IBA.3D OSA Orthotown 1.17 Orthodontic Symmetry Analysis Article
2013-08-05
: Pdf Orthodontic Symmetry Analysis Article Orthodontic_Symmetry_Analysis_Article 8 2013 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 18

Are Contemporary
Occlusion Concepts Valid
In An Asymmetric World?
Paul L. Ouellette, DDS, MS
Jason P. Ouellette, DDS
Jonathan P. Ouellette, DDS
Dental Specialists Team for Smiles
Rivers Edge Professional Center
455 Magnolia Avenue
Merritt Island, Florida 32952
800 76-SMILE

Introduction
Having practiced orthodontics for more than four decades, I have been continually searching for answers! Is there unequivocal evidence of the existence of “ideal
occlusion”? Are current or past prosthetic-driven occlusion principals valid? Do anterior guidance, CPO “cuspid protected occlusion” and other occlusion concepts really
exist? Why do some orthodontic cases finish with near perfect interdigitation with “ideal” anterior guidance, bilateral balanced or canine protected occlusal schemes? Can
occlusion principals really exist without skeletal symmetry?
General dentists and dental specialists can be profoundly influenced by their dental school education, expert-espoused occlusion dogma and personal clinical experiences.
In some cases occlusion becomes their obsession or religion. We all strive to create healthy beautiful smiles with the best possible function. Sometimes we may not be able
to achieve “ideal occlusion”. Why?
This preliminary study of orthodontic pre-treatment asymmetry is an attempt to “quantify” the “Why”
Evolution of the 3D Symmetry Analysis – Visual 3D OSA
This project started in January of 2008. This was the year I was initially introduced to 3D CBCT imaging by my dental student sons, Jonathan and Jason. Their dental
schools were early adopters of CBCT imaging. When developing the orthodontic symmetry analysis (Visual 3D OSA) we consulted several well-known educators and
technical experts in their fields. We worked very closely with Anatomage, San Jose, California. At the time, Brendon Bengsten was one of CEO, Jack Choi’s, first Invivo
Application Specialists. Brendon was instrumental in helping us design and implement Visual 3D OSA. In addition, we attended several 3D imaging conferences. Doctor
Paul Ouellette conducted on site and long distant telephone interviews with CBCT experts such as Ed Lin, DDS, MS, Sean Carlson, DDS, MS, Randy Womack, DDS, Robert
Boyd, DDS, MS, Ed Mills, DDS, Scott Ganz, DDS, MS, Marty Levin, DDS, MS and numerous other 3D imaging pioneers. Doctor James Mah, Chairman UNLV Orthodontic
Department helped us with the statistical analysis of our data. We attended a Bioblock Orthotropics Symposium that featured the well-known American Anthrologist, Professor
Emeritus, Robert Corruccini, Southern Illinois University-Carbondale. We also communicated by email with his esteemed colleague, Peer Moore-Jansen, Chairman
Department of Anthropology, Wichita State University. At the Orthotropics Symposium we had the opportunity to consult with Doctors John and Michael Mew from London.
Doctor William Hang’s presentation was enlightening and helpful. Selection of anatomical landmarks, analysis protocol and proposed study conclusions evolved using many
of our consultant’s clinical experiences and suggestions. Visual 3D OSA is just the beginning of our search for evidence that will hopefully support our conclusions.
Paul L. Ouellette, DDS, MS, Jason P. Ouellette, DDS, and Jonathan P. Ouellette, DDS
Are Contemporary Occlusion Concepts Valid In An Asymmetric World?
Smile Enhancement Therapy
Dentofacial Traits - Does Ideal Occlusion Exist?
Orthodontic patients present with diverse mixtures of "dentofacial traits”. A dentofacial trait is a hard or soft-tissue characteristic, or combination
of characteristics, that distinguish an individual’s facial appearance and determines their level of oral and social function. Some traits are directly in-
herited from biological parents, while other traits come from previous generations. These traits make each of us unique and beautiful from within our
own personal genome.
The orthodontist attempts to treat every case to the current “standard of care”, or to current occlusion (bite) philosophies proposed or mandated by
universities, dental literature, clinical studies, textbooks, dental boards, as well as communications with other orthodontic and cosmetic dentist col-
leagues. Current orthodontic philosophy has evolved from concepts related to Prosthetic Dentistry (replacement and modification of missing or dam-
aged teeth) and to Victorian Era concepts espoused by Edward Angle (Angle 1899) and others.
The concept of what is normal occlusion (a normal bite relationship) by Doctor Angle has been the foundation of the orthodontic and cosmetic
dental profession for over 100 years. Previously accepted concepts of occlusion are rapidly changing as we become aware of evidence-based studies
and the evolution of contemporary occlusion concepts.
Anatomage Invivo5, San Jose, Ca
Reference: Marc Ackerman’s paperback book, Enhancement Orthodontics, Amazon
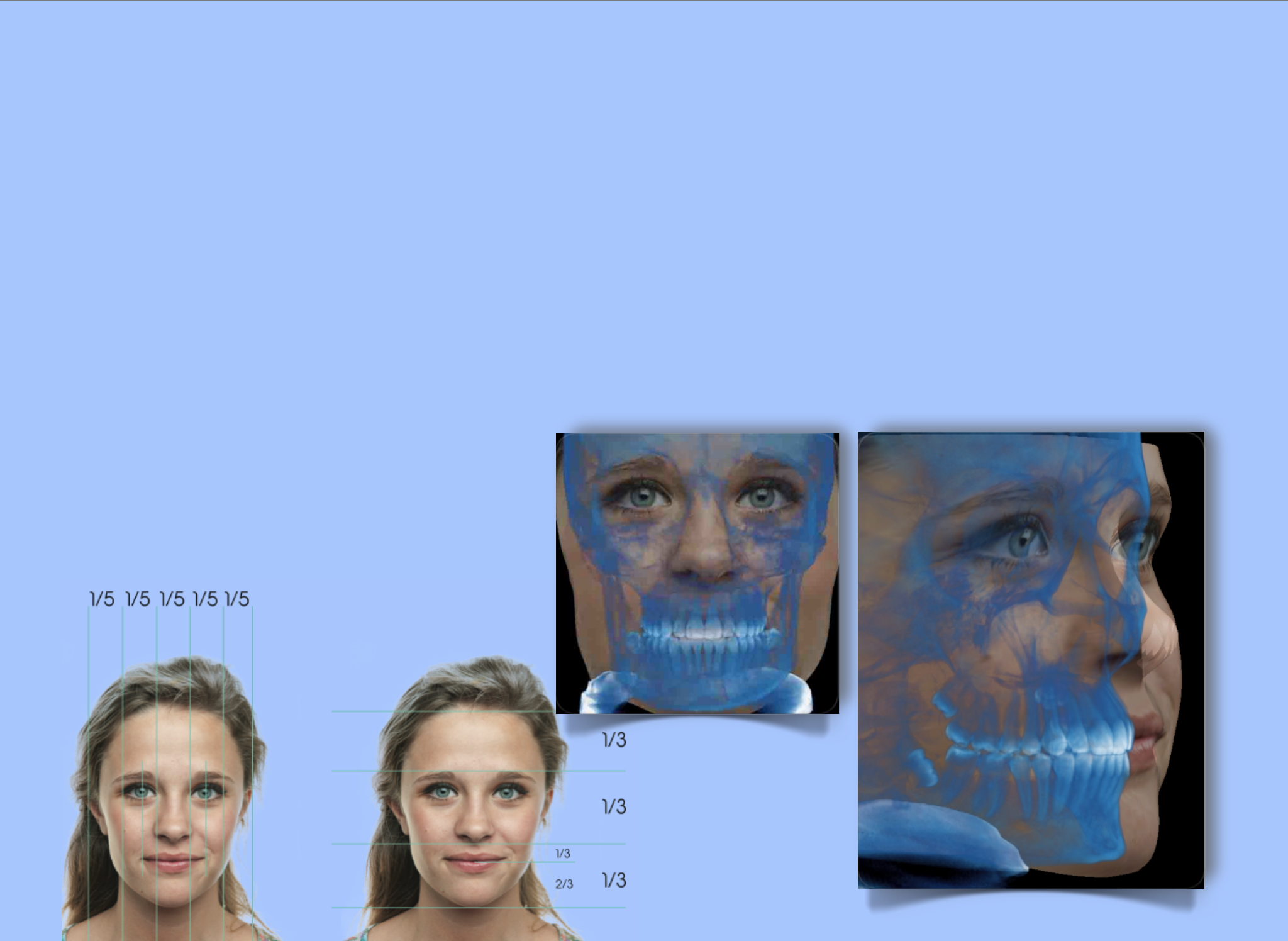
Lindsey’s Near
Perfect Symmetry
The Polymorphic Cuboidal Analysis
Cephalometrics (Cephalo = Skull; Metrics = Measure) is the scientific
analysis of anatomical dimensions of the human skull using medical type
radiographs. Orthodontists, Oral and Plastic Surgeons are the biggest users of
cephalometrics. For more than 70 years orthodontists have used 2D
cephalometrics to measure and treatment plan 3D problems. The advent of 3D
CBCT imaging has now made it possible to use 70 years of 2D cephalometric
research to aid in the development of modern 3D cephalometric analyses. 3D
imaging has taken much of the “guesstimating” out of orthodontic diagnosis and
treatment planning.
