The Successful Future Of TKA Digging Your Way Through Bundle Syllabus
2015-10-05
: Pdf The Successful Future Of Tka Digging Your Way Through The Bundle Syllabus The_Successful_Future_of_TKA__Digging_Your_Way_Through_The_Bundle_Syllabus 10 2015 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 39
10/5/2015
1
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Migration of care in TJA
Steven B. Haas MD, MPH
Chief, Knee Service
John N. Insall Chair, Knee Surgery
The Hospital for Special Surgery
New York, NY
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Disclosure
•Smith & Nephew Orthopaedics
•Designer (Royalty income), Consultant and Research
Support on Knee Products
•APOS Therapy
•Medical Advisory Board
•SandDance Technology
–Ownership
•IMP
–Royalty
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Migration of care in TJA in 2015
●Improved knowledge
●Entire care pathway practices
●Improved technology
●Patient factors
●Increasing life expectancy
●Expanding indications
●Millennium patient
●No longer primarily geriatric orthopedics
●More demanding patients
●ALL ROADS LEAD TO RAPID RECOVERY
●Both in ASCs & Hospitals
10/5/2015
2
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Why do we care about rapid
recovery?
●Is it for the science?
●Current consensus is that mid-term
to long-term results are similar
regardless of short-term results
●Available resolution of measurement tools?
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Why do we care about rapid
recovery?
●“It’s not about how much money you spend, it’s about where you
spend the money you have.” - Fred Cushner, MD
●COST CONTAINMENT
●Global endeavor
●Decrease in healthcare $
●Decrease available patient resources
●If you’re not careful:
●Can affect patient care
●Your quality
●Disempowers surgeon
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Why do we care about rapid
recovery?
●COST CONTAINMENT = improve efficiencies
●Technique
●Implant cost
●Pharmacy
●OR utilization
●Ancillary services
●Nursing utilization
●Discharge status
●Acute Rehab
●Nursing facility
●Home
●Hospital Length of Stay
10/5/2015
3
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Implant
Technologies Technique
Factors that may matter for recovery
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Technique is important
●But not enough by itself
●MIS approaches
●Most important to do the surgery well
●Blood conservation techniques
●Alternative anesthesia
●Multimodal pain control
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Implant
Technique
Factors that may matter for recovery
Technologies
10/5/2015
4
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
New Technologies to Improve
Efficiency & Outcome
•Visionaire –PSI
•FastPaK –Disposable Instruments
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
New Technologies that
May Improve Outcome
•Orthosensor - Intraop Balancing Sensors
•Blue Belt –Robotic Navigated Surgery
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
TechniqueTechnologies
Factors that may matter for recovery
Implant
10/5/2015
5
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Technology needs to
meet patient expectations
and demands
•Our Younger Active Patients
want to:
Skiing Golfing Racket Sports
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
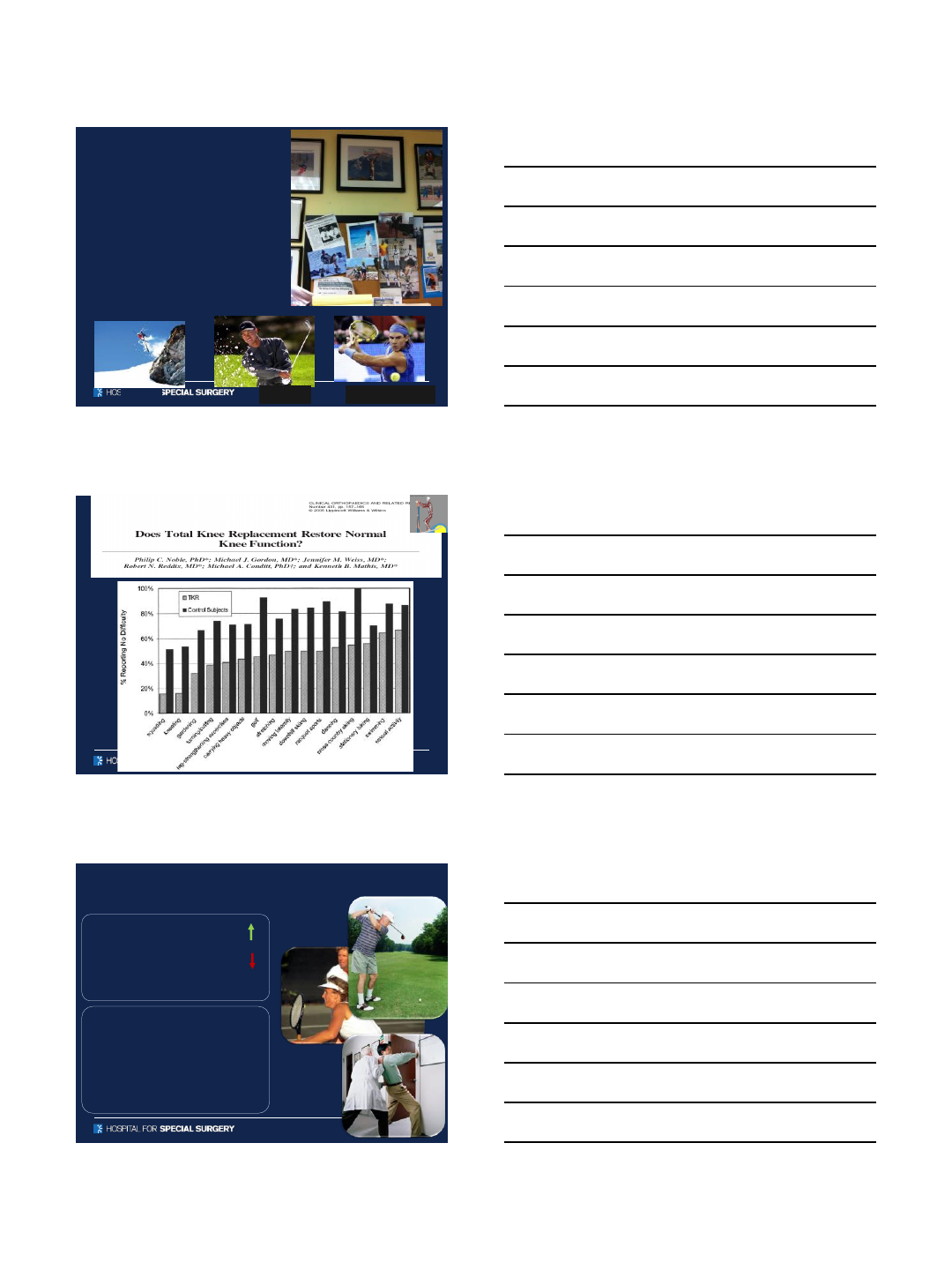
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Performance/Satisfaction of TKA’s v THA?
•Post THA: sports activities increased
from 36% to 52%
•Post TKA: sports activities decreased
from 42% to 34%
The Ulm Osteoarthritis Study- K Huch
•Up to 20% of patients are not satisfied
with the outcome following total knee
replacement
•Only 82% to 89% of primary TKA
patients are satisfied
J Bone Joint Surg Br. 2010 Sep;92(9): Scott CE,
Howie CR, MacDonald D, Biant LC
Clin Orthop Relat Res. 2010 Jan;468(1):57-63: Bourne
RB, Chesworth BM, Davis AM, Mahomed NN, Charron
KD
10/5/2015
6
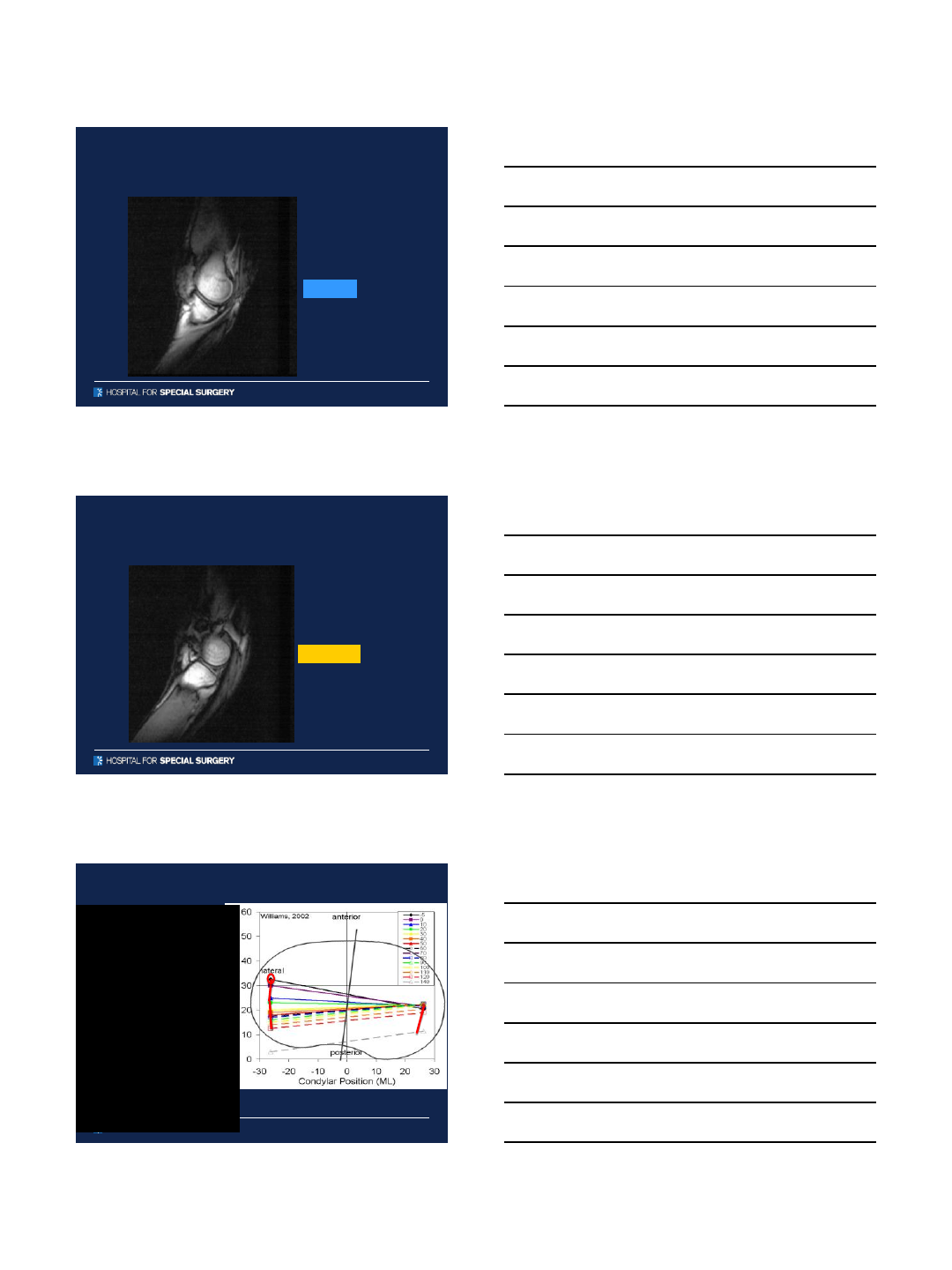
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
“Understanding Normal Knee Kinematics
Better –A Dynamic MRI Study”
A. Williams M.D. JBJS 2002
MEDIAL
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
“Understanding Normal Knee Kinematics
Better –A Dynamic MRI Study”
A. Williams M.D. JBJS 2002
LATERAL
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
•0°(Full Extension)
–Screw-home
(5°femoral internal axial
rotation)
–Posterior femoral condyle
nearly flush with posterior tibia
•0-90°
–Medial pivot
(rollback + femoral external
axial rotation)
–Q-angle minimized
(quad mechanism in straight
line)
•90-155°
–Posterior femoral translation
–Axial rotation ceases
Kinematics –Normal Knee
10/5/2015
7
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Kinematics –Normal Knee
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Traditional TKA limitations
Non-anatomic (abnormal) positioning
•Paradoxical motion (anterior sliding)
8-13 mm
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Conventional TKA limitations
Non-anatomic (abnormal) motion
•Paradoxical motion (anterior sliding)
•No Rotation or even Lateral pivoting
Conventional Knee
10/5/2015
8
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Abnormal kinematic patterns
•Forward sliding of the femur
–Posterior impingement
–Extensor mechanism lever arm
•
Victor J, Banks S, Bellemans J: Kinematics of posterior cruciate
ligament retaining and substituting total knee replacements. J Bone Joi nt
Surg Br. 2005 May; 87 (5)
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Abnormal kinematic patterns
•Forward sliding of the femur
–Posterior impingement
–Extensor mechanism lever arm
•Axial rotation
–Limited or Reverse femoral/tibial rotation ~ Q-angle
Victor J, Banks S, Bellemans J: Kinematics of posterior cruciate
ligament retaining and substituting total knee replacements. J Bone Joi nt
Surg Br. 2005 May; 87 (5)
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Reverse tibial rotation
–lateral pivot
LATERAL MEDIAL
Q
Patellar ML Shear Force
-50
0
50
100
150
200
250
030 60 90 120 150
Flexion Angle (deg)
Force (N)
10/5/2015
9
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Correct tibial rotation
LATERAL MEDIAL
Q
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Solutions?
