S://www.aarc.org/wp Content/uploads/2015/04/aerosol_guide_rt Aerosol Guide Rt
User Manual: Pdf s://www.aarc.org/wp-content/uploads/2015/04/aerosol_guide_rt How to get your COPD initiative funded
Open the PDF directly: View PDF ![]() .
.
Page Count: 61

A Guide To
Aerosol Delivery Devices
for Respiratory Therapists
4th Edition
Douglas S. Gardenhire, EdD, RRT-NPS, FAARC
Dave Burnett, PhD, RRT, AE-C
Shawna Strickland, PhD, RRT-NPS, RRT-ACCS, AE-C, FAARC
Timothy R. Myers, MBA, RRT-NPS, FAARC
Copyright ©2017 by the American Association for Respiratory Care
Platinum Sponsor

2
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
A Guide to Aerosol
Delivery Devices for
Respiratory Therapists,
4th Edition
Produced by the
American Association
for Respiratory Care
Douglas S. Gardenhire, EdD, RRT-NPS, FAARC
Dave Burnett, PhD, RRT, AE-C
Shawna Strickland, PhD, RRT-NPS, RRT-ACCS, AE-C, FAARC
Timothy R. Myers, MBA, RRT-NPS, FAARC
With a Foreword by
Timothy R. Myers, MBA, RRT-NPS, FAARC
Chief Business Ofcer
American Association for Respiratory Care
DISCLOSURE
Douglas S. Gardenhire, EdD, RRT-NPS, FAARC has served as a consultant for the following
companies: Westmed, Inc. and Boehringer Ingelheim.
i
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Foreward
Aerosol therapy is considered to be one of the corner-
stones of respiratory therapy that exemplies the nuances
of both the art and science of 21st century medicine. As
respiratory therapists are the only health care providers
who receive extensive formal education and who are tested
for competency in aerosol therapy, the ability to manage
patients with both acute and chronic respiratory disease as
the experts in aerosol therapy allows the concept of “art”
and “science” to take on a practical reality.
Respiratory therapists continue to be the experts when it
comes to the art and science of aerosol therapy. With the
rapidly changing eld of aerosol medications and delivery
systems, it is imperative that we not only share this expertise
with patients but also other members of the health care
delivery team across the continuum of care. With a renewed
focus on wellness and prevention within the U.S. health care
system and a determined focus to minimize cost and waste,
the choice of appropriate respiratory medications and deliv-
ery devices makes selection of both the drug and optimum
delivery device even more critical.
How does a therapeutic intervention around for centuries
still combine the art with science in the context of aerosol
therapy? The “science” component includes many different
aspects such as pharmacology, cardiopulmonary anatomy
and physiology, physics, and a thorough understanding of
the different aerosol delivery technologies on the market
today. In order to claim expertise in the science of aerosol
therapy and optimize it for patients, the respiratory therapist
must have concrete knowledge and understanding of the
numerous drug formulations, their mode of action, and an
understanding of the respiratory conditions where the drug
and delivery is recommended and supported by the scientic
evidence.
While the “art” of aerosol delivery is much more abstract
than the science, it is as equally important to the appropri-
ate delivery of respiratory medications for optimal outcomes.
For aerosol therapy, the interaction between technology
and human behavior is where “art” comes into play. There
is ample scientic evidence of sub-optimal or ineffective
use of aerosols when self-administered in large part due to
lack of knowledge about proper technique by patients. All
too often, patients do not receive optimum (or sometimes
any) benet from their prescribed metered-dose inhalers,
dry-powder inhalers, and nebulizers simply because they are
not adequately trained or evaluated on their proper use.
The combination of the right medication and the most
optimal delivery device with the patient’s cognitive and
physical abilities is the critical juncture where science inter-
sects with art. For aerosol therapy to be effective, the appro-
priate delivery system for the medication must be matched
to the patient’s ability to use it correctly. The art of aerosol
therapy does indeed arise from the science. When these two
different, but synergistic components of medicine do not
properly align, patient adherence decreases. Medication is
wasted. Minimal patient benet is derived.
Because aerosol therapy is integral to our scope of prac-
tice and because we are considered the experts in this area,
we have a professional obligation to our patients to continue
our learning and competencies in the delivery of aerosolized
medicines. Respiratory therapists must take advantage of
this opportunity to reinforce their value by updating their
knowledge of aerosol delivery systems and combining that
knowledge with effective assessment of patients requiring
this therapy. Recommending an appropriate delivery system
tailored specically to the patient’s abilities is part of that
assessment.
This guide will provide you the opportunity to advance
your knowledge and expertise in aerosol delivery. Mastery
of both the art and science of aerosol delivery can have a
profound impact on appropriately matching medications and
delivery devices to optimize your patients’ clinical outcomes.
You will also contribute to more cost-effective use of health
care system resources.
The fourth edition of this Aerosol Guide delivers detailed
and comprehensive information that, when combined with
your dedication and commitment to be the professional
experts in this important area, will empower you to provide
guidance to your physician, nurse, and pharmacist colleagues
— but, most importantly, to your patients.
Timothy R. Myers, MBA, RRT-NPS, FAARC
Chief Business Ofcer
American Association for Respiratory Care
ii
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Continuing Respiratory
Care Education (CRCE)
As part of your membership benets in the American
Association for Respiratory Care® (AARC), the Association:
• provides you with continuing education opportunities;
• keeps track of all the CRCE® hours you earn from CRCE-
approved programs; and
• allows you to print online a transcript of your CRCE
records.
These services are available to you 24 hours a day, seven
days a week, on the AARC web site (www.AARC.org).
The contents of this book are approved for six CRCE con-
tact hours; and as an AARC member, there is no charge to
you. To earn those CRCE contact hours, please go to the
AARC web site at:
http://c.aarc.org/go/adu
Further instructions will be given on that web site, including:
• how to register to take an examination to assess your
mastery of course objectives;
• how to update your e-mail address so that registration
conrmation can be sent to you.
Learning Objectives
As you read this book, you will be able to:
1. Identify the terminology used in aerosol medicine.
2. State approximate amount of aerosol deposited in
the lower respiratory tract for nebulizers, pressurized
metered-dose inhalers (pMDIs), and dry-powder
inhalers (DPIs).
3. List advantages and disadvantages of inhalation
compared to other routes of drug administration.
4. Identify hazards of aerosol therapy that can impact the
patient receiving therapy as well as care providers and
bystanders.
5. List advantages and disadvantages of nebulizers for
aerosol delivery.
6. Compare the principle of operation of a jet nebulizer,
mesh nebulizer, and ultrasonic nebulizer.
7. Describe types of pneumatic jet nebulizer designs and
methods that are used to decrease aerosol loss from a
jet nebulizer during exhalation.
8. Learn steps for correct use of jet, ultrasonic, and mesh
nebulizers.
9. Describe the basic components of a metered-dose
inhaler.
10. List advantages and disadvantages of metered-dose
inhalers.
11. Compare and contrast performance of pMDIs with HFA
and CFC propellants.
12. Discuss factors affecting the pMDI performance and
drug delivery.
13. Explain the importance of priming and tracking the
number of doses for a metered-dose inhaler.
14. Compare and contrast the design of holding chambers
and spacers.
15. Identify factors that affect dose delivery from a holding
chamber/spacer.
16. List advantages and disadvantages of dry-powder
inhalers.
17. Describe the principle of operation of various
commercially available dry-powder inhalers.
18. Identify factors affecting the DPI performance and drug
delivery.
19. Explain how you know that each DPI is empty.
20. List the correct steps for use of a nebulizer, metered-
dose inhaler, metered-dose inhaler with holding
chamber/spacer, and dry-powder inhaler.
21. Describe causes and solutions of problems seen with
nebulizers, pMDIs, and DPIs.
22. Discuss criteria to assist clinicians in selecting an
aerosol delivery device.
23. Identify special considerations for neonatal and pediat-
ric drug delivery.
24. Explain how to establish an infection control manage-
ment system in aerosol drug delivery.
25. Describe the proper technique of cleaning aerosol
delivery devices.
26. Discuss the importance of occupational health and
safety for respiratory therapists.
27. List common problems and errors with each type of
inhaler.
28. Describe how to instruct and evaluate patients in the
use of inhaler devices.
iii
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Table of Contents
Foreword ..............................................................................i
Acronyms .............................................................................iv
The Science of Aerosol Drug Delivery ......................................................1
Terminology
Mechanisms of Aerosol Deposition and Particle Sizes
Types of Aerosol Generators
Where Does an Inhaled Aerosol Drug Go?
Equivalence of Aerosol Device Types
Advantages and Disadvantages of Inhaled Aerosol Drugs
Hazards of Aerosol Therapy
Currently Available Aerosol Drug Formulations
Small-Volume Nebulizers ................................................................9
Advantages and Disadvantages of SVNs
Types of SVNs
Factors Affecting Jet Nebulizer Performance and Drug Delivery
Nebulizers for Specic Applications
Continuous Aerosol Therapy
Drug-Delivery Technique
Inhalers . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Pressurized Metered-Dose Inhalers .......................................................21
Advantages and Disadvantages of pMDIs
Types of pMDIs
Currently Available pMDI Formulations
Factors Affecting pMDI Performance and Drug Delivery
Drug-Delivery Technique
Metered-Dose Inhaler Accessory Devices ..................................................29
Advantages and Disadvantages of pMDI Inhaler Accessory Devices
Spacers
Valved Holding Chambers
Drug-Delivery Technique
Dry-Powder Inhalers ...................................................................32
Advantages and Disadvantages of DPIs
Types of DPIs
Currently Available DPI Formulations
Factors Affecting the DPI Performance and Drug Delivery
Drug-Delivery Technique
Criteria to Select an Aerosol Generator ...................................................40
Patient-Related Factors
Drug-Related Factors
Device-Related Factors
Environmental and Clinical Factors
Neonatal and Pediatric Aerosol Drug Delivery ..............................................42
Age and Physical Ability
Age and Cognitive Ability
Aerosol Drug Delivery in Distressed or Crying Infants
Patient-Device Interface
Parent and Patient Education
Infection Control......................................................................44
IC Management System in Aerosol Drug Delivery
Preventing Infection and Malfunction of Aerosol Generators at Hospitals or Clinics
Occupational Health and Safety of Respiratory Therapists
Educating Patients in Correct Use of Aerosol Devices........................................48
Patient Adherence
Common Patient Errors with pMDIs
Common Patient Errors with Holding Chambers/Spacers
Common Patient Errors with DPIs
Common Patient Errors with SVNs
Instructing and Evaluating Patients in the Use of Inhaler Devices
References ...........................................................................52
iv
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Acronyms
CDC Centers for Disease Control and Prevention
CDER Center for Drug Evaluation and Research
CDRH Center for Devices and Radiological Health
CF cystic brosis
DPI dry-powder inhaler
FDA U.S. Food and Drug Administration
FPF ne-particle fraction
GSD Geometric Standard Deviation
HFA hydrouoroalkane
IC infection control
MMAD mass median aerodynamic diameter
MMD mass median diameter
pMDI pressurized metered-dose inhaler
SPAG small particle aerosol generator
SVN small-volume nebulizer
VHC valved holding chamber
1
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
The Science of
Aerosol Drug Delivery
Aerosols exist everywhere there is gas to breathe. From
pollen and spores, to smoke and pollution, to man-made
chemicals, the aerosol category includes any ne liquid or
solid particles. A “medical aerosol” is any suspension of liq-
uid (nebulizer or pMDI) or solid drug particles (pMDI or DPI)
in a carrier gas.1 Our respiratory systems evolved to have
ltration and elimination systems that must be overcome
or bypassed in the process of providing local delivery of
medications to the lung. Methods for generating aerosols,
formulating drugs, and administering medications effec-
tively to the desired site of action constitute the science of
aerosol drug delivery. As is the case in any scientic disci-
pline, one must rst understand the terms and denitions
used to describe the principles of aerosol medicine in order
to subsequently master its methods.
Terminology
Denitions of key terms used in aerosol drug delivery are
listed in alphabetical order below.
aerosol: a suspension of liquid and solid particles produced
by an aerosol generator such as the small-volume
nebulizer (SVN), the pressurized metered-dose inhaler
(pMDI), or the dry-powder inhaler (DPI)
aerosol deposition: process of aerosol particles depositing
on absorbing surfaces
aerosol generator: a device used for producing aerosol
particles
aerosol output: mass of medication exiting an aerosol gen-
erator
aerosol therapy: delivery of solid or liquid aerosol particles
to the respiratory tract for therapeutic purposes
dead volume (or residual volume): the amount of medica-
tion that remains in the nebulizer after a treatment is
complete
diffusion: the mechanism of aerosol deposition for small
particles less than 3 µm (Diffusion is also called
Brownian motion.)
dry-powder inhaler: an aerosol device that delivers the
drug in a powdered form, typically with a breath-actu-
ated dosing system
emitted dose: the mass of medication leaving an aerosol
generator as aerosol
ne-particle fraction (FPF): percentage of the aerosol
between 1–5 µm that deposits in the lung
heterodisperse: aerosol particles of different sizes
hydrouoroalkane (HFA): a nontoxic liqueed gas propel-
lant developed to be more environmentally friendly
than CFCs and used to administer the drug from a
pMDI
inhaled dose: the proportion of nominal or emitted dose
that is inhaled
inhaled mass: the amount of medication inhaled
inhaler: device used to generate an aerosolized drug for a
single inhalation
inertial impaction: the mechanism of aerosol deposition
for particles larger than 5 µm
gravitational sedimentation (gravitational settling): the
settling rate of an aerosol particle due to gravity, parti-
cle size, and time
geometric standard deviation (GSD): one standard devi-
ation above and below the median particle sizes in
an aerosol distribution that indicates the variability in
aerosol particle size
mass median aerodynamic diameter (MMAD): average
aerosol particle size as measured by a cascade impac-
tor
monodisperse: aerosol particles of same or similar sizes
nebulizer: an aerosol generator producing aerosol particles
from liquid-based formulations
nominal dose: the total drug dose placed in the nebulizer
plume: a bolus of aerosol leaving the pMDI or other aero-
sol devices
pressurized metered-dose inhaler (pMDI): a drug device
combination that dispenses multiple doses by means
of a metered value; used interchangeably with pMDI
respirable mass: the product of the ne particle fraction
multiplied by the inhaled mass
residual volume (or dead volume): the amount of med-
ication that remains in the nebulizer at the end of a
treatment
spacer: a valveless extension device that adds distance
between the pMDI outlet and the patient’s mouth
valved holding chamber: a spacer with a one-way valve
used to contain aerosol particles until inspiration occurs

2
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Mechanisms of Aerosol Deposition and
Particle Sizes
The major mechanisms of aerosol deposition include
inertial impaction, gravitational sedimentation (settling),
and diffusion. Inertial impaction occurs with larger (>3 µm),
fast-moving particles. Gravitational settling is a function of
particle mass and time, with the rate of settling proportion-
al to particle size and mass. Diffusion occurs with particles
smaller than 1 µm. These mechanisms come into play as
aerosol particles are inhaled orally or through the nose.
Larger particles (> 10 µm) are ltered in the nose and/or
the oropharynx, largely by inertial impaction; particles of
5–10 µm generally reach the proximal generations of the
lower respiratory tract, and particles of 1–5 µm reach to
the lung periphery.
Particle size plays an important role in lung deposition,
along with particle velocity and settling time. As particle
size increases above 3 µm, aerosol deposition shifts from
the periphery of the lung to the conducting airways.
Oropharyngeal deposition increases as particle size increas-
es above 6 µm. Exhaled loss is high with very small particles
of 1 µm or less. Consequently, particle sizes of 1–5 µm are
best for reaching the lung periphery, whereas 5–10 µm
particles deposit mostly in the conducting airways, and
10–100 µm particles deposit mostly in the nose.
Aerosol devices in clinical use produce heterodisperse
(also termed polydisperse) particle sizes, meaning that
there is a mix of sizes in the aerosol. Monodisperse
aerosols, which consist of a single particle size, are rare
in nature and medicine. A measure that quanties a
polydisperse aerosol is the mass median diameter (MMD).
This measure determines the particle size (in µm) above
and below which 50% of the mass of the particles is con-
tained. This is the particle size that evenly divides the mass,
or amount of the drug in the particle size distribution. This
is usually given as the mass median aerodynamic diameter,
or MMAD, due to the way sizes are measured. The higher
the MMAD, the more particle sizes are of larger diameters.
As seen in Figure 1, larger particles between 10–15 µm
deposit mostly in the upper airways, particles within the
5–10 µm range reach the large bronchi, and particles of
1–5 µm penetrate to the lower airways and lung periph-
ery.2
Types of Aerosol Generators
Three common types of aerosol generators are used for
inhaled drug delivery: the small-volume nebulizer (SVN), the
pressurized metered-dose inhaler (pMDI), and the dry-pow-
der inhaler (DPI). Each device type is described below.
• Small-Volume Nebulizer: The SVN is an aerosol gener-
ator that converts liquid drug solutions or suspensions
into aerosol and is powered by compressed air, oxy-
gen, a compressor, or an electrically powered device.
• Pressurized Metered-Dose Inhaler: The pMDI is a
small, portable self-contained drug device combina-
tion that dispenses multiple doses by a metered value.
Because of high medication loss in the oropharynx and
hand-held coordination difculty with pMDIs, holding
chambers and spacers are often used as ancillary devic-
es with the pMDI.
• Dry-Powder Inhaler: The DPI is an aerosol device that
delivers drug in a powdered form, typically with a
breath-actuated dosing system.
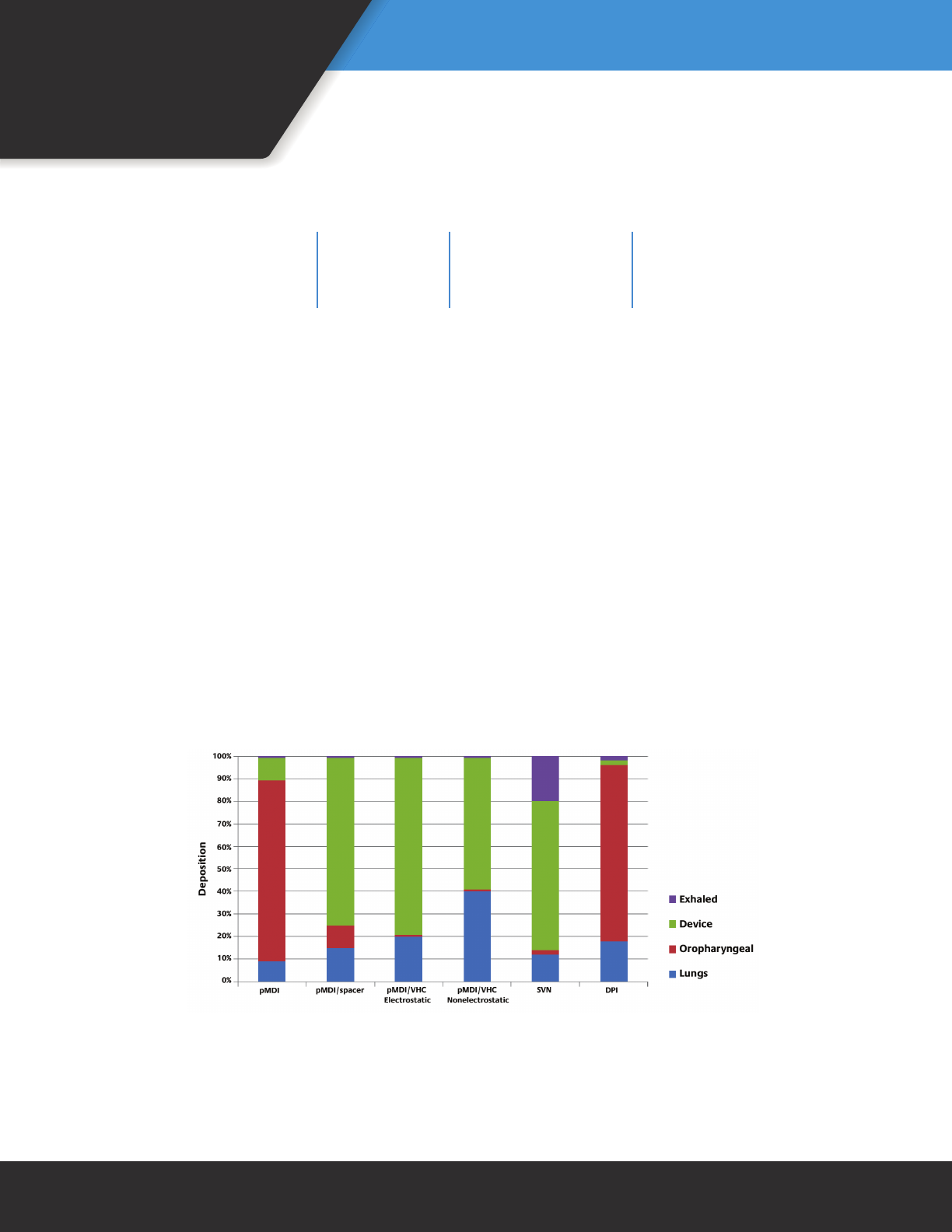
Where Does an Inhaled Aerosol Drug Go?
Lung deposition may range from 1–50% with clinical
aerosol delivery systems.3–7 Deposition is dependent on a
variety of factors such as the device, the patient, the drug,
and the disease. For example, out of 200 micrograms (µg)
of albuterol in two actuations or puffs from a pMDI, only
about 20–40 µg reach the lungs with correct technique.
The remaining drug is lost in the oropharynx, in the device,
or in the exhaled breath. Figure 2 indicates the percentag-
es of drug deposition for different aerosol systems, show-
ing that oropharyngeal loss, device loss, and exhalation/
ambient loss differ among aerosol device types, as do lung
doses.
Figure 1. A simplied view of the effect of aerosol particle
size on the site of preferential deposition in the airways
(From Reference 2, with permission)
3
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
It is important to realize that different types of aerosol
devices deposit a different fraction of the total dose of a
given drug (also termed “nominal” dose) in the lungs. In
addition, different types of aerosol devices such as nebuliz-
ers and pMDIs do not have the same nominal dose. Using
albuterol as an example, the typical pMDI nominal dose is
two actuations, or about 200 µg, while the typical nebuliz-
er nominal dose is 2.5 mg, or 12 times more drug. Table 1
lists both the pMDI and nebulizer nominal doses for several
drugs, showing this difference.
Equivalence of Aerosol Device Types
Historically, nebulizers were thought to be more effec-
tive than pMDIs, especially for short-acting bronchodilators
in acute exacerbations of airow obstruction. Contrarily,
evidence has shown equivalent clinical results whether
a pMDI, a nebulizer, or a DPI is used, provided that the
patient can use the device correctly.8 For bronchodila-
tors, the same clinical response is often achieved with
the labeled dose from the pMDI or nebulizer, despite the
higher nominal dose for the nebulizer. Because any of
these aerosol generators, if used properly, can be effective
with their label dose, dosage should be device specic and
based on the label claim.
Newer aerosol devices and drug formulations are increas-
ing the efciency of lung deposition when compared
to the traditional devices commonly used. For example,
lung deposition for HFA-beclomethasone dipropionate
(QVAR™, Teva Pharmaceuticals, North Wales, PA) is in
the range of 40–50% of the nominal dose using a pMDI
formulation with hydrouoroalkane propellant, which
replaces the older chlorouorocarbon (CFC) propellants.9
New devices such as the Respimat® inhaler (Boehringer
Ingelheim Pharmaceuticals, Ridgeeld, CT) have shown lung
depositions of 40%.10 Although lung dose efciency varies
between devices, inhalers with relatively low lung depo-
sition fraction have been clinically proven to achieve the
desired therapeutic effect in the target audience.
Figure 2. Drug deposition with common aerosol inhaler devices. Shown by color are the
varying percentages of drug lung deposition and drug loss in the oropharynx, device, and
exhaled breath.
pMDI = pressurized metered-dose inhaler; VHC = valved holding chamber;
SVN = small-volume nebulizer; DPI = dry-powder inhaler
(Modied, with permission, from Reference 1 and Reference 7)
Table 1. Differences in nominal (total) dose between a pMDI and an SVN
for different drug formulations (Modied, with permission, from Reference 1)
Drug pMDI Nominal Dose SVN Nominal Dose
Albuterol 0.2 mg (200 µg) 2.5 mg
Ipratropium 0.04 mg (40 µg) 0.5 mg
Levalbuterol 0.045 mg – 0.09 mg 0.31 mg – 1.25 mg