When developing the OSA- Orthodontic Symmetry Analysis the concept of
the “Polymorphic Cube” was proposed by the authors. Utilizing bilateral (both
sides of the skull) paired (same landmark on each side of skull) anatomical
landmarks, a virtual Rubik’s-like Polymorphic cube is constructed in the maxillary
and mandibular anatomical space. If one exhibits “perfect symmetry”, ALL cuboidal
measurements would be equal in ALL planes of space. In addition, the
“Polymorphic Cube” would be precisely positioned at right angles (90 degrees) in
the space it occupies between the right and left condyles of the mandible. Our
interpretation of a patient’s orthodontic problem also takes into consideration the
influence of genetics, postural and environmental influences. The Polymorphic
cube is subject to changes or “morphing” and it can be quantified in exact
measure.
Polymorphic Cube “Anterior” the position of the maxillary and mandibular
central incisors is analyzed. 3D OSA measures the interincisal angle using right
upper and lower central incisors. Polymorphic Cube ”Posterior” the patient’s
airway is easily viewed and analyzed. Total airway volume and the most
constricted point is measured in the 3D OSA. Thus, we screen our patients for
potential OSA problems (Obstructive Sleep Apnea). See images that follow:
Malocclusion (Bad Bite) is NOT a disease state! A closer look at occlusion concepts.
For more than 40 years Doctor Ouellette Sr. has had the privilege of modifying and creating more than 15,000 beautiful smiles. Throughout
Dr O’s career he frequently noticed some cases did not completely correct. “We were not able to achieve ideal occlusion”. Why did this happen?
In 2008, the authors began using 3D CBCT imaging with the goals of providing a more comprehensive pre-treatment diagnosis and to identify evi-
dence to document patients’ symmetry or asymmetries. Is it possible to predict which cases can be completely resolved to a “perfect bite”. Do asym-
metries play a role in treatment outcomes? Is it possible to “describe - and preferably quantify - variations in occlusion”? (Ref: Isaacson et al, 1975)
Doctor Paul Ouellette and his two sons, Doctors Jason and Jonathan developed a 3D Cephalometric analysis of 121 pre-treatment CBCT images.
Their goal was to identify and “quantify” existing asymmetries and create the OSI – Orthodontic Symmetry Index.
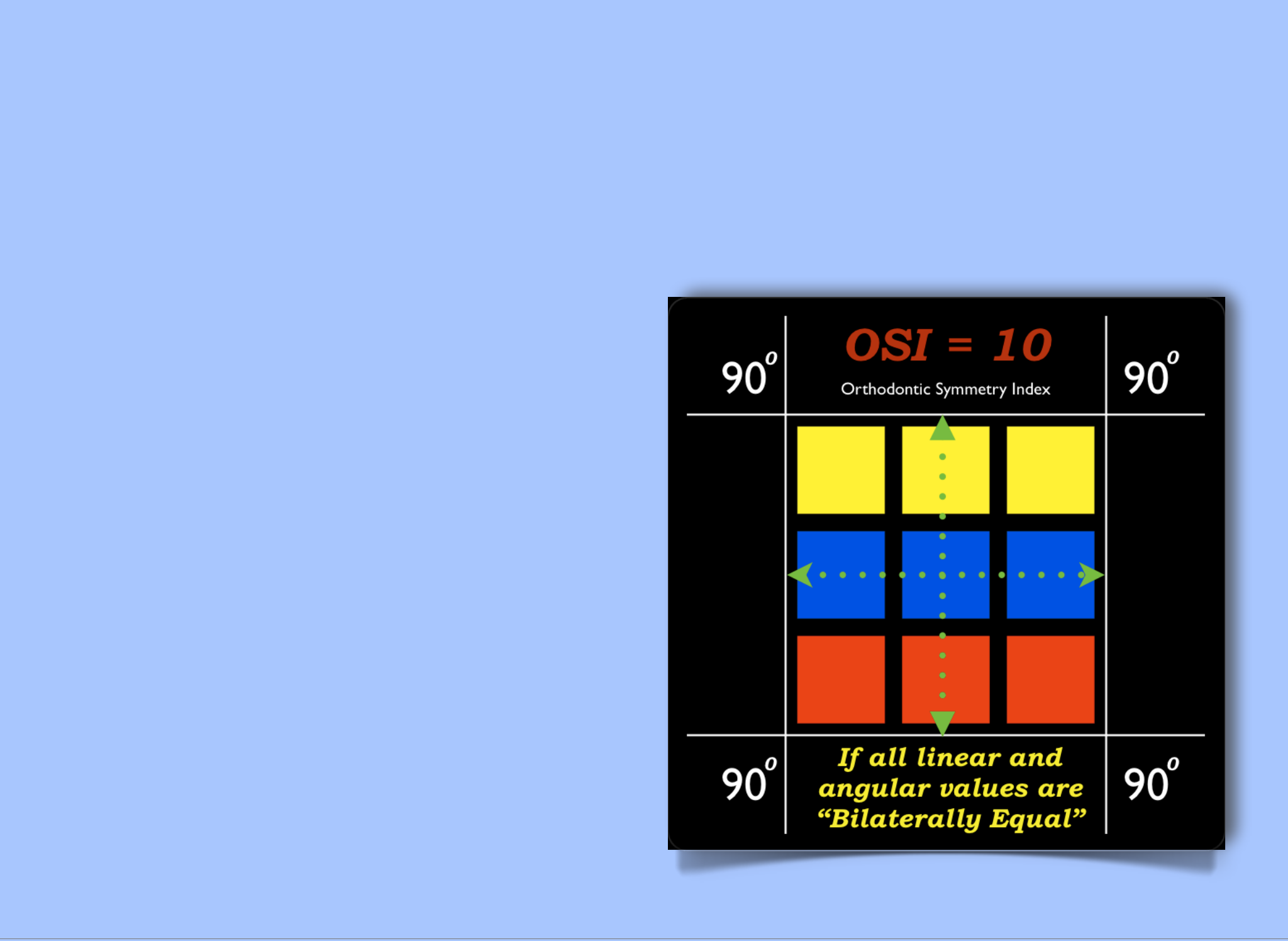
Does the perfect 10 exist?
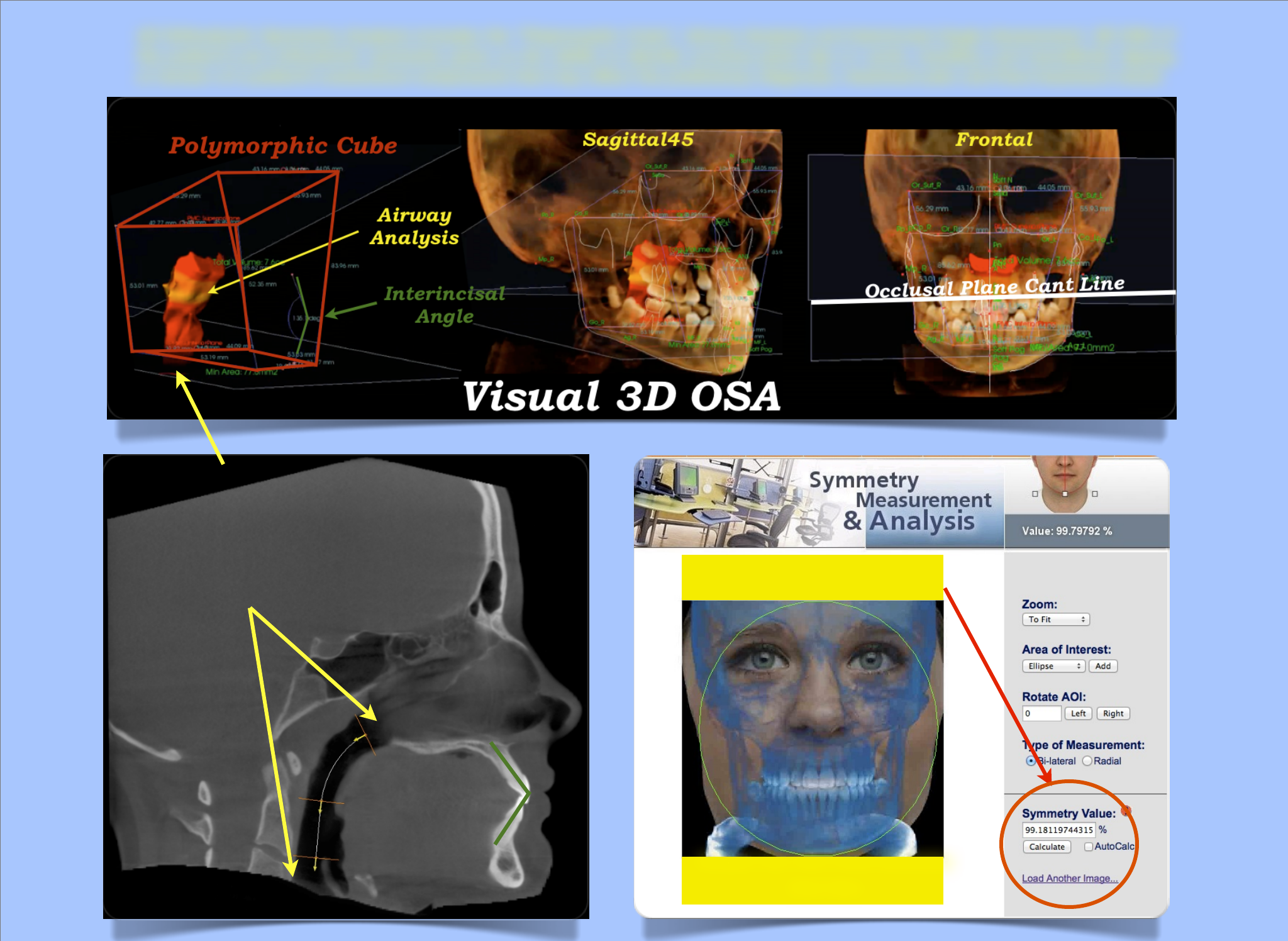
Upper and Lower Limits of
Lindsey’s “Normal Airway”.
