Cervical Radiculopathy Syllabus
2014-08-27
: Pdf Cervical Radiculopathy Syllabus Cervical_Radiculopathy_Syllabus 8 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 37
8/21/2014
1
The Case for Posterior Foraminotomy
Michael Y. Wang, MD
Professor
Departments of Neurological Surgery & Rehab Medicine
The Miller School of Medicine at the
University of Miami
Disclosure
Consultant: Depuy Spine
Royalties: Depuy Spine
Springer Publishing
Quality Medical Publishing
Stock: Innovative Surgical Devices
Spinicity
Grants: Department of Defense
C4/5
Today’s Case
8/21/2014
2
Thanks Sheeraz !
This is a perfect case for a
posterior foraminotomy:
1. Young patient
2. Unilateral symptoms
3. Single level
4. Minimal neck pain
5. No abnormal alignment
6. No abnormal motion
Pro Con
No approach problems
No need to stabilize
Decreased adjacent level
disease
Possibility of recurrence
No treatment of instability
Unilateral treatment
Interrupts neck musculature
Is it Effective?
8/21/2014
3
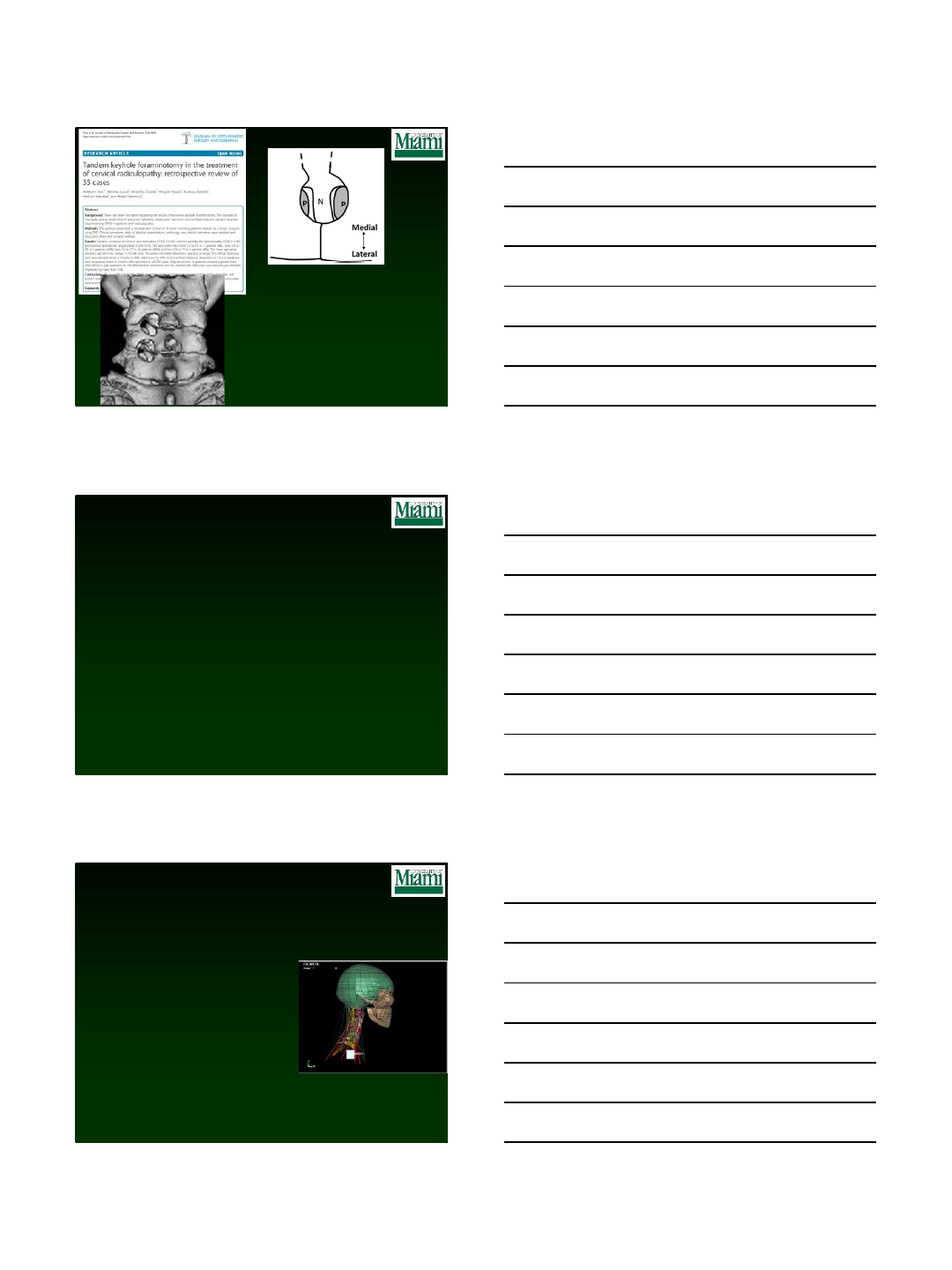
•44 patients followed for 6 or more years (mean 8.8 years)
•98% of patients experienced symptomatic relief
•No index level reoperations
•Two cases of adjacent level disease
Does it Work for Two
Levels?
8/21/2014
4
35 patients
1. 99 minutes
2. 55 g Blood loss
3. 88% had relief at 3 months
4. 97% had relief at final F/U
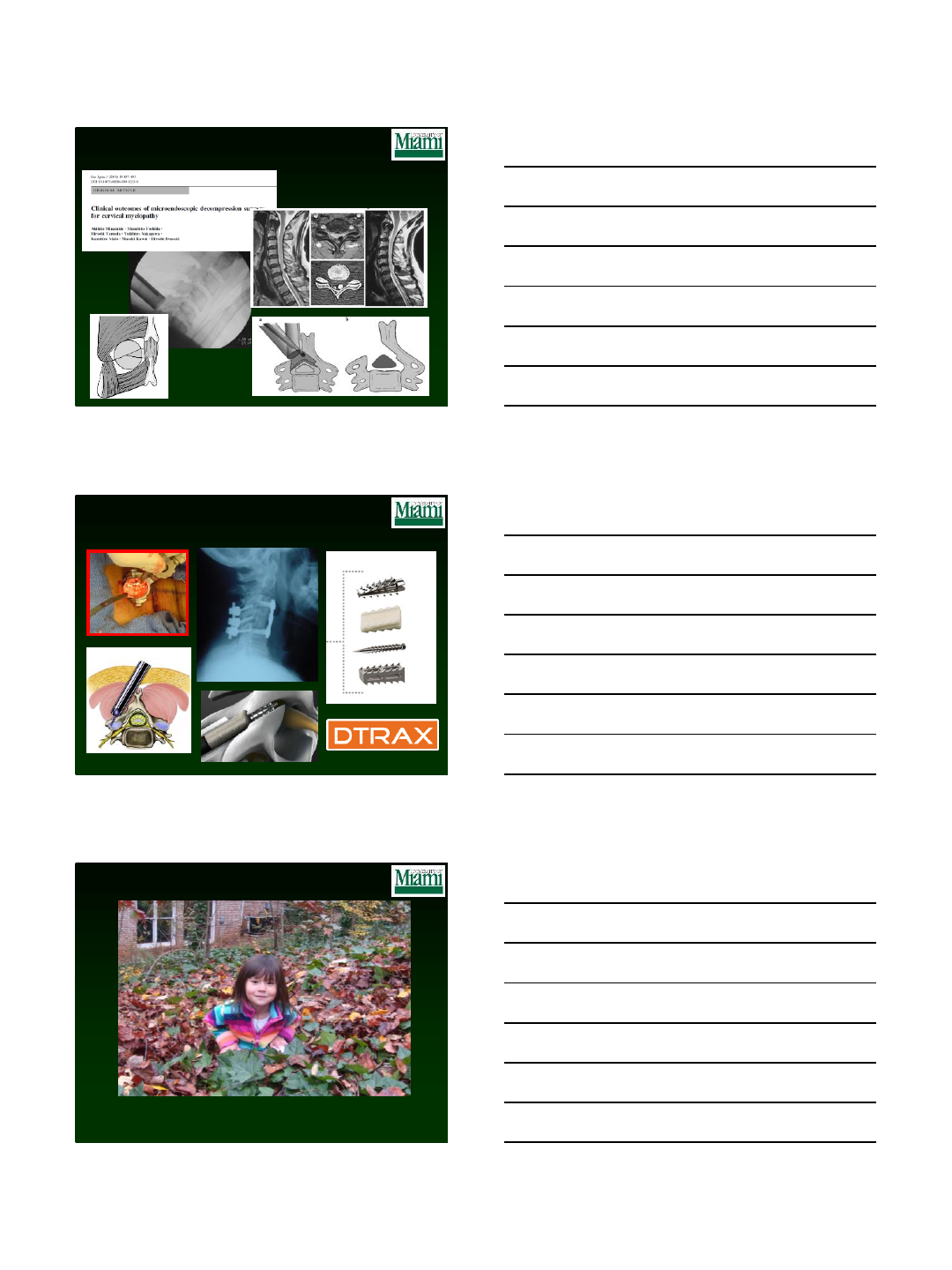
What About MIS?
What About the
Posterior Approach ?
Standard open techniques require extensive
disruption of dorsal musculoligamentous
resulting in :
Incision-related pain
Devitalization of neck musculature
Poor cosmesis
Interruption of the posterior “dynamic tension
band”
Minimal access approaches attempt to overcome
these drawbacks of conventional open surgery Finite element analysis
8/21/2014
5
Tubular Dilator Retractors
1. Utilizes serial expansion of
muscles over a guide wire
2. Spreads muscles instead of
cutting them
3. Final dilation to 16 mm to 24
mm in diameter
4. Serves essentially as an
access port
“Mom…look what I did
through the Tube !”
