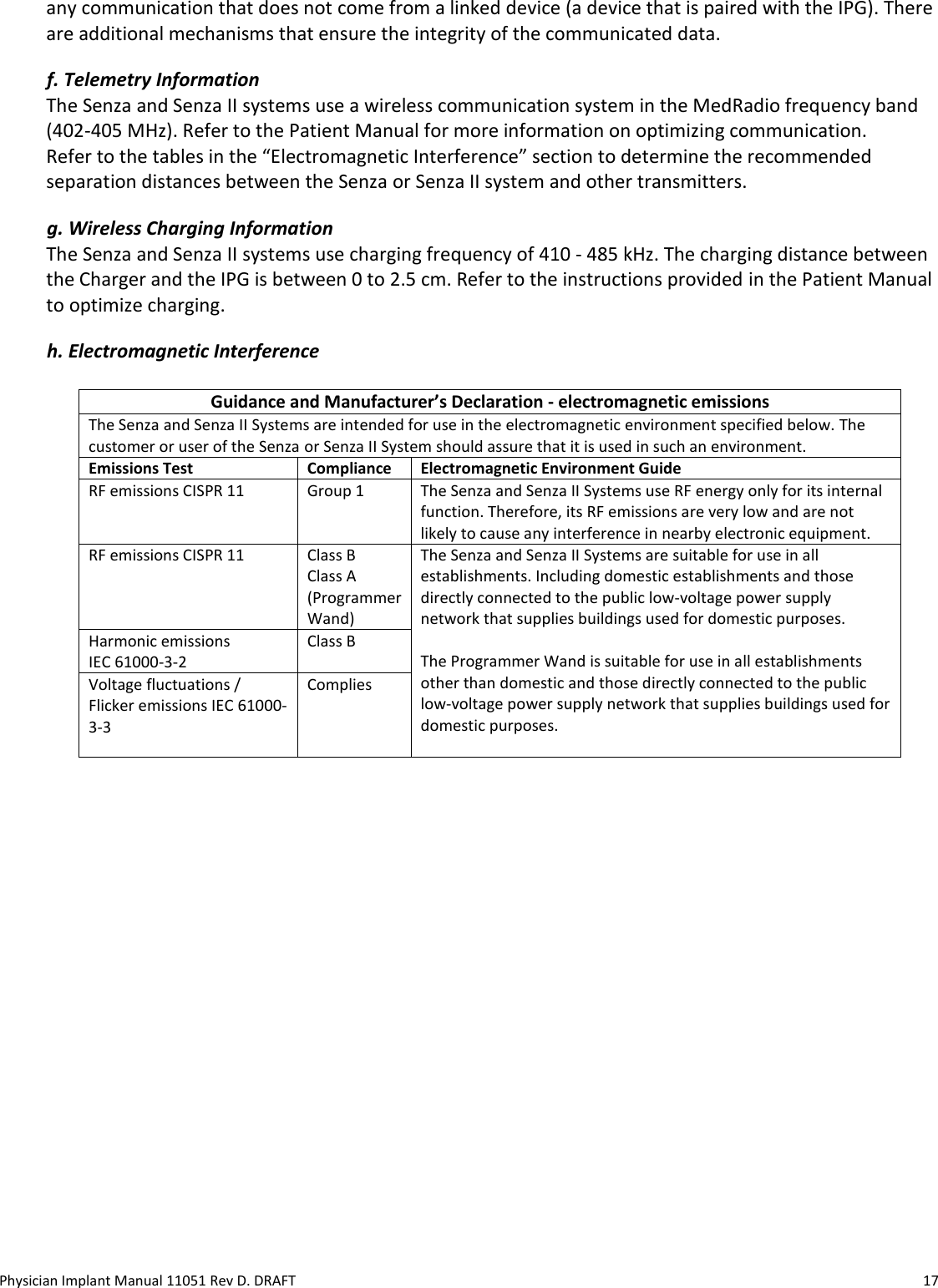
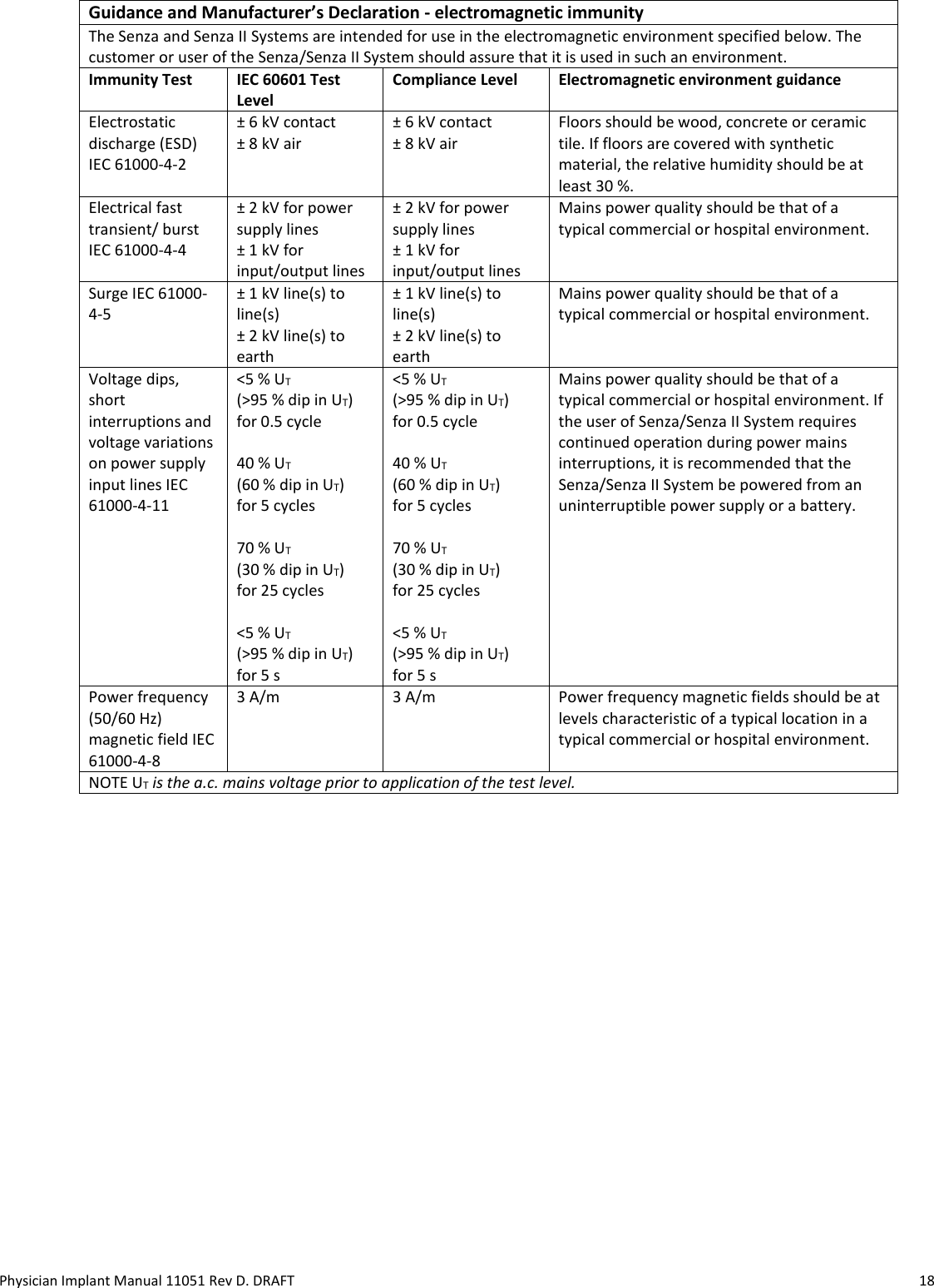
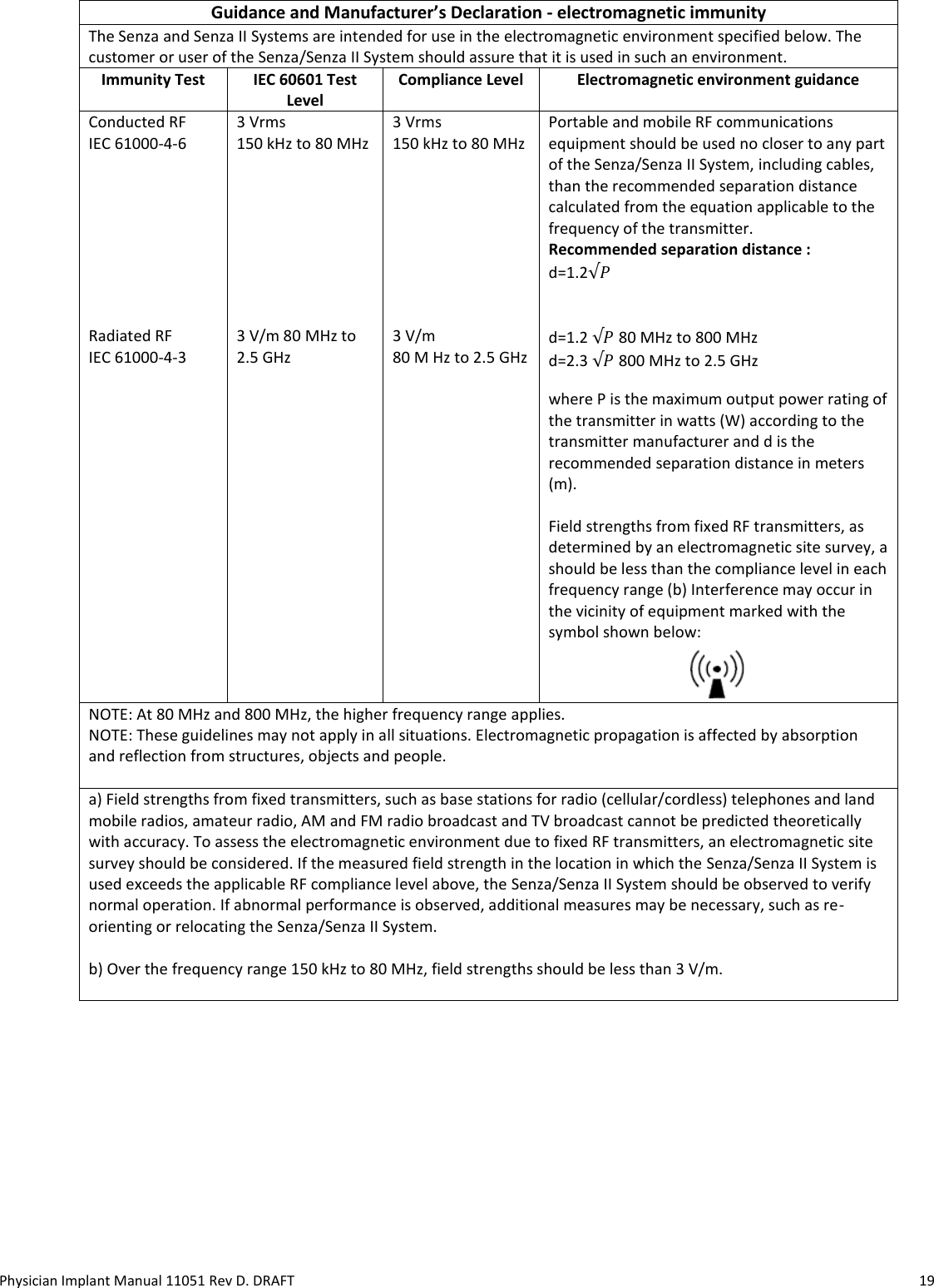
