Zimmer MotionLoc Screw For The Periarticular Locking Plate System Surgical Technique, 97 2347 035 00 Technique
2016-04-01
: Pdf Zimmer Motionloc Periarticular Surgical Technique Zimmer_Motionloc_Periarticular_Surgical_Technique 3 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 8

Zimmer®
MotionLoc® Screw
for the Periarticular
Locking Plate
System
Surgical Technique
Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System
Background
A plating construct needs to be strong enough to support the damaged bone while the fracture heals. However, too
much stiffness forces the body to heal through osteonal or primary/direct healing. Primary healing requires nearly
perfect anatomic reduction and rigid compression for absolute stability which has proven to be a very complex and
unforgiving procedure.1 In animal studies, Far Cortical Locking Technology provides controlled axial flexibility to promote
fracture healing through callus formation, or secondary healing, by stressing the fracture with micromotion at the
fracture site.2 The idea of Far Cortical Locking Technology motivated Zimmer to create Zimmer® MotionLoc® Screws for
NCB® Plates and now, a stainless steel version for use with Zimmer Periarticular Locking Plates.
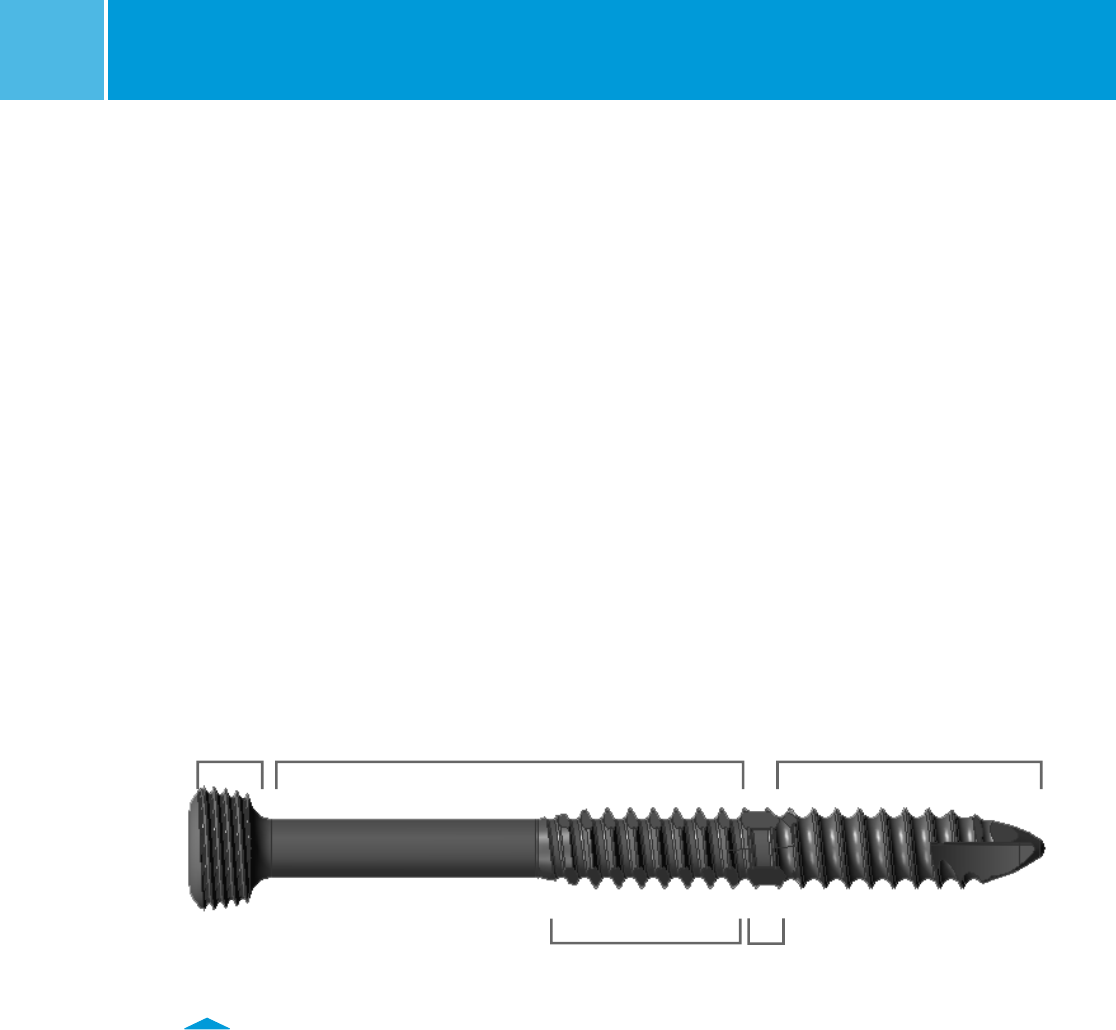
ZIMMER MotionLoc SCREW DESIGN
MotionLoc Screws look different than most cortical screws. The picture below outlines the different design aspects.