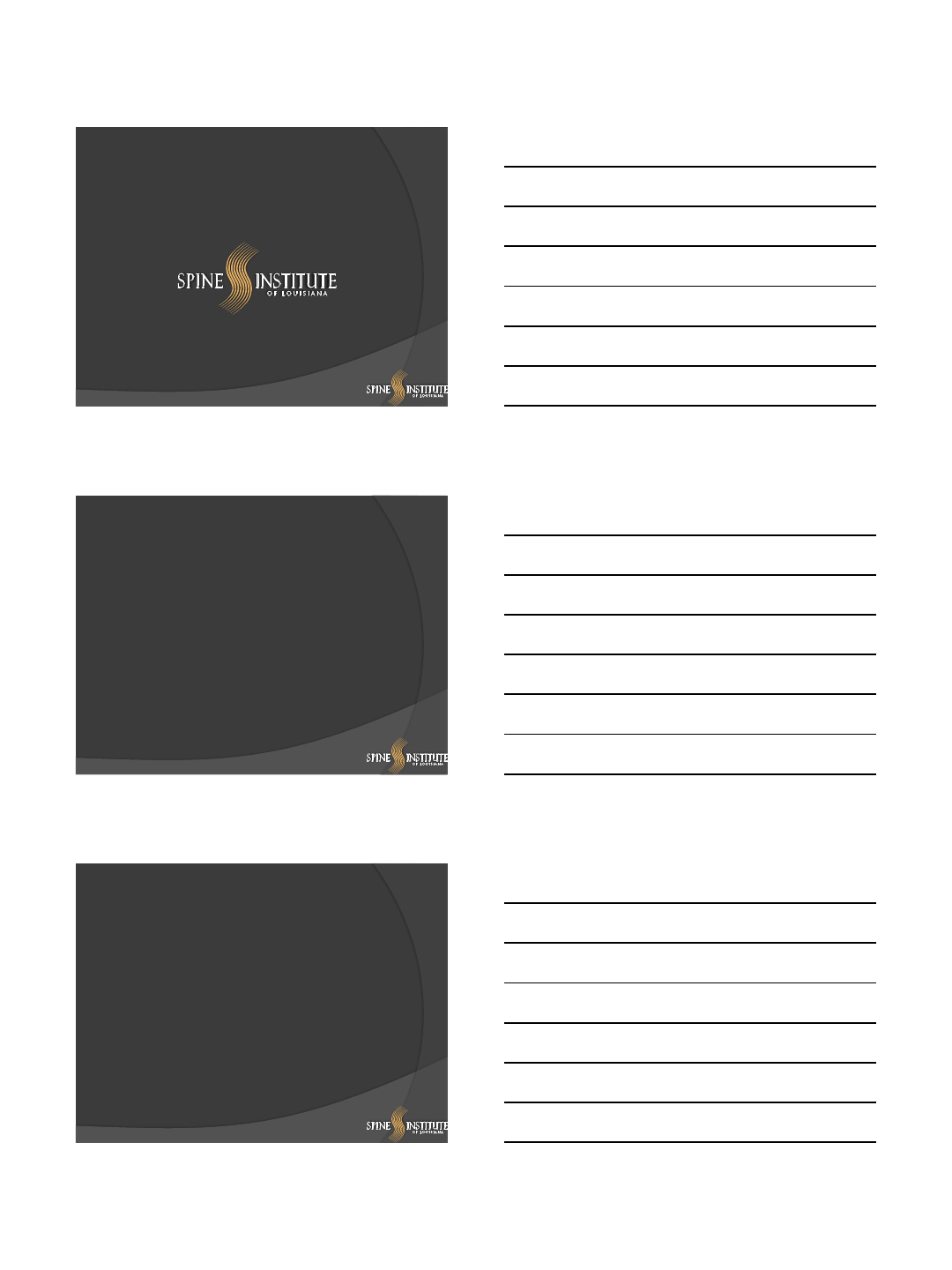
Minimally invasive techniques are being
used for:
1. Odontoid screw fixation
2. Transarticular screw placement
3. C1-2 Harms techniques
4. Tumor removal
5. Laminectomy
6. Trans-facet fixation
Cervical Foraminotomy
•100 consecutive patients
undergoing minimally invasive
cervical foraminotomy
• 97 patients reported as “good” or
“excellent” results
•Typical discharge home in 3 hours
•60 patients able to return to work
within one week.
•Two dural tears
•One wound infection
8/21/2014
6
•19 open and 22 tubular foraminotomies
•Groups were similar in all respects
What is the Rate of
Reoperation or
Adjacent Disease?
Thanks Sheeraz !
•178 patient followed a mean of 31.7 months
•9 (5%) of patients underwent reoperation at index level
•Associated factors: young, thin, anxious patients
8/21/2014
7
70 patients:
1. No secondary intervention
2. 5 patients had ACDF
3. ACDF was a mean of 44
months later
4. 1.1% per year same level
5. 0.9% per year adjacent
level surgery
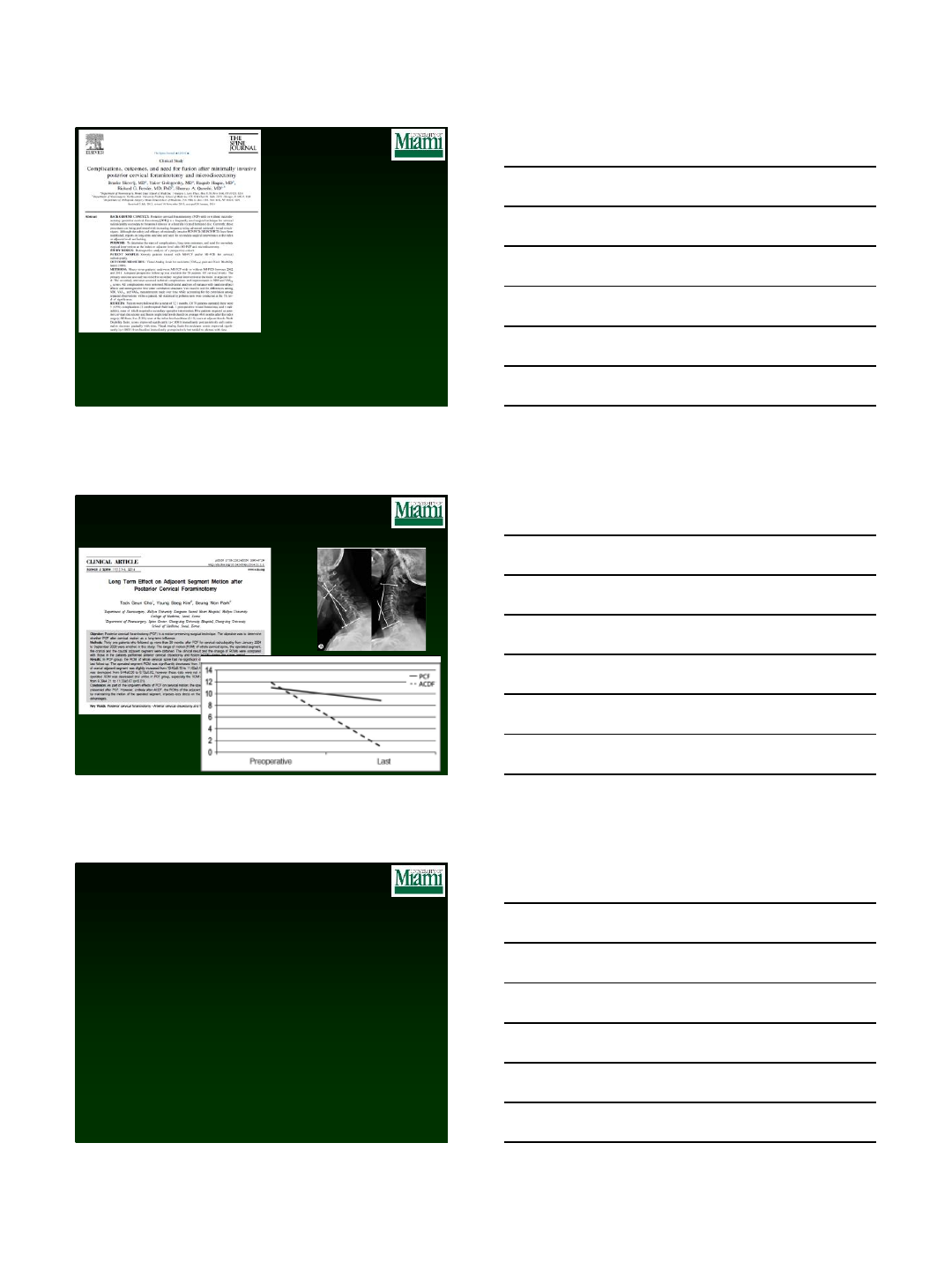
Biomechanical Effects in vivo
Cost Utility Analysis
Alvin, et al (JSDT)
The Cleveland Clinic experience w/ foraminotomy:
•45 ACDF vs 25 foraminotomy patients
•Assessed with VAS, NDI, EQ-5D & PHQ-9
•Both groups showed improved outcomes and MCID
•At one year, foraminotomy was more cost effective
ACDF $131,951 / QALY
Foraminotomy $ 79,856 / QALY
8/21/2014
8
Military Experience
ACDF Foraminotomy
Number of patients 19 19
Mean Age 39.3 41.5
OR Time 151.6 153.9
Blood Loss 32.6 39.7
Complications 2 0
Direct Costs 10,078 3,570
Return to work (weeks) 19.6 4.8
Foraminotomy has been around for over
50 years, so what does the future hold?
Use of smaller tubes
•Randomized trial of ACDF vs. Foraminotomy
•N=175 with f/u 2 years
•Dx: Radiculopathy
•6 complications, 3 revisions
•87.4% resolution of symptoms
•No difference between groups
{kind=link}
8/26/2014
1
Cervical Radiculopathy: Case Based Debate
CERVICAL TDR
Pierce D. Nunley MD
Director, Spine Institute of Louisiana
Assistant Professor, Louisiana State University
Disclosures
Research Funding
LDR Spine
Speaker’s Bureau
LDR Spine
K2M
Smith and Robinson introduced anterior cervical discectomy and
arthrodesis in 1958 as a surgical option for the management of
cervical disc disorders.
Smith GW, Robinson RA. The treatment of certain cervical spine disorders by anterior removal of
the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 1958; 40: 607-24
ACDF has gained acceptance as standard of care for patients with
persistent radicular and/or myelopathic symptoms that have failed
to improve with conservative treatments.
Rao RD, Currier BL, Albert TJ et al. Degenerative cervical spondylosis: clinical syndromes,
pathogenesis and management. J Bone Joint Surg Am 2007; 89: 1360-78
History

8/26/2014
2
20-32% of patients undergoing ACDF would develop ASP
during the next 10 years
As longer term results became available, the outcome studies
increasingly focused on the adverse effects of this procedure.
ASP –Adjacent Segment Pathology
Similar stress profiles were recorded from intact
specimens and those with the artificial joint inserted.
The artificial joint resulted in reduced stresses in the
annulus compared with spines with a simulated
fusion.
The concern that spinal fusion may be a contributing
factor to accelerated ASP led to increased interest in
“motion preservation”
Rationale
This immediately led the scientists and surgeons
to focus their attention towards developing
alternative procedures to ACDF
The concept of “motion preservation
technology” was thus born and subsequently led
to the development of cervical total disc
replacement (c-TDR).
Since then several total disc arthroplasty implants
have been used for treating cervical degenerative
disc disease and the clinical outcomes have been
published in the literature.
