L5 S1 Controversies Syllabus
2015-09-08
: Pdf L5-S1 Controversies Syllabus L5-S1_Controversies_Syllabus 9 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 55
1
Choosing Levels in Adult Scoliosis
Indications to Extend Fusion to the Sacrum and
Pelvis
Sigurd Berven, MD
Professor in Residence
UC San Francisco
Disclosures
•Research/Institutional Support:
–NIH, AO Spine, OREF, AOA
•Consultancies/Scientific Advisory:
–Medtronic, DePuy, Stryker, Globus
•Ownership/Stock/Options:
–Providence Medical, Simpirica
•Royalties: Medtronic
Challenges in Adult Scoliosis
Surgery
•Choosing Levels
•Junctional Complications
•When can we do less?
–When should we do more?
2
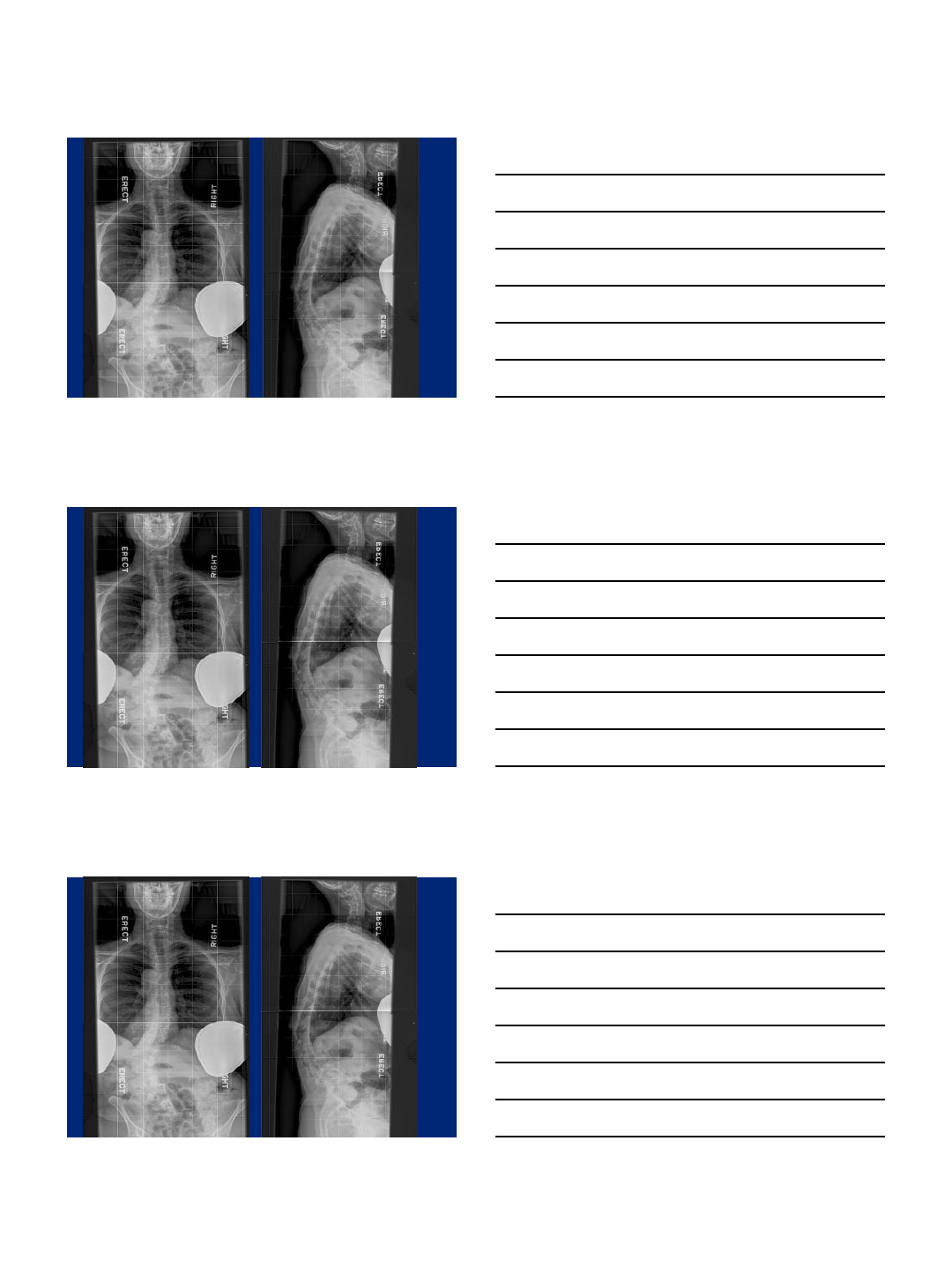
How High
How High
How Low
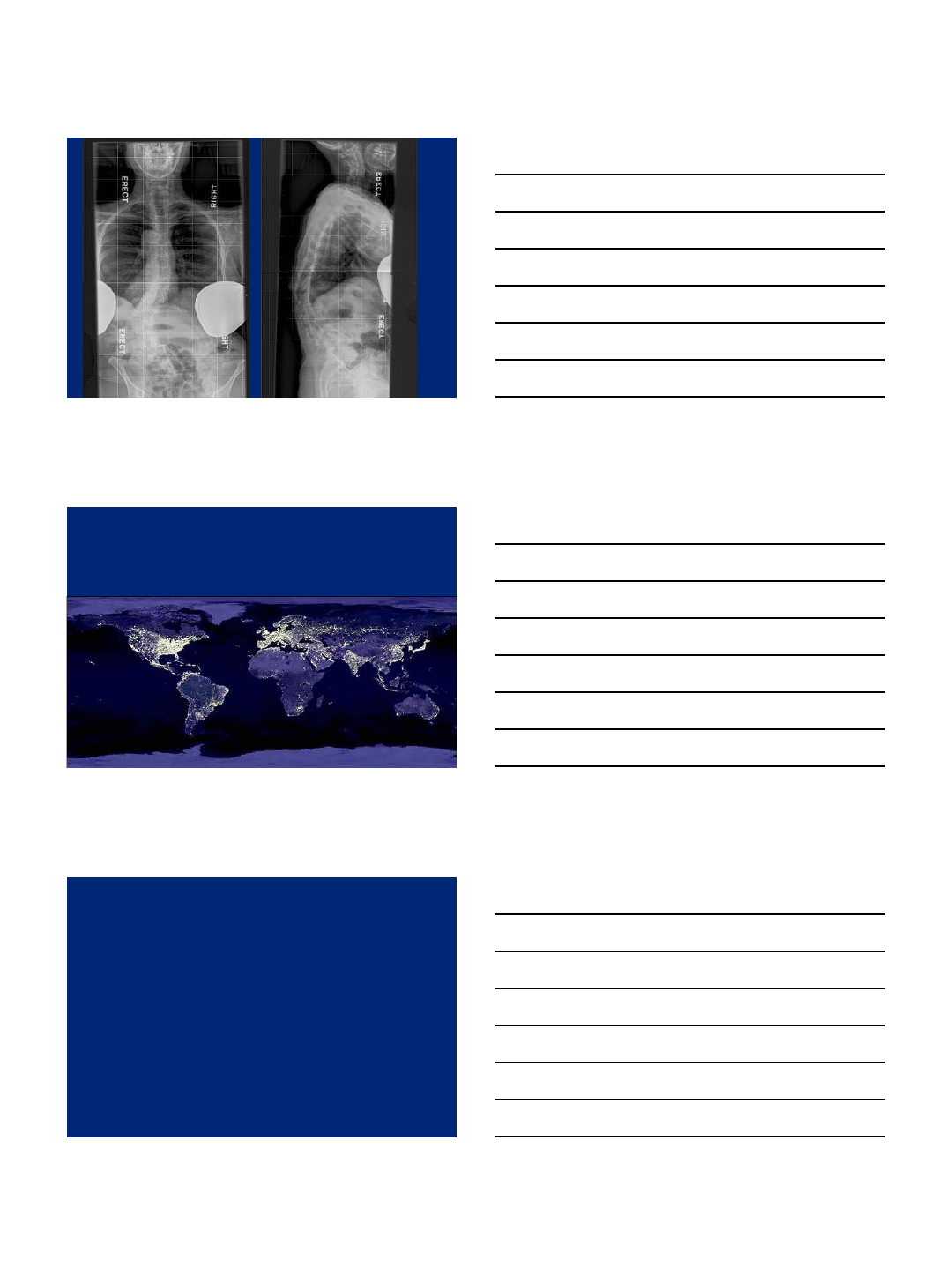
3
How High
How Low
When to go front and back
Surgical Strategies
•Characterized by significant variability
•Outcomes studies required for an Evidence-based approach
Overview
•The challenge of the lumbosacral junction:
–Strain on S1 screws
–Solid arthrodesis at L5-S1
•Biomechanics of the Pivot Point
•Techniques and Limitations
4
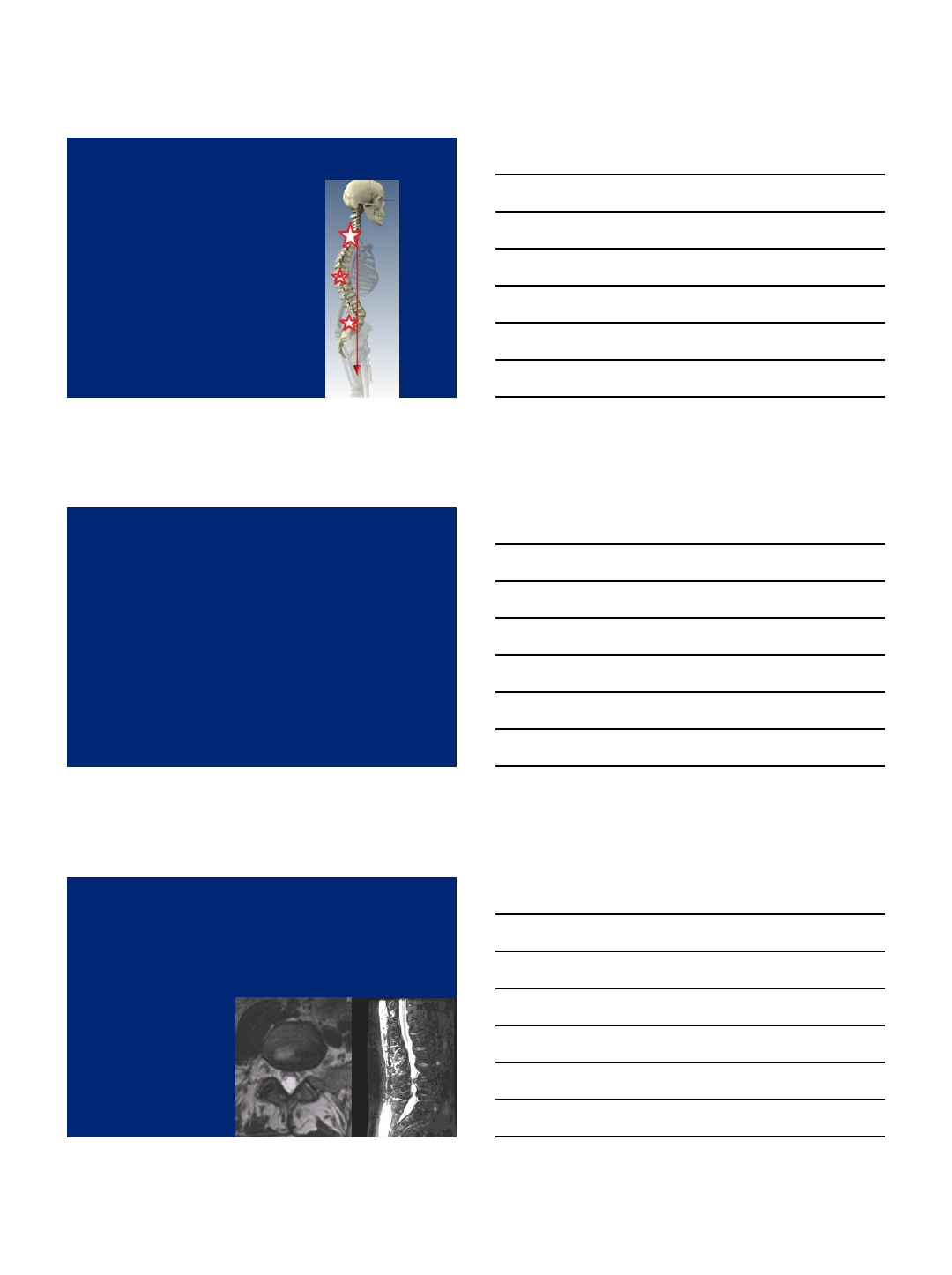
Hazards of the Junctions
•Thoracolumbar
•Lumbosacral
•Cervicothoracic
The Lumbosacral Junction
Two modes of failure:
1) Symptomatic degeneration below a
long fusion to L4 or L5
2) Nonunion or Malunion at L5-S1
Preoperative Assessment
•Localization of Pain on Physical Exam
•Advanced Imaging- MRI or CT
•Dynamic Imaging
•Provocative testing
–Facet Block
–Discography

5
The Case to Fuse to L5
•Better Function
•Less complications
•Good Survival of the L5-S1 motion segment
•Revision considerations
•Leaving options open for new technologies in the
future
•The loss of range of motion resulting from spinal fusion might lead to low back pain, trunk rigidity, and a negative
impact on quality of life. Nonetheless, these outcomes have not been conclusively demonstrated because lumbar
mobility and LIV have not been correlated with validated outcome instruments.
•METHODS:
•Forty-one patients (mean age, 27 y) with idiopathic scoliosis treated by spinal fusion (mean time since surgery, 135
mo) were included. Patients were assigned to 3 groups according to LIV level: group 1 (fusion to T12, L1, or L2)
14 patients; group 2 (fusion to L3) 13 patients, and group 3 (fusion to L4, L5, or S1) 14 patients. At midterm
follow-up, patients completed the Scoliosis Research Society (SRS)-22 Questionnaire and Quality of Life Profile
for Spine Deformities to evaluate perceived TF, and rated LBPi with a numerical scale. Lumbar mobility was
assessed using a dual digital inclinometer.
•RESULTS:
•Group 3 (fusion to L4, L5, or S1) showed statistically significant differences relative to the other groups, with less
lumbar mobility and poorer scores for the SRS subtotal (P = 0.003) and SRS pain scale (P = 0.01). Nevertheless,
LBPi and TF were similar in the 3 groups. TF correlated with SRS-22 subtotal (r = -0.38, P = 0.01) and pain scale
(r = -0.42, P = 0.007) scores, and with LBPi (r = 0.43, P = 0.005).
•CONCLUSIONS:
•LIV correlated moderately with lumbar mobility, health-related quality of life (SRS-22), and spinal pain (SRS-22
pain subscale), but not with intensity of pain in the lumbar area or perceived TF.
6
7
The slippery slope of extending
fusion to the sacrum
•Anterior column support
•Role of iliac fixation
Fusion to L5 vs. S1
8
L5 vs S1 Paradox
Thoracolumbar deformity arthrodesis to L5 in adults: the fate of the L5-
S1 disc.
- Edwards, Bridwell, et al. Spine 2003 Sep 15;28(18):2122-31.
•61% developed advanced disc degeneration at L5-S1
•Associated with loss of sagittal balance, need for revision surgery and lower
scores of SRS-24
•18% loss of fixation at L5
Higher incidence of complications in patients fused to S1
Edwards, Bridwell et al, SRS 2003
Failure of Fixation at L5
Purpose
Determine long-term radiographic and clinical
outcome of long (>T12) fusions to L5
The selection of L5 versus S1 in long fusions for adult
idiopathic scoliosis.
Swamy, Berven, Bradford.
Neurosurg Clin N Am 2007 Apr;18(2):281-8.

9
Survivorship Analysis
5 year: 75%
10 year: 70%
If include pts
considering
revision
5 year: 70%
10 year: 65%
Overall: 50% at
latest FU
The selection of L5 versus S1 in long fusions for adult idiopathic scoliosis.
Swamy, Berven, Bradford. Neurosurg Clin N Am 2007 Apr;18(2):281-8.
Conclusions
•Primary long fusions to L5 associated with
–25% revision rate at 5 years
–30% revision rate at 10 years
•Fusion to L5 is most reliable in patients with good
sagittal balance and bone quality
Indications to Extend Fusion to the Sacrum
•Symptomatic degenerative changes at L5-S1
–Spondylolisthesis at L5-S1
–Stenosis requiring decompression at L5-S1
•Significant sagittal plane realignment
•Osteoporosis
•Fixed obliquity of the L5-S1 motion segment
–Trunk translation
10
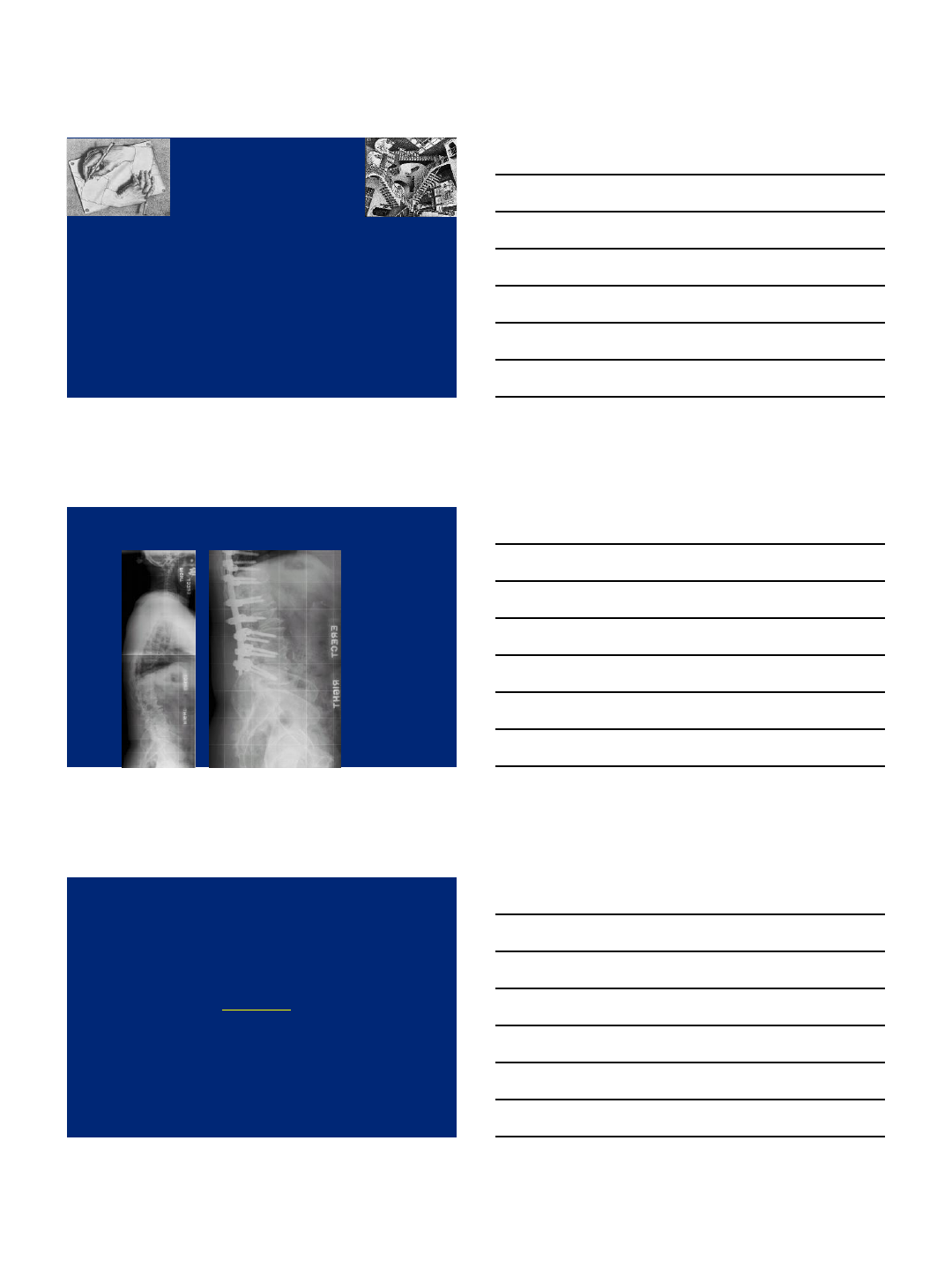
Sacral Fixation Considerations
•Sacrum is a poor fixation point due
to the large cancellous component
•Bicortical or tricortical fixation needed
•Sacrum exposed to large cantilever forces
•Fixation to the sacrum eliminates most
important sagittal compensatory mech.
