SNOMED CT Starter Guide Doc Current En US INT 20140731
User Manual: Pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 57

SNOMED CT Starter Guide
July 2014
2 | P a g e
TABLE OF CONTENTS
1. Introduction ............................................................................................................................... 3
2. SNOMED CT Benefits .................................................................................................................. 4
3. Using SNOMED CT in Clinical Information .................................................................................. 6
4. SNOMED CT Basics ..................................................................................................................... 9
5. SNOMED CT Logical Model ....................................................................................................... 14
6. SNOMED CT Concept Model ..................................................................................................... 20
7. SNOMED CT Expressions........................................................................................................... 27
8. SNOMED CT Implementation ................................................................................................... 34
9. Content Development .............................................................................................................. 38
10. Extension and Customization ................................................................................................... 40
11. Translations and Language Preferences ................................................................................... 44
12. Mapping ................................................................................................................................... 46
13. Release Schedule and File Formats ........................................................................................... 51
14. IHTSDO – The Organisation Behind SNOMED CT ...................................................................... 53
15. Learning More About SNOMED CT ........................................................................................... 56
The SNOMED CT Starter Guide is a publication of the International Health Standards Development Organisation
(IHTSDO), the association that owns and maintains SNOMED Clinical Terms. IHTSDO acknowledges the work
undertaken by Anne Randorff Højen and Robyn Kuropatwa in preparing this guide as an assignment during their
participation in the SNOMED CT Implementation Advisor (SIA) scheme.
© Copyright 2014 International Health Terminology Standards Development Organisation (IHTSDO), all rights
reserved.
SNOMED, SNOMED CT and IHTSDO are registered trademarks of the International Health Standards Development
Organisation. SNOMED CT licensing information is available at www.ihtsdo.org/licensing. For more information about
IHTSDO and IHTSDO Membership, please refer to www.ihtsdo.org or contact us at info@ihtsdo.org.
The July 2014 version contains minor corrections and clarifications addressing comments made on the first version
published in January 2014 and revised in February 2014. Future updates of this and other documents will be
accessible from the document library at www.snomed.org/doc.
SNOMED CT Starter Guide
July 2014
3 | P a g e
1. INTRODUCTION
Goals and objectives
The vision for the SNOMED Clinical Terms (SNOMED CT) Starter Guide is for it to be a practical and useful
starting point from which anyone with a general interest in healthcare information can begin learning
about SNOMED CT.
Target audience
The target audience for this Starter Guide includes people from various disciplines who may be involved at
any point in the SNOMED CT information management cycle – from initial planning, clinical content
definition and implementation through to use of the resulting clinical information. This spans people
involved with planning and deciding to proceed and resource a SNOMED CT implementation, people
involved in reference set development, terminology management, technical implementation and all
aspects of deployment and use. It also includes people involved in clinical information retrieval, analyses,
decision support and other aspects of knowledge representation. The characteristics common to all
members of the target audience are that they have a reason for wanting to understand SNOMED CT and
are seeking a high-level initial overview of topics of which they need to be aware. The Starter Guide does
not provide in depth knowledge but does provide an informative and authoritative foundation on which to
build.
Topics
The topics covered in this SNOMED CT Starter Guide include:
SNOMED CT Benefits
Using SNOMED CT in Clinical Information
SNOMED CT Basics
SNOMED CT Logical Model
SNOMED CT Concept Model
SNOMED CT Expressions
Content Development
Extension and Customization
Translations and Language Preferences
Mapping
Release Schedule and File Formats
Implementation
IHTSDO
Learning More
For each topic the questions addressed include:
Why is this important?
What is this?
Supporting references are included in the final chapter of the guide.
SNOMED CT Starter Guide
July 2014
4 | P a g e
2. SNOMED CT BENEFITS
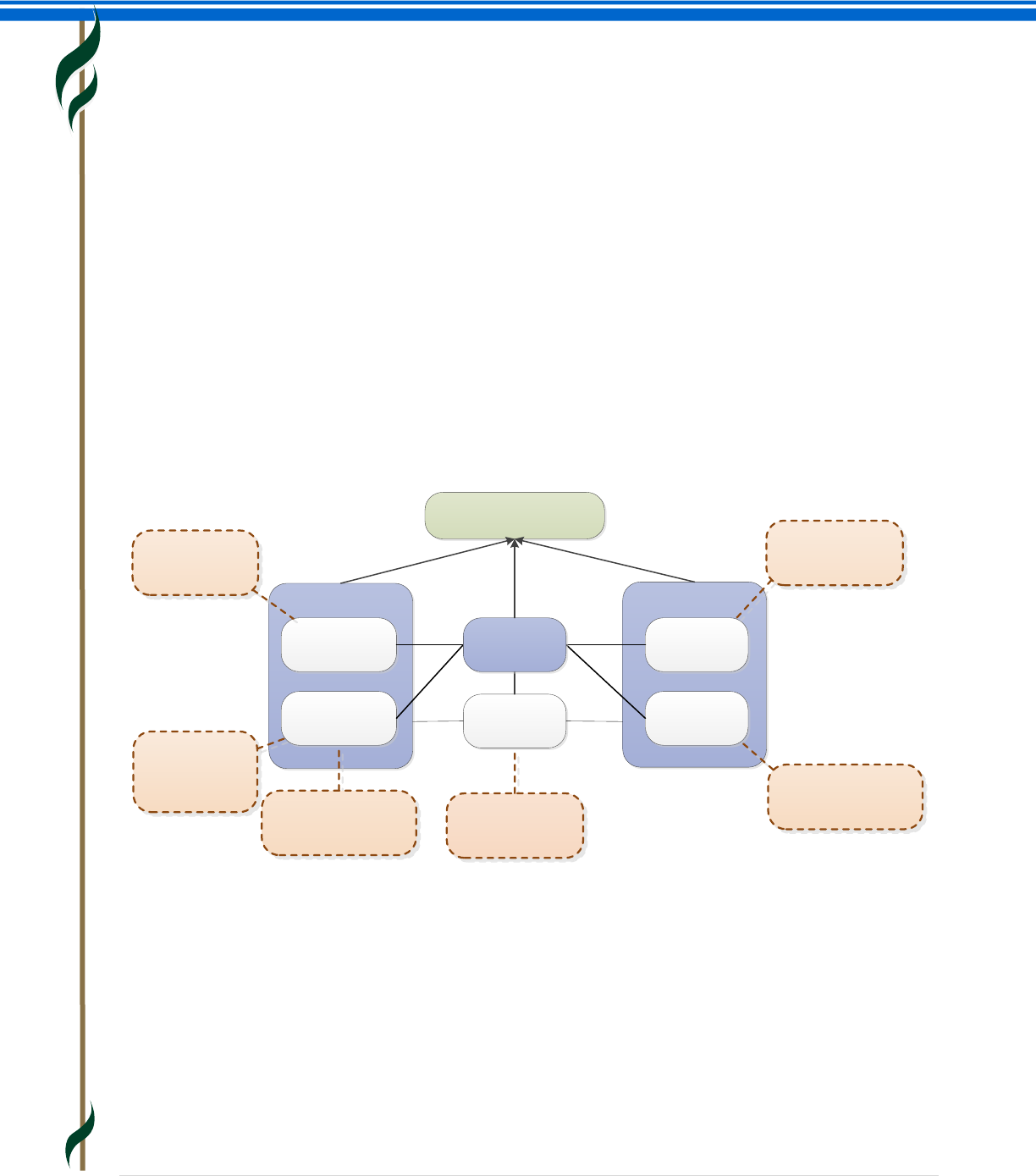
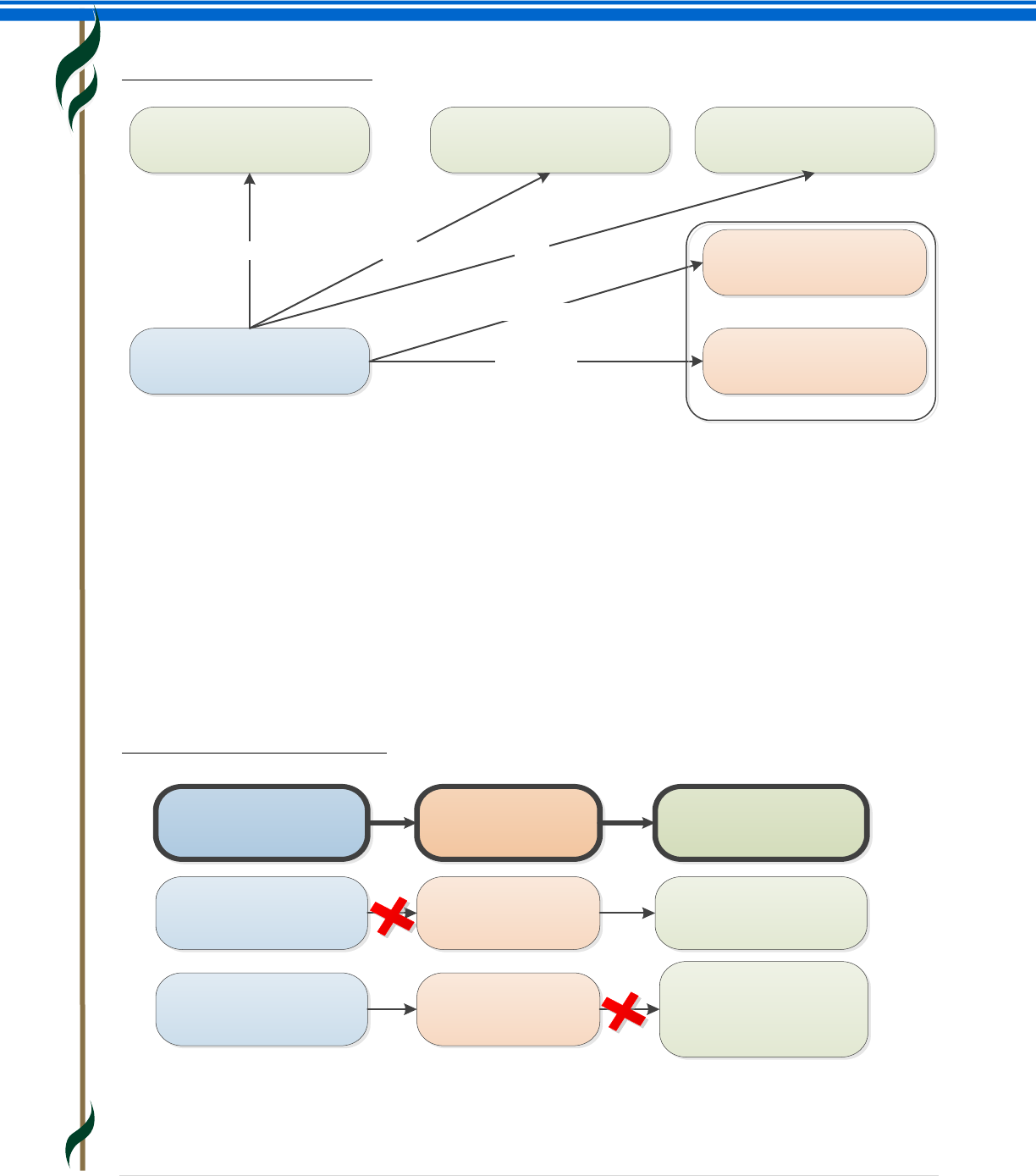
This section provides an overview of how effective use of SNOMED CT:
Benefits populations
Benefits individual patients and clinicians
Supports evidence based healthcare
Why is this important?
Understanding the benefits of SNOMED CT will inform key decisions and the development of strategies for
adoption, implementation and use of this clinical terminology.
What is this?
SNOMED CT supports the development of comprehensive high-quality clinical content in health records. It
provides a standardized way to represent clinical phrases captured by the clinician and enables automatic
interpretation of these. SNOMED CT is a clinically validated, semantically rich, controlled vocabulary that
facilitates evolutionary growth in expressivity to meet emerging requirements.
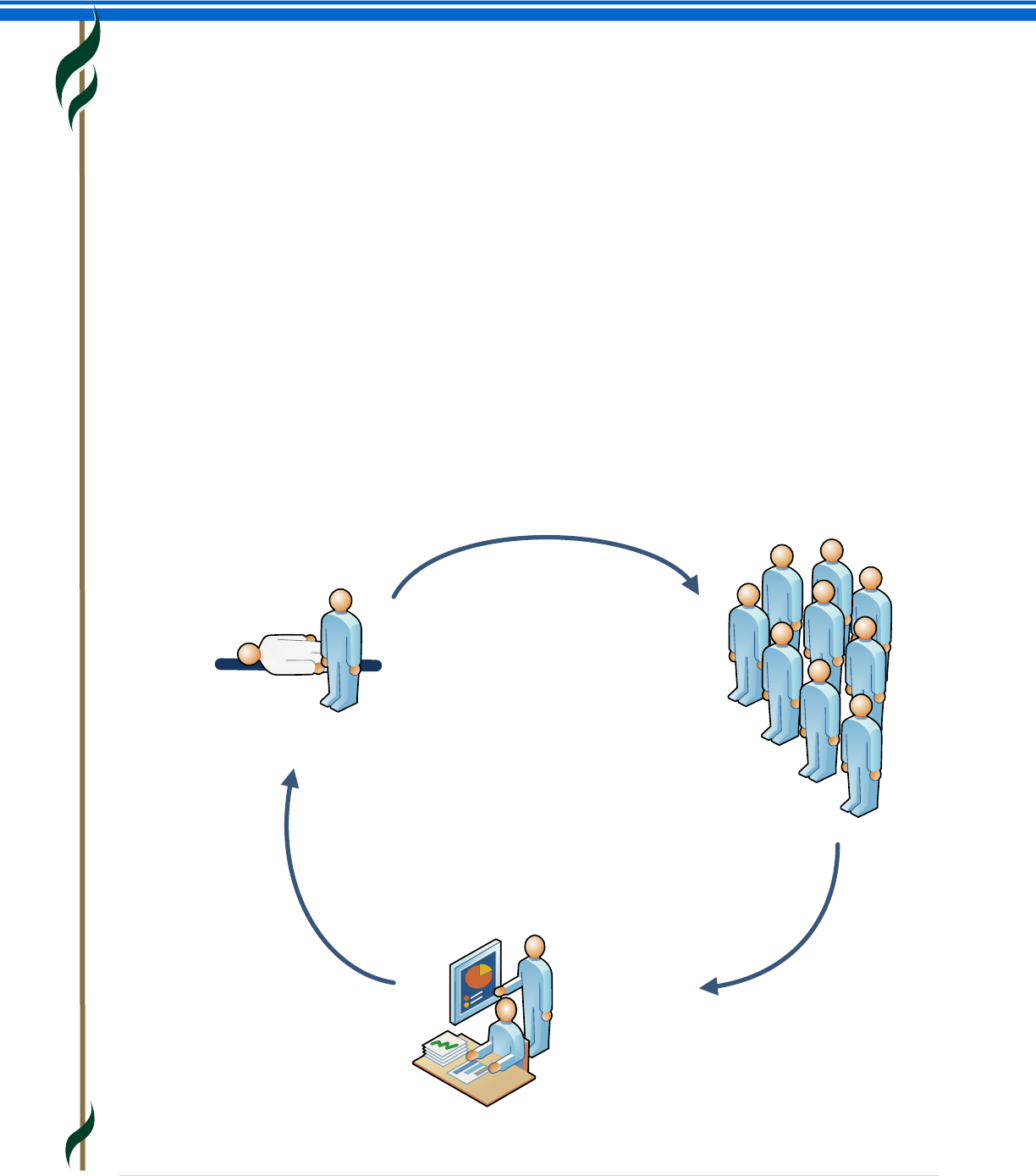
Benefit Individuals
Patients and Clinicians
Benefit Populations
Evidence-Based Healthcare
RESEARCH
(Clinical knowledge)
CLINICAL ASSESSMENT AND
TREATMENT
POPULATION
MONITORING
SNOMED CT Starter Guide
July 2014
5 | P a g e
Electronic Health Records
SNOMED CT based clinical information benefits individual patients and clinicians as well as populations and
it supports evidence based care.
The use of an Electronic Health Record (EHR) improves communication and increases the availability of
relevant information. If clinical information is stored in ways that allow meaning-based retrieval, the
benefits are greatly increased. The added benefits range from increased opportunities for real time
decision support to more accurate retrospective reporting for research and management.
SNOMED CT Enabled Health Records Benefit Individuals
SNOMED CT enabled clinical health records benefit individuals by:
Enabling relevant clinical information to be recorded using consistent, common representations
during a consultation.
Enabling guideline and decision support systems to check the record and provide real-time advice,
for example, through clinical alerts.
Supporting the sharing of appropriate information with others involved in delivering care to a
patient through data capture that allows understanding and interpretation of the information in a
common way by all providers.
Allowing accurate and comprehensive searches that identify patients who require follow-up or
changes of treatment based on revised guidelines.
Removing language barriers (SNOMED CT enables multilingual use).
SNOMED CT Enabled Health Records Benefit Populations
SNOMED CT enabled clinical health records benefit populations by:
Facilitating early identification of emerging health issues, monitoring of population health and
responses to changing clinical practices.
Enabling accurate and targeted access to relevant information, reducing costly duplications and
errors.
Enabling the delivery of relevant data to support clinical research and contribute evidence for
future improvements in treatment.
Enhancing audits of care delivery with options for detailed analysis of clinical records to investigate
outliers and exceptions.
SNOMED CT Enabled Health Records Support Evidence-Based Healthcare
SNOMED CT enabled health records inform evidence based health care decisions by:
Enabling links between clinical records and enhanced clinical guidelines and protocols.
Enhancing the quality of care experienced by individuals.
Reducing costs of inappropriate and duplicative testing and treatment.
Limiting the frequency and impact of adverse healthcare events.
Raising the cost-effectiveness and quality of care delivered to populations.
SNOMED CT Starter Guide
July 2014
6 | P a g e
3. USING SNOMED CT IN CLINICAL INFORMATION
This section provides an overview of:
How SNOMED CT supports reuse of clinical information
Extent of practical use
Approaches to implementation
Lessons learnt
Challenges
Why is this important?
The objective of IHTSDO and all users of SNOMED CT is to facilitate the accurate recording and sharing of
clinical and related health information and the semantic interoperability of health records.
What is this?
How SNOMED CT supports reuse of clinical information
SNOMED CT is a clinical terminology with global scope covering a wide range of clinical specialties,
disciplines and requirements. As a result of its broad scope, one of the benefits of SNOMED CT is a
reduction of specialty boundary effects that arise from use of different terminologies or coding systems by
different clinicians or departments. This allows wider sharing and reuse of structured clinical information.
Another benefit of SNOMED CT is that the same data can be processed and presented in ways that serve
different purposes. For example, clinical records represented using SNOMED CT can be processed and
presented in different ways to support direct patient care, clinical audit, research, epidemiology,
management and service planning. Additionally, the global scope of SNOMED CT reduces geographical
boundary effects arising from the use of different terminologies or coding systems in different
organizations and countries.