•Either retain both cruciates
•Either substitute for both cruciates
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Saving Both Cruciates
•Limited number of
ideal patients
•Technically difficult
for most surgeons
•Potential new
complications
(ACL avulsion / fx)
•Anatomic shapes
likely more desired
10/5/2015
10
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
HYPOTHESIS
•As TKA is a surface replacement within
an existing soft tissue envelope, we
assume that the lack of restoration of
normal anatomic contours and kinematic
patterns is the reason for impaired
function
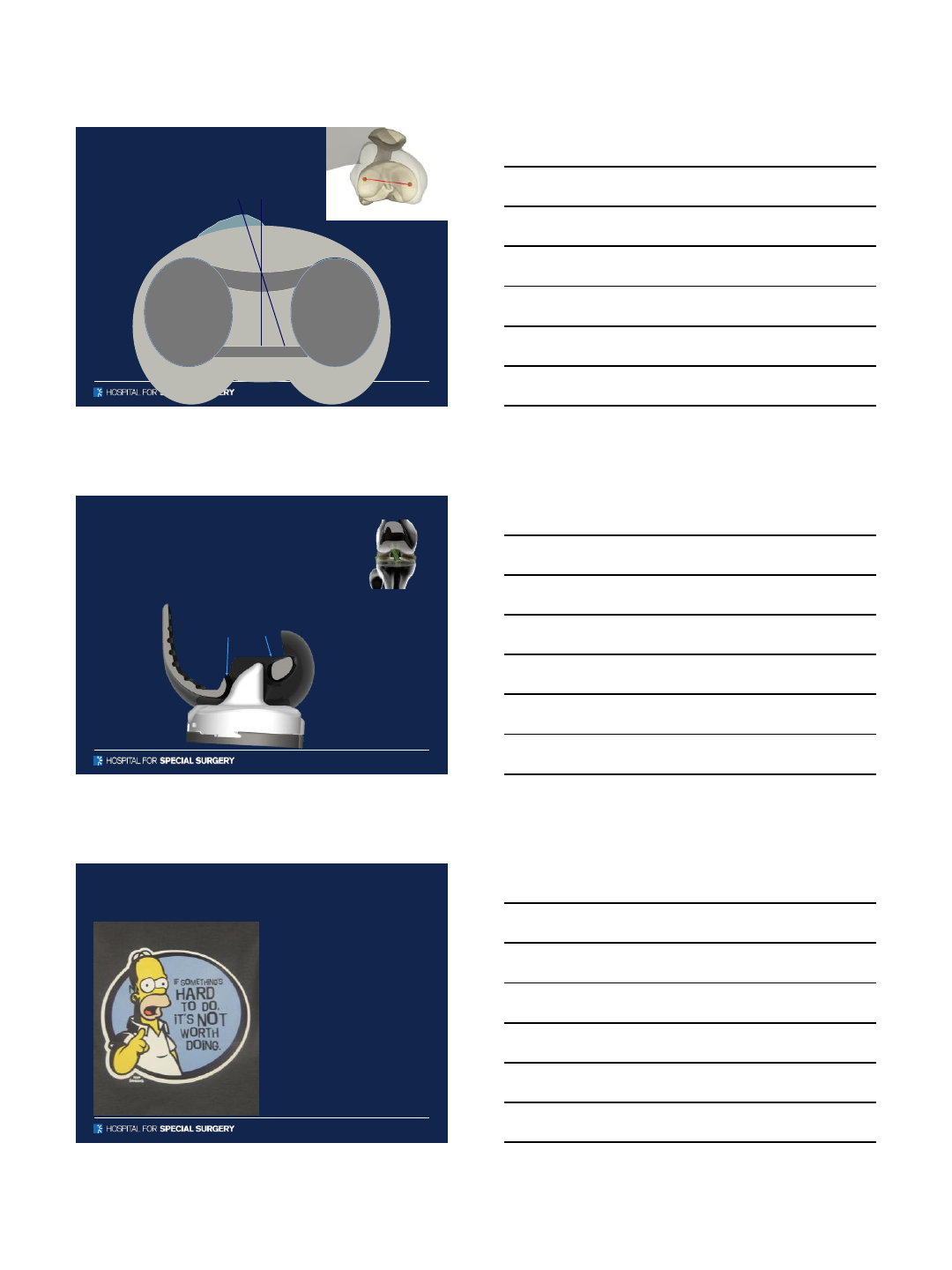
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Normal anatomic
contours
•CT and MRI antropomorphic
data
•Computer modeling and
simulation
•Femoral/Tibial geometry
controlled with over 80
parameters
lateral
medial
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
•Reproduces Normal Kinematics Flexion and Stability
–Precise Matching of Normal Anatomy
•Most Anatomically Correct for Females & Males
–Differing Tibial Geometry Medial / Lateral
