Dr. Patrick Meere NYU Langone Medical Center New York NY
2015-08-18
: Pdf Dr. Patrick Meere Nyu Langone Medical Center New York Ny Dr._Patrick_Meere_NYU_Langone_Medical_Center_New_York_NY 8 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 8
1
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery
NYU Hospital for Joint Diseases
New York, NY
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
The Use of Sensor Technology
Allowing Implant Salvage
In Selected Cases of Revision Total Knee Arthroplasty
A TWO-CASE RETROSPECTIVE CASE SERIES
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
2
INTRODUCTION
The revision burden associated with total knee
arthroplasty (TKA) is projected to reach a staggering
13 billion dollars, annually [3, 4, 5]. Complications
reported by TKA recipients include: pain (44%
overall), sensation of instability (21% reason for
revision), and joint stiness (17% reason for revision);
problems that may be attributed to soft-tissue
imbalance [6, 7, 8]. One of the possible reasons
for the substantial prevalence of such complications
is the traditional subjectivity associated with
defining intraoperative soft-tissue balance [9].
The use of pressure sensors imbedded in tibial
trial liners is proving an ecient method for soft
tissue envelope calibration and rebalancing at the
time of TKA [2]. When used in a revision case of
a compatible implant, it may prevent the need for
the exchange of all components. It is also critical
that such methods are developed to diagnose
specific problems during revision TKA, thereby
facilitating surgical correction and implant salvage
when feasible. Therefore, the purpose of this
consecutive, two-patient case series was to test
the ecacy of using intraoperative sensing
technology to eectively guide revision surgery
in patients with chronic instability.
METHODS
A case series of two patients is presented.
The inclusion criteria for this series were:
1) satisfactory radiographic alignment,
2) suspected soft tissue imbalance in the
coronal plane.
In both cases the contingency plan consisted of
a revision total knee arthroplasty (rev TKA) with
