Lead Management Syllabus
2013-07-08
: Pdf Lead Management Syllabus Lead_Management_Syllabus 7 2013 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 40
1
Charles J. Love, MD FACC FAHA FHRS CCDS
Professor of Medicine
Director, Cardiac Rhythm Device Services
Wexner Medical Center at The Ohio State University
Columbus, OH USA
President, International Board of Heart Rhythm Examiners
Optimal Lead Selection:
An Extractor’s Guide to Lead Choice
and Implant Technique
Disclosures
Honoraria, research support and/or consulting with:
Boston Scientific
Cook Medical
Leadexx
Lake Region Medical
Medtronic
Spectranetics
St. Jude Medical
No off label uses of devices
or drugs will be part of this
presentation.
Extraction “Experts” Have Learned!
Those that do a lot of extraction begin to
think!
What causes the problems to arise that result
in a need for an extraction
How to modify our implant techniques and
device choices
Avoid increased risk of mechanical, vascular and
infectious complications.
What hardware might result in an easier and
safer extraction experience (for patient AND
doctor).
2
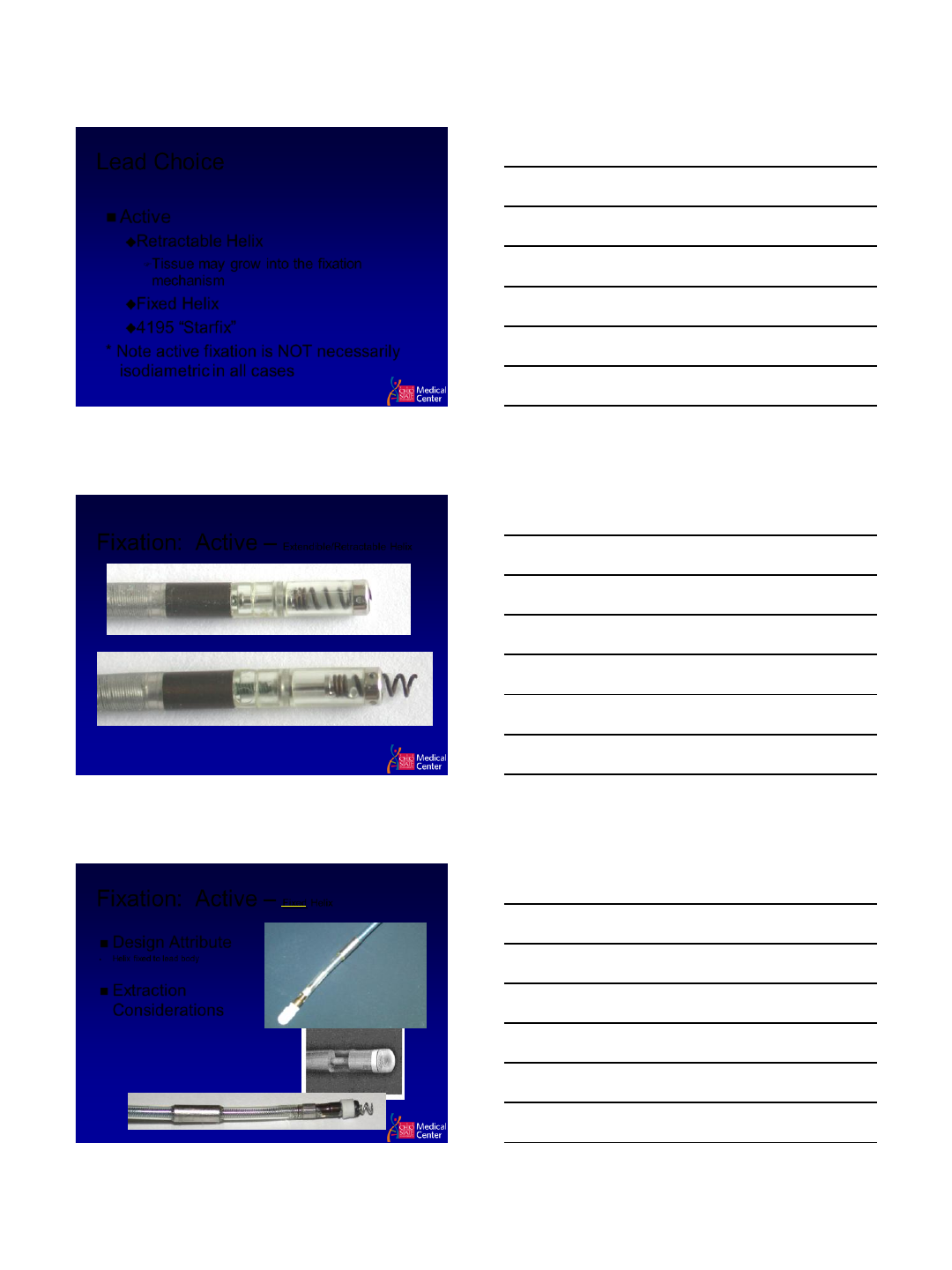
Many choices for many issues
First, understand where and how
complications occur
This will affect
Implant site
Venous Access Techniques
Lead choice
Pocket tissue plane
Lead Crush
Lead Crush
3
Fixation – Active versus Passive
Active Fixation
Passive Fixation
Lead Choice
Fixation
Passive
Tine Length
•Longer tines are more difficult to extract
Tined leads in general more difficult to
extract due to fibrosis around tines!
LV Lead Designs
4
Lead Choice
Active
Retractable Helix
Tissue may grow into the fixation
mechanism
Fixed Helix
4195 “Starfix”
* Note active fixation is NOT necessarily
isodiametric in all cases
Fixation: Active – Extendible/Retractable Helix
Helix deploys with rotation of terminal pin
Fixation: Active – Fixed Helix
Design Attribute
•Helix fixed to lead body
Extraction
Considerations
Ex. Fixed Helix
•BSC FINELINE®*
•BSC THINLINE®*
•BSC SWEET TIP®
* - coradial

6
4195 Starfix
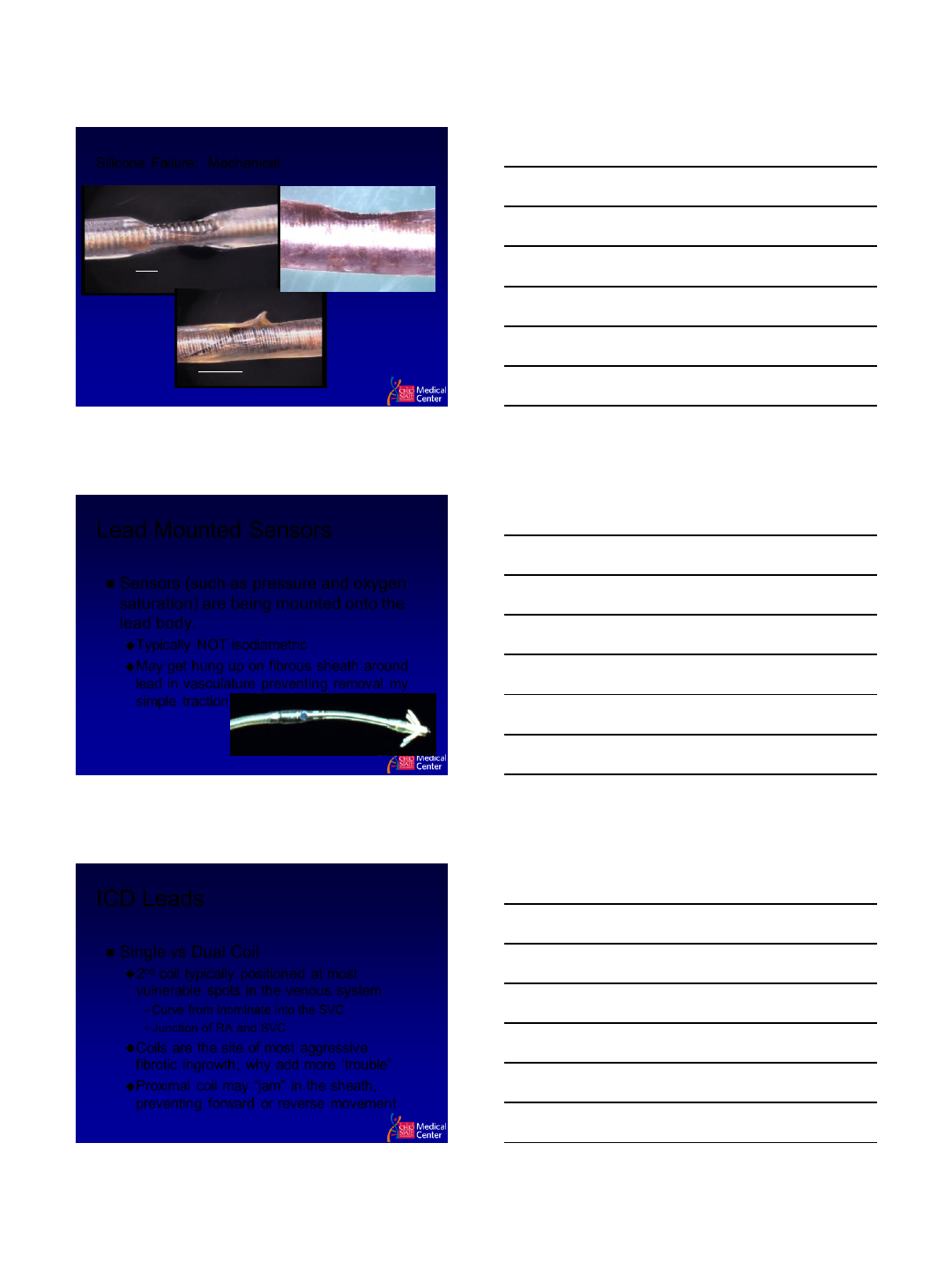
Connector
IS-1 / DF-1
Has a “yoke” around
which tissue grows
and has to be
dissected before the
lead can be pulled
through the tissues
IS-4/DF-4
Eliminates yoke and
reduces need for more
extensive dissection of
the lead from the
pocket
Lead Length
Leads that are longer than necessary
create a “plate of spaghetti” in the
pocket. Leads that are just the right
length need much less work to free
them from the fibrous pocket tissue.
