Pedal Loop Reconstruction Syllabus
2016-06-06
: Pdf Pedal Loop Reconstruction Syllabus Pedal_Loop_Reconstruction_Syllabus 6 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 35
6/6/2016
1
Anand Prasad, MD, FACC, FSCAI, RPVI
Associate Professor of Medicine
Freeman Heart Association Endowed Professor in Cardiovascular Disease
Associate Program Director Cardiovascular Diseases Fellowship Program
Associate Editor Catheterization and Cardiovascular Interventions
Interventional Cardiology and Vascular Medicine
University of Texas Health Science Center San Antonio
Pedal Loop Reconstruction: A Crash Course in 60 minutes
“Pedal-Plantar Anatomy”
Research Funding:
Osprey Medical
Mike Hogg Fund
Freeman Heart Association
Medtronic
Speaking Honoraria:
St Jude Medical
AstraZeneca
Gilead
Disclosures
•Implications for targeting angiosome guided therapy.
•Understanding anatomic variants which may be congenital and non-pathologic
•Avoiding confusing branches or collaterals with true vessels –which may lead to
complications.
•Intact pedal plantar loop allows for the most robust filling of the distal vessels.
•Rates of healing appear to be higher with an intact pedal plantar loop
(Rashid H et al J of Vasc Surgery 57(5):1219-1226, 2013. and Manzi M et al J Cardiovasc Surg, 50(3):331-7,2009.)
Why is it important to know tibial and pedal anatomy?
6/6/2016
2
Tibial and Popliteal Anatomy: Implications for the Pedal Circulation
Anterior tibial artery anterior circulation
Lateral originating vessel –represents first branch off of P3 segment of popliteal artery.
Superiorly passes through tibialisanterior and extensor hallicus longus muscles.
Lies in the anterior compartment –therefore perforations have implications for compartment syndrome.
At the level of the ankle, crosses under extensor retinaculum and supplies dorsum of the foot at the dorsalis pedis.
Tibial anatomy Pedal Anatomy
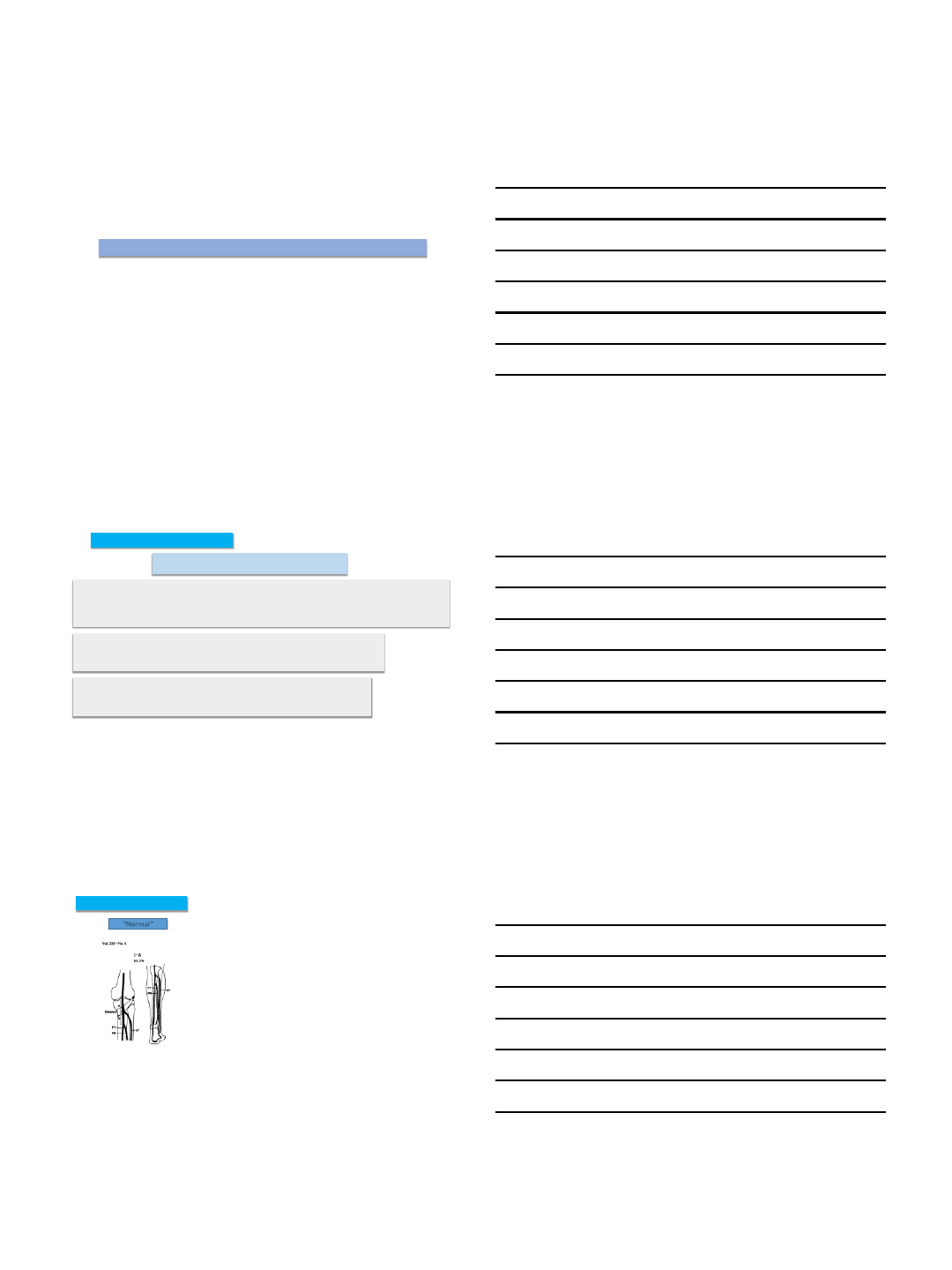
Vast majority of individuals have (at birth) three primary tibial
vessels:
Posterior tibial artery posterior circulation
Originates off tibo-peroneal trunk.
Lies in the deep posterior compartment.
Traverses behind the medial malleolus and then divides into medial a nd lateral plantar vessels.
Peroneal artery communicating branches to the primary tibial vessels, calcaneal perfusion
