MRI Of The Hand And Wrist Syllabus
2015-07-27
: Pdf Mri Of The Hand And Wrist Syllabus MRI_of_the_Hand_and_Wrist_Syllabus 7 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 75
7/16/2015
1
Imaging in the Diagnosis of Ulnar
Sided Wrist Pain
Kimberly K. Amrami, MD
Professor of Radiology
Chair, Division of Musculoskeletal Radiology
Mayo Clinic
Rochester, Minnesota
Sources of Ulnar Sided Wrist Pain
•TFCC –foveal attachment –UT
Ligament
•Distal Radioulnar Joint
•Extensor Carpi Ulnaris
•LT ligament
•Ulnocarpal Impaction
•Arthritis
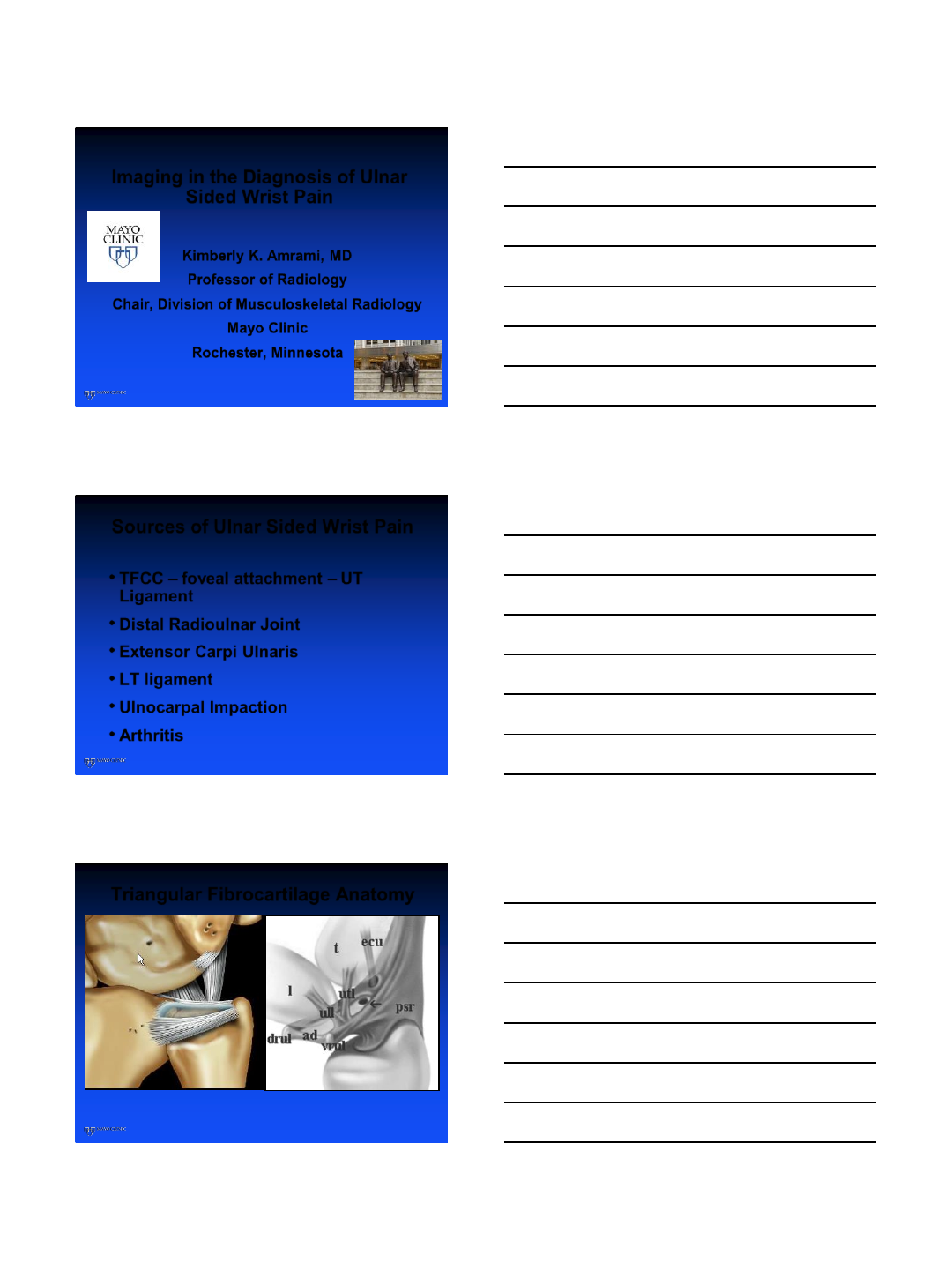
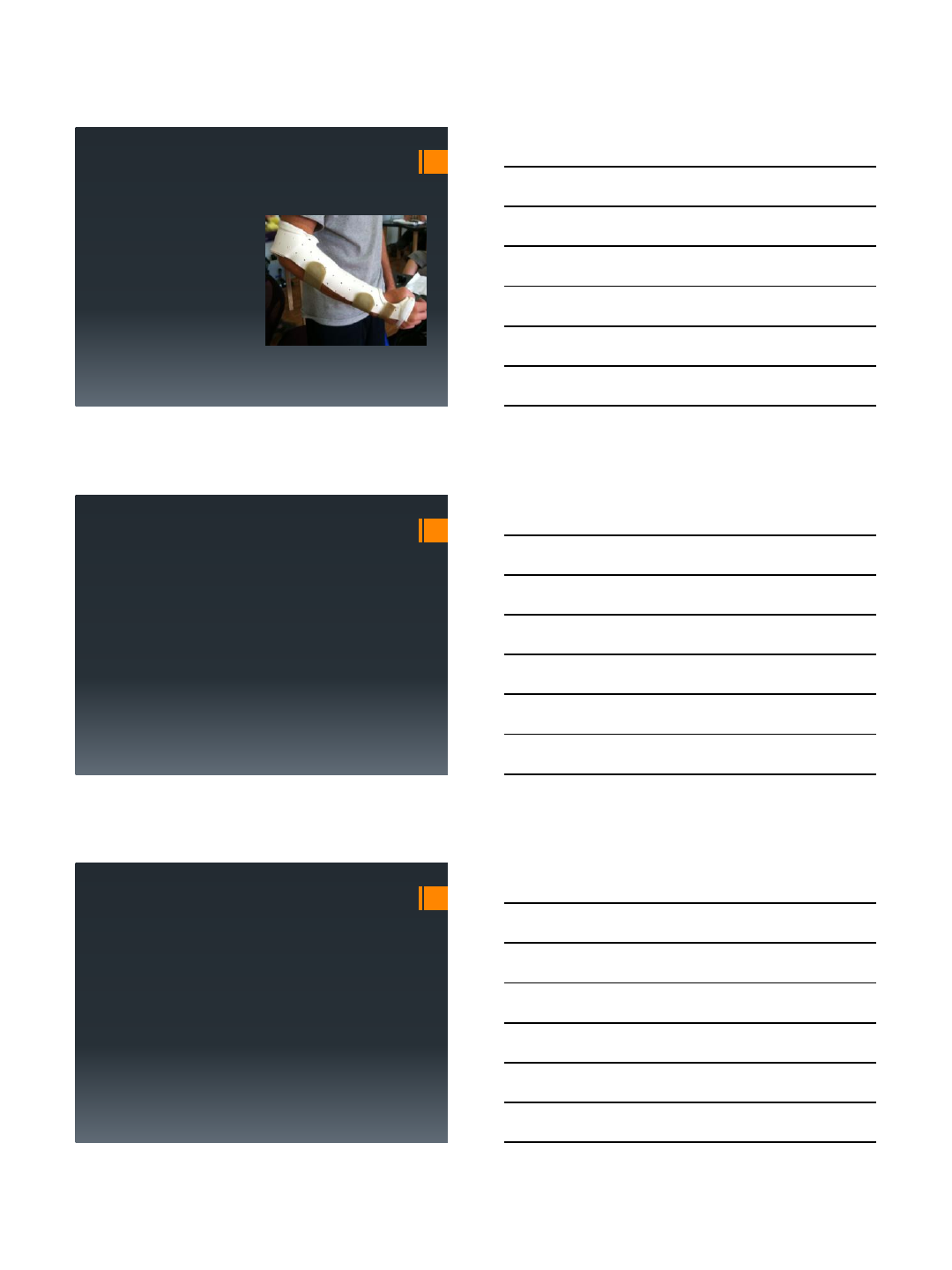
Triangular Fibrocartilage Anatomy
7/16/2015
2
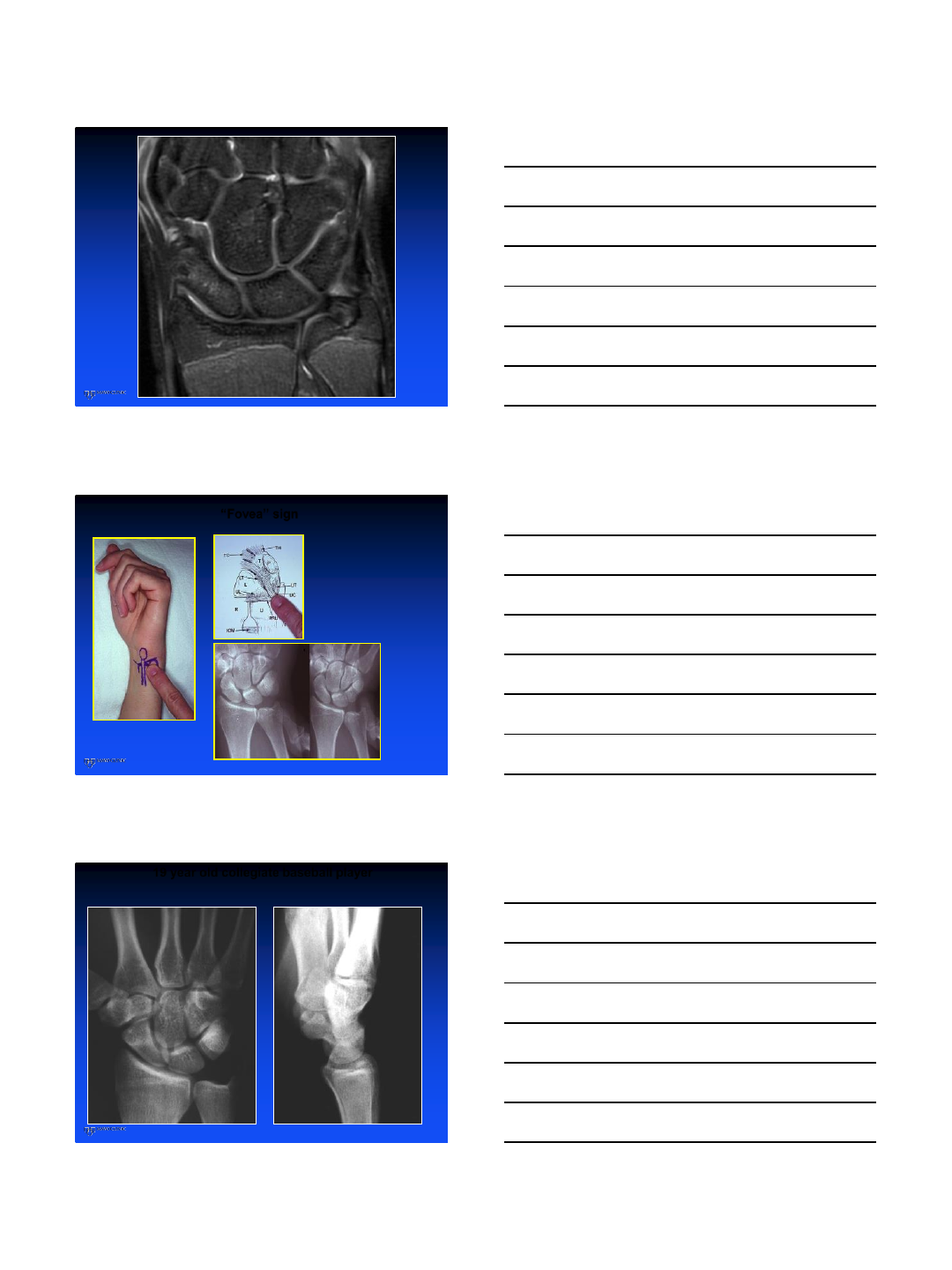
“Fovea” sign
S.C. Tay, K. Tomita, R.A. Berger
The “ulnar fovea” sign for defining
ulnar wrist pain: an analysis of
sensitivity and specificity
J Hand Surg Am 32(4) (2007), pp
438-44
SN 95.2%
SP 86.5%
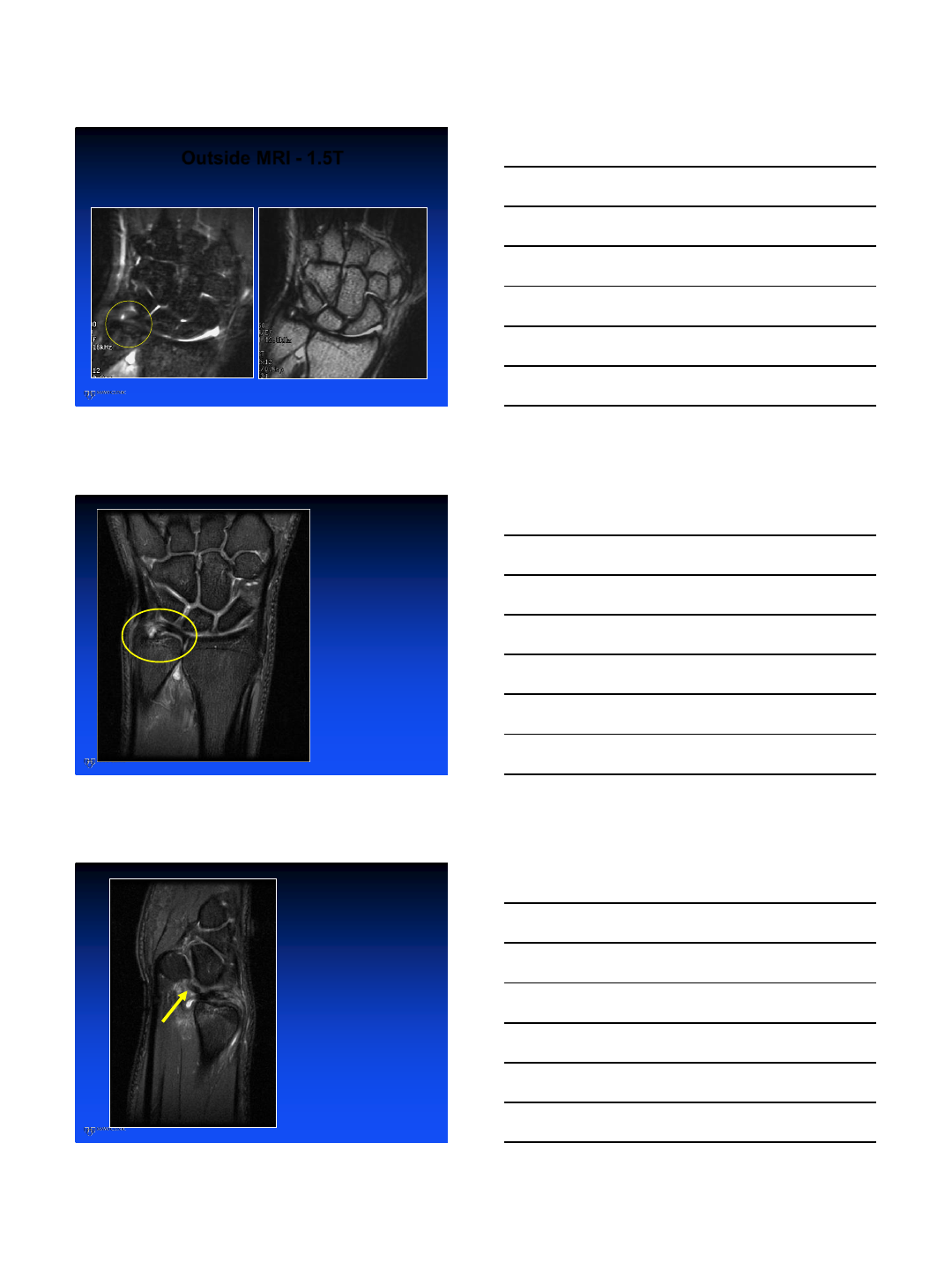
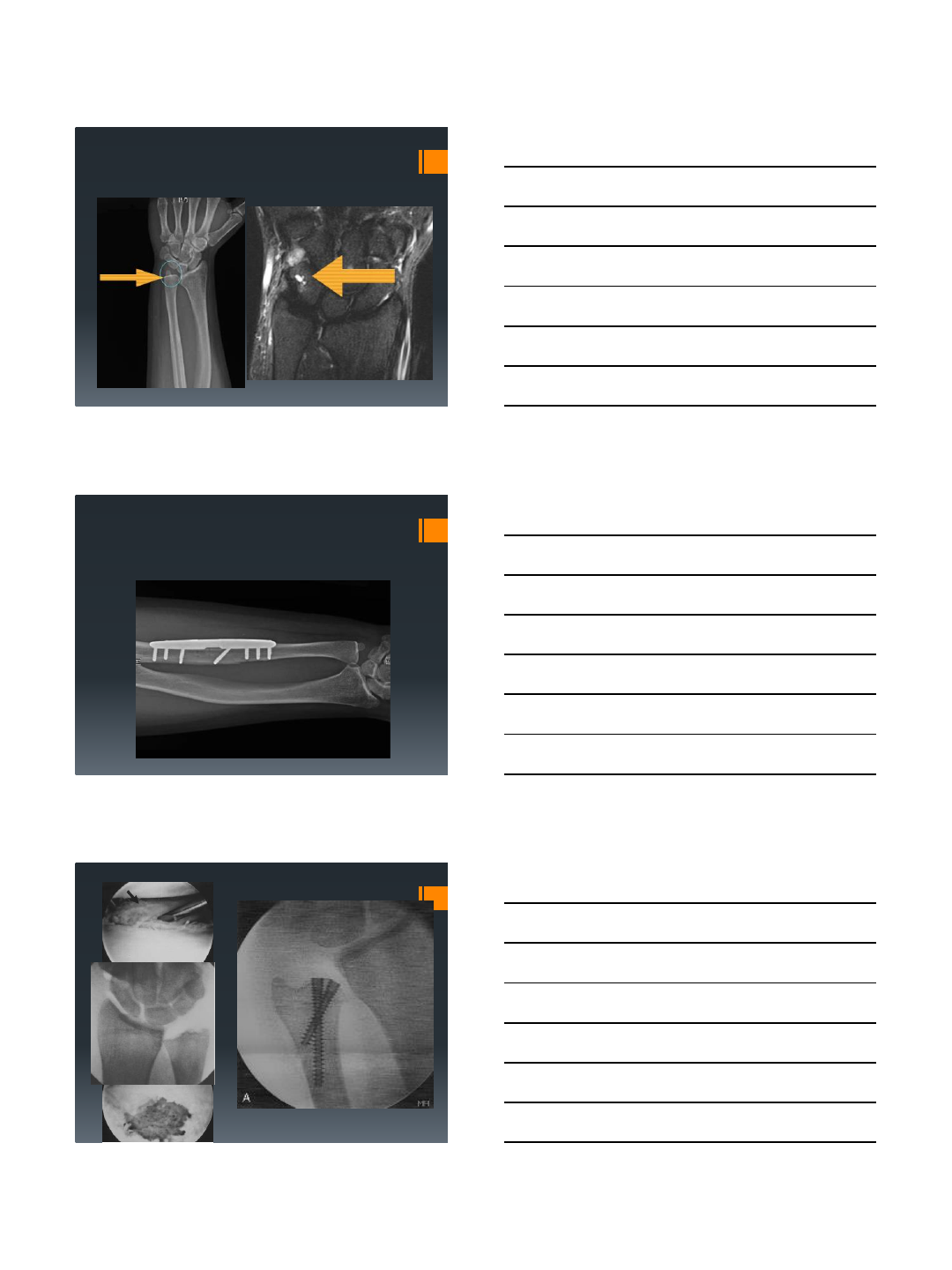
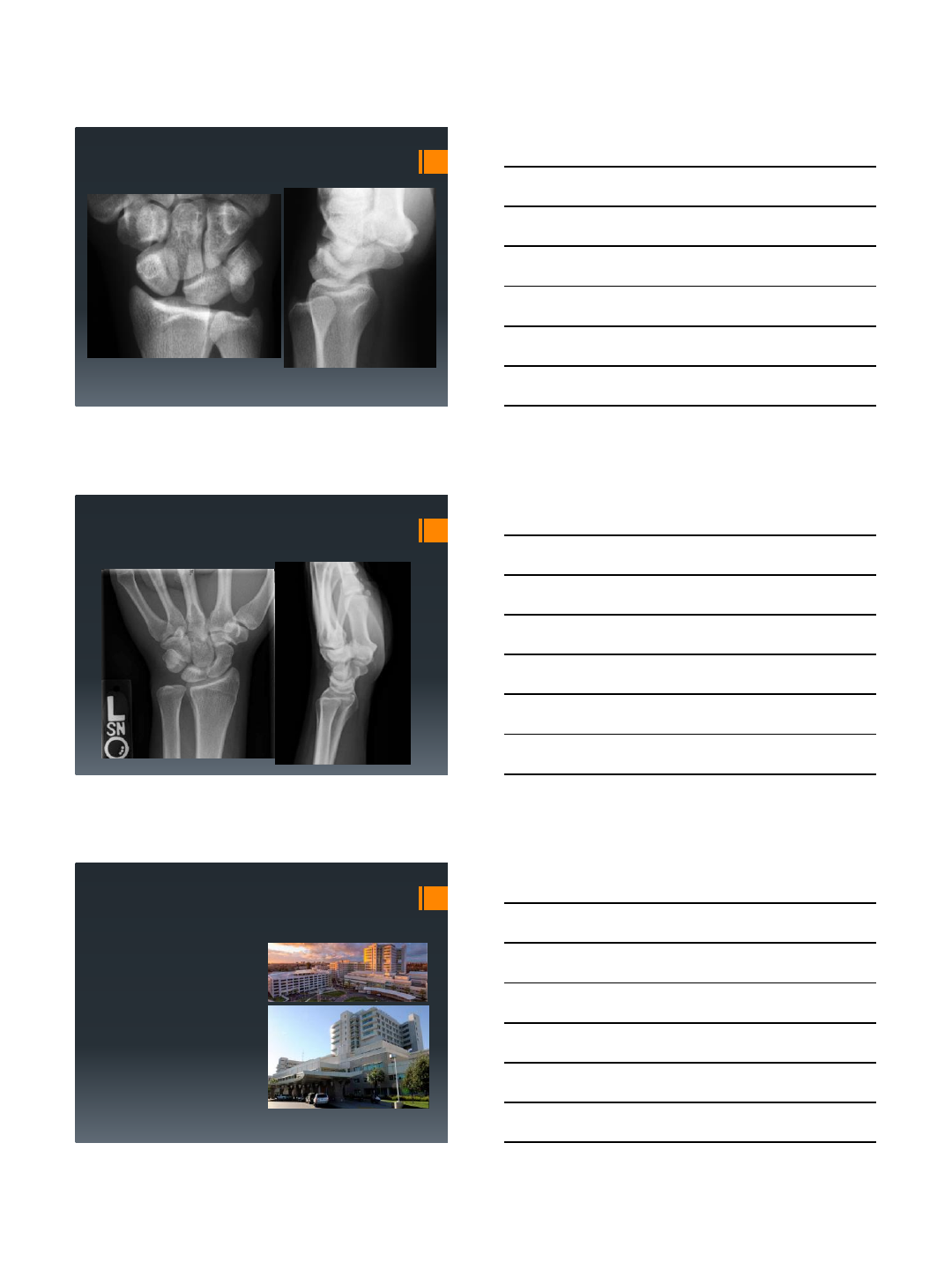
19 year old collegiate baseball player
Being recruited by the Yankees Nephew of a colleague
X-ray slightly supinated
7/16/2015
3
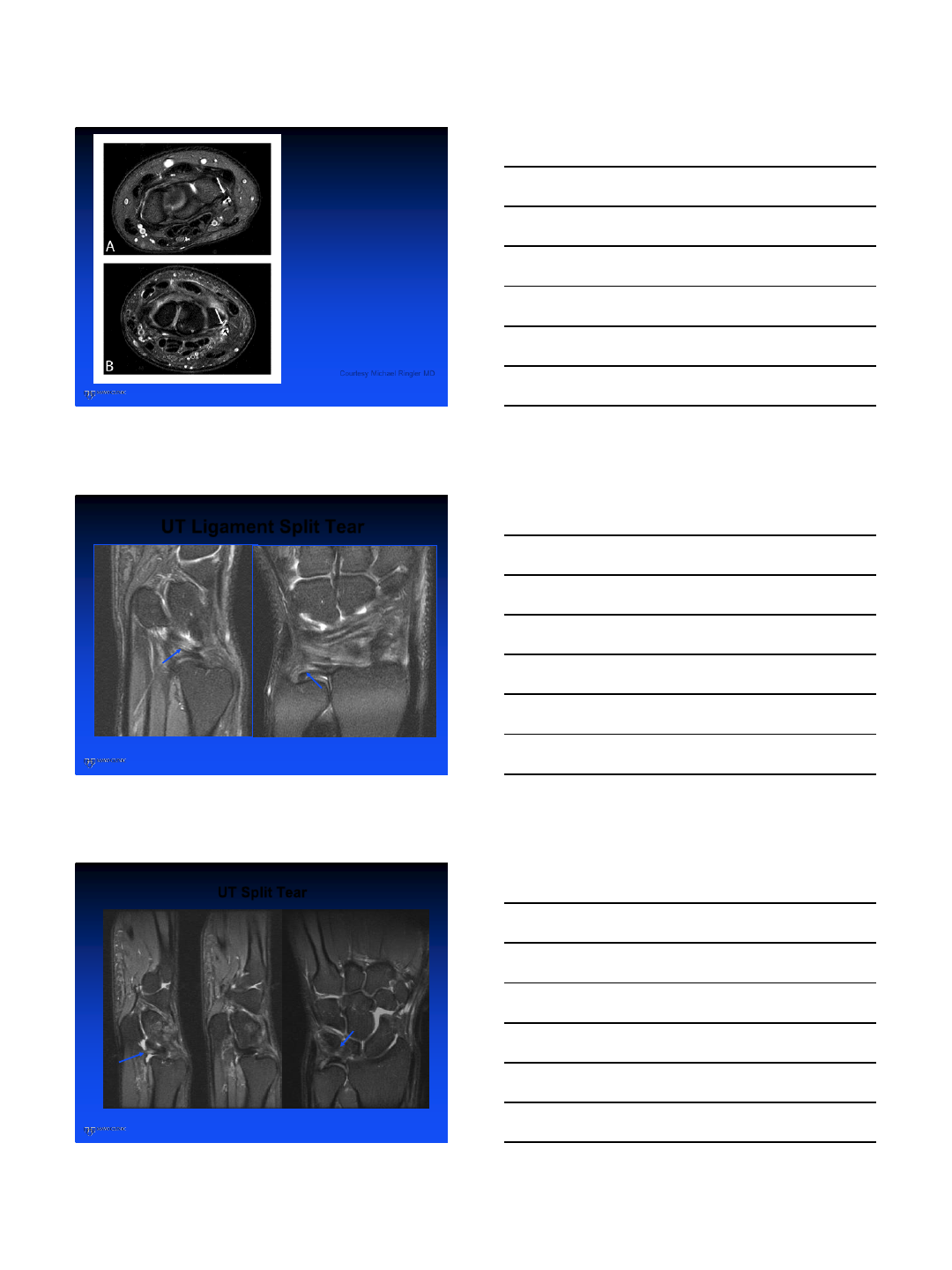
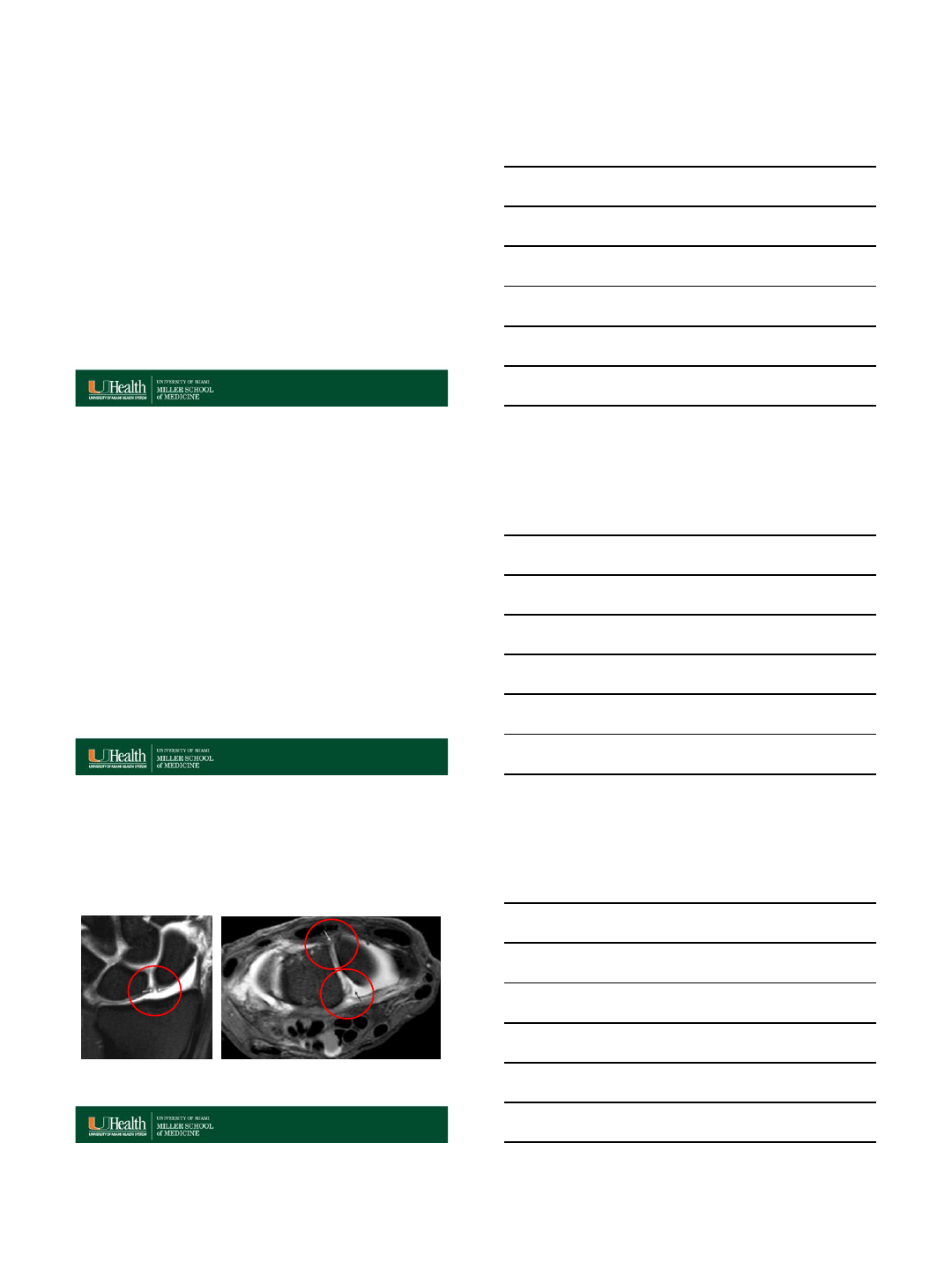
Outside MRI - 1.5T
STIR FSE T2
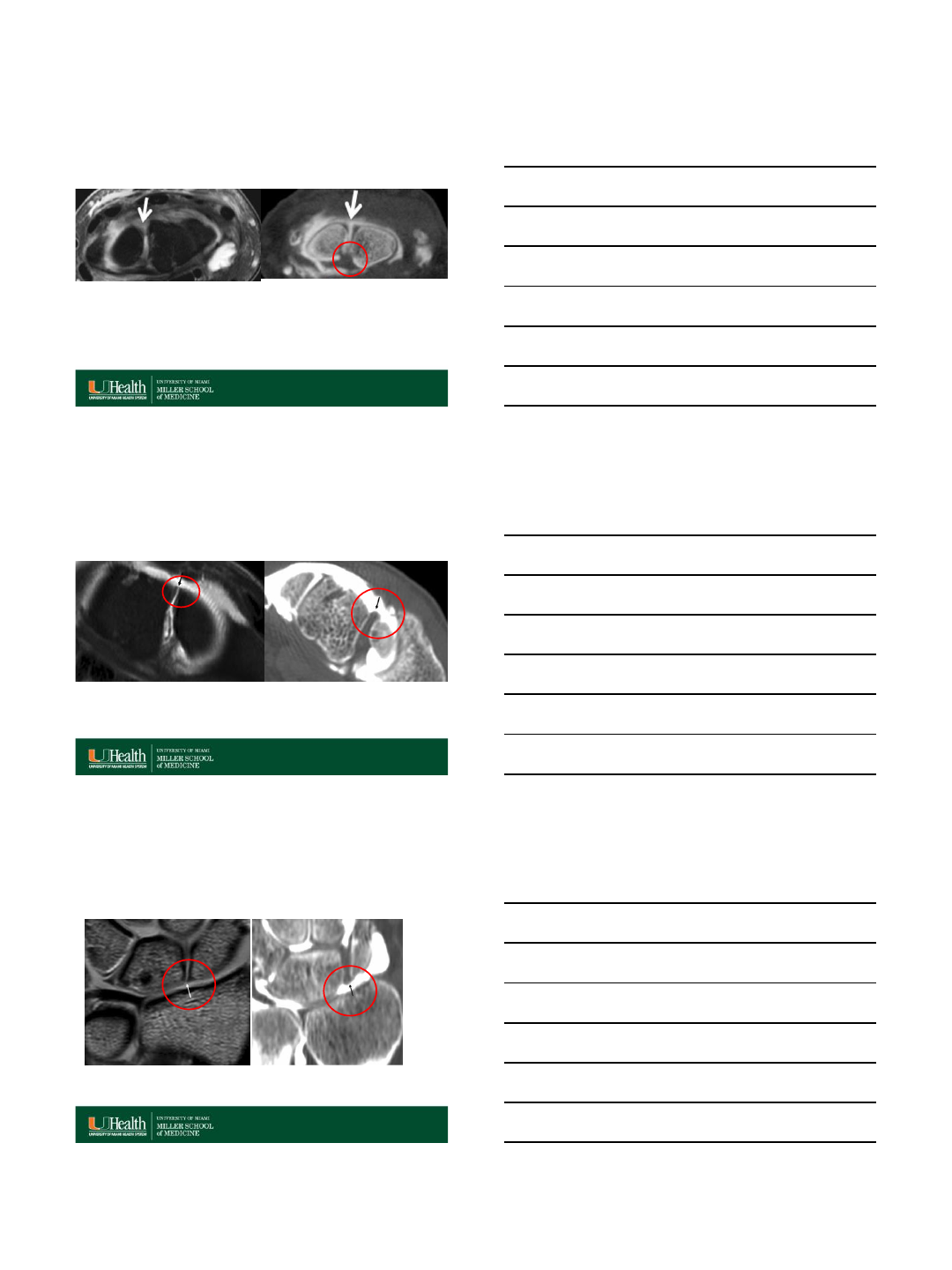
Outside Diagnosis –Foveal Tear
Diagnosis:
Ulnotriquetral
ligament tear -
Partial foveal
tear
Tx: TFCC and
UT repair
Returned to
collegiate play
after surgery

7/16/2015
4
TFCC –Ulnotriquetral Ligament
•Important stabilizer of the ulnar wrist
•But tears may not lead to gross
instability
•Important source of pain
•Complete, partial and “split tears”
significant
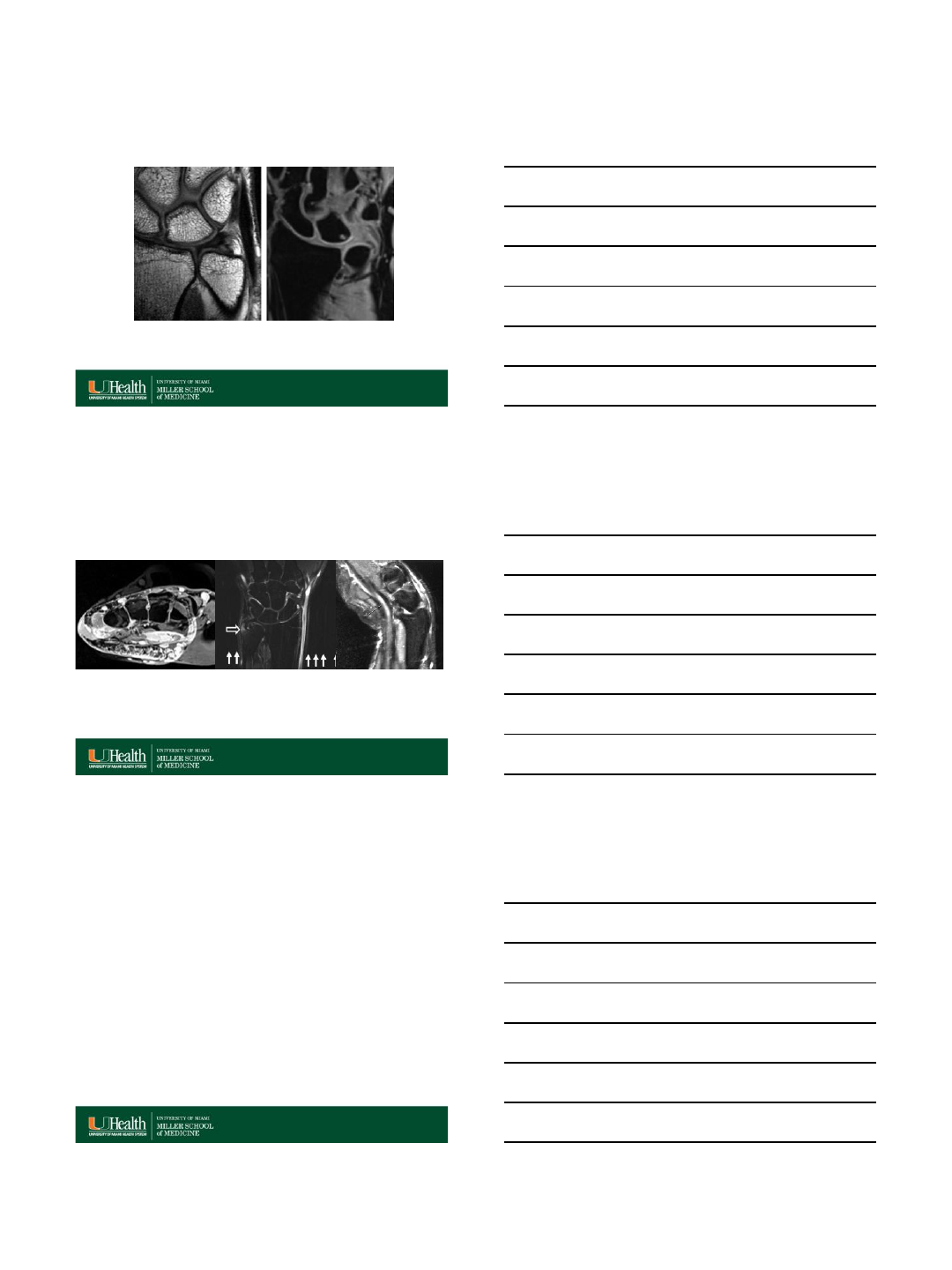
Can you really see the UTL?