Excess lead also causes additional
pressure points and may lead to “Cold
Flow”
7
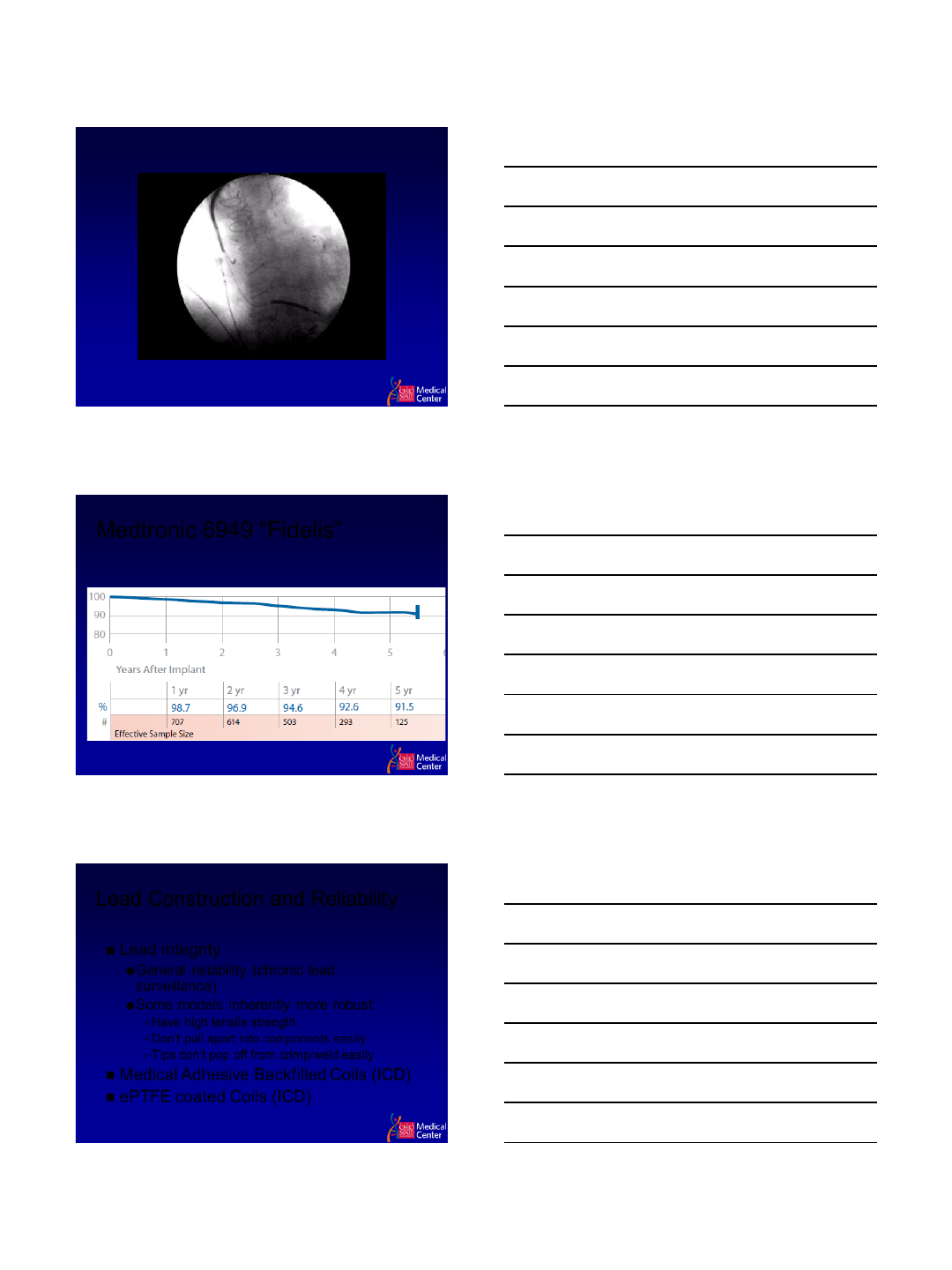
Silicone Failure: Mechanical
Abrasion: 4 years
Cold Flow comes from
repetitive forces or pressure
Wear comes from contact with
other leads, yoke, device
Abrasion: 11 Months
Cold Flow: 1 year
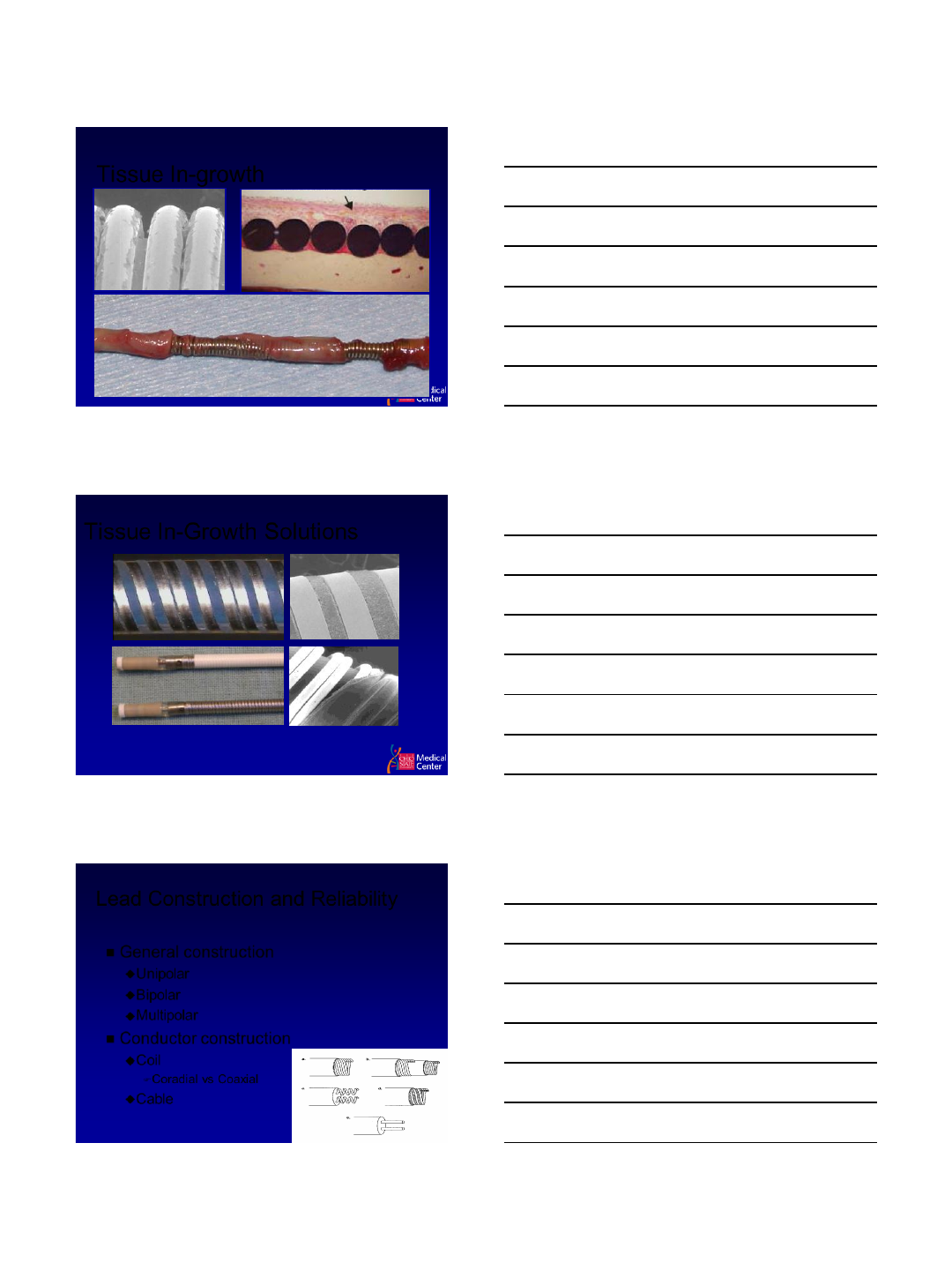
Lead Mounted Sensors
Sensors (such as pressure and oxygen
saturation) are being mounted onto the
lead body.