partial or total revision of the metallic components.
The revision TKA surgery technique focused on
balance restoration through critical analysis of
pressure mapping technique of tibio-femoral
contact point loads in the functional range. Pre-
operative and post-operative functional scores
along with clinical findings were prospectively
documented.
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
3
CASE 1
PATIENT
57 year old female, 18 months after a primary total
knee arthroplasty.
CLINICAL PRESENTATION
Persistent pain, swelling and instability. Inability to
stand, walk or perform stairs without significant
pain and stiness. No improvement despite diligent
and supervised physiotherapy for over a year.
Complains of inability to fully stretch. Positive
antalgic gait with 10 degrees lack of extension
contracture, further passive flexion range up to 95
degrees. Positive chronic eusion and periarticular
swelling. No gross opening during varus or valgus
stress test. Negative sag, less than 2 mm anterior
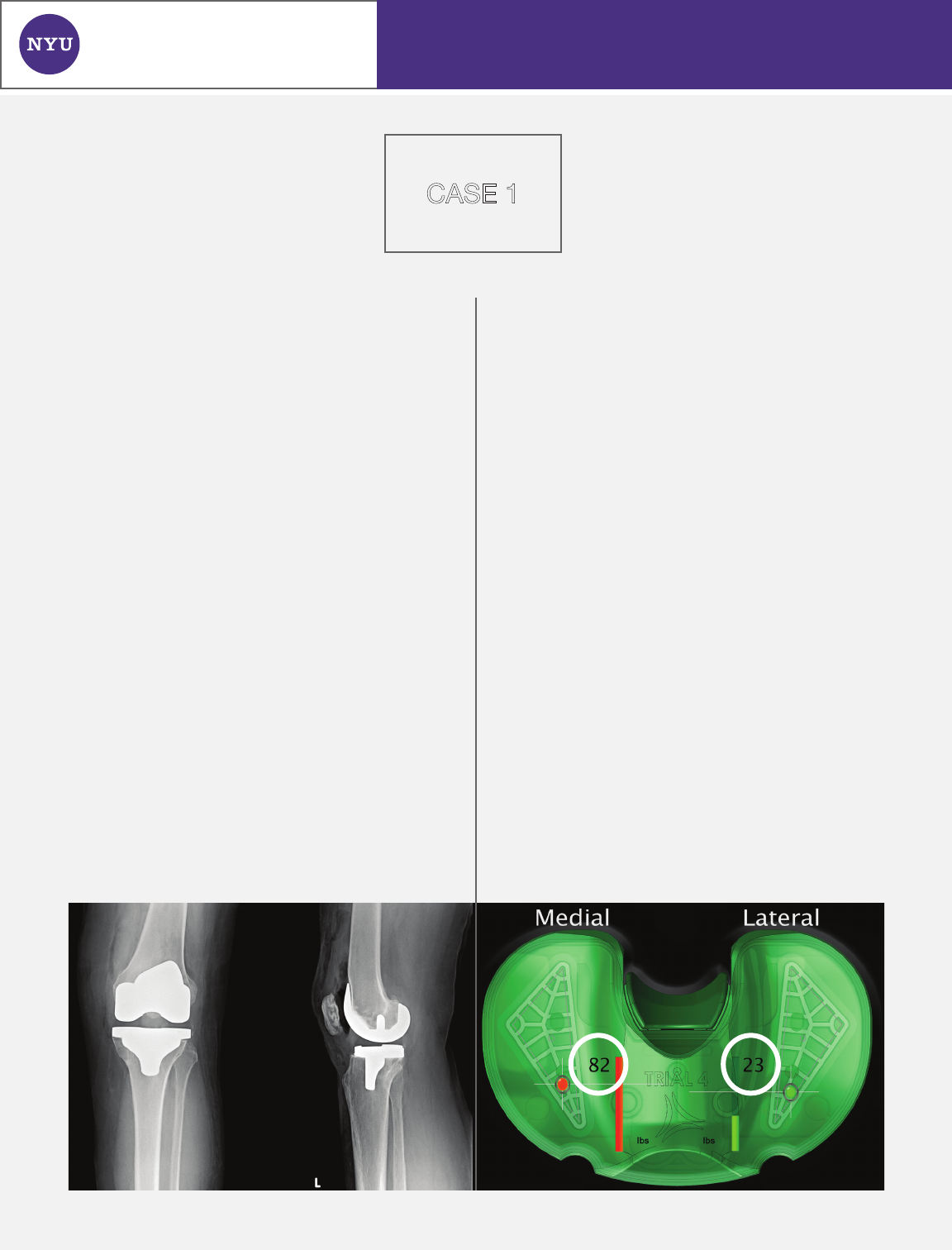
draw in flexion. Radiographs show a satisfactory
alignment and sizing with no evidence of
malrotation (Figure 1).
INTENDED PLAN
Open arthrotomy, lysis of adhesions, probable
femoral revision with distal femoral recession to
regain flexion / extension balance.
OPERATIVE FINDINGS
At the time of surgery pressure mapping identified
the dominant instability as excessive medial
tightness in extension with an excessively high-
pressure differential: 82 lbs medially v. 23 lbs
laterally (Figure 2). The medial and lateral pressures
in flexion were tensioned appropriately (Figure 3).
Pie-crusting of the posterior medial collateral
ligamentous fibers selectively corrected the
coronal imbalance and restored complete
extension. Simple liner thickness then suced to
restore pressure balance. The resultant pressures
in supported extension were 36 lbs medially v. 32lbs
laterally and in flexion (90 degrees) 10 lbs medially
v. 13 lbs laterally (Figures 4-5). The intra-operative
PROM measured 0-123 degrees. The metallic
implant components were preserved.