A. B. E.
Locking Motion Cortical
Threads Control Collar Threads
C.
Reverse Cutting
Threads
D.
Expanded
Core Section
Fig. 1
2
3
Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System
A. Locking Threads
This is the portion of the screw that locks into the
plate. The head of the screw is threaded to match the
threaded holes in the plates.
B. Motion Control Collar
This is the portion of the MotionLoc Screw that makes
it unique. The diameter of this portion has been
reduced in comparison to the distal end of the screw.
This allows the screw within the drilled hole to flex
through elastic deformation without permanently
deforming the screw. This is called the working length
of the screw because this is the area that flexes a
controlled amount to create the desired micromotion
at the fracture site (Fig. 2).
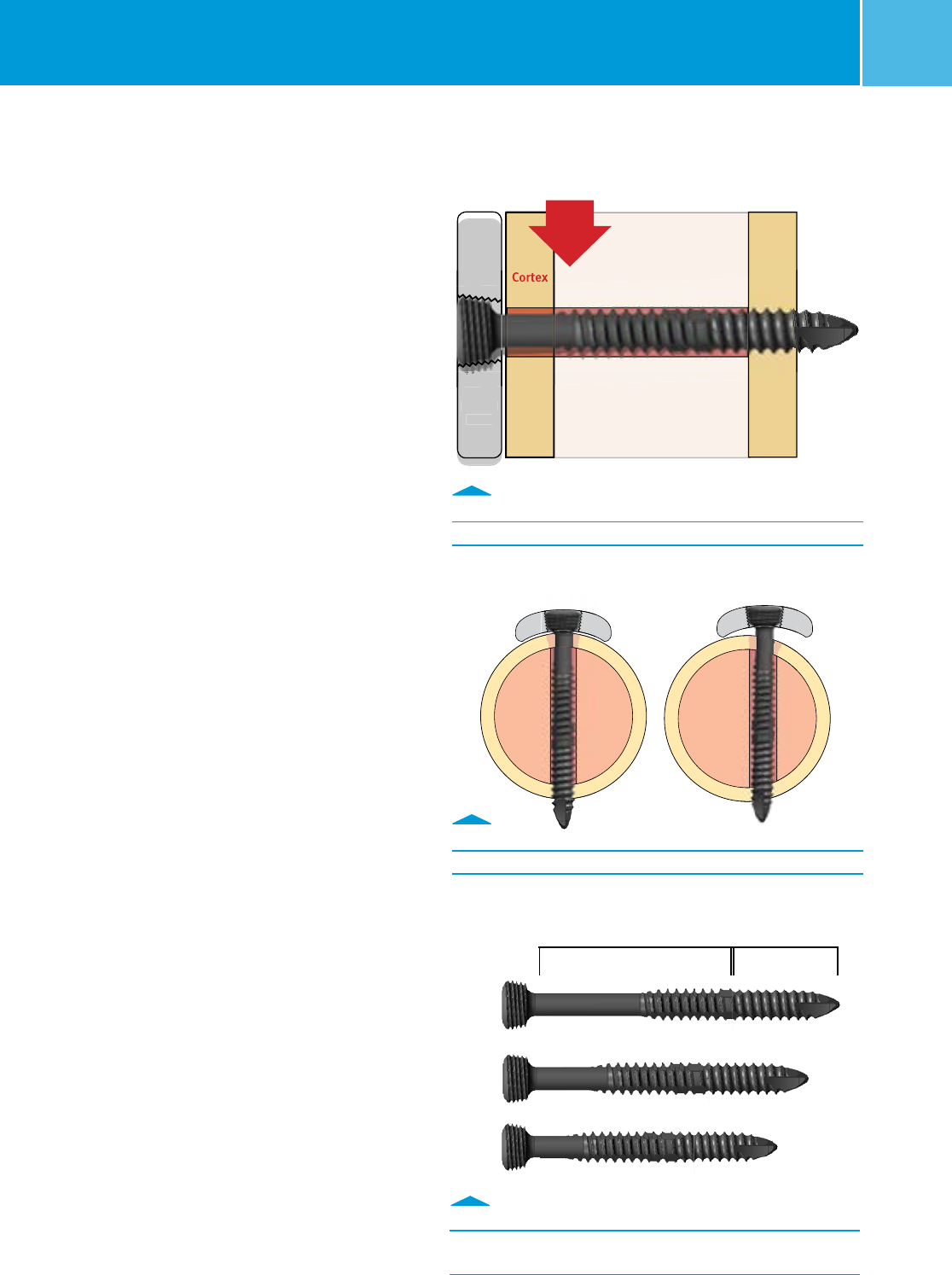
NOTE: Working Length
Increased flexibility of the screw is directly
proportional to the length of the screw. Mechanically,
MotionLoc Screws behave in a manner similar to a
