Zimmer Nexel Total Elbow Surgical Technique 97 8401 002 00
2014-06-20
: Pdf Zimmer Nexel Total Elbow Surgical Technique zimmer_nexel_total_elbow_surgical_technique 6 2014 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 36

97-8401-002-00 7-8-13 Printed in USA ©2013 Zimmer, Inc.
Zimmer®
Nexel™
Total Elbow
Surgical Technique
Table of Contents
PAGE
Indications / Contraindications ............................1
Pre-Operative Considerations ...............................2
Surgical Technique Summary ................................3
SECTION
1. Surgical Preparation and Exposure 5
2. Humeral Preparation 7
3. Ulnar Preparation 12
4. Trial Reduction 16
5. Component Implantation 17
6. Final Assembly 22
7. Closure 25
8. Postoperative Management 26
9. Poly Revision 27
10. Component Removal 29
Zimmer® Nexel™ Total Elbow Surgical Technique
Zimmer® Nexel™ Total Elbow Surgical Technique
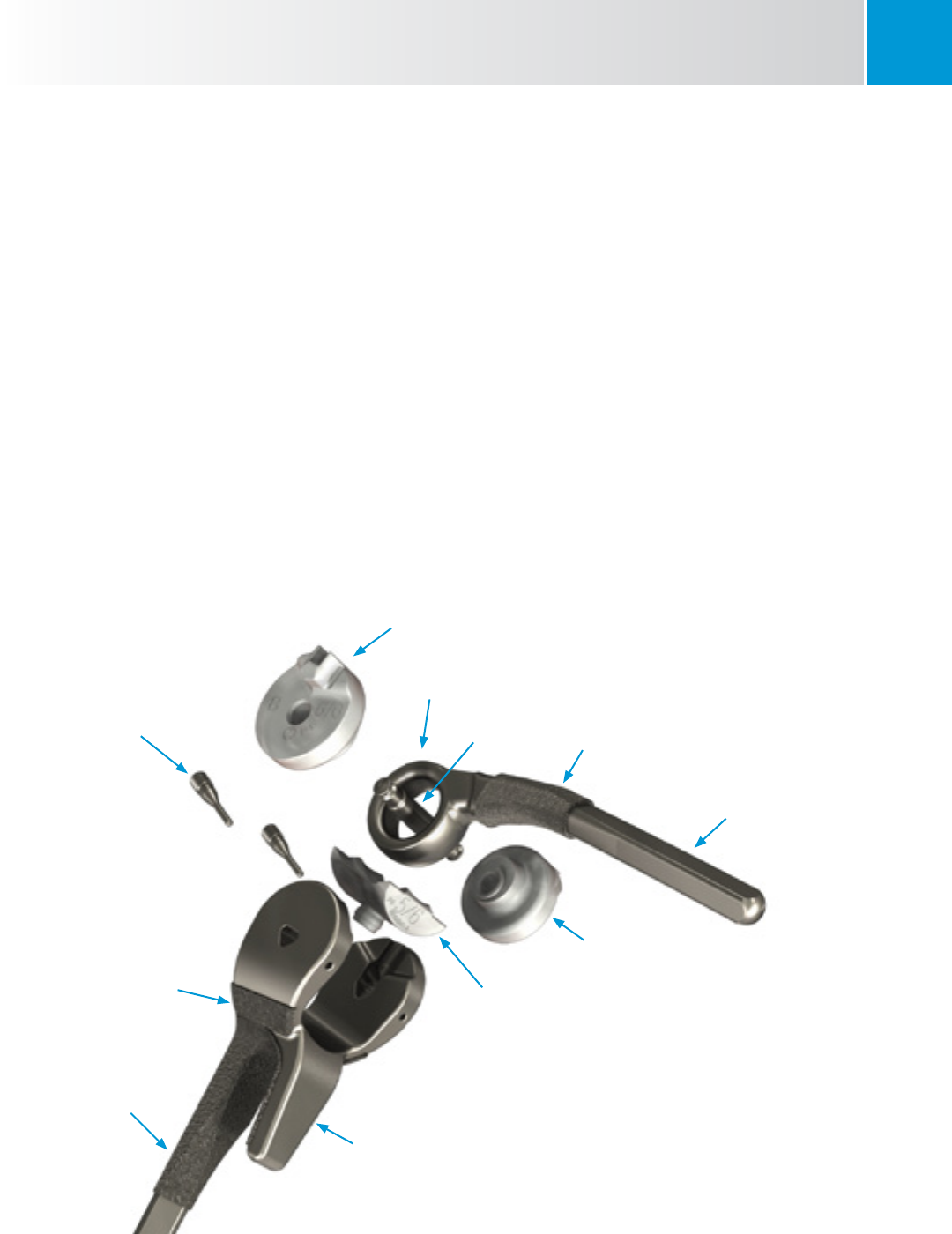
Device Description
This device is a total elbow prosthesis designed for use with
bone cement. It is available in sizes 4, 5 and 6, in left and
right configurations. The Ulnar and Humeral Components are
manufactured from Tivanium® (Ti-6Al-4V) alloy. The Ulnar
Component has a porous coating of Ti-6Al-4V plasma spray and
is curved to facilitate implantation. The Humeral Component
has a porous coating of Ti-6Al-4V plasma spray and has an
anterior flange to accommodate a bone graft. The Axle-Pin and
Humeral Screws are manufactured from Zimaloy® (Co-Cr-Mo)
alloy. Vitamin E highly cross-linked ultra-high molecular weight
polyethylene (Vivacit-E®) bearings prevent metal-to-metal
articulating contact.
Note: Size 4, 5 and 6 are numerical relative descriptions of the
available girths of the Implant stems. 4,5 and 6 do not imply or
equate to a dimension. 4 does not equal 4 mm, and so on.
Plasma Spray
Humeral
Component
Humeral Screws
Ulnar Bearing
Ulnar Eye
Axle-Pin Plasma Spray
Ulnar Component
Ulnar Bearing
Humeral Bearing
Anterior Flange

1
Zimmer® Nexel™ Total Elbow Surgical Technique
Indications / Contraindications
INDICATIONS
Indications for use include:
• Elbowjointdestructionwhichsignicantlycompromisesthe
activities of daily living
• Post-traumaticlesionsorbonelosscontributingtoelbow
instability
• Ankylosedjoints,especiallyincasesofbilateralankylosis
from causes other than active sepsis
• Advancedrheumatoid,post-traumatic,ordegenerative
arthritis with incapacitating pain
• Instabilityorlossofmotionwhenthedegreeofjointorsoft
tissue damage precludes reliable osteosynthesis
• Acutecomminutedarticularfractureoftheelbowjoint
surfaces that precludes less radical procedures, including
13-C3 fractures of the distal humerus
• Revisionarthroplasty
Caution: This device is intended for cemented use only
CONTRAINDICATIONS
Use of the Zimmer® Nexel™ Total Elbow is
contraindicated in patients with:
• Currentlyactive,orhistoryofrepeated,localinfectionat
the surgical site
• Paralysisordysfunctionalneuropathyinvolvingtheelbow
joint
• Signicantipsilateralhanddysfunction
• Excessivescarringoftheskinorsofttissuethatcould
prevent adequate soft tissue coverage
• Dailyactivitiesthatwouldsubjectthedevicetosignicant
stress (i.e., heavy labor, torsional stress, and/or
competitive sports)
Relative contraindications include:
• Distantfociofinfection(e.g.genitourinary,pulmonary,skin
[chronic lesions or ulcerations], or other sites). In cases of
distant infection, the foci of infection should be treated
prior to, during and after surgery.
• Ancientpriorsepsis
2
Zimmer® Nexel™ Total Elbow Surgical Technique
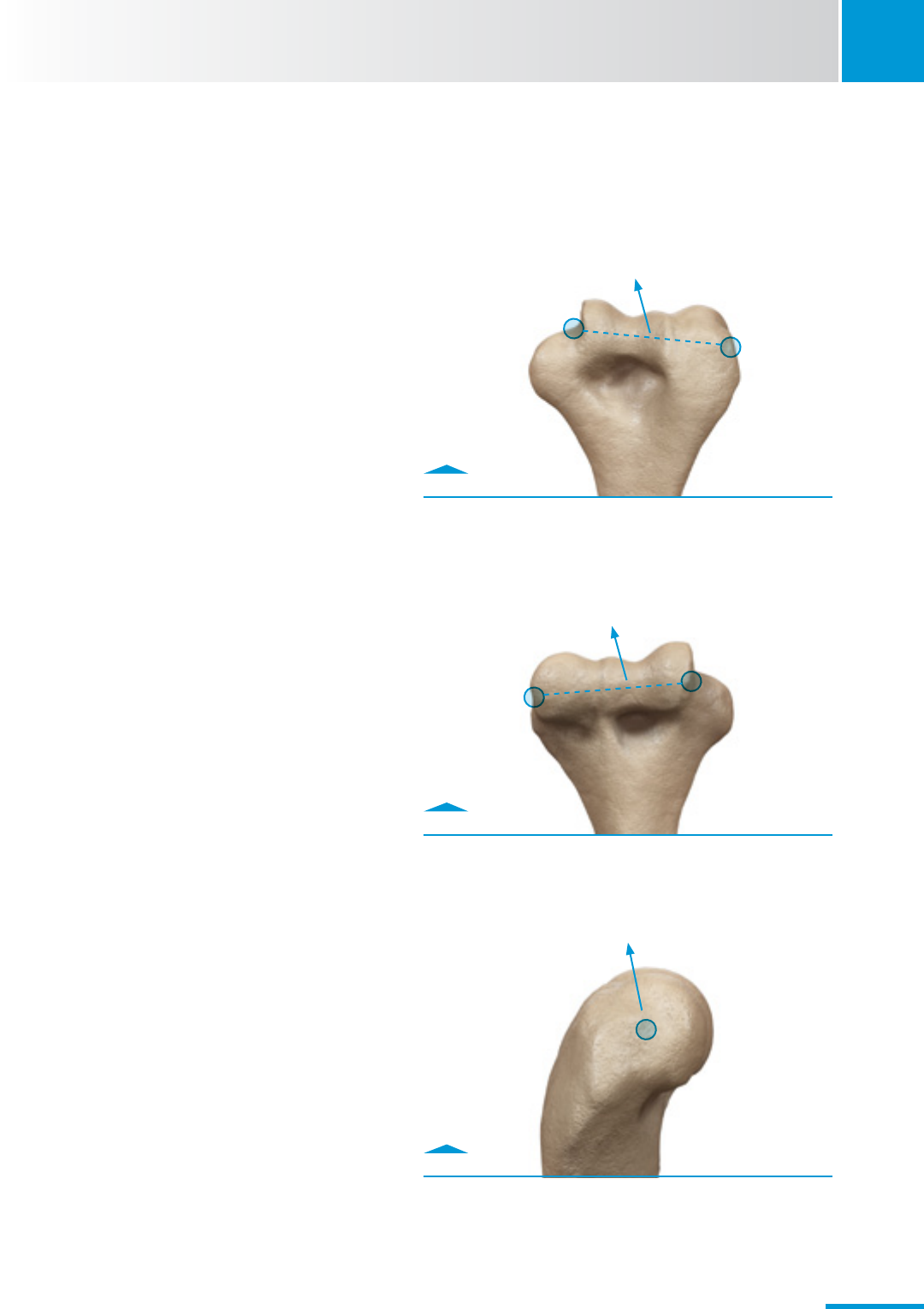
Fig. 0.0
Posterior View
Fig. 0.1
Anterior View
Fig. 0.2
Lateral View
Pre-Operative Considerations
• Forthoseinexperiencedinthetechniqueofelbow
arthroplasty, training with a cadaver specimen(s) is
recommended to appreciate the soft tissue implications of
the technique.
• Beawareofexistingshoulderpathology;assessshoulder
stiffness, avoid forceful rotation.
• Avoidoverlappingcementmantlesand/orinterference
between shoulder and elbow humeral stems, and/or a short
cement gap between shoulder and elbow humeral stems as
these are known fracture risks.
• Understandifarevisionlengthstemistobeusedand
assess/accommodate for the amount of anterior bowing of
the humerus on the lateral pre-operative radiographs.
• Toaddressexioncontracture,considercountersinkingthe
Humeral Component to the extent that does not produce a
fracture of the medial condyle.
• Forproperorientationofthehumeralcomponent,
understand the humeral osseous landmarks establishing
the axis of flexion of the elbow. Medially, the landmark is a
point at the anterior/inferior aspect of the medial condyle.
Laterally, the landmark is the center of the capitellum
(Fig. 0.0-0.2).
M L
L M
P A
CenterofRotation
Axis of Flexion
Axis of Flexion
A A
Axis of
Flexion
3
Zimmer® Nexel™ Total Elbow Surgical Technique
Create notch
with rongeur
Anterior View
Fully seat
Trephine
Stabilizer
1
2
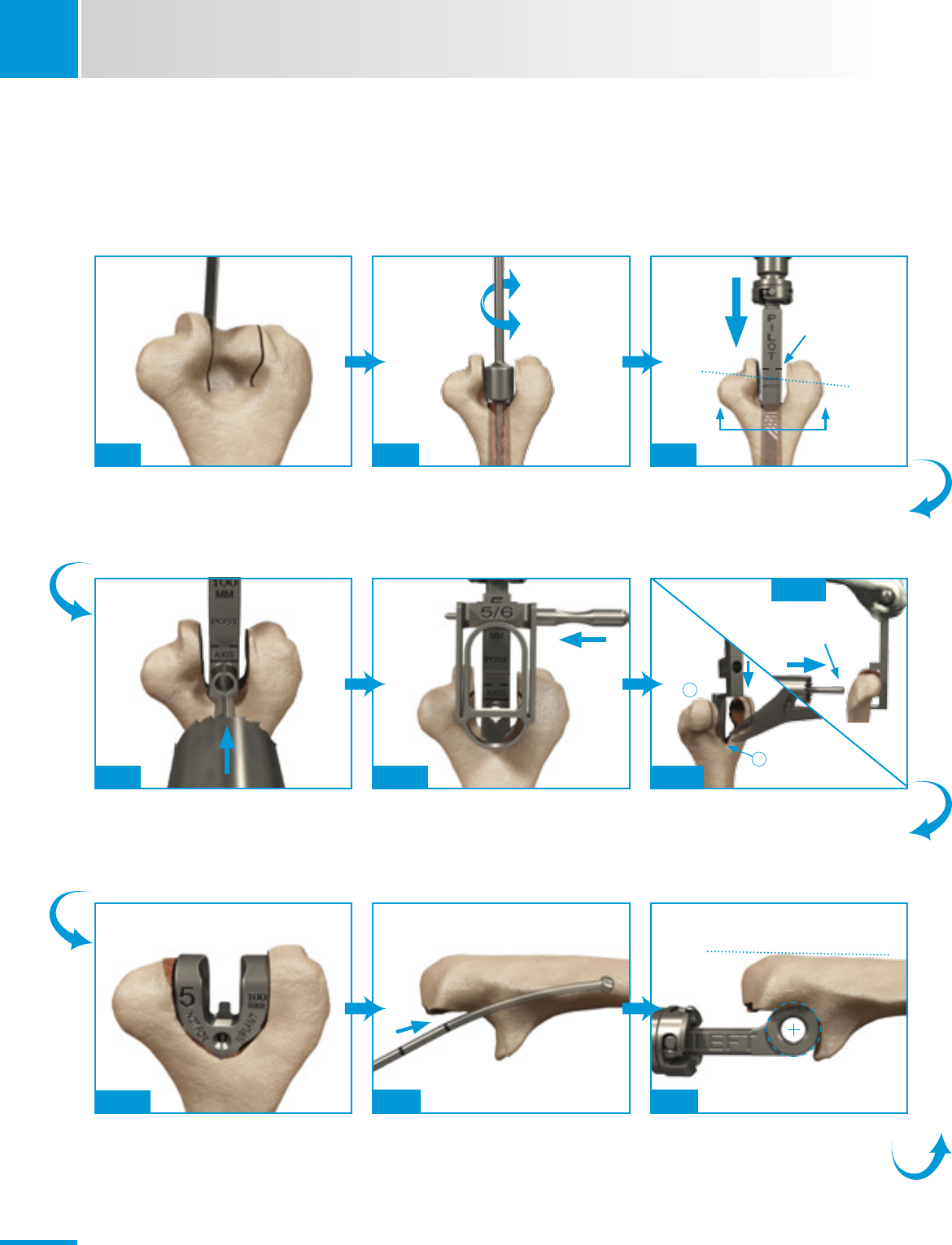
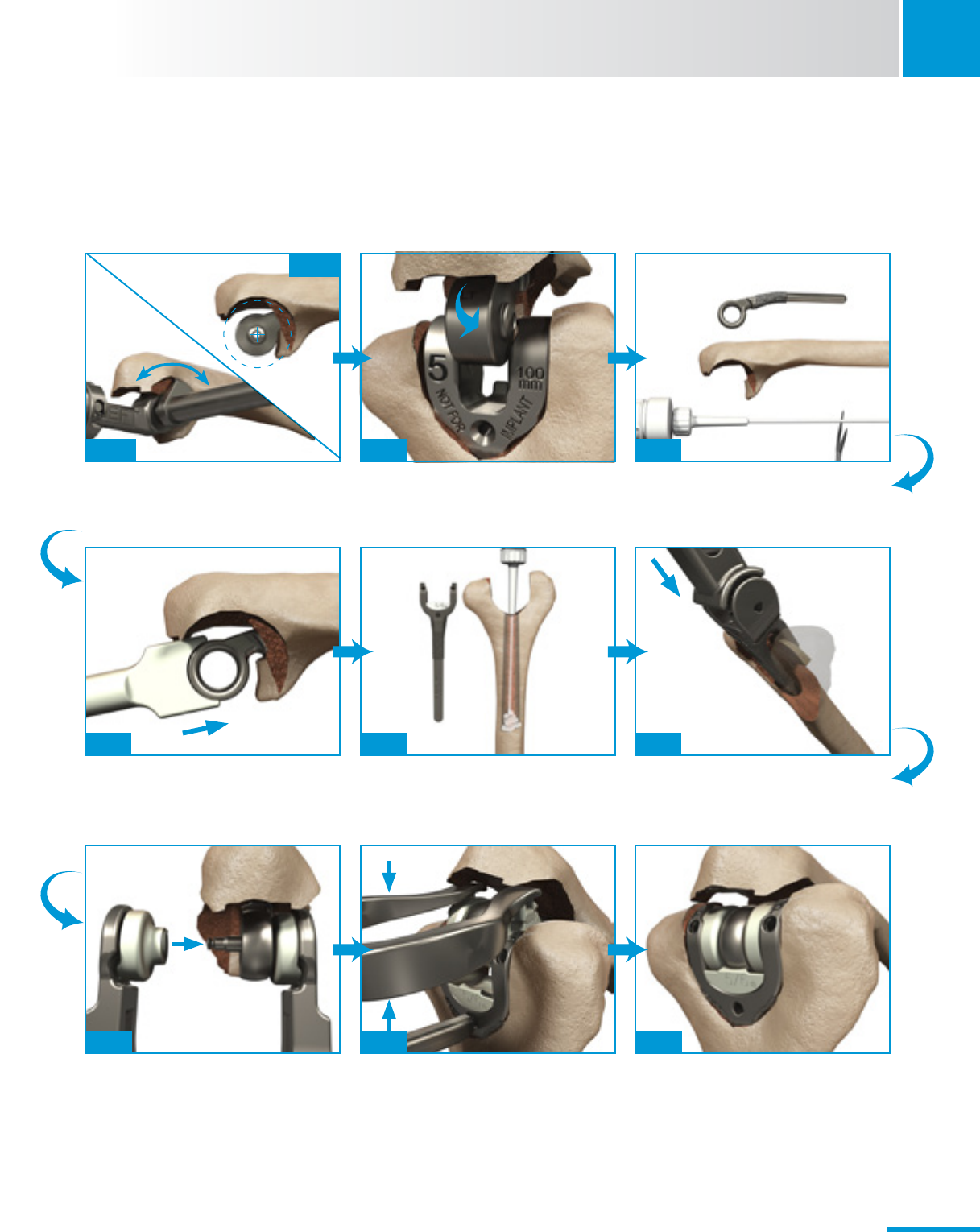
Surgical Technique Summary
Use saw or ronguers to remove trochlea and
access humeral canal.