8/26/2014
3
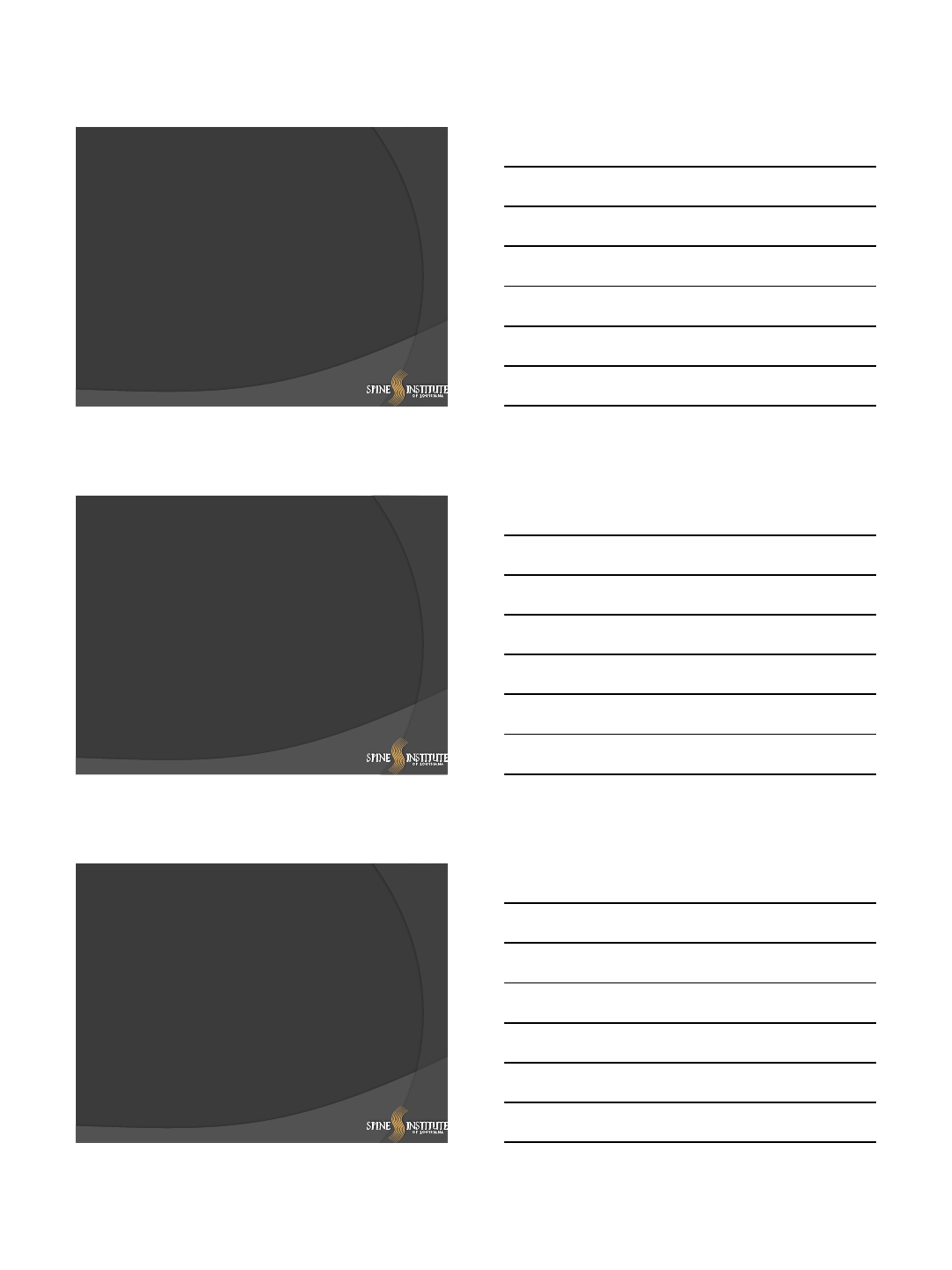
FDA Clearance of Cervical Discs in U.S.
1. Garrido BJ, Taha TA and Sasso R. Clinical outcomes of Bryan cervical disc arthroplasty: a
prospective, randomized, controlled, single site trial with 48-month follow-up. J Spinal
Disord Tech. 2010 Aug;23(6):367-71
2. Quan GM, Vital J, Hansen S. Eight –year clinical and radiological follow-up of the Bryan
cervical disc arthroplasty. Spine 2011; 36(8): 639-646
3. Sasso RC, Anderson PA, Riew KD and Heller JG. Results of cervical arthroplasty compared
with anterior discectomy and fusion: Four-year clinical outcomes in prospective randomized
controlled trial. J Bone Joint Surg Am 2011; 93: 1684-92
4. Coric D, Nunley PD, Guyer RD, Mustane D et al. Prospective randomized multicenter study
of cervical arthroplasty: 269 patients from the Kineflex/C artificial disc investigational
device exemption study with a minimum 2-year follow-up. J Neurosurg: Spine/ June 24,
2011; epub ahead of print
5. Huppert J, Beaurain J, Steib JP and Bernard P et al. Comparison between single and multi-
level patients: clinical and radiological outcomes 2 years after cervical disc replacement.
Eur Spine J. 2011; Sep 20(9): 1417-26
6. Zechmeister I, Winkler R, Mad P. Artificial total disc replacement versus fusion for the
cervical spine: a systematic review). Eur. Spine J. 2011; 20(2): 177-84
A review of the published literature raises the following
basic questions:
1. Are the short or long term clinical outcomes better in patients with disc
replacement as compared to ACDF?
2. Is there a significant difference in the incidence of Clinical adjacent segment
pathology (CASP) after the two procedures?
3. Is there a strong, evidence-based rationale to perform total disc replacement
instead of ACDF?
4. Are there specific patient subsets in which either of the procedures may
provide better longer term outcomes (index level or adjacent segment
disease)?
8/26/2014
4
Primary Outcome Comparisons
Problems
1. the longest published follow-up period for total disc
replacement is about 8 years
2. Most of the published data for total disc replacement consists
of patients with one or two level disease
3. The data for total disc replacement is usually gathered from
the patients who have participated in the randomized
controlled trials (RCT) for particular implants. (Such trials have
very stringent inclusion/exclusion criteria for selecting patients and are
often criticized as not representing the general patient population.)
1. Most published results of the ACDF procedure
are retrospective and/or anecdotal from
experience of a single surgeon or institution,
(class III studies at best.)
2. The outcome instruments used and success
criteria used for the ACDF studies have varied
according to the different authors’ judgment and
tools available at the time of data acquisition.
ACDF Outcomes
Problems
Comparable success rates for both procedures at the average
follow-up of 2-4 years
Clearly established the non-inferiority of the TDR procedure
to the ACDF,
Questionable rationale for utilizing TDR as an alternative to
the fusion procedure**.
** Bartels RHMA, Donk R and VerBeek ALM. No justification
for cervical disc prostheses in clinical practice: a meta-analysis
of randomized controlled trials. Neurosurgery, 66(6): 1153-
1160; 2010
Bottom Line
8/26/2014
5
Adjacent Segment Pathology (CASP)
Hilibrand’s follow-up study: Admitted that the scientific literature
was unclear whether the ASP is a result of the spinal fusion with
iatrogenic motion restriction or whether it represented a
progression of the natural history of degeneration
Hillibrand AS, Robbins M: Adjacent segment degeneration and adjacent segment disease: the
consequences of spinal fusion? Spine J 2004; 4: 190S-194S
The primary end points of TDR clinical trials are focused on
improvements in patient’s symptoms attributable to the index-level.
The published results are mostly focused on the outcomes at 24-
month follow-up, the period being too short to assess ASD.
Our Experience
Total disc arthroplasty is equivalent to ACDF for providing relief from
symptoms
The risk of developing adjacent segment degeneration is equivalent after
both procedures but is significantly higher in patients with concurrent
DDD in lumbar spine.
Our Experience
At a projected follow-up of up to 54 months, the risk of
developing symptomatic adjacent segment disease (CASP) does
not significantly vary between patients receiving total disc
arthroplasty or anterior fusion.
Other factors including bone mineral density and presence of
concurrent lumbar degeneration have a more significant effect in
the incidence of adjacent segment degeneration.
8/26/2014
6
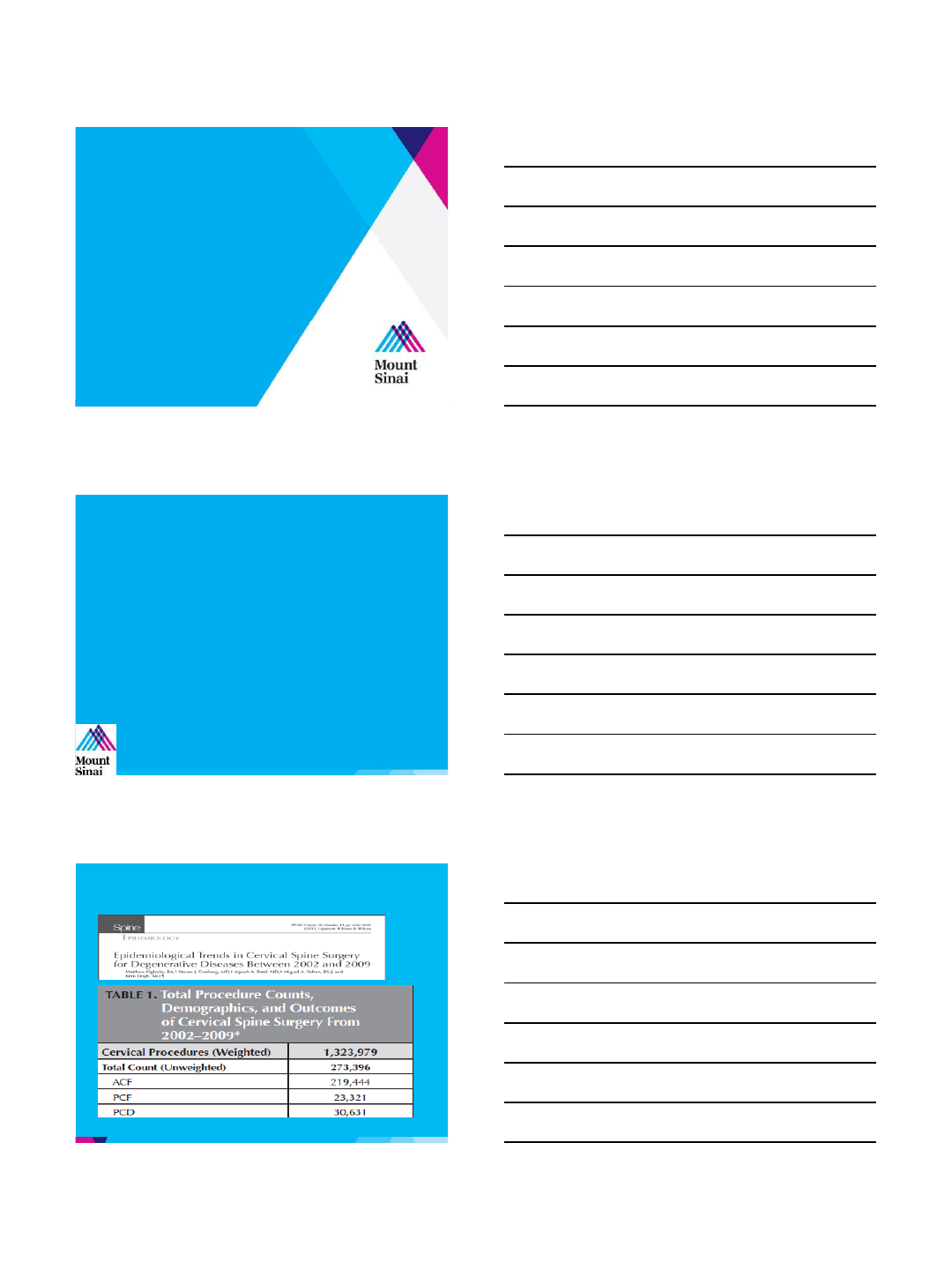
Comparison of artificial cervical arthroplasty versus
anterior cervical discectomy and fusion for one-level cervical degenerative
disc disease: a meta-analysis of randomized controlled trials.
Luo, et al - Eur J Orthop Surg Traumatol –Jul 2014
•13 RCT’s, 24 month f/u
•Statistical significant improvement TDR over
ACDF in
•Neurological Success
•Secondary Surgical Procedures
•VAS –Neck & Arm
•NDI –Statistically similar
Artificial cervical disc arthroplasty versus anterior
cervical discectomy and fusion: a systematic review
Mroz, et al SPINE 25:1 2014
“Level I evidence suggests that artificial
cervical disc arthroplasty has relatively low
complication, reoperation, and heterotopic
ossification rates and that quality of life
measures such as Neck Disability Index, visual
analogue scale, and Short Form 36 (SF36)
significantly improved ….”
Two-level Total Disc Replacement with Mobi-C® Cervical Artificial Disc
versus Anterior Discectomy and Fusion: A Prospective, Randomized,
Controlled Multicenter Clinical Trial with 4 Year Follow-up Results
N=389 f/u 4-7 years
Patients receiving treatment with TDR at
TWO LEVELS had statistically significantly
greater improvement than ACDF for:
NDI
SF-12 PCS
Patient Satisfaction
Overall Success
Revision Surgeries
Radiographic ASP
Davis RJ, Nunley PD, et al J. of Neurosurgery –Spine 2014
8/26/2014
7
Cervical TDR vs Foraminotomy
Patient Symptoms
Radiculopathy vs Neck Pain
Myelopathy?