4
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Advantages and Disadvantages of
Inhaled Aerosol Drugs
There are a number of advantages and disad-
vantages that go along with the inhalation of
drugs to treat pulmonary disease (Table 2). The
primary advantage of inhaled aerosol therapy
is treating the lung directly with smaller doses,
resulting in fewer side effects than with oral
delivery.11 As seen in Figure 3, inhalation of terbu-
taline, a short-acting beta-2 agonist, from a pMDI
resulted in better airow than with a much larger
oral dose or even with a subcutaneous injection
of drug.
Hazards of Aerosol Therapy
Hazards associated with aerosol drug therapy may occur
as a result of inhaled medication, an aerosol generator
being used, the aerosol administration technique, and the
environment. Hazards of aerosol therapy can impact the
patient receiving therapy, as well as care providers and
bystanders.
Hazards for Patients
Adverse Reaction: Most hazards associated with aerosol
therapy are attributed to adverse reactions to the drug
being used. Therefore, inhaled medications should be
administered with caution. Types of adverse reactions
Figure 3. Changes in FEV1 for three different routes of
administration with terbutaline. Greater clinical effect was seen
with drug delivered as inhaled aerosol from a pMDI, compared
to similar or larger doses delivered orally or by subcutaneous
injection. (From Reference 6, with permission)
Table 2. Advantages and disadvantages of the inhaled aerosolized drugs
(Modied, with permission, from Reference 1)
Advantages
Aerosol doses are generally smaller than systemic
doses.
Onset of effect with inhaled drugs is faster than
with oral dosing.
Drug is delivered directly to the lungs, with
minimal systemic exposure.
Systemic side effects are less frequent and severe
with inhalation when compared to systemic
delivery.
Inhaled drug therapy is less painful than injection
and is relatively comfortable.
Disadvantages
Lung deposition is a relatively low fraction of the
total dose.
A number of variables (correct breathing pattern,
use of device) can affect lung deposition and dose
reproducibility.
The difculty of coordinating hand action and
inhalation with the pMDIs reduces effectiveness.
The lack of knowledge of correct or optimal use of
aerosol devices by patients and clinicians decreases
effectiveness.
The number and variability of device types confuses
patients and clinicians.
The lack of standardized technical information on
inhalers for clinicians reduces effectiveness.
5
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
include headache, insomnia, and nervousness with adren-
ergic agents, local topical effects with anticholinergics, and
systemic/local effects of corticosteroids.12,13 If any of these
adverse reactions are seen during aerosol drug therapy, the
treatment should be ended and the physician should be
notied.
Bronchospasm: Administering a cold and high-density
aerosol may induce bronchospasm in patients with asthma
or other respiratory diseases.13-15 If bronchospasm occurs
during aerosol therapy, the therapy should be immediately
discontinued for 15-20 minutes. If it persists, the physician
should be notied.
Drug Concentration: In both jet and ultrasonic nebulizers,
drug concentration may increase signicantly during aero-
sol therapy.16-18 An increase in drug concentration may be
due to evaporation, heating, or the inability to efciently
nebulize suspensions.13,16,18,19 As a result of changes in drug
concentration, the amount of the drug remaining in the
nebulizer at the end of aerosol therapy is increased and
the patient is exposed to higher concentrations of inhaled
medications. This is a great problem with continuous-feed
nebulization.
Infection: It has been well documented that aerosol gener-
ators can become contaminated with bacteria and increase
the risk of infection in patients with respiratory diseases.20-25
The risk of transmission of an infection is dependent upon
duration of exposure of drugs with pathogens and the pro-
cedures taken by respiratory therapists to avoid pathogen
exposure. Proper practices of medication handling, device
cleaning, and sterilization can greatly reduce this risk.
Eye Irritation: Inhaled medications delivered with a face
mask may inadvertently deposit in the eyes and result in eye
irritation. Improving the interface between the face mask
and patient may eliminate this problem and increase the
amount of drug delivered to the distal airways. Therefore,
caution should be exercised when using a face mask during
aerosol drug administration.
Hazards for Care Providers and Bystanders
Exposure to Secondhand Aerosol Drugs: Care providers
and bystanders have the risk of exposure to inhaled medica-
tions during routine monitoring and care of patients. While
workplace exposure to aerosol may be detectable in the
plasma,26 it may also increase the risk of asthma-like symp-
toms and cause occupational asthma.27-29 The development
and implementation of an occupational health and safety
policy in respiratory therapy departments can minimize
exposure to secondhand aerosol drugs.
Infection: Care providers, bystanders, and even other
patients have the risk of inhaling pathogens during aerosol
therapy. The risk of infection can be minimized with the
development and implementation of an infection control
management system including use of masks, lters, and
ventilation systems.30-32
Currently Available Aerosol Drug
Formulations
Some aerosol drugs are available in more than one for-
mulation. Others (often newer drugs) are available only in a
single formulation. Table 3 provides currently available aero-
sol drug formulations, their brand names, their FDA-approved
aerosol delivery devices, and their costs.
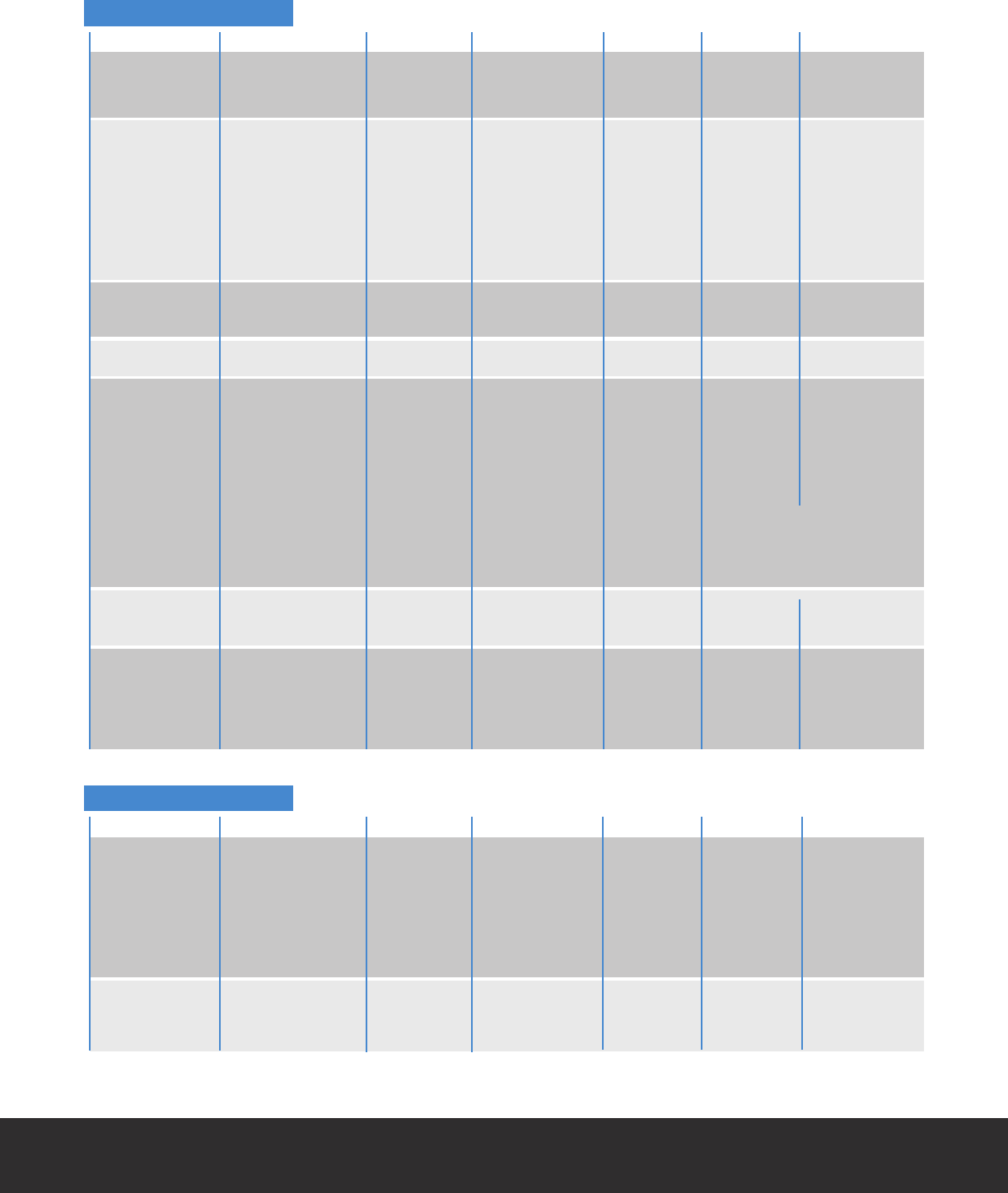
Table 3. Currently available aerosol drug formulations with corresponding inhaler devices and costs
for use in the United States.
HFA = hydrouoroalkane; pMDI = pressurized metered-dose inhaler; SVN = small-volume nebulizer; DPI = dry-powder inhaler
Cost information from www. goodrx.com. Prices used were from WalMart in 2017.
6
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Short-Acting Bronchodilator
Long-Acting Bronchodilator
Drug Brand Device Strength Doses Cost Cost/Dose
Albuterol AccuNeb® SVN 0.63 25 $50.20 $2.01
Sulfate 1.25 25 $50.20 $2.01
Albuterol Sulfate SVN 2.5 25 $15.30 $0.61
ProAir® HFA pMDI 200 $58.99 $0.30
ProAir RespiClick® DPI 200 $55.73 $0.28
Proventil® HFA pMDI 200 $73.74 $0.37
Ventolin® HFA pMDI 200 $56.42 $0.28
Levalbuterol Xopenex® SVN 0.31/3ml 24 $39.16 $1.63
Inhalation 0.63/3ml 24 $39.16 $1.63
Solution 1.25/3ml 24 $39.16 $1.63
1.25/0.5ml 24 $23.08 $0.96
Xopenex HFA™ pMDI 200 $61.61 $0.31
Ipratropium Ipratropium SVN vial 25 $4.57 $0.18
Bromide Bromide
Atrovent HFA® pMDI 200 $331.32 $1.66
Ipratropium Ipratropium SVN 120 $59.57 $0.25
Bromide and Bromide and
Albuterol Sulfate Albuterol Sulfate
DuoNeb® SVN 120 $284.54 $2.37
Combivent® pMDI 120 $336.97 $2.81
Respimat®
Drug Brand Device Strength Doses Cost Cost/Dose
Aclidinium Tudorza Pressair® DPI 400 mcg 60 $318.10 $5.30
Bromide
Arformoterol Brovana® SVN 15 mcg/2ml 30 $457.06 $15.24
60 $907.12 $15.12
Formoterol Perforomist® SVN 20 mcg/2ml 60 $873.92 $9.57
Indacaterol Arcapta® DPI 75 mcg 30 $227.70 $7.59
Salmeterol Serevent® DPI 50 mcg 60 $340.31 $5.67
Tiotropium Spiriva® DPI 18 mcg 30 $359.25 $11.98
Spiriva Respimat® pMDI 1.5 mcg 30 $359.25 $11.98
Spiriva Respimat® pMDI 2.5 mcg 30 $359.25 $11.98
Olodaterol Stiverdi pMDI 2.5 mcg 60 $180.74 $3.01
Respimat®
Umeclidinium Incruse® Ellipta® DPI 62.5 mcg 30 $314.17 $10.47
Glycopyrrolate Seebri Neohaler DPI 15.6 mcg 60 $313.67 $5.23
7
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
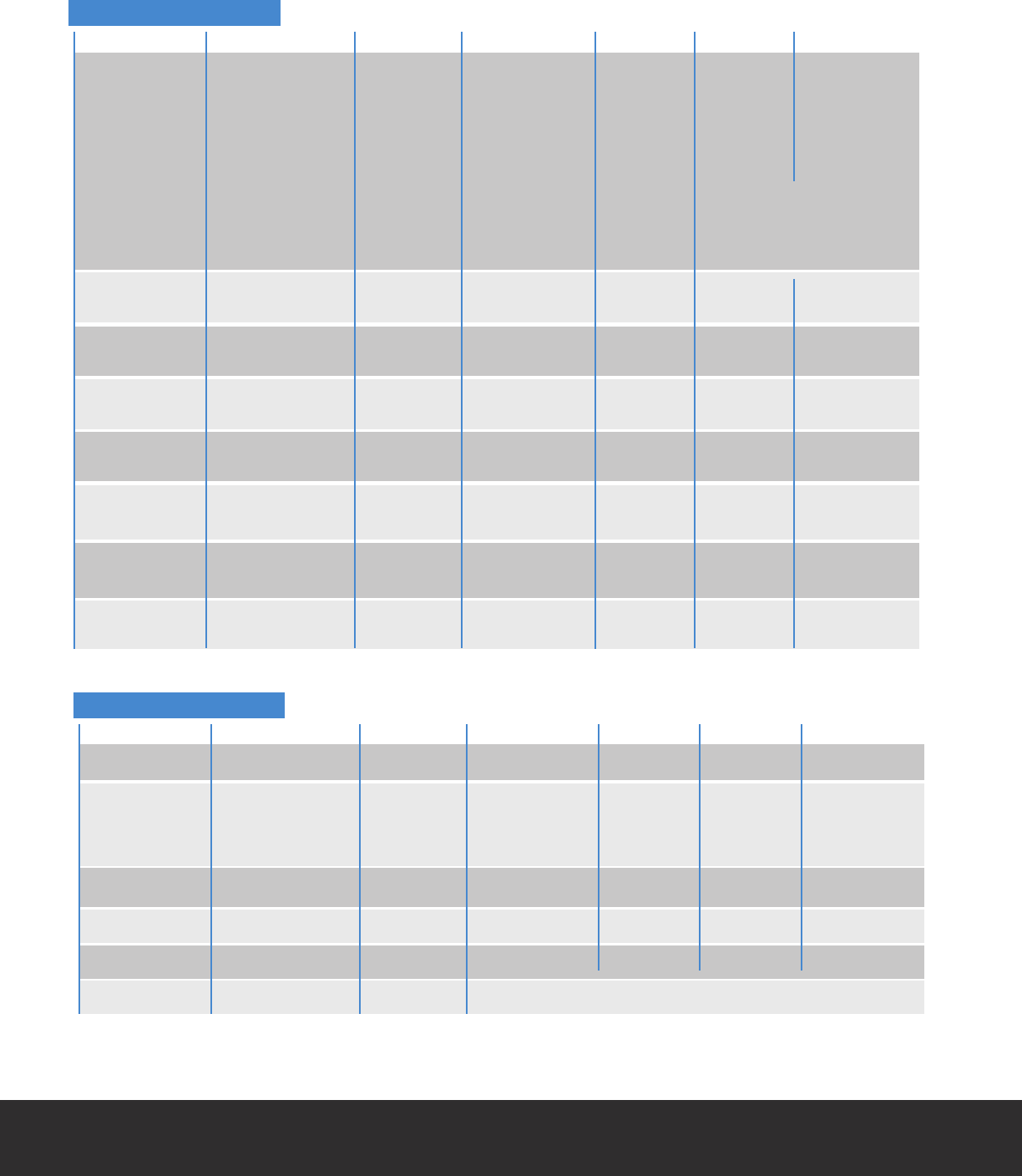
Table 3. (continued)
Corticosteroids
Drug Brand Device Strength Doses Cost Cost/Dose
Beclomethasone QVAR™ 40 pMDI 40 mcg 120 $162.14 $1.35
QVAR™ 80 pMDI 80 mcg 120 $211.57 $1.76
Budesonide Pulmicort SVN 0.25 mg 30 $277.14 $9.24
Respules 0.5 mg 30 $324.93 $10.83
1.0 mg 30 $642.92 $21.43
Generic SVN 0.25 mg 30 $63.48 $2.12
0.5 mg 30 $73.47 $2.45
1.0 mg 30 $145.49 $4.85
Pulmicort® DPI 90 mcg 120 $164.14 $1.37
Flexhaler® 180 mcg 120 $214.12 $1.79
Ciclesonide Alvesco® pMDI 80 mcg 60 $243.51 $4.06
160 mcg 60 $243.51 $4.06
Flunisolide Aerospan® pMDI 80 mcg 120 $214.56 $1.79
Fluticasone Flovent Diskus® DPI 50 mcg 60 $165.03 $2.75
propionate 100 mcg 60 $173.96 $2.90
250 mcg 60 $226.57 $3.78
Flovent HFA® pMDI 44 mcg 120 $173.96 $1.45
110 mcg 120 $226.57 $1.89
220 mcg 120 $348.05 $2.90
ArmonAir® DPI 55 mcg 60 Newly approved
RespiClick® 113 mcg 60 No pricing available
232 mcg 60
Fluticasone Arnuity® Ellipta® DPI 100 mcg 30 $164.41 $4.48
furoate 200 mcg 30 $214.43 $7.15
Mometasone Asmanex® HFA pMDI 100 mcg 120 $191.68 $1.60
furoate 200 mcg 120 $224.06 $1.87
Asmanex® DPI 110 mcg 30 $190.00 $6.33
220 mcg 30 $205.00 $6.83
Mucoactive Drugs
Drug Brand Device Strength Doses Cost Cost/Dose
Dornase Alpha Pulmozyme® SVN 2.5mg/2.5ml 30 $3173.13 $105.77
N-Acetylcysteine SVN 4ml/10% 1 $2.46 $2.46
10ml/10% 1 $4.16 $1.64
30ml/10% 1 $9.81 $1.31
4ml/20% 1 $3.21 $3.21
10ml/20% 1 $6.02 $2.41
30ml/20% 1 $12.00 $1.60
Hyperosmolar HyperSal® SVN 3.5% 60 $52.99 $0.88
Saline 7% 60 $91.94 $1.03
PulmoSal™ (ph 7.4) SVN 7% 60 $51.94 $0.87
8
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Table 3. (continued)
Other Drugs
Drug Brand Device Strength Doses Cost Cost/Dose
Zanamivir Relenza® DPI 5 mg 20 $65.49 $3.28
Tobramycin TOBI® SVN 300mg/5ml 56 $7,578.95 $135.33
generic 300mg/5ml 56 $1590.21 $28.40
Bethkis SVN 300mg/4ml 56 $5862.93 $209.40
Tobi Podhaler DPI 28 mg 224 $9152.54 $40.85
Aztreonam Cayston® SVN 75 mg 84 $8254.28 $98.27
Cromolyn Sodium SVN 20mg/2ml 60 $211.63 $3.53
Ribavirin Virazole® SPAG 6g 1 $25766.30 $25766.30
Mannitol Aridol® DP Bronchial Challenge Test Kit, No pricing available
Combination Drugs
Drug Brand Device Strength Doses Cost Cost/Dose
Fluticasone and Advair HFA® pMDI 45/21 mcg 120 $285.26 $2.38
Salmeterol 115/21 mcg 120 $352.74 $2.94
230/21 mcg 120 $461.72 $3.85
Advair Diskus® DPI 100/50 mcg 60 $285.26 $4.75
250/50 mcg 60 $352.74 $5.88
500/50 mcg 60 $461.72 $7.70
AirDuo RespiClick® DPI 55/14 mcg 60 Newly approved
113/14 mcg 60 No pricing available
232/14 mcg 60
Budesonide and Symbicort® pMDI 80/4.5 mcg 120 $270.22 $2.25
Formoterol 160/4.5 mcg 120 $307.87 $2.57
Mometasone/ Dulera® pMDI 100/4 mcg 120 $290.54 $2.42
Formoterol 200 120 $290.54 $2.42
Fluticasone furate/ Breo® Ellipta® DPI 100/25 mcg 60 $314.80 $5.25
Vilanterol 200/25 mcg 60 $314.80 $5.25
Tiotropium/ Stiolto® Respimat® pMDI 2.5/2.5 mcg 60 $333.16 $5.55
Olodaterol
Umeclidinium/ Anoro® Ellipta® DPI 62.5/25 mcg 60 $333.16 $5.55
Vilanterol
Indacaterol/ Utibron Neohaler® DPI 27.5/15.6 mcg 60 $313.67 $5.23
Glycopyrrolate
Formoterol/ Bevespi pMDI 9/4.8 mcg 120 $333.16 $2.78
Gylcopyrrolate Aerosphere®
9
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Small-Volume
Nebulizers
Small-volume nebulizers (SVNs) are popular aerosol gen-
erators in acute care settings with clinicians and patients
as they convert drug solutions or suspensions into aerosols
that deposit into the patient’s lower respiratory tract while
requiring minimal patient cooperation.
Advantages and Disadvantages of SVNs
Nebulizers have long been the cornerstone of medical
aerosol therapy in the acute and critical care setting. Also,
they are frequently the device selected for patients such as
infants, small children, and the elderly who are unable to
operate, coordinate, or cooperate with the use of various
inhalers that require active participation and hand-eye-
breath coordination. This functionality offsets the issues of
portability, weight, noise, cost, and time of administration
associated with nebulizers. Table 4 lists the advantages and
disadvantages of small-volume nebulizers.
Nebulizers are regulated as medical devices by the U.S.
Food and Drug Administration (FDA) Center for Devices and
Radiological Health (CDRH). They are tested in accordance
with applicable standards for medical device electrical safe-
ty, electromagnetic compatibility, environmental tempera-
ture and humidity, shock and vibration, as well as for their
biocompatibility of materials.
Nebulizers are designed to be used with a broad range
of liquid formulations. Drugs for use with nebulizers are
approved by the FDA and the Center for Drug Evaluation
and Research (CDER). Historically, drug solutions for inha-
lation were approved based on studies using standard jet
nebulizers (the rst type of SVN) ranging in efciency from
6–12%. The use of more efcient nebulizers created the risk
of delivering inhaled dose above the upper threshold of the
therapeutic window, increasing the risk of side effects and
toxicity. Consequently, the FDA requires that the drug label
of new liquid formulations identify the nebulizers used in
the clinical studies (Table 5). Because drug delivery varies
with different nebulizer types, it is important to use the
nebulizer cited on the drug “label” when possible. At the
Table 4. Advantages and disadvantages of SVNS (Modied, with permission, from Reference 1)
Advantages
Ability to aerosolize many drug solutions
Ability to aerosolize drug mixtures (>1 drug), if
drugs are compatible
Minimal patient cooperation or coordination is
needed.
Useful in very young, very old, debilitated, or
distressed patients
Drug concentrations and dose can be modied.
Variability in performance characteristics among
different types, brands, and models
Normal breathing pattern can be used, and an
inspiratory pause (breath-hold) is not required for
efcacy.
Disadvantages
Treatment times may range from 5–25 minutes.
Equipment required may be large and
cumbersome.
Need for power source (electricity, battery, or
compressed gas)
Potential for drug delivery into the eyes with face
mask delivery
Potential for drug delivery exposure to clinicians
and caregivers
Assembly and cleaning are required.
Contamination is possible with improper handling
of drug and inadequate cleaning.
10
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
very least, clinicians should be aware of the relative perfor-
mance of the “label” nebulizer.
Pneumatic jet nebulizers most commonly used in the
hospital or clinic are low-cost, mass-produced, single-pa-
tient-use disposable devices. Newer, more efcient nebuliz-
ers that operate at a higher efciency and require shorter
treatment durations tend to be more expensive (Table 6).
Nebulizer systems may include a nebulizer hand set, com-
pressor or power pack, tubing, and accessories. In general,
the compressor or electronics are durable and long-lasting,
whereas handsets and accessories require more frequent
replacement. Replacement costs are shown in Table 7.
Table 5. Drug formulations and approved nebulizers for that formulation
(Modied, with permission, from Reference 1)
Drug Formulation
Bronchodilator
Acetylcysteine
Arformoterol
Formoterol
Budesonide (Pulmicort Respules®)
Tobramycin (TOBI®)
Dornase alfa (Pulmozyme®)
Pentamadine (NebuPent)
Ribavirin (Virazole®)
Iloprost (Ventavis®)
Aztreonam (Cayston®)
Treprostinil (Tyvaso®)
Approved Nebulizer
Nebulizer type not specied
Nebulizer type not specied
Nebulizer type not specied
Nebulizer type not specied
Should not be used with ultrasonic nebulizer
Pari LC®, Sidestream Plus
Hudson T Up-draft II, Marquest Acorn® II, Pari LC®,
Durable Sidestream®, Pari Baby™
Marquest Respirgard II
Small Particle Aerosol Generator
I-neb Adaptive Aerosol (AAD) System
Altera™ Nebulizer System
Tyvaso® Inhalation System
Table 6. Relative costs of different nebulizer systems
(Modied, with permission, from Reference 1)
Nebulizer Type Approximate Cost Range
Pneumatic compressor nebulizer $30–$200
Ultrasonic nebulizer $70–$250
Vibrating mesh/horn nebulizer $200–$1,200
Microprocessor-controlled breath-actuated nebulizer $750–$2,000
Table 7. Replacement costs of nebulizer components
(Modied, with permission, from Reference 1)
Nebulizer Components (Interval) Approximate Cost Range
Disposable jet nebulizer (1–7 days in acute care, longer use at home) $1–3
Jet nebulizer with bag reservoir (1–3 days) $4–15
Jet nebulizer with lter (1–3 days) $10–12
Breath-enhanced nebulizer $4–20
Breath-actuated jet nebulizer $4–6
Ultrasonic nebulizer medication chamber (daily or weekly) $1–5
USN handset replacement (3–12 months) $100–250
Vibrating mesh replacement (3–12 months) $40–150
11
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Types of SVNs
Jet Nebulizers
Jet nebulizers are
operated by com-
pressed air or oxygen
in order to aerosolize
liquid medications.
They are commonly
used because they are
the least expensive
kind of nebulizer. A
jet nebulizer delivers
compressed gas through a jet, causing a region of negative
pressure. The solution to be aerosolized is entrained into
the gas stream and is sheared into a liquid lm. This lm is
unstable and breaks into droplets due to surface tension
forces. A bafe located in the aerosol stream impacts these
droplets producing smaller particles. The operating perfor-
mance of jet nebulizers is affected by both the technical
and patient-related factors described in Table 8.
Factors Affecting Jet Nebulizer
Performance and Drug Delivery
There are many factors for respiratory therapists to keep
in mind during aerosol therapy. Nebulizer design holds a
key determining factor in the size of particles and output
performance produced, which results in the ultimate ef-
ciency of medication according to the factors discussed
below. Various types of nebulizers are available on the
market, and several studies have indicated that perfor-
mance varies between manufacturers and also between
nebulizers from the same manufacturer.1,33,34
• Gas Flow and Pressure: Jet nebulizers are designed
to operate by means of varied levels of compressed
gas ow and pressure. Each model of jet nebulizer is
designed to work best at a specic ow, ranging from
2–8 L/min, which should be listed on the device label.
Operating any jet nebulizer at a lower ow or pressure
will increase particle size. For example, a jet nebulizer
designed to operate at 6–8 L/min at 50 psi will pro-
duce larger particles if driven by a compressor pro-
ducing 13 psi. Consequently, jet nebulizers should be
matched with a compressor or gas source that match-
es their intended design. Gas ow is also inversely relat-
ed to nebulization time. Using a higher gas ow rate in
aerosol therapy will decrease the amount of treatment
time needed to deliver the set amount of drug.
• Fill and Dead Volumes: Altering the ll volume is
another factor that impacts the efciency of jet neb-
ulizers. Studies report increased efciency with this
due to nebulizers with a xed dead volume, and thus
an increase in ll volume reduces the proportion of
dead volume within the nebulizer. Although efciency
increases with a greater ll volume, there is also an
increase in nebulization time.34
Likewise, these nebu-
lizers do not function well with small ll volumes like
2 mL or less because this is close to dead volume (also
termed residual volume). Jet nebulizers do not aerosol-
ize below dead volume; therefore, it is recommended
to use a ll volume of 4–5 mL unless the nebulizer is
specically designed for a smaller ll volume.1,34 This
precaution dilutes the medication, allowing for a great-
er proportion to be nebulized, though it increases the
treatment time. Dead volume, the amount of medi-
cation remaining in the jet nebulizer at the end of a
treatment, can range from 0.5 to 2.0 mL. The greater
the dead volume, the less drug is nebulized.
• Gas Density: By a similar offsetting, the density of gas
used to run a jet nebulizer can impact aerosol deposi-
tion by affecting aerosol output and particle size. For
example, delivering aerosol with helium-oxygen (heliox)
gas mixtures can increase lung deposition by as much
as 50%. Using heliox at the same ow rate as with air
or oxygen reduces particle size and aerosol output, ulti-
mately increasing treatment times. Consequently, the
ow with heliox should be increased by 1.5–2 times to
bring particle size and output back to levels achieved
with air or oxygen.
• Humidity and Temperature: Humidity and tempera-
ture can also affect particle size and residual volume.
Table 8. Factors affecting penetration and deposition of therapeutic
aerosols delivered by jet nebulizers (Modied, with permission, from Reference 1)
Technical Factors
Design and model of nebulizer
Flow used to power nebulizer
Fill volume of nebulizer
Solution characteristics
Composition of driving gas
Designs to enhance nebulizer output
Continuous vs. breath-actuated
Patient Factors
Breathing pattern
Nose vs. mouth breathing
Composition of inspired gas
Airway obstruction
Positive pressure delivery
Articial airway and mechanical ventilation
12
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Specically, water evaporation
during aerosol therapy can
reduce the temperature of an
aerosol, which results in an
increase in solution viscosity and
a decrease in the nebulizer out-
put of drug.
• Breathing Pattern: Breathing
pattern inuences aerosol depo-
sition in the lower respiratory
tract. The patient should be
instructed to do tidal breath-
ing with periodic deep breaths
during aerosol therapy.
• Device Interface: Medical
aerosols can be administered using
either a mouthpiece or a face mask. Ideally, a mouth-
piece should be used. The nose tends to lter more
aerosol than the mouth, so use of a mouthpiece should
be encouraged, when appropriate. Mouthpieces can-
not be used for infants and small children. In addition,
the use of a mouthpiece may be uncomfortable for
longer aerosol therapy. Use of a mask increases the
amount of aerosol deposited on the face, in the eyes,
and into the nose. Whether a mouthpiece or a face
mask is used, it is important to instruct the patient
to inhale through the mouth during aerosol therapy.
Proper mask t and design can optimize the inhaled
dose and reduce deposition to the eyes. The respira-
tory therapist must keep all of these factors in mind
when practicing or equipping patients.
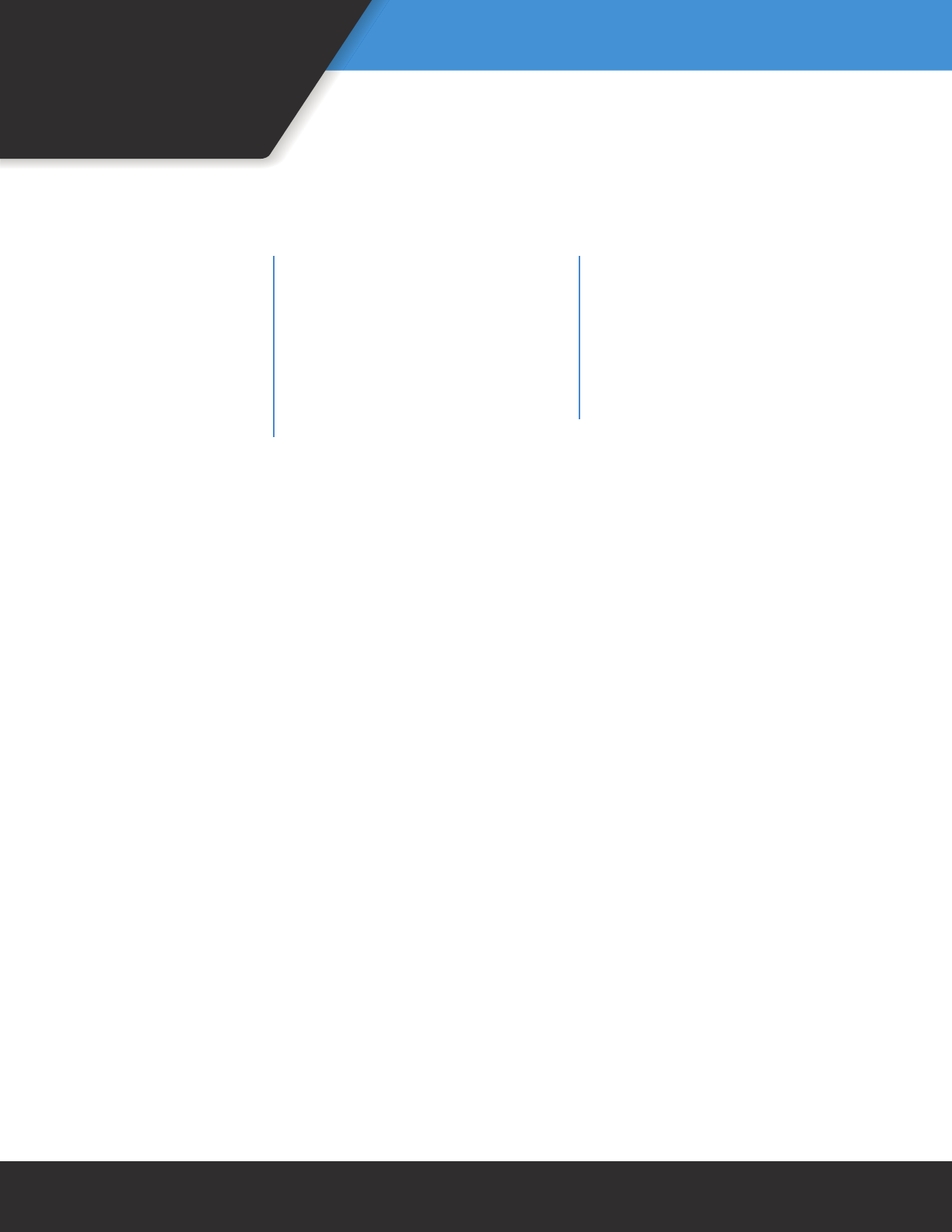
Types of Pneumatic Jet Nebulizer Designs
Nebulizer design changes over the past decade have
created different nebulizer categories.35,36 There are four
different designs of the pneumatic jet nebulizer: jet nebu-
lizer with reservoir tube, jet nebulizer with collection bag
or elastomeric reservoir ball, breath-enhanced jet nebuliz-
er, and breath-actuated jet nebulizer. All four of these are
depicted in Figure 4 and described below.
A. Jet Nebulizer with a Reservoir Tube: This is the least
expensive and most widely used nebulizer. It provides
continuous aerosol during inhalation, exhalation, and
breath-hold, causing the release of aerosol to ambient air
during exhalation and anytime when the patient is not
breathing (Figure 4-A).36-37 Consequently, only 8-15% of
the emitted aerosol is inhaled. In order to decrease drug
loss and increase inhaled mass, a t-piece and large bore
tubing are attached to the expiratory side of the nebuliz-
er. These types of nebulizers have been considered to be
inefcient due to their providing a low percentage of the
dose to the patient.38 Figure 5 illustrates the functioning of
a jet nebulizer. Examples of a jet nebulizer with a reservoir
tube model include the Sidestream Nebulizers™ (Philips,
Murrysville, PA) and the Micro Mist® (Teleex Medical,
Research Triangle Park, NC).
Figure 4. Different types of pneumatic jet nebulizer designs and their aerosol
output indicated by the shaded area: A. pneumatic jet nebulizer with reservoir
tube; B. jet nebulizer with collection bag; C. breath-enhanced jet nebulizer; D.
breath-actuated jet nebulizer. (From Reference 1, with permission)
Figure 5. Schematic illustration of the function of a jet
nebulizer (From Reference 1, with permission)
13
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
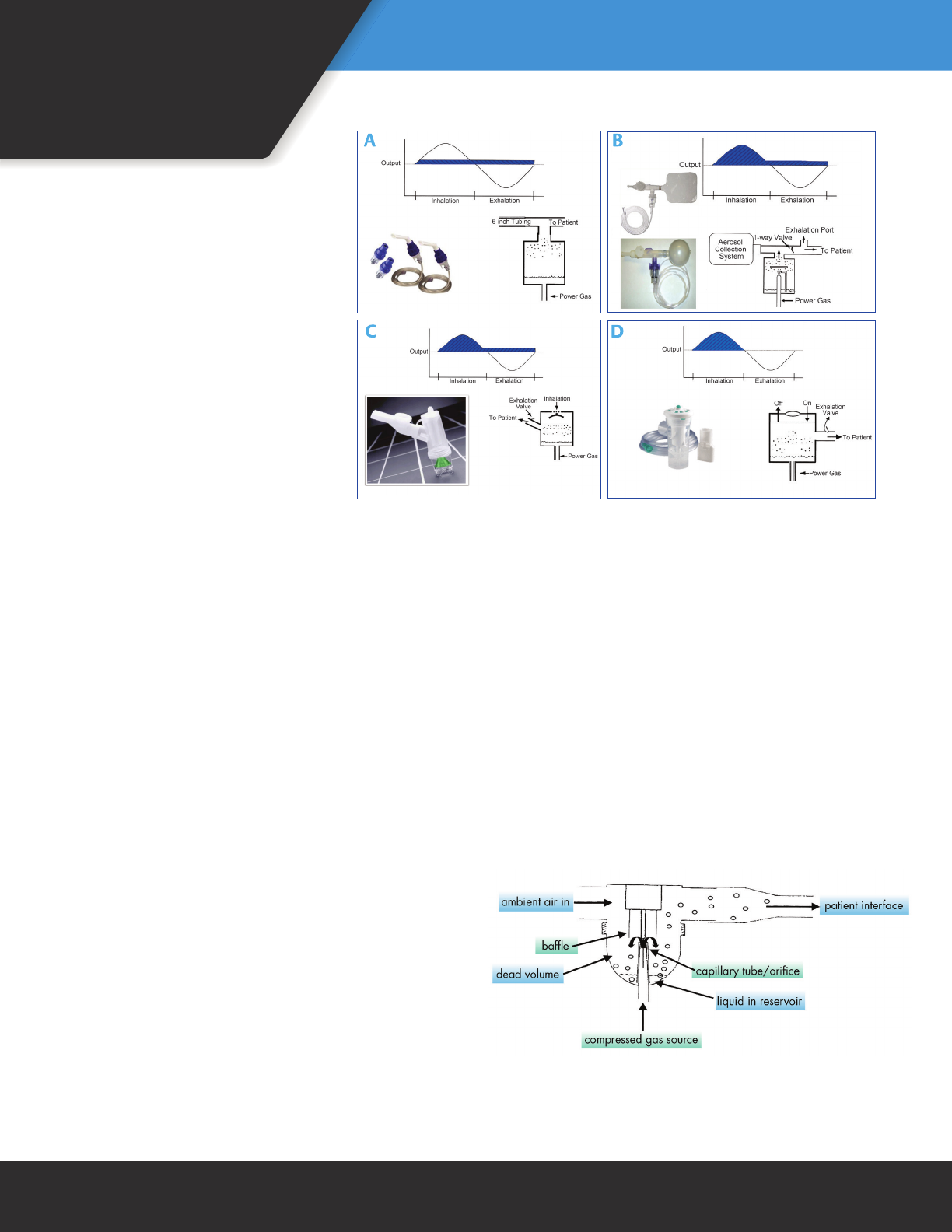
B. Jet Nebulizer with Collection Bag or Elastomeric
Reservoir Ball: These types of nebulizers generate
aerosol by continuously lling a reservoir (Figure 4-B).
The patient inhales aerosol from the reservoir through
a one-way inspiratory valve and exhales to the atmo-
sphere through an exhalation port between the one-
way inspiratory valve and the mouthpiece.35,37 Figure
6 illustrates the principle of operation and patterns
of gas ow during inhalation and exhalation with
the Circulaire® II (Westmed, Tucson, AZ) which is one
model of the nebulizer with a collection bag or elasto-
meric reservoir ball.
C. Breath-Enhanced Jet Nebulizer: Breath-enhanced
nebulizers use two one-way valves to prevent the
loss of aerosol to environment (Figure 4-C). When
the patient inhales, the inspiratory valve opens and
gas vents through the nebulizer. Exhaled gas passes
through an expiratory valve in the mouthpiece. Figure
7 illustrates the operation principle of the breath-en-
hanced nebulizer. PARI LC® Sprint (PARI, Midlothian,
VA), NebuTech HDN® (Salter Labs, Arvin, CA), and
SideStream Plus® (Philips, Murrysville, PA) are the
breath-enhanced nebulizers available on the market.
D. Breath-Actuated Jet Nebulizer: Breath-actuated
nebulizers are designed to increase aerosol drug
delivery to patients by generating aerosol only during
active inspiration. Consequently, loss of medication
during expiration phase is greatly reduced, as shown
in Figure 4-D.37 Whereas breath actuation can increase
the inhaled dose by more than three-fold, this ef-
ciency is achieved only by an increase in dosing time.
Breath-actuation mechanisms can be classied as man-
ual, mechanical, and electronic:
1. Manual Breath-Actuated: The rst generation of
breath-actuated nebulizers uses a thumb control to
regulate aerosol production during inspiration and
expiration. Blocking the patient-controlled thumb port
directs gas to the nebulizer only during inspiration;
releasing the thumb at the port pauses the nebuliza-
tion (Figure 8). The thumb control breath-actuated
nebulizer wastes less of the medication being aerosol-
ized, but it signicantly increases the treatment time
and requires good hand-breath coordination.
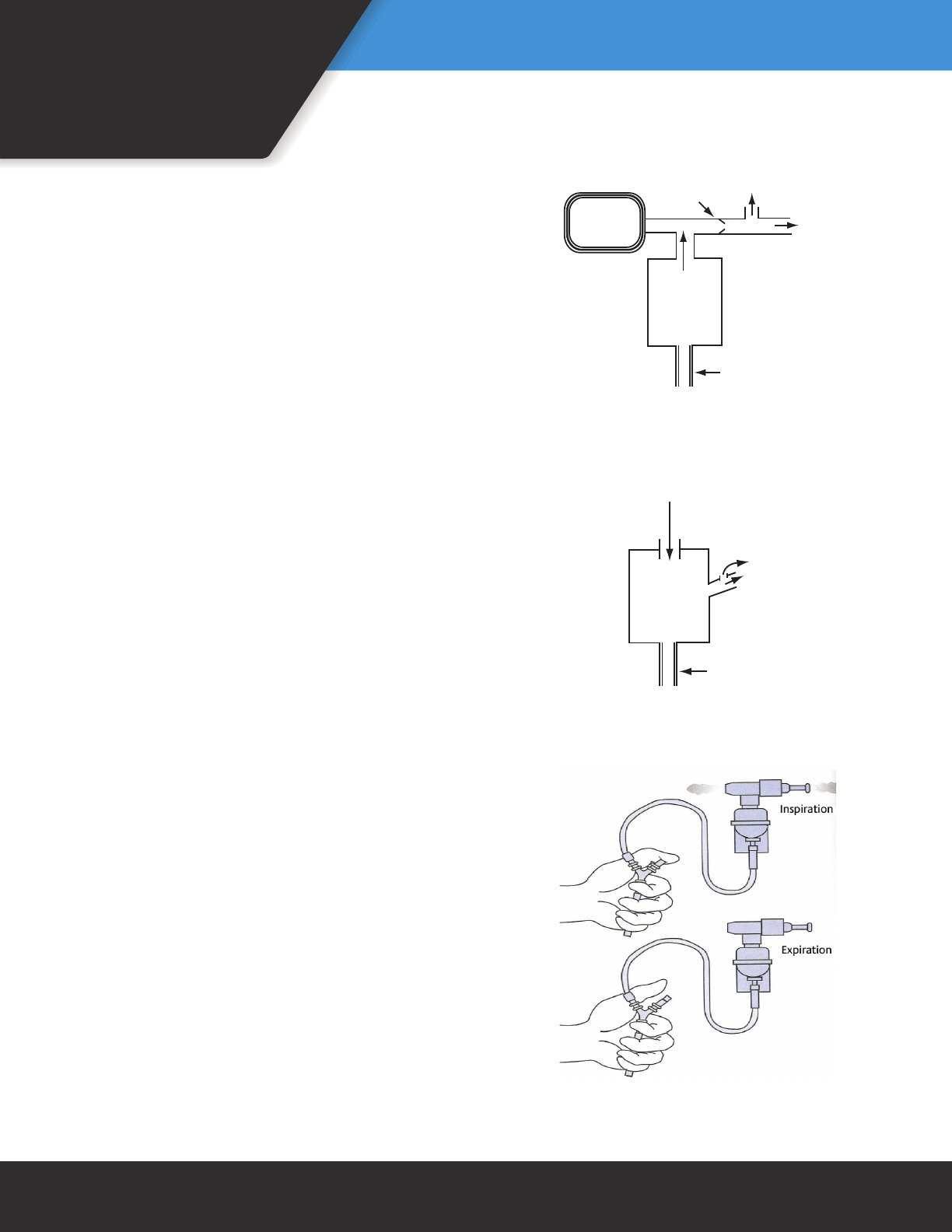
2. Mechanical Breath-Actuated: The AeroEclipse® II BAN
Figure 6. Schematic illustration of the function
of a jet nebulizer with collecting bag
(From Reference 37, with permission)
Figure 7. Schematic illustration of the
function of a breath-enhanced jet nebulizer
(From Reference 37, with permission)
Figure 8. Schematic illustration of the function of
a manual breath-actuated jet nebulizer
(From Reference 7, with permission)
aerosol
storage bag
one-way valve exhale
inhale
power gas
open vent
air intake
exhale
inhale
power gas
14
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
(Monaghan Medical Corporation, Plattsburgh, NY) is an
example of mechanical breath-actuated nebulizers. As
shown in Figure 9, the mechanical breath-actuated neb-
ulizer has a breath-actuated valve that triggers aerosol
generation only during active inspiration and eliminates
the need for a storage bag or reservoir. Patients must
be able to generate a sufcient inspiratory ow to
trigger the nebulizer. Therefore, the sensitivity of this
mechanism makes it suitable only for some children and
adults.
3. Microprocessor Breath-Actuated: The nal type of
breath-actuated jet nebulizer is more complex but
more appropriate to a wider range of users. In this
type, compressor-driven jet nebulizers are actuated by
an electronic circuit, commonly triggered by a pres-
sure transducer sensing inspiratory effort. For several
decades these devices have been used in pulmonary
function and research labs to administer precise boluses
of aerosol for methacholine challenge. A newer gener-
ation of “smart” microprocessor-controlled breath-ac-
tuated nebulizers uses computer programs and sensing
technology to control the pattern of aerosol generation
and even to calculate and track the delivered dose. The
I-neb AAD® system (Philips) is one model of the micro-
processor, breath-actuated that uses vibrating mesh
nebulization.
Ultrasonic Nebulizers
Ultrasonic nebulizers convert electrical energy to
high-frequency vibrations using a transducer. These
vibrations are transferred to the surface of the solution,
creating a standing wave that generates aerosol (Figure
10). Ultrasonic nebulizers were initially introduced as
large-volume nebulizers most commonly used to deliver
hypertonic saline for sputum inductions. Small-volume
ultrasonic nebulizers are now commercially available for
delivery of inhaled bronchodilators but should not be
used with suspensions such as budesonide. Ultrasonic
nebulizers tend to heat medication. This raises concerns
about disrupting proteins, but that does not affect com-
monly inhaled medications. The MicroAir® Ultrasonic
Model (Omron Healthcare, Bannockburn, IL) and MABIS®
NebPak™ and MiniBreeze™ Ultrasonic Nebulizers (Mabis
Healthcare, Waukegan, IL) are different models of the
ultrasonic nebulizer.
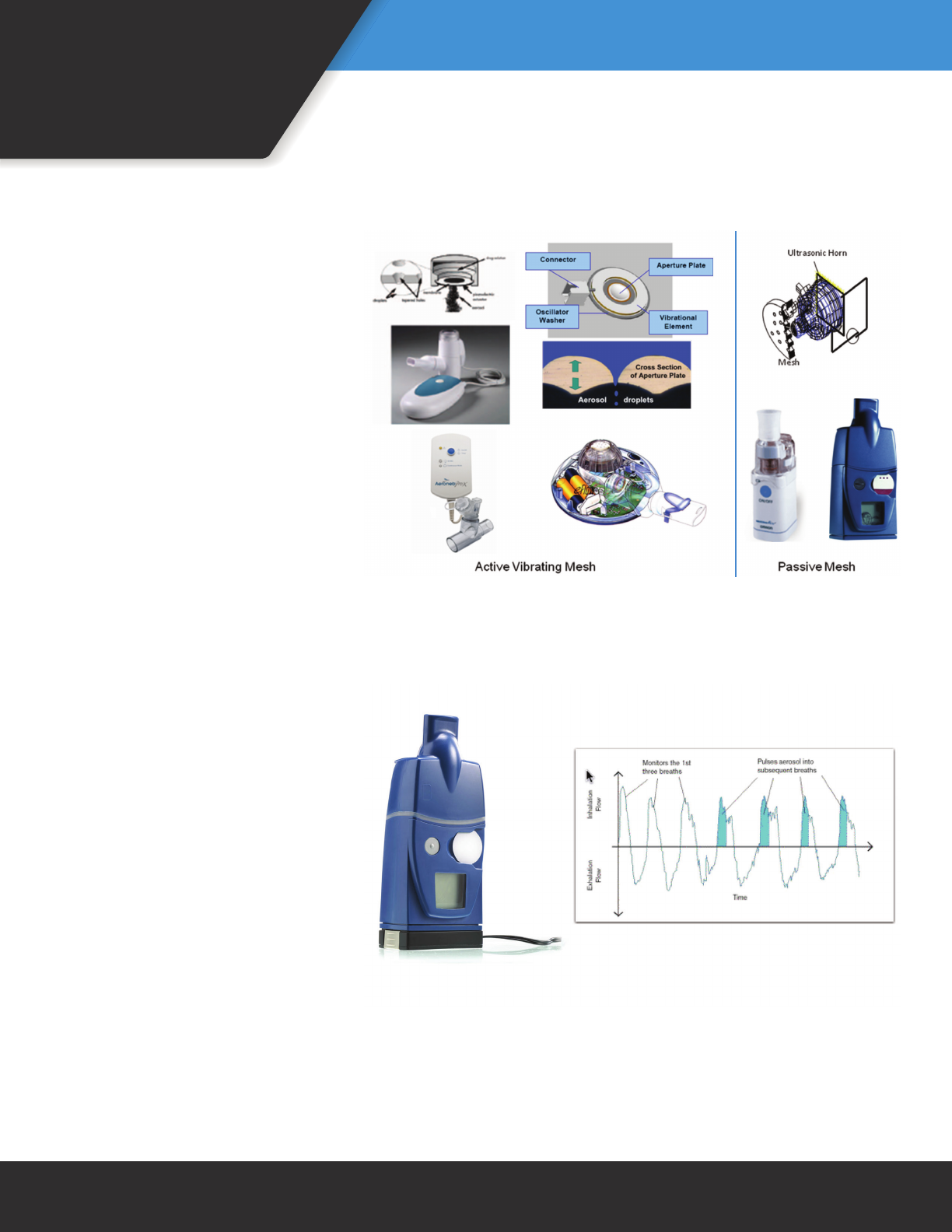
Mesh Nebulizers
Mesh nebulizers use electricity to vibrate a piezo (at
approximately ~128 KHz) element that moves liquid
formulations through a ne mesh to generate aerosol.
The diameter of the mesh or aperture determines the
size of the particle generated. Mesh nebulizers are very
efcient and result in minimal residual volume (0.1–0.5
mL). As seen in Figure 11, mesh nebulizers utilize two
basic mechanisms of action: active vibrating mesh and
passive mesh.
Figure 9. Schematic illustration of the function of
a mechanical breath-actuated nebulizer
(From Reference 37, with permission)
Figure 10. Components and operation principle of an ultrasonic
nebulizer (From Reference 1, with permission)
air intake
(spring-loaded valve)
exhale
inhale
power gas
15
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Active Vibrating Mesh: Active vibrat-
ing mesh nebulizers have an aperture
plate with 1,000–4,000 funnel-shaped
holes vibrated by a piezo-ceramic ele-
ment that surrounds the aperture plate.
The Aeroneb® Ultra and Solo (Aerogen,
Galway, Ireland), Akita® Jet (Inamed,
Germany) and eRapid® (PARI, Midlothian,
VA) are models of the active vibrating
mesh nebulizers (Figure 11, left).
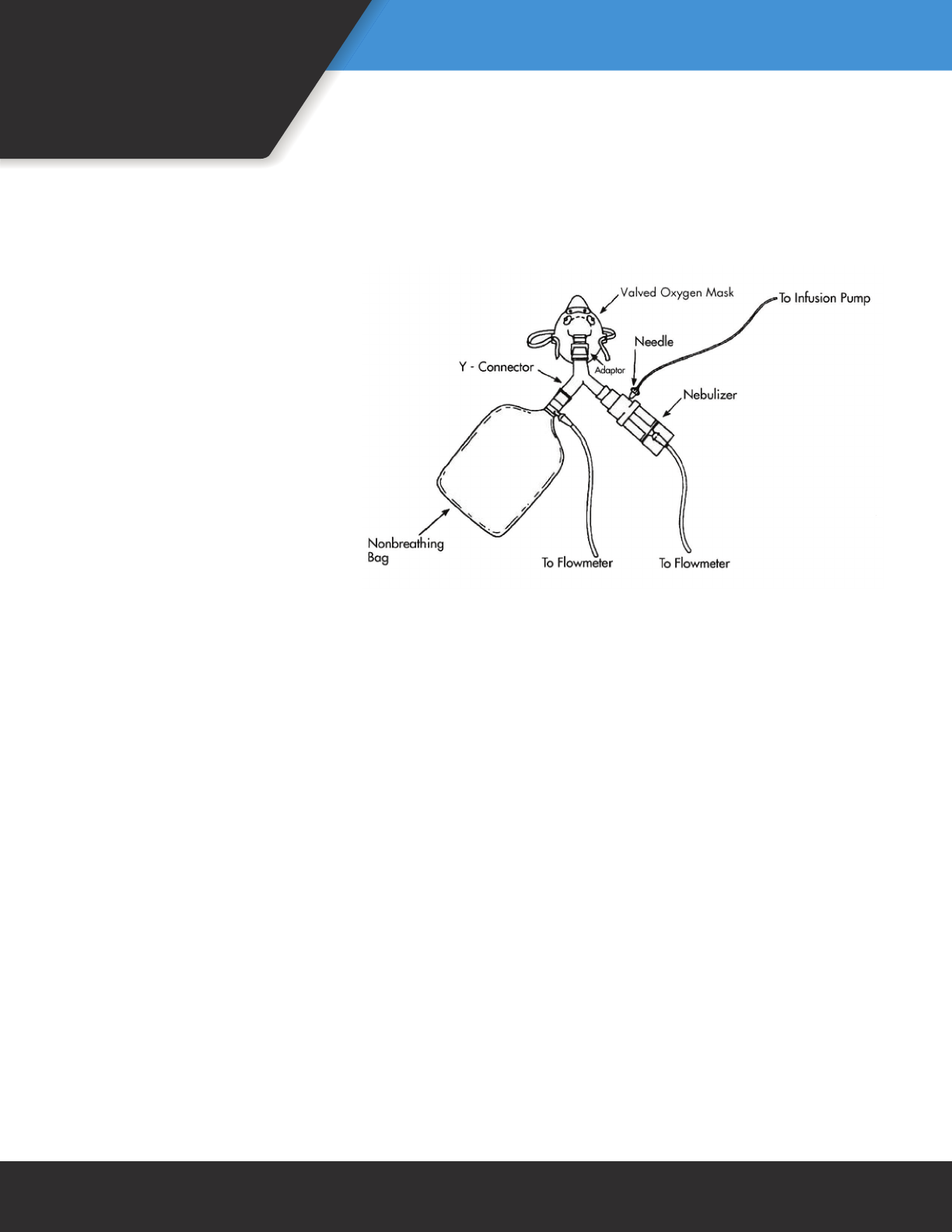
Passive Mesh: These types of nebulizers
utilize an ultrasonic horn to push uid
through a mesh (Figure 11, right). I-neb®
AAD System® (Philips) and MicroAir™ U22
(Omron Healthcare) are models of the
passive mesh nebulizer. A third-gener-
ation adaptive aerosol delivery (AAD)
system such as the I-neb® has a small,
battery-powered, lightweight, and silent
drug delivery device designed to deliver
a precise, reproducible dose of drug. The
aerosol is created by a passive mesh, and
aerosol is injected into the breath at the
beginning of inhalation (Figure 12). The
dosage of the drug is controlled through
specic metering chambers. The meter-
ing chambers can deliver a pre-set vol-
ume ranging from 0.25 to 1.7 mL with
a residual volume of about 0.1 mL. The
I-neb® model incorporates an AAD algo-
rithm that pulses medication delivery
into 50–80% of each inspiration, based
on a rolling average of the last three
breaths. Throughout the treatment, the
I-neb® provides continuous feedback to
the patient through a liquid crystal dis-
play; and upon successful delivery of the
treatment, the patient receives audible
and tactile feedback.
Nebulizers for Specic
Applications
Nebulizer for Ribavirin Administration
The small-particle aerosol
generator (SPAG) is a large-volume
nebulizer designed solely to deliver
Figure 11. Basic congurations of mesh nebulizers
Figure 12. Adaptive aerosol delivery as provided by the Philips I-neb®. As illustrated,
aerosol is injected into the breath at the beginning of inhalation.
(With permission of Philips)
16
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
aerosolized ribavirin (Virazole®, Valeant
Pharmaceuticals, Aliso Viejo, CA) for
prolonged periods of nebulization. It
consists of a nebulizer and a drying
chamber that reduces the MMAD to
about 1.3 µm. Because of teratogenic
characteristics of ribavirin, a scavenging
system is strongly recommended for use
during its administration.
Nebulizer for Aerosolized Pentamidine
Administration
When administering aerosolized pent-
amidine, an SVN tted with inspiratory
and expiratory one-way valves and with
expiratory lter is used. These valves
prevent exposure of secondhand pent-
amidine aerosol and contamination of
the ambient environment with exhaled
aerosol. In 2014, the National Institute
for Occupational Safety and Health
(NIOSH) removed pentamidine from
its hazardous drug list indicating it no longer requires
these devices or aerosol treatments to be delivered in a
negative pressure room.
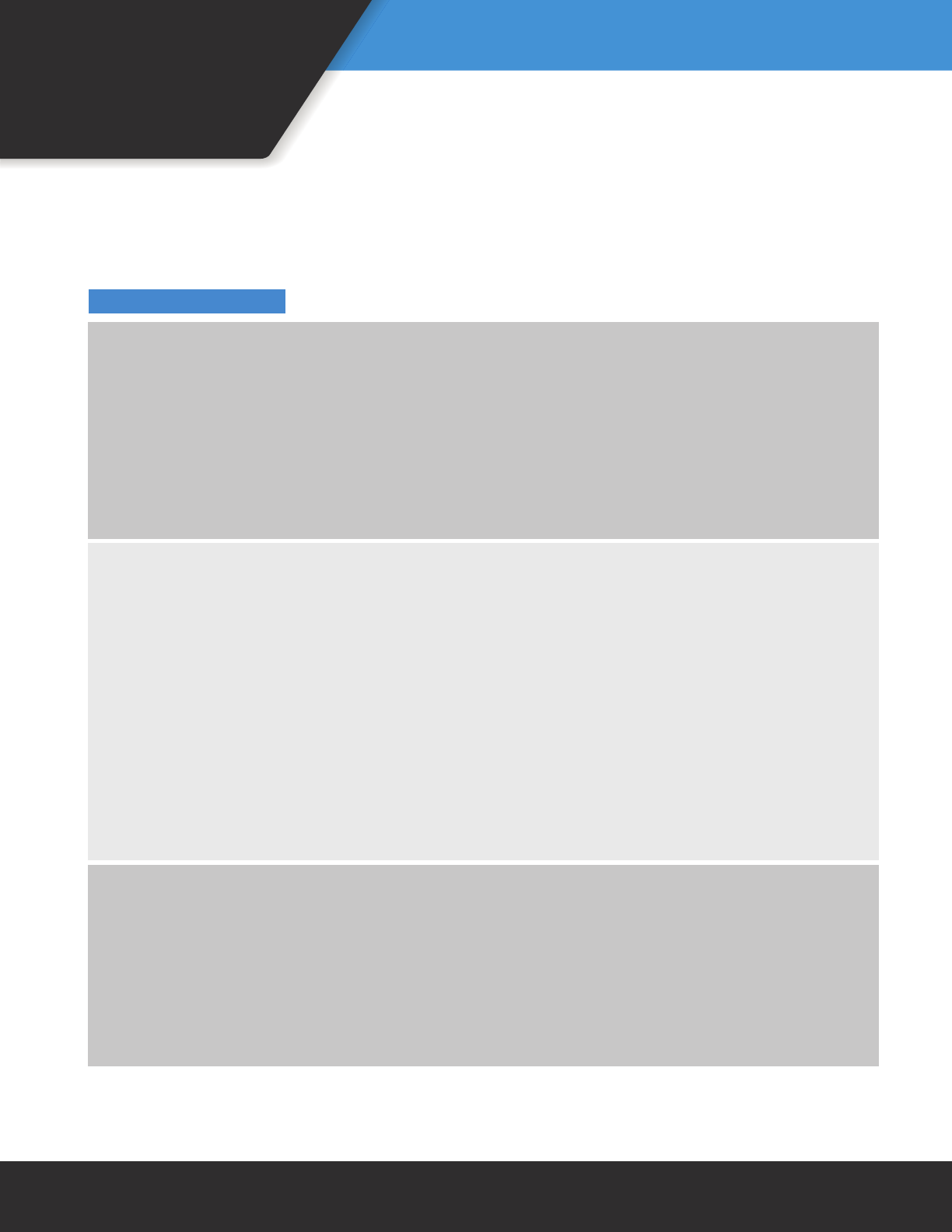
Continuous Aerosol Therapy
Continuous aerosol drug administration is a safe
treatment modality and is used to treat patients suffer-
ing acute asthma exacerbations. Researchers reported
that it may be as effective as intermittent aerosol ther-
apy or may, in fact, be superior to intermittent nebuli-
zation in patients with severe pulmonary dysfunction.39
Figure 13 illustrates a basic setup for continuous aero-
sol therapy that includes an infusion pump, a one-way
valved oxygen mask, and a reservoir bag. Commercial
nebulizers used in continuous nebulization common-
ly have luer lock ports designed for use with infusion
pumps. The nebulization is most commonly adminis-
tered using standard aerosol masks.
Drug-Delivery Technique
Because different types of nebulizers are available on
the market, the respiratory therapist should carefully
review operation instructions prior to giving aerosol
therapy and certainly prior to instructing patients in
at-home aerosol delivery. Proper technique is provided
in Technique Box 1.
Figure 13. Setup for continuous aerosol therapy (From Reference 1, with permission)

