XIFIN Pay For Value White Paper
2015-05-08
: Pdf Xifin Payforvaluewhitepaper XIFIN_PayForValueWhitePaper 08 2013 clpmag uploads wp-content
Open the PDF directly: View PDF ![]() .
.
Page Count: 28
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
WWW.XIFIN.COM
A Pay-For-Value, Data-Driven
Approach for the Coverage of
Innovative Genetic Tests
Co-Authors:
Paul Billings,
Chief Medical Ofcer, Life Technologies
Richard Ding,
Chief Executive Ofcer, bioTheranostics, Inc.
Lâle White,
Chief Executive Ofcer, XIFIN, Inc.
Rina Wolf,
Vice President of Commercialization Strategies,
Consulting & Industry Affairs, XIFIN, Inc.
David Lorber,
Director of Business Development, XIFIN, Inc.
WHITE PAPER

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
CONTENTS
Summary 1
Introduction 2
Centers for Medicare & Medicaid Services (CMS) Recognizes the Need for Change 2
The Rise of Coverage with Evidence Development (CED) 2
CED and Molecular Diagnostics 4
Molecular Diagnostics: Unique Considerations and Unique Opportunities 4
Critical Concepts for Coverage 7
Clinical Utility 7
Prognostic Rather Than Predictive Results 8
Intellectual Property: Business Constraints 9
Proposal: A Market-Driven, Self-Regulating Approach 10
A Self-Regulating System 10
Shared Risk 11
Data Exchange Supports an Outcomes-Driven Reimbursement Model 14
Take Advantage of the Shift Toward Pay for Value Instead of Fee for Service 18
Considerations for Reimbursement Rates 19
Conclusion 21
Acknowledgements 21
References 22
About the Authors 24
pg i

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 1
SUMMARY
The Coverage with Evidence Determination (CED) methodology is necessary
for treatments and appropriate for traditional diagnostics. However, when
applied to innovations in personalized medicine and molecular diagnostics,
CED (in its current form and with proposed modications) fails to capture the
benets of improved health care and decreased costs that are possible from
the new technology and the data generated from these services. Given the
speed of innovation in this important clinical area, CED methods may make new
tests obsolete before they are commercialized, hindering investment in their
development. Current registry systems have demonstrated promising concepts
for an alternative to CED, but have also uncovered additional challenges, as
would be expected by pioneering new ideas.
This paper proposes an alternative model for coverage determination that
builds upon programs like MolDx by Palmetto and capitalizes on the knowledge
gleaned from early registries, addresses the key underlying nancial motivations
that drive coverage determinations, and advocates for a shift to a Pay-For-Value
(PFV) model based on risk sharing between parties. This proposed model is
intended to move forward the discussion on a design for coverage determination
that encourages innovation in the agile environment of molecular diagnostics.
Changes are urgently needed to allow health care to meet the new demands
posed by increased medical personalization and for accountability of all parties
in the US healthcare system. A technology-enabled coverage determination
process presents a unique opportunity for a self-regulating system that inherently
optimizes patient outcomes, payor costs, and developer prots.
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 2
INTRODUCTION
Centers for Medicare & Medicaid Services (CMS) Recognizes the Need
for Change
One in four Americans receives benets through CMS.1 Thus CMS is in a unique
position to not only make coverage determinations and negotiate low pricing
for its beneciaries, but also to establish the coverage and pricing precedents
most other payors follow. The mission of CMS is to “ensure effective,
up-to-date health care coverage and to promote quality care for
beneciaries.”2 In 2000, CMS (then known as the Health Care
Financing Administration) needed to develop coverage policies for
procedures “where we believed that the enthusiasm of interested
parties was disproportionate to the persuasiveness of the then-current
evidence base.”3 Put more bluntly, diagnostic providers held out higher
hope for certain diagnostics and therapies and therefore recommended
their prescription even when there was no direct evidence of benet. In 2000,
CMS recognized several key shortcomings4 that are still at issue today:
1) For many emerging technologies, seemingly insufcient utilization
evidence had been collected to support a coverage policy; a clear
denition of “sufcient evidence” has yet to be seen in 2013.
2) In many cases CMS beneciaries could benet from early access to an
emerging technology, and by covering an emerging technology CMS
could itself expedite the collection of the necessary data to support a
coverage decision; this is still true in 2013.
3) Randomized Controlled Trials (RCTs), previously considered the gold
standard, are neither a good t, nor are feasible, for the rapid pace
of development of some medical innovations. Applied to molecular
diagnostics, it may increase the cost of development substantially. In
2013, retrospective data, not garnered from RCTs, is becoming more
acceptable as illustrated by a recent reference from Novitas Draft LCD
DL33138 (see Figure 1).5
The Rise of Coverage with Evidence Development (CED)
In 2006, the Coverage with Evidence Development (CED) program6 formalized
a control mechanism to allow CMS to provide cutting-edge health care coverage
CMS is one of the
largest purchasers
of health care in the
world, covering one
in four Americans
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
while still evaluating the clinical utility of new procedures. The CED process, with
its classically designed studies and data collection techniques, was created for
drugs and biologics and is not well suited to molecular diagnostics.
CED approaches t best in a medical system akin
to an assembly line stage-gate supply chain model:
Not only is this stage-gate process not optimal for
molecular diagnostics, but it negates (by providing
no incentive or collection mechanism for) the vast
amount of data the tests can produce and must
freely ow between the stages.
In early 2012, CMS solicited feedback about
updating the program and at about the same time
the President released the National Bioeconomy
Blueprint that specically stated, “Expanding the Coverage with Evidence
Development program to drive innovation: reimbursement for medical treatments
is a powerful driver of industry investment.”7 The draft guidance for CED8, the
review of which ended in January 2013, makes recommendations that are
based on the feedback from the existing CED program, and are in alignment
with the Blueprint. While these recommendations provide some minor tweaks to
the current CED program, they do not address the unique considerations and
opportunities of molecular diagnostics (outlined below). This results in molecular
diagnostics developers being saddled with untenable returns on investment
delaying potentially life-saving (and cost-saving) diagnostics.9
pg 3
Novitas Draft LCD
DL33138
Comparative cohort designs are critical for
assessing predictive ability, and randomization
is highly desirable, although nonconcurrent
randomized cohorts can speed the evaluation
process. The sufficiency of nonrandomized cohorts
must be very carefully scrutinized, on a case by
case basis. This is a reflection of the fact that
alternative approaches to more conventional
randomized prospective controlled trials—such as
prospective-retrospective study designs—may be
able to support predictive biomarker CVU, as long
as they are appropriately conducted. Per above,
there are currently NO standardized thresholds
and/or benchmarks for evaluating the CVU/medical
necessity of emerging biomarkers.
Figure 1: This dra LCD from Novitas indicates alternaves to
randomized controlled trials are viable, if appropriately conducted.5
01 Validation of
diagnostic
02 Clinical utility
03 Reimbursement
determination
04 If additional
indications, go
to stage 01
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 4
CED and Molecular Diagnostics
The CED process, in efforts to ensure correct utilization, can
unnecessarily stie innovation for smaller, venture-backed companies
that do not have the resources to survive the extended period of data-
gathering and potential non-coverage dictated by the CED process.
Given that a great deal of innovation in the molecular diagnostic
space is done by these venture-backed companies, the CED process
has the effect of dampening the entire molecular diagnostics industry.
CED—by design—can take years, and the diagnostics going through
the process may be saddled with an unrecoverable cost burden,
private insurer non-coverage, and be eclipsed by another technology
before reaching market (similar to why labs oppose the FDA process
in favor of the more agile Clinical Laboratory Improvement Act
(CLIA) process for Laboratory Developed Test (LDT) oversight). The
proposed CED process requires the services of a protocol “expert,”
such as the independent Center for Medical Technology Policy
(CMTP)11 further increasing the cost. With these burdens imposed by
CED protocols, the risk-adjusted ROI for developing new diagnostics
such as NexGen Sequencing may not be favorable to produce
desirable rapid development and deployment.
Finally, there is growing recognition of the value of longitudinal
studies, which can capture real world clinical practice, outside
of a sometimes “articial” study environment. Another system
(not CED) that embraces broader data collection and analysis
capabilities and delivers a revamped incentive system is needed.
It should be parsimonious and let research physicians explore how
new diagnostics can be most valuable and allow producers to be
innovative and agile.
Molecular Diagnostics: Unique Considerations and Unique
Opportunities
Genetic testing, molecular diagnostics, genomic testing, and
personalized medicine are fundamentally different from, and will
change, traditional diagnostics and medicine. The difference
Food and Drug
Administration Regulation
Could Add Additional
Burden
The role of the Food and Drug
Administration (FDA) should also be
considered. Currently through a trial
parallel review program, parts of the
clinical trial process can be run in
parallel with early validity studies.
While this may help accelerate the
FDA-approval path, it further codifies
a path that the majority of molecular
diagnostics do not currently follow.