With SNOMED CT, clinical information is recorded using identifiers that refer to concepts that are formally
defined as part of the terminology. SNOMED CT supports recording of clinical information at appropriate
levels of detail using relevant clinical concepts. The structures of SNOMED CT allow information to be
entered using synonyms that suit local preferences while recording the information in a consistent and
comparable form. Additionally, the hierarchical nature of SNOMED CT permits information to be recorded
with different levels of detail to suit particular uses (e.g. |pneumonia|, |bacterial pneumonia| or
|pneumococcal pneumonia|). SNOMED CT allows additional detail to be added by combining concepts
where the available concepts are not sufficiently precise (e.g. |pneumococcal pneumonia| with a |finding
site| of |right upper lobe of lung|).
SNOMED CT allows a range of different options for immediate retrieval and subsequent reuse to address
immediate and longer term clinical requirements and the requirements of other users. The nature of
SNOMED CT hierarchies allow information to be selectively retrieved and reused to meet different
requirements at various levels of generalization (e.g. retrieval of subtypes of |lung disorder| or |bacterial
infection| would both include |bacterial pneumonia|).
SNOMED CT Starter Guide
July 2014
7 | P a g e
The SNOMED CT concept model also allows additional details to be considered when retrieving data. For
example, the concept |pneumococcal pneumonia| is a subtype of |bacterial pneumonia| which has a
defining relationship that specifies that the |causative agent| is |streptococcus pneumoniae| and this
allows the organism causing this disease to be analyzed.
Extent of practical use
Many systems use SNOMED CT to represent some types of clinical information. The extent of use is varied
in terms of:
The clinical content captured (i.e. what is included and what is not).
How the structure of this content relates to the structures in the records.
The scope and consistency of use and reuse (i.e. within and across national and local organizations,
across departments, within proprietary applications or specifically configured instances of
proprietary applications).
Approaches to implementation
SNOMED CT has been implemented in a variety of ways which differ in the extent to which they harness
particular features of the terminology. In some cases, these differences merely reflect the specific
requirements of a particular use. Other factors include the design of existing systems prior to the
introduction of SNOMED CT, sophistication of available technology and support for a range of other health
informatics standards.
Key determinants for effective benefits realization include:
Representation of stored clinical information.
o To enable effective reuse of clinical information, SNOMED CT should be used within a
record structure (or information model) that stores similar information consistently and in
ways that can be readily queried.
Ease of data entry
o Different approaches to data entry are valuable and may be mediated in a variety of ways
to enable ease of data entry.
o The method of data entry should not result in inconsistent representations of the same
types of clinical information.
o The most effective approaches constrain data entry specific to the clinical context and
reason for use.
o Unconstrained searches across the entire content of SNOMED CT are rarely appropriate for
routine data entry.
o Constraints that limit data entry to a fixed set of SNOMED CT concepts are useful where
the clinical context and reasons for use are narrow.
o Constraints that alter dynamically to meet requirements of a particular data entry context
offer a more generalizable approach that can be configured to meet different
requirements.
o Natural Language Processing (NLP) to parse and tag text with SNOMED CT expressions has
been found useful in some applications.
SNOMED CT Starter Guide
July 2014
8 | P a g e
Communication
o Communication interfaces, including message structures, need to be designed to retain the
common elements of clinical content structure and coding. Communication should enable
the receiving system to reuse the clinical information effectively based on the SNOMED CT
expressions within it.
Retrieval, analysis and reuse
o Record storage and indexing can be designed to optimize use of the semantic features of
SNOMED for selective retrieval and to support flexible analytics.
o Retrieval in the patient care setting should result in the display of clinical records including
highlighting of critical information selected taking account of the computer processable
expressivity of SNOMED CT.
o Real time decision support ranges from simple flagging of contraindications to guidelines
for investigation and management.
o Batch mode decision support identifies patients with chronic diseases and risk factors who
require recalls for review and other scheduled interventions.
o Analysis of data can be completed for selected populations of patients for a variety of
purposes including audit, service planning, epidemiology and clinical research.
Lessons learnt
The features of SNOMED CT support reusability of clinical information. However, reusability also requires a
consistent structured representation of clinical information that complements the meaning supported by
SNOMED CT. Without this, overlaps and conflicts between structural and terminological representations of
clinical content can result in ambiguous and potentially conflicting interpretations.
The way in which the use of terminology and structure together contribute to the representation of
meaningful information is sometimes referred to as the “model of meaning”. To enable widespread clinical
information reuse, queries need to be consistently formulated in ways that take account of the way the
information is structured and coded. A common model of meaning facilitates widespread reuse of clinical
information, ability to reuse queries and a consistent approach to linkage between clinical information and
knowledge resources.
Human factors may result in inconsistent recording of similar clinical information. This issue can be
minimized by effectively constraining data entry.
Challenges
An important limitation is the diversity of views related to the structure of clinical information and the
overlap between information models and terminology. There are also differing views on application design,
different requirements for collection of clinical information and different views on record structures and
data entry methods appropriate to different use cases.
IHTSDO is working with other standards bodies including the International Organisation for Standardisation
(ISO) and Health Level 7 (HL7), as well as various collaborative efforts exploring the relationship between
terminology and structured clinical information. The objective is to ensure that the role of SNOMED CT as a
key component of clinical information and systems is understood as part of overall efforts towards
harmonization and interoperability.
SNOMED CT Starter Guide
July 2014
9 | P a g e
4. SNOMED CT BASICS
This section provides an overview of:
SNOMED CT features
Exploring SNOMED CT
SNOMED CT design and development
SNOMED CT components and hierarchies
SNOMED CT characteristics
SNOMED CT supporting different languages
SNOMED CT products and services
Why is this important?
An awareness of SNOMED CT features, components, characteristics and products provides an initial
foundation on which to build greater understanding. It also informs discussions leading to decisions about
adoption, implementation and use of this terminology.
What is this?
SNOMED CT features
SNOMED CT:
Is the most comprehensive, multilingual clinical healthcare terminology in the world.
Is a resource with comprehensive, scientifically validated clinical content.
Enables consistent, processable representation of clinical content in electronic health records.
Is mapped to other international standards.
Is already used in more than fifty countries.
When implemented in software applications, SNOMED CT can be used to represent clinically relevant
information consistently, reliably and comprehensively as an integral part of producing electronic health
information.
Implementation requires an understanding of the way that SNOMED CT content is represented by
Components and supported by Reference Sets (Refsets).
Exploring SNOMED CT
While reading the guide, you may find it useful to explore the content of SNOMED CT. You can do this using
one of a range of online browsers listed on our web site at www.snomed.org/browsers. Note that the listed
browsers are not endorsed by IHTSDO and they should only be used to a get feel for the content and
structure of the terminology. It is useful to experiment with several different browsers as they vary in the
way they present particular features of the terminology.
SNOMED CT Starter Guide
July 2014
10 | P a g e
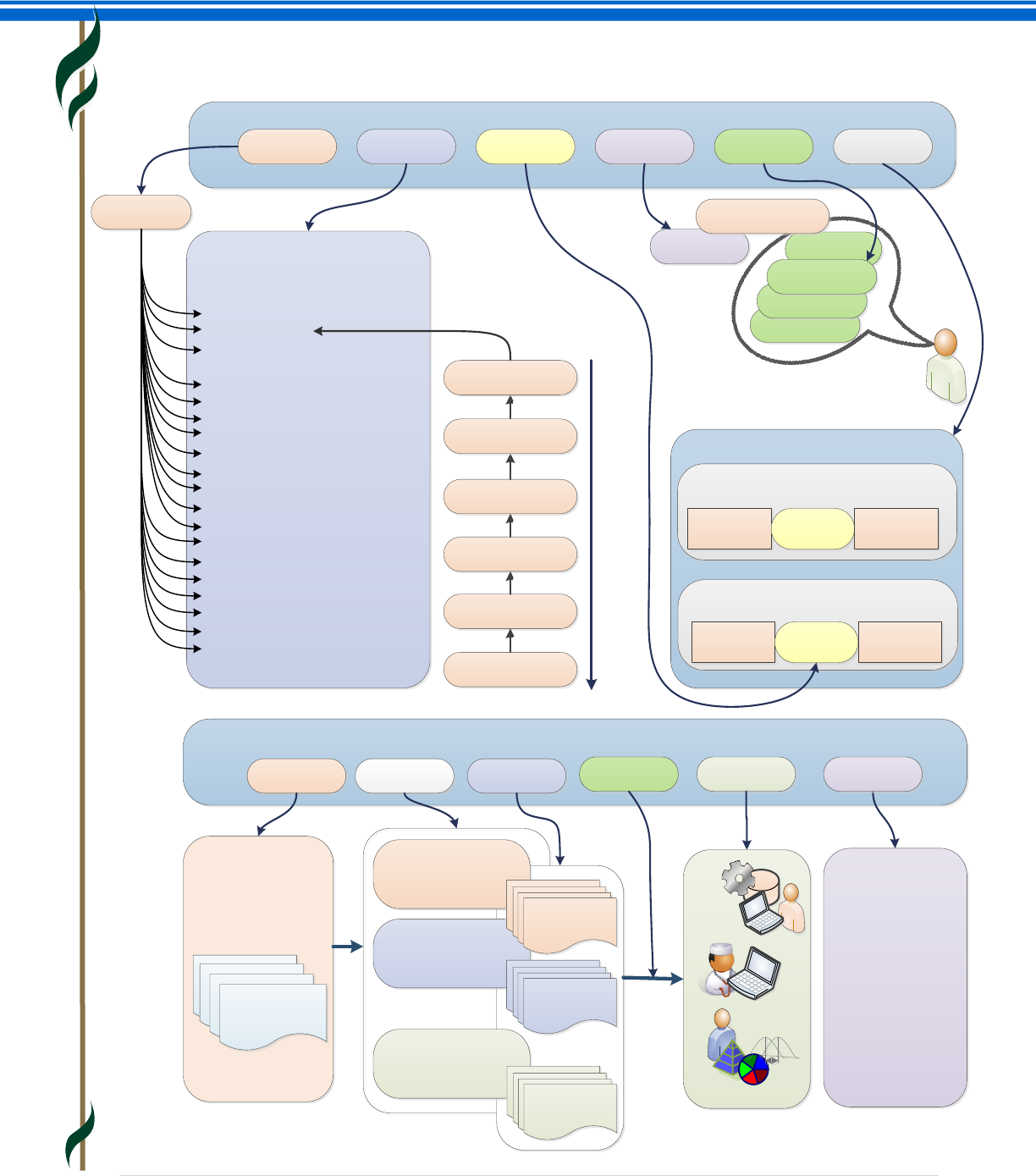
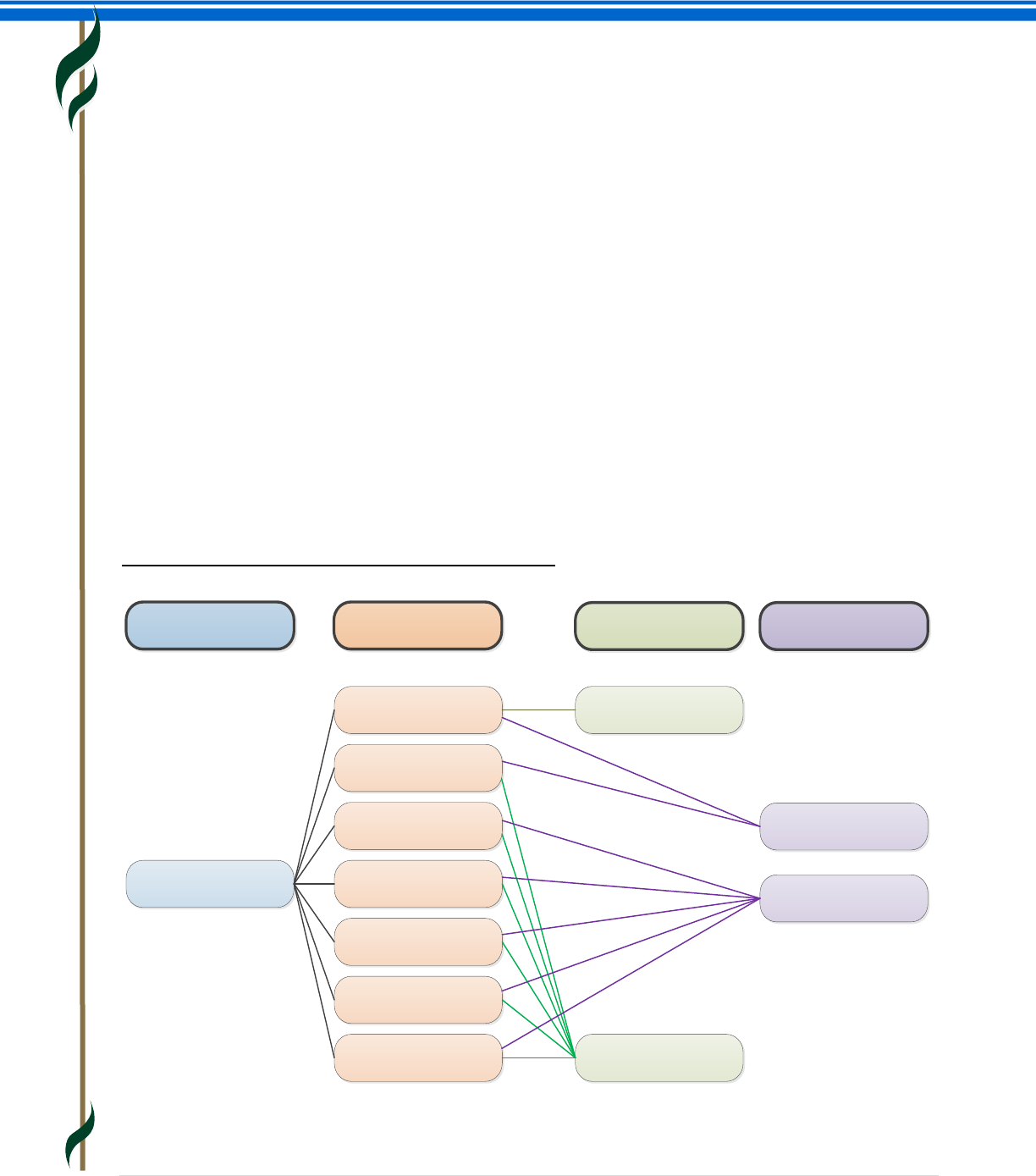
SNOMED CT design and development
Member country ZZ
National Release Center
Member country XX
National Release Center
Member country YY
National Release Center
84114007
· Clinical
documentation
· Semantic
interoperability
· Decision support
· Data retrieval
· Analytics
· Statistics
· Information
management
· Etc.
Weak heart
Myocardial failure
HF – Heart failure
Cardiac failure
SNOMED CT HIERARCHIES
Concepts are organized into top-level
hierarchies
SNOMED CT DESIGN
Concepts DescriptionsHierarchies RelationshipsIdentifiersAttributes
SNOMED CT
Joint finding
Arthropathy
Arthropathy of knee joint
Arthritis of knee
ROOT
CONCEPT
Is a
Is a
Is a
Is a
Is a
Is a
RELATIONSHIPS
Is a relationships connect
concepts in a hierarchy
Arthropathy Is a
High granularity
Low granularity
Attribute relationships connect concepts
in different hierarchies
Appendicitis Associated
morphology Inflammation
Heart failure (disorder)
SNOMED CT DEVELOPMENT AND RELEASES
· Body structure
· Clinical finding
· Environment or geographical
location
· Event
· Linkage concept
· Observable entity
· Organism
· Pharmaceutical / biologic product
· Physical force
· Physical object
· Procedure
· Qualifier value
· Record artifact
· Situation with explicit context
· Social context
· Special concept
· Specimen
· Staging and scales
· Substance
· Body structure
· Clinical finding
· Environment or geographical
location
· Event
· Linkage concept
· Observable entity
· Organism
· Pharmaceutical / biologic product
· Physical force
· Physical object
· Procedure
· Qualifier value
· Record artifact
· Situation with explicit context
· Social context
· Special concept
· Specimen
· Staging and scales
· Substance
· Development
· Maintance
· Education
· Distribution
· Releases
SNOMED CT international
‘SNOMED CT Core’
Release: month/year
SNOMED CT international
‘SNOMED CT Core’
Release: month/year
SNOMED CT international
‘SNOMED CT Core’
Release: month/year
SNOMED CT international
‘SNOMED CT Core’
Release: month/year
....
....
SNOMED CT ‘XX
National’ Edition
Release: month/year
SNOMED CT ‘ZZ
National’ Edition
Release: month/year
SNOMED CT ‘YY
National’ Edition
Release: month/year
20%
20%
20%
20%
20%
Joint finding
IHTSDO Members Implementation
Reference Sets Users
Finding by site
Musculoskeletal finding
Purposes
SNOMED CT Starter Guide
July 2014
11 | P a g e
SNOMED CT Components
SNOMED CT is a core clinical healthcare terminology that contains concepts with unique meanings and
formal logic based definitions organized into hierarchies.
SNOMED CT content is represented using three types of component:
Concepts representing clinical meanings that are organized into hierarchies.
Descriptions which link appropriate human readable terms to concepts.
Relationships which link each concept to other related concepts.
These components are supplemented by Reference Sets, which provide additional flexible features and
enable configuration of the terminology to address different requirements.
Concepts
SNOMED CT concepts represent clinical thoughts, ranging from |abscess| to |zygote|. Every concept has a
unique numeric concept identifier. Within each hierarchy, concepts are organized from the general to the
more detailed. This allows detailed clinical data to be recorded and later accessed or aggregated at a more
general level.
Descriptions
SNOMED CT descriptions link appropriate human readable terms to concepts. A concept can have several
associated descriptions, each representing a synonym that describes the same clinical concept. Each
translation of SNOMED CT includes an additional set of descriptions, which link terms in another language
to the same SNOMED CT concepts. Every description has a unique numeric description identifier.
Relationships
SNOMED CT relationships link concepts to other concepts whose meaning is related in some way. These
relationships provide formal definitions and other properties of the concept. One type of relationship is the
|is a| relationship which relates a concept to more general concepts. These |is a| relationships define the
hierarchy of SNOMED CT concepts.
For example, the concepts |bacterial pneumonia| and |viral pneumonia| both have an |is a|
relationship to |infective pneumonia| which has an |is a| relationship to the more general concept
|pneumonia|.
Other types of relationships represent aspects of the meaning of a concept.
For example, the concept |viral pneumonia| has a |causative agent| relationship to the concept
|virus| and a |finding site| relationship to the concept |lung|.
Every relationship has a unique numeric relationship identifier.
Reference sets
Reference sets (Refsets) are a flexible standard approach used by SNOMED CT to support a variety of
requirements for customization and enhancement of SNOMED CT. These include the representation of
subsets, language preferences for use of particular terms and mapping from or to other code systems.
Every reference set has a unique numeric concept identifier.
SNOMED CT Starter Guide
July 2014
12 | P a g e
SNOMED CT hierarchies
SNOMED CT concepts are organized in hierarchies. Within a hierarchy, concepts range from the more
general to the more detailed. Related concepts in the hierarchy are linked using the |is a| relationship.
Examples of some of the hierarchies include |clinical finding|, |procedure|, |observable entity|,
|body structure| and |organism|.
SNOMED CT characteristics - comprehensive, scalable and flexible
SNOMED CT has a broad coverage of health related topics. It can be used to describe a patient's medical
history, the details of an orthopedic procedure, the spread of epidemics, and much more. At the same
time, the terminology has an unmatched depth, which enables clinicians to record data at the appropriate
level of granularity.