cantilever beam. As the length of the beam/screw
increases so does the beam/screw flexibility.
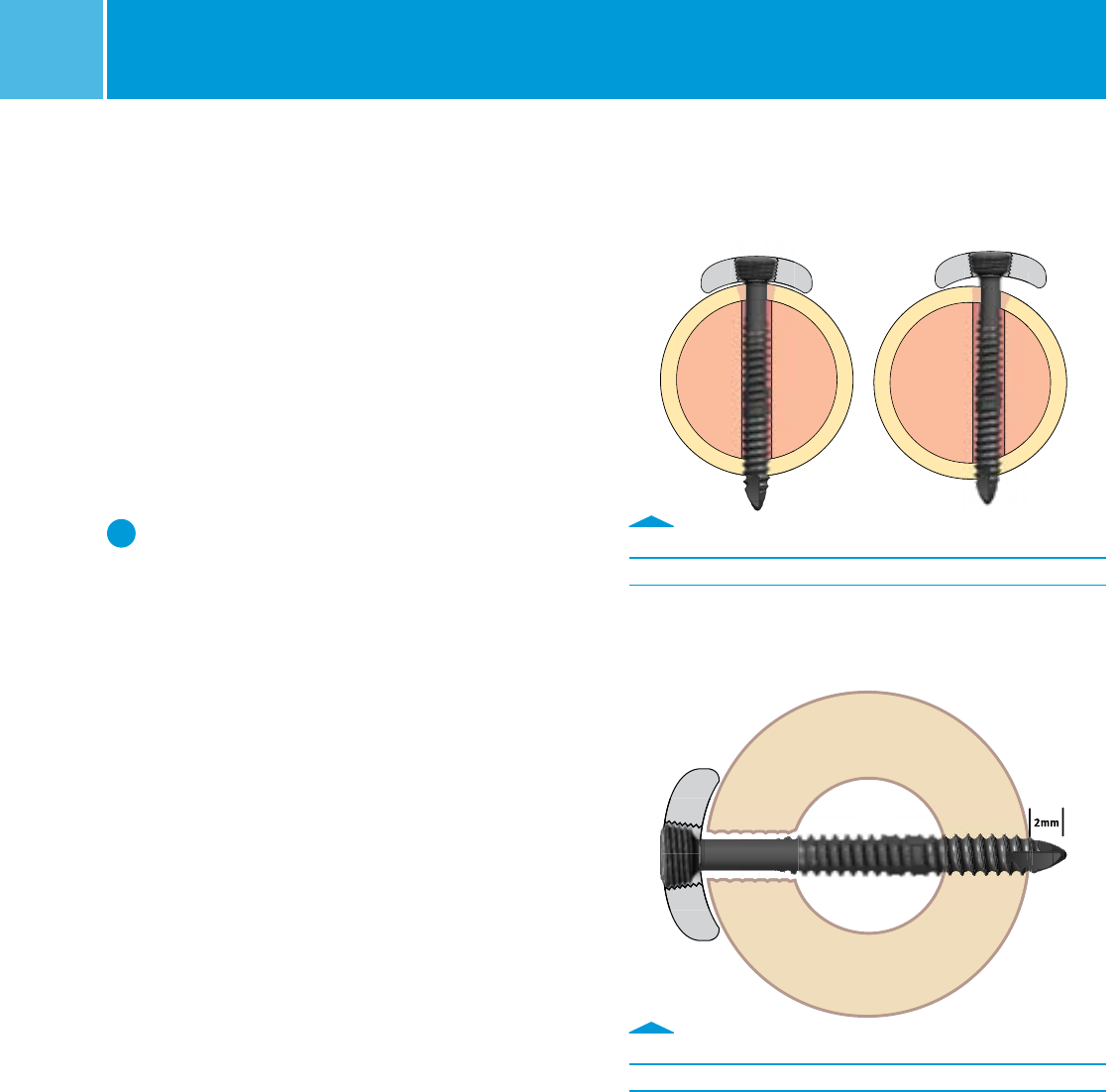
It is important to maximize the working length of the
screw, so centering the screw in the bone is key. The
figure below shows how the screw is affected when
placed off-center (Fig. 4).
Fig. 2
Motion Control Collar
Fig. 3
To maximize working length, center screw in bone.
High
Load
Near
Cortex
Far
Cortex
Locked
Plate
Locked
Plate
Fig. 4
As the screw length increases, the working length increases,
