Print Human Touch Wheelchair HT 2580/i Joy 2580 3 Yr ASQ
User Manual: Human Touch Wheelchair HT-2580/iJoy-2580
Open the PDF directly: View PDF ![]() .
.
Page Count: 8
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
P101360100
Person filling out questionnaire
Child’s information
Date ASQ completed:
Relationship to child:
Parent
Street address:
Names of people assisting in questionnaire completion:
Grandparent
or other
relative
Guardian
Foster
parent
Teacher Child care
provider
Other:
Ages & Stages
Questionnaires®
Month Questionnaire
34 months 16 days through 38 months 30 days
Please provide the following information. Use black or blue ink only and print
legibly when completing this form.
36
Child’s first name: Child’s last name:
Child’s date of birth:
First name: Last name:
Middle
initial:
City:
Home
telephone
number:
State/
Province: ZIP/
Postal code:
Other
telephone
number:
E-mail address:
Child’s gender:
Male Female
Middle
initial:
Country:
Program Information
Child ID #:
Program ID #:
Program name:
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
page 2 of 7
E101360200
Month Questionnaire
36
34 months 16 days
through 38 months 30 days
Important Points to Remember:
❑
✓Try each activity with your child before marking a response.
❑
✓Make completing this questionnaire a game that is fun for
you and your child.
❑
✓Make sure your child is rested and fed.
❑
✓Please return this questionnaire by _______________.
Notes:
____________________________________________
____________________________________________
____________________________________________
____________________________________________
On the following pages are questions about activities children may do. Your child may have already done some of the activities
described here, and there may be some your child has not begun doing yet. For each item, please fill in the circle that indicates
whether your child is doing the activity regularly, sometimes, or not yet.
COMMUNICATION
1. When you ask your child to point to her nose, eyes, hair, feet, ears, and
so forth, does she correctly point to at least
seven
body parts?
(She can
point to parts of herself, you, or a doll. Mark “sometimes” if she cor-
rectly points to at least three different body parts.)
2. Does your child make sentences that are three or four words long?
Please give an example:
3. Without giving your child help by pointing or using gestures, ask him to
“put the book
on
the table” and “put the shoe
under
the chair.” Does
your child carry out both of these directions correctly?
4. When looking at a picture book, does your child tell you what is hap-
pening or what action is taking place in the picture (for example, “bark-
ing,” “running,” “eating,” or “crying”)? You may ask, “What is the dog
(or boy) doing?”
5. Show your child how a zipper on a coat moves up and down, and say,
“See, this goes up and down.” Put the zipper to the middle and ask
your child to move the zipper
down.
Return the zipper to the middle
and ask your child to move the zipper
up.
Do this several times, placing
the zipper in the middle before asking your child to move it up or
down. Does your child consistently move the zipper up when you say
“up” and down when you say “down”?
6. When you ask, “What is your name?” does your child say both her first
and last names?
YES SOMETIMES NOT YET
COMMUNICATION TOTAL
GROSS MOTOR
1. Without holding onto anything for support, does your child
kick a ball by swinging his leg forward?
2. Does your child jump with both feet leaving the floor at the
same time?
3. Does your child walk up stairs, using only one foot on
each stair?
(The left foot is on one step, and the right foot
is on the next.)
She may hold onto the railing or wall.
(You
can look for this at a store, on a playground, or at home.)
4. Does your child stand on one foot for about 1 second
without holding onto anything?
5. While standing, does your child throw a ball
overhand
by
raising his arm to shoulder height and throwing the ball
forward?
(Dropping the ball or throwing the ball underhand
should be scored as “not yet.”)
6. Does your child jump forward at least 6 inches with both
feet leaving the ground at the same time?
FINE MOTOR
1. After your child watches you draw a line from the top of
the paper to the bottom with a pencil, crayon, or pen,
ask her to make a line like yours. Do not let your child
trace your line. Does your child copy you by drawing a
single line in a vertical direction?
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
36 Month Questionnaire
page 3 of 7
E101360300
YES SOMETIMES NOT YET
GROSS MOTOR TOTAL
YES SOMETIMES NOT YET
Count as “yes”
Count as “not yet”
FINE MOTOR
(continued)
2. Can your child string small items such as beads,
macaroni, or pasta “wagon wheels” onto a string
or shoelace?
3. After your child watches you draw a single circle, ask him
to make a circle like yours. Do not let him trace your
circle. Does your child copy you by drawing a circle?
4. After your child watches you draw a line from one
side of the paper to the other side, ask her to make
a line like yours. Do not let your child trace your
line. Does your child copy you by drawing a single
line in a horizontal direction?
5. Does your child try to cut paper with child-safe scissors?
He does not need to cut the paper but must get the
blades to open and close while holding the paper with
the other hand.
(You may show your child how to use
scissors. Carefully watch your child’s use of scissors for safety reasons.)
6. When drawing, does your child hold a pencil, crayon, or pen between
her fingers and thumb like an adult does?
PROBLEM SOLVING
1. While your child watches, line up four objects like
blocks or cars in a row. Does your child copy or
imitate you and line up
four
objects in a row?
