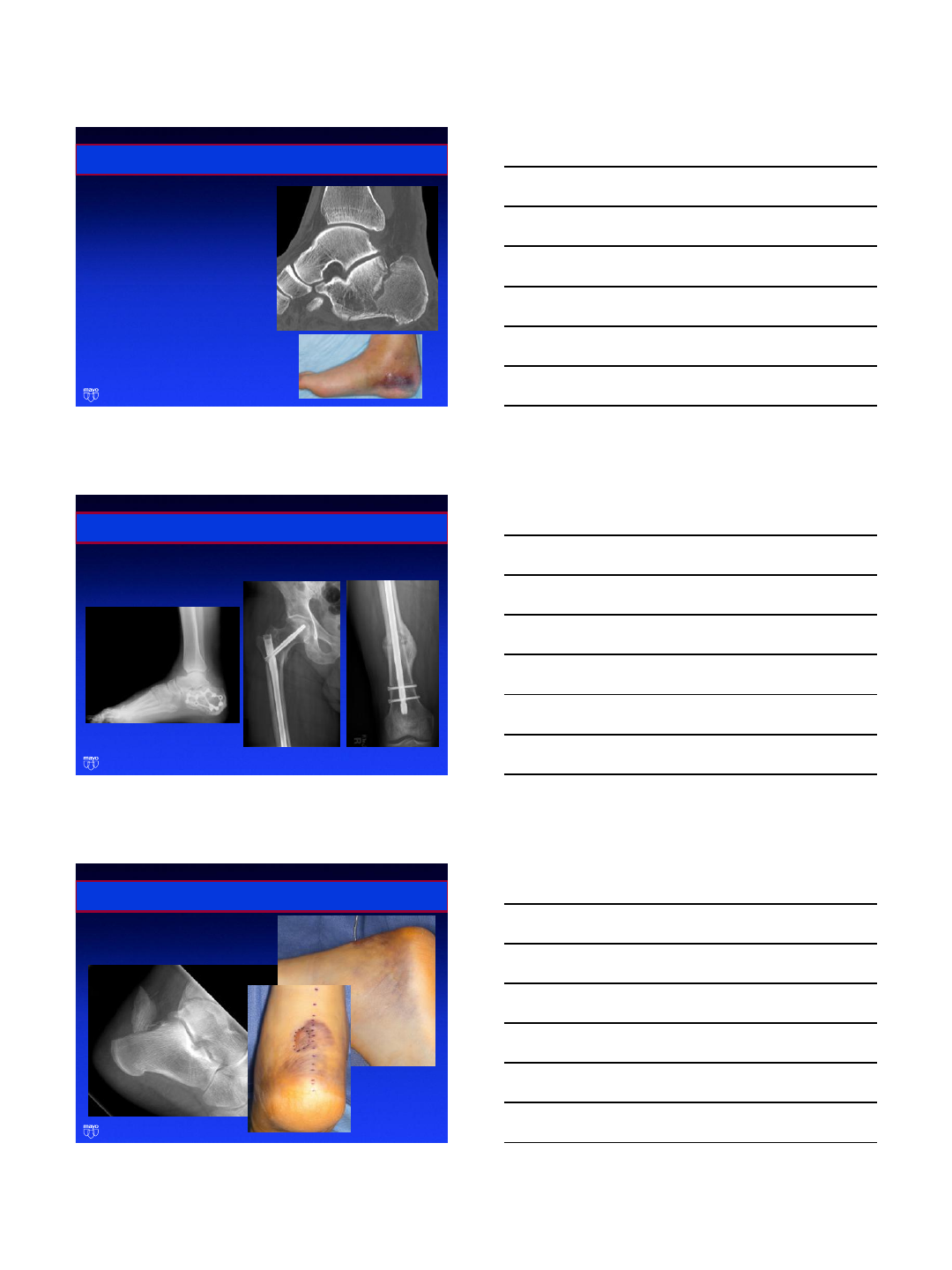
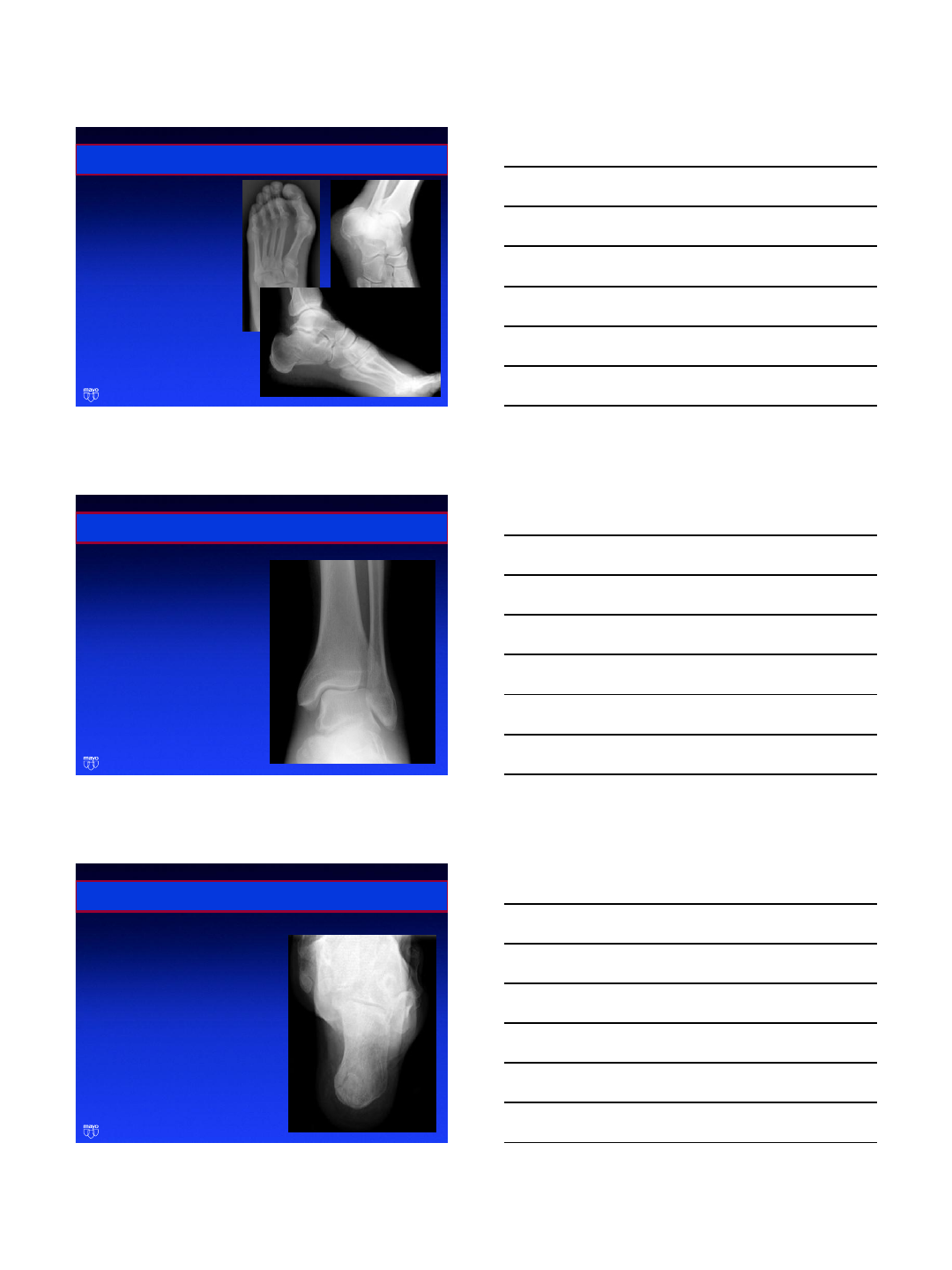
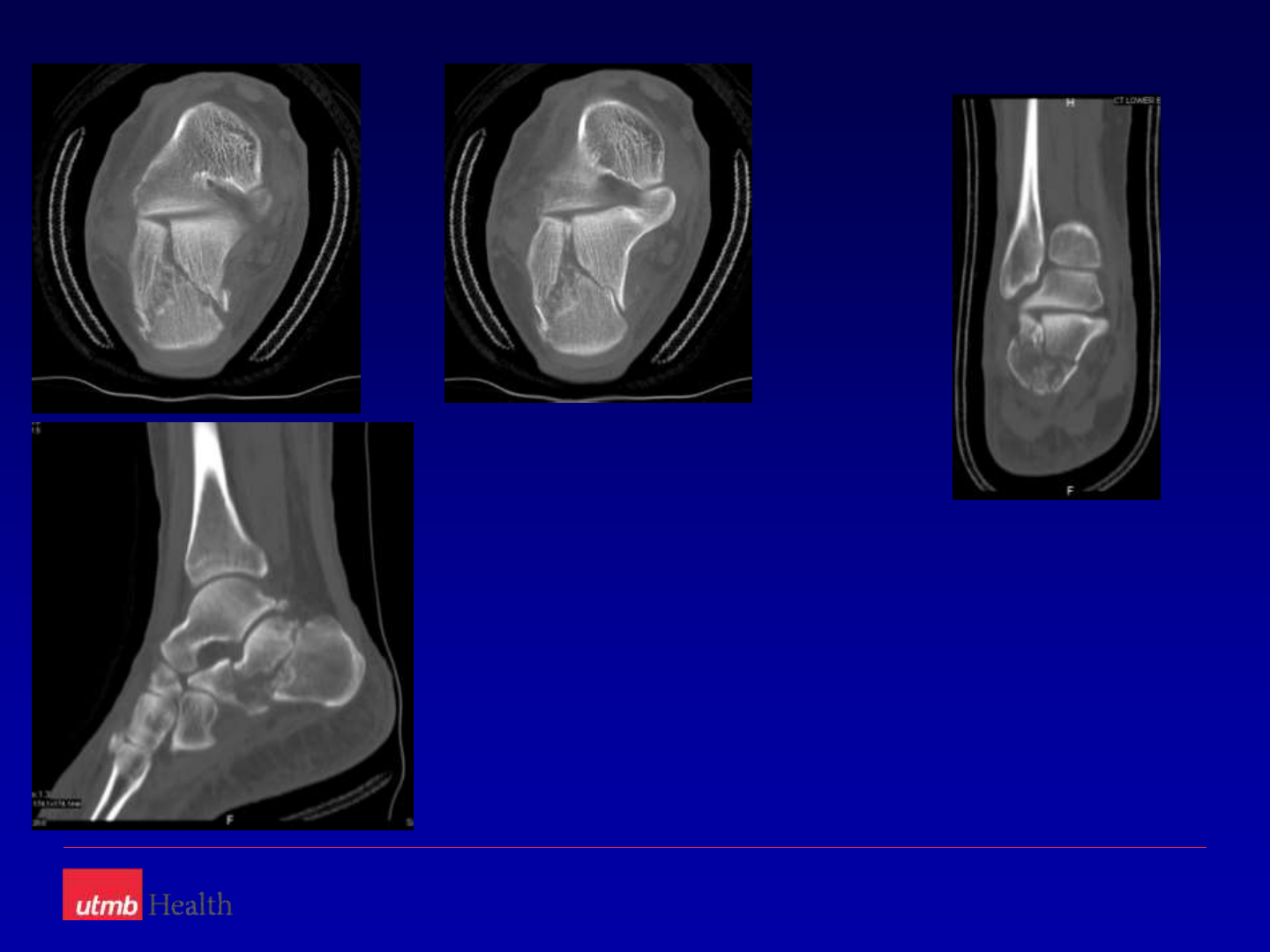
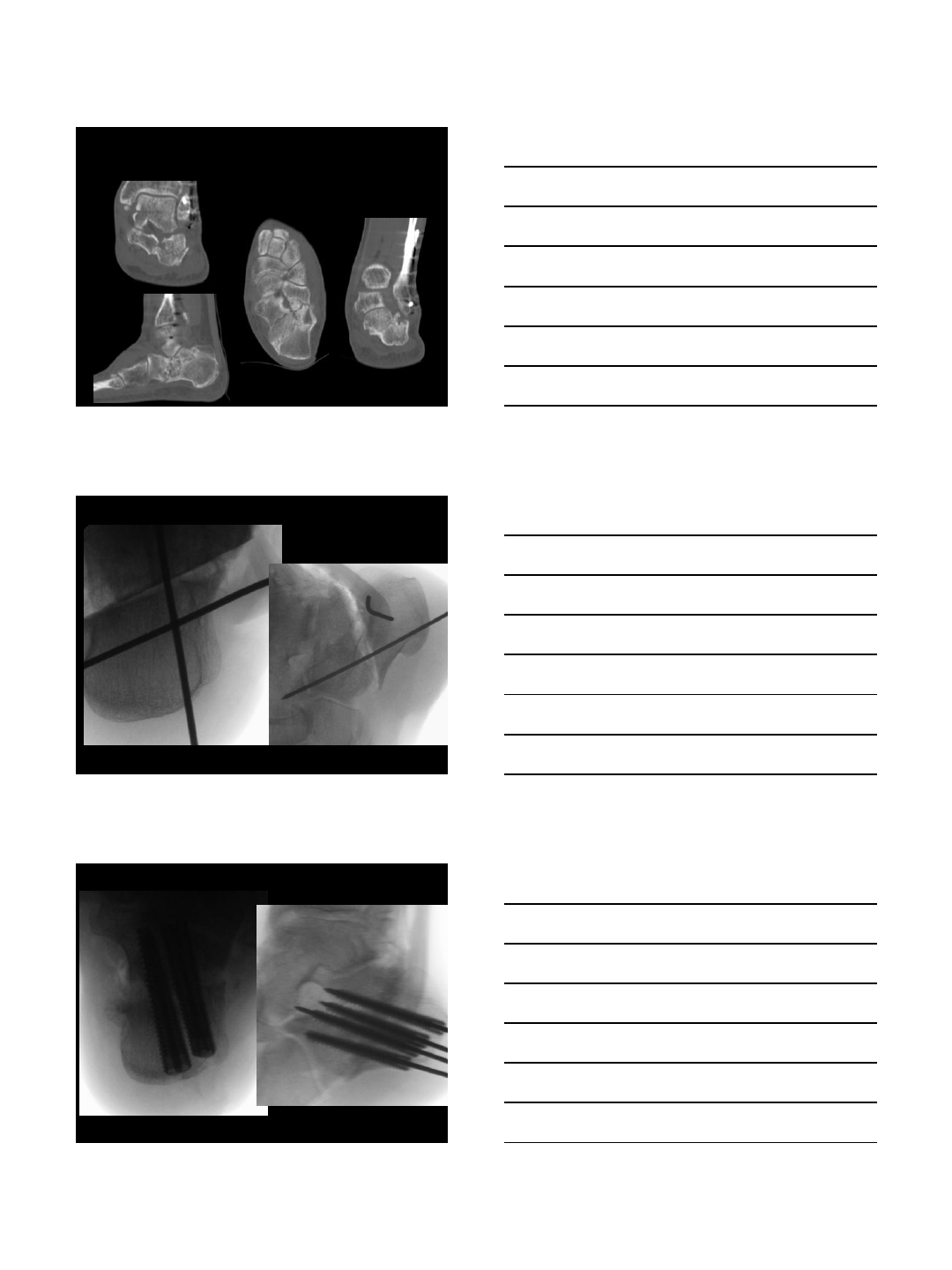
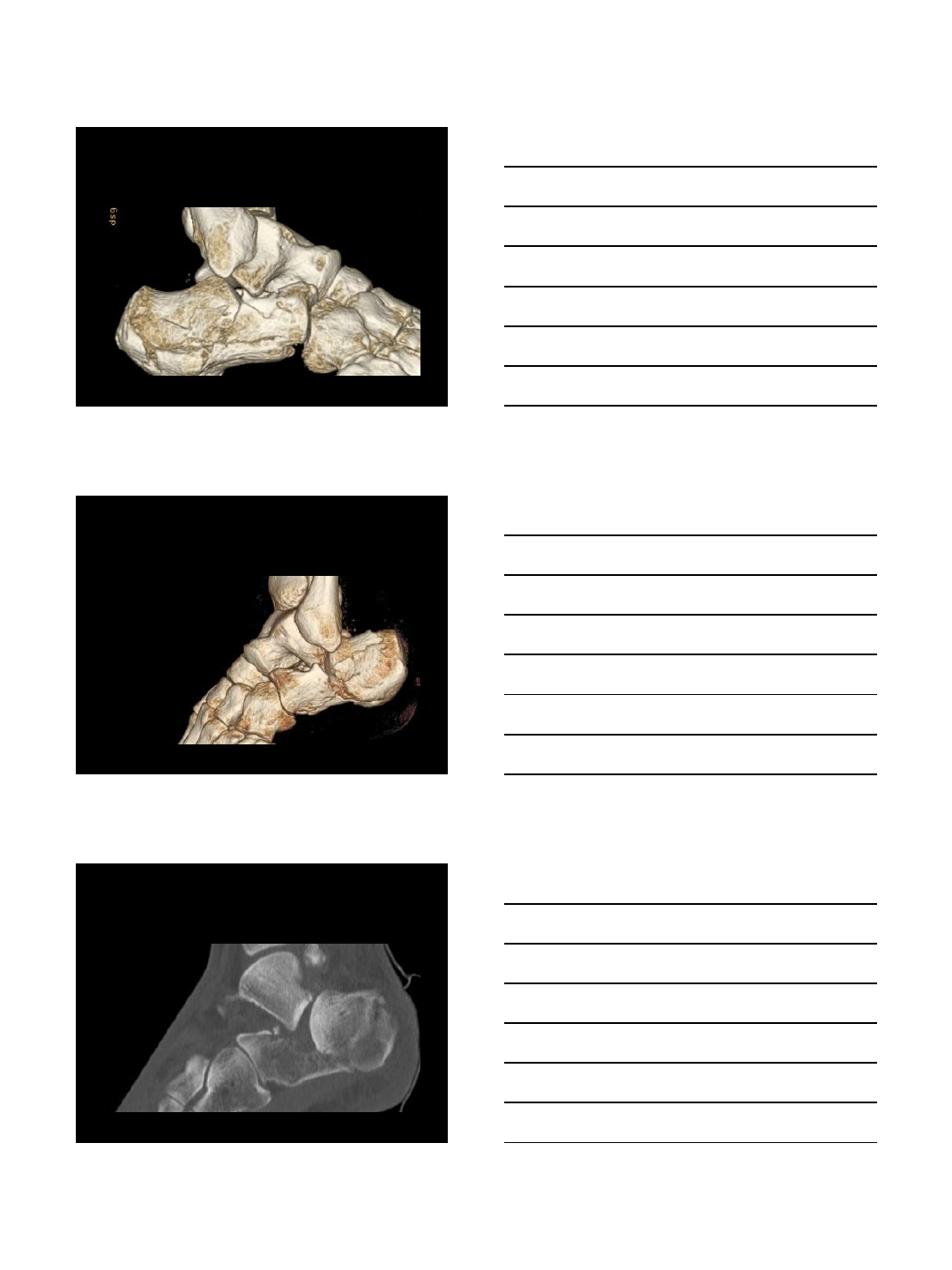
CT scan
3D reconstruction
MRI
Bone Scan
Fractures of the Calcaneus
Evaluation
•Radiographs:
Foot, 3 views
AP ankle
Harris view
CT scan
3D reconstruction
MRI
Bone Scan
Fractures of the Calcaneus
Evaluation
•Radiographs:
Foot, 3 views
AP ankle
Harris view
CT scan
3D reconstruction
MRI
Bone Scan
2/4/2014
4
Fractures of the Calcaneus
Evaluation
•Radiographs:
Foot, 3 views
AP ankle
Harris view
CT scan
3D reconstruction
MRI
Bone Scan
Fractures of the Calcaneus
Evaluation
•Radiographs:
Foot, 3 views
AP ankle
Harris view
CT scan
3D reconstruction
MRI
Bone Scan
Fractures of the Calcaneus
Evaluation
•Radiographs:
Foot, 3 views
AP ankle
Harris view
CT scan
3D reconstruction
MRI
Bone Scan
2/4/2014
5
Fractures of the Calcaneus
Evaluation
•Radiographs:
Foot, 3 views
AP ankle
Harris view
CT scan
3D reconstruction
MRI
Bone Scan
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Always
Never
Maybe
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Always
2/4/2014
6
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Always
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Never
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Maybe
2/4/2014
7
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Maybe