UseHumeralAwlReamertoopencanaland
conrmreadinessforRasps.
SequentiallyRaspthecanal;solidlineneeds
to align with the axis of flexion.
Score the bone, and create rounded humeral
cut by using the Trephine saw.
Secure the Humeral Cut Guide by inserting
the Pin, then make vertical cuts using
oscillating saw.
Fully seat the Trephine Stabilizer until the marking
aligns with the axis of Flexion (notch anterior
humerus), and finish the Trephine cut.
Fig. 2.3 Fig. 2.4Fig. 2.1
Assess Humeral bone preparation with
Provisional.
PreparethedistalulnausingFlexibleReamers,
Solid followed by Cannulated, until marking
aligns with chosen length Implant.
Prepare the proximal ulna using sequential
Rasps,untilholefeatureonRaspaligns
with axis of flexion.
Fig. 2.11 Fig. 2.12
Fig. 2.13
Fig. 2.7
Fig. 2.14 Fig. 3.7Fig. 3.5
Dashedlinedenotes
top of Implant
Donotstartdrill
until pin in hole.
Flat of the Olecranon
4
Zimmer® Nexel™ Total Elbow Surgical Technique
Surgical Technique Summary
Fig. 4.1 Fig. 5.1Fig. 3.9
Fig. 3.11
Fig. 5.4
Fig. 6.4
Fig. 5.5
Fig. 6.6
Fig. 5.2
Fig. 6.1
After using the Ulnar Bearing Clearance
Template to confirm adequate clearance for
Implant, assess the ulnar preparation using
the Ulnar Provisional.
Reducejointandperformatrialrangeof
motion.
Retrogradellthehumeralcanalwithcement.
Partiallyreducethejointwithhandpressure,
then fully reduce it using the Articulation
Inserter. (Alternate: Ulnar Bearing Tamp is
used with the triceps-on exposure.)
Use Ulnar Stem Inserter to fully seat implant.
After the scrub nurse has loaded the Ulnar
Bearing Assembly Tool (UBAT) with Bearings/
Axle-Pin, attach the assembly to Ulnar
Implant in situ.
Retrogradelltheulnarcanalwithcement.
Insert bone graft under the anterior flange
and use the Humeral Stem Inserter to fully
seat the Implant.
Bearings will be flush with top of Implant
when fully seated, and Humeral Screws will
threadineasilyusingElbowTorqueDriver.
1
SECTION
5
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 1.1
Incision just lateral to medial epicondyle.
1. Surgical Preparation and Exposure
1.1 Patient Preparation
• Positionthepatient.
· Position patient in supine with a sandbag under
the scapula.
· Place the arm across the chest.
• Placearolledtowelunderelbow.
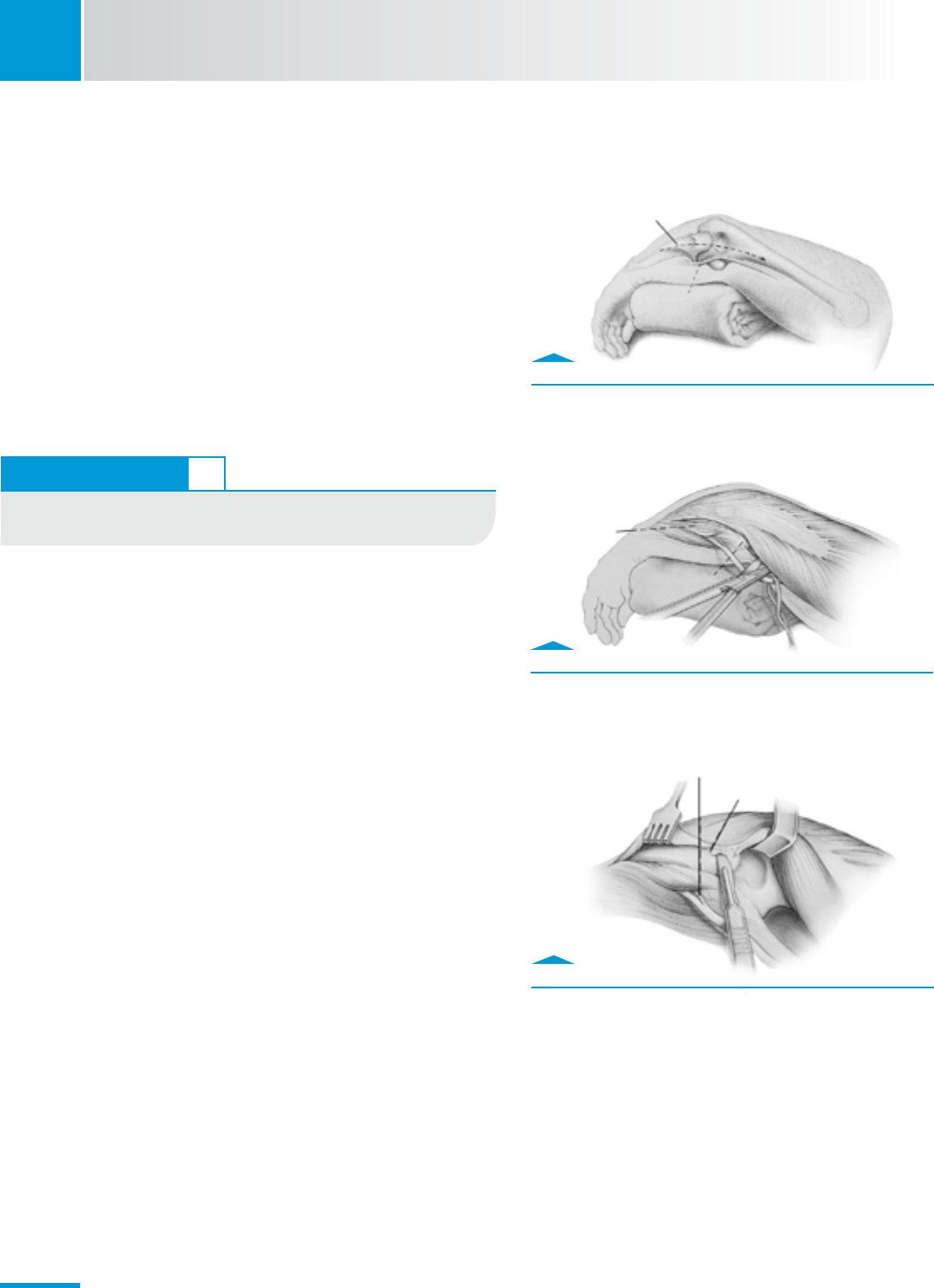
1.2 Incision
• Makeastraightincisionapproximately15cminlength.
· Centerincisionovertheelbowjointjustlateraltothe
medialepicondyleandjustmedialtothetipofthe
olecranon (Fig. 1.1).
1.3 Ulnar Nerve Protection
• Isolatetheulnarnerve.
· Identify the medial aspect of the triceps mechanism.
· Use ocular magnification and a bipolar cautery
as necessary.
• Mobilizetheulnarnervetotherstmotorbranch.
• Verycarefullytranslocatethenerveanteriorlyintothe
subcutaneous tissue (Fig. 1.2).
Note: Carefully protect the nerve throughout the remainder of
the procedure.
TECHNIQUE TIP 1.2
A more midline positioned incision decreases the need for
elevating an extensive flap.
Fig. 1.3
Remove triceps from the proximal ulna.
Fig. 1.2
Translocate ulnar nerve to subcutaneous tissue.
Ulnar Crest
Ulnar Nerve
Flexor carpi
ulnaris m.
Medial epicondyle
Motor branch
of ulnar m.
Sharpey’s fibers
SECTION
1
6
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 1.5
Release medial and lateral collateral ligaments.
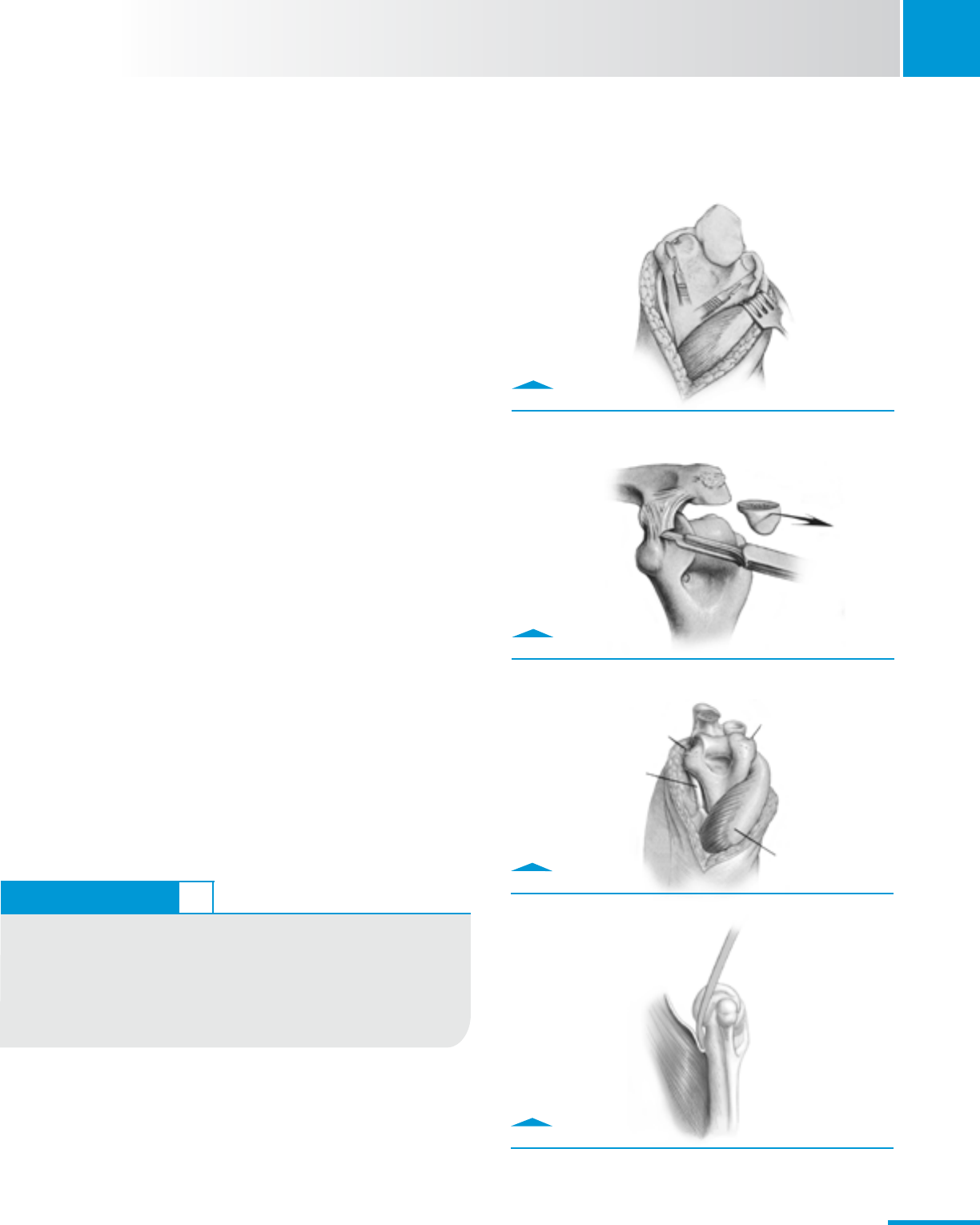
1.4 The Bryan/Morrey Approach*
The Bryan/Morrey approach is recommended for new and
inexperienced users of the Nexel Total Elbow System. This
approach employs a meticulous repair of the triceps that is
detailed at the end of this surgical technique. Once experience
is gained, other exposures (e.g., Triceps-On/Sparing) can be
employed at the surgeon’s discretion.
• Releasethetriceps(Fig.1.3previouspage).
· Make an incision over the medial aspect of the ulna.
· Elevate the ulnar periosteum along with the forearm fascia.
• Exposedistalhumerus,proximalulnaandradialhead
(Fig 1.4)
· Retractthemedialaspectofthetricepsalongwiththe
posterior capsule.
· Removethetricepsfromtheproximalulnabyreleasingthe
Sharpey’s fibers from their insertion
· Further reflect the extensor mechanism laterally including
the anconeus.
· Transpose the entire extensor mechanism (triceps, ulnar
periosteum, and anconeus) as a single soft-tissue sleeve
laterally.
• Exposeanddislocatethejoint.
· Releasethemedialandlateralcollateralligamentsfrom
their humeral attachment (Fig. 1.5).
· Flex the elbow to disarticulate the ulna from the humerus
(Fig. 1.6).
· Externally rotate the forearm to allow further flexion
and separation of the articulation.
· Releasetheanteriorcapsuleandcontractedsofttissue
from the distal humerus (Fig. 1.7).
Fig. 1.4
Transpose the extensor mechanism laterally.
Fig. 1.6
Flex elbow to disarticulate ulna from humerus.
Fig. 1.7
Release anterior capsule from distal humerus.
ReleasedLCL
ReleasedMCL
Ulnar nerve
Triceps
TECHNIQUE TIP 1.4
A complete release of the soft tissues from the medial aspect of the
distal humerus protects the medial epicondyle from fracture during
flexion and manipulation of the forearm. Elbows with severe arthritis,
post-traumatic surgery, and/or extensive soft-tissue contractures
should undergo releases of the capsule and extensor/flexor origins
to facilitate motion and soft tissue balance.
* Morrey, Bernard F., The Elbow and its Disorders. 4th. Philadelphia, PA:
Saunders Elsevier, 2009.
Instruments
2
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
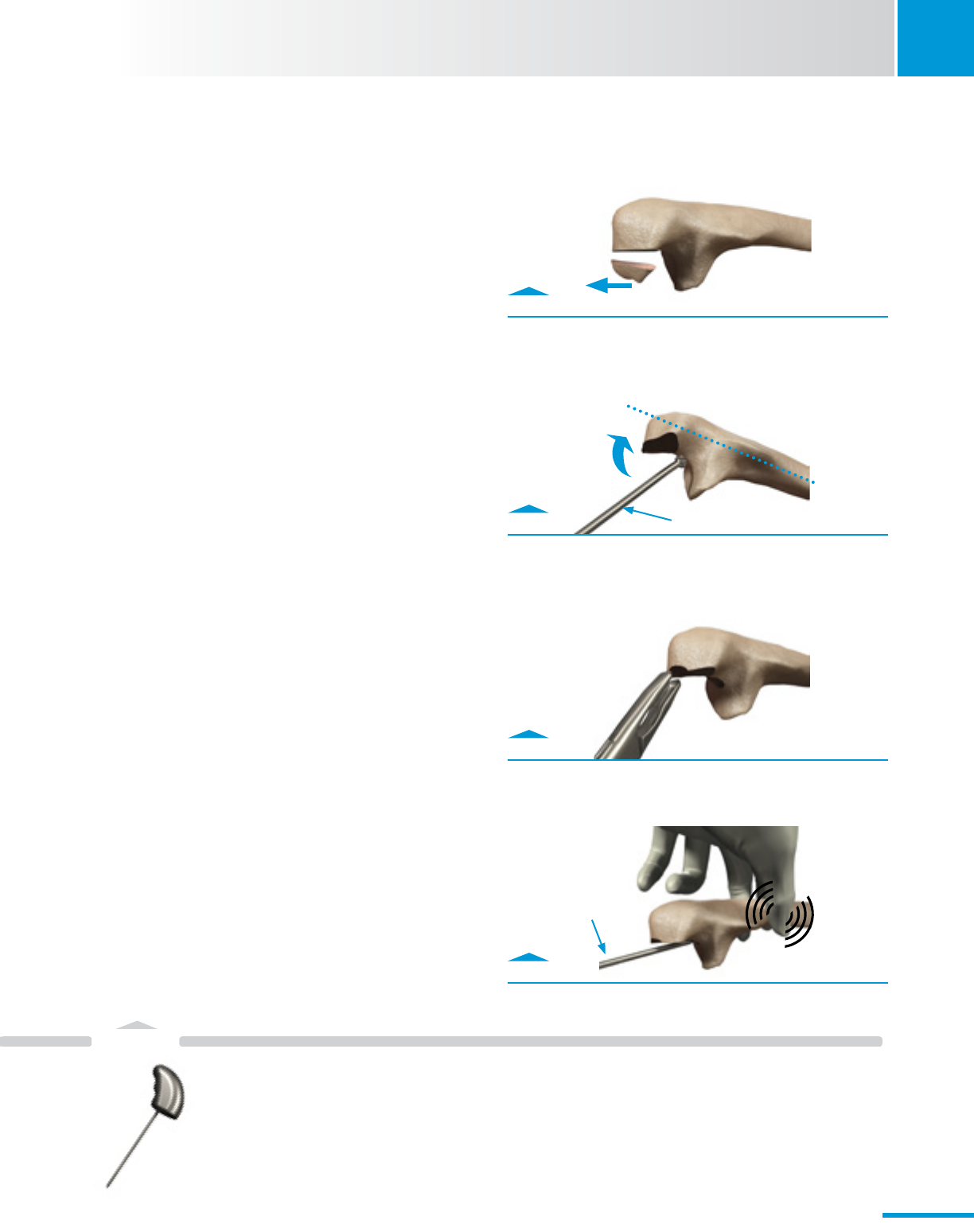
Fig. 2.1
Use oscillating saw to remove trochlea.