17
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Technique Box 1. Steps for Correct Use of Nebulizers
Technique for Jet Nebulizers: When a jet nebulizer is used, the patient should:
1. Assemble tubing, nebulizer cup, and mouthpiece (or mask).
2. Place medicine into the nebulizer cup.
3. Sit in an upright position.
4. Connect the nebulizer to a power source.
5. Breathe normally with occasional deep breaths until sputter occurs or until the end of nebulization.
6. Keep the nebulizer vertical during treatment.
7. Rinse the nebulizer with sterile or distilled water and allow to air dry.
Technique for Mesh and Ultrasonic Nebulizers: When a mesh or ultrasonic nebulizer is used,
the patient should:
1. Correctly assemble the nebulizer per manufacturer’s specications.
2. If applicable, follow manufacturer’s instructions in performing a functionality test prior to the rst use
of a new nebulizer as well as after each disinfection to verify proper operation.
3. Pour the solution into the medication reservoir. Do not exceed the volume recommended by the
manufacturer.
4. Sit in an upright position.
5. Turn on the power.
6. Hold the nebulizer in the position recommended by the manufacturer.
7. Follow the instructions for breathing technique that is recommended by the manufacturer for these
uniquely designed mesh and ultrasonic nebulizers.
8. If the treatment must be interrupted, turn off the unit to avoid waste.
9. At the completion of the treatment, disassemble and clean as recommended by the manufacturer.
10. When using a mesh nebulizer, do not touch the mesh during cleaning. This will damage the unit.
11. Once or twice a week, disinfect the nebulizer following the manufacturer’s instructions.
General Steps To Avoid Reduced or No Dosing for All Nebulizers: When using nebulizers, the following
steps should be used in order to avoid reduced or no dosing during aerosol treatment. The patient should:
1. Read and follow the instructions.
2. Make sure that the nebulizer is properly assembled and all connections are secured tightly.
3. Make sure that the nebulizer is cleaned and dried between uses.
4. Make sure that the nebulizer operated in its proper orientation.
18
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Technique Box 1. Steps for Correct Use of Nebulizers (continued)
*Cleaning: Please refer to the Infection Control section on pages
44–47 for the cleaning instructions of small-volume nebulizers.
When Does the Treatment Need To Be Ended?
Troubleshooting
Problem with Jet Nebulizers: Absent or Low Aerosol
Causes Solutions
Loose or unattached connections Check the connections and make sure that they are
properly attached.
Inappropriate owmeter setting Check the owmeter setting and adjust the ow
if it is not appropriate.
Obstruction in the orice of the Check the orice of the jet nebulizer and
jet nebulizer clear obstructions when needed.
Problems with Mesh and Ultrasonic Nebulizers: The Unit Does Not Operate
Causes Solutions
Incorrect battery installation (seen in both Check the battery installation and reinstall if needed.
mesh and ultrasonic nebulizers)
External power source connection (seen Check the connections with the AC adapter
in both mesh and ultrasonic nebulizers) and the electrical output.
Overheated unit (seen in ultrasonic Turn off the unit, wait until it cools down, and restart
nebulizers) the unit.
Incorrect connection of the control module Check the connections with the control module cable
cable (seen in mesh nebulizers) and attach them properly, if needed.
Malfunctioning electronics (seen in both mesh Replace the unit.
nebulizers and ultrasonic nebulizers)
Nebulizers are commonly used for intermittent
short-duration treatments and typically have a set vol-
ume of drug formulation placed in the medication res-
ervoirs. The drug remaining in a nebulizer after therapy
ranges from 0.1 to 2 mL.18 Whereas some respiratory
therapists and patients tap the nebulizer in order to
reduce dead volume and increase nebulizer output,40
others continue aerosol therapy past the point of sput-
tering in an effort to decrease dead volume.18 Some
nebulizers will sputter for extended periods of time
after the majority of the inhaled dose has been adminis-
tered. Evidence suggests that after the onset of sputter,
very little additional drug is inhaled.18,41 Because the
time it takes to administer the drug is a critical factor
for patient adherence to therapy, some clinicians have
adopted recommendations to stop nebulizer therapy
at, or one minute after, the onset of sputter. Newer
nebulizers may use microprocessors to monitor how
much dose has been administered and automatically
turn off the nebulizer at the end of each dose.
19
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Inhalers
The pressurized metered-dose inhaler and dry-powder
inhaler are medical aerosol delivery devices that combine
a device with a specic formulation and dose of drug. Each
actuation of the inhaler is associated with a single inspira-
tion of the patient. These are typically single-patient-use
devices dispensed from the pharmacy with a specic quan-
tity of medication and disposed of when the medication
has been depleted.
Inhalers are approved by the FDA Center for Drug
Evaluation Research (CDER) as drug and device combina-
tions. They typically are required to go through the com-
plete drug development process from pre-clinical to pivotal
trials in hundreds to thousands of patients. Inhaler-based
drugs must have reproducible doses (+/- 20) from rst to
last dose and have a shelf life with drug of at least 12–24
months. Once an inhaler enters the Phase III trials, the
design and materials are set and cannot be changed with-
out additional expensive clinical trials.
There is a large variety of inhaler designs, and many
drugs are available only in a single inhaler form (Figure
14). Patients are commonly prescribed several types of
inhalers with different instructions for operation. Confusion
between device operation can result in suboptimal therapy.
For example, pMDIs typically require slow inspiratory ow
(<30 L/min) with a breath-hold, while a DPI may require
signicantly high ows (30–90 L/min) based on their resis-
tive properties to disperse a full dose. Patients may confuse
which inspiratory ow to use with which device and may
get much less drug from both devices. Therefore, educa-
tion and repetitive return demonstration is the key to prop-
er inhaler use.

