Charcot Arthropathy Syllabus
2014-07-14
: Pdf Charcot Arthropathy Syllabus Charcot_Arthropathy_Syllabus 7 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 49

1
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Jeremy J. McCormick, M.D.
Assistant Professor - Foot and Ankle Surgery
Washington University
St. Louis, MO
My disclosures are listed in the AAOS database.
I have no potential conflicts with this presentation.
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Jeremy J. McCormick, M.D.
The life of a foot and ankle surgeon…
Glamourous Not so glamourous…
Each equally important…
http://w ww.presentdiabetes.co m http://sportsillu strated.cnn .com/nhl/n ews/20131228/alex-steen-
blu es-concussion -injury.ap/

2
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Overview on Charcot
Staging and classification
Approach to treatment
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Overview on Charcot
Staging and classification
Approach to treatment
Jean-Martin Charcot
French neurologist
1836 described unique
arthropathy in patients with
neurosyphilis
http://www.sciencemuseum.org.uk/broughttolife/
people/jeanmartincharcot.aspx
3
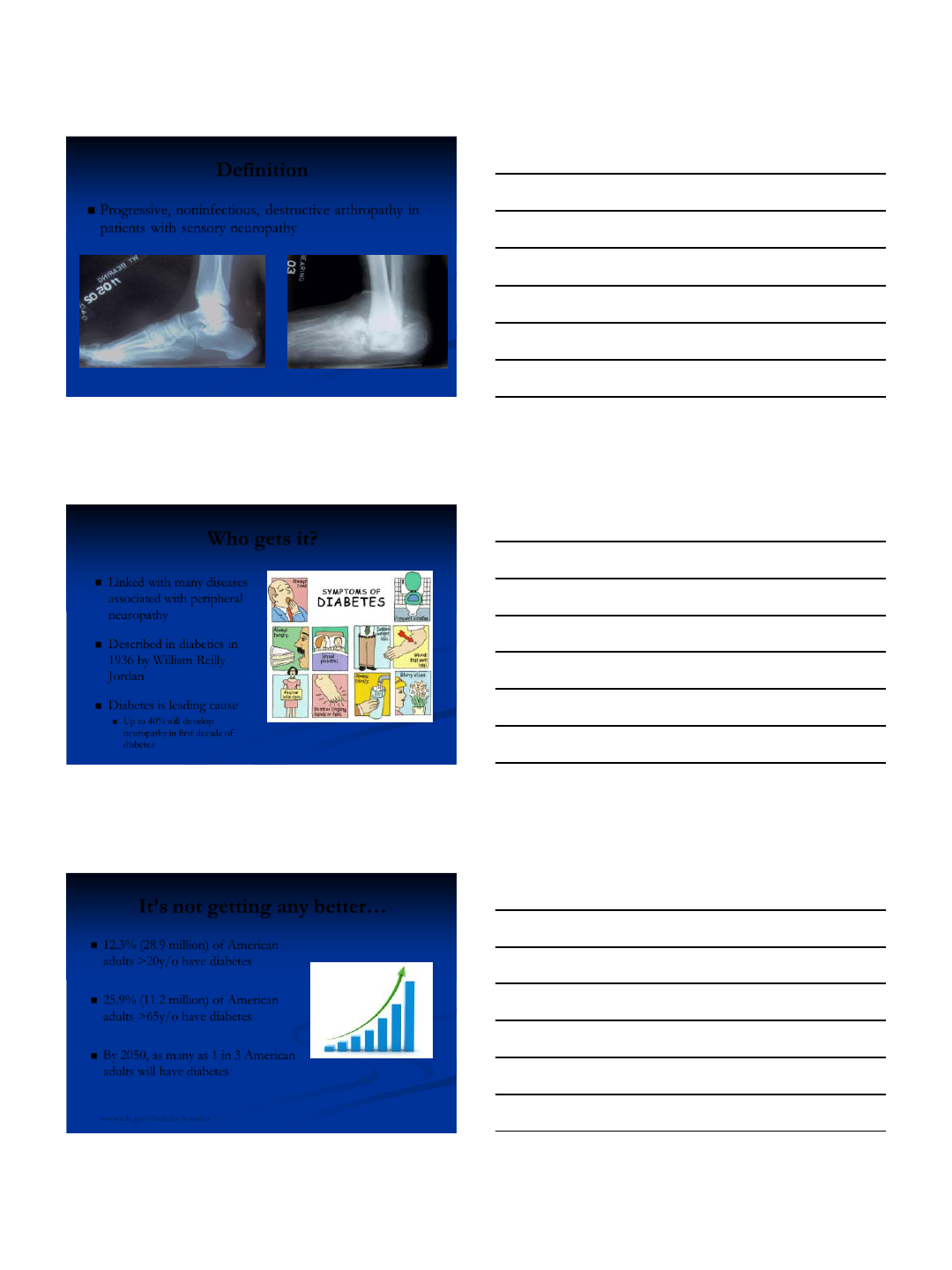
Definition
Progressive, noninfectious, destructive arthropathy in
patients with sensory neuropathy
Courtesy of Carroll P. Jones, MD
Who gets it?
Linked with many diseases
associated with peripheral
neuropathy
Described in diabetics in
1936 by William Reilly
Jordan
Diabetes is leading cause
Up to 40% will develop
neuropathy in first decade of
diabetes
http://www.healthisfuture.com/wp-content/uploads/symptoms-of-diabetes.jpg
It’s not getting any better…
12.3% (28.9 million) of American
adults >20y/o have diabetes
25.9% (11.2 million) of American
adults >65y/o have diabetes
By 2050, as many as 1 in 3 American
adults will have diabetes
www.cdc.gov/diabetes/statistics
http://jaxrealestatefacts.com/2012/03/23/anothe
r-700k-house-goes-under-contract-in-
ortega/increasing-sales/
4
Why diabetes?
Leads to neuropathy
Loss of nitric oxide function
Vasoconstriction/Ischemia
Injury to nerve cells/function
Will not protect weightbearing
Will not sense a problem
Wukich and Kline – JBJS Am, 2008
http://www.mynewtown.co.uk/newsviewer/tabid/1
387/ArticleId/1013/Hot-footing-for-charity.aspx
Etiology – Multiple Theories
Neurotraumatic
Repetitive micro-trauma
Neurovascular
Autonomic dysfunction that causes increases
in blood flow
Inflammatory mediated
Increase in cytokines >> osteoclastic activity
Baumhauer et al, 2006
http://www.everyvotecou
nts.org.uk/pack-
content/politics-
works/factsheets/political
-parties.php
Likely a Combination of Events
Peripheral neuropathy
Unrecognized injury
Repetitive stress on injured structures
Increased local blood flow
http://www.sfmconsulting.co.uk/blog/entry/the_whole_is_great
er_than_the_sum_of_its_parts
5
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Overview on Charcot
Staging and classification
Approach to treatment
Eichenholtz Classification
Radiographic natural history of changes that occur
From destructive to consolidation
I – Fragmentation
II – Coalescence
III – Reconstruction
A fourth stage (O) has been added
Eichenholtz SN (1966) General considerations. In: Eichenholtz SN (ed)
Charcot joint. Thomas, Springfield, pp 3–20 http://edtreatmenttoday.com/ed-
treatment-guide/steps-to-follow-in-
ed-treatment/
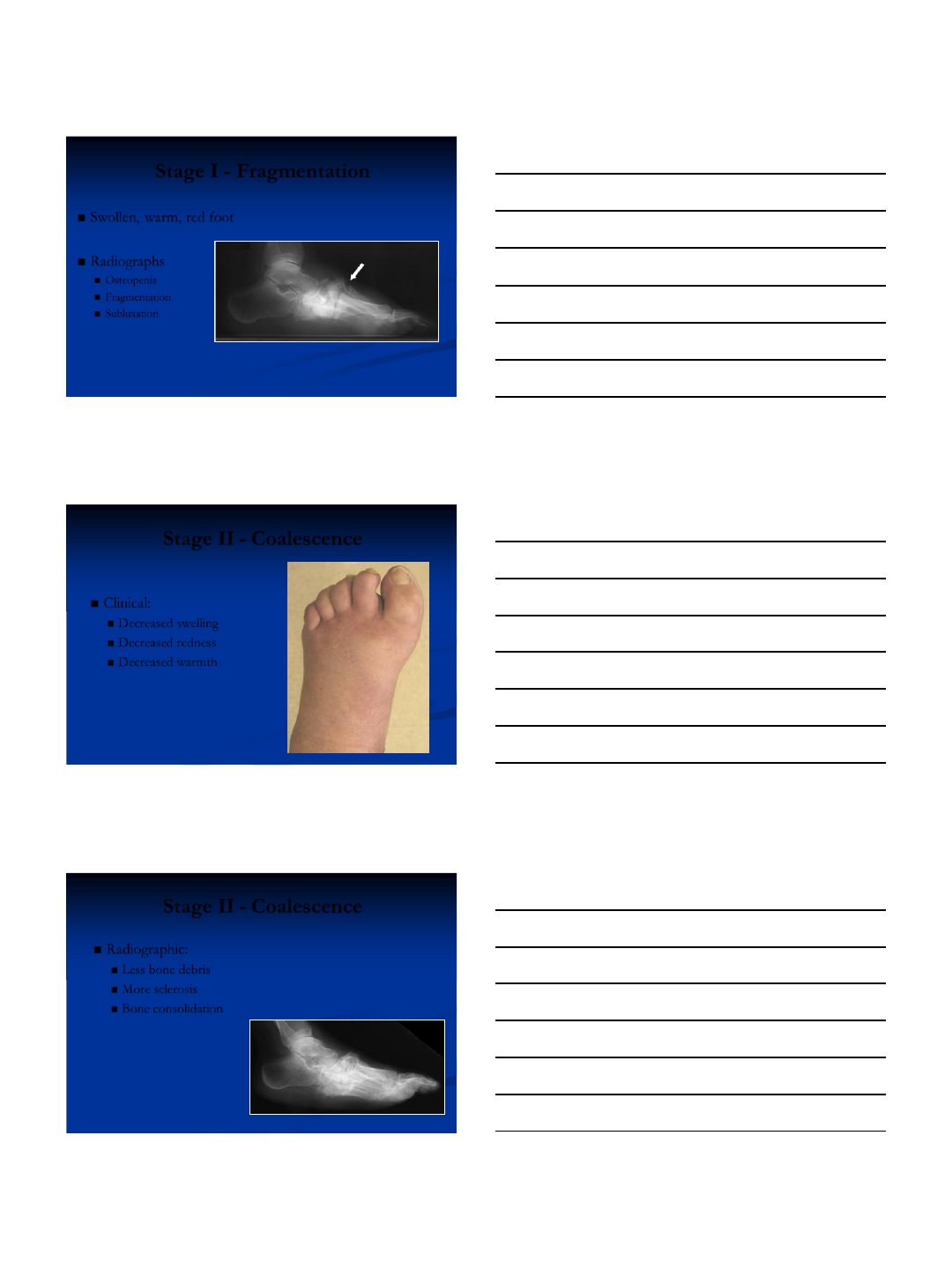
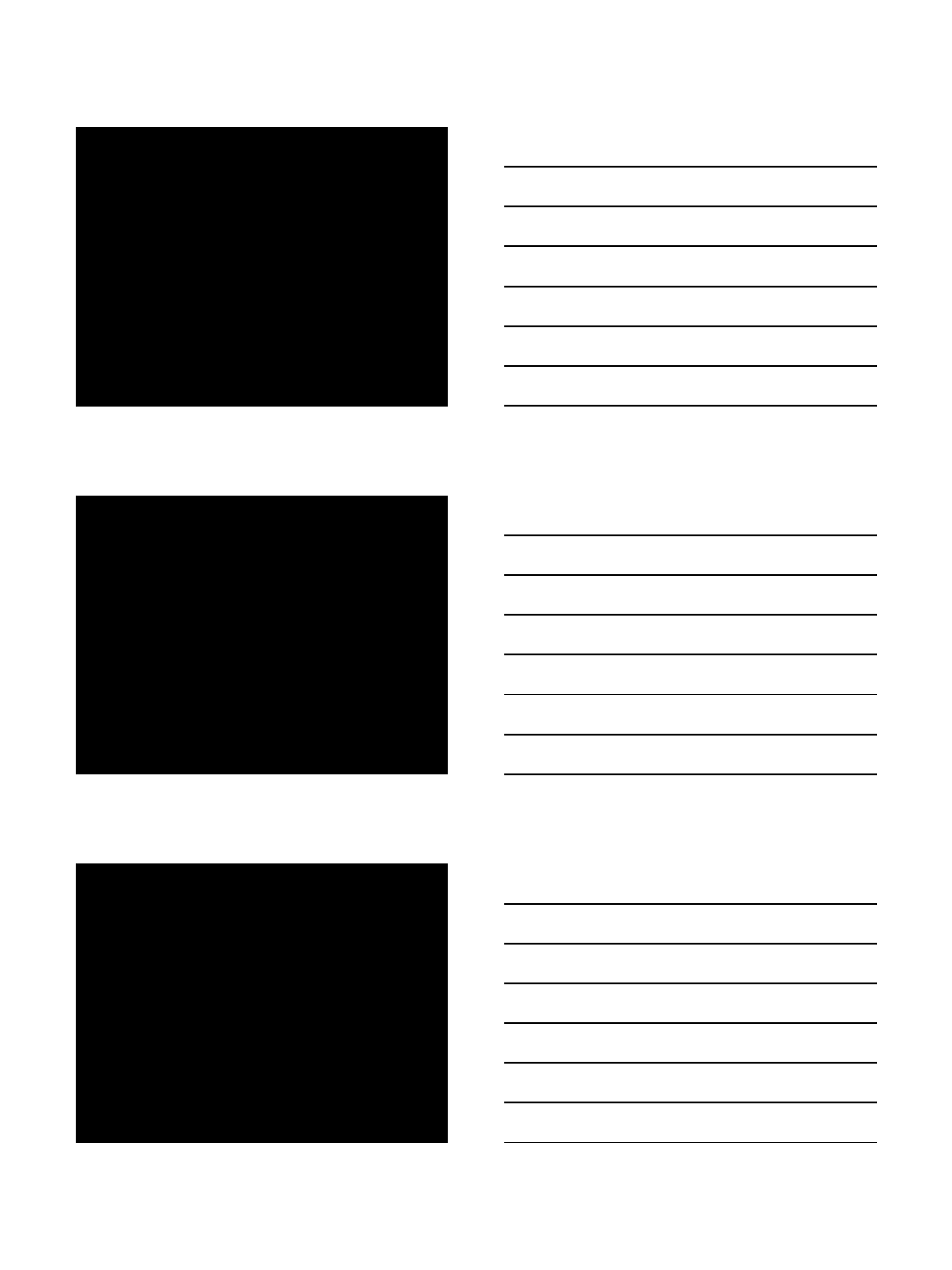
Stage 0
Swollen, red, warm foot
Normal x-rays
Different than infection
Elevation decreases swelling
No systemic symptoms
Courtesy of Carroll P. Jones, MD
6
Stage I - Fragmentation
Swollen, warm, red foot
Radiographs
Osteopenia
Fragmentation
Subluxation
Courtesy of Carroll P. Jones, MD
Stage II - Coalescence
Clinical:
Decreased swelling
Decreased redness
Decreased warmth
Courtesy of Carroll P. Jones, MD
Stage II - Coalescence
Radiographic:
Less bone debris
More sclerosis
Bone consolidation
Courtesy of Carroll P. Jones, MD
7
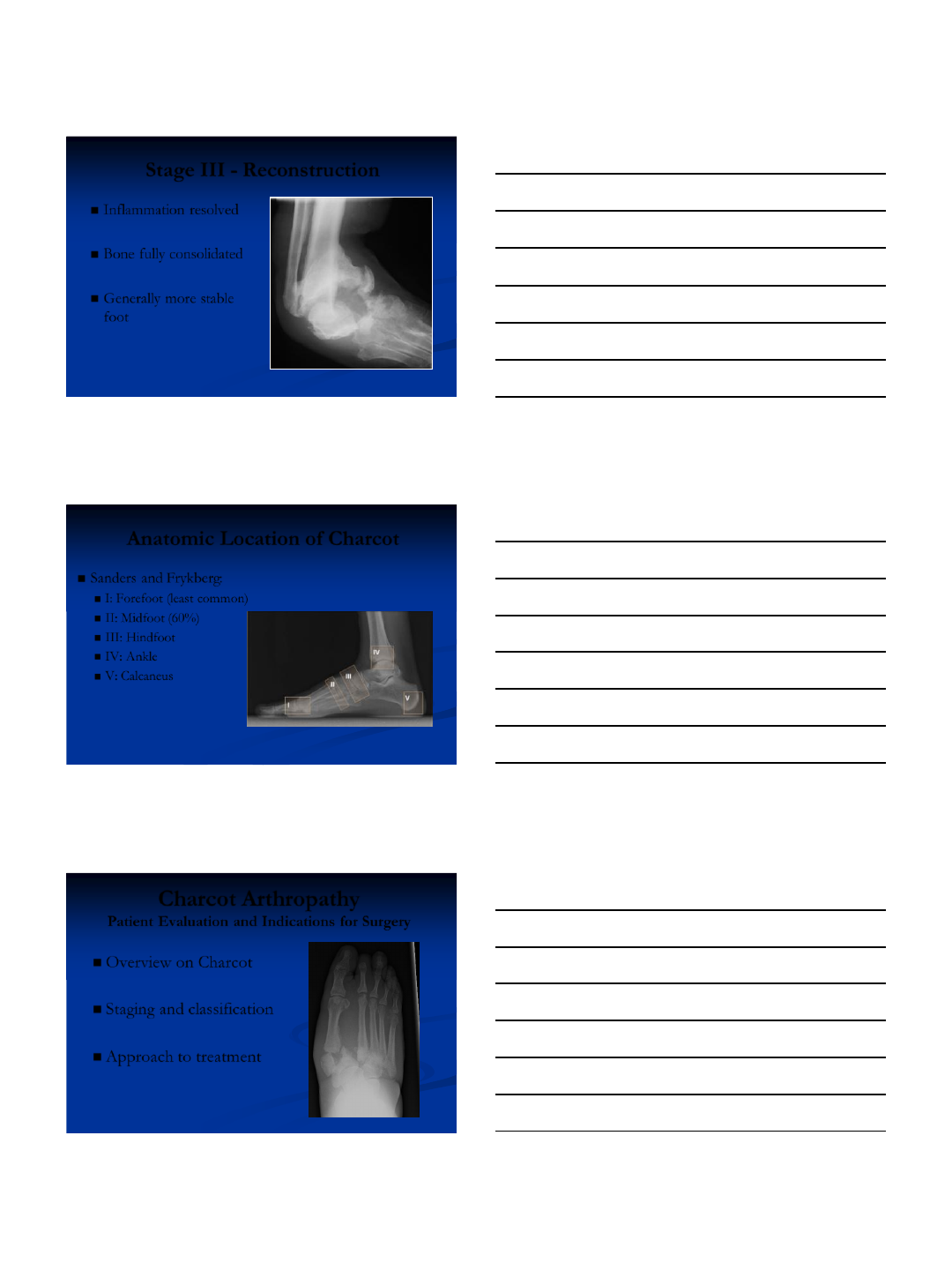
Stage III - Reconstruction
Inflammation resolved
Bone fully consolidated
Generally more stable
foot
Courtesy of Carroll P. Jones, MD
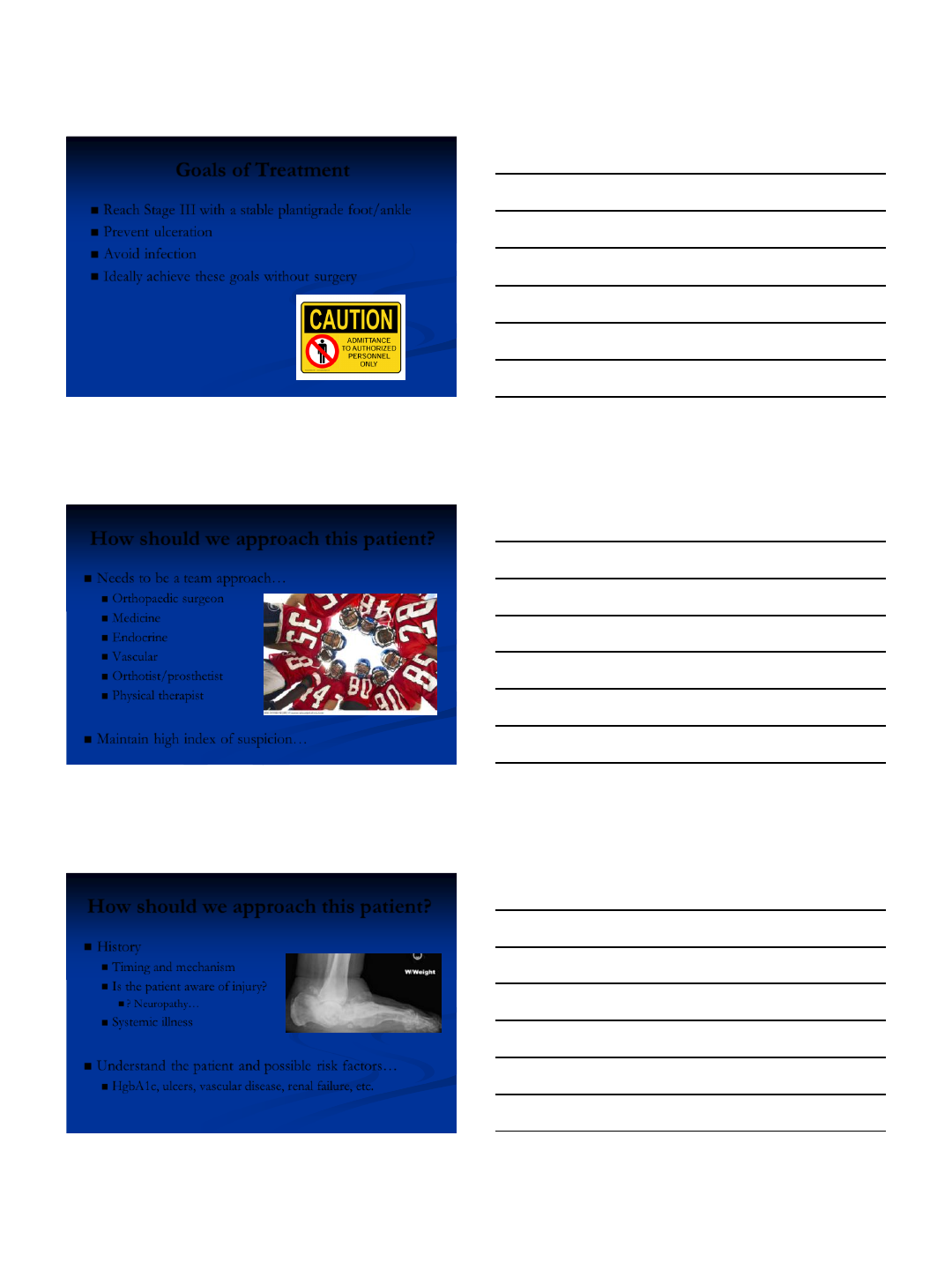
Anatomic Location of Charcot
Sanders and Frykberg:
I: Forefoot (least common)
II: Midfoot (60%)
III: Hindfoot
IV: Ankle
V: Calcaneus
http://diabeticfootandankle.net/index.php/dfa/rt/printerFriendly/21884/html
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Overview on Charcot
Staging and classification
Approach to treatment
8
Goals of Treatment
Reach Stage III with a stable plantigrade foot/ankle
Prevent ulceration
Avoid infection
Ideally achieve these goals without surgery
http://blackras.wordpress.com/about/
How should we approach this patient?