Laboratory Developed Tests (LDTs),
subject to more industry appropriate,
agile regulations and oversight by
CLIA have, and for the foreseeable
future will (due to the structure of
the industry), provide a rich source
of new diagnostics. LDTs, regulated
under the Clinical Laboratory
Improvement Amendments (CLIA) of
1998, have historically been able to
deliver critical tests of public health
importance before FDA approval
is received. An LDT diagnostic for
HIV viral load testing was available
six years before an FDA approved
kit was available. Similarly, an LDT
diagnostic for KRAS to determine
which patients would respond to
cancer treatments was available
years before the FDA kit. A recent
ACLA petition stated that “FDA’s
regulation of LDTs as devices would
adversely affect patient care in the
US.”10
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 5
between traditional and molecular diagnostics is comparable to that between
devices and “smart” devices; a room “knows” when someone enters and turns
on the lights, a car knows when it is skidding and applies the anti-locking break
system. Very specic technology-provided information (motion detection, skid
recognition) alters outcomes in a manner completely impossible without the
added information. Similarly, very specic information provided by molecular
diagnostics for specic patients, can alter the course of medical treatment in a
manner completely impossible without the added information.
Molecular diagnostics presents unique nancial, timetable, and scientic
benets relative to other diagnostics, which are not leveraged by the CED
process:
1. Financial – molecular diagnostics target small markets with high
development costs
• Unit costs are higher – The development costs for molecular diagnostics
and treatments are commonly on par with, or higher than, non-molecular
tests and treatments, but generally are only given to a relatively small
number of patients exhibiting very specic indicators.
• Benetsaregreater – Molecular diagnostics can be more precise than
traditional diagnostics, allowing appropriate therapies to be delivered
sooner, resulting in better outcomes and less waste.
• Relative value is greater – As treatments and diagnostics evolve (Figure
2), their costs generally increase, as does the value of knowing when to
utilize a treatment. In other words, a $20 test to determine if $50 worth
Visual See a lesion/growth
See the bacteria
Stain for specific
structures
Micro-
scopic
Chemical
Marker
Evolution of Diagnostics
Genetic Identify underlying
genetic cause
Physical Remove lesion / growth
Tree bark, Penicillin
Broad-based chemical
agents
Natural
Synthetic
Evolution of Treatments
Genetic Drugs targeted at
specific mutations
Figure 2: Both diagnoscs and treatments connue to evolve to higher-cost, more complex protocols that also possess higher potenal value to
the paent.

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 6
of antibiotics should be prescribed is a benecial test; a $3,000 test to
determine if $100,000 worth of a cancer therapy should be prescribed is
a more benecial one. This results in the personalized test being more
valuable from a purely nancial perspective.
The CED process does not take into account the increased development costs
to the developer, the improved health outcomes for the patient, the potential
for waste reduction or cost control, or the decreased costs for payors. It
additionally assumes that costs will be offset in the long run when the diagnostic
is disseminated for usage by the general public. The entire point and value of
genetics is that they will never be broadly disseminated. Markets will be smaller
and even more personalized.
2. Timetable of molecular diagnostics – studies are slow, trials need not
be slow
• Conductingstudiesismoredifcult–Because molecular diagnostics
are narrowly targeted, the group of patients who have the correct set of
highly specic risk factors that indicate appropriate use of a diagnostic is
necessarily small. Identifying a patient population large enough to support
statistically signicant results can prove time-consuming and difcult, and
could delay access. The challenge of nding suitable patients increases
the value of data from each patient and speaks directly to the need for
increased data federation through electronic health records.
• Trial periods – While studies can be slow, trials, and the inception of
data gathering, can happen more quickly. It is benecial and preferred to
begin gathering data immediately rather than in a drawn out trial process.
Unlike treatment trials, diagnostic trials can, by appropriate weighting of the
results, present no health risk to patients. It is important to note that in the
absence of decision support tools to help physicians determine the weight
that should be applied to diagnostics results, the diagnostics may not be
used in an efcacious manner.12
The CED process makes no allowance for the rapidity with which molecular
diagnostics evolve or the dearth of test subjects who can contribute to the
knowledge pool (and the data these test subjects can provide).
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 7
3. Scientic–moleculardiagnosticsinvolveshugenumbersofvariables
Because of the virtually limitless combinations of genetic markers possible, it
is likely that during the course of evaluating a specic molecular diagnostic,
useful variations will be identied. These variations are far more numerous
than could be reasonably addressed by sequential independent studies.
The variations may:
• Increase the accuracy or specicity of a diagnostic
• Identify new applications in test subjects (e.g., identifying the presence of
HER2 in colon cancer patients who subsequently respond to Herceptin)
The CED process does not allow tests to evolve dynamically based on the
cornucopia of data that can be provided by slight biomarker variations, or
newly-discovered indications.
CRITICAL CONCEPTS FOR COVERAGE
Clinical Utility
The core element to determining appropriate coverage centers on clinical utility.
There is little dispute that for analytic or clinical validity, measurements should
be done accurately and be reproducible in varying
clinical environments.13 The disputes arise around
the concept of utility or clinical utility—what does it
mean? How is it measured? Who pays to measure
it? How is it used as both a yardstick and gate for
payment?
All parties have slightly varying denitions of utility;
utility can have different meanings when applied
to inherited conditions vs. reproductive decision-
making vs. public health, and there is uncertainty around when an appropriate
quantity of data has been accumulated to measure utility. In the context of CED,
the payors’ denition that a clinically useful result is one that alters the course of
treatment (e.g., identifying the right type of intervention or changes in monitoring
methods or frequency), is probably most relevant.
Measuring clinical utility, or determining when it needs to be measured
through the CED process, is not clearly dened. The historical code-stacking
A study done by McKinsey & Co for the Personalized
Medicine Coalition revealed that of $292B spent on
medications in 2008, approximately $145B went to
drugs that were ineffective for the patients who took
them. Further findings estimate the cost of adverse
drug events to range between $45 to $135B per
year. An estimated 25% of these costs could be
averted through the use of diagnostic tests for the
appropriate biomarkers.
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 8
reimbursement methodology (the use of which we are not advocating) largely
circumvented the need to dene clinical utility by allowing diagnostics, still lacking
complete clinical utility studies, to be reimbursed. In fact, under the code-stack
methodology, tests were frequently reimbursed before much, if any, clinical
utility data were generated—allowing information
to be collected after commercialization. Since
diagnostics are ordered by physicians, adoption
of new diagnostics is generally driven by expert
specialty physicians or key opinion leaders integral
to the research process and the generation of
data for more widespread publication. The end
of code-stacking at the beginning of 2013, and
the concomitant introduction of specic codes for
various diagnostics, resulted in limiting the scope
of use of some diagnostics (e.g., EGFR) and
requiring new tests to be coded as miscellaneous
requiring appeals. Without reimbursement for new
tests, physicians may be unnecessarily constrained
in using their best judgment for medical care.
Additionally, under the code-stacking model, slight
variations of tests could be used and reimbursed.
Code-stacking, while far from ideal, provided a mechanism by which patients
could benet from innovative diagnostics.
An increased reliance on cost-prohibitive, xed CED utilization studies, when
combined with the discontinuation of code-stacking provides impediments
to: investment in new molecular diagnostics (costs are higher and revenue is
delayed); the collection of data so new diagnostics can be approved; and most
importantly, providing the best care. Diagnostics that fulll unmet medical needs
are not properly incented or nanced.
Prognostic Rather Than Predictive Results
There is an important distinction between predictive and prognostic factors
in relation to the utilization of diagnostics.14 Prognostic factors speak to the
probable course and outcome of a disease, while predictive factors address
Clinical utility is in the eye of the
beholder
For patients, relief or cure is a shared goal with
the provider. But utility might be the end of wasteful
payments, palliative care provision, or estate
planning.
For providers, utility may be a simple change of
guidelines or atrophied standards of care but could
also mean changes in office or hospital workflows,
simpler and more targeted test ordering or less
iatrogenic illness.
For hospitals, utility is better Diagnosis related
group management and facility optimization as well
as potentials for marketing and differentiation.
For payors, utility is cost saving, improved
outcomes and more informed management of
groups.

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
the likely effectiveness of a therapy. The coverage decision for a diagnostic
should be based on the test’s ability to provide prognostic guidance that impacts
patient care, (a so called “actionable result”), not on the predicted (or realized)
effectiveness of the resultant therapy. The prognostic guidance is realized
as soon as the physician sees the results. The results could range from the
avoidance of an unnecessary therapeutic intervention to simply a change in
surveillance.15 This “instantaneous” value of diagnostics makes them ideal for a
PFV payment structure.
Due to the complexity of molecular diagnostic results, the determination of
“standard of care” and coverage should to some extent be based on the
decision support provided to the physician along with the result. For example,
if a physician decides on a course of action different than one that would have
been taken without the diagnostic, then the test demonstrates utility and the
diagnostic provider should be reimbursed. If the physician takes appropriate
action as a result of a diagnostic and its associate decision support, the physician
should be considered to have delivered the standard of care and should also be
reimbursed.