Originates off tibo-peroneal trunk.
Lies in the deep posterior compartment but supplies blood to the lateral compartment.
Important source of collaterals when primary tibial vessels are occluded.
Mousa e t al. JA NUA RY 2012 I SUPPLEMENT TO END OVASCUL AR TODAY
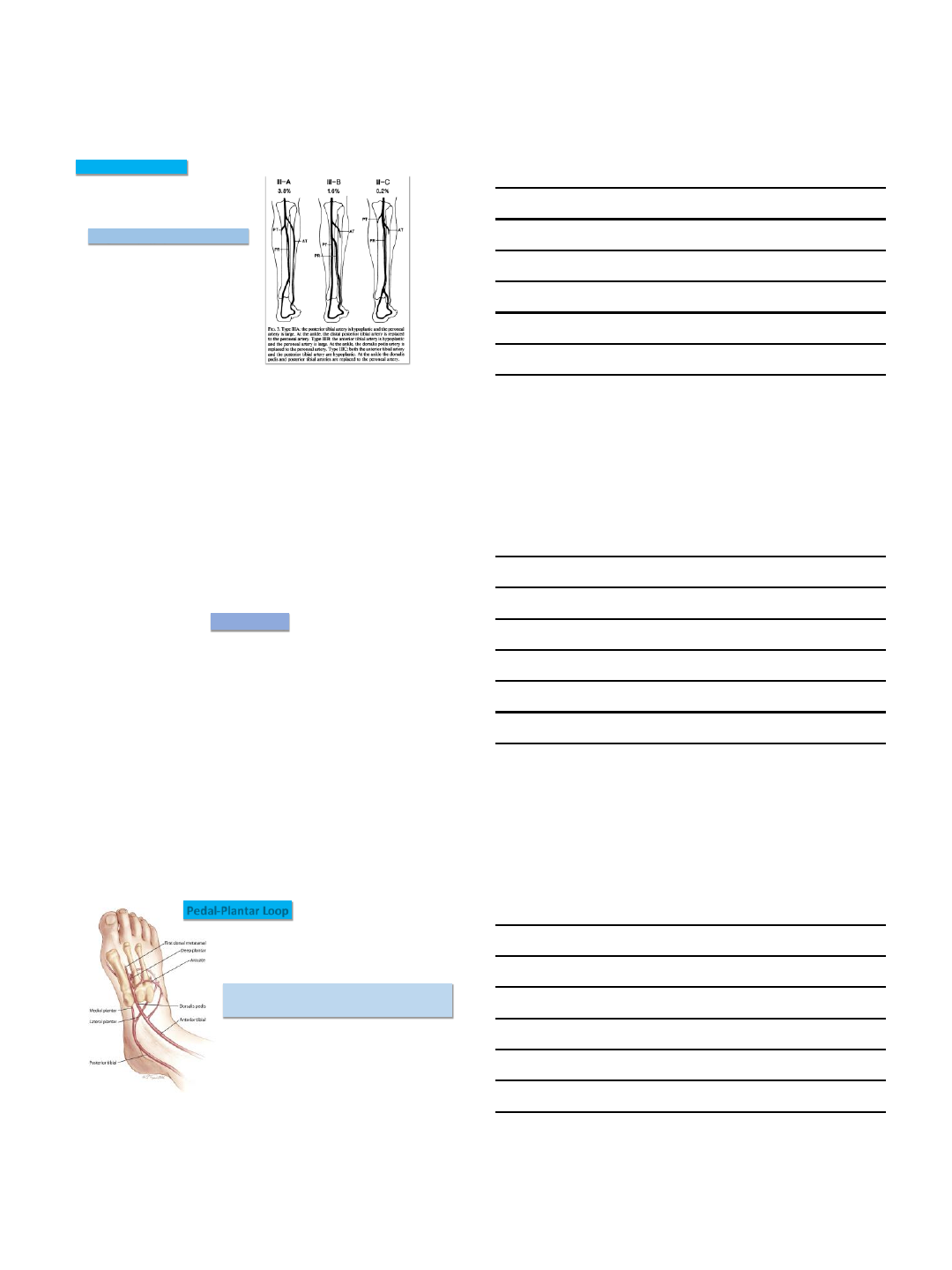
“Normal” Tibial “shared” origin Tibial high take off
Tibial anatomic variations
Kim D et al. Ann. Surg. - December 1989
6/6/2016
3
Congenitally hypoplastic tibial vessels
Tibial anatomic variations
Kim D et al. Ann. Surg. - December 1989
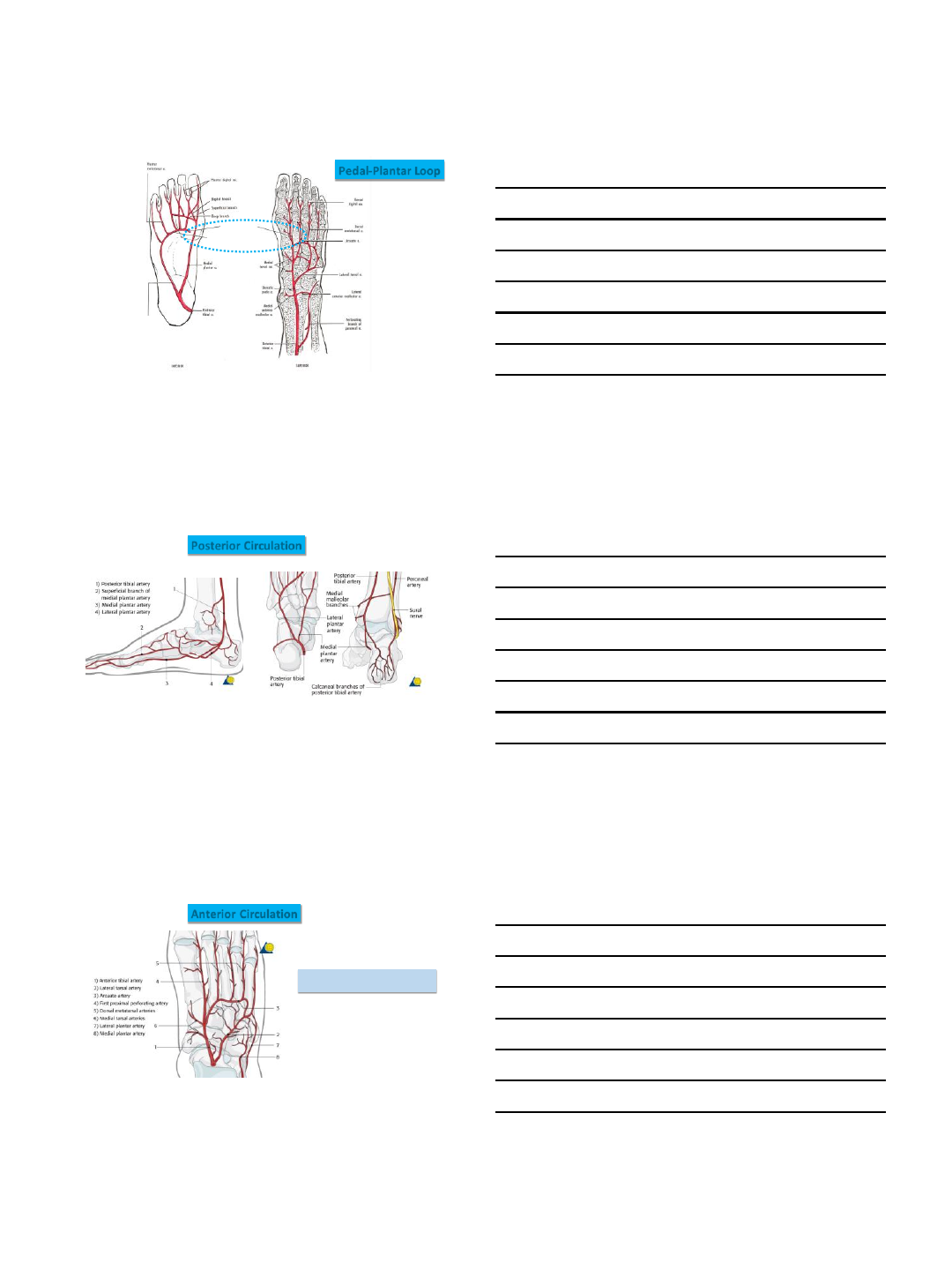
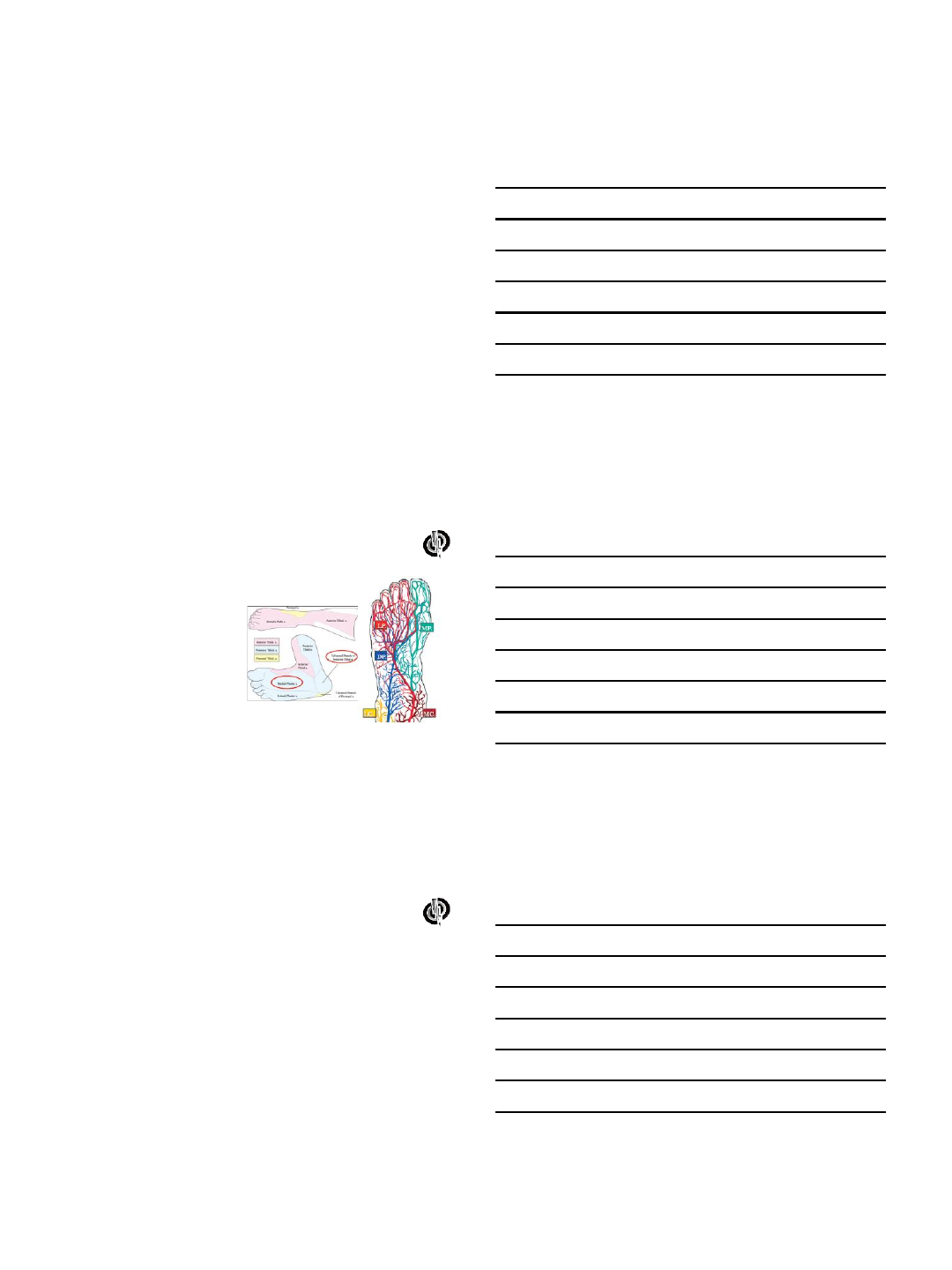
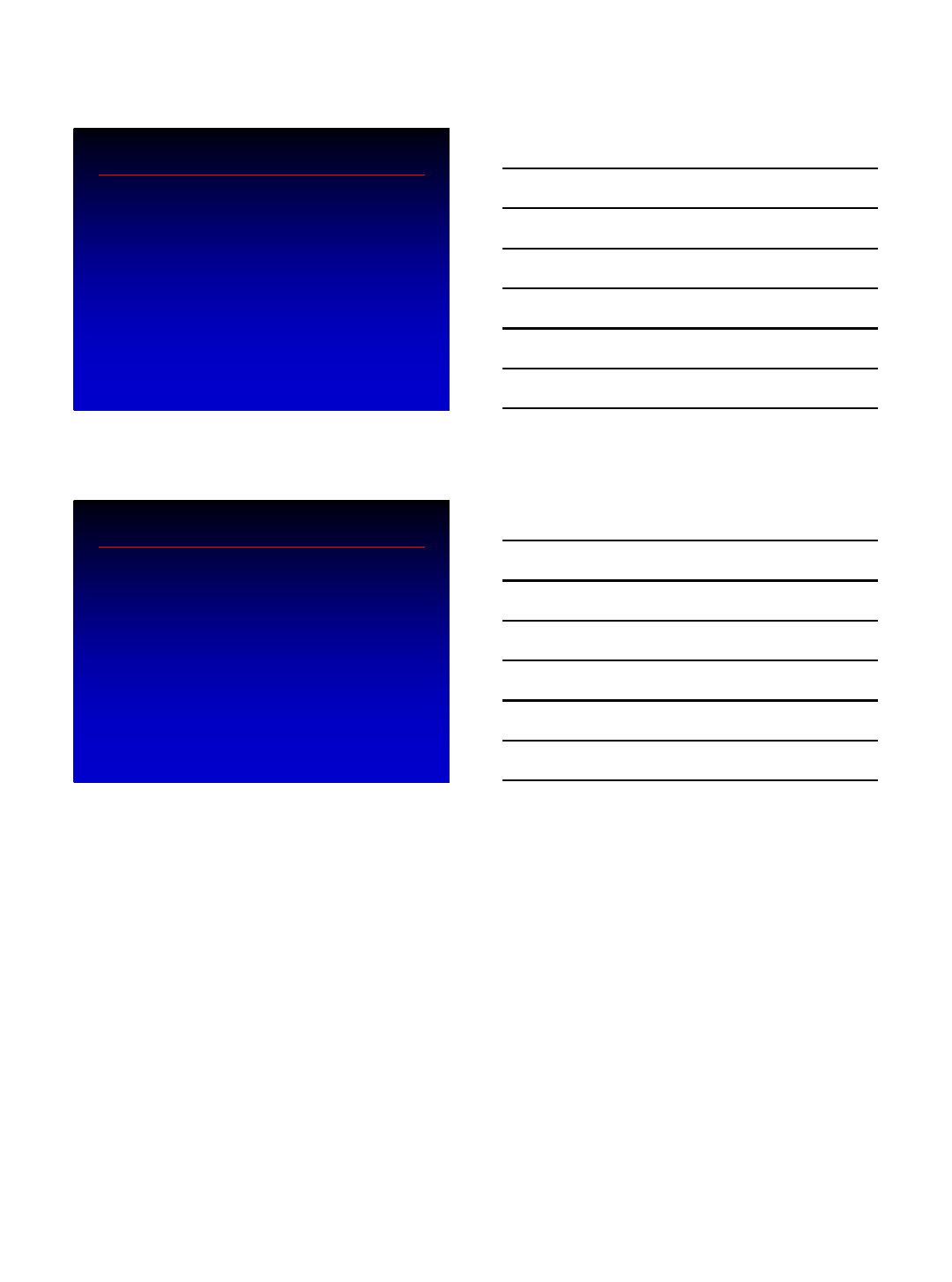
Pedal Anatomy
Foot Posterior Tibial Artery . Source: classconnection.s3.amazonaws.com
Deep plantar arch:
•Receives supply from the anterior circulation (dorsalis pedis)
•And the posterior circulation (lateral plantar artery)
Pedal-Plantar Loop
6/6/2016
4
Anatomy of L eft Foot and Ankle. S ourc e: www.medicalexhibits.com
Pedal-Plantar Loop
Authors: Ri ck B uckley, Andrew Sands, https://www2.aofou nd atio n.org
Posterior Circulation
Authors: Ri ck B uckley, Andrew Sands, https://www2.aofou nd atio n.org
Anterior Circulation
Lateral tarsal artery and plantar
arteries have communications
6/6/2016
5
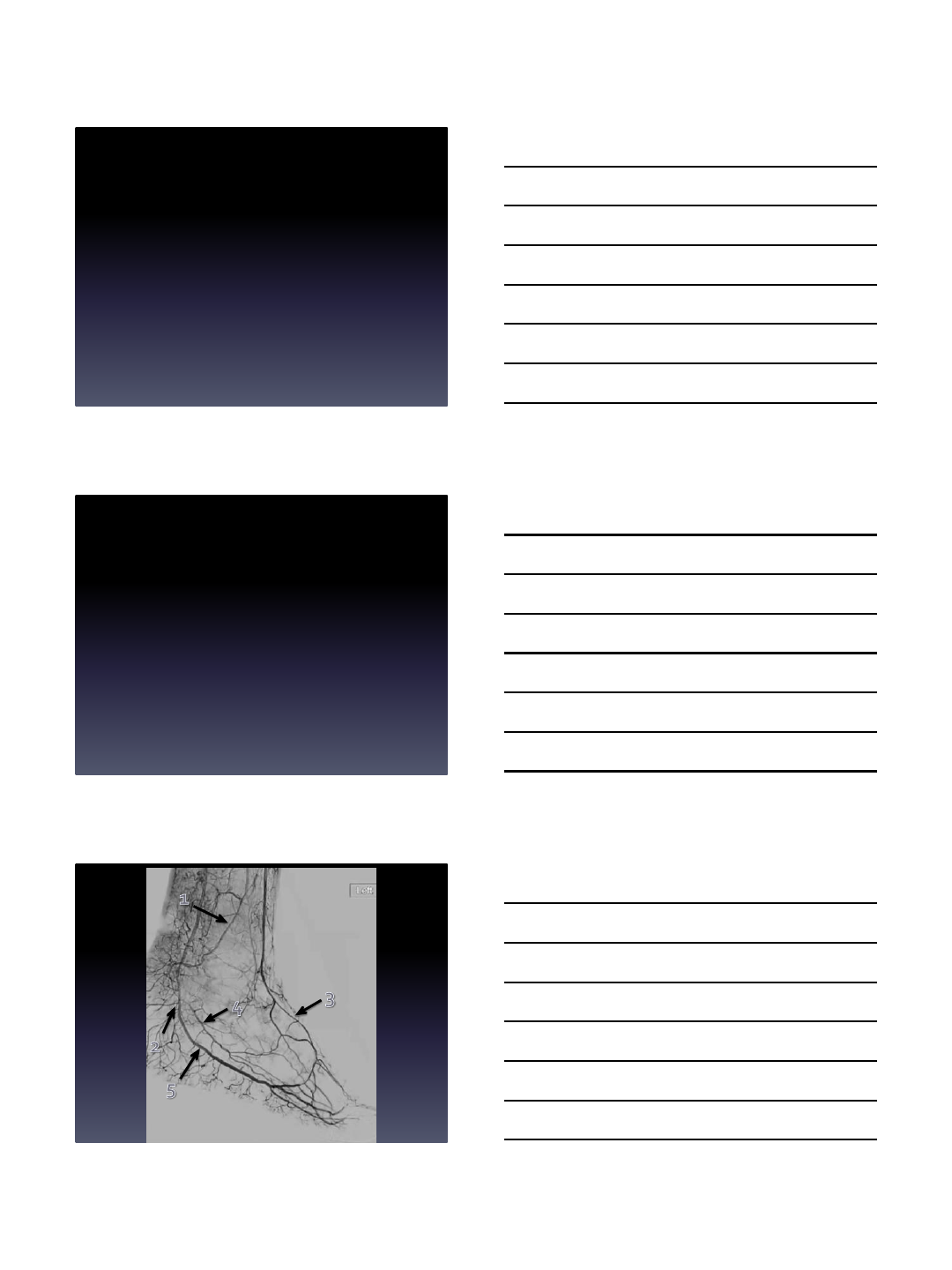
Malleolar arteries
Anteri or Tibial
Dorsalis Pedi s
Lateral Tarsal
Com mu nicatio n
Medial P lantar
Lateral Plantar
Calcaneal
Pos terior Tibial
Manzi et al. RadioG raphics 2011; 31:1623–1636
5th Meta -tarsal bone
mus t be separated
Lateral Oblique View
1st Meta tarsal space
mus t be visible
Anterior Posterior View
Medial P lantar
Lateral Plantar
Dorsalis Pedi s
Lateral Tarsal
Manzi et al. RadioG raphics 2011; 31:1623–1636
Metatarsal access
6/6/2016
6
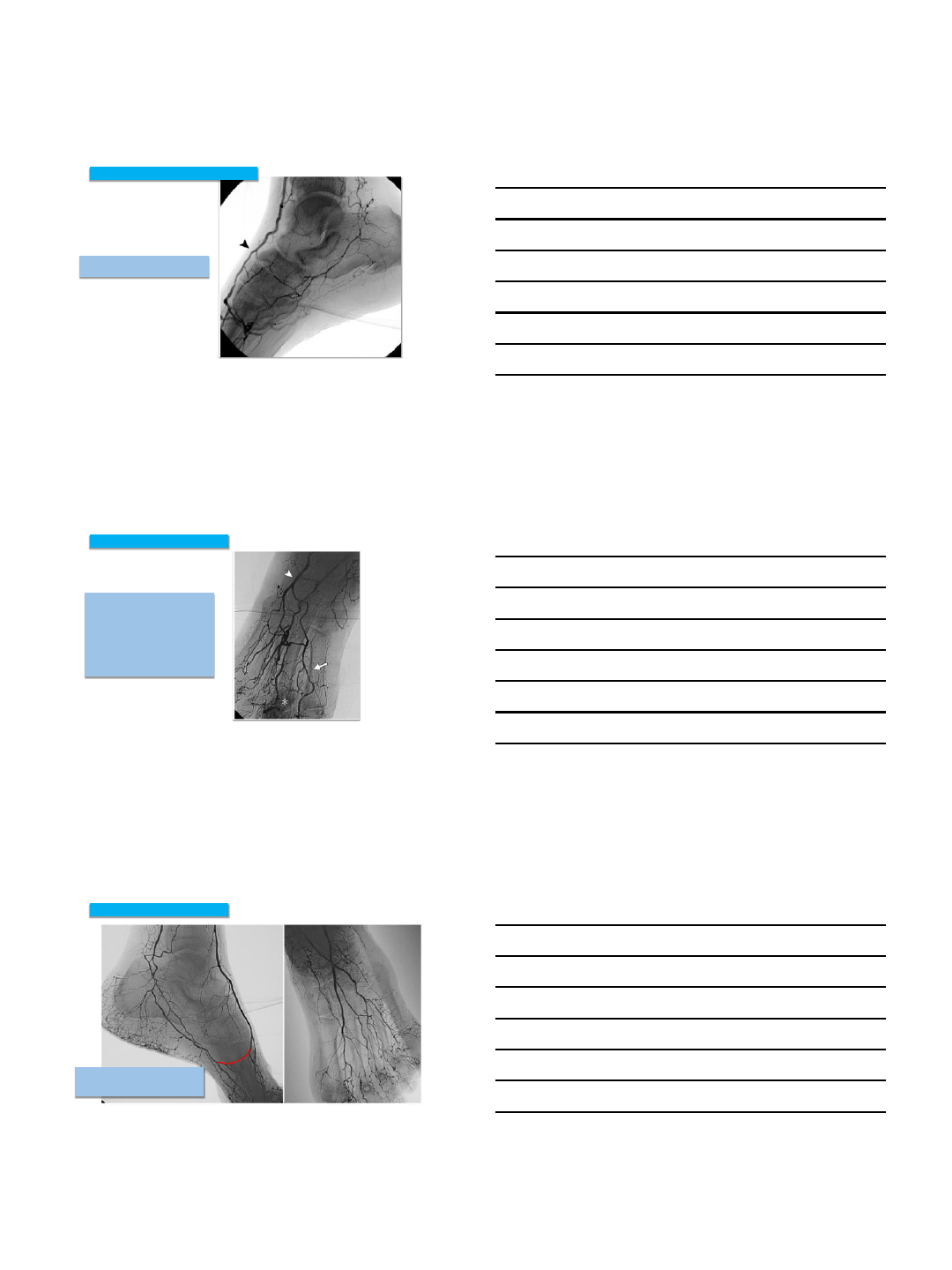
Pedal Anatomy: Occlusions, Collaterals, Variations
Anteri or Tibial
Dorsalis Pedi s
Lateral Tarsal
Medial P lantar
Superficial
Branch of
Medial
Plantar
Pos terior Tibial
Calcaneal
Lateral Plantar
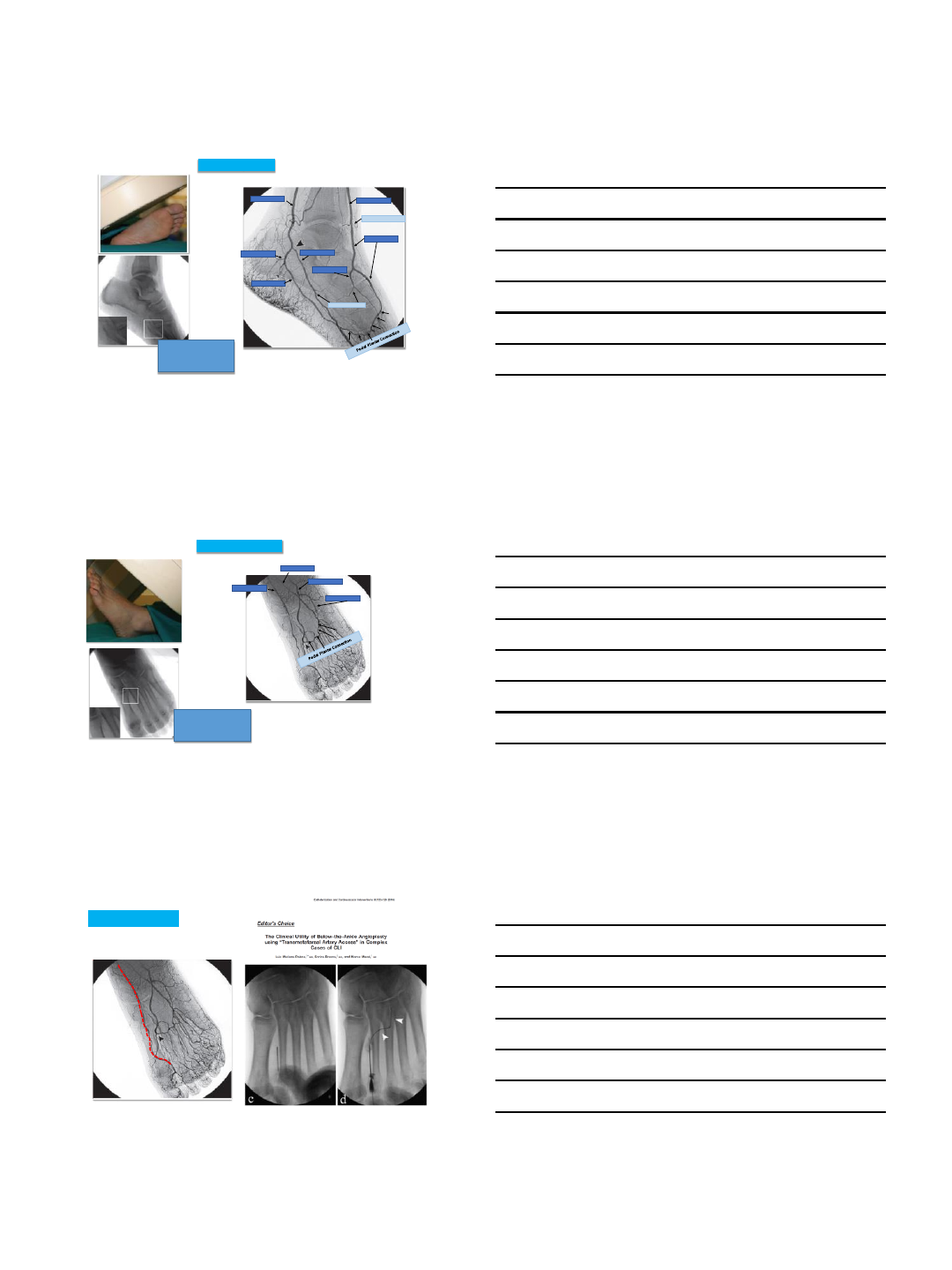
Pedal Plantar Loop: Connections and Collaterals
Manzi et al. RadioG raphics 2011; 31:1623–1636
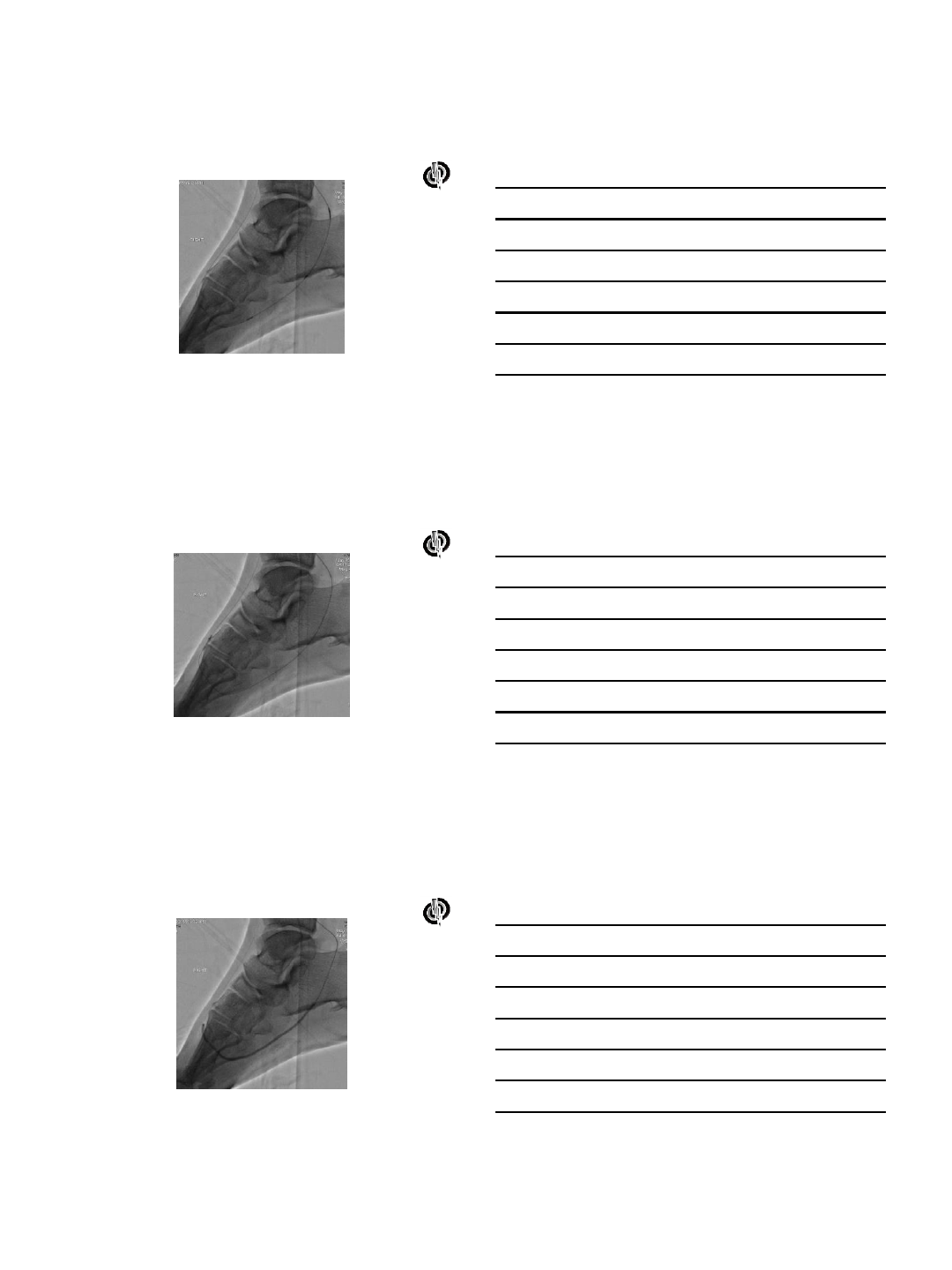
Anterior circulation is occluded and the
medial plantar provides sole pedal
blood flow.
