The Scapholunate Ligament Complex Syllabus
2013-03-17
: Pdf The Scapholunate Ligament Complex Syllabus the_scapholunate_ligament_complex_syllabus 3 2013 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 71
10/17/2012
1
The Scapholunate Ligament
Complex
David J. Slutsky MD
Assistant Professor
Dept of Orthopedics
Harbor- UCLA
The Hand & Wrist Institute
Torrance, CA
DISCLOSURES
~ There is no commercial support for this
Talk
And….
~There are no conflicts of interest.
The Scapholunate ligament
Complex
-the stability of the scapholunate joint is not
dependent wholly upon the scapholunate
interosseous ligament (SLIL) but rather upon
both primary and secondary stabilizers, which
form a scapholunate ligament complex (SLLC).
-Each case of SL instability is unique and
therefore should be treated with tissue specific
repairs, which may partly explain why one
procedure cannot successfully restore joint
stability in every case.
10/17/2012
2
The Scapholunate ligament
Complex
-Elsaidi et al sequentially divided the RSC, LRL,SRL, SLIL and
finally the dorsal capsule insertion on the scaphoid.1 There was
no appreciable change in the radiographic appearance of the
wrist.
-When the DRCL was then divided, a DISI deformity occurred
-Short et al determined that the SLIL is the primary stabilizer of
the SL articulation and that the DRCL, DIC, ST and RSC
ligaments are secondary stabilizers.2
-The SL joint is therefore dependent on a complex of ligaments,
each having a separate role but working in concert.
1.Elsaidi GA, Ruch DS, Kuzma GR, et al: CORR:152-7, 2004
2. Short WH, Werner FW, Green JK, et al: J Hand Surg 32:297-309, 2007
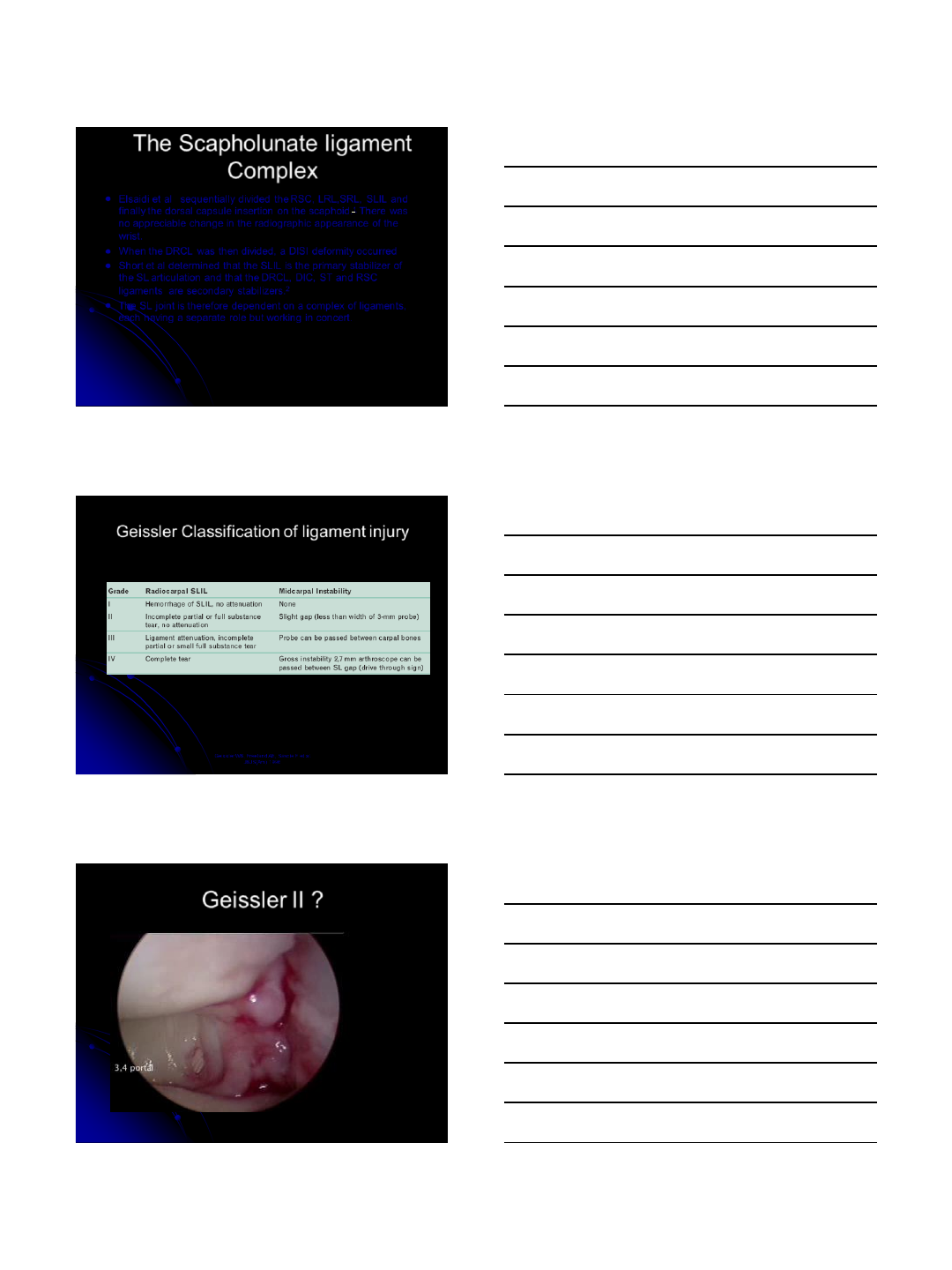
Geissler WB, Freeland AE, Savoie F et al.
JBJS(Am) 1996
Geissler Classification of ligament injury
This classification quantifies the resultant instability and not
the actual size of the tear.
Geissler II ?
10/17/2012
3
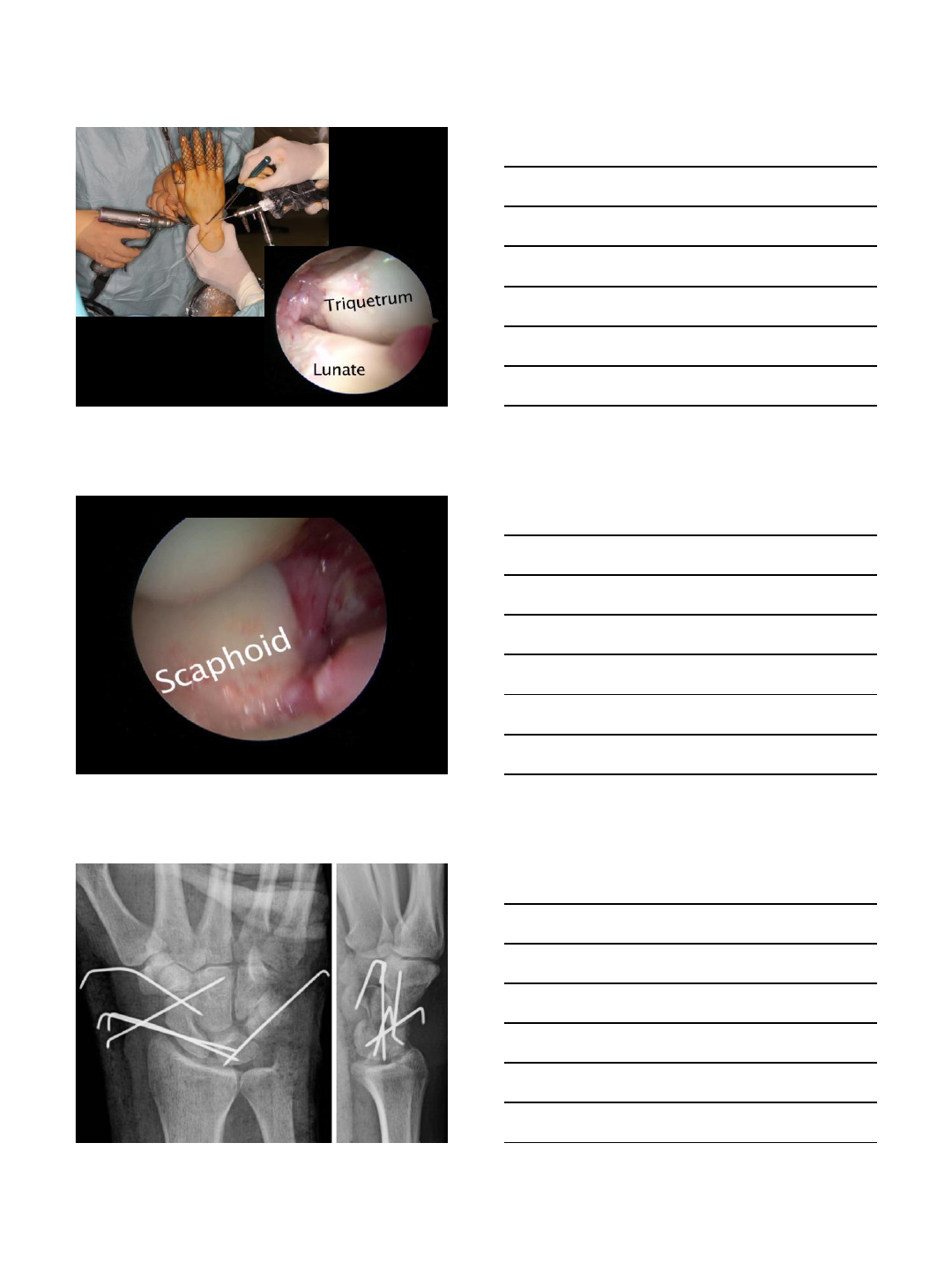
Dynamic Wrist Arthroscopy
Hagert E, Lalonde DH. Wide-awake wrist arthroscopy and open
TFCC repair. Journal of Wrist Surgery 2012;1:63– 68.
Ong M, Ho PC, Wong C, Cheng S, Tse W. Wrist Arthroscopy under Portal Site
Local Anesthetic without tourniquet. Journal of Wrist Surgery November 2012.
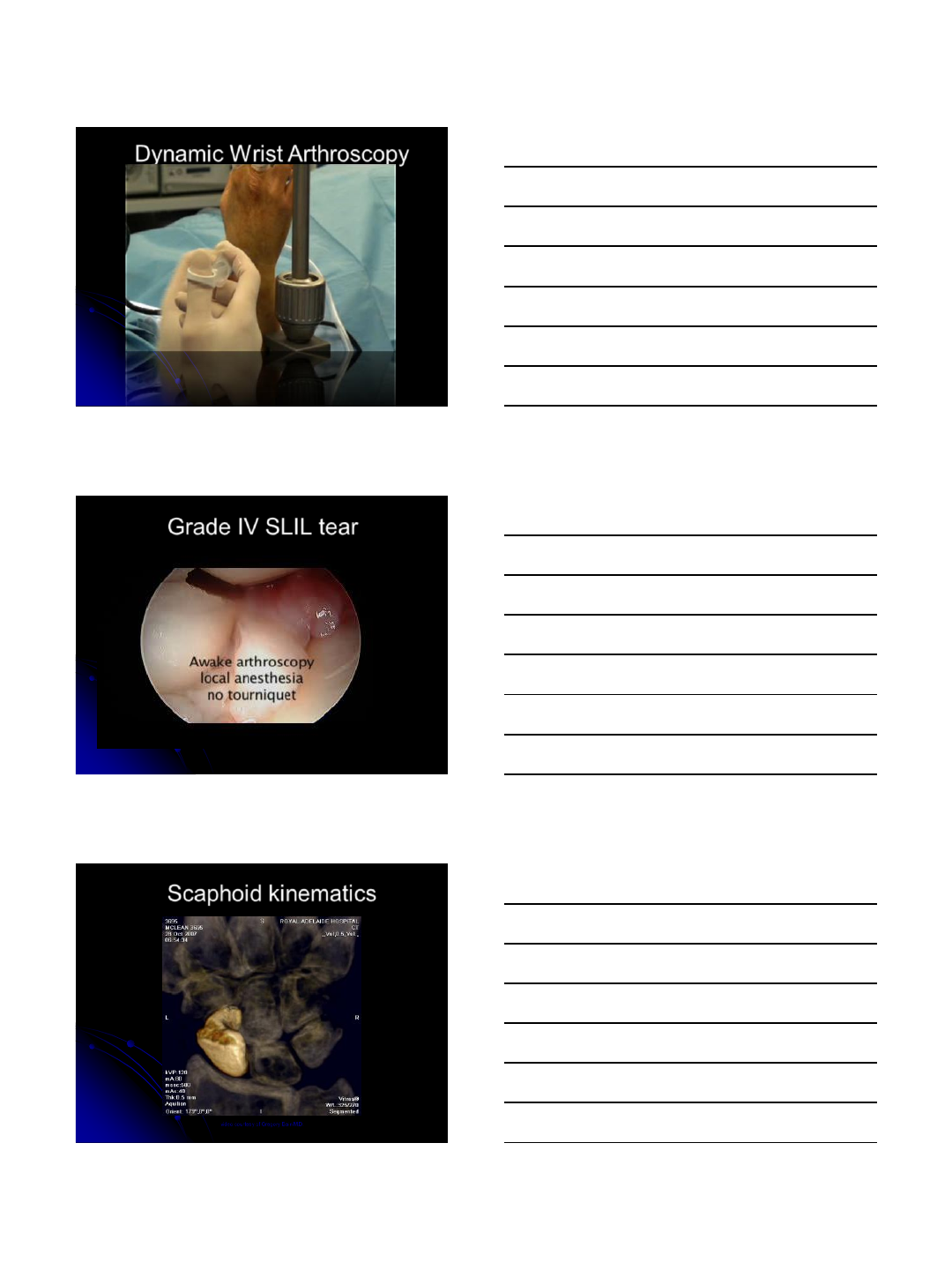
Grade IV SLIL tear
Scaphoid kinematics
video courtesy of Gregory Bain M.D.
10/17/2012
4
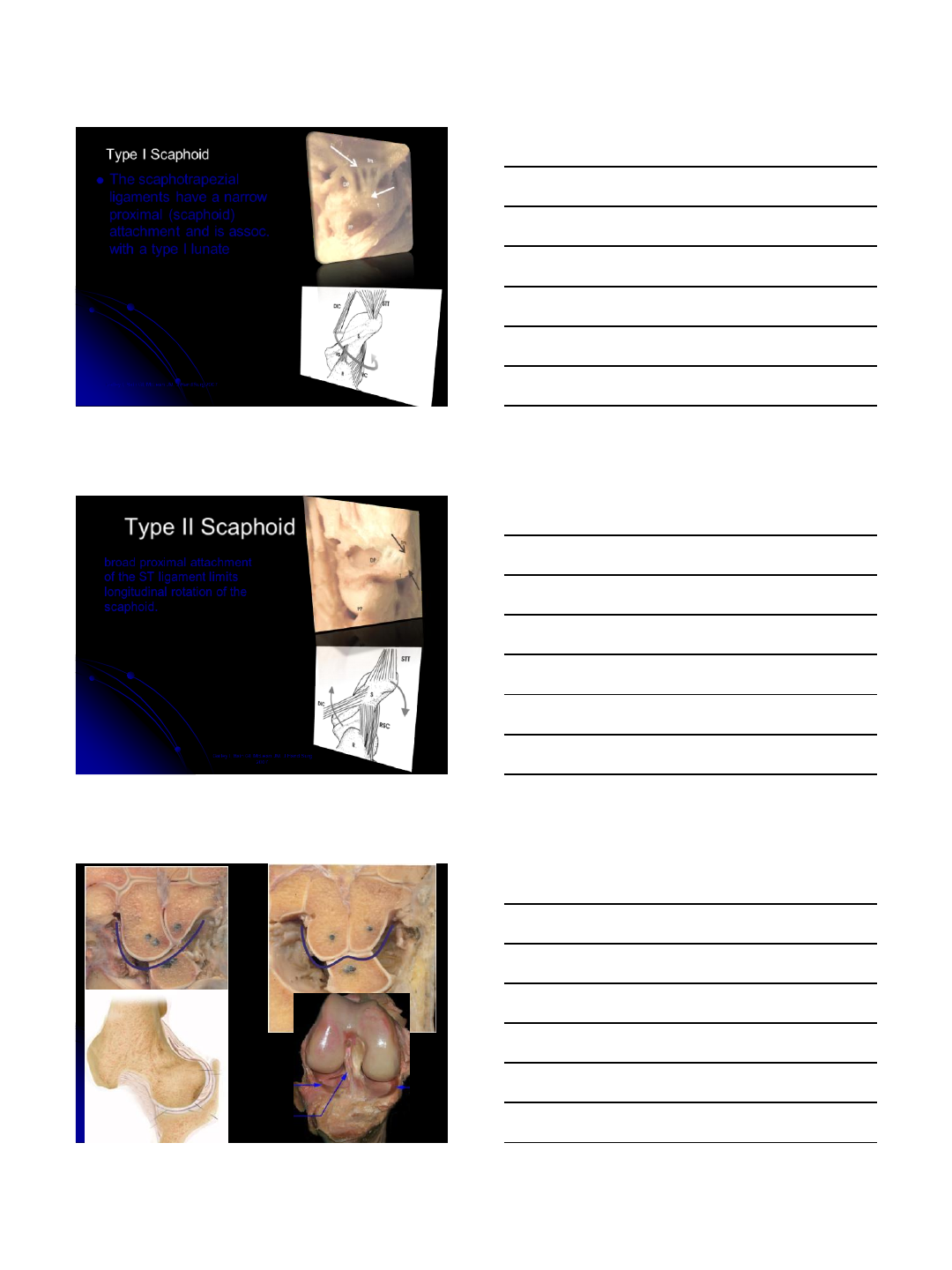
Type I Scaphoid
-The scaphotrapezial
ligaments have a narrow
proximal (scaphoid)
attachment and is assoc.
with a type I lunate
Galley I, Bain GI, McLean JM. J Hand Surg 2007
This facilitates rotation
around the longitudinal
axis of the scaphoid, as
well as limiting flexion
and extension of the
bone.
Type II Scaphoid
broad proximal attachment
of the ST ligament limits
longitudinal rotation of the
scaphoid.
Galley I, Bain GI, McLean JM. J Hand Surg
2007
These scaphoids are associated
with type II lunates and therefore
are limited from rotation and
Translation
Type I
“rotating unicondylar
scaphoid”
Type II
“flexing bicondylar scaphoid”
10/17/2012
5
Type I lunate – SL injury with a
rotating scaphoid will exhibit
abnormal flexion and requires a
procedure to limit scaphoid flexion
- dorsal capsulodesis
- DIC capsulodesis
Type II lunate – SL injury with a
flexing scaphoid will exhibit
abnormal rotation and require
procedures to limit
scaphoid pronation
- Bone-ligament-bone
- Tri-ligament tenodesis
- Brunelli
Volar
Palmar SLIL plication
Palmar capsulodesis
STT ligament plication
STT fusion
shrinkage
Brunelli
Tri-ligament
tenodesis
Dorsal
Capsulodesis
DRCL repair
Arthroscopic
capsuloplasty
Interosseous
Tendon graft
RASL
Bone-ligament-bone
Slutsky DJ. Current Innovations in Wrist Arthroscopy. J Hand Surg Sept 2012
SLLC arthroscopic assessment
-Palmar SLIL – volar radial portal, MCR
-Dorsal SLIL – 3,4 and 4,5 portal, MCU
-Dorsal capsule – volar radial portal, 6R
-ST ligaments – MCR, STT portal
10/17/2012
6
Structure
Instability
Classification
A = ≤ 6
mths
no midcarpal
step
B = ≥ 6
mths
Midcarpal step drive
through sign
Treatment Options
Palmar SLIL
Geissler
I/II
Geissler
III/IV
P
-1A
P
-1B
Shrinkage, volar plication, LRL transfer,
SL pinning
RASL, interosseous graft, limited fusion
Dorsal SLIL
Geissler
I/II