Fig. 2.2
Use bur to expose humeral canal.
Fig. 2.3
Use Humeral Awl Reamer to open canal.
2. Humeral Preparation
Note: Be aware that instruments labeled size “5/6” can be
used for a size 5 or 6 implant; likewise, instruments labeled
size “4/5” can be used for a size 4 or 5 implant.
2.1 Trochlear Resection
• Resectthecentralportionofthetrochlea(Fig.2.1).
· Use a saw or a rongeur as appropriate.
· Retainresectedbonefortheanteriorbonegraft
(Section 5.1).
2.2 Humeral Canal Exposure
• Identifyandexposethehumeralcanal(Fig.2.2).
· Use a bur or rongeur at the proximal base of the
olecranon fossa.
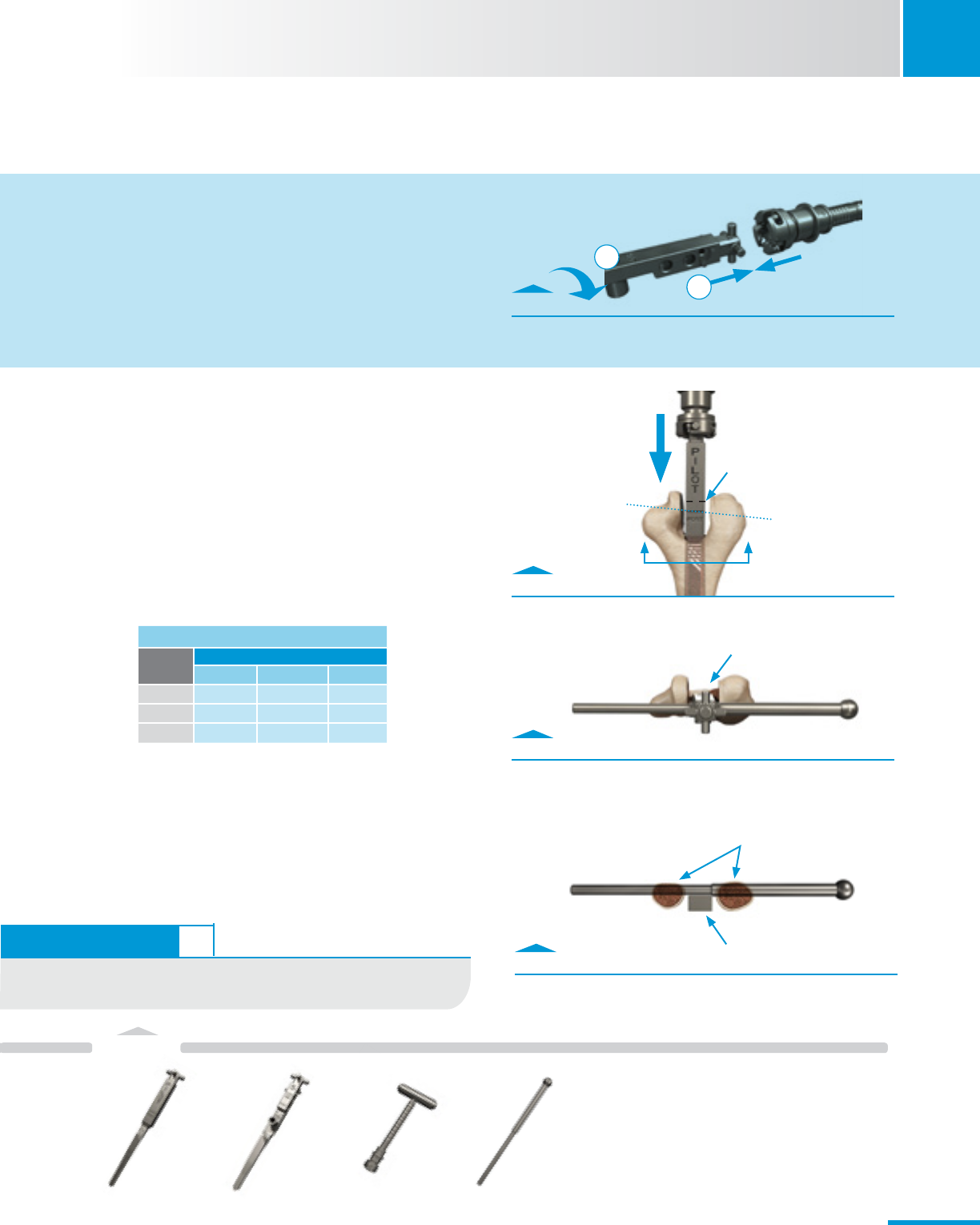
2.3 Humeral Canal Reaming
• UsetheHumeralAwlReamertoopenthehumeralcanal
(Fig. 2.3).
Note: The Humeral Awl Reamer should be centered and
fit through the previously resected middle portion of the
trochlear cut, otherwise remove more bone until it fits; this
ensures clearance for the width of the Humeral Rasp.
TECHNIQUE TIP 2.1
The bone graft can be harvested at this time by first making a
center cut, followed by additional medial or lateral cuts.
Base of
olecranon fossa
Bur
Ensure proper width.
Check for bony
interferences.
Humeral Awl
Reamer
00-8401-060-00
7
Instruments
SECTION
2
Zimmer® Nexel™ Total Elbow Surgical Technique
A A
TECHNIQUE TIP 2.1
FlexibleCannulatedReamersareavailableifdifcultyisencountered
duringrasping.(Sizes8-12mmlocatedintheRevisionCase.)
Fig. 2.5
Use Internal/External Alignment Rod to assess axial
alignment.
Fig. 2.4
Sequentially Rasp the canal; solid line needs to align with
the axis of flexion.
Fig. A
Connect Rasps to T-Handle.
Fig. 2.6
Cross-section A-A with Internal/External Alignment Rod
inserted through Rasp.
2.4 Humeral Canal Rasping
• UsethePilotHumeralRasptoinitiatecanalpreparation.
· GentlyimpacttheRaspuntilthesolidetchedlineis
coincident with the axis of flexion (Fig. 2.4).
• Progressivelyraspuntilthedesiredsizeandtisachieved
(see table).
· PlacetheInternal/ExternalAlignmentRod
perpendicularlythroughtheRasptoassistwith
determination of axial alignment (Fig. 2.5).
• DonotremovethenalHumeralRasportheT-Handle.
Note: While rasping, keep the flat posterior side of the Humeral
Rasp approximately parallel to the plane formed by the
posterior cortices of the medial and lateral columns at the level
of the roof of the olecranon fossa (Fig. 2.6). If these landmarks
are not available, use the relatively flat posterior surface of the
distal humeral shaft to approximate this plane.
SCRUB NURSE
Rasp Connections
A. TheRaspsattachtotheT-Handlebypushingandtwisting
them together. An audible click will be heard.
1
2
Plane formed by medial and lateral columns
Axis of Flexion
Dashedlinedenotes
top of Implant
T-Handle removed for clarity
Rasp
Final Rasp by Implant Size/Length
Implant
Size
Implant Length (mm)
100 150 200
44-100 4-150 n/a
55-100 5-150 5-150
66-100 6-150 6-150
Humeral
PilotRasp
00-8401-064-00
Humeral
Rasp
00-8401-065-15
T-Handle
00-8401-002-00
Internal/External
AlignmentRod
00-8401-061-00
8
Instruments
2
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
2.5 Initial Trephine Cut
• Identifythepositionoftheroundedhumeralcut.
· Use the appropriate size-matched Trephine based
onthenalRasp.(Size5-100Raspand5/6Trephine
shown for example - Fig. 2.7).
· InsertthepilotpinintotheRaspandcarefullyadvance
the Trephine’s pilot pin until the depth stop is reached
(Fig. 2.7).
· Score the posterior surface of the distal humerus (Fig.
2.8). This provides a reference for the final preparation.
Note: Irrigation should be employed during cutting to reduce
heat generation.
Note: The Size 4 Trephine has a slightly different pilot
pin diameter than the Size 5/6 to prevent mismatch from
occurring between the Trephine and Humeral Rasps.
Fig. 2.7
Advance until Trephine reaches depth stop.
Fig. 2.8
View of bone after initial Trephine cut.
Pilot Pin
Size 5/6 Trephine
Humeral
Rasp
00-8401-065-10
Trephine
00-8401-075-00
9
Instruments
SECTION
2
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 2.10
Insert the Pin to secure the Guide in place.
Fig. 2.9
Attach the Humeral Cut Guide to the Rasp.
2.6 Trochlear Excision
• ExcisetheremainingtrochleausingtheHumeralCutGuide.
· Attach the size-matched Humeral Cut Guide to the
HumeralRasp(Fig.2.9).
· Stabilize the Humeral Cut Guide with the Humeral
BearingDriverPinifdesired(Fig.2.10).
· Use an oscillating or reciprocating saw through the
Humeral Cut Guide slots (Fig. 2.11).
Note: Assess the preliminary humeral preparation. If it is
determined that the Humeral Component needs to be inserted
further proximally, the T-Handle/Rasp can be impacted to the
desired depth and steps 2.4–2.6 are repeated as necessary.
Choose closest peg
option that allows full
seating of cut guide.
Humeral
Rasp
00-8401-065-10
Humeral Bearing
DriverPin
00-8401-079-00
Humeral
Cut Guide
00-8401-005-00
10
Fig. 2.11
Secure the Humeral Cut Guide by inserting the Pin, then
make vertical cuts using oscillating saw.
Donotimpact
Cut Guide.
Oscillating saw fits
inside the closed-
ended slots.
Blade thickness =
.050 in. (1.27mm)
Instruments
2
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
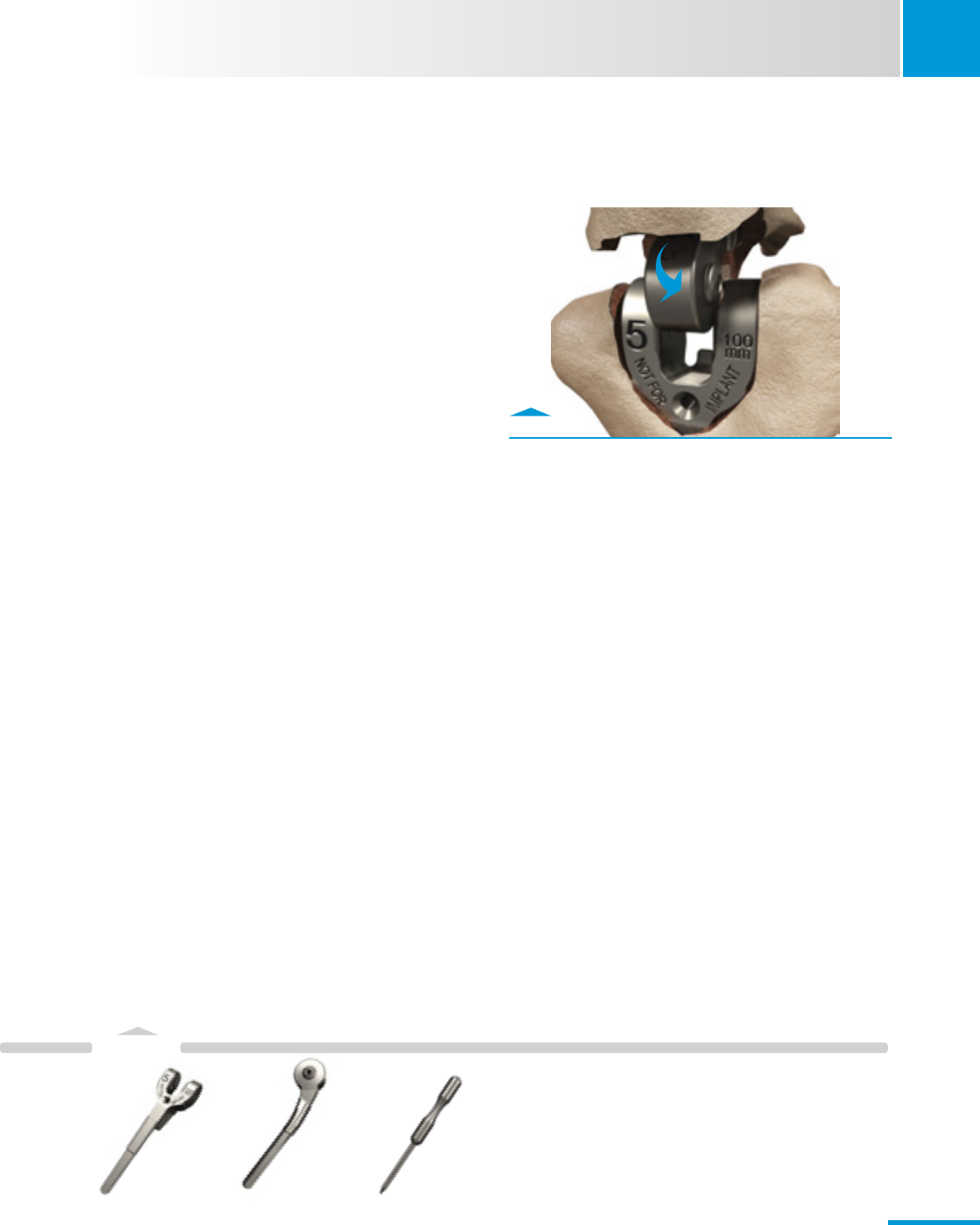
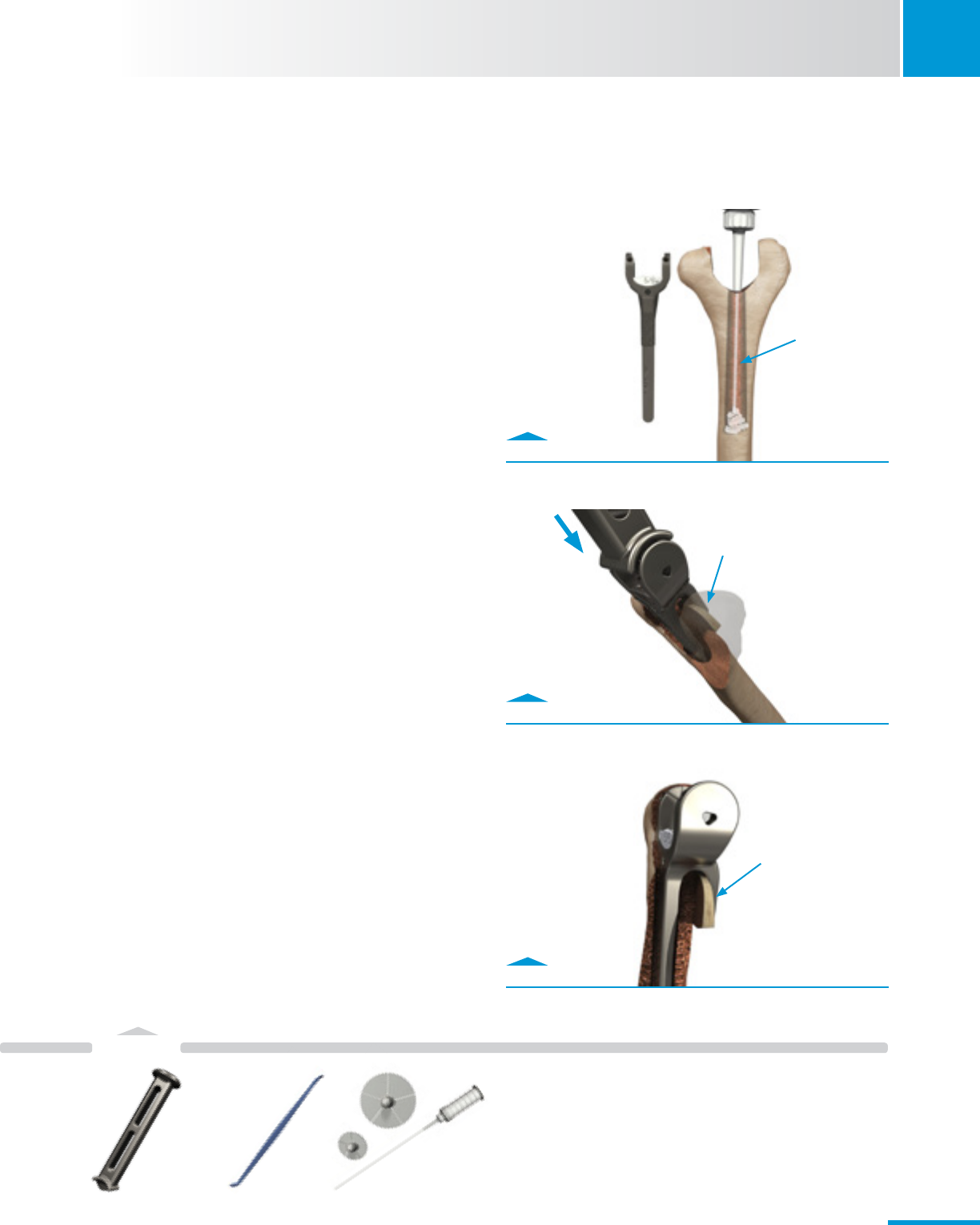
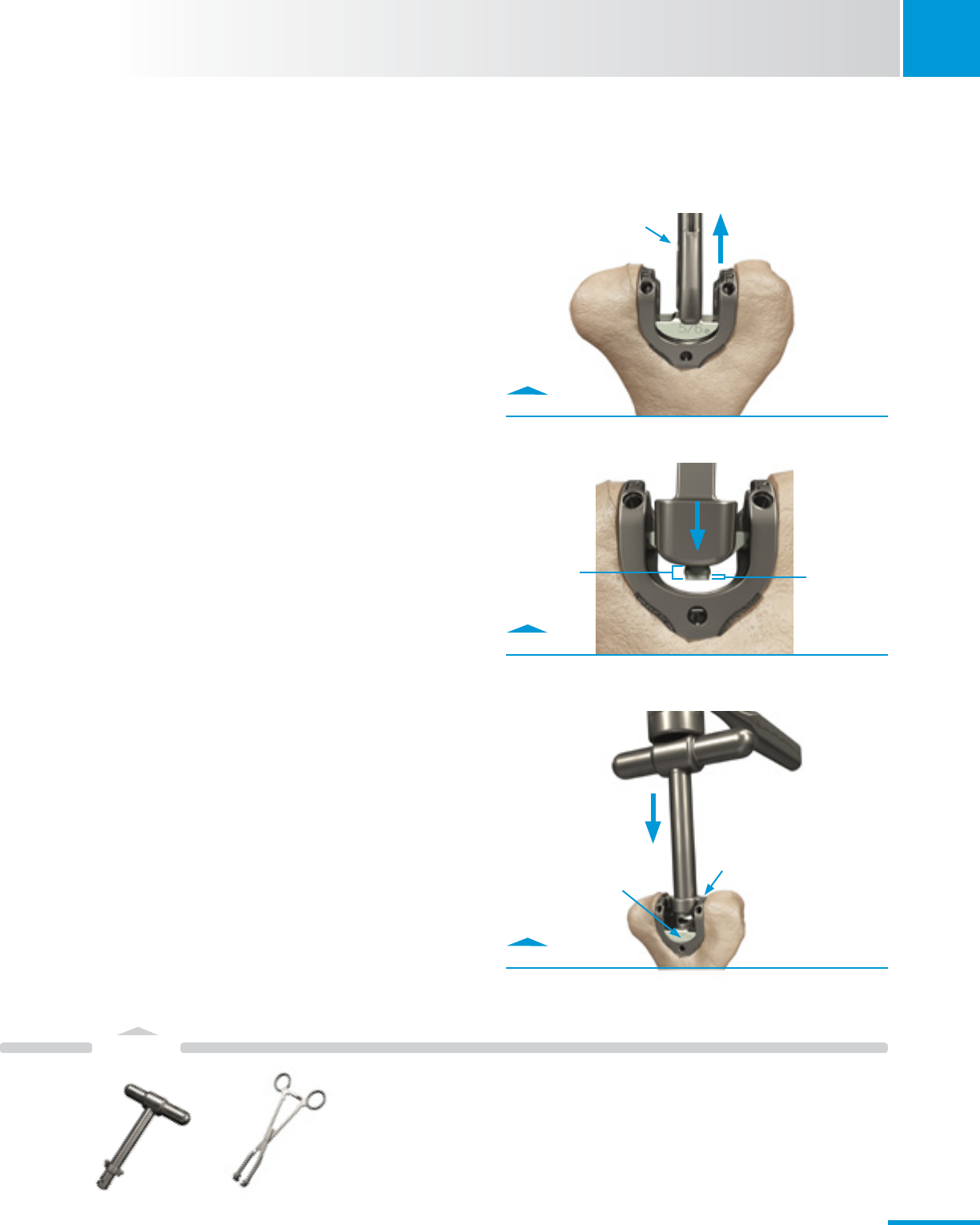
2.7 Final Trephine Cut
• Completetheroundedhumeralcut.
