BIOTRONIK SE and KG TACHBORAX implantable cardioverter defibrillator User Manual
BIOTRONIK SE & Co. KG implantable cardioverter defibrillator
15_TACHBorax UserMan

BIOTRONIK SE & Co. KG
Woermannkehre 1
12359 Berlin · Germany
Tel +49 (0) 30 68905-0
Fax +49 (0) 30 6852804
sales@biotronik.com
www.biotronik.com
Inlexa 1
VR-T, DR-T, HF-T
ICD-Familie | Tachyarrhythmietherapie |
Kardiale Resynchronisationstherapie
Gebrauchsanweisung
420651
Revision: A (2015-12-09)
© BIOTRONIK SE & Co. KG
Alle Rechte vorbehalten.
Technische Änderungen vorbehalten.
® Alle verwendeten Produktnamen können Marken oder eingetragene Marken von
BIOTRONIK oder dem jeweiligen Eigentümer sein.
Index 420651GebrauchsanweisungInlexa 1 VR-T , DR-T, HF-T,

1
1 Product Description
Product Description1403736Technical Manual
Intended Medical Use
Intended use Inlexa 1 is part of a family of implantable cardioverter-defibrillators (ICDs). The
primary objective of the therapy is to prevent sudden cardiac death. Furthermore,
the device is capable of treating bradycardia arrhythmias and cardiac resynchroni-
zation therapy with multisite ventricular pacing.
The implantation of an ICD is a symptomatic therapy with the following objectives:
• Termination of spontaneous ventricular fibrillation (VF) through shock delivery
• Termination of spontaneous ventricular tachycardia (VT) through antitachy-
cardia pacing (ATP); in case of ineffective ATP or hemodynamically not tolerated
VT, with shock delivery
• Cardiac resynchronization through multisite ventricular pacing (triple-chamber
devices)
• Compensation of bradycardia through ventricular (single-chamber devices) or
AV sequential pacing (dual- and triple-chamber devices)
Diagnosis and
therapy forms
The device monitors the heart rhythm and automatically detects and terminates
cardiac arrest resulting from ventricular tachyarrhythmia. All major therapeutic
approaches from the field of cardiology and electrophysiology are included.
BIOTRONIK Home Monitoring® enables physicians to perform therapy manage-
ment at any time.
Required expertise In addition to having basic medical knowledge, the user must be thoroughly familiar
with the operation and the operation conditions of a device system.
• Only qualified medical specialists having this required special knowledge are
permitted to use implantable devices.
• If users do not possess this knowledge, they must be trained accordingly.
Indications Inlexa 1 can treat life-threatening ventricular arrhythmias with antitachycardia
pacing and defibrillation.
Generally approved differential diagnostics methods, indications, and recommen-
dations for ICD therapy apply to BIOTRONIK devices. See the current guidelines of
cardiology associations for guidance.
We recommend observing the indications published by the German Cardiac Society
(Deutsche Gesellschaft für Kardiologie, Herz- und Kreislaufforschung) and the ESC
(European Society of Cardiology). This also applies to the guidelines published by
the Heart Rhythm Society (HRS), the American College of Cardiology (ACC), the
American Heart Association (AHA), and other national cardiology associations.
Single-chamber and
dual-chamber
Single-chamber and dual-chamber ICDs are indicated for patients with the
following risk:
• Sudden cardiac death caused by ventricular arrhythmias
Triple-chamber Triple-chamber ICDs are indicated for patients with the following risks:
• Sudden cardiac death caused by ventricular arrhythmias
• Congestive heart failure with ventricular asynchrony
2
Contraindications Known contraindications:
• Tachyarrhythmia caused by temporary or reversible irritation, e.g. poisoning,
electrolyte imbalance, hypoxia, sepsis or acute myocardial infarction
• Such frequent VT or VF that the therapies would cause an unacceptably rapid
depletion of the device batteries
• VT with few or without clinically relevant symptoms
• VT or VF treatable by surgery
• Concomitant diseases that would substantially limit a positive prognosis
• Accelerated intrinsic rhythm
System Overview
Device family The complete Inlexa 1device family consists of several device types with a DF-1/IS-1
connection.
•Single-chamber: VR-T
•Dual-chamber: DR-T
• Triple-chamber: HF-T
Device The device's housing is made of biocompatible titanium, welded from outside and
thus hermetically sealed. The ellipsoid shape facilitates implantation in the pectoral
muscle area.
The connections for bipolar pacing and sensing (and unipolar connections for the
triple-chamber device) as well as for shock delivery are found in the device header.
The housing serves as a potential antipole during shock delivery or in the case of
unipolar lead configuration.
DF-1/IS-1 The labeling on each device provides information pertaining to the connector port
assignment in the header.
