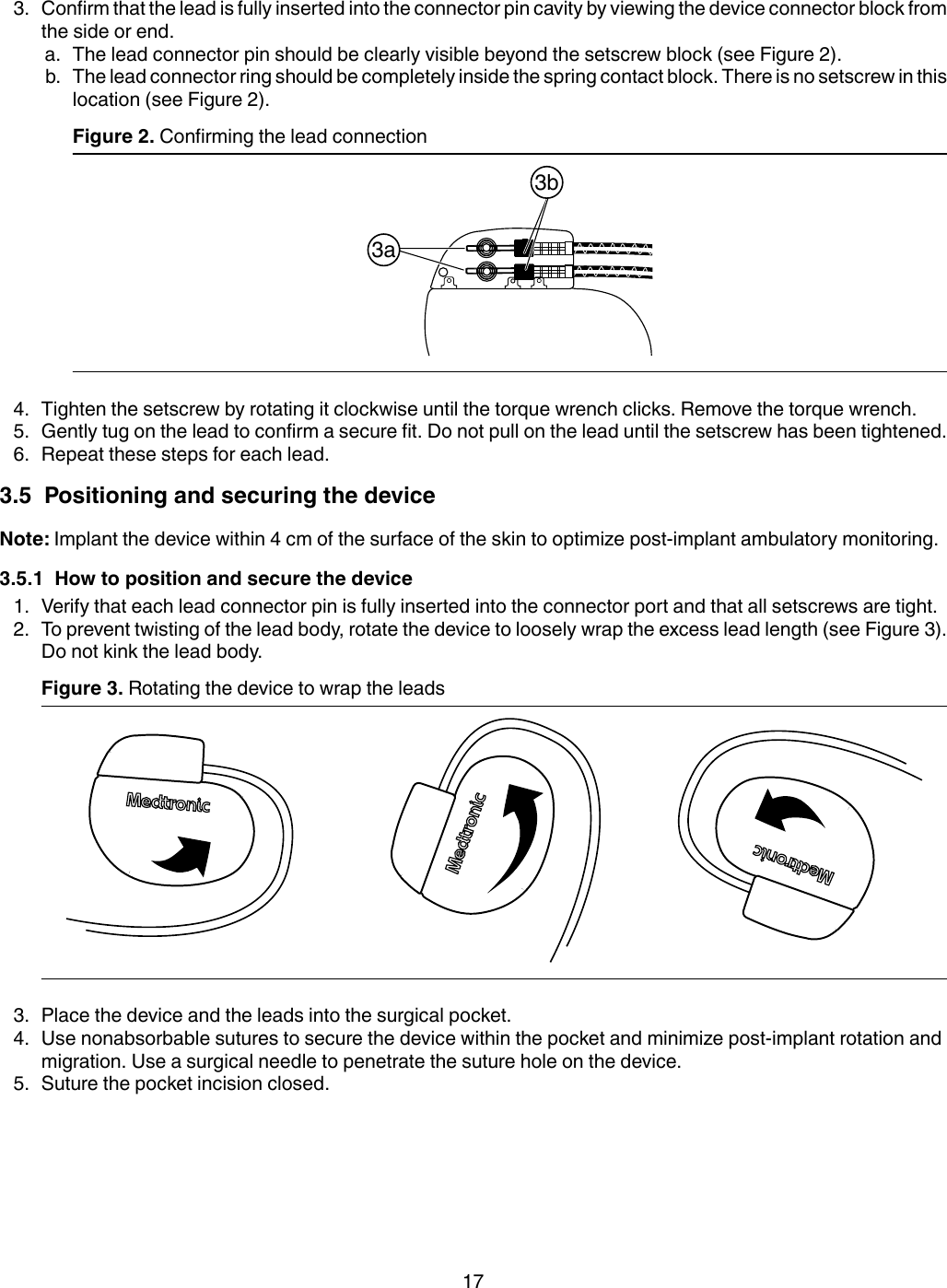
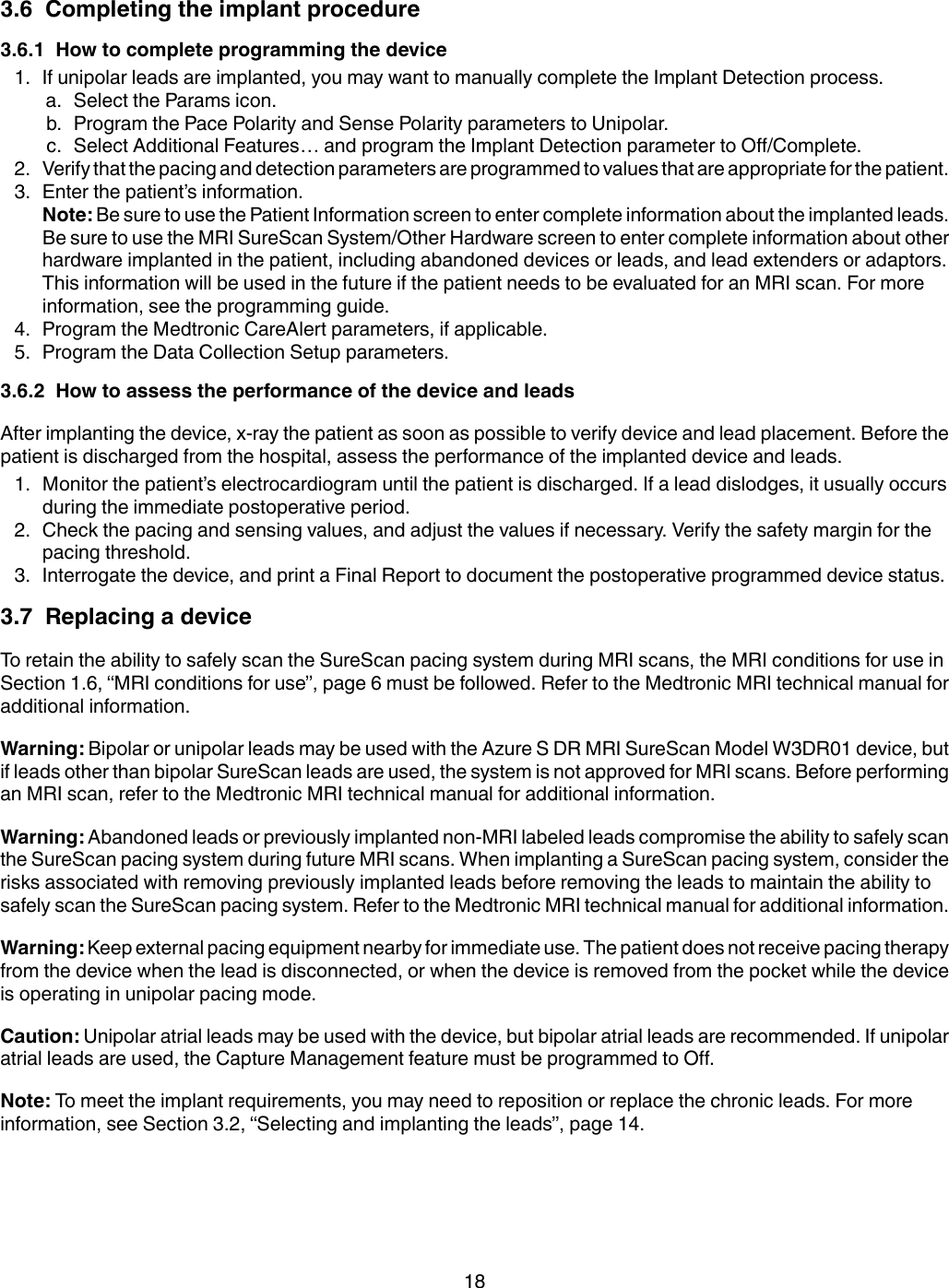