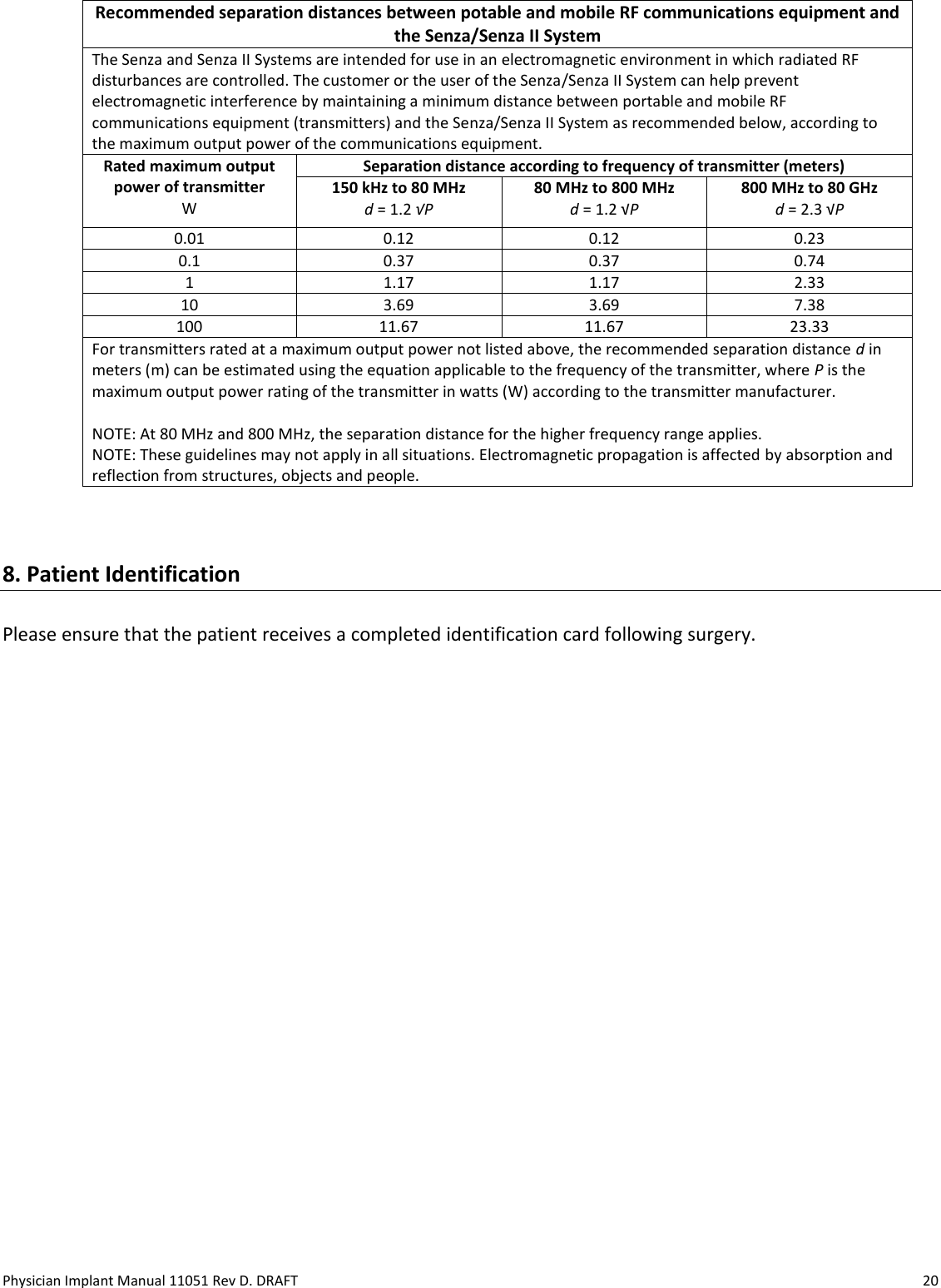
Nevro IPG2000 Implantable Spinal Cord Stimulator