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Maybe
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Maybe

2/4/2014
8
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Maybe
Fractures of the Calcaneus
Treatment
•Operative: 3 groups
Maybe
Fractures of the Calcaneus
Open Reduction of Calcaneus Fractures
Prof. V. K. Panchbhavi MD, FACS
Chief Division of Foot & Ankle Surgery
Director Foot & Ankle Fellowship Program
University of Texas Medical Branch
Galveston, Texas, USA
Department of Orthopedic Surgery and Rehabilitation
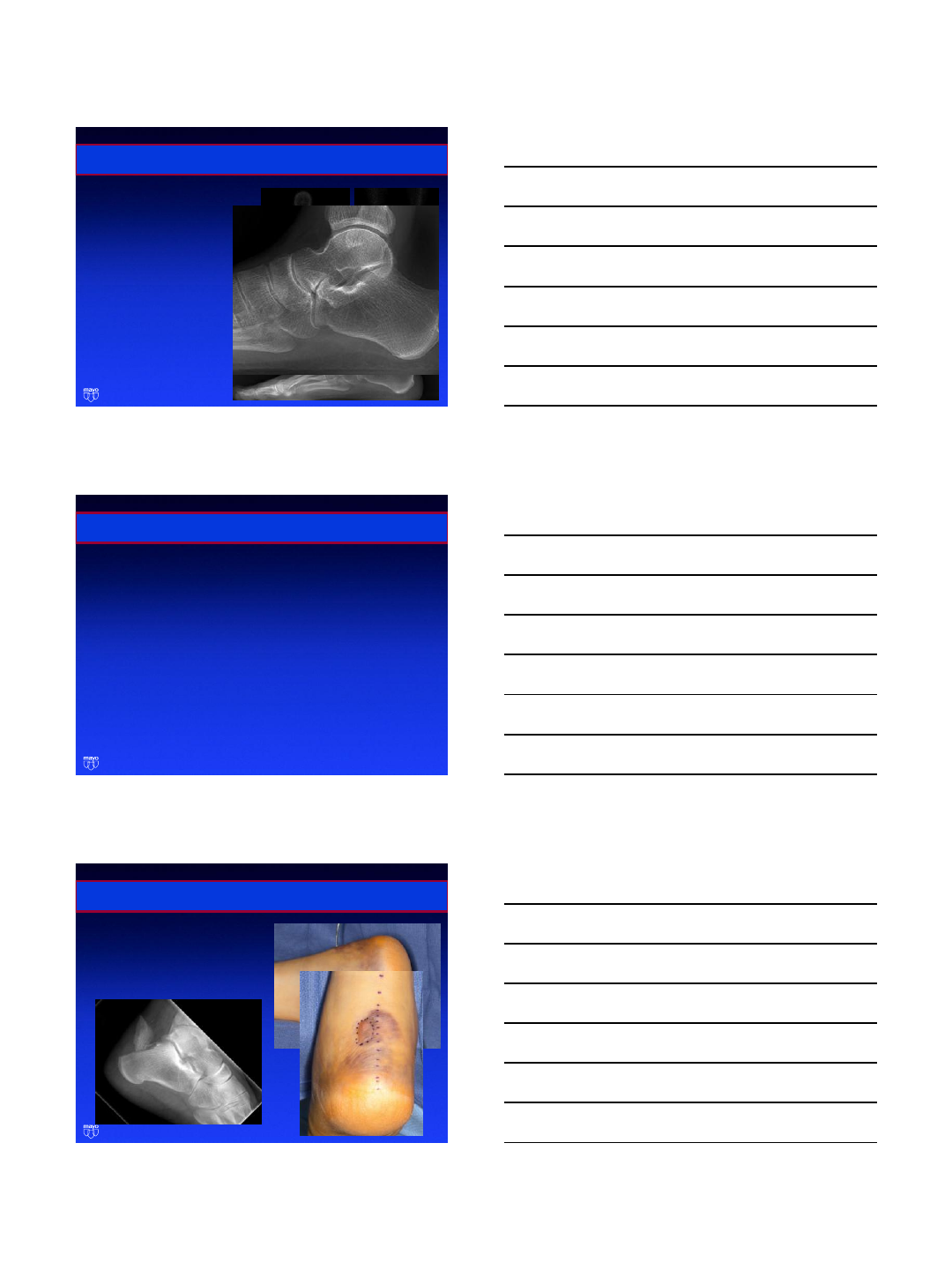
Objectives
Patient positioning
Surgical approaches
Reduction maneuvers
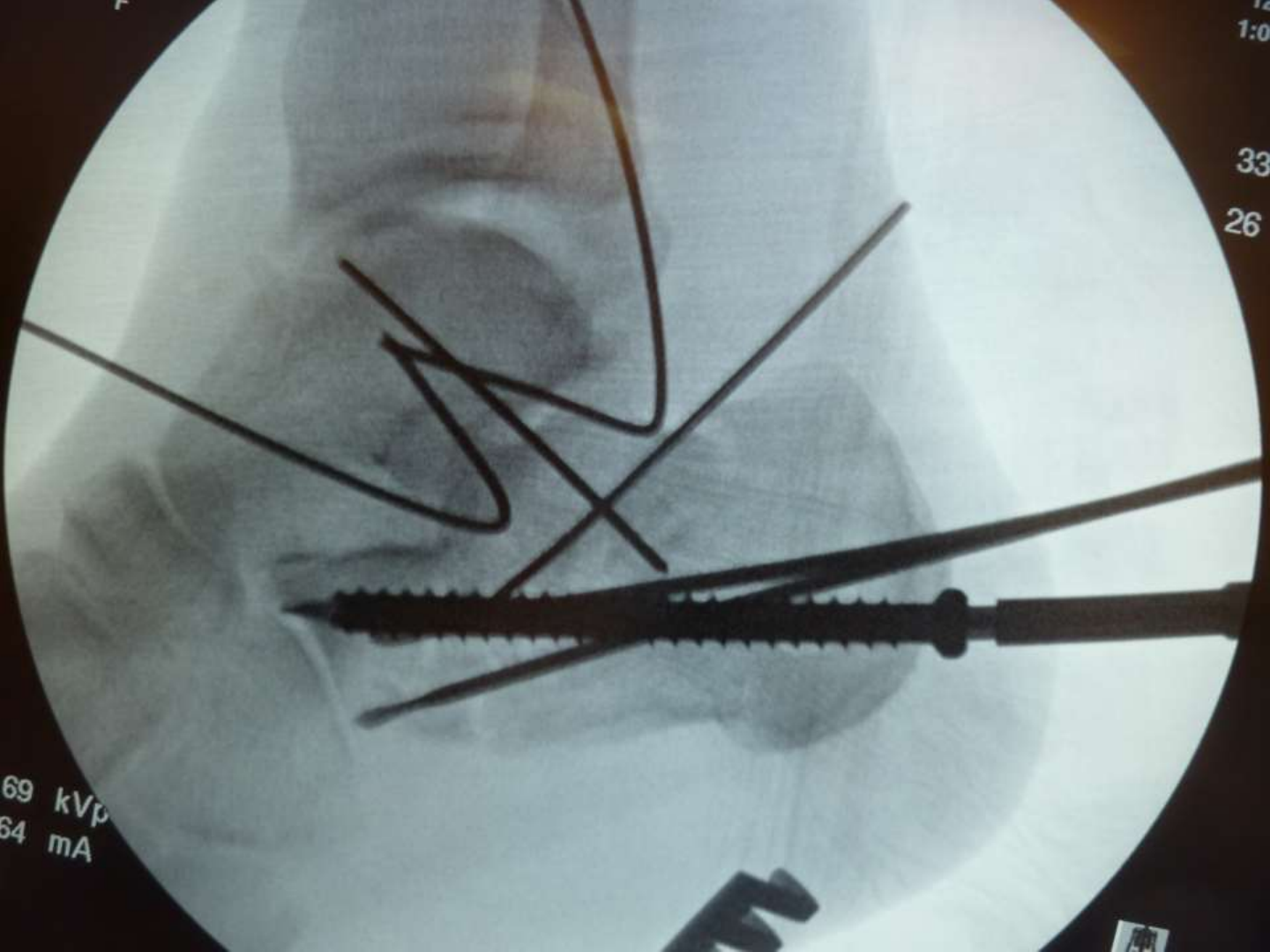
Internal fixation methods
Department of Orthopedic Surgery and Rehabilitation
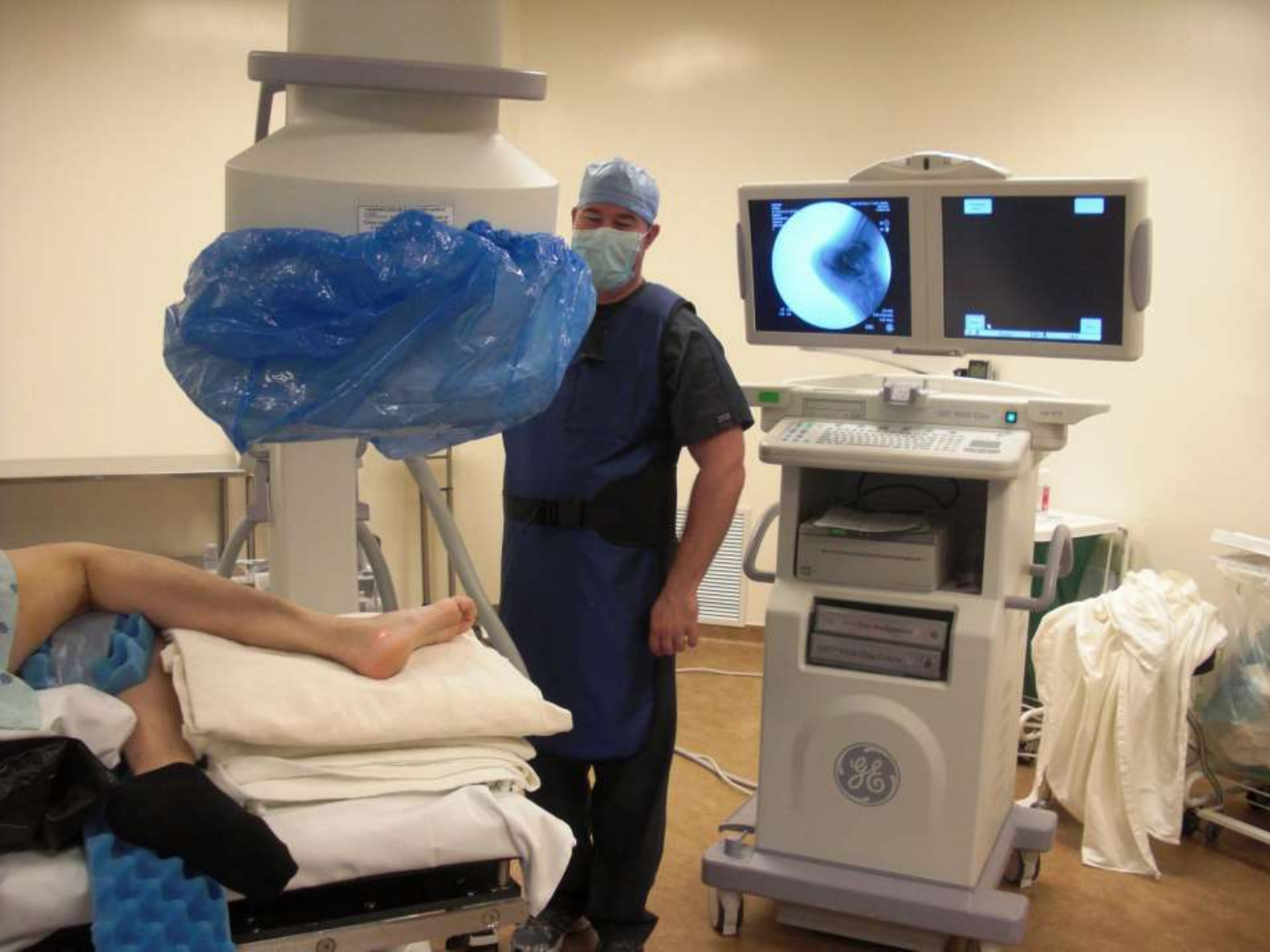
Positioning –consideration


Department of Orthopedic Surgery and Rehabilitation
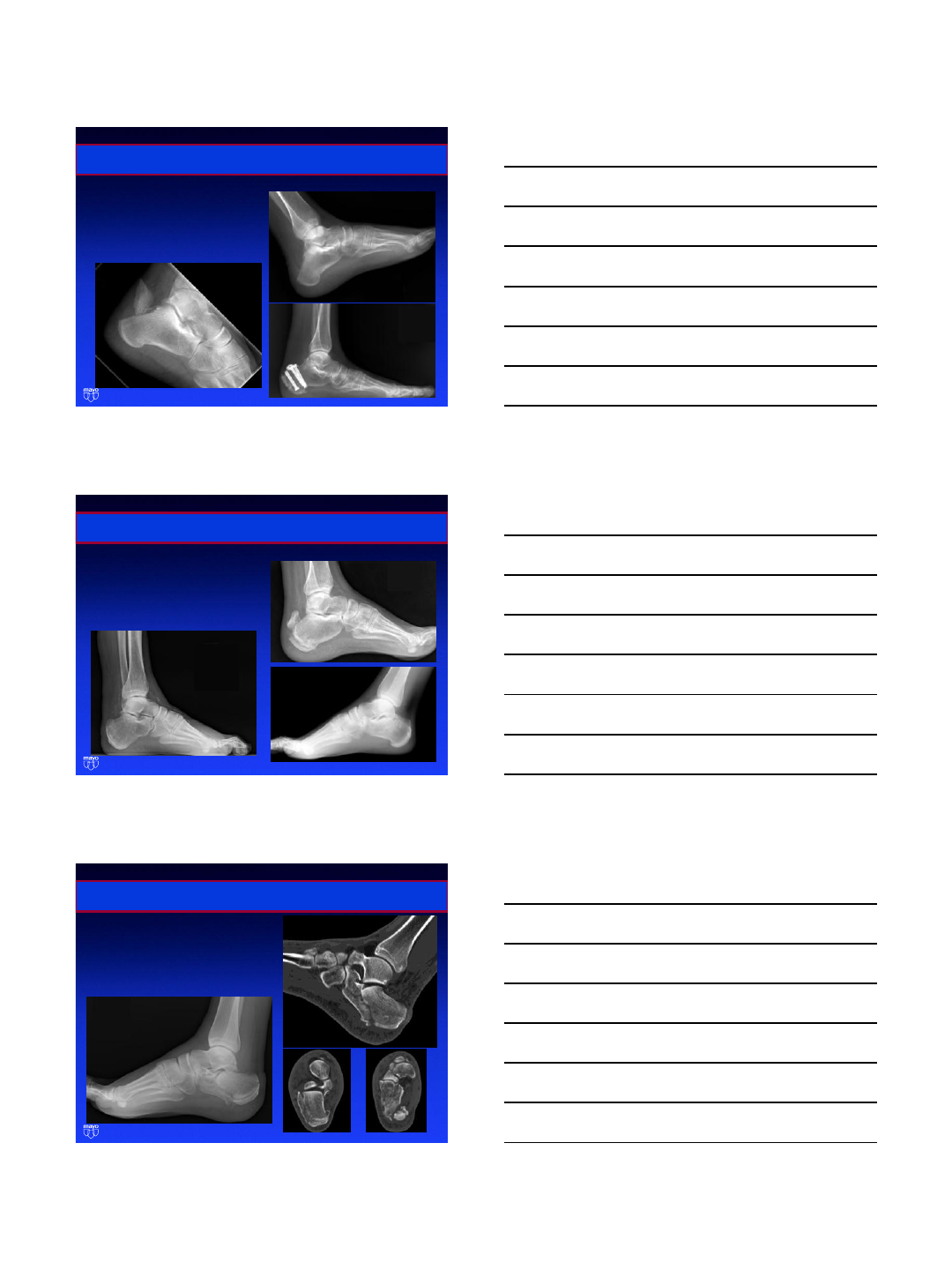
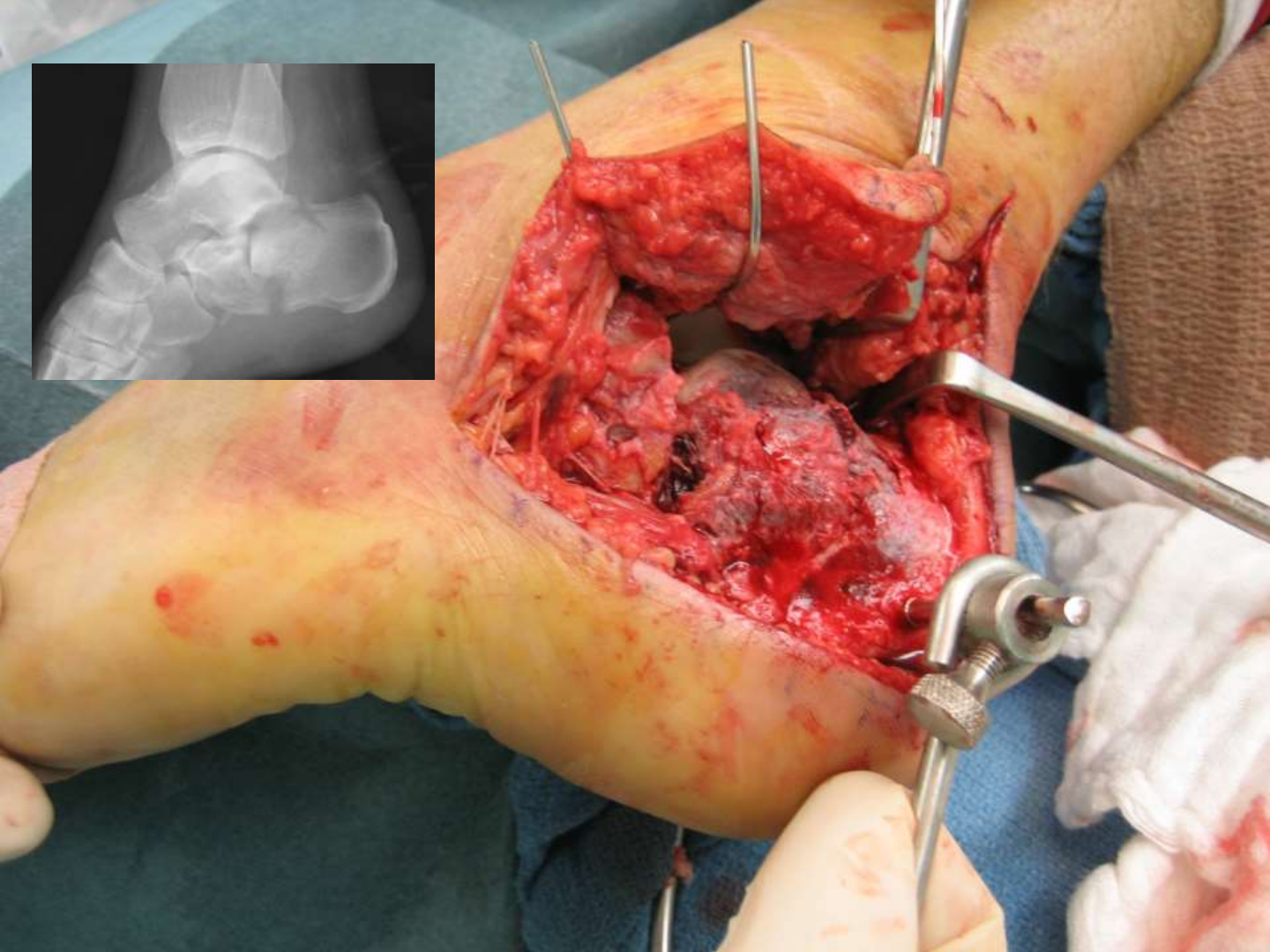
Surgical approach - considerations

Department of Orthopedic Surgery and Rehabilitation
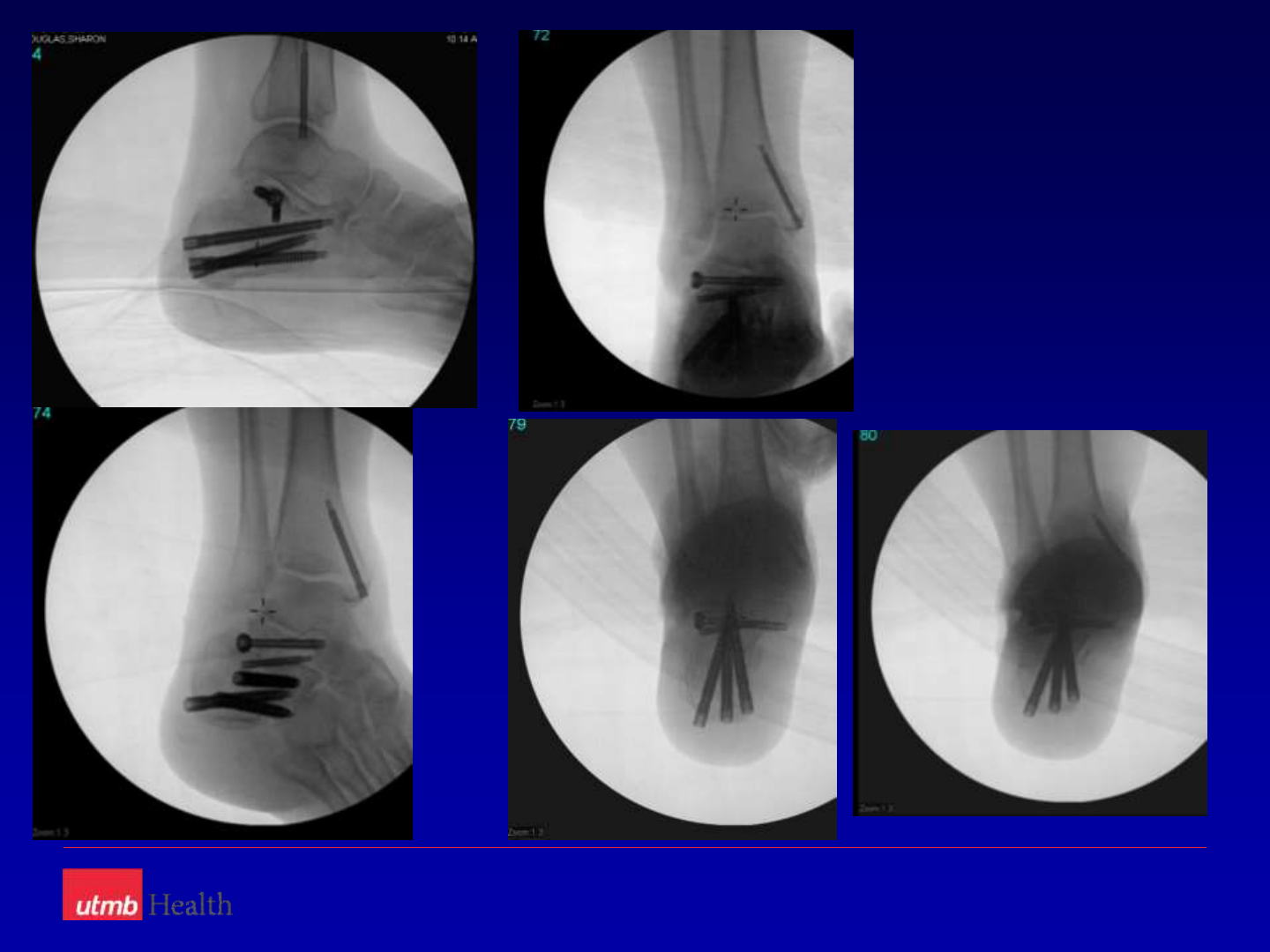
Surgical Approach
Department of Orthopedic Surgery and Rehabilitation
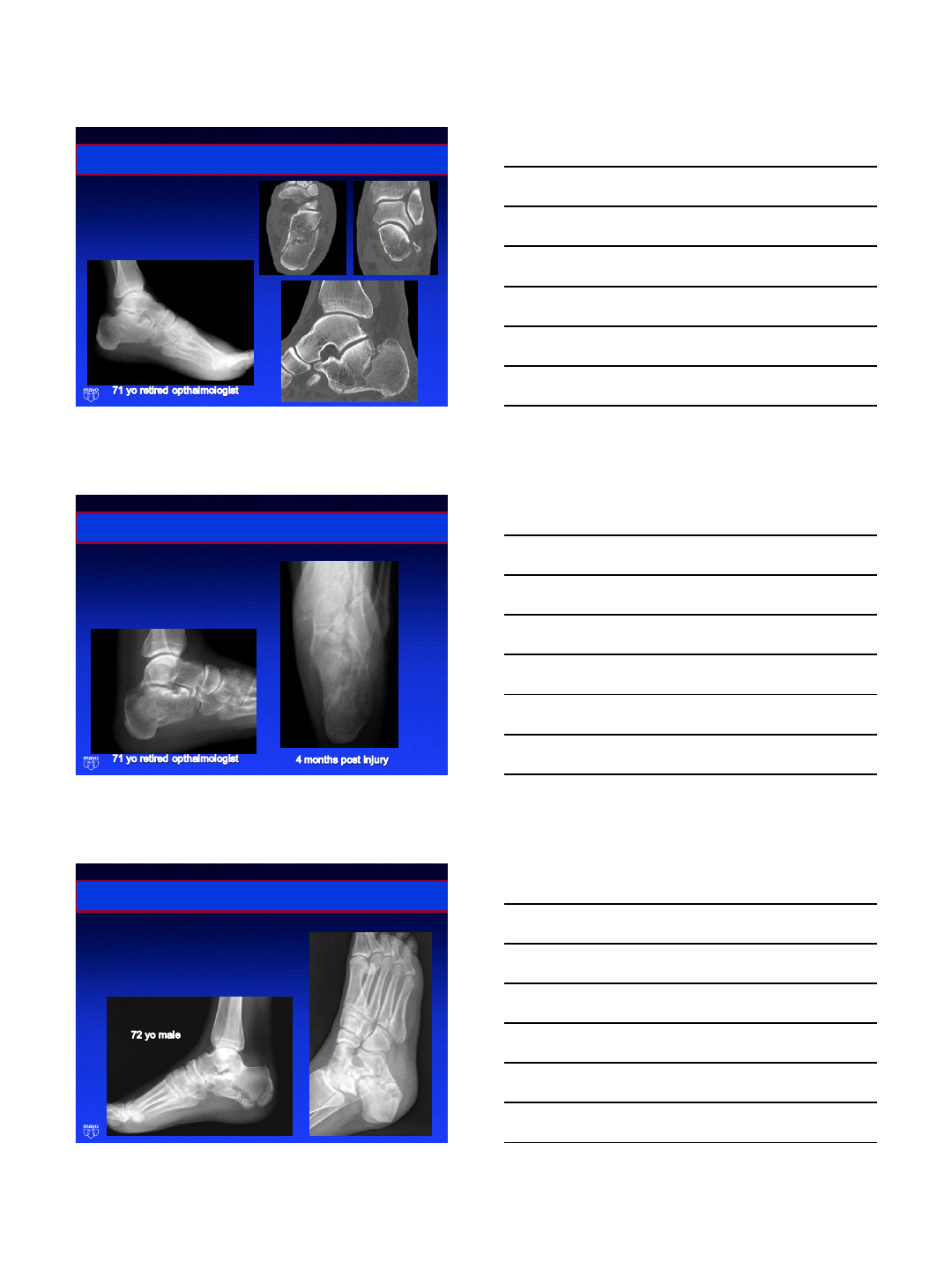
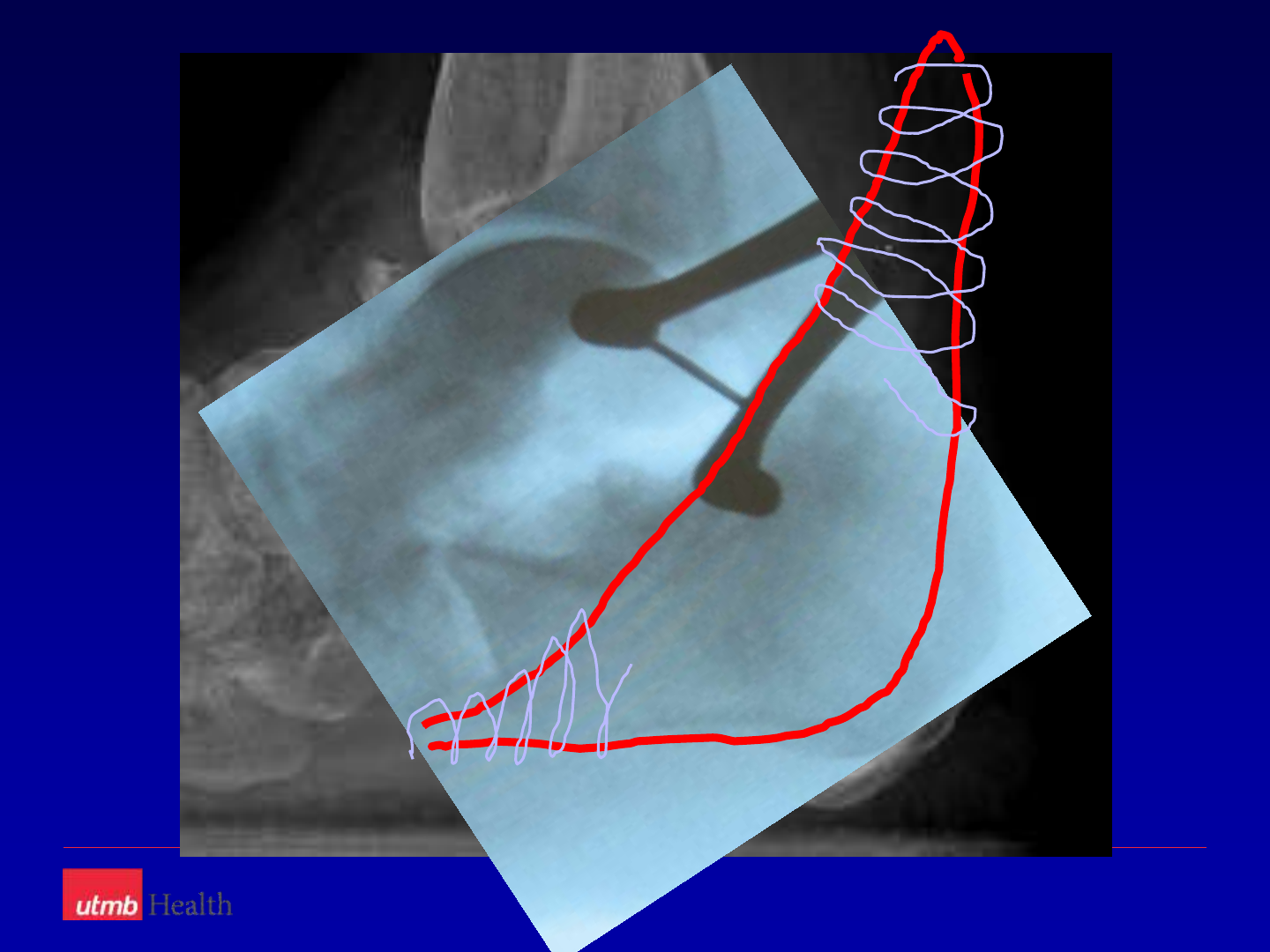
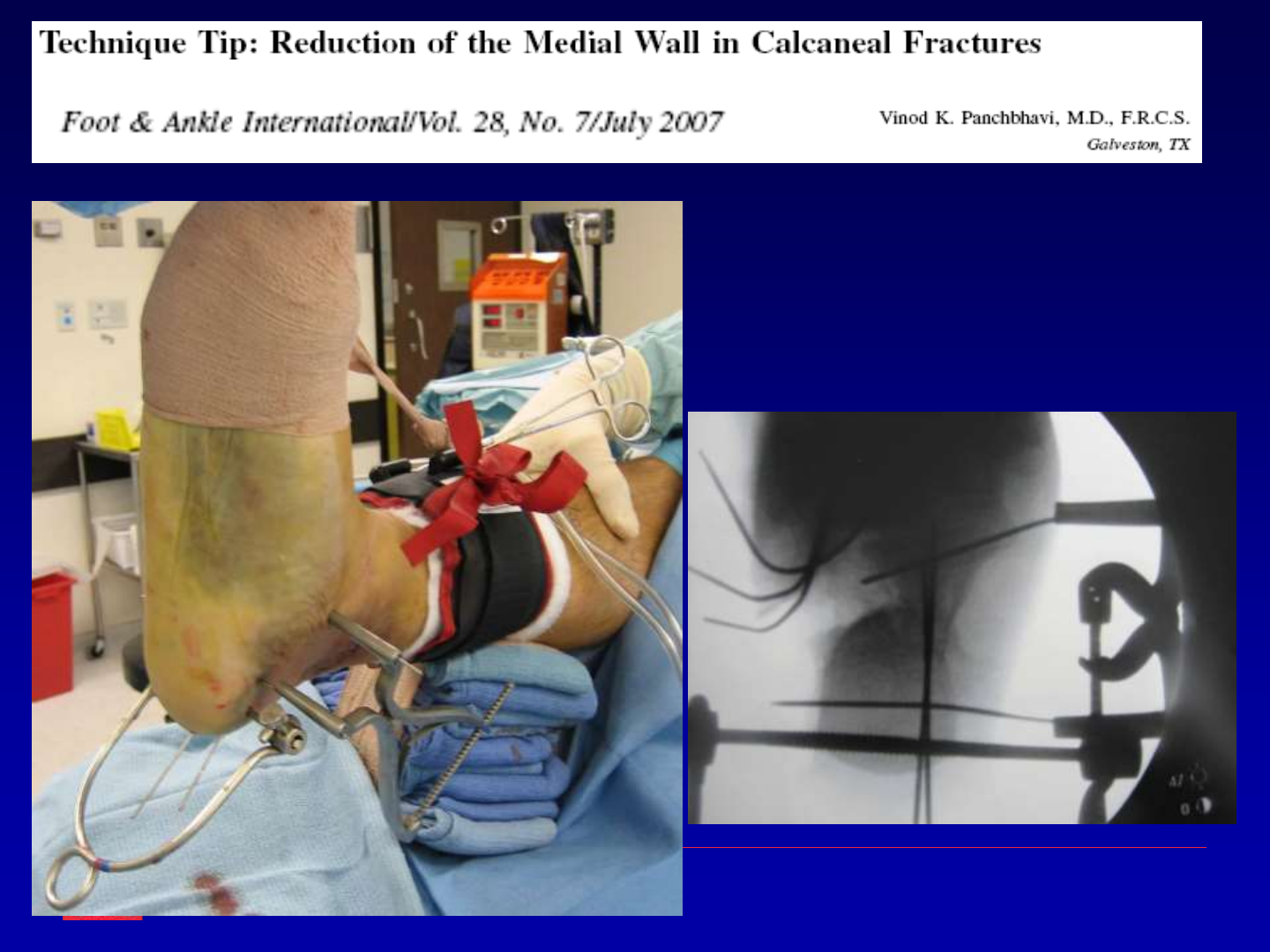
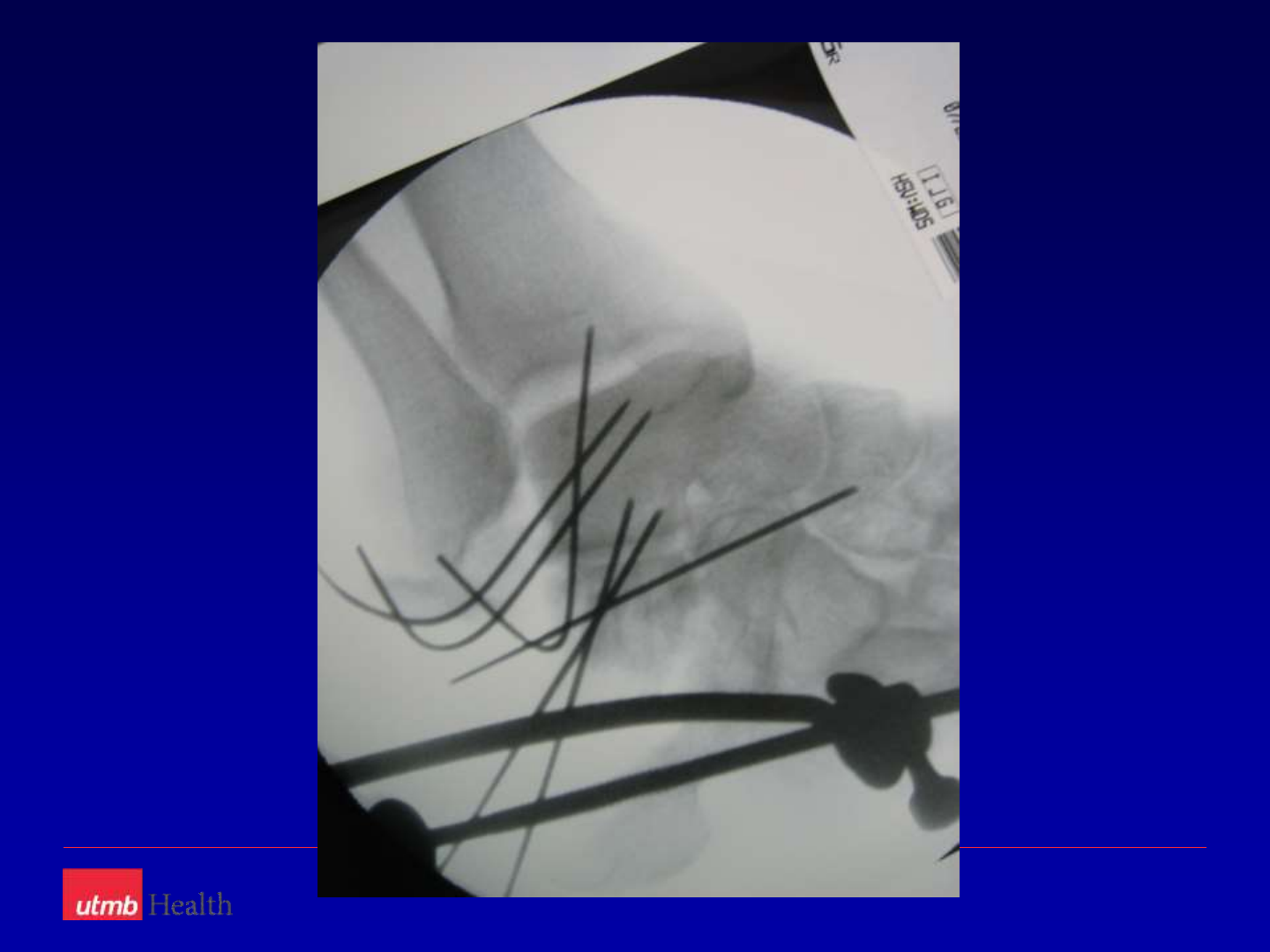
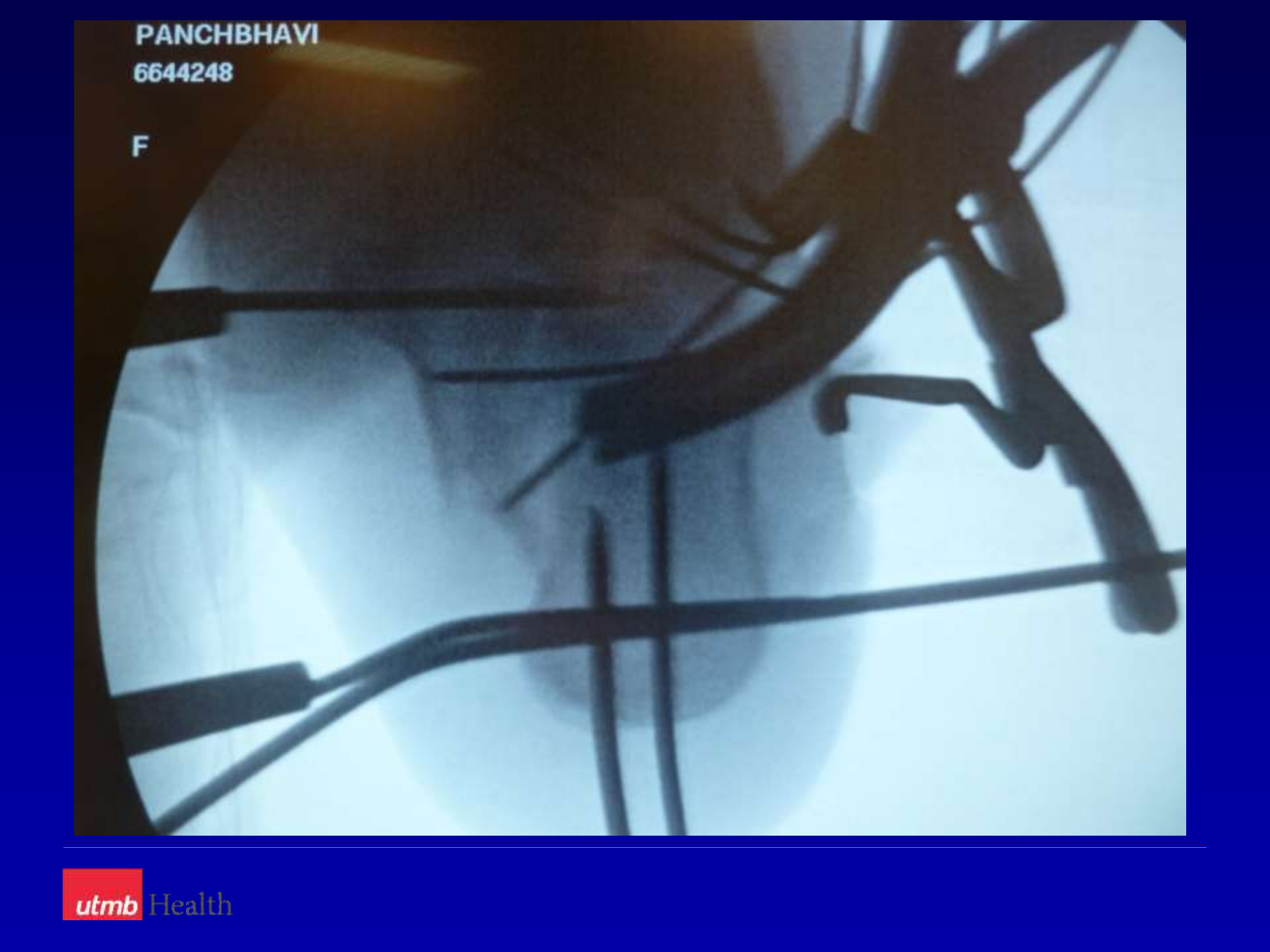
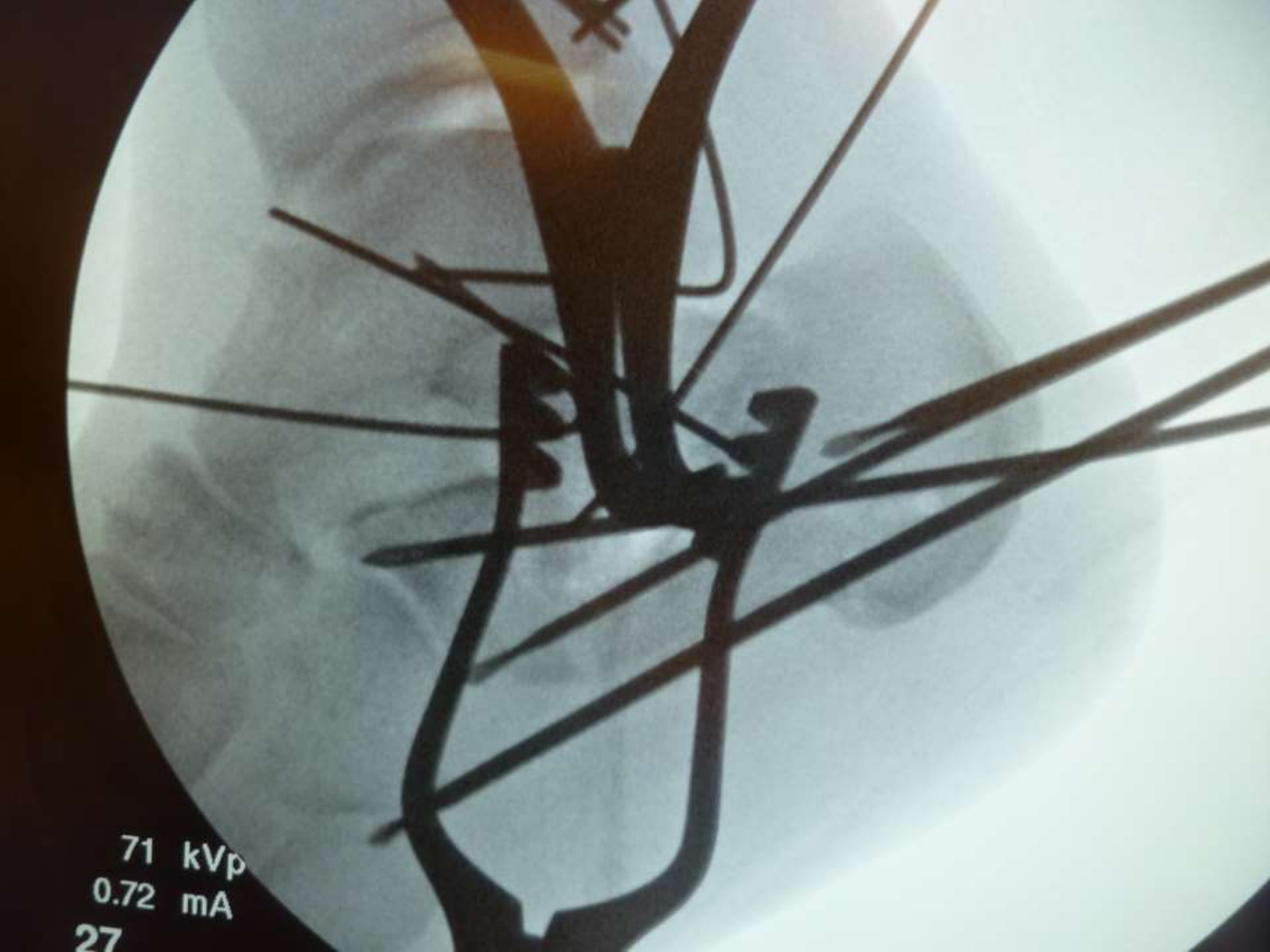
