New Horizons HSi S6W2 Ey Health Care Industry Report 2014
User Manual: HSi S6W2
Open the PDF directly: View PDF ![]() .
.
Page Count: 116 [warning: Documents this large are best viewed by clicking the View PDF Link!]

Health Care Industry Report 2014
New horizons
Voyage to value
Featuring exclusive interviews with
the International Consortium for Health Outcomes Measurement,
the Center for Healthcare Quality and Payment Reform
and the Robert Wood Johnson Foundation
To our clients
and other friends
Jonathan G. Weaver
EY Americas Health Care Sector Leader
Jim Costanzo
National Practice Leader
EY Health Care Advisory Services
A profound tidal shift is under way in the
US health care system. In the wake of
uneven quality and unsustainable spending,
the old volume-driven model is being
jettisoned. A new tide is rolling in to
transform how care is delivered and paid
for, rewarding those who improve patient
outcomes and do so at lower costs. The
ultimate destination is a more efcient,
higher-quality, consumer-focused health
care system — one rmly anchored in value.
“Like sailboats at sea, health
care organizations will need
to steer condently through
the shifting winds and changing
currents that continue to
challenge their course.”
The journey forward is an arduous one.
Ongoing implementation of the Affordable
Care Act, emerging health insurance
exchanges, mounting pressures for price
transparency, a heightened focus on
population health, massive investments
in health information technology,
an increased impetus to gain scale and
market share, a growing call to engage
patients in their care — these are among
the converging forces the industry must
deftly navigate.
And they are only the beginning. In the
years ahead, health care providers and
payers can expect rising pressures from
every direction. Like sailboats at sea, they
will need to steer condently through the
shifting winds and changing currents that
continue to challenge their course.
This edition of New horizons is focused
on how health care organizations can
best nd their way on the voyage to
value. Along with an overview of recent
industry developments, we include brief
proles of several organizations and
programs that are in the vanguard of value
creation. Questions are also provided to
serve as a gauge of today’s initiatives — and
tomorrow’s imperatives.
As your organization sails toward the
new horizon, we hope this report will help
inform your discussions and enrich your
decisions. If you have any questions about
the issues explored in New horizons, please
contact your local EY executive.
i
1
Prelude
Value and viability
Setting sail
Feature
Value-based health care:
measuring outcomes that
matter to patients
A conversation with
Jens Deerberg‑Wittram, MD,
President, the International
Consortium for Health
Outcomes Measurement
31
Chapter 2
Value in delivery
Changing tack
43
Chapter 3
Value in information
technology
Supporting the journey
Feature
The move to meaningful
use and ICD-10: finding
the bearings
A roundtable discussion with
EY Health Care Advisory
Services leaders
71
Chapter 5
Value in transactions
Gaining the wind
59
Chapter 4
Value in compliance
Heeding the warnings
11
Chapter 1
Value in payment
Making headway
Feature
Accountable payment
models: paying to support
higher-quality, lower-cost
health care
A conversation with
Harold D. Miller, President
and CEO, the Center for
Healthcare Quality and
Payment Reform
Contents
ii New horizons: voyage to value
93
Postscript
Value in leadership
Taking the helm
Feature
Leadership in transformative
times: navigating the
changing tides
A conversation with
Risa Lavizzo‑Mourey, MD, MBA,
President and CEO, the Robert
Wood Johnson Foundation
83
Chapter 6
Value in measurement
Sounding the depth
107
EY thought leadership
publications
99
Appendix
Value in government
initiatives
Reading the forecast
106
Frequently used
acronyms
108
Acknowledgments
iii

{ }
“To reach a port we must set sail — sail, not tie
at anchor; sail, not drift.”
Franklin D. Roosevelt, 32nd US President
Prelude
Value and viability
Setting sail
The demand to derive greater value from health care, producing the best patient outcomes
at the lowest cost, is pervasive and urgent. Compared with the rest of the world, the US
spends the most money for health care. Yet our overall health is not improving, especially
within the most costly patient populations — those with chronic diseases.
Value Outcomes
Cost
To close the value gap, the health care industry today has set sail on a new course.
Since passage in 2010 of the Patient Protection and Affordable Care Act (ACA),
where the term “value” appears prominently, the pursuit of value-based care has rapidly
emerged in industry and policy discussions. The ultimate goal on the “voyage to value” is
to create an economically sustainable approach to how care is delivered and how it is paid
for. Advocates maintain that costs can best be controlled by re-engineering care delivery
and rewarding improved value: keeping people healthy, using medical interventions
appropriately, and preventing and managing the chronic illnesses that consume a large
part of our health care dollars.
“Value is the only goal that unites the interests of all the parties in the
healthcare system.”
Michael E. Porter, PhD
Bishop William Lawrence University Professor
The Institute for Strategy and Competitiveness
Harvard Business School
1
In the consumer world, value is a familiar
concept. Consumers tend to equate
good value with products of the highest
quality for the lowest price. When applied
to health care, however, value is more
complex, as the consumer — from patients
and providers to payers and purchasers,
and the product — patient outcomes, can
vary widely. According to the Institute of
Medicine (IOM), an organization that has
studied the issue closely, value is in the
eye of the beholder, representing different
things to different stakeholders.
Value for health care providers, for
example, hinges on making decisions
based on appropriateness of care.
For payers, it means using evidence-
based interventions and paying based on
outcomes. For employers, value is keeping
workers and their families healthy and more
productive at lower costs. And for patients,
value is having a high-quality relationship
with care providers, meeting personal
health goals and being assured that out-
of-pocket payments are targeted to these
goals. Reconciling stakeholder perspectives
in a way that creates value for all is a
challenge requiring thoughtful discussion,
diligent focus and unied action.
Driven by the value challenge, industry
stakeholders are pursuing a variety of
strategies. Health care providers are
embracing payer incentives to deliver
high-value care through such models as
pay-for-performance, bundled-payment,
global budgets and nancial-risk-sharing
within accountable care organizations
(ACOs). Payers are nding new ways to
partner with providers to add value to the
patient experience. Employers are striving
to rein in rising health care premiums while
pursuing affordable, high-value products
and services that enhance employee health
and productivity. Product manufacturers
are investing in innovations that deliver
value by improving quality of life. Patients
are looking to access tools and transparent
information that help them make the most
informed value-based decisions.
In this edition of New horizons, we look at
the voyage to value in health care and the
course ahead in delivering on the value
promise. Throughout, “Value vignettes”
prole real-world examples of how payers,
providers and industry groups are pursuing
value. “Viewnder” questions at the end of
each chapter offer considerations for your
board and leadership team as you pursue
value initiatives within your organizations
and with partners across the continuum
of care.
Our launching point is a conversation
with Dr. Jens Deerberg-Wittram, who
leads the International Consortium for
Health Outcomes Measurement. His
organization has been instrumental in
dening and driving the adoption of a
global set of outcome measures for a full
range of medical conditions. In focusing
on the outcomes that matter most to
patients —the center of the health care
universe — these efforts are helping the
industry set sail toward the full potential
of value-based care.
2New horizons: voyage to value

3
Feature
Value-based health
care: measuring
outcomes that
matter to patients
A conversation with
Jens Deerberg‑Wittram, MD,
President, the International
Consortium for Health Outcomes
Measurement (ICHOM)
(www.ichom.org)
Dr. Deerberg‑Wittram leads ICHOM,
a global organization cofounded
by Professor Michael Porter of
the Institute for Strategy and
Competitiveness at Harvard Business
School, the Karolinska Institute in
Sweden and the Boston Consulting
Group to help advance value‑
based health care. We talked with
Dr. Deerberg‑Wittram about the
concept of value and the importance
of measuring outcomes that matter
to patients.
You’ve observed health care systems
around the world. What does value
mean, from your perspective? Why
has it been so difficult to consistently
deliver health care value — and
measure it?
The term “value” was best dened for
health care by Professor Michael Porter of
the Harvard Business School: the outcomes
we achieve for the money we spend. The
term “outcome” hasn’t been clearly dened
in the past. If we look at different sources
that deal with outcome measurement,
what is called an outcome is really an
output. An outcome from our perspective
is only one thing: the results that matter
to a patient after a care delivery process.
It’s an exciting formula because it offers a
new perspective on value with a different
measure of success.
“An outcome from our perspective
is only one thing: the results that
matter to a patient after a care
delivery process.”
Although physicians are striving to improve
patients’ health, historically, the more
broad measures of health care system
outcomes have not been aligned with
specic patient health outcomes. In an
outcomes-based world focused on patients’
health, we say: “Let’s do this differently.
Let’s move away from volume and measure
value based on the results that matter to
patients. To what extent can we achieve
these results? And how much money do
we need to get there?”
Let’s look at an example. If you have a
patient who is suffering from prostate
cancer, and you ask physicians what kind of
outcomes they are measuring, they will tell
you that they measure a lot of things — for
example, length of stay, appropriate MRI
scans, PSA level, number of procedures
and patient satisfaction. All these kinds
of measures may be interesting, but
not relevant. They are not what matter
to patients.
If you ask patients their denition of an
outcome, they will tell you clearly and
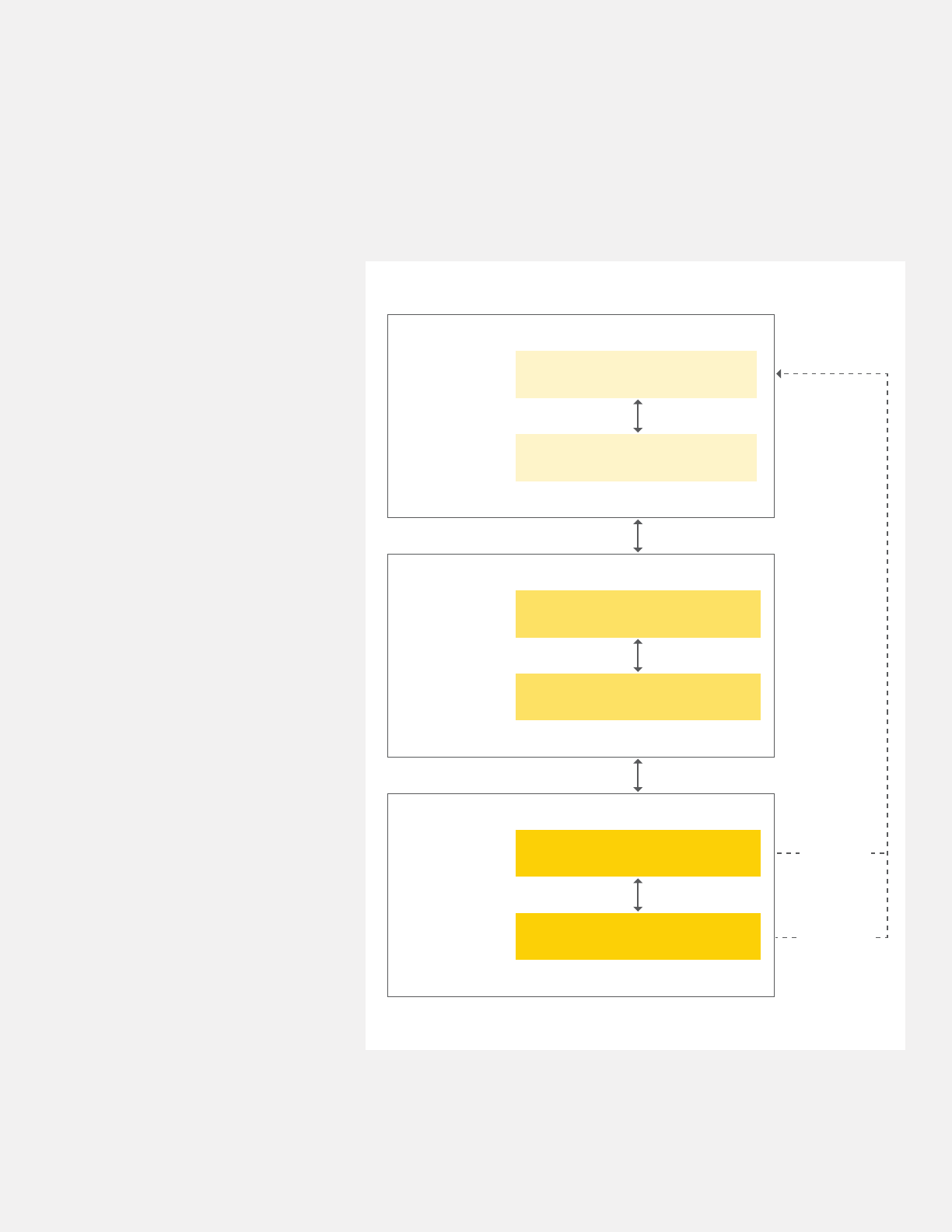
consistently. Michael Porter has rendered
these responses as an outcome measures
hierarchy (see diagram on the next page).
The rst tier is the health status achieved
or retained. Do I survive as a patient who
is suffering from cancer? What will be
the status of my health or degree of my
recovery? Will my quality of life be good?
Will I be in pain? Will I be able to sleep?
What about anxiety?
The second tier is the process of recovery.
How much time will it take to return to
normal activities? What difculties and
complications might I face in my care
or treatment?
The third tier is health sustainability. Will my
illness recur? Will my treatment have any
long-term consequences? For example,
apatient with cancer treated with beam
radiotherapy may see great results for a
year, but two or three years later may be
complaining about complications caused
by the treatment.
We believe that if you want to determine
value, you need to measure the outcome
of every medical condition from the patient
perspective. Standardized outcomes can
help clinicians decide on treatments that
improve patients’ quality of life.
4New horizons: voyage to value
What is the process for obtaining these
outcomes that matter to patients?
Measuring outcomes systematically
requires having the right data sources.
Some outcomes can be determined
only by asking the patient directly — for
example, “Do you have pain?” and “How
would you rate your quality of life?” We call
these “patient-reported outcomes,” and
they are an essential part of outcomes
measurement. Yet patients can’t report
on a number of other outcomes that
matter to them, such as complications
that happen during surgery. You have
to ask the physician about that, because
the patient doesn’t know. These are
“physician-reported outcomes.” One of
the most difcult outcomes to measure
is mortality —a patient with cancer who
dies two years after treatment, for instance.
The patient by denition is not able to
report. In this case it might be helpful to
get access to the national death registry,
if it is available.
At ICHOM, in dening health outcomes,
we directly involve patients in the process.
All of our patient representatives have been
treated for the condition being evaluated.
We also bring together leading physicians
from across the globe who specialize in
treating this condition. As patients and
physicians discuss and reach consensus
on the outcomes that matter most to them,
the ICHOM team serves as facilitator.
What role does technology play
in this process?
We’re looking more and more at technology
solutions to collect meaningful outcomes
data. For example, a key resource is mobile
devices. If you want to measure the mobility
of a patient after orthopedic surgery,
Tier 1
Health status
achieved or
retained
The outcome measures hierarchy
Survival
Degree of health or recovery
Tier 2
Process
of recovery
Time to recovery and time to return
to normal activities
Difficulty of care or treatment process (e.g.,
diagnostic errors, ineffective care, treatment-
related discomfort, complications, adverse effects)
Tier 3
Sustainability
of health
Sustainability of health or recovery
and nature of recurrences
Source: Professor Michael Porter, “What is value in health care?”
New England Journal of Medicine, December 23, 2010. Used with permission.
Recurrences
Care-induced
illnesses
Long-term consequences of therapy
(e.g., care-induced illnesses)
5
it’s probably much easier to look at GPS
data on his or her mobile phone than to ask
how many miles or meters were walked this
week. This new measuring and reporting
capability is a huge step forward and one
that will help greatly in collecting more
relevant data on outcomes.
However, in the outcome measurement
eld today, we’ve found that large
information technology vendors are not
the drivers of innovation. Numerous smaller
companies are making the greatest strides
in this space, developing ready-to-use
plug-and-play apps for outcomes collection.
The challenge will be to integrate their
solutions into larger systems.
Tell us more about the mission of
ICHOM. How did your organization
come together? What are your plans
for the future?
In the early ’90s, Michael Porter began
writing the rst paper about creating
value-based competition in health care.
In 2006, he published a book on this topic,
Redening Health Care. It provides the
argument for using health outcomes data
to redene the nature of competition in the
industry. Over the past eight years, we have
offered many courses at Harvard and other
institutions worldwide where we teach
the value concept to providers, payers,
pharmaceutical companies and medical
technology companies.
People quickly “got it.” They agreed
we needed to move to value as the
new denition of success in health care.
Further discussions led to the idea of
standardization. It doesn’t make sense
to tell surgeons around the world that
they should measure incontinence, for
example —and then nd years later they’re
all measuring it in a different way. We would
have no chance to compare outcomes.
We concluded we needed a standard set
of measures ready to use, simple to handle
and comprehensive enough to cover the
relevant aspects of a patient’s condition
from a patient’s perspective — but not
too complex to overstretch organizations.
And, we needed to offer these measures for
free. In the summer of 2012, we launched
ICHOM as a nonprot organization and
started our work.
Our rst goal was to show that it’s possible
to dene meaningful patient outcome
standards and test them in the eld.
We agreed to begin with four medical
conditions, and for these reasons:
1. Coronary artery disease, which is the
number one cause of death globally and
also one of the most costly conditions to
treat. But it’s also preventable through
patients’ lifestyle changes.
2. Localized prostate cancer, one of
the most common types of cancer
in men. It has different ways of being
treated — from active surveillance
to radical prostatectomy — and can
produce wide variations in outcomes
that matter to patients. For example,
the average incontinence level
one year after prostate surgery in
Germany and Sweden is around 50%,
while organizations performing best
in this procedure worldwide show
a post-surgery incontinence level
of 5% — a tenfold difference.
3. Cataracts, a health issue found in
patients around the globe. Cost for
treatment shows wide variations.
In India, for example, the cost is 1% of
what it is in the most expensive centers
in the US.
4. Low back pain, a condition that is
one of the greatest causes of sick
leave in the workforce and has a
huge impact on global economies.
It is also a condition involving
different medical specialties and many
different treatments. We need to
better understand which options offer
patients the best long-term outcomes.
“Our ve-year goal is to cover 50
medical conditions that represent
about 70% of the disease burden
in industrialized countries.”
Within a year, we completed four Standard
Sets of outcomes for our rst four medical
conditions. In November 2013, we unveiled
these at a Harvard conference drawing
health care leaders from more than 20
countries. These standards have also been
submitted to leading journals and are in
the process of being published. In 2014,
we’re studying more medical conditions
6New horizons: voyage to value
and plan to have Standard Sets for 12 more
conditions by the end of the year. Our ve-
year goal is to cover 50 medical conditions
that represent about 70% of the disease
burden in industrialized countries.
You’ve had the opportunity to observe
health care value in many countries
around the world. How does the US
measure up?
I would say the US has a long way to go
but is denitely on its way. Historically, it’s
been a nation willing to try new approaches.
We see lots of interest and energy to move
forward and improve. The momentum
is coming from providers — from small
organizations that want to begin measuring
value, to well-known leaders that have the
bandwidth and funding for pilot testing.
It’s also coming from payer organizations
that want to reimburse based on outcomes,
and from the ACA itself, which has opened
many opportunities to measure and pay
for outcomes.
You’ve had considerable experience
as a hospital executive and
understand the unique challenges
faced by C-suites and board members.
How can executive leadership best
support outcomes measurement in
their own organizations?
Perhaps my personal experience can shed
some light. For eight years, I ran a 4,800-
bed for-prot system and was also a health
care consultant. I saw rsthand the impact
outcomes can have on managing health
care costs, and I came to believe that health
care should be organized around improving
outcomes and value.
Before this realization, I tried everything
I could to change clinician behavior in a
systematic way, from clinical pathways
to lean management. But it didn’t work.
If you tell a physician, “The antibiotics
you use cost 25% more than those of your
colleagues,” they may not care. If you
say, “I have a clinical pathway in my
computer that tells me what to do,” they
may not take it. They’ll say, “I’m not a
technician. I’m a physician.”
“I have found the only thing that
works — and drives organizational
change — is providing outcomes
information.”
I have found that the only thing that works —
and drives organizational change — is
providing outcomes information. This is
something you must believe or experience
as a health care executive. Then you will
take the right steps.
The rst step is to commit yourself
to outcomes measurement. Walk the
walk. Tell your people, “I want you to
measure outcomes. I want you to know
how to do this, and I want to discuss
with you how we can do better from a
patient perspective.”
Second, don’t wait for a big-bang
information technology x. It isn’t coming.
Third, try to nd payer partners who
are ready to tie money to outcomes.
The ACA gives most organizations room
to do just that.
Last, seek out the “evangelists” in your
organization who are already measuring
outcomes. Give them the bandwidth,
support and funds to run pilots. Celebrate
their successes. In the new world of value-
based health care systems, one successful
pilot can position your organization for
lasting leadership.
7

8New horizons: voyage to value

Viewfinders
Considerations for your board and executive leaders
•Is value the “wind in the sails” of your
organization’s mission and leadership?
•Have you dened your organization’s
core value proposition and
overarching strategy to succeed
in avalue-based world?
•How are you building your reputation in
the community as a provider of value?
•Have you developed a culture of
collaboration and accountability to
support value-based approaches?
In what ways are your employees at
every level empowered to deliver value
in their daily work?
•What tools have you built into your
processes for continuous feedback
and action to support the voyage from
volume to value?
•How do you know you are delivering the
outcomes that matter to patients?
9

{ }
“Price is what you pay. Value is what you get.“
Warren Buffett, 20th‑century American investment entrepreneur
Chapter 1
Value in payment
Making headway
Voyage to value
In pursuing value-based health care, payers are partnering with
providers to create high-value payment systems that reward quality over
quantity. Varied routes are being tried to shape the payment model of
the future, from changing payment incentives to adopting performance
measurements. Value-based payments can spur the health care system
to make delivery more efcient, steer clear of waste and reward
providers for helping patients stay healthy.
Meanwhile, with mounting nancial pressures, health care organizations
are “battening down the hatches” through a range of methods designed
to streamline operations and better manage their bottom lines. This dual
focus — looking externally to leverage new payment opportunities and
internally to curtail costs — is a promising approach in making headway
toward the value destination.
11
Government and market forces are propelling the health
care industry in a new direction — one that moves away
from paying for volume and toward paying for value.
In these deep currents of change, health care providers
and payers must pilot a variety of nancial decisions, new
business processes and strategic opportunities. In this
chapter, we look at payment systems driven by policy and
by the market. We also explore several approaches health
care organizations are taking to lower their costs in a
world of reduced margins and value-driven operations.
Value-based payment models:
considering the options
The move toward value-based payment,
in motion for many years, has been
accelerated by the Affordable Care Act.
The law includes several nancial incentives
for providers to better coordinate
health care delivery. Different payment
methodologies have been proposed as
the prime solution for stimulating delivery
system change. A range of government
initiatives are in play to improve quality
through payment models (see Exhibit 1-1
on page 13). Commercial payers, too, are
pairing payment incentives with changes
aimed at producing better-coordinated,
higher-quality and more-efcient care.
According to Catalyst for Payment Reform,
a national organization for health care
purchasers, 10.9% of commercial payments
today are value-oriented, designed to
either improve performance or cut waste.
This marks a signicant leap from 2010,
when 1%–3% of payments were value-based.
Exhibit 1-2 on page 14 illustrates the
continuum of value-based payment models,
from lowest to highest risk, accompanied by
a discussion of how these models are being
pursued today.
Fee-for-service (FFS)
Paying health care providers on an FFS
basis has been cited as a key contributor
to the nation’s cost and quality challenges.
In the FFS system, each procedure or
service is billed and paid for separately.
These payments may encourage the use
of more, and more expensive, services and
fail to reward high-quality care. FFS also
makes coordination of care across multiple
providers and varied settings difcult and
burdensome for patients, as they receive
different bills from different clinicians and
may not have a designated care manager
to help them with treatment decisions.
Pay-for-performance (P4P)
The P4P model typically pays fees for
individual services, with some form of a
nancial incentive payment to physicians
based on their performance compared with
a set of performance metrics. While early
P4P programs used quality and access
measures to determine incentive awards,
current models often include measures of
physician practice efciency, such as use
of lower-cost generic pharmaceuticals.
In the government sector, the P4P
model is implemented through hospital
value-based purchasing, penalties for
readmissions and penalties for hospital-
acquired infections (see Exhibit 1-1 on
page 13). In the private payer sector, P4P
is evident in a wide range of quality-based
commercial contracts.
“The way we price health care
cannot be understood by a human
being of average intelligence and
limited patience.”
Michael Leavitt
Former Secretary
US Department of Health and Human
Services (HHS)
Care management fees
In this model, health plans pay providers,
typically organized as patient-centered
medical homes, for better care coordination.
Payments are intended to provide an
investment in practice functions that
traditionally have not been reimbursed,
such as educating patients in self-
management.
12 New horizons: voyage to value

Exhibit 1-1. Government initiatives in the shift from volume-driven to value-driven payment
•Bundled Payment for Care Initiative
(BPCI). A total of 299 hospitals and
166 post-acute care organizations are
part of BPCI, a Medicare pilot program.
Providers are reimbursed for certain
care episodes through single case rates
and can participate in gainsharing.
•Comprehensive Primary Care
Initiative (CPCI). A four-year public-
private partnership, CPCI is designed
to test a model of improved access
to quality health care at lower cost.
Atotal of 500 primary care practices
in eight states are participating.
CMS is paying primary care practices
a care management fee to coordinate
services for Medicare fee-for-service
beneciaries.
•Hospital Acquired Condition (HAC)
Reduction Program. Beginning
October 1, 2014, the HAC Reduction
Program, mandated by the ACA,
requires the Centers for Medicare &
Medicaid Services (CMS) to reduce
hospital payments by 1% for hospitals
that rank among the lowest-
performing 25% in HACs.
•Hospital Value-Based Purchasing
(HVBP) Program. Created under the
ACA and launched in October 2012,
the HVBP Program lays the groundwork
for Medicare to become a value-based
purchaser of health care services.
Payment adjustments, up or down
by as much as 1.25%, are based on
hospital performance across two dozen
measures of clinical processes, patient
satisfaction and outcomes.
•Medicare Hospital Readmissions
Reduction Program. Under this
program, the government is looking
at the number of heart attack, heart
failure and pneumonia patients who
return to the hospital within 30 days
of discharge. The program will be
expanded in October 2014 to add
two additional conditions, elective
hip or knee replacements and chronic
obstructive pulmonary disease.
Hospitals with more readmissions than
Medicare expected given their mix of
patients were penalized by losing up
to 1% of their regular payments during
the program’s rst year, scal 2013.
The maximum penalty ramped up to
2% beginning October 2013 and is 3%
beginning October 2014 — rising to 8%
in 2017.
•Medicare Shared Savings Program
(MSSP) ACOs. In December 2013,
CMS named 123 new ACOs as
members of its MSSP, the largest
group announced since the program
started in 2012. These ACOs will cover
1.5 million Medicare beneciaries.
CMS will begin accepting applications
for its 2015 class of MSSP participants
in the summer of 2014.
•Pioneer ACOs. In July 2013, CMS
released the rst-year results from
the Pioneer program, sponsored by
the Center for Medicare & Medicaid
Innovation. All 32 Pioneer ACOs
improved quality, but only 13 were able
to save enough money to share in the
savings with Medicare. In the wake of
these results, nine Pioneers announced
they were dropping out of the program.
Seven of those ACOs planned to
transition to the lower-risk MSSP, while
two left the sea of Medicare ACOs
entirely. CMS is considering opening
the application process to allow more
organizations to join the program.
•Value-Based Physician Payment
Modier (VBPPM). Applied by CMS
to physician performance, the VBPPM
is a method for paying physicians
differentially based on the quality and
cost of their care, as reported through
Medicare’s Physician Quality Reporting
System. Using quality and cost
data reported for 2013, differential
payment is scheduled to begin in 2015
for large group practices and in 2017
will be applied to most or all physicians
who submit claims under the Medicare
physician fee schedule.
Source: CMS, 2014.
13
Since mid-2011, when the Obama
Administration began promoting the
medical home model, the number of
medical home practices has been growing
rapidly (see Chapter 2, page 34). According
to Modern Healthcare, Medicare and
43 other payers, including commercial
plans and state Medicaid programs, are
supporting 500 medical home practices
with per-member, per-month, care
management fees.
Bundled payments
Under the bundled payment model,
sometimes referred to as an “episode
of care” payment, instead of being paid
separately for each individual service,
providers receive one payment for all
services delivered to a patient during a
single episode of care — for example, a hip
replacement or a coronary artery bypass
graft. The payment is made for all services
that the patient is expected to use, from
physician and hospital services to post-
discharge services such as home health
and rehabilitation. Bundled payments
are also applied to treating such chronic
conditions as diabetes, with payments
made in anticipation of all services to be
received in treating the condition over a
dened timeframe.
If the costs of care are less than the
bundled payment amount, participating
providers keep the difference. If costs
exceed payment, they absorb the loss.
Bundled payments give participating
providers an incentive to coordinate their
activities, eliminate unnecessary services
and avoid complications that require
additional services.
In the government payer sector, CMS
has piloted bundled payments through
its Acute Care Episode Demonstration
project and Bundled Payment for Care
Initiative (see Exhibit 1-1 on page 13).
In 2012, bundled payments made their
way into the state-driven Medicaid sector
with the Arkansas Health Care Payment
Improvement Initiative. Currently the
country’s only Medicaid bundled payment
model, it is mandated for state providers
within ve episodes of care.
Exhibit 1-2. Spectrum of payment models
Providers are paid
Fee-for-service Pay-for-
performance
Care
management
fees
Bundled
payments
Shared savings
and shared loss
Global
payments
Provider-
sponsored
health plans
A specic price
for each service
rendered
Fee-for-service
payments
plus incentive
payments for
quality and
efciency
Per-member,
per-month
fees — typically
for providers
organized
as patient-
centered
medical homes —
to fund
investments
in care
coordination
One lump sum
for all services
rendered to a
patient during a
hospitalization
or episode
of care — or
to treat a
particular
disease for a
dened time
period
Payments
closely tied to
controlling the
overall cost of
the care that
patients receive
while achieving
quality targets —
sharing in
savings if
costs are less
than target
and sharing in
losses if costs
are greater than
target
A xed dollar
amount, usually
prepaid monthly,
designed to
account for
most or all of
the expected
cost of care
for a group of
patients for a
dened time
period; may be
supplemented
with incentive
payments
for achieving
quality goals
Through
ownership of
the provider’s
own health plan,
assuming 100%
of the nancial
risk for insuring
a patient
population
Less risk, less value More risk, more value
Source: EY analysis, 2014.
14 New horizons: voyage to value
The private payer sector also reects a
wide range of bundled payment initiatives.
For example:
•Geisinger Health System in Danville, PA,
developed its ProvenCare as a bundled
payment model for coronary artery
bypass graft surgery and has since added
additional bundles.
•Horizon Healthcare Services, Inc.,
New Jersey’s oldest and largest health
insurer, started its bundled payment
program with total joint replacements
and has expanded to include such
episodes of care as pregnancy and
adjuvant breast cancer treatment.
•The PROMETHEUS Payment model,
launched in 2006 with the support of the
Robert Wood Johnson Foundation, now
includes 21 bundles with the potential
to affect payment for almost 30% of the
insured adult population.
•Several major national employers
have started their own bundled
payment arrangements with hospitals
(see Value vignette above).
Shared savings and shared loss
In the shared savings and shared loss
model — the payment strategy for such
structures as ACOs — providers are paid
based on achieving dened performance
goals. Those that meet or exceed certain
quality and cost performance benchmarks
can share in any resulting cost savings.
Those that do not meet goals will share
in losses.
Value vignette
Employers Centers of Excellence Network: bundling payments for value
Beginning January 1, 2014, a
rst-of-its-kind coalition of large US
employers — including Lowe’s and
Walmart — began offering knee- and
hip-replacement surgeries to more
than 1.5 million employees and their
dependents. The companies joined
the Pacic Business Group on Health
(PBGH) Negotiating Alliance to create
the Employers Centers of Excellence
Network (ECEN).
According to PBGH, these elective
surgeries represent a growing portion of
employer health care spending. Prices can
vary between $15k and $125k, without
correlation to quality. As of early 2014,
the network is offering these procedures
at four US health care systems:
• Johns Hopkins Bayview Medical Center
in Baltimore, MD
• Kaiser Permanente Orange County-
Irvine Medical Center in Irvine, CA
• Mercy Hospital in Springeld, MO
• Virginia Mason Medical Center in
Seattle, WA
ECEN assists members that want their
employees to have high-quality elective
surgical care by providing information on
which surgeons perform best on these
procedures. The network evaluates and
selects centers of excellence (COEs),
negotiates bundled payments and
encourages member organizations to
promote use of these COEs to their
employees. According to ECEN, each
COE is committed to the highest-quality
standards and has performed far better
than national norms for complications,
reoperations and patient experience.
In addition to total hip and knee
replacements, other elective surgeries
such as spine/low back and cardiac
surgeries will be added. Participating
employers receive discounted rates
for care.
For employees, participation in ECEN is
voluntary. Those who take part receive
100% coverage for their surgical care,
with no deductibles or co-pays, as well as
travel, lodging and living expenses for the
patient and a caregiver. Each employee
is assigned to a patient advocate, who
schedules the surgery and selects the
center. After surgery, the same advocate
assists with insurance claims, as well as
the transition back to the patient’s home
physician. The COE also assigns a patient
navigator to guide the patient while he or
she is on-site.
“[ECEN] is designed to serve as a
model for delivering high-quality
health care with transparent and
predictable costs.”
David Lansky
PBGH President and CEO
Lowe’s and Walmart have tested the
waters before with bundled payments.
Lowe’s entered into a bundled-payment
agreement with Cleveland Clinic for
cardiac surgery, and Walmart and six
hospitals, including Cleveland Clinic and
Mayo Clinic, have launched bundled
payments for workers’ cardiac and
spinal surgeries.
Sources: PBGH website; Walmart website; “Wal‑Mart, Lowe’s, PBGH form network for ‘no‑cost’ knee/hip replacements,” San Francisco Business Times,
October 8, 2013, via The Business Journals, www.bizjournal.com; “Wal‑Mart, Lowe’s to offer employees leg up on knee and hip work — at certain systems,”
Modern Healthcare, October 8, 2013.
15
The concept behind ACOs is that by linking
provider payment to cost and quality
outcomes, the provision of unnecessary
treatments and services is discouraged
while prevention, care coordination, quality
and value are emphasized.
Along with the Medicare Shared Savings
Program and Pioneer ACO program in
the public sector, several commercial
ACO contracts have emerged. Current
estimates (Leavitt Partners, May 2014)
put the number of ACOs in the US at
626; 329 have government contracts,
210 have commercial contracts
and 74 have both government and
commercial contracts. The remaining
13 ACOs have not yet made specic
announcements about their contracts or
are still in the process of nalizing them.
Among recent developments:
•Anthem Blue Cross and Blue Shield plans
to form an ACO with Franciscan Alliance,
a Catholic health care system in Indiana.
•Memorial Healthcare and Florida Blue
have formed a new ACO, Memorial
Health Networks. The ACO marks the
tenth accountable care arrangement
between Florida Blue and hospital
systems throughout the state — and the
fth in south Florida.
•UnitedHealthcare, the Minnetonka,
MN–based health insurer subsidiary
of UnitedHealth Group, plans to more
than double its accountable care
health plan contracts with hospitals
and physicians over the next four
years. UnitedHealthcare currently ties
$20 billion of its contract payments to
quality and cost efciency, and plans
to allocate $50 billion by 2017.
Global payments
A comprehensive payment to a group of
providers, global payments are meant to
account for most or all of the expected cost
of care for a group of patients for a dened
timeframe. These agreements pay on a
per-member, per-month basis. The model
offers providers incentives to keep their
patient populations healthy and maintain
low utilization of clinical services.
While generally synonymous with the term
“capitation,” the term “global payment” is
preferred by advocates to distinguish it
from early capitation models, under which
some providers suffered nancial losses.
Today, global payments have evolved
considerably compared with earlier
efforts. For example, some payers are
using risk-adjustment methods to account
for the relative illness burden of the
population and risk sharing to protect
the provider if costs are higher than
anticipated. This way, providers are not
facing potential catastrophic nancial
losses — or an incentive to curtail care,
acommon concern with early versions
of capitation arrangements. A leading
example of a global payment model is the
Alternative Quality Contract (AQC) from
Blue Cross Blue Shield of Massachusetts
(see Value vignette below).
“Ending fee-for-service payment
in favor of accountable care
organizations and bundled payment
once and for all is unlikely to be
feasible for quite some time, but
gradually increasing disincentives for
providers that do not participate in
reformed payment approaches is a
practical way to move forward.”
Paul B. Ginsburg
President
Center for Studying Health System Change
“Achieving health care cost containment through
provider payment reform that engages patients
and providers”
Health Affairs, May 2013
Value vignette
The Alternative Quality Contract: increasing value through accountability
The Alternative Quality Contract,
apayment model from Blue Cross
Blue Shield of Massachusetts (BCBSMA),
illustrates current trends in payer-
provider cost-saving initiatives. Launched
in 2009, the AQC is one of the largest
commercial payment reform initiatives
in the US. It includes more than three-
quarters of BCBSMA’s overall network
of contracted primary care providers and
specialists who care for nearly 700,000
BCBS members. BCBSMA notes that
the AQC arrangement is a ve-year
agreement that encourages providers
to invest in long-term initiatives —
signicantly longer than BCBSMA’s
traditional contracts, which are typically
three years for hospitals and one year
for physicians.
The model combines a per-patient global
budget with signicant performance
incentives based on nationally endorsed
quality measures. BCBSMA links its
contracts with providers to dozens
of quality metrics that track whether
patients get the right screenings
and exams, whether physicians and
hospitals prescribe the correct drug and
whether patients are satised with their
care. A study nds that this approach
improved quality of care while cutting
costs as much as 10% below their fee-for-
service level.
Source: BCBSMA, http://www.bluecrossma.com/visitor/about‑us/affordability‑quality/aqc.html
16 New horizons: voyage to value