The Polymorphic Cube Airway
Analysis Demonstrates A 3D
Volumetric Rendering.
Interincisal Angle
Normal = 1300
Analyze Your Own Facial Symmetry
Click Here
Lindsey is 9.91
3D Orthodontic Symmetry Analysis includes the “Polymorphic Cube”, Airway Analysis and Interincisal Angle Assessment. 3D OSA of
the patient’s pre-orthodontic symmetry gives us the ability to identify occlusal plane tips or cants, maxillary and mandibular tipping
or torsion of a patient’s anatomical components that may affect the preliminary diagnosis, treatment plan and final treatment result.
Subject: 3D CBCT Study
Date: Fri, 22 Oct 2010 22:05:18 PM
Hi Doctor Corruccini:
I really enjoyed your presentation today. My sons (both future orthodontists) and I are doing a study using Anatomage Invivo5 software (Anatomage.com) San Jose, Ca) to analyze 120+ Cone
Beam Volumes (Orthodontic patients) to study anatomical variation. We plan to use paired bilateral landmarks to be measured in relation to the midsagittal plane. Our thesis is "Anatomical
Variation is the Norm". Class I occlusion may be the treatment goal for all orthodontists. but in nature Class I may not be the norm. Only a small percentage of the population has "ideal Class I
occlusion".
As you know the lateral cephalogram has been historically used as the "gold standard" in orthodontic cephalometric analysis. Many of the speakers at the Orthotropics Symposium this week
stated that conventional cephalometrics using a lateral cephalogram is not a dependable measure of true anatomical morphology. Our 3D CBCT analysis will hopefully create a new "standard of
care" for cephalometric analysis. Initially, we want to create the "Symmetry Index" for the orthodontic patient using 3D CBCT scans.
As I said to you after your presentation, I would hope you could help us create an accurate 3D cephalometric analysis that would quantify the degree of anatomical variation an orthodontic pa-
tient has prior to the orthodontist formulating his preliminary diagnosis and treatment plan. You mentioned the "F "/ Variation test in your presentation today. Would it be possible to create a
"symmetry index" for an orthodontic patient prior to formulating a treatment plan?
With your permission, I plan to spotlight your previous contributions to the orthodontic literature in our study. In addition, I have been communicating with one of your colleagues, Doctor Peer
Moore-Jansen. We also hope to work with Doctor Moore-Jansen as we design our study and report our results to our colleagues.
Thank you again for any help you can provide.
Paul
Paul L. Ouellette, DDS, MS
On 9/10/2010, Doctor O wrote:
Hi Peer:
Again thank you for your comments!! The only reason I use Basion is due to the widespread acceptance in my profession of this landmark as one of the tried and true (probably not true) land-
marks in cephalometrics.! I am very open to considering other more easily reproducible landmarks.! I will start looking for hormion in my next 3D tracings.! If it is easier to find than basion I will
use it in our analysis.!
I have a teleconference with Brendon at Anatomage this week.! I will discuss your suggestion with him. In addition, what would you suggest for the most easily reproducible "paired
landmarks"...i.e....R L mental foramen, R L gonion, R L condylion, R L zygomatic lateral landmarks, etc.?!
Have a great weekend!
Paul
5
Are Contemporary Occlusion Concepts Valid In An Asymmetric World?
Pre-Study Email Communications
We used an “out of the box” research protocol to gather
information for our study. In addition to a thorough
online literature search, we visited several universities
and practices of early adopters of CBCT imaging. We
attended every possible 3D imaging meeting. Telephone
interviews, exchanging emails and live interviews with
pioneers in 3D technology were performed by Dr. O Sr.
SIDEBAR
Sent: Fri, Sep 10, 2010
Subject: Re: landmarks/asymmetry
Paul:
I watched the video you sent me. I am definitely interested in providing you with whatever help I can. You refer to basion as your 2rd point for the plane, and I suggest that you consider
my comments about the differences among the definitions of basion and select the more reproducible and consistent of them. Have you considered hormion at the base of the vomer? It
is more anterior than is basion, but it is easy to define.
!
Peer!
Peer H. Moore-Jansen
Subject: Re: landmarks/asymmetry
Date: Tue, 7 Sep 2010 09:07:36 AM
Hi Peer,
Thank you for your help as we navigate through our project.! I like the idea of the transmeatal axis as a transverse plane.! Orthodontists in the past used the ear positioning rods on the
Cephalometer as a cephalometric landmark -- Porion.! With the 3D analysis (and 2D Digital Images) we now use the superior rim of the external auditory meatus for Porion Right and Po-
rion Left..."paired landmarks."! In order to create a plane in the Anatomage 3D software you have to choose a third point, probably basion.! What do you suggest?
I do not want to begin the tracing of all our volumes until Anatomage creates a way of adjusting landmark positions at the end of the tracing session prior to saving the data.! As I stated
before, my sons and I were not able to produce consistent tracings from one operator to the other, at least in our hands.!
I contacted Brendon at Anatomage last week and asked if he and one of his colleagues, Roger would be able to trace the 120 volumes using our Orthodontic Symmetry Index analysis.!
Prior to outsourcing the volume tracing to Anatomage I would like to work with you and your team to select the most reproducible "paired landmarks" for the analysis.!
I will put together a list of our proposed landmarks and have you give us your feedback.! Of course, we will give you and your department full credit in any future publications for your con-
tributions to the study.
Thank you again for your help!
Paul
Sent: Mon, Sep 6, 2010 11:58 PM
Subject: RE: landmarks/asymmetry
Paul:
If you stay in touch. I will work with you along the way. What did you think of the "transmeatal axis" as a transverse reference plane? Either way I am glad to!know you are in receipt of my
email.
!
Peer!
Peer H. Moore-Jansen
6

Subject: Re: landmarks/asymmetry
Date: Sun, 5 Sep 2010 11:01:44 AM
Hi Peer,
Thank you for your comments.!
I will carefully read your email and take all your suggestions into consideration.!! I agree with your suggestion to use the Basion Nasion sagittal plane as one of our main reference
planes.! My problem has been to consistently &!accurately locate Basion with the current version of the Anatomage 3D Cephalometric application.!! When the user completes his or her
landmark inputs in the 3D application selected planes can be displayed on the monitor screen.! Most of my early 3D analysis tracings exhibited landmarks that were slightly off by 1 to 3
mm.! Currently, the user can not easily adjust the position of a "missed landmark" without starting all over at the beginning of the 3D analysis.! I have talked with Brendon at Anatomage
about this problem and the Anatomage development team will eventually provide a fix.!
When your time permits please send me the links to the Forensic Databank and any other pertinent research.! Prior to publishing our results I want to make sure that our study is not
flawed in any way.
If you have any reference or published papers that are not available online, I would be glad to pay your research assistant the cost of duplicating the materials.!
Again, THANK YOU!
Paul
Re: landmarks/asymmetry
September 10, 2012 10:47 AM
Hi Peer:
Thank You !! for remembering me.! My colleagues and I have compiled data on 121 orthodontic patient CBCTs and have fully developed the 3D Orthodontic Symmetry Analysis (OSA).!