Typically NOT isodiametric
May get hung up on fibrous sheath around
lead in vasculature preventing removal my
simple traction
ICD Leads
Single vs Dual Coil
2nd coil typically positioned at most
vulnerable spots in the venous system
Curve from inominate into the SVC
Junction of RA and SVC
Coils are the site of most aggressive
fibrotic ingrowth; why add more ‘trouble”
Proximal coil may “jam” in the sheath,
preventing forward or reverse movement
8
ICD Coil Attachment to the Venous System
Medtronic 6949 “Fidelis”
Lead Construction and Reliability
Lead integrity
General reliability (chronic lead
surveillance)
Some models inherently more robust
Have high tensile strength
Don’t pull apart into components easily
Tips don’t pop off from crimp/weld easily
Medical Adhesive Backfilled Coils (ICD)
ePTFE coated Coils (ICD)
9
Tissue In-growth
Tissue In-Growth Solutions
Flatwire Design
+ Backfill
e-PTFE
Covering
Sleeve
Extraction Considerations
•Non-backfilled coils may have more tissue ingrowth possibly resulting in snow-
plowing of tissue: Try upsizing extraction sheath
Lead Construction and Reliability
General construction
Unipolar
Bipolar
Multipolar
Conductor construction
Coil
Coradial vs Coaxial
Cable
10
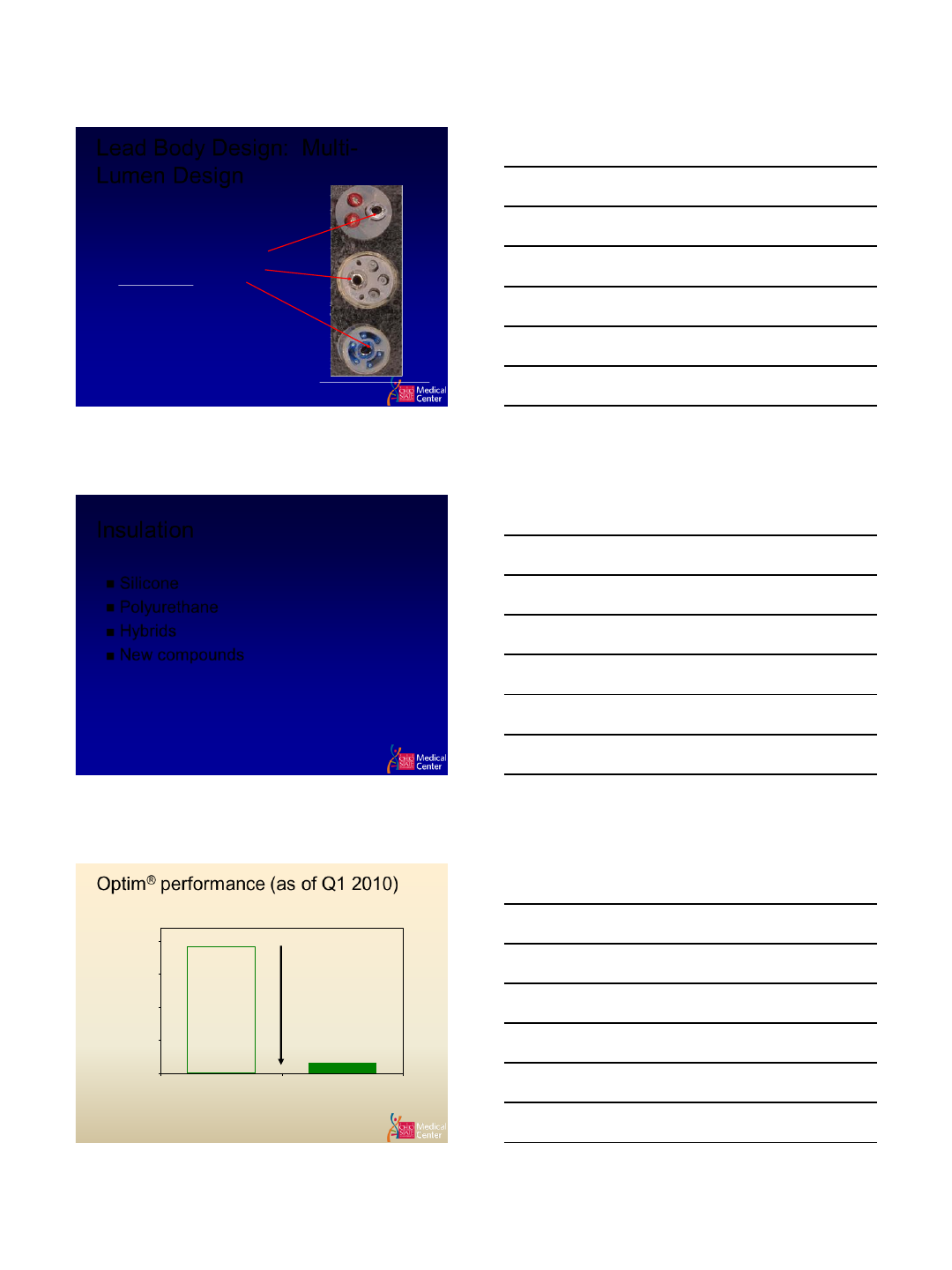
Lead Body Design: Multi-
Lumen Design
Ellenbogen, Kenneth A., et al. “Engineering and Clinical As pects of Defibrillation Leads.” Clinical Cardiac Pacing and Defibrillation, 2nd Ed.
151-165. W.B. Saunders Company, Philadelphia 2000.
Design Attribute
•ICD leads have multiple lumens for High
Voltage Cables, Electrode conductors and
Crush lumens
Extraction Considerations
•Strip back insulation to verify distal
electrode conductor lumen insert lead
locking device for Lead Locking
Deployment.
Integrated bipolar
uses RV coil as anode
for P/S Guidant
BSX
MDT
STJ
Insulation
Silicone
Polyurethane
Hybrids
New compounds
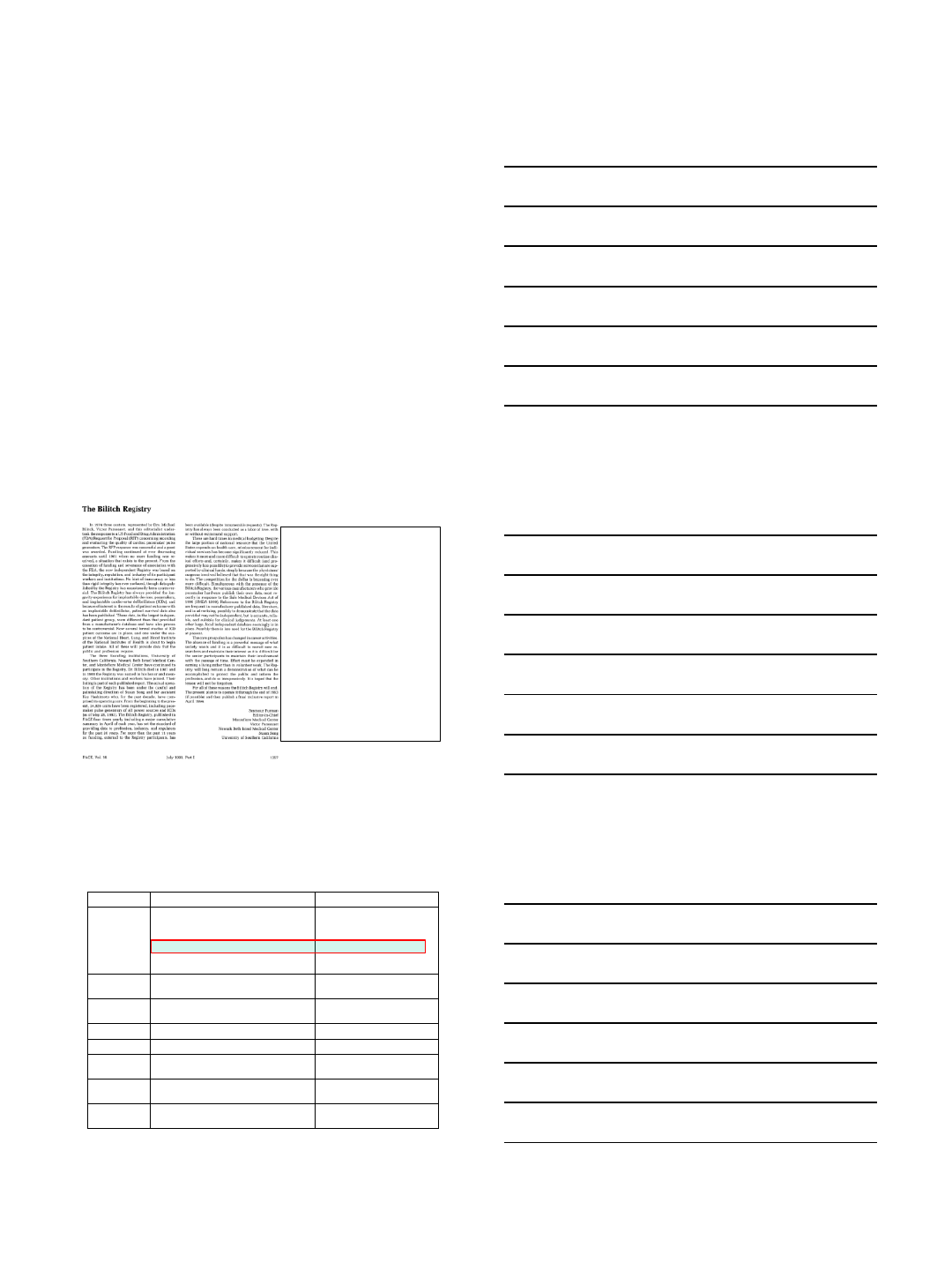
Optim® performance (as of Q1 2010)
Optim® Effects on SJM Tachy Lead Abrasion
(Kaplan-Meier Analysis of US Data)
0.00191
0.00016
0.0000
0.0005
0.0010
0.0015
0.0020
SILICONE Tachy Leads
(Riata 8F & Riata ST) OPTIM® Tachy Leads
(Riata ST Optim & Durata)
Abrasion Failure Probability
After 38 Months of Implant
>90% Reduction
Optim ® Provides a Significant
Reduction in Abrasion Risk
(p<0.0001 by log-rank test)
Courtesy Dr. Mark Carlson
11
Sterile Technique
Meticulous attention to Sterile
Technique
All involved in the lab or admitted to the lab
during the operation should be thoroughly
educated in sterile technique
This is NOT Cathlab sterile technique, it is
Operating Room sterile technique
Minimize personnel traffic in and out of the
room, as well as number of people in the
room
Sterile Technique
Proper use of prophylactic antibiotics
Type
Time of administration
Irrigation
Not clear whether this helps or not
However: Every person on the jury during
your malpractice trial will know you were an
idiot for not irrigating with antibiotic solution
TyRx antibiotic pouch
Conclusion
Planning prospectively for an extraction
can make the subsequent operation
more rapid and safe, and may reduce
the need for counter-traction and cutting
sheaths
Lessons learned from why leads fail can
lead to lead choices and implant
techniques that reduce the need for
subsequent lead extraction
7/1/2013
1
Early Lead Failures and
Recalls
Andrew E. Epstein, MD
Professor of Medicine, Cardiovascular Division
University of Pennsylvania
Chief, Cardiology Section
Philadelphia VA Medical Center
Philadelphia, PA
•In response to a FDA
RFP, registry founded in
1974 by Drs. Bilitch,
Parsonnet and Furman.
•Maintained data on
devices, leads and
programmers.
•Funding ceased 1981.
•Registry continued at
USC, NBIMC, and
Montefiore.
•Dr. Bilitch died in 1987.
•Registry ceased in 1994.
Major CRM Lead Advisories / Recalls
Manufacturer
Lead / Lead Family
Issue
Medtronic
6972 Family 80A Poly U Leads
4002 Family 80A Poly U Leads
4012 Family 80A Poly U Leads
4004 Family 80A Poly U Leads
4504 & 4504M / 4582 Poly U CapSure
/ Target Tip Tined Atrial J Leads
80A Poly U degradation
80A Poly U degradation
80A Poly U degradation
80A Poly U degradation
80A Poly U degradation
St Jude Med.