Medial Plantar fills Lateral Tarsal
and anterior pedal circulation
Pedal Plantar Loop: Connections and Collaterals
Manzi et al. RadioG raphics 2011; 31:1623–1636
6/6/2016
7
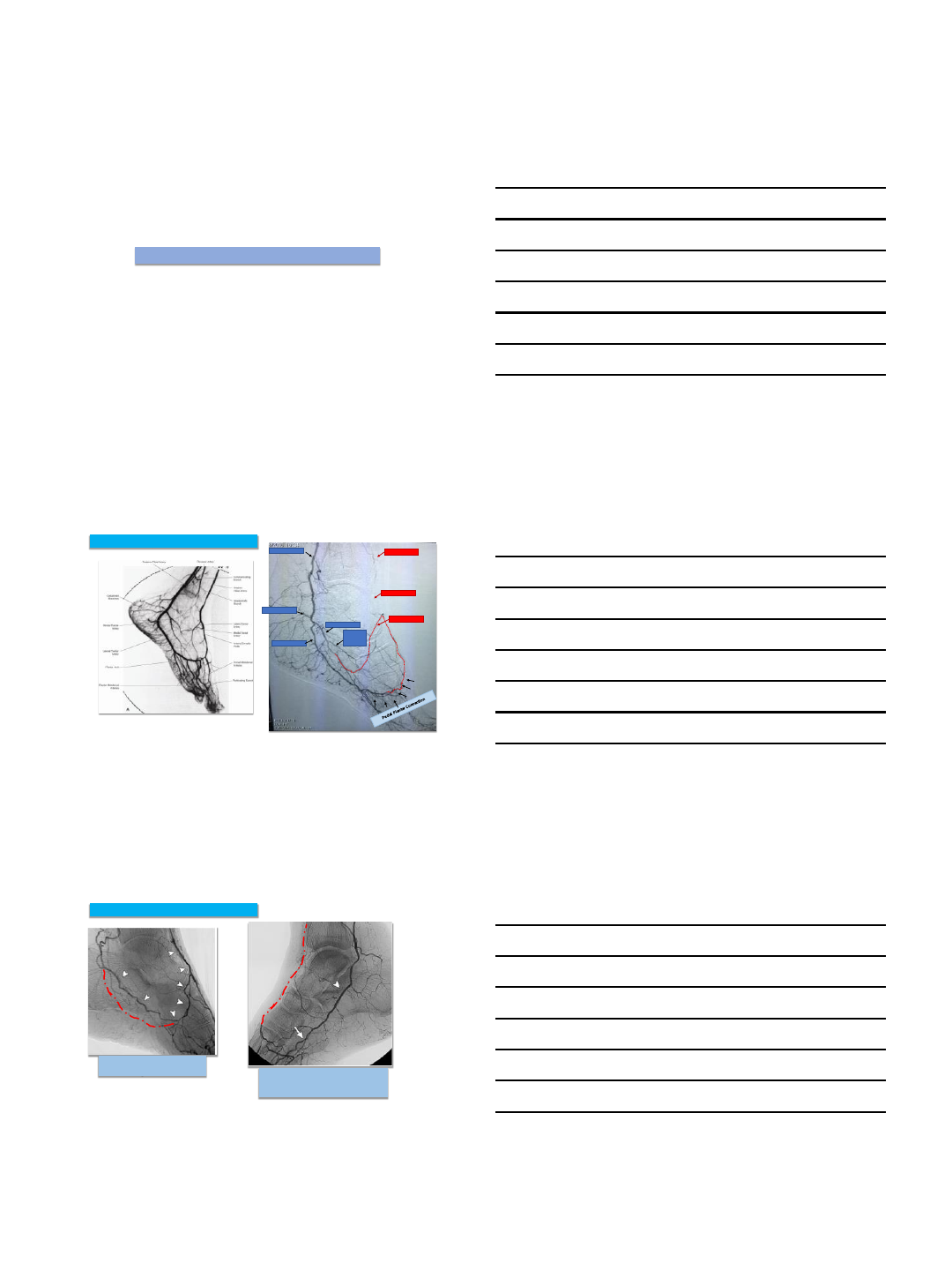
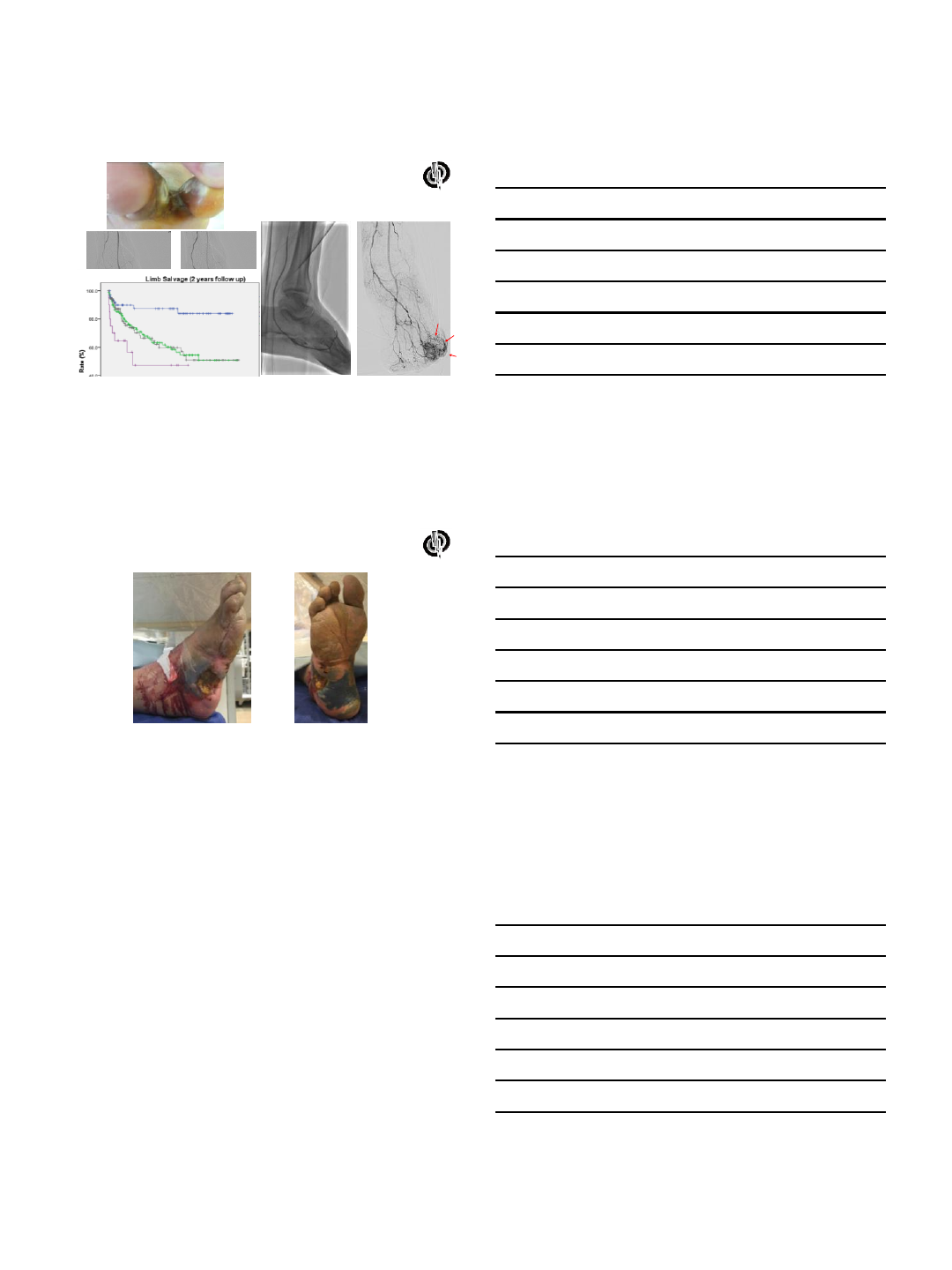
Posterior circulation is occluded but
fills from anterior circulation
Pedal Plantar Loop: Connections and Collaterals
Manzi et al. RadioG raphics 2011; 31:1623–1636
Anatomic variation:
No dorsalis pedis: Lateral tarsal
artery is the dominant anterior
vessel: 6-12% individuals.
The arcuate artery which normally
originates from the dorsalis pedis is
missing: ~ 30% of individuals.
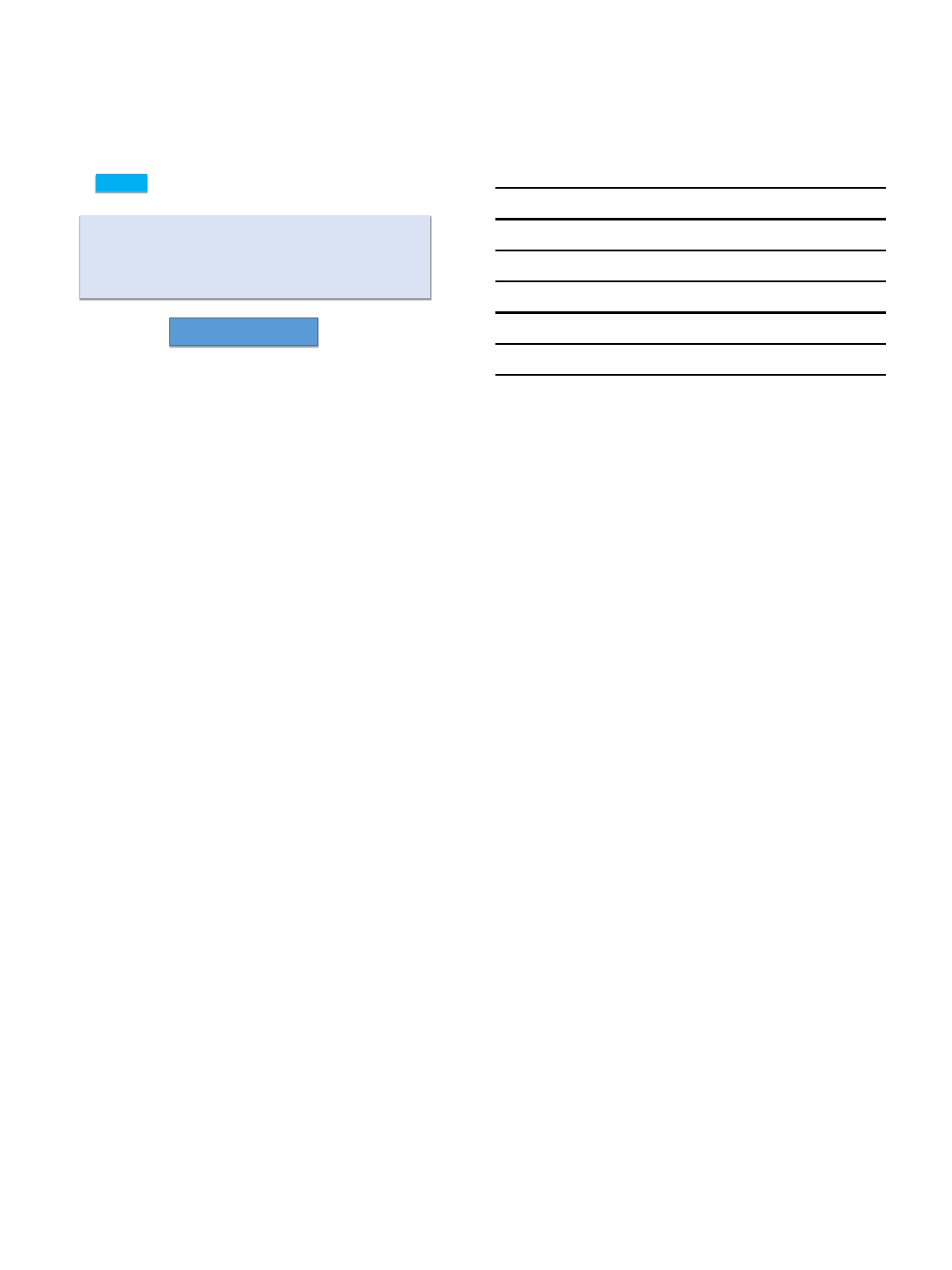
Pedal Plantar Loop: Anatomic Variation
Manzi et al. RadioG raphics 2011; 31:1623–1636
Pedal Plantar Loop: Anatomic Variation
Anatomic variation:
Anterior and Posterior circulations do
not communicate: ~ 10% of individuals.
Manzi et al. RadioG raphics 2011; 31:1623–1636
6/6/2016
8
Summary
Tibial and pedal anatomy i n the majority of patients will be reproducible, however variations exist that can
impact interpretation of angiograms.
