Efficiencies Of Block Graft Syllabus
2014-09-04
: Pdf Efficiencies Of Block Graft Syllabus Efficiencies_of_Block_Graft_Syllabus 9 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 85
9/4/2014
1
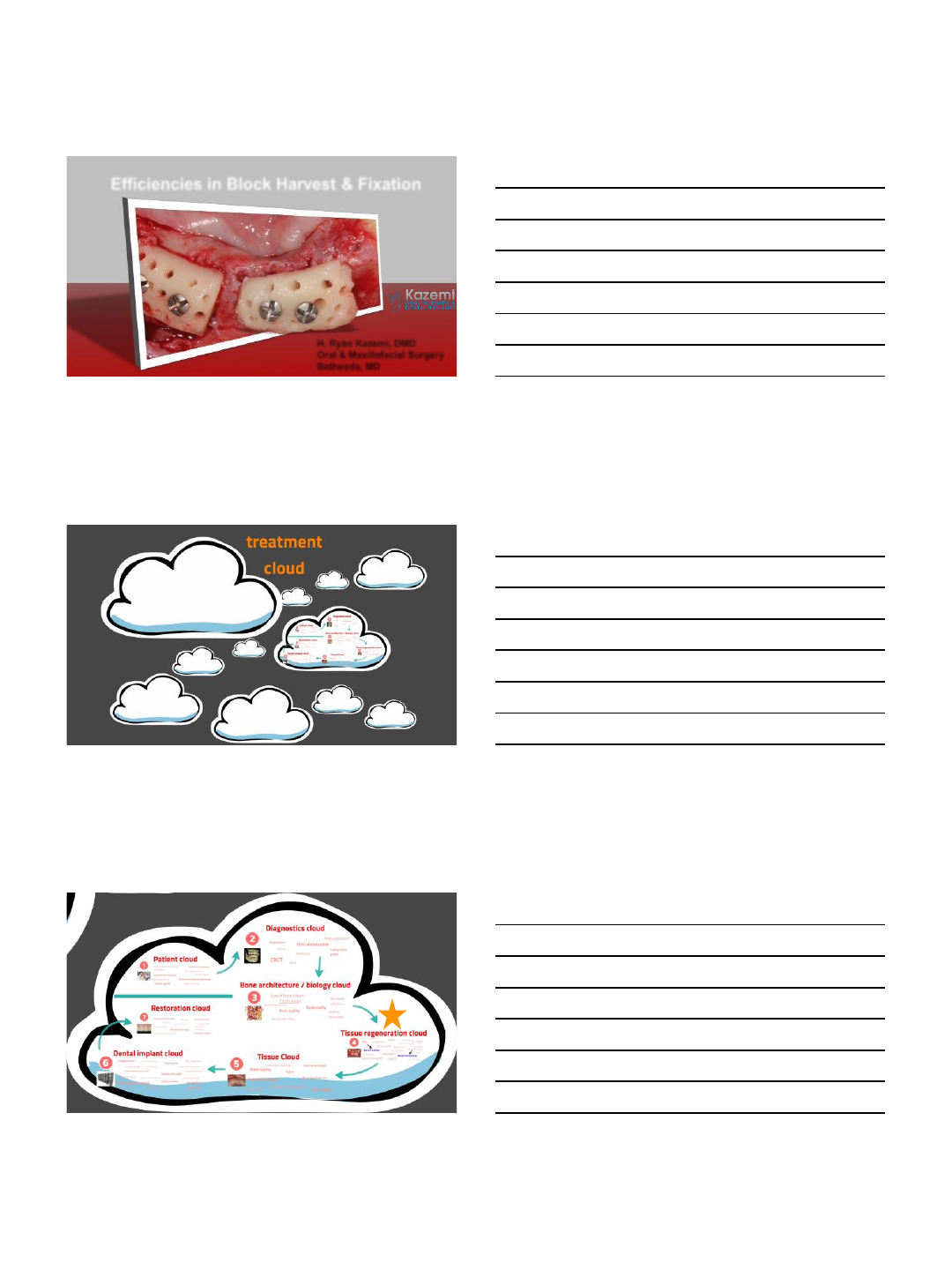
H. Ryan Kazemi, DMD
Oral & Maxillofacial Surgery
Bethesda, MD
Efficiencies in Block Harvest & Fixation
implant cloud
9/4/2014
2
block graft
available bone?
stability?
implant survival?
9/4/2014
3
block graft
donor site bone volume
tuberocity 2-5 cc
chin / ramus 5-10 cc
autogenous
collection < 1cc
iliac crest
- anterior
- posterior
- trephine
30-40 cc
70-140 cc
10-20 cc
available bone?
stability?
implant survival?
ramus
good volume
low morbidity
block graft
long-term block graft stability in thin periodontal biotype patients
97% of augmented width
maintained after 3.3 years
verdugo etal, Int j oral maxillofac implants 2011; 26:325-
332
osseointegration
critical to preservation of
grafted bone
available bone?
stability?
implant survival?
block graft
the potential of the horizontal ramus of the mandible as a donor site
for block and particular grafts in pre-implant surgery
99% implant survival rate
soehardi a, et al. ijomi 2009 nov; 38 (11)
available bone?
stability?
implant survival?
greatest stress of implant at neck / crest
+
increased bone density of block graft (D1)
=
distinct biomechanical advantage
9/4/2014
4
deficiency type
defect size
soft tissue biotype
inter-septal bone
vestibular depth
<<
>>
clinical cbct
defect form
defect size
anatomy
recipient
siebert
horizontal: Ivertical: II mixed: III
allen vertical: Ahorizontal: Bmixed: C
Cologne
Orientation, graft needs, relation of graft to
defect
classification
IAN
width
height
recipient
site
9/4/2014
5
shape
of ideal
block
graft
recipient
site
recipient site
IAN
width
height
donor
site
9/4/2014
6
0º 10º20º
planning block form
donor recipient
donor recipient
9/4/2014
7
9/4/2014
8
⃣
draw
blood
for prgf
⃣
open
recipient
site
⃣
open
donor site
& harvest
block
⃣
fixate
block to
recipient
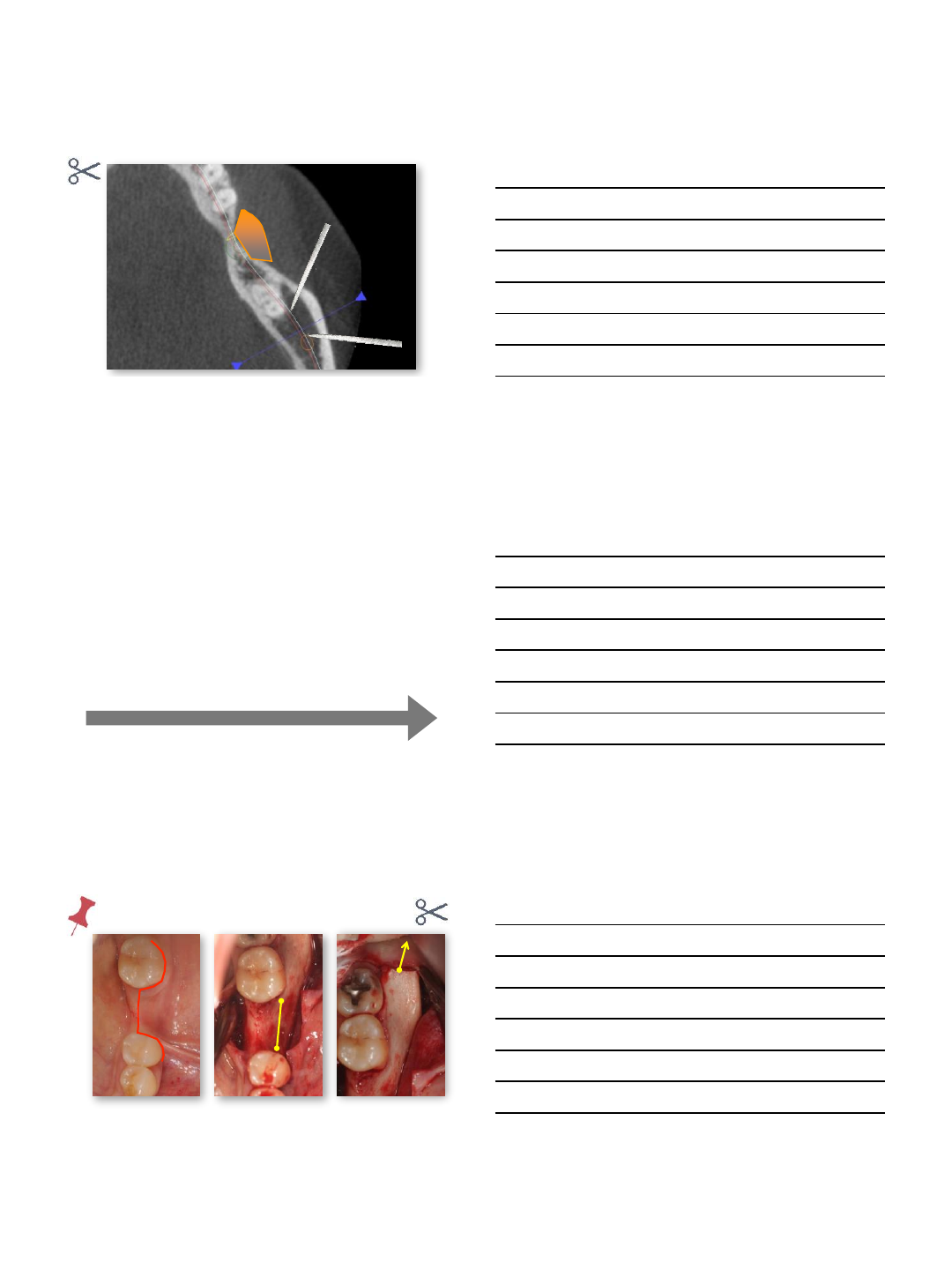
surgical order
incision & flap
9/4/2014
9
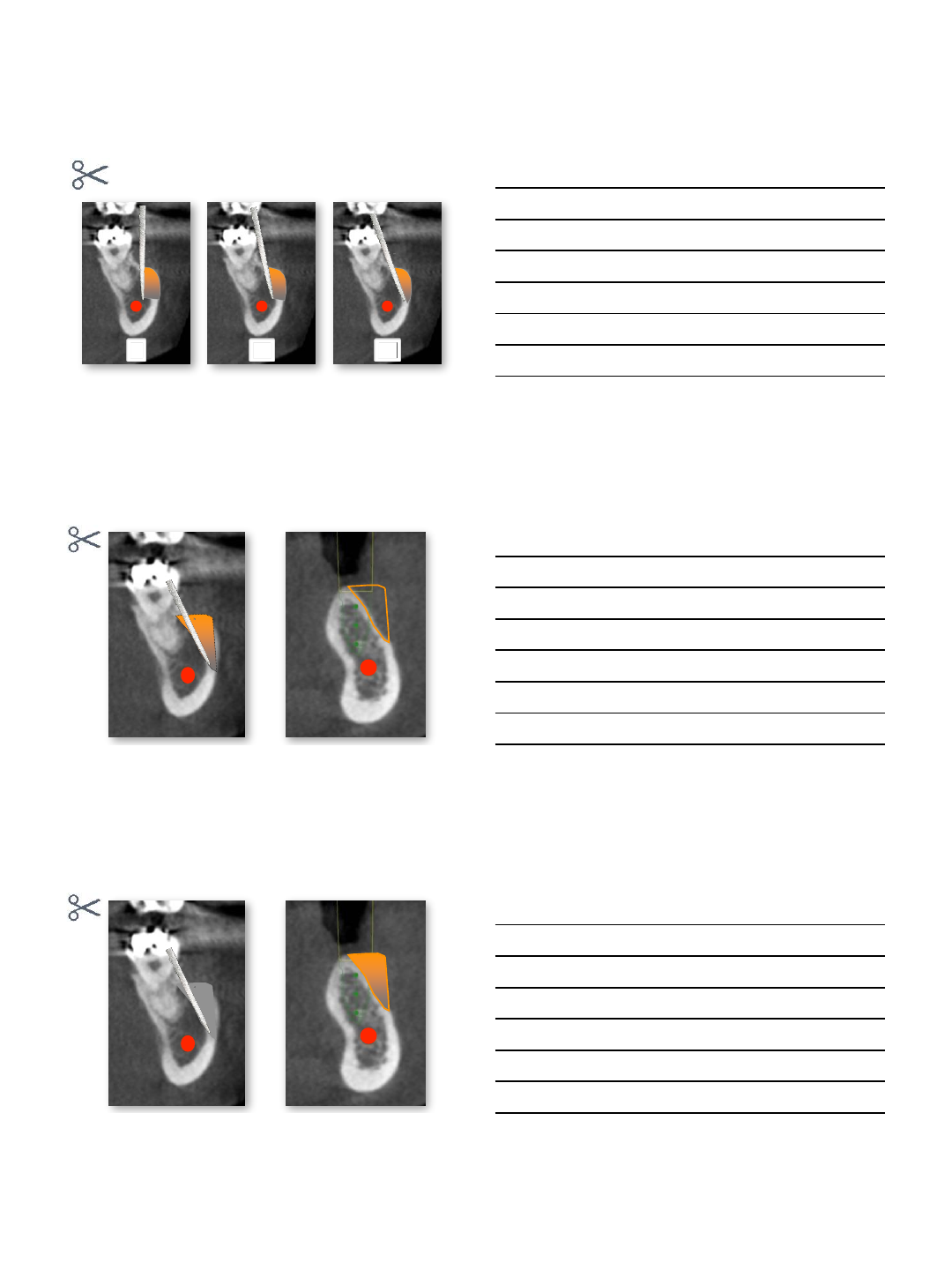