UTL –3 planes
7/16/2015
5
Courtesy Michael Ringler MD
Intact
Split Tear
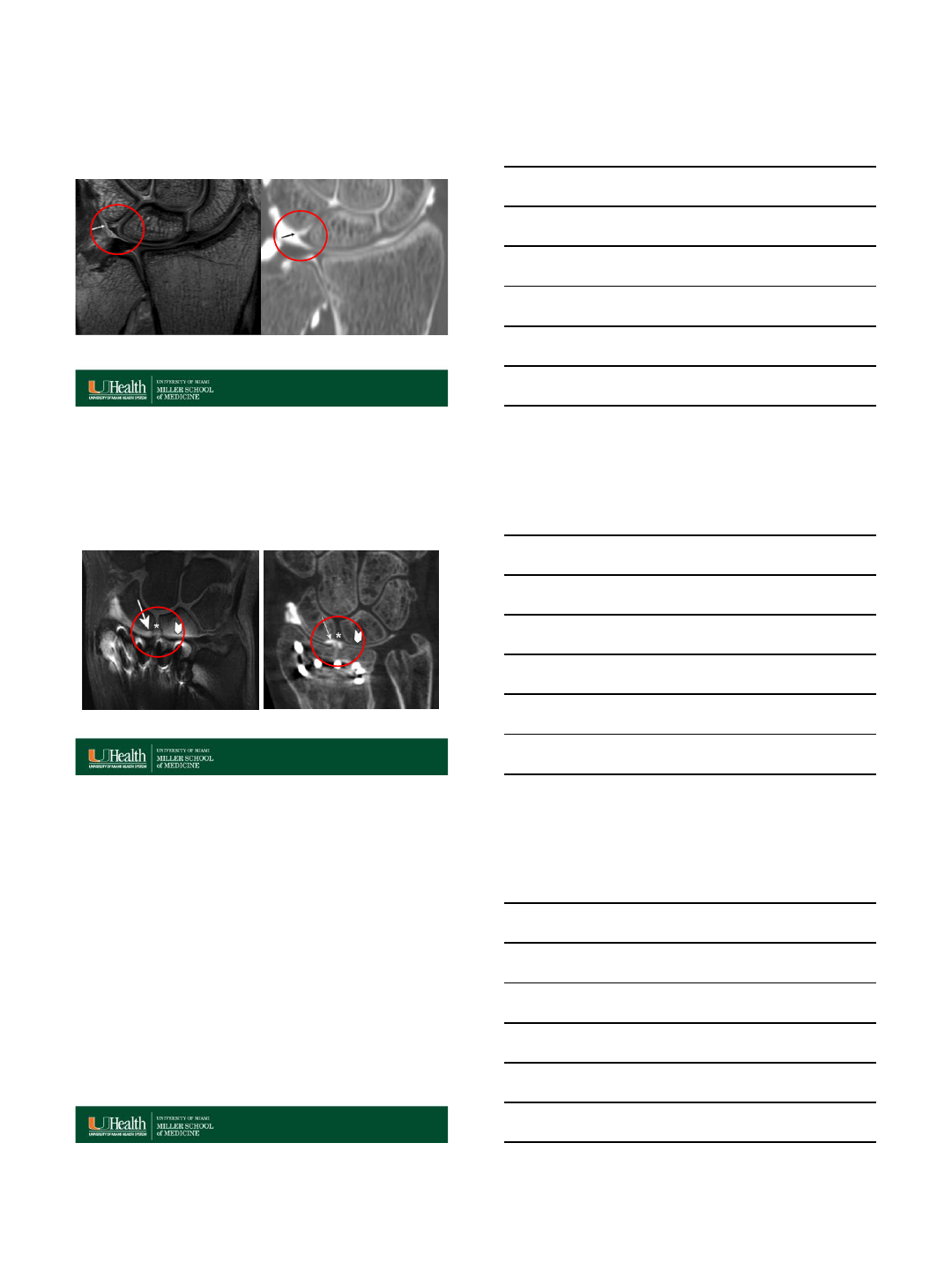
UT Ligament Split Tear
Called Prospectively
UT Split Tear
Missed Prospectively
7/16/2015
6
75 100 100 100 94.9 100
0
20
40
60
80
100
SN 1.5T SN 3.0T SP 1.5T SP 3.0T Acc 1.5T Acc 3.0T
UT
M.L. Anderson, J.A. Skinner, J.P. Felmlee,
R.A. Berger, K.K. Amrami
Diagnostic comparison of 1.5 Tesla and
3.0 Tesla preoperative MRI of the wrist in
patients with ulnar-sided wrist pain
J Hand Surg Am, 33 (7) (2008), pp. 1153–
1159
M.D.Ringler, B.M.Howe, K.K.Amrami, C.E.
Hagen, R.A. Berger
Utility of magnetic resonance imaging for
detection of longtudinal split tear of the
ulnotriquetral ligament
J Hand Surg Am, 38 (9)(2013), pp.1723-7
100% sensitivity
at 3T
30-58% sensitivity
1.5 and 3T
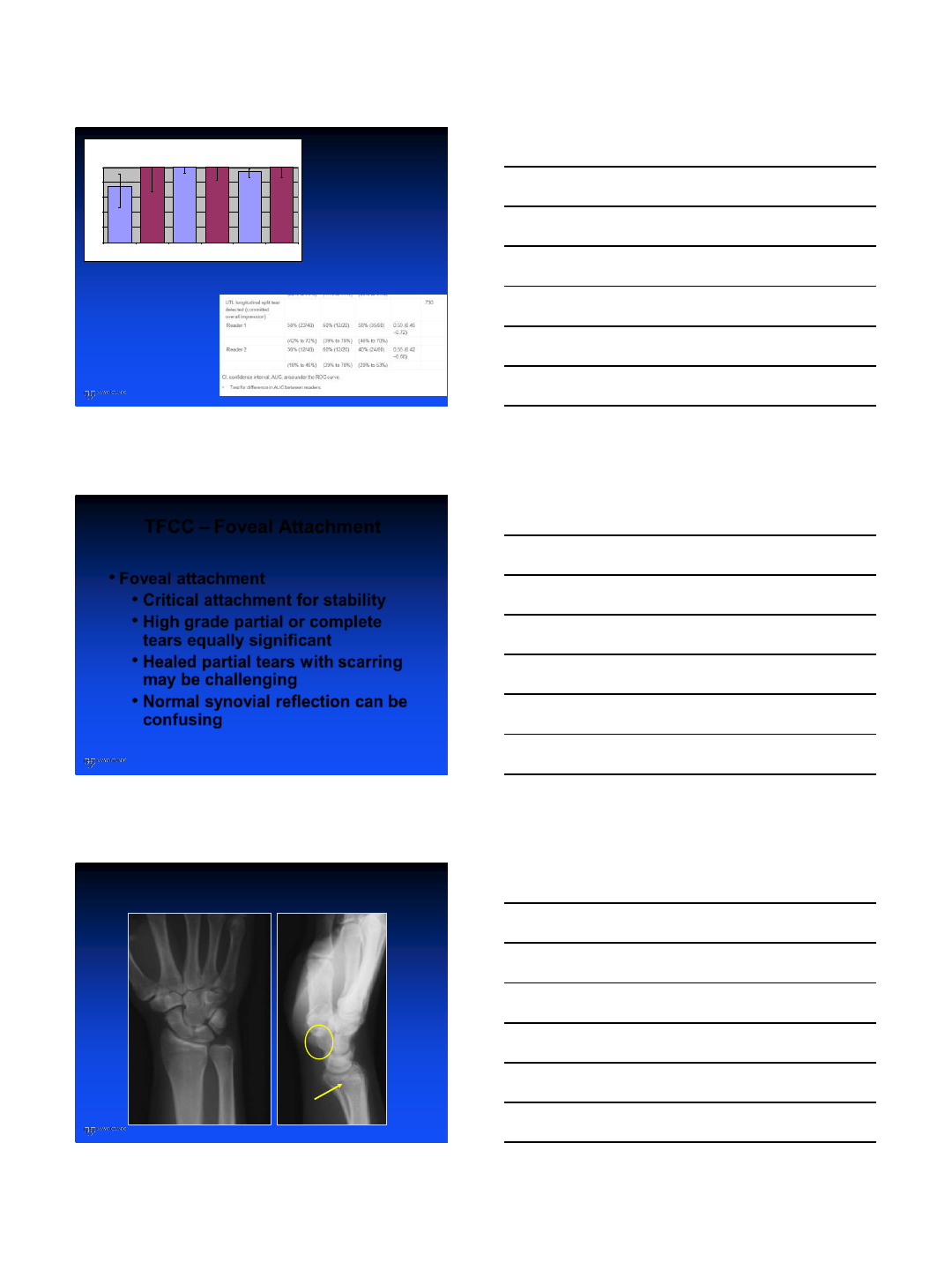
TFCC –Foveal Attachment
•Foveal attachment
•Critical attachment for stability
•High grade partial or complete
tears equally significant
•Healed partial tears with scarring
may be challenging
•Normal synovial reflection can be
confusing
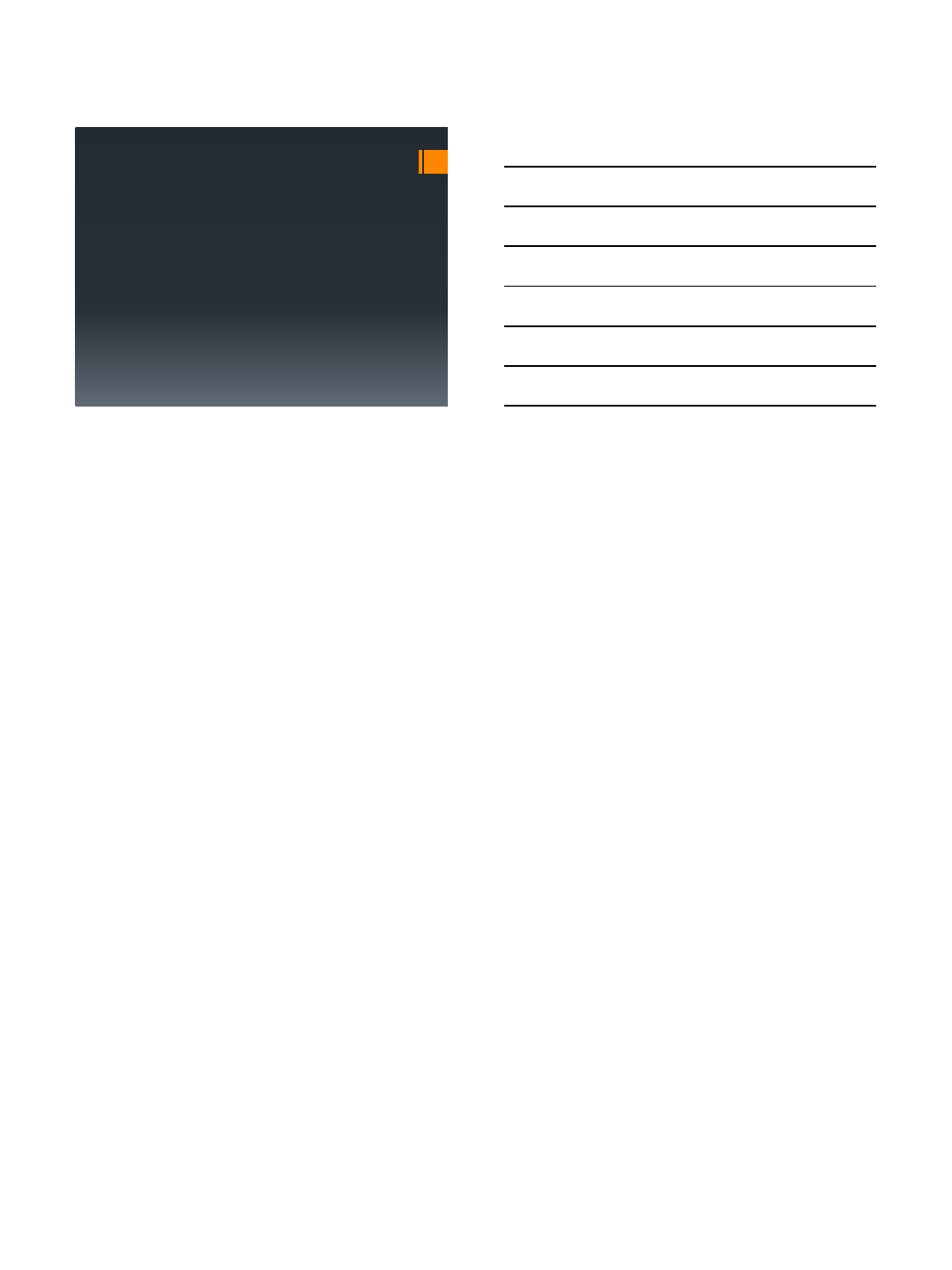
55 yo male with ulnar wrist pain –fell while gardening
7/16/2015
7
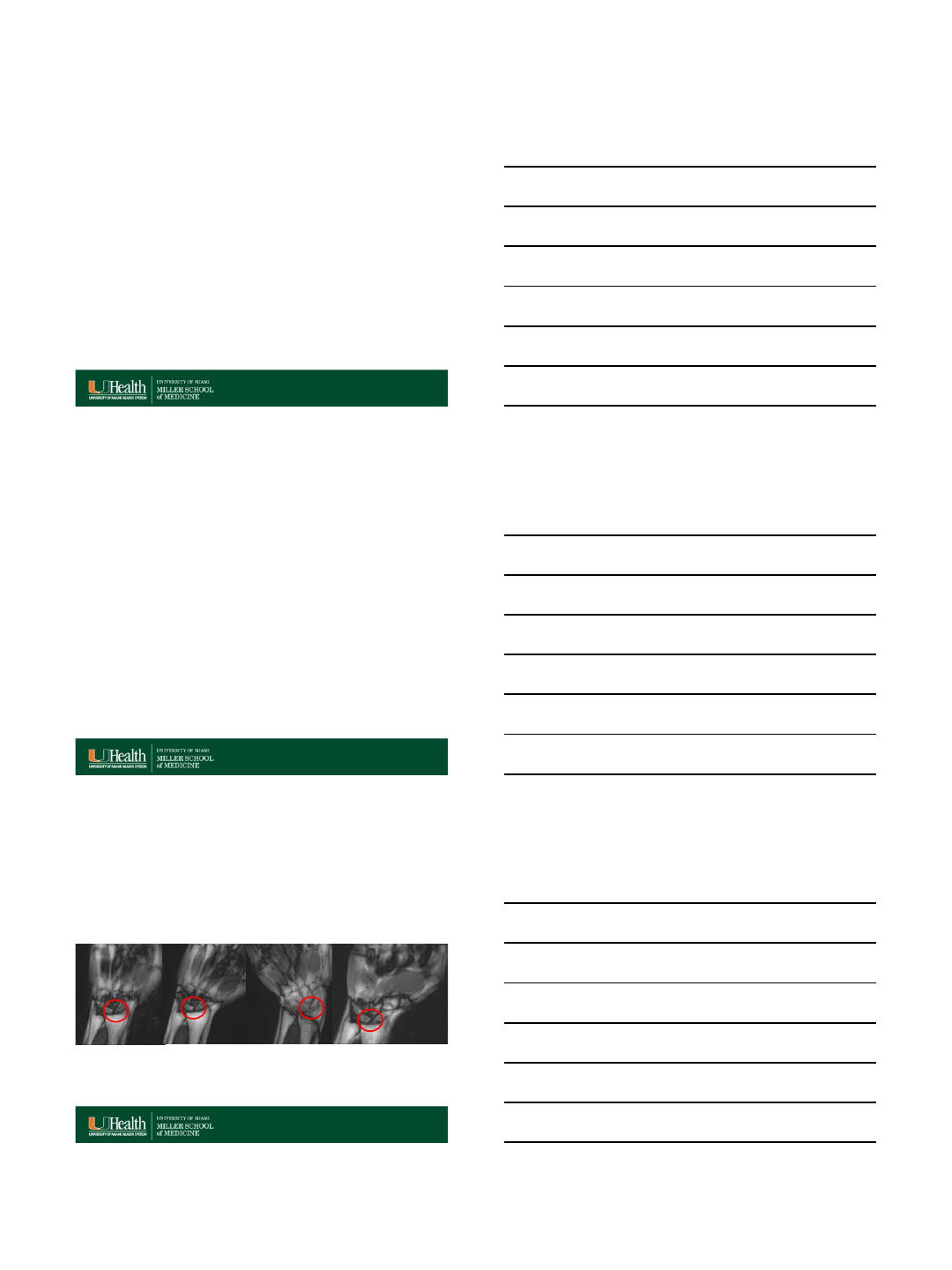
Foveal Dissociation –UT Intact
7/16/2015
8
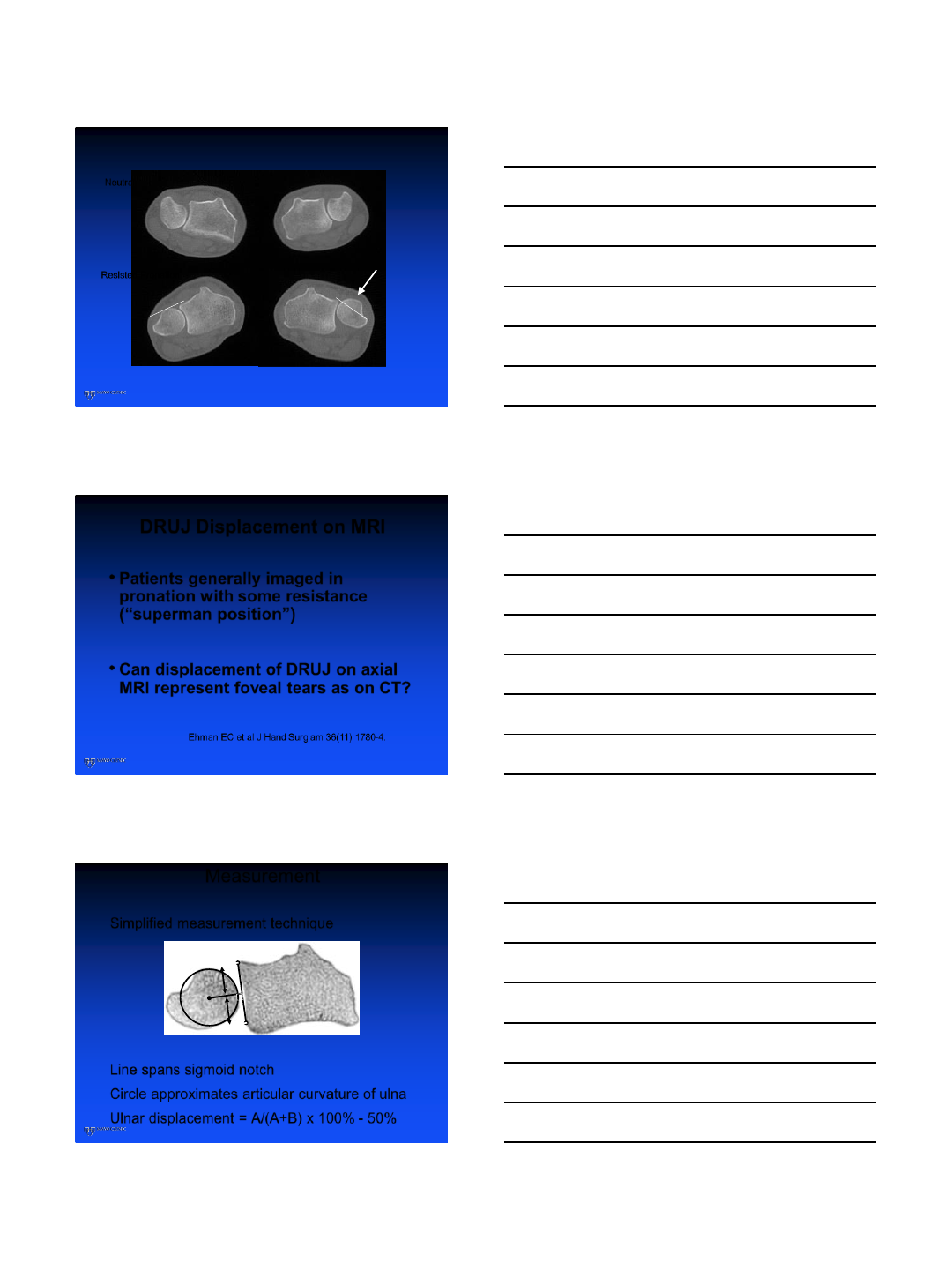
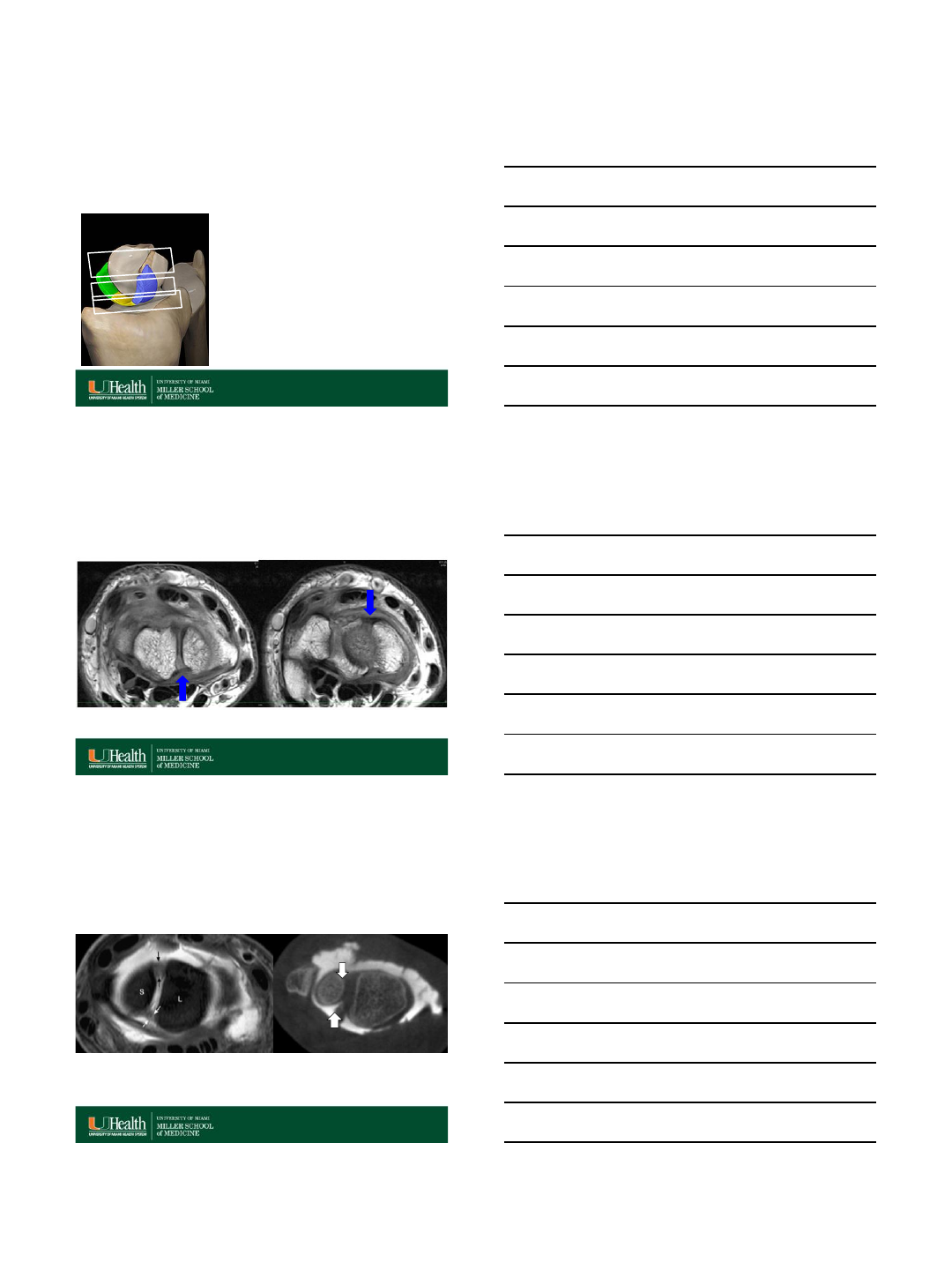
Neutral
Resisted Pronation
DRUJ Displacement on MRI
•Patients generally imaged in
pronation with some resistance
(“superman position”)
•Can displacement of DRUJ on axial
MRI represent foveal tears as on CT?
Ehman EC et al J Hand Surg am 36(11) 1780-4.
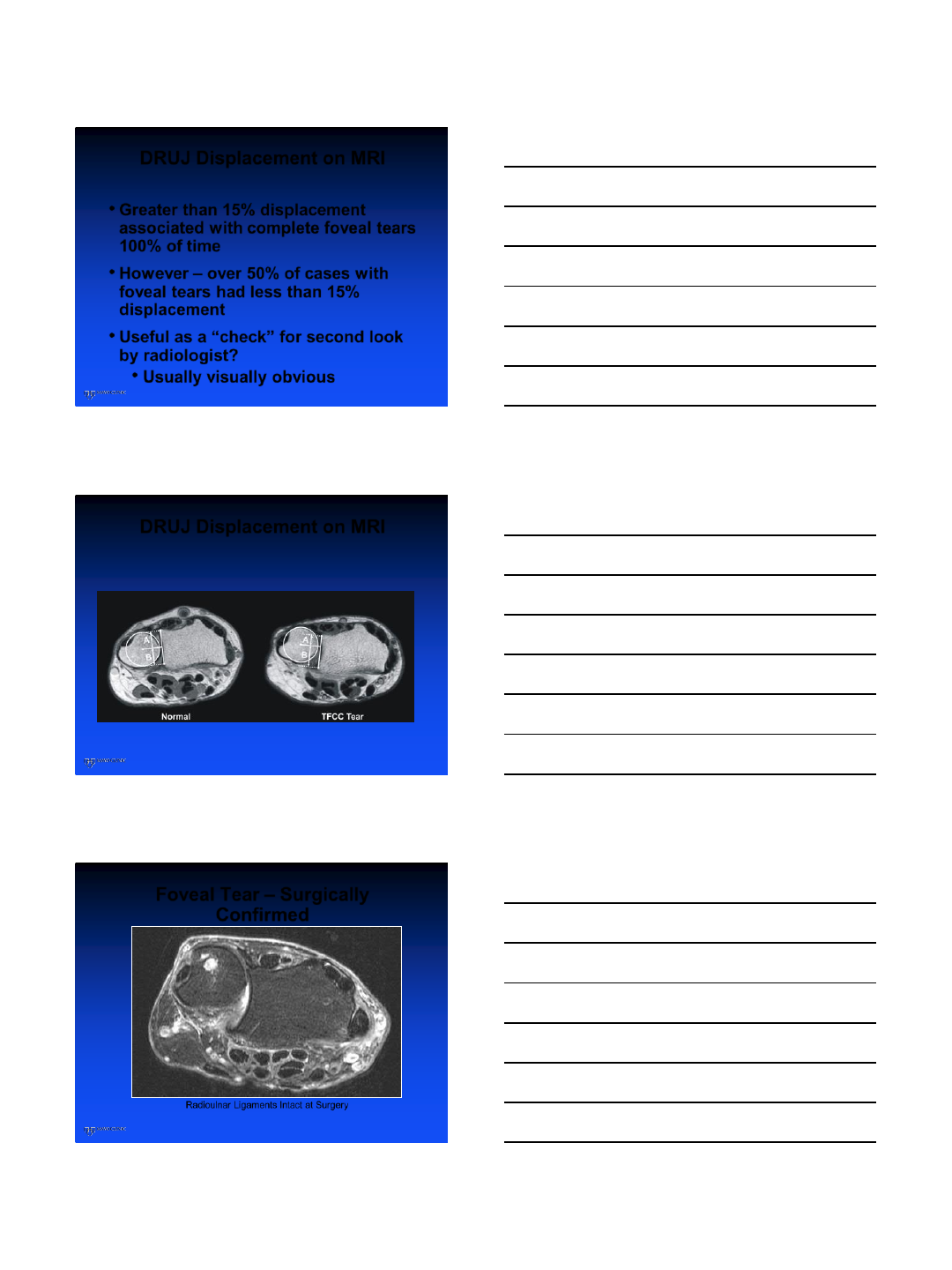
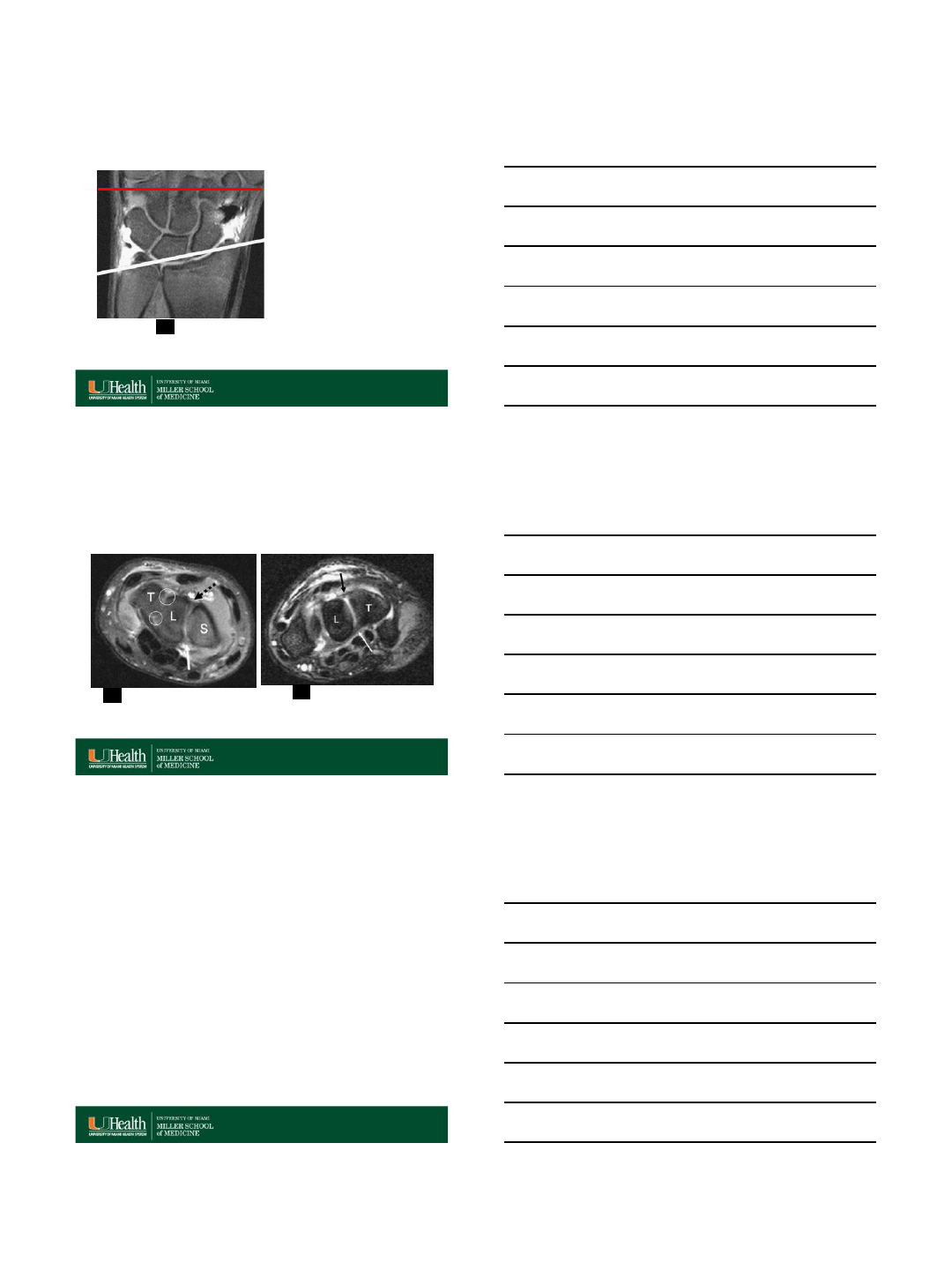
Measurement
Simplified measurement technique
Line spans sigmoid notch
Circle approximates articular curvature of ulna
Ulnar displacement = A/(A+B) x 100% - 50%
A
B
7/16/2015
9
DRUJ Displacement on MRI
•Greater than 15% displacement
associated with complete foveal tears
100% of time
•However –over 50% of cases with
foveal tears had less than 15%
displacement
•Useful as a “check” for second look
by radiologist?