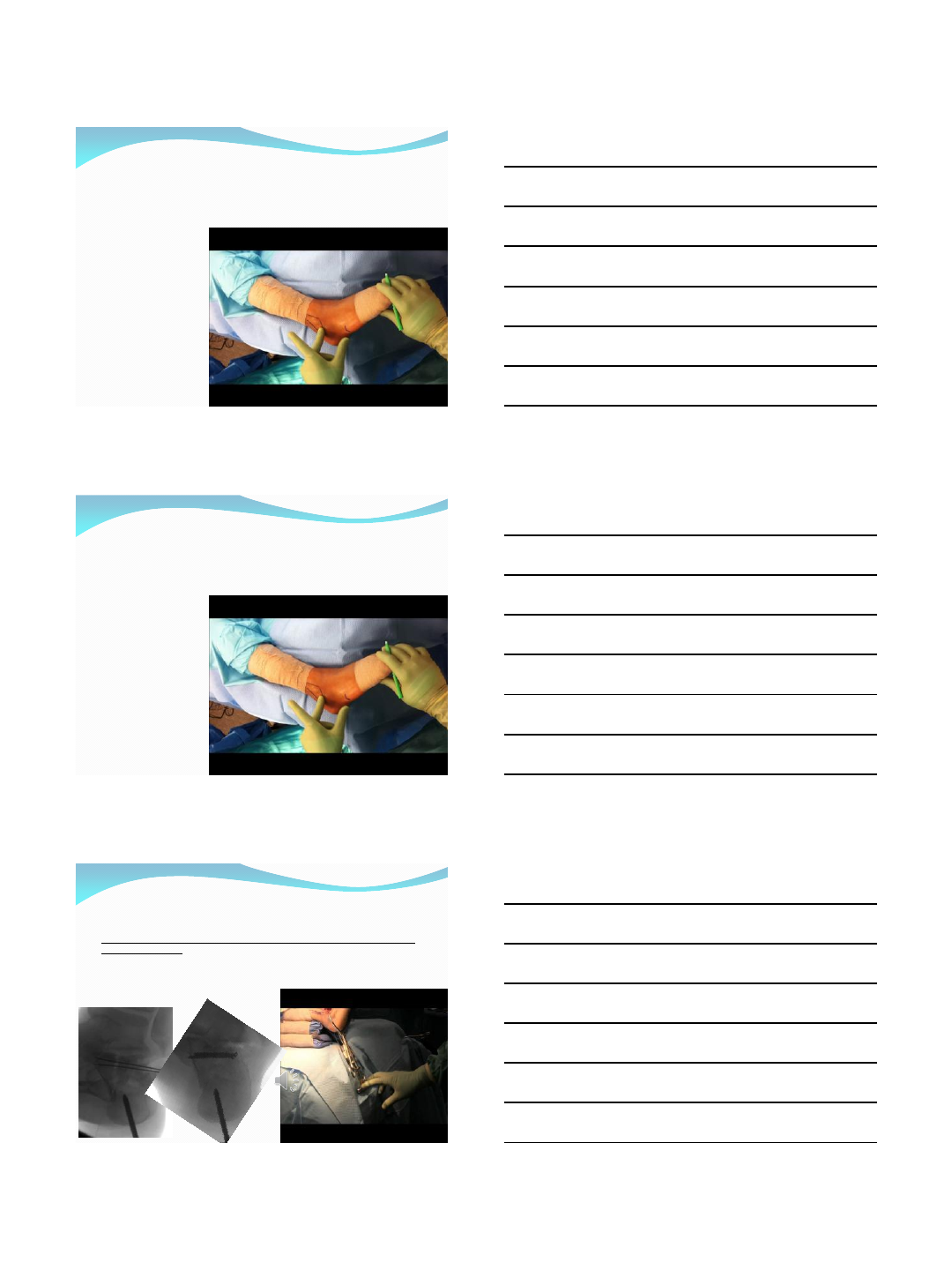
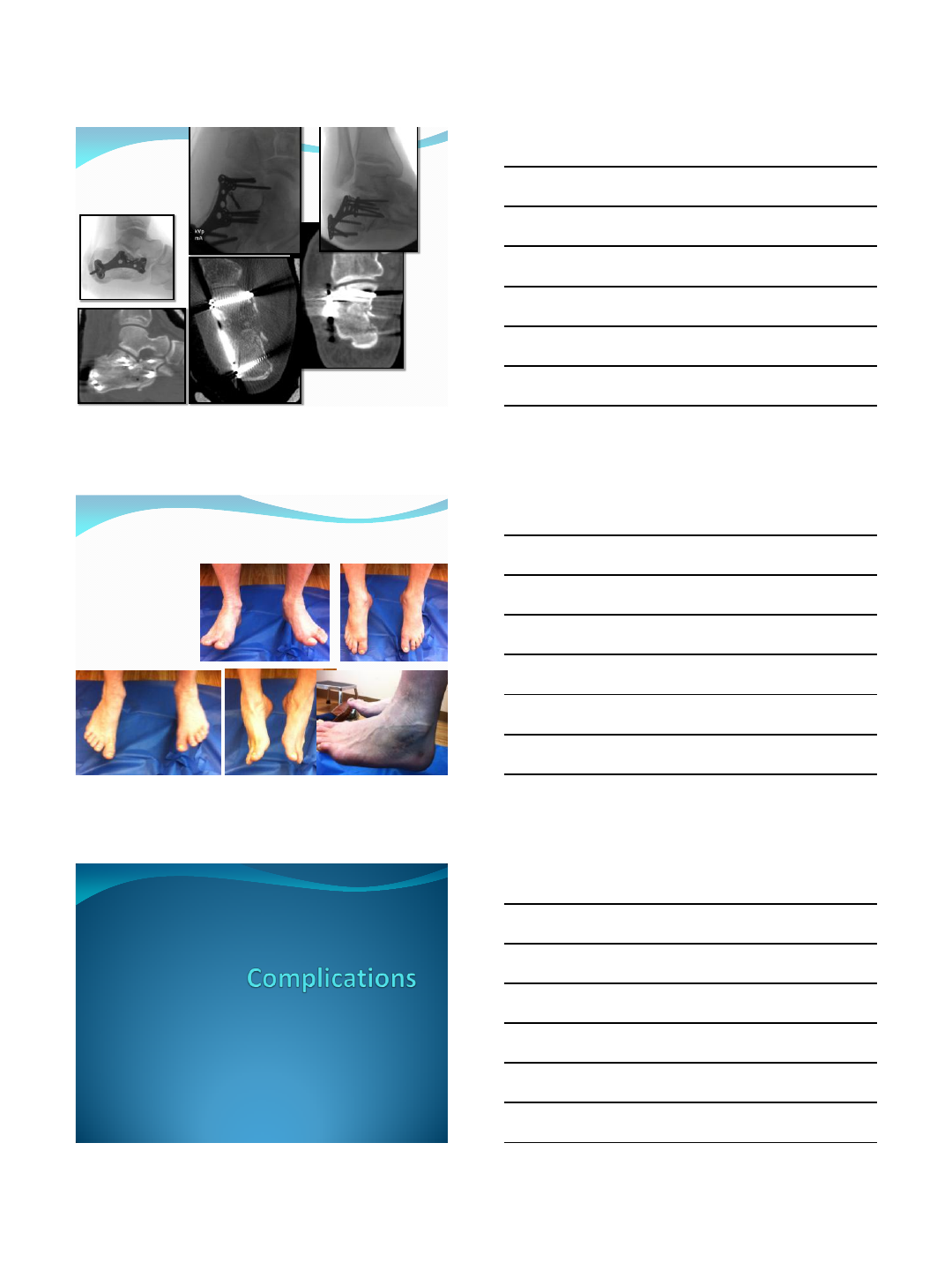
Reduction maneuvers






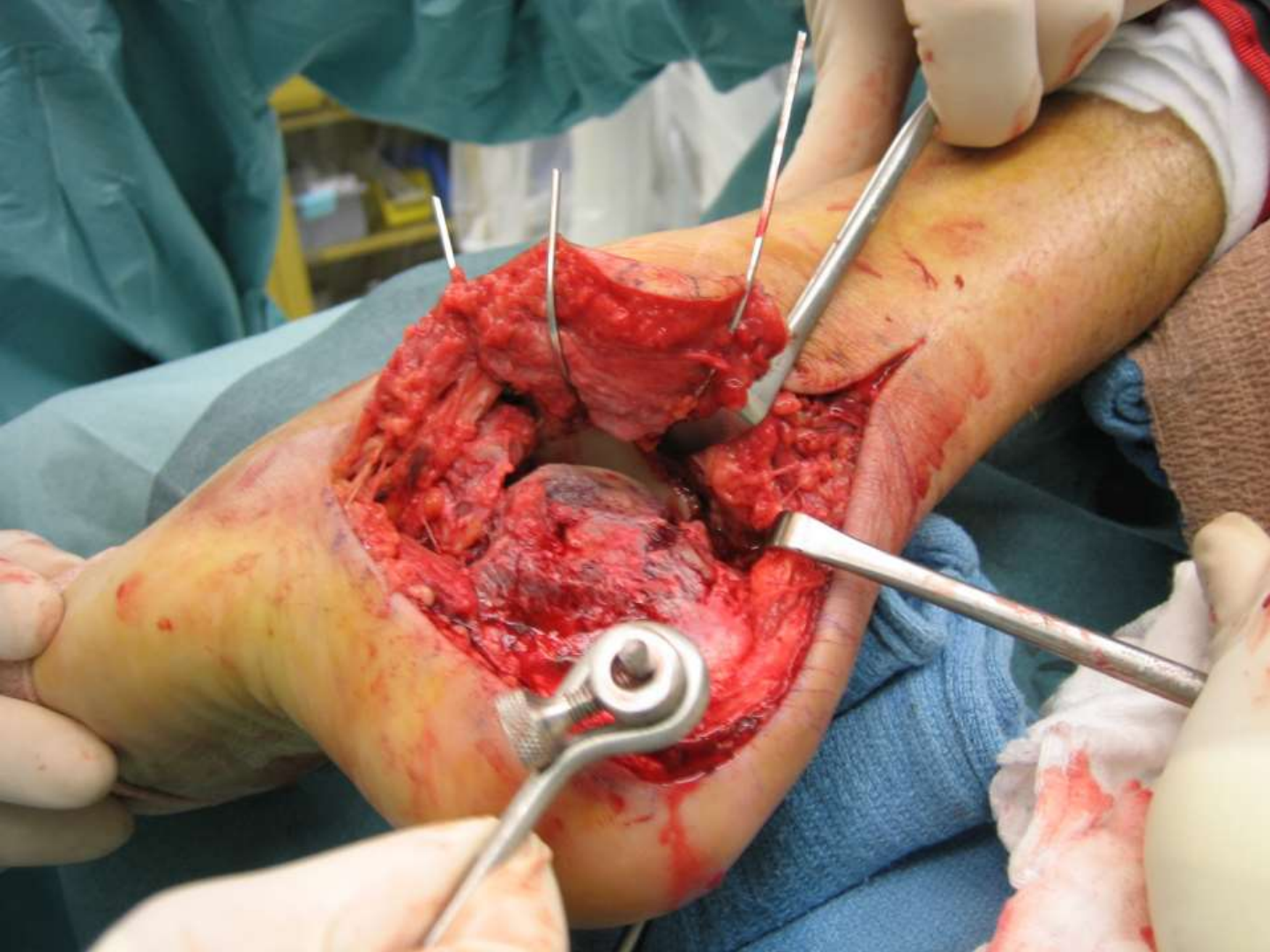
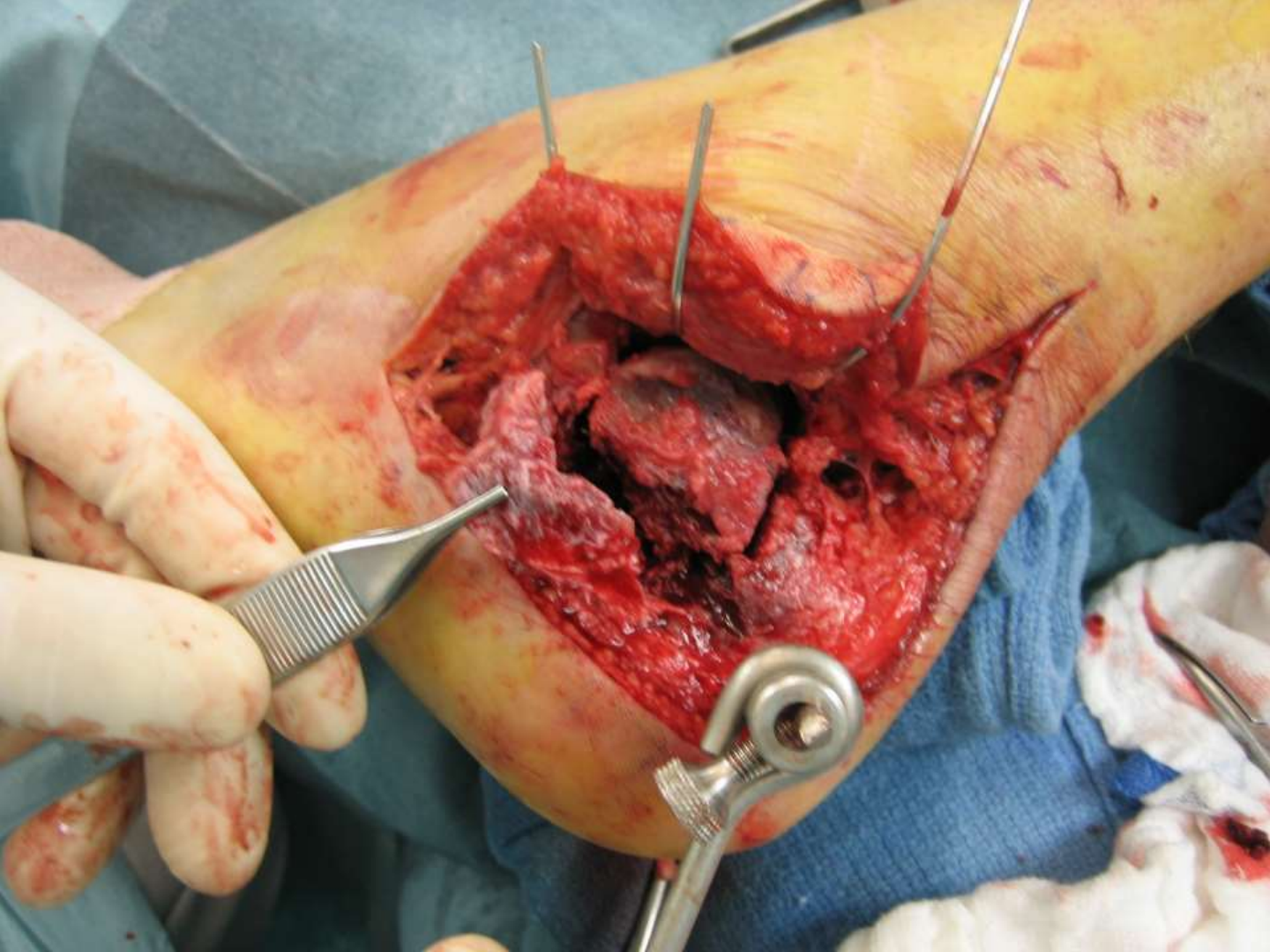
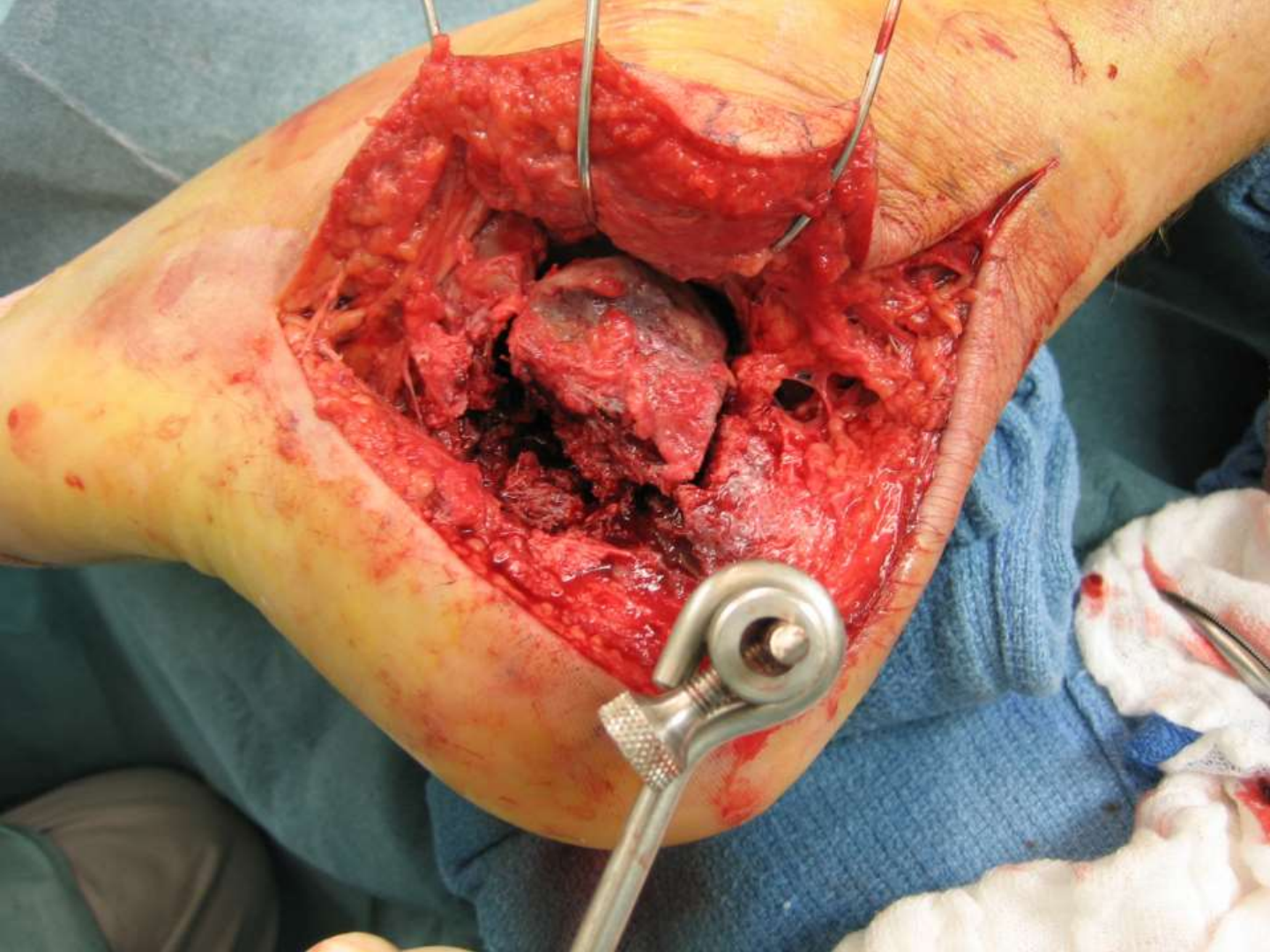
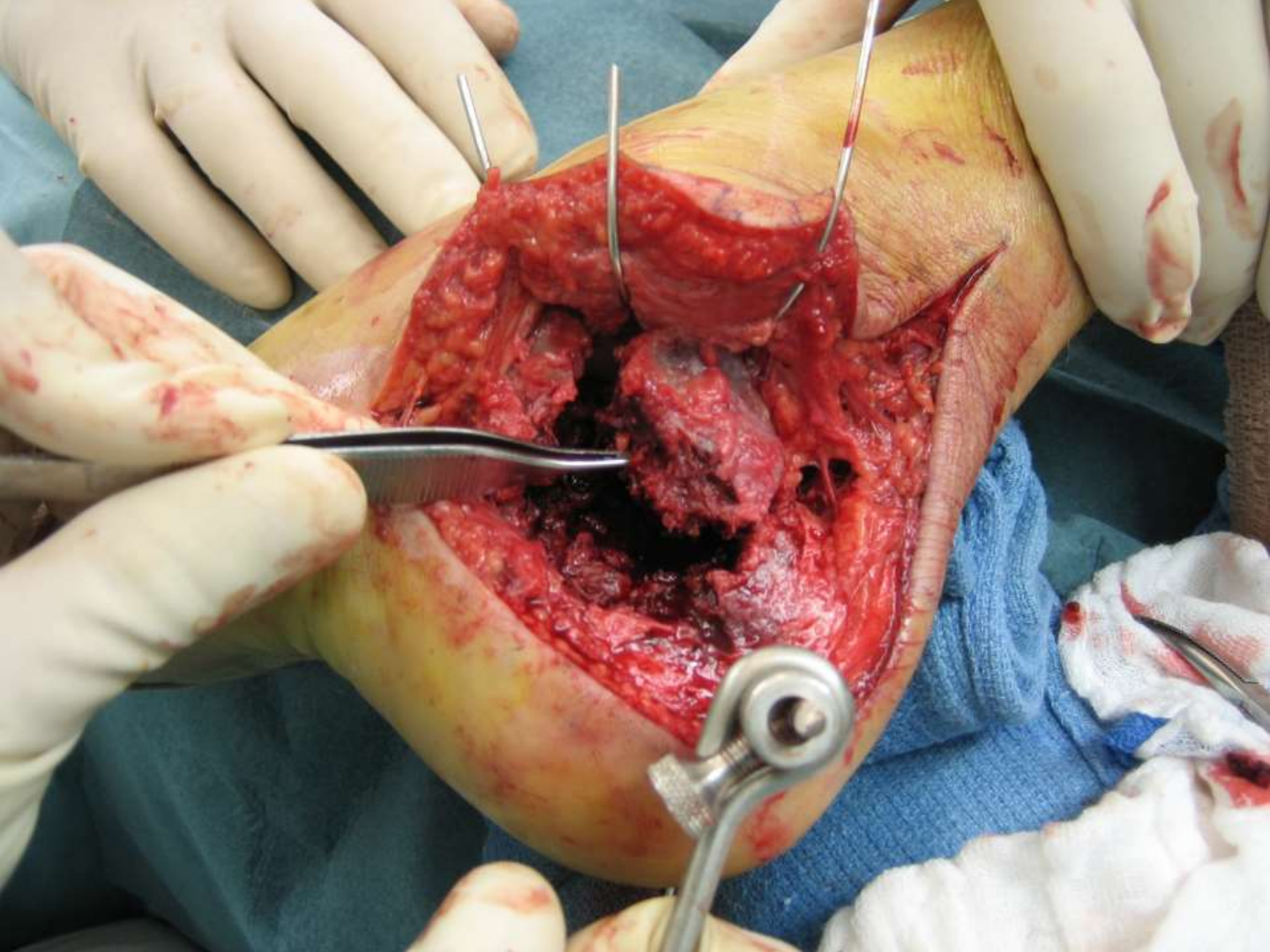


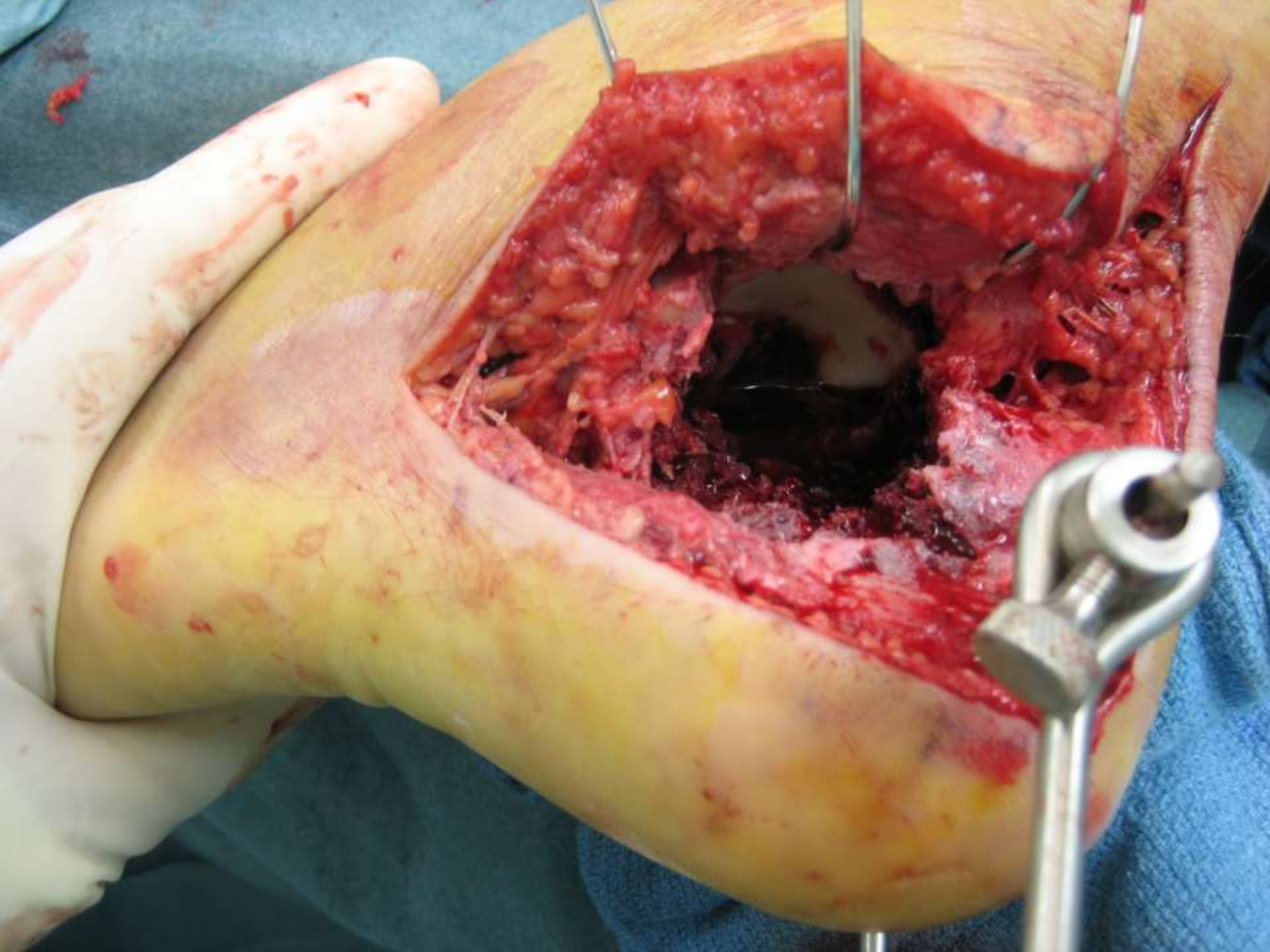

Department of Orthopedic Surgery and Rehabilitation
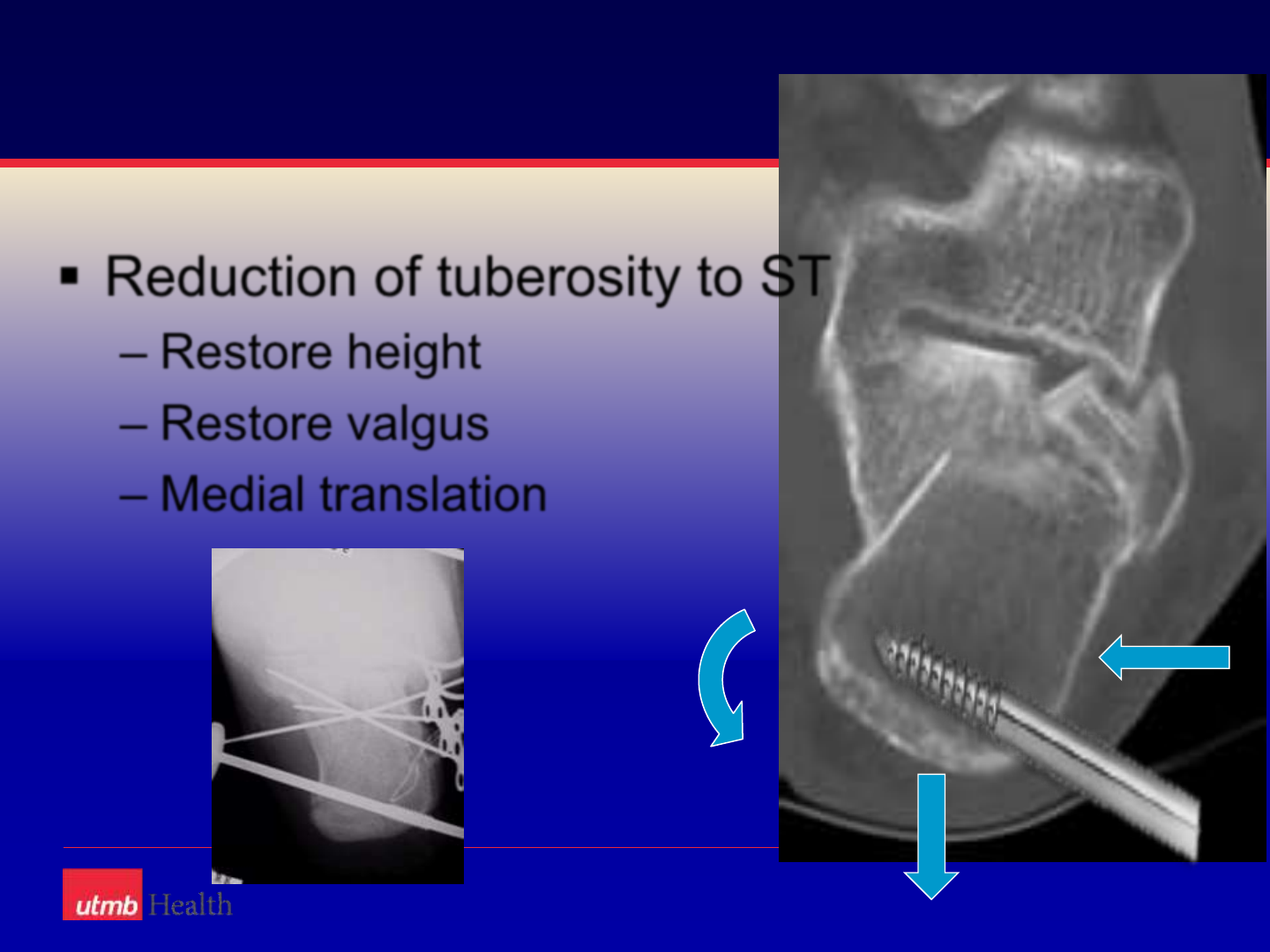
Reduction of tuberosity to ST
–Restore height
–Restore valgus
–Medial translation

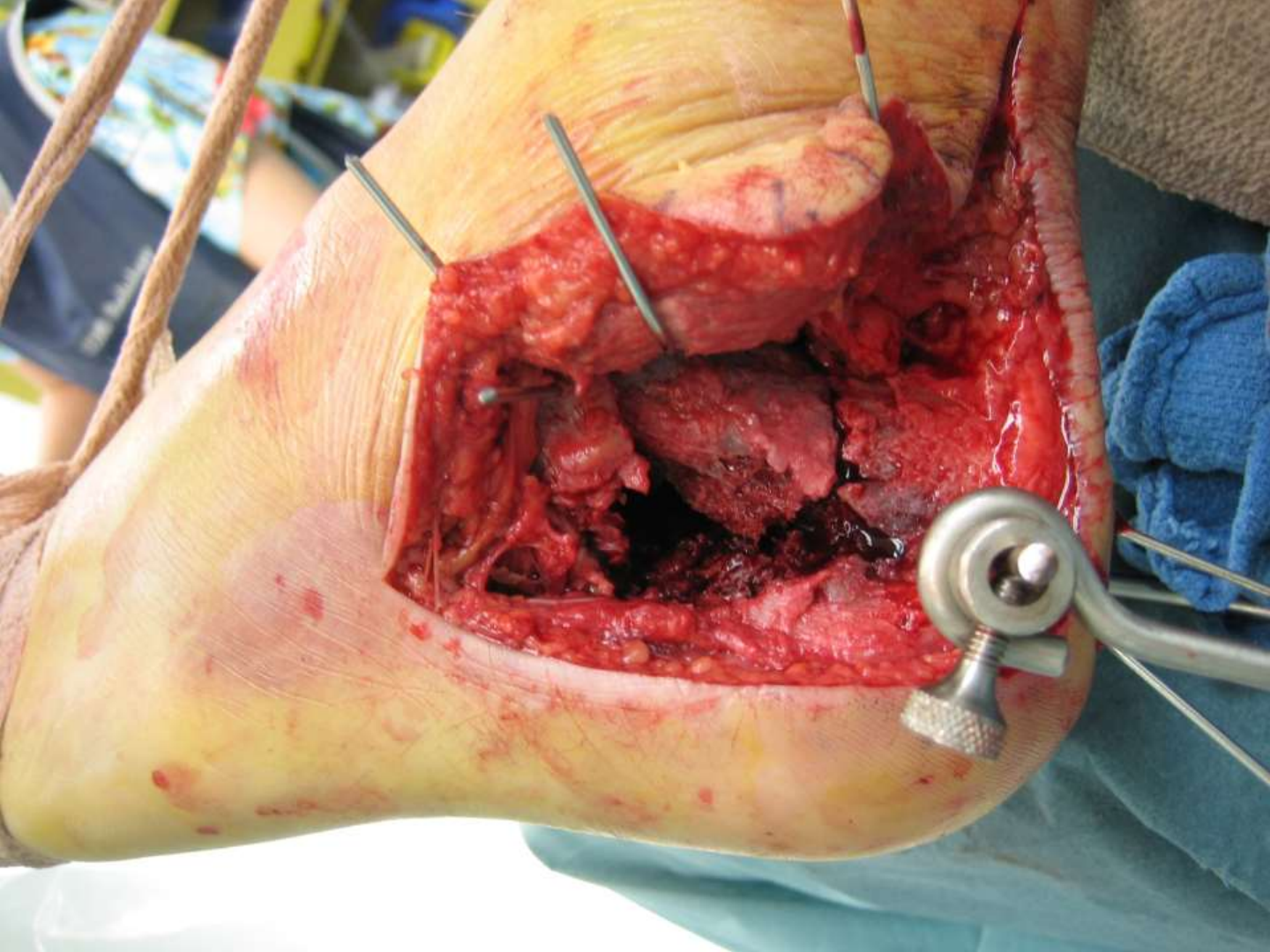





Donati-Allgower Stitch




















Department of Orthopedic Surgery and Rehabilitation
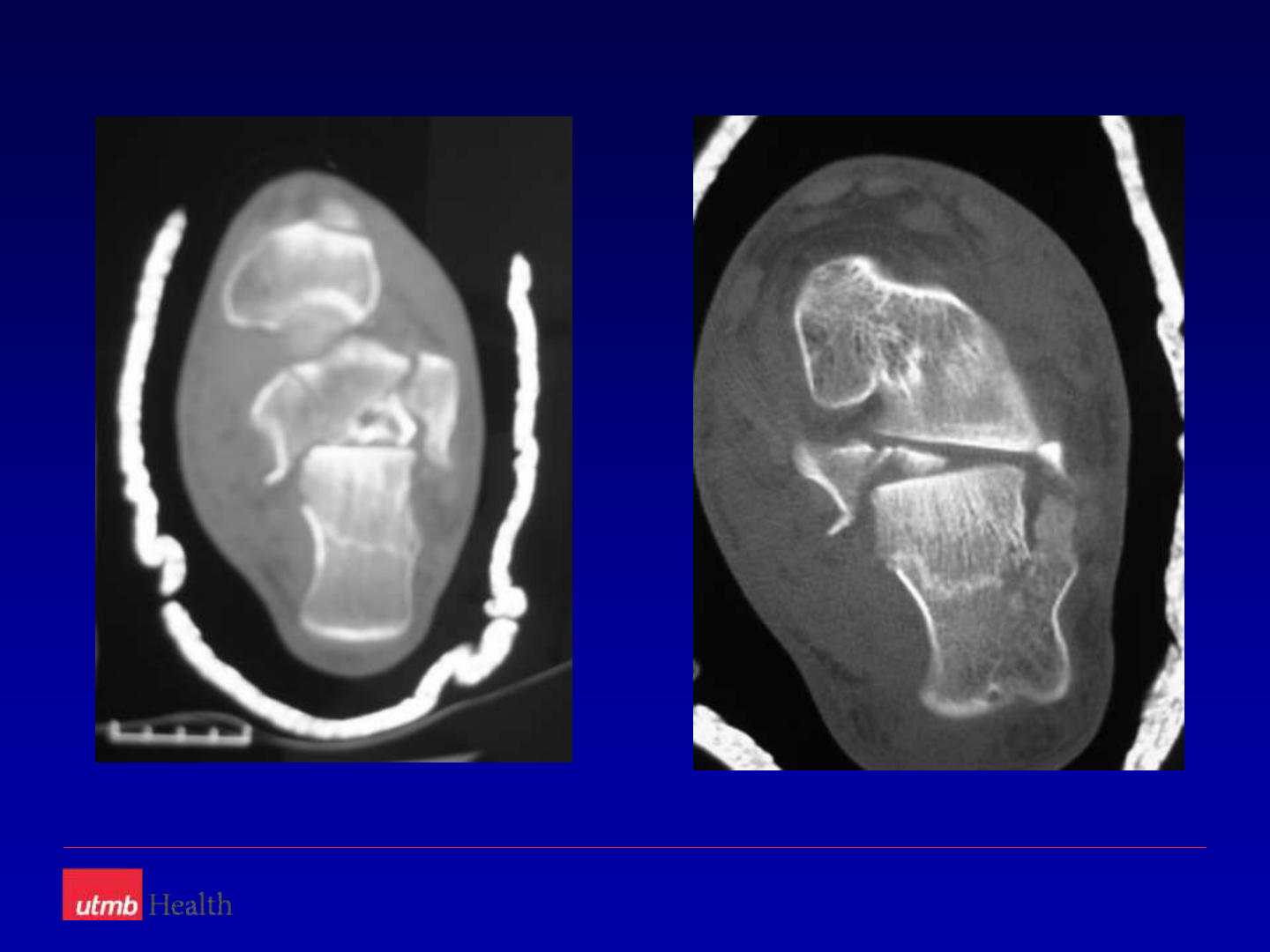
Take Home Messages
Understand 3 D anatomy
Study the fracture planes and displacement
Plan the approach
Reduce the articular surface
Restore the height
Restore the tuberosity

Thank You
2/4/2014
1
Calcaneal Fractures
•Dr. Alastair Younger
•Associate Professor,
•University of British Columbia
Disclaimers
•Institutional support from Linvatec, Smith
and Nephew, Cartiva, Wright Medical,
Integra foundation, BMTI, Acumed, Bioset,
Synthes.
•Consultant Biomimetics (Wright), Acumed
and Cartiva
Background
•Buckley paper
•Early reports
–No difference with
OR
•Final paper
–Beneficial in select
groups
2/4/2014
2
Rates of ORIF British Columbia
0
20
40
60
80
100
120
140
2000 2002 2004 2006 2008 2010 2012 2014
Calcaneus ORIF BC
Calcaneus ORIF BC
Aims of ORIF
•Surgeon must:
–Restore the tuberosity fragment
–Restore the subtalar joint
–Reconstruct the medial wall
–Reduce the peroneal tendons
–Restore height
–Avoid wound complications
–Release tendons and nerves from the fracture
Why less invasive
•Wrinkle test
•Elevate
•Cryocuff
•After fracture blisters
resolve
2/4/2014
3
Technical factors
•Dissection and approach
Technical factors
•Assessment of reduction
•Fixation
Reduction
2/4/2014
4
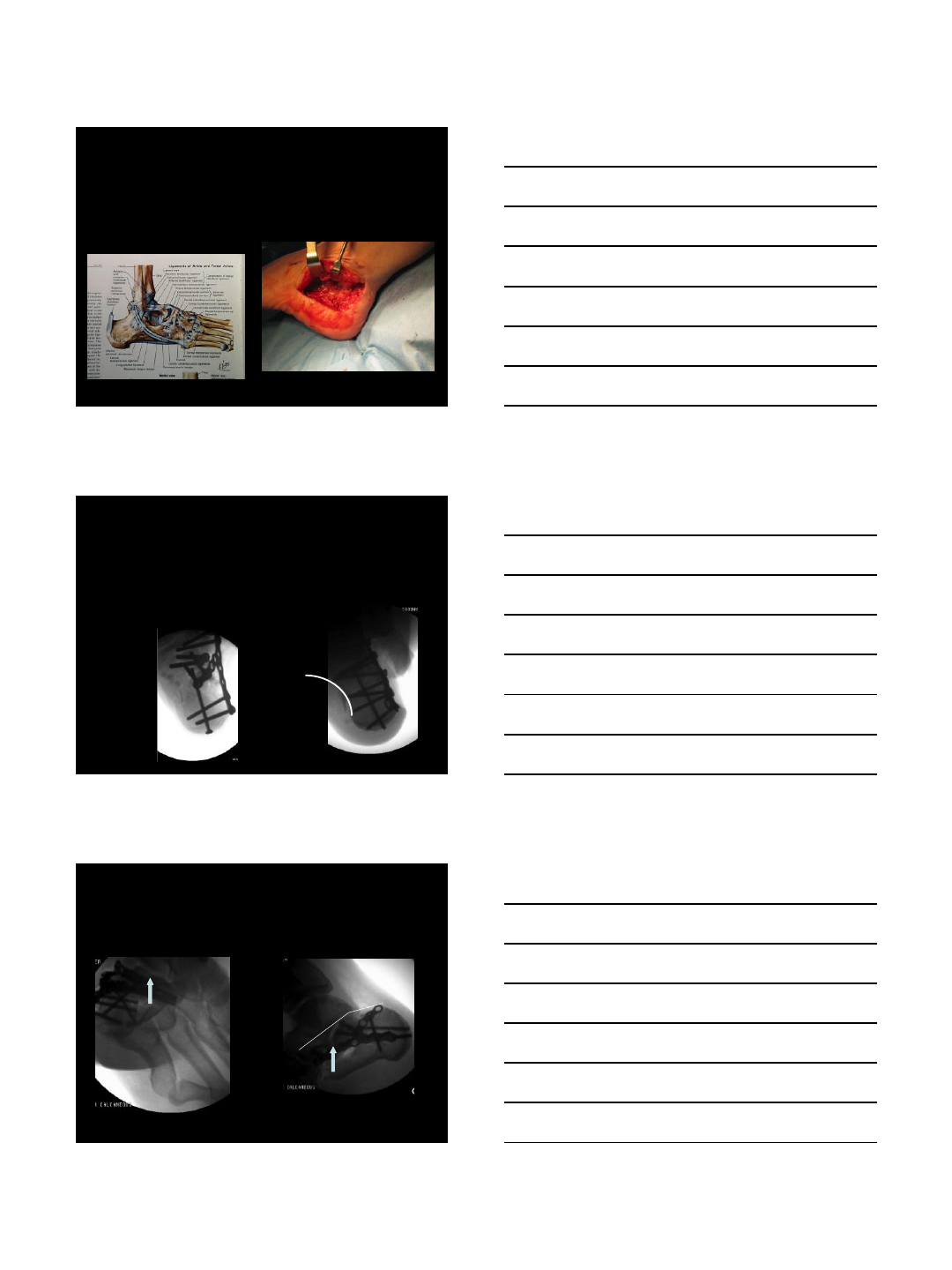
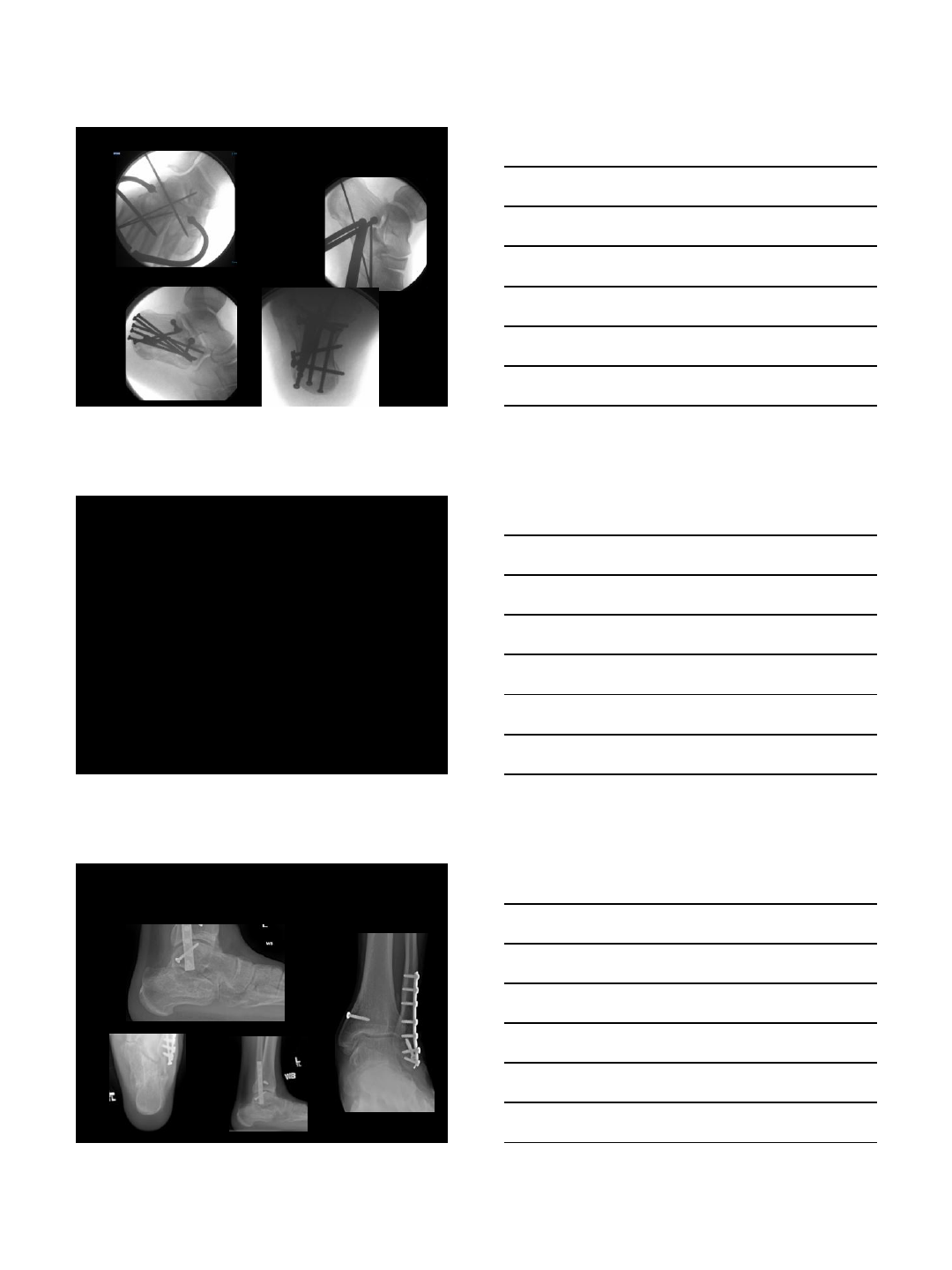
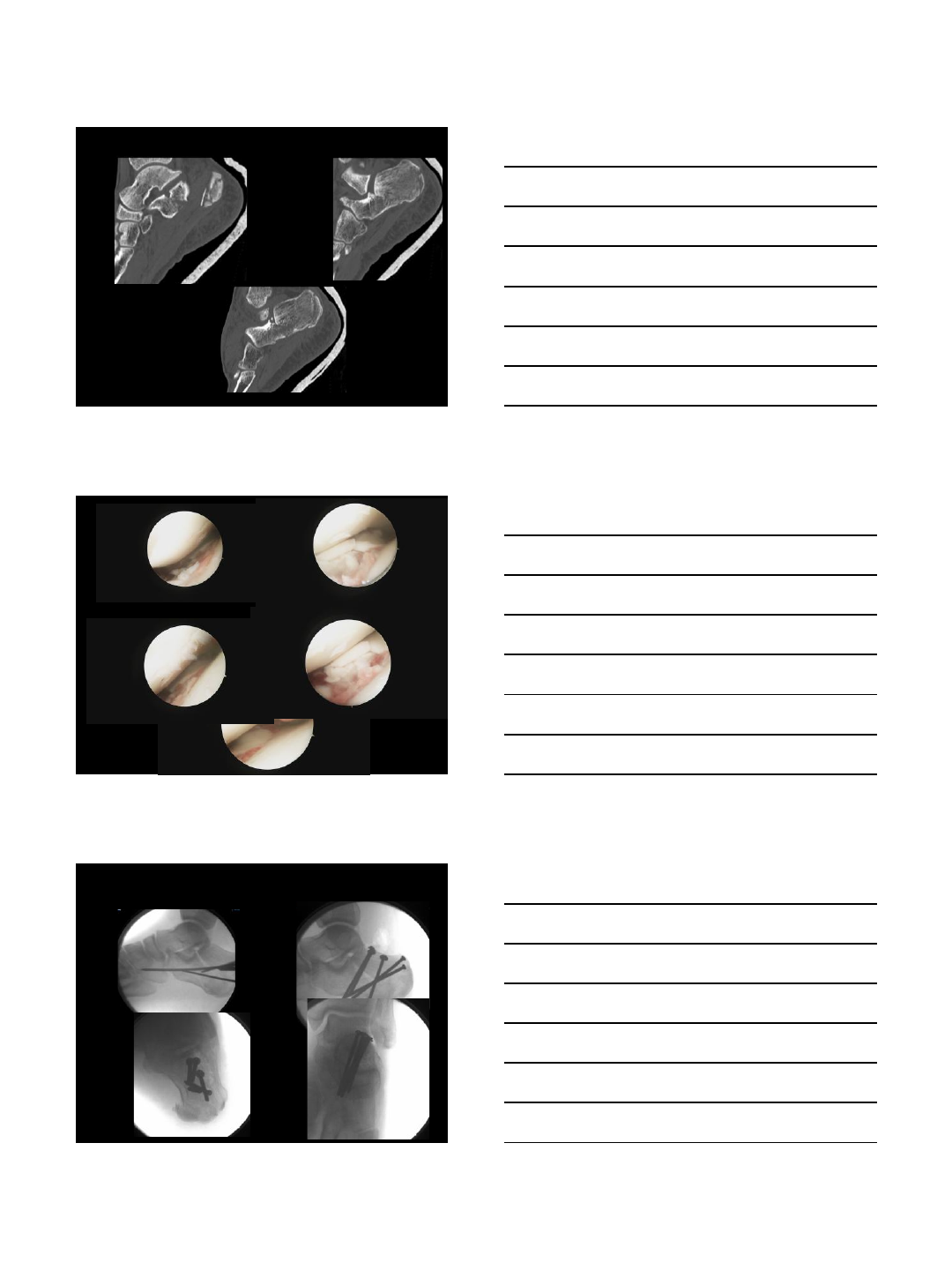
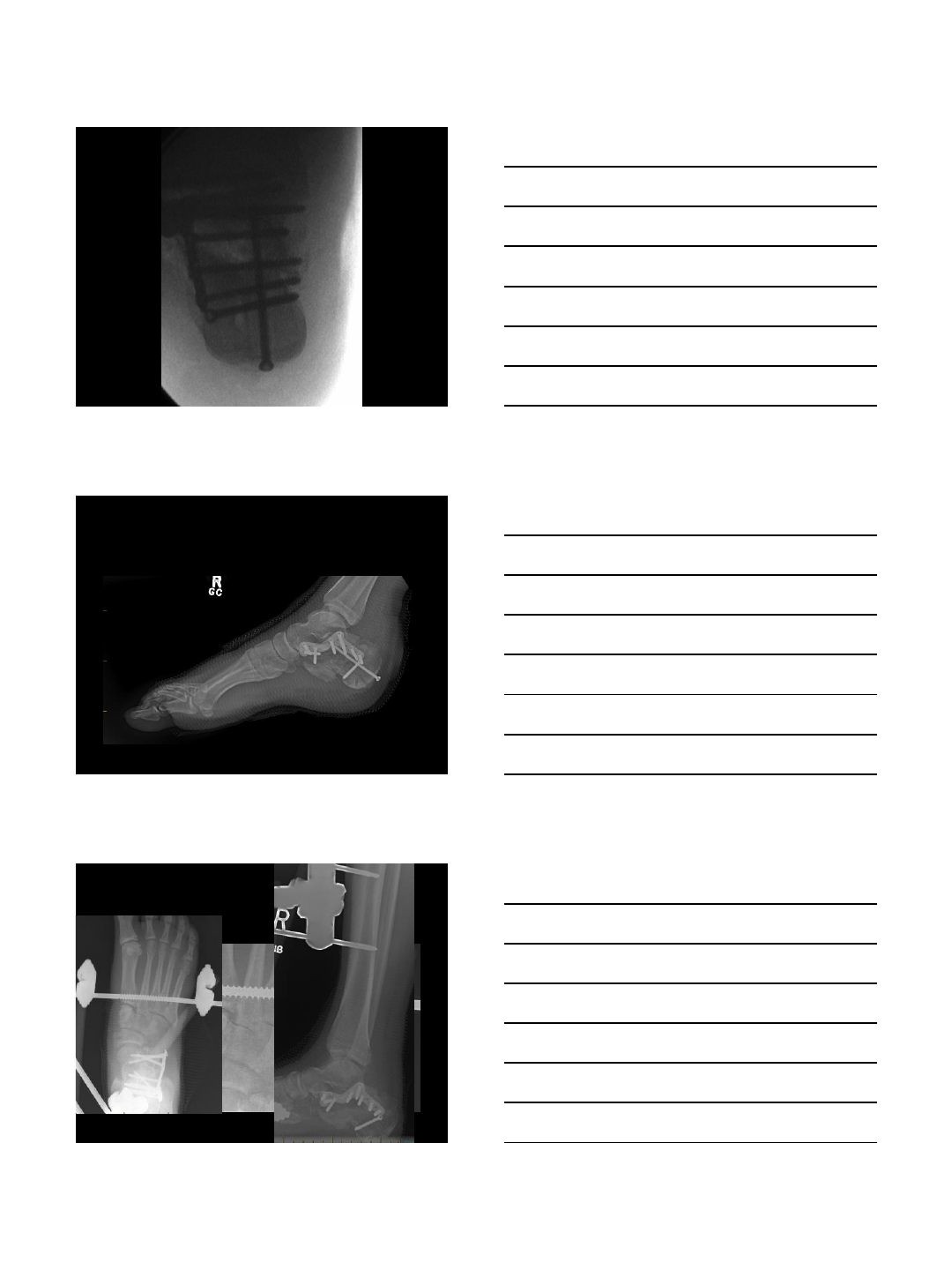
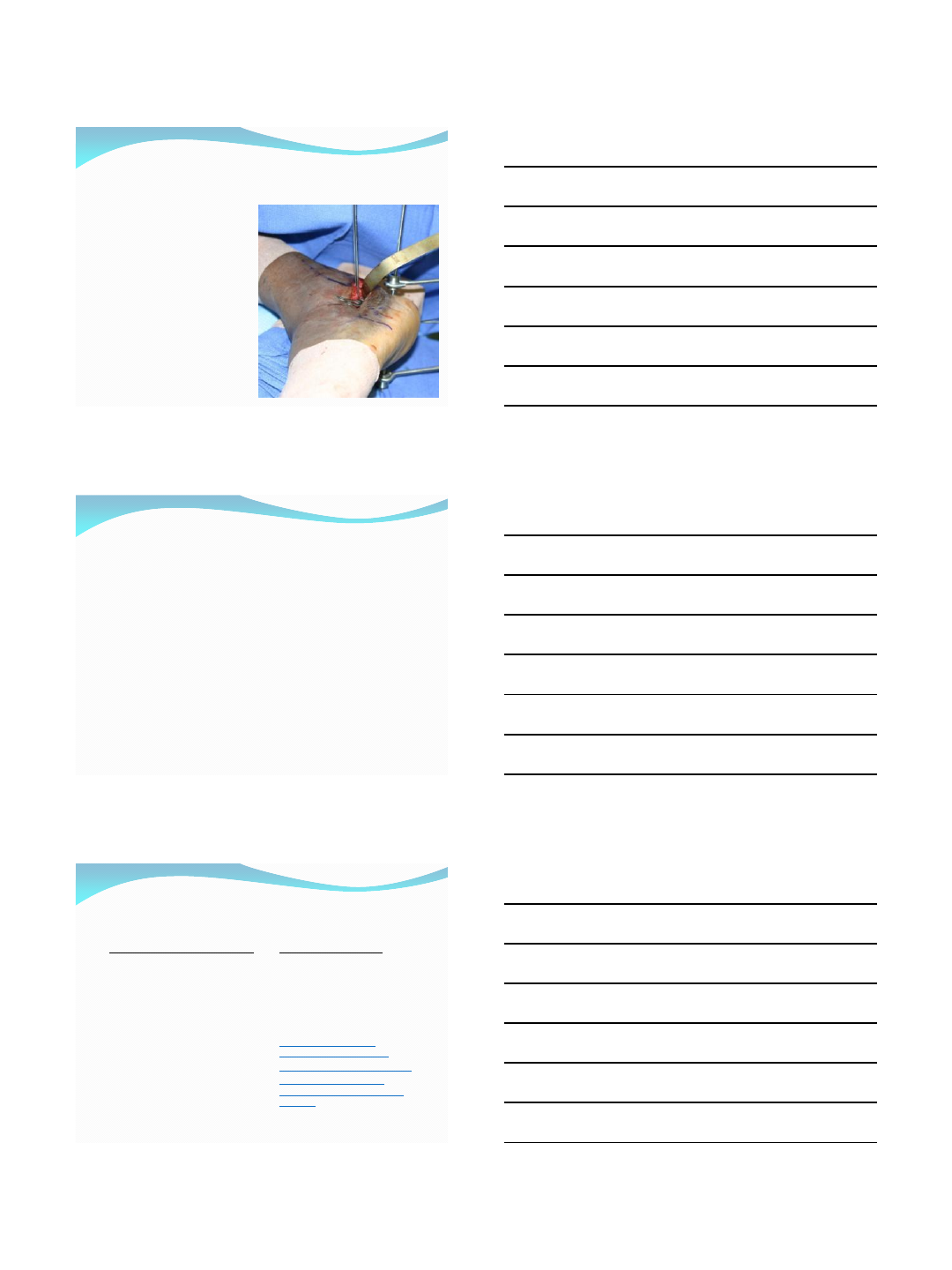
Case – tuberosity #
•Running from Hooker
•Skin issues urgent
•Reduction using large
fragment clamp
•Held with ex fix
•Medial and lateral bar
Less invasive – still need to
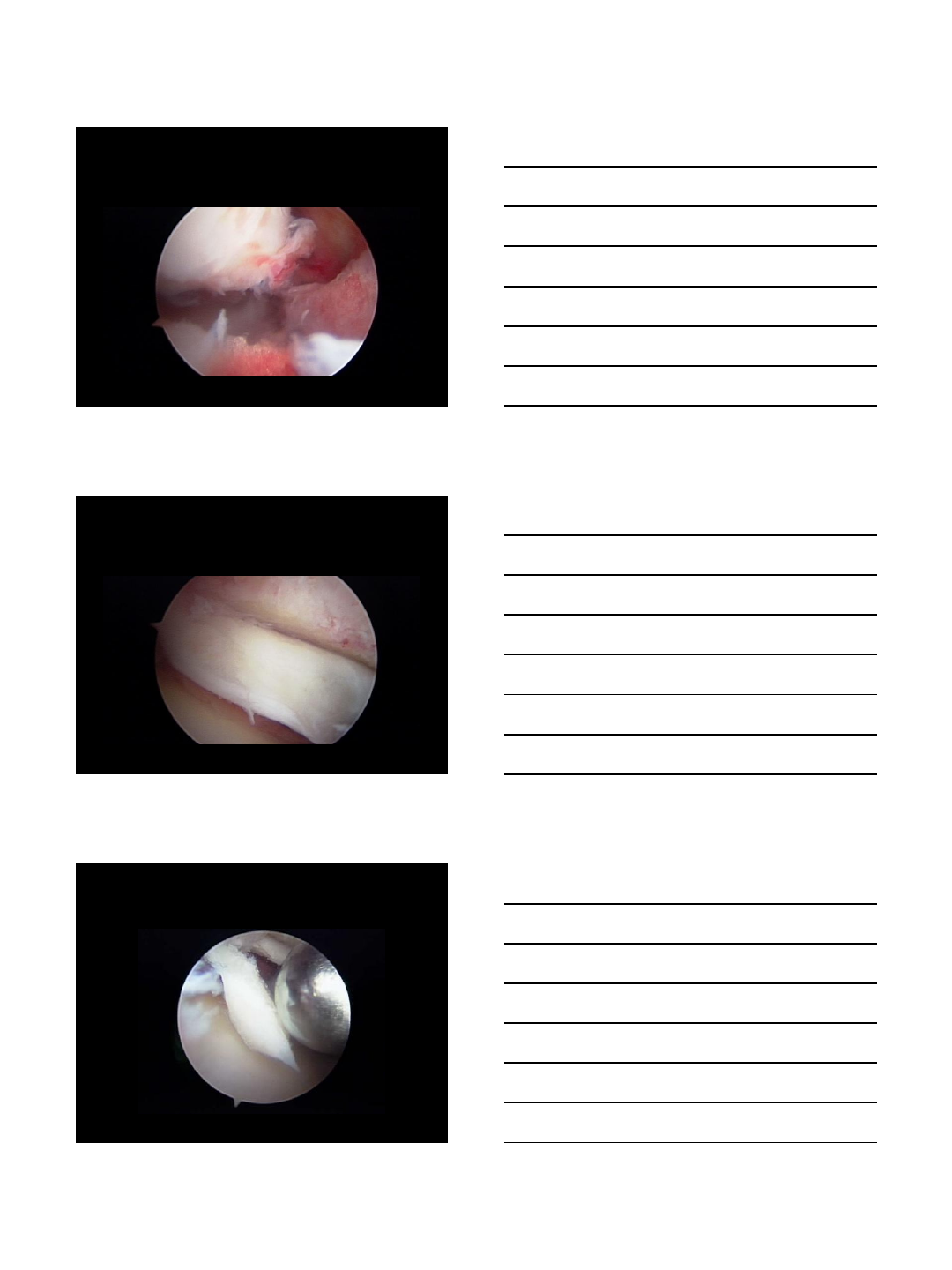
reduce the peroneal tendons
•Reduction of peroneal tendons
Calc fracture – arthroscopic
reduction
2/4/2014
5
2/4/2014
6
2/4/2014
7
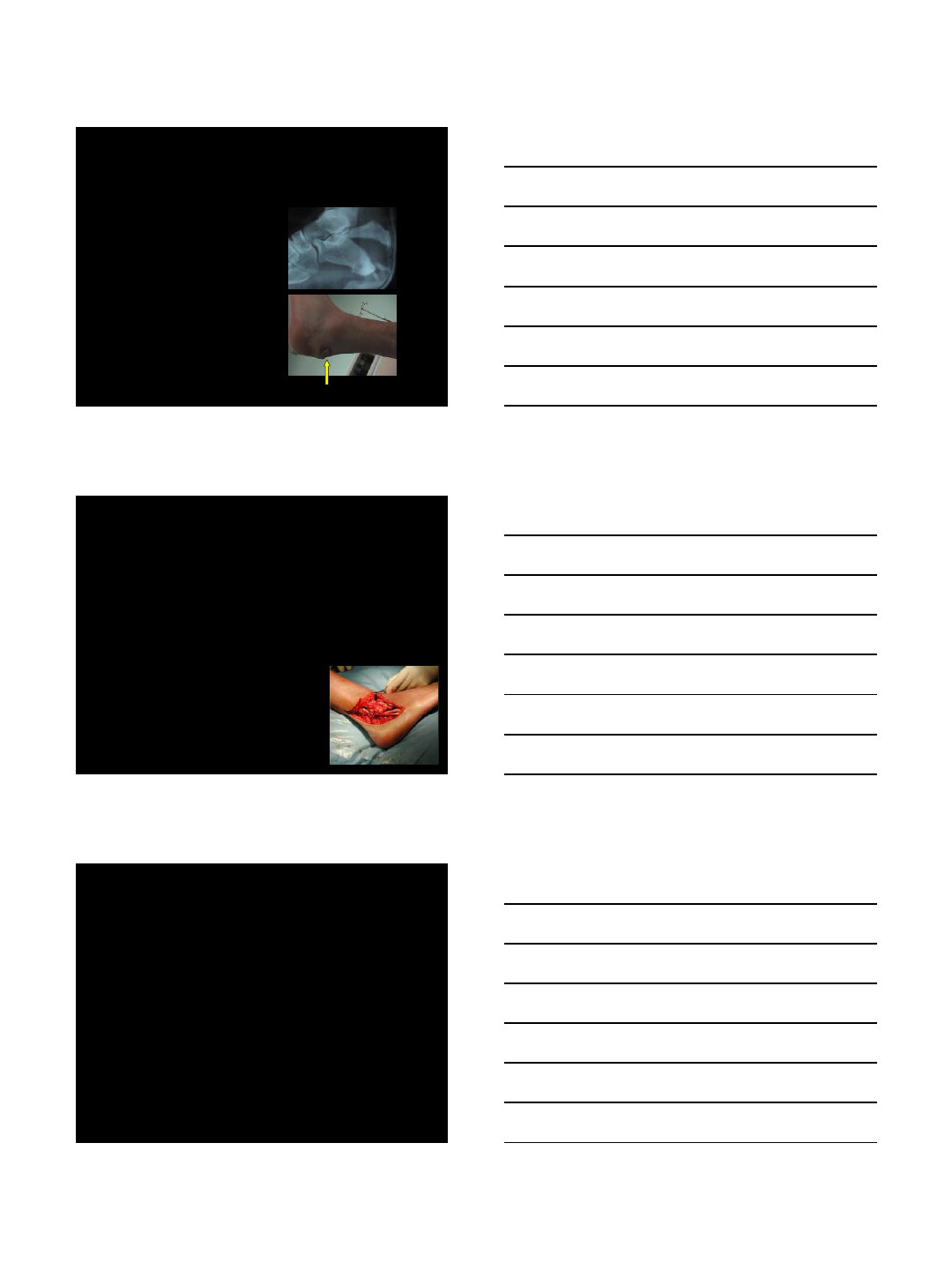
Missed calcaneal fracture
•4 months out
2/4/2014
8
2/4/2014
9
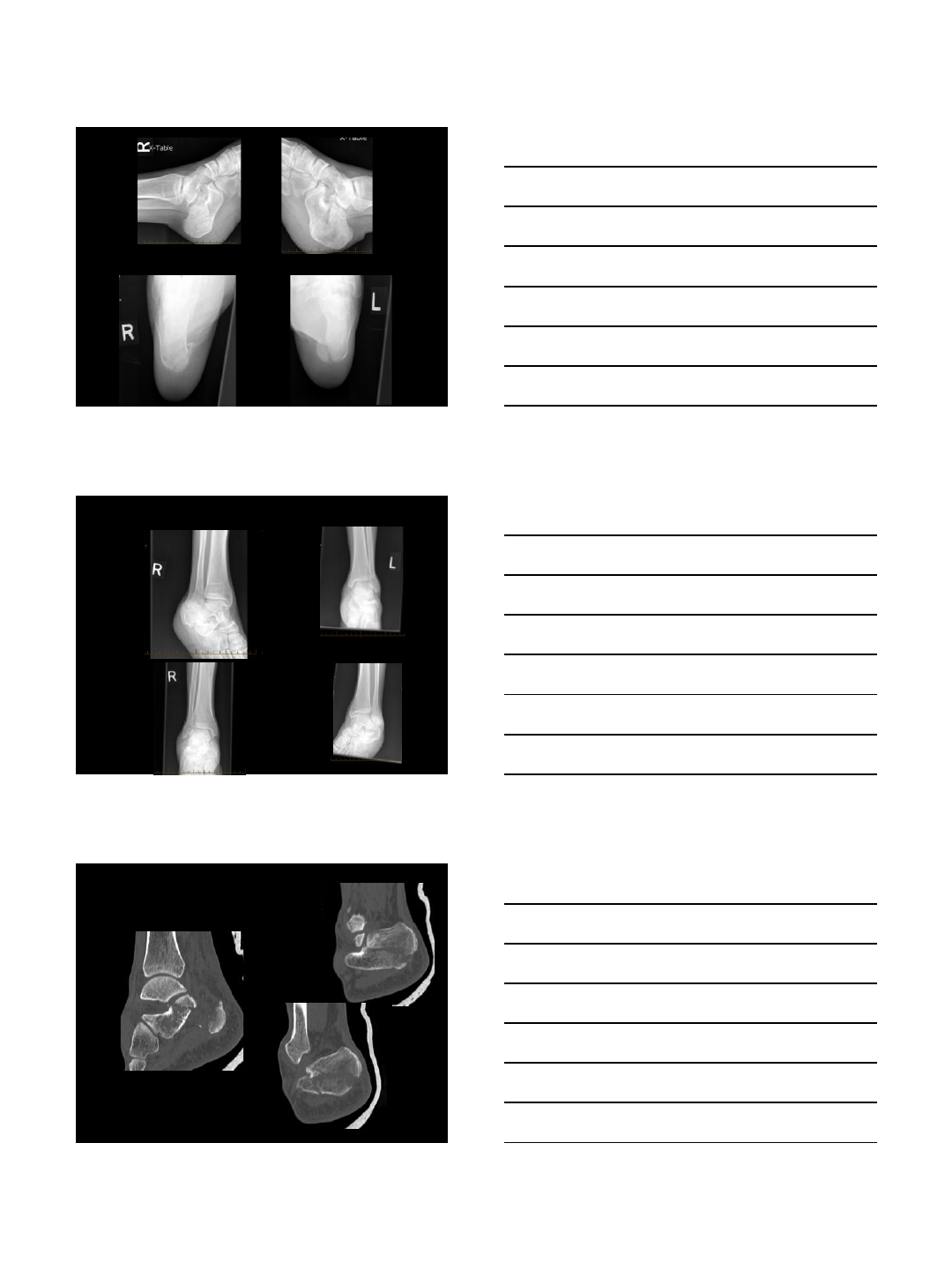
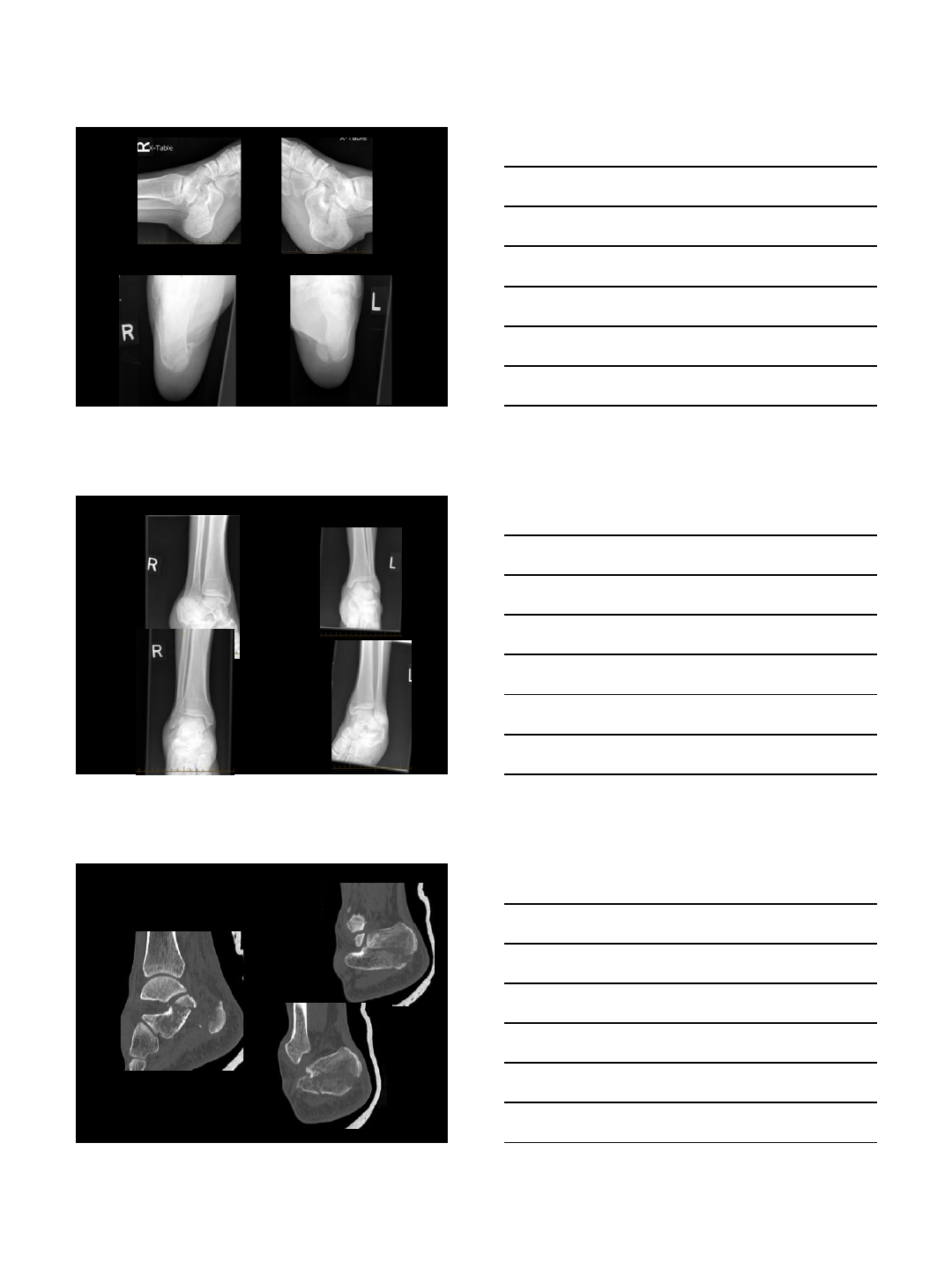
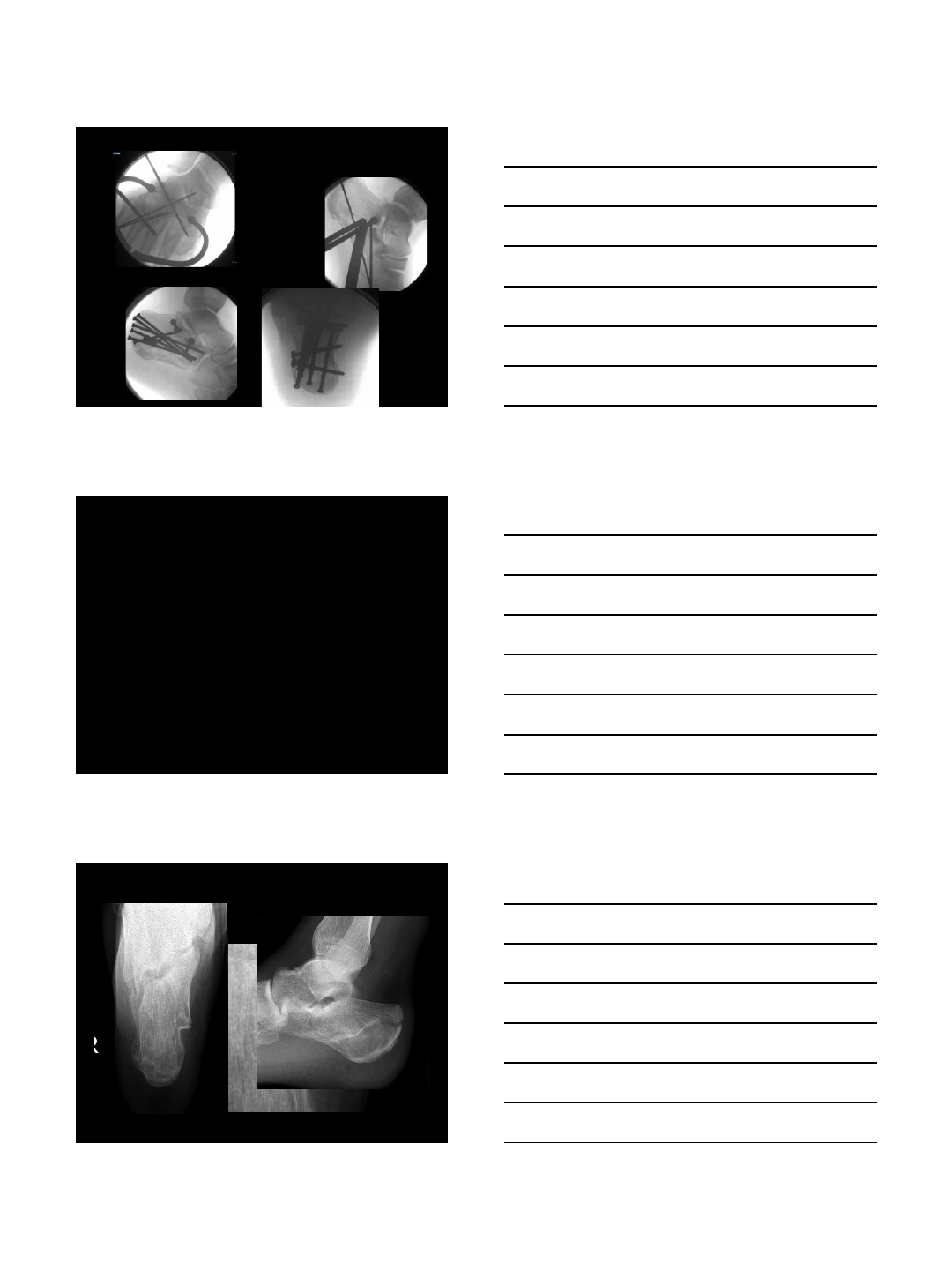
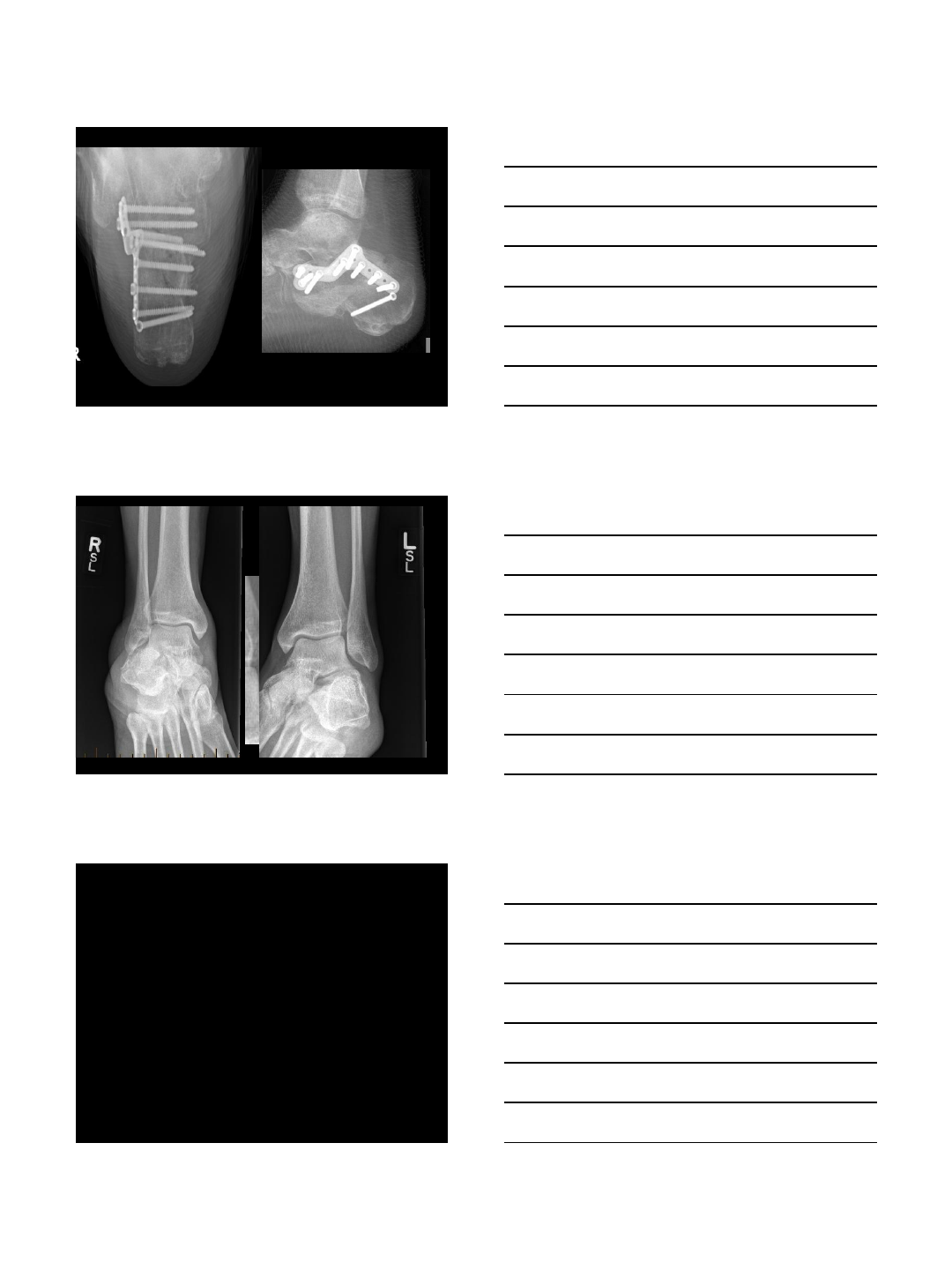
Calcaneal fracture – 3 weeks out
•60 year old
•Fell from boxes in a storage locker
•Healthly – enjoys golf
2/4/2014
10
Minimally invasive calcaneus
45 year old
•Movie set constructor
