Philips Dose Tracking Systems In Radiation Safety Programs White Paper V2?func=doc
895001 Product Whitepaper Philips DoseWise Portal 2.0 Radiation dose management solution 9db27534b13340dea26fa77c0154cf88 Philips - DoseWise Portal 2.0 Radiation dose management solution895001
895001 Product Brochure Philips DoseWise Portal 2.0 Radiation dose management solution 91c8cb76af3d47d68509a77c014830a9 Philips - DoseWise Portal 2.0 Radiation dose management solution895001
User Manual: Philips dose tracking systems in radiation safety programs DoseWise Portal
Open the PDF directly: View PDF ![]() .
.
Page Count: 3

DoseWise
Customer Services
The role of dose tracking systems
in radiation safety programs
Authors: Christopher Martel, CHP, Dominic Siewko, CHP
In 2009 dozens of patients undergoing CT head examinations were accidentally
overexposed leading to hair epilation and concerns for cancer induction. These events
were an eye-opener for the radiology industry, as up to this point no other signicant
diagnostic radiology incident had occurred. This drove the need for far more attention
on how to manage radiation exposure for patients, not necessarily from a clinical
image quality perspective, but from a patient safety perspective. What the industry
quickly realized is that within the current healthcare framework there is no clear owner
of managing cumulative radiation dose to patients and how this information should be
used throughout their care. The goal of this whitepaper is to drive this conversation and
oers the Philips perspective on how we use the data available from radiation dose
tracking solutions to contribute to patient care.

What is dose tracking and why is it important?
We have been exposing patients to medical radiation in
the healing arts for over 100 years. The focus up until now
has primarily been on image quality to ensure an accurate
diagnosis and deservedly so, as the lack of evidence
regarding low levels of medical radiation exposure are largely
unknown to this day. The key to medical radiation exposure
is ensuring that the procedure is justied for the patient
and that the radiation exposure is managed for the desired
balance between image quality and radiation dose to that
patient. This has always been done on an individual basis,
per patient and per procedure. It has not been common
practice to use this exposure data retrospectively as part
of the patient’s care or as part of the hospital’s equipment
quality or safety program at a larger level.
This is where dose tracking is important and can be a
value-added tool to hospitals, providing improved quality
control and cumulative dose management (managing patient
risk). Hospitals and imaging clinics have never before been
able to capture radiation dose across all their equipment,
regardless of modality or vendor. The advent of dose tracking
software allows radiology departments to assess variability
across their equipment. This also allows for the patient’s
dose to be sent to the EMR and attached to their records via
the radiology dictation system, which is a convenience to
the radiologist while simultaneously reducing transcription
errors. Surprisingly, to this day, most patient radiology exam
radiation doses are not recorded as part of their medical
records.
Regulatory requirements and standards
In the United States, the Nuclear Regulatory Commission
is the regulating authority for all radioactive materials
(including Nuclear Medicine radiopharmaceuticals), and the
States are the regulating authority for radiation generating
machines such as X-ray machines and linear accelerators.
In many instances, States have also been delegated the
authority over radioactive materials (called “Agreement
States”), therefore having responsibility for all sources of
radiation.
Historically, the only regulations that existed with regard
to medical patient radiation exposure were specically for
excessive dose in Nuclear Medicine, reportable to either
the NRC or the local Agreement State, but no standards
existed for reporting X-ray exposure. In recent years, partly
in response to the overexposure events and also due to
heightened awareness of radiation exposure in general,
Agreement States began to adopt local regulations such
as California where AB510 was adopted in 2012, requiring
hospitals to report excessive CT exposures to the state -
a rst in the nation. Other states, such as New York and
Texas, have begun to add local State requirements for CT
image quality and protocol optimization, a trend that is likely
to continue.
As of 2015, the Joint Commission requires routine analysis
of patient exposures in CT in an eort to optimize and
normalize exam protocols (and dose) across their enterprise.
It is likely that these standards and regulations will continue
to evolve and cover other X-ray modalities and applications
over time, particularly in uoroscopy.