Leads BIOTRONIK leads are sheathed with biocompatible silicone. They can be flexibly
maneuvered, are stable long-term, and are equipped for active or passive fixation.
They are implanted using a lead introducer set. Some leads are coated with poly-
urethane which is known to increase the sliding properties for the lead. Leads with
steroids reduce inflammatory processes. The fractal design of the electrodes
provides for low pacing thresholds. BIOTRONIK provides adapters to connect
already implanted leads to new devices.
Note: Not all device types are available in every country.
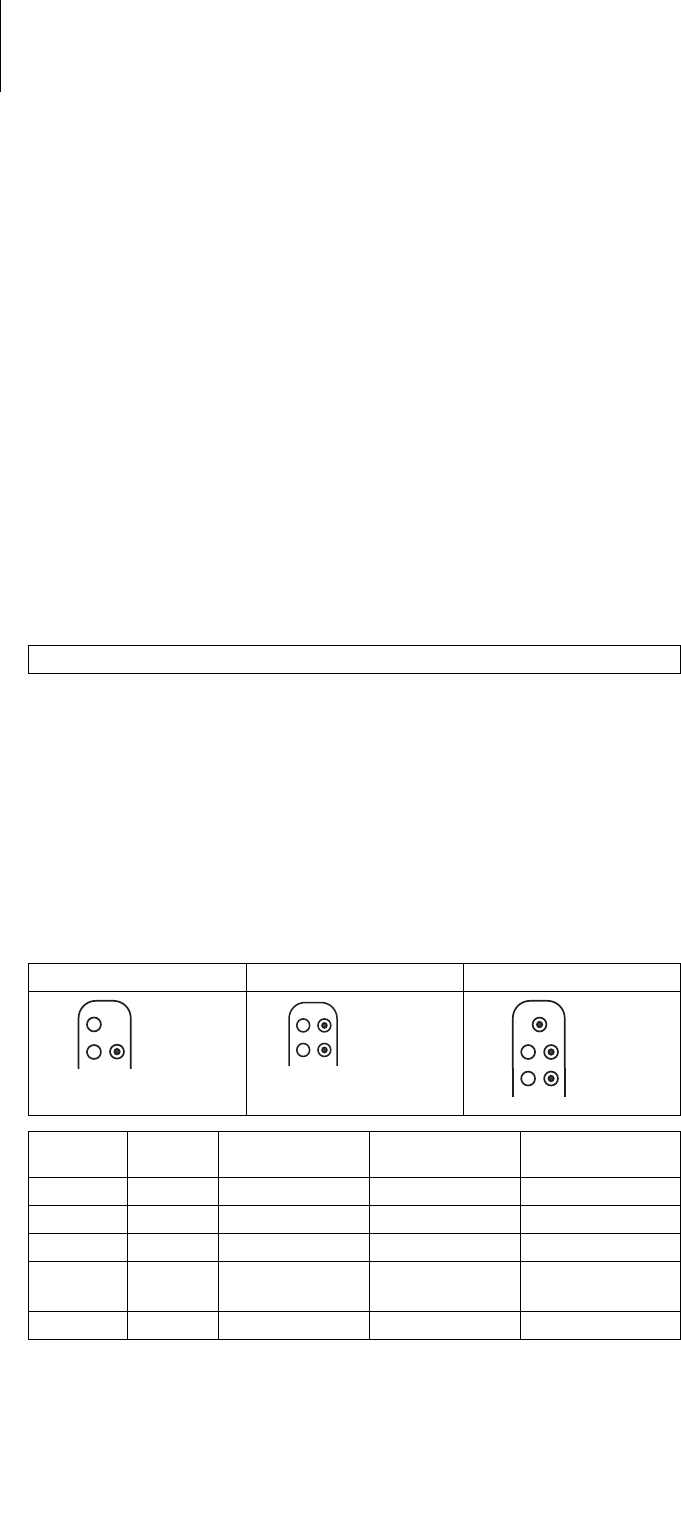
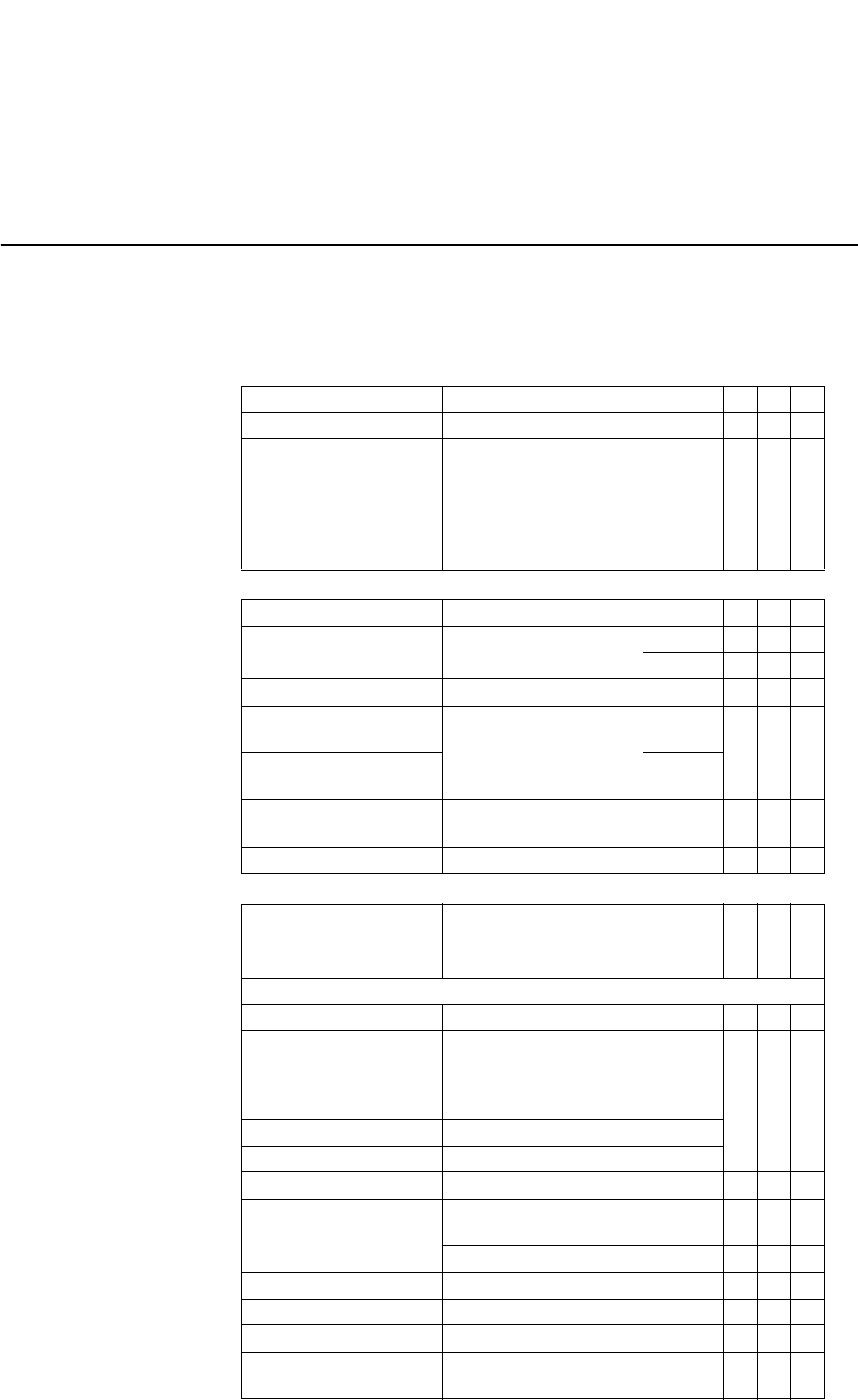
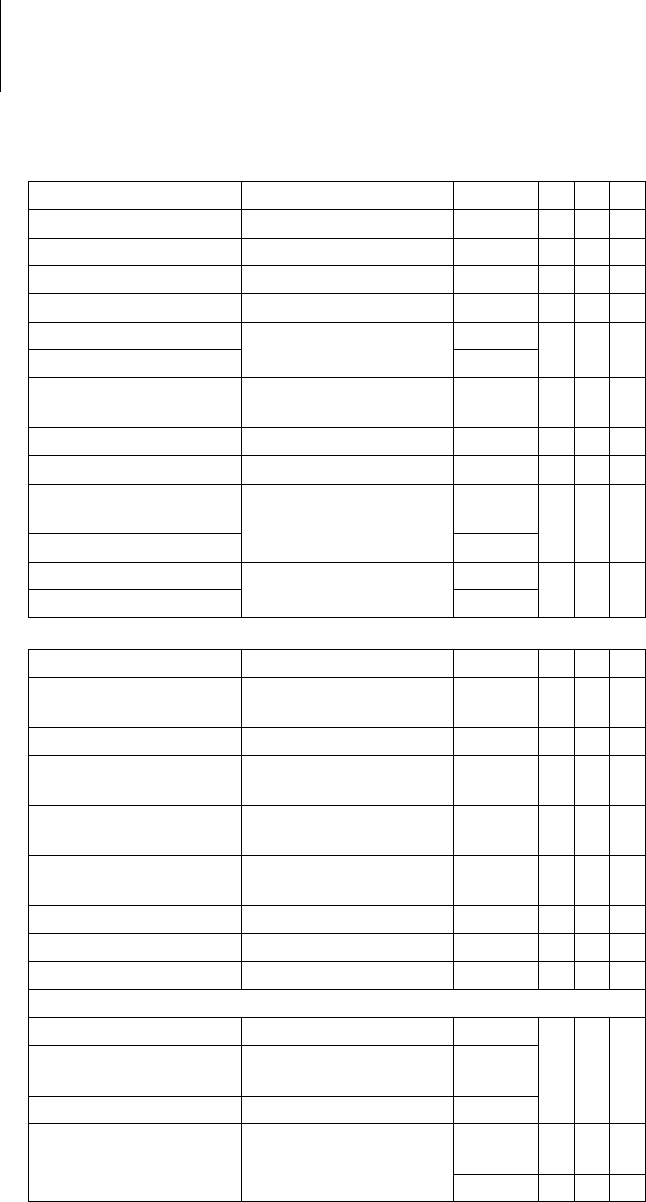
VR DR HF
Connector
port Lead
connector Configuration Implantation site Device type
RA IS-1 Bipolar Atrium DR, HF
(R)V IS-1 Bipolar (Right) ventricle VR, DR, HF
RV DF-1 Shock coil Right ventricle VR, DR, HF
SVC DF-1 Shock coil Superior vena
cava
VR, DR, HF
LV IS-1 Unipolar, bipolar Left ventricle HF
DF-1
RV
SVC
DF-1
IS-1
RV
DF-1
RV
SVC
DF-1 IS-1
RA
IS-1
RV
DF-1
RV
SVC
DF-1 IS-1
RA
IS-1
RV
LV
IS-1
3
Telemetry Telemetric communication between the device and the programmer can be carried
out following initialization either by applying the programming head (PGH) to the
device or by using wireless radio frequency (RF) telemetry in the programmer.
BIOTRONIK calls this function SafeSync®.
Programmer Implantation and follow-up are performed with BIOTRONIK's portable
programmer: Programmer software PSW version N.N. and higher
There is a programmer with integrated RF telemetry and one with a separate
SafeSync Module.
Leadless ECG, IEGM, markers and functions are displayed simultaneously on the
color display.
Using the programmer, the pacing thresholds can be determined and all tests can
be performed during in-office follow-up. If necessary, the current software is trans-
ferred to the device during implantation.
In addition to this, the programmer is used to set mode and parameter combina-
tions, as well as for interrogation and saving of data from the device.
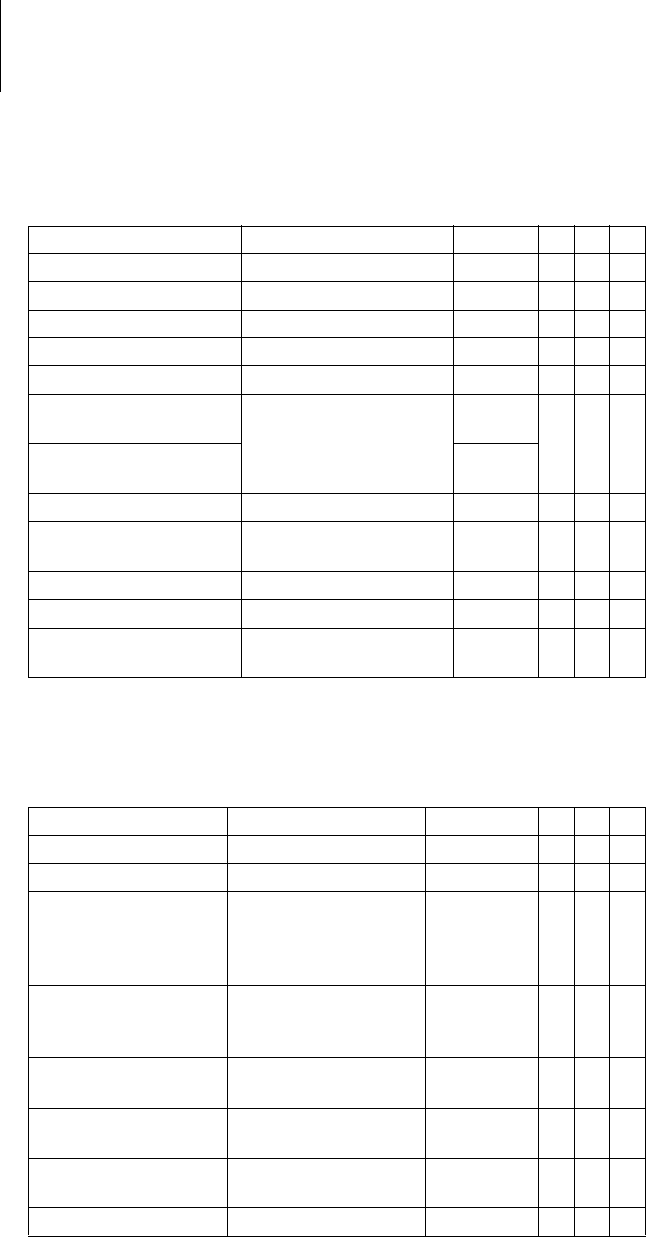
Modes The mode setting depends on the individual diagnosis:
NBD and NBG codes VVE is the NBD code for the antitachycardia mode of the single-chamber, dual-
chamber, and triple-chamber devices:
DDDR is the NBG code for the antibradycardia mode of the dual-chamber devices:
DDDRV is the NBG code for the antibradycardia mode of the triple-chamber devices:
VVIR is the NBG code for the antibradycardia pacing modes of the single-chamber
device:
Device type Modes
VR VVI; VVIR; VOO; OFF
DR, HF DDD; DDDR; DDDR-ADIR; DDD-ADI; DDI; DDIR;
VDD; VDDR; VDI; VDIR
VVI; VVIR; AAI; AAIR; VOO; DOO; OFF
V Shock in the ventricle
V Antitachycardia pacing (ATP) in the ventricle
E Detection via IEGM analysis
D Pacing in the atrium and ventricle
D Sensing in the atrium and ventricle
D Pulse inhibition and pulse triggering
R Rate adaptation
D Pacing in the atrium and ventricle
D Sensing in the atrium and ventricle
D Pulse inhibition and pulse triggering
R Rate adaptation
V Multisite pacing in both ventricles
V Ventricular pacing
V Sensing in the ventricle
I Pulse inhibition in the ventricle
R Rate adaptation
4
BIOTRONIK
Home Monitoring®
In addition to effective pacing therapy, BIOTRONIK provides a complete therapy
management system:
• With Home Monitoring, diagnostic and therapeutic information as well as
technical data are automatically sent to a stationary or mobile transmitter via an
antenna in the device header. The data are encrypted and sent from the trans-
mitter to the BIOTRONIK Service Center via the cellular phone network.
• The received data are deciphered and evaluated. Each physician can set the
criteria for evaluation to be used for each patient and can configure the time of
notification via e-mail, SMS or fax.
• A clear overview of the results of this analysis is displayed for the attending
physicians on the protected Internet platform Home Monitoring Service Center
(HMSC).
• Data transmission from the device is performed with a daily device message.
• Device messages which indicate special events in the heart or in the device are
forwarded immediately.
• A test message can be initiated at any time using the programmer to immedi-
ately check the Home Monitoring function.
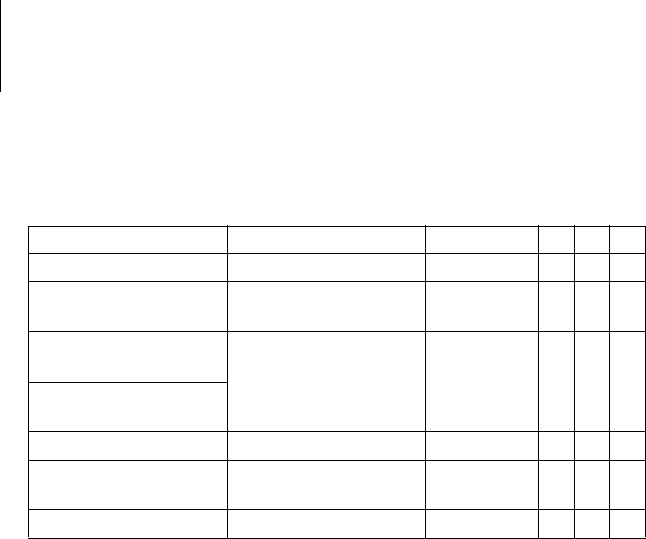
Inlexa 1order numbers Not all device types are available in every country:
Package contents The storage package includes the following:
• Sterile packaging with device
• Serial number label
• Patient ID card
• Warranty booklet
The sterile container includes the following:
• Device, blind plugs (if applicable)
• Screwdriver
VR-T DR-T HF-T
405797 405796 40579
Note: The technical manual pertaining to the device is either included in hard copy
form in the storage package or in digital form on the internet.