and so does the screw flexibility.
Screw
Length
46
44
42
Working Length Cortical Length
Cortex
Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System
4
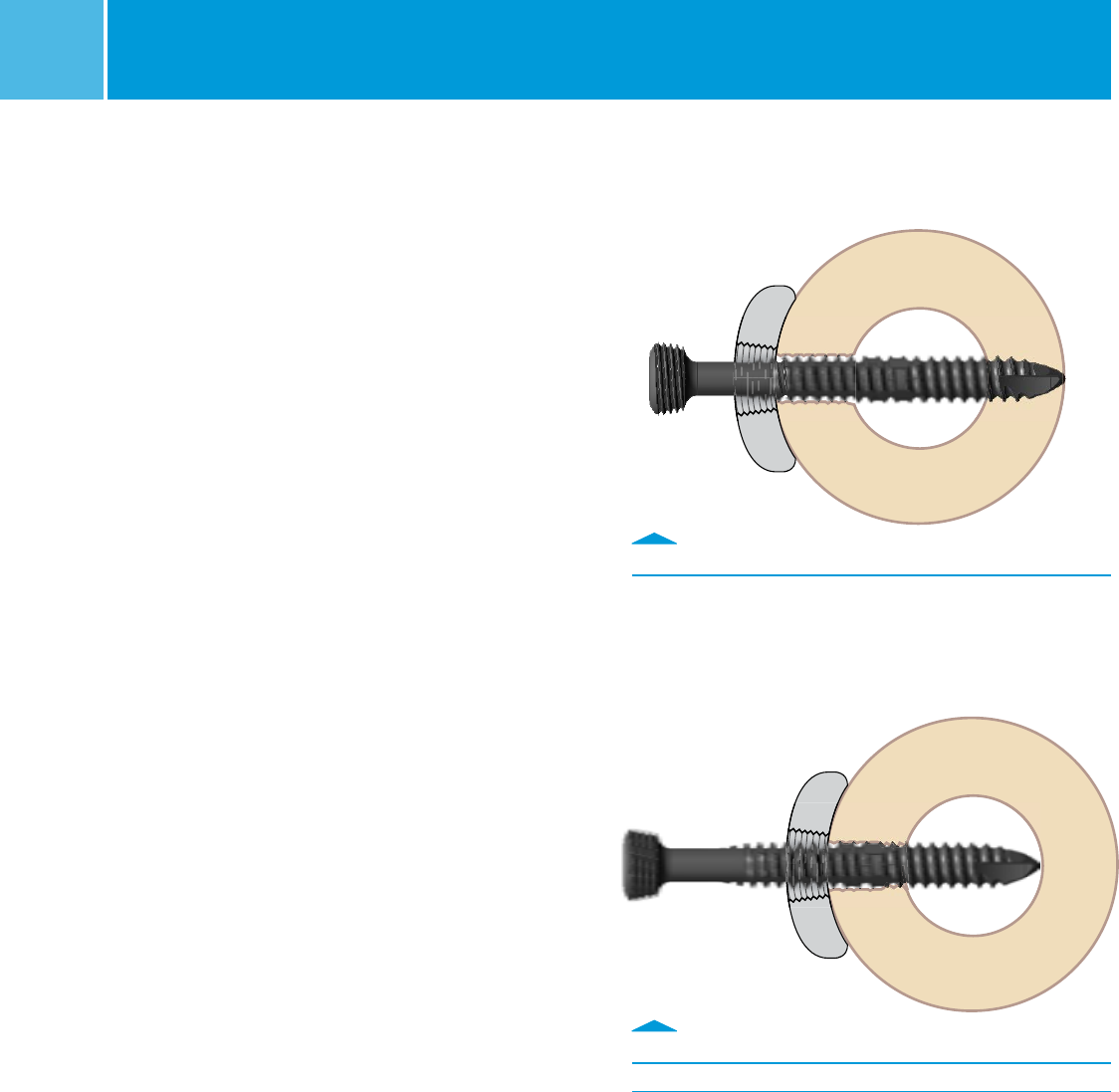
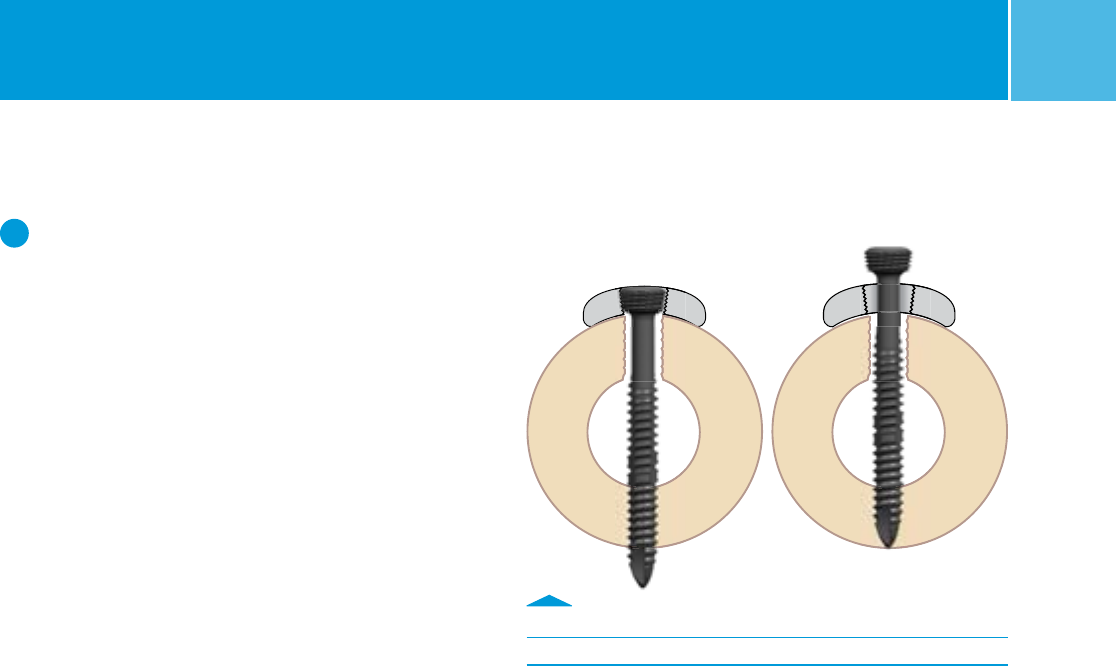
C. Reverse Cutting Threads
The reverse cutting threads on the working length of
the screw ease screw removal. The reverse cutting
threads are designed to engage with the near cortex
before the threads on the tip of the screw disengage
with the far cortex, so the screw can be backed out
(Fig. 5).