Identification of primary tibial vessels, perfusion to the wound angiosome, a nd understanding of collaterals is
ke y to planning interventions.
Important arteries and landmarks include the first metatarsal space, the medial and lateral plantar course, the
la teral tarsal branch off of the dorsalis pedis, and the union of the lateral plantar with the dorsalis pedis to
complete the pedal plantar loop
THANK YOU
5/23/2016
1
With Pedal Loop Reconstruction,
Any Need For Angiosome
GuidedTherapy?
John H. Rundback MD FAHA FSVM FSIR
Medical Director, Interventional Institute
Holy Name Medical Center, Teaneck, NJ
Angiosomes
•First described by Taylor in
2007
•Not specifically intended to
describe pedal arch
vessel
•In fact, the pedal arch is the
terminal distribution of the
named angiosomes
•The extent of name pedal
vessels is limited Alexandrescu. J
Endovasc Ther 2011
Angiographosomes
•A better term for angiographically mediated revascularization
•Requires distal injections, vasodilator, AP and lateral projections
•Goal is to assess regional and wound specific PERFUSION
•Most pedal wounds are watershed…
•Multivessel contribution including pedal arch branches supply
ischemic tissue
5/23/2016
2
Angiographosome
AP
LAT PT LAT DP
Case 1
•Lateral calcaneal foot ulcer
•Prior posterior tibial intervention
•Normal posterior tibial ABI, normal hallux TBI
5/23/2016
3
5/23/2016
4
5/23/2016
5
5/23/2016
6
PRE POST
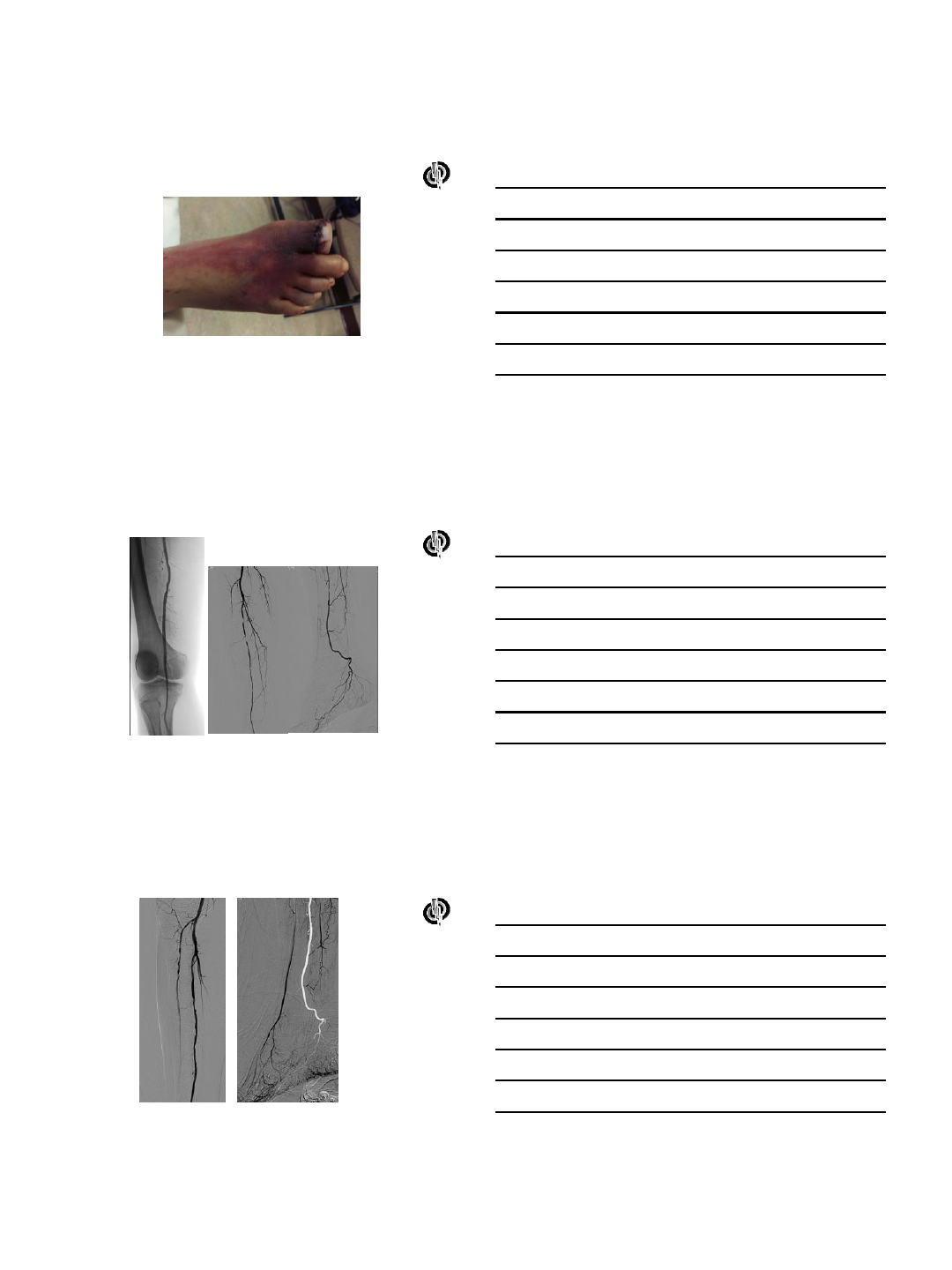
Case 2
•Distal hallux wound in March revascularized peroneal with PT
continuation, and AT PTA with sluggish flow.
•Had Distal hallux amp with plantar flap
•Presents with Regional Ischemia, rest pain, cellulitis on dorsum of foot
5/23/2016
7
Prior angio
5/23/2016
8
5/23/2016
9
5/23/2016
10
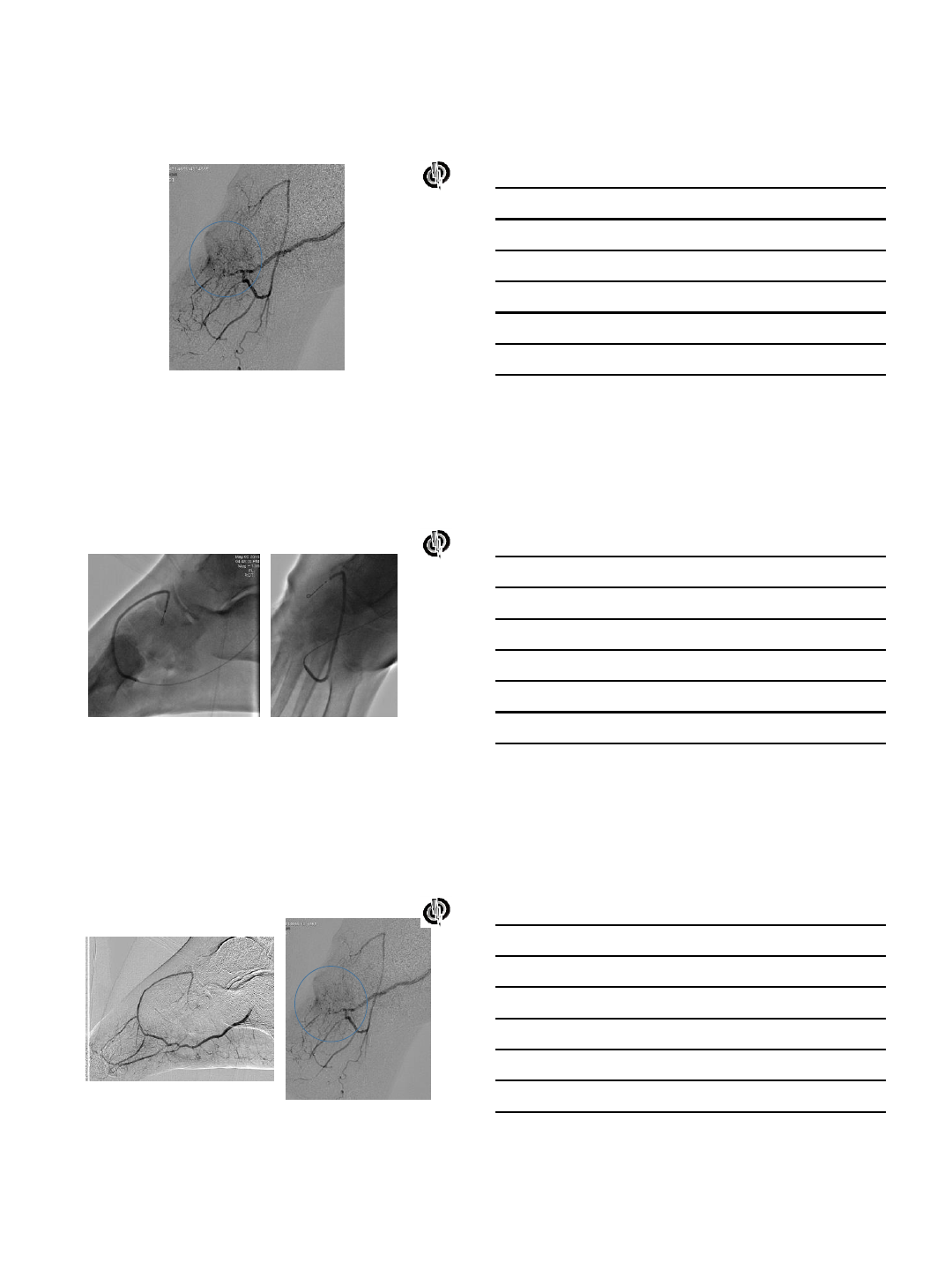
Case 3. Pedal Arch
wound supply
Absent plantar arch
Partial arch –dorsalis pedis
Partial arch –plantar artery
P=0.012
Complete plantar arch
ANT TIB
INJECTION
POST TIB
INJECTION
(PROX TO
COLLATS)
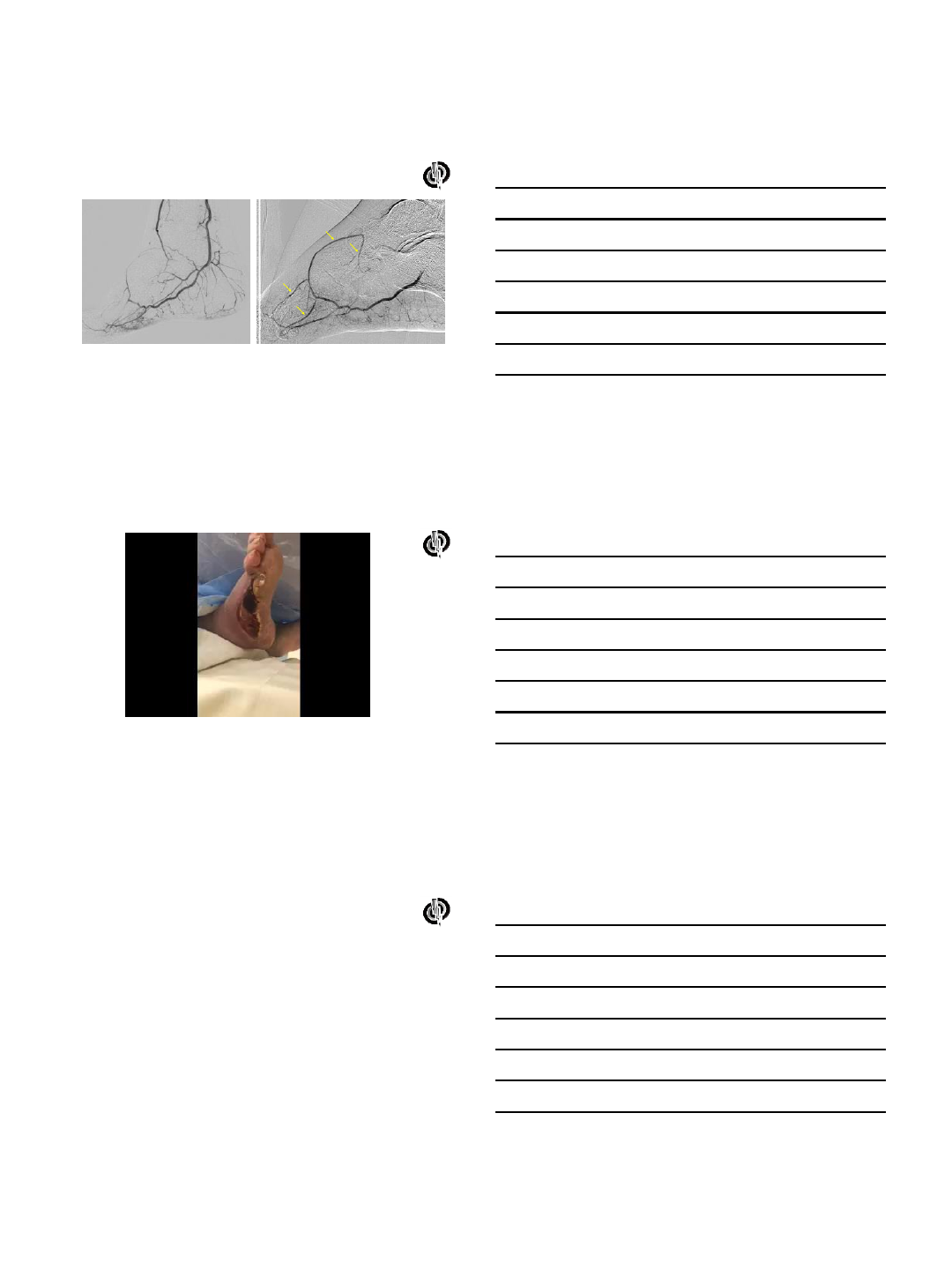
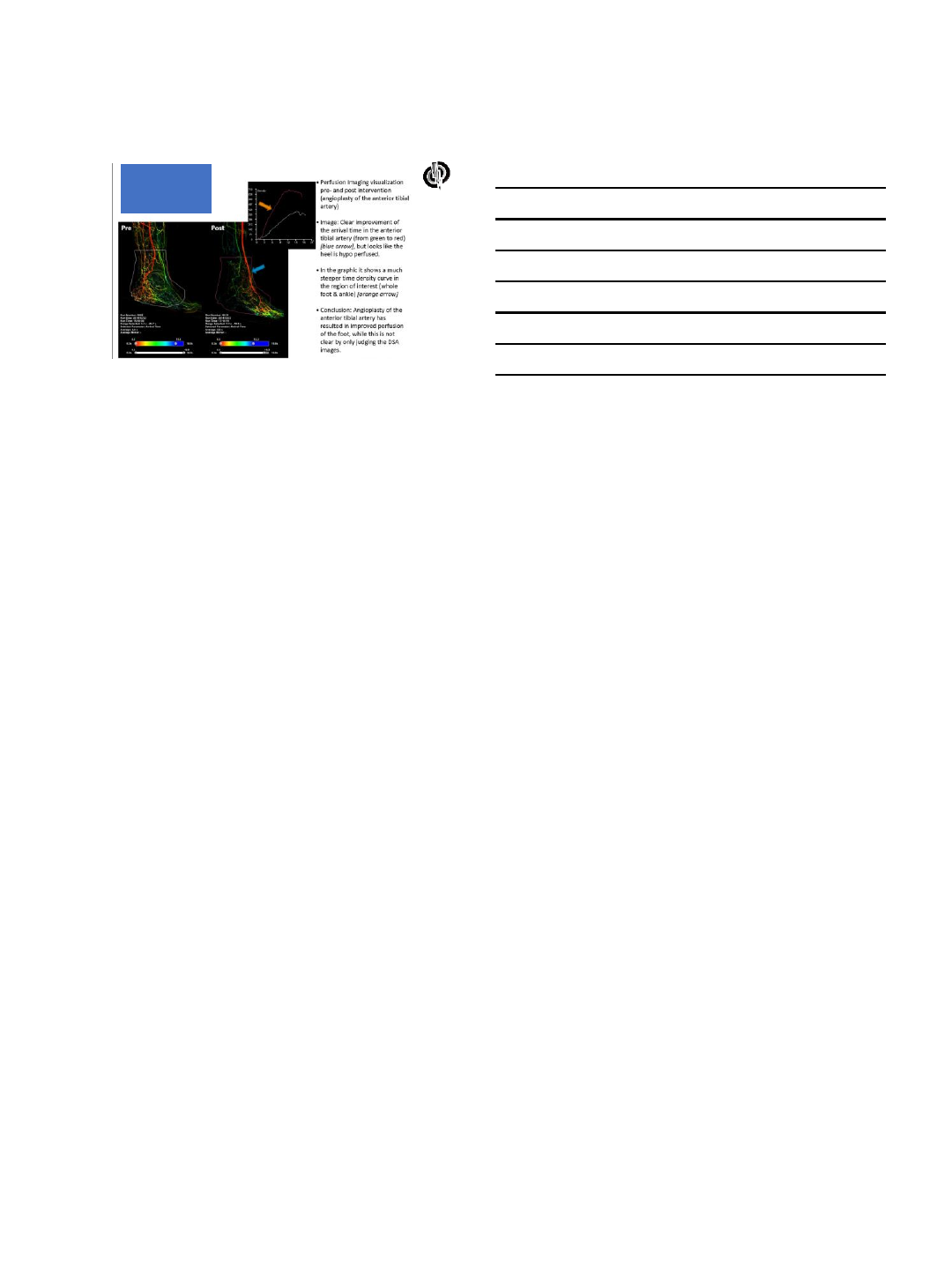
Case 4. Wound blush –watershed –
multivessel contribution –methylene blue angiography
Conclusion
•ANGIOGRAPHOSOMES –angiographically mediated revascularization
remains relevant for pedal arch interventions
•Wound blush is the main objective measure
•Methylene blue or indocyanine green (Luna systems) can further
define patterns of pedal arch perfusion
•Evolving perfusion systems will provide more optimized
determination of real time interventional success
5/23/2016
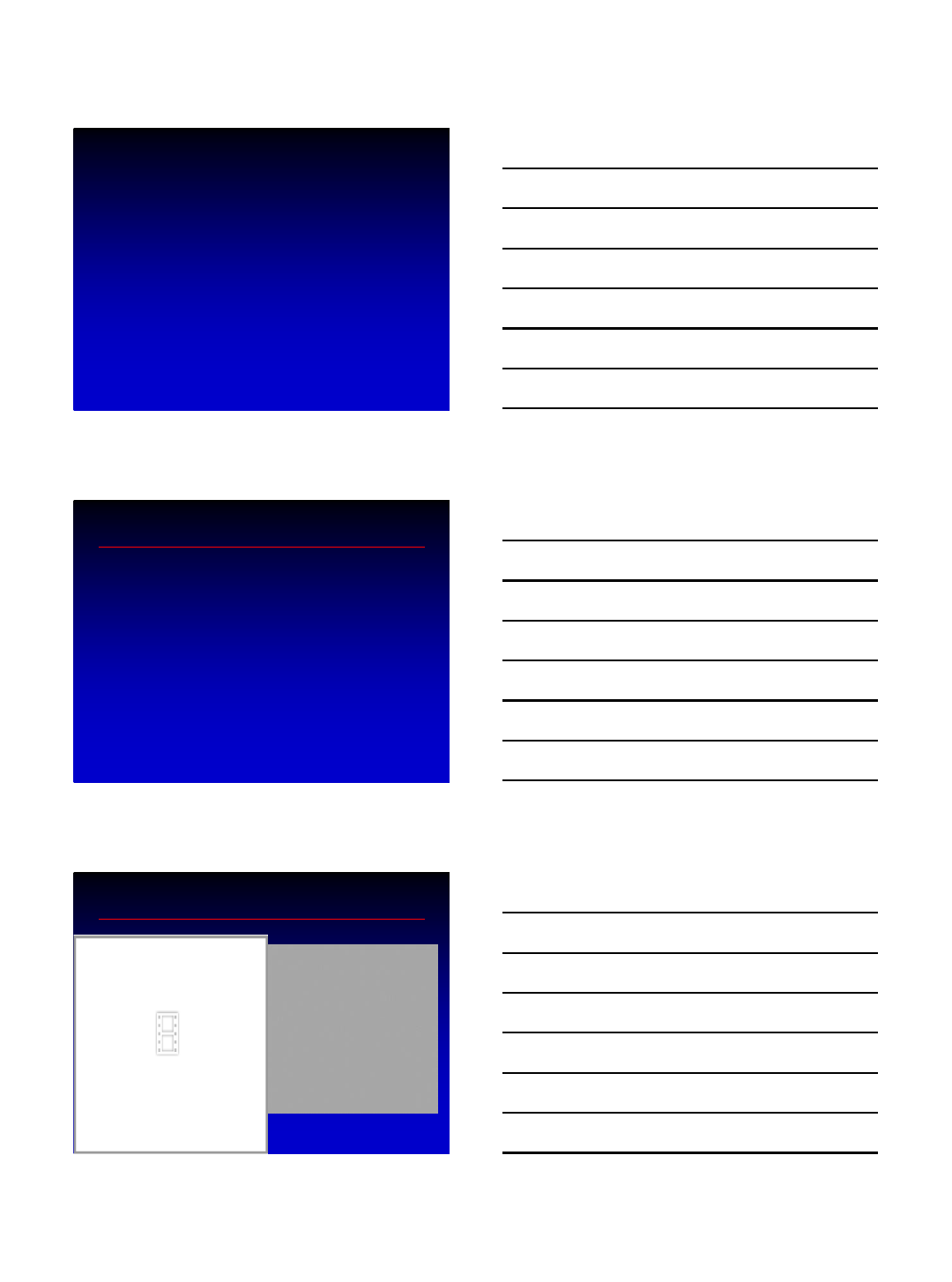
11
2D Perfusion
-time
-AUC
-opacification
1
Pedal loop reconstruction: what are the tools?