Needs to be a team approach…
Orthopaedic surgeon
Medicine
Endocrine
Vascular
Orthotist/prosthetist
Physical therapist
Maintain high index of suspicion…
http://dailystrugglesandupliftingscriptures.blogspot.com/2012/07
How should we approach this patient?
History
Timing and mechanism
Is the patient aware of injury?
? Neuropathy…
Systemic illness
Understand the patient and possible risk factors…
HgbA1c, ulcers, vascular disease, renal failure, etc.
{kind=link}
9
How should we approach this patient?
Physical exam
Vascular
Motor
Sensory – neuropathy?
Protective sensation?
Semmes-Weinstein monofilament
Associated with risk of Charcot
Look for other signs
Claw toes
Ulcer/amputation
http://shanesfootcom fort.weebly.com/ claw-toe.html
http://w ww .diabetesindia.com/diabetes/the_feet_diabetes1.htm
The Challenge…
Majority are morbidly obese
Extreme difficulty complying with treatment
Medical comorbidities
Poor potential for healing
Immunocompromised
High risk of ulceration
http://visionaryfam.com/2014/02
/time-for-a-challenge/
Stage I – Non-op Treatment
Total Contact Cast
Immobilization is critical
Minimize deformity
Control swelling
Offload foot
2-3 months if possible
Follow closely
http://www.o-
wm.com/content/total-contact-cast-
system-simplifies-application-process
{kind=link}
10
Can You Keep Them NWB?
Very difficult
Probably only 50% compliance
Even if WB may still achieve
good result
De Souza, et al – JBJS, 2008
Err on the side of casting for
too long… http://www.confusereviews.com/?p=3729
Stages II – Non-op Treatment
Charcot Restraint
Orthotic Walker
(CROW)
Other AFO
http://www.mccleveop.com/orthotic
s/crow-boots/
http://lermagazine.com/article/evi
dence-based-orthotic-management-
of-pttd
Stages III – Non-op Treatment
In-depth shoe
Custom insert
Life long
Educate the patient
http://www.valentineorthotics.com/medicare-shoe-program.html

11
Non-op is NOT Easy!
23% required bracing > 18 months
49% risk of recurrent ulceration
Ulceration increases risk of amputation
2.7% annual rate of amputation
Saltzman – CORR, 2005
http://www.thegodboxproject.com/blog/2012/03/
16/fun-friday-the-secret-to-saying-no/fingers-
crossed-2/
Surgical Indications
Unstable, unbraceable deformity
Recurrent ulceration
Deep infection
Deformity at high-risk for ulceration
http://www.idlehearts.com/if-plan-a-didnt-work/559/
Charcot Arthropathy
Patient Evaluation and Indications for Surgery
Overview on Charcot
Staging and classification
Approach to treatment
{kind=link}
12
Take Home Points