20
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
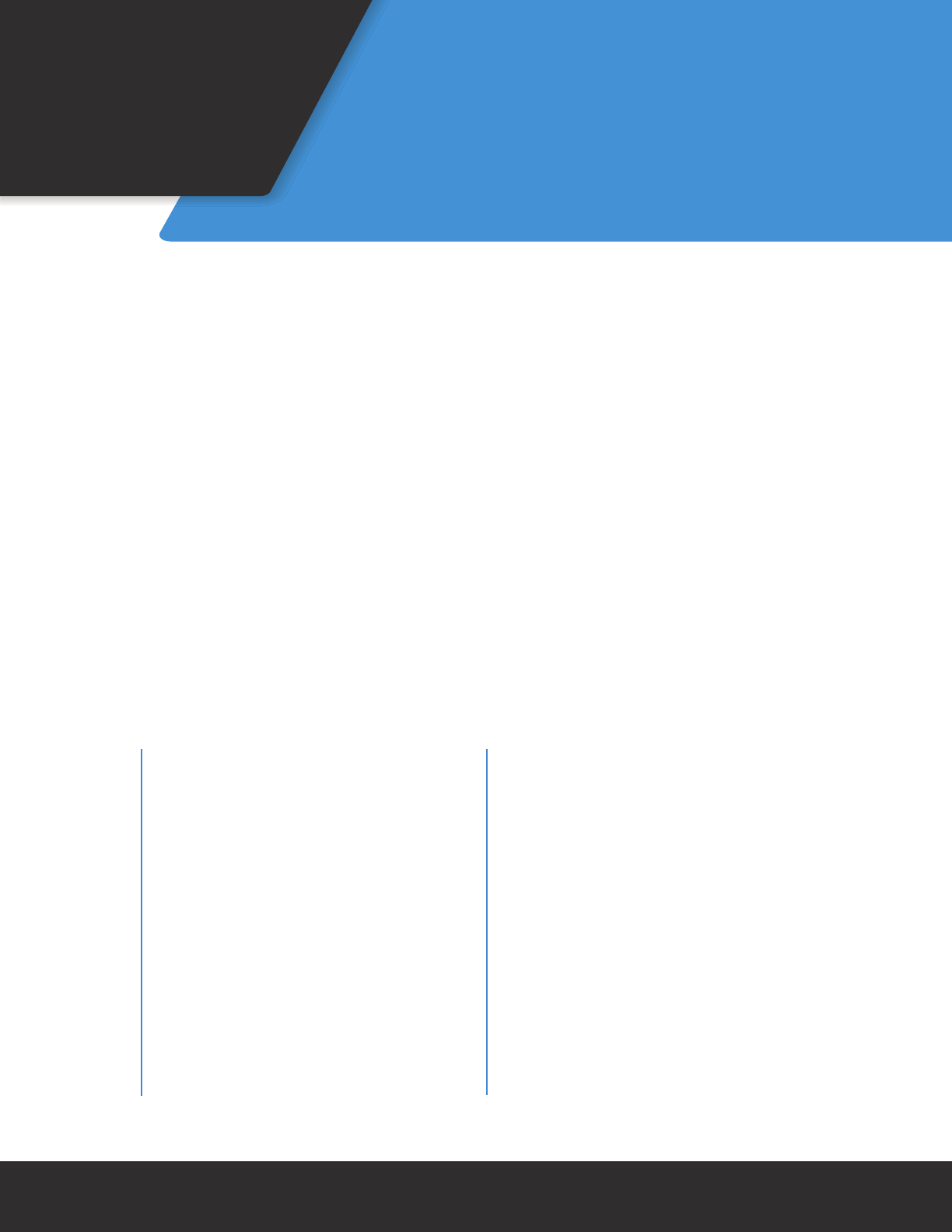
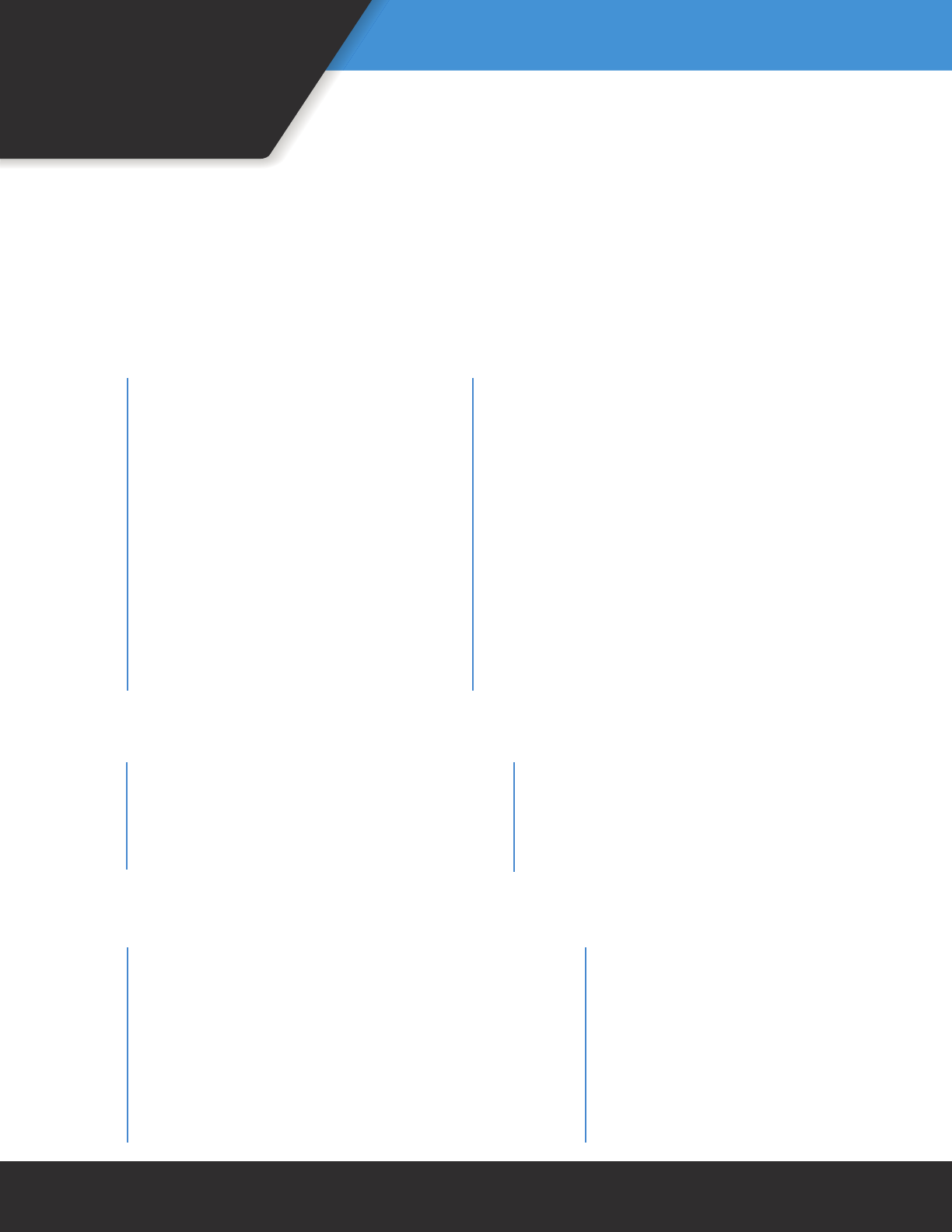
Figure 14. Common Inhalers Available in the United States
Spiriva®
Handihaler®
(tiotropium
bromide)
Inhalation Powder
Boehringer Ingelheim
Pharmaceuticals, Inc.
Atrovent® HFA
(ipratropium
bromide HFA)
Inhalation
Aerosol
Boehringer Ingelheim
Pharmaceuticals, Inc.
Anticholinergics/b2-Agonist Combination
Combivent®
Respimat®
(ipratropium
bromide and
albuterol sulfate)
Inhalation Spray
Boehringer Ingelheim Pharmaceuticals, Inc.
Stiolto®
Respimat®
(tiotropium
bromide
and olodaterol)
Inhalation Spray
Boehringer Ingelheim Pharmaceuticals, Inc.
Utibron™
Neohaler®
(indacaterol
and
glycopyrrolate)
Inhalation Powder
Sunovion Pharmaceuticals Inc.
Anoro®
Ellipta®
(umeclidinium
and vilanterol)
Inhalation
Powder
GlaxoSmithKline
Bevespi
Aerosphere™
(glycopyrrolate
and formoterol
fumarate)
Inhalation Aerosol
AstraZeneca Pharmaceuticals
Alvesco®
(ciclesonide)
Inhalation
Aerosol
Nycomed
Flovent® Diskus®
(uticasone
propionate)
Inhalation
Powder
GlaxoSmithKline
ArmonAir™ RespiClick®
(uticasone propionate)
Inhalation Powder
Teva Specialty Pharmaceuticals
Flovent® HFA
(uticasone
propionate)
Inhalation
Aerosol
GlaxoSmithKline
Arnuity®
Ellipta®
(uticasone
furoate)
Inhalation
Powder
GlaxoSmithKline
Pulmicort®
Flexhaler®
(budesonide)
Inhalation Powder
AstraZeneca LP
Asmanex
Twisthaler®
(mometasone)
Inhalation
Powder
Schering Corporation
QVAR®
(beclomethasone
dipropionate)
Inhalation
Aerosol
Teva Specialty Pharmaceuticals
Aerospan®
(unisolide)
Inhalation
Aerosol
Mylan Pharmaceuticals
Corticosteroids
Anticholinergics
ProAir® HFA
(albuterol sulfate)
Inhalation Aerosol
Teva Specialty
Pharmaceuticals
ProAir® RespiClick®
(albuterol sulfate)
Inhalation Powder
Teva Specialty
Pharmaceuticals
Arcapta™
Neohaler™
(indacaterol)
Inhalation Powder
Novartis Pharmaceuticals
Striverdi®
Respimat®
(olodaterol)
Inhalation Spray
Boehringer Ingelheim
Pharmacueticals, Inc.
Ventolin® HFA
(albuterol sulfate HFA)
Inhalation Aerosol
GlaxoSmithKline
Serevent® HFA
(salmeterol xinafoate)
Inhalation Aerosol
GlaxoSmithKline
Xopenex® HFA
(levalbuterol tartare)
Inhalation Aerosol
Sunovion Pharmaceuticals Inc.
Serevent® Diskus®
(salmeterol xinafoate)
Inhalation Powder
GlaxoSmithKline
b2-Agonists
Proventil® HFA
(albuterol sulfate)
Inhalation Aerosol
3M Pharmaceuticals Inc.
Advair® Diskus®
(uticasone
propionate and
salmeterol)
Inhalation Powder
GlaxoSmithKline
Advair® HFA
(uticasone propionate
and salmeterol
xinafoate)
Inhalation Aerosol
GlaxoSmithKline
Breo® Ellipta®
(uticasone furoate
and vilanterol)
Inhalation Powder
GlaxoSmithKline
Symbicort®
(budesonide and
formoterol fumarate
dihydrate)
Inhalation Aerosol
AstraZeneca
AirDuo
RespiClick®
(uticasone
propionate
and salmeterol)
Inhalation Powder
Teva Specialty Pharmaceuticals
b2-Agonist/Corticosteroid Combination Other
Dulera®
(mometasone
furoate/
formoterol
fumarate
dihydrate)
Inhalation Aerosol
Merck
Tudorza™
Pressair™
(aclidinium
bromide)
Inhalation Powder
Forest Pharmaceuticals, Inc.
Incruse®
Ellipta®
(umeclidinium)
Inhalation
Powder
GlaxoSmithKline
Seebri™
Neohaler®
(glycopyrrolate)
Inhalation
Powder
Sunovion Pharmaceuticals Inc.
TOBI® Podhaler®
(tobramycin)
Inhalation
Powder
Novartis Pharmaceuticals
Relenza®
(zanamivir)
Inhalation Powder
GlaxoSmithKline
21
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Pressurized
Metered-Dose Inhalers
Since its development by Dr. George Maison in 1955,
the pMDI has been the most common aerosol generator
prescribed for patients with asthma and COPD. This is
because it is compact, portable, easy to use, and provides
multi-dose convenience in a single device.
Advantages and Disadvantages of pMDIs
The pMDI was designed and developed as a drug and
device combination that delivers precise doses of specic
drug formulations. Unlike nebulizers, drug preparation
and handling is not required with pMDIs, and the internal
components of pMDIs are difcult to contaminate. Table
9 gives the advantages and disadvantages associated with
the use of pMDIs.
Types of pMDIs
There are two major types of pMDIs: conventional pMDIs
and soft-mist inhalers. Regardless of manufacturer or active
ingredient, the basic components of the pMDI include the
canister, propellants, drug formulary, metering valve, and
actuator. The characteristics of each pMDI component are
described in Table 10.
Conventional pMDI
As seen in Figure 15, the pMDI consists of a canister, the
medication, the propellant/excipient, a metering valve, the
mouthpiece, and actuator.42 The medication represents
only 1–2% of the mixture emitted from the pMDI and is
either suspended or dissolved in the propellant/excipient
mixture. The propellant of the pMDI makes up 80% of the
mixture. These agents prevent aggregation of the drug
particles and lubricate the metering valve. They also ensure
that the drug is well suspended in the canister. The meter-
ing valve acts to prepare a pre-measured dose of medica-
tion along with the propellant. The volume of the metering
valve changes from 25–100 µL and provides 50 µg to 5 mg
of drug per actuation, depending on the drug formulation.
The conventional pMDI has a press-and-breathe design.
Depressing the canister into the actuator releases the
drug-propellant mixture, which then expands and vaporizes
to convert the liquid medication into an aerosol. The initial
vaporization of the propellant cools the aerosol suspension.
The canister aligns the hole in the metering valve with the
metering chamber when it is pressed down. Then, the high
propellant vapor pressure forces a pre-measured dose of
Table 9. Advantages and disadvantages of pMDIs (Modied, with permission, from Reference 1)
Advantages
Portable, light, and compact
Multiple dose convenience
Short treatment time
Reproducible emitted doses
No drug preparation required
Difcult to contaminate
Disadvantages
Hand-breath coordination required
Patient activation, proper inhalation pattern, and
breath-hold required
Fixed drug concentrations and doses
Reaction to propellants in some patients
Foreign body aspiration from debris-lled
mouthpiece
High oropharyngeal deposition
Difcult to determine the dose remaining in the
canister without dose counter
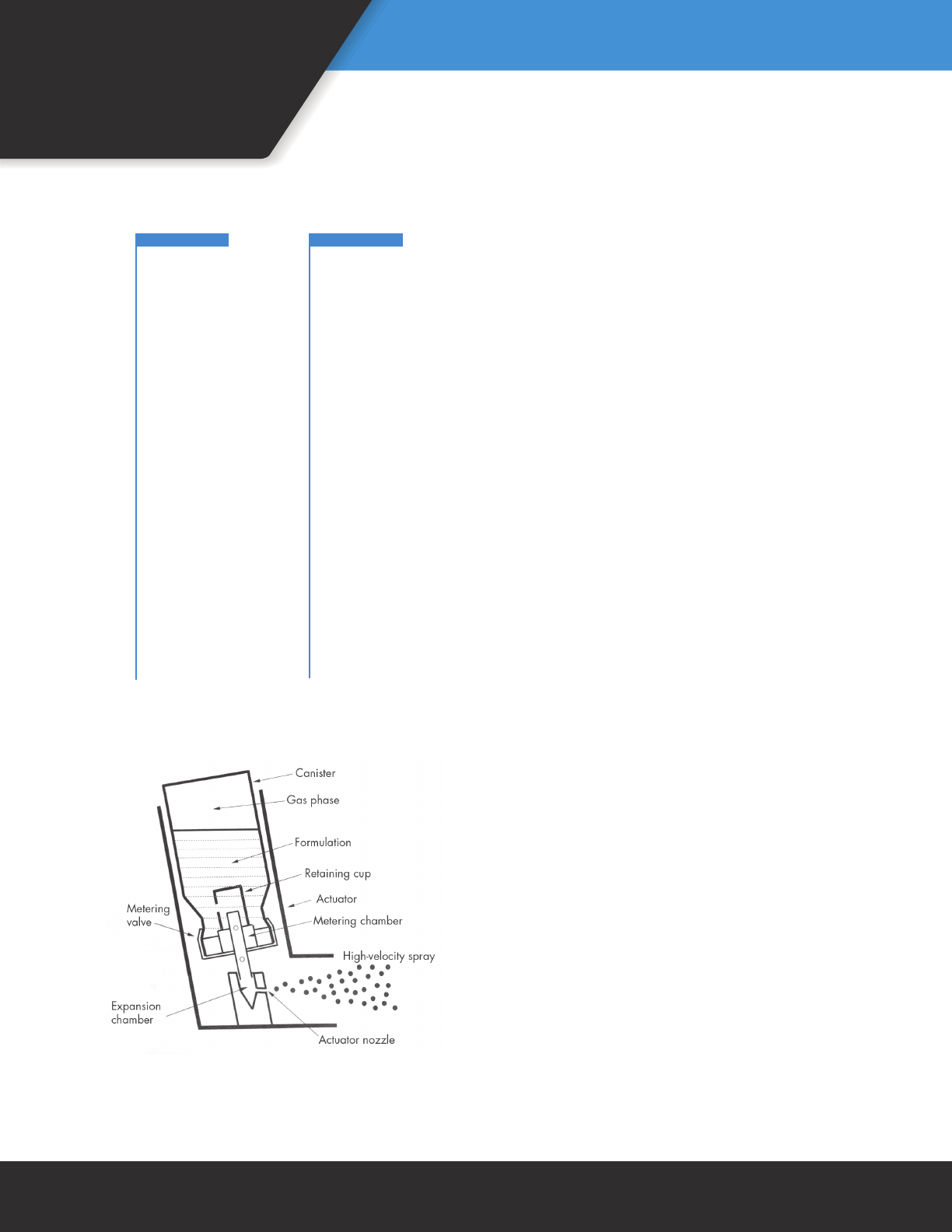
22
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
medication out of this hole and through the actuator noz-
zle. Last, releasing the metering valve rells the chambers
with another dose of the drug-propellant mixture. The pro-
pellants used with pMDIs are HFAs. HFAs are pharmacolog-
ically inert and do not contain surfactant or use alcohol for
this purpose.
Soft-Mist pMDI
The Respimat® (Boehringer Ingelheim Pharmaceuticals,
Ridgeeld, CT) is a propellant-free soft-mist inhaler. The
Respimat® utilizes mechanical energy in the form of a ten-
sioned spring to generate the soft aerosol plume. The ener-
gy from turning the transparent base to the right one-half
turn draws a predetermined metered volume of solution
from the medication cartridge through a capillary tube into
a micro-pump. When the dose release button is depressed,
the energy from the spring forces the solution to the
mouthpiece, creating a soft aerosol plume that lasts approx-
imately 1.5 seconds. Similar to pMDIs, the Respimat® will
need to be primed before use and at times when the device
has had no use. If not used for more than 3 days, actuate
the inhaler once. After more than 21 days of no use, it is
Figure 15. Standard components of pMDI (Modied with
permission from Reference 42)
Table 10. Basic components of the pMDI (From Reference 1 with permission)
Component Particulars
Canister Inert, able to withstand high internal pressures and utilize a coating to prevent
drug adherence
Propellants Liqueed compressed gases in which the drug is dissolved or suspended
Drug Formulary Particulate suspensions or solutions in the presence of surfactants
or alcohol that allocate the drug dose and the specic particle size
Metering Valve Most critical component that is crimped onto the container and is responsible for
metering a reproducible volume or dose
Elastomeric valves for sealing and preventing drug loss or leakage
Actuator Frequently referred to as the “boot,” partially responsible for particle size based
on the length and diameter of the nozzle for the various pMDIs (Each boot is
unique to a specic pMDI/drug.)
Dose Counter This component provides a visual tracking of the number of doses remaining in
the pMDI