5
Therapeutic and Diagnostic Functions
Diagnostic functions • Data from implantation and the most recent interrogations and follow-ups are
recorded as well as arrhythmia episodes; they are stored together with other
data to assess both the patients' and the device's state at any time.
• To check the lead for proper functioning, an automatic impedance measure-
ment using subthreshold pacing pulses is performed in the device.
• Leadless ECG function: For all device types, far-field derivation can be
measured without external leads between the right ventricular shock coil and
housing, which, depending on the implantation site, corresponds to ECG
derivation II or III (Einthoven).
• Once a telemetry connection has been established during a test procedure in an
in-office follow-up, the leadless ECG and the IEGM are displayed with markers.
Antitachycardia pacing • The ICD can treat ventricular tachycardia with antitachycardia pacing (ATP); ATP
can also be delivered in the VF zone (ATP One Shot) when the stability criterion
indicating that this will be effective before shock delivery (monomorphic
rapid VTs) is met.
• Depending on the device type, the device program contains not only the ICD
functions but also all pacemaker functions for 1, 2 or 3 chambers. The heart
rhythm is continuously monitored; each arrhythmia is classified according to
the heart rate and the adjustable detection criteria. Depending on the preset
values, antibradycardia as well as antitachycardia therapy is inhibited or
delivered.
Cardioversion, defibrillation • The ICD can treat ventricular tachyarrhythmia with cardioversion and/or defi-
brillation. Shock polarity and energy can be programmed individually. Shock
energies between 2.0 and 40 J are possible depending on the device family.
Before delivery of the shock, the ICD can be set to only deliver a shock when
ongoing tachyarrhythmia is confirmed; during this time period the device can
identify spontaneous conversion of the tachyarrhythmia and cancel the charging
process if necessary.
• The shock paths can be set between the different shock coils (SVC/RV) and/or
the housing.
Antibradycardia pacing
and CRT
• Innovative rate hystereses, automatic sensor functions, and a night program
promote the patient's intrinsic rhythm, avoid overdrive pacing, and facilitate
adaptation of the device to the individual needs of the patient.
• Thresholds: atrial as well as ventricular pacing thresholds are automatically
determined in the device, automatic threshold monitoring (ATM) for trend
analysis.
• Setting an upper tracking rate for the atrium prevents unspecific atrial pacing,
thus reducing the risk of pacemaker-mediated tachycardia.
• Positive AV hysteresis functions support intrinsic conduction and thus the
natural contraction sequence. Negative AV hysteresis functions support the
cardiac resynchronization therapy by maintaining pacing in stress situations.
• For resynchronization of the ventricles, triple-chamber implants have functions
for multisite pacing with possible VV delays in either direction.
• To ensure that no additional surgery is necessary in case of a left-sided increase
of pacing threshold or undesired phrenic nerve stimulation, different pacing
polarities can be set for the left ventricular lead with a triple-chamber device.
Storing programs There are different therapy programs:
• Parameter settings effective for the most common indications in pre-configured
programs (Program Consult).
• For special indications, individual parameter settings can be stored in up to
three therapy programs.

6
Home Monitoring functions • The device automatically sends information to the transmitter once a day. It also
sends messages related to events, which are immediately forwarded to the
Service Center. In addition to this, test messages can be initiated using the
programmer.
• Appointments for Home Monitoring-supported follow-ups can be scheduled via
the HMSC.
• Important medical information in the device messages include the following:
— Atrial and ventricular arrhythmias
— Parameters relevant to leads in the atrium and ventricle: pacing thresholds,
sensing amplitudes, impedances
— Current statistics
—IEGM online HD
® with up to 3 high definition channels
7
2 General Safety Instructions
General Safety Instructio ns2403736Technical Manual
Operating Conditions
Technical manuals The following technical manuals provide information about usage of the device
systems:
— Technical manual for the device
— Technical manual for the HMSC
— Technical manual for the electrodes
— Technical manuals for the programmer and its accessories
— Technical manuals for the user interface
— Technical manuals for cables, adapters and accessories
• Technical manuals are either included in hard copy form in the storage package
or in digital form on the internet: manuals.biotronik.com
• Follow all relevant technical manuals.
• Reserve technical manuals for later use.
Care during shipping
and storage
• Devices must not be stored or transported close to magnets or sources of elec-
tromagnetic interference.
• Note the effects of the storage duration; see Battery Data.
Delivery in shipment mode The device is delivered in shipment mode to protect the battery; capacitor reforming
required during storage could result in controlled extended charge times of the
shock capacitors.
• The shipment mode is displayed on the programmer after the initial interroga-
tion (it is deactivated during implantation by the first valid (in-range) measure-
ment of the pacing impedance).
Temperature Extremely low and high temperatures affect the service time of the battery in the
device.
• Temperatures of +5°C to +45°C are permitted for transport, storage, and use.
Sterile delivery The device and the screwdriver have been gas-sterilized. Sterility is guaranteed only
if the blister and quality control seal have not been damaged.
Sterile packaging The device and screwdriver are packaged in two separately sealed blisters. The
inner blister is also sterile on the outside so that it can be transferred in a sterile
state during implantation.
Single use only The device and screwdriver are intended for single use only.
• Do not use the device if the package is damaged.
• The device must not be resterilized and reused.

8
Possible Complications
General information on
medical complications
Complications for patients and device systems generally recognized among practi-
tioners also apply to BIOTRONIK devices.
• Normal complications may include fluid accumulation within the device pocket,
infections, or tissue reactions. Primary sources of complication information
include current scientific and technological knowledge.
• It is impossible to guarantee the efficacy of antitachycardia therapy, even if the
programs have proven successful during tests or subsequent electrophysio-
logical examinations. In rare cases the set parameters may become ineffective.
It is possible for therapies to induce or accelerate tachycardia and cause
sustained ventricular flutter or fibrillation.
Skeletal myopotentials Bipolar sensing and control of sensitivity are adapted by the device to the rate range
of intrinsic events so that skeletal myopotentials are usually not recorded. Skeletal
myopotentials can nonetheless be classified as intrinsic events especially at very
high sensing sensitivity and, depending on the interference, may cause inhibition or
antiarrhythmia therapy.
In the case of undesired myopotentials, the device switches to asynchronous pacing
if the interference rate is exceeded.
Possible technical failures Technical failure of a device system cannot be entirely ruled out. Possible causes
can include the following:
• Lead dislodgement, lead fracture
• Insulation defects
• Device component failures
• Battery depletion
• Interrupted telemetry
Electromagnetic
interference (EMI)
Any device can be sensitive to interference if external signals are sensed as intrinsic
rhythm or if measurements prevent rate adaptation.
• BIOTRONIK devices have been designed so that their susceptibility to EMI is
minimal.
• Due to the intensity and variety of EMI, there is no guarantee for safety. It is
generally assumed that EMI produces only minor symptoms, if any, in patients.
• Depending on the pacing mode and the type of interference, sources of inter-
ference may lead to pulse inhibition or triggering, an increase in the sensor-
dependent pacing rate or asynchronous pacing.
• Under unfavorable conditions, for example during therapeutic or diagnostic
procedures, interference sources may induce such a high level of energy into
the pacing system that the cardiac tissue surrounding the lead tip is damaged.
Device behavior in
case of EMI
In case of electromagnetic interference, the device switches to asynchronous
pacing for as long as the interference rate is exceeded.
Static magnetic fields The magnetic sensor in the device detects magnetic fields starting at a magnetic
flux density of approximately 1.5 mT. Magnetic fields below 1 mT do not affect the
sensor.

9
Possible Risks
Procedures to avoid The following procedures must be avoided, as they may cause harm to the patient
or damage the device and, as a result, put the system functionality at risk:
• Transcutaneous electrical nerve stimulation
• Hyperbaric oxygen therapy
• Applied pressures higher than normal pressure
Risky therapeutic and
diagnostic procedures
If electrical current from an external source is conducted through the body for diag-
nostic or therapeutic purposes, then the device can be subjected to interference,
which can place the patient at risk.
Arrhythmia or ventricular fibrillation can be induced during diathermic procedures
such as electrocautery, HF ablation or HF surgery. For example, damaging
pressure levels may arise during lithotripsy. For example, excessive warming of
body tissue near the device system may occur during therapeutic ultrasound. Influ-
ences on the device are not always immediately clear.
If risky procedures cannot be avoided, the following should be observed at all times:
• Electrically insulate the patient.
• Switch off the ICD's detection function. The pacemaker function can remain
active. The device may need to be switched to asynchronous modes for this.
• Do not introduce energy near the device system.
• Additionally check the peripheral pulse of the patient.
• Monitor the patient during and after every intervention.
External defibrillation The device is protected against the energy that is normally induced by external defi-
brillation. Nevertheless, any implanted device may be damaged by external defibril-
lation. Specifically, the current induced in the implanted leads may result in necrotic
tissue formation close to the electrode/tissue interface. As a result, sensing prop-
erties and pacing thresholds may change.
• Place adhesive electrodes anterior-posterior or perpendicular to the axis
formed by the device to the heart at least 10 cm away from the device and from
implanted leads.
Radiation therapy The use of radiation therapy must be avoided due to possible damage to the device
and the resulting impaired functional safety. If this type of therapy is to be used
anyway, prior risk/benefit analysis is absolutely necessary. The complexity of influ-
encing factors such as different sources of radiation, a variety of devices and
therapy conditions makes it impossible to issue directives that guarantee radiation
therapy without an impact on the device. The EN 45502 standard pertaining to active
implantable medical devices requires the following measures during the adminis-
tration of therapeutic ionizing radiation:
• Adhere to instructions for risky therapy and diagnosis procedures.
• Shield device against radiation.
• After applying radiation, double-check the device system to make sure it is func-
tioning properly.
Magnetic resonance
imaging
Magnetic resonance imaging must be avoided due to the associated high frequency
fields and magnetic flux density: Damage or destruction of the device system by
strong magnetic interaction and damage to the patient by excessive warming of the
body tissue in the area surrounding the device system.
Note: Please contact BIOTRONIK with questions during the risk/benefit analysis.
10
3 Implantation
Implantation3403736Technical M anual
Implantation Procedure
Having parts ready The following parts that correspond to the requirements of the EC Directive 90/385/
EEC are required:
• BIOTRONIK device with blind plug and screwdriver
• BIOTRONIK leads and lead introducer set
— Single-chamber device: one bipolar ICD lead with 1 or 2 shock coils for the
ventricle
— Dual-chamber device: one bipolar lead for the atrium and one bipolar ICD
lead for the ventricle with 1 or 2 shock coils
— Triple-chamber device: an additional unipolar or bipolar LV lead
• The lead connections DF-1 and IS-1 are permitted. Use only adapters approved
by BIOTRONIK for leads with different lead connections or leads from other
manufacturers.
