Shoulder Arthroplasty Syllabus
2013-09-23
: Pdf Shoulder Arthroplasty Syllabus Shoulder_Arthroplasty_Syllabus 9 2013 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 38
C
I I I
ISTITUTO CLINICO
HUMANITAS
Disclosures and Potential Conflict of Interest
Royalties:
MD Services
Consultant:
LIMA Corporate
Conmed Linvatec
Tornier Biologics
C
I I I
ISTITUTO CLINICO
HUMANITAS
Complications of
Uncemented Metalback
Glenoid Implants:
Personal Experience &
Literature Analysis
A.Castagna, M.Borroni,
G.Delle Rose, C.F.De Biase
IRCCS CLINICAL INSTITUTE HUMANITAS
Milano - Italy
C
I I I
ISTITUTO CLINICO
HUMANITAS
Background
Total shoulder arthroplasty is an effective procedure for:
•Degenerative arthropathy
•Some inflamatory arthropathies
•Certain proximal humeral fractures
C
I I I
ISTITUTO CLINICO
HUMANITAS
TSA Vs. Hemi
The results of total shoulder arthroplasty
are better than hemiarthroplasty
JSES 2007
JBJS 2000
... BUT ….
C
I I I
ISTITUTO CLINICO
HUMANITAS
Glenoid Failure
•60% of failed TSA is the result of loosening
of the glenoid component
JSES 2002
C
I I I
ISTITUTO CLINICO
HUMANITAS
Evolution
•1975 English & McNab
•1981 Smith & Nephew Cofield
•1988 Biomet Biomodular
• Kirschner II C
•1990 Zimmer Mark 2 Copeland
•1993 Biomet Mark 3 Copeland
•1994-1998 Biomet Nottingham I - II Wallace
•1994 Aequalis Tornier
•1994-2002 Randelli - SMR Lima Randelli
•1998 Arthrex Univers 3D Habermeyer
•2000 Zimmer Sulmesh Gerber
C
I I I
ISTITUTO CLINICO
HUMANITAS
English & McNab
1975
•21 glenoid
•FU 3 years
•1 loosening
CORR 1987
C
I I I
ISTITUTO CLINICO
HUMANITAS
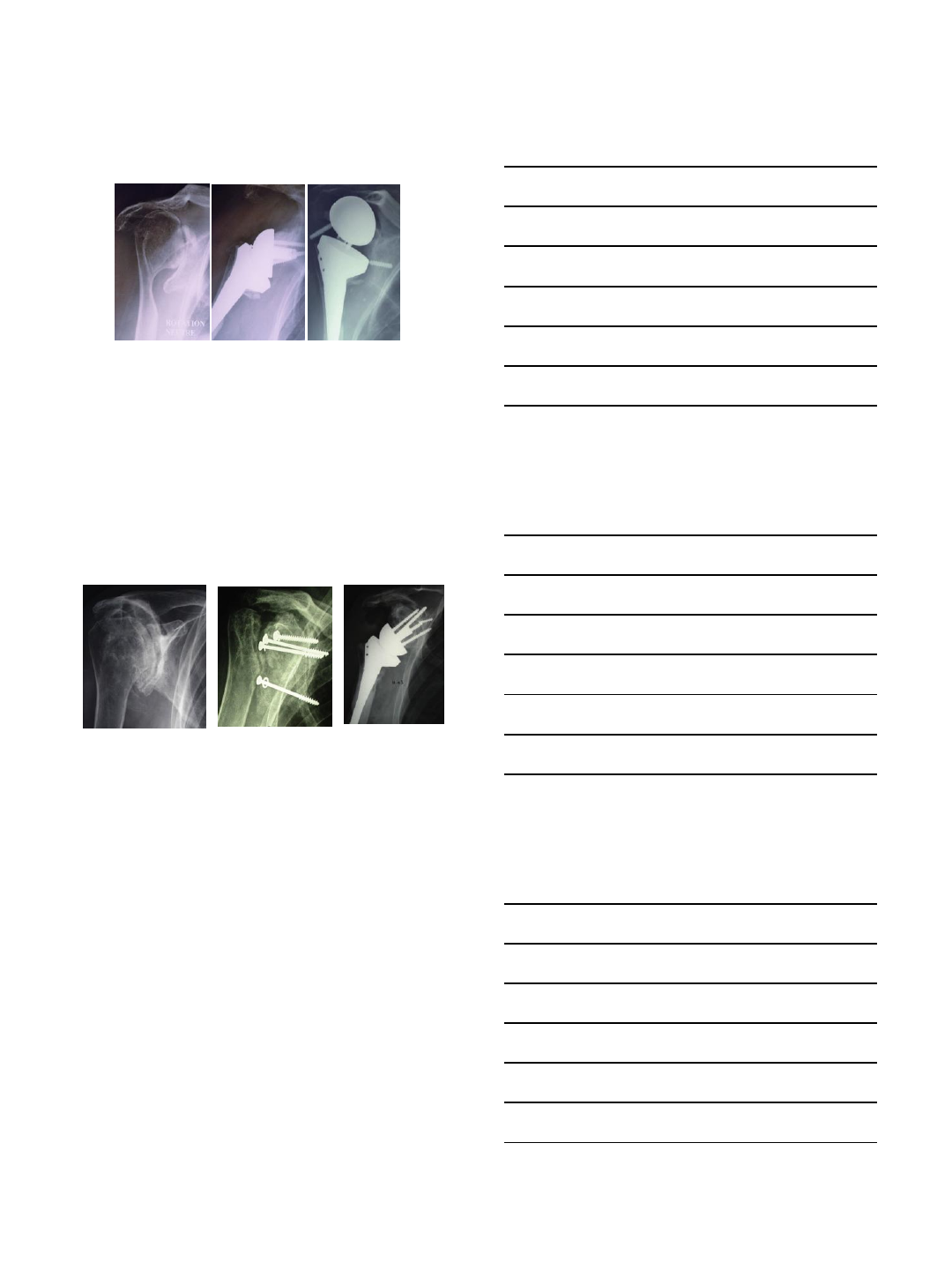
Smith&Nephew Cofield I
1981
•180 tissue ingrowth glenoid components
•16% complication of the glenoid
component
•Conforming radius of curvature
•One small central peg
•Main Fixation: screw
CORR 1994
C
I I I
ISTITUTO CLINICO
HUMANITAS
•83 ingrowth total shoulder
•Medium FU 9.5 years
•33 (39.7%) glenoid loosening
•26 (31.3%) glenoid revision
JBJS 2008
Smith&Nephew Cofield II
C
I I I
ISTITUTO CLINICO
HUMANITAS
Biomet Biomodular
1988
•32 cemented and 26 MB glenoid
•FU 5 years
•High rate dissociation PE/MB
•Same clinical results
•Higher rate of radiolucent lines in cemented
group
JBJS 1999
C
I I I
ISTITUTO CLINICO
HUMANITAS
Biomet Biomodular
•36 TSA in Rheumatoid patients
•Mean FU 132 months (96-168)
•Survivorship: 89% at 10 years
•1 (2.7%) glenoid loosening
•Cone peg
•Initial fixation: 2 screws
JSES 2010
C
I I I
ISTITUTO CLINICO
HUMANITAS
Kirschner II C
140 uncemented glenoid;7.5 years FU
16 (11%) Clinical failures
21 (15%) Radiological failures
16 (11%) Fractured screws
53 (38%) Radiolucent line<1 mm
40 (29%) Radiolucent line 1> <2
2 (1.4%) Radiolucent line >2 mm
JBJS 2005
C
I I I
ISTITUTO CLINICO
HUMANITAS
Zimmer Mark 2
1993
•42 TSA
•FU 7.6 years
•3 (7.1%) radiological loosening
•3 glenoid revision
–1 PE/MB disassociation (Design change in Mark 3)
–1 traumatic loosening
–1 primamry glenoid lossoening
JSES 2004
C
I I I
ISTITUTO CLINICO
HUMANITAS
Aequalis Tornier
1994
•354 total shoulder arthroplasty with a cementless glenoid
•Primary fixation was granted by 2 expansion screw
•Flat glenoid
•Hydroxyapatite on the porous back
•Glenoid Complication 16,5%
•Glenoid revision 6,4%
2000
C
I I I
ISTITUTO CLINICO
HUMANITAS
•40 double blinded randomized TSA
•20 PE cemented - 20 metal back
•FU minimum 3 years
•Radiolucent lines 85% PE - 25% MB
•Revision: 0 PE (0%) - 3 MB (15%)
•Failure between 1st-4th year
JSES 2002
Aequalis Tornier
C
I I I
ISTITUTO CLINICO
HUMANITAS
Arthrex Univers 3D
1998
•24 patients with cementless glenoid since
1998
•26% associated with glenoid bone graft
•95% no radiolucency
•4% radiolucent line < 1 mm
•Cage screw
•No locked connection between cage and
MB
•No loosening
SECEC 2003
C
I I I
ISTITUTO CLINICO
HUMANITAS
Zimmer Sulmesh
•22 TSA
•Mean FU 50.0 months (24-89)
•Multiple layers of highly porous titanium
•3 (13.6%) failure but with broken peg
•No other loosening
JSES 2010
C
I I I
ISTITUTO CLINICO
HUMANITAS
Biomet Nottingham
1994/1998
•90 Biomodular:
–75.6% (8y) 71.7% (11y)
•103 Nottingham I
–81.8% (8y)
•Loosening mainly occured in the
first 4 y
•34 Nottingham II
–93.1% (4y)
BMC Muskoloskeletal Disorders 2007
C
I I I
ISTITUTO CLINICO
HUMANITAS
•We reviewed from 1996 to 2005, 35 consecutive TSA with
SMR MB glenoid:
–27 (77.1%) primary arthritis
–5 (14.2%) post traumatic arthritis
–3 (8.5%) rheumatoid arthritis
•Mean age : 62.7 years (53.9-70.8) Titanium alloy shell with
hydroxyapatite coating
Convex back side of MB
base-plate. Lima Lto
JBJS Br 2010
Our Experience
C
I I I
ISTITUTO CLINICO
HUMANITAS
Pre Op: X ray and CT scan
•77,1% A1-A2 (slightly or severe concave glenoid)
•17,1% B1 (slightly biconcave glenoid)
•5,7% B2 (severely biconcave glenoid)
Our Experience
C
I I I
ISTITUTO CLINICO
HUMANITAS
Mean follow-up of 6.2 years (48-154 months)
Clinical data:
–Constant Score
–Vas
–SST
Radiological data:
–Implant position
–Radiolucent lines (Molè classification)
Our Experience
C
I I I
ISTITUTO CLINICO
HUMANITAS
SCORE PREOP POSTOP
CS 35.2 70.8
VAS 7.8 3.1
SST 8.4 4.4
Our Experience
C
I I I
ISTITUTO CLINICO
HUMANITAS
27 cases (77.1%)
no radiolucent lines
8 cases (22.8%)
radiolucent lines <2mm
Our Experience
C
I I I
ISTITUTO CLINICO
HUMANITAS
•No PE disassembly
•No glenoid revision or loosening
Our Experience
C
I I I
ISTITUTO CLINICO
HUMANITAS
•Shape: convex, not flat
•Polyethylene: material and
sterilization
•Stabilizing system: central
hollow peg, not only screws
•HA also on the peg (not only on
the MB)
•???
Why such different results?
C
I I I
ISTITUTO CLINICO
HUMANITAS
•Shape: convex, not flat
•Stabilizing system: central
hollow peg, not only screws
•HA also on the peg (not only
on the MB)
•???
Why such different results?