•Usually visually obvious
DRUJ Displacement on MRI
Foveal Tear –Surgically
Confirmed
Radioulnar Ligaments Intact at Surgery

7/16/2015
10
Complex tears
•Fovea –body of TFCC –UT ligament
•Tears commonly extend up and down
this axis
•Fall on an outstretched hand is a
common mechanism
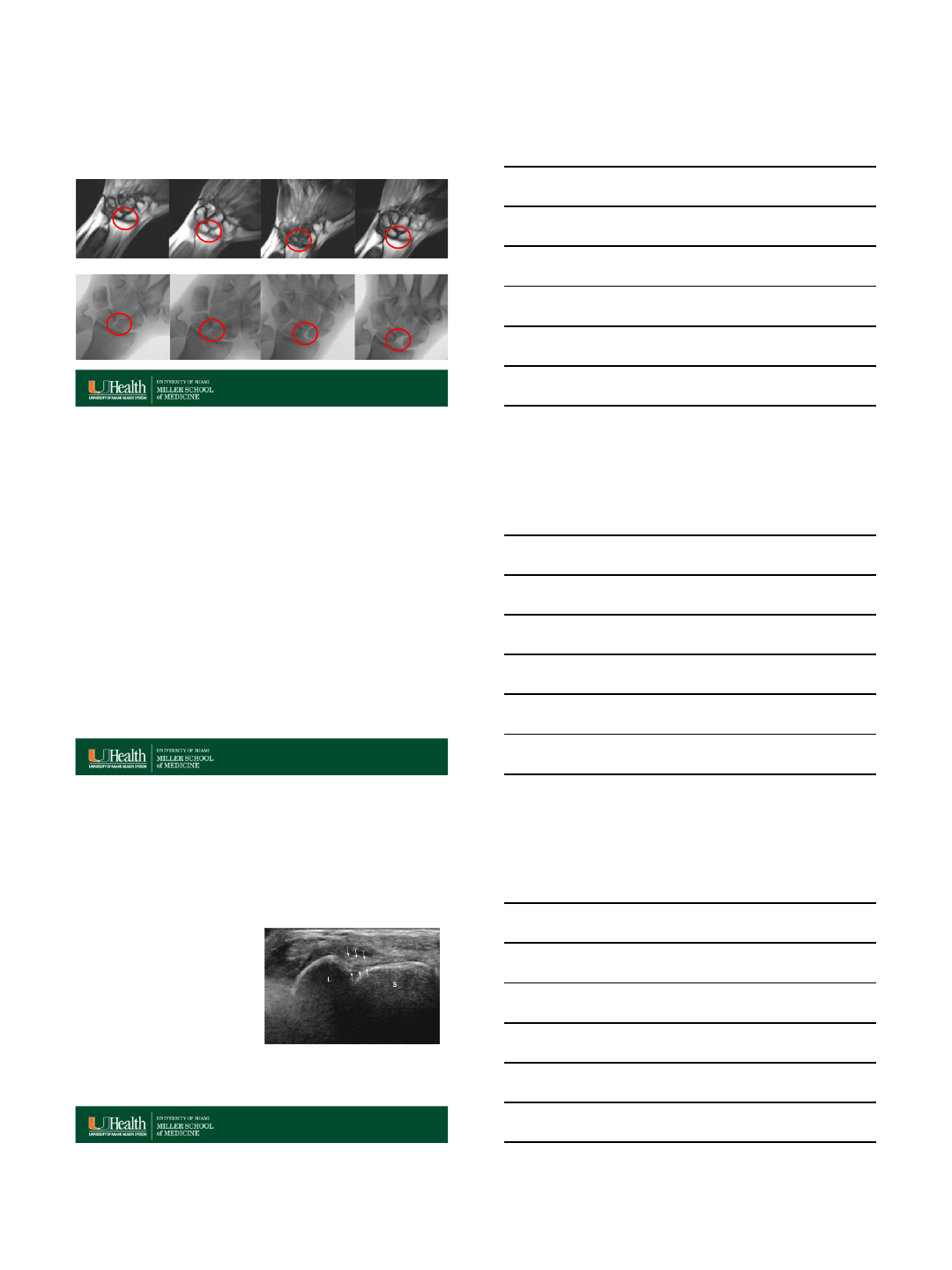
UT, TFCC and Foveal Tears
Foveal Tear is Complete
29 yo woman
Complete foveal Tear
ECU Subsheath Tear and Subluxation
Subluxation of the ECU
7/16/2015
11
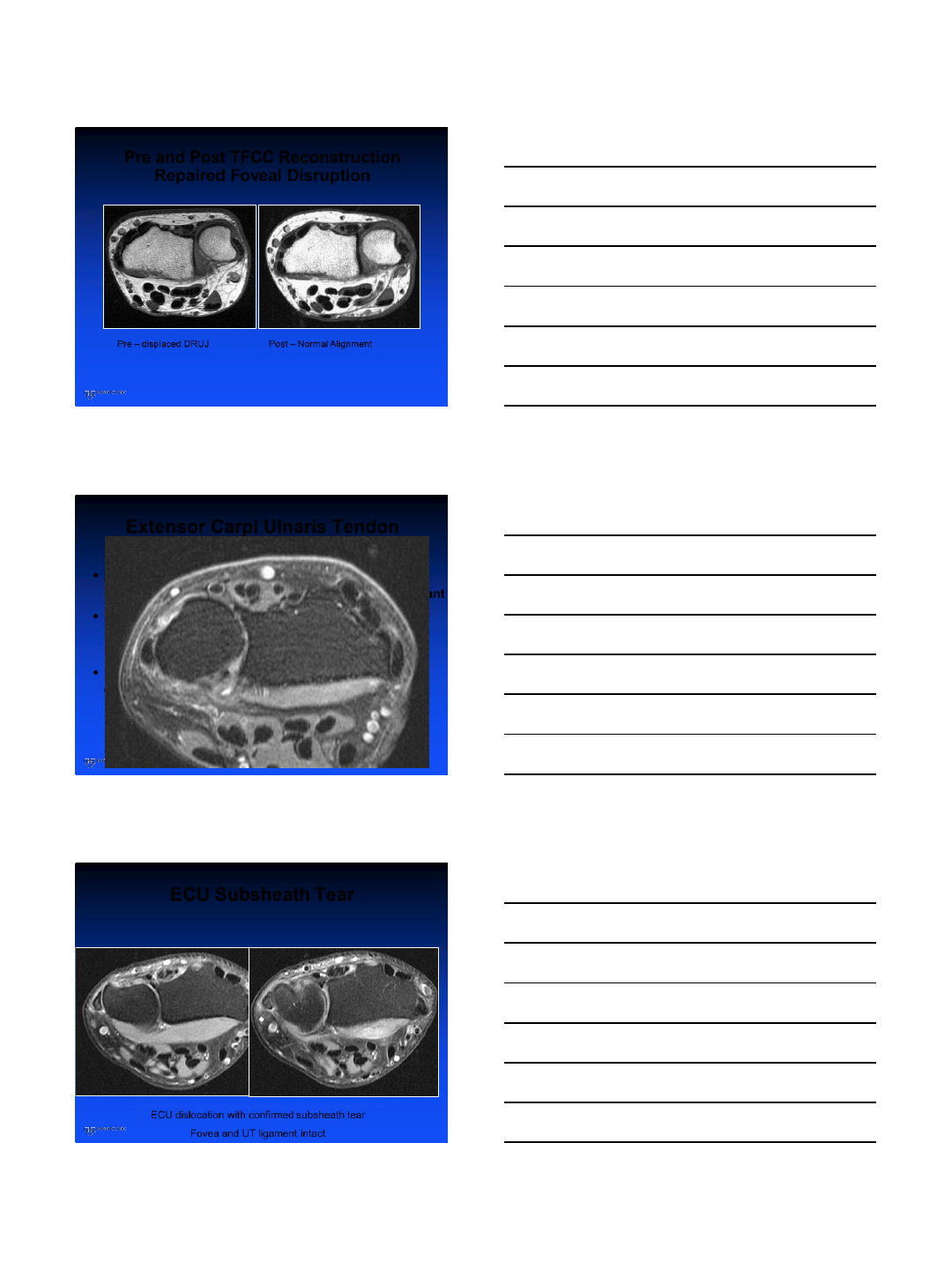
Pre and Post TFCC Reconstruction
Repaired Foveal Disruption
Pre –displaced DRUJ Post –Normal Alignment
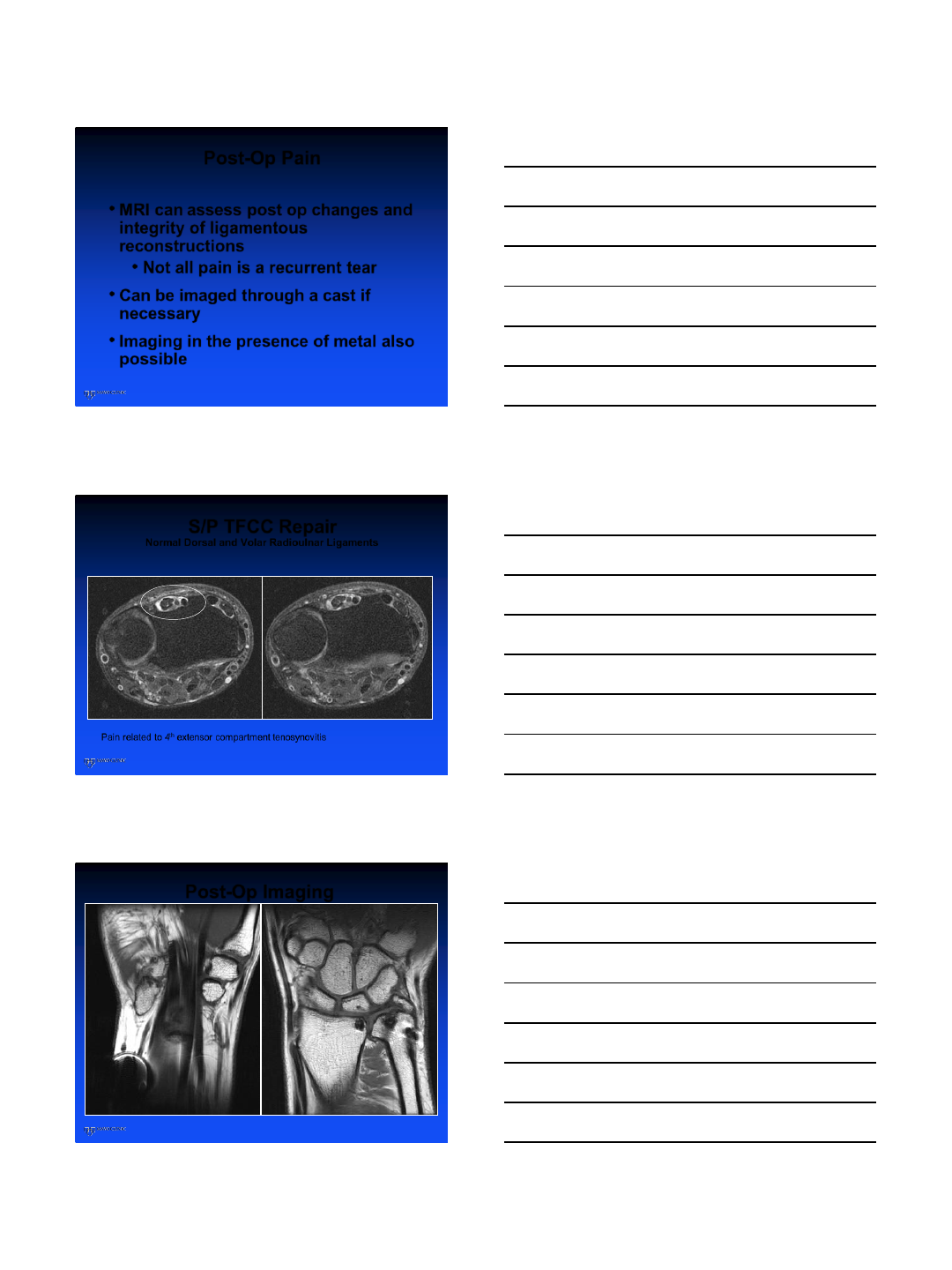
Extensor Carpi Ulnaris Tendon
•Some subluxation likely physiologic/positional
•In the absence of pain or instability not really relevant
•ECU subluxations may occur with subsheath
intact
•Dislocations usually mean subsheath is
disrupted
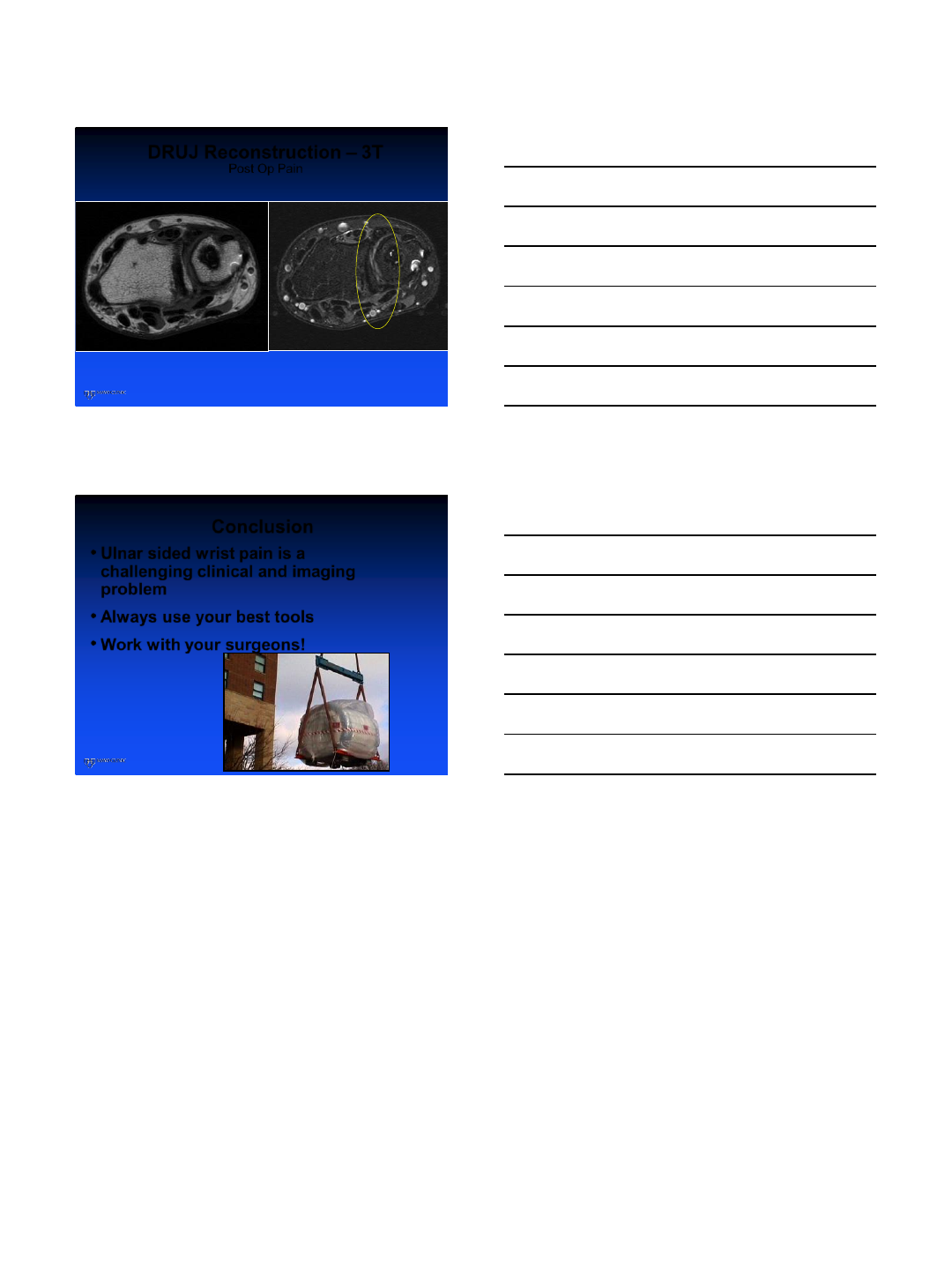
ECU Subsheath Tear
ECU dislocation with confirmed subsheath tear
Fovea and UT ligament intact
7/16/2015
12
Post-Op Pain
•MRI can assess post op changes and
integrity of ligamentous
reconstructions
•Not all pain is a recurrent tear
•Can be imaged through a cast if
necessary
•Imaging in the presence of metal also
possible
S/P TFCC Repair
Normal Dorsal and Volar Radioulnar Ligaments
Pain related to 4th extensor compartment tenosynovitis
Post-Op Imaging
U-head (3T) DRUJ Reconstruction (3T)
7/16/2015
13
DRUJ Reconstruction –3T
Post Op Pain
Intact Reconstruction –degenerative arthritis at the DRUJ
Conclusion
•Ulnar sided wrist pain is a
challenging clinical and imaging
problem
•Always use your best tools
•Work with your surgeons!
Thanks to:
Richard Berger, MD, PhD
Joel Felmlee, PhD
7/27/2015
1
Wrist MRI and Ulnar
Sided Wrist Pain
Christopher O. Bayne, MD
UC Davis Medical Center
July 27, 2015
Disclosures
None
Ulnar Sided Wrist Pain
Diagnostic
challenge
Complex anatomy
Small size of structures
Can cause vague,
intermittent sx
7/27/2015
2
Ulnar Sided Wrist Pain
Differential Diagnosis
Osseous
Ligamentous
Tendinous
Vascular
Neurologic
Magnetic Resonance Imaging
Can be useful
Diagnosis/Treatment
Soft tissue lesions
Ligament
Cartilage
Soft tissue tumor
Tendonitis
Effusions
Bone (Less osseous detail
than CT)
Edema/Occult fractures
Magnetic Resonance Imaging
DIAGNOSES:
TFCC/Ulnar impaction
Tendonopathy
ECU
Lunotriquetral Ligament
Tear
7/27/2015
3
Triangular Fibrocartilage Complex
Anderson et al, JHS 2008
1.5 T MRI--85% sens/ 75% spec
3.0 T MRI--94% sens/88% spec
Lee et al, MR Imaging 2013
MR Arthrogram
Sensitivity: 93-94%
Specificity: 97-100%
Anderson ML, et al. J Hand Surg Am. 2008
Shin AY, et al. JBJS 2004
Triangular Fibrocartilage Complex
CLASSIFICATION
Type 1 (Traumatic)
1A- Central
1B- Ulnar
1C- Distal
1. Transverse *
2. Longitudinal (UT Split)*
1D -Radial
Type 2 (Degenerative)
2A- TFCC wear/thinning
2B- Lunate/Ulna
2C- Perforation
2D- Ligament disruption
2E- Ulnocarpal/DRUJ arthritis
Triangular Fibrocartilage Complex
CLASSIFICATION
Type 1 (Traumatic)
1A- Central
1B- Ulnar
1C- Distal
1. Transverse *
2. Longitudinal (UT Split)*
1D -Radial
Type 2 (Atraumatic)
2A- TFCC wear/thinning
2B- Lunate/Ulna
2C- Perforation
2D- Ligament disruption
2E- Ulnocarpal/DRUJ arthritis
Tay SC MD, Berger RA, et al. Hand Clin. 2010
7/27/2015
4
Triangular Fibrocartilage Complex
CLASSIFICATION
Type 1 (Traumatic)
1A- Central
1B- Ulnar
1C- Distal
1. Transverse *
2. Longitudinal (UT Split)*
1D -Radial
Type 2 (Atraumatic)
2A- TFCC wear/thinning
2B- Lunate/Ulna
2C- Perforation
2D- Ligament disruption
2E- Ulnocarpal/DRUJ arthritis
Citation
Tay SC MD, Berger RA, et al. Hand Clin. 2010
Ulnar Fovea Sign
95 % sen si t iv it y, 86% sp ec if ic i ty
*Tay SC MD, Berger RA, et al. JHS (Am). 2007
Triangular Fibrocartilage Complex
*Ringler MD, Berger RA, et al. JHS (Am). 2013
CONSIDERATIONS
UT split: low
sensitivity/specificity
MR may be more helpful
to exclude concomitant
injury
Ulnar positive variance
Check lunate and ulnar
head –impaction signs
7/27/2015
5
Triangular Fibrocartilage Complex
TREATMENT
Non-operative
Acute Type 1
First line Type 2
Steroid injection x 1-3
Oral and topical NSAIDs
Splinting/Casting
(Muenster, if tolerated)
Triangular Fibrocartilage Complex
OPERATIVE
Arthroscopy vs Open
Central: Debridement
Ulnar: Repair
Distal: repair if mechanical instability/ persistent
pain (UT split)
Radial: ? Repair
Ulnar Impaction: ulnar shortening
Triangular Fibrocartilage Complex
REPAIR OPTIONS:
Arthroscopy assisted with extra capsular knot
All-inside anchor
Thermal Shrinkage (less favored)
+/- Ulnar shortening
7/27/2015
6
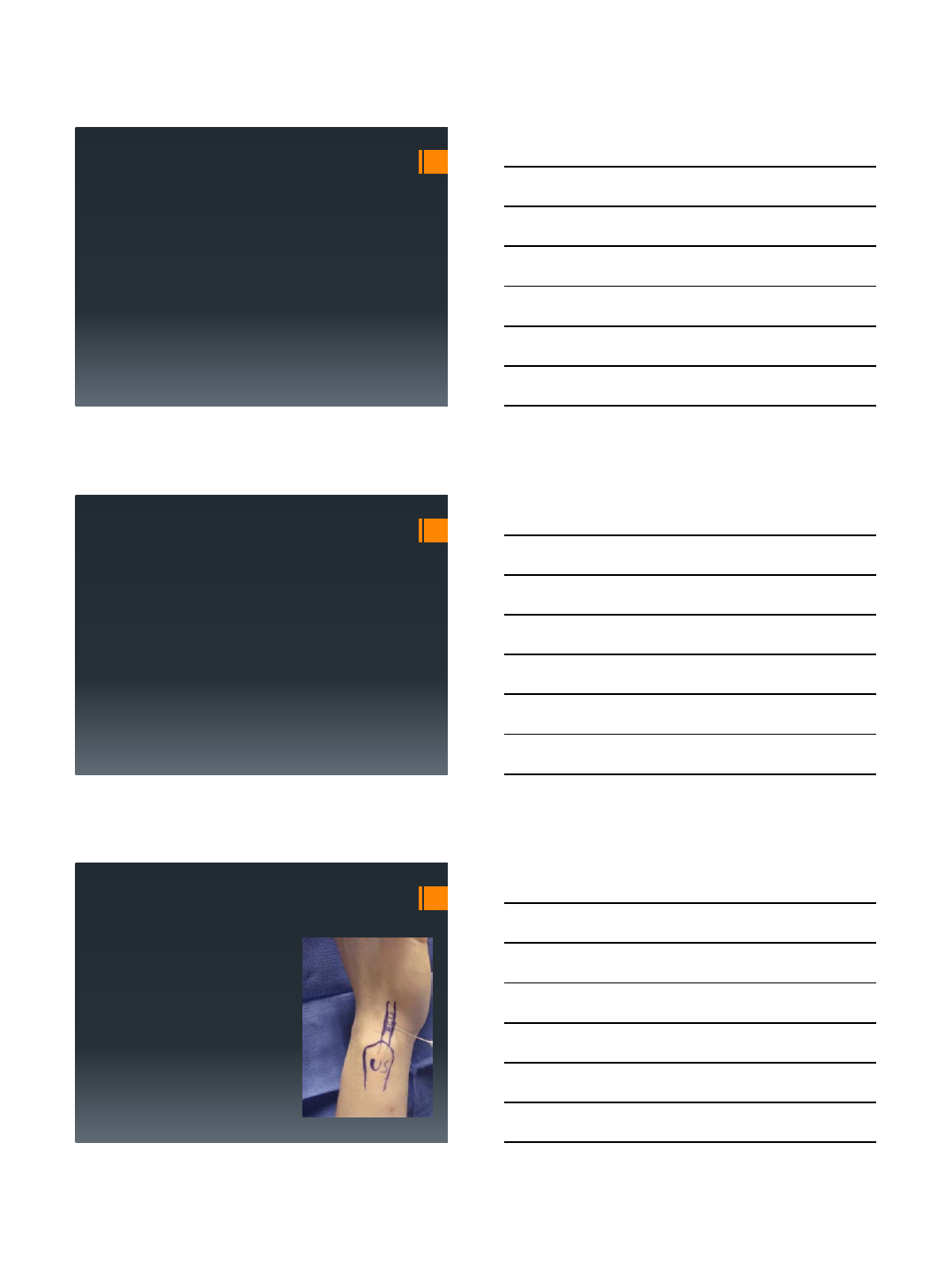
Ulnar Shortening
Ulnar Shortening
Ulnar Shortening
Wafer procedure Osteochondral osteotomy
7/27/2015
7
Tendinopathy
Extensor Carpi Ulnaris
Pathology:
Tenosynovitis
Rupture
Subluxation
Tendinopathy
Extensor Carpi Ulnaris
MRI:
Tenosynovitis - Thickened tendon. Fluid within sheath
Rupture - Discontinuity of tendon fibers
Subluxation –Nonspecific, consider dynamic study
Tendinopathy
Extensor Carpi Ulnaris
Treatment:
Non-operative
-NSAIDS
-Immobilization: (Muenster Cast/splint
6-8 weeks)
Tenosynovitis (Consider steroid
injection)
ECU Subluxation
Acute injuries
1st line chronic injuries
7/27/2015
8
Tendinopathy
Extensor Carpi Ulnaris
Operative Treatment
Tenosynovitis (Recalcitrant) –Tx to dorsum of hamate
Rupture - Repair
Subluxation –Reconstruction of ECU subsheath/groove
deepening
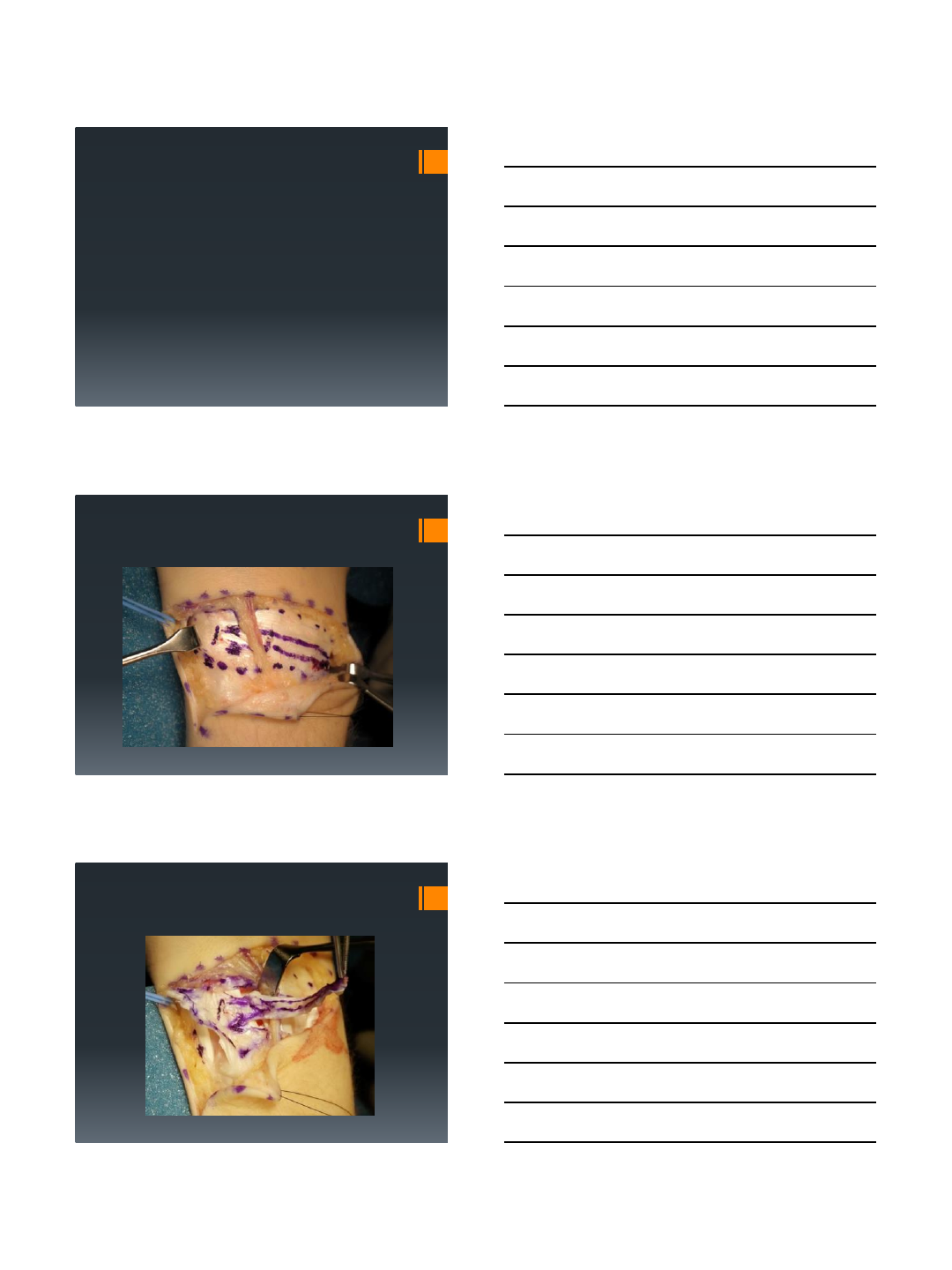
ECU Stabilization
ECU Stabilization
7/27/2015
9
ECU Stabilization
ECU Stabilization
ECU Stabilization
7/27/2015
10
Lunotriquetral Ligament Tear
Images from Alexander Y Shin M.D.
Lunotriquetral Ligament Tear
Summary
Ulnar Wrist Pain
Can be challenging
History
Exam
Imaging
MRI
7/27/2015
11
Thank you
7/17/2015
1
Imaging of the Scapholunate
and Lunotriquetral Ligaments:
Normal anatomy, anatomic variants, and
injury assessment
Dr. Jean Jose
Associate Professor Radiology
Associate Section Chief, Musculoskeletal Division
University of Miami
Miller School of Medicine
TITLE: Imaging of Scapholunate and Lunotriquetral
Ligaments
NAME: Jean Jose
DISCLOSURE OF COMMERICAL INTEREST: My
disclosure is in the Final VuMedi Program.
I have no relevant disclosures.
Disclosure of Commercial Interest
Introduction
•Carpal instability is often a confusing and challenging topic, in part
related to many different patterns of instability and also to the
existence of countless intrinsic and extrinsic ligaments.
•Such instability relates to biomechanical alterations with multiple
causes that, if not identified and treated in a timely fashion, will lead
to gradual articular collapse.