•Fixation to the sacrum alters gait
Pedicle Fixation in
the Sacrum
•S1 pedicle screw is the
strongest fixation point
- unicortical fixation
- bicortical fixation
- tricortical fixation
•S2 pedicle screw
- short
- weak bone
0
1
2
3
4
5
6
7
8
9
020 40 60 80 100
Average Torque (in-lbs)
Percent Screw Length
Bicortical vs Tricortical Average Insertional Torque
Tricortical
Bicortical
Linear
(Tricortical)
Linear
(Bicortical)
Polly, Kuklo, et al
Limitations of Long Fusion to the Sacrum
•Cantilever forces for long segment constructs becomes
critical when sacral fusion extends to L3 or higher
–Shono, et al. Spine 1998
–Cunningham, et al. Spine, 2003
•Clinical correlation with a high incidence of symptomatic
pseudarthroses in long fusions to S1
•Kostuik 1983, 40% pseudarthrosis
•Boachie 1991, 41% pseudarthrosis
•Delvin 1991, 33% pseudarthrosis
•Lenke 2004, 23% pseudarthrosis
•Balderston 1986, 28% good result
11
Long fusions to the sacrum require anterior
column support +/- iliac crest extension
•Cantilever forces for long segment
constructs becomes critical when sacral fusion
extends to L3 or higher
–Anterior interbody decrease S1 screw strain 30-40 %
–S2 fixation decreases S1 screw strain by 15%
–Iliac fixation decreases S1 screw strain by 50 to 300 %
Limitations of Long Fusion to the Sacrum
•Cantilever forces for long segment constructs becomes
critical when sacral fusion extends to L3 or higher
–Shono, et al. Spine 1998
–Cunningham, et al. Spine, 2003
•Clinical correlation with a high incidence of symptomatic
pseudarthroses in long fusions to S1
•Kostuik 1983, 40% pseudarthrosis
•Boachie 1991, 41% pseudarthrosis
•Delvin 1991, 33% pseudarthrosis
•Lenke 2004, 23% pseudarthrosis
•Balderston 1986, 28% good result
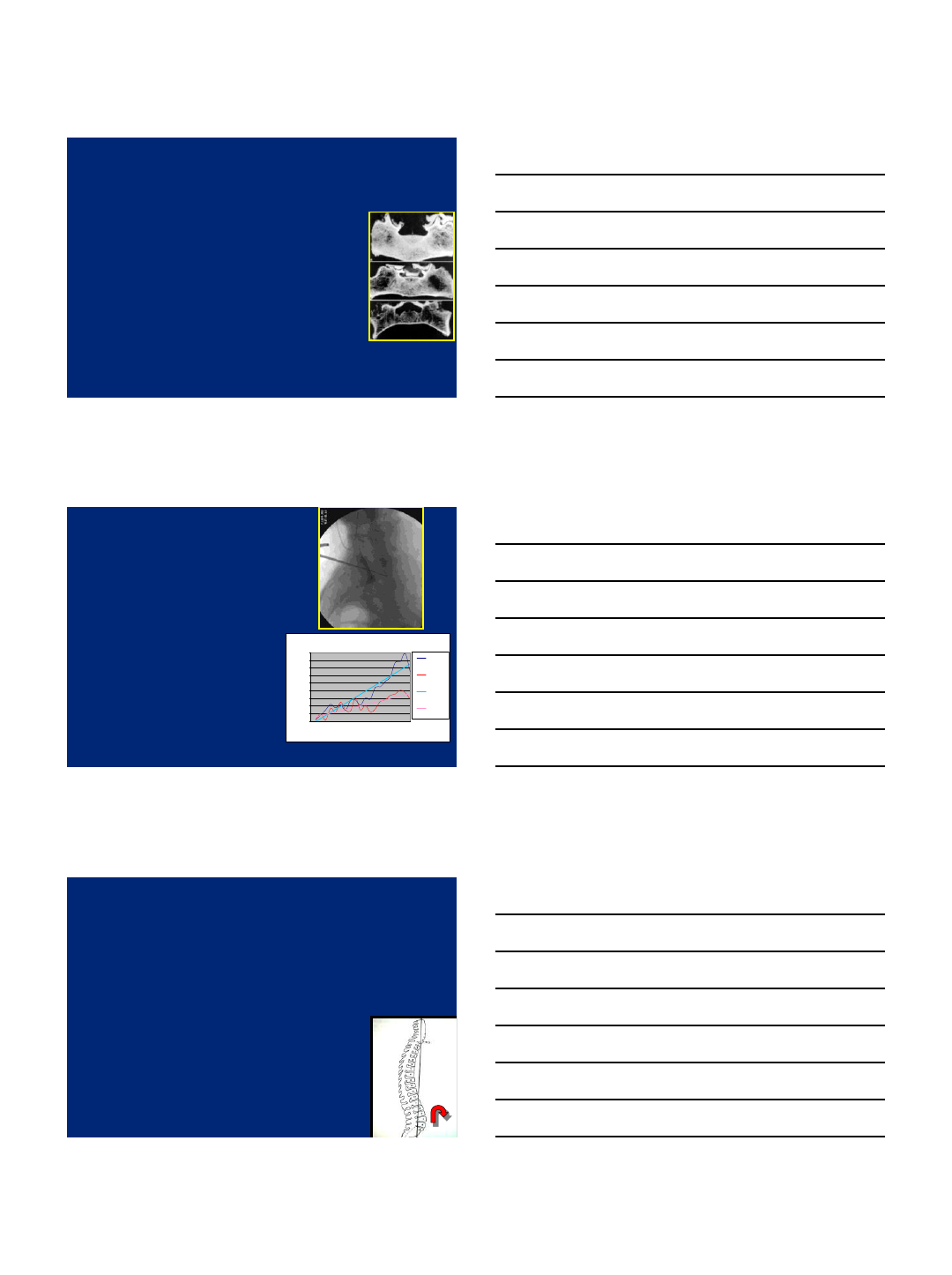
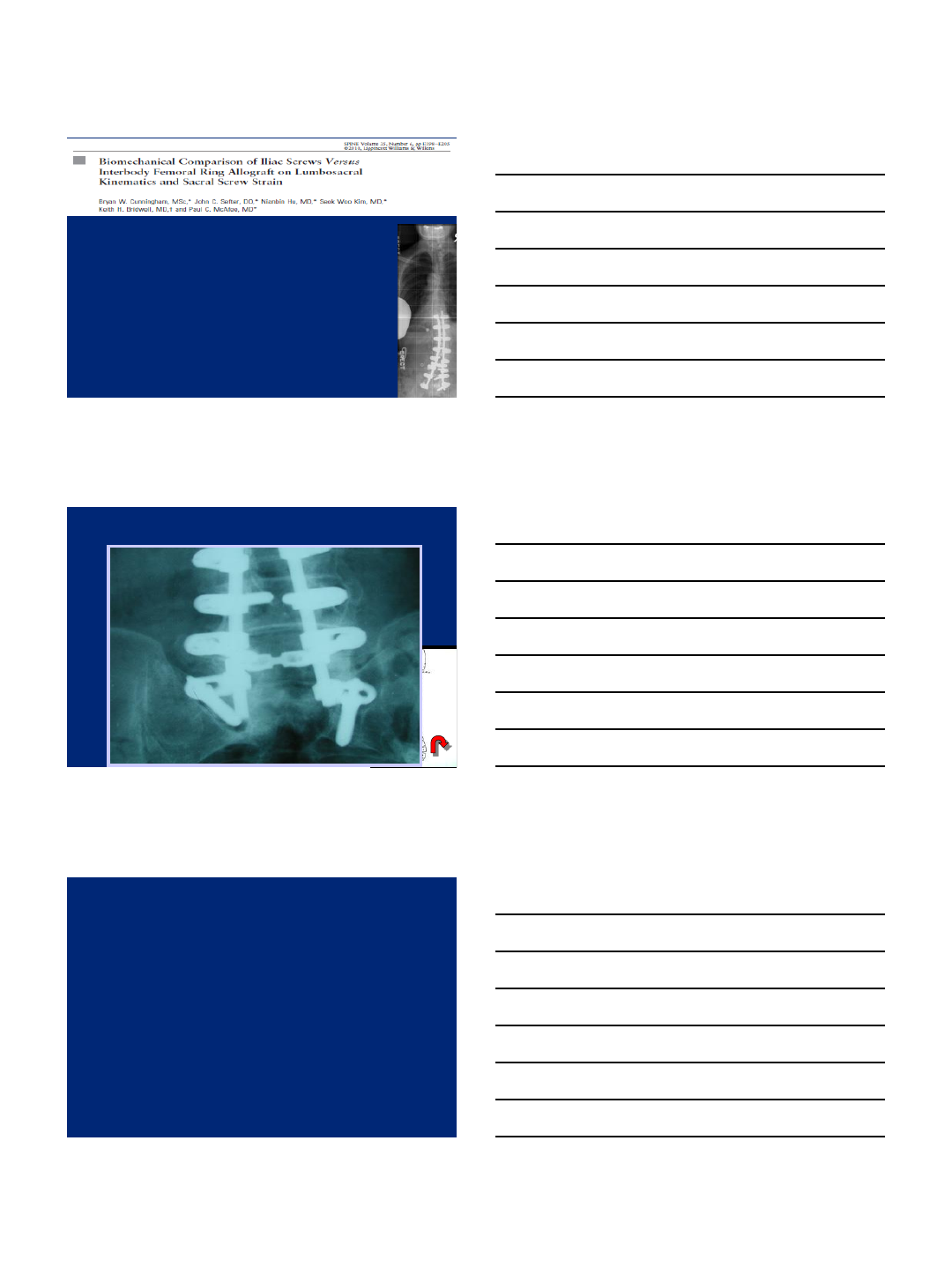
McCord DH et al
Spine 1992
•66 bovine specimens/10 instrumentation
techniques
•Established pivot point at the lumbosacral
joint at the intersection of the middle
osteoligamentous column (sagittal plane) and
the lumbosacral intervertebral disc
(transverse plane)
12
Reducing Strain on Sacral Screws
in Long Fusions to the Sacrum
0
50
100
150
200
250
S1 Sublami nar
Wire S1 Hook S1 Pedicle
Screw S1 Screw with
S2 Hook Ch opin Block Iliosacral
Screw Iliac Screw with
S1 Screw Galveston wi th
S1 Screw Control
Moment (Nm)
MAXIMUM MOMENT AT FAILURE
S1 Fixation
S1/S2 Fixation
Sacro-Pelvic
Control
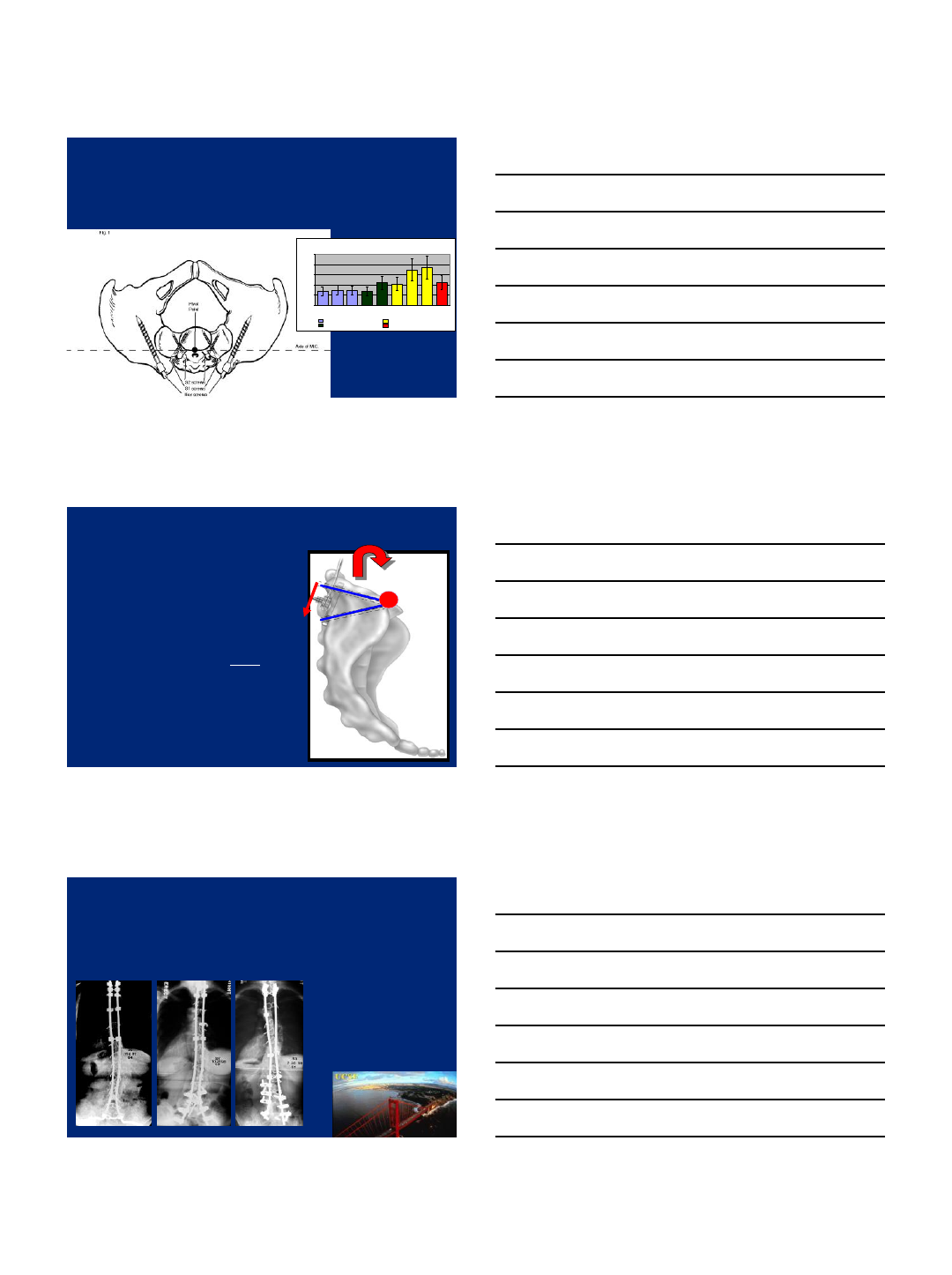
S2 SCREW
•“Biomechanical comparison of
lumbosacral fixation
Techniques in a calf spine
model”
Spine 2002, Lebwohl et al
•S2 screw extends fixation distal to
the pivot point thus extending lever
arm and providing additional
support
•However, the S2 screw does not
extend anterior to the pivot point
and thus not as good as iliac screw
fixation
PI
VOT
PIVOT
Long Fusion To The Sacrum in Adult Spinal
Deformity: Luque Galveston vs. Iliac Screws
vs. Sacral Screws
Emami et al:Spine 2003
UCSF Spinal Disorders Service
13
Iliac Bolt Fixation
•Bolt or screw is passed
into the ilium at the PSIS
•Bolt or screw is affixed
directly to the spine construct
•Effective in high demand
construct
•Failure rate half of traditional
Galveston
How Many Iliac Screws?