Radiological Considerations
Central vs Peripheral
Soft vs Hard
Adjacent Segements
Long Term Consequences
Bridge Burning?
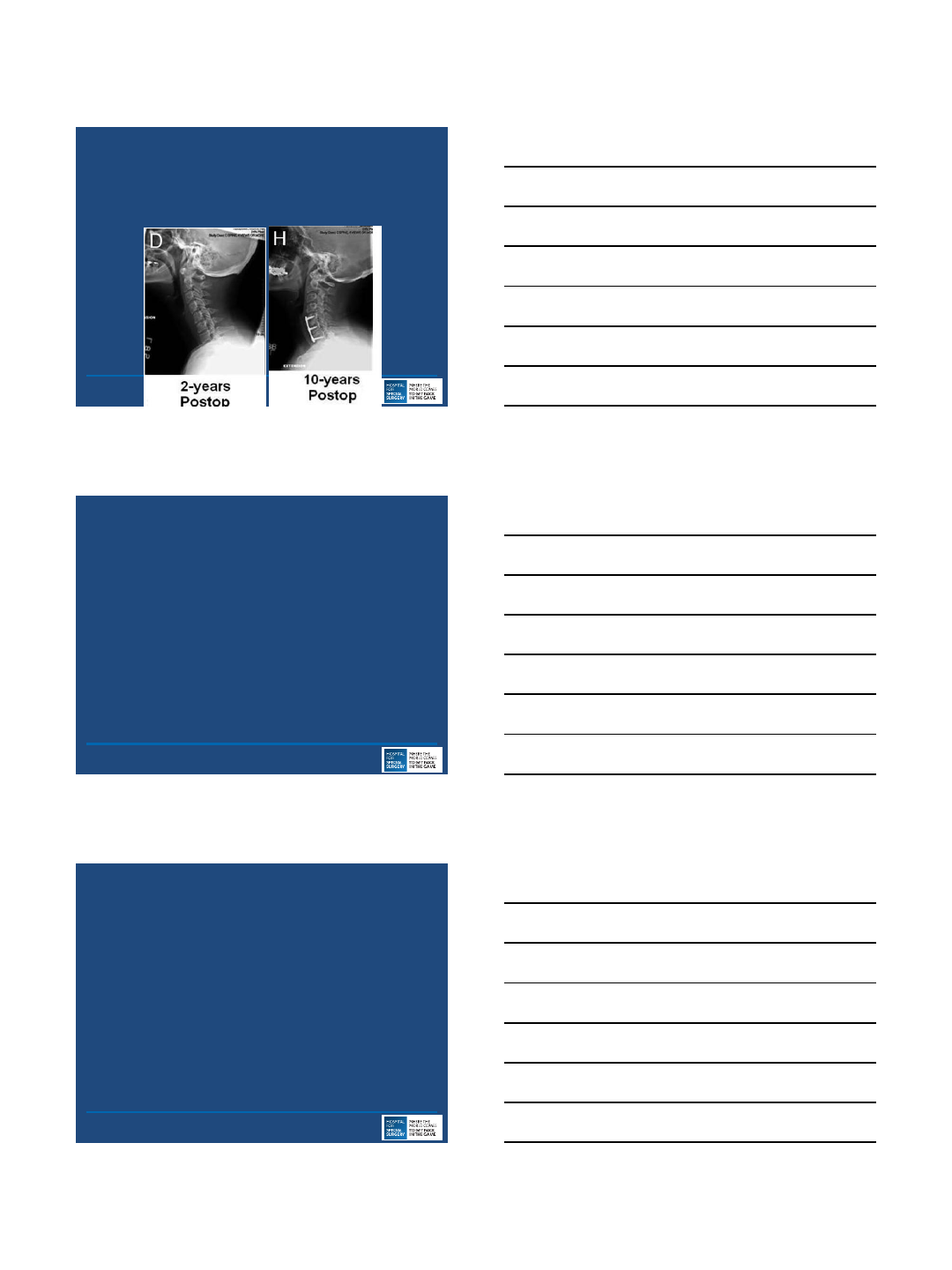
Long-term patient outcomes after posterior
cervical foraminotomy: an analysis of 151 cases
Bydon, et al –J Neursurgery Spine 15:1-5 2014
n=151, f/u 4 to 15 years
Reoperation Rates:
18.3% f/u > 2 years
24.3% f/u > 10 years
“Patients with no preoperative neck pain
had the lowest rates of revision surgery
after PCF.”
Reoperation Rates After Anterior Cervical Discectomy and Fusion vs
Posterior Cervical Foraminotomy: A Propensity Matched Analysis.
Mroz, et al Neurosurgery 2014
N=790, f/u 2 –6 years
Reoperation rate at the index level was:
4.8% for the ACDF
6.4% for the PCF group (p = 0.7),
8/26/2014
8
Cervical arthroplasty after previous surgery: results of treating
24 discs in 15 patients.
Sekhon et al - J Neurosurg Spine. 2005 Nov;3(5):335-41.
“provided encouraging early clinical
results, although patients with preoperative
hypermobility should be treated with
caution. Issues such as accelerated
device-related wear and the use of
arthroplasty after aggressive facetectomy
resection will need further study”
The Effect of Posterior Decompressive Procedures on Segmental
Range of Motion Following Cervical Total Disc Arthroplasty.
Patwardhan AG, et al –SPINE June 2014
Human Cadaver Biomechanical Study
Unilateral Hemilaminotomy MAY be safe, but
warned against cyclic loading in In-Vivo state
Bilateral Hemi and Laminectomy UNSTABLE
By performing Hemilaminotomy, what FUTURE
are we relegating our patients to?
Debate Case
C4/5
More Pathology
Hypermobile
8/26/2014
9
Conclusions
c-TDR is a safe and efficacious procedure for
the indications of cervical myeloradiculapathy
in appropriately selected patients
c-TDR at two levels has shown superiorty
over 2 level ACDF (Class I Evidence)
PCF may lead to as many or more revision
surgeries as well as prevent conversion to
c-TDR
THEREFORE: c-TDR is the best choice
Thank You!
8/24/2014
1
For Single Level Disease With
Radiculopathy, ACDF is the Best Option
Todd J. Albert, MD
Surgeon-in-Chief and Medical Director
Korein-Wilson Professor
Hospital for Special Surgery
Chairman, Department of Orthopaedic Surgery
Weill Cornell Medical College
NY , NY
Todd J Albert, MD
DISCLOSURES
INDUSTRY
(c,e) DePuy, Biomet; (d) Vertech, In Vivo Therapeutics, Paradigm Spine, Biomerix,
Breakaway Imaging, Crosstree, Invuity, Pioneer, Gentis, ASIP, PMIG; (e) Facetlink
•a)Research or institutional support received; b) Miscellaneous non-income support (e.g., equipment or services),
commercially derived honoraria, or other non-research related funding (e.g., paid travel); c) Royalties; d) Stock or
stock options held; e) Employee or Consultant; n) Nothing of value received
EXTERNAL ADVISORY ROLE
SIC HSS
MAB –United Healthcare
CSRS –Past President
SRS-BOD
IMAST Past Chair
AOA –Chair Development Committee
Agenda
•ACDF Has a Long Track
Record of Outstanding
Outcome
•CDA Data Cannot Be Trusted
•Laminoforaminotomy Not Ideal
8/24/2014
2
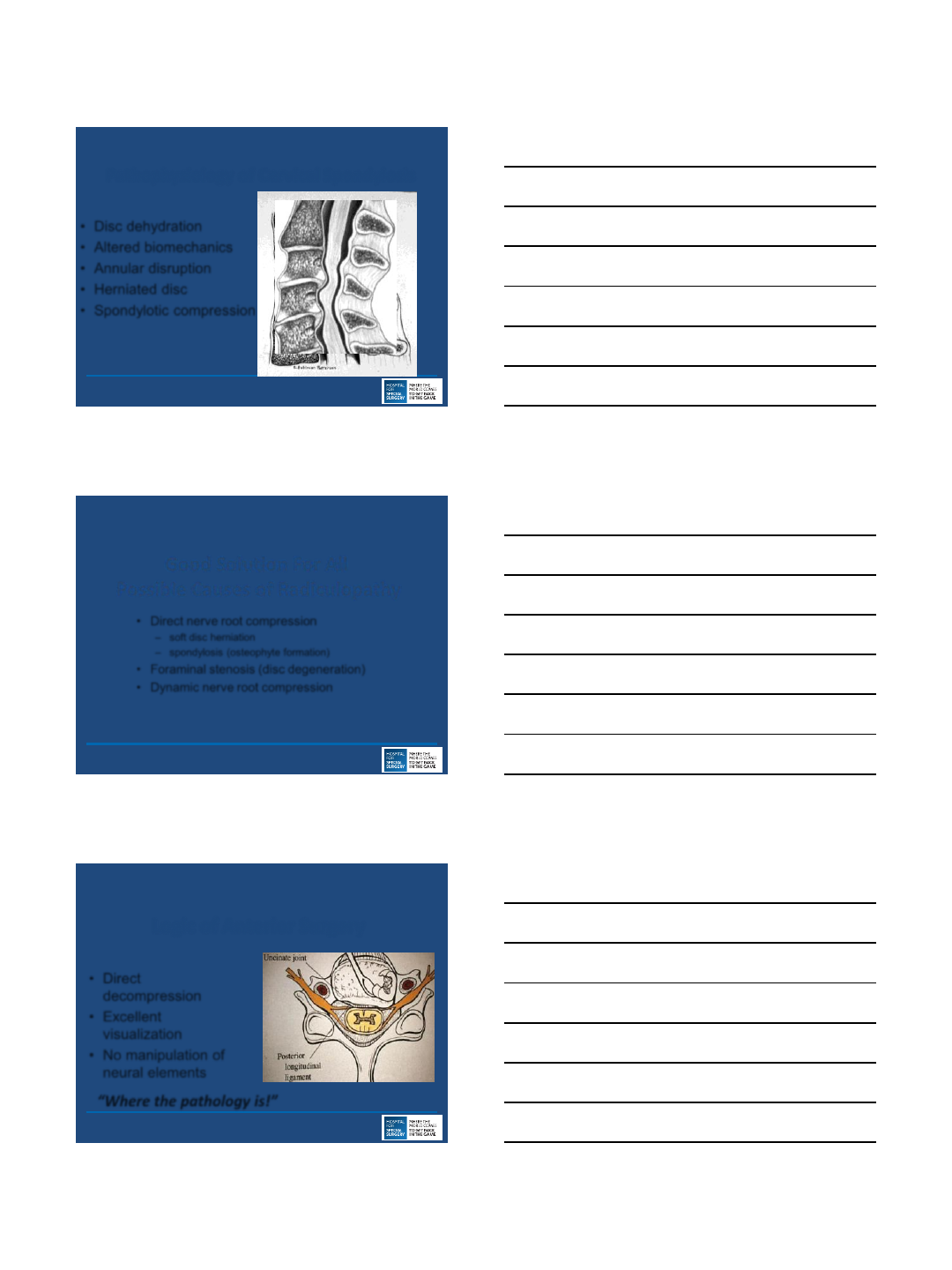
ACDF
•Disc dehydration
•Altered biomechanics
•Annular disruption
•Herniated disc
•Spondylotic compression
Pathophysiology of Cervical Spondylosis
ACDF for Radiculopathy
•Direct nerve root compression
–soft disc herniation
–spondylosis (osteophyte formation)
•Foraminal stenosis (disc degeneration)
•Dynamic nerve root compression
Good Solution For All
Possible Causes of Radiculopathy
ACDF for Radiculopathy
•Direct
decompression
•Excellent
visualization
•No manipulation of
neural elements
Logic of Anterior Surgery
“Where the pathology is!”