D. Expanded Core Section
The expanded core section of the screw is a little larger
than the outer diameter of the motion control collar.
As the screw advances through the drilled hole upon
insertion, it leaves a bigger motion envelope behind it
for the working length of the screw (Fig. 6).
E. Cortical Threads
This is the portion that fixes into the cortical bone
for hold. It has the same thread form as a standard
cortical screw and is inserted using a standard surgical
procedure. Since MotionLoc screws are only fixed in the
far cortex, radiographs must be inspected to confirm
the screw tip has completely engaged that cortex.
The MotionLoc Screws are intended for use in the
diaphyseal segment of a fracture where screw purchase
in the far cortex opposite the plate can be obtained.
They are not for use in the metaphysis or epiphysis
of the bone. Fig. 6
Expanded Core section passing through the near cortex.
Fig. 5
Reverse cutting threads
5
Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System
Reducing Stiffness of Locked
Plating Constructs
MotionLoc Screws reduce the locked plating construct
stiffness by more than 58% while retaining construct
strength.3 The stiffness reduction through the screws
creates nearly parallel micromotion at the fracture site.
Indications for Use
MotionLoc Screws, when used with the Periarticular
Locking Plate System, are indicated for temporary
internal fixation and stabilization of osteotomies and
fractures of long bones, including:
• Comminuted fractures
• Supracondylar fractures
• Intra-articular and extra-articular condylar fractures
• Fractures in osteopenic bone
• Nonunions
• Malunions
Contraindications
Contraindications include:
• All concomitant diseases that may impair the fixation
of the implant and/or the success of the intervention.
• Acute or chronic, local or systemic infections.
• Severe muscular, neural, or vascular diseases that
endanger the extremities involved.
• Lack of bone substance or bone quality, which makes
stable seating of the screws impossible or results
in an unstable screw/plate construct.
• Allergy to the implanted material.
Preoperative Preparation
After assessing the fracture radiographically
and preparing a preoperative plan, position the
patient on the appropriate table. Ensure that the
fluoroscope can be positioned to visualize the
appropriate bone in both the lateral and anterior/
posterior views. For specific preoperative positioning,
refer to the surgical technique for the appropriate
Zimmer Periarticular Locking Plate being used.
Plate Selection
Two factors to consider when choosing plate length:
(1) Location of the fracture and (2) the number and
distribution of the screws around the fracture site.
W WARNING: When considering the number and
distribution of screws, remember that a minimum
of 3 MotionLoc screws must be placed on the
diaphyseal side of the fracture to use the product.
MotionLoc screws should be placed (1) distal to
the fracture in proximal humerus and proximal tibia
fractures; and (2) proximal to the fracture for distal
femur and distal tibial fractures. The remainder
of the Periarticular Locking Plate is secured as
described in the Periarticular Locking Plate package
insert and corresponding surgical technique
(Proximal Tibial Plates, Distal Tibial Plates, Proximal
Humeral Plates, and Distal Femoral Plates).