Normal anatomic contour matching
10/5/2015
11
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
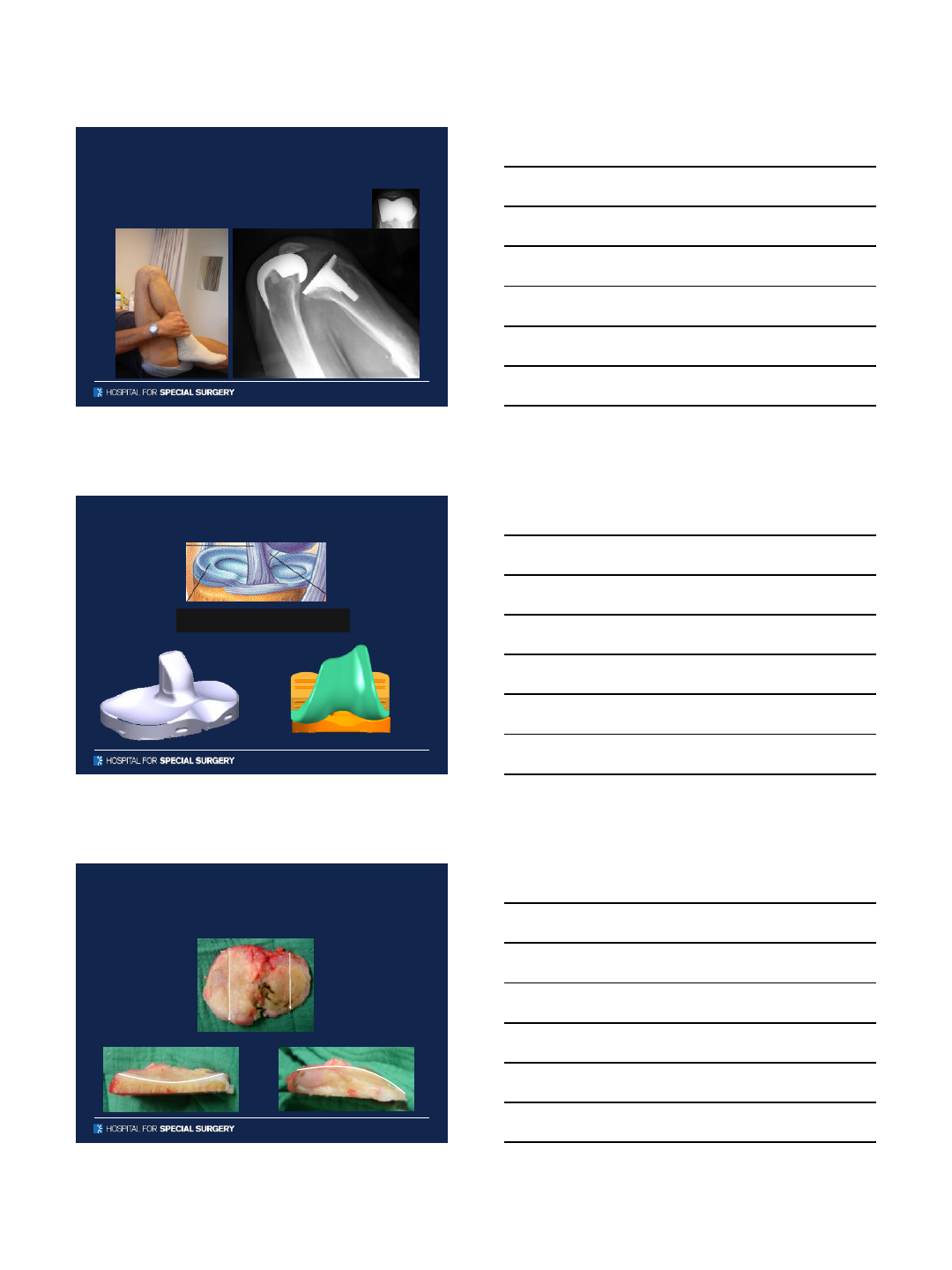
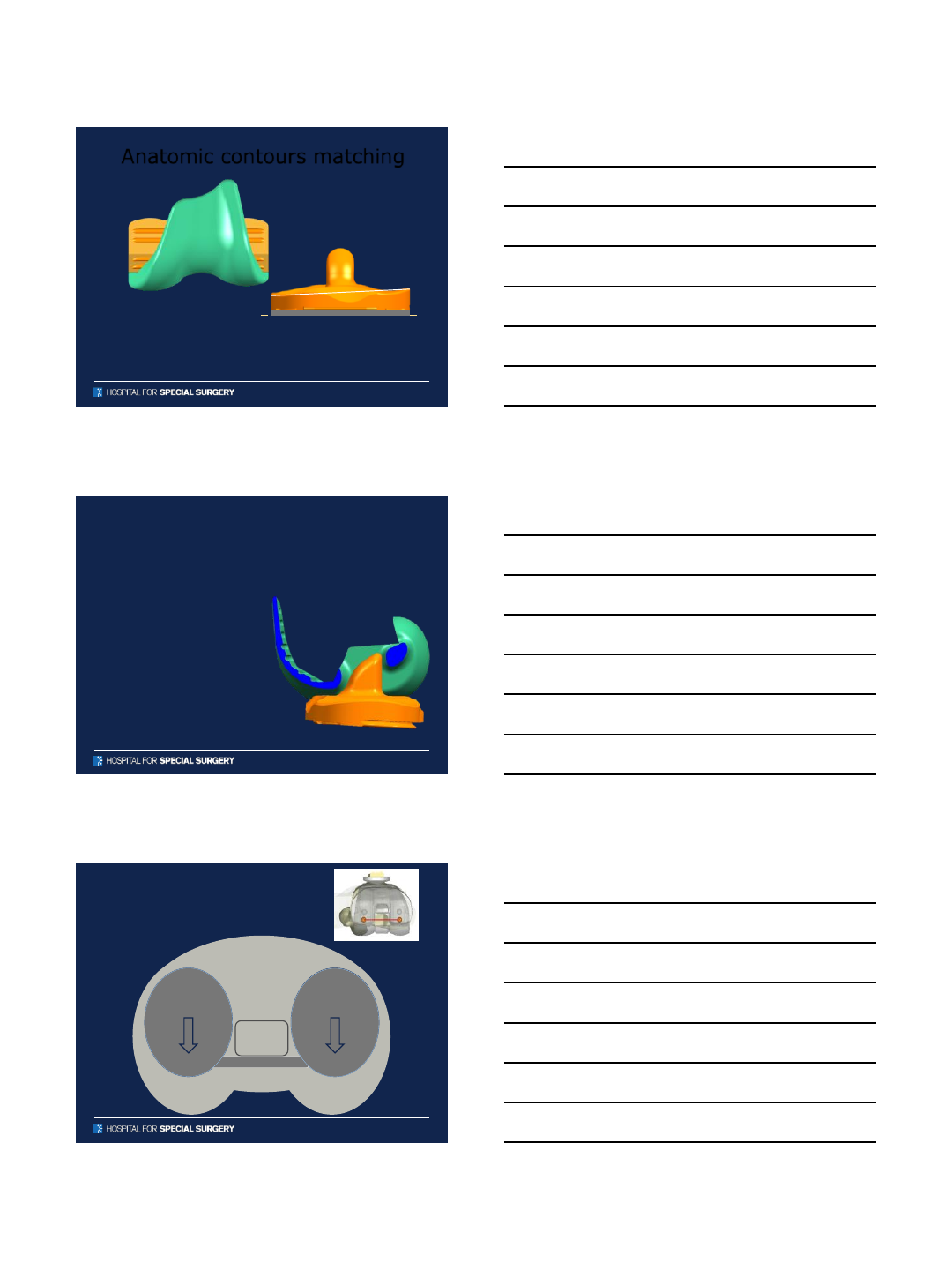
Anatomic contours matching
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Anatomic contours matching - tibia
High ML Conformity
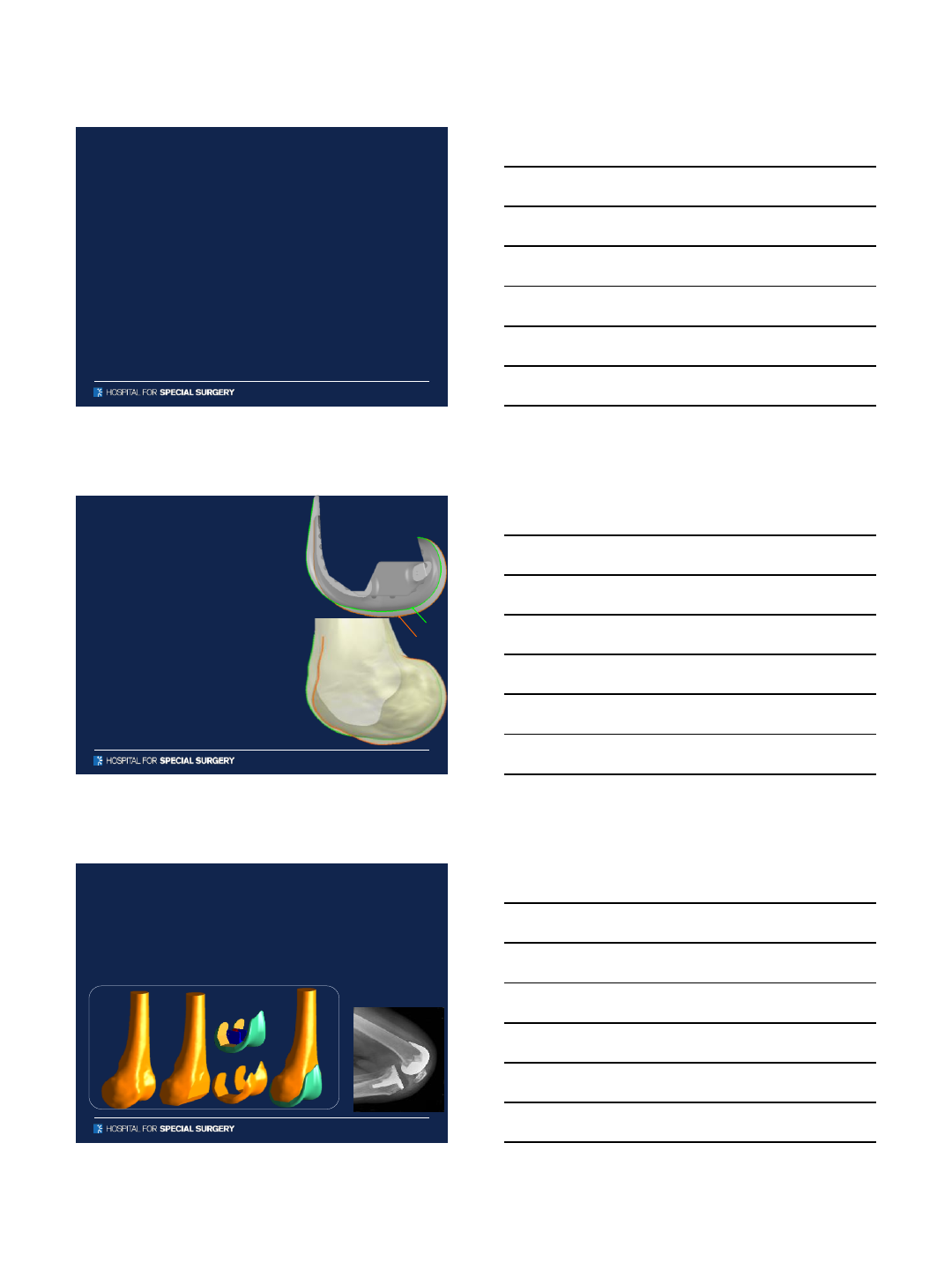
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Anatomic contours matching - tibia
medial lateral
10/5/2015
12
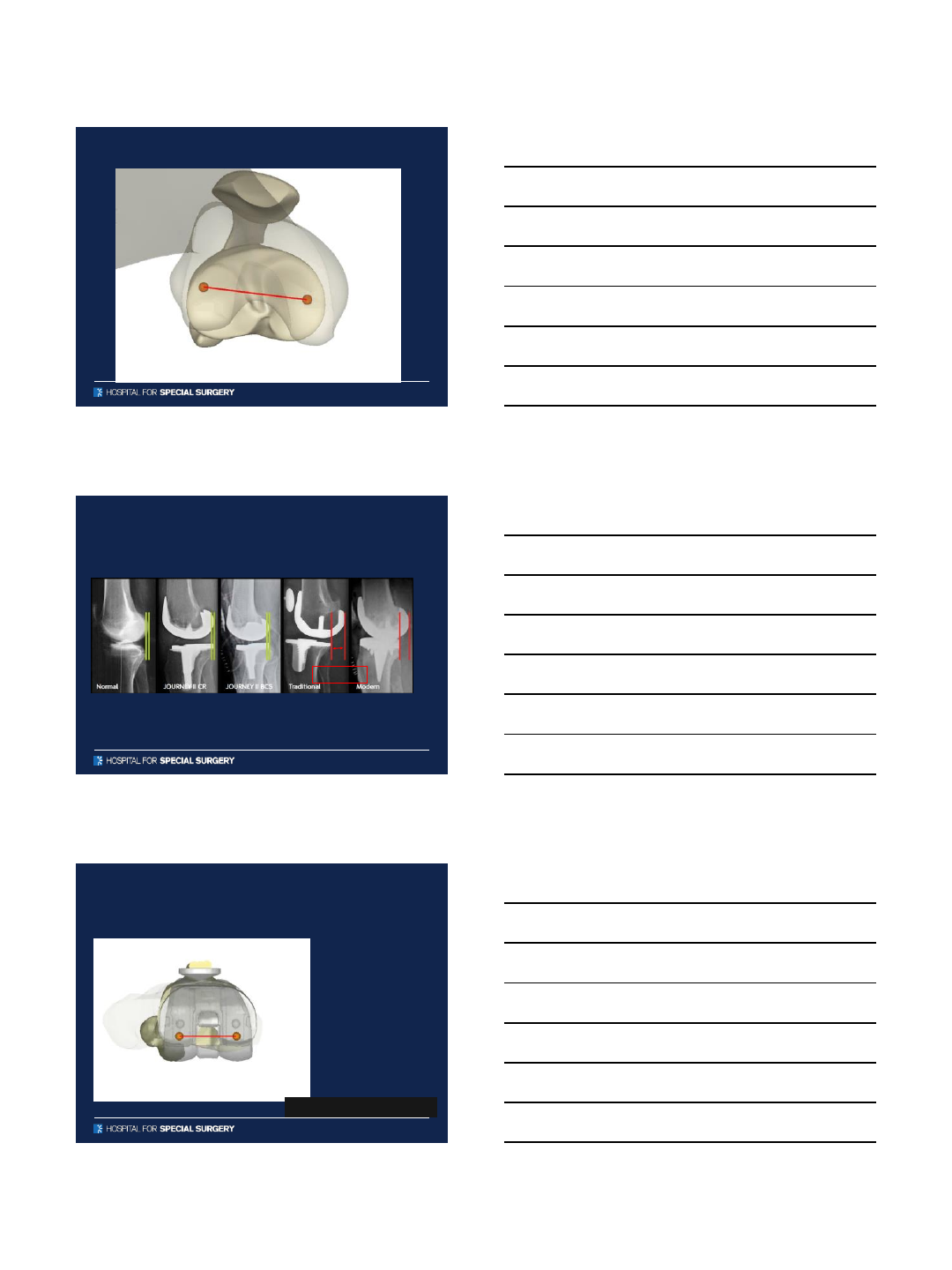
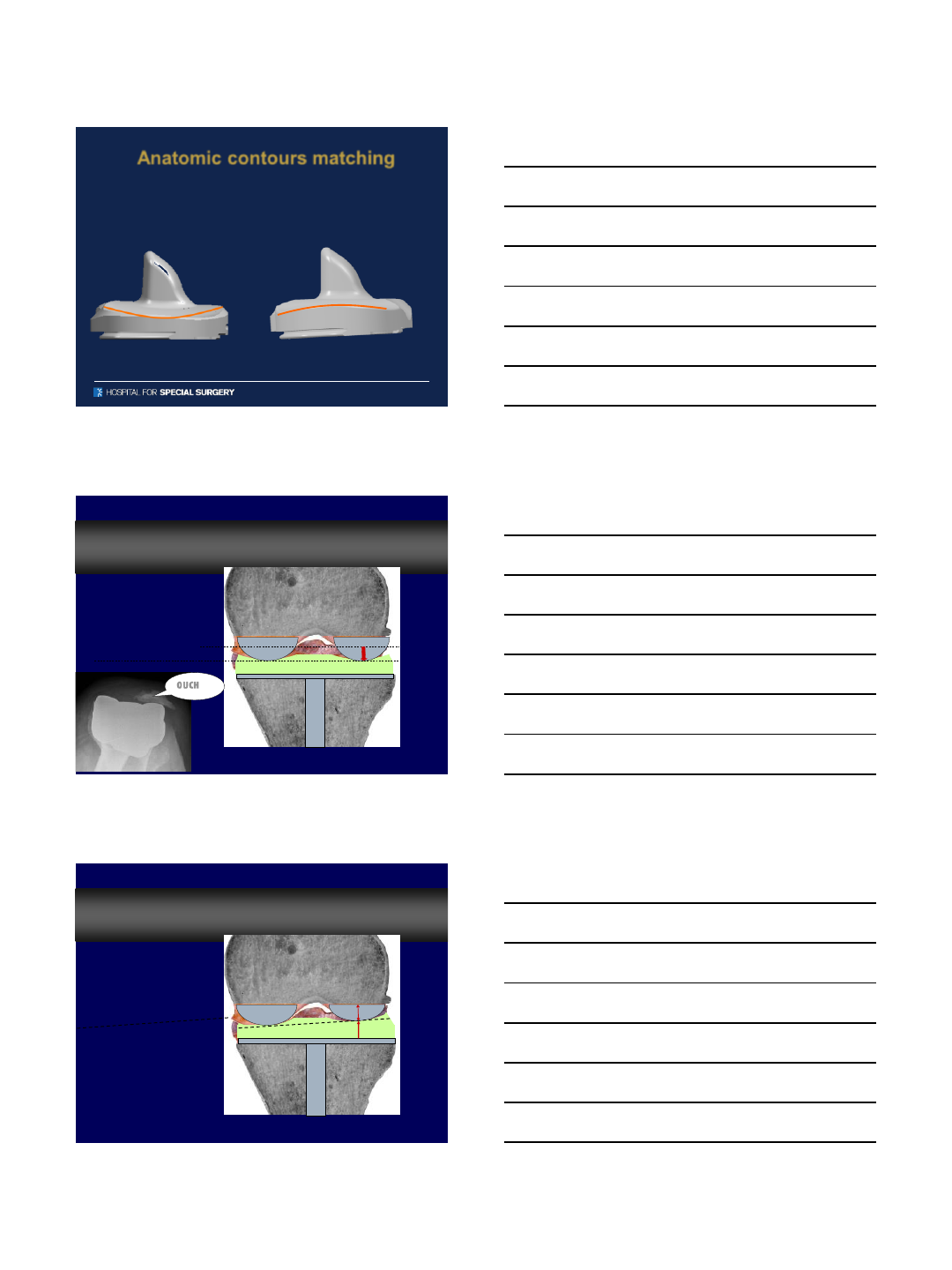
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Anatomic contours matching
•Cupped medial
compartment
•Sloped lateral
compartment
medial joint line level
lateral joint line level
OUCH
Normal Anatomy, TKA and Joint Line
Normal Anatomy, TKA and Joint Line
10/5/2015
13
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
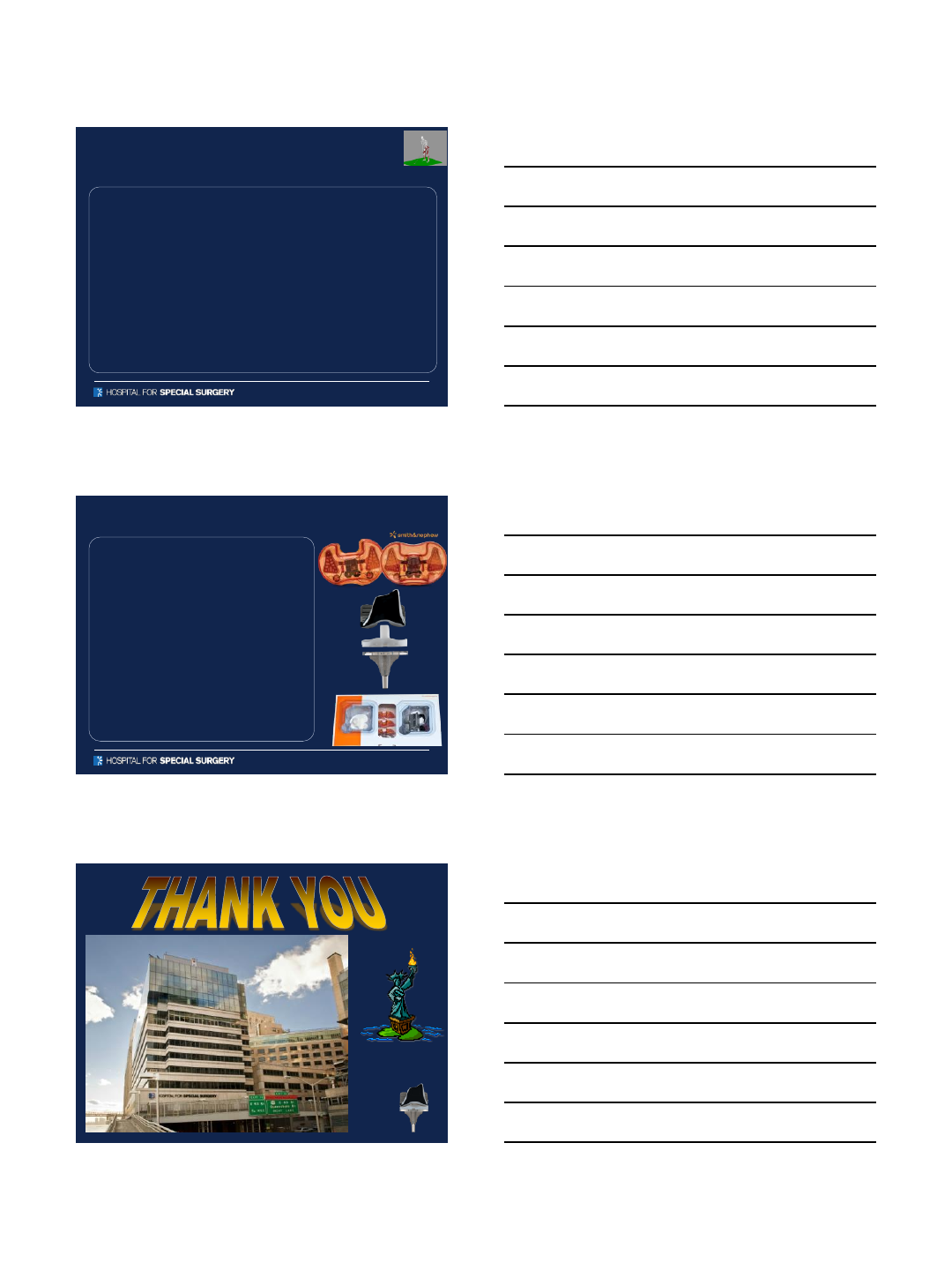
Bone resection
Bone resection
Anatomic contours matching
–If you want kinematic alignment, why not do it the right way?