Intellectual Property: Business Constraints
Pharmaceuticals and other therapies generally enjoy a relatively long period
of post-approval patent protection, and consumption patterns that may last for
several years. The rate at which molecular diagnostics are evolving means that
the useful lifetime of diagnostic patents could be signicantly shorter than for
therapeutic patents. Further, molecular diagnostics are almost always deployed
as a single instance (i.e., one set of biomarkers). Even if a patent remains viable,
it is likely that an enhanced version of the diagnostic would become available
prior to the protocol endpoint. In other words, because molecular diagnostic
technology evolves so rapidly, patents for these diagnostics are much more
likely to be obsolete than are patents for medical devices or slower-moving
technologies.
pg 9
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
PROPOSAL: A MARKET-DRIVEN, SELF-REGULATING APPROACH
The alternative to CED proposed herein leverages advances in technology
to exchange information, and the vast amounts of data created by molecular
diagnostics, to allow for a more market-driven, self-regulating, PFV approach to
health care.
A Self-Regulating System
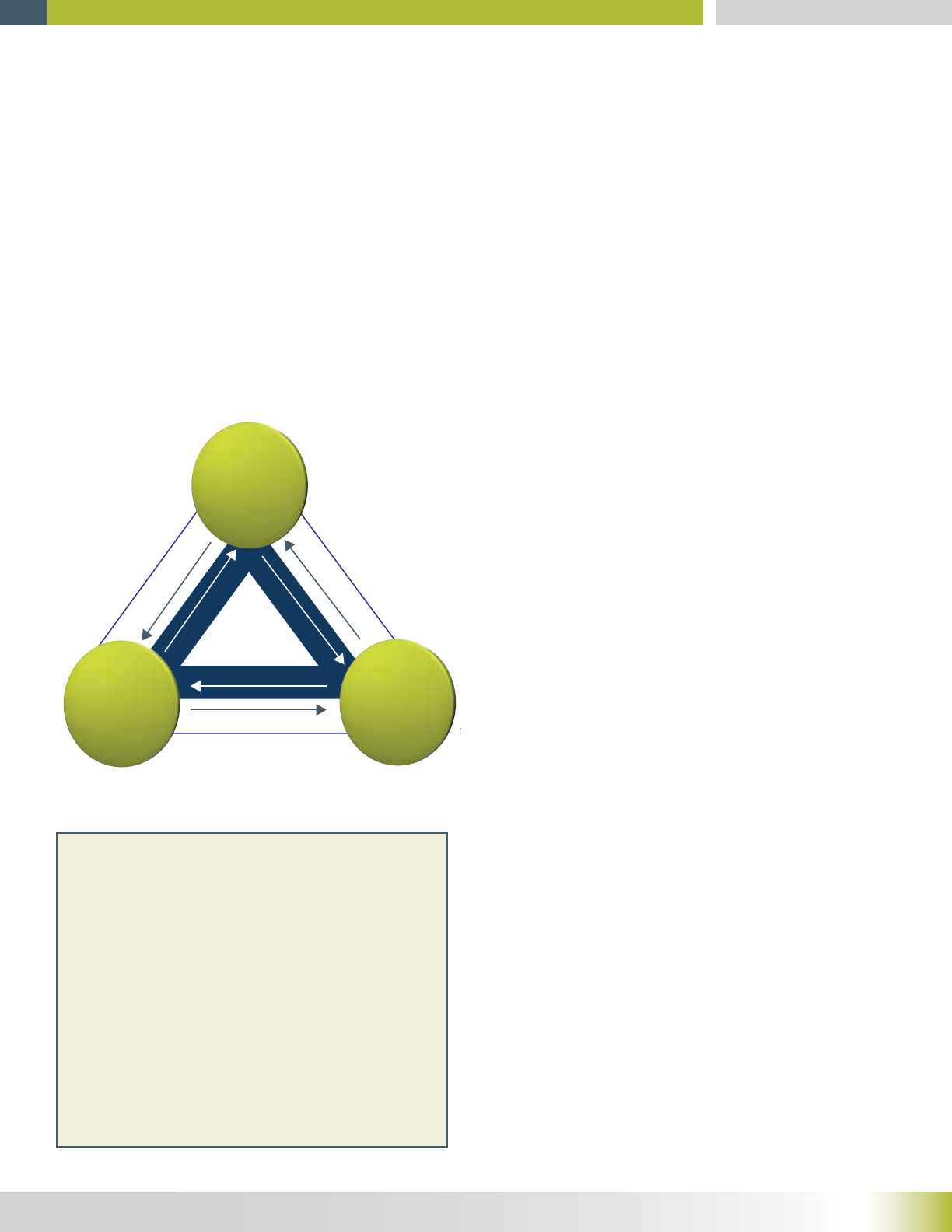
The driver for the interactions between the payor, diagnostic provider and the
physician/patient is reimbursement (in addition to the more altruistic desires to
improve outcomes). Reimbursement drives two opposite, but complementary
cycles (Figure 3).
Counter clockwise cycle:
• Patients and physicians want diagnostic
providers to develop tests that improve
treatment decisions.
• Payors want patients and physicians to
efciently use nascent diagnostics (i.e.,
correctly order and interpret results leading to
lower overall costs, less waste and improved
outcomes).
• Diagnostic providers want payors to provide
reimbursement for their innovations (a driver
for this cycle).
For the complementary clockwise cycle:
• Diagnostic providers want data supporting the
clinical utility of their new tests.
• Payors want decision support systems from
diagnostic providers to help physicians
correctly 1) order diagnostics, 2) interpret the
results, and 3) select the most appropriate
treatments.
• Physicians want payors to provide
reimbursement for efciently practicing
medicine (a driver for this cycle).
pg 10
Diagnostic Tests
Data
Physician/
Patient
Diagnostic
Provider
Eciency
Decision Support
Reimbursement
Reimbursement
Payor
Figure 3: Two cycles acvely linking payors, physicians, and providers to
eciently deliver health care.
The need for decision support systems to help
physicians improve use and interpretation of tests
was highlighted in a recent study of US medical
records by the Centre for Health Systems and Safety
Research, at the University of New South Wales. The
investigators found that doctors in the United States
fail to follow up as many as 62% of clinical pathology
laboratory tests and up to 35% of radiology reports.
This means that they are missing critical diagnoses.
In turn, this causes delays in treatments for many
conditions, including cancer.16
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
These complementary cycles provide a unique opportunity for a paradigm
shift in how molecular diagnostics are developed, approved, reimbursed, and
continually studied. Molecular diagnostics are particularly poorly suited to CED
and Fee-For-Service (FFS) reimbursement and are particularly well suited to an
alternative process and
pay-for-performance
reimbursement (Figure 4).
The key elements
that allow molecular
diagnostics to advance
from series of static
stages of development
to the more uid market-
driven cycle described in
Figure 4 are risk sharing
and data exchange.
The end result should
be a model that allows
the agile renement
of practice guidelines
that efciently optimize
healthcare.
Shared Risk
Risk sharing for medical
coverage is a relatively
new concept. After
Johnson & Johnson
received a coverage
rejection in 2006 for
its multiple myeloma agent, Velcade, from the UK’s National Institute of Health
& Clinical Excellence (NICE), it proposed the Velcade Response Scheme.17
This scheme essentially placed the payment burden back on the developer in
cases where the therapy was ineffective. About the same time, Genomic Health
pg 11
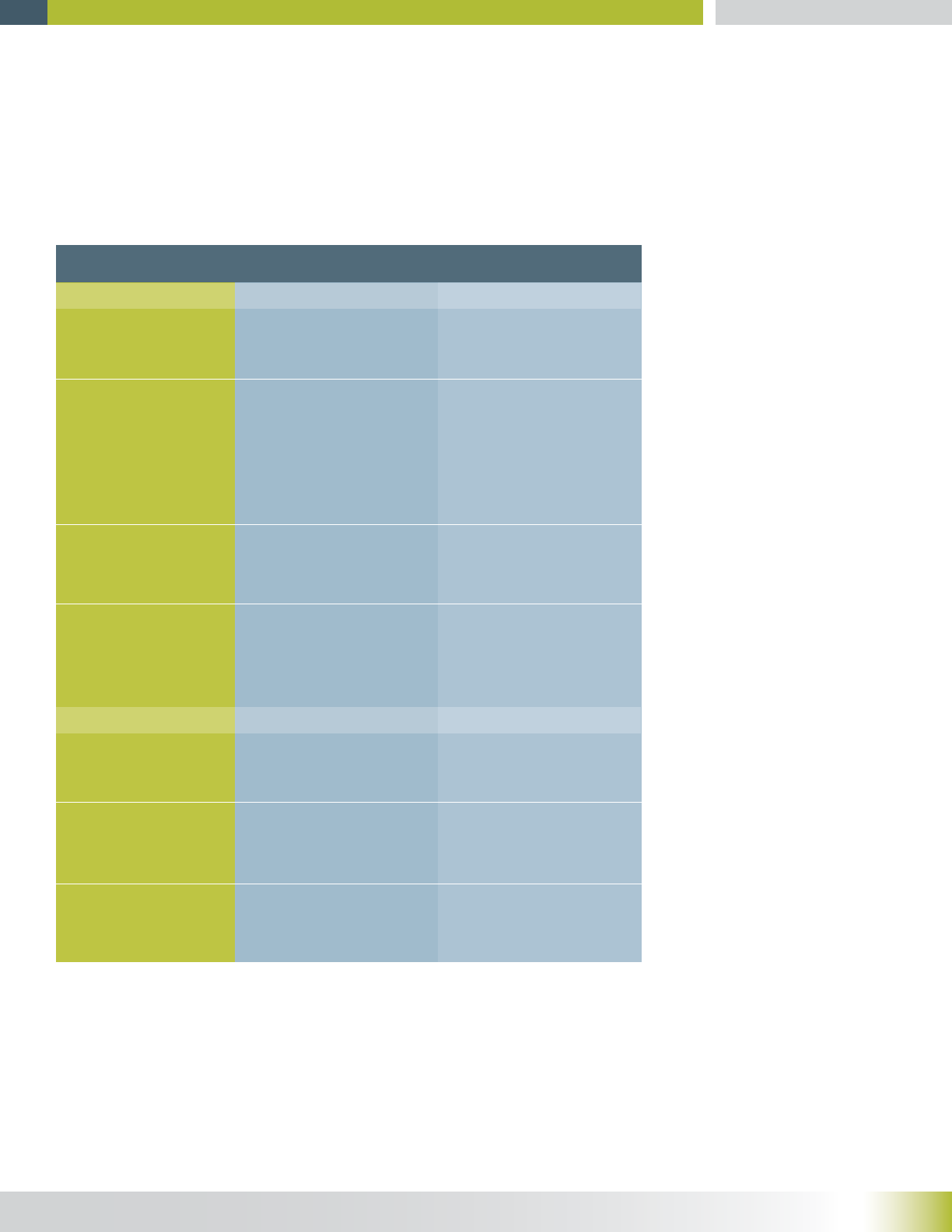
CED and FFS
Stages of Development
Design…likely to continu-
ally morph as more data
is collected
Approval…likely to be
required for many very
similar variations
Reimbursed or not, regard-
less of appropriateness of
the test
Reimbursed on a sliding
scale if treatment is altered.
