MXCSRecon Osteo Defect J11837A
2015-06-08
: Pdf Mxcsreconosteodefectj11837A MXCSReconOsteoDefectJ11837A 6 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 11
Case Report
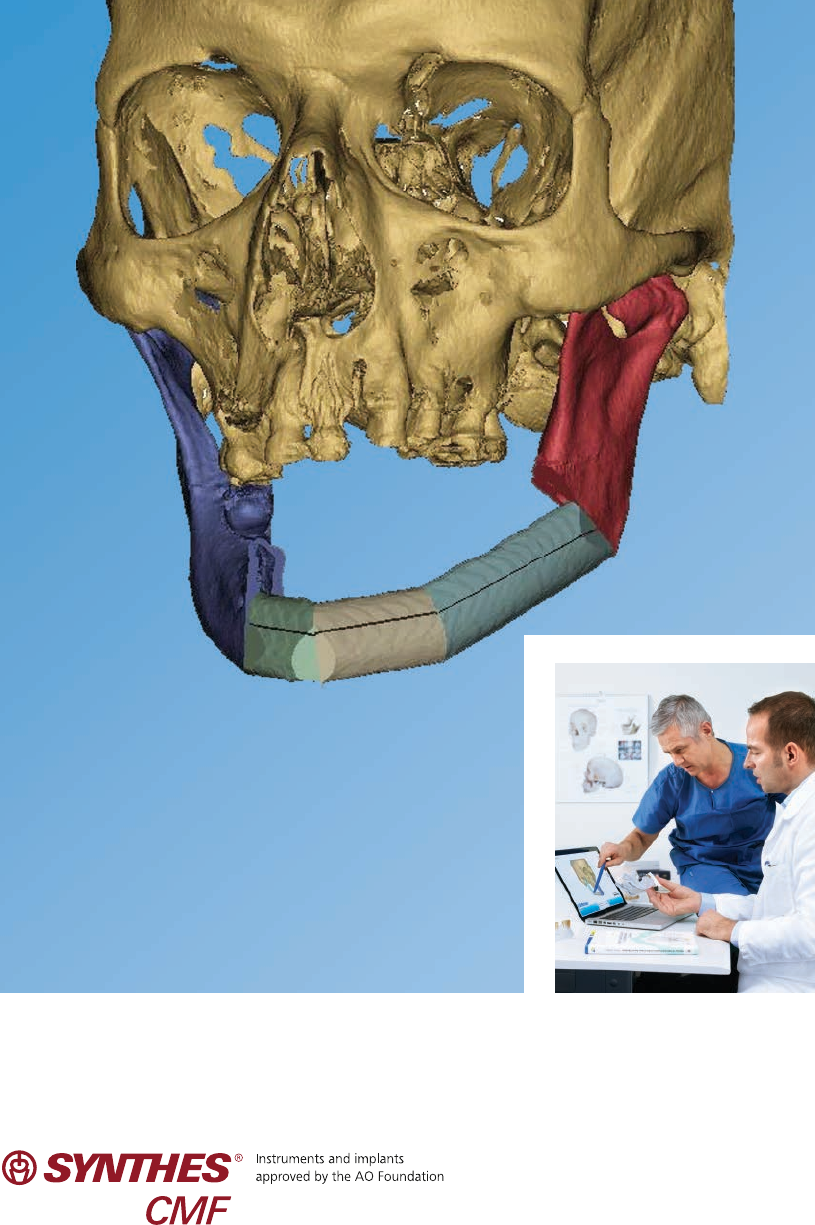
Reconstruction of a Mandibular
Osteoradionecrotic Defect with a Fibula
Osteocutaneous Flap. Using Synthes ProPlan
CMF, Patient Specific Plate Contouring (PSPC)
and the MatrixMANDIBLE Plating System.
Synthes Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report
Patient Profile
The patient is a 63 year old male with a history of squamous
cell carcinoma of the left floor of mouth which was treated
with local resection, ipsilateral neck dissection, and post op-
erative radiation therapy twelve years ago.
During his initial consultation, he complained of left mandib-
ular pain and intermittent drainage from his left mental area.
No recent history of facial trauma was noted but he reported
a “crack” sound followed by pain while eating one week
prior to office visit.
Clinical examination showed mandibular instability of the left
parasymphyseal area, anesthesia in the distribution of the
mental nerve as well as deviation of the chin to the left.
Furthermore, extensive radiation damage was noted on the
skin of the left neck and mandible area. Intra-oral exam
revealed exposed bone on the left mandibular ridge as well
as poor dentition with multiple caries and generalized
periodontal disease.