OSA is "fully" developed pending any suggestions from you and other collaborators.
See YouTube link for most recent OSA video:!http://www.youtube.com/watch?v=VcWlwg2IXqM
My sons and I also developed a preliminary 3/4 CT analysis.! There is much controversy in our field today related to higher (than 2D image) absorbed dose values used in orthodontic
imaging.! In addition, children are prone to more potential problems from excessive radiation (ie thyroid and brain exposures).! The 3/4 analysis has a smaller FOV and radiation levels are
dramatically less.! Imaging Sciences (iCat) is steadily reducing exposure with changes to their CT generation 3 imagers (27-36 mSv versus over 100 mSv for older machines).! In the fu-
ture, 3D CBCT imagers will have radiation exposure values the same or less than 2D x-rays.
In our to be soon published study in Orthotown (pending acceptance) we will reference your 1994 work as we found in the Standards paper (see below).! Brendon is compiling our data
case by case due to a glitch in the Anatomage application. At this time Anatomage's data export to Excel is not functioning. He promises to be finished in two weeks. At that time I will
evaluate the data and would like to talk with you about running statistical analyses.! In addition, I recently presented a lecture at UNLV two weeks ago and talked with Dr. James Mah, Or-
tho Chair about our project.! He agreed to help us with analyzing the data and make his suggestions.
In our publication, we plan to give proper credit to all collaborators.
Thank you again, for your help!
Paul
7

Subject: Re: landmarks/asymmetry
Date: Wed, 20 Jun 2012 12:31:36 PM
Hi Peer...!
We are nearing completion of our first 121 volume CBCT symmetry study. We have several more volumes to analyze, but want to get our preliminary study published ASAP.! The Lawrence
Andrews Straightwire study used 120 orthodontic study models.! We plan to present our first paper using a similar number of patients (121).! When I was in my orthodontic residency at
Loyola, Chicago our department provided several of Dr. Andrew's ideal occlusion cases.!
My colleague, Brendon Bengsten, formerly with Anatomage as the one of the developers of their 3D cephalometric analysis, has done all the 3D cephalometric tracings. We are looking for
your guidance in analyzing the data.! Would you have a statistics grad student or other experts in your department that could help us look at our data to come up with a meaningful contri-
bution to orthodontic cephalometrics.! My initial goal was to come up with an Orthodontic Symmetry Index (OSI), e.g.. 1 to 3 (or 4,5).! If a patient has little variation between the right and
left sides the Symmetry Index would be 1.! A moderate variation would be 2 and severe 3.! I hope to keep the concept simple and useful for the user.
I have also coined the term / concept "polymorphic cube"...! Bilateral paired landmarks create a polygon / cube or the "skeletal base" in the center of the patient's Maxillo-Mandibular com-
plex. Recently, we added an airway analysis to our study.! The airway is conveniently positioned at the bottom of the cube and is in most cases centered.! We also added the interincisal
angle using the right upper and lower central incisors. (125-130 norm).! My thought process includes a quick analysis of the position of the anterior teeth, the initial status of the airway
volume and is there asymmetries that may affect our predicted final result.
We also want to create a volumetric analysis of the polymorphic cube, mapping each side and comparing the volumes in mm2 or cm2; Like a finite element analysis, skeletal mapping! or
a grid analysis of an object.! Perhaps you can think of a way to do this using your experience in scientific research.! After 40 years in private orthodontic practice my scientific method
needs major help!!
If your time permits, please give us your suggestions and guidance.
Thank you for your help!
Paul
Hi James,
Brendon Bengston of iHub3D completed the compiling of our 3D OSA study data this week. We analyzed 121 FFOV 3D CBCT orthodontic patient volumes. !As we discussed during my
recent visit to UNLV,!I would like your guidance in the statistical analysis of our data. !There are approximately 430 cephalometric measurements. We used Excel spreadsheet columns to
organize the data into bilateral paired landmarks. We measured anatomical skull landmarks in millimeters to the midsagittal plane. !In addition, we measured several bilateral paired land-
marks to construct the proposed "Polymorphic Cube". !The virtual 3D polymorphic cube is located within the maxillary-mandibular center of the skull just below the cranial base. !If a pa-
tient exhibits an asymmetry from one side of the skull to the other it will be evident if there is a difference in mm and/or angular measurements. !If a patient has a tilting or cant of a con-
structed plane such as the occlusal, mandibular or condylar planes the “paired angles” will be significantly unequal. !We also included airway volumes and most constricted AW point
measurements for each volume.
The last time I analyzed a data set was more than 40 years ago. !(Ref: TMJ sound prints: electronic auscultation and sonographic audio-spectral analysis of the temporomandibular joint,
Paul L Ouellette, JADA September 1, 1974 89(3): 623-628). !I used the Sonagraph, Bell Laboratories, Chicago, to analyze right and left temporomandibular joint sound waves. !Sound was
recorded using bone conduction hearing aids (transducers). !The FBI prior to advancements in computer sound analysis used the Sonagraph to analyze human voice sound waves. !The
capture of Pablo Escobar in Medellín, Colombia, December 2, 1993 utilized this technology during the surveillance operations. !When analyzing TMJ data individual patient “Sound
Prints” were organized into four distinct groups. !Perhaps a similar protocol could be considered for the 3D OSA study.
Brendon and I used 2 mm and 2-degree ranges on each side of a visual representation of the measurements. !For example, condylion right may be 50 mm to the midsagittal and condylion
left could be 44 mm, a 6 mm difference. !If we use a range of 2 mm per side or a 4 mm total range, the patient would have one of the sides 2 mm outside the range. Brendon used a color
spectrum guide (e.g.: red = asymmetry) to visually display asymmetries (outside the 4mm range).
Our goal is to create an easy to diagnose and locate areas of asymmetry by "Visual Representation" (i.e.: Rickett’s VTO) of significant differences in mm and angular measurements.
Hopefully, your vast experience in research, data organization and analysis will help us find a simple solution. !Brendon will be sending you the data set for your review. Please call or
email to discuss this project when you have time.
My sons and I would be honored to include you as one of the principal authors or give you credit as a contributor. !Let me know if you have the time and want to participate in this study.
Thank you for your time and help!
Paul
8

Dr. Mah’s response:
Hi Paul, in order to design appropriate statistical approaches to analyzing the data, we'll need to know your hypothesis(es) with respect to what is the reference standard and which vari-
able is being tested. In other words,!is!it the correlation between difference in the paired landmarks and angle to respective plane (occlusal, mandibular, condylar) that you are after? Or is
it the difference between the paired measurement and landmarks on the cube.
!
Regards,
!
James Mah
Dr. Ouellette’s response:
Hi James,
Thank you for your quick response.
My original hypothesis, subject to modification:
Every orthodontic patient has multiple asymmetries and unequal angular values that may result in tipping or cants of anatomical planes (occlusal, mandibular, condylar, etc).!
Human asymmetry (anatomical variation) is the Norm !
The purpose of quantifying a patient's asymmetry(s) is to provide our dental colleagues accurate CBCT evidence that further challenge, "Occlusion Dogma" such as the possibility that
anterior guidance, canine protected occlusion and other gnathological principals (concepts) can not exist in an asymmetrical patient. Patients have to ADAPT to the occlusal scheme they
have inherited and/or the environment created when modified by treatments such as corrective orthodontics or full mouth reconstruction. !!
References:! Rinchuse's papers that question “evidence” of occlusion dogma.!
Akerman’s papers and book that state, “Malocclusion is NOT a disease”,
“Modification of dentofacial traits” and “Roll, Pitch and Yaw”
Brendon used the difference between landmark measurements to the midsagittal plane.! He used the same protocol for the angular measurements.
What would you use if you designed the study?!
Paul
Subject: Re: Dr. Mah’s response to statistic question
Date: Tues, 23 Oct 2012 12:50 PM
Hi Everyone,
After reviewing!the research description and!looking at the examples provided by Brendon, it appears that you have interval data drawn from a normally distributed population. Paired t-
tests are appropriate since the measurements are within the same individual. Paired t-tests could be run for the left and right differences and the left and right distance to the constructed
cube measurements. If the hypothesis calls for a correlation between measurements to estimate asymmetry of another region, linear regression or Bland-Altman analyses may be per-
formed. But I am not sure if this is needed since one could simply measure the distance rather than predict it from another.
!
James
9
Hi Peer:
We are nearing completion of our first 121 volume CBCT symmetry study. We have several
more volumes to analyze, but want to get our preliminary study published ASAP.! The Law-
rence Andrews Straightwire study used 120 orthodontic study models.! We plan to present
our first paper using a similar number of patients (121).! When I was in my orthodontic resi-
dency at Loyola, Chicago our department provided several of Dr. Andrew's ideal occlusion
cases.!