1016 & 1026 Pacing Leads
55D Poly U (very thin) inner
insulation degradation
Telectronics
AccuFix & Encor “J” lead Family (The
“801” lead)
J shape retention wire
extruded thru insulation
Medtronic
Transvene ICD family leads
80A Poly U degradation
BSI
Endotak DSP Family ICD Leads
IS-1 connector failures
Medtronic
Fidelis Family ICD Leads
Pace-sense & high V cables
and coil fractures
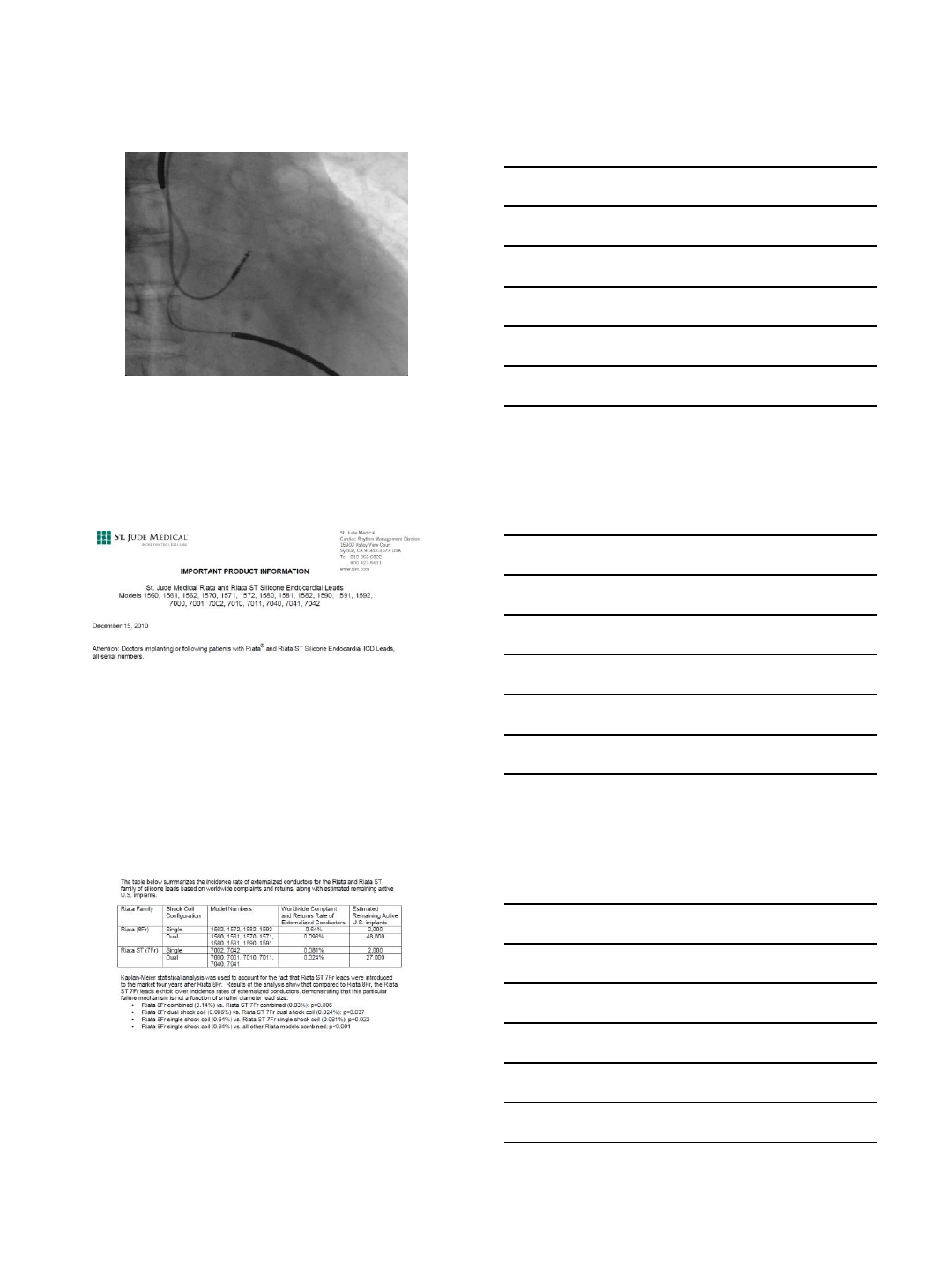
St Jude Med.
Riata & Riata ST silicone ICD leads
Inside-out silicone abrasion
externalized cables
St Jude Med.
QuickSite & QuickFlex Bipolar Lds
Inside-out silicone abrasion
externalized cables (distal)
Courtesy of Mr. John Helland
7/1/2013
2
80A Polyurethane
2 year explant
MDT 4058M
External Surface
Contacts blood / tissue
Environmental Stress
Cracking (ESC)
Internal Surface
Contacts metal
conductors
Metal-Ion Induced
Oxidation (MIO)
Polyurethane Failure Mechanisms
Courtesy of Mr. John Helland
MDT 4004
Pellethane 80A
MDT CRM Product Performance Report, 2006.
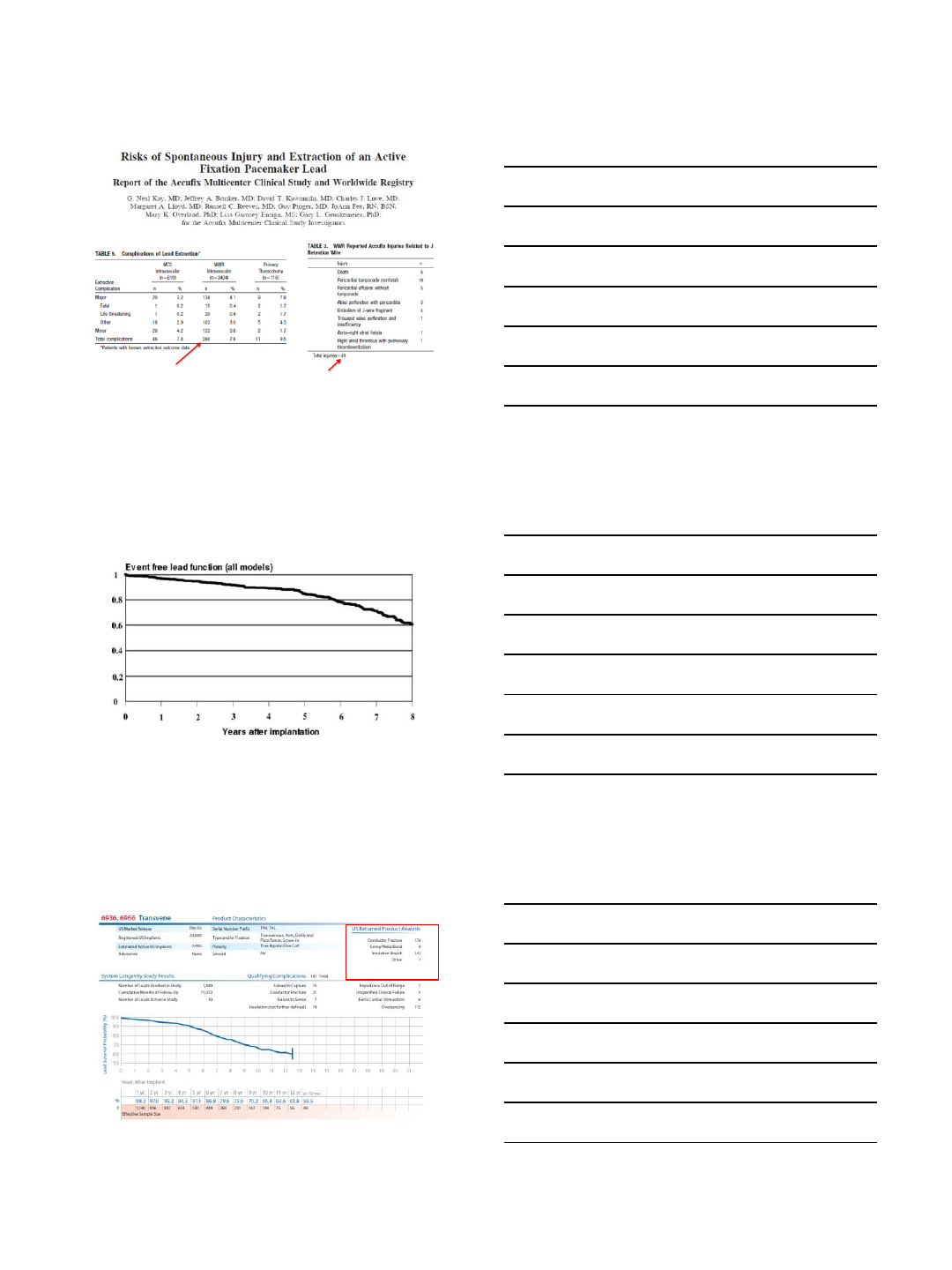
Telectronics AccuFix Lead
•Recalled in November
1994 after 2 deaths, 2
non-fatal injuries
•45,000 worldwide
implants
•Risk of wire
fracture/protrusion
•Issue: More deaths
documented due to
extraction than lead
malfunction
7/1/2013
3
40
Kay GN, et al. Circulation 1999;100:2344-2352.
260
Event-free Lead Function
(n=990)
Kleemann T, et al. Circulation 2007;115:2474-2480.