14
Study Aims and Design
Goals
Pelvic versus Sacral + ALIF
Unilateral iliac versus bilateral iliac
Methods
Seven cadavers instrumented up to L1
Multi-axial bending with pure moment
S1 screws modified with strain gauges for
pullout force
L1-S1, uni-iliac, bi-iliac… with and without
ALIF at L5/S1
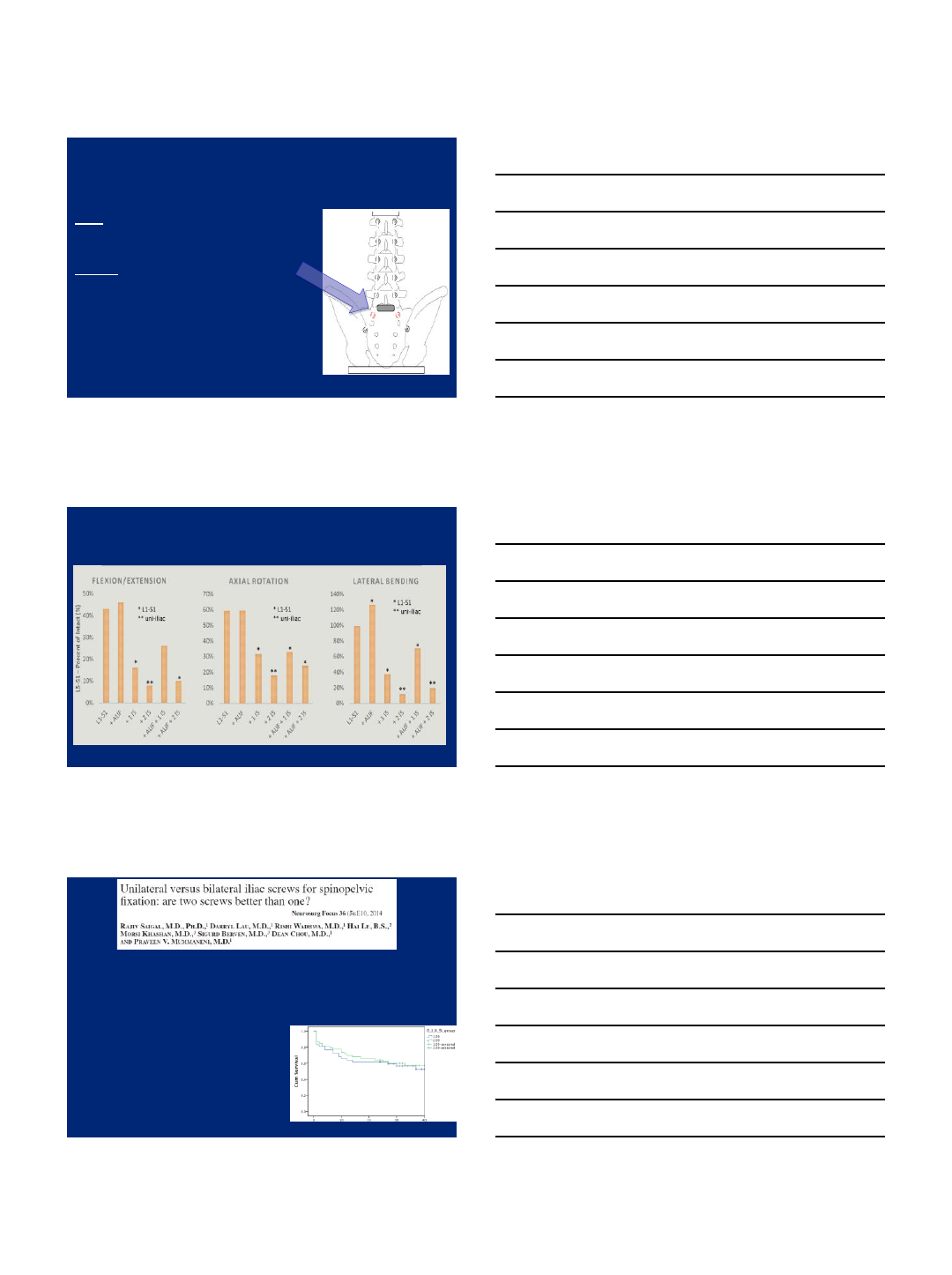
Multi-axial bending
0%
10%
20%
30%
40%
50%
L5-S1 –Percent of Intact (%)
FLEXION/EXTENSION
*
** *
* L1-S1
** uni-iliac
0%
20%
40%
60%
80%
100%
120%
140%
LATERAL
BENDING
*
*
** **
** L1-S1
** ni-iliac
0%
10%
20%
30%
40%
50%
60%
70%
AXIAL ROTATION
**
**
* L1-S1
** uni-iliac
*
One vs Two Iliac Screws
•100 patients with long fusions from thoracic spine
to the sacrum
–53patients with 2 iliac screws
–47 patients with 1 iliac screws
15
Limitations of Iliac Fixation
•Higher incidence of perioperative complications
–Wound infection
•Abdul-Jabbar A, et al.
•Higher incidence of need for revision surgery
–Screw removal
•Emami A, et al.
Evidence-based approach to the use
of Iliac Fixation
•Extension of fixation to ilium in:
–Compromised anterior column support at L5-S1
•TLIF at L5-S1
–Revision fixation to the sacrum in a long construct
•Above L3
–Compromised sacral fixation
–Incomplete correction of sagittal and coronal balance
–Pelvic obliquity/Long thoracolumbar (c-shaped) deformity corrected
with cantilever maneuver
–Ankylosing Spondylitis
Conclusions
•Fixation at the lumbosacral junction is challenging and
important for stable reconstructions in deformity
•High strain on the sacral screws may lead to screw
loosening and nonunion
•Pelvic fixation reduces strain on the sacral screws
•Role of biologics and new technologies in limiting need
for iliac fixation requires further investigation
16
UCSF Center for Outcomes Research

1
Spino-Pelvic Parameters:
How Do They Affect My
Decision to Extend a Fusion to
the Sacrum/Pelvis
Han Jo Kim MD
Frank J. Schwab, MD
Bassel G. Diebo, MD
Virginie Lafage, PhD
Hospital for Special Surgery
New York, NY
Disclosures
•Consultant
–K2M, Biomet, Medtronic
•Speaker Bureau (not present, within last 36 months)
–Depuy, Stryker
•Board Membership
–ASJ, HSS Journal
SPINOPELVIC PARAMETERS
2
Setting Surgical Goals
Regional
Loss of lordosis
Versus PI
Global
SVA
Compensatory
Pelvic tilt
PI-LL < 10°SVA < 5cm PT < 20-25°
Literature Review
•34 consecutive adult deformity patients fused from the
thoracic spine to L5
•Subsequent L5-S1 DDD developed in 66% of patients
after long adult fusions to L5
Literature Review
•High percentage of patients subsequently degenerated the L5-
S1 disc
•With degeneration of the L5-S1 disc, sagittal balance was
frequently lost
•Prevalence of breakdown of the L5-S1 disc much greater in
the “long”fusions (T4-L5) vs. the “short”fusions (T10-L5)
3
Literature Review
Kim YJ, Bridwell KH, Lenke LG, Cho K, Edwards II C,
Rinella AS: Pseudarthrosis in adult spinal deformity following
multisegmental instrumentation and arthrodesis. J Bone Joint
Surg 2006;88(4):721-728
•A clinical and radiographic assessment of 232 adults
•Factors found to be significantly associated were preop
thoracolumbar kyphosis of >20°, age of >55 years,
arthrodesis to S1 compared to L5
•Patients with a pseudarthrosis had lower total outcome scores
on SRS questionnaire
•Prevalence of pseudarthrosis following long arthrodesis was
17%. Close to 30% for fusions to sacrum.
Literature Review
Islam NC, Wood KB, Transfeldt EE, Winter RB,
Denis F, Lonstein JE, Ogilvie JW. Extension of
fusions to the pelvis in idiopathic scoliosis. Spine
2001;26(2):166-173.
•41 patients (40 female; 1 male)
•39 of 41 had combined anteroposterior fusion extension
•Pseudarthrosis rate was 37% (15/41)
•With sacral fixation only, the rate was 53% (8/15), with
iliac fixation only 42% (3/7) and with both iliac and
sacral fixation 21% (4/19; p<0.05)
Enami A, Deviren V, Berven S, Smith JA, Hu SS,
Bradford DS. Outcome and complica-tions of long
fusions to the sacrum in adult spinal deformity. Spine
2002;27:776-686.
Literature Review
•54 consecutive patients who underwent elective combined anterior
and posterior surgical reconstruction for acute spine deformity were
studied
•Attention to sagittal balance is critical
•Luque-Galveston fixation technique has an unacceptably high rate
of pseudarthrosis. Currently, the authors are using bicortical and
triangulated sacral screws with anterior interbody support
•They recommend using iliac fixation, although there is a higher rate
of painful implants, requiring removal
4
McCord DH, Cunningham BW, Shono Y,
Myers JJ, McAfee PC. Biomechanical analysis
of lumbosacral fixation. Spine
1992;17(8S):S235-243
Long fixation points in the ilium that extend
anterior to the axis of rotation of L5-S1 provide
the most stable fixation of the lumbosacral
joint.
Literature Review
Literature Review
Cunningham BW, Lewis SJ, Long J, Dmitriev
AE, Linville DA, Bridwell KH. Biomechanical
evaluation of lumbosacral reconstruction
techniques for spondylo-listhesis: An in vitro
porcine model. Spine 2002;27(21):2321-2327
In a spondylolisthesis model, both the iliac screws and
the interbody cages at the lumbo-sacral junction
protected the S1 screws, but the iliac screws were far
more valuable.
•Age
–Bone quality
–Degenerative changes in disc, foramen, canal
•Deformity
–Large SVA
–Large Coronal Decompensation
–Large Curve Magnitude
–Rigid vs. Flexible Deformity
–Presence of L5/S1 Spondylolisthesis
–Laminectomy Defects at L5/S1
Factors that Dictate my Decision to Fuse
to Sacrum/Ilium
5
Factors that Dictate my Decision to Fuse
to Sacrum/Ilium
•Age
–Bone quality
–Degenerative changes in disc, foramen, canal
•Deformity
–Large SVA
–Large Coronal Decompensation
–Large Curve Magnitude
–Rigid vs. Flexible Deformity
–Presence of L5/S1 Spondylolisthesis
–Laminectomy Defects at L5/S1
•Spino-Pelvic Parameters
–High PT
–High PI
High PT
•PT will be very difficult to correct without
fusion to S1 and Iliac Fixation in Adult
Spinal Deformity
High PI
• “Guillotine Effect” of Fusion to L5 on
L5/S1 Disc Space
–High shear stresses

6
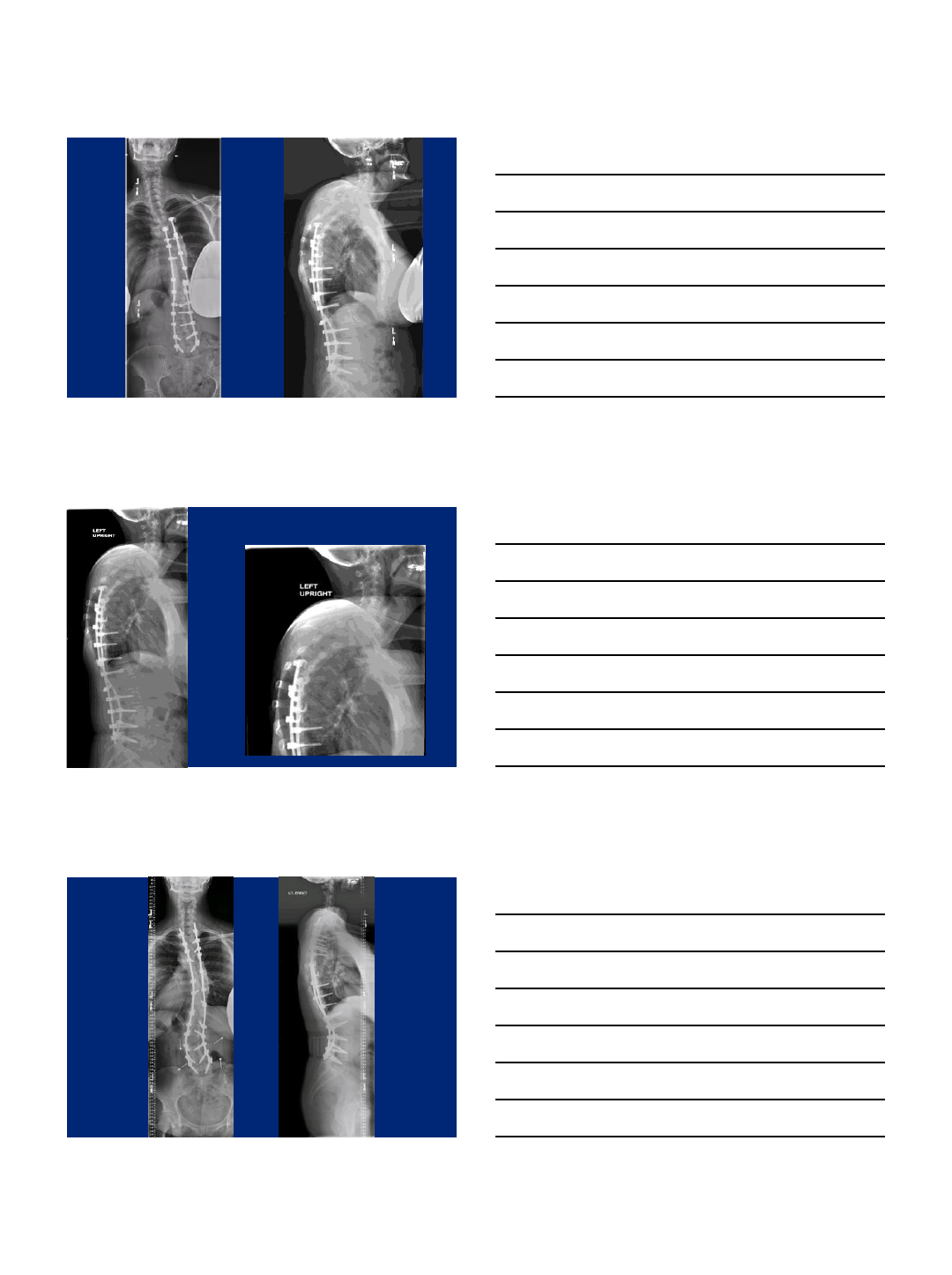
Substantial sagittal imbalance, back pain, inability to
ambulate
PT 36
LL 20
PI 55
SVA 20cm
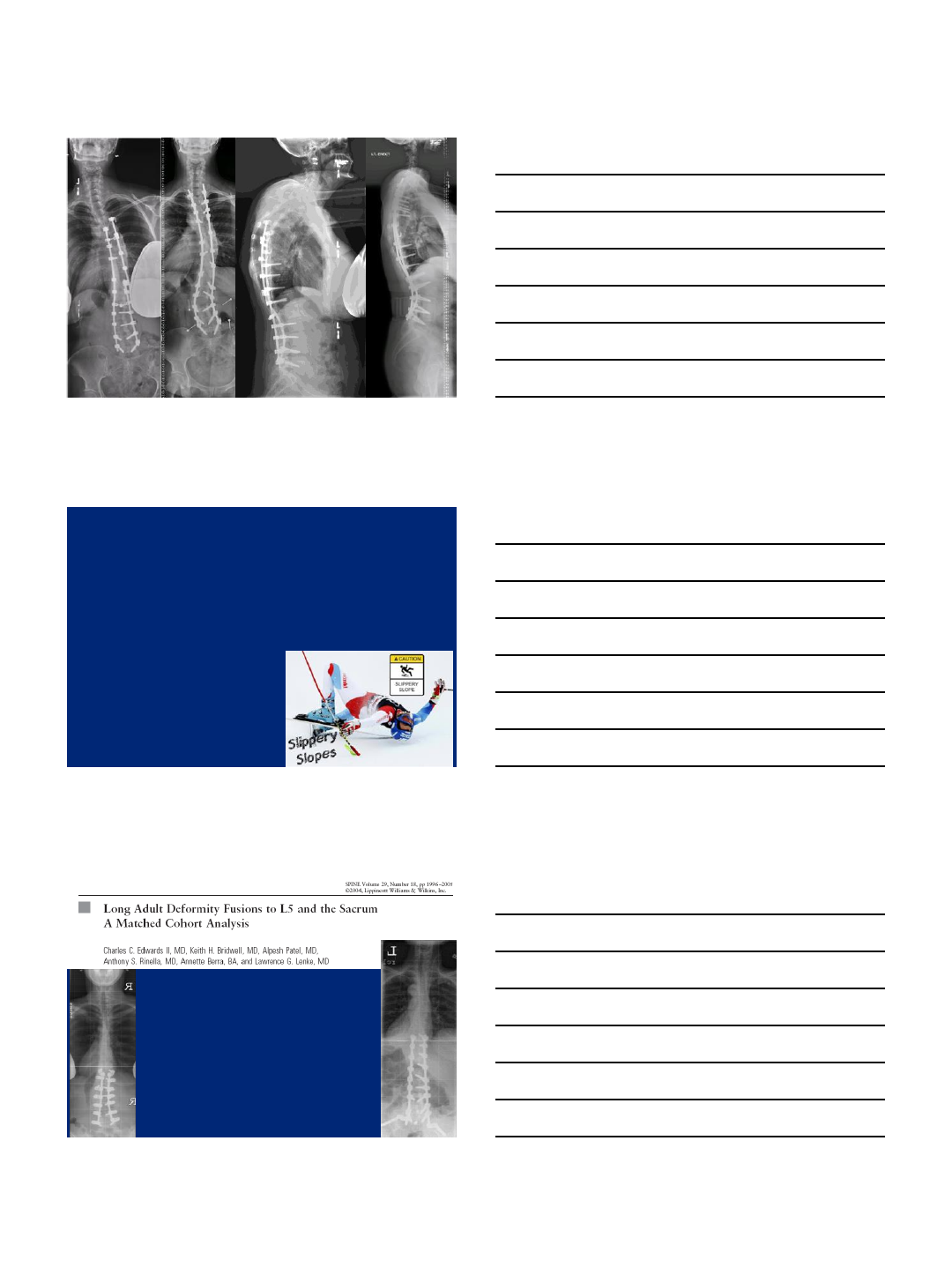
Cantilever to “Dial In” Pelvic
Anteversion
PT 36
LL 20
PI 55
SVA 20 cm
PT 8
LL 55
PI 55
SVA 1cm
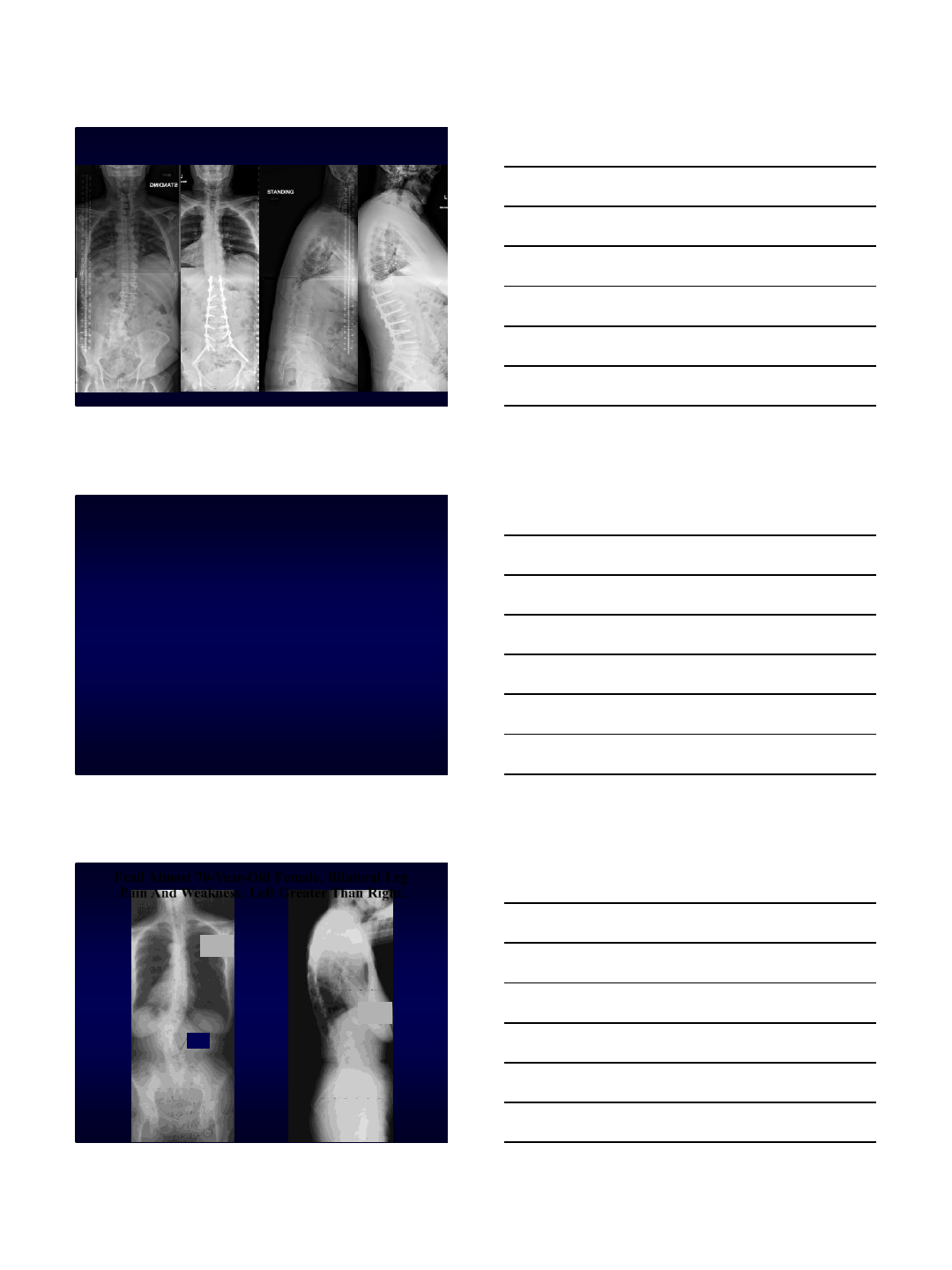
Case
•79M with bilateral leg and back pain
–10% back, 90% leg pain
•50% Left, 50% Right
–Exacerbated by standing/walking
–Improved with sitting, lying down (some
positions)
–No bowel/bladder symptoms
–Subjective weakness/numbness when
ambulating
–Failed PT/Injections
7
Exam
•Marked Positive Sagittal Balance
•Can only stand for a short period of time
•Static Motor Exam intact
•Sensory exam normal
PI 50
PT 26
LL 9
TK 27
CL 4
SVA 17
8
L1/2 L2/3 L3/4 L4/5
Questions
•Osteotomy? Can you do PCOs? Or will this
need a PSO?