Specific applications tend to focus on a restricted set of SNOMED CT, such as concepts related to
ophthalmology. These subsets can be used to present relevant parts of the terminology, depending on the
clinical context and local requirements. This means for example, that a drop down list to select diagnoses in
an electronic health record in a mental health facility can be tailored to that setting. Similarly, subsets can
be defined for problem lists for physician specialties or to provide appropriate medication lists for nurses in
community care.
When individual jurisdictions have needs beyond those that can be reflected in a global terminology,
perhaps due to requirements in local legislation, they can develop local or national extensions. Thus, even
though SNOMED CT is global in scope, it can be adapted to each country's or areas requirements.
SNOMED CT maps work to provide explicit links to health related classifications and coding schemes in use
around the world, e.g. statistical classifications such as ICD-9-CM, ICD-10, and ICD-O3. Maps to or from
several national code systems are also available from, or under development, by IHTSDO Members. Maps
to or from clinical domain specific code systems are also maintained by specialty groups with which IHTSDO
has collaborative agreement. Maps facilitate reuse of SNOMED CT based clinical data for other purposes,
such as reimbursement or statistical reporting.
Supporting different languages
SNOMED CT is a multinational, multilingual terminology. It has a built-in framework to manage different
languages and dialects. The International Release includes a set of language independent concepts and
relationships. Today, SNOMED CT is available in US English, UK English, Spanish, Danish and Swedish. Partial
translations into Canadian French, Lithuanian, and several other languages are currently taking place, and
further language translations are being planned by IHTSDO Members.
The basic objective of any SNOMED CT translation is to provide accurate representations of SNOMED CT
concepts in a way that is understandable, usable, and safe. Translations must be concept based.
Translators need to analyses concepts based on the fully specified name and take account of its position
within the hierarchy, its descriptions, and its relationships to other concepts. This enables a meaningful
translation of a concept based on phrases that are well used and clearly understood in all countries. The
IHTSDO maintains guidelines and other materials to support countries undertaking translations.
SNOMED CT Starter Guide
July 2014
13 | P a g e
SNOMED CT products and services
IHTSDO Members and organizations covered by the SNOMED CT Affiliate License have access to a range of
products and services, including:
SNOMED CT terminology files consisting of:
o Concepts
o Descriptions
o Relationships
Derivative works that help in the uptake and use of SNOMED CT, including Reference Sets that
support:
o Identification of subsets of SNOMED CT content
o Language or dialect preferences for use of particular descriptions
o Maps to other code systems and classifications
o Other relevant metadata to support use of SNOMED CT components.
Implementation guidance for successful use of SNOMED CT including:
o Implementation guidance
o Translation guidance
o Editorial guidance for content development
Access to services supporting submission of requests for changes or additions to content and
documentation.
Participation in the global IHTSDO community through an electronic collaborative space and
meeting of special interest groups.
SNOMED CT Starter Guide
July 2014
14 | P a g e
5. SNOMED CT LOGICAL MODEL
This section provides an overview of:
Logical Model Components – representing the core content of the terminology
Reference Sets – configuring and enhancing terminology content
Why is this important?
The SNOMED CT logical model provides the fundamental structure of SNOMED CT and specifies how the
components can be managed in an implementation setting to meet a variety of primary and secondary
uses.
What is this?
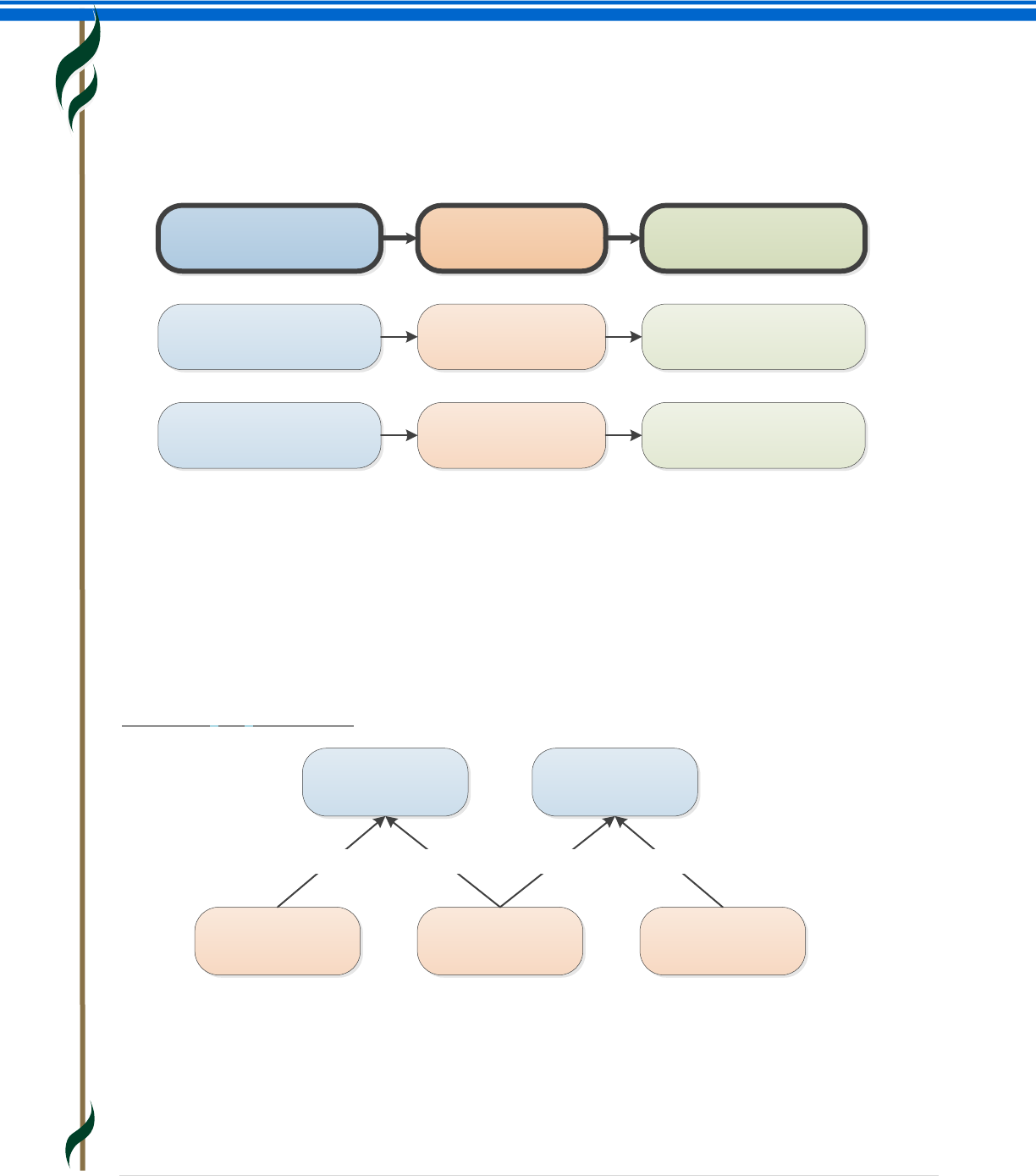
The SNOMED CT logical model defines the way in which each type of SNOMED CT component and
derivative is related and represented. The core component types in SNOMED CT are concepts, descriptions
and relationships. The logical model therefore specifies a structured representation of the concepts used to
represent clinical meanings, the descriptions used to refer to these, and the relationships between the
concepts.
Concepts
Every concept represents a unique clinical meaning, which is referenced using a unique, numeric and
machine-readable SNOMED CT identifier. The identifier provides an unambiguous unique reference to each
concept and does not have any ascribed human interpretable meaning.
Other types of components also have unique identifiers – however, the concept identifier has a
specific role as the code used to represent the meaning in clinical records, documents, messages
and data.
SNOMED CT
identifier
Descriptions
Fully Specified
Name (FSN)
Synonym
Relationships
|Is a|
relationship
Attribute
relationship
Concept
Components
One FSN Is marked
as “Preferred” in
each language
One Synonym is
marked as
“Preferred” in
each language
Each concept has at
least one |is a|
relationship
Each concept can have
as many attribute
relationships as needed
Each component has
a unique identfier
There may also be any
number of Synonyms
marked as “Acceptable”
SNOMED CT Starter Guide
July 2014
15 | P a g e
Descriptions
A set of textual descriptions are assigned to every concept. These provide the human readable form of a
concept. Two types of description are used to represent every concept - Fully Specified Name (FSN) and
Synonym.
The FSN represents a unique, unambiguous description of a concept’s meaning. The FSN is not intended to
be displayed in clinical records, but is instead used to disambiguate the distinct meaning of each different
concept. This is particularly useful when different concepts are referred to by the same commonly used
word or phrase. Each concept can have only one FSN in each language or dialect.
A synonym represents a term that can be used to display or select a concept. A concept may have several
synonyms. This allows users of SNOMED CT to use the terms they prefer to refer to a specific clinical
meaning. Concepts can have multiple synonyms, and the associated terms are not necessarily unique –
thus two concepts can have the same synonym term. Interpretation of a synonymous term therefore
depends on the concept identifier.
Each concept has one synonym which is marked as |preferred | in a given language, dialect, or context of
use. This is known as the “preferred term” and is a word or phrase commonly used by clinicians to name
that concept. In each language, dialect or context of use, one and only one synonym can be marked as |
preferred |. Any number of other synonyms that are valid in a language, dialect or context of use can be
marked as | acceptable |.
Example of descriptions for a single concept (US - English)
Concept Id Description Description type
myocardial infarction
(disorder)
22298006
myocardial infarction
Infarction of heart
cardiac infarction
heart attack
myocardial infarct
MI – Myocardial
infarction
Fully Specified Name
(FSN)
Synonym
Acceptability
(US English Language Ref Set)
Preferred
Acceptable
SNOMED CT Starter Guide
July 2014
16 | P a g e
Relationships
A relationship represents an association between two concepts. Relationships are used to logically define
the meaning of a concept in a way that can be processed by a computer. A third concept, called a
relationship type (or attribute), is used to represent the meaning of the association between the source
and destination concepts. There are different types of relationships available within SNOMED CT.
Subtype relationships
Subtype relationships are the most widely used type of relationship. Subtype relationships use the |is a|
relationship type and are therefore also known as |is a| relationships. Almost all active SNOMED CT
concepts are the source of at least one |is a| relationship. The only exception is the root concept
|SNOMED CT Concept| which is the most general concept. The |is a| relationship states that the source
concept is a subtype of the destination concept. SNOMED CT relationships are directional and the |is a|
relationship read in the reverse direction states that the destination concept is a supertype of the source
concept.
Example of |is a| relationships
The |is a| relationships form the hierarchies of SNOMED CT. They are therefore also known as hierarchical
relationships. The source concept of the |is a| relationship has a more specific clinical meaning than the
target concept. This means that the level of clinical detail of the concepts increases with the depth of the
hierarchies.
Concept
(source) Relationship type Concept
(destination)
44054006
diabetes mellitus type 2
(disorder)
116680003
Is a
(attribute)
73211009
diabetes mellitus
(disorder)
44054006
diabetes mellitus type 2
(disorder)
363698007
Finding site
(attribute)
113331007
structure of endocrine system
(body structure)
385627004
Cellulitis
128276007
Cellulitis of foot
118932009
Disorder of foot
|Is a||Is a|
62837005
Cellulitis of hand
|Is a|
95345008
Ulcer of foot
|Is a|
SNOMED CT Starter Guide
July 2014
17 | P a g e
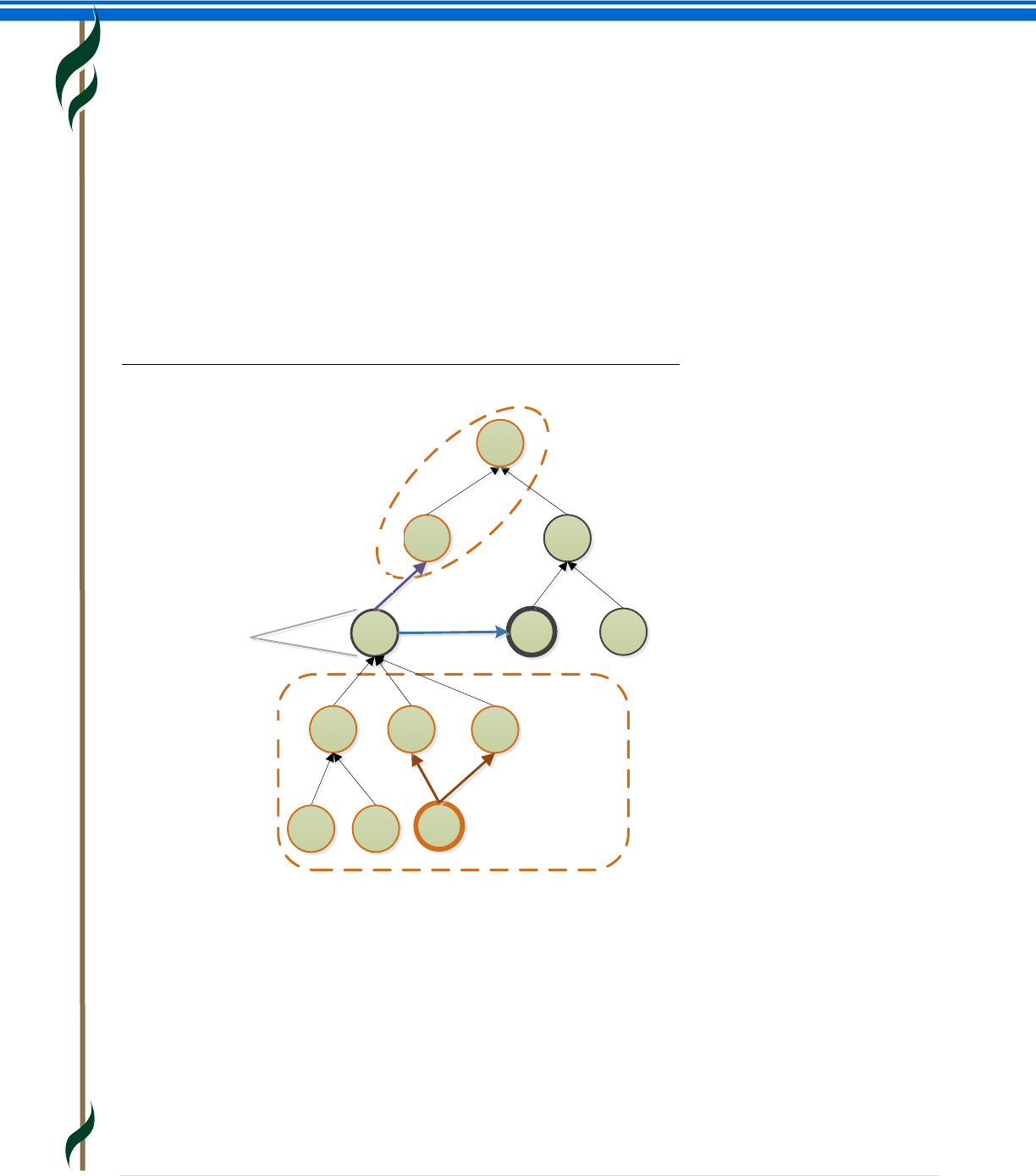
If two concepts are directly linked by a single |is a| relationship, the source concept is said to be a “subtype
child” of the destination concept. The destination concept is referred to as a “supertype parent”. Any
concept that is the source of a sequence of one or more |is a| relationships leading to a specified
destination concept, is a “subtype descendant” of that concept. Similarly, any concept that is the
destination of a sequence of one or more |is a| relationships leading to a specified source concept, is a
“supertype ancestor” of that concept. It is also said that the source concept of an |is a| relationship “is
subsumed by” the target concept, and that the target concept of an |is a| relationship “subsumes” the
source concept.
Each concept can have |is a| relationships to several other concepts (i.e. a concept may have multiple
supertype parent concepts). As a result the SNOMED CT hierarchy is not a simple tree but has a structure
that is known as a “polyhierarchy”.
Illustration of SNOMED CT subtype hierarchy and terms used to describe it
Attribute relationships
An attribute relationship contributes to the definition of the source concept by associating it with the value
of a defining characteristic. The characteristic (attribute) is specified by the relationship type and the value
is provided by the destination of the relationship.
The following example shows the defining relationships of the concept |abscess of heart|. The attribute
relationships |associated morphology| and |finding site| are used to associate the source concept
|abscess of heart| to respectively the target concepts |abscess|, and |heart structure|.
Top level hierarchy
Multi-parent /
Acyclic graph
Subtype descendants
Attribute
relationship
Supertype ancestors
Supertype parent
Root Concept – SNOMED CT
|is a| relationship
Subtype child
Concept in focus
SNOMED CT Starter Guide
July 2014
18 | P a g e
Example of defining relationships
Unlike |is a| relationships, which are used to define all concepts, the applicability of each type of attribute
relationship is limited to a defined domain and range. The domain refers to the concepts that can serve as
source concepts for that type of attribute relationship. The range refers to the concepts that can serve as
destinations (values) for those attributes. The domain and range specification ensure consistent definitions
that can be used to infer additional semantic relationships to deliver reliable meaning-based retrieval of
the composed meanings.
The first example below violates the domain constraint of |causative agent|, as descendants of |body
structure| are not in the domain of |causative agent|. The second example below is valid with respect to
the domain constraint of |causative agent|, because |disorder| is in the domain of |causative agent|.
However, this example violates the range constraint of |causative agent|, as descendants of morphological
abnormality are not in the range of |causative agent|.
Example of erroneous relationships
42522007
abscess of mediastinum
(disorder)
128998007
inflammatory disorder of the
cardiovascular system (disorder)
128599005
structural disorder of heart
(disorder)
|is a|44132006
abscess
(morphological abnormality)
|associated morphology|
425548001
abscess of heart
(disorder)
80891009
heart structure
(body structure)
|finding site|
|is a| |is a|
Group
Concept Relationship type Concept
6142004
influenza
(disorder)
246075003
causative agent
(attribute)
182046008
entire femur
(body structure)
246075003
causative agent
(attribute)
115650001
Renotrophic virus
(organism)
44132006
abscess
(morphological
abnormality)
SNOMED CT Starter Guide
July 2014
19 | P a g e
Fully defined and primitive concepts
In SNOMED CT every concept is specified as either fully defined or primitive.
A concept is fully-defined if its defining characteristics are sufficient to distinguish its meaning from other
similar concepts. One example is that the concept |acute disease| is fully-defined by its two defining
relationships. The first relationship is |is a| |disease| and the second relationship is |clinical course|
|sudden onset AND/OR short duration|. Stating that this concept is fully-defined means that any concept
that |is a| |disease| and has a |clinical course| of |sudden onset AND/OR short duration| is a subtype of
this concept (or the concept itself).
A concept is primitive (not fully-defined) if its defining characteristics are not sufficient to uniquely
distinguish its meaning from other similar concepts. One example is that the primitive concepts |disease|
and |drug action| share the same defining characteristics: namely a relationship of type |is a| to the
concept |clinical finding|. This is despite the fact that the concepts |disease| and |drug action| represent
different clinical ideas.