Lawrence A. Garcia, MD
Chief, Section Interventional Cardiology
and Vascular Interventions
Director, Vascular Medicine
St. Elizabeth’s Medical Center
Tufts University School of Medicine
Boston, MA
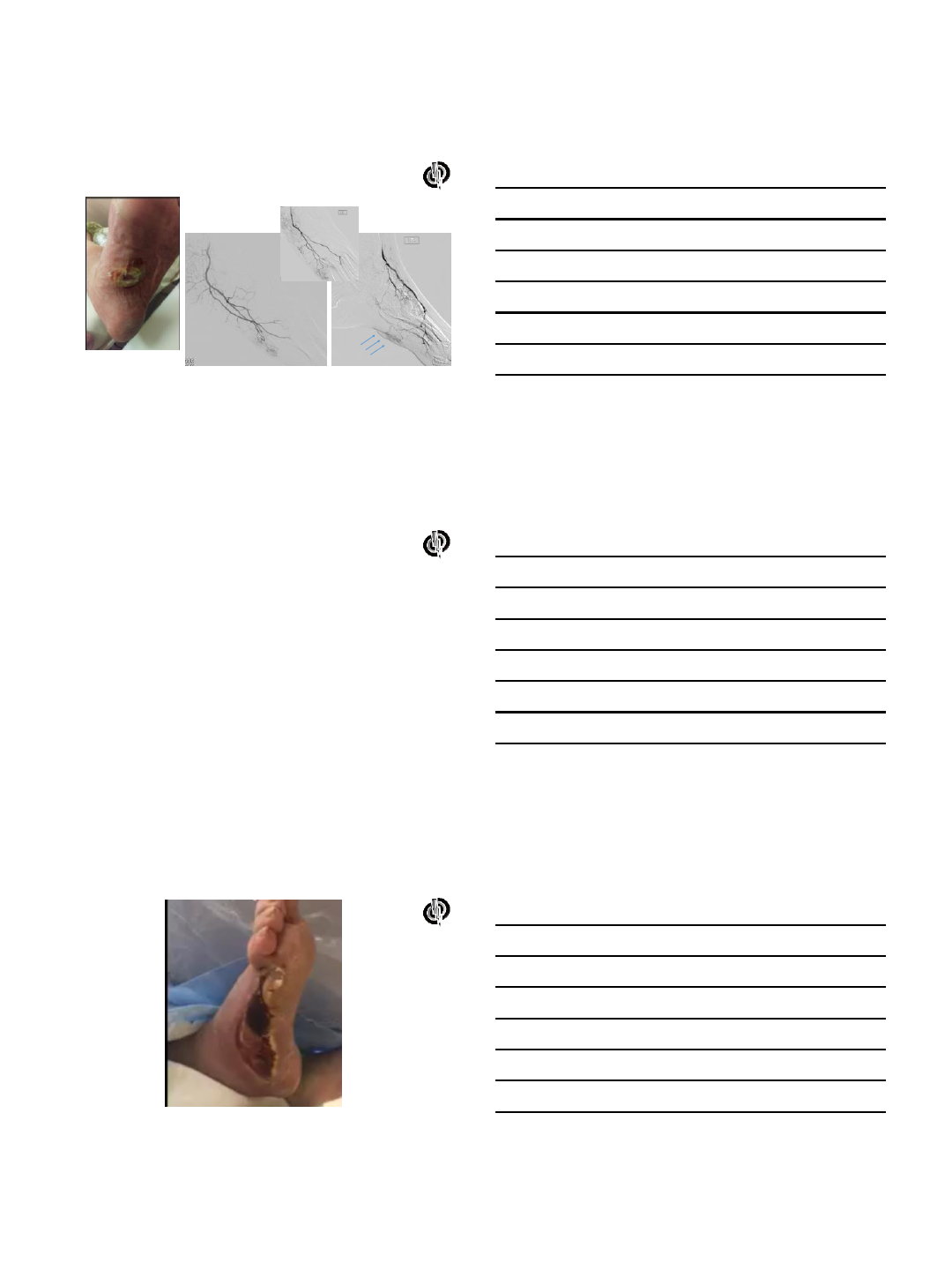
Case PT
•88 year old female with history HTN, HLP,
DM and PVD with L great toe ulceration and
chronic pain with infection at site with MRSA
•Non-invasive work-up included ABI/duplex
with non-compressible. Pre-occlusive Doppler
in all tibial vessels distally with outflow
appearing to be PT
•Angiography planned and images taken
2
3
What do you need?
•Access tools
•Sheaths
•Wires
•Support catheters
•Ballloons
–Non-DCB
–DCB
•Stents
–Balloon expandable
–SES
–DES
•Athrectomy
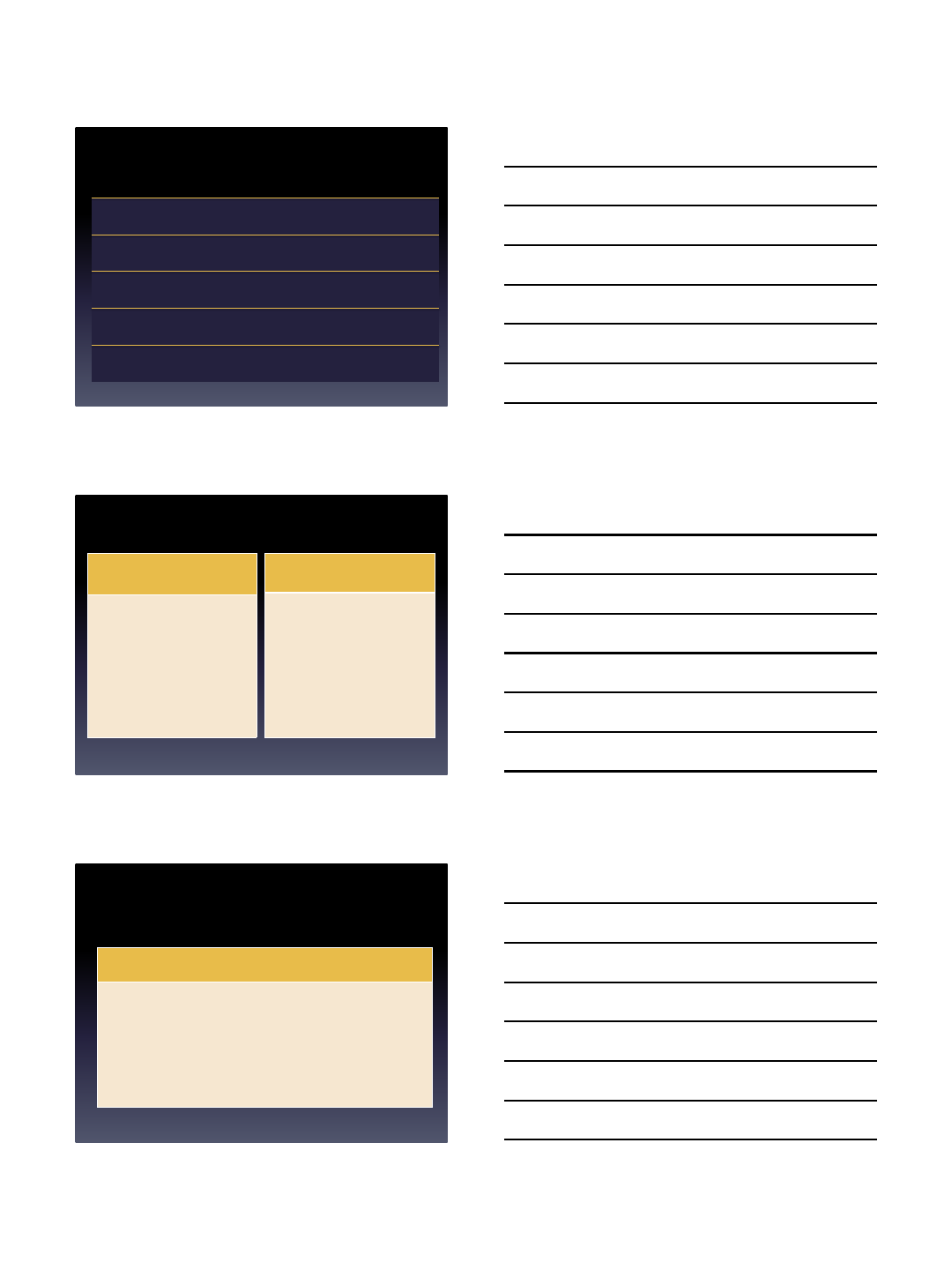
Access tools
• Access and “bear
back” your wire and
support catheter
•Can use angiocath
–Simple IV catheter
•Cook systems check-
flo 4 Fr
•Larger sheaths have
been used (5-6 Fr)
Wires
•Depends on your tastes
• 0.035” rarely used in the tibial circulation
• 0.018” useful and supportive
• 0.014” most commonly used
4
Industry
Name
Support
Tip
Wt
Use
Abbott
SpartaCore
Strong
<1.0 gm
WorkHorse
Command/Winn
series
Medium
Up to 10 gm
Crossing
Connect
Strong
Up to 30 g
Crossing
SteelCore
Strong
<1.0 gm
WorkHorse
Asahi
Regalia
Low
1.0 gm
Crossing
Astato
20
Medium
20 gm
Crossing
GrandSlam
High
<1.0 gm
Position
Treasure/
Astato 30
Medium
12
-30gm
Crossing
BSC
V14
High
3 gm
Crossing
V18
Medium
3
-6 gm
Crossing
Victory
14/18
Medium
12,18,25,30 g
Crossing
Support catheters
•Either for position or
increase force of distal
wire
• 0.018” and 0.014”
systems most often
used
•Straight or angled
Devices
•Balloons
–POBA
–DCB?