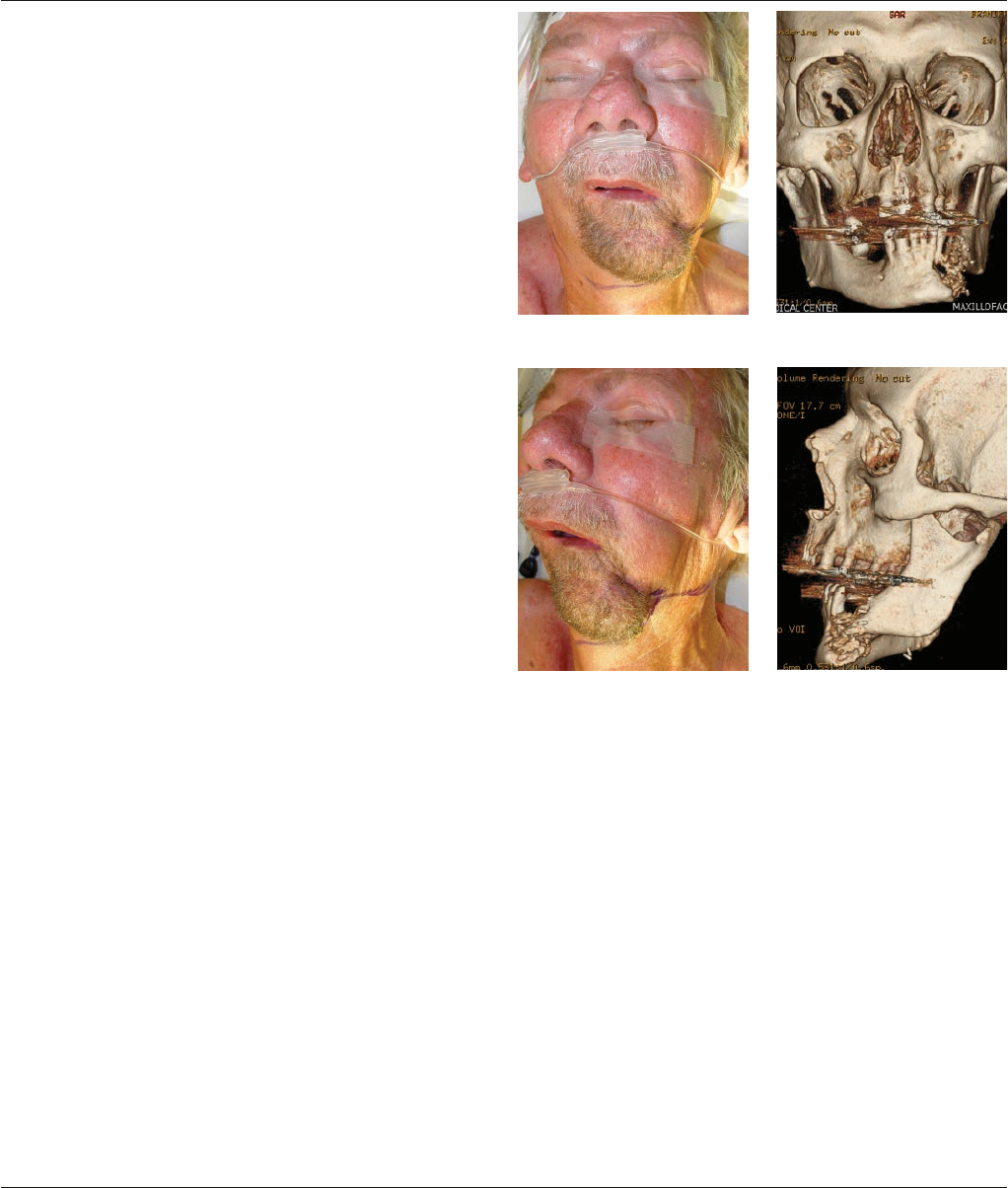
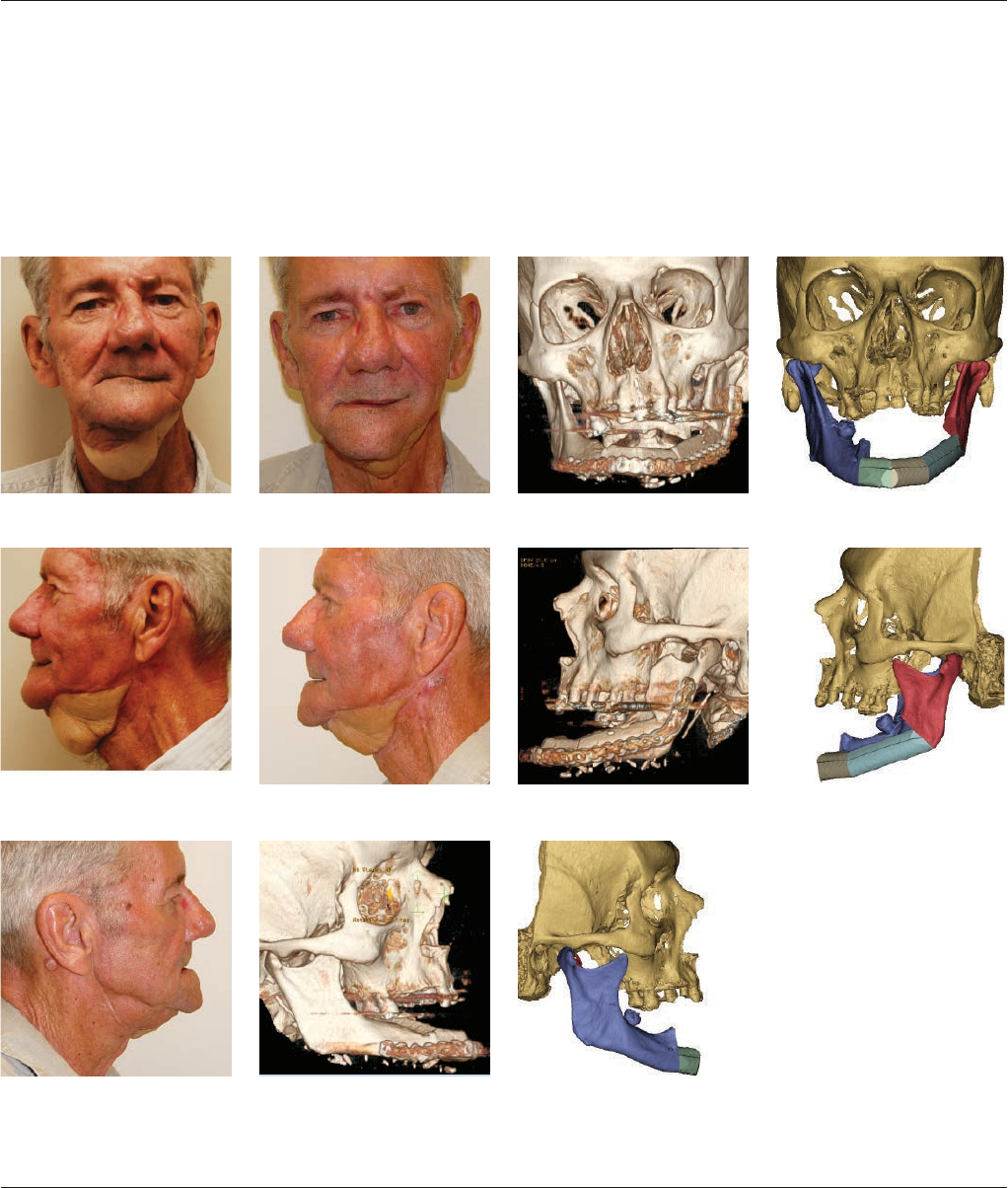
His CT scan revealed a fracture of the left mandibular para-
symphyseal area with significant areas of osteolysis involving
the body of the left mandible and extending almost to the
symphysis. Over-rotation of the left proximal segment as well
as anterior displacement of the condylar head was observed.
Furthermore, significant collapse of mandibular width was
noted as seen by the displacement of the genial tubercle to
the left of the sagittal midline. Figures 1–4.
Biopsies were taken to rule out malignant disease. Clinical
impression of osteoradionecrosis was confirmed with no
evidence of malignancy on histopathology.
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula
Osteocutaneous Flap. Using Synthes ProPlan CMF, Patient Specific Plate
Contouring (PSPC) and the MatrixMANDIBLE Plating System.
Figure 1 Figure 2
Figure 3 Figure 4

Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report Synthes 1
Treatment Plan
In consideration of the previous radiation therapy and
surgical entry, a free tissue transfer was necessary to ensure
success of this reconstruction. A CTA of bilateral extremities
was obtained to evaluate the potential of using the fibula as
a reconstructive tool.
CT scans were uploaded into Synthes ProPlan CMF to create
three-dimensional images for preoperative planning. The
appropriate CT scanning protocol, as defined by Synthes