Understand the natural progression of Charcot
Early recognition and treatment
Maintain a high index of suspicion
Achieve early stability and maintain alignment through
casting
Thank you…
7/14/2014
1
Charcot Arthropathy:
Internal Fixation
VuMedi Webinar July 2014
Carroll P. Jones MD
OrthoCarolina Foot and Ankle Institute
Charlotte, NC
Disclosures: AAOS Website.
Paid consultant for Wright Medical
Technology and have been involved
in the development of Charcot-
specific implants.
Goals of Treatment
•Reach consolidation phase with a stable
plantigrade foot/ankle
•Prevent ulceration/infection
•Ideally achieve these goals
nonoperatively
7/14/2014
2
•Nonop treatment 70% successful
–Clinically plantigrade foot
–Radiographically plantigrade
•Pinzur et al; FAI 1993
•Fabrin et al; Diabetes Care 2000
•Pinzur et al; FAI 2004
Surgical Indications
•Unstable, unbraceable deformity
•Recurrent ulceration
•Deep infection
•Deformity at high-risk for ulceration
Clinical Challenge
•Limited Level-I evidence
•Effective clinical algorithm
–Nonop (total contact cast)
–Exostectomy
–Surgical correction: internal fixation
–Surgical correction: external fixation
7/14/2014
3
Algorithm
•Plantigrade •Nonplantigrade
Total Contact Cast/Brace
Low Risk High Risk
Corrective osteotomy:
Internal Fixation
Thin-wire Fixation
Ankle/Hindfoot Charcot
•Arthrodesis provides the most reliable
and durable correction and stability
•Most deformities can be corrected
intraoperatively
•Typically include both ankle and ST
joints for levels of fixation
•Internal fixation reserved for relatively
“clean” cases
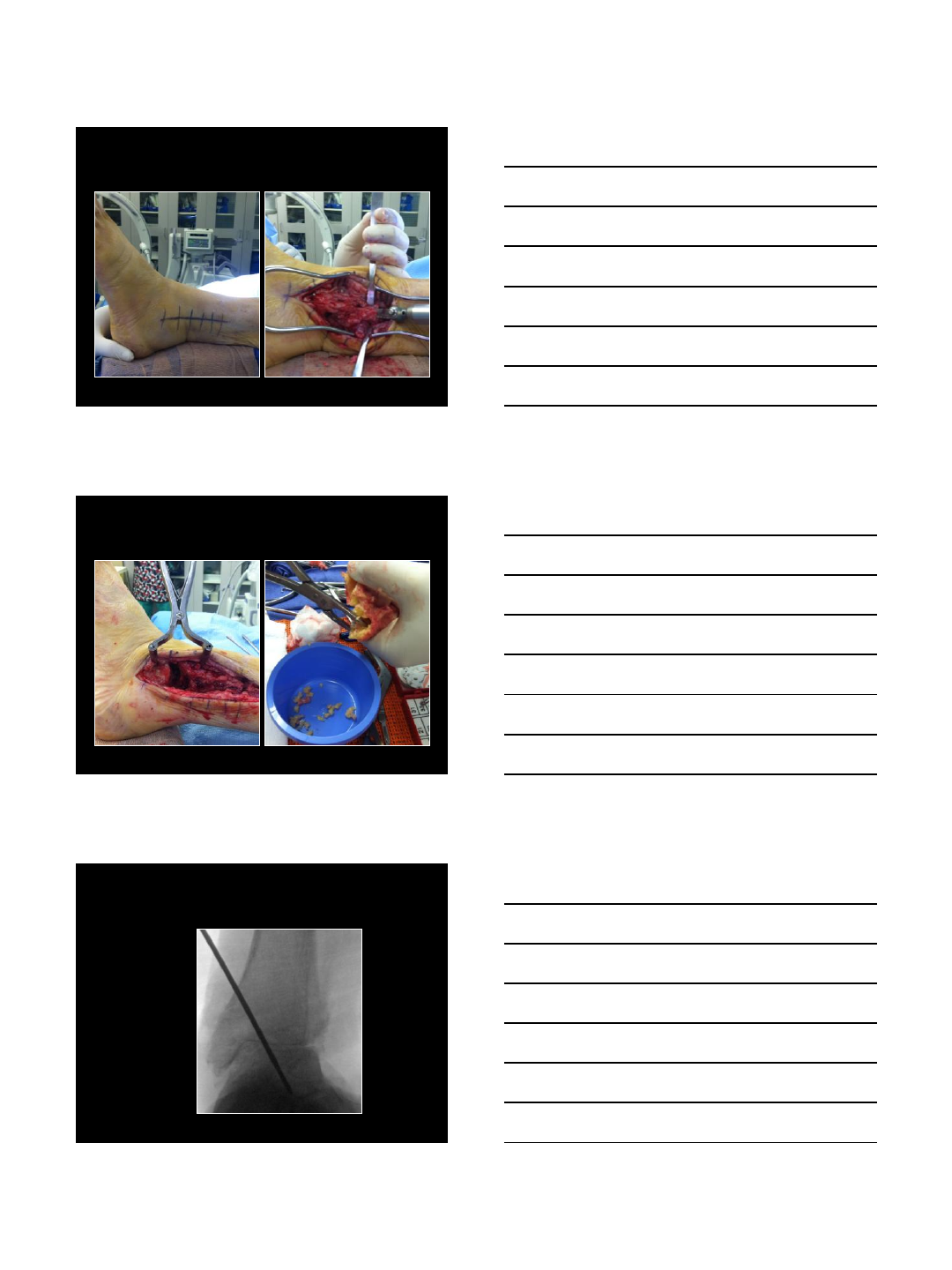
Case Example
•70 yo diabetic
neuropathy
•4 month h/o ankle
deformity
•Unable to ambulate
7/14/2014
4
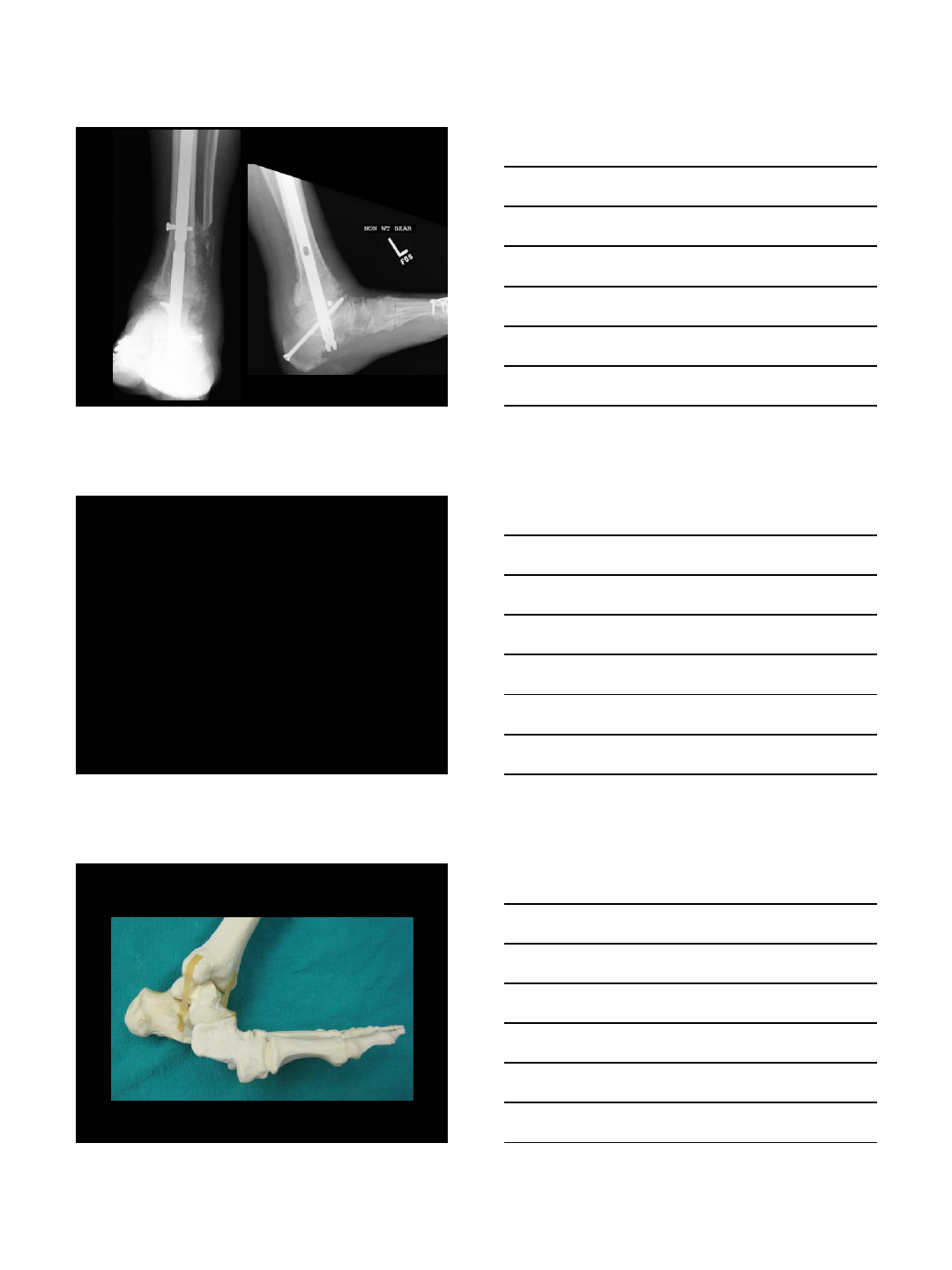
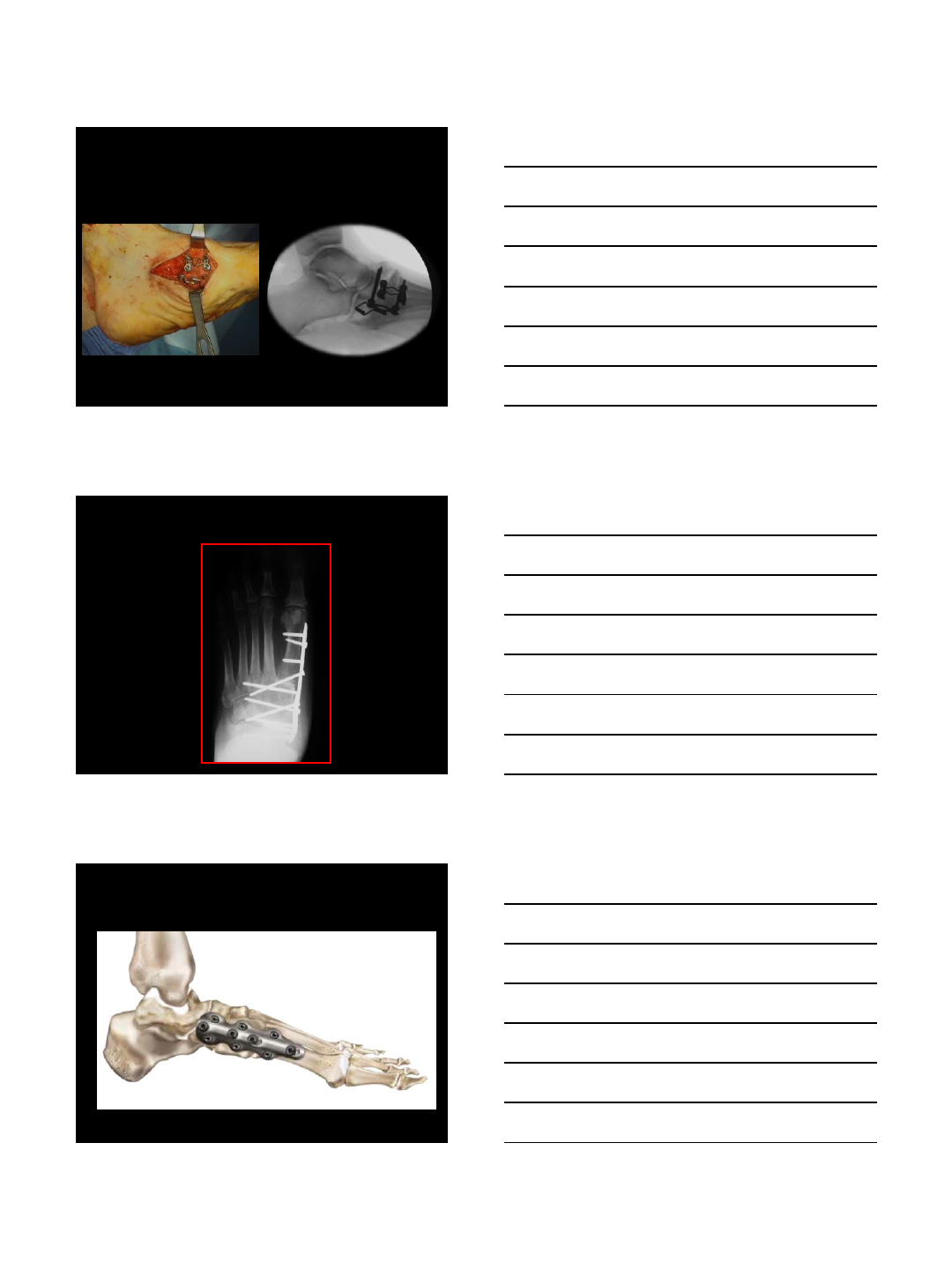
Transfibular Approach
Joint Preparation
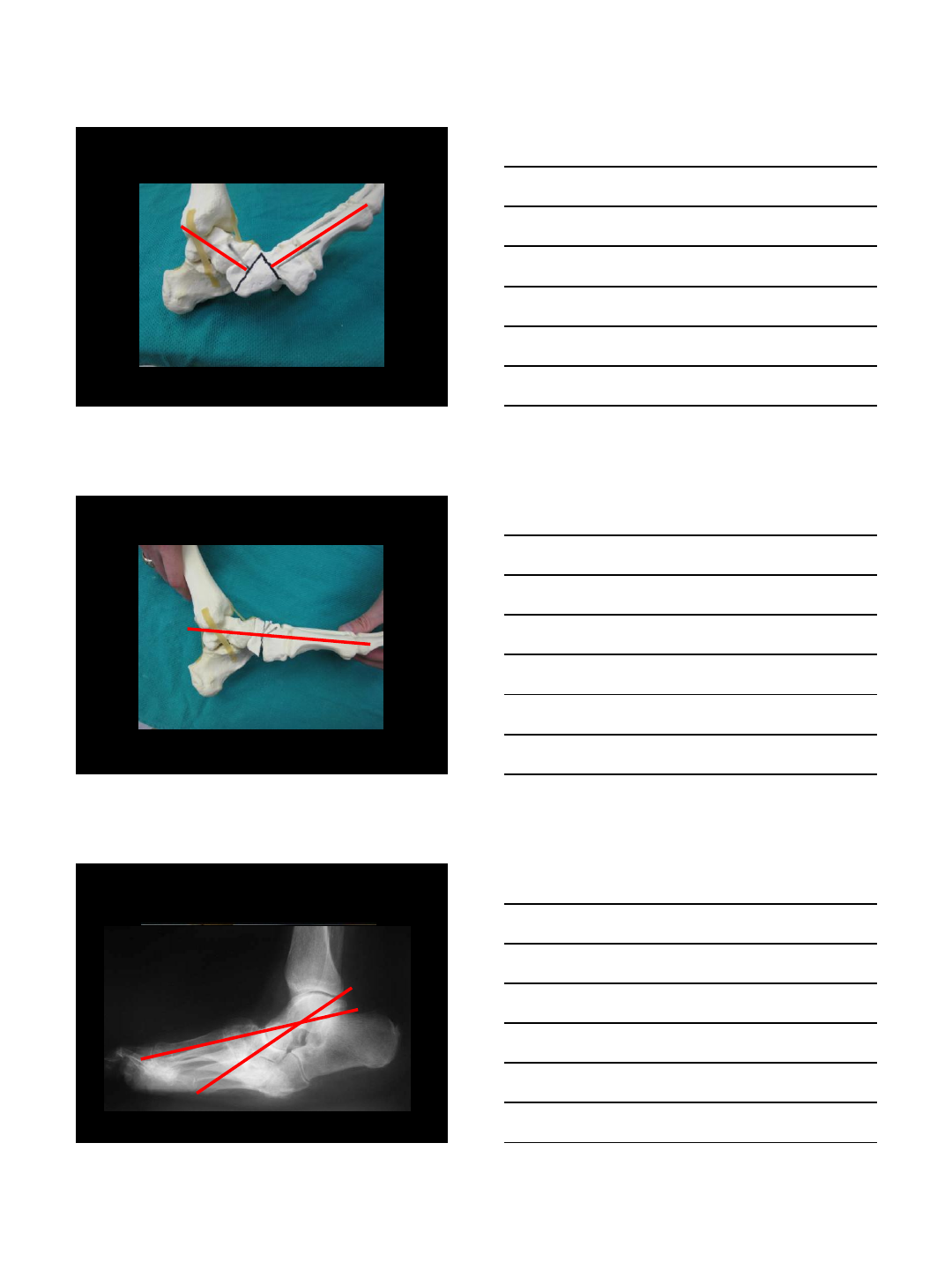
Reduced Mortise
7/14/2014
5
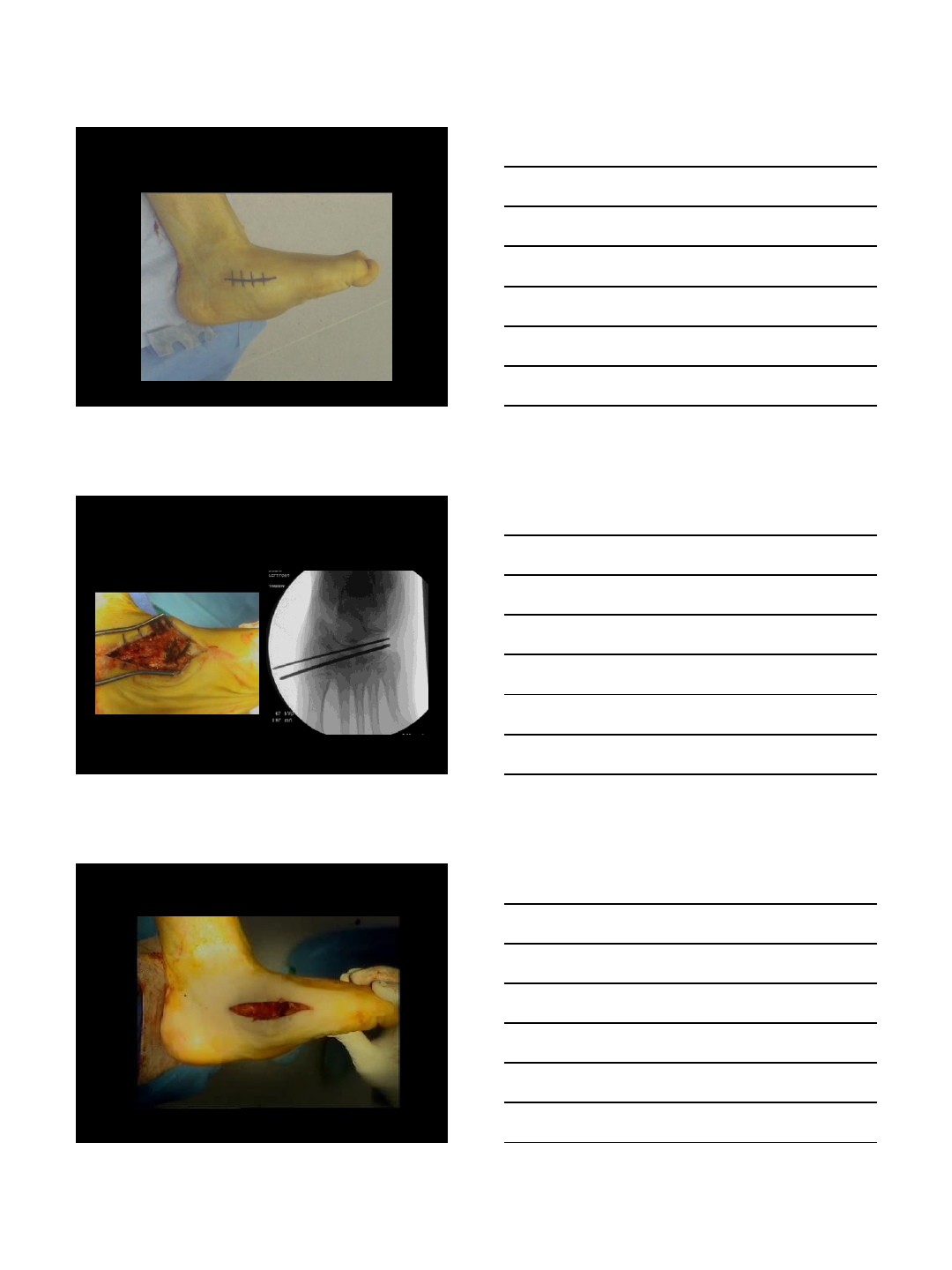
TTC Intramedullary Rod
•Load-sharing device (vs plate/screw
fixation)
•Bridge ankle and ST joints
•Percutaneous insertion
•Soft-tissue friendly
•Low metal/hardware exposure
(intraosseous)
•Frame can be added if necessary
Midfoot Charcot
7/14/2014
6
Technique
Closing-wedge osteotomy
Technique
Remove wedge and close
Low Risk Charcot
-32°
7/14/2014
7
Surgical Approach
Surgical Approach
Video
7/14/2014
8
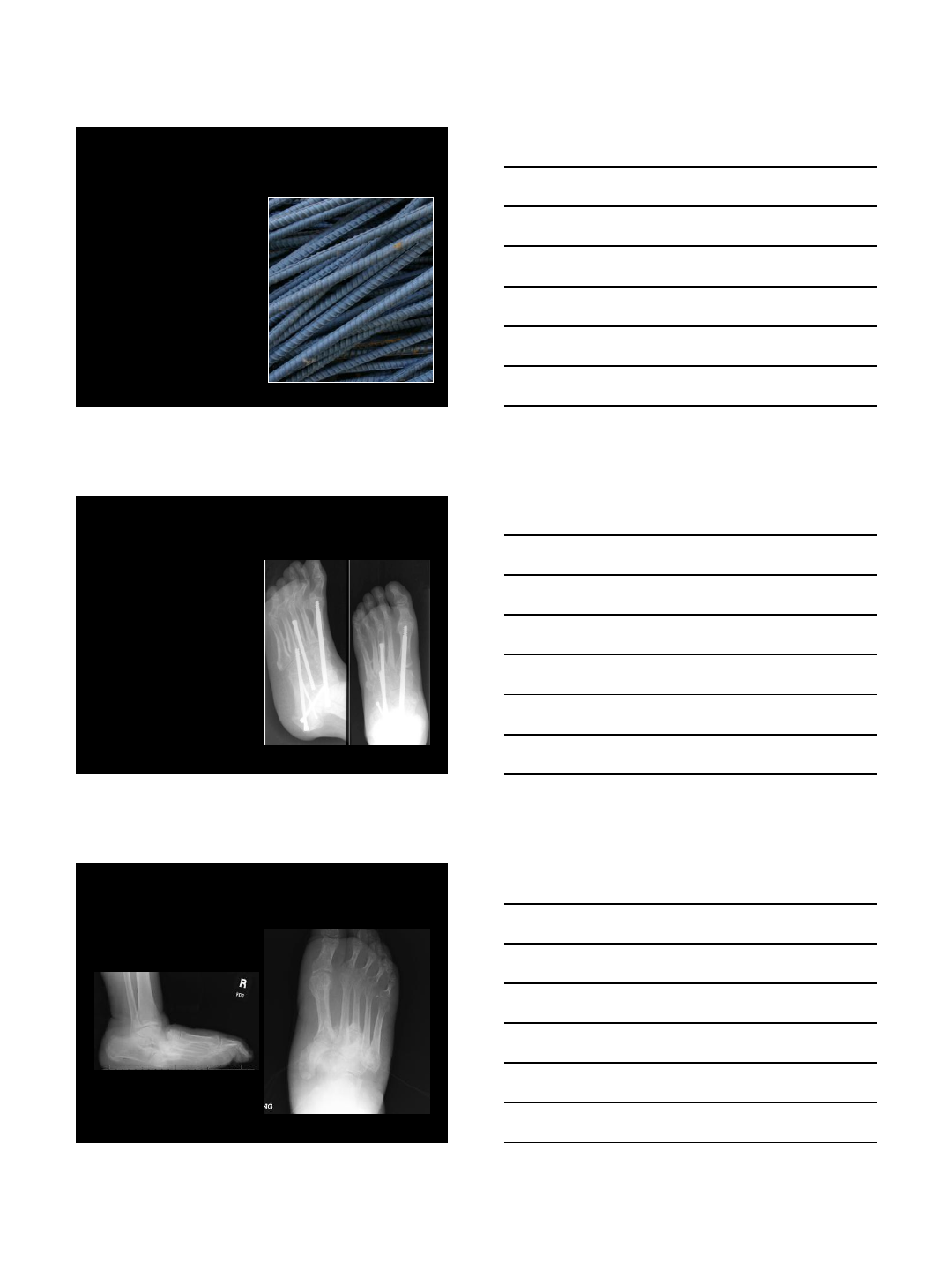
Internal Fixation
How Much Fixation?
Charcot-Indicated Plates
7/14/2014
9
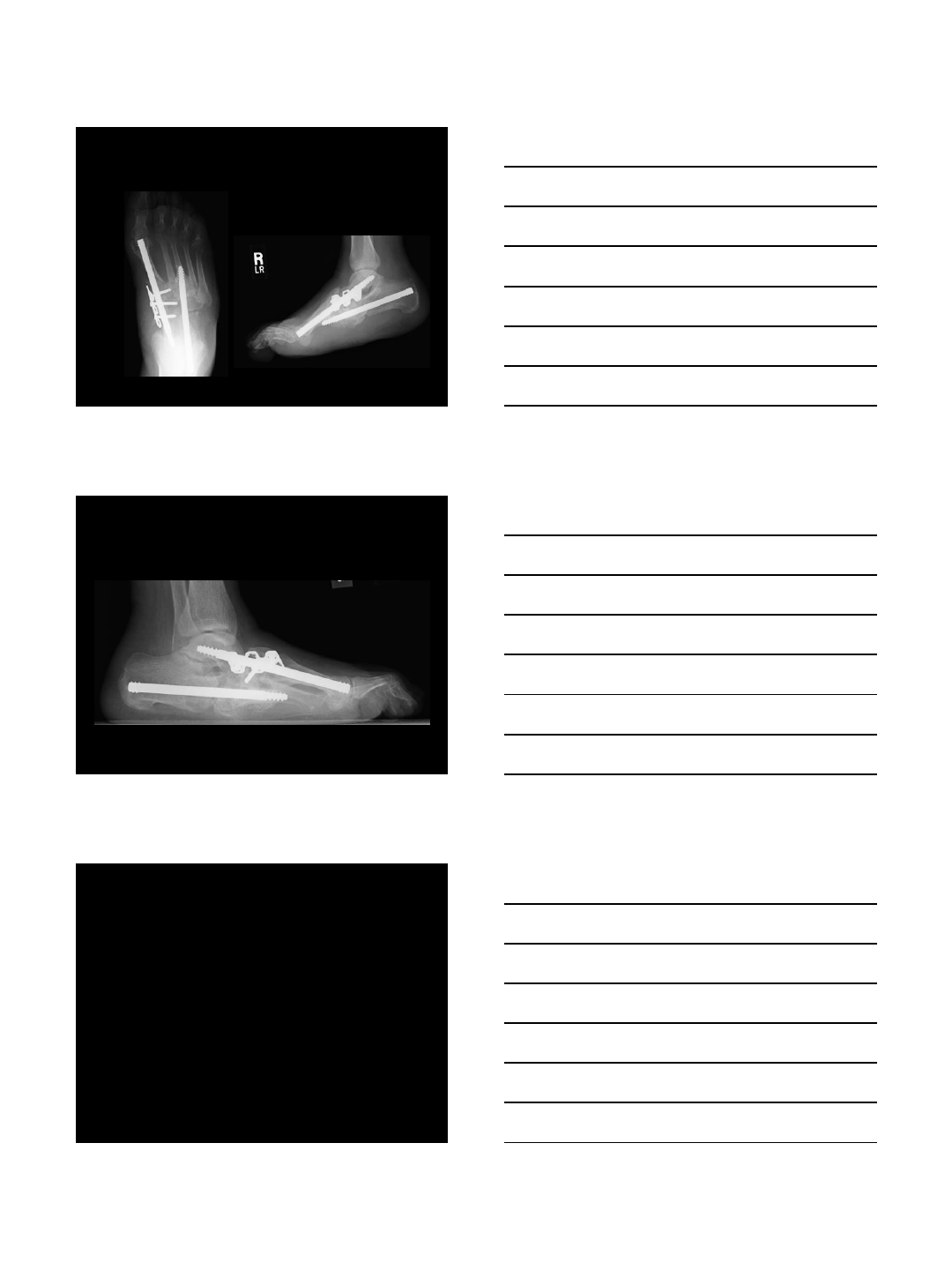
What About Beaming?