Provider-sponsored health plans
As many health care providers are
assuming risk through new contracts with
payers, others are taking risk-bearing
to a higher level by becoming provider-
sponsored health plans. Financial pressures,
the wave of new entrants in the insurance
market and the move toward population
health have spurred several health systems
to launch their own health insurance plans.
Now isn’t the rst time providers have
taken on the payer side of business.
The most notable example of provider
initiatives in the payer space is California’s
Kaiser Permanente, which started as
a hospital in the 1930s and has since
grown to nearly 8.9 million health plan
members — making it the largest US health
plan by medical enrollment. Today’s four
largest provider-sponsored health plans
after Kaiser, according to data from AIS’s
Directory of Health Plans: 2013, were also
early risk-bearing pioneers: University of
Pittsburgh Medical Center (UPMC) Health
Plan (founded 1998), Healthrst (founded
1993), Henry Ford Health System’s
Health Alliance Plan (founded 1960) and
Spectrum’s Priority Health (founded 1992).
Since the shift to value-based care, the
concept is again attractive to many
providers, who are nding that creating
and offering their own health plans is a
route to achieving competitive advantage.
According to the American Hospital
Association, about one in eight hospitals —
primarily not-for-prot health systems and
nonacademic systems — operated health
plans in 2011.
Recent activity reects the growing trend.
For example:
•In Massachusetts, Partners Healthcare
in Boston, the state’s largest hospital
and physician organization, acquired
Neighborhood Health Plan, a nonprot
organization insuring more than
240,000 mostly low-income residents
across the state.
•In New York, North Shore–Long Island
Jewish Health System — with 16
hospitals and more than 300 outpatient
centers — has launched its own health
plan, CareConnect, on the state health
insurance exchange (HIX).
•In Ohio, Cincinnati-based Catholic Health
Partners is selling health plans through
its subsidiary, HealthSpan, on the
Ohio exchange.
•In Texas, Baylor Scott & White recently
expanded the nonprot Scott & White
Health Plan to portions of Baylor’s
market area, covering more than
240,000 members across 71 counties
in the central part of the state.
•In Virginia, Falls Church–based Inova
Health System has partnered with
Aetna to establish a 50-50 ownership
joint venture, the Innovation Health
insurance plan.
Providers that are considering forming a
health plan need to carefully weigh the
benets against the risks (see Exhibit 1-3).
The quest for efficiency:
controlling costs in a value-
driven world
Regardless of which payment model
organizations adopt or where they are
in their voyage to value, increasing
efciencies and reducing operating costs
are always worthwhile goals. A survey
from the Health Information Management
Systems Society and AVIA (The 2013
Healthcare Provider Innovation Survey)
reveals that while providers have numerous
priorities — from reducing medical errors
to improving patient satisfaction — cutting
costs is still at the top of the list. As margins
tighten for US hospitals, especially for
Exhibit 1-3. Potential benefits and risks for providers considering health
plan formation
Potential benets Potential risks
• Greater nancial rewards. With a
projected drop in inpatient service
utilization, forming a health plan can
help providers hedge against potential
revenue loss.
• Improved market share. Incentives
are created to keep patients within the
system, providing the opportunity for
deeper market penetration.
• Better population health
management. Critical decisions
around what care to provide and what
to pay for are under the provider’s
control. With more tightly integrated
clinical and nancial performance
data and metrics, health systems
may be better positioned to improve
outcomes and lower costs around
specic patient populations.
• High start-up costs. Providers need to
have enough funds to cover start-up
costs and regulatorily required capital
thresholds, and enough potential
covered lives to absorb actuarial and
other risks.
• Payer pull-outs. Hospitals that
start their own health plans will be
competing with other plans in their
markets. Commercial payers may
choose to end contracts, posing a new
set of challenges for hospitals.
• New responsibilities. Changing from
being a provider to being a provider-
payer will require a different mindset,
skill set and knowledge base with a
corresponding learning curve.
Source: EY analysis, 2014.
17
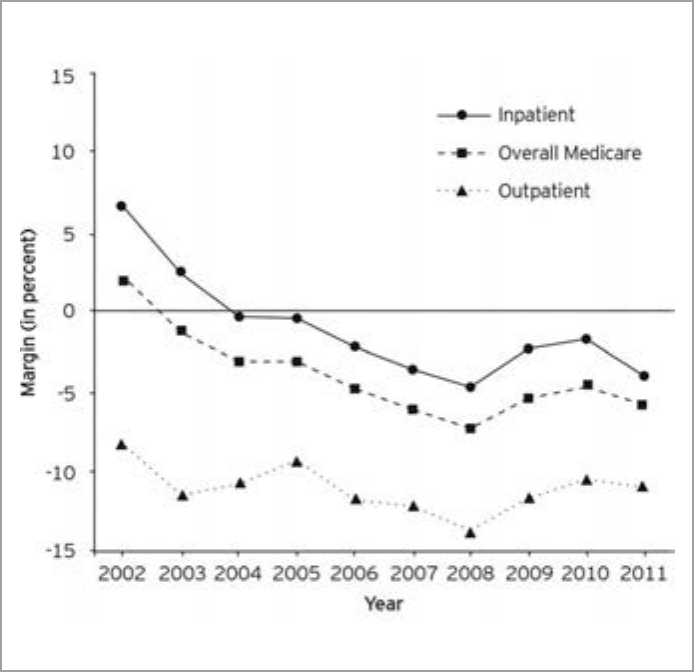
those with higher levels of Medicaid and
Medicare patients (see Exhibit 1-4), hospital
executives are using a range of strategies
to control costs. Highlighted below are
prevalent approaches.
Readmission reduction
Nearly one in ve Medicare patients
returns to the hospital within a month
of discharge. From the government’s
vantage point, readmissions are a leading
symptom of inadequate quality and a
costly, uncoordinated system. The ACA
charged the Department of Health and
Human Services (HHS) with creating
the Hospital Readmissions Reduction
Program, effective for discharges beginning
October 1, 2012. With an initial penalty
rate of 1% of Medicare payments for
failure to substantially reduce readmission
rates, the penalty continues to rise (see
page 13). CMS reports an estimated 2,225
hospitals were penalized $227 million in
2013 because of excess readmissions.
What are the causes of unnecessary
readmissions? A seminal report from
the Robert Wood Johnson Foundation
highlights a variety of catalysts
(see Exhibit 1-5 on page 20).
A scan of the health care horizon nds a
range of cost-effective solutions to reduce
readmission rates. For example:
•In California, Napa’s Queen of the
Valley Medical Center uses the Case
Management, Advocacy, Resource/
Referral, Education (CARE) Network,
through which a social worker and
nurse visit patient homes to make
sure the patient understands post-
discharge care plans. Over a one-year
span, the CARE program yielded a
60% reduction in ED visits and a 40%
reduction in hospitalizations for the
patient population.
•In Ohio, Cincinnati’s Mercy Health has
used nurses specially trained to act as
patient guides through the discharge
process. In less than a year, the
program has yielded savings in avoided
readmissions of about $495,000 and
a 15% drop in all-cause readmission
rates for heart failure, acute myocardial
infarction and pneumonia.
•In Utah, Salt Lake City’s University of
Utah Health Care hired a hospital-based
transitions navigator to help patients
transition safely from hospital to medical
home. Over three months, the program
yielded a 23% reduction in the hospital’s
30-day readmission rate.
To prevent hospital-acquired infections
(HAIs), a major cause of readmission, many
providers are implementing automated
infection control and patient surveillance
systems. These systems provide real-time
alerts, pushing time-sensitive patient
information directly to the treating
physician to act quickly in reducing adverse
events. Studies have found 10%–70%
of HAIs could be prevented through
systematic surveillance and standard
preventive guidelines.
Exhibit 1-4. Trending of Medicare margins
Source: Medicare Payment Advisory Commission (MedPAC) report, March 2013.
18 New horizons: voyage to value

19
Patient flow improvement
Regardless of how many hospital beds are
available, inefcient processes, inadequate
care transitions and a eet of other
challenges can lead to poor use of capacity.
Patient-ow problems not only create
operational bottlenecks, but they often
set the course for patients’ perceptions of
their entire stays. If the hospital encounter
starts with a long wait to get a bed, the
hospital may already have lost the battle
for delivering a positive patient experience.
Providers nationwide are taking action
to address the patient-ow challenge.
For example:
•In Connecticut, Yale-New Haven Hospital
implemented process changes that led
to an 84% improvement in discharges by
11:00 a.m., a decreased length of stay
from 5.23 to 5.05 days and the ability
to accommodate 45 additional patients
each day.
•In Ohio, Cincinnati Children’s Hospital
Medical Center improved surgical
scheduling practices, resulting in fewer
delays and cancellations of elective
surgeries because beds were not
available, as well as a more predictable
ow of patients through the intensive
care unit. The changes also saved the
facility $100 million in capital costs by
eliminating the need for 75 new beds.
•In Washington, at Seattle-based Virginia
Mason Health System, nurses analyzed
their workows and took steps to
improve efciency. A key change was
reorganizing nurses’ care patterns on
the hospital oor so that they could
care for patients who were in groups of
rooms rather than spread across a unit.
In areas where this change has been
implemented, Virginia Mason reports its
nurses now spend 90% of their time on
direct patient care and attend to patients’
needs faster and more effectively.
A key area of focus for improving patient-
ow is the Emergency Department.
Automated patient-ow solutions are
helping relieve ED overcrowding by
speeding up throughput processes.
To reduce heavy patient volumes in the
ED, some health care systems have also
created transfer centers — hubs for patient
referrals between the system and all the
clinics, hospitals and physician ofces in
the region. These centers enable referring
providers to make one phone call to send
their patients directly from their facilities
to the appropriate level of acute care,
bypassing an unnecessary ED visit. Patients
can readily receive the care they need, while
hospitals can decrease the number of patients
entering the hospital through the ED.
Supply chain retooling
On average, the supply chain represents the
second-highest component of a hospital’s
operating costs — eclipsed only by the
cost of labor. More and more hospitals
are recognizing the value that the supply
chain can bring to their organizations and
have moved to add supply chain strategic
initiatives to their overall goals. Approaches
range from rightsizing inventory, to joining
purchasing collaboratives for best-price
negotiation, to building and automating
warehouses and ordering directly from
manufacturers. For example:
•In Arizona, Phoenix-based Banner Health
saved $226 million in ve years by
aligning supply chain management with
efforts to improve quality, remove waste
and disseminate best practices.
•In Florida, University of Florida and
Shands Teaching Hospital in Gainesville
are collaborating with Orlando Health
in joint supply purchasing decisions —
resulting in millions of dollars in savings
for both organizations.
•In Mississippi, Meridian’s Anderson
Regional Medical Center rightsized its
inventory levels and gained savings
of $1.5 million.
Exhibit 1-5. What leads to needless hospital readmissions?
1. Some patients leave the hospital with
a treatment plan for one illness when
other problems of equal importance
are ignored.
2. Many patients are discharged without
understanding their illnesses or
treatment plans or they inadvertently
discontinue the medicines needed to
stay well.
3. Family members who may be the
patient’s central caregivers are often
not included in discharge planning.
4. The physicians caring for the patient
may not communicate with each other
or may not develop a coordinated plan
for care after discharge.
5. Patients may not have the right
prescriptions or cannot ll them.
6. Appointments with primary care
clinicians or with specialists may not
occur soon enough after discharge.
Missed clinician visits lead to missed
opportunities to recognize that the
patient is not improving.
7. Information about a patient’s hospital
stay does not always go to the
appropriate community clinicians.
8. Clarity is lacking on which clinician
is responsible for care after patient
discharge; accountability is spread
among hospital staff, community
physicians and nurses, skilled nursing
facilities and families. Without clear
accountability, problems that could be
prevented are missed, leading to ED
visits and repeat hospitalizations.
Source: The Revolving Door: A Report on U.S. Hospital Readmissions, RWJF, February 2013.
20 New horizons: voyage to value
Many hospitals have found the most
effective way to reduce costs for
those supplies over which physicians
have the greatest inuence, such as
implants, medical devices and high-cost
pharmaceuticals, is to involve them
vigorously in cost-saving initiatives.
“Hospitals have got to start engaging
the right executives and physicians
and share data with them. They’re
scientists by nature. You’ve got
to give doctors input on what is
being used.”
Brent Johnson
Vice President of Supply Chain & Support Services
Intermountain Healthcare
Healthcare Finance News, September 2013
Revenue cycle re-engineering
From offering online scheduling to issuing
easy-to-understand bills, the revenue
cycle presents a distinct opportunity to
make the transactional side of health care
more nancially sound for providers — and
more satisfying for patients. The goal is
to transform the process from reactive to
proactive, from one that begins after the
patient receives care to one that starts
with the patient’s rst interaction with the
provider organization.
Forward-thinking providers are unlocking
the value in their revenue cycles by
becoming more patient-centric at all patient
touch points. They are empowering patients
through self-service communication tools
such as patient account portals, scheduling
apps and registration kiosks; using
analytics to improve processes and patient
communications; keeping patients informed
of, and prepared for, their nancial
obligations; and making the billing process
more consumer friendly. For example:
•In Nebraska, Omaha’s Bergan Mercy
Medical Center offers “My Cost,” a
customized, online tool. Patients can
obtain out-of-pocket cost information
By the numbers
• Without major health care redesign
or intervention, by 2022, health care
costs in the US could make up as much
as 19.9% of GDP — up from 17.2%
in 2012 (source: CMS, 2014).
• According to an annual survey of
governance structure and practices
in the nation’s nonprot hospitals and
health systems, 52% of respondents
have added value-based payment
goals to their strategic and nancial
plans (source: Governance Institute,
2013 biennial survey).
• The US health care system wastes
30 cents of every dollar spent
(source: IOM, 2012).
• The number of physicians accepting
new Medicare patients increased by
3% between 2007 and 2012 and is
higher than the number of physicians
accepting new private insurance
patients (source: HHS Ofce of the
Assistant Secretary for Planning
and Evaluation).
• Family premiums increased 4% in
2013, the same as in 2012, and
individual premiums increased 5%
versus 3% in 2012 (source: Kaiser
Family Foundation, “2013 Employer
Health Benets Survey”).
• High-deductible plans can reduce
health care costs by 5% to 14%
(source: Robert Wood Johnson
Foundation, 2012 report).
• A recent study nds that although
20% of health plans say value-based
payment models support more
than half of their business today,
60% of respondents anticipate they
will support more than half their
business within ve years (source:
Availity, “Health Plan Readiness to
Operationalize New Payment Models,”
May 2013).
• A recent survey nds that only 14%
of adults understand basic insurance
(source: Carnegie Mellon survey,
July 2013).
• Despite increasing health care costs,
less than 15% of internal medicine
residency programs feature curricula
aimed at teaching residents to
be more cost-conscious (source:
Journal of the American Medical
Association (JAMA), research letter,
December 27, 2013).
• 5% of all inpatients will develop a
hospital-associated infection — at an
average cost of tens of thousands of
dollars (source: Agency for Healthcare
Research and Quality (AHRQ), 2014).
• The $2.4 billion hospital revenue cycle
management industry for software
and services is expected to see double-
digit increases in 2014 (source: Black
Book Rankings LLC, 2013).
• Patients satised with hospital
billing processes are ve times more
likely to recommend the hospital
to a friend (source: Connance,
December 14, 2011).
• A cost analysis of more than
10.2 million patient discharges for
various conditions revealed that,
at 24.2% of costs, supplies and
devices were the leading contributors
to the increase in average cost per
discharge — surpassing intensive
care unit charges, imaging and other
advanced technological services
(source: Jared Lane Maeda, PhD,
et al., “What Hospital Inpatient
Services Contributed the Most to the
2001 to 2006 Growth in the Cost Per
Case?” Health Services Research,
August 29, 2012).
21
Value vignette
An employer view on value: exploring leading practices
The Towers Watson/National Business
Group on Health Employer Survey on
Purchasing Value in Health Care, now
in its 19th year, tracks strategies and
practices employers are using in the quest
for health care value. The 2014 report,
The New Health Care Imperative: Driving
Performance, Connecting to Value,
proles the activities of high-performing
companies, as well as current trends in
the health care benet programs of US
employers with at least 1,000 employees.
The survey was completed by 595
employers between November 2013 and
January 2014. Respondents collectively
employ 11.3 million full-time employees,
have 7.8 million employees enrolled in
their health care programs and represent
all major industry sectors.
The survey found that employers are
committed to providing subsidized health
care benets to active employees —
even in an environment of continued
health care cost increases, uncertainty
about some provisions of health care
reform and a slow-to-recover economy.
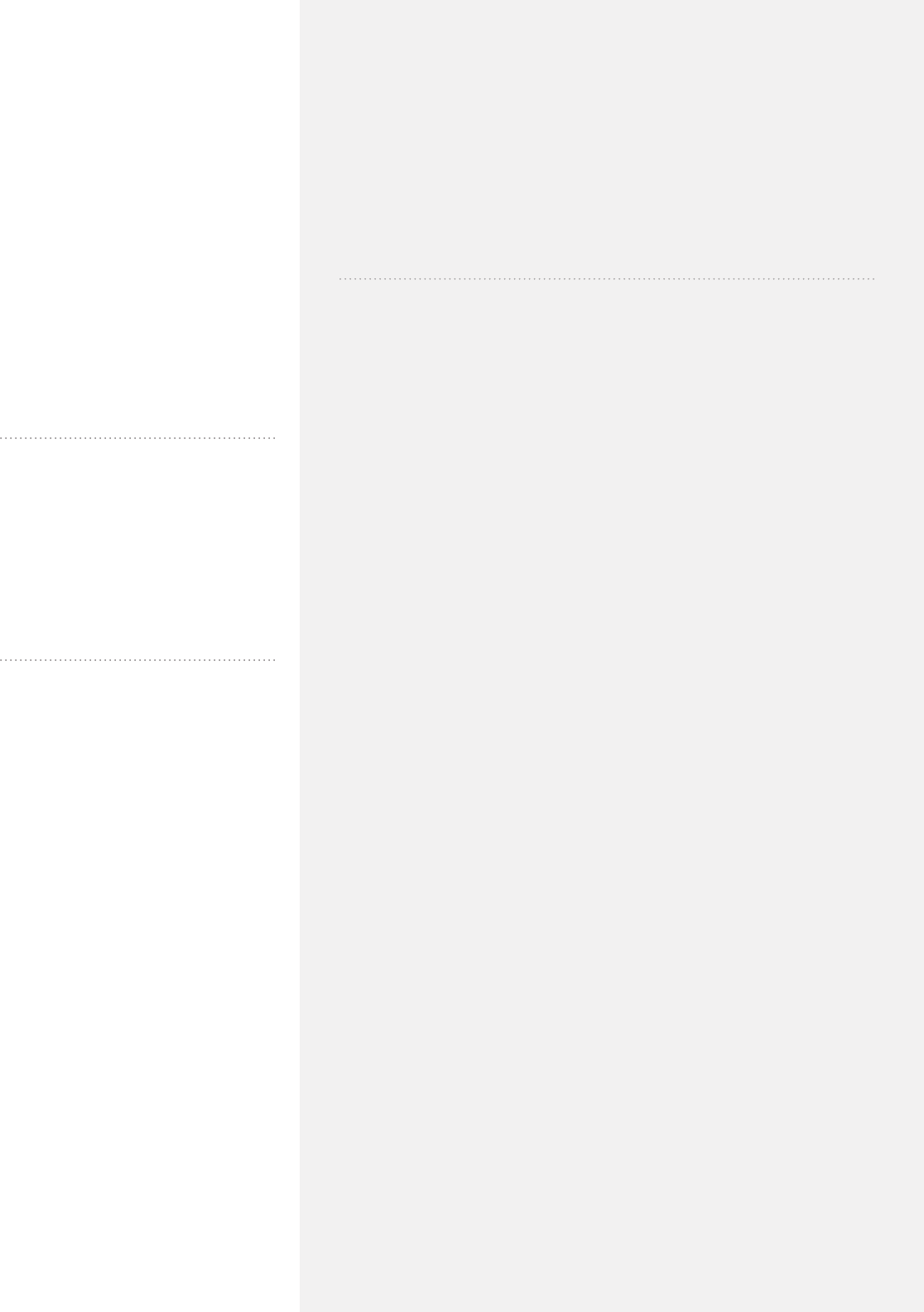
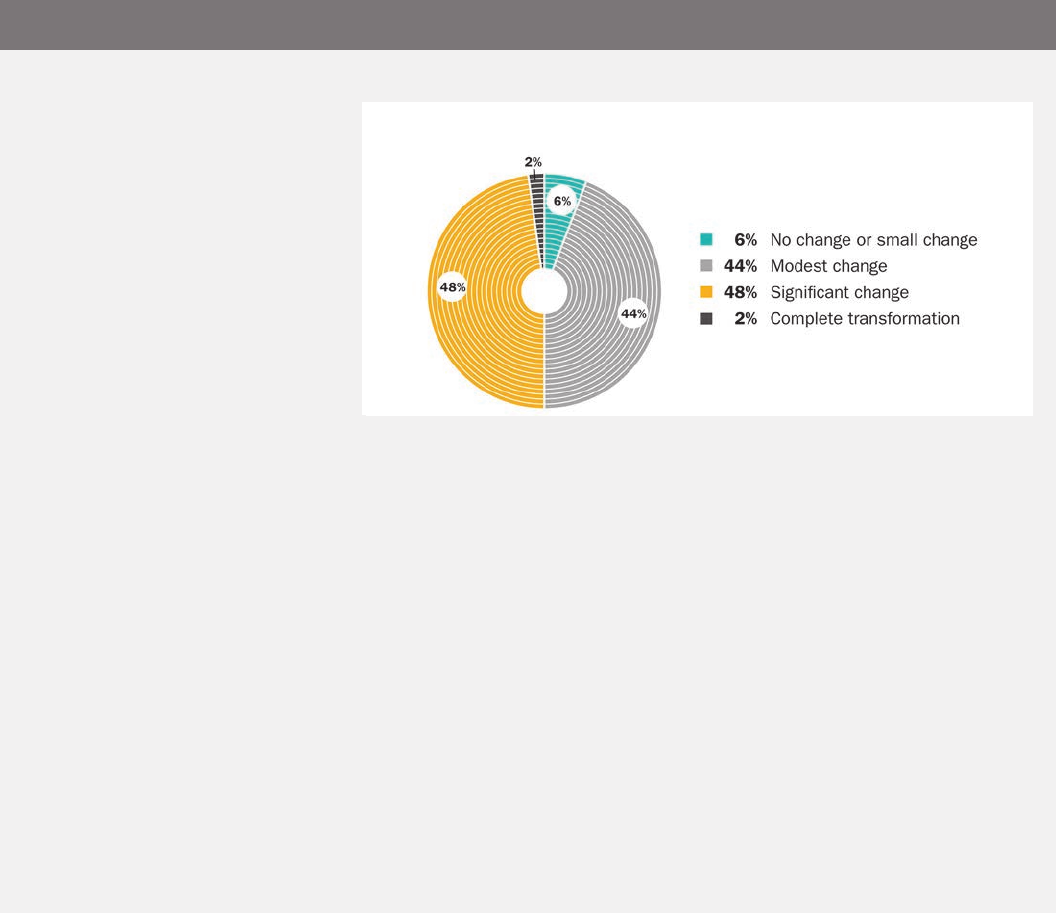
Yet 94% of respondents expect employer-
sponsored health care benets to undergo
modest or major changes over ve
years’ time (see chart).
Survey responses indicate that employers
are taking steps to derive the most value
from their health benet programs. In the
view of the report’s authors, employers
who want their health plans to stay
viable over the long term will need to
take a holistic approach that includes
ve key steps:
1. Optimize benet delivery channels.
Improve self-managed programs and
explore alternatives such as private
exchanges or hybrid arrangements.
2. Restructure benets. Consider
offering new plan options, redesigning
benets, recalibrating contribution
strategy and tier structures, and linking
health savings account strategies
with your approach to retiree
health benets.
3. Enhance network and value-
based contracting. Reduce unit
costs, and improve efciency,
quality outcomes, and risk-transfer
arrangements to providers.
4. Focus on population health
management. Improve chronic-
condition management, reduce risk
factors and improve care gaps.
5. Engage employees and improve
their accountability. Use quality and
transparency tools, point-of-care
cost-sharing designs, account-based
strategies and incentive approaches.
Source: Towers Watson, www.towerswatson.com/en‑US/Insights/IC‑Types/Survey‑Research‑Results/2014/03/towers‑watson‑nbgh‑employer‑survey‑on‑purchasing‑value‑
in‑health‑care
Nearly all employers anticipate signicant or modest changes in health benet
programs by 2018
22 New horizons: voyage to value
for specic medical tests or procedures,
customized to their insurance
plan designs.
•In Ohio, Riverside Methodist Hospital in
Columbus has made nancial counseling
a priority in its revenue cycle, including
all patient accounts in one seamless
discussion of patient responsibility and
nancial aid resources, as opposed to
discussions with every visit. Hospital
executives report Riverside has increased
point-of-service collections by an average
of $50,000 per month.
•In Oklahoma, Saint Francis Hospital,
the agship facility for Tulsa’s Saint
Francis Health System, has taken steps
to limit how often it asks for patient
information and to integrate registration
systems throughout the organization
so that — regardless of setting — patient
information can be collected in a
unied way.
In a value-based world, creating a positive
care experience is integral not only to
building lasting patient relationships
but also to maintaining a healthy cash
ow. Putting the patient at the center of
the revenue cycle brings an unparalleled
opportunity to generate loyalty today — and
provide for viability tomorrow.
No turning back: sailing
to tomorrow
US health care is at a pivotal point in its
journey. The realities of rapidly surging
health care costs, attening Medicare
reimbursement and the rising tide of
demand for services from the newly insured
are forcibly coming together, leaving
the industry with no easy route to make
headway toward the new horizon. Most
agree the best course forward is to continue
to pursue value-based approaches — while
looking carefully within to better manage
operating costs. The conditions are often
uncertain. Yet for those whose sails are well
set, the voyage to value can be a perfect
opportunity for creating a stronger, more
efcient and more resilient organization.
Our chapter concludes in a conversation
with Harold Miller, who leads the Center for
Healthcare Quality and Payment Reform.
He offers his viewpoint on which payment
models are the most effective in delivering
long-term value.
Value vignette
Capacity management: reducing bottlenecks for a better patient experience
A recent study from software provider
Central Logic — featuring input from
such health care leaders as UPMC,
Dartmouth-Hitchcock and Memorial
Sloan-Kettering — offers six tips for how
hospitals can better manage capacity to
reduce length of stay and improve the
patient-care experience:
1. Focus on accurate patient placement.
Conrm that patients are in the right
bed, at the right level of care, at the
right time.
2. Conduct daily, multidisciplinary
rounds and bed meetings. Make
sure care teams work cohesively,
appropriate tests are ordered,
procedures are completed promptly,
discharge plans are followed and
capacity is optimized.
3. Discharge patients as soon
as possible, at any time of
the day. Focus on helping patients
reach discharge as quickly as is
clinically feasible.
4. Smooth patient census. Look at peak
census patterns by time of day and
day of week. Consider scheduling
elective surgeries on weekends to
relieve congestion, free up resources
and reduce length of stay.
5. Communicate consistently with
staff and patients. Streamline
communication through case
managers to facilitate communication
across silos. Help patients manage
expectations for length of stay.
6. Measure and distribute the correct
metrics. Evaluate such indicators as
30-day readmission rates, average
daily admits, observation volumes,
case mix index and length of stay by
diagnostic group against the impact
on your organization’s overall capacity
management. Discuss metrics to
ensure hospital administrators
understand data implications for
optimizing capacity.
Source: Central Logic, www.centrallogic.com/check-gate resource?le=/public/uploads/global/2013/10/
CapacityManagementSixThoughts.Final.pdf
23
Accountable payment
models: paying to
support higher-quality,
lower-cost health care
A conversation with Harold D. Miller,
President and CEO, the Center for
Healthcare Quality and Payment
Reform (CHQPR) (www.chqpr.com)
Harold Miller is a nationally recognized
expert on health care payment and
delivery systems and has worked with
the federal government and several
states and regions in designing and
implementing system reforms. Along
with his role in leading CHQPR, he
also serves as adjunct professor of
public policy and management at
Carnegie Mellon University. We talked
with him about how new payment
models can improve the quality of
care for patients, lower costs for
employers and improve the nancial
viability of health care providers.
You have said that the biggest need in
health care today is to change the way
doctors and hospitals are paid, and the
second-biggest need is to change the
benefit designs for patients. Why are
these the greatest concerns? And how
should we address them?
Both the public and private sectors need
to nd a way to control health care
spending — but to do it without harming
patients. The biggest barrier to higher-
quality, lower-cost care is that we don’t pay
physicians and hospitals for many services
that would help patients stay well, and the
fee-for-service payment system penalizes
providers nancially for achieving better
outcomes and avoiding unnecessary tests
and procedures.
Patient benet designs also tend to do just
the opposite of what is needed to support
higher-quality, lower-cost care. High cost-
sharing and high deductibles discourage
people from getting services that will
help them stay healthy, such as seeing a
primary care physician early when they
have a health problem and taking their
medications regularly. On the other hand,
if patients need an expensive procedure,
such as a knee replacement or a cardiac
stent, they will likely pay the same amount
whether they go to a high-cost provider
or a low-cost provider, because the cost
is typically well above their deductible or
out-of-pocket limit. So if they believe that
higher cost means higher quality (even
though evidence shows it doesn’t), they will
have a natural incentive to use the higher-
cost provider.
We need to start paying doctors and
hospitals for keeping patients healthy and
to reward them for delivering high-quality,
affordable care. And we need to change
benet designs so that patients also have
the ability and incentives to use lower-cost,
higher-quality services and providers.
You advocate for accountable payment
models. What are these?
An accountable payment model has
two main characteristics: exibility and
accountability. It gives providers the
exibility to decide what the patient
needs rather than limiting the patient to
narrowly dened procedures that a health
plan is willing to pay for. But in return,
the providers assume accountability for
delivering high-quality care at an equal or
lower cost than under traditional fee-for-
service payment.
Examples of accountable payment
models include:
•Bundled payments: making a single
payment to two or more providers
who are now paid separately, such as
physicians and hospitals
•Warrantied payments: paying providers
more for high-quality care, with no extra
payment for correcting preventable
errors and complications
•Condition-based payments: paying
providers based on the patient’s
condition, rather than based on how
many procedures were used to treat the
condition, so that providers have the
exibility to use fewer or lower-cost tests
and procedures if they will achieve the
same outcomes
Central to making these accountable
models work are physicians. I’ve found
that physicians in all specialties have ideas
for how to change care in ways that would
be better for patients and save money
for purchasers, but they need to be paid
in ways that support that. A challenge is
that it’s difcult to get physicians more
involved because they’re busy taking
care of patients. We need to support their
leadership in redesigning payment and
delivery systems and make sure they don’t
lose money by devoting time to this effort.
Feature
24 New horizons: voyage to value
“An accountable payment model
has two main characteristics:
exibility and accountability.”
Are there any payment models in
existence today that illustrate what
you describe?
I’ve seen several examples of how
accountable payment models can
signicantly improve quality and reduce
costs. For example, physicians and
hospitals that are being paid for surgeries
and procedures using bundles and
warranties have been able to redesign
care in ways that dramatically reduce
infections, complications and readmissions.
The patients get better care, the payers
spend less money for the care, and
the physicians and hospitals do better
nancially —a win-win-win.
There are other examples around the
country where multiple small physician
practices are working together through
an independent practice association (IPA)
to manage overall costs for a group of
patients. One multi-specialty IPA manages
global payment contracts from several
payers and has even created its own
Medicare Advantage preferred provider
organization (PPO) plan. The IPA pays its
primary care physicians 250% of what
Medicare pays because investing in strong
primary care has meant that patients need
fewer hospitalizations, enabling the group
to reduce total spending. Moreover, even
though patients in the PPO plan are not
restricted to using the physicians in the IPA,
most choose to do so because the different
payment structure for those physicians
has enabled them to provide better, more
coordinated care.
A lot of what is driving consolidation
of hospitals and physicians is the
continuing focus on price discounts
and “shared savings” models. You have
said that those structures are a barrier
to innovative care delivery. Why?
What should matter to payers is spending,
not price alone. If you demand large price
discounts under fee-for-service payment,
ahospital may be forced to try to increase
the number of services it delivers in
order to cover its costs. Conversely,
if we’re successful in reducing avoidable
hospitalizations, it may actually cost more
per patient to take care of the patients who
do still need to be hospitalized, but overall
spending will still be lower.
Discounts and shared savings don’t change
the underlying payment system, and that’s
what’s really broken. For example, we want
our hospitals to always be ready for us:
to have the emergency room open if we
need emergency care; to have a cath lab
that gives us a short door-to-balloon time
if we have a heart attack; to be prepared
if our community experiences a disaster.
But we don’t pay the hospitals for this
readiness —we pay only when the hospital
treats someone. So if we demand that
hospitals reduce the prices of individual
services they deliver, they’ll be forced to
look for ways to deliver more and more
services to make up for those discounts
and to cover that standby capacity.
“Shared savings” sounds like a collaborative
approach to payment, but it’s really not
because it doesn’t change the underlying
fee-for-service structure. If a hospital
or physician practice performs fewer
procedures, it will lose 100% of the revenue
for those procedures, but its costs won’t go
down proportionally. Telling providers that
a year from now they may or may not get
back a small portion of that money isn’t an
attractive nancial proposition, particularly
for a provider that is already operating on
thin margins.
How about accountable care
organizations — are they a step
in the right direction?
The concept of the ACO — providers
working together to manage the overall
cost and quality of care — is a good one,
but the problem is that most ACOs are
being paid fee-for-service plus shared
savings, which doesn’t really change
anything. Physicians and hospitals in
these models need to be paid differently
so they can actually redesign the way
they’re delivering care. “Coordination” is
only part of the answer. In a true ACO,
every physician in every specialty would
be looking for ways to redesign care for
higher quality and lower cost. That’s what
I call “building ACOs from the bottom
up” — changing how front-line providers
are delivering care instead of adding yet
another layer of management on top of the
same approach to delivery and payment.
In the marketplace today, we’re seeing
a lot more providers and payers
combining. How do you see that
working or not working in the future?
There are huge advantages if payers and
providers can work more closely together,
and many providers have found that
having their own health plan is a natural
way to achieve that. It’s more problematic,
though, when a large payer acquires one
provider or when a provider creates a
health plan that tries to sell insurance
covering other providers. In those cases,
the organization is trying to be two things
at once: a general health plan and a
general provider. If they’re trying to sell
two different products — health care and
health insurance — to two different sets of
customers, which is the most important?
The real goal should be to try to create a
closer connection between providers and
employers. A growing number of employers
are looking to do direct contracting with
25
provider organizations, and vice versa.
Any time you can take out the middleman,
you have a more efcient structure.
“The real goal should be to try
to create a closer connection
between providers and purchasers.”
How far along are we on the
timeline of moving from volume-
to value-based care?
I don’t think we’re very far, unfortunately.
Providers can’t redesign care for higher
quality and lower costs without a payment
model that supports that, but Medicare
and private health plans haven’t made the
payment changes needed to support them.
Too many payers are claiming that pay-for-
performance and shared savings programs
are “payment reforms” when they’re not.
We could go a lot farther a lot faster if we
enabled providers to implement different
payment models more rapidly than is being
done today. If the most innovative providers
can’t make any progress, we won’t have the
diffusion of innovation we need to really
change the system. With the right kind of
support, I think we could see a signicant
fraction of providers using new models
within ve years.
What other obstacles are standing in
the way of payment reform, and how
can they be hurdled?
First, we need a fundamental change in
how we view new payment and delivery
models. Many see them as a win-lose.
But they’re potentially a win-win-win for all
involved. The win for patients is better care;
for purchasers, it’s reduced spending or a
slower trend in spending; and for providers,
it’s a way for them to be more nancially
viable when they succeed in delivering
quality care.
At the Center for Healthcare Quality and
Payment Reform, we’ve identied 10
barriers to implementing health care
payment reforms, along with potential
solutions (see chart on the next page).
An overriding theme weaving through the
list of barriers is a general lack of trust.
In many cases, physicians don’t trust
hospitals, hospitals don’t trust physicians
and neither physicians nor hospitals trust
payers. And the true purchasers, the
employers, rarely if ever talk to the true
providers, the physicians and hospitals.
When employers actually talk with
providers, however, they typically nd that
their interests are more aligned than they
thought. One employer coalition that has
started talking directly with physicians told
me, “We’ve found that the care we want
to buy is what the physicians want to sell.”
That kind of conversation can lead to the
win-win-win we’re all looking for.
Because of the lack of trust, it helps to
have a neutral convener. A growing number
of communities are fortunate enough to
have a multi-stakeholder regional health
improvement collaborative that can
bring purchasers and providers together,
facilitate their discussions and also provide
the trusted data needed to create win-
win-win changes in payment and benet
designs. People who don’t have one in their
community should form one, and those who
do have one should support and use it.
How can executives and board members
in provider and payer organizations
best support accountable payment
models at their organizations?
Providers need to develop a vision of their
future that’s aligned with where the country
needs to go. In the years ahead, a smaller
hospital as opposed to a larger one may
be the mark of success if fewer patients
coming to your hospital means you’re doing
a better job of improving the health of your
community’s residents.
If hospitals and physicians improve their
ability to keep people healthy, affordably,
they can be an essential catalyst in
the economic development of their
communities. A healthier workforce and
lower health insurance premiums will draw
more employers to a community; more
jobs and higher-quality, more affordable
health care will draw more residents. As a
result, hospitals will grow, but in a different
way — not because they’re hospitalizing
a higher proportion of the community’s
residents, but because the population
of the community is growing.
“Unlike other industries, success
in health care means selling less
products and services, not more.”
It will be difcult to get health insurers
to implement new payment models unless
they think it’s good for their business,
too. Payers will need to spend money to
negotiate new contracts with providers and
implement new payment systems, yet most
of the savings will go back to their self-
insured employer customers. There won’t
be a direct return on investment for the
insurer unless employers begin to demand
the use of accountable payment models,
so that health plans that truly commit to
and invest in these models will retain and
gain customers.
Bottom line: unlike other industries, success
in health care means selling less products
and services, not more. It’s a different
mindset, requiring an entirely different
payment system for future sustainability.
26 New horizons: voyage to value