In February 2018 the EU is slated to also codify new laws
through a European Commission Council Directive “laying
down basic safety standards for protection against the
dangers arising from exposure to ionizing radiation” that
will implement very similar rules for tracking and monitoring
patient exposure. These new rules are even more explicit
than the 2015 Joint Commission Standards, calling for
medical providers to exercise justication, optimization,
protocol management, additional sta training and clinical
audits.
In the US there is a new law being enacted referred
to as “MACRA”, short for Medicare Access and CHIP
Reauthorization Act, which went into eect April 2015.
This is a bold move for Medicare that shifts reimbursement
from a pay-per-service model to a “value-based care”
system. Value-based care will be measured by metrics that
healthcare providers must keep to ensure reimbursement
from CMS. While the scope of MACRA is massive, buried in
the metrics are patient radiation dose requirements which
dose tracking software can help manage.
Framework of existing hospital process
Radiation is ubiquitous in today’s worldwide healthcare
environment; X-ray machines are standard tools employed
by clinicians in diagnosis and in treating people; and
radioactive materials are used in diagnosing symptoms,
in treating cancer, and in sterilizing blood. The hazards
associated with radiation requires that the sources of
radiation be tightly regulated and controlled.
Hospitals are required to have the administrative resources to
manage the purchase, use and disposal of radiation sources,
including policies, programs and procedures. They must also
have the facilities and personnel needed to implement these
policies, programs and procedures. The standard model
is to have a Hospital Radiation Safety Committee (RSC)
that essentially works on the State’s behalf to oversee the
implementation of programs, and ensure that all activities
are performed in compliance with applicable regulations.
The RSC is required in the United States per Federal Code
10 CFR 35.24 (and local Agreement State regulations) to
provide this organization.
The hospital or imaging clinic is also required to delegate
the authority to manage all radiation safety related activities
to a Radiation Safety Ocer (RSO). The RSO is usually an
employee that has been delegated the responsibilities either
as part of their part-time job, or as their full-time job and
must meet minimum educational and practical experience.
The RSO usually has a sta to assist with the day-to-day
implementation of the programs and procedures. In the US
this is usually a dedicated role within the hospital and in
Europe it is usually a role owned by the Medical Physicist or
Radiologist.
As part of radiation dose management in general, the RSC
legally requires a routine meeting of the following hospital
sta to provide oversight of all byproduct radioactive
materials used in the hospital:
• The Radiation Safety Ocer
• A representative of the nursing sta
• A management representative (non-radiology)
• At least one authorized user for each type of radioactive
material use by the hospital
In the US, the terms “authorized users” and “byproduct
material” may be foreign to most people:
• Authorized users are hospital sta with specialty academic
and practical training in radiation dosimetry, protection,
radiobiology, mathematics, medical use and research use
of radioactive materials, to name a few.
• Byproduct materials are radioactive materials that
are produced by a nuclear reactor. These are usually
“byproducts” of nuclear fuel such as uranium and thorium
that are recovered to make medical radio-isotopes.
Iodine-131 and Molybdinum-99 generators are examples
of these materials.
Notice, however, in these denitions that X-rays are NOT
covered in the Radiation Safety Committee requirements.
This is the gap that has left out X-ray medical radiation dose
to patients from being supervised and reviewed as part of a
formal process.
Who assumes responsibility for patient radiation safety?
Who actually carries out the duties of the RSO often is
related to an individual’s professional area of expertise.
It is not uncommon for the RSO to have radiation safety
responsibilities for radioactive materials only, and a
diagnostic imaging Medical Physicist having responsibilities
for X-ray machines. Radiation used for therapeutic purposes
are most commonly the responsibility of Medical Physicists
that specialize in radiation therapy. So although the RSO may
be responsible for radiation safety across the institution in
name, in practice, there are other individuals that may have
narrow responsibilities in their specic area of expertise
and report program status to the RSO. It’s worth mentioning
that even though the regulatory framework requires that the
RSO be delegated this authority of oversight of radioactive
materials, that delegation is made usually by the CEO/
President of the organization. This is because the application
to the NRC or Agreement State to use radiation is signed by
the highest oce in the institution.