FIGURE 1 FIGURE 2, extension

Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
RESULTS
CASE 1
4
POST-OPERATIVE COURSE
The WOMAC scores improved from 46.2 (pre-op)
to 86.2 at 6 weeks and 88.6 at 8 months post-
operatively. The total Knee Society Score (KSS)
improved from 70 points (pre-op) to 169 points
at 8 months. The KSS pain and function separately
improved from 25 to 89 points and 45 to 80 points
respectively. The passive range of motion (PROM)
improved from 10-90 degrees (pre-op) to 0-122
and 0-127 for the same post-op intervals. The
improved range was preserved to date.
FIGURE 3, flexion
FIGURE 4, extension
FIGURE 5, flexion
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
5
CASE 2
PATIENT
77-year-old female with recent MCL injury on
10-year-old left TKA.
CLINICAL PRESENTATION
Three months of instability, persistent pain diusely
in the left knee after sustaining an accidental fall
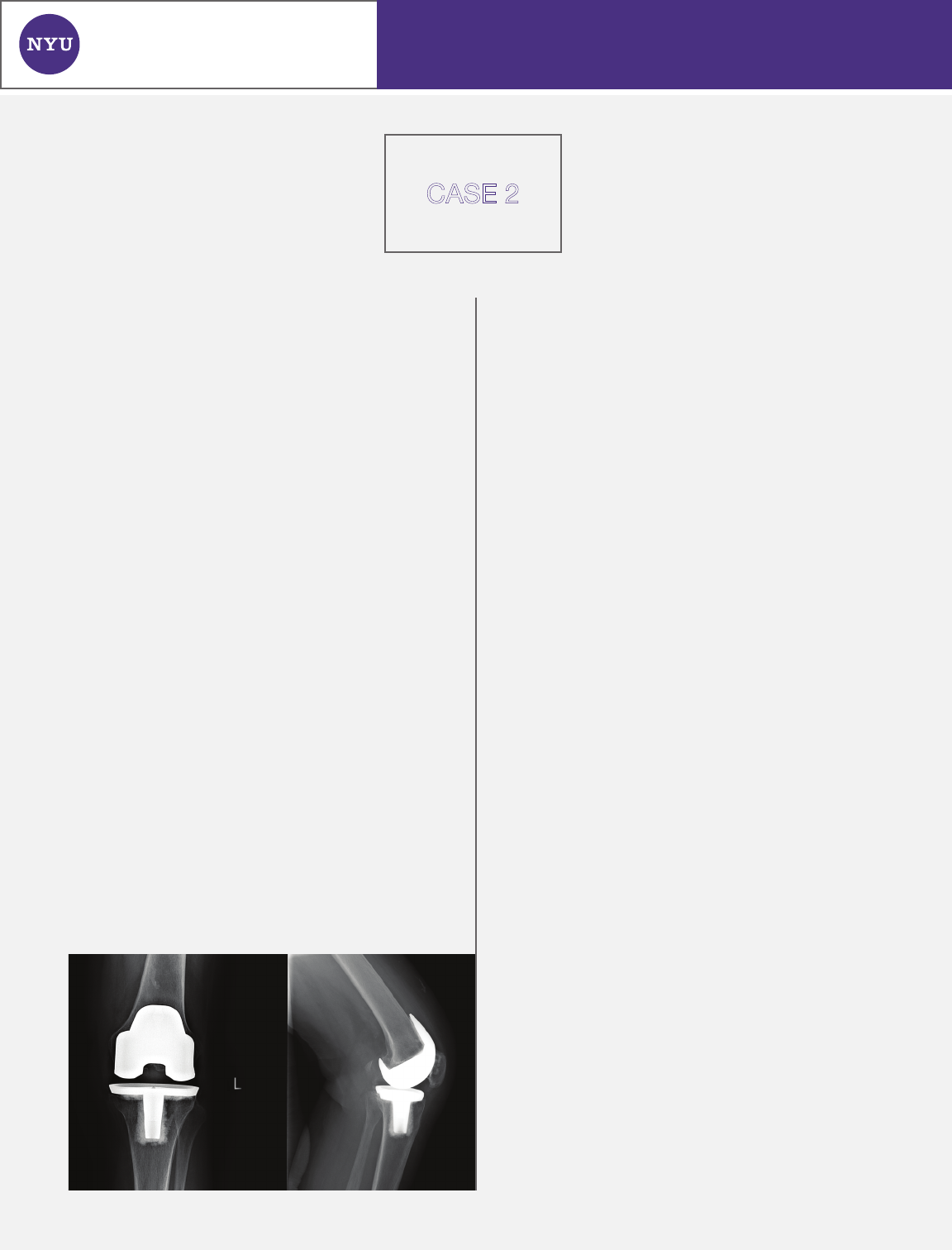
in a department store. Prior to this the clinical
function was good and there was no radiological
evidence of wear on her posterior stabilized left
knee total knee arthroplasty performed over 10
years ago (Figure 6). Subsequent to the fall with
hypervalgus and forceful flexion, the patient
developed recurrent and persistent instability of
the left knee. Physical exam confirmed a grade II
laxity of the medial collateral ligament with dull
point tenderness at the femoral insertion point.