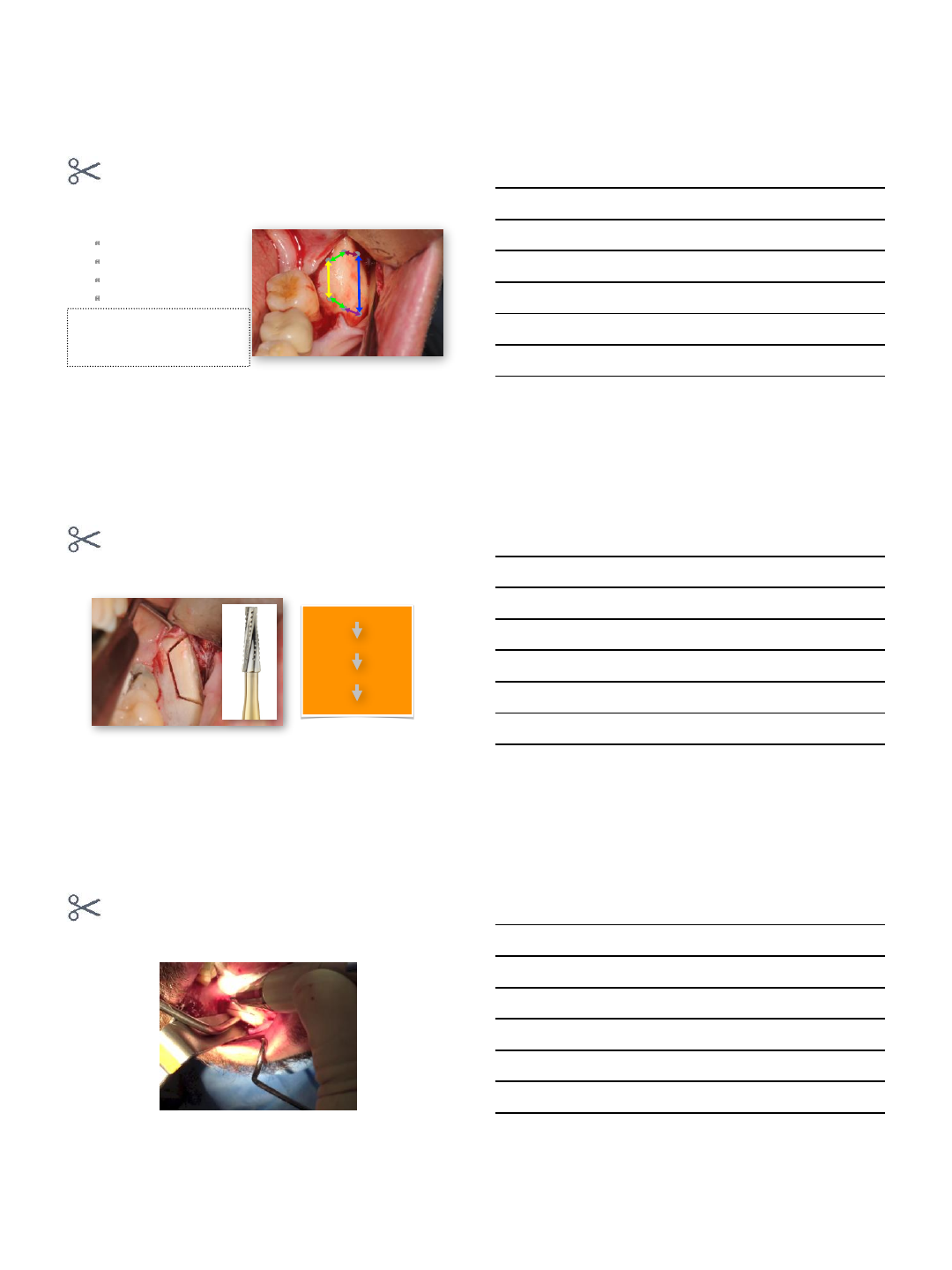
block harvest
⃣measure
sagittal
medio-lateral
vertical
caudal
over extension
sagittal, vertical, & caudal >> 10%
medio-lateral >> 20%
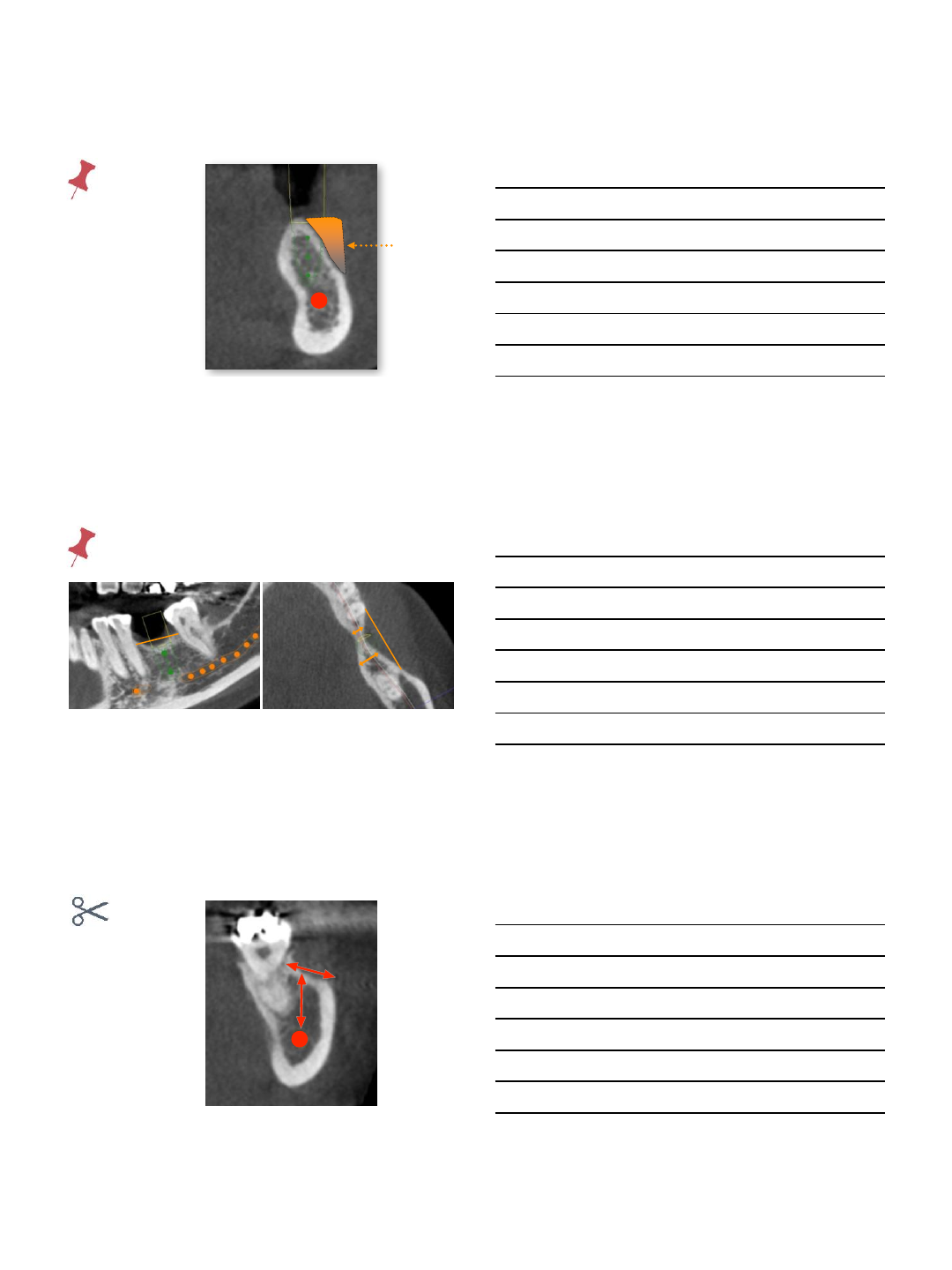
block harvest
⃣outline
sagittal cut
medio-lateral cut
vertical cut
caudal cut
block harvest
⃣outline
9/4/2014
10
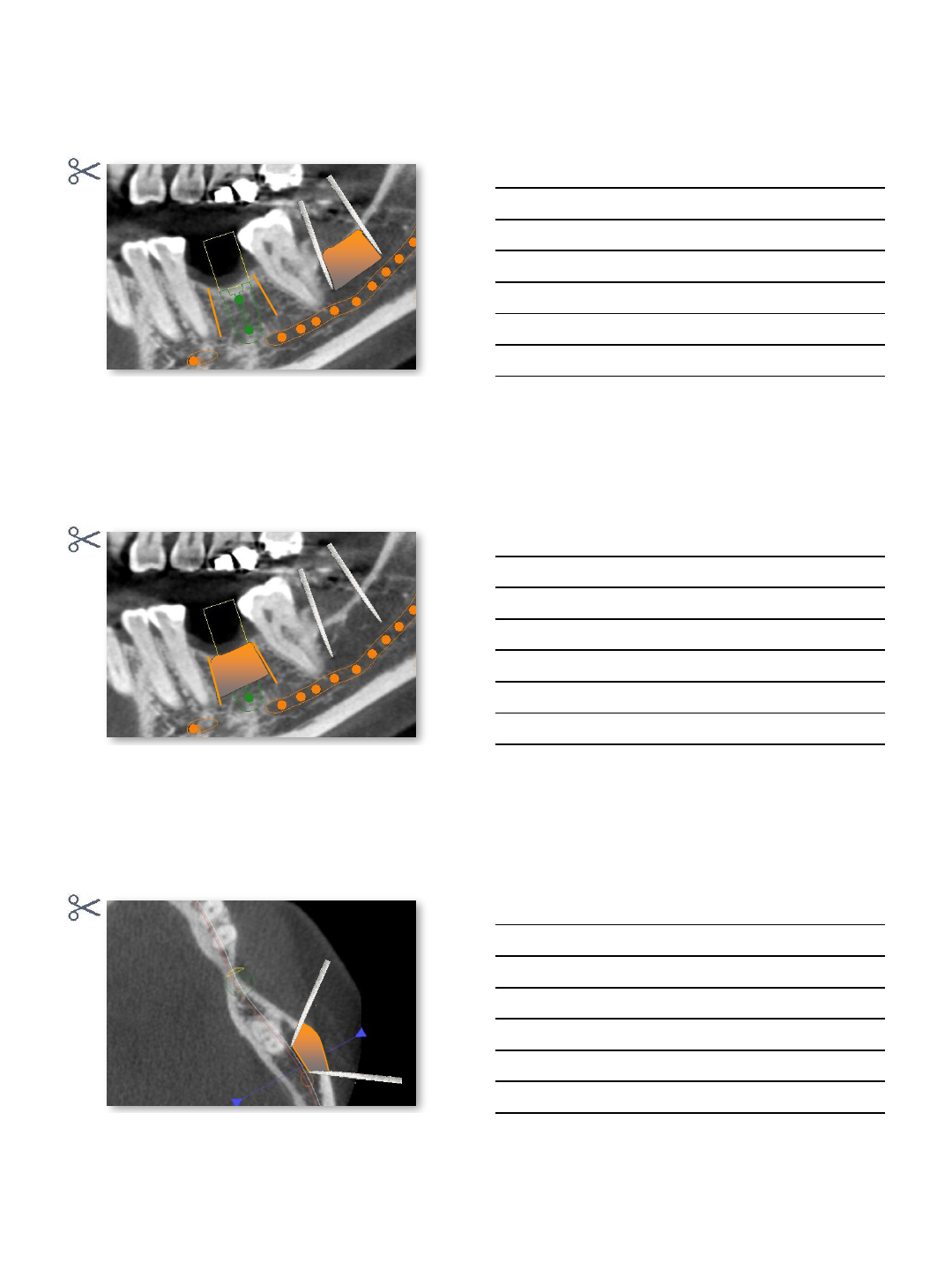
block harvest
⃣outline-caudal
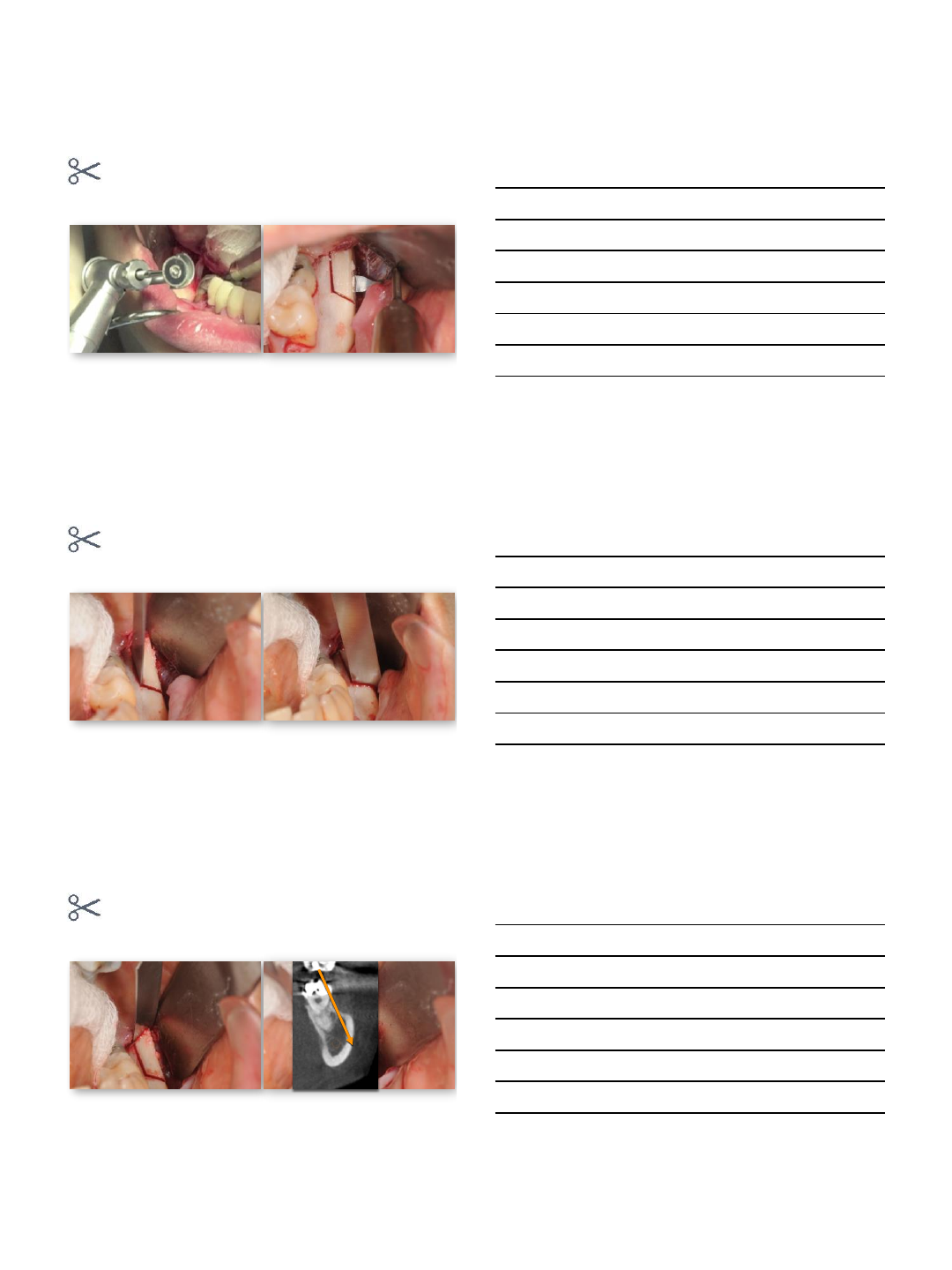
block harvest
⃣complete osteotomy
block harvest
⃣complete osteotomy
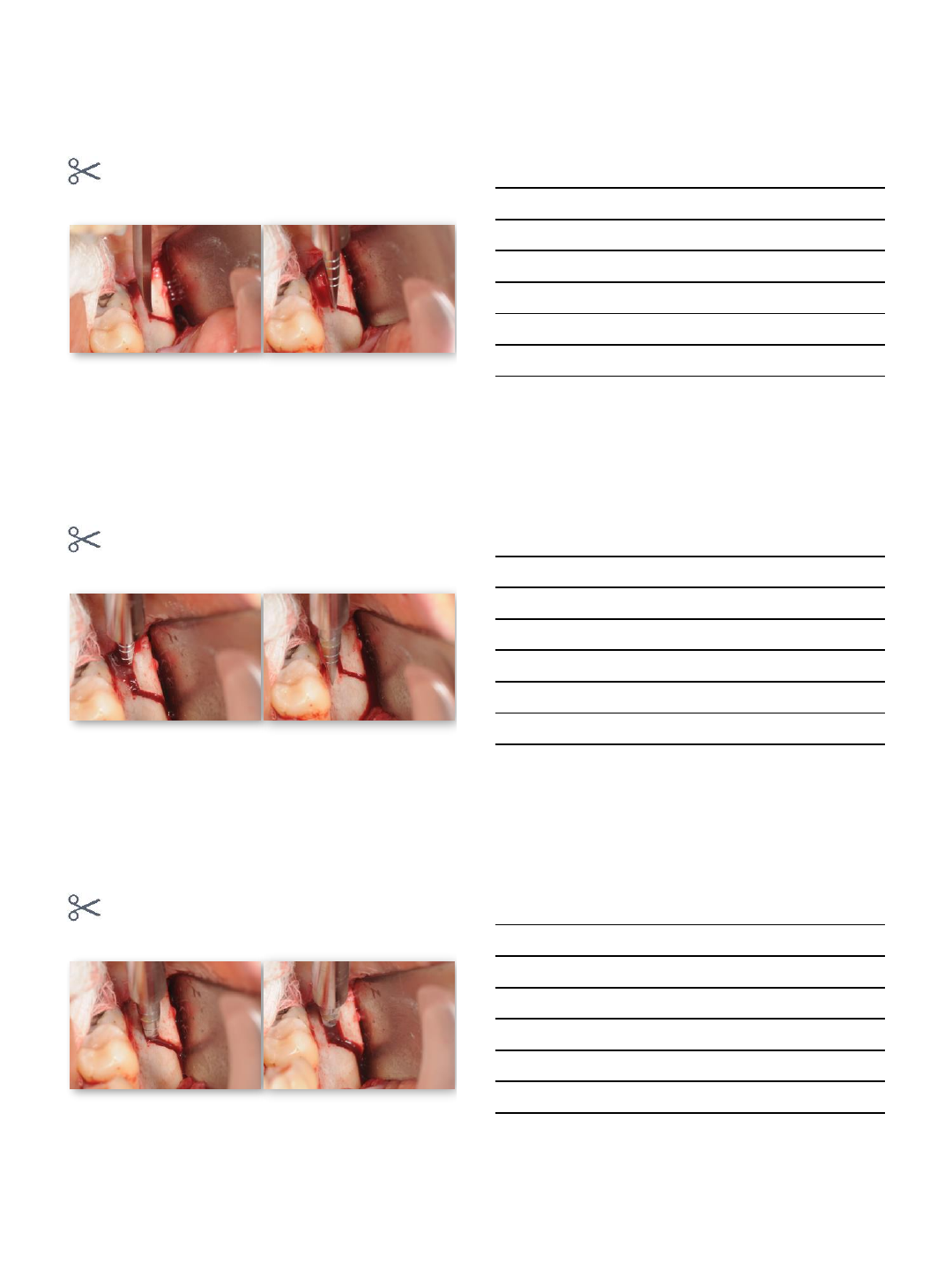
9/4/2014
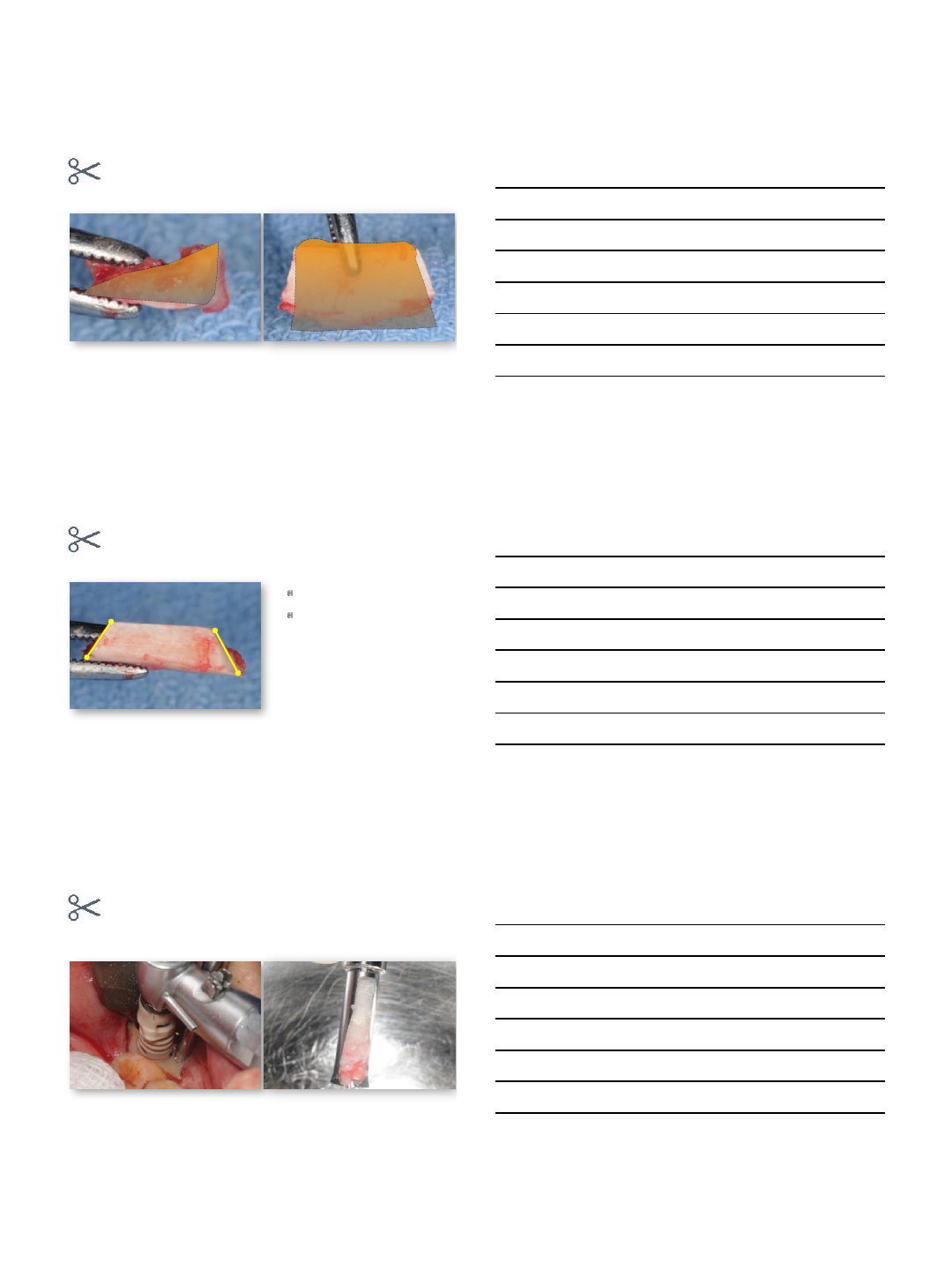
11
block harvest
⃣split
block harvest
⃣split
block harvest
⃣split
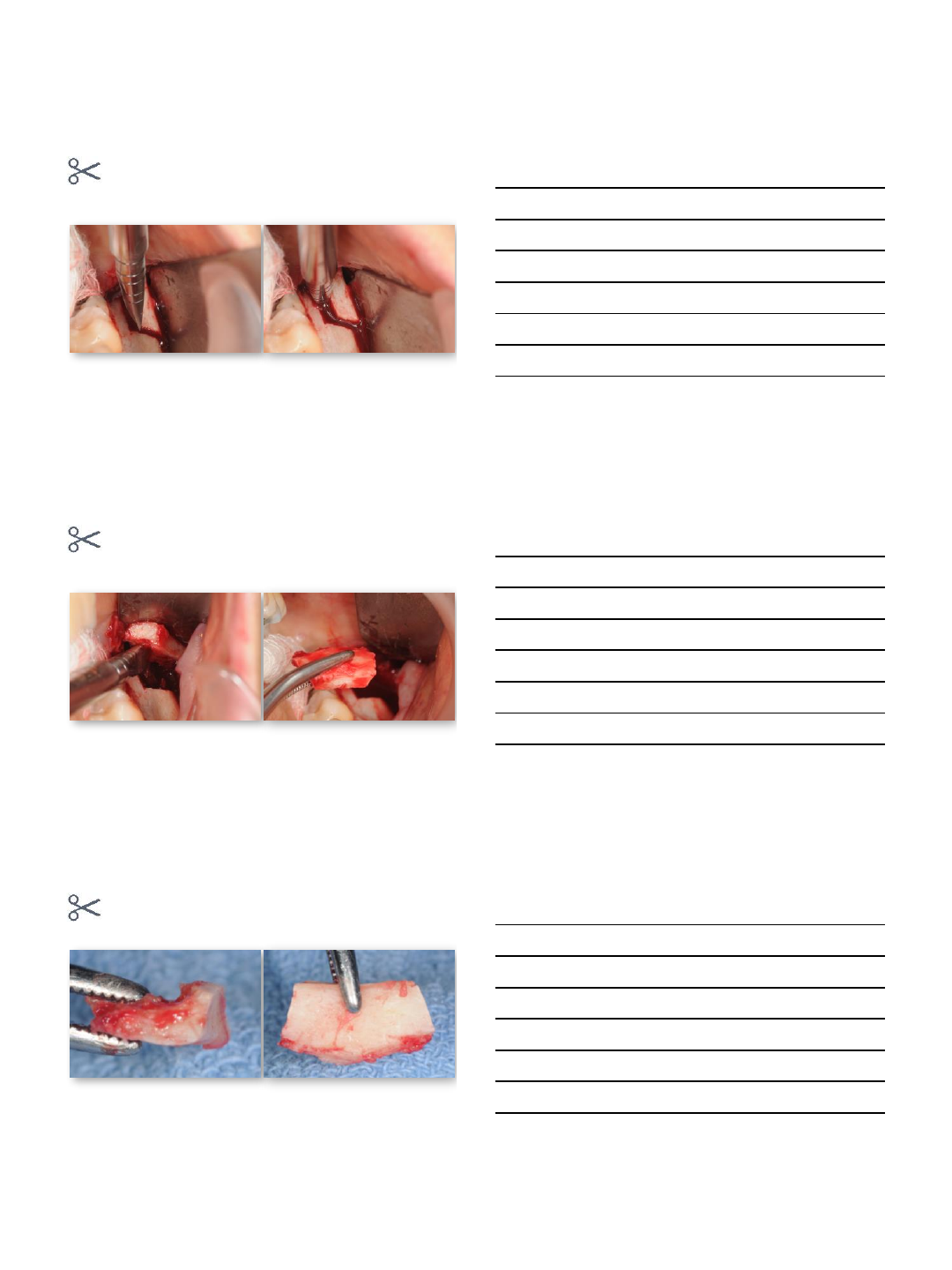
9/4/2014
12
block harvest
⃣split
block harvest
⃣block fracture
9/4/2014
13
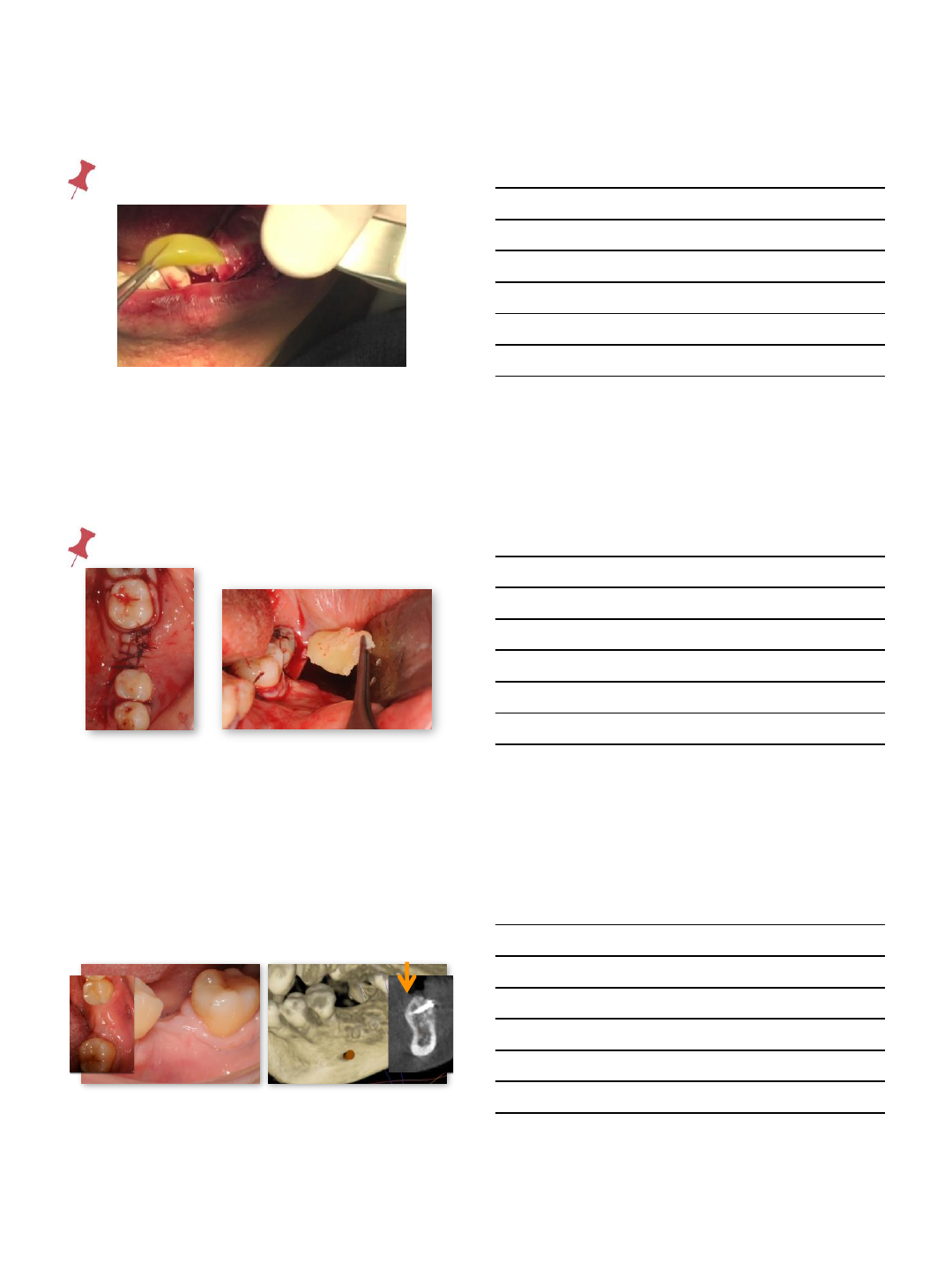
storage
moist guaze
prgf
NO saline
immersion
particulate harvest
trephine burs
9/4/2014
14
particulate harvest
bone scraper
particulate harvest
bone scraper
autogenous bone +mineralized bone +prgf bone complex
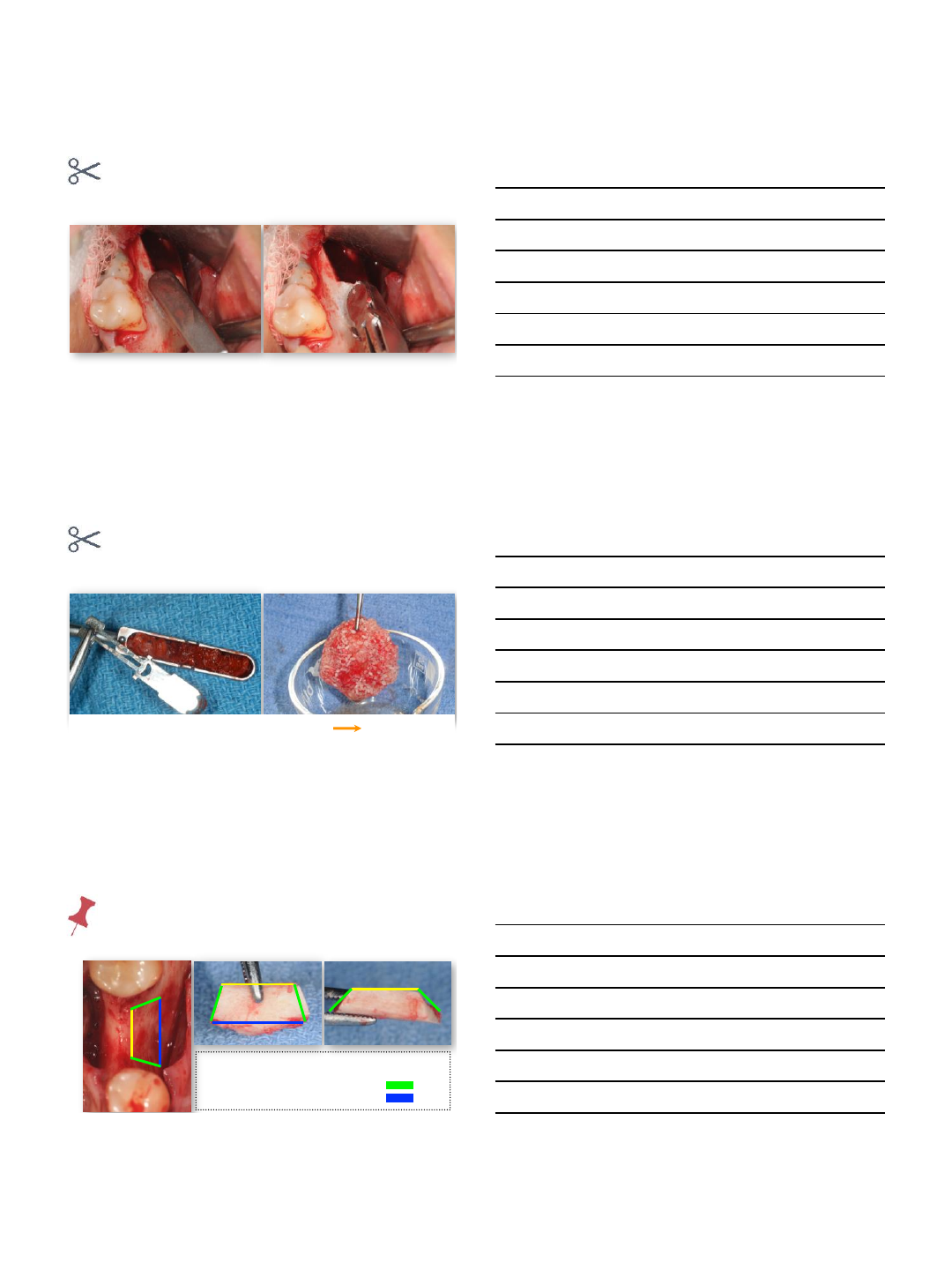
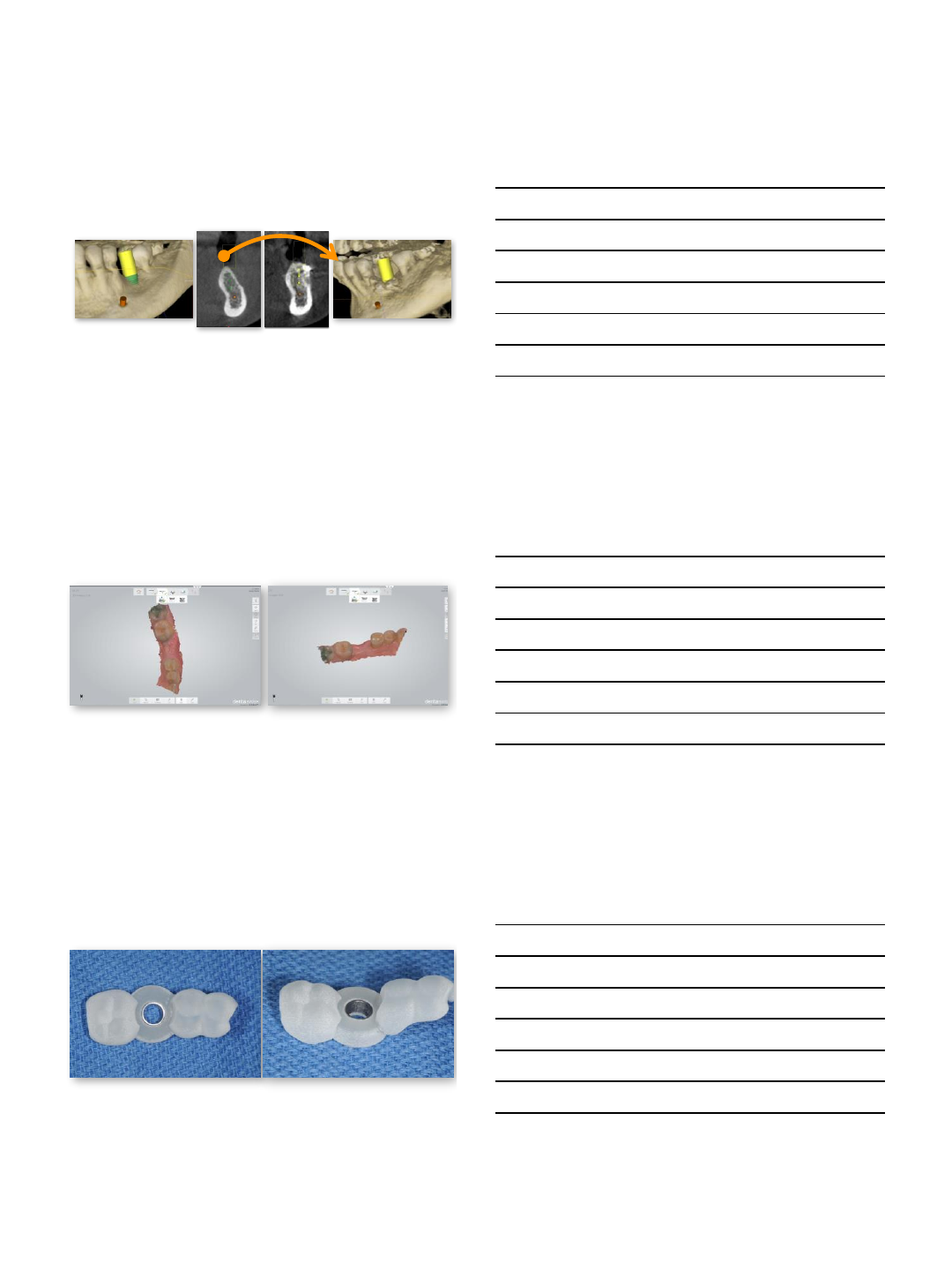
prepare recipient
maximal interface & stability
butt joints at the recipient bed
medio-lateral line angle
caudal line angle
9/4/2014
15
prepare recipient
maximal interface & stability
decorticate
perforation
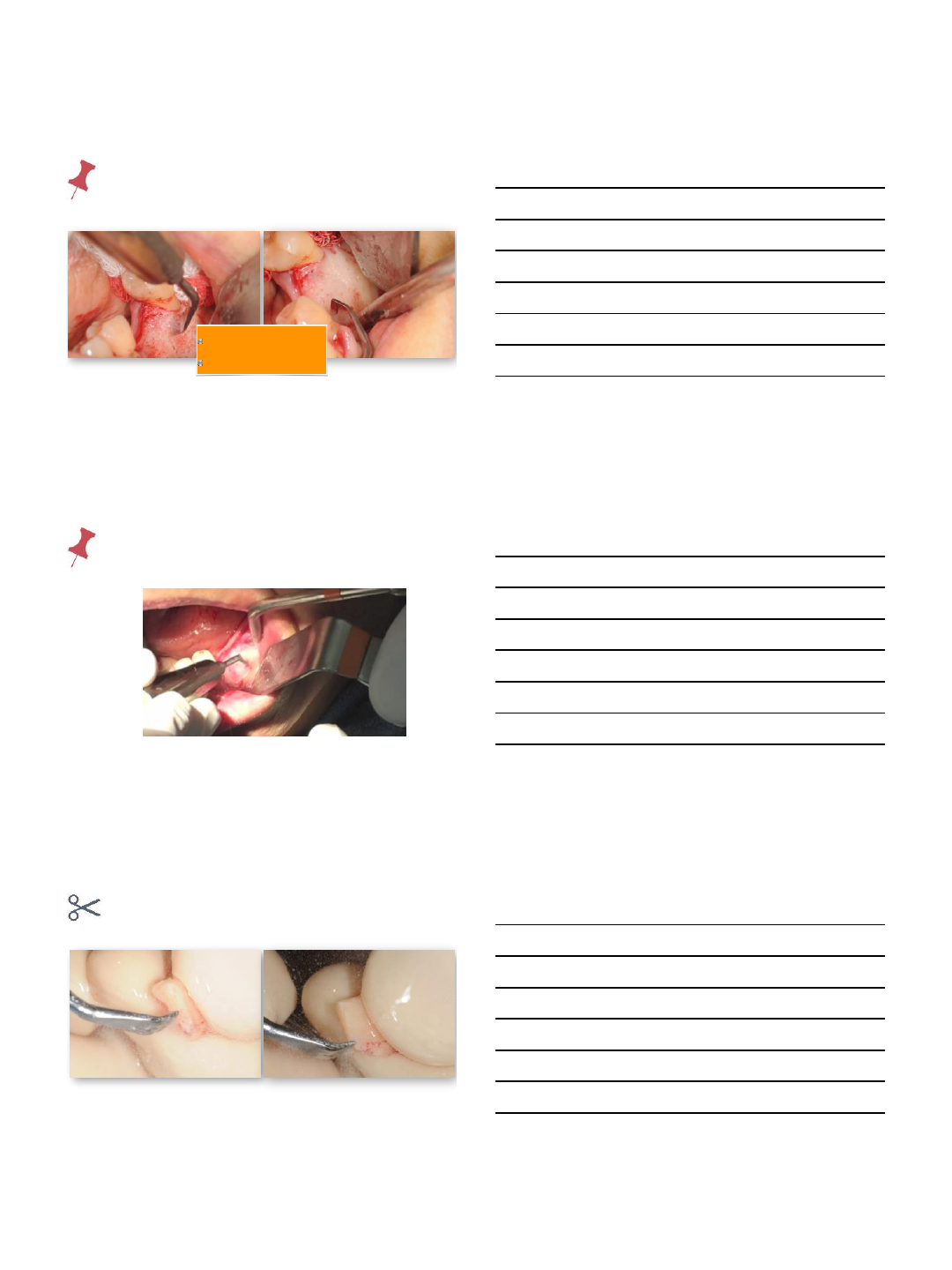
prepare recipient
maximal interface & stability
modify block
9/4/2014
16
adapt block
adapt block
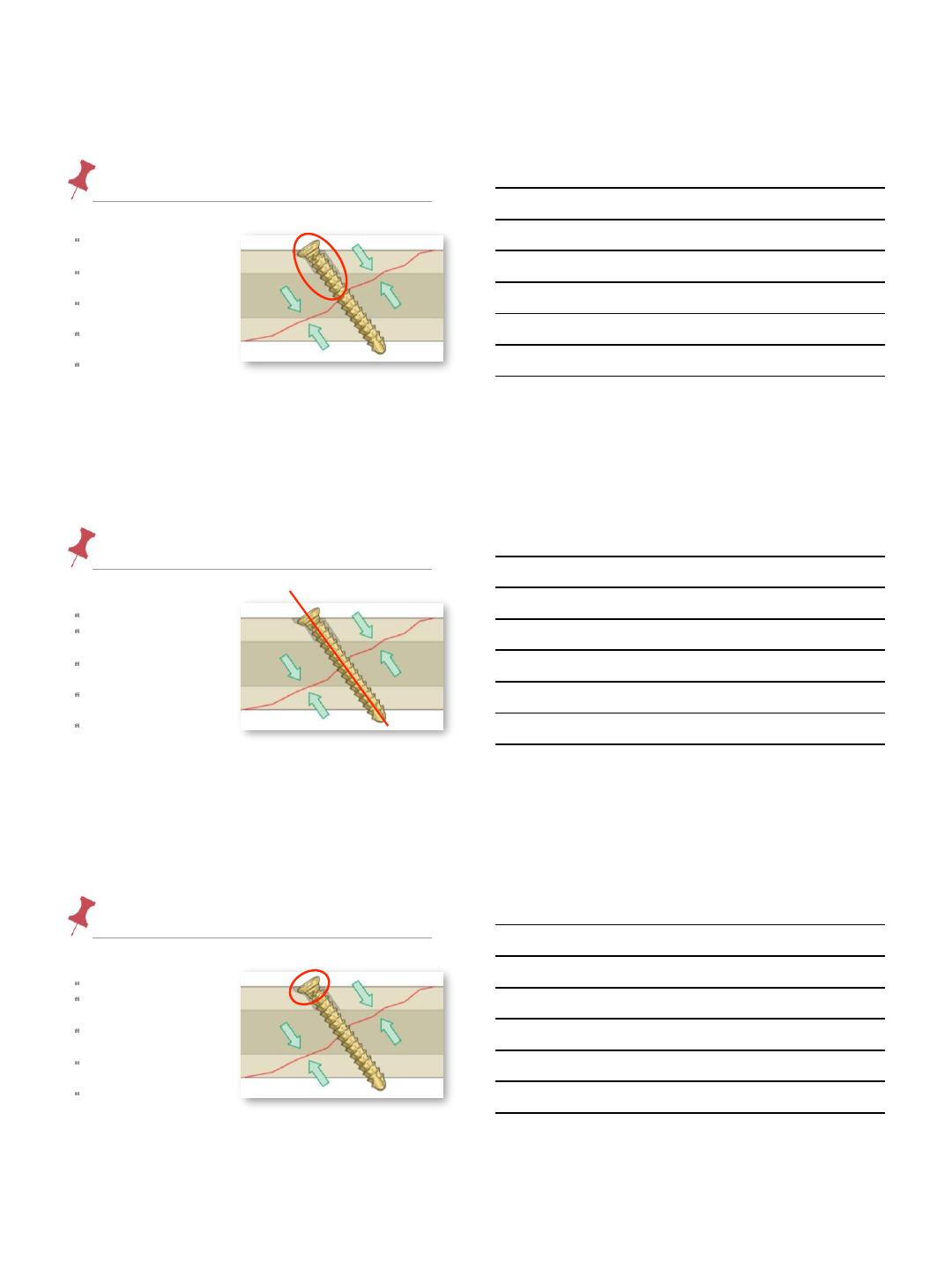
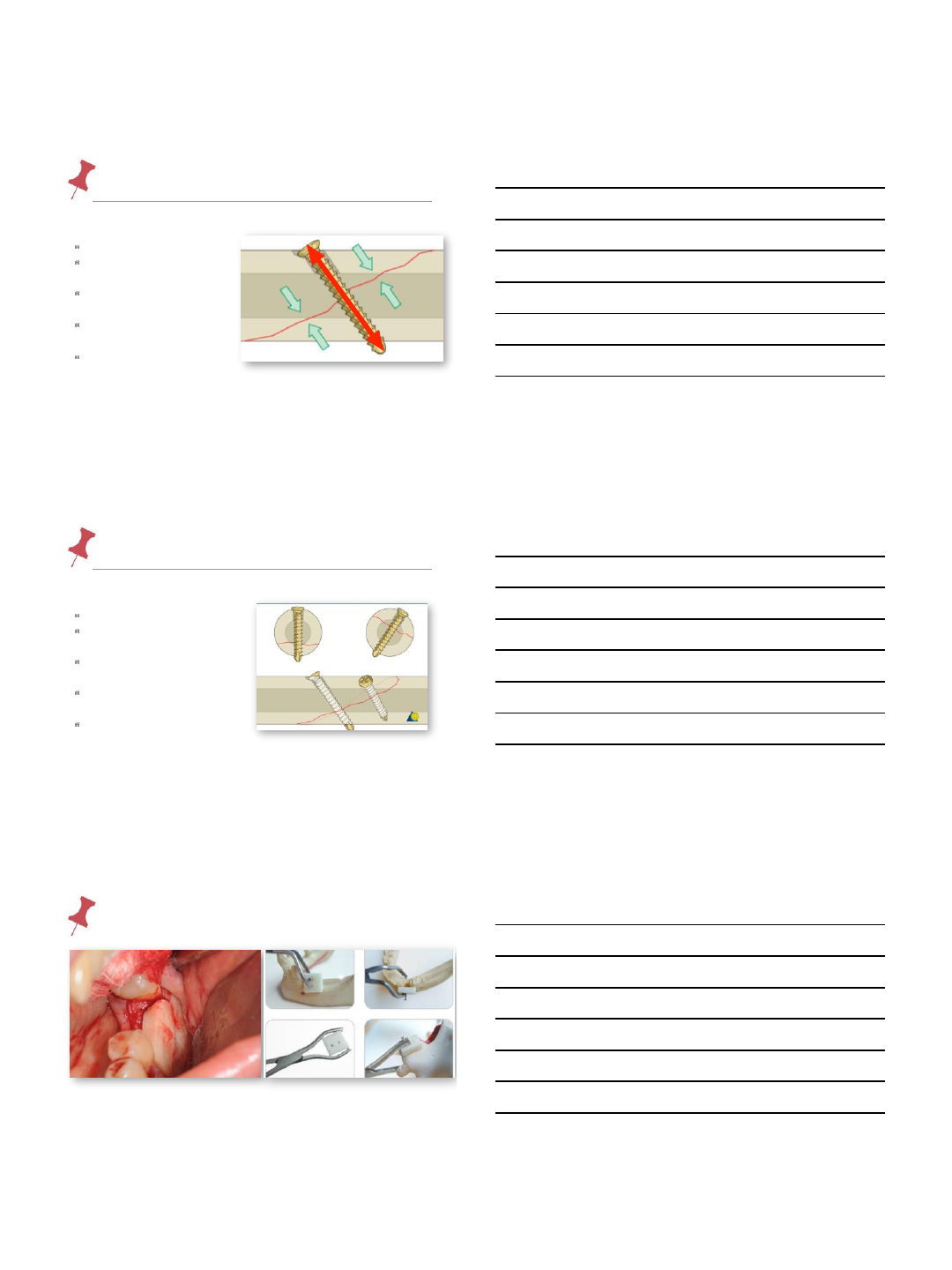
fixation AO- Arbeitsgemeinschaft fur
Osteosynthesefragen
lag techniquecompression lag screw
primary bone healing
decreases gap
increases stability
>>
overdrill near cortex to
size of the external
diameter of the screw
reduction (contact)
rigid fixation
compression
9/4/2014
17
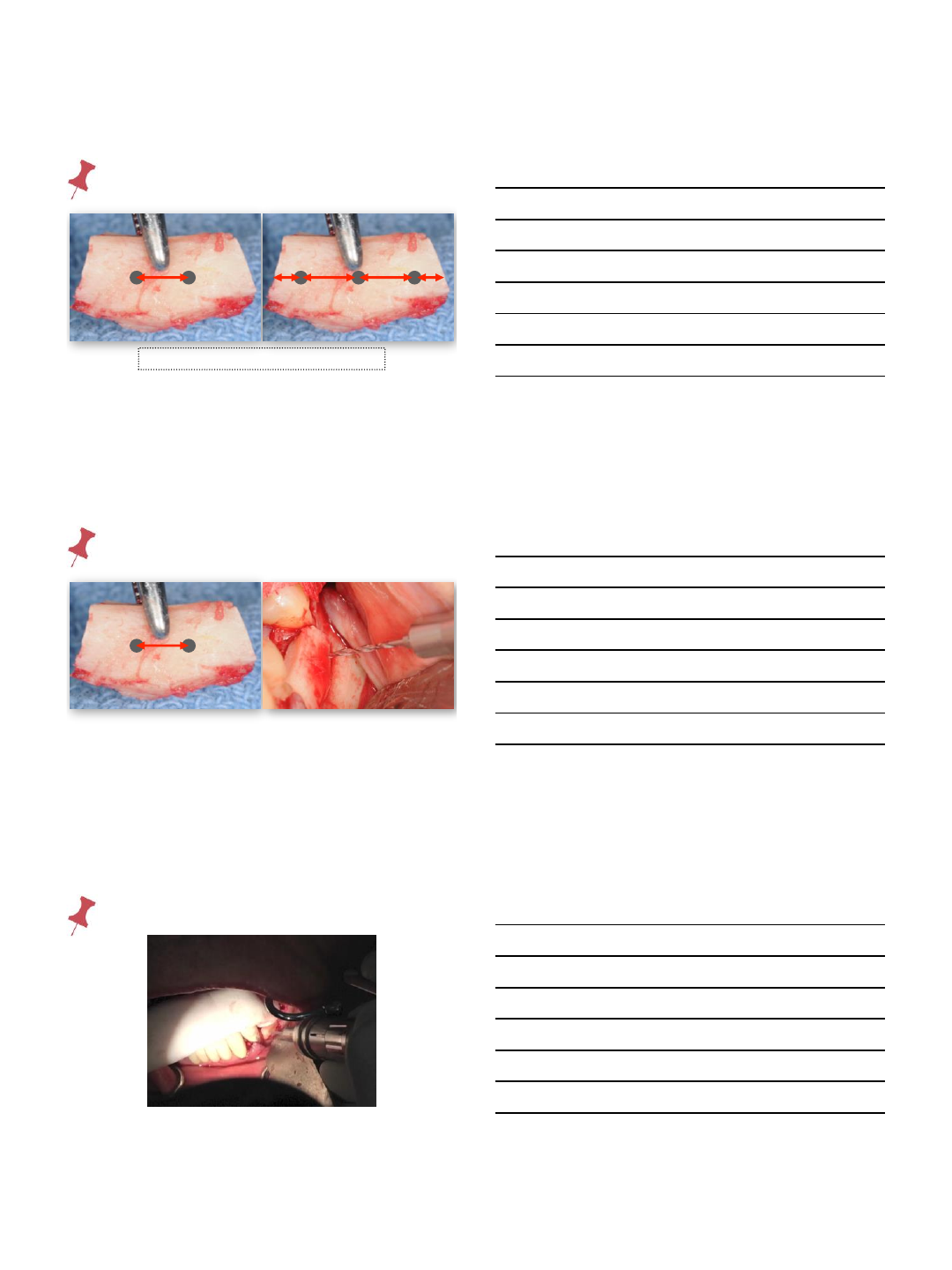
screw
stability and compression of block / recipient
overdrill the block
hole
screw perpendicular to
‘fracture site’
countersink to create a
platform
select the right screw
length
two-point fixation
screw
stability and compression of block / recipient