C
I I I
ISTITUTO CLINICO
HUMANITAS
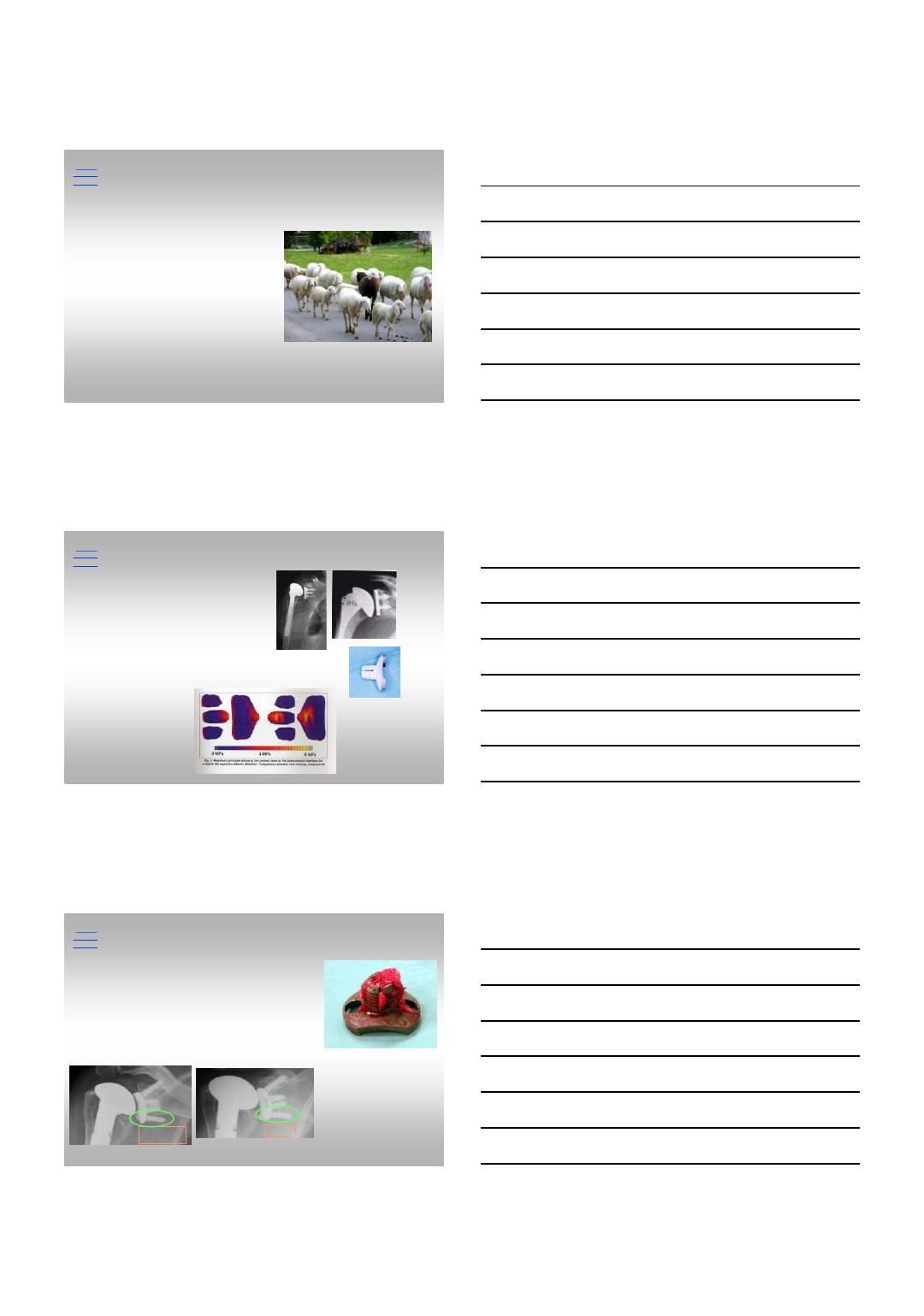
Glenoid Stabilization Elements
•2 screws (first phase)
•Central hollow peg
Discussion
Post op 5 aa
3 poor positioning
of the screws
with no
negative effect
C
I I I
ISTITUTO CLINICO
HUMANITAS
•Component
–Stability
–Disassembly
–Breakage
•Overstuffing
–Soft tissue tension
•Poliethilene wear
Open Issues
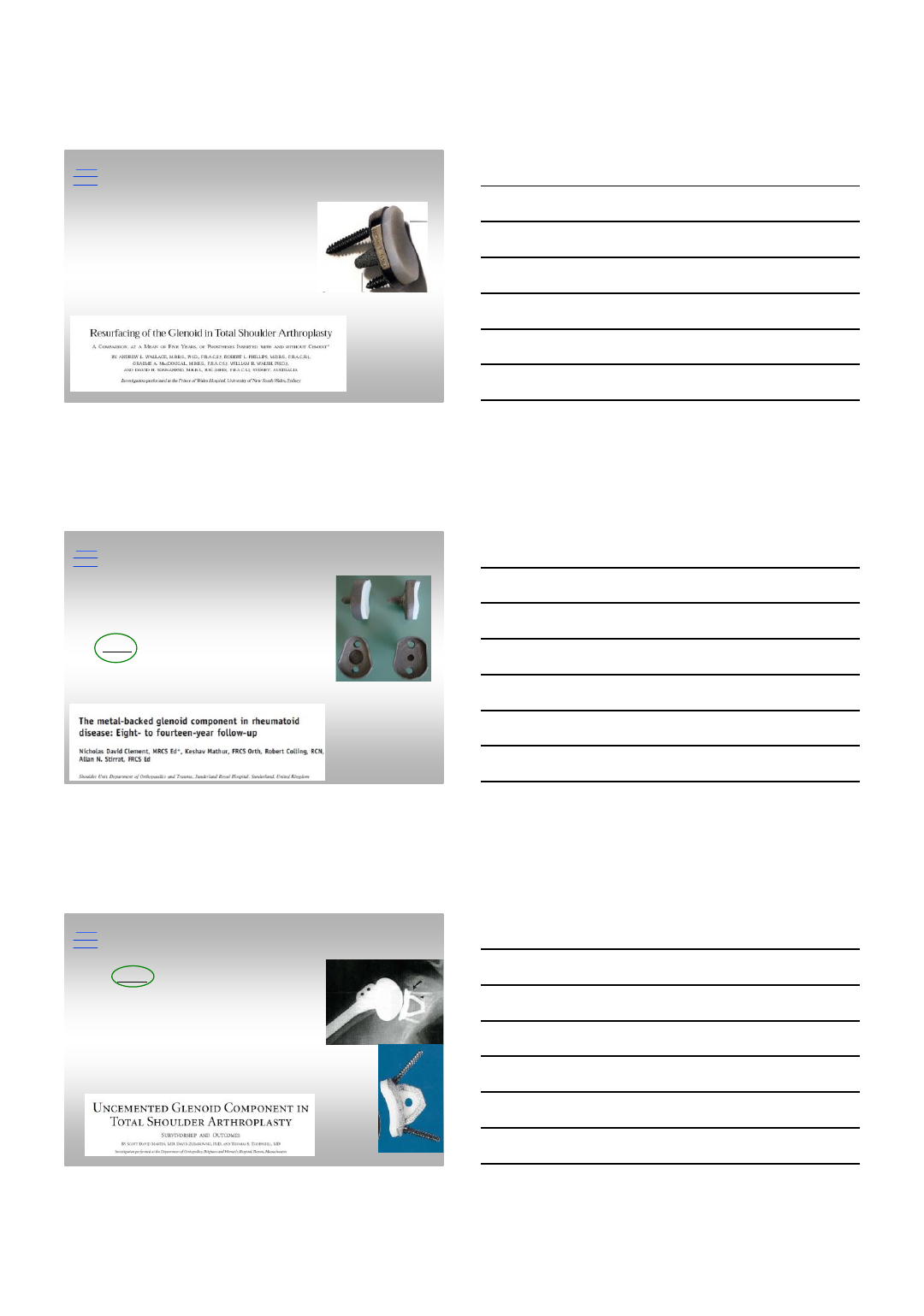
Polietilene wear
Metal wear
Osteolysis
Loosening
C
I I I
ISTITUTO CLINICO
HUMANITAS
Take Home Message
Glenoid is still the weak point in TSA!
–Needs more investigation, new ideas
–Do not compare pears with apples
… On the other hand ..
–Revision surgery is every day more frequent
–Metal Back glenoid may help to face the revision problems
C
I I I
ISTITUTO CLINICO
HUMANITAS
Istituto Clinico HUMANITAS
alex.castagna@tin.it
9/22/2013
1
Periprosthetic Humeral Fractures
Avoiding Complications with
Shoulder Arthroplasty
9-23-2013
Tom R Norris, MD
VuMedi Webinar
Disclosures: Tornier, Inc. consultant, design surgeon, royalties, stock
Risk Factors for PPF
•Osteopenia-older age, RA
•Soft tissue contractures
•Polyethylene osteolysis
•Cemented, on-growth, in-growth
implant stems
•Stress riser with ipsilateral total elbow
•Technical factors
–Reaming, oversize implant, forceful
rotation
Campbell 1998, Wright, Cofield 1995, Bonutti, Hawkins 1992
Incidence: Humeral fractures in
shoulder arthroplasty
•Intraoperative fractures occurs in 0.6-3%- Primary
•Intraoperative fractures 24.1% - Revision humeral stems
–All intraoperative complications were fractures in RSA series
–Occurred during prosthesis and/or cement removal in revisions.
–Overall, this resulted in decreased patient function and
satisfaction.
•Postoperative fractures occurred in 1.4% – Primary
–All postoperative fractures, as found in most studies, were
secondary to trauma
Zumstein, Pinedo, Old, Boileau. Problems, complications, reoperations, and revisions in 782 reverse total shoulder
arthroplasty: JSES. 2011.
Wright, Cofield: Humeral fractures after shoulder arthroplasty. JBJS Am 1995.
Iannotti, Williams J Arthroplasty 2002
Campbell, Iannotti et al. JSES 1998
9/22/2013
2
Multiple classification systems
Campbell et al 1998
Classification
•Angulation
–0-15°
–16-30 °
–> 30 °
•Displacement
–Mild < 1/3 shaft diameter
–Mod 1/3 to 2/3 shaft diameter
–Severe > 2/3 shaft diameter
Wright TW, Cofield RH: Humeral fractures after shoulder arthroplasty. JBJS Am 1995; 77:1340-1346.
Classifications of Humeral PPF
Wright and Cofield-1995
Type
Description
Treatment
A
Above
tip of stem
Conservative
; functional splint
B
At
tip of stem
Poor
healing potential with conservative treatment.
In
low demand patients, if closed reduction can be obtained, trial
of
conservative
management for max 90 days; if no evidence of
union,
surgical
intervention.
For
healthy, active patients, immediate surgical intervention.
C
Distal
to tip of stem
If
closed reduction can be obtained, trial of conservative
treatment
for
up to 90 days.
If
no evidence of healing, surgical intervention.
New category: Planned osteotomies in stem removal or exchange
9/22/2013
3
Proximal humeral periprosthetic fracture
classifications derive and expanded from the
Johansson 1981 classifications of PPF in the femur