There was associated multidirectional instability,
recurrent eusion, synovitis and periarticular tissue
edema. The PROM was -3 to 107. The valgus stress
test at 10 degrees of flexion showed 5 mm medial
opening with a soft endpoint. On varus stress the
lateral joint opened by 3mm. The anterior drawer
test showed anterior translation by 4mm (grade 2).
The posterior draw was stopped by the post.
INTENDED PLAN
The patient was indicated for a left knee open
arthrotomy, synovectomy, and lysis of adhesions,
possible primary medial collateral ligament repair,
probable augmentation of tibial liner with soft
tissue recalibration with the use of pressure
mapping technology, possible full revision to a
Total Stabilized TKA based on medial opening
stability and ability to generate sufficient and
functional contact resting pressures.
OPERATIVE FINDINGS
The patient was found to have the anticipated
diuse synovitis secondary to chronic multidirec-
tional instability. The MCL was found to be plasti-
cally deformed by approximately 10% but with very
good residual elasticity. There was no evidence
of mechanical dissociation of the implants. The
patient was found to have significant patella baja
with arthrofibrosis of the infrapatellar ligament.
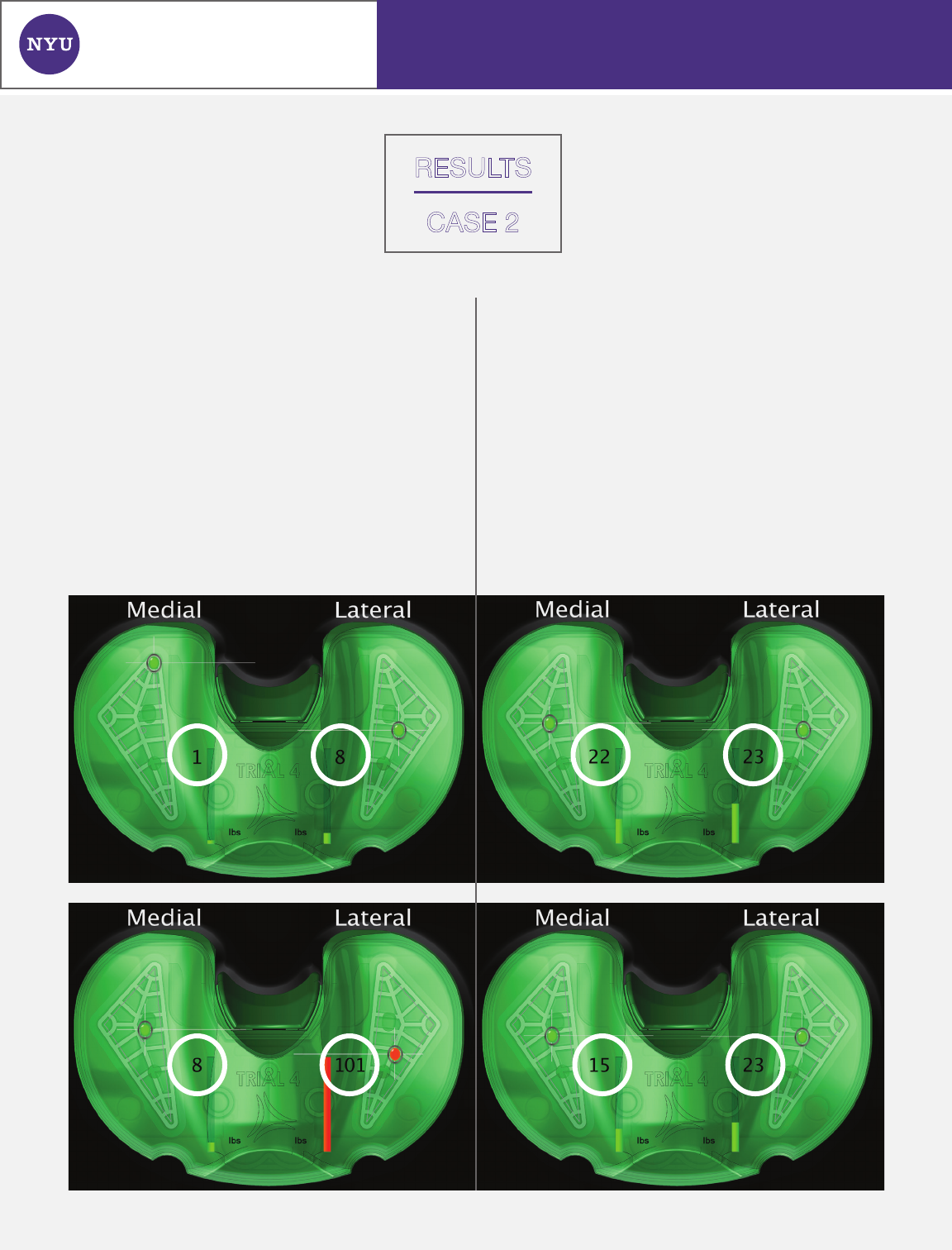
Compartmental tibial load pressure mapping
indicated insufficient load on the medial side,
reflecting the known traumatic laxity of the medial
collateral ligament in extension (Figure 7). To
increase the contact pressure to an acceptable