8/24/2014
3
ACDF for Radiculopathy
•Directly remove pathology
•Distraction indirect decompression
•Eliminates motion = root irritation (ACDF only)
Benefits of Procedure
ACDF for Radiculopathy
•Eliminates motion
•Removes arthritic
stimulus
•Regression of
osteophytes
Arrests Progression of Cervical Spondylosis
CRITICAL DISTINCTION
Adjacent Segment Disease
Reoperation Rate Lowest In
Patients With Most Fusion
Levels
-Contradicts Theory That Fusion
ASD
Length of fusion
single level = 18%
multilevel = 12%
Hilibrand et al., (Am), 1999JBJS
8/24/2014
4
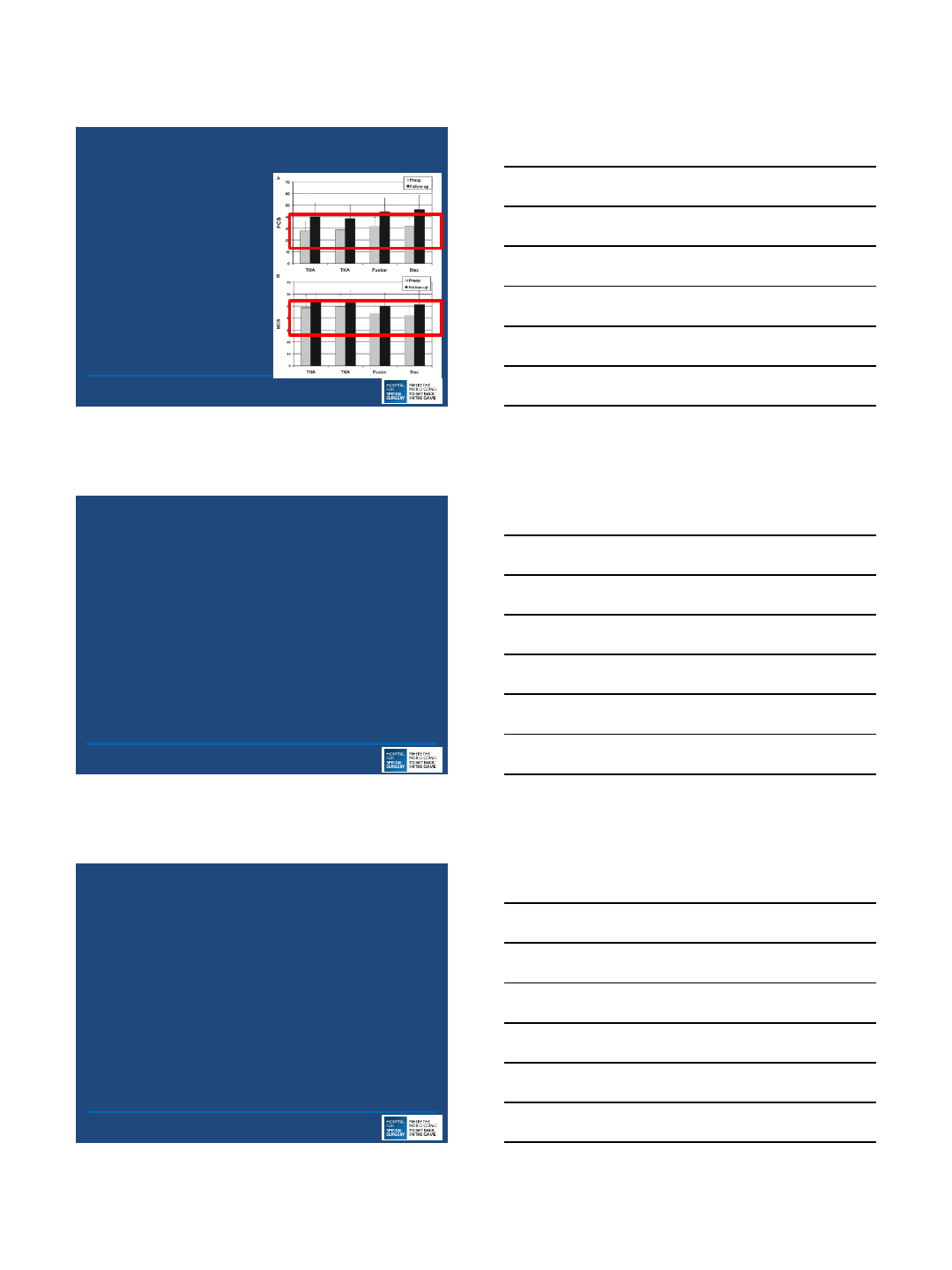
ACDF Effective, Safe, Procedure
Proven Outcome
Comparable to Hip/Knee
Replacement
Anderson Spine 2009
ACDF Improves Sagittal Balance
–ACDF Corrects Kyphosis
•Uchida JNS 2009
•Song JBJS Br 2010
•Shamji Spine 2013
•Important Factor Anterior Reconstruction
•Kyphosis Poor Outcome
•Kyphosis Increased Incidence of ASD
•Sagittal Balance Associated with Myelopathy
Ferch JNS Spine 2004
Kawakami JSDT 1999
Villavicencio Neurosurgery 2011
Gum AJO 2012
Faldini CORR 2011
Hansen Spine 2012
Park MS Spine 2014
Smith Spine 2013
Agenda
•ACDF Has a Long Track Record of
Outstanding Outcome
•CDA Data Cannot Be Trusted
•Laminoforaminotomy Not Ideal
8/24/2014
5
My Opponent Will Cite Data Supporting CDA
•Try To Create Mass Confusion With Charts, Tables, and
Meta Analyses
–ProDisc C 5 Year Results
•Zigler JE Spine 2013
–Prestige 7 Year Results
•Burkus JNS 2014
DON’T BELIEVE IT
REOPERATION RATES SUSPECT
UNDERREPORTING COMPLICATIONS
NOT ALL CDAs Do Well
Reoperation Data Is Unreliable
•Reoperation Rates at the same institution
different for ACDF patients in the control
arm of an IDE study (9%) versus outside
of IDE study (2.1%)
CDA Patients Highly Selected
•Only 43% percentage of patients are
candidates for CDA
–Auerbach Spine 2008
•Cannot extrapolate CDA results to general
population
8/24/2014
6
Reports of CDA Complications
Increasing
•Early
–Dislocation
•Late
–Osteolysis
–Subsidence
Hacker Spine 2013
Where Are These
Complications In
IDE Study Data?
Tsermoulas Br J Neurosurg 2013
Other Late Complications
•Wear Osteolysis
•Ossification
Tumilian Spine 2011
Where Are These
Complications In
IDE Study Data?
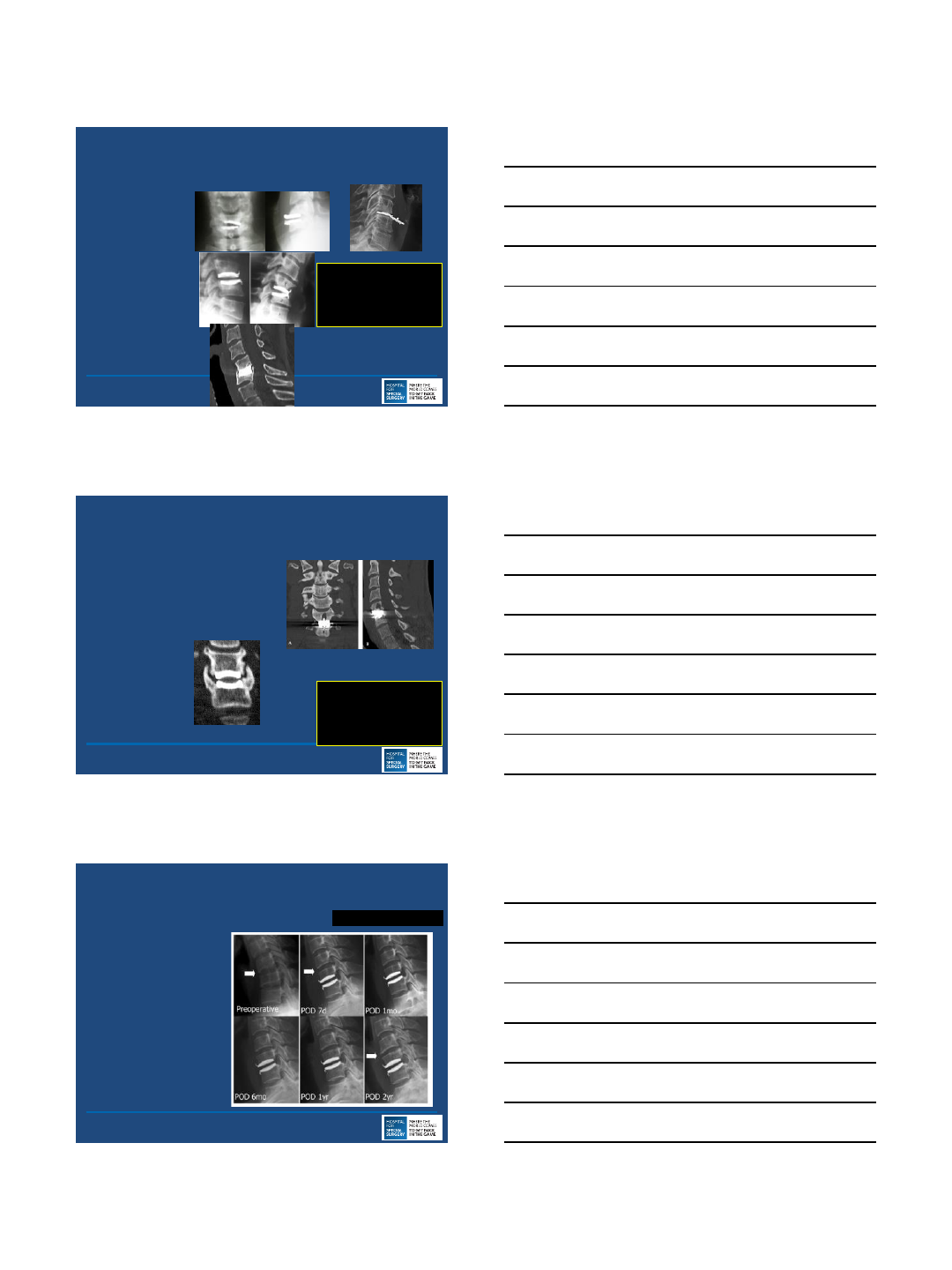
ASD Occurs After CDA
9/72 Adjacent
Segment
Degeneration
(12.5%)
Bryan
No Industry Funding
Yi Surg Neurol 2009