Treatment options
•Non-operative B and C level fractures
•prolonged healing and delay rehab up to 7
months
•Implant sparing
–ORIF with plate/cables/screws
–Strut allografts cable constructs
•Conversion to long stem
–Biomechanically stronger
–Removal well fixed implant problematic
•Alloprosthetic replacement
Kligman, Roffman 1999, Campbell et al 1998, Wirth, Rockwood 1996
Kelly, Purchase, Kam, Norris 2009, Norris, McElheney 1990
Avoiding Periprosthetic Fx in TSA
•Adequate capsular release
•Avoid forceful ER of the arm
•Proper patient positioning to allow exposure
•Avoid endosteal notching during canal preparation
•Avoid aggressive reaming—cortical breach
•Avoid underreaming followed by oversized prosthesis
•Preoperative templating to avoid overreaming
•Beware of patient factors
–RA, osteoporosis/osteopenia, cortical thinning, previous fracture
malunion with deformity
•Creation of humeral windows or humeral unicortical
osteotomy parallel to long axis to facilitate controlled
removal of well-fixed humeral stem during revisions
9/22/2013
4
Considerations
•Will the fracture heal with non-operative
treatment?
–Fracture location, displacement, component
fixation
•Does the humeral component need to be
exchange for a different type?
•Is there bone support for the prosthesis, or is
auto or allograft support/replacement
necessary?
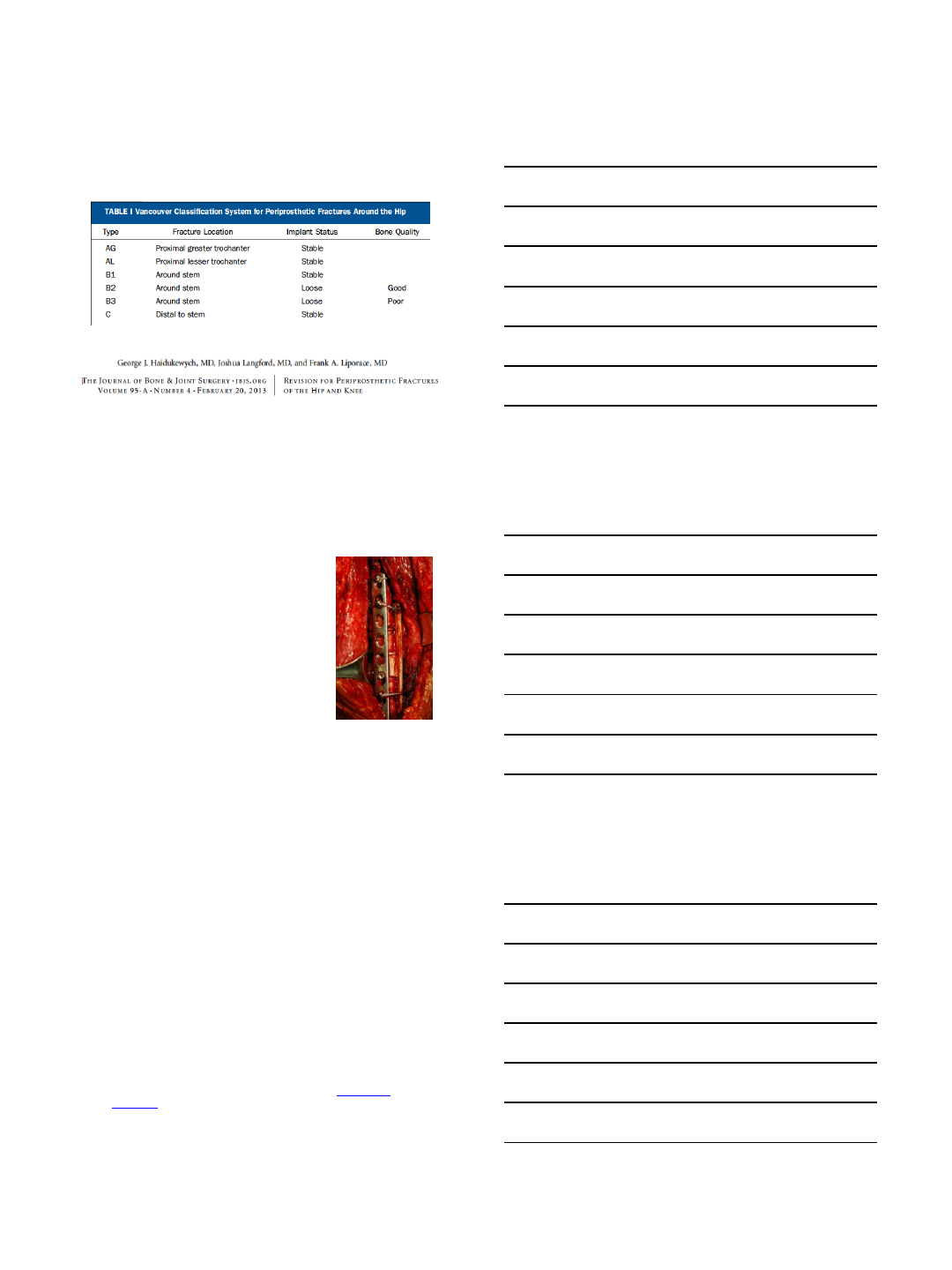
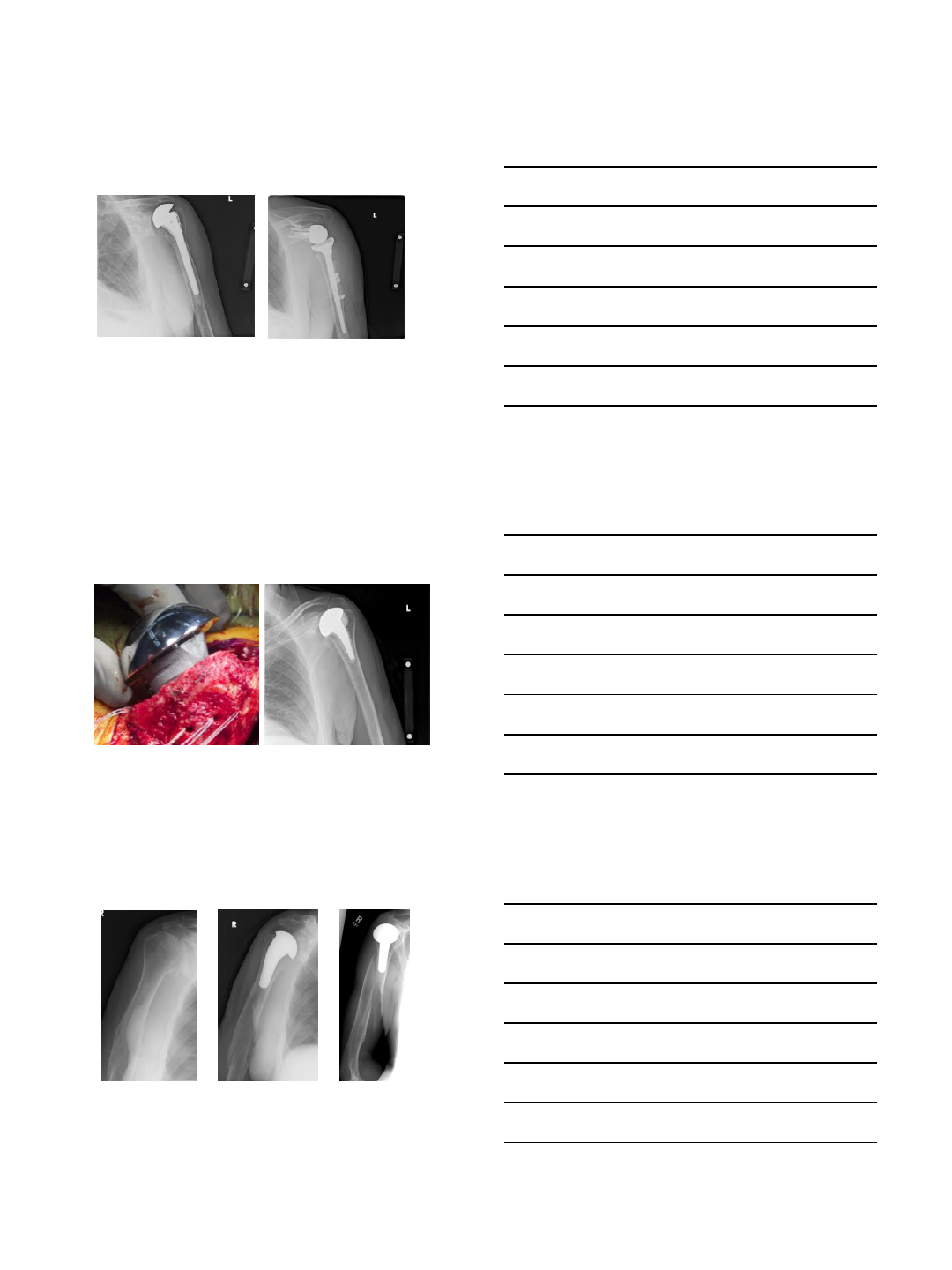
Stress Shielding + Osteolysis
in implant for revision
Meticulous use of flexible osteotomes
around the posterior fin at the GT
results successful stem removal without
fracture and preservation of bone stock
High implant, RCT, stress
shielding, and osteolysis
Words of caution
–When working proximally,
beware the tuberosities
•It can be easy with the sclerotic, thinned
bone to causes fractures of GT and LT
•Cut notches for the fins
–If tri-flange more likely to need
osteotomy 83% vs. 8%
•Phipatanakul J Shoulder Elbow Surg. 2009 Sep-
Oct;18(5):724-7
•If they fracture/When they fracture
–Tag the cuff
–Prepare to fix it at stem implantation
–Use same techniques as hemi for fx
9/22/2013
5
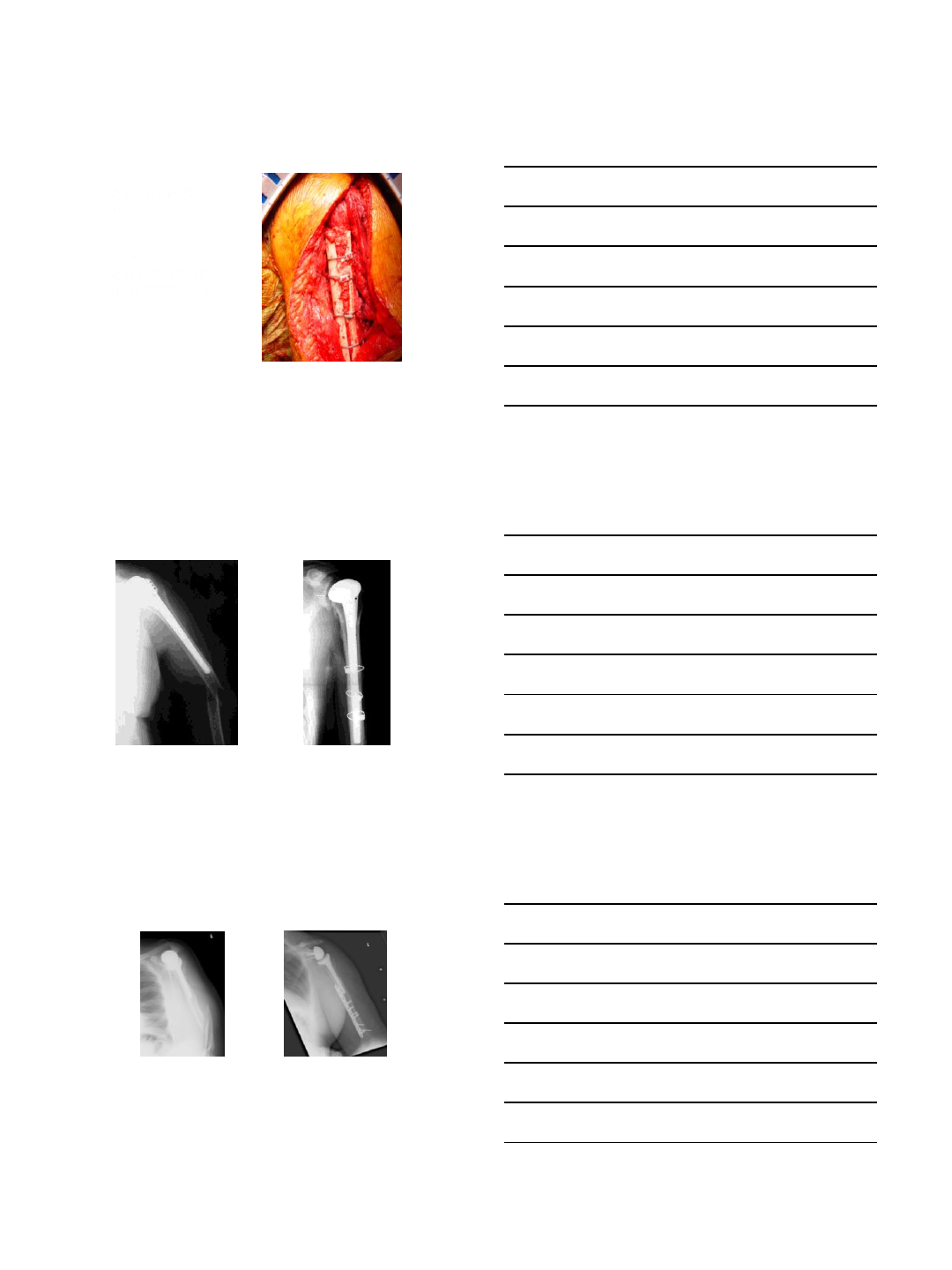
Tuberosity fixation
•Racking hitch heavy
nonabsorable suture
•Place at cuff insertion to
tuberosity
•Cerclage around
humeral stem
•Tuberosity overlap shaft
•Then held with SS-
rotator interval closure
14
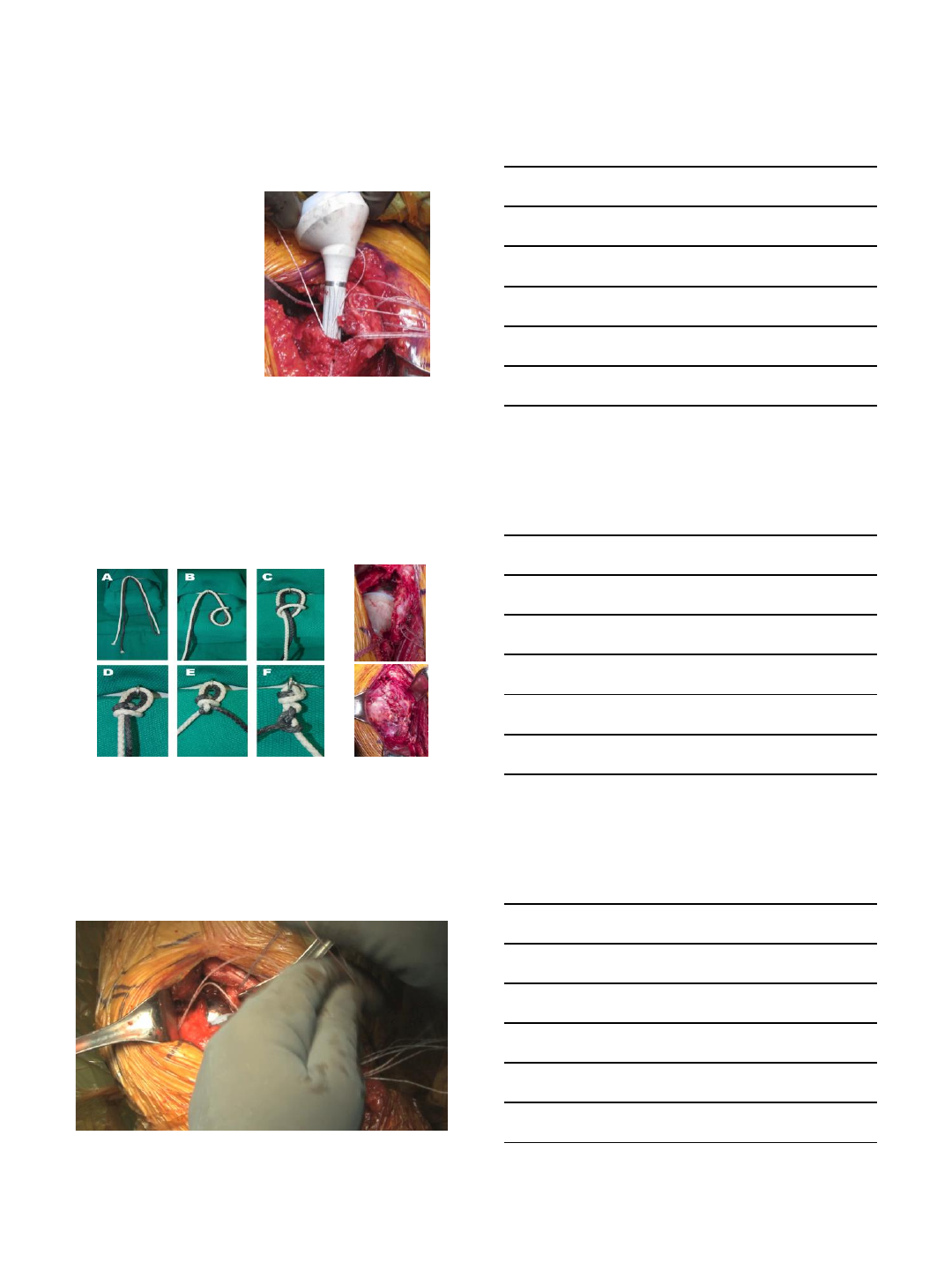
Techniques for tuberosity
reconstruction: Racking Hitch Knot
Racking hitch suture for tuberosity and
cerclage shaft fracture fixation
9/22/2013
6
Revision Surgery
10 x risk of fracture than primary!
•Much of revision is implant extraction!
•Inadvertent as well as planned controlled
fractures run risks of unanticipated nerve
injuries
Bone Preservation in Revision
•GOAL: preserve the humeral shaft circumferential
integrity and muscle attachments during stem removal.
•TECHNIQUES:
–Use flexible osteotomes around GT to loosen the implant
sufficiently for an in-line extraction
–Obtain implant specific extraction device to insert on the
top of the humeral stem with an attachable slap hammer -
-OR–
–stem extractor
–gouges for in-line disimpaction
–longitudinal controlled osteotomy or window
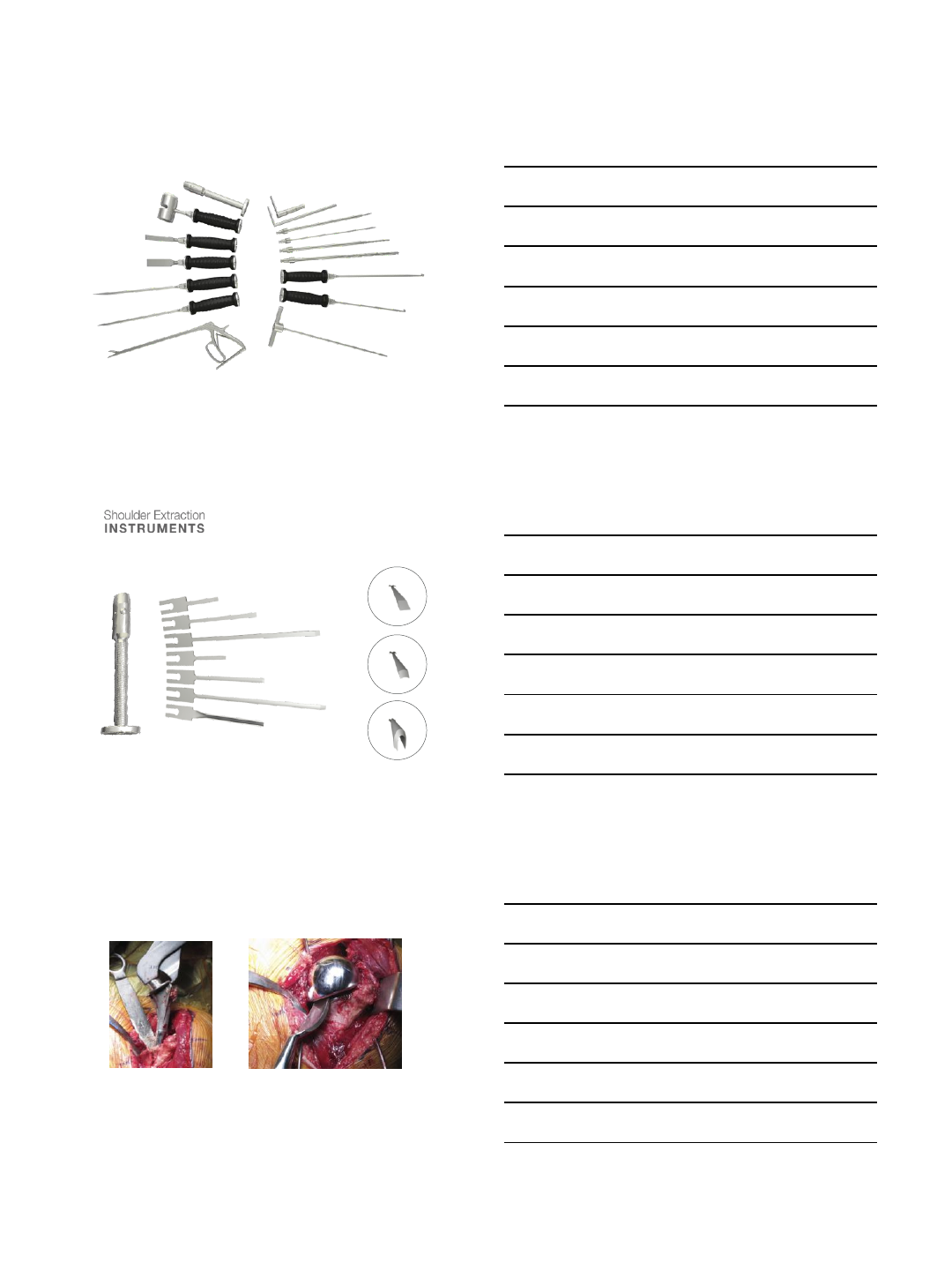
Revision Instruments
be prepared!