· Insert the Trephine Stabilizer into the humeral canal.
· Notch the coronoid fossa (anterior cortex) with a bur
or rongeur to achieve proper depth of insertion of the
Trephine Stabilizer (Fig. 2.12).
· Insert the Trephine’s pilot pin into the Trephine
Stabilizer and drill while gently advancing the Trephine
to its depth stop (Fig. 2.13).
2.8 Humeral Canal Assessment
• Inserttheappropriatesize-matchedHumeralProvisional
into the humeral canal.
· Ensure the Humeral Provisional is fully seated. If
necessary, use a mallet to lightly tap Provisional to
final depth.
· The distal aspect of the Humeral Provisional should
not sit proud relative to the distal aspect of the lateral
humeral condyle.
• Usearongeurstotrimanyexcesscondylarbonedistalto
the Provisional (Fig. 2.14).
• RemovetheHumeralProvisional.UsetheHumeralBearing
DriverPintoassistasneeded(Fig.2.14).
Fig. 2.12
Notch anterior cortex to allow Stabilizer to fully seat.
Fig. 2.13
Finish the Trephine cut using Stabilizer.
Fig. 2.14
Assess Humeral bone preparation with Provisional.
Create notch with
rongeur
Anterior View
Fully seat Trephine
Stabilizer
Donotstartdrill
until pin in hole.
Trim any bone
as necessary to
be flush with
Provisional.
HumeralBearingDriver
Pin can be inserted
here to assist with
removal of Provisional.
Humeral
Provisional
00-8401-045-10
Trephine
00-8401-075-00
Trephine
Stabilizer
00-8401-012-05
Humeral Bearing
DriverPin
00-8401-079-00
TECHNIQUE TIP 2.2
SimilartotheHumeralRasps,theTrephineStabilizerhasetchlines
on its posterior side indicating the axis of flexion (solid line), and the
distal “top” of the Humeral Component (dashed line).
1
2
11
Instruments
SECTION
3
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 3.2
Enter ulnar canal with bur.
Fig. 3.4
Enter ulnar canal with Ulnar Awl Reamer.
Fig. 3.1
Remove tip of olecranon.
Fig. 3.3
Create notch with rongeur.
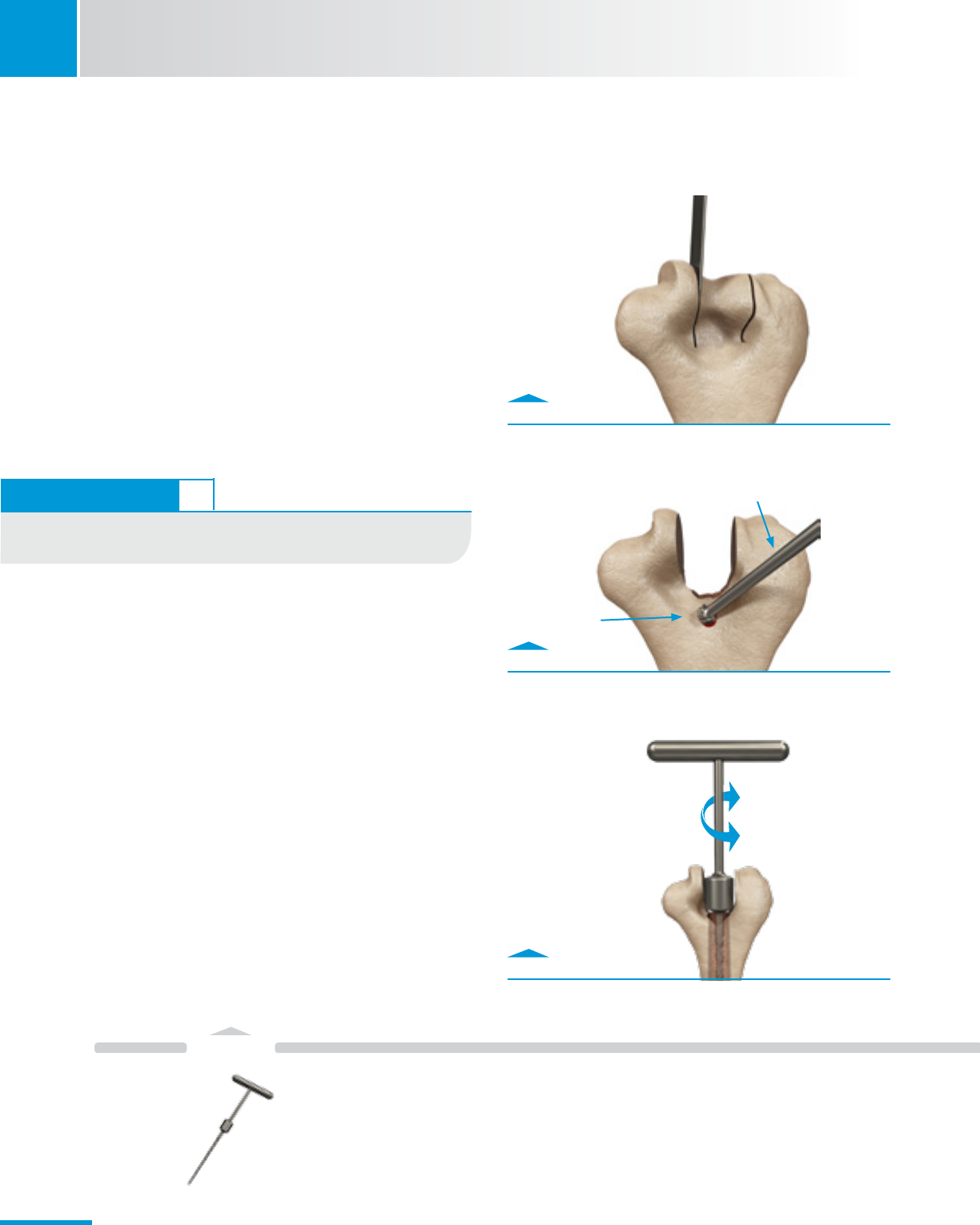
3. Ulnar Preparation
Note: Be aware that instruments labeled size “5/6” can be
used for a size 5 or 6 implant; likewise, instruments labeled size
“4/5” can be used for a size 4 or 5 implant.
Note: Excessive resection of the olecranon compromises the
re-attachment of the triceps mechanism and weakens the
olecranon process. Inadequate resection tilts the intramedullary
Rasp causing malalignment of the Ulnar Component and risks
perforation of the dorsal ulnar cortex.
3.1 Ulnar Canal Exposure
• Removethetipoftheolecranonusinganoscillatingsaw
(Fig. 3.1).
• Useahigh-speedburtoopenthemedullarycanalatthe
base of the coronoid (Fig. 3.2).
3.2 Ulnar Canal Reaming
• “Notch”theolecranon.
· Notch the olecranon using a bur or rongeur (Fig. 3.3).
· The notch should be aligned and deep enough such that
in-line access to the ulnar canal can be achieved with the
Reamers/Rasps.
• OpenthecanalusingtheUlnarAwlReamer(Fig.3.4).
· Place fingers along the exposed shaft of the ulna to
help identify the location of the ulnar shaft distal to the
coronoid to prevent violation of the cortices distally.
Ulnar Awl
Reamer
31-8106-168-00
bur
UlnarAwlReamer
12
Instruments
3
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
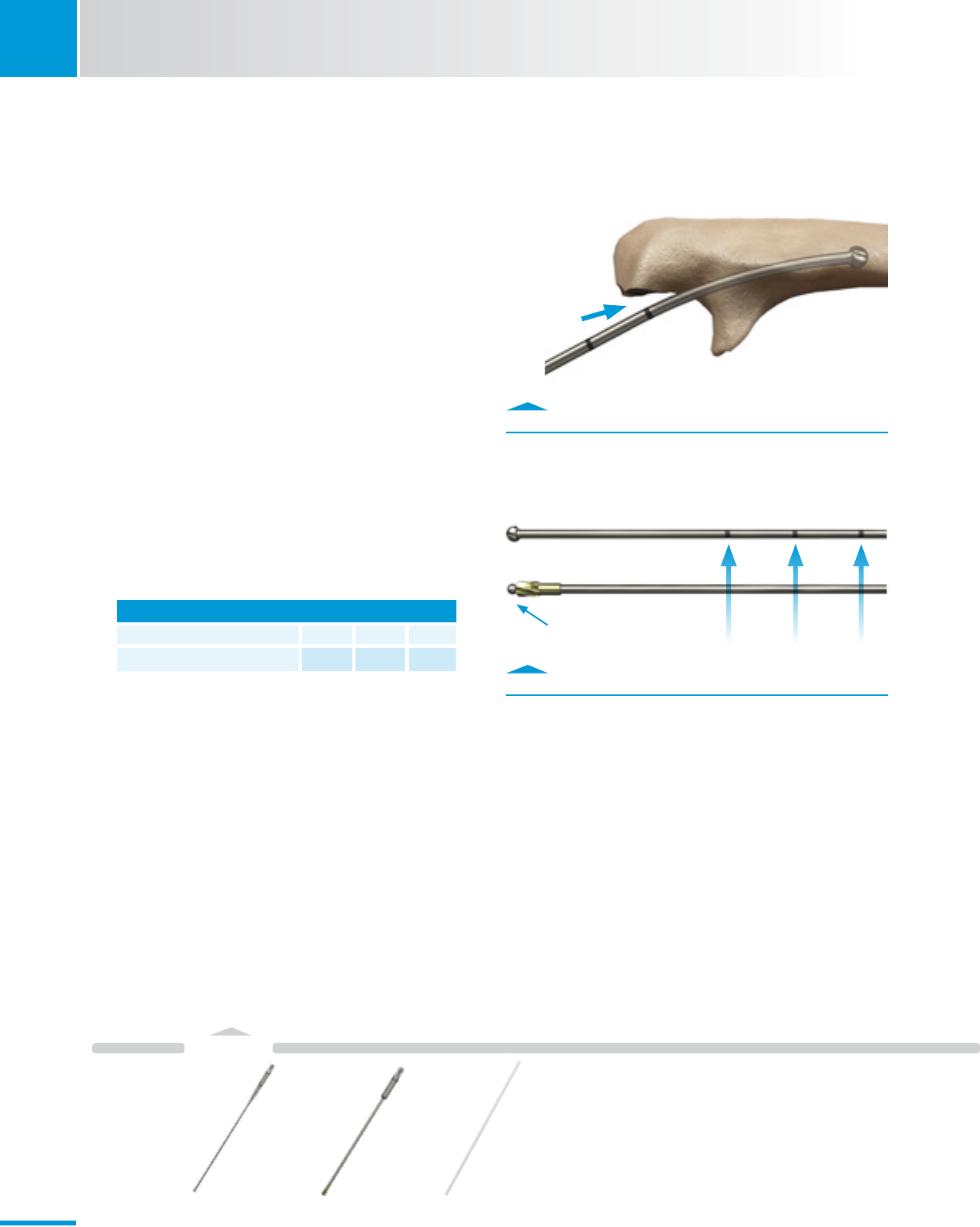
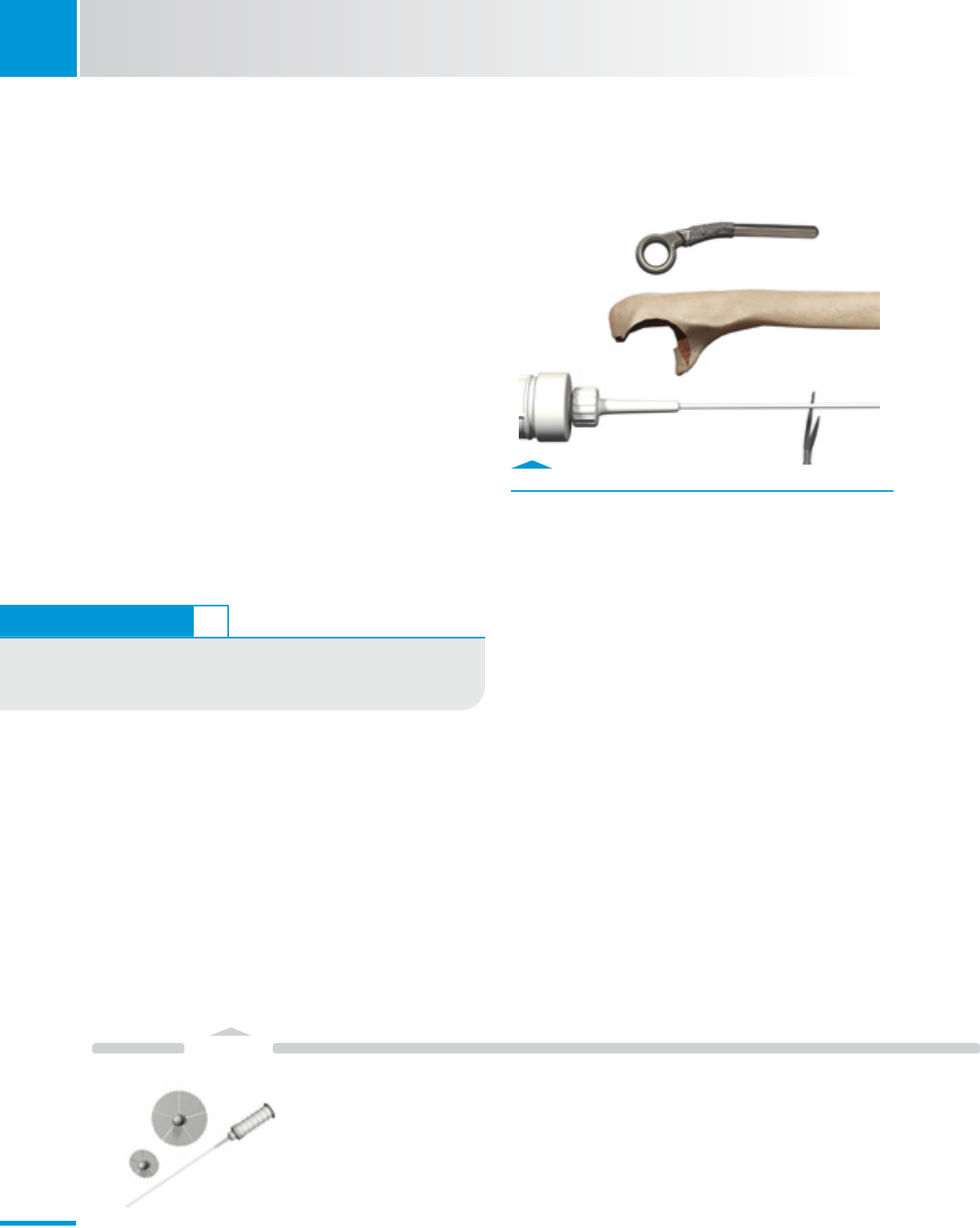
Fig. 3.5
Ream canal with Flexible Reamers to depth mark.
Fig. 3.6
Mark Cannulated reamers with surgical marker.
Note: Flexible Reamers must be used for ulnar canal
preparation. They are used to expand the canal prior to
rasping and fully prepare the distal portion of the canal for
implantation. They must be used progressively beginning with
the smallest 4.5mm Flexible Solid Reamer. DO NOT skip sizes,
or attempt to begin with larger cutting head sizes.
• Progressivelyreamtheulnarcanaluntilthedesiredsizeis
achieved (see table).
· StartwiththeFlexibleSolidReamers.
- Reamtothedepthmarking(75,90or115mm)
based on the desired Implant length (Fig. 3.5).
· ContinuereamingwithFlexibleCannulatedReamersas
necessary depending on chosen implant size.
- Use with Sterile Ball Tip Guide Wire 2.4 x 70 to avoid
cortical penetration as necessary depending on
chosen implant size.
Note: Flexible Cannulated Reamers do not have depth
markings and can be marked with a surgical marker (Fig. 3.6).