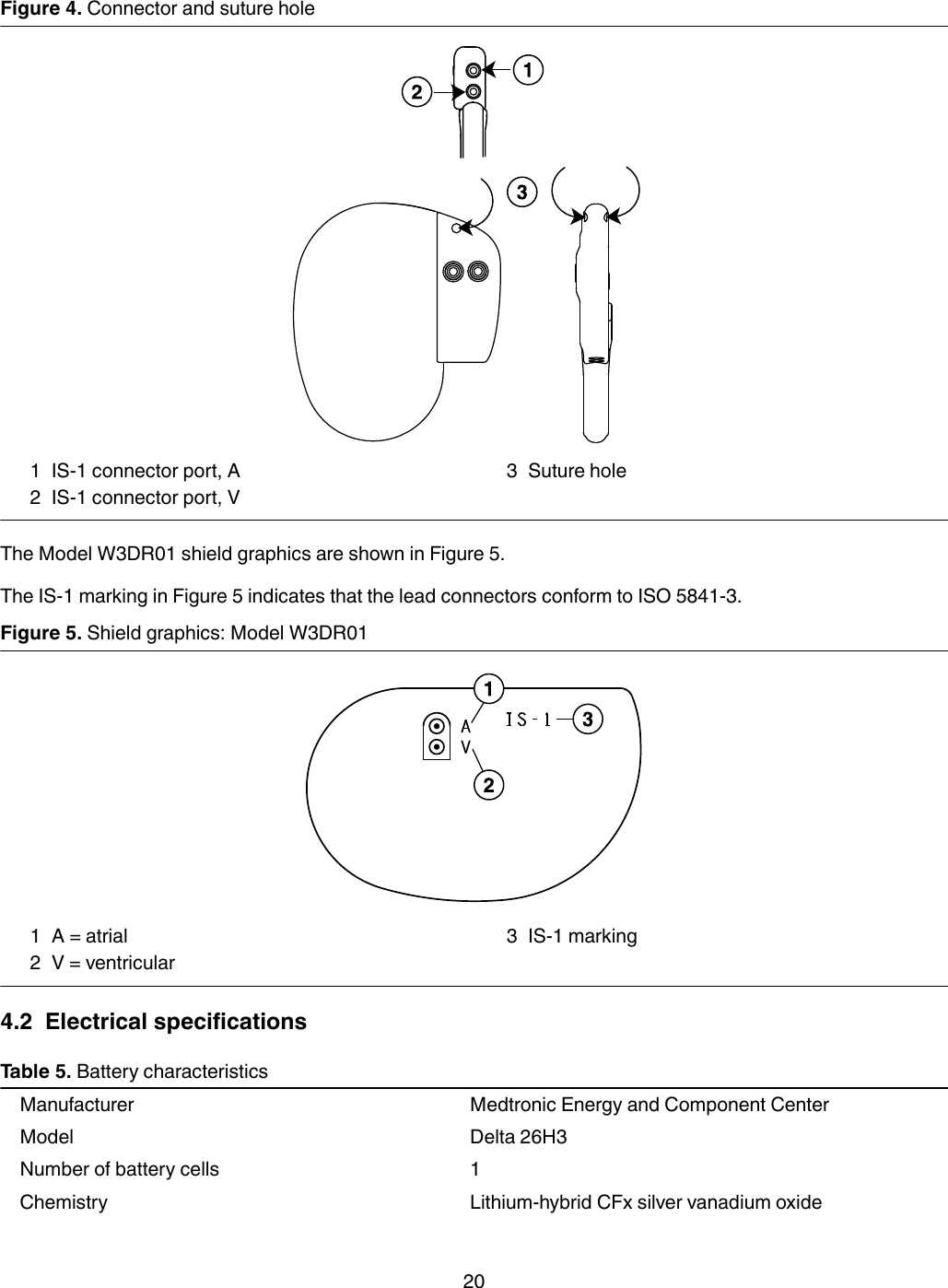
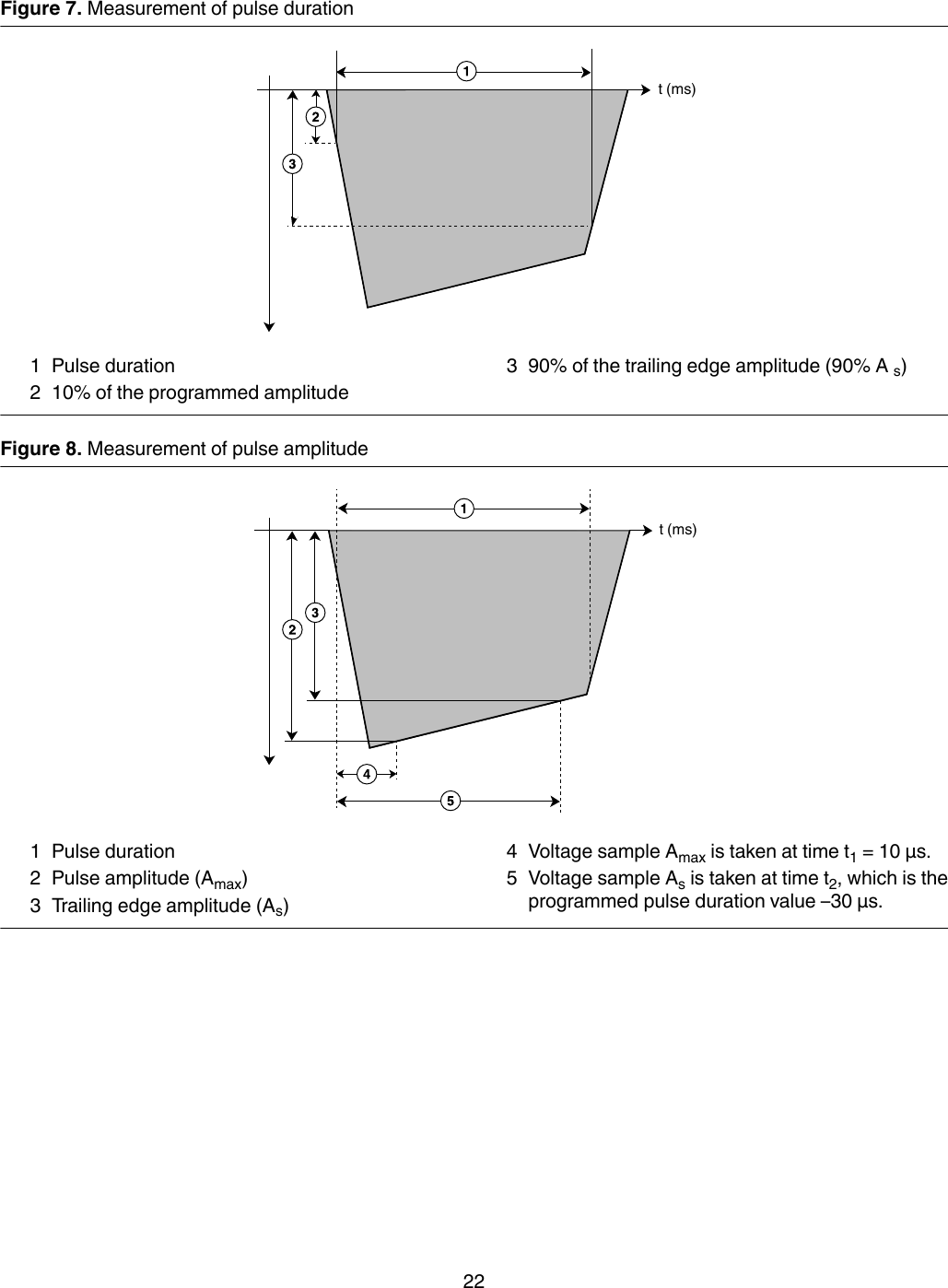