10 barriers to implementing health care payment reforms — and how to overcome them
Barrier Solution
1. Continued use of FFS
payment in payment
reforms
• Use episode-of-care payments, condition-based payments, and risk-adjusted global payments
to eliminate undesirable incentives under fee-for-service and to give providers the exibility
and accountability for reducing costs and improving quality
2. Expectation that
providers will be
accountable for costs
they cannot control
• Use risk adjustment and risk limits to keep insurance risk with payers but transfer performance
risk to providers
• Use risk exclusions to give providers accountability only for the types of costs they can control
• Make provisions for contract adjustments to deal with unforeseen events
3. Compensation of
physicians based on
volume, not value
• Change physician compensation systems to match incentives under payment reform
• Modify federal and state fraud and abuse (F&A) laws to permit gain-sharing between hospitals
and physicians
4. Lack of data to set
payment amounts
• Give providers access to timely analyses of utilization and cost data through community multi-payer
claims databases
5. Lack of patient
engagement
• Ask patients to designate their primary care physicians rather than using statistical attribution
rules based on FFS claims to assign them retrospectively
• Use value-based benet designs to enable and encourage patients to improve health, adhere
to treatment plans and choose high-value providers and services
6. Inadequate measures
of quality of care
• Develop quality measures for all of the conditions and procedures that drive signicant amounts of cost
• Use outcomes measures instead of process measures to give providers exibility in redesigning care and
supporting effective patient choice
• Use regional health improvement collaboratives (RHICs) to collect patient-reported information
on outcomes
7. Lack of alignment
among payers
• Ask physicians and other providers to dene lower-cost, higher-quality ways to deliver care and
the payment changes needed to support them
• Encourage employers to support regional payment reforms and to choose health plans that will
implement them in a coordinated way
• Offer Medicare payment reforms to a broad range of providers on an ongoing basis
• Use state government and/or RHICs to facilitate agreement among payers
8. Negative impacts
on hospitals
• Reduce xed costs and improve efciencies in hospitals
• Change payment levels to hospitals to reect higher costs per admission that may accompany
lower admission rates
• Increase transparency about hospital costs to ensure that prices for hospital care are adequate,
but not excessive
9. Policies favoring large
provider organizations
• Remove anti-trust barriers to small physician practices joining together to manage new payment models
• Combat anti-competitive practices by large providers
• Avoid unnecessary standards for structure and processes in payment systems and accreditation systems
that increase costs and favor large organizations
10. Lack of neutral convening
and coordination
mechanisms
• Support the creation and operation of multi-stakeholder RHICs in all regions
Source: Center for Healthcare Quality and Payment Reform, “Ten barriers to implementing healthcare payment reforms and how to overcome them,” rst edition,
December 2012.
27

New horizons: voyage to value28

Viewfinders
Considerations for your board and executive leaders
For providers
•How are you managing the transition
from fee-for-service to value-based
payment systems? Are you prepared to
take on more responsibility for containing
costs while demonstrating continuous
improvements in patient outcomes?
Do these plans include educating
physicians and staff on the implications
of value-based payment?
•Are you seeking out payers who are open
to value-based contracts? What service
lines best position your organization
for a value-based bundled payment
arrangement?
•If you are considering forming a provider-
sponsored plan, have you evaluated risk,
regulatory concerns and market position?
•Have you identied opportunities
for reducing waste, determining
which clinical areas can benet from
increased standardization and evidence-
based practices?
•Are you building value-creating
partnerships with your physicians? Are
you engaging physicians in developing a
true accounting of all costs and the value
of each step involved in a procedure?
Is physician compensation tied to value,
efciency and quality?
•Have you assessed the effectiveness
of your admission, discharge and
transfer protocols?
•What measures have you taken to
enhance your organization’s ability to
reduce hospital-acquired conditions and
readmissions and improve other key
performance measures?
•Have your nancial metrics and
management reporting tools changed
to adapt to new models of care, with
broader metrics that include all aspects
of the care continuum?
For payers
•Are you working with providers to
develop new models of care that put
incentives in the right place — and ensure
the care delivery changes providers
would like to see are incorporated
into revised nancial structures? Are
incentives large enough to drive changes
in provider behavior?
•Does your value-based payment model
consider your current and future
technology base, including automation
and scalability?
•Have you developed scalable payment
models that can be implemented
seamlessly, along with toolkits providers
can use to help them succeed under
these models?
•How are you pursuing opportunities
to pool your data and combine it with
data from Medicare and Medicaid, to
facilitate analyses of health cost drivers
and enable a more granular assessment
of provider performance?
•Are you developing tools and support
that enable providers to deliver more
cost-effective care and track their
performance — for example, are member-
specic care alerts and care guidelines
integrated into physician workows?
•Are you embracing opportunities
to develop a more collaborative
relationship with providers by creating
the infrastructure for coordinated care
models that have more sophisticated
informatics and decision support systems
to assist providers in improving care and
reducing costs?
•Are you positioning yourself as a trusted
source for patients’ clinical and lifestyle
information needs, providing better
tools to help your members manage
their health?
29

{ }
“The art of the sailor is to leave nothing to chance.”
Annie Van De Wiele, 20th‑century Belgian author and voyager
31
Chapter 2
Value in delivery
Changing tack
Voyage to value
Providers and payers have a clear directive: to maximize health care
value for patients as they journey through the health care system.
For providers, that means planning and delivering the best possible
care, partnering across the care continuum through seamless teams
and making sure effective transitions take place. For payers, it means
collaborating with providers in new ways, and it means empowering
patients with coverage options that focus on high-performing providers
and with incentives for better managing chronic illness and for
maintaining health and wellness.
Just as sailing upwind requires a change in tack — back and forth across
the wind — health care organizations must be nimble in their voyage to
high-value care, ready to adjust their positions and approaches to adapt
to rapidly changing conditions.
Today’s move toward value-based care represents another
step in the evolution from isolated to integrated delivery.
Providers and payers are encouraged to work together at
unprecedented levels of collaboration. The new horizon
of care focuses on communicating fully with patients,
anticipating their needs and treating them before costly
complications occur. The journey forward also demands
developing new programs and services designed to keep
people healthy and help those with chronic conditions
better manage their own care. In this chapter, we provide
an overview of industry initiatives to improve care
coordination, optimize quality and safety, and enhance
the value of the patient experience.
Value in care management:
learning from emerging models
Historically, for US health care consumers,
the care experience has been a fragmented
one. As patients move from clinician
to clinician, they have struggled with
navigating complex waters. They may
be adrift in a sea of information, with
little guidance in making sense of it all.
This lack of coordination has added
unnecessary risks, as test results may not
be communicated accurately, prescriptions
from multiple physicians may conict, and
follow-up after hospital discharge may
be insufcient. Uncoordinated care has
also added costs to the system — through
duplicate or unnecessary testing and
services, overused intensive procedures
and preventable hospital readmissions.
Emerging models of care integration are
demonstrating how health care can be
delivered more seamlessly, accurately
and effectively, particularly for people
with chronic illnesses and complex needs.
Built on a foundation of strong clinical
and organizational support, these models
are designed to provide continuous,
well-coordinated care across health care
services and from acute to long-term
settings. As discussed in Chapter 1,
value-based payment models provide
incentives for coordinating care and
delivering value — and encourage patients
and their support networks to be the center
of care planning and delivery.
Evidence-based care and
standardized practice guidelines
Providing high-value care hinges on having
the best information on what treatment
works best for which patient, and under
what circumstances. Evidence-based
protocols can help providers diagnose
and treat various conditions — enabling
care to be standardized yet tailored to
unique patient needs. Integrated within an
electronic health record, these protocols
automatically provide clinicians with the
best evidence about a particular condition
as well as a pathway for decision-making.
A scan of the health care horizon nds
many initiatives focused on evidence-based
care. For example:
•At Boston Children’s Hospital, the
hospital’s cardiovascular department
developed standardized clinical
assessment and management plans
(SCAMPs) in 2009. SCAMPs are
described as practical and exible tools
for “narrowing practice variability” while
still enabling providers to use their
clinical judgment and adapt treatment
pathways to individual patient needs.
Since the program’s creation, more
than 12,000 patients have been
enrolled in 49 SCAMPs in pediatric and
adult medicine, and 19 institutions are
currently collecting SCAMPs data.
•Kaiser Permanente’s Healthy Bones
Program identies and proactively treats
patients at risk for osteoporosis and hip
fractures, using standardized practice
guidelines for managing osteoporosis.
Patients are treated in accordance with
the latest clinical evidence, provided with
osteoporosis education and supported
through at-home care programs.
According to Kaiser, the program has
reduced hip fracture rates over ve years
by an average of almost 50%.
•Virginia Mason Medical Center in Seattle,
WA, incorporated evidence-based
decision rules into provider workows
at the point of ordering an advanced
imaging test to reduce variability. If the
provider cannot cite an appropriate
evidence-based decision rule, the test
cannot be ordered. The medical center
reports this initiative has resulted in
32 New horizons: voyage to value
reduced delays for necessary imaging,
as well as no unnecessary tests and
substantial decreases in imaging use.
The team approach
Just as teamwork is crucial in sailing —
requiring all crew members to skillfully
perform their assigned tasks — a high-
performing team in health care is essential
to achieving a more patient-centered,
coordinated and effective health care
delivery system (see Exhibit 2-1 on
page 34). The concept has been advanced
through the ACA and such initiatives
as the Patient-Centered Primary Care
Collaborative and the Interprofessional
Education Collaborative, as well as
exemplary programs in individual health
systems such as:
•Daily huddles: In Ohio, the Cleveland
Clinic’s care enhancement program for
lung transplant patients calls for daily
huddles of caregivers, patients and their
families. The goal is to keep all informed
of each patient’s prognosis and recovery
and enable development of a cohesive
care plan. According to the Clinic, the
program has reduced costs and lengths
of stay, improved survival rates, and
enhanced patient satisfaction with
clinician communication by nearly 30%.
•Multidisciplinary rounds: In Texas, at the
MD Anderson Cancer Center, integrated
teams coordinate several specialties to
develop a comprehensive cancer care
plan. Disease-specic centers have
multidisciplinary meetings to discuss
new and complex cases and also conduct
multidisciplinary rounds. Team members
coordinate care through an electronic
health record that the patient can
also access.
“The clinician operating in isolation
is now seen as undesirable in health
care — a lone ranger, a cowboy, an
individual who works long and
hard to provide the care needed,
but whose dependence on solitary
resources and perspective may put
the patient at risk.”
IOM
“Core Principles & Values of Effective
Team -Based Health Care”
October 2012
•Collaborative care units: In Wisconsin,
community health system ThedaCare
leverages collaborative care units that
organize care delivery around the
patient’s experience. When a patient is
admitted, an interdisciplinary care team
coordinates with him or her to agree on
Value vignette
The VALUE framework: teaching value to future physicians
Teaching hospitals, academic medical
centers and residency programs have a
useful tool for training future physicians
in delivering high-value care: the VALUE
framework. The tool was developed by
Mitesh Patel, MD, a physician and Robert
Wood Johnson Foundation Clinical
Scholar, along with colleagues at the
Perelman School of Medicine at the
University of Pennsylvania.
VALUE is an acronym for 1) validation
and variability, 2) affordability and access,
3) long-term benets and less side effects,
4) utility and usability and 5) effectiveness
and errors. According to the tool’s
developers, this framework can be used
with physicians in training to assess the
benets of medical interventions, from
tests and medications to surgeries.
Patel points to ndings that less than
half of medical students feel they are
appropriately trained in health care
policy topics, such as medical economics.
Residents can use VALUE, he notes, as
they’re seeing patients to select those
options that generate high value and
reduce unnecessary costs.
“Training residents to practice
medicine using concepts of value-
based care is like learning a new
language for both residents
and their teachers. The VALUE
framework can bridge this gap and
become a useful tool for improving
the care of our patients.”
Mitesh Patel, MD
Robert Wood Johnson Foundation
Clinical Scholar
Source: University of Pennsylvania news release, http://www.uphs.upenn.edu/news/news_releases/2012/08/value/; Journal of General Internal Medicine,
September 2012; www.amednews.com/article/20120919/profession/309199996/8/
33
a care plan. ThedaCare reports that the
program has reduced hospital lengths of
stay, errors in patient care and inpatient
care costs by 25%, while improving
provider compliance with care protocol
and achieving a patient satisfaction rate
of 5out of 5, 95% of the time.
As discussed in Chapter 3, robust health
information technology (HIT) is essential
to a team-based approach — enabling the
care team to share and act on patient
information among disparate care
providers. Technology also supports team-
based care through advanced analytics to
identify and manage risk, real-time clinical
analytics at the point of care and online and
mobile applications that engage patients
between ofce visits.
From medical homes to medical
neighborhoods
The patient-centered medical home
(PCMH) model continues to show
promise as an anchor for patient care.
The National Committee for Quality
Assurance (NCQA) has recognized more
than 37,000 clinicians at more than
7,500 sites throughout the country in
its PCMH program (see Exhibit 2-2).
Today, the focus on the medical home
model has expanded to include “medical
neighborhoods” —dened by the Patient-
Centered Primary Care Collaborative
(PCPCC) as a “clinical community
partnership.”
“[A successful medical neighborhood
will] focus on meeting the needs
of the individual patient, but also
incorporate aspects of population
health and overall community
health needs.”
AHRQ
“Coordinating Care in the Medical Neighborhood:
Critical Components and Available Mechanisms”
June 2011
Exhibit 2-1. Five principles of team-based health care
Principle The team
1. Shared goals Sets shared goals that reect patient and family priorities and
can be clearly articulated, understood and supported by all
team members
2. Clear roles Has in place clear expectations for each team member that can
optimize team efciency and facilitate division of labor — so
that the team can accomplish more than the sum of its parts
3. Mutual trust Engenders trust, creating strong norms of reciprocity and
greater opportunities for shared achievement
4. Effective
communication
Prioritizes and continuously renes its communication
skills, with consistent channels for candid and complete
communication that are used by all team members across
all settings
5. Measurable
processes and
outcomes
Agrees on and implements reliable and timely feedback on
how the team functions and achieves its goals, and uses this
feedback to track and improve performance immediately and
over time
Source: Adapted from Pamela Mitchell et al., “Core Principles & Values of Effective Team‑Based Health
Care” (IOM discussion paper), October 2, 2012.
Exhibit 2-2. NCQA PCMH growth, 2009–14
28 383
1,606
3,302
5,198
6,762
7,525
37,757
34,492
24,544
16,194
7,676
1,976
214
4/1/20144/1/20134/1/20124/1/20114/1/20104/1/2009
Sites
Clinicians
Source: NCQA, 2013.
34 New horizons: voyage to value

According to PCPCC, medical neighborhoods
include the medical and social supports
needed to enhance health, with the PCMH
serving as the patient’s primary hub
and coordinator of health care delivery.
Beyond the medical home, neighbors in
the medical neighborhood range from
hospitals and specialty clinics to health
plans and ancillary service providers that
are part of the continuum of care. All work
together to enable PCMHs to reach their
full potential in improving patient outcomes
and managing population health.
Patient-centricity: enhancing the
customer experience
To transition from FFS to value-based
reimbursement models, health care
organizations are becoming more patient-
centric — at the individual and population
levels. Through providing ongoing
education, proactive prevention measures
and a consistently positive customer
experience, providers and payers can help
patients become better advocates for their
own health.
“We need to ip from focusing on
the medical condition to focusing
on the patient.”
Maureen Bisognano
President and CEO
Institute for Healthcare Improvement
Many aspects of health reform effectively
mandate patient centricity. The Hospital
Consumer Assessment of Healthcare
Providers and Systems measures the
quality of caregiver-patient interactions,
and payment is based in part on patients’
perceptions of their hospital care. The
success of the Hospital Readmissions
Reduction Program (see Chapter 1,
page 18) and ACOs also hinges on keeping
patients connected to providers. Patient-
centric initiatives are varied and numerous.
For example:
•Bedside communications: In Michigan,
Spectrum Health has installed an
interactive care console with the goal of
enhancing communication at the patient
bedside. The console integrates medical
information with customizable features
through which patients can learn more
about their medical conditions. It also
serves as a tool to help patients adhere
to recommended treatment plans.
•Chief experience ofcer: In Ohio,
the Cleveland Clinic has created the
position of chief experience ofcer
to determine what changes would
improve the patient’s physical and
Value vignette
The Joslin Diabetes Center: creating a value-driven model
The Joslin Diabetes Center in Boston,
MA — afliated with Harvard Medical
School since its founding in 1898 — is
the world’s largest diabetes research and
clinical care organization. It is focused on
providing efcient, coordinated care for
24,000 patients with diabetes.
A value-driven model for helping contain
and manage chronic disease, Joslin
follows dened principles to create a
streamlined treatment system. A full
range of diabetes services are provided
in a single location, with convenient
scheduling and easy access to related
medical services. Adult and pediatric
patients can be seen by a team of
medical experts — an endocrinologist,
ophthalmologist, podiatrist and
diabetes educator — all in the same day.
Electronic medical records keep track
of quality results.
Joslin’s team care has resulted in
dramatically improved outcomes and
lowered costs. For example:
•Early intervention has decreased late-
stage blindness from 60% to about 1%
•Patients cared for at Joslin incur on
average $1,465 less in total health
care costs each year
“[Joslin] represents an evolution …
from care delivered reactively
at high cost to care delivered
proactively and preventatively,
which reduces longer-term
costly complications.”
Ranch C. Kimball
Former CEO
Joslin Diabetes Center
Through its “Joslin Inside” program,
Joslin works with US and worldwide
afliate organizations to provide care,
education and tools for patients to
manage their own diseases. Another
program, “Joslin Everywhere,” leverages
mobile apps and decision-support
algorithms to provide patients with
avirtual care experience. Joslin is also
teaming with American Well™ in a global
telehealth initiative that brings diabetes
care to patients at home.
Sources: Harvard Business School, www.hbs.edu/centennial/businesssummit/healthcare/value‑based‑health‑
care‑delivery.html; Diabetes Mine, www.diabetesmine.com/2013/04/behind‑the‑scenes‑with‑the‑ceo‑of‑
joslin‑diabetes‑center.html
35
emotional experience. One of the rst
actions the ofcer recommended was
redesigning patient gowns to make them
more “dignied.”
•Care experience working groups:
In Pennsylvania, UPMC has developed
a six-step methodology and practice
to deliver ideal care experiences
and improve clinical outcomes while
decreasing waste and costs. Working
groups and project teams strive to
identify — and close — the gaps between
current and ideal care experiences.
The program has been adopted by
numerous health care organizations
outside of UPMC, nationally
and internationally.
“The most important predictor
of patient loyalty is a patient’s
condence in their provider.
Practices that foster trust between
providers and patients not only
can attract new patients, but
will also optimize the impact of
[patient satisfaction scores] and
value-based payments.”
Thomas H. Lee, MD
Chief Medical Ofcer
Press Ganey
Advances in home care
As technology enhances the ability to treat
illness at home, as well as to remotely
monitor and coach patients on health,
home care is coming of age. According
to home care management industry
statistics, 12 million patients are receiving
home health care services, with more
than 428 million patient visits each year.
About 70% of those using these services
By the numbers
• Between 2013 and 2025, the
population over 65 years will grow
by close to 45%; the number of
patients with chronic diseases will
increase between 21% and 27%;
and demand for adult primary
care services will increase by
14% (source: Health Affairs,
November 2013).
• More than 15% of patients are likely
to leave their current physician and
practice, according to a recent survey
(source: Press Ganey, “Protecting
Market Share in the Era of Reform:
Understanding Patient Loyalty in
the Medical Practice Segment,”
December 10, 2013).
• The average American is 25 pounds
overweight and does not exercise
(source: Centers for Disease Control
and Prevention, 2014).
• In improving population health
management, lifestyle and wellness
coaching is the most popular resource
to invest in, a recent survey nds.
More than 71% of survey respondents
indicated their hospital invested in this
resource (source: Premier, 2013 Fall
Economic Outlook report).
• The average American visits the
doctor three times a year but spends
52 hours a year searching for
health information on the internet
(source: Makovsky Health and Kelton,
third annual national consumer
survey, 2013).
• About 1 in 25 hospital patients
acquired an infection during his or her
stay in 2011 (source: S. Magill et al.,
“Multistate Point-Prevalence
Survey of Health Care — Associated
Infections,” New England Journal
of Medicine, March 27, 2014).
• Nearly 4 in 10 hospitalists responding
to a survey from Johns Hopkins
University School of Medicine said
they struggle with unsafe workloads
at least once a week. Almost a
quarter believed their workload “likely
contributed” to patient complications
and even deaths. Most of them
dened a safe workload as up to 15
patients per shift (source: Henry J.
Michtalik et al., “Impact of Attending
Physician Workload on Patient Care:
A Survey of Hospitalists,” JAMA Intern
Med., 173(5), 2013, pp. 375-377).
• According to the American College
of Healthcare Executives (ACHE),
turnover among hospital CEOs rose to
20% in 2013 — the highest it has been
since ACHE began compiling data in
1981 and 3% higher than in 2012
(source: ACHE, 2014).
• Two-thirds of hospital CEOs hired in
2014 will come from a non-health
care background, according to a
poll of more than 1,400 human
resources professionals at health care
organizations (source: Black Book
Rankings poll, December 18, 2013).
36 New horizons: voyage to value
are age 65 and older, most being treated
for heart disease, diabetes and cerebral
vascular diseases.
Leading health care providers reect
a range of home care approaches.
For example:
•The Hospital at Home® model, developed
by researchers at the Johns Hopkins
Schools of Medicine and Public Health
in Baltimore, MD, provides home care
as a full substitute for acute hospital
care. Patients who meet specic medical
eligibility criteria can receive hospital-
level care — including diagnostic tests
and treatment therapies from physicians
and nurses — at home. Clinicians and
pharmacists visit daily to coordinate
the medical care plan and work with
family caregivers, while teleheath nurses
provide additional support remotely.
The program has been adopted by
numerous health systems, home care
providers and managed care programs
as a tool to cost-effectively treat acutely
ill older adults.
•At Partners HealthCare in Massachusetts,
the Connected Cardiac Care Program,
aself-management and telemonitoring
program, helps patients with heart
failure manage their health at home.
Through advanced care coordination,
patient education and technology,
patients can report their weight, blood
pressure, heart rate and symptoms daily
to telemonitoring nurses — reducing
the need for trips to the hospital.
In its 10 years in operation, the program
has yielded an estimated $10 million
in savings and a 51% reduction in
hospital readmissions for patients
with heart failure.
Value vignette
Mobile apps: adding value to wellness programs by engaging consumers
As the industry shifts from volume- to
value-based reimbursement models,
payers have a greater nancial stake
in keeping members healthy. More
health plans are turning to mobile
apps to engage patients in their own
care and offer incentives for adopting
and maintaining healthy habits. Many
are using digital health trackers and
tness apps to create positive customer
experiences and inuence healthy
behavior choices. For example:
• Aetna’s What’s Your Healthy?
campaign features a fully integrated
consumer website and mobile
platform, CarePass, through which
consumers can track health and
wellness apps conveniently from one
online hub. CarePass connects apps
on its platform, enabling users to
manage their tness and set health
and wellness goals.
• CareFirst Blue Cross Blue Shield’s
Ready, Step, Go! app lets users count
steps, distance traveled and calories
burned for each workout.
• Cigna and MyFitnessPal, a free
personal health and tness resource,
have joined forces to combine Cigna’s
health coaching programs with
MyFitnessPal’s nutrition, physical
activity and weight management
resource. Customers can connect
their MyFitnessPal accounts with
their coach to share their diet and
exercise activity. Coaches can view a
participating user’s progress and offer
advice and support.
• Humana t for Android uses the
built-in GPS of mobile devices to track
tness activities.
• Kaiser Permanente has created
several mobile apps to help its
members better manage their diet
and exercise programs, including
Mix It Up, an online nutrition program;
Thrive Across America, a physical
activity challenge; Everybody Walk!,
a personalized walking program; and
KP Preventive Care, an app offering
personalized health reminders.
• UnitedHealthcare’s NOT ME diabetes
prevention program helps customers
at risk for developing type 2 diabetes
to eat healthier, exercise and lose
weight. OptimizeMe, another United-
Healthcare app, lets users track health
and tness goals and share them on
social networks.
“Any time you engage a consumer,
you’re not only going to help that
consumer live a healthier life,
you’re going to help the payer
lower their costs as well.”
Nick Martin
Vice President of Innovation
UnitedHealthcare
Speaking to FierceHealthIT
Sources: FierceHealthIT, www.ercemobilehealthcare.com/slideshows/payers-invest-mhealth-7-mobile-
health-and-wellness-apps; www.ercehealthit.com/special-reports/unitedhealthcare-reward; HuffPost Healthy
Living, www.hufngtonpost.com/shaan-gandhi/smartphones-health_b_4450403.html
37
•At Virginia Commonwealth University
Medical Center in Richmond, the House
Calls program has reduced hospital
costs for patients with multiple chronic
conditions by 60%. Described as a
“doctor’s ofce on wheels,” it serves those
who can’t easily come to the medical
center for scheduled appointments.
Patient safety: taking action
Preventing harm is fundamental to
delivering high-value care, and the industry
continues to move forward in improving
patient safety. Through system-level
initiatives, such as procedures to guide
the delivery of care, checklists and care
protocols, and tools built into the electronic
health record (EHR) to help reduce errors,
health care organizations are striving to
create an environment that guards against
human mistakes and supports a culture
of consistently reliable care.
“An institution could have the best
surgeons in the world, but if the
aftercare is lacking and the patient
develops an infection as a result,
then the hospital has failed to
protect its patient.”
Leah Binder
President and CEO
The Leapfrog Group
A May 2014 report from HHS indicates
these efforts are beginning to show results:
a 9% decrease in harms experienced by
patients in hospitals in 2012 compared
with the 2010 baseline and an 8%
decrease in Medicare fee-for-service
30-day readmissions. The report estimates
that national reductions in adverse drug
events, falls, infections and other forms
of harm have prevented nearly 15,000
deaths in hospitals as well as 560,000
patient harms — and saved $4.1 billion
in costs in 2011 and 2012. HHS credits
these improvements to “strong public-
private partnerships, active engagement
by patients and families, and a wide
range of aligned federal programs and
initiatives —including new tools provided
by the Affordable Care Act — working in
concert towards shared aims.”
Recent improvements in patient safety are
cited also in the Leapfrog Group’s spring
2014 update. The report notes nearly
one in three hospitals improved its safety
scores by 10% since 2012, most through
safer practices and processes. Of the
2,522 scored hospitals, 804 received an
A in safety, 668 a B, 878 a C, 150 a D
and 22 an F. States with the highest
percentage of A hospitals were Maine
(74%), Massachusetts (70%), South Dakota
(67%), Illinois (57%) and Hawaii (50%).
The Leapfrog Group notes, however, that
alongside improvement in many hospital
scores, other hospitals — some with national
name recognition — continue to have a poor
safety record.
The approaching implementation of a key
ACA provision is also ramping up safety
initiatives. The law requires that, starting
in 2015, hospitals with more than 50 beds
Value vignette
Four guidelines from the Lucian Leape Institute: helping patients feel valued
A new report from the National Patient
Safety Foundation’s Lucian Leape
Institute offers four recommendations
for improving patient engagement:
1. Core values: Make engagement a core
goal and value for your organization.
Create standards of dignity and
respect for all. Implement policies
that facilitate patient engagement,
such as providing open access to
clinical records and establishing open
visitation policies.
2. Patient and family participation:
Involve patients and their families in
designing and improving care. Invite
them to serve on safety, quality and
personnel review committees.
3. Staff training: Train all staff in patient
and family engagement. Enable
clinicians to learn from patients and
families about the experience of
illness, as well as the communication
skills needed in patient/family
partnerships, shared decision-making,
and disclosure and apology.
4. Community collaboration: Raise
public awareness by collaborating
with community and patient advocacy
groups. Inspire a strategic alignment
across the communities of health
care consumers and advocates, policy
makers, researchers and health care
leaders and clinicians to commit to
increasing patient engagement and
reducing harm.
Source: Lucian Leape Institute, “Safety Is Personal: Partnering with Patients and Families for the Safest
Care,” 2014.
38 New horizons: voyage to value
that want to contract with a health plan in
the ACA’s insurance exchanges participate
in a patient safety organization (PSO).
They will also be required to establish a
patient safety evaluation system, dened
as “the collection, management, or analysis
of information for reporting to or by a
patient safety organization.” In addition
to complying with the law, participating
in a PSO can increase internal reporting
and knowledge about adverse events and
enable providers to better collaborate in
preventing medical errors.
“We are on the cusp of the golden
age of healthcare delivery.”
George C. Halvorson
Former Chairman and CEO
Kaiser Permanente
From silos to synergies: rounding
the cusp
The voyage to value-based care is an effort
that calls for all hands on deck. Health care
providers and payers must continue to
eliminate silos, create synergies and align
strategies, structures and practices for
delivering value to patients through the full
cycle of care. The ultimate destination is a
patient-centric system — one of relentless
collaboration to improve health outcomes,
keep people healthy and enhance the
care experience.
Value vignette
Mobile health clinics: delivering value in serving high-risk populations
Each year, mobile vans and clinics
provide health services to an estimated
7.5 million people, targeting those
who typically do not have a physician
or insurance, or are otherwise outside
the conventional health care system.
According to the Mobile Health Clinics
Association, 2,000 mobile health
clinics are currently operating in the US.
For example:
• In California, Napa’s St. Joseph Health
invests $5 million each year in mobile
health clinics, about 11% of which is
offset by reimbursements.
• In southeastern Massachusetts and
East Bay, RI, Southcoast Health
System’s mobile health system serves
seniors, teens and families who do not
have access to medical care.
• In Virginia, Bon Secours Health Systems
has had mobile clinics since 1984.
The initiative was recently expanded
with a fth mobile clinic — and plans
for a sixth focused on nutrition in areas
lacking access to healthy foods.
• The Family Van program based
at Harvard Medical School has
demonstrated a return on investment
of $36 for every $1 spent.
• Breathmobile, a group of mobile
asthma clinics, provides free care to
underserved children in different cities
across the nation.
Most mobile units are run by hospitals,
medical centers, public health
departments, community health centers,
private foundations and faith-based
organizations. Many nonprots have
funds set aside for mobile vans as part
of their community benet requirements.
Proponents note that mobile units
can reduce ED visits and keep chronic
conditions from advancing to the degree
where patients need higher-cost care.
Trust for America’s Health, a health
advocacy organization, has shown a
return of $5.60 for every $1 spent
on prevention.
Source: Healthcare Finance News, www.healthcarenancenews.com/news/mobile-health-vans-value-proposition, H&HN Magazine, May 2014
39
Value vignette
Value centers: focusing on solutions
“Think tanks” for health care value serve
as resource hubs for advancing value-
driven health care solutions. Proled
below are ve leading centers.
Colorado Center for Improving
Value in Health Care (CIVHC)
Denver, CO
Created in 2008 by Executive Order
of the Governor, CIVHC is a nonprot
organization designed to advance
statewide initiatives for improving
Colorado’s health care quality and
containing costs. It is funded by some
of the state’s leading health foundations.
With a 28-member board of directors
and a broad base of support from
more than 60 organizations statewide,
CIVHC convenes diverse constituencies of
consumers, providers, payers, businesses,
policy makers and government
agencies to work together in improving
value across the health care system.
The organization also administers an
all-payer database.
Mayo Clinic Robert D. and Patricia E. Kern
Center for the Science of Health Care
Delivery (CSHCD)
Rochester, MN
Established in 2011, the CSHCD is
focused on the science of care delivery.
Combining data analysis, health care
engineering principles and health care
delivery research, the center tests
theories, models and methods to
determine if they can improve patient
care, outcomes and cost. The center
includes ve major programs: Value
Analysis, Health Care Delivery Research,
Health Care Systems Engineering,
Population Health Science and Surgical
Outcomes. Each program plays a role in
the center’s quest to improve patient care
while working to contain costs.
University of California, San Francisco
(UCSF) Center for Healthcare Value (CHV)
Launched in early 2013, the UCSF CHV
is designed to advance rational, science-
driven and clinician-tested health care
solutions that improve health care value.
Its work includes initiatives in delivery
systems, research and policy, and training.
For example, through its Caring Wisely
campaign, CHV is working with delivery
system leaders to inspire and support
front-line proposals that lower health
care costs. Another initiative, the
Action Research Program, partners a
multidisciplinary team of implementation
scientists and medical students with a
clinical practice to help design and test
new system strategies for care delivery.
The UPMC Center for High-Value
Health Care (CHVHC)
Pittsburgh, PA
A nonprot organization owned by UPMC,
CHVHC translates the work of UPMC
into evidence-based practice and policy
change for improving health care quality
and efciency. Many CHVHC activities
are supported through grants and
contracts and conducted in partnership
with community organizations and
government agencies. Representative
projects range from expanding the
patient-centered medical home model
to addressing the unmet medical needs
of adults with mental illness.
Wisconsin’s ThedaCare Center
for Healthcare Value (TCHV)
Appleton, WI
TCHV is focused on improving value for
patients by collaborating with patients
and leaders in the provider, employer,
payer and government communities.
TCHV reports that, combined, its
61 member hospitals have eliminated
millions of dollars of waste and thousands
of defects in medical processes within
their organizations. These lean provider
health care organizations often become
“centers of value” sought out by employers
seeking high-quality outcomes and
competitive prices.
Source: Program websites.
40 New horizons: voyage to value