–If PSO, what level?
–If PCO, what level(s)?
•Is an Interbody necessary?
–Lateral? Transforaminal? Anterior?
•Choice for UIV? Lower or Upper Thoracic?
•Iliac Fixation?
•Will you need Biologics?
9
PSF T11-Ilium, PCO L1-L5, TLIF L5/S1
PI 50
PT 8
LL 50
TK 40
SVA -5mm
2 yrs post-op 2 yrs post-op
Do We Always Have To
Go To The Sacrum? Are
There Select
Circumstances Where
We’d Be Better Off
Stopping At L5?
Case following Courtesy of Dr. Keith H. Bridwell MD
10-7-05
69+11
10-7-05
69+11
56°
Frail Almost 70-Year-Old Female. Bilateral Leg
Pain And Weakness, Left Greater Than Right.
Good Sagittal Parameters!
10
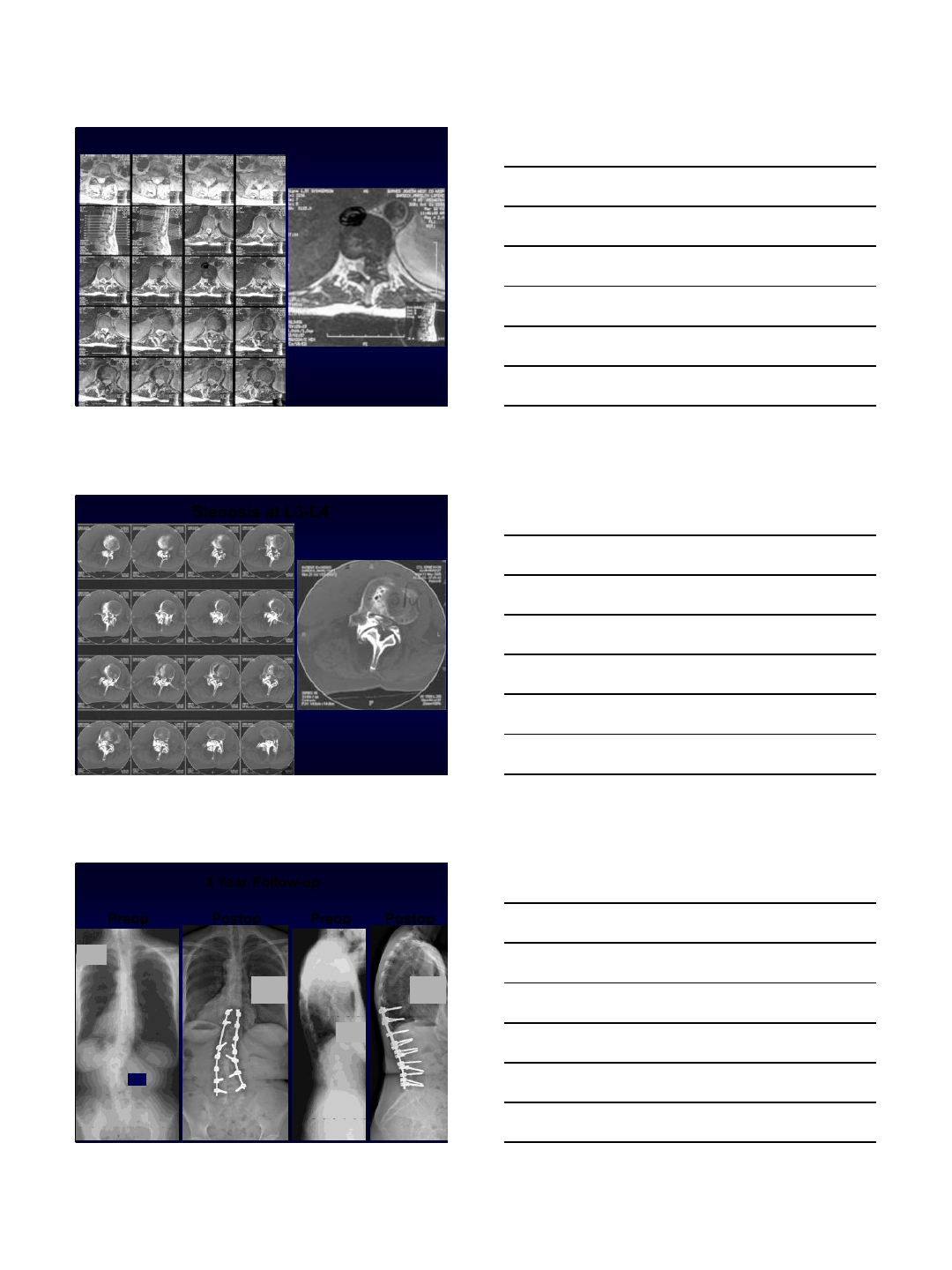
Large Calcified Disc Herniation at T11-T12 on the Left Side
Stenosis at L3-L4
10-7-05
69+11
Preop Postop Preop Postop
10-7-05
69+11
56°
9-14-09
73+10
3+9 yr po
9-14-09
73+10
3+9 yr po
4 Year Follow-up
11
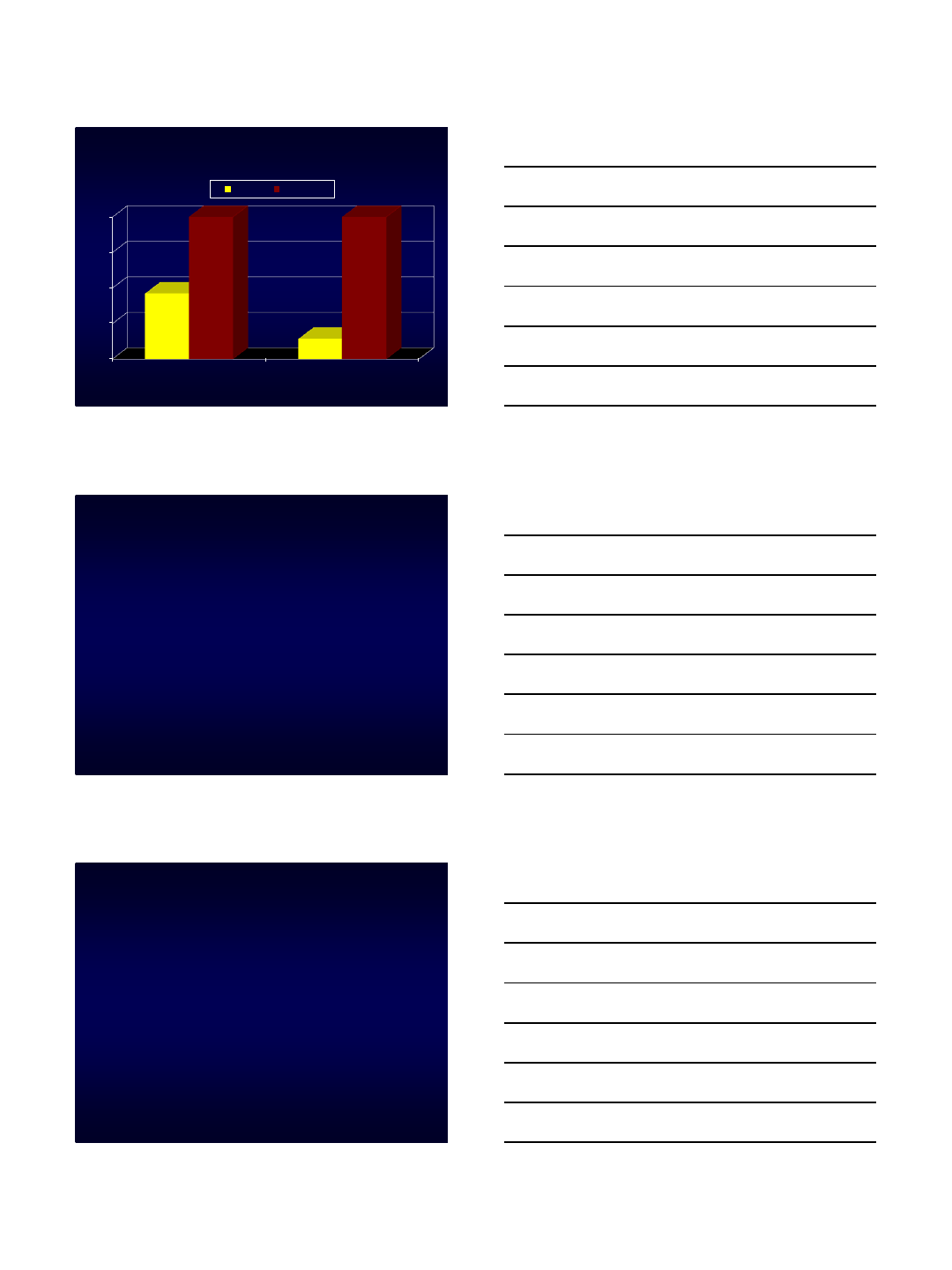
Oswestry Scores
0
25
50
75
100
Preop Ultimate Postop
46
14
100 100
Score Potential
Balance Risks/Benefits
•Large PI-LL mismatch
•Large PT
•Large PI (natural anatomy)
Balance Risks/Benefits
•Large PI-LL mismatch
•Large PT
•Large PI (natural anatomy)
•Need fusions to Sacrum/Ilium
•Pseudo Risk

9/8/2015
1
L5-S1 Fusion options
Approach, Interbody
support, & Graft
Options
Jason W. Savage, MD
Cleveland Clinic
Center for Spine Health
9/8/2015
Disclosures
•Consultant: Stryker Spine
•Editorial Board: JSDT
•Off-label use of BMP
outline
•Approach
–Anterior
–Posterior
•Interbody Support
–ALIF/PLIF/TLIF/OLIF
–Advantages/Disadvantages
–Is it necessary ???
•Graft Options
–Bone vs. PEEK vs. Metal
–BMP
9/8/2015
2
Goals of surgery
•Restore regional lordosis
• “Fix”the fractional curve
•Achieve a solid fusion
Up to 25% pseudarthrosis
rate at L5-S1
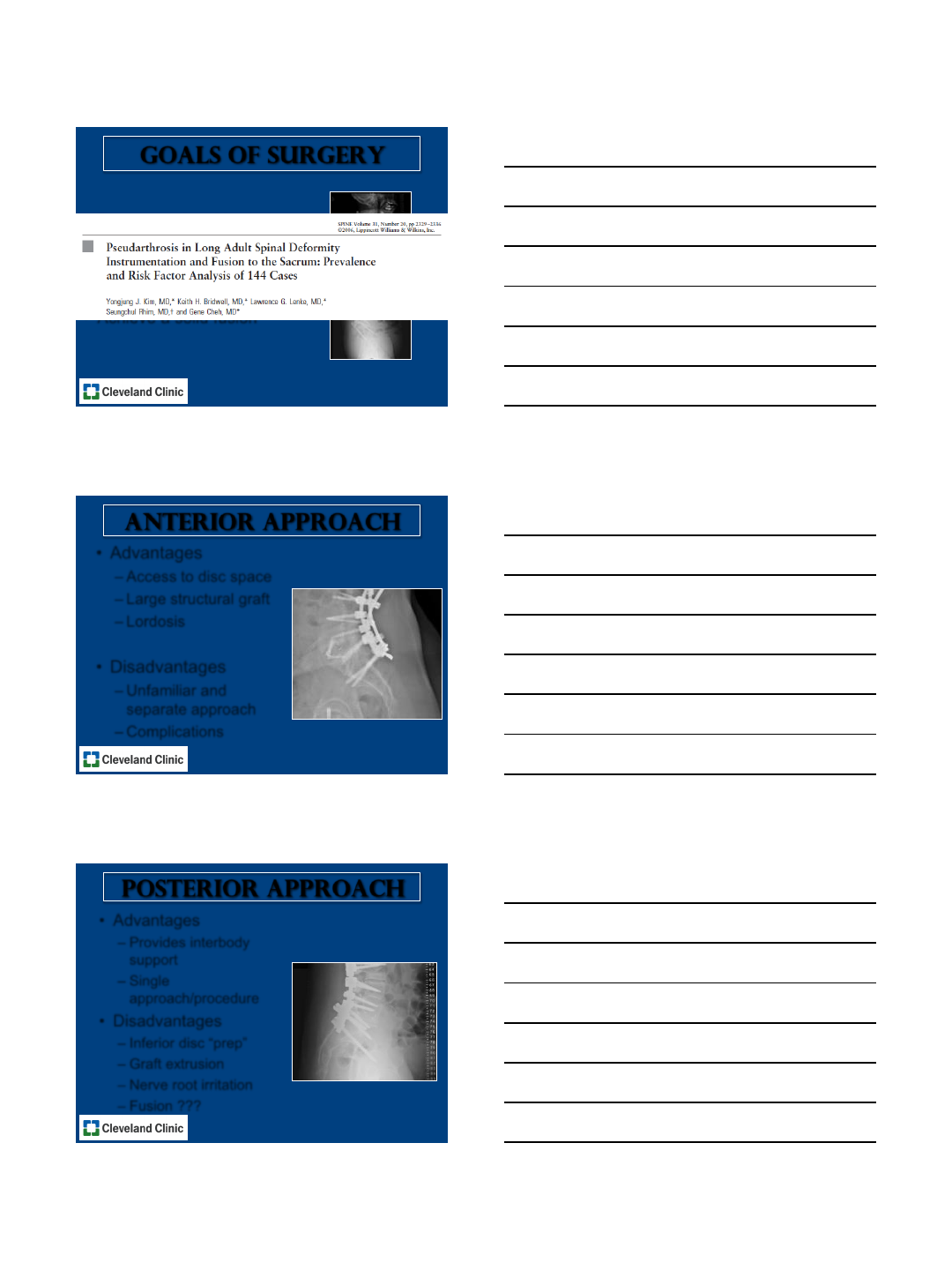
Anterior approach
•Advantages
–Access to disc space
–Large structural graft
–Lordosis
•Disadvantages
–Unfamiliar and
separate approach
–Complications
Posterior approach
•Advantages
–Provides interbody
support
–Single
approach/procedure
•Disadvantages
–Inferior disc “prep”
–Graft extrusion
–Nerve root irritation
–Fusion ???
9/8/2015
3
Anterior vs. posterior
J Neurosurg Spine 2007;7:379-386.