Geissler
III/IV
D
-1A
D
-1B
Shrinkage, DIC
capsulodesis
Acute repair,
tenodesis, bone-lig-bone, limited fusion
Combined
Geissler
I/II
Geissler
III/IV
C
– 1A
C
- 1B
Shrinkage, combined volar/dorsal plication
Interosseous graft, RASL, limited fusion
Dorsal Capsule
Geissler
I/II
Geissler
III/IV
DC
– 1A
DC
– 1B
Shrinkage, dorsal
capsuloplasty
ST ligaments
Geissler
I/II
Geissler
III/IV
ST
– 1A
ST
– 1B
Blatt
capsulodesis, ST ligament shrinkage/plication
STT/SC fusion
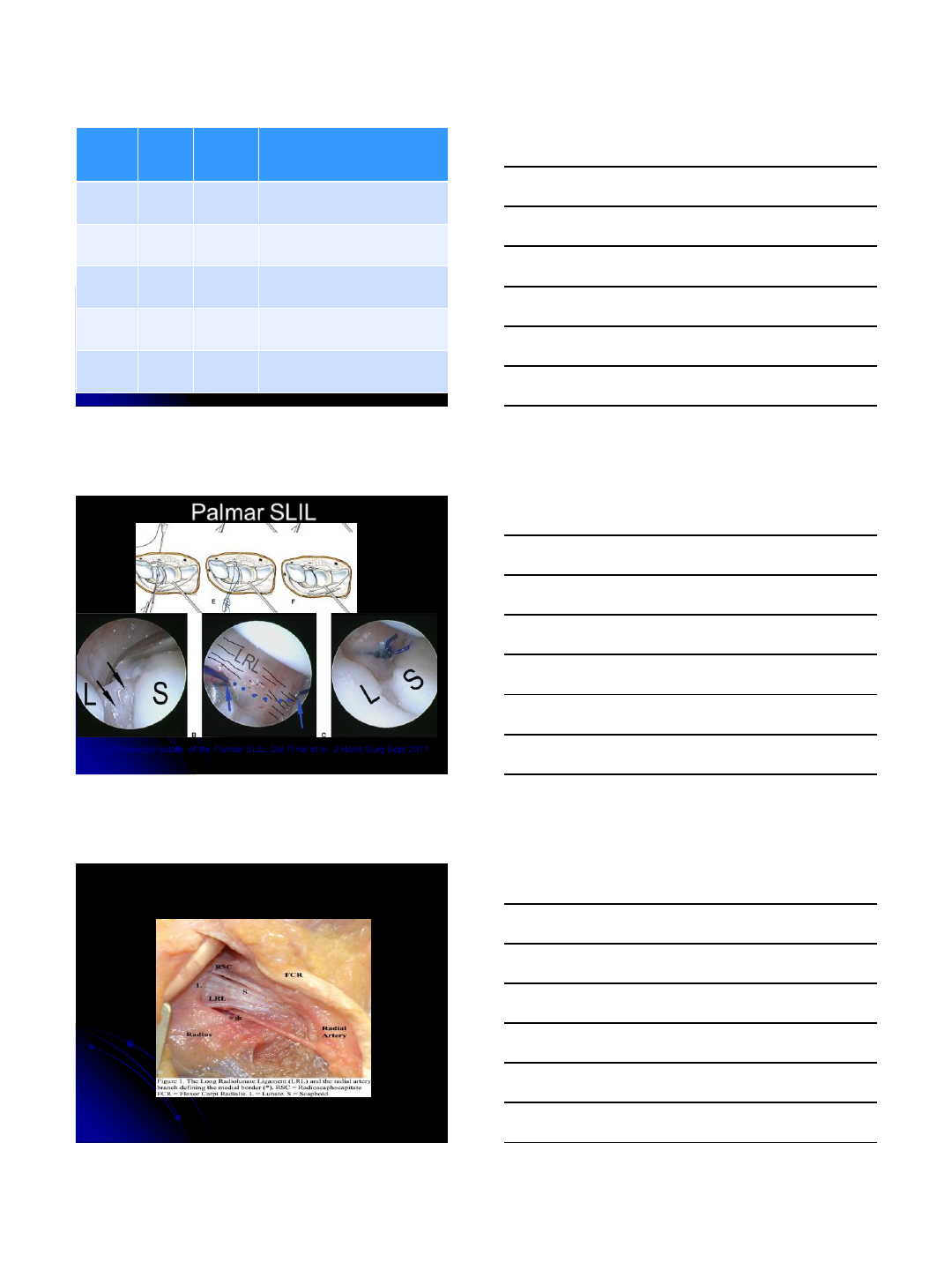
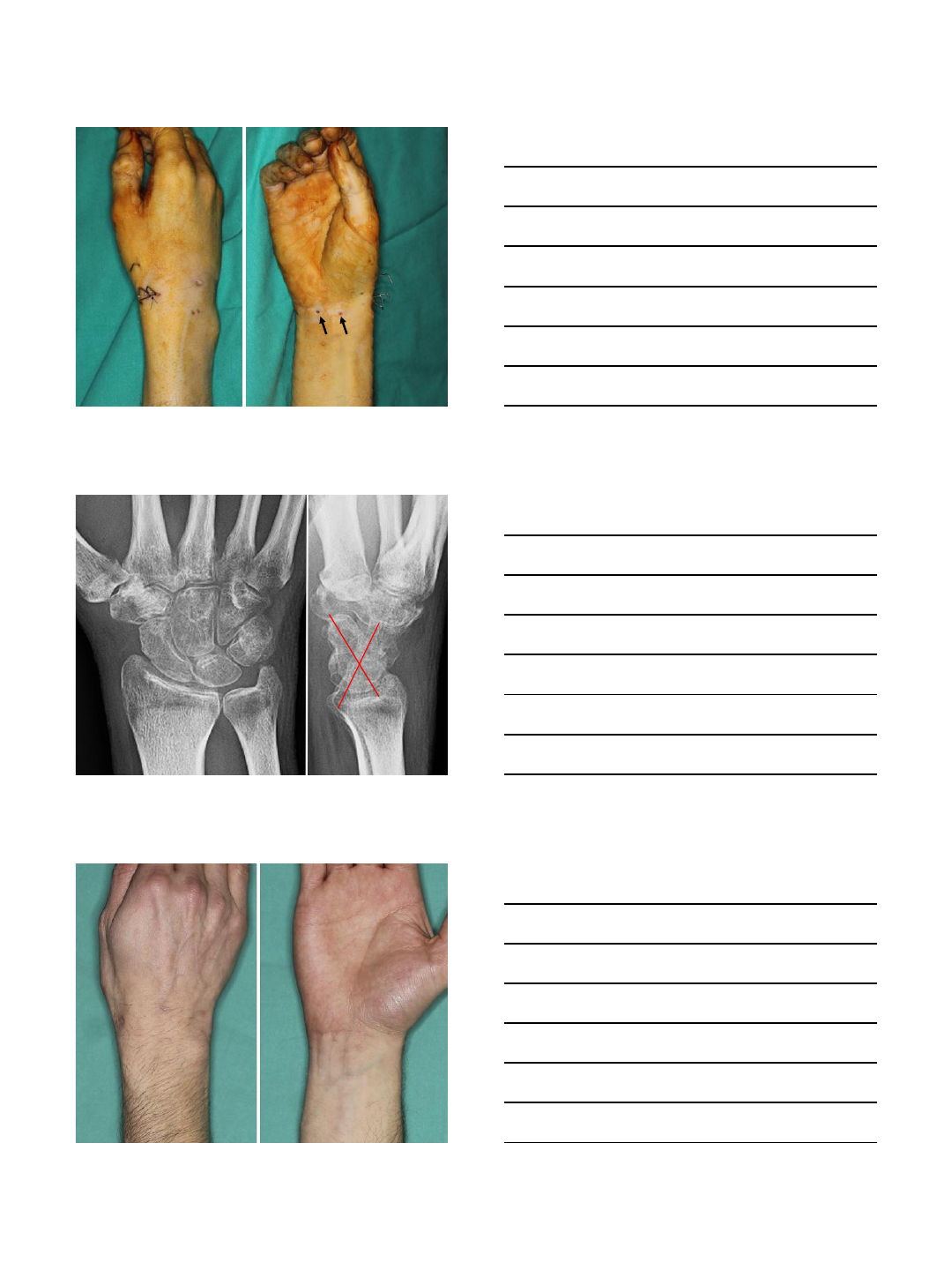
Palmar SLIL
Arthroscopic suture of the Palmar SLIL. Del Pinal et al. J Hand Surg Sept 2011
VOLAR CAPSULODESIS FOR
SCAPHOLUNATE DISSOCIATION
Van Campen RJ, Moran SL. IWIW Chicago 2012
10/17/2012
7
DRCL TEAR
10/17/2012
8
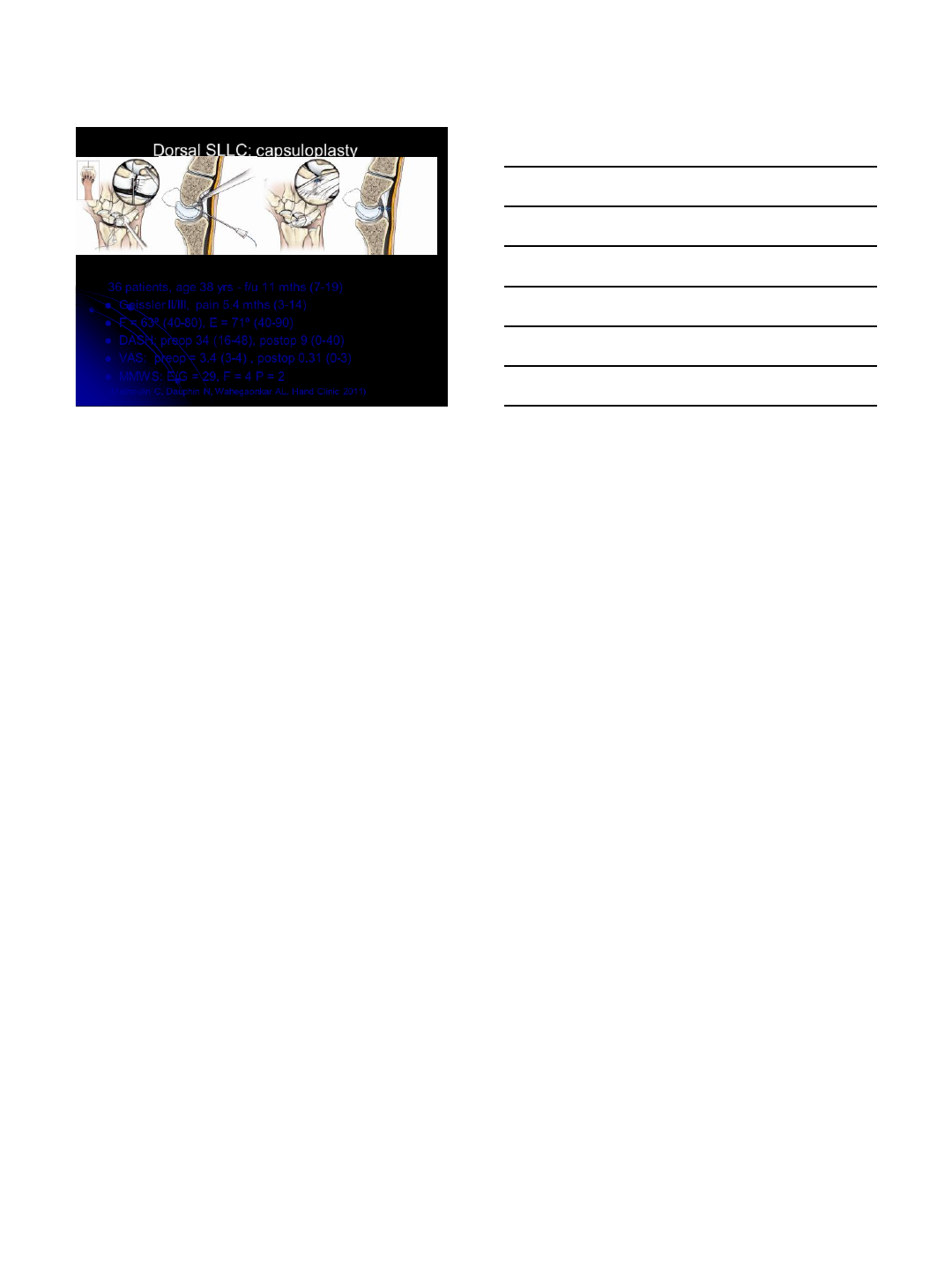
Dorsal SLLC: capsuloplasty
36 patients, age 38 yrs - f/u 11 mths (7-19)
-Geissler II/III, pain 5.4 mths (3-14)
-F = 63º (40-80), E = 71º (40-90)
-DASH: preop 34 (16-48), postop 9 (0-40)
-VAS: preop = 3.4 (3-4) , postop 0.31 (0-3)
-MMWS: E/G = 29, F = 4 P = 2
(Mathoulin C, Dauphin N, Wahegaonkar AL. Hand Clinic 2011)
1
Institut
de la Main
Arthroscopic Dorsal Capsuloplasty
Ch. Mathoulin, Adeline Cambon-Binder
Acknowledgements to all EWAS members,
Especially : Jane Messina (Italy)
Abhijeet Wahegaonkar(India)
Luc Van Overstraeten (France)
Emmanuel Camus (France)
David Slutsky (USA)
Pak-Cheong Ho (Hong-kong, SAR China)
Loris Pegoli (Italy)
Max Haerle (Germany)
Andrea Tandara (Germany)
Marc Garcia-Elias (Spain)
Marina Carrara (Brazil)
Gustavo Mantovani (Brazil)
Martin Caloia (Argentina)
Gabriel Clemboski (Argentina)
Tanya Burgess (Australia)
Antonio Pagliei (Italy)
Institut
de la Main
S L
TFCC
rsl
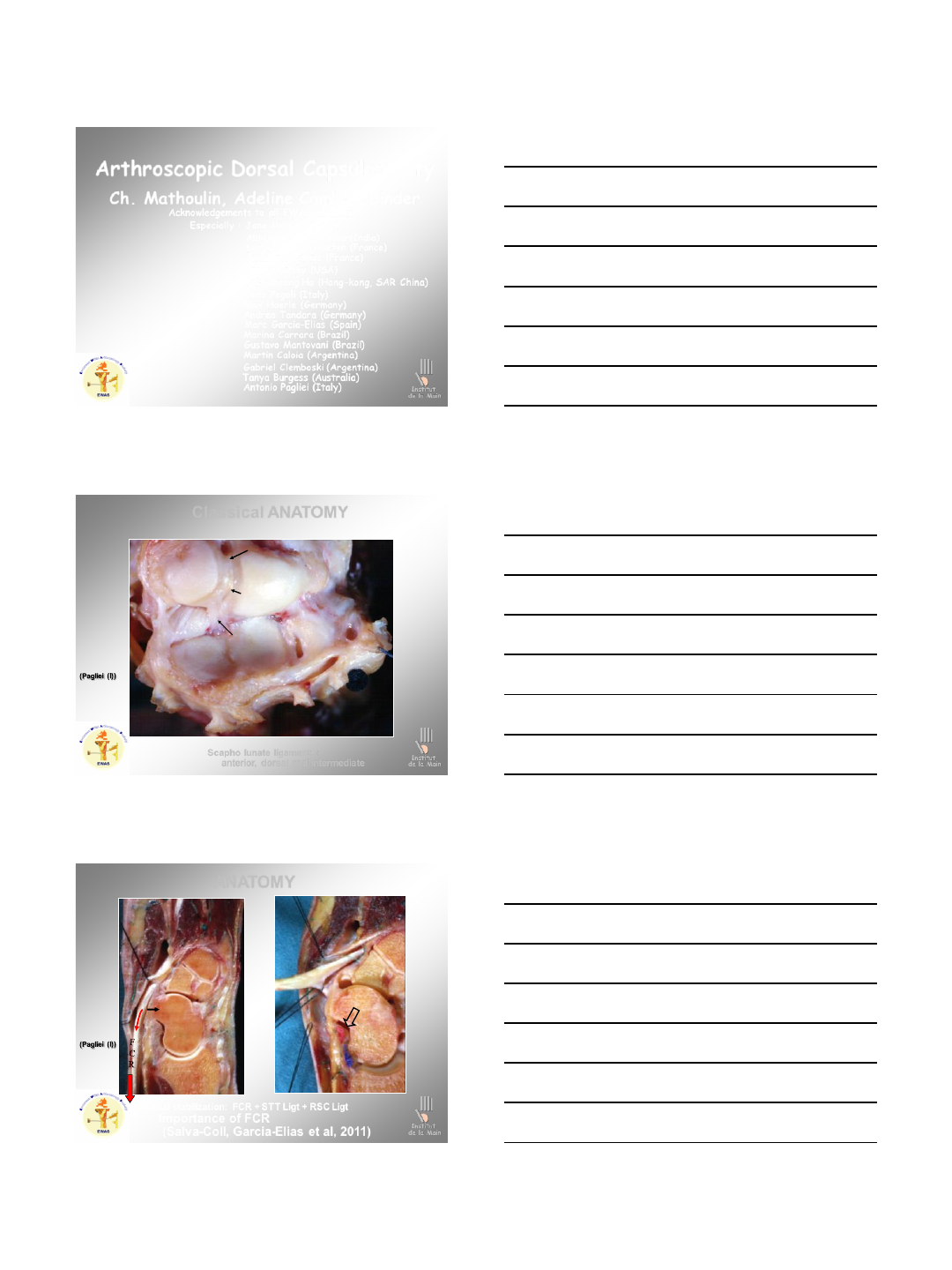
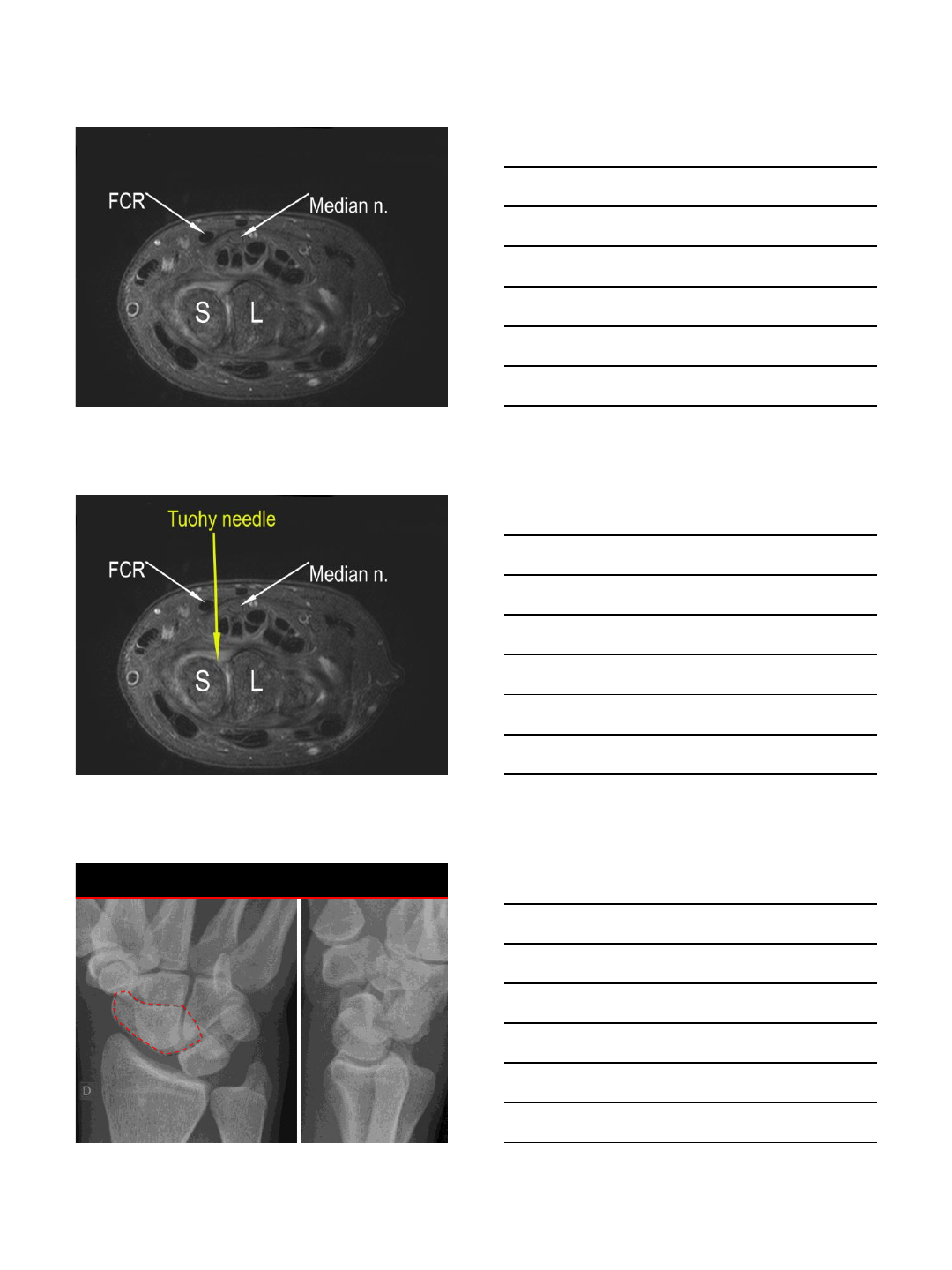
Scapho lunate ligament :
anterior, dorsal and intermediate
Classical ANATOMY
Institut
de la Main
R
IIM
S
Tp
Distal stabilization: FCR + STT Ligt + RSC Ligt
Importance of FCR
(Salva-Coll, Garcia-Elias et al, 2011)
ANATOMY
2
Institut
de la Main
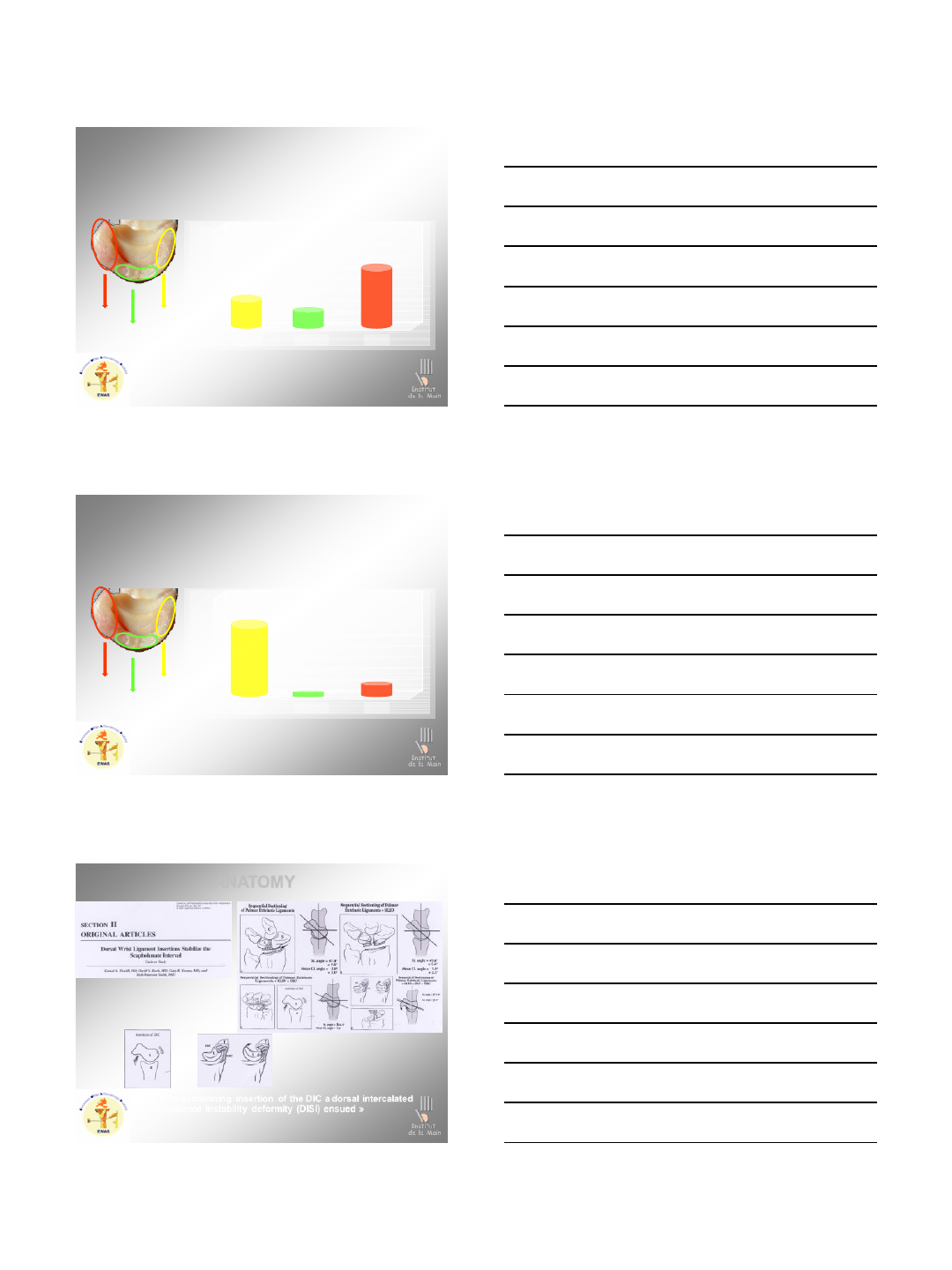
SCAPHOLUNATE LIGAMENT
Main scapholunate joint stabilizer
Meade et al 1990 – Short et al. – Looi et al. 2001
DORSAL
PROXIMAL
PALMAR
0
50
100
150
200
250
300
350
400
450
Palmar Proximal Dorsal
Yield Strength
118 +/-
21 63 +/- 32
260 +/-
18
Berger et al. ‘99
Institut
de la Main
SCAPHOLUNATE LIGAMENT
Contributes to carpal proprioception
DORSAL
PROXIMAL
PALMAR
Palmar Proximal Dorsal
Mainly
proximal
part
Mataliotakis et al. ‘09
Sensory innervation
Mataliotakis et al. ’11
Importance of AIO nerve and PIO nerve too !!!!
Institut
de la Main
« Only with sectionning insertion of the DIC a dorsal intercalated
scapholunate instability deformity (DISI) ensued »
ANATOMY
3
Institut
de la Main
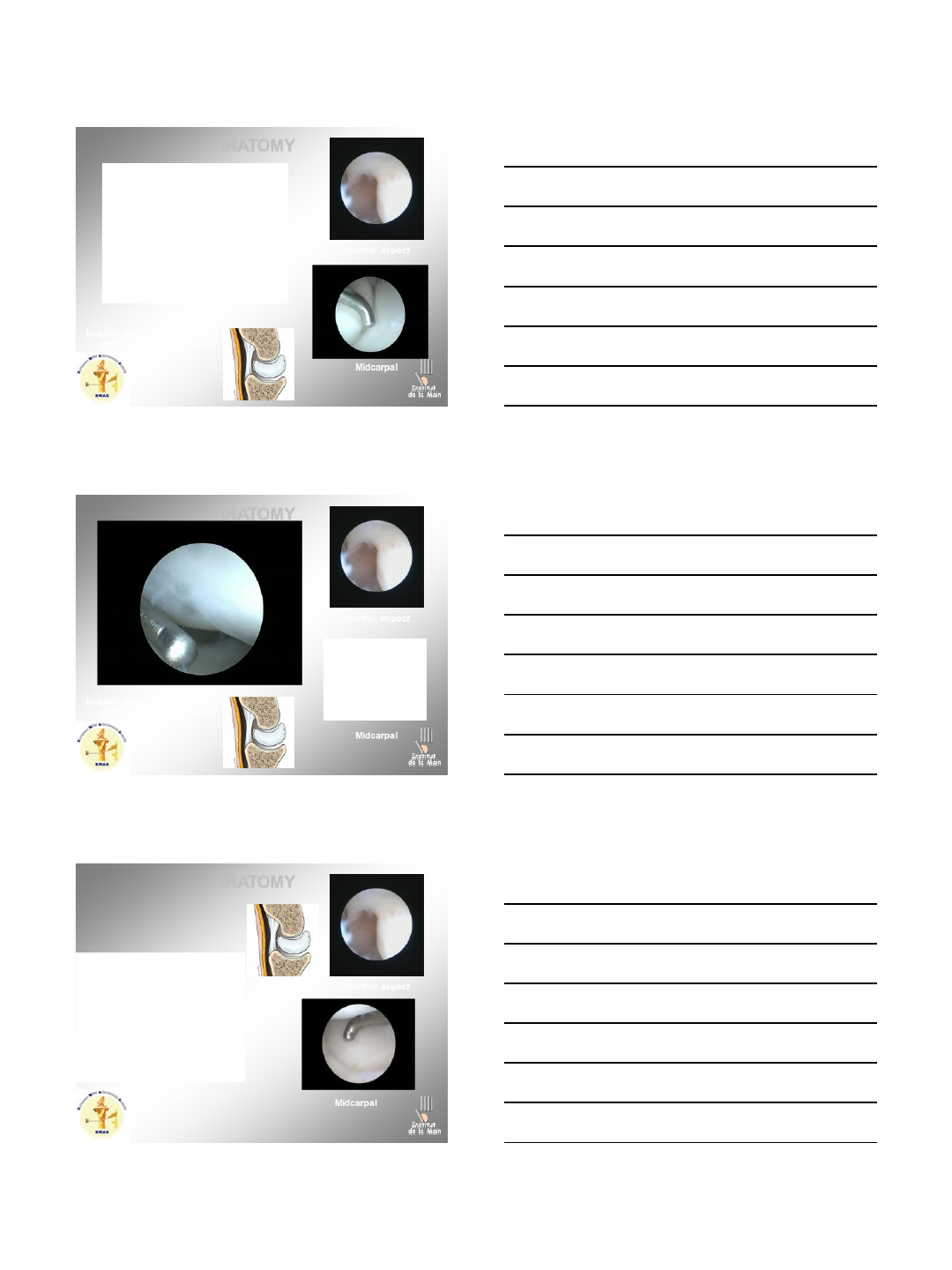
ANATOMY
Isolated dorsal capsule tear
with midcarpal SL spacing
Midcarpal
Institut
de la Main
Normal aspect
Institut
de la Main
ANATOMY
Isolated dorsal capsule tear
with midcarpal SL spacing
Midcarpal
Institut
de la Main
Normal aspect
Institut
de la Main
ANATOMY
Radiocarpal Midcarpal
Institut
de la Main
Normal aspect
4
Institut
de la Main
ANATOMY
Radiocarpal Midcarpal
Institut
de la Main
Normal aspect
Institut
de la Main
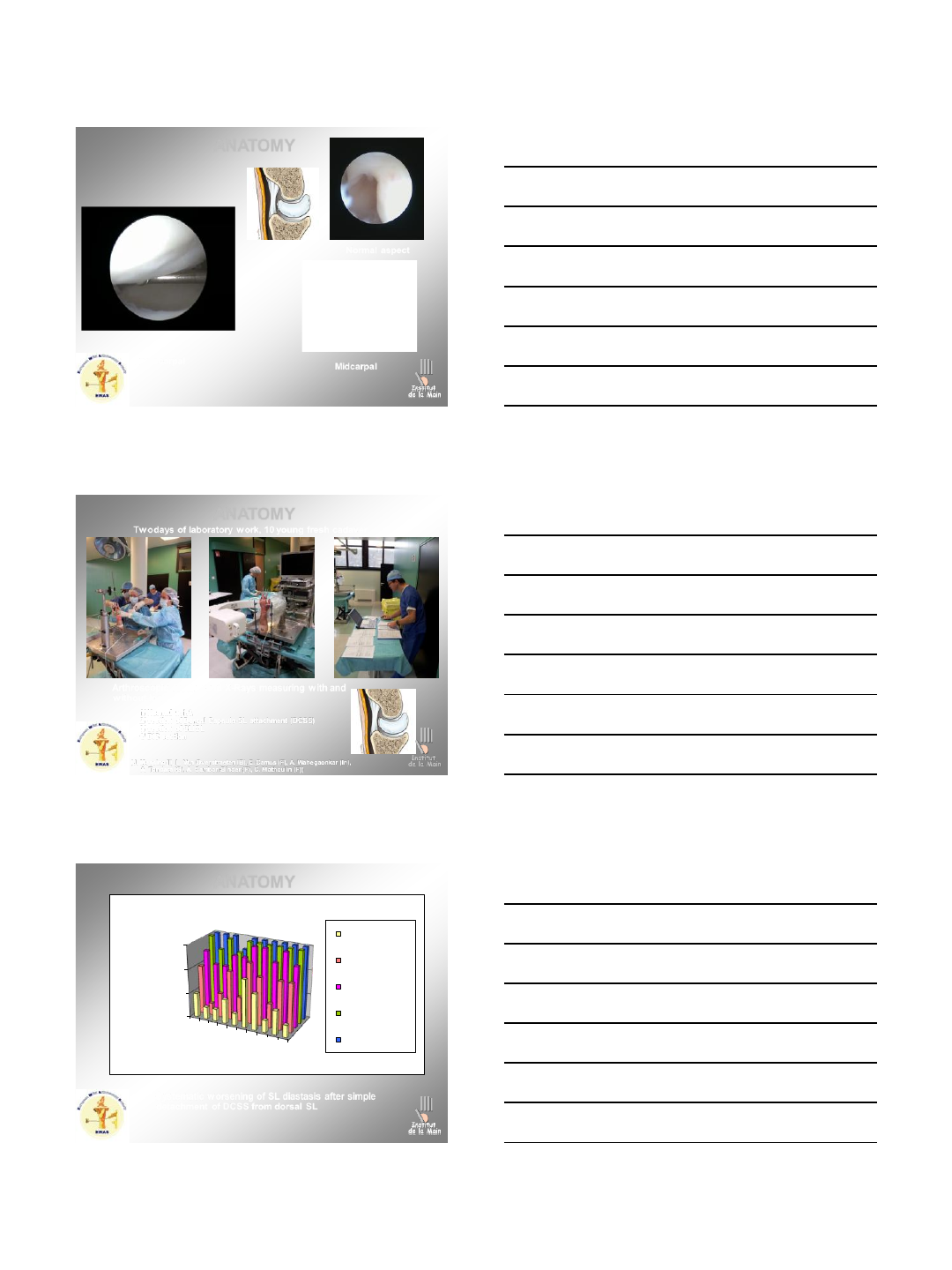
ANATOMY
Arthroscopic testing and X-Rays measuring with and
without load
1/ Normal wrist,
2/ section of Dorsal Capsulo-SL attachment (DCSS)
3/ section of SLIOL
4/ DIC section
( (J. Messina (I), L. Van Overstraeten (B), E. Camus (F), A. Wahegaonkar (In),
A. Tandara (G), A. Cambon-Binder (F), C. Mathoulin (F))
Two days of laboratory work, 10 young fresh cadaver
Institut
de la Main
ANATOMY
Systematic worsening of SL diastasis after simple
detachment of DCSS from dorsal SL
Two days of laboratory work, 10 young fresh cadaver
Institut
de la Main
0
2
4
6
1
3
5
7
9
SEVERITY
SL LAXITY
GRADE
CASES
CASES EVOLUTION AFTER SECTIONS
Initial
section aDIC/SL
section SL
section DIC
section DRC
5
Institut
de la Main
ANATOMY
This structure (Dorsal capsulo-
scapholunate Septum) is a bridge
between the DST ligt and the
dorsal SL ligt, and seems to be
essential to the SL stability, and
probably its tears could be
considered as a first stage of SL
instability…!!!