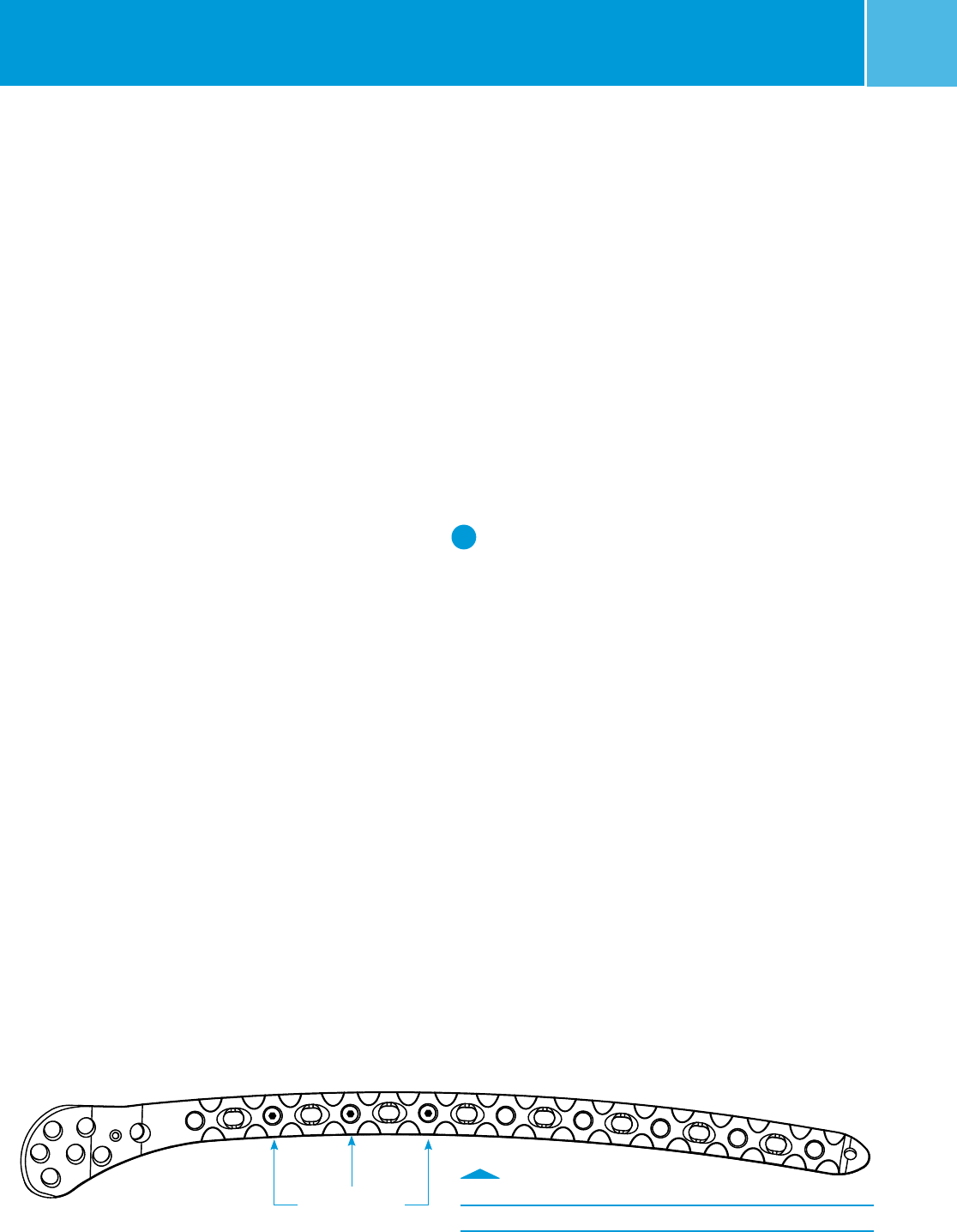
With the Zimmer Periarticular Locking Plate System, the
threaded-round holes in the shaft are the locking holes.
MotionLoc Screws must lock into the plate and must be
inserted into the threaded-round shaft holes (Fig. 7).
MotionLoc screws may be grouped more tightly around
the fracture than with standard locking screws as
they reduce the stiffness and translate micromotion
into the fracture site. This allows them to be placed in
consecutive locking holes.
MotionLoc Screw placement
Fig. 7
3 MotionLoc screws
6Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System
Plate Placement and Fracture Reduction
Center the plate on the bone as much as possible.
MotionLoc screws function best when the working length
is maximized across the widest portion of the bone
(Fig. 8).
Provisional fixation with k-wires or drill bits may be used
to more accurately place the plate.
Fix the metaphyseal and epiphyseal segments of the
fracture as described in the surgical techniques for the
corresponding plate used.
W WARNING: Standard Periarticular Locking screws
or cortical screws should NOT be used in the same
fracture segment as the MotionLoc Screws as this
may lead to a stress riser and potential failure.
Compression technique should only be used in the
metaphysis.
4.5mm Zimmer MotionLoc Screw Technique
To insert the 4.5mm Zimmer MotionLoc Screws, thread
the 3.7mm Standard Cannula (Blue Ring) into the
desired locking hole.
Use the 3.7mm Standard Drill through the cannula to
drill a pilot hole. Use the fluoroscope to confirm the drill
position in both the A/P and lateral planes. Remove the
cannula.