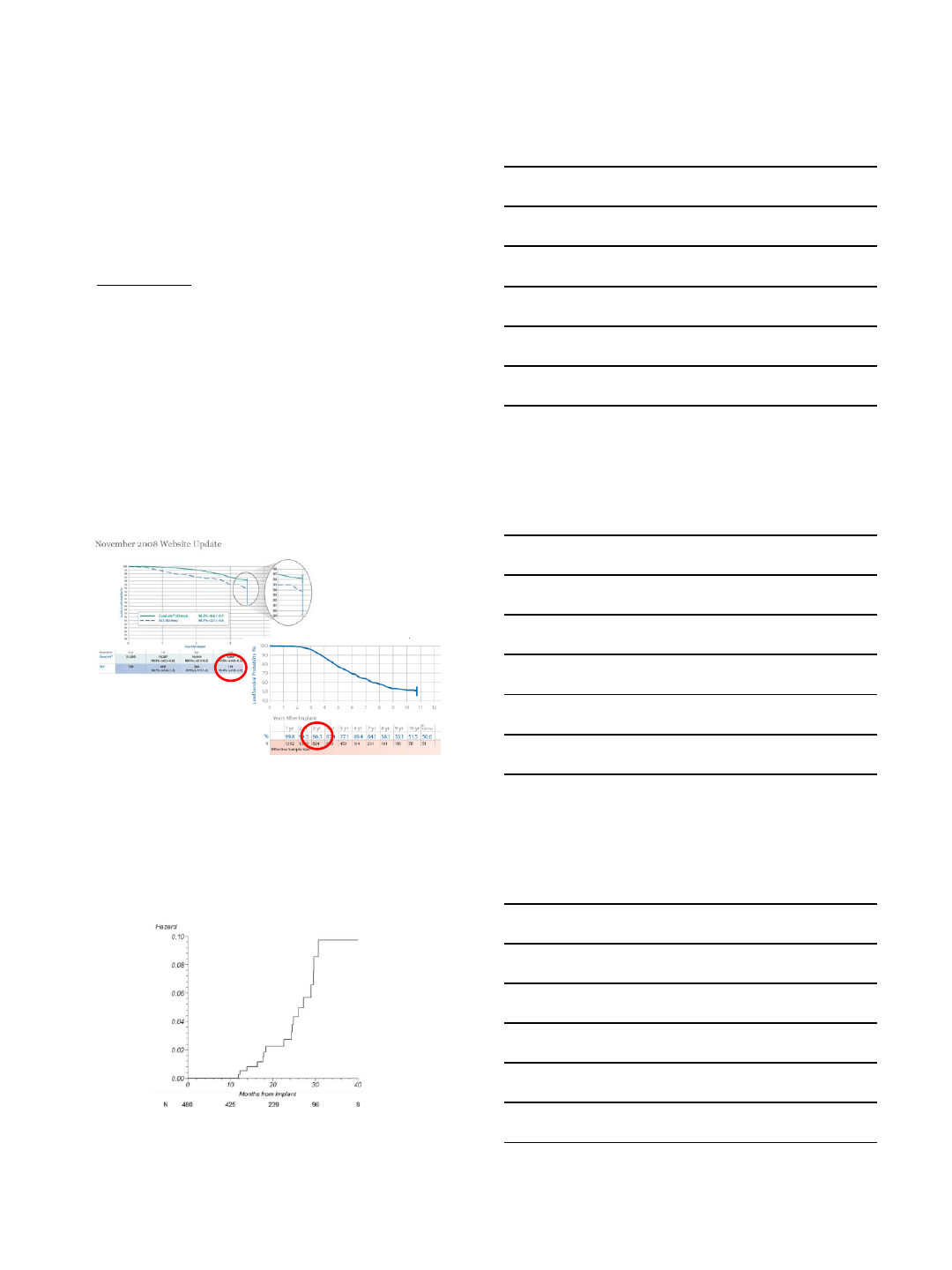
Transvene ICD Lead
Medtronic Product Performance Report, 2012.
7/1/2013
4
Sprint Fidelis ICD Leads
•6930, 6931, 6948, and 6949
•Market released in 2004
•Smaller than previous ICD leads
•268,000 implanted worldwide
•172,000 implanted in the US
October 15, 2007
Voluntary suspension of distribution of Sprint Fidelis leads
High incidence of conductor fractures
90%: Low voltage conductor
•Distal portion of the lead, affecting the anode (ring electrode)
•Near anchoring sleeve, primarily affecting the cathode (tip/helix
electrode)
10%: High voltage conductor
Sprint Fidelis versus 4004
Medtronic Product Performance Reports
Fidelis
4004
Risk of Model 6949 Lead Failure
Farwell D, et al. Heart Rhythm 2008;5:1375-1379.
7/1/2013
5
0.47% silicone abrasion over 9 years
Approximately 10% were inside-out
0.47% (abrasion) x 10% (externalization) =
0.047% Riata leads show externalized conductors
•Usual monitoring
•Lead parameters
•Provocative testing: maneuvers, possibly fluoroscopy
•Remote monitoring
•Not prophylactic explant
St Jude Medical November 28, 2011.
7/1/2013
6
Analysis of OPTIMUM, SCORE, and
SJ4 Registries of Patients with
Durata and Riata ST Optim ICD Leads
Parameter
OPTIMUM
SCORE
SJ4
TOTAL
Enrollment years
2006-2009
2007-2012
2009-2010
—
Enrolled (n)
5929
3357
1534
10 820
Unique leads (n)
6016
3416
1573
11 005
Median follow-up (y)
3.5
2.3
2.7
3.0
Cairns J, et al. HRS LBCTs, May 9, 3013.
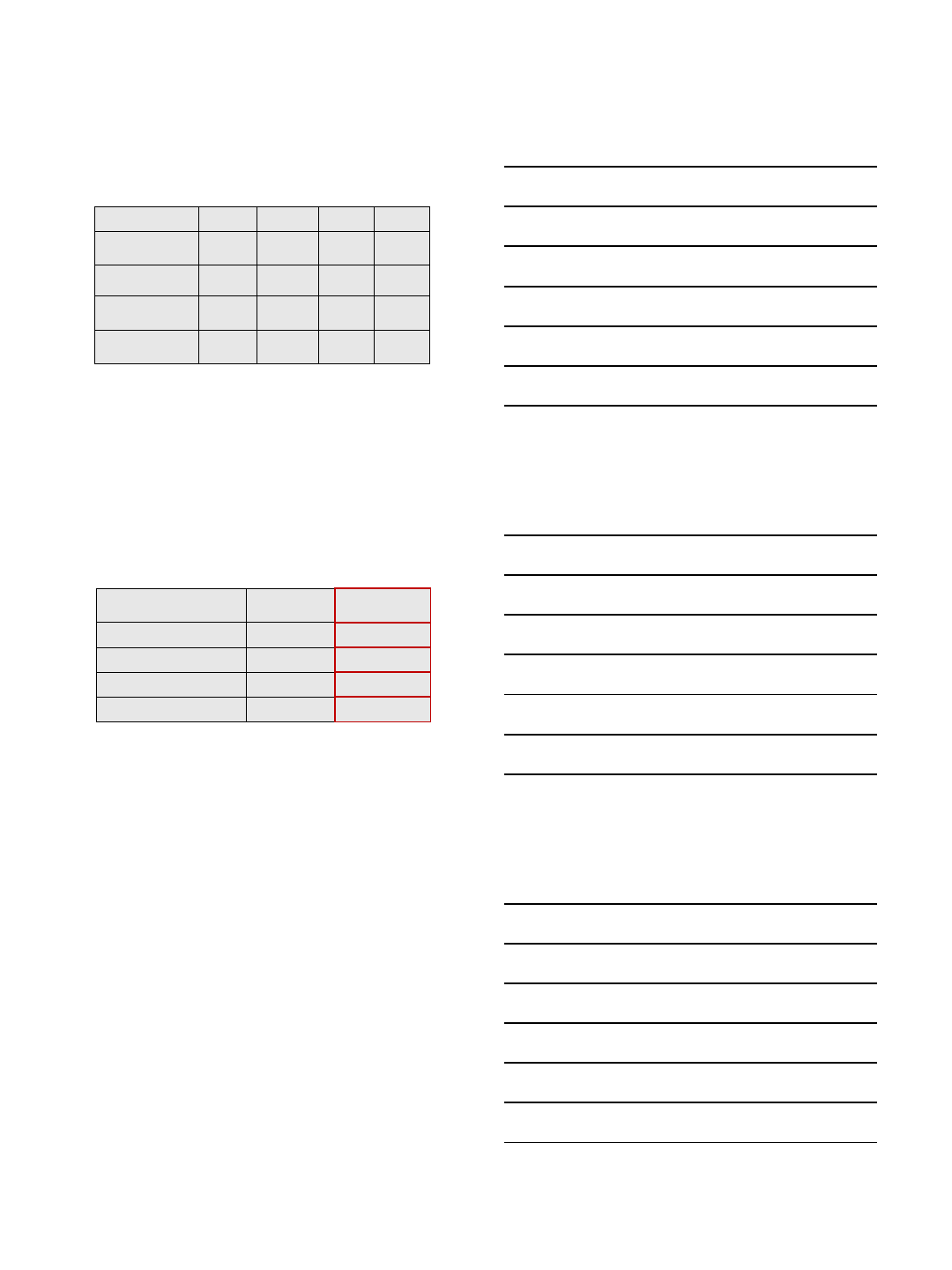
PHRI Analysis of St Jude Medical
Registries of Patients with Optim-
insulated ICD Leads
End point
Failure Rate (%)
Freedom from
Failure at 5 y (%)
All-cause mechanical failure
0.35
99.4
Conductor fracture
0.22
99.6
Insulation abrasion
0.07
99.9
Externalized conductor
0
100
Cairns J, et al. HRS LBCTs, May 9, 3013.
Risk of Overreaction: Complications
Associated with ICD Replacement in
Response to Advisories
•17 Canadian centers, 2915 recalled devices
•533 (18.3%) replaced
•66% primary prevention
•Complications in 43 pts (8.1%)
•Major requiring reoperation: 31 pts (5.8%)
•Death: 2 pts
•Minor complications: 12 pts (2.3%)
•Of explanted devices, 3 (0.1%) had malfunction
(early battery depletion), none with clinical
consequence
Gould PA, et al. JAMA 2006;295:1907-1911.
7/1/2013
7
Lessons Learned
•All leads have a finite failure rate.
•Goal of zero failure rate is unattainable.
•Resolution is in how failures are managed.
•Need post-marketing surveillance, not absence
of approval of new technology by requiring long-
term follow-up before approval.
•Our responsibilities are to weigh the evidence
and make judgments of risk benefit ratios. This
requires data and understanding.
7/5/2013
1
Techniques for Lead Extraction
Cardiac Electrophysiology
Cleveland Clinic
Oussama M. Wazni
Scope
250,000-275,000 ICD devices are implanted
yearly throughout the world.
Up to 10% of all leads implanted may
require removal.