My colleague, Brendon Bengsten, formerly with Anatomage as the one of the developers of
their 3D cephalometric analysis, has done all the 3D cephalometric tracings. We are looking
for your guidance in analyzing the data.! Would you have a statistics grad student or other
experts in your department that could help us look at our data to come up with a meaningful
contribution to orthodontic cephalometrics.! My initial goal was to come up with an Ortho-
dontic Symmetry Index (OSI), eg.1 to 3 (or 4,5).! If a patient has little variation between the
right and left sides the Symmetry Index would be 1.! A moderate variation would be 2 and
severe 3.! I hope to keep the concept simple and useful for the user. (We reversed the varia-
tion index (OSI) using numbers 10 - 7 in the 3D Visual OSA.)
I have also coined the term / concept "polymorphic cube"...! Bilateral paired landmarks cre-
ate a polygon / cube or the "skeletal base" in the center of the patient's Maxillo-Mandibular
complex. Recently, we added an airway analysis to our study.! The airway is conveniently
positioned at the bottom of the cube and is in most cases centered.! We also added the inter-
incisal angle using the right upper and lower central incisors. (125-130 norm).! My thought
process includes a quick analysis of the position of the anterior teeth, the initial status of
the airway volume and is there asymmetries that may affect our predicted final result.
We also want to create a volumetric analysis of the polymorphic cube, mapping each side
and comparing the volumes in mm2 or cm2; Like a finite element analysis, skeletal mapping!
or a grid analysis of an object.! Perhaps you can think of a way to do this using your experi-
ence in scientific research.! After 40 years in private orthodontic practice my scientific
method needs major help!!
If your time permits, please give us your suggestions and guidance.
Thank you for your help! Paul (End of Email Communications)
10
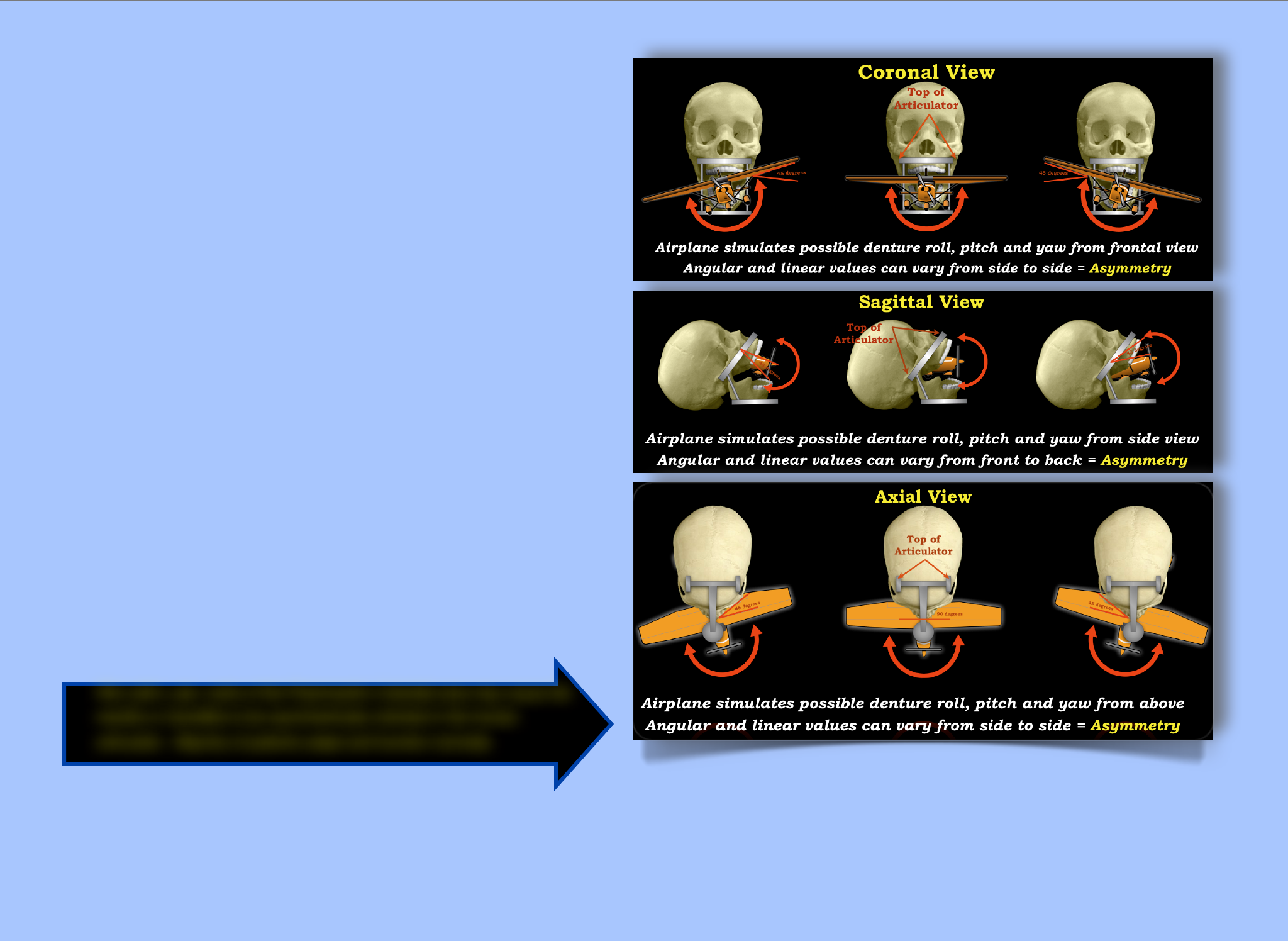
Roll, pitch, yaw, cants of the Polymorphic Cuboidal area may cause the
maxilla or mandible to be asymmetrically oriented in the human
articulator. Majority of patients adapt and function normally.
“FUNCTIONAL ADAPTATION”
Dentists use articulators to simulate “estimated positions” of the maxillary and mandibular dental arches in the skull. The 3D CBCT view of the human skull
makes it possible to measure bilateral dimensions and angulations related to the center of or mid-sagittal plane of the skull. In the “Perfect 10” all linear and
angular measurements would be equal.
Abstract
This study is focused on the statistical analysis of orthodontic symmetry based on pre-treatment evaluation of 121 randomly selected orthodontic patients using Anatomage 3D cepha-
lometric Analysis of full volume (FFOV) CBCT images. Cephalometric measurements, linear and angular, were obtained from anthropologically recognized anatomical bilateral paired
landmarks. hub 3D diagnostic services performed 3D cephalometric analysis using for the study.
Allowing H₀: µ₀= 0 to represent perfect orthodontic symmetry as measured by the virtual construction of a Polymorphic Cube (def: multi-sided object subject to morphological
change). H₁: µ₁≠ 0 to represent orthodontic asymmetry, we are testing to what statistical significance, if any, we can reject or not reject the null hypothesis.
Study Design
Brendon Bengston was one of the first Anatomage software engineers that helped develop the Anatomage 3D Cephalometric application and trained orthodontists to use 3D CBCT
analysis. Brendon helped my sons and I learn how to use Invivo5 3D Cephalometric Analysis. Brendon subsequently left Anatomage to form Conebeaminfo.com, a CBCT knowledge-
base website and iHub3D.com, a 3D diagnostics portal for orthodontic case workups. Our practice exclusively uses iHub3D for every orthodontic patient. iHub3D provides a very af-
fordable menu of diagnostic services and his partner, Larry Chan, MD, Radiologist, provides radiological reporting services. Prior to initiating an orthodontic treatment plan it is impor-
tant to know the degree of asymmetry a patient possesses. Also if a case does not finish with an ideal occlusion, the orthodontist could order the 3D Orthodontic Symmetry Analysis
(OSA) to look for areas of asymmetry. iHub3D also provides 3D animations that we use for patient education and practice marketing.