•Wheel burr
•Sagittal saw
•Flexible osteotomes
•Rigid osteotomes
•Ultra Drive
•Drills (6-9mm)
•cement extraction
sets
•System specific
extraction devices
•Reverse cutting
curettes
•Universal extraction
gouges
•Fluoroscopy
•Cerclage cable system
(metallic or polymer)
9/22/2013
7
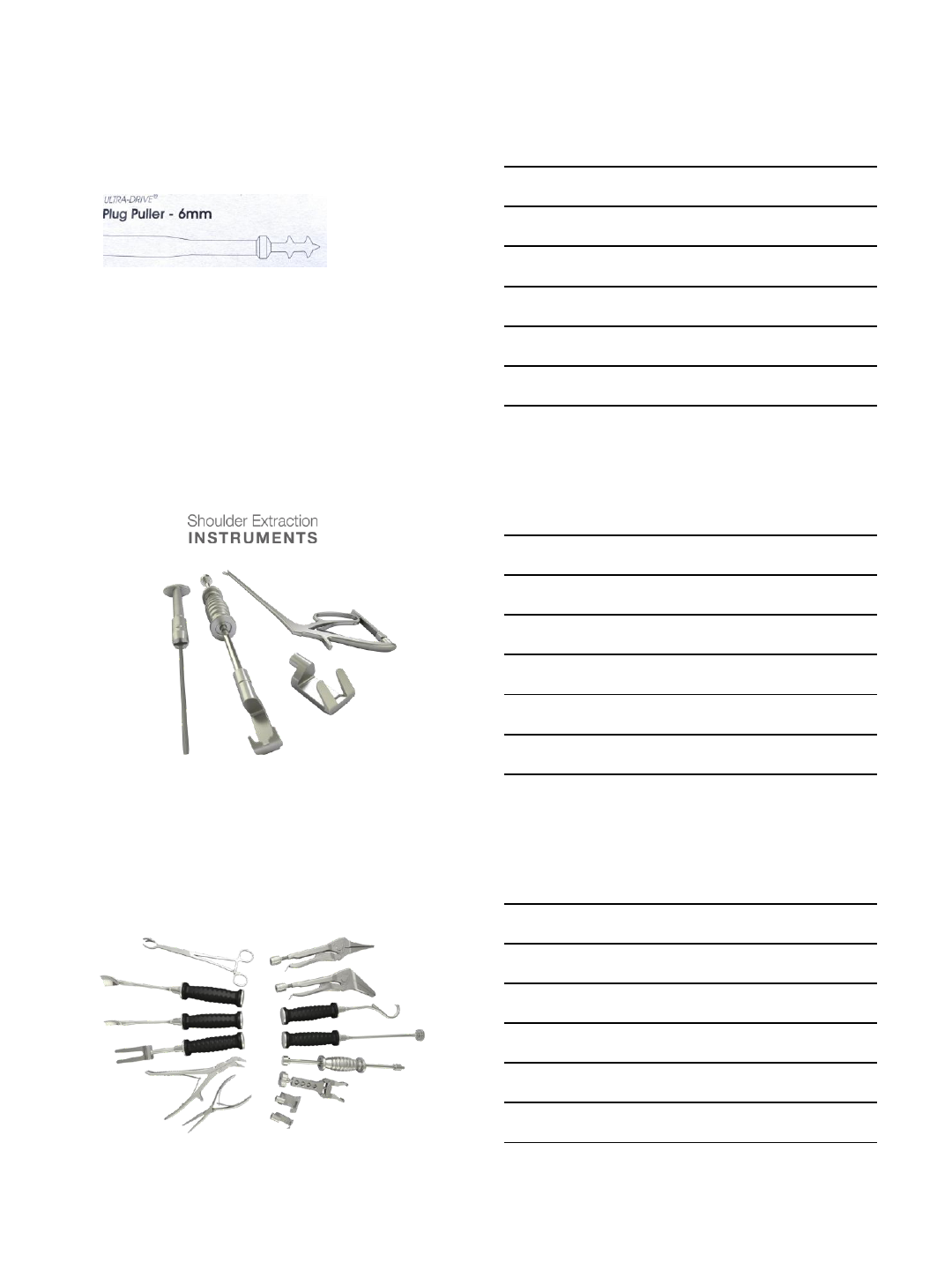
Cement Removal
distal to implant if long IM fixation needed
•6mm Ultra-Drive plug puller is used to make a central perforation in
the humeral cement mantle.
•ALT: use increasing size drills (6-9mm)
•Subsequent use of reverse cutting curettes
•Caution: cortical perforation can occur and cause injury to the radial
nerve.
•Use table so fluoroscopy can be used
•Cement can deflect ultra drive and drills out thru weaker cortex!
Component Removal/Utility Instruments
9/22/2013
8
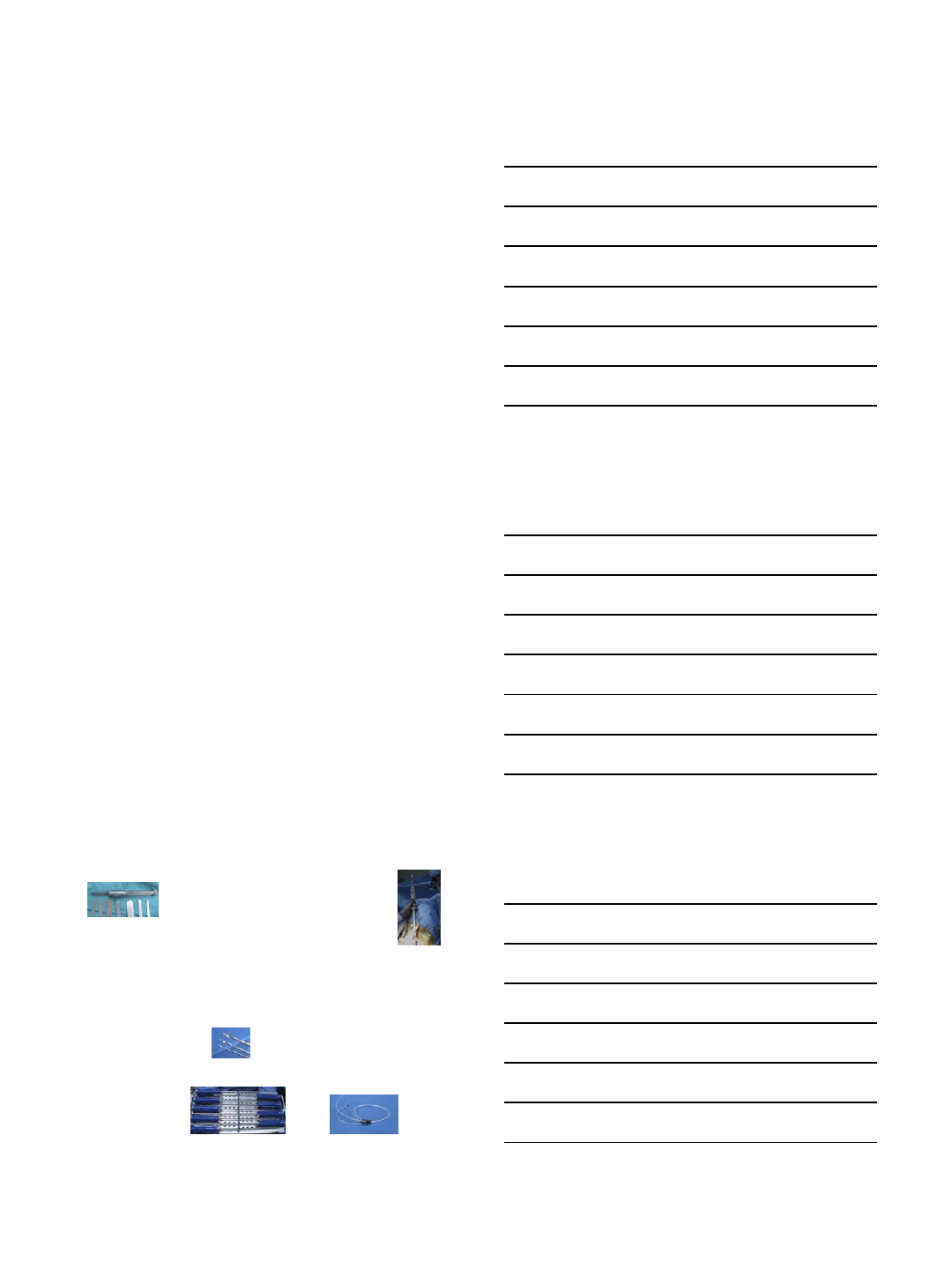
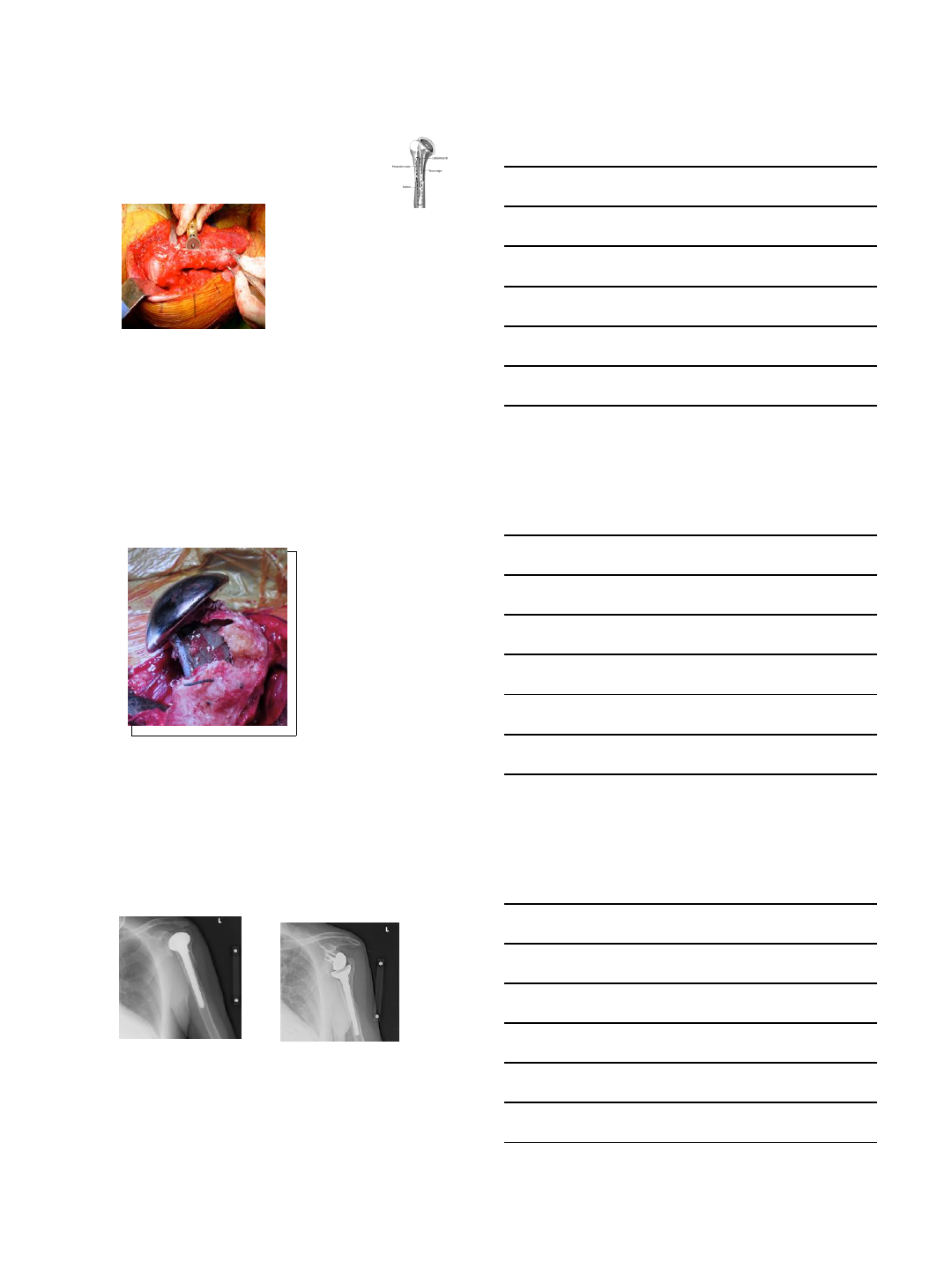
Cement Removal Instruments
Flexible Osteotomes & Handle
Fin
Radial
Flat
Revision strategies for implant removal
In-Line extraction to preserve shaft
Implant specific extraction device gouge for in line disimpaction
9/22/2013
9
Humeral Osteotomy or Window
-For stem removal, a high
speed circular saw is used to
make a controlled
longitudinal humeral
osteotomy.
-Make the early decision to
osteotomize to preserve bone
and avoid additional fractures
and comminution
Preserve muscle attachments,
especially the deltoid
Sperling JW, Cofield RH: Humeral windows in revision shoulder arthroplasty. JSES
2005; 14:258-263.
Increasingly popular: Gohlke, Nicholson, Romeo, Kelly G9MD, Tech Shoulder Elbow
Intra-Operative GT Fx
Inadvertent greater
tuberosity fracture during
disimpaction of a straight
humeral stem with
posterior fin. This can be
avoided by either using
flexible osteotomes to
better expose the fin or
with a controlled
osteotomy in cases with
poor bone stock.