Alternative Process and PFV
Reimbursement…values
are likely to be strongly
contested—high value
results
Fixed set of experiments
using a fixed protocol
Granted or not granted
based on the protocol
Let the biomarker set morph
and guide physicians in the
use of the evolving results
Remove the concept of
approval for molecular
diagnostics. The physician
makes informed decisions
about the appropriateness
of a diagnostic given the
indicators and available
data
Additional studies need to
be funded and undertaken
Incentivized to:
Have the diagnostic ordered
as much as possible
Not prescribe the diagnostic
because it might not alter
the course of treatment
Limit access to diagnostics;
difficulty in getting coverage
for their patients
The developer can promote
use of the diagnostic, by
assuming varying amounts
of the risk associated with
the cost
Incentivized to:
Have the diagnostic ordered
only where it might alter the
course of treatment
Have the diagnostic ordered
whenever the physician
believes it will alter
treatment
Prescribe any diagnostic
and provided with all
available data to make an
informed decision
Additional indications …
likely to be discovered as
more data is collected
Interested parties
Developers
Payors
Physicians
Figure 4: Comparing the status quo (CED and FFS) to an alternave process based on PFV from the perspecve
of development of a diagnosc and each of the interested pares.
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
launched OncotypeDX. This molecular diagnostic for the determination of
recurrent invasive breast cancer in estrogen receptor positive and lymph node
negative women, had signicant validation, but lacked clinical utility data. Lee
Newcomer at United Healthcare led an effort with Genomic Health to develop a
risk sharing model for OncotypeDX.
An important aspect of risk sharing as it applies to molecular diagnostics involves
managing risk through decision support tools (discussed below). Both the
ordering of diagnostics (e.g., when to use a molecular diagnostic, which specic
analytes should be tested) and the interpretation of results are complex. As part
of sharing risk, payors must collaborate with diagnostic providers to ensure they
can provide correct guidance for physicians so that the right tests are ordered at
the right time and so that the right treatment decisions result.
There are two important notes about risk sharing, a relatively labor-intensive
methodology. First, risk sharing is not being proposed as a primary, long-term
solution, but rather a model that allows clinical utility data to be accumulated
while providing appropriate remuneration in the dynamic molecular diagnostics
market. Second, to avoid the complexities of risk sharing but still allow for
some non-covered procedures, a pre-
authorization process is sometimes
used. While pre-authorization does
avoid some complexities it is highly
inefcient, time-consuming, and can
signicantly increase costs.18
As an example of how a risk sharing
model might work, assume a
hypothetical diagnostic, ABC-test
(Figure 5). The risk sharing model is based on the idea that the lab should
be paid (see the Considerations for Reimbursement section) if the diagnostic
produces actionable results. ABC-test has three indicators, each with equal
prognostic weight (row A). The lab, using its own data, expresses the risk it
is willing to take that the diagnostic will produce actionable results (row B). If
the lab is highly condent that the diagnostic will produce actionable results, it
pg 12
Indicators present
Lab’s confidence /
interest in results
Cost distribution if
treatment is not altered
Lab
Payor
Patient
1
5%
2
60%
3
90%
New
70%
100%
Negotiated Diagnostic Risk Sharing for ABC-test
The payor pays 100% if the diagnostic produces actionable results
—whatever treatment is provided is known to be the right one.
A
D
C
B
Figure 5: Hypothecal negoated diagnosc risk sharing. Provider expresses its condence
in its test, guiding coverage and cost distribuon.

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
could make this percentage high—effectively saying that if the diagnostic fails to
produce actionable results, the lab will absorb the cost. This condence level can
then be used by payors to make a coverage determination (row D).
For ABC-test:
• For one indication, the diagnostic provider has very low condence that the
diagnostic will alter treatment. It expresses this by indicating that if the test
does not alter the course of treatment, it will only absorb 5% of the cost—a
clear signal from the lab to the payor that the test should not be covered in
this case.
• The payor will likely follow the lab’s guidance and not provide coverage for
the test in this case.
• The physician and patient can then determine if they feel the test will be
benecial, knowing that the patient will likely be responsible for the bill.
• For three indications, the diagnostic provider is condent (90%) that the
diagnostic will alter the standard treatment. It expresses this by indicating
that if the test does not alter the course of treatment, it will absorb 90% of the
cost—a clear signal from the lab to the payor that the test should be covered.
• The payor will likely follow the lab’s guidance and provide coverage;
the lab has already placed a large bet on the test altering the course of
treatment.
• The physician and patient have high condence that the payor and
diagnostic provider believe the diagnostic is appropriate and one of them
will cover the cost.
• For a new indication, one for which the diagnostic provider thinks the test
might be useful but lacks clinical utility data; the lab can also place a bet. The
extent to which the lab wants the data and believes that its diagnostic can
alter treatment is expressed by the risk it is willing to take.
• The payor will likely follow the lab’s guidance. If the lab has high
condence in the diagnostic’s ability to alter treatment, the payor will
probably cover the diagnostic—either it alters treatment (good for the
payor; although it will pay for the diagnostic, it will get a better outcome) or
it does not (good for the payor, since the lab will absorb most of the cost).
• The physician and the patient have a condence level in the diagnostic
informed by the willingness of the lab and payor to cover the cost.
pg 13

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
• The lab must only be held accountable for these pricing mechanisms if
the physician has followed criteria that have been agreed to between the
payor and the lab for appropriate patient selection, timing of use of test
along care continuum, and treatment guidelines.
It is through this coverage determination that payors must incentivize providers
to design appropriate practice guidelines, and incentivize physicians to use new
and emerging technologies appropriately. In order for this balance to work fairly,
payors must:
• Compel test providers to develop appropriate protocols that clearly
demonstrate where and how these tests should be used in the continuum of
diagnosis and care;
• Work with providers to facilitate the educational process and to set policies
that encourage appropriate and effective use, and discourage less effective,
often older, modalities (e.g., limits on number of IHC stains prior to a
molecular alternative being mandated);
• Provide mechanisms to measure the effectiveness of these protocols. As an
example, Aetna is involved in a program with eviti Inc., to provide participating
Aetna oncologists in two states with access to eviti’s evidence-based decision
support tool.19
Together, payors, physicians, and laboratories hold the key to ensuring optimal
ordering of new diagnostics.
DATA EXCHANGE SUPPORTS AN OUTCOMES-DRIVEN
REIMBURSEMENT MODEL
Data exchange involves 1) the collection of data, 2) a repository in which the data
is federated, and 3) the expert analysis and formulation of the data into decision
support tools for physicians guiding the ordering of molecular diagnostics and the
interpretation of the results. The current regulatory environment forces diagnostic
providers to be passive purveyors of tests, not involved in the discipline of their
ordering. This forced separation results in the Ofce of the Inspector General
(OIG) preventing the free ow of data between the needed parties. The CED
process does not support, and by failing to create an enabling mechanism
effectively prohibits, this data exchange.
pg 14

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
Data Collection
The collection of data would need to include outcomes, phenotypes exhibited or
indicators observed, and specic biomarkers and methodologies. Outcomes, in
reference to diagnostics, are probably better referred to as actionable results.