overdrill the block hole
screw perpendicular
to ‘fracture site’
countersink to create a
platform
select the right screw
length
two-point fixation
screw
stability and compression of block / recipient
overdrill the block hole
screw perpendicular to
‘fracture site’
countersink to create
a platform
select the right screw
length
two-point fixation
9/4/2014
18
screw
stability and compression of block / recipient
overdrill the block hole
screw perpendicular to
‘fracture site’
countersink to create a
platform
select the right screw
length
two-point fixation
screw
stability and compression of block / recipient
overdrill the block hole
screw perpendicular to
‘fracture site’
countersink to create a
platform
select the right screw
length
two-point fixation
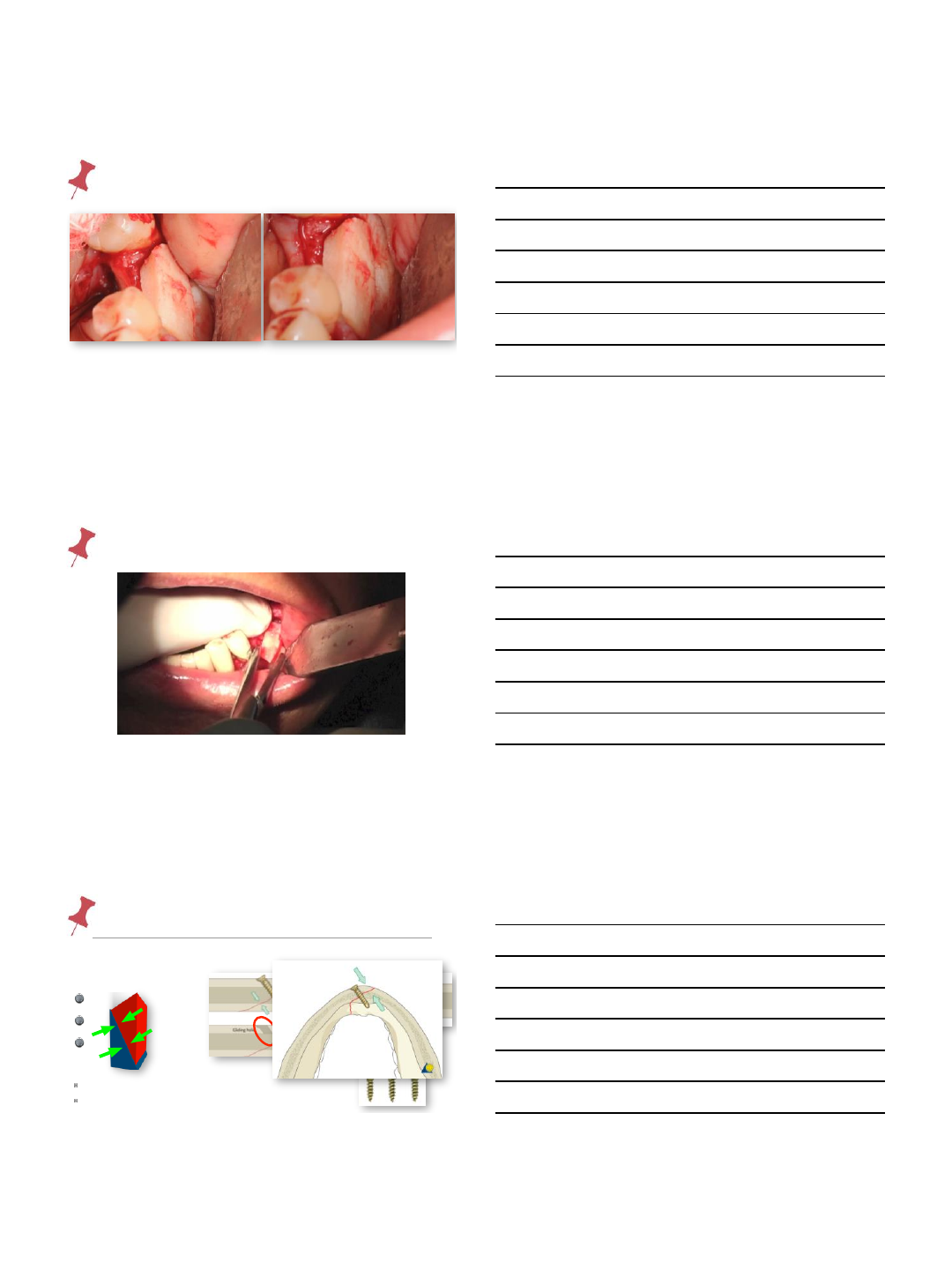
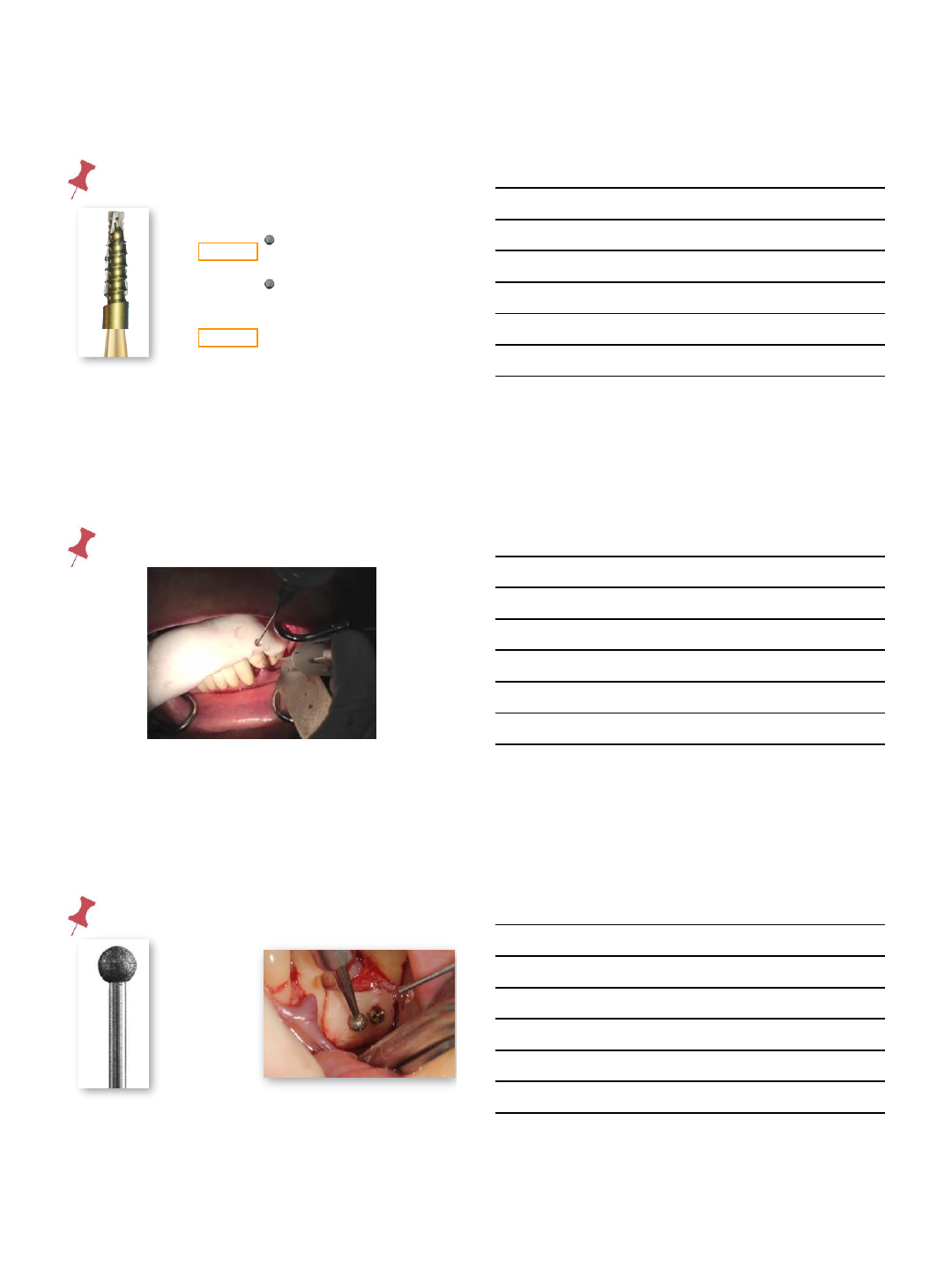
fixation- ⃣hold block
9/4/2014
19
fixation- 2 vs 3 point
min 3 mm 2 23 3
prevent stress fracture of block
fixation- ⃣first drill
min 3 mm
fixation- ⃣first drill
9/4/2014
20
fixation- ⃣over-drill
702 bur
tip 1.1 mm
head 1.6 mm
length 4.5 mm
701 bur
tip 0.8 mm
head 1.2 mm
length 3.8 mm
lag technique
easy rotation of
screw without block
displacement
fixation- ⃣over-drill
fixation- ⃣countersink
8 round
diamond
diameter
3 mm
9/4/2014
21
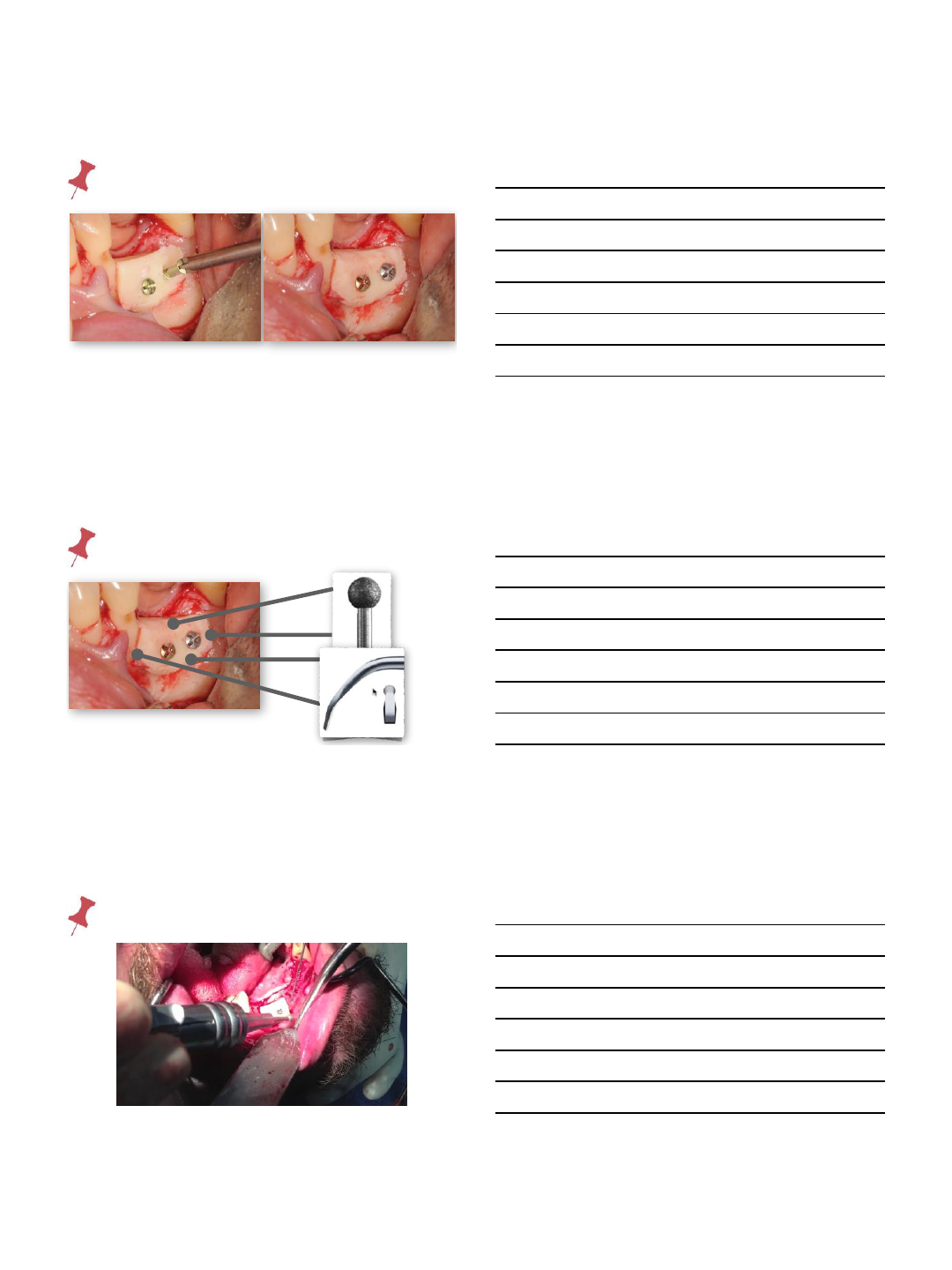
fixation- ⃣screw
fixation- ⃣osteoplasty
fixation- ⃣osteoplasty
9/4/2014
22
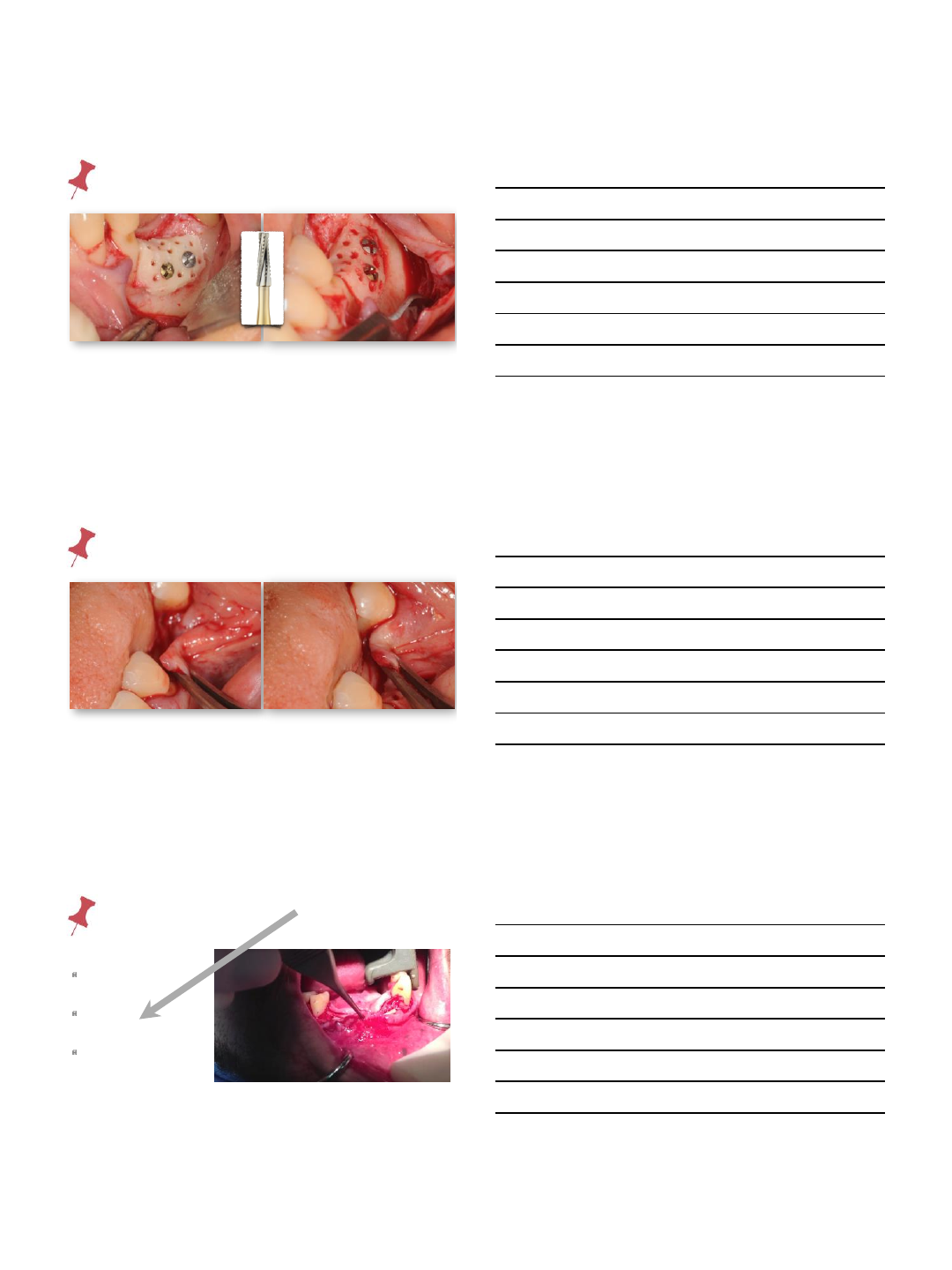
fixation- ⃣perforations
flap release- tensionless
flap release- tensionless
complete flap
elevation
periosteal
scoring
supra-periosteal
dissection
9/4/2014
23
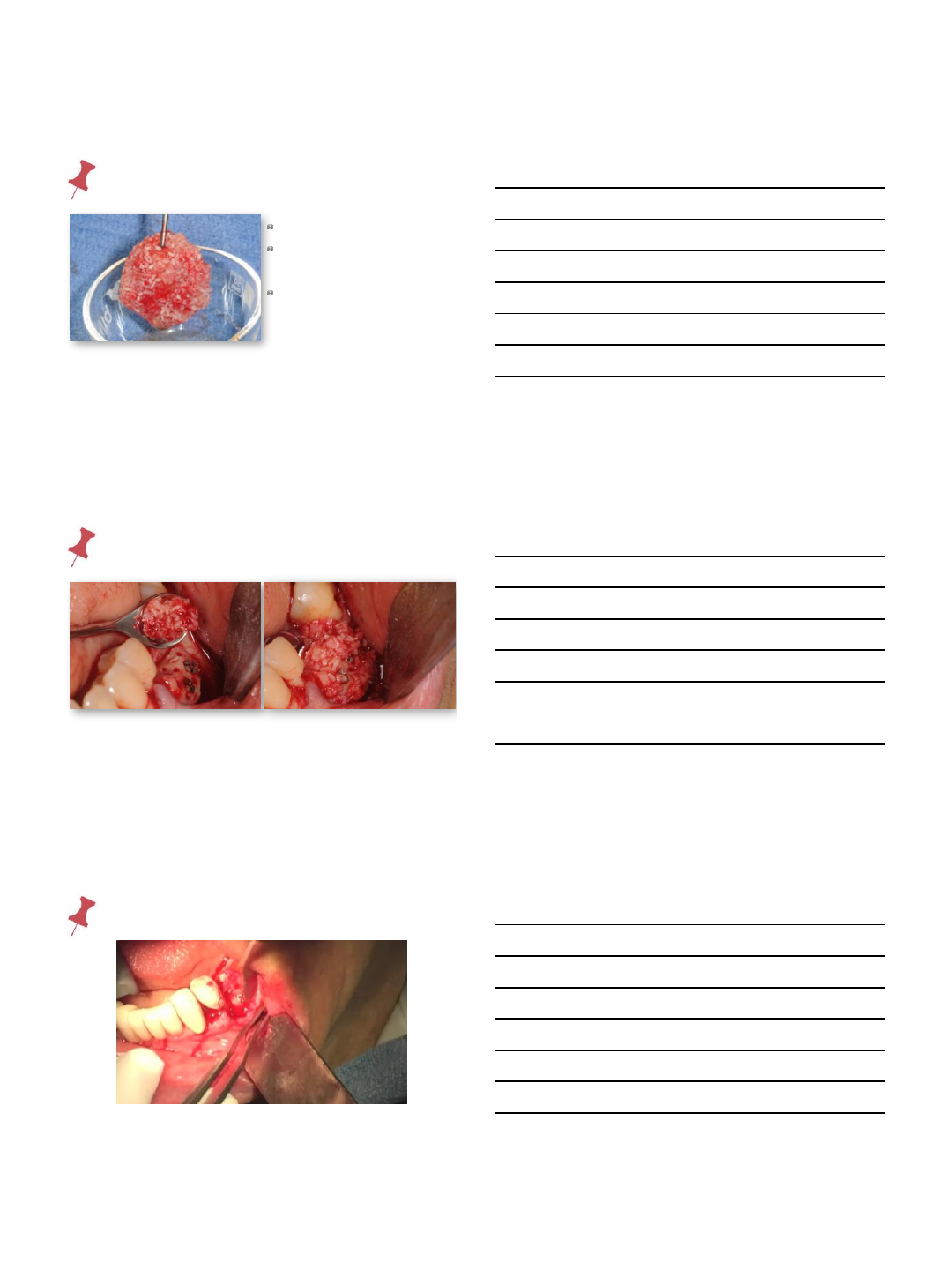
bone gap fill
prgf
autogenous
particulate bone
mineralized
allogenic bone to
expand
bone gap fill
bone gap fill
9/4/2014
24
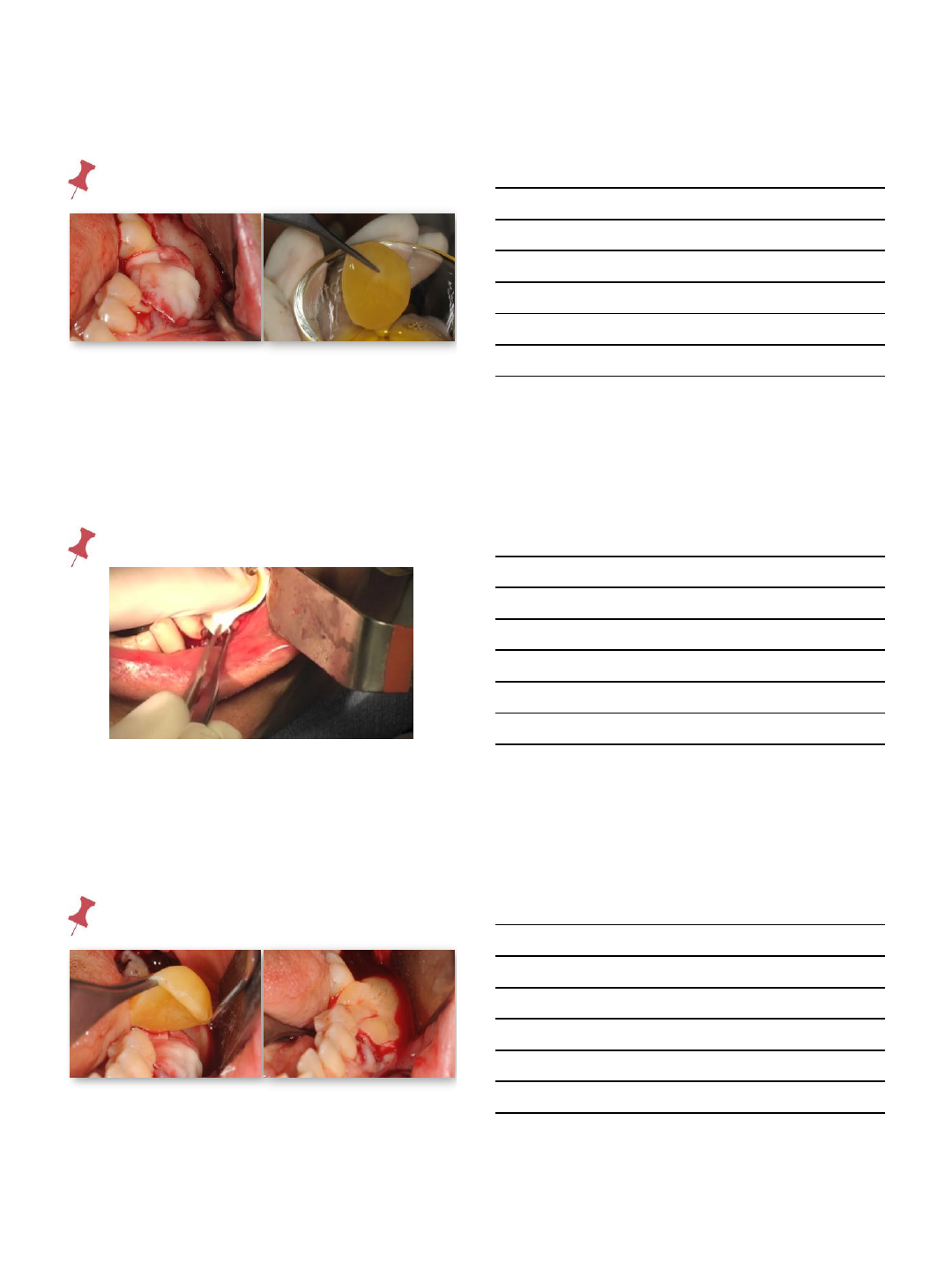
membrane
membrane
prgf membrane
9/4/2014
25
prgf membrane
tension-less closure
prgf clot in donor site
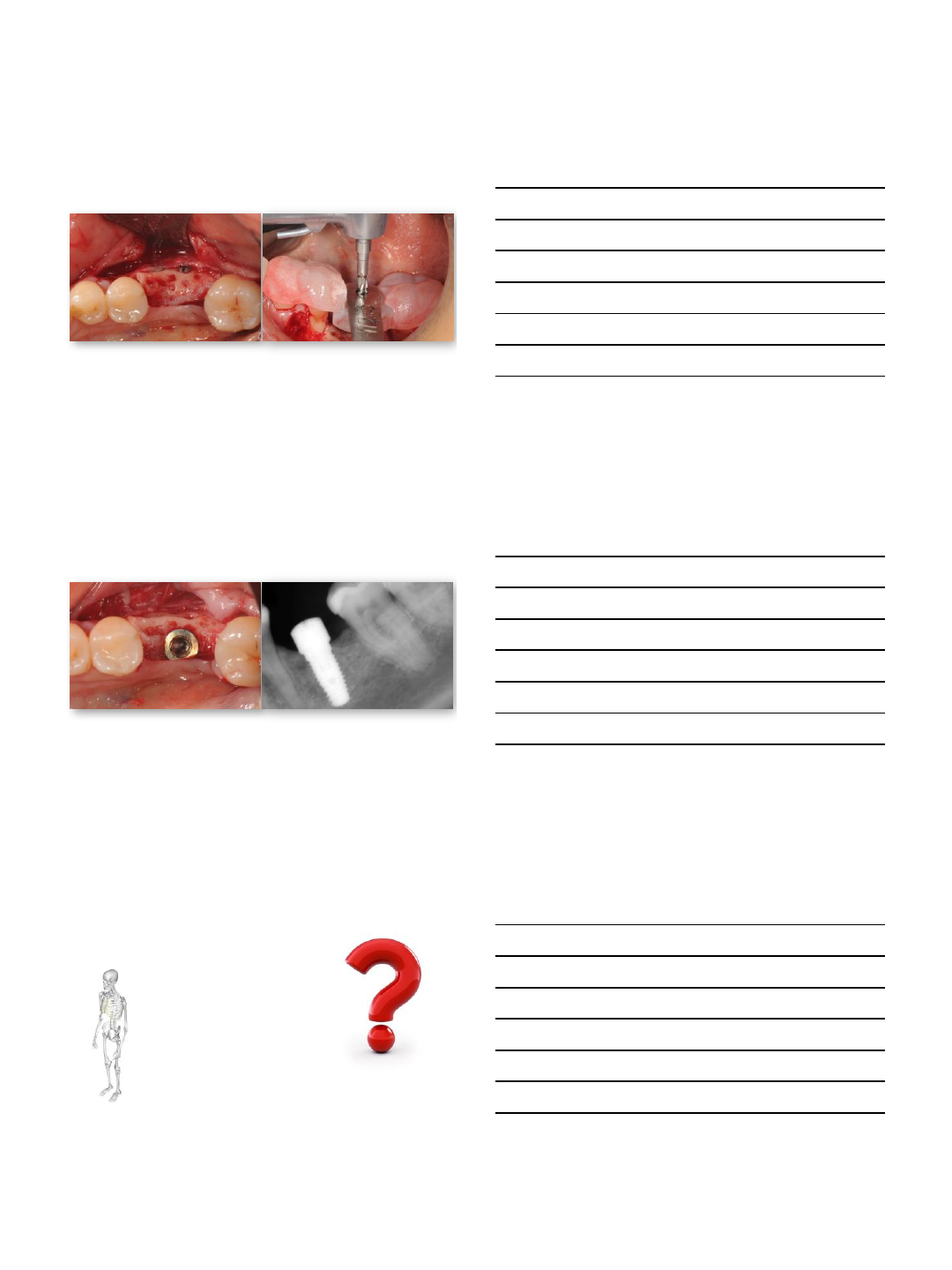
implant planning
9/4/2014
26
before after
implant planning
Implant Placement
Implant Placement
9/4/2014
27
Implant Placement
Implant Placement
cad / cam
customized
bone
blocks
9/4/2014
28