ProPlan CMF, was followed for the maxillofacial and lower
extremity scans. In this protocol the patient is aligned with-
out a gantry tilt. The head is stabilized to prevent motion
with the jaws slightly opened, with or without a bite block.
A DICOM compliant scanner is required with parameters set
for unidirectional, 1 mm slices supplied in CD or MOD media.
Preoperative Planning Session
Through a web-based meeting with a Synthes ProPlan CMF
clinical engineer, the area to be resected was identified. The
extent of the resection was characterized according to the
radiographic findings, keeping in mind the three-dimensional
morphology of the neo-mandible and length of segments
of fibula to be used. The resection was planned from the
left mandibular angle to just anterior of the right mental
foramen in order to preserve sensation to the right lower lip.
Figures 5–7.
Surgical guides were virtually generated and created using
CAD-CAM technology. The distorted anatomy of the re-
sected native mandible was then restored virtually to ensure
appropriate position of the proximal and distal segments.
The repositioned neo-mandible created a more normal
occlusion with the mandibular dentoalveolar complex in
preparation for osteointegrated implants. Figures 8–10.
Figure 5 Figure 6
Figure 7
Figure 8 Figure 9
Figure 10
2 Synthes Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap. Using Synthes
ProPlan CMF, Patient Specific Plate Contouring (PSPC) and the MatrixMANDIBLE Plating System.