•Fell off the top of a 14 foot cowboy set
building
2/4/2014
11
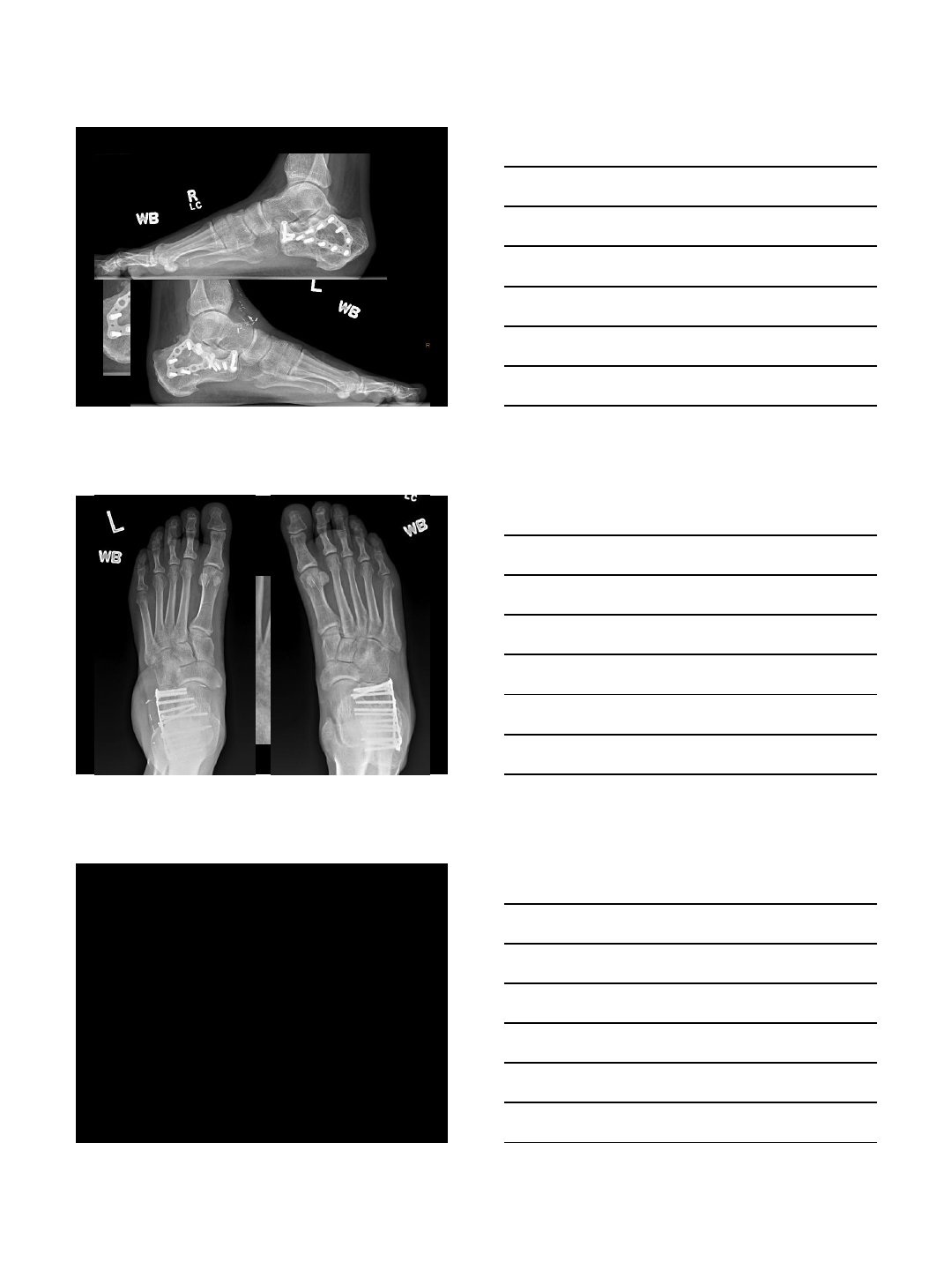
Bilateral calcaneal fractures
Left side
2/4/2014
12
2/4/2014
13
Bilateral calc orif
Calc fracture – arthroscopic
reduction
Bilateral calcaneal fracture case
2/4/2014
14
2/4/2014
15
2/4/2014
16
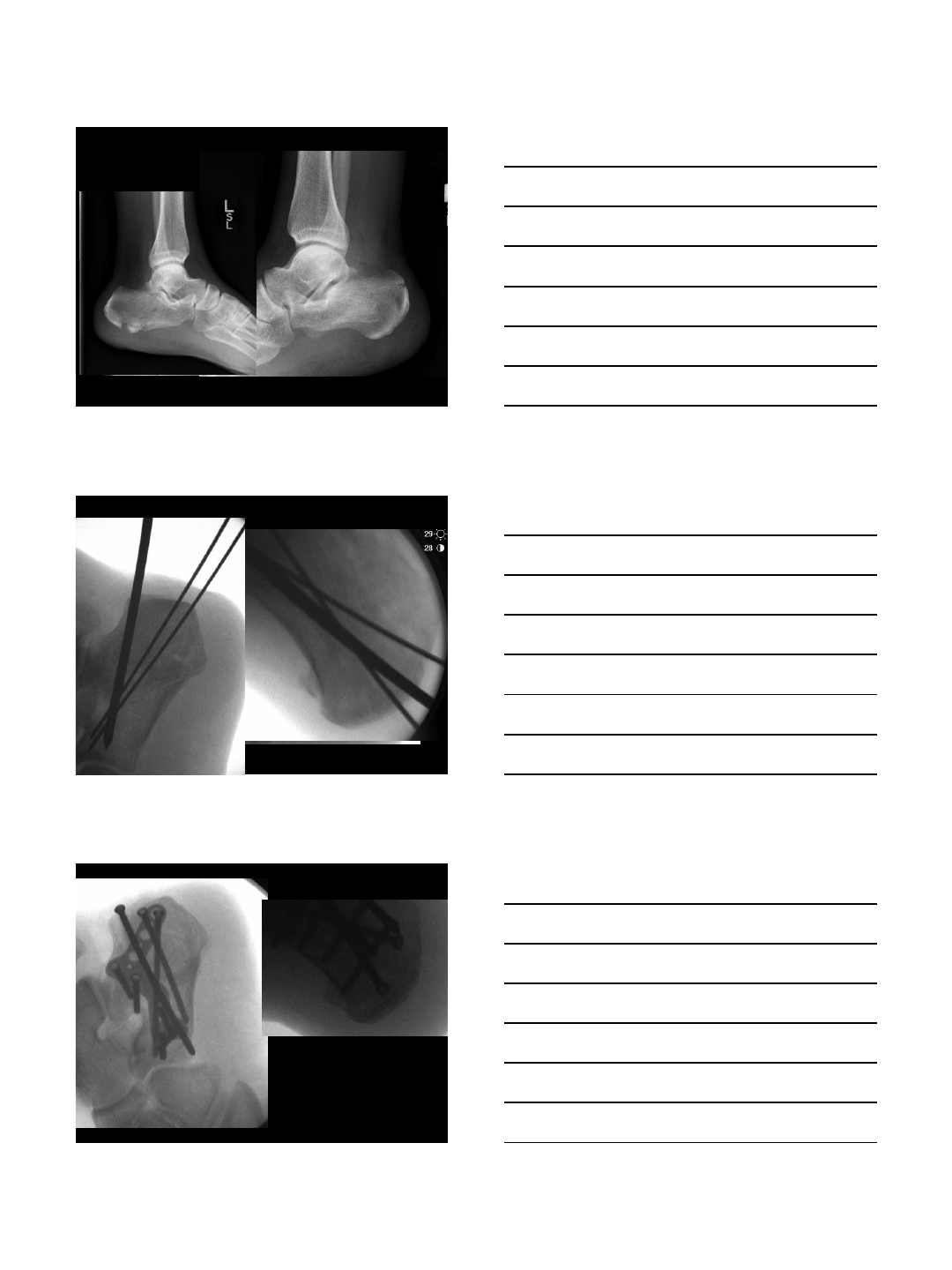
28 year old male
•Fell off bus stop
•Plays hockey
•Works as a doorman downtown hotel

2/4/2014
17
2/4/2014
18
2/4/2014
19
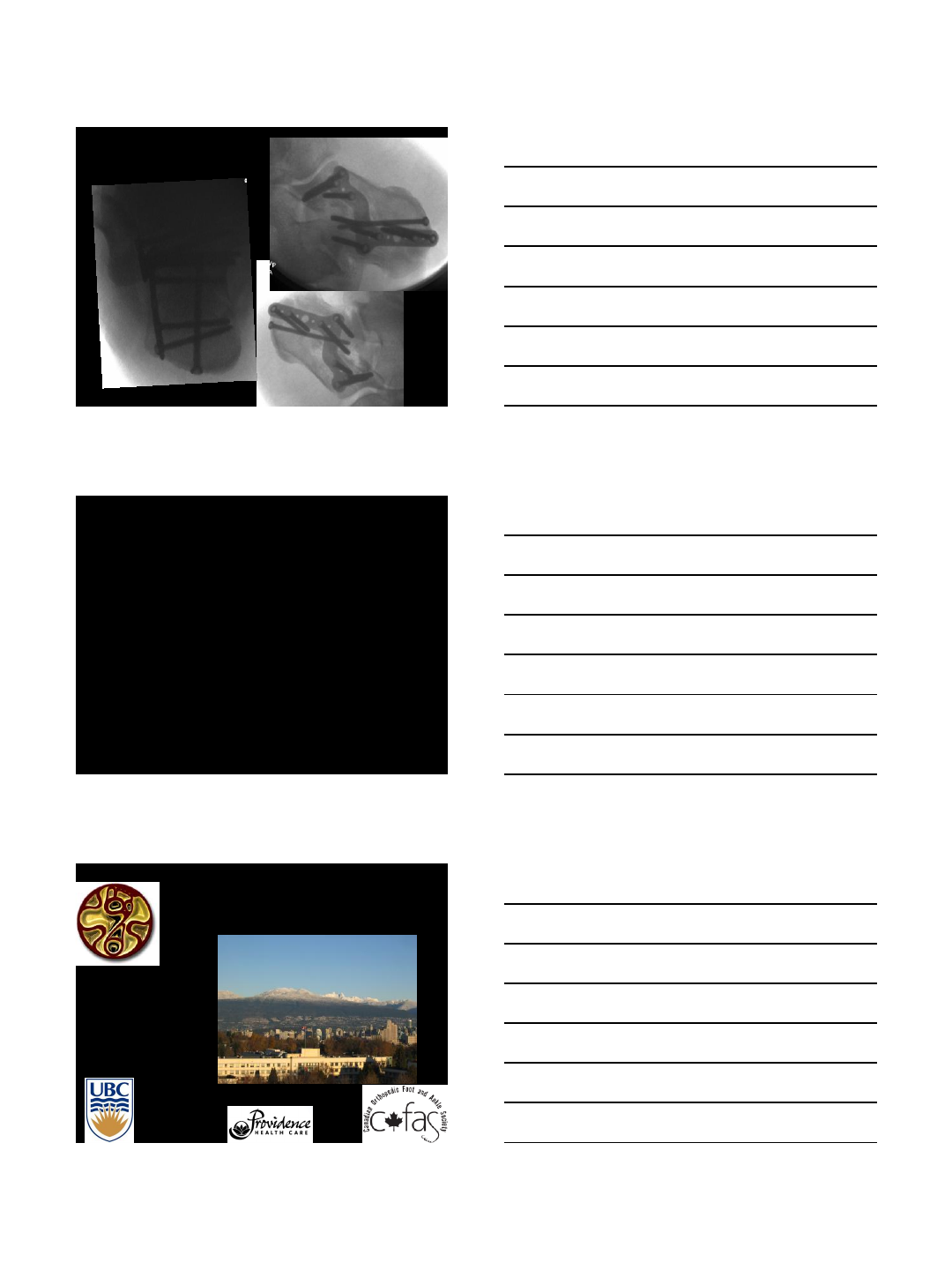
Compound calcaneus
•Fell from height
•Large medial compound wound
•Drug abuse, smoker, not employed
2/4/2014
20
2/4/2014
21
Bilateral calcaneal fractures
•Fell from tree
•45 year old male
2/4/2014
22
2/4/2014
23
Summary
•ORIF beneficial in most cases
•Techniques are changing to reduce
morbidity and expanding indications
•Late reconstruction is difficult and may not
restore function
•Make sure you restore normal anatomy
–Early and late
–Open or percutaneous
Thank You
2/4/2014
1
Steven Steinlauf, MD
The Orthopaedic Foot and Ankle Institute of South Florida
Clinical Assistant Professor University of Miami
Memphis, TN October 2013
Disclosure
I am a consultant and designer for Smith and Nephew
(VLP Foot System)
I Instruct for the AO
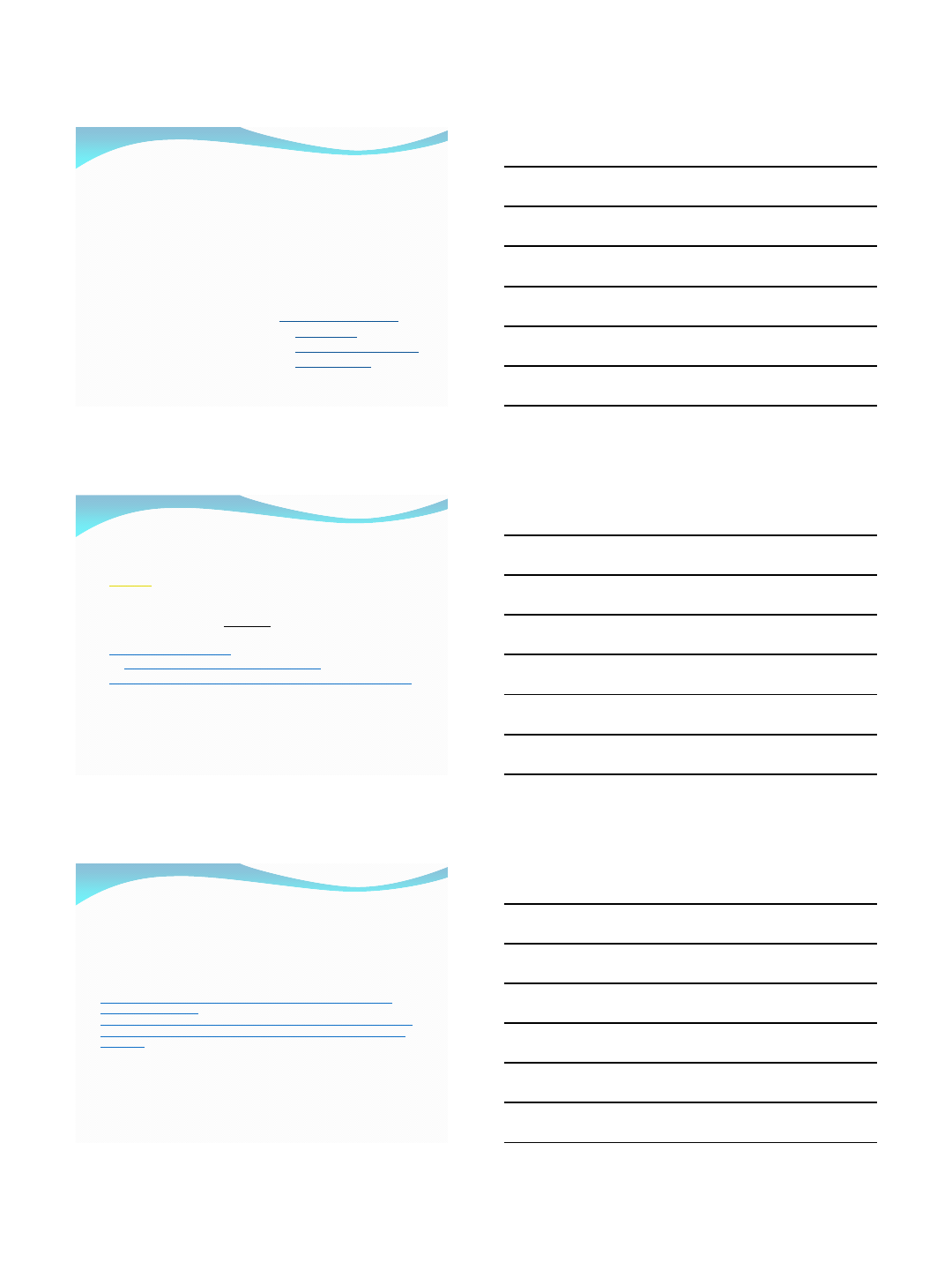
Complications of Extensile
Lateral Approach
Poor wound
healing
Risk of infection
Significant scar
tissue
Decreased ROM
2/4/2014
2
A Better Solution?