Ulnar Reaming
Size Ulnar Component 4 5 6
Final Flexible Reamer (mm) 4.5 6.5 7.0
SolidReamer
CannulatedReamer
Flexible Cannulated
Reamer
00-8401-072-01
Ball Tip
Guidewire
47-2255-008-00
Flexible Solid
Reamer
00-8401-070-05
Ball at end of
Guide Wire
75mm 90mm 115mm
13
Instruments
SECTION
3
Zimmer® Nexel™ Total Elbow Surgical Technique
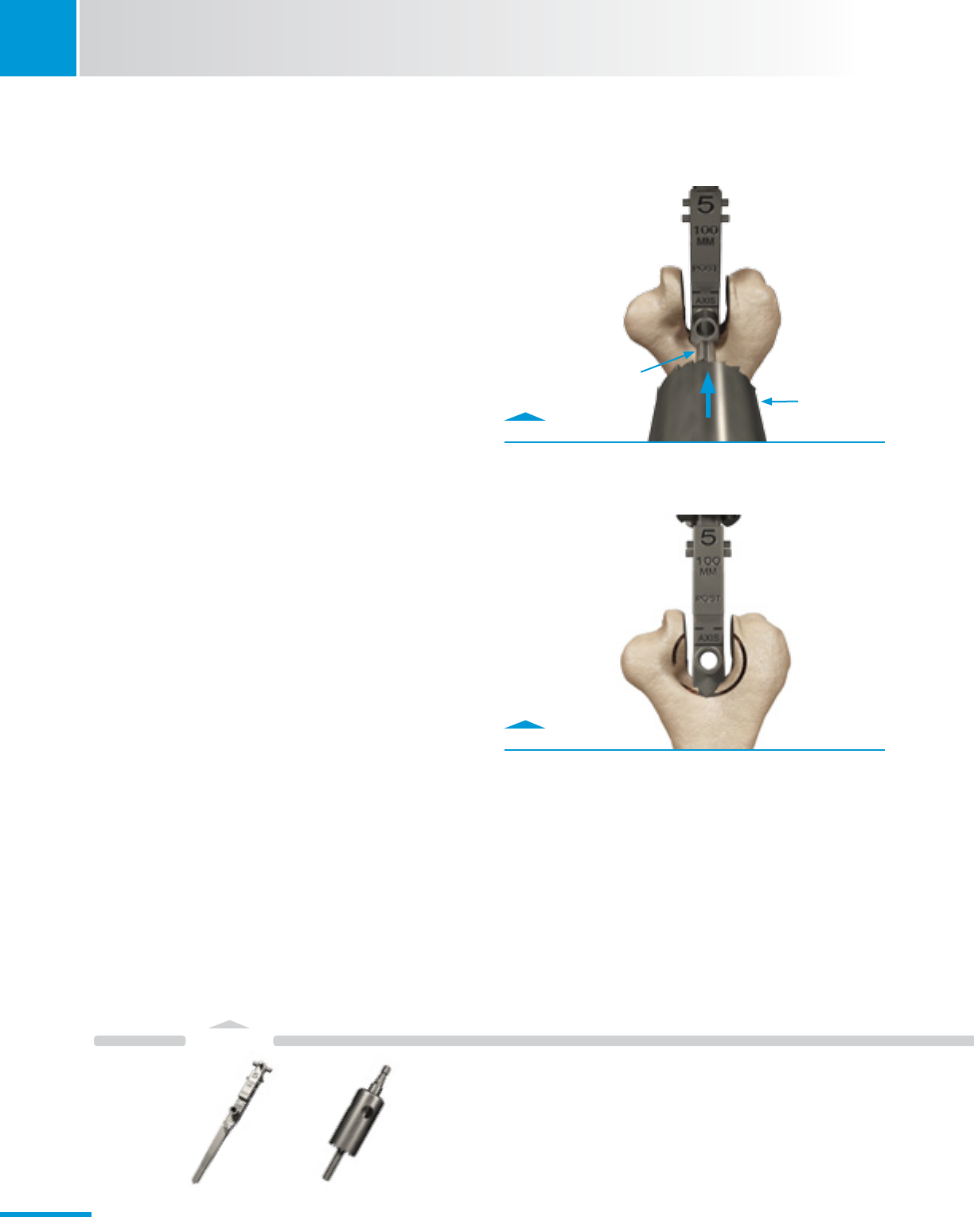
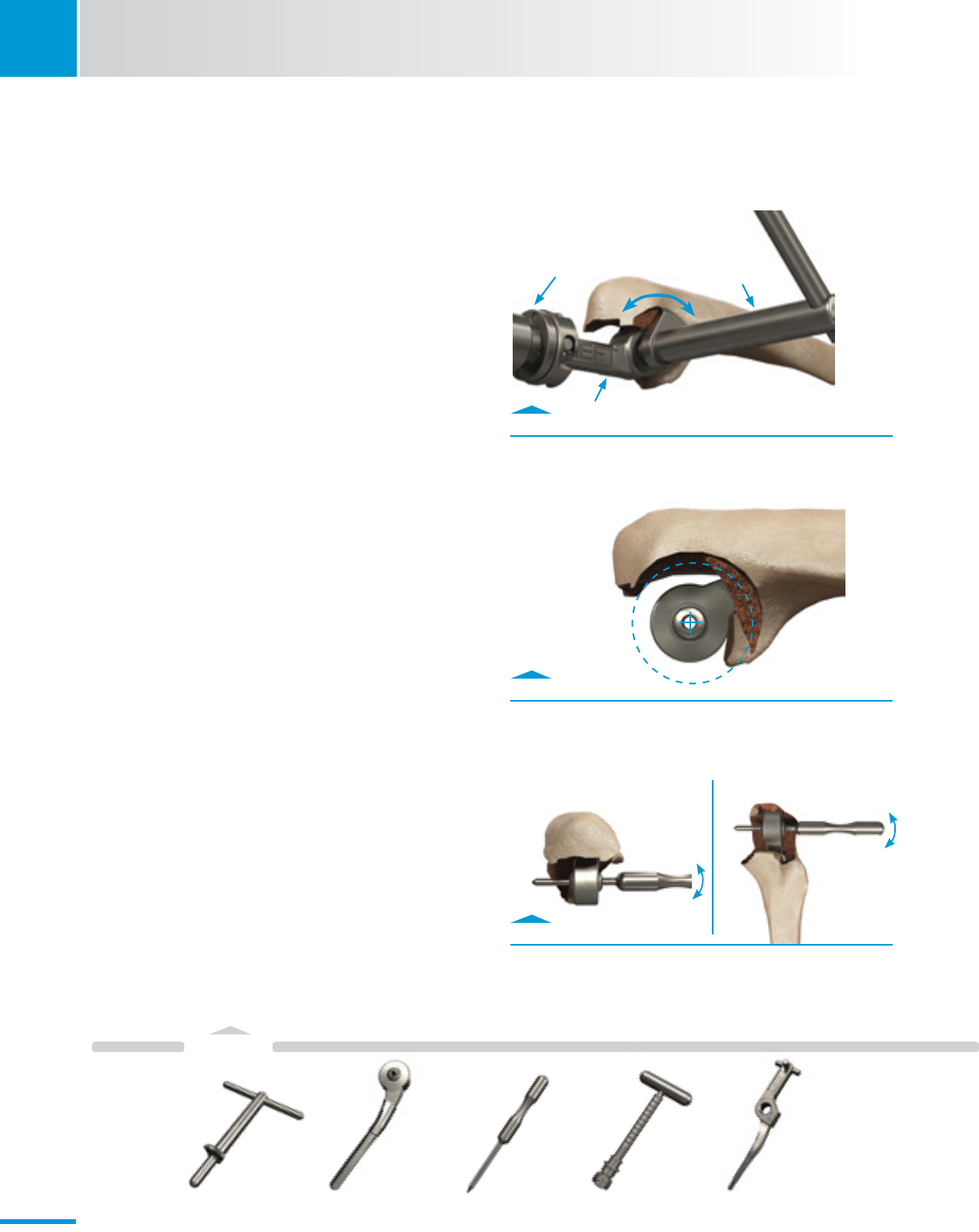
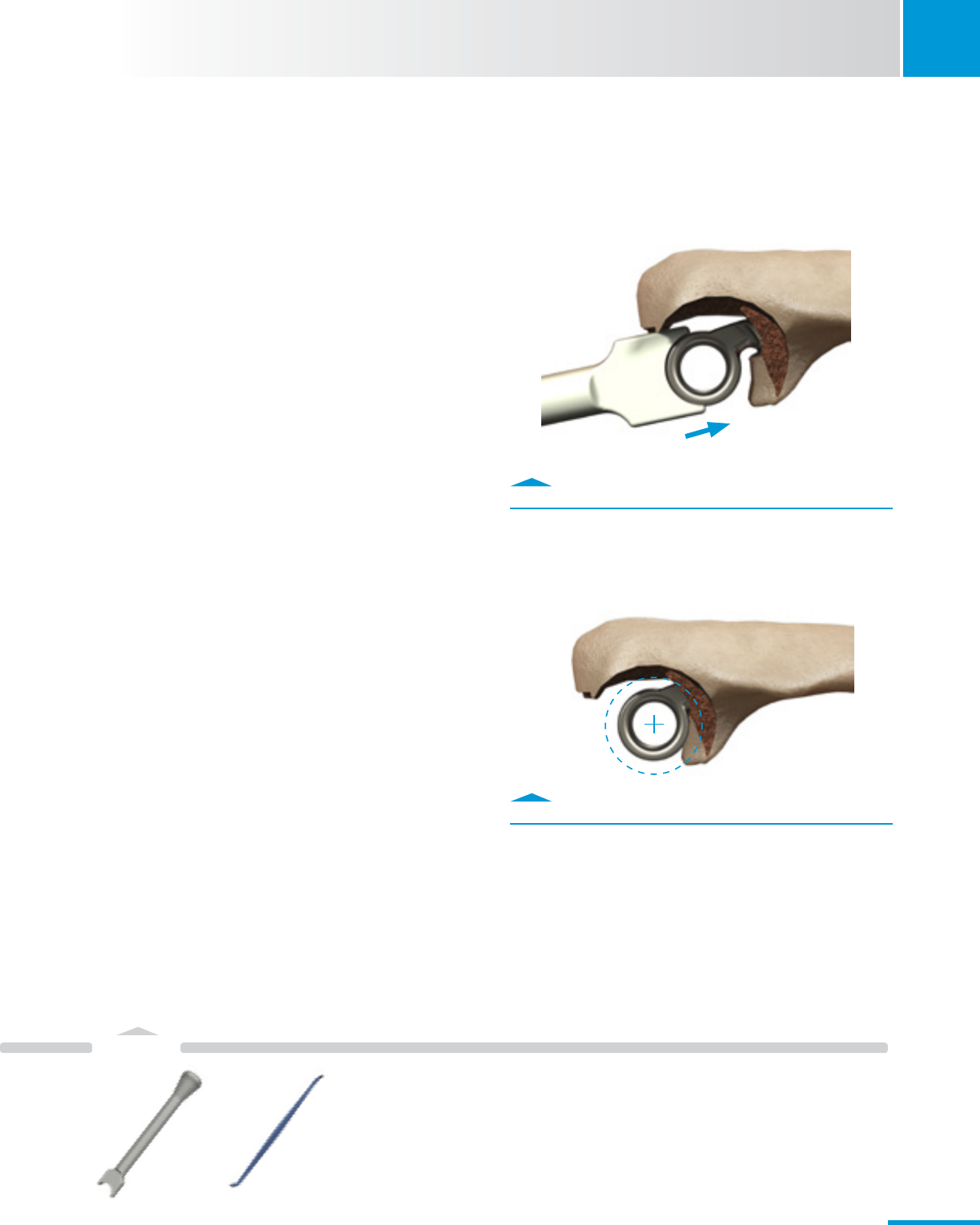
3.3 Ulnar Canal Rasping
Note: Keep the flat posterior surface of the Rasp parallel to the
relatively flat surface of the posterior aspect of the olecranon in
both the coronal and sagittal planes (Fig. 3.7 & 3.8).
• ContinueulnarcanalpreparationwiththePilotUlnarRasp.
· GentlyimpacttheT-Handleuntilthe“eye”oftheRasp
isconcentricwiththeprojectedcenterofthesigmoid
notch in the sagittal plane (Fig. 3.7).
• Progressivelyraspuntilthedesiredsizeortisachieved.
• DonotremovethenalRasporT-Handle.
Fig. 3.8
Rasp is parallel to flat of the olecranon.
Fig. 3.7
Rasp canal until the “eye” is concentric with center of sig-
moid notch.
Flat of the Olecranon
“Eye”oftheRaspmatchesthe
diameter of the Ulnar Component.
T-Handle
removed
for clarity
Flat of the Olecranon
UlnarRasp
Pilot
00-8401-033-01
T-Handle
00-8401-002-00
14
Instruments
3
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
T-Handle Ulnar Clearance
Template
Rasp
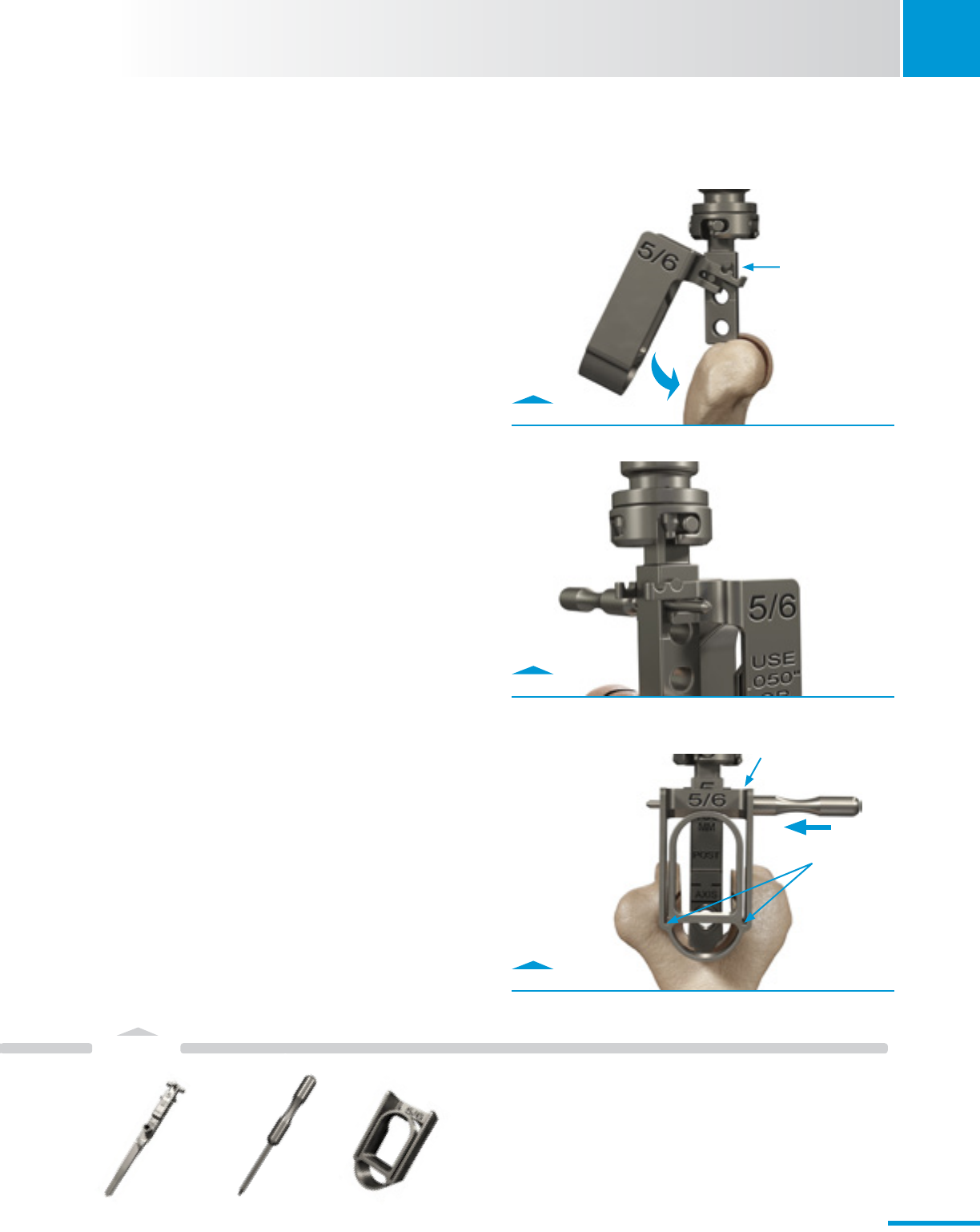
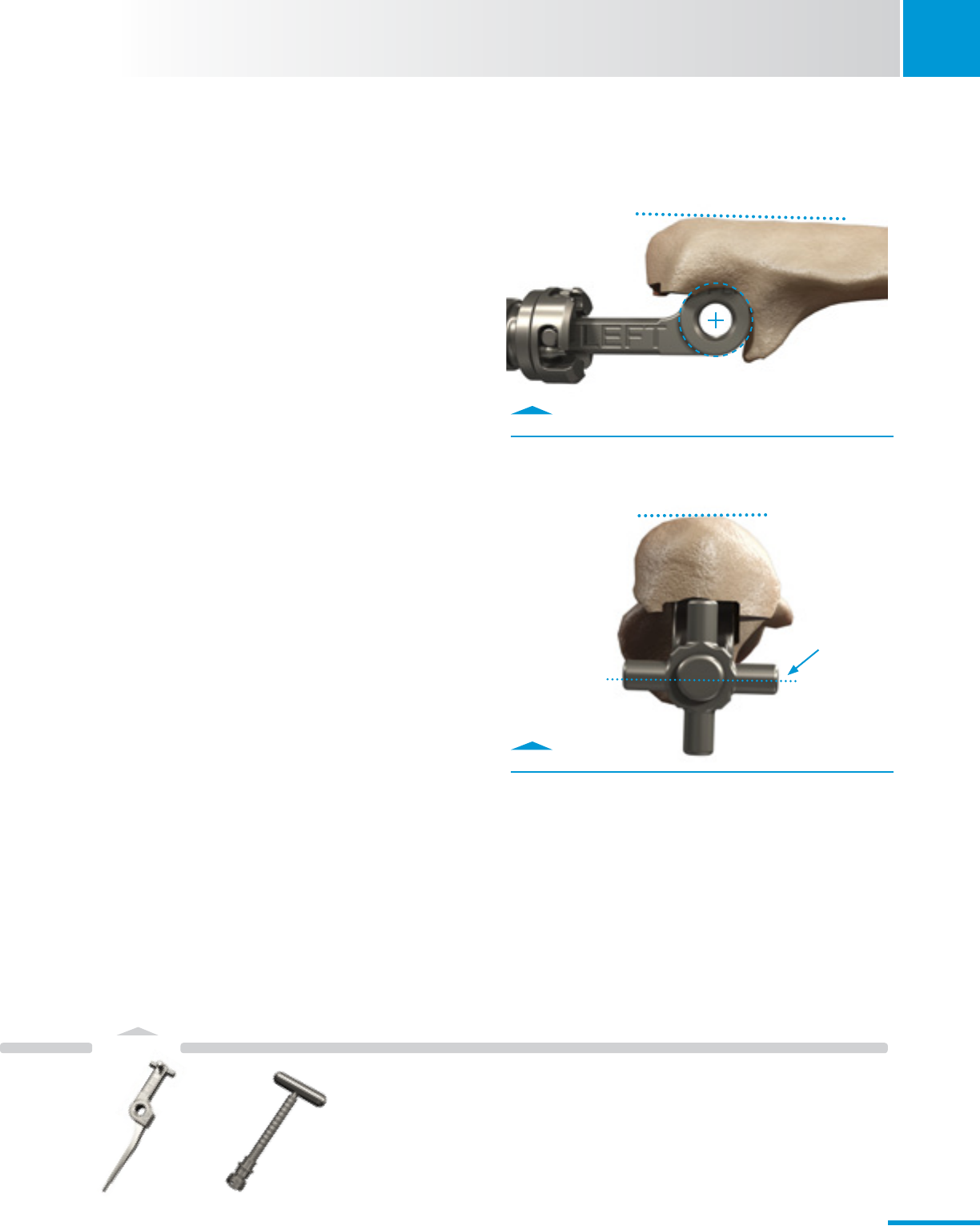
3.4 Sigmoid Notch Preparation
• Ensureadequateclearanceexistsaroundthesigmoidnotch
to allow articulation.