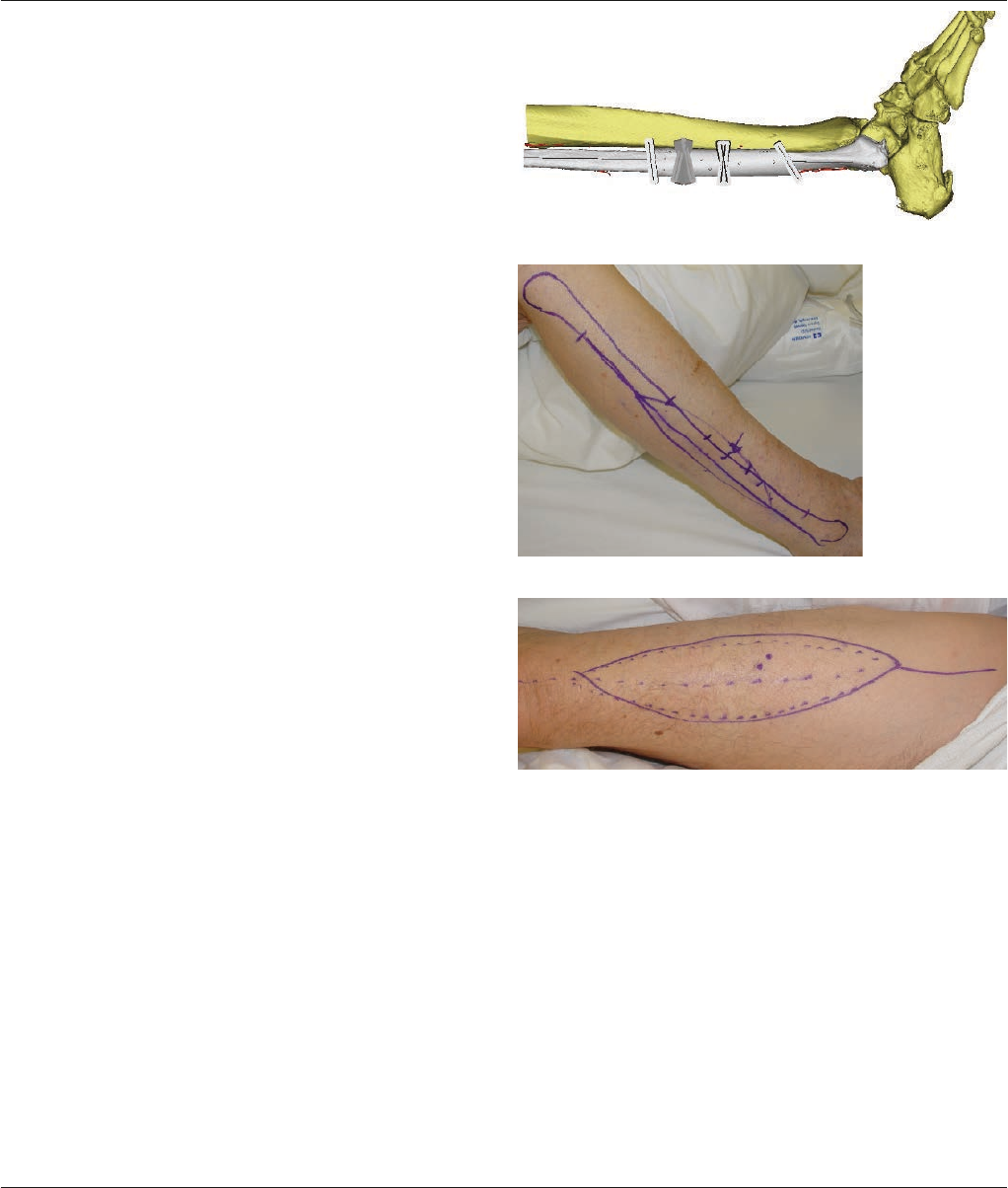
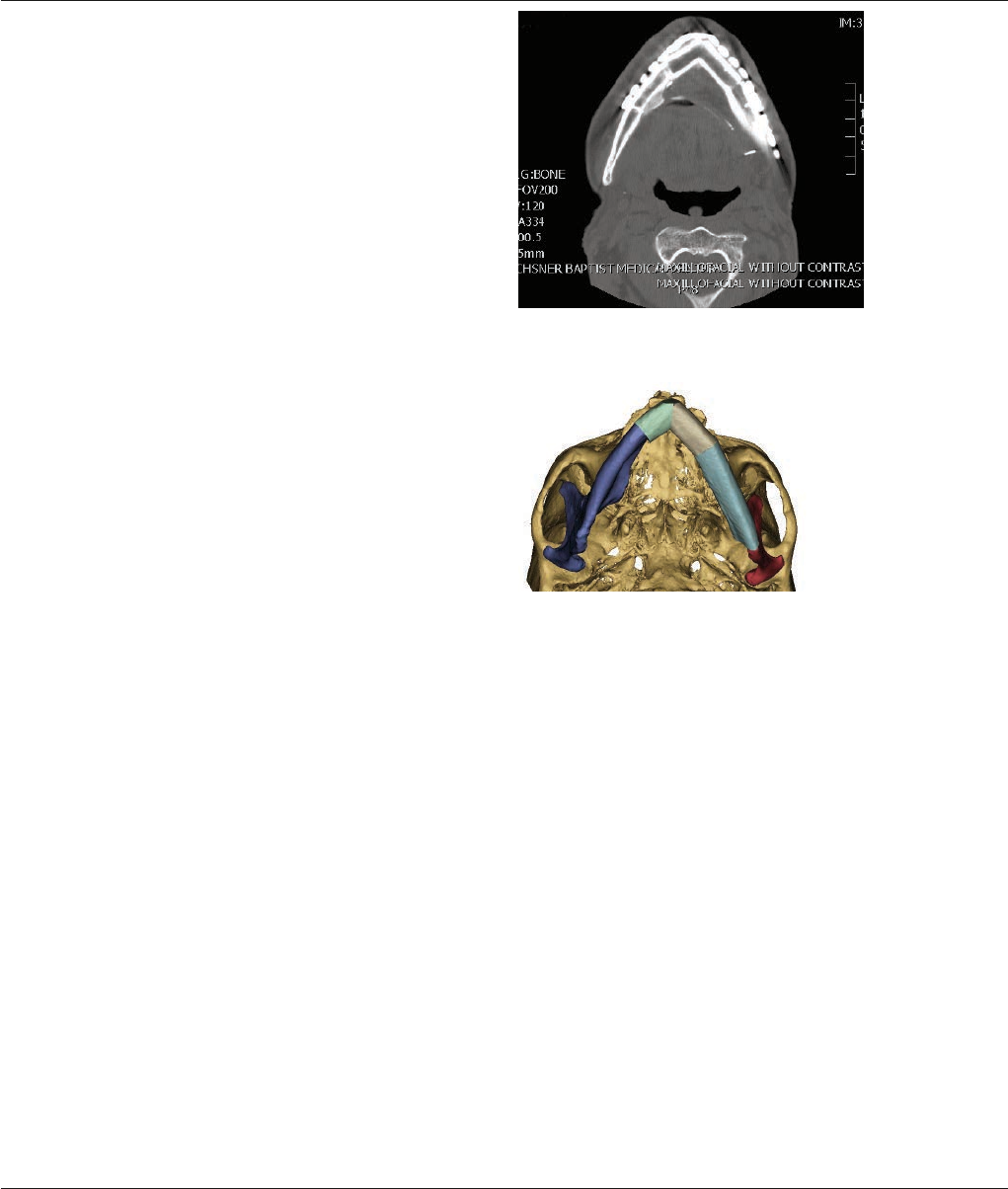
The right fibula was selected to reconstruct the mandible to
allow for the vascular anastomosis to the right neck, away
from the zone of injury and facilitate favorable inset of the
skin paddle intra-orally. A three-segment fibular graft was
planned to reconstruct the defect with the vascular pedicle
running medially. Once the virtual contouring was completed,
a patient specific surgical guide was generated to identify
the location of the osteotomies. Figure 11. The distal osteotomy
was placed 7 cm from the ankle to ensure stability of the
joint while maximizing vascular pedicle length. A stereolithic
model of the neo-mandible was created. A Patient Specific
Plate Contouring (PSPC) plate was provided to match the
contour of the neo-mandible. The precontoured mandible
plate, mandible resection guide, fibula osteotomy guide,
anatomic model and Case Report were provided preopera-
tively as a kit.
Intraoperative Surgical Details
Marking for an osteocutaneous right fibular free flap as well
as a right anterolateral thigh flap were made pre-operatively.
Figures 12–13. Due to the extensive post-radiation soft
tissue damage and the required expansion of the soft tissue
envelope following restoration of the skeletal anatomy, an
anterolateral thigh flap was chosen to resurface the antici-
pated external skin deficit.
Figure 12
Figure 13
Figure 11
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report Synthes 3
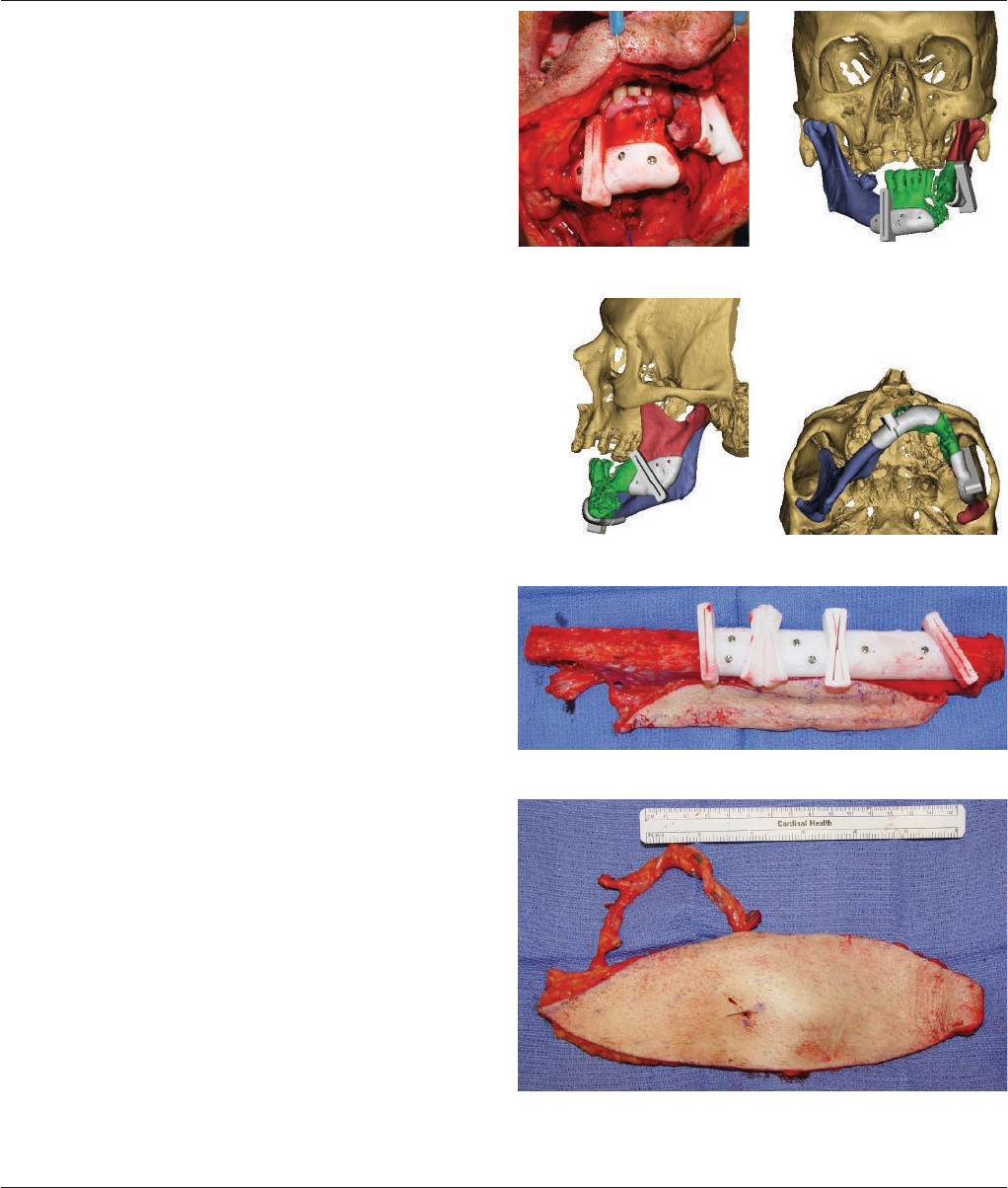
Access was gained through a cervical incision including exci-