Institut
de la Main
0
1
2
3
4
5
6
7
Initial section aDIC/SL section SL section DIC
INDICE GRAVITE
SECTIONS
Institut
de la Main
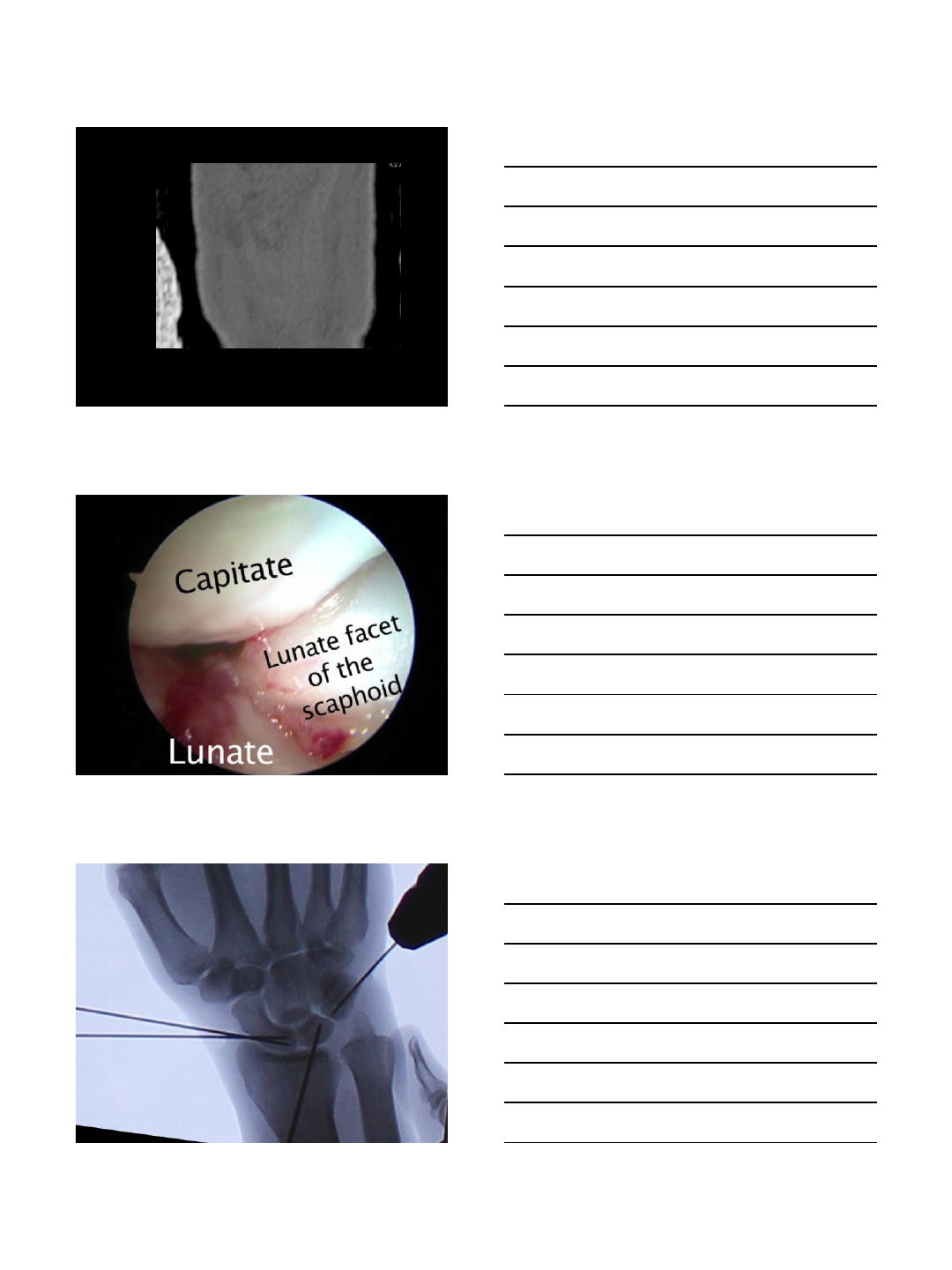
L
R
S
R
C
C
ANATOMY
Prominent role of dorsal radiocarpal ligaments:
DIC/Dorsal ScaphoTriquetral Ligt
Dorsal Scapholunate Ligt
Dorsal Capsulo-Scapholunate Septum
Institut
de la Main
DIC/DST
DSL
DCSS
Institut
de la Main
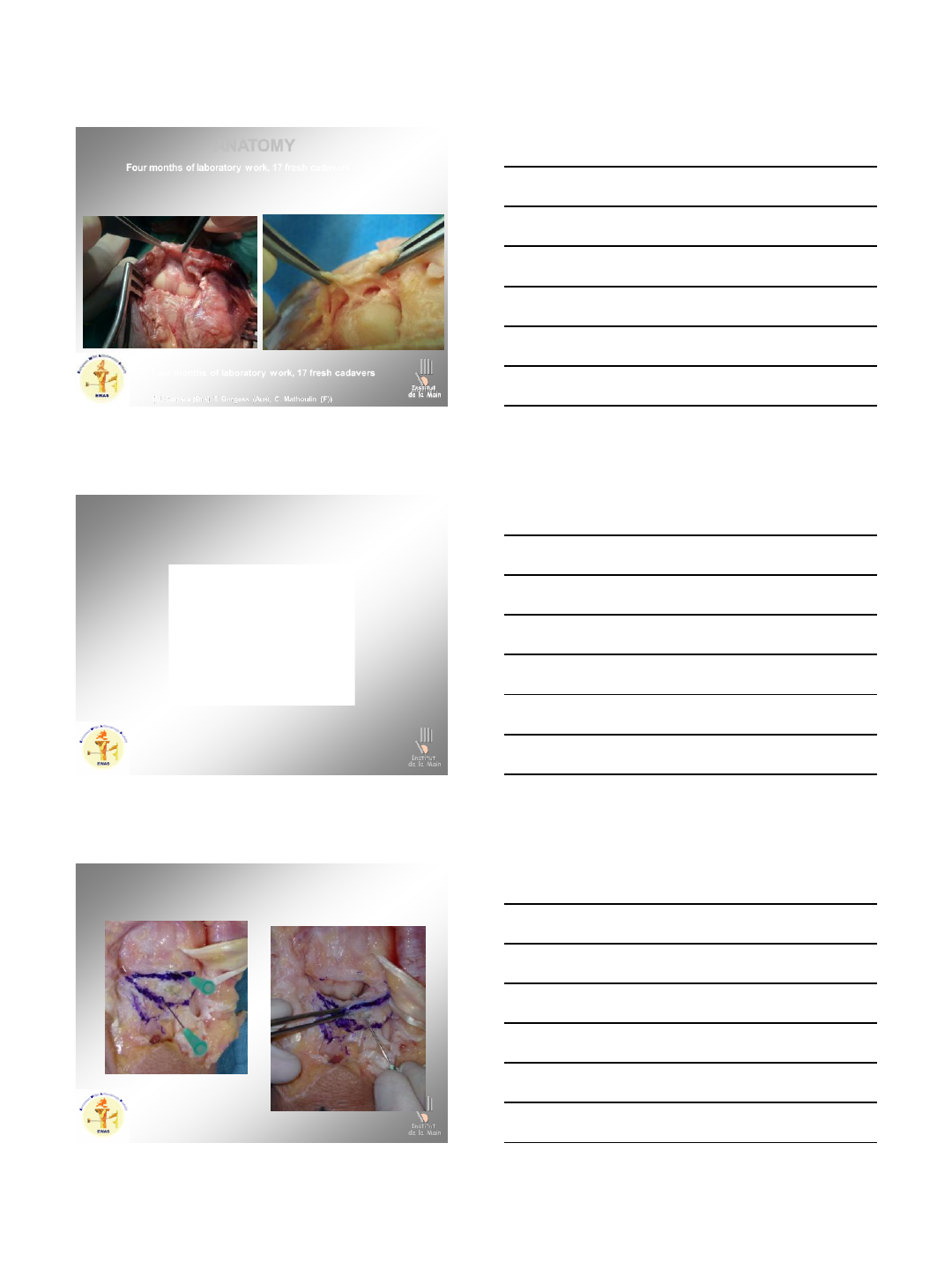
ANATOMY
The DCSS structure was identified between the scapholunate ligament and the DIC
DCSS always identified, consisting of three arches (two transverse arches in series
along the distal line of the scapholunate interval, forming a confluence into the third
which was larger than the previous mentioned)
Four months of laboratory work, 17 fresh cadavers
Institut
de la Main
(M. Carrara (Bra), T. Burgess (Aus), C. Mathoulin (F))
6
Institut
de la Main
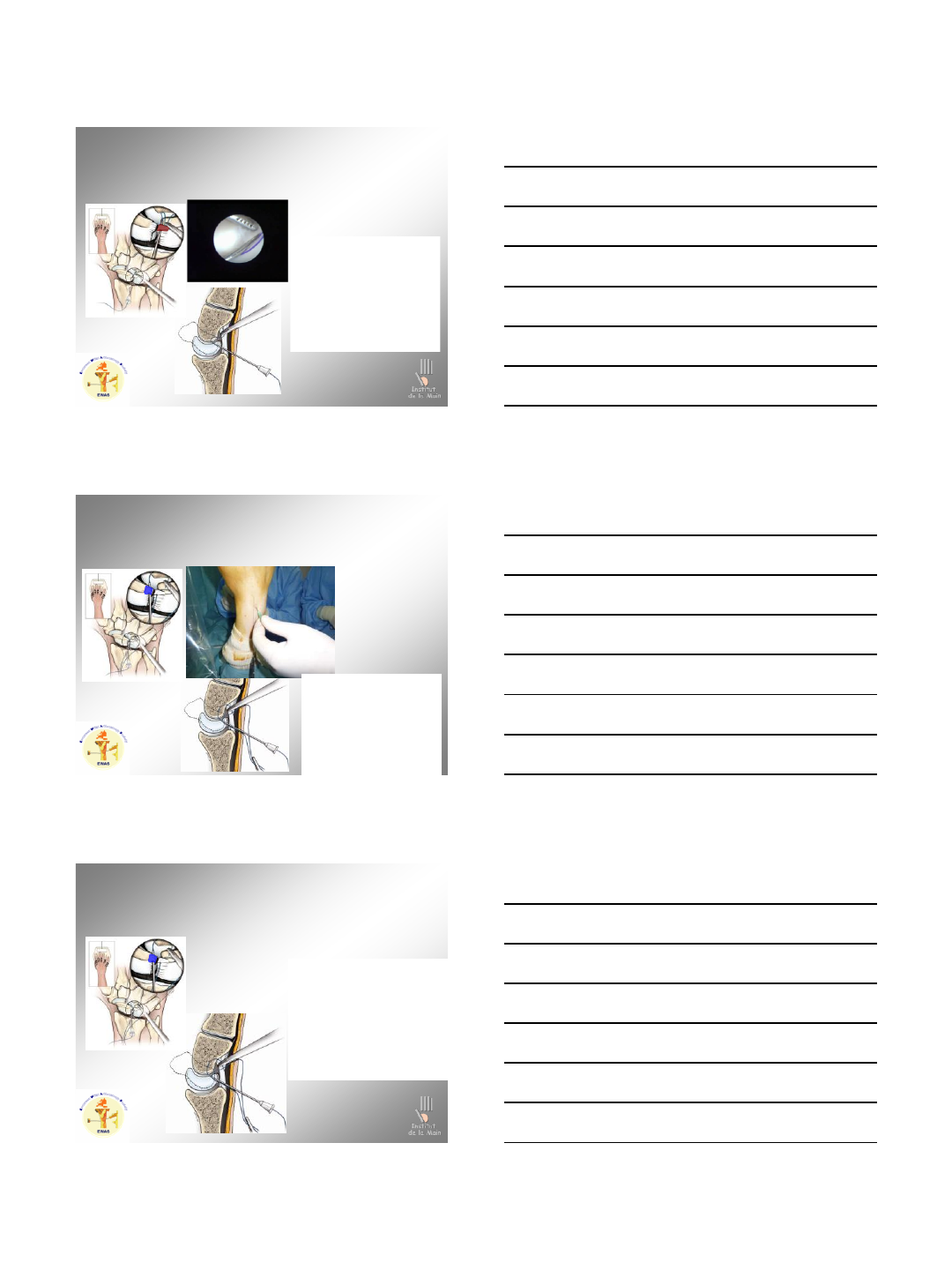
ANATOMY
It demonstrated a wide diffuse attachment along the scapholunate ligament and
then arced dorsally fanning out to a longer insertion into the dorsal capsule.
Four months of laboratory work, 17 fresh cadavers
Institut
de la Main
Four months of laboratory work, 17 fresh cadavers
(M. Carrara (Bra), T. Burgess (Aus), C. Mathoulin (F))
Institut
de la Main
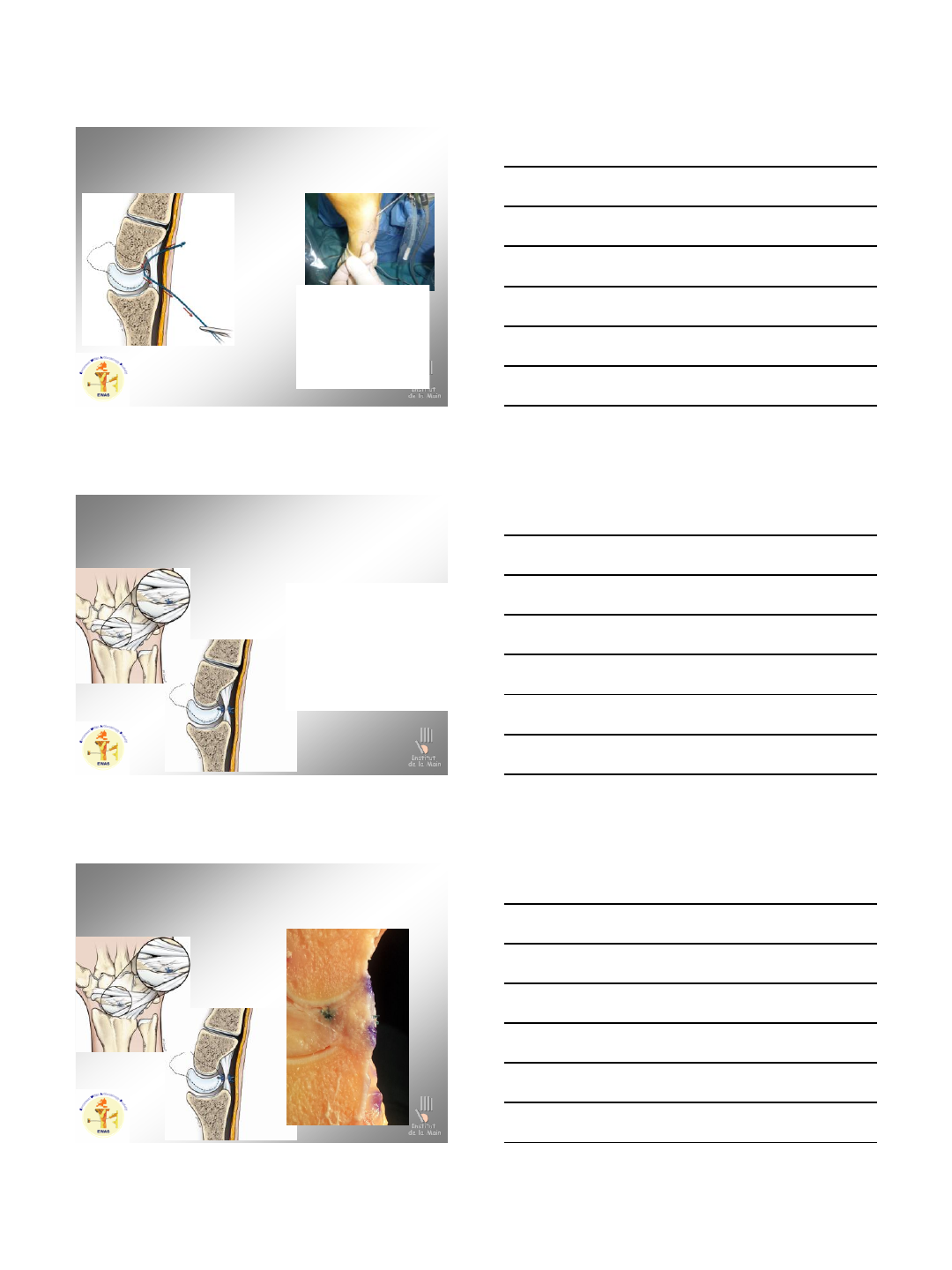
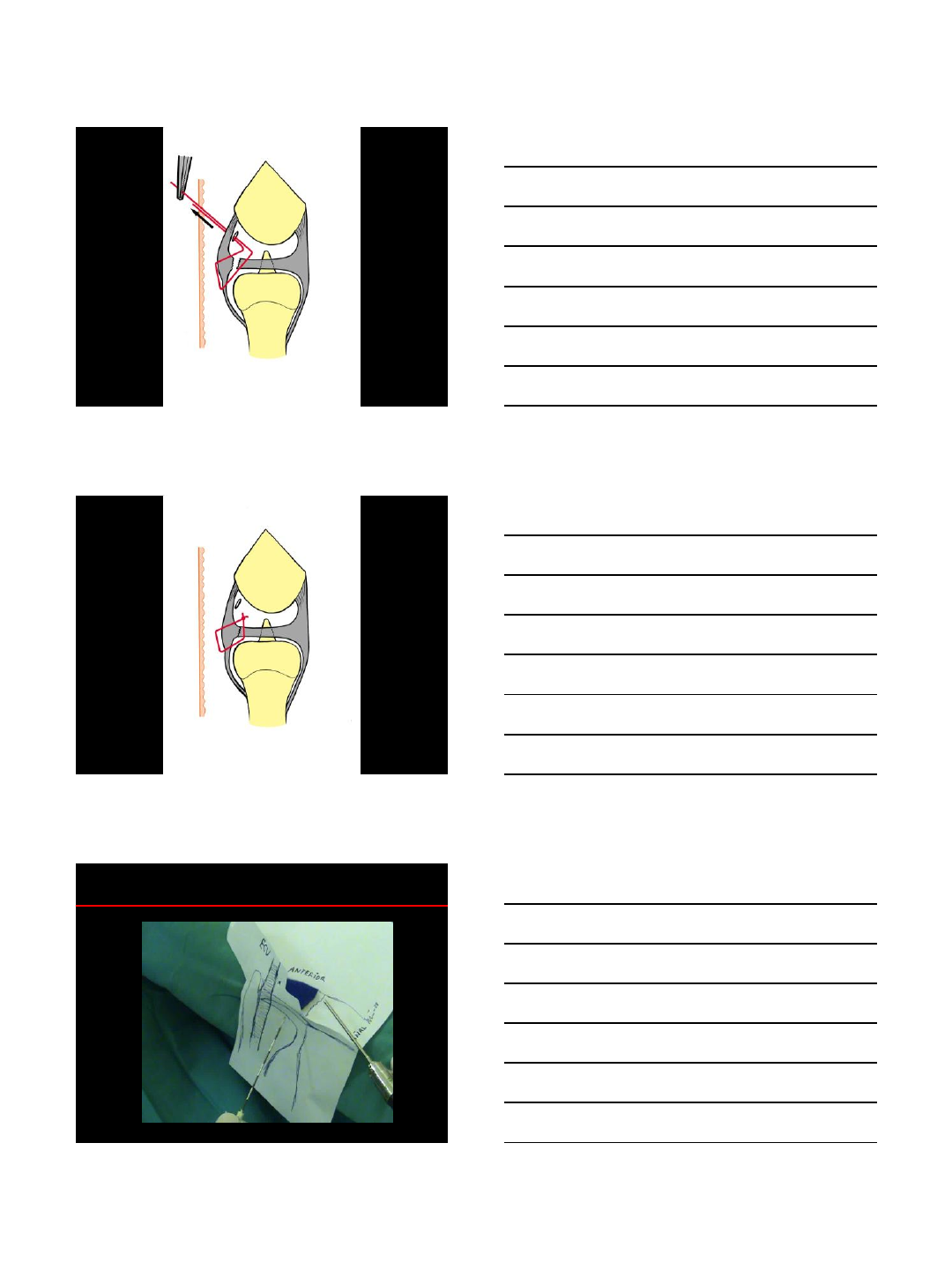
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
7
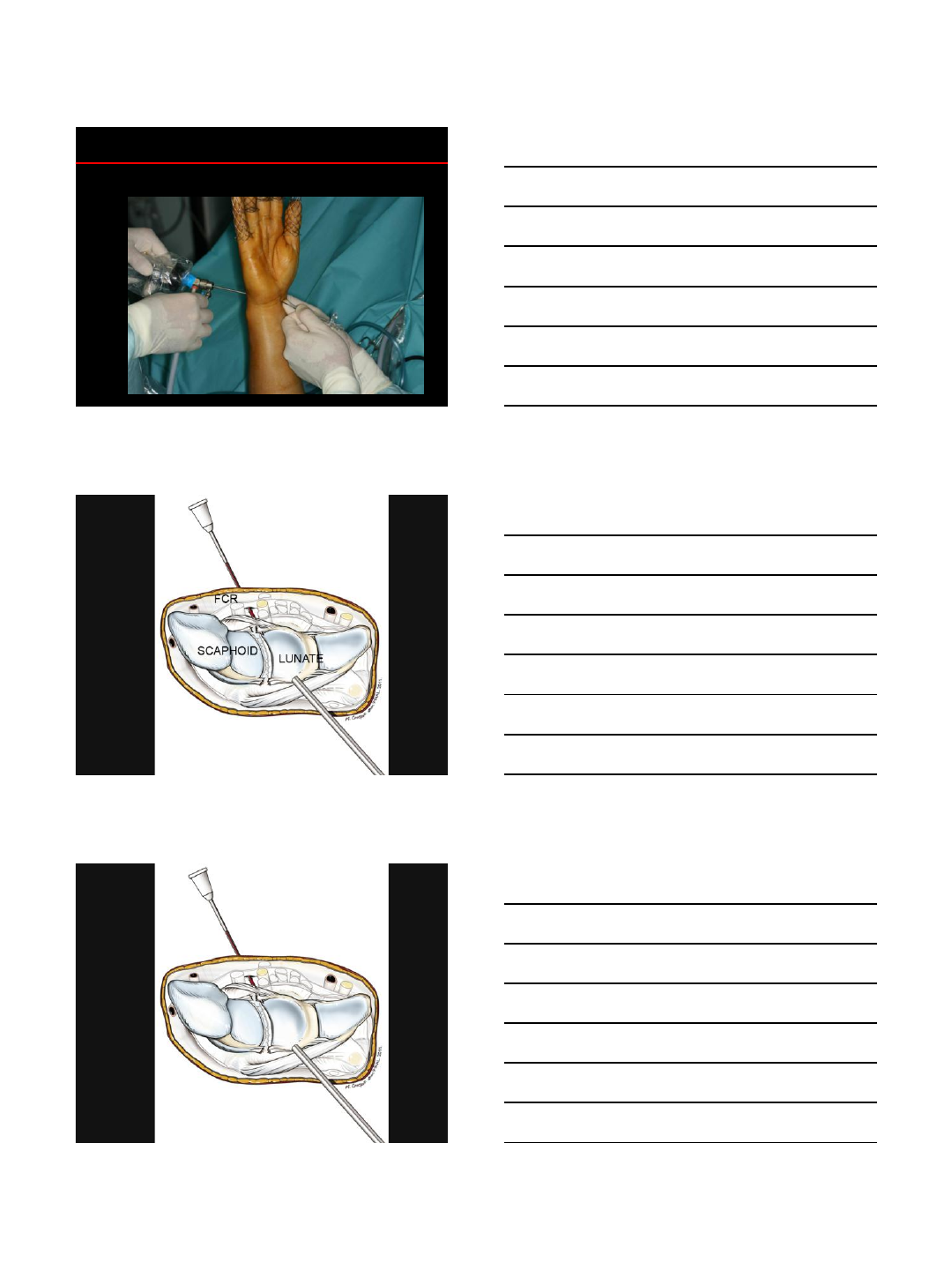
Institut
de la Main
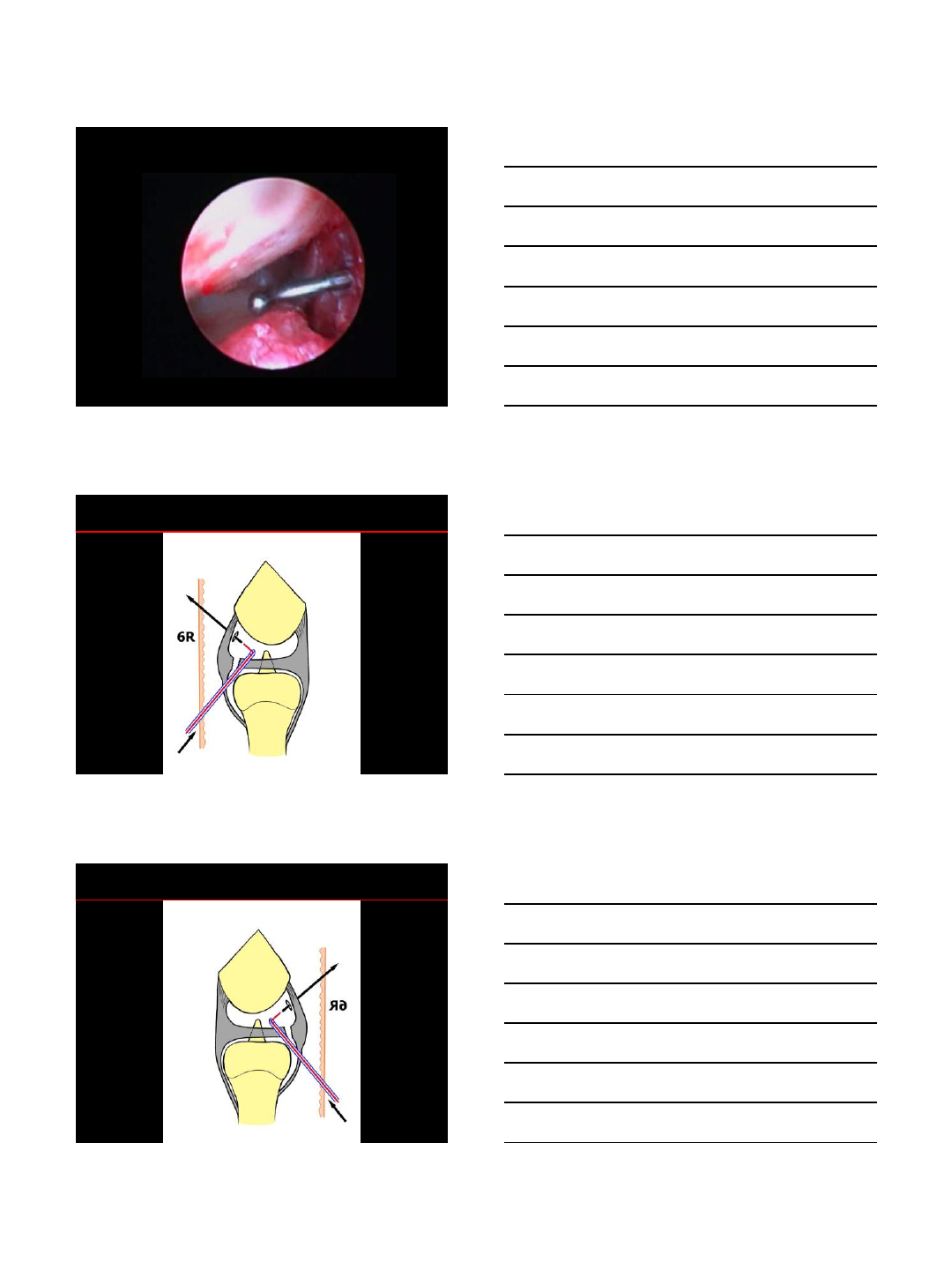
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
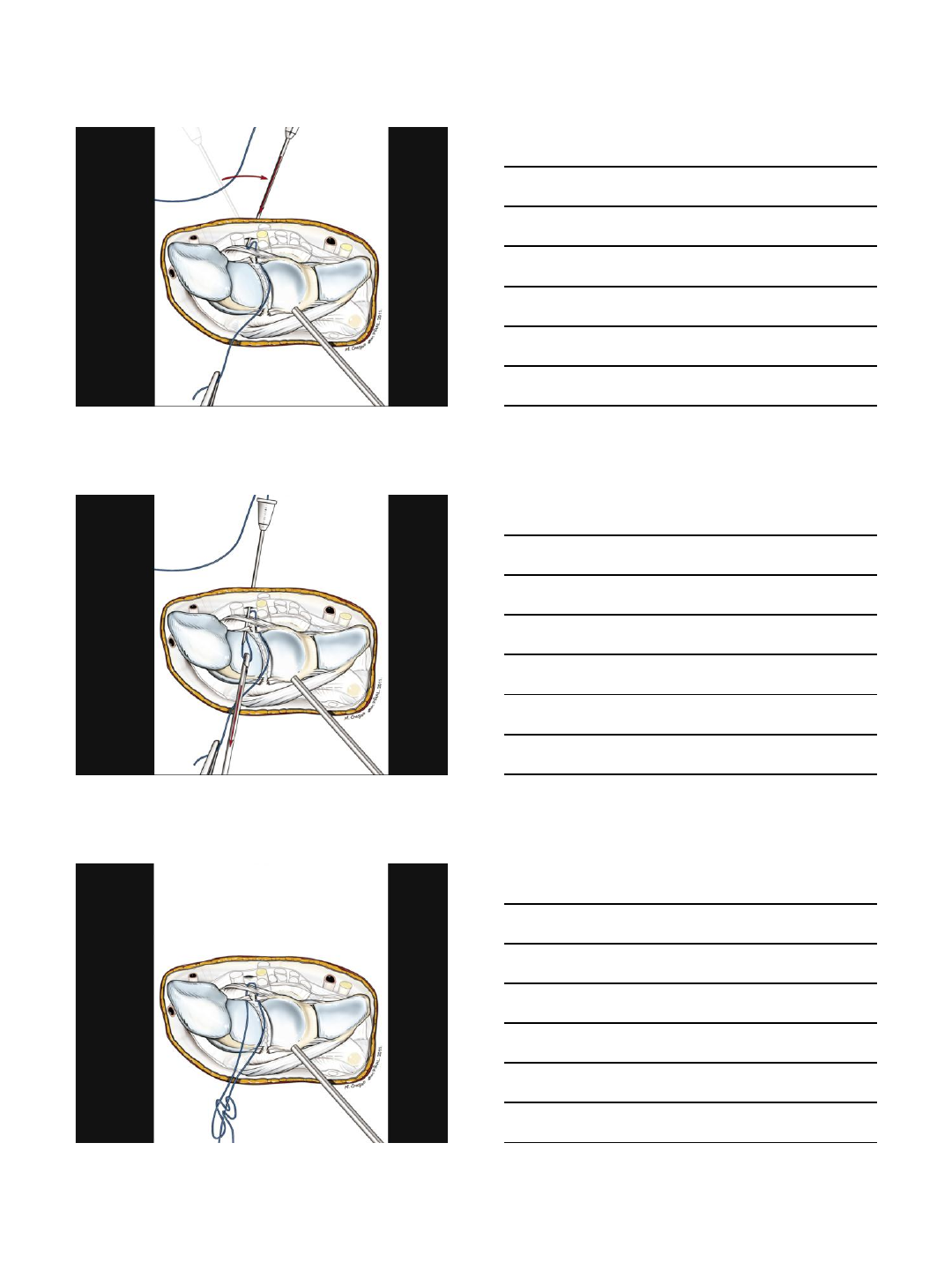
1 thread through 3,4 P, then DWC and ULNAR remnant
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
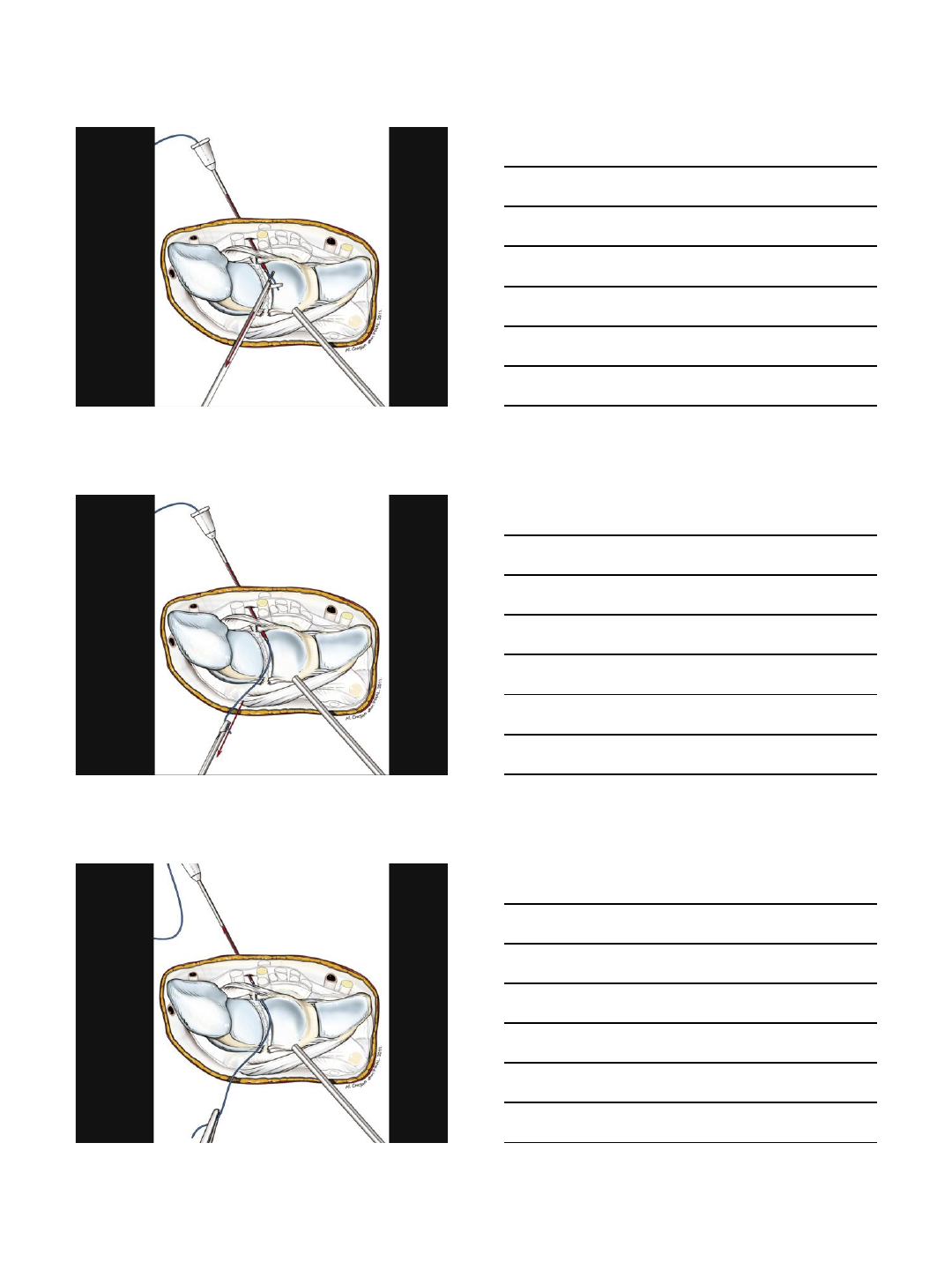
Institut
de la Main
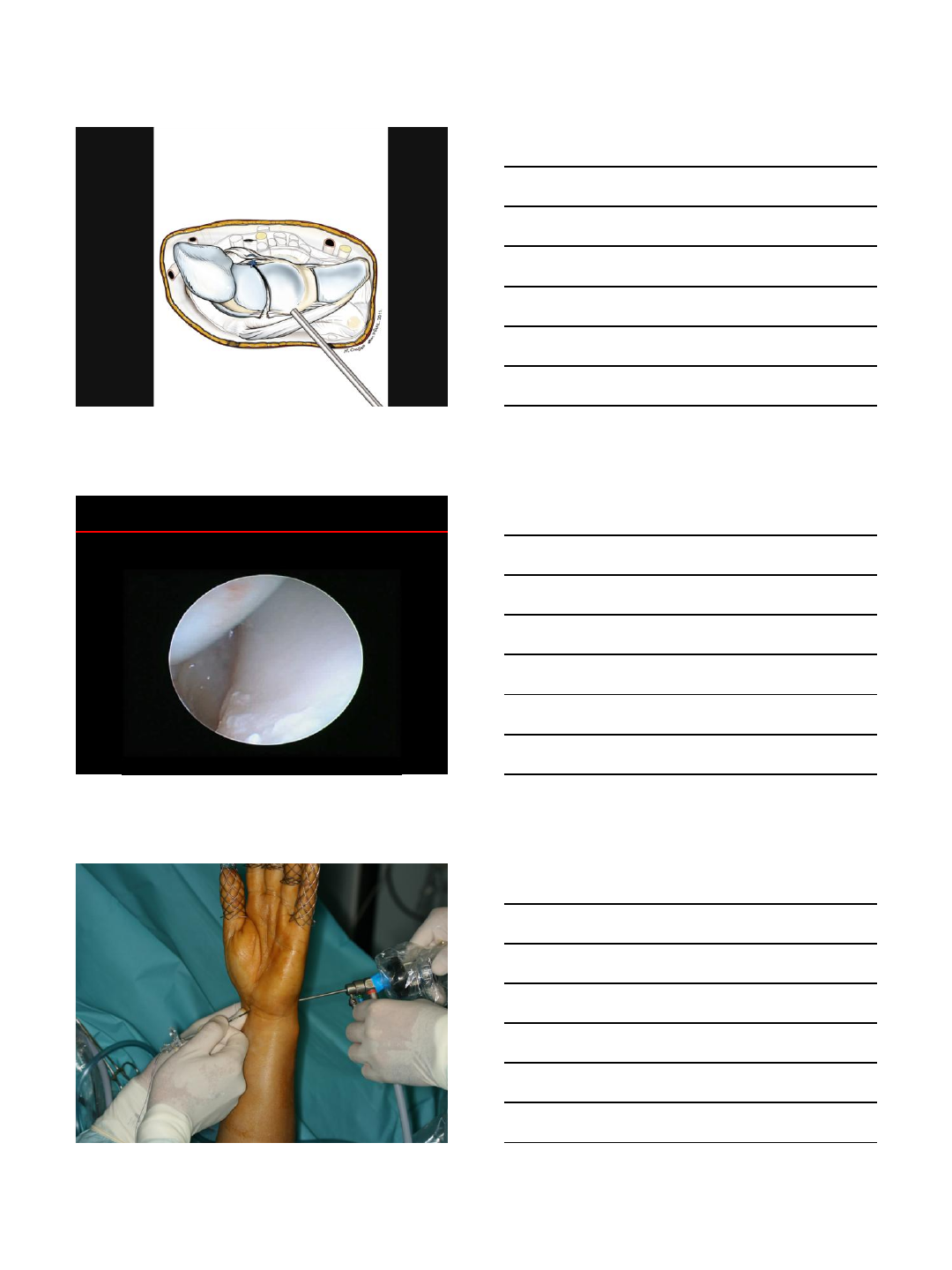
Retrieval through RMCP
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
8
Institut
de la Main
Retrieval through RMCP
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
2nd thread through DWC and RADIAL remnant
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
Retrieval through the same RMCP
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
9
Institut
de la Main
Pulled inside MCJ by proximal traction
Knot made outside patient (Nicky’s knot)
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
Second knot subcutaneous in 3,4 Portal
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
Second knot subcutaneous in 3,4 Portal
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
10
Institut
de la Main
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Institut
de la Main
SL K-Wires +/- SC K-Wires only if unreductible
Arthroscopic Dorsal Capsuloligamentous Repair
ADCLR
Without pinning!!!
Institut
de la Main
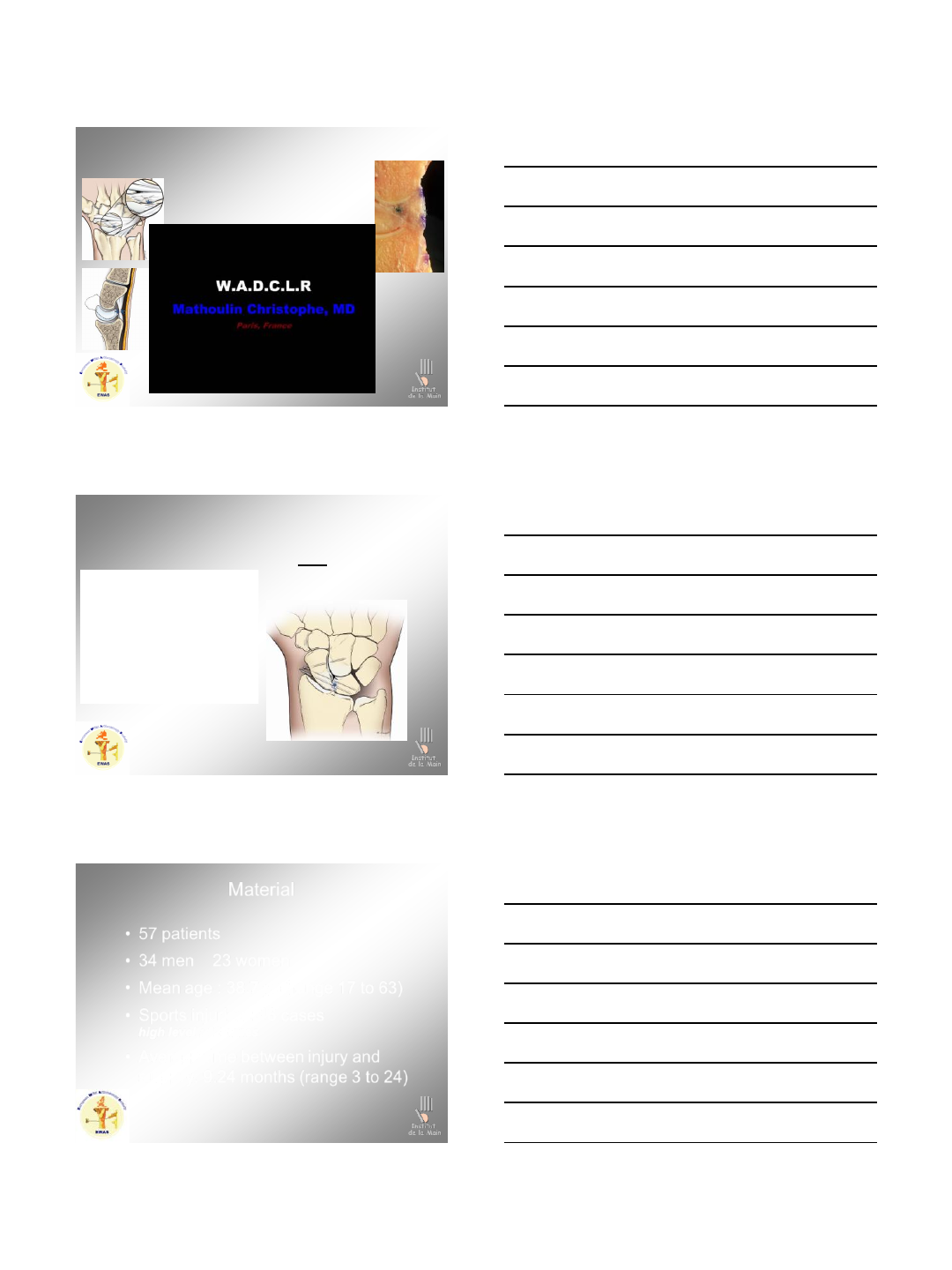
Material
•57 patients
•34 men 23 women
•Mean age : 38.7 yo (range 17 to 63)