-3
-2
-1
0
1
2
3
4
5
6
7
1 2
ALIF
TLIF
•Retrospective
•32 ALIF vs. 25 TLIF
•Foraminal Height
•18.5% vs. -0.4% (p<0.01)
•Segmental Lordosis
•8.3 vs. -0.1°(p<0.01)
•Regional Lordosis
•6.2 °vs. -2.1°(p<0.01)
Lumbar Lordosis
Anterior vs. posterior
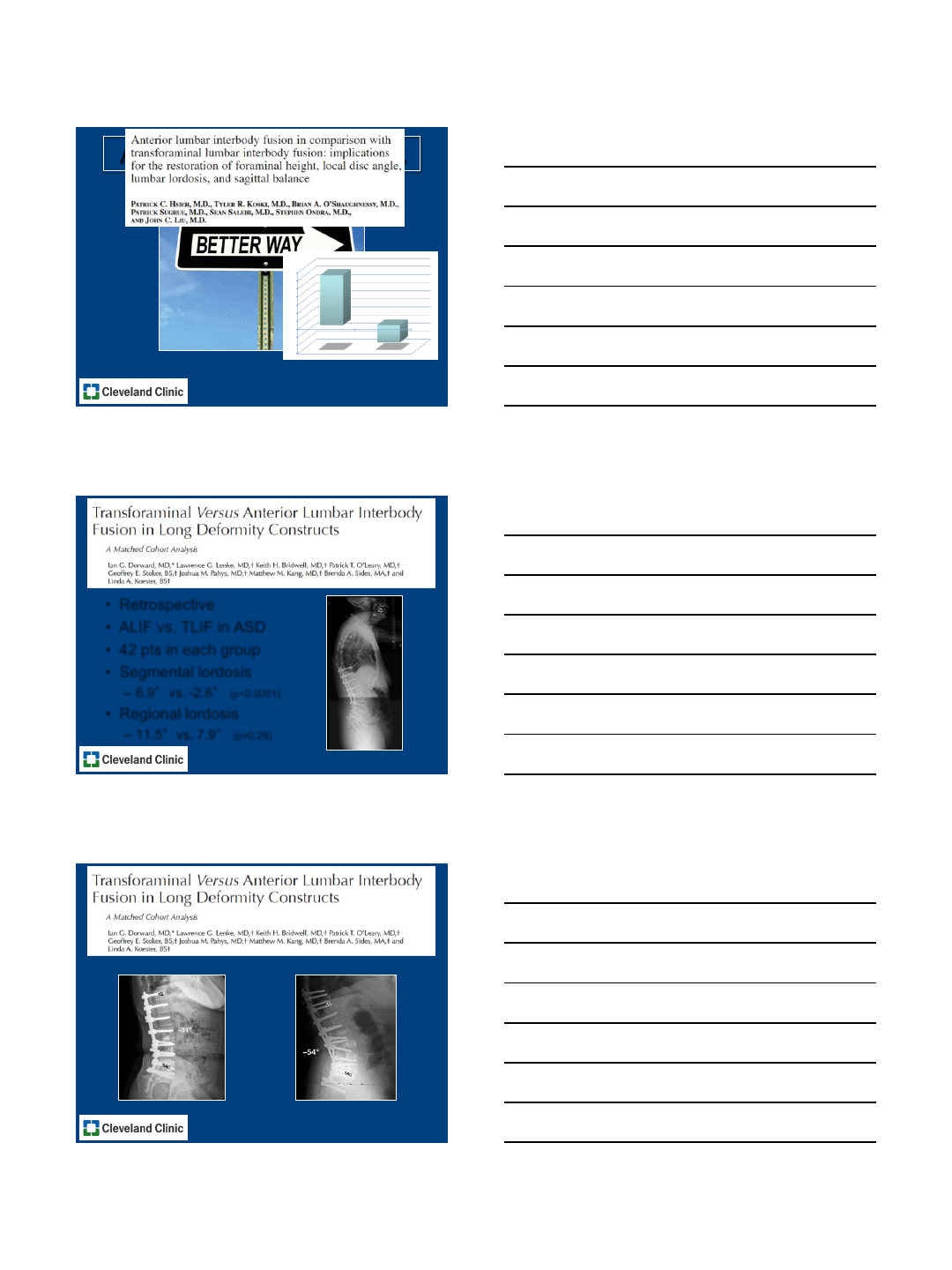
•Retrospective
•ALIF vs. TLIF in ASD
•42 pts in each group
•Segmental lordosis
–6.9°vs. -2.6°(p<0.0001)
•Regional lordosis
–11.5°vs. 7.9°(p=0.29)
Spine 2013;38:E755-E762.
Spine 2013;38:E755-E762.
NO DIFFERENCE IN RATE OF PSEUDARTHROSIS
9/8/2015
4
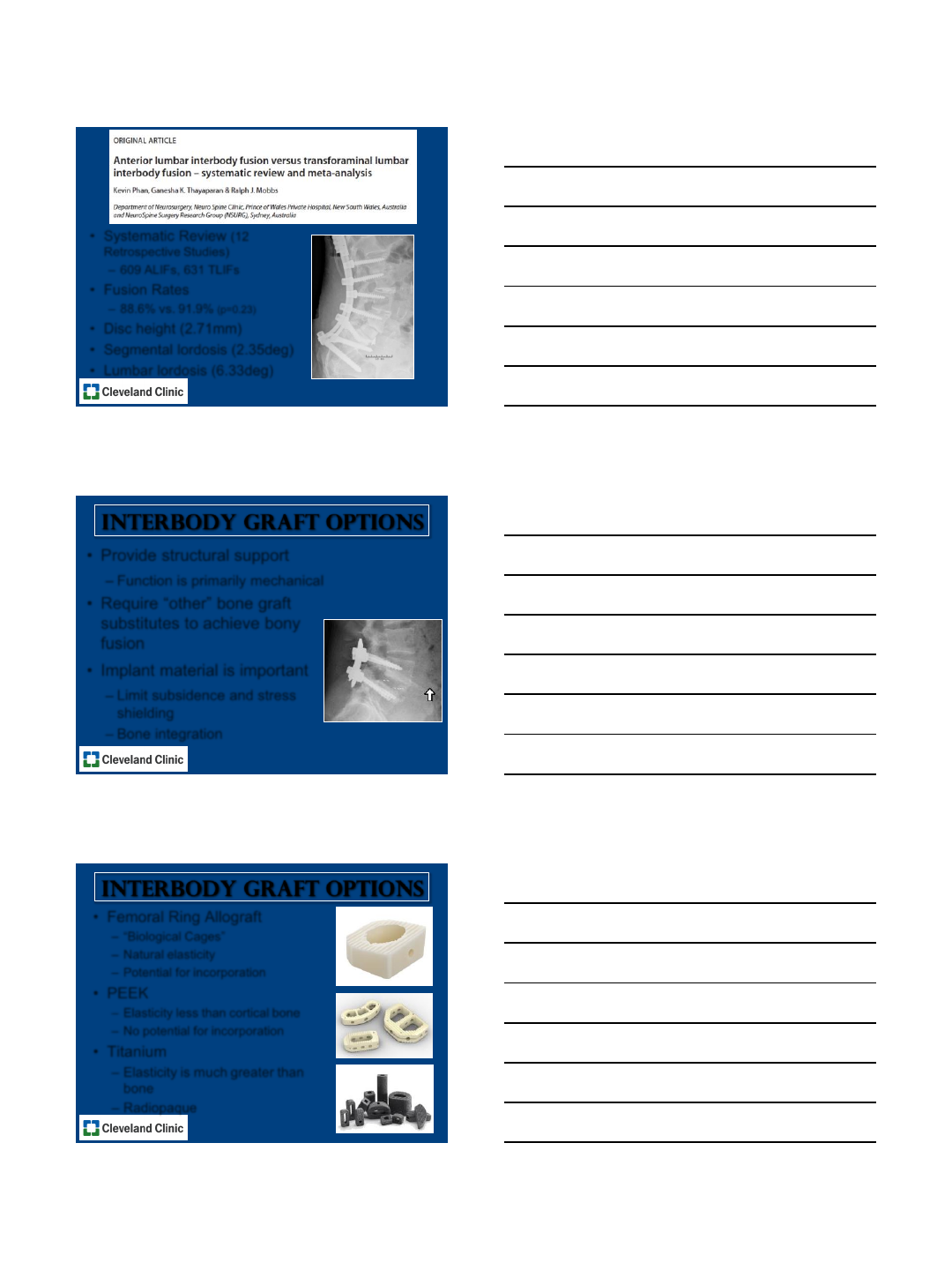
Br J Neurosurg 2015;Early Online:1-7.
•Systematic Review (12
Retrospective Studies)
–609 ALIFs, 631 TLIFs
•Fusion Rates
–88.6% vs. 91.9% (p=0.23)
•Disc height (2.71mm)
•Segmental lordosis (2.35deg)
•Lumbar lordosis (6.33deg)
Interbody graft OPTIONS
•Provide structural support
–Function is primarily mechanical
•Require “other”bone graft
substitutes to achieve bony
fusion
•Implant material is important
–Limit subsidence and stress
shielding
–Bone integration
Interbody graft OPTIONS
•Femoral Ring Allograft
– “Biological Cages”
–Natural elasticity
–Potential for incorporation
•PEEK
–Elasticity less than cortical bone
–No potential for incorporation
•Titanium
–Elasticity is much greater than
bone
–Radiopaque
9/8/2015
5
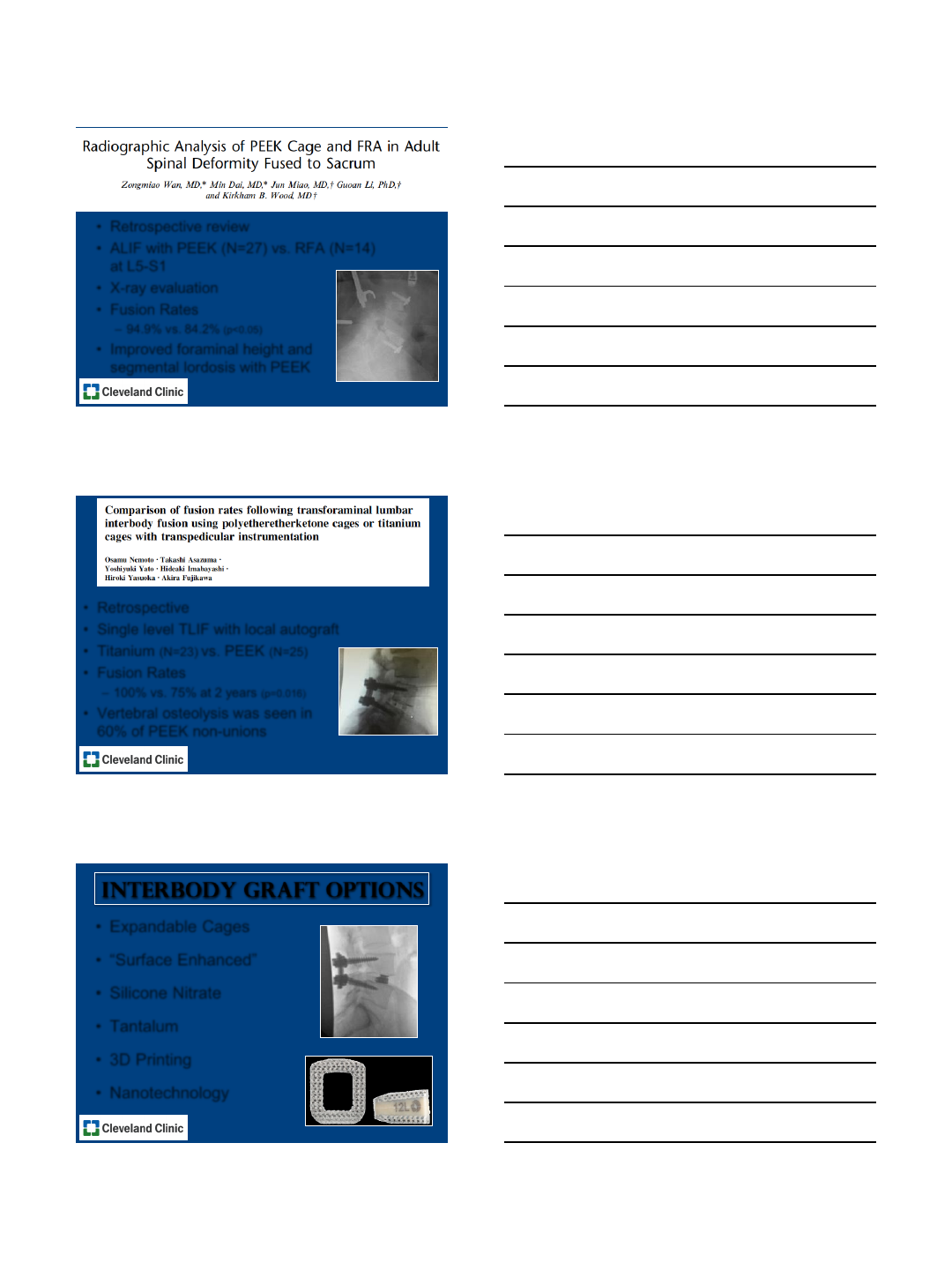
J Spinal Disord Tech 2014;27:327-335.
•Retrospective review
•ALIF with PEEK (N=27) vs. RFA (N=14)
at L5-S1
•X-ray evaluation
•Fusion Rates
–94.9% vs. 84.2% (p<0.05)
•Improved foraminal height and
segmental lordosis with PEEK
Eur Spine J 2014;23:2150-2155.
•Retrospective
•Single level TLIF with local autograft
•Titanium (N=23) vs. PEEK (N=25)
•Fusion Rates
–100% vs. 75% at 2 years (p=0.016)
•Vertebral osteolysis was seen in
60% of PEEK non-unions
•Expandable Cages
• “Surface Enhanced”
•Silicone Nitrate
•Tantalum
•3D Printing
•Nanotechnology
Interbody graft OPTIONS
9/8/2015
6
MSC
DBM BMP
Ceramics
Allograft Autograft
Efficacy Safety
RegulatoryCost
The world of biologics
Courtesy of Wellington K. Hsu, MD
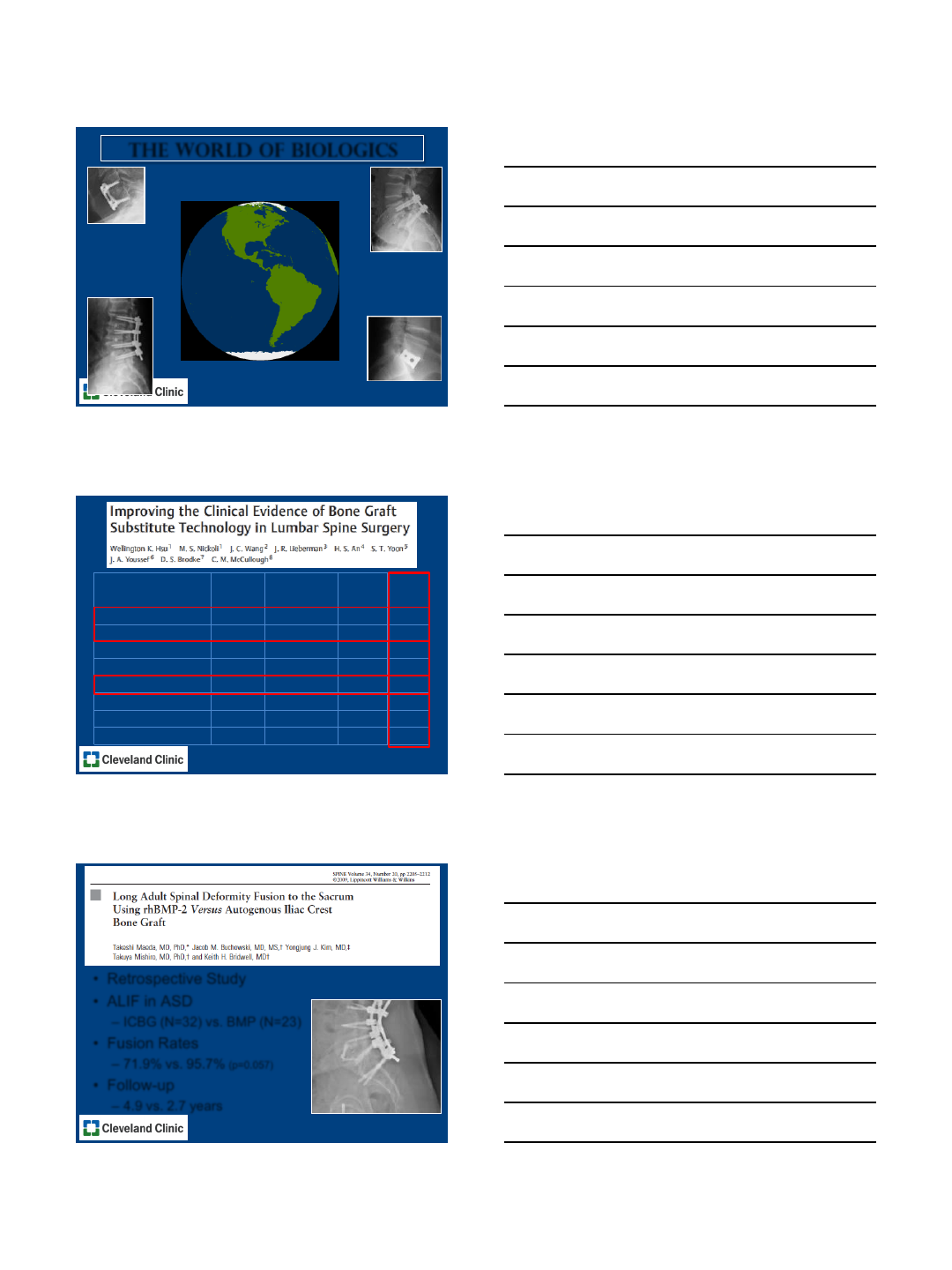
# Studies # Patients # Fused
Rate
(%)
ICBG 23 1389 1103 79%
Local Autograft 8 714 637 89%
Allograft alone 4 269 141 52%
BMA 2 40 34 85%
BMP - 2 3 213 201 94%
Ceramics 16 697 603 87%
DBM13192 171 89%
PRP 4 209 154 74%
•Retrospective Study
•ALIF in ASD
–ICBG (N=32) vs. BMP (N=23)
•Fusion Rates
–71.9% vs. 95.7% (p=0.057)
•Follow-up
–4.9 vs. 2.7 years
Spine 2009;34:2205-2212.

9/8/2015
7
•Retrospective Case Series
•L5-S1 Interbody fusion vs. PLF
–IF (N=35) vs. PLF (N=26)
•Average BMP
–4.1mg in IF vs. 3.2mg in PLF
•Fusion Rates
–97% vs. 96% (p=1.0)
Spine 2015;11:E634-E639.
•ALIF
–Sagittal plane deformity (mostly from
L4-L5 and/or L5-S1)
–Adjacent segment pathology below a
previous fusion (i.e. AIS)
•TLIF
–De novo scoliosis with “tall”disc or
spondy
–Fractional curve
•PLF alone
–De novo scoliosis with collapsed disc
My algorithm at L5-S1
Case example
Courtesy of Doug Orr, MD
9/8/2015
8
Case example
•Historically high rate of
pseudarthrosis at L5-S1
•Iliac Fixation, 360°, and
Biologics have improved
fusion rates
•ALIF improves disc height,
segmental lordosis, and LL
better than TLIF
•Likely no difference in
fusion
•Still a lot of questions ???
Conclusions
Thank you
1
Department of Orthopedic Surgery
Johns Hopkins University
Sacroplevic Fixation
Options, Techniques and
Complications
Khaled M. Kebaish, M.D., FRCSC
Professor of Orthopedic & Neurosurgery
DISCLOSURE
Depuy Spine Consultant, Royalty
K2M Consultant
Orthofix Consultant
WHY PELVIC FIXATION?