•Stents
–DES
–SES (BMS/DES)
•Atherectomy
–Directional
–Orbital
–Rotational
5
•To date there are no meaningful data
regarding outcomes with atherectomy in the
pedal loop
•Definitive LE
–78% patency 6 cm LL CLI
•LIBERTY 360
–To be presented 2016
Primary Patency in Subgroups
Subgroup Claudicants (n=743) CLI (n=279)
Patency
(PSVR < 2.4) Lesion
Length (cm) Patency
(PSVR < 2.4) Lesion
Length (cm)
All (n=1022) 78% 7.5 71% 7.2
By Lesion Length
< 4 cm (n=318) 81% 2.2 84% 2.3
4-9.9 cm (n=418) 83% 6.5 62% 6.6
≥ 10 cm (n=283) 67% 14.4 65% 15.1
SFA Only By Lesion Length
< 4 cm (n=184) 78% 2.3 82% 2.3
4-9.9 cm (n=253) 83% 6.5 60% 6.9
≥ 10 cm (n=232) 65% 14.6 63% 15.5
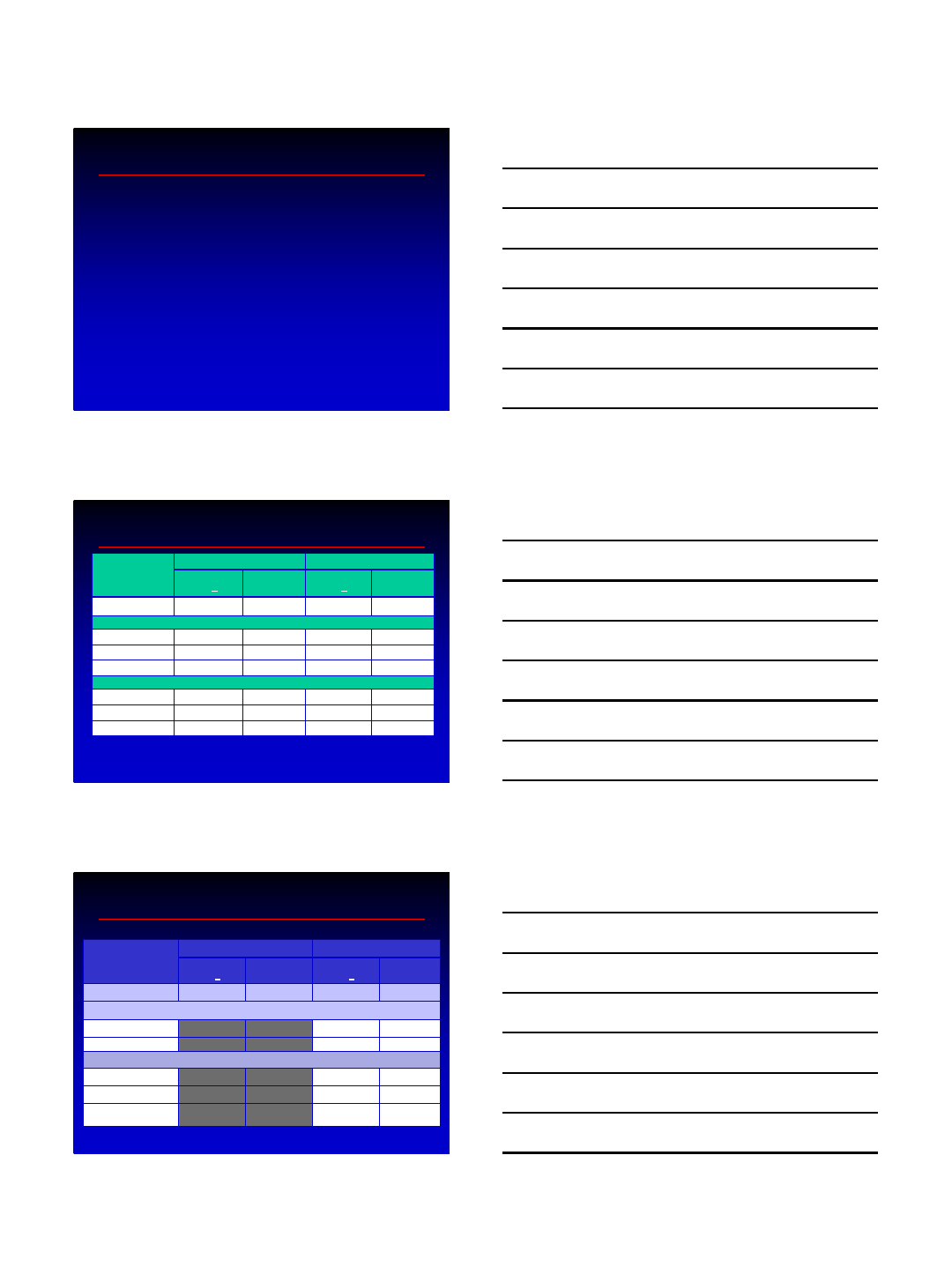
Primary Patency in Subgroups
Subgroup Claudicants (n=743) CLI (n=279)
Patency
(PSVR < 2.4) Lesion
Length (cm) Patency
(PSVR < 2.4) Lesion
Length (cm)
All (n=1022) 78% 7.5 71% 7.2
Lesion type
Stenoses (n=806) 81% 6.7 73% 5.8
Occlusions (n=211) 64% 11.1 66% 10.3
Lesion Location
SFA (n=671) 75% 8.1 68% 8.6
Popliteal (n=162) 77% 6.0 68% 5.4
Infrapopliteal
(n=189) 90% 5.5 78% 6.0
6
LIBERTY 360
•Prospective, observational, multi-center clinical study to
evaluate acute and long-term clinical, functional and economic
outcomes of endovascular device intervention in patients with
distal outflow peripheral arterial disease (PAD)
•No inclusion and exclusion
•Independent core laboratory analyses and adjudications
–Angiographic
–Duplex Ultrasound
–Six Minute Walk Test
–Health Economics
•Includes separate analyses for
–Claudicants
–Critical limb ischemia (RB4 and 5)
–Critical limb ischemia (RB6)