•Sports injuries : 46 cases
high level : 12 cases
•Average time between injury and
surgery: 9.24 months (range 3 to 24)
11
Institut
de la Main
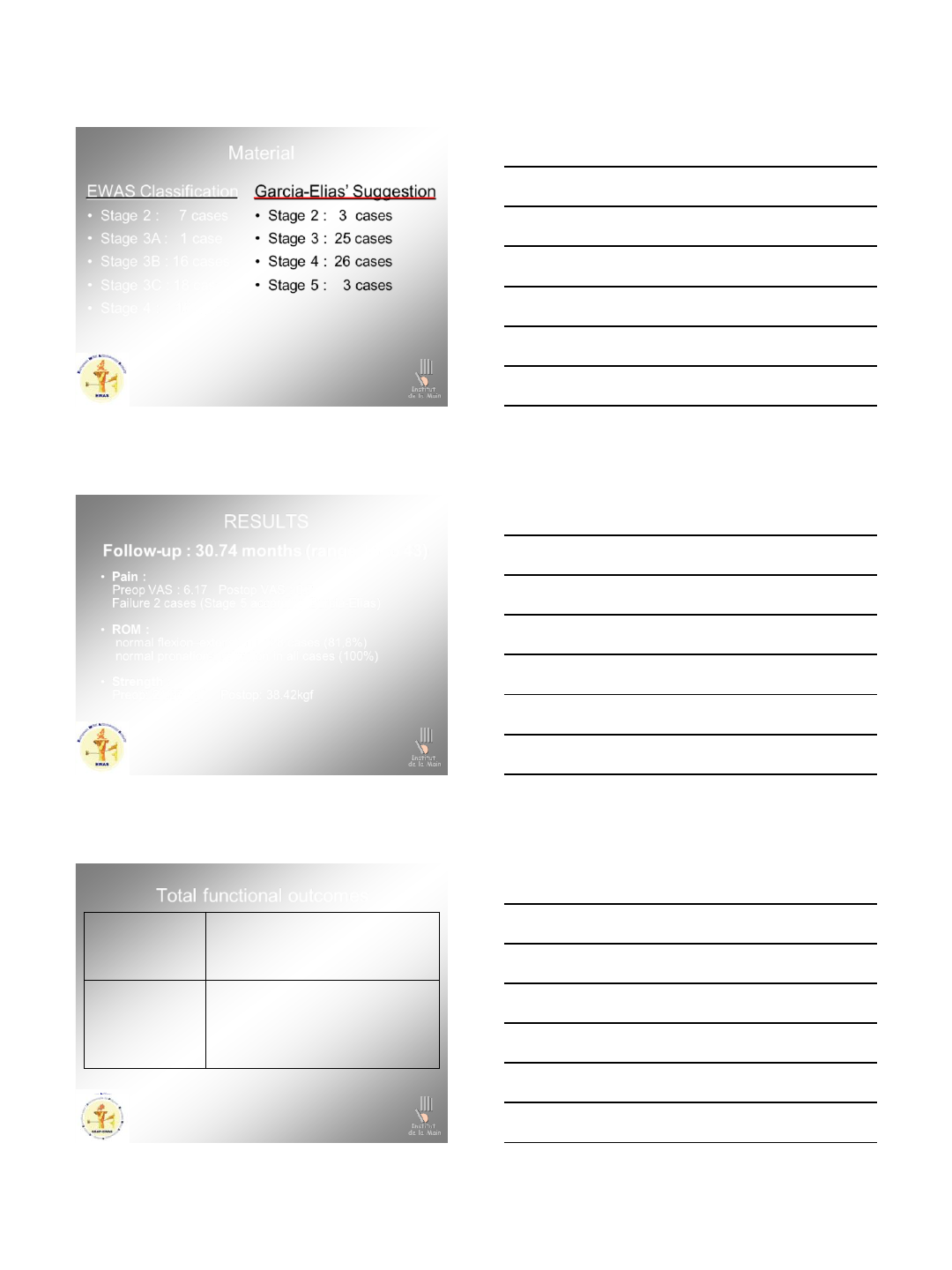
Material
Garcia-Elias’ Suggestion
•Stage 2 : 3 cases
•Stage 3 : 25 cases
•Stage 4 : 26 cases
•Stage 5 : 3 cases
EWAS Classification
•Stage 2 : 7 cases
•Stage 3A : 1 case
•Stage 3B : 16 cases
•Stage 3C : 18 cases
•Stage 4 : 16 cases
Institut
de la Main
RESULTS
•Pain :
Preop VAS : 6.17 Postop VAS : 0.7
Failure 2 cases (Stage 5 according Garcia-Elias)
•ROM :
normal flexion–extension in 28 cases (81,8%)
normal pronation-supination in all cases (100%)
•Strength :
Preop: 24.07 kgf Postop: 38.42kgf
Follow-up : 30.74 months (range 18 to 43)
Institut
de la Main
Total functional outcomes
Flexion
Extension
Pre-op post-op controlateral
52.45 63.55(p<0,01) 71.43(p=0,26)
50.62 74.56 (p<0,01) 77.89 (p=0,35)
Radial deviation
Ulnar deviation
Pronation supination
Wrist strength
15.7 21.82 (p<0,01) 27.36 (p=0,48)
26.75 35.52 (p<0,01) 37.28 (p=0,27)
0-160 0-178 (p<0,02) 0-179 (p=0,16)
24.07 38.42 (p<0,01) 40.81(p=0,18)
•No problem with sporty level +++
12
Institut
de la Main
Results
Outcome was related to :
–Stage 5 Garcia-Elias (2/3)
Outcome was related to :
–delay surgery (better outcome if short delay)
Complications:
- Slight flexion stiffness 6 cases (range 40° to 60°)
- One Sudeck (healed)
Institut
de la Main
Results
DASH:
PreOp : Average 46.05 (range 13.64 to 90.91)
PostOp : Average 8.29 (range 0 to 40.91)
Mayo WS:
Excellent : 35 cases
Good: 18 cases
Average : 2 cases
Poor: 2 cases
Institut
de la Main
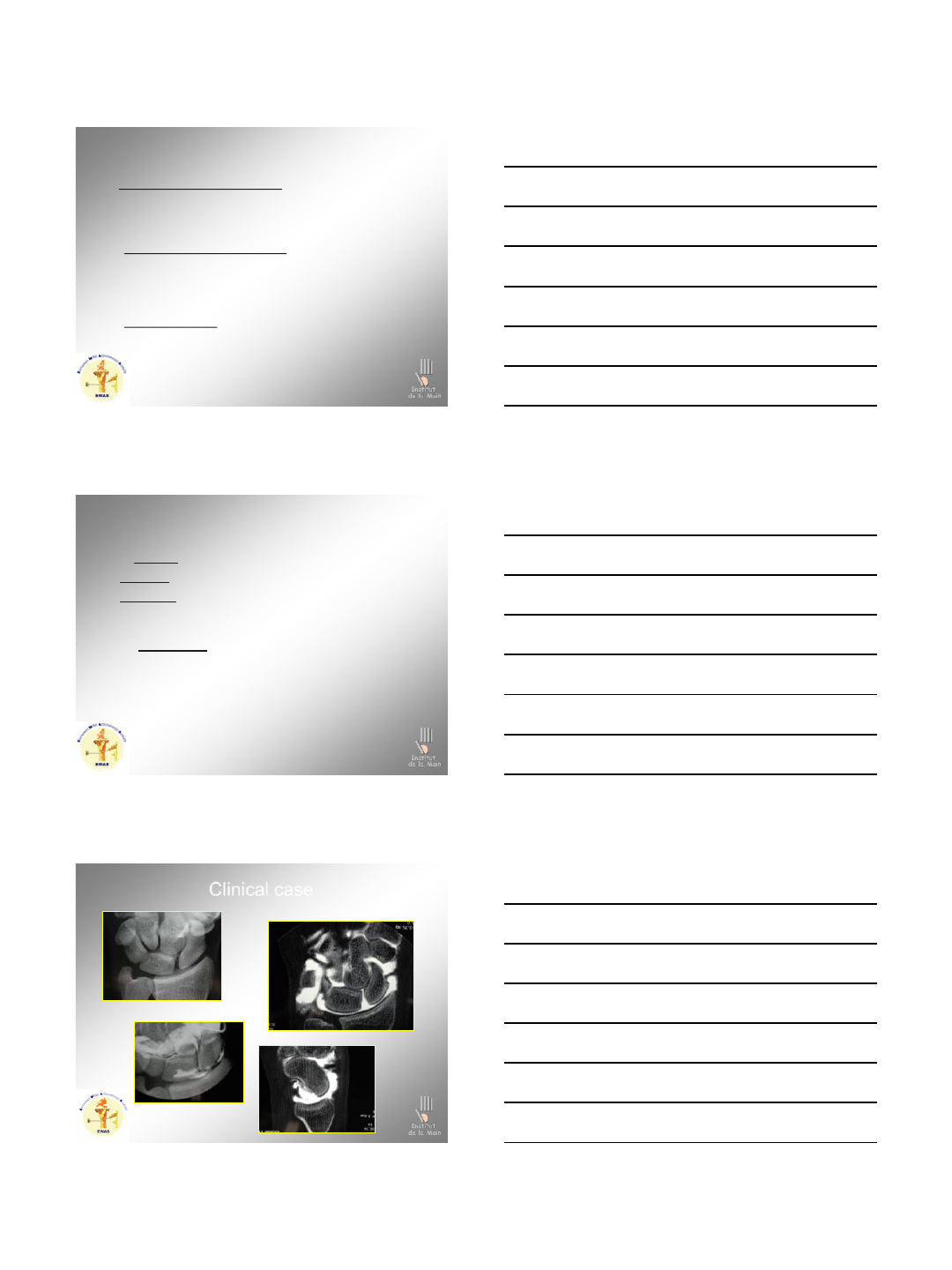
Clinical case
13
Institut
de la Main
ADCLR
Stage EWAS 4, Geissler 4, Garcia-Elias 4
Clinical case
Institut
de la Main
ADCLR
Stage EWAS 4, Geissler 4, Garcia-Elias 4
Clinical case
Institut
de la Main
ADCLR
SL pinning + Scapho-capitate pinning
Clinical case

14
Institut
de la Main
ADCLR
SL pinning + Scapho-capitate pinning
Clinical case
Institut
de la Main
ADCLR
SL pinning + Scapho-capitate pinning
Clnical case
Post ADCLR
Pre ADCLR
Institut
de la Main
ADCLR
SL pinning + Scapho-capitate pinning
Clnical case
Post ADCLR
Pre ADCLR
15
Institut
de la Main
ADCLR
SL pinning + Scapho-capitate pinning
Clinical case
Institut
de la Main
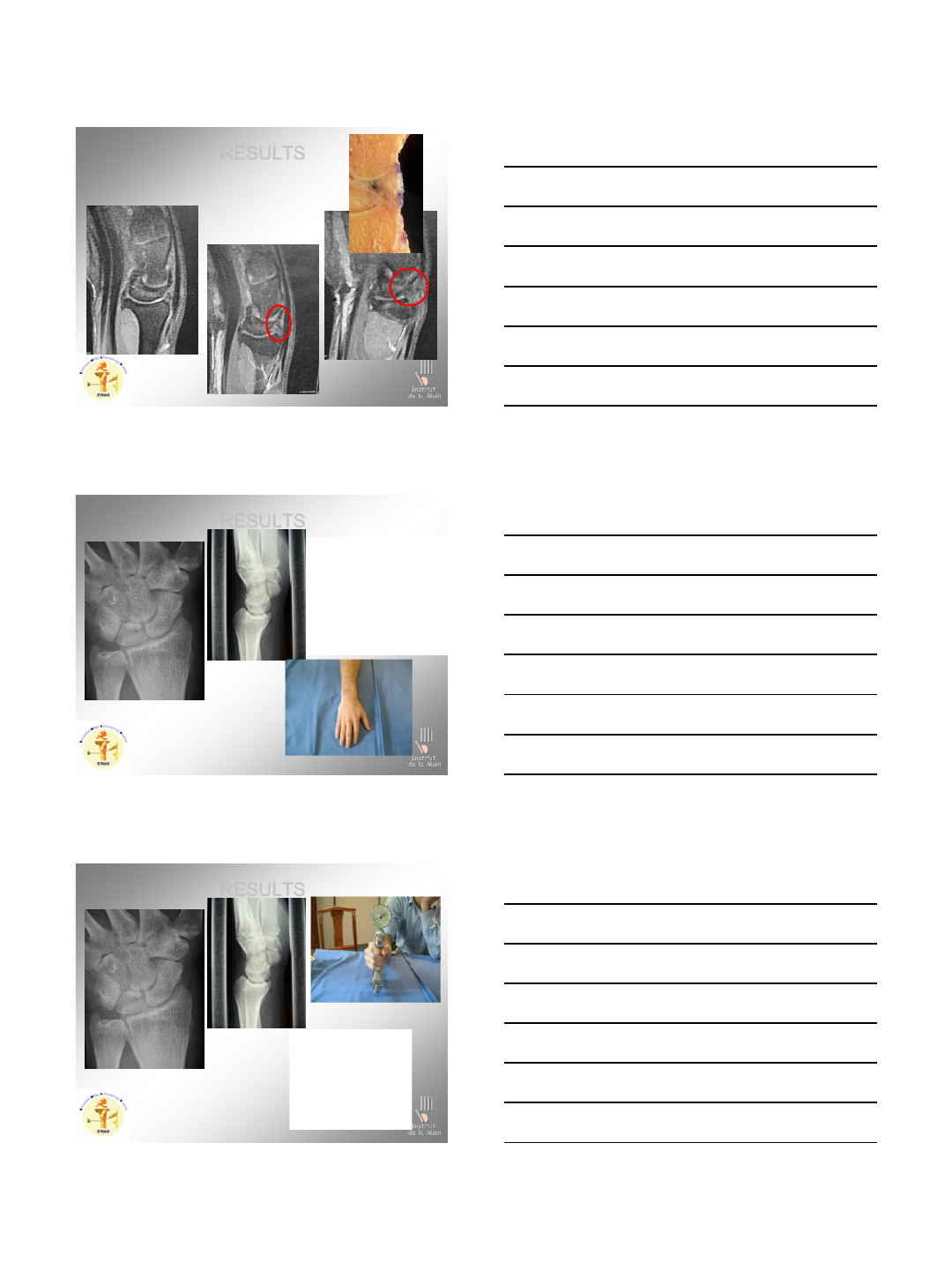
D + 2 months
RESULTS
SLIOL unrepaired, Stability of dorsal part
Normal aspect
Institut
de la Main
D + 2 months
RESULTS
SLIOL unrepaired, Stability of dorsal part
Normal aspect
16
Institut
de la Main
D + 9 months
RESULTS
Institut
de la Main
D + 19 months
RESULTS
Institut
de la Main
D + 19 months
RESULTS
17
Institut
de la Main
OUTSTANDING ISSUES
Is the SLIOL really useless ? YES
What is the real importance of proprioception? Do we act on
proprioception with arthroscopic repair? YES
Does the distal volar ligamentous lesions (stt) exist? ??