23
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
recommended to actuate the device until aerosol is seen,
then actuate 3 more times. Since the device is propellant
free, there is no need to shake it. The Respimat® has a dose
indicator and will lock once all medication is used. Figure
16 shows the standard components of the Respimat®.
Currently Available pMDI Formulations
A number of aerosol formulations are available for use in
pMDIs today (Figure 14). Pressurized metered-dose inhalers
are presently used to administer beta-2 agonists, anticho-
linergics, anticholinergic/beta-2 agonist combinations, cor-
ticosteroids, and anti-asthmatic drugs.
Factors Affecting pMDI Performance and
Drug Delivery
Most pMDIs are designed to deliver a drug dose of 100
µm per actuation. Just like other aerosol generators, drug
delivery with the pMDIs is approximately 10–20% of the
nominal dose per actuation. The particle size of aerosols
produced by the pMDI is in the ne particle fraction range
in which the aerodynamic diameter of aerosols is less than
5 µm. Several factors inuence the pMDI performance and
aerosol drug delivery. Understanding the effects of these
factors will improve the efcacy of pMDIs when used for
patients with pulmonary diseases. Therefore, both respira-
tory therapists and patients must actively control the fol-
lowing effects:
• Shaking the Canister: Not shaking a pMDI canister that
has been standing overnight decreases total and respi-
rable dose by 25% and 35%, respectively, because the
drugs in pMDI formulations are usually separated from
the propellants when standing.43 Therefore, pMDIs must
be shaken before the rst actuation after standing in
order to rell the metering valve with adequately mixed
suspension from the canister.12
• Storage Temperature: Outdoor use of pMDIs in very
cold weather may signicantly decrease aerosol drug
delivery. Dose delivery was constant with HFA pMDIs
over the range of -20º to 20ºC.
• Nozzle Size and Cleanliness: The amount of med-
ication delivered to the patient is dependent upon
nozzle size, cleanliness, and lack of moisture. Actuator
nozzle is pMDI specic, and the coordination of the
nozzle with the medication will inuence both inhaled
dose and particle size. In general, there is an inverse
relationship between the inner diameter of the nozzle
extension and the amount of drug delivered to the
patient.44 A nozzle extension with an inner diameter < 1
mm increases drug delivery.44 White and crusty residue
due to crystallization of medication may inuence drug
delivery. Therefore, the nozzle should be cleaned peri-
odically based on the manufacturer’s recommendations.
• Timing of Actuation Intervals: The rapid actuation of
more than two puffs with the pMDI may reduce drug
delivery because of turbulence and the coalescence
of particles.43 A pause between puffs may improve
bronchodilation, especially during asthma exacerba-
tions with episodes of wheezing and poor control of
symptoms.45 In other cases, such as in the day-to-day
management of pre-adolescents with a beta agonist
(terbutaline) and a corticosteroid (budesonide), pauses
between puffs have not been found to be benecial.46
Although early research was mixed regarding the impor-
tance of a pause between the two actuations, recent
literature suggests a pause of one minute between
actuations for effective aerosol therapy.1,7,13
• Priming: Priming is releasing one or more sprays into
the air. Initial and frequent priming of pMDIs is required
in order to provide an adequate dose. The drug may be
Figure 16. Soft-mist inhaler
24
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
separated from the propellant and other ingredients in
the canister and metering valve when the pMDI is new
or has not been used for awhile. Because shaking the
pMDI will mix the suspension in the canister but not
the metering chamber, priming of the pMDI is required.
Table 11 provides the recommended guidelines for
priming the various pMDIs available on the market.
• Characteristics of the Patient: Characteristics of the
patient using the pMDI will result in a variability of aero-
sol deposition. For example, aerosol deposition will be
lower in infants and children due to differences in their
anatomy and their physical and cognitive abilities.
• Breathing Techniques: There are two primary tech-
niques for using a pMDI without a spacer: the open-
mouth technique and the closed-mouth technique.
The manufacturers of pMDIs universally recommend
the closed-mouth technique for using a pMDI. In this
method, the mouthpiece of the boot is placed between
the sealed lips of the patient during drug administra-
tion. On the other hand, some researchers and clini-
cians have advocated an open-mouth technique in
an attempt to reduce oropharyngeal deposition and
increase lung dose.47,48
Table 11. Priming requirements for commercially available pMDIs (Modied, with permission, from Reference 1)
Short-Acting Bronchodilators
Inhaled Corticosteroids
Combination Drugs
Generic Name Brand Name Time to Prime No. of Sprays
Albuterol Sulfate HFA Proventil® HFA New and when not used for 2 weeks 4
Ventolin® HFA New and when not used for 14 days 4
Levalbuterol HCl Xopenex® HFA New and when not used for 3 days 4
Ipratropium Bromide HFA Atrovent® HFA New and when not used for 3 days 2
Ipratropium Bromide/ Combivent® HFA New and when not used for 24 hours 3
Albuterol Sulfate Combination
Generic Name Brand Name Time to Prime No. of Sprays
Beclomethasone QVAR™ New and when not used for 10 days 2
Propionate HFA
Ciclesonide Alvesco® New and when not used for 10 days 3
Fluticasone Propionate Flovent® HFA New 4
Not used more than 7 days or if dropped 1
Generic Name Brand Name Time to Prime No. of Sprays
Budesonide combined Symbicort® HFA New and not used more than 7 days or 2
with Formoterol if dropped
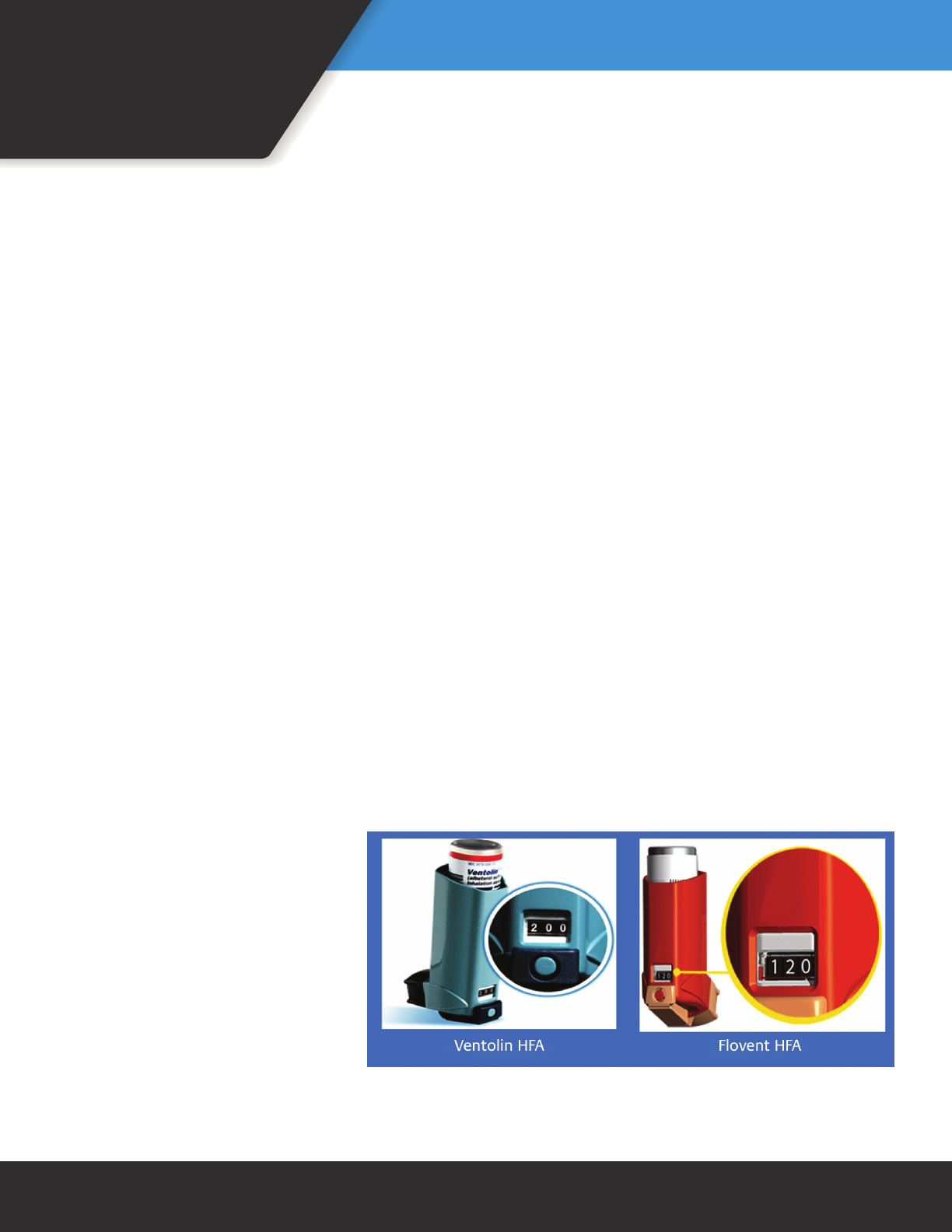
25
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
When using the open-mouth technique, the inhaler is
placed two nger widths away from the lips of an open
mouth and aimed at the center of the opening of the
mouth. Studies suggest that the open-mouth technique
reduces unwanted oropharyngeal deposition by allow-
ing aerosol plume more distance to slow down before
reaching the back of the mouth and up to two-fold more
drug deposition to the lung than with use of the closed-
mouth technique.47,49 In contrast, other researchers
suggest that the open-mouth technique does not offer
any advantage over the closed-mouth technique,50,51 but
that it does create additional hazards such as the aerosol
plume being misdirected from the mouth and into the
eye or elsewhere.52 Therefore, the best technique should
be determined based on the patient’s physical abilities,
coordination, and preference. If the patient is well coordi-
nated and can master the open-mouth technique better,
it can be used by following the directions below. Also,
the patient’s aerosol administration technique should be
observed continuously and corrected when appropriate.
Proper technique is provided in Technique Box 2.
Drug-Delivery Technique
Because different types of pMDIs are available on the
market, the respiratory therapist should carefully review
operation instructions prior to giving aerosol therapy
and certainly prior to instructing patients in at-home use.
Proper technique is provided in Technique Box 2.
How To Know the pMDI Is Empty: Since their intro-
duction in the 1950s, pMDIs have not been packaged
with dose counters that allow patients
to determine when a pMDI should be
discarded.53-55 After the pMDI delivers
the number of puffs stated on their
label, it may look, taste, and feel like it
is still working, but the dose delivered
may be very low. This “tailing off effect”
may last long after the pMDI is “empty
of drug.”13,56 Also, the pMDI without a
dose counter could lead to waste if the
inhaler is discarded prematurely. Indirect
methods such as oating the canister in
water are misleading and can reduce the
ability of the pMDI to work properly.55,57,58
Therefore, they should not be used to
determine the amount of medication remaining in the
canister.
The only reliable method to determine the number of
doses remaining in a pMDI is counting the doses given
either manually or with a dose counter. Manual methods
include reading the label to determine the total number
of doses available in the pMDI and using a log to indicate
every individual actuation given (including both priming
and therapy doses). This tally is subtracted from the num-
ber of actuations on the label until all have been used.
At that time, the pMDI should be properly discarded.
Unfortunately, manually counting doses may be imprac-
tical and undependable, especially in patients who use
reliever medications on the go.
Therefore, the U.S. Department of Health and Human
Services FDA requires new pMDIs to have integrated
dose counters and recommends that all pMDIs have
dose counting devices that indicate when the pMDI
is approaching its last dose.59 The dose counter is a
counting device attached to the top of the pMDI can-
ister or to the boot of the device. When the pMDI is
actuated, it counts down the number of actuations
from the total remaining in the canister. The Ventolin®
HFA (GlaxoSmithKline, Research Triangle Park, NC) and
Flovent® HFA (GlaxoSmithKline) have built-in dose count-
ers (Figure 17).
Also, mechanical or electronic dose counters have been
available from third parties for use by attachment to a
range of pMDIs. Although research has conrmed accept-
able performance and patient satisfaction by pMDIs with
(continued on page 28)
Figure 17. Counter on Ventolin® HFA and Flovent® HFA pMDIs

Technique Box 2. Steps for Correct Use of pMDIs
Technique for pMDIs
Open-Mouth Technique: The patient should be instructed to:
1. Remove the mouthpiece cover and shake the pMDI thoroughly.
2. Prime the pMDI into the air if it is new or has not been used for several days.
3. Sit up straight or stand up.
4. Breathe all the way out.
5. Place the pMDI two nger widths away from their lips.
6. With mouth open and tongue at (tip of tongue touching inside of their lower front teeth), tilt outlet
of the pMDI so that it is pointed toward the upper back of the mouth.
7. Actuate the pMDI as she/he begins to breathe in slowly.
8. Breathe slowly and deeply through the mouth and hold their breath for 10 seconds. If she/he cannot
hold their breath for 10 seconds, then for as long as possible.
9. Wait one minute if another puff of medicine is needed.
10. Repeat Steps 2–10 until the dosage prescribed by the physician is reached.
11. If taking a corticosteroid, she/he should rinse their mouth after the last puff of medicine, spit out the
water, and not swallow it.
12. Replace the mouthpiece cover on the pMDI after each use.
Closed-Mouth Technique: The patient should be instructed to:
1. Remove the mouthpiece cover and shake the inhaler thoroughly.
2. Prime the pMDI into the air if it is new or has not been used for several days.
3. Sit up straight or stand up.
4. Breathe all the way out.
5. Place the pMDI between their teeth; make sure that their tongue is at under the mouthpiece and
does not block the pMDI.
6. Seal their lips.
7. Actuate the pMDI as they begin to breathe in slowly.
8. Hold their breath for 10 seconds. If they cannot hold their breath for 10 seconds, then for as long as
possible.
9. Wait one minute if another puff of medicine is needed.
10. Repeat Steps 2–10 until the dosage prescribed by the patient’s physician is reached.
11. If taking a corticosteroid, she/he should rinse the mouth after the last puff of medicine, spit out the
water and not swallow it.
12. Replace the mouthpiece cover on the pMDI after each use.
Breath-Actuated pMDI (Autohaler™) Technique: When using the Autohaler™, the patient
should be instructed to:
1. Remove the mouthpiece cover and check for foreign objects.
2. Keep the Autohaler™ in a vertical position while the arrow points up, and do not block the air vents.
3. Prime the Autohaler™ into the air if it is new or has not been used recently.
4. Push the lever up.
5. Push the white test re slide on the bottom of the mouthpiece for priming the Autohaler™.
6. Push the lever down in order to release the second priming spray.
7. Return the lever to its down position and raise the lever so that it snaps into place.
8. Sit up straight or stand up.
9. Shake the Autohaler™ three or four times.
10. Breathe out normally, away from the Autohaler™.
11. Place the pMDI between their teeth. Make sure that their tongue is at under the mouthpiece and
does not block the pMDI.
12. Seal their lips around the mouthpiece.
13. Inhale deeply through the mouthpiece with steady moderate force,
14. Pay attention to the click sound and the feel of a soft puff when the Autohaler™ triggers the release of
medicine.
15. Continue to inhale until the lungs are full.
16. Remove the mouthpiece from the mouth.
17. Hold breath for 10 seconds or as long as possible.
18. Repeat steps above until the dosage prescribed by the patient’s physician is reached.
19. Replace the mouthpiece cover and make sure the lever is down.
26
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
27
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Technique Box 2. Steps for Correct Use of pMDIs (continued)
Technique for pMDIs
Soft Mist pMDI (Respimat™) Technique: When using the Respimat™, the patient
should be instructed to:
Preparation:
1. With the cap closed, press the safety catch while pulling off the clear base. Be careful not to touch the
piercing element located inside the bottom of the clear base.
2. Push the narrow end of the cartridge into the inhaler. The base of the cartridge will not sit ush with
the inhaler. About 1/8 of an inch will remain visible when the cartridge is correctly inserted.
3. The cartridge can be pushed against a rm surface to ensure it is correctly inserted.
4. Do not remove the cartridge once it has been inserted into the inhaler.
5. Write the discard by date on the label of the inhaler. The discard by date is 3 months from the date the
cartridge is inserted.
6. Put the clear base back into place. Do not remove the clear base again. The inhaler should not be
taken apart after they have inserted the cartridge and put the clear base back.
Priming:
7. Hold the inhaler upright with the cap closed to avoid accidental release of dose.
8. Turn the clear base in the direction of the white arrows on the label until it clicks (half a turn).
9. Flip the cap until it snaps fully open.
10. Point the inhaler toward the ground. Press the dose-release button. Close the cap.
11. Repeat steps 7–10 until a spray is visible.
12. Once the spray is visible, repeat steps 7–10 three more times to make sure the inhaler is ready for use.
Patient-Use Instructions:
1. Hold the inhaler upright with the cap closed to avoid accidental release of dose.
2. Turn the clear base in the direction of the white arrows on the label until it clicks (half turn).
3. Flip the cap until it snaps fully open.
4. Breathe out slowly and fully, and then close lips around the end of the mouthpiece without covering
the air vents.
5. Point inhaler toward the back of mouth.
6. While taking in a slow, deep breath through the mouth, press the dose-release button and continue to
breathe in slowly for as long as possible.
7. Hold breath for 10 seconds or for as long as comfortable.
8. Close the cap until next prescribed dose.
General Steps To Avoid Reduced or No Dosing for pMDIs: The patient should:
1. Remove the cap of the pMDI from the boot.
2. Prime as directed (Table 11 on page 24).
3. Clean and dry the boot of the pMDI based on the manufacturer’s guidelines.
4. Track remaining doses.
Troubleshooting
Problem with Jet Nebulizers: Absent or Low Aerosol
Causes Solutions
Incorrect pMDI assembly Check the assembly and reassemble when needed.
Incorrect pMDI and spacer assembly Check the assembly of the pMDI/spacer and reassemble if
needed.
Empty the pMDI Check the dose counter or daily log sheet to ensure there is
enough medicine in the canister. Otherwise, replace the
pMDI.
28
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Figure 18. Currently available pMDI dose counters on the market
(continued from page 25)
dose counters,60-62 care must
be taken to assure that a
third-party dose counter works
with the specic pMDI being
used.18,63 Some of the built-
in counters may not t the
spacer, and improper t to the
canister may interfere with
proper actuation, resulting
in no or partial drug being
emitted and in a miscount
of remaining doses.63 Using
a third-party dose-counting
device increases the cost of
aerosol therapy, which may
limit their wide acceptance.
Figure 18 shows currently
available pMDI dose counters
in the United States.
With any third-party counter, read the product label and accompanying package
information for each pMDI before use and follow the manufacturer’s recommend-
ed doses. When attempting to keep track of the number of doses remaining in the
pMDI, Table 12 outlines monitoring recommendations with and without integrated
dose counters.
Cleaning: Please refer to the Infection Control section on page 44 for the cleaning
instructions for inhalers.
Table 12. Monitoring remaining pMDI doses
Without Dose Counter: The user should:
1. Determine the number of puffs that the pMDI has when it is full.
2. Calculate how long the pMDI will last by dividing the total number of puffs in the pMDI by the total puffs used. Also
remember that the medication will run out sooner if the pMDI is used more often than planned.
3. Identify the date that the medication will run out and mark it on the canister or on the calendar.
4. Keep track of how many puffs of medicine administered on a daily log sheet and subtract them to determine the
amount of medication left in the pMDI.
5. Keep the daily log sheet in a convenient place such as bathroom mirror.
6. Replace the pMDI when all of the puffs have been administered.
With Dose Counter: The user should:
1. Determine how many puffs of medicine that the pMDI has when it is full.
2. Track the pMDI actuations used and determine the amount of medication left in the pMDI by checking the counter
display.
3. Learn to read the counter display. Each dose counter has a specic way of displaying doses remaining in the canis-
ter. For example, turning red indicates that the number of actuations is less than 20 puffs and it is time to rell the
pMDI. Reading the manufacturer’s guidelines to interpret the counter display is recommended before its use.
4. When the last dose is dispensed, properly dispose of the pMDI.
29
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Metered-Dose Inhaler
Accessory Devices
Metered-dose inhaler accessory devices were designed
to overcome the difculties experienced when using a
pMDI and are available in different forms and sizes.
Advantages and Disadvantages of pMDI
Inhaler Accessory Devices
The use of these devices improves the effectiveness of
aerosol therapy and reduces oropharyngeal deposition by
adding volume and space between the metering valve and
the patient’s mouth. They overcome problems with hand-
breath coordination. Table 13 lists both advantages and
disadvantages seen with valved holding chambers (VHCs)
and spacers used in conjunction with pMDIs.
While the term spacer is used in clinical practice to refer
to all types of extension add-on devices, these devices are
categorized into spacers or holding chambers (or valved
holding chambers) based on their design. A spacer is a sim-
ple tube or extension device which adds space and volume
between the pMDI and mouth with no one-way valves to
contain the aerosol plume after pMDI actuation. A holding
chamber (valved holding chamber) is an extension spacer
device with one-way valve(s) to contain the aerosol until
inhaled and direct exhalation away from the aerosol in the
chamber, reducing aerosol losses with poor hand-breath
coordination. In addition to the major design difference
that denes spacers versus (valved) holding chambers,
there are other design differences among brands of hold-
ing chambers and spacers. Volume may vary, although in
the United States most holding chambers/spacers are less
than 200 mL. Direction of spray may vary between forward
(toward the mouth) and reverse (away from the mouth).
The AeroChamber® (Monaghan Medical Corporation),
OptiChamber Diamond® and the OptiChamber® Advantage
(Philips) are examples of forward sprays. The ACE® Aerosol
Cloud Enhancer (Smiths Medical, Dublin, OH) is an example
of reverse spray. Some holding chambers/spacers accept
the manufacturer’s mouthpiece-actuator (the boot), while
others have a nozzle receptacle for accepting only the can-
ister. As an example, the ACE® has a canister nozzle recep-
tacle, while the AeroChamber®, OptiChamber Advantage®
and OptiChamber Diamond® have malleable openings to
accept the pMDI mouthpiece. While boots are designed
specic to each pMDI, the canister nozzles vary and may
not t any one specic nozzle receptacle, reducing drug
efcacy. Figure 19 shows examples of spacers and holding
chambers.
Table 13. Advantages and disadvantages of holding chambers or spacers (“add-on”
devices) used with pMDIs (Modied, with permission, from Reference 64)
Advantages
Reduced oropharyngeal drug impaction and loss
Increased inhaled drug by two to four times than
the pMDI alone
Allows use of the pMDI during acute airow
obstruction with dyspnea
No drug preparation required
Simplies coordination of pMDI actuation and
inhalation
Helps reduce local and systemic side effects.64
Disadvantages
Large and cumbersome compared to the pMDI
alone
More expensive and bulky than a pMDI alone
Some assembly may be needed
Patient errors in ring multiple puffs into chamber
prior to inhaling or there is a delay between
actuation and inhalation
Possible contamination with inadequate cleaning
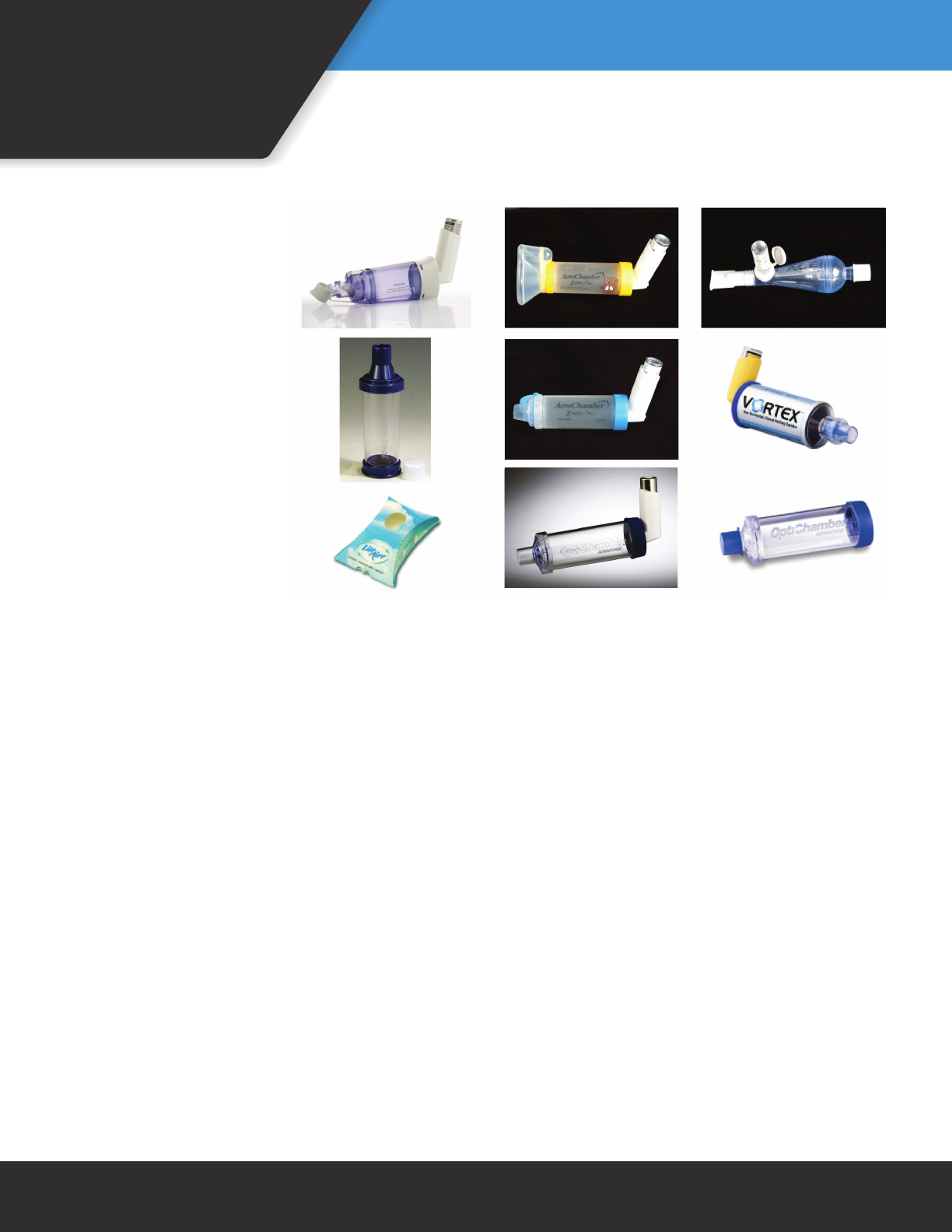
30
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Figure 19. Examples of VHCs and spacers
Spacers
The use of a spacer with
pMDIs should produce at
least an equivalent inhaled
dose and clinical effect to
that of a correctly used
pMDI alone. A spacer pro-
vides additional volume that
slows the aerosol velocity
from a pMDI, allowing a
reduction in particle size.
Aerosol retention and dis-
charged dose depends on
the size and shape of the
spacer, and electrostatic
charge on the inner walls
of plastic spacers. Spacers
decrease oral deposition,
but they only provide limit-
ed protection against poor
hand-breath coordination.
When using a spacer, it is
important for the patient
to coordinate their inhalation to occur slightly before
actuating the inhaler. Some spacers require removal of
the inhaler canister from the manufacturer’s actuator
and incorporation into a special orice on the spacer. It is
important to understand that dose delivery can be affected
in some spacer designs if the device does not t the pMDI
properly or if the design uses a special orice or actuator
incorporated into the spacer itself. Occasionally, clinicians
or patients construct homemade holding chambers from
plastic containers (e.g., soda bottle) or other devices (e.g.,
toilet paper roll). These may function as a spacer and pro-
vide protection against reduced dose with pMDI actuation
before inhalation, but they do not protect against actua-
tion during exhalation. Also, their performance is variable,
so they should not be considered as suitable replacements
for a commercially available spacer.
Valved Holding Chambers
A valved holding chamber (VHC) has a low-resistance
one-way valve that allows aerosol particles to be contained
within the chamber for a short time until an inspiratory
effort opens the valve. Although the presence of a one-way
valve prevents aerosol particles from exiting the chamber
until inhalation begins, optimal aerosol dosing still depends
on inhaling as close to or simultaneously with pMDI actua-
tion into the chamber. Time delays can signicantly reduce
the available dose for inhalation from a VHC. The one-way
valve should have a low resistance so that it opens easily
with minimal inspiratory effort. Valves placed between the
chamber and the patient also act as an impaction point,
further reducing oropharyngeal deposition. It’s important
to assure the valve works properly, as dysfunctional valves
can cause ineffective delivery of medication.65 Ideally,
there should be a signal to provide feedback if inspiratory
ow is too high. Children with low tidal volumes (less than
device dead space) may need to take several breaths from
a VHC through a face mask for a single pMDI actuation. In
this case, the VHC should incorporate one-way valves for
both inhalation and exhalation to decrease rebreathing
and avoid blowing aerosol from the chamber. A VHC with
mouthpiece costs as little as $15–$20, and a static-free
device with mask can cost as much as $50–$60.
Drug-Delivery Technique
While spacers and VHCs provide many benets for opti-
mal drug delivery with pMDIs, there are also potential
problems with their use (Table 13). Improper technique
may decrease drug delivery or, in some cases, cause the
dose to be lost. Possible causes of decreased drug delivery
include multiple actuations into the device, electrostatic
charge, inhaling before actuating the pMDI, delay between
31
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
actuation and inhaling the dose, or improper insertion of
actuator into spacer and/or VHC.66 It has been shown that
improper insertion of the actuator can contribute to a
spray of medication that does not follow the optimal axis
of the chamber and a good proportion of medicine ends
up deposited on the inside of the chamber.67 Also, it has
been suggested that spacer size and shape may provide
better deposition of specic particle sizes.66 More research
is needed on length, shape, and volume of spacers. In
children, lack of a proper mask t, a spacer volume that is
greater than tidal volume (mechanical dead space), and
crying are problematic. Proper technique is provided in
Technique Box 3.
Cleaning: Please refer to the Infection Control section on
page 44 for cleaning instructions for the pMDI chamber
and collapsible bag device.
Technique Box 3. Steps for Correct Use of pMDI with Spacer/VHC
Technique for pMDIs with Spacer/VHC: The patient should be instructed to:
1. Remove the mouthpiece cover and shake the inhaler thoroughly.
2. Prime the pMDI into the air if it is new or has not been used for several days.
3. Assemble the apparatus and check for foreign objects.
4. Keep the canister in a vertical position.
5. Sit up straight or stand up.
6. Breathe all the way out.
7. Follow the instructions below based on the type of device interface used:
With the mouthpiece:
a. Place the mouthpiece of the spacer between their teeth and seal their lips. Make sure that their
tongue is at under the mouthpiece and does not block the pMDI.
b. Actuate the pMDI as they begin to breathe in slowly. Also make sure to inhale slowly if the device
produces a “whistle” indicating that inspiration is too rapid.
c. Move the mouthpiece away from the mouth and hold their breath for 10 seconds. If they cannot
hold their breath for 10 seconds, then hold for as long as possible.
With the mask:
d. Place the mask completely over the nose and mouth and make sure it ts rmly against the face.
e. Hold the mask in place and actuate the pMDI as they begin to breathe in slowly. Also make sure to
inhale slowly if the device produces a “whistle” indicating that inspiration is too rapid.
f. Hold the mask in place while the child takes six normal breaths (including inhalation and exhalation),
then remove the mask from the child’s face.
8. Wait 15–30 seconds if another puff of medicine is needed.
9. Repeat steps above until the dosage prescribed by the patient’s physician is reached.
10. If taking a corticosteroid, rinse the mouth after the last puff of medicine, spit out the water, and do not
swallow it.
11. Replace the mouthpiece cover on the pMDI after each use.
General Steps To Avoid Reduced or No Dosing for pMDIs with Spacer/VHC: The patient should:
1. Assure proper t of the pMDI to the spacer or VHC.
2. Remove cap from the pMDI boot.
3. Clean and reassemble the pMDI spacers and VHCs based on the manufacturers’ instructions.