Conclusions
•Pedal loop reconstruction is an attractive intervention for
limb salvage and foot preservation
•Devices and selection of method of intervention remain at
the discretion of the operator
•Access and contemporary interventional approach allows a
myriad of technologies and devices for ultimate
revascularization
•Issues that remain
–Still may be too aggressive to the pedal loop without
current long term data seems an important issue
–Is drug elution/delivery an important part of the
intervention?
6/6/2016
1
Pedal Loop Reconstruction
Step by Step Case
Presentation
Fadi Saab MD, FACC,FASE,FSCAI
Associate Director of Cardiovascular Laboratories
Co-Director of Pulmonary Embolism and Deep Venous Thrombosis Services
Clinical Assistant Professor-Michigan State University
School of Medicine
Metro Heart and Vascular
Metro Health Hospital
Disclosures
•Bard Peripheral Vascular - Research, Consultant,
•Cardiovascular Systems, Inc. - Research, Consultant,
•Cook Medical - Research, Consulting
•Covidien –Consulting
•Terumo –Consulting
•Spectranetics –Research, Consulting
6/6/2016
2
Advantage of Retrograde Tibial
Access
Increase success rate of crossing
Shorten treated segment
Preserve options of therapy : Surgery, atherectomy
Utilize hibernating lumen
Preserve tibial vessels flow
Saab et al
Pedal Loop Reconstruction
Antegrade Approach
•
Critical Limb Ischemia patients
•
Patients with Short Pedal CTO’s
•
Requires at Least 5 Fr Sheath
•Adequate Flow through the opposite
vessel (PT or AT)
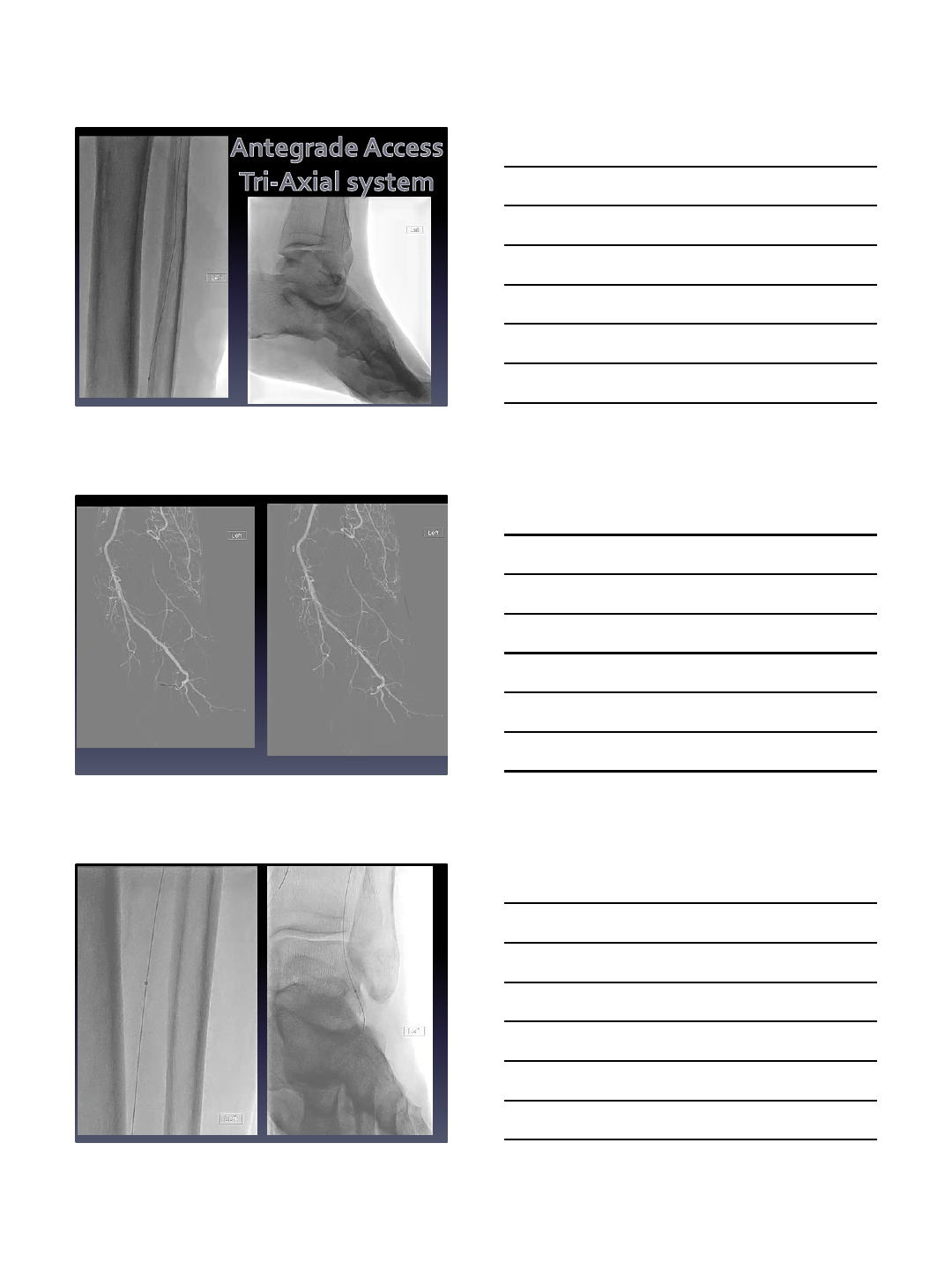
Retrograde Approach
•
Usually for longer CTO’s
•