S1 Pedicles capacious & short
Sacrum bone is osteopenic
Failure rate of S1 Screws
Up to 44%
Inadequate as the only means
of fixation in long fusion
Camp et al, Spine 1990
2
INDICATIONS FOR
PELVIC FIXATION
Expected significant biomechanical
stresses
Long fusions to the sacrum
Definition: > 4 levels
Osteoporosis
Sacral Fracture
3
Sacro-Pelvic Fixation Options
Casting and bracing
Sacral Sublaminar
devices
Wires
Cables
Hooks
Sacral pedicle screws
S1 pedicle screws
S2 Pedicle screws
S1 Alar screws
S1 and Alar screw
blocks
Dunn-McCarthy S-
Rod
Jackson intra-sacral
rod
Kostuik sacral bar
Galveston technique
Iliac Screws
Sacral Alar Iliac
screws (S2AI)
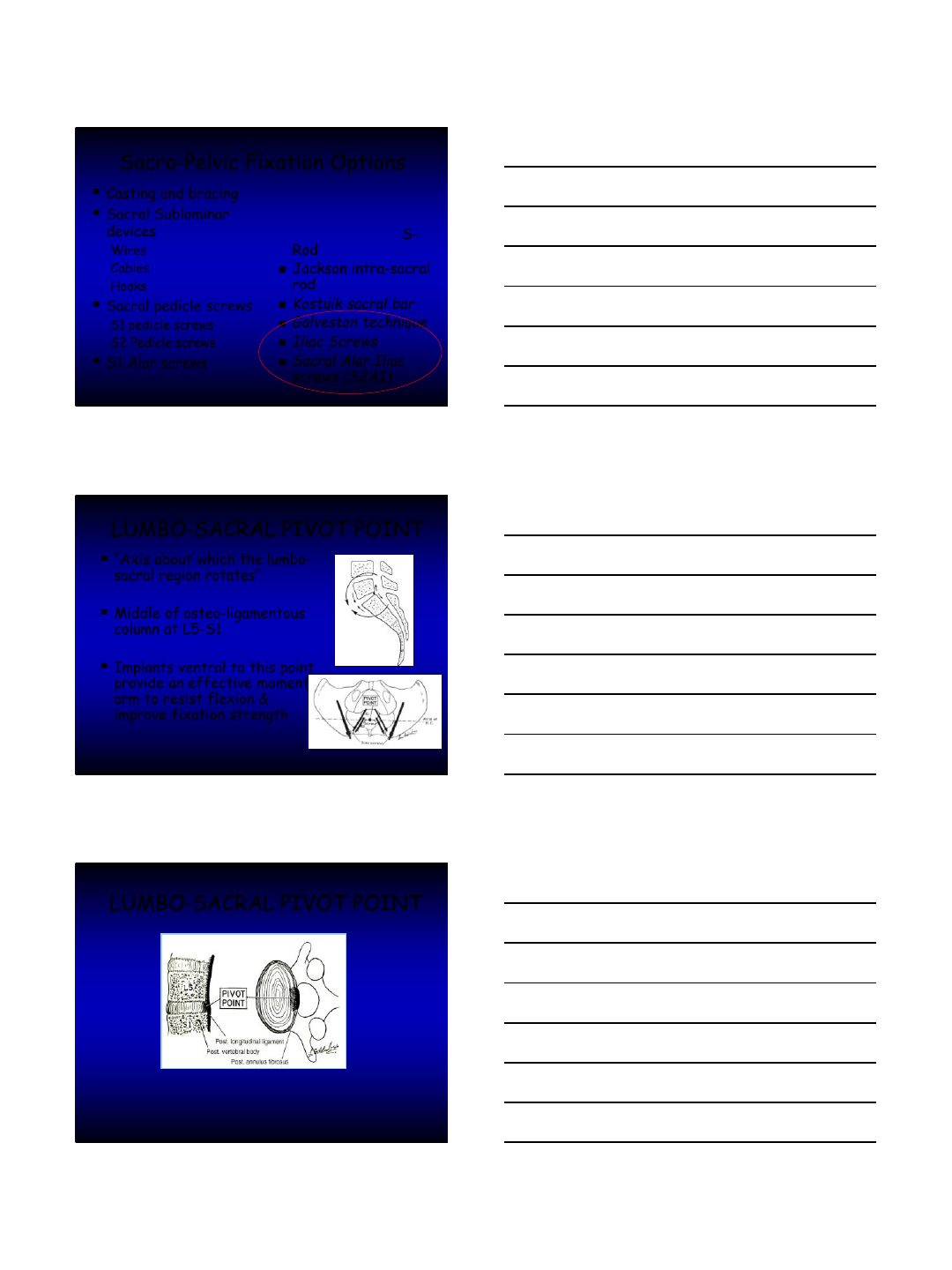
LUMBO-SACRAL PIVOT POINT
“Axis about which the lumbo-
sacral region rotates”
Middle of osteo-ligamentous
column at L5-S1
Implants ventral to this point
provide an effective moment
arm to resist flexion &
improve fixation strength
McCord et al, Spine, 1992.
LUMBO-SACRAL PIVOT POINT
McCord et al, Spine, 1992.

4
GALVESTON TECHNIQUE
Most commonly used in NM Spinal
deformities
Inexpensive
Difficult to get the correct angle
Loss of correction
Windshield wiper effect
Broom MJ, et al, JBJS (A), 1989.
Gau Y, et al, J Spinal Disord, 1991.
Moseley C, et al, Orthop Trans, 1986.
Jackson Technique
S1 pedicle screws
Rod placed in S1 screw and
into sacral ala
Not crossing the SI joint
Technically difficult
Biomechanically weaker
than iliac fixation
Jackson RP, et al, Spine, 1993.
Lebwohl NH, Spine, 2002.
Iliac Screws
Commonly used
Fixation with screws
Implants easier to place
Reduction in LS motion
More Protective of S1
than IB cages
Cunningham BW, et al, Spine, 2002.
5
67 patients ( 81 initial Cohort)
5 years Follow-up
Iliac screws removed in 23 pts
7 broken screws
Screws halos in 29 pts
No SI joint arthritis
Woojin et Al. paper 46,
IMAST 2011
67 of 190 patients
Iliac screws
Minimum 2 ys follow-up
34.3 % failure
11.9 Major failure
S2 Alar –Iliac S2AI
“SAI”
6
Surgical Technique
How it all started?
Surgical Technique
How it all started?
Surgical Technique
How it all started?
7
Surgical Technique
How it all started?
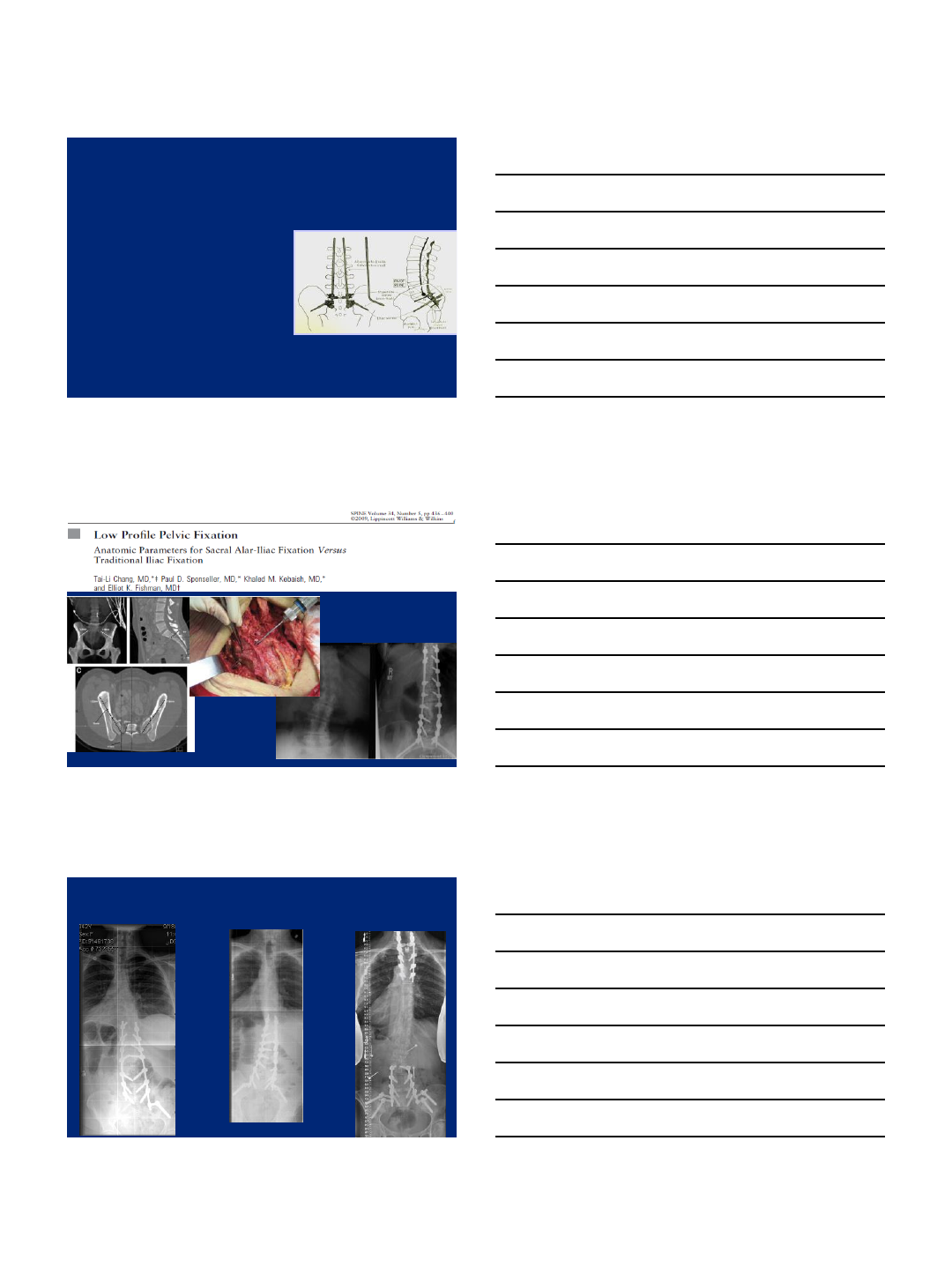
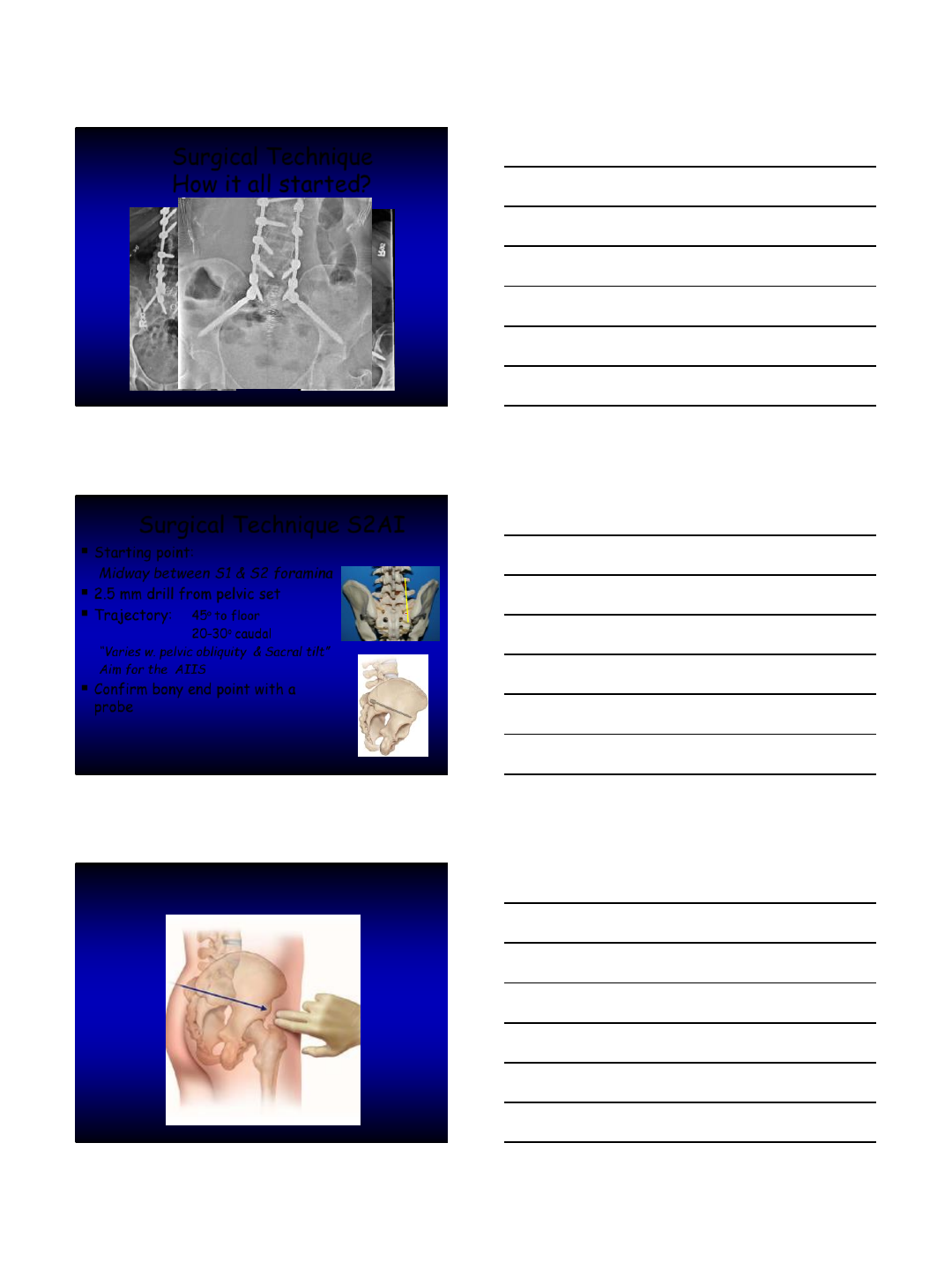
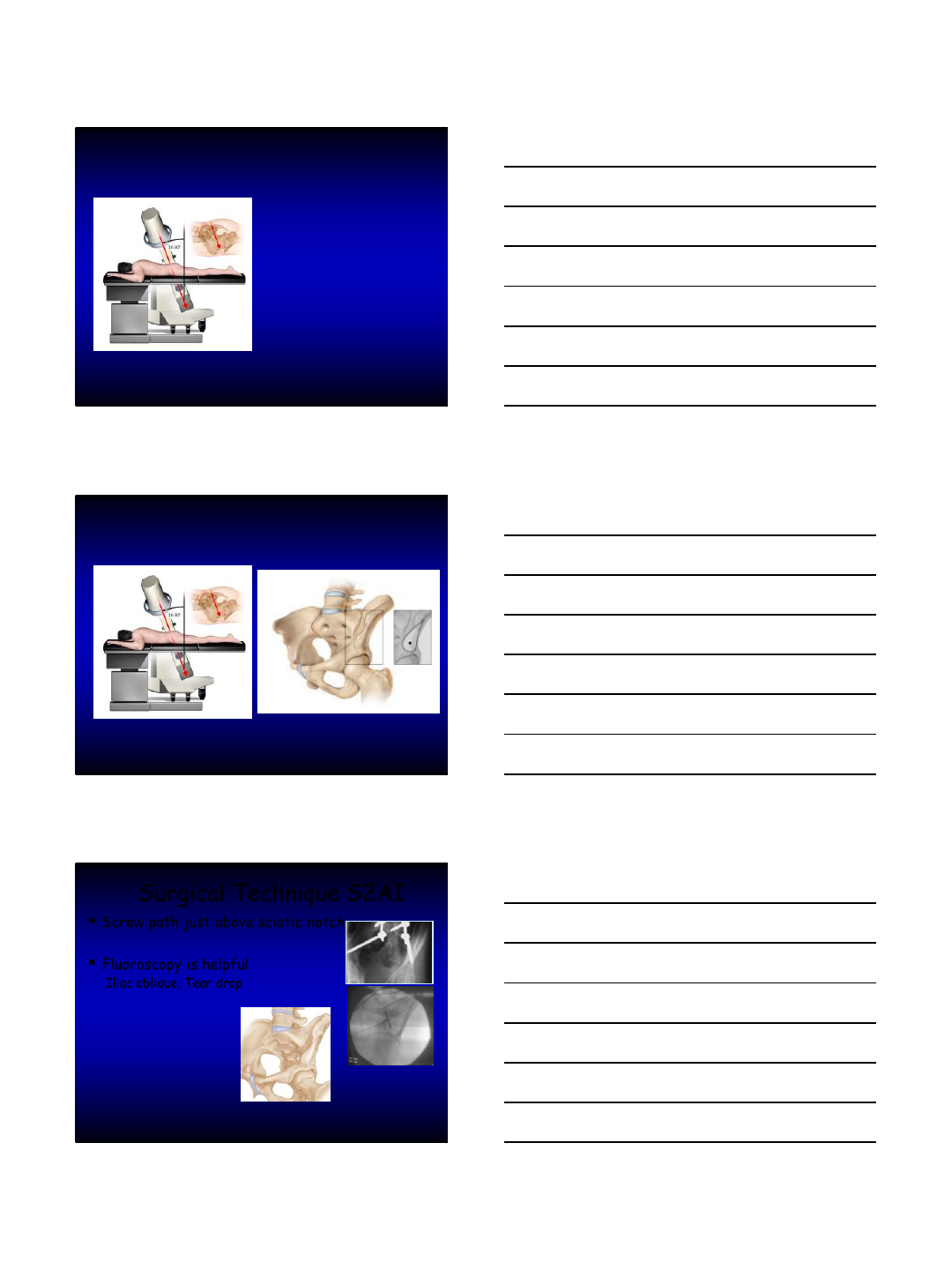
Surgical Technique S2AI
Starting point:
Midway between S1 & S2 foramina