32
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Dry-Powder Inhalers
Dry-powder inhalers (DPIs) are portable, inspiratory-
ow-driven inhalers that administer dry-powder formula-
tions to the lungs. DPIs do not contain propellant and are
breath-actuated. The patient’s inspiratory effort, both their
inspiratory ow rate and the volume inhaled, creates the
energy to disaggregate the small drug particles from larger
carrier particles and disperse the particles as aerosol emit-
ted from the device. DPIs coordinate release of the drug
with the act of inhalation. They have been developed to
overcome the difculties of using metered-dose inhalers
and are often prescribed with the intention of providing
the patient with an overall more user-friendly and predict-
able therapy.
Advantages and Disadvantages of DPIs
Dry-powder inhalers have both advantages and disad-
vantages as seen in Table 14. Because they do not require
hand-held coordination, the patient’s inspiratory ow
should be adequate enough to draw the drug from the
device. It is important that the patient understands how
the DPI works and how it should be used. For example,
the patient should know that they should not exhale into
the device. This will prevent the introduction of ambient
humidity into the mouthpiece and the resulting negative
effect to the medication. Such precautions and others,
explored in greater detail below, should be considered by
clinicians when prescribing a DPI for individual patients and
when performing follow-up evaluations of patient success
with a DPI.
Types of DPIs
Currently, DPIs can be classied into three categories
based on the design of their dose containers, i.e., sin-
gle-dose DPIs, multiple unit-dose DPIs, and multiple-dose
DPIs (Figure 20). While the single-dose DPIs have individually
wrapped capsules that contain a single-dose of medication,
multiple unit-dose DPIs disperse individual doses that are
premetered into blisters of medication by the manufacturer.
The third type, the multiple-dose DPI, either measures the
dose from a powder reservoir or uses blister strips prepared
by the manufacturers to deliver repeated doses. Regardless
of the type of DPI, they all have the same essential compo-
nents incorporated within the inhaler. They all have a drug
holder, an air inlet, an agglomeration compartment, and a
mouthpiece. The design of these components allows DPIs to
induce sufcient turbulence and particle-to-particle collision
Table 14. Advantages and disadvantages of DPIs (Modied, with permission, from Reference 1)
Advantages
Small and portable
Built-in dose counter
Propellant free
Breath-actuated
Short preparation and administration time
Disadvantages
Dependence on patient’s inspiratory ow
Patient less aware of delivered dose
Relatively high oropharyngeal impaction
Vulnerable to ambient humidity or exhaled
humidity into mouthpiece
Limited range of drugs
Different DPIs with different drugs
Easy for patient to confuse directions for use with
other devices

33
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Figure 20. Currently available dry-powder aerosol formulations in the United States
categorized by design features (see text description of design features)
that detaches particles from
their carrier surface and deag-
glomerates larger particles into
smaller particles.
Single-Dose DPIs
Single-dose DPIs operate
by evacuating powder med-
ication from a punctured
capsule. The HandiHaler®
(Boehringer Ingleheim), The
TOBI Podhaler® (Novartis),
and the Neohaler (Sunovion)
are examples of single-dose
DPIs (Figure 20). While the
HandiHaler® is used for the
delivery of tiotropium bro-
mide, the TOBI Podhaler is uti-
lized for the administration of
tobramycin. The Neohaler® is
used for the delivery of glyco-
pyrrolate as well as Utibron®,
the combination of indacaterol
and glycopyrrolate. Although
the HandiHaler®, Podhaler,
and Neohaler® have different congurations, their principle
of operation is similar. When using a single-dose DPI, the
user places each capsule into the drug holder. Then, the
user must prime the device by piercing the single-dose
capsule and allowing entrainment of air into the device
for dispersion with inhalation. The primary disadvantage of
single-dose DPIs is the time needed to load a dose for each
use. Also, patients should be instructed not to swallow the
capsules.
Multiple Unit-Dose DPIs
The Diskhaler® (GlaxoSmithKline) is an example of the
multiple unit-dose DPI. It is used for the administration of
zanamivir through a rotating wheel that contains a case
with four or eight blisters of medication. Each blister is
mechanically punctured when the cover is lifted, allowing
the medication to be inhaled though the mouth. When
using the Diskhaler®, the inspiratory ow rate should be
greater than 60 L/min to achieve an adequate drug deposi-
tion into the lungs.
Multiple-Dose DPIs
Multiple-dose DPIs measure doses from a powder res-
ervoir or disperse individual doses through pre-metered
blister strips. The most common types of multi-dose DPIs
include the RespiClick®, the Flexhaler® and the Pressair®
(AstraZeneca, Wilmington, DE), and the Diskus® and Ellipta®
(GlaxoSmithKline). The Twisthaler® is a multi-dose DPI used
to deliver mometasone furoate. The Flexhaler® delivers
budesonide, and the Diskus® administers salmeterol, utica-
sone, or a combination of salmeterol and uticasone.
In the Twisthaler® and the Flexhaler®, the DPI nozzle
is comprised of two parts: a lower swirl chamber and an
upper chimney in the mouthpiece. Their uted chimney
designs produce a stronger vortex with an increased num-
ber of particle collisions with the chimney for deagglomer-
ation. When using a new Flexhaler®, it should be primed by
holding it upright and then twisting and clicking the brown
grip at the bottom twice. The Twisthaler® does not require
priming before use.
The Diskus® is a multi-dose DPI that contains 60 doses of
dry-powder medication individually wrapped in blisters. The
wrapping in blisters protects the drug from humidity and
other environmental factors. Sliding the dose-release lever
punctures the wrapped blister on a foil strip and prepares
the dose for inhalation. When the Diskus® cover is closed,
the dose release lever is automatically returned to its start-
ing position. As with the Twisthaler®, no priming is neces-
sary with the Diskus®.
34
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
The Ellipta® is similar to the Diskus® and is used in the
delivery of various long-acting beta agonists and combina-
tion medications such as Brea® and Anoro® as well as other
drugs such as Incruse®, an ultra-long-acting anticholinergic,
and Arnuity®, a corticosteroid. Similar to the Diskus®, this
multi-dose DPI utilizes two coiled blister strips containing
individually wrapped doses of dry-powder medication.
Opening the mouthpiece cover peels the foil to expose
the medication dosage. After inhaling the medication, the
mouthpiece cover is returned to its closed position. It is
important to note that, if the mouthpiece cover is opened
and the dose is prepared, closing the mouthpiece cover
without inhalation of the medication will result in a lost
dose.
The Pressair® is multi-dose dry power inhaler that admin-
isters aclidinium bromide in 30 or 60 doses. The device
utilizes a button that once depressed loads the medication.
This can be conrmed visually by checking the control
window that changes from red to green once a new dose
is ready. Once the patient inhales a click can be heard,
noting the dose was inhaled. The individual may conrm by
looking at the control window that changes from green to
red to indicate a dose has been taken. Patients will need to
have a minimum peak inspiratory ow of 35 L/min to effec-
tively use this device.
Currently Available DPI Formulations
As seen in Figure 20, the device design largely deter-
mines whether a DPI model is single dose (loading a single
dose prior to each use), multiple unit-dose (loading four or
eight blisters of medication), or multiple-dose (containing
an entire month’s prescription).
Factors Affecting DPI Performance and
Drug Delivery
Respiratory therapists and patients must actively control
the following effects:
• Intrinsic Resistance and Inspiratory Flow: Each type
of DPI has a different intrinsic resistance to airow that
determines how much inspiratory ow needs to be
created in the device to release the correct amount of
drug. For example, the HandiHaler® has a higher resis-
tance than the Diskus® and therefore requires a greater
inspiratory effort. When the patient inhales through
the DPI, she/he creates an airow with a pressure drop
between the intake and exit of the mouthpiece. Thus,
the patient can lift the powder from the drug reser-
voir, blister, or capsule depending on the model being
used. The patient’s inspiratory effort is also important
in its deaggregating of the powder into ner particles.
Whereas higher inspiratory ows improve drug deag-
gregation, ne-particle production, and lung delivery,
excessive inspiratory ow can increase impaction on
the oral cavity and thus decrease total lung deposition.
• The Patient’s Inspiratory Flow Ability: DPIs depend
on the patient’s ability to create adequate inspiratory
ows. Very young children and patients with acute
airow obstruction due to asthma or COPD may not be
able to generate an adequate inspiratory ow when
using the DPI. Because very low inspiratory ows result
in reduced drug delivery, especially ne-particle deliv-
ery, potential DPI patients should be evaluated for the
ability to generate a minimal inspiratory ow.
• Exposure to Humidity and Moisture: Because all DPIs are
affected by humidity and moisture, which can cause pow-
der clumping and reduce deaggregation and ne-particle
development during inhalation, they must be kept dry.
Capsules and drug blisters generally offer more protection
from ambient humidity than a reservoir chamber contain-
ing multiple doses for dispensing. Therefore, designs with
a reservoir chamber such as the Twisthaler® and Pressair ®
should be protected from humidity and moisture as much
as possible. Whereas it is easy to keep the Twisthaler® and
Pressair ® out of the bathroom, avoiding use in ambient
humidity is difcult if it is carried to the beach, kept in a
house with no air conditioning, or left in a car. An alter-
native DPI design or availability of the drug in a different
aerosol system, such as a pMDI, might be considered for
such situations. All DPIs are also affected by exhaled air
introduced into the mouthpiece, especially after the device
is cocked and loaded and when the powder is exposed.
Therefore, patients must be instructed to exhale away
from the DPI prior to inhalation.
Drug-Delivery Technique
Because different types of DPIs are available on the mar-
ket, respiratory therapists should carefully review operation
instructions prior to giving aerosol therapy and certainly
prior to instructing patients in at-home use. Proper tech-
nique is provided in Technique Box 4.
35
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Technique Box 4. Steps for Correct Use of Each Model of DPIs
Technique for Single-Dose DPIs
HandiHaler®: The patient should be instructed to:
1. Peel back the aluminum foil and remove a capsule immediately before using the HandiHaler®.
2. Open the dust cap by pulling it upward.
3. Open the mouthpiece.
4. Place the capsule in the center chamber; it does not matter which end is placed in the chamber.
5. Close the mouthpiece rmly until they hear a click; leave the dust cap open.
6. Hold the HandiHaler® with the mouthpiece up.
7. Press the piercing button once and release; this makes holes in the capsule and allows the medication to
be released during inhalation.
8. Exhale away from the HandiHaler®.
9. Place the mouthpiece into the mouth and close lips tightly around the mouthpiece.
10. Keep head in an upright position.
11. Breathe in at a rate sufcient to hear the capsule vibrate, until the lungs are full.
12. Remove the mouthpiece from the mouth and hold breath for 10 seconds or as long as comfortable.
13. Exhale away from the HandiHaler®.
14. Repeat the inhalation from the HandiHaler®.
15. Open the mouthpiece, remove the used capsule, and dispose of it. Do not store capsules in the
HandiHaler®.
16. Close the mouthpiece and dust cap for storage of the HandiHaler®.
17. Store the device in a cool, dry place.
Neohaler®: The patient should be instructed to:
1. Remove the mouthpiece cover.
2. Hold the base of the inhaler and tilt the mouthpiece to open the Neohaler®.
3. Remove the capsule from the blister pack immediately before use.
4. Place the capsule into the chamber in the base of the Neohaler®.
5. Close the inhaler; a click will sound to indicate the inhaler is closed.
6. Simultaneously press both buttons on the side of the Neohaler® to pierce the capsule and then release.
7. Keep the head in a neutral, upright position.
8. Do not exhale into the device.
9. Hold the device horizontal, with the buttons on the left and right.
10. Place the mouthpiece into the mouth and close lips tightly around the mouthpiece.
11. Breathe in a full breath rapidly and deeply; the capsule should be heard vibrating in the device.
12. Remove the mouthpiece from the mouth and perform a 10-second breath hold (or as long as comfort-
able).
13. Do not exhale into the device.
14. Open the chamber and examine the capsule; if there is powder remaining, repeat the inhalation process.
15. After use, remove and discard the capsule. Do not store the capsule in the Neohaler®.
16. Close the mouthpiece and replace the cover.
17. Store in a cool, dry place.
Podhaler: The patient should be instructed to:
1. Hold base of Podhaler and unscrew lid in a counter-clockwise direction, setting aside lid once complete.
2. Stand Podhaler upright in the base of the case.
3. Hold body of Podhaler and unscrew mouthpiece in a counter-clockwise direction, setting aside mouth-
piece on a clean, dry surface.
4. Take blister card and tear the pre-cut lines along the length and width.
5. Peel foil that covers one Podhaler capsule on blister card.
6. Remove capsule one at a time and place in capsule chamber at the top of Podhaler.
7. Place mouthpiece back on Podhaler and screw mouthpiece in a clockwise direction until tight.
8. Hold Podhaler pointing mouthpiece down.
9. Placing the thumb on the blue button, pressing the blue button all the way down once.
10. Exhale as completely as possible away from the inhaler.
11. Place the mouthpiece into the mouth and close lips tightly around mouthpiece.
12. Breathe in a full breath deeply and slowly and perform a 10-second breath hold (or as long as
comfortable).
13. Exhale away from the device.
14. To ensure the entire dose has been inhaled, repeat steps 10 through 12.
15. Unscrew the mouthpiece and remove capsule from chamber and throw away.
16. Repeat steps 4 to 15 three more times until all four doses (4 capsules) have been used.
36
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Technique Box 4. Steps for Correct Use of Each Model of DPIs (continued)
Technique for the Multiple Unit-Dose DPI
Diskhaler®: The patient should be instructed to:
1. Remove the cover and check that the device and mouthpiece are clean.
2. Extend tray and push ridges to remove tray.
3. Load medication disk on the rotating wheel.
4. Pull the cartridge all the way out and then push it all the way in until the medication disk is seen in the
dose indicator. This will be the rst dose that will be given.
5. Keep the device at and lift the back of the lid until it is lifted all the way up to pierce the medication
blister.
6. Click back into place.
7. Move the Diskhaler® away from the mouth and breathe out as much as possible.
8. Place the mouthpiece between the teeth and lips and make sure the air hole on the mouthpiece is not
covered.
9. Inhale as quickly and deeply as possible.
10. Move the Diskhaler® away from the mouth and perform a 10-second breath hold or as long as
comfortable.
11. Breathe out slowly.
12. If another dose is needed, pull the cartridge out all the way and then push it back in all the way in order
to move the next blister into place. Then repeat Steps 4 through 12.
13. Place the mouthpiece cover back on after the treatment. Make sure the blisters remain sealed until
inspiration in order to protect them from humidity and loss.
Technique for Multiple-Dose DPIs
Diskus®: The patient should be instructed to:
1. Open the device.
2. Slide the lever from left to right.
3. Breathe out normally; do not exhale into the device.
4. Place the mouthpiece into the mouth and close lips tightly around the mouthpiece.
5. Keep device horizontal while inhaling dose with a rapid and steady ow.
6. Remove the mouthpiece from the mouth and perform a 10-second breath hold or as long as comfort-
able.
7. Be sure not to exhale into the device.
8. Store the device in a cool dry place.
9. Observe the counter for the number of doses remaining and replace when appropriate.
Twisthaler®: The patient should be instructed to:
1. Hold the inhaler straight up with the pink portion (the base) on the bottom.
2. Remove the cap while it is in the upright position to ensure the right dose is dispensed.
3. Hold the pink base and twist the cap in a counter-clockwise direction to remove it.
4. As the cap is lifted off, the dose counter on the base will count down by one. This action loads the dose.
5. Make sure the indented arrow located on the white portion (directly above the pink base) is pointing to
the dose counter.
6. Breathe out normally; do not exhale into the device.
7. Place the mouthpiece into the mouth and close the lips tightly around the mouthpiece.
8. Inhale the dose with a rapid and steady ow while holding the Twisthaler® horizontal.
9. Remove the mouthpiece from the mouth and perform a ve to 10-second breath hold or as long as
comfortable.
10. Do not exhale into the device.
11. Immediately replace the cap, turn in a clockwise direction, and gently press down until a click is heard.
12. Firmly close the Twisthaler® to assure that the next dose is properly loaded.
13. Be sure that the arrow is in line with the dose-counter window.
14. Store device in cool, dry place.
37
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Technique Box 4. Steps for Correct Use of Each Model of DPIs (continued)
Technique for Multiple-Dose DPIs (continued)
Flexhaler®: The patient should be instructed to:
1. Twist the cover and lift it off.
2. Hold the Flexhaler® in the upright position (mouthpiece up) while loading a dose.
3. Do not hold the mouthpiece when the inhaler is loaded.
4. Twist the brown grip fully in one direction as far as it goes. It does not matter which way is turned
rst.
5. Twist it full back in the other direction as far as it goes.
6. Make sure to hear a click during each of the twisting movements.
7. Do not exhale into the device.
8. Place the mouthpiece into the mouth, close the lips tightly around the mouthpiece, and inhale deeply
and forcefully through the inhaler.
9. Remove the inhaler from the mouth and exhale.
10. Do not exhale into the device.
11. If more than one dose is required, repeat the steps above.
12. Put the cover back on the inhaler and twist it shut.
13. Rinse the mouth with water after each dose to reduce the risk of developing thrush. Do not swallow
the rinse water.
Tudorza Pressair: The patient should be instructed to:
1. Wash and dry hands thoroughly.
2. Remove the protective cap by gently squeezing the marked arrows on each side of the cap and pulling
outward.
3. Hold the inhaler with the mouthpiece facing toward the patient and the green button on top. DO NOT
place in the mouth yet.
4. Press the green button all the way down and release it. DO NOT hold the button down.
5. Check the control window on the device (above the mouthpiece) to ensure the color has changed
from red to green, indicating the dose and device are ready for use.
6. Exhale away from the device before placing the mouthpiece into the mouth.
7. Place the mouthpiece into the mouth and breathe in quickly and deeply.
8. A click is heard when the dose is delivered, but continue the deep breath until at full capacity.
9. Remove the device from the mouth and breathe out.
10. Check the control window on the device (above the mouthpiece) to ensure the color has changed
from green to red. IF NOT, repeat Step 7.
11. Replace the protective cap on the mouthpiece.
RespiClick®: The patient should be instructed to:
1. Hold the inhaler upright with the red mouthpiece cover facing the patient.
2. Remove the red mouthpiece cover in the upright position until a click is heard. This exposes the
mouthpiece as well as loads the medication. The dose counter on the back of the device will count
down one number each time the medication is delivered.
3. Exhale away from the device.
4. Place the mouthpiece into the mouth and close lips tightly around the mouthpiece.
5. Do not block the air vent above the mouthpiece.
6. Inhale deeply through the RespiClick®.
7. Remove the mouthpiece from the mouth and perform a 10-second breath hold or as long as comfort-
able.
8. Check the dose counter on the back of the device to make sure the dose was delivered.
9. Firmly close the cap over the mouthpiece.
10. Store the device in a cool dry place.
11. Observe the counter for the number of doses remaining and replace when appropriate.
38
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
How To Know the DPI Is Empty
Single-Dose DPI: Single-dose DPIs such as the HandiHaler®
use a single capsule for each dose, and only full capsules
should be used when each dose is given. The capsule
should be inspected to assure that the patient took the full
dose. If there is powder remaining, the capsule should be
returned to the inhaler and inhalation should be repeat-
ed.68 Then, the capsule should be disposed of after treat-
ment. Prescription renewal should be based on the remain-
ing capsules.
Multiple Unit-Dose DPI: The Diskhaler® is a multiple unit-
dose DPI with a rell disk that contains 4- or 8-unit-dose
blisters.69 Because there is not a dose counter on the DPI,
doses must be tracked manually. Therefore, visual inspec-
tion will conrm use of all packets. The disk is disposed of
when all the doses have been used.
Technique Box 4. Steps for Correct Use of Each Model of DPIs (continued)
Technique for Multiple-Dose DPIs (continued)
Ellipta®: The patient should be instructed to:
1. Open the device by sliding the mouthpiece cover down until a click is heard. This exposes the mouth-
piece as well as loads the medication. The center dose counter will count down one number each
time the mouthpiece cover is opened.
2. Hold the Ellipta® in an upright position.
3. Exhale away from the Ellipta®.
4. Place the mouthpiece into the mouth and close lips tightly around the mouthpiece. Do not block the
air vent on the device,
5. Keep the device horizontal while inhaling the dose with a rapid and steady breath.
6. Remove the mouthpiece from the mouth and perform a 10-second breath hold or as long as comfort-
able.
7. Do not exhale into the device.
8. Close the mouthpiece cover.
9. Store the device in a cool dry place.
10. Observe the counter for the number of doses remaining and replace when appropriate.
General Steps To Avoid Reduced or No Dosing for DPIs: The patient should:
1. Read and follow the instructions for proper assembly.
2. Make sure to keep the DPI clean and dry.
3. Keep the DPI in proper orientation during the treatment.
4. Be sure to puncture the capsule or blister pack.
5. Do not exhale into the DPI.
6. Make sure to generate adequate inspiratory ow.
7. Track the doses remaining in the DPI.
Troubleshooting
Problem with DPIs: Malfunctioning DPIs
Causes Solutions
Incorrect DPI assembly Check the assembly and reassemble, when needed.
Failure to discharge medicine Replace the unit.
Empty DPI Check the dose counter to ensure that it is not empty.
Otherwise, replace the DPI.

39
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Multiple-Dose DPIs: Multiple-dose DPIs historically come with
integrated mechanical devices that indicate the number of
doses remaining in the inhaler.68 The devices give a particular
display when the doses are coming to an end so that a new
DPI can be ordered from the pharmacist. The dose counter of
each type of multiple-dose DPI is explained in Table 15.
Cleaning: Please refer to the Infection Control section on
page 44 for the cleaning instructions for DPIs.
Table 15. Monitoring remaining doses of multiple-dose DPI
Dose No. of Type of Meaning of
Container Doses Indicator Dose Indicator
Flexhaler® Reservoir 60 or 120 “0” Although the indicator counts down every time a dose is
loaded, it will not move with each individual dose but
intervals of ve or so doses.
The indicator is marked in intervals of 10 doses, alternating
numbers and dashes. When it is down to “0,” it must
be thrown away.
Twisthaler® Reservoir 30 “01” The dose display showing “01”indicates the last dose of
medicine in the Twisthaler®, and the medicine must be
relled.
Diskus® Blister Strip 60 Red The numbers turning red in the dose display indicates that
numbers there are ve doses left.
When the dose window shows “0,” there is no medicine
left, and the discus should be disposed.
RespiClick® Reservoir 60 or 200 “0” When the dose counter displays “0,” there is no
medicine left and the device should be disposed.
Ellipta® Blister strip 30 “0” When the dose counter displays “0”, this is the
last dose. Discard the device after inhalation.
Pressair® Reservoir 30 or 60 “0” When dose counter displays “0,” there is no
medicine left and the device should be disposed.
40
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Criteria To Select
an Aerosol Generator
The selection of the delivery device is very important for
optimizing the results of aerosol drug therapy. Evidence
indicates that all three types of aerosol generators can be
equally effective if they are used correctly by the patient.8
The criteria to select an aerosol generator can be divid-
ed into four categories: patient-related, drug-related,
device-related, and environmental and clinical factors.
Patient-Related Factors
Age, Physical, and Cognitive Ability of Patients
An aerosol generator should be selected in accord with
the patient’s age, physical, and cognitive ability. Age
changes anatomic and physiologic factors such as airway
size, respiratory rate, and lung volume.13,69-76 The patient’s
cognitive ability to understand how and when to use a
device and drug as well as his/her physical ability and
coordination in using an aerosol generator should guide
the selection of an aerosol generator.8,13,18,69,75,77-79 Aerosol
devices have different requirements for proper use. For
guidance about the device selection in infants and pediat-
rics, see “Neonatal and Pediatric Aerosol Drug Delivery” on
pages 42-43.
As for adults and the elderly who cannot manage hand-
held coordination or proper inhalation technique,77,80-82
pMDIs may not be a good option. Also, the inability to gen-
erate sufcient inspiratory ow (>40–60 L/min) eliminates
the use of aerosol generators such as DPIs.77,83
Preference of Patients
Patient preference is a critical factor in the selection of
an aerosol generator and the effectiveness of aerosol ther-
apy. Patients tend to use devices they prefer more regularly
than devices they dislike.84-87 Therefore, the selection of
an aerosol generator should be tailored according to the
patient’s needs and preferences.
Drug-Related Factors
Availability of Drug
Some drug formulations are available with only one type
of aerosol generator. If a drug can be administered with
the three types of aerosol generators, the clinician should
select an aerosol generator based on the patient’s needs
and preference.8,18,79,87 Otherwise, a drug formulation that
can be used with only a single aerosol generator dictates
which aerosol generator to choose.
Combination of Aerosol Treatments
Many patients are prescribed more than one inhaled
drug. In that case, using the same type of aerosol genera-
tor may increase the patient’s adherence to therapy while
minimizing the patient’s confusion caused by the use of
different aerosol devices.8,18,87-88
Device-Related Factors
Convenience of Aerosol Generator
Selecting the most convenient aerosol generator for the
patient is very important to adherence. Ease of use, treat-
ment time, portability, cleaning, and maintenance required
for each device should guide the selection process. For
example, a rescue medication needs to be small, light, and
portable so the patient can easily have it available when
needed.69,79 Also, nebulizers may be less preferable to deliv-
er inhaled medications as they are more expensive, require
a power source, and need regular maintenance.69,87,89-90
When all other factors are equal, the most convenient
device should be chosen for patients.
Durability of Aerosol Generator
A selected aerosol generator should have good durability
so that it can withstand rigorous treatment and cleaning
procedures every day. Devices that require extensive clean-
ing are not a good choice for patients unwilling to routine-
ly clean and maintain the device.
41
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Cost and Reimbursement of Aerosol Generator
It is very important to select an aerosol generator that is
the least out-of-pocket expense for the patient. Patients do
not use drugs and devices they cannot afford.91-93 As shown
in Table 3, Table 6, and Table 7, costs of aerosol generators
and drug formulations vary widely. The cost to the patient
will depend on the presence and type of medical insurance
they have.79 If the “best” device/drug is not one that the
patient can afford, the least costly aerosol generator and
drug combination should be identied in order to meet
the patient’s needs. Therefore, it is important to work with
the patient to identify strategies to access affordable drug/
device options in order to meet their clinical needs. If all
the other factors are constant, the least costly aerosol gen-
erator and drug combination should be selected.
Environmental and Clinical Factors
When and where the aerosol therapy is required can
impact device selection. For example, therapy that is given
routinely, once or twice a day, before or after bedtime does
not need to be as portable as rescue medications that may
be required at anytime. Also, noisy compressors may not be
good in small homes where a late-night treatment might
awaken other members of the family. In environments
where patients are in close proximity to other people, sec-
ondhand exposure to aerosols may be a factor, and devices
that limit or lter exhaled aerosol should be selected.
42
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Neonatal and Pediatric
Aerosol Drug Delivery
Infants are not simply anatomically scaled-down adults.
Therefore, aerosol drug administration differs fundamen-
tally in infants and children. Cognitive ability (i.e., under-
standing how and when to use a device and drug) and
physical ability (i.e., coordination to use that device) as
well as age-related anatomic and physiologic factors (i.e.,
airway size, respiratory rate, lung volumes) create substan-
tial challenges for effective aerosol delivery at each stage
of development.70-73,94-95 When respiratory therapists gain a
clear understanding of these challenges, they can optimize
aerosol drug delivery and its therapeutic outcomes in less
developed patients. This section explores the challenges
and solutions that may optimize aerosol drug delivery in
infants and pediatrics.
Age and Physical Ability
Selection of an aerosol device is critical to successful
aerosol therapy in infants and children.70,78,95 Children
under the age of three may not reliably use a mouthpiece,
making delivery via mask necessary for both nebulizers and
pMDIs.95-99 Especially at low tidal volumes, VHCs are the
preferred method for pMDI delivery in infants and small
children.97-98 Breathing patterns, inspiratory ow rates,
and tidal volumes change with age. Even healthy children
below four years of age cannot reliably generate sustained
inspiratory ow rates of 60–90 L/min required for optimal
use of many DPIs. Thus, the use of breath-actuated nebu-
lizers or DPIs may not be reliable in children younger than
four years.73,100
Age and Cognitive Ability
The choice of aerosol device should be tailored to the
patient’s age and to cognitive ability to use the device
correctly. Table 16 presents the recommended ages for
introducing different types of aerosol generators to chil-
dren.69-71,100-103 Small-volume nebulizers and pMDIs with
VHCs are recommended for use with infants and children up
to ve years of age.70-71,100 Since children up to three years
of age typically cannot use a mouthpiece, both nebulizers
and pMDIs with holding chambers should be administered
via masks.70,97-98 Independent of age, a face mask should
be used until the child can comfortably use a mouthpiece.
A child below ve years of age may not be able to master
specic breathing techniques.70-71,100 With low tidal volumes
and short inspiratory times, breath-actuated nebulizers
may increase inhaled dose compared to continuous neb-
ulization.104 However, it may take three-fold more time to
administer that dose. Also, time constraints and portability
of compressor nebulizers make them less desirable for pre-
school children.70 It is generally accepted that the cognitive
ability to control breathing and hand/breath coordination
develops by age ve or six.69,70,101 Once children reach age
four and above, they may have a sufcient understanding of
how to use a pMDI or DPI successfully.73,100
Table 16. Age guidelines for use of aerosol delivery device types
Aerosol Generator Age
SVN with mask or hood Infant94
SVN with mask ≤ 3 years
SVN with mouthpiece ≥ 3 years
pMDI with valved holding chamber/spacer and mask < 4 years
pMDI with valved holding chamber/spacer ≥ 4 years
Dry-powder inhaler ≥ 4 years
Metered-dose inhaler ≥ 5 years
Breath-actuated MDI (e.g., Autohaler®) ≥ 5 years
Breath-actuated nebulizer ≥ 5 years