Historically, radiation safety was applicable to the hospital’s
workers and the general public that visited the hospital;
radiation safety for patients was considered “not applicable”
because they were intentionally being exposed to radiation
for their benet. The only exception to this was radiation
therapy because the high levels of radiation exposure to
kill cancers also carry a signicant risk to the patient if their
personal safety was not addressed as part of the treatment
protocol. However, recent data has forced the diagnostic
imaging community to also address patient radiation safety.
As a result, computer technology now allows the healthcare
community to monitor and track radiation exposures to
patients to ensure their safety is maximized.
The question facing healthcare professionals today is “what
data are clinically important and useful for monitoring,
tracking and controlling patient radiation exposures?” and,
more importantly, “what should we do with this data?” The
answer to the question as to who owns patient radiation
dose therefore depends on the resources available in
the hospital. Some hospitals will not employ a Medical
Physicist, and although some hospitals contract RSO work
to consultants they are more likely to have a resource. RSOs
also own the management of hospital sta occupational
dose, so it is preferable that they manage patient dose and
have the responsibility to track patient dose and bring it to
the RSC meetings for discussion in close collaboration with
Medical Physicists and other radiology professionals.
NCRP report 172 also prescribes the creation of a “Clinical
Dose Optimization Team”, or CDOT, to own this responsibility.
Their responsibility is to review image quality, patient
radiation doses, procedures and imaging protocols as
compared to national values. This team should consist of:
• Imaging Physicians
• Qualied Medical Physicist
• Radiographic Technologist
• Ancillary sta from imaging department
Working with the data from dose tracking software
Integrating patient radiation safety related data into the
institution’s Radiation Safety Program is a great challenge
for many. The primary focus has been rst on patient
radiation dose delivered by CT scanners, and second from
the uoroscope used for guided interventional procedures.
The reason why these modes of radiation exposure were
chosen over the others is because they are performed on a
larger proportion of the worldwide population as compared
to the other modalities, and the exposure to each patient
can be a signicant amount of radiation compared to
other radiology modalities such as digital radiography and
mammography.
Radiation dose tracking software brings all patient exposures
into one place allowing hospitals to segment, analyze and
track dose to individual patients. It also allows hospitals to
discover trends in their data across their imaging suite of
machines, allowing protocol adjustments and normalizing
exam exposure.
DRL/Achievable dose targets
The National Commission on Radiation Protection Report
172 established levels for general types of procedures that
most institutions perform using X-rays for the purpose
of providing benchmark values. They produce average
values for a variety of procedures from all modalities for
comparison allowing institutions to generate average values
of their own, and if they are higher than the published values,
then they should take steps to possibly manage radiation
exposure. These benchmark or reference values are referred
to as Diagnostic Reference Levels (DRLs). These DRLs are
typically the 75th percentile of the dose distribution for
patients in that exam protocol.
Report 172 also provided more challenging lower levels that
institutions should try to attain, referred to as Achievable
Doses (ADs). The intention is that when the institution is
hovering at or below the DRL, there should be a lower target
to aim for. The ADs are typically dened as 50th percentile
of the dose distribution and meant to manage dose even
further while maintaining adequate image quality.
Certain countries in Europe, such as France’s ASN Guide
No. 11, have also established local DRLs that healthcare
institutions should target. In fact, there are many ways of
managing the data. For example, the UK PM77 Guidance re
a complete rescan needed this would be a recordable (and
potentially reportable) event to the government agency.
We still have a ways to go to harmonize the best approach
to managing patient exposure, however DRLs seem like the
most probable path.
One thing should remain clear however, that DRLs are not
meant to be for regulatory or commercial purposes nor are
they to limit exposure to patients for a certain procedure.
Justication and optimization are the keys to managing
dose to a particular patient. DRLs are valuable to manage
equipment optimization and protocol management.
2 3
© 2016 Koninklijke Philips N.V. All rights reserved.
Specications are subject to change without notice.
Trademarks are the property of Koninklijke Philips N.V.
or their respective owners.
4522 991 23551 * NOV 2016
How to reach us
Please visit www.philips.com/healthcare
healthcare@philips.com
Methods of analyzing data
The RSC is responsible for ensuring that the use of radiation
for diagnostic purposes in the hospital is purchased, used
and disposed of according to applicable regulations, and
that the safety of workers, the public, and now patients
are appropriately managed. The collected data is used for
two purposes. The rst are as quality measures – to ensure
that the programs and procedures are being performed as
intended and that the outcomes are consistent with the
respective design goals. The second is to identify outliers, i.e.,
those instances where things did not go as expected.