· Place the Ulnar Clearance Template through the Ulnar
Rasp(Fig.3.9).
· Score the bone surface by rotating the Template around
thesigmoidnotch,whilesupportingRasp/T-Handle.
· Withdraw the Template and remove the remaining bone
within the scoring and any other osseous impingements
with a bur.
· Repeatontheoppositeside.
• ReinserttheTemplateoneachsideoftheRasptoconrm
adequate bone has been removed and to achieve
impingement-free device articulation.
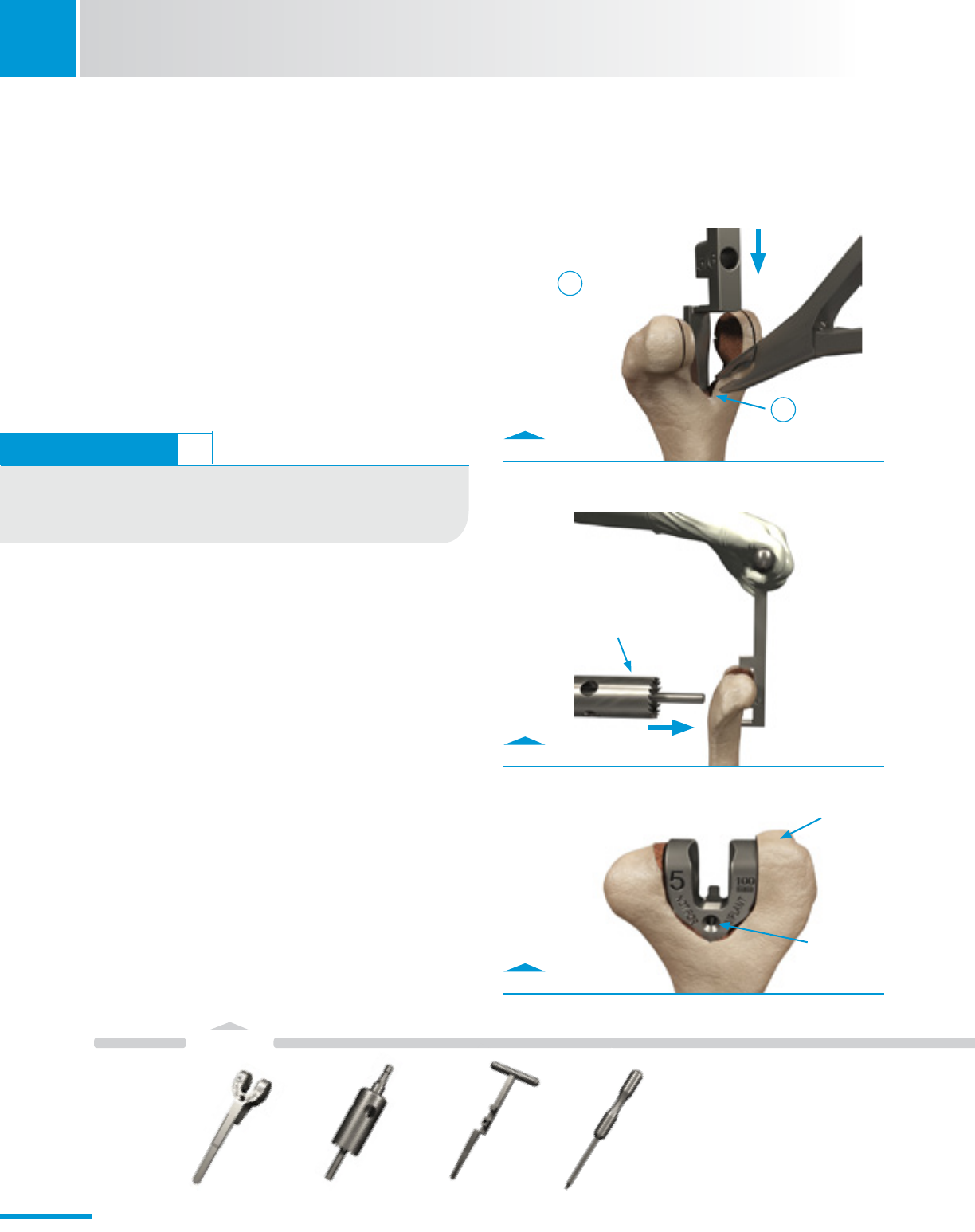
3.5 Ulnar Canal Assessment
Warning: Do not cement the Ulnar Provisional
• Assessulnarcanaldepthofpreparation.
· Insert the appropriate size/length Ulnar Provisional into
the Ulnar canal.
· If necessary, use a mallet to lightly impact the Ulnar
Provisional to final depth.
· Confirm that the center of the Ulnar Provisional is
concentricwiththeprojectedcenterofthegreater
sigmoid notch (Fig. 3.10).
• AssessproperrotationofUlnarProvisional.
· UsetheHumeralBearingDriverPintoconrmrotational
and varus/valgus alignment (Fig. 3.11).
Fig. 3.10
Insert Ulnar Provisional to assess ulnar bone preparation.
Fig. 3.11
Use Pin to assess alignment.
Fig. 3.9
Use Ulnar Clearance Template to confirm sufficient bone
removal.
Ulnar Clearance
Template
00-8401-039-00
Ulnar
Provisional
00-8401-015-07
Humeral Bearing
DriverPin
00-8401-079-00
T-Handle
00-8401-002-00
UlnarRasp
00-8401-034-01
15
Instruments
SECTION
4
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 4.1
Reduce the joint.
4. Trial Reduction
4.1 Link Provisionals
• ConnecttheProvisionalsandreducethejoint.
· Re-inserttheappropriateHumeralProvisional.
· Slide the Ulnar Provisional into the Humeral Provisional
(Fig. 4.1).
4.2 Evaluate Range of Motion
• Performatrialrangeofmotion.
· Removeanyosseousimpingements.Thiscouldinclude
all or portions of the radial head and coronoid process.
· Perform any additional soft tissue releases as needed.
• RemoveProvisionals
· UsetheHumeralBearingDriverPintoaidinUlnarand
Humeral Provisional removal as needed.
Note: Provisionals will provide varus/valgus and internal/
external rotation laxity at the coupling similar to the
final Implants.
Note: Causes for incomplete restoration of elbow extension
include: inadequate depth of insertion of the Humeral
Component, inadequate depth of insertion of the Ulnar
Component, unresolved angular deformity, inadequate release
of anterior, medial or lateral soft-tissue contracture and
posterior bone impingement. Assess these factors prior to final
component implantation.
Humeral
Provisional
00-8401-045-10
Ulnar
Provisional
00-8401-015-07
Humeral Bearing
DriverPin
00-8401-079-00
16
Instruments
SECTION
5Zimmer® Nexel™ Total Elbow Surgical Technique
5. Component Implantation
5.1 Prepare the bone graft
• Fashionabonegraftfromtheexcisedtrochleaor
radial head.
• Ifnobonefromtheelbowisavailable(inmostrevision
cases) use either a bone graft from the radial head if still
present, or the iliac crest or an allograft.
5.2 Prepare Canals for Cementing
• Preparethehumeralandulnarcanalsforcementing.
· Use copious irrigation to clean both medullary canals,
then dry.
· InsertCementRestrictorsasneeded.
5.3 Cement Ulnar Component
• Injectcementintotheulnarcanal.
· Cut the Cement Nozzle to the length of the Ulnar
Component.
- Leave approximately 1 cm of the proximal canal free
of cement to avoid excessive backflow (Fig. 5.1).
Fig. 5.1
Retrograde fill canal with cement.
TECHNIQUE TIP 5.2
The use of high viscosity cement is difficult in smaller diameter
cementnozzlesusedinelbowreplacement.Besuretoinjectthe
cement when still in the viscous state.
CementRestrictor
with Nozzle
32-8105-038-00
17
Instruments
SECTION
5
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 5.2
Use Ulnar Stem Inserter to fully seat Implant.
• InserttheUlnarComponentintothecanal.
• FullyseatandaligntheUlnarComponent(Fig.5.2).
· Use the Ulnar Stem Inserter to protect the articular
surface of the Ulnar Component from damage during
insertion.
· Ensure the implant is perpendicular with the flat plane of
the olecranon.
· CentertheUlnareyeontheprojectedcenterofthe
greater sigmoid notch (Fig. 5.3).
• RemoveexcesscementfromaroundtheUlnarComponent.
· Use the plastic Quik-Use® Curette to avoid scratching the
Implant.
Note: Excess/loose cement can lead to third-body wear of
the articulation.
Note: DO NOT install the Axle-Pin and Ulnar Bearings until after
the Ulnar Component has been placed properly in the canal, all
bone cement has been removed from the exposed articulation
area, and the cement has fully cured. Only use the Ulnar Stem
Inserter to seat the Ulnar Implant.
Fig. 5.3
Implant eye is concentric with the projected center of
sigmoid notch.
Ulnar Stem
Inserter
00-8401-028-00
Quik-Use
Curette
00-5049-053-00
18
Humeral Bearing
DriverPin
00-8401-079-00
Fig. A
Place Humeral Bearing using Humeral Placement Tool.
Fig. B
Position Driver, slide collar into Humeral slots, insert pin,
turn Driver handle.
Fig. C
No Gaps should be present when bearing is fully seated.
SECTION
5Zimmer® Nexel™ Total Elbow Surgical Technique
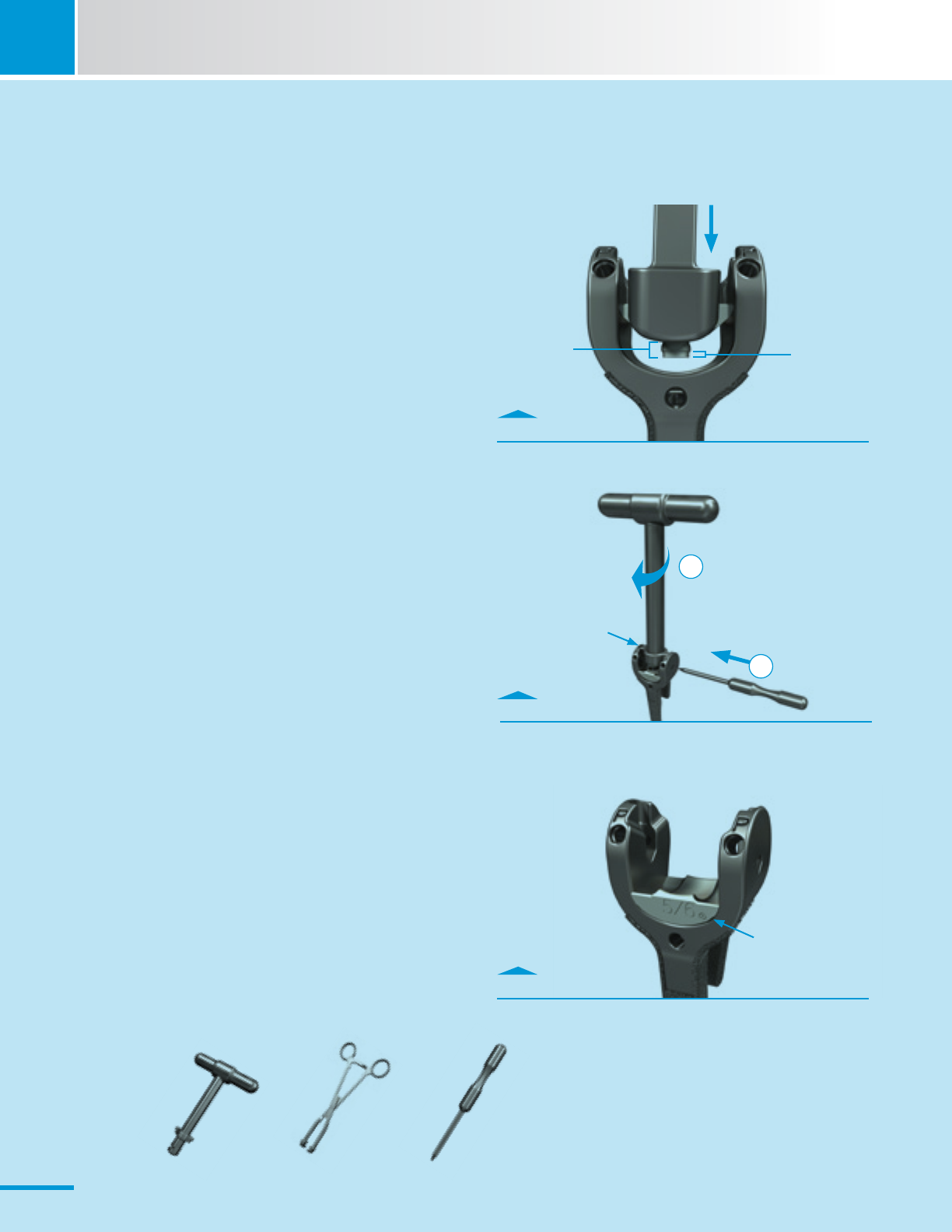
SCRUB NURSE
Install the Humeral Bearing
A. Place the appropriate-sized Humeral Bearing into the
Humeral Component using the Humeral Bearing Placement
Tool.
· The Humeral Bearing will not be fully seated
at this stage.
· Only the “pilot cylinder” of the peg feature should be
inserted into the hole in the base of the yoke of the
Humeral Component.
· See last figure for proper orientation of the Humeral
Bearing.
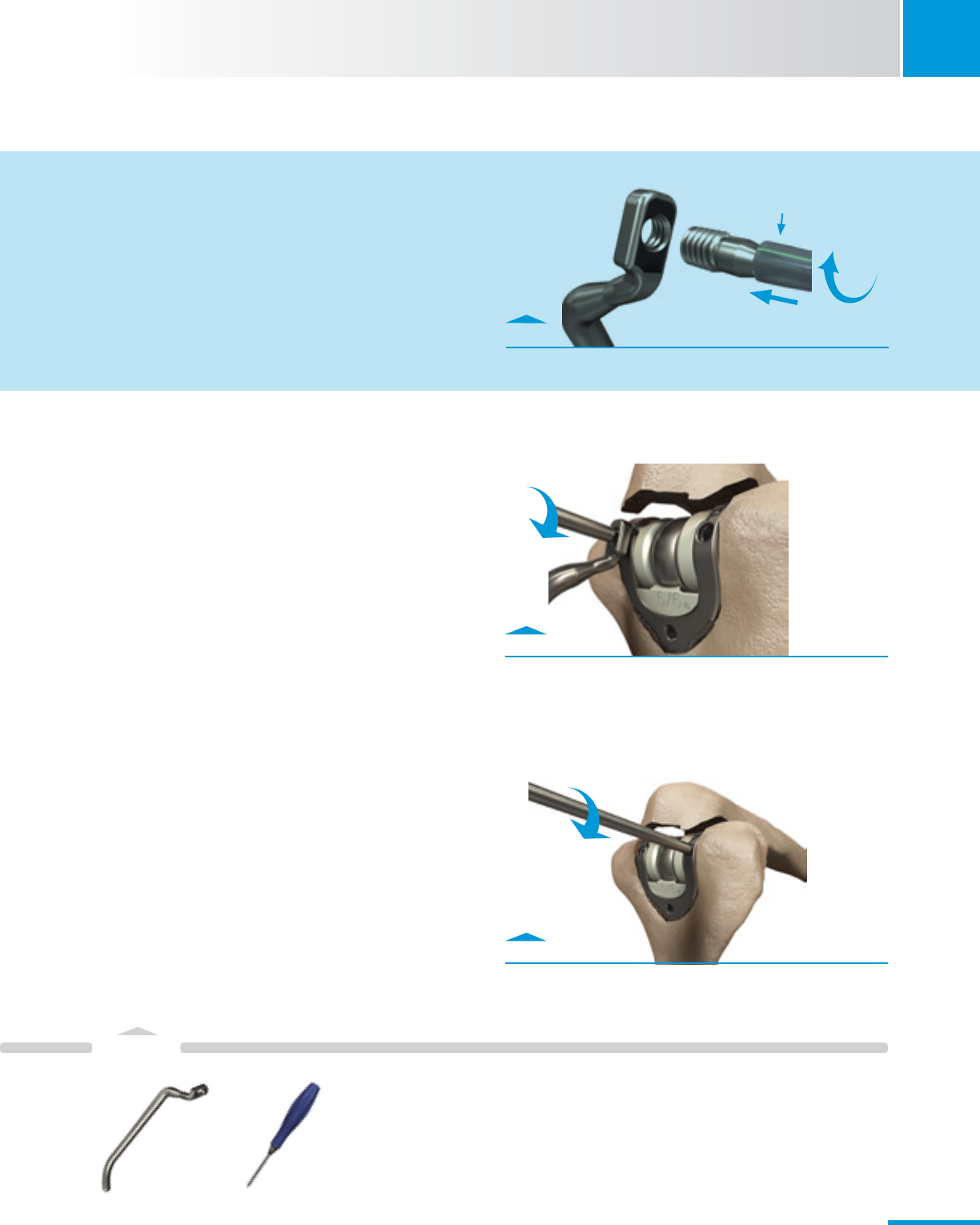
B.PositiontheHumeralBearingDriveragainstarticulation
surface of the Humeral Bearing and insert the Humeral
BearingDriverPinsimultaneouslythroughtheHumeral
ImplantandtheslotsintheshaftoftheDriver.
· ThehandleofHumeralBearingDrivershouldbeparallel
to flat posterior face of Humeral Component.
· Turn the T-Handle 90 degrees clockwise.