Reference sets
Reference Sets (Refsets) are a standard way to represent additional non-defining information about
members of a set of components. Reference Sets are important as they can be used in SNOMED CT
enabled applications to constrain, configure and enhance functionality to match requirements for different
use cases. Some examples of the many uses of reference sets are to represent:
Language and dialect preferences for use of particular terms to describe a concept. Language
Reference Sets allow the preferred and acceptable descriptions to be configured for a language,
dialect or context of use.
Subsets of components that are included in or excluded from the set of values that can be used in
a particular country, Organisation, specialty or context.
Value sets of concepts limiting the permitted content of a field in line with requirements of
standard message or communication interface.
Frequently used descriptions or concepts that can be prioritized for searches in a particular
country, Organisation, specialty or context.
Structuring and ordering of lists and hierarchies to display concepts in convenient structured lists
or tree-view controls to assist entry of particular data items.
Maps to or from other code systems the maps supported by Reference Sets includes simple one-
to-one maps and more complex maps requiring human-readable advice or machine processable
rules to resolve ambiguities.
SNOMED CT Starter Guide
July 2014
20 | P a g e
6. SNOMED CT CONCEPT MODEL
This section provides an overview of:
Concept Model – Top Level Hierarchies
Concept Model Attributes – Representing Characteristics of a Concept
Why is this important?
The SNOMED CT concept model specifies the way in which SNOMED CT concepts are defined using a
combination of formal logic and editorial rules. Concept model rules specify the top level concepts under
which concepts are arranged in the subtype hierarchy and the types of relationships that are permitted
between concepts in particular branches of the hierarchy.
What is this?
Concept model – top level hierarchies
The top of the SNOMED CT hierarchy is occupied by the root concept (|SNOMED CT concept|). All concepts
are descended from this root concept through at least one sequence of |is a| relationships. This means
that the root concept is a supertype of all other concepts and all other concepts are subtypes of the root
concept.
The direct subtypes of the root concept are referred to as ‘Top Level Concepts’. These concepts are used to
name the main branches of the hierarchy. Each of these Top Level Concepts, together with their many
subtype descendants, forms a major branch of the SNOMED CT hierarchy and contains similar types of
concepts. As the hierarchies descend (that is, more |is a| relationships are added below the Top Level
Concepts) the concepts within them become increasingly specific.
Below is a list of the Top Level Concepts with a brief description of the content represented in their branch
of the hierarchy.
|Clinical finding| represents the result of a clinical observation, assessment or judgment and
includes normal and abnormal clinical states (e.g. |asthma|, |headache|, |normal breath
sounds|). The |clinical finding| hierarchy includes concept used to represent diagnoses.
|Procedure| represents activities performed in the provision of health care. This includes not only
invasive procedures but also administration of medicines, imaging, education, therapies and
administrative procedures (e.g. |appendectomy|, |physiotherapy|, |subcutaneous injection|).
|Situation with explicit context| represents concepts in which the clinical context is specified as
part of the definition of the concept itself. These include presence or absence of a condition,
whether a clinical finding is current, in the past or relates to someone other than the subject of the
record (e.g. |endoscopy arranged|, |past history of myocardial infarction|, |family history of
glaucoma|).
|Observable entity| represents a question or assessment which can produce an answer or result
(e.g. | systolic blood pressure|, |color of iris|, |gender|).
SNOMED CT Starter Guide
July 2014
21 | P a g e
|Body structure| represents normal and abnormal anatomical structures (e.g. |mitral valve
structure|, |adenosarcoma|).
|Organism| represents organisms of significance in human and animal medicine (e.g.
|streptococcus pyogenes|, |beagle|, |texon cattle breed|).
|Substance| represents general substances, the chemical constituents of
pharmaceutical/biological products, body substances, dietary substances and diagnostic
substances (e.g. |methane|, |insulin|, |albumin|).
|Pharmaceutical / biologic product| represents drug products (e.g. |amoxicillin 250mg capsule|,
|paracetamol + codeine tablet|).
|Specimen| represents entities that are obtained (usually from the patient) for examination or
analysis (e.g. |urine specimen|, |prostate needle biopsy specimen|).
|Special concept| represents concepts that do not play a part in the formal logic of the concept
model of the terminology, but which may be useful for specific use cases (e.g. |navigational
concept|, |alternative medicine poisoning|).
|Physical object| represents natural and man-made physical objects (e.g. |vena cava filter|,
|implant device|, |automobile|).
|Physical force| represents physical forces that can play a role as mechanisms of injury (e.g.
|friction|, |radiation|, |alternating current|).
|Event| represents occurrences excluding procedures and interventions (e.g. |flood|,
|earthquake|).
|Environments and geographical locations| represents types of environments as well as named
locations such as countries, states and regions (e.g. |intensive care unit|, |academic medical
center|, |Denmark|).
|Social context| represents social conditions and circumstances significant to health care (e.g.
|occupation|, |spiritual or religious belief|).
|Staging and scales| represents assessment scales and tumor staging systems (e.g. |Glasgow Coma
Scale|, |FIGO staging system of gynecological malignancy|).
|Qualifier value| represents the values for some SNOMED CT attributes, where those values are
not subtypes of other top level concepts. (e.g. |left|, |abnormal result|, |severe|).
|Record artefact| represents content created for the purpose of providing other people with
information about record events or states of affairs. (e.g. |patient held record|, |record entry|,
|family history section|).
|SNOMED CT Model Component| contains technical metadata supporting the SNOMED CT
release.
SNOMED CT Starter Guide
July 2014
22 | P a g e
Concept model attributes – representing characteristics of a concept
SNOMED CT attributes (or relationship types) are used to represent a characteristic of the meaning of a
concept. SNOMED CT currently uses more than fifty defining attributes when defining the meaning of
concepts. Each SNOMED CT attribute can be applied to concepts in one or more branches of the hierarchy.
The set of concepts to which an attribute can be applied is called the ‘domain’ of the attribute. The
permitted set of values for each attribute is called the ‘range’ of the attribute.
Domain
The domain is the hierarchy to which a specific attribute can be applied.
For example:
The domain of the attribute |associated morphology| is the |clinical finding| hierarchy.
Therefore, a |procedure| cannot have an |associated morphology|.
However, a |procedure| can have a |procedure morphology|.
Range
The range is the set of SNOMED CT concepts that are allowed as the value of a specified attribute.
For example:
The range for the attribute |associated morphology| is the concept |morphologically abnormal
structure| and its subtype descendants.
The range for the attribute |finding site| is |anatomical or acquired body structure| and its
subtype descendants in the |body structure| hierarchy.
Examples of the domain and range specified for the attributes |finding site| and |laterality|
DOMAIN
(hierarchy) ATTRIBUTE RANGE
(concept or hierarchy)
|Clinical finding| |FINDING SITE|<< 442083009 |Anatomical or
acquired body structure|
<< This Concept or
one of its and
descendants.
|Body structure| |LATERALITY|< 182353008 |Side| < Descendants only.
Not the concept
itself.
A specific domain to which
the attribute may be applied.
Typically this is a top-level
hierarchy.
A relationship type used to
characterize the semantic
meaning of the source
concept.
The allowable values that can
be applied to each Attribute.
SNOMED CT Starter Guide
July 2014
23 | P a g e
Some SNOMED CT attributes (or relationship types) have a hierarchical relationship to one another. The
hierarchy formed from such relationships is known as an ‘attribute hierarchy’. In an attribute hierarchy,
one general attribute is the parent of one or more specific subtypes of that attribute. Subtypes of a
concept defined using the more general attribute can be defined using a more specific subtype of that
attribute. For example, |after|, |causative agent| and |due to| are subtypes of |associated with|, because
they have a more specific meaning.
Attributes used to define SNOMED CT concepts
The SNOMED CT defining attributes are used to represent the meaning of concepts in these 9 hierarchies:
Clinical finding concepts
Procedure concepts
Evaluation procedure concepts
Specimen concepts
Body structure concepts
Pharmaceutical/biologic product concepts
Situation with explicit context concepts
Event concepts
Physical object concepts
Attributes used to define clinical finding concepts
Below is a list of attributes used to define |clinical finding| concepts, and a brief description of their
meaning:
|Finding site| specifies the body site affected by a condition
|Associated morphology| specifies the morphologic changes seen at the tissue or cellular level
that are characteristic features of a disease.
|Associated with| represents a clinically relevant association between concepts without either
asserting or excluding a causal or sequential relationship between the two.
|After| represents a sequence of events where a clinical finding occurs after another |clinical
finding| or a |procedure|.
|Due to| relates a |clinical finding| directly to a cause such as another |clinical finding| or a
|procedure|.
|Causative agent| identifies the direct causative agent of a disease such as an |organism|,
|substance| or |physical force|. (Note: This attribute is not used for vectors, such as mosquitos
transmitting malaria).
|Severity| used to sub-class a |clinical finding| concept according to its relative severity.
|Clinical course| represents both the onset and course of a disease.
SNOMED CT Starter Guide
July 2014
24 | P a g e
|Episodicity| represents episodes of care provided by a physician or other care provider, such as a
general practitioner. This attribute is not used to represent episodes of disease experienced by the
patient.
|Interprets| refers to the entity being evaluated or interpreted, when an evaluation, interpretation
or judgment is intrinsic to the meaning of a concept.
|Has interpretation|, when grouped with the attribute |interprets|, designates the judgment
aspect being evaluated or interpreted for a concept (e.g. presence, absence etc.)
|Pathological process| provides information about the underlying pathological process for a
disorder, but only when the results of that process are not structural and cannot be represented by
the |associated morphology| attribute.
|Has definitional manifestation| links disorders to the manifestations (observations) that define
them.
|Occurrence| refers to a specific period of life during which a condition first presents.
|Finding method| specifies the means by which a clinical finding was determined. This attribute is
frequently used in conjunction with |finding informer|.
|Finding informer| specifies the person (by role) or other entity (e.g. a monitoring device) from
which the clinical finding information was obtained. This attribute is frequently used in conjunction
with |finding method|.
Attributes used to define procedure concepts
|Procedure site| describes the body site acted on or affected by a procedure.
|Procedure morphology| specifies the morphology or abnormal structure involved in a procedure.
|Method| represents the action being performed to accomplish the procedure. It does not include
the surgical approach, equipment or physical forces.
|Procedure device| describes the devices associated with a procedure.
|Access| describes the route used to access the site of the procedure.
|Direct substance| describes the |substance| or |pharmaceutical / biologic product| on which the
procedure’s method directly acts.
|Priority| refers to the priority assigned to a procedure.
|Has focus| specifies the |clinical finding| or |procedure| which is the focus of a procedure.
|Has intent| specifies the intent of a procedure.
|Recipient category| specifies the type of individual or group upon which the action of the
procedure is performed.
|Revision status| specifies whether a procedure is primary or a revision.
SNOMED CT Starter Guide
July 2014
25 | P a g e
|Route of administration| represents the route by which a procedure introduces a given
substance into the body.
|Surgical approach| specifies the directional, relational or spatial access to the site of a surgical
procedure.
|Using substance| describes the substance used to execute the action of a procedure, but it is not
the substance on which the procedure’s method directly acts.
|Using energy| describes the energy used to execute an action.
Attributes used to define evaluation procedure concepts
|Has specimen| specifies the type of specimen on which a measurement or observation is
performed.
|Component| refers to what is being observed or measured by a procedure.
|Time aspect| specifies temporal relationships for a measurement procedure.
|Property| specifies the kind of property being measured.
|Scale type| refers to the scale of the result of an observation of a diagnostic test.
|Measurement method| specifies the method by which a procedure is performed.
Attributes used to define specimen concepts
|Specimen procedure| identifies the procedure by which a specimen is obtained.
|Specimen source topography| specifies the body site from which a specimen is obtained.
|Specimen source morphology| specifies the morphologic abnormality from which a specimen is
obtained.
|Specimen substance| specifies the type of substance of which a specimen is comprised.
|Specimen source identity| specifies the type of individual, group or physical location from which
a specimen is collected.
Attributes used to define body structure concepts
|Laterality| provides information on whether a body structure is left, right, bilateral or unilateral. It
is applied only to bilaterally symmetrical body structures which exist on opposite sides of the body.
Attributes used to define pharmaceutical/biologic product concepts
|Has active ingredient| indicates the active ingredient of a drug product, linking the
|pharmaceutical / biologic product| hierarchy to the |substance| hierarchy.
|Has dose form| specifies the dose form of a product.
SNOMED CT Starter Guide
July 2014
26 | P a g e
Attributes used to define situation with explicit context concepts
|Associated finding| Links concepts in the |situation with explicit context| hierarchy to their
related |clinical finding|.
|Finding context| represents a situation in which a |clinical finding| is known, or unknown, and if
known, whether it is present, absent or uncertain (possible), and to also express the meaning that
the finding is not actual but is instead an anticipated or possible future finding.
|Associated procedure| links concepts in the |situation with explicit context| hierarchy to
concepts in the |procedure| hierarchy for which there is additional specified context.
|Procedure context| indicates the degree of completion, or status of a |procedure|, as well as its
various possible future states prior to its being initiated or completed.
|Temporal context| indicates the time of the occurrence of the situation, by indicating whether
the associated procedure or finding is actual and therefore occurred in the present, in the past, or
at a specified time; or that it is planned or expected in the future.
|Subject relationship context| specifies the subject of the |clinical finding| or |procedure| being
recorded, in relation to the subject of the record.
Attributes used to define event concepts
|Associated with| represents a clinically relevant association between concepts without either
asserting or excluding a causal or sequential relationship between the two.
|Occurrence| refers to the specific period of life during which a condition first presents.
Attributes used to define physical object concepts
|has active ingredient| indicates the active ingredient of a drug product, linking the
|pharmaceutical / biologic product| hierarchy to the |substance| hierarchy.
SNOMED CT Starter Guide
July 2014
27 | P a g e
7. SNOMED CT EXPRESSIONS
This section provides an overview of:
Precoordinated Expressions
Postcoordinated Expressions
Why is this important?
SNOMED CT provides a mechanism that enables clinical phrases to be represented, even when a single
SNOMED CT concept does not capture the required level of detail. This is important as it enables a wide
range of clinical meanings to be captured in a record, without requiring the terminology to include a
separate concept for every detailed combination of ideas that may potentially need to be recorded.
Application software that supports the use of SNOMED CT expressions enables detailed clinical information
to be recorded, retrieved and analyzed.
What is this?
Clinical expressions using SNOMED CT concepts can be of two types: precoordinated expressions, which
use a single SNOMED CT concept identifier; and postcoordinated expressions, which contain more than one
SNOMED CT identifier.
SNOMED CT support of the postcoordination technique allows additional clinical detail to be represented if
required. For example, |pneumococcal pneumonia| has a |finding site| of |lung structure|, which can be
refined to |right upper lobe of lung|.
Postcoordination greatly increases the depth of detail that SNOMED CT can represent without having to
include every possible specific site for every possible disorder via a concept. For example, the concept
|bacterial pneumonia| has a defining relationship specifying its |causative agent| as |bacteria| and this
can be refined to |Streptococcus pneumoniae|.
SNOMED CT expressions are a structured combination of one or more concept identifiers used to represent
a clinical idea in a logical manner, which is automatically processable. Expressions are represented using
the SNOMED CT compositional grammar, which is a lightweight syntax for the representation of SNOMED
CT expressions.
The logic on which the SNOMED CT concept model is based allows alternative representations of the same
or similar information to be recognized and compared. For example, |pneumococcal pneumonia| refined
by |finding site| |right upper lobe of lung| can be computed to have the same meaning as |right upper
lobe pneumonia| refined by |causative agent| |Streptococcus pneumoniae|.
SNOMED CT Starter Guide
July 2014
28 | P a g e
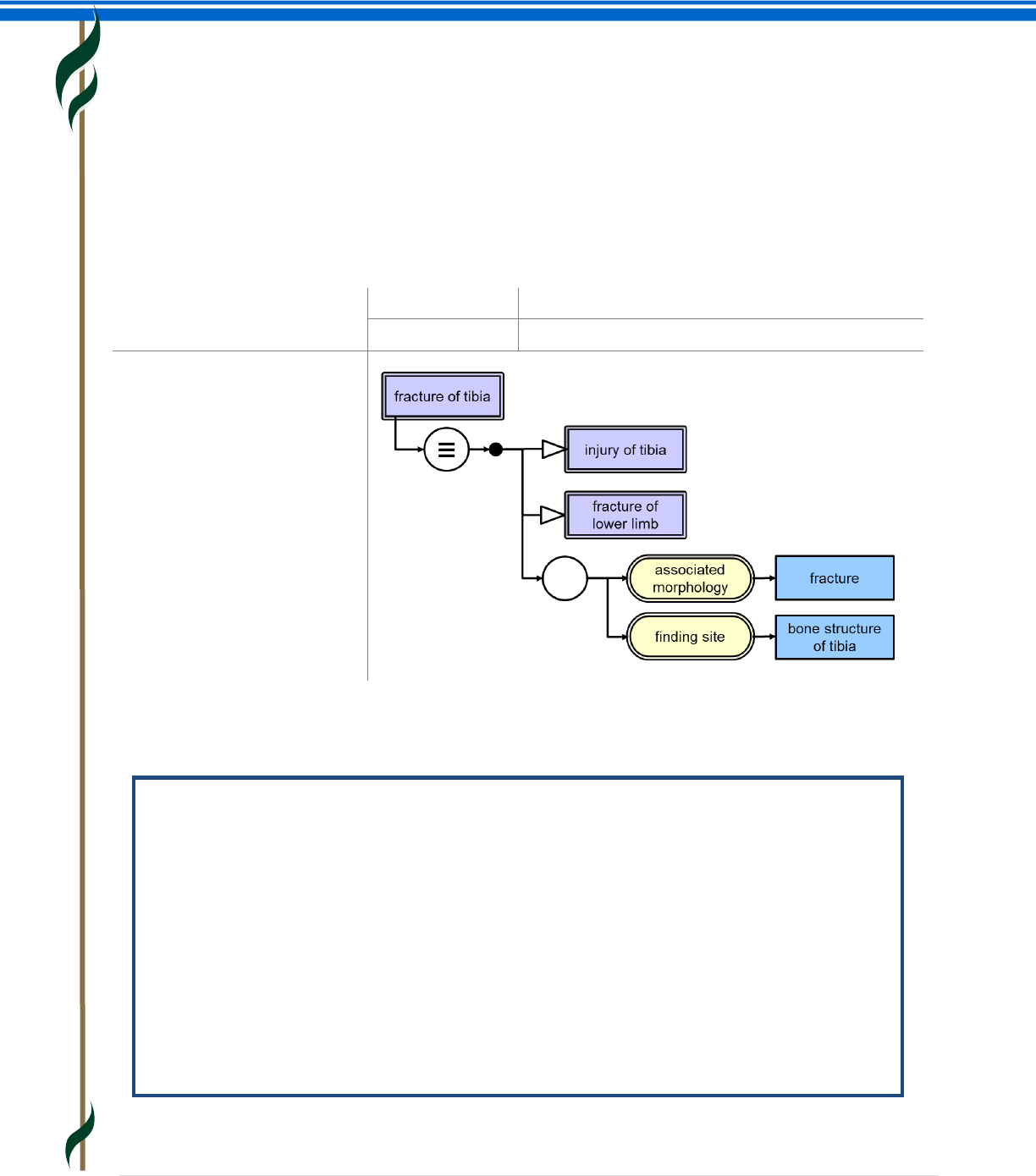
Precoordinated expressions
Precoordinated expressions are expressions that represent the meaning of individual concepts which are
predefined in SNOMED CT. Besides the unique concept identifier and descriptions, each concept also has a
formal logic definition represented by a set of defining relationships to other concepts. The figure below
shows the precoordinated expression used to record |fracture of tibia|. It illustrates that this can be
represented by a single identifier, with or without an accompanying human-readable term. It also
illustrates the defining relationships of the concept identified in the expression. This is the precoordinated
definitional knowledge which is conveyed by this expression.