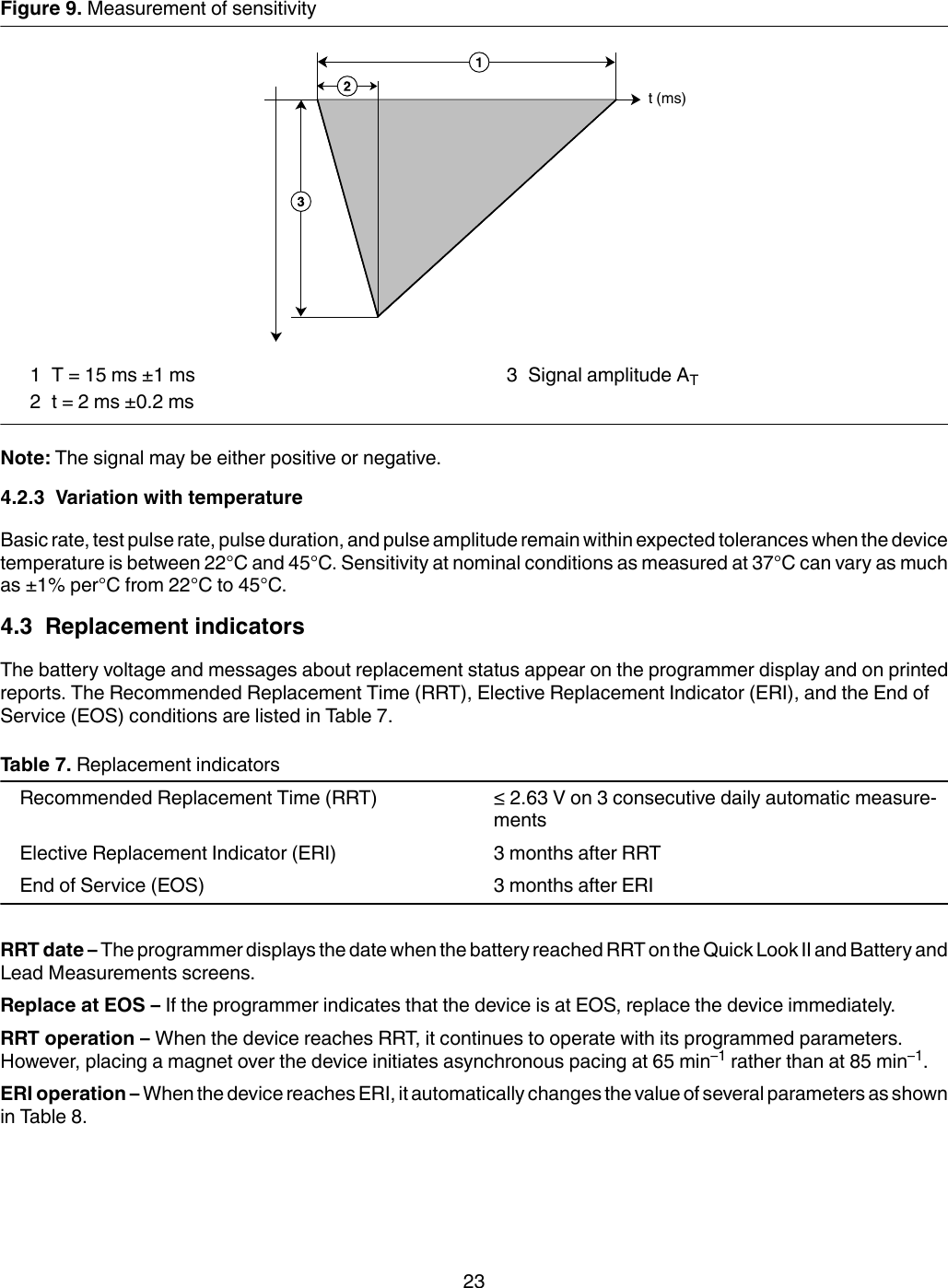
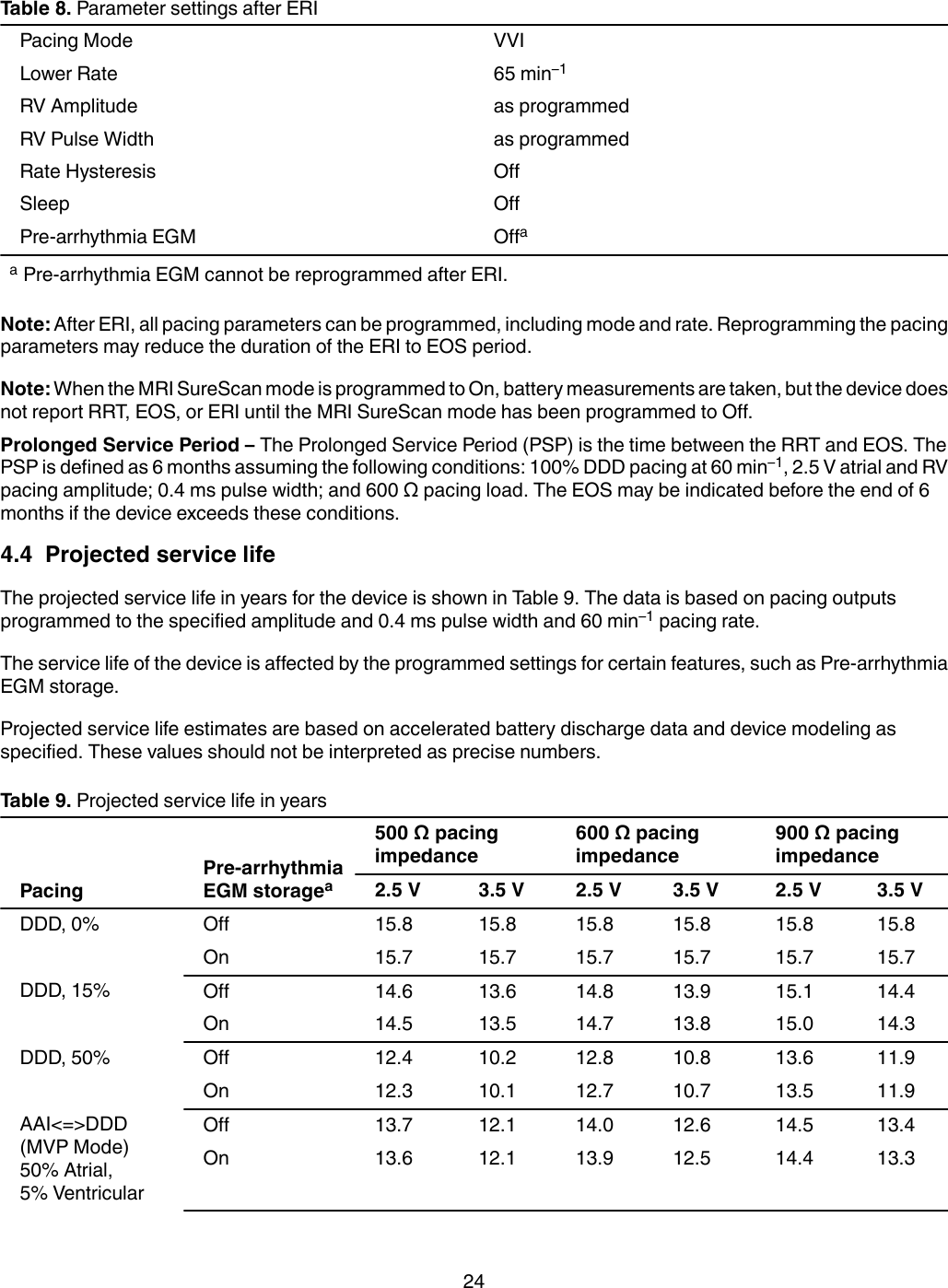
Medtronic BLEIMPLANT Azure S SR MRI SureScan, Azure S DR MRI SureScan, Azure XT SR MRI SureScan, Azure XT DR MRI SureScan User Manual MAPS ID 502381 042
Medtronic, Inc. Azure S SR MRI SureScan, Azure S DR MRI SureScan, Azure XT SR MRI SureScan, Azure XT DR MRI SureScan MAPS ID 502381 042
User Manual