MergedFile 3981846f Dee5 420a 8934 De1f9256c421
2018-06-13
: Pdf 3981846F-Dee5-420A-8934-De1F9256C421 3981846f-dee5-420a-8934-de1f9256c421 6 2018 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 40
6/12/2018
1
Global Neurosurgery:
Building Neurosurgery, Training, and
Research
Michael M. Haglund MD, PhD, MACM, FAANS, FCS (ECSA)
Distinguished Professor of Neurosurgery, Neurobiology, and Global Health
Division Chief, Duke Global Neurosurgery and Neurology
Program Director, Duke Neurosurgery Training Program
Program Director Uganda East African Neurosurgery Training Program
Chief External Examiner, Fellowship in Neurosurgery COSECSA
Duke Division of Global
Neurosurgery and Neurology
Disclosures: Nuvasive for DGNN Grant Funding for East
Africa, UCB Pharmaceuticals for Epilepsy Centers of
Excellence
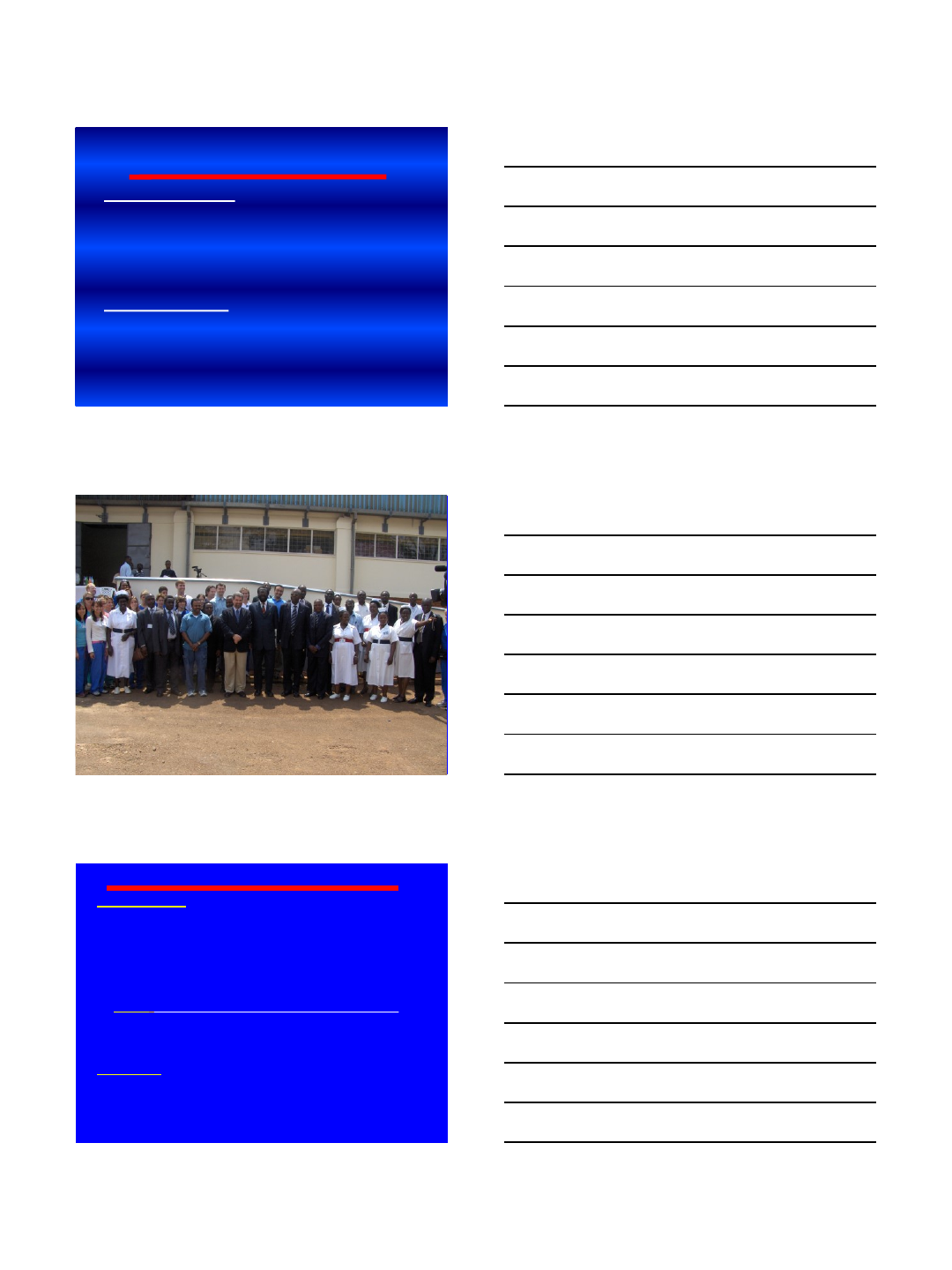
World Population
Worldmapper.org
6/12/2018
2
World Physicians
Africa: 565 Neurosurgeons
US: 3,600 Neurosurgeons
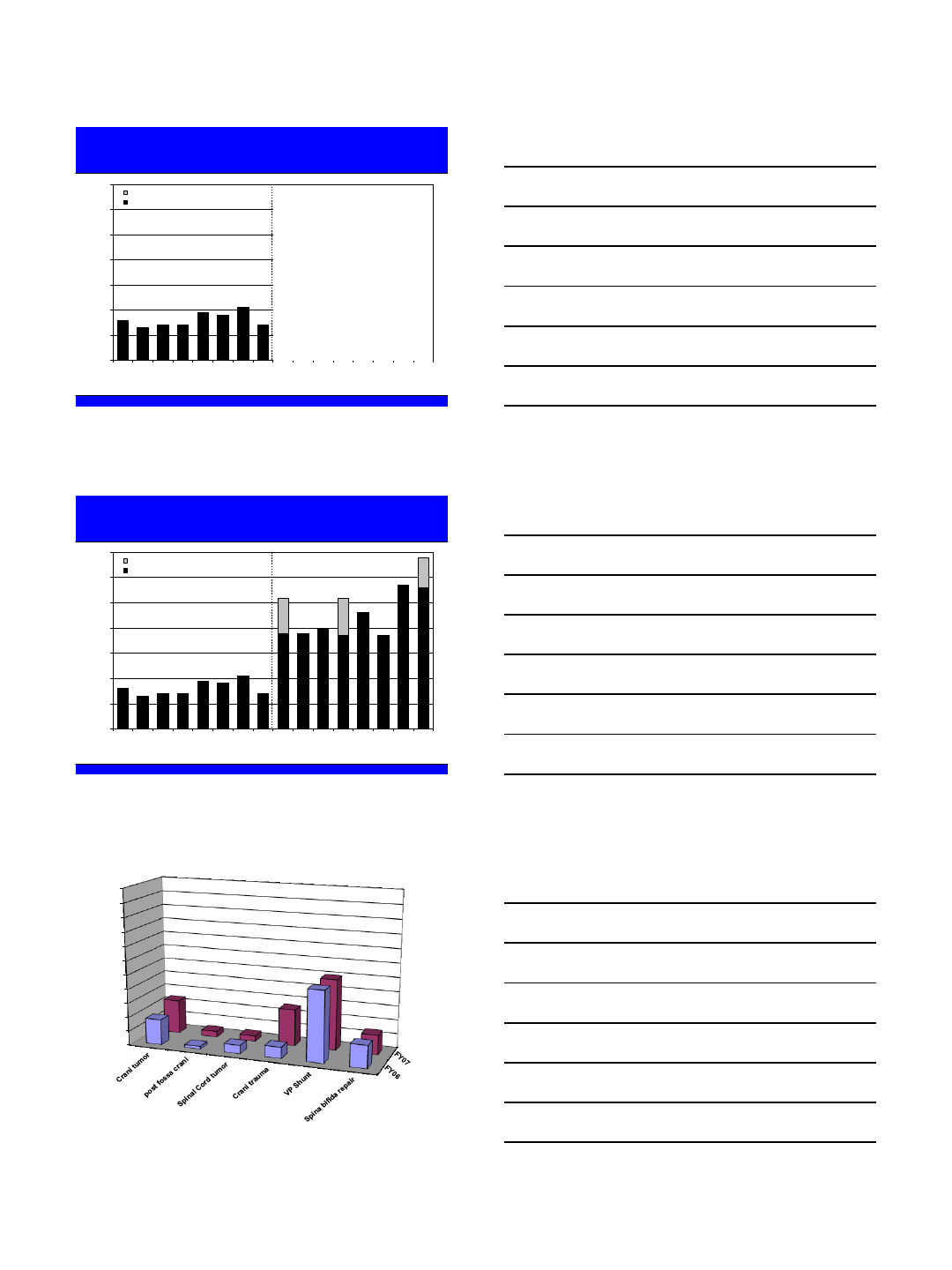
Northern
Eastern
Southern
Central
Western
African Regions
Countries in
East Africa
Total
Population
No. of
Neurosurgeons
Ration
Neurosurgeons
to population
Neuro-
surgical
Centers
Neurosurgery
Training
Program(s)
Northern
Africa and
South Africa:
486 of 563
NSUs
Morocco
Uganda
East Africa
United States
32 million
30 million
270
million
320
million
171
5
27
3,600
1:187,000
1:6 million
1:10 million
1:88,000
15
2
13
17 in NC
6
0
5
95
Neurosurgery in Africa 2007
6/12/2018
3
Problems: 2007
1) Only 1 Neurosurgeon for 6 million people in Uganda
2) No technology (one ventilator in 1,500 bed hospital)
3) No operating room dedicated to Neurosurgery
4) No Neurosurgery training program to train more
neurosurgeons
Solutions: 4-Ts
1) Technology: Duke Global Health PLUS (Placement of Life-giving
Useable Surplus): Dr. Dzau, Dr. Merson, Jane Pleasants
2) Twinning: Teams of 23-55 medical professionals (1-2 trips/year)
3) Training: Neurosurgery Training Program in Uganda (FIENS)
4) Top Down Approach: All specialties and their patients benefit
Duke Neurosurgery
East Africa Project
Duke Twinning: One on One Training
2007- 2017: 438 Volunteers on 16 trips
31,600 hours, $2.1 million in donated time
417 surgeries
Duke Technology Transfer:
–Total Ten Years:
•2007: $1,275, 000/ 9 tons equipment/supplies & $90,000 donations
•2008: $1,875,000/ 8 tons equipment/supplies & $150,000 donations
•2009: $ 750,000 / 4 tons equipment/supplies & $140,000 donations
•2010: $ 1,3750,000/ 7 tons equipment/supplies & $135,000 donations
•2012 (2): $ 875,000/ 8 tons equipment/supplies & $175,000 donations
•2013 (2): $ 850,000/ 10 tons equipment/supplies & $240,000 donations
•2014 (2): $1,125,000,000/ 11 tons equipment/supplies & $200,000 donations
•2015 (2): $1,005,000/13 tons equipment/supplies & $375,000 donations
•2016 (2):$ 950,000/12 tons equipment/supplies & $500,000 donations
•2017 (2): $ 1,050,000/11 tons equipment/supplies & $275,000 donations
Total: 44,118,536,000 UGX and 11,880,000,000 UGX in donations
Total: $12,255,000 and 93 tons of equipment & supplies,
$3,300,000 donations to develop three Neurosurgery Hospitals
–Benefactors:
–Duke University Health System: Former Chancellor Victor Dzau, Jane Pleasants,
–Chancellor Eugene Washington
–Duke University: President Richard Brodhead
–Duke Global Health Institute: Director Michael Merson
–Division of Neurosurgery: Dr. Allan Friedman, Dr. John Sampson
–Corporate Support: Nuvasive, Synthes Spine, Integra Neuroscience, Biomet, K2M
6/12/2018
4
0
10
20
30
40
50
60
70
FY06 qtr 1
FY06 qtr 2
FY06 qtr 3
FY06 qtr 4
FY07 qtr 1
FY07 qtr 2
FY07 qtr 3
FY07 qtr 4
FY08 qtr 1
FY08 qtr 2
FY08 qtr 3
FY08 qtr 4
FY09 qtr 1
FY09 qtr 2
FY09 qtr 3
FY09 qtr 4
Cases (n)
Elective OR + Duke NSU Camp
NSU Elective OR
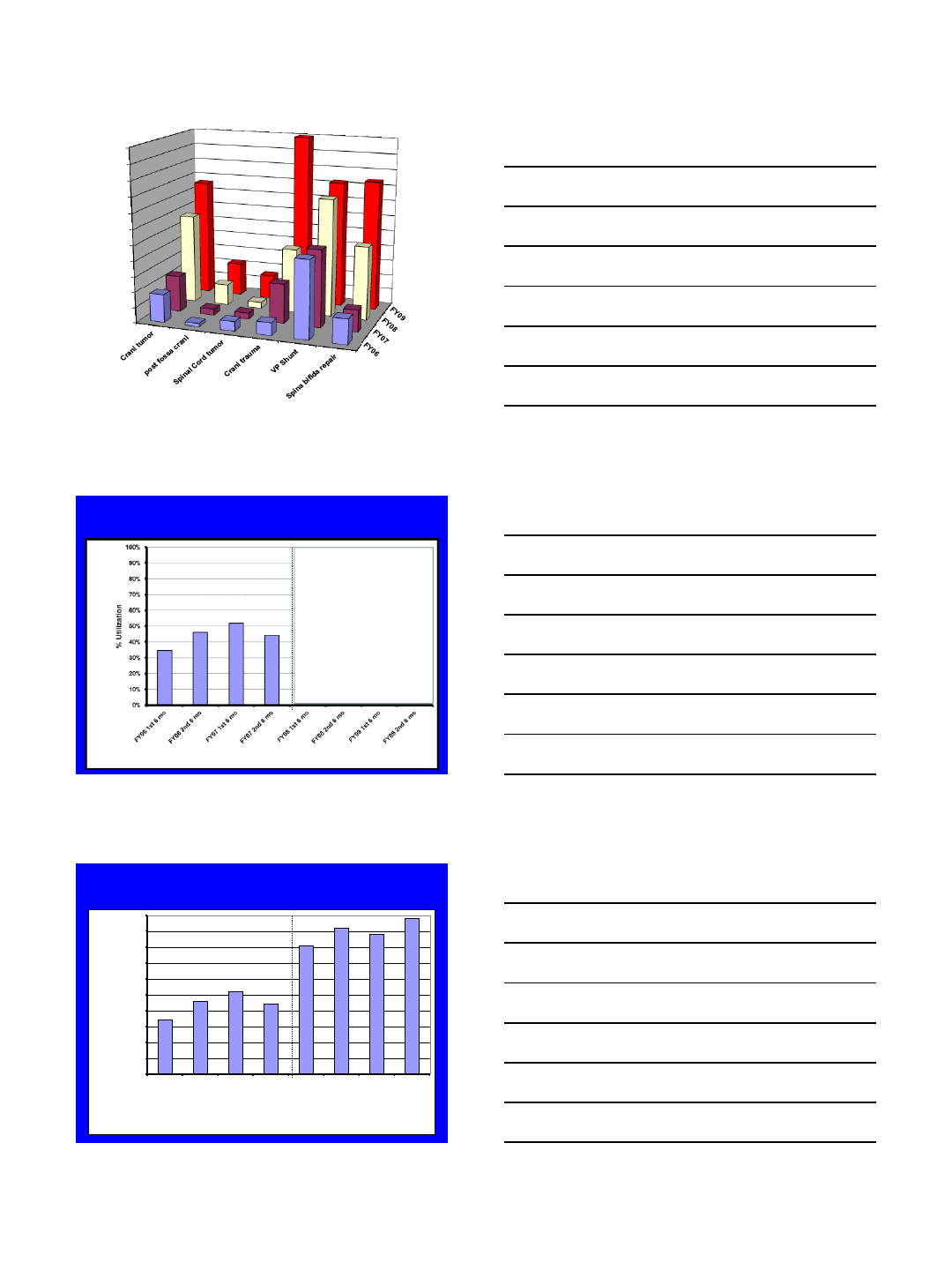
Neurosurgical Cases per Qtr
Initiation Duke NSU Program
0
10
20
30
40
50
60
70
FY06 qtr 1
FY06 qtr 2
FY06 qtr 3
FY06 qtr 4
FY07 qtr 1
FY07 qtr 2
FY07 qtr 3
FY07 qtr 4
FY08 qtr 1
FY08 qtr 2
FY08 qtr 3
FY08 qtr 4
FY09 qtr 1
FY09 qtr 2
FY09 qtr 3
FY09 qtr 4
Cases (n)
Elective OR + Duke NSU Camp
NSU Elective OR
Neurosurgical Cases per Qtr
0
5
10
15
20
25
30
35
40
45
50
55
Cases (n)
6/12/2018
5
0
5
10
15
20
25
30
35
40
45
50
55
Cases (n)
Elective Neurosurgery OR Utilization
Start of Duke Neurosurgery Program
Elective Neurosurgery OR Utilization
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
FY06 1st 6 mo
FY06 2nd 6 mo
FY07 1st 6 mo
FY07 2nd 6 mo
FY08 1st 6 mo
FY08 2nd 6 mo
FY09 1st 6 mo
FY09 2nd 6 mo
% Utilization
Start of Duke Neurosurgery Program
6/12/2018
6
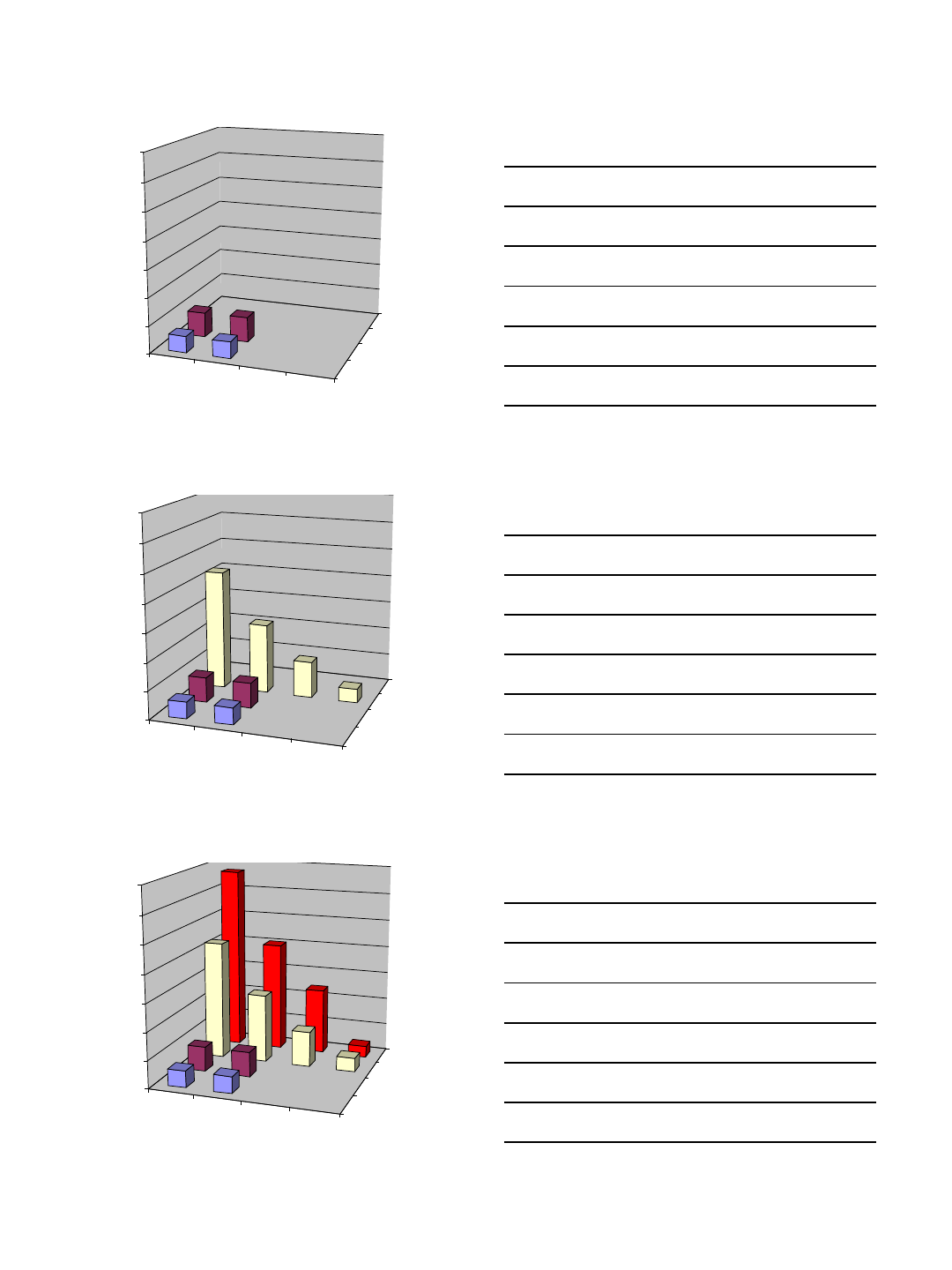
multiple
case days 2 case
days 3 case
days 4 case
days
FY06
FY07
FY08
FY09
0
10
20
30
40
50
60
70
Cases (n)
multiple
case days 2 case
days 3 case
days 4 case
days
FY06
FY07
FY08
FY09
0
10
20
30
40
50
60
70
Cases (n)
multiple
case days 2 case
days 3 case
days 4 case
days
FY06
FY07
FY08
FY09
0
10
20
30
40
50
60
70
Cases (n)
6/12/2018
7
73,000
83,000
93,000
103,000
113,000
123,000
133,000
143,000
153,000
163,000
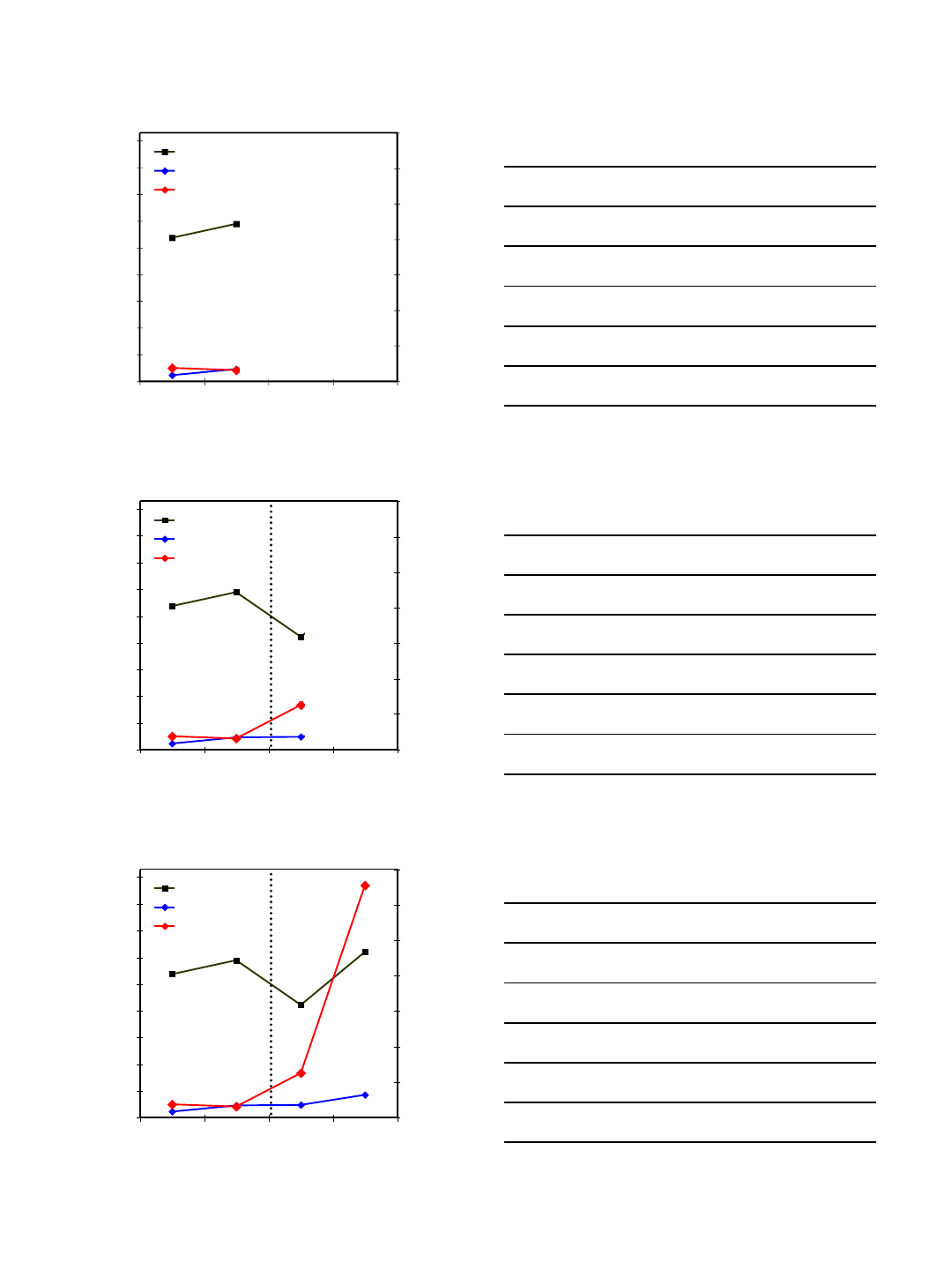
FY06 FY07 FY08 FY09
Admissions (n)
1100
1300
1500
1700
1900
2100
2300
2500
Total Surgical Cases (n)
Total Admits
New Admits
Total Surgical Cases
Initiation of Duke Project
73,000
83,000
93,000
103,000
113,000
123,000
133,000
143,000
153,000
163,000
FY06 FY07 FY08 FY09
Admissions (n)
1100
1300
1500
1700
1900
2100
2300
2500
Total Surgical Cases (n)
Total Admits
New Admits
Total Surgical Cases
Initiation of Duke Project
73,000
83,000
93,000
103,000
113,000
123,000
133,000
143,000
153,000
163,000
FY06 FY07 FY08 FY09
Admissions (n)
1100
1300
1500
1700
1900
2100
2300
2500
Total Surgical Cases (n)
Total Admits
New Admits
Total Surgical Cases
Initiation of Duke Project
6/12/2018
8
Uganda Neurosurgery Training Program:
Co-Directors: Dr. Michael Muhumuza and Professor Michael Haglund
Duke Neurosurgery Curriculum and East African NSTP Curriculum
Start first two Ugandan residents Aug 2009: Dr. Obiga and Dr. Muhindo,
Second set of two residents started August 2012
MMed Neurosurgery at Makerere University, Fall 2018
Currently 5 more in program, 2 starting summer 2018, total 7 residents
Uganda East African Neurosurgery Training Program: Twinning
Uganda residents spend one month at Duke observing in year 4 COSECSA
Duke Neurosurgery Residents spend one week to 1 month Uganda PGY-5/6
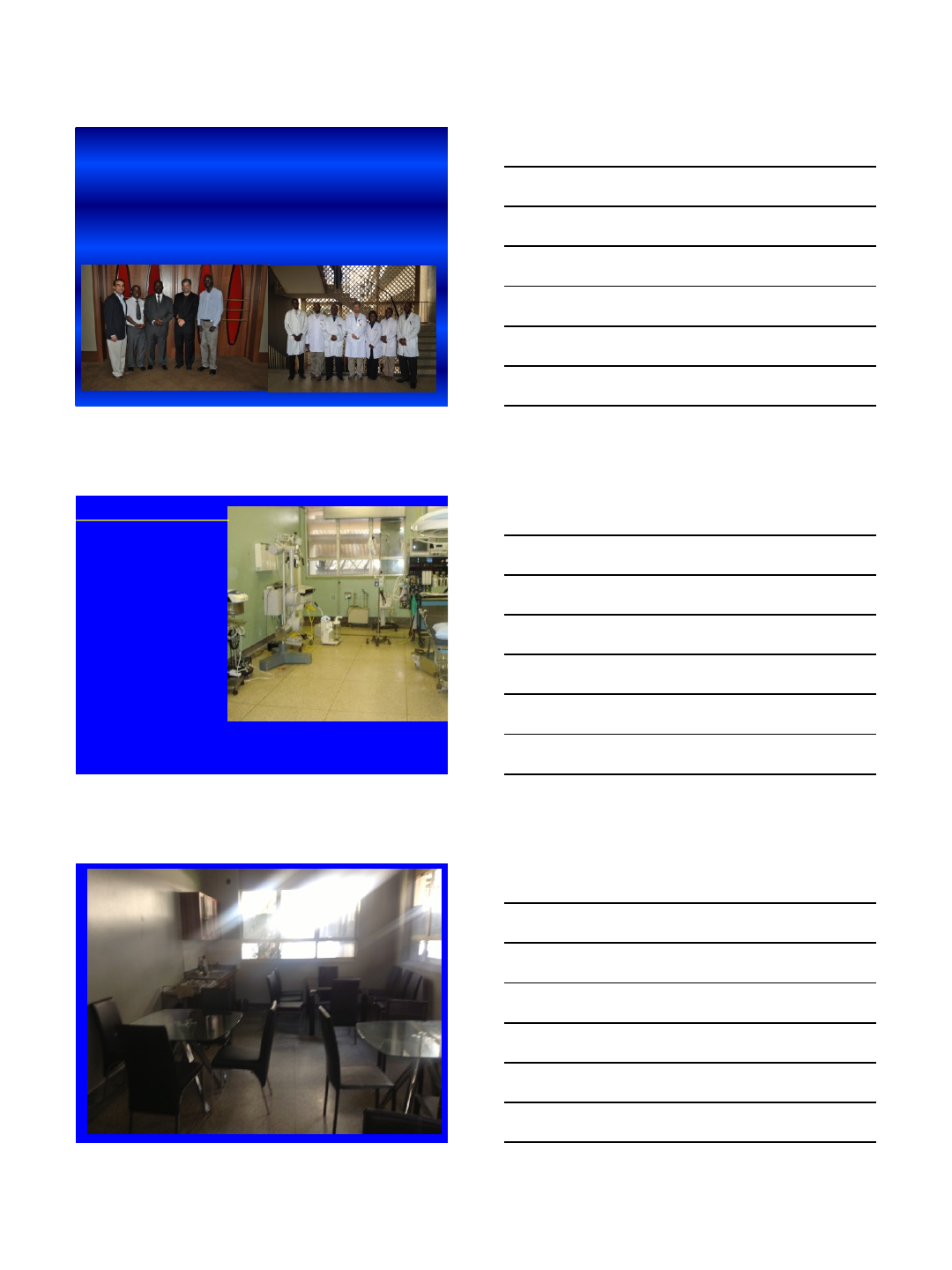
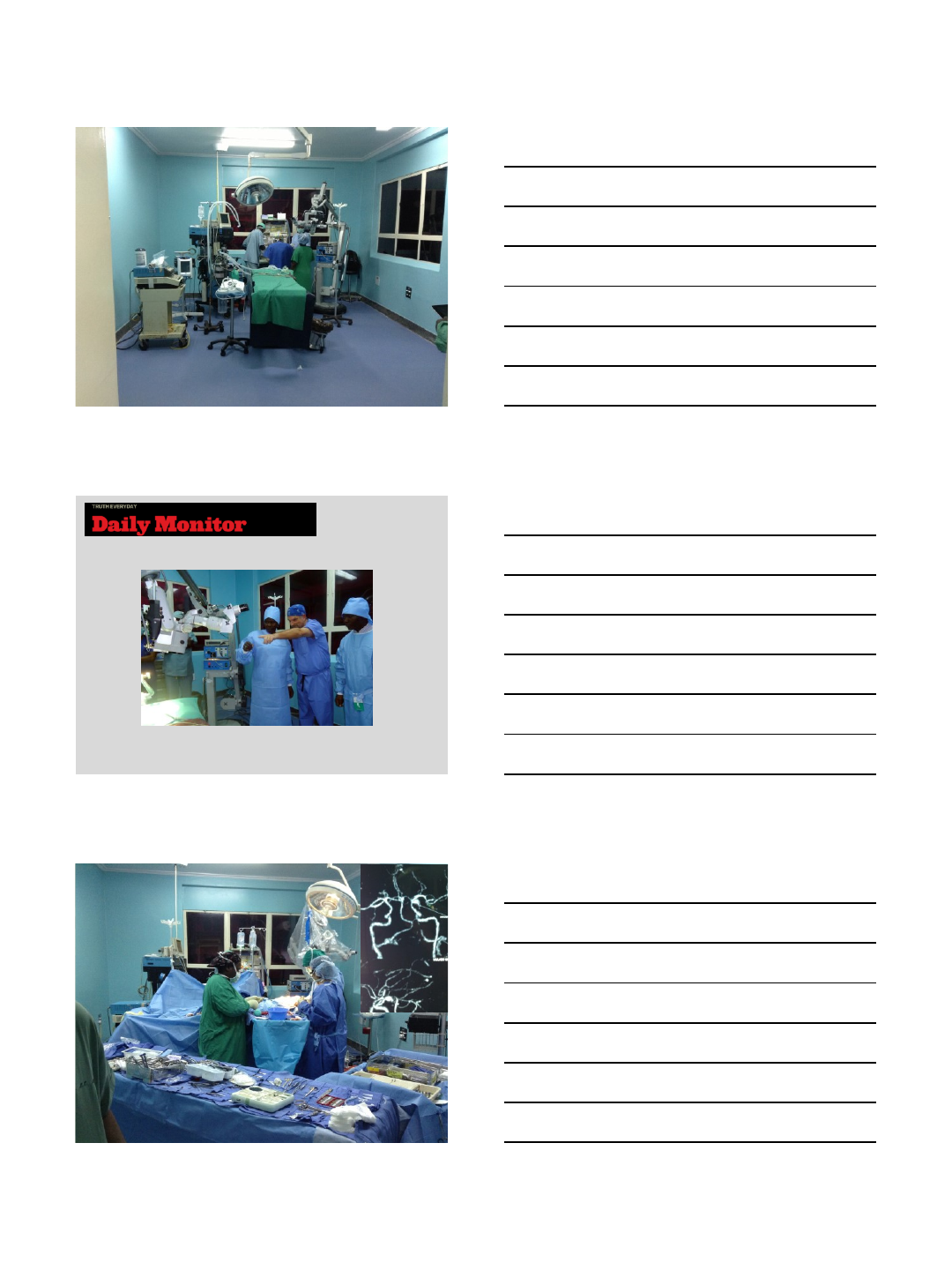
Before new Neurosurgery Theater:
Neurosurgeons operate 2 days/wk
Trauma cases build up on Ward 3A
Elective cases best for resident
training pushed off for
clearing Ward 3A trauma
Hope to build capacity and training
by building new NSU Theater
{kind=link}
6/12/2018
10
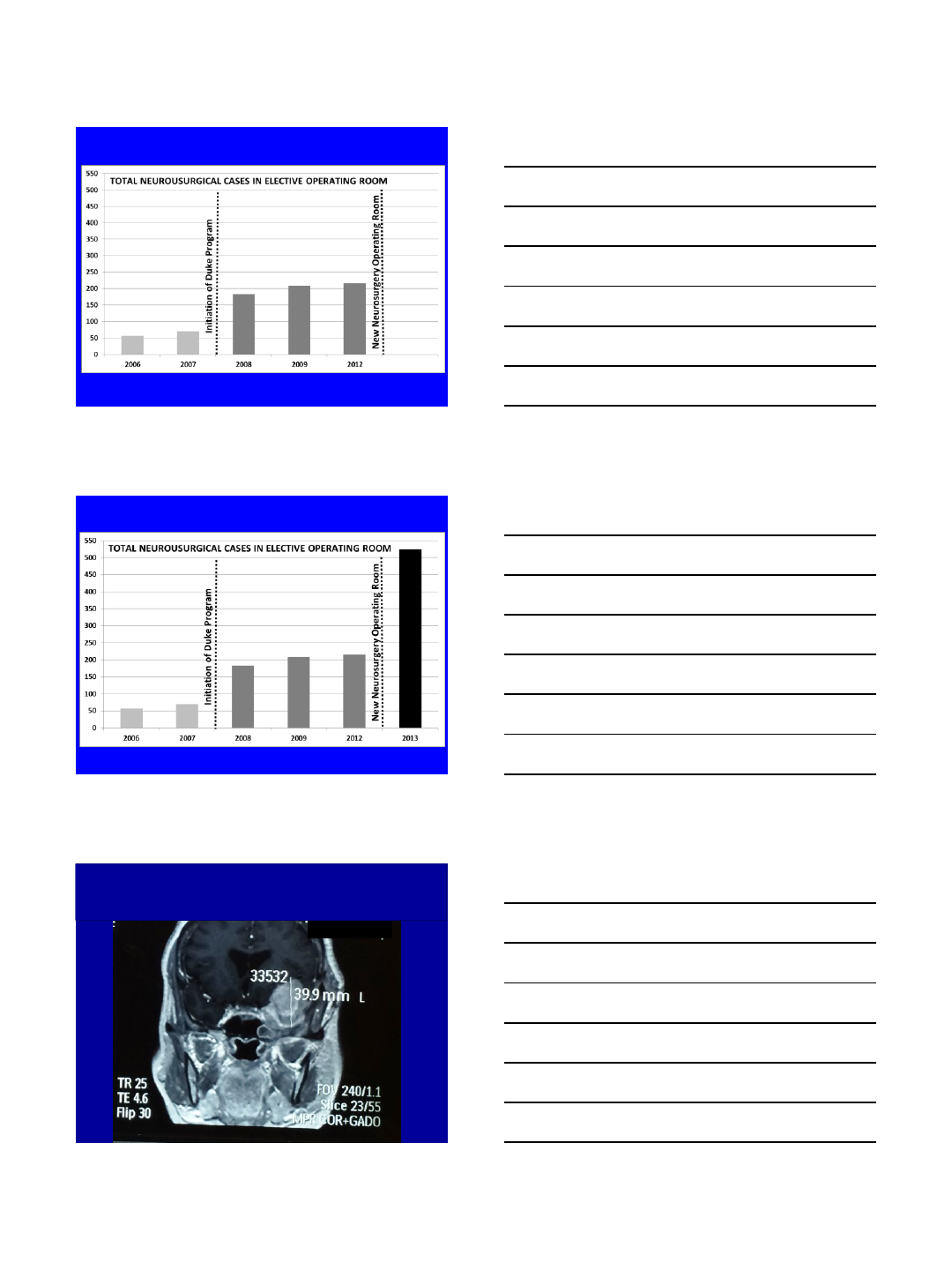
Operating Theater #4: Alex Muhindo, Professor
Haglund
Thursday Case #7

6/12/2018
11
Duke Global Neurosurgery..
..training Ugandans in Uganda
Duke Global Neurosurgery..
..training Ugandans in Uganda
TRAINING: 7 Neurosurgeons in Uganda 2013 Trained
5 graduates, 7 more in training,
Goal: 50 neurosurgeons by 2030
2016
2013
2013
2020
2023
2022
2024
2025
V
I
S
I
O
N
2022
COSECSA/ MMed TRAINED NEUROSURGEONS
50 Neurosurgeons for 62 million
1 NSU for 1.24 million
2
0
3
0
2026
2015
2011
2011
2017
2018
2019
2021
2022
V
I
S
I
O
N
2
0
3
0
2020
COSECSA TRAINED NEUROSURGEONS
2016
2011
2011
2020
2023
2022
2024
2025
V
I
S
I
O
N
2
0
2022
2025
2025
2025 2025
2025
2025
2025
2024
2024
2024
2025
2021
2024
2023
2023
2020
2021
2020
2021
2021
2021
2025
2021
2023
2021
2021
2021
300 General Surgeons Trained by 50 Neurosurgeons
2030
2030
2030
2030
2030
2030
2030
2030
2030
2030
2030
2030
2030 2030
2030
2030
2030
2030
2030
2030
2030
2030
2030
2030
2030
350 NSU trauma surgeons for 62 million
1 NSU trauma for 171,000 people
6/12/2018
12
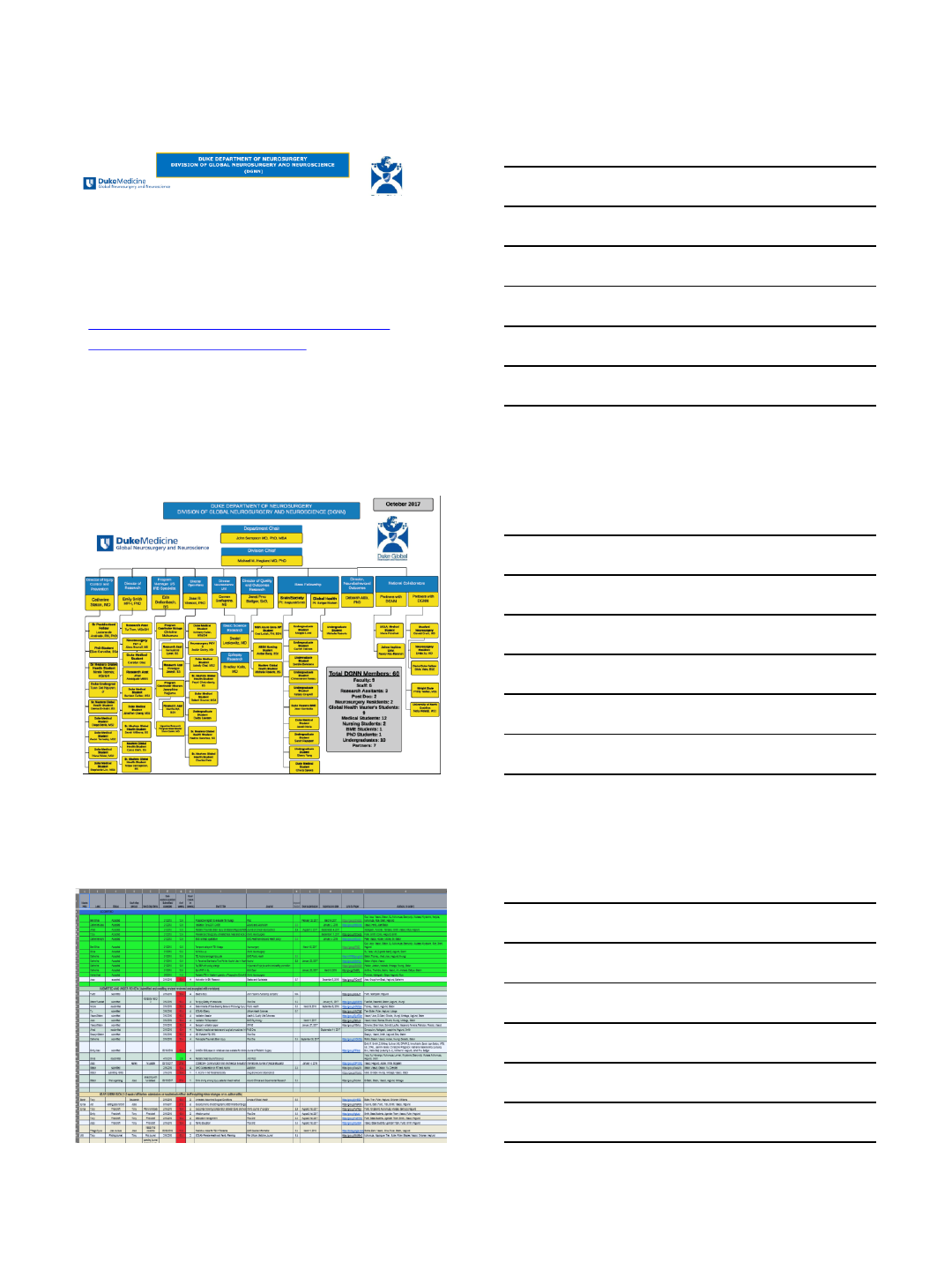
The New Vision for Global Neurosurgery
June 28, 2014
Meeting with new Chair of Neurosurgery,
John Sampson, MD, PhD, MHS, MBA
6/12/2018
13
Published/Accepted (October 2014 –December 2015): 15 manuscripts
1. High Road Utilizers Surveys Compared to Police Data for Road Traffic Crash Hotspot Localization in Rwanda and Sri Lanka.
Staton C, De Silva V, Krebs E, Andrade L, Rulisa S, Mallawaarachchi B, Jin K, Vissoci J, Ostbye T. BMC Public Health acceptance
13Dec2015
2. Road Traffic Injury Prevention Initiatives: a systematic review and metasummary of effectiveness in low and middle income
countries Staton CA, Vissoci JRN, Gong E, Toomey N, Wafula R, Abdelgadir J, Zhou Y, Liu C, Pei F, Zick B, Ratliff C, Rotich C,
Jadue N, Andrade L, von Isenburg M, Hocker M.Plos One acceptance 18Nov 2015 (Output of Global Injuries Course)
3. Building Neurosurgical capacity in low and middle income countries Anthony Fuller, Tu Tran, Michael Muhumuza, Michael M.
Haglund Published online: November 3, 2015, eNeurologicalSci.
4. Surgeons OverSeas Assessment of Surgical Need (SOSAS) Uganda: update for household survey. Fuller A, Butler E, Tran T,
Makumbi F, Luboga S, Muhumuza C, Chipman J, Groen R, Gupta S, Kushner A, Galukande M, Haglund M. World Journal of
Surgery 2015 Dec, 39(12):2900
5. A prospective registry evaluating the epidemiology and clinical care of Traumatic Brain Injury patients presenting to a Regional
Referral Hospital in Moshi, Tanzania: challenges and the way forward. Staton, Msilanga, Kiwango, Vissoci, Lester, Hocker,
Gerardo, Mvungi Int J Inj Contr Saf Promot. 2015 Aug 4:1-9. PMID: 26239625
6. Burden of Surgical Conditions in Uganda: Pilot Study of a Population-Based Survey in Wakiso District, Uganda. Butler E, Tran T,
Fuller A, Makumbi F, Luboga S, Kisakye S, Haglund M, Chipman J, Galukande M. Surgery. 2015 Sep;158(3):764-72. doi:
10.1016/j.surg.2015.05.011. Epub 2015 Jun 16. PMID: 26088920
7. Distribution and characteristics of severe traumatic brain injury at Mulago National Referral Hospital in Uganda. Tran TM, Fuller AT,
Kiryabwire J, Mukasa J, Muhum uza M, Ssenyojo H, Haglund MM.World Neurosurg. 2015 Mar;83(3):269-77. doi:
10.1016/j.wneu.2014.12.028. Epub 2014 Dec 19. PMID: 25529531
8. Central nervous system tumor distribution at a tertiary referral center in Uganda. Hatef J, Adamson C, Obiga O, Taremwa B,
Ssenyojo H, Muhum uza M, Haglund M, Schroeder K. World Neurosurg. 2014 Sep-Oct; 82(3-4):258-65. doi:
10.1016/j.wneu.2014.06.040. Epub 2014 Jun 19. PMID: 24953304 Accepted with revisions.
9. Quality of the Development of Traumatic Brain Injury Clinical Practice Guidelines: A Systematic Review
Patel, Abraham, Reid, Tran, Toomey, Vissoci, Rodrigues, Viera, Gerardo, Euker, Mvungi, Staton
Accepted with revisions to PLoS One
10. Qualitative Evaluation of Trauma Delays in Road Traffic Injury Patients in Maringa, Brazil. Patel A, Vissoci JRN, Hocker M, Molina
E, Morales Gil N, Staton C Accepted with minor revisions to PloS One
DGNN Google Docs on April 27, 2018, 48 manuscripts in 24 months
6/12/2018
14
Thanking Julie and other faculty
Put in grants for Bass, others,
UCB-Belgium grant, Nuvasive
Grant
Neurosurgical Camp
Mbarara, Uganda
2016
Uganda Neurosurgery
Residency
Mbarara, Uganda
April 2016
Duke University Bass Foundation
Research Group
Kampala, Uganda
July 2016
6/13/2018
1
O. Boachie-Adjei, M.D. DSc.
President and Founder FOCOS
CEO, Medical Director and Surgeon in Chief
FOCOS Hospital
Past President
Scoliosis Research Society
Prof. Orthopedic Surgery
Weill Medical College of Cornell University
Chief Emeritus Scoliosis Service
Hospital For Special Surgery, New York
Spinal Surgery in Ghana:
How We Create A Center of Excellence
Author’s Disclosure Information
Oheneba Boachie-Adjei, MD
DePuy Spine, (a,b,e)
K2M, (a,b,d)
Weigao Co (b,c)
a) Grants/Research
Support
b) Consultant
c) Stock/Shareholder
d) Speakers’Bureau
e) Other Financial Support
The fourth greatest impact on the health of the world
population, considering both death and disability (DALYs)
(Lancet 15 December 2012)
–Ranking of major causes of death and disability (%
DALYs)
•Cardiovascular and circulatory diseases 11.8%
•All neoplasms 7.6%
•Mental and behavioural disorders 7.4%
•Musculoskeletal disorders 6.8%
Global Health and Orthopedics
6/13/2018
2
FOCOS Orthopaedic Hospital
MISSION: To provide optimum orthopaedic
care and improve quality of life in Ghana and
other countries
VISSION: A Sustainable infrastructure
for state of the art orthopaedic care and
education.
Challenges
•Human Resources
•Finances
•Infrastructure
•Complex Orthopedic and medical
conditions
•Sustainability
Human Resource Challenge
6/13/2018
3
USA, Mexico, Argentina. Spain, Italy, Norway, Japan, Turkey, Australia
,India, Nigeria, Sierra Leone, New. Zealand, Kenya, Greece
Funding Challenge
•Ghana fares poorly among African and
global averages for total Expenditure on
health.
•The average Ghanaian cannot afford
major orthopedic surgical care and the
NHIS doesn't cover such surgical
services.
Fee For service and sponsorship program via
Fundraising (30% patients subsidized)
6/13/2018
4
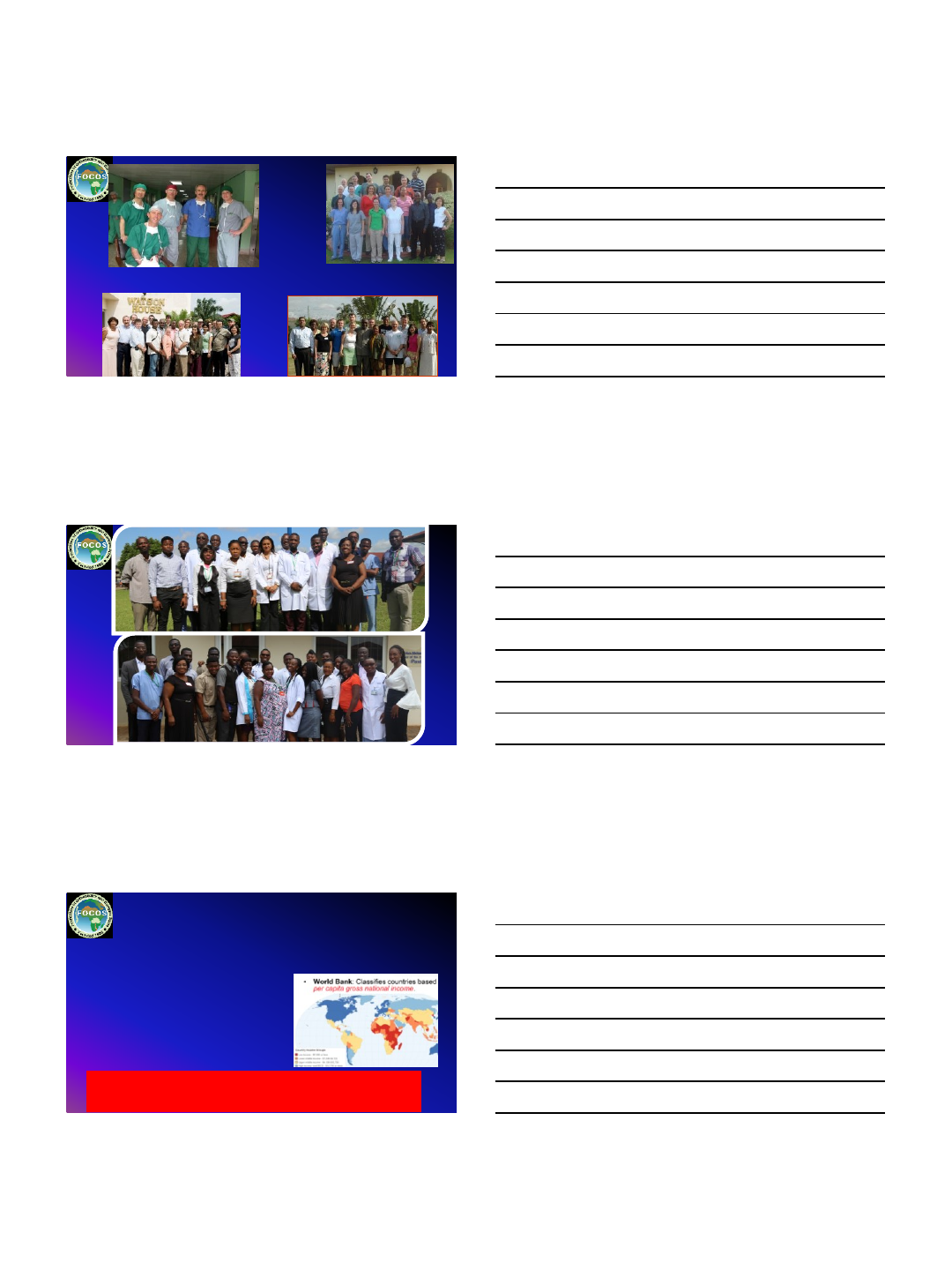
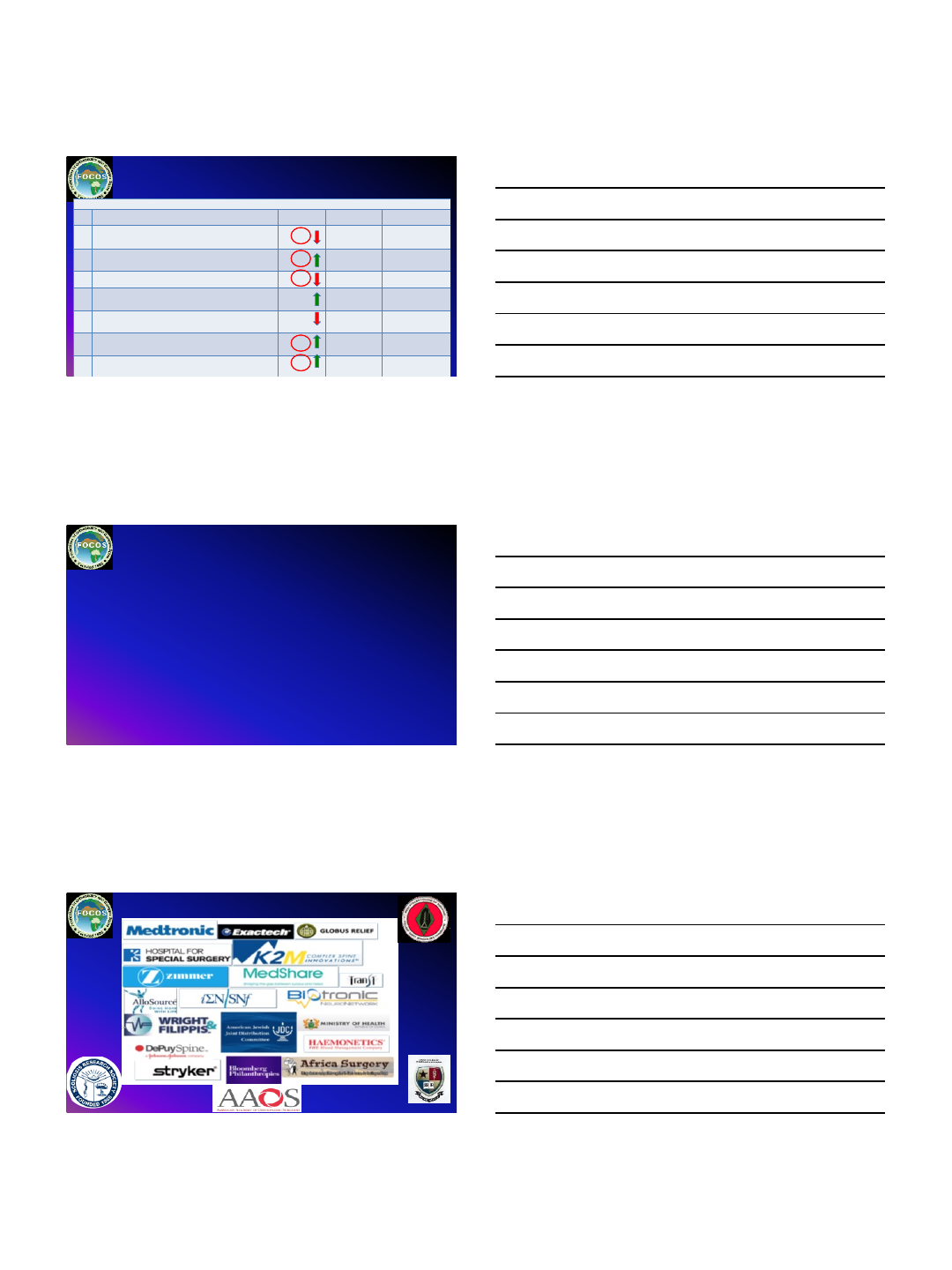
Health Expenditure Indicators
No
Indicator
Ghana Value Africa Average Global Average
1
Total Expenditure on health as % of gross domestic product ( 2014)
3.6
5.5 10.0
2
General government expenditure on health as % of total
expenditure on health (2014)
59.8
47.8 60.1
3
Private expenditure on health as % of total expenditure on health
(2014)
40
52.2 39.9
4
General government expenditure on health as % of total
government expenditure ( 2014)
7.0
10.0 15.5
5
Out
-of-
pocket expenditure on health as % of private expenditure on
health(2014)
67 60.1 45.5
6
Per Capita total expenditure on health at average exchange rate
(US$) (2014)
58
107 1057
7
Per capita government expenditure on health at average exchange
rate (US$) (2014)
35
51 635
Health Expenditure Indicators 2014
FOCOS Funding strategies
•Government Seed Grant
•FOCOS-MOH CO-Consignment initiatives for imports
•International Volunteerism
•International Multi-industry partnership
•Global Private donors and Benefactors
•Private foundation sponsorships of patients
•FOCOS USA GRANTS
•Private Loans
Global Partners
6/13/2018
5
STATE OF THE ART HOSPITAL
FOCOS Surgical THEATRE
•Twin operating theaters with state of the art equipment
–Advanced anaesthesia machines, cell savers, neuro-monitoring devices, C-
arms, high definition cameras.
•Headed by a qualified perioperative nurse manager
INTENSIVE CARE UNIT/RECOVERY
•Full coverage by anesthetists and 5 critical care nurses
•A 6 bed unit with patient nurse ratio of 2:1 when in full capacity
•All the essential equipment of a first class ICU including ventilators, monitors,
defibrillators, perfusers, infusion pumps and other critical care equipment in
optimum working condition
6/13/2018
6
LAB, Phisiotherapy and Radiology
Manned by qualified biomedical scientists , laboratory technician
•Fully automated with capacity to do most investigations
•hematological analysis,
•serologies ,blood banking and biochemistries.
Pharmacy/Nutrition and Dietetics
The pharmacy is manned by
•One (1)Senior Pharmacist and Two (2)Pharmacy Technicians
•It offers a full complement of various classes of drugs available to patients
•Staffed by qualified nutritionists/dietician Develops meal plans to suit individual
patient needs including nutritional rehabilitation for our malnourished patients
6/13/2018
7
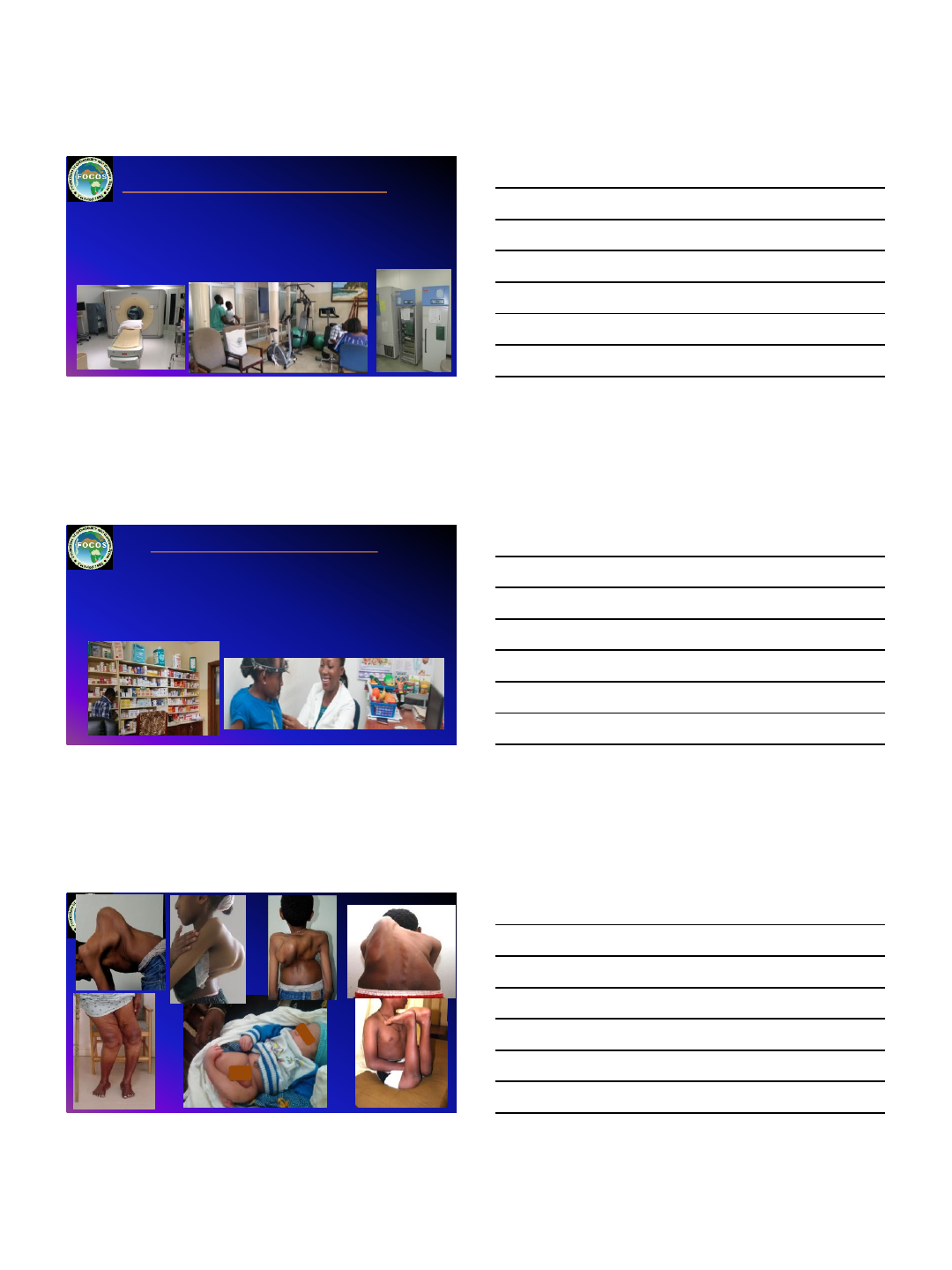
15%
39%
19%
22%
5% Spine cases
(Degenerative)
Spine cases (Deformity)
Halo traction
Major joint cases
Trauma cases
Types of Surgery
COUNTRIES OF ORIGIN OF FOCOS PATIENTS
IN-PATIENTS (21 countries)
Africa Europe Others
D.R.C Albania Canada
Ethiopia Russia China
Gambia Haiti
Ghana India
Liberia Philippines
Niger Uruguay
Nigeria USA
Sierra Leone
Tanzania
Togo
Uganda
Zambia
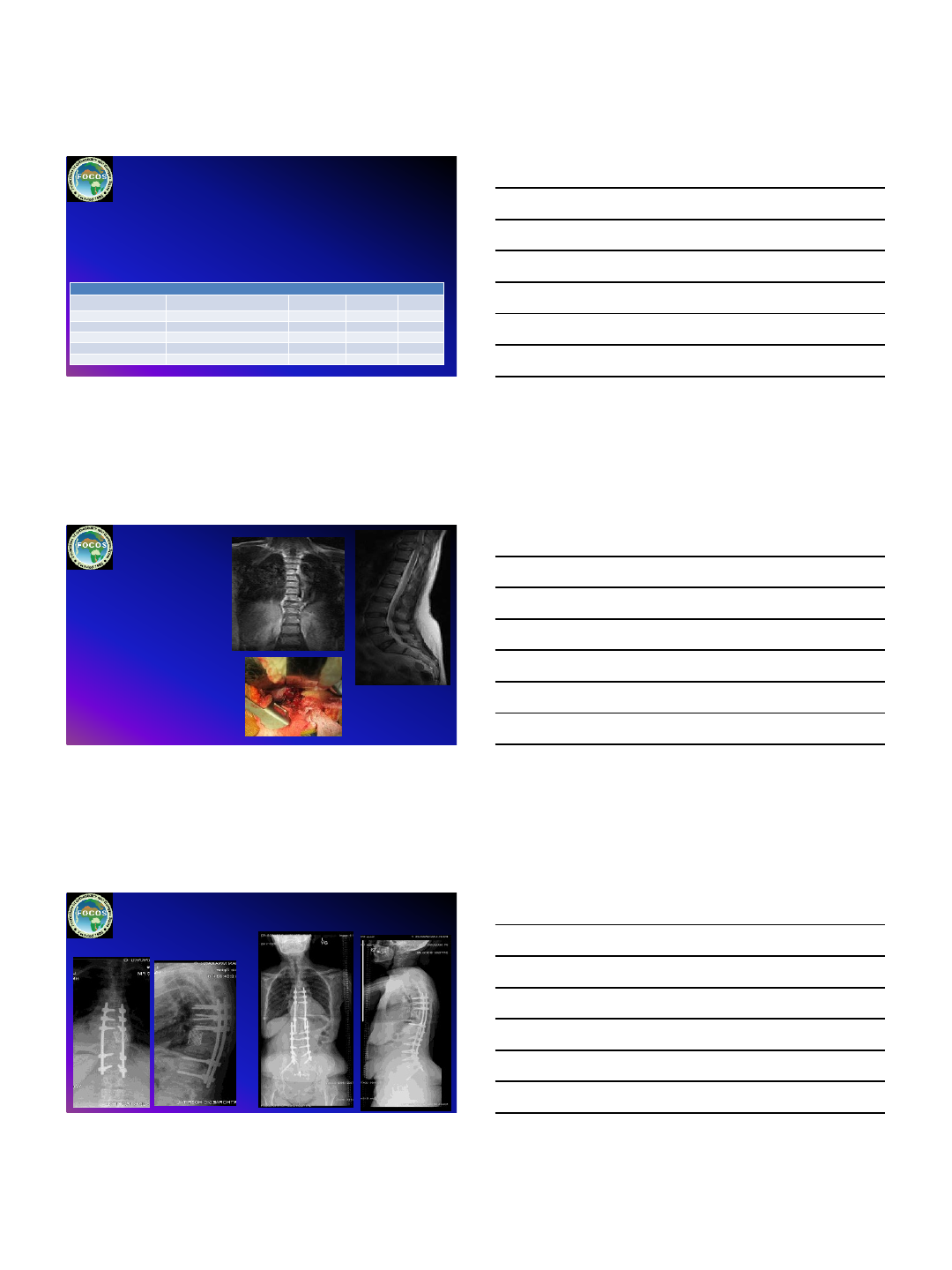
COUNTRIES OF ORIGIN OF FOCOS PATIENTS
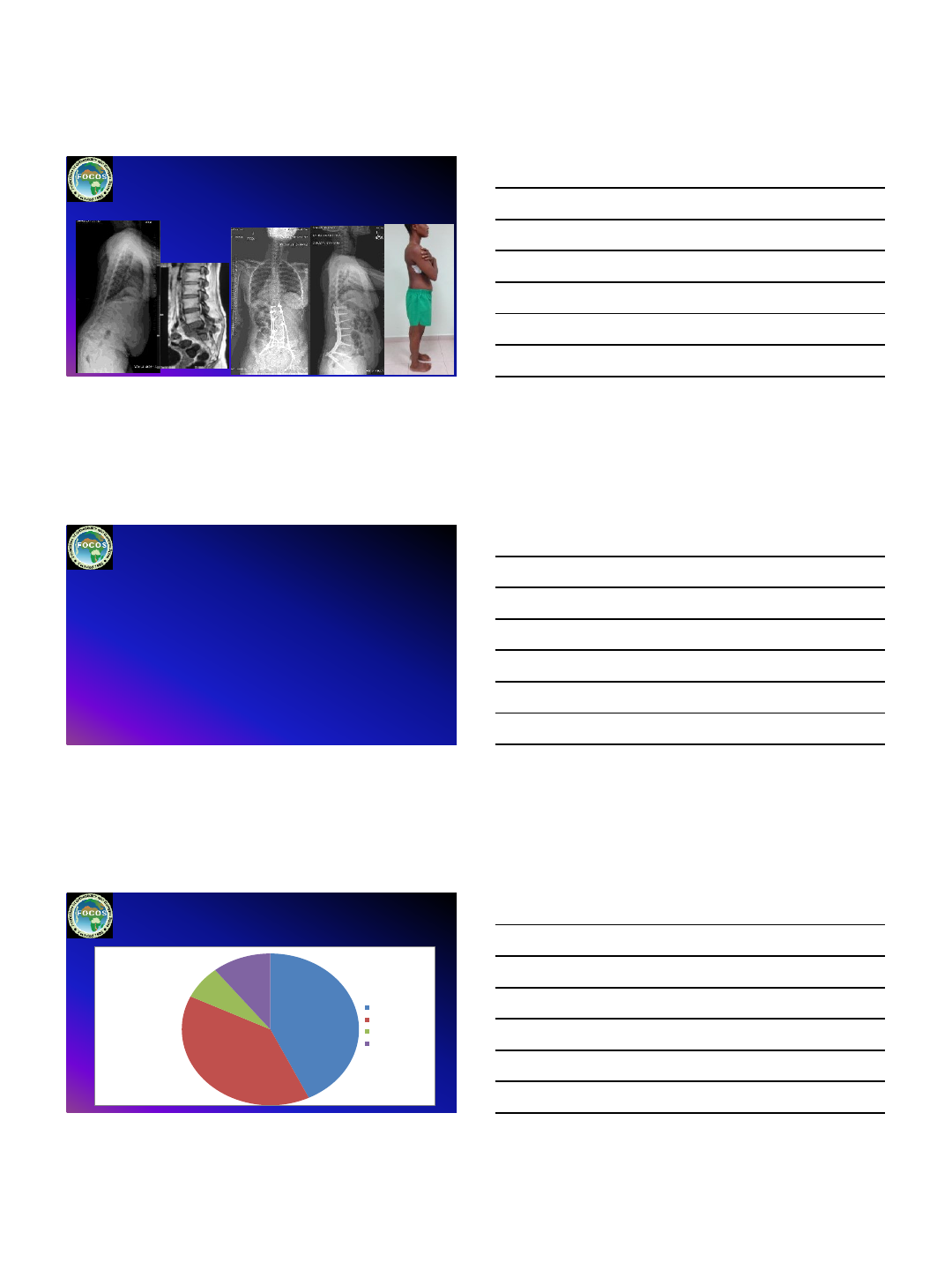
SS063 33F
Progressive back pain and difficulty standing and walking
Tuberculous Spondylitis:
6/13/2018
8
Posterior decompression PLIF PSSI ,
FOCOS Nutritional Pathways
•Nutrition status is a significant factor in the perioperative
care of the orthopedic patient
•90% orthopedic patients from Ethiopia seen at the
department were undernourished or small for their age
•Early identification of patients who are malnourished or
at risk is essential which leads to timely nutrition
interventions
PEDIATRIC PATIENTS CHANGE IN WEIGHT
42.86%
39.29%
7.14%
10.71%
WT GAIN≥1KG
WT GAIN≤ 1KG
WTMAINTANCE
WT LOSS≤1KG
6/13/2018
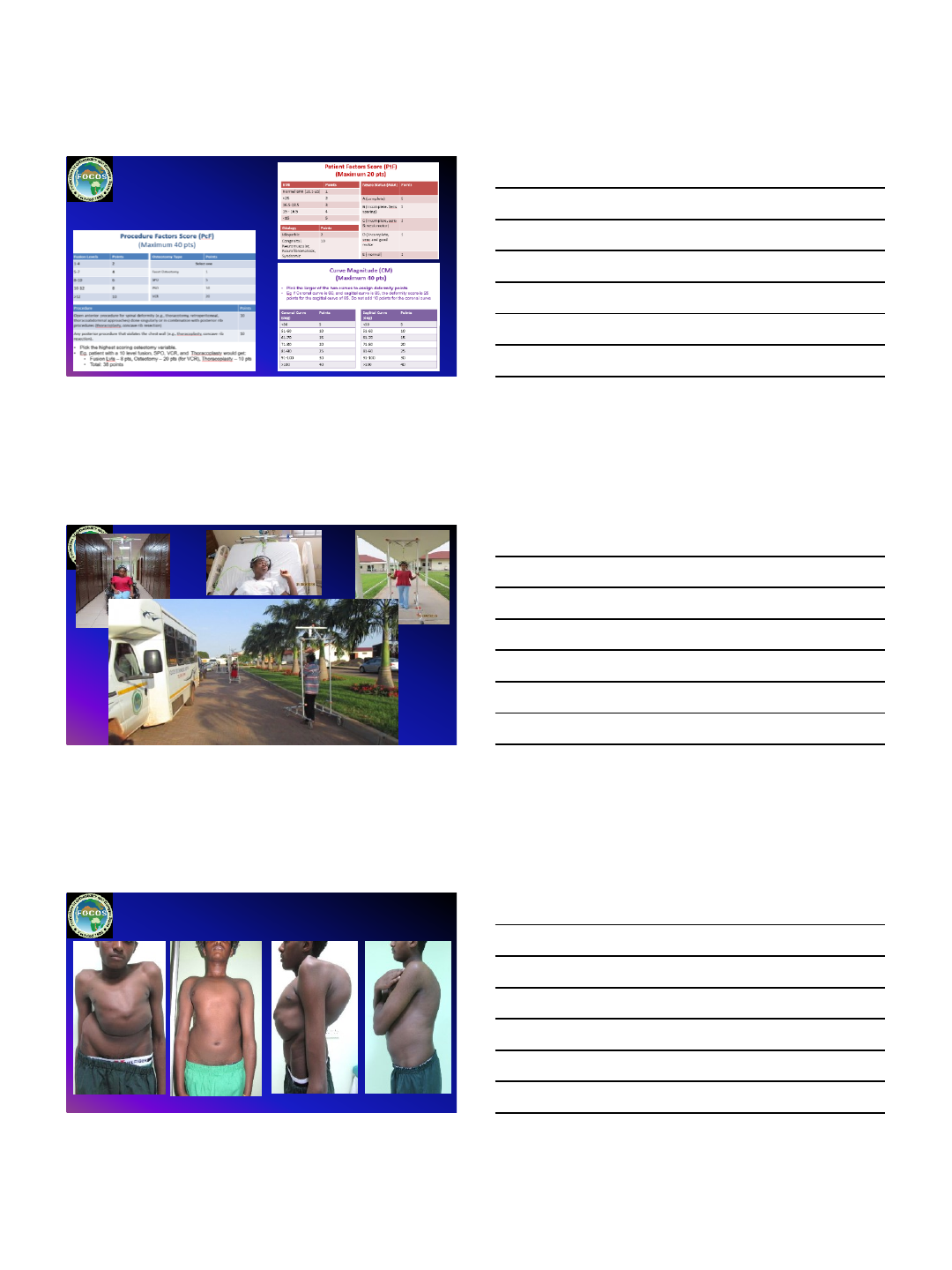
9
FOCOS RISK SCORE
FOCOS Traction, Feeding and surgical, program
6/13/2018
10
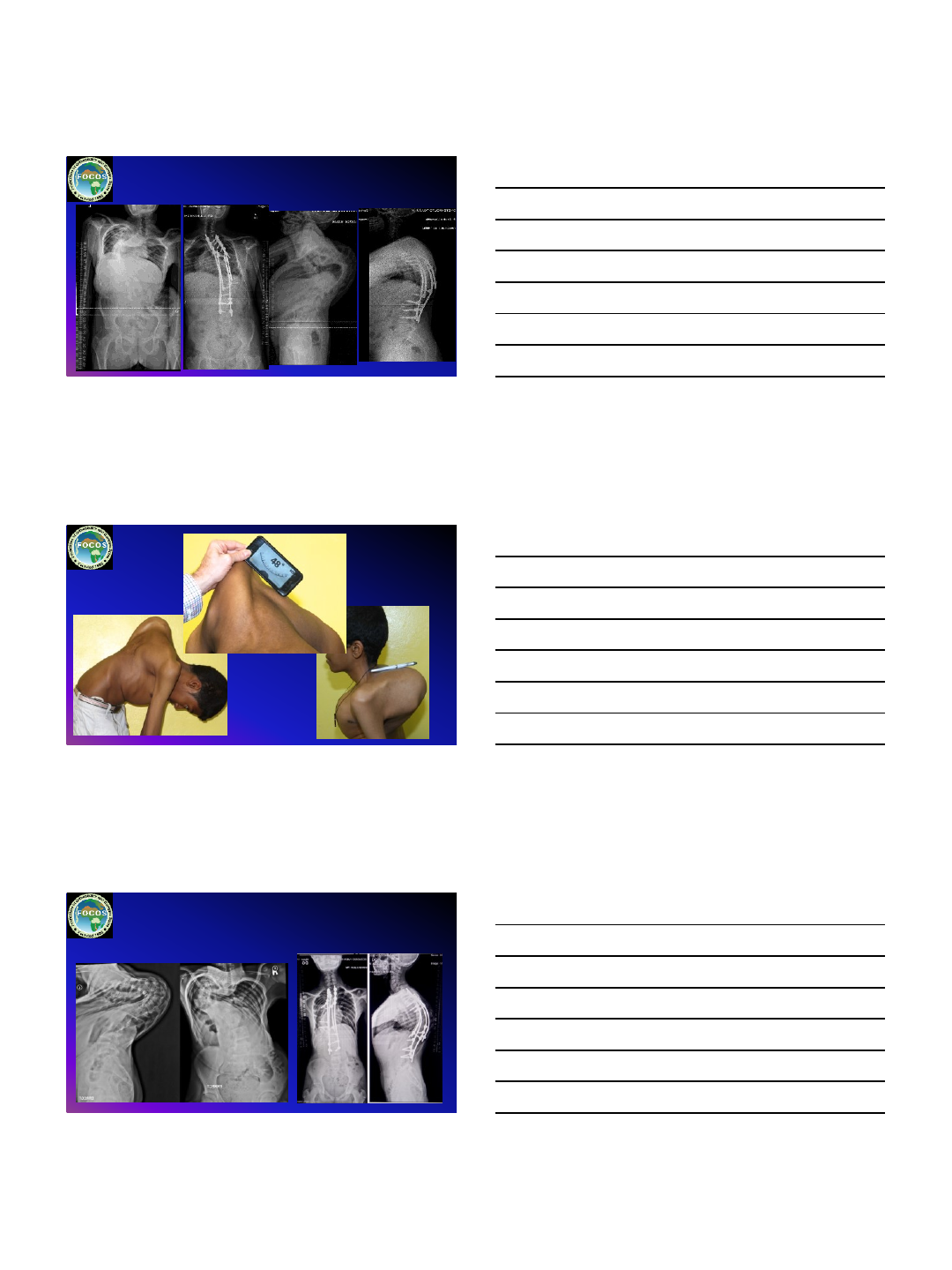
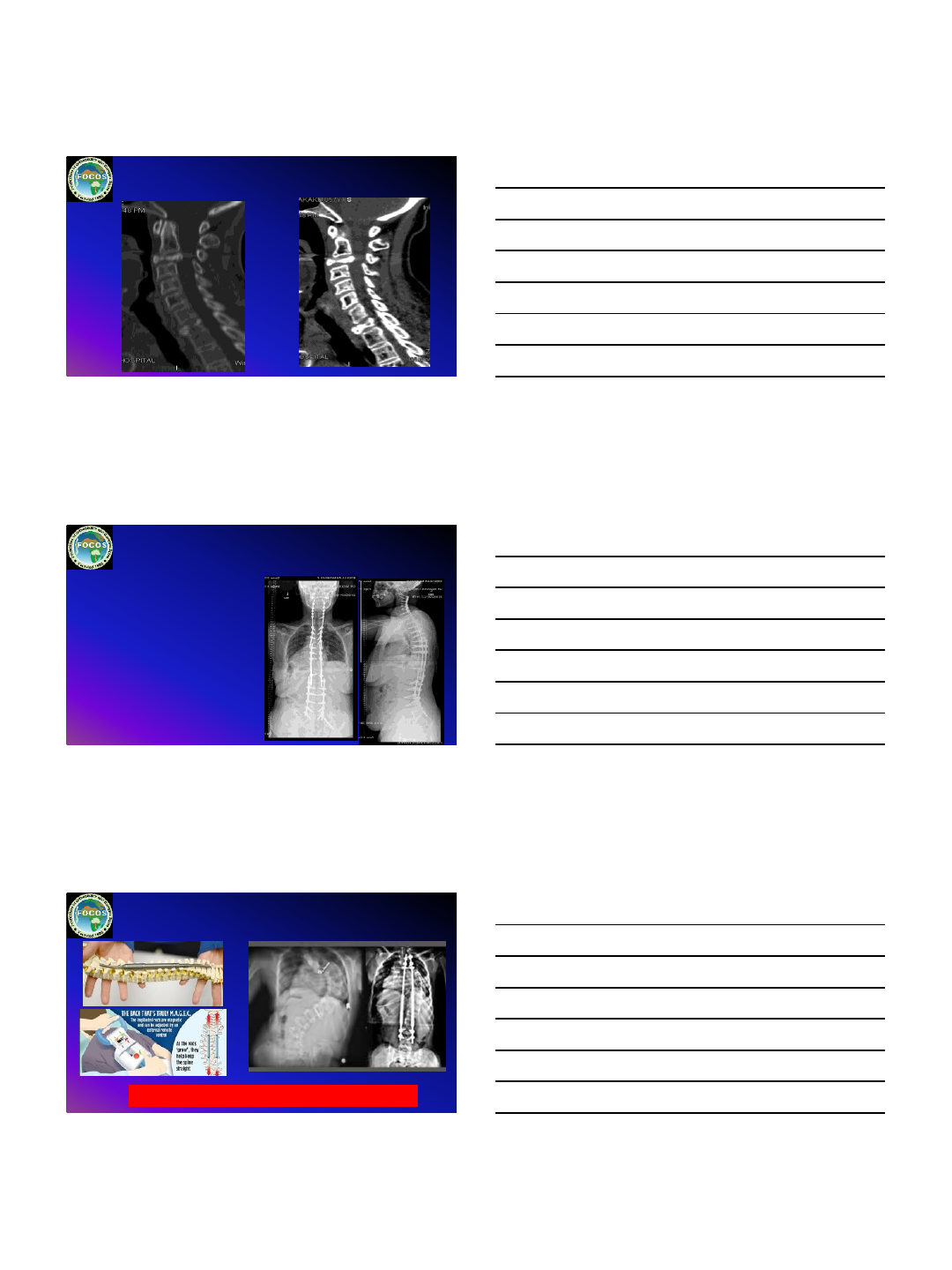
140°
178°
AIS Kyphoscoliosis
Severe and rigid
4 months HGT, PSF PCO, Thoracoplasty and SSI
Balanced Correction
6/13/2018
11
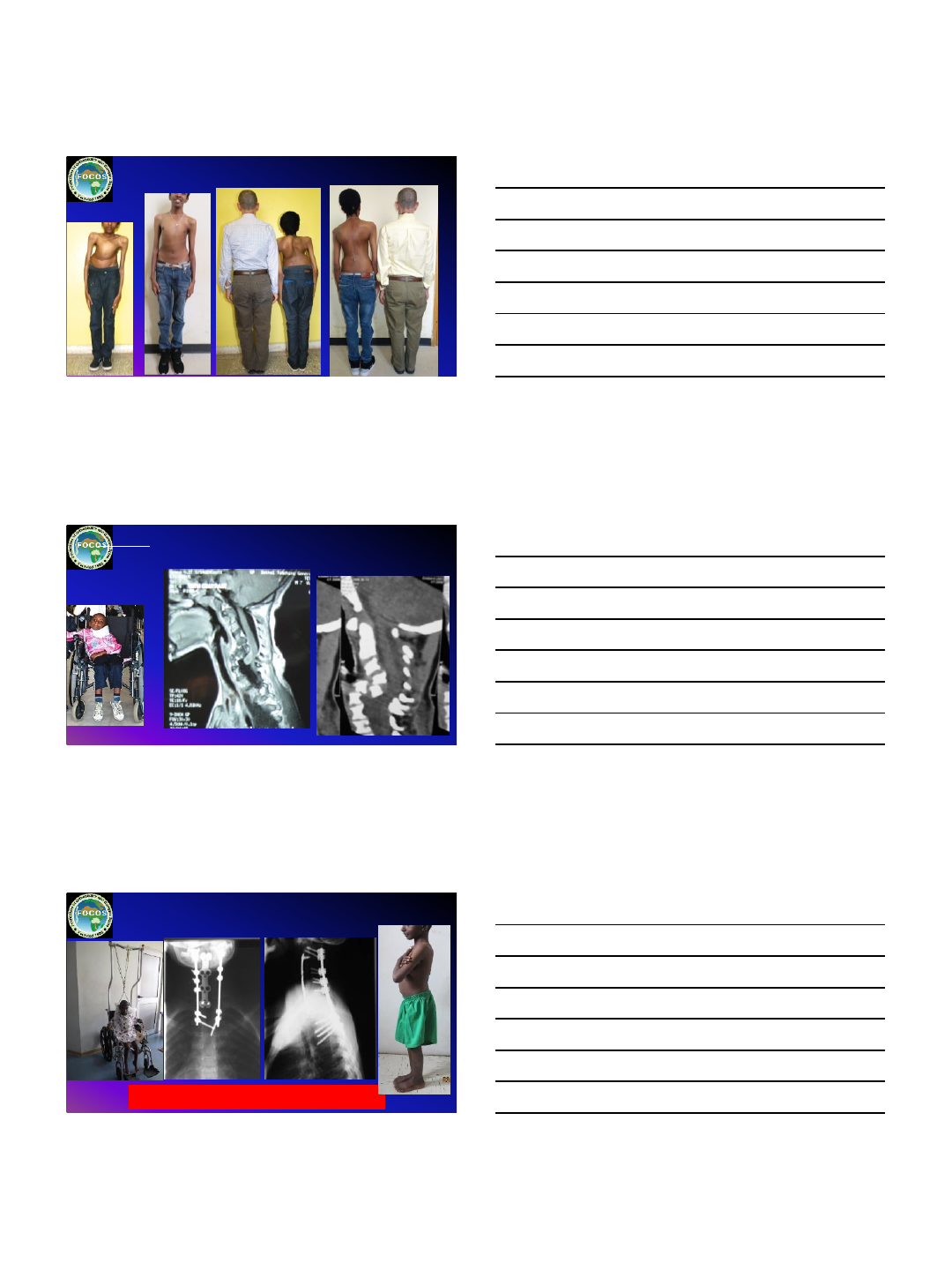
Dia8YM : NF, Cervical Kyphosis / Dislocation, Quadriplegia
ASIA –A C6 level
Procedure: ASF C3-C7, Corpectomy C4-C6, Fibular Strut graft C3-C7,
Instrumentation C2-T1
3 years post op
6/13/2018
12
Patient Details
Date Comment Ht (cm) Wt (kg) BMI
09
-03-2015 Pre-op
WCB
WCB
WCB
21
-09-2015 6 mo
155.3
61.7
25.6
26
-09-2016 1 yr
155.3
72.2
29.9
27
-06-2017 2 yr
153.5
58.9
25
19
-02-2018 3yr
155.3
72.3
30
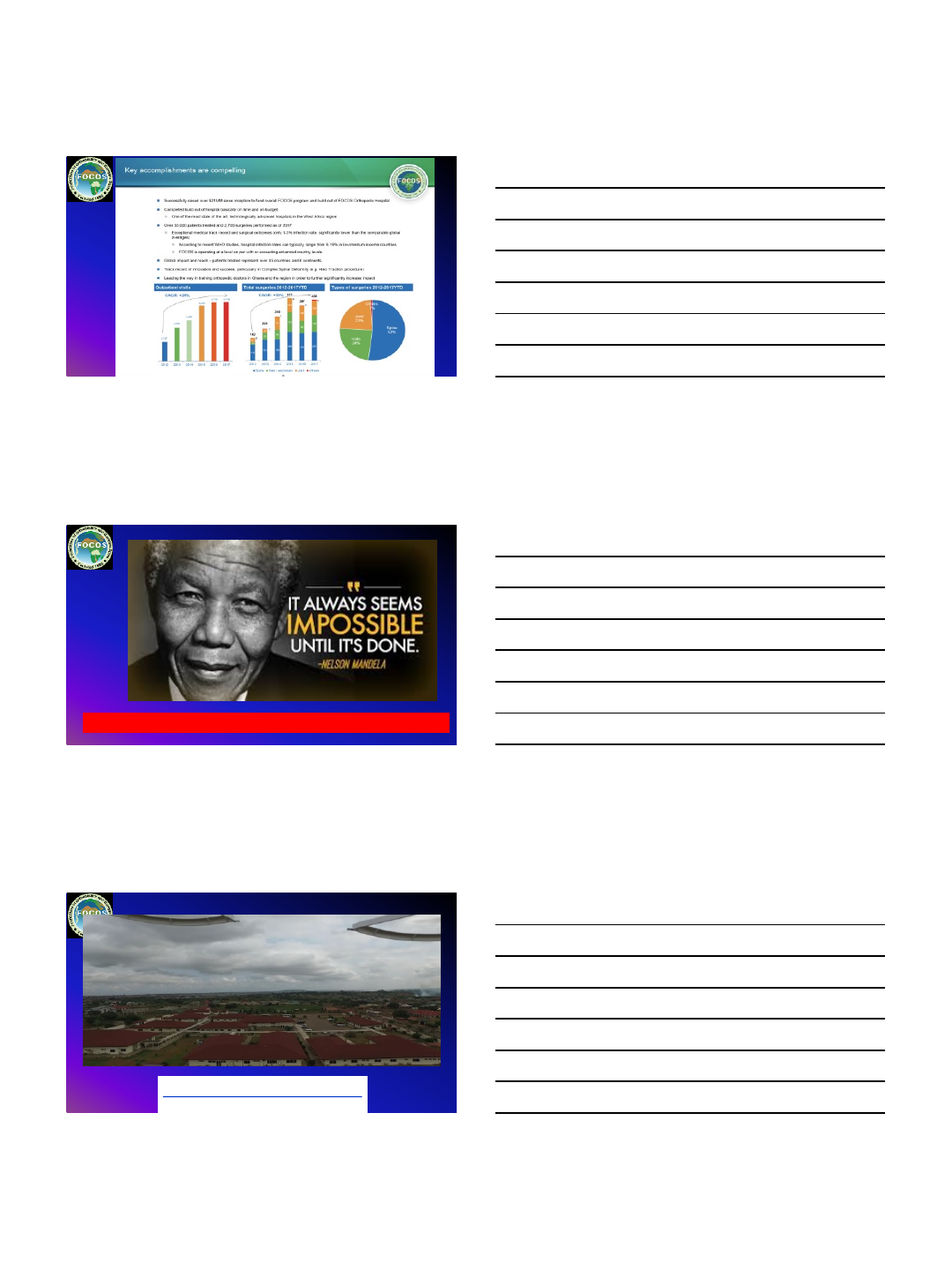
ENL968 57F 12-05-1960 NG
•A known case of multiple myeloma with Myelopathy
•She previously had T10 Corpectomy + ASF T9-T11, PSF T7-L1 done in 2015.
•Two years Post op she was noticed to have collapsed L2 Vertebra and subsequently had
Extension of PSF T11-S1.
•She currently presents with complaints of neck pain and upper back pain as well as
occasional numbness in both hands.
•2018 Collapsed C3 Treated with PSF C2-T5
•Past Medical History:
I. Appendicectomy (1973)
II. 3 Cervical Cerclage
III. T10 Corpectomy + ASF T9-T11, PSF
T7-L1
IV. 6 Cycle of Chemotherapy for
multiple myeloma
V. Hypertensive
•Medications:
I. Exforge 10/160mg
II. Tramadol
Oncology Patients
2015 2017
6/13/2018
13
2018 Collapsed C3
Op Note: 21-02-18
•Diagnosis: Collapsed C2 and T1
Vertebra
•Procedure: PCF C2-T5, C7/T1
Foraminotomies Bonegraft (Local +
Allograft.
•Complications: None
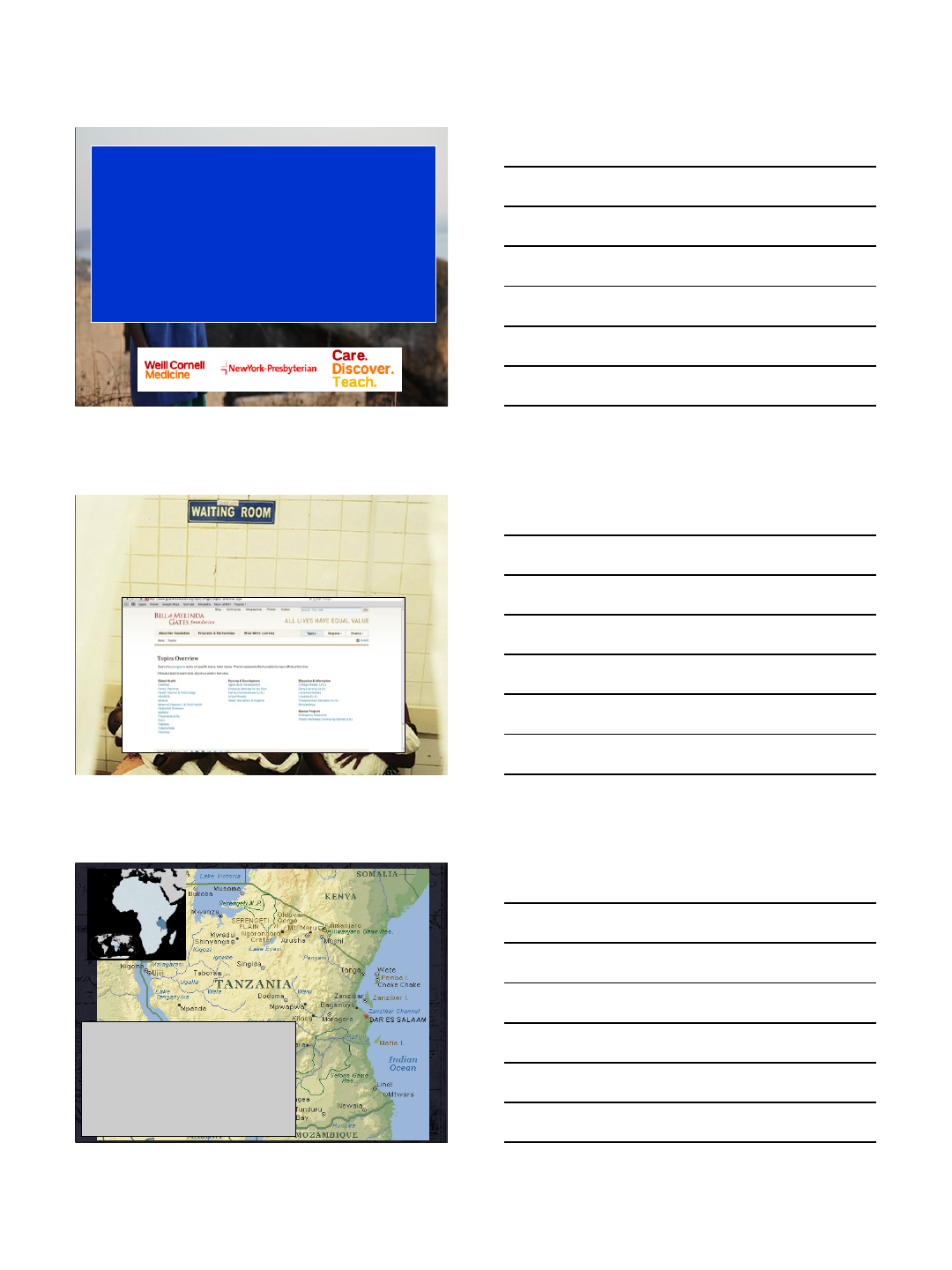
SCOLIOSIS CORRECTION BY REMOTE CONTROL
MAGEC: Only Center in West Africa
Donation by San Diego Spine Foundation
6/13/2018
14
When Life Throws You a Curve FOCOS will Help Straighten It
www.focoshospitalgh.com
www.orthofocos.org
THANK YOU
1
Spinal Trauma
in Tanzania
Roger Härtl, MD
Professor of Neurosurgery
Director of Spinal Surgery
Director of the Weill Cornell Center for Comprehensive
Spine Care
Department of Neurosurgery
Weill-Cornell Medical College
New York, NY
USA
“Surgery is the neglected stepchild
of global public health”
•45-50 million people
–>100 tribes
–45% Muslim
–45% Christian
–Tribal religions
•Economy
–Agriculture, Service industry, mining, industry
–Avg. salary $60-70/month
2
Photographs by Andre Liohn
Photographs by Andre Liohn
3
4
5
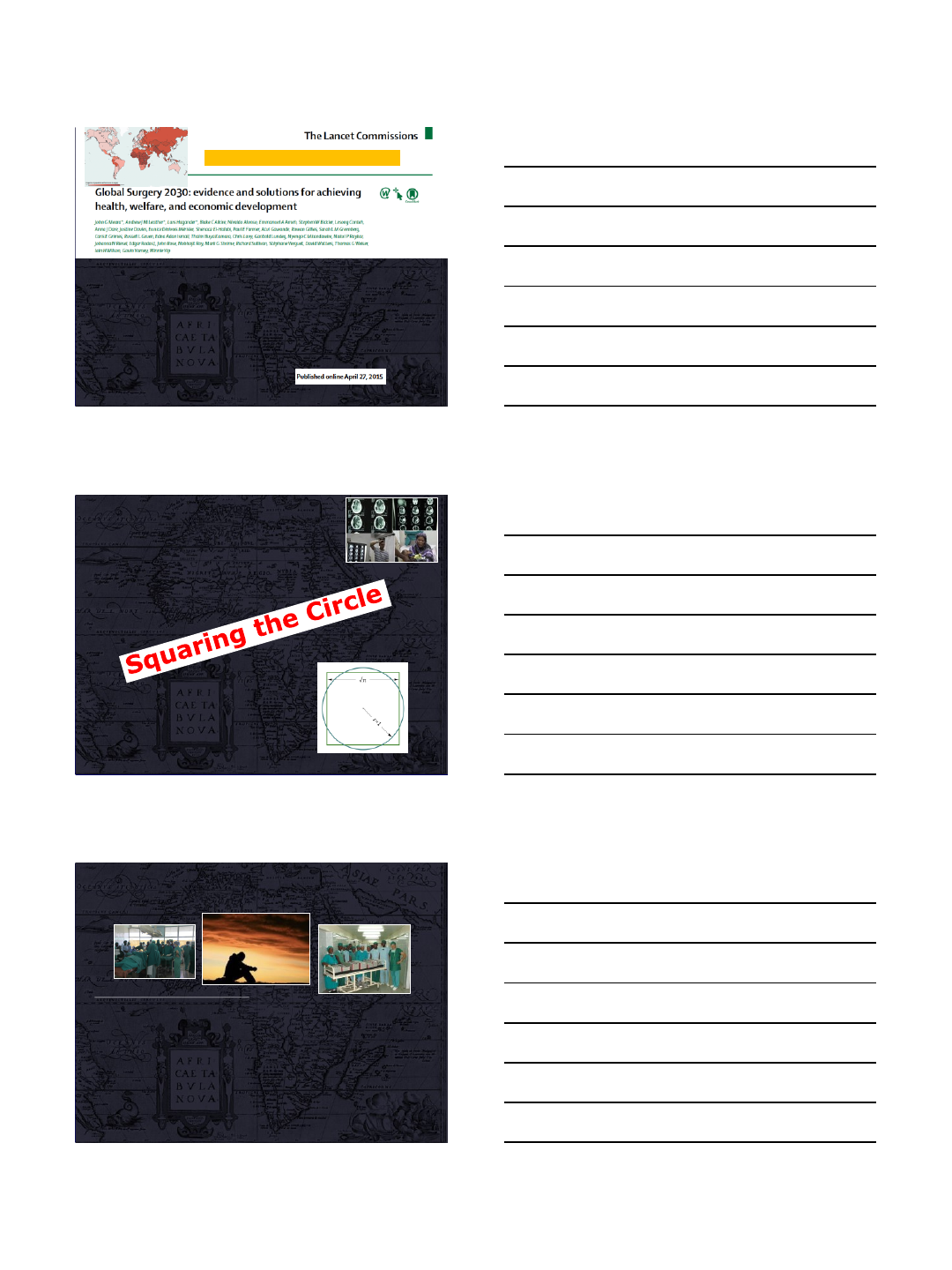
•5 billion people do not have access to surgical and
anaesthesia care
•143 million additional surgical procedures are
needed
•Investing in surgical services in LMICs is affordable,
saves lives, and promotes economic growth
•Surgery is an “indivisible, indispensable part of
health care
Why Does Surgery Matter?
Questions
•How can we have an impact from overseas?
•Limited time –1 week/year…
•Limited resources
•Cultural barriers
•Language barriers
•Do our goals, priorities, expectations align?
–Who is right, who is wrong?
•Fragmented groups in NA & Europe
–little coordination
•Communication challenges: Equipment,
WIFI
Weill Cornell Neurosurgery Initiative
Definition of achievable goals
•To…
–assess the current management of neurosurgical
diseases
–develop a close network that fosters exchange, teaching
and communication
–train physicians and health care workers in best
management practices
–implement stepwise and reasonable changes that will
improve neurosurgical care
6
7-point SUSTAINABLE
Weill Cornell Global Neurosurgery Initiative
1.Yearly visits to teach & train
2.Yearly Neurosurgery symposium
in Tanzania
3.Observational fellowship at Weill
Cornell: TZ→Cornell 6 fellows so
far
4.One year Global Neurosurgery
Fellowship Cornell →TZ
5.Clinical research
6.Weekly Skype conferences
7.Publications
Maria Santos
Andreas Leidinger
•2011
•2013
•2014
•2015
•2016
•2017
7
Images by Andre Liohn
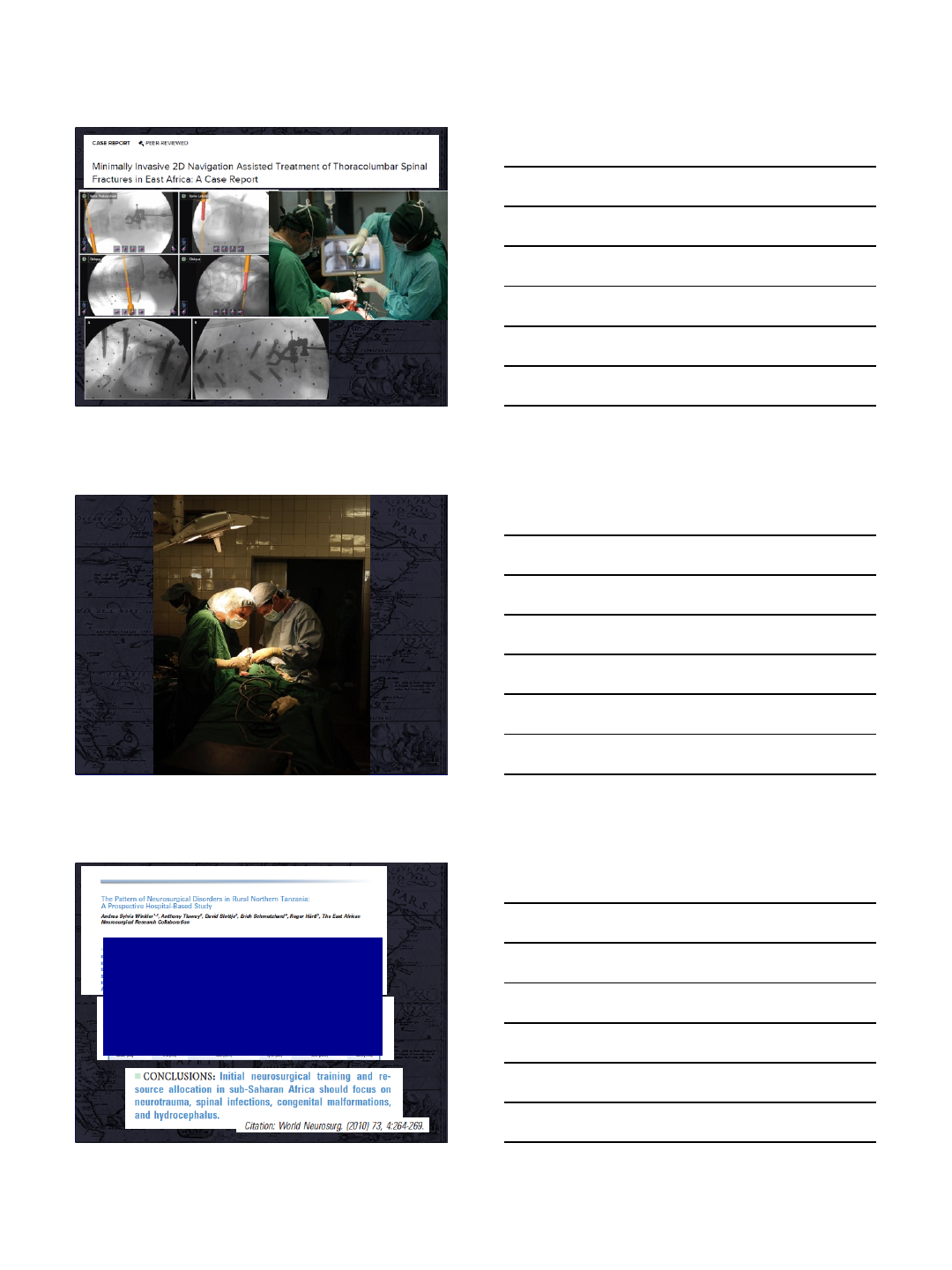
Neurosurgical diseases
•Neurotrauma
•Spinal infections
•Congenital malformations
•Hydrocephalus
8
Study Objectives
•Prospective collection of data of all
spinal trauma admitted to MOI.
•To:
–Describe the general demographics
–Understand the overall management and patient flow
–Identify bottlenecks and critical points
–Identify deficits and aspects in need of foreign
support
–Assess surgical outcome
Muhimbili Orthopedic
Institute (MOI)
From 2015-2017
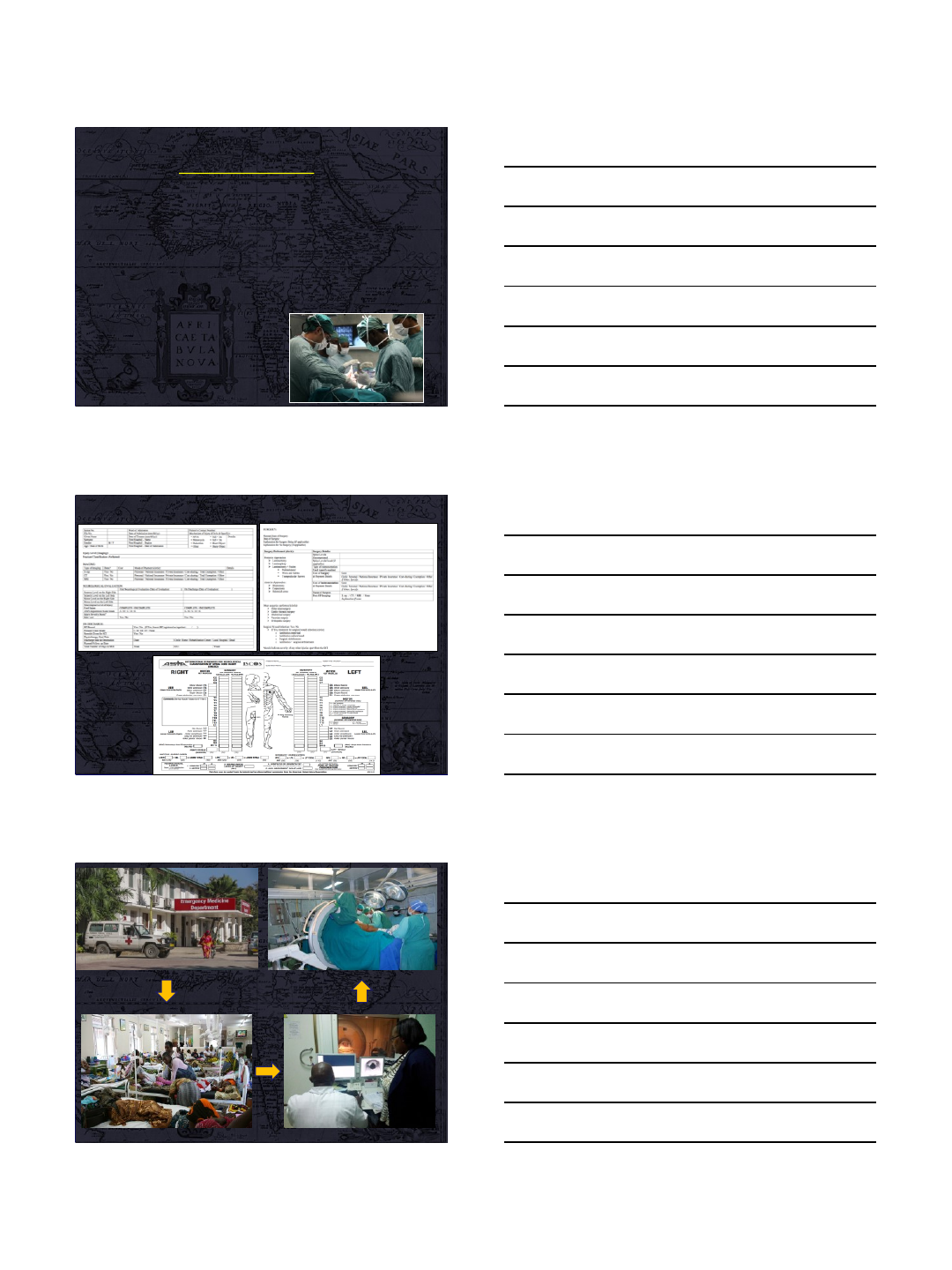
Data Collection Tools
9
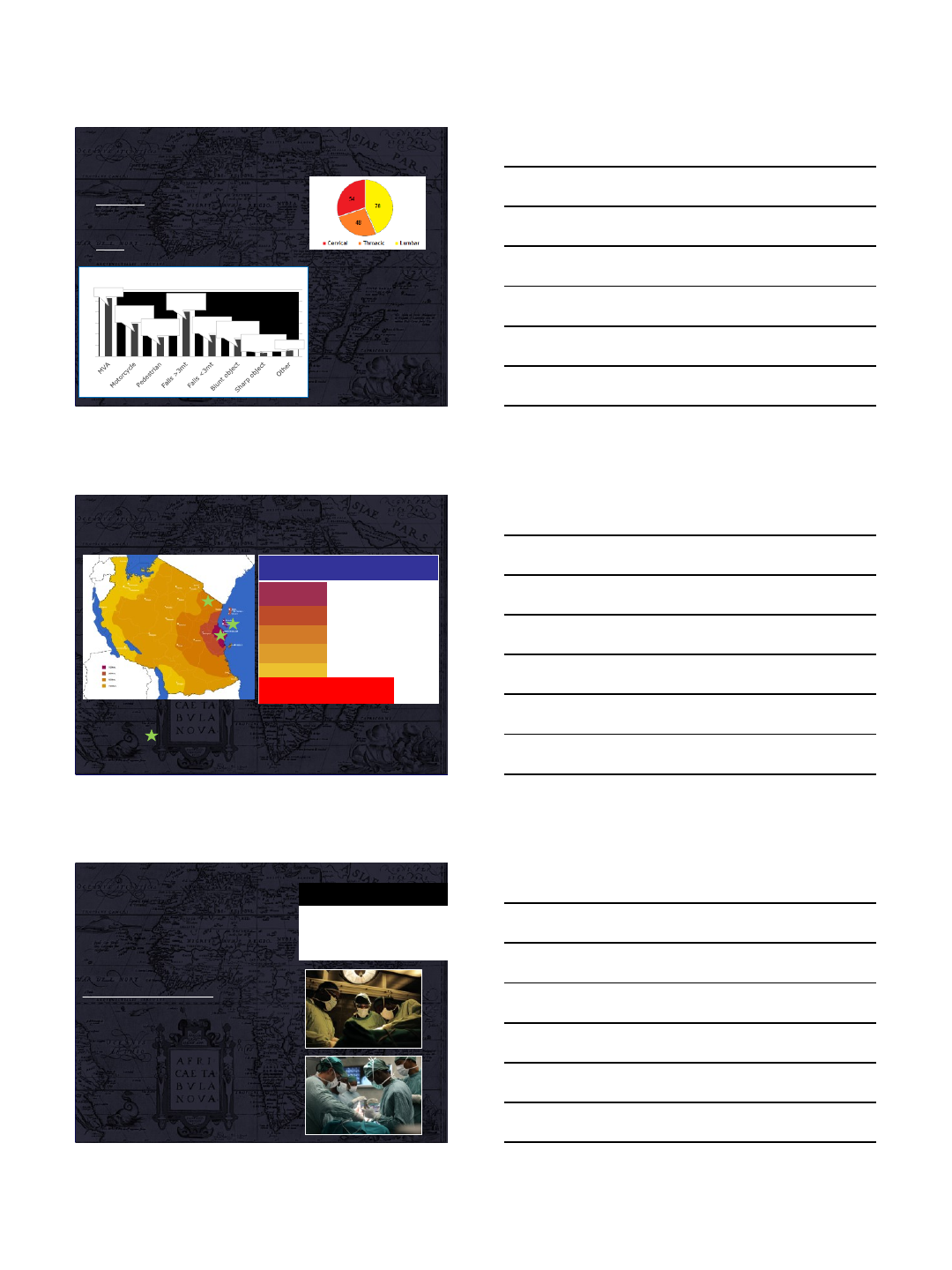
Demographics & Epidemiology
•n= 180 ST patients collected
•GENDER
- Male 149 (82.8%)
- Female 31 (17.2%)
•AGE: 35.7±12 years old
1. Primarily affects young
males
2. High incidence of falling
from heights
3. Low incidence of ST
secondary to violence
MVA, 52
Motorcycle,
29
Pedestrian,
17
Falls >3mt,
40
Falls <3mt,
19
Blunt object,
15
Sharp object,
3
Other, 5
0
10
20
30
40
50
60
Mechanism of Injury
Few hospitals
Long waiting list
Distance Referral
time
(days)
n
<100km 1 55
Dar
es
Salaam
100-200km 7 2
Regions
200-500km 11 36
500-1000km 8 32
1000+km 9 5
Averange
time
7.09
Three neurosurgical centers:
KMCM (Moshi), Muhimbili (Dar es Salaam) and NED Institute
(Zanzibar).
Results: Surgery
40% of all patients received surgery.
◦45% of all complete injury patients.
◦36% of incomplete injury patients.
Average time to surgery: 28 days.
1. No patient received surgery within 24 hrs.
2. Time to surgery for patients with incomplete
injuries was 36 days versus 30 days for those
with complete injuries.
3. 90% of incomplete injuries that arrived within
24 hours post trauma did not receive surgery
within one week.
Factors associated with
shorter time to surgery
ICU Stay (p=0.252)
AO Type C (p=0.504)
MVA accident as mechanism of
injury (p=0.493)
10
Results: Primary Outcome
Factors related to positive
change in AIS Grade
Shorter time to surgery
Surgery (p=0.003)
Younger age
Falling mechanism <3mts
Private insurance
AIS Improvement at
discharge (p=0.03)
Mortality
(p=0.007)
Surgery Group
21.4%
1.6%
Conservative Group
8.2%
16.1%
•Overall, surgery was the
only factor associated with
improvement in AIS score
from admission to discharge
(p<0.003).
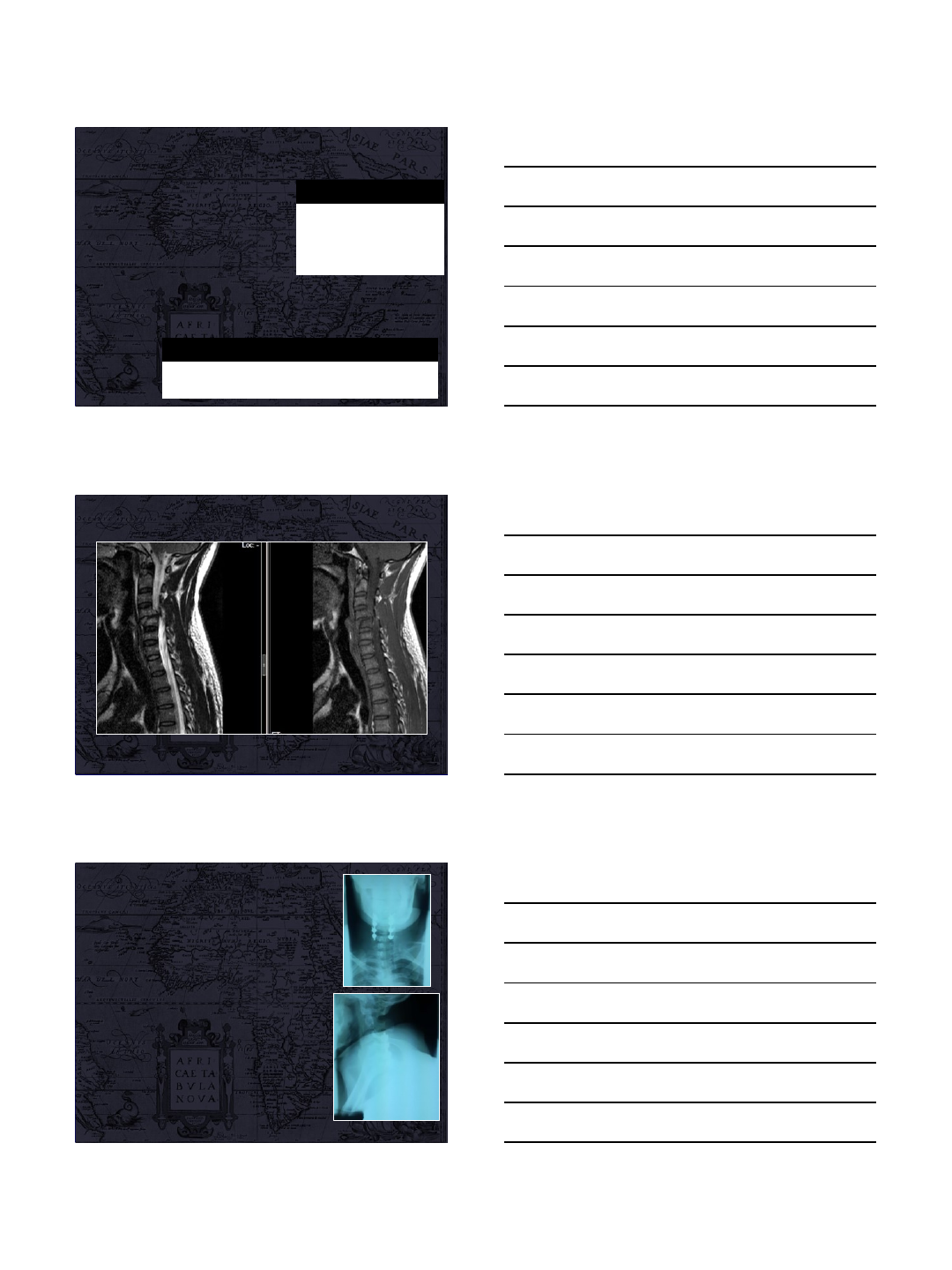
C3-C6 CERVICAL REDUCTION AND FUSION +
C4-C6 DECOMPRESSION WITH CORTICAL
SCREWS.
•Patient was operated 12 days after
arrival.
•Postoperatively:
–Patient kept with soft neck collar
–Started physiotherapy 5 days after the
surgery
•Total admission: 32 days
•Complications: NONE
•ON DISCHARGE:
–ASIA C
11
Costs and Financing
•Private patients: 2322.2 USD
•Public status: 873.0 USD.
•Private patients were more likely
to receive surgery (57%) compared
to public patients (37.7%, p=0.088).
Hospital Bed ICU Bed X-ray CT/MRI Surgical
table
Lumbar screw
(unit)
Public
4.47 USD/day 13.40 USD/day 11.17 USD 70-93 USD 89.3 USD 69 USD
Private
33.5 USD/day 53.60 USD/day 11.17 USD 70-93 USD 670 USD 69 USD
NHIF
2188 USD
flat rate inclusive of all expenses (medication, hospital bed, ICU
bed, laboratory workups, imaging, surgery, surgical implants and
rehabilitation.)
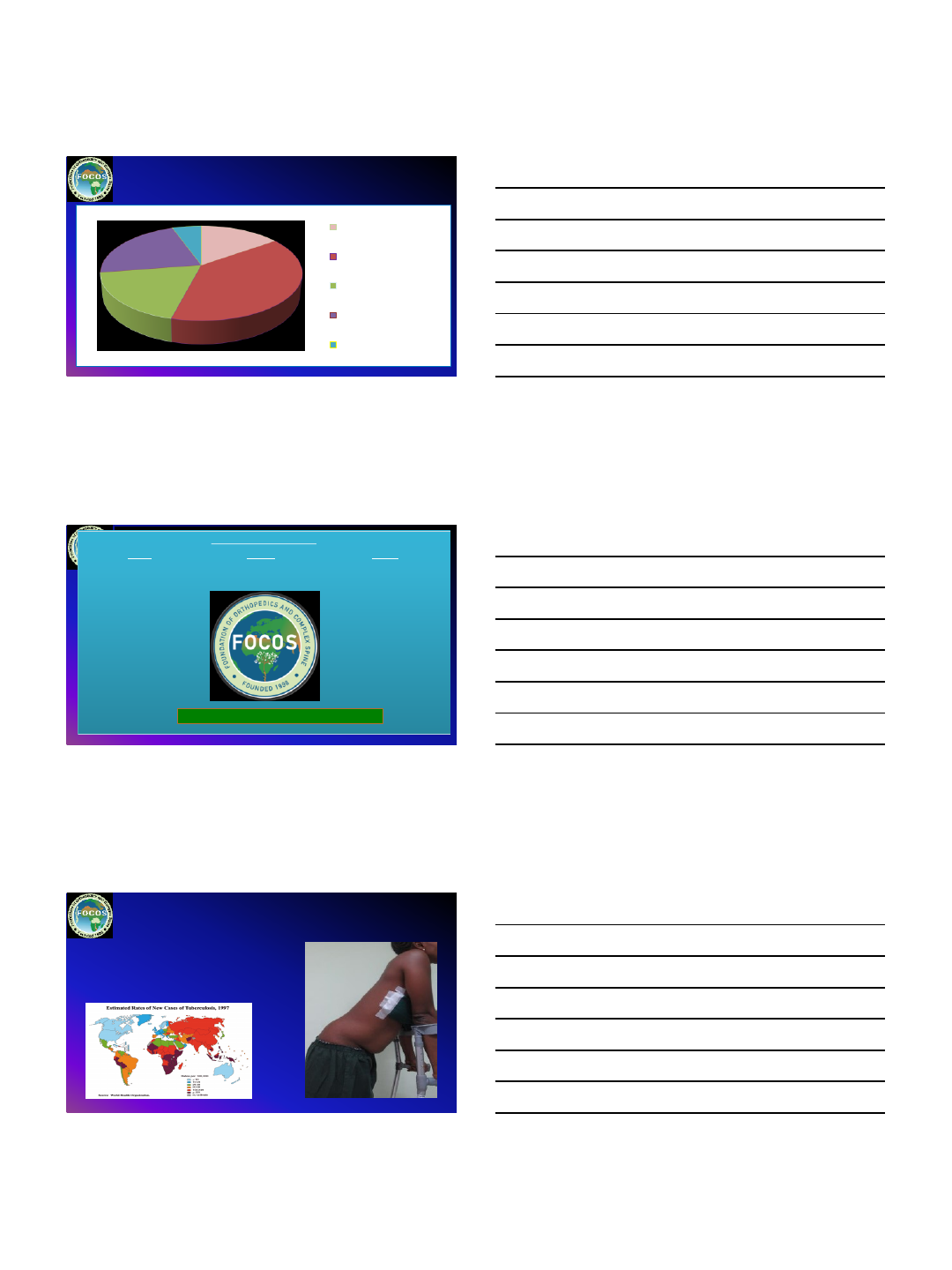
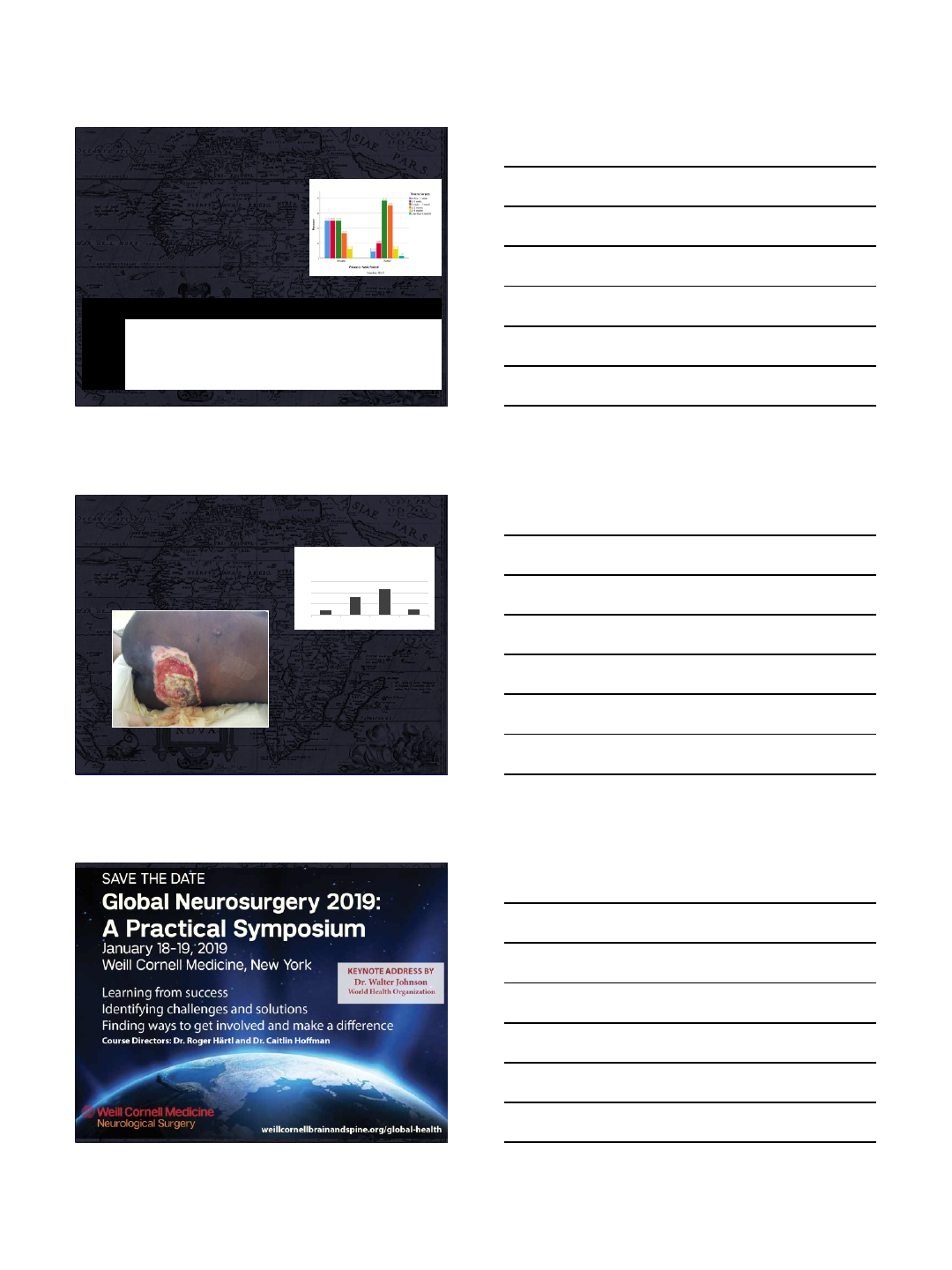
Complications
•Mortality (8.8%)
•Complications:
–Pressure ulcers (19.2 %)
–Wound infection (2.6 %)
Longer waiting lists and lack of
human resources contribute to
pressure ulcers like this 43 year old
male suffering an ASIA A lesion
after MVA.
8.8
32.4
47.1
11.8
0
20
40
60
III III IV
Pressure Ulcer
Grading
•Mortality (%) was associated with cervical injuries (p=0.001)
and complete lesions (p=0.016)
•Physiotherapy was done for 87.5% of patients.
12
Conclusion
•Surgery matters
–“Investing in surgical services in LMICs is affordable, saves
lives, and promotes economic growth” LANCET
•Surgical training and education takes time and
happens “one-on-one”
•Identify champion surgeons
•Weill Cornell Neurosurgery SUSTAINABLE Model To
Maximize impact:
1. Regular visits
2. Courses
3. Permanent fellowships in TZ
4. 3 months fellowships in NYC
5. Research:
1. collect data and measure impact
6. Skype calls: communication
7. Publications
http://weillcornellbrainandspine.org/tanzania