The second example shown below illustrates the fact that some SNOMED CT concepts provide quite a lot of
detailed refinement, some of which might otherwise be captured separately. We will return to this
example when considering postcoordination.
Example: Precoordinated representation of “Laparoscopic emergency appendectomy”
SNOMED CT contains the concept 174041007|laparoscopic emergency appendectomy|. The
identifier of this concept (174041007) can be used (with or without the associated term) as a
precoordinated expression to record an instance of this procedure.
The procedure ‘laparoscopic emergency appendectomy’ has at least three distinct facets:
‘removal of appendix’, ‘using a laparoscope’ as ‘emergency procedure’. The SNOMED CT
concept 174041007|laparoscopic emergency appendectomy| precoordinates these facets as its
definition includes the following defining relationships:
116680003|is a| = 80146002|appendectomy|
260870009|priority|=25876001|emergency|
425391005|using access device| = 86174004|laparoscope|
Precoordinated expression
representing fracture of tibia
Identifier only
31978002
With display term
31978002 |fracture of tibia |
Graphic view of the defining
relationships of the concept
|fracture of tibia|
SNOMED CT Starter Guide
July 2014
29 | P a g e
Postcoordinated expressions
Expressions that contain two or more concept identifiers are referred to as postcoordinated expressions.
Postcoordination combines concepts and allows more detail to be added to the meaning represented by a
single concept. A postcoordinated expression is not just a list of concept identifiers, it follows a set of rules
that mimic the way attributes and values are used to define SNOMED CT concepts.
Example: Postcoordinated representation of “Laparoscopic emergency appendectomy”
Although SNOMED CT contains the concept |laparoscopic emergency appendectomy|, it is also
possible to represent this clinical phrase using the following postcoordinated expression.
80146002|appendectomy|:260870009|priority|=25876001|emergency|, 425391005|using
access device|=86174004|laparoscope|
This postcoordinated expression has exactly the same meaning as the precoordinated
expression
174041007|laparoscopic emergency appendectomy|
The fact that the two expressions have the same meaning can be computed because
174041007|laparoscopic emergency appendectomy| is a fully-defined subtype descendant
of 80146002|appendectomy| ; and
the only differences between the defining attributes of these concepts are the addition of
o 260870009|priority|=25876001|emergency|
o 425391005|using access device| = 86174004|laparoscope|
The example above shows that postcoordination can be applied even when a single concept is available to
represent the required means. However, the real strength of postcoordination is that it allows a clinical
phrase to be represented even when the precise concept is not present in SNOMED CT. In these cases,
postcoordinated refinements can be applied to an existing concept to more precisely capture the required
meaning.
Example: Postcoordinated representation of “Laparoscopic removal of device from
abdomen”
SNOMED CT does not contain a concept that represents this clinical idea. However, it is possible
to represent it using the following postcoordinated expression.
68526006|removal of device from abdomen|:425391005|using access device|= 6174004|laparoscope|
Postcoordinated expressions may be created at run-time by selection of individual facets of a concept. For
example, to indicate the nature and location of a fracture for a particular bone and, where relevant,
whether the bone affected is on the right or left. Some applications allow generation of postcoordinated
expression using natural language processing. Alternatively, postcoordinated expression can be selected
during user interface design and bound to simple data entry options. In these cases, the user may not be
aware that the information is being captured in a postcoordinated form.
SNOMED CT Starter Guide
July 2014
30 | P a g e
Representing postcoordination
There are several valid ways to represent and store postcoordinated expressions. However, to support
interoperability, IHTSDO has specified a standard SNOMED CT compositional grammar form that is both
human-readable and computer processable. The examples of expression that you see in this guide use this
grammar.
The basics of SNOMED CT compositional grammar
At its simplest level a single SNOMED CT concept identifier is a valid expression.
o 80146002
A concept identifier can optionally be followed by a term associated with that concept
enclosed between two pipe characters
o 80146002|appendectomy|
A concept identifier (with or without a following term) can be followed by a refinement.
The refinement follows a colon
o 80146002|appendectomy|: <refinement>
A refinement consists of a sequence of one or more attribute-value pairs. Both the
attribute and the value are represented by a concept identifier (with or without a
following term). The attribute is separated from the value by an equals sign
o 80146002|appendectomy|:260870009|priority|=25876001|emergency|
If there is more than one attribute-value pair, the pairs are separated by commas
o 80146002|appendectomy|:260870009|priority|=25876001|emergency|,
425391005|using access device|=86174004|laparoscope|
Curly braces represent grouping of attributes within a refinement, for example to indicate
that the method applies to a specific site
o 80146002|appendectomy|:{ 260686004|method|=129304002|excision - action|,
405813007|procedure site - direct|= 181255000|entire appendix|}
Round brackets represent nesting to allow the value of an attribute to be refined
o 161615003|history of surgery|:363589002|associated procedure|=
(80146002|appendectomy|: 260870009|priority|=25876001|emergency)
Postcoordination and the concept model
The refinements used in postcoordinated expressions should follow the same concept model rules that are
applied when concepts are defined. Attributes should only be applied to concepts that are in the specified
‘domain’ for that attribute. The values applied to attributes should be limited to the specified ‘range’ for
that attribute. These rules may sometimes seem to limit flexibility but these rules are important, because if
they are followed, it is possible to compute similarities and subtype relationships between different
expressions. This ability to compute subtypes is the key to effective meaning-based retrieval of
postcoordinated expressions.
SNOMED CT Starter Guide
July 2014
31 | P a g e
Example: Postcoordination and concept model rules
A disease with a particular morphological abnormality at a particular site is represented in the
following way:
64572001|disease|: { 363698007|finding site|= 91723000|anatomical structure|,
116676008|associated morphology|= 49755003|morphologically abnormal structure|}
It must not be represented in other ways that conflict with concept model rules such as:
49755003|morphologically abnormal structure|: 363698007|finding site|=
91723000|anatomical structure |
64572001|disease|: 363698007|finding site|= (91723000|anatomical structure|:
116676008|associated morphology|= 49755003|morphologically abnormal structure|)
64572001|disease|: 116676008|associated morphology|= (49755003|morphologically
abnormal structure|: 363698007|finding site|=91723000|anatomical structure |)
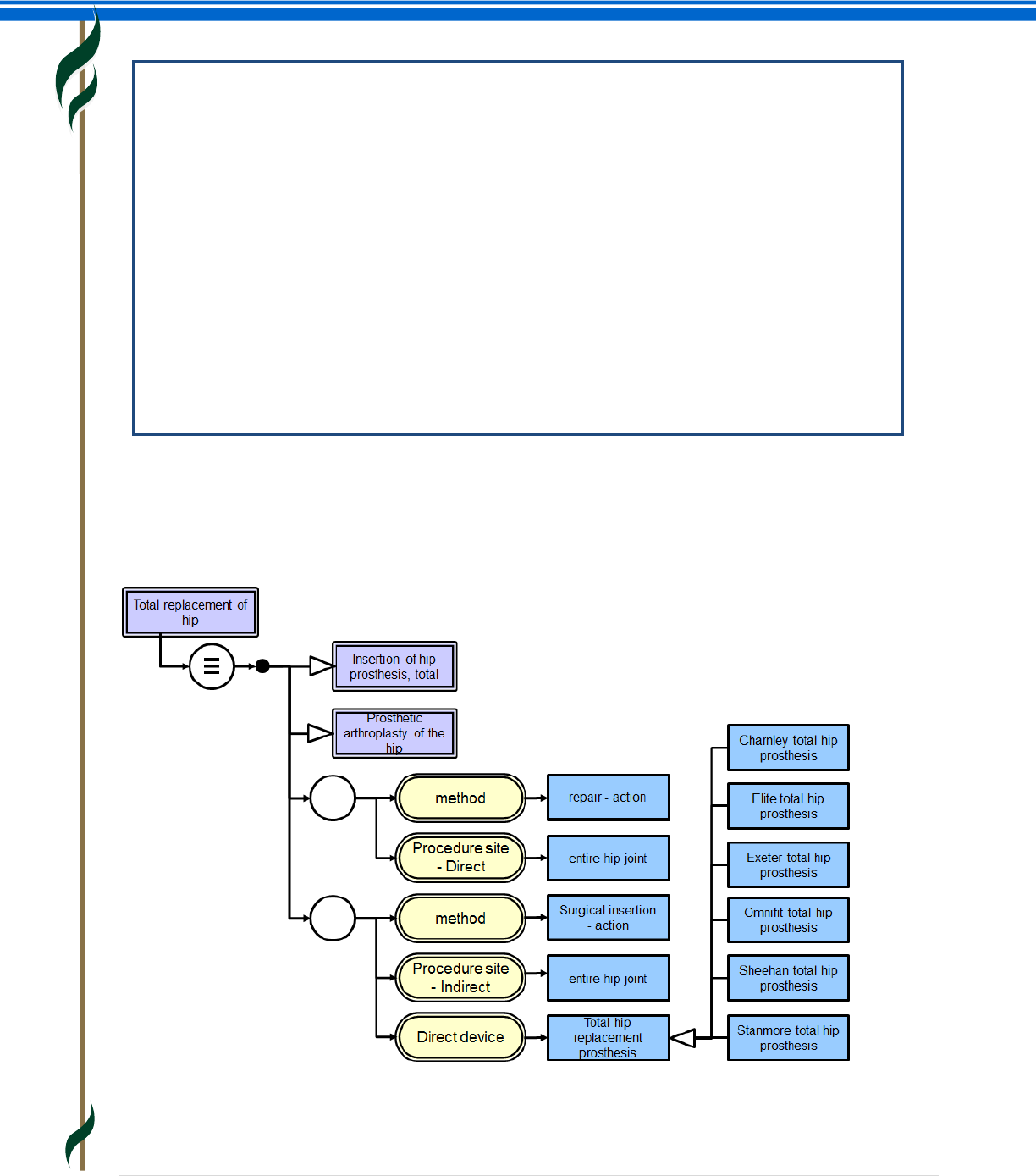
In some cases, postcoordination may be simply a matter of choosing one of the subtypes of a defining
attribute value. For example the definition of |total hip replacement| includes the attribute |direct device|
with the value |total hip replacement prosthesis|. The subtypes of this value include different types of
prosthesis, some of which are shown in the graphical view of the concept definition below. One of these
more specific values can be selected to specify the type of prosthesis actually used.
SNOMED CT Starter Guide
July 2014
32 | P a g e
In the same way clinical situations, such as family history, can be recorded for any disorder and are not
limited to a predefined set of conditions.
Example: Postcoordination of family history
The definition includes 246090004|associated finding|=246090004|disease|. This value can be refined
to refer to a particular disease. For example:
281666001|family history of disorder|:246090004|associated finding|=22298006|myocardial
infarction|
The definition of |family history of disorder| specifies that the |subject relationship context| is
|person in family of subject|. This value indicates that the finding applies to a family member
rather than the patient and can be refined to refer to a particular family member. For example:
281666001|family history of disorder|:{246090004|associated finding|=22298006|myocardial
infarction|,408732007|subject relationship context|=444295003|father of subject|}
Consistent retrieval of precoordinated and postcoordinated expressions
SNOMED CT expressions support consistent and comparable representation of meaning using both
precoordinated and postcoordinated expressions. This facilitates retrieval of all instances of expressions
that match a set of criteria specified using the subtype hierarchy and other defining relationships.
Example: Laparoscopic procedures
Several earlier examples in this chapter have represented procedures. If there was a requirement
to retrieve all laparoscopic procedures the first step would be to establish the criteria for inclusion.
The requirement could be expressed as follows.
51316009|laparoscopic procedure| and all its subtypes
In some cases, it is simply a question of looking at the subtype hierarchy.
For example
174041007|laparoscopic emergency appendectomy| is the source of a sequence of |is a|
relationships which lead to 51316009|laparoscopic procedure|.
In other cases, it is necessary to look at the definition of |laparoscopic procedure| and compare
this with the equivalent expression. |Laparoscopic procedure| is fully-defined as follows.
71388002|procedure|:425391005|using access device|=86174004|laparoscope|
Therefore, queries looking for instances of laparoscopic procedures should also retrieve
postcoordinated expressions in which both of the following are true:
The focus concept is a subtype of 71388002|procedure|
The attribute 425391005|using access device| is present with the value
86174004|laparoscope| or a subtype of that concept.
This rule would include postcoordinated representations, such as the following expression, for
which there is no existing SNOMED CT concept:
68526006|removal of device from abdomen|:425391005|using access device|=
6174004|laparoscope|
SNOMED CT Starter Guide
July 2014
33 | P a g e
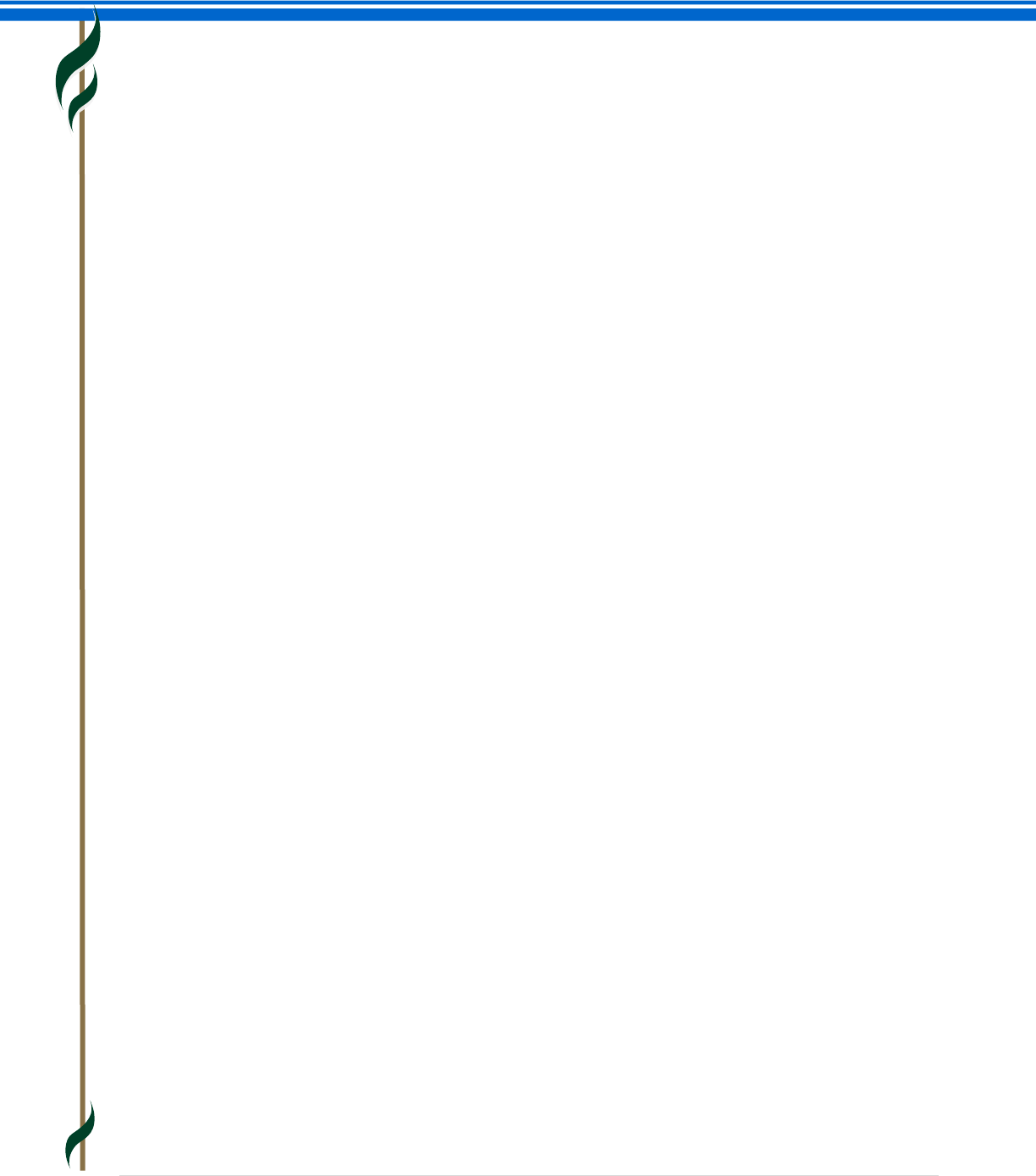
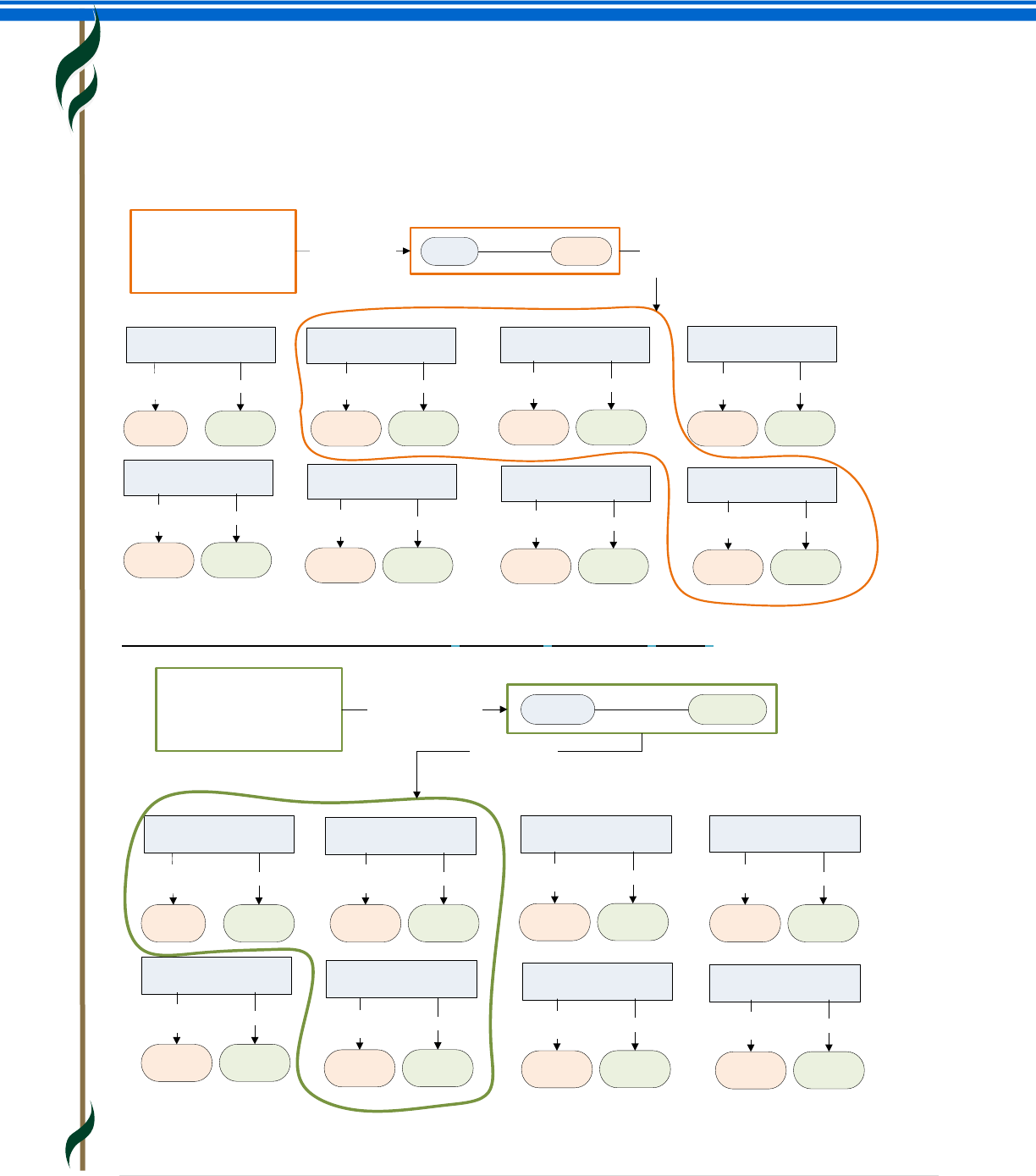
The following graphics illustrate the ways in which query predicates based on SNOMED CT concept
definitions can be used to retrieve data based on different criteria. In each case, the data retrieved includes
expressions that either have attributes matching the criteria or refer to a concept with defining
relationships that match the query criteria.