• BIOTRONIK programmer (with integrated SafeSync RF telemetry or with
separate SafeSync Module) and approved cables
• External multi-channel ECG device
• Keep spare parts for all sterile components.
Keeping an external
defibrillator ready
To be able to respond to unforeseeable emergencies or possible technical failures
of the device:
• Keep an external defibrillator and paddles or patch electrodes ready.
Unpacking the device
• Peel the sealing paper off of the outer blister at the marked position in the
direction indicated by the arrow. The inner blister must not come into contact
with persons who have not sterilized their hands or gloves, nor with non-sterile
instruments!
• Take hold of the inner blister by the gripping tab and take it out of the outer
blister.
• Peel the sealing paper off of the sterile inner blister at the marked position in
the direction indicated by the arrow.
Checking parts Damage to any of the parts can result in complications or technical failures.
• Check for damage before and after unpacking all parts.
• Replace damaged parts.
• Upon delivery, the tachyarrhythmia therapy function in the ICD is deactivated.
The ICD must only be implanted in this state.
• Leads must not be shortened.
!
!
WARNING
Inadequate therapy due to defective device
If an unpacked device is dropped on a hard surface during handling, electronic
parts could be damaged.
• Use a replacement device.
• Return the damaged device to BIOTRONIK.
11
Implantation site • Depending on lead configuration and the patient's anatomy, the ICD is generally
implanted subpectorally on the left side.
Preventing leakage
currents
Leakage currents between the tools and the device must be prevented during
implantation.
• Electrically insulate the patient.
Preventing unintentional
shock delivery
Avoiding damage
to the header
Set screws and blind plugs (if applicable) must be tightened or loosened with care.
• Loosen set screws with the supplied screwdriver. Use only BIOTRONIK screw-
drivers with torque control!
• Do not forcibly pull out the blind plug!
• If lead revision is necessary, re-order sterile screwdrivers from BIOTRONIK.
Preventing short circuits
in the header
Ensure that connector ports
are clean
In case of contamination during implantation:
• Clean lead connectors with a sterile cloth.
• Rinse connector port only with sterile water.
Overview: Implanting
Connecting the device The lead connectors are connected to the ports in the header of the device:
!
!
WARNING
Shock delivery with activated ICD
There is a risk of unintended shock delivery when handling an activated ICD.
• Deactivate ICD therapy before touching the device during implantation, device
replacement and explantation.
!
!
WARNING
Short circuit due to open lead connector ports
Connector ports in the header which are open and thus not electrolyte-proof may
cause undesired current flows to the body and penetration of body fluid into the
device.
• Close unused connector ports with blind plugs.
1 Prepare the vein.
2 Implant the leads, perform the measurements, and fixate the leads.
3 Form the device pocket.
4 Connect the lead connector to the device.
5 Insert the device.
6 Guide the fixation suture through the opening in the header and fixate the
device in the prepared device pocket.
7 Close the device pocket.
8 Check the device with standard tests.
1 Disconnect stylets and stylet guides.
2 DF-1/IS-1 connection:
• Connect the DF-1 connector for the right-ventricular shock coil to RV.
• Connect the DF-1 connector for the supraventricular shock coil to SVC.
Or connect a subcutaneous array to SVC.
12
Keeping distance
between leads
Applying the
programming head
The programming head (PGH) features a diagram of the device. This is used to
assist in positioning the head to ensure proper telemetry.
• Make sure the PGH is positioned correctly.
Establishing
telemetry contact
The programmer (or the SafeSync Module) can be no more than 3 m from the
device; ideally there should be no hindrances between the patient and the
programmer.
• Switch on RF telemetry on the programmer.
• Apply the programming head for about 2 s until successful initialization is
displayed on the programmer:
The SafeSync symbol is displayed in the navigator and the signal
strength is displayed in the status line.
• Remove the programming head.
Activating ICD therapy • Load the software that is suitable for the device type in the programmer.
• Activate ICD therapy.
• Shipment mode is permanently deactivated once the leads have been connected
and initial measurement of the pacing impedance has been performed success-
fully. The device data are saved.
• Take precautionary measures while programming.
• If the device induces tachycardia while programming ATPs or does not deliver
adequate therapy in the DFT test: use emergency shock or an external defibril-
lator.
3 DF-1/IS-1 connection:
• Connect the bipolar IS-1 connector for the atrium to RA.
• Connect the bipolar IS-1 connector for the right ventricle to RV.
• Connect the unipolar or the bipolar IS-1 connector for the left ventricle to
LV.
4 Push the lead connector into the header without twisting or bending the
connector or conductor until the connector tip (on the DF-1 connector)
becomes visible behind the set screw block. This indicator can vary
depending on the manufacturer of the lead used.
5 If you cannot easily plug the lead connector into the connection:
• Use only sterile water as lubricant.
6 If the lead connector cannot be inserted completely, the set screw may be
protruding into the drill hole of the set screw block.
• Use the screwdriver to perpendicularly pierce through the slitted point in
the center of the silicone plug until it reaches the set screw.
• Carefully loosen the set screw without completely unscrewing it, so that
it does not become tilted upon retightening.
7 Turn the set screw clockwise until torque control starts (you will hear a
clicking sound).
8 Carefully withdraw the screwdriver without retracting the set screw.
• In case of IS-1 connections with 2 set screws, tighten both screws!
• When you withdraw the screwdriver, the silicone plug automatically seals
the access to the screw head safely.
!
!
WARNING
Inadequate therapy
When leads are not spaced sufficiently apart or are positioned inappropriately, this
can lead to far-field sensing or insufficient defibrillation.
• The distance between 2 shock coils must be greater than 6 cm.
• Tip and ring electrodes must not have contact with each other.

13
Precautionary Measures while Programming
Performing standard tests
and monitoring the patient
Critical conditions can occur for the patient even during standard tests due to
inadequate parameter settings or interrupted telemetry.
• Ensure sufficient patient care even during tests.
• After the threshold test, check to determine whether the threshold is clinically
and technically justifiable.
• Continuously monitor the ECG and the patient's condition.
• Cancel testing if necessary.
Cancelling telemetry Programmer interference or interrupted telemetry during performance of
temporary programs (follow-up tests) can result in inadequate pacing of the
patient. This is the case if the programmer can no longer be operated due to a
program error or a defective touch screen and therefore the temporary program
cannot be terminated. Under these circumstances, it is helpful to cancel telemetry,
in which case the device automatically switches to the permanent program.
• In the case of telemetry with programming head: lift the PGH by at least 30 cm.
• In the case of RF telemetry: switch off and reposition the programmer.
• Turn off possible sources of interference.
Avoiding critical
parameter settings
No modes and parameter combinations that pose a risk to the patient should be set.
• Prior to setting rate adaptation, determine the patient's capacity for exertion.
• Check compatibility and effectiveness of parameter combinations after making
settings.
• When setting atrial therapies after an AT or AF has been detected, note that no
ventricular tachyarrhythmia can be detected for the duration of atrial therapy
delivery.
Checking for electrodes
suitable for the shock path
Three different shock paths can be set. Two of these form an electrical path to the
housing of the implanted device.
• For the RV -> SVC shock path, a second shock coil must be available (dual shock
coil).
Monitoring the patient
when setting
asynchronous modes
The asynchronous modes V00 and D00 can only be set if tachyarrhythmia sensing is
deactivated. This would leave the patient without sensing and therefore without ICD
therapy.
• Continually monitor the patient.
• Keep an external defibrillator ready.
Setting sensing Manually set parameters can be unsafe. For example, unsuitable far-field protec-
tion may impede sensing of intrinsic pulses.
• Note automatic sensitivity control.
Preventing device-induced
complications
BIOTRONIK devices feature several functions to prevent device-induced complica-
tions to the greatest extent possible:
• Measure the retrograde conduction time.
• Set PMT protection.
• Set the VA criterion.
Preventing conduction of
atrial tachycardia
BIOTRONIK devices feature several functions to prevent conduction of atrial tachy-
cardia to the ventricle(s):
• Set mode switching for indicated patients.
• Set the upper rate and the refractory periods to prevent abrupt ventricular rate
switching.
• Prefer Wenckebach response and avoid 2:1 behavior.
• Set all parameters so as to prevent constant changing between atrial and
ventricular-controlled modes.
14
Note the reduced
pulse amplitude due to a
battery voltage drop
If the rate and amplitude are set very high and the pulse width is set too long at the
same time, the battery voltage may temporarily drop so low that the actual pulse
amplitude drops well below the selected level.
• Continuously check the pacing efficiency using ECG monitoring.
Observe when inducing
short-term cardiac arrest
To permit TAVI (transcatheter aortic valve implantation), the pressure in the heart
must be reduced so that the heart valve can be correctly positioned. Intentional
cardiac arrest by high-rate pacing (rapid pacing) should be brief, must be tolerated
by the patient and can trigger a life-threatening arrhythmia.
• Take all necessary precautionary measures and keep required emergency
equipment ready.
• Continually monitor the patient by ECG.
• Complete the TAVI procedure before high-rate pacing ends. Extend the pacing
duration if necessary.
• Abort the procedure if it is not successfully completed within the maximum
pacing duration so that cardiac arrest can be stopped.
• Reactivate ICD therapy at a clinically indicated point in time when the TAVI
process is completed.
Avoiding AV crosstalk When pacing using atrial ATP parameters, atrial pacing pulses can either be
conducted into the ventricle or be sensed such that ventricular pacing is prevented.
• Check the settings for the presence of crosstalk.
• If necessary, temporarily set VVI and a rate for backup stimulation so that no
ventricular pulses are prevented.
Observing the shock
impedance limit
The implanted device could be damaged if the shock impedance is too low.
• The shock impedance must be > 25 Ω.
Preventing recurrence
after therapy shock
After a therapy shock, pacing can be performed with a post-shock program if there
is no intrinsic rhythm.
• The following post-shock program parameters can be adjusted: Post-shock
duration, basic rate, rate hysteresis, ventricular pacing, LV T-wave protection,
triggering, AV delay (fixed, not dynamic)
• The default settings for the post-shock program are as follows:
A and RV: 7.5 V, 1.5 ms
LV: settings from the permanent program
Phrenic nerve stimulation
that cannot be terminated
In rare cases, chronic phrenic nerve stimulation cannot be terminated by repro-
gramming the available left ventricular pacing configuration or using other
measures.
• Set a right ventricular mode both in the permanent program as well as the ATP,
in the post-shock program and for mode switching if need be.
Avoiding risks in the case of
exclusive LV pacing
Lead dislodgement in the case of exclusive left ventricular pacing could pose the
following risks: loss of ventricular pacing and ATP therapy, induction of atrial
arrhythmias.
• Consider sensing and pacing parameters with reference to loss of therapy.
• Exclusive LV pacing is not recommended for patients who depend on the device.
• Please note that capture control is not available.
• In the case of follow-ups and threshold tests, take loss of synchronized ventric-
ular pacing into consideration.