8/24/2014
7
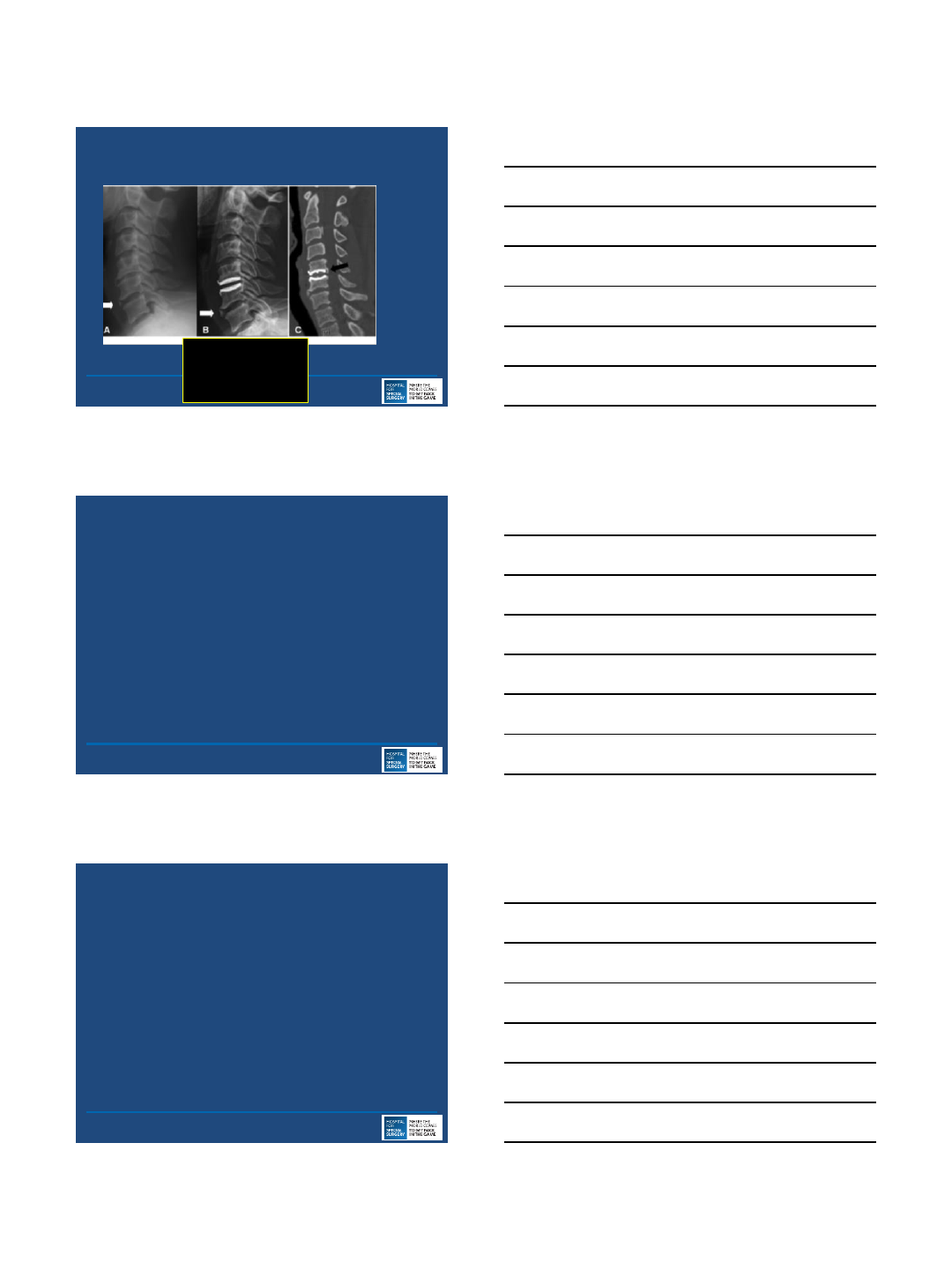
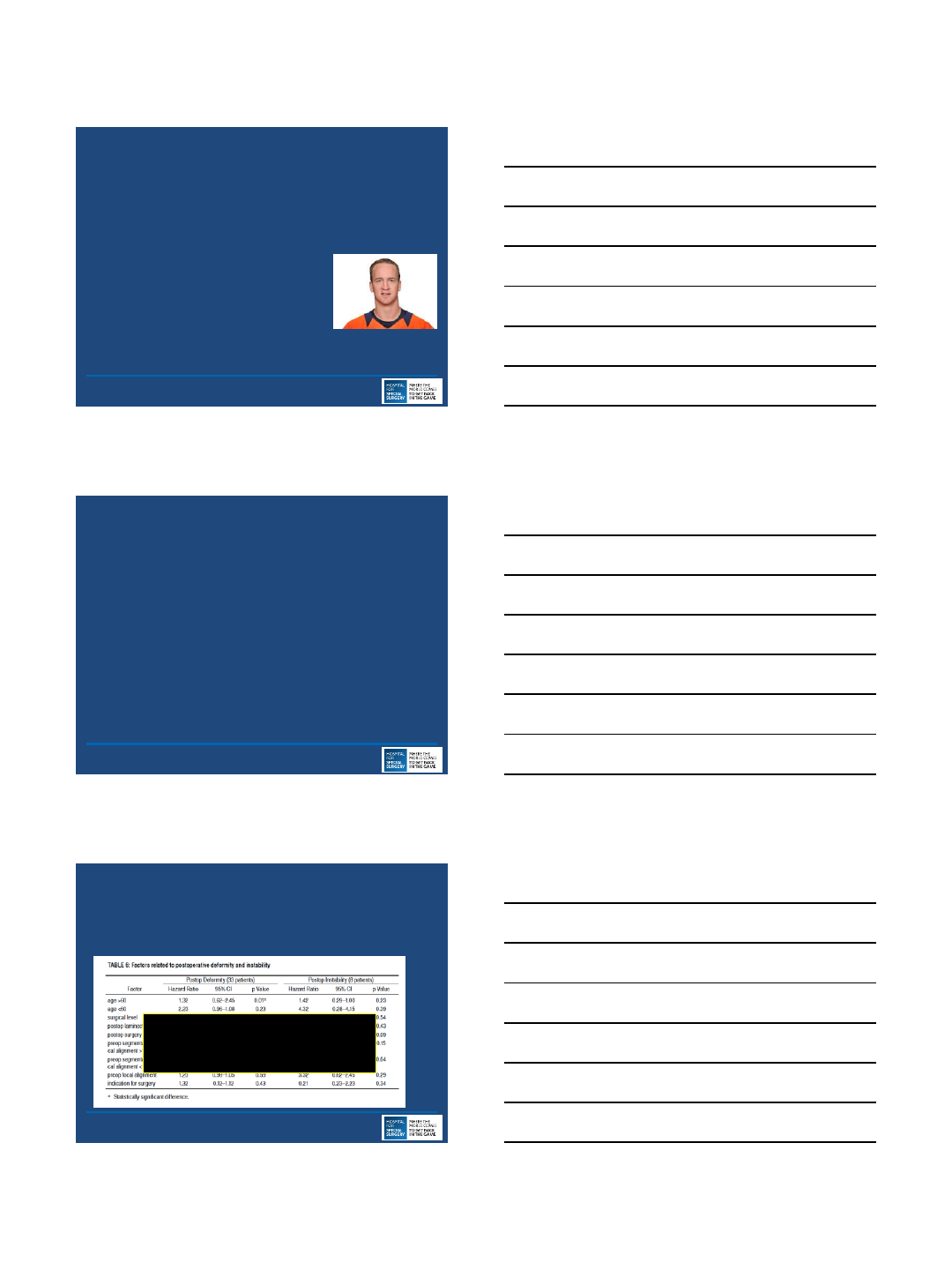
Same Segment Disease After CDA
Yi Surg
Neurol 2009
Where Are These
Complications In
IDE Study Data?
Not All CDAs Do Well
•Review of Discover Data
•Decreased Disk Height Poor Outcome
•Excessive Lordosis Poor Outcome
Rihn JSDT 2014
Laminoforaminotomy
•High Neurological Injury
•High Reoperation Rate
•Kyphosing
8/24/2014
8
Laminoforaminotomy
•Neurological Injury
–2.3% Palsy
•Choi World Neurosurgery 2013
–2.1% Palsy
–But if you are part of that 2% it’s a big deal
Jagannathan JNS 2009
High Reoperation After
Laminoforaminotomy
•N=790, Cleveland Clinic, n=627 ACDF, 163 PCF
•2 year reop rate (p=0.7)
•ACDF 4.8%
•PCF 6.4%
Lubelski Neurosurgery 2014
Laminoforaminotomy Kyphosing Procedure
•N=162, UVA, Postop Kyphosis 20% of Patients at 5
Years
–Jagannathan JNS 2009
Laminoforaminotomy
Flat Neck Deformity
8/24/2014
9
Progressive Kyphosis After
Laminoforaminotomy
•Described Even In Paper Favorable to Laminoforaminotomy
•Had to Be Rescued with ACDF Jagannathan JNS 2009
Summary
•ACDF Great, Safe, Effective Durable Procedure
•Need More Independent Verification of CDA Data
•Laminoforaminotomy Potential To Be Cost Effective
Conclusion
•Need Better Understanding of the Drivers of Outcome of
Cervical Surgery
–Sagittal Balance?
–Fusion Rate?
–Motion?
–Reoperation Rate?

8/24/2014
10
Thank You
8/24/2014
1
Current Surgical
Strategies for Cervical
Radiculopathy
Sheeraz Qureshi, MD,MBA
Associate Professor,
Orthopaedic Surgery
Spinal Surgery, Mount Sinai
Hospital
Icahn School of Medicine at
Mount Sinai
Co-Director, Spinal Surgery
Fellowship
Disclosures
1. Committee Appointments
1. AAOS Evaluations Committee
2. CSRS Research Committee
3. NASS Evidence-Based Guidelines Committee
4. CSRS Survey Committee
5. NASS Value Committee
2. Journals
1. Spine Journal (Reviewer)
2. Spine (Reviewer)
3. CORR (Reviewer)
4. Global Spine Journal Reviewer
3. Royalties
1. Zimmer
4. Consulting
1. Medtronic
2. Stryker
3. Zimmer
4. Orthofix
5. Teaching
1. Medtronic
2. Stryker
3. Globus
6. Advisory Boards
1. Zimmer Scientific Advisory Board
2. Orthofix Scientific Advisory Board
3. MTF Medical Board of Directors
4. Axiomed Data Safety Monitoring Board
Increasingly Common Problem
8/24/2014
2
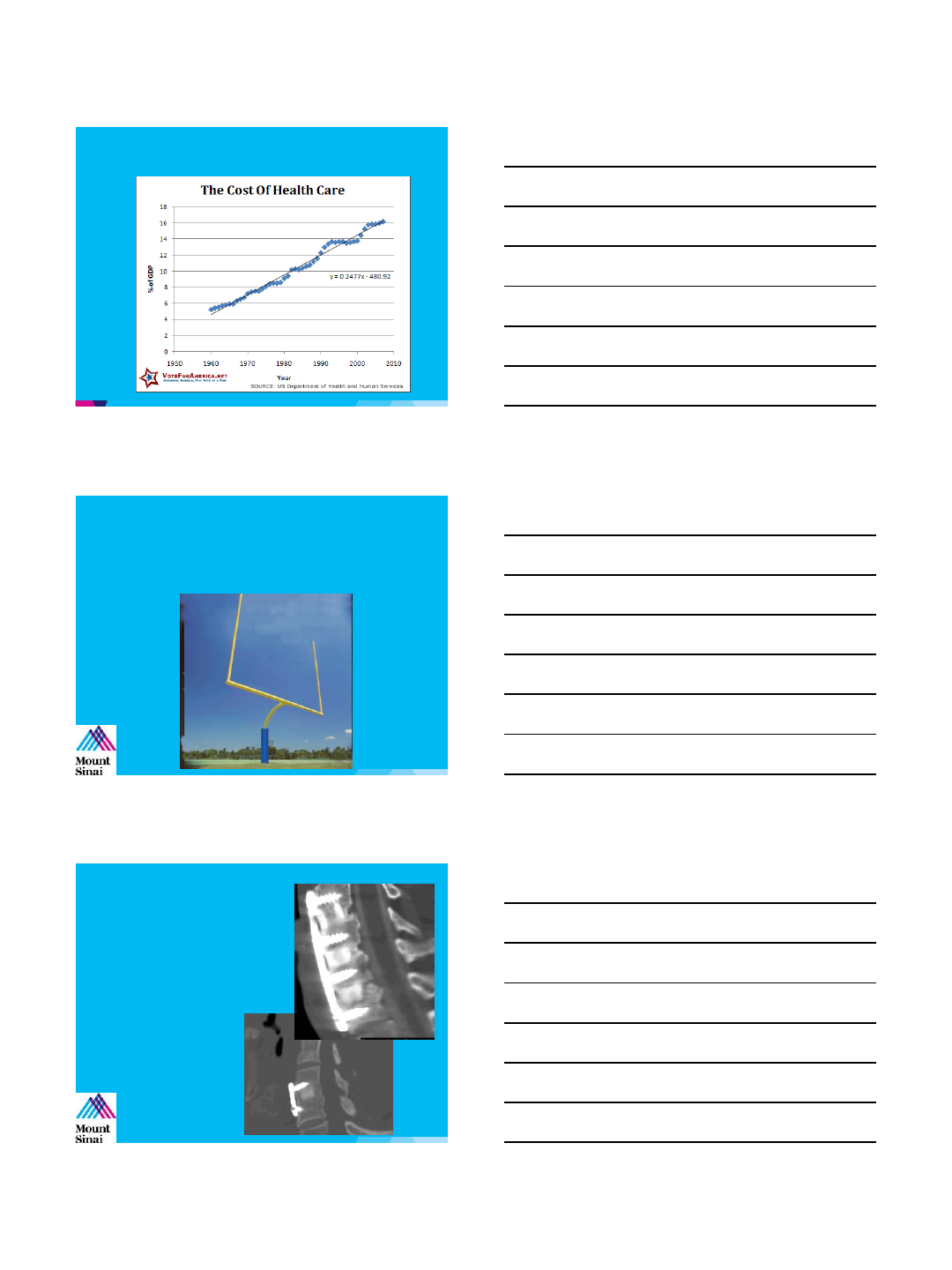
Economic Crisis
What is Value?