•Relatively new
technique for
Charcot (1997?)
•Similar to rebar in
construction
•Concrete has very
poor tensile
properties
•Rebar + concrete:
magnitudes
stronger
What is Beaming?
•Intraosseous
fixation bridging
one or multiple
joints
•Screw, rod , or bolt
•Most commonly
used in the medial
column
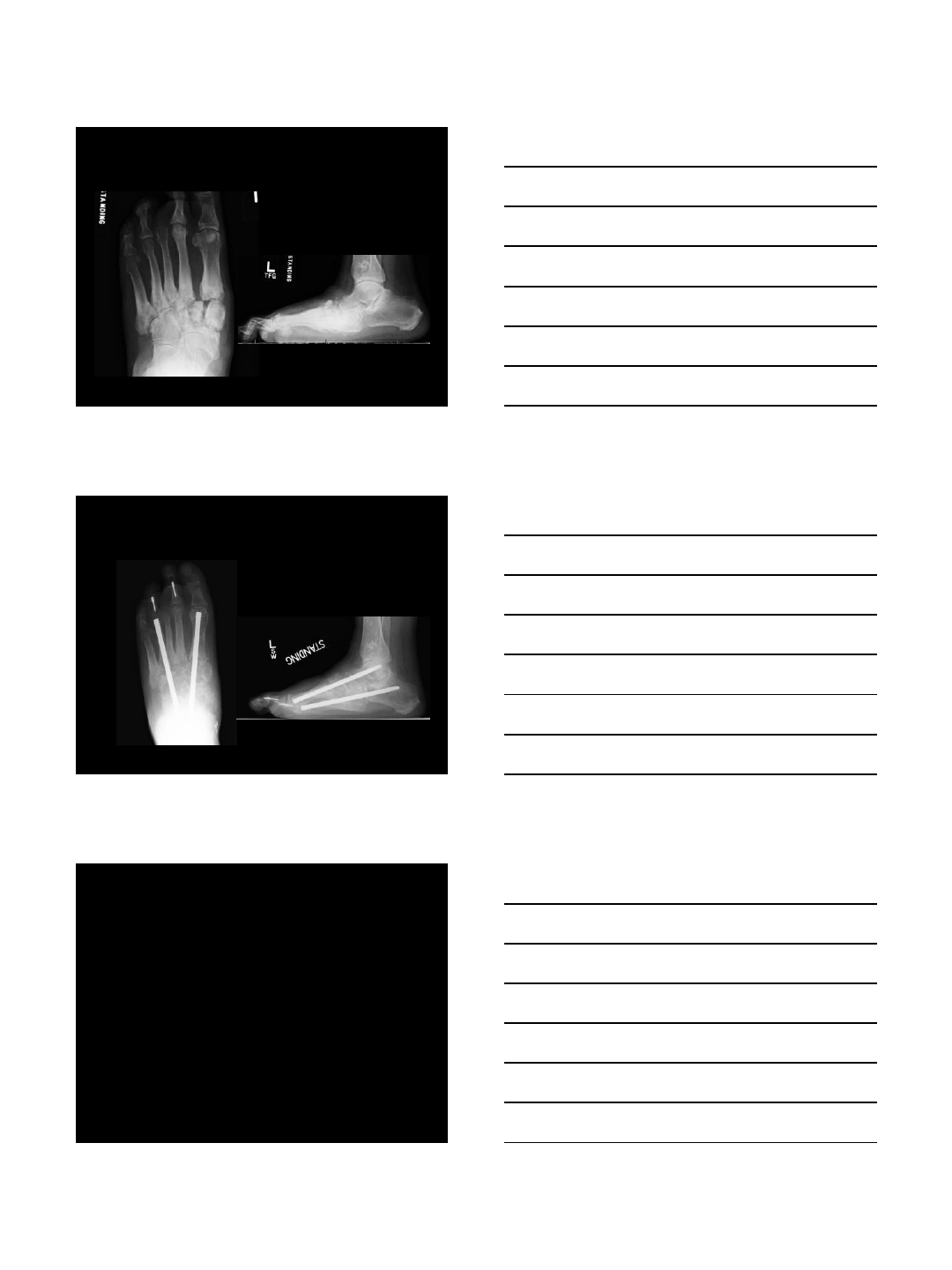
62 yo Recurrent Ulceration
7/14/2014
10
62 yo Recurrent Ulceration
6 Months Postop
My Technique
•Evolving…
•6.5 mm solid bolt stainless steel
system
•Retrograde 1st ray/talus bolt
•Retrograde lateral column bolt
•Rarely augment with plate fixation
7/14/2014
11
55 yo Painful Charcot
9 Months Postop
Caveats
•TAL critical
•Prepare all joints that the bolts cross
•Bone graft defects (typically allograft)
•NWB in TCC for 8-10 weeks
•Transition to extra-depth shoe/insert
7/14/2014
12
Results
Charlotte experience
•6 patients
•Minimum 6 month f/u
•All clinically/radiographically healed
•No deep infections
•One required plantar lateral
exostectomy 4 months postop
Conclusions
•Consider internal fixation for unstable
ankle and mid/hindfoot Charcot in
absence of deep infection
•Adjunctive external fixation should be
considered
•Beaming very promising for midfoot –
need for greater variety of sizes
Thank You!
1
Charcot Foot Treated with a Static
Circular External Fixator
Michael S. Pinzur, MD
Professor of Orthopaedic Surgery
Loyola University health System
Disclosure
Consultant
Small Bone Innovations
Wright Medical
Lecturer
Smith-Nephew
Stryker
Favorable Outcome
Ulcer and Infection-Free
Able to ambulate independently with
commercially-available therapeutic shoes
custom accommodative foot orthoses
2
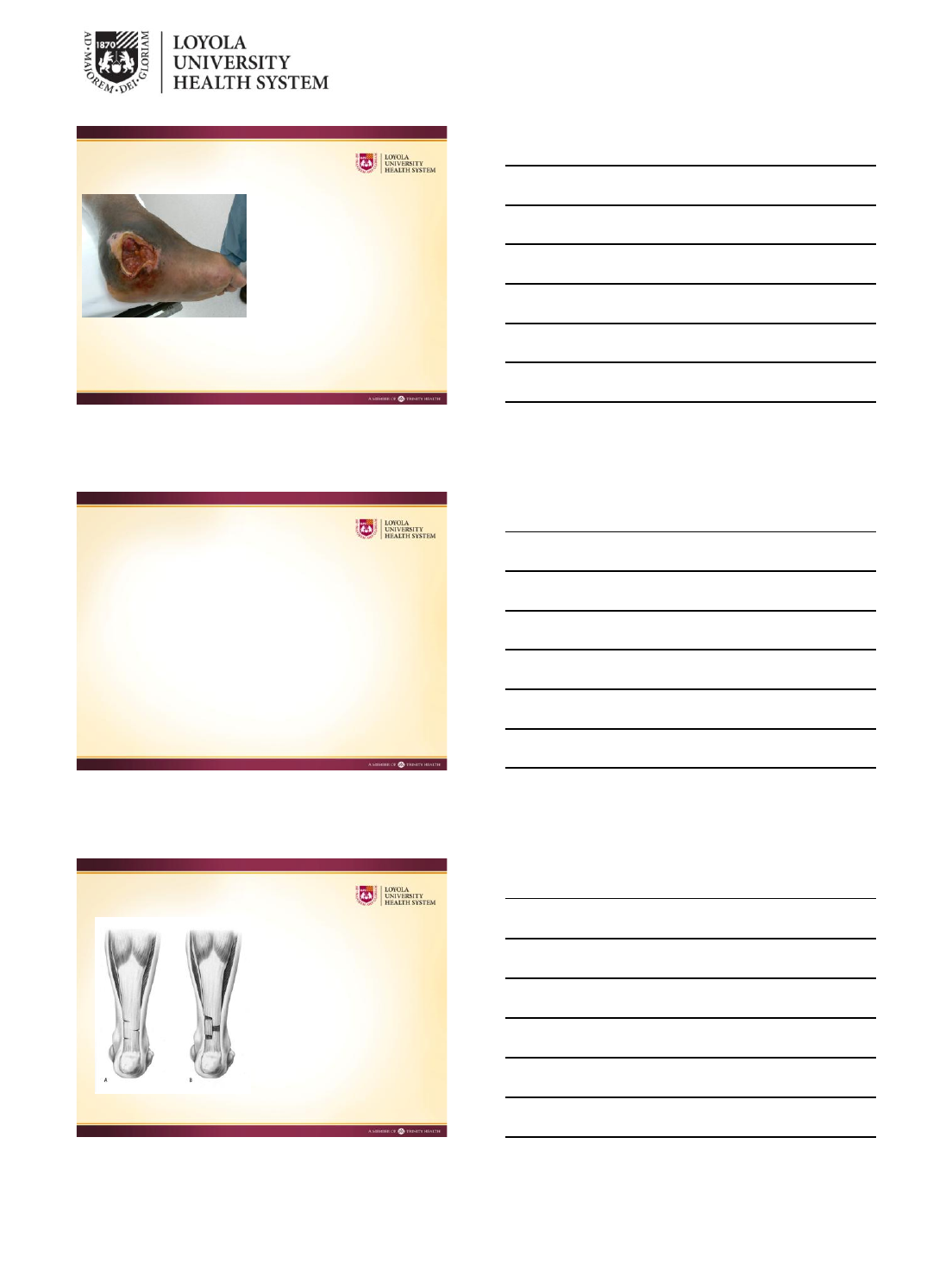
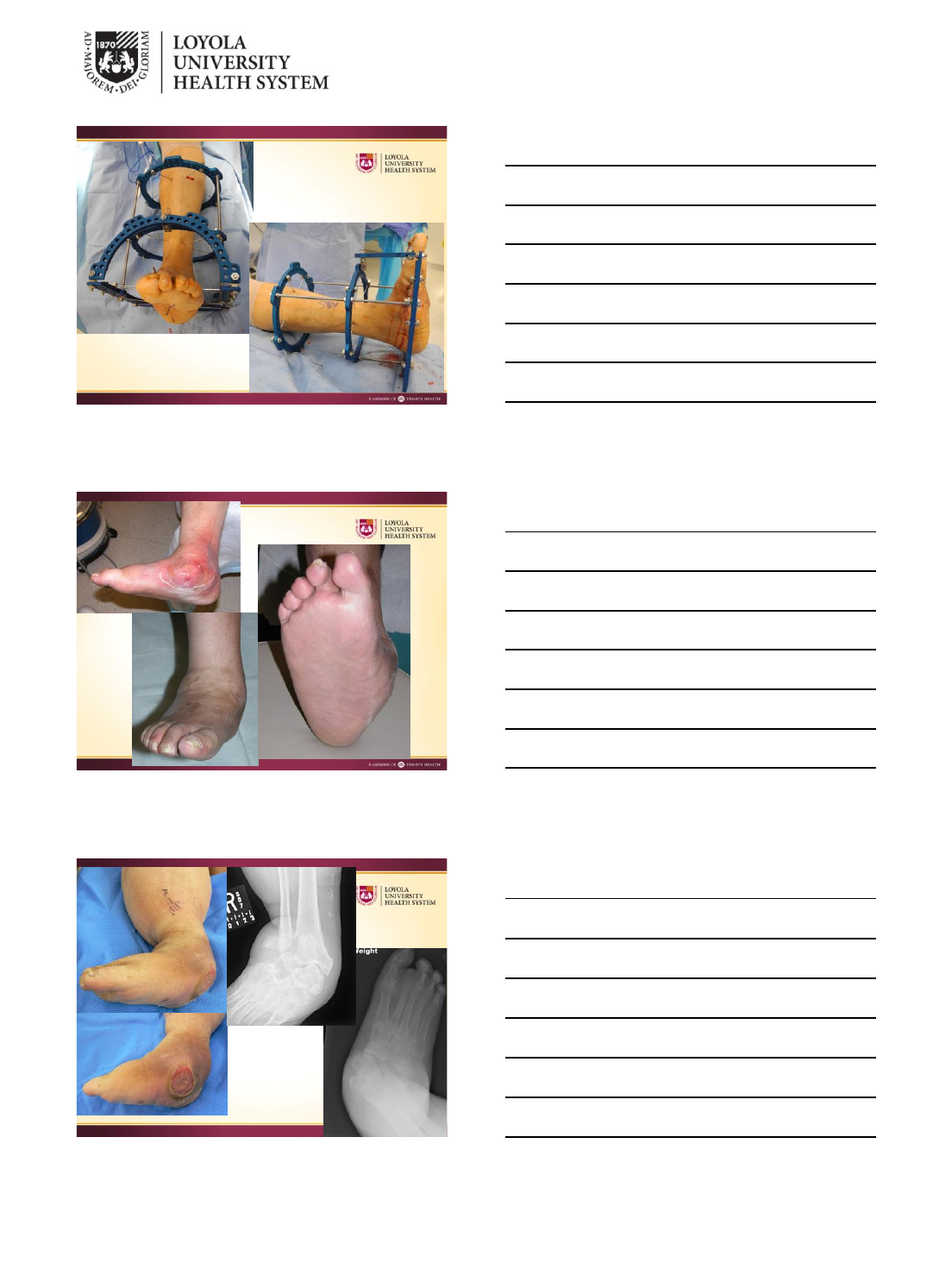
Who needs surgery?
1. Non-plantigrade foot
with overlying ulcer and
osteomyelitis
2. Clinically and
radiographically non-
plantigrade foot
3. Painful neuropathic
non-union
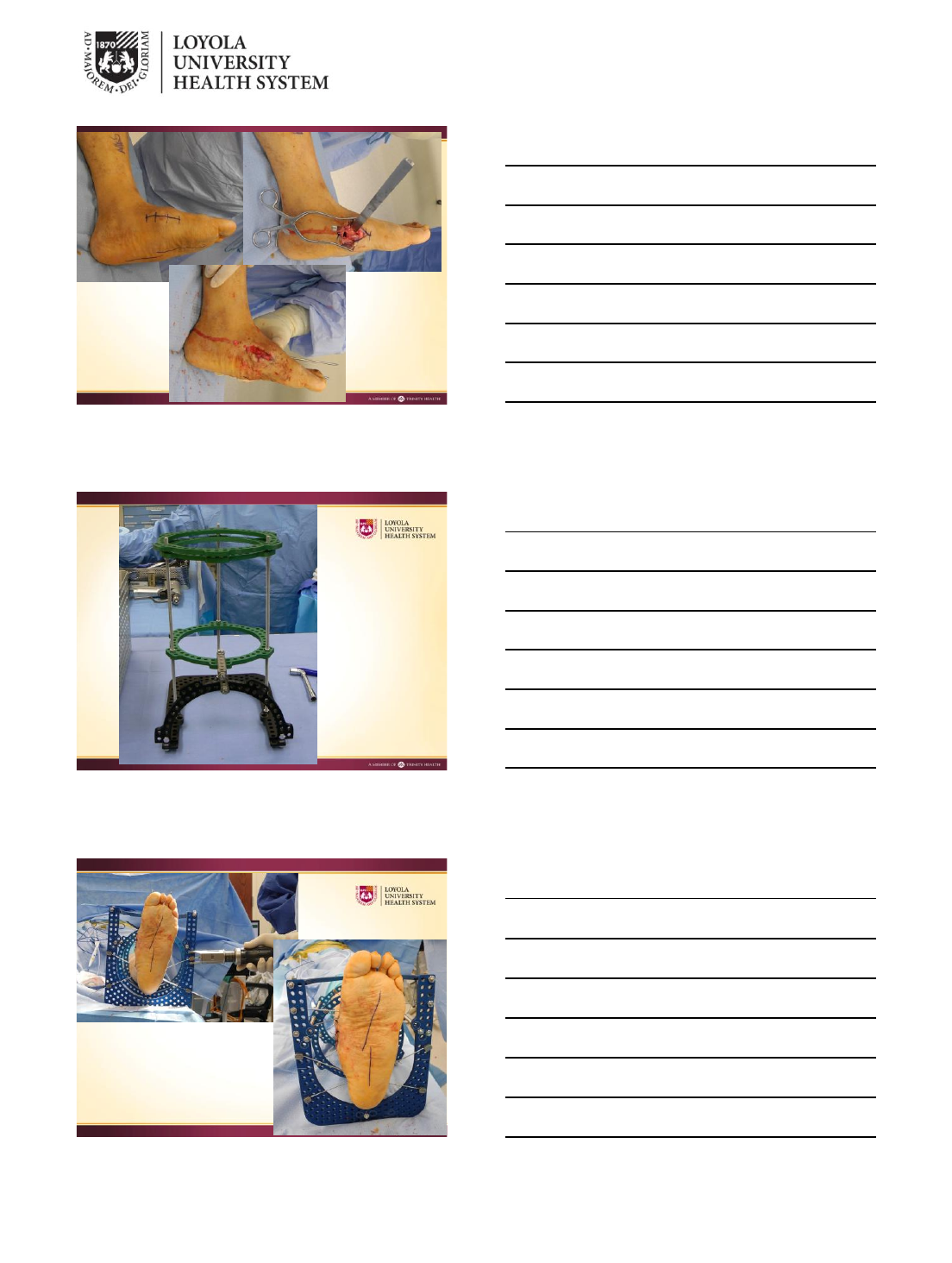
Principles of Static Ring
Able to OBTAIN correction of deformity
Obstacles to MAINTAIN correction:
vitamin D deficient / poor quality bone
poor host
Motor Balancing
Gastrocnemius muscle
lengthening
or
Tendon Achilles
lengthening
3
4
5
6

7
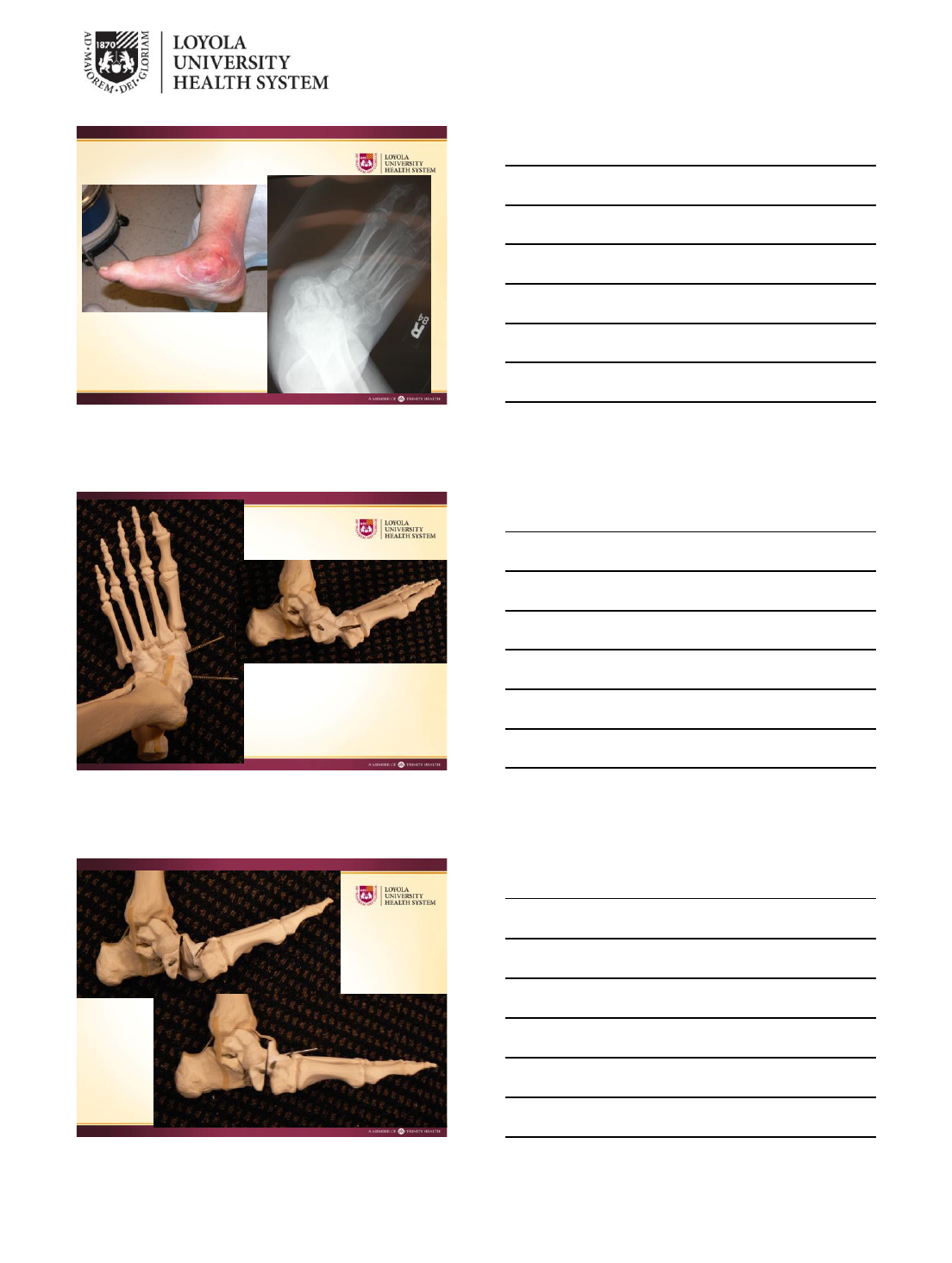
Static Ring Fixation
Obtain correction at
surgery
Difficulty with
maintaining
correction
7/12/2014
1
Richard Gellman, MD
Summit Orthopaedics
Portland, OR
Dynamic = gradual deformity correction
using Ilizarov multiplanar external fixation
Most corrections with Taylor Spatial Struts
Simple lengthenings or distraction with threaded
rods
Some ankle equinus corrections in lighter patients
with universal hinges
Create a stable, plantigrade,
ulcer-free foot below an aligned
leg
7/12/2014
2
Unbraceable, unstable
deformity
+ Recurrent ulceration
Non ambulatory patients
wanting alternative to
amputation
Patients need to
understand that this is
limb salvage surgery.