level, a liner thickness augmentation is required.
This however caused overstung of the lateral
compartment in extension (Figure 8). This was
then corrected by a rim coronary ligament release
(Arcuate plus 3mm of the lateral Iliotibial band
insertion up to Gerdy’s tubercle) on the lateral side
and final liner thickness augmentation by 5mm.
The coronal pressure balance was thus optimized
to less than 10 pounds dierential in extension and
in flexion (Figure 9-10).
The above pathway pertains to static loads.
FIGURE 6
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
6
RESULTS
CASE 2
Dynamic load evaluation through a varus / valgus
maneuver (at 10 degrees of flexion) can produce
pressure dierentials that reflect the tension in the
ligaments opposite to the direction of the applied
force. Varus loading with 25 N force created a
20 lbs load dierential on the medial compartment,
representing the tightness of the lateral collateral
ligament. Valgus loading with the same 25 N force
generated a 17 lbs load dierential, confirming the
sucient resiliency of the MCL. This ligamentous
stability was deemed to be very acceptable and
preferable to a full revision to a TS component.
POST-OPERATIVE COURSE
Discharged on post-operative day (POD) 2. Single
cane on POD 10. Unassisted ambulation by POD
20 with walking tolerance of 6 blocks, no assist
on stairs. Post-operative exam at 21 days reveals
minimal pain or tenderness. Medial opening on
valgus stress of less than 3mm. PROM: -3 to 112
degrees. The WOMAC score improved from 47.7
(pre-op) to 84.8 at 6 weeks.