▶“Goalposts around which we define outcomes”
The Past …
▶Spine surgery outcomes
–Technical concepts
•Fusion Rates
•Complications
8/24/2014
3
The Past …
▶Goal of surgery
–Technically successful procedure
Outcomes Measures
McCormick et al, 2013, JAAOS
The Surgeon’s Task
▶Choose the procedure that results in the best
possible outcome for the patient
8/24/2014
4
Emphasis
▶Cost
▶Cost Effectiveness
▶Value
How is Value Defined
▶Value
–Quality of an intervention divided by the cost
measured over time
▶Key factors
–Quality
–Cost
–Time
Obligation
▶Goal of healthcare is NOT simply to achieve
lowest cost treatment for given pathology
8/24/2014
5
What’s the CHEAPEST
treatment?
▶NSAIDs
▶Tylenol
▶PT
▶Home exercise program
▶Injections
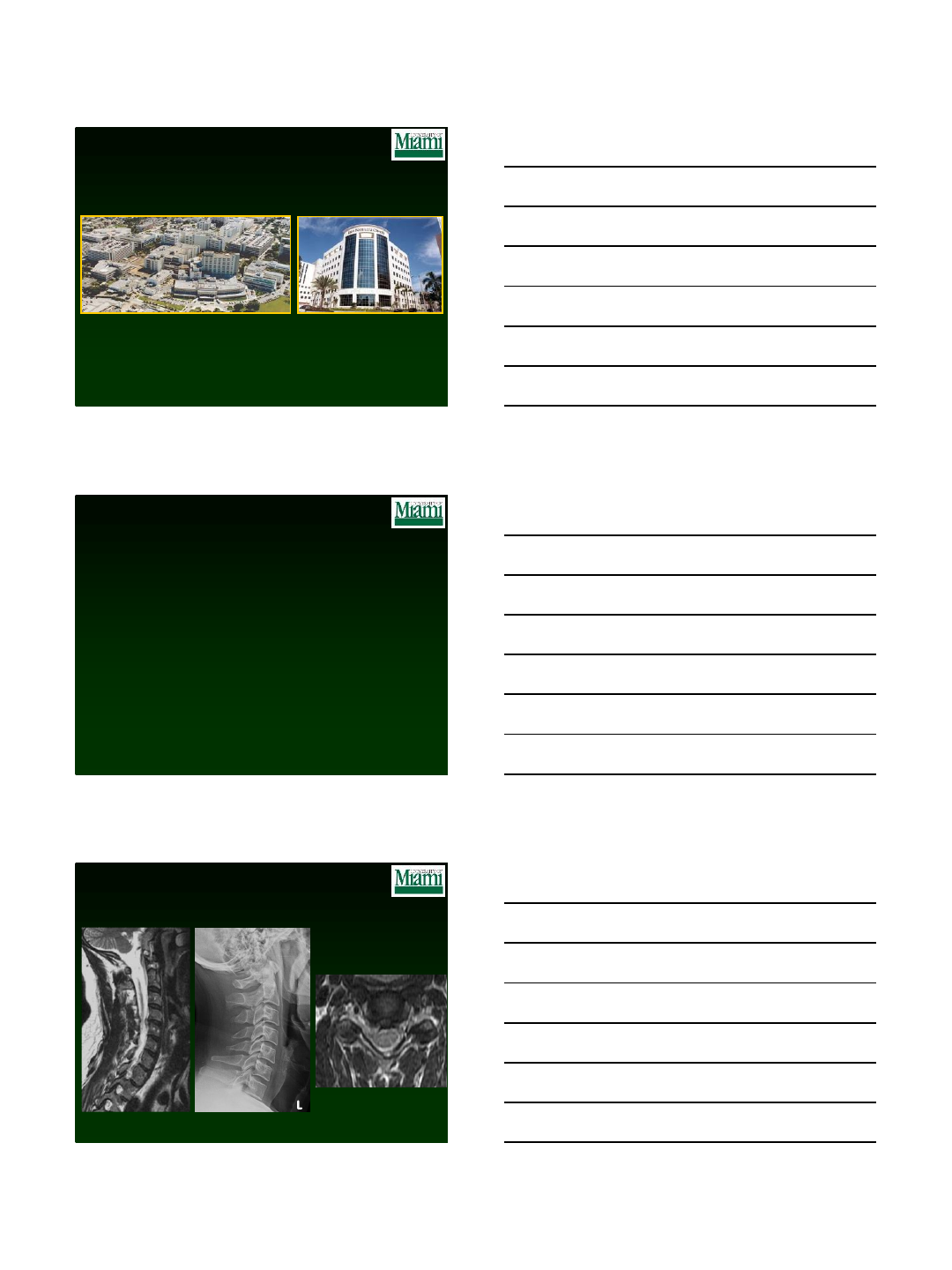
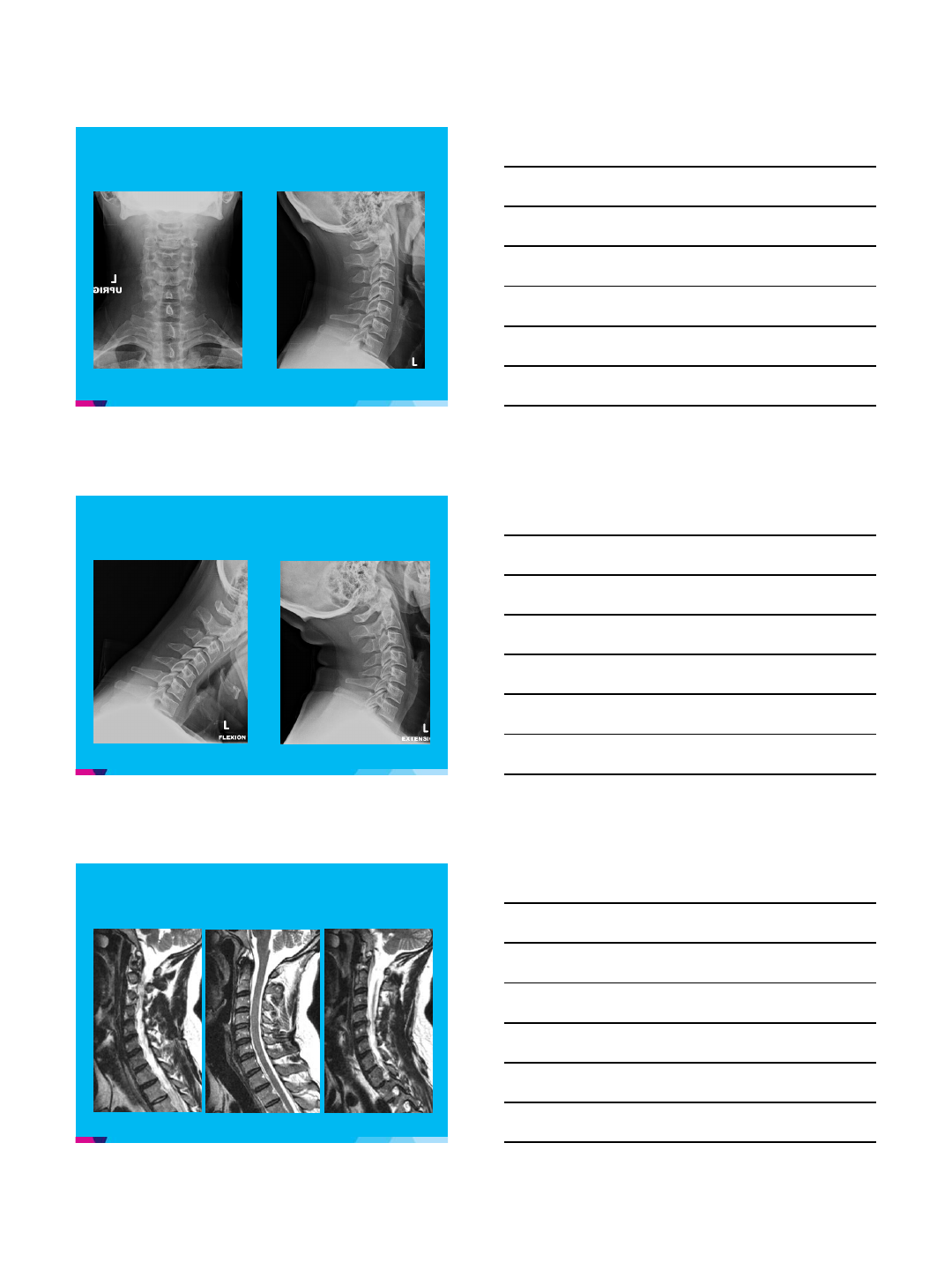
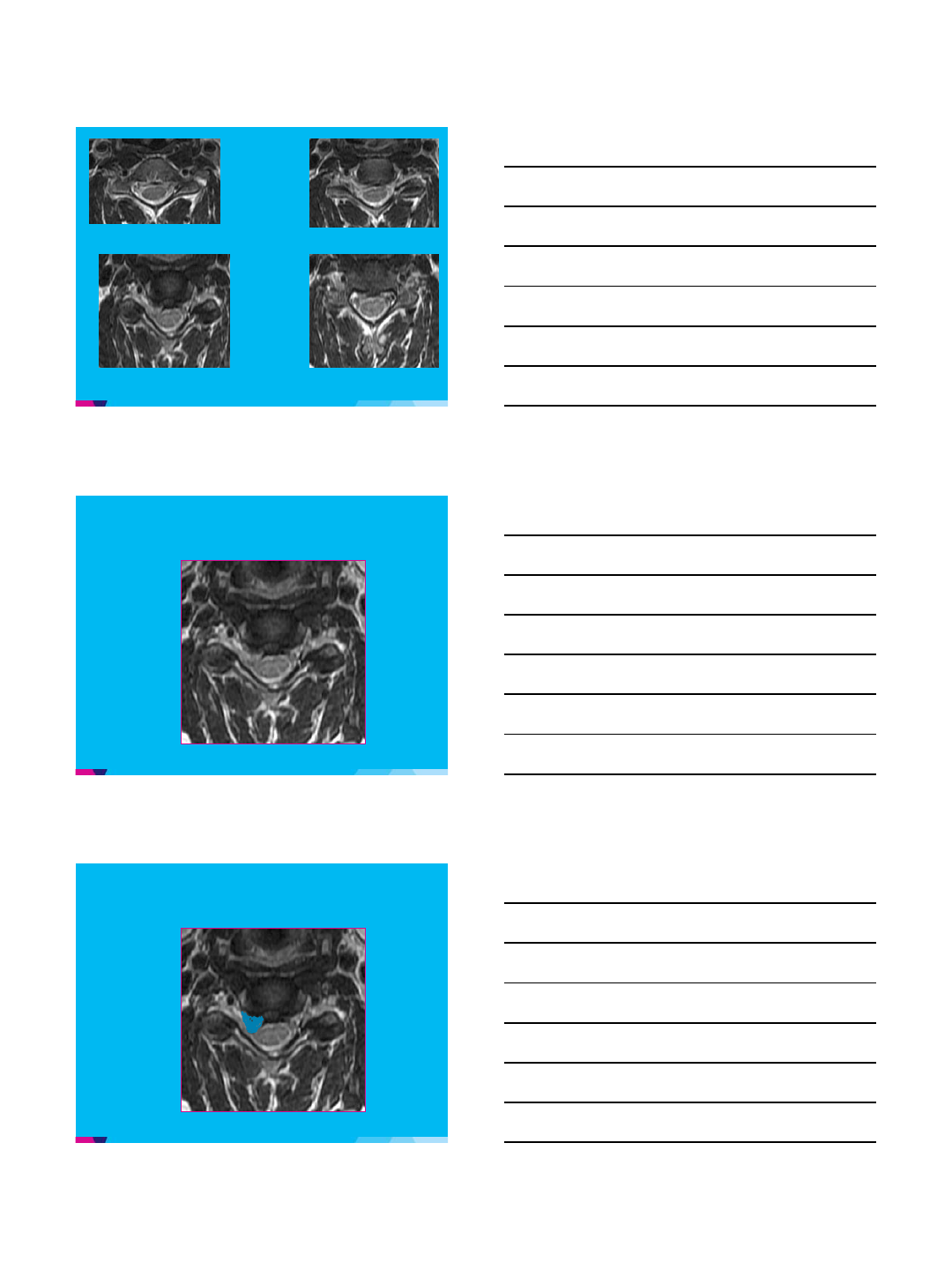
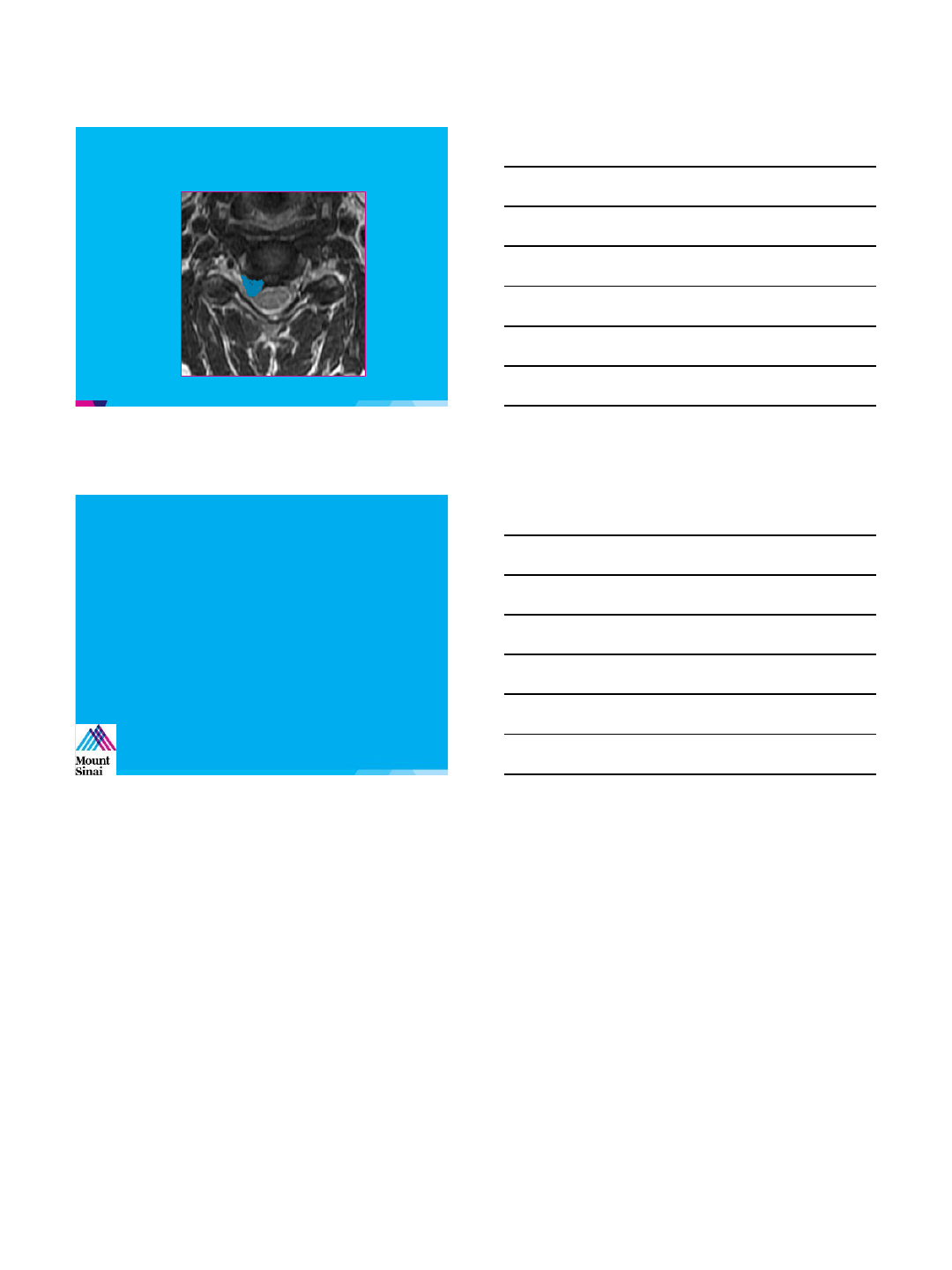
Case
1. 37 year old right hand dominant attorney with 4 week