2.5 mm drill from pelvic set
Trajectory: 45oto floor
20-30ocaudal
“Varies w. pelvic obliquity & Sacral tilt”
Aim for the AIIS
Confirm bony end point with a
probe
8
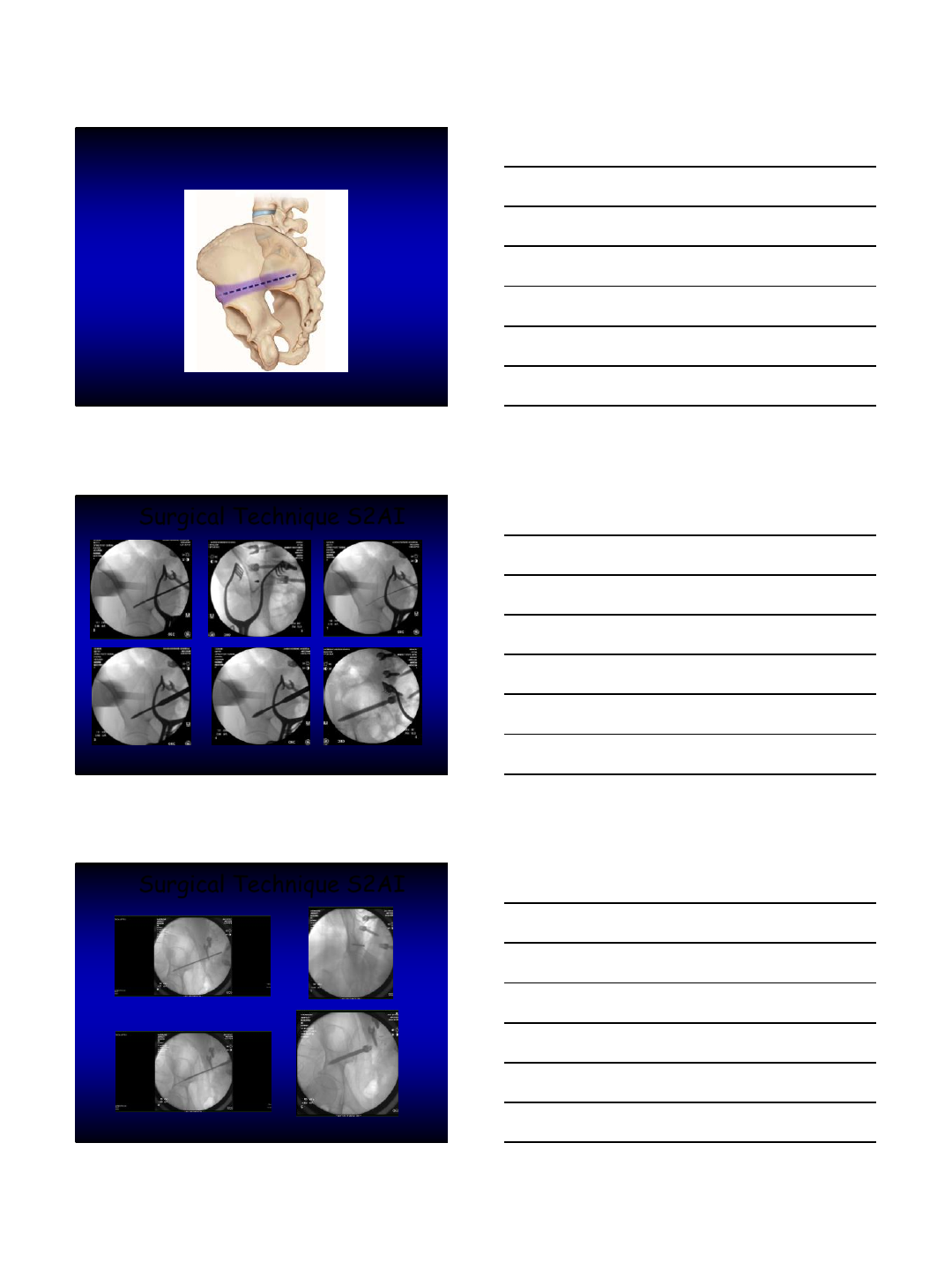
Surgical Technique S2AI
Surgical Technique S2AI
9
Surgical Technique S2AI
Screw path just above sciatic notch
Fluoroscopy is helpful
Iliac oblique, Tear drop
10
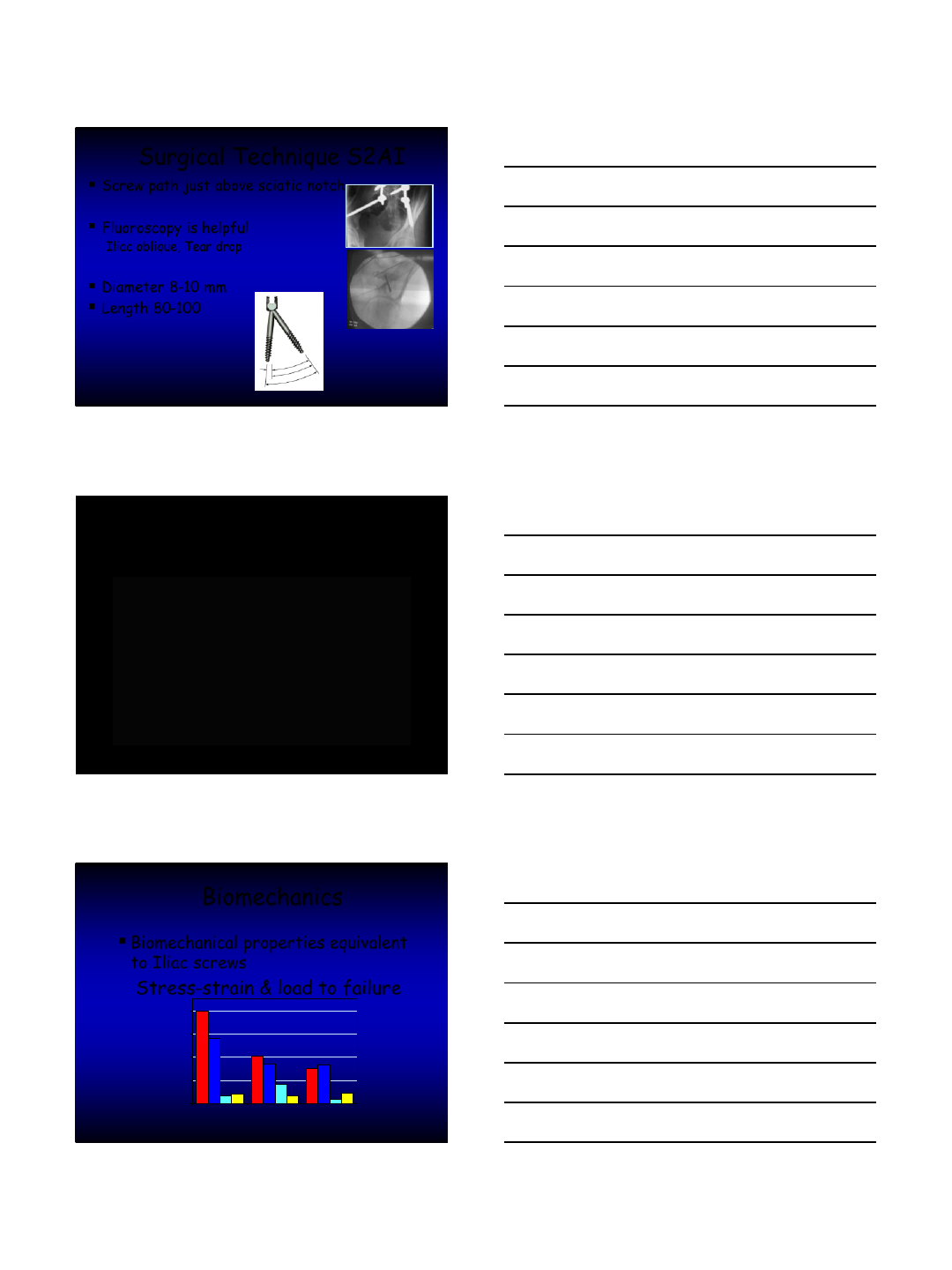
Surgical Technique S2AI
Screw path just above sciatic notch
Fluoroscopy is helpful
Iliac oblique, Tear drop
Diameter 8-10 mm
Length 80-100
Biomechanics
Biomechanical properties equivalent
to Iliac screws
Stress-strain & load to failure
0
50
100
150
200
S1+S2 Screw S1+S2 Portal S1+Iliac Screw
11
Department of Orthopaedic Surgery
Johns Hopkins University
Outcomes and Complications of Sacro-Pelvic Fixation Using
S2 Alar-Iliac (S2AI) Fixation in Adult Deformity patients:
A prospective Study with 2-Year Follow-Up
Khaled Kebaish, MD
Mostafa El Dafrawy,,M.D
Hamid Hassanzadeh, M.D
Philip Neubauer, M.D
Roosevelt Offoha, BS
Eric Tan, M.D
Paul Sponseller, MD
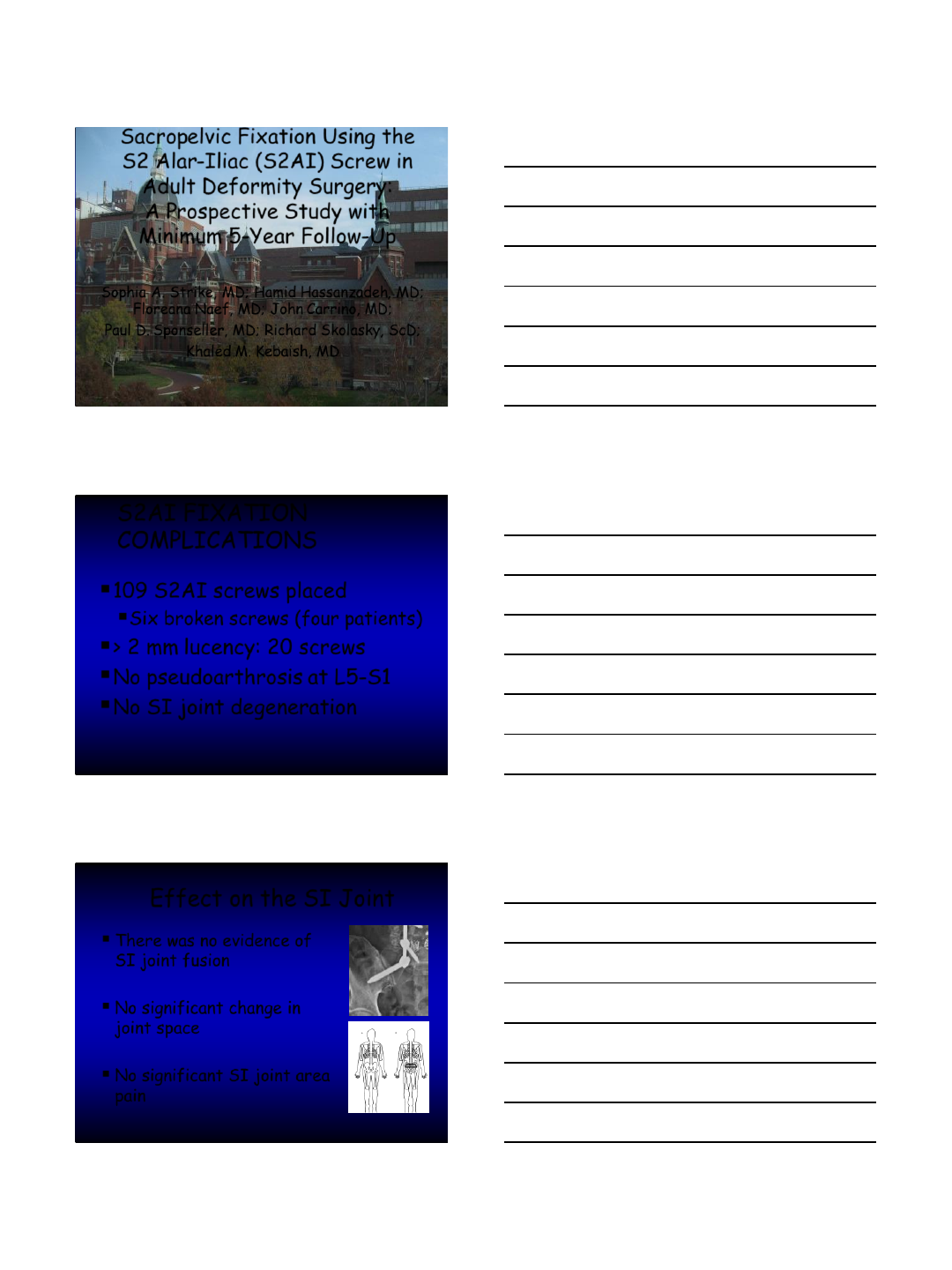
RESULTS
146 patients were included
2 year clinical & radiographic F/U
2 patient were lost to follow up
Average age: 59 ys (21-80)
35% of patients had > one co-
morbidity
S2AI Fixation specific complications
Screw Breakage
8 (5 pts)
Screw
Misplacement 2
Minimal Screw
loosening
(<2mm) 13 patients
16 screws (6%)
Reoperation
4
12
Sacropelvic Fixation Using the
S2 Alar-Iliac (S2AI) Screw in
Adult Deformity Surgery:
A Prospective Study with
Minimum 5-Year Follow-Up
Sophia A. Strike, MD; Hamid Hassanzadeh, MD;
Floreana Naef, MD; John Carrino, MD;
Paul D. Sponseller, MD; Richard Skolasky, ScD;
Khaled M. Kebaish, MD
S2AI FIXATION
COMPLICATIONS
109 S2AI screws placed
Six broken screws (four patients)
> 2 mm lucency: 20 screws
No pseudoarthrosis at L5-S1
No SI joint degeneration
Effect on the SI Joint
There was no evidence of
SI joint fusion
No significant change in
joint space
No significant SI joint area
pain
Corlett EN, Bishop RP. Ergonomics 1976

13
Concerns of Fusion Across SI Joint
Anatomic studies
Minimal motion in
pediatric cadavers
No motion in adult
cadavers
75% auto fused in
adults over 50 years
Asher MA, et al, CORR, 1986.
Kostuik JP, et al, CORR, 1986.
White AA, et al, Surgery of Musculoskeletal System, 1990.