• Mode switching and post shock do not permit exclusive LV pacing. Please note
the effects when programming mode switching and the post shock parameters.
Permanent program Post-shock program
DDD
DDI, AAI
DDI
VDD, VDI VDI
VVI and OFF VVI

15
Recognizing lead failure Automatic impedance measurement is always switched on.
• Impedance values that indicate technical failure of a lead are documented in the
event list.
Considering power
consumption and
service time
RF telemetry requires somewhat more power: Consumption during implantation
corresponds to approximately 10 days of service time and consumption during a
20-minute follow-up corresponds to approximately 3 days.
• Do not establish unnecessary RF telemetry.
• After 5 minutes without input, SafeSync switches to the economy mode.
• Check the battery capacity of the device at regular intervals.
Magnet Response
Application of the
programming head when
ICD therapy is set
If a connected programming head is applied and is communicating with the
programmer and ICD therapy is permanently set, detection and therapy remain
intact except during the diagnostic tests. If ICD therapy is not set as permanent, no
therapy is delivered when the programming head is applied.
Programming head
application
When the programming head is applied, time remains for device interrogation and
for manual activation or deactivation of the therapy before the device switches back
to the previously set permanent therapy mode. The same applies to programming
head application to establish RF telemetry contact.
Application of a
permanent magnet
Applying a permanent magnet interrupts detection and therapy of tachycardia
events. After 8 hours of this type of deactivation, the device automatically reacti-
vates the therapy functions to prevent accidental permanent deactivation.
• If detection interruptions of longer than 8 hours are required, the magnet has to
be briefly removed from the device. The 8 hour countdown restarts when the
magnet is applied again.
• Use BIOTRONIK magnets: type M-50 permanent magnets.

16
Follow-up
Follow-up intervals Follow-ups must be performed at regular, agreed intervals.
• The first follow-up should be carried out by the physician using the programmer
(in-office follow-up) approximately 3 months after implantation following the
lead ingrowth phase.
• The next in-office follow-up should be carried out once a year and no later than
12 months after the last in-office follow-up.
Follow-up with BIOTRONIK
Home Monitoring®
Monitoring using the Home Monitoring function does not serve to replace regular
in-office appointments with the physician required for other medical reasons.
Follow-up supported by Home Monitoring can be used to functionally replace in-
office follow-up under the following conditions:
• The patient was informed that the physician must be contacted despite use of
the Home Monitoring function if symptoms worsen or if new symptoms arise.
• Device messages are transmitted regularly.
• The physician decides whether the data transmitted via Home Monitoring with
regard to the patient's clinical condition as well as the technical state of the
device system are sufficient. If not, an in-office follow-up needs to be carried
out.
Possible early detection due to information gained via Home Monitoring may neces-
sitate an additional in-office follow-up. For example, the data may indicate at an
early stage lead problems or a foreseeable end of service time (ERI). Furthermore,
the data could provide indications of previously unrecognized arrhythmias or modi-
fication of the therapy by reprogramming the device.
Follow-up with the
programmer
Use the following procedure for in-office follow-up:
1 Record and evaluate the ECG.
2 Interrogate the device.
3 Evaluate the status and automatically measured follow-up data.
4 Check the sensing and pacing functions.
5 Possibly evaluate statistics and IEGM recordings.
6 Manually perform standard tests if necessary.
7 Possibly customize program functions and parameters.
8 Transmit the program permanently to the device.
9 Print and document follow-up data (print report).
10 Finish the follow-up for this patient.
17
Patient Information
Patient ID card A patient ID card is included in delivery.
• Provide the patient with the patient ID.
• Request that patients contact the physician in case of uncertainties.
Prohibitory signs Premises with prohibitive signs must be avoided.
• Draw the patient's attention to prohibitory signs.
Possible sources of
interference
Electromagnetic interference should be avoided in daily activities. Sources of inter-
ference should not be brought into close proximity with the device.
• Draw the patient's attention to special household appliances, security check-
points, anti-theft alarm systems, strong electromagnetic fields, cell phones,
and transmitters among other things.
• Request patients to do the following:
— Use cell phones on the side of their body that is opposite of the device.
— Keep the cell phone at least 15 cm away from the device both during use and
when stowing.
18
Replacement Indications
Possible battery levels • BOS: Beginning of Service: > 90% charge
• MOS 1: Middle of Service: 90% to 40% residual charge
• MOS 2: Middle of Service: < 40% residual charge
• ERI: Elective Replacement Indication (i.e. RRT: Recommended Replacement
Time)
• EOS: End of Service
Elective Replacement
Indication (ERI)
Elective Replacement Indication can be detected by Home Monitoring.
• The device can monitor the heart rhythm for at least 3 more months.
• At least 6 maximum energy shocks can be delivered until EOS occurs.
• The selected parameters in the software do not change.
EOS replacement indication End of Service can be detected by Home Monitoring.
• VT and VF detection and all therapies are deactivated!
• The antibradycardia function remains active in the VVI mode:
— Ventricular pacing: RV; basic rate 50 bpm; without special pacemaker
functions such as hysteresis, etc.
— Pulse amplitude of 6 V; pulse width of 1.5 ms
— Cycle duration for BIOTRONIK Home Monitoring®: 90 days
!
!
CAUTION
Temporally limited therapy
If ERI occurs shortly after follow-up and is only detected during the subsequent
follow-up, then the remaining service time can be much less than 3 months.
• Replace device soon.
!
!
WARNING
Patient at risk of death
If EOS replacement indication occurs before replacement of the device, then the
patient is without therapy.
• Replace device immediately.
• Monitor patient constantly until immediate replacement of the device!
19
Explantation and Device Replacement
Explantation •Interrogate the device status.
• Deactivate VT and VF therapies prior to explantation.
• Remove the leads from the header. Do not simply cut them loose.
• Use state-of-the-art techniques to remove the device and, if necessary, the
leads.
• Explants are biologically contaminated and must be disposed of safely due to
risk of infection.
Device replacement If, upon replacing the device, already implanted leads are no longer used but left in
the patient, then an additional uncontrolled current path to the heart can result.
• Deactivate VT and VF therapies prior to device replacement.
• Insulate connector ports that are not used.
Basic principles:
• The device must not be resterilized and reused.
Cremation Devices must not be cremated.
• Explant the device before the cremation of a deceased patient.
Disposal BIOTRONIK takes back used products for the purpose of environmentally safe
disposal.
• Clean the explant with a solution of at least 1% sodium hypochlorite.
• Rinse off with water.
• Fill out explantation form and send to BIOTRONIK together with the cleaned
device.
Note: Normal oxidation processes may cause ICD housing discolorations. This is
neither a device defect nor does it influence device functionality.
20
4 Parameters
Parameters4403736Technical Manual
Bradycardia / CRT
General ICD therapy
Timing: Basic rate day/night
and rate hystereses
Timing: AV delay
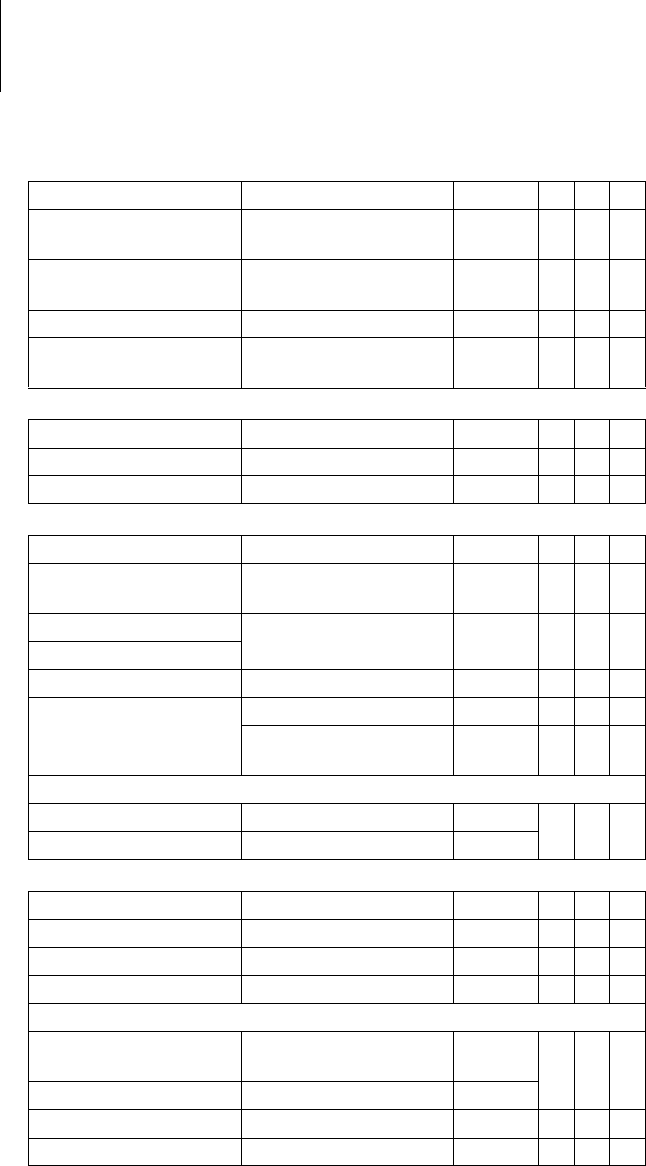
Parameter Range of values Standard VR DR HF
ICD therapy OFF; ON ON x x x
Programs Display standard
program; Display safe
program; Display first
interrogated program;
Individual 1, 2, 3;
Program Consult
— xxx
Parameter Range of values Standard VR DR HF
Basic rate 30 ... (5) ... 100 ... (10)
... 160 bpm
40 bpm x
60 bpm x x
Night rate OFF; 30 ... (5) ... 100 bpm OFF x x x
Night begins 00:00 ... (00:01)
... 23:59 hh:mm
22:00 hh:
mm
xxx
Night ends 06:00 hh:
mm
Rate hysteresis OFF; -5 ... (-5) ... -25 ...