Unlike therapeutics, where outcomes (quality of life, survival rate, etc.) may not be
known for years, the “outcomes” of most diagnostics are known within days—the
physician reads the report, and either takes the same action s/he would have
without the diagnostic, or takes a different action. An incentive system must be
put in place, potentially as part of the nal laboratory report, where reimbursement
is tied to improved stratication or diagnosis, prognosis, monitoring or predicting
response.
Data Repository
Currently, physicians struggle to keep abreast of the subtle differences between
similar diagnostics and then to ensure they are correctly interpreting and acting
on them. Developers attempt to collect data about the set of conditions that led
to the diagnostic’s prescription and the set of actions taken as a result of the
diagnostic. Payors struggle to understand the correct ordering of diagnostics
and if the diagnostic impacted the course of treatment. Driven by the need for
coverage, diagnostic providers are opting-in to Palmetto’s MolDx program (PTI
codes), the McKesson Z-Codes, and other registry systems. These systems
provide a promising beta test for how such registry systems might work (e.g.,
they provide the additional specicity that was lacking from code stacks), but they
also identied a new challenge by being so specic that they prevent variants
of the diagnostic from easily being ordered or reimbursed. If during the course
of use, a clinically useful biomarker variant is identied, current registry systems
set up the variant as a new diagnostic rather than creating a branch. Additionally,
the current systems may suffer from a perceived lack of independence needed
to be a universal, impartial “single source of truth.” This may result in some
diagnostic providers being somewhat reticent to contribute the desired level of
data needed to optimize healthcare decisions: 1) indications and decision support
leading to diagnostic ordering and 2) results and decision support to guide results
interpretation.
The National Institutes of Health (NIH) has created the Genetic Testing Registry
(GTR)20 and ClinVar21 to aggregate test-related information. GTR provides
pg 15
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
detailed information about the purpose of the test and the indications (primarily
diagnoses) leading to use. ClinVar aggregates information about sequence
variation and its relationship to health. Together, these two data resources can
provide the foundation for a collaborative, easy to use and impartial repository,
with the caveat that the data in any repository is inherently limited by the honesty
of the submitters. A solution to facilitate the free exchange of data may be
relatively close.
The GTR accumulates clinical utility statements and citations for individual
tests and curates professional practice guidelines, position statements, and
recommendations. A results database, maintained by the developer, could utilize
the GTR to refer to accessioned tests that explicitly describe the diagnostic.
With versioning, changes in biomarkers or methodologies—or other factors—
could be delineated clearly for an evolving test and would enable the reporting
of outcomes to continue. The GTR currently allows physicians to see a list of
molecular diagnostics; view information about validity, prociency testing, and
utility; understand the appropriate use cases (phenotypes/indications); and
access a wide variety of resources (relevant trials/studies, molecular details,
drug labeling related to companion diagnostics). Developers of diagnostics could
also be required to provide a feedback/reporting mechanism as a condition of
coverage. HIT vendors would utilize the public, open source data to provide
content for optimizing ordering and reporting through EMRs, CPOEs, PMS,
etc. The foundation for the proposed paradigm shift in diagnostic prescription,
development, and reimbursement is predicated upon the free exchange of
data. Physicians must provide data to developers so developers can provide
effective decision support tools that allow payors to know diagnostics are being
prescribed and interpreted correctly, and payors, in turn, will provide coverage
for the diagnostic the physician wants to prescribe. The payor’s role must shift
from simply paying the bills, to strategically investing in (covering the cost of)
diagnostics.
Decision Support
Diagnostic developers—labs—have the most complete information about
when to order their diagnostics and how the results should be interpreted. To
pg 16
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
ensure physicians have the best possible information, the burden of creating
and providing decision support should be placed with the diagnostic provider.
An appropriate risk sharing model can ensure that labs provide unbiased
information. Registry information will facilitate the timely renement of such
decision support and the eventual establishment of practice guidelines.
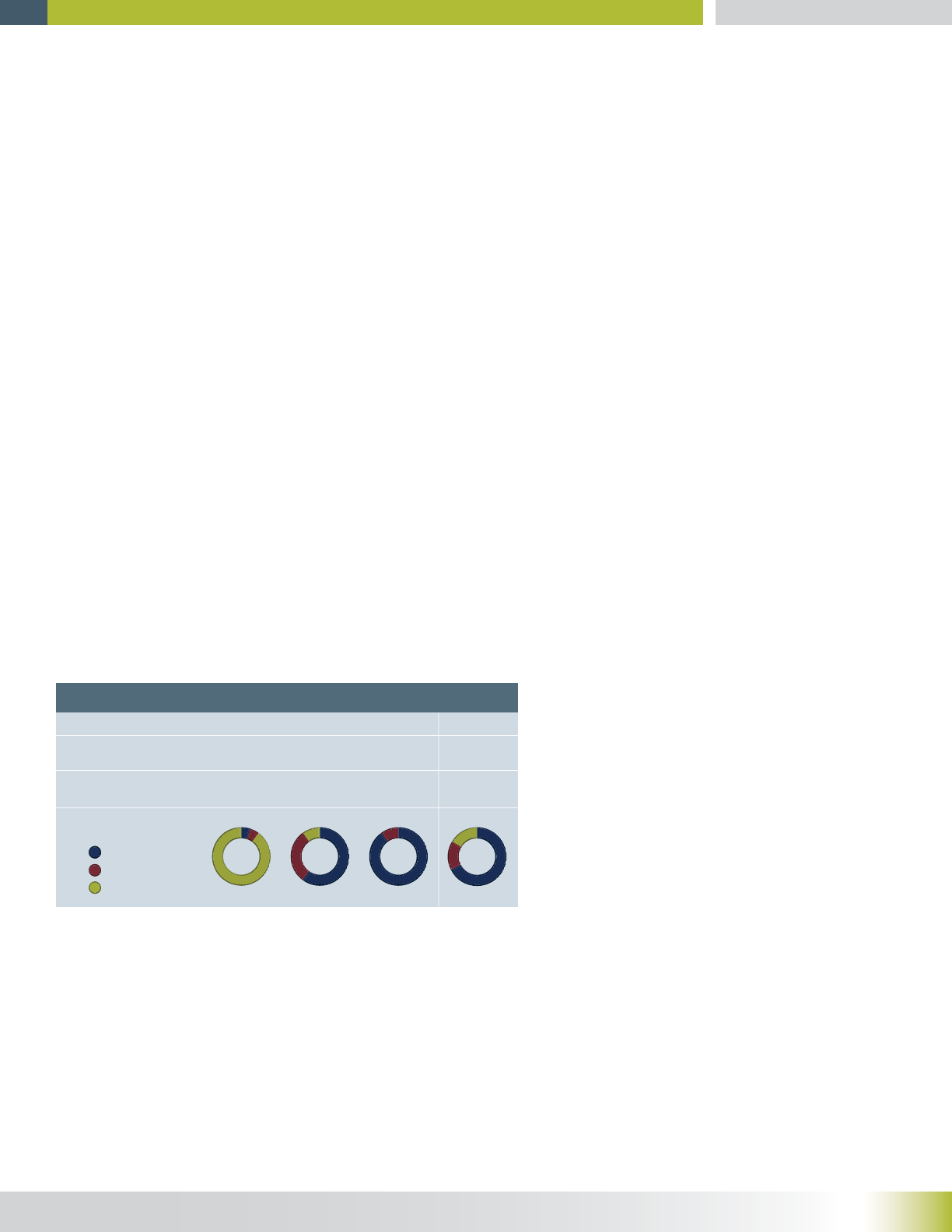
Figure 6 shows a highly simplied example of decision support for ordering the
hypothetical molecular diagnostic, ABC-test. The data in the table is a summary
of physician-reported utilization and treatment decisions. In this example there
are again three established indicators,
each with equal prognostic weight,
and one new, relatively unutilized
indicator. Additionally, treatment in this
case is assumed to be binary (altered
or unaltered), when in practice, there
is likely to be a sliding scale as to the
extent treatment has been altered.
These data, combined with the payors’
current coverage decision, allows the physician, with the patient, to make an
informed decision about the appropriateness of the diagnostic.