history of right upper extremity pain, numbness, and mild
weakness
2. Attempted oral steroid with minimal relief only and
currently doing PT
3. Physical exam confirms positive Spurling’s on the right,
with 4+/5 weakness of deltoid and biceps
4. No physical exam findings of spinal cord irritation
8/24/2014
6
8/24/2014
7
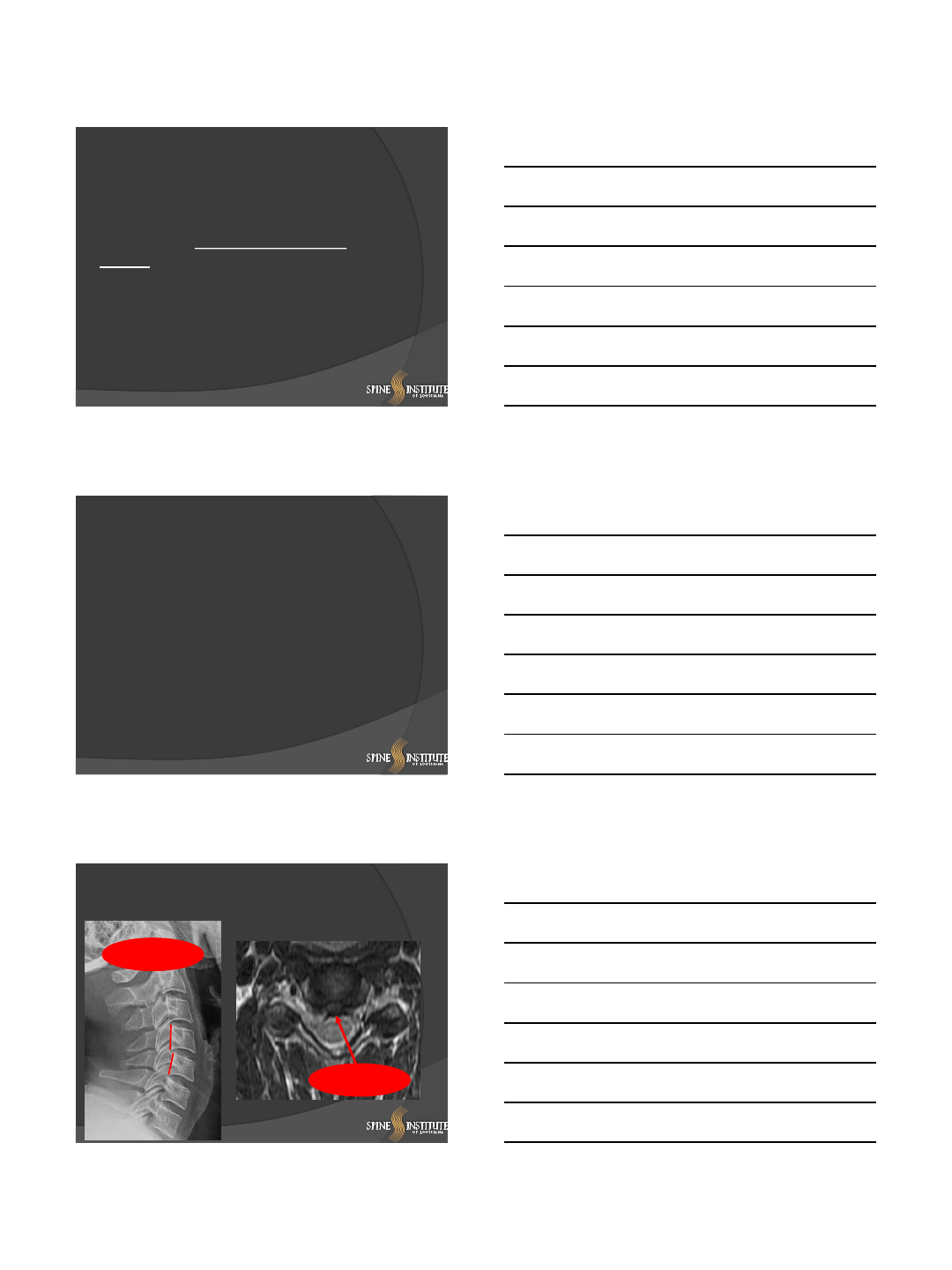
C4 C4/5
C4/5 C5
8/24/2014
8
Esteemed Faculty
Mike Wang Pierce Nunley Todd Albert
22
Mount Sinai / Presentation Slide / December 5, 2012 23
Case
1. 37 year old right hand dominant attorney with 4 week
history of right upper extremity pain, numbness, and mild
weakness
2. Attempted oral steroid with minimal relief only and
currently doing PT
3. Physical exam confirms positive Spurling’s on the right,
with 4+/5 weakness of deltoid and biceps
4. No physical exam findings of spinal cord irritation
8/24/2014
9
What Would You Do?
1. ACDF
2. CDR
3. PCF
26