•Avoid internal rotation of femur
•Avoid excessive valgus/varus tibia resections
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
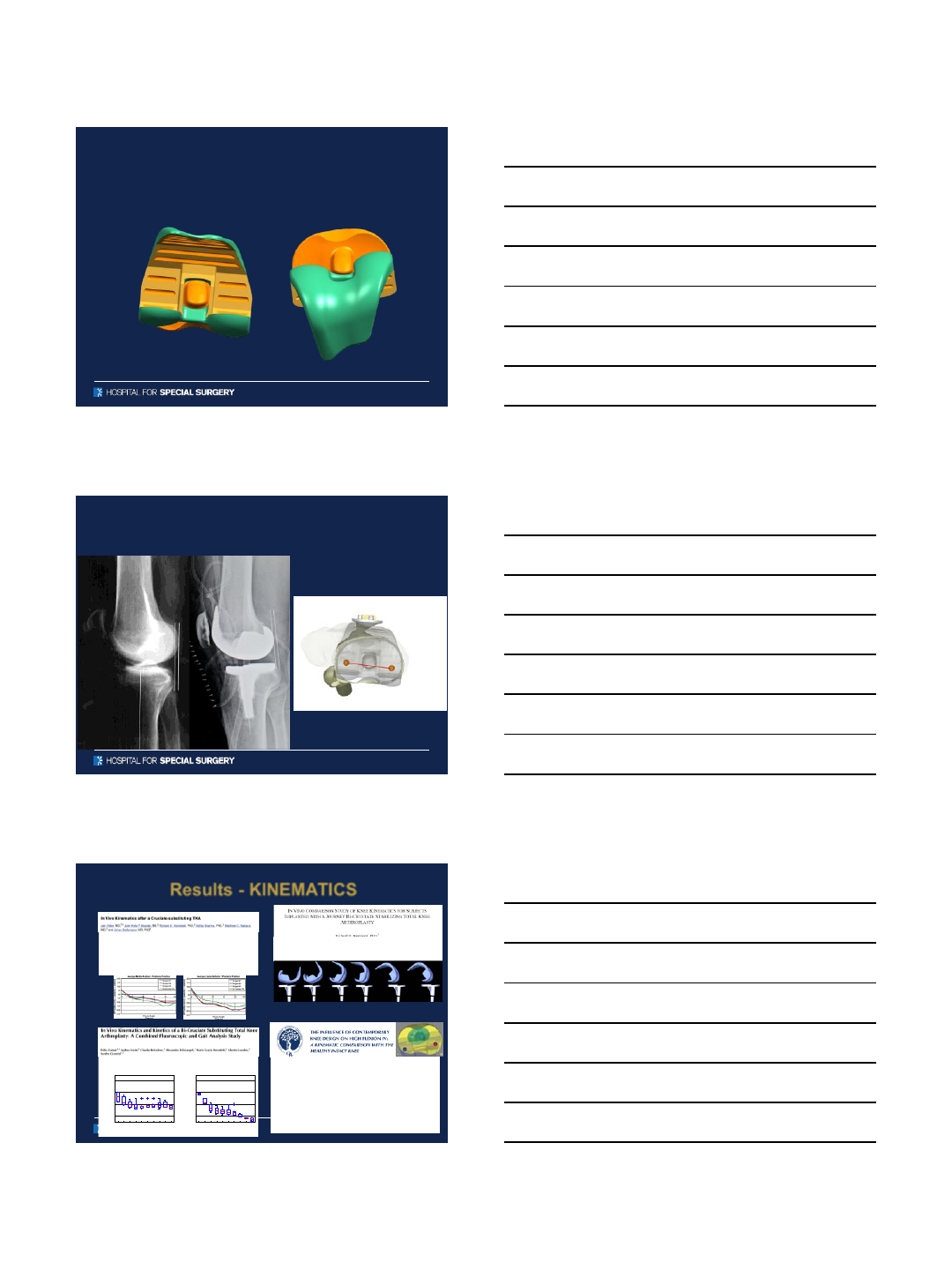
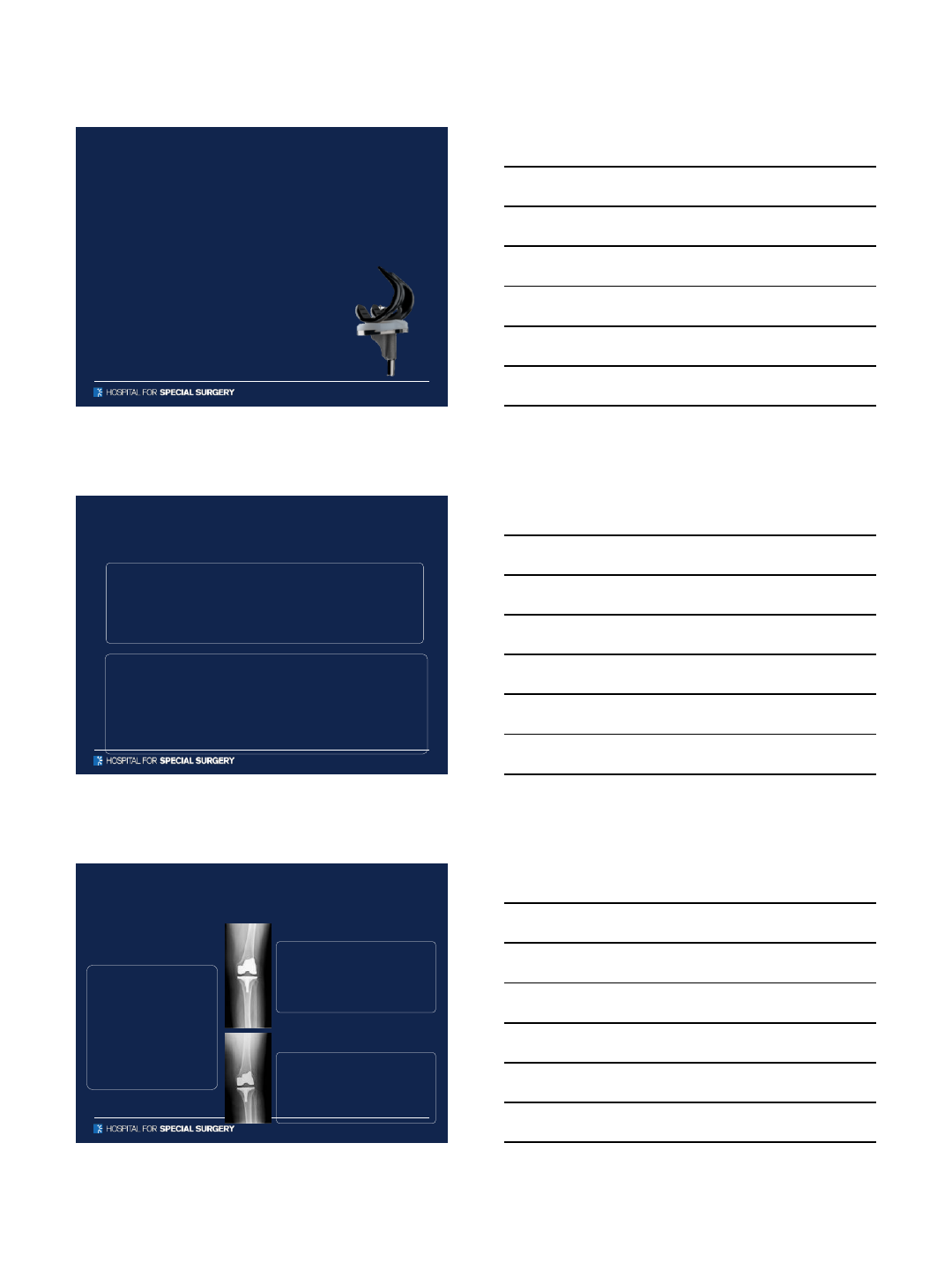
Anterior Cam
–Provides anterior
stabilization during early gait
(up to 20°flexion)
–Maximized contact area
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Designed Roll Back –
Traditional PS knee
10/5/2015
14
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
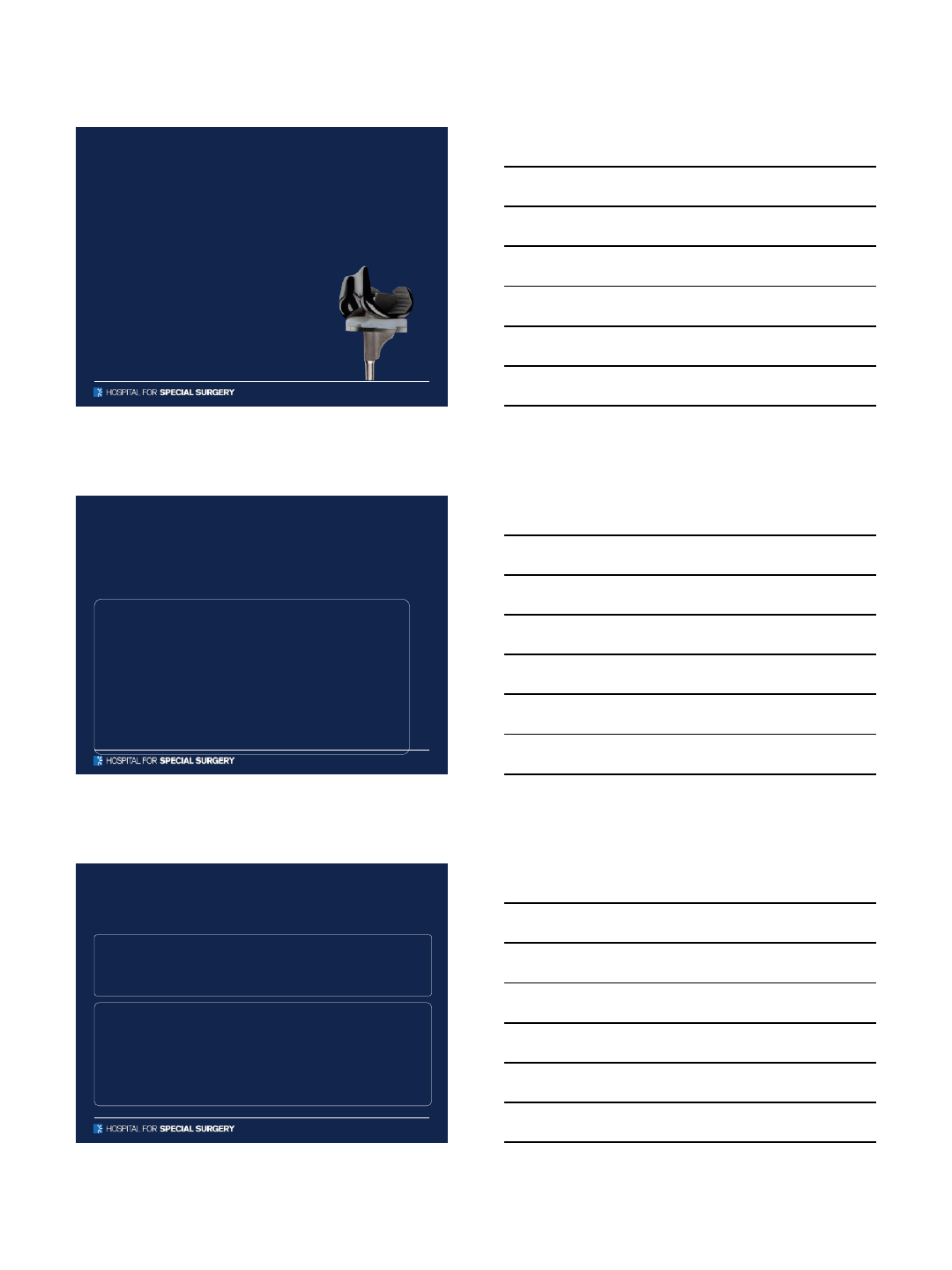
Asymmetric Posterior Cam
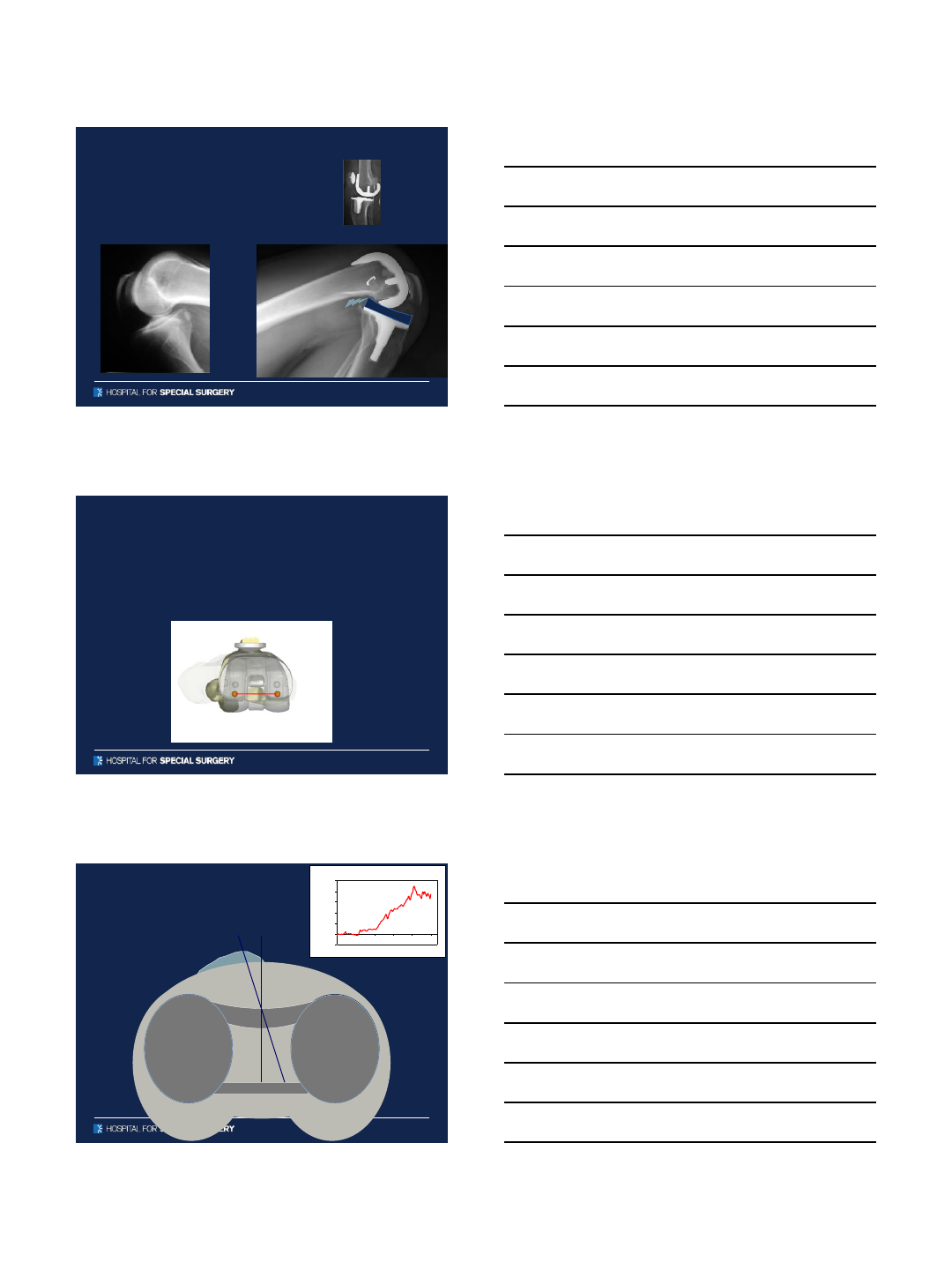
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Bicruciate Substituting & Retaining
AP Position and Rotation
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
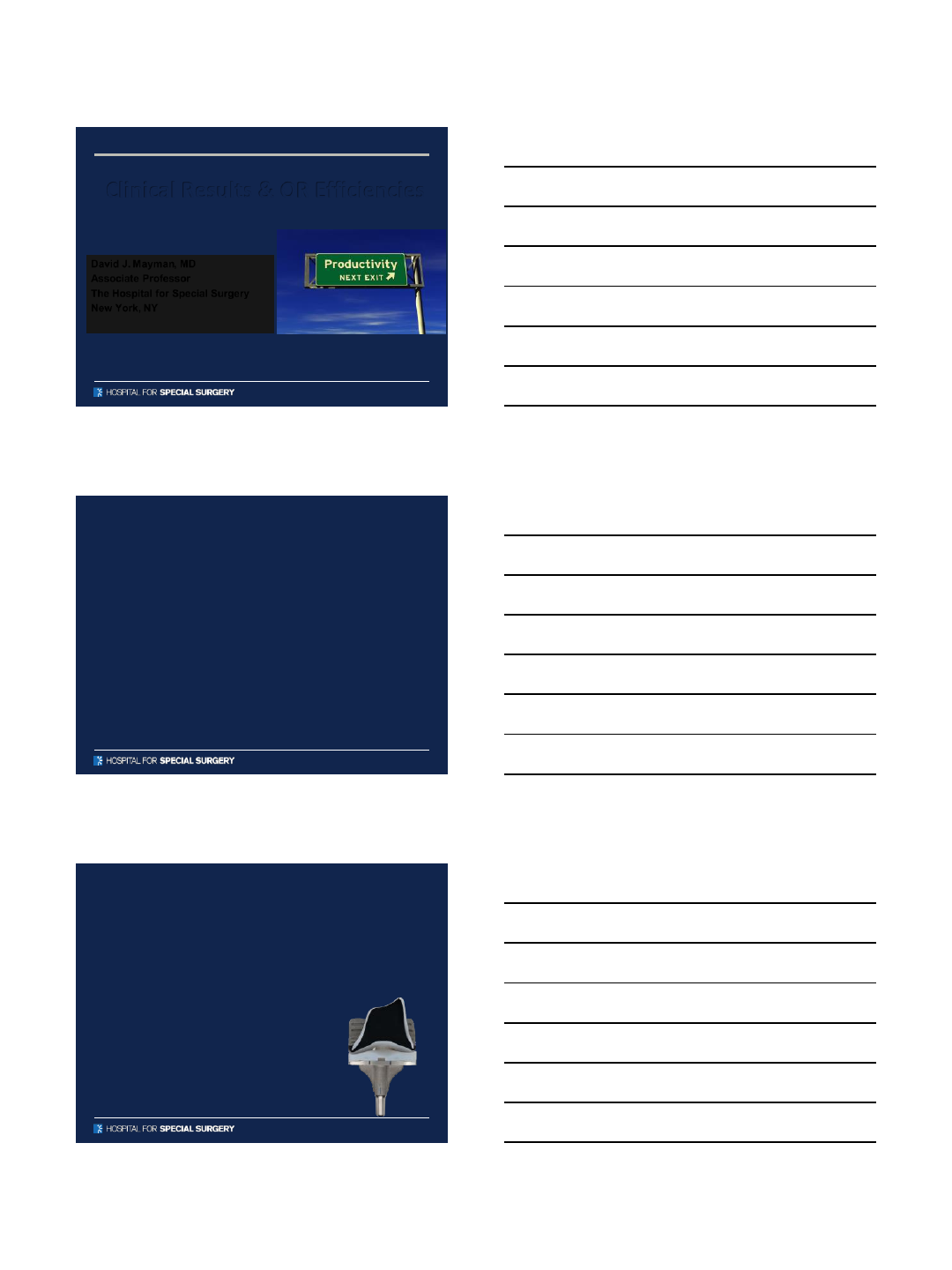
Results - KINEMATICS
• “BCS designs were able to
achieve early femoral rollback
and external femoral rotation,
both hallmarks of healthy intact
knee motion”
•95% normal axial rotation patterns
•100% posterior femoral translation
•The average axial tibiofemoral
rotation from full extension to
maximum flexion for all TKAs was
10.8°
010 20 30 40 50 60 70 80 90
20
40
60
80
A/P medial CP [%TibSize]
<--Pos A/P location [%TibSize] Ant-->
Flexion [Deg]
010 20 30 40 50 60 70 80 90
20
40
60
80
A/P lateral CP [%TibSize]
<--Pos A/P location [%TibSize] Ant-->
Flexion [Deg]
10/5/2015
15
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Implant Conclusion
•While successful, TKR patients are frequently limited in
higher level activity
•Traditional TKR do NOT reproduce normal kinematics
•JOURNEY II BCS is designed to allow for more normal
kinematics
•Improvements in kinematics may lead to improved
performance of higher level activity
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Overall summary
●Business of medicine affects your quality of care
●Rapid recovery model for TJA
●Little to do with “kicking patients out”
●More to do with adopting best clinical practices
●It’s a clinical, scientific & financial shift
●TJA landscape is changing
●Multiple variables affect recovery speed
●We all are learning from each other’s experiences
●NEW TECHNOLOGY CAN IMPROVE BOTH
●Efficiency
●Quality
10/5/2015
16
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Clinical Results & OR Efficiencies
David J. Mayman, MD
Associate Professor
The Hospital for Special Surgery
New York, NY
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
Disclosures
Consultant: Mako/Stryker
Consultant: Smith and Nephew
OrthAlign Stock Options
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
•Single Site Registry –Early reports
•2 Single-Site: Early outcome reports
–Dr. Bill Huang
–Dr. Dave Mayman
JOURNEY II TKA: Excelling in The Bundle
10/5/2015
17
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: Patient Satisfaction
Dr. Mark Snyder
Registry Experience
•Redcap Registry Database, level-3 data
•JOURNEY II BCS outcomes data at 1 year
•n = 56
•Mean age = 59
Mark A Snyder, MD
Director, Orthopaedic Center of Excellence
Good Samaritan Hospital
Med Exec, Trihealth Orthopaedic & Spine Institute
Cincinnati, Ohio
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: Patient Satisfaction
Dr. Mark Snyder
Registry Experience
•Pre-op EuroQol5: 50 (35 to 70)
•Post-op EuroQol5: 93 (60 to 100)
•Statistically insignificantly different from THA in young
patients!
•Mean flexion 130.7o(115oto 145o)
•Patient satisfaction (VAS 1-10 Scale) 9.4 (98.7 %)
•Risk Adjusted 30-day Readmission Rate: 0%
•Relevant Surgical Complication Rate: 0% (National range
4-6%)
•No transfusions and no venous thromboembolisms
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: Patient Satisfaction
Dr. Mark Snyder
Registry Experience
•Pre-op UCLA activity score: 4.7 (3 to 6)