Viewfinders
Considerations for your board and executive leaders
For providers
•How is your organization integrating care
to provide value? What technologies and
analytics are you applying to support
integrated care? How are you pursuing
strategies to align physicians and manage
care beyond your walls?
•What procedures are in place to
continuously monitor patient ow,
occupancy and stafng levels for each
major service line?
•How are you treating your patients like
valued customers? Are you offering
patients decision aids that clearly
outline the risks and benets of
medical interventions — and help them
make choices that are consistent with
their preferences?
•How do you dene the patient care team
and ensure that each step in a patient’s
plan of care is delivered by the most
appropriate team member? How are
you assessing which care setting is most
cost-effective and appropriate to the
patient experience and outcome? What
tools are being provided to your clinicians
to aid in communicating complex
medical information to patients and their
families — and to engage patients as
fully informed, active decision makers in
planning and receiving care?
•What procedures are in place to ensure
optimal care transitions within hospital
units and between the hospital and
community sites?
•Have you considered adding a chief
experience ofcer to your executive
leadership team?
•How are you collaborating with post-
acute entities to make sure patients are
compliant with treatment plans? What
steps do you take to transfer discharge
and follow-up instructions, along with
treatment plans, to the appropriate post-
acute community providers?
•Do you have evidence-based care
protocols for all your common and
highest-cost conditions and procedures?
If all are not yet in place, what is your
strategy for lling these gaps and
keeping others current?
For payers
•What initiatives are in place to let your
members know they are valued? Do you
survey individual members as well as plan
sponsors to determine how well the plan
meets the personal needs of each insured
individual and the sponsor organization’s
overall employee health goals?
•How are you providing physicians with
information? Are you participating
in development of evidence-based
care protocols with health systems
or physician groups in your market
area, sharing your information to help
them in identifying best practices for
their population?
•How are you supporting members
with information? Do you have a
customer portal where patients can
view their specic claims information
and access generic health education
and disease management information?
Do you provide health coaching as an
option, with coaches able to access a
customer’s specic relevant data (with
the customer’s consent) in order to make
personalized recommendations?
•Are you advancing value in delivery
by empowering members with
coverage options that focus on high-
performing providers?
•What incentives are you offering
customers for managing chronic
conditions and for maintaining health
and wellness?
•Does your organization track
developments in telemonitoring and
eHealth initiatives and participate in
demonstrations of these products
to determine whether they are a
cost-effective strategy for reducing
readmissions or otherwise lowering
the cost of care? When such initiatives
are proven benecial to the delivery
of quality care and cost-effectiveness,
how do you incorporate them as part
of your plans’ benets and inform your
customers of their availability?
41

{ }
“The winds and the waves are always on the side
of the ablest navigators.”
Edward Gibbon, 18th‑century British historian

43
Chapter 3
Value in information technology
Supporting the journey
Voyage to value
In the voyage to value, HIT — and the data it yields — serves as ballast,
holding the ship steady in its journey forward. HIT supports a full range
of value-based goals, from improving quality and outcomes to assisting in
clinical decision-making, developing evidence, tracking costs, enhancing
coordination and facilitating patient engagement. New systems and
capabilities have proliferated, making it possible to collect outcomes
data, analyze and convert it into useful information and share the
information broadly with industry stakeholders.
To maximize the value of HIT, health care information technology (IT)
staff are moving far beyond installing, supporting and repairing
computer hardware and software. They are aggregating and reporting
health data, delivering information needed by various clinical areas of
their organizations and educating clinicians in how to make the most
meaningful use of the data available to them. The ultimate goals are to
buoy improvements in care delivery and to optimize patient engagement.
Health care organizations must continue to invest
signicant capital — human resources, time and
money — in information systems design, implementation
and training. These investments in EHRs and other
health information technologies are essential to comply
with government mandates. As their implementation
becomes more widespread, and staff more skilled in
their use, many health care organizations are realizing
signicant value from their IT investments. The data
being captured today can yield salient insights into
achieving better care management, more effective and
efcient practices and improved outcomes. In this chapter,
we provide an overview of key HIT initiatives and their role
in value creation.
ICD-10 and EHR meaningful use:
pushing back the deadlines
With the latest delay in the deadline for
changing over to International Classication
of Diseases, 10th Edition (ICD-10), health
care chief information ofcers and IT staff
now face the imperative to complete and
continue readiness for this major transition.
At the same time, they need to balance this
effort with demands for time and resources
to meet upcoming deadlines for achieving
EHR Stage 2 meaningful use (MU).
The transition to value-based health care
strains IT capacity even further because
of the need for billing, management and
point-of-care patient information access to
support ACOs and other collaborative care
initiatives. Provided below is an update on
the status of these two major initiatives,
discussed in further detail in the roundtable
discussion at the end of the chapter.
ICD-10
Despite pleas for further delays from
several trade associations representing
various segments of the health care
provider industry, CMS stood rm on the
October 1, 2014, deadline for ICD-10
implementation — only to see Congress take
an opposing stance and impose a one-year
delay as part of the sustainable growth rate
(physician payment x) legislation in early
2014. CMS estimates that this one-year
delay could cost as much as $6.6 billion,
about 30% of what has already been
invested by providers, payers and vendors.
In March 2014, the American Academy
of Family Physicians released results of a
survey reporting that most major national
commercial health insurers were ready for
the transition to ICD-10 claims processing.
All surveyed payers have set up “ICD-10
preparedness pages” on their websites
dedicated to assisting providers with the
transition. Most reported that they were
currently testing systems coordination
with their larger clients — hospital chains
and large physician practices — and had
plans to move toward readiness testing for
small and individual physician practices
before October 1. The delay will help
those smaller provider organizations
achieve readiness in preparing for the
transition, now scheduled for no sooner
than October 1, 2015. But for those
organizations already well prepared to
transition, the delay will require new
demands, such as providing additional
or refresher training and managing the
requirements of two different coding
systems, to make sure clinicians and
IT staff comply with current ICD-9 system
requirements while still preparing and
training for the eventual switch.
“The delay is going to be disruptive
and costly for healthcare delivery
innovation, payment reform,
public health, and healthcare
spending, and uncertainty on the
implementation date only adds to
the disruption and cost.”
Coalition for ICD-10
Letter to CMS Administrator Marilyn Tavenner
April 11, 2014
While most health care providers already
have the IT infrastructure and systems
in place for the ICD-10 conversion,
testing the interaction of these systems
between providers and payers is crucial
before implementation. In February, CMS
announced that it would conduct “end-to-
end” testing for some selected providers,
followed by an announcement in March
that this testing would be scheduled for the
end of July. CMS requested more than 500
provider testing volunteers, but only 32 will
actually be chosen to participate. With the
delay in ICD-10 implementation, it is not
clear now when this testing will take place.
Many payer organizations had also planned
to conduct signicant system testing in
the spring and summer of 2014, leaving
time to work through any problems in time
for the prior October 1, 2014, transition
date. With the delay, payer system testing
schedules may be revised.
44 New horizons: voyage to value
For health care providers, a necessary
investment for efciently transitioning to
ICD-10 is providing training for clinicians
and information management staff, as well
as post-implementation processes to test
the effective use of ICD-10. Effectiveness
testing will identify specic re-training and
optimizing needs to help organizations gain
the most value from the conversion while
minimizing cash ow delays. Since much of
this training has already started, the delay
in the transition deadline requires providers
to assess how best to use the additional
year to achieve a successful transition.
There is no mandate to wait until October
2015 to put into practice the training that
has occurred or is scheduled near term.
Those providers most likely to succeed in
Value vignette
Beacon Community health IT pilot project: shining the light
Over three years, from 2010 to
2013, the HHS Ofce of the National
Coordinator for Health Information
Technology (ONCHIT) provided
$250 million of funding to 17 selected
Beacon Communities nationwide. The
communities selected had already made
progress using HIT as a foundation
for local improvement and innovation.
Funding was to be used to further
leverage the value of their HIT and health
information exchanges (HIEs) in better
coordinating patient care.
At the February 2014 Health Information
Management Systems Society (HIMSS)
conference, leaders from the Beacon
Communities and ONCHIT presented
results of the pilot project, along
with ways these programs could be
implemented in other communities.
The initiatives improved cost, quality
and population health, with measurable
results over the three-year period,
and tested innovative approaches
to performance measurement,
technology integration and care
delivery. The pilot project:
•Involved more than 8,500 health care
providers and 8 million patient lives
•Covered a variety of federal and state
value-based health care payment
initiatives, including:
•State Innovation Model activities in
Minnesota, Maine and Washington
•Comprehensive Primary Care
initiatives in Colorado, Ohio
and Oklahoma
•Pioneer ACOs in Maine, California
and New York
•Medicare Shared Savings
Programs in Indiana, Louisiana
and Pennsylvania
•Produced six “Beacon Nation
Learning Guides” covering such
topics as “Capturing High Quality
Electronic Health Records Data to
Support Performance Improvements”
and “Driving Clinical Transformation
in a Practice Setting with Health
Information Technology,” all of which
can be downloaded at no cost from
www.healthit.gov
Highlighted below are representative
results achieved by various Beacon
Communities:
•Pediatric asthma improvement with
the Cincinnati Children’s Beacon
team. Using a combination of clinical
interventions and alerts, the time
between utilizations increased from
173 days to 311 days for Medicaid high-
risk patients.
•Care transition initiative for emergency
services with the San Diego Beacon
team. Various initiatives — connecting
ambulances to EDs, providing patient
event notication to providers and
payers, and developing a Beacon
Community health information
exchange (HIE) that made patient
information available to providers
across systems at the point of care,
whether ED, hospital or clinic —
together resulted in a more than
fourfold drop in calls. Over a two-year
period, for a pre-identied group of
1,171 frequent emergency medical
service users, calls per month to 911
dropped from 3,077 to 690.
•Re-admissions reduced for patients
with chronic heart failure and chronic
obstructive pulmonary disease — and
patient and clinician satisfaction
improved — at Keystone Beacon
Communities (ve counties in
Pennsylvania). A web-based HIE was
developed by 24 organizations with
38 unique delivery settings, including
hospitals, long-term care (LTC)
facilities, physician practices, home
health agencies and a pharmacy.
The system has been used to publish
health information, share notications
and direct messages related to care
transitions, and develop a patient
portal. This HIE is now a nationally
available web-based service.
More information about the Beacon
Community Program can be found at
www.beaconcommunityprogram.com/
Source: www.healthit.gov/policy‑researchers‑implementers/beacon‑community‑program
45

asmooth transition, with minimal cash ow
delays, will be those that start practicing
ICD-10 documentation and coding skills
sooner rather than later. Physicians can
certainly document in ICD-10 terms, and
coders can dual-code sets of charts under
both ICD-9 and ICD-10 requirements,
to practice what was covered in training
and to minimize the need for extensive
retraining next year. With clinicians and
coders practicing ICD-10 standards, this
strategy will allow time to assess the
effectiveness of training to date, as well as
to identify specic weaknesses that require
retraining or refreshing between now and
October 2015. Practicing ICD-10 coding
and documentation over the next year will
help address major problems before the
transition date.
Health payers and providers can also use
the additional time for end-to-end testing
to conrm that systems are ready to
le and accept claims under the ICD-10
standards and that the exchange of data
through claims clearinghouses will go
smoothly. Efforts made now to test all
affected IT systems will help to minimize
the disruption in cash ow that can be
expected when ICD-10 conversion goes live.
EHR meaningful use
HIT teams were given a bit of breathing
room with CMS’ proposed rule, announced
May 20, 2014, to extend Stage 2 MU
through 2016, with Stage 3 pushed back
to 2017. Also provided is some exibility in
meeting Stage 1 or Stage 2 requirements
in 2014. As a result, the start of Stage 3
will be delayed until at least federal scal
year 2017 for hospitals and calendar year
2017 for physicians and other eligible
professionals. CMS and the Ofce of the
National Coordinator for Health Information
Technology (ONCHIT) decided to push
back the Stage 2 timeframe to allow more
time for Stage 3 preparation. During
the extended time, ONCHIT will focus on
helping health care providers meet Stage 2
requirements for patient engagement,
interoperability and health information
exchange. CMS and ONCHIT will also use
this time to collect and analyze Stage 2
data in order to make more informed policy
decisions for Stage 3.
“The phased approach to program
participation helps providers move
from creating information in Stage 1,
to exchanging health information
in Stage 2, to focusing on improved
outcomes in Stage 3. This approach
has allowed us to support an
aggressive yet smart transition
for providers.”
Robert Tagalicod, Director, Ofce of E-Health
Standards and Services, CMS
Jacob Reider, Acting National Coordinator
for Health Information Technology, ONC
Blog post, December 13, 2013
http://www.cms.gov/eHealth/ListServ_
Stage3Implementation.html
The proposed rule would provide additional
exibility by allowing eligible professionals
and hospitals to use the 2011 edition of
certied EHR technology (CEHRT), or a
combination of the 2011 and 2014 editions
of CEHRT, for the 2014 EHR reporting.
Providers would be able to attest to
meaningful use under the 2013 reporting
Value vignette
Connected providers: creating new lines in the “Old Line State”
Now in its fth year, Chesapeake Regional
Information System for our Patients
(CRISP) functions as Maryland’s state-
designated HIE. Hospitals and authorized
health care professionals access CRISP
more than 12,000 times a month for
real-time sharing of patient information.
Maryland’s efforts to establish an HIE
began before the federal government’s
efforts to stimulate adoption of EHRs
and HIEs. As Maryland Governor Martin
O’Malley explained, “Even before the
American Recovery and Reinvestment
Act authorized the Medicare and Medicaid
Electronic Health Record incentive
program, we took the lead and funded
our Maryland HIE efforts with $10 million
of state-level programs. The federal law
has continued to backstop our efforts.”
To date, 37 of the 46 acute care hospitals
in Maryland are using EHRs and all 46 can
share with other providers in real time.
CRISP has recently adopted an alerting
system aimed at reducing readmissions
by directing the most vulnerable patients
to the most appropriate follow-up care.
The system plans to increase the number
of users as well as clinicians’ ability to
access and use the data. CRISP has also
deployed a prescription drug monitoring
program to integrate prescription drug
use information in real time. As the
access point to Maryland’s Prescription
Drug Monitoring Program for health care
providers, CRISP can help providers track
potential drug abuse habits and connect
patients with treatment that could lower
potential future costs and enhance the
likelihood of recovery.
Source: www.crisphealth.org
46 New horizons: voyage to value
year denition and use the clinical quality
measures from 2013. Also, providers
scheduled to begin attesting to Stage 2 in
2014 could use the 2014 edition of CEHRT
to meet the 2014 Stage 1 objectives if they
attest that they ran into vendor problems.
The proposed rule also formalizes the
agencies’ plans to extend Stage 2 through
2016 and push back the start of Stage 3
until 2017, as previously announced
last December.
The delay primarily impacts those hospitals
that had achieved Stage 1 MU for two or
three years by the start of the Stage 2
phase on October 1, 2013, and physicians
who met Stage 1 for two or three years
by January 1, 2014, the start of their
Stage 2 window. Those providers required
to step up to Stage 2 in 2014 will not be
affected by the delay, as they already faced
the start of Stage 3 in scal or calendar
year 2017. All providers must demonstrate
that they have met Stage 2 MU within their
applicable year, either federal or scal.
In February, CMS also delayed for one
month the reporting deadline for physicians
to attest to meaningful use for the 2013
reporting year, with a new deadline of
March 31, 2014. Hospitals had been
required to submit their attestation data for
scal year 2013 by November 30, 2013,
but CMS allowed a “one-time opportunity”
to submit retroactively if they were
unable to meet the deadline because
they “experienced difculty attesting,” as
long as they contacted CMS for assistance
by March 15, 2014. The 2013 reporting
deadlines are signicant because meeting
them not only allows providers to receive
Medicare incentive payments for 2013 but
will also result in avoiding the 2015 penalty
adjustment to payments.
More details about Stage 3 requirements,
along with more details on the revised
attestation timeline, are expected to be
released in fall 2014. Upcoming important
dates for the EHR incentive programs are:
•September 30, 2014: end of 2014 scal
year and end of the 2014 reporting
period for eligible hospitals
•November 30, 2014: attestation
deadline for Medicare-eligible hospitals
for the 2014 program year
•December 31, 2014: end of 2014
calendar year and end of the 2014
reporting period for eligible professionals
Data analytics: connecting
the community
As health care providers invest signicant
funds into building electronic health
records, they are realizing returns on
investment through more informed health
decisions and better patient outcomes and
satisfaction. The value of HIT investments is
optimized when physicians, other clinicians
and community providers partnering in
medical homes and bundled care demos,
or simply trying to best manage high-risk
patients, can access data in real time, in a
useable format. The health care industry is
also looking to provide realistic insights into
population health, patient management
and best practices, all of which can be
facilitated through optimal use of available
data. The Value vignettes in this chapter
provide several examples of specic
initiatives that have been proven to achieve
real value from HIT.
But connecting to and sharing data
with other providers in the community
is not a simple exercise. Despite the
industry’s movement to a common
messaging standard — Health Level
Seven International — and the standard
requirement that EHRs exchange a
common type of patient summary
document, information sharing is far from
uniform. The messaging standard is more
a framework than a specic, detailed set of
rules. And different IT vendors apply the
standard differently. In another example,
one set of clinician groups may use certain
medical terms differently than the hospital
or other physician groups. Although
this is really a matter of semantics,
these differences can lead to errors and
problems to be addressed before data can
be effectively shared. Another complicating
factor is that many post-acute providers still
have limited information system capability
and limited ability to send or receive data
electronically.
In order to collect data efciently and
accurately for analyzing patterns in care
delivery, the system needs to go beyond
basic data interchange, which simply sends
and receives “snapshots” of information as
of a specic point in time. The value to be
gained through analysis of data to identify
practice patterns and provide decision
support tools can be achieved only through
an interface that builds a well-organized
data warehouse and operates more like
aprivate HIE.
A recent survey conducted by the eHealth
Initiative and College of Healthcare
Information Management Executives
found that while 80% of health care
chief information ofcers believe data
analytics are important to achieving their
organization’s strategic goals, 84% felt
using big data presents a challenge. Only
17% reported that they had staff trained
to collect and analyze data.
Achieving the value of HIT is a time-
consuming and costly process, requiring
input, understanding and agreement from
the hospital, physician practices and other
community providers involved. Several
steps should be considered in this process
(see Exhibit 3-1 on page 48).
Telehealth: optimizing IT value
in health care delivery
With the industry’s move toward a value-
based model, care coordination is a major
driver — one that can be well supported by
47

HIT. Ideally, each patient should receive
the right care, in the right setting, at the
right time from a health care provider who
understands the patient’s needs. HIT can
facilitate data sharing to make sure each
patient’s history, needs, limitations and
resources are considered by all providers
when making care decisions. Telehealth
provides many benets in supporting this
effort, including:
•Ensuring the most appropriate caregivers
are involved, regardless of a patient’s or
physician’s physical location
•Providing a new way to share specialty
expertise over a broad geographic area —
including getting specialists to places
they couldn’t physically get to in the
crucial timeframe, assisting in covering
shortages in health care personnel and
providing patients more convenient
options for follow-up care, possibly
resulting in better compliance with post-
discharge instructions
•Monitoring and tracking specic
symptoms of recently discharged
patients at risk for readmission or those
with chronic conditions
•Potentially, in a widespread facility
campus, eliminating the need to move
across the campus by enabling physicians
to participate in an examination or
emergency consult simply by using their
laptops for a much quicker response time
Although telehealth is growing, with more
than half of all US hospitals using some
form of it, according to the American
Telemedicine Association, many regulatory
and legal hurdles need to be managed.
Measures to facilitate telehealth have
been gaining bipartisan support in
Congress. In February 2014, several
former US senators launched the Alliance
for Connected Care to advocate for federal
and state regulatory changes to support
telehealth, especially extending these
programs to rural providers.
“Telehealth services are rapidly
becoming a very important part of
healthcare delivery under the new
paradigm, but we unfortunately
don’t have a regulatory environment
or policy environment that
accommodates the new technology.”
Former Senator Tom Daschle
Co‑founder, Alliance for Connected Care
Along with the investment in technology
to support a telehealth initiative,
telehealth faces other nancial — and
regulatory —challenges. Even though
20 states have parity laws requiring that
some primary care telehealth services
be reimbursed on par with face-to-face
services, many payers do not yet cover
remote consultations and other telehealth
services. Currently, 43 states and the
District of Columbia provide at least some
Medicaid coverage for telehealth services.
Medicare generally pays only for telehealth
services provided in rural areas. As payers
increasingly see the value of telehealth —in
reducing ED visits and readmissions,
increasing the quality of care, especially
in remote areas, and providing measurable
cost savings — insurance coverage for
telehealth services is expected to rise.
Other regulatory challenges include
licensure and credentialing requirements.
The Federation of State Medical Boards
is working on an interstate compact and
plans to hold a vote at its 2014 annual
Exhibit 3-1. Steps in achieving HIT value
1. Identify all available sources of
data, whether or not part of the
hospital’s EHR, including items such
as pharmacy records, billing systems,
physician schedules and appointment
logs, and patient health information
from all providers involved.
2. Assess the accuracy of the available
data from these sources.
3. Develop a plan to integrate clinical
data from a patient’s hospital records
with clinical data from outpatient and
clinic visits, claims data, physician
encounters and services of other
community providers.
4. Determine if the project will be done
in-house or whether outside vendors
will be used.
5. If an in-house data analytics
deployment team will be used, involve
representatives from hospitals,
physician practices representing
all major specialties, and other
community providers to create a
system-wide team. Offer sufcient
career opportunities to keep
team members committed to the
analytics effort.
6. Get commitments from leaders of all
participating organizations to make
data-based decisions rather than
relying on past personal experiences.
7. Identify goals and uses of data for
specic end users so they will know
what is expected of them, and can
contribute to the design format
and content to optimize the use of
the data provided. Customize each
analytical project for the specic
department or service involved —
for example, a readmission risk factor
scorecard for discharge planners or
a population-health tracking tool for
primary care physicians to assess
and track those patients with a
specic chronic disease to prevent
nonemergency hospital admissions.
Source: EY analysis, 2014
48 New horizons: voyage to value

meeting on a proposed telehealth policy
codifying standards and principles for
state boards and legislatures to use
in developing telehealth policies and
regulations. The proposed compact claries
that “the practice of medicine occurs where
the patient is located at the time telehealth
technologies are used.” This would
result in physicians being required to
be licensed in each state where their
telehealth patients are located. Other less
controversial items included in the compact
are designed to make sure that patient
privacy is protected, telehealth information
is securely stored and there is no difference
in the standards of care between a digital
and face-to-face patient encounter.
For an in-depth look at telehealth
initiatives, see EY’s Health Care Industry
Post, “Shaping your telehealth strategy”
(www.ey.com/US/en/Industries/United-
States-sectors/Health-Care/EY-shaping-
your-telehealth-strategy).
A view to the future: riding
the momentum
As the industry moves toward value-
driven health care, payer and provider
organizations will nd more ways to mine
the intrinsic value of HIT. Many IT systems
can readily collect vast amounts and types
of data — procedures ordered, costs of care,
volumes of services provided by diagnosis,
post-discharge activity and much more.
By analyzing, sharing and using this data,
health care organizations can determine
best practices, support care management
decisions and continue to work toward
achieving health care value’s “holy grail”:
improved outcomes at lower costs.
We conclude this chapter with a roundtable
discussion featuring leaders of EY’s HIT
Advisory Services practice. Together, they
offer further insights on the strategic role
of HIT in creating and enabling system
transformation.
By the numbers
• Using data analytics helped Kaiser
Permanente’s Southern California
hospitals achieve mortality rates
26% lower than other hospitals in the
system (source: Kaiser’s chief medical
information ofcer John Mattison
presentation to VentureBeat Data
Science Summit, December 2013).
• The global health care analytics market
is projected to be worth $21 billion by
2020 (source: MarketsandMarkets
report, December 2013).
• In 2013, 170 data breach incidents
affected about 6.4 million individuals,
compared with 2012’s 200 incidents,
which affected about 2.8 million
individuals (source: HHS).
• Nearly 80% of family medicine and
internal medicine practitioners
surveyed in April 2013 use
smartphones in their “day-to-day
practice.” In the same survey, 61%
reported using mobile tablets (souce:
Ipsos survey conducted for Wolters
Kluwer Health, 2013).
• By 2013, 59% of hospitals had
adopted at least a basic EHR system,
an increase from 34% in 2012 (source:
ONCHIT Data Brief, May 2014).
• In 2013, 78% of ofce-based
physicians used an EHR system, an
increase from 18% in 2001 (source:
National Center for Health Statistics,
January 2014).
• About 13% of all ofce-based
physicians reported that they intended
to participate in meaningful use
incentives and also had EHR systems
with the capabilities to support 14
of the Stage 2 Core Set objectives
for meaningful use (source: National
Center for Health Statistics,
January 2014).
• The estimated costs for small
physician practices to implement
ICD-10 ranges from $56,639 to
$226,105 (source: American Medical
Association, January 2014).
• Through April 2014, more than
408,000 health care providers
received more than $23.7 billion
in EHR incentive payments from
Medicare or Medicaid (source:
Medicare and Medicaid Incentive
Programs HIT Policy Committee
presentation, June 2014).
• A total of 51,000 health IT
professionals will be needed to
implement EHRs, support the
conversion to ICD-10 and implement
federal health care initiatives such
as patient-centered medical homes
(source: US Bureau of Labor Statistics,
January 2014).
• Health information technician
positions are expected to increase
22% from 2012 to 2022 (source:
US Bureau of Labor Statistics,
January 2014).
49