•Understanding requires a basic knowledge of anatomy and
pathophysiology, which is critical for the proper prompt diagnosis
and treatment of carpal instability.
•Such knowledge can then be applied to the analysis of imaging
studies, including MRI, CT and US, allowing a more complete and
meaningful diagnosis in cases of wrist instability and a more
meaningful conversation between the radiologist and the referring
physician.
http://radsource.us/carpal-instability/
7/17/2015
2
Dissociative vs. Nondissociative
injuries
•Dissociative:
–Results from tear of the intrinsic ligaments.
–SL or LT dissociation leads to DISI (SLAC) or
VISI, respectively.
•Nondissociative:
–Results from a tear of the extrinsic ligaments.
http://radsource.us/carpal-instability/
Wrist Instability
•Pre-dynamic:
–Partial ligament tear.
–Plain radiographs are normal.
–Soft tissue injury seen with MRI, US, CT, or arthroscopy.
•Dynamic:
–Incompetent or complete ligament tear.
–Static (non-stress) plain radiographs are normal.
–Abnormal changes in carpal alignment are seen on stress
radiographs/dynamic US/cine MRI.
•Static (i.e. Scapholunate dissociation):
–Complete SLIL and volar or dorsal extrinsic disruption.
–Abnormal changes in carpal alignment seen on non-stress
radiographs.
http://radsource.us/carpal-instability/
Mayo Clinic Classification
•CID (carpal instability dissociative)- Intrinsic ligaments
–Disruption within a row; e.g., SL or LT disruptions/dissociation,
scaphoid fracture, and Kienbock’s disease (proximal carpal row);
or axial carpal dislocations (distal carpal row).
•CIND (carpal instability nondissociative)- Extrinsic ligaments
–Symptomatic carpal dysfunction between the radius and the
proximal row, or between the proximal and distal carpal rows,
without disruption within or between the bones of the proximal or
distal carpal row.
–CIND is subdivided into radiocarpal and midcarpal patterns.
•Radiocarpal- insufficiency or disruption of the obliquely orientated extrinsic
radiocarpal ligaments –RS, RSC, LRL ligaments- (i.e. RA, Madelung’s)
•Midcarpal- insufficiency or disruption of the triquetro-hamate-capitate (THC),
dorsolateral STT, dorsal radiocarpal and RSC ligaments.
http://radsource.us/carpal-instability/
7/17/2015
3
•CIC (carpal instability complex):
–Features of CID & CIND
–Lesser Arc (pure ligament injury) and Greater Arc (transosseous
injury)
–Five groups identified.
•Dorsal perilunate dislocation (lesser arc injury)
•Dorsal perilunate fracture-dislocation (greater arc injury)
•Palmar perilunate dislocation (lesser or greater arc injury)
•Axial dislocation Isolated carpal bone dislocation
•CIA (carpal instability adaptive):
–Extrinsic to wrist (result from extracarpal pathology); e.g.,
Malunion of distal radius fracture
Mayo Clinic Classification
http://radsource.us/carpal-instability/
Natural History of SL and LT Instability
•Static Instability (Scapholunate and Lunotriquetral dissociation)
–Interval diastasis > 3 mm
–Scapholunate dissociation- most common ligamentous cause of carpal
instability.
–Lunotriquetral dissociation- second most common ligamentous cause of
carpal instability.
•Increased frequency of lunotriquetral ligament tears in association with degenerative
tears of the triangular fibrocartilage (70% of cases).
•Dorsal Intercalated Segment Instability (DISI)-
–Most common form of carpal instability (dissociative type).
–Complete SLIL and failure of scaphoid stabilizers (volar extrinsic rupture,
with secondary changes in volar RSC, radiolunate, STT
(scaphotrapezoid), and dorsal intercarpal ligaments).
–Scaphoid tilts volarly and the lunate tilts dorsally, both the SL and CL
angles are increased (SL > 60°, CL > 30°).
http://radsource.us/carpal-instability/
•Volar Intercalated Segment Instability (VISI)
–Second most common type of carpal instability (dissociative type).
–Secondary to disruption of the lunotriquetral ligamentous complex.
–Results in volar rotation of the lunate and extension of the triquetrum.
–The SL angle is decreased (SL < 30°) and the CL angle is increased
(> 30°).
–The dorsal radiocarpal ligament is also injured in VISI.
•Scapholunate Advanced Collapse (SLAC), degenerative changes
typically in the following stages:
–Stage I: Styloid-scaphoid DJD
–Stage II: DJD of the proximal scaphoid facet
–Stage III: Capitolunate DJD
–Stage IV: Radiolunate/Pancarpal DJD
Natural History of SL and LT Instability
http://radsource.us/carpal-instability/
7/17/2015
4
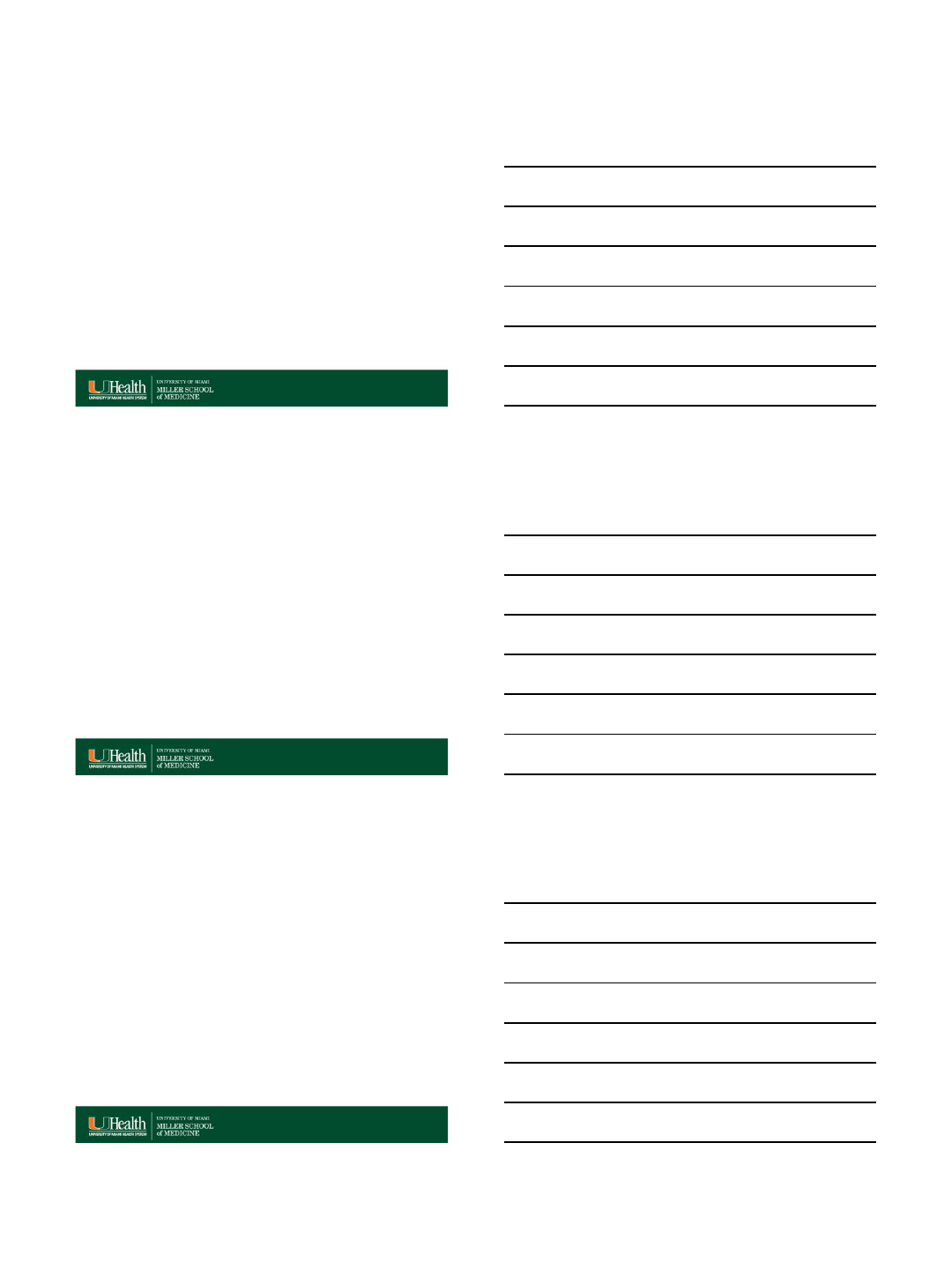
Anatomy: Scapholunate Ligament
•C-shaped Ligament: 3
portions
–Dorsal
–Membranous (proximal)
–Volar
•Dorsal Component
–Transversely oriented collagen
(collagenous structure)
–Thickest and Strongest (300 N
failure force) Component
SL
http://radsource.us/sll-tear-and-disi-deformity/
•Dorsal component
–Most critical of the SL stabilizers
–Primary restraint not only to
distraction, but also to torsional
and translational moments.
–SLL tear can lead to scapholunate
dissociation, which together with
dorsal intercarpal ligament (DICL)
tear results in DISI and SLAC.
J Hand Surg 2008;33A:998–1013.
Anatomy: Scapholunate Ligament
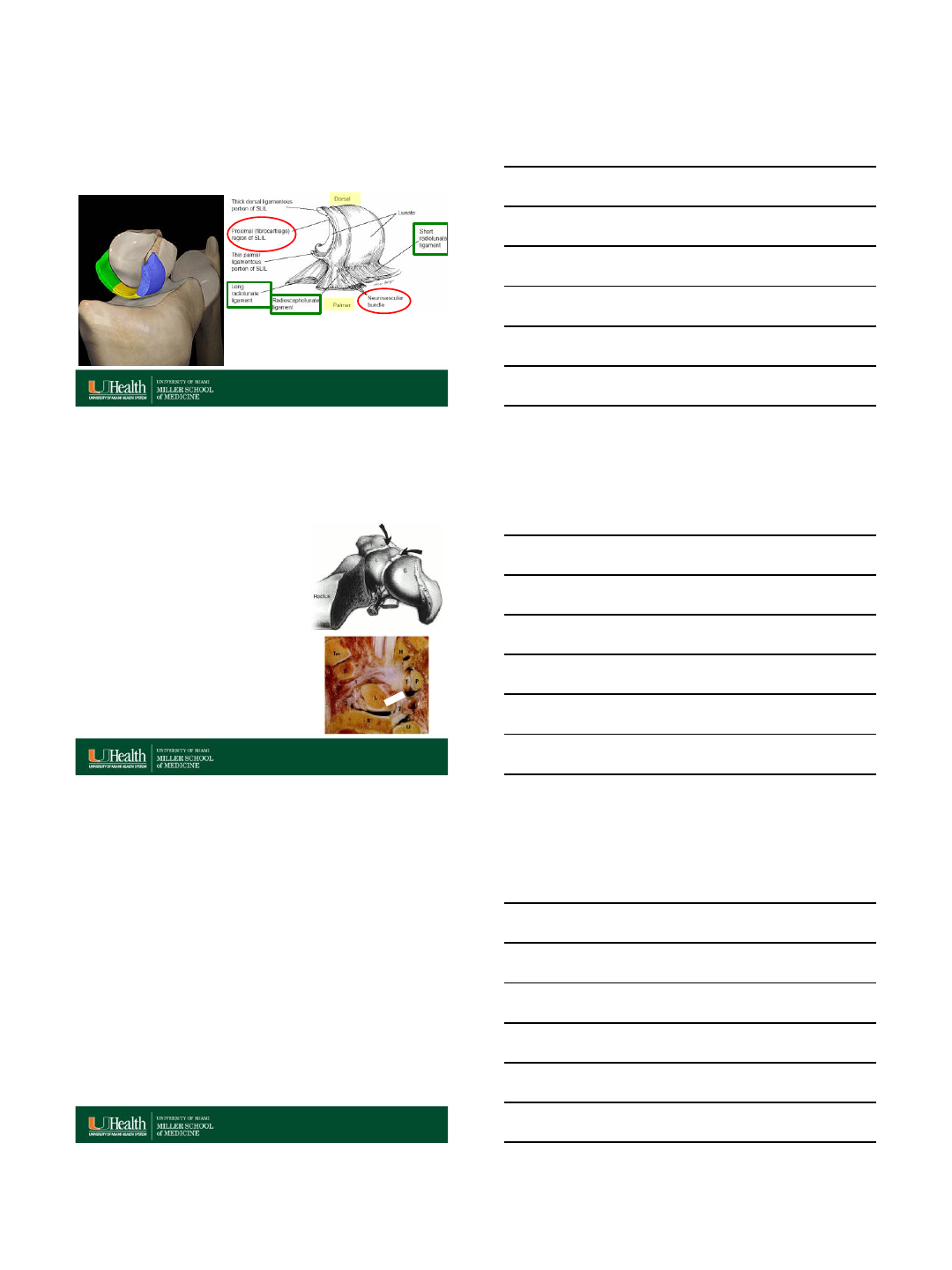
Anatomy: Scapholunate Ligament
•Volar (palmar):
–Collagenous structure
–Considerably thinner
–Important contribution to
rotational stability
•Membranous (proximal):
–Fibrocartilaginous structure
–Little to no restraint to abnormal
motion
SL
http://radsource.us/sll-tear-and-disi-deformity/
7/17/2015
5
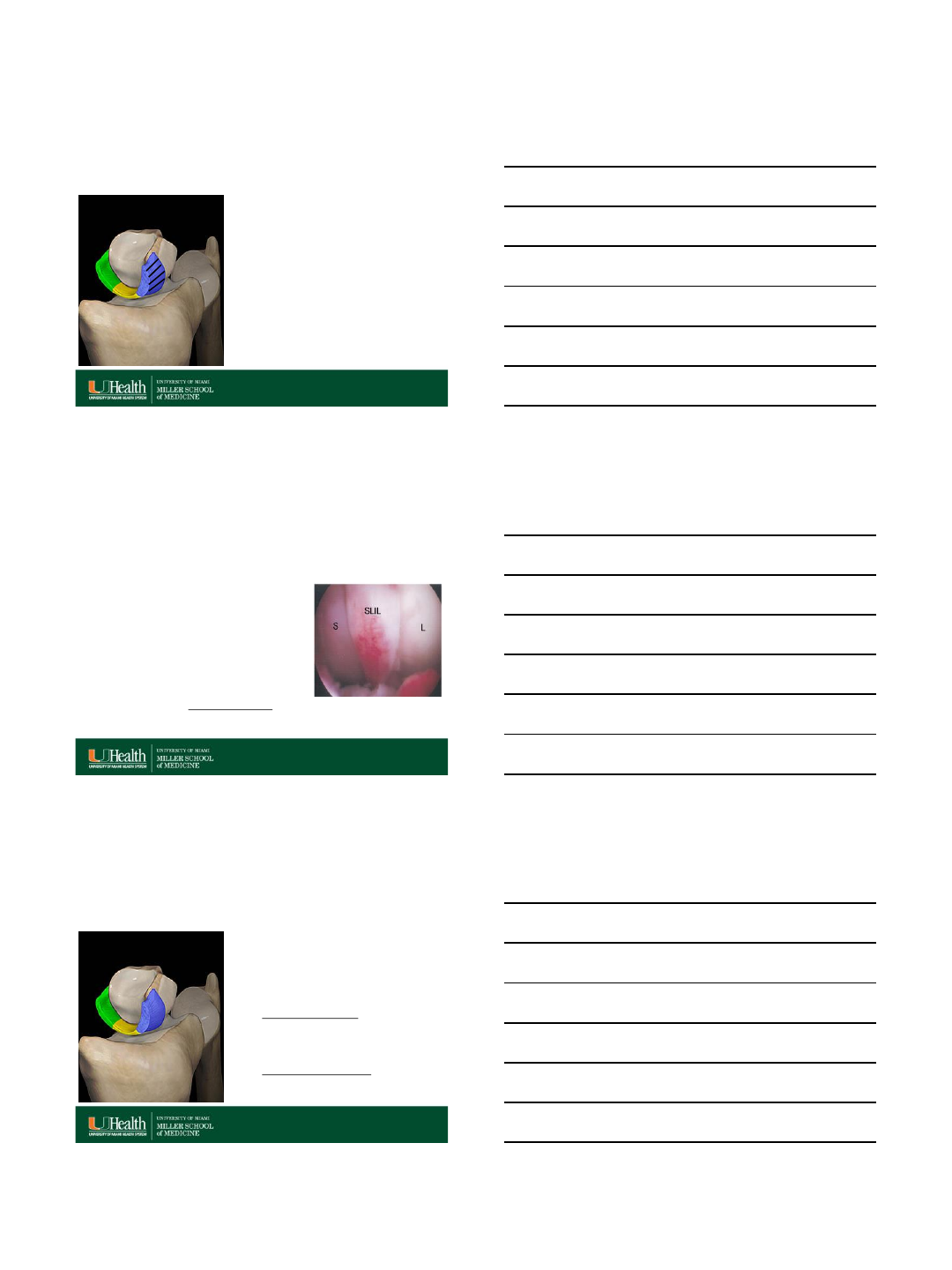
Scapholunate Ligament (SLIL)
http://radsource.us/sll-tear-and-disi-deformity/
Interosseous Lunotriquetral Ligament
•V-Shaped ligament
•Together with the SLIL, links the bones of
the proximal carpal row, allowing
synchronous motion.
•Dorsal and volar bands (true ligamentous
components, consisting of collagen
fascicles) and structurally weaker proximal
(central) membranous parts
(fibrocartilaginous tissue similar to that of
the triangular fibrocartilage).
•The thickest and functionally most
important part of the LTL is the volar band,
with contributions from fibers of the
ulnocapitate ligament. Transmits extension
moment of the triquetrum
•LTL tear can lead to lunotriquetral
dissociation, which together with a tear of
the extrinsic dorsal radiocarpal ligament
(DRCL) results in VISI.
RadioGraphics 2011 31:1, 79-80
J Bone Joint Surg Am, 2000 Apr; 82 (4): 578 -578
http://radsource.us/sll-tear-and-disi-deformity/
•Imaging findings require correlation with the
clinical examination results, as ligamentous
perforations or tears of the SLL and LTL can
also be seen in asymptomatic patients.
•On radiographs, widening of the scapholunate
interval of more than 2 mm may indicate SLL
disruption.
•However, widening of the scapholunate interval
may not occur in all cases of SLL disruption, and
widening may occur as a normal variation with
lunotriquetral coalition.
RadioGraphics 2011 31:1, 79-80
Interosseous SLL and LTL
7/17/2015
6
MRI
•Accurate assessment of SLL and LTL injury with
MR imaging is often a diagnostic dilemma.
•Factors that contribute to this difficulty in
diagnostic assessment include:
1. Low image spatial resolution,
2. Low signal to noise ratio (SNR),
3. Low contrast resolution,
4. MRI artifacts (i.e. wrap, pulsation, motion etc),
5. Suboptimal imaging technique
6. Normal variant morphology of the ligaments.
RadioGraphics 2011; 31:63–78
Spatial resolution
RadioGraphics 2011; 31:63–78
Low and high spatial resolution. Note the marginal blurring of anatomic
structures and the loss of detail.
Signal to noise ratio (SNR)
RadioGraphics 2011; 31:63–78
Low and high SNR. Note the increased granularity and the loss of structural
information in low SNR image.
7/17/2015
7
Contrast to noise ratio (CNR)
RadioGraphics 2011; 31:63–78
Coronal gradient-echo (GRE) MR image of the wrist, obtained with low
contrast-to-noise ratio, shows preferential loss of small structure detail (eg,
the bone trabeculae).
MRI artifacts
RadioGraphics 2011; 31:63–78
J Magn Reson Imaging. 2011 Apr; 33(4): 908–915
•Nonuniform fat
saturation over the
ulnar styloid
•Pulsation artifact
adjacent to the radial
artery
•Wrap around artifact
AJNR 2004 25: 431-440
•Magic angle artifact
Interosseous scapholunate and
lunotriquetral ligament MR assessment
•MRI allows assessment of the three
SL and LT ligament components:
–Volar and dorsal components are best
assessed in the axial plane,
–Membranous segment is best assessed on
the coronal plane.
Skeletal Radiol (2014) 43:713–724
7/17/2015
8
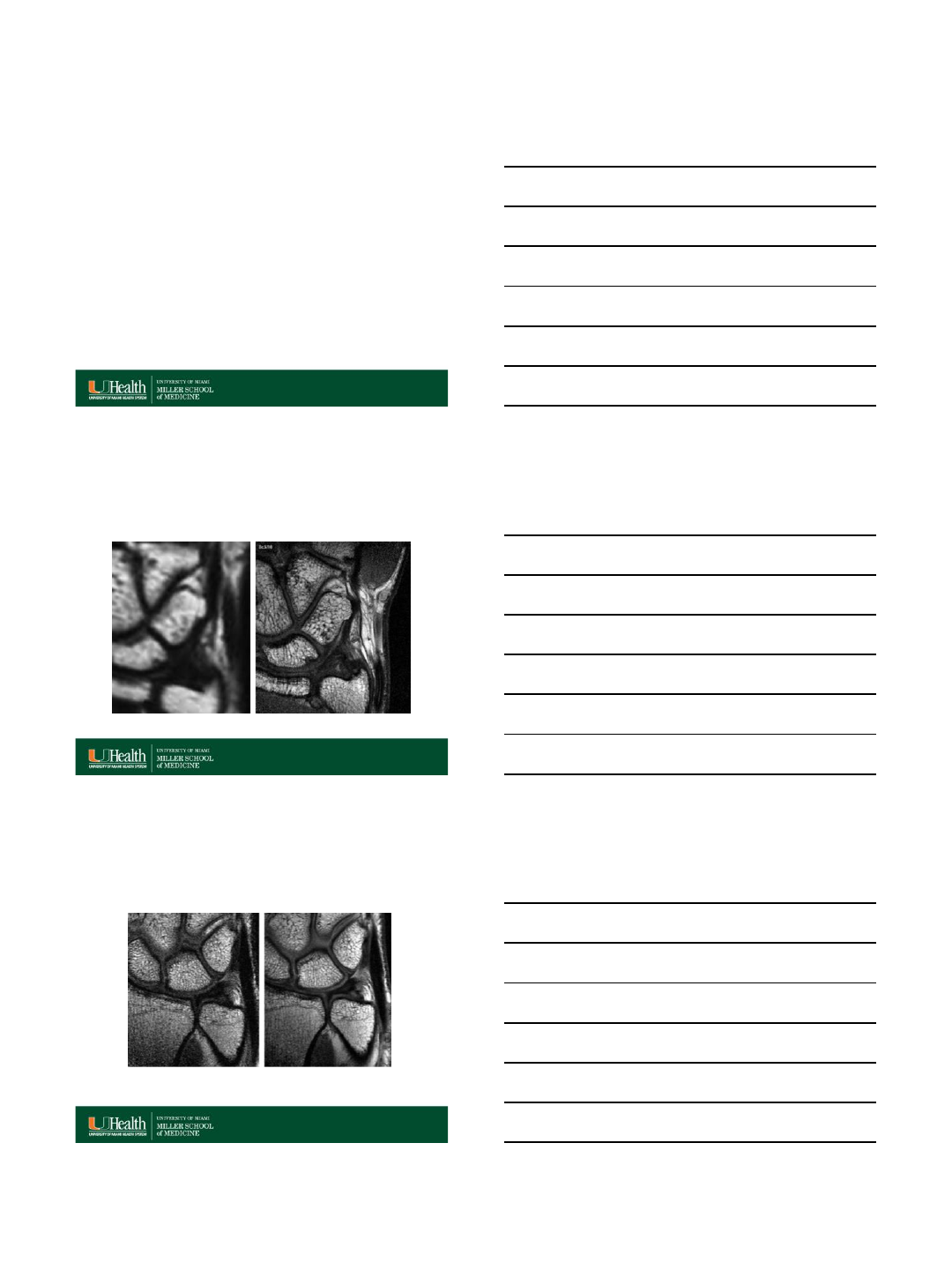
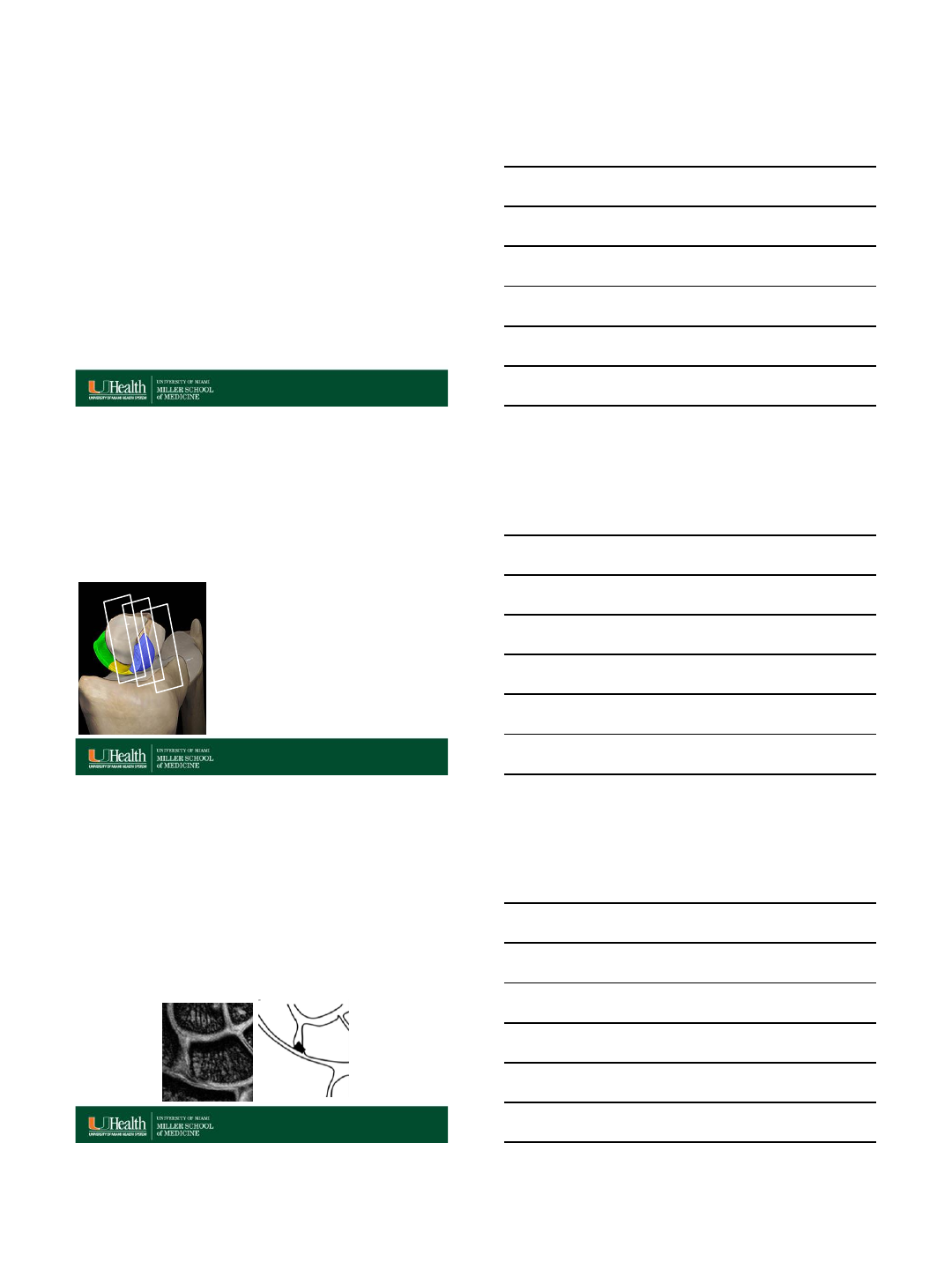
Axial MRI:
Scapholunate Ligament
•In the axial plane:
–Ligament does not take on
strange shapes
–Easy to see volar and dorsal
portions as bands
–Suboptimal view of
membranous ligament
Skeletal Radiol (2014) 43:713–724
Axial MRI:
Scapholunate Ligament
Proton Density Fast Spin Echo (TE 28, TR 3000; slice thickness 3.00mm, 0.0 gap)
SS
LL
Skeletal Radiol (2014) 43:713–724
Normal dorsal and volar components of the SL
ligament “band-like” configuration
Skeletal Radiol (2014) 43:713–724
CTA
Skeletal Radiol (2013) 42:649–657
MRA
7/17/2015
9
Oblique axial MR imaging
•Improves assessment of the individual ligament components.
Skeletal Radiol (2006) 35: 765–773
SL LT
Oblique axial MR imaging
•Improves assessment of the individual SL and
LT ligament components.
Skeletal Radiol (2006) 35: 765–773
Conventional true axial axial oblique
SL LT
Normal Variant Anatomy
•Lack of familiarity with normal variant anatomic
MR imaging appearances of the LTL and SLL
may contribute to the suboptimal sensitivity and
specificity for lesion detection.
•Therefore, it is important to become familiar with
the morphology and signal intensity of the LTL
and SLL at high resolution MR imaging to
improve the accuracy of diagnosis of
ligamentous disease, and to differentiate actual
disease from normal or variant appearances.
RadioGraphics 2011; 31:63–78
7/17/2015
10
•The SLL varies in shape on coronal images from
trapezoidal in its volar aspect to triangular
centrally to band-like in its dorsal aspect, all with
heterogeneous internal signal intensity.
•On coronal images, the LTL varies in shape from
symmetrically triangular to a distorted triangle to
a linear conformation, with variable patterns of
curvilinear increased internal signal intensity.
RadioGraphics 2011; 31:63–78
Normal Variant Anatomy
(Coronal Images)
SL : MRI
•In the coronal plane:
–Volar portion: trapezoidal
and intermediate signal
intensity
–Membranous portion:
triangular in shape and lower
in signal
–Dorsal portion: band-like
shape
Coronal MRI
Skeletal Radiol (2014) 43:713–724
MRI Shape of SL Ligament
•Dorsal and volar components of the SLL are band-like.
•The proximal or membranous component of the SLL varies in shape
from its volar to its dorsal aspect on coronal images.
–Volar aspect of the membranous component has a trapezoidal
conformation, and attaches scaphoid and lunate cortex.
RadioGraphics 2011; 31:63–78
7/17/2015
11
MRI Shape of SL Ligament
•Dorsal and volar components of the SLL are band-like.
•The proximal or membranous component of the SLL varies in shape
from its volar to its dorsal aspect on coronal images.
–Volar aspect of the membranous component has a trapezoidal
conformation, and attaches scaphoid and lunate cortex.
–The central portion of the membranous component is triangular,
and attaches to the hyaline cartilage of the scaphoid and lunate
in most cases.
RadioGraphics 2011; 31:63–78
MRI Shape of SL Ligament
•Dorsal and volar components of the SLL are band-like.
•The proximal or membranous component of the SLL varies in shape
from its volar to its dorsal aspect on coronal images.
–Volar aspect of the membranous component has a trapezoidal
conformation, and attaches scaphoid and lunate cortex.
–The central portion of the membranous component is triangular,
and attaches to the hyaline cartilage of the scaphoid and lunate
in most cases.
–The dorsal aspect of the membranous component is band-like
on coronal images, and is variable in attachment, attaching to
the cartilage or cortex of the scaphoid and lunate in various
combinations.
RadioGraphics 2011; 31:63–78
Coronal MRI:
Scapholunate Ligament
•Volar portion:
trapezoidal and
intermediate signal
intensity
•Membranous portion:
triangular in shape and
lower in signal
•Dorsal portion: band-
like shape
SL
S
L
7/17/2015
12
MR and CT Arthrogram
Skeletal Radiol (2014) 43:713–724
Intact membranous segment of the scapholunate ligament
MRI Signal Intensity SLL
•The volar portion of the SLL, with its band-like ligamentous
structure separated by loose vascular connective tissue,
demonstrates striated heterogeneous increased signal
intensity.
•Similarly, the fibrocartilaginous membranous portion has
been reported to predominantly demonstrate heterogeneous
signal intensity, which ranges from high-intermediate signal
intensity in its volar aspect to low signal intensity in its dorsal
aspect.
•The dorsal portion of the SLL has low internal signal
intensity, which is probably due to its constituent elements of
homogeneous transversely oriented collagen fascicles.
RadioGraphics 2011; 31:63–78 •
Shape and Signal Intensity LT
MRI
•A modified V- shaped configuration, with the dorsal and
volar components best seen on axial images, and with
the membranous portion best seen in on coronal images.
•The volar and dorsal components appear band-like on
axial images.
•The membranous portion (proximal zone) of the LTL has
a variety of normal variant shapes and signal
intensity on coronal images.