Minimal Incision Techniques
The concept = Less damage
to the soft tissues
Biologic fixation principles
Medial – Bordeaux, no
direct reduction of post
facet or ant calcaneus
Medial and limited lateral
Percutaneus Fixation
Tongue and Tuberosity
fractures
Sinus tarsi approach
Screws only
Screws and mini-plates
Custom plates
Which is better?
Kline AJ, et. Al. FAI 2013, June, Sinus Tarsi Vs. extensile
lateral
Retrospective
79 - extensile lateral approach
33 - minimally invasive
Wound complication –
29% extensile vs. 6% minimally invasive
20% extensile - secondary surgery, 2% minimally invasive
FFI - 31 extensile group vs. 22 minimally invasive
VAS pain - 36 extensile, 31 minimally invasive
84% extensile satisfied, 94% minimally invasive
no differences - Bohler's angle and angle of Gissane.
The sinus tarsi approach in
displaced intra-articular calcaneal
fractures: a systematic review.
•Schepers T Int Orthop, 2011
•8 case series reporting on 256 patients with 271 calcaneal fractures
•good to excellent – ¾
•minor wound complications of 4.1% was reported and major wound
complications in 0.7%.
•The results, i.e. functional outcome and complication rates, of the sinus
tarsi approach compare similarly or favourably to the extended lateral
approach.
2/4/2014
3
Mini-incision Treatment for
calcaneal fractures
Workup - same
Radiographs and CT – same
Timing – different
Extensile lateral incision – Once swelling goes down
(usually within 3 weeks)
Mini-incision techniques - 1 – 14 days (The earlier
the better, soft tissues permitting)
Preop –
RICE
Jones dressing
Indications
Very Narrow at first
A learning curve exists
Easier if you have performed many through an extensile
lateral exposure
Understand the anatomy and the fracture
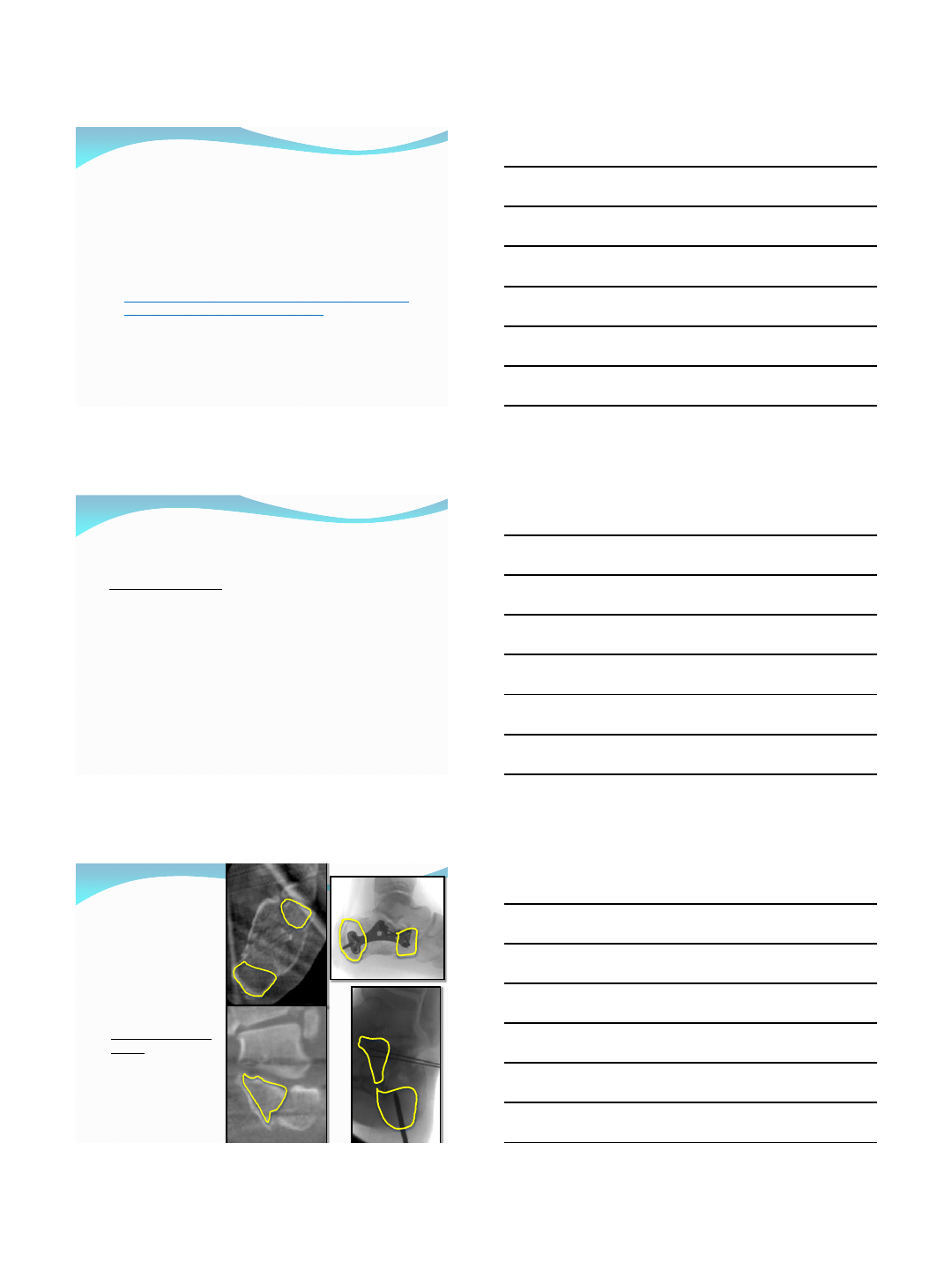
Indications
You must have good
bone in 3 locations:
Anterior, Posterior
tuberosity, Constant
fragment
These are the areas for
needed screw fixation
Specific percutaneus
plate - fracture lines
extending to these
regions – locking
screws help
2/4/2014
4
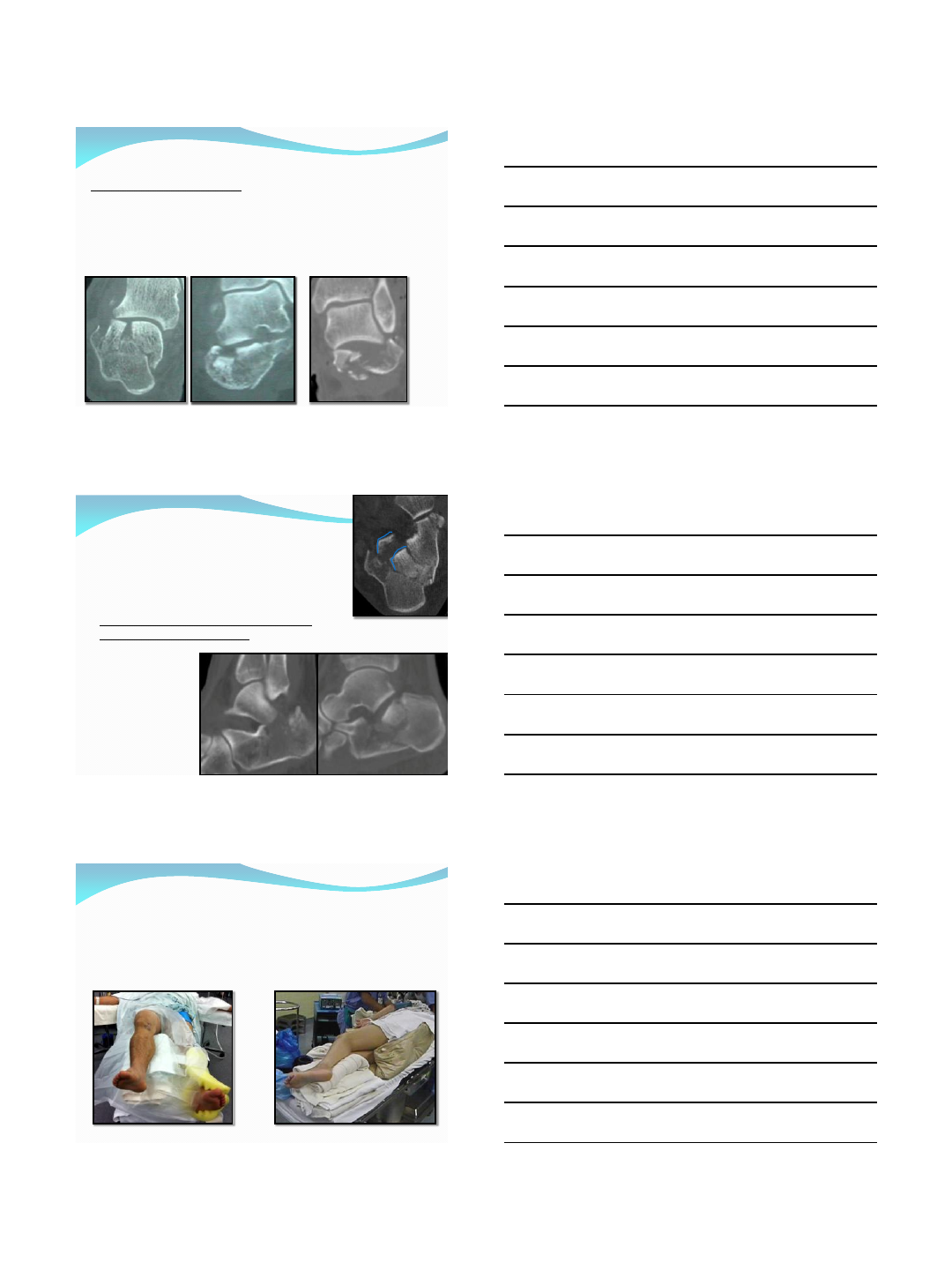
Indications
Specific Fracture Patterns:
Sander’s 2 part (Easiest)
Sander’s 3 Part with an anterior central part (Difficult)
Sander’s 4 part (Fairly Straight forward)
Need to reestablish articular anatomy grossly and then fuse
Excellent for open injuries in the correct setting
Contraindications
Sander’s 3 part fractures with posterior fragments
You cannot get to them from the sinus tarsi incision
Fractures where you do not think that you can
achieve an anatomic reduction of the joint
Remember – Small Incisions with a poor
reduction achieve nothing!!!
Positioning
Supine for unilateral or
bilateral
Lateral decubitus
2/4/2014
5
Percutaneus Plate
Sanders 2 Part
Step 1 -Medial Ex-Fix Placement
Placement of medial ex- fix:
Enables you to “pull” the
posterior tuberosity out of
the way.
This allows for:
Easier reconstruction of
the posterior facet
Easier correction of
height and varus
No need for a medial
screw
Greatest advance in
technique
Steps 2 -
Incision /
Disimpaction
Sinus tarsi incision –
Dorsal to the peroneals
Keep the peroneals in
their sheath
Compress Lateral wall
“blow-out”
Make path for the plate –
stay on the outside of the
posterior tuberosity
Disimpact medial wall –
Curved elevator
Correct varus and height
2/4/2014
6
Steps 2 - Incision / Disimpaction
Steps 2 - Incision / Disimpaction
Step 3 -Reduction and
stabilization of posterior facet
Pulling the posterior tuberosity out of the way makes the posterior facet
reduction possible
Lag the posterior facet with 2.0 to 3.0mm screws as needed (canulated vs. solid)
Aim towards sustentaculum as much as possible
Confirm reduction with scope and fluro

2/4/2014
7
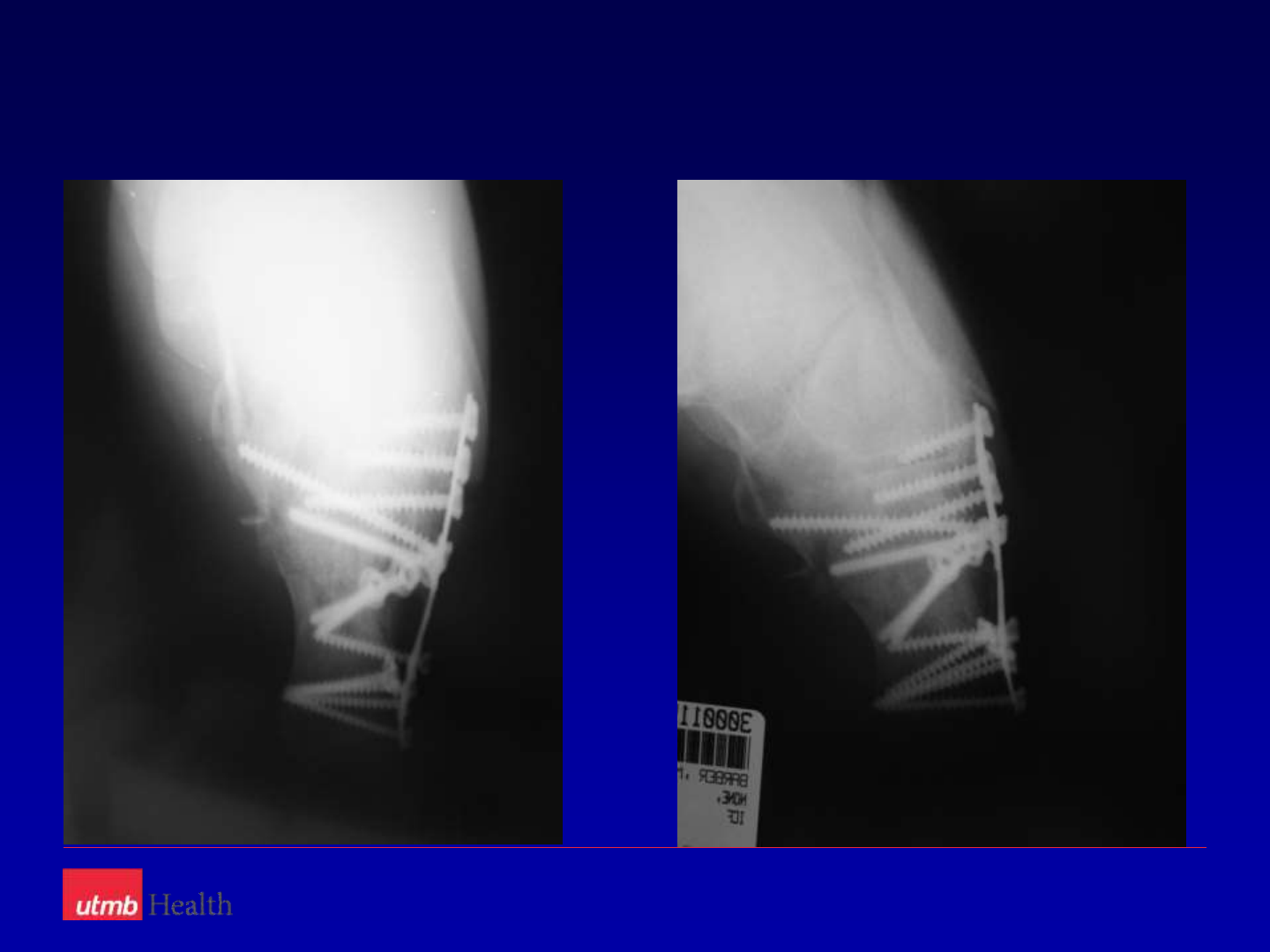
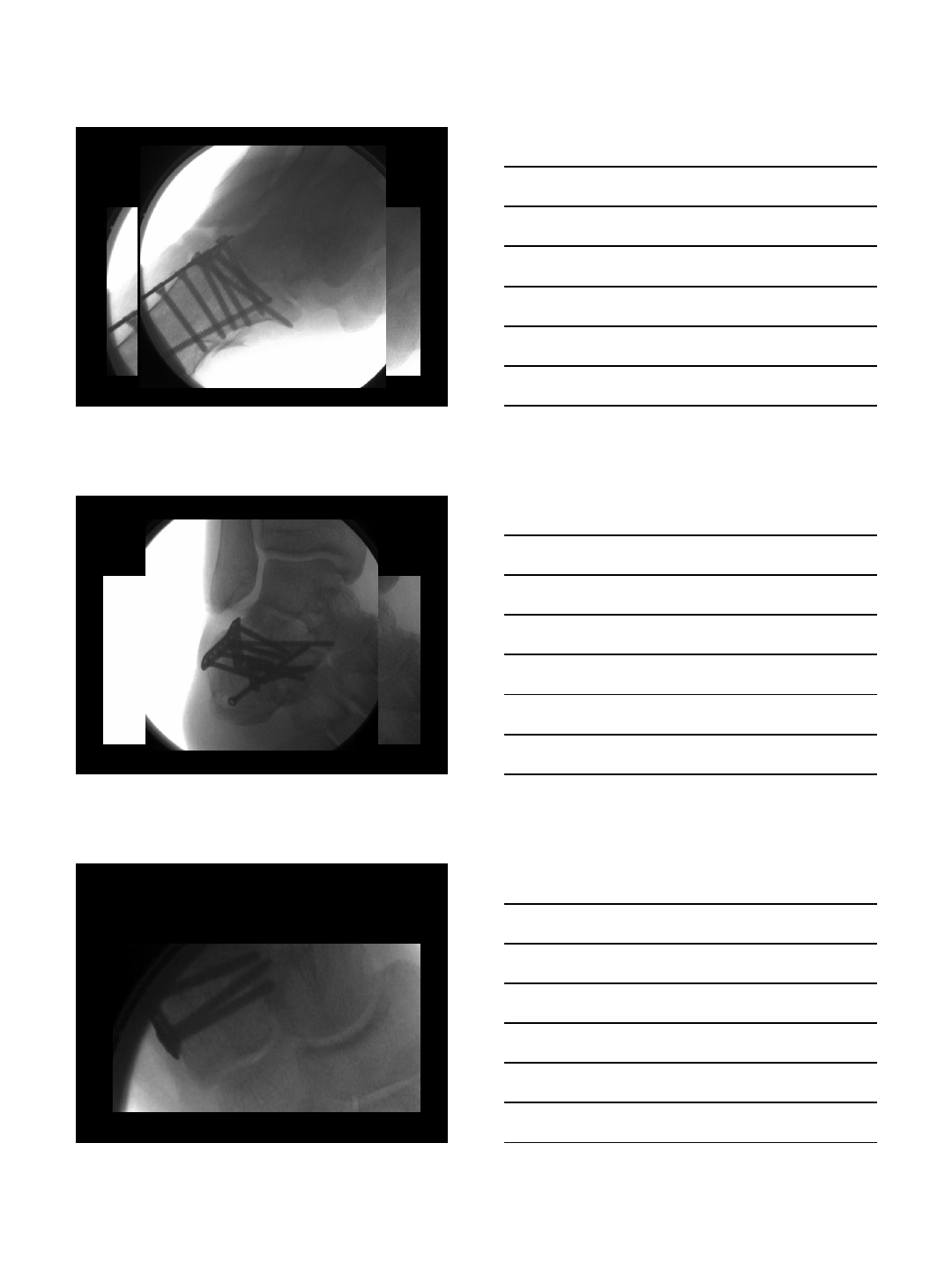
Step 4 - Plate Placement
Step 4 - Plate Placement
Step 4 - Plate Placement
2/4/2014
8
Finals
Post-op Protocol
Start Early
Motion – 7 days
+/- (when the
wound is ready)
Better final
ROM?

2/4/2014
9
Delayed Wound Healing
Rough with tissues
Incision too small
Fix after 2 weeks
Move too soon (less
than 1 week)
Stop movement until
wound is healed
Infection
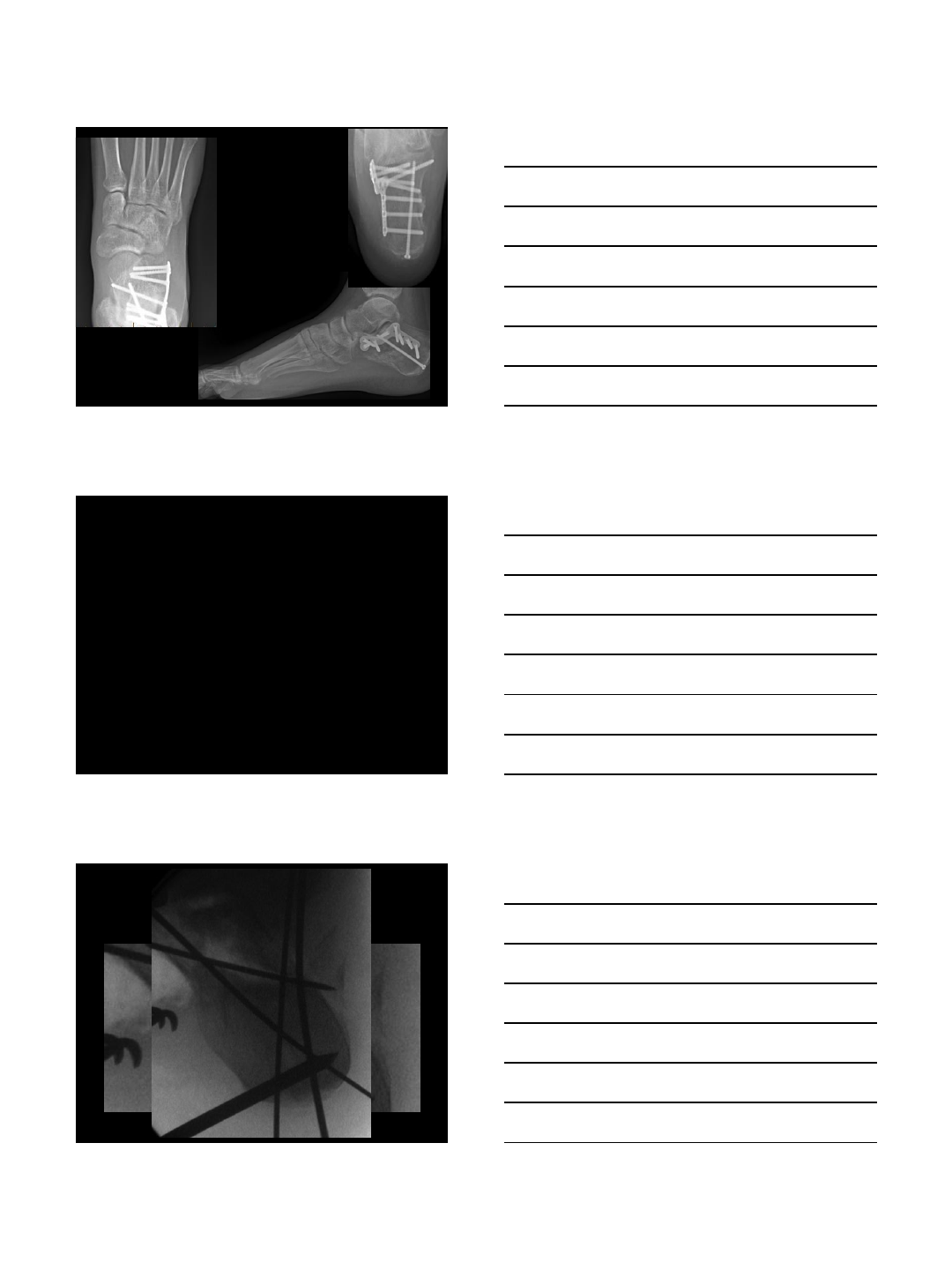
Mini incision
ORIF and primary fusion
for an open Sander’s 4
fracture
Vac
Abx
No need for a flap
Hopefully risk will be
less
Sural Nerve Injury
Take care to
place screws
dorsal or plantar
to the nerve
2/4/2014
10
Peroneal Tendonitis
Protect the tendons
throughout the case
Keep them in their
sheath
Possibly more pain
and need for ROH?