•Post-op UCLA activity score: 7.3 (6 to 9)
•Competes with THA and RHA improvements in patients!
–Groin pain after metal on metal hip resurfacing: a mid-term
follow-up of a prospective cohort of patients. Illical E, et a. HSS J
2012;8(3):257
–Physical activity before and after primary total hip arthroplasty: A
registry-based study. Lubbeke A, et al. Arthritis Care Res 2013
Aug 7 [Epub]
•At 1 year 88% in sports and 100% back to work!
10/5/2015
18
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
•Single Site Registry –Early reports
•2 Single-Site: Early outcome reports
–Dr. Bill Huang
–Dr. Dave Mayman
JOURNEY II TKA: Excelling in The Bundle
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: LOS Reduction
Bill Huang , MD
•Almost exclusively PS TKR user
•2007-2009 –Legion, Journey 1 BCS, & PFC Sigma RP
•2009 -2013 –Legion
•2013 -2015 –Legion & Journey 2 BCS
•Fellowship-trained arthroplasty surgeon
•Practices exclusively in hip and knee replacements
•Private practice in a community hospital
•Averages 250 TKR/UNI and 200 THA per year
•50 revisions per year
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: LOS Reduction
Bill Huang MD -- early outcome
Methods:
•Functional scores
–Knee Society Score
•Radiographic follow-up
–Pre op
–1 months
–4 months
•Complications
•Technical Data
Legion PS Primary PS
•n: 50
•Mean age: 61.9
•Average BMI: 34
•M/F ratio: 54%/46%
Journey 2 BCS
•n: 50
•Mean age: 60.4
•Average BMI: 36.1
•M/F ratio: 51%/49%
10/5/2015
19
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: LOS Reduction
Bill Huang MD
LEGION Primary PS
•Tourniquet time: 42 minutes
•LOS: 2.4 days
JOURNEY II BCS
•Tourniquet time: 45 minutes
•LOS: 1.8 days
ROM
•Pre Op: 6.8 –110.1
•1 month: 3.2 –90.1
•4 months: 0.66 –122.4
•Pre Op: 6.5 –108
•1 month: 3.7 –108
•4 months: 0.58 –127.4
•Wound issues: 2
•Infection: 0
•VTE: 0
•Reoperation: 0
•MUA: 3
•Wound issues: 1
•Infection: 0
•VTE: 0
•Reoperation: 0
•MUA: 1
Complications
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: LOS Reduction
Bill Huang MD -- Knee Society Scores
Legion PS Primary PS
KNEE SCORE
•Pre Op: 42.8
•1 month: 64
•4 months: 87.6
Journey 2 BCS
KNEE SCORE
•Pre Op: 43.2
•1 month: 69.6
•4 months: 92.6
FUNCTION SCORE
•Pre Op: 59
•1 month: 76
•4 months: 98
FUNCTION SCORE
•Pre Op: 62
•1 month: 79
•4 months: 98
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: LOS Reduction
Bill Huang, MD
Early Outcome Experience
Key Points:
•JOURNEY II BCS Achieved:
–Earlier, Greater ROM
–Higher KS Scores
–Less MUA rate
•Anecdotal Patient Comments:
–Less pain and less narcotic usage in first 4 months
–Less joint swelling/effusion in first 1 months
–Easier getting up from seated position
– Feels less “mechanical”
10/5/2015
20
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
•Single Site Registry –Early reports
•2 Single-Site: Early outcome reports
–Dr. Bill Huang
–Dr. Dave Mayman
JOURNEY II TKA: Excelling in The Bundle
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: Functional
Improvement
David Mayman, MD
Early Outcome Experience
Methods:
•N= 200 retrospectively reviewed
•100 TKA with Legion
•100 TKA with Journey
•113 females and 87 males
•Mean age 51 years ( range 43-66)
•All patients underwent a clinical exam and post-operative ROM was
recorded at 6 weeks
ADULT RECONSTRUCTION AND JOINT REPLACEMENT
JOURNEY™ II BCS: Functional
Improvement
David Mayman, MD
Results:
•Average ROM
•Legion 96°(range 85-116)
•Journey 119°(range 95-125)
•Average Pain (KSS)
•Legion: 30
•Journey: 37
Conclusion:
•There was a significant and clinically relevant improvement in flexion in patients who
underwent a TKA with a JOURNEY II TKA implant (p<.0001)
•Patients who undergo a TKR with a Journey implant have better range of motion and less pain
post-operatively at 6 weeks.