Are isolated lesions of the DCSS pre-unstable lesions, or are
they another entity? YES
What is the real place of extrinsic ligaments? SLLComplex
Institut
de la Main
Conclusion
DSL, DST, DCSS ligts seem essential in SL stability
SLLComplex: a new concept!!!!!!
Arthroscopic
capsuloligamentous
repair is a simple and reliable procedure
convenient for the patient
with chronic scapho-lunate tears,
except in stage 5 (GE)
These encouraging first results
need a longest follow-up.
Institut
de la Main
3/9/2013
1
A TECHNIQUE FOR
ARTHROSCOPIC REPAIR
OF THE VOLAR S-L
LIGAMENT
Francisco del Piñal, MD, Dr Med. (*)
Hand and Plastic Surgery. Private practice.
Hand-Wrist Unit and Department of Plastic Surgery. Mutua Montañesa.
SANTANDER. SPAIN.
(*) nothing to disclose.
A TECHNIQUE FOR ALL-
INSIDE SUTURING IN THE
WRIST .
Francisco del Piñal
Hand and Plastic Surgery. Private practice.
Hand-Wrist Unit and Department of Plastic Surgery. Mutua Montañesa.
SANTANDER. SPAIN.
pacopinal@gmail.com
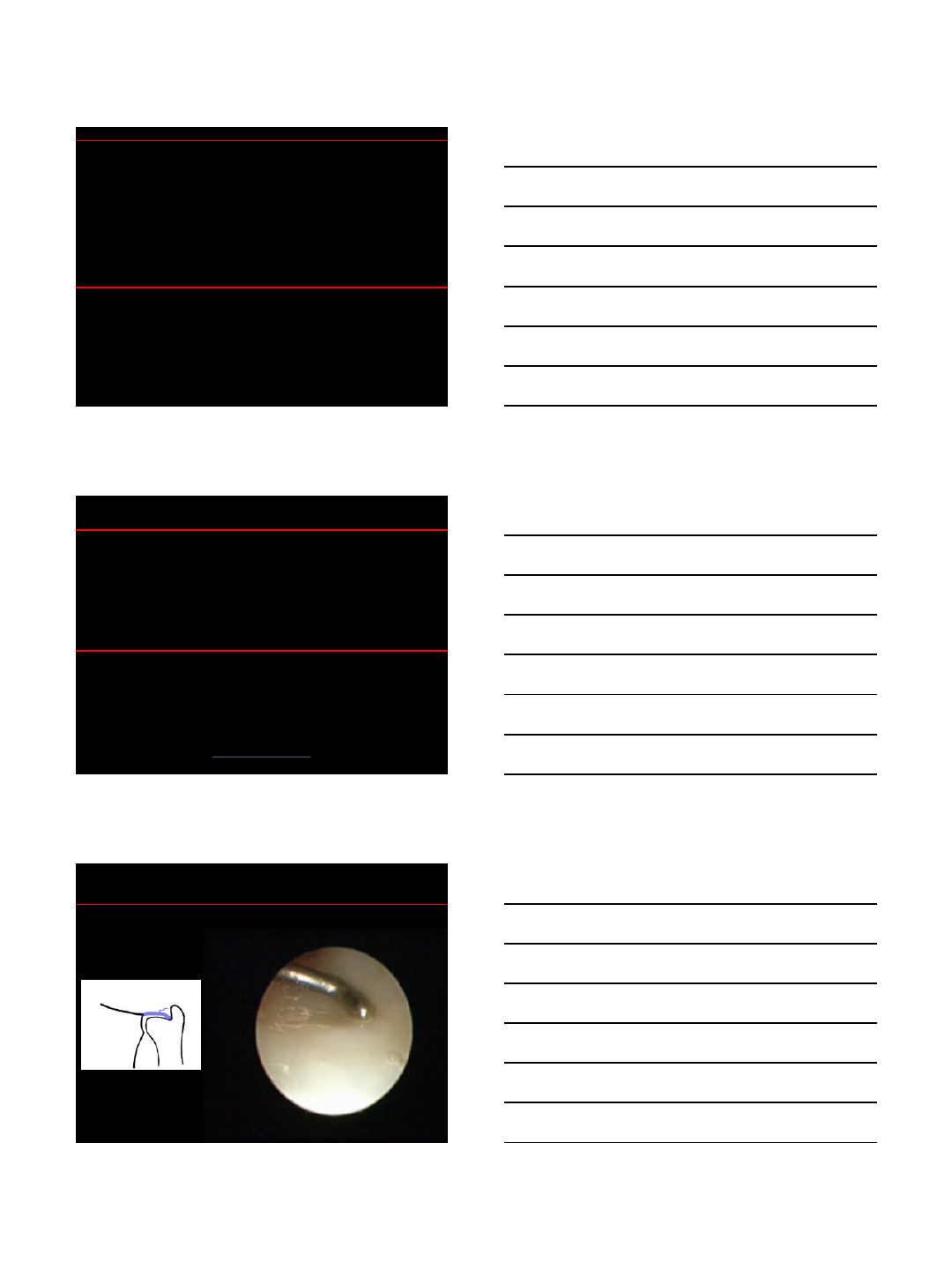
PERIPHERAL COMPLETE FOVEAL
1B tear without instability
3/9/2013
2
1B tear without instability
De Araujo, Poehling, Whipple. Arthroscopy .1995.
DORSAL BRANCH OF THE
ULNAR NERVE
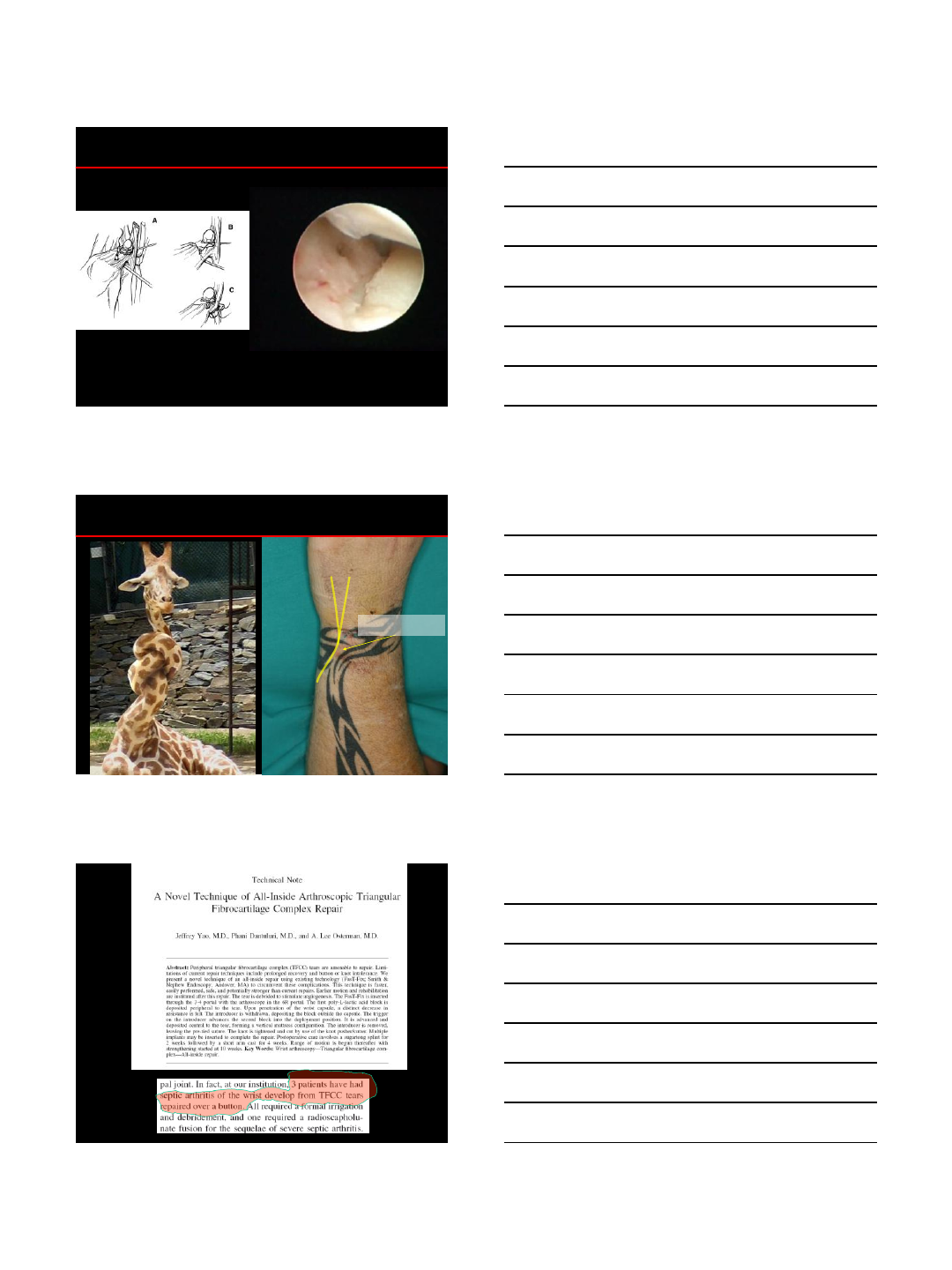
The problem…THE KNOT
Arthoscopy 2007.

3/9/2013
4
TRIQUETRUM
ULNAR HEAD
TFC
3/9/2013
5
3/9/2013
6
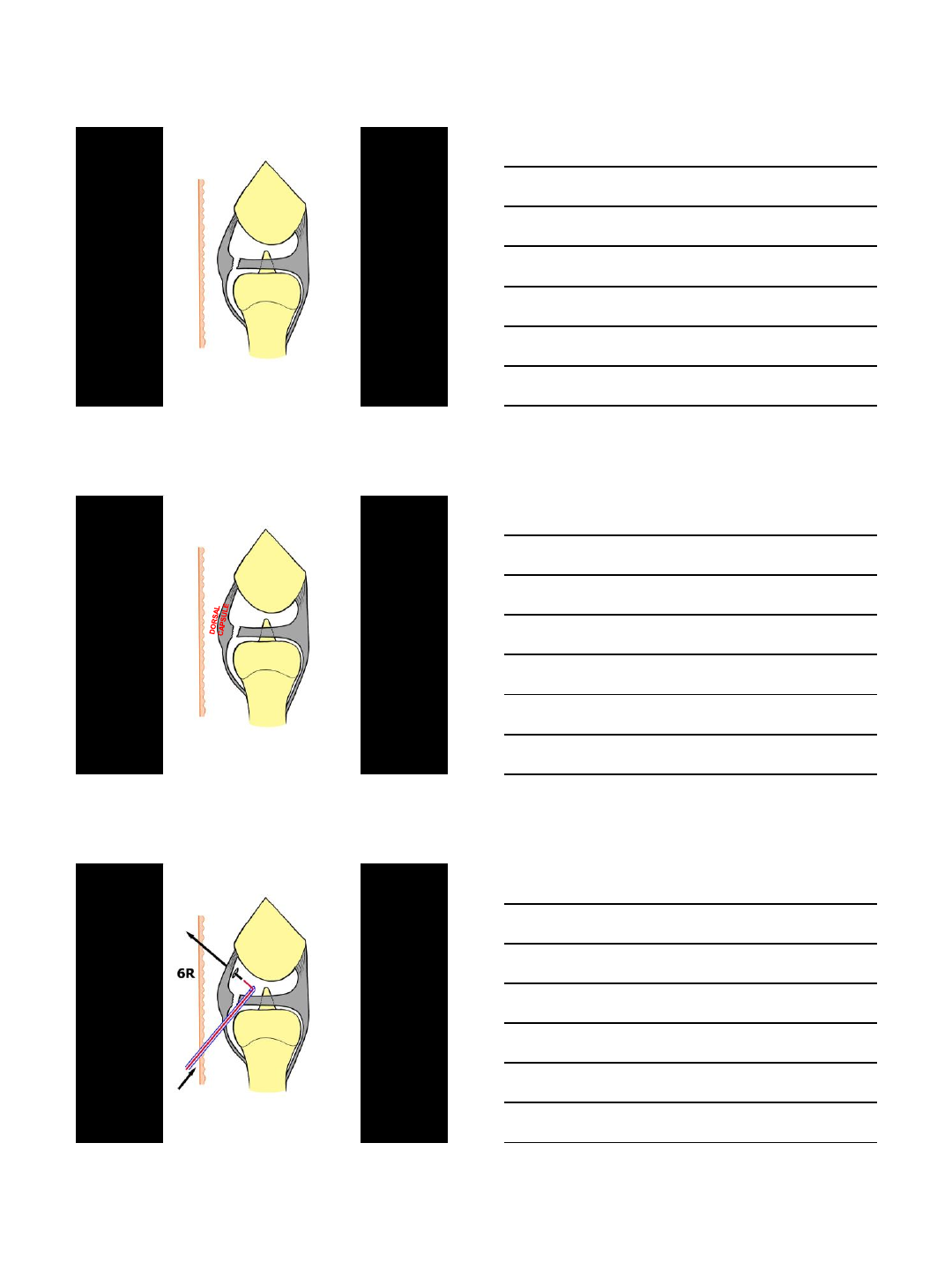
TECHNIQUE
3/9/2013
7
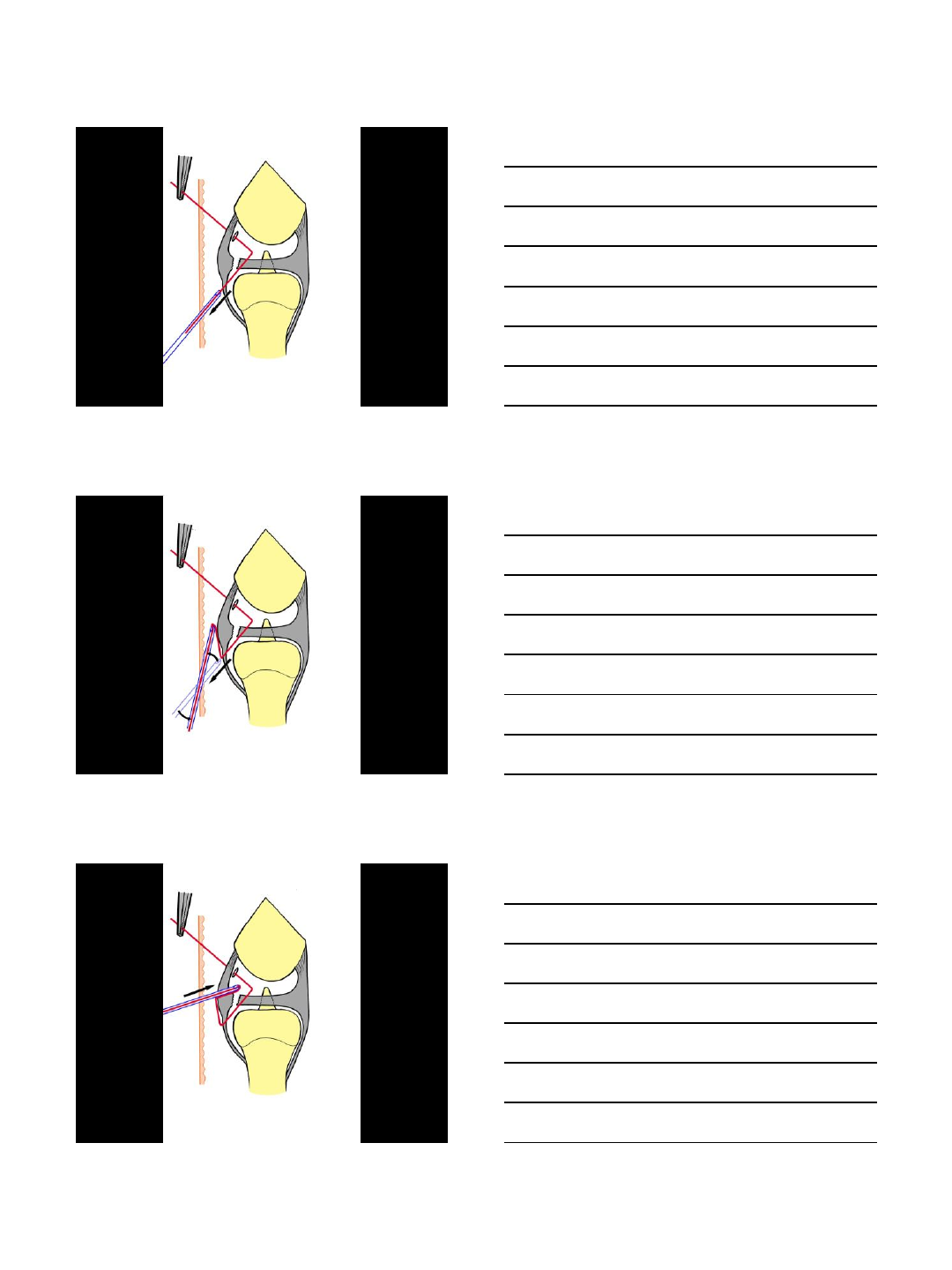
ALL-IN REPAIR
All-in VOLAR S-L suturing
All-in VOLAR S-L suturing
3/9/2013
8
All-in VOLAR S-L suturing
3/9/2013
9
3/9/2013
10
3/9/2013
11
All-in VOLAR S-L suturing
3/9/2013
12
CLOSURE SL- SPACE OF POIRIER-LT
3/9/2013
13
3/9/2013
14
3/9/2013
15
3/9/2013
16
1 year postoper.
CLINICAL EXPERIENCE…
8 Volar S-L Repair.
6 Volar and Dorsal S-L Repair.
4 Volar capsule and Ligaments repair (PLFD).
S L
CLINICAL EXPERIENCE…
3/9/2013
17
In summary, …
Sardinero’s Beach. View from the Operating Room.