43
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Aerosol Drug Delivery in Distressed or
Crying Infants
Inhaled drugs should be given to infants when they are
settled and breathing quietly. Crying children receive vir-
tually no aerosol drug to the lungs,94,96,102,105-106 with most
of the inhaled dose depositing in the upper airways or
pharynx, which is then swallowed.71-72,94,106-107 Therefore, it
is essential to develop approaches that minimize distress
before administering aerosol drugs. These approaches
include, but are not limited to, playing games, comforting
babies, and providing other effective forms of distraction.
Also, aerosol drugs can be administered while the infant is
asleep as long as administration does not wake up or agi-
tate the infant. Although sleep breathing patterns indicated
a higher lung dose in an infant-model study,108 an in-vivo
study showed that 69% of the children woke up during
aerosol administration and 75% of them were distressed.109
Patient-Device Interface
Even infants and small children can make known their
preferences for specic devices. This should be a consider-
ation in device selection. Using a device that is preferred by
the child and parent can increase adherence, inhaled dose,
and desired clinical response.
Mouthpiece or Face Mask?
Mouthpieces and face masks are commonly used for
aerosol drug delivery in children above three years of age.
Studies suggest that the mouthpiece provides greater
lung dose than a standard pediatric aerosol mask104,110 and
is effective in the clinical treatment of children.104,111-112
Consequently, the use of mouthpieces should be encour-
aged, but a mask that is consistently used is better than a
mouthpiece that is not.
Importance of a Closely Fitting Face Mask
A good face mask seal is a critical factor in achieving
optimal drug deposition and avoiding getting aerosol into
eyes. Even small leaks of 0.5 cm around the face mask
decrease drug inhaled by children and infants by more
than 50%.113-117 Initially, a small child may refuse to use a
face mask when feeling sick or irritable. However, parental
education, play activities, encouragement to hold the mask
rmly against the child’s face, and close supervision can
reduce poor tolerance of face masks and improve aerosol
drug delivery.
Face Mask or Blow-by?
Blow-by is the administration of aerosolized drug
through the nebulization port of a nebulizer that is direct-
ed toward the patient’s face. Although blow-by is a tech-
nique commonly used for crying babies or uncooperative
children, it has been documented that it is less efcient
compared with a face mask as aerosol drug deposition
decreases signicantly as the distance from the device
to the child’s face is increased. Therefore, evidence sug-
gests blow-by to be ineffective and use should be discour-
aged.97,113,118-119
Parent and Patient Education
As children grow and their aerosol device needs to be
changed, they and their care providers should be taught
the best techniques for the use and maintenance of aerosol
devices. Also, children may demonstrate poor adherence to
aerosol drug delivery because they lack the ability to use
a device correctly or contrive to use it ineffectively.120-121
Therefore, respiratory therapists should explain the effects
of medications prescribed, the importance of aerosol
therapy, and the proper use of aerosol generators to the
patient and the parent. After initial training is provided,
frequent follow-up demonstration is essential to optimize
aerosol drug delivery and adherence to prescribed therapy
in infants and children.
44
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Infection Control
Aerosol generators can become contaminated with
pathogens from the patient, the care provider, and the
environment. The contamination of nebulizers has been
documented in patients with cystic brosis (CF),20-22 asth-
ma,23-24 and immunodeciency.122 A survey of respiratory
therapists and cystic brosis patients found a wide dispar-
ity of nebulizer cleaning methods.123 In another survey, it
was shown that only 60% of cystic brosis caregivers were
aware of infection control guidelines.124 In the absence of
infection control (IC), an aerosol generator will be contam-
inated and may cause bacterial colonization in the respira-
tory tract.20-22,25,125 Therefore, it is essential to establish an
IC management system that will reduce nosocomial infec-
tions, length of stay in the hospital, and costs associated
with hospitalization.24,125-126
IC Management System in Aerosol Drug
Delivery
Patient Education and Awareness
Patient Education: It has been documented that aerosol
generators used at home are frequently contaminated with
bacteria.23-24,127-128 Therefore, the importance of cleaning
and maintaining aerosol equipment should be emphasized
in IC education programs129 with patients and caregivers
through repeated oral and written instructions.
Patient Adherence: Approximately 85% of patients with
CF fail to disinfect their nebulizers at home.130 It has been
determined that, in addition to the constraints of cleaning
and disinfecting instructions provided by the manufactur-
ers, adherence can be inuenced by personal, socio-cul-
tural, and psychological factors.131 Furthermore, a major-
ity of cystic brosis health care workers reported a low
self-efcacy with using infection control guidelines, which
can be linked to poor adherence.124 Changing aerosol gen-
erators every 24 hours, using disposable equipment with
health insurance approval, and partnering with patients to
increase adherence85 can increase patient compliance to IC
and minimize the risk of infection.
Cleaning and Maintenance of Aerosol Generators
Cleaning: The cleaning instructions for the different types
of aerosol generators are given below.
• Pressurized Metered-Dose Inhalers: The plastic container
of pMDIs should be cleaned at least once a week132-133
as shown in Table 17.
• Metered-Dose Inhalers Accessory Devices: When a spac-
er is used with a pMDI, it should be cleaned before rst
use and then periodically cleaned based on the manu-
facturer’s suggestions. Table 18 provides the steps for
cleaning the pMDI accessory devices.
• Dry-Powder Inhaler: It is important to note that DPIs
should not be submerged in water. Also, they should
be kept dry as moisture will decrease drug delivery.
Although there is no clear evidence about the DPI
cleaning practice, each manufacturing company has
Table 17. Cleaning instructions for the pMDI
Cleaning the pMDI
Clean once a week and as needed. Look at the hole where the drug sprays out from the inhaler.
Clean the inhaler if you see powder in or around the hole.
Remove the pMDI canister from the plastic container so it does not get wet.
Rinse the plastic container with warm water and shake out to remove excess water.
Dry overnight.
Replace the canister back inside the mouthpiece and recap the mouthpiece.

45
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
recommendations for periodic cleaning and suggests
wiping the mouthpiece of the DPI with a clean dry
cloth.
• Nebulizers: In the home, nebulizers should be cleaned
after every treatment. A study showed that 73% of
nebulizers were contaminated with microorganisms
and 30% had potentially pathogenic bacteria.134
Moreover, there was a signicant increased risk of
COPD exacerbation in COPD patients that had nebuliz-
ers with pathogens versus those with non-pathogenic
bacteria. However, nebulizer contamination can be
signicantly improved with proper instruction on infec-
tion control.135 The longer a dirty nebulizer sits and is
allowed to dry, the harder it is to thoroughly clean.
Rinsing and washing the nebulizer immediately after
each treatment can go a long way in reducing infec-
tion risk. According to the Cystic Fibrosis Foundation
guidelines,136 parts of aerosol generators should be
washed with soap and hot water after each treatment,
with care taken not to damage any parts of the aerosol
generator. Table 19 provides the cleaning instructions
for the jet nebulizer. Mesh and ultrasonic nebulizers
should be cleaned and disinfected based on the man-
ufacturer’s recommendations. Also, it is important to
remember not to touch the mesh during the cleaning
of mesh nebulizers because this will damage the unit.
Disinfection: Periodic disinfection and nebulizer replace-
ment is highly recommended to minimize contamination.
Each manufacturer suggests a different method of disinfec-
tion for its product. Therefore, the manufacturer’s specic
instructions on disinfecting aerosol generators should be
followed. It is also important to note that all solutions
should be discarded after disinfection. The varied methods
for disinfection include having the patient:
Heat methods:
1. Boil or microwave137 the nebulizer parts for ve minutes.
This disinfection process does not require a nal rinse.
2. Wash in a dishwasher if the dishwasher achieves a tem-
perature of > 158°F or 70°C for 30 min.137
Cold Methods:
1. Soak them in solution of one-part household bleach and
50-parts water for three minutes.
2. Soak the parts in 70% isopropyl alcohol for ve minutes.
3. Soak them in 3% hydrogen peroxide for 30 minutes.
4. Soak them in one-part distilled white vinegar in three-
parts hot water for one hour (not recommended for CF
patients).
The patient should disinfect the nebulizer once or twice
a week by using one of the methods for disinfection listed
above. Evidence suggests that a quaternary ammonium
compound can also be used for disinfecting jet nebulizers
as it has comparable effectiveness with the combined dis-
infection procedure of a detergent pre-wash and 1.25%
acetic acid soak. Also, a quaternary ammonium compound
Table 18. Cleaning instructions for the pMDI chamber
Cleaning the Chamber Device
Clean every two weeks and as needed.
Disassemble the device for cleaning.
Soak the spacer parts in warm water with liquid detergent and gently shake both pieces back and forth.
Shake out to remove excess water.
Air dry spacer parts in the vertical position overnight.
Do not towel dry the spacer as this will reduce dose delivery because of static charge.
Replace the back piece on the spacer when it is completely dry.

46
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
soak need only be 10 minutes, while the acetic acid soak
should not be less than one hour. Another advantage of
using the quaternary solution is that it can be reused for up
to one week, as opposed to the acetic acid solution that
cannot be reused.138
Final Rinse: The patient should use sterile water (not dis-
tilled or bottled) for the nal rinse.136 Sterile water can be
made by boiling tap water for ve minutes.
Drying and Maintenance: Because bacteria grow in wet,
moist places, nebulizers should be thoroughly dried and
stored in a clean dry place between treatments. Drying
can be enhanced by attaching gas ow to the nebulizer
for a short time after it is rinsed. It has been reported that
nebulizer performance may change in time due to incor-
rect cleaning, maintenance, and disinfection procedures.139
Nebulizers must be kept from being contaminated by fol-
lowing the manufacturer’s instructions for care and clean-
ing. This is necessary for all aerosol generators used for
inhaled medication.
Preventing Infection and Malfunction of
Aerosol Generators at Hospitals or Clinics
Aerosol Generators: Bacterial contamination of nebulizers
at the hospital has been associated with nosocomial infec-
tions.140-141 The Centers for Disease Control and Prevention
(CDC) recommends that nebulizers be cleaned, rinsed with
Table 19. Cleaning instructions for the jet nebulizer
Cleaning After Each Use
Wash hands before handling equipment.
Disassemble parts after every treatment.
Remove the tubing from the compressor and set it aside.
The tubing should not be washed or rinsed.
Rinse the nebulizer cup and mouthpiece with either sterile
water or distilled water.
Shake off excess water.
Air dry on an absorbent towel.
Store the nebulizer cup in a zippered plastic bag.
Cleaning Once or Twice a Week
Wash hands before handling equipment.
Disassemble parts after every treatment.
Remove the tubing from the compressor and set it
aside. The tubing should not be washed or rinsed.
Wash nebulizer parts in warm water with liquid dish soap.
Disinfect the nebulizer based on the manufacturer’s rec-
ommendations. The nebulizer parts may be soaked in one
of the following solutions:
1. One-part household bleach and 50-parts water
for three minutes
2. 70% isopropyl alcohol for ve minutes
3. 3% hydrogen peroxide for 30 minutes
4. One-part distilled white vinegar in three-parts hot water
for one hour (not recommended for CF patients).
Rinse parts with sterile or distilled water.
Shake off excess water and place all parts on a clean paper
towel.
Allow them to air dry completely on an absorbent towel.
Reassemble the nebulizer and store in a clean, dry bag
container.

47
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
sterile water, and air-dried between treatments.142 Also,
each hospital or out-patient clinic should have an infection
surveillance program that can determine local IC practices
based on the continuous and systematic collection, analy-
sis, and interpretation of infection data. Nebulizers should
be changed every 24 hours.143-144 If an aerosol generator is
labeled “For Single Patient Use,” it should be used on a sin-
gle patient and then discarded.
MDI – Common Canister Use: Many hospital pharmacies
see a robust number of MDI canisters still containing med-
ication returned, leading to strategies for reducing cost.10
As a result, some hospitals practice common canister pro-
tocol for specic patient populations. A review focusing on
common canister protocol and the risk of infection found
some evidence of cross-contamination.145 However, the
evidence from the studies in this review is weak since none
of the research is in the form of peer-reviewed publications.
A recent study indicated a common canister protocol was
associated with signicant cost savings when compared
to single-patient MDI, and reported similar rates of venti-
lator assisted pneumonia, mortality, and length of stay.146
Hospital decision makers must perform a full risk-benet
evaluation before incorporating a common canister pro-
tocol in their institution, as more work needs to be done
in this area before best-practices can be suggested with a
high degree of condence.
Inhaled Drugs: Multi-dose drug containers have been asso-
ciated with contaminated nebulizers and are a potential
source of spreading nosocomial infections.149-151 Therefore,
unit-dose medications are recommended when possible.142
Also, it is important to avoid contaminating drug solutions.
Infection Transmission: The transmission of infection from
therapist to patient can be reduced by therapists washing
their hands with water and soap or cleaning hands with
hand sanitizers before and after treatment.151-152 The use of
gloves should be considered an adjunct to hand hygiene. A
respiratory therapist must change gloves between patients
and clean hands after gloves are removed due to the fact
that gloves create a warm and moist environment that sup-
ports the growth of microbial contamination and, thereby,
the transmission of infection.30,153 Goggles, face masks, and
face shields should be used alone or in combination to seal
out airborne pathogens that therapists may inhale with
aerosol drug therapy.
Compliance to IC Management System: The IC manage-
ment system can be effective only with the practice of the
dedicated and knowledgeable respiratory therapists who
implement it. Therefore, respiratory therapists should be
trained appropriately in using set protocols established by
the IC management system in aerosol drug delivery.
Infection Surveillance: It is essential for hospitals to estab-
lish simple and sensible infection surveillance measures to
periodically evaluate the IC activities used by respiratory
therapists.
Occupational Health and Safety of
Respiratory Therapists
Respiratory therapists undergo not only the risk of expo-
sure to inhaled medications but are also faced with the risk
of inhaling pathogens during aerosol therapy. The elements
of occupational health and safety for the respiratory thera-
pist are shown below.
Health Assessment and Immunization: Screening respira-
tory therapists for infection and immunization must occur
from the beginning to the end of employment.
Hand Hygiene: It has been documented that hand hygiene
is effective in decreasing the transmission of respiratory
viruses.31,152,154-156 Also, the World Health Organization’s
guidelines suggest that inadequate hand hygiene is the
leading cause of nosocomial infection and spread of multi-
drug resistant organisms.157 Health care workers who self-
reported handwashing during patient care had a lower risk
of having respiratory infections.31,154-156
Protective Equipment: Respiratory therapists must have
access to the appropriate personal protective equipment,
such as masks and eye protectors, when needed.30
Ventilation System: These systems exchange room air
six to 10 times per hour31 and create a negative-pressure
environment in patient rooms that is effective in removing
99.9% of airborne contaminants in 69 minutes.32
Filtered Nebulizers: Placing a lter on the exhalation part
of a nebulizer may protect respiratory therapists from infec-
tion and reduce secondhand aerosol breathing in hospitals
and out-patient clinics.

48
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Educating Patients
in Correct Use of
Aerosol Devices
A number of problems occur with patient use of aerosol
devices. Knowledge of these problems can help the respira-
tory therapist better instruct patients. Understanding there
are problems with use of aerosol devices can also direct
the therapist in evaluating a patient who has poor manage-
ment of airways disease. Either poor patient adherence to
prescribed aerosol therapy or errors in the use of aerosol
devices can reduce the effectiveness of inhaled drug ther-
apy. Both of these problem areas should be evaluated and,
if possible, ruled out in a patient who presents with poor
control of their airway disease before other changes in
their disease management are initiated.
Patient Adherence
A general problem with the use of inhaled medications
is patient adherence with prescribed use, although this
problem is not unique to inhaled drugs. “Adherence”
refers to a patient’s choice to follow prescribed therapy,
whereas “compliance” implies following of orders and pas-
sivity on the patient’s part. Lack of adherence can result in
poor health outcomes and increased healthcare costs.158
Both long- and short-term adherence may be inuenced
by patient and social factors.158-159 There are a number of
ways to monitor patient adherence with prescribed aero-
sol therapy such as provider interview, patient self-report,
dose counting, and electronic monitoring devices attached
to the inhaler. Monitoring devices attached to inhaler
devices are considered the most accurate and objective.
In one study, diary reports from patients showed a median
use of beta agonists of 78%, while data from an electron-
ic pMDI monitor reported only 48%.160 Therapists should
be aware that patients tend to over-report use of inhaled
drugs compared to data obtained from device monitors.
Failure to adhere to prescribed therapy is categorized as
“unintentional” or “intentional.” Table 20 lists both types
of non-adherence with denitions and examples.131 Upon
assessing poor patient adherence, a strategy incorporating
patient-centered care may help the caregiver understand
patient beliefs, views, and concerns about their treatment.
Goal setting and action plans are two motivational tools
Table 20. General types of non-adherence to prescribed aerosol therapy and potential factors that
can predispose to each type (Modied, with permission, from Reference 1 and Reference 131)
Unintentional Factors:
Not Understanding Therapy Correctly
Misunderstanding prescribed drug regimen:
• Poor physician-patient communication
• Poor therapist-patient communication
Language barriers
Intentional Factors:
Understanding Therapy But Not Adhering Correctly
Patient beliefs:
• Do not really require regular medication
• Are not really sick
• Gain attention from parents and kept at home (children)
• Medication too expensive
• Concern about side effects
• Perceived lack of effect from medication
Patient forgetfulness
Patient stress and busy lifestyle
Complex and demanding aerosol regimens
Psychological factors (e.g., depression)

49
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
that may improve patient adherence and can be discussed
in a supportive bi-directional conversation with the patient
during the patient-centered approach.
Note that one example of unintentional non-adherence
is incorrect aerosol device technique due to misunder-
standing prescribed drug regimen, which can be corrected
through patient training. There is no perfect, fail-safe,
error-proof inhaler on the market today. The pMDI is rec-
ognized as a difcult inhaler for patients to use without
proper training. Even holding chambers and spacers intro-
duced to address these issues present additional problems
(Table 21). DPIs were also introduced, in part, with the
rationale that their use would be simpler than with a
pMDI.161-162 Nebulizers are probably the simplest inhaler
type for a patient to use if we assume that assembly, prop-
er cleaning, and maintenance is not a problem. However,
Table 21. Common problems, disadvantages, and errors with each type of aerosol generator
(Modied, with permission, from References 1 and 132)
Pressurized Metered-Dose Inhalers
Errors in technique
• Failure to coordinate pMDI actuation on inhalation
• Too short a period of breath hold after inhalation
• Too rapid an inspiratory ow rate
• Inadequate priming/shaking/mixing before use
• Abrupt discontinuation of inspiration as aerosol hits throat
• Actuating pMDI at total lung capacity
• Actuating pMDI prior to inhalation
• Firing pMDI multiple times during single inhalation
• Firing pMDI into mouth but inhaling through nose
• Exhaling during actuation
• Putting wrong end of inhaler in mouth
• Holding canister in the wrong position
• Failing to remove cap before use
• Excessive use of pMDI beyond rated capacity (loss of dose count)
• Failure to clean boot
• Wasting remaining doses
Lack of adequate patient training in use of pMDI
Cognitive impairment of users
Lack of adequate hand strength or exibility to activate pMDI
Ideomotor dyspraxia
Valved Holding Chambers/Spacers
Incorrect assembly of add-on device
Failure to remove electrostatic charge in non-electrostatic holding
chambers/spacers can decrease emitted dose in new holding chamber/
spacer
Lengthy delay between pMDI actuation and inhalation from holding
chamber/spacer
Inhaling too rapidly
Firing multiple puffs into holding chamber/spacer before inhaling
Lack of patient instruction in assembly or use
Dry-Powder Inhalers
Errors in technique
• Not holding device correctly while loading dose
• Failure to pierce or open drug package
• Using the inhaler in wrong orientation
• Failure to prime
• Exhaling through the mouthpiece
• Not exhaling to residual volume before inhaling
• Not inhaling forcefully enough
• Inadequate or no breath hold
• Exhaling into mouthpiece after inhaling
Use of multi-dose reservoir designs in high ambient
humidity, which can reduce ne-particle dose
Lack of patient instruction in assembly or use
Nebulizers
Failure to assemble equipment properly
Spillage of dose by tilting some nebulizers
Failure to keep mouthpiece in mouth during nebulization
Failure to mouth breathe

50
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
there can be problems with all types of inhaler devices.
Table 20 lists the common errors and mistakes that can
occur with each type of device.131,161-162
Common Patient Errors with pMDIs
Although hand-breath coordination with a pMDI has long
been recognized as a problem, there are a number of other
potential mistakes a patient can make when using a pMDI
(Table 21). A large systematic review on errors in inhaler
use revealed that incorrect inhaler technique is frequent
and has not improved over the last 40 years.163 Lack of
coordination, improper inhalation (speed and/or depth),
and no post-inhalation breath hold were the most frequent
MDI technique errors.163 Also, failure to shake a pMDI
before each use can interfere with correct drug release.
Failure to prime a pMDI can also affect correct drug
release. A very practical problem and a real inconvenience
for users is the lack of a built-in dose counter to indicate
when a pMDI is empty. Dose counters are commercially
available, but this involves purchasing an additional item. In
one survey, 72% of patients said they continued to use their
pMDI until there was no sound when it was actuated.94
A pMDI can continue to produce a spray with propellant
and little or no drug if it is actuated after its rated capac-
ity, whether that is 120 or 200 puffs. Therapists should
instruct patients in the importance of tracking the number
of doses remaining in the pMDI (see page 39). It has been
shown that MDI’s without a counter results in signicantly
poorer adherence (underuse and overuse) when compared
to MDI’s with a counter.164 Furthermore, signicantly more
asthma and COPD patients visited the ED when not using
a dose counter when compared to a group using a dose
counter.165
Common Patient Errors with Holding
Chambers/Spacers
Common errors that can occur with holding chambers/
spacers are also listed in Table 21. Incorrect assembly of
the holding chamber/spacer is a potential problem. Many
patients mistakenly believe that pausing before inhaling
from a holding chamber/spacer after the MDI is actuated
has no effect on the delivered dose. This technique can
cause reduced drug availability. The ideal technique is to
place the mouthpiece between the lips and take a slow,
deep inhalation beginning when the pMDI is actuated.
Available dose can also be reduced if multiple puffs are
red into a holding chamber/spacer followed by a single
inhalation. Electrostatic charge is present on the chamber
walls of a new plastic holding chamber/spacer, which can
be removed by pre-washing with an ionic detergent or by
actuating 10–20 puffs from the pMDI through the cham-
ber.33,166 An alternative is to purchase a non-electrostatic
holding chamber/spacer.
Common Patient Errors with DPIs
Problems have also been identied with patient use of
DPIs (Table 21). Error rates, dened as failure to correctly
perform an essential step, have been shown to be similar
for pMDIs and DPIs.167 In contrast, another study revealed
that the DPI had a signicantly lower rate of improper
handling compared to the MDI.167 A large study on asthma
patient errors with a DPI showed that the most common
mistakes included failure to exhale prior to inhalation, insuf-
cient breath hold at end of inhalation, and lack of forceful
inhalation.168 Moreover, factors signicantly associated with
one or more of these major errors included an asthma-re-
lated hospitalization or no inhaler technique review during
the previous year.167 One of the unfortunate aspects of DPIs
is that the models currently available in the United States
all have a somewhat different design. They look different,
and there are differences in the details of cocking and load-
ing the DPIs.161 One of the highest error rates is failing to
hold the device correctly, which is an aspect of loading and
cocking the device for use.
Common Patient Errors with SVNs
The usual problems cited with SVNs are not problems
of patient use but rather general disadvantages with this
type of aerosol device (Table 21). Disadvantages include
bulk and size of equipment, need for external power source
(compressed gas or electricity), and lengthy treatment
times. Also, aerosol generators can function at suboptimal
levels for providing adequate medication delivery.169 Of all
the inhaler devices, however, nebulizers are the simplest
for patients to use. In addition, newer nebulizer technology
is directed at reducing the overall size of devices, elimi-
nating the need for an external power source, providing
shorter treatment times, and eliminating drug loss during
exhalation.