•This study suggests that an implant design that more closely replicates the normal anatomic
joint line and knee kinematic patterns may help reduce some of the dissatisfaction following
TKA.
10/5/2015
21
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Efficiency Has Not Been Addressed
•Why do we have trial implants in the room for right
and left knees?
•Why do we have trials for every size implant in the
room?
•Relies on sterilizing many trays
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
10/5/2015
22
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
What can we do to improve this?
Smith and Nephew has come up with three options to
address as many surgeons and hospitals as possible
•Option 1
–Template Derived Instrumentation
•Option 2
–VISIONAIRE™
•Option 3
–Disposable instruments with VISIONAIRE™
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
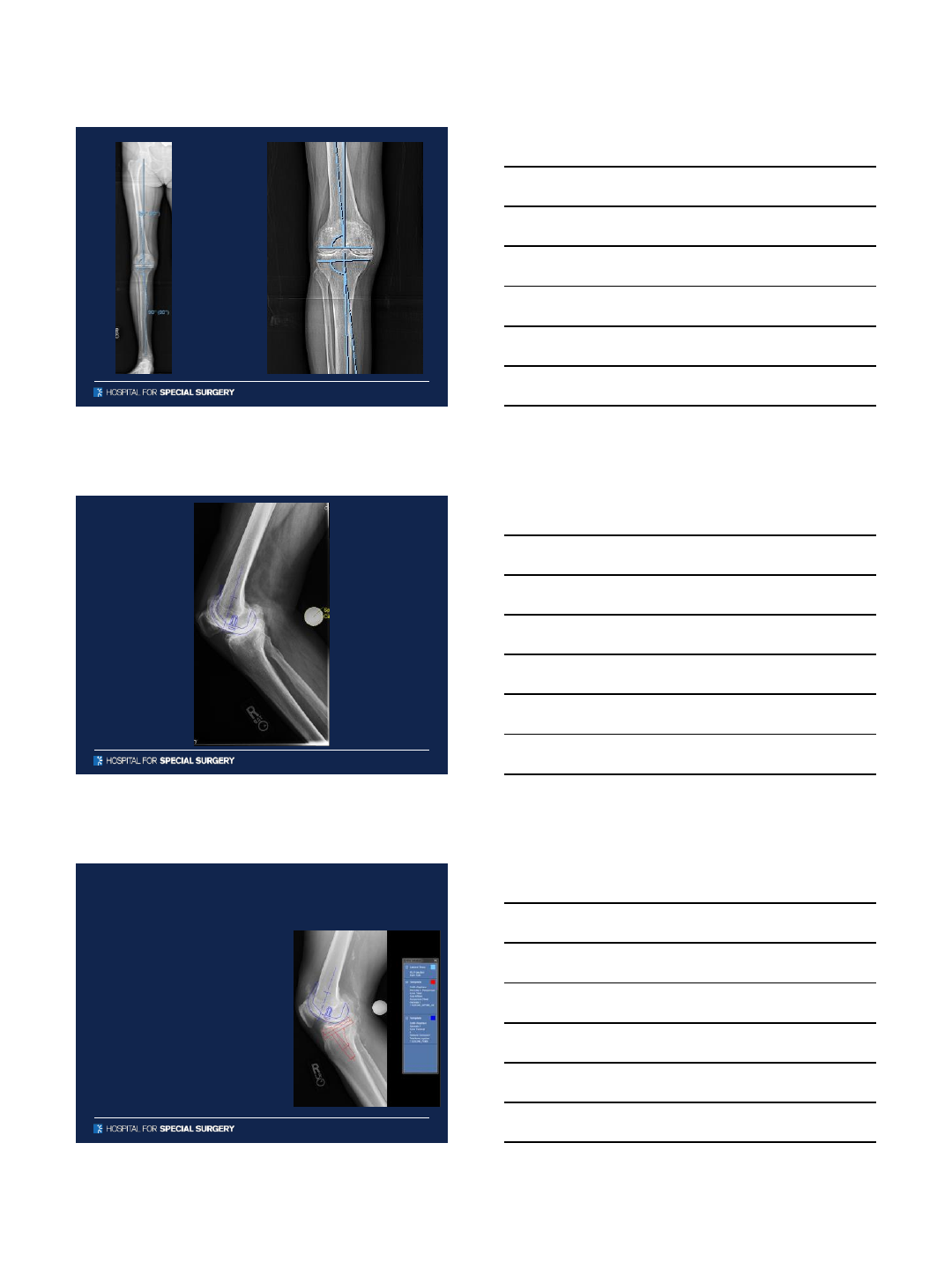
Pre-Operative Templating
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Digital Templating
•Anticipate sizes of components
•Avoid leg length discrepancy
•Restore offset
•Avoid femoral fracture
•Avoid instability
10/5/2015
23
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
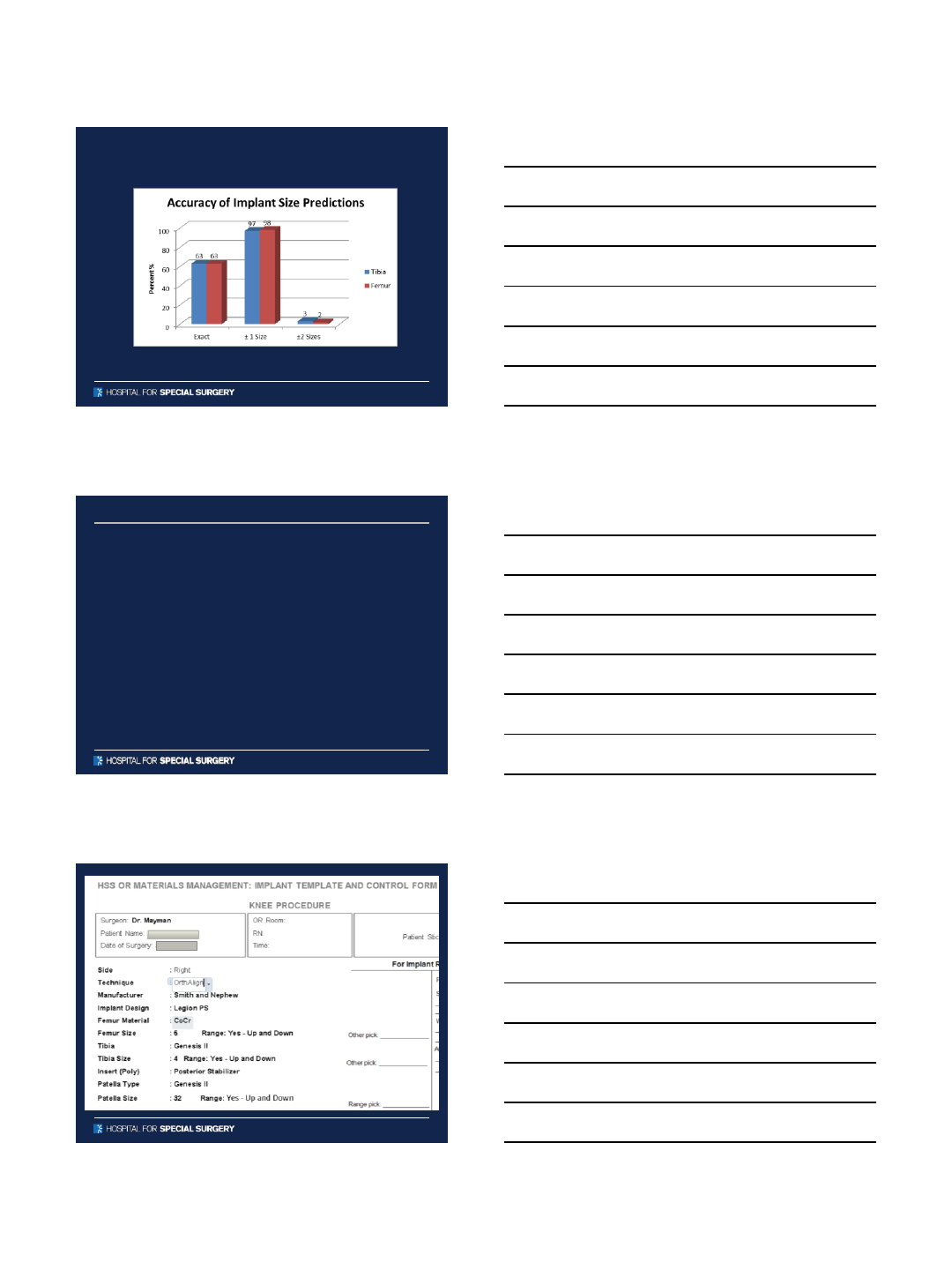
Accuracy of Digital Templating for
TKA
•N=71 patients (76 knees)
•Standing anteroposterior and
lateral knee digital
radiographs
•Calibrated using a 25mm
calibration marker
•Templated sizes for the
femoral and tibial
components compared to
implanted sizes.