(You
can also use spools of thread, small boxes, or other
toys.)
2. If your child wants something he cannot reach, does he find a chair or
box to stand on to reach it (for example, to get a toy on a counter or to
“help” you in the kitchen)?
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
36 Month Questionnaire
page 4 of 7
E101360400
YES SOMETIMES NOT YET
FINE MOTOR TOTAL
YES SOMETIMES NOT YET
Count as “not yet”
Count as “yes”
Count as “yes”
Count as “not yet”
PROBLEM SOLVING
(continued)
3. When you point to the figure and ask your child, “What is
this?” does your child say a word that means a person or
something similar?
(Mark “yes” for responses like “snowman,”
“boy,” “man,” “girl,” “Daddy,” “spaceman,” and “monkey.”)
Please write your child’s response here:
4. When you say, “Say ‘seven three,’” does your child repeat
just
the two
numbers in the same order?
Do not repeat the numbers.
If necessary,
try another pair of numbers and say, “Say ‘eight two.’”
(Your child must
repeat just one series of two numbers for you to answer “yes” to this
question.)
5. Show your child how to make a bridge with blocks, boxes,
or cans, like the example. Does your child copy you by
making one like it?
6. When you say, “Say ‘five eight three,’” does your child repeat
just
the
three numbers in the same order?
Do not repeat the numbers.
If neces-
sary, try another series of numbers and say, “Say ‘six nine two.’”
(Your
child must repeat just one series of three numbers for you to answer
“yes” to this question.)
PERSONAL-SOCIAL
1. Does your child use a spoon to feed herself with little spilling?
2. Does your child push a little wagon, stroller, or toy on wheels, steering
it around objects and backing out of corners if he cannot turn?
3. When your child is looking in a mirror and you ask, “Who is in the mir-
ror?” does she say either “me” or her own name?
4. Does your child put on a coat, jacket, or shirt by himself?
5. Using these exact words, ask your child, “Are you a girl or a boy?”
Does your child answer correctly?
6. Does your child take turns by waiting while another child or adult takes
a turn?
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
36 Month Questionnaire
page 5 of 7
E101360500
YES SOMETIMES NOT YET
PROBLEM SOLVING TOTAL
YES SOMETIMES NOT YET
PERSONAL-SOCIAL TOTAL
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
36 Month Questionnaire
page 6 of 7
E101360600
OVERALL
Parents and providers may use the space below for additional comments.
1. Do you think your child hears well? If no, explain:
2. Do you think your child talks like other children her age? If no, explain:
3. Can you understand most of what your child says? If no, explain:
4. Can other people understand most of what your child says? If no, explain:
5. Do you think your child walks, runs, and climbs like other children his age?
If no, explain:
6. Does either parent have a family history of childhood deafness or hearing
impairment? If yes, explain:
YES NO
YES NO
YES NO
YES NO
YES NO
YES NO
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
36 Month Questionnaire
page 7 of 7
E101360700
OVERALL
(continued)
7. Do you have any concerns about your child’s vision? If yes, explain:
8. Has your child had any medical problems in the last several months? If yes, explain:
9. Do you have any concerns about your child’s behavior? If yes, explain:
10. Does anything about your child worry you? If yes, explain:
YES NO
YES NO
YES NO
YES NO
Ages & Stages Questionnaires®, Third Edition (ASQ-3
™
),
Squires & Bricker
© 2009 Paul H. Brookes Publishing Co. All rights reserved.
P101360800
3. ASQ SCORE INTERPRETATION AND RECOMMENDATION FOR FOLLOW-UP: You must consider total area scores, overall
responses, and other considerations, such as opportunities to practice skills, to determine appropriate follow-up.