predesign &
prefabricate
an ideal block
simplify
improve adaptation
decrease operative time
cad allografts
Ridge Augmentation Using Customized
Allogenic Bone Blocks: Proof of Concept
and Histological Findings
Customized Allogenic
Bone Blocks
Schlee, M, Rothamel, D:
Implant Dent 2013; 0: 1-7
CBCT
3-D planning software
defect drawn on 3-D surface
3-D information converted
CNC programming
graft milled out of a single block
cad allografts
Ridge Augmentation Using Customized Allogenic Bone Blocks: Proof of Concept and Histological Findings
Schlee, M, Rothamel, D:Implant Dent 2013; 0: 1-7
9/4/2014
29
cad allografts
Ridge Augmentation Using Customized Allogenic Bone Blocks: Proof of Concept and Histological Findings
Schlee, M, Rothamel, D:Implant Dent 2013; 0: 1-7
cad allografts
Ridge Augmentation Using Customized Allogenic Bone Blocks: Proof of Concept and Histological Findings
Schlee, M, Rothamel, D:Implant Dent 2013; 0: 1-7
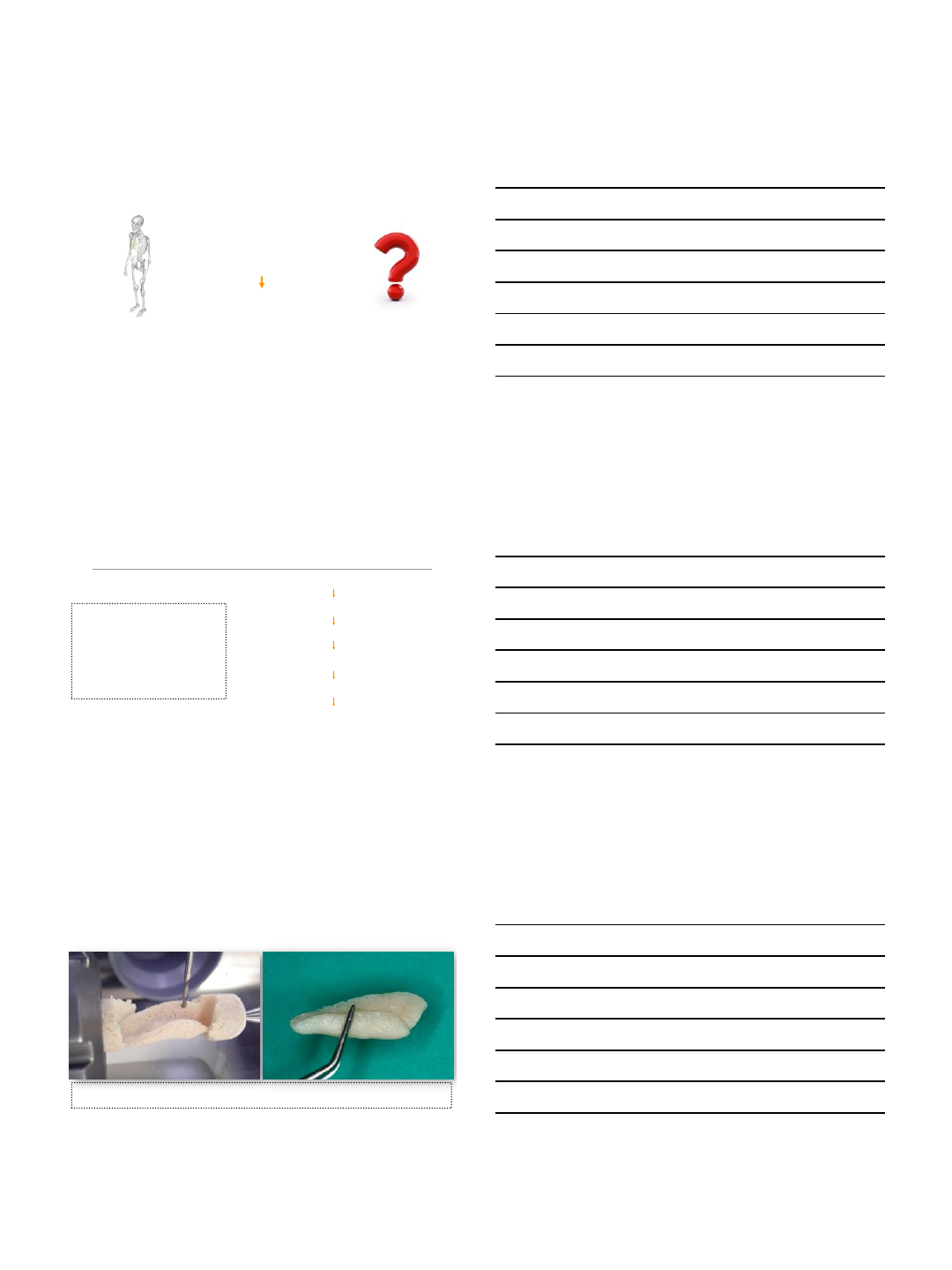
cad /cam
customized
autogenous
bone
blocks
9/4/2014
30
CBCT
3-D design
of block
harvest block
immediate
placement
❓bone handling
❓sterility
❓cellular response
❓cost
stay
tuned
chair-side
milling machine
www.facialart.com
9/4/2014
1
V. Broumand, DMD, MD
Assistant Professor of Surgery
Director of Resident Medical Education
University of Miami
Miller School of Medicine
Complications during surgery,
immediate post operative and
long term for the harvest site
Autogenous Bone
Harvesting For Ridge
Augmentation
1. Tibia
2. Symphysis
3. Ramus
4. Maxillary Tuberosity
9/4/2014
2
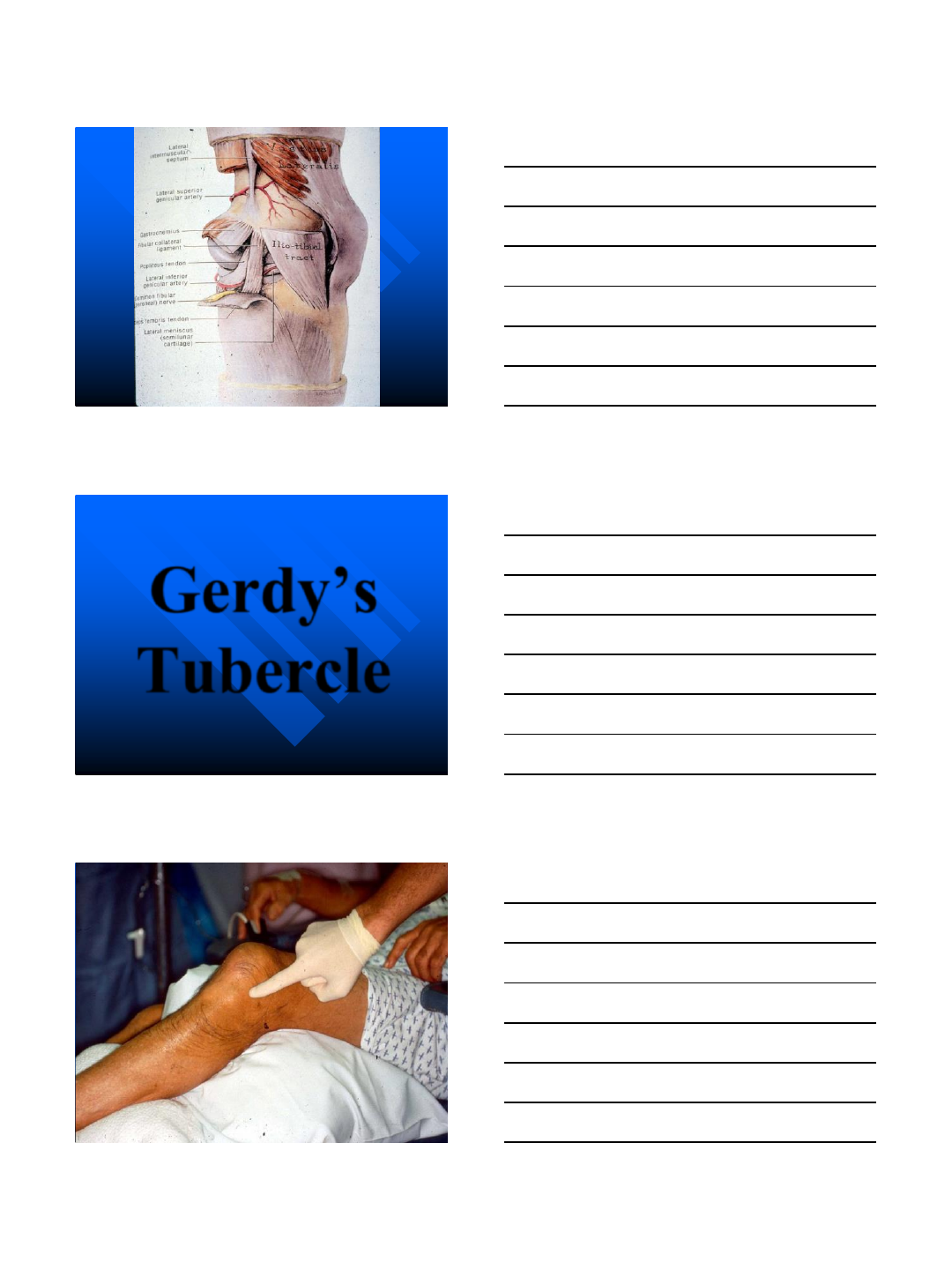
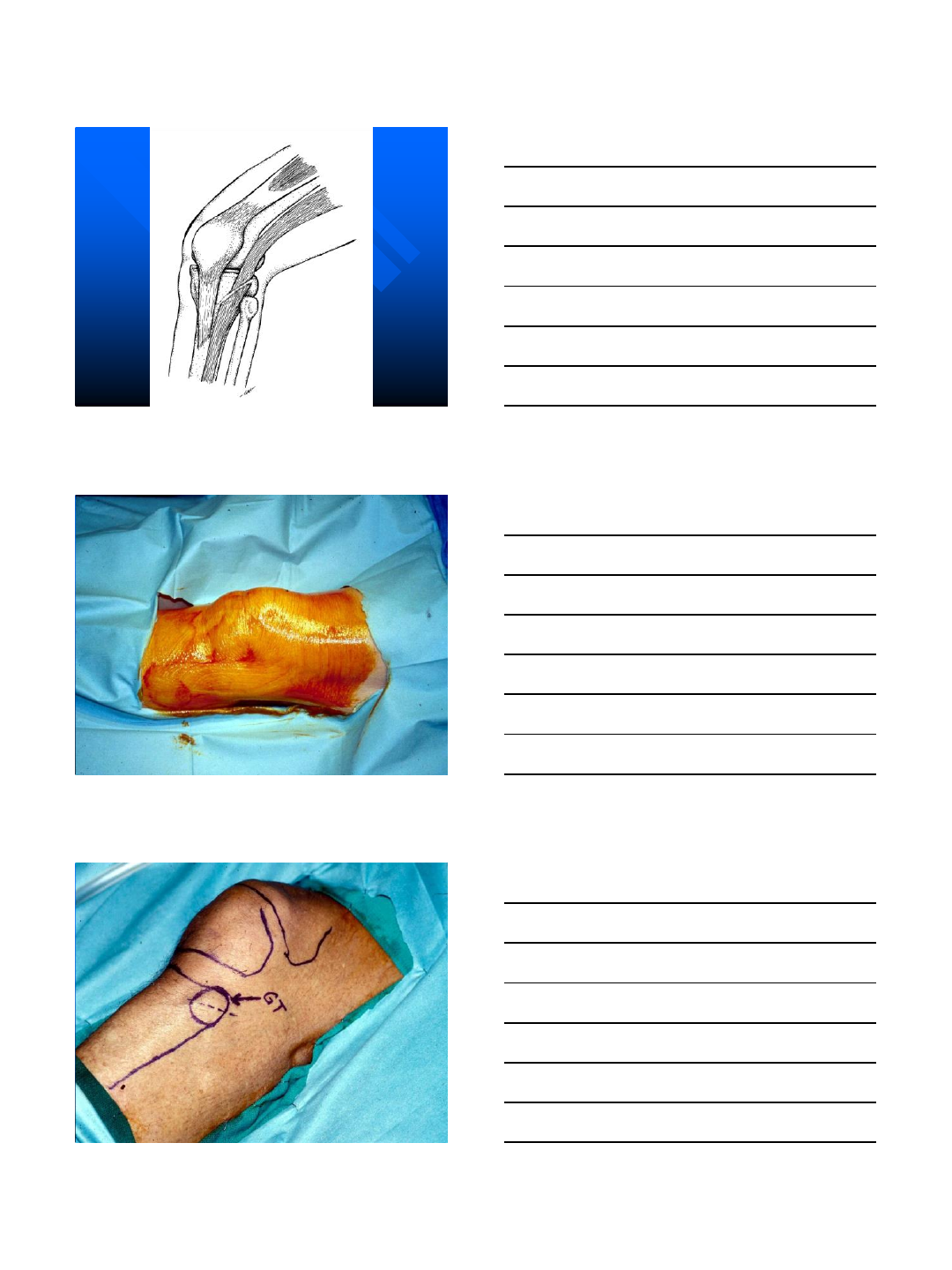
Tibia Bone Harvest
An Office
Procedure
9/4/2014
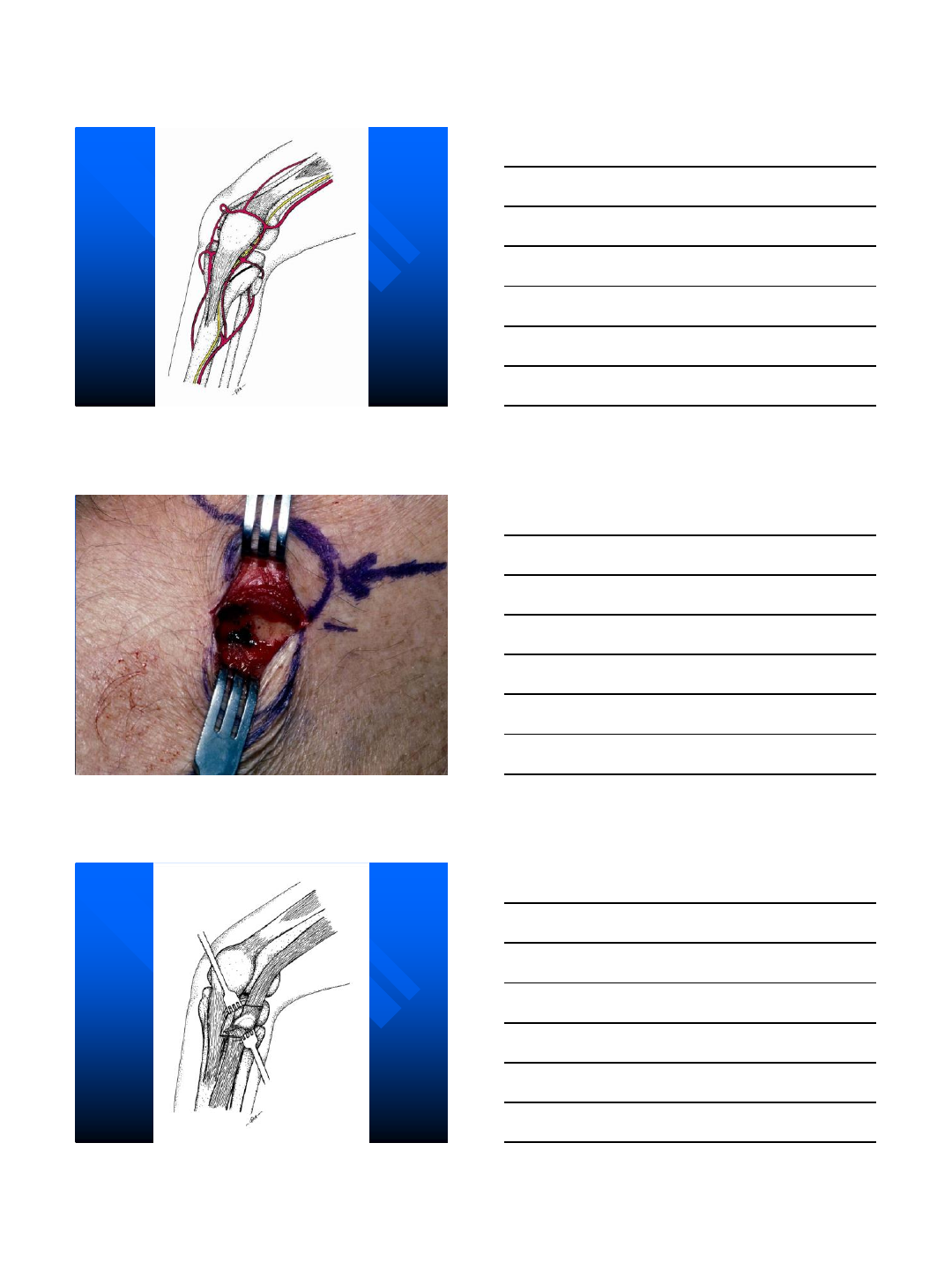
3
Gerdy’s
Tubercle
9/4/2014
4
9/4/2014
5
9/4/2014
6
9/4/2014
7
Post Op Instructions
1. Normal activity
2. No sports, running, or stairs
for 6 weeks
3. Ice x 48 hours
4. Elevate leg at night
9/4/2014
8
9/4/2014
9
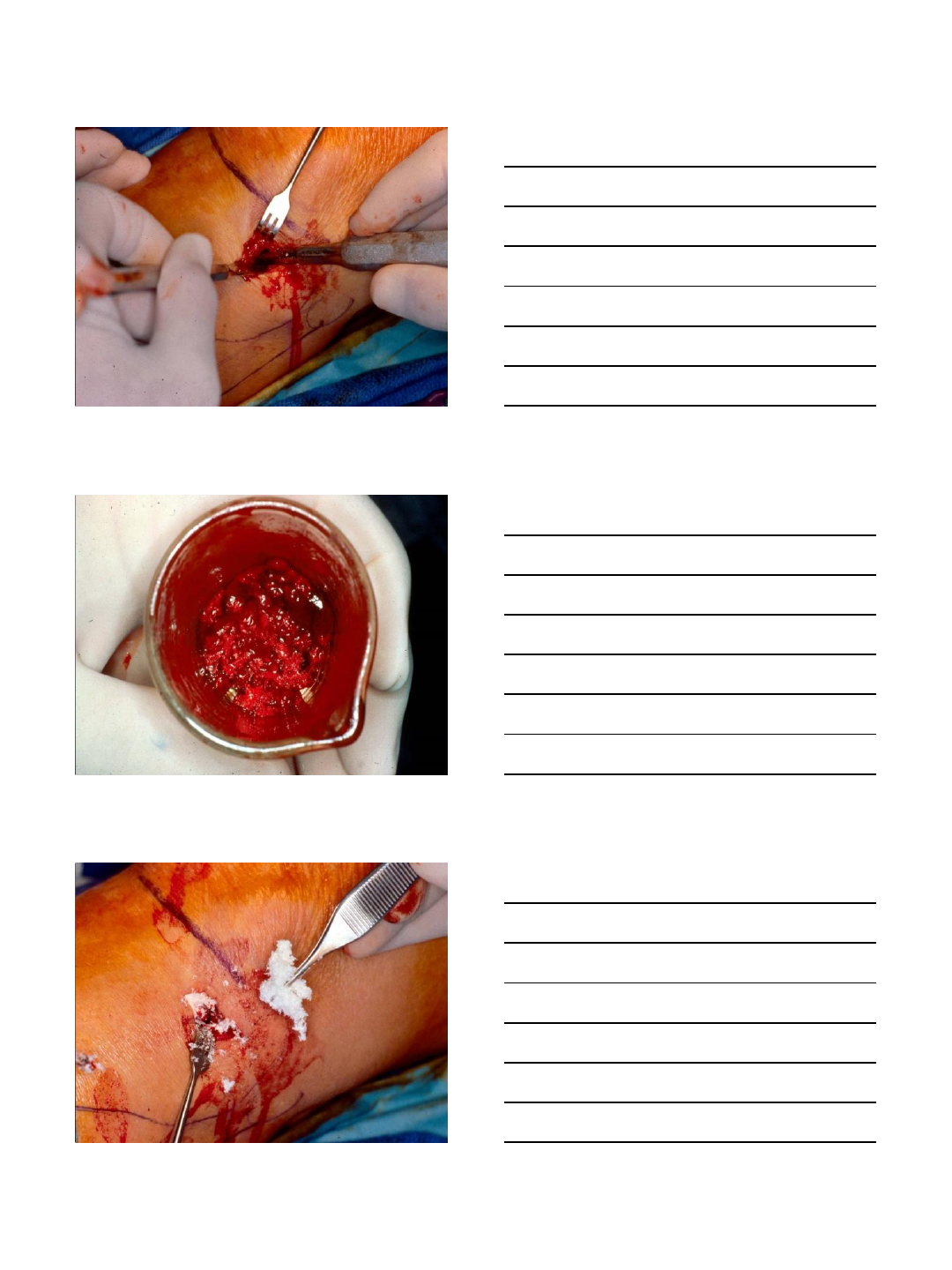
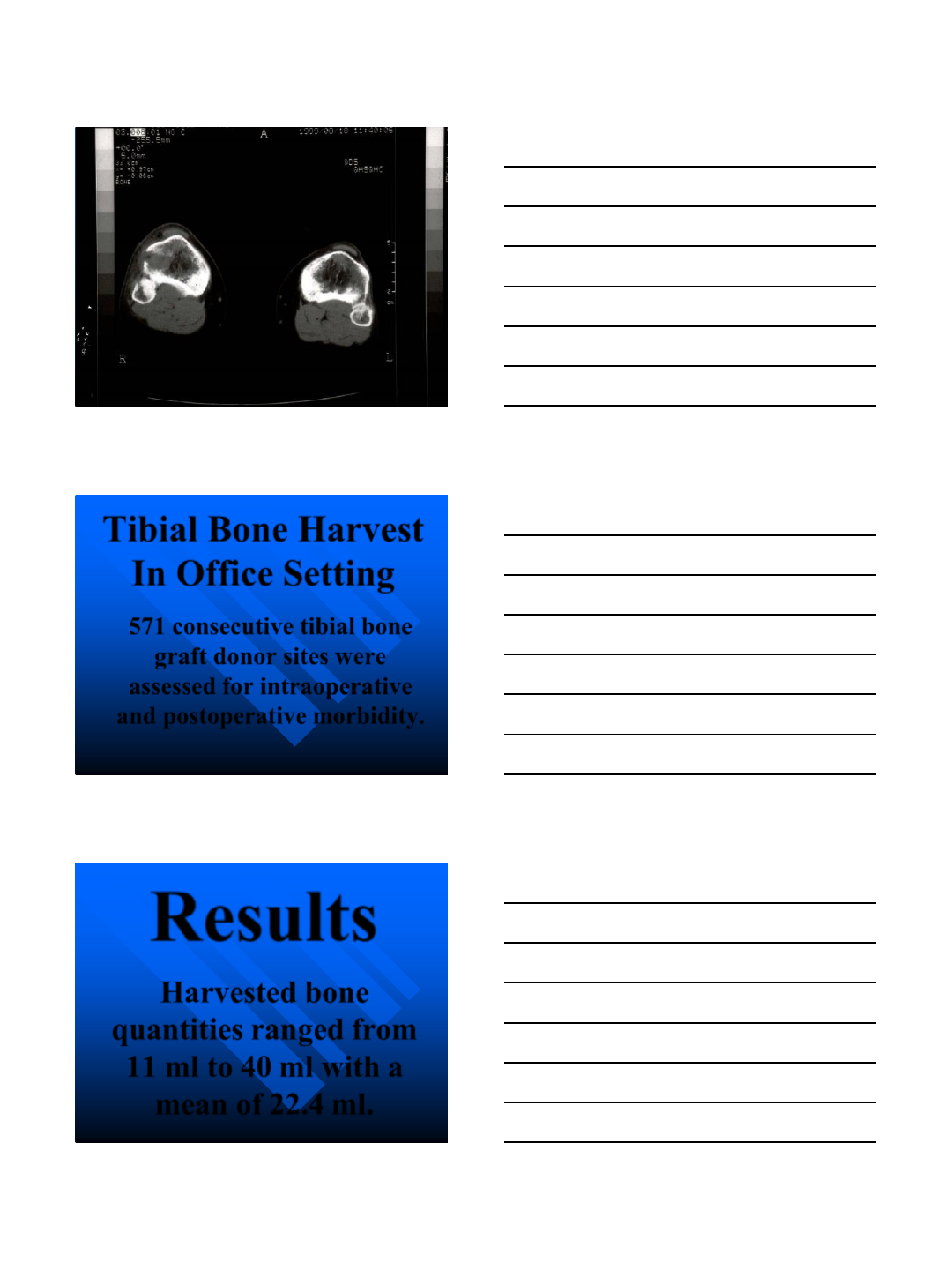
Tibial Bone Harvest
In Office Setting
571 consecutive tibial bone
graft donor sites were
assessed for intraoperative