10/5/2015
24
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Results
Tibia and Femur were both exact = 43/76 (63%)
Tibia and Femur ±1 size = 74/76 ( 97%)
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Template Derived Instrumentation
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
™
™

10/5/2015
25
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Instruments Picked From Plan
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT

10/5/2015
26
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
10/5/2015
27
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
10/5/2015
28
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
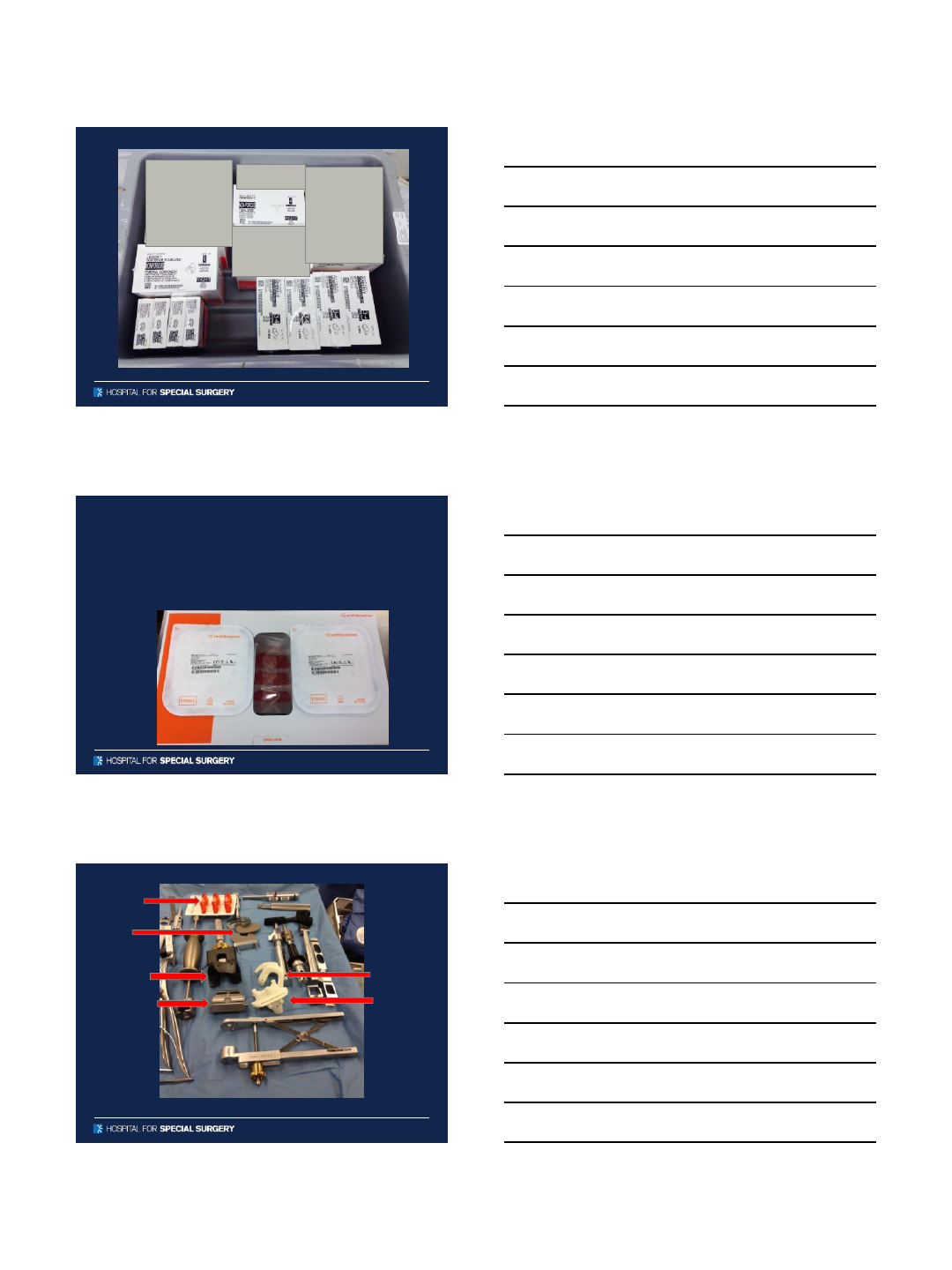
Visionaire
•Takes the pre-operative templating and advances
the accuracy
•Has the potential to improve efficiency further
•MRI and long leg x-rays required
•Must be done at least 3 weeks prior to surgery
•Surgeon receives a plan from an engineer that is
approved by the surgeon and then patient
specific cutting guides are created
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
10/5/2015
29
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
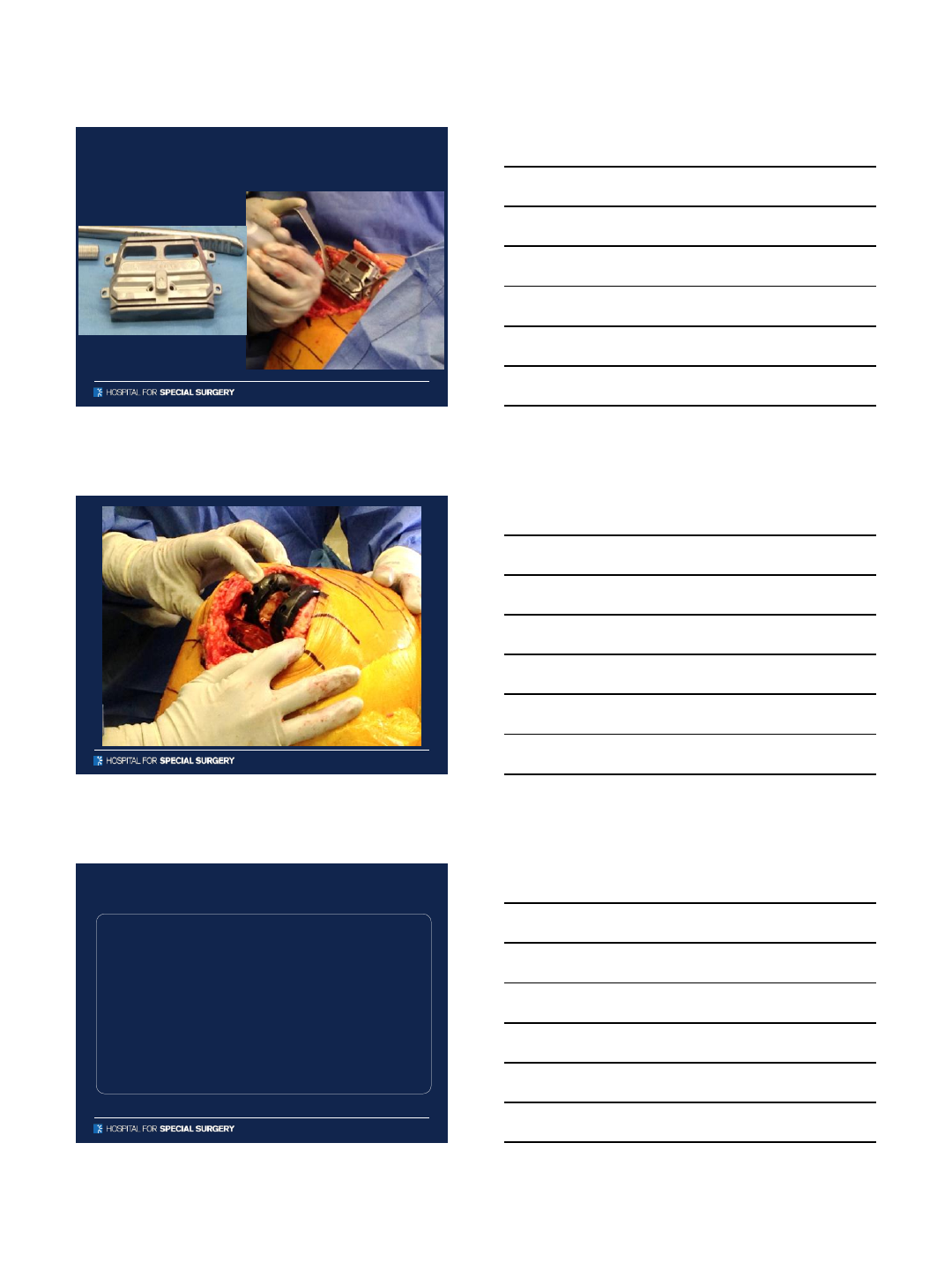
Disposables
•Disposable instruments build on the experience
of VISIONAIRE™and takes efficiency in the OR to
the next step
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Poly
Trials
Tibial Trial
Femoral Trial
Femoral cutting
Block
Tibial cut
block
Distal femoral
Cutting block
10/5/2015
30
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Summary
•Pre-operative templating is an accurate method
for predetermining implants w/I 1 size
•Patient specific instrumentation of some sort can
help improve the efficiency of delivery
•As demand increases and reimbursement
decreases we need to improve efficiency while
maintaining or improving quality.
10/5/2015
31
ADULT RECONSTRUCTION AND JOINT REPLACEMENTADULT RECONSTRUCTION AND JOINT REPLACEMENT
Thank you
10/5/2015
1
New Developments in CMS Policy 2015 and Beyond
Digging Your Way Through the Bundle
Peter C. Geagan –Director of Commercialization, Smith & Nephew, Inc. 1
Inspired Leadership Facilitates Change
Do you know the true costs of your episode of care?
•“When TDABC is fully embraced we will know the
true cost of an episode of care”
–Michael Porter, Bishop William Lawrence University Professor at The Institute
for Strategy and Competitiveness, Harvard Business School 1
•“If you cannot measure your outcomes & quality, then
someone will report what they measure and report it”
- Dr. Joseph Iannotti, Professor and Chair Orthopaedic and Rheumatologic
Institute, Clinical Transformation, Cleveland Clinic 1
2
1 “Shifting From Volume to Value, AAOS Bundled Payment Summit, 5/28/15, Washington, DC
Culture Change Is Key
Agenda
3
Bundled
Payment
Programs
What
WhyWhen
10/5/2015
2
2015
History of Bundled Payments
2013
2012
2010
2010
2000
1980
4
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014-Fact-sheets-items/2014-01-30-2.html
acceleratingaccelerating
Impact of the Affordable Care Act (2010)
Payment reform is the pace of change
Shifting from volume based payments to value based
payments
More emphasis on quality metrics & outcomes & less on RVUs
Moving toward shared risk contracts and capitation models 5
BPCI CCJR HRRP HAC VBP ACOs MSSP
accelerating
Why the Shift to Bundles in TJA?
•2014 over 475,000 inpatient primary TJA were paid for
through CMS
•TJA accounts for over $15 Billion in annual CMS spend
•Tremendous variance in cost and quality of care for TJA in the
90 day episode
•$16,500 to $33,000 across geographic areas
•Post Acute Care utilization & quality varied by site of service
•Rate of infections and implant failures varied greatly -3x in
some cases requiring readmission to hospital
6
http://innovation.cms.gov/initiatives/ccjr/

10/5/2015
3
Wide cost variances
currently exist across a
TJA episode of care
With the most variation
occurring during the
post-acute aspect of
the bundle
7
$30,000
$25,000
$20,000
$15,000
$10,000
$5,000
$-
Lowest Cost Highest Cost Variation
Hip Replacements
Key Findings
Why Shift? –Variation within the bundle
Miller, D.C., et al (2011). Large Variations in Medicare Payments for Surgery Highlight Savings Potential From Bundled Payment Programs. Health Affairs, 30 (11). 2107-2115.
Index Hospitalization
Physician Services
Readmissions
Post Discharge Care
8
$$$
$
$
$
$
Fee-For-Service Bundled Payment
Payment for each service regardless of quantity or quality Payment for comprehensive, coordinated intervention
Vs.
Bundled Payment - Overview
Pre-Admission
Services
Part A Inpatient
Services (Hospital)
Part B Inpatient
Services (MDs)
Post-Acute Costs
(Part A & Part B)
Readmissions
http://innovation.cms.gov/initiatives/bundled-payments
Target percentage of Medicare Fee for Service payments linked to quality
and bundled payment models
10
All Medicare FFS
85% - Payments
linked to quality
30% -
Bundled
Payments
All Medicare FFS
90% - Payments
linked to quality
50% - Bundled
Payments
2016 2018
Change
Medicare Payment Method Shift
Center for Medicare and Medicaid Innovation, 8/1/ 2013 (CMS.gov)
10/5/2015
4
MSSP BPCI CCJR
National
Reach
Gain
Sharing
Timeline Annual 3-Pre
90-Post
Admission
90-Post
Various
Models
Mandatory
Alternative Payment Models
75 MSA’s
11
http://innovation.cms.gov/initiatives/bundled-payments/
http://innovation.cms.gov/initiatives/ccjr/
https://www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014-Fact-sheets-items/2014-01-30-2.html
Participation
Agreement
12
BPCI: Brief overview
Covers 48 different episodes of care (DRGs)
•78% participants chose lower extremity joint
replacement
Bundled Payment for Care Improvement
•4 different voluntary models (Models 1, 2, 3, and 4)
•Controlled by (any)
‐Physician group (295)
‐Hospital (403)
‐3rd Party Convener
•Outcome Measures
‐Implementation Plan (IP) proposed by awardee outlines quality
metrics to be improved
‐Goal of aligning inpatient and post-acute care pathways to
increase quality and reduce costs
•Bundle Price Target (2-3% off 3 yr avg of account’s
history):
‐If costs less than historical spend, savings may be
retained/shared
‐If costs are more than historical spend, payment owed to
CMS
‐Physician Gain Sharing up to 50% of FFS
Episode of Care Horizon
All Medicare Part A / B fee-for-service payments
Admission Discharge
30, 60, 90 days
http://innovation.cms.gov/initiatives/bundled-payments/
(Participants as of
July 1,2015)
13
Model 1 (11)
(retrospective)
Model 2 (741)
(retrospective)
Model 3 (1,353)
(retrospective)
Model 4 (10)
(prospective)
CMMI BPCI Models
Pre-Admission
Services
(3 days*)
Part A Inpatient
Services
(Hospital)
Part B Inpatient
Services (MDs)
Related Readmissions
(Part A / B) & Unrelated
Readmissions (Part B only)
Post-Acute Costs
(Part A & Part B)
Model 2 presents the broadest opportunity to improve care by focusing on the entire continuum
of care for targeted DRGs
http://innovation.cms.gov/initiatives/bundled-payments
10/5/2015
5
BPCI Update Model 2–August 2015
BPCI Participant motivation:
1. Wanting to learn about payment reform
2. Pursuing the financial opportunities of BPCI
3. Urging of leadership and wanting to be innovative
4. BPCI opportunities to improve quality
5. Alignment with participation in other initiatives.
Early results Q4,2013: note –small sample size
•Inpatient and PAC alignment with 23 of 24 Model 2 awardees
•Decrease in anchor LOS from 4.6 days to 4.3 days
•90 Day Episode of care costs dropped from $37,275 to $32,369 –
statistically significant
•30 Day Unplanned Readmissions from 8.6% to 6.7%
•Emergency Dept (no hospital admit) visits from 6.9% to 8.7%
•No change in Mortality rates
The Lewin Group, CMS Bundled Payments for Care Improvement (BPCI) Initiative Models 2-4: Year 1 Evaluation & Monitoring Annual Report, Feb 2015
14
• “It’s about making changes that matter clinically…if we get away from patient care & it’s all about
finances, we lose.” -Dr. Jim Weinstein, CEO of Dartmouth/Hitchcock 1
• “No one wants the low-cost/low-quality option”
-Dr. Daniel Murrey, CEO of Orthocarolina 1
• “If you cannot prove your outcomes and quality of care is better, then you will compete only on price”
-Dr. Joseph Iannotti, Professor and Chair Orthopaedic and Rheumatologic Institute, Clinical
Transformation, Cleveland Clinic 1
• “How do you inspire change? Strong physician clinical process leadership integrated with
administrative support“ -Dr. Mark Snyder, Medical Executive Tri-Health Orthopedics and Spine Institute
1
• “Make data denial impossible…& keep riveting people on the why (outcomes/efficiency improvement)
to overcome the aversion to change.”
-Michael Porter, Bishop William Lawrence University Professor at The Institute for Strategy and
Competitiveness, Harvard Business School 1
15
1 “Shifting From Volume to Value, AAOS Bundled Payment Summit, 5/28/15, Washington, DC
2 “Crossing the Chasm” Geoffrey A. Moore, HarperBusiness, 1991.