Example: Result of retrieving concepts with |associated morphology| specified as |benign neoplasm|
Example: Result of retrieving concepts with |finding site| specified as |kidney|
Abscess of bladder Lung cyst
Benign neoplasm
of bladder
Renal cyst Abscess of lung
Benign tumor of
lung
Cyst
Associated
morphology
Kidney
Finding site
Abscess
Associated
morphology
Kidney
Finding site
Abscess
Associated
morphology
Lung
Finding site
Benign
neoplasm
Associated
morphology
Lung
Finding site
Abscess
Associated
morphology
Bladder
Finding site
Cyst
Associated
morphology
Lung
Finding site
Benign
neoplasm
Associated
morphology
Bladder
Finding site
Renal abscess
Query formulation:
”Retrieve the findings
which have a benign
tumor morphology”
Query predicate Concept Benign
neoplasm
Associated
morphology
Benign tumor of
kidney
Benign
neoplasm
Associated
morphology
Kidney
Finding site
Query
result
Abscess of bladder Lung cyst
Benign neoplasm
of bladder
Renal cyst Abscess of lung
Benign tumor of
lung
Cyst
Associated
morphology
Kidney
Finding site
Abscess
Associated
morphology
Kidney
Finding site
Abscess
Associated
morphology
Lung
Finding site
Benign
neoplasm
Associated
morphology
Lung
Finding site
Abscess
Associated
morphology
Bladder
Finding site
Cyst
Associated
morphology
Lung
Finding site
Benign
neoplasm
Associated
morphology
Bladder
Finding site
Renal abscess
Benign tumor of
kidney
Benign
neoplasm
Associated
morphology
Kidney
Finding site
Query formulation:
”Retrieve the findings
located in the kidney”
Query predicate Concept Kidney
Finding
site
Query result
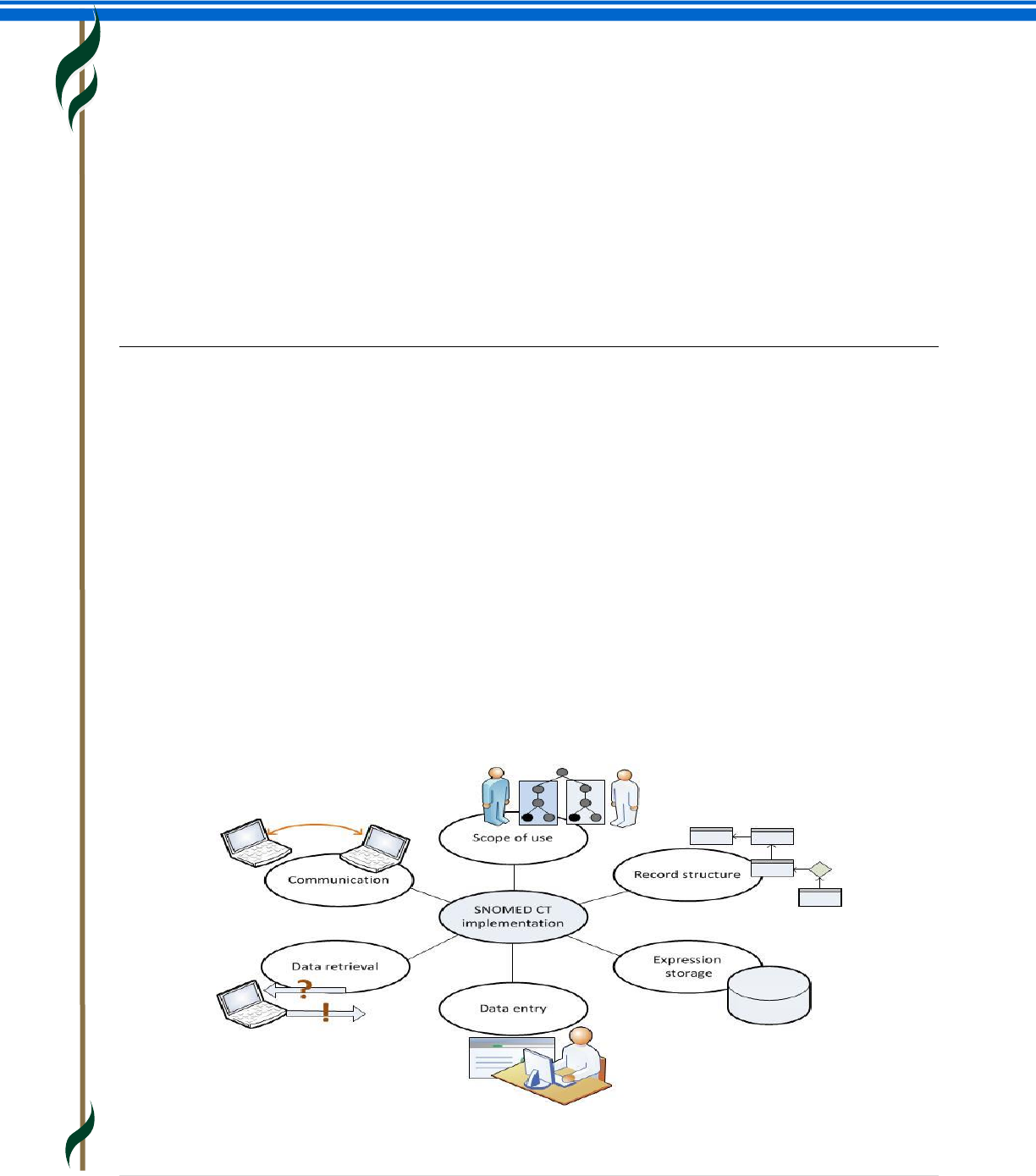
SNOMED CT Starter Guide
July 2014
34 | P a g e
8. SNOMED CT IMPLEMENTATION
This section provides an overview of:
How is SNOMED CT used?
Implementation Examples
o Clinical Record Applications
o Clinical Decision Support
o Enabling Interoperability
o Reporting
SNOMED CT in action
Why is this important?
Realization of the benefits described in Chapter 2 - SNOMED CT Benefits, depends on using the terminology
in software applications. The extent of benefits realization depends on the effectiveness of implementation
and the way SNOMED CT is used within the system and by users and organizations.
What is this?
How is SNOMED CT used?
SNOMED CT itself is only a part of the solution to addressing the requirements for effective electronic
clinical records. A terminology on its own ‘does nothing’. To benefit from a terminology, it must be
implemented and used as part of an application. The design of the software application in which it is used,
and the objectives and motivation of its users, are key factors in determining success.
SNOMED CT is useful for clinical documentation, as it supports the representation of detailed clinical
information, in a way that can be processed automatically. Realization of the capability of SNOMED CT to
support clinical information and meaning based retrieval requires careful consideration of the actual
setting, in terms of scope of use, record structure, data entry, data retrieval and communication.
SNOMED CT Starter Guide
July 2014
35 | P a g e
Implementation Examples
Clinical record applications
SNOMED CT can be implemented in a wide range of clinical record applications. These include systems
developed for use with other code systems that have been adapted to support SNOMED CT as well as
systems designed with the assumption that SNOMED CT would serve as the primary terminology. The
SNOMED CT features that applications support and use may vary, partly due to differences in user
requirements and partly due to development priorities.
A terminological resource is only one part of a software application. The functions required to implement a
terminology can be divided into:
Terminology services: Functions that can be performed without reference to data stored in a
particular application record structure.
Record services: Functions that involve storing, retrieving or processing application data (e.g.
patient health records).
Different applications may make use of different aspects of SNOMED CT. Applications that only require
SNOMED CT for a very limited range of uses and may not require all the features of SNOMED CT. However,
by using SNOMED CT, these applications benefit from an enhanced ability to exchange data with other
more terminology rich applications. These applications can also evolve to meet emergent requirements by
making increasing use of the power of SNOMED CT.
Most users only require a small subset of the content of SNOMED CT. However, use of a terminology that
spans a wide range of specialties delivers the benefits that arise from consistency, and interoperability.
Clinical decision support
How can the use of SNOMED CT assist in clinical decision support?
Clinical decision support is defined broadly as a clinical system application or process that helps health
professionals make clinical decisions to enhance patient care. An example of clinical decision support
would be the use of alerts to identify specific clinical contraindications in the administration of
thrombocytopenia therapy after a stroke.
The use of SNOMED CT makes clinical information available in a computable form which can be queried
and used to trigger decision support rules and prompts. The hierarchies of SNOMED CT enable complex
reasoning to support decision support rules. For example, in SNOMED CT the concept |stroke| is
synonymous with |cerebrovascular accident| and subsumes all lower level concepts including |paralytic
stroke|, |thrombotic stroke| etc. This means that decision support queries are easier to develop and
implement because they do not need to identify all the individual terms and codes which may be relevant.
Has it been implemented?
Yes. SNOMED CT is known to be used for Clinical Decision Support in a number of organizations including
Kaiser Permanente, Duke University Medical Hospital in the US; National Health Service Hospitals in the UK
and Hospital Italiano in Buenos Aries, Argentina.
Kaiser Permanente has a central terminology service which develops and maintains clinical decision
support rules and prompts. These can be quickly distributed for implementation throughout the
SNOMED CT Starter Guide
July 2014
36 | P a g e
Organisation. In addition to using this type of approach for clinical decision support, Kaiser Permanente
also use it to identify potential cohorts for clinical trials etc.
Enabling interoperability
How can you ensure that clinical information entered in one context can be safely and accurately
transmitted to another system in another context?
Information can be recorded using SNOMED CT concepts and descriptions that are independent of the
clinical information system being used and either independent of or tied to the context of use, depending
on the user requirements. SNOMED CT is a common clinical terminology covering a wide range of
requirements and its use. SNOMED CT allows meaning-based computation to be applied to information in
messages sent between systems, and provides a foundation for interoperable interpretation of clinical
information.
For example, subtype descendant concepts that may be relevant to prescribing decisions (e.g. |allergy to
substance|, |kidney disease|) can be used to trigger alerts and reminders in the recipient system, such as
medication allergy alerts and drug level investigation warnings. These preventative health care reminders,
enable the quality of care to be improved.
Has it been implemented?
Yes. In the United States, Kaiser Permanente (KP), The Veterans Health Administration (VHA), and the
Department of Defense (DoD) health systems currently interoperate using SNOMED CT. A consortium
comprised of Kaiser Permanente, the Mayo Clinic, Intermountain Health Care, Geisinger Health System,
and Group Health Cooperative of Puget Sound has announced they will interoperate using SNOMED CT and
techniques established by KP, the VHA and DoD.
Reporting
How can clinical information encoded as SNOMED CT concepts be used for reporting purposes?
Information encoded as SNOMED CT concepts is semantically consistent. In other words, there is one
unique SNOMED CT identifier representing each separate meaning. This lends itself to reporting through
specifying the SNOMED CT identifiers of interest. SNOMED CT supports recording at appropriate levels of
detail and using relevant terms. This also means that reports can be generated at the appropriate levels of
detail using relevant terms for display in the report.
The hierarchical nature of SNOMED CT means that information can be aggregated at the appropriate levels
of generalization. That same information can also be used in reporting to provide the same level of detail.
SNOMED CT is a common clinical terminology covering a wide range of requirements and supporting a
wide variety of use cases for reporting, including patient care, clinical audit, quality improvement,
outcomes, epidemiology, patient safety, etc. As SNOMED CT is a clinical terminology with a global scope,
reports using SNOMED CT can be compared across boundaries.
Where required, SNOMED CT may also be mapped to other code systems and classifications to support
existing reporting requirements.
SNOMED CT Starter Guide
July 2014
37 | P a g e
Has it been implemented?
Yes, many clinical information systems use SNOMED CT to varying degrees and many standards mandate or
recommend that SNOMED CT be used. Such cases include reports sent using HL7 messages, microbiology
results reporting, and genetic database reports.
Other examples of SNOMED CT in action
You can see other examples of implementations using SNOMED CT in a dynamically maintained list at
www.snomedinaction.org. This site also allows you to add summaries of implementations that you are
involved in.
SNOMED CT Starter Guide
July 2014
38 | P a g e
9. CONTENT DEVELOPMENT
This section provides an overview of:
SNOMED CT International Release Content Development
Request Submission
Why is this important?
Understanding the quality and rigor of the approach to SNOMED CT content development ensures user
confidence in the quality of the content when implementing or using SNOMED CT.
What is this?
SNOMED CT international release content development
SNOMED CT‘s content development is based on four basic principles that have and continue to guide
development of its clinical content and technical design including:
Development efforts must encompass broad, inclusive involvement of diverse clinical groups and
medical informatics experts.
The clinical content must be quality focused and adhere to strict editorial rules.
The quality improvement process must be open to public scrutiny and vendor input, to ensure that
the terminology is truly useful within health care applications.
There must be minimal barriers to adoption and use.
The content of SNOMED CT evolves with each release. The types of changes made include new concepts,
new descriptions, new relationships between concepts, and new reference sets, as well as updates and
retirement of any of these components. Drivers of these changes include changes in understanding of
health and disease processes; introduction of new drugs, investigations, therapies and procedures; and
new threats to health, as well as proposals and work provided by SNOMED CT users.
The three basic operational criteria that help determine whether new content is following the principle of
creating and sustaining semantic interoperability are that SNOMED CT must be:
Understandable: The meaning must be able to be communicated, to be understood by an average
health care provider without reference to inaccessible, hidden or private meanings.
Reproducible: It is not enough for one individual to say they think they understand the meaning. It
must be shown that multiple people understand the meaning in the same way.
Useful: The meaning must have some demonstrable use or applicability to health or health care.
Recognizing the goal that SNOMED CT should become the accepted international terminological resource
for health care, it must therefore be capable of supporting multilingual terminological renderings of
common concepts. For the terminology to be acceptable to the widest possible range of users it must
include translations as well as alternative spellings and other variations that arise from a national and
regional dialect. Furthermore it must be capable of representing differences between the underlying
concepts that arise from cultural, ethnic or linguistic variations.
SNOMED CT Starter Guide
July 2014
39 | P a g e
Clinical terminology development is challenging for a variety of reasons. Even in a single country or
language people often use the same words to mean different things, as well as using different words for
the same thing. The names assigned to some clinical conditions are sometimes based on an earlier
incomplete or erroneous understanding and often these misleading names remain in use long after
knowledge has moved on. Progress of medical knowledge and evolution of pathogenic organisms creates a
continual, growing requirement to add new content and revise definitions. Efforts by specialty bodies to
establish diagnostic criteria and staging scales also lead to changes, and sometimes to divergence between
different or overlapping sources of authority. In the face of these challenges, content development is
directed to address current and emerging priorities identified by IHTSDO Members and other stakeholders.
Continuous quality improvement is the aim of IHTSDO. Quality processes are included as part of the work
completed by the team of modeler’s involved in SNOMED CT development. A documented scientific
process is followed and content is defined and reviewed by multiple clinician editors. Conflicts between
editors are resolved through an iterative process, based on achieving agreement and consensus, before
being entered into the terminology. As necessary, the authoring team consult with additional experts to
review the scientific integrity of the content.
Requesting content additions and changes
IHTSDO provides a request submission service to gather and process requests for additions and changes to
the content of the SNOMED CT International Edition. This service is directly accessible by National Release
Centers (NRC) in Member countries and recognized Terminology Authorities within organizations with
whom IHTSDO is actively collaborating. Organizations within Member countries can submit their requests
for additions and changes to the National Release Centre. In some cases, requests with particular local
relevance may be added to a National Extension. The NRC forwards requests that it considers have
international relevance to the IHTSDO for a decision. If a request is deemed to have high priority it should
result in action in the next release cycle. However, requests that require significant changes that would
impact on other content may take longer.
SNOMED CT Starter Guide
July 2014
40 | P a g e
10. EXTENSION AND CUSTOMIZATION
This section provides an overview of:
Extension Content
Reference Sets
Why is this important?
SNOMED CT is designed to allow the International Edition to be enhanced by adding Extensions that
address national or local requirements. Additional content required to support national, local or
organizational needs that may not have international relevance or may not meet the editorial guideline for
inclusion in the International Edition.
SNOMED CT design also includes the Reference Set mechanism which provides a standard way to
customize and enhance content for use in a particular country, language, specialty, application or context.
Reference Sets developed nationally or locally can modify search and display of content from the
International Edition as well as enhancing Extension content.
What is this?
Extension content
Many clinical concepts are relevant in all countries, organizations and specialties but some concepts are
relevant only to a particular environment. SNOMED CT is designed to allow the International Edition to be
enhanced by adding Extensions to meet national or local requirements without compromising the main
body of SNOMED CT. This is intended to meet the needs of different specialties and countries, regions,
vendors and healthcare institutions.
Extensions are managed by IHTSDO Members or Affiliates who have been issued with a Namespace
Identifier. A Namespace Identifier distinguishes the Identifiers of the Components created by an
Organisation. The responsibilities of organizations that create an Extension and provide it for use by other
organizations include:
Maintaining Concept, Descriptions, Relationships, and Reference Sets that they create.
Inactivating these components as appropriate (duplication, ambiguous, outdated, etc.)
The Concepts, Descriptions, Relationship and Reference Sets that form an Extension use a namespace
identifier, which ensures that their SNOMED CT identifier is different from components in:
SNOMED CT International Release,
Other SNOMED CT Extensions
The namespace identifier is part of the component identifier. Therefore, components are distinguishable
not only in the thesaurus, but also when stored in a patient record, query or decision support protocol.