Risk of amputation or
need for future
reconstructions 20%
Deformities that can’t be acutely corrected
Too severe
▪ plantigrade foot not obtainable despite heroic attempts
at soft tissue release, bone shortening,
Poor soft tissue, unsafe to make requisite surgical
dissections
Acute correction would lead to unwanted
arthrodesis such as a pantalar or TCC
Safe to operate on contracted or previously
operated soft tissue
Maintains bone length, may limit need for
arthrodesis
Lower deep infection rate
Ability to allow limited weight bearing due to
strength of frames
7/12/2014
3
Best to have applied quite a few static
Holding Frames before attempting dynamic
frames
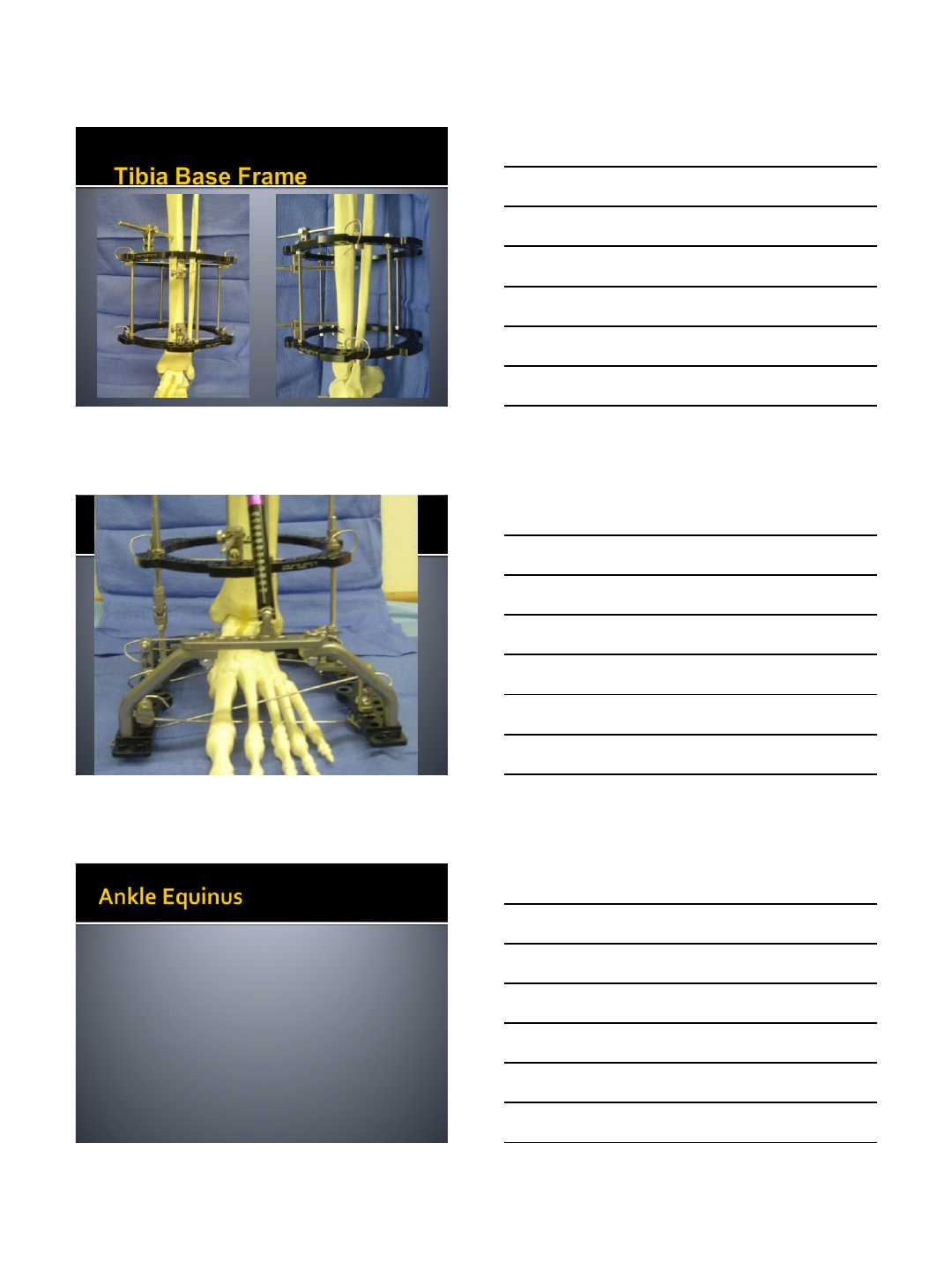
Ankle
Combined Foot Deformity = hindfoot and
midfoot deformities
Midfoot
Examples: ankle equinus contracture,
neuropathic ankle fx/dx, AVN talus, distal
tibia collapse
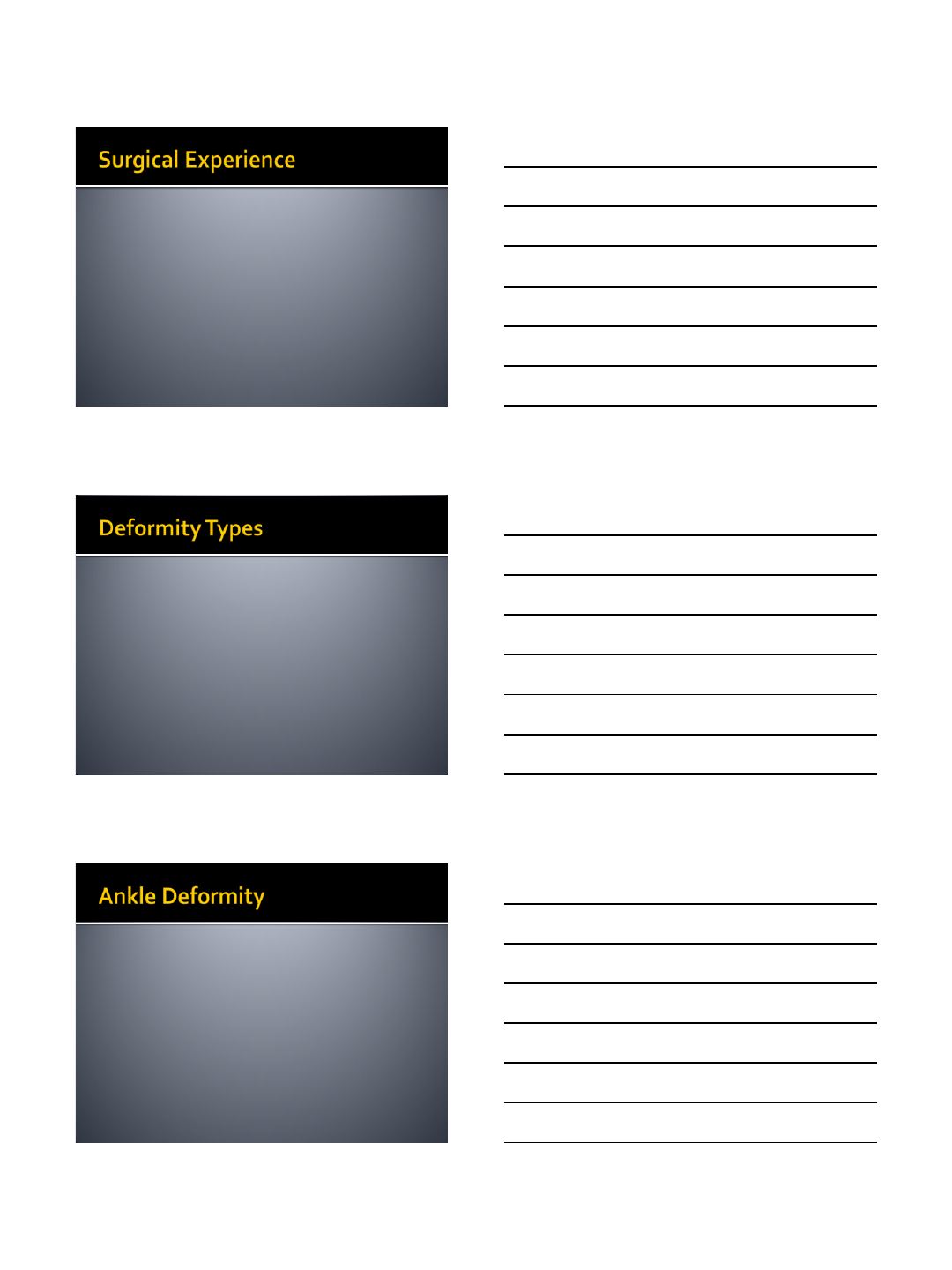
Apply standard 2 ring tibial base frame, one
long foot ring and connect lower tibial ring to
foot ring with Taylor Spatial struts
If deformity at tibiotalar joint, insert a talar
neck wire and attach to foot ring. This focuses
distraction, correction across ankle joint
7/12/2014
4
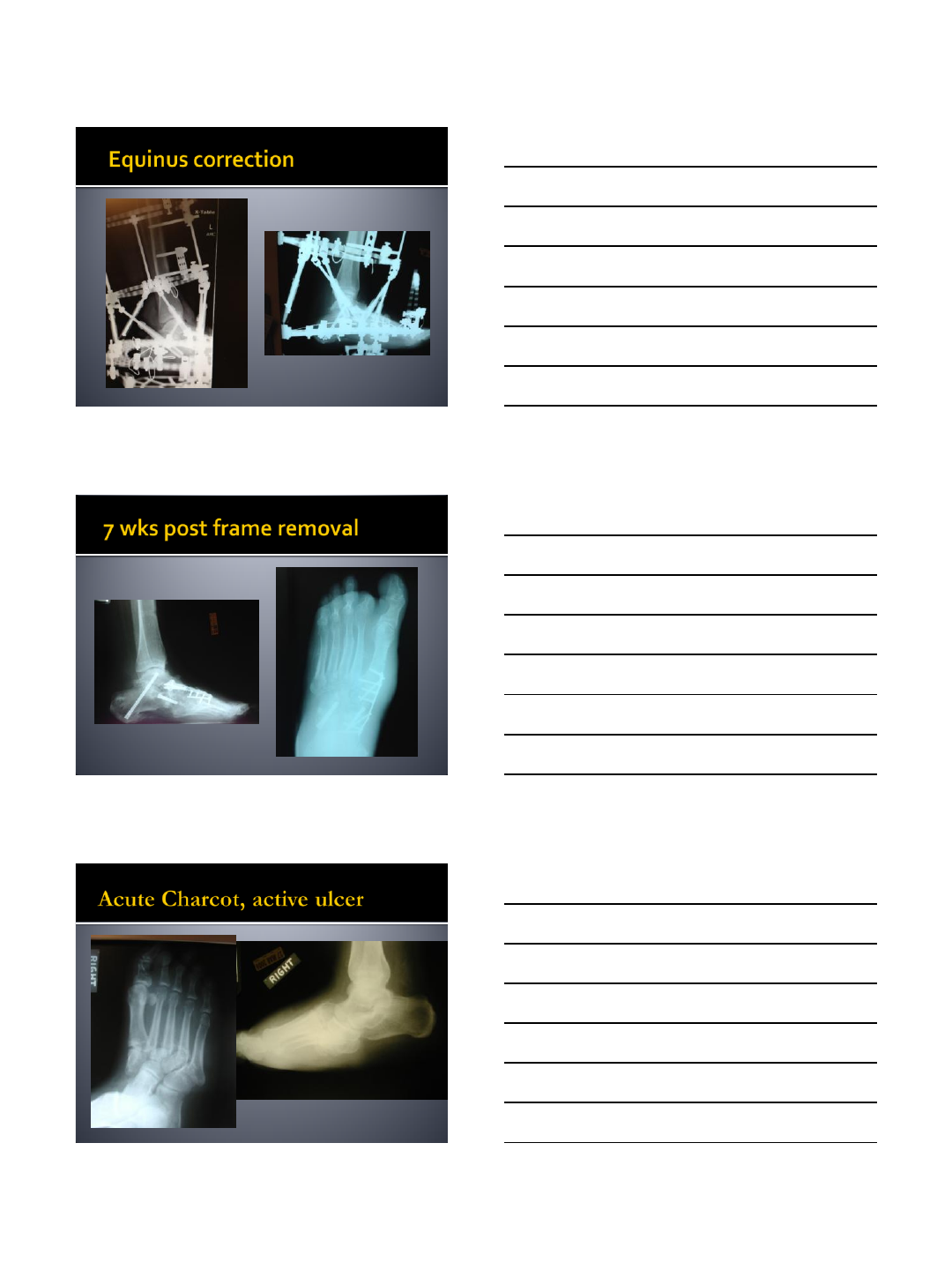