RadioGraphics 2011; 31:63–78 •
7/17/2015
13
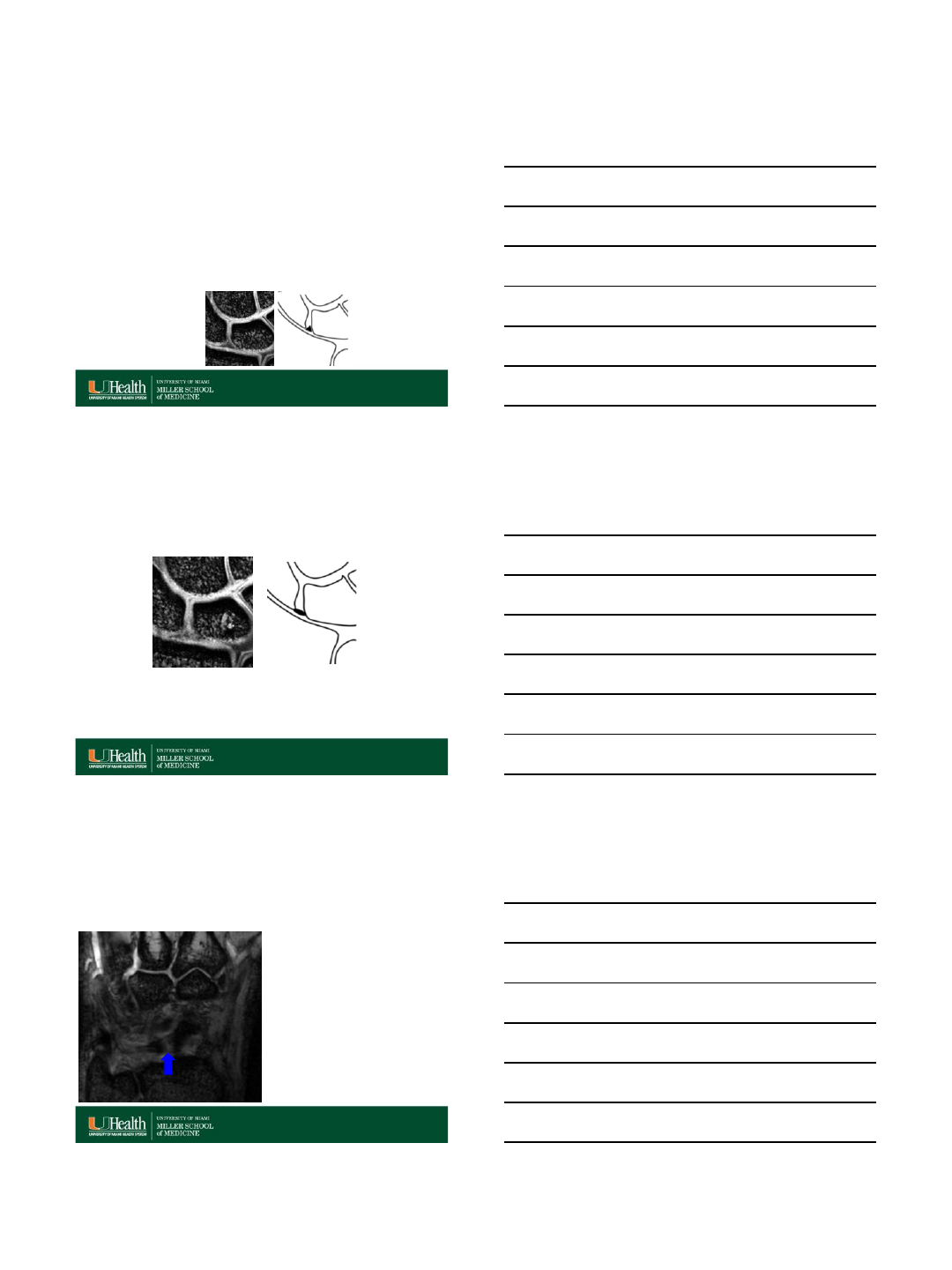
Lunotriquetral ligament (LT)
“Band-Like Configuration”
Dorsal and volar components axial images
–Axial: easiest to see dorsal and volar portions
–Coronal: easiest to see proximal portion
Skeletal Radiol (2014) 43:713–724
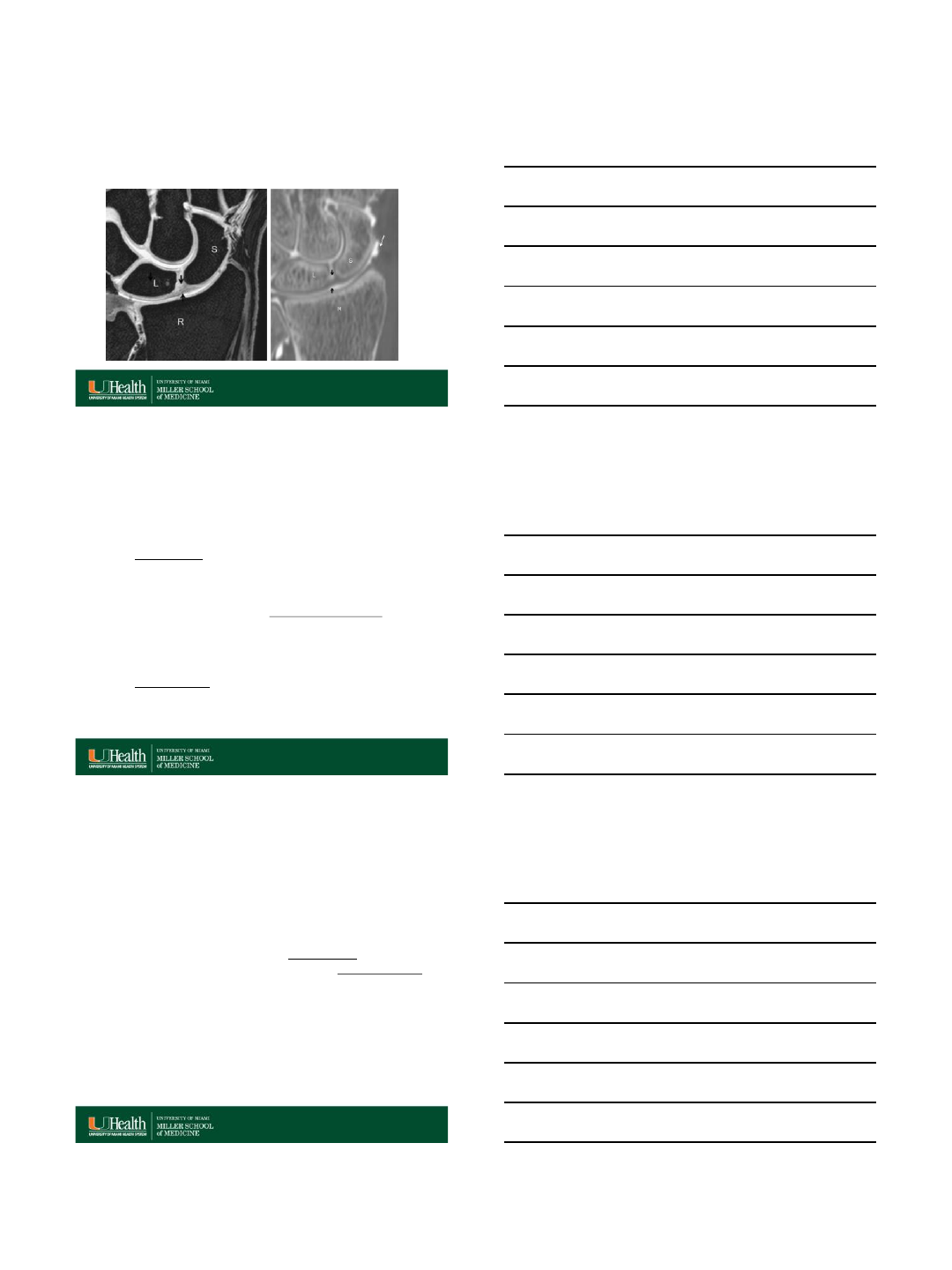
Shape Variations Membranous
Portion (proximal zone) of the LTL
•Most commonly triangular or deltoid
region (geometry) of low signal
intensity (85.6% of cases).
•An alternative conformation of the
ligament is a linear or bar-like
geometry, which may mimic a tear
owing to absence of its distal vertex.
•An indistinct or amorphous shape of
the ligament may be seen in
asymptomatic older patients;
probably the result of degenerative
change.
RadioGraphics 2011; 31:63–78
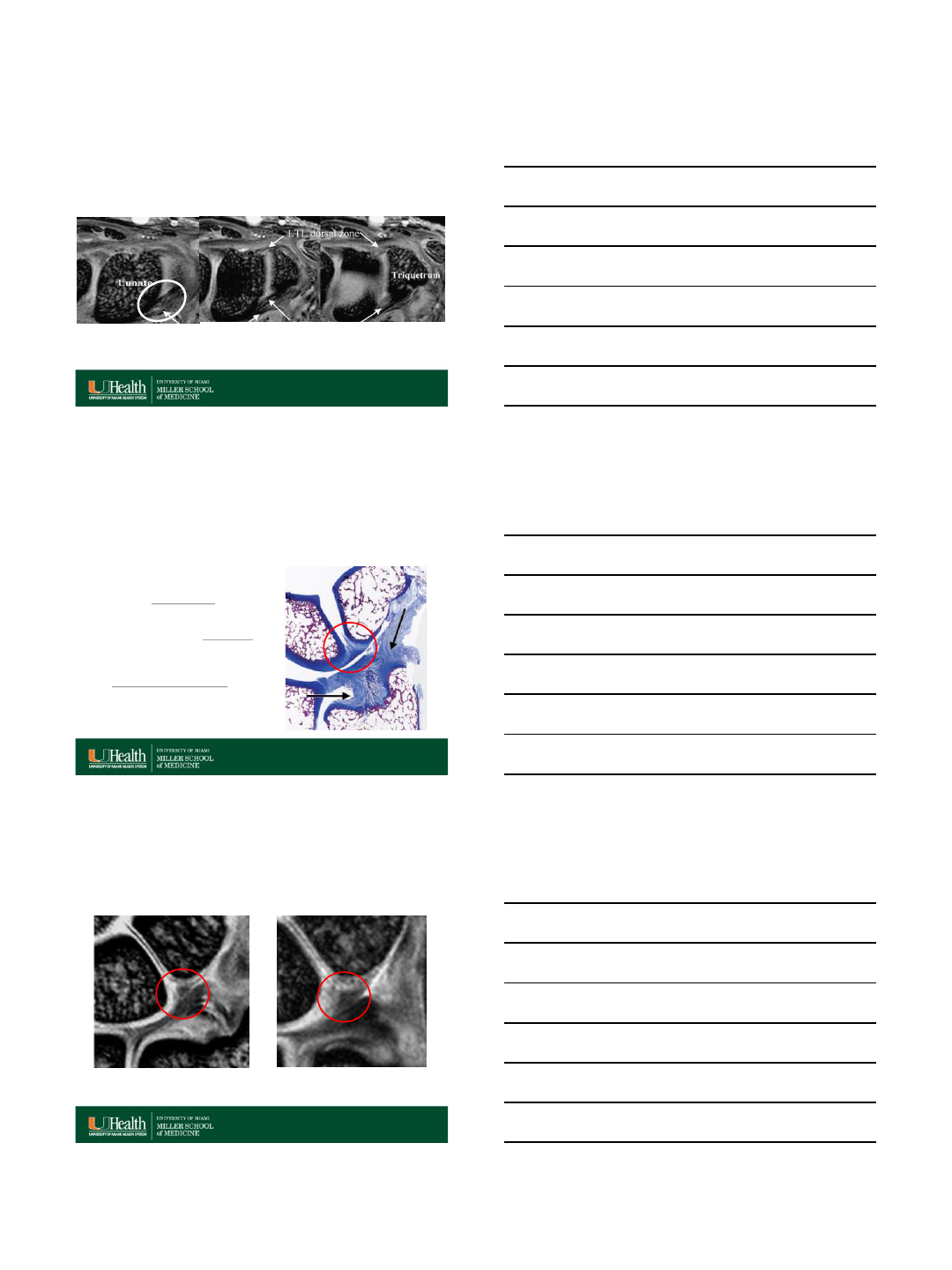
Variations in LTL shape
Triangular Morphology
RadioGraphics 2011; 31:63–78
Regular (equilateral triangle) (41.1%) Broad-based isosceles triangle (20.0%)
7/17/2015
14
RadioGraphics 2011; 31:63–78
Narrow-based isosceles triangle (6.7%)Asymmetric (scalene) triangle (17.8%)
Variations in LTL shape
Triangular Morphology
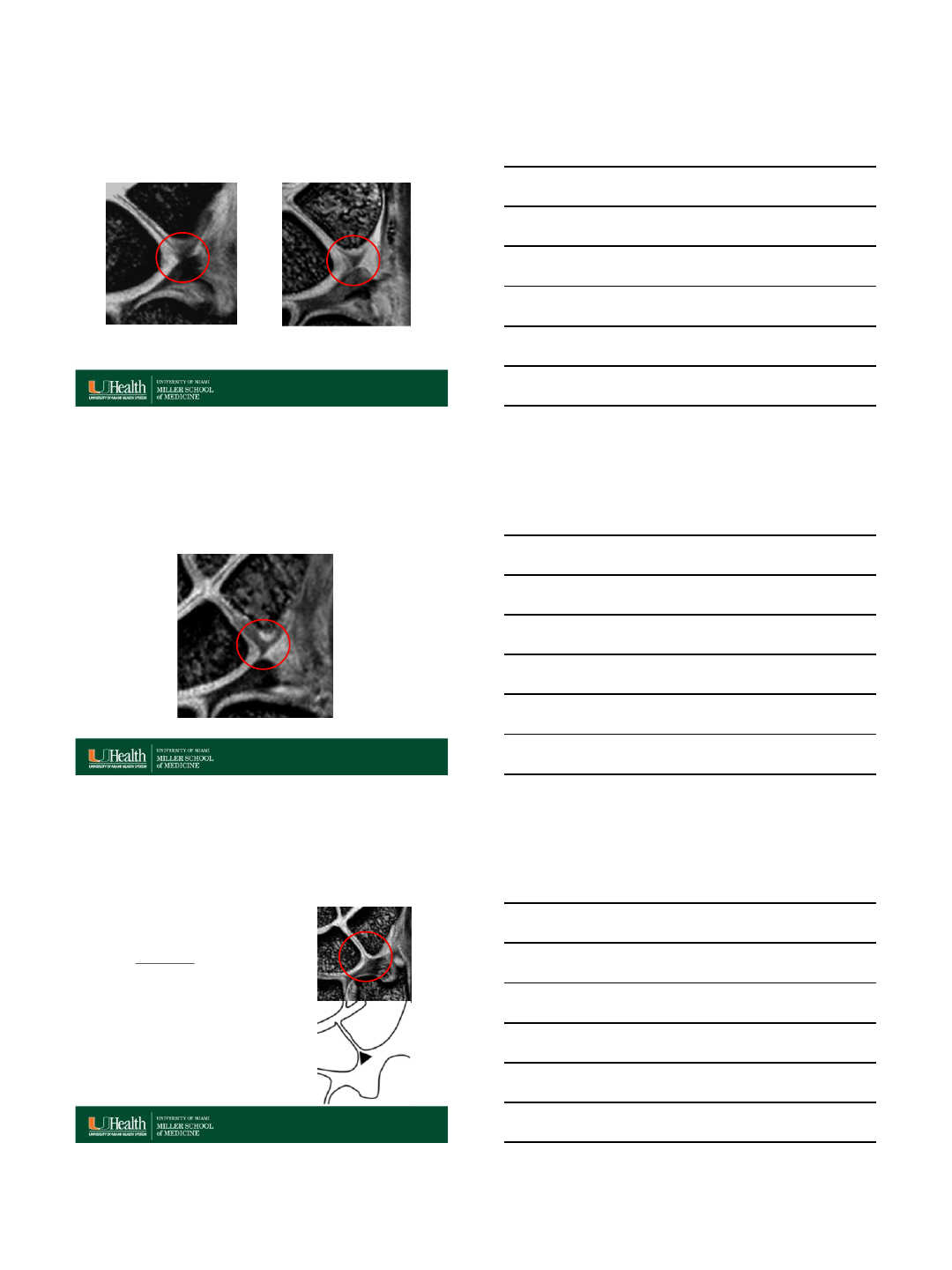
RadioGraphics 2011; 31:63–78
Variations in LTL shape
Linear or bar-like morphology
Signal Intensity
•Variation in the internal signal
intensity of the membranous portion,
categorized as follows:
–The type 1 variant: uniform low
internal signal intensity (33.8% of
patients).
RadioGraphics 2011; 31:63–78
7/17/2015
15
Signal Intensity
•Variation in the internal signal
intensity of the membranous portion,
categorized as follows:
–The type 1 variant: uniform low
internal signal intensity (33.8% of
patients).
–The type 2 variant: thin line of
increased signal intensity inside
the triangular body (45.5%).
RadioGraphics 2011; 31:63–78
Signal Intensity
•Variation in the internal signal
intensity of the membranous portion,
categorized as follows:
–The type 1 variant: uniform low
internal signal intensity (33.8% of
patients).
–The type 2 variant: thin line of
increased signal intensity inside
the triangular body (45.5%).
–The type 3 variant: linear
increased signal intensity through
the triangle and traversing both
the proximal (base) and distal
margins of the membranous
component (20.8%).
RadioGraphics 2011; 31:63–78
Shape and signal intensity changes in
the LTL with different wrist positions
•The shape and signal intensity of the membranous
portion of the LTL change when the wrist is positioned in
ulnar or radial deviation, as the ligament is very flexible.
•With the wrist in ulnar deviation, the triangular shape is
distorted and decreased in size in comparison to the
appearance with the wrist in the neutral position.
•With the wrist in radial deviation, the triangular body
becomes wider and higher in internal signal intensity in
comparison to the appearance with the wrist in the
neutral position.
RadioGraphics 2011; 31:63–78
7/17/2015
16
Shape and Signal Intensity LTL Changes in Ulnar
and Radial Deviation
RadioGraphics 2011; 31:63–78 •
Ulnar deviation Neutral Radial deviation
MRI SL and LT Tear Findings
•Tears of the LTL and SLL are
diagnosed on the basis of MR
imaging findings of:
1. Irregular morphology,
2. Abnormal signal intensity,
3. Fluid (contrast) partially or completely
transecting the ligamentous
structures.
RadioGraphics 2011; 31:63–78
SLL disruption
•While complete disruption with static instability may
be identified on plain radiographs, less severe
injuries may pose a diagnostic dilemma.
•Different imaging modalities such as arthrography,
ultrasound, computed tomography (CT)
arthrography, and magnetic resonance imaging
(MRI) with or without MR arthrography have been
proposed for the detection of SLD.
•MRI is the imaging of choice of detection of SL
ligament tear.
•Arthroscopy remains the diagnostic gold standard.
Skeletal Radiol (2015) 44:1103–1110
7/17/2015
17
Interosseous Ligament Tears
•Tears of SLIL and LTL may occur
following acute trauma, such as a
fall on the outstretched hand,
from repetitive stress,
inflammatory disease, or
degeneration.
•Categorized as:
–Complete Tear: All portions are
disrupted.
–Full Thickness Tear: Focally
extends through the entire
thickness of the ligament.
–Partial Thickness Tear: Involves
a portion of the thickness of the
ligament.
Skeletal Radiol (2014) 43:713–724
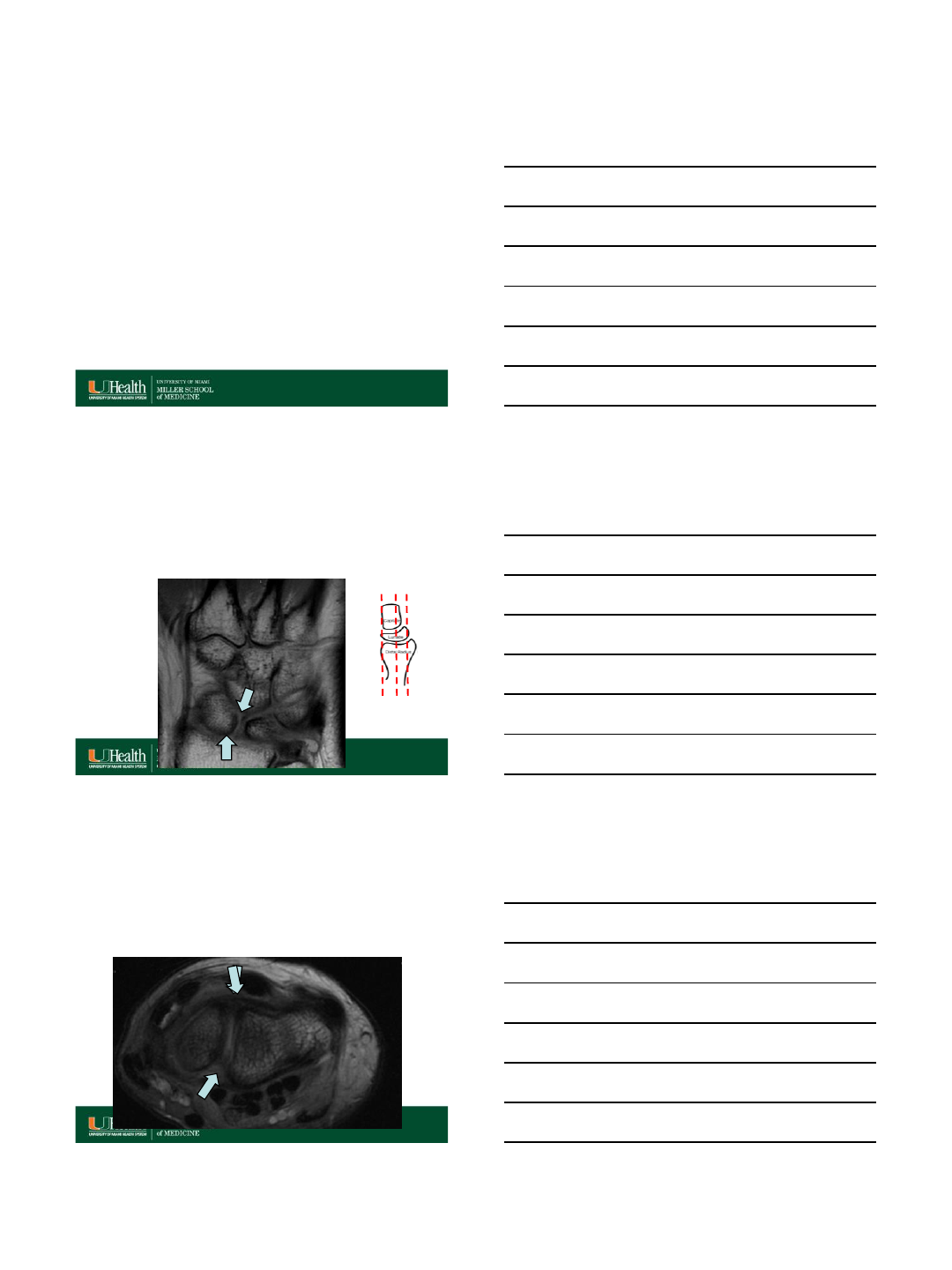
Tear of the scapholunate ligament with
carpal stability maintained
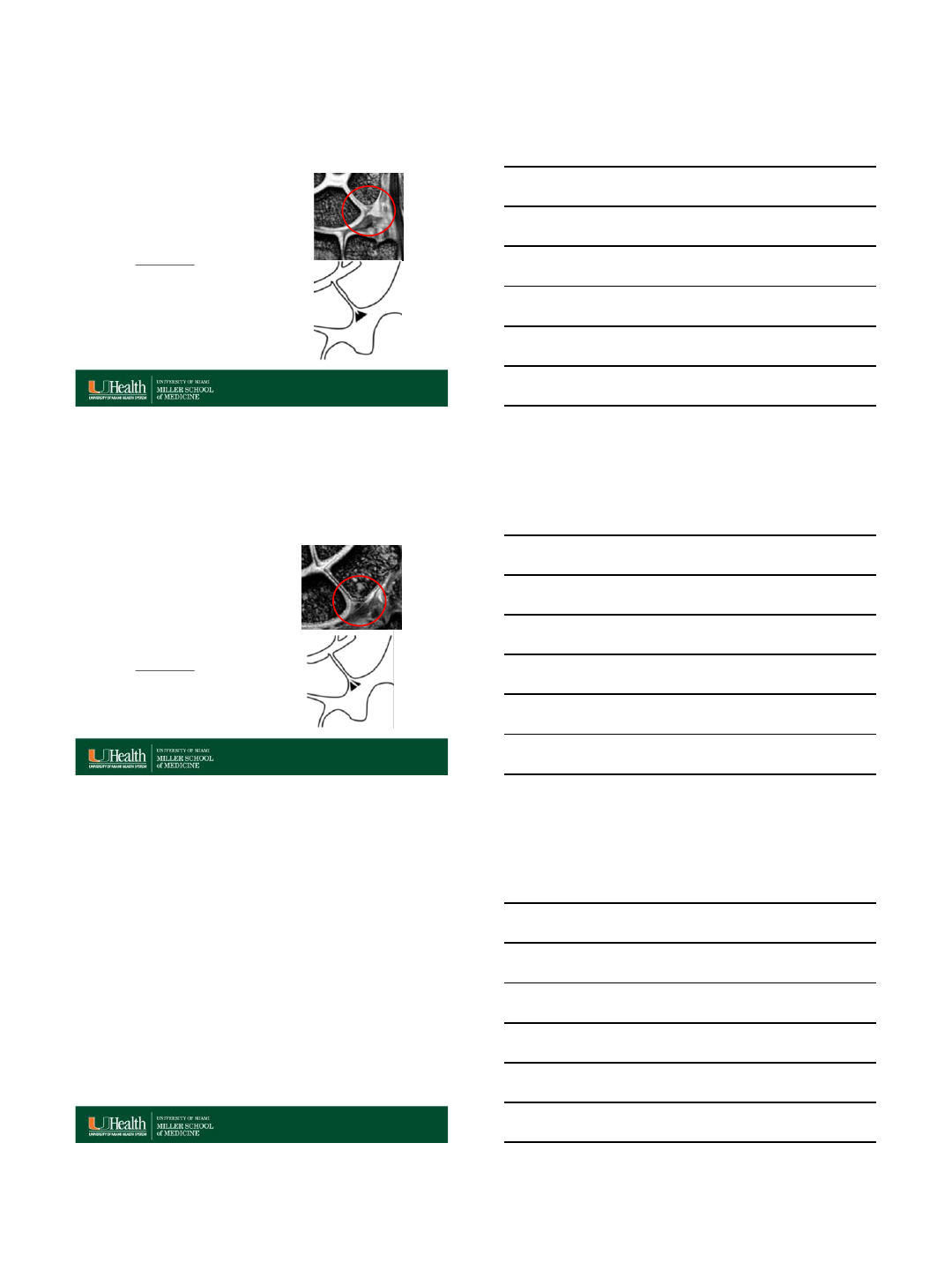
RadioGraphics 1995: 15:575-587
Interval normal (< 3 mm) SL and CL angles are normal
(SL < 60°, CL < 30°) RSC, RLT , SRL ligaments are normal
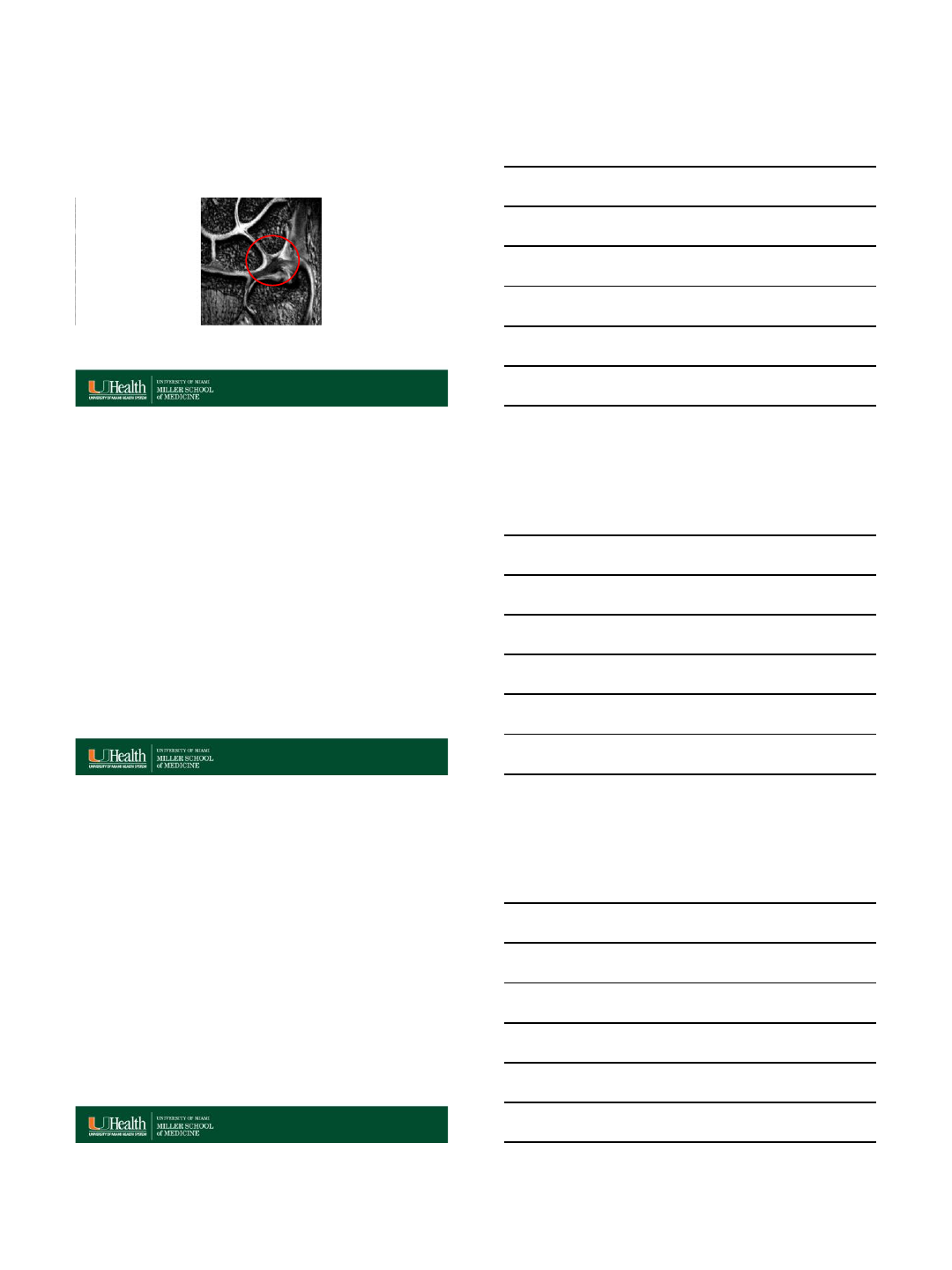
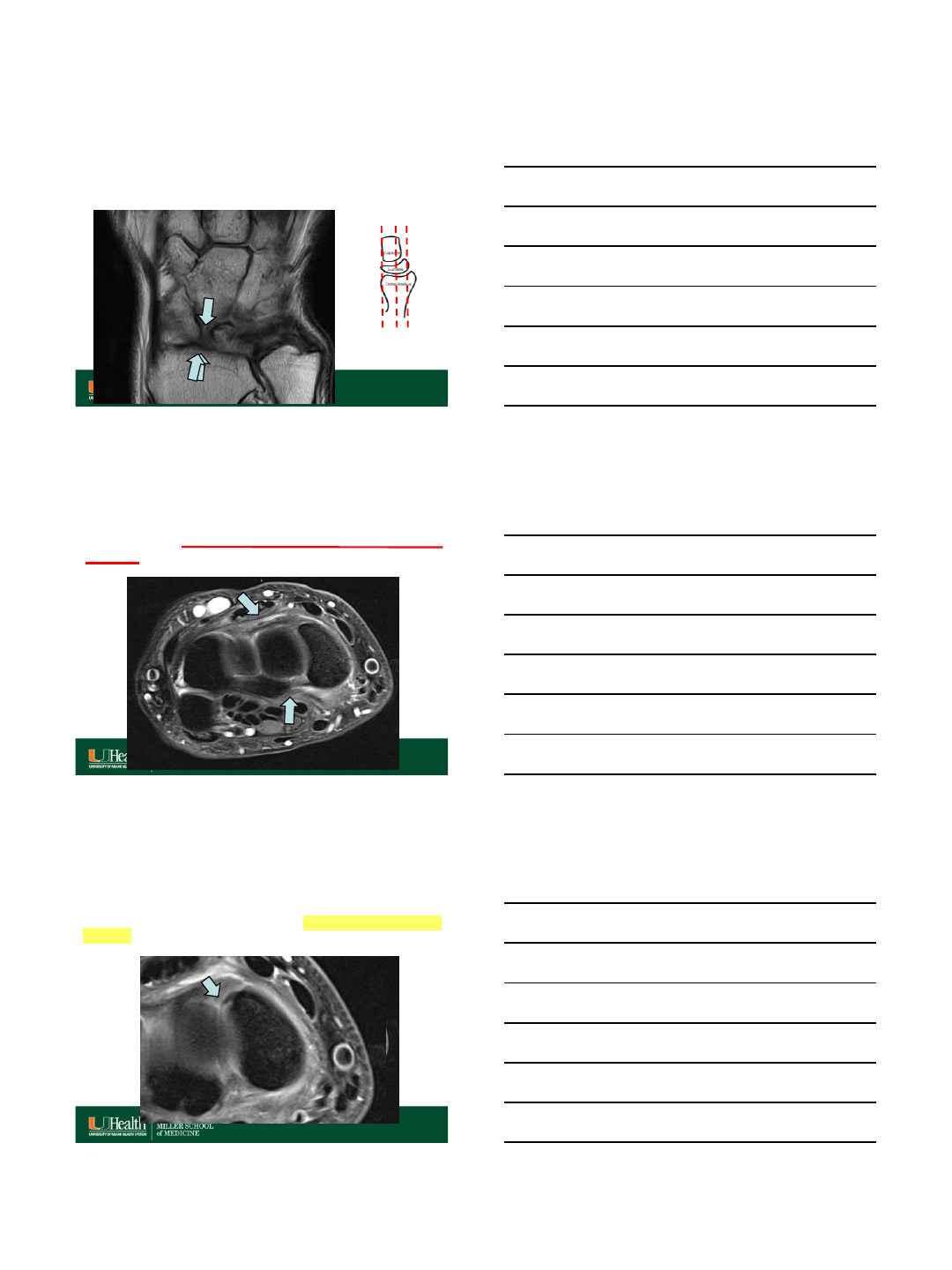
Tear of the scapholunate ligament
with carpal instability (DISI)
RadioGraphics 1995: 15:575-587
Interval diastasis > 3 mm SL and CL angles are increased
(SL > 60°, CL > 30°).
7/17/2015
18
Caution
•Normal lunate appears more dorsally tilted on sagittal MR images
than on lateral radiographs, due to wrist positioning in coil. This is
particularly exacerbated when the wrist is in ulnar deviation or in
pronated position.