SNOMED CT Starter Guide
July 2014
41 | P a g e
Extensions use the same file structure as the core International Release. This ensures that:
SNOMED CT enabled implementations can benefit from the content in these Extensions without
the need for any additional software development;
The same application software can be used to enter, store and process information from different
extensions;
Reference Sets can be constructed that refer to content from the International Release and a
variety of Extensions.
Software applications should allow the users or user communities to specify the Extensions to be
recognized by their systems.
An Extension should only be recognized if:
It has been supplied by the IHTSDO or another Organisation authorized by the IHTSDO to provide
such Extensions;
The recognizing Organisation is satisfied with the quality control procedures of the providing
Organisation.
The fact that an Organisation is permitted to produce Extensions does not imply any seal of approval
related to the quality of Extensions provided by that Organisation. Therefore a person or Organisation that
recognizes or installs an Extension does so entirely at their own risk.
Reference sets
SNOMED CT has a broad clinical coverage and includes a depth of detail appropriate to a range of health
care disciplines and clinical specialties. As a result, it has extensive content, different parts of which are
needed in particular environments. The SNOMED CT design includes the Reference Set mechanism, which
provides a standard way to refer to a set of SNOMED CT components and to add customized information to
a component.
Organizations implementing SNOMED CT benefit from Reference Sets because they allow requirements for
use of particular descriptions and concepts to be represented in a standard form that can be applied to any
SNOMED CT enabled application. This allows Reference Sets to be shared throughout and between
organizations, even when different software is used to meet local or departmental requirements.
Software developers and vendors benefit because Reference Sets provide a common, machine processable
representation of requirements for different patterns of use of SNOMED CT. This simplifies local
configuration and enhances interoperability with other SNOMED CT enabled applications.
Reference sets can be used for many different purposes, including:
Language and dialects are represented as Language Reference Sets (see Chapter 11 - Translations
and Language Preferences).
Maps to and from other code systems and classifications are represented as Simple, Complex or
Extended Map Reference Sets (see Chapter 12 - Mapping).
SNOMED CT Starter Guide
July 2014
42 | P a g e
Subsets of concepts, description or relationships are represented as Simple Reference Sets. The
only information that a Simple Reference Set provides is that a component is part of this subset.
Subsets may be used for a variety of general and specific purposes, some of which are identified in
the following examples.
Ordered lists and navigation hierarchies are represented as Ordered Reference Sets. These offer
additional functionality to meet advanced variants of the requirements addressed by component
subsets.
General use cases for subsets represented as Simple Reference Sets
Excluding content
o For example, the “Non-human Reference Set” excludes content which is only
relevant in veterinary medicine.
Including content
o Limiting searches to content of specific interest to a specialty or specific data entry
context
o In some cases very limited subsets can be presented as dropdown lists or option
boxes rather than searches.
Prioritizing content
o In some cases, a subset represents an initial priority list of options but the full
content of SNOMED CT is searchable when required.
o Note that Ordered Reference Sets support more flexible prioritization.
Managing use of codes in messages and communications
o A Simple Reference Set may represent a value set applicable to a particular field in
a message.
Specific use cases for subsets represented as Simple Reference Sets
National, jurisdictional or organizational requirements
o Collecting particular minimum sets of data using specific codes.
Regional variations in disease prevalence
o Providing prioritized access to diseases that are prevalent in the region where data
is being collected.
Specialty and discipline variations
o The frequency of use of particular concepts depends on the professional discipline
and/or clinical specialty of the user. Specialty subsets can optimize data entry.
Supporting data entry protocols
o Different subsets of concepts are relevant at different points in different data
entry protocols. Subsets represented as Simple Reference Sets can be used to
restrict the available options to match the requirements at particular points in a
data entry protocol.
SNOMED CT Starter Guide
July 2014
43 | P a g e
Reference set development
Generic data structures for Reference Sets have been used to create a simple core structure that can be
extended to meet a variety of requirements. This has been done rather than developing a complex and
inextensible structure that can only be used in a finite and constrained number of ways to enforce editorial
policy.
Creating a new Reference Set requires access to a namespace in order to generate SNOMED CT Ids. Within
that namespace, at least one module ID concept (with an FSN and Preferred Term) should be added under
the |module| sub-hierarchy (within the Core Metadata) for each of the authoring organizations. The steps
required to create a new reference set include:
1. Create the Reference Set Concept in the Foundation Metadata hierarchy.
2. Define the Reference Set Attributes within the metadata hierarchy.
3. Create the Descriptor for the Reference Set (by adding members to the Reference Set Descriptor
Reference Set).
4. Add members to the Reference Set.
Please note that step 2 does not need to be performed if using one of the standard Reference Set types
that have been predefined in the international release of SNOMED CT. The Reference Set Attributes for
these predefined Reference Set types have already been added to the international release.
It is recommended that for each reference set, there is formal documentation that records (at a minimum)
the rules, principles and approach used to determine the members of that reference set.
Reference Sets need to be maintained and the content re-examined when new releases of SNOMED CT are
made available. Processes need to be established to address the concepts that have become inactive and
the new concepts added in each new release.
SNOMED CT Starter Guide
July 2014
44 | P a g e
11. TRANSLATIONS AND LANGUAGE PREFERENCES
This section provides an overview of:
Requirements for translations and language preferences
Translation approaches
How SNOMED CT represents translations
Why is this important?
The basic objective of any SNOMED CT translation is to provide accurate and unambiguous descriptions of
SNOMED CT concepts in the target language.
What is this?
SNOMED CT is a multinational, multilingual terminology. It has a built-in framework to manage different
languages and dialects. Today, SNOMED CT is available in several languages, including US English, UK
English, Spanish, Danish and Swedish, and more translations are continuously being done by member
countries.
The goal of any SNOMED CT translation is to provide accurate representations of SNOMED CT concepts in a
way that is understandable, usable, and safe. Translations must be concept-based, as term-to-term
translations may yield literal expressions that are often meaningless. Instead, the translator analyses each
concept based on the position within the hierarchy, the descriptions, and relationships to other concepts
before deciding on the most meaningful translation of a concept. IHTSDO provides guidelines to support
countries undertaking translations.
Translation approaches
SNOMED CT translation is an interdisciplinary collaboration which requires careful attention to content,
structure and clinical relevance. These factors are of foremost importance in order to ensure the usability
of the terminology in connection with implementation in electronic health record systems. Both linguistic
and semantic quality must be assured.
The core SNOMED CT is not perfect and its structure and content continue to evolve. These facts call for
vigilance on the part of the translation team members who need to review and analyses the relationships
of each concept in order to elucidate the meaning of a term within the terminological context. Looking at
the preferred term in English is not sufficient to enable accurate concept-based translation.
Close collaboration between specialists in health informatics, linguistics and terminology is essential for the
translation process. A translation based solely on linguistic, morphological-syntactical analysis might result
in a seemingly correct term which may not adequately represent the concept in question, nor be used by
healthcare professionals. On the other hand, compliance with linguistic, systematic, and orthographic
principles is necessary in order to avoid confusion and ensure the practical applicability of the terminology.
SNOMED CT Starter Guide
July 2014
45 | P a g e
It is crucial that those involved in the translation, verification, validation, and approval processes are
familiar with the terminological principles on which SNOMED CT is based. It is equally important that they
comply with IHTSDO Style Guides and that they are conscious of issues such as the choice of lexical variant,
term requirements, translation techniques, and the importance of ensuring linguistic consistency.
Additionally, it is important that those involved in the translation process are aware that sometimes, their
inability to understand a given term or concept may be caused not by their own lack on insight, but actually
by a mistake or an ambiguity in the core terminology (international release) that needs to be corrected.
SNOMED CT undergoes constant improvement, mistakes are corrected, and ambiguities are addressed. To
ensure this constant enhancement of SNOMED CT, any translation team should register questions,
comments or suggestions and forward these to the IHTSDO in order to avoid spending extra time on
unsolvable issues and at the same time contribute to discovering any mistakes and ambiguities. Currently,
questions and remarks from the translation teams are dealt with by the IHTSDO request submission
process.
How SNOMED CT represents translations
From a practical perspective, the deliverables from SNOMED CT translation include:
Descriptions – each of which contains a term in the target language which accurately reflects the
meaning of the concept with which it is associated.
A Language Reference Set – containing references to each of the descriptions and an indication of
whether it is preferred or acceptable for use in the particular language or dialect.
This approach allows the same descriptions to be used in other local variants of the language. In this case
another Language Reference Set is provided indicating which descriptions contain the preferred and
acceptable terms. Descriptions not referenced by a Language Reference Set are not used in that language
or dialect.
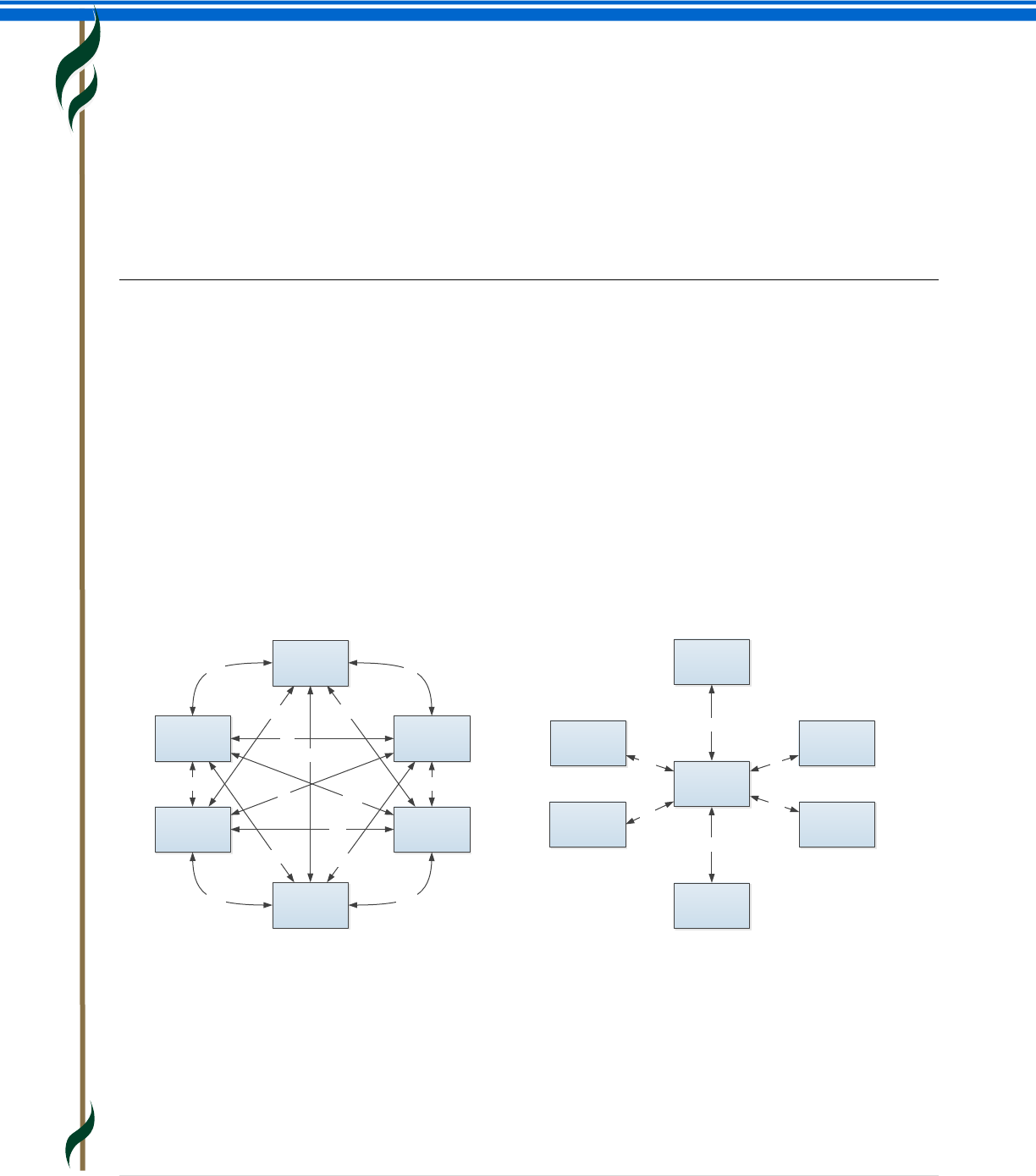
SNOMED CT Starter Guide
July 2014
46 | P a g e
12. MAPPING
This section provides an overview of:
Mapping approaches
How SNOMED CT represents maps
Steps in a mapping process
Why is this important?
Clinical information recorded using SNOMED CT may include data that is relevant to reports, statistical
returns, billing claims, etc. that need to be encoded using a specific code system or a statistical
classification such as ICD-10. Mapping allows relevant information to be used for those purposes,
minimizing the requirement for additional manual data entry.
Organizations planning to implement SNOMED CT based solutions may also be faced with data
transformation and migration challenges which lead them to consider mapping their existing clinical data,
code systems or classifications to SNOMED CT.
As a common global reference terminology, SNOMED CT limits the need for development of “everything to
everything” maps between multiple different code systems.
Problem: Map Everything to Everything
Solution: Map to a SNOMED Clinical Terms
What is this?
Maps are associations between particular codes, concepts or terms in one code system and codes,
concepts or terms in another code system that have the same (or similar) meanings. Mapping is the
process of defining a set of maps. Maps are developed in accordance with a documented rationale, for a
given purpose and as a result there may be different maps between the same pair of code systems to meet
different uses cases.
A
M
IQ
UE
A-Q A-I
I-U
U-M
M-E
E-Q
Q-I
Q-M
A-E A-U
E-I
E-U
I-M
A-M
Q-U
A
M
IQ
UE
Q-S
A-S
I-S
U-S
M-S
E-S
SNOMED
Clinical Terms
SNOMED CT Starter Guide
July 2014
47 | P a g e
There are a number of different types of mapping activities that an Organisation may need to undertake.
These include mapping:
SNOMED CT to a statistical classification (such as ICD-10)
Classifications to SNOMED CT
Other standard code systems to or from SNOMED CT
Locally developed code systems to SNOMED CT
Locally collected clinical data documented as free text to SNOMED CT
The completeness of mapping between two code systems depends on the scope, level of detail provided by
the two schemes and the precision of mapping required to safely meet the intended mapping use case.
Mapping approaches
The approaches used when undertaking mapping include human mapping, automatic mapping or a
combination of both of these.
Automatic mapping is when computer algorithms are used to create maps between concepts and or terms
- for example between local clinical content and SNOMED CT. Lexical mapping, where the structure of the
words in the clinical term is compared and analyzed as to whether the words are the same, similar or
different, is often incorporated within automatic mapping. Significant care must be taken with automatic
mapping, because severe mapping errors can result if not done in a controlled way. Automatic mapping, in
conjunction with human review (and manual remapping where necessary), is likely to achieve better
results than automatic mapping alone.
Human mapping is the use of human knowledge and skill to author maps. Each map is built singly and
individually. The process requires examination of each and every concept in the coding system. Informed
judgments or decisions are made about the shared meaning of concepts. Electronic or computational tools
are used, but only in support of work process.
How SNOMED CT represent maps
SNOMED CT specifications and content include resources that support mapping to and from other code
systems, classifications and terminologies. These resources support simple, complex and extended
mappings. Simple maps, where there is a one-to-one Relationship between a SNOMED CT concept and
code in a target scheme, are represented using a Simple Map Reference Set. Complex and Extended Map
Reference Sets enable the representation of:
Maps from a single SNOMED CT concept to a combination of codes (rather than a single code) in
the target scheme.
Maps from a single SNOMED CT concept to choice of codes in the target scheme. In this case, the
resolution of the choices may involve:
o Manual selection supported by advisory notes.
o Automated selection based on rules that test other relevant characteristics in the source
data (e.g. age and sex of the subject, presence or absence of co-existing conditions, etc.).
o A combination of automated processing with manual confirmation or selection where rules
are insufficient to make the necessary decisions.
SNOMED CT Starter Guide
July 2014
48 | P a g e
Steps in a mapping process
The main steps to be completed and documented when completing a mapping process include:
Evaluate mapping as a solution
Produce mapping requirements
Develop and review the maps
Use the maps
Review activity
Evaluating mapping as a solution
When approaching the creation of a map, the first step is to understand the data which needs to be
transformed or migrated and the requirements for use of that data. Key questions to address include:
Are the business requirements well understood?
Are there other options for meeting the business requirements without mapping?
To what extent can the source data contribute value to the target data?
What are the options?
What requirements are there beyond developing and delivering the maps? (e.g. enabling
appropriate use of the maps for data conversion).
What is the scope of the mapping exercise?
What are the expert resource requirements and costs of creating, quality assuring and maintaining
the maps?
What are the potential risks arising from using the maps?
Produce mapping requirements
It is essential to fully understand the structure, content and semantics of both the source and target code
systems. It is also important to understand how the meaning of the codes is affected by the structure and
functionality of the source and target systems. Once the code system and how it has been used is fully
understood, a document should be created which defines the rules to be applied when creating maps to or
from SNOMED CT. These rules will address for example, the approach to inexact mappings, the use of
synonyms, postcoordinated expressions and others. In order to be able to understand the evolution of the
maps, an audit trail of the map creation and maintenance activity should be maintained.
Evaluate
mapping as a
solution
Produce
mapping
requirements
Develop and
review the
Maps
Use the Maps Review
Activity
SNOMED CT Starter Guide
July 2014
49 | P a g e
Human resource requirements are dependent on the mapping scale, the model used for mapping and the
type and complexity of the map being developed. The roles that may be required could include mapping
sponsor, mapping manager, mapping specialist, clinical specialists and a mapping advisory group.
Once all requirements have been defined, appropriate software tools to support the creation of the maps
must be decided upon. The tools required depend on the complexity of the map and mapping process.
Three main alternatives include the use of simple multipurpose tools like Excel, dedicated map
maintenance applications and/or custom built applications.
Develop the map
The process of map development needs to be done in a controlled manner and involves:
Data preparation
Algorithmic mapping (where possible and deemed to be safe)
Human mapping, including map verification
Publication
Life cycle management
Checks and balances should be used at each stage to ensure that the process is technically accurate and
any maps created should be checked either using a map verification process or by parallel independent
mapping. Once maps are created and published a cycle of testing should be performed to validate that the
results obtained through the use of the maps to transform or migrate data meets the defined
requirements.
Use the maps
Having created the maps to or from SNOMED CT, there are various aspects to consider when using the
maps to migrate or transform clinical data. The actual specific use case needs to influence the final
requirements of how this is undertaken. Specific attention needs to be paid to reporting, interoperability
and data migration. The more common use cases are:
Identifying records to include in reports.
Transforming the original clinical data to meet the messaging specification for sending data to
another system.
Migrating existing clinical data either because a system is being upgraded to use SNOMED CT or to
introduce a new system that uses SNOMED CT.
Throughout the use of maps, there are fundamental principles and best practices that should be adhered
to including:
Consider all design elements of the system.
Maintain an audit trail for transformation or migration.
Manage future amendments to the mapping table.
Ensure visibility of original text of mapped items (as recorded prior to mapping).
Support clinical safety.
SNOMED CT Starter Guide
July 2014
50 | P a g e
Review activity
As with any process, a post-activity review stage is recommended. This should ensure that:
Appropriate lessons are learnt and documented and thus can be referred to in any future mapping
activity.