Value vignette
Healtheway: developing strategies for innovative information exchange
A nonprot public-private partnership,
Healtheway is “in the business of
providing cost-effective HIE operational
services.” The partnership supports the
eHealth Exchange, a rapidly growing
community of exchange partners who
securely share health information.
Currently, nearly 50 participants —
including four federal agencies, six state
health information networks, eight
Beacon communities and more than 20
health information organizations and
health systems — collaborate across the
industry to develop implementation
strategies enabling secure and
interoperative, standards-based HIEs.
The eHealth Exchange has a presence
in all 50 states covering more than 800
hospitals, 6,000 medical groups and
more than 1 million patient records.
While Healtheway was formed in
2012, the eHealth Exchange began in
February 2009 with just two participants,
the Social Security Administration and
MedVirginia, exchanging transactions
to expedite processing of benets to the
disabled. By the end of 2014, eHealth
Exchange expects to have nearly 100
participants, connecting 1,600 hospitals,
10,000 medical groups and nearly
100 million patients.
In 2012, Healtheway began a collaboration
with the Care Connectivity Consortium
(CCC) to enhance HIE capabilities and
services. Founded by ve early adopters
of electronic medical records — Geisinger
Healthcare System, Group Health
Cooperative, Intermountain Healthcare,
Kaiser Permanente and Mayo Clinic —
CCC is designed to improve and advance
the technology for comprehensive,
secure, reliable and innovative electronic
exchange of health information across the
country. It has a presence in 18 states
with 18 million members and more than
23,000 physicians.
The collaboration between CCC and
Healtheway is intended to achieve
widespread connectivity, efciently
and effectively at the lowest cost,
while addressing critical challenges to
information exchange. Both organizations
are pursuing innovations to improve HIE
interoperability and efcacy. CCC has
developed advanced patient-centered
care technology that will be supported
by Healtheway’s network services
and shared with eHealth Exchange
participants as part of the collaboration.
This has made available to participants:
• Enhanced content management
services
• A trait sensitivity study to optimize
demographic traits for patient matching
• Patient identity management services
As CCC continues to develop information-
sharing services, these services will be
made available to all eHealth Exchange
participants.
Source: www.healthewayinc.org; www.careconnectivity.org/wp‑content/uploads/2014/02/CCC‑Healtheway‑Overcoming‑Challenges‑in‑HIE‑HIMSS.2014‑Web.pdf
50 New horizons: voyage to value
Value vignette
HIMSS: quantifying the value of health IT
Unveiled in July 2013, the HIMSS Health
IT Value Suite™ is a knowledge repository
of value-focused, evidence-based data to
guide providers, policy makers and payers
in assessing the value of investments in
health IT. The Suite offers examples to
help stakeholders evaluate the success
of their IT investments, emphasizing
performance improvements by
considering numerous clinical, business
and nancial factors. Because the value
of health IT can be demonstrated in many
different ways, the Suite organizes a
“common vocabulary to identify, classify
and discuss the many known examples
of health IT value.”
The Suite contains hundreds of provider
case studies that can be researched to
measure value and educate users on the
ndings. Based on these studies, HIMSS
has identied ve kinds of value that
health IT creates to benet patients,
health care providers and communities
(see table below).
Using the Suite, health care organizations
can determine how health IT can
help reduce:
• Redundancies in testing, labs and x-rays
• Hospital-acquired infections
• ED admissions
• Costs, while maintaining or improving
the quality and safety of patient care
Source: www.himss.org; table adapted from “HIMSS Introduces Health IT Value Suite to Realize the Value of Health IT,” July 16, 2013,
www.himss.org/News/NewsDetail.aspx?ItemNumber=21536
STEPS Subtypes Documented examples in Health IT Value Suite
Satisfaction Patient, provider, staff • Improving patient satisfaction scores
• Improving internal communications with providers and staff
Treatment/clinical Safety, quality of care, efciency • Reducing medical errors
• Reducing readmissions
• Improving scheduling
Electronic information/data Evidence-based medicine, data
sharing and reporting
• Increasing use of evidence-based guidelines
• Increasing population health reporting
Prevention and patient
education
Prevention, patient education • Increasing immunizations
• Improving patient compliance
Savings Financial/business, efciency
savings, operational savings
• Reducing days in accounts receivable
• Reducing patient wait times
• Improving inventory control
51
The move to
meaningful use
and ICD-10: finding
the bearings
A roundtable discussion
Craig Kappel, Partner
Health Care Advisory Services
Ernst & Young LLP
Rob Wallace, Executive Director
Health Care Advisory Services
Ernst & Young LLP
Practice leaders Craig Kappel and
Rob Wallace offer their perspectives
on today’s most pressing HIT
challenges — and how organizations
can realize the most value from their
meaningful use and ICD‑10 initiatives.
As we look at the role of health
information technology in delivering
value, how should organizations
view value through the significant
investments in meaningful use
and ICD-10?
Rob Wallace: Meaningful use is a key effort
by the federal government to deliver value
by moving from a fee-for-service health
care system to one that is outcomes-based.
Each stage brings a different level of value.
Stage 1 was all about capturing data
and sharing it by implementing certied
electronic health record systems. Stage 2 is
focused on advanced clinical processes and
patient engagement. Stage 3 is designed to
measurably improve health outcomes.
Meaningful use also brings value in helping
providers deliver safer care. No longer
do they need to deal with handwriting
that can’t be deciphered or medical
chart information that isn’t well dened.
Accepted protocols, built into software
applications, make decisions easier. And
hospitals and physicians — working from
shared information — have incentives to
improve their ability to serve patients.
Craig Kappel: The move to ICD-10
can yield signicant value for health
care organizations. It can be used to
improve not only medical management
and claims processing but other core
business processes. As health care moves
toward outcomes-based payment models,
population health and comparative
effectiveness, the more granular ICD-10
codes — along with more availability of
digital clinical information that meaningful
use is prompting — can be a catalyst
for accelerating adoption of these
evolving models.
In the midst of competing HIT priorities,
how high is the sense of urgency for
both these initiatives?
Rob Wallace: A proposed rule from CMS —
announced May 20, 2014 — would extend
Stage 2 through 2016 and begin Stage 3
in 2017, as well as allow exibility for
meeting 2014 Stage 1 and 2 requirements.
This could provide some much-needed
relief based on the readiness of many EHR
vendors and providers. However, some
key dates are imminent and priorities
should reect these timeframes. Unless
successful with a hardship exception,
eligible hospitals (EHs) must attest by
July 1, 2014, and eligible professionals
(EPs) by October 1, 2014, to avoid
penalties in 2015.
Craig Kappel: Now that we’ve been delayed
twice with ICD-10, the concern is that the
industry will not take the October 1, 2015,
compliance date seriously — and will
approach readiness half-heartedly.
If the 2015 deadline becomes a reality,
although we can’t know for certain that
it will, this lack of full focus could be
detrimental to providers and payers alike.
It’s interesting that the current wording
of the new compliance date includes
the phrase, “at the earliest.” That could
lead to lukewarm efforts to meet the
October 1, 2015, date.
Part of the cause of the most recent delay
is that small physician practices and sole
proprietors were not ready for ICD-10.
Now that the delay has been announced,
we’re seeing varied responses from small
organizations. Some are now dismissing
ICD-10 as a priority — a focus they may
return to next year. Or they may lobby
again to delay it.
Feature
52 New horizons: voyage to value
Although not seeming to be, another
major challenge is that in the IT space,
aplethora of systems are already ICD-10
compliant. If changes are required, the
window between now and the October
2015 deadline isn’t wide enough to make
any other major revisions to IT systems.
No IT function wants to be in the midst of
a major implementation when the ICD-10
compliance date kicks in.
How are the best-performing
organizations maintaining their
ICD-10 readiness?
Craig Kappel: Instead of parking the
project on the side, leading organizations
are continuing a measured march toward
ICD-10 readiness. They are looking at it
less as a compliance exercise and more
as a way to improve their operations — by
getting physicians and coders trained,
implementing computer-assisted coding
and creating stronger systems for
documentation. Improving the quality of
medical information will also likely improve
their payments.
Payers have a different challenge. They
can’t “ip the switch” and start asking for
bills to be rendered in ICD-10 format until
the compliance date is locked and loaded.
In general, they need to continue testing
with as many providers as they can.
Medicare meaningful use timeline
First
payment
year
Stage and reporting period
2011 2012 2013 2014 2015* 2016 2017** 2018 2019 2020 2021
2011
1
90 days
1
365 days
1
365 days
1 or 2
calendar
qtr.
2
365 days
2
365 days
3
90 days
3
365 days
TBD TBD TBD
2012
1
90 days
1
365 days
1 or 2
calendar
qtr.
2
365 days
2
365 days
3
90 days
3
365 days
TBD TBD TBD
2013
1
90 days
1
calendar
qtr.
2
365 days
2
365 days
3
90 days
3
365 days
TBD TBD TBD
2014
1
90 days
1
365 days
2
90 days
2
365 days
3
90 days
3
365 days
TBD TBD
2015
1
90 days
1
365 days
2
90 days
2
365 days
3
90 days
3
365 days
TBD
2016
1
90 days
1
365 days
2
90 days
2
365 days
3
90 days
3
365 days
2017
1
90 days
1
365 days
2
90 days
2
365 days
3
90 days
Notes: In 2014, regardless of stage, if performing subsequent attestation, the reporting period is a calendar quarter. If rst attestation, the reporting period is a
continuous 90 days. For EPs, attestation must be completed by October 1, 2014, to avoid penalties beginning January 1, 2015. EHs must attest by July 1, 2014,
to avoid penalties beginning October 1, 2014.
* According to the proposed rule, the Stage 2 reporting period will be 365 days in 2015.
** Data collection for attestation periods and MU requirements are yet to be dened. Dates shown for 2017 and beyond are subject to change when Stage 2 and Stage 3
MU nal rules are issued.
53
give patients incentives for taking a greater
role in their care. The rst step is educating
them on how they can access their
information. Many organizations are using
portals for this purpose and measuring
patient use.
As more and more providers actively
seek opportunities for consolidation,
what part will meaningful use play?
Rob Wallace: Smaller organizations that
can’t adopt MU criteria may be open
to aligning with larger organizations
that are successfully meeting MU
requirements. If the newly consolidated
entity doesn’t meet MU thresholds, buyers
could be putting their progress at risk.
For example, if the acquiring hospital is
demonstrating MU and the target hospital
isn’t, the buyer may be at risk of losing
incentive payments or may face payment
adjustments. Executive teams should
involve their IT leadership early in the M&A
process to mitigate any nancial risks of
MU misalignment and prepare properly for
IT integration.
CMS’ meaningful use audits are
expected to affect between 5% and
10% of providers. How can providers
best prepare?
Rob Wallace: Two areas of documentation
typically scrutinized are an electronic
snapshot of EHR capabilities and use
and a security risk analysis of the EHR
system during the reporting period. CMS is
using an external rm for many of these
MU audits. Although we’ve found that
the information the external resource is
looking for isn’t always as restrictive as
CMS guidelines, as organizations prepare
for an audit, our advice is to always follow
the frequently asked questions guidance
and other guidelines from CMS. No provider
wants to be surprised in a subsequent audit
that may be more rigorous.
Given the revised timeframes for
both meaningful use and ICD-10,
how should executives and board
members proceed?
Rob Wallace: Know exactly where your
organization is in MU implementation and
have condence in your monitoring and
reporting mechanisms. What gaps need
to be lled and what plans are in place to
mitigate risks? It’s a tremendous risk to
attest that you’ve met MU measures and
then nd out through an external audit
or through your own discovery that you
haven’t. Perform your own internal audit
before attesting.
Craig Kappel: Organizations need to move
forward with as many of the activities as
they can to stay on course for ICD-10.
But they need to approach ICD-10 as an
opportunity to improve their operations
and strengthen their ability to demonstrate
quality in their organization. If we fast-
What metrics are providers and payers
using to gauge how well their HIT
investments are delivering value?
Craig Kappel: In the ICD-10 world,
measures are different than day-to-
day operational metrics of nancial
performance and productivity. ICD-10
measurements gauge whether physicians
and coders are being trained on time,
whether IT systems are being remediated
and tested on time and whether the
revenue cycle is being adjusted as needed.
These macro-operational milestones need
to be monitored along the way.
“Smaller organizations that can’t
adopt MU criteria may be open to
aligning with larger organizations
that are successfully meeting
MU requirements.”
Rob Wallace: Meaningful use has clear
thresholds for measurement. Providers
who started Stage 1 in 2011 or 2012 — and
who are transitioning to Stage 2 in 2014 —
need to assess the costs and benets
of the program and potential incentives
and penalties. Meeting MU requirements
becomes more difcult with Stage 1, 2014
measures and Stage 2. The new measures
include patient engagement requirements.
We’re just beginning to understand how to
54 New horizons: voyage to value
forward a year from now and the deadline
is postponed again, then if I were a board
member, I would be highly distraught if my
organization had spent countless hours and
millions of dollars on a compliance exercise
that has brought no benet. But I would
be delighted if our investment resulted in
improved operations and strengthened our
ability to measure quality.
“Organizations need to approach
ICD-10 as an opportunity to
improve their operations and
strengthen their ability to
demonstrate quality.”
How can the board and executives best
support IT strategies and initiatives at
their organizations?
Craig Kappel: For any health care
organization, IT is an important enabler.
If I were a board member I would be less
interested in someone reporting to me
that an application has been successfully
implemented or will be successfully
implemented. I’d be more interested in
knowing that the entire organization — the
business as well as IT — has jointly enabled
this new technology for the overall benet
of the organization.
Each organization is different. In some,
IT is a world unto itself and doesn’t
always involve the business as much as it
should. All too often, we see organizations
implementing 50% to 60% of the
capabilities of any given application, and
the rest are never really used. Focusing
on leveraging all capabilities these
technologies offer is key.
Rob Wallace: The sheer volume of
information health care organizations have
to work with can be daunting. They need
to sift through all of it, decide what matters
most and set priorities. And they can’t
forget about the fundamentals of HIPAA
security and to consider the overall risk
of any data breaches — balancing the
imperative to keep sensitive information
secure while giving clinicians access to
track and share the data needed for more
effective care delivery.
55

New horizons: voyage to value56

Viewfinders
Considerations for your board and executive leaders
For providers
•Has your organization assessed the many
signicant issues facing your IT staff over
the next two years, setting priorities for
competing demands?
•Have you assessed ICD-10 implementation
plans and adjusted them to address
the delay in conversion? Have you
arranged to test systems with payers
and claims processors?
•Are opportunities in place for patient
charts to be coded under ICD-9 and
ICD-10 conventions so that staff
maintain skills learned in training, and
areas of weakness can be identied and
addressed before the conversion date?
•Have clinicians been encouraged to
document to ICD-10 standards, with
staff or consultants available to assess
their efforts and provide one-on-one
consultation, making sure that patient
documentation will be adequate to
support ICD-10 coding before the
conversion date?
•Do you have processes in place to
conrm you meet Stage 2 MU reporting
requirements? Have you assessed
the value of any remaining incentive
payments you may receive as well as
potential payment penalties if Stage 2
MU is not achieved — and determined that
this value exceeds the cost of compliance
with Stage 2 MU? For example, the
requirement for active use of a patient
portal may be exceedingly expensive,
if not impossible to achieve, for some
medical practices dealing primarily with
elderly patients.
•Are IT representatives participating
on implementation teams for all new
payment models, such as ACOs and
medical homes?
•Have you implemented data analytics?
Do you have staff trained in collecting
and analyzing data or do you plan to rely
on consultants to set up data collection,
analysis and monitoring processes? Are
end users involved in developing data
reporting and data analytic projects?
•Do you need to hire a new breed of IT
staff skilled in decision support, clinical
areas and strategic planning to move
forward with unearthing the value in the
data your HIT systems capture?
•Are your patient privacy and data
security guidelines and standards
reviewed and updated regularly
to conrm that new data-sharing
arrangements, remote access and
telehealth initiatives are addressed, and
that staff involved in these arrangements
are well trained in patient privacy and
data security requirements?
•Does the team assessing the feasibility
and viability of telehealth services for
your organization include representatives
of all stakeholders involved? Have they
identied safe, high-quality services
when deciding which telehealth services
to support? Are they tasked with
determining the coverage available for
telehealth services by the most likely
payer organizations?
For payers
•Have you assessed your ICD-10
implementation plans and adjusted them
to address the delay in conversion?
Have you arranged to test your claims
acceptance and processing systems with
participating providers in adequate time
to address and correct any issues before
the conversion date?
•Are you effectively using the claims,
outcomes and cost data processed
to identify opportunities for starting
new payment initiatives with specic
providers, or for use in contract
negotiations and coverage decisions?
Do you have staff trained in collecting
and analyzing data or do you plan to rely
on consultants to set up data collection,
analysis and monitoring processes?
•Are participating providers consulted
in your data analytics efforts when
considering causes behind variations
in costs and outcomes and in
developing opportunities for new
payment initiatives?
•Do you seek out and support
opportunities for providers in your
market to implement telehealth initiatives
where the expected result is cost savings
or improved outcomes?
•Do you share with plan sponsors
information about the telehealth
coverage your plans provide as a
marketing tool, particularly those
telehealth programs that can save
patients travel time and time needed
to be away from work for consultations
with specialists?
•Do you conrm that all medical services
your plans cover are appropriately
reimbursed — whether provided face
to face or remotely?
•Are your health information privacy
and data security guidelines reviewed
and updated regularly to conrm that
new data-sharing and remote access
arrangements with providers are
properly addressed, and that staff are
well trained in privacy and data security
requirements?
57

{ }
“Never go into strange places on a falling tide
without a pilot.”
Thomas Gibson Bowles, 19th‑ and 20th‑century British journalist

Chapter 4
Value in compliance
Heeding the warnings
Voyage to value
As health care organizations sail on their voyage to value, growing
demands — for greater transparency, increased collaboration and
seamless transitions in providing quality services across the care
continuum — require heightened vigilance in complying with a myriad
of rules and regulations, some familiar and some new. An effective
compliance program, like a lighthouse in a storm, helps health care
organizations steer clear of dangerous waters — curtailing risk, reducing
penalties and proactively protecting them from running aground with
the law.
The compliance programs of tomorrow, however, will need to do
more than shield organizations from government investigations.
They will need to move beyond the minimum standards set by
laws and regulations to reect the full value of the compliance
investment —supporting efforts to lower costs, deliver better patient
care and enhance employee engagement.
59
Understanding and meeting the expectations of industry
stakeholders is paramount to demonstrating integrity
and delivering value to all who are onboard the health
care voyage. In the rolling seas of high risk, it could
mean the difference between sinking and sailing. In this
chapter, we provide a summary of recent enforcement
activity in the battle against health care F&A and how
organizations are responding by strengthening — and
achieving value through — their compliance programs.
Along with provider imperatives, issues unique to payers
are highlighted, including new compliance requirements
mandated by the ACA.
CMS oversight: setting direction
CMS is responsible for overseeing
compliance with an enormous cache
of regulations that govern the Medicare,
Medicaid and Children’s Health Insurance
programs. Also under its purview are
regulations spawned by the ACA that
govern the health insurance exchanges.
In fact, CMS oversees more pages of
regulations for the Medicare program
alone than the Internal Revenue Code.
Over the past decade, new health
care legislation expanded or added
new responsibilities for CMS in
compliance oversight:
•The Decit Reduction Act of 2005 created
a Medicaid Integrity Program to address
fraud and abuses in Medicaid.
•The Tax Relief and Health Care Act
of 2006 established a physician
quality reporting program and quality
improvement initiatives, and enhanced
CMS’ program integrity efforts through
the Recovery Audit Contractor
(RAC) program.
•The American Recovery and Reinvestment
Act of 2009 provided incentives for
investing in technological advances,
prevention and wellness activities, and
a concurrent burden on CMS to monitor
compliance and reporting activities
related to these incentives.
•The ACA holds CMS responsible for
implementing its consumer protections
and private health insurance provisions.
Most of these initiatives are directly
attributable to determining whether the
federal government — and the American
population — receives appropriate value for
its large investment in health care.
“[Compliance is] the process of …
helping health care professionals
understand and meet the
expectations of those who grant
us money, pay for our services,
regulate our industry …”
The Health Care Compliance Association
2013 enforcement overview
Continuing a trend of the past several years,
well over half of all government recoveries
in 2013 resulted from health care fraud
cases. Most of these settlements were
from lawsuits brought under the qui tam
provisions of the False Claims Act (FCA).
The number of qui tam lawsuits has grown
signicantly, with more than 750 new cases
led in 2013 — about double the annual
number ve years ago.
FCA lawsuits are civil cases, but federal
and state governments also pursue
criminal cases under health care F&A
laws. The Department of Justice (DOJ)
generally pursues such cases, often
involving the cross-agency Medicare Fraud
Strike Force. The HHS Ofce of Inspector
General (OIG) conducts criminal, civil and
administrative investigations of fraud and
misconduct against individuals and health
care organizations, assessing penalties
ranging from exclusion from participating
in Medicare and Medicaid to civil monetary
penalty settlements and administrative
recoveries of overpayments. The OIG also
oversees settlements of provider self-
disclosure matters.
Exhibit 4.1 on page 61 provides a brief
summary of the types of enforcement
activities in 2013 by organization type.
60 New horizons: voyage to value
“We will also produce savings for
taxpayers by continuing to crack
down on waste, fraud and abuse.
Every dollar we invest in the Health
Care Fraud and Abuse Control
initiative, for example, returns
$8.10 in money we recover, which
last year was a record-breaking
$4.3 billion.”
Kathleen Sebelius
HHS Secretary
Oral Testimony before the Committee on Ways &
Means, United States House of Representatives
March 12, 2014
Reviewing the types of cases settled in
2013, as well as the enforcement activities
of the DOJ, OIG and CMS over time, can
guide health care organizations as they
steer through regulatory waters. To stay
on course, then, in developing an effective
compliance program, organizations should
devote part of their efforts to consistently
monitoring regulations.
FCA
CMS and other federal ofcials have often
referred to the FCA as the most effective
tool in ghting against fraud because of its
provisions to reward those who go public
with information about allegedly abusive
practices. The FCA allows the government
to recoup up to three times the actual
damages, plus up to $11,000 per violation.
Federal enforcement of the FCA has been
expanding from overbilling or inappropriate
billing to cover such concerns as off-
label drug marketing and cases involving
violations of good manufacturing practices
and other broad applications. We can
expect federal enforcement activities to
continue to encompass new and wide-
ranging applications of the FCA.
Exhibit 4.1. 2013 enforcement activity summary
Hospitals Most settlements in 2013 were related to FCA claims of improper billing for short stays and
misclassication as inpatient/outpatient/observation. Cases involving the Stark Law and Anti-Kickback
Statute (AKS) increased in 2013. Most stemmed from allegations of improper payments to physicians for
consulting, rent or bonuses.
Long-term care (LTC) With a growing number of qui tam lawsuits, LTC cases ranged from allegations of providing medically
unnecessary services to hospice patients who did not meet the required prognosis of six months or less to
live, to cases of inadequate nursing care or unnecessary therapy services. The Medicare Fraud Strike Force
brought several actions involving home health providers for fraudulent claims.
Physician practices In this segment, enforcement actions primarily related to upcoding for higher levels of physician
services than were actually provided, as well as AKS violations in physician relationships with labs and
other ancillary service providers, particularly those in which physicians held an investment interest.
The Medicare Fraud Strike Force takedowns resulted in charges being led against many individual
physicians as well as group practices.
Pharmaceuticals Unlike the previous year, no blockbuster multibillion-dollar settlements were made in 2013. Cases were
primarily related to off-label marketing allegations and AKS violations for inducements to physicians to
prescribe certain drugs through consulting arrangements, free continuing education courses and other
forms of payment.
Medical device
companies
Cases ranged from encouraging physicians and other providers to submit claims with incorrect diagnosis
and procedure codes, lack of medical necessity for devices, and AKS allegations of rebates or free medical
equipment in exchange for prescribing certain medical devices. Increased scrutiny by CMS resulted in
many denials of medical device providers’ initial applications to participate in Medicare and Medicaid.
Health plans Only one notable settlement was reached with a health plan in 2013. It was related to allegations that the
plan articially inated its patient risk adjustment scores to receive higher payments.
Source: Compiled from DOJ statements, www.justice.gov
61
The Stark Law
Growing activity in the Stark Law and
AKS violations also can be expected to
continue, along with increasing focus on
the Stark Law’s application to Medicaid
claims. Historically, enforcement of Stark
was centered on claims submitted to
Medicare, due to specic wording in the
law that prohibits federal payments for
self-referrals. With Medicaid payments
made by the states, there is no direct
federal payment to prohibit. Amendments
to Stark expanded its reach to Medicaid by
prohibiting federal matching fund payments
to the states for Medicaid claims that would
have been prohibited by Stark if made for
Medicare claims.
A proposed rule to implement this
provision stated that each state would
have to establish its own sanctions for such
violations. A nal rule implementing this
provision has not been issued, and CMS has
not provided any further guidance on how
the Stark Law applies to Medicaid claims.
However, in two signicant 2013 cases,
the US District Court in both the Middle and
Southern Districts of Florida upheld the
government’s argument that under the FCA,
certain referral practices prohibited under
Stark can be applied to both Medicare
and Medicaid claims. The government is
expected to rely on these rulings, greatly
expanding the sizes of potential settlements
in Stark Law cases by imposing penalties
on Medicare and Medicaid claims.
Physician activities
With CMS’ focus on physicians as
the “gatekeepers” of the health care
system, and based on increasing numbers
of enforcement activities directed at
individual physicians and physician
group practices, we can anticipate
increasing scrutiny of physician activities,
relationships and actions. In particular,
continuing investigations into payments
by pharmaceutical and medical device
companies to physicians as paid speakers,
consultants and advisory board members
can be expected. CMS has stepped up
activities to increase physicians’ awareness
of their responsibilities in combatting health
care fraud and abuse as part of their role
in providing quality medical care. For an
update, see the Value vignette on page 63.
Along with CMS, other federal agencies
are engaging physicians in identifying
instances of health care fraud or
noncompliance with applicable statutes.
Part of the compliance education effort
involves providing examples of compliance
problems and advising physicians how they
can report such concerns. For example,
the US Food and Drug Administration is
seeking help from physicians in its Bad
Ad program, asking doctors to report
misleading advertisements for drugs,
biologicals or medical equipment as
well as advertisements for off-label use
of drugs. Off-label marketing cases will
continue to be an area of high interest
in enforcement activities.
Health insurance exchanges
As the federal and state insurance
exchanges begin their second national
open enrollment period, CMS is expected
to increase its oversight and enforcement
activities related to adequacy of networks,
minimum loss ratios and other provisions
intended to hold payers responsible
for complying with the ACA’s insurance
plan requirements. Also, all payments
made through, or in connection with,
the exchanges are subject to the FCA.
This signicantly expands enforcement
opportunities over a much broader universe
than Medicare and Medicaid claims.
Health care payers can expect greater
enforcement activity than they have
experienced in the past.
CMS fraud detection initiatives
CMS uses a wide variety of initiatives
to help detect and prevent fraudulent
programs — from low tech, such as
the Senior Medicare Patrol, to high
tech, such as predictive modeling in
the agency’s Fraud Prevention System.
For the Senior Medicare Patrol, the
Administration is expanding its activities
to educate Medicare beneciaries on how
to prevent, detect and report Medicare
fraud, waste and abuse. Government
ofcials have stepped up educational
initiatives and raised nancial incentives
for beneciaries to enlist their help in
battling fraudulent claims. In 2013, more
than 49,000 complaints from Medicare
beneciaries were reported and referred
for further evaluation.
CMS reported that its Fraud Prevention
System helped to stop, prevent or identify
about $115 million in fraudulent payments
in its rst year of operation. The system
uses predictive modeling and data analytics
to review Medicare fee-for-service claims
for indicators of fraud. Highlighted claims
are bumped for review and scrutiny.
In addition to enforcement measures,
CMS can also use its authority to suspend
payments to providers and suppliers
suspected of fraudulent activities, moving
from the effort of collecting overpayments
to preventing inappropriate payments.
Over the past several years, the OIG has
increasingly focused its investigations on
the responsibilities of corporate executives.
Under the “Responsible Corporate Ofcer,”
or Park doctrine, a responsible corporate
ofcer’s liability “does not depend on their
62 New horizons: voyage to value
approval or knowledge of wrongdoing, but
hinges instead on whether they had the
responsibility and authority to prevent or
correct the violation and failed to do so.”
This doctrine permits the OIG to exclude
individual ofcers or owners of companies
investigated for F&A violations from
participating in Medicare and Medicaid.
Few individuals have been excluded under
this doctrine to date, but the OIG continues
to emphasize that it intends to use
exclusion to hold executives and owners
accountable for their companies’ conduct.
The OIG has also indicated its intent to
actively enforce “corporate integrity
agreements,” seeking exclusion from
Medicare or Medicaid for any breaches.
In March 2014, the OIG issued a notice
of exclusion for numerous breaches of
a national health care organization’s
corporate integrity agreement.
“OIG is committed to driving
positive change through work that
is relevant, innovative, customer-
focused, and high impact. During
this reporting period, we continued
to advance our core mission of
protecting HHS programs and the
people they serve.”
Daniel Levinson
HHS Inspector General
Semiannual Report to Congress, Fall 2013
Value vignette
Physician education: enlisting the gatekeepers
CMS has launched a major compliance
education initiative for physicians, who
are described as the health care system’s
“principal gatekeepers.” According to the
agency, formal education on program
integrity will help increase awareness
and compliance. As a result, physicians
will be less likely to submit inappropriate
claims or to become victims of fraud
schemes themselves.
Although physician compliance with
Medicare and Medicaid legislation and
regulation has always been subject to
review and oversight by the HHS OIG and
other agencies, the ACA upped the stakes
by requiring all physicians, as well as all
health care providers who treat Medicare
or Medicaid patients, to establish an
effective compliance program as a
condition of enrollment.
To help physician practices in creating
an effective compliance program, as
well as increase their overall awareness
of compliance matters, the OIG issued
Compliance Program Guidance for
Individual and Small Group Physician
Practices (available at: http://oig.hhs.
gov/authorities/docs/physician.pdf).
The OIG has also compiled a wealth of
compliance education materials on its
website “Compliance 101” (http://oig.
hhs.gov/compliance/101/). This site was
designed to help health care providers
and suppliers understand F&A laws and
the consequences of violating them, as
well as offer ways to cultivate a culture
of compliance. It includes a variety of
webcasts, videos, documents and other
training materials, available at no cost.
To further educate physicians on
compliance and other Medicare
concerns, CMS established the Medicare
Learning Network (MLN). A one-stop
site, it includes ofcial CMS information,
education and resources for Medicare
fee-for-service providers. Information
is also available from other federal
agencies to promote physician awareness
of fraudulent, or otherwise illegal,
activities. The MLN provides a variety
of informational and educational products,
including web-based training courses,
many of which offer continuing medical
education credits.
One of the many educational documents
included on the MLN is “Avoiding
Medicare Fraud & Abuse: A Roadmap
for Physicians” (available at www.cms.
gov/Outreach-and-Education/Medicare-
Learning-Network-MLN/MLNProducts/
Downloads/Avoiding_Medicare_FandA_
Physicians_FactSheet_905645.pdf).
This document aims to help physicians
in complying with federal laws by
outlining “red ags” in relationships
with payers, fellow physicians and
vendors. Summaries are provided of
applicable laws with related enforcement
measures and penalties, along with
recommendations for how physicians
can respond to potential red ags.
The document also includes links to other
sources for further information, including
where to go for help and what to do if a
physician identies a problem in a current
business relationship.
Sources: Websites cited.
63

Summary of benefits and
coverage: complying with
a new mandate
The ACA requires that a summary of
benets and coverage (SBC) be provided to
employees eligible for employer-sponsored
health insurance with written health plan
enrollment materials when coverage is
renewed, by the rst day coverage is in
force (if any changes have been made
since enrollment) or upon request. Group
health plans, individual health plans and
self-insured plans are all required to comply
with this mandate. Intended to help insured
individuals make an informed choice, the
SBC must summarize health coverage
options in a standard format to enable
comparisons across plan options.
Effective January 1, 2014, SBCs are
required to indicate whether the plan
meets the minimum essential coverage as
required by the ACA’s individual mandate.
They need to indicate also whether the plan
meets the minimum value requirement —
that the plan pay at least 60% of allowed
charges for covered services. The SBC must
also include a notice of coverage options.
Because of the nature of health insurance
operations, the Department of Labor (DOL),
HHS and the Treasury Department were all
involved in developing and implementing
regulations for SBCs. These departments
are also working together on implementing
and overseeing this mandate. As explained
in “FAQs About Affordable Care Act
Implementation Part VIII,” posted on the
DOL website (www.dol.gov/ebsa/faqs/faq-
aca8.html), the departments’ approach to
ACA implementation is “[to work] together
with employers, issuers, states, providers
and other stakeholders to help them come
into compliance with the new law and [to
By the numbers
• In the rst two years that the ACA’s
screening and review requirements
were in effect, CMS revoked the
Medicare participation agreements
of 14,633 providers and suppliers
compared with only 6,307
revocations in the two previous
years (source: CMS, 2013).
• In the rst half of 2013, Medicare
RACs collected $1.37 billion
in overpayments and returned
$65.4 million in underpayments
(source: CMS, 2013).
• Each day, CMS’ Fraud Prevention
System monitors 4.5 million claims
(Medicare Part A, B and durable
medical equipment) using a variety
of analytic models (source: Center
for Program Integrity, CMS, 2012).
• A nationwide takedown by the
Medicare Fraud Strike Force in six
cities resulted in charges against
90 individuals — including 27
doctors, nurses and other medical
professionals — for their alleged
participation in Medicare fraud
schemes involving about $260
million in false billings (source: DOJ,
May 2014).
• A New Jersey medical center paid
$435,640 to settle allegations that it
violated the FCA by making improper
rent payments to a cardiology practice
that referred large numbers of
patients to the medical center (source:
US Attorney, District of New Jersey,
April 2014).
• In 2013, Health Care Fraud Prevention
and Action Team efforts resulted in
ling charges against 274 individuals
or organizations, 251 criminal actions
and $333 million in investigative
receivables (source: OIG, Semiannual
Report to Congress, 2013).
• In the federal scal year ended
September 30, 2013, the federal
government recovered nearly
$3.8 billion in settlements and
judgments from civil cases involving
fraud; $2.9 billion of this recovery
resulted from qui tam lawsuits.
The whistleblowers in these cases
recovered $388 million (source: DOJ,
December 2013).
• In 2013, only one FCA settlement
was made against a health insurance
plan. It concerned allegations that the
plan articially inated its patient risk
adjustment scores to receive higher
payments (source: DOJ, 2013).
• The government’s decision to
intervene (join with the whistleblower)
in a qui tam lawsuit greatly increases
the potential value of settlements
and recoveries. In cases in which the
government intervened in 2013, more
than $2.87 billion was recovered,
but only $109 million was recovered
in cases in which the government
did not intervene (source: DOJ,
December 2013).
64 New horizons: voyage to value
work] with families and individuals to help
them understand the new law and benet
from it, as intended.”
The departments have agreed not to
impose penalties on health plans and
issuers that are “working diligently and
in good faith” to provide the required SBC
content consistent with the nal rule’s
requirements and to work with health
plans and employers over time to achieve
maximum uniformity in SBCs. An initial,
two-year, safe harbor and enforcement
relief period has ended, with employers
expected to provide employees with
SBCs consistent in format and length
with the template provided by the DOL.
However, the departments will work with
the plans/insurers to help them come
into compliance and will allow some
modication for conditions that do not t
within SBC requirements.
Compliance program best
practices: following the leaders
With the additional onus on health care
organizations to have in place an effective
compliance program, due to provisions
of the ACA, every organization needs
to periodically assess its compliance
practices and procedures. Compliance
programs cannot be effective as stand-
alone silos of review; they need to be
woven throughout an organization’s
systems and operations. The emphasis
of federal sentencing guidelines on having
a culture of compliance lends further
support to the need for organizations to
embed compliance processes throughout
their operations.
By implementing and maintaining an
effective compliance program, health
care organizations benet from an
improved ability to detect and remediate
potential compliance violations and to
demonstrate their ongoing process of
self-assessment and commitment to
ethical and compliance practices. This will
enhance the organization’s perception
by its stakeholders and foster a positive
public image. Having a viable compliance
process in place will also help to mitigate
damages from any violations that may
occur. Self-reporting problems can result
Value vignette
Value-based purchasing: addressing compliance issues
Medicare’s Hospital Value-Based
Purchasing Program, authorized by the
ACA (see Chapter 1, page 13), now links
hospital payments to outcomes, process
of care and patient satisfaction. As a
result, the accuracy of clinical and patient
satisfaction data has become a signicant
compliance risk — compelling compliance
ofcers to monitor the accuracy of
this data. Failure to keep accurate
and complete HVBP data can result in
underpayments or overpayments.
In HVBP’s rst year, Medicare
redistributed almost $1 billion to hospitals
based on their reported outcomes,
process and patient satisfaction measures.
While the maximum payment gain or loss
to a hospital was limited to 1% of regular
Medicare payments (with that percentage
growing over the rst ve years of HVBP),
1,557 hospitals received increases while
1,427 saw payment reductions.
With payment partially based on
performance data, failure to report
accurate and complete data can be
considered submitting a false claim or
making a false statement. For example,
failure to document that a medication
was administered or a procedure
performed, or failure to include a
patient in the documentation counts,
can impact payment and be considered
fraudulent. HVBP compliance reviews
must determine that all patients who
should be included are, in fact, taken into
account. HVBP compliance audits should
also consider who can access and edit
the data, and review any questionable
data access. The patient satisfaction
survey process should also be part of the
compliance review process to determine
that answers were not coerced in any way.
Adding the review of HVBP processes
of care and patient satisfaction survey
reporting to the compliance team’s
responsibilities may at rst be like sailing
in uncharted waters, but — with the
widespread impact of the False Claims
Act — it is a necessary precaution.
Source: “Medicare Discloses Hospitals’ Bonuses, Penalties Based on Quality,” Kaiser Health News, http://www.kaiserhealthnews.org/stories/2012/december/21/
medicare‑hospitals‑value‑based‑purchasing.aspx; Nina Youngstrom, “Medicare Value‑Based Purchasing Opens a Large New Can of Compliance Worms,” Report on
Medicare Compliance, Volume 20, Issue 11, March 28, 2011.
65