User Manual Users manual
Nevro Corporation Implantable Spinal Cord Stimulator Users manual
UserManual.wiki
>
Nevro
>
IPG2000 User Manual
Users manual
Navigation menu
Upload a User Manual
Namespaces
Wiki Guide
HTML
PDF
Info
Views
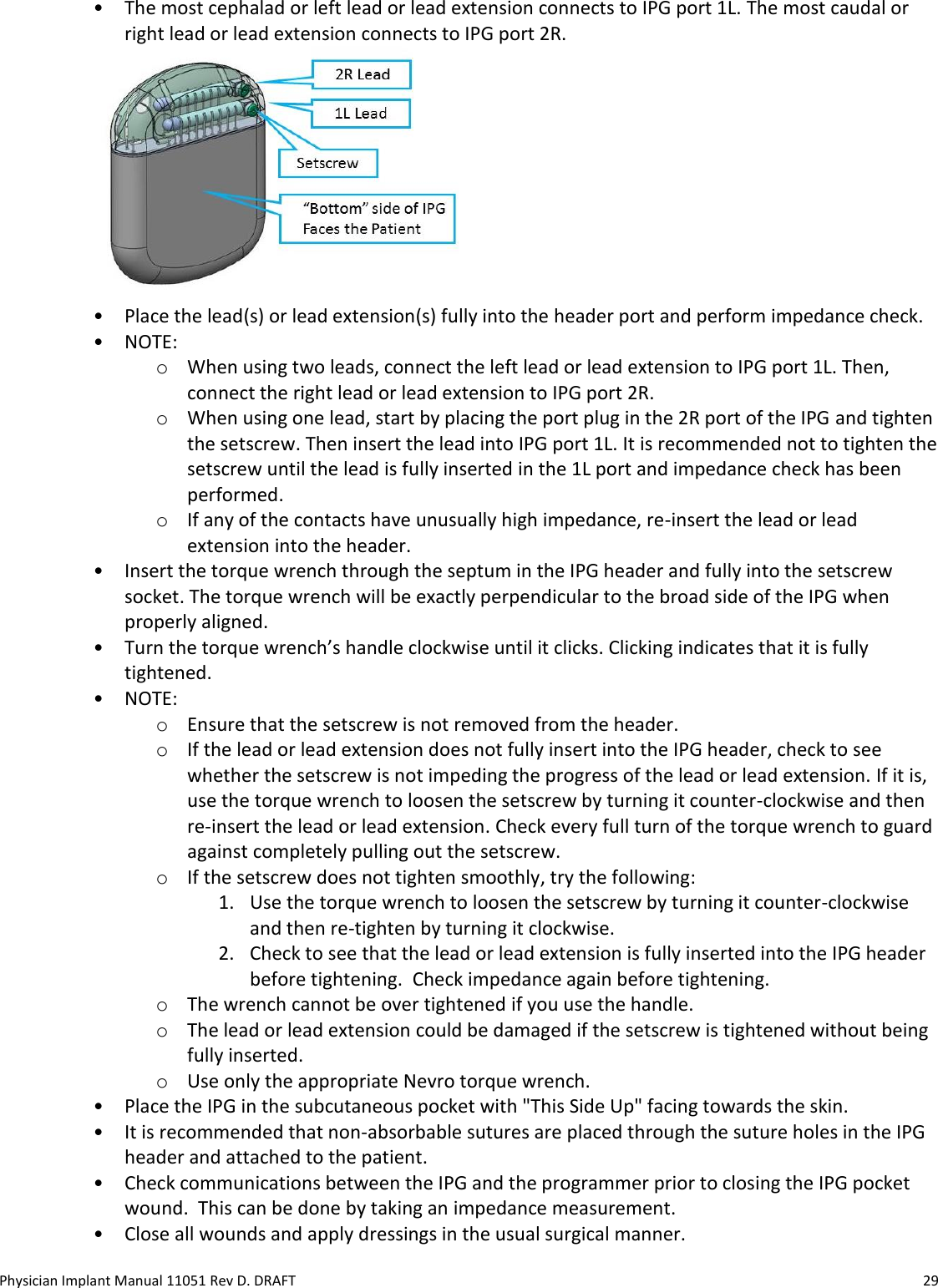
User Manual
Discussion / Help
Navigation