and postoperative morbidity.
Results
Harvested bone
quantities ranged from
11 ml to 40 ml with a
mean of 22.4 ml.
9/4/2014
10
Morbidity
Blood loss range from 25 ml to 122
ml with a mean of 45 ml.
There were no intraoperative
misadventures such as knee joint
entrance, cartilage damage, or affect
to patellar tendon.
Potential Complications
Tibia Harvest
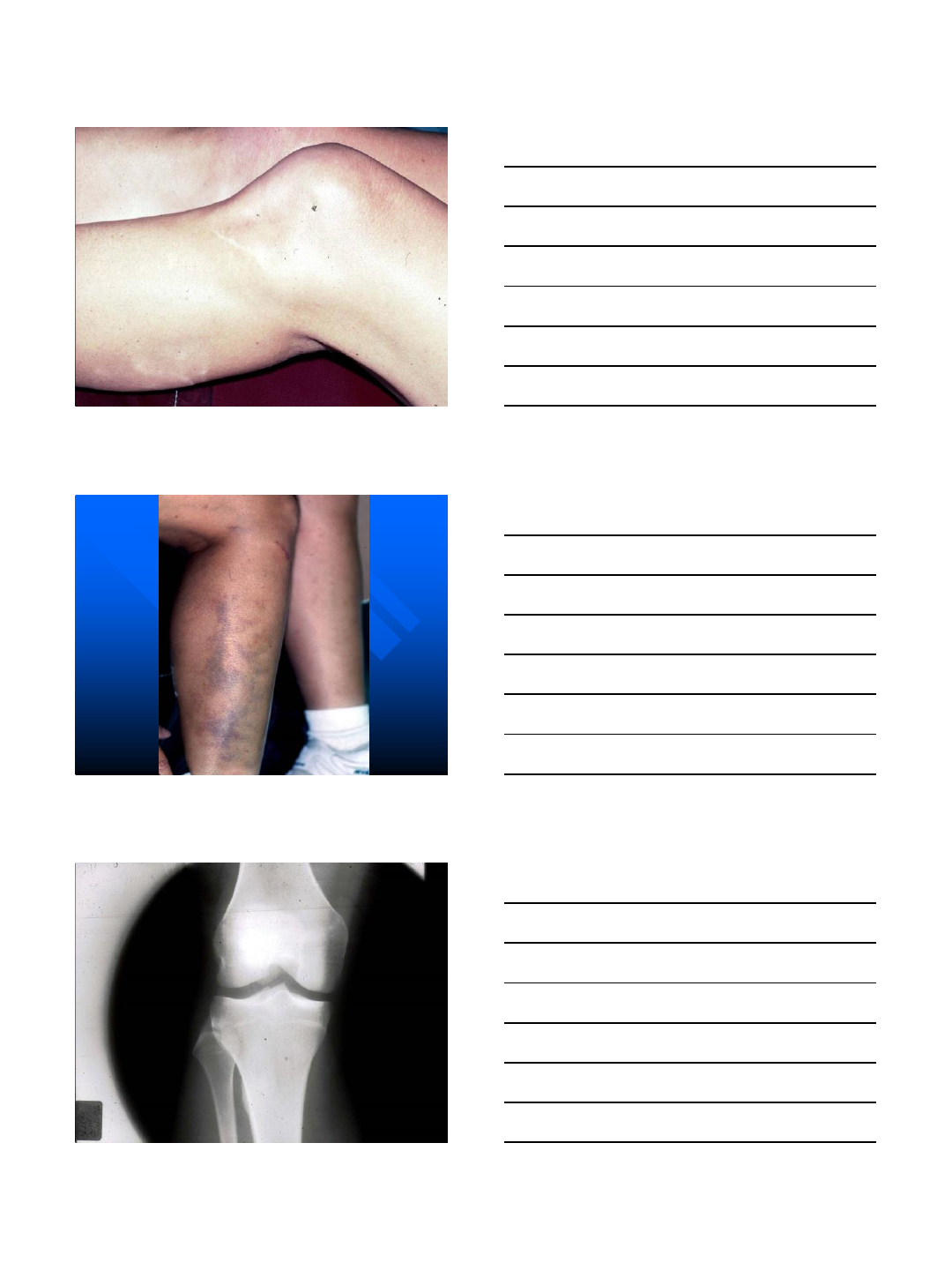
1. Ecchymosis
2. Dehiscence
3. Hematoma
4. Entering the knee joint
5. Scar
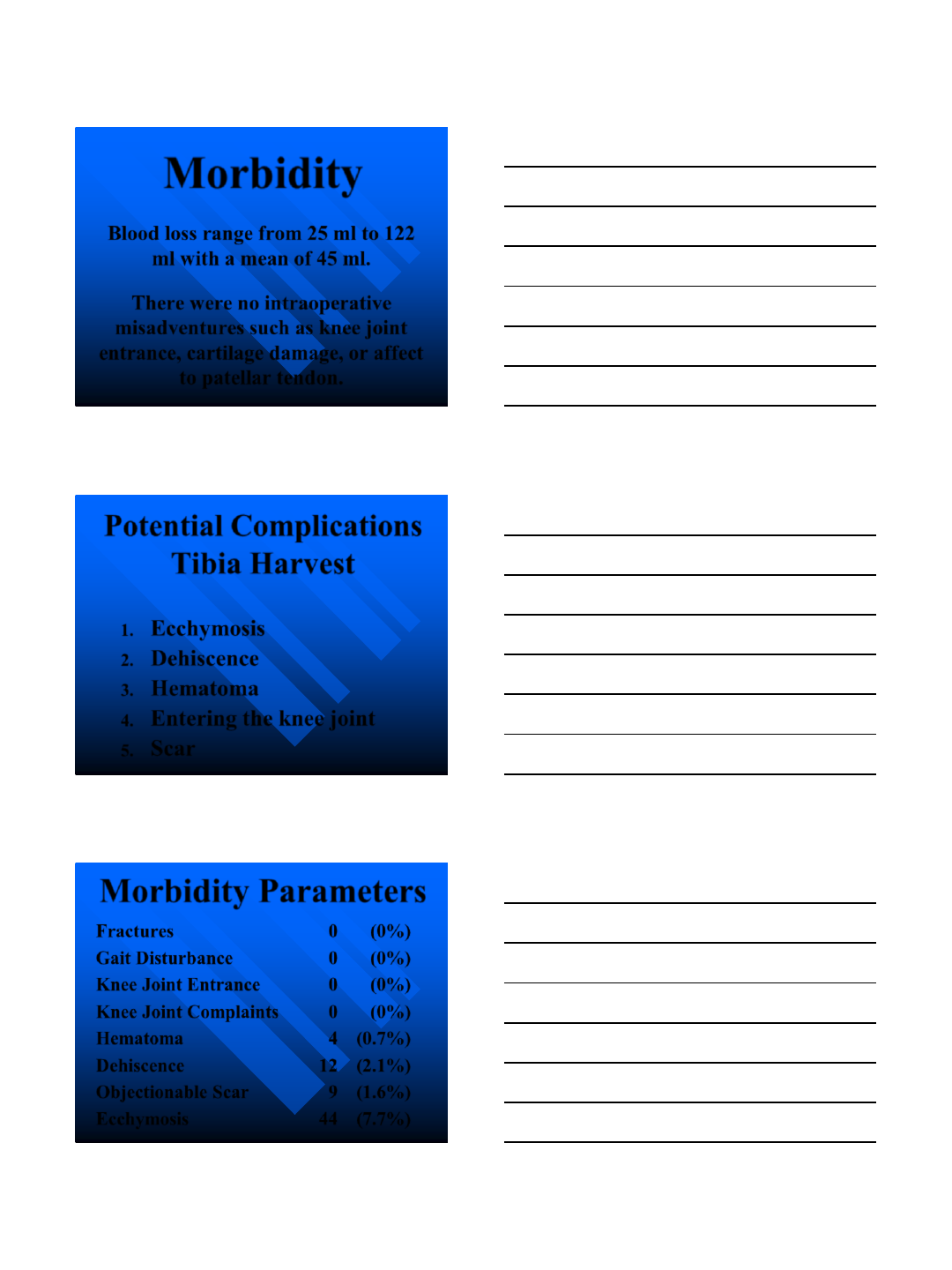
Morbidity Parameters
Fractures 0 (0%)
Gait Disturbance 0 (0%)
Knee Joint Entrance 0 (0%)
Knee Joint Complaints 0 (0%)
Hematoma 4 (0.7%)
Dehiscence 12 (2.1%)
Objectionable Scar 9 (1.6%)
Ecchymosis 44 (7.7%)
9/4/2014
11
Tibial Harvest
Complications
O’Keefe in 1991 –230 grafts
for orthopedic reconstruction
in operating room setting.
Complication rate 1.4%.
Tibial Harvest
Complications
Marx, Schalit, Bartholomew
1997 –2004
571 grafts in office setting for
oral and maxillofacial surgery
Complication rate 1.1%
Tibia Bone Harvest
Advantages
1. Minimal morbidity
2. Good quality bone (note, slightly less than
ilium)
3. Office or operating room procedure
4. Straightforward anatomy and technique
5. Requires minimal instrumentation
6. Can be accomplished under IV sedation
9/4/2014
12
Tibia Bone Harvest
Disadvantages
1. Limited to 30 cc of bone
2. Edema about ankles
3. No block graft capability
Symphysis
Graft
Harvest
9/4/2014
13
9/4/2014
14
Potential Complications
Symphysis Harvest
1. Parasthesia *
2. Fracture
3. Tooth root damage
4. Change in lip position
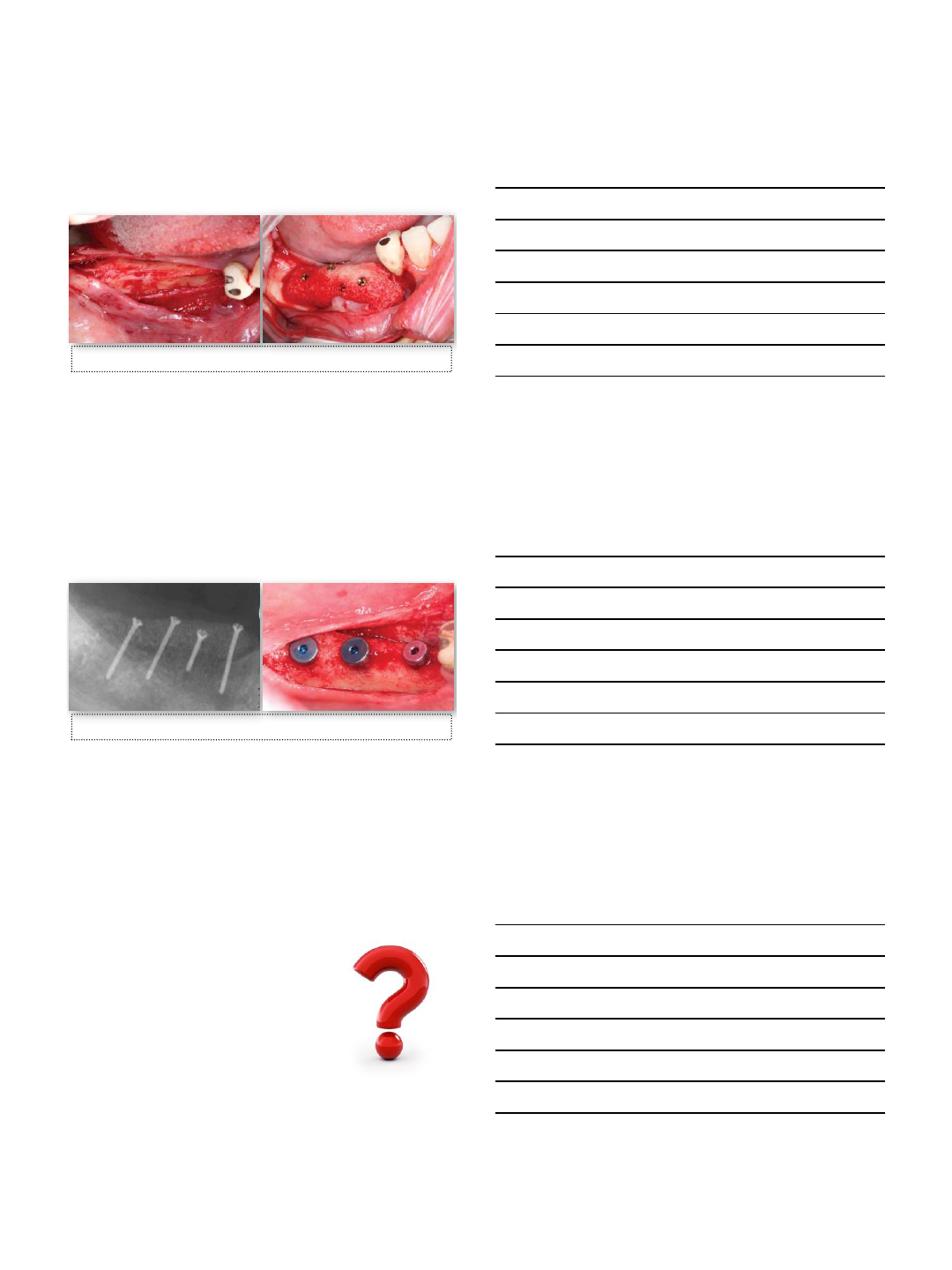
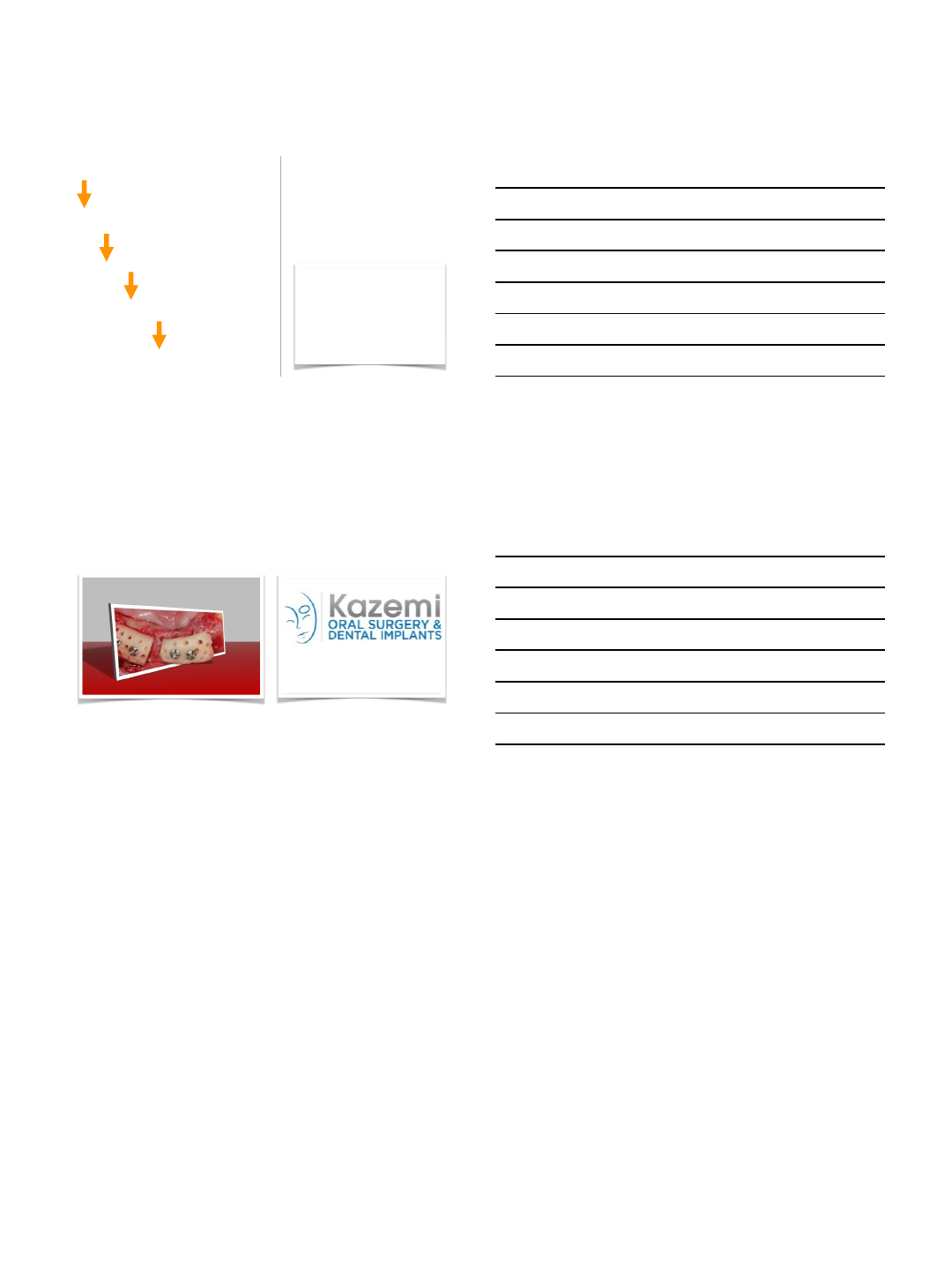
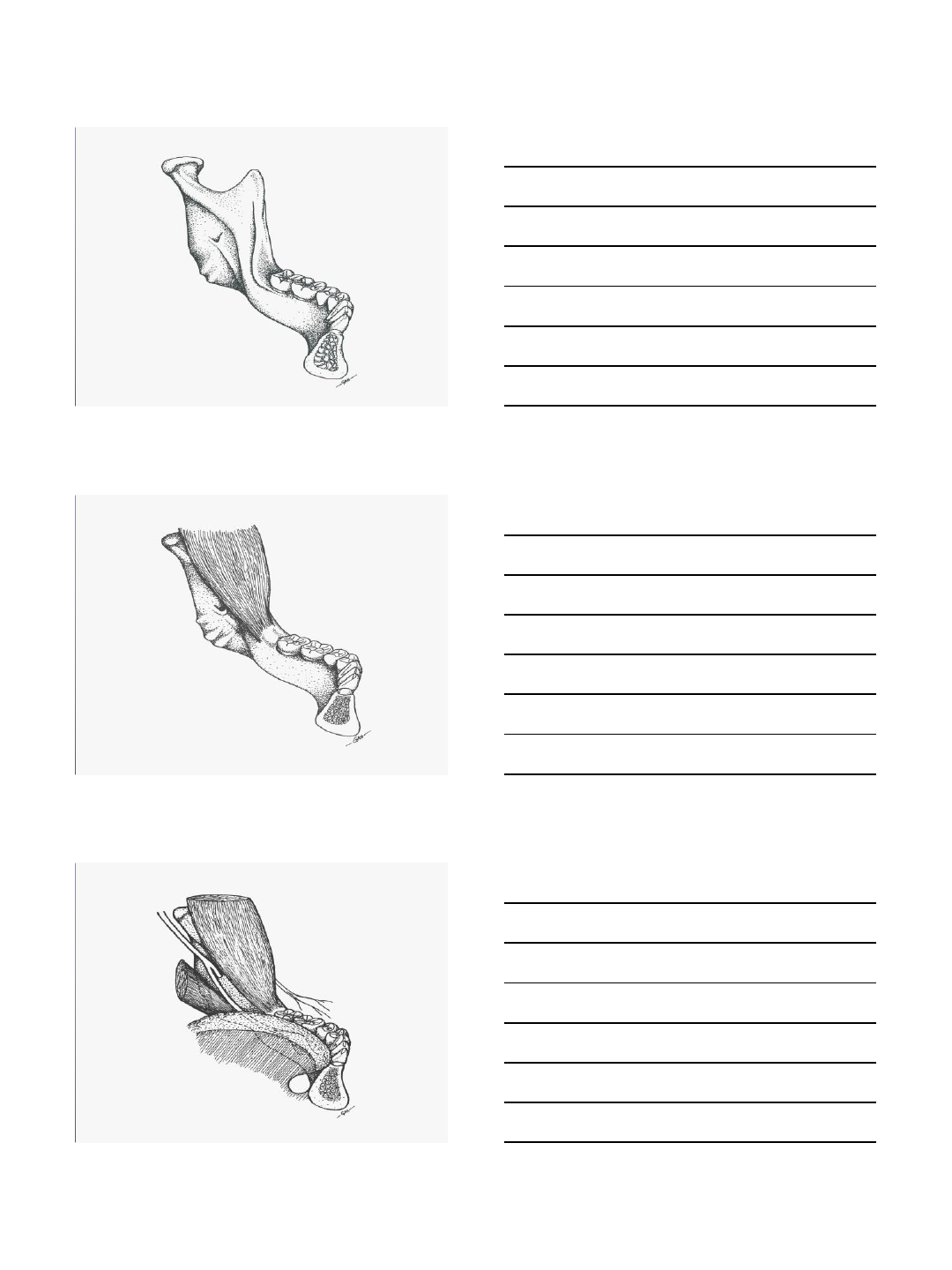
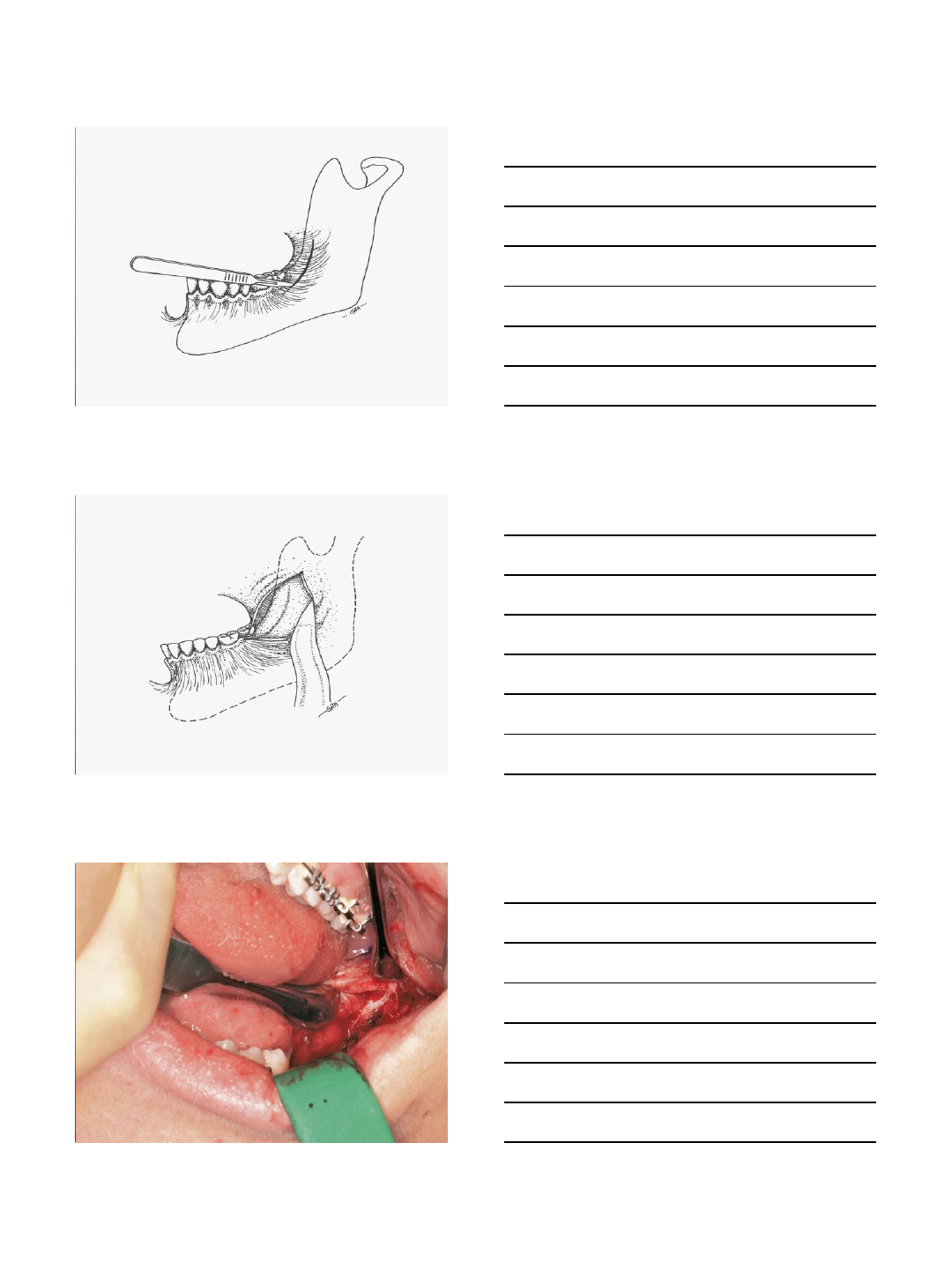
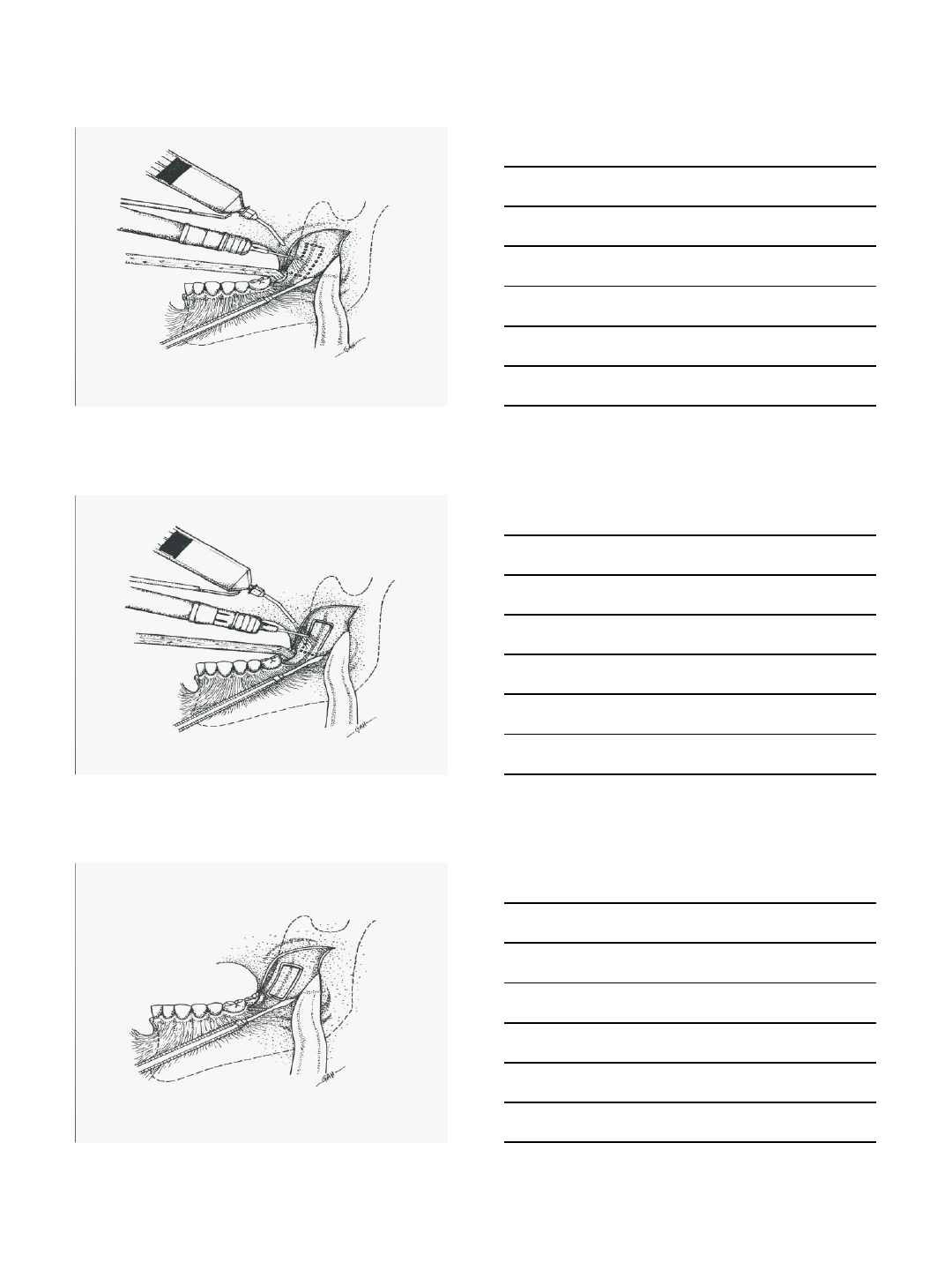
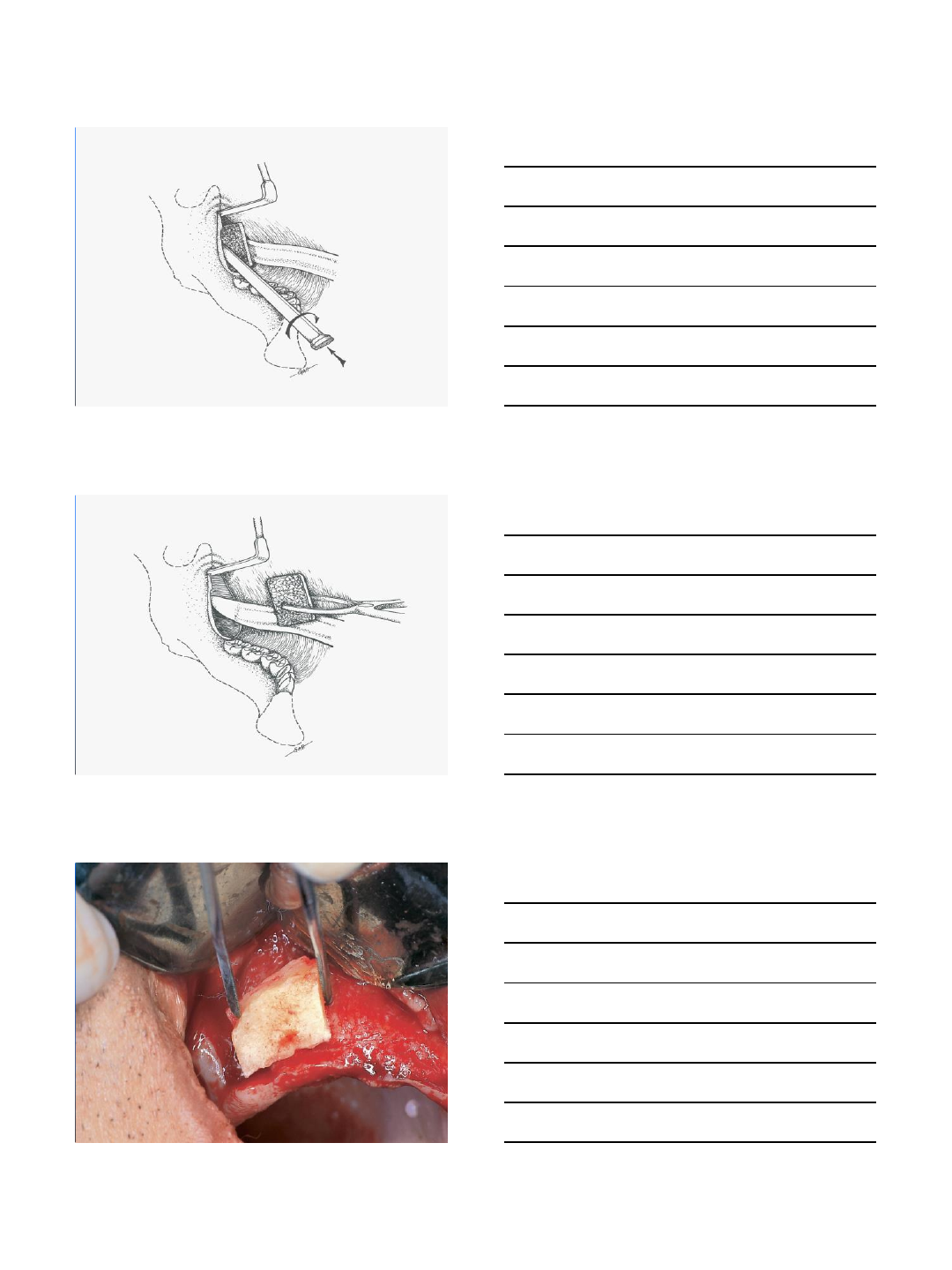
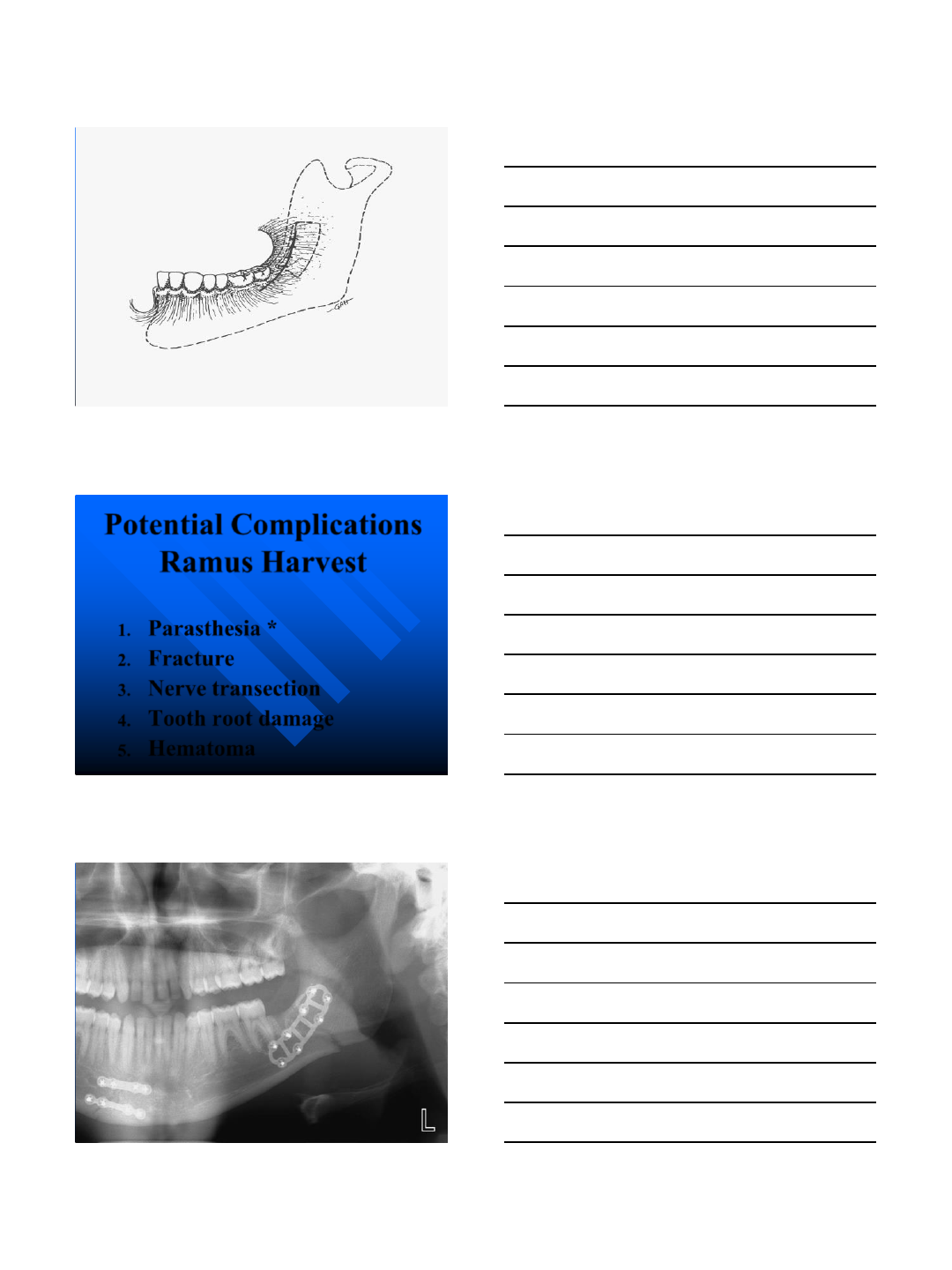
Ramus
Graft
Harvest
9/4/2014
15
9/4/2014
16
9/4/2014
17
9/4/2014
18
9/4/2014
19
Potential Complications
Ramus Harvest
1. Parasthesia *
2. Fracture
3. Nerve transection
4. Tooth root damage
5. Hematoma
9/4/2014
20
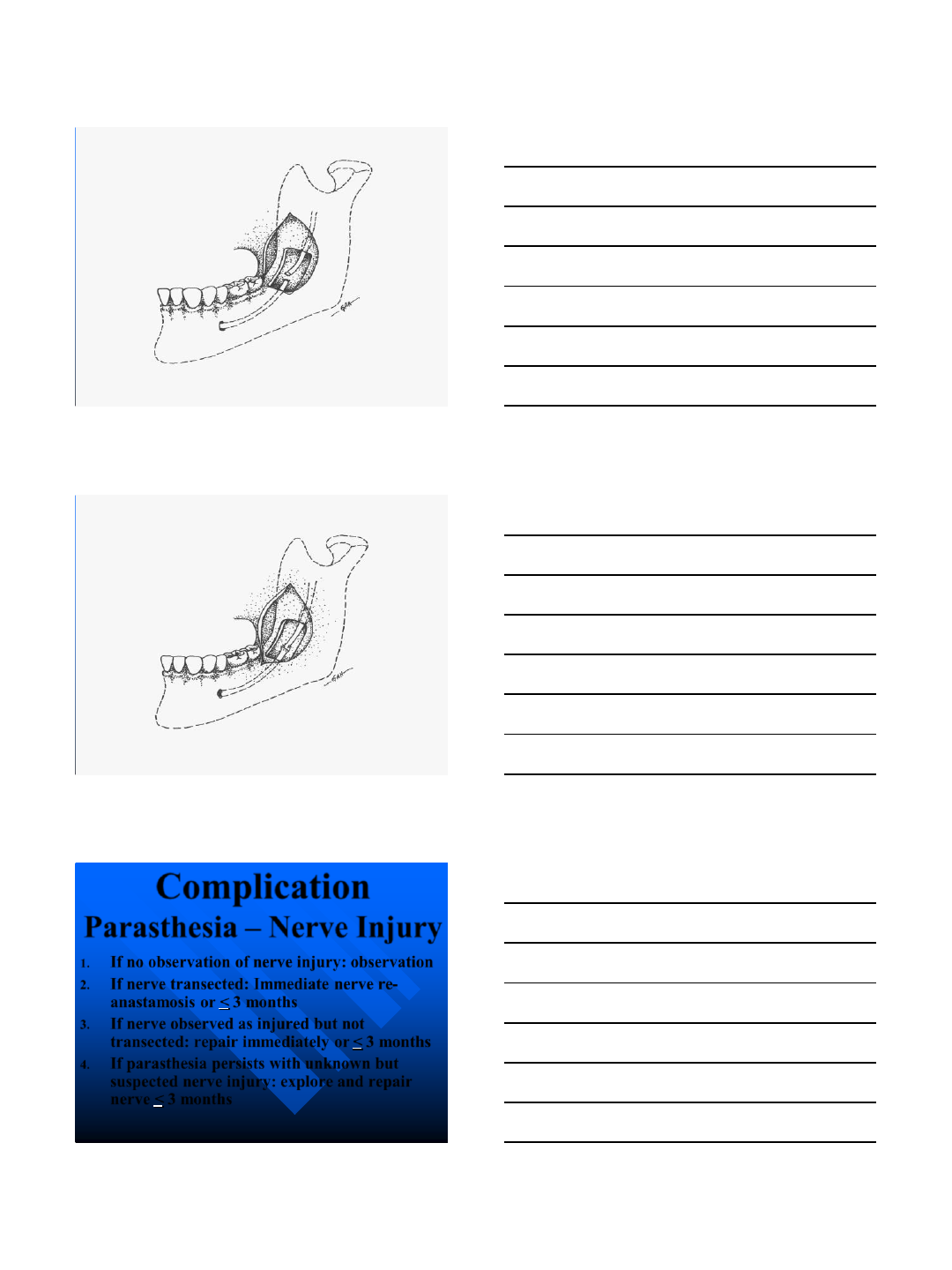
Complication