Always perform percutaneous achilles
lengthening or tenotomy first in equinus
corrections
Set up TSF program as apex anterior
deformity with origin at center of talar dome
Hold in corrected position of at least 10
degrees dorsiflexion for 6 weeks to prevent
recurrence
7/12/2014
5
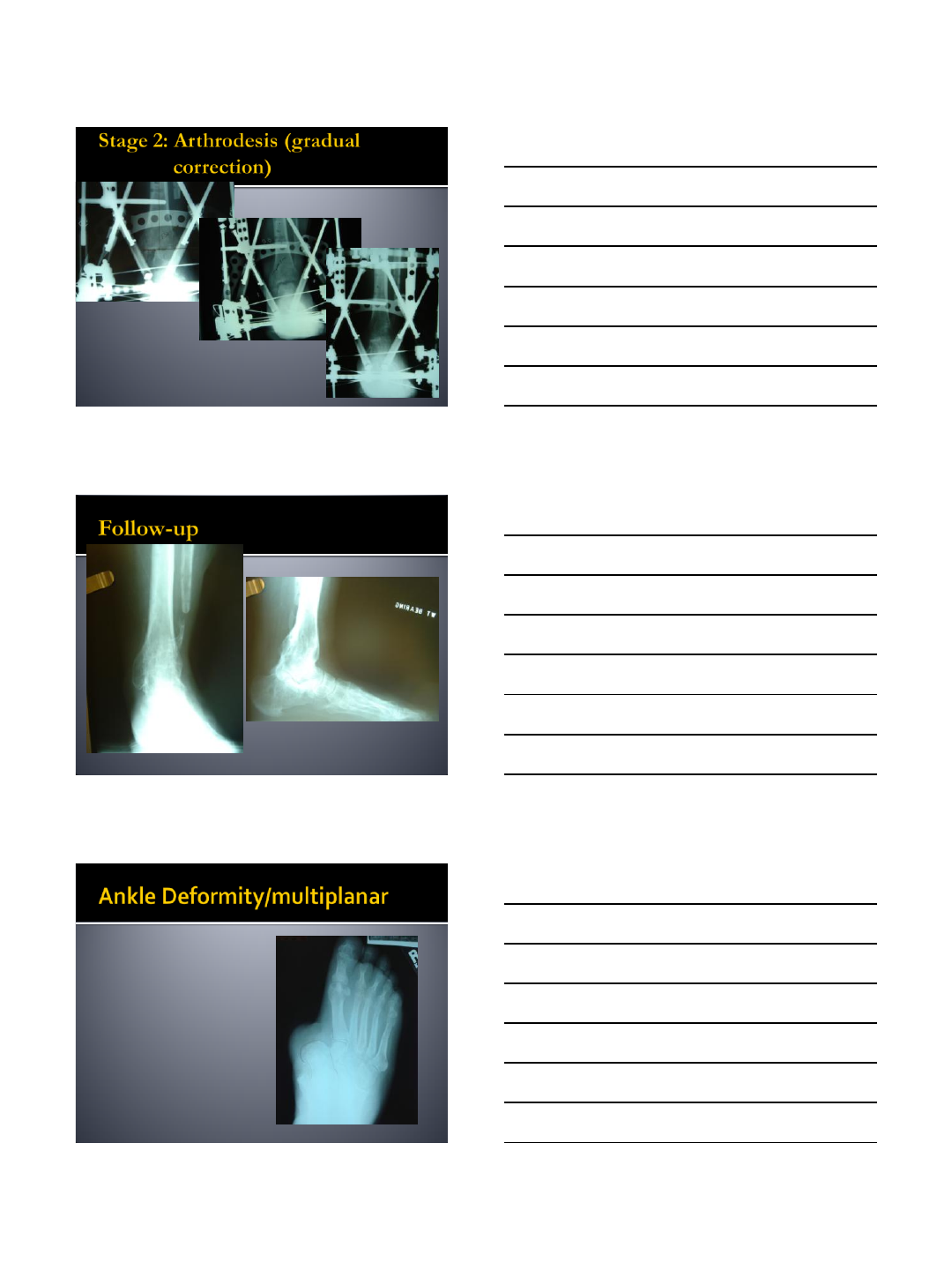
Ideal for contracted longstanding
ankle/hindfoot dislocations
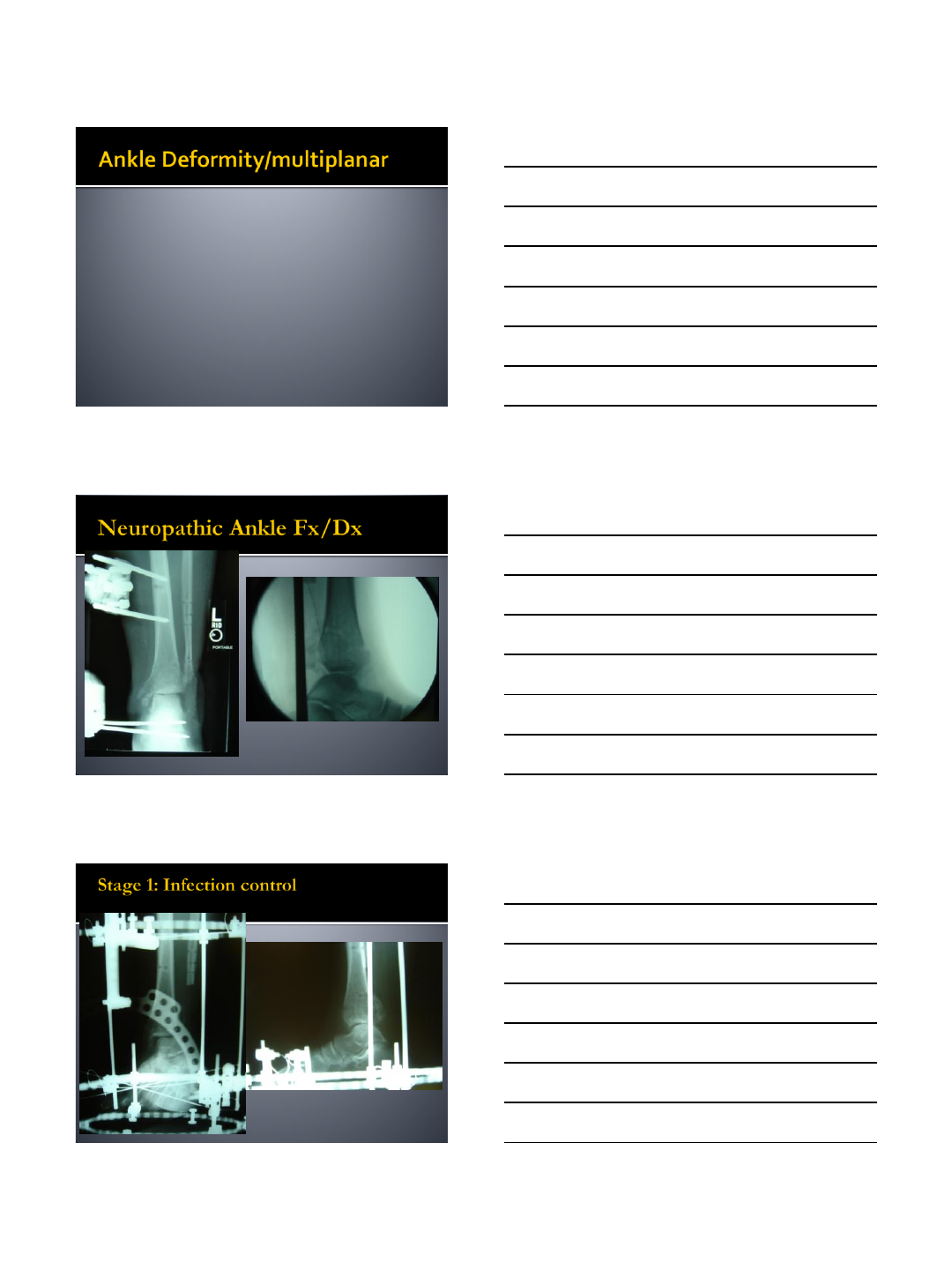
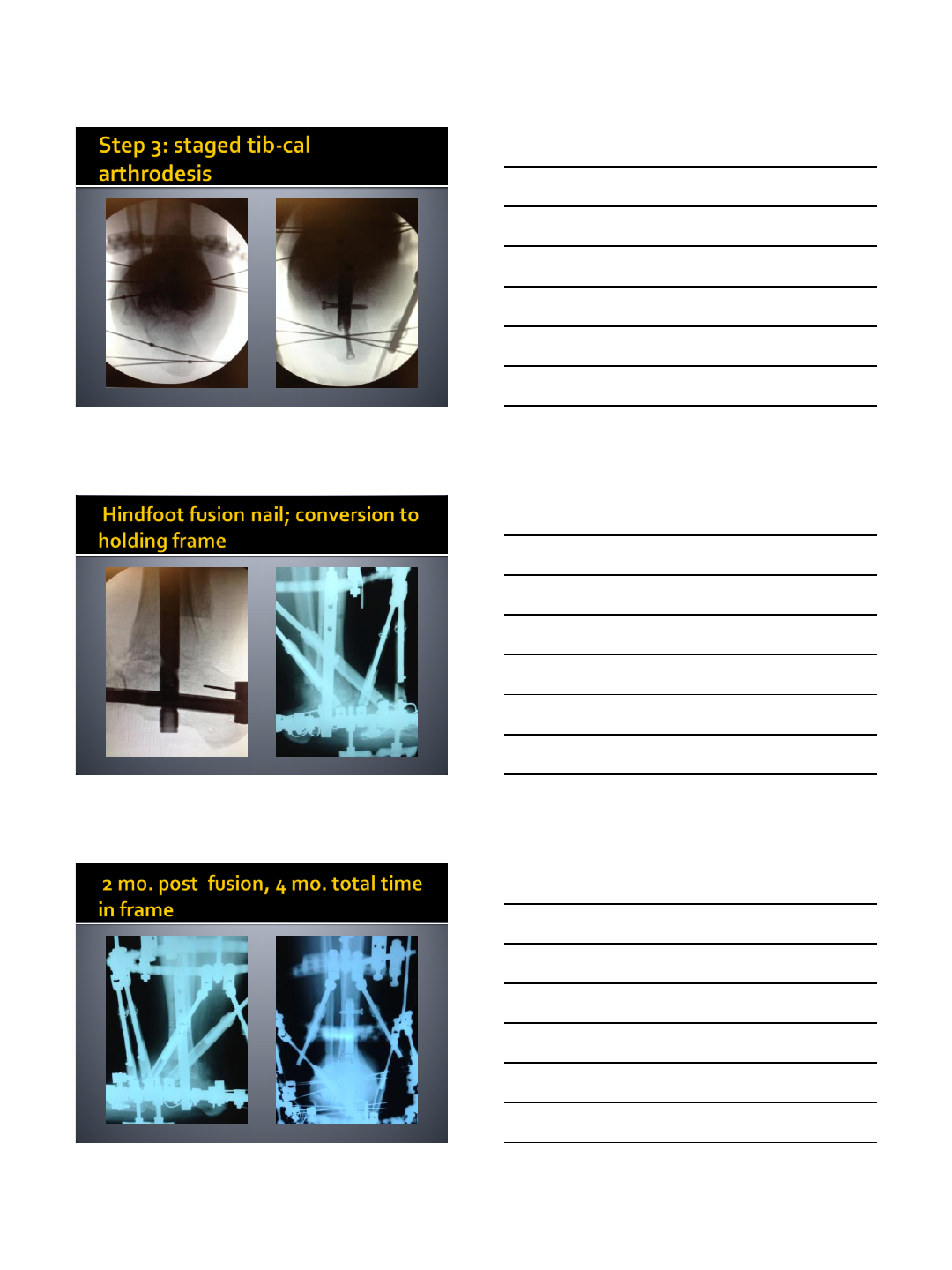
For a more rapid correction, especially with
infected cases, I perform talectomy,
antibiotic bead placement, deformity
correction
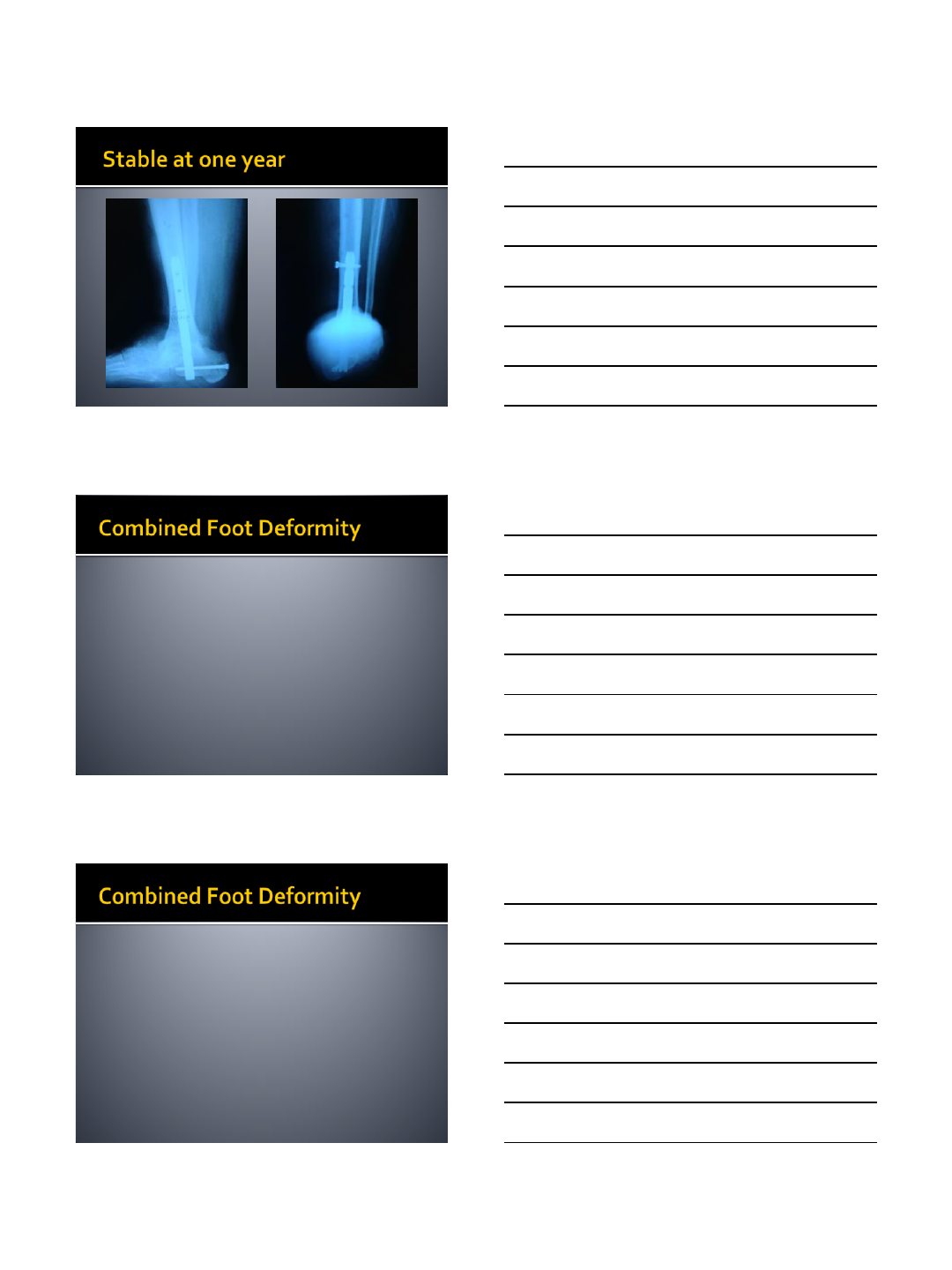
Stage Tibia-Calcaneal fusion in 4-6 weeks
Frames can be set up to allow insertion of 16
cm hindfoot fusion nails
7/12/2014
6
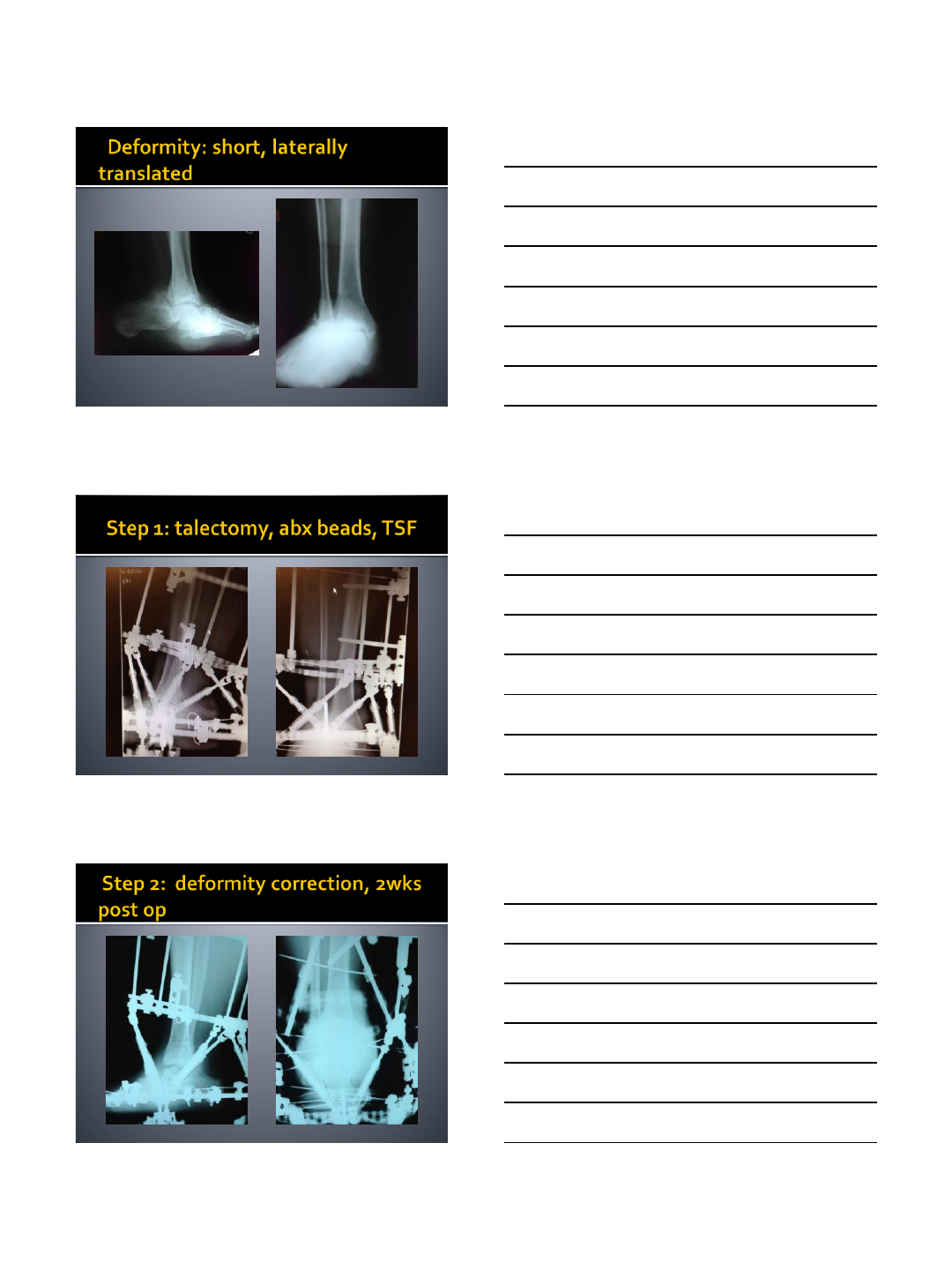
59 yom DM
Morbid obesity
Longstanding lateral
peritalar dislocation
(PTTD gone wild)
Active MSSA infection
over ulcer breakdown
on talar head, I&D site
by his podiatrist
Not able to walk
7/12/2014
7
7/12/2014
8
7/12/2014
9
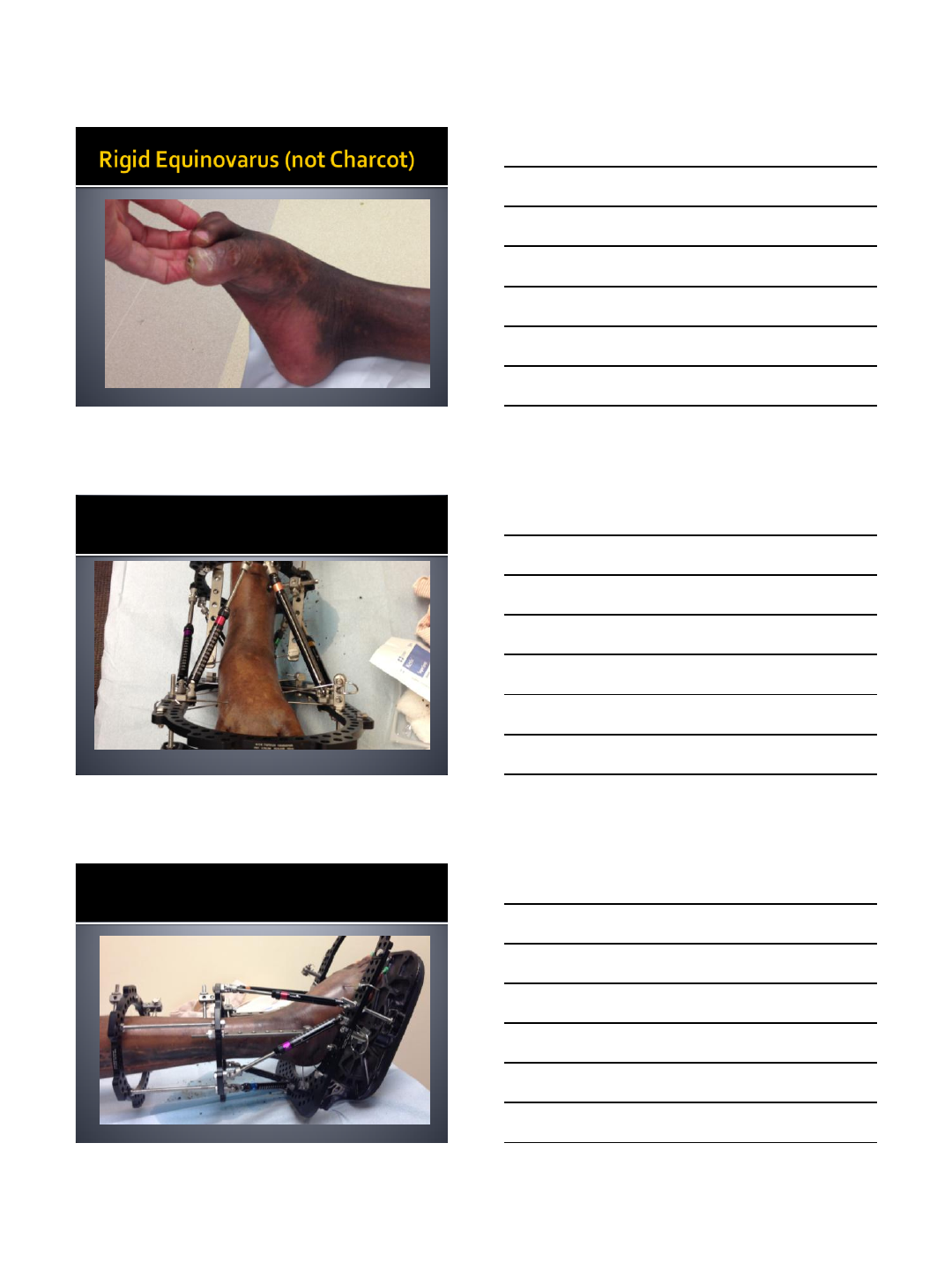
Severe valgus peritalar dislocation, rigid
equinovarus foot
Hindfoot and midfoot both in varus or valgus
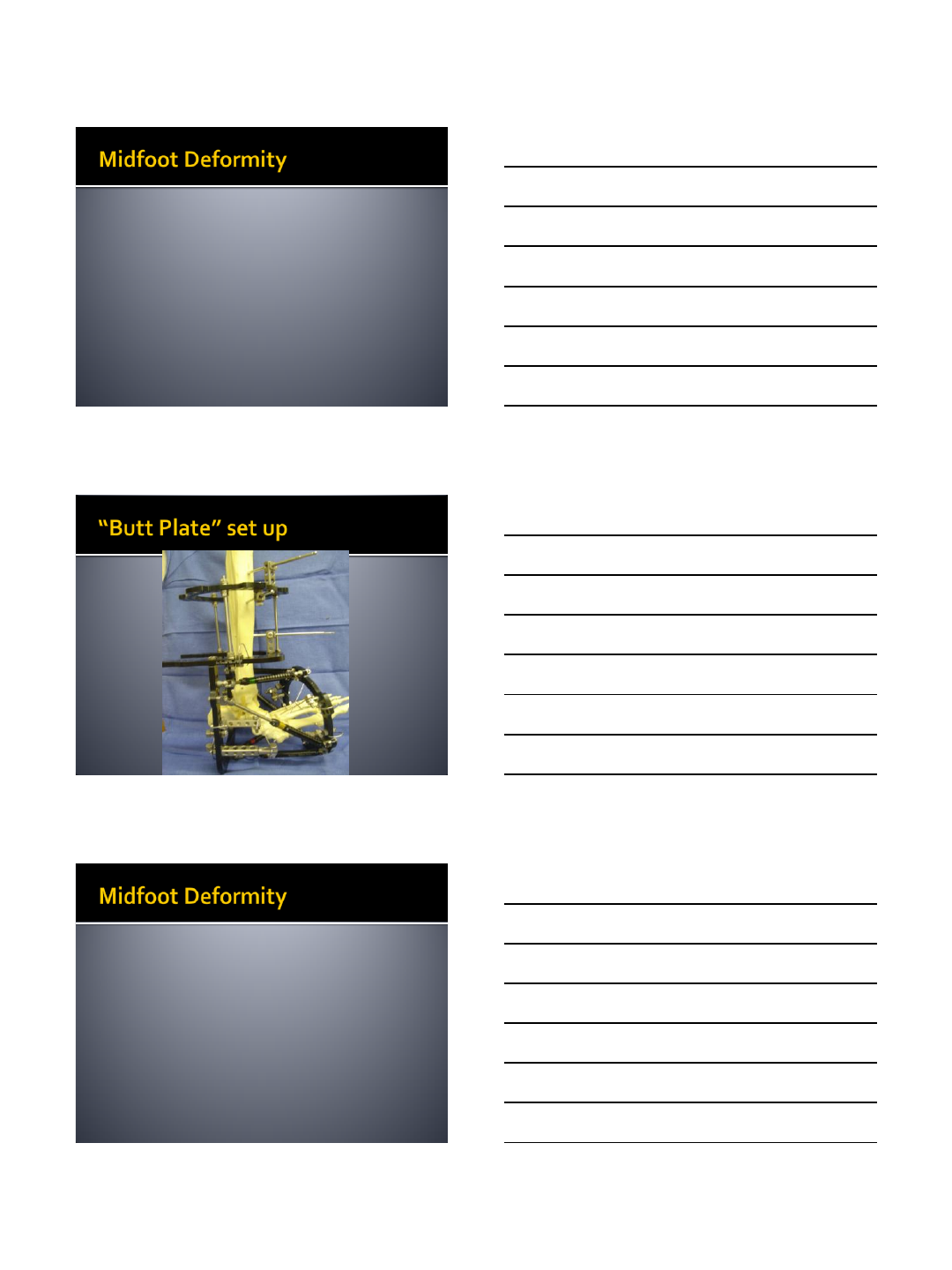