Issues that can be addressed within the current mapping are appropriately managed. For example,
where the maps are being used for transformation then lessons learnt should be fed back into the
process to improve the quality of the transformed data. The same is true in a data migration
scenario where maps are reapplied subsequent to the initial migration.
SNOMED CT Starter Guide
July 2014
51 | P a g e
13. RELEASE SCHEDULE AND FILE FORMATS
This section provides an overview of:
Release schedule and process
Release files and formats
Release types
Why is this important?
SNOMED CT is distributed to IHTSDO Members and Affiliate Licensees as a set of downloadable files. Those
wishing to implement SNOMED CT in software applications should understand the release schedule and
the structure and content of the release files. Users should be aware that regular updates of SNOMED CT
are made available and should be used in their systems to benefit from continuous improvements to
coverage and quality.
What is this?
Release schedule and process
The SNOMED CT International Edition is currently released twice a year on the 31st of January and the 31st
of July. The release files are made available to Members in advance of the formal release date and Affiliate
Licensees gain access either through their National Member or via the IHTSDO Affiliate Licensing system.
Many IHTSDO Members supplement the International Edition with releases of their national Extension. The
Extensions may be released at the same time as the International Edition but in some cases are released on
different dates and at different intervals.
Release files and formats
Release Format 2 (RF2) is the primary format used for SNOMED CT release files. This format includes
valuable additional data that was not supported by the earlier format.
The SNOMED CT International Edition is released as a set of files:
The release files are:
o Tab-delimited text files
o Encoded in accordance with the Unicode UTF-8 specification (which supports a wide range
of characters, symbols and accented characters)
There are individual files with specified columns for each of the core components of SNOMED CT:
o Concepts
o Descriptions
o Relationships
All components in the release files have permanent unique SNOMED CT Identifiers.
There are also individual files with specified columns for each type of Reference Set
o These files contain essential information about language preferences, subsets, maps and
metadata to support technical implementations
The same file formats are also used for SNOMED CT Extensions.
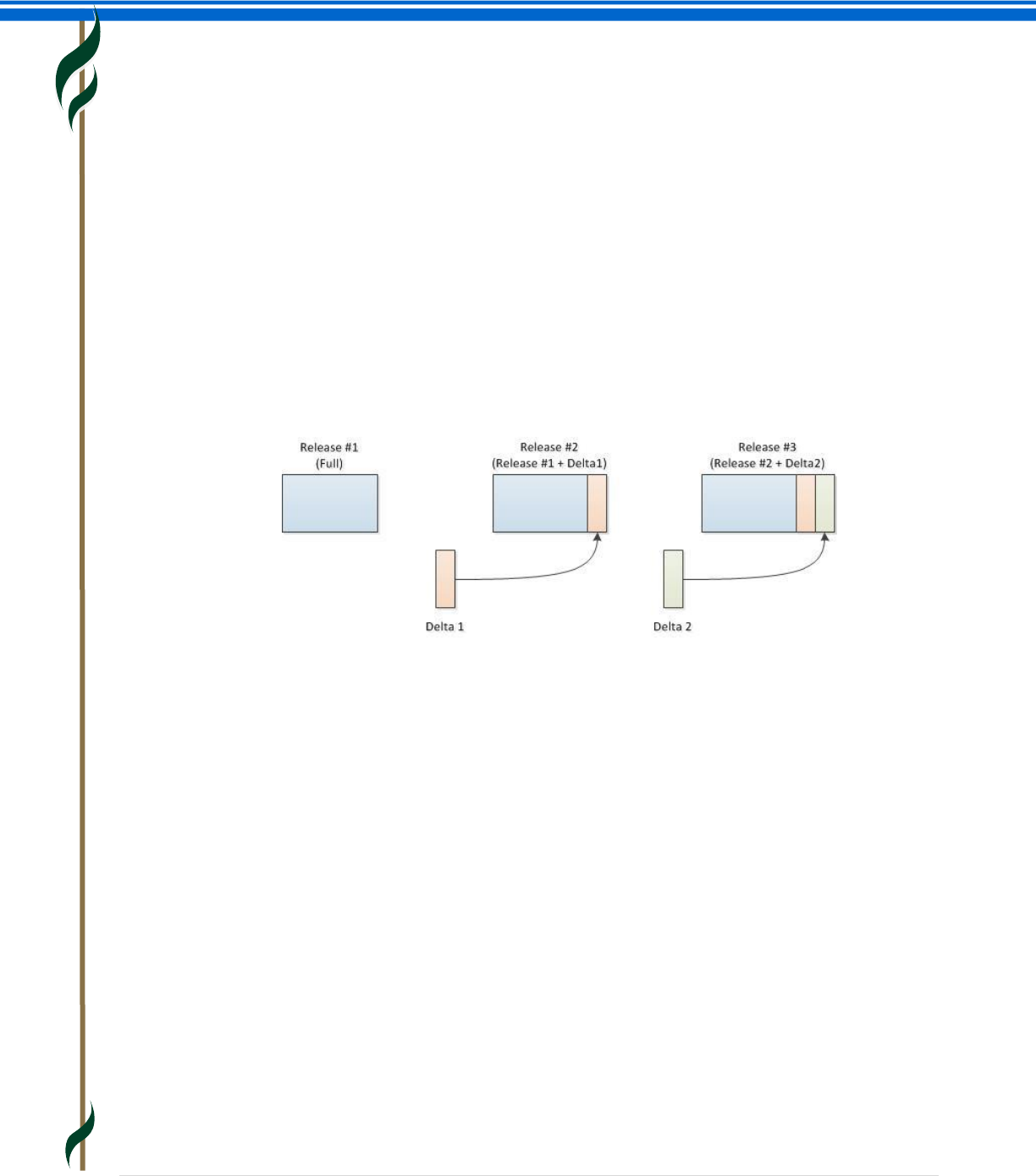
SNOMED CT Starter Guide
July 2014
52 | P a g e
Release types
The RF2 specification provides a history tracking mechanism within the distributed files. This enables
different release types to be provided using the same file format and utilizing this mechanism to optimize
installation and updating.
Full Release: A ‘Full’ release contains every version of every component that has ever been released prior
to or in the specified Edition. This release provides a full historical record and can be used to obtain views
of the state of any component at any point in time since its first release. The ‘Full’ release is the easiest way
to install and initialize SNOMED CT. However the files are large and in each release only a small fraction of
the content will have changed.
Delta Release: A ‘Delta’ release contains only those component versions created, inactivated or changed
since the previous release. The ‘Delta’ release is much smaller than a ‘Full’ release and is ideal for updating
a ‘Full’ release of the previous version. Adding a ‘Delta’ release to the previous version’s ‘Full’ release will
update the installation to a ‘Full’ release of the current Version.
Snapshot Release: A ‘Snapshot’ release contains the most recent version of every component released up
to the time of the snapshot. The version of each component contained in a snapshot is the most recent
version of that component at the release time. The ‘Snapshot’ release is useful for a simple installation but
does not provide a history or retrospective view of the terminology.
There are valid use cases for each Release Type. Each International release will incorporate all three of
these Release Types, allowing users to choose the most appropriate format for their needs. Extensions
should always be available as a full release and other Release Types may also be made available.
Relationships between files
In Snapshot Release files
Each SNOMED CT concept is held as a single row in the concept file. Each row represents a clinical
concept.
Each description is held as a single row in the description file, and is associated with a single
concept.
Each relationship, from a source concept to a destination concept, is held as a single row in the
relationship file. Each row also refers to the concept that represents the relationship type
In Full Release files, concepts, descriptions and relationships may be represented by more than one row. In
this case each row represents the state of the component at a stated point in time.
SNOMED CT Starter Guide
July 2014
53 | P a g e
14. IHTSDO – THE ORGANISATION BEHIND SNOMED CT
This section provides an overview of:
The International Health Terminology Standards Development Organisation (IHTSDO)
Members of IHTSDO
IHTSDO Standing Committees and Working Groups
National Release Centers
Why is this important?
IHTSDO is the international not-for-profit Organisation that owns and administers SNOMED CT, and owns
the rights to SNOMED CT and related terminology standards.
What is this?
IHTSDO is an association governed by a General Assembly that contains one representative of each of its
national Members.
IHTSDO seeks to improve the health of humankind by fostering the development and use of suitable
standardized clinical terminologies, notably SNOMED CT, in order to support safe, accurate, and effective
exchange of clinical and related health information. The focus is on enabling the implementation of
semantically accurate health records that are interoperable.
The purpose of IHTSDO is to develop, maintain, promote and enable the uptake and correct use of its
terminology products in health systems, services and products around the world, and undertake any or all
activities incidental and conducive to achieving the purpose of the Association for the benefits of the
members.
Members of IHTSDO
IHTSDO now has more than 25 national Members. An updated list of the current members can be found at
the IHTSDO web page (www.ihtsdo.org/members). Members of the IHTSDO can be either an agency of a
national government or another body endorsed by an appropriate national government authority within
the country it represents. The IHTSDO welcomes new Members.
The IHTSDO Members pay a fee, based on national wealth, to the IHTSDO which gives them the right to a
seat on the General Assembly. IHTSDO does not charge Affiliate Licensees for use of the SNOMED CT
International Edition within Member countries. Licensing is also free in the poorest countries and for
certain approved public-good uses in other countries. In other cases, low-cost per-institution charges apply
to the use of SNOMED CT in operational systems involved in data creation and/or analysis. All use of
SNOMED CT is subject to the acceptance of the terms of the SNOMED CT Affiliate License agreement
(www.ihtsdo.org/license.pdf) and the terms of sublicenses issued to end-user organizations by Affiliate
Licensees. Members may also impose additional conditions on use of SNOMED CT within their countries.
For example, a Member may require licensees to support and include its National Extension in its
implementations.
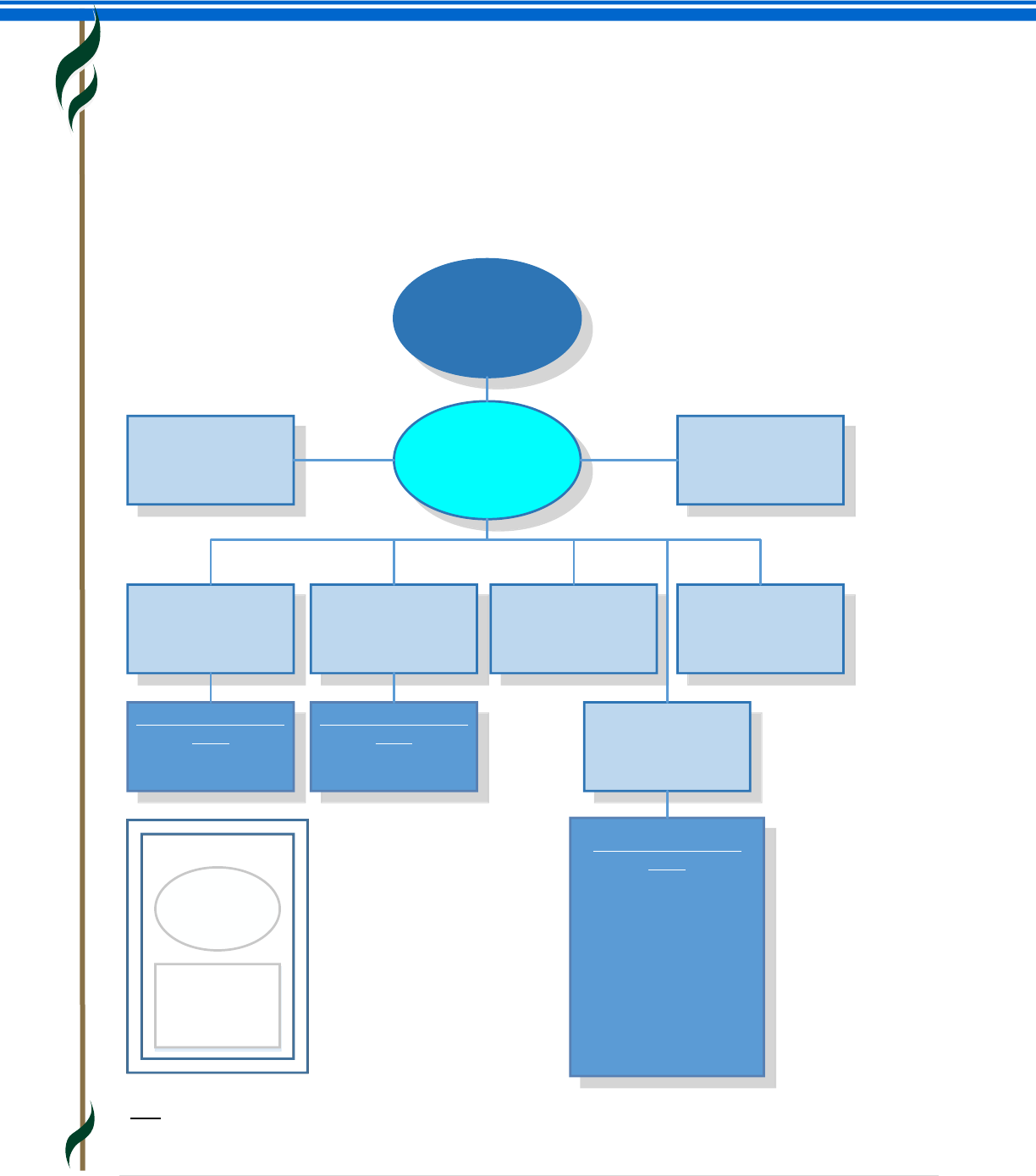
SNOMED CT Starter Guide
July 2014
54 | P a g e
IHTSDO governance
The highest governance body of the IHTSDO is the General Assembly which includes a formally appointed
representative of each IHTSDO Member. The General Assembly appoints a Management Board which
directs the Association and has responsibility for key business decisions. The Chief Executive Officer (CEO)
is appointed by the Management Board and has day-to-day responsibility for the conduct of the business.
The CEO is supported by a team of senior staff responsible for particular lines of business.
General
Assembly
Management
Board Member Forum
Content Committee
Implementation &
Education
Committee*
Quality Assurance
Committee
Technical
Committee
Healthcare
Professional
Coordination Group
Special Interest Groups
(SIGs)
· Nursing SIG
· International Family
Practice/General
Practice SIG
· Dentistry SIG
· Anesthesia SIG
· International Pathology
& Laboratory Medicine
(IPALM) SIG
· Pharmacy SIG
Special Interest Groups
(SIGs)
Translation SIG
Mapping SIG
Special Interest Groups
(SIGs)
Implementation SIG
Education SIG
Vendor Liaison
Forum*
Updated 13 December 2013
Note* Diagram includes provisional changes to the names of the Affiliate Forum (shown as Vendor Liaison Forum)
and the Implementation and Innovation Committee (shown as Implementation and Education Committee) which are
expected to be formally adopted in 2014)
Key:
Rectangle:
Advisory Body
Ellipse:
Governance
Body
SNOMED CT Starter Guide
July 2014
55 | P a g e
IHTSDO advisory bodies
Standing Committees
The IHTSDO has four Standing Committees which provide advice to the Management Board. Committee
members are elected by the General Assembly. They meet face to face twice a year, and between those
meetings have regular conference calls. Meetings of these committees are generally open to observers.
Content Committee: Is responsible for providing advice on issues related to the definition and
maintenance of the clinical content and structure of SNOMED CT and its related standards.
Implementation and Education Committee: Is responsible for providing advice, assistance and education
to enable effective practical implementation of SNOMED CT in ways that aid the management of clinical
information and assist clinical decision making.
Quality Assurance Committee: Is responsible for the development and quality assurance of SNOMED CT
and its related standards and the Association’s other Terminology Products in harmony with proper respect
to external standards.
Technical Committee: Is responsible for focusing on technology related issues relating to the use and
application of SNOMED CT, the fitness for purpose of frameworks and tools adopted in the application of
SNOMED CT.
Working Groups
Working groups include
Special Interest Groups (SIGs) which are open forums that examine issues on particular topics or
healthcare specialty areas; and
Project Groups which have defined time-limited objectives.
There are two distinct types of Special Interest Group
Topic Based SIGs cover a general topic area (e.g. implementation, translation) and report to one of
the Standing Committees; and
Professional Specialty SIGs focus on requirements of a particular clinical discipline or specialty (e.g.
Nursing, Anesthesia). These SIGs report to the Healthcare Professional Coordination Group which
includes the chairs of each of the professional SIGs.
To join a Special Interest Group or to access information about one of the other groups you need to create
an account on the IHTSDO Collaborative Space (see www.ihtsdo.org/collabnet).
National release centers
IHTSDO Members undertake a range of activities related to their involvement in the IHTSDO and their role
in distributing, extending and supporting the use of SNOMED CT in their country. The Organisation or
agency that coordinates this role in each country is referred to as a National Release Centre (NRC). National
Release Centers provide a single point of contact for communications with IHTSDO and other IHTSDO
Members. Within their own countries, NRCs manage the use of SNOMED CT and communicate with a range
of stakeholders, including SNOMED CT Affiliate Licensees, healthcare institutions, clinical groups and end
users.
SNOMED CT Starter Guide
July 2014
56 | P a g e
15. LEARNING MORE ABOUT SNOMED CT
The Starter Guide is intended as a practical and useful starting point from which anyone with a general
interest in healthcare information can begin learning about SNOMED CT. It provides a broad overview of
SNOMED CT from which to start a more detailed exploration of areas that are of particular interest.
IHTSDO provides many other materials on its website that you are welcome to explore. These include
specifications and more detailed guides on which this Starter Guide is based. In addition there are FAQs,
“how to” guides and brief summaries of benefits. Training slide sets, recorded tutorials and online self-
assessment tests are also available and these resources are set to grow significantly during 2014.
The website also provides access to presentations and tutorial slide sets from the annual SNOMED CT
Implementation Showcase events held over the last three years.
Topic
Key reference
Information about IHTSDO
Find out more about the Organisation, members,
committees, special interest groups, newsletter and
events.
www.ihtsdo.org
· www.ihtsdo.org/about-ihtsdo
· www.ihtsdo.org/members
· www.ihtsdo.org/committee
· www.ihtsdo.org/sig
· www.ihtsdo.org/newsletter.pdf
· www.ihtsdo.org/events
General information about SNOMED CT
Materials include a benefits paper, a very short
introductory presentation and information about
licensing.
www.snomed.org
· www.snomed.org/benefits.pdf
· www.snomed.org/snomedintro.pdf
· www.snomed.org/license
Documentation Library
Access to detailed documents, including the
Technical Implementation Guide, Editorial Guide
and FAQs.
www.snomed.org/doc
SNOMED CT Browsers
A range of online and offline tools to search
SNOMED CT content.
www.snomed.org/browsers
SNOMED CT in action
Examples of how SNOMED CT is being used around
the world.
www.snomedinaction.org
SNOMED CT Starter Guide
The latest version of this guide.
(The guide can also be found in the Documentation
Library - see above).
www.snomed.org/snomedct_starter.pdf
SNOMED CT E-Learning Center
www.snomed.org/elearning
SNOMED CT Online Assessment Tests
www.snomed.org/challenge
SNOMED CT Starter Guide
July 2014
57 | P a g e