Parasthesia –Nerve Injury
1. If no observation of nerve injury: observation
2. If nerve transected: Immediate nerve re-
anastamosis or < 3 months
3. If nerve observed as injured but not
transected: repair immediately or < 3 months
4. If parasthesia persists with unknown but
suspected nerve injury: explore and repair
nerve < 3 months
9/4/2014
21
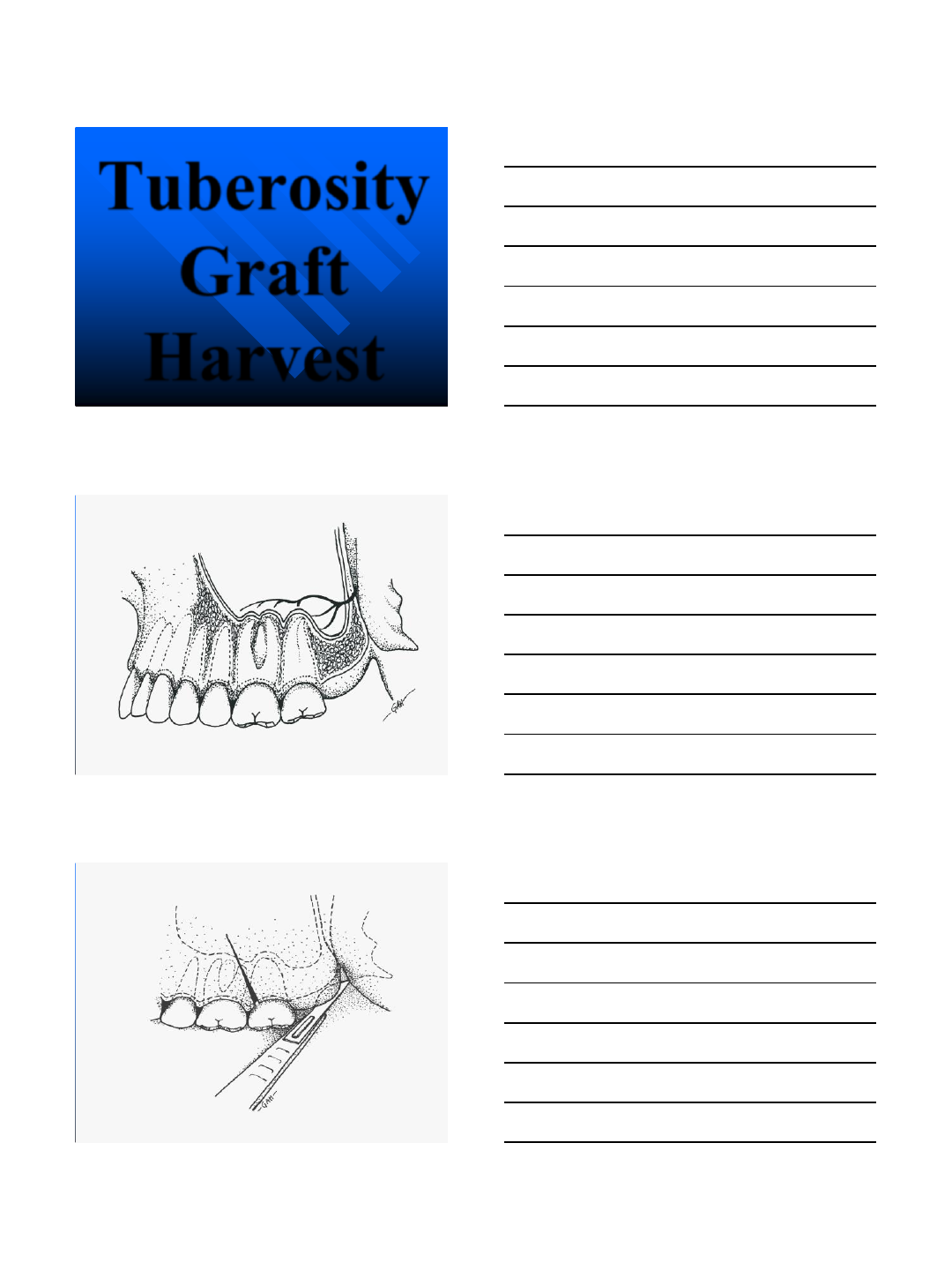
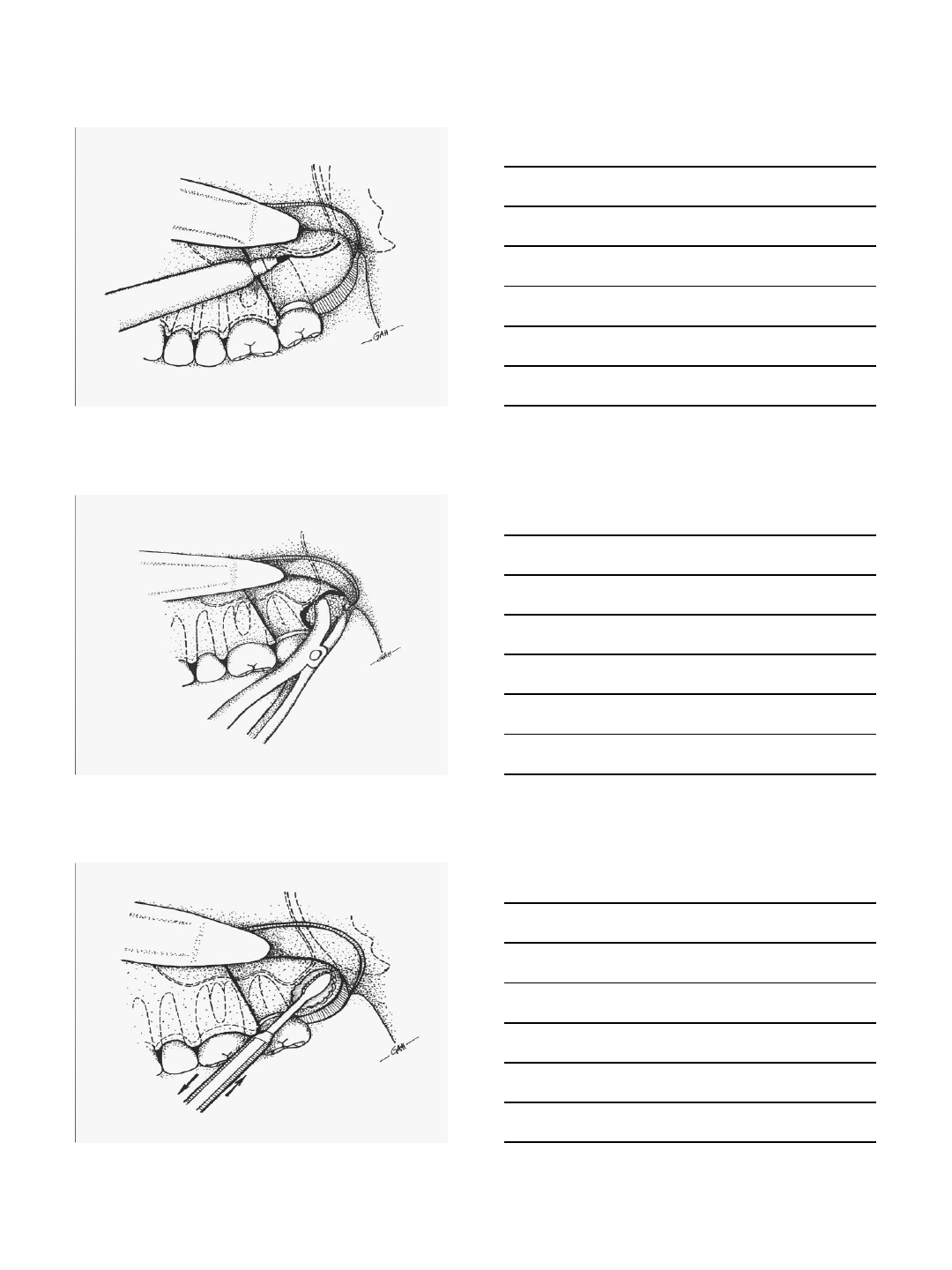
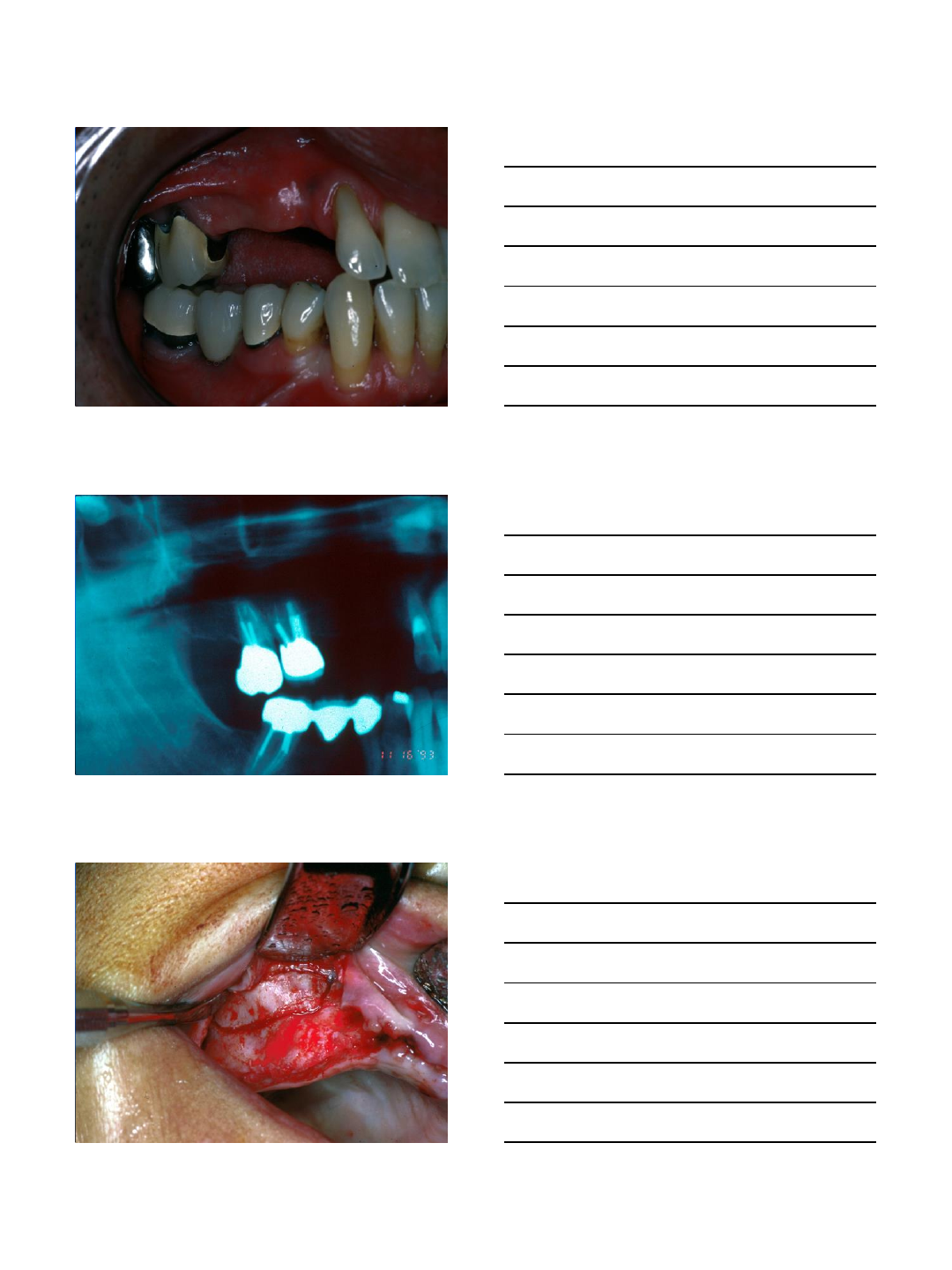
Tuberosity
Graft
Harvest
9/4/2014
22
9/4/2014
23
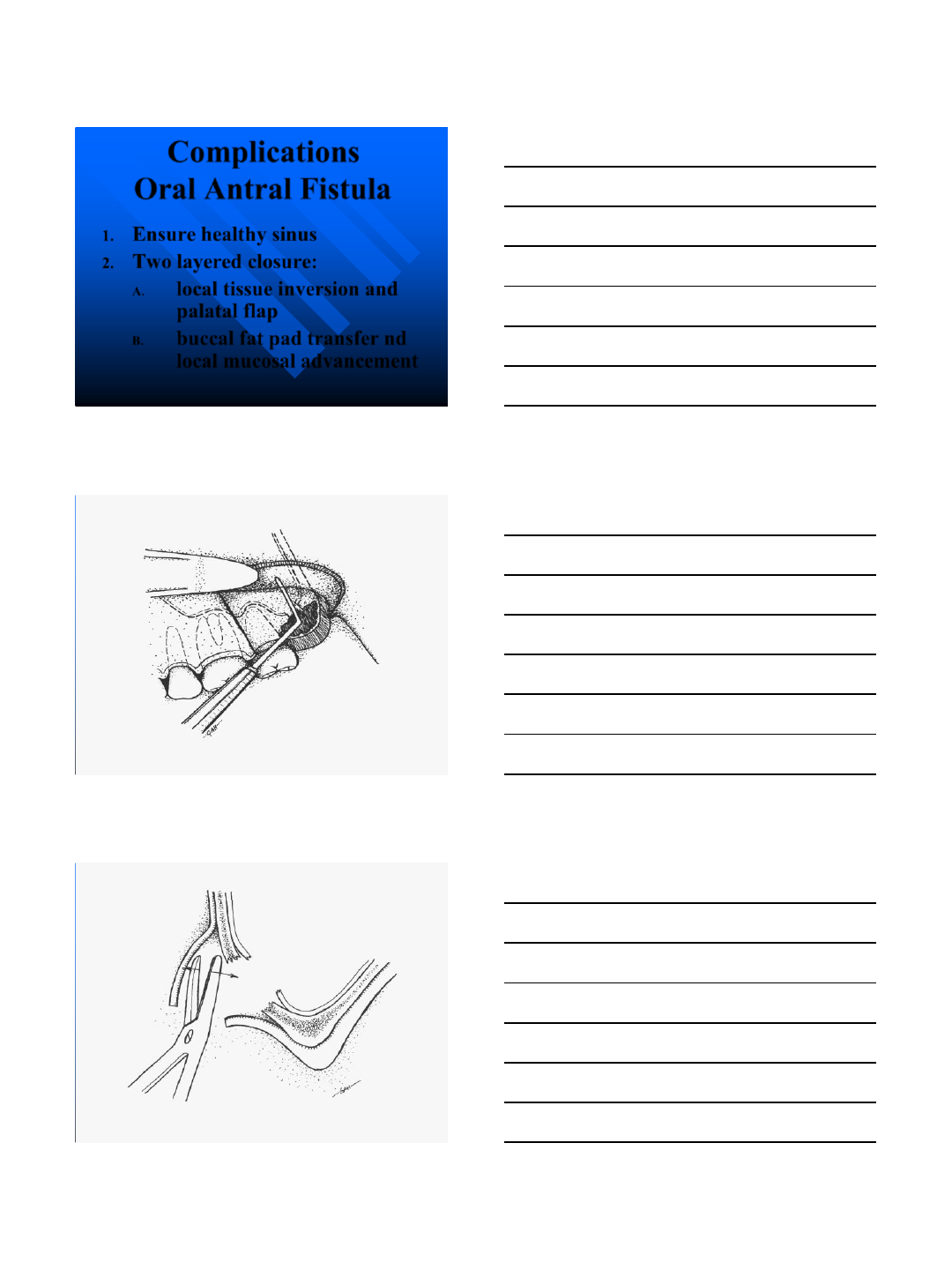
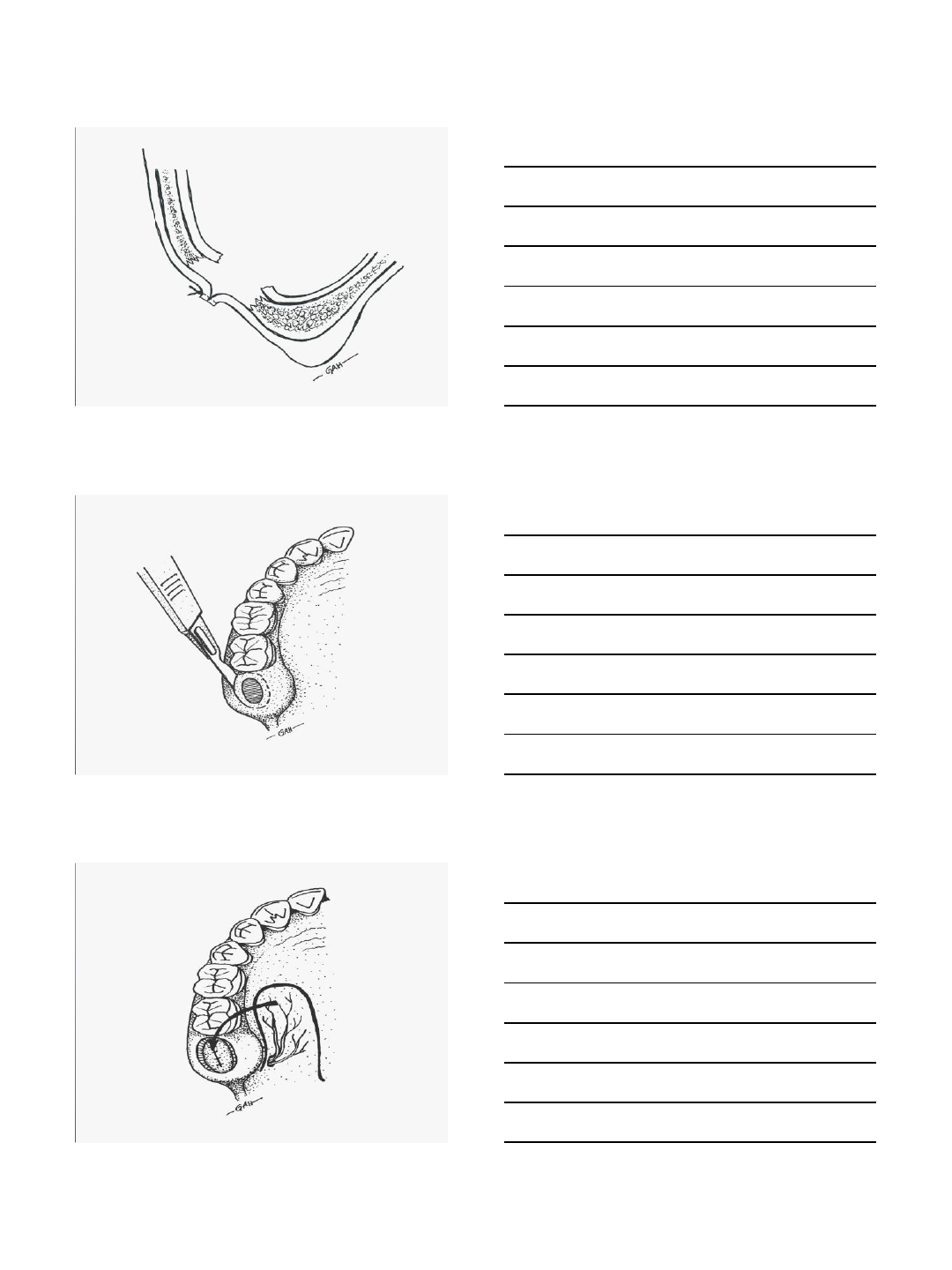
Complications
Oral Antral Fistula
1. Ensure healthy sinus
2. Two layered closure:
A. local tissue inversion and
palatal flap
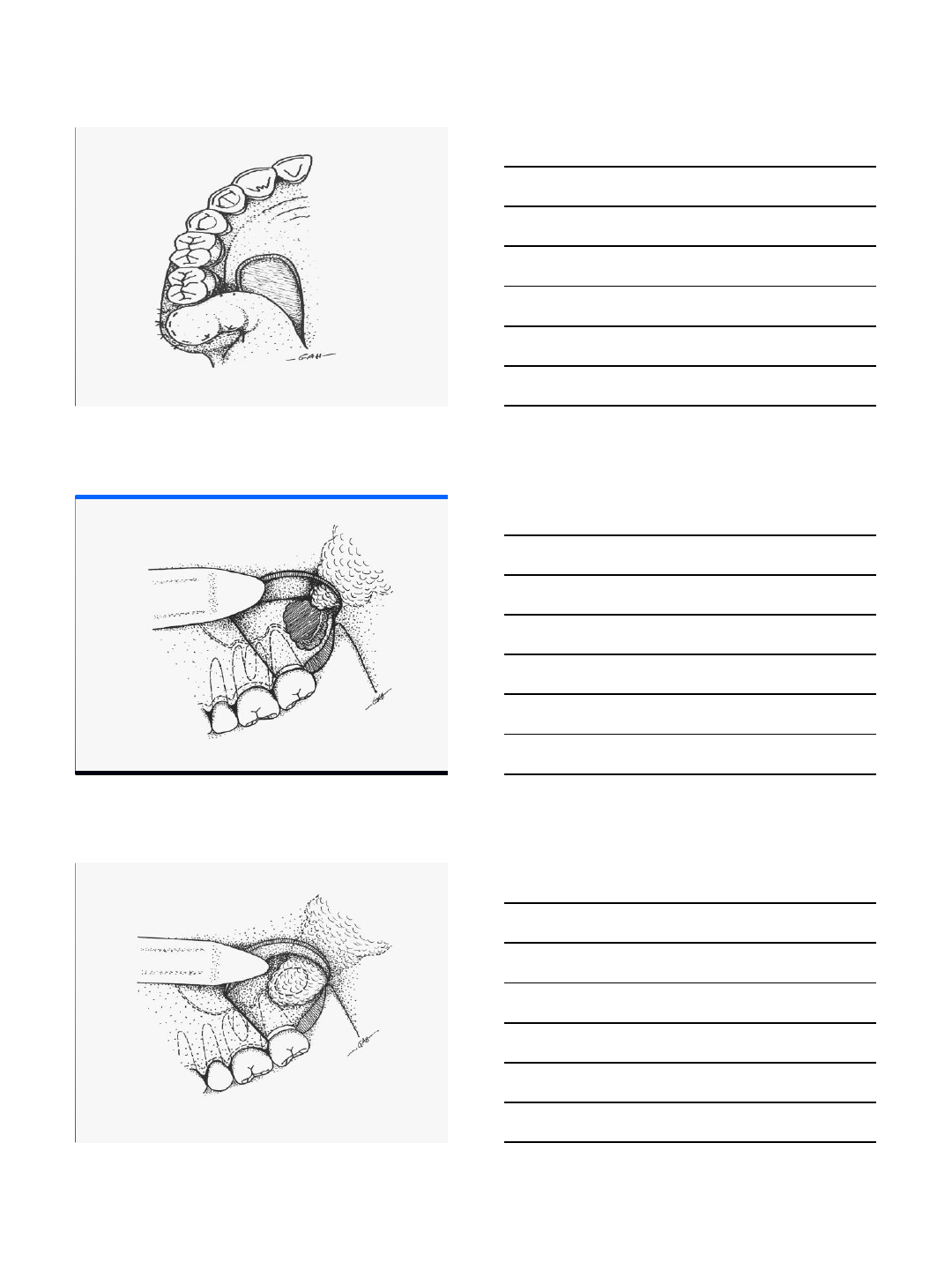
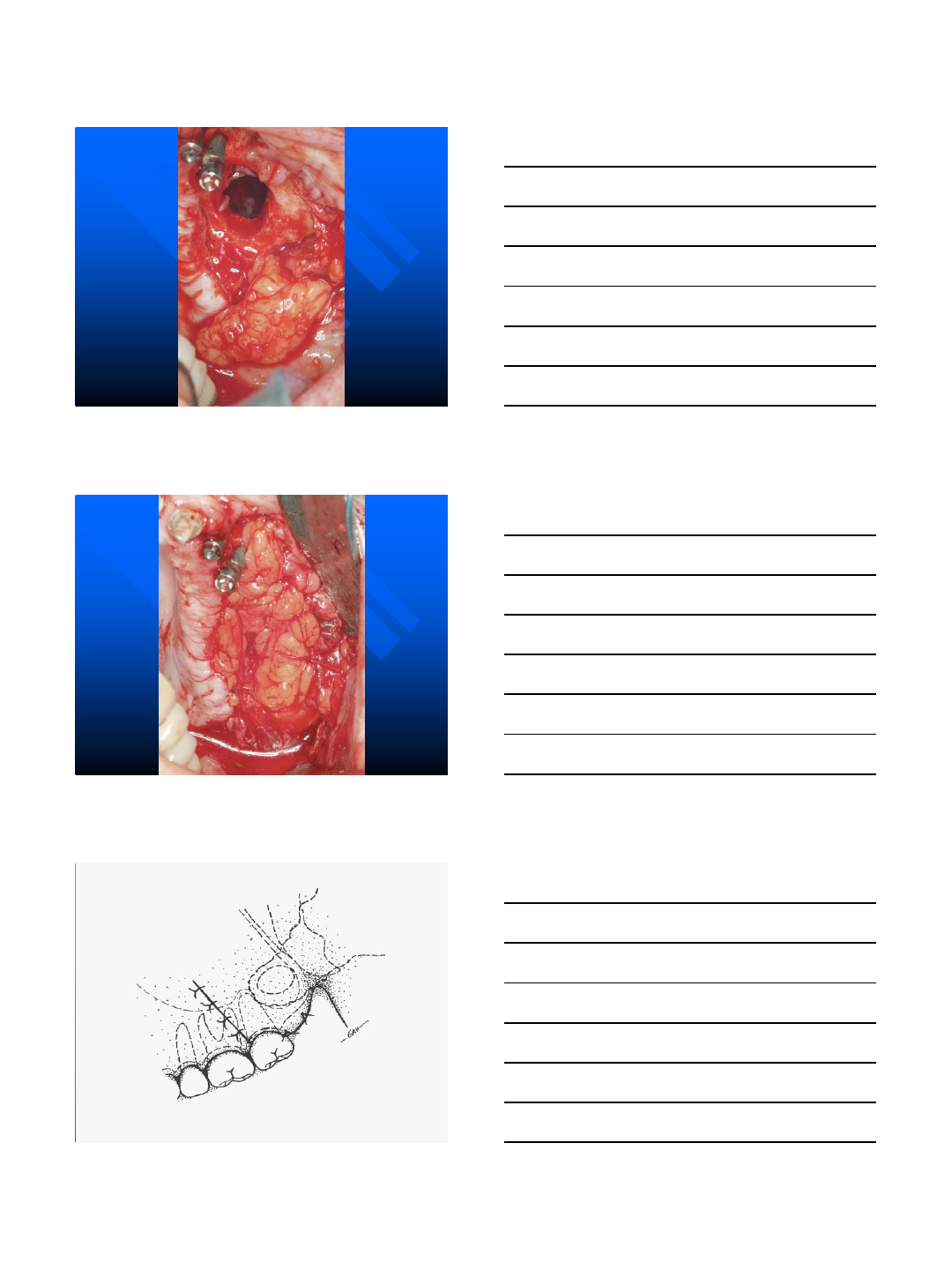
B. buccal fat pad transfer nd
local mucosal advancement
9/4/2014
24
9/4/2014
25
9/4/2014
26
9/4/2014
27
Potential Complications
Tuberosity Harvest
1. Oral-antral fistula
2. Sinusitis
3. Tooth root damage
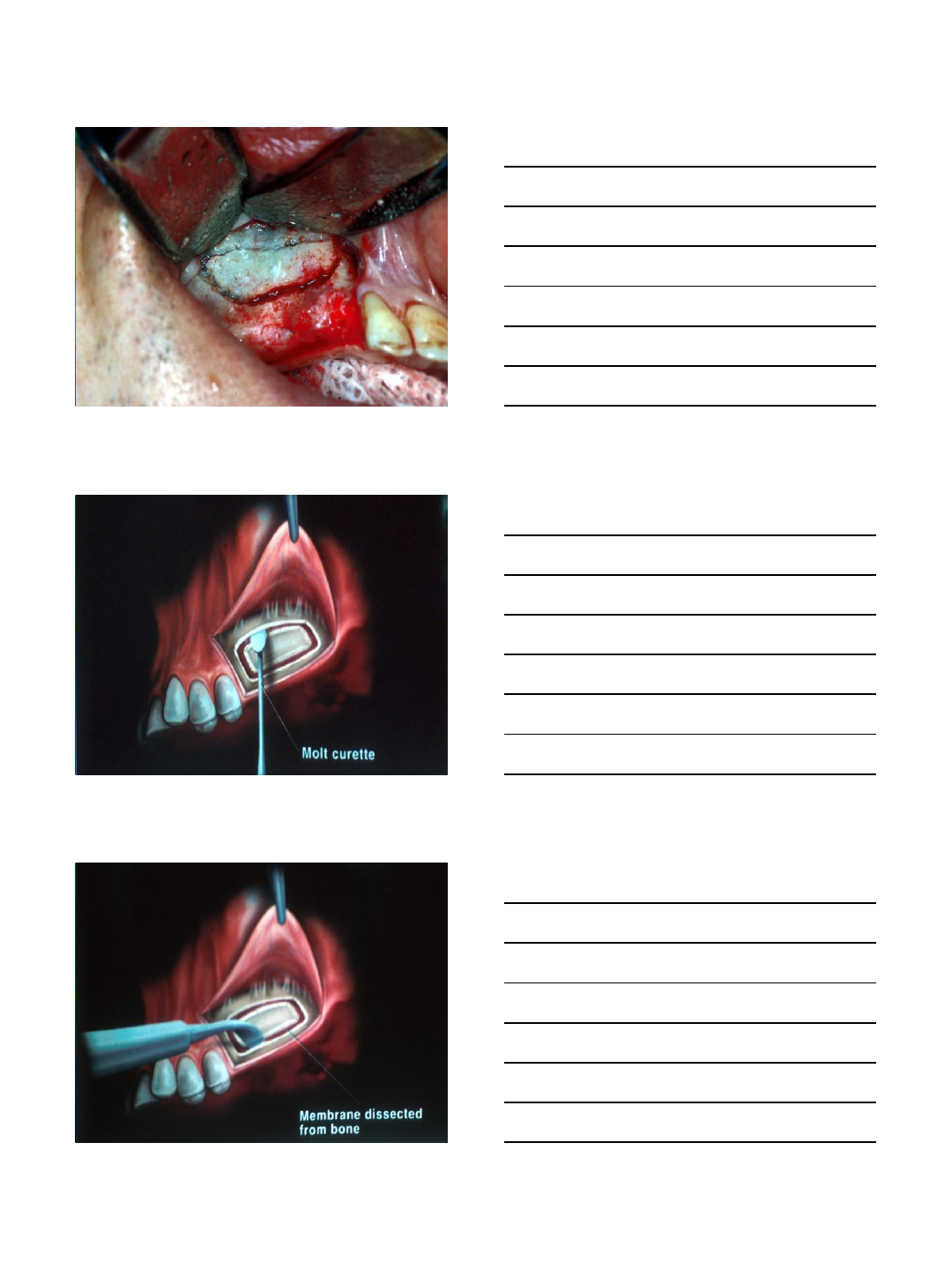
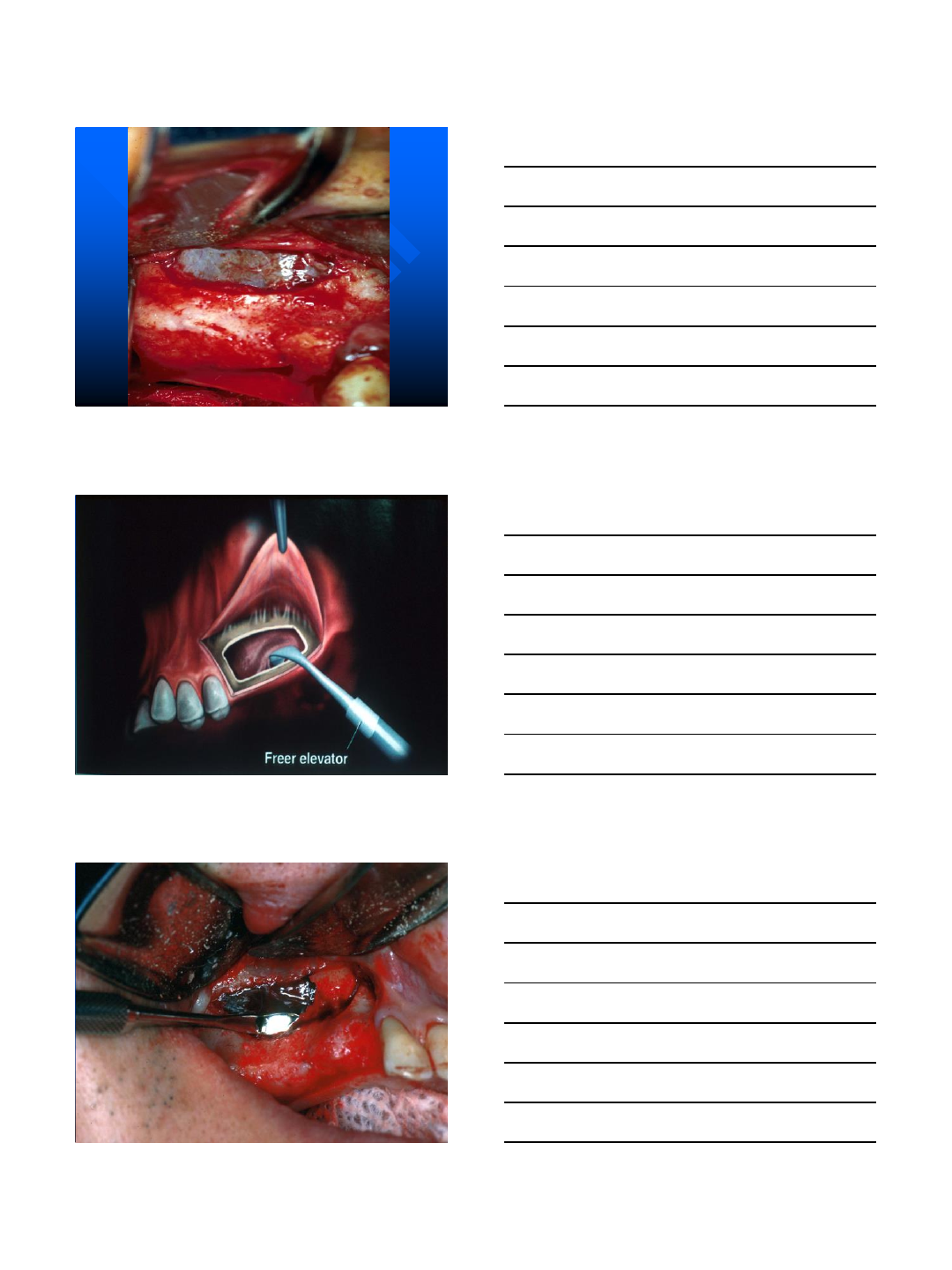
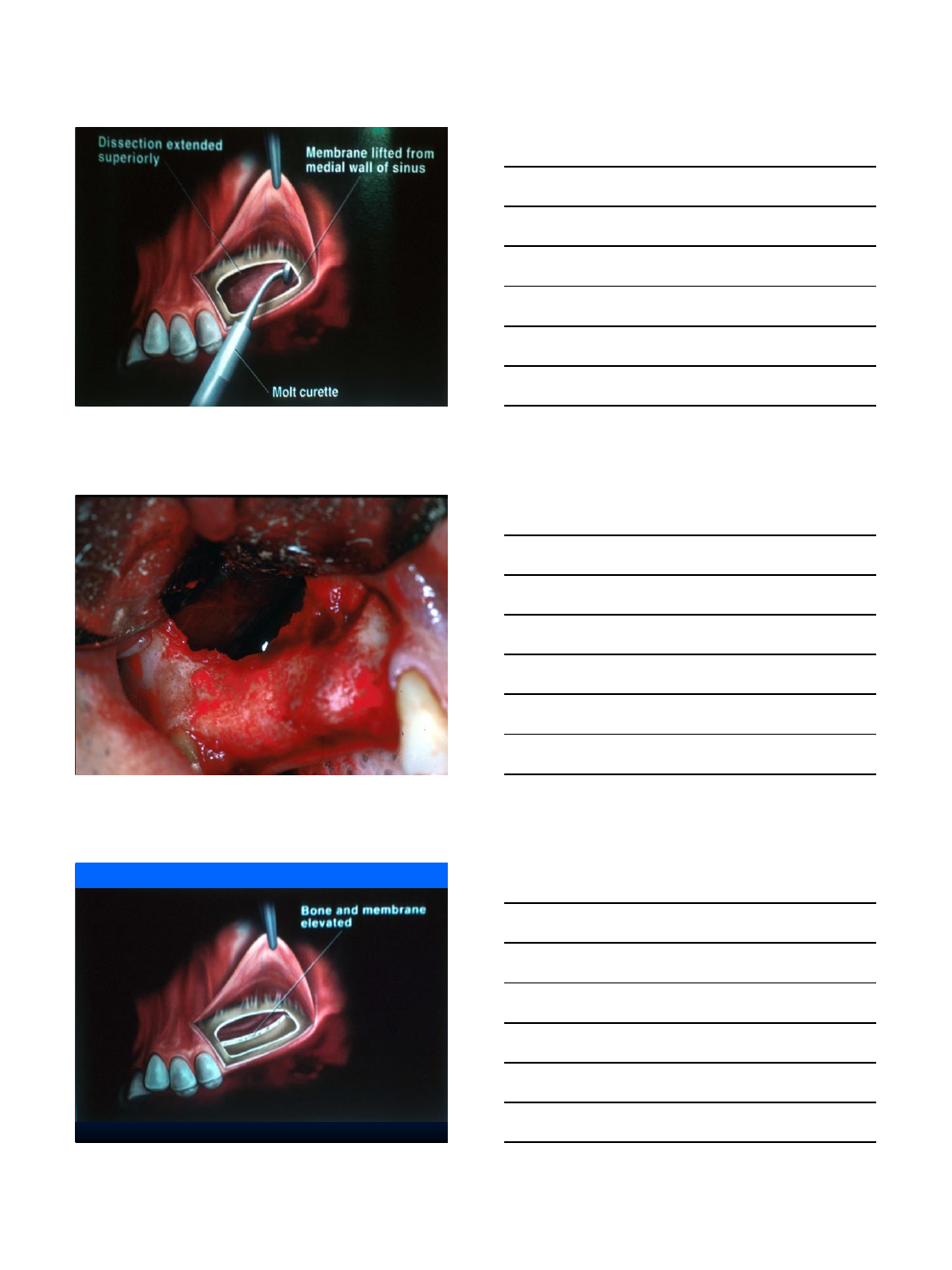
Sinus Lift
9/4/2014
28
9/4/2014
29
Contraindications of Maxillary
Sinus Grafting
Acute sinusitis
Cysts
Tumors
Foreign Bodies
9/4/2014
30
9/4/2014
31
9/4/2014
32
9/4/2014
33
9/4/2014
34
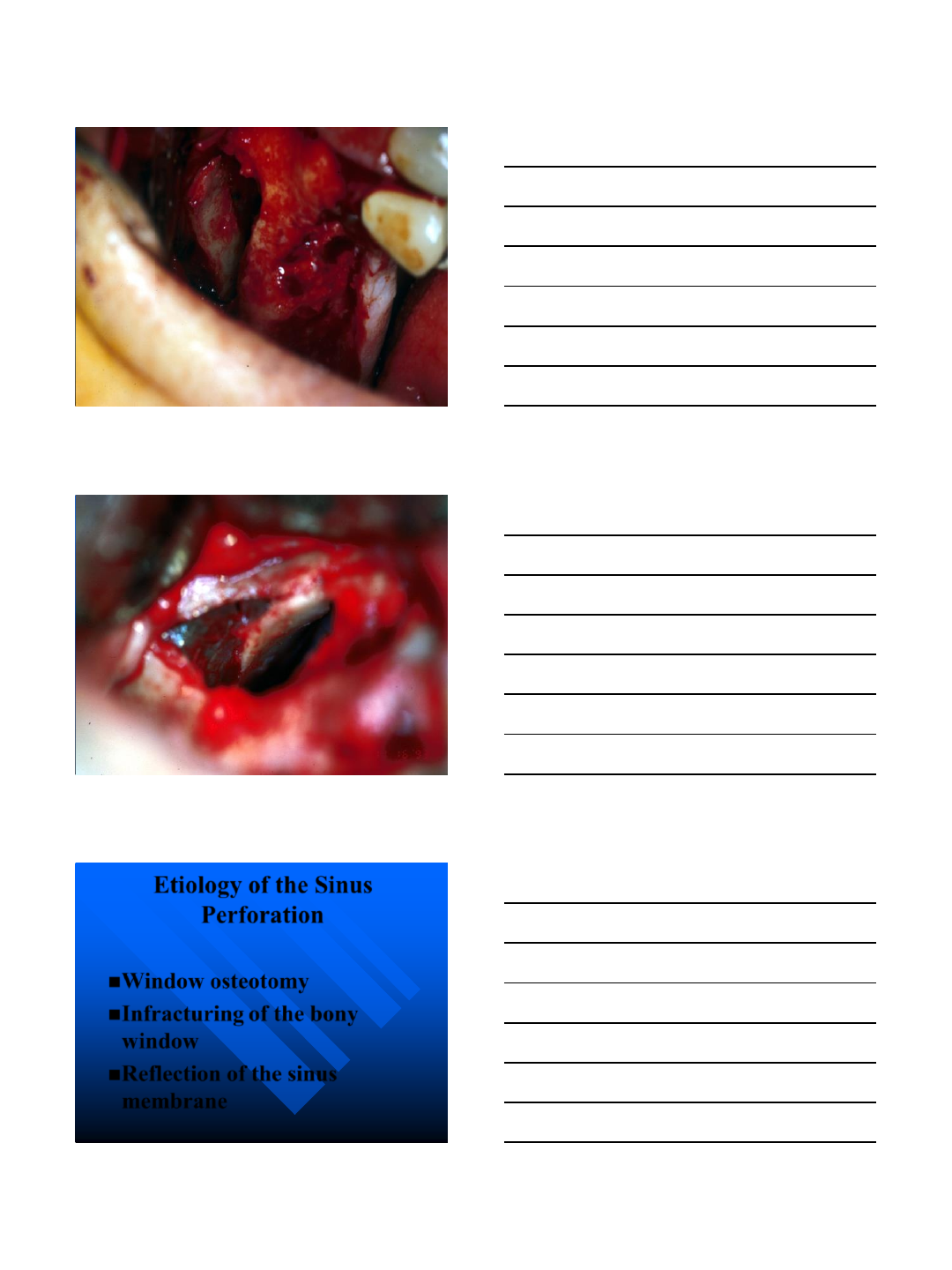
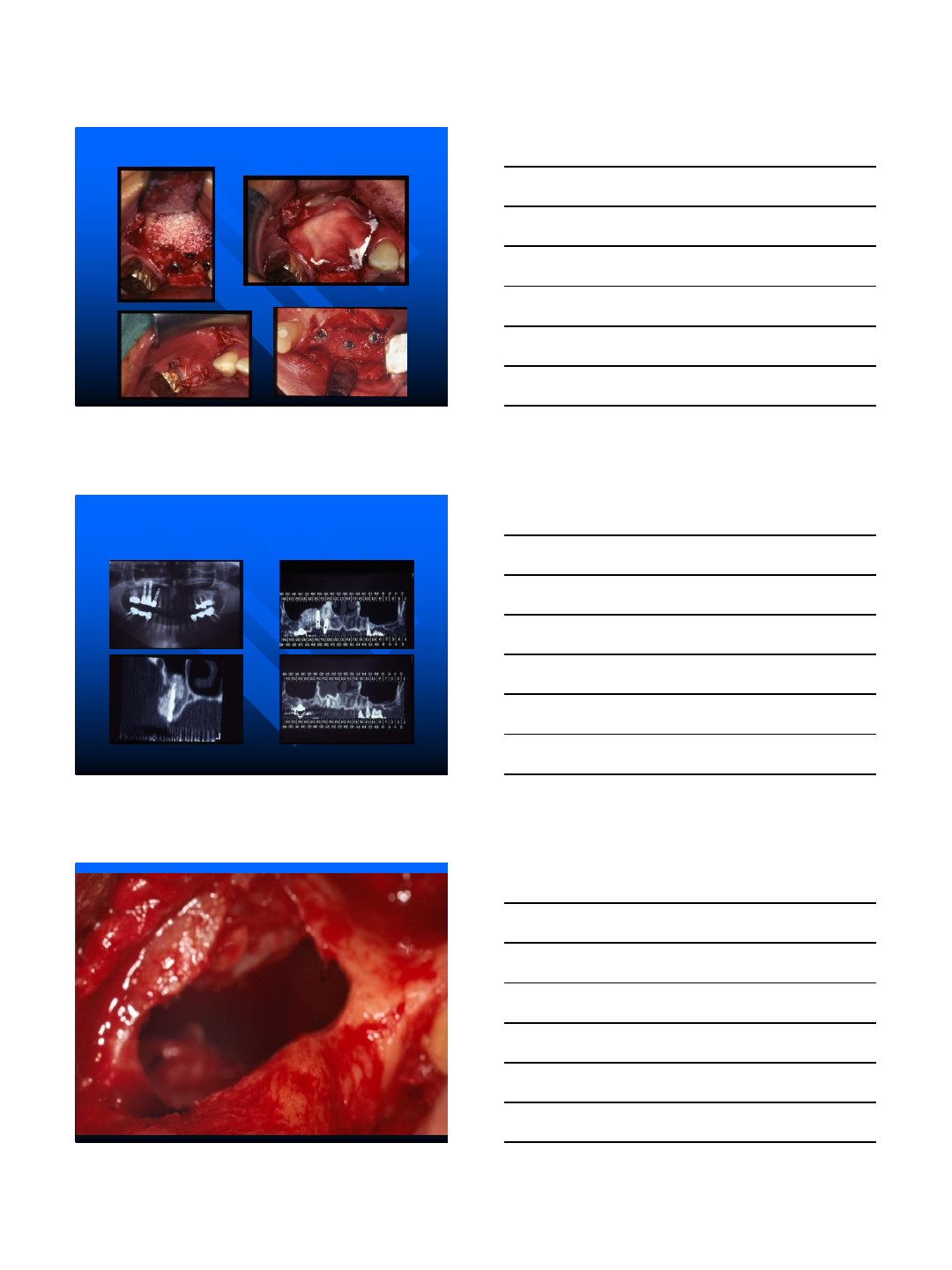
Etiology of the Sinus
Perforation
Window osteotomy
Infracturing of the bony
window
Reflection of the sinus
membrane
9/4/2014
35
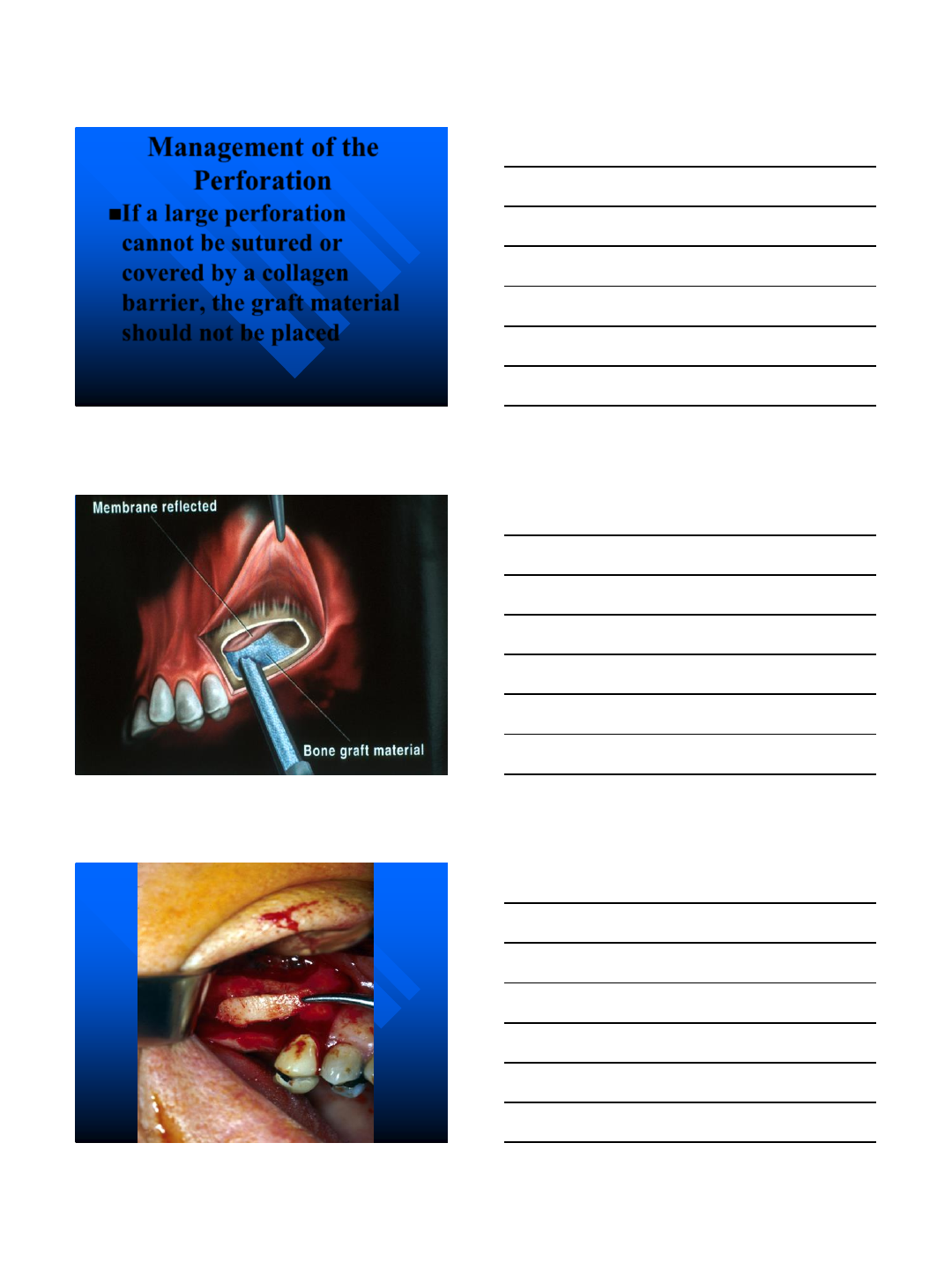
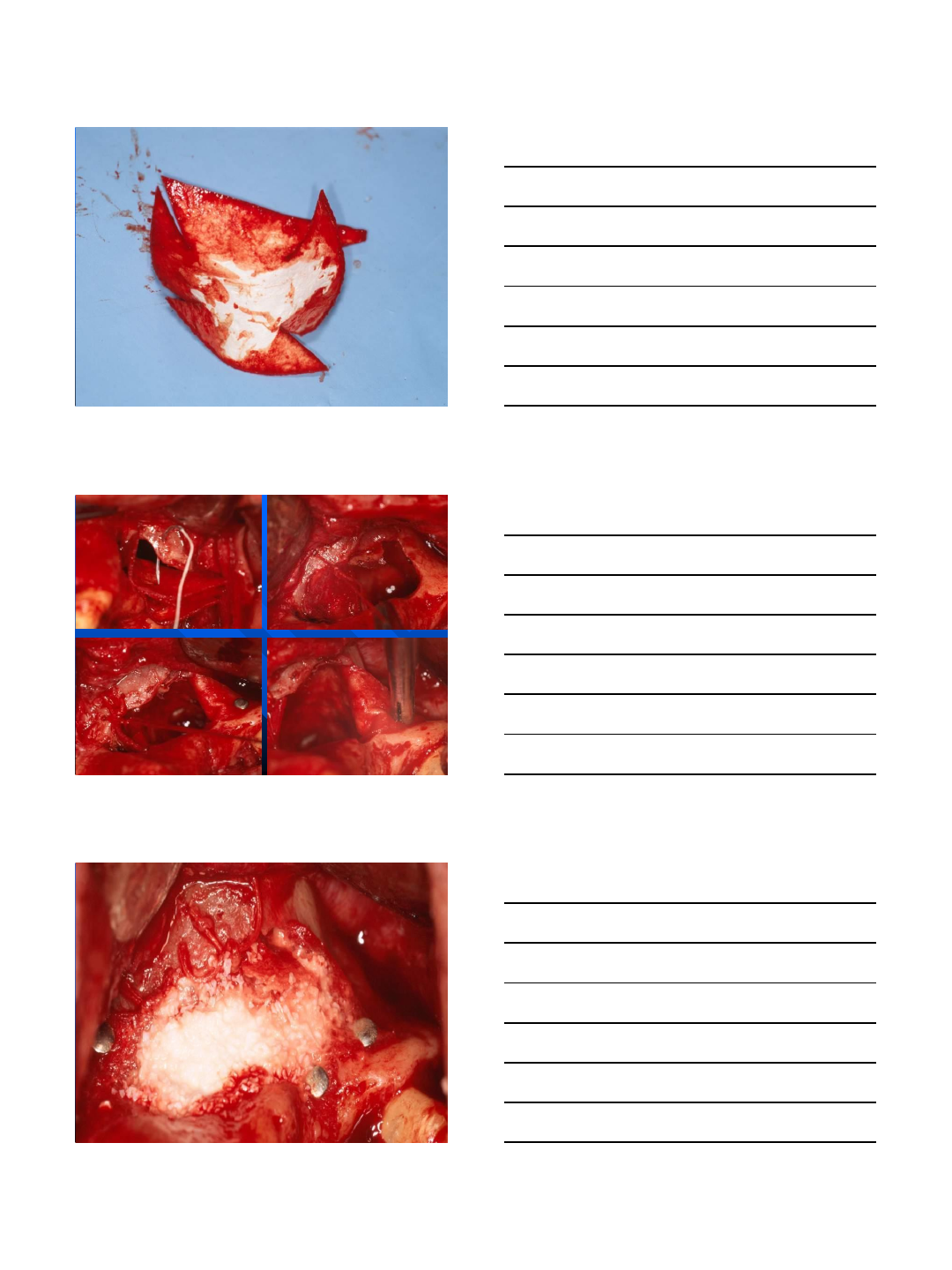
Management of the
Perforation
If a large perforation
cannot be sutured or
covered by a collagen
barrier, the graft material
should not be placed
9/4/2014
36
9/4/2014
37
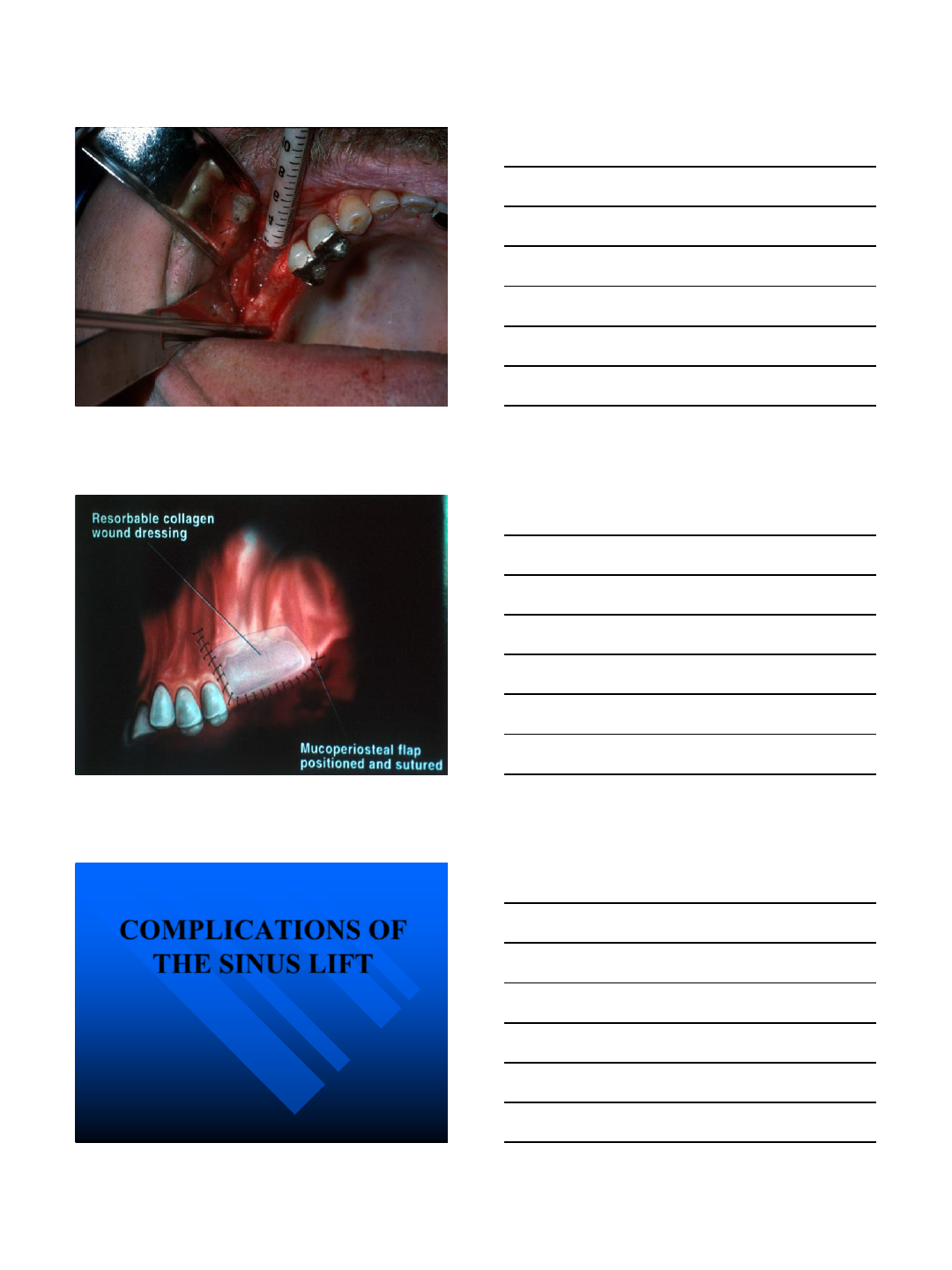
COMPLICATIONS OF
THE SINUS LIFT
9/4/2014
38
INTRAOPERATIVE
COMPLICATION
BLEEDING
MEMBRANE
PERFORATION
DAMAGE TO
ADJACENT
DENTITION
MAXILLARY SINUS VASCULAR
SUPPLY
BRANCHES OF THE
MAXILLARY ARTERY
INFRA ORBITAL
ARTERY
SPHENOPALATINE
ARTERY
POSTERIOR
SUPERIOR
ALVEOLAR ARTERY
Solar et al COIR 1998.