· Resistancewillbefelt,butnoaudibleclickwilloccur.
C. The Humeral Bearing will be fully seated when there are
no visual gaps when viewing from the posterior and the
anterior sides of the Humeral yoke.
No gaps
Peg
Peg Pilot Cylinder
Collar
2
1
Humeral
BearingDriver
00-8401-078-00
Humeral Bearing
Placement Tool
00-8401-082-00
19
Instruments
SECTION
5
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 5.4
Retrograde fill canal with cement.
Fig. 5.5
Insert bone graft and fully seat the Humeral Component
using Humeral Stem Inserter.
Fig. 5.6
Cross-section view.
5.4 Cement Humeral Component
• Injectcementintothehumeralcanal.
· Cut the Cement Nozzle to the length of the
Humeral Component.
· Leave approximately 1 cm of the distal canal free of
cement to avoid excessive backflow (Fig. 5.4).
• ImplanttheHumeralComponentintothehumeralcanal.
· Before fully seated, wedge a bone graft between the
flange of the Humeral Component and the anterior distal
humeral cortex (Fig. 5.5).
· Carefully impact the Humeral Component with the
appropriate size-matched Humeral Stem Inserter to fully
seat the Component (Figs. 5.5-5.6).
• Clearanyexcessbonecementwiththeplastic Quik-Use
Curette.
• Allowcementtofullycure.
Cement
nozzle
Insert bone graft
Bone graft
Quik-Use
Curette
00-5049-053-00
Humeral
Stem Inserter
00-8401-058-05
CementRestrictor
with Nozzle
32-8105-038-00
20
6
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
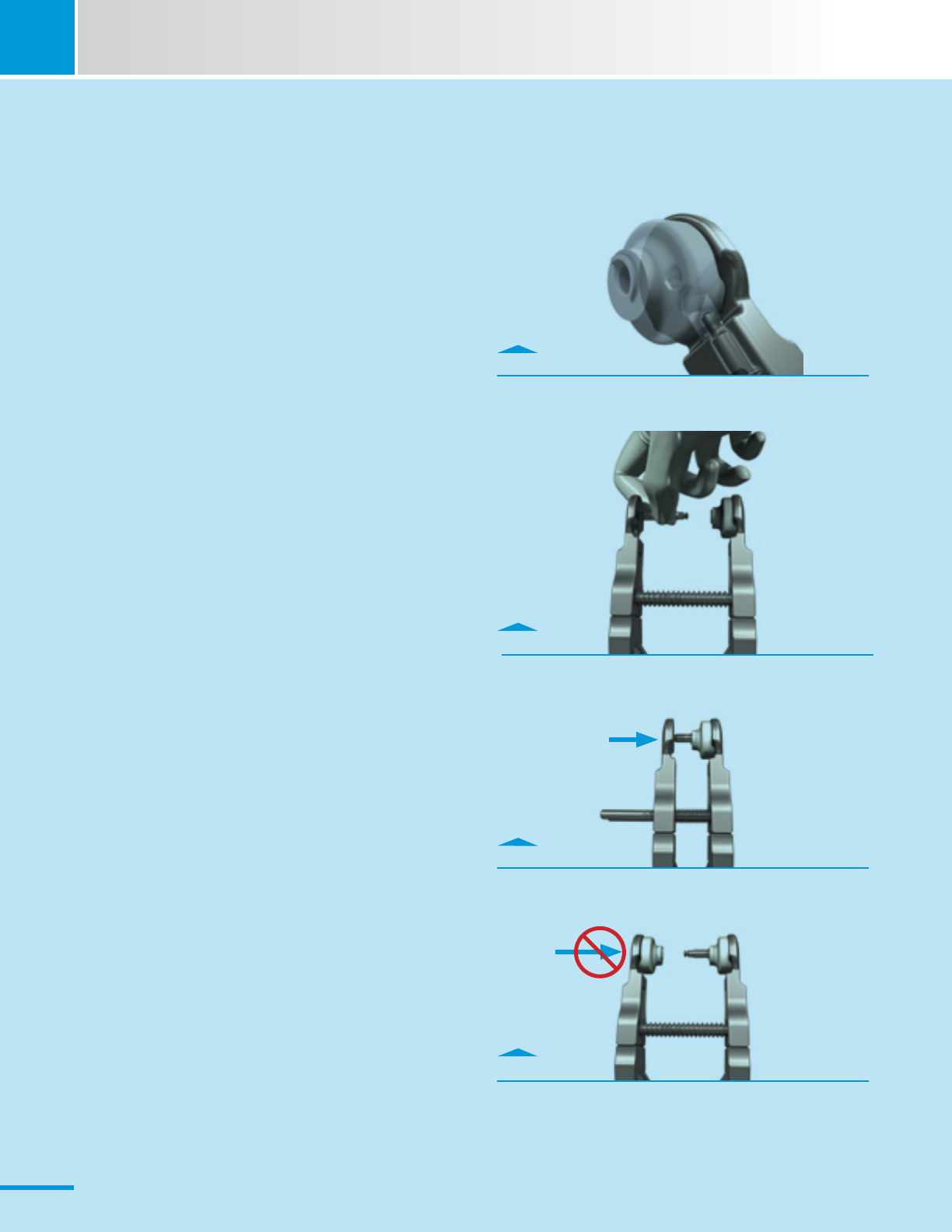
SCRUB NURSE
Install the Humeral Bearing
A. Load an Ulnar Bearing into one side of the Ulnar Bearing
Assembly Tool (UBAT).
B.LoadtheAxle-Pinintotheoppositejawofthetool
maintaining a finger-hold on the Axle-Pin.
C. Squeeze the handles.
· Stop when hard resistance is felt – no audible click will
be heard.
D. Load the second Ulnar Bearing.
· DONOTsqueezethesecondBearingontotheAxle-Pin.
· Carefully hand the pre-loaded instrument to the surgeon
after the Ulnar Component has been cemented and
cleared of any debris.
Donotsqueeze.
Fig. A
Lock bearings into spring loaded part of UBAT.
Fig. B
Maintain finger-hold on Axle-Pin.
Fig. C
Squeeze UBAT to press Axle-Pin into Bearing.
Fig. D
Load second Ulnar Bearing.
21
Instruments
SECTION
6
Zimmer® Nexel™ Total Elbow Surgical Technique
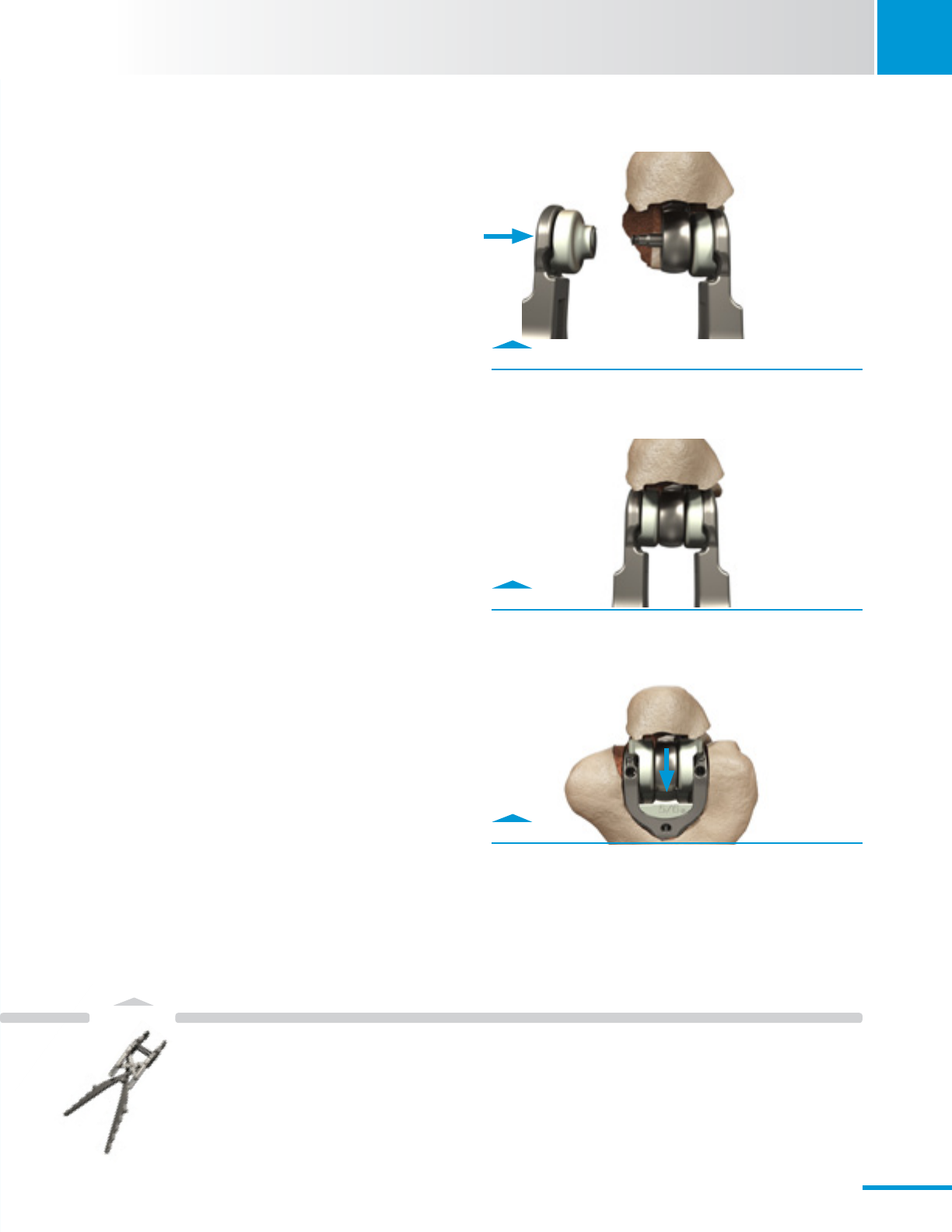
6. Final Assembly
6.1 Ulnar Bearing Assembly
• AttachtheBearing/Axle-PinassemblytotheUlnar
Component.
· Carefully place the Axle-Pin through the eye of the
Ulnar Component in-situ (Fig. 6.1).
· Squeeze the handles of the pre-loaded Ulnar Bearing
Assembly Tool (UBAT) until hard resistance is felt.
No audible click will be heard (Fig. 6.2).
Note: Bearings/Axle-Pin assembly is designed to be loose
fitting to the Ulnar eye.
Note: Use caution to avoid contact between the Axle-Pin and
the Ulnar Component to avoid scratching the Implant.
6.2 Elbow Reduction
• Begintoreducethejoint.
· Align the Axle-Pin and the tabs of the Ulnar Bearings to
the slots in the Humeral Component (Fig. 6.3).
· Partiallyreducethejointbyapplyinghandpressureto-
the forearm to drive the Axle-Pin and Bearings into the
Humeral Implant.
Fig. 6.1
Use UBAT to place Bearings.
Fig. 6.3
Align Bearing tabs and partially reduce joint.
Fig. 6.2
Use UBAT to attach bearings.
Ulnar Bearing
Assembly Tool
00-8401-081-00
22
Instruments
6
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
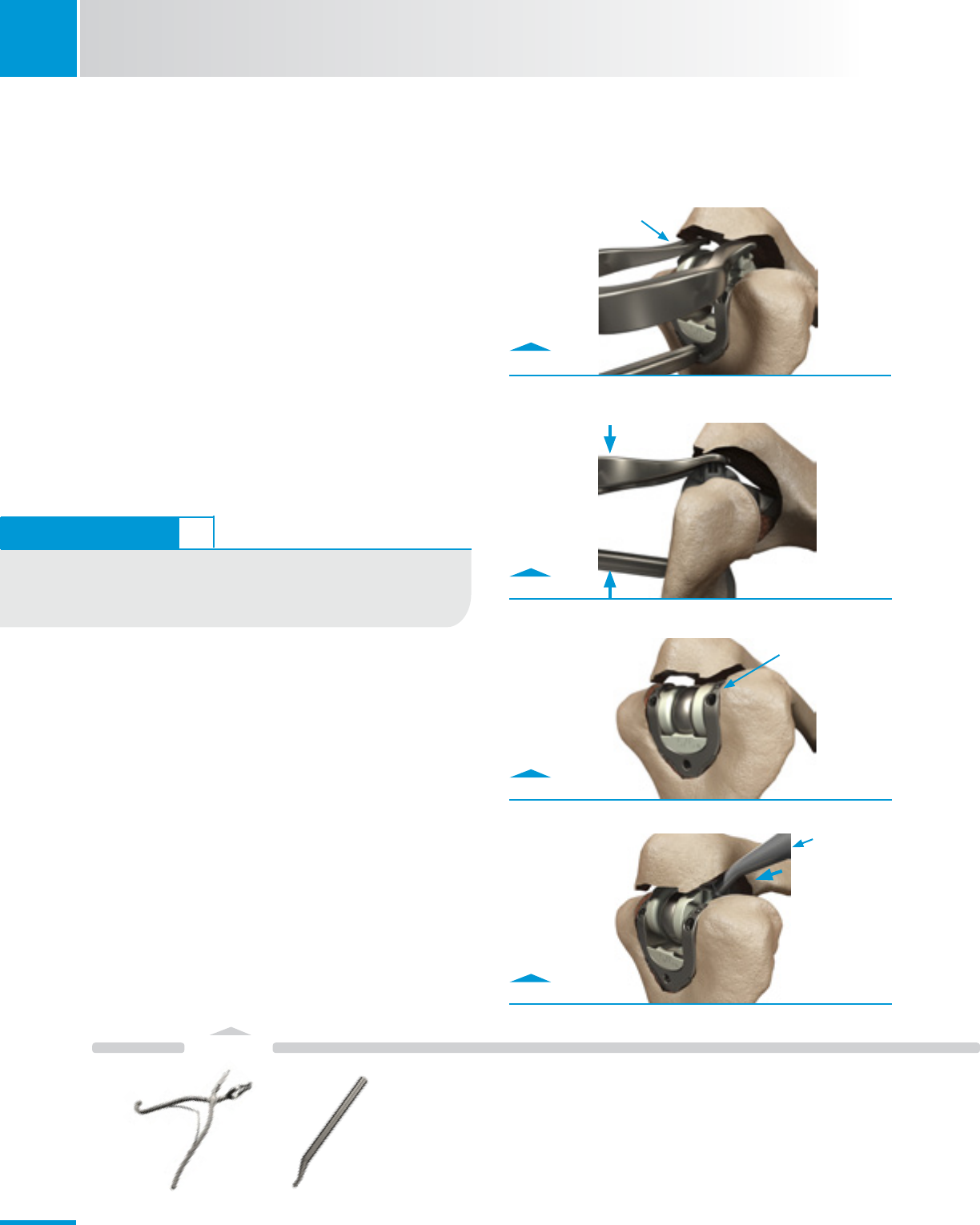
Fig. 6.5
Use Articulation Inserter to squeeze together implants.
Fig. 6.6
Bearings will be flush with top of implant when fully seated.
Fig. 6.7
Use Ulnar Bearing Tamp to press bearings in place if needed.
• Finishreductionofjoint.
· Tocompletereductionofthejoint,applytheArticulation
Inserter.
- Top of the Articulation Inserter fits into the Ulnar
Bearing tab pockets.
- Bottom of the Articulation Inserter fits into the
proximal posterior hole in the Humeral Component
(Fig. 6.4 & 6.5).
· Squeeze the instrument until resistance is felt and
Bearings are fully seated. No audible click will be heard.
- The Ulnar Bearings should appear flush with the
curved distal surfaces of the Humeral Component
(Fig. 6.6).
Fig. 6.4
Insert Peg in hole of Humeral Component and feet into the
Bearing pockets.
Align Bearing
tabs with slots in
Humeral Implant
Feet fit into Bearing
tab pockets.
Bearings should
be flush with top
of implant
Gently push or tap
Bearing tabs on each
side of the olecranon.
Ulnar
Bearing Tamp
00-8401-018-00
Articulation
Inserter
00-8401-019-00
TECHNIQUE TIP 6.5
The Ulnar Bearing Tamp is an alternate tool available to assist with
alignment and insertion of the articulation, if access is unachievable
with the Articulation Inserter (Fig. 6.7).
23
Load Humeral Screw into Humeral Screw Holder.
SCRUB NURSE
Screw Loading
A. Load Humeral Screw
· Use the flexible plastic tubing to grasp the Humeral Screw.
· Thread Humeral Screw into the black-etched side of a Screw Holder.
· Removeanddiscardthetubing.
· RepeatwithsecondScrewandsecondScrewHolder.
Instruments
SECTION
6
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 6.8
Use Elbow Torque Driver to insert screws.
Fig. A
Use Elbow Torque Driver to insert screws.
6.3 Humeral Screw Insertion
Note: Proper application of torque to install the Humeral Screws
is required for a successful prosthesis; only use the tools
provided in the instrument set to apply torque.
Note: If Bearings are not flush with the Humeral Component,
difficulty might be encountered during Humeral Screw inser-
tion. Ensure Bearings are fully seated prior to inserting Screws
(see section 6.2, Fig. 6.6).
Note: Never reuse any Humeral Screw after it has been installed
to its prescribed torque, even if during same surgery. The Elbow
Torque Driver is designed for single-surgery.
• Insertthescrews.
· Place the loaded Humeral Screw Holder against the
posterior face of the Humeral Component and drive the
ScrewfreeoftheScrewHolder;repeatontheotherside.
• SequentiallytightentheScrewstotheprescribedtorque.
· Lightly snug each Screw before final torquing either one.
· DriveeachScrewtothenaltorquewiththeElbow
TorqueDriveruntilanaudible“click”isheard(Fig.6.9).
· DisposeofElbowTorqueDriverwhennished.
6.4 Final Range of Motion
• Performanalrangeofmotion.
· Removeanyimpingingboneandaddressanysofttissue
contractures.
Fig. 6.9
Lightly snug each Screw then achieve final torque “click.”
Tighten until “Click” is heard.