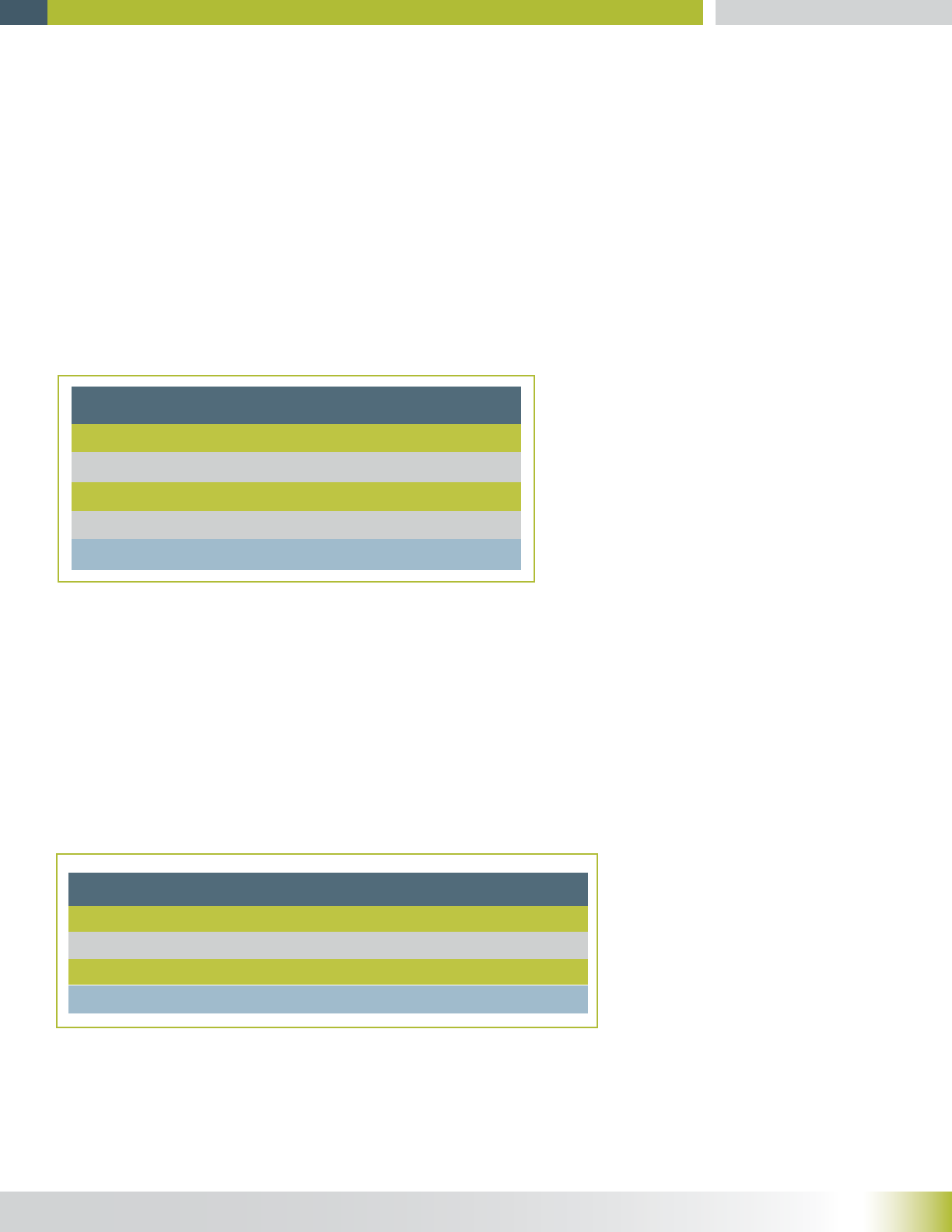
The second critical aspect to a decision support system for molecular diagnostics
is the results decision support. Figure 7 shows a highly simplied example of
decision support for interpreting the results from ABC-test. The data in the table
is a summary of physician reported results and treatment decisions. In this
example there are three sets
of biomarkers observed,
the number of cases each
set was observed and the
percentage of those cases
where treatment was altered.
Again, treatment is assumed
to be binary. Importantly, the
data also includes a physician retrospective—does the physician feel s/he made
the right decision. The higher percentage of physicians that feel they made the
pg 17
1
2
3
New
Total
100
200
390
10
700
25%
32%
80%
90%
410
Indicators Present # of Prescriptions Altered Treatment
Figure 6: ABC-Test decision support for ordering. Empirical data to guide physicians in
prescribing the diagnosc and to set payment raos.
50%
70%
90%
Total
300
250
150
700
Biomarkers
Matched
33%
68%
94%
410
(n=99) 50% Yes
(n=170) 80% Yes
(n=141) 90% Yes
(n=201) 50% Yes
(n=80) 30% Yes
(n=9) 20% Yes
Altered
Treatment
Physician Retrospective
Altered Unaltered
# of Patients
Figure 7: ABC-Test results decision support. Empirical data guides physician in selecng a treatment.
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
right decision based on the results of the diagnostic further validates the decision
support tool. This data quickly and easily provides physicians with the latest
utilization data.
Ideally, a data exchange system supporting data collection, curation, and
decision support could be implemented that would allow coverage decisions for
new molecular diagnostics with little or no regulation/oversight.
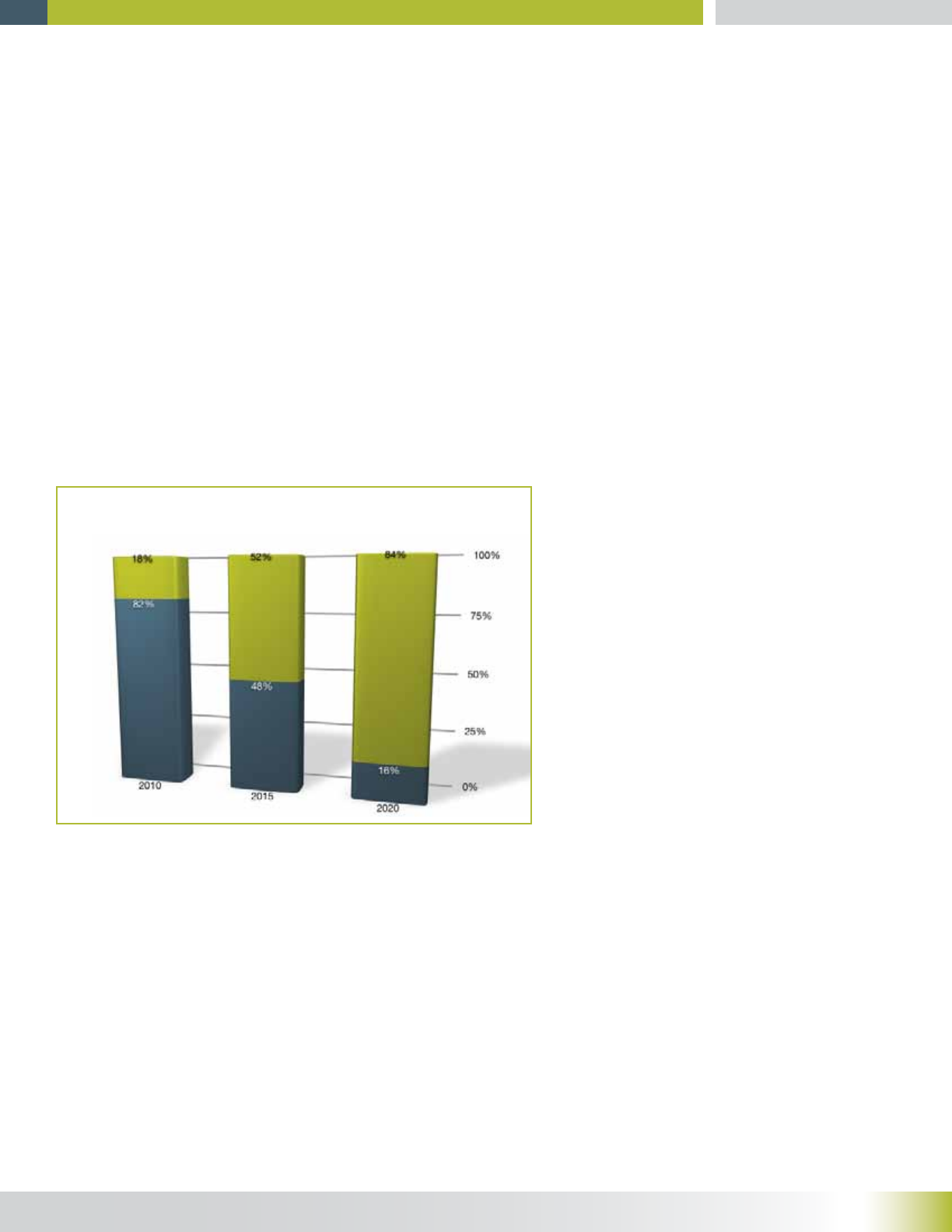
Take Advantage of the Shift Toward Pay for Value (PFV) Instead of Fee
For Service (FFS)
As shown in Figure 8, Fee for Service (FFS), the most prevalent reimbursement
model in the US healthcare system, is projected to rapidly give way to Pay for
Value22 (PFV). The change is being
driven by the exploding costs of
health care and is being enabled by
the relative ease of data sharing. An
FFS system is simpler than a PFV
system; under FFS, a service (checkup,
diagnostic, treatment) is provided and
payment is rendered, whereas PFV
requires a feedback loop to determine
payment. This feedback loop is a
challenge because it requires all
parties to use more data; physicians,
diagnostic providers, and payors need
to consider it.
The processes already in place for molecular diagnostics reimbursement allow
for a limited PFV system. As part of the negotiation between developers and
payors, conditions for reporting use patterns can be established directly, tying
coverage to correct use of the diagnostic. These conditions are almost always
part of the CED process while clinical utility is being demonstrated, but do not
have to be limited to that process; they can be required after clinical utility has
been established. Extending reporting after the demonstration of clinical utility
pg 18
Projected Decline in Fee-for-Service
Percent of Hospital-based Physicians
Figure 8: Fee-for-service reimbursement models are expected to be rapidly replaced
over the next decade by pay-for-value models.22

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
would allow for the collection of additional data about similar variations on
approved use conditions.