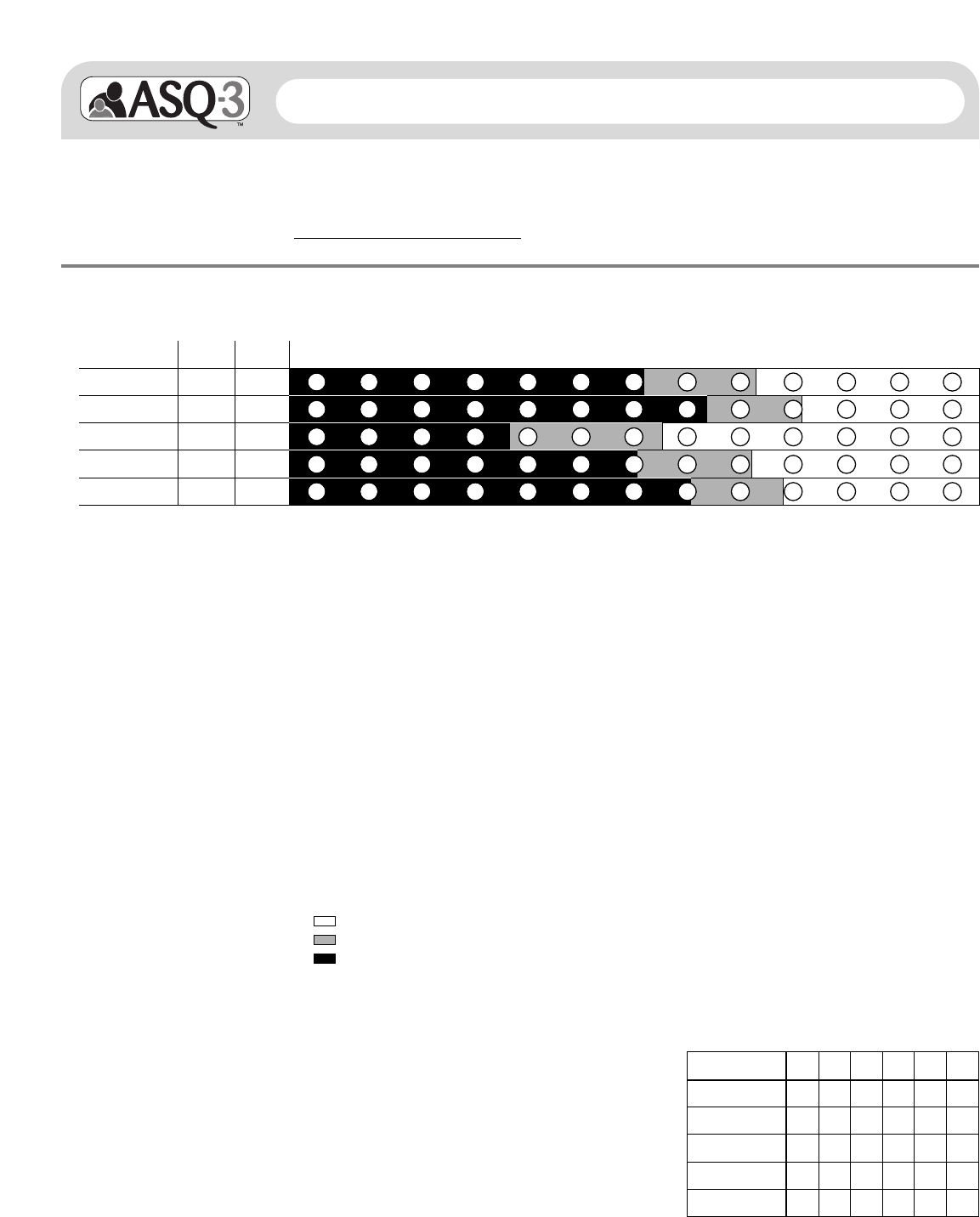
If the child’s total score is in the area, it is above the cutoff, and the child’s development appears to be on schedule.
If the child’s total score is in the area, it is close to the cutoff. Provide learning activities and monitor.
If the child’s total score is in the area, it is below the cutoff. Further assessment with a professional may be needed.
Child’s name: ________________________________________________________
Child’s ID #: ______________________________________________________
Administering program/provider:
Month ASQ-3 Information Summary
36
34 months 16 days through
38 months 30 days
Communication
Gross Motor
Fine Motor
Problem Solving
Personal-Social
123456
2. TRANSFER OVERALL RESPONSES: Bolded uppercase responses require follow-up. See
ASQ-3 User’s Guide,
Chapter 6.
1. SCORE AND TRANSFER TOTALS TO CHART BELOW: See
ASQ-3 User’s Guide
for details, including how to adjust scores if item
responses are missing. Score each item (YES = 10, SOMETIMES = 5, NOT YET = 0). Add item scores, and record each area total.
In the chart below, transfer the total scores, and fill in the circles corresponding with the total scores.
Communication
Gross Motor
Fine Motor
Problem Solving
Personal-Social
0 5 10 15 20 25 30 35 40 45 50 55 60
Total
Area Cutoff Score
30.99
36.99
18.07
30.29
35.33
4.FOLLOW-UP ACTION TAKEN: Check all that apply.
______ Provide activities and rescreen in _____ months.
______ Share results with primary health care provider.
______ Refer for (circle all that apply) hearing, vision, and/or behavioral screening.
______ Refer to primary health care provider or other community agency (specify
reason): __________________________________________________________.
______ Refer to early intervention/early childhood special education.
______ No further action taken at this time
______ Other (specify): ____________________________________________________
5. OPTIONAL: Transfer item responses
(Y = YES, S = SOMETIMES, N = NOT YET,
X = response missing).
1. Hears well? Yes NO
Comments:
2. Talks like other children his age? Yes NO
Comments:
3. Understand most of what your child says? Yes NO
Comments:
4. Others understand most of what your child says? Yes NO
Comments:
5. Walks, runs, and climbs like other children? Yes NO
Comments:
6. Family history of hearing impairment? YES No
Comments:
7. Concerns about vision? YES No
Comments:
8. Any medical problems? YES No
Comments:
9. Concerns about behavior? YES No
Comments:
10. Other concerns? YES No
Comments:
Date ASQ completed: __________________________________________
Date of birth: ______________________________________________