Our Study:
Total patients undergoing percutaneus plating
(minimum f/u 3 mos.): 49 pts.
Total Fxs.: 51
2 patients with Bilateral fxs had both sides tx with ORIF
Males – 33 (34fxs), Females – 16 (17 fxs)
Patients
Not at high risk for infection -
26 pts. (26 fxs.)
1 infection at operative site
1 infection at site of posterior
skin necrosis near tongue fx.
High Risk Patients” –
Smokers: 14 pts. (16fxs.)(No
infecs)
Diabetic: 3 pts. (No infecs)
Smokers (plus diabetes /
HIV): 2 pts. (No infecs)
Open Fractures: 4 pts. (1
infection)
High Risk Group 1
infection in 25 cases.
No infections since 2008.
9 pts - extension for
stabilization of pers – 0
infecs.
2/4/2014
11
Our Study:
Delayed wound Healing – 5 pts.
None required additional surgery or special treatment
Painful hardware requiring removal – 4 pts.
Conclusions
The sinus tarsi approach offers the following benefits:
Fewer serious wound complications
Lower risk of infection
Especially in high risk groups
Anatomic reduction of Sanders type II and some type III
fractures (confirmed with an arthroscope)
Able to use for Type IV fractures (primary subtalar fusion)
Functional outcome is likely similar to extensile lateral
approach (We need to complete phase 2)
2/3/2014
1
SURGICAL MANAGEMENT OF
THE CALCANEAL MALUNION
MICHAEL P. CLARE, M.D.
FLORIDA ORTHOPAEDIC INSTITUTE
TAMPA, FLORIDA, USA
VUMEDI CALCANEUS WEBINAR 2014
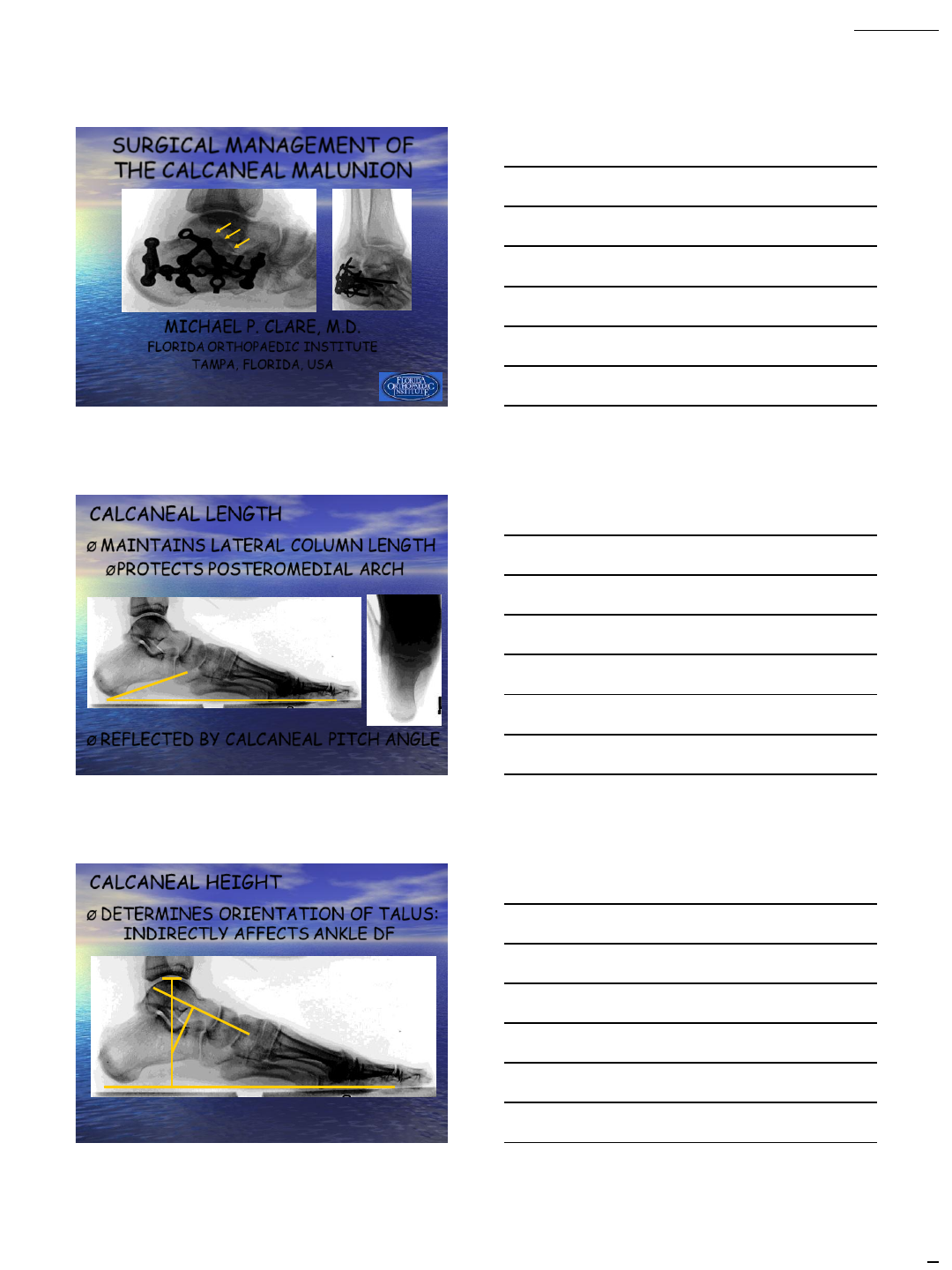
CALCANEAL LENGTH
ØMAINTAINS LATERAL COLUMN LENGTH
ØPROTECTS POSTEROMEDIAL ARCH
ØREFLECTED BY CALCANEAL PITCH ANGLE
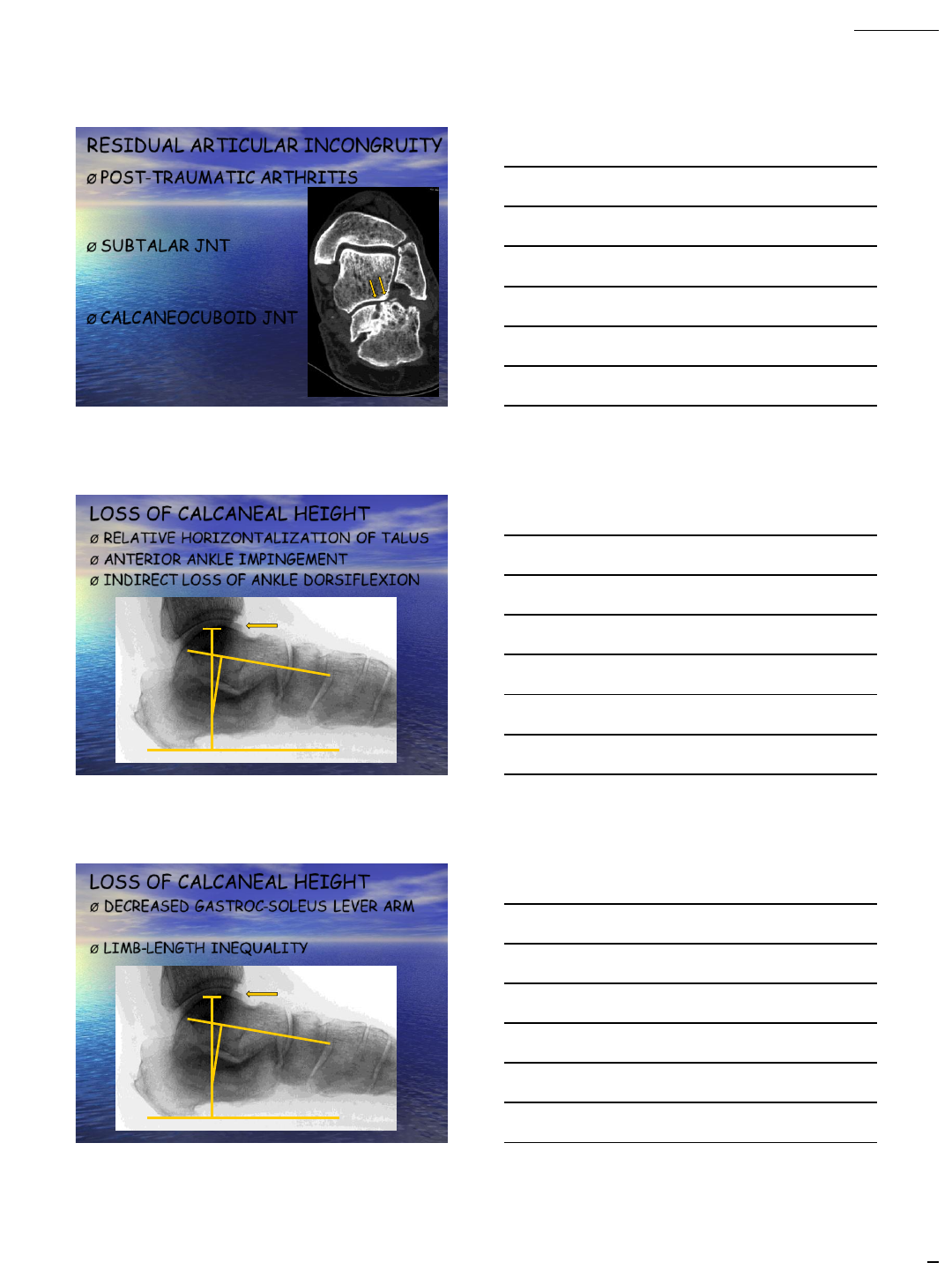
CALCANEAL HEIGHT
ØDETERMINES ORIENTATION OF TALUS:
INDIRECTLY AFFECTS ANKLE DF
2/3/2014
2
RESIDUAL ARTICULAR INCONGRUITY
ØPOST-TRAUMATIC ARTHRITIS
ØSUBTALAR JNT
ØCALCANEOCUBOID JNT
LOSS OF CALCANEAL HEIGHT
ØRELATIVE HORIZONTALIZATION OF TALUS
ØANTERIOR ANKLE IMPINGEMENT
ØINDIRECT LOSS OF ANKLE DORSIFLEXION
LOSS OF CALCANEAL HEIGHT
ØDECREASED GASTROC-SOLEUS LEVER ARM
ØLIMB-LENGTH INEQUALITY
2/3/2014
3
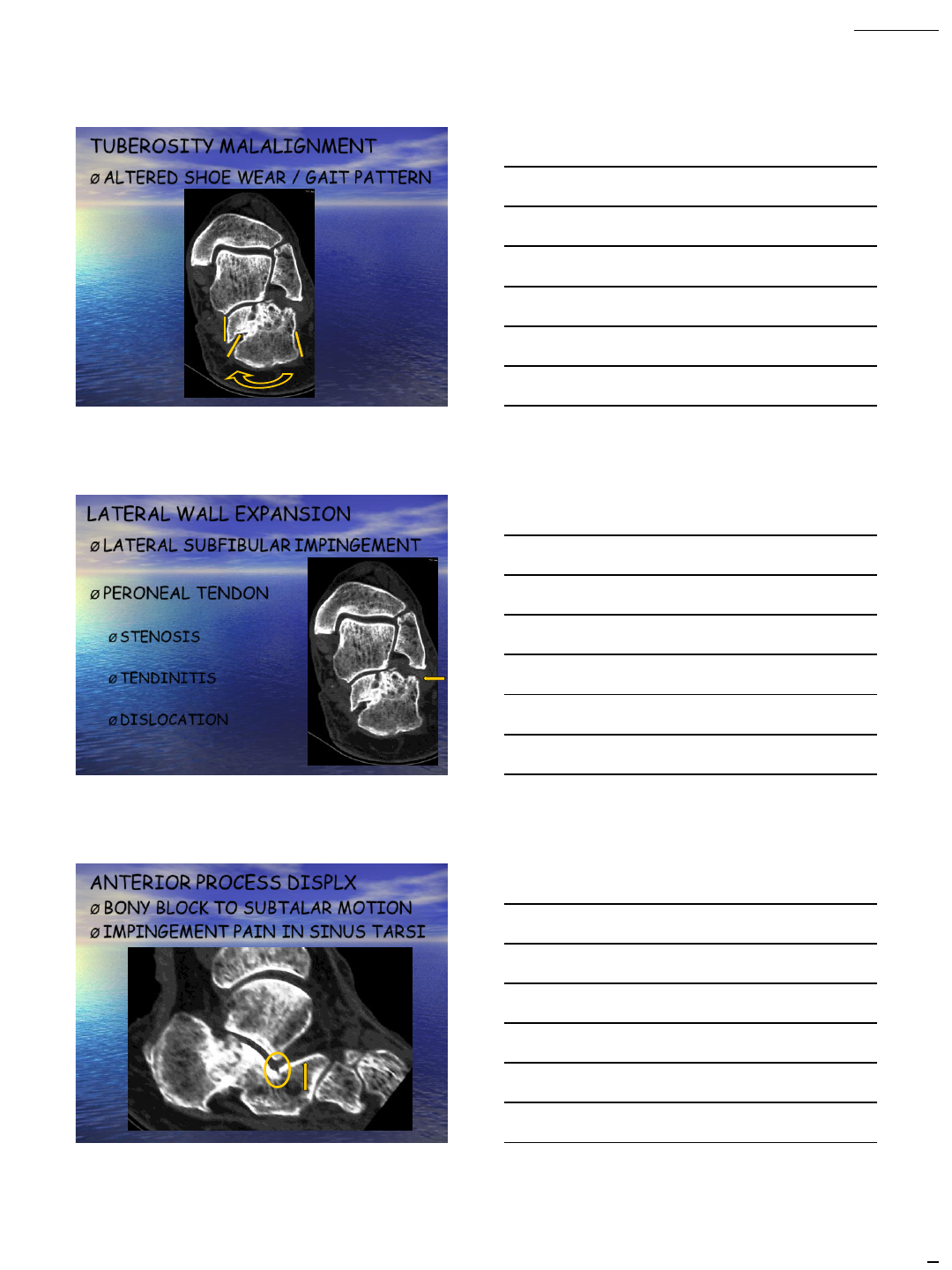
TUBEROSITY MALALIGNMENT
ØALTERED SHOE WEAR / GAIT PATTERN
LATERAL WALL EXPANSION
ØLATERAL SUBFIBULAR IMPINGEMENT
ØPERONEAL TENDON
ØSTENOSIS
ØTENDINITIS
ØDISLOCATION
ANTERIOR PROCESS DISPLX
ØBONY BLOCK TO SUBTALAR MOTION
ØIMPINGEMENT PAIN IN SINUS TARSI
2/3/2014
4
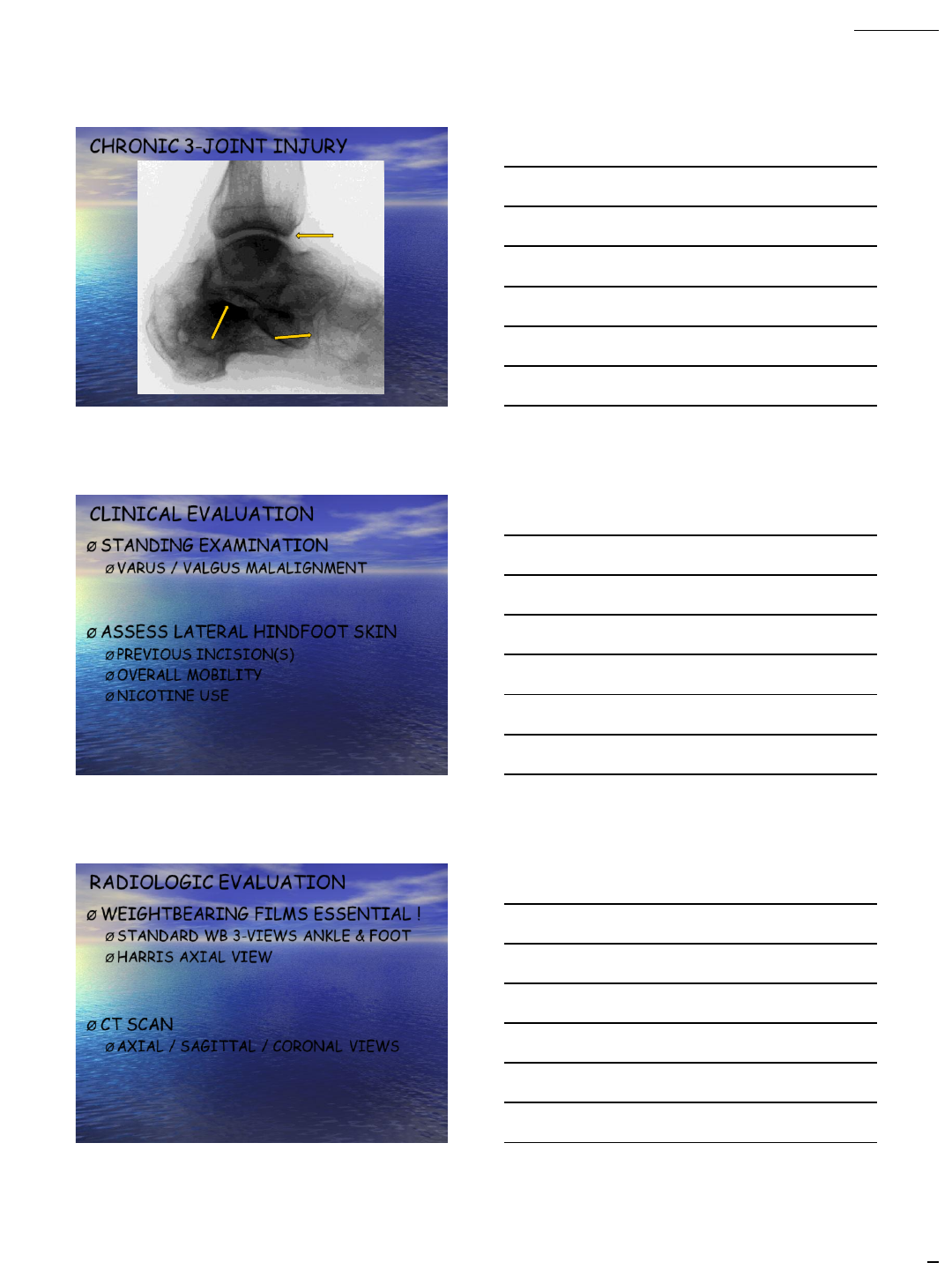
CHRONIC 3-JOINT INJURY
CLINICAL EVALUATION
ØSTANDING EXAMINATION
ØVARUS / VALGUS MALALIGNMENT
ØASSESS LATERAL HINDFOOT SKIN
ØPREVIOUS INCISION(S)
ØOVERALL MOBILITY
ØNICOTINE USE
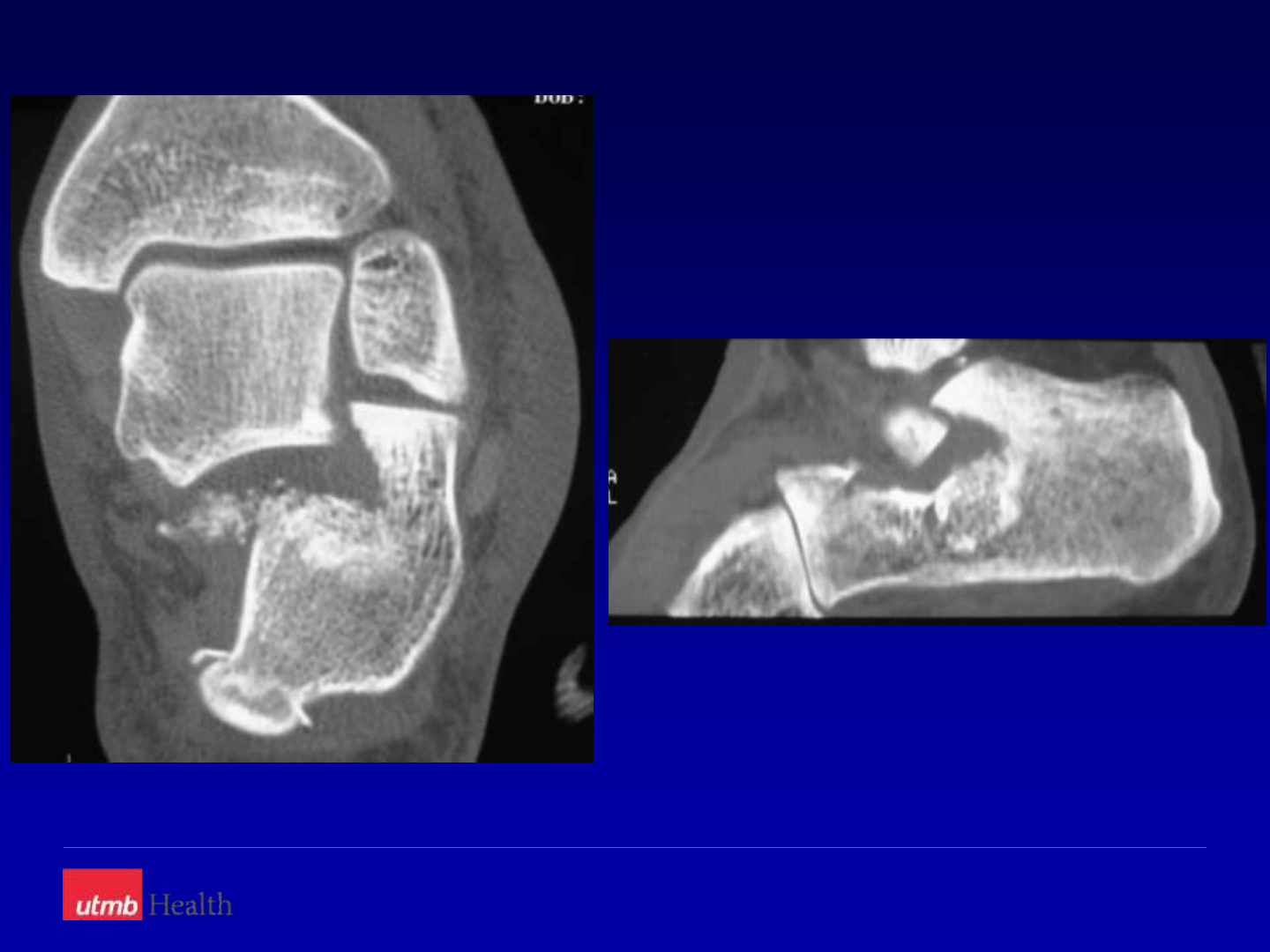
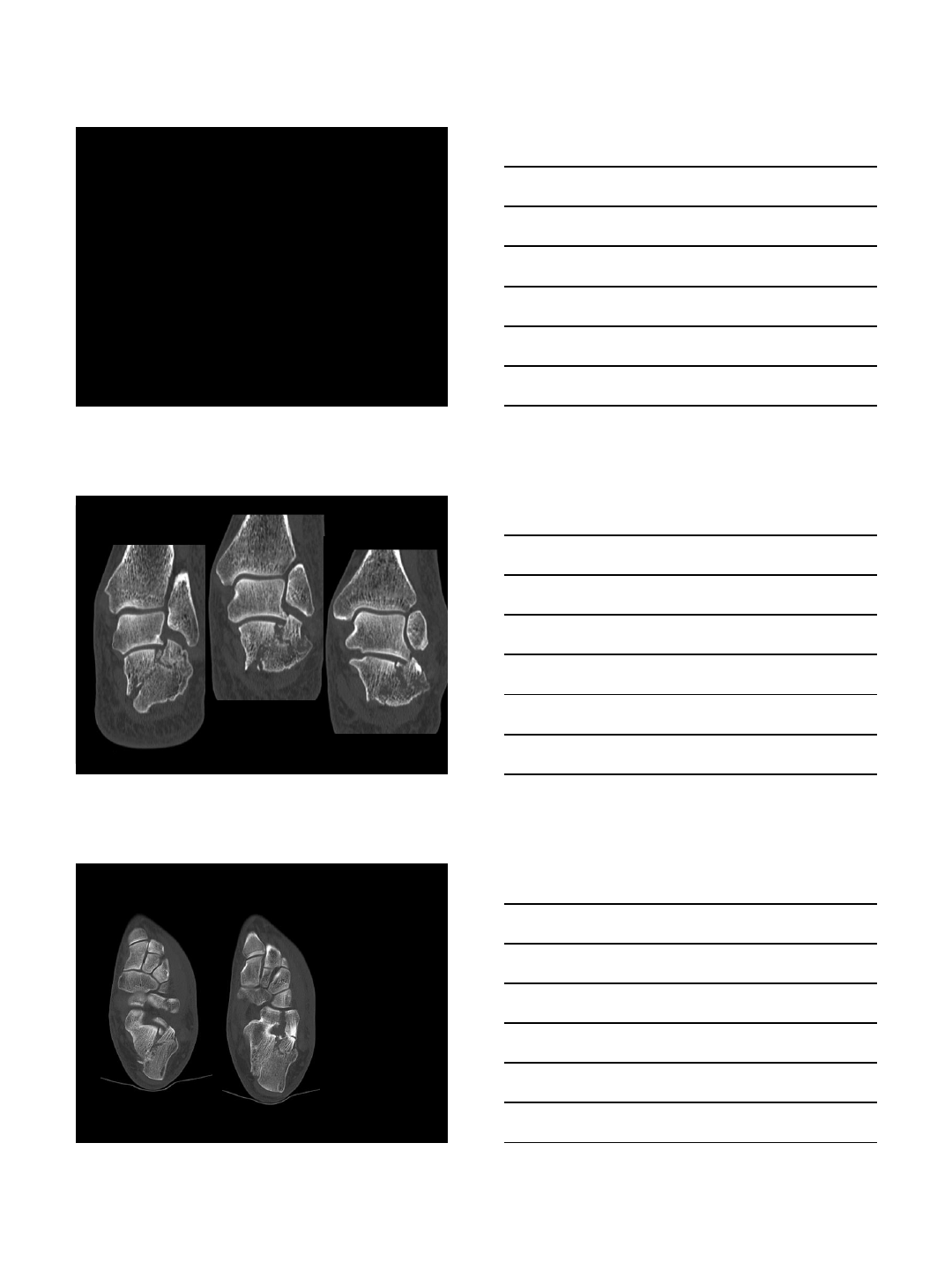
RADIOLOGIC EVALUATION
ØWEIGHTBEARING FILMS ESSENTIAL !