Dose monitoring and tracking is extremely useful for both
purposes. For example, the patient-specic radiation dose
metric for CT scans (i.e., Dose Length Product, volumetric
Computed Tomography Dose Index or Size Specic Dose
Estimate) can be aggregated by protocol type (e.g., head
scan, abdomen scan, etc.) and described and compared
through statistics. Comparing actual values to appropriate
benchmarks can reveal whether the institution is comparable
to other institutions performing the same types of scans on
the same types of patients. The data can also be used to
identify outliers. Dose metrics used on the individual level
can be used to identify those patients that received far more
radiation than the protocol or other controlling factors can
explain. This can help Medical Physicists to identify areas of
improvement, or unknown operational practices, that could
help manage equipment use and normalize dose per exam
across the patient population.
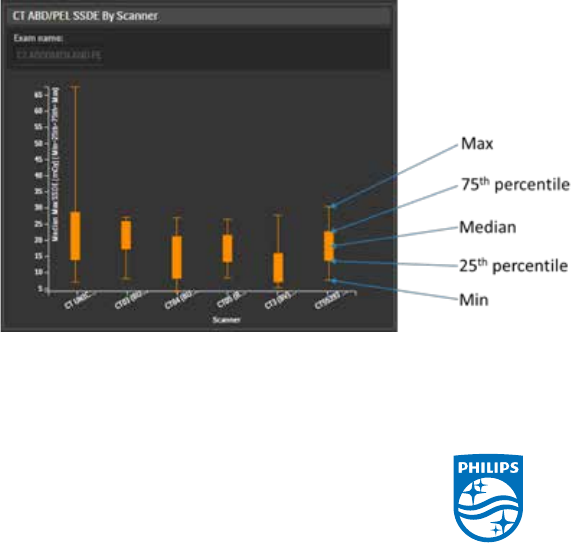
Because DRLs and Achievable Dose work within the concept
of “percentile” of the dose distribution, the statistical boxplot
graph is a very eective method of analyzing the data.
A boxplot indicated the distribution of data with a min/max/
median while also identifying the 75th percentile and also the
25th percentile. If you participate in the American College of
Radiology’s Dose Index Registry (DIR) then you are probably
already familiar with this type of graph, as this is what they
use to distribute data to participants. See Figure 1 below for
an example of a box plot.
Goals/Review of progress
Healthcare institutions are expected to manage patient
exposure having probably never done it before, so where
do you start?
The concept of dose management is one that entails
patient safety, risk, regulatory compliance and now facility
accreditation As such, it is important that hospital executives
“buy-in” to this philosophy to ensure that stang, funding and
other adequate resources are available with accountability
established. A robust hospital infrastructure builds the
foundation for success. This is where the concept of the CDOT,
as mentioned above, comes into play. The CDOT should serve
as the central owner of patient dose that reports into the
Radiation Safety Committee for that institution. Vendors and
manufacturers are keen on the needs of users and can also
help provide training, content and support for developing your
patient radiation safety program. Education of stakeholders
is key after programs are established and infrastructure is
complete. Of course all relevant sta should be educated on
the processes and teams established to monitor dose, but
patients should also be included. Patients have never been
as educated on dose as they are today. The reality is that the
internet is full of content that may be either too technical,
or misleading based on the source, for patients to educate
themselves. A proactive and transparent patient education
campaign with factual data is a good path to follow.
The rst step to managing patient dose is data. Using a
commercial dose tracking software, or data mining from
your PACS or RIS, allows you to benchmark yourself with
retrospective data. Set goals to understand your current
dose results against DRL values and make modest targets to
improve aggregate dose. Reviewing the data will also identify
unknown practices, such as variation among Technologists,
and help standardize ways of working in an environment with
equipment from multiple vendors and with dierent levels of
technology due to age.
The path forward for patient dose management will take
some time, but small steps with some organizational support
will begin to yield successful results. This is the expectation
from organizations such as Joint Commission as well as
individual States as they promulgate more regulation in this
area.
Figure 1. Example of a boxplot data distribution