Tipping point –Law of Diffusion of Innovation
2
16
CCJR: Brief overview
Lower Extremity Joint Specific
•With and without complications
(DRG 469 470)
Mandatory Bundled Pay Program by
CMS
•Hospital Controlled
•Fee - Weighted (shifting to Regional)
•4 Outcome Measures
‐Readmissions
‐Complications
‐Patient Experience (HCAHPS)
‐Additional Financial Incentive for Functional PROs
•75 MSA Covered Areas
•20% Cap on bonus for savings to hospital
•50% Cap on physician FFS
Episode Horizon
All Medicare Part A / B fee-for-service payments
Admission Discharge
90 days
10/5/2015
6
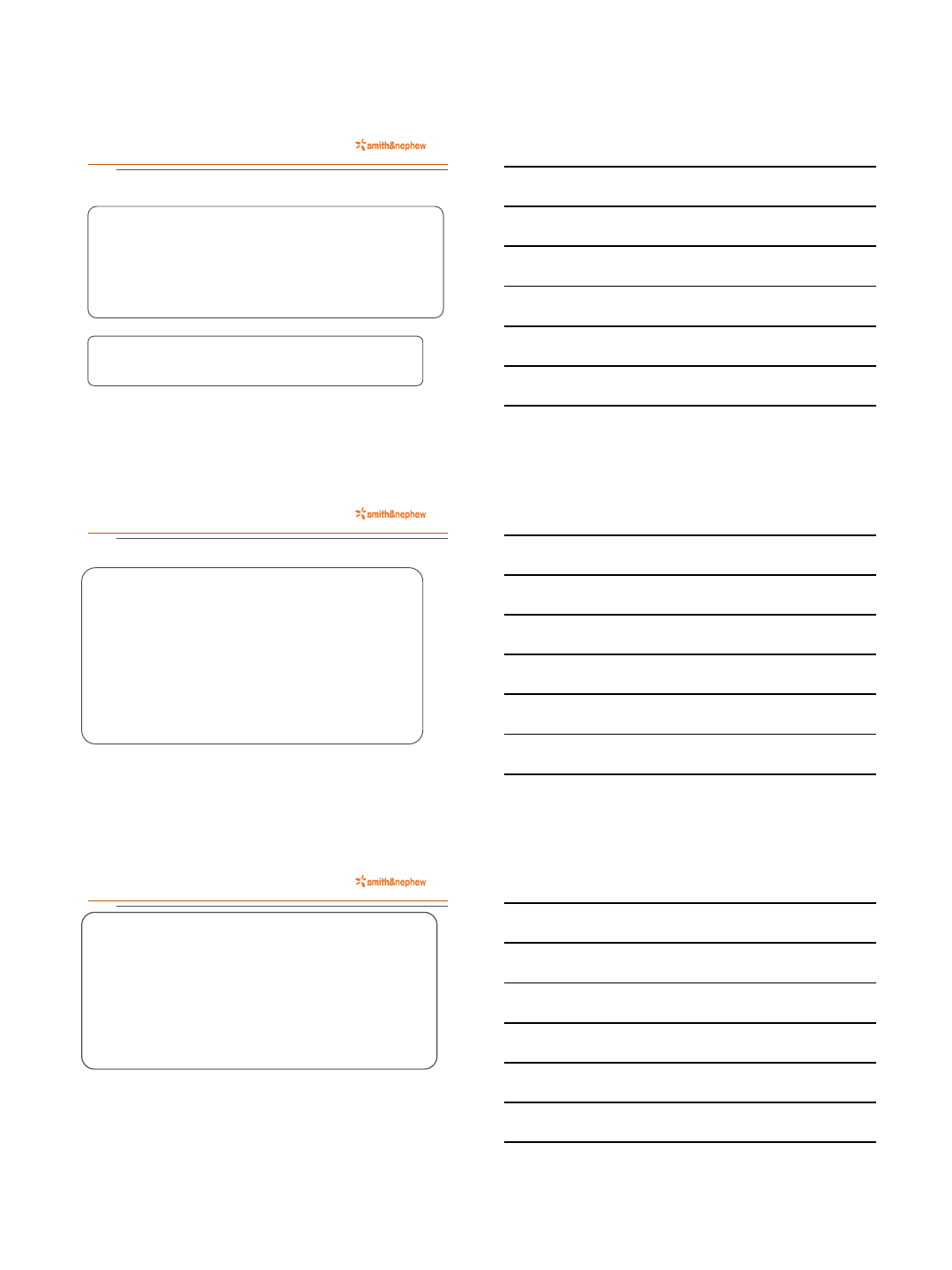
HRRP
Hospital Readmit
Reduction Program
HAC
Hospital Acquired
Condition
VBP
Value Based
Purchasing
Penalty
Only
Improve
Quality/Safety
Timeline Annual Annual Annual
Mandatory
Quality Programs –Above and Beyond BPCI/CCJR
Bonuses
30 Day
Readmits
% at Risk 3% 1% 1.75%
17
https://www.cms.gov/medicare/medicare-fee-for-service-payment/acuteinpatientpps/readmissions-reduction-program.html
https://www.cms.gov/Medicare/Medicare-Fee-for-Service-Payment/AcuteInpatientPPS/HAC-Reduction-Program.html
https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/hospital-value-based-purchasing/index.html
Affordable Care Act Penalty Avoidance
2016 -Up to 6.75 % of total Medicare FFS Inpatient revenues hospital
wide potentially at risk
8/1/15 - Press Ganey Associates Knowledge Brief Hospital Pay for Performance 2015 Update
18
Quality Programs - Affordable Care Act
$428 Million in Penalties experienced by Hospitals
in 2015 (eroding FFS Medicare Inpatient Revenue)
Re-Admissions (HRRP) –up to 3% penalties for highest rates
•2,610 were penalized in 2015 (433 more than 2014)
‐Potentially Avoidable Readmissions
result in approx. $17B Medicare spend
‐2015 - $13.3 million was largest
penalty for Single Hosp - Avg was -.63%1
•Hip/Knee Replacements added as a measure in 2015 based on July
2010-June30 2013 data collection
‐The three main causes of 30 day readmissions (for TJA) were2
‐Wound complications
‐Surgical site infections (SSIs) –Most Costly
‐Medical issues
1The Bottom Line of Hospital Readmissions, The Camden Group Insights Blog, Matthew Smith, Setember 18,2015.
2Cost Burden of 30-Day Readmissions Following Medicare Total Hip and Knee Arthroplasty, Joseph A. Bosco III, et al. The Journal of Arthroplasty 2013.
19
10/5/2015
7
HACs –Hospital Acquired Conditions –¾ of hospitals with lowest HAC rates
held harmless, bottom ¼ get 1% penalty
•Domain 1:Pressure ulcer rate (PSI 3); Iatrogenic pneumothorax rate (PSI
6); Central venous catheter-related blood stream infection rate (PSI 7);
Postoperative hip fracture rate (PSI 8); Postoperative pulmonary
embolism (PE) or deep vein thrombosis rate (DVT) (PSI 12);
Postoperative sepsis rate (PSI 13); Wound dehiscence rate (PSI 14);
and Accidental puncture and laceration rate (PSI 15).
•Domain 2: Central Line-Associated Blood Stream Infection and
Catheter-Associated Urinary Tract Infection.
VBP –Value Based Purchasing –1.5% withheld for FY 2015; 1.75% for 2016
•2016 Score Weighted as follows: Process of Care (SCIPs) (10%), Experience of
Care (HCAHPS) (25%), Clinical Outcomes (AMI-HF-PN Mortality-CAUTI-
CLABSI-SSI)(40%), Medicare spending per beneficiary-Efficiency (25%)
Quality Programs - Affordable Care Act
20
http://innovation.cms.gov/
Quality Metrics
CMMI released a list of quality metrics for monitoring
•Measures pull largely from existing reporting programs and fall
into:
–Case Mix
–Utilization and Efficiency
–Clinical Quality: Process
–Clinical Quality: Outcome
–Care Experience
•Measures are for hospitals, home health, SNF, IRF, and LTCH
•CMMI has not released information on evaluation and
performance benchmarks
•6 provider-submitted measures 21
Provider/Physician Response
•BPCI/CCJR/HRRP/VBP/HACs Creates visibility to Quality
of care such as Complications/Readmissions/excessive
Use of Post acute Resources (Bending the Cost Curve)
•How will the Episode of Care Redesign process increase
functional and quality of life and pain scores? (ICHOM) *
•Embrace Culture Change driving Episode of Care Re-
design
•TDABC (Bozic/Porter), outcomes improvement data, and be
willing to employ BPs from early adopters like HSS, CJRI,
Geisinger, NOSA
22
* “Shifting From Volume to Value, AAOS Bundled Payment Summit, 5/28/15, Washington, DC The International Consortium for Health
Outcomes Measurement (ICHOM), Slide 215.
10/5/2015
8
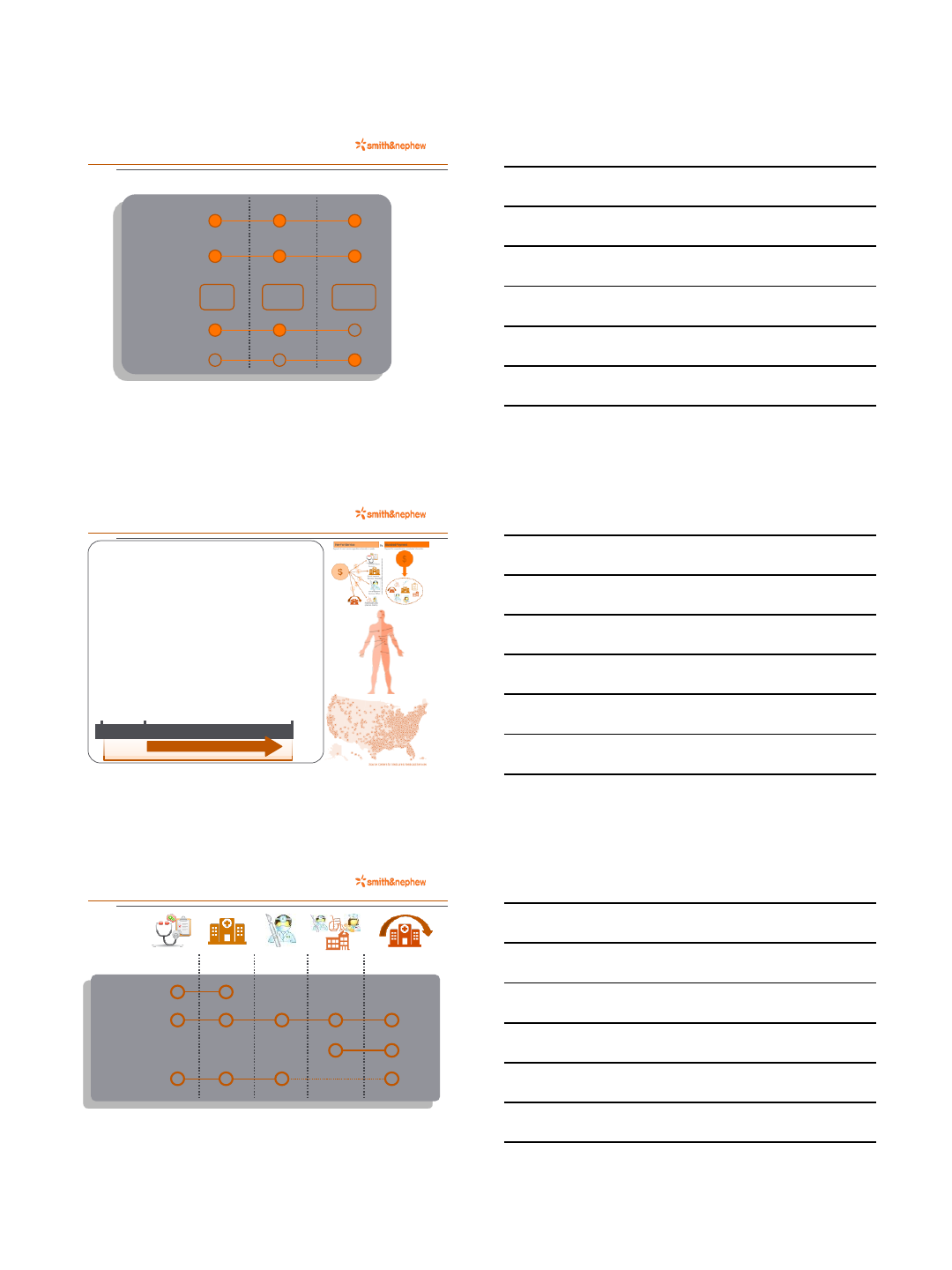
All Medicare Part A / B fee-for-service payments
Rehabilitatio
n and
Recovery
Acquisition Cost /
Hospital
Efficiencies
Long Term
Follow Up
‘Prehab’
Phase
Medicare FFS Part A and B Breakdown of Cost Across Care Continuum THA (2011-2013).
One more look at TJA cost drivers…
23
Admission Discharge 90 Day 10 Year
90 days
•Implant and
Device
Acquisition
•Hospital Fees
•LOS
•Physician Fees
•Post-Acute Care and Rehabilitation
•Readmission Costs
•Facility Costs (SNF, Home Health)
Know Your Why
24
1 “Shifting From Volume to Value, AAOS Bundled Payment Summit, 5/28/15, Washington, DCJim Weinstein, MD –CEO of Dartmouth-
Hitchcock
Simon Senick , https://www.youtube.com/watch?v=sioZd3AxmnE
Thank you!
25