(-20) ... -65 bpm
OFF xxx
Scan/repetitive OFF; ON ON x x x
Parameter Range of values Standard VR DR HF
AV dynamics Low; Medium; High;
Fixed; (Individual)
Low x x
AV delay (1 or 2) after:
– Pacing 15; 40 ... (5) ... 350 ms – x x
– Sensing Either automatic:
AV delay after pacing +
sense compensation
Or: 40 ... (5) ... 350 ms
–xx
– At rate 1 50 ... (10) ... 130 bpm 60 bpm
– At rate 2 60 ... (10) ... 140 bpm 130 bpm
Sense compensation OFF; -5 ... (-5) ... -120 ms -40 ms x x
AV hysteresis mode OFF; Positive; Negative;
IRSplus
OFF x
OFF; Positive; Negative OFF x
AV hysteresis (positive) 70; 110; 150; 200 ms 70 ms x x
AV hysteresis (positive) 70; 110; 150 ms 110 ms x x
AV hysteresis (negative) 10 ... (10) ... 150 ms 50 ms x x
AV scan and repetitive
(positive)
OFF; ON ON x x
21
Timing: Post-shock pacing
Timing: Upper rate
Timing: Mode switching
Timing: Ventricular pacing
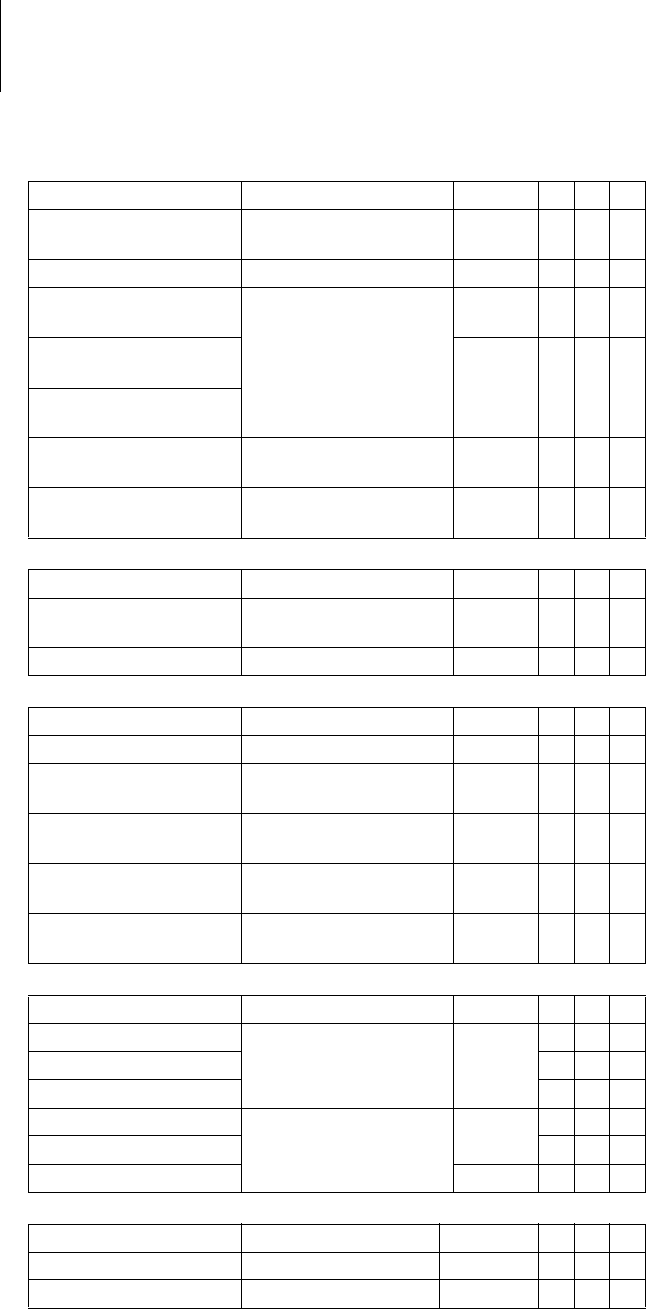
Parameter Range of values Standard VR DR HF
Post-shock duration OFF; 10 s; 30 s; 1 min;
2 min; 5 min; 10 min
10 s x x x
Post-shock basic rate 30 ... (5) ... 100 ... (10)
... 160 bpm
60 bpm x x x
AV delay post shock 50 ... (10) ... 350 ms 140 ms x x
Ventricular post-shock
pacing
RV; BiV RV x
Parameter Range of values Standard VR DR HF
Upper rate 90 ... (10) ... 160 bpm 130 bpm x x
Atrial upper rate OFF; 175; 200; 240 bpm 200 bpm x x
Parameter Range of values Standard VR DR HF
Intervention rate OFF; 120 ... (10) ...
200 bpm
160 bpm x x
Onset criterion 3 ... (1) ... 8 (out of 8) 5 x x
Resolution criterion
Modification of basic rate OFF; 5 ... (5) ... 30 bpm 10 bpm x x
Mode After mode VDD(R): VDI(R) VDIR x x
After mode DDD(R):
DDI(R)
DDIR x x
After mode switching:
– Rate OFF; 5 ... (5) ... 50 bpm 10 bpm x x
– Duration 1 ... (1) ... 30 min 1 min
Parameter Range of values Standard VR DR HF
Permanent RV; BiV; LV BiV x
Triggering OFF; RVs; RVs+PVC RVs x
LV T-wave protection OFF; ON ON x
Maximum trigger rate:
– DDD(R) and VDD(R) UTR + 20; 90 ... (10)
... 160 bpm
UTR + 20 x
– DDI(R), VDI(R) and VVI(R) 90 ... (10) ... 160 bpm 130 bpm
Initially paced chamber RV; LV LV x
VV delay after Vp 0 ... (5) ... 100 ms 0 ms x
22
Timing: Refractory periods
and blanking periods
Timing: PMT protection
Timing: Rate adaptation via
accelerometer
Pacing: Pulse amplitude
and pulse width
Pacing:
Atrial capture control
Parameter Range of values Standard VR DR HF
PVARP AUTO; 175 ... (25) ...
600 ms
225 ms x x
PVARP extension OFF; ON ON x x
Blanking after atrial
pacing
50 ... (10) ... 100 ms 50 ms x x
LV blanking after
RV pacing
80 ms x
RV blanking after
LV pacing
Far-field protection
after Vs
OFF; 25 ... (25) ... 225 ms 75 ms x x
Far-field protection
after Vp
50 ... (25) ... 225 ms 75 ms x x
Parameter Range of values Standard VR DR HF
PMT detection/termina-
tion
OFF; ON ON x x
VA criterion 250 ... (10) ... 500 ms 350 ms x x
Parameter Range of values Standard VR DR HF
Maximum sensor rate 80 ... (10) ... 160 bpm 120 bpm x x x
Sensor gain AUTO; Very low; Low;
Medium; High; Very high
Mediumxxx
Sensor threshold Very low; Low; Medium;
High; Very high
Mediumxxx
Rate increase 1; 2; 4; 8 bpm/cycle 2 bpm/
cycle
xxx
Rate decrease 0.1; 0.2; 0.5; 1.0 bpm/
cycle
0.5 bpm/
cycle
xxx
Parameter Range of values Standard VR DR HF
Pulse amplitude A 0.5 ... (0.25) ... 4.0 ... (0.5)
... 6.0; 7.5 V
AUTO x x
Pulse amplitude V/RV x x x
Pulse amplitude LV x
Pulse width A 0.4; 0.5 ... (0.25) ... 1.5 ms 0.4 ms x x
Pulse width V/RV xxx
Pulse width LV 0.4 ms x
Parameter Range of values Standard VR DR HF
Atrial capture control OFF; ATM ON x x
Threshold test start 2.5 ... (0.5) ... 5.0 V 3.5 V x x
23
Pacing:
Ventricular capture control
Lead configuration LV
on IS-1 connection
Parameter Range of values Standard VR DR HF
Ventricular capture
control
OFF; ATM ON xxx
Threshold test start 2.5 ... (0.5) ... 5.0 V 3.5 V x x x
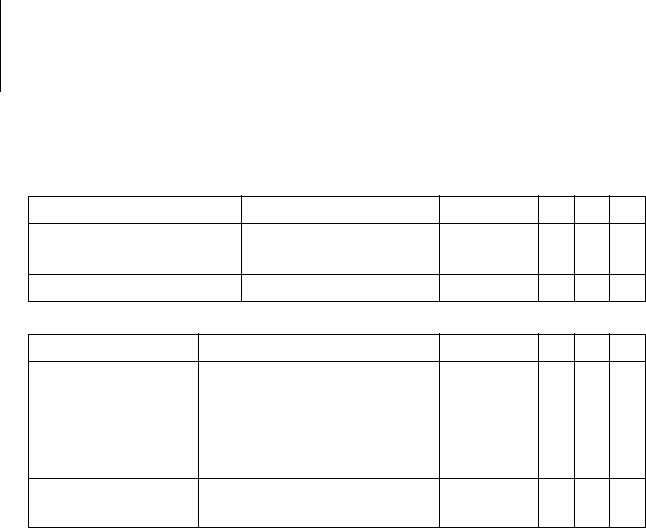
Parameter Range of values Standard VR DR HF
Pacing polarity LV
(IS-1)
LV tip -> LV ring
LV tip -> RV shock coil
LV ring -> LV tip
LV ring -> RV shock coil
UNIP
LV tip -> RV
shock coil
x
Sensing polarity LV
(IS-1)
UNIP; BIPL UNIP x
24
Tachycardia
Detection Parameter Range of values Standard VR DR HF
Interval AT/AF 240 ... 600 ms 300 ms x x
Interval VT1 OFF; 270 ... (10) ... 600 ms OFF x x x
Interval VT2 OFF; 270 ... (10) ... 500 ms
Interval VF OFF; 240 ... (10) ... 400 ms 300 ms
Detection counter VT1 10 ... (2) ... 100 28 x x x
Detection counter VT2 10 ... (2) ... 80 20
Detection counter VF 6 out-of 8; 8 out-of 12;
10 out-of 14; 12 out-of 16;
16 out-of 20; 18 out-of 24;
20 out-of 26; 22 out-of 30;
24 out-of 30; 30 out-of 40
18 out of
24
Redetection counter VT1 10 ... (2) ... 50 20 x x x
Redetection counter VT2 10 ... (2) ... 40 14
Redetection counter VF 6 out-of 8; 8 out-of 12;
10 out-of 14; 12 out-of 16;
16 out-of 20;
18 out-of 24; 20 out-of 26;
22 out-of 30; 24 out-of 30
8 out
of 12
xxx
SMART detection VT1/VT2 OFF; ON ON x x
SMART detection ON:
– Onset VT1/VT2 4 ... (4) ... 32% 20% x x
– Stability VT1/VT2 8 ... (4) ... 48% 12%
SMART detection OFF:
– Onset VT1/VT2 4 ... (4) ... 32% 20% x x x
– Stability VT1/VT2 OFF; 8 ... (4) ... 48 ms 24 ms
MorphMatch OFF; Monitoring; ON OFF x x x
Sustained VT OFF; 1; 2; 3; 5; 10; 20;
30 min
OFF xxx
Forced termination OFF; 1 ... (1) ... 10 min 1 min x x
25
Therapy: ATP
Therapy: Shock
Parameter Range of values Standard VR DR HF
Attempts OFF; 1 ... (1) ... 10 OFF x x x
ATP type for VT1/VT2 Burst; Ramp Burst x x x
ATP type for VF OFF; Burst; Ramp Burst x x x
ATP optimization OFF; ON OFF x x x
Number S1 for VT1/VT2 1 ... (1) ... 10 5 x x x
Number S1 for VF 8
S1 decrement for VT1/VT2
and for VF
5 ... (5) ... 40 ms 10 ms x x x
Scan decrement OFF; 5 ... (5) ... 40 ms OFF x x x
Add S1 for VT1/VT2 OFF; ON ON x x x
Ventricular pacing
for VT1/VT2
RV; LV; BiV RV x
Ventricular pacing for VF RV
R-S1 interval for VT1/VT2 70 ... (5) ... 95% 80% x x x
R-S1 interval for VF 85 %
Parameter Range of values Standard VR DR HF
Number of shocks
VT1/VT2
0; 1; 2; 6; 8 8 x x x
Number of shocks VF 6; 8 8 x x x
1st Shock for VT1/VT2 OFF; 2 ... (2) ... 20 ... (5) ...