Set up like Ankle equinus frame except talar
neck wire attaches to distal tibia by long
hinges. This stabilizes the ankle joint (talus in
the mortise) so that correction occurs
through the subtalar, talonavicular, calcaneal-
cuboid joint complex
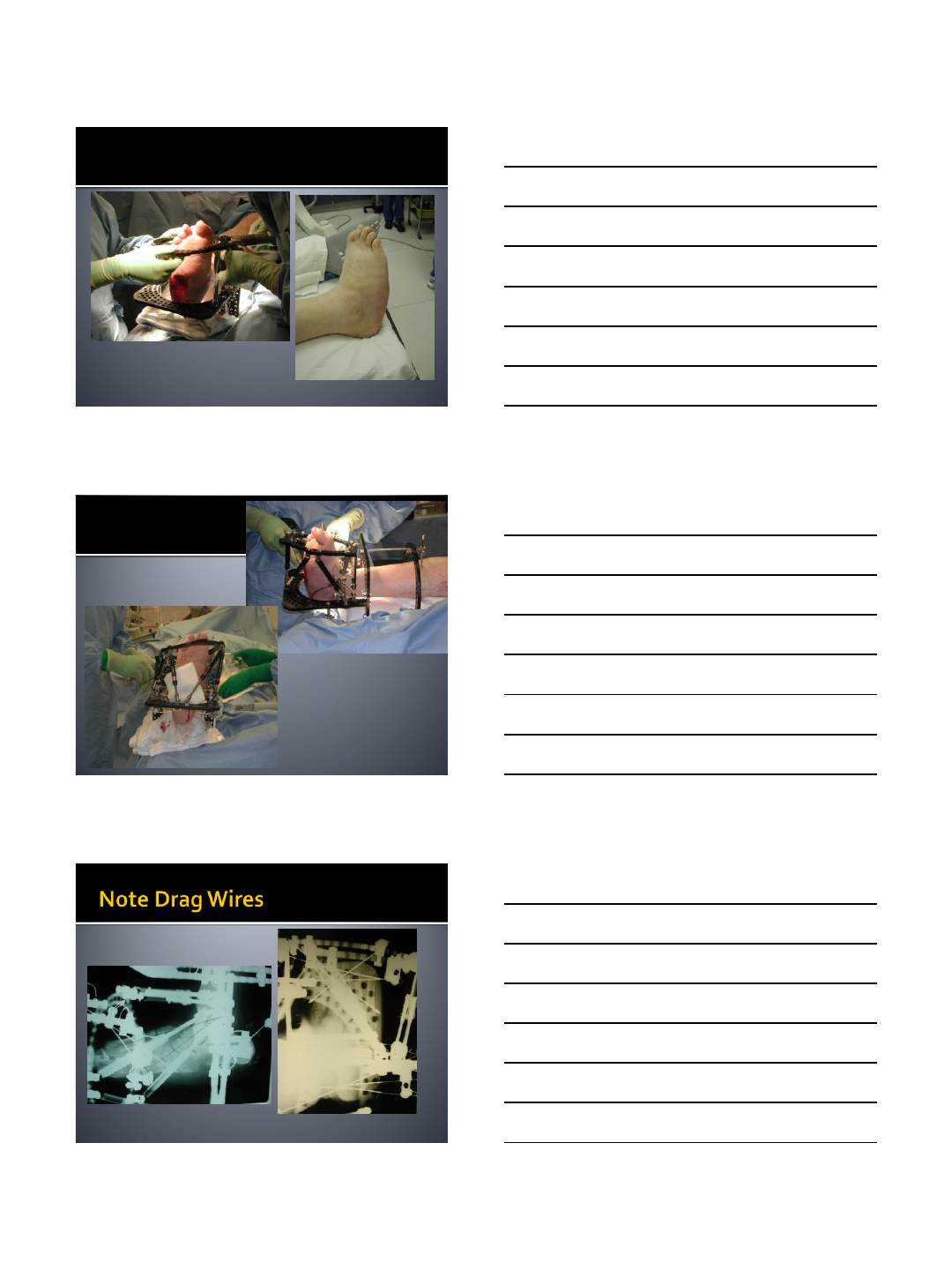
Forefoot deformity of aDduction or
aBduction can be acutely corrected with
“drag” olive wires
May need to pin toes
In severe deformities, may need to prevent
weight bearing for first 1-2 weeks until the
sole of the foot is more plantigrade
7/12/2014
10
7/12/2014
11
Apply tibial base frame
Place U-ring along posterior aspect of distal
tibia on lateral view
Attach full ring that encircles the forefoot
Place at least 3 wires into metatarsals for
sufficient strength of fixation
Attach struts after insertion of first forefoot
wire to make strut attachment easier
May need to first distract (lengthen) 10-15
mm in order to disengage midfoot bones
prior to correction of angular or translational
deformity
TSF software pretty good for midfoot
correction
Option to set up as tibia but have forefoot
correlate to proximal tibia
7/12/2014
12
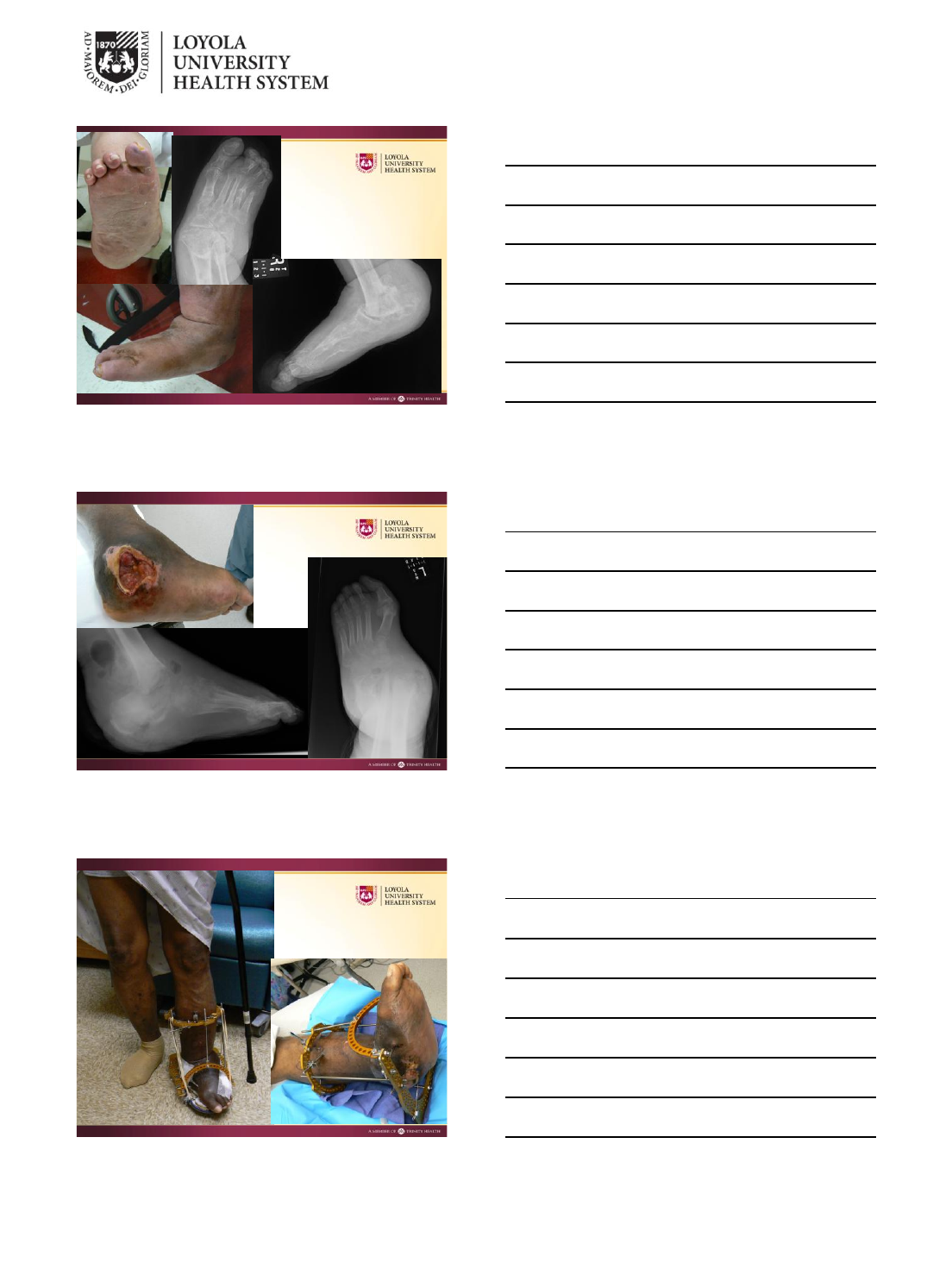
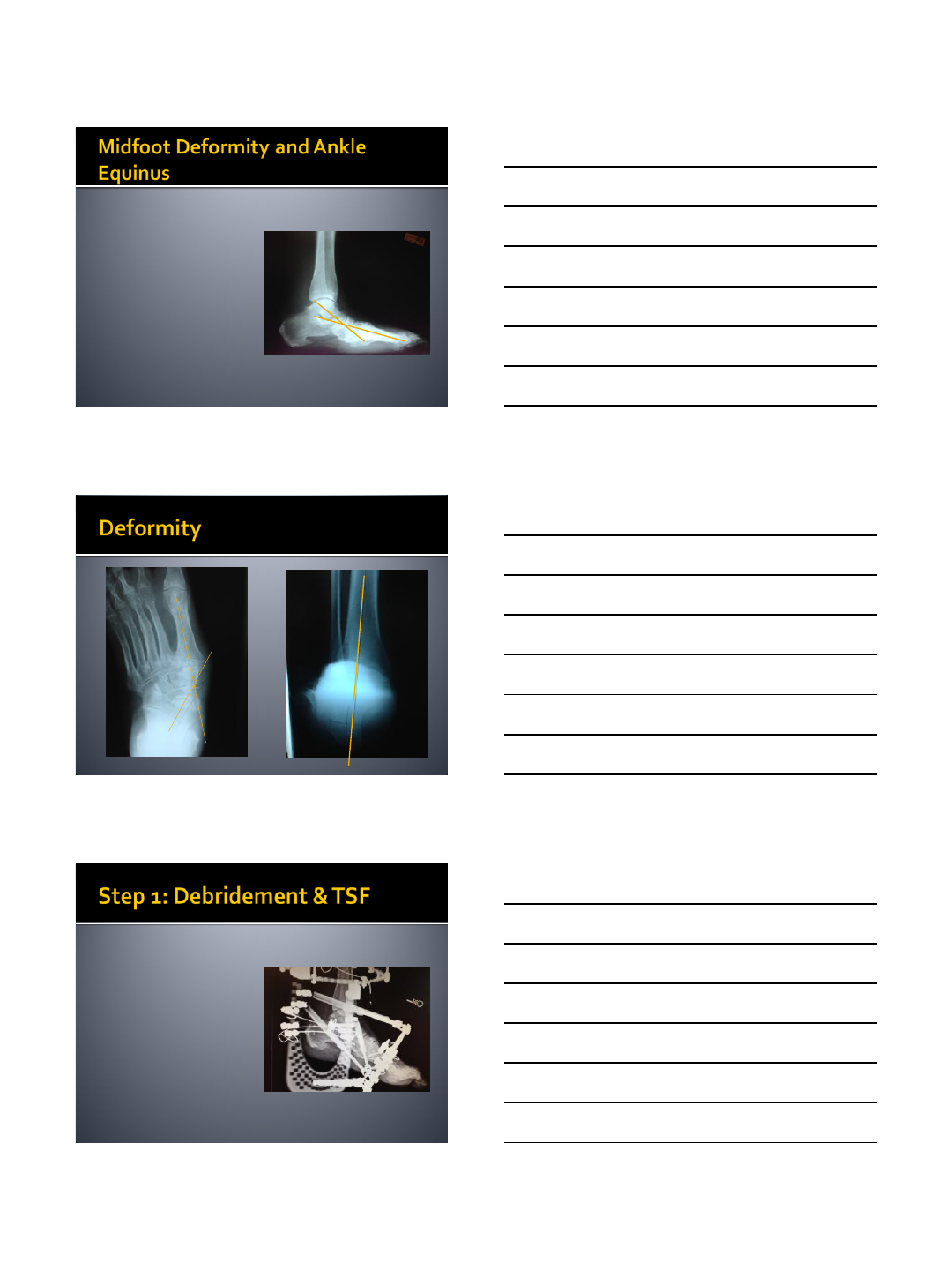
57 yom with DM.