Posterior fin rests with greater tuberosity
Preserve GT
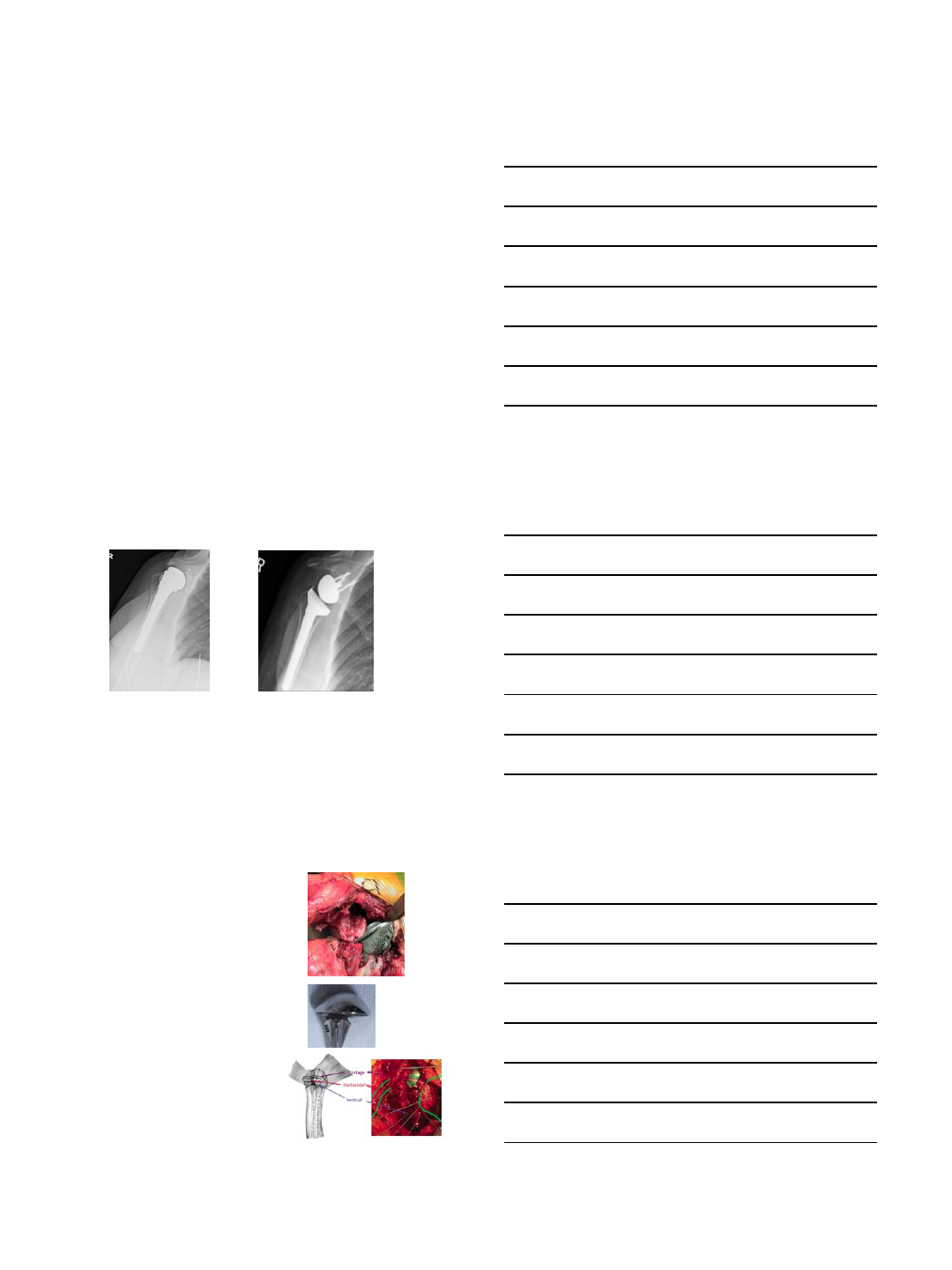
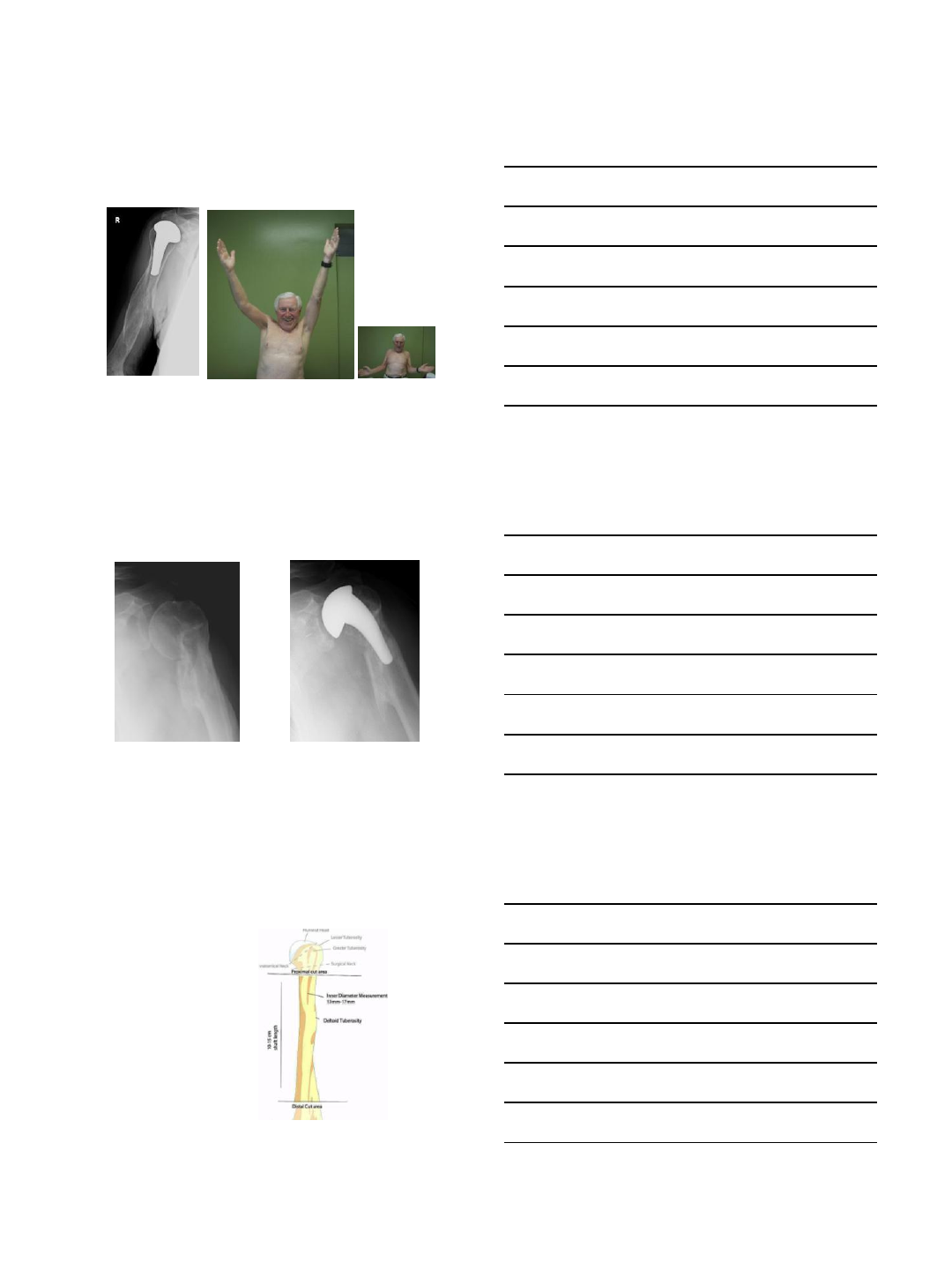
PF HHA for PHF malunited
greater tuberosity over HH and
glenoid arthrosis
There is a malunion of the
greater tuberosity; Despite the
malunion, the patient has
active FF to 115 degrees, and
maintenance of ER.
9/22/2013
10
Intraoperative GT Fx, Humeral
Osteotomy in revision
Removal of anatomic TSA with RCT, intraoperative greater tuberosity fracture,
and humeral shaft controlled osteotomy, PMMA removal, placement of polymer
cerclage cables and conversion to RSA with racking hitch GT fixation.
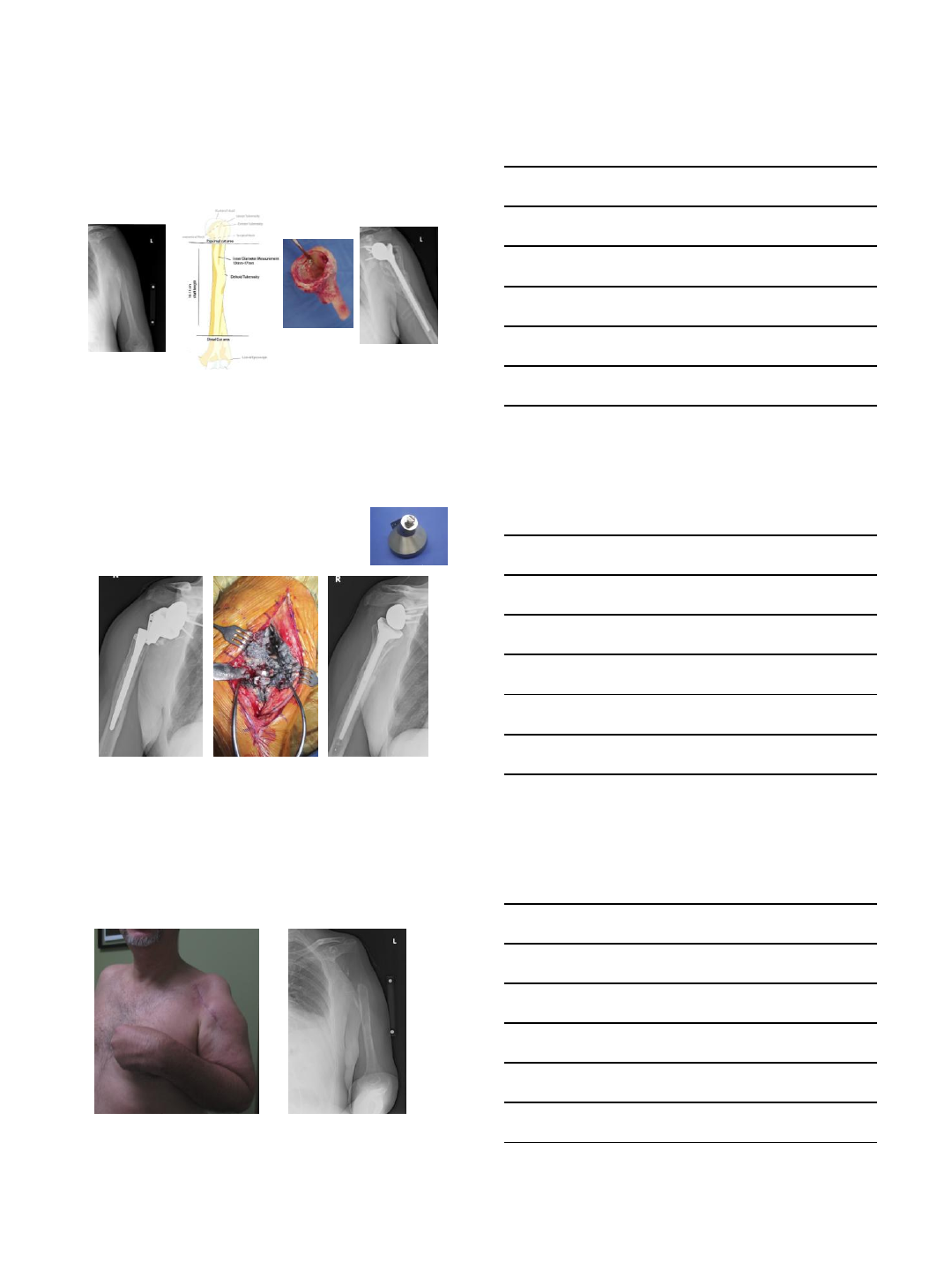
Avoid cx in prosthesis selection
No posterior fin-easier insertion
and removal
Short stem as ABX spacer
removable with humeral preservation
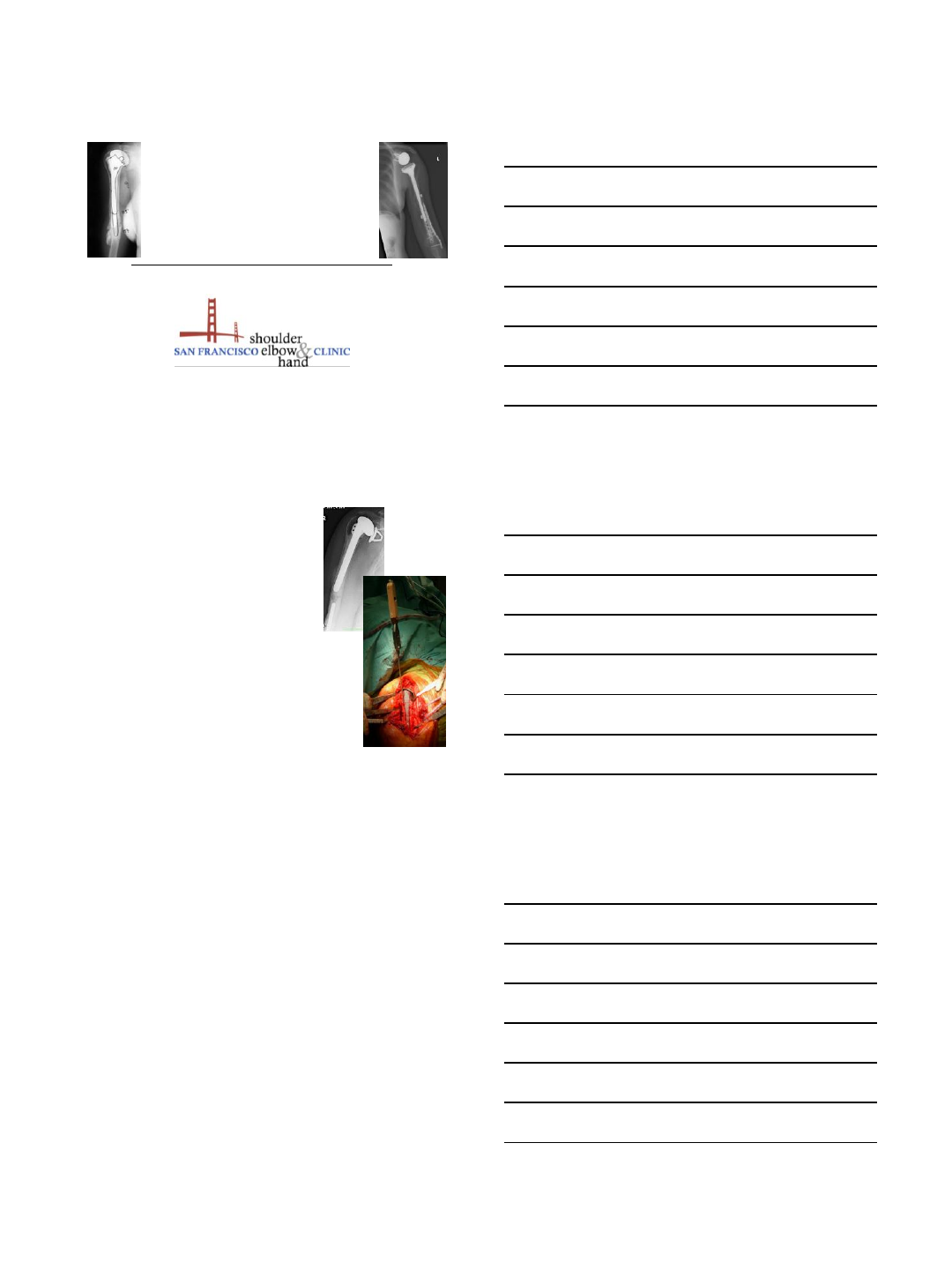
Complications-PPF with short stem
81 yo skier 8 months post-op
Periprosthetic fracture
Pre-op healed old
humeral shaft fracture
OA
Prior HS fracture Post op 8 mo
9/22/2013
11
Healed 3 m post closed rx
11 mo
Short Stem TSAs
Bypass deformity in proximal humeral MU
Avoids new fracture
Be Prepared
Revision-bone replacement
•Allograft humerus
–R and L available
•Tubular or can create
struts
•Save native deltoid
muscle attachment with
bone and wrap around
allograft prn
9/22/2013
12
Management of Proximal bone loss
Humerus – less bow than femur to pass long straight stem
RSA preferred in revisions with cuff and bone loss
Chacon J Bone Am. 2009 Jan;91(1):119-27
Tubular allograft for additional support and muscle attachments indicated for
humeral deficiency
Risk of absent proximal bone support
Prosthesis removal for sepsis
radial nerve palsy
Thermal injury
9/22/2013
13
Etiology radial nerve palsy
•Drill perforate humeral
shaft
•Ultra drive- heat + shaft
perforation
•Cerclage cable for
fracture fixation
•Trephine-heat with
retained stem removal
•Cement extrusion mid
shaft
Posterior triceps split
Posterior approach
•D-P approach-radial
nerve posterior at
deltoid insertion
•Safest to isolate nerve
posteriorly
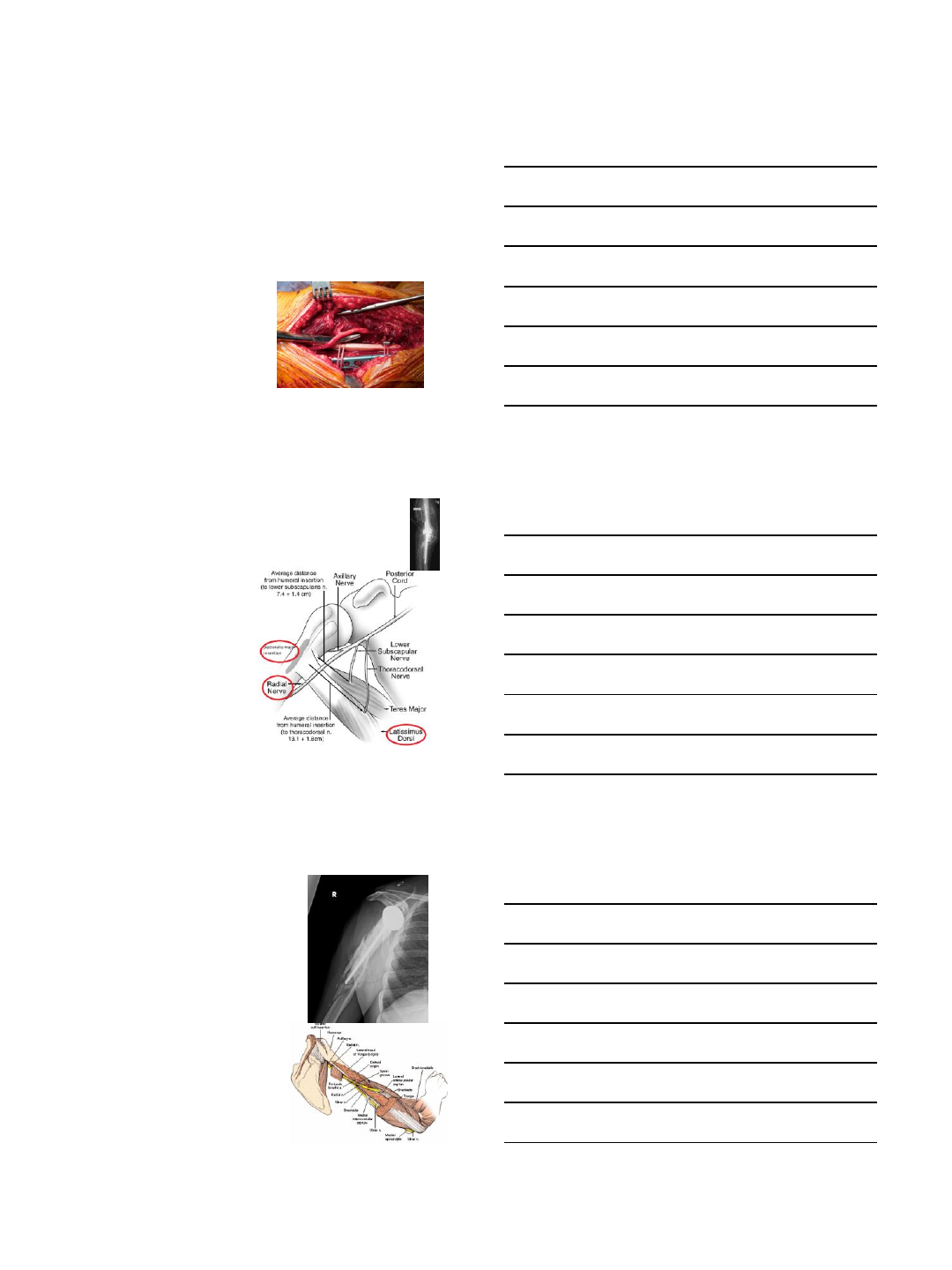
Radial Nerve!