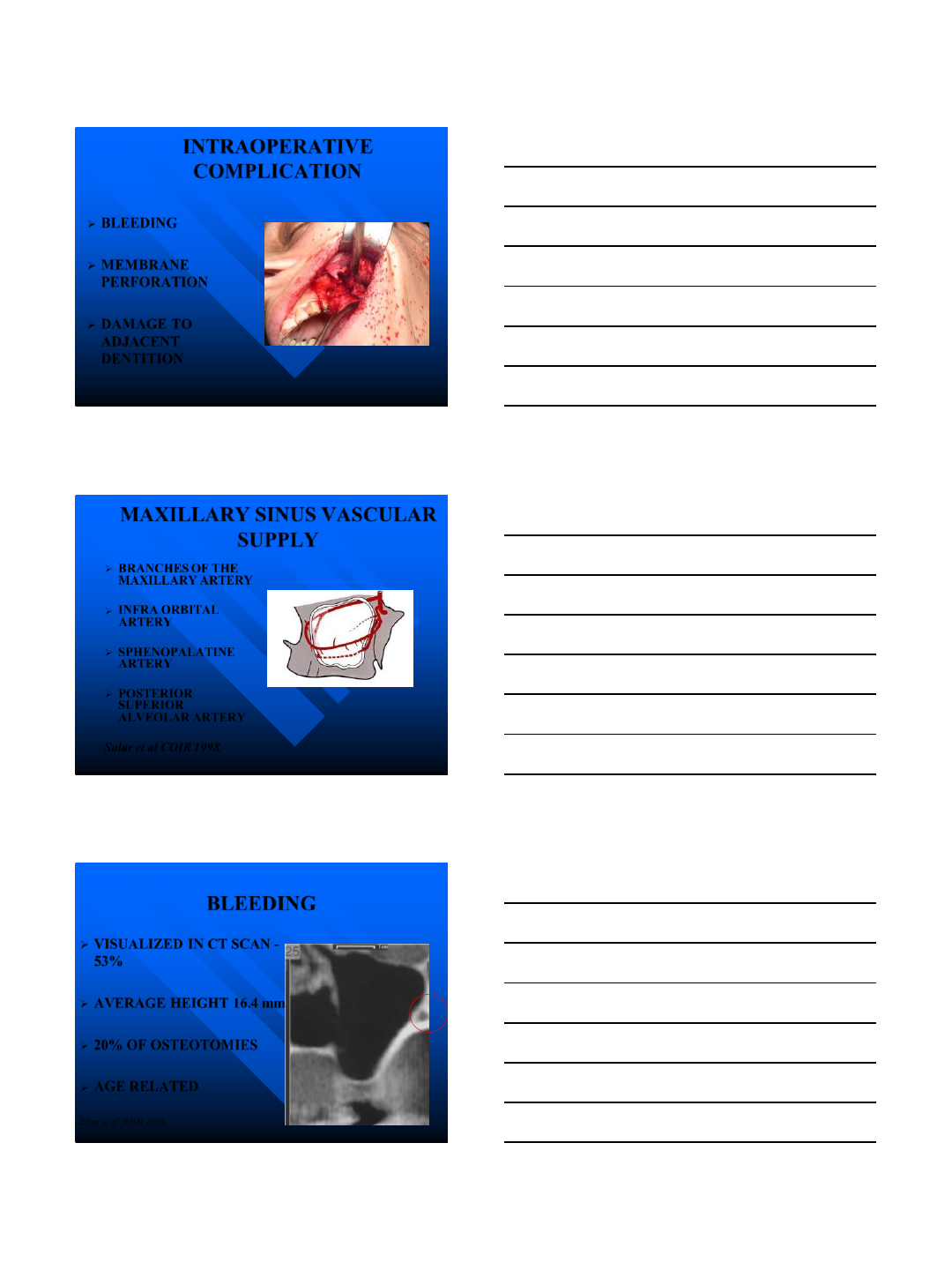
BLEEDING
VISUALIZED IN CT SCAN -
53%
AVERAGE HEIGHT 16.4 mm
20% OF OSTEOTOMIES
AGE RELATED
Elian et al JOMI 2005.
9/4/2014
39
BLEEDING
MEMBRANE ELEVATION BECOMES
MORE DIFFICULT
INTERFERES WITH PLACEMENT OF
GRAFT MATERIAL
HEMATOMA FORMATION
ELIAN et al JOMI 2005.
NICOLAAS et al J OMS Surg 2001.
BLEEDING
PREVENTION:
PREOP
IDENTIFICATION
SMALL WINDOW
TWO WINDOWS
MANAGEMENT
PRESSURE
BONE WAX
CAUTERIZATION
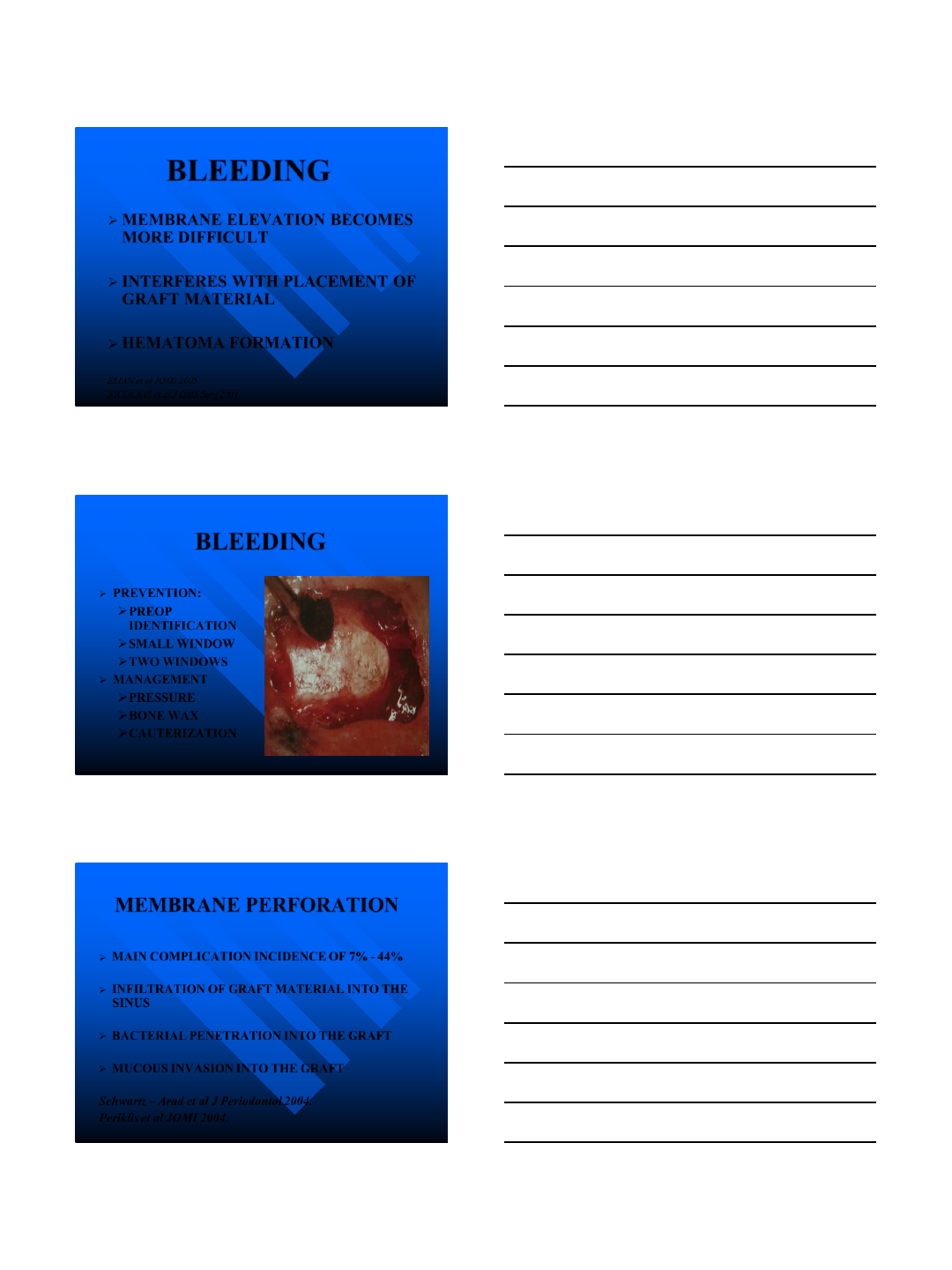
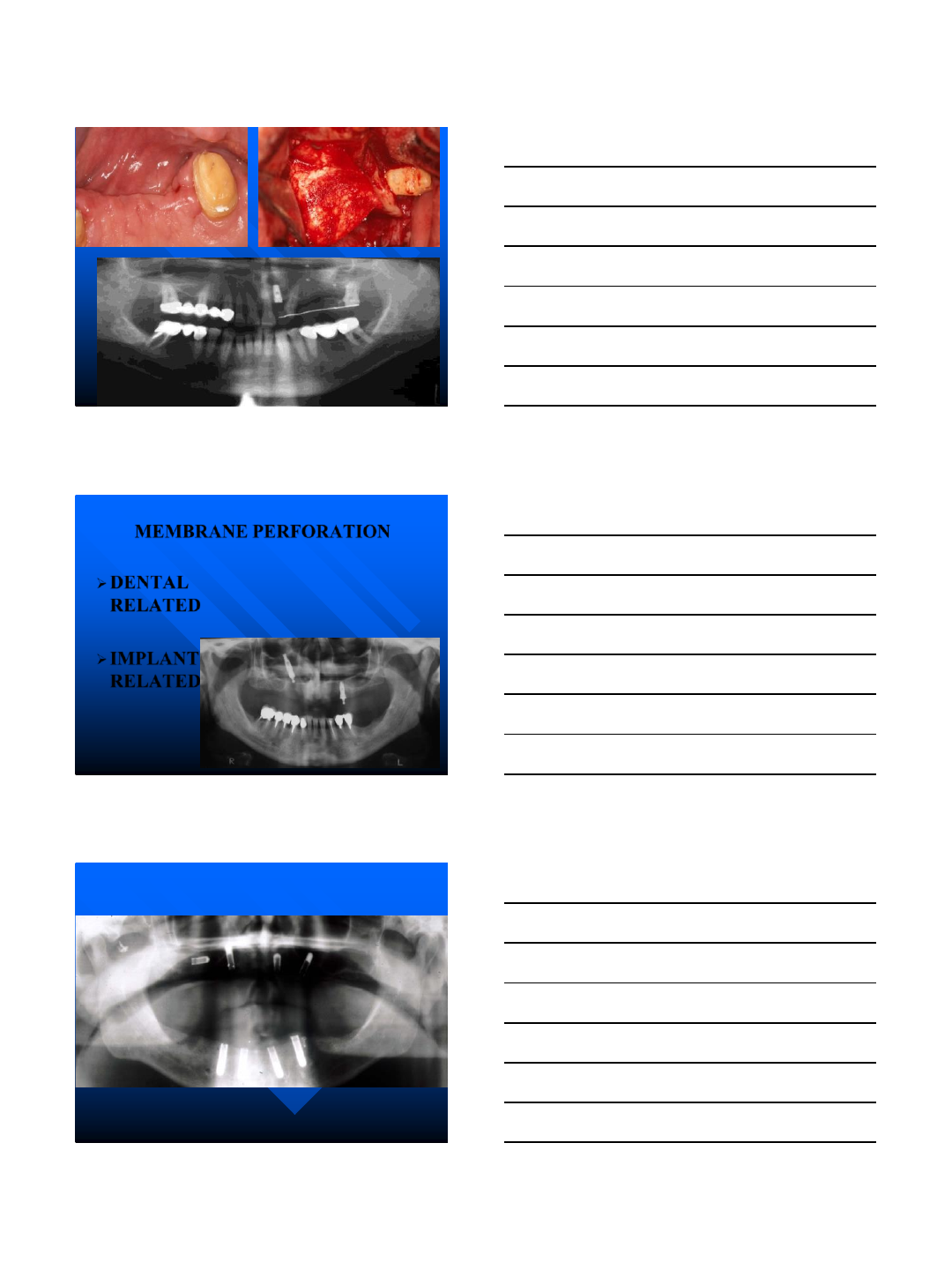
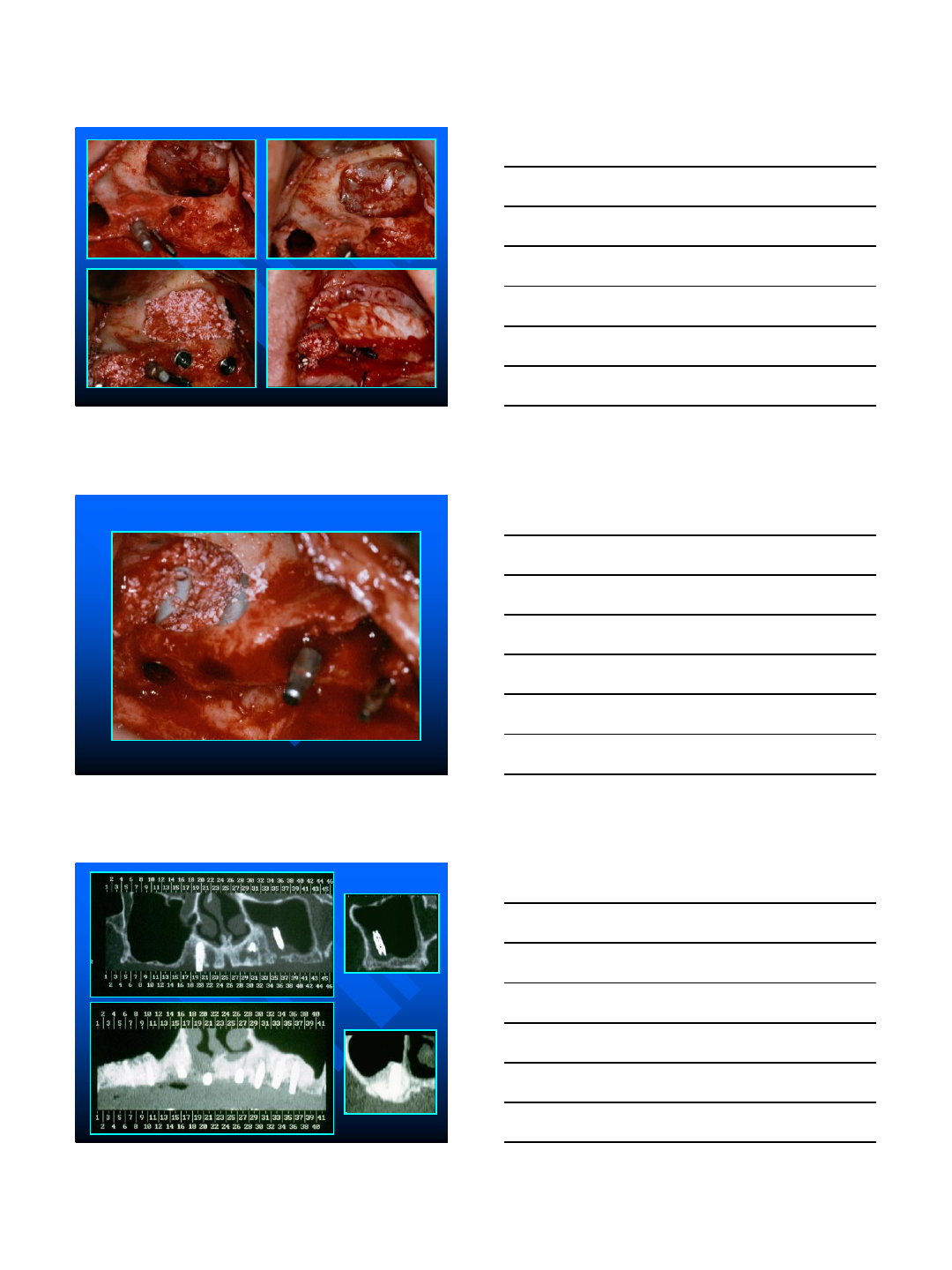
MEMBRANE PERFORATION
MAIN COMPLICATION INCIDENCE OF 7% - 44%
INFILTRATION OF GRAFT MATERIAL INTO THE
SINUS
BACTERIAL PENETRATION INTO THE GRAFT
MUCOUS INVASION INTO THE GRAFT
Schwartz –Arad et al J Periodontol 2004.
Periklis et al JOMI 2004.
9/4/2014
40
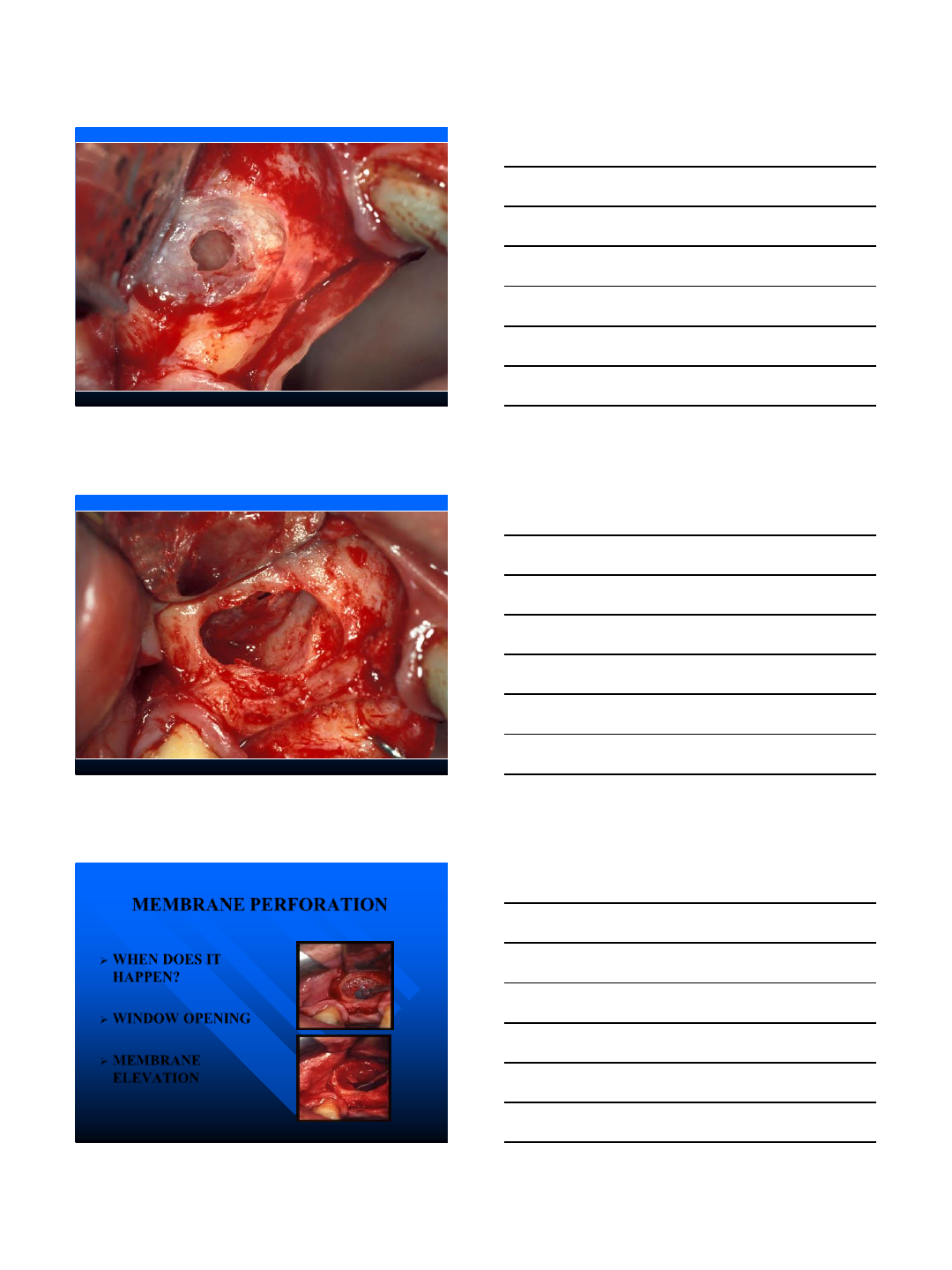
MEMBRANE PERFORATION
WHEN DOES IT
HAPPEN?
WINDOW OPENING
MEMBRANE
ELEVATION
9/4/2014
41
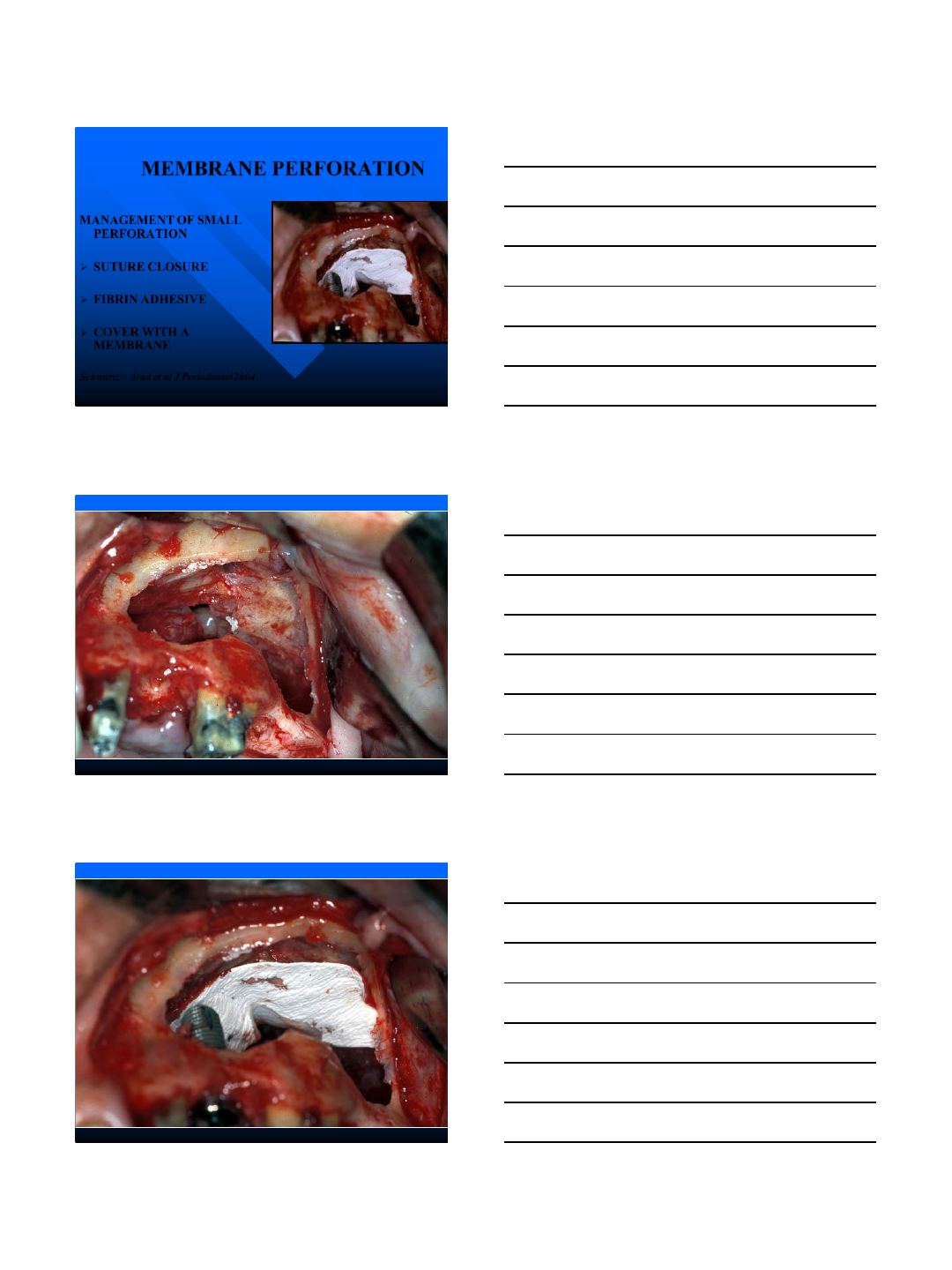
MEMBRANE PERFORATION
MANAGEMENT OF SMALL
PERFORATION
SUTURE CLOSURE
FIBRIN ADHESIVE
COVER WITH A
MEMBRANE
Schwartz –Arad et al J Periodontol 2004.
9/4/2014
42
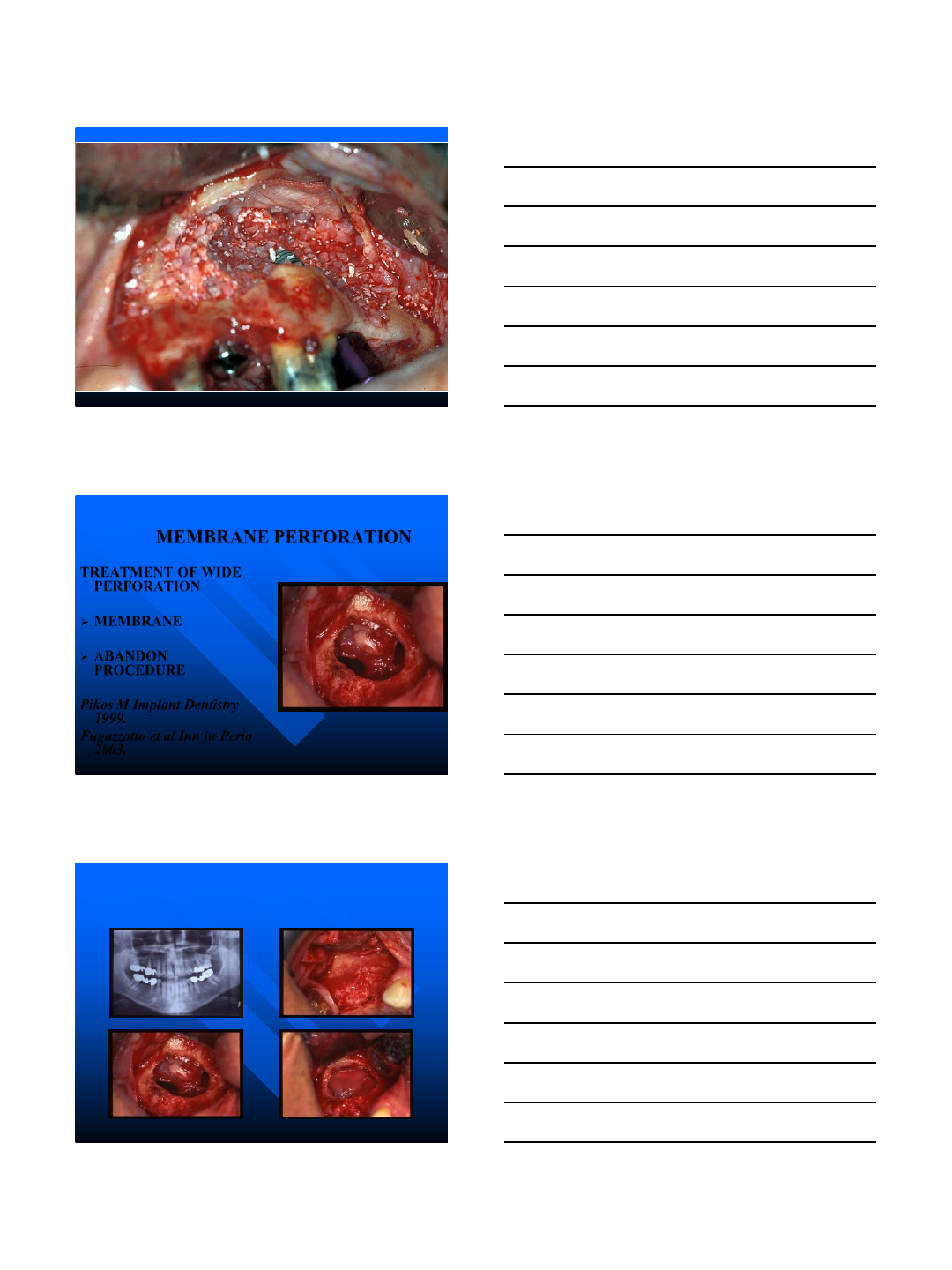
MEMBRANE PERFORATION
TREATMENT OF WIDE
PERFORATION
MEMBRANE
ABANDON
PROCEDURE
Pikos M Implant Dentistry
1999.