CONSIDERATIONS FOR REIMBURSEMENT RATES
In simple terms, there should be a sliding scale for payment responsibility. A
test that has little impact on the course of treatment, arguably has little value,
and should be reimbursed at a correspondingly low rate. Similarly, a test that
signicantly alters the course of treatment (compared
to without the test) has signicant value and should be
reimbursed at a correspondingly higher rate (Figure 9). Of
course payment for medical services is not this simple and
straightforward.
Assuming a philosophy of shared risk/payment for
molecular diagnostics based on the degree to which the
diagnostic altered the course of treatment, there is still the
core question, “What is an appropriate price for a test?” To
begin answering this question, look to the analyte being
measured (Figure 10).
If the key analytes or sequences being studied by a new diagnostic are
new, it is important to understand if there is a similar diagnostic for the same
indicated use (different gene, identical condition). If there is a similar diagnostic,
with less sensitivity or specicity for the identical condition (traditional PSA
vs. ultra-sensitive PSA, CTID vs. IHC), then the new diagnostic should be
reimbursed incrementally more than the existing, less sensitive, diagnostic. The
reimbursement uptick should be based on the relative superiority of the new
diagnostic over its predecessor. If the new analyte is equal to or no better than
the existing diagnostic they both should be reimbursed at a discount as they are
commodities.
If there is no similar diagnostic for the condition, then the impact on the standard
of care must be determined. The new diagnostic should be reimbursed at a
rate appropriate for the value it delivers. When the clinical utility is anticipated
but not proven, the diagnostic initially should be reimbursed at cost plus, until
pg 19
Figure 9: A sliding scale of cost responsibility based on
“aconability” of results.
Payor
Responsibility
Developer
Responsibility
% of Cost
Treatment as a result of diagnosis
Unchanged Somewhat
changed
Significantly
changed
100%
75%
50%
25%
0%
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
clinical utility and overall health economic value is determined. At this time the
test should be reimbursed based on its value. There are a number of established
methods for determining the value of specic diagnostics that should be used.23, 24
Finally, if the analyte being studied is not new, or clinical utility of the existing
diagnostic is not obvious or available, the reimbursement rate is essentially cost-
plus—there is no justication for anything else. If the clinical utility is known, then
a value-based price with cost consideration would be appropriate.
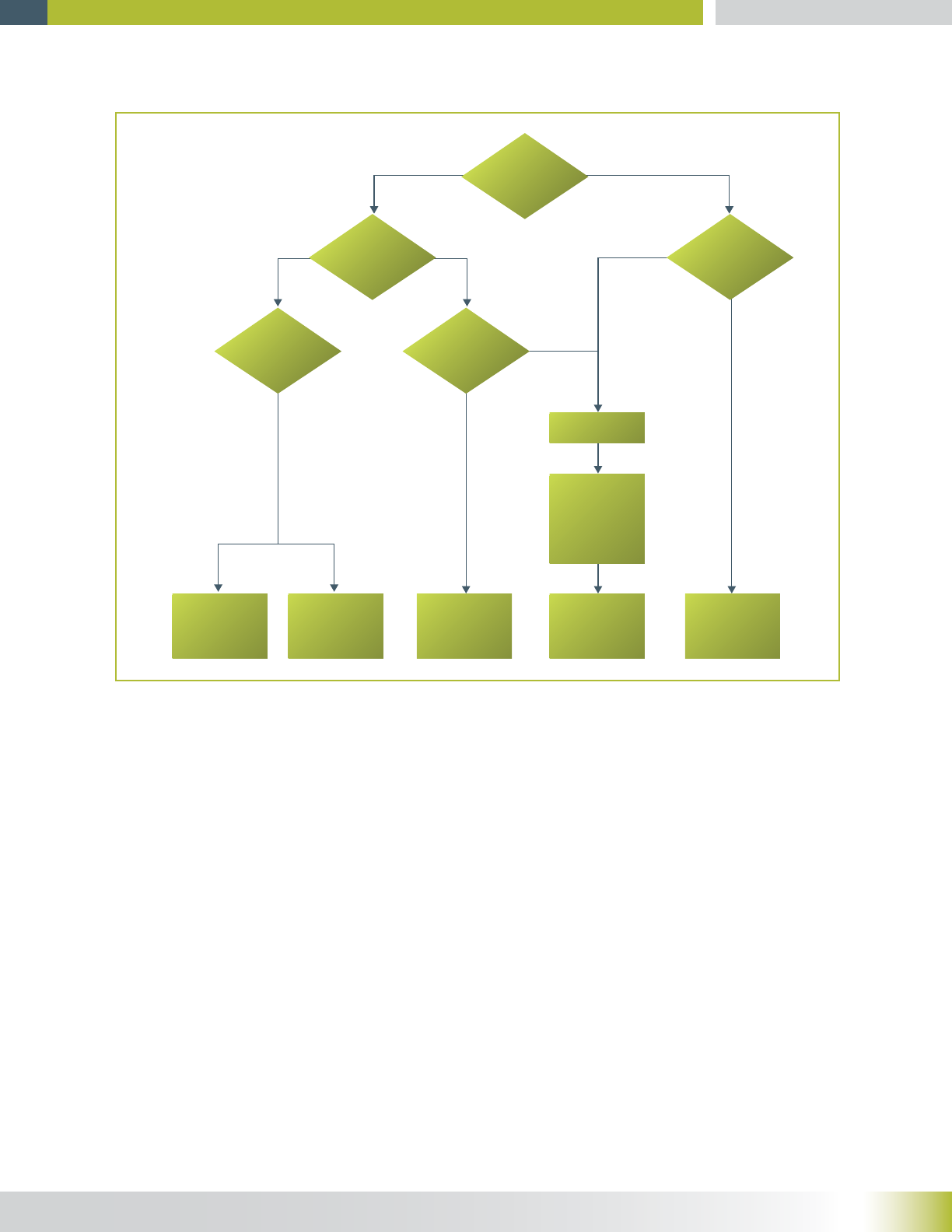
pg 20
New
Analyte?
Similar
Diagnostic?
Superiority
Over Standard?
Known
Care Impact?
Clinical
Utility?
Cost Plus
Not obvious
or available
Value-BasedValue-BasedDiscountPremium
Yes
Yes
Yes
No
Yes
Yes
No
No
Demonstrate
Clinical Utility
&
Health
Economics
Value-based
with Cost
Consideration
Figure 10: Proposed price determinaon decision methodology for an analyte.
Price Determinaon Decision Factors

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
CONCLUSION
For gradually evolving science, therapies and medical equipment that can
jeopardize the health and well-being of the patient, the more cautious and
lengthy process of a CED may provide an excellent scientic validation assuring
that payor resources are not wasted on ineffective treatments.25 However, in
the fast-paced world of molecular diagnostics, the very controls that make CED
so effective become a hindrance for the development of a diagnostic that can
protect against the misapplication of a therapy. The rigid testing protocols, long
testing periods, and the de facto use of CED as a means for private payors to
avoid coverage, all make the current and formally proposed changes to CED a
roadblock to the development of new molecular diagnostics. Just as is the case
with software development and analysis of big data, a new, faster, more dynamic
process is needed to ensure that CMS remains a leader in outcomes-based
medicine and fullls the meaning of the National Bioeconomy Blueprint.
A more efcient process providing the speed and agility demanded by patients
and physicians, the real-world utilization data needed by laboratories, and the
cost assuredness demanded by payors is possible for molecular diagnostics by
relying on:
• A risk-sharing, market-driven, pricing structure;
• The free exchange of data including collection, an unbiased repository, and
decision support; and
• The healthcare-wide push for pay for value business model.
ACKNOWLEDGEMENTS
We gratefully acknowledge Wendy Rubinstein, Director, NIH Genetic Testing
Registry, for reviewing the content related to NIH’s Genetic Testing Registry and
ClinVar.
© 2013, XIFIN, Inc. All rights reserved. XIFIN and the XIFIN logo,are registered trademarks of XIFIN, Inc. All
other marks are property of their respective owners. XMD-3034-13
pg 21

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
REFERENCES
1. “CMS Financial Report: Fiscal Year 2012” Centers for Medicare and Medicaid. November 15, 2012.
http://tinyurl.com/bc6qbpg, Accessed February 12, 2013.
2. U.S. Department of Health and Human Services. http://tinyurl.com/by7lbeq, Accessed February 12,
2013.
3. “Draft Guidance for the Public, Industry, and CMS Staff Coverage with Evidence Development in
the context of coverage decisions.” Centers for Medicare & Medicaid Services. November 29, 2012,
http://tinyurl.com/cyp3jkd, accessed January 28, 2013.
4. “Draft Guidance for the Public, Industry, and CMS Staff Coverage with Evidence Development in
the context of coverage decisions.” Centers for Medicare & Medicaid Services. November 29, 2012,
http://tinyurl.com/cyp3jkd, accessed January 28, 2013.
5. “Novitas LCD DL33138 – Biomarkers for Oncology” Novitas Solutions, January 29, 2013. http://
tinyurl.com/ae82wcd, accessed February 19, 2013.