at risk with the humeral shaft procedures
•In revisions, there is
distorted, scarred anatomy;
nerve can be difficult to
identify in its normal
location along the humerus.
•Release the pectoralis, the
nerve can be traced from a
normal area on the belly of
the latissimus dorsi and
follow it as it courses
posterior to the humeral
spiral groove, then lateral
and distal.
Radial nerve palsy after humeral revision in total elbow arthroplasty. Throckmorton TW, Zarkadas PC,
Sanchez-Sotelo J, Morrey BF. JSES 2011. 20(2), 199-205.
Words of caution
•When making osteotomy
be weary of the risks of
–Uncontrolled extension of
the fracture down the
humerus
–Nerve injury
•Radial nerve is especially at
risk when fixing the
osteotomy/ placing cables
•Radial nerve is straight
posterior at the level of
deltoid
–Suggest getting full
exposure before beginning
osteotomy
9/22/2013
14
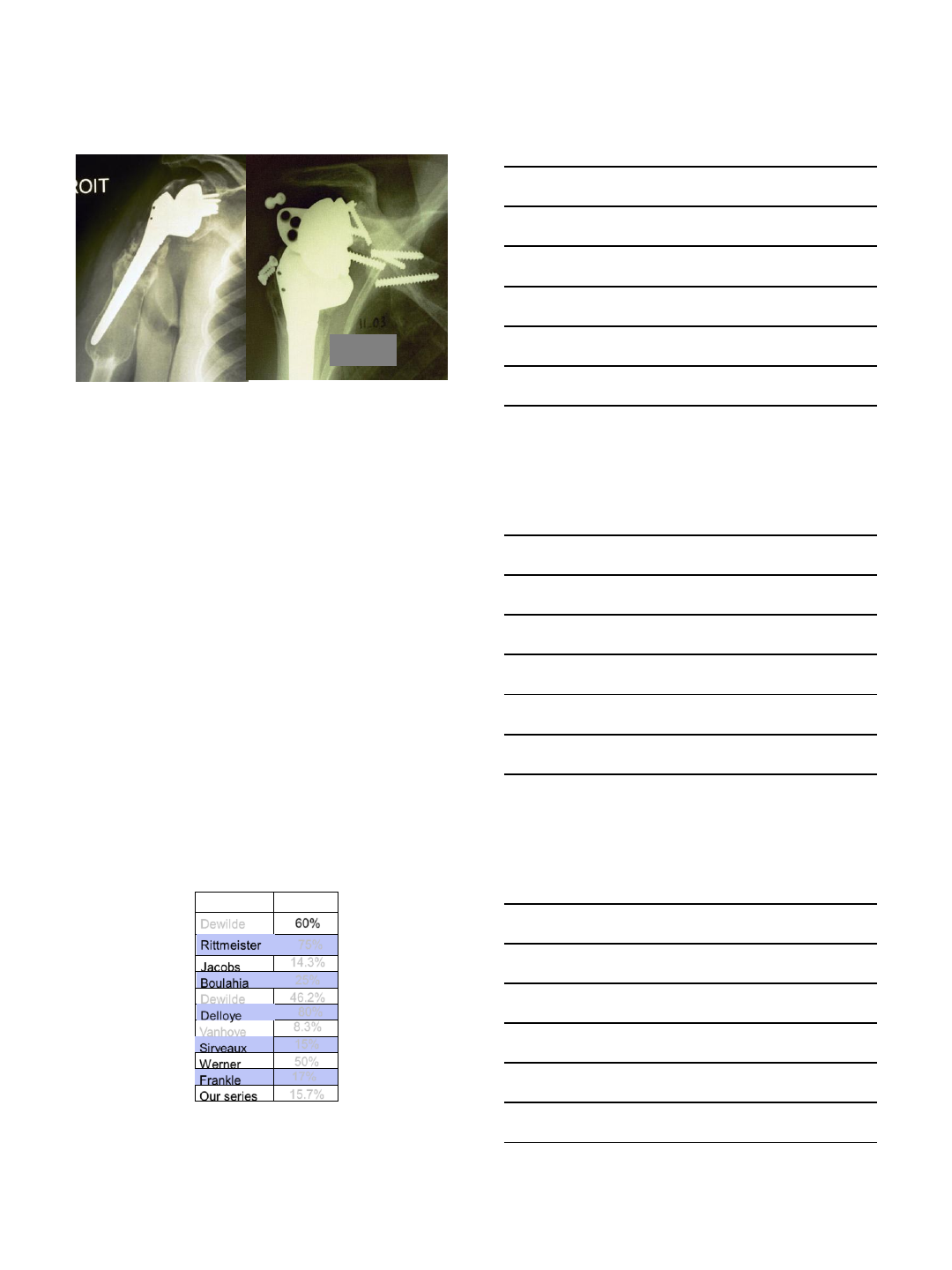
Humeral component unscrewing
due to lack of bone support
Avoid radial nerve
Cerclage racking hitch
Post Operative PHF – Type B
error to wait
Type B fx, obese body habitus
14 weeks after a fall, abundant
callus, 15 degrees varus angulation.
The fracture site is not united.
New lucency formation around the
humeral stem.
Early fixation of Type B fractures allow return to function sooner and lower
chance of nonunion.
Also allow direct examination of stem stability.
ORIF-save the stable implant
9/22/2013
15
ORIF cortical struts
•Allograft provides
immediate bone
support
•Ultimately increase
bone stock
•Aids in load dispersal
by increasing surface
area
Chandler et. Al Semin Arthroplasty 93: 17/19 fracture treated with allograft struts & cables healed
Haddad et. Al. JBJS 2002: 40 fractures treated with allograft struts secured with cables or plates. 98% union
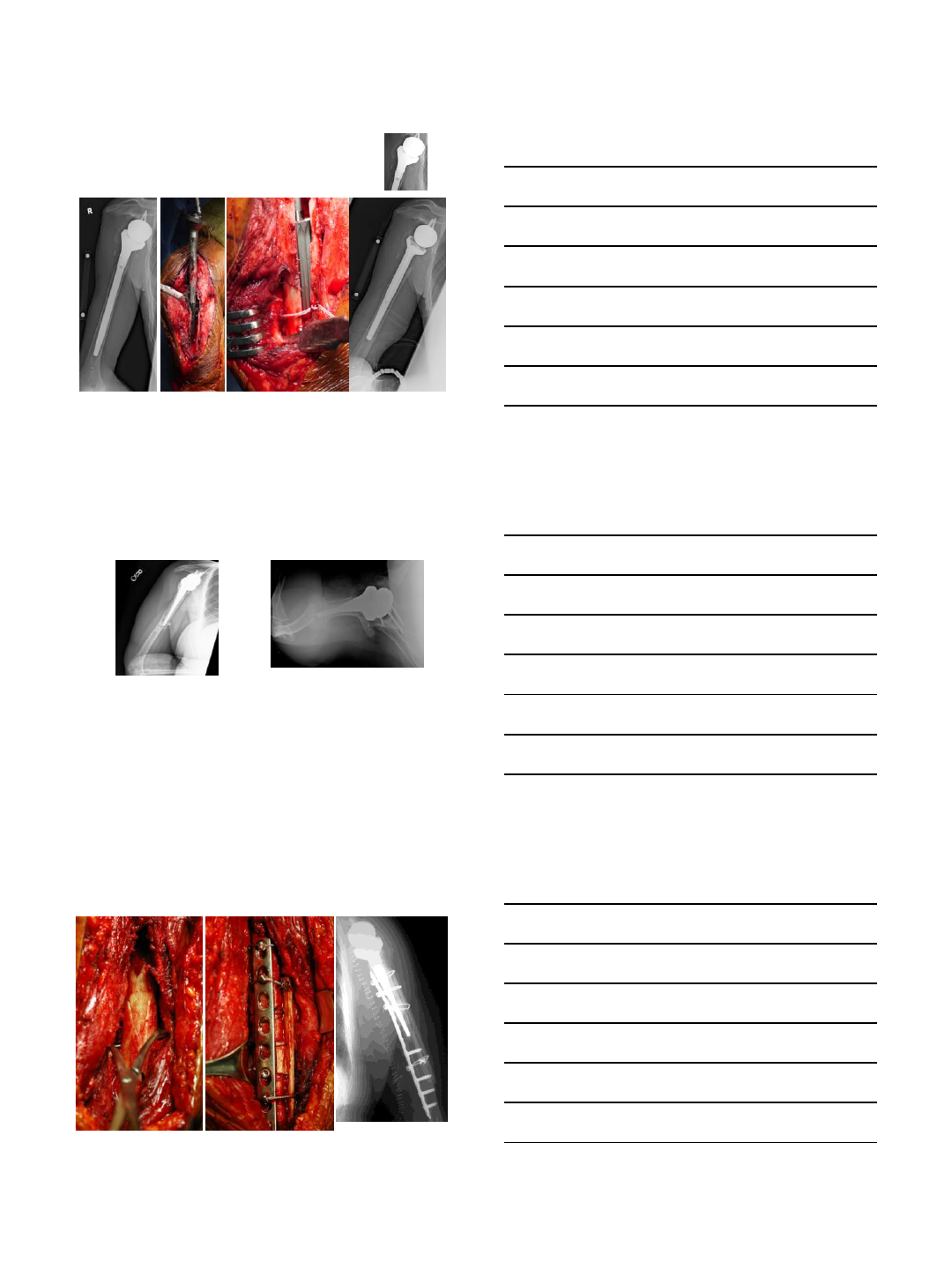
Longer stem for IM fixation
Post-Operative PPF
Type C displaced
muscle interposition
ORIF -preserve prosthesis

9/22/2013
16
Bone loss from revision
humeral cemented stem,
sepsis
Then humeral allograft,
Longer IM stem fixation,
PMMA
distal plate for more distal
fracture
Many of the problems begin with mid humeral length stems
Short stems or no stems will reduce
complications with PPF
•Easy to insert/remove
•Press fit
•Convertible or exchangeable
•More proximal PPF
•Less interference with TER
Periprosthetic Fractures and how to Avoid or Minimize Complications
Summary
•Periprosthetic fractures 1-3 % primary
•Up to 24% in revision surgery
•Frequently associated with treatment to preserve
or exchange standard humeral stems
•PMMA and in-growth fixation complicate revisions
•Radial nerve at risk in humeral shaft
•More instruments and techniques needed for
revisions-be prepared!