66 New horizons: voyage to value

in considerably lesser penalties and help to
avoid long-running, resource-demanding
investigations and settlement negotiations.
An effective compliance program must
ow from the top down, with the board
and executives rmly committed to a
culture of compliance and accountability.
Compliance ofcers need to have authority
to oversee a robust program but need to
work as partners within the organization,
not strictly policing but educating,
strategizing and encouraging compliance
efforts. The compliance ofcer, working
with each department or division, should
identify areas of compliance risk unique
to the operations and functions of that
department or division. When risks have
been identied, compliance staff needs
to work with operational staff to develop
effective policies, identify necessary
training and establish ongoing monitoring
programs specic to the risks identied.
Compliance ofcers also need to create a
structure for employees to anonymously
report any noted violations or instances
of noncompliance.
Value vignette
Employee surveys: benchmarking the effectiveness of compliance programs
In its compliance guidance documents,
the HHS OIG calls for benchmarking and
showing evidence of compliance program
effectiveness. One recommended
method of benchmarking is surveying
employees. Surveys can demonstrate
how well employees understand their
organization’s compliance program and
their obligations to it.
Two types of employee surveys can be
used to gauge program effectiveness:
•A culture survey, measuring
employees’ perceptions, attitudes
and beliefs about their organization’s
compliance environment. These
questions are typically asked in
the form of a statement, with the
respondent selecting from choices
such as completely agree, agree
somewhat, neutral, disagree
somewhat and completely disagree.
Starting with a baseline survey taken
early in program development and
re-surveying periodically after it is
implemented —with employees trained
and working within the compliance
program guidelines — can demonstrate
an organization’s progress in
establishing a culture of compliance.
•A knowledge survey, measuring
employees’ understanding of the
compliance program’s structure,
operations and the role of the
compliance ofcer. Typically, these
surveys are structured as questions
or statements with yes/no/don’t
know answers. Such surveys can
demonstrate how effective the
compliance program is in reaching
all employees. They can also be
supplemented with selected open-
ended questions to provide more
in-depth assessment of employees’
knowledge of specic program aspects.
For a survey to be effective, the
questions should:
•Be short and simple
•Be specic and unambiguous
•Use familiar terms
•Avoid hypothetical questions
•Be written in the present tense
•Avoid cultural bias
Surveys should be a reasonable length
to hold employees’ interest and avoid
careless responses. To avoid bias in
responses, employee identity needs
to be protected — and respondents
assured of their anonymity.
The OIG’s Compliance Program
Guidance for Hospitals notes that “the
compliance ofcer or reviewers should
consider techniques such as … using
questionnaires developed to solicit
impressions of a broad cross-section
of the hospital’s employees and staff.”
The US Sentencing Guidelines state
that businesses must promote an
organizational culture that “encourages
ethical conduct and a commitment to
compliance with the law.” Both guidelines
stress the importance of understanding
and documenting an organization’s
culture of compliance.
Surveys can provide insight into how
effective an organization’s compliance
program has been in changing and
improving compliance throughout the
organization. They can also illuminate
the program’s strengths and weaknesses,
as well as provide a way to let employees
know that their opinions are valued and
that their input is being used to make
positive changes.
Source: Richard P. Kusserow, “Measuring and Benchmarking Compliance Program Effectiveness,” Journal of Health Care Compliance, Vol. 15, No. 2, March – April 2013.
67
An effective compliance program will also
maintain appropriate documentation of
its compliance processes and procedures,
results of reviews, evidence of training and
education, and any manuals or guidelines
developed. The compliance ofcer should
report to the board to help members
fulll their obligation for overseeing the
organization’s compliance efforts. Once
CMS issues regulations implementing
the ACA’s compliance provisions, each
organization should carefully assess the
policies and operating and reporting
practices of its compliance plan to conrm
it will meet CMS’ denition of an effective
compliance program.
Beyond compliance: adding value
As health care organizations voyage
forward, effective compliance programs
can do more than create safeguards. They
can add value by establishing processes
and procedures directed toward delivering
better patient care, lowering costs and
improving employee engagement —
following the same protocols for program
monitoring, tracking, oversight and
reassessment. A logical starting point
could involve monitoring compliance
with tracking and reporting outcomes,
operational care practices and patient
satisfaction for value-based purchasing
initiatives, moving toward encompassing
system-wide efforts to improve the quality
of care. Together, these efforts can lead to a
culture of compliance not only in regulatory
matters but also in an organization’s overall
commitment to value in health care delivery.
“By going after the practices that
shake our trust in the marketplace
and risk harm to us when we need
medical care, we seek to make our
health care system work better.”
Stuart F. Delery
US Assistant Attorney General
Keynote address, CBI Pharmaceutical
Compliance Congress
January 29, 2014
Value vignette
Compliance and long-term care: tracking the ACA mandate
The ACA requires owners, operators
and administrators of LTC facilities to
operate, by March 23, 2013, an effective
compliance and ethics program that
prevents and detects criminal, civil and
administrative violations and promotes
quality of care. Since CMS has not
yet issued implementing regulations,
compliance will not be enforced until the
rule is in place. This rule will eventually
be enforced through LTC surveys and the
certication process. The ACA identied
eight elements of an effective compliance
and ethics program:
• Develop compliance standards
and procedures that reduce the
prospect of criminal, civil and
administrative violations
• Assign executives within the organization
responsibility for monitoring and
overseeing compliance
• Avoid assigning or delegating
responsibility to individuals likely
to commit criminal, civil or
administrative violations
• Communicate compliance standards
to all employees and agents through
publications and training programs
• Implement measures to achieve
compliance, such as monitoring
and auditing procedures to detect
noncompliance and a reporting system
where employees can report violations
• Consistently enforce compliance
standards, including effective
disciplinary measures in cases
of noncompliance
• Take reasonable steps to respond to
violations and institute mechanisms
to correct and prevent recurrences
of noncompliance
• Periodically assess the compliance
program to determine if modications
are needed to reect changes within
the organization
Source: Amy Runge, “How the Affordable Care Act Impacts Compliance and Ethics Programs of Long‑Term Care Facilities,” Washington Healthcare News, 2013,
www.wahcnews.com/newsletters/wa‑arunge‑0613.pdf
68 New horizons: voyage to value

Viewfinders
Considerations for your board and executive leaders
For all health care organizations
•Does your board foster a culture of
compliance, looking beyond regulatory
compliance to incorporate compliance
as a way of enhancing the value of the
services you provide?
•Does your board hold everyone in your
organization accountable for conforming
to compliance policies and procedures?
•Does the executive responsible for your
compliance plan report directly to the
CEO or board? Is this executive required
to report periodically to the board on
compliance efforts, results of compliance
reviews, results of employee surveys on
compliance efforts and resolution of any
reported potential violations?
•Do you have procedures in place that
encourage employees to safely and
anonymously report potential F&A
concerns or events of noncompliance,
along with a clear process to follow up
on any reported issues?
•Do you use employee surveys to assess
the effectiveness of your compliance
program and your progress in fostering
aculture of compliance?
•Do you have a designated individual
or team that monitors developments
in enforcement activities by state
and federal agencies, assessing the
implications if such investigations were
extended to your organization?
•Does this individual or team also
monitor federal and state legislative
and regulatory activity so that your
organization can proactively address
compliance with new laws or regulations
that apply to your operations? Does
this individual or team follow pending
legislation so that your organization can
proactively plan for changes that may
affect future operations?
For providers
•Does your organization have an effective
compliance program that meets the eight
requirements for a provider’s compliance
plan as dened in the ACA?
•Has your compliance program been
customized to suit the needs and
operations of your organization?
•Do you review the annual OIG Work Plan
to understand the issues the OIG plans
to focus on each year, assessing the
implications for your organization as well
as your organization’s ability to comply
with all applicable regulatory guidelines?
•Do you actively monitor the federal
Medicare and state Medicaid exclusion
lists to conrm that your organization
does not contract with, hire or
otherwise work with anyone excluded
from participating in the Medicare or
Medicaid programs?
•Do you coordinate compliance and
quality assurance functions to meet
requirements of HVBP programs while
avoiding any inadvertent violations of
F&A regulations?
•Do you conduct a self-assessment of
your billing, coding and documentation
efforts each year and evaluate the
results to determine where modications
are needed to your compliance plan or
employee education efforts?
•Do you have a clear process in place
to thoroughly and promptly assess
any potential improprieties and, where
applicable, self-report any violations
to appropriate government agencies?
For payers
•Does your compliance team review
the terms of contracts each year to
determine that your organization is
in compliance with existing contracts,
particularly in such areas as utilization
management, data tracking and
reporting, customer education and
timely claims processing?
•Are you prepared for increased
oversight and review activities by CMS
for plans sold on the federal or state
insurance exchanges?
•Have you analyzed the claims data
your organization maintains to identify
patterns of potentially fraudulent
activity? Do you track your competitors’
initiatives to identify best practices or
to curb fraudulent activity and assess
whether those practices would be
effective for your organization?
•Do you educate your members to show
them how they can be involved in
preventing health care fraud and abuse
and to arm them with the ability to
identify potentially abusive practices?
Do you provide a hotline or other
mechanism for members to report
unusual or potentially fraudulent claims
or practices?
•Do you work with employers or other
plan sponsors for the group health
insurance plans you provide to create
summaries of benets and coverage that
comply with ACA requirements and the
DOL template?
69

{ }
“The real voyage of discovery consists not in seeking
new landscapes, but in having new eyes.”
Marcel Proust, 20th‑century French author
Chapter 5
Value in transactions
Gaining the wind
Voyage to value
Mergers and acquisitions (M&As), afliations and even divestitures
offer organizations the opportunity to create signicant nancial,
operational and strategic value. Providers and payers are nding value
in transforming their business models to expand scope and diversify their
market and revenue sources. Nontraditional players are entering the
health care waters to gain share in new or existing markets. The success
of today’s transactions is no longer measured by size but by the ability
to create value.
Health care organizations need to maneuver carefully, however, through
the potentially turbulent winds of M&As and other afliations, aiming
for high-value transactions while avoiding risks inherent in any deal — for
example, the wrong choice of partner, a awed transaction structure,
inadequate due diligence or a lack of compatible cultures. On the other
hand, staying on the shore of a promising transaction brings risk also.
As the tide to value rolls out, those who fail to capitalize on opportunities
to transform their business models may be left behind.
71

Health care reform demands that providers meet
performance and quality goals and payers implement
methodologies to tie payments to high-quality outcomes.
As a result, many are seeking partners on their voyage
to value — to extend networks, provide a wider range of
services and products, and share nancial and operational
practice data in determining the most cost-effective
and high-value options for care delivery. In this chapter,
we provide an overview of the year’s developments in
transaction activities. Also explored is the synergistic
value of provider-provider, provider-payer and payer-payer
M&As and other kinds of afliations and combinations.
M&A activity overview: rolling
with the changing tides
Over the past decade, health care
organizations have seen a variety of
opportunities to collaborate, at times
informally, but increasingly as part of a
structured agreement — be it a merger,
acquisition, partnership or other non-
traditional afliation. While M&As continue
to be a viable option for extending market
area, other afliation strategies can help
achieve an organization’s long-term goals
by adding services not currently in an
organization’s portfolio, or providing an
opportunity to reduce operating costs.
In the past two years, trends in health
care M&A transactions have ebbed and
owed. Overall, health care M&A activity
in 2013 decreased from 2012, which had
the greatest number of transactions since
2007. However, even with fewer deals,
some sectors saw an increase in the dollar
value of transactions closed.
The fourth quarter of 2013 did show an
uptick in the number of deals compared
with the rst half of the year. Continuing
into the rst quarter of 2014, both the
health care services and health care
technology sectors overall have seen a
slight drop in the number of transactions
compared with the fourth quarter of 2013,
but a slight increase over the rst quarter
of 2013. While we will continue to see
some large deals announced, generally,
current deals trend toward smaller and
more strategic transactions, as health care
organizations look for opportunities to ll
gaps in service coverage or specialties, or
to cover all segments of a redened market
area. While nding the right strategic t
may result in fewer deals and the possibility
of higher prices, strategic deals promise
greater potential for adapting current
business models to meet the demands of
health care reform, providing greater value
for acquiring organizations.
“The health care market is moving
beyond the uncertainty that
surrounded implementation of
the Affordable Care Act. Acquirers
now are investing in improving
patient outcomes, whether it’s
buying a long-term care facility or
a data analytics company that will
help to streamline operations and
contain costs.”
Lisa E. Phillips
Editor
Health Care M&A News
February 3, 2014, press release
Services sector overview
Compared with other health care sectors,
the hospital sector reects a different
trend in M&A activity. Although hospital
transactions had been steadily increasing
since 2009, a slight drop in 2013 appears
to be continuing into 2014. Transaction
activity in the rst quarter of 2014, with
12 deals completed, shows a signicant
decrease compared with the rst
quarter of 2013, when 21 transactions
were completed. Yet despite hospital
transactions’ drop in number in 2013, their
value spiked more than eightfold — from
$1.9 billion in 2012 to $18.6 billion in
2013. The big increase is due primarily
to two multibillion-dollar deals: the
acquisition by Community Health Systems
of Health Management Associates and
Tenet Healthcare Corp.’s acquisition of
Vanguard Health Systems.
As hospital organizations assess the impact
of the ACA and the movement toward
value-based purchasing, the decrease in the
number of hospital transactions suggests
that other provider segments are currently
72 New horizons: voyage to value
more valuable targets than hospital
consolidations. Acquiring complementary
organizations may also be quicker and
easier than consolidating hospitals,
as there may be fewer management and
governance issues to resolve. Increases
in transactions of LTC providers and
ancillary services providers support this
observation. However, acquisitions of
smaller rural hospitals are expected to
continue as those hospitals struggle to
raise the capital necessary to meet health
care reform’s demands for a more robust
IT infrastructure.
Physician group practice deals show trends
similar to those of hospitals. In the rst
quarter of 2014, transactions decreased
compared with the rst quarter and the
fourth quarter of 2013. A look at who is
acquiring physician group practices shows
another interesting trend. While hospital
organizations continue to show strong
interest in acquiring physician group
practices, in 2013, only 14% of physician
group acquisitions were completed by
Exhibit 5-1. Deal volume by health care sector, quarterly comparison
Q1:14 Q4:13 Q1:13
Sector Deals Deals Change Deals Change
Services
Behavioral health care 3 2 50% 7–57%
Home health and hospice 610 -40% 9–33%
Hospitals 12 17 –29% 21 –43%
Labs, MRI and dialysis 11 922% 922%
Long-term care 60 65 -8% 44 36%
Managed care 5 4 25% 2150%
Physician medical groups 10 20 –50% 13 –23%
Rehabilitation 2 6 –67% 20%
Other health providers and clinical research organizations 27 15 80% 24 13%
Services subtotal 136 148 –8% 131 4%
Technology
Biotechnology 26 30 –13% 12 117%
e-health 19 24 –21% 16 19%
Medical devices 25 30 –17% 25 0%
Pharmaceuticals 33 46 –28% 28 18%
Technology subtotal 103 130 –21% 81 27%
Grand total 239 278 –14% 212 13%
Source: Levin Associates, The Health Care M&A Report, April 2014.
73
hospital organizations compared with 51%
in 2011. Publicly traded physician practice
management companies represented 54%
of physician group acquisitions; several
managed care companies and an LTC
provider also acquired physician group
practices in 2013. As the uncertainties of
the ACA are sorted out and health care
providers continue to assess how best
to manage population health, strategic
transactions can be expected to increase
in the market’s voyage to value.
Technology and life sciences
sector overview
The health care technology segments
show almost exactly the same trend: in
the rst quarter of 2014, the number
of transactions fell compared with the
Value vignette
Health IT companies: leveraging emerging technologies for value
Health care providers and payers are
moving swiftly to capture the value
of the information they maintain in
their HIT — developing strategies for
optimizing the impact of participating
in pay-for-value models and achieving
operational efciencies. They are also
continually seeking opportunities to
engage patients through data access,
information portals and mobile health
care applications. In the quest to realize
HIT value, health care organizations are
increasingly relying on HIT companies to
provide software, data structure and data
analysis and are adopting new technology
offerings at unprecedented rates. As a
result, HIT companies providing these
services and products are increasingly
targets for acquisition.
Of particular interest for acquisition
are those companies that facilitate
health information sharing and the
interoperability of systems between
providers, as well as those that develop
new software and technology applications.
Many of these technology companies
are private, smaller businesses that
focus on a niche specialty or emerging
technology. The acquiring companies
look to supplement their current software
offerings with additional capabilities,
reach new target markets through
specialized product suites, capture new
technologies, broaden their distribution
channels and achieve their own
operational efciencies.
A sample of HIT acquisitions over the
past year illustrates the high demand
by buyers looking to add a new niche to
their existing service lines, or investors
looking for prots and growth in a high-
demand market.
Adding a niche
Roper Industries, a diversied company
providing engineered products and
solutions for global niche markets,
acquired several HIT companies in the
past two years, broadening its current
offering by targeting companies operating
in specic niche markets. In the largest
strategic HIT transaction of 2013,
Roper acquired Managed Health Care
Associates, Inc., a company providing
services, software and technology to
pharmacies and LTC providers and
sponsoring a network that connects
post-acute and alternate-site health
care providers with ACOs nationwide.
Roper also had the largest strategic HIT
acquisition in 2012 with its purchase of
Sunquest Information Systems, a market
leader in laboratory IT services.
Aiming for investment value
In 2013, private equity buyers were
responsible for 51% of acquisitions of HIT
companies based on acquisition value,
or 25% based on number of transactions.
Private-equity interest in HIT continues
to be strong in 2014. In the rst quarter
of 2014, private equity rms completed
163 health care IT deals. Technology
companies that focus on the practice
of health care accounted for about 53%
of these transactions. Consumer-focused
HIT companies represent about 46%,
and telehealth, scheduling and rating
companies make up the balance.
The largest private equity HIT deal of the
rst quarter of 2014 was the acquisition
by Kohlberg Kravis Roberts of a majority
interest in Sedgwick Claims Management
Services for $2.4 billion. Sedgwick
provides technology-enabled claims
and productivity management solutions.
The largest HIT initial public offering
in the rst quarter of 2014, raising
$1.3 billion, was IMS Health Holdings,
ahealth care data analytics company.
Sources: Roper Industries, Managed Health Care Associates, Sunquest Information Systems, Sedgwick Claims Management Services and Mercom Capital Group;
BerkeryNoyes Investment Bankers, “An overview of M&A in the Healthcare/Pharma Information and Technology Industry,” 2014; “Strong Start for Healthcare IT Sector
with $858 Million in VC Funding in Q1 Executive Summary,” Modern Healthcare.
74 New horizons: voyage to value
prior quarter but increased from the
year-ago quarter (except that medical
device organizations held constant
over the previous year). Although the
pharmaceuticals segment saw an increase
in the number of transactions, there were,
unlike previous years, no multibillion-dollar
deals announced in 2013. Generic drug
makers and specialty drug companies
showed signicant activity.
As population health management grows
and efforts intensify to revamp health
delivery and reduce health care spending,
e-health and medical device companies —
with their potential to readily meet these
demands — are particularly attractive
targets. In the rst quarter of 2014, private
equity companies invested about $858
million in e-health companies. A sell-off can
be anticipated as these companies grow
and mature over the next several years and
private equity companies move on to their
next horizon.
And it appears the growth in health care
technology and pharmaceutical deals this
year is just getting started. The last week
of April 2014 saw a major spurt with three
large pharmaceutical deals and one major
medical device transaction announced.
A big deal — in health care real estate
investment trust transactions
Another signicant acquisition, announced
in early June 2014, is Ventas’ plan to
acquire American Realty Capital Healthcare
Trust in a $2.6 billion transaction. Ventas is
currently one of the country’s larger health
care real estate investment trusts (REITs),
as measured by market capitalization. If this
acquisition, planned to close in the fourth
quarter of 2014, is completed, Ventas will
become the nation’s largest health care
REIT. Both Ventas and American Realty
Capital Healthcare Trust invest in medical
ofce buildings and senior housing.
By the numbers
• In the past two years, the health
care industry’s most active M&A
segment was health care IT, with 280
transactions (source: BerkeryNoyes
Investment Bankers, April 2014).
• Fitch Ratings predicts hospitals in the
25 states that did not expand Medicaid
in 2014 will “face greater nancial
challenges and rating pressure”
compared with hospitals in states
with Medicaid expansions. Overall,
hospitals in the 25 non-expansion
states are expected to lose out on
over $200 billion in additional revenue
over the next decade, which may
spur interest in nding a strategic
merger partner to derive operating
efciencies or as a source of capital.
(source: Fitch Ratings, October 2013).
• Acquisitions of physician medical
groups dropped from a high of 108 in
2011 to 65 in 2013. In 2011, 51% of
the transactions saw hospitals or
an integrated health system as the
acquiring organization. In contrast,
in 2013, only 14% of the acquisitions
were by hospitals or integrated
health systems. The remainder were
acquired by managed care companies
(payers) or publicly traded practice
management corporations (source:
Health Care M&A News, April 2014).
• In September 2013, a health system
in Chicago committed $230.5 million,
plus annual payments of $118.5
million through 2016, to acquire a
900-physician practice, in one of the
largest sums ever paid for a medical
practice acquisition (source: Modern
Healthcare, February 2014).
• As many as 1,000 health care facilities
are expected to undergo an M&A
between 2013 and 2020 (source:
Booz & Company, March 2013).
• 88% of health care provider executives
plan to pursue an M&A within the next
12 months (source: GE Capital survey,
January 2014).
• Hospital markets in 71% of the
country’s metropolitan statistical
areas are already considered
“highly concentrated” under Federal
Trade Commission (FTC)/DOJ
guidelines (source: American Medical
Association, Competition in Health
Insurance: A Comprehensive Study
of U.S. Markets, 2013 Edition).
• 86% of insurance executives expect
to see an increase in the volume of
M&As over the next one to three
years (source: Towers Watson survey,
March 2014).
• Just one insurer accounted for
more than 50% of the market in 15
states and just two health insurance
organizations accounted for more than
50% of the health insurance market in
45 of the 50 states (source: American
Medical Association, Competition in
Health Insurance: A Comprehensive
Study of U.S. Markets, 2013 edition).
• A recent study — covering mergers
in the 10-year period from 1998 to
2008 — revealed that only 41% of
acquired hospitals outperformed
their market peers and most M&A
deals failed to live up to expectations
(source: S.B. Saxena, A. Sharma and
A. Wong, “Succeeding in Hospital &
Health Systems M&A: Why So
Many Deals Have Failed and How
to Succeed in the Future,” Booz &
Company, 2013).
75

76 New horizons: voyage to value
Antitrust laws and M&As:
sounding the foghorn
In January 2014, a federal judge ruled
in favor of the FTC in deciding that a
health system in Idaho violated antitrust
laws when it acquired the state’s largest
independent physician practice. The judge
ruled that the acquisition must be
unwound — a difcult and expensive task
to accomplish.
Although the judge acknowledged that
the acquiring system sought to improve
patient outcomes through the acquisition,
he also ruled that it would result in an
“unfair and illegal marketplace advantage”
by dominating primary care and would
increase the risk of price increases.
This decision will likely inuence future
acquisitions of physician groups by hospital
organizations. Each potential acquisition
should anticipate raising antitrust concerns
if it will result in high market shares, even
if limited to a localized area. According to
this ruling, organizations seeking to achieve
integrated care in their communities do
not have to purchase a group practice to
achieve this goal; they should consider
alternatives such as integrated networks
or co-management arrangements that stop
short of an acquisition.
“Keeping health care costs low and
quality high by ensuring vigorous
competition between providers
is, and will continue to be, a top
commission priority.”
Edith Ramirez
Chair, FTC
In April 2014, the FTC continued its
winning streak with a victory in a federal
appeals court case. An Ohio health system’s
acquisition of a hospital was determined
to be “extremely likely to illegally increase
prices.” The acquiring organization
argued that the acquisition was the only
way to keep the nancially struggling
Value vignette
Transaction alternatives: merging efforts, not assets
Sometimes an alternative to a full
merger of two organizations’ assets
may accomplish the merging entities’
goals while eliminating the need for
antitrust approval that an asset merger
would require. A recent example of an
alternative solution is the creation of
Together Health Network (Together),
a new company jointly founded by
two large, competing health systems,
Ascension Health and CHE Trinity Health.
Together was formed in response to
the need for value-based payments
and population health management for
managed care contracting in Michigan.
It is a closely aligned, clinically integrated
network, uniting 27 hospitals, more
than 12 physician organizations and
5,000 physicians across Michigan.
In all, 75% of the state’s residents will
be 20 minutes or less from at least one
of the network facilities.
Moving forward, Together plans to:
•Offer health insurance products to
health insurers and also directly to
employers by fall 2014
•Sell a variety of managed care plans
on private health exchanges and also
on the federally run HIX in Michigan
•Offer managed care contracts with
shared-savings arrangements, pay-
for-performance payments and global
budgets with bundled payments tied
to specic procedures and narrow
provider networks
•Provide patient care through its
network by January 2015
“We believe this one-of-a-kind
collaboration between two of
the state’s largest healthcare
organizations will set a new
standard for providing value-
based healthcare in Michigan.”
Patricia Maryland, PhD
President of Health Care Operations and
Chief Operating Ofcer
Ascension Health
Press release, May 9, 2014
Together will be physician-run, with plans
to hire a physician CEO. The managing
board will include nine physicians, four
Trinity and Ascension executives and two
members representing the community.
In the initial start-up period, staff from
both health systems will support the
new company.
Source: “Ascension Health, CHE Trinity form integrated network in Michigan,” Modern Healthcare,
May 7, 2014.
77
acquiree from closing; the FTC argued it
had enough cash to pay its obligations.
The court upheld an earlier FTC ruling that
the acquired hospital must be divested.
This case is expected to be appealed to the
US Supreme Court. The decision will likely
prompt hospitals to consider alternative
strategies, such as reducing services or
other cost-cutting moves, if a potential
merger may raise antitrust concerns.
In a recent interview with Modern
Healthcare, Markus Meier, Assistant
Director for Health Care Enforcement
in the FTC’s Bureau of Competition, was
asked about the FTC’s apparent efforts
to discourage M&As despite the ACA’s
goals to create networks that coordinate
care. He responded by explaining, “We’re
worried about organizations that are not
much more than a price-xing cartel, or
organizations that are fairly integrated
but are so large that they dominate
their marketplace and have the ability to
exercise signicant market power. Both of
these types of behavior have a very high
likelihood of harming consumers, raising
prices and not improving quality at all.”
When asked if he thought it was fair that
the FTC was stepping up enforcement
efforts in this era of reform, he replied,
“I sometimes have to remind physicians
and hospitals that the antitrust laws aren’t
there to protect their interests as producers
of health care services, they’re intended
to protect consumers, including patients,
health plans and self-insured employers.
By promoting competition, we hope that
leads to lower prices, better quality, more
choices and innovation.”
Do payers need to sail together?
Achieving economies of scale
Health care payers are likely to consider
whether scale and efciencies that can
be achieved through mergers are needed
to thrive under the ACA. The law requires
health insurers’ claims and allowable
costs for quality improvement activities
to account for a specied percentage of
premiums charged (the minimum medical
loss ratio). Payers that fail to meet the
required ratio must issue rebates to their
members. Also, the increased transparency
and ability to compare costs of various
plans facilitated by the health insurance
exchanges (HIXs) is expected to increase
payer competition. These factors increase
the incentive to generate efciencies in
operations, cut costs and keep revenue on
track. Given these pressures, payers may
nd mergers a viable option for achieving
their goals.
Through a merger or acquisition, payers
can expand their markets, achieve
operational efciencies and spread their
risk over a larger pool of customers.
Potential acquisition candidates can range
from strategic targets such as another
payer operating in a different market or
providing niche insurance products to a
vertical target, such as a physician practice
or other health care provider. Finding the
right strategic t is critical (see Exhibit 5-2).
Divestitures: cutting the sails free
Often when looking to cut costs or improve
quality, health care organizations consider
divesting certain services from their
portfolios. Sometimes, arrangements are
Exhibit 5-2. Payer questions in
searching for the right M&A fit
To nd the best strategic t and select
an effective target for acquisition,
payers should consider several factors.
Does the acquisition target:
•Have a product line that
complements yours?
•Offer your organization access to
new markets or new technology?
•Have the current medical
expertise, systems or programs
to better manage the health of
your population?
•Provide expertise that could help to
reduce your current administrative
costs — for example, a claims
processing rm or call center?
•Have an insured population that
will help to reduce your current
acuity risk?
•Have an acceptable medical loss
ratio? And will you be able to
reduce medical costs through
combining your operations to
ensure minimum medical loss ratios
will be achieved?
•Provide an opportunity to increase
vertical integration, delivering
medical services or products
necessary to meet your customers’
health care needs — such as a
physician practice or pharmacy
company — with the potential to
increase revenues or lower costs?
Source: EY analysis, 2014
78 New horizons: voyage to value
made to transfer or sell service lines to
competitors better situated to provide
them cost effectively. Other times, specic
service lines are simply shut down and no
longer offered.
The state of Louisiana has taken divestiture
of costly services to a new level. After
several years of extensive budget cuts to
the Louisiana State University (LSU) Health
Care Services Division (formerly known as
Louisiana’s Charity Hospitals), the cost of
maintaining the Division’s 10 hospitals was
still considered too expensive for the state
budget. In a move to cut state costs, in
2013 the governor of Louisiana proposed
closing or divesting most of these hospitals
and their afliated clinics. The hospitals
divested would be converted from public
to private entities and leased to private
operators. Several hospitals would be
closed and their operations transferred to
existing private health care organizations.
The university’s board of supervisors
approved the plans and the Louisiana State
Civil Commission has approved eight of the
privatization plans with one deal pending.
The state intends to retain only one LSU
hospital as a public entity.
Lease payments from the newly privatized
hospitals are expected to generate about
$100 million per year for the state. Further
budget “savings” are expected through
layoffs of all hospital and clinic employees.
About 90% of these former state employees
were rehired by the private entities running
the hospitals, although with signicantly
reduced benet packages. All privatizations
are planned to be complete by the end
of 2014.
In May, CMS took the wind out of the
privatization plan, rejecting the nancing
plans for the rst six hospitals privatized.
CMS determined that the “advance
lease payments” the private operators
paid up front as part of their no-bid
contracts do not meet federal guidelines
for how Medicaid funds can be spent.
CMS indicated that the structure of the
contracts “amounted to Louisiana trying
to get extra federal Medicaid dollars to
repay private managers” for the advance
lease payments. The state is planning to
appeal the ruling and work on changing the
nancial structure of the privatization deals
to gain CMS approval. Should the appeal
and restructuring attempts fail, estimates
of amounts the state would have to repay
the federal government range from
$200 million to $500 million.
Value vignette
Achieving high value: building a formal alliance without a merger
In 2012, the Central Georgia Health
System and Tift Regional Health
System created a formal partnership
intended to develop a regional care,
integrated services network. The goal
of the partnership was to work as equal
partners to “enhance the level of medical
service delivery in the region and
position both systems for the challenges
of health care reform.”
With the growing need to manage
population health, these organizations
decided to broaden their geographic
reach. In late summer 2013, they
joined with 21 other hospitals in south
and central Georgia to create a not-
for-prot limited liability corporation,
Stratus Healthcare. Along with
combining resources to reduce costs,
the collaborative alliance is designed
to exchange best practices, develop
coordinated information systems and
manage population health.
Today, a total of 29 hospitals, 14 health
systems, about 2,000 physicians and
more than 18,700 employees make
up Stratus Healthcare. Through this
formalized alliance, members can “take
advantage of a shared service model, yet
remain independent,” according to the
company. Stratus’ work is conducted by
work groups formed with representatives
of each partner hospital.
Stratus work groups have already been
analyzing primary care, emergency
medicine, hospitalist and specialty care
networks to assess the development of
consistent clinical guidelines, coordinate
transfer arrangements, launch
telemedicine programs and share
outcomes data. Future work groups will
consider computer technology platforms
and data warehouse capabilities to
enable the seamless exchange of
electronic health information, collective
purchasing, shared business resources
and an integrated clinical network.
Source: Stratus Healthcare.
79
Toward a new horizon: achieving
high-value transactions
Health care provider and payer organizations
have set sail on a rigorous journey — one
fraught with nancial and operational
challenges. Many are nding it a critical
imperative to seek partners, assessing
the potential of various forms of afliation.
But to fare successfully in the shifting
winds, any such arrangement must yield
high value.
Achieving value is much more than a larger
organization swallowing a troubled entity;
it is a strategic deal deliberately designed
to align incentives and share successes.
In assessing opportunities to collaborate,
EY’s Capital Agenda can serve as a guide
(see Value vignette). Those that seek
out best-t partners to build a stronger
organization have the greatest chance of
sailing through the changes reform and
the market demand — and reaching the
destination of true value delivered.
Value vignette
EY’s Capital Agenda: evaluating strategies
To gain the wind in their voyage
to value, health care organizations
should continually evaluate their
capital strategies, review their capital
investment methods and focus on their
capital assets. EY’s Capital Agenda
includes four dimensions of evaluation
to facilitate this process:
• Preserve: assess the potential impact
of evolving market conditions on
your operational performance and
capital base
• Optimize: drive cash and working
capital, and manage your portfolio
of core and noncore assets to
accelerate return
• Raise: consider future capital
requirements and determine how
funding sources can be diversied
to increase options
• Invest: strengthen investment
appraisal and execution methods
to manage risk while realizing
opportunities
How organizations manage their capital
today will dene their competitive
positions tomorrow. The Capital Agenda
serves as a resource for evaluating
opportunities, making strategic decisions
and creating efcient transactions.
Source: EY, Provider Post, Health care’s Capital Agenda. For more guidance, request a copy from your local
EY executive.
80 New horizons: voyage to value