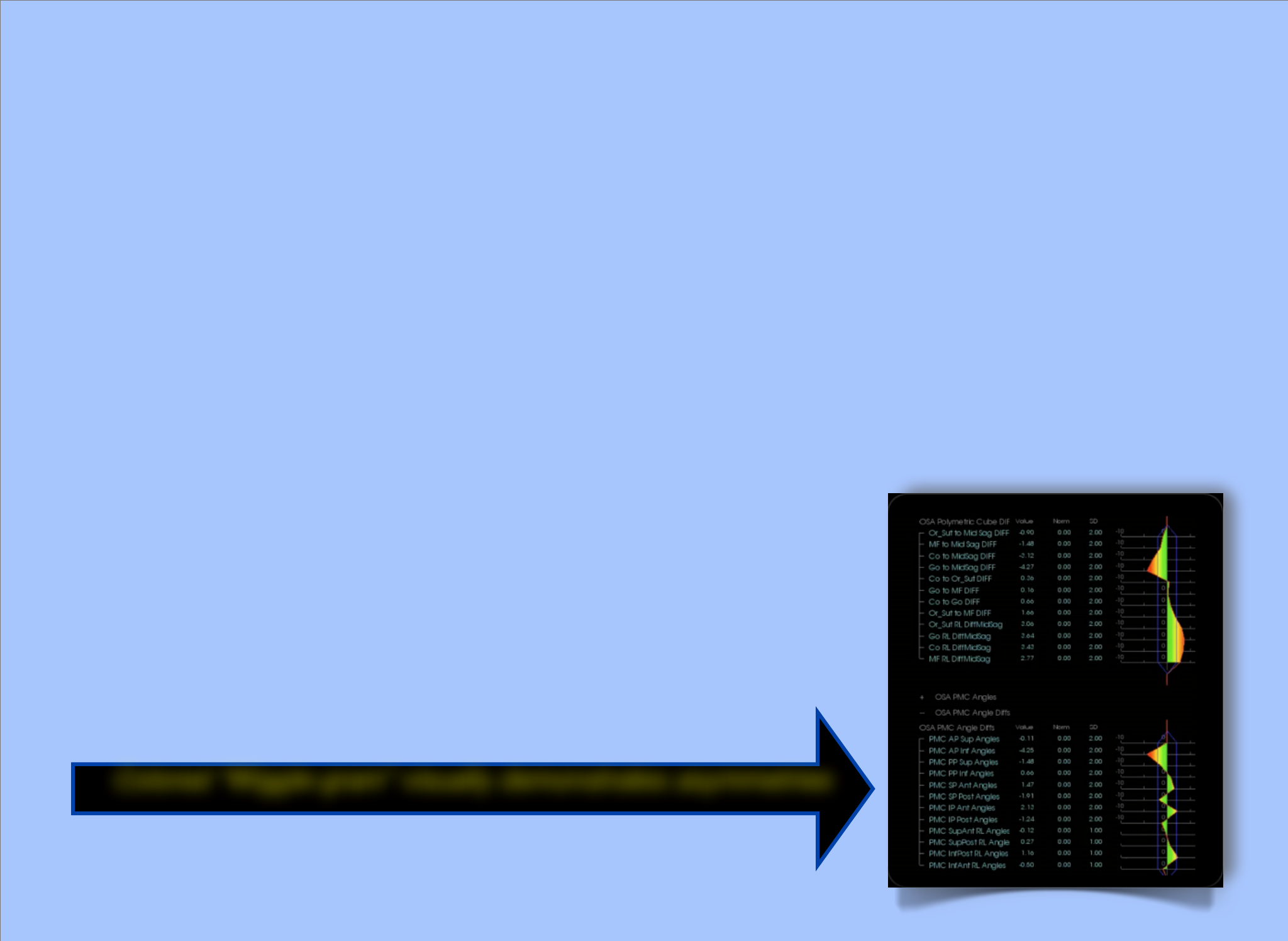
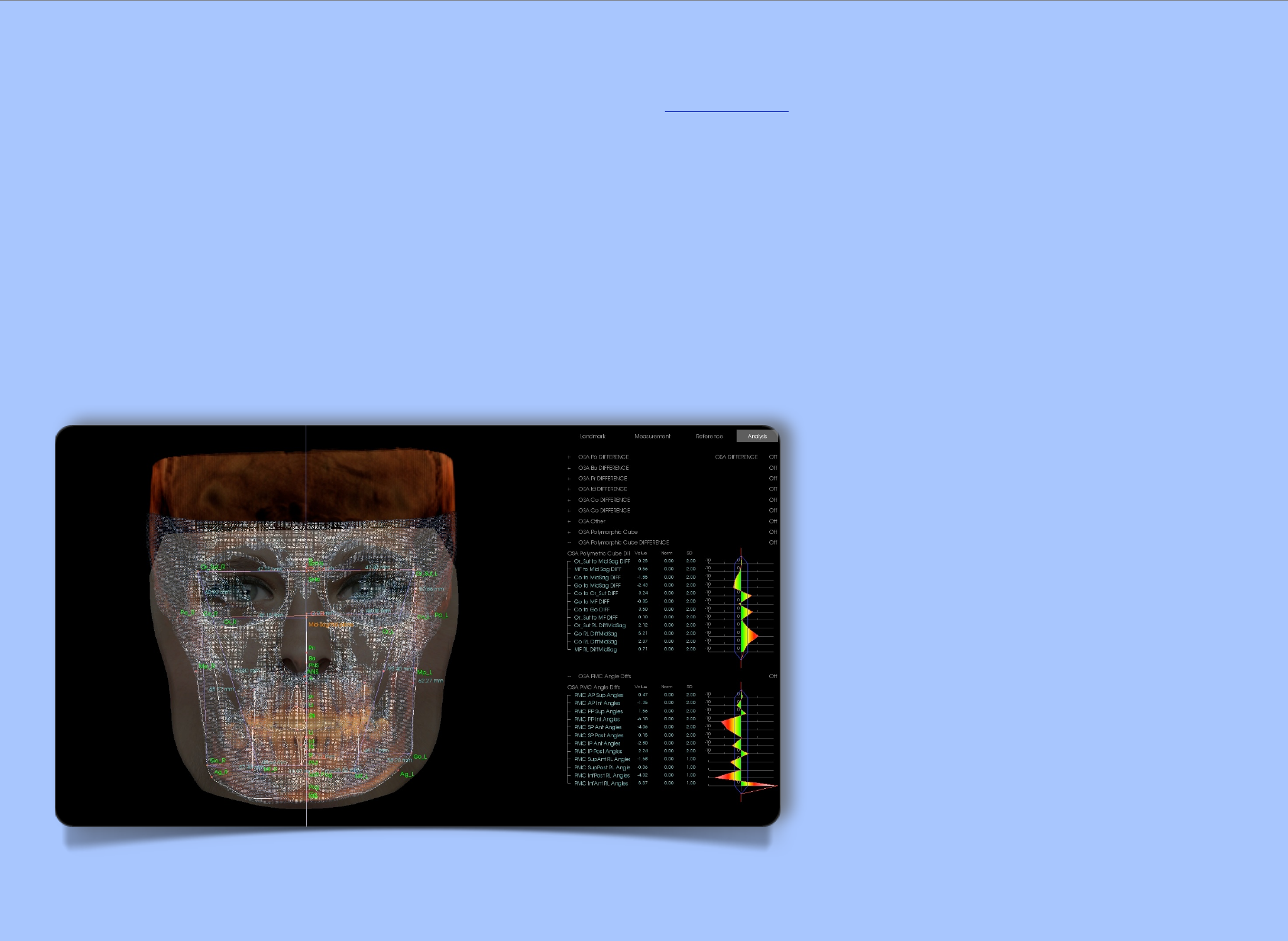
When developing OSA we asked Brendon to make our analysis easy for the non-professional to understand. An “outside the norm” color spectrum “wiggle-gram” is used to clearly
demonstrate asymmetrical areas of the patient’s maxillo-mandibular complex. (see Wiggle-gram Image ) We do not emphasize linear or angular values with patients or referring doc-
tors. Visually identifying areas of asymmetry allows us to create a pre-treatment disclaimer, “We may not be able to finish this case with an “ideal” bite, but we will do the best we can
considering your “genetic” traits and asymmetries. Our goal is to fully inform the patient and assign “ownership” of the orthodontic problem to the patient.
OSA steps using Anatomage 3D Cephalometric Analysis
1. Establish the Cartesian coordinate system: MidSag plane = Ba, N, A point; Horizontal plane = Po_R, Or_R, Perp to MidSag
2. Establish bilateral key source landmarks: Po, Co, & Go
3. Establish key MidSag source landmarks: Ba, Pr, & Id
4. Establish secondary landmarks and planes to measure key source landmarks to
Planes - MidSag plane, FH plane, & Frontal Plane Landmarks - Ba, Sella, Or, Or_Sut (Zygomatic Process), Po, Go, A, B, Pog, Me, Pr, Id, ANS, & PNS
5. Create singular measurements then compare them bilaterally to corresponding measurements. i.e. Co_R to Go_R and Co_L to Go_L - then measured the Difference between the two.
All measurements are Right minus Left
Norm = 0 SD = 2mm (built in user tracing error)
6. Estimate PMC (Polymorphic Cube): Or_Sut, Co, Go, MF - Bilateral difference measurements distance angular
7. Colored wiggle-gram - ALL measurements are R minus L
Polymorphic Cube Linear Measurements
Analyzing 121 samples (patients) we used two-tailed, paired t-tests to analyze eight significant differences in distances between corresponding landmarks and the appropriate plane
of symmetry in each sample.