MRI of the Upper Extremity: Shoulder, Elbow, Wrist and
Hand. Christine B. Chung, Lynne S. Steinbach -
Wolters Kluwer Health 2009
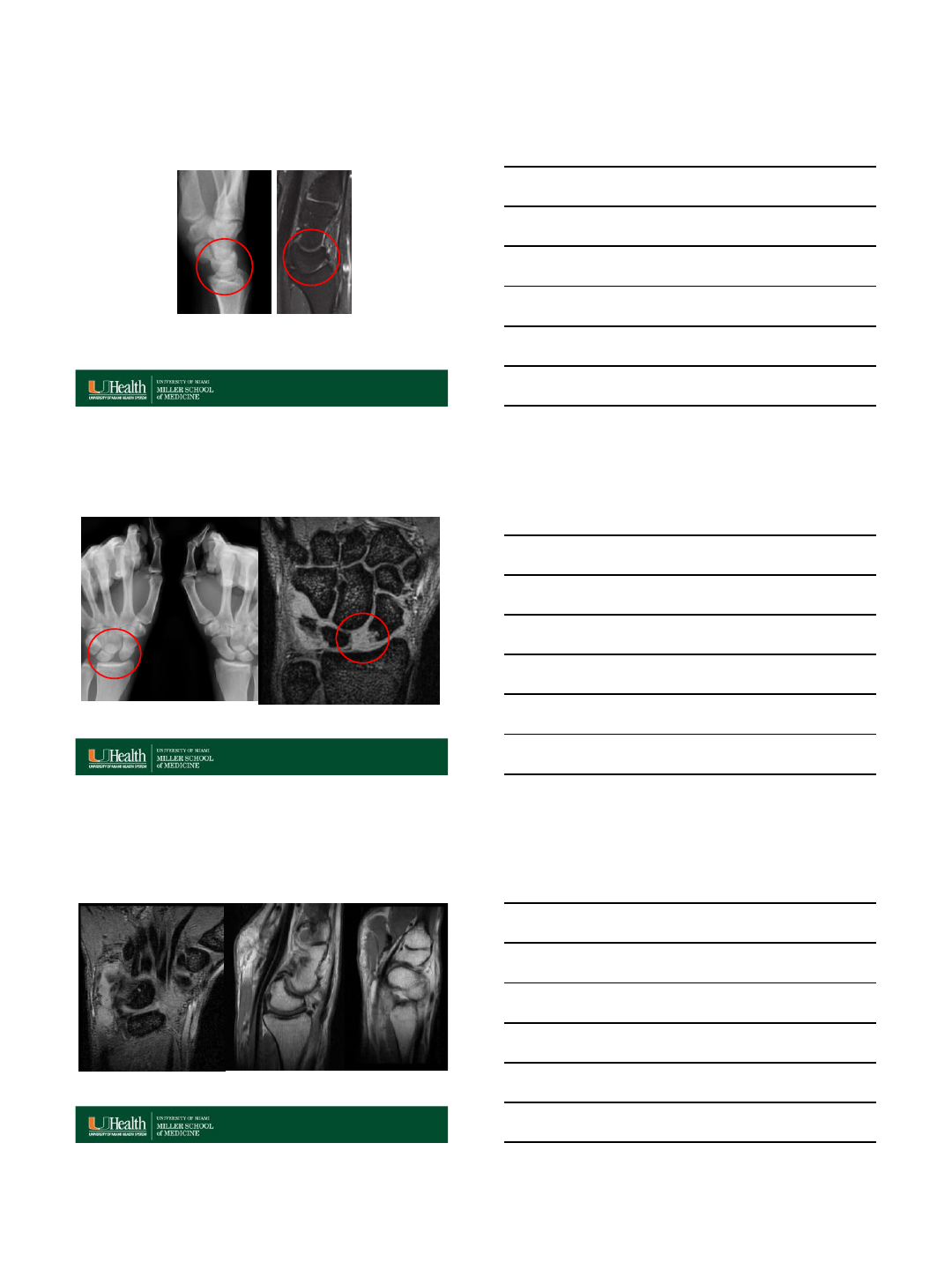
Interval diastasis > 3 mm
Interval diastasis > 3 mm SL and CL angles
are increased (SL >
60°, CL > 30°)
RSC, RLT , SRL
ligaments are
abnormal
7/17/2015
19
MRI vs MRA for SL tear
•Non contrast MRI.
–Sensitivity (41-71 %)
–Specificity (60-100%)
–Accuracy (53-100%)
–Even with the 3.0-T field strength, differentiation between partial and complete
dorsal lesions remains difficult.
•MRA allows better evaluation of the SL ligament.
–Higher sensitivity (50–89 %),
–Higher specificity (52–100 %)
–Higher accuracy (60–98 %)
•Axial and coronal views are necessary for thorough evaluation of the
C-shaped fibers’ continuity.
•In general, the accuracy of diagnosing tears in the volar and dorsal
fibers is similar to those of the membranous fibers.
Skeletal Radiol (2014) 43:725–743
J Wrist Surg. 2013 Feb; 2(1): 69–72
Accuracy of LT tears MRI
•Accuracy of nonarthrographic MR imaging in diagnosing
tears of the LTL in clinical studies has also been widely
variable and suboptimal,
–Reported sensitivities of 40%–75%
–specificities of 64%–100% when arthroscopy was used as the
standard of reference.
•Direct MR arthrography appears to be more sensitive in
detection of LT lesions
–sensitivities of 86%–92%) but is not necessarily more specific
–(specificities of 46%–100%).
RadioGraphics 2011; 31:63–78
SL Ligament tear MRA
Skeletal Radiol (2014) 43:725–743
Full-thickness tear (arrows) of membranous and volar component of scapholunate
ligament, with by abnormal communication between the radiocarpal and mid-carpal
compartments.
Dorsal SL component is intact.
7/17/2015
20
UM Institutional Review
• We retrospective reviewed MRI’s of SL
tears and correlated with arthroscopy
findings.
•We identified several mistakes in MRI
interpretations.
Retrospective Mistake #1
Original Dictation: Full thickness tear of the dorsal portion
based on the coronal sequence
Tear??
volar dorsal
Retrospective Mistake #1
Original Dictation: full thickness tear of the dorsal portion
based on the coronal sequence
False Positive: No evidence of SLIL tear!!!
7/17/2015
21
Retrospective Mistakes # 2
Original Dictation: Full thickness tear of the volar and
proximal ligament
volar dorsal
?
Retrospective Mistake # 2
Original Dictation: full thickness tear of the volar and proximal
ligament
False Negative: Full thickness tear of the volar and proximal
ligament Complete tear of the SLIL
Operative Report…
“…the dorsal portion of the scapholunate ligament was
intact to its scaphoid attachment, but not to the lunate
side…”
LS
7/17/2015
22
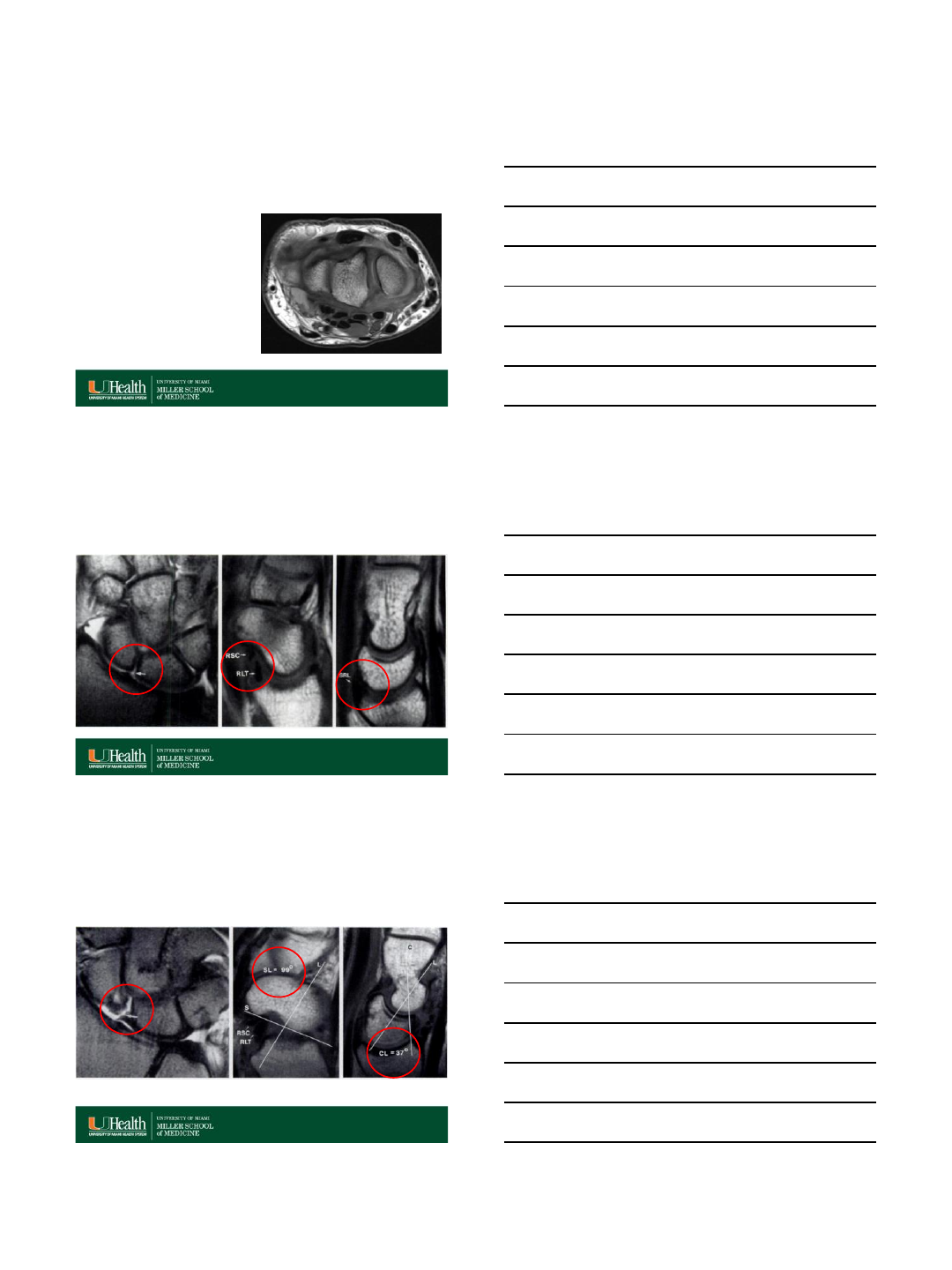
Lunotriquetral ligament tear with
carpal instability (VISI)
RadioGraphics 1995: 15:575-587
The SL angle is decreased (SL < 30°) and the CL angle is increased (> 30°).
The dorsal radiocarpal ligament is also injured in VISI.
MRA and CT Arthrogram (CTA)
In certain cases, CTA may increase sensitivity, specificity and accuracy compared with MRA.
Skeletal Radiol (2013) 42:649–657
Normal CTA- Intact LT, SLL, TFCC Abnormal CTA- Torn LT and TFCC
MRA of same patient showing torn LT and TFCC
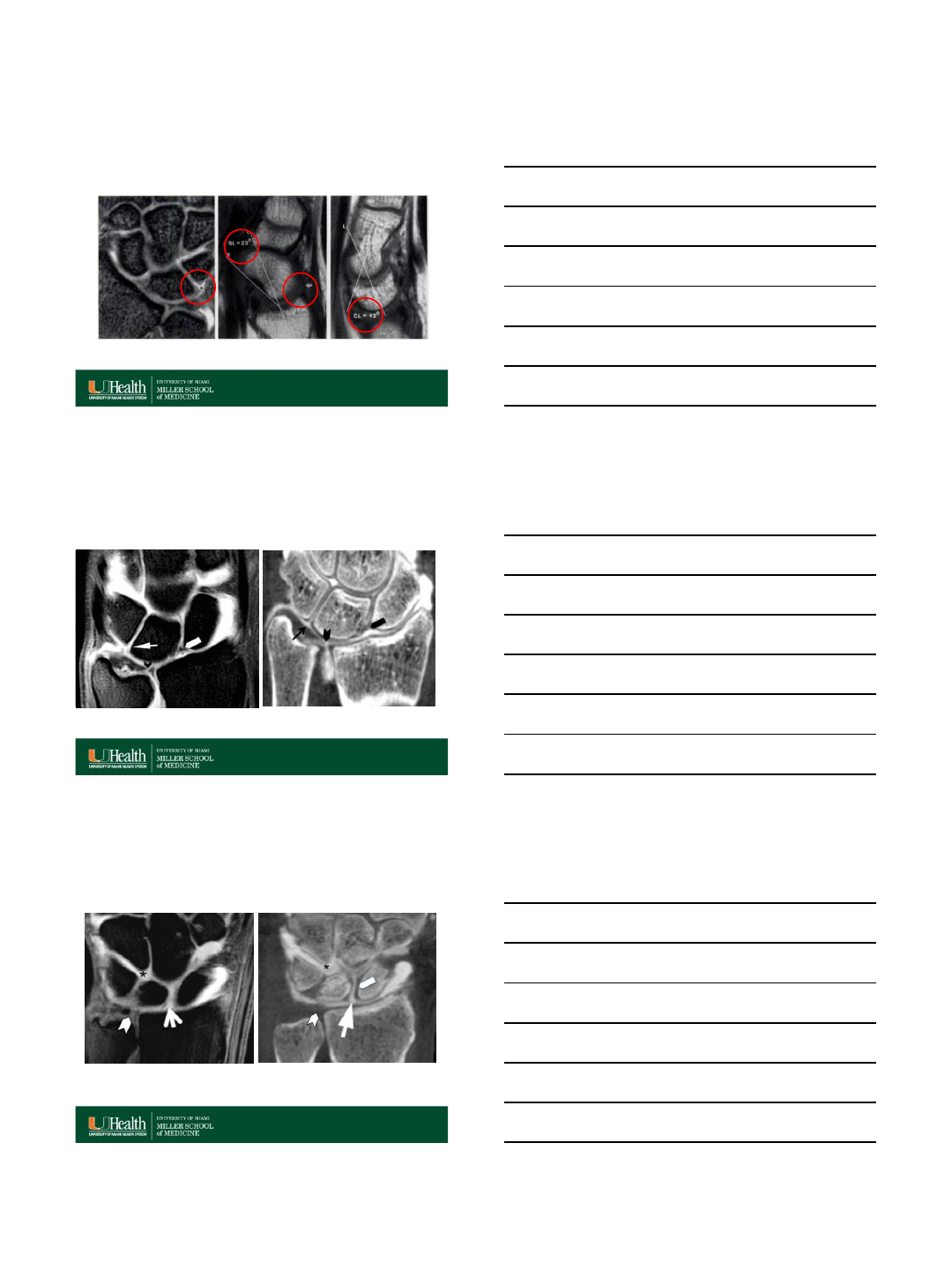
MRA and CTA
Coronal
Skeletal Radiol (2013) 42:649–657
SL membranous component tear, with intact LT and TFCC.
Contrast extends into midcarpal space (asterisk) through SL tear.
7/17/2015
23
MRA and CTA
Coronal
Skeletal Radiol (2013) 42:649–657
SL dorsal and membranous component tear, with
intact volar component.
SLL tear MRA vs CTA
False Positive
Skeletal Radiol (2013) 42:1277–1285
Both CT and MR arthrography have a very high degree of accuracy for diagnosing
tears of the SLL and LTL, with both being more accurate than conventional MR
imaging.
Axial MRA - suspicious tear dorsal SLL Axial CTA- normal dorsal SLL
Skeletal Radiol (2013) 42:1277–1285
Occasionally, CTA will confirm ligament tears not appreciable with MRA
SLL tear MRA vs CTA
False Positive
7/17/2015
24
Skeletal Radiol (2013) 42:1277–1285
LTL tear MRI vs CTA
False negative
Occasionally, CTA will confirm ligament tears not appreciable with MRA
MRA vs CTA Post-Op
Skeletal Radiol (2013) 42:649–657
Scaphoid cartilage defect (arrow) is better delineated on the coronal CT-image
due to fewer metal artifacts. SL, LT and TFCC are intact.
Conclusion
•Intrinsic and extrinsic ligament defects may be small and
insignificant, or lesions that cause significant instability,
pain, and chronic disability.
•MRI, US and CT are all useful in the assessment of wrist
ligament tears, allowing sensitive detection and detailed
assessment, but the examination must be tailored based
on clinical considerations.
•Knowledge of the anatomy, dynamic function, and
instability patterns is central to evaluating these lesions.
•Accurate assessment of these injuries is important for
promptly determining the best conservative or surgical
approach to the injured patient.
http://radsource.us/sll-tear-and-disi-deformity/
7/17/2015
25
Questions and Answers
Section
•Cine MRI is an imaging technique that
allows acquisition of continuous MR
images with high spatial and temporal
resolution.
•May be useful in detecting dynamic
instability.
Skeletal Radiol (2015) 44:1103–1110
Cine MRI in diagnosis
of scapholunate dissociation
Skeletal Radiol (2015) 44:1103–1110
Cine MRI
Normal Volunteer
Normal SL interval
Neutral Radial Deviation Ulnar Deviation Clenched Fist
7/17/2015
26
Skeletal Radiol (2015) 44:1103–1110
Cine MRI Scapholunate dissociation
Increase SL interval with Ulnar Deviation and Clenched Fist
Neutral Radial Deviation Ulnar Deviation Clenched Fist
Sensitivity of US
•Visibility of the SLL and LTL at US varies depending on the equipment and
the operator’s experience
•Complete visibility of the dorsal band of the SLL in 48-97% and partial
visibility in 3-30% of wrists, and complete visibility of the volar band of the
SLL in 7-81% and partial visibility in 9-12% of those same wrists.
•Complete visibility of the dorsal band of the LTL in 61% and partial visibility
in 39% of normal wrists, and complete visibility of the volar band in 33% and
partial visibility in 7% of normal wrists.
•The reported sensitivity of US in depicting lesions of the dorsal band of the
SLL varies from 46% to 100%, while specificity varies from 92% to 100%.
•The results are less promising for LTL lesions, with sensitivity varying from
25% to 50% and specificity from 90% to 100%.
•Sonoarthrography in the presence of radiocarpal joint effusion improves the
visibility.
RadioGraphics 2011 31:1, 79-80
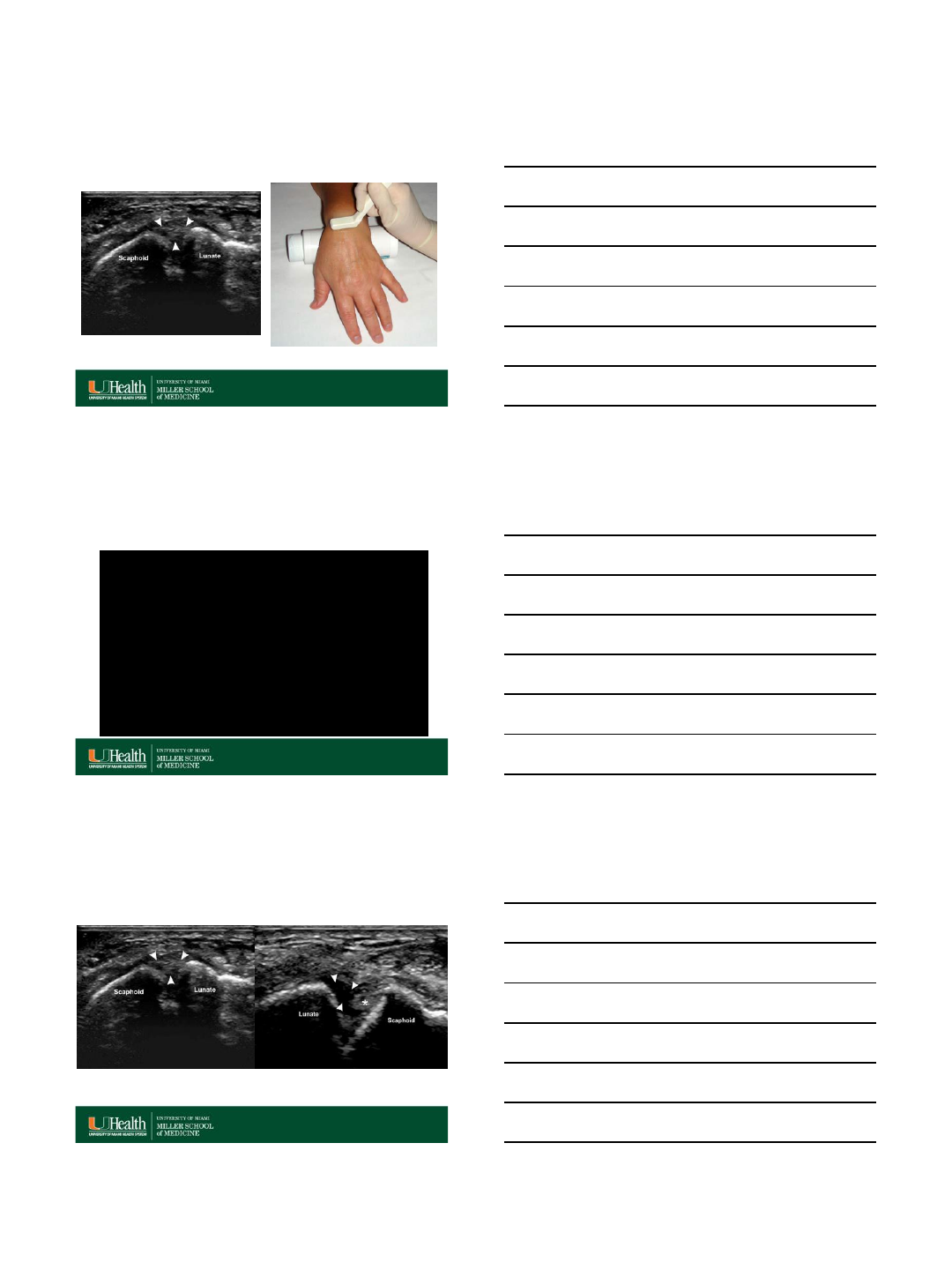
SL Ligament Ultrasound
•The SLL and LTL are considered
normal if they are seen as echogenic,
frequently fibrillar bands in their
expected anatomic locations.
•Partially torn ligaments show some
irregularity of the fibers.
•The ligaments are considered torn if
their fibers are not seen in the
expected anatomic locations between
the scaphoid and lunate or between
the lunate and triquetrum, or if
discontinuity of their fibers is seen.
•If a joint effusion is present or
sonoarthrography is performed, fluid
can be seen in the regions of torn
ligaments.
Skeletal Radiol (2014) 43:713–724
7/17/2015
27
RadioGraphics 2011 31:1, 79-80
SL Ligament Ultrasound
US of the dorsal band of the scapholunate ligament with
the wrist in pronation and slight flexion.
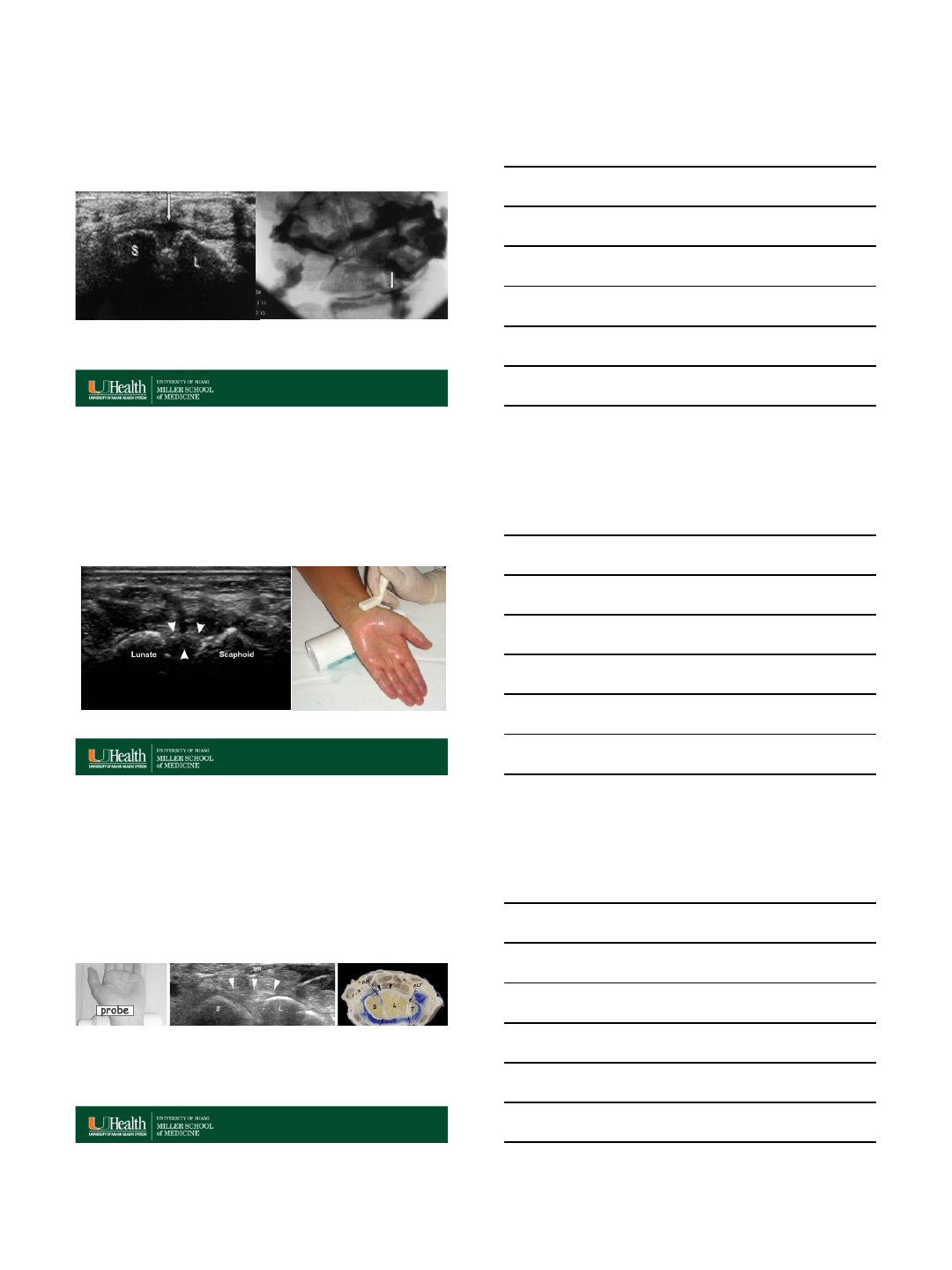
RadioGraphics 2011 31:1, 79-80
RadioGraphics 2011 31:1, 79-80
SL Ligament Ultrasound
Normal SL tear
7/17/2015
28
Scapholunate ligament tear
Skeletal Radiol (2004) 33:85–90
Arthrogram with contrast injected into the
midcarpal joint space confirms SL tear, with
contrast appearing in the radiocarpal joint space
(arrow)
SL tear
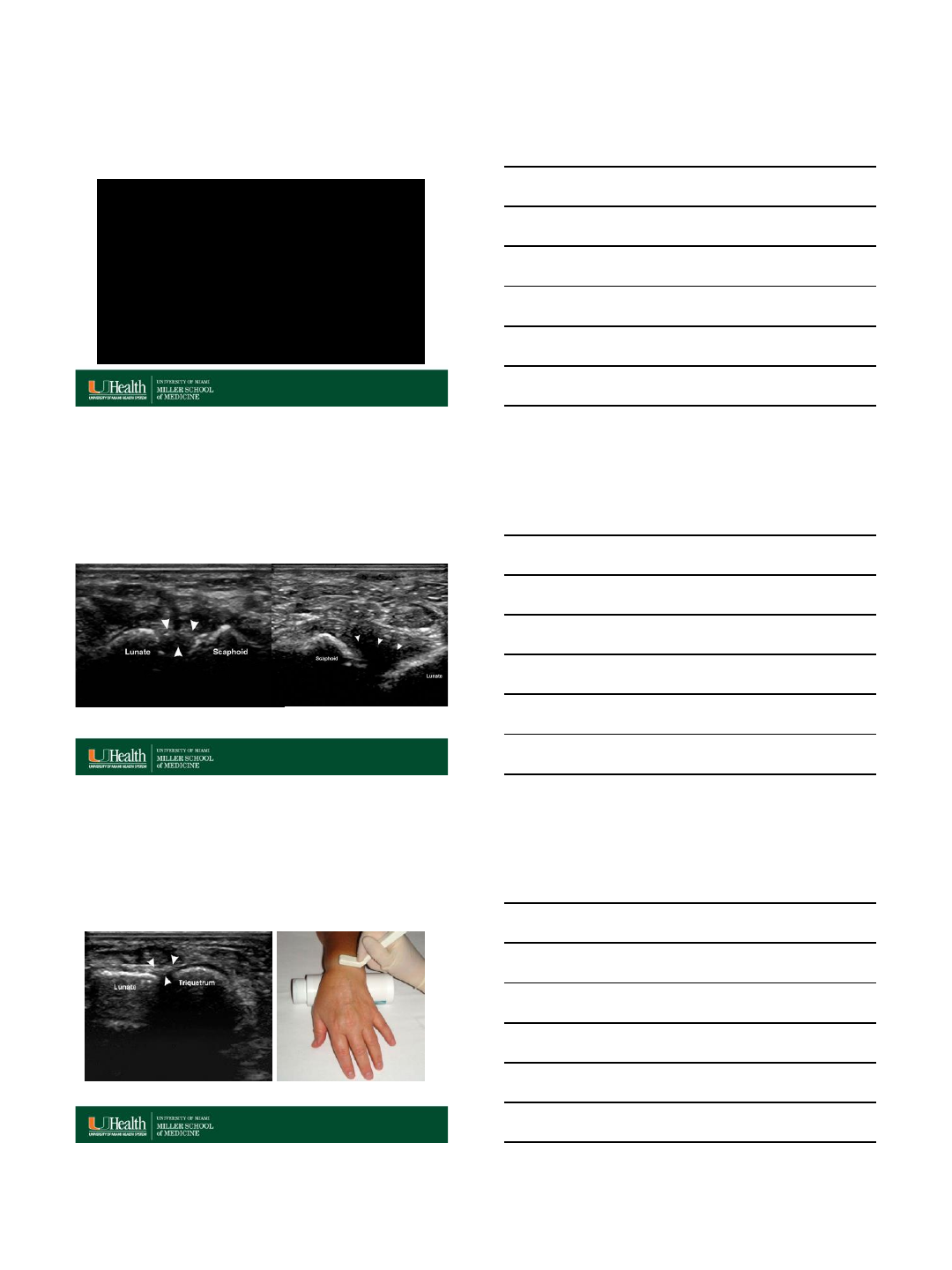
Volar band of the scapholunate
ligament
RadioGraphics 2011 31:1, 79-80
Normal
Skeletal Radiol (2005) 34: 513–521
Volar band of the scapholunate
ligament
7/17/2015
29
US of the volar band of the scapholunate ligament
with the wrist in supination and slight extension.
RadioGraphics 2011 31:1, 79-80
RadioGraphics 2011 31:1, 79-80
Volar band of the scapholunate
ligament
Normal SL tear
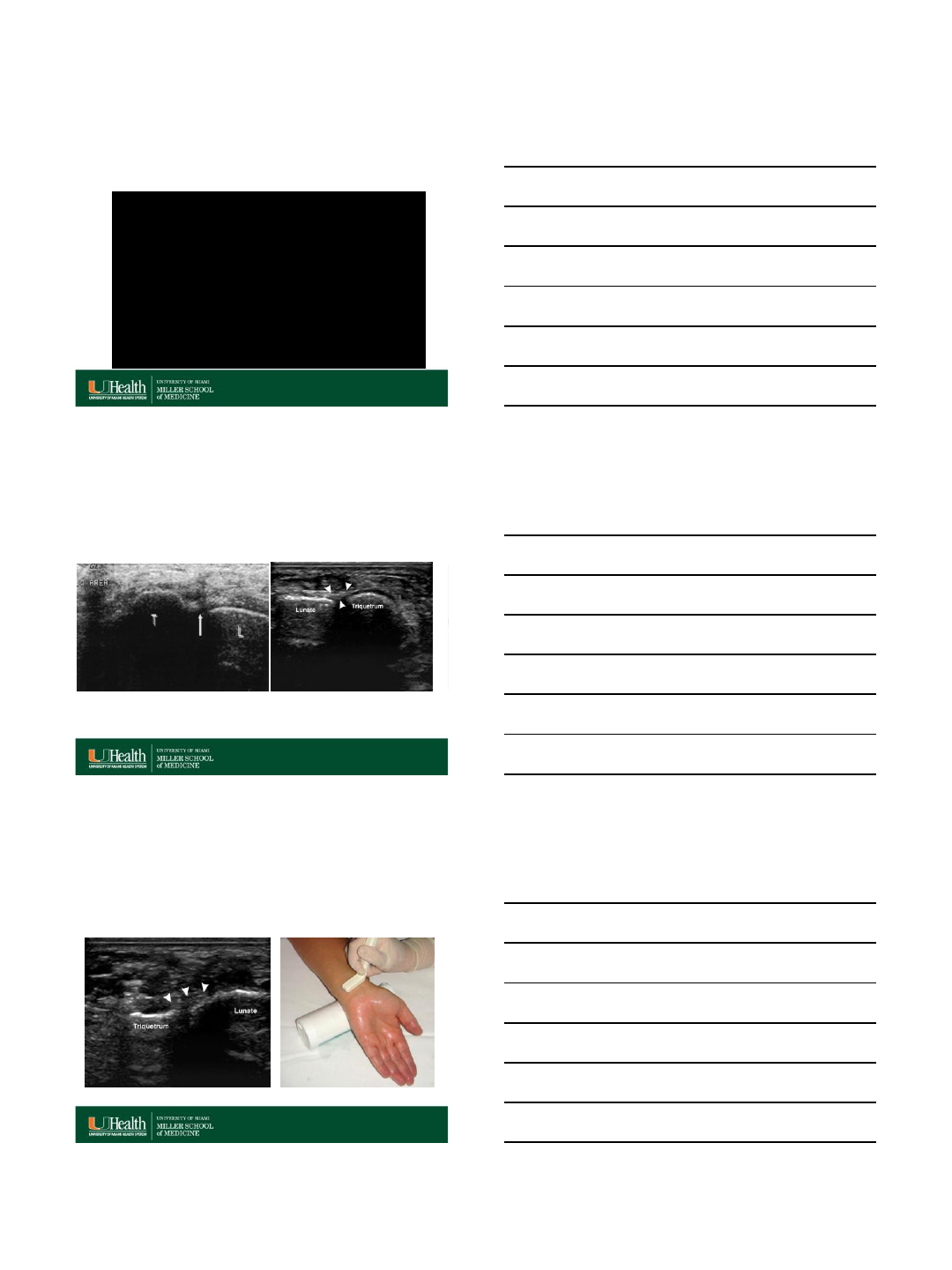
RadioGraphics 2011 31:1, 79-80
US Dorsal band of the
lunotriquetral ligament
7/17/2015
30
US of the dorsal band of the lunotriquetral ligament
with the wrist in pronation and slight flexion.