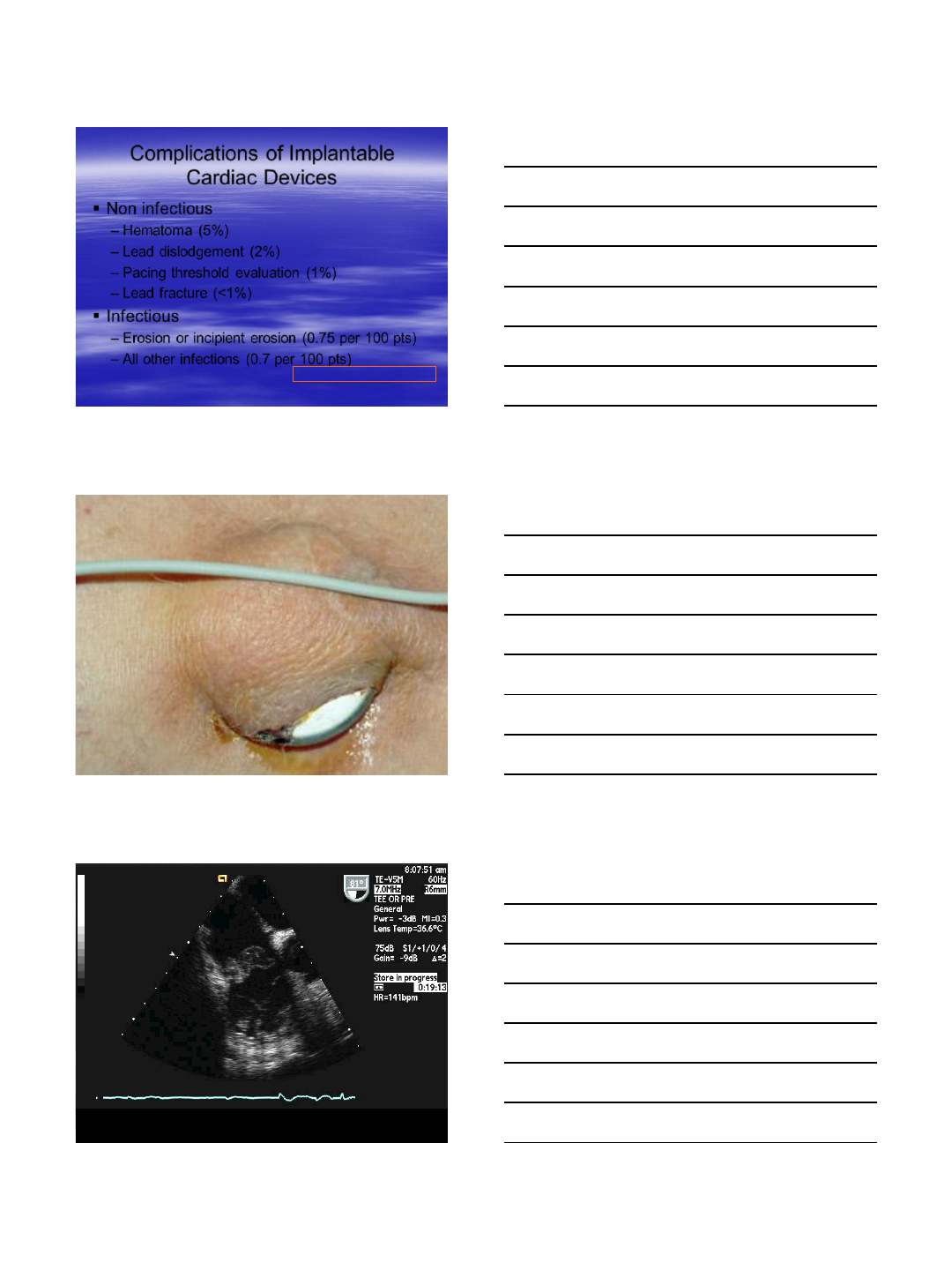
EPS: A growing demand
3 million implanted ICDs
180,000 pacing systems
Increasing indications
Aging population
7/5/2013
2
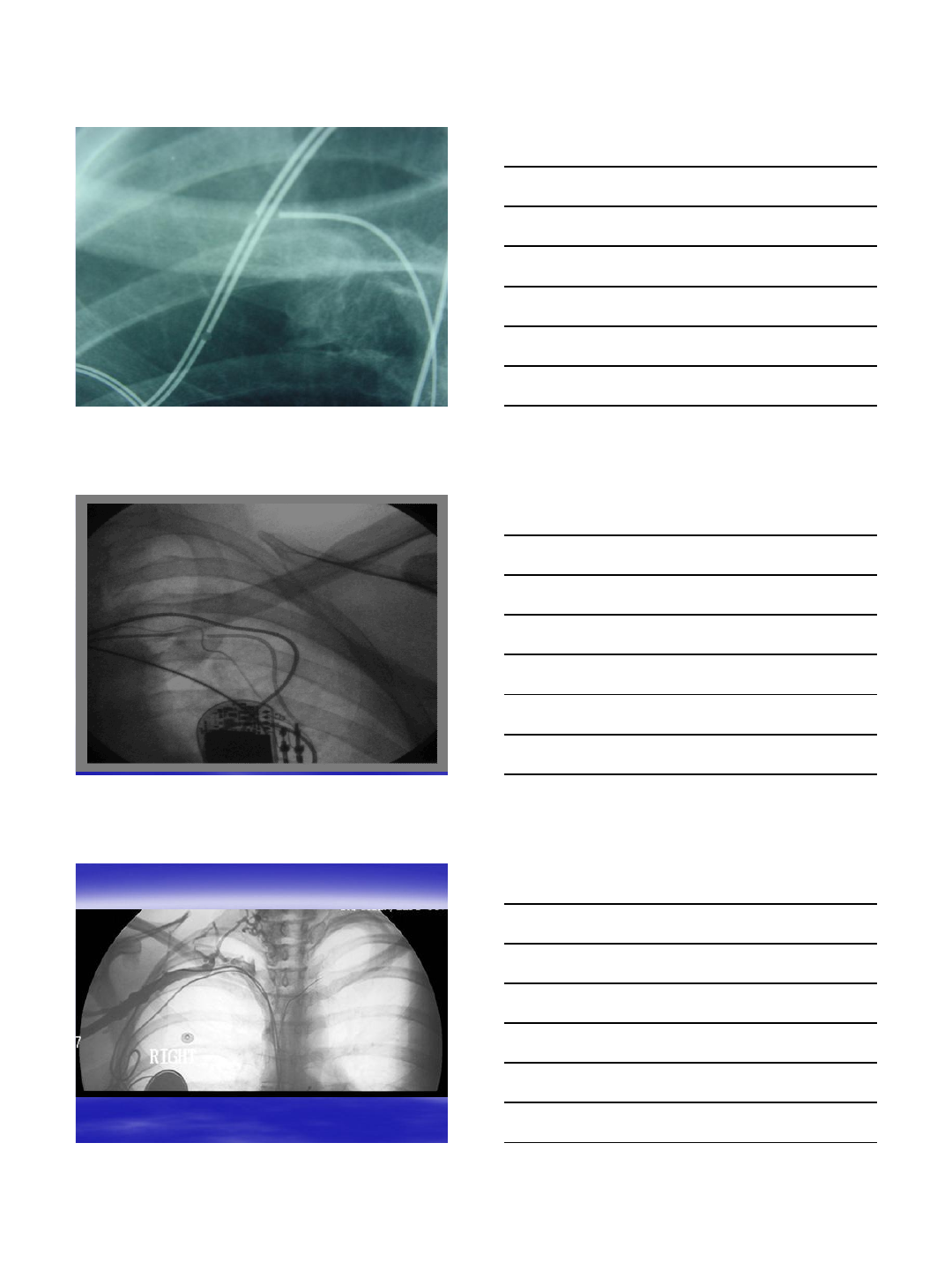
Complications of Implantable
Cardiac Devices
Non infectious
–Hematoma (5%)
–Lead dislodgement (2%)
–Pacing threshold evaluation (1%)
–Lead fracture (<1%)
Infectious
–Erosion or incipient erosion (0.75 per 100 pts)
–All other infections (0.7 per 100 pts)
Klug et al Circulation 2007;116
Infection
Infection
7/5/2013
3
Lead Fracture
Technique Failure
Venous Occlusion
7/5/2013
4
Bilateral Occlusion
Poor
Judgment