sion of the fistulous tract. Once the mandible was accessed,
the surgical guides were secured to the mandible using
monocortical screws and the resection was performed with a
sagittal saw. Figures 14–17, actual and virtual images. A
right coronoidectomy was performed and the PSPC plate
secured using bicortical fixation with 2.4 mm Titanium
MatrixMANDIBLE Self-Tapping screws. Next, the right
superior thyroid and facial artery were prepared for micro-
vascular transfer along with the right external jugular vein
and a branch of the internal jugular vein.
Harvesting Fibular Osteocutaneous Flap
The right fibular flap was harvested in standard fashion
under tourniquet. A skin paddle of 10 X 4 cm was included
to resurface the intra-oral defect created by the expansion
of the soft tissue envelope, while allowing primary closure of
the donor site. The harvested fibula was then taken to the
back table and the surgical guide was secured to its lateral
aspect using monocortical screws. Figure 18. The osteoto-
mies were performed using a sagittal saw while protecting
the vascular pedicle. The three segments were positioned on
the PSPC plate according to the pre-surgical plan and fixated
using 2.4 mm Titanium MatrixMANDIBLE Locking Screws.
The intra-oral skin paddle was placed and microvascular
anastomosis performed under microscope. An 18 X 8 cm
anterolateral thigh flap was then harvested, inset at the left
neck and revascularized without complication. Figure 19.
Figure 14 Figure 15
Figure 16 Figure 17
Figure 18
Figure 19
4 Synthes Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report
Results