If drilling in hard cortical bone, tap the far cortex with the
4.5mm Locking Screw Tap.
Screw Length Measurement
MotionLoc screws should fully engage the far cortex (Fig.
9). Use the 4.5mm Locking Screw Depth Gauge to obtain
a screw length reading. Add 2mm to that reading to
select the appropriate MotionLoc screw length.
Screw Insertion
Select the appropriate MotionLoc Screw from the
MotionLoc Screw Caddy for Zimmer Periarticular Locking
Plate System. Insert the screw using the 5.0mm Hex
Screwdriver until it has threaded into the locking hole of
the Periarticular Locking Plate.
Fig. 8
Center the MotionLoc Screws
Fig. 9
Screw Length Measurement
2mm
2mm
7
Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System Zimmer® MotionLoc® Screw for the Periarticular Locking Plate System
N NOTE: To ensure that the MotionLoc Screw finds
the drilled hole in the far cortex, it is important to
align the screw in the direction of the drilled hole
while inserting the screw. Use alignment of the
depth gauge prior to its removal to determine proper
orientation of screw prior to placement.
Follow the same procedure to insert a MINIMUM of three
(3) MotionLoc Screws into the shaft of the bone. Ensure
that all screws are securely tightened.
3.5mm MotionLoc Screw Technique
To insert the 3.5mm MotionLoc Screws, thread the
2.7mm Standard Cannula (Black Ring) into the desired
locking hole.
Use the 2.7mm Standard Drill through the cannula to
drill a pilot hole. Use the fluoroscope to confirm the drill
position in both the A/P and lateral planes. Remove the
cannula.
If drilling in hard cortical bone, tap the far cortex with the
3.5mm Locking Screw Tap.
Screw Length Measurement
Use the 3.5mm Locking Screw Depth Gauge to obtain a
screw length reading. Add 2mm to that reading to select
the appropriate screw length. MotionLoc screws should
fully engage the far cortex.
Screw Insertion
Select the appropriate MotionLoc Screw from the
MotionLoc Screw Caddy for Zimmer Periarticular Locking
Plate System. Insert the screw using the Small Hex
Screwdriver until it has threaded into the locking hole of
the Periarticular Locking Plate.
Follow the same procedure to insert a MINIMUM of three
(3) MotionLoc Screws into the shaft of the bone. Ensure
that all screws are securely tightened.
Fig. 10
Screw removal
Implant Removal
MotionLoc screws have been designed to aid in the
removal process. A portion of the screw has reverse
cutting threads to engage in the near cortex bone as the
cortical threads disengage from the far cortex of bone
(Fig. 10).
To remove the Zimmer Periarticular Locking Plate, back
off all bone screws. This prevents rotation of the plate
when removing the last screw. Then completely remove
all screws with the screwdriver, ensuring that the tip of
the screwdriver is completely seated in the hex drive of
the screw. Failure to do so could damage the hex drive
and complicate the extraction of the implant.
97-2347-035-00 Rev. 2 MC 120978 1-29-15 Printed in USA ©2015 Zimmer, Inc.
Contact your Zimmer representative or visit us at www.zimmer.com
The CE mark is valid only if it is also printed on the product label.
References
1. Skirving AP, Day R, Macdonald W, McLaren R: Carbon fiber reinforced plastic (CFRP) plates versus stainless steel dynamic compression
plates in the treatment of fractures of the tibiae in dogs. Clin Orthop Relat Res 1987; 224:117-124.
2. Bottlang M, et al. Far cortical locking can improve healing of fractures stabilized with locking plates.
J Bone Joint Surg (A), 92:7,2010.
3. Data on file at Zimmer. (ZRR 2671-13 & ZRR 2674-13)
DISCLAIMER:
This documentation is intended exclusively for physicians and is not intended for laypersons. Information on the products and
procedures contained in this document is of a general nature and does not represent and does not constitute medical advice or
recommendations. Because this information does not purport to constitute any diagnostic or therapeutic statement with regard
to any individual medical case, each patient must be examined and advised individually, and this document does not replace
the need for such examination and/or advise in whole or in part.
Please refer to the package inserts for important product information, including, but not limited to, indications,
contraindications, warnings, precautions, and adverse effects.