11
We allowed the null hypothesis for each difference to read,
!H₀: µ₀= 0,
and tested against the alternative hypothesis,
!H₁: µ₁≠ 0.
We found that for 6 of the 8 differences, there is statistically significant data to suggest that we should reject the null hypothesis (samples are symmetric) at an α = .10 significance
level and accept the alternative hypothesis (samples are asymmetric). It should be noted that in the remaining 2 measurements, we have failed to reject the null hypothesis at the stated α
= .10 significance interval.
The data tables in the associated spreadsheets contain the p-value for each of the 8 distance differences. If the p-value is less than .10 then we reject the null hypothesis and accept
the alternative.
Polymorphic Cube Angle Measurements
Measurements of angles created by the surfaces of the Polymorphic Cube can likewise be compared to their corresponding opposites in order to assess orthodontic symmetry. We
analyzed the differences between corresponding angles in the same way we analyzed the distances. We allowed the null hypothesis to read,
!H₀: µ₀= 0,
and tested against the alternative hypothesis,
!H₁: µ₁≠ 0.
In this case, we found far less statistically significant data to reject the null hypothesis. In fact, using the α = .10 significance interval, we found that only 2 of 12 measurements were
significantly different enough for us to reject the null hypothesis. Therefore, we must state that we failed to reject the null hypothesis in 10 of 12 angle difference measurements.
The data tables in the associated spreadsheets contain the p-value for each of the 12 angle differences. If the p-value is less than
.10 then we reject the null hypothesis and accept the alternative.
Symmetry Index based on the Polymorphic Cuboidal Analysis
Along with ascertaining the statistical significance of different distances between landmarks, we evaluated the data to arrive at a
“Symmetry Index” based on the 121 samples. Our evaluation of the data found the mean of 8 difference measurements used in the
Polymorphic Cube for linear distance of each patient. We then found the sample mean and sample standard deviation of the 121 dif-
ference means. Since the difference means approximately follow a Normal distribution, we assigned a scale score according to the
Normal curve. That is, if a patient had a difference mean that fell between 1 sample standard deviation of the sample mean in either
direction, we assigned them a 9, which indicates “average orthodontic symmetry.” If the patient had a difference mean that fell be-
tween 1 and 1.5 sample standard deviations in either direction, we assigned them a 8, which indicates “moderate orthodontic asymme-
try”. If the patient had a difference mean that fell outside of 1.5 sample standard deviations in either direction, we as-
signed them a 7, which indicates “severe orthodontic asymmetry.
12
Colored “Wiggle-gram” visually demonstrates asymmetries
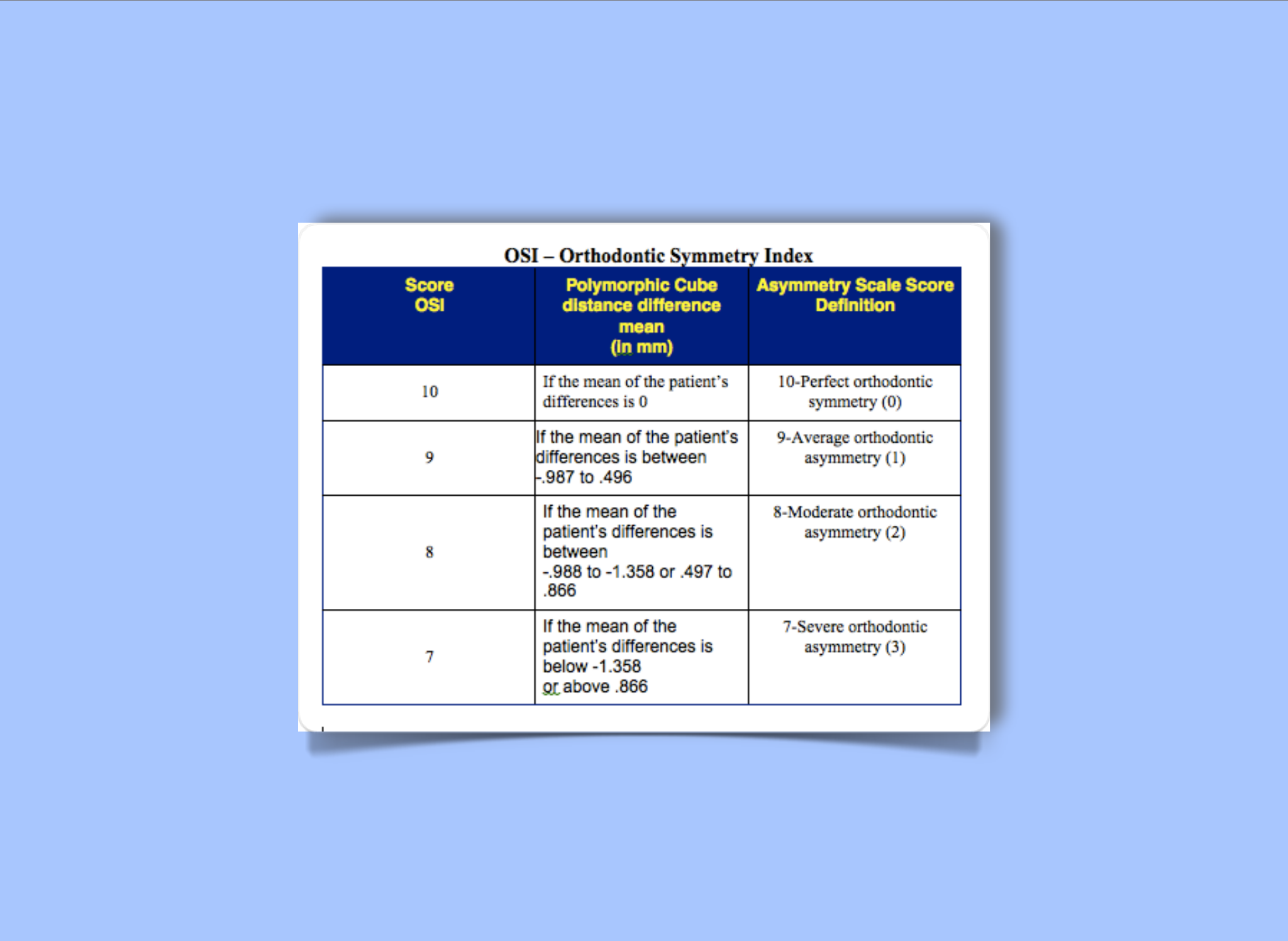
Statistical Analysis of OSA Polymorphic Cube Data
Doctor James Mah, UNLV Orthodontic Chairmen, gave us assistance in designing the OSA statistical analysis. To assure the accuracy and validity of the statistical formulas we
also utilized the services of a local mathematics expert, Mr. Chad Pinnick. Below is a chart that illustrates the mathematical parameters used to compute the OSI - Orthodontic
Symmetry Index.
13
Macro Analysis
When analyzing an orthodontic case we ask patients to upload their frontal image to the website www.symmeter.com. The free online symmetry tool allows the patient or doctor
quickly identify the degree of facial asymmetry present. Patients can see for themselves they are not perfectly symmetrical. Anatomage also has a superimposition tool that visually
demonstrates bilateral right and left skeletal variations.
Mini Analysis
The OSA analysis uses a series of cephalometric landmarks to construct the virtual polymorphic cube. This study of 121 subjects yielded data that we organized into four levels of
asymmetry. Level 0 = Perfect Symmetry, Level 1 = Minor Asymmetries present, Level 2 = Moderate Asymmetries present and Level 3 = Severe Asymmetries present. For purposes of
patient communication we substituted 10, 9, 8 and 7 because our society rates good-looking people as “perfect 10s”. As anticipated there were no perfect 10s in our study!
Micro Analysis
In future articles we will present, The “Three-Quarter 3D Symmetry Analysis” for MFOV CBCT Volumes and another study of “Pointcloud Topographic Skull Mapping” that will
demonstrate the presence of “pockets of asymmetry”. The image below demonstrates Pointcloud Skull Mapping. Colored areas of asymmetry are visually illustrated in the Wiggle-
gram.
Discussion
Considering the data and the results of the analysis, we do
not expect the patient to have orthodontic symmetry based on
the differences in corresponding distances measured on the
Polymorphic Cube. The data generally indicates that while the
distances significantly vary to demonstrate general skeletal
asymmetry in the population; whereas angular values on the
surfaces of the Polymorphic Cube do not significantly vary. We
are not saying that there is no difference in corresponding an-
gle measures, simply that the difference is not sufficient to re-
ject the hypothesis of perfect symmetry among angle measures
at the chosen α = .10 significance interval.