ØSTANDARD WB 3-VIEWS ANKLE & FOOT
ØHARRIS AXIAL VIEW
ØCT SCAN
ØAXIAL / SAGITTAL / CORONAL VIEWS
2/3/2014
5
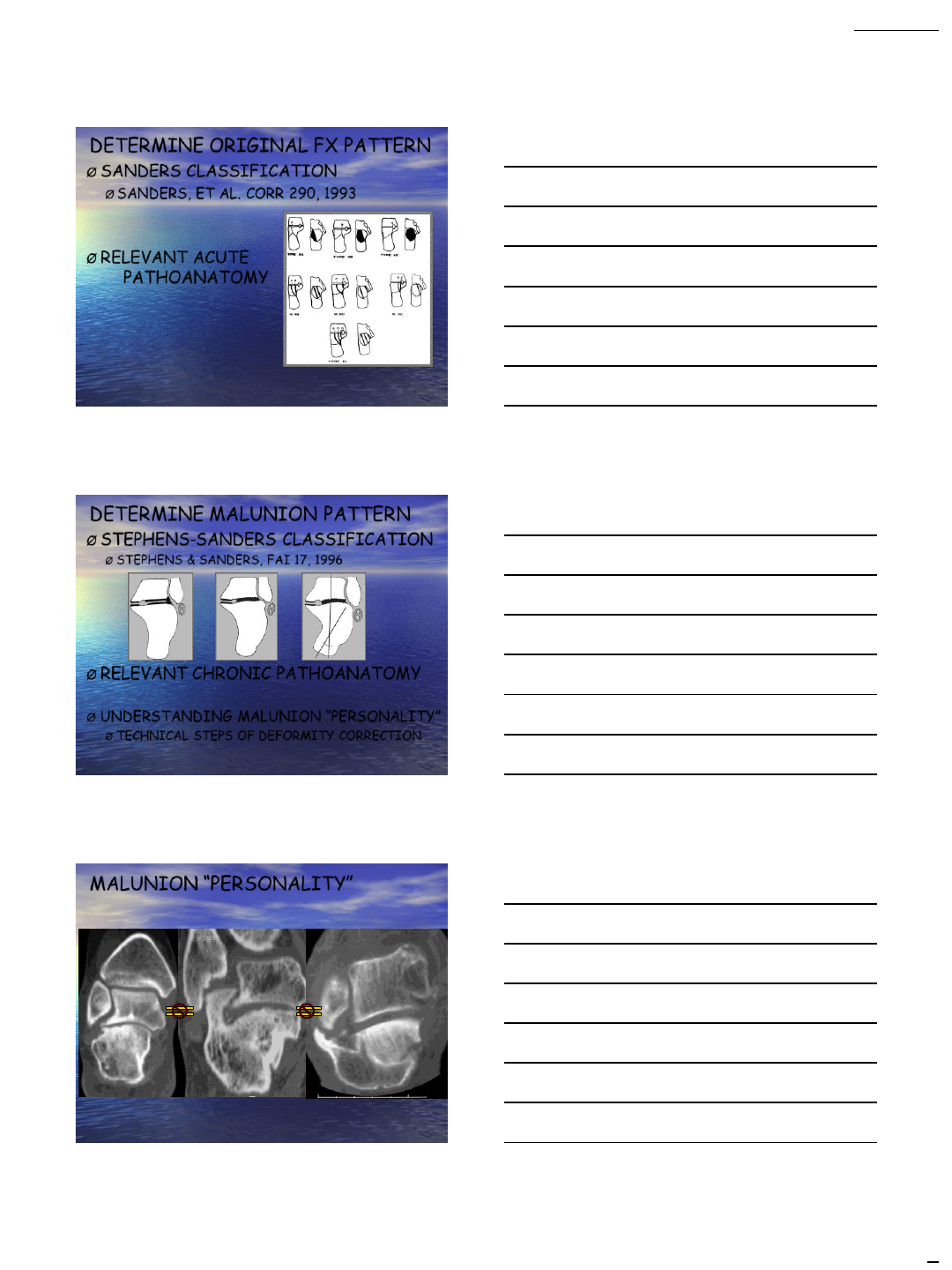
DETERMINE ORIGINAL FX PATTERN
ØSANDERS CLASSIFICATION
ØSANDERS, ET AL. CORR 290, 1993
ØRELEVANT ACUTE
PATHOANATOMY
DETERMINE MALUNION PATTERN
ØSTEPHENS-SANDERS CLASSIFICATION
ØSTEPHENS & SANDERS, FAI 17, 1996
ØRELEVANT CHRONIC PATHOANATOMY
ØUNDERSTANDING MALUNION “PERSONALITY”
ØTECHNICAL STEPS OF DEFORMITY CORRECTION
MALUNION “PERSONALITY”
2/3/2014
6
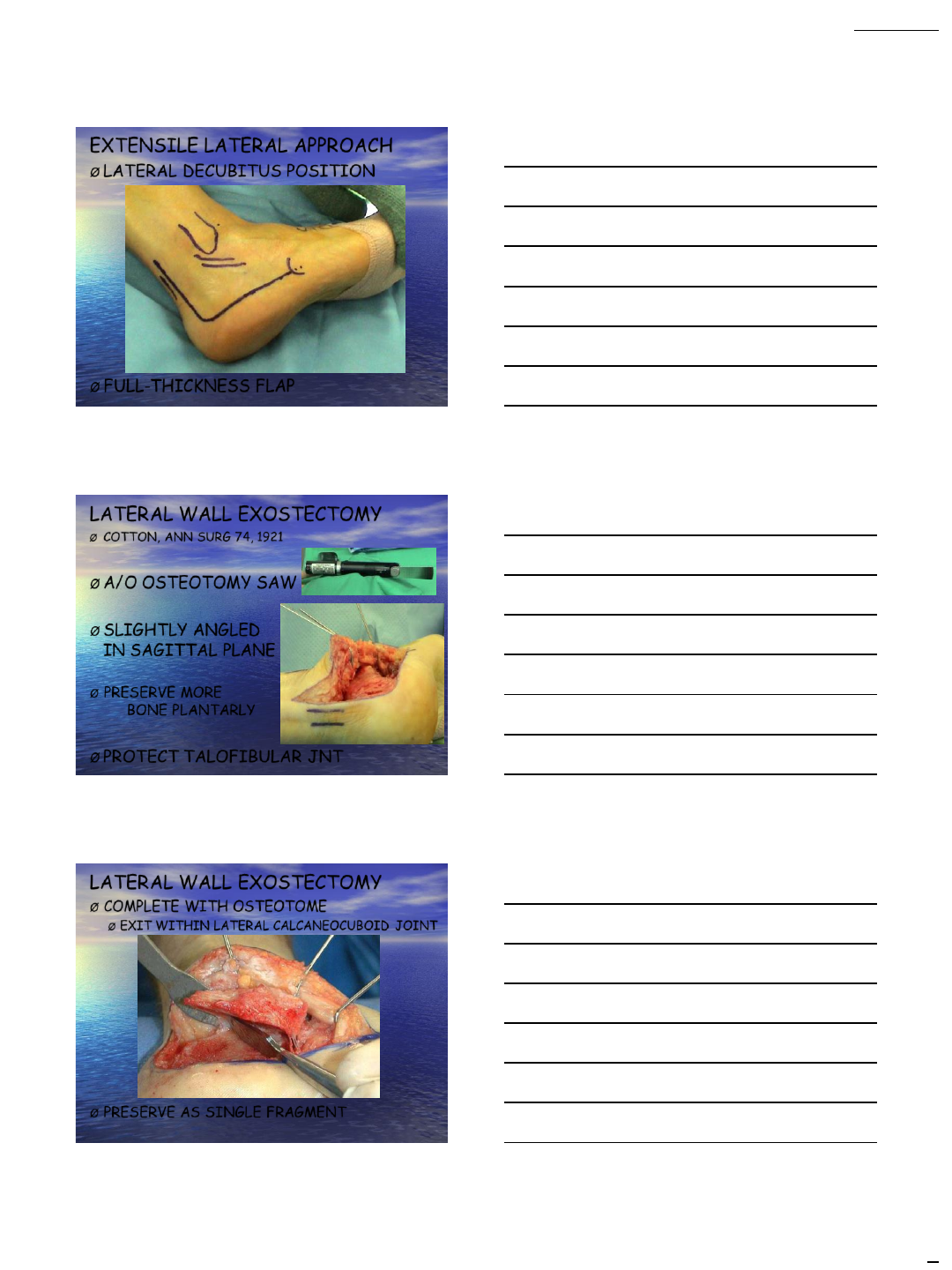
EXTENSILE LATERAL APPROACH
ØLATERAL DECUBITUS POSITION
ØFULL-THICKNESS FLAP
LATERAL WALL EXOSTECTOMY
ØCOTTON, ANN SURG 74, 1921
ØA/O OSTEOTOMY SAW
ØSLIGHTLY ANGLED
IN SAGITTAL PLANE
ØPRESERVE MORE
BONE PLANTARLY
ØPROTECT TALOFIBULAR JNT
LATERAL WALL EXOSTECTOMY
ØCOMPLETE WITH OSTEOTOME
ØEXIT WITHIN LATERAL CALCANEOCUBOID JOINT
ØPRESERVE AS SINGLE FRAGMENT
2/3/2014
7
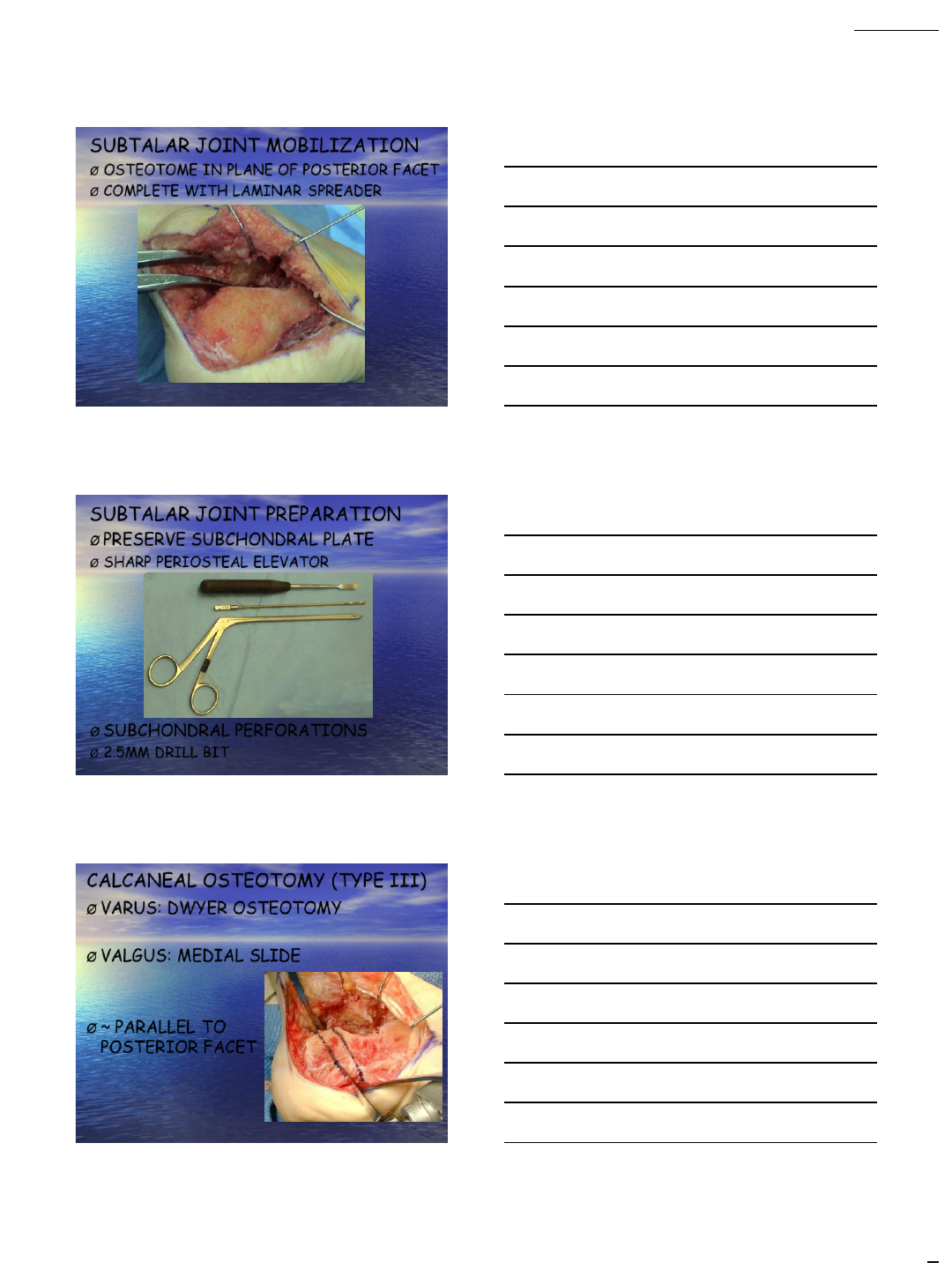
SUBTALAR JOINT MOBILIZATION
ØOSTEOTOME IN PLANE OF POSTERIOR FACET
ØCOMPLETE WITH LAMINAR SPREADER
SUBTALAR JOINT PREPARATION
ØPRESERVE SUBCHONDRAL PLATE
ØSHARP PERIOSTEAL ELEVATOR
ØSUBCHONDRAL PERFORATIONS
Ø2.5MM DRILL BIT
CALCANEAL OSTEOTOMY (TYPE III)
ØVARUS: DWYER OSTEOTOMY
ØVALGUS: MEDIAL SLIDE
Ø~ PARALLEL TO
POSTERIOR FACET
2/3/2014
8
BONE BLOCK INSERTION
ØKALAMCHI & EVANS, JBJS-BR 59, 1977
ØLAMINAR SPREADER POSTEROMEDIALLY
ØSHAPE GRAFT WIDTH-WISE
ØBROADEST PORTION POST-MED
ØSUPPLEMENTAL VOID FILLER / GF
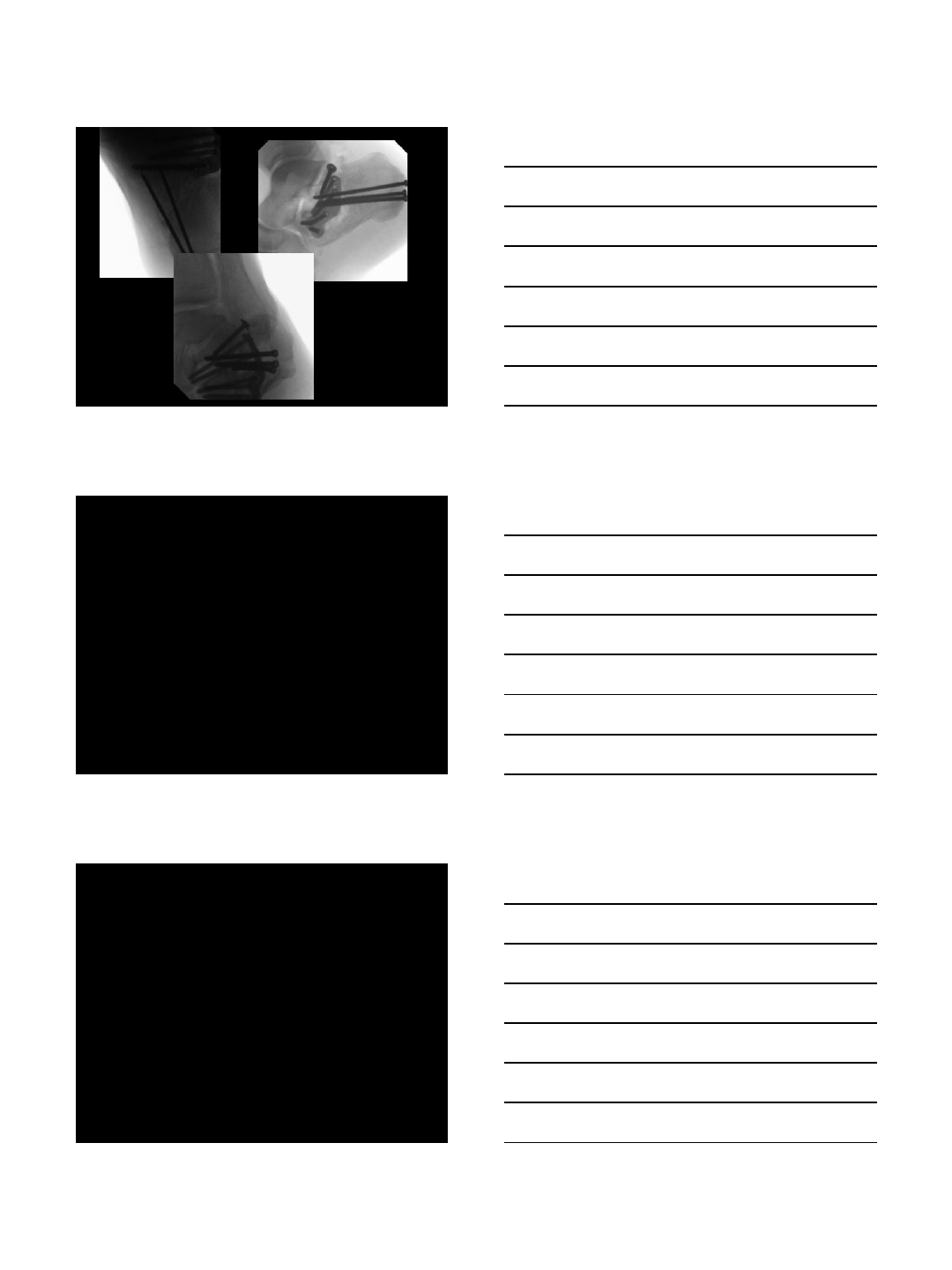
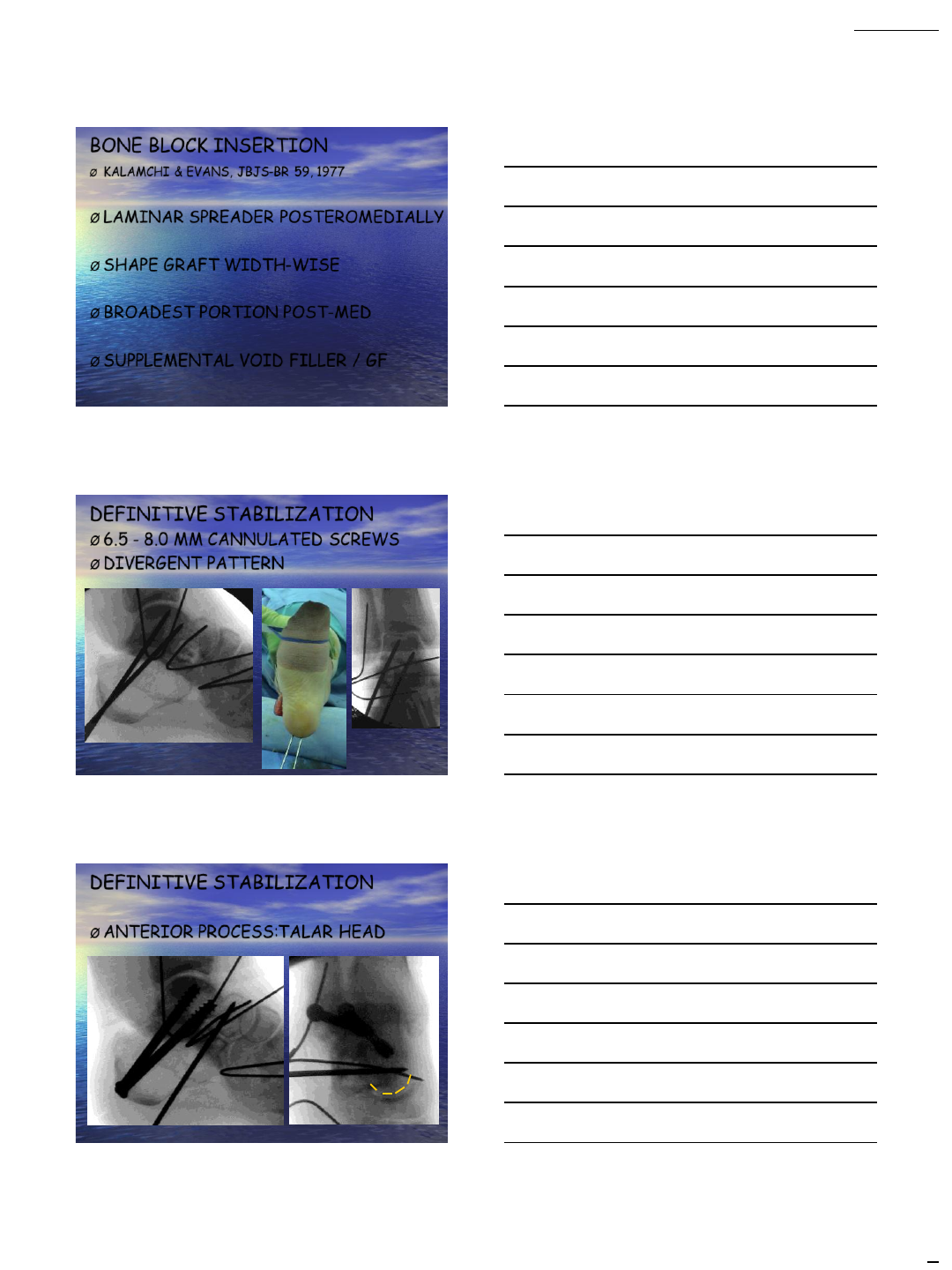
DEFINITIVE STABILIZATION
Ø6.5 - 8.0 MM CANNULATED SCREWS
ØDIVERGENT PATTERN
DEFINITIVE STABILIZATION
ØANTERIOR PROCESS:TALAR HEAD
2/3/2014
9
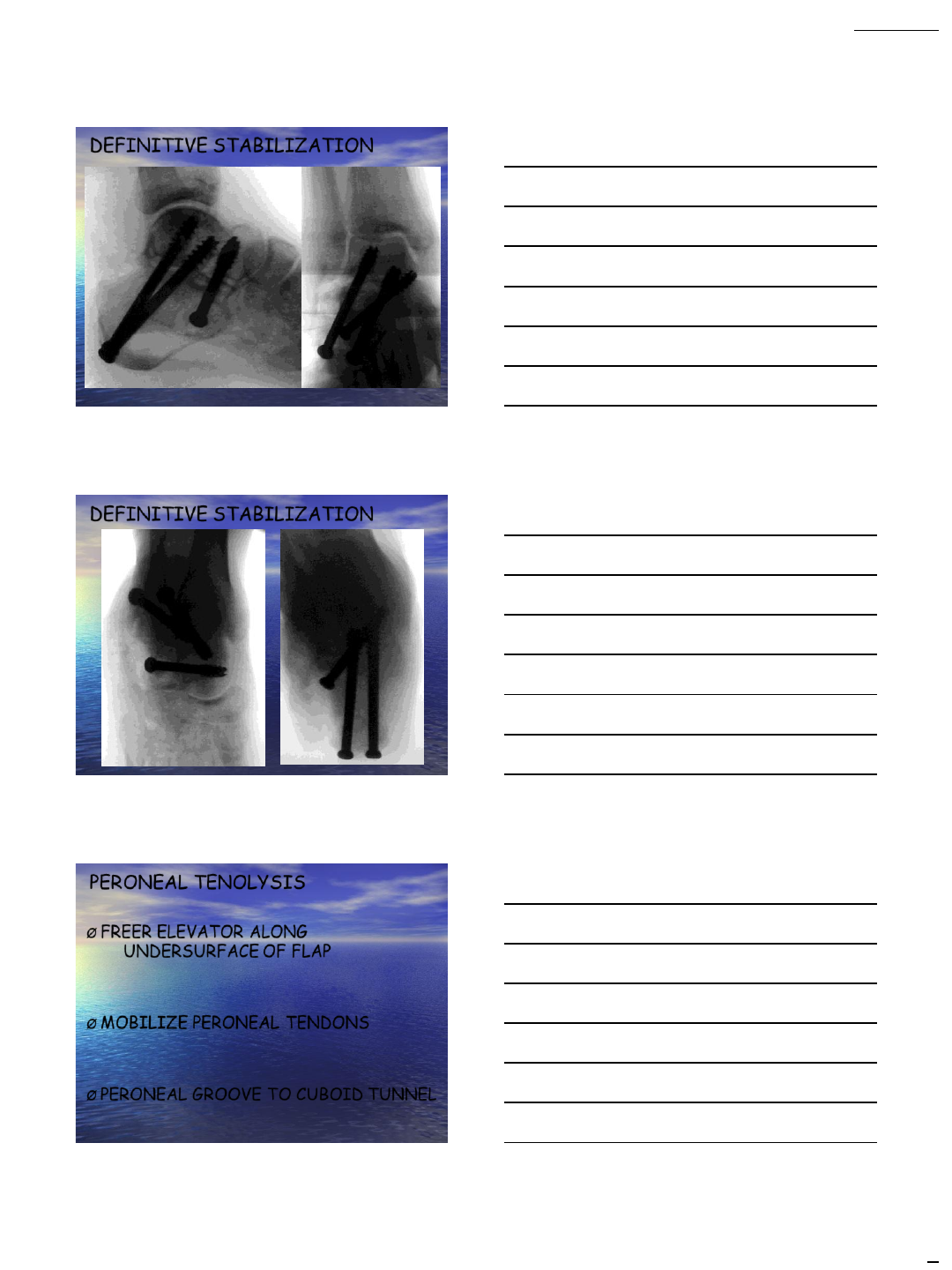
DEFINITIVE STABILIZATION
DEFINITIVE STABILIZATION
PERONEAL TENOLYSIS
ØFREER ELEVATOR ALONG
UNDERSURFACE OF FLAP
ØMOBILIZE PERONEAL TENDONS
ØPERONEAL GROOVE TO CUBOID TUNNEL
2/3/2014
10
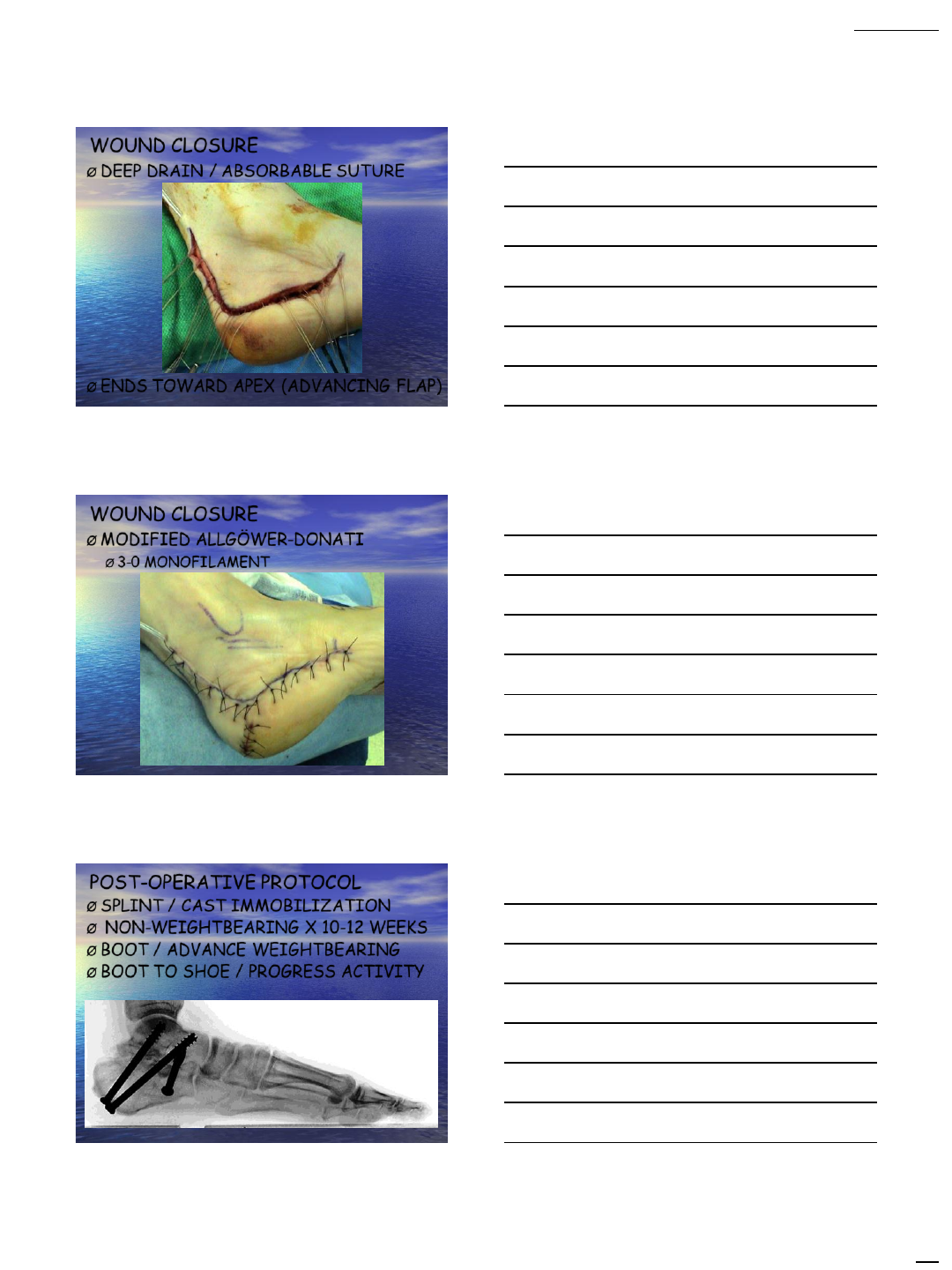
WOUND CLOSURE
ØDEEP DRAIN / ABSORBABLE SUTURE
ØENDS TOWARD APEX (ADVANCING FLAP)
WOUND CLOSURE
ØMODIFIED ALLGÖWER-DONATI
Ø3-0 MONOFILAMENT
POST-OPERATIVE PROTOCOL
ØSPLINT / CAST IMMOBILIZATION
Ø NON-WEIGHTBEARING X 10-12 WEEKS
ØBOOT / ADVANCE WEIGHTBEARING
ØBOOT TO SHOE / PROGRESS ACTIVITY
2/3/2014
11
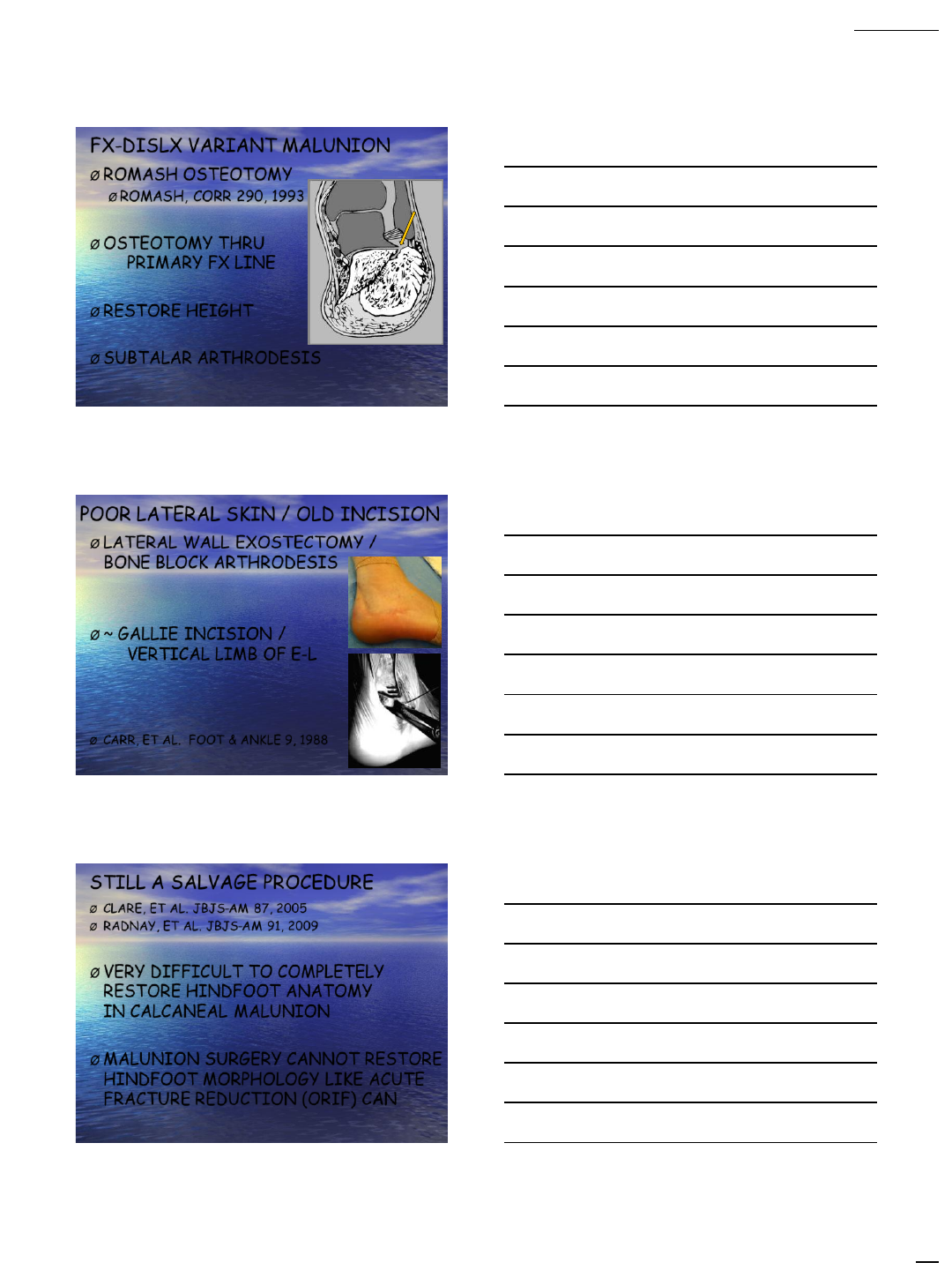
FX-DISLX VARIANT MALUNION
ØROMASH OSTEOTOMY
ØROMASH, CORR 290, 1993
ØOSTEOTOMY THRU
PRIMARY FX LINE
ØRESTORE HEIGHT
ØSUBTALAR ARTHRODESIS
POOR LATERAL SKIN / OLD INCISION
ØLATERAL WALL EXOSTECTOMY /
BONE BLOCK ARTHRODESIS
Ø~ GALLIE INCISION /
VERTICAL LIMB OF E-L
ØCARR, ET AL. FOOT & ANKLE 9, 1988
STILL A SALVAGE PROCEDURE
ØCLARE, ET AL. JBJS-AM 87, 2005
ØRADNAY, ET AL. JBJS-AM 91, 2009
ØVERY DIFFICULT TO COMPLETELY
RESTORE HINDFOOT ANATOMY
IN CALCANEAL MALUNION
ØMALUNION SURGERY CANNOT RESTORE
HINDFOOT MORPHOLOGY LIKE ACUTE
FRACTURE REDUCTION (ORIF) CAN
2/3/2014
12
ACUTE ORIF BENEFICIAL
ØCLARE, ET AL. JBJS-AM 87, 2005
ØRADNAY, ET AL. JBJS-AM 91, 2009
ØRESTORATION OF CALCANEAL HEIGHT /
LENGTH / OVERALL MORPHOLOGY
ØEVEN IN THE EVENT OF LATE PTOA:
IN-SITU SUBTALAR ARTHRODESIS
SUMMARY
Ø3-JOINT INJURY: 3-JOINT MALUNION
ØDETERMINE ACUTE PATHOANATOMY:
CHRONIC PATHOANATOMY
ØINDIVIDUALIZE TREATMENT
ØRESTORING CALCANEAL HEIGHT / WIDTH
ØELIMINATING LATERAL WALL EXPANSION
ØMOBILIZING PERONEAL TENDONS