6. “National Coverage Determinations with Data Collection as a Condition of Coverage: Coverage with
Evidence Development.” Centers for Medicare & Medicaid Services. July 12, 2006, http://tinyurl.com/
athoyo2, accessed January 28, 2013.
7. “National Bioeconomy Blueprint.” White House. April 26, 2012 http://tinyurl.com/cd9j485, accessed
January 28, 2013
8. “Draft Guidance for the Public, Industry, and CMS Staff Coverage with Evidence Development in
the context of coverage decisions.” Centers for Medicare & Medicaid Services. November 29, 2012,
http://tinyurl.com/cy3jkd, accessed January 28, 2013.
9. “Invention reinvented: McKinsey perspectives on pharmaceutical R&D 2010” McKinsey & Company,
p.92 http://tinyurl.com/nhqx9zj, accessed July 11, 2013
10. “Lab Group Submits Citizen Petition against FDA Regulation of Lab Developed Tests” GenomeWeb
June 5, 2013, http://tinyurl.com/km7ldnm, accessed June 6, 2013
11. “Evaluation of Clinical Validity and Clinical Utility of Actionable Molecular Diagnostic Tests in Adult
Oncology” Center for Medical Technology Policy, May 1, 2013. http://www.cmtpnet.org/effectiveness-
guidance-documents/molecular-diagnostics-egd/, accessed May 16, 2013
12. “The Gap in Medical Testing,” New York Times, the Editorial Board, July 7, 2013, http://tinyurl.com/
lgr9w6y, accessed July 11, 2013
13. “The Value of Laboratory Screening and Diagnostic Tests for Prevention and Health Care
Improvement” The Lewin Group, Inc. September 2009. http://tinyurl.com/k4af3tv, accessed March 4,
2013
14. Italiano, Antione. “Prognostic or Predictive? It’s Time to Get Back to Denitions!” Journal of Clinical
Oncology, Dec. 10, 2011. 29:35, p. 4718 http://jco.ascopubs.org/content/29/35/4718.1.full, accessed
March 2, 2013.
15. “PROPOSED/DRAFT Local Coverage Determination (LCD): Molecular Diagnostic Testing (DL33219)”
Centers for Medicare and Medicaid Services, http://tinyurl.com/nfyfvde, accessed July 1, 2013
16. Callen, J, et al. “Failure to Follow-Up Test Results for Ambulatory Patients: A Systematic Review”
Journal of General Internal Medicine, Dec 20, 2011. http://link.springer.com/article/10.1007/s11606-
011-1949-5/fulltext.html, accessed June 20, 2913
17. “Risk Sharing Schemes in Oncology: Future or Fad?” Oncology Business Review. March 2010, p. 16.
http://obroncology.com/documents/OBR_MAR10_RS(1).pdf, accessed June 24, 2013
18. “Payers Try New Approaches To Manage Molecular Diagnostics” Biotechnology Healthcare, Fall
2010; 7(3) p.26. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2957737/, accessed June, 24, 2013
pg 22

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
19. “Aetna, eviti Launch A Decision Support Program To Make Cancer Care More Effective And Efcient”
Aetna News Hub. August 28, 2012. http://tinyurl.com/o6vloz4, accessed June 24, 2013
20. Rubinstein, W. et al. “The NIH genetic testing registry: a new, centralized database of genetic tests
to enable access to comprehensive information and improve transparency” Nucleic Acids Research
2012; 41:D1 D925-D935 http://nar.oxfordjournals.org/content/41/D1/D925.full, accessed July 5, 2013
21. “ClinVar” National Center for Biotechnology Information, U.S. National Library of Medicine. http://www.
ncbi.nlm.nih.gov/clinvar, accessed July 5, 2013
22. “The View from Healthcare’s Front Lines: An Oliver Wyman CEO Survey” Oliver Wyman, http://
www.oliverwyman.com/media/The_View_from_Healthcares_Front_Lines_An_Oliver_Wyman_CEO_
Survey.pdf, accessed March 8, 2012
23. Di Ruffano, Lavinia, et al. “Assessing the value of diagnostic tests: a framework for designing and
evaluating trials” BMJ 2012; 344:e686 http://www.bmj.com/content/344/bmj.e686, accessed March 8,
2013
24. Moons, K, et al. “Quantifying the Added Value of a Diagnostic Test or Marker” Clinical Chemistry
2012; 182550 http://www.clinchem.org/content/58/10/1408.full.pdf+html, accessed March 8, 2013
25. Daniel, G.et al. “Coverage With Evidence Development for Medicare Beneciaries: Challenges
and Next Steps,” Journal of the American Medical Association, July 22, 2013. 173:14 p 1281 http://
archinte.jamanetwork.com/article.aspx?articleid=1685892, accessed July 22, 2013
pg 23

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 24
ABOUT THE AUTHORS
Paul Billings, CMO, Life Technologies
Board certied internist and clinical geneticist Dr. Paul R. Billings serves as
Chief Medical Ofcer at Life Technologies. Dr. Billings brings extensive expertise
and clinical experience in the areas of genomics and molecular medicine. Most
recently, he served as Director and Chief Scientic Ofcer of the Genomic
Medicine Institute at El Camino Hospital, the largest community hospital in the
Silicon Valley. He currently serves as a member of the United States Department
of Health and Human Services Secretary’s Advisory Committee on Genetics,
Health and Society, where he helps shape policy in the rapidly evolving eld of
genomic medicine. Dr. Billings has had a distinguished career as a physician
and researcher. He has been a founder or chief executive ofcer of companies
involved in genetic and diagnostic medicine, including GeneSage, Omicia
and CELLective Dx Corporation. Previously, he was senior vice president
for corporate development at Laboratory Corporation of America Holdings
(LabCorp). He is the author of nearly 200 publications and books on genomic
medicine. Dr. Billings holds an MD from Harvard Medical School and a PhD in
immunology, also from Harvard University.
Richard Ding, CEO, bioTheranostics
Richard Ding has over 20 years of management experience in the diagnostics
and pharmaceutical industry. As a member of the team at Myriad Genetics
that cloned BRCA1 gene, Richard Ding made contribution to the development
of BRAC tests. Prior to becoming CEO of bioTheranostics, Richard Ding had
taken various cross-functional positions at Eli Lilly and Company. More recently,
Richard serves on the Executive Committee at bioMérieux as Senior VP, Strategy
and Business Development. Major achievements include twelve M&A deals and
a number of companion diagnostics collaboration with major pharmaceutical
companies. Richard holds an MBA from the University of Utah and received his
undergraduate education and scientic training at Fudan University, China.
Lâle White, CEO, XIFIN, Inc.
Lâle White is a nationally recognized expert in the eld of medical nancial
management and regulatory compliance, with over 25 years of experience in
A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests
information systems development and medical billing. She lectures extensively
on these topics and has consulted for major laboratories and laboratory
associations throughout the US. She worked with HCFA and the US Ofce of
the Inspector General to develop the rst OIG Model Compliance Program.
Ms. White was previously Vice President - Finance of Laboratory Corporation
of America (NYSE: LH), one of the largest clinical reference laboratories in the
US, and its predecessor National Health Laboratories (NYSE: NHLI), where she
led the software development of several accounts receivable, inventory, cost
accounting and nancial management systems for the laboratory industry. Ms.
White has a BA in nance and an MBA from Florida International University.
Rina Wolf, Vice President of Commercialization Strategies, Consulting &
Industry Affairs, XIFIN, Inc.
Rina Wolf is a nationally recognized expert in the eld of laboratory
commercialization and reimbursement, with over 20 years of experience in the
diagnostic laboratory industry, specializing in Molecular Diagnostic Laboratories.
She lectures extensively on these topics and has consulted for major laboratories
and laboratory associations throughout the US. She is a former president
and board member of the California Clinical Laboratory Association and is an
active participant with the American Clinical Laboratory Association and the
Personalized Medicine Coalition. Ms. Wolf also advises and presents to investor
audiences, recent speaking engagements include Piper Jaffray, Cowen Group
and Bloomberg’s G2 Intelligence Lab Investment Forum. Most recently Ms. Wolf
held the position of Vice President of Reimbursement and Regulatory Affairs at
Axial Biotech, Inc. where she was responsible for creating and implementing their
successful reimbursement strategies. Prior to joining Axial Biotech, Inc., Ms. Wolf
held executive positions in the area of commercialization and reimbursement at
RedPath Integrated Pathology, Inc., Genomic Health, Inc., and Esoterix (now
LabCorp). Ms. Wolf has a Bachelor of Arts degree from UCLA and a Masters of
HealthCare Administration.
David Lorber, Director of Business Development, XIFIN, Inc.
David Lorber is the Director of Business Development at XIFIN.
Before joining XIFIN, he was the Director of Global Sales Operations at Accelrys;
a leading scientic informatics company. He also held various marketing
pg 25

A Pay-For-Value, Data-Driven Approach for the Coverage of Innovative Genetic Tests pg 25
and product management roles at Accelrys, bringing new products to market
and redesigning the corporate pricing strategy. He began his career as a
computational chemist designing early-stage drug leads for oncology targets. He
holds a PhD in Computational Chemistry from Northwestern University and an
MBA from the Rady School of Management at UC San Diego.