3/8/2013
1
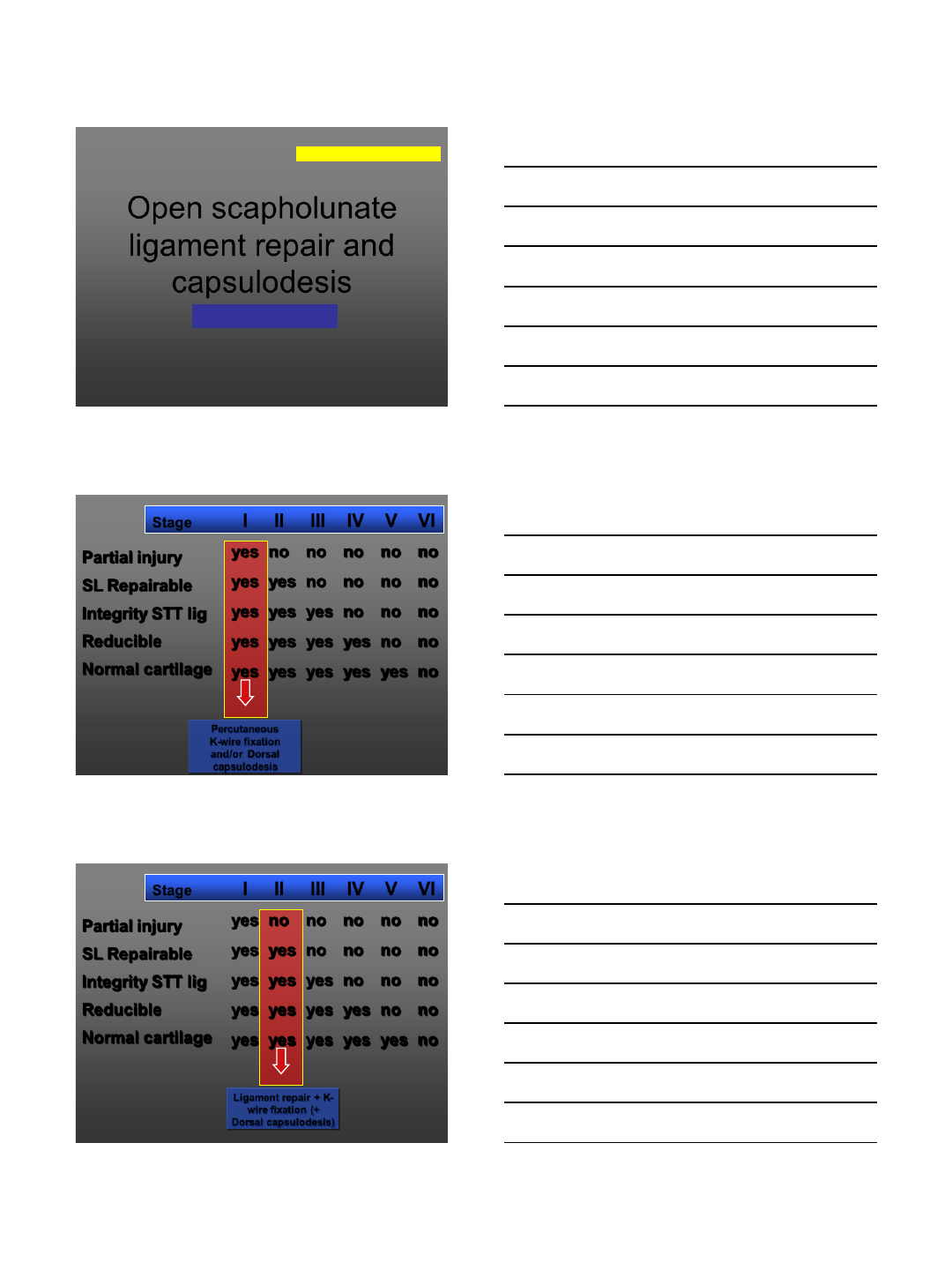
Open scapholunate
ligament repair and
capsulodesis
Luchetti Riccardo
WEBMINAR on SL lesion, 2013
Rimini (Italy)
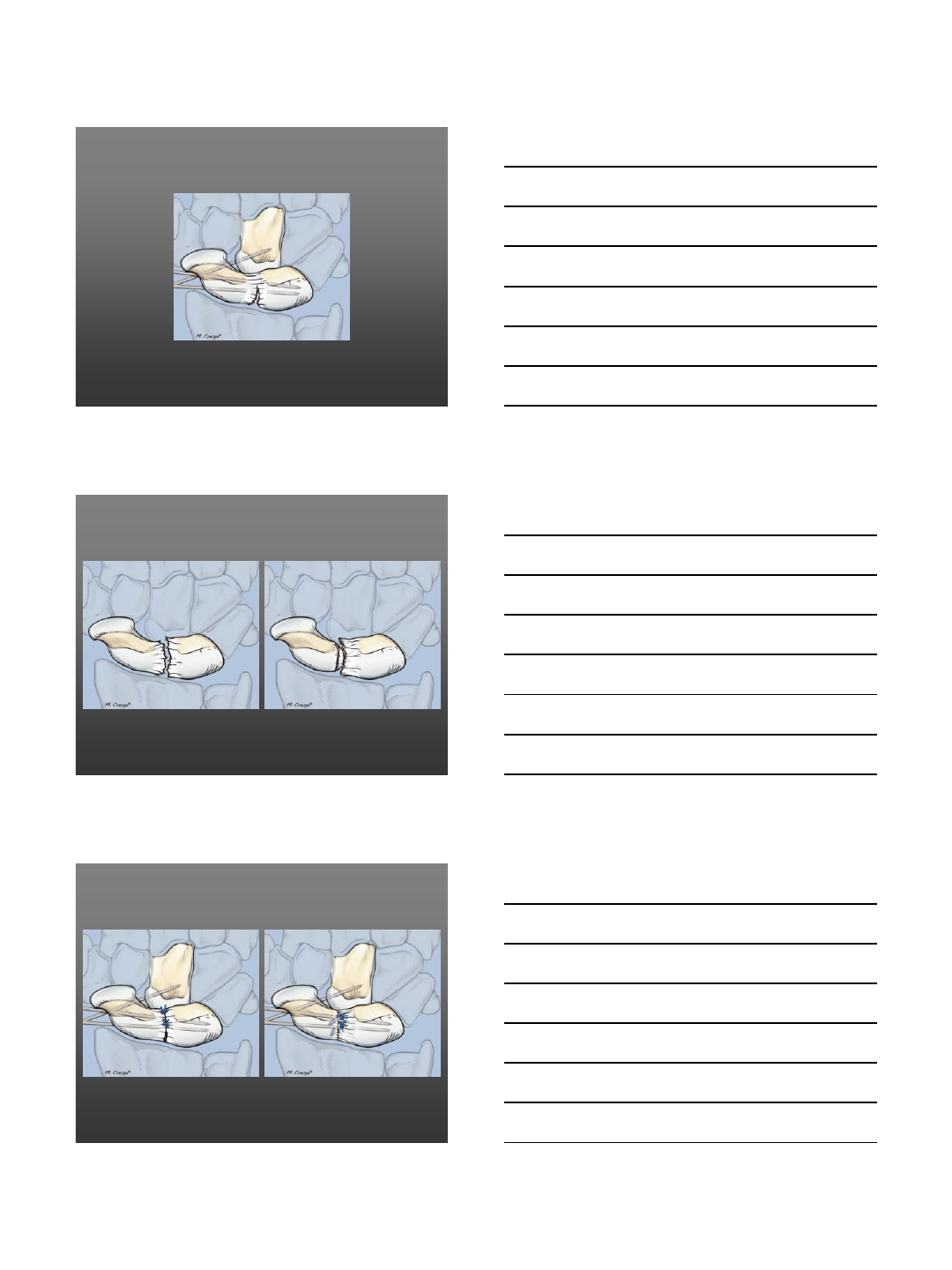
Partial injury
SL Repairable
Integrity STT lig
Reducible
Normal cartilage
yes no no no no no
yes yes no no no no
yes yes yes no no no
yes yes yes yes no no
yes yes yes yes yes no
Stage I II III IV V VI
Percutaneous
K-wire fixation
and/or Dorsal
capsulodesis Garcia Elias M
Partial injury
SL Repairable
Integrity STT lig
Reducible
Normal cartilage
yes no no no no no
yes yes no no no no
yes yes yes no no no
yes yes yes yes no no
yes yes yes yes yes no
Stage I II III IV V VI
Ligament repair + K-
wire fixation (+
Dorsal capsulodesis) Garcia Elias M
3/8/2013
2
3/8/2013
3
Algorithm of Treatment
•Arthroscopic Shrinkage & Pinning
•Open Repair
•Augmentation by Capsulodesis
•Reconstruction by B-L-B graft
•Reconstruction by Tenodesis
SLIL Tears
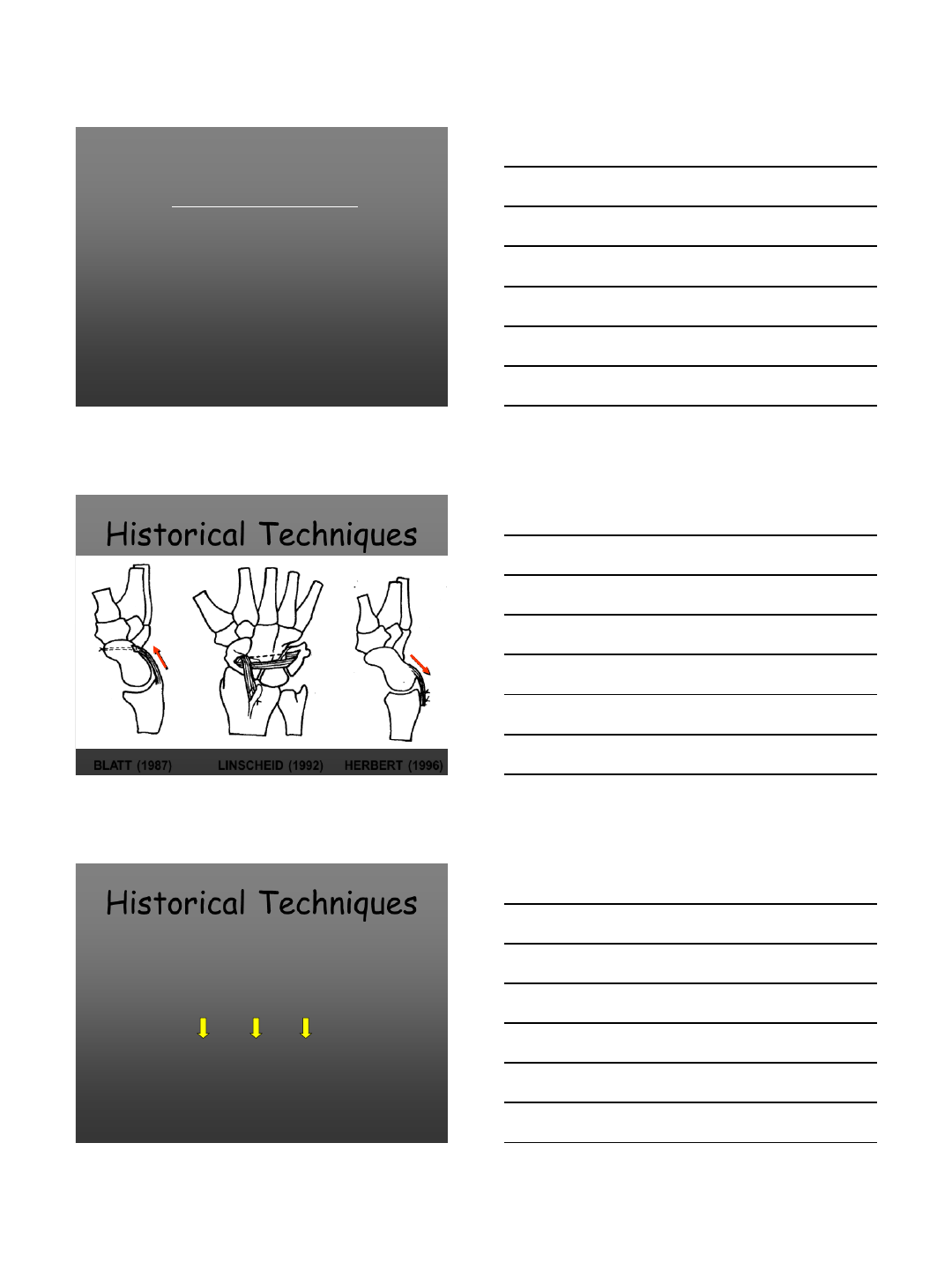
Historical Techniques
BLATT (1987) LINSCHEID (1992) HERBERT (1996)
•All of them crossed the radio
carpal joint
•Reduction of wrist flexion
Historical Techniques
3/8/2013
4
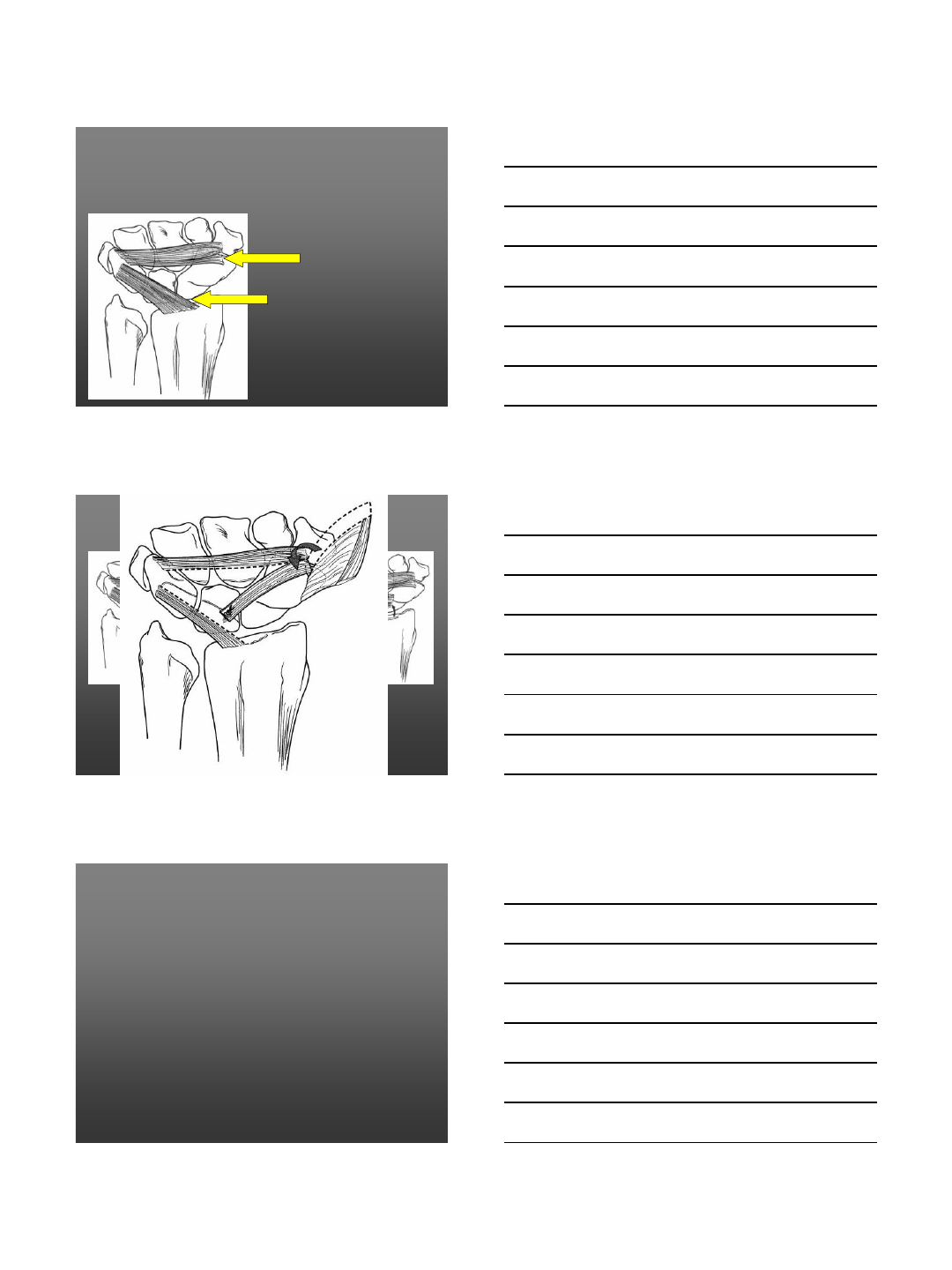
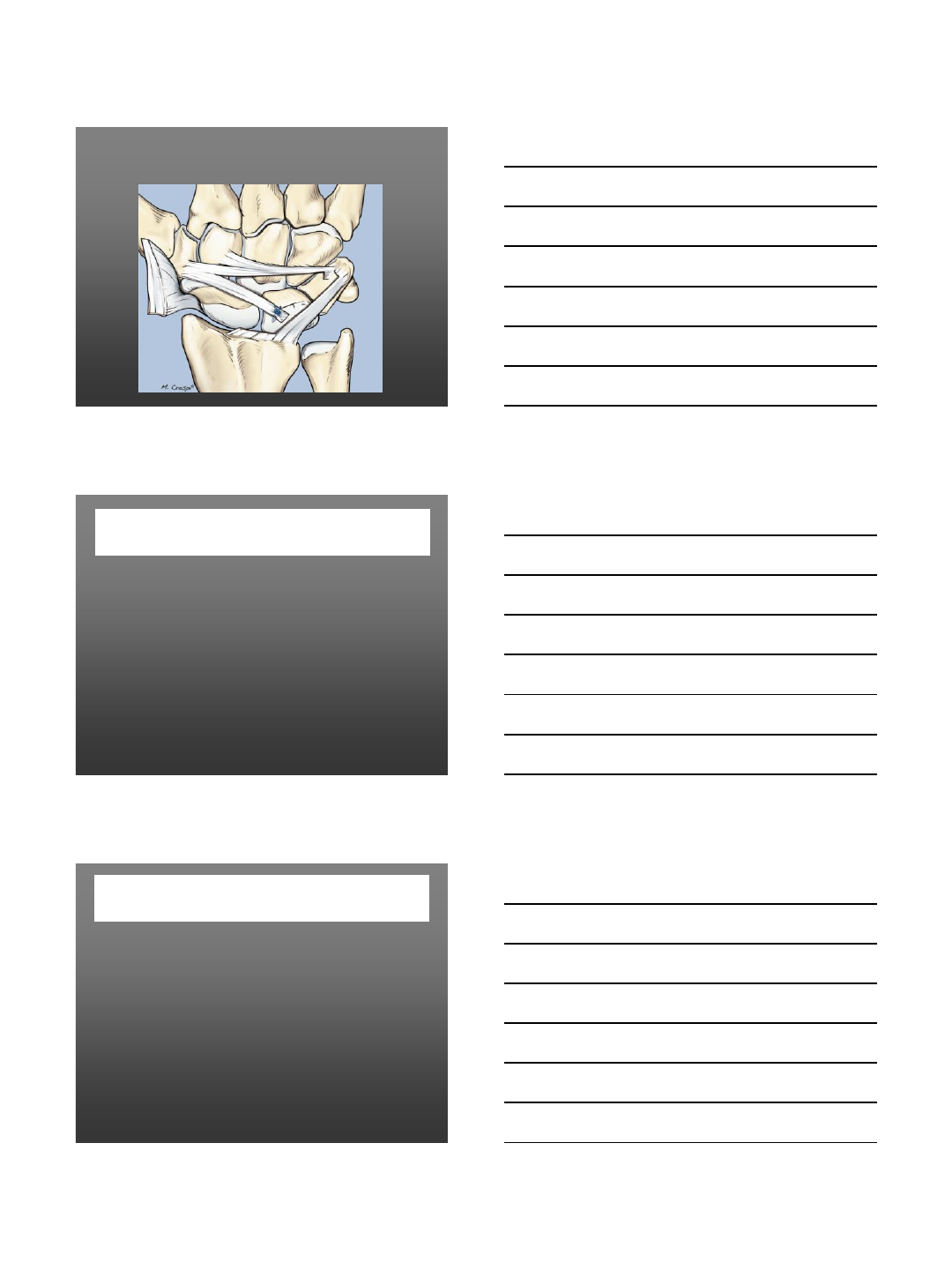
Dorsal ligaments
of the wrist
Dorsal Intercarpal Lig
Radio Triquetral Lig
Szabo Cohen Viegas
Options
Berger
Procedure
•Isolated
•Associated, with SLIL repair
3/8/2013
5
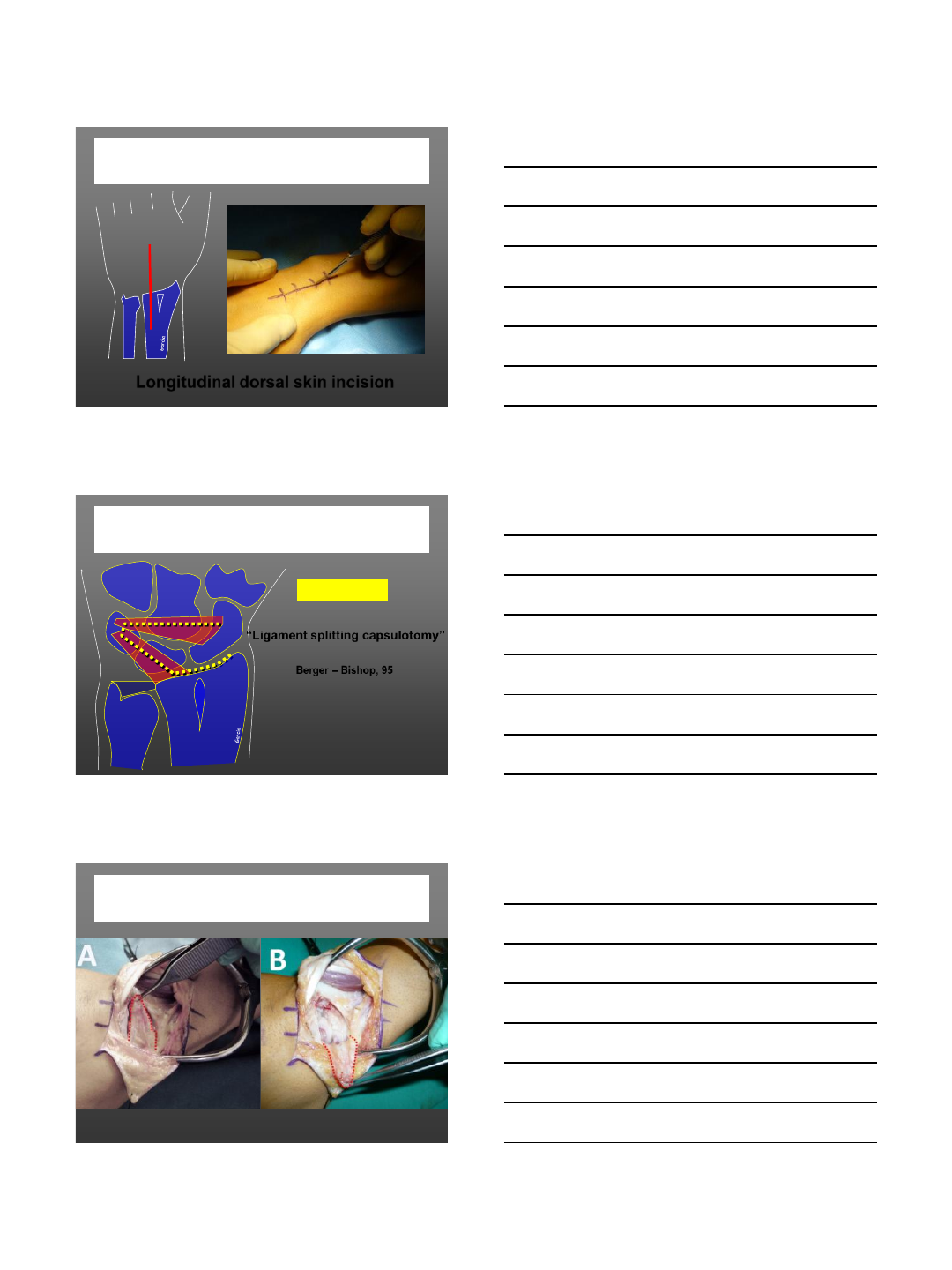
Surgical Technique
•Longitudinal skin incision
(Traditional)
•Transverse skin incision
(Short)
Surgical Technique
Traditional Technique
3/8/2013
6
Longitudinal dorsal skin incision
Surgical Technique
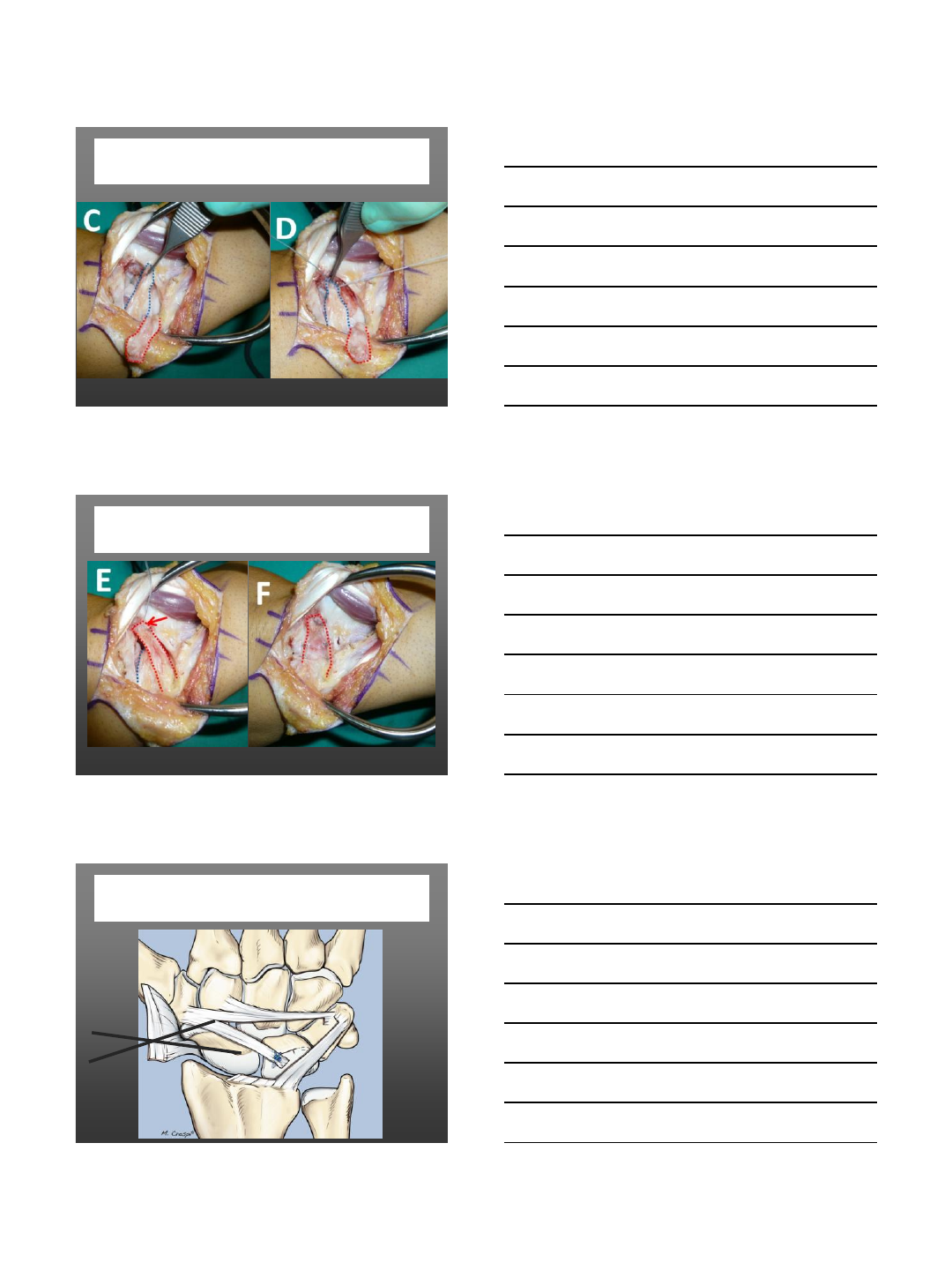
“Ligament splitting capsulotomy”
Berger – Bishop, 95
Capsulotomy
Surgical Technique
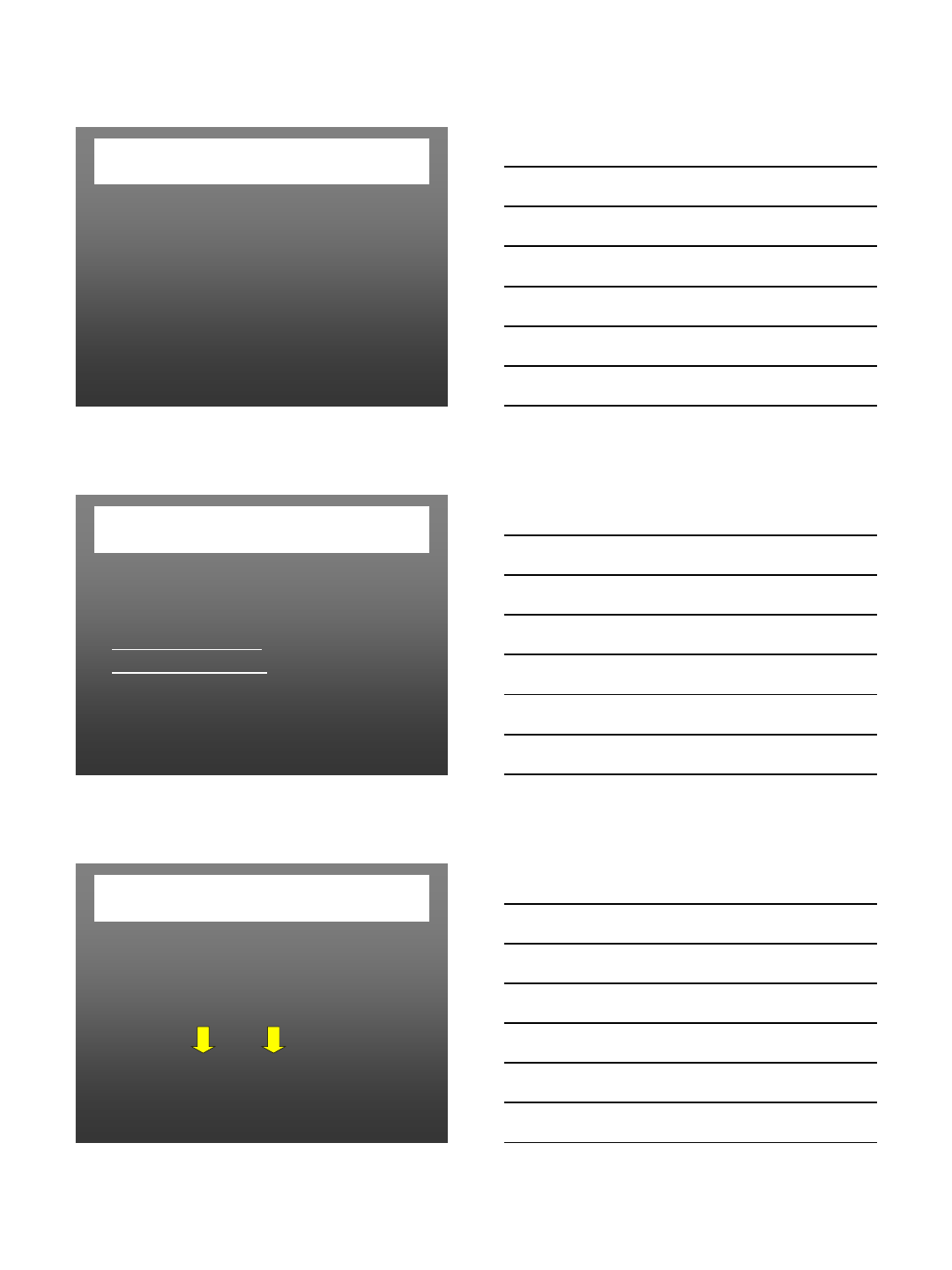
Surgical Technique
Step 1
3/8/2013
7
Surgical Technique
Step 2
Surgical Technique
Step 3
SL and SC pins fixation
3/8/2013
8
Present Series
•2001- 2004
•Cases : 18 (9 F, 9 M)
•Age (mean) : 35 y.o. (15 to 57 y.o.)