Screw
Holder
Elbow
TorqueDriver
Removeanddiscard
plastic tubing
Humeral
Screw Holder
00-8401-084-00
Elbow
TorqueDriver
00-8401-080-00
24
7
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
7. Closure
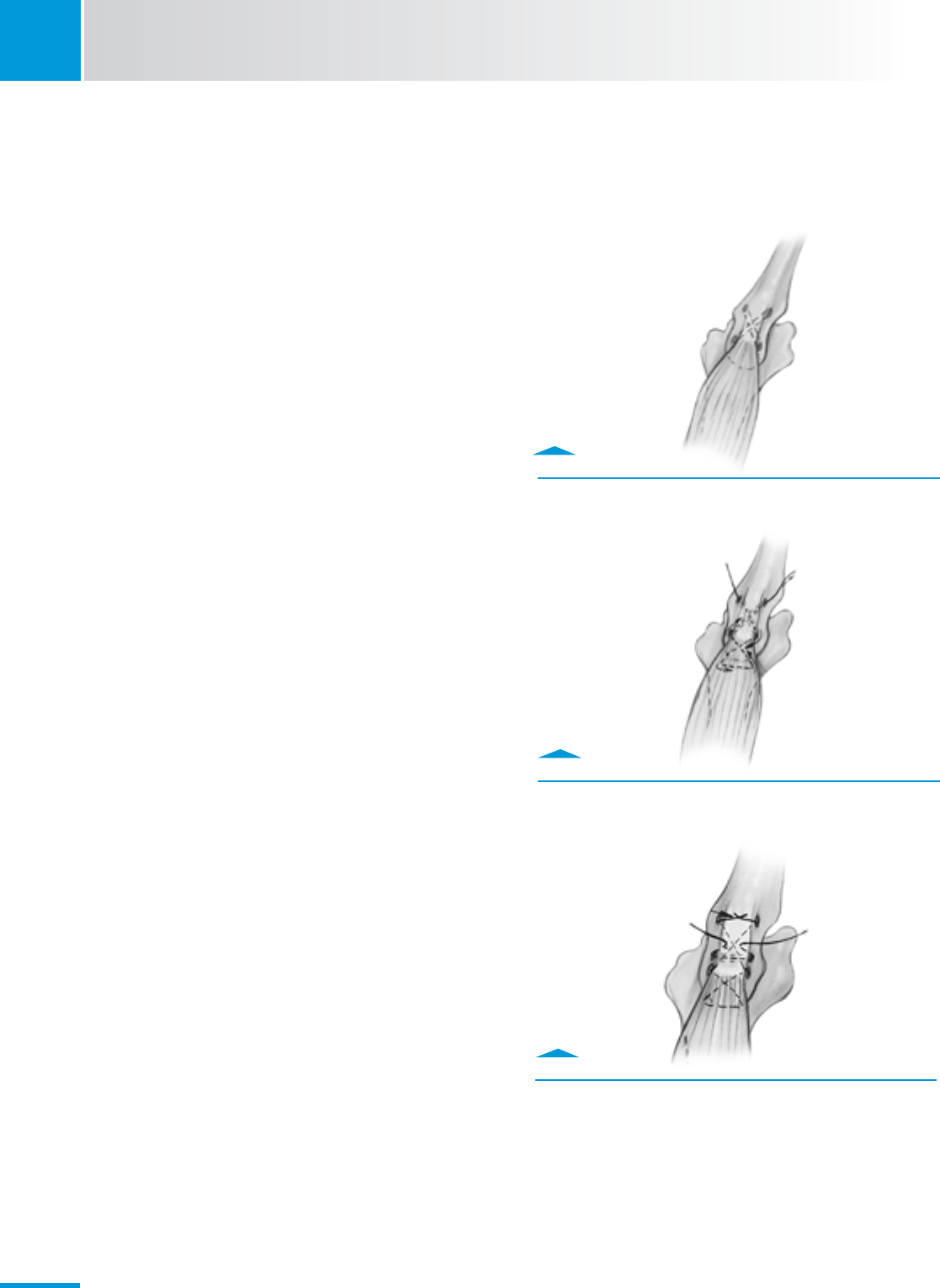
• Repairthetriceps.
· Place cruciate and transverse drill holes in the proximal
ulna (Fig. 7.1).
• Performcruciaterepairofthetriceps.
· Repositiontriceps.
· Returntricepstoapositionthatisslightlyover-
corrected from its anatomic position.
· Pull the sleeve medially about 2 cm.
• Begintosutureandrstlockingstitch.
· Start suture medially and directed laterally through the
drill hole to capture the lateral triceps tendon with a
locking stitch (Fig 7.2).
· Use a #5 nonresorbable suture.
• Secondlockingstitch.
· The suture is brought to the midline of the triceps and
a second locking stitch is placed slightly more proximal
and in the triceps tendon’s midline.
• Thirdlockingstitch.
· The third locking stitch aligns with the medial tunnel
in the olecranon and the suture is drawn through the
tunnel emerging on the lateral aspect of the reflected
mechanism.
· It is brought through the sleeve of tissue from lateral to
medial.
• TransverseRepair.
· Start to suture medial to lateral through the olecranon
(Fig. 7.3).
· After piercing the lateral sleeve of tissue, it is brought
to the midportion of the triceps tendon and a locking
stitch is placed slightly proximal to the attachment after
which it again pierces the medial aspect of the margin
of the triceps.
- Use #5 nonresorbable suture.
- Tie sutures with the elbow in approximately 45
degrees of flexion.
Fig. 7.1
Drill holes in proximal ulna.
Fig. 7.2
Capture triceps tendon with locking stitch.
Fig. 7.3
Suture medial to lateral through the olecranon.
25
SECTION
8
Zimmer® Nexel™ Total Elbow Surgical Technique
• Completetheclosureinaroutinefashion.
· Stabilize the ulnar nerve in the anterior subcutaneous
pocket.
· Obtain hemostasis with bipolar cautery.
· Close the wound in layers.
· Insert a drain, if desired.
• Finishclosure.
· Apply a compressive dressing, use an anterior splint
with the elbow in full extension and elevate the arm.
8. Postoperative Management
• Removethedrain,ifused,thenextday.
• Removethecompressivedressingontherstorsecond
day after surgery.
• Instructthepatientonactivitiesofdailyliving.
· Typically, no formal physical therapy is required.
· Avoid strengthening exercises.
· Allow elbow flexion and extension as tolerated.
• Ifgreaterthan45degreeexioncontracturewaspresent
before surgery, use a static extension brace at night for 4-8
weeks.
• Thepatientmustavoidforcibleextensionfor6-8weeks.
• Liftinglimitations
· The patient must not lift more than one pound (~0.5
kg)duringtherstthreepost-operativemonths;and,
thereafter, not more than five pounds (~2.25 kg) with
the operated arm.
26
Instruments
9
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
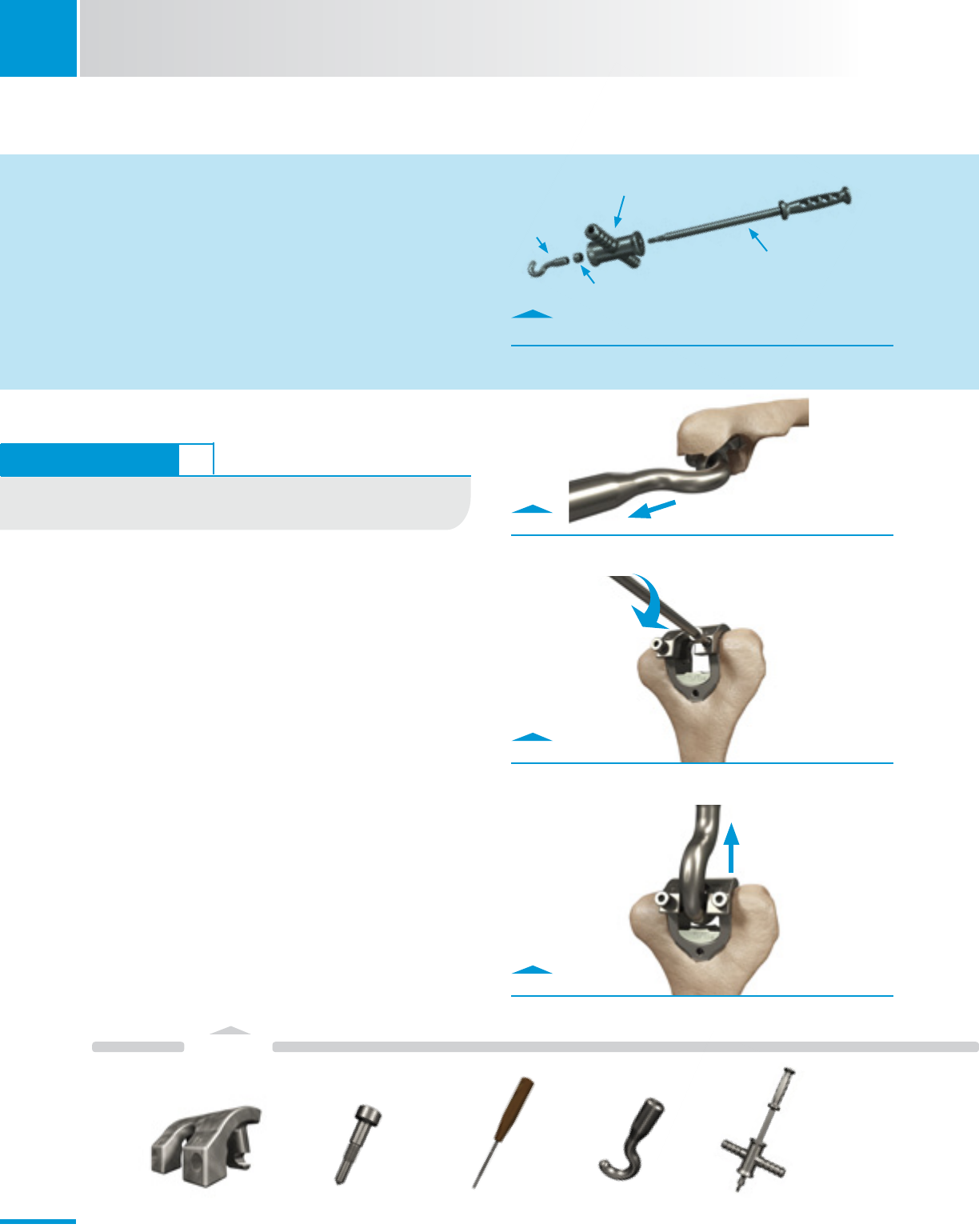
9. Poly Revision
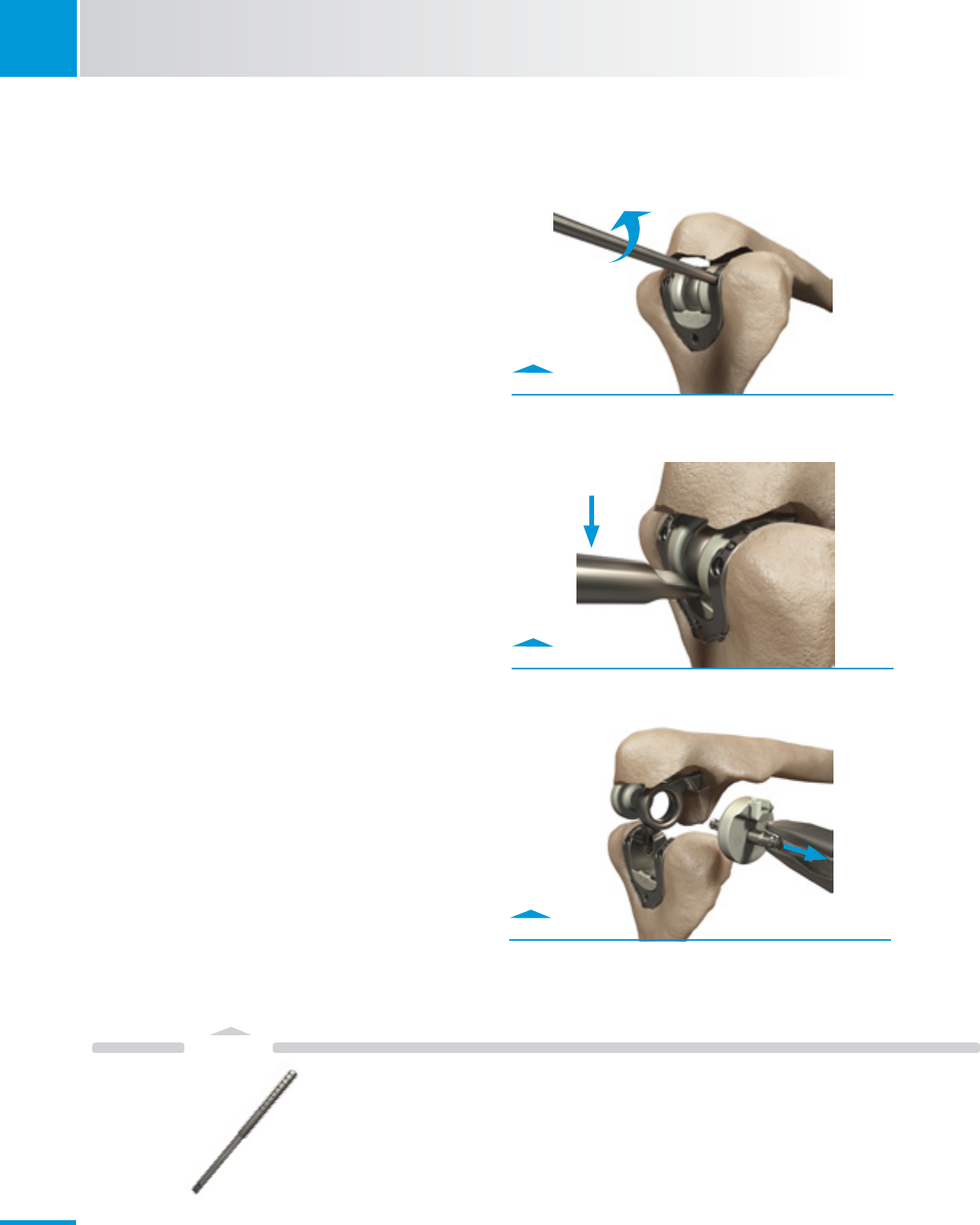
9.1 Unlink Implant
• RemovebothHumeralScrewsusingtheElbowTorque
Driver(Fig.9.1).
• Hyperextheforearmtocreateaseparationbetween
Implants.
• ApplythetipoftheArticulationExtractorbetweenthe
UlnareyeandtheHumeralBearing(Fig.9.2.);Leverthe
Articulation Extractor to separate the articulation (Fig. 9.2.).
9.2 Remove Bearings
• RemoveUlnarBearings.
· Firmly grasp the Axle-Pin with a rongeur and pull it
through the opposite Bearing to release the Ulnar
Bearings. A second rongeur can be used to secure the
opposing Ulnar Bearing (Fig. 9.3).
Fig. 9.1
Remove the screws with the Elbow Torque Driver.
Fig. 9.2
Use Articulation Extractor to separate the implants.
Fig. 9.3
Remove Ulnar Bearings using rongeurs.
Pull Axle-Pin
Push Articulation
Extractor handle down.
Articulation
Extractor
00-8401-092-00
27
Instruments
SECTION
9
Zimmer® Nexel™ Total Elbow Surgical Technique
• RemoveHumeralBearing.
· Use a rongeur to remove the Humeral Bearing by
grasping the Bearing and rocking the rongeur fore or aft
(Fig 9.4).
- Confirm no fragments of the Bearing remain in the
Implant.
9.3 Replace Bearings
• Placetheappropriatesize-matchedHumeralBearing
into the Humeral Component using the Humeral Bearing
Placement Tool (Fig. 9.5).
· The Humeral Bearing will not be fully seated at this
stage.
· Only the “pilot cylinder” of the peg feature should be
inserted into the hole in the base of the yoke of the
Humeral Component.
• PositiontheHumeralBearingDriveragainstthearticulation
surface of the Humeral Bearing.
• CarefullyimpacttheHumeralBearingDriverwithamalletto
seat the Humeral Bearing (Fig. 9.6).
· Confirm there are no gaps between the Humeral Bearing
and the Humeral Component.
• Finishtheprocedureusingtheprimarytechniquestarting
at Section 6: Final Assembly.
Fig. 9.4
Remove the Humeral Bearing using rongeurs.
Fig. 9.5
Use Humeral Bearing Placement Tool to place bearing.
Fig. 9.6
Position Driver, slide collar into Humeral slots, tap Driver to
fully seat Bearing.
Rongeur
Sliding collar drops into
slots of Humeral Component
to stabilize tool
No gaps when
fully seated
Humeral
BearingDriver
00-8401-078-00
Humeral Bearing
Placement Tool
00-8401-082-00
Peg Pilot Cylinder
28
Instruments
10
SECTION
Zimmer® Nexel™ Total Elbow Surgical Technique
Fig. 10.2
Attach Humeral Extractor Plate.
Fig. 10.1
Extract Ulnar Implant.
Fig. A
Assemble the Slide Hammer
10. Component Removal
10.1 Ulnar Component Removal
• PlacetheImplantExtractorHookthroughtheUlnareye(Fig.
10.1).
• RemovetheUlnarComponentwiththeSlideHammer.
10.2 Humeral Component Removal
Note: If the Humeral Component is well fixed, remove the
cement from around the implant as extensively as possible
before attempting extraction.
• Attachthesize-matchedHumeralExtractorPlate.
· Insert the Humeral Extractor Screws through the
openings in the Humeral Extractor Plate and into the
Humeral Implant threaded holes (Fig. 10.2).
· Lightly tighten the Screws using the Small Hex
Screwdriver – no audible click will be heard.
• PlacetheImplantExtractorHookundertheHumeral
Extractor Plate (Fig. 10.3).
• RemovetheHumeralComponentwiththeSlideHammer. Fig. 10.3
Extract Humeral Implant.
SCRUB NURSE
Slide Hammer Assembly
A. Assemble Slide Hammer
· Place the Hammer on the shaft and lock in place by
threading the nut onto the shaft.
· Thread the Implant Extractor Hook on the end of the shaft.
hammer
Implant
Extractor
Hook
nut
shaft
Humeral
Extractor Plate
00-8401-059-05
Humeral Extractor
Screws
00-8401-093-00
Small Hex
ScrewDriver
00-4812-035-00
Extractor
Hook
00-8401-029-00
Slide
Hammer
00-8401-009-00
TECHNIQUE TIP 6.5
If the Ulnar Component is well fixed, remove the cement from around
the Implant as extensively as possible before attempting extraction.
29

Zimmer® Nexel™ Total Elbow Surgical Technique
Zimmer® Nexel™ Total Elbow Surgical Technique
Zimmer® Nexel™ Total Elbow Surgical Technique

97-8401-002-00 7-8-13 Printed in USA ©2013 Zimmer, Inc.
Contact your Zimmer representative or visit us at www.zimmer.com
The CE mark is valid only if it is also printed on the product label.
This documentation is intended exclusively for physicians and is not intended for laypersons.
Information on the products and procedures contained in this document is of a general nature
and does not represent and does not constitute medical advice or recommendations. Because
this information does not purport to constitute any diagnostic or therapeutic statement with
regard to any individual medical case, each patient must be examined and advised individually,
and this document does not replace the need for such examination and/or advice in whole or
in part. Please refer to the package inserts for important product information, including, but not
limited to, contraindications, warnings, precautions, and adverse effects.