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap. Using Synthes
ProPlan CMF, Patient Specific Plate Contouring (PSPC) and the MatrixMANDIBLE Plating System.
Figure 20–Postop 3 months Figure 21–Postop 6 months Figure 22 Figure 23
Figure 24– Postop 3 months Figure 25–Postop 6 months Figure 26 Figure 27
Figure 28– Postop 6 months Figure 29 Figure 30
The patient did well post-operatively. At six months follow-
ing his surgery, he underwent debulking and re-inset of the
external anterolateral thigh flap. CT scans indicated good
contour and union at all osteotomy sites. Accurate alignment
of the patient’s bone using Synthes ProPlan CMF ensured
that the mandibular symmetry and function were restored as
planned preoperatively. Figures 20–30 show the patient and
compare post-operative 3D reconstruction models with
virtual planning images.
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report Synthes 5
Figure 31
Figure 32
Figures 31–32 compare a post-operative segmental CT scan
with its virtual planning image. In the CT scan, note the
symphysis in the midline and radiographic evidence of bony
union at the osteotomies.

6 Synthes Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap. Using Synthes
ProPlan CMF, Patient Specific Plate Contouring (PSPC) and the MatrixMANDIBLE Plating System.
1 Chrcanovic BR, Reher P, Sousa AA, Harris M,
Osteoradionecrosis of the jaws—a current overview—
part 1: Physiopathology and risk and predisposting factors.
Oral Maxillofac Surg, 2010 Mar;14(1): 3-16
Results from case studies are not predictive of results in other cases.
Results in other cases may vary.