•Affected side : 11 L, 7 R
•Type of lesion : all hyperext. but one
•Time elapse from injury to surgery : 10 mo
(2 to 24 mo)
•Watson test ++ in all cases
Wrist ARS
•RC and MC ARS (18 cases)
–SL instability: 100% (Geissler type 3)
•Correlation with MRI : 87%
•Correlation with x-ray : 56%
ARS: gold standard
Type of SLIL lesion
•Partial (stage 1) = 14
•Complete (stage 2) = 4
with SLIL tear
but still repairable
3/8/2013
9
Postop Rehab
•Spica cast immobilization for 4 weeks
–Immediate finger mobilization
–Hand edema drenage
•Rehab after first month
–Active and passive wrist mobilization
•Wrist splint protection for one month more
•Return to work after 3 months
•Sport activity after 3 months
Case # 1
•AA, f, 32 years old,
right dominant.
•Right partial SLIL tear
•MRI positive
•Watson test: positive
•MWS: 70
Wrist Arthroscopy
•SLIL instability
type 3° according
with Geissler
RC
MC
Case # 1

3/8/2013
10
Results
•Pain: 2
•Complete wrist ROM
•Grip strength increased
•Retur to previous work
•Watson test: negative
•MWS: 100
Case # 1
Case # 2
•CAS, f, 55 years old, right
dominant.
•Right wrist partial SLIL
tear
•X-rays: positive
•MRI: doubtful
•Watson test: positive
•MWS: 85
Case # 2
3/8/2013
11
Case # 2
Follow up at 1 month
Case # 2
•Pain: 0
•Incomplete wrist ROM
•Grip strength: 100%
•MWS: 95
•Return to prev. work
F-up: 10 months
Pain (VAS) 8 5 <0,005
Flex – Ext (°) 127 123 ns
Grip Strength (Kg / %) 24 / 75 27 / 87 <0,05 / ns
MWS (Cooney) 62 84 <0,005
MWS (Krimmer) 72 90 <0,005
DASH 38 20 ns
Preop Postop Parameters p
Clinical Results
(F-up 15 mo)
Pts didn’t require any
more surgical procedure
18 cases
3/8/2013
12
AUTHORS # F-up Pain F/E
Grip
strength MWS
Comparison with literature
(months) (VAS) (%) (%)
Moran 31 54 83 70 73
Minami 17 49 87 93 83
Kobayashi 21 14 ? 81 ?
Luchetti 18 15 80 87 84
(Dorsal capsulodesis by using the DIC ligament)
Modification of the
Surgical Technique
According to the SLIL lesion
Clinical eval: Watson test +/-
X-ray: no DISI def
Arthroscopy: stage 2/3
Transversal dorsal skin incision
with ext. retinaculum preservation
Surgical Technique
Dreant, 2009
3/8/2013
13
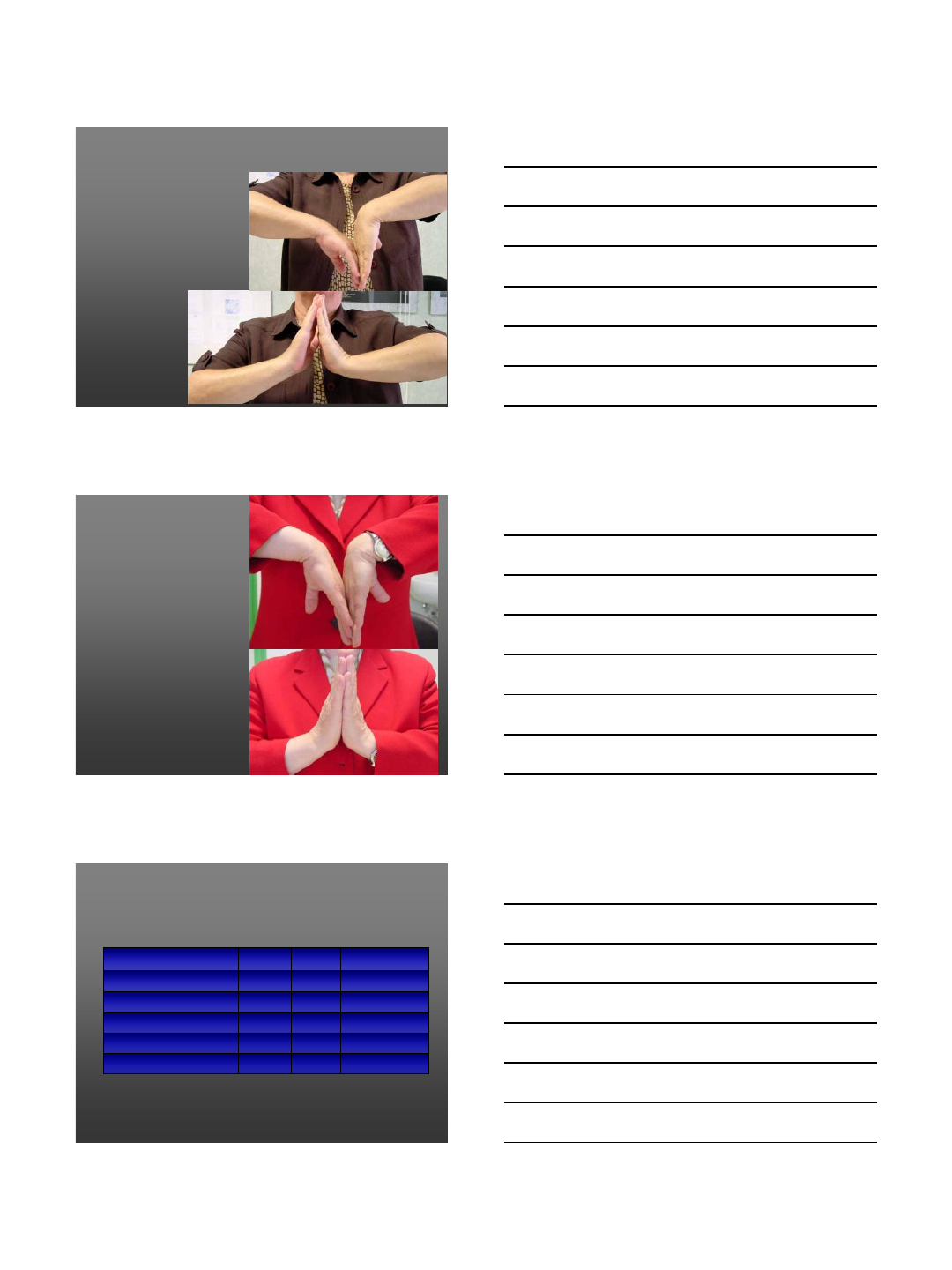
Double parallel incision with
dorsal capsule preservation
Surgical Technique
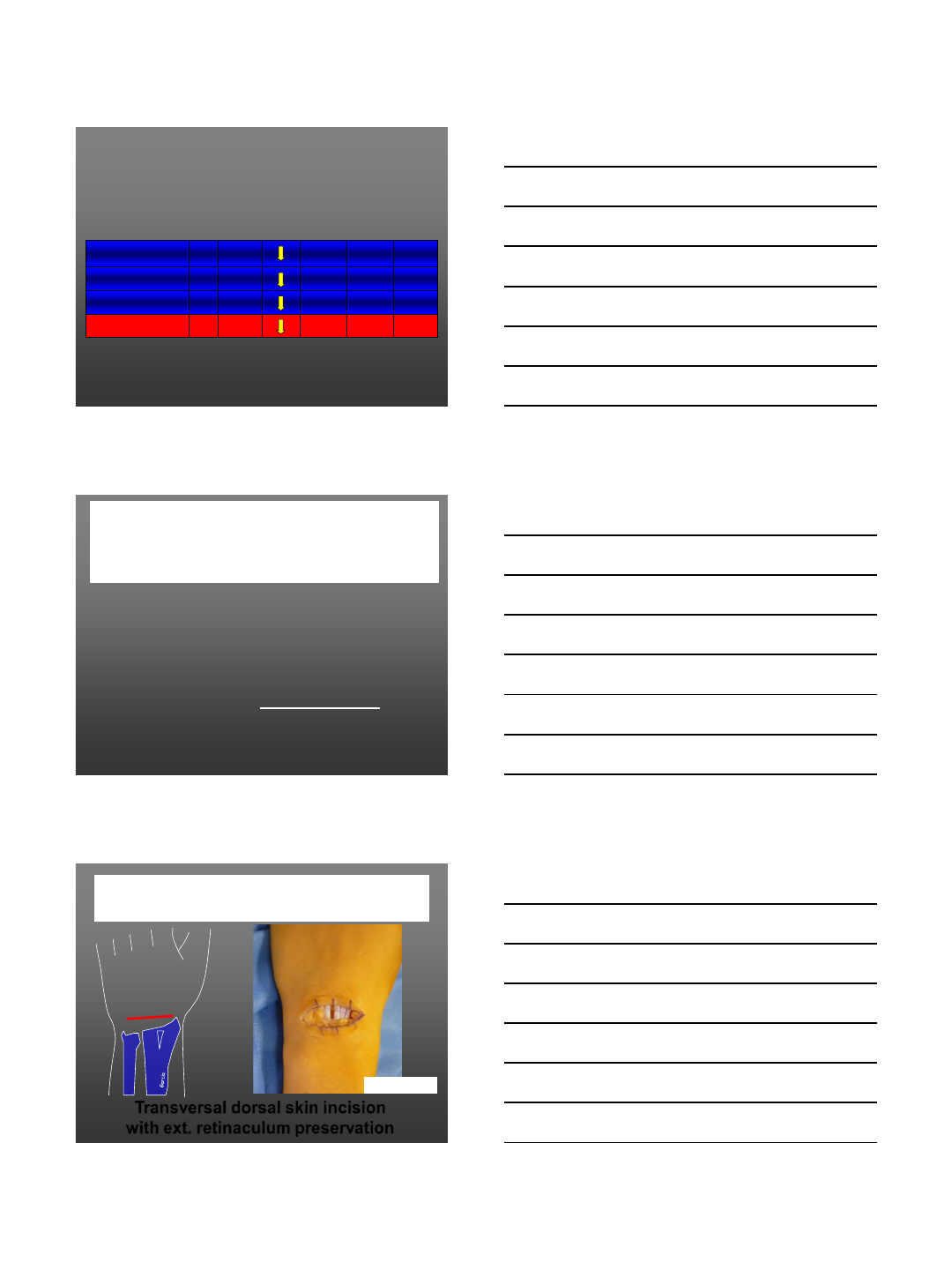
“Double parallel capsular incisiones
Capsulotomy
Surgical Technique
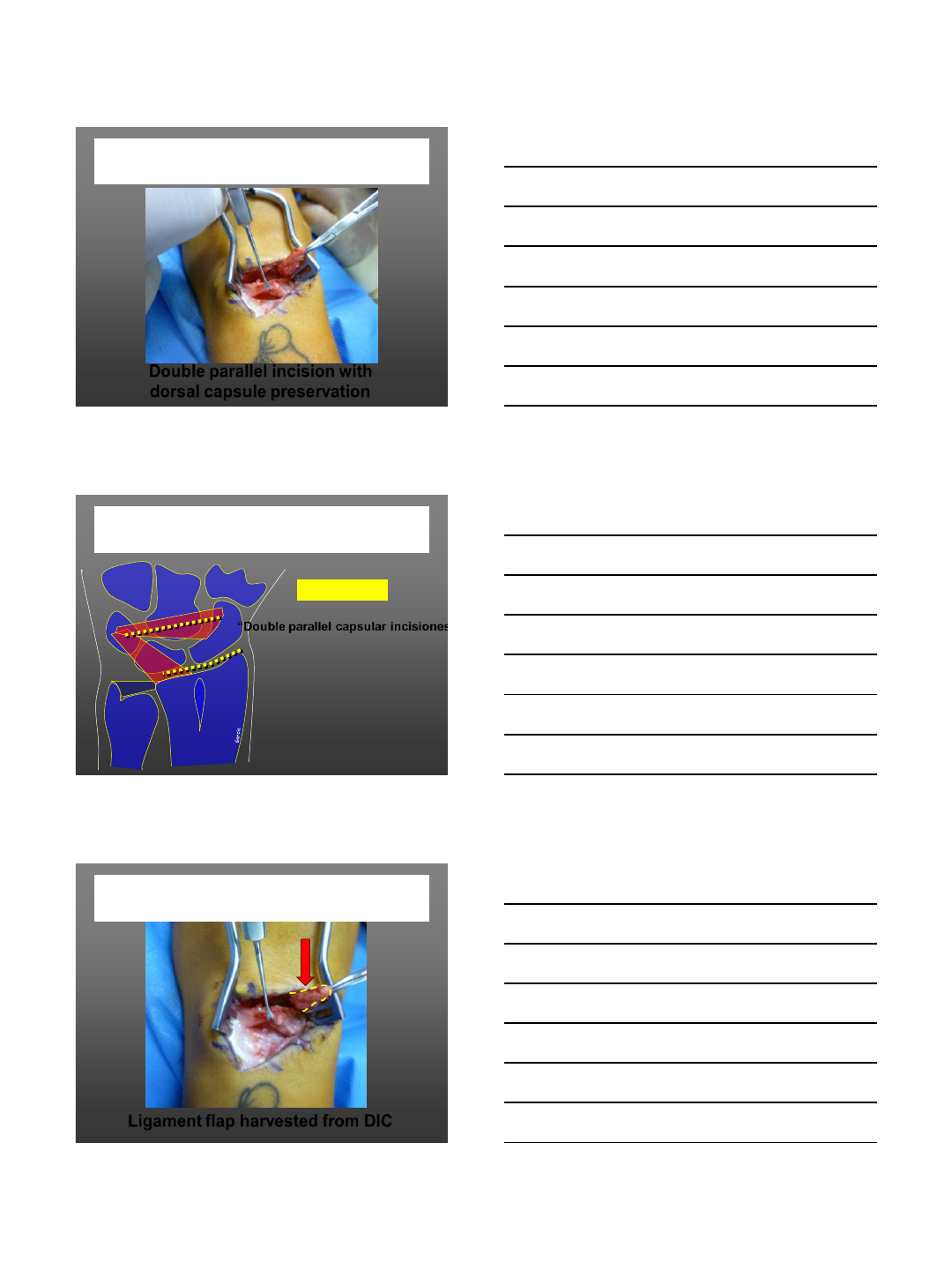
Ligament flap harvested from DIC
Surgical Technique
3/8/2013
14
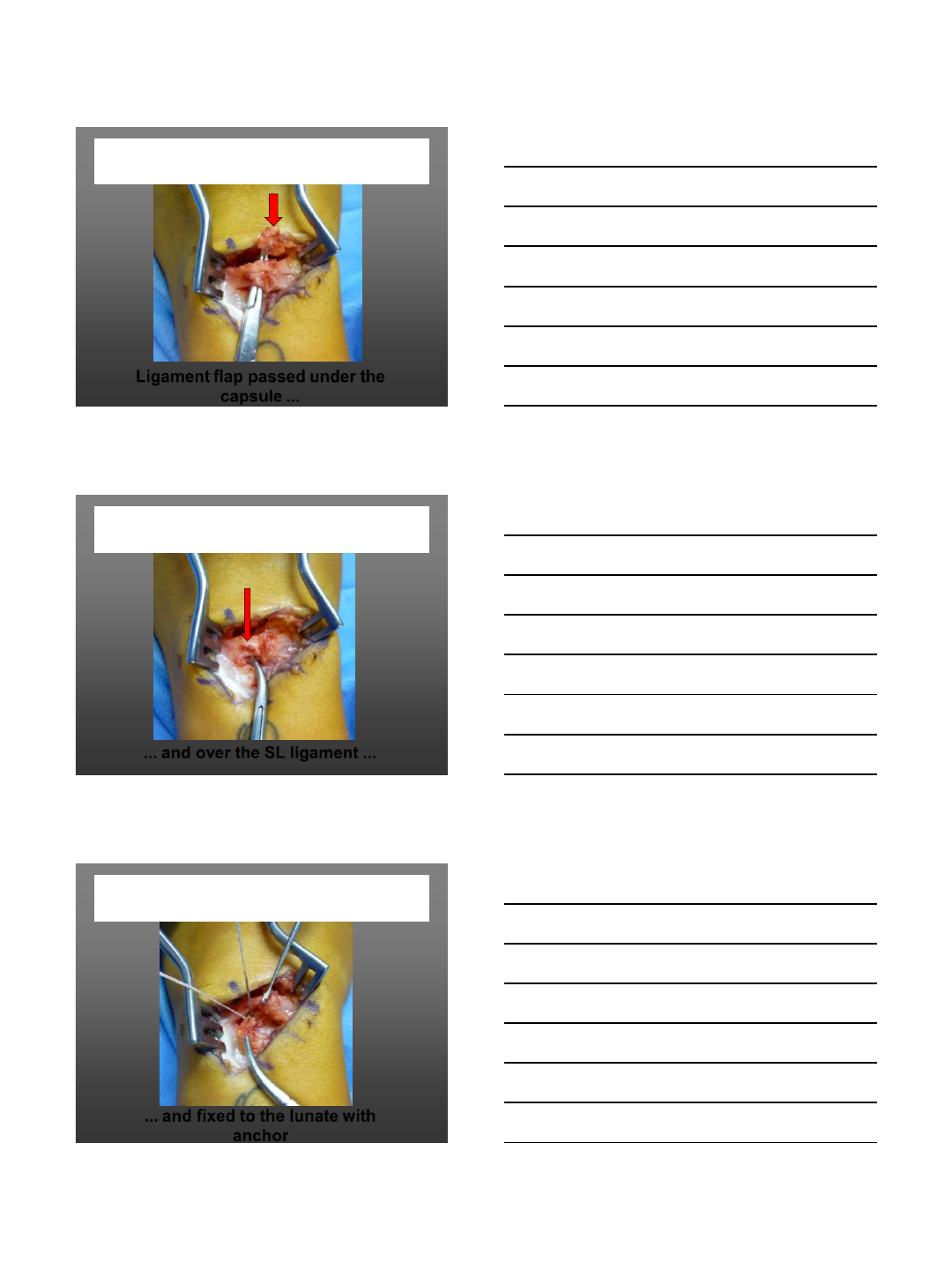
Ligament flap passed under the
capsule ...
Surgical Technique
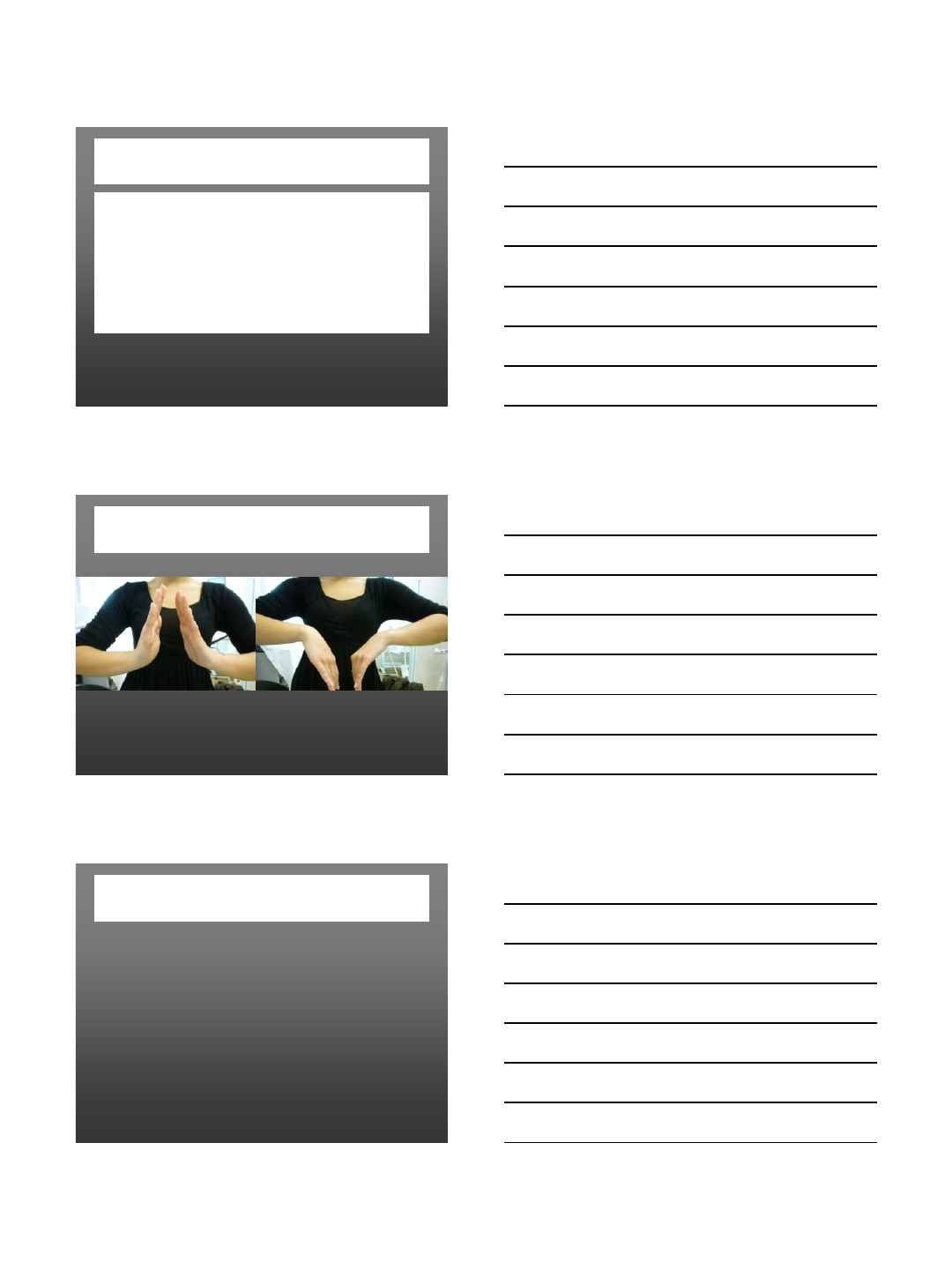
... and over the SL ligament ...