Fugazzotto et al Inn in Perio
2003.
9/4/2014
43
MEMBRANE PERFORATION
BLEEDING CONTROL
9/4/2014
44
9/4/2014
45
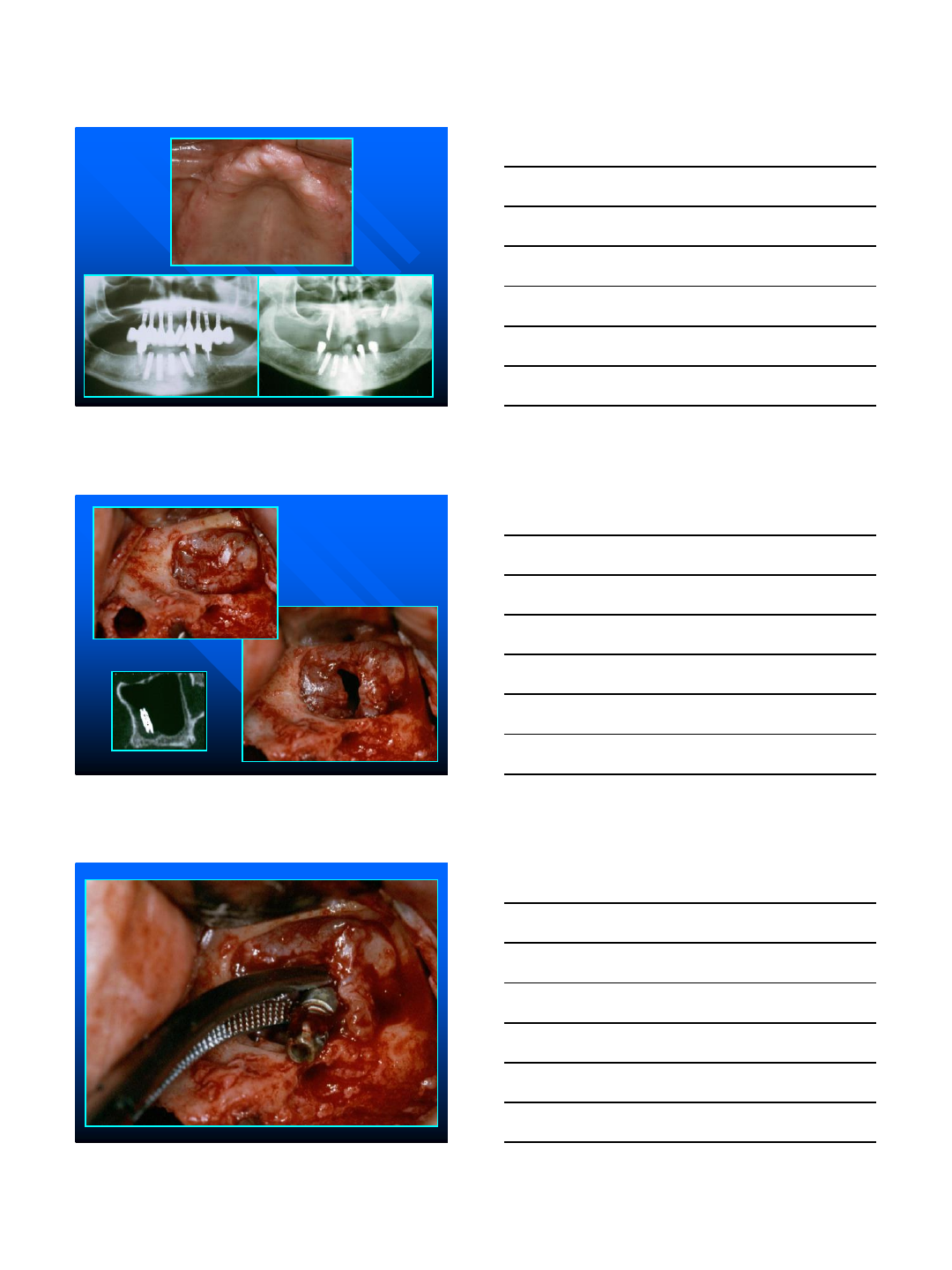
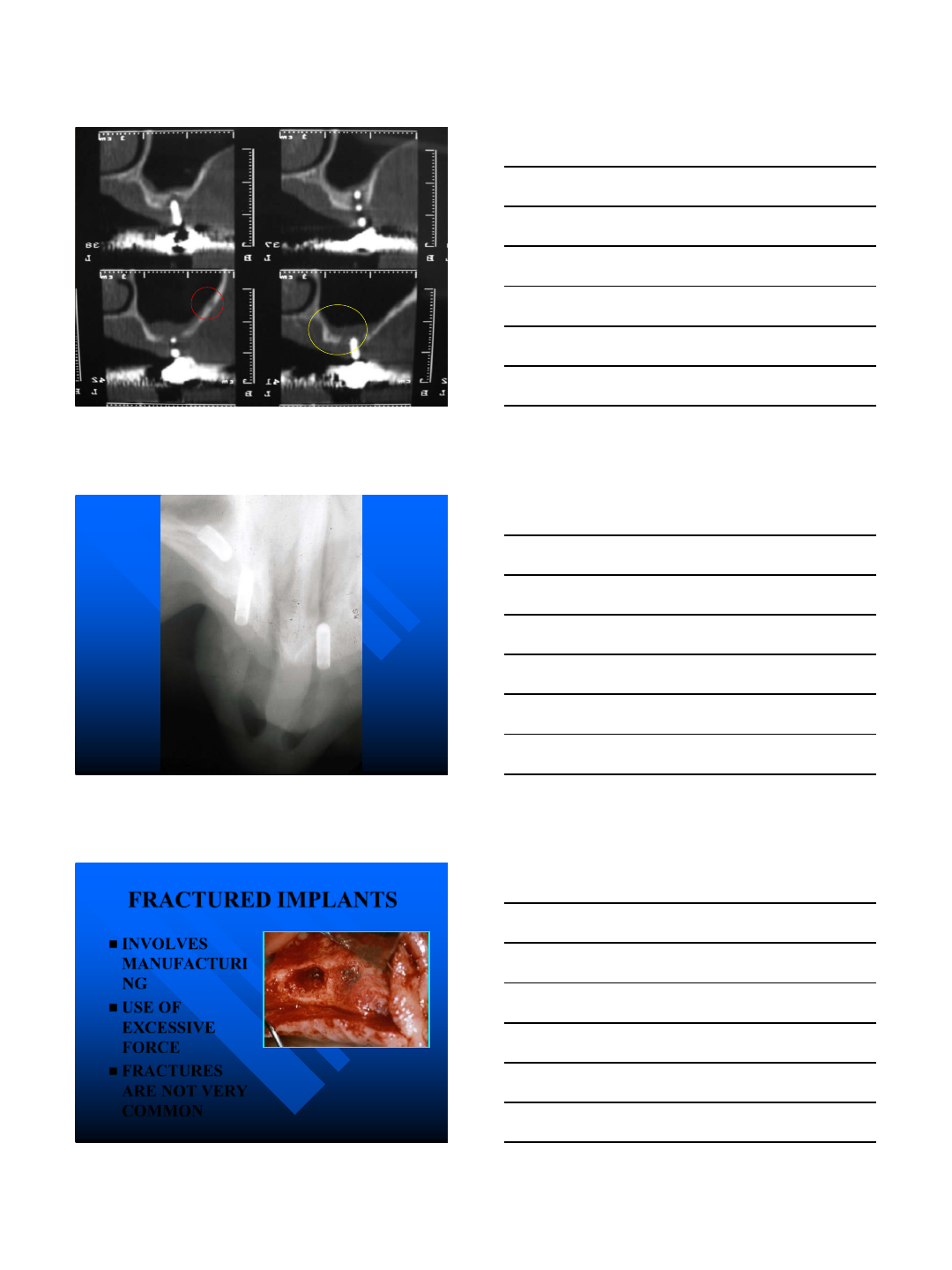
MEMBRANE PERFORATION
DENTAL
RELATED
IMPLANT
RELATED
9/4/2014
46
9/4/2014
47
9/4/2014
48
FRACTURED IMPLANTS
INVOLVES
MANUFACTURI
NG
USE OF
EXCESSIVE
FORCE
FRACTURES
ARE NOT VERY
COMMON
9/4/2014
49
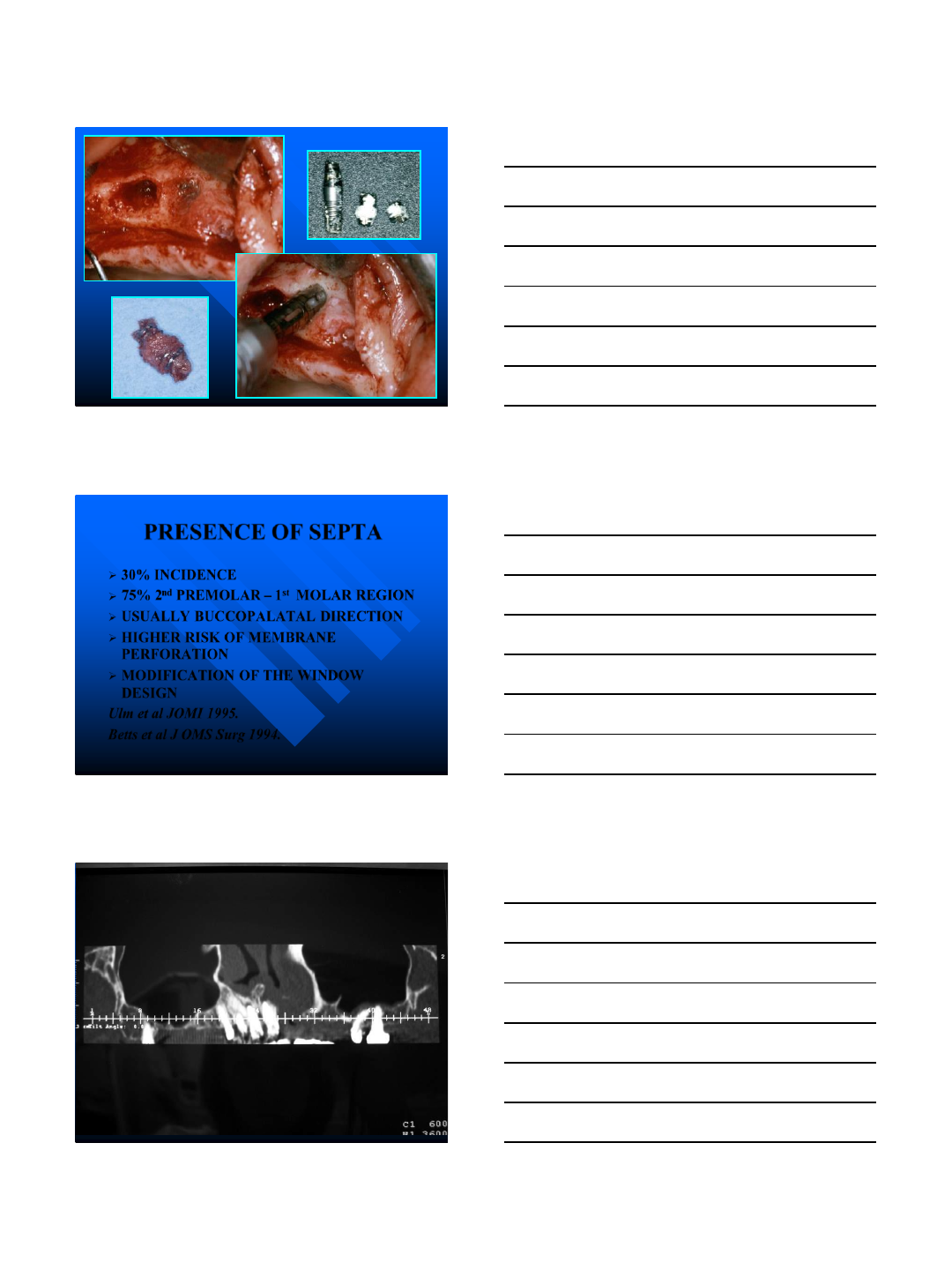
PRESENCE OF SEPTA
30% INCIDENCE
75% 2nd PREMOLAR –1st MOLAR REGION
USUALLY BUCCOPALATAL DIRECTION
HIGHER RISK OF MEMBRANE
PERFORATION
MODIFICATION OF THE WINDOW
DESIGN
Ulm et al JOMI 1995.
Betts et al J OMS Surg 1994.
9/4/2014
50
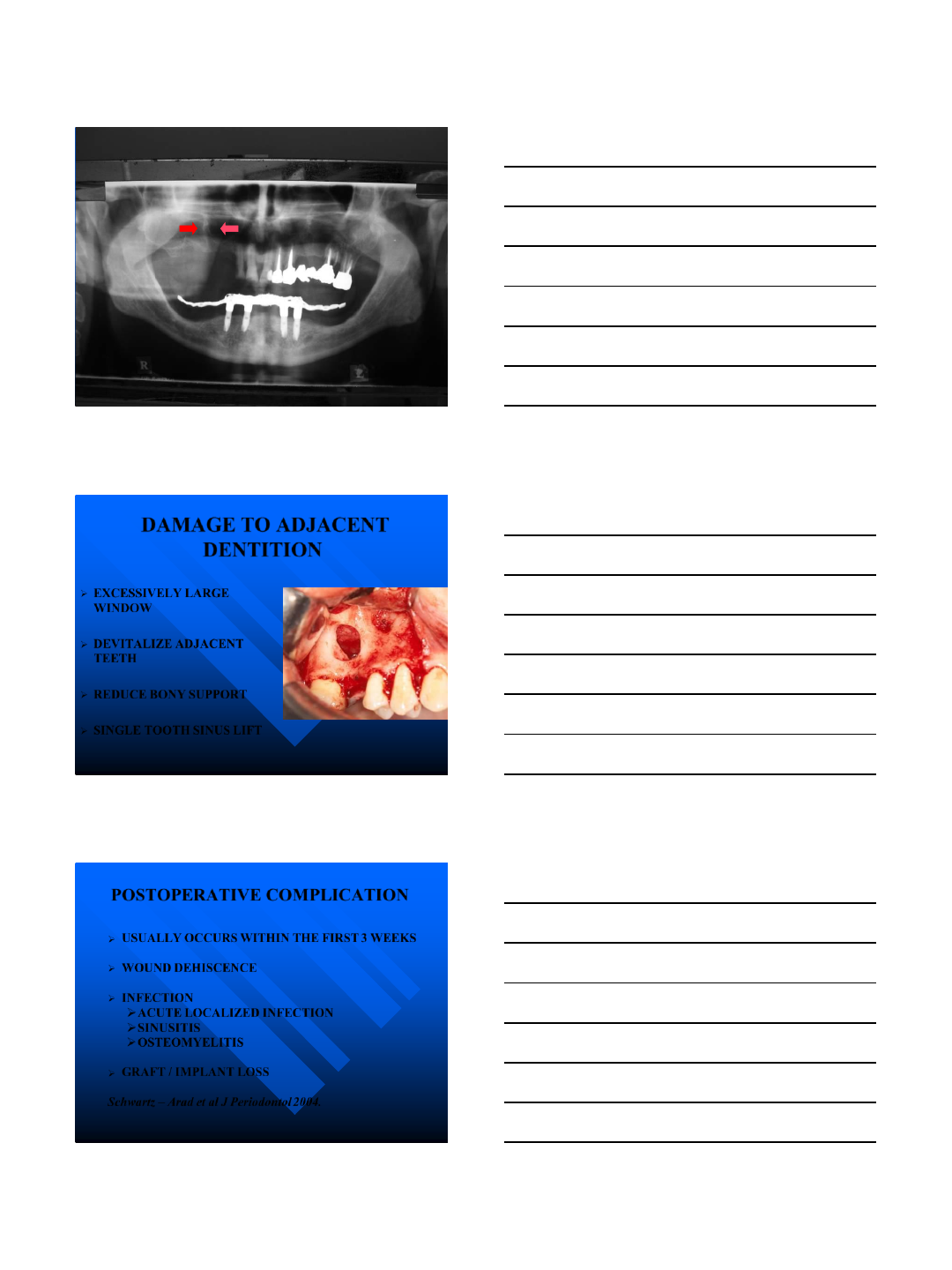
DAMAGE TO ADJACENT
DENTITION
EXCESSIVELY LARGE
WINDOW
DEVITALIZE ADJACENT
TEETH
REDUCE BONY SUPPORT
SINGLE TOOTH SINUS LIFT
POSTOPERATIVE COMPLICATION
USUALLY OCCURS WITHIN THE FIRST 3 WEEKS
WOUND DEHISCENCE
INFECTION
ACUTE LOCALIZED INFECTION
SINUSITIS
OSTEOMYELITIS
GRAFT / IMPLANT LOSS
Schwartz –Arad et al J Periodontol 2004.
9/4/2014
51
POSTOPERATIVE COMPLICATION
PREVENTION
ANTIBIOTICS
NASAL DECONGESTANTS
MOUTH RINSES
SINUS PRECAUTIONS
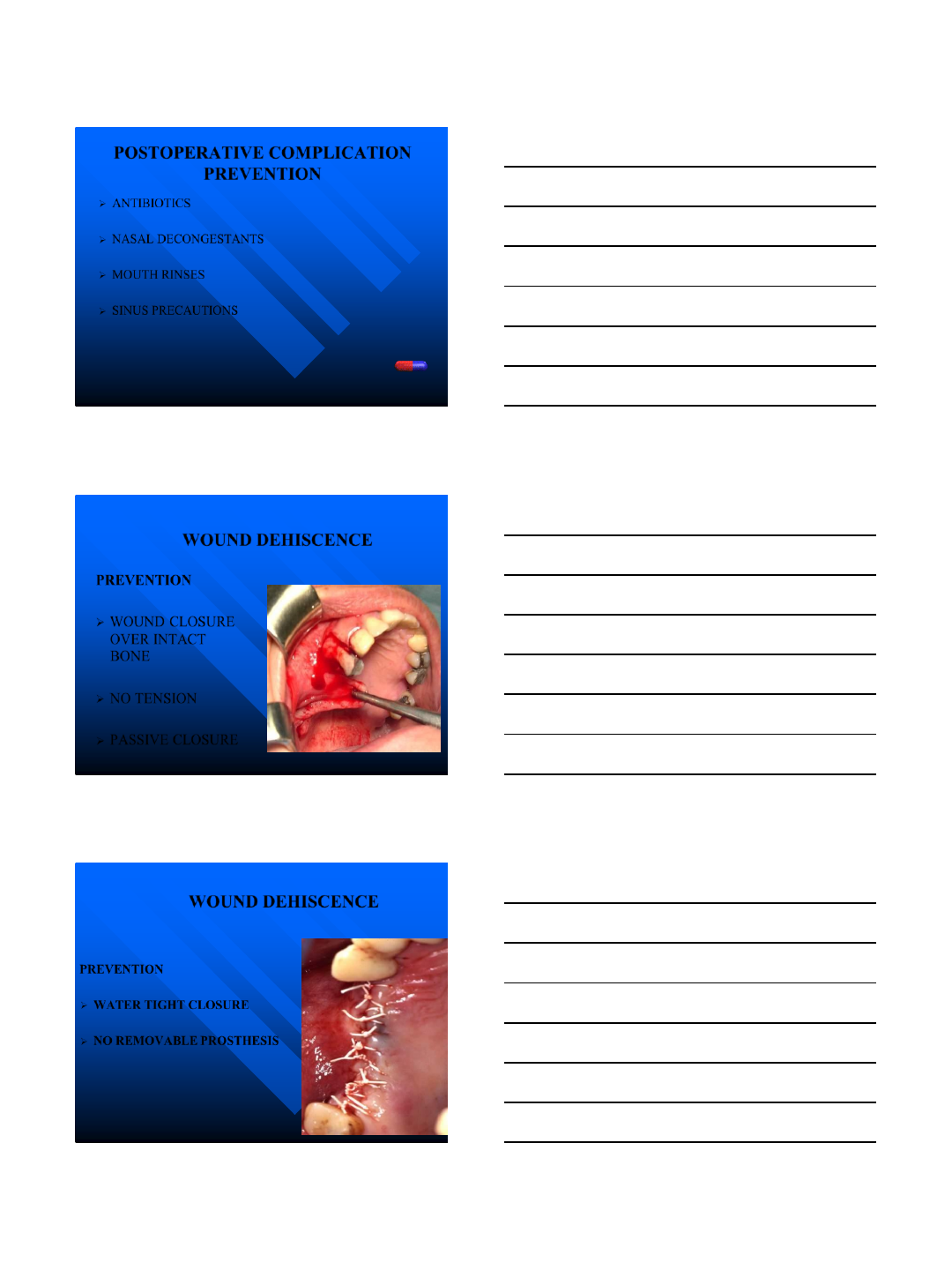
WOUND DEHISCENCE
PREVENTION
WOUND CLOSURE
OVER INTACT
BONE
NO TENSION
PASSIVE CLOSURE
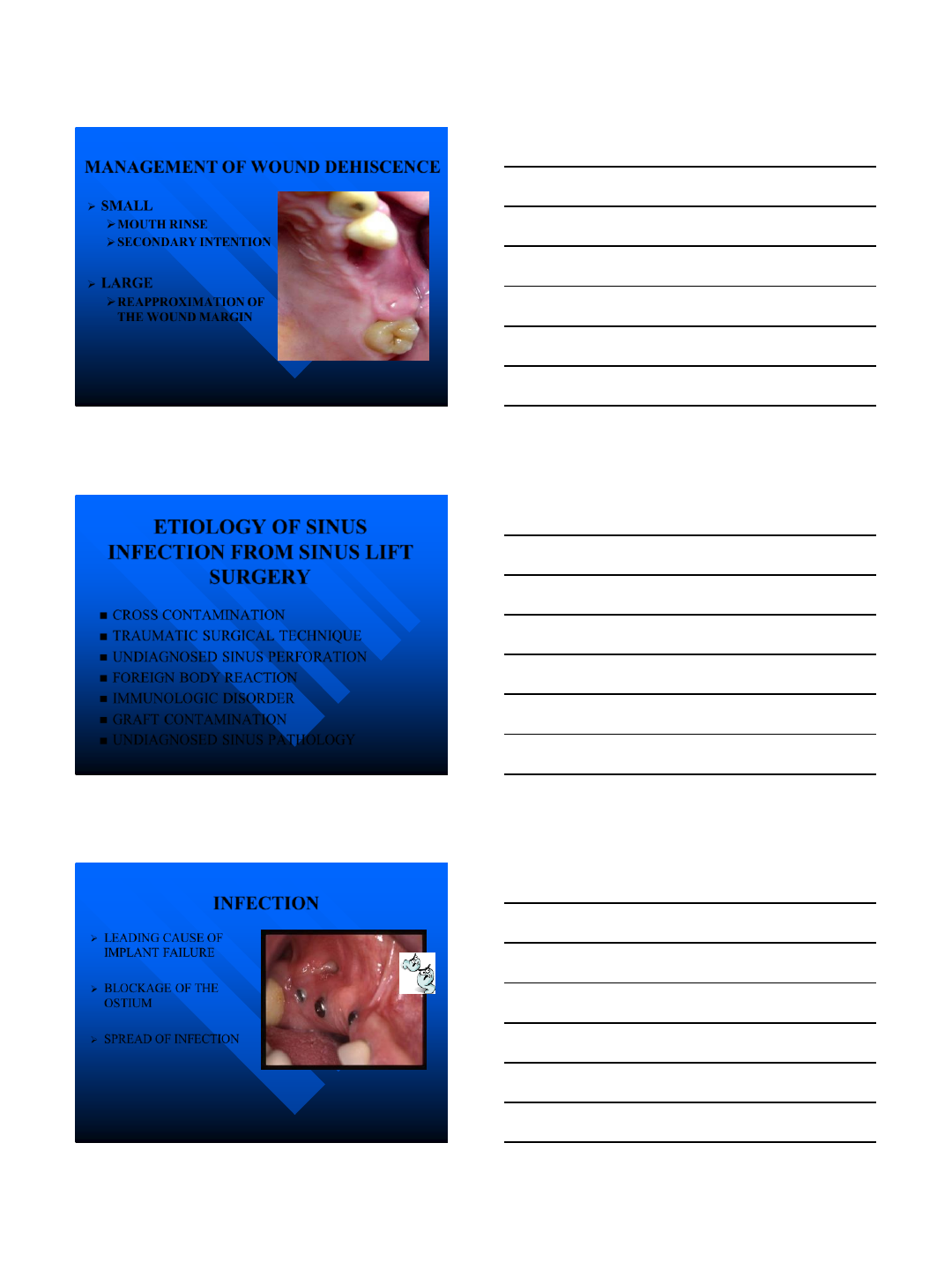
WOUND DEHISCENCE
PREVENTION
WATER TIGHT CLOSURE
NO REMOVABLE PROSTHESIS
9/4/2014
52
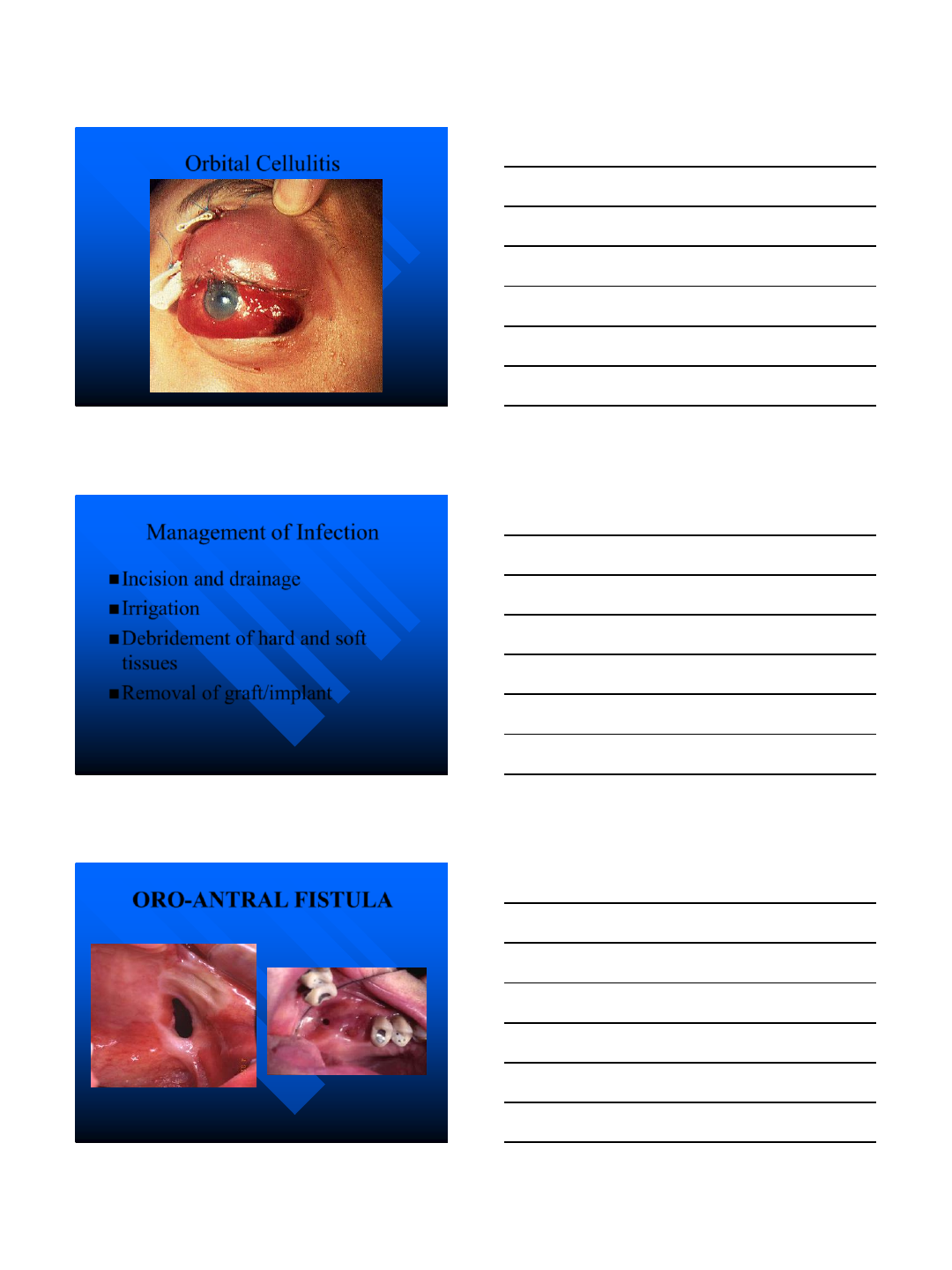
MANAGEMENT OF WOUND DEHISCENCE
SMALL
MOUTH RINSE
SECONDARY INTENTION
LARGE
REAPPROXIMATION OF
THE WOUND MARGIN
ETIOLOGY OF SINUS
INFECTION FROM SINUS LIFT
SURGERY
CROSS CONTAMINATION
TRAUMATIC SURGICAL TECHNIQUE
UNDIAGNOSED SINUS PERFORATION
FOREIGN BODY REACTION
IMMUNOLOGIC DISORDER
GRAFT CONTAMINATION
UNDIAGNOSED SINUS PATHOLOGY
INFECTION
LEADING CAUSE OF
IMPLANT FAILURE
BLOCKAGE OF THE
OSTIUM
SPREAD OF INFECTION
9/4/2014
53
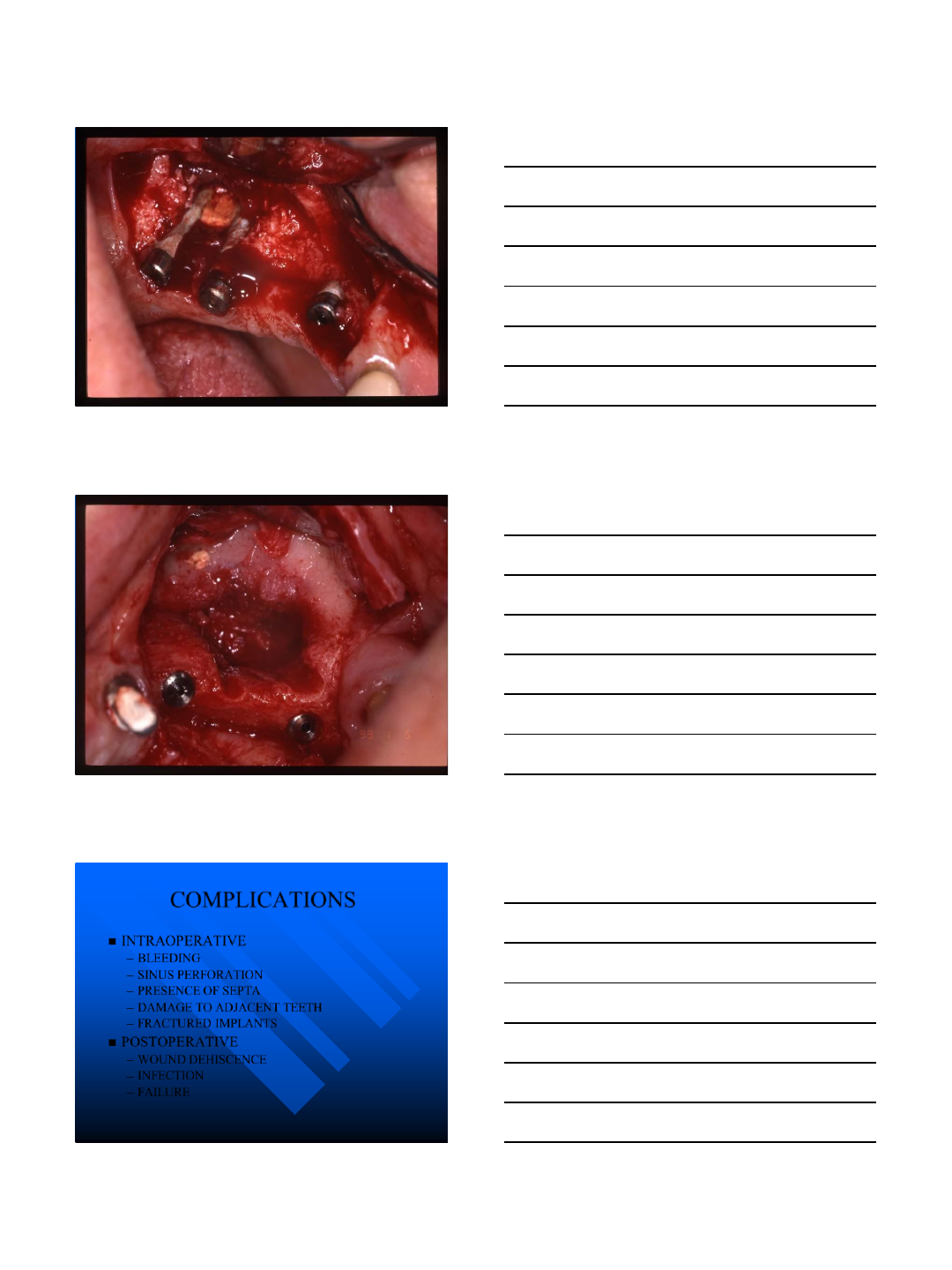
Orbital Cellulitis
Management of Infection
Incision and drainage
Irrigation
Debridement of hard and soft
tissues
Removal of graft/implant
ORO-ANTRAL FISTULA
9/4/2014
54
COMPLICATIONS
INTRAOPERATIVE
–BLEEDING
–SINUS PERFORATION
–PRESENCE OF SEPTA
–DAMAGE TO ADJACENT TEETH
–FRACTURED IMPLANTS
POSTOPERATIVE
–WOUND DEHISCENCE
–INFECTION
–FAILURE
9/4/2014
55
Thank you
References
Fonseca, R.J. Walker, R.V. Betts, N.J. Barber, H.D. Oral and Maxillofacial
Trauma. Saunders. 1997
Miloro, M. Ghali, G.E. Larsen, P.E. Waite, P.E. Peterson’s Principles of Oral
and Maxillofacial Surgery. BC Decker INC. 2004
Marx, R.E. Philosophy and particulars of autogenous bone grafting. Oral and
Maxillofacial Surgery Clinics of North America. 5:599-612, 1993
Marx, R.E. Biology of Bone Grafts. Oral and Maxillofacial Surgery
Knowledge Update. 1:3-17. 1994
Piecuch,J.F. Silverstein, K. Quinn, P.D. Bone grafts in Preprosthetic Surgery.
Oral and Maxillofacial Surgery Knowledge Update 2:11-35. 1998
Stevens, M.E. Bone Harvesting Techniques. Oral and Maxillofacial
Knowledge Update. 1:19-34. 1994
Roberts, W.E. Roberts, J.A. Epker, B.N. Burr, D.B. Remodeling of
Mineralized Tissues, Part I: The frost Legacy. Seminars in Orthodontics
12:216-237. 2006
Roberts, W.E. Roberts, J.A. Epker, B.N. Burr, D.B. Remodeling of
Mineralized Tissues, Part:II Control and Pathophysiology. Seminars in
Orthodontics 12:238-253. 2006
The End