Viewfinders
Considerations for your board and executive leaders
For all organizations
•Whether you are pursuing an M&A
target or are considering offering your
organization as an acquisition candidate,
do you have a strategic plan in place?
Does it include a SWOT analysis? How are
you documenting that you are following
your plan?
•Before pursuing a transaction, as either
the acquiring or selling company, does
your organization take into account
who will be responsible for transaction-
related tasks, such as gathering and
organizing data for due diligence,
communicating with other parties, and
analyzing and synthesizing acquisition-
related documents? If an internal team
will be used, who will be responsible for
their day-to-day activities? Have you
considered hiring an interim executive
or team to assist in this process?
•When considering a potential M&A
candidate, do you carefully assess
whether aligning with the candidate
will advance your long-term strategies
and help your organization better serve
your stakeholders?
•Early in the process, do you determine
whether the candidate meets
criteria for cultural alignment with
your organization?
•Have you considered whether an
alternative to a merger or acquisition
would better meet your needs and goals?
•Do you start drafting a post-merger
transition/action plan early in the
process, during due diligence, as well
as identifying transition team members
and responsibilities?
•Does your transition plan include
responsibility for monitoring quality and
performance throughout the process to
make sure day-to-day operations stay
on schedule, are consistent and do not
suffer as a result of efforts to integrate
the newly acquired organization?
•Do you have a process in place to provide
any required notications to federal
and state agencies and to assess the
probability of FTC challenges to your
planned merger or acquisition?
For providers
•When considering an M&A candidate,
do you understand what value
this organization will bring to your
organization? Will the candidate provide
lasting value to help your organization
in managing risks related to pay-for-
performance contracts or ll a strategic
gap that meets a clearly dened need?
•Do your due diligence process and
integration plans include detailed review
and inventory of all HIT systems, both
clinical/operational and nancial,
to identify redundant systems and
software and to determine the adequacy
of systems planned to be used by the
newly merged entity? Are decisions
about which systems will be retained and
plans for necessary conversions made
early in the process to best achieve a
smooth transition?
For payers
•When evaluating an M&A candidate,
does your team carefully assess their
participation in state and federal HIXs,
the plans offered, the demographics of
enrollees and the networks with which
they have contracted? Will the networks
be broad enough to stand up to CMS’
scrutiny intended to make sure networks
are not so narrow as to discourage
or prohibit enrollees from obtaining
needed care?
•Do you consider acquisitions of
companies that can enhance your
organization’s capabilities in e-health,
risk management, data analytics and
population health management of
healthy individuals as well as specic
categories of chronic care populations?
•Do you assess the impact an M&A
candidate will have on your member
engagement and satisfaction?
81

{ }
“Everything that can be counted does not necessarily
count; everything that counts cannot necessarily
be counted.”
Albert Einstein, 20th‑century German physicist
Chapter 6
Value in measurement
Sounding the depth
Voyage to value
The concept that cost and quality determine value in health care has
remained a constant. Yet historically, value has been difcult to measure.
Unlike in many other industries, the end user of health care’s product,
the patient, has often been displaced from purchasing decisions while
the value equation has typically focused on cost or quality, but rarely the
two together.
With today’s industry sea change — including the ACA’s expansion
and renement of measurement and reporting requirements — new
methods are emerging to measure value in its many dimensions. These
measures are core to “sounding the depth” of cost and quality challenges
and enabling system transformation: care reorganized, processes
continuously improved and new routes taken to enhance value for
all industry stakeholders.
83
Measuring value in health care has been an earnest yet
often elusive pursuit. Typically, measures have centered
on the provider rather than the patient. They have
often fallen short of gauging the things that matter
most to health care consumers, such as clear and
respectful communication, early and timely treatment
and stronger, quicker recoveries. In this chapter, we
highlight organizations that are making waves in value
measurement, along with methods being tried across the
waterfront to calculate health care value.
Measurement leaders: meeting
the challenge
A variety of organizations have taken on
the mission of developing metrics for value.
Proled below are the contributions of
several leaders in value measurement.
American Hospital Association (AHA)
AHA has offered 19 metrics to help health
care providers measure their progress
toward value-based care (see Exhibit 6-1
on page 85). These measures are focused
on meeting four value-based strategies
as the industry transitions from pay for
volume to pay for value.
AHA has also published a “road map” to
help health care leaders assess and score
their progress in achieving these strategies
(available at www.hpoe.org/resources/
hpoehretaha-guides/1360).
High Value Healthcare
Collaborative (HVHC)
A consortium of 19 top US medical
centers and the Dartmouth Institute
for Health Policy and Clinical Practice,
HVHC provides a forum for sharing data
to reduce variance and improve value.
The collaborative collects and exchanges
data on quality, outcomes and cost for
expensive, high-variation conditions and
treatments; identies and evaluates
best-practice health care models and
innovative, value-based payment models;
and shares with the public the knowledge
and lessons learned. The group is currently
focused on nine high-volume, high-cost
and high-variation conditions: total knee
replacement, diabetes, congestive heart
failure, depression, spine surgery, labor
and delivery, asthma, hip surgery and
bariatric surgery.
HVHC’s rst research, studying nearly
11,000 total knee replacements performed
across ve health systems, found
considerable differences in procedures and
outcomes. According to the group, ndings
are intended to spur value improvements,
including more coordinated management
of complex patient cases, more consistent
operative teams for surgeons and a process
for better managing patient expectations.
Integrated Healthcare
Association (IHA)
For 13 years, IHA has served as the
convening organization for California’s
statewide pay-for-performance program.
Eight commercial health plans and
about 200 physician organizations (POs)
participate in the program, which covers
an estimated 9 million Californians
enrolled in commercial health maintenance
organization (HMO) and point-of-service
(POS) products. According to IHA, seven
of the plans — Aetna, Anthem Blue Cross,
Blue Shield of California, Cigna Healthcare
of California, Health Net, UnitedHealthcare,
and Western Health Advantage — have paid
out more than $450 million in incentives
through 2012 based on the results,
which have shown over time a steady
improvement in quality metrics.
Recently, IHA has started to transition
to value-based P4P. This shared-savings
model holds POs accountable not only for
the quality of care provided to their HMO
and POS members, but also for the cost,
cost trend and resources used for care
provided. In 2013, one participating health
plan — Blue Shield of California — fully
implemented the new program design;
several others are planning to adopt it
in 2014. IHA notes that standardized
measures of quality and cost will help in
assessing health care value, supporting the
development of value-based network tiers,
informing consumer selection and serving
as a key resource for HIXs.
“I have been struck … by how
important measurement is to
improving the human condition.
You can achieve amazing progress
if you set a clear goal and nd a
measure that will drive progress
toward that goal …”
Bill Gates
Co‑Chair, Bill & Melinda Gates Foundation
2013 Annual Letter
84 New horizons: voyage to value

Value vignette
Why is health care value so hard to gauge? Assessing the need for new measures
From HHS to local business coalitions,
many organizations are rigorously
attempting to measure value. But efforts
often ounder in addressing value from a
patient outcome perspective. According
to ThedaCare’s Center for Healthcare
Value, measures fall short when they are:
1. Department- or process-centric.
Metrics arising from internal patient
surveys or provider reviews often look
at a single department or function,
for example, the ED and patients’
satisfaction with their experience there.
Although these are worthy measures
for teams working to improve a
specic area of care, they do not
reect the full value continuum of the
patient experience.
2. Too broad. Health care rankings
such as Thomson-Reuters’ 100 Top
Hospitals or U.S. News Best Hospitals
typically look at care throughout the
organization or in large specialty areas.
National rankings are too broad for
patients in evaluating value for the
specic treatments they need, where
they need them.
3. Subjective. Health care grading
websites such as HealthGrades have
proliferated, reecting the growing
consumer quest for local health
care information. Yet these services
typically deliver subjective information
provided by patients and their family
members as opposed to objective data
for decision-making.
4. Focused on half the value equation.
Many public and private organizations
have focused on improving health care
quality, exploring ways to quantify
and improve outcomes. These efforts,
however, often exist in isolation of
costs. Conversely, many initiatives
document and report costs but do
not measure the effectiveness of care.
Claims data, for example, can yield
a clear picture of costs, but has not
been intricately linked to the quality
of patient care for specic spending.
Source: ThedaCare’s Center for Healthcare Value, Measuring Healthcare Value: Linking cost and quality of patient outcomes to drive organization and industry
improvements, February 2012, www.createhealthcarevalue.com
Exhibit 6-1. Measures of progress toward value-based care
Strategy 1. Align hospitals, physicians
and other clinical providers across the
continuum of care
1. Percentage of aligned and
engaged physicians
2. Percentage of physician and other
clinical provider contracts containing
performance and efciency incentives
aligned with ACO-type incentives
3. Availability of non-acute services
4. Distribution of shared savings and
performance bonuses or gains to
aligned physicians and clinicians
5. Number of covered lives accountable
for population health (e.g., ACOs or
patient-centered medical homes)
6. Percentage of clinicians in leadership
Strategy 2. Use evidence-based practices
to improve quality and patient safety
7. Effective measurement and
management of care transitions
8. Management of utilization variation
9. Reduction of preventable
admissions, readmissions, ED visits,
complications and mortality
10. Active patient engagement in design
and improvement
Strategy 3. Improve efciency through
productivity and nancial management
11. Expense per episode of care
12. Shared savings, nancial gains or
risk-bearing arrangements from
performance-based contracts
13. Targeted cost-reduction and risk-
management goals
14. Management to Medicare
payment levels
Strategy 4. Develop integrated
information systems
15. Integrated data warehouse
16. Lag time between analysis and
availability of results
17. Understanding of population
disease patterns
18. Use of electronic health information
across the continuum of care
and community
19. Real-time information exchange
Source: AHA, Health Research & Educational Trust, and Hospitals in Pursuit of Excellence, Metrics for the Second Curve of Health Care, April 2013.
85
International Consortium for Health
Outcomes Measurement
ICHOM’s mission is to dene a global
standard set of outcome measures that
matter to patients for the most relevant
medical conditions, and to drive adoption of
these measures worldwide to unlock the full
potential of value-based health care. ICHOM
denes outcomes as “the results people
care about most when seeking treatment,
including functional improvement and the
ability to live normal, productive lives.”
The ICHOM website (www.ichom.org) offers
a searchable metrics repository designed
to increase the comprehensiveness of
measures in use and to standardize existing
measures across registries.
For more information on ICHOM’s
activities, see the conversation with
D r. Jens Deerberg-Wittram, pages 4–7.
National Quality Forum (NQF)
A standard-setting organization, NQF
endorses measures that are considered the
gold standard for health care measurement
in the US. Expert committees made up
of varied stakeholders, including patients,
evaluate measures for NQF endorsement
that are used by the federal government
and private sector.
NQF has endorsed several resource-use
measures designed to gauge health
care value. These measures are dened
as “comparable measures of actual
dollars or standardized units of resource
in the care of a specic population or
event.” Current resource-use measures
span a variety of conditions, including
asthma, cardiovascular conditions, chronic
obstructive pulmonary disease, diabetes,
hip and knee replacements and pneumonia.
Measures also include a population-based
per-member-per-month index and a total
cost population-based per-member-per-
month index.
Network for Regional Healthcare
Improvement (NRHI)
A national membership association, NRHI
works to support the efforts of the 30
regional health improvement collaboratives
in the US (see page 26 of the conversation
with Harold Miller). NRHI reports that the
collaboratives help communities covering
nearly 40% of the US population to improve
their quality of health care services while
controlling costs.
Intended to serve as neutral, trusted
sources of actionable information about
health care value and population health,
the collaboratives publish reports for the
public and health care providers on aspects
of quality and cost of care. Measurements
and reporting initiatives are developed
and operated with the participation and
supervision of the physicians and hospitals
whose performance is being measured.
According to NRHI, the involvement of
participating providers increases their
willingness to change care processes with
the goal of performance improvement.
Pacific Business Group on Health
Founded in 1989, the nonprot PBGH
is one of the nation’s leading nonprot
business coalitions focused on health
care (see Value vignette, page 15). PBGH
represents 60 large companies, such as
Boeing, Target and Wells Fargo, as well as
public agencies such as CalPERS. Together,
these organizations provide health care
coverage to 10 million Americans and their
dependents in all 50 states.
PBGH has led efforts to have private
employers and government reach
consensus on quality care and value
measures. For example, the group has
advocated for measures beyond those that
gauge clinical processes and structure to
those that measure outcomes. It has called
for Congress to direct CMS to identify and
adopt “useful, standardized measures that
address consumer and purchaser concerns.”
Methods for measurement:
capturing the value equation
A variety of methods have been developed
and implemented to measure the value
delivered by providers and payers alike.
Proled below are several approaches.
Diabetes value metric
Work from the Wisconsin Collaborative
for Healthcare Quality (WCHQ) breaks
new waves in blending quality and cost
into a single, actionable health care value
measure specic to a health care condition.
In late 2010, WCHQ formed a Resource
Use Work Group to develop a value
metric linking quality data and cost data
for a specic condition — diabetes — and
episode of care. The diabetes value metric
used quality data provided from WCHQ
provider organizations, along with diabetes
standards cost data provided by the
Wisconsin Health Information Organization
(WHIO) consisting of claims-based data
submitted by WHIO payer organizations.
According to WCHQ, the diabetes value
metric demonstrates that a condition-
specic value measure is possible, showing
the way for developing and disseminating
health care value measures more broadly.
The metric will eventually be provided
to the public for use in assessing the
value that organizations provide to their
diabetic patients.
Global cardiovascular risk (GCVR)
Under a grant from the Robert Wood
Johnson Foundation, the National
Committee for Quality Assurance (NCQA)
is evaluating a new measurement tool that
focuses on enhancing patient value by
improving the health outcomes of patients
86 New horizons: voyage to value
with heart disease and diabetes. The GCVR
measure has been co-developed by the
NCQA and health care modeling software
company Archimedes, Inc. GCVR has
been called a “next generation” quality
improvement tool, measuring how well
providers reduce the risk of future adverse
outcomes — such as heart attacks, strokes
and diabetic complications — in the
populations they serve. The measure will
draw on clinical information from electronic
health records to provide the data needed
to assess improvement in preventing
adverse outcomes.
“[GCVR] has the potential to become
the rst customized, outcomes-
based electronic health record
measure used by Medicare and
commercial payers. Its widespread
adoption could have a profound
impact on health care costs because
it assesses how well providers
engage in prevention and goal-
setting for their high-risk patients.”
Margaret E. O’Kane
President
NCQA
Patient-reported outcomes
measures (PROMs)
PROMs capture patient perceptions of the
outcomes of their care. These measures
reect whether patients believe the
services they received actually delivered
value by improving their overall health and
well-being.
With the growing focus on patient-
centered care and value-based payment
approaches, PROMs are expected to play
a larger role for providers in assessing
their performance and determining the
By the numbers
• In a 2014 survey of health care
executives, nearly three-quarters
(72%) of respondents believe the
industry can make the shift from
volume-based reimbursements
to value-based care, while more
than one quarter (28%) do not
(source: HealthLeaders Media, 2014
Industry Survey, Forging Healthcare’s
New Financial Foundation,
February 21, 2014).
• The value of care offered to hospital
patients can vary by as much as
40% across the US (source: Data
Advantage’s Hospital Value Index™
study, 2009).
• According to a recent report,
10 cities — Boston, Portland (OR),
Philadelphia, St. Louis, Charlotte,
New York, Washington, DC,
Minneapolis, Chicago and Atlanta —
have the best health care in the
country, based on market and hospital
performance for populations. The
study notes that if lower-scoring
markets improve their performance,
they could save nearly 4 million
years of potential lives lost — the
equivalent of an extra year of life for
the entire population of Los Angeles
(source: iVantage Health Analytics,
March 2014).
• By 2030, the number of primary
total knee replacements is expected
to increase by 673%, to 3.48 million
procedures annually, and the number
of primary total hip replacements
will increase by 174%, to 572,000
procedures annually (source: S. Kurtz
et al., “Projections of primary and
revision hip and knee arthroplasty
in the United States from 2005 to
2030,” J Bone Joint Surg Am., 2007
Apr, 89(4):780-785).
• In 2013, 20% of covered workers were
enrolled in high-deductible health
plans — up from 13% in 2010 (source:
Kaiser Family Foundation, 2013,
Health Benets survey).
87
comparative effectiveness of different
treatments. By 2015, for example,
providers participating in ACOs will need
to demonstrate that the care they have
delivered produced value for the patient,
as reported by the patient. The HHS
ONCHIT also plans to incorporate PROMs
into meaningful use standards, which is
expected to accelerate their use.
“These are things that matter
to patients: do I feel better? Can
my mom go up the stairs after
hip surgery?”
Mary Barton, MD
Vice President for Performance Measurement
NCQA
Provider Peer Grouping
(PPG) system
This initiative from the Minnesota
Department of Health (MDH) is designed
to offer a clearer picture of the value
of services offered by the state’s
providers. According to MDH, Minnesota
is the rst state in the nation to develop
a comprehensive system offering
information about health care value — both
cost and quality. With this data, payers
and consumers can compare provider
performance and choose high-quality,
low-cost providers.
The PPG initiative is authorized by the
state’s 2008 reform law, which calls
for developing an all-payer database
and risk-adjustment methodology for
measuring quality and prices for hospital
and physician services. PPG draws on
provider information across all payers,
offering a standardized approach to value
measurement and reporting. The initiative
includes a rapid response team of
providers, purchasers and consumers who
provide input on issues that arise in PPG
implementation.
Quality-adjusted life year (QALY)
QALY is a measure of health improvement
used worldwide in guiding decisions for
health care resource allocation. This metric
combines quality of life with quantity
of life. Quality of life is measured on a
scale of 0 to 1; one year in perfect health
yields 1QALY.
Although QALYs have been used by many
countries — most notably, the UK — in cost-
effectiveness analyses to guide coverage
and reimbursement decisions, their use
is a matter of long-standing debate in
the US. Proponents maintain that QALYs
provide a reliable gauge for measuring and
comparing the health effects of different
interventions across a diverse range of
diseases and conditions. Opponents cite
concerns that QALYs discriminate on the
basis of age and disability, unfairly favoring
younger and healthier populations that
have more potential QALYs to gain.
In 1996, the US Panel on Cost-Effectiveness
in Health and Medicine recommended
that cost-effectiveness analyses use QALYs
as a standard measure for identifying
and assigning value to health outcomes.
The ACA, however, contains language
specically forbidding the use of cost
per QALY “as a threshold to establish
what type of health care is cost effective
or recommended.” Many industry
observers note that strict adherence to a
QALY approach is unlikely in the US, but
amodied approach — coupled with other
criteria — may help illuminate the value of
health interventions.
Relative resource use (RRU)
For more than two decades, the NCQA has
reported on care quality received by health
plan members. Its new measure, RRU, is
a pioneering effort to better understand
the value of care delivered. RRU combines
two indexes, one measuring quality and
another measuring service utilization.
It is based on the concept that patients
who receive high-quality care for certain
chronic conditions are more likely to be
able to manage their health and thus
avoid expensive services such as ED visits,
surgery and hospitalization. NCQA reports
RRUs for ve common chronic diseases:
asthma, cardiovascular disease, chronic
obstructive pulmonary disease, diabetes
and hypertension.
In calculating RRU components for diabetes,
for example, the quality index assesses
whether patients receive guideline-
recommended care and adequate control
of blood glucose, cholesterol and blood
pressure. The utilization component is
calculated by multiplying the number of
times a patient receives a specic service
by a standardized price, not a plan’s
negotiated provider rate. The utilization
component is risk-adjusted for age, gender
and health conditions. NCQA calculates
averages for plans nationally and compares
them to individual plans. Several major
health plans, such as Aetna, Cigna Corp.,
Health Net and UnitedHealth Group, are
participating in the RRU program.
Time-driven, activity-based
costing (TDABC)
Developed by Harvard Business School
professors Robert Kaplan and Michael
Porter, TDABC is a costing method for
assessing value. In health care, the cost
of looking after a patient along the care
88 New horizons: voyage to value
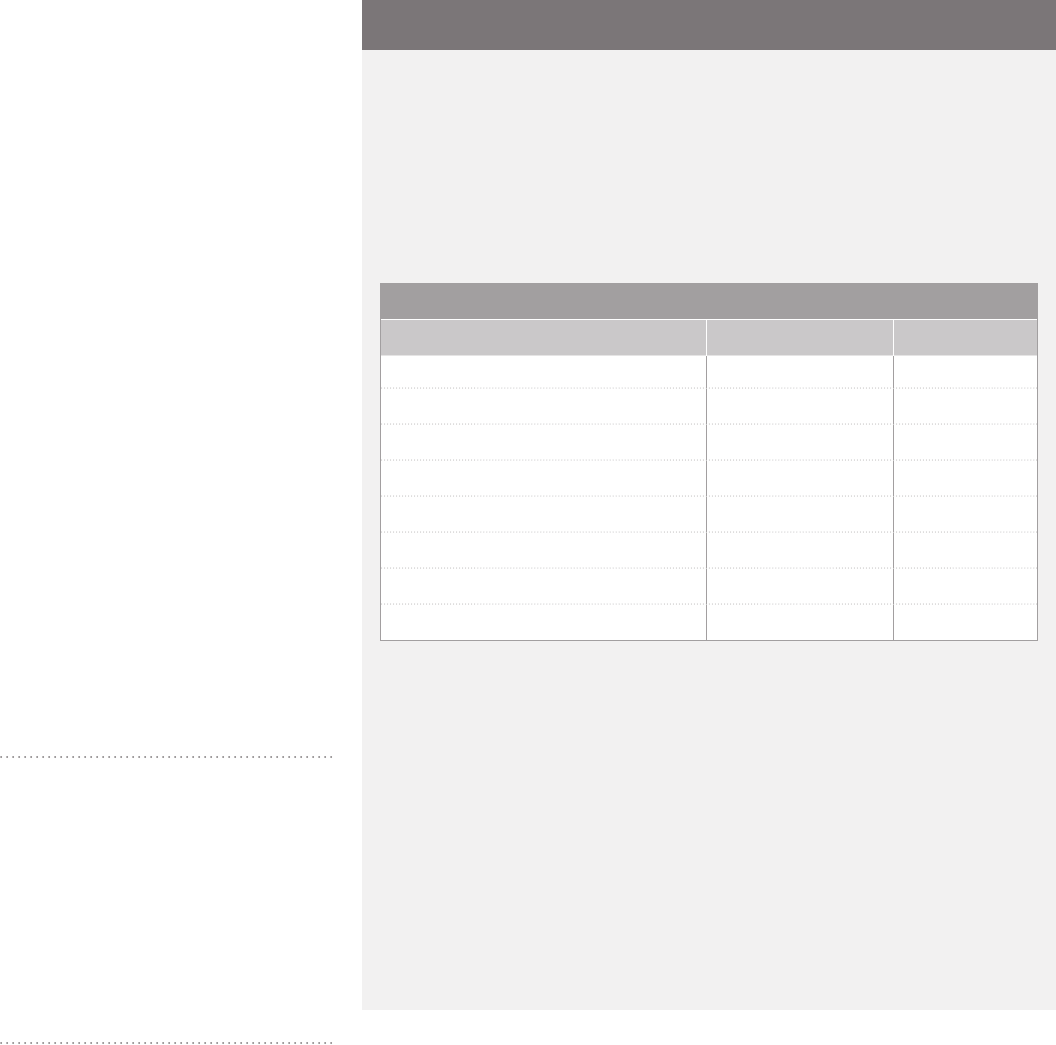
continuum is calculated by multiplying the
time spent at each step by the cost per unit
of time associated with the step. According
to Kaplan and Porter, TDABC requires
health care providers to 1) trace the path
of a patient through the care experience;
2) identify the actual cost of each resource
that the patient uses through the full
cycle of care, from personnel to space and
equipment; and 3) document how much
time the patient spends with each resource.
The methodology has been used by such
leading health care providers as Boston
Children’s Hospital, the Cleveland Clinic,
the Mayo Clinic, MD Anderson Cancer
Center and UPMC. At UPMC’s Bone and
Joint Center, for example, TDABC is being
used to help assess the true cost of knee
and hip replacements. Real-time metrics
are gathered through “shadowing,” where
an unbiased observer follows the patient
and family as they journey through the care
experience. UPMC is participating in an
Institute for Healthcare Improvement effort
with 31 other medical facilities to share
cost and outcome data. Participants in this
initiative, called the Joint Replacement
Learning Community, will use the TDABC
metric to measure costs, analyze and
review data, and set improvement targets.
“One goal of this effort is to
enhance efciencies and process
improvement along with clinical
outcomes in order to nally answer
the ‘value equation’ of outcomes
divided by true costs.”
Anthony M. DiGioia III, MD
Medical Director
Bone and Joint Center at Magee‑Womens
Hospital of UPMC
Speaking to Pittsburgh Business Times
Value vignette
Healthcare Transparency Index: finding better value for health care dollars
Eight health care services that are high
cost as well as highly variable in price
present the greatest opportunity to
save on health care costs, according
to Change Healthcare Corporation,
a Brentwood, TN, company focused
on consumer engagement and cost
transparency. The company’s Healthcare
Transparency Index (HCTI) measures
price variability for different procedures.
Leading the list of opportunities for cost
savings is CT scans, which vary in price
from $300 to more than $2,600.
Change Healthcare’s HCTI tracks cost
variability of common health care
services across various prescription,
medical, dental and vision services from
quarter to quarter. Certain services,
when analyzed at the most granular
level, can vary by as much as tenfold,
according to the report.
The company notes that health plan
sponsors can leverage this information
by applying the Transparency Index to
their own populations. By reviewing
services that are high cost, highly
variable in price and used often within
the plan, plan sponsors can better target
communications to employees to help
them nd better value for their health
care dollars.
The HCTI report, updated quarterly,
is based on more than 167 million
claims arising from more than
5.5 million patients obtaining health
insurance through Change Healthcare
member organizations.
Source: www.changehealthcare.com
Services offering the greatest opportunity for health care savings
Service Price range Price variability
CT scans $300–$2,681 794%
MRIs $485–$2,708 458%
Colonoscopies and upper GI endoscopies $1,290–$4,035 213%
Mammograms $118–$402 242%
Ultrasounds $100–$572 472%
C-section deliveries $6,128–$23,526 284%
Ofce visits with lipid screening $179–$506 182%
Ofce visits with diabetes screening $118–$470 298%
89

Value-driven outcomes (VDOs)
In 2012, the University of Utah Health Care
(UUHC) launched VDOs as a tool to create
cost and outcomes data at a granular level.
Led by an executive team, the initiative is
designed to illuminate what it costs to care
for a patient for a given episode of care —
with a focus on hospital, physician and
professional costs across the inpatient and
outpatient spectrum.
With costs on an x-axis and outcomes on
a y-axis, users can see direct correlations
between the cost of every choice made and
how it affects the quality of care. By looking
at information in the aggregate, UUHC
leaders note they can ask larger questions
about overall health care delivery — and nd
new ways to redesign care pathways. From
these standardized care pathways, clinical-
decision support tools can be designed
that hardwire best practices into the EHRs.
Protocol-based computer reminders can
then help guide practitioners to make
evidence-based decisions at the point of
care. The VDO technology may eventually
be shared with other institutions for
measuring costs and outcomes throughout
patient cycles of care. The tool received a
2013 Innovator Award from Hospitals &
Health Networks magazine.
Value Quotient® (VQ)
University of California, Los Angeles (UCLA)
Health System has created a Value Quotient
to compare the value of services to patients
with health care costs. The measure has
been piloted in helping patients manage
chronic intestinal ailments, with plans to
expand to other chronic diseases such as
heart failure and diabetes.
The VQ incorporates the annual burden
of the patient’s disease, including
such factors as disease activity,
complications, medication side effects
and hospitalizations; quality of life; and
work productivity. Each year, an individual
patient’s VQ is analyzed by health system
staff to determine factors that inuence
the score and to develop a plan for the year
ahead. The health system is also creating
apps for tablets and smartphones to help
manage these chronic diseases.
“Words can spearhead social
transformation. Let’s hope that’s
true for value in health care.
Where other mantras — such as
quality or managed care — have
failed to galvanize the system’s
diverse stakeholders, value may
have a chance.”
David Blumenthal, MD
President, The Commonwealth Fund
Kristof Stremikis
Senior Researcher, The Commonwealth Fund
“Getting real about health care value”
Blog, September 17, 2013
The measurement movement:
collaborating for better outcomes
Creating the value-based health care
system of tomorrow calls for new
measures — metrics that all stakeholders
view as fair, consistent and patient-focused;
that unite cost and quality dimensions into
standard measures; and that require robust
methods of collecting information and
reporting on the value of specic providers,
health plans and technologies.
As the demand intensies for value
measures, the trends discussed in this
chapter are sure to accelerate. Clearly,
patients and employers want to make
health decisions based on useful measures
of the outcomes they care most about.
Working together, providers, payers and
policy makers can catch the wind in setting
these industry standards and delivering on
the value promise.
90 New horizons: voyage to value

Viewfinders
Considerations for your board and executive leaders
For providers
•What metrics are you using to gauge
value in your organization’s health
care delivery? Have you identied
measurable factors that contribute to
variability in costs? Are you participating
in any regional or national initiatives in
developing value metrics?
•Are you participating in any initiatives
aimed at developing outcomes metrics
for patients that gauge improvements
in quality of life?
•How are you engaging physicians in
establishing value metrics for their
services? Are you providing tools to help
them understand how they practice and
the costs of care they are providing?
How will these value metrics incorporate
a measure of patient well-being —
determining which services contribute
positively and which are unnecessary
or even counterproductive?
•Are you collecting, analyzing and linking
accurate quality and nancial data to
support your organization’s decision-
making through integrated clinical and
management information systems?
•Are you collaborating with other
health care organizations in your
market to gather comparable cost and
outcomes data to develop broad value
measurements for a total episode of care
or time period? Are you comparing and
contrasting the value provided across
the market to identify best practices and
reassess your current practices?
•How are you using value measurements
to make strategic decisions about new
investments and business initiatives?
•Are you leveraging measurements to
negotiate with payers in a more informed
way, demonstrating what it costs your
organization to provide high-value care?
For payers
•What metrics are you using to evaluate
providers to identify those most
capable of succeeding in a high-value
contracting network?
•Are you supporting providers with care
management tools, patient information
and education resources, timely data
analysis and reimbursement systems
that encourage value delivery?
•How are you using outcomes and
cost data to establish and measure
the effectiveness of bundled
reimbursement models?
•Are you monitoring the various initiatives
in value measurement across the country
and incorporating any such initiatives,
at least on a demonstration basis, with
selected providers in your markets?
•Are you measuring members’ satisfaction
with the care they received and regularly
sharing these measures with providers?
How are these scores used in negotiating
contracts with providers? Are the results
shared with health plan sponsors and/or
directly with your insured members?
91