FIGURE 7, extension FIGURE 9, extension
FIGURE 8, extension FIGURE 10, flexion
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
7
DISCUSSION
In this short case series, two patients presented
with chronic instability, pain, and eusion in an
established TKA joint. All asymmetric loading was
confirmed and corrected through the use of the
intraoperative sensor system. The initial operative
plan for both cases indicated a potential need for
exchange of metal components. However, digital
guidance provided by the sensor system obviated
the need for the surgeon to exchange any metal
components, thereby avoiding patient morbidities
and excess cost associated with revision surgery.
In Case I, the patient presented with coronal soft-
tissue imbalance, driven by excessive tension in
the posterior medial collateral ligament fibers. In
such cases, pressure mapping sensor technology
helps the surgeon to define the specific deficiency
and probable best correction. In many revision
cases, the imbalance is coronal rather than sagittal.
Thus, implant salvage may be feasible, sparing the
patient the morbidity associated with a complete
revision of all TKA components.
In Case II, the decision to convert an unstable TKA
after a serious MCL injury relied on the subjective
impression of medial joint line opening and
shearing upon valgus stress testing. The adjunct
use of sensor technology in this case allowed for
quantified evidence of the morbid imbalance and
assisted in the performance of titrated release of
the relatively tighter contralateral ligament and
capsule upon liner thickness augmentation.
Finally, the response to physiological loading of
the collateral ligaments showed symmetrical ΔP’s
(rapid pressure dierentials during the load
impulse application and recoil). This confirmed
the restoration of functional stability to the joint.
Of note was the fact that the implant salvaged in
this case was of a dierent manufacturer than that
for which the sensor was design. Nonetheless,
undersizing by one size allowed for a good fit
and translational stability for compression load
testing purposes.
This small case series provides promising results
for the ecacy of using intraoperative sensor
technology during revision cases requiring the
correction of instability. Further case studies and
longer follow-up will need to be obtained to
understand long-term outcomes.
Hospital for Joint Diseases
NYU LANGONE MEDICAL CENTER
PATRICK A. MEERE, MD
Department of Orthopaedic Surgery, NYU Hospital for Joint Diseases, New York, NY
8
REFERENCES
1 Weinstein AM, Rome BN, Reichmann WM, et
al. Estimating the burden of total knee
replacement in the United States. Journal
Bone Joint Surg. 2013; 95(5): 385-392.
2 Gustke KA, Golloday GJ, Roche MW, et al. A
new method for defining balance: promising
short-term clinical outcomes of sensor-
guided TKA. J Arthroplasty. 2013; [E-Pub
ahead of print] DOI: 10.1016/j.art.2013.10.020.
3 Bhandari M, Smith J, Miller LE, et al. Clinical
and economic burden of revision knee
arthroplasty. Clin Med Insights Arthritis
Musculoskelet Disord. 2012; 5: 89-94.
4 Bourne RB, Maloney WJ, Wright JG. An AOA
critical issue: the outcome of the outcomes
movement. J Bone Joint Surg Am. 2004; 86:
633-640.
5 Maloney WJ. An American implant registry:
has the time come? J Bone Joint Surg Am.
2001; 83: 1582-1585.
6 Sharkey PF, Hozack WJ, Rothman RH, et al.
Insall award paper: why are total knee
arthroplasties failing today? Clin Orthop Relat
Res. 2002; 404: 7-13.
7 Muhall K, Ghomrawi H, Scully S, et al. Current
etiologies and modes of failure in total knee
arthroplasty revision. Clin Orthop Relat Res.
2005; 446: 45-50.
8 Wylde V, Hewlett S, Learmonth ID, et al.
Persistent pain after joint replacement:
prevalence, sensory qualities, and
postoperative determinants. Pain. 2011;
152(3): 566-572.
9 D’Lima DD, Patil S, Steklov N, et al. Dynamic
intraoperative ligament balancing in total
knee arthroplasty. Clin Orthop Relat Res.
2007; 463: 208-212.