40 J
40 J x x x
2nd Shock for VT1/VT2 OFF; 4 ... (2) ... 20 ... (5) ...
40 J
40 J x x x
3rd - nth shock for VT1/
VT2
OFF; 4*40 J; 6*40 J 6*40 J x x x
1st Shock for VF 2 ... (2) ... 20 ... (5) ... 40 J 40 J x x x
2nd Shock for VF 4 ... (2) ... 20 ... (5) ... 40 J 40 J x x x
3rd - nth shock for VF 4*40 J; 6* 6*40 J x x x
For shock in VT1/VT2 and VF:
– Confirmation OFF; ON ON x x x
– Polarity Normal; Reverse; Alter-
nating
Normal
– Shock form Biphasic; Biphasic 2 Biphasic
– Shock path RV -> ICD+SVC
RV -> ICD
RV -> SVC
RV->
ICD+SVC
xxx
RV -> ICD
26
Sensing
Sensitivity and thresholds
Diagnostics
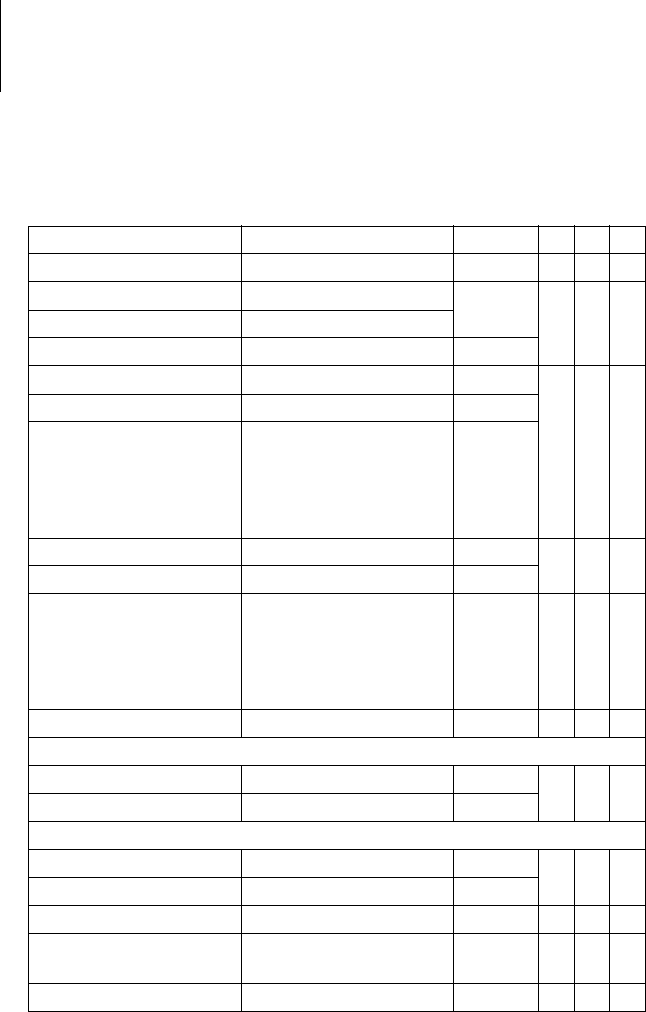
The following can be set:
Parameter Range of values Standard VR DR HF
Sensing A STD; OFF STD x x
Sensing RV STD; TWS; VFS; IND STD x x x
Sensing LV STD; OFF; IND STD x
Upper threshold RV 50; 75% 50% x x x
Upper threshold LV 50; 75% 50% x
Upper threshold duration
after detection
110; 150 ... (50) ... 500 ms
VFS: 110 ms
350 ms x x x
Upper threshold duration
after pacing
400 ms
Lower threshold RV 25; 50% 25% x x x
T-wave suppression
after pacing
OFF; ON OFF x x x
Minimum threshold A 0.2 ... (0.1) ... 2.0 mV 0.4 mV x x
Minimum threshold RV 0.5 ... (0.1) ... 2.5 mV 0.8 mV x x x
Minimum threshold LV 0.5 ... (0.1) ... 2.5 ... (0.5)
... 5.0 mV
1.6 mV x
Parameter Range of values Standard VR DR HF
For AT/AF OFF; ON ON x x
For SVT OFF; ON ON x x
Periodic recording When Home Monitoring
OFF:
OFF; 30 ... (30) ...
180 days
90 days x x x
IEGM configuration RA, RV, LV
RA, RV, FF
FF; RV; LV
RA, RV, LV x
Start resting period 00:00 ... (1:00 AM) ...
23:00 hh:mm
2:00
AM hh:mm
xxx
Duration of resting
period
0.5 ... (0.5) ... 12 h 4 h x x x
AV delay adjusted in
sensing test
OFF; 300 ms 300 ms x x
Thoracic impedance (TI) OFF, ON OFF x x x
27
Home Monitoring
Parameter Range of values Standard VR DR HF
Home Monitoring OFF; ON OFF x x x
Time of transmission STD; 00:00 ... (1:00 AM)
... 23:00 hh:mm
STD xxx
IEGM for therapy
episodes
OFF; ON ON x x x
IEGM for monitoring
episodes
Ongoing atrial episode OFF; 6; 12; 18 h 12 h x x
Transmission date XX.XX.XXXX Follow-up
+ 91 days
xxx
Cycle duration 20 ... (1) ... 366 days 91 days x x x
28
5Technical Data
Technical Data5403736Technical M anual
Mechanical Characteristics
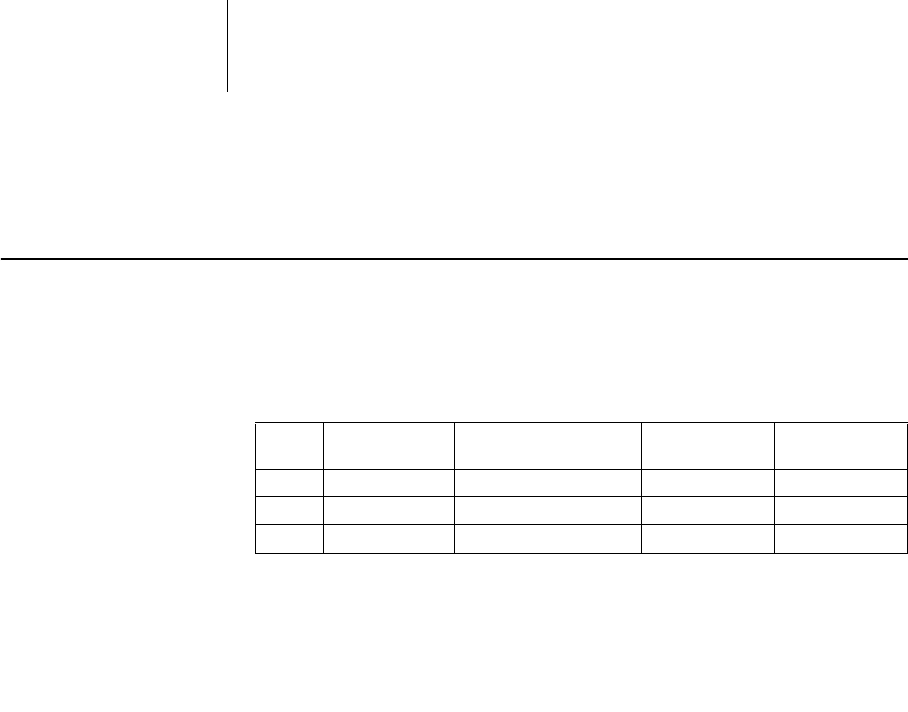
Housing Devices with header for DF-1 connector:
Materials in contact with
body tissue
• Housing: Titanium
• Header: Epoxy resin
• Silicone plugs and blind plugs (if applicable): Silopren or silastic
X-ray identification HK
Type Lead
connector W x H x D in mm Volume cm3Mass g
VR DF-1 69 x 55 x 12,5 38 71
DR DF-1 69 x 55 x 12,5 39 71
HF DF-1 69 x 58.5 x 12,5 40 73

29
Electrical Characteristics
Standards The specifications are made according to EN 45502-2-2:2008.
Measuring conditions If not indicated otherwise, all specifications refer to the following conditions:
• Ambient temperature: 37ºC ± 2ºC
• Pacing/sensing: 500 Ω ±1%
• Shock: 50 Ω ±1%
Factory settings • Arrhythmia zones VT1, VT2, VF: OFF
• Antibradycardia pacing: OFF
• Home Monitoring: OFF
Telemetry data • MICS frequencies: 402-405 MHz
• Maximum power of transmission: < 25 µW (–16 dBm)
International
radio certificationDevices with BIOTRONIK Home Monitoring® are equipped with an antenna for
wireless communication.
Telemetry information for Canada:
This device must neither interfere with meteorological and earth resources tech-
nology satellites nor with meteorological stations working in the 400,150 to 406,000
MHZ band, and it must accept any interference received, including interference that
may cause undesired operation.
• This device will be registered with Industry Canada under the following number:
IC: 4708A-TACHBORAX
The code IC in front of the certification/ registration number only indicates that
the technical requirements for Industry Canada are met.
Telemetry information for the USA:
This transmitter is authorized by rule under the Medical Device Radiocommunica-
tion Service (in part 95 of the FCC Rules) and must not cause harmful interference
to stations operating in the 400.150-406.000 MHz band in the Meteorological Aids
(i.e., transmitters and receivers used to communicate weather data), the Meteoro-
logical Satellite, or the Earth Exploration Satellite Services and must accept inter-
ference that may be caused by such stations, including interference that may cause
undesired operation. This transmitter shall be used only in accordance with the FCC
Rules governing the Medical Device Radiocommunication Service. Analog and
digital voice communications are prohibited. Although this transmitter has been
approved by the Federal Communications Commission, there is no guarantee that
it will not receive interference or that any particular transmission from this trans-
mitter will be free from interference.
This device will be registered with Federal Communications Commission under the
following number:
FCC ID: QRITACHBORAX
Telemetry data for Japan:
In accordance with Japanese law, this device has been assigned an identification
number under the "Ordinance concerning certification of conformity with technical
regulations etc. of specified radio equipment", Article 2-1-8.