RadioGraphics 2011 31:1, 79-80
Lunotriquetral ligament tear
Skeletal Radiol (2004) 33:85–90
Midcarpal joint injection demonstrating
contrast in the radiocarpal joint at the
level of a lunatotriquetral tear (arrow)
NormalTear
RadioGraphics 2011 31:1, 79-80
US Volar band of the
lunotriquetral ligament
7/17/2015
31
US of the volar band of the lunotriquetral ligament
with the wrist in supination and slight extension.
RadioGraphics 2011 31:1, 79-80
Thank You
7/16/2015
1
Intercarpal Injuries
VuMedi Webinar
Robert RL Gray
July 27, 2015
Disclosures
•Reviewer, Injury
•Committee Member, ASSH Clinical Outcomes
Committee and Flatt Fellows Conference
Committee
•Speakers Bureau, Skeletal Dynamics
•Employee, NorthShore University HealthSystem
Mayo Classification of Carpal
Instability
•CID (Carpal Instability
Dissociative)
•CIND (Carpal
Instability
Nondissociative)
•CIC (Carpal Instability
Combined/Complex)
•CIA (Carpal Instability
Adaptive)
•CIND—Nearly 100%
overlap w Diagnosis of
Midcarpal Instability
•Implies extrinsic
Ligament
Derangement
•Think Ligamentous
Laxity
CID—Most Common
Proximal and Distal
Carpal Row Variants
Implies Ligament
Disruption or
Scaphoid Fracture
CIC—A Little from
Column A, A Little
from Column B
Perilunate injries,
Tire explosions
CIA—Adaptive
Changes secondary to
Distal Radius
Malalignment
Fracture Malunion
Madelung’s
Deformity
7/16/2015
2
Ganglionectomy
•Open
•Arthroscopic
•US-guided aspiration/injection
Recurrence rate 5-13%
7/16/2015
3
SL treatment
•Non-op
•Non-op
•Non-op
•Direct repair (book only)
•Capsulodesis
•Tenodesis (Brunelli or variant)
•SL reassociation (RASL, SLAM)
•Intercarpal fusion (STT, SC, SL)
Moran, S.L., Ford, K.S., Wulf, C.A., and Cooney,
W.P. Outcomes of dorsal capsulodesis and
tenodesis for the treatment of scapholunate
instability. J Hand Surg. 2006; 31A: 1438–1446
91% of contralateral grip strength
7/16/2015
4
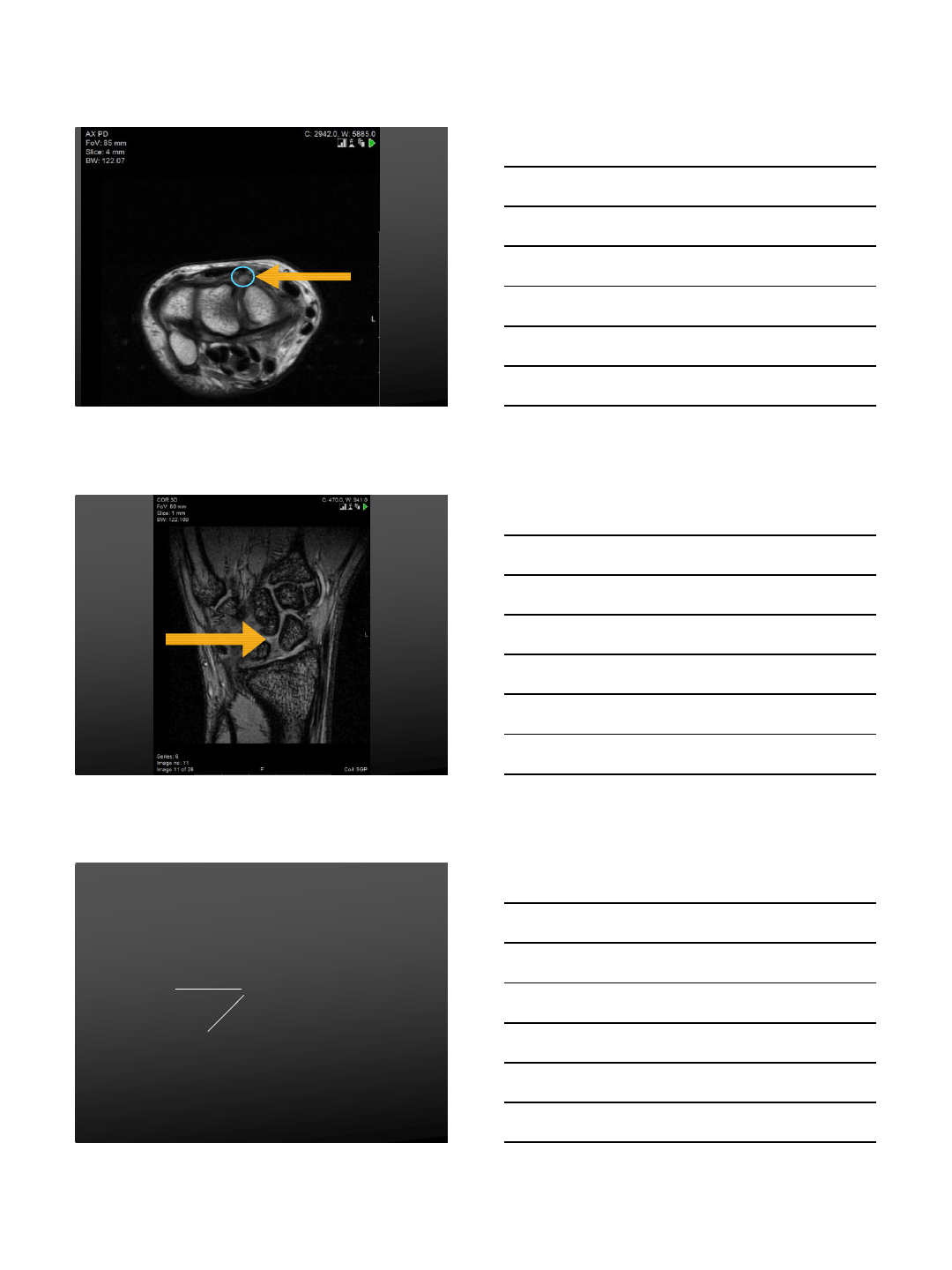
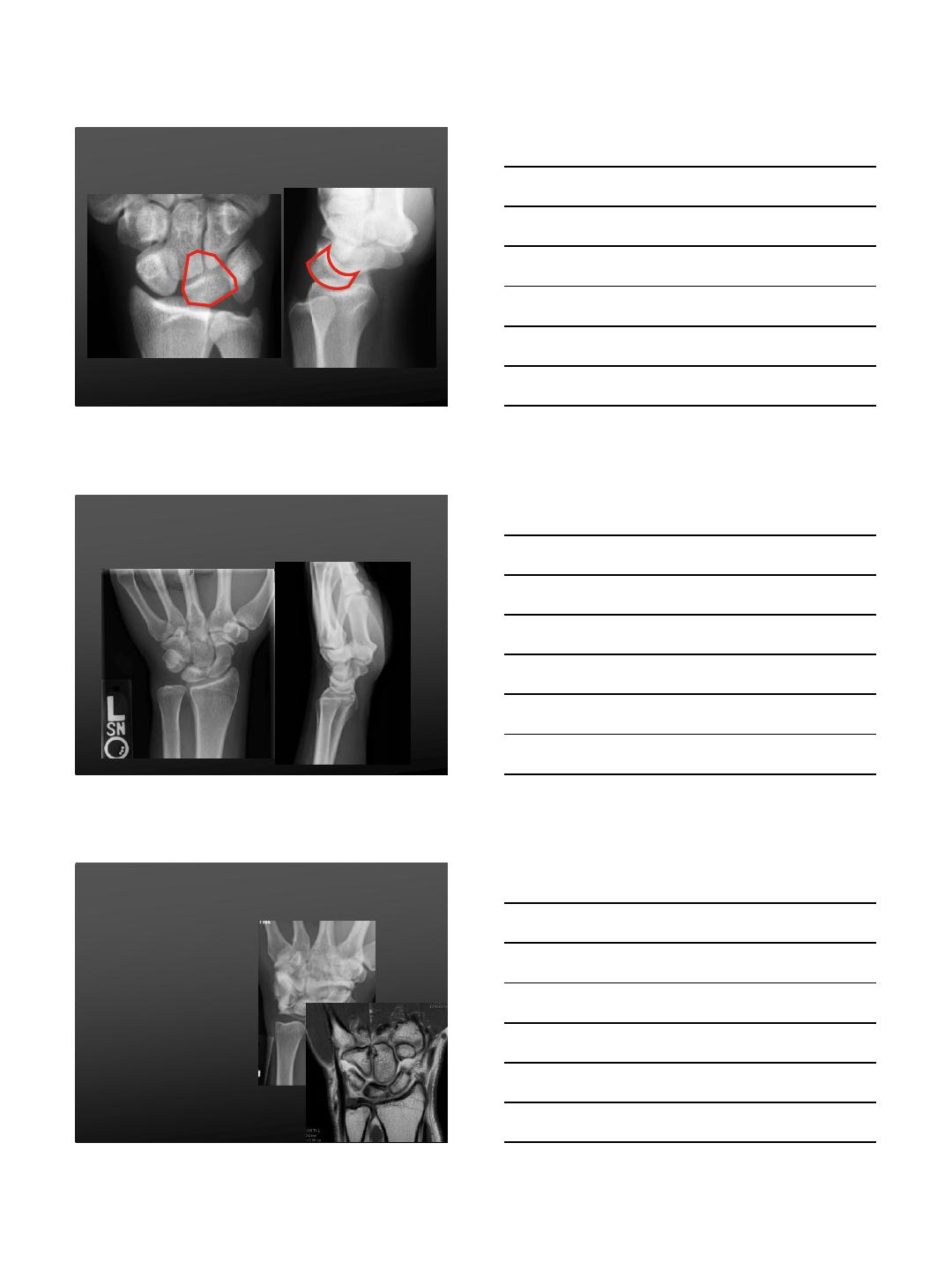
Lunotriquetral Ligament
Tear
Images from Alexander Y Shin M.D.
Lunotriquetral Ligament
Tear
Lunotriquetral Ligament
Tear
MRI:
Sensitivity 30-50%
Specificity: 94-97%
MR Arthrography:
Sensitivity 50-60%
Specificity 94-97%
Moser T, Dosch JC, et al. Musk Imag 2007
7/16/2015
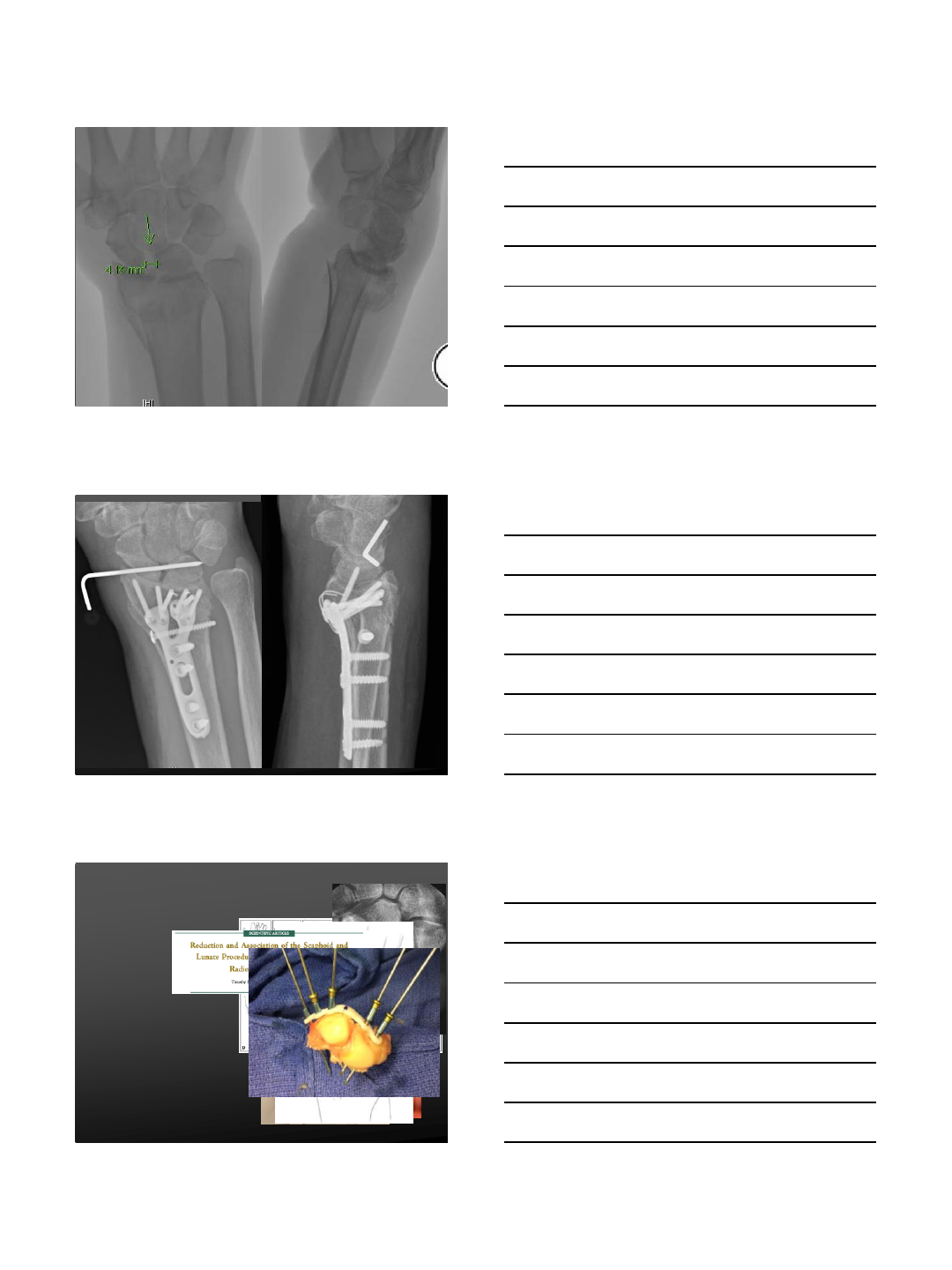
5
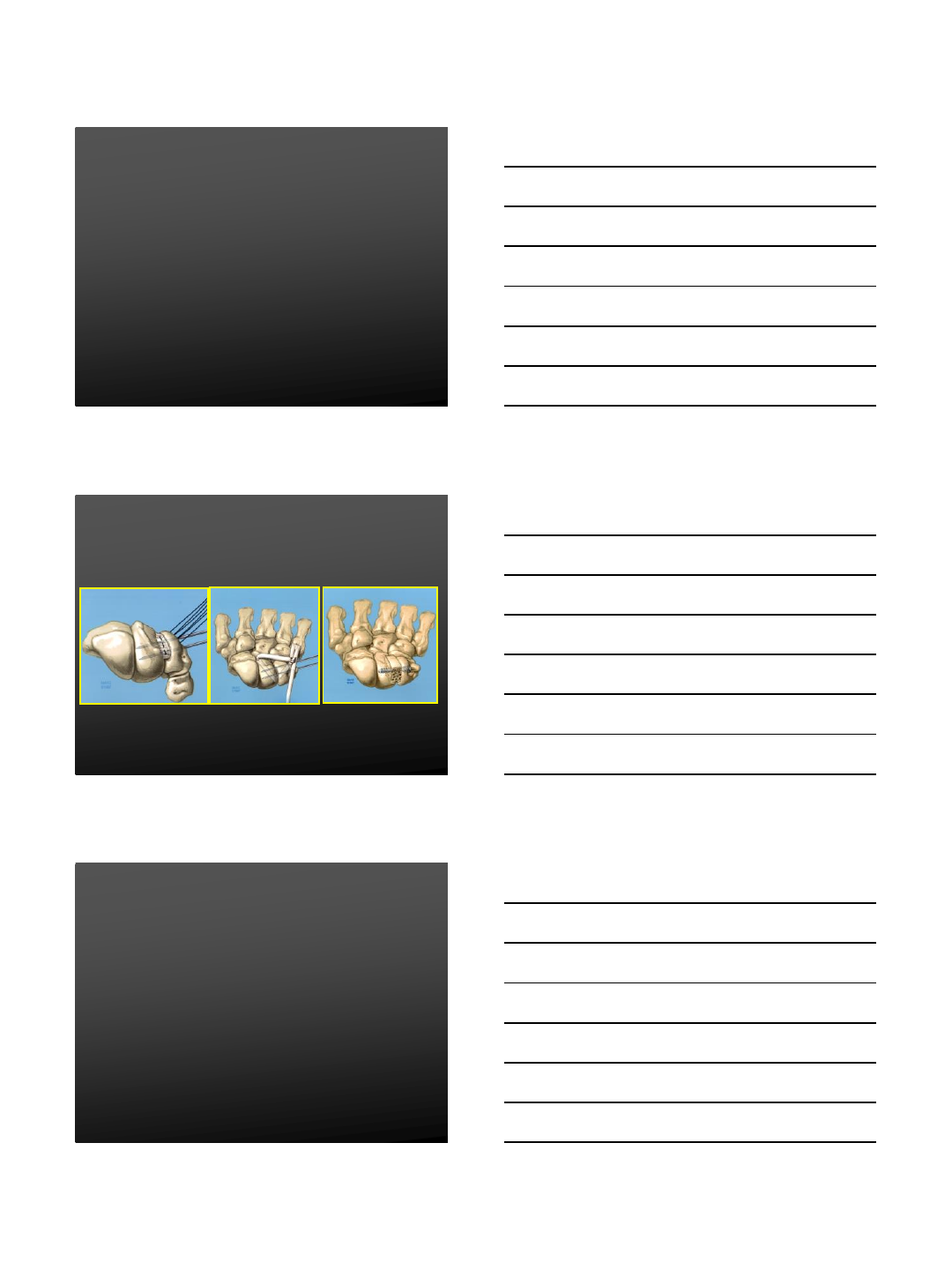
Lunotriquetral Ligament
Tear
Non-Operative
Cast immobilization
Initial management
(Acute/Chronic)
Pre-Dynamic
Dynamic
Operative
Static instability
Dynamic tears not
responsive to non-operative
treatment
Operative Treatment
Images from Alexander Y Shin M.D.
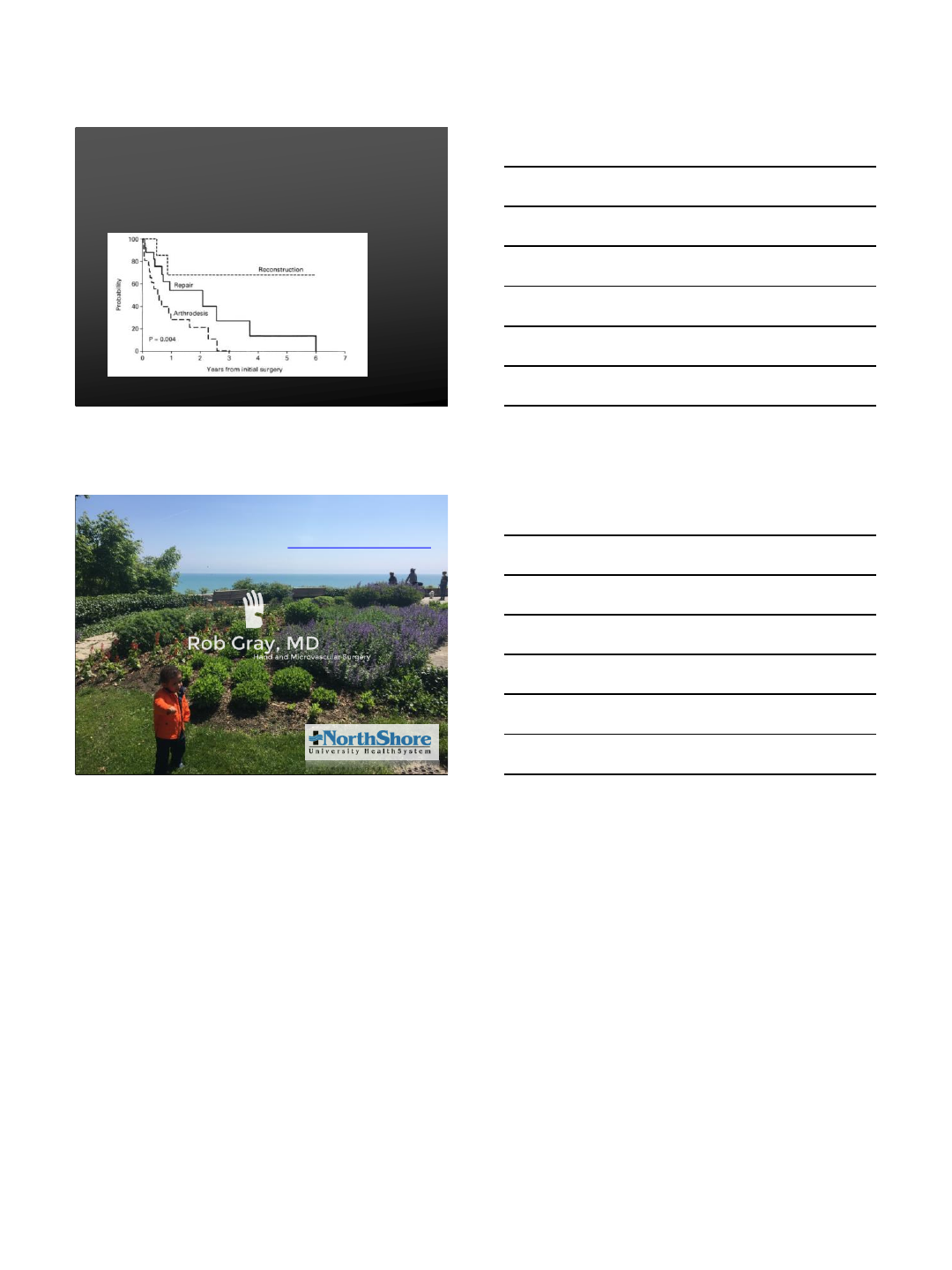
LT Instability Outcomes
Shin et al 2001
Reconstruction or repair:
•Better strength, motion, pain relief, satisfaction
Arthrodesis more likely to require further surgery at 5
years
(Probability of not requiring further surgery):
•Reconstruction 68.6%
•Repair 23.3%
•Arthrodesis 21.8%
Shin AY, Berger RA, Bishop AT et a. JBJS 2001.
7/16/2015
6
LT Instability Outcomes
Shin et al 2001
COMPLICATIONS:
Shin AY, Berger RA, Bishop AT et a. JBJS 2001.
T H A N K S . RGREEZY@GMAIL.COM
WWW.ROBGRAYMD.COM
7/27/2015
1
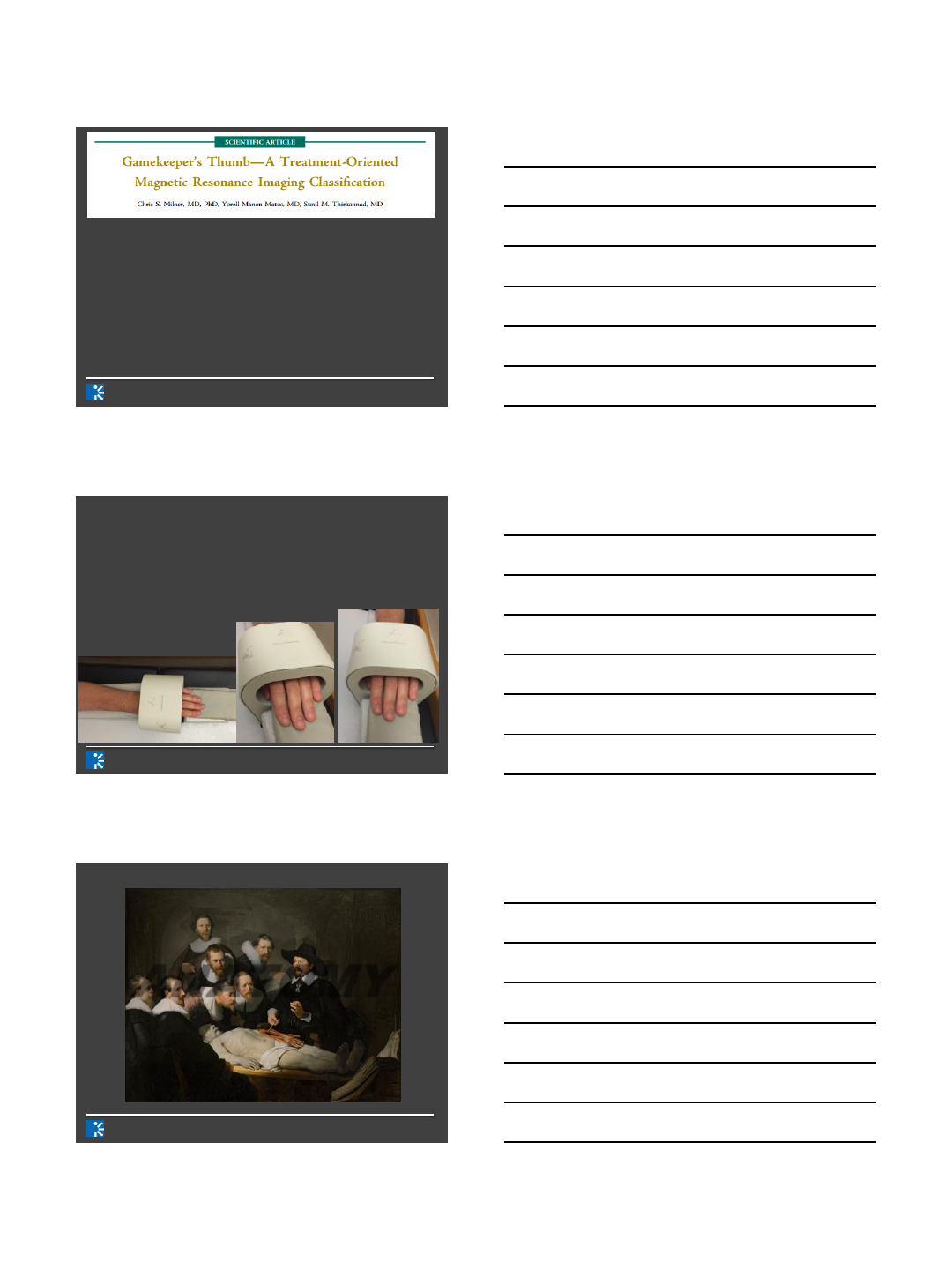
Magnetic Resonance Imaging
(MRI) of Ligamentous Injury
of the Thumb
Harry ‟Tate” G. Greditzer, IV MD, MSc
Department of Radiology and Imaging
Hospital for Special Surgery
New York, NY
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
TITLE: Magnetic Resonance Imaging (MRI) of Ligamentous
Injury of the Thumb
NAME: Harry G. Greditzer IV, M.D.
DISCLOSURE OF COMMERICAL INTEREST: My
disclosure is in the Final VuMedi Program.
I have no relevant disclosures
Disclosure of Commercial Interest
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Introduction
•The ulnar collateral ligament (UCL) and radial
collateral ligament (RCL) are primary
stabilizers of the thumb metacarpophalangeal
(MP) joint
•Injury to these ligaments may result in joint
instability, leading to significant disability and
pain
•The diagnosis is best established clinically,
though MRI is the imaging modality of choice
for grading.