Requires a Tri-Axial system
•
Usually safer
•
At least a 6 Fr sheath
•
Retrograde crossing under
Flouroscopy with a 0.014 loop
technique
Saab et al
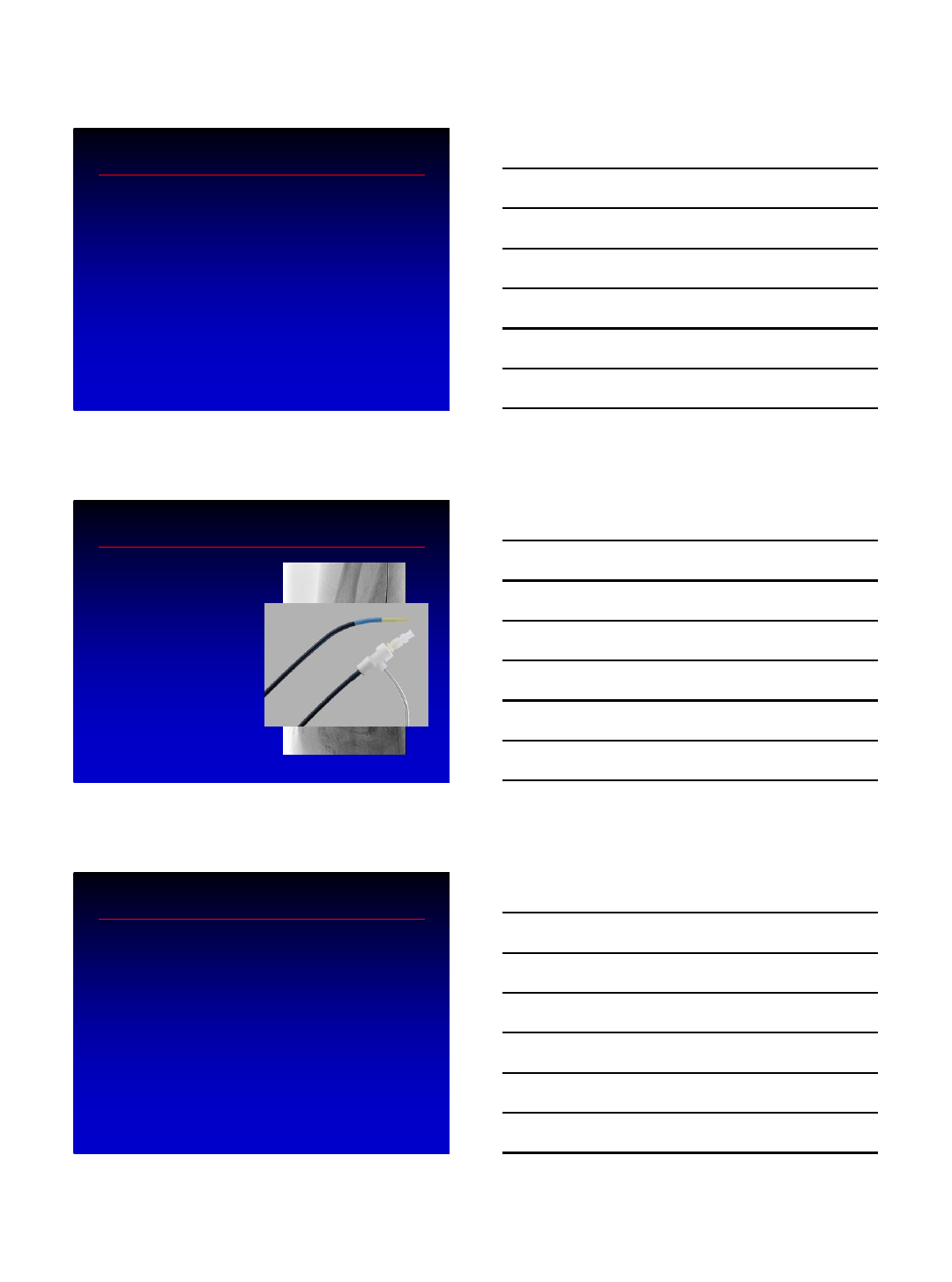
Pedal Loop Reconstruction
Wires
•
Journey Wire (BSCN)
•
Regalia Wire (Asahi)
•
Glide Advantage (0.014) (Terumo)
•
Runthrough (Terumo)
•
Gladius (Asahi)
Saab et al
6/6/2016
3
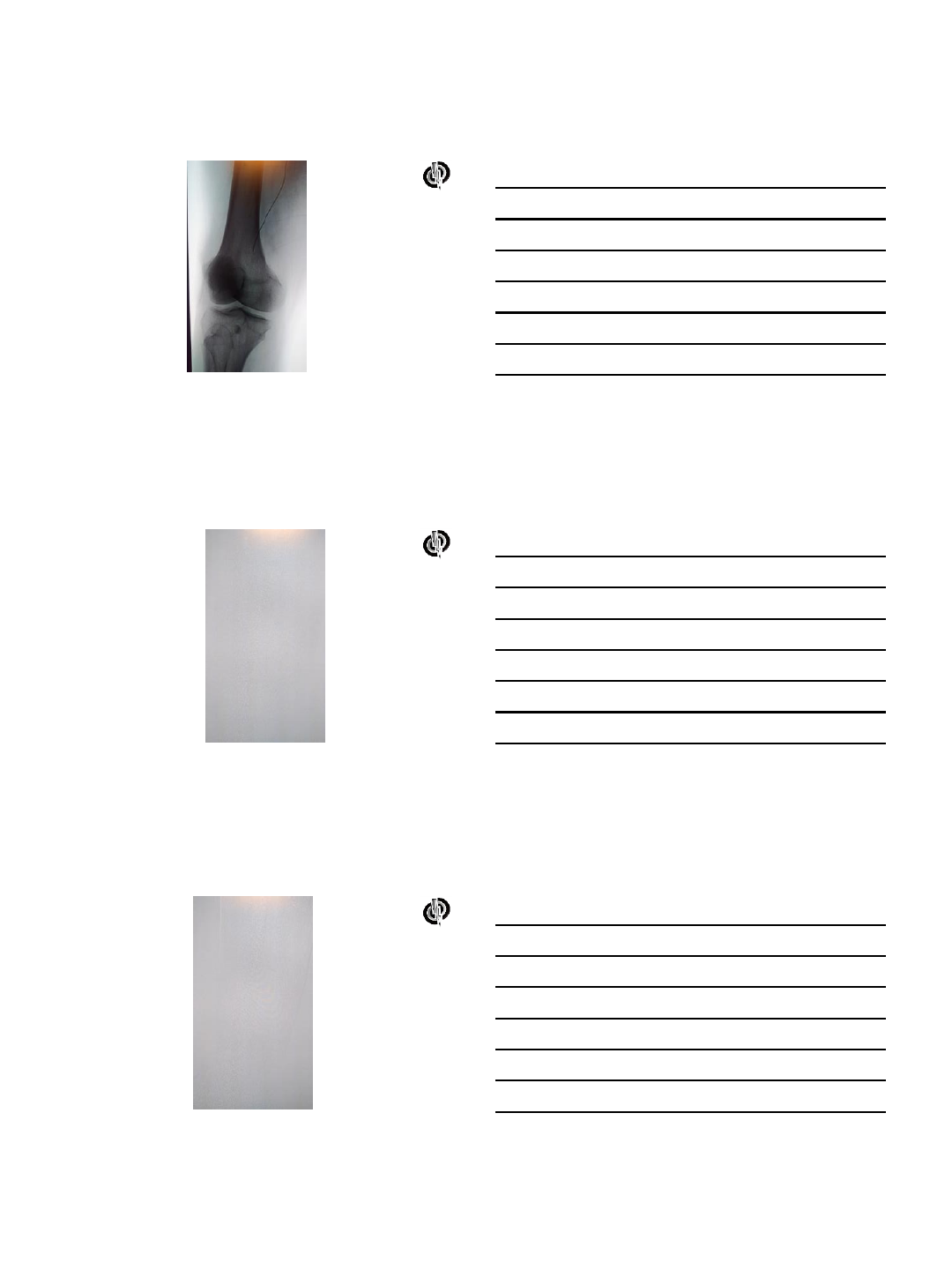
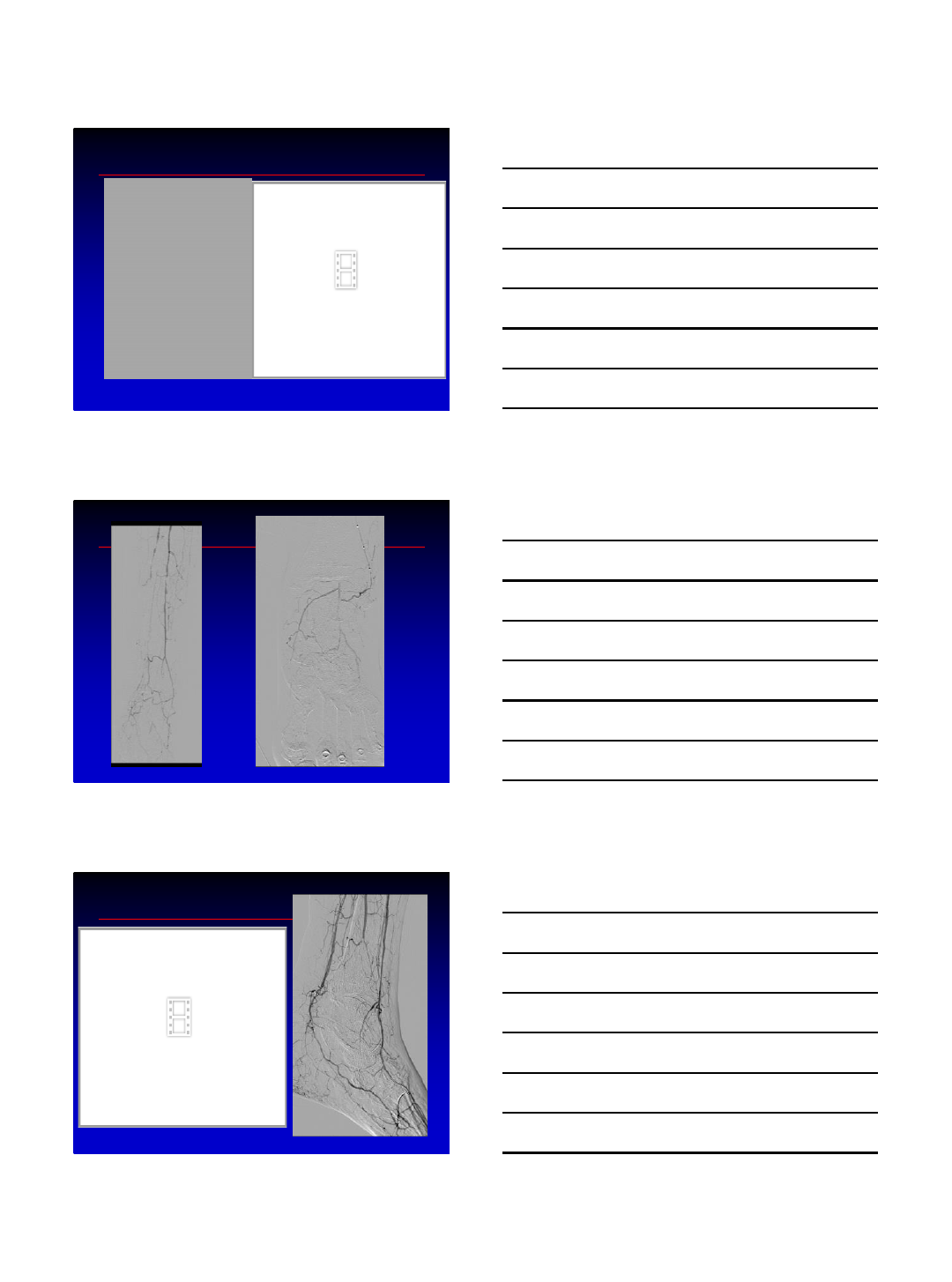
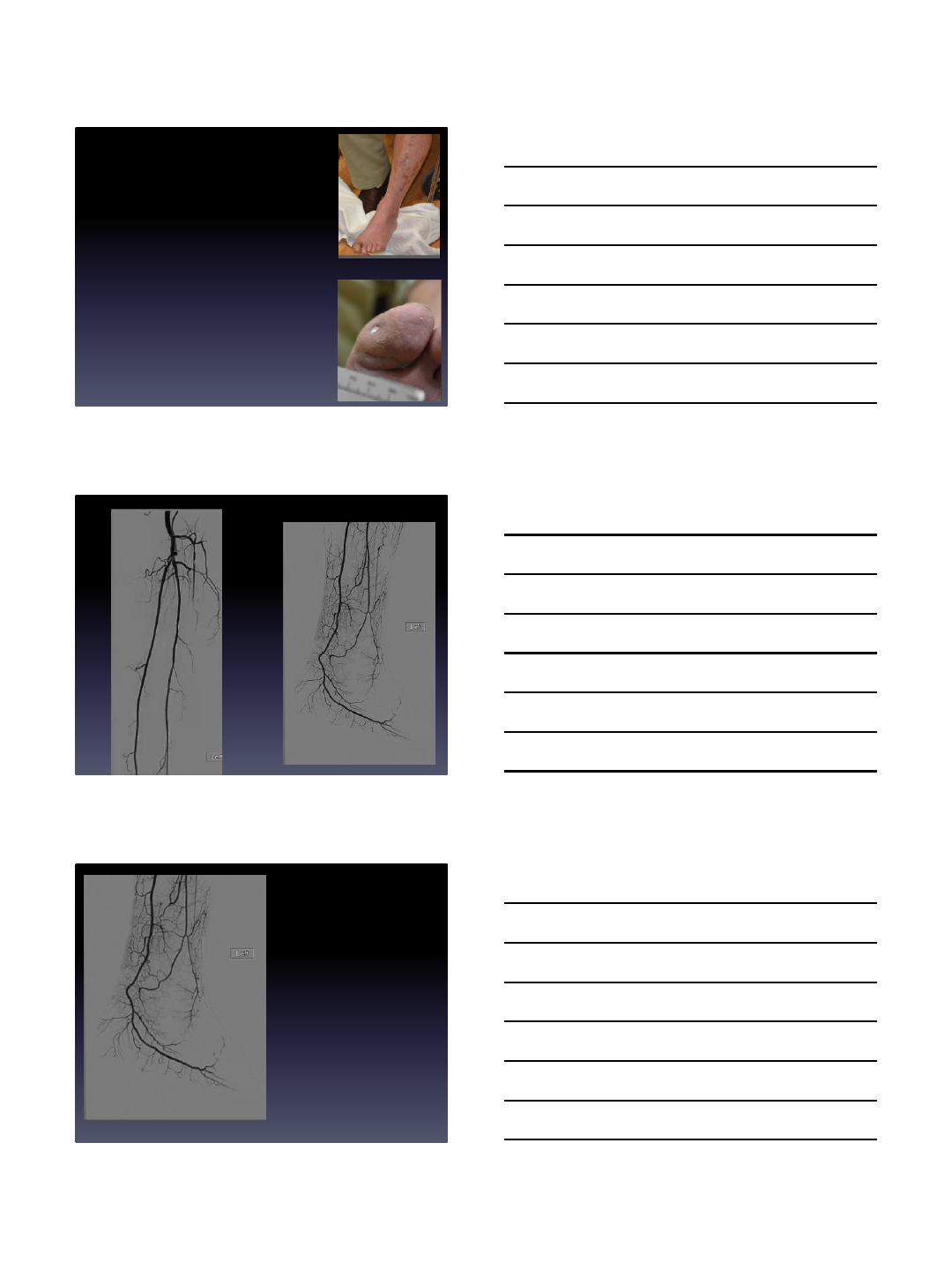
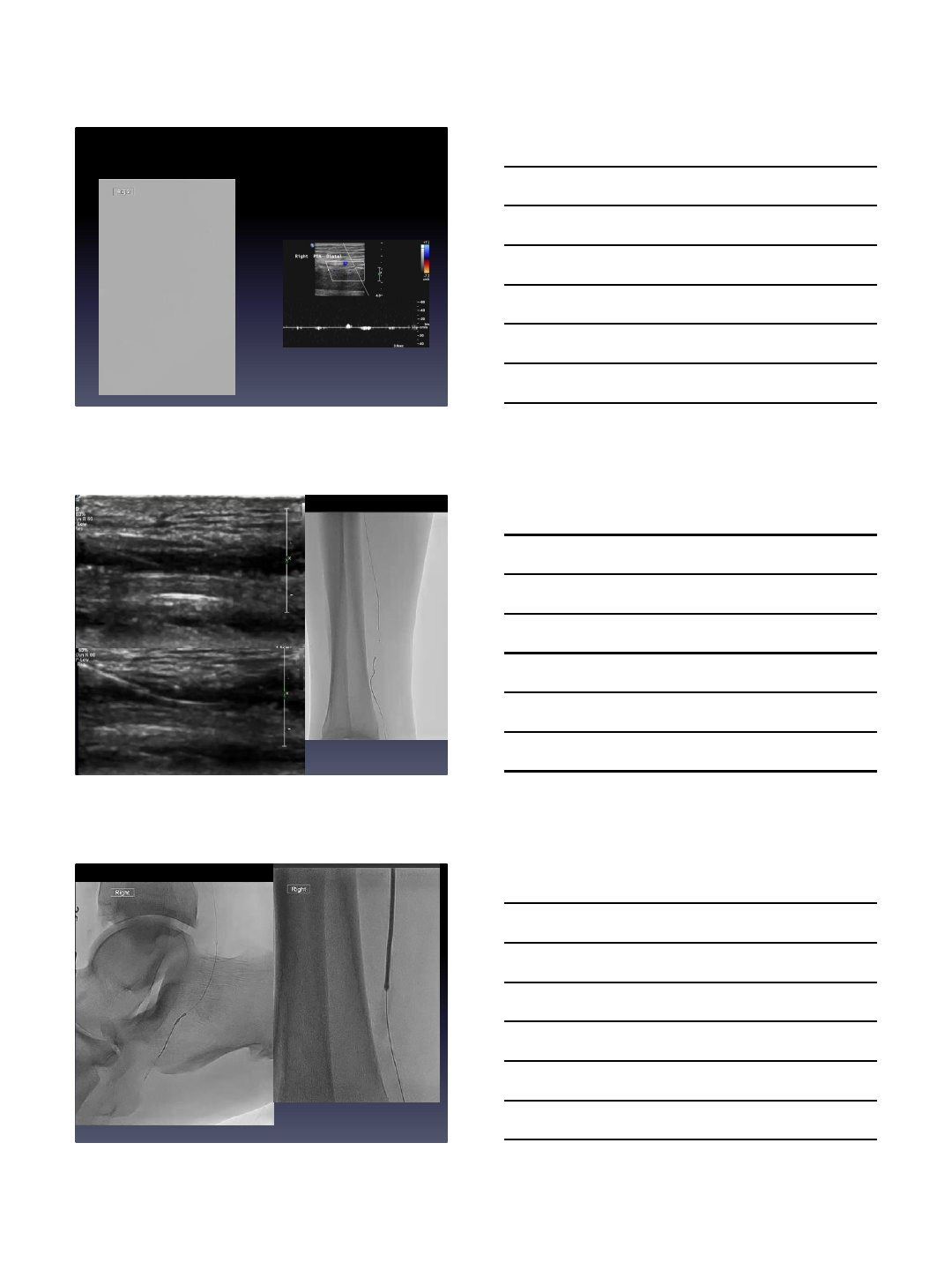
Case Presentation
•69 year old that presented
with a non healing wound over
the Plantar and dorsal aspect
of the great toe
•Risk factors include: HTN, DM,
Ischemic cardiomyopathy with
an EF of 40%
•Despite 6 months of wound
care, no healing
• Non compressible ABI’s
Antegrade
VS
Retrograde?
6/6/2016
4
6/6/2016
5
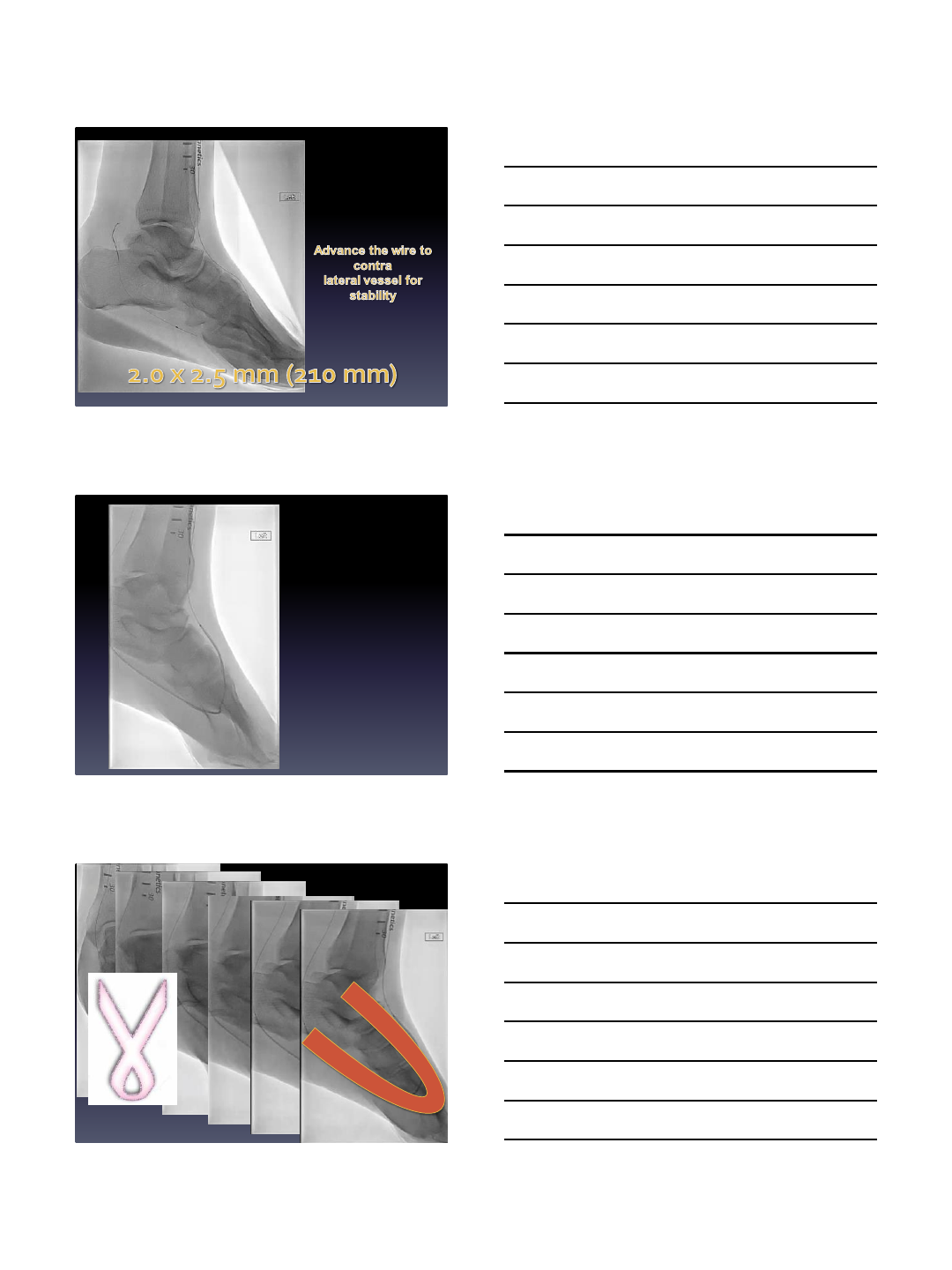
Visual Illusion
6/6/2016
6
6/6/2016
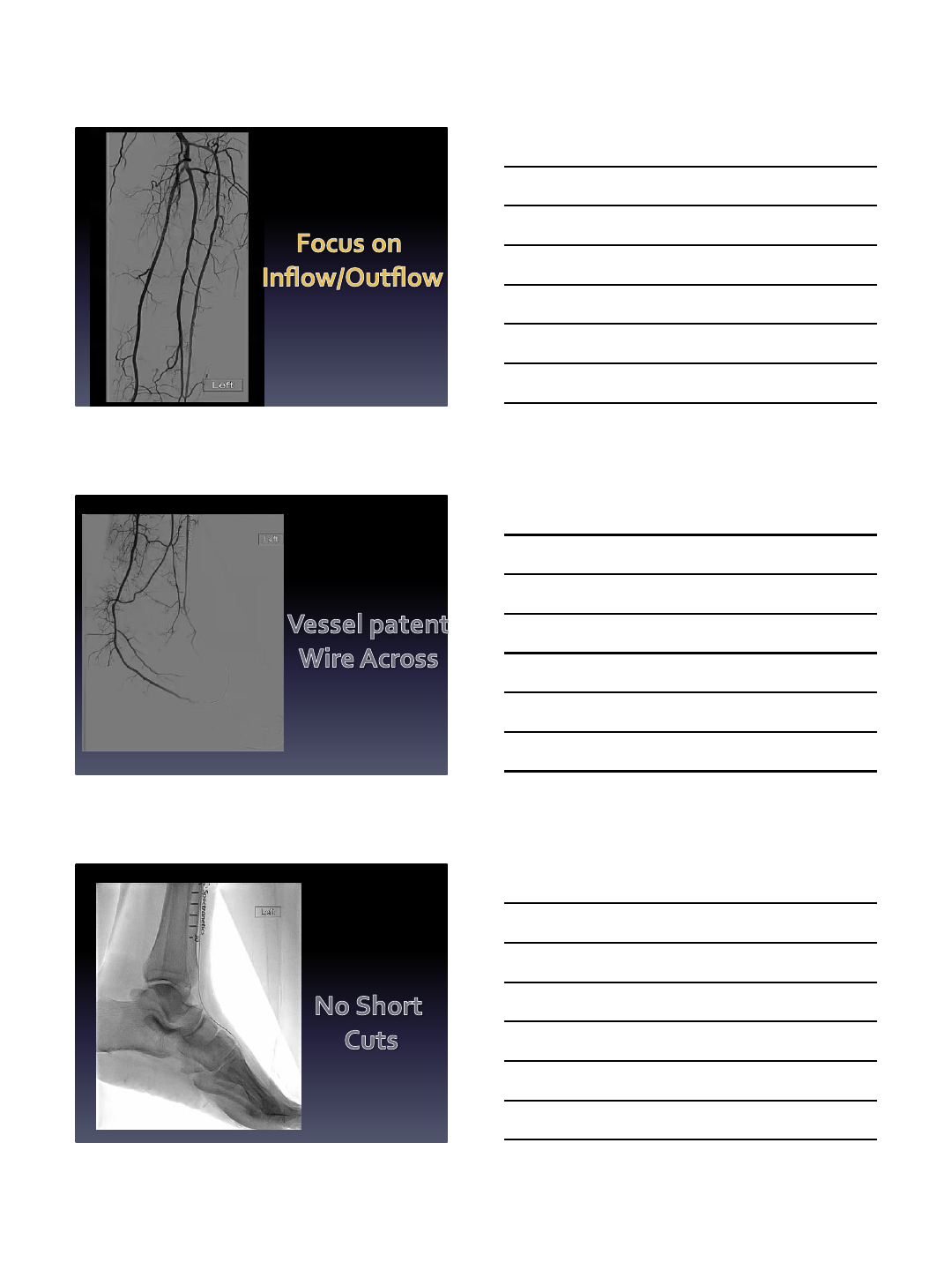
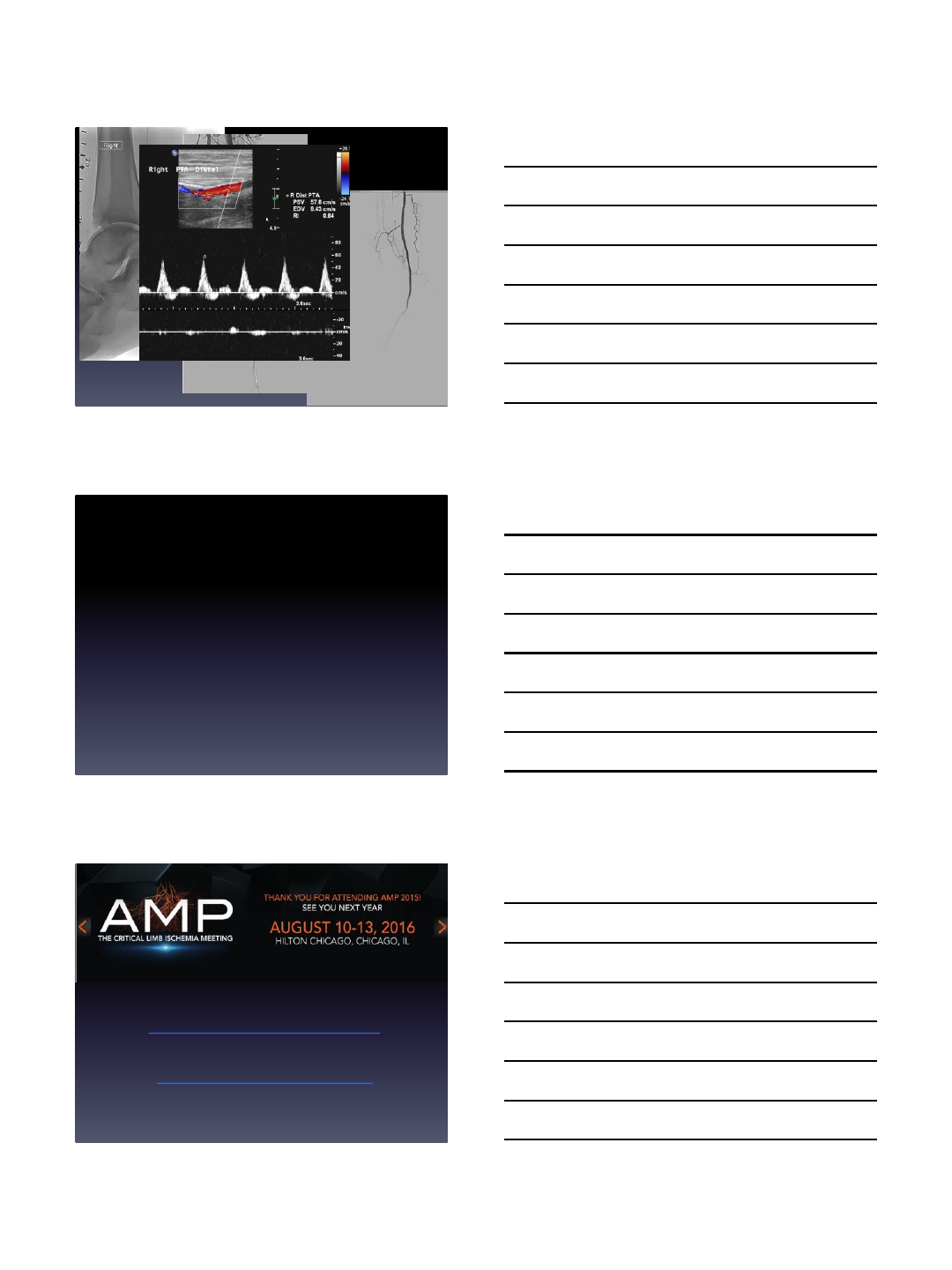
7
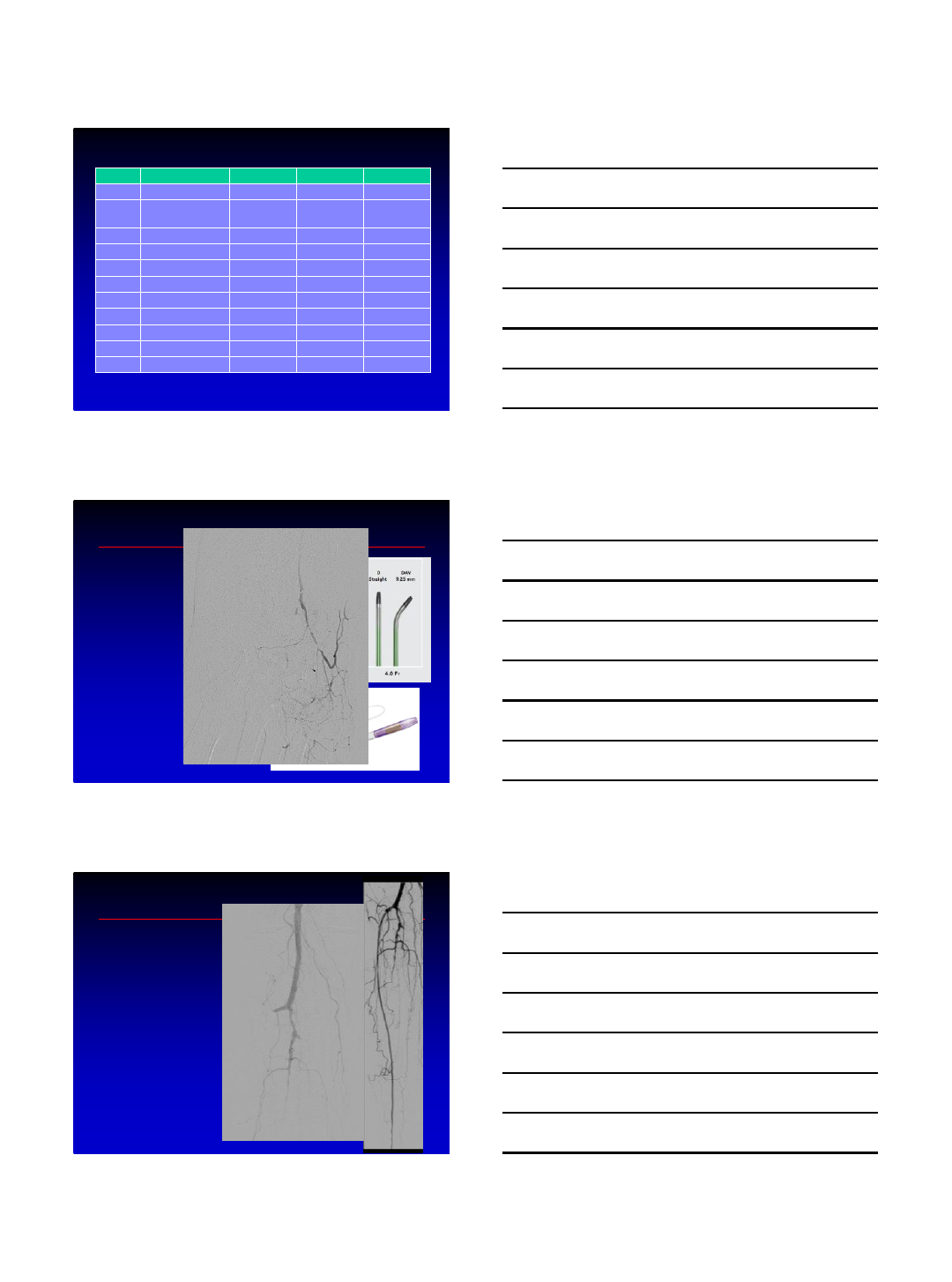
Retrograde Crossing
6/6/2016
8
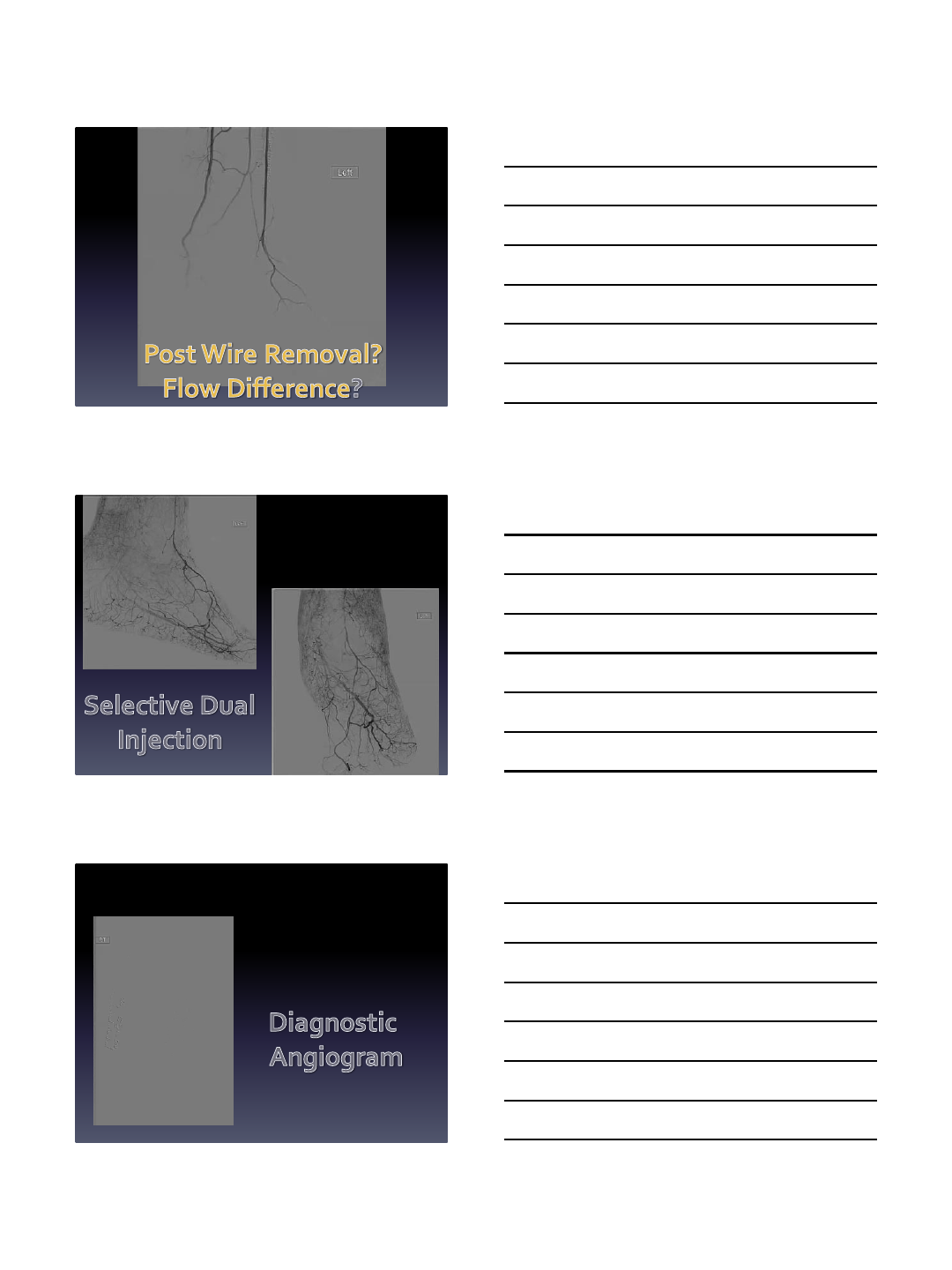
6/6/2016
9
Another Option
6/6/2016
10
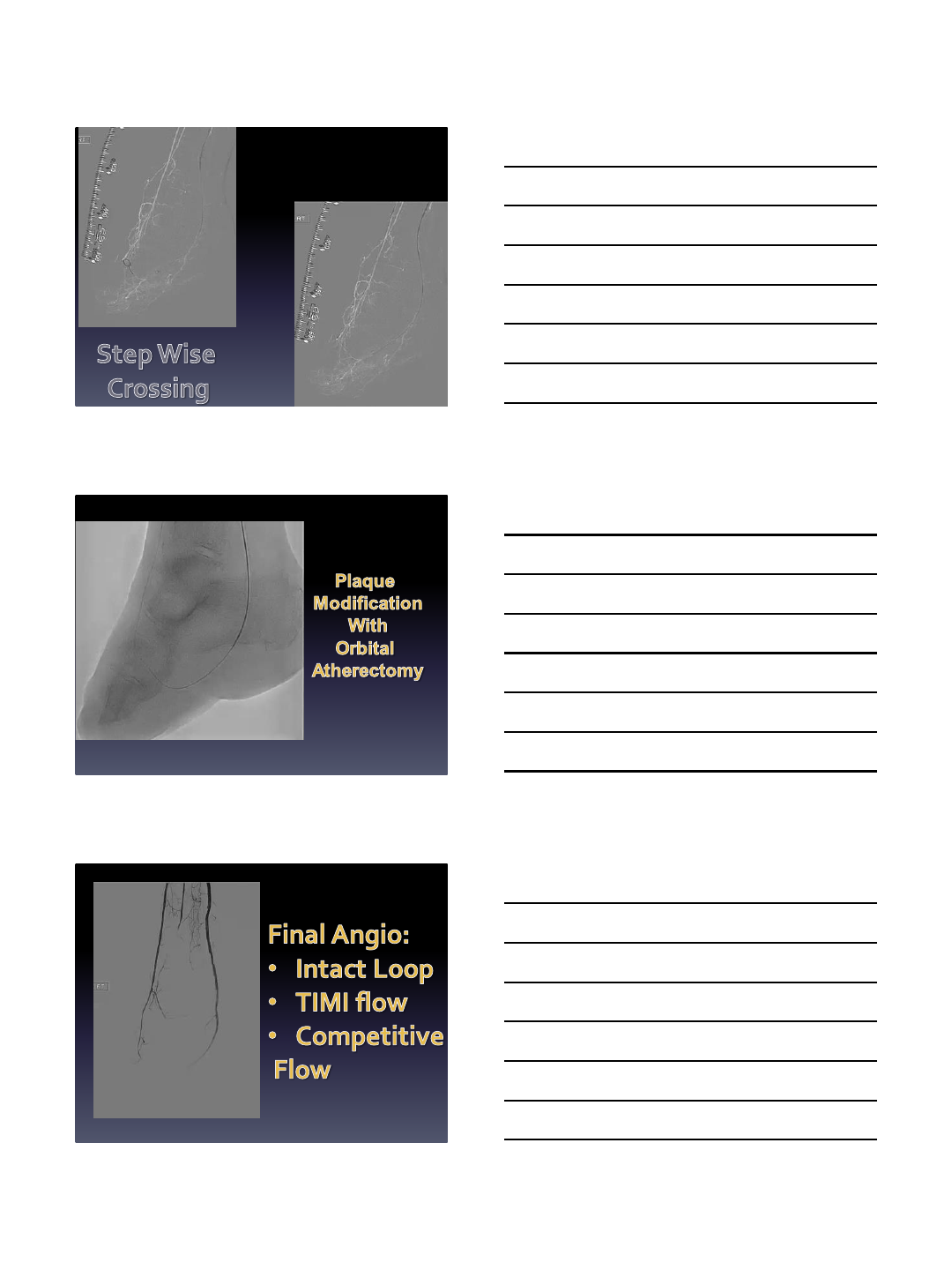
Conclusion
•Pedal Loop reconstruction is the next phase in CLI therapy
•Current available plaque modification technology for the
pedal loop is expanding.
•Current technologies include Laser atherectomy, Orbital
atherectomy and Phoenix atherectomy
•Long term benefits will need to be tracked and
documented in trials and registries (PRIME Registry)
fadisaab17@hotmail.com
Fadi.saab@metrogr.org
313-590-5902