Surgical Technique
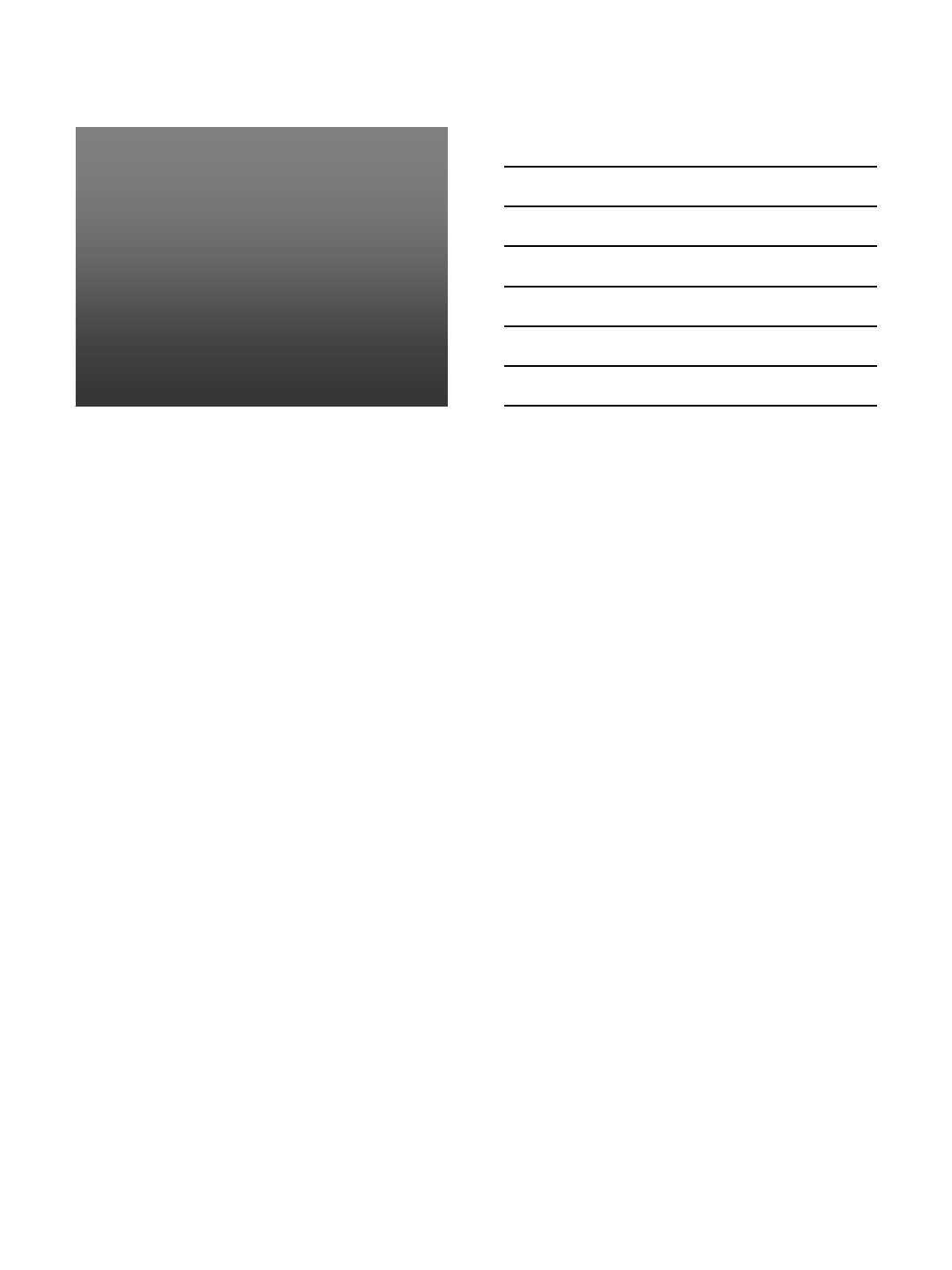
... and fixed to the lunate with
anchor
Surgical Technique
3/8/2013
15
Postop Rehab
•Immobilization (for 3 weeks)
•Earlier rehabilitation
Same results
… even better, related to minor SL lesion
Conclusion
•Valid surgical procedure
•Indication for stage 1 to 3 (with
SLIL repair)
•Easy technique
• Patients’ informed consent
about the risk of partial lost of
wrist flexion
3/8/2013
16
Thanks for your attention
3/8/2013
1
www.wrightington.com 1
Results of a Modified Brunelli Procedure
for Chronic Scapholunate Instability
www.wrightington.com 2
Wrightington Hospital, UK
www.wrightington.com 3
Sir John Charnley
“Never operate on a bone that you can swallow”
3/8/2013
2
www.wrightington.com 4
Some things have changed
www.wrightington.com 5
Some things have changed
www.wrightington.com 6
3/8/2013
3
www.wrightington.com 7
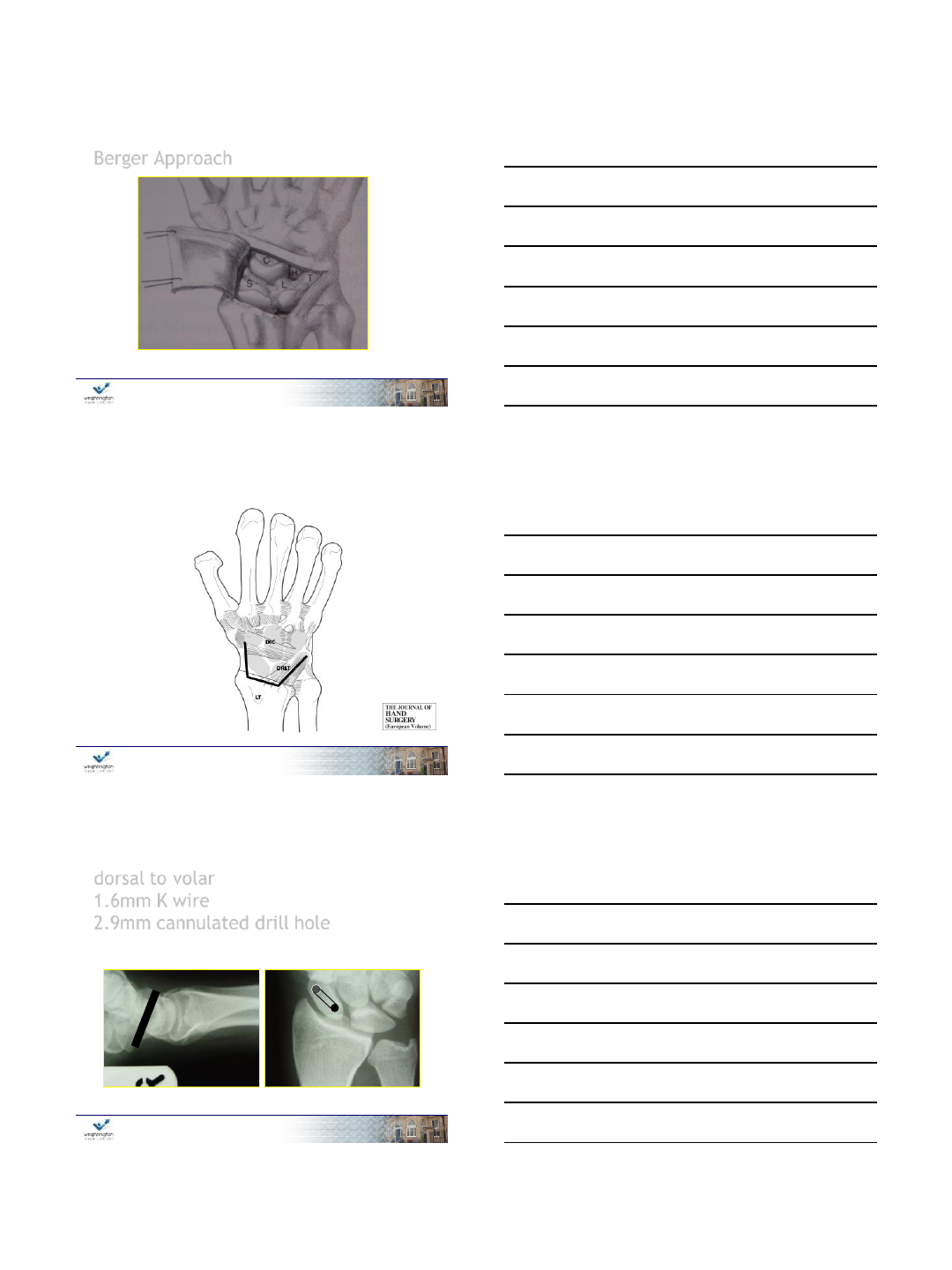
Berger Approach
www.wrightington.com 8
Anakwe R E e t al. J Hand Surg Eur Vol
2012;1753193412453414
Copyright © by The British Society for Surgery of the Hand
www.wrightington.com 9
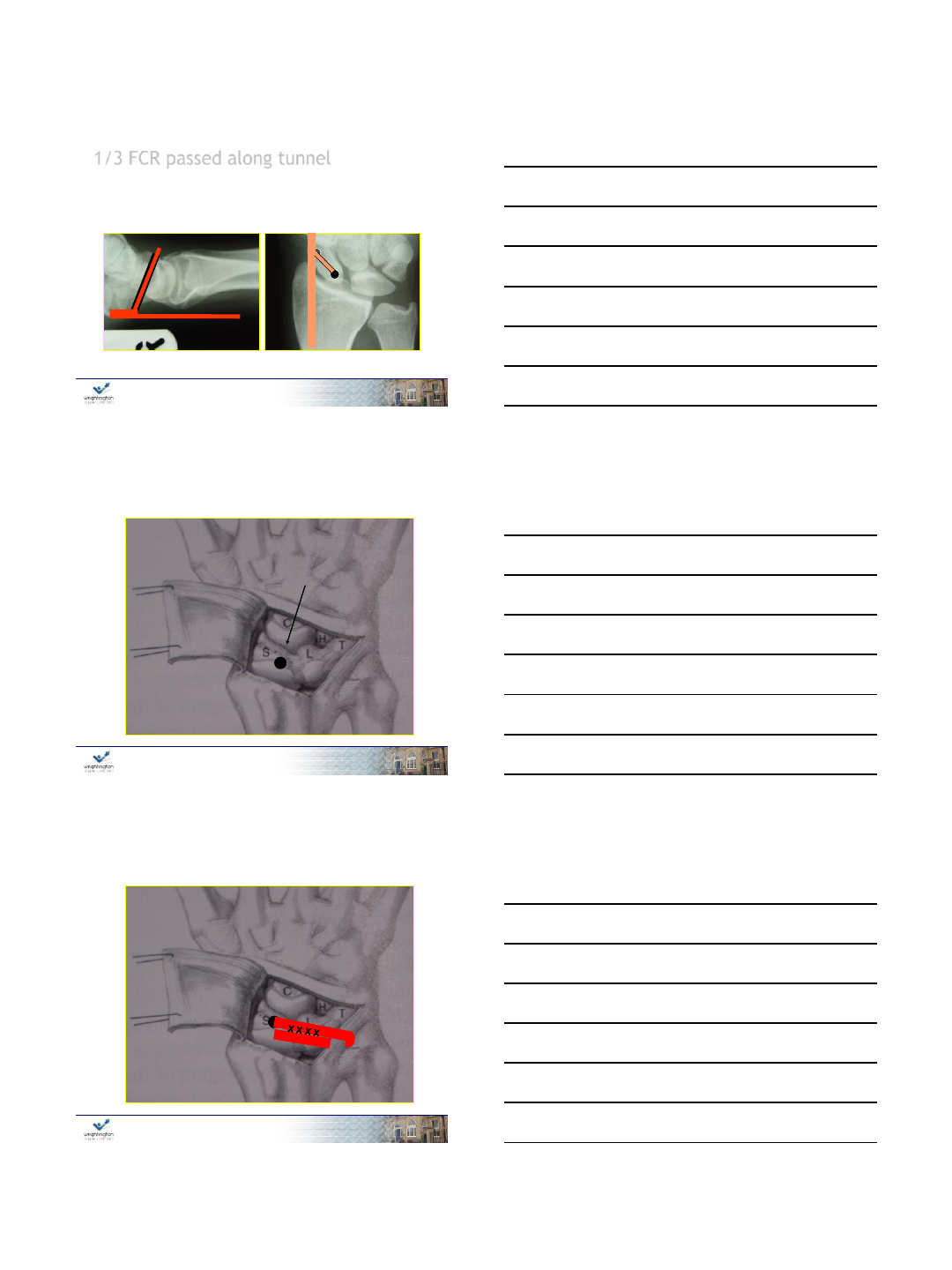
dorsal to volar
1.6mm K wire
2.9mm cannulated drill hole
3/8/2013
4
www.wrightington.com 10
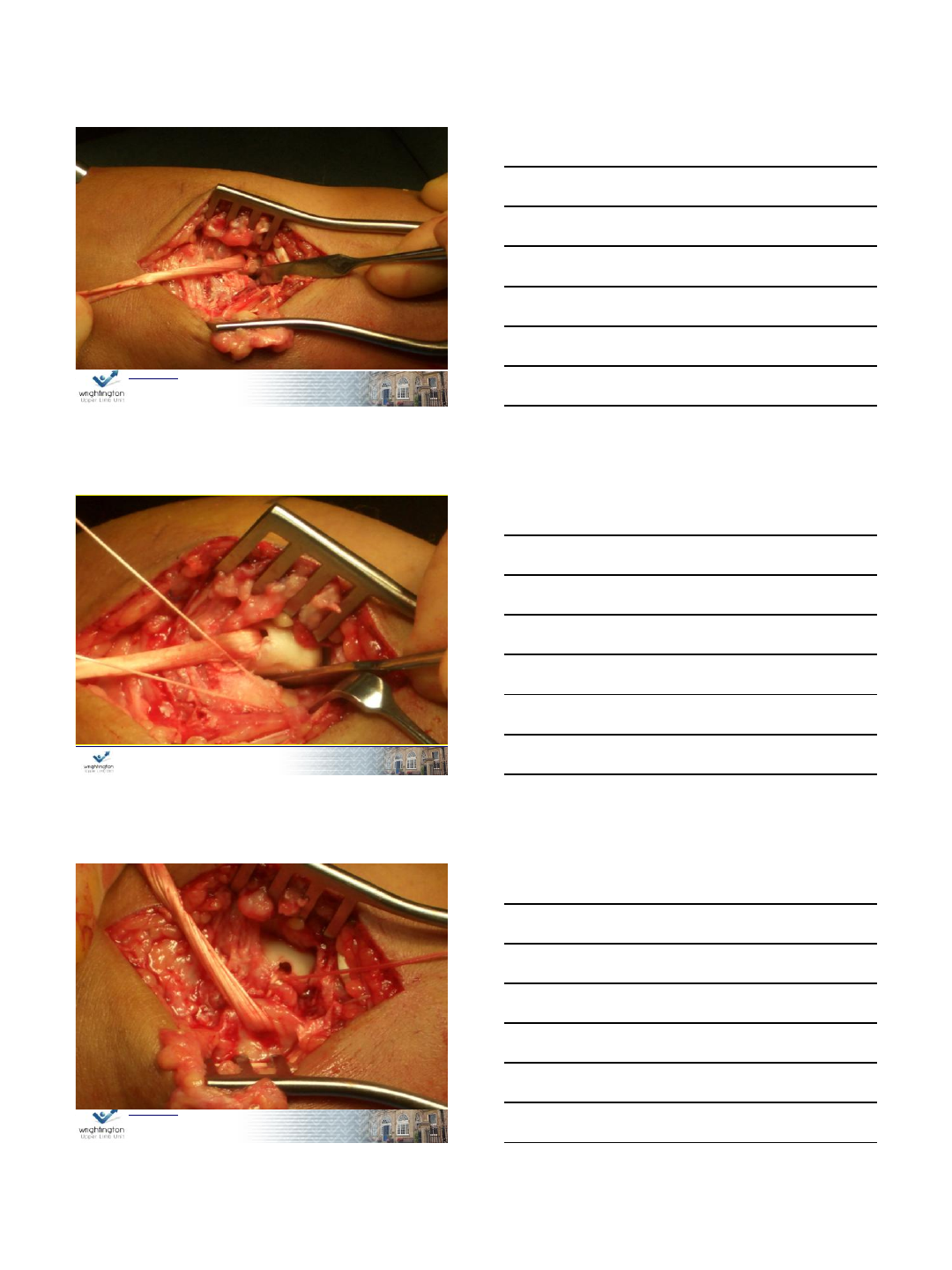
1/3 FCR passed along tunnel
www.wrightington.com 11
Emerges here
www.wrightington.com 12
Brunelli IV
Tri Ligament tenodesis
Stanelli
3/8/2013
5
13
www.wrightington.com 13
www.wrightington.com 14
15
www.wrightington.com 15
3/8/2013
6
16
www.wrightington.com 16
www.wrightington.com 17
www.wrightington.com 18
Methods
162 patients with chronic SLD ‘95-02
Part 1
Postal questionnaire
VAS
Problem solve
WWS
Satisfaction
Surgery again
Compensation
3/8/2013
7
www.wrightington.com 19
Methods
162 patients with chronic SLD ‘95-02
74 Male 88 Female
Part 2
Clinical review
Grip Strength
Range of movement
Employment status
www.wrightington.com 20
Results
Part 1 Questionnaire
117 replied (72%)
Male 52 Female 65
Mean follow up 50.2 months (9-100)
Part 2 Clinical Review
55 Reviewed
Male 25 Female 30
Mean follow up 45.1 months (10-98)
www.wrightington.com 21
Wrightington Wrist Score
Hand in back pocket
Straight lift grip
Take change
Personal care
Hand to face
Use a screw driver
Do usual work
Rise from a chair
•1=no problem
•2= with difficulty
•3= with aid
•4= unable
8 = best score
32 = worst score
3/8/2013
8
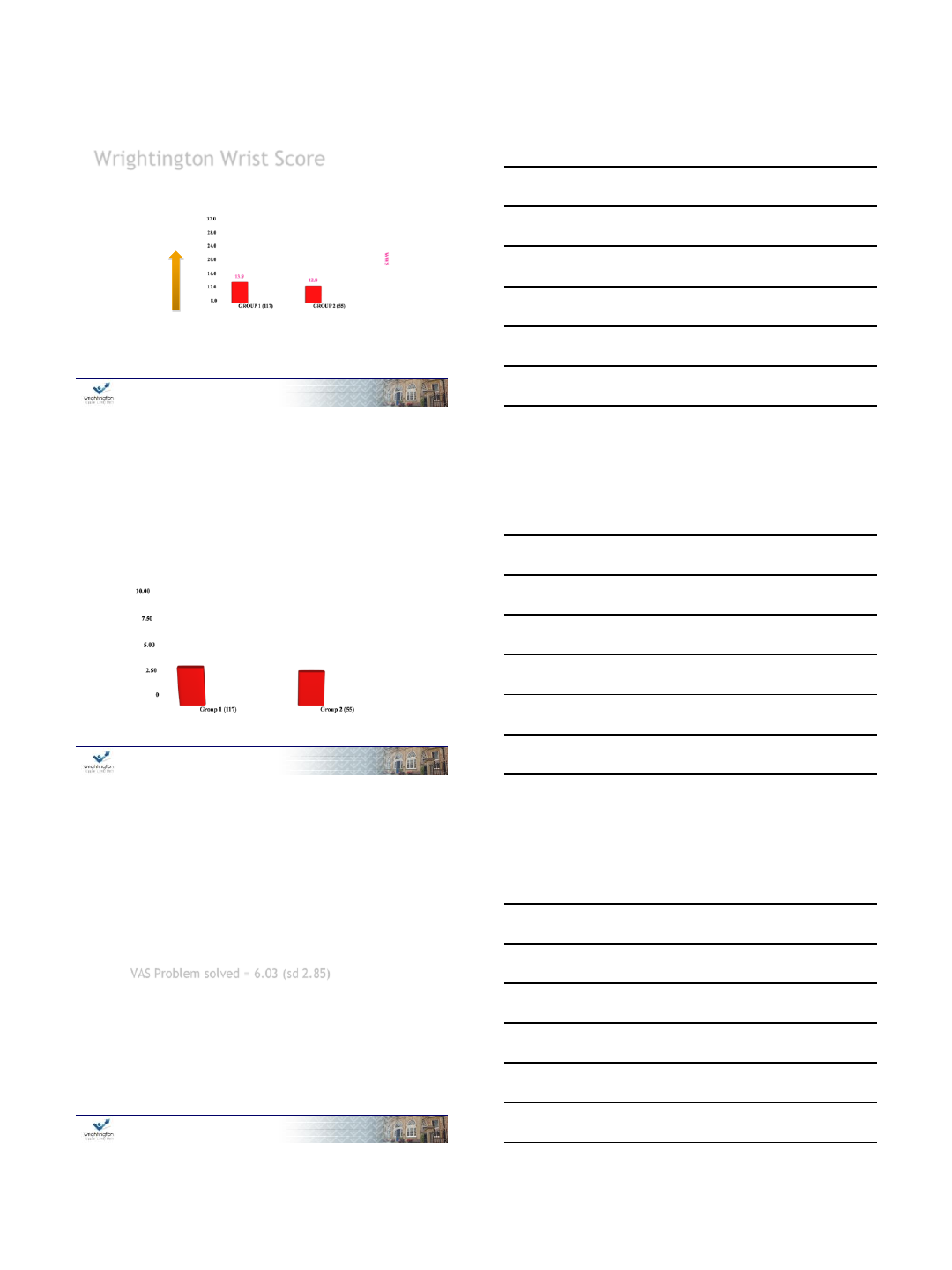
www.wrightington.com 22
Wrightington Wrist Score
Worse
www.wrightington.com 23
VAS PAIN
VAS PAIN
www.wrightington.com 24
VAS Problem solved = 6.03 (sd 2.85)
Completely cured
Not at
all
VAS Problem solved = 6.77
S.D. = 2.71
3/8/2013
9
www.wrightington.com 25
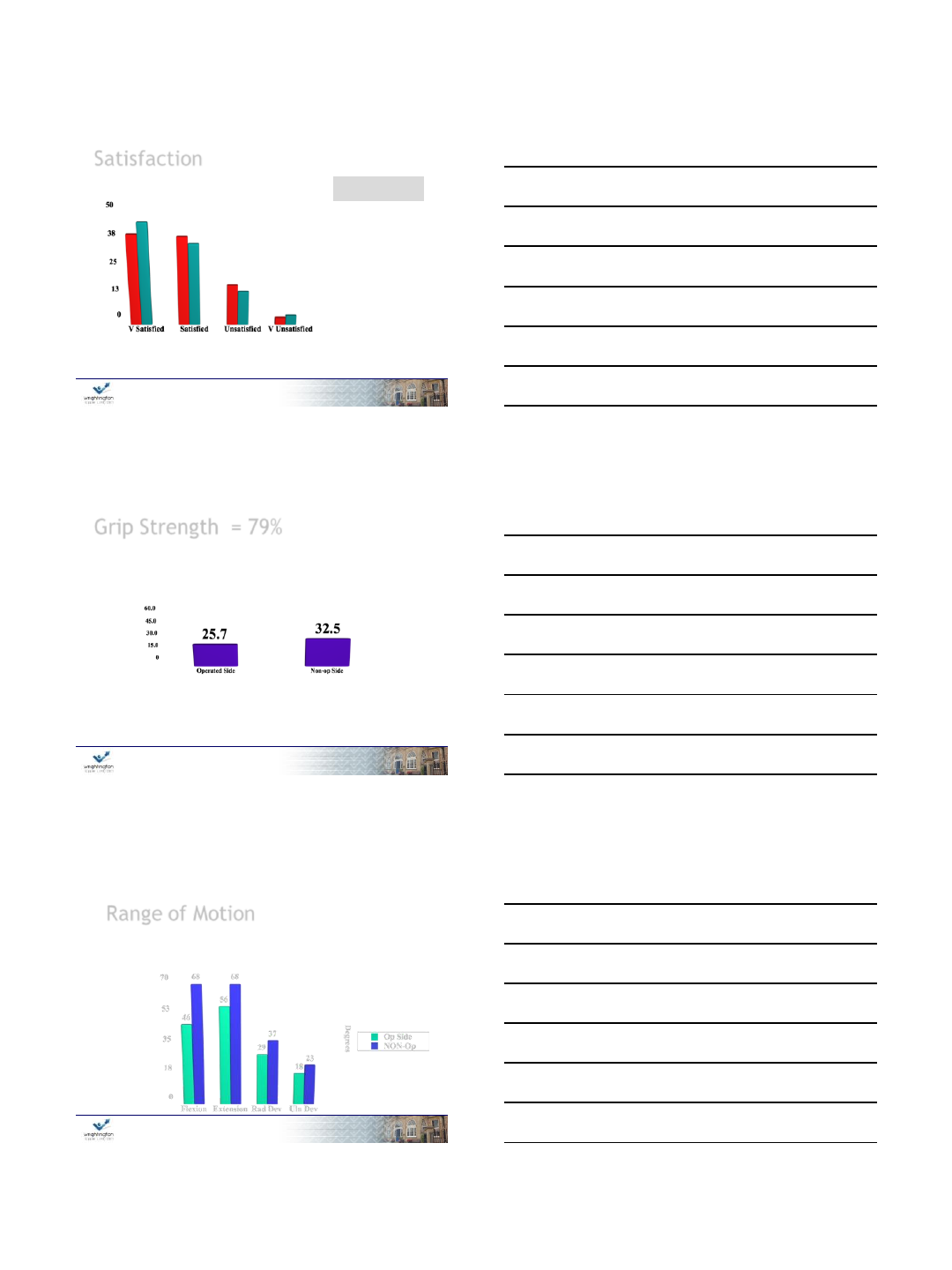
Satisfaction
%
81%
19%
All responders
Reviewed
www.wrightington.com 26
Grip Strength = 79%
www.wrightington.com 27
Range of Motion
35˚ Loss of Flexion - Extension (26% of non operated side)
13˚ Loss of Radial - Ulnar deviation (12%)
3/8/2013
10
www.wrightington.com 28
Employment
21 (34%) of those reviewed were taking part in
heavy or light manual labour
4% unemployed
24 patients (43%) had changed their occupation
or duties
www.wrightington.com 29
Surgery again ?
88% would have the same again overall
30
www.wrightington.com 30
30
3/8/2013
11
Ashleigh Williams1, Chye Yew Ng 2, Mike Hayton 2
Outcomes of Modified Brunelli
Procedure in Professional
Athletes with Scapholunate
Instability
1 University of Manchester, Manchester, UK.
2 Wrightington Hospital, UK.
Presented BSSH 2012 York
www.wrightington.com 32
Methods
Retrospective review
All procedures performed by senior author (MJH)
16 professional athletes who underwent a modified Brunelli
procedure between 2008 - 2011 identified from the database
Patients were emailed a
questionnaire and Fup
telephone interview
11 rugby 1 golf
15 patients replied
1 motor cycling
(bilateral wrist)
2 boxing
www.wrightington.com 33
Results
Patient demographics
Number of operations 16
Age Mean 30 years (range 18 - 42)
Gender All male
Dominance of hand operated on 9 dominant, 7 non dominant
Level of competition before injury 9 international, 7 national
Time to surgery after injury Mean 30 weeks (range 2 - 78)
Follow up Mean 24 months (range 3 - 43)
3/8/2013
12
www.wrightington.com 34
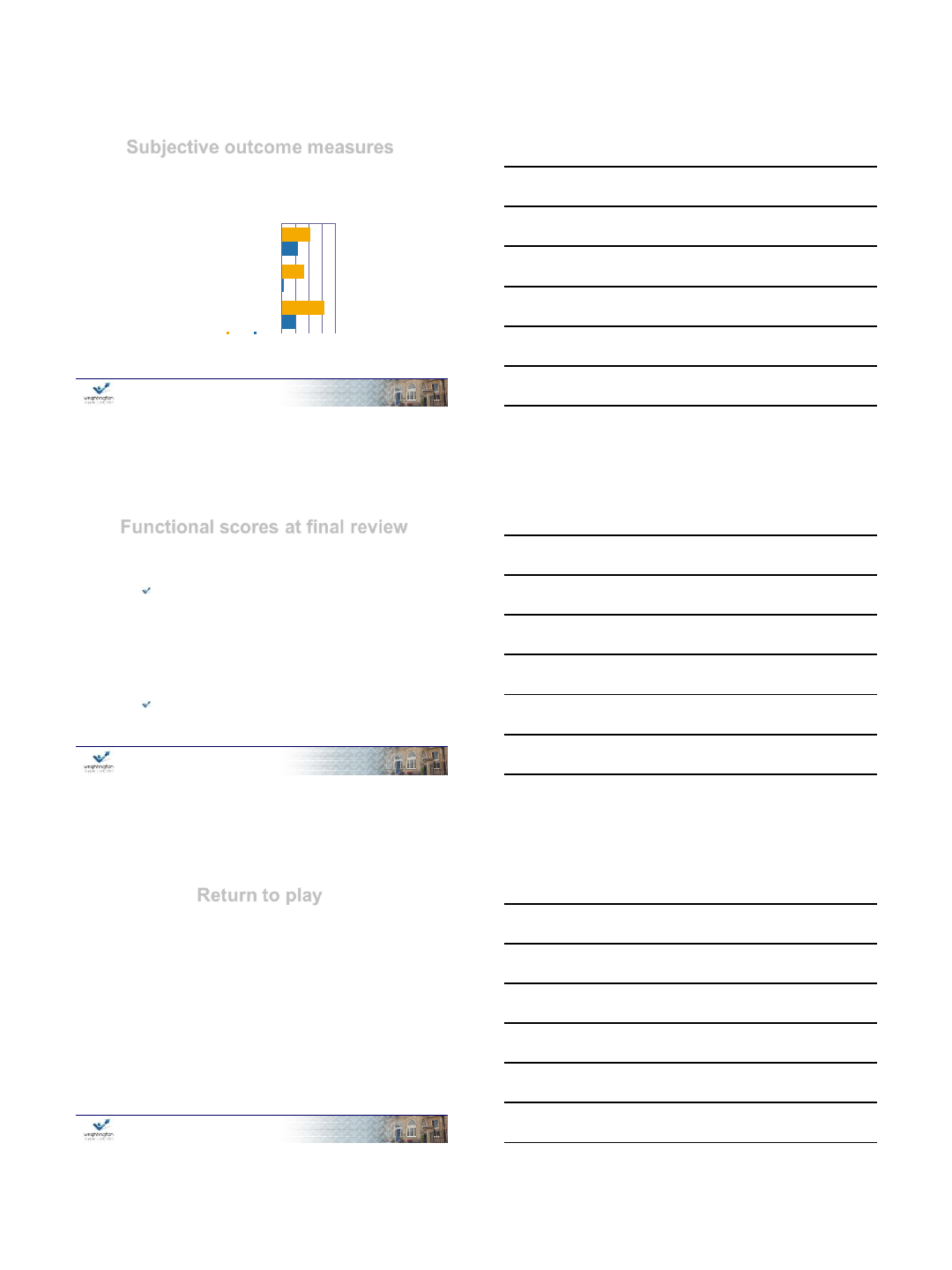
Subjective outcome measures
0.0000 2.5000 5.0000 7.5000 10.0000
Instability
VAS pain
score at
REST
VAS pain
score
ACTIVITY
Preoperative Postoperative
VAS (Visual Analogue Score)
Error bar showing SEM (standard error of mean)
Mann-Whitney U test
p value
0.047
<0.001
<0.001
www.wrightington.com 35
Functional scores at final review
Quick DASH
7.66 SEM 2.11 (range 0-25)
Wrightington activity of daily living,
assessment for wrist function2
(8 is normal – 32 most abnormal)
9.25 SEM 0.38 (range 8-13)
2 Talwalkar SC, et al. J Hand Surgery (British and European Volume) 2006; 31: 110-117.
www.wrightington.com 36
Return to play
• 10 of 15 (67%) returned to play at their pre-injury
level of competition.
•5 of 15 (33%) returned to a lower competition
level: - 3 directly related to the wrist injury
- 2 due to other unrelated injuries
But for other injuries 12 out of 15 (80%)
returned to playing
3/8/2013
13
www.wrightington.com 37
Summary
Modified Brunelli procedure in professional
athletes generally
Relieves wrist pain with (p<00.1)
Appears to improve stability (not significant)
Improves functional outcome scores
But for other injuries 12 out of 15 (80%)
returned to playing
www.wrightington.com 38
Thank you