7/27/2015
2
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
•Magnetic resonance imaging sensitivity and
specificity for UCL injury detection
approaches 100%
•With the latest generation of dedicated
extremity coils, it offers a level of detail that
can show the precise location of the torn
ligament within the accuracy of a millimeter
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
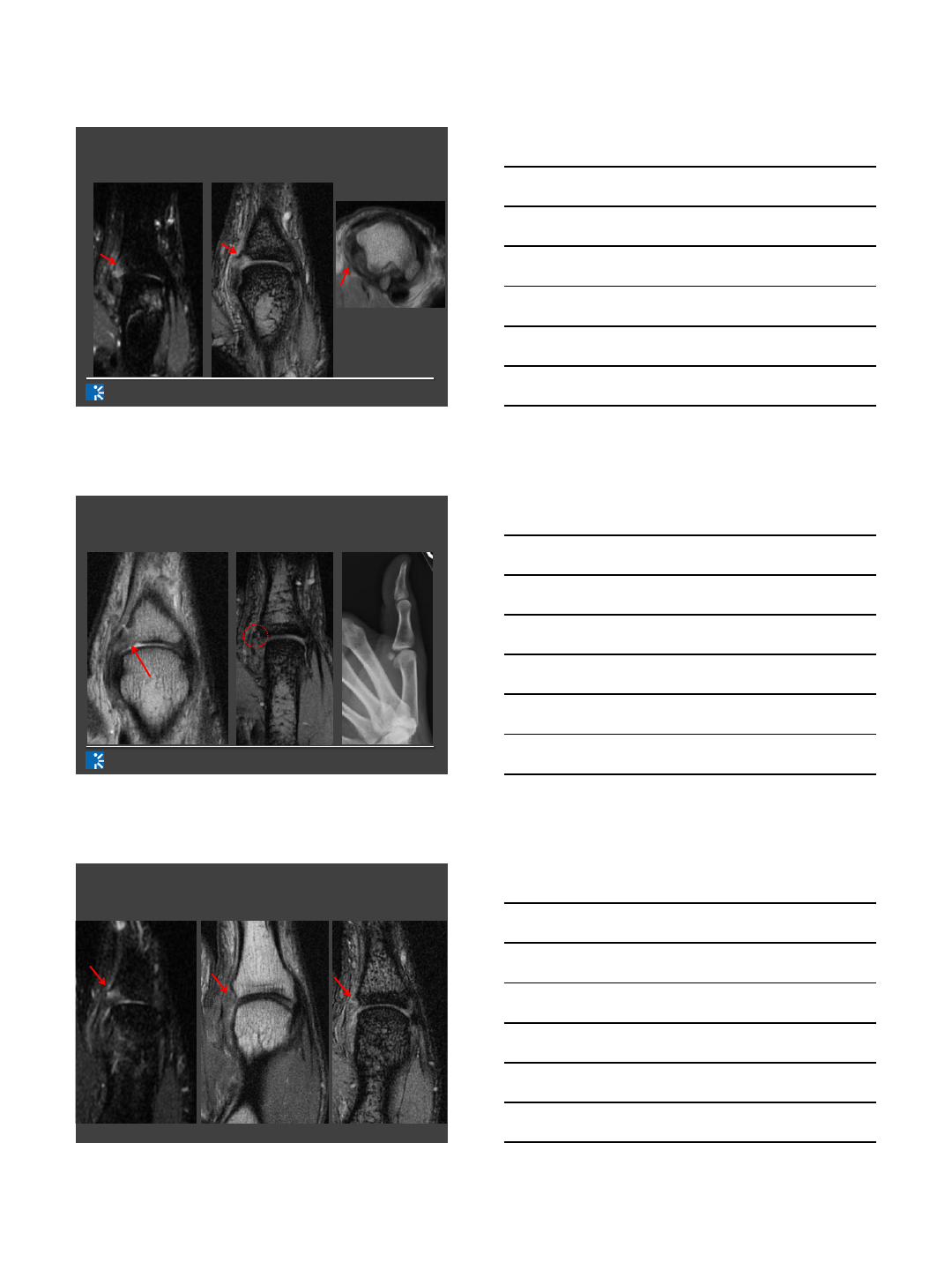
MRI Protocol
•Patient supine with arm at their side
•Palm down with thumb in neutral position
•Place in dedicated wrist coil
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
ANATOMY

7/27/2015
3
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Aponeurosis of Abductor
Pollicis Brevis tendon
Ulnar Collateral
Ligament
Aponeurosis of Adductor
Pollicis Tendon
Radial Collateral
Ligament
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Aponeurosis
of Abductor
Pollicis Brevis
tendon
Ulnar
Collateral
Ligament
Aponeurosis
of Adductor
Pollicis
Tendon
Radial Collateral
Ligament
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
CASES
7/27/2015
4
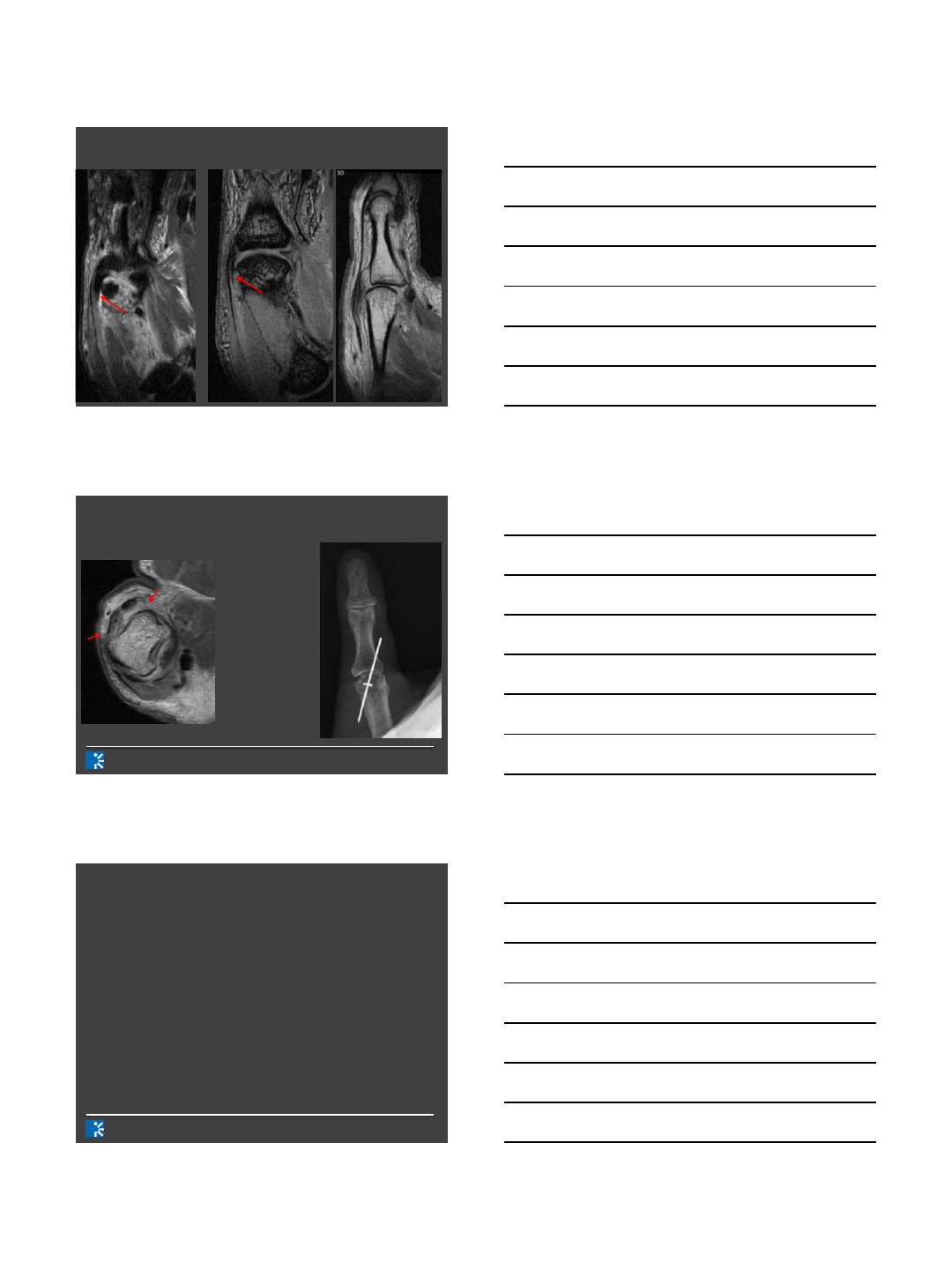
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Case 1: Fall after skiing 11 days ago
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Case 1: Fall after skiing 11 days ago
Case 2: Skiing injury 1 month ago
7/27/2015
5
U
R
Case 3: NFL Running Back Injured
Thumb During Practice
Yo-Yo on
a String
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
7/27/2015
6
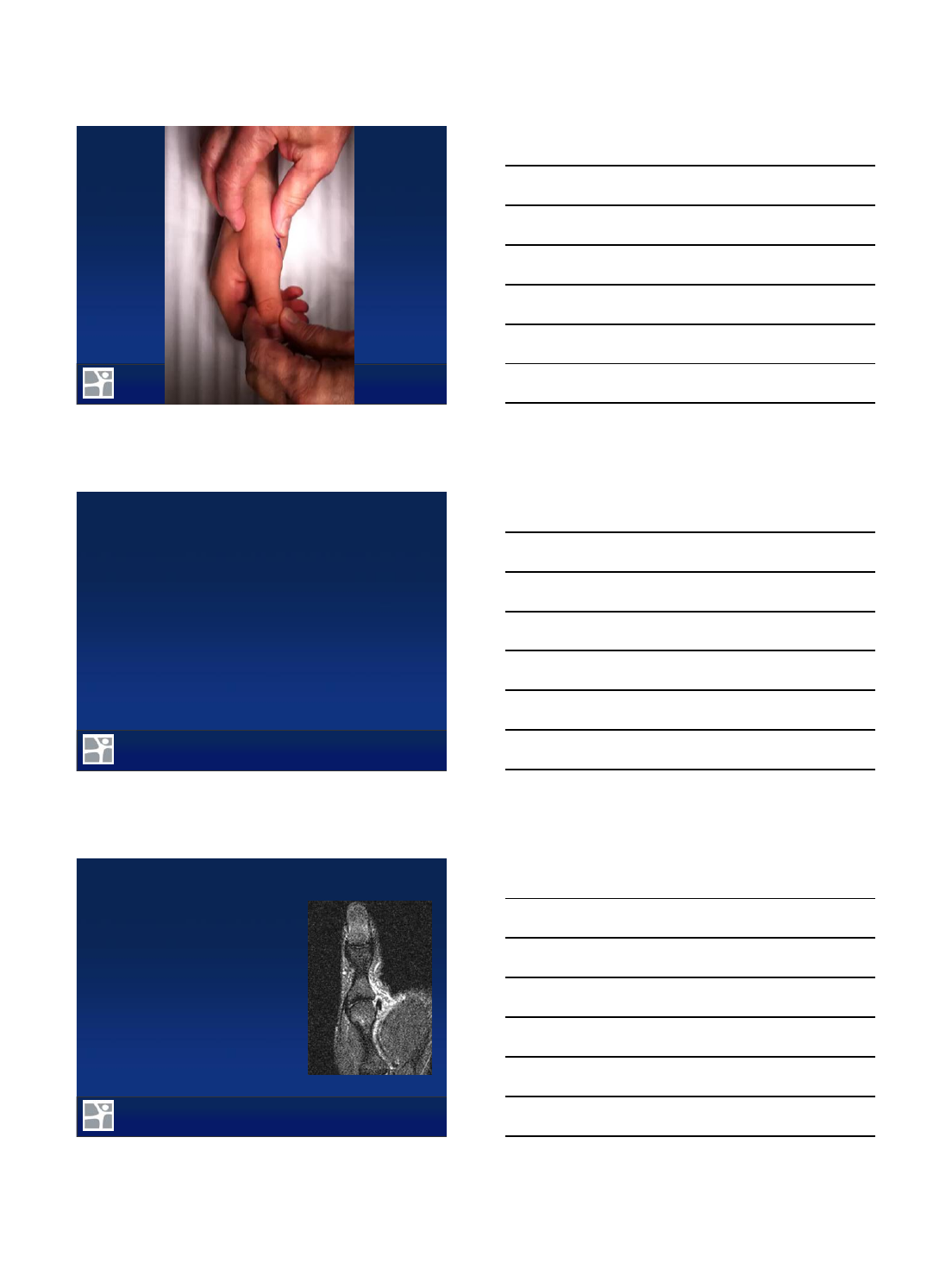
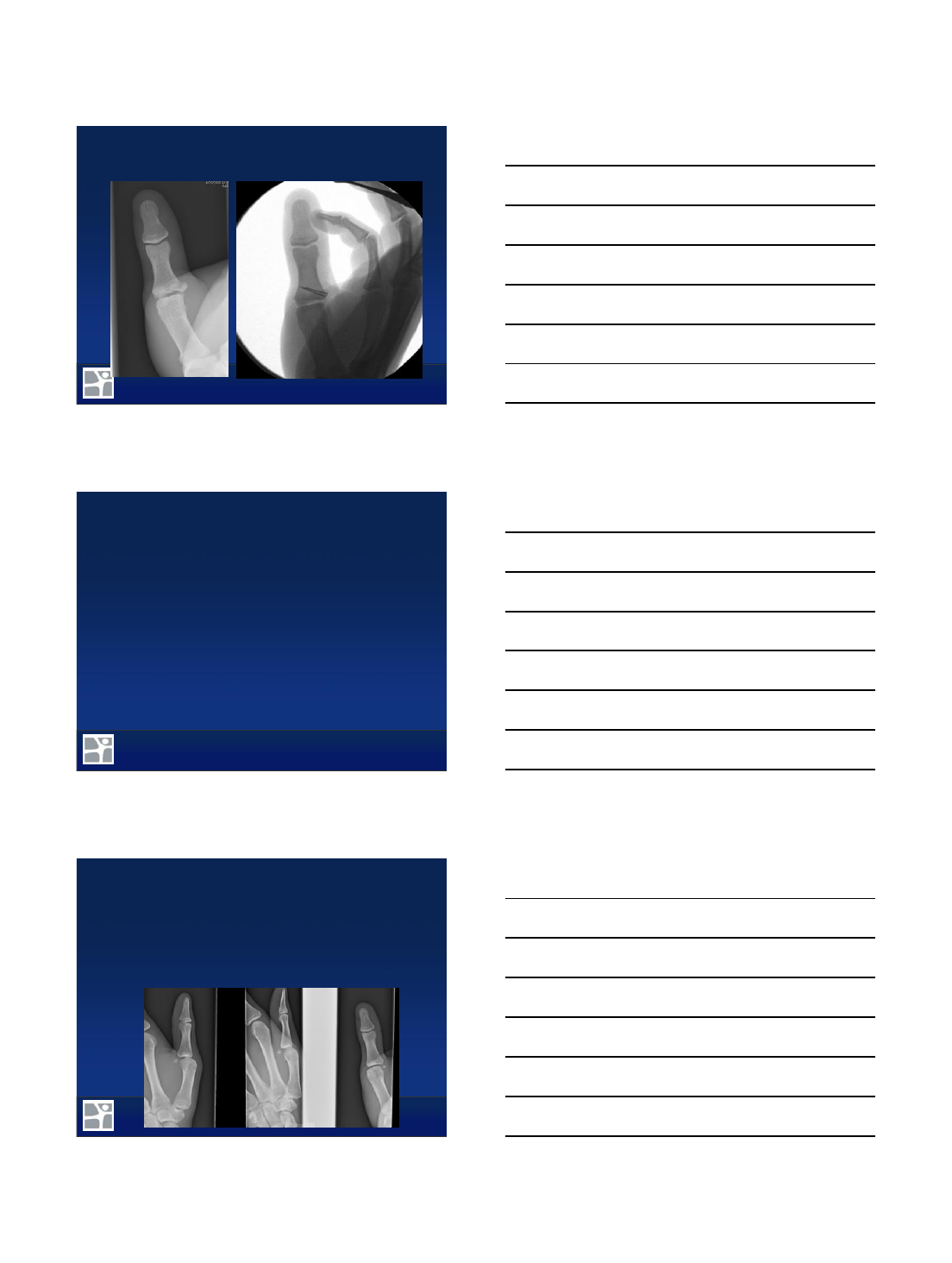
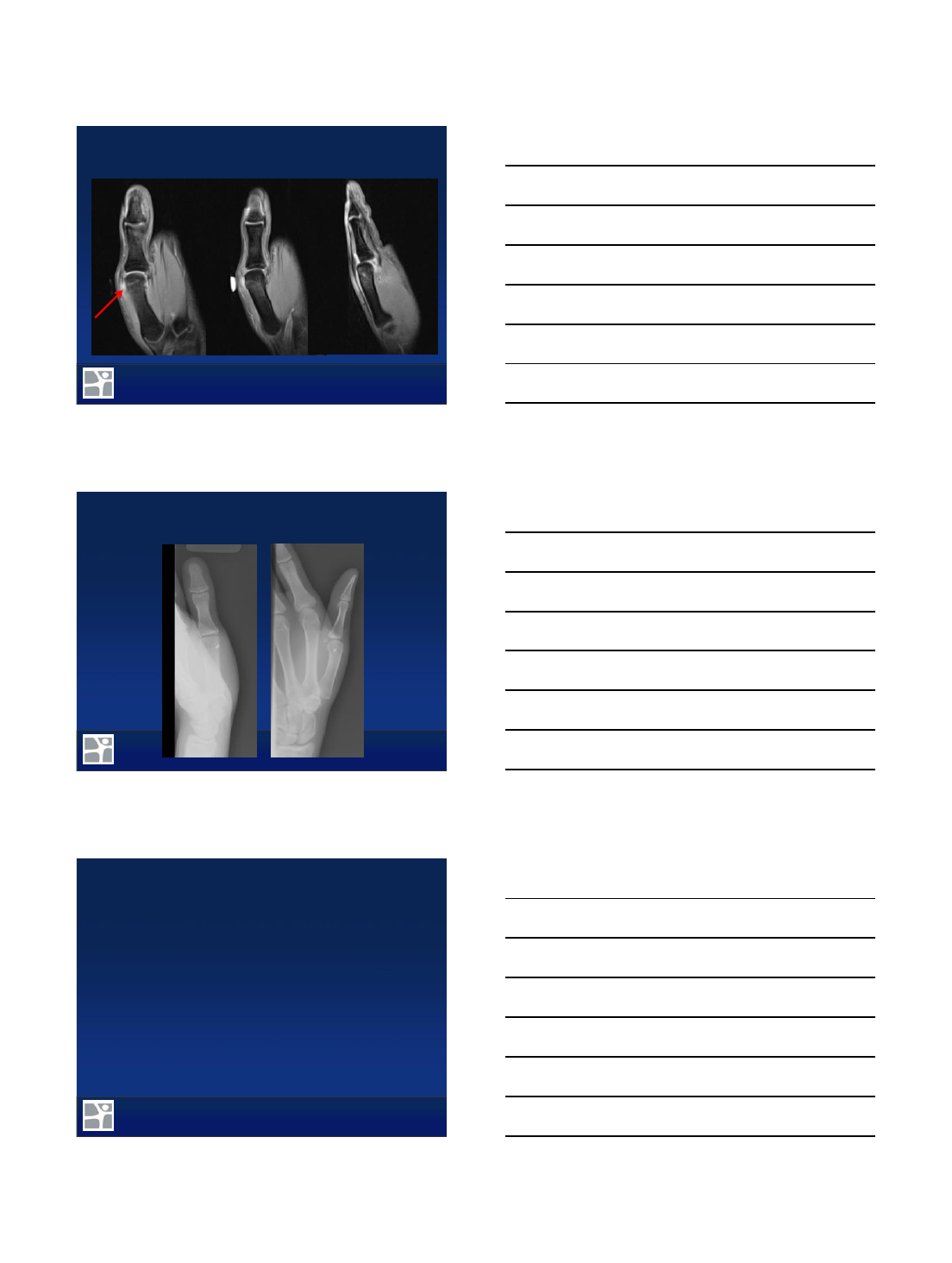
Case 4: 48 y/o male suffers basketball injury
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Case 4: 48 y/o male suffers basketball injury
•Radial
collateral
ligament
repair
•Sagittal
band
repair
•Reduced
K-wire
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
Summary
•MRI thumb positioning is paramount
•Small FOV and thin slices
•IR first to find the acute injury!
•Coronal plane is useful for ligamentous
injury
•Axial and sagittal planes for the plates and
sagittal bands
7/27/2015
7
HOSPITAL FOR SPECIAL SURGERY IMAGING & INTERVENTION
THANK YOU!
1
Surgical Treatment of
Thumb MCP Collateral
Ligament Injuries
Vumedi Webinar
July 27, 2015
Mark A. Vitale, MD, MPH
ONS Foundation for Clinical Research and Education
ONS, Greenwich, CT;
Attending Orthopaedic Surgeon
Greenwich Hospital
Yale-New Haven Health
Columbia Orthopaedics
2
I have no disclosures for potential conflicts of interest
specific to this presentation
Speaker’s bureau for Auxilium Pharmaceuticals (Xiaflex)
Disclosures
Columbia Orthopaedics
3
Ligamentous anatomy
Exam of thumb stability
When to order advanced imaging
How to treat surgically
–Acute versus chronic injuries
–Bony avulsions
–UCL versus RCL
–Postop protocol
Overview
2
Columbia Orthopaedics
4
Ligamentous Anatomy MCP Joint
Designed to be stable in extension AND flexion
Dynamic stability
Extrinsic stabilizers: EPL, EPB, FPL
Intrinsic stabilizers: APB, FPB and adductor pollicis
Static stability
Dorsal capsule and volar plate
UCL
Proper and accessory
Adductor aponeurosis volar and adjacent to UCL
RCL
Proper UCL originates more dorsally on MC head
Abductor aponeurosis dorsal to RCL
Columbia Orthopaedics
5
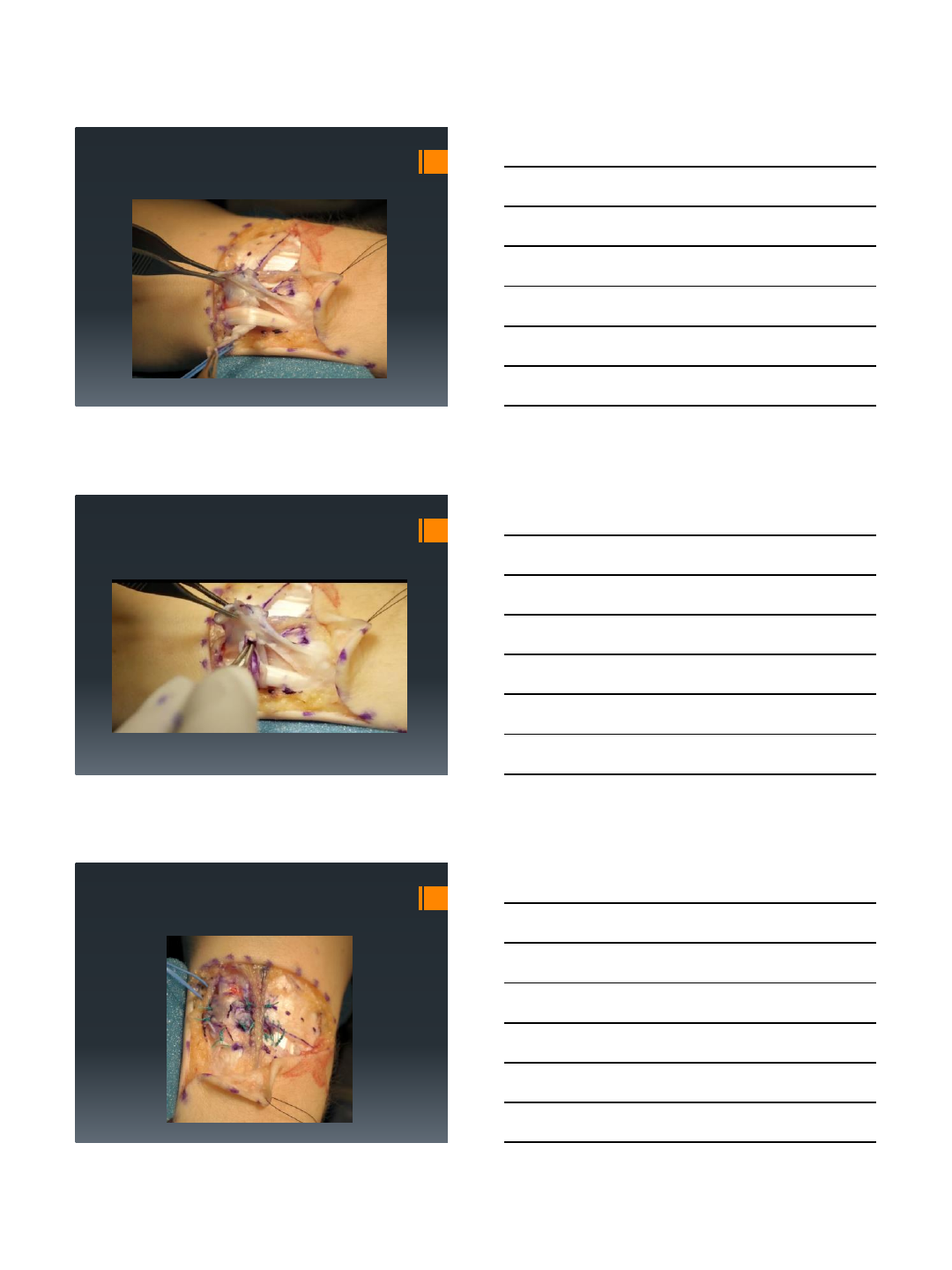
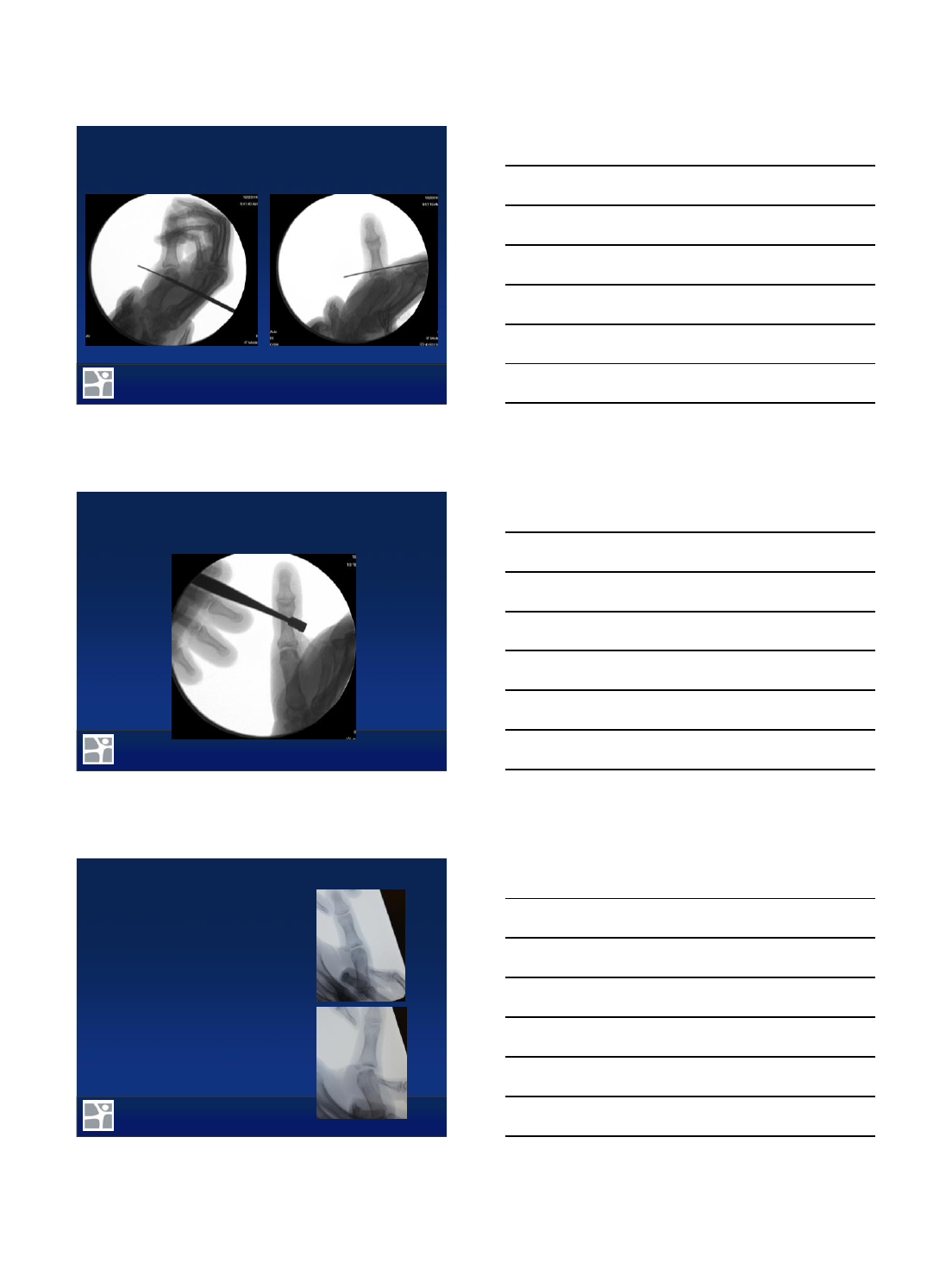
Physical Exam –UCL Rupture
Resting position of ulnar deviation
Tenderness to palpation at ligament
Palplable mass suggests but does not r/o Stenar lesion
Most importantly test joint stability . . .
Columbia Orthopaedics
6
Physical Exam –UCL Rupture
Evaluation of joint stability to radial/ulnar stress
Test MPJ in extension and 30°flexion
Instability = radial deviation > 35°or > 15°asymmetry
Flexion to test proper collateral ligament
Extension to test accessory ligament + volar plate
Instability > 35°implies tear of proper + accessory collaterals and
Stenar’s lesion present in 90% (Heyman et al 1993)
More reliable bc easy to be deceived by rotation of MC in flexion
Local local anesthetic to avoid guarding (Cooper et al 2005)
3
Columbia Orthopaedics
7
Columbia Orthopaedics
8
Advanced Imaging
My indications for MRI:
Difficult to get good exam because of guarding
Borderline degree of instability (e.g. 25°-30°)
Possible Stenar’s lesion (e.g. palpable mass)
Assess cartilage in chronic injuries to decide between
reconstruction vs fusion
NOT needed when clear instability with no form endpoint
Will change my surgical decision making when:
Stenar’s lesion
Relative indication if highly retracted tear w/o Stenar’s lesion
Articular injury/arthrosis
Columbia Orthopaedics
9
Acute UCL Rupture
Surgical indications:
Opening > 35°or 15°from
contralateral thumb
Stenar’s lesion
No discrete endpoint to radial stress
Relative indication: MRI reveals
significant retraction but borderline
instability and no Stenar’s lesion
4
Columbia Orthopaedics
10
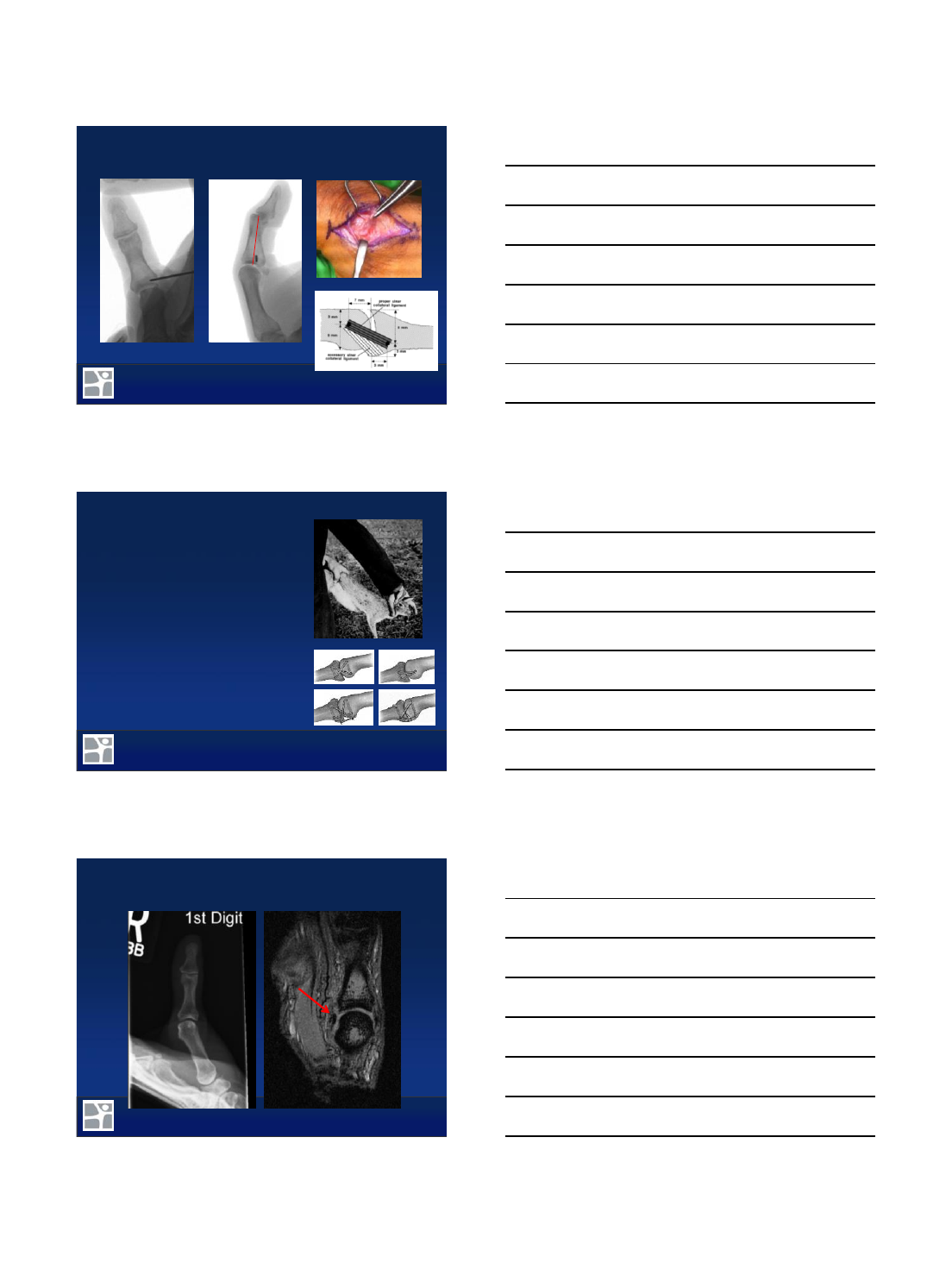
Surgical Treatment –Acute UCL Rupture
(Trumble et al 1999)
Columbia Orthopaedics
11
Chronic UCL Rupture
May be attenuated and difficult to
mobilize to anatomic insertion
Textbook = approx 6 weeks
Reality = usually some robust local
tissue even months later
If poor local tissue present, may be
treated with
Dynamic stabilization (EIP/EPB
transfer, adductor advancement)
Static stabilization with tendon graft
(many configurations)
MCP fusion if arthritic –important to
assess cartilage (XR or MRI)
Columbia Orthopaedics
12
Surgical Treatment –Chronic UCL Rupture
5
Columbia Orthopaedics
13
Surgical Treatment –Chronic UCL Rupture
Columbia Orthopaedics
14
Surgical Treatment –Chronic UCL Rupture
Columbia Orthopaedics
15
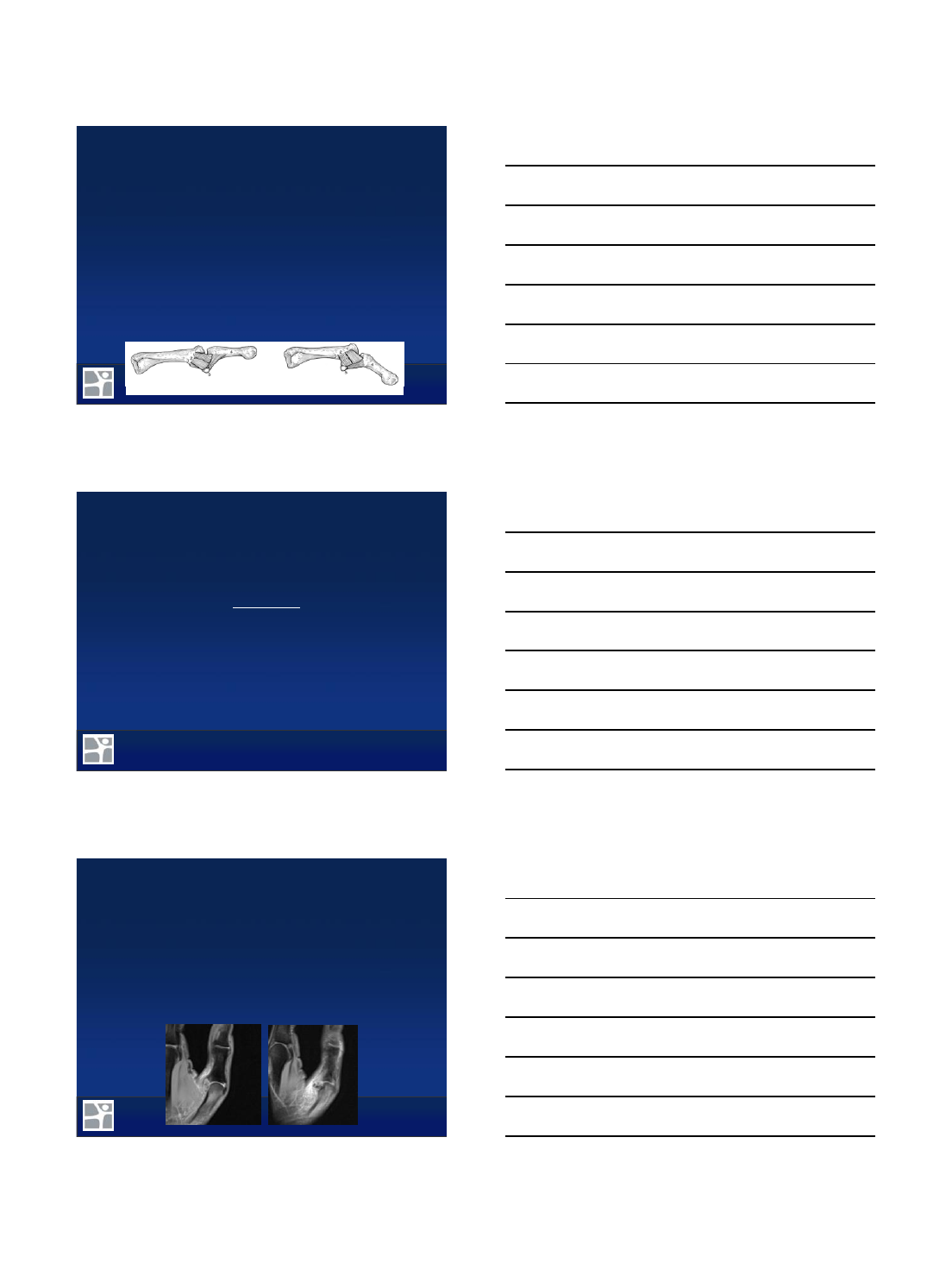
Bony Avulsion
Often compromise stability if
involves entire ligament insertion
Nonunion rates of 25 –60%
Significant rotational deformity
My surgical indications:
Fractures a/w significant instability
Fractures with significant articular
displacement
6
Columbia Orthopaedics
16
Surgical Treatment –Bony Avulsion
Columbia Orthopaedics
17
RCL Rupture
RCL less common, “reverse gamekeeper’s”
10 –42% of thumb collateral ligament injuries
Pathoanatomical considerations
RCL avulses from MC head 55%, proximal phalanx 29%,
midsubstance 16%
Greater distal insertional area of RCL
No true Stenar’s lesion bc abductor aponeurosis dorsal to RCL
and much broader
Physical Exam
Stress testing
AP drawer test
More likely volar and rotatory subluxation
Columbia Orthopaedics
18
RCL Rupture
My surgical indications
Opening > 35°or 15°from contralateral thumb
No discrete endpoint to valgus stress
Significant radiographic volar subluxation or ulnar translation
No true Stenar’s lesion equivalent
7
Columbia Orthopaedics
19
Surgical Treatment –RCL Rupture
Columbia Orthopaedics
20
Surgical Treatment –RCL Rupture
Columbia Orthopaedics
21
Thumb spica splint/cast with IP free for 3 weeks
Removable orthoplast splint with therapy supervised by
therapist weeks 3 –6
Special attention to the patient with the stiff MP joint
Splint only for heavy activities weeks 6 - 12
Return to sport/heavy activity 3 –4 months
Postop Procotol