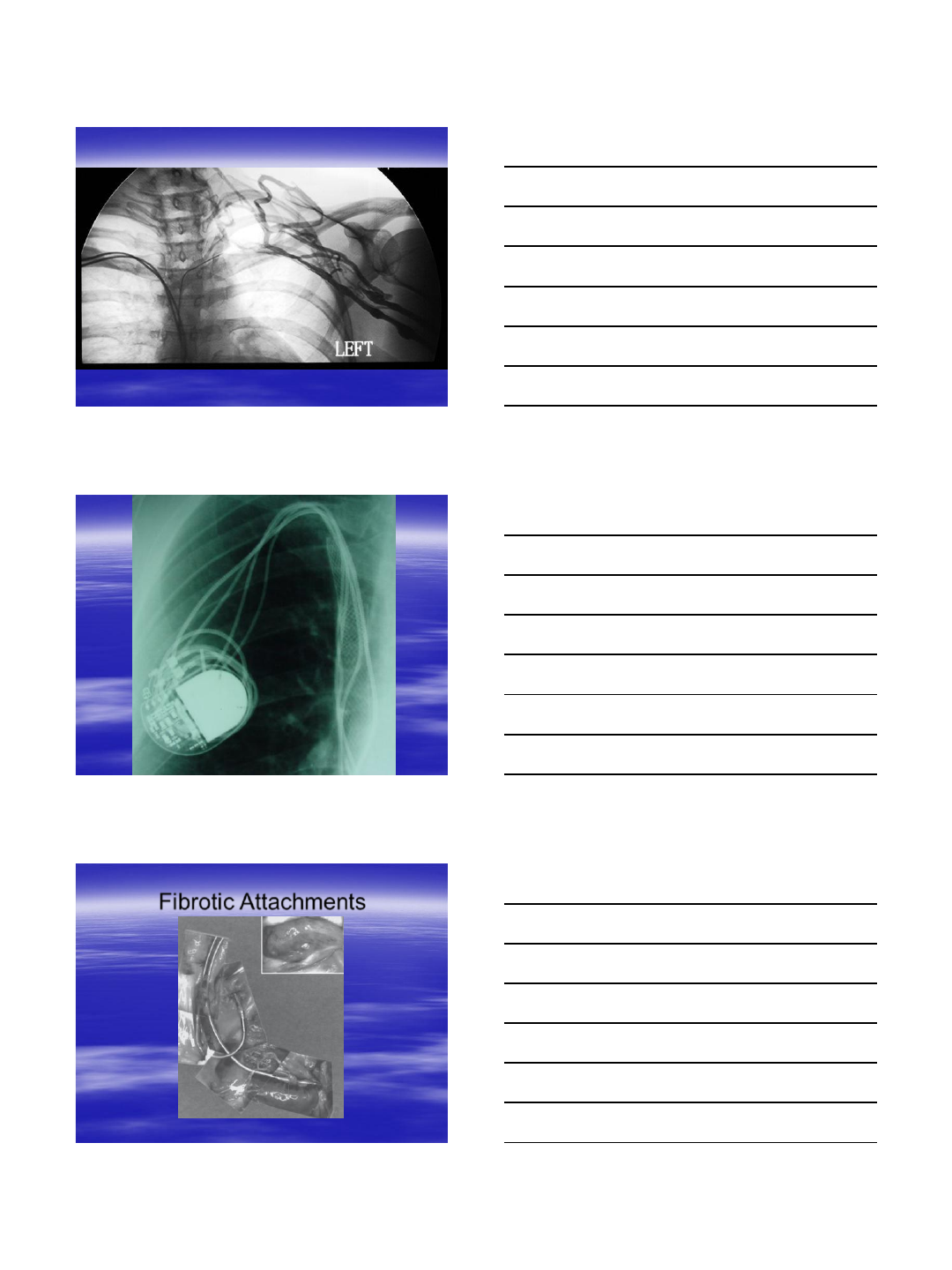
Fibrotic Attachments
7/5/2013
5
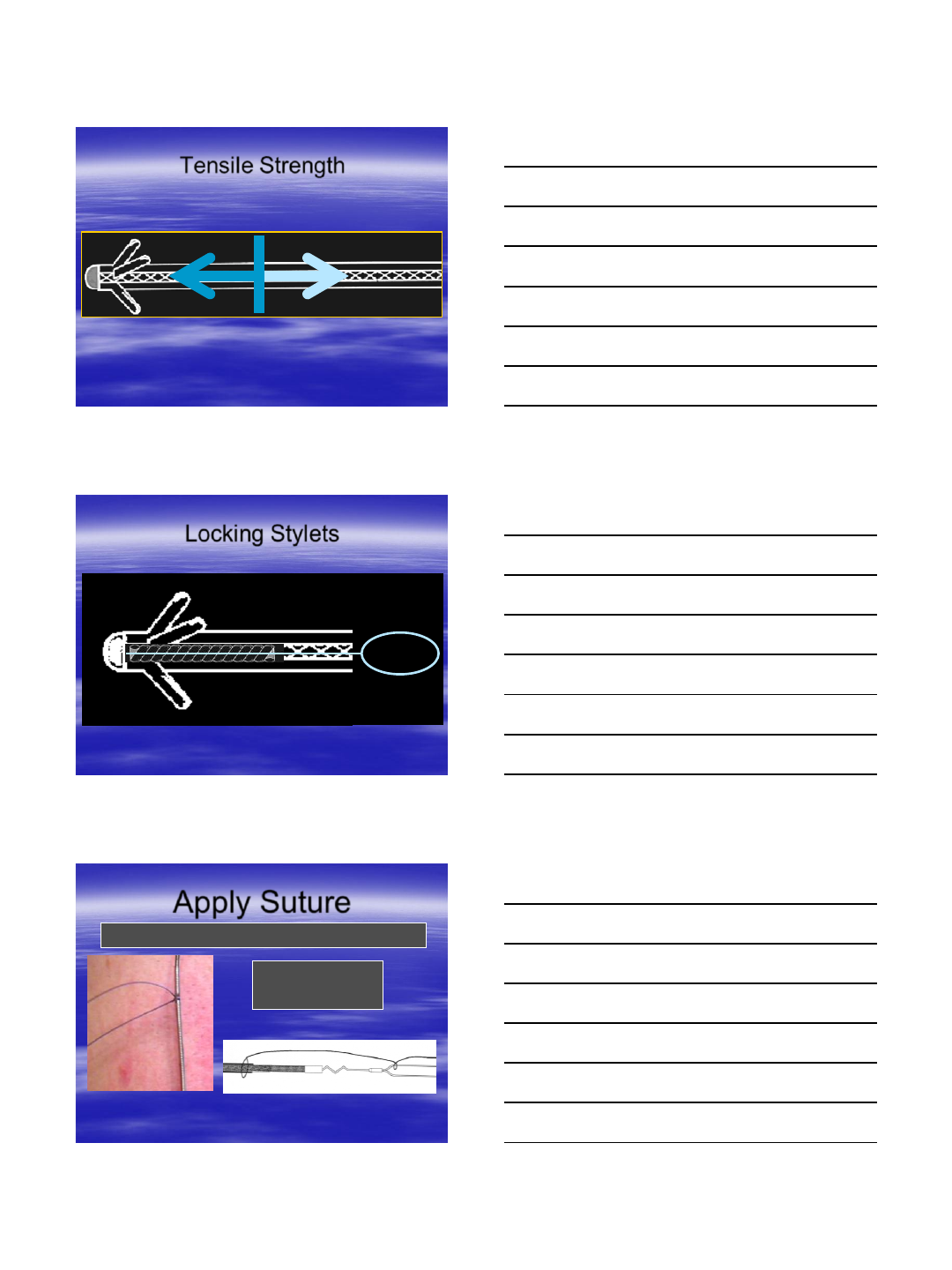
Tissue Ingrowth
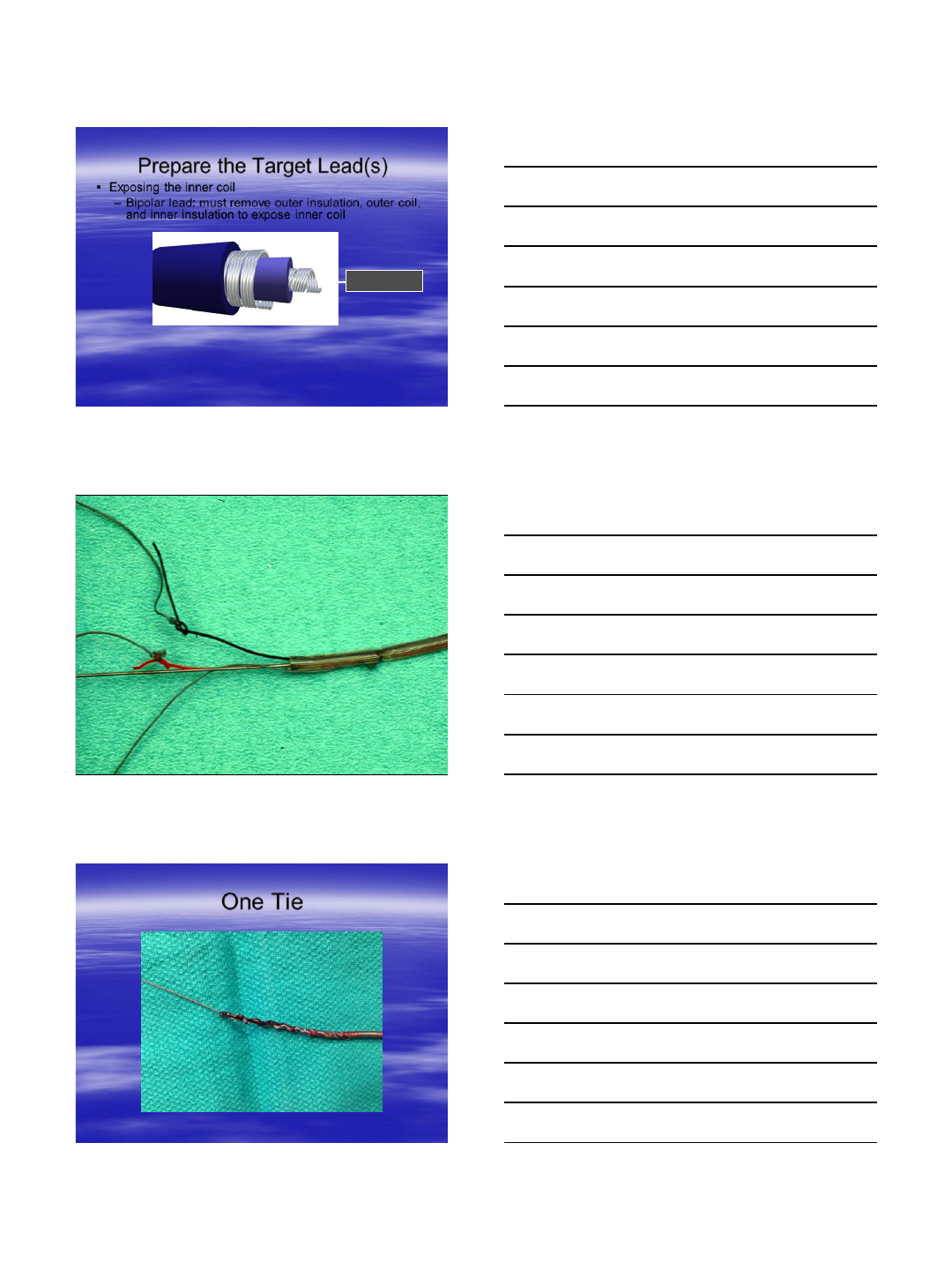
Extraction Risks
Lead extraction risks:
–Rupture of SVC
–Perforation (with tamponade) of SVC with new lead
placement
–Cardiac tamponade
–Failure to extract an infected lead
–Low cardiac output
–Lead breakage and migration
–Avulsion of veins and myocardial tissue
–Death
7/5/2013
6
Tensile Strength
Locking Stylets
Apply Suture
Example: 0 Ethibond
tied with 2 “throws”
for low profile
Connect suture from lead outer insulation to closest LLD loop.