We must also address the creation of the Orthodontic Symme-
try Index. OSI was created as a guide for the user to quickly
access a patient’s overall level of pre-treatment asymmetry. It
is based on the mean of the differences in distances observed
between anatomical landmarks used to create the Polymorphic
Cube. The index is there as a tool to assist the user in deciding
the overall severity of asymmetry, not to evaluate the cause of
the asymmetry or anatomical variation (i.e. enlarged growth on
one side versus lack of growth on contralateral side).
14

Conclusion
Visual 3D OSA helps one better communicate with patients and referring doctors by putting all on notice that ideal occlusion may NOT be always obtainable. The majority of pa-
tients have an innate ability to functionally adapt to the esthetically modified occlusion. Failure to functionally adapt may result in future problems that require additional modification.
I have had “occlusion-passionate” referring doctors instruct me to NOT remove braces without a “little more CPO, group function and/or anterior guidance”. Can there be ideally engi-
neered occlusion if the patient has substantial asymmetry, especially angular variations that may create occlusal cants, tips, rolls, yaw (ref: Ackerman) or unequal condylar linear meas-
urements to the midsagittal plane? Visual 3D OSA now makes it possible to identify and quantify a credible reason for less than ideal occlusion.
15
Click Here
Blue reveals asymmetrical areas
Powered by Anatomage Invivo5
Occlusion Concepts Are Nonetheless Very Important!
Evidence that old concepts may not be valid in an asymmetrical world does not lessen the importance of using time-tested “occlusion engineering principals” as guidelines, not absolutes, when
treatment planning an orthodontic or reconstruction case. Occlusion engineering concepts can be compared to general building principals. A building properly designed should have squared
walls with all structural components in balance or equilibrium. Occlusion modification by the dentist uses similar construction guidelines everyday. Construction principals such as fulcrums,
levers, moments, resistance, stress relaxation, static equilibrium, inclined planes, constant force, working, balancing, parallelism, cantilever, resultant force theory, vector analysis, tension,
material strength, deformation, resilience and other principals are universally used by dentists, the architects of the maxillo-mandibular space. Most important, a building structure, like the
human denture, has to have a sound foundation. The “Polymorphic Cube”, if symmetrical and stable (little or no morphing), is the foundation for functional adaptation to homeostasis.

3D Cephalometrics - Occlusion Concepts References - Recommended Reading List
1. Ackerman, Marc B.: Orthodontics and Its Discontents, International Journal of Periodontics & Restorative Dentistry, Guest Editorial, Quintessence Publishing Co Inc, 2005
2. Ackerman, Marc B.: The myth of Janus: Orthodontic progress faces orthodontic history, American Journal of Orthodontics and Dentofacial Orthopedics, June 2003.
3. Ackerman, James L., Ackerman, Marc B.: A Philadelphia Fable: How Ideal Occlusion Became the Philosopher’s Stone of Orthodontics, Angle Orthodontist, Vol. 77, No. 1, 2007
4. Ackerman, Marc B.: Enhancement Orthodontics; Theory and Practice (Paperback Book), Publisher, Blackwell Munksgaard, May 2007.
5. Jantz, Richard J., University of Tennessee, Department of Anthropology; Moore-Jansen, Peer H., University of Tennessee, Department of Anthropology: Database for Forensic Anthropology in the United
States: structure, content and analysis, 1962-1991 (ICPSR 2581)
6. Haas, Jonathan, Organizer; Volume Editors: Jane E. Buikstra and Douglas H. Ubelaker, Assistant Editor: David Aftandilian, Contributions by: D. Aftandilian, J. E. Buikstra, M. Finnegan, J. Hass, D. A.
Kice, C. R. Nichol, D. W. Owsley, J. C. Rose, M. J. Schoeninger, G. R. Scott, C. G. Turner II, D. H. Ubelaker, P. L. Walker and E. Weidl STANDARDS FOR DATA COLLECTION FROM HUMAN SKELE-
TAL REMAINS, Proceedings of a Seminar at The Field Museum of Natural History, ARKANSAS ARCHEOLOGICAL SURVEY RESEARCH SERIES Nº 44 1994.
7. Huang, John C., HyeRan, Choo, Mah , James K: Three-Dimensional Cephalometrics in Clinical Practice: CBCT for You and Me, Faculty Files, Spring 2 0 0 8 • P C S O Bulletin.
8. Isaacson, RJ, Christiansen, RL, Evans, Ca, Riedel, RA: Research on variation in dental occlusion; a “state-of-the-art” workshop conducted by the Craniofacial Anomalies Program, The National Institute of
Dental Research, Am J. Orthodontics, Vol. 68, 1975.
9. McCoy, Gene: Occlusion Confusion, San Francisco, Ca., 3D Dentists, Chapter 20, iPad Interactive Book, Publisher DentalSpecialists.com, May 2012.
10. Redmond and Cho: The Cutting Edge: A Three-Dimensional Cephalometric Analysis, JCO, Volume, XLIII Number 4, April 2009
11. Rinchuse, Donald J. and Kandasamy, Sanjivan: Clinical Practice-Practical Science: Centric relation: A historical and contemporary orthodontic perspective, J Am Dent Assoc, Vol 137, No 4, 494-501,
2006 American Dental Association.
12. Rinchuse, Donald J., Du, Sinh Q., Zullo, Thomas G. and Rinchuse, Daniel J.: Reliability of three methods of occlusion classification, American Journal of Orthodontics and Dentofacial Orthopedics, April
1998.
13. Rinchuse, Donald J., Sweitzer, Emily M., Rinchuse, Daniel J. and Rinchuse, Dara L.: Understanding science and evidence-based decision making in orthodontics, American Journal of Orthodontics and
Dentofacial Orthopedics, May 2005.
14. Rinchuse, Daniel J., Kandasamy, S and Sciote, J: A contemporary and evidence-based view of canine protected occlusion, American Journal of Orthodontics and Dentofacial Orthopedics July 2007.
15. Rinchuse, Daniel J and Kandasamy, S: Centric relation: A historical and contemporary orthodontic perspective, JADA, Vol. 137, April 2006.
16. Rinchuse, Daniel J. and Kandasamy, S: Myths of orthodontic gnathology, American Journal of Orthodontics and Dentofacial Orthopedics, September 2009.
17. Rinchuse, Daniel J and Kandasamy, S: Articulators in orthodontics: An evidence-based perspective, American Journal of Orthodontics and Dentofacial Orthopedics, February 2006.
18. Rinchuse, Daniel J. and McMinn: Summary of evidence-based systematic reviews of temporomandibular disorders, American Journal of Orthodontics and Dentofacial Orthopedics, December 2006.
19. Vig, Peter, Is craniofacial asymmetry and adaptation for masticatory function an evolutionary process, Nature, Volume 248, No. 5444, p. 165, March 8, 1974.
20. Vig PS, Hewitt AB: Asymmetry of the human facial skeleton. Angle Orthod. 1975;45:125–129.
Acknowledgments
We would like to thank Doctor Peer Moore-Jansen, Professor and Chair, Department of Anthropology Wichita State University, Kansas for his recommendations and contributions to the National Anthropo-
logical Forensic Database. We would also like to thank Doctor James Mah, Professor and Chair, Department of Orthodontics, University of Nevada, Las Vegas for his help in study design, statistical analysis
and valuable comments. Mr. Brendon Bengston, iHub3D, San Jose, California, was an invaluable resource for 3D CBCT diagnostic services and providing help in designing the OSA - OSI applications. Our
thanks to Mr. Chad Pinnick for developing the statistical analysis of our study data and computing the Orthodontic Symmetry Index. Thank you Doctor Peter Vig for reviewing our study, giving guidance and
providing two of our early references for craniofacial asymmetry and functional adaptation. We thank Doctor Randy Womack for publishing our study. 16

17
About The Authors
Jason P. Ouellette, DDS
Paul L. Ouellette, DDS, MS
Email
4BracesDro@gmail.com
Jonathan P. Ouellette, DDS
A TRUE DENTAL FAMILY - Doctor Paul Ouellette works with his two sons, Doctors Jason and Jonathan of the DentalSpecialists.com. Jason is a senior orthodontic
resident at Jacksonville Florida University. Jonathan is a senior AEGD resident at University of Florida, Miami. Jonathan has been accepted to a one year implant dentistry
fellowship in Alabama. The doctors have developed a practice model that includes Orthodontics, Implant Dentistry and Prosthetic Rehabilitation of complex cases. Doctor
Ouellette’s daughter, Danielle, a college senior pre-dental student, applied her creative writing talents to help the family develop the first 700 page interactive ebook, “3D
Dentists: The Future of Dentistry is Now!” Being so close-knit as a family who literally work and play together, they felt compelled to create a book geared to first year
dental students and experienced healthcare professionals new to or considering acquisition of 3D imaging technology. 3D Dentists is written for inquisitive dental patients
that want to be fully informed before making a life changing decision for themselves or a family member. 3D Dentists is available for download at
www.EarnYourSmile.org
.
CLICK HERE