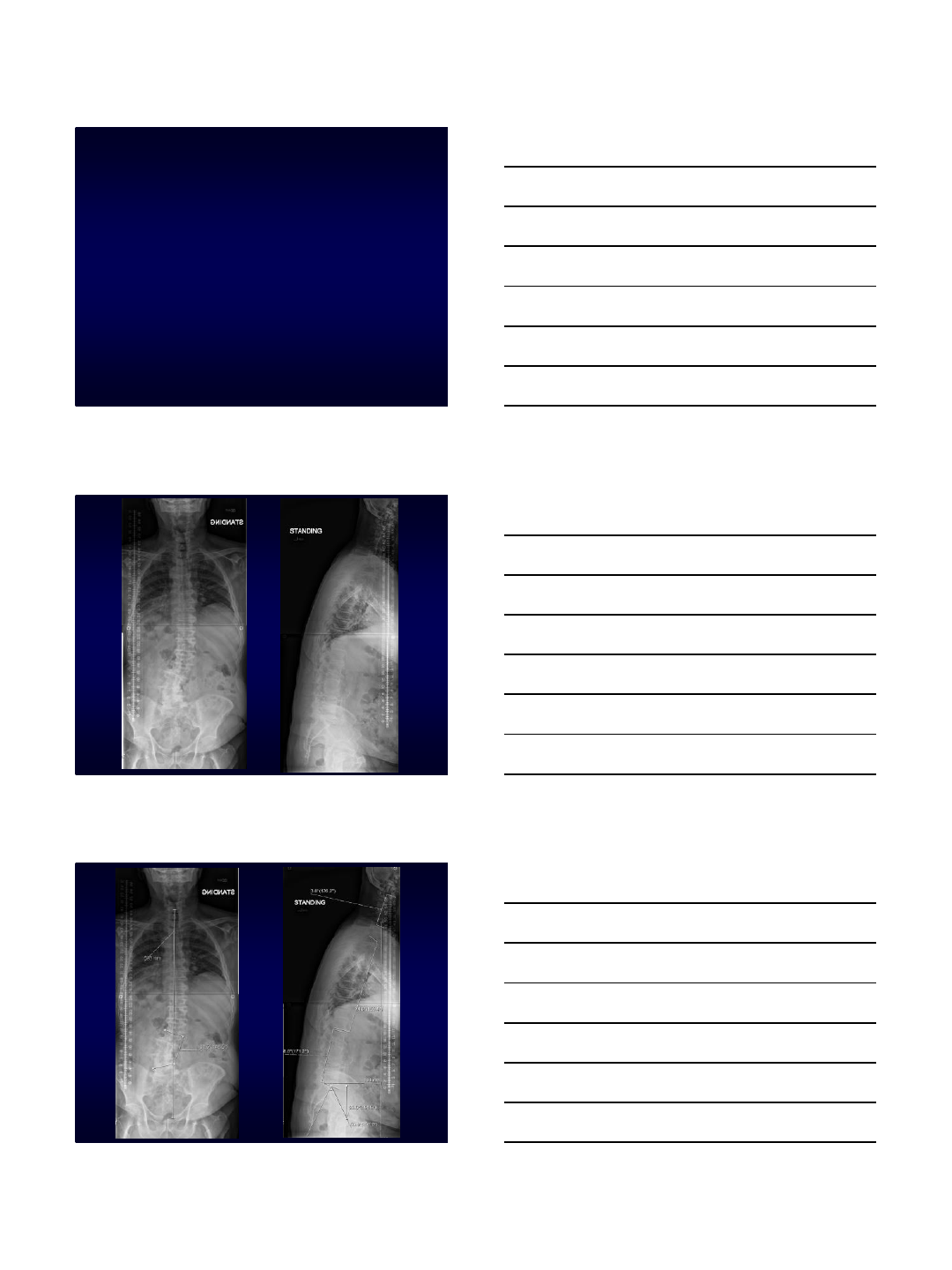
Adult Scoliosis
71 YO M
Retired Physician
Severe Back Pain
and Rt Buttock
Used to be very
active now
Limited by his
symptoms
No Prior Rx
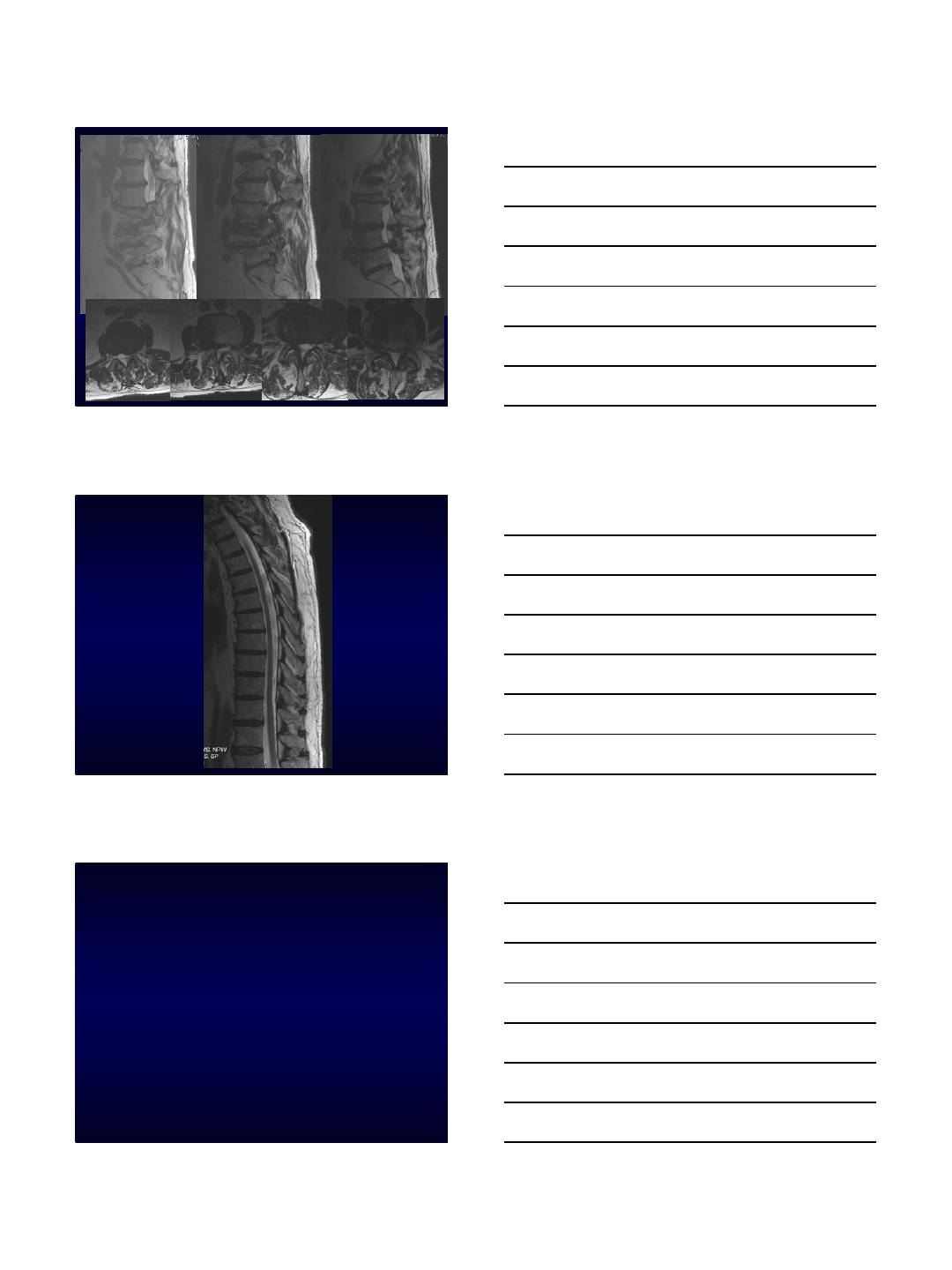
14
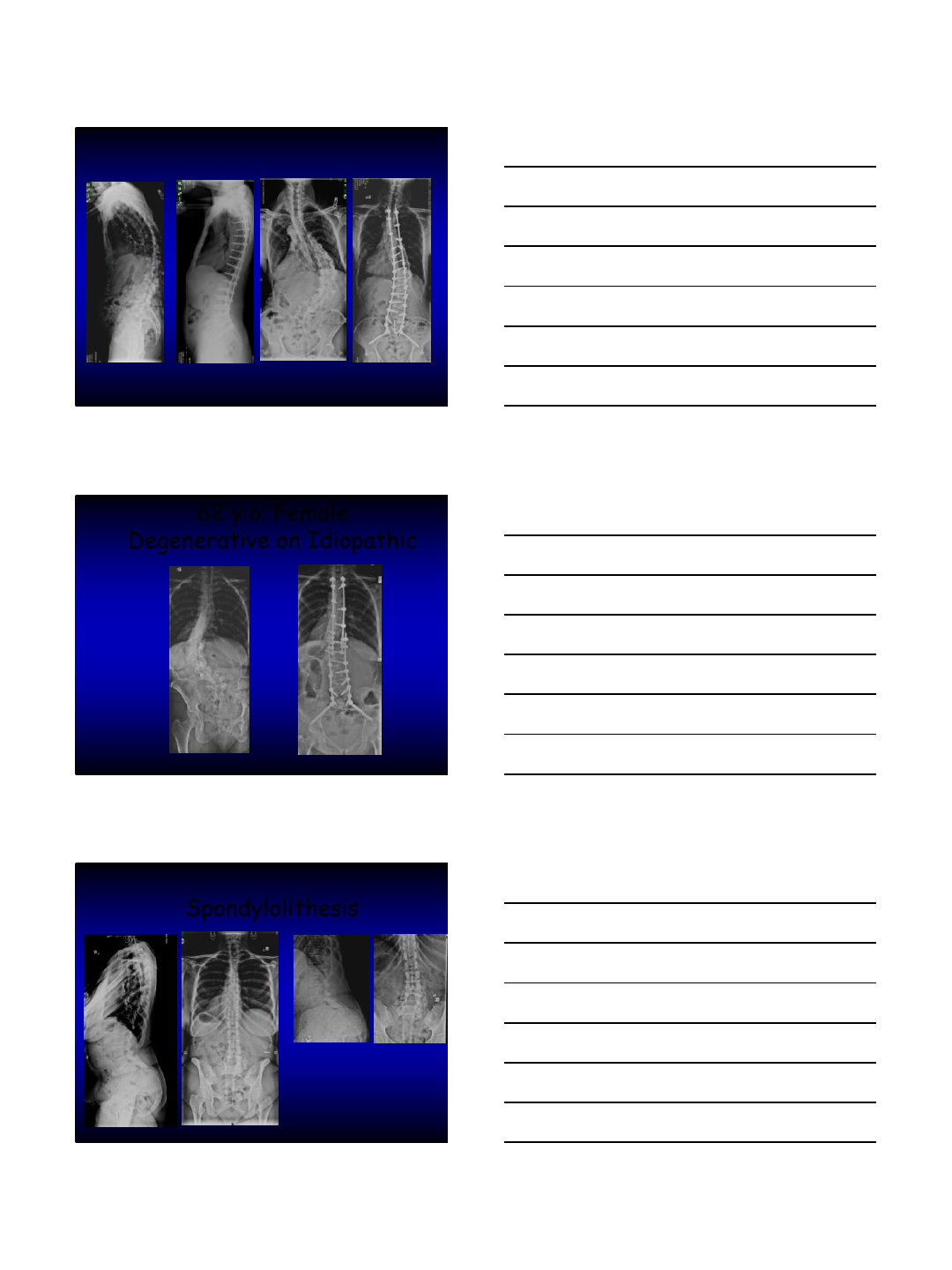
62 y.o. Female
Degenerative on Idiopathic
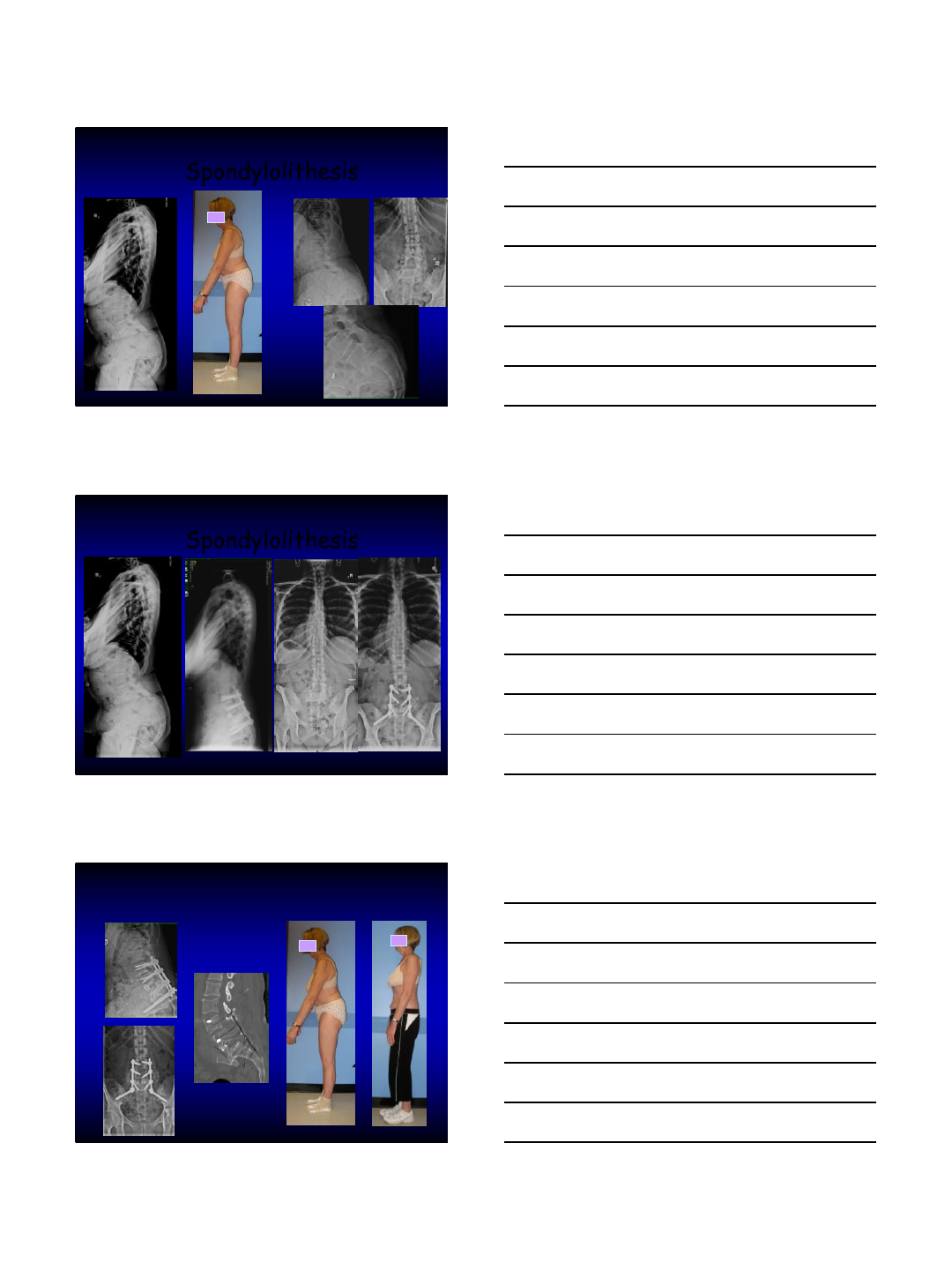
Spondylolithesis
15
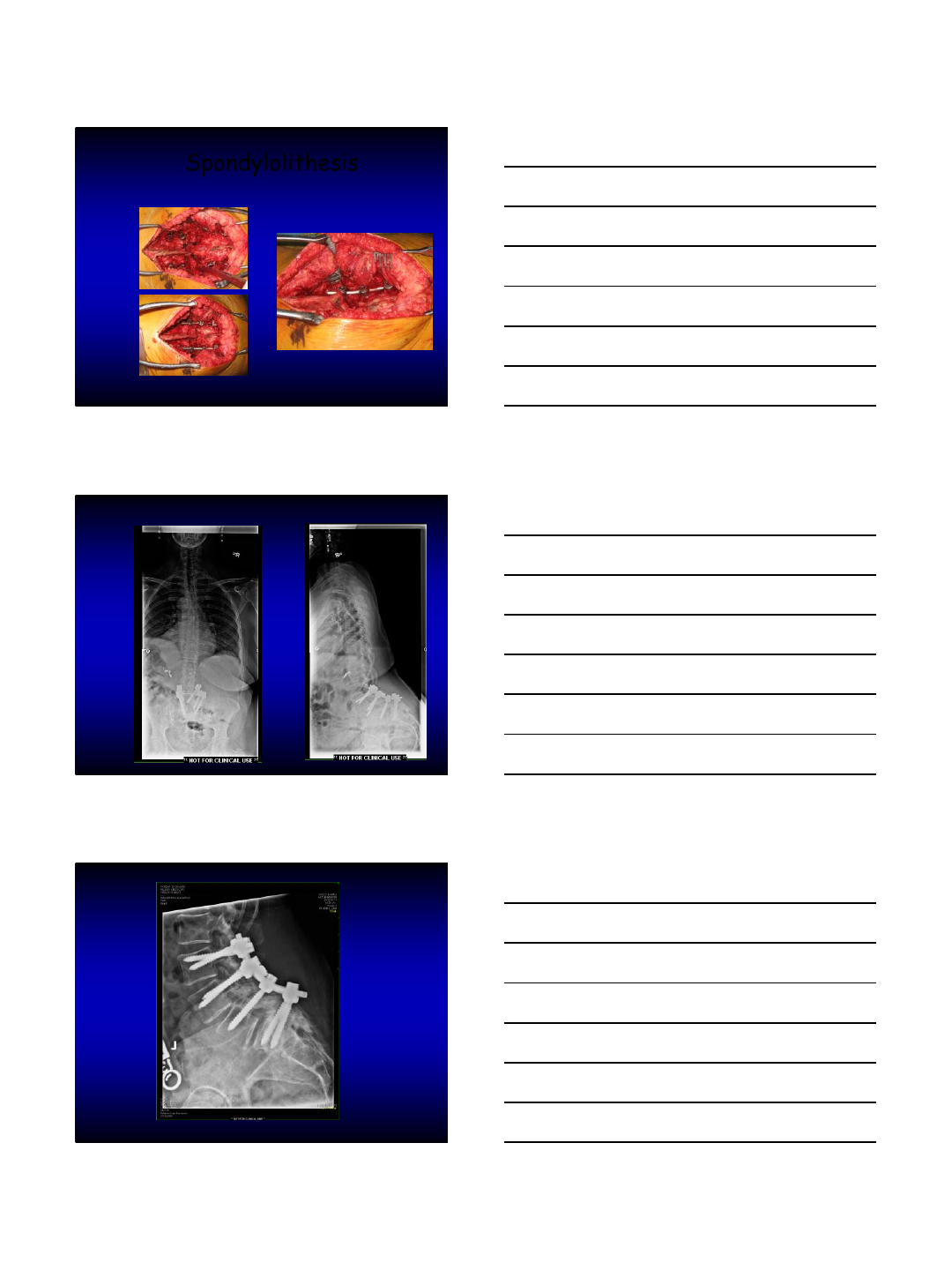
Spondylolithesis
Spondylolithesis
16
Spondylolithesis
Sacral Fracture

17
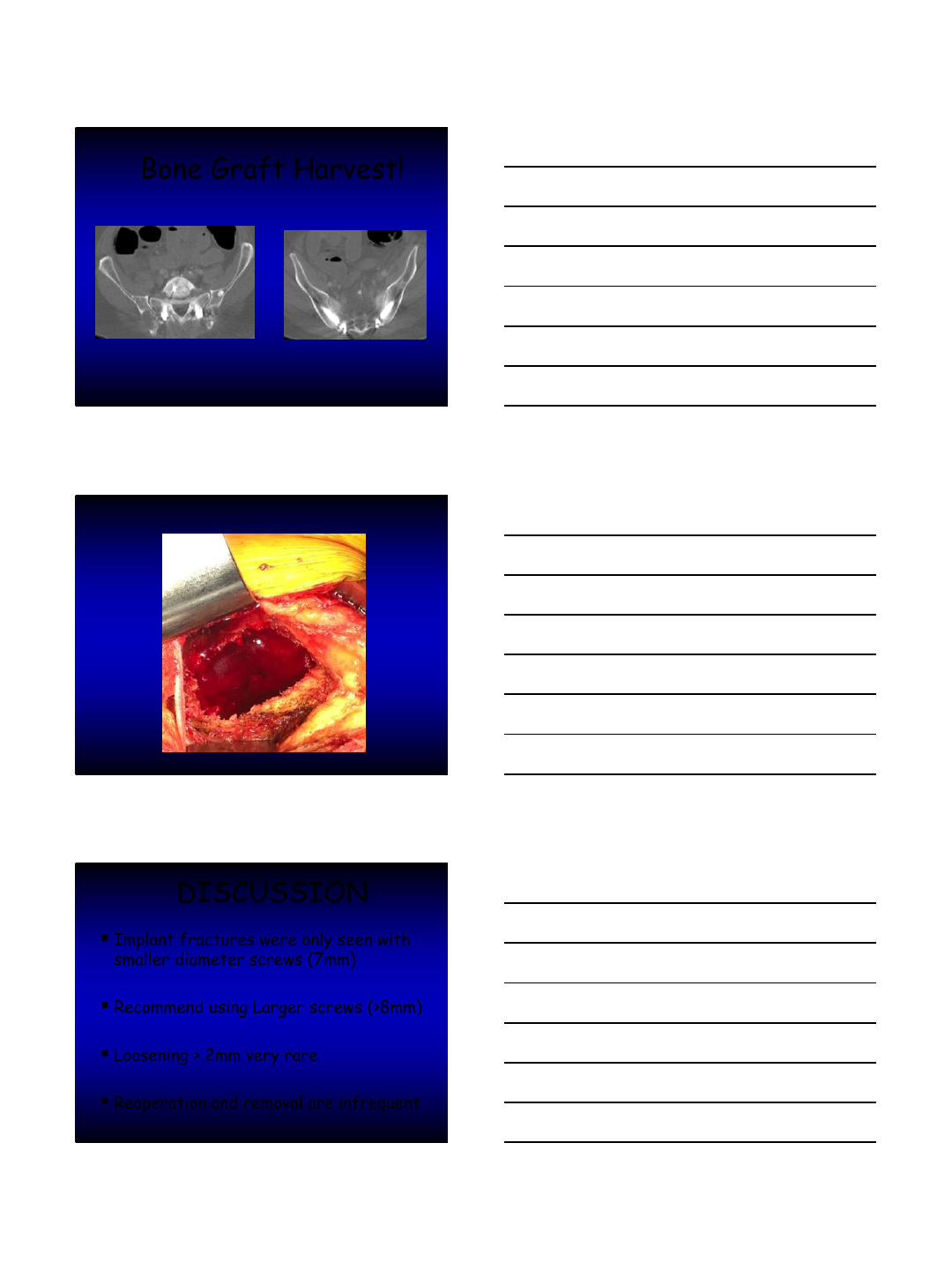
Bone Graft Harvest!
18
Bone Graft Harvest!
DISCUSSION
Implant fractures were only seen with
smaller diameter screws (7mm)
Recommend using Larger screws (>8mm)
Loosening > 2mm very rare
Reoperation and removal are infrequent
19
S2AI Technique
Relatively easy and safe
Minimal offset from the axis of
spine
Less prominent
One rod no connectors
Better control of the pelvis
S2AI Technique
Relatively easy and safe
Minimal offset from the axis of
spine
Less prominent
One rod no connectors
Better control of the pelvis
EASIER TO PERFORM
RECONSTRUCTIVE PROCEDURES AT
THE LS JUNCTION
Conclusion
Many techniques for PELVIC FIXATION
High Rate of implant related problems
S2 Alar Iliac (SAI) technique easy & safe
Lower Complications
Effective in distal LS corrective
procedures
No effect on the SI joint at 5 ys!
Can be done through an MIS approach
20
THANK YOU