Discussion
Osteoradionecrosis is one of the most devastating complica-
tions of head and neck cancer treatment. A tumor in the
floor of mouth nearly doubles the rate of incidence. Whether
or not a patient is a smoker and has poor immunologic and
nutritional health at the time of treatment may also increase
the risk.1 The effects of therapeutic external beam radiation
are chronic as well as progressive and lead to an hypoxic,
hypovascular and hypocellular environment that decreases
healing potential. Insult to the mandible, either from chronic
infection, dental extraction or surgical entry may contribute
to osteoradionecrosis in this patient population. Contempo-
rary surgical management of osteoradionecrosis of the
mandible involves radical debridement of non-viable bone
with simultaneous reconstruction using well-vascularized
tissue from a distant site. Often this debridement will be
extensive to ensure healthy native mandibular margins.
The use of pre-operative virtual surgical planning allows
restoration of normal skeletal anatomical contour and
evaluation of the length of segments for the neomandible
to ensure adequate vascularity to the reconstruction. The use
of pre-fabricated cutting guides which identify the location
of the closing osteotomies and a pre-contoured plate
decrease operative time as it simplifies the reconstruction
process.
Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report Synthes 7
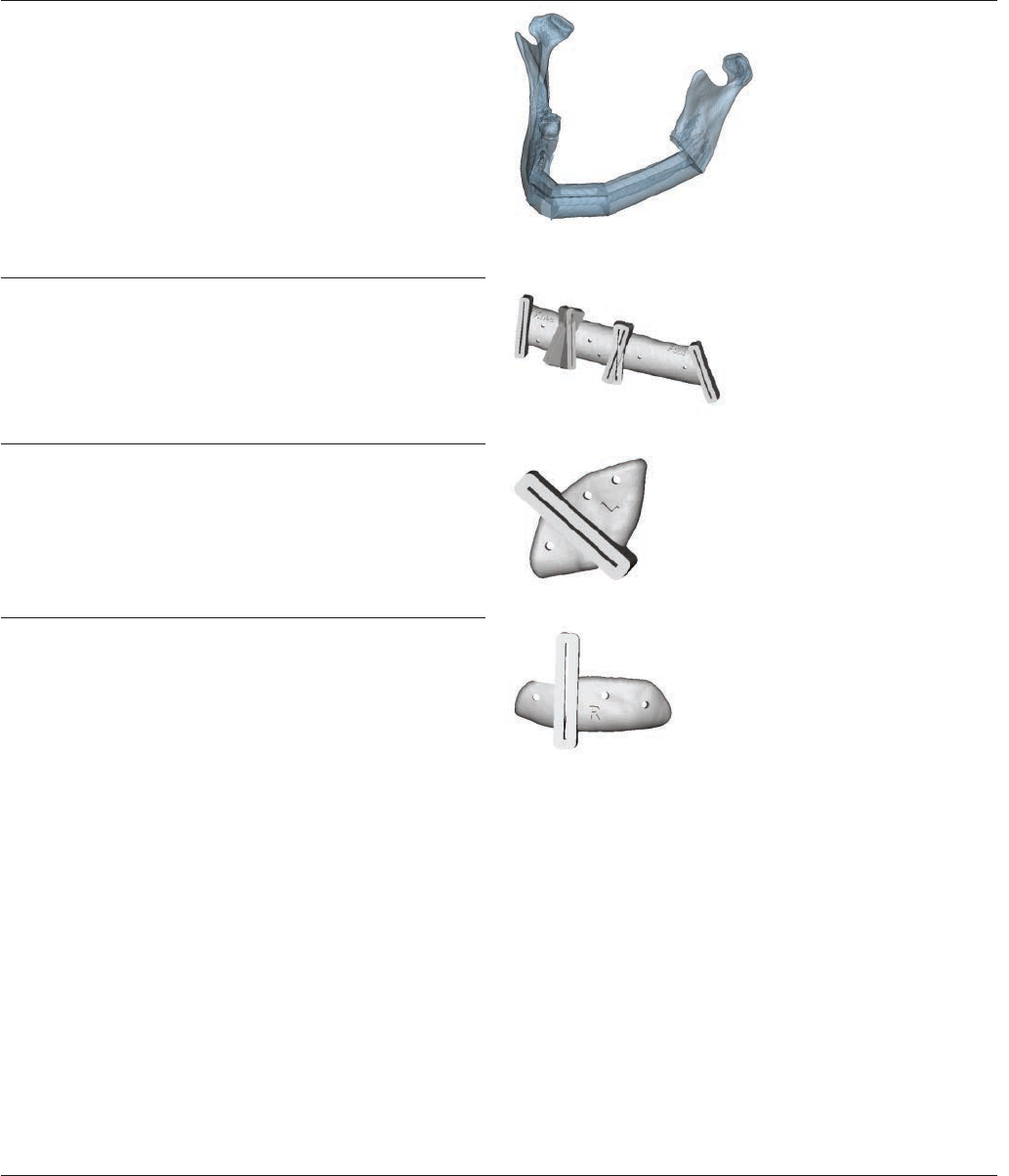
Osteotomy Guides and Model
Product Information
SD900.231 Planned Outcome Model
SD900.102 Fibula Guide
SD900.101 Mandible Guide–Left
SD900.101 Mandible Guide–Right
8 Synthes Reconstruction of a Mandibular Osteoradionecrotic Defect with a Fibula Osteocutaneous Flap Case Report
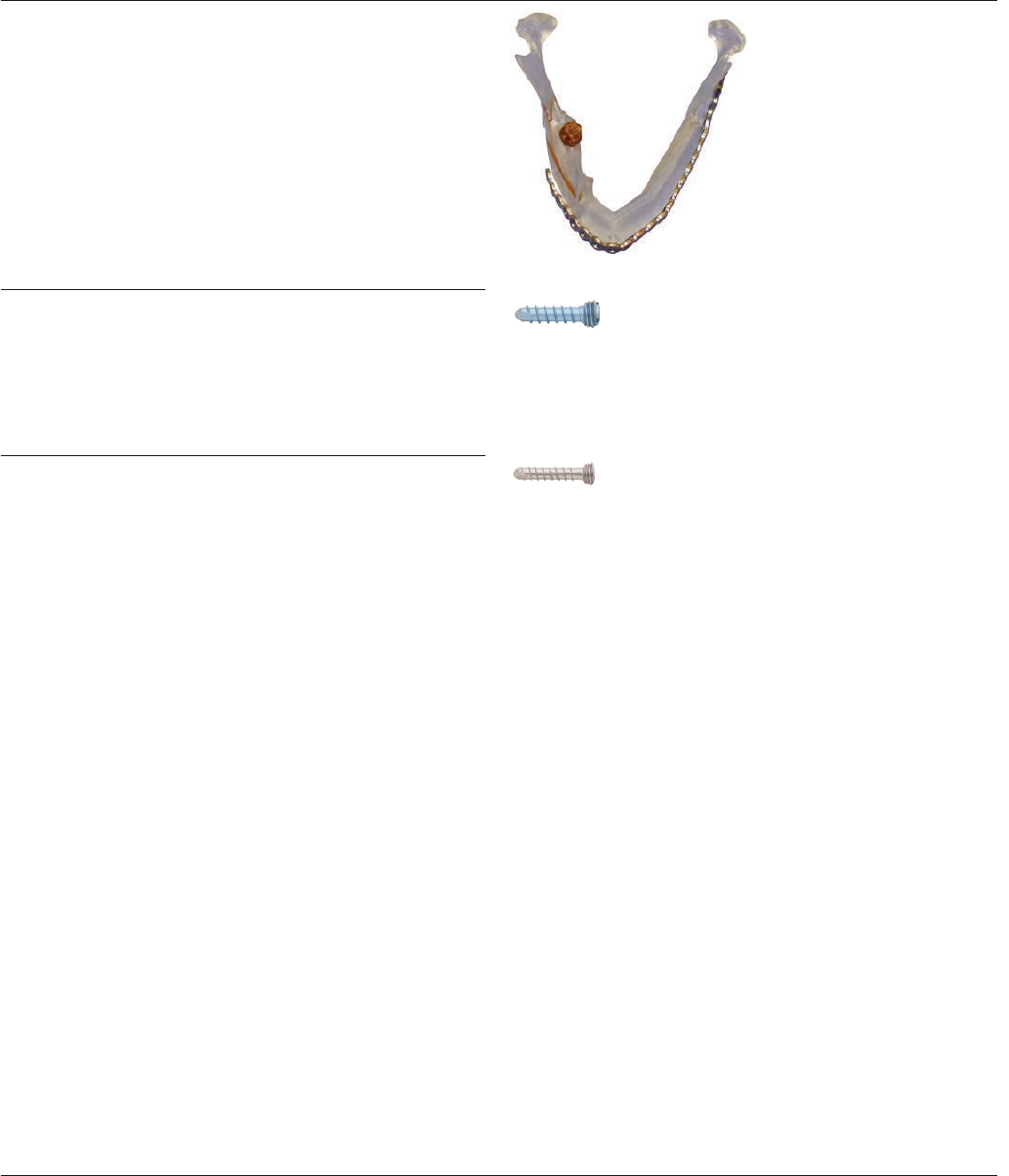
Implants Used
Product Information
SD449.510 Titanium MatrixMANDIBLE Angle
Reconstruction Plate, 2.5 mm thick,
7 x 23 holes, left
04.503.638– 2.4 mm Titanium MatrixMANDIBLE
04.503.648 Locking Screws, self-tapping
04.503.605– 2.0 mm Titanium MatrixMANDIBLE
04.503.618 Locking Screws, self-tapping

© 2012 Synthes, Inc. or its affiliates. All rights reserved. ProPlan CMF and Synthes are a trademark of Synthes, Inc. or its affiliates. Printed in U.S.A. 9/12 J11837-A
Surgeon Profile
Hugo St-Hilaire, MD, DDS, FACS
Assistant Professor, Clinical Surgery
Division of Plastic and Reconstructive Surgery
LSU Health Sciences Center
School of Medicine at New Orleans
New Orleans, Louisiana
Cutting Guides and Planned
Outcome Model Manufactured by:
Distributed by Synthes CMF
Imported by Synthes (Canada) Ltd.
Synthes CMF
1302 Wrights Lane East
West Chester, PA 19380
Telephone: (610) 719-5000
To order: (800) 523-0322
Fax: (610) 251-9056
Synthes (Canada) Ltd.
2566 Meadowpine Boulevard
Mississauga, Ontario L5N 6P9
Telephone: (905) 567-0440
To order: (800) 668-1119
Fax: (905) 567-3185 www.synthes.com