• R: 202-SMD021
30
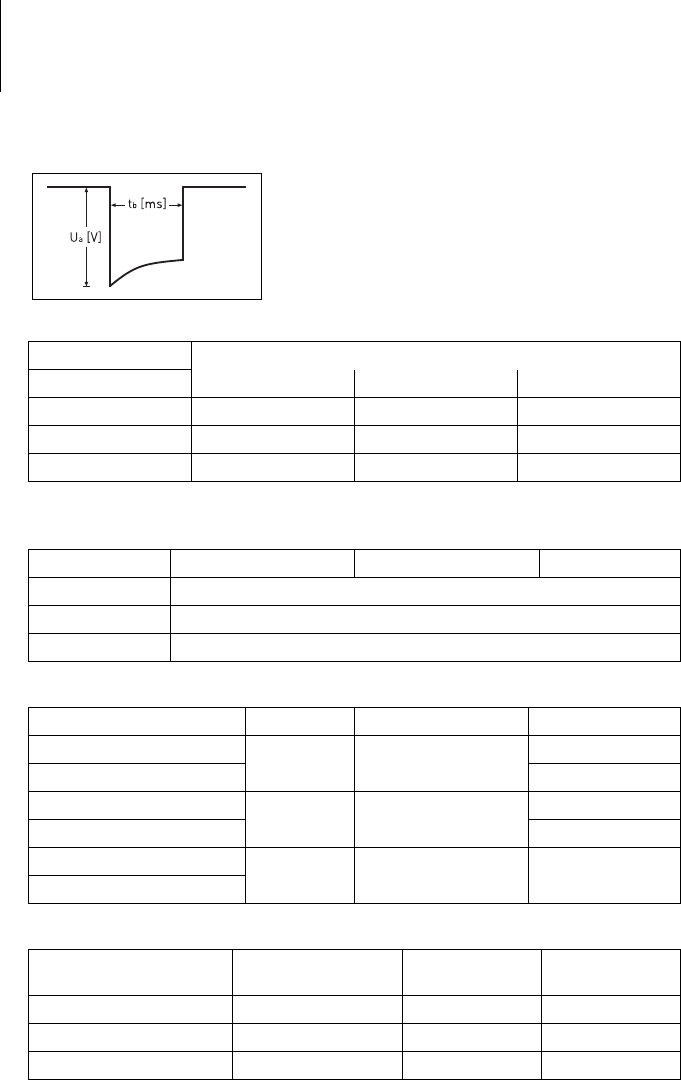
Pulse form The pacing pulse has the following form:
The pulse amplitude reaches its maximum value at
the beginning of the pulse (Ua). With increasing
pacing duration (tb), the pulse amplitude is reduced
dependent on the pacing impedance.
Common mode
rejection ratio
ATP amplitude A burst was measured at 500 Ω, an amplitude of 7.5 V (tolerance ±1.5 V), pulse width
of 1.5 ms, R-S1 interval of 300 ms and an S1 count of 5:
Automatic
sensitivity control
Measurement of actual values and test signal wave shape: standard triangle.
Shock energy / peak voltage With shock path: RV to housing + SVC
Rate Common mode rejection ratio
Atrium: DR, HF V right: VR, DR, HF V left: HF
16.6 Hz 72 dB 59 dB 57 dB
50 Hz 73 dB 66 dB 57 dB
60 Hz 71 dB 66 dB 62 dB
ATP amplitude Measured minimum Measured maximum Mean value
RA 7.57 V 7.49 V 5.1 V
RV 7.54 V 7.49 V 5.1 V
LV 7.55 V 7.51 V 5.1 V
Sensitivity Value Tolerance Measured value
A: positive 0.2 mV 0.2 ... 0.5 0.23 mV
A: negative 0.24 mV
RV: positive 0.5 mV 0.3 ... 0.7 0.55 mV
RV: negative 0.58 mV
LV: positive 0.5 mV 0.3 ... 0.7 0.52 mV
LV: negative
Shock energy
(Tolerance) Tolerance
Peak voltage Measured value
Shock energy Measured value
Peak voltage
1 J (0.7 ... 1.18) 100 ... 140 V 0.89 J 125,0 V
20 J (15.9 ... 21.6) 500 ... 550 V 16,62 J 530,4 V
40 J (32.0 ... 43.2) 710 ... 790 V 33,84 J 750,9 V
31
Battery Data
Battery characteristics The following data is provided by the manufacturers:
Storage period The storage period affects the battery service time.
• Devices should be implanted within 19 months between the manufacturing date
and the use by date (indicated on the package).
• If the ICD is implanted shortly before the use by date, the expected service time
may be reduced by up to 17 months.
Calculation
of service times
• The services times have been calculated as follows – in all chambers depending
on the device type:
— Pulse amplitude: 2.5 V
— Pulse width: 0.4 ms
— Pacing impedance: 500 Ω
— Basic rate: 60 bpm
— Home Monitoring: ON,
1 device message each day and 12 IEGM online HD transmissions per year
— Diagnostic functions and recordings: permanently set
• Capacitor reforming is performed 4 times per year and therefore at least
4 maximum charges for shocks have to be assumed per year even if less than 4
are delivered.
Calculation
of the number of shocks
Calculation of the number of shocks: Service time [in years] x number of shocks per
year
Inlexa 1 VR-T Service times with LiS 3410 RR battery:
Manufacturer LITRONIK Batterietechnologie GmbH & Co
01796 Pirna, Germany
Battery type LiS 3410 RR
System LiMnO2
Battery ID number
shown on the programmer
6
Device type VR-T, DR-T, HF-T
Battery voltage at ERI 2.85 V
Charge time at BOS 8 s
Charge time at ERI 10 s
Usable capacity until ERI:
VR, DR, HF
1390 mAh
Usable capacity until EOS 1520 mAh
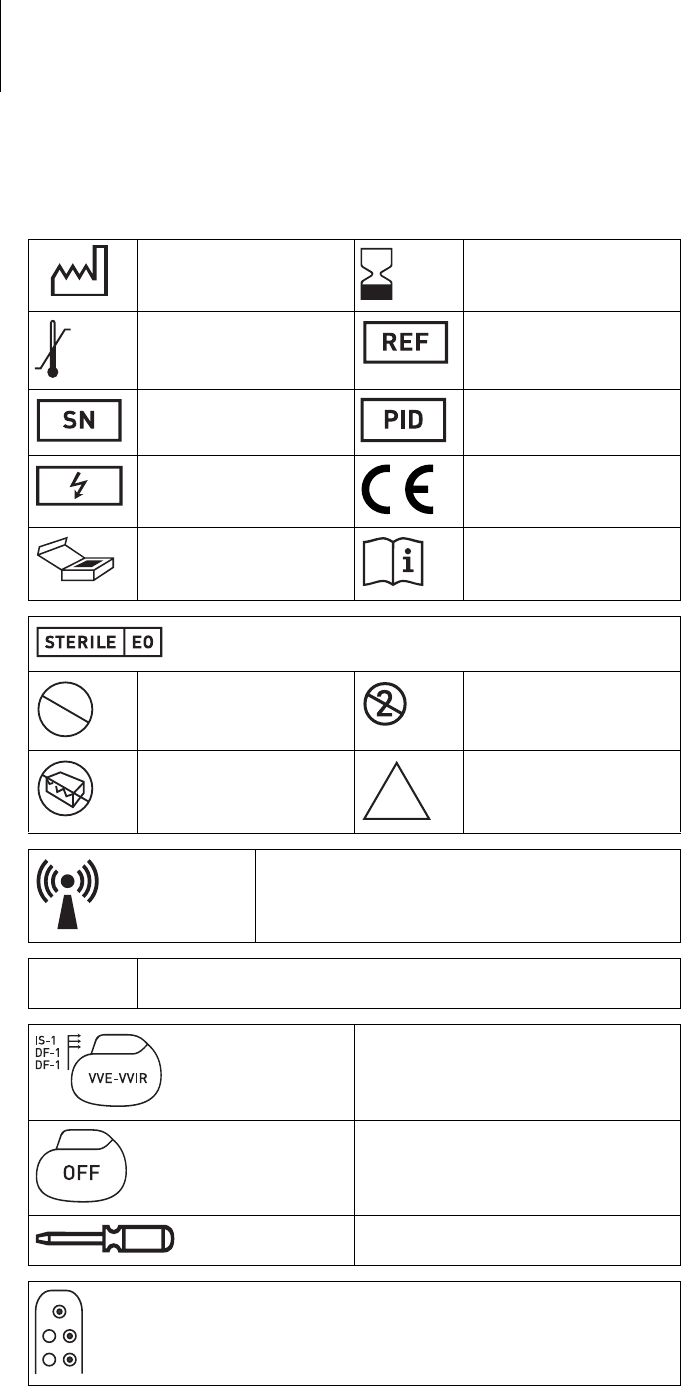
Pacing Service time [in years] at number of shocks per year
48121620
0% 10.3 8.3 7.0 6.0 5.3
15% 10.1 8.1 6.8 5.9 5.2
50% 9.5 7.8 6.6 5.7 5.0
100% 8.8 7.3 6.2 5.4 4.8
32
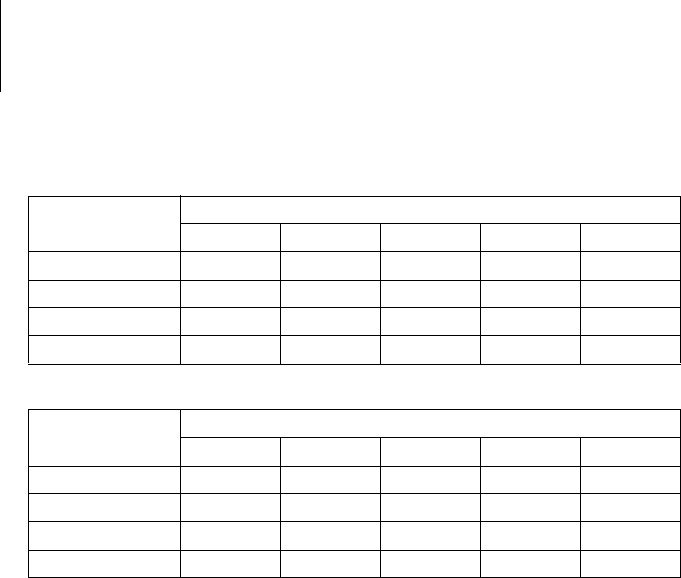
Inlexa 1 DR-T Service times with LiS 3410 RR battery:
Inlexa 1 HF-T Service times with LiS 3410 RR battery:
Pacing Service time [in years] at number of shocks per year
48121620
0% 9.4 7.7 6.5 5.7 5.0
15% 9.0 7.4 6.3 5.5 4.9
50% 8.1 6.8 5.9 5.2 4.6
100% 7.1 6.1 5.3 4.7 4.3
Pacing Service time [in years] at number of shocks per year
48121620
0% 8.9 7.4 6.3 5.5 4.9
15% 8.3 7.0 6.0 5.2 4.7
50% 7.2 6.1 5.4 4.8 4.3
100% 6.0 5.3 4.7 4.2 3.9
33
Legend for the Label
Label on the package The label icons symbolize the following:
Manufacturing date Use by
Storage temperature Order number
Serial number Product identification
number
Dangerous voltages! CE mark
Contents Follow the instructions for
use
Sterilized with ethylene oxide
Do not resterilize Single use only.
Do not reuse!
Do not use if packaging is
damaged
Non-sterile
Transmitter with non-ionizing radiation at designated
frequency
TP2 Compatibility with telemetry protocol version 2
of BIOTRONIK Home Monitoring
Example
Device:
NBG code and compatible leads
Example
Factory settings for therapy: OFF
Screwdriver
Example of lead connection: DF-1/IS-1
STERILIZE
2
NON
STERILE