Fd9c8528 2542 48af B376 7df366f018d7
2017-03-29
: Pdf Fd9C8528-2542-48Af-B376-7Df366F018D7 fd9c8528-2542-48af-b376-7df366f018d7 3 2017 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 2
25
20
15
10
5
0 to 40 55 to 6050 to 55 65 to 7060 to 65 75 to 8070 to 75 85 to 9080 to 85 95 to 100
2
90 to 9545 to 50
40 to 45
SVC Length in mm
Number of Patients
3
4
11
13 14
1616
22
23
4
SVC Tears Can Be Intra- and Extra-Pericardial
• The pericardium extends above the right atrium and covers
between 30-45% of the SVC.
• TEE may identify an intra-pericardial tear, but not recognize
the tear also extends above the pericardium in the SVC.
• Tears that extend into both areas can bleed into
pericardium and the right chest.
• Bleeding in the pericardium should not rule out a tear that
extends higher in the SVC.
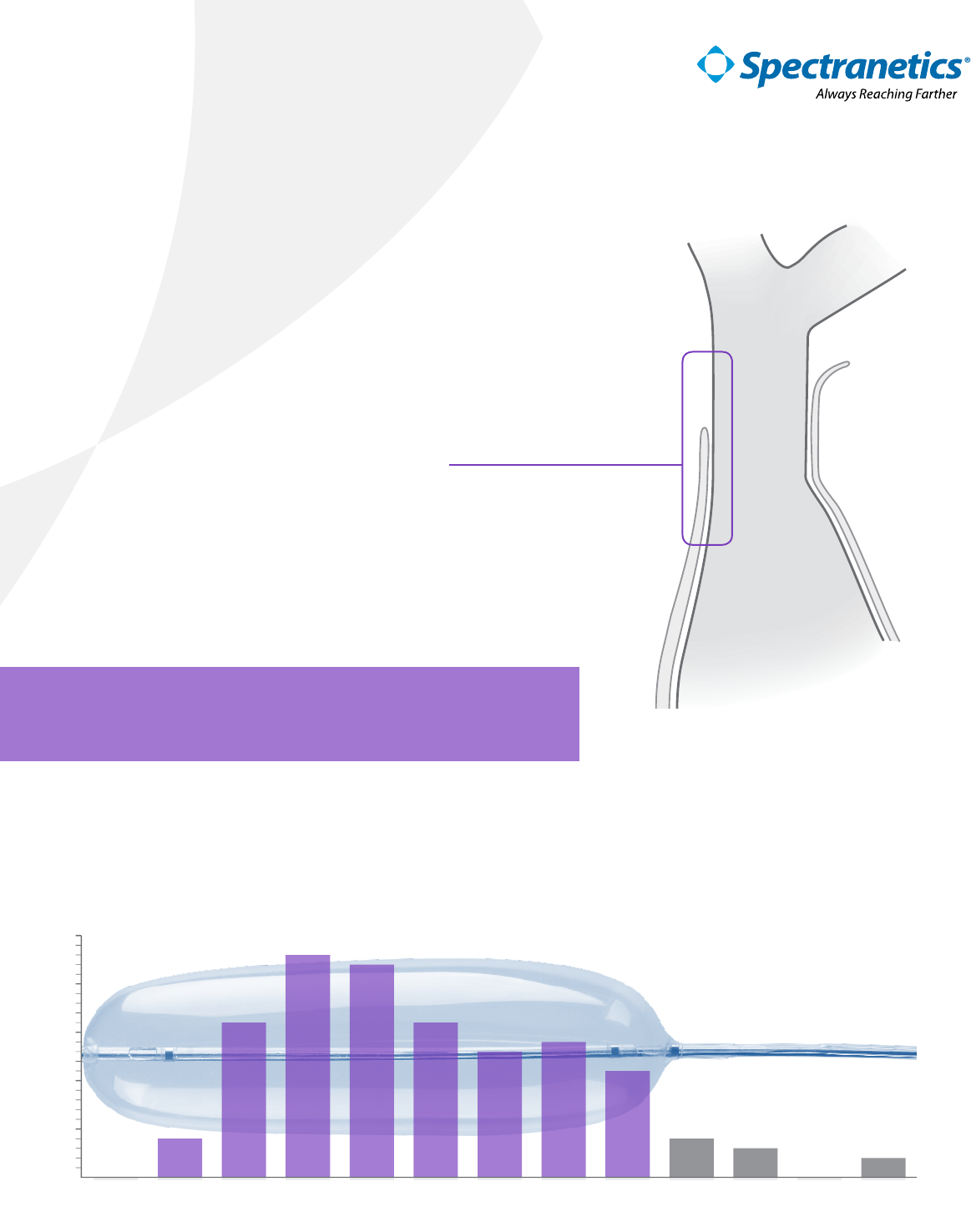
SVC Anatomy & Bridge™ Deployment
Diagram of the pericardium covering about 1/3 of the SVC. The right atrium (RA)
and brachiocephalic vein (BC, also known as the innominate vein) are also shown for
reference.
“When in doubt, inate Bridge.”
- Dr. Roger Carrillo, MD. University of Miami
SVC lengths of patient population at University of Miami
93% of patients would be completely covered by the Bridge Balloon. The
remaining 7% of patients would be mostly covered by the 8cm Bridge Balloon.
Courtesy of Roger Carrillo, MD.
Bridge™ Occlusion Balloon has proven to be a life-saving technology.1
Procedural planning that considers superior vena cava (SVC) anatomy in
relation to the pericardium can help ensure successful deployment and
utilization.
93%
119 out of 128 patients had
SVC lengths that would be
completely covered by Bridge.
BC BC
RA
SVC
Pericardium
Bridge is designed to cover the entire length of the SVC,
including tears in the intra- and extra-pericardial space.
DEPLOYS IN
UNDER
2 MINUTES2
STOPS ON
AVERAGE 90%
OF BLOOD
LOSS3
30 MINUTES
OF ACCEPTABLE
HEMOSTASIS4
©2016 Spectranetics. All Rights Reserved. Approved for External Distribution. D032863-00 112016
“I cannot overstate that this is a tool that saves lives.1”
- Dr. Roger Carrillo, MD., University of Miami
References
1. Elrod, Jodia. Use of Bridge™ Occlusion Balloon in Lead Extraction: Interview with Dr. Roger Carrillo. EP Lab Digest.
November, 2016.
2. Document on le D027562. Bridge can be fully deployed in under one minute (53 seconds) in an animal model
when pre-positioned on a guidewire, or in under two minutes (1 minute, 46 seconds) when not pre-positioned.
3. Document on le D027561. When deployed, the Bridge occlusion balloon reduces blood loss by up to 90%, on
average, in an animal model of an SVC tear. Testing was conducted in a heparinzed porcine model which has
shorter SVC length than is typical in humans. A balloon design scaled for use specically in the porcine model was
used in generating this data.
4. Document on le, D026197. In an animal model with SVC tears up to 3.5 cm, with 2 pacing leads and 1 ICD lead.
Important Safety Information
INDICATIONS
The Bridge Occlusion Balloon Catheter is indicated for use for temporary
vessel occlusion of the superior vena cava in applications including
perioperative occlusion and emergency control of hemorrhage. Any use
for procedures other than those indicated in these instructions is not
recommended
CONTRAINDICATIONS
None known.
WARNINGS
Do not position the Bridge Occlusion Balloon Catheter in a manner that
would obstruct the right atrium. Obstruction of the atrium could lead to
arrhythmias and/or hemodynamic compromise.
Prior to initiating the lead extraction procedure, a Bridge Occlusion Balloon
Catheter compatible guidewire should be placed through a venous access
site and across the length of the superior vena cava. Attempting to place a
compatible guidewire after a venous tear occurs may result in an inability to
traverse the superior vena cava with the guidewire, result in the guidewire
Always Reaching Farther
Corporate Headquarters
The Spectranetics Corporation
9965 Federal Dr., Colorado Springs, CO 80921
Tel: 719-447-2000 • Fax: 719-447-2022
Customer Service: 800-231-0978
German Oce
Spectranetics Deutschland GmbH
Schweinfurter Str. 7
97080 Würzburg, Germany
Phone: +49 931/4520080 • Fax: +49 931/45200811
Spectranetics International B.V.
Plesmanstraat 6, 3833 LA Leusden
The Netherlands
Tel: +31 33 4347 050 • Fax: +31 33 4347 051
exiting the vasculature at the tear site, result in an inability to place the Bridge
Occlusion Balloon Catheter or delay or prevent the ability to achieve occlusion.
Lead extraction should be performed at institutions with cardiothoracic
surgical capabilities by physicians knowledgeable in the techniques
and devices for lead or catheter removal. Complication prevention and
management protocols should be in place and routinely practiced. It is strongly
suggested that the recommendations for lead management of the Heart
Rhythm Society (HRS) and European Heart Rhythm Association (EHRA) be
followed for best results.
Failure to observe recommended ination techniques may result in formation
of contrast crystals which could prevent deation. Do not over-inate the
Bridge Occlusion Balloon Catheter after fully occluding the vessel. Over
ination may result in damage to the vessel Do not exceed the Maximum
Ination Volume. Over ination may result in damage to the vessel or rupture
of the balloon. Occlusion of the superior vena cava beyond 30 minutes is
not recommended as this may increase the risk of adverse physiologic or
neurologic complications.
Refer to the IFU for additional information.