•Short stems will likely decrease potential
complications associated with longer stems

9/22/2013
17
Thank you
9/16/2013
1
Avoiding complications with
Reverse Shoulder Arthroplasty
My best tips
VuMedi Webseminar Sept 2013
I receive
Royalties from TORNIER Inc
for patents on Shoulder Prosthesis
DISCLOSURE
Complications in Reverse SA
About 516 cases, the average complication rate is 22%
15.7%
Our series
Frankle
50%
Werner
Sirveaux
8.3%
Vanhove
Delloye
46.2%
Dewilde
Boulahia
14.3%
Jacobs
Rittmeister
60%
Dewilde
Complic. rate
75%
25%
80%
15%
17%
9/16/2013
2
Total rate of complications
(Intraop + postop)
Primary
arthroplasty Revision
Arthroplasty
15.3% 64.7%
Intraoperative complications
Primary Arthroplasty:
2.7%
Intraoperative glenoid fracture
- no reaming
- cancellous graft
Intraoperative complications
Revision Arthroplasty
30.9%
Humerus fracture: 28%
cement removal,
osteopenia,
old ladys…
a humeral window
is preferable
9/16/2013
3
Postoperative complications
Revision
Arthroplasty
33.8%
Primary
Arthroplasty
12.6%
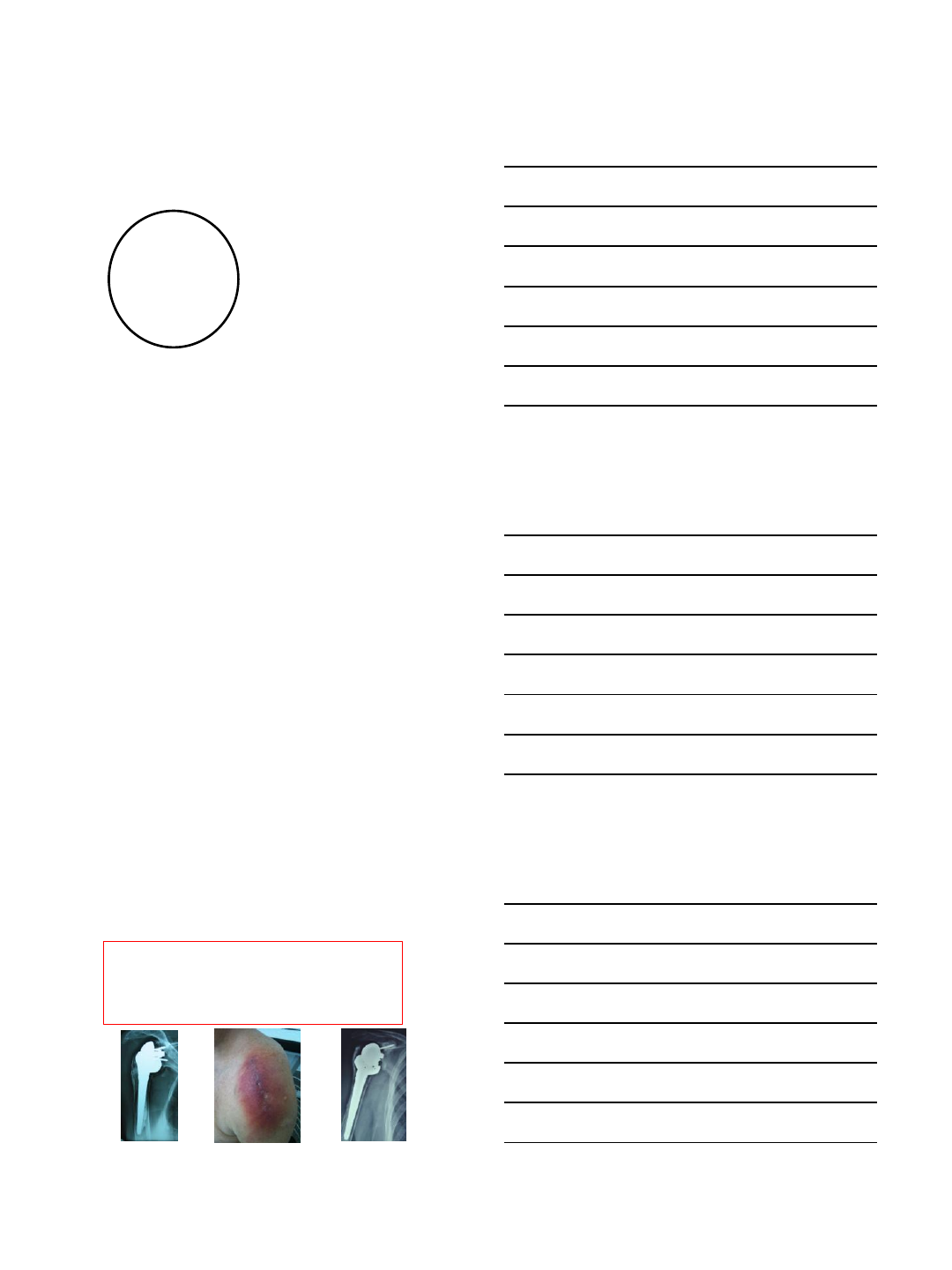
Postoperative complications
Instability 3.3%
Infection 3%
PO hum fc 2.6%
Glen loose 1.3%
Neuro 0.8%
Hum loose 0.6%
Iary Reverse
Arthroplasty
Instability 10.6%
Hum pb 10.6%
Infection 6.4%
Hematoma 2.1%
Glen pb 1%
Revision
Arthroplasty
How to avoid infections ?
Reoperations are at risk +++
- Cement with Antibiotics (R Gobezie)
- Two stages surgery in case of doubt
(cultures & spacer for 6 weeks)
9/16/2013
4
How to avoid infections ?
Systematic cultures for any reoperation
if more than one positive
=> oral ATB for 6 weeks
How to avoid instability
with DP approach
- Use a 42 mm glenosphere
- Correct deltoid tension
- Subscapularis repair
and protection
What is deltoid « tension »?
An intraop subjective criteria (conjoint tendon’s
tension, difficult to reduce , no pistonning, complete
adduction…..)
which depends on :
etiology (Post Trauma Arthr, Rev Arthrop…. are stiffer)
anesthesia (degree of sleep, interscalene block)
Therefore assessment of deltoid length is a better
objective approach than deltoid tension
9/16/2013
5
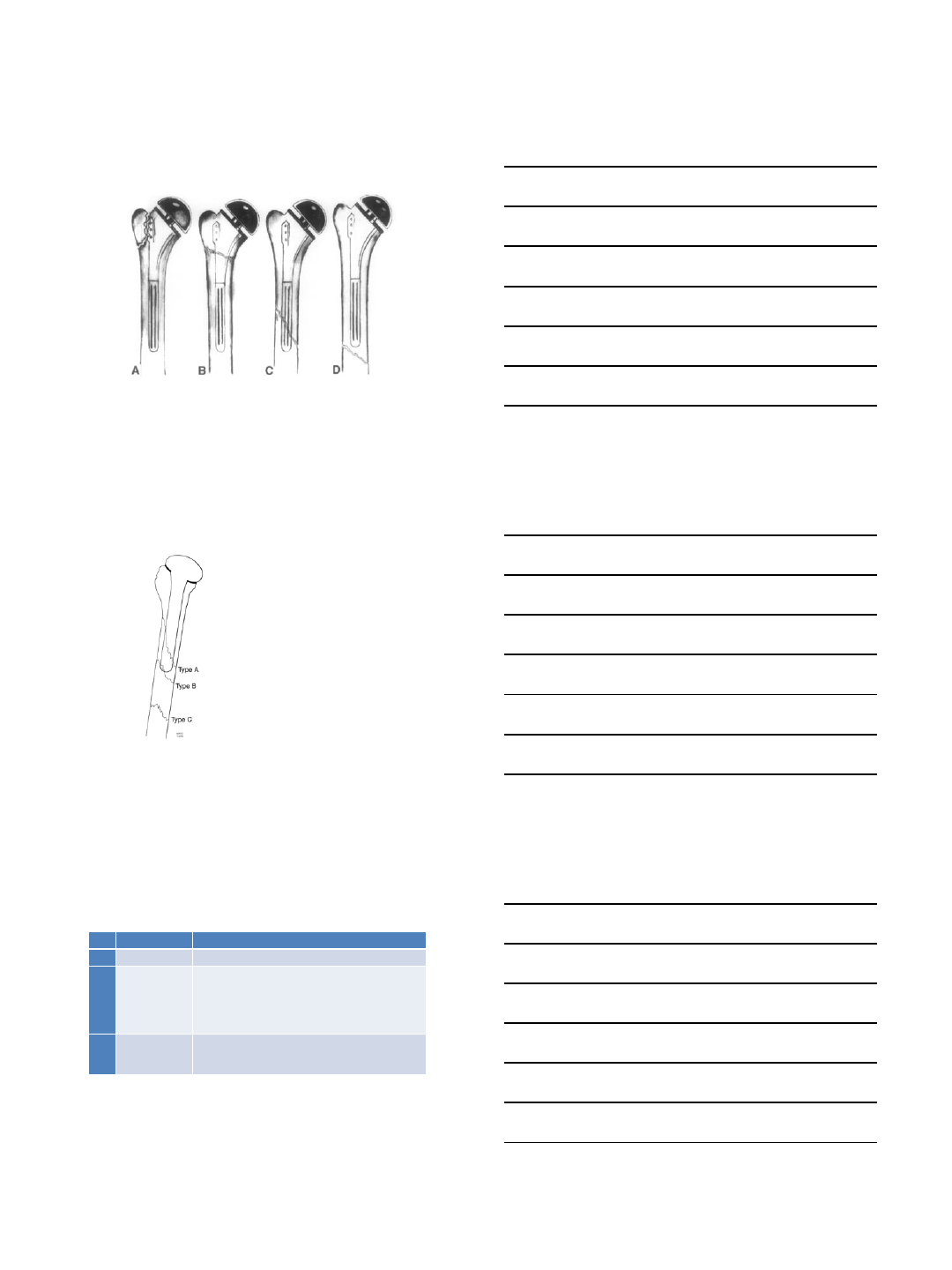
Deltoid length
-position of the glenosphere
-height of the stem
A B C D
you really control only few factors !
- Position of the glenosphere in the vertical plan (you don’t choose)
- Glenosphere size (3§ or 42 mm) (arm > 300 mm = 1%)
- Eccentric glenosphere (2 to 4 mm)
- Stem height (cut, spacer, poly) several cm: >10% Key!
small cut generous cut
c c
H
P
… if CH = CP, average arm lengthening is 2.4 cm
=> deltoid tension is OK
Laedermann - JSES 2008
9/16/2013
6
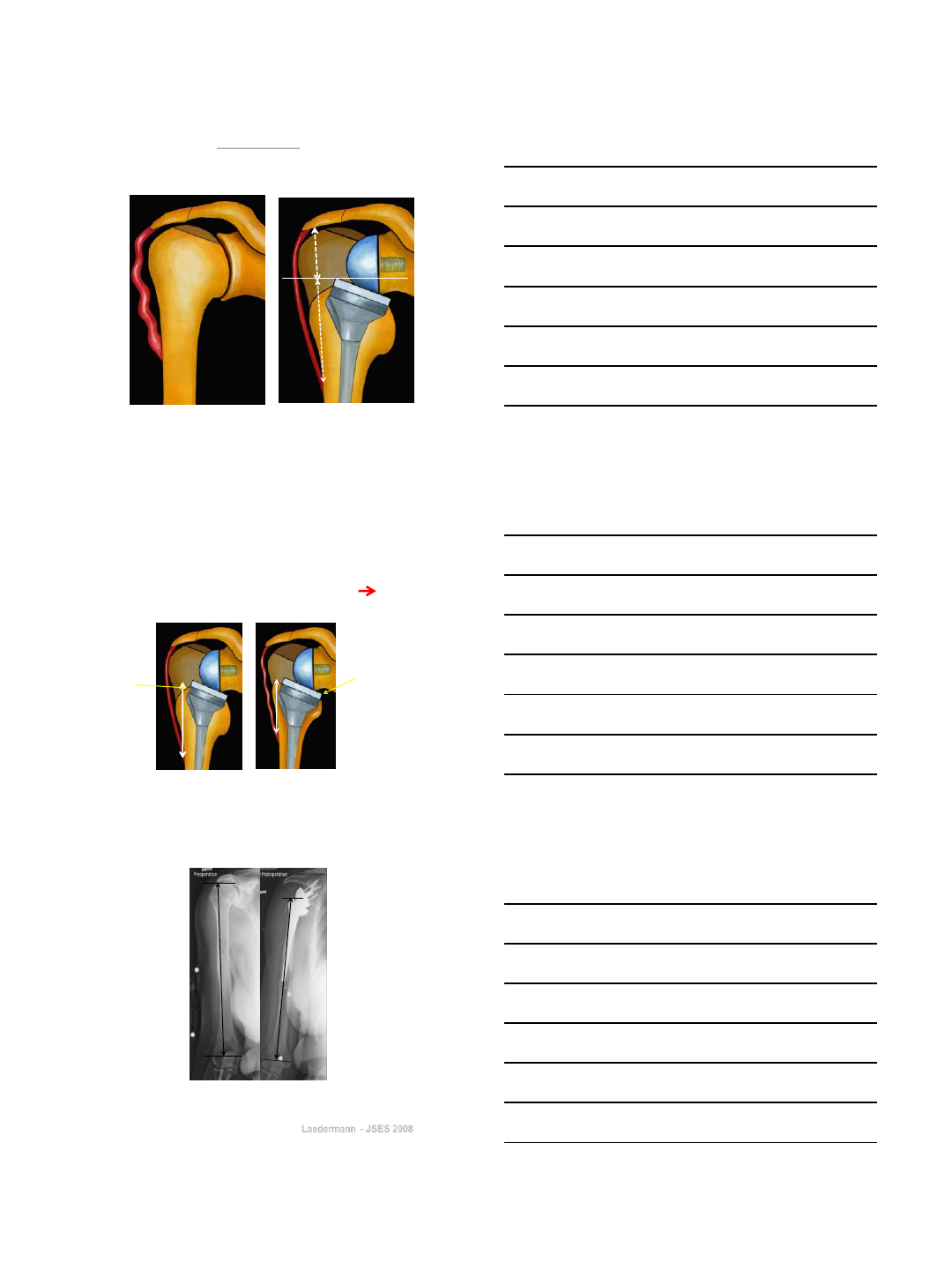
Ideally the metallic top
of the prosthesis should
be just above the GT
Laedermann
JSES 2008
H
C C
R
A B
Rather than to check the « tension »
of the deltoid,, better to respect the
length of the Humerus.