7/5/2013
7
Prepare the Target Lead(s)
Exposing the inner coil
–Bipolar lead: must remove outer insulation, outer coil,
and inner insulation to expose inner coil
Inner Coil
One Tie
7/5/2013
8
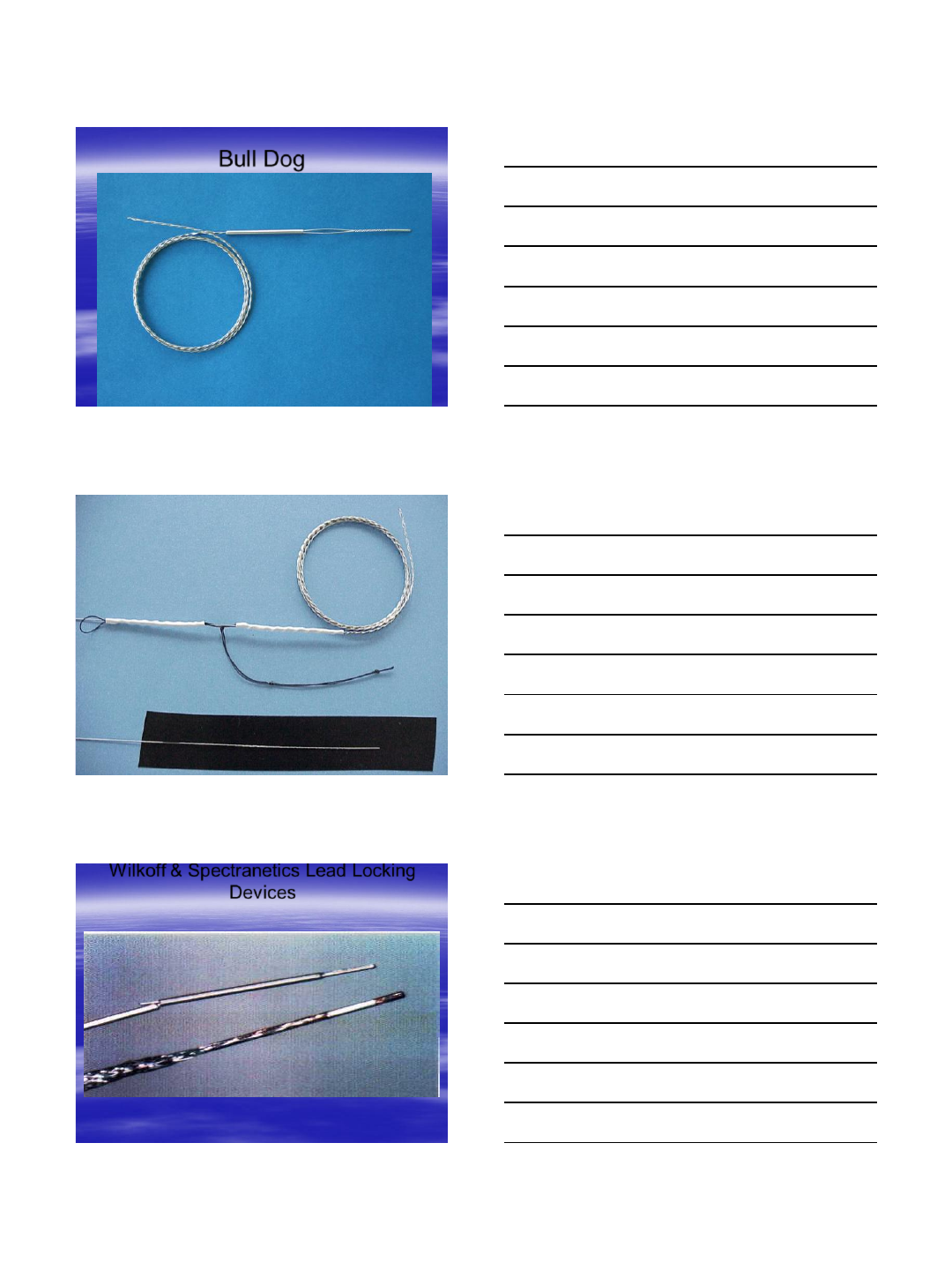
Bull Dog
Liberator™
Wilkoff & Spectranetics Lead Locking
Devices
Wilkoff™ Locking Stylet 0.17” – 0.19”
Lead Locking Device® or LLD2
7/5/2013
9
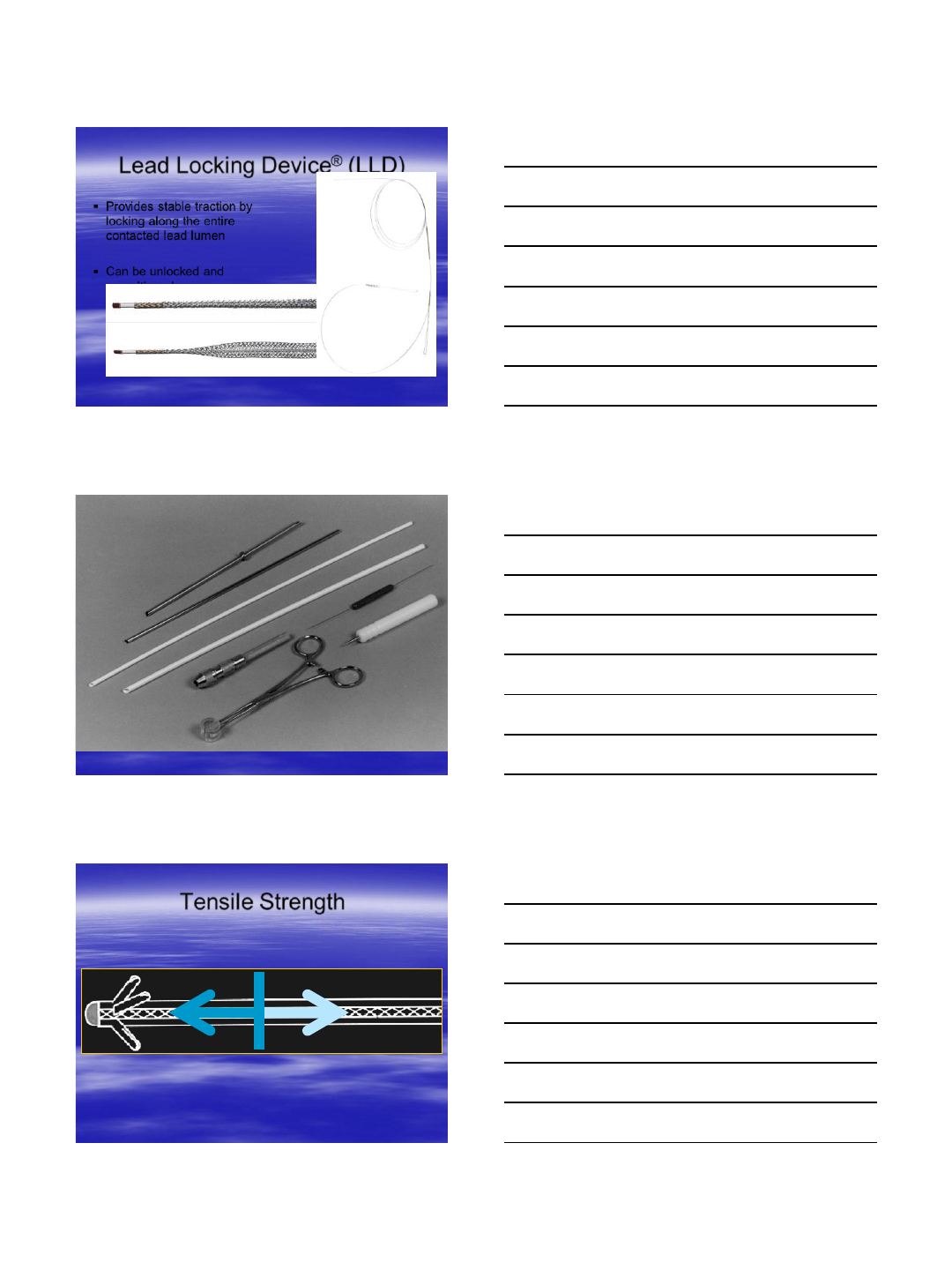
Provides stable traction by
locking along the entire
contacted lead lumen
Can be unlocked and
repositioned
Unlocked
Locked
Lead Locking Device® (LLD)
Tensile Strength
7/5/2013
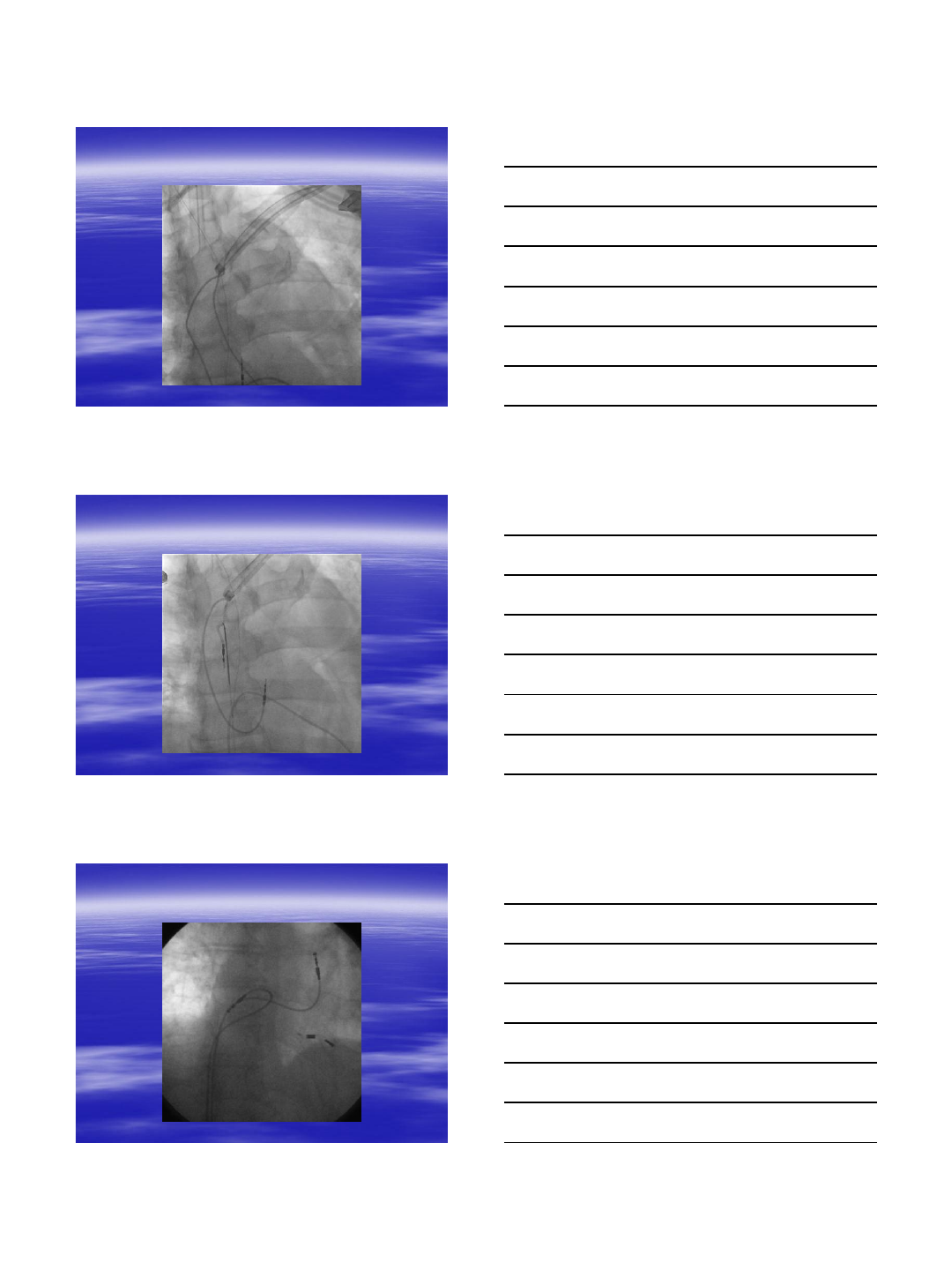