Chronic midfoot
ulceration over 10
years
Failed debridements
and CROW
MR negative for deep
bone involvement
Teaches nursing at
local college
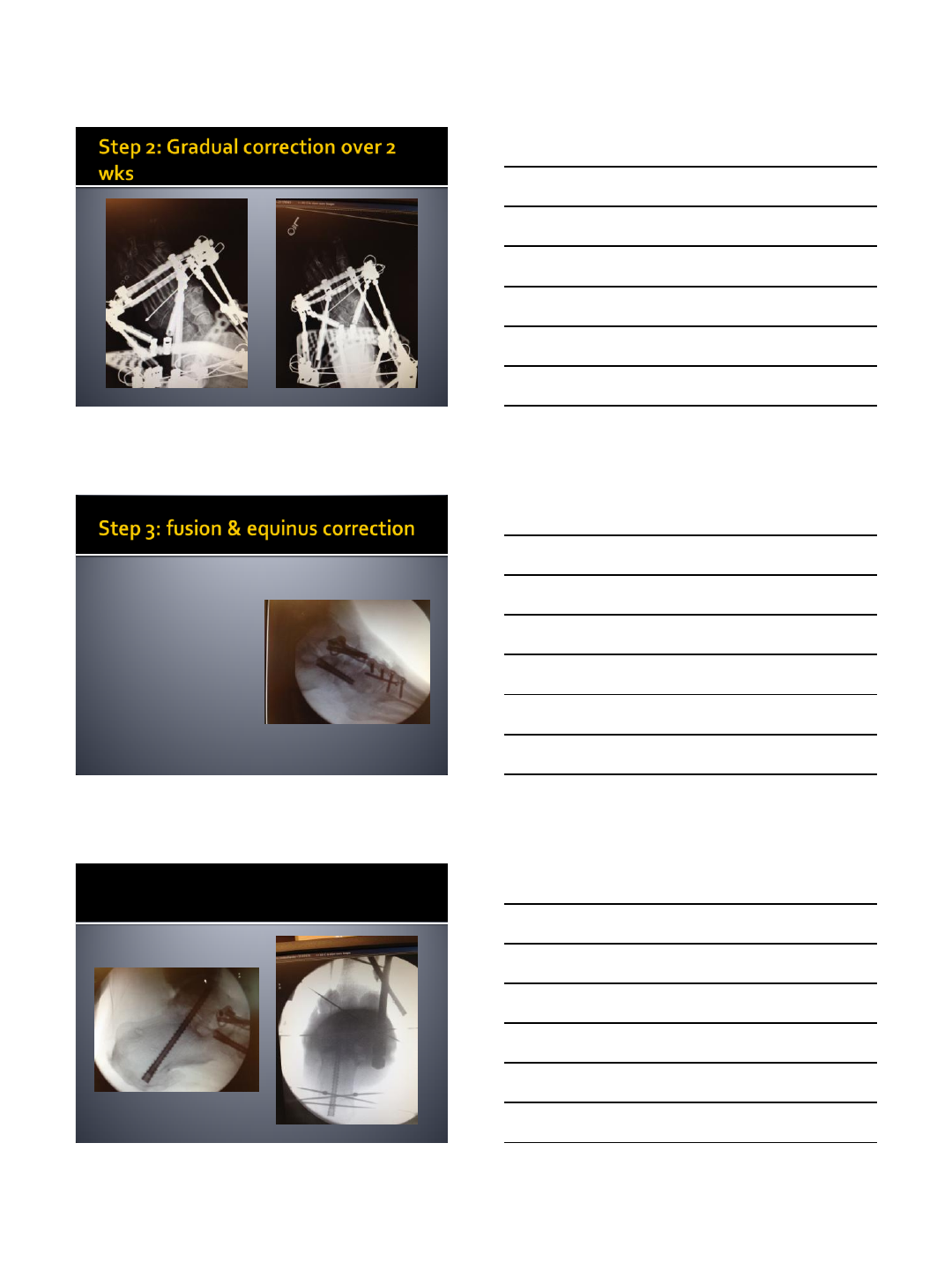
25 degree Talo-1st Met
40 degrees Talo-1st Met
No significant hindfoot malalignment
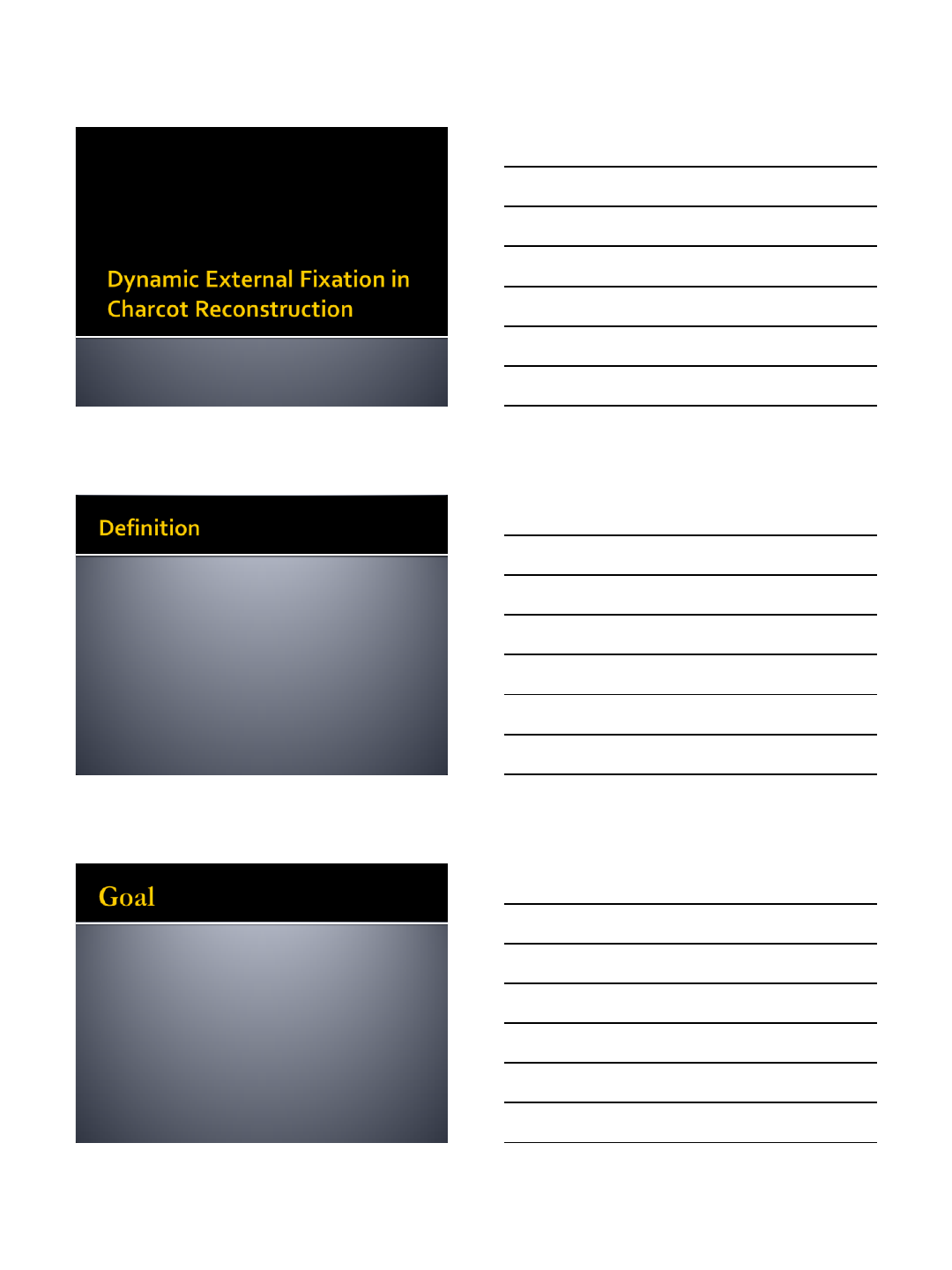
Debridement and
closure of ulcer
Gradual correction of
midfoot rocker bottom
and abduction
contracture with frame
Safer for lateral skin
7/12/2014
13
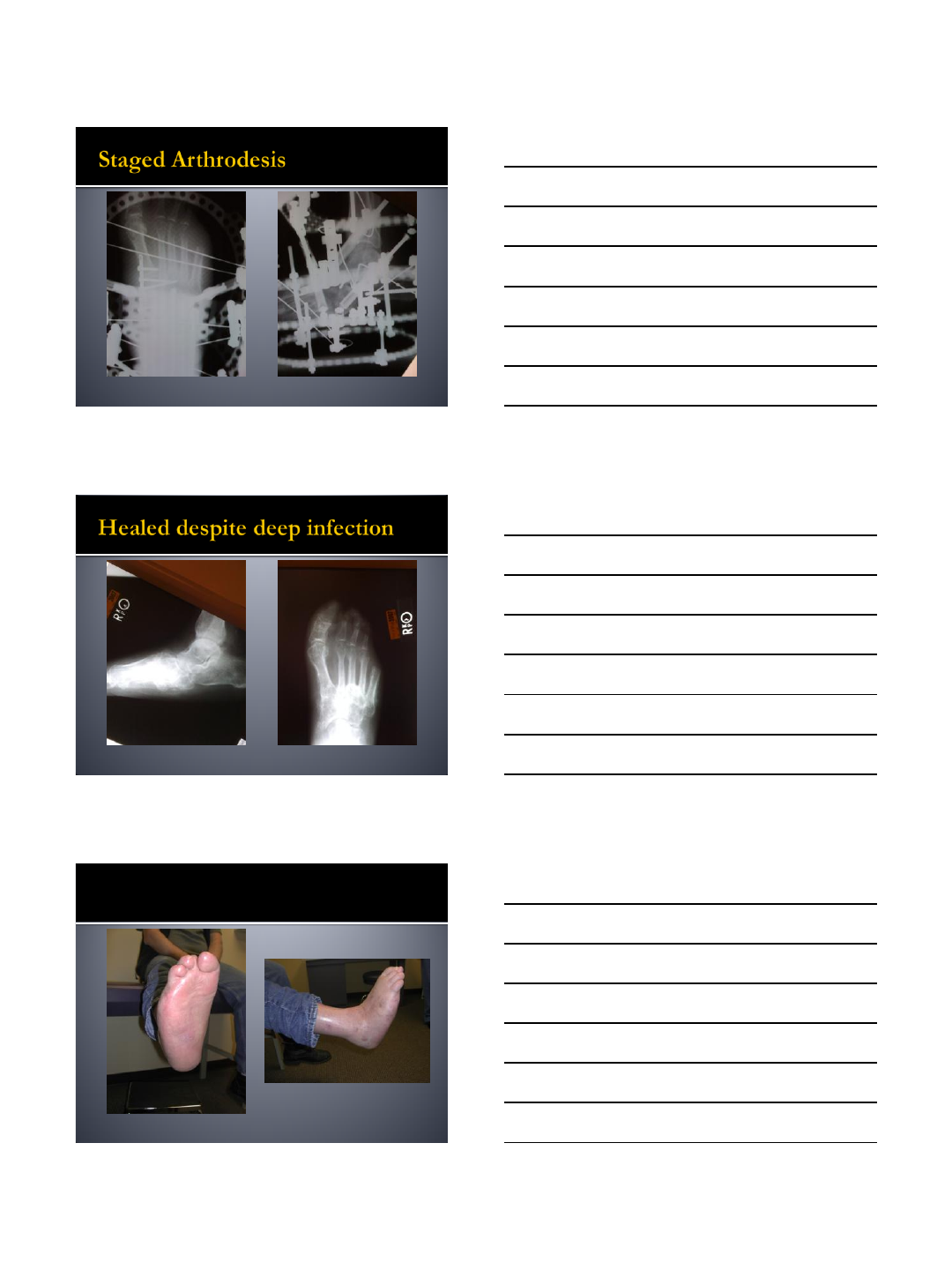
3 weeks after frame
application
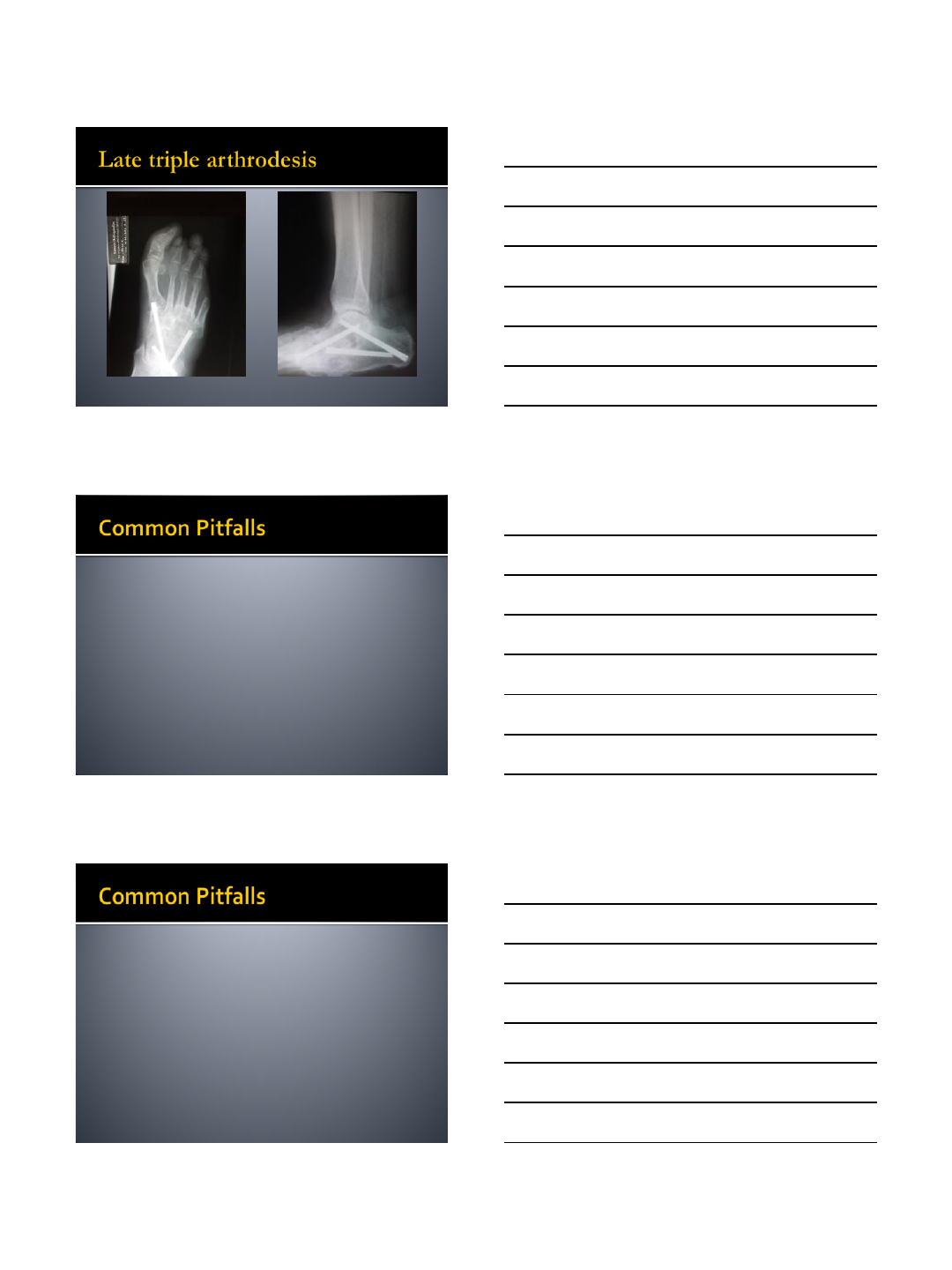
Staged triple and 1st
TMT arthrodesis
Frame modification to
correct equinus
contracture
7/12/2014
14
Plantigrade, ulcer healed
7/12/2014
15
Stretched the soft tissue,
incomplete reduction
7/12/2014
16
7/12/2014
17
Lack of experience with static frames prior to
attempting dynamic frames
Challenges of placing sufficient number of
wires to create a stable and strong frame in
small areas of the foot
Challenge of working around struts
Experience in running TSF programs
Experience in applying frames in a manner to
allow strut application and decrease strut
changes
Keeping wire fixation away from osteotomies
and internal fixation
Aggressively managing pin site infections
Planning frame modifications in the OR to
replace broken or loose wires before
catastrophic failure occurs
Need to perform staged arthrodesis to
maintain correction
Gradual transitions after frames are removed
with walking casts and AFOs
7/12/2014
18
gellman@summitdocs.com