{ }
“It is not the ship so much as the skillful sailing
that assures the prosperous voyage.”
George William Curtis, 19th‑century American writer
Postscript
Value in leadership
Taking the helm
The future of American health care is no longer a blur on the distant horizon. It is coming
rapidly into focus. Today’s convergence of market, economic and government pressures
requires bold responses from health care executives and board members to secure their
organizations’ long-term viability.
In the journey toward a value-based health care system, leaders are asked to navigate
through often volatile conditions. The ability to read the wind and the waters — foreseeing
changes and responding with agility and resilience — is vital to effective leadership.
As you reect on this edition of New horizons, consider how your leaders are piloting your
organization’s course to a prosperous future, including:
•Pursuing payment systems that reward high-value care while looking internally
to curtail costs
•Maximizing care delivery and the patient experience
•Making strategic use of information technology
•Staying the course in compliance programs to avoid hazards and create value
•Considering transaction opportunities for their potential to yield nancial, operational
and strategic returns
•Using measures for gauging the outcomes that matter to patients
•Watching the legislative and regulatory forecast — and responding proactively
In today’s sea change of reforms and transformations, executive leaders and board
members are the most visible champions for value. Although they can’t change the
direction of the winds above or the currents beneath, those with staying power — and strong
partnerships — will be able to continuously adjust their sails for a successful journey.
The endpoint of this edition of New horizons is a conversation with the president and CEO
of the Robert Wood Johnson Foundation, Dr. Risa Lavizzo-Mourey. Under her leadership,
the Foundation has launched a variety of value-based programs to address the nation’s
most pressing health care challenges. She offers her insights on taking the lead in the
continuous voyage to value.
93
Feature
Leadership in
transformative
times: navigating
the changing tides
A conversation with
Risa Lavizzo‑Mourey, MD, MBA,
President and CEO, the Robert Wood
Johnson Foundation (RWJF)
(www.rwjf.org)
Since 2003, Dr. Lavizzo‑Mourey
has led the Robert Wood Johnson
Foundation, the nation’s largest
philanthropy dedicated solely to
health and health care. We talked with
her about her perspective on pursuing
value, creating a culture of health and
developing the next generation of
health care leaders.
In your varied roles as a practicing
physician, a contributor to developing
national health policy and an executive
leader of the Robert Wood Johnson
Foundation, you’ve had many
opportunities to observe and advocate
for value. What is your concept of value
in the health care world?
The starting point for me is always what
value means for patients — those we are
seeking to serve in our health care system.
In short, if you’re a patient, it means getting
the care you need so you can actually
get better.
A patient I encountered early in my career
as a physician taught me this. She had
a number of challenges. But the one
that brought her into the hospital was a
swollen leg that had been infected many
times. Each time she was admitted, she
received the same things — good care, a
change in her dressing, IV antibiotics and a
warm place to sleep for the night. But after
treatment, discharge and a few more
days, she would be back again with the
same problem.
“In my view, value is not only
high-quality care for the price
you pay; it is high-quality care
that gets patients the outcomes
they want.”
Beyond her medical issues, she had other
life challenges: chronic behavioral health
problems, no stable living situation and
no one from outside the hospital to help
her with her care. We were paying a lot of
money for care that was suboptimal, and
ultimately, we were not delivering the
outcomes that mattered to the patient.
If we are going to provide high-value care,
we need to look beyond what happens in
the health care setting and determine what
we can change that will help people get to
the functional status they want.
In my view, then, value is not only high-
quality care for the price you pay; it is
high-quality care that gets patients the
outcomes they want.
What stands in the way of getting more
value out of our health care system?
How can these obstacles be overcome?
A person’s ability to stay healthy
is inuenced largely by his or her
environment. So we need to create the
kinds of environments that are conducive
to the kinds of individual behaviors and
outcomes we want to see.
If you have cardiovascular disease and
are advised to quit smoking, you have a
much better chance of being able to be
smoke-free if your environment supports
your goal — for example, if the pharmacy
where you have your prescriptions lled
decides it’s not going to sell cigarettes.
In designing a system that delivers high-
quality outcomes, we need to make sure
people understand the kinds of services
they need and where these services are
provided in the community. We need to
rigorously pay for care that will lead to
a decrease in the need for higher-cost
care. And, we need to realize that often,
particularly in the complex world we live
in, providers, patients and payers don’t
have enough information about the prices
being paid for services, the quality they’re
getting for those prices and how likely it
is that these services will lead to positive
outcomes. This lack of information is the
biggest barrier to having a truly sustainable,
high-quality health system.
94 New horizons: voyage to value
You talk often of the need to create
an American “culture of health.” Paint
the picture for us of what that would
look like.
A culture of health means having access
to the care you need where and when you
need it and preferably in a setting that
is the most convenient for you. It means
creating an environment that promotes
prevention and wellness to all members
of the population.
If you’re a child, you should be able to walk
to school and be safe. You should know
when you get to school what you learn
there will help you grow up to be healthy.
If you’re an employee, you should be
condent your employer will help you make
healthy choices for you and your family.
For all, it means knowing your community
has a stake in the kinds of infrastructure
that support good health. That can be
as simple as a store that provides fresh
produce, a place where you can exercise
safely and community services that help
you address the stresses of life. It’s the
assurance that the issues that diminish
health — from inadequate housing to
unsafe streets — will be addressed by
community leaders. In a culture of health,
good health is a national value, one that
keeps us focused on being healthy and
staying healthy.
Many of the Foundation’s initiatives
have been exemplary in their pursuit
of value. Tell us about some of your
key programs and what we can learn
from them.
We’ve worked in many areas that are
thresholds for improving the culture
of health and achieving value. The rst
is making sure that as many people as
possible have insurance coverage so they
can begin to address their health care
needs. Our goal at RWJF is coverage for
95% of all Americans by 2020.
When a signicant part of the population
is not covered, we tend to see a lower
health status for everyone. This is part
of the reason that the ACA was enacted.
The Foundation has been working on
this issue for more than 40 years —
demonstrating to individuals and
communities the consequences when
people cannot get the health care they
need when they need it. For most people,
being sick is, gratefully, a relatively
infrequent event. So, because they
are rarely ill, they haven’t focused on
what could happen when they are sick.
Educating the public about the importance
of health care coverage is work that should
never stop.
We have also learned that working at the
community level is critical to improving value.
At RWJF, our best learning laboratories
have been in local environments.
For example, we’re supporting the
Boston-based Health Leads program
(www.healthleadsusa.org). Through this
initiative, health care providers
can “prescribe” food, heat and other
basic resources their patients need to
be healthy — as well as medications.
Health Leads is making it easier for
providers to address social factors affecting
their patients’ health and to connect
low-income patients with resources and
services in their communities.
Today, the program is in place at 20 adult,
pediatric and prenatal clinics and in
community health centers across the
country. It is providing health care leaders
and policy makers with a working example
of how community programs can address
the nonmedical factors that affect health
and well-being.
What are the Foundation’s top priorities
today, and what might they be over the
next 10 years in the voyage to value?
If we’re really going to improve the value we
get from health care, we need to do a better
job in several areas — from reversing the
epidemic of childhood obesity to creating
asmoke-free culture nationwide.
Improving health care value:
10 characteristics of an American
culture of health
1. Good health ourishes across
geographic, demographic and
social sectors.
2. Being healthy and staying healthy
is valued by our entire society.
3. Individuals and families have the
means and the opportunity to
make choices that lead to healthy
lifestyles.
4. Business, government, individuals
and organizations work together
to foster healthy communities
and lifestyles.
5. Everyone has access to affordable,
quality health care.
6. No one is excluded.
7. Health care is efcient and
equitable.
8. The economy is less burdened by
excessive and unwarranted health
care spending.
9. The health of the population
guides public and private
decision-making.
10. Americans understand that we
are all in this together.
Source: Robert Wood Johnson Foundation, 2014.
95
We need to make sure patients are more
engaged in the value they receive for their
health care dollars. That means paying
attention to prices and quality in a way we
haven’t before.
We need to invest in the health of the
population and to continue to nd ways
for people to make health the easy or
default choice.
And we need to prevent violence. We can’t
be a healthy nation if we continue to be a
violent one. At RWJF, we have supported
several initiatives to prevent domestic and
community violence and are broadening
our focus so that nonviolent behaviors
can be inculcated in children at a very
young age —and will become the behaviors
that endure.
How can businesses help employees
derive more value from their health
care dollar — and drive accountability
for providers and payers?
First, businesses can provide complete
and transparent information — along with
the analytics to help employees make the
best choices in health care. We have been
living in a world where the information
people need to make decisions is treated in
a proprietary way. The more we can share
that information and develop the analytics
to measure value, the closer we will be to
reaching our goals.
Second, we know that comprehensive
worksite wellness programs bring strong
returns for employers, especially when
they’re extended to families. The numbers
are staggering: for every dollar invested in
these programs, there is an average return
of more than three dollars, through lower
medical costs, reduced turnover rates and
increased employee retention. We hope to
see more and more employers investing in
and promoting these programs.
Third, we must recognize that the kinds of
coverage benets that will be provided over
the next few years will — by necessity — be
evolving. Employers, since they cover such
a signicant part of the cost, will need to
take a rigorous approach to analyzing the
most high-value benets they can provide
and their impact. I would argue the impact
they need to look at is not just services
provided but the overall health of their
populations. Providers and payers should
be helping employers demonstrate the
value of population health.
In this time of industry transition,
what are the greatest challenges — and
opportunities — in developing the
next generation of health care leaders
to “navigate the changing tides”?
It’s critical that our leaders be able to reach
across sectors and silos to create a value-
based world — not only health care value
but the value of broader systems. When we
talk about the value proposition, we tend
to refer almost exclusively to the value we
get from the services health care systems
provide. But we need to recognize that the
health care dollar is inextricably tied to
the money we invest in many other areas,
such as public health, education and public
infrastructure. Often we don’t put a health
value on those investments. Health needs
to be considered in all policies, not just
health care policies.
“It’s critical that our leaders be
able to reach across sectors
and silos to create a value-
based world — not only health
care value but the value of
broader systems.”
An already complex health care system
becomes even more so when you start
asking how to make the system work with
communities and businesses to promote
the health of a population. Whether it’s
an individual organization or a city or
region that has succeeded in achieving
this goal, all have tended to have leaders
from sectors and areas that we don’t think
of as being related to health — architects
who know how to create healthy spaces,
for instance, or transportation specialists
who understand the importance of
the infrastructure in contributing to
population health.
This collaboration among disciplines is
sometimes difcult to cultivate. But it’s
absolutely essential. Building networks of
people who understand and are committed
to health outcomes in their communities
will help achieve high value and enable all
people to live long and healthy lives.
96 New horizons: voyage to value

97

{ }
“A change in the weather is sufcient to recreate
the world and ourselves.”
Marcel Proust, 20th‑century French novelist
99
Appendix
Value in government initiatives
Reading the forecast
Voyage to value
“Show me the value” are the abiding watchwords of health care policy
makers. The way toward the industry’s future will continue to be guided
by government policies to reduce cost, create greater efciencies
and maximize value for system stakeholders. While federal and state
lawmakers of both parties may have different visions of how to achieve
health care value, they share the belief that the US health care system
must readily embark on the value journey.
As legislators negotiate health care laws — from new payment
methods to treatment options, insurance parameters to reporting
requirements —the overall course should veer toward opportunities that
will enhance the value of care provided for money spent. Legislative and
regulatory initiatives provide direction as health care organizations read
the forecast on their voyage to value.
March 31, 2014, was a signicant date for the US
health care industry. The ACA initial enrollment period
ended that day with more than 7 million Americans
selecting health insurance plans through the federal
or state health insurance exchanges (HIXs). On the same
date, the US Congress passed the Protecting Access
to Medicare Act of 2014 (PAMA), which implements a
variety of provisions affecting virtually every health care
organization. In this Appendix, we provide a high-level
review of these and other developments and government
activities. Highlights are intended to help you assess the
current legislative environment and gain perspective on
initiatives affecting your operations and strategies.
The ACA: launching new health
care coverage
Although estimates of 7 million new
health care enrollees were met by the
original March 31, 2014, ACA deadline,
in late March, CMS announced a special
enrollment extension period through
April 15, 2014. Qualifying for the special
extension were those who tried to enroll by
the deadline but could not complete their
applications in time and those who had
previously encountered website problems
that prohibited them from enrolling
earlier. In the last week of March, a surge
of enrollees caused slow processing and
activated a “virtual waiting room” when
the number of people trying to sign up
exceeded the exchange’s capacity. Those
who chose to take advantage of this special
enrollment extension period had to attest
that they had trouble signing up before the
original deadline. In total, about 8 million
Americans selected health plans through
the federal and state exchanges by the
end of the ACA’s rst open enrollment,
April 15, 2014.
Sustainable growth rate: adding
another temporary fix
The PAMA provided a temporary patch to
the sustainable growth rate (SGR) physician
payment update formula, preventing the
24% Medicare payment cut scheduled to
go into effect April 1. This bill represents
the 17th deferment of payment cuts
resulting from the SGR formula since its
implementation in 1997. Physician groups
had hoped that a permanent x to the SGR
formula would be enacted instead, and they
continue to push for this.
While legislators of both parties attempted
to implement a permanent x, these efforts
failed largely because of the inability to
fund such a measure. The Congressional
Budget Ofce (CBO) now estimates that
a permanent repeal of the SGR will cost
$138 billion to $180 billion, depending
on other payment policies included in the
package and whether some temporary
Medicare payment rules are made
permanent. Although the issue will likely
be revisited in 2015, no further action is
expected in 2014.
“Full repeal of the sustainable
growth rate formula is the answer
to strengthening the Medicare
program, not another patch.”
Ardis Dee Hoven, MD
President
American Medical Association
ICD-10 implementation: delaying
the start again
The PAMA also includes a variety of other
measures with signicant impact on
the US health care system — including,
somewhat unexpectedly, mandating a delay
in ICD-10 diagnostic and procedure codes
for one more year.
While physician trade associations actively
worked to prevent the 24% SGR cut in
physician payments, preferably through
apermanent x, the addition of a delay in
ICD-10 implementation to this legislation
surprised many. Most major health
insurance organizations have indicated
that they were well-prepared for the
switch to ICD-10 on October 1, 2014.
And, shortly before the delay was enacted,
CMS — as a nal step in its readiness
agenda — issued a request for health care
provider organizations to apply to be part
of ICD-10 “end-to-end” testing.
However, some physician trade associations
had lobbied for a delay. They cited the
lack of available/affordable systems and
100 New horizons: voyage to value
the signicant cost of implementation and
training as factors preventing a reasonable
conversion to ICD-10 by October 2014,
especially for small physician groups or
individual physician practices. Despite
the availability of CMS’ eHealth University,
designed to help health care providers —
particularly smaller groups — to implement
the conversion successfully, many small
physician groups were not expected
to be ready by the October 1, 2014,
conversion date.
With the date for conversion to this
signicantly more complex coding system
now set for October 1, 2015, health
care providers and payers will need to
re-evaluate their training and testing
plans to make sure the key points of
conversion are top of mind when the actual
switch to ICD-10 is nally implemented.
Provider and payer organizations that
have already invested in training sessions
to prepare their clinicians and health
information management staff for ICD-10
implementation now must assess whether
those efforts will need to be repeated
next year to bring staff up to speed.
And HIT staff will need to reassess their
priorities, changing the schedule for ICD-
10 conversion activities and postponing
planned moves to take on other initiatives.
For more on ICD-10, see chapter 3 of this
edition of New horizons.
“Even if you slow down, don’t stop …
use [the ICD-10 delay] to your
advantage. Strengthen your clinical
documentation programs.”
Lynne Thomas Gordon
CEO
American Health Information
Management Association
Speaking to Modern Healthcare, April 5, 2014
Other provisions: spanning
a range of industry sectors
The PAMA further extends until 2023
the 2% reduction in Medicare payments
imposed by the federal budget sequester,
which was rst extended in the federal
funding deal agreed to in December 2013.
This is two years longer than the original
budget sequester imposed.
Also included in the PAMA are a number
of other health care provisions. Some
measures are geared to further implement
pay for value or otherwise reform current
payment methodologies. Key provisions,
by industry sector, are highlighted below.
Hospitals
•Postponing until March 15, 2015,
compliance with Medicare’s controversial
“Two-Midnight Rule” for determining
inpatient versus observation
patient status
•Suspending until March 15, 2015,
RAC audits of allegedly medically
unnecessary claims
•Preserving until 2017 disproportionate
share payments for safety-net hospitals
Physicians
•Implementing a 0.5% Medicare update
for physician services with claims
dated during calendar 2014 and a 0%
update to the 2015 Medicare physician
fee schedule
•Reducing certain “misvalued” physician
payment codes and creating a program
designed to promote proper use of
diagnostic tests and treatments, while
discouraging overuse
Skilled nursing facilities (SNFs)
•Establishing a new value-based
purchasing program for SNFs based
on their performance on hospital
readmissions — readmission scores
will be posted on the Nursing Home
Compare website (www.medicare.gov/
nursinghomecompare/) beginning in
2017, with the value-based purchasing
program starting in 2018
•Reducing payments to SNFs by $2 billion
over 10 years
Clinical labs
•Reforming the current clinical laboratory
fee schedule used to determine payment
for Medicare diagnostic lab services
through changes in the process of
setting rates and in the identication
codes used to enable better assessment
of the efcacy of individual tests —this
provision will forestall another round
of across-the-board cuts in lab
payment rates
Medical imaging
•Requiring providers to consult “physician-
developed appropriateness provisions,”
such as clinical decision support tools,
before ordering advanced medical
imaging procedures for Medicare
patients; backed by the American College
of Radiology, this quality initiative
is intended to reduce duplicate and
unnecessary scans
Outpatient therapy
•Extending the outpatient therapy caps
exceptions process through March 31,
2015, and extending the outpatient
therapy caps (and exceptions process)
to hospital outpatient therapy services;
these caps have been extended a
number of times since they were rst
implemented in 2006
101

102 New horizons: voyage to value

Mental health
•Authorizing a multistate pilot program
designed to raise standards for mental
health services and improve integration
of care
•Establishing a new grant program,
with up to $60 million available over
four years, to improve outpatient
treatment for individuals with serious
mental illnesses
Payers
•Extending for an additional year
(to 2017) Medicare Advantage Special
Needs Plans, which provide services to
beneciaries who are institutionalized,
have chronic conditions or are dually
eligible for Medicare and Medicaid
•Eliminating the cap on deductibles for
employer-sponsored health plans
The legislative/regulatory horizon:
looking ahead
A variety of other health care-related
initiatives can be expected in the months
ahead, some as potential legislation
by the US Congress or state legislatures
and others as regulations issued and
implemented by CMS and other agencies.
Proled below are upcoming considerations.
A new captain at the helm
After seeing the ACA through its rst
open enrollment and a vast number
of implementing regulations, Kathleen
Sebelius resigned as Secretary of Health
and Human Services. President Obama
nominated Sylvia Mathews Burwell, Director
of the Ofce of Management and Budget, to
be her replacement. Burwell’s conrmation
hearings presented another opportunity
for Senate Republicans to raise concerns
about the ACA, revisit problems with the
initial enrollment process and critique
extensions and delays in ACA provisions.
The Senate conrmed Burwell as Secretary
on June 5, 2014.
Through the eyes of some observers the
new Secretary will be jumping headrst
into churning waters. With the federal and
state exchanges gearing up for the second
enrollment period, she will also need to
address funding and staff shortages at CMS
and the need to replace several senior
CMS staffers who have recently resigned.
HIX premium rates and plans
for 2015
Now that commercial insurers participating
in the HIXs have initial enrollment
information, they must move quickly to set
their rates for the next open enrollment
period. While premiums are expected to
increase, the extent of the increase is not
yet known. Insurers are still in the process
of evaluating the age, health status and
plan selections of those newly insured,
as well as those expected to enroll in 2015.
Initial reports from insurers participating
in the HIXs indicate that most expect to
stay in the exchanges they participated in
during 2014. Some are also considering
participating in additional HIXs for 2015.
Premiums for HIX plans were lower than
the CBO had originally predicted for
2014. Some insurers are believed to have
offered lower rates in some of their plans
to help persuade the uninsured to sign
on. In some plans, narrower networks and
tight plan limitations contributed to the
lower-than-expected premiums. Some
insurers may choose to keep 2015 rates
low to build market share, while others
may increase rates to improve protability
or to offset adverse selection, especially
in the rate of younger, and presumably
healthier, individuals.
While preliminary demographic analyses
show younger people signed up at a lower
rate than older people, some insurers
indicate that more young people enrolled
than they had expected when they
submitted their bids for 2014. For 2015,
the CBO projects that new enrollees will
be younger and healthier than those who
enrolled during 2014, which will help
reduce the costs of insurance plans —
perhaps somewhat mitigating the need for
large premium rate increases.
In April 2014, the CBO issued an analysis
on the cost of the ACA’s insurance
subsidies, predicting that over the next
10 years, the subsidies will total about
$1 trillion, compared with the $1.2 trillion
originally estimated. This revised estimate
is partially due to new projections of
the cost of health insurance plans sold
through the HIXs. The CBO expects the
average premium to rise about $100 for
2015, and to then grow about 6% per year
through 2024.
Another consideration in setting premium
rates is the provider networks included in
each health insurance plan. Insurers are
expected to limit networks in negotiations
with providers to help soften the increases
in premium rates for 2015. In March, CMS
issued proposed regulations under which
CMS would no longer defer to the states
to certify adequate provider networks.
It would instead establish its own process
to make sure networks include a sufcient
number of hospitals and other health
providers so that the insurer meets
the reasonable access review standard.
Plans would, in general, be expected to
contract with at least 30% of the essential
community providers in their market.
Comments on this proposed rule were
103
accepted until April 14, 2014. CMS is
reviewing them and will issue a nal rule
later this year.
Insurers are under pressure to consider
these factors to determine soon which
markets they intend to offer plans in,
as well as 2015 premium rates. Some state
HIXs require that plan information and
premium rates be submitted as early as
May 1, 2014, while the federal HIXs have
adeadline of June 27.
CMS oversight
Now that the new health insurance plans
offered on the HIXs are in effect, many
participating insurers face oversight by
CMS. Yet it is unclear just how much
scrutiny CMS will apply. CMS is responsible
for enforcing market reforms in states that
are not enforcing them directly, or have not
entered into a collaborative enforcement
agreement with CMS.
CMS oversight for Medicare Advantage
plans has been comprehensive in reviewing
services covered, rates charged and
customer service issues. Insurers that have
not previously participated in Medicare
Advantage may nd the oversight from
CMS more rigorous than they typically
experience with state insurance
commissioners. Final regulations dening
essential health benets have been issued,
and throughout 2014, insurers will learn
just how aggressively CMS will interpret
its requirements to monitor these health
insurance plans.
HIX changes
Several state-run HIXs have indicated
plans to make changes after the initial
enrollment period. For example, Oregon’s
state-run exchange was unable to sign up
any enrollees online, although it did enroll
applicants over the phone and by mail.
After consultant analyses showed that it
would be far less expensive to move to the
federal exchange and abandon the state’s
exchange rather than refurbishing it, CMS
has informed Oregon ofcials that it does
not believe Oregon can repair its exchange.
Oregon will likely operate under the federal
exchange for the 2015 enrollment period.
On the other hand, two states, Idaho and
New Mexico, plan to move from the federal
exchange to their own state exchanges
for the 2015 enrollment period. Both
had initially planned to offer a state-run
exchange but decided they could not get
their own exchanges established in time
to meet the 2014 deadlines.
Employer mandate
In February 2014, the Administration
issued long-awaited nal regulations on
the employer mandate and employer
requirements for information reporting.
With this issuance, the IRS can begin
enforcing these provisions. The employer
mandate and information reporting will
generally take effect on January 1, 2015,
although the Administration has provided
an additional year, to 2016, for smaller
employers, i.e., those with 50–99 full-time
equivalent (FTE) employees, to comply
with the ACA’s mandate to provide health
coverage to their FTEs. Businesses and
insurers will have to begin collecting
data on January 1, 2015, although the
rst reports will not be due to individuals
(January 31) and the IRS (March 31) until
2016. The effective date of the employer
mandate and the information reporting
requirements results from a one-year delay
of the provisions that the Administration
announced in July 2013.
The nal employer mandate rules phase
in the percentage of full-time workers who
must be provided coverage in order to
avoid penalties, from 70% in 2015 to 95%
in 2016 and beyond. They also include
other transition policies for the rst year
of the employer mandate.
The nal regulations on information
reporting generally incorporate the
reporting method outlined in proposed
rules issued in September 2013. They
include limited options for streamlined
reporting for large employers in specic
circumstances.
Medicaid plan changes
Most states will assess their current
Medicaid programs for opportunities to
save money and best handle increased
enrollments, particularly those states
that enacted Medicaid expansions funded
through ACA provisions. A number of
states have begun considering changes
in payment structures to value-based
programs such as ACOs or medical homes,
moving away from fee-for-service models.
Some of the 24 states that initially decided
not to expand Medicaid are reconsidering
their decisions. Pennsylvania has requested
approval to use federal Medicaid expansion
funds to subsidize private health insurance
policies. One controversial provision of this
plan requires able-bodied, working-age
Medicaid applicants to complete certain
work-search activities as a condition of
receiving Medicaid-funded health insurance.
Initial reaction from CMS is that a work-
104 New horizons: voyage to value
search requirement will not be permitted.
Indiana is considering a consumer-driven
model in which beneciaries would
contribute some of their own money
toward health coverage. Utah and Virginia
are contemplating private insurance
coverage options, similar to the Arkansas
expansion plan that was approved by
CMS and implemented in 2014. Other
states are assessing a variety of options,
from traditional Medicaid to premium-
assistance models.
Federal budget
The Administration has presented to
Congress a budget proposal for 2015 that
reduces federal decits to 1.6% of GDP over
10 years. It also adheres to the spending
levels agreed to in the Bipartisan Budget
Act of 2013 while shifting spending toward
domestic initiatives President Obama would
like to implement during the remainder
of his term. House Budget Committee
Chair Paul Ryan has released a budget
proposal that cuts more than $5 trillion in
spending over 10 years and would balance
the federal budget. It includes many of
the same initiatives proposed in prior-
year Republican budget proposals. It is
unlikely that either of these comprehensive
proposals will proceed.
The rough waters of the past several
years surrounding the federal budget —
with scal cliffs, sequesters and battles
over the debt ceiling — are today much
calmer. An improving economy and
impacts of the last several budget
battles have signicantly decreased the
federal decit. The CBO now predicts the
2014 federal decit will be $514 billion,
asignicant decrease from the 2009 high
of $1.4 trillion. However, the CBO also
projects that health care spending will be
the key driver of a return to increasing
decits in just a few years. The federal
debt ceiling has been suspended through
March 15, 2015, raising the possibility that
renewed attempts to rein in health care
spending may arise next year — and bring
turbulence to the calmer seas.
Greater transparency
In April 2014, the Administration released
for the rst time physician payment
data showing procedures provided and
payments received by 880,000 distinct
health care providers. This data enables
comparisons by physician, specialty,
location, and types of services and
procedures provided. The release adds a
new level of transparency to health care
costs, supplementing the hospital inpatient
and outpatient charge data released
last ye a r.
“Data transparency is a key aspect
of transformation of the health care
delivery system.”
Marilyn Tavenner
Administrator
CMS
Health care issues and the
upcoming elections
Another wave to dismantle the ACA
could arise after the fall elections if the
Republican Party retains a majority
in the House and gains control of the
Senate. As the campaign season gets
under way, the ACA appears to be a major
issue in a number of races across the
country and is expected to play heavily
in candidate debates.
Vigilance and visibility: sailing
with the wind
Health care provider and payer
organizations have a broad range of federal
and state legislation and regulation to
monitor, understand and comply with —
from the PAMA to the continuing, although
delayed, move toward EHR Stage 2 MU.
Also, they need to keep up with ongoing
initiatives in health care payment, delivery,
IT and compliance discussed in this
edition of New horizons. Regardless of the
challenges ahead, staying informed can
help health care organizations see clearly
through any conditions.
As new regulations are issued throughout
the year, EY will continue to keep you
informed. For an analysis of the latest
developments, visit www.ey.com/US/
en/Industries/United-States-sectors/
Health-Care
105
ACA Affordable Care Act
ACO accountable care organization
CMS Centers for Medicare &
Medicaid Services
DOJ US Department of Justice
DOL US Department of Labor
ED Emergency Department
F&A fraud and abuse
FCA False Claims Act
FFS fee-for-service
HHS US Department of Health and
Human Services
HIE health information exchange
HIMSS Health Information
Management Systems Society
HIT health information technology
HIX health insurance exchange
ICD-10 International Classication
of Diseases, 10th edition
ICHOM International Consortium
for Health Outcomes
Measurement
IOM Institute of Medicine
IT information technology
LTC long-term care
M&As mergers and acquisitions
MU meaningful use
OIG Ofce of Inspector General
ONCHIT Ofce of the National
Coordinator for Health
Information Technology
PAMA Protecting Access to Medicare
Act of 2014
P4P pay-for-performance
RWJF Robert Wood Johnson
Foundation
SBC summary of benets and
coverage
Frequently used acronyms
106 New horizons: voyage to value
EY thought leadership publications
Along with New horizons, EY provides a variety of other thought leadership resources to keep our provider care, payer and life sciences
clients up-to-date on government activities and market developments:
5 Insights for executives series
Brief overviews asking ve questions that get
to the core of an issue — and answering them
at a glance. For example:
• “Bringing patients into focus: using analytics to
create a 360-degree view (SCORE No. BT0327)
Access le at:
www.ey.com/Publication/vwLUAssets/
Bringing_patients_into_focus_-_5_Insights_for_
executives/$FILE/Bringing_patients_into_focus_
Optimized.pdf
Health Care Industry Posts
Succinct, timely news briefs and analysis on a wide
range of issues affecting health care providers and
payers. For example:
• “Shaping your telehealth strategy: leveraging
telehealth technologies to lower costs, improve
quality outcomes and enhance the patient
experience” (SCORE No. EC0023)
Access our full library of Health Care Industry Posts
at: www.ey.com/US/en/Industries/United-States-
sectors/Health-Care/Provider-Post-library_news-
and-analysis
BoardMatters Quarterly
A quarterly publication highlighting critical issues
for today’s audit committees across industries
worldwide. For example:
• “Balancing the risk and rewards of digital
technology” (SCORE No. CJ0237)
Access le at:
http://www.ey.com/US/en/Issues/Governance-
and-reporting/Audit-Committee/BoardMatters-
Quarterly---April-2014---1---Balancing-the-risks-
and-rewards-of-digital-technology
Progressions: global pharmaceutical
report 2014
EY’s 10th pharmaceutical industry report,
“Navigating the payer landscape,” focusing on the
critical relationship between pharma companies
and health insurers (EYG No. FN0137)
Access le at:
www.ey.com/Publication/vwLUAssets/
EY_-_Progressions_2014:_Navigating_the_payer_
landscape/$FILE/EY-progressions-2014.pdf
Beyond borders: global
biotechnology report 2013
EY’s 27th annual biotechnology report, “Matters
of evidence,” proling strong performance by
major players but a challenging environment for
the rest of the industry — and an urgent need to
focus on demonstrating value (EYG No. FN0016)
Access le at:
www.ey.com/Publication/vwLUAssets/Beyond_
borders/$FILE/Beyond_borders.pdf
Pulse of the industry: medical
technology report 2013
EY’s sixth annual report on the state of the medical
technology industry, highlighting and analyzing
current trends and a future of industry innovation
(SCORE No. CW0076)
Access le at:
www.ey.com/Publication/vwLUAssets/Pulse_of_the_
industry_–_medical_technology_report_2013_-_
Redening_innovation/$FILE/Pulse_Redening_
medical_technology_innovation.pdf
107

Project leadership
Jon Weaver, EY’s Americas Health Care
Sector Leader, served as executive sponsor
of New horizons: voyage to value, providing
strategic vision and overall guidance.
He also offered valued input on chapter
drafts and served as lead interviewer
for our conversations with external
contributors Jens Deerberg-Wittram, MD,
Howard Miller and Risa Lavizzo-Mourey, MD,
as well as with our Health Care Advisory
Services leaders Craig Kappel and
Rob Wallace.
We are grateful also to EY’s Americas
Health Care Sector Region Leaders —
Carole Faig, David Copley, JoEllen Helmer,
Laura Freitag, Tom Grifth and
Tony Bielawski — and to Jim Costanzo,
National Practice Leader, Health Care
Advisory Services, for co-sponsoring
this project.
Sue Carrington, Managing Editor,
developed the theme, visuals and chapter
direction for New horizons, engaged
project resources and managed the book’s
production. She researched, wrote and
edited chapters and interviews and was
responsible for the publication’s overall
content and quality.
Cindy Shimko, contributing writer,
conducted signicant research, wrote
several chapters and offered key input on
chapter drafts and Viewnder questions.
Bill Fera reviewed book content and
offered helpful feedback. Chip Clark,
Craig Kappel, Greg Park, Rob Wallace
and Tom Gregory provided input on
specic chapters. Carole Faig, Chip Clark,
Christine Quintana, Susan Flaherty and
Tom Grifth reviewed the entire publication
before press.
Anne Phelps and Daniel Esquibel offered
helpful insights on the legislative and
regulatory Appendix.
Design, editorial and other assistance
Ryan La served as lead designer. He was
assisted by Jeff Wolnowitz. Carl Byrne
and Don Batting offered design guidance
and review. Hollie Gantzer created the
web edits.
Heather McKinley, Jane Spencer,
Lucia Barzellato, Mark Bushell,
Peter McKinley and Rachel Buck
facilitated nal approvals.
Russ Colton served as copy editor and
Sue Brown as proofreader. Tori Decker
provided administrative support.
John La Place and Lauren Verdery led the
public relations outreach for New horizons.
Acknowledgments
108 New horizons: voyage to value
New horizons is published by EY’s Health
Care Industry practice. It is designed to help
the rm’s health care clients successfully
navigate the challenges and opportunities
that market changes, government activities
and technology innovations present.
For more information, contact a partner
in your local EY ofce. Access additional
resources at www.ey.com/US/en/Industries/
United-States-sectors/Health-Care

EY | Assurance | Tax | Transactions | Advisory
About EY
EY is a global leader in assurance, tax, transaction
and advisory services. The insights and quality
services we deliver help build trust and confidence
in the capital markets and in economies the world
over. We develop outstanding leaders who team
to deliver on our promises to all of our stakeholders.
In so doing, we play a critical role in building a better
working world for our people, for our clients and for
our communities.
EY refers to the global organization, and may refer
to one or more, of the member firms of Ernst & Young
Global Limited, each of which is a separate legal entity.
Ernst & Young Global Limited, a UK company limited
by guarantee, does not provide services to clients.
For more information about our organization, please
visit ey.com.
Ernst & Young LLP is a client-serving member firm
of Ernst & Young Global Limited operating in the US.
© 2014 Ernst & Young LLP.
All Rights Reserved.
SCORE No. EC0024
1401-1180329 NY
ED None
In line with EY’s commitment to minimize its impact
on the environment, this document has been printed
on paper with a high recycled content.
This material has been prepared for general informational
purposes only and is not intended to be relied upon as
accounting, tax, or other professional advice. Please refer
to your advisors for specific advice.