51
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
Instructing and Evaluating Patients in the
Use of Inhaler Devices
There is an increasing variety of aerosol devices and oper-
ation, even within the same category of device type (e.g.,
DPIs). Confusion and errors of use can result. The following
general steps are recommended for clinicians to ensure
correct patient use:
1. Review device instructions carefully and practice with a
placebo device prior to teaching others.
2. Demonstrate assembly and correct use of device to
patients using a checklist.
3. Provide the patient with written instructions on how
to use the device, and include a written plan for use of
the medication (frequency based on symptoms).
a. Written instructions should be accompanied by pic-
tures for patients with low literacy.
4. Have the patient practice use of the device while being
observed by the clinician.
5. Review patient use of the device at each return visit.
6. Review the patient’s understanding of the inhaled med-
ications at each return visit (when to use, purpose of
drug, prescribed frequency).
7. Have a high index of suspicion for incorrect use or
non-adherence if poor management of airway disease
occurs.
52
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
References
1. Hess DR, Myers TR, Rau JL. A guide to aerosol delivery devices for respi-
ratory therapists. American Association for Respiratory Care, Dallas,
Texas 2005.
2. Gardenhire, D.S. Rau’s Respiratory Care Pharmacology. St. Louis:
Elsevier, 2016.
3. Newman S, Hollingworth A, AR C. Effect of different modes of inha-
lation on drug delivery from a dry powder inhaler. Int J Pharm 1994;
102:127-132.
4. Newman SP, Pavia D, Moren F, et al. Deposition of pressurised aerosols
in the human respiratory tract. Thorax 1981; 36(1):52-55.
5. Newman SP, Woodman G, Clarke SW, Sackner MA. Effect of InspirEase on
the deposition of metered-dose aerosols in the human respiratory tract.
Chest 1986; 89(4):551-556.
6. Lewis RA, Fleming JS. Fractional deposition from a jet nebulizer: how
it differs from a metered-dose inhaler. Br J Dis Chest 1985; 79(4):361-
367.
7. Fink JB. Humidity and aerosol therapy. In: Mosby’s respiratory care
equipment. St. Louis MO: Mosby-Elsevier Inc; 2010:91-140.
8. Dolovich MB, Ahrens RC, Hess DR, et al. Device selection and out-
comes of aerosol therapy: evidence-based guidelines: American
College of Chest Physicians/ American College of Asthma, Allergy, and
Immunology. Chest 2005; 127(1):335-371.
9. Leach CL, Davidson PJ, Hasselquist BE, Boudreau RJ. Inuence of
particle size and patient dosing technique on lung deposition of HFA-
beclomethasone from a metered dose inhaler. J Aerosol Med 2005;
18(4):379-385.
10. Geller DE. New liquid aerosol generation devices: systems that force
pressurized liquids through nozzles. Respir Care 2002; 47(12):1392-
1404.
11. Dulfano MJ, Glass P. The bronchodilator effects of terbutaline: route of
administration and patterns of response. Ann Allergy 1976; 37(5):357-
366.
12. Gardenhire DS. Airway pharmacology. In: Egan’s fundamentals of respi-
ratory care. St Louis MO: Mosby Elsevier; 2009:667-692.
13. Fink JB. Aerosol drug therapy. In: Egan’s fundamentals of respiratory care.
St Louis MO: Mosby Elsevier; 2009:801-842.
14. Babu KS, Marshall BG. Drug-induced airway diseases. Clin Chest Med
2004; 25(1):113-122.
15. Leuppi JD, Schnyder P, Hartmann K, et al. Drug-induced bronchospasm:
analysis of 187 spontaneously reported cases. Respiration 2001;
68(4):345-351.
16. Steckel H, Eskandar F. Factors affecting aerosol performance during
nebulization with jet and ultrasonic nebulizers. Eur J Pharm Sci 2003;
19(5):443-455.
17. O’Callaghan C, Barry PW. The science of nebulised drug delivery.
Thorax 1997; 52(Suppl 2):S31-S44.
18. Hess DR. Aerosol delivery devices in the treatment of asthma. Respir
Care 2008; 53(6):699-723.
19. Ip AY, Niven RW. Prediction and experimental determination of solute
output from a Collison nebulizer. J Pharm Sci 1994; 83(7):1047-1051.
20. Pitchford K, Corey M, Highsmith A, et al. Pseudomonas species contam-
ination of cystic brosis patients’ home inhalation equipment. J Pediatr
1987; 111(2):212-216.
21. Rosenfeld M, Emerson J, Astley S, et al. Home nebulizer use among
patients with cystic brosis. J Pediatr 1998; 132(1):125-131.
22. Vassal S, Taamma R, Marty N, et al. Microbiologic contamination study
of nebulizers after aerosol therapy in patients with cystic brosis. Am J
Infect Control 2000; 28(5):347-351.
23. Barnes KL, Clifford R, Holgate ST, et al. Bacterial contamination of
home nebuliser. Br Med J (Clin Res Ed) 1987; 295(6602):812.
24. Wexler MR, Rhame FS, Blumenthal MN, et al. Transmission of gram-neg-
ative bacilli to asthmatic children via home nebulizers. Ann Allergy
1991; 66(3):267-271.
25. Jakobsson BM, Onnered AB, Hjelte L, Nystrom B. Low bacterial contam-
ination of nebulizers in home treatment of cystic brosis patients. J
Hosp Infect 1997; 36(3):201-207.
26. Carnathan B, Martin B, Colice G. Second hand (S)-albuterol: RT expo-
sure risk following racemic albuterol (Abstract). Respir Care 2001;
46(10):1084.
27. Dimich-Ward H, Wymer ML, Chan-Yeung M. Respiratory health survey
of respiratory therapists. Chest 2004; 126(4):1048-1053.
28. Christiani DC, Kern DG. Asthma risk and occupation as a respiratory
therapist. Am Rev Respir Dis 1993; 148(3):671-674.
29. Kern DG, Frumkin H. Asthma in respiratory therapists. Ann Intern Med
1989; 110(10):767-773.
30. Rhinehart E, Friedman MM. Personal protective equipment and staff
supplies. In: Infection control in home care (An ofcial APIC publica-
tion). Gaithersburg MD: Aspen Publishers, Inc.; 2006:61-69.
31. Gamage B, Moore D, Copes R, et al. Protecting health care workers
from SARS and other respiratory pathogens: a review of the infection
control literature. Am J Infect Control 2005; 33(2):114-121.
32. Segal-Maurer S, Kalkut G. Environmental control of tuberculosis: con-
tinuing controversy. Clin Infect Dis 1994; 19(2):299-308.
33. Dennis JH. Standardization issues: in vitro assessment of nebulizer per-
formance. Respir Care 2002; 47(12):1445-1458.
34. Hess D, Fisher D, Williams P, et al. Medication nebulizer performance.
Effects of diluent volume, nebulizer ow, and nebulizer brand. Chest
1996; 110(2):498-505.
35. Dennis JH. A review of issues relating to nebulizer standards. J Aerosol
Med 1998; 11(Suppl 1):S73-S79.
36. Welch MJ. Nebulization therapy for asthma: a practical guide for the
busy pediatrician. Clin Pediatr (Phila) 2008; 47(8):744-756.
37. Rau JL, Ari A, Restrepo RD. Performance comparison of nebulizer
designs: constant-output, breath-enhanced, and dosimetric. Respir
Care 2004; 49(2):174-179.
38. Alvine GF, Rodgers P, Fitzsimmons KM, Ahrens RC. Disposable jet nebu-
lizers. How reliable are they? Chest 1992; 101(2):316-319.
39. Camargo CA Jr, Spooner CH, Rowe BH. Continuous versus intermittent
beta-agonists in the treatment of acute asthma. Cochrane Database
Syst Rev 2003; (4):CD001115.
40. Everard ML, Evans M, Milner AD. Is tapping jet nebulisers worthwhile?
Arch Dis Child 1994; 70(6):538-539.
41. Malone RA, Hollie MC, Glynn-Barnhart A, Nelson HS. Optimal duration
of nebulized albuterol therapy. Chest 1993; 104(4):1114-1118.
42. Newman SP. Principles of metered-dose inhaler design. Respir Care
2005; 50(9):1177-1190.
43. Everard ML, Devadason SG, Summers QA, Le Souef PN. Factors affecting
total and “respirable” dose delivered by a salbutamol metered dose
inhaler. Thorax 1995; 50(7):746-749.
44. Niven RW, Kacmarek RM, Brain JD, Peterfreund RA. Small bore nozzle
extensions to improve the delivery efciency of drugs from metered
dose inhalers: laboratory evaluation. Am Rev Respir Dis 1993; 147(6 Pt
1):1590-1594.
45. Pedersen S. The importance of a pause between the inhalation of two
puffs of terbutaline from a pressurized aerosol with a tube spacer. J
Allergy Clin Immunol 1986; 77(3):505-509.
46. Pedersen S, Steffensen G. Simplication of inhalation therapy in asth-
matic children. A comparison of two regimes. Allergy 1986; 41(4):296-
301.
53
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
47. Dolovich M, Rufn RE, Roberts R, Newhouse MT. Optimal delivery of
aerosols from metered dose inhalers. Chest 1981; 80(6 Suppl):911-915.
48. Lawford P, McKenzie. Pressurized bronchodilator aerosol technique:
inuence of breath-holding time and relationship of inhaler to the
mouth. Br J Dis Chest 1982; 76(3):229-233.
49. Thomas P, Williams T, Reilly PA, Bradley D. Modifying delivery technique
of fenoterol from a metered dose inhaler. Ann Allergy 1984; 52(4):279-
281.
50. Unzeitig JC, Richards W, Church JA. Administration of metered-dose
inhalers: comparison of open- and closed-mouth techniques in child-
hood asthmatics. Ann Allergy 1983; 51(6):571-573.
51. Chhabra SK. A comparison of “closed” and “open” mouth techniques
of inhalation of a salbutamol metered-dose inhaler. J Asthma 1994;
31(2):123-125.
52. Newman S, Clark A. Inhalation techniques with aerosol bronchodilators.
Does it matter? Pract Cardiol 1983; 9:157-164.
53. Holt S, Holt A, Weatherall M, et al. Metered dose inhalers: a need for
dose counters. Respirology 2005; 10(1):105-106.
54. Ogren R, Baldwin J, Simon R. How patients determine when to replace
their metered dose inhalers. Ann Allergy Asthma Immunol 1995; 75(6
Pt 1):485-489.
55. Rubin BK, Durotoye L. How do patients determine that their metered-
dose inhaler is empty? Chest 2004; 126(4):1134-1137.
56. Schultz RK. Drug delivery characteristics of metered-dose inhalers. J
Allergy Clin Immunol 1995; 96(2):284-287.
57. Cain WT, Oppenheimer JJ. The misconception of using oating patterns
as an accurate means of measuring the contents of metered-dose
inhaler devices. Ann Allergy Asthma Immunol 2001; 87(5):417-419.
58. Brock TP, Wessell AM, Williams DM, Donohue JF. Accuracy of oat test-
ing for metered-dose inhaler canisters. J Am Pharm Assoc (Wash) 2002;
42(4):582-586.
59. U.S. Department of Health and Human Services, U.S. Food and Drug
Administration. Guidance for industry: integration of dose-counting
mechanisms into MDI drug products. Rockville MD, 2003.
60. Sheth K, Wasserman RL, Lincourt WR, et al. Fluticasone propionate/
salmeterol hydrouoroalkane via metered-dose inhaler with integrated
dose counter: Performance and patient satisfaction. Int J Clin Pract
2006; 60(10):1218-1224.
61. Simmons MS, Nides MA, Kleerup EC, et al. Validation of the Doser, a
new device for monitoring metered-dose inhaler use. J Allergy Clin
Immunol 1998; 102(3):409-413.
62. Julius SM, Sherman JM, Hendeles L. Accuracy of three electronic moni-
tors for metered-dose inhalers. Chest 2002; 121(3):871-876.
63. Williams DM, Wessell A, Brock TP. The Doser external counting device.
Chest 1999; 116(5):1499.
64. Momeni S, Nokhodchi A, Ghanbarzadeh S, et al. The effect of spacer
morphology on the aerosolization performance of metered-dose inhal-
ers. Adv Pharm Bull 2016; 6(2):257-260.
65. Mitchell JP, Nagel MW. Valved holding chambers (VHCs) for use with
pressurised metered-dose inhalers (pMDIs): a review of causes of
inconsistent medication delivery. Prim Care Respir J 2007; 16(4):207-
214.
66. Yazdani A, Normandie M, Youse M, et al. Transport and deposition
of pharmaceutical parti cles in three commercial spacer-MDI combina-
tions. Comput Biol Med 2014; 54:145-155.
67. Ogrodnik N, Azzi V, Sprigge E, et al. Nonuniform deposition of pressur-
ized metered- dose aerosol in spacer devices. J Aerosol Med Pulm Drug
Deliv 2016; 29(6):490-500.
68. American College of Chest Physicians. Patient instructions for inhaled
devices in English and Spanish. Northbrook IL, 2006.
69. Rau JL. The inhalation of drugs: advantages and problems. Respir Care
2005; 50(3):367-382.
70. Fink JB, Rubin BK. Aerosol and medication administration. In: Czerviske
MP, Barnhart SL, editors. Perinatal and pediatric respiratory care. St
Louis MO: Elsevier Science; 2003.
71. Everard ML. Aerosol delivery to children. Pediatr Ann 2006; 35(9):630-
636.
72. Everard ML. Inhalation therapy for infants. Adv Drug Deliv Rev 2003;
55(7):869-878.
73. Ahrens RC. The role of the MDI and DPI in pediatric patients: “Children
are not just miniature adults”. Respir Care 2005; 50(10):1323-1328.
74. Pongracic JA. Asthma delivery devices: age-appropriate use. Pediatr Ann
2003; 32(1):50-54.
75. Boe J, Dennis JH, O’Driscoll BR, et al. European Respiratory Society
Guidelines on the use of nebulizers. Eur Respir J 2001; 18(1):228-242.
76. Rubin BK, Fink JB. Optimizing aerosol delivery by pressurized metered-
dose inhalers. Respir Care 2005; 50(9):1191-1200.
77. Rau JL. Practical problems with aerosol therapy in COPD. Respir Care
2006; 51(2):158-172.
78. Rubin BK. Nebulizer therapy for children: the device-patient interface.
Respir Care 2002; 47(11):1314-1319.
79. Geller DE. Comparing clinical features of the nebulizer, metered-dose
inhaler, and dry powder inhaler. Respir Care 2005; 50(10):1313-1321.
80. Gray SL, Williams DM, Pulliam CC, et al. Characteristics predicting incor-
rect metered-dose inhaler technique in older subjects. Arch Intern Med
1996; 156(9):984-988.
81. Allen SC, Ragab S. Ability to learn inhaler technique in relation to
cognitive scores and tests of praxis in old age. Postgrad Med J 2002;
78(915):37-39.
82. McFadden ER Jr. Improper patient techniques with metered-dose
inhalers: clinical consequences and solutions to misuse. J Allergy Clin
Immunol 1995; 96(2):278-283.
83. Atkins PJ. Dry powder inhalers: an overview. Respir Care 2005;
50(10):1304-1312.
84. Fink JB, Rubin BK. Problems with inhaler use: a call for improved clini-
cian and patient education. Respir Care 2005; 50(10):1360-1375.
85. Lewis RM, Fink JB. Promoting adherence to inhaled therapy: building
partnerships through patient education. Respir Care Clin N Am 2001;
7(2):277-301, vi.
86. Fink JB. Inhalers in asthma management: is demonstration the key to
compliance? Respir Care 2005; 50(5):598-600.
87. Berlinski A. Assessing new technologies in aerosol medicine. Respir Care
2015;60(6):833-849.
88. van der Palen J, Klein JJ, van Herwaarden CL, et al. Multiple inhalers
confuse asthma patients. Eur Respir J 1999; 14(5):1034-1037.
89. Castro-Rodriguez JA, Rodrigo GJ. Beta-agonists through metered-dose
inhaler with valved holding chamber versus nebulizer for acute exac-
erbation of wheezing or asthma in children under 5 years of age: a
systematic review with meta-analysis. J Pediatr 2004; 145(2):172-177.
90. Meadows-Oliver M, Banasiak NC. Asthma medication delivery devices. J
Pediatr Health Care 2005; 19(2):121-123.
91. Chan PW, DeBruyne JA. Parental concern towards the use of inhaled thera-
py in children with chronic asthma. Pediatr Int 2000; 42(5):547-551.
92. Apter AJ, Reisine ST, Afeck G, et al. Adherence with twice-daily dosing
of inhaled steroids. Socioeconomic and health-belief differences. Am J
Respir Crit Care Med 1998; 157(6 Pt 1):1810-1817.
93. Rubin BK. What does it mean when a patient says, “my asthma medica-
tion is not working?” Chest 2004; 126(3):972-981.
94. DiBlasi RM. Clinical controversies in aerosol therapy for infants and chil-
dren. Respir Care 2015;60(6):894-916.
95. Everard ML. Inhaler devices in infants and children: challenges and solu-
tions. J Aerosol Med 2004; 17(2):186-195.
96. Tal A, Golan H, Grauer N, et al. Deposition pattern of radiolabeled
salbutamol inhaled from a metered-dose inhaler by means of a spacer
with mask in young children with airway obstruction. J Pediatr 1996;
128(4):479-484.
97. Everard ML, Clark AR, Milner AD. Drug delivery from holding chambers
with attached facemask. Arch Dis Child 1992; 67(5):580-585.
98. Nikander K, Berg E, Smaldone GC. Jet nebulizers versus pressurized
metered dose inhalers with valved holding chambers: effects of the
facemask on aerosol delivery. J Aerosol Med 2007; 20(Suppl 1):S46-S55.
54
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
99. Bower L, Barnhart S, Betit P, et al. American Association for Respiratory
Care. AARC Clinical Practice Guideline: selection of an aerosol deliv-
ery device for neonatal and pediatric patients. Respir Care 1995;
4(12):1325-1335.
100. National Asthma Education and Prevention Program. Expert Panel
Report III: guidelines for the diagnosis and management of asthma.
Bethesda MD: National Institutes of Health; 2007.
101. Everard ML. Guidelines for devices and choices. J Aerosol Med 2001;
14(Suppl 1):S59-S64.
102. Ritson S JD, Everard ML. Aerosol delivery systems acceptable to young chil-
dren improve drug delivery. Thorax 1998; 53:A55.
103. Fink JB. Aerosol delivery to ventilated infants and pediatric patients.
Respir Care 2004; 49(6):653-665.
104. Nikander K, Agertoft L, Pedersen S. Breath-synchronized nebulization dimin-
ishes the impact of patient-device interfaces (face mask or mouthpiece) on
the inhaled mass of nebulized budesonide. J Asthma 2000; 37(5):451-459.
105. Iles R, Lister P, Edmunds AT. Crying signicantly reduces absorption of
aerosolised drug in infants. Arch Dis Child 1999; 81(2):163-165.
106. Everard ML. Trying to deliver aerosols to upset children is a thankless task.
Arch Dis Child 2000; 82(5):428.
107. Murakami G, Igarashi T, Adachi Y, et al. Measurement of bronchial
hyperreactivity in infants and preschool children using a new method.
Ann Allergy 1990; 64(4):383-387.
108. Janssens HM, van der Wiel EC, Verbraak AF, et al. Aerosol therapy and
the ghting toddler: is administration during sleep an alternative? J
Aerosol Med 2003; 16(4):395-400.
109. Esposito-Festen J, Ijsselstijn H, Hop W, et al. Aerosol therapy by pressured
metered-dose inhaler-spacer in sleeping young children: to do or not to
do? Chest 2006; 130(2):487-492.
110. Restrepo RD, Dickson SK, Rau JL, Gardenhire DS. An investigation of
nebulized bronchodilator delivery using a pediatric lung model of spon-
taneous breathing. Respiratory Care 2006; 51(1):56-61.
111. Kishida M, Suzuki I, Kabayama H, et al. Mouthpiece versus facemask for
delivery of nebulized salbutamol in exacerbated childhood asthma. J
Asthma 2002; 39(4):337-339.
112. Lowenthal D, Kattan M. Facemasks versus mouthpieces for aerosol treat-
ment of asthmatic children. Pediatr Pulmonol 1992; 14(3):192-196.
113. Smaldone GC, Berg E, Nikander K. Variation in pediatric aerosol deliv-
ery: importance of facemask. J Aerosol Med 2005; 18(3):354-363.
114. Amirav I, Newhouse MT. Aerosol therapy with valved holding chambers
in young children: importance of the facemask seal. Pediatrics 2001;
108(2):389-394.
115. Janssens HM, Tiddens HA. Facemasks and aerosol delivery by metered-
dose inhaler valved holding chamber in young children: a tight seal
makes the difference. J Aerosol Med 2007; 20(Suppl 1):S59-S65.
116. Everard ML, Clark AR, Milner AD. Drug delivery from jet nebulisers. Arch Dis
Child 1992; 67(5):586-591.
117. Esposito-Festen JE, Ates B, van Vliet FJ, et al. Effect of a facemask leak
on aerosol delivery from a pMDI-spacer system. J Aerosol Med 2004;
17(1):1-6.
118. Kesser B, Geller D, Amirav I, Fink J. Baby don’t cry: in vitro comparisons
of “baby’s breath” aerosol delivery hood vs. face mask or blow-by using
the “Saint” infant upper airway model and “Aeroneb Go” vs. T-piece
nebulizer (Abstract). Respir Care 2003; 48(11):1079.
119. Rubin BK. Bye-bye, Blow-by. Respir Care 2007; 52(8):981.
120. Everard ML. Aerosol therapy: regimen and device compliance in daily
practice. Paediatr Respir Rev 2006; 7(Suppl 1):S80-S82.
121. Everard ML. Regimen and device compliance: key factors in determin-
ing therapeutic outcomes. J Aerosol Med 2006; 19(1):67-73.
122. Craven DE, Lichtenberg DA, Goularte TA, et al. Contaminated medi-
cation nebulizers in mechanical ventilator circuits. Source of bacterial
aerosols. Am J Med 1984; 77(5):834-838.
123. Lester MK, Flume PA, Gray SL, et al. Nebulizer use and maintenance by
cystic brosis patients: a survey study. Respir Care 2004; 49(12):1504-
1508.
124. Garber E, Desai M, Zhou J, et al. Barriers to adherence to cystic brosis
infection con trol guidelines. Pediatr Pulmonol 2008; 43(9):900-907.
125. Hutchinson GR, Parker S, Pryor JA, et al. Home-use nebulizers: a poten-
tial primary source of Burkholderia cepacia and other colistin-resistant,
gram-negative bacteria in patients with cystic brosis. J Clin Microbiol
1996; 34(3):584-587.
126. Saiman L, Siegel J. Infection control recommendations for patients with
cystic brosis: microbiology, important pathogens, and infection con-
trol practices to prevent patient-to-patient transmission. Infect Control
Hosp Epidemiol 2003; 24(5 Suppl):S6-S52.
127. Cohen HA, Kahan E, Cohen Z, et al. Microbial colonization of nebulizers
used by asthmatic children. Pediatr Int 2006; 48(5):454-458.
128. Blau H, Mussaf H, Mei Zahav M, et al. Microbial contamination of neb-
ulizers in the home treatment of cystic brosis. Child Care Health Dev
2007; 33(4):491-495.
129. Saiman L, Siegel J. Infection control in cystic brosis. Clin Microbiol Rev
2004; 17(1):57-71.
130. Lester MK, Flume PA, Gray SL, et al. Nebulizer use and maintenance by
cystic brosis patients: A survey study. Respir Care 2004; 49(12):1504-
1508.
131. Rau JL. Determinants of patient adherence to an aerosol regimen.
Respir Care 2005; 50(10):1346-1359.
132. Chew NY, Reddel HK, Bosnic-Anticevich SZ, Chan HK. Effect of mouth-
piece washing on aerosol performance of CFC-free Ventolin. J Asthma
2004; 41(7):721-727.
133. American College of Chest Physicians. Priming and cleaning your MDI
and spacer, 2006.
134. Jarvis S, Ind PW, Thomas C, et al. Microbial contamination of domicil-
iary nebulisers and clinical implications in chronic obstructive pulmo-
nary disease. BMJ Open Respir Res 2014; 1(1):e000018.
135. Della Zuana A, Garcia Dde O, Juliani RC, et al. Effect that an educa-
tional program for cystic brosis patients and caregivers has on the
contamination of home nebulizers. J Bras Pneumol 2014; 40(2):119-
127.
136. The Cystic Fibrosis Foundation. Stopping the spread of germs, 2009.
137. Saiman L, Siegel JD, LiPuma JJ, et al. Infection prevention and con-
trol guideline for cystic brosis: 2013 update. Infect Control Hosp
Epidemiol 2014; 35 Suppl 1:S1-S67.
138. Chatburn RL, Kallstrom TJ, Bajaksouzian S. A comparison of acetic acid
with a quaternary ammonium compound for disinfection of hand-held
nebulizers. Respir Care 1988; 33(3):179-187.
139. Le Brun PP, de Boer AH, Heijerman HG, Frijlink HW. A review of the
technical aspects of drug nebulization. Pharm World Sci 2000;
22(3):75-81.
140. Grieble HG, Colton FR, Bird TJ, et al. Fine-particle humidiers. Source of
Pseudomonas aeruginosa infections in a respiratory-disease unit. N Engl
J Med 1970; 282(10):531-535.
141. Mertz JJ, Scharer L, McClement JH. A hospital outbreak of Klebsiella
pneumonia from inhalation therapy with contaminated aerosol solu-
tions. Am Rev Respir Dis 1967; 95(3):454-460.
142. Tablan OC, Anderson LJ, Besser R, et al. Guidelines for preventing health
care-associated pneumonia, 2003: recommendations of CDC and the
Healthcare Infection Control Practices Advisory Committee. MMWR
Recomm Rep 2004; 53(RR-3):1-36.
143. O’Malley CA, VandenBranden SL, Zheng XT, et al. A day in the life of a
nebulizer: surveillance for bacterial growth in nebulizer equipment of
children with cystic brosis in the hospital setting. Respir Care 2007;
52(3):258-262.
144. American Association for Respiratory Care. AARC Clinical Practice
Guideline: selection of an aerosol delivery device. Respir Care 1992;
37(8):891-897 (retired August 2006).
145. Larson T, Gudavalli R, Prater D, et al. Critical analysis of common can-
ister programs: a review of cross-functional considerations and health
system econom ics. Curr Med Res Opin; 2015; 31(4):853-860.
146. Gowan M, Bushwitz J, Watts P, et al. Use of a shared canister protocol
for the delivery of metered-dose inhalers in mechanically ventilated
subjects. Respir Care 2016; 61(10):1285-1292.
147. Estivariz CF, Bhatti LI, Pati R, et al. An outbreak of Burkholderia cepacia
associated with contamination of albuterol and nasal spray. Chest 2006;
130(5):1346-1353.
55
A Guide to Aerosol Delivery Devices for Respiratory Therapists, 4th Edition
American Association for Respiratory Care, © 2017
148. Hamill RJ, Houston ED, Georghiou P, et al. An outbreak of Burkholderia
(formerly Pseudomonas) cepacia respiratory tract colonization and
infection associated with nebulized albuterol therapy. Ann Intern Med
1995; 122(10):762-766.
149. Rau JL, Restrepo RD. Nebulized bronchodilator formulations: unit-dose
or multi-dose? Respir Care 2003; 48(10):926-939.
150. U.S. Food and Drug Administration, Center for Drug Evaluation and
Research. Public health advisory: contamination of multi-dose bottles of
Albuterol Sulfate Solution for Inhalation (0.5%), 2002.
151. Center for Disease Control and Prevention. Clean hands save lives, 2008.
152. Center for Disease Control and Prevention. Guideline for hand hygiene
in healthcare settings, 2008.
153. Larson EL. APIC guideline for handwashing and hand antisepsis in
health care settings. Am J Infect Control 1995; 23(4):251-269.
154. Paes BA. Current strategies in the prevention of respiratory synctial
virus disease. Pediatr Respir Rev 2003; 4(1):21-27.
155. Purssell E. Preventing nosocomial infection in paediatric wards. J Clin
Nurs 1996; 5(5):313-318.
156. Hall CB. Nosocomial respiratory syncytial virus infections: the “Cold
War” has not ended. Clin Infect Dis 2000; 31(2):590-596.
157. World Health Organization (WHO). WHO Guidelines on Hand Hygiene
in Health Care: First Global Patient Safety Challenge Clean Care Is
Safer Care. World Health Organization: Geneva; 2009.
158. Braido F, Baiardini I, Blasi F, et al. Adherence to asthma treatments:
‘we know, we intend, we advocate’. Curr Opin Allergy Clin Immunol
2015; 15(1):49-55.
159. Bourbeau J, Bartlett SJ. Patient adherence in COPD. Thorax 2008;
63(9):831-838.
160. Milgrom H, Bender B, Ackerson L, et al. Noncompliance and treatment
failure in children with asthma. J Allergy Clin Immunol 1996; 98(6 Pt
1):1051-1057.
161. Melani AS, Zanchetta D, Barbato N, et al. Inhalation technique and
variables associated with misuse of conventional metered-dose inhal-
ers and newer dry powder inhalers in experienced adults. Ann Allergy
Asthma Immunol 2004; 93(5):439-446.
162. McFadden ER Jr. Improper patient techniques with metered-dose
inhalers: clinical consequences and solutions to misuse. J Allergy Clin
Immunol 1995; 96(2):278-283.
163. Sanchis, J., I. Gich, and S. Pedersen, Systematic Review of Errors in
Inhaler Use: Has Patient Technique Improved Over Time? Chest, 2016.
150(2): p. 394-406.
164. Koehorst-ter Huurne K, Moviq K, van der Valk P, et al. The inuence of
type of inhalation device on adherence of COPD patients to inhaled
medication. Expert Opin Drug Deliv 2016; 13(4):469-475.
165. Price DB, Rigazio A, Buatti Small M, et al. Historical cohort study
examining comparative effectiveness of albuterol inhalers with and
without integrated dose counter for patients with asthma or chronic
obstructive pulmonary disease. J Asthma Allergy 2016; 9:145-154.
166. Wildhaber JH, Devadason SG, Eber E, et al. Effect of electrostatic
charge, ow, delay and multiple actuations on the in vitro delivery
of salbutamol from different small volume spacers for infants. Thorax
1996; 51(10):985-988.
167. Khassawneh BY, Al-Ali MK, Alzoubi KH, et al. Handling of inhaler devic-
es in actual pulmo nary practice: metered-dose inhaler versus dry pow-
der inhalers. Respir Care 2008; 53(3):324-328.
168. Westerik JA, Carter V, Chrystyn H, et al. Characteristics of patients
making serious inhaler errors with a dry powder inhaler and associa-
tion with asthma-related events in a primary care setting. J Asthma
2016; 53(3):321-329.
169. Rau JL. Practical problems with aerosol therapy in COPD. Respir Care
2006; 51(2):158-172.