If deltoid length is insufficient => instability
29cm 33cm
How
to avoid
glenoid
loosening
9/16/2013
7
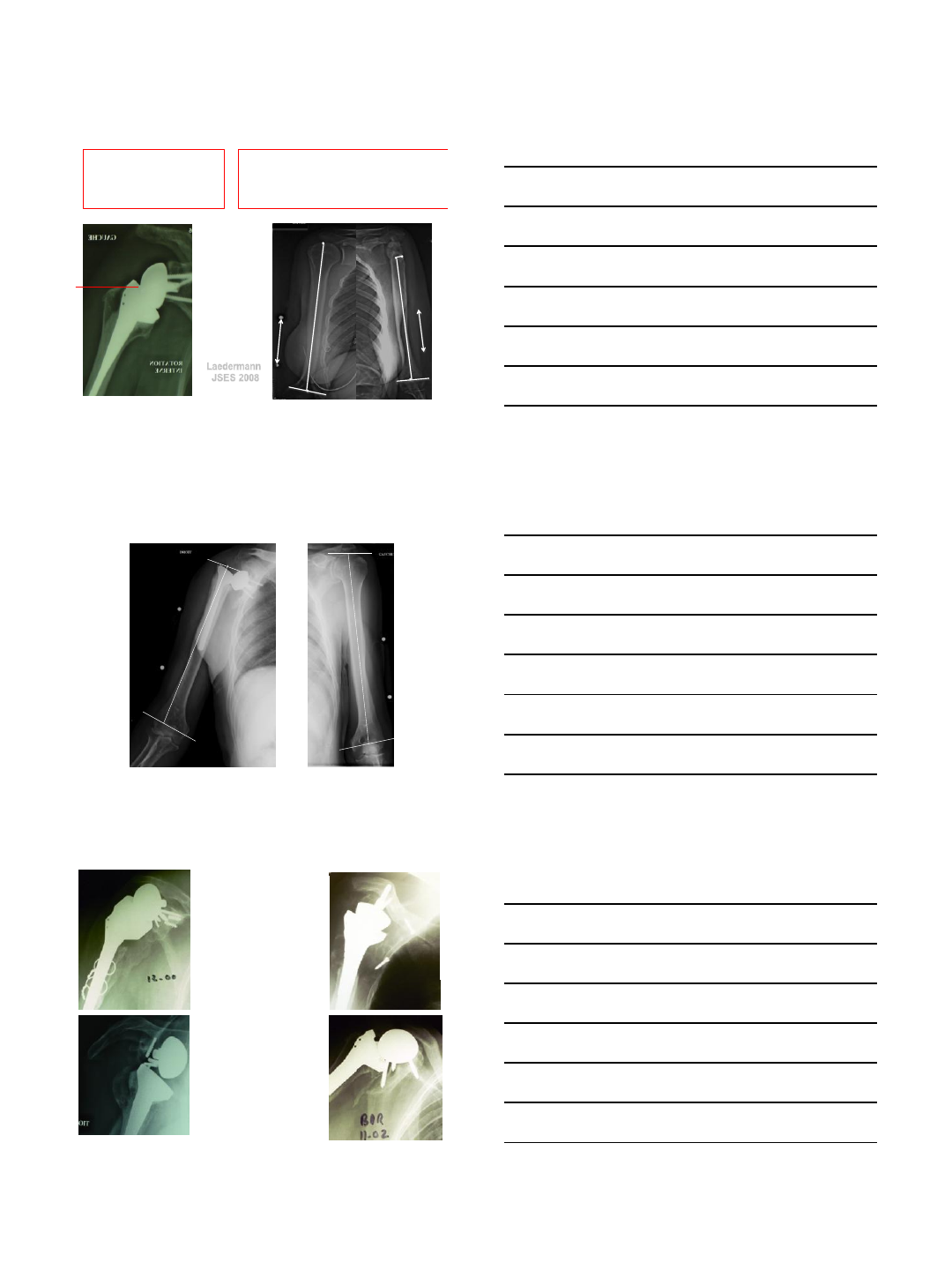
Glenoid loosening
causes
• superior tilt, central post not in the
native glenoid (technical error)
- insufficient glenoid bone stock
(excessive indication)
1996
Superior tilt
central Post not in the native glenoid
9/16/2013
8
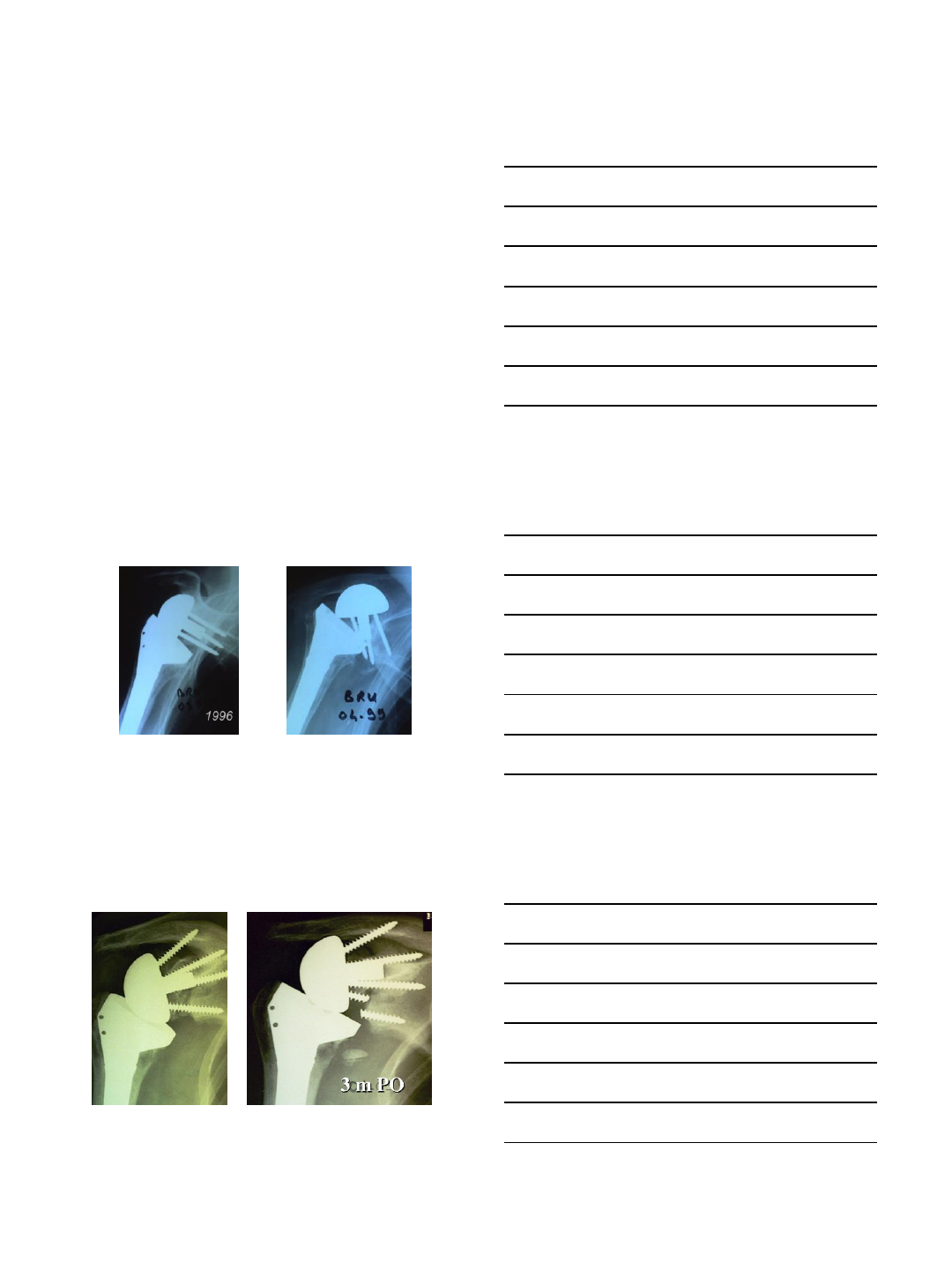
Insufficient glenoid bone stock
If insufficient glenoid bone stock
better to do 2 stage surgery
Influence of learning curve
- 2 consecutive cohorts of 240 Reverse SA
implanted by the same two surgeons (LNJ & GW):
• Sept 1995 -> June 2003 (8y) (J Bone Joint Surg Am. 2007).
• July 2003 -> March 2007 (4y) (J Shoulder Elbow Surg. 2012)
To evaluate if surgeon’s experience
modifies complications ?
9/16/2013
9
Cohort 1 Cohort 2
Infection 8 1
Dislocation 15 4
Glenoid loosening 2 2
Spine fracture 2 2
Neuro complic 5 7
Humeral loosening 0 1
TOTAL complic 32 =16% 17 =9%
Revisions 11 cases
4.5%
7 cases
2.9%
Avoiding complications: experience
1995-2003 2003-2007
P= 0.07
lowering
the sphere
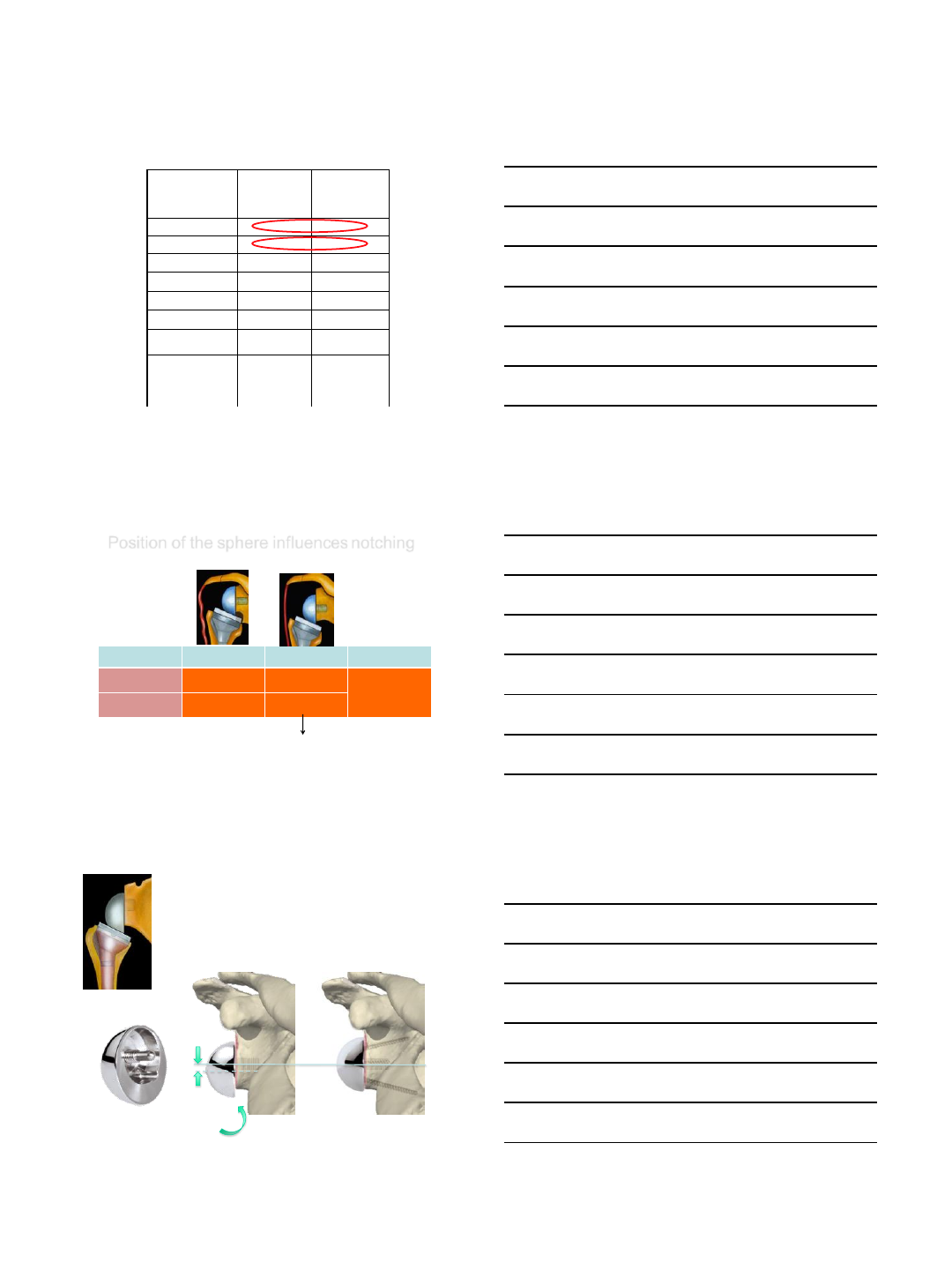
cohort 1 cohort 2 P =
Notch Gr 0, 1 49.3% 82.3%
p= 0.012
Notch Gr 3,4 30% 8.7%
Whatabout Notching ?
Position of the sphere influences notching
Excentric sphere gives
more inferior clearance
+4mm
Lowered design
9/16/2013
10
Cohort 1
95-03
152 c; fu: 41m
Cohort 2
03-07
198 c; fu: 40m
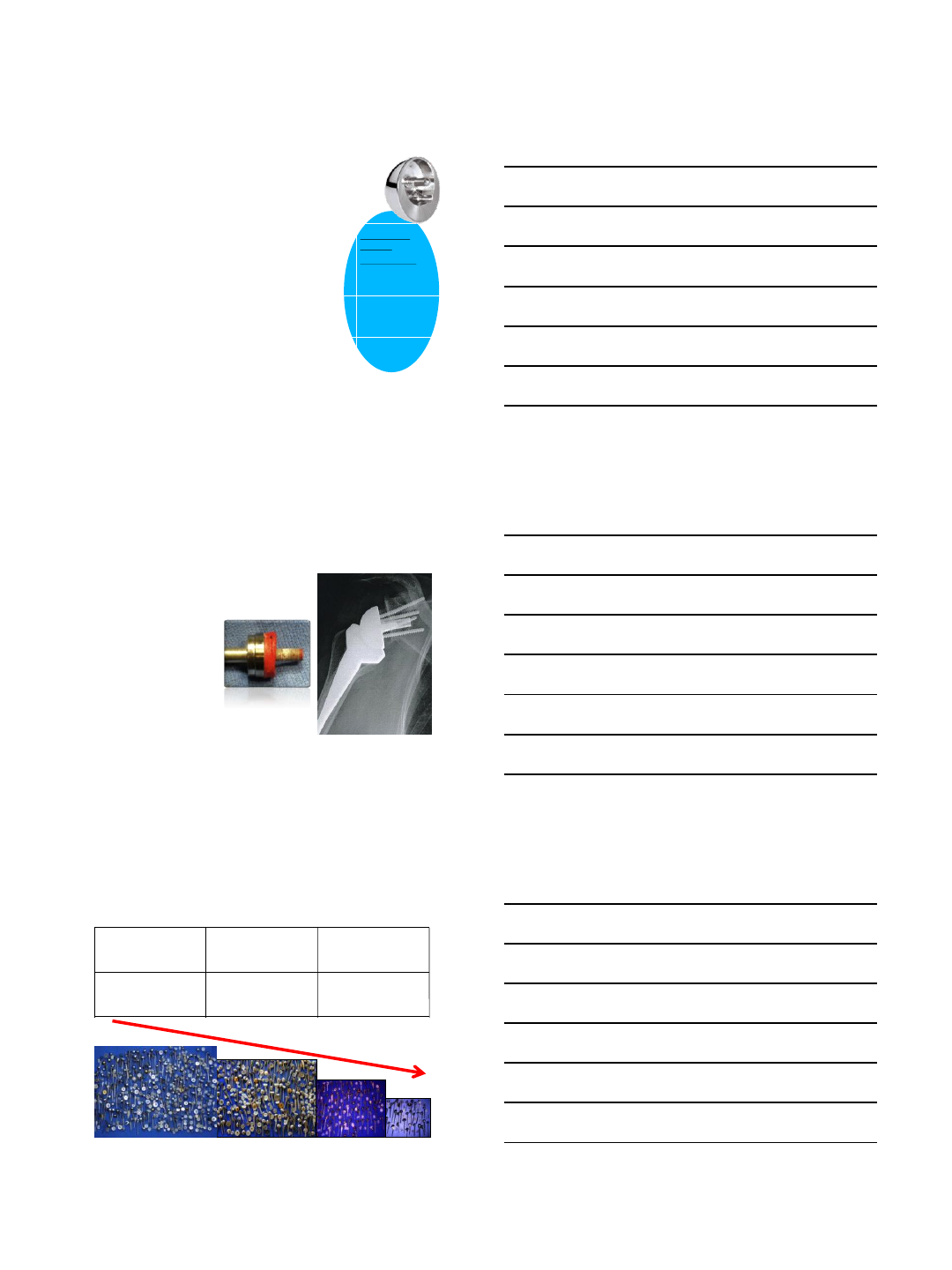
Cohort 3
07-08
52 c; fu: 30m
Notch 0-1 49.3%
82.3%
85.7%
Notch 3-4 30% 8.7%
2.4%
Influence of excentric sphere
on notching
glenoid lateralization (Boileau)
An other way to limit notching:
Revision Arthroplasty decreased
(dramatically)
First cohort Second cohort
22,5 %
(54 cases)
7 %
(17 cases)
Revision
Arthroplasty
9/16/2013
11
Summary
The main complications are: instability, infection
intraoperative fracture and glenoid loosening
Although notching is not a real complication, it is a concern
that can be addressed by improving surgical technique
The rate of complication depends on
definition, etiology, intra vs postop, surgeon experience
Thank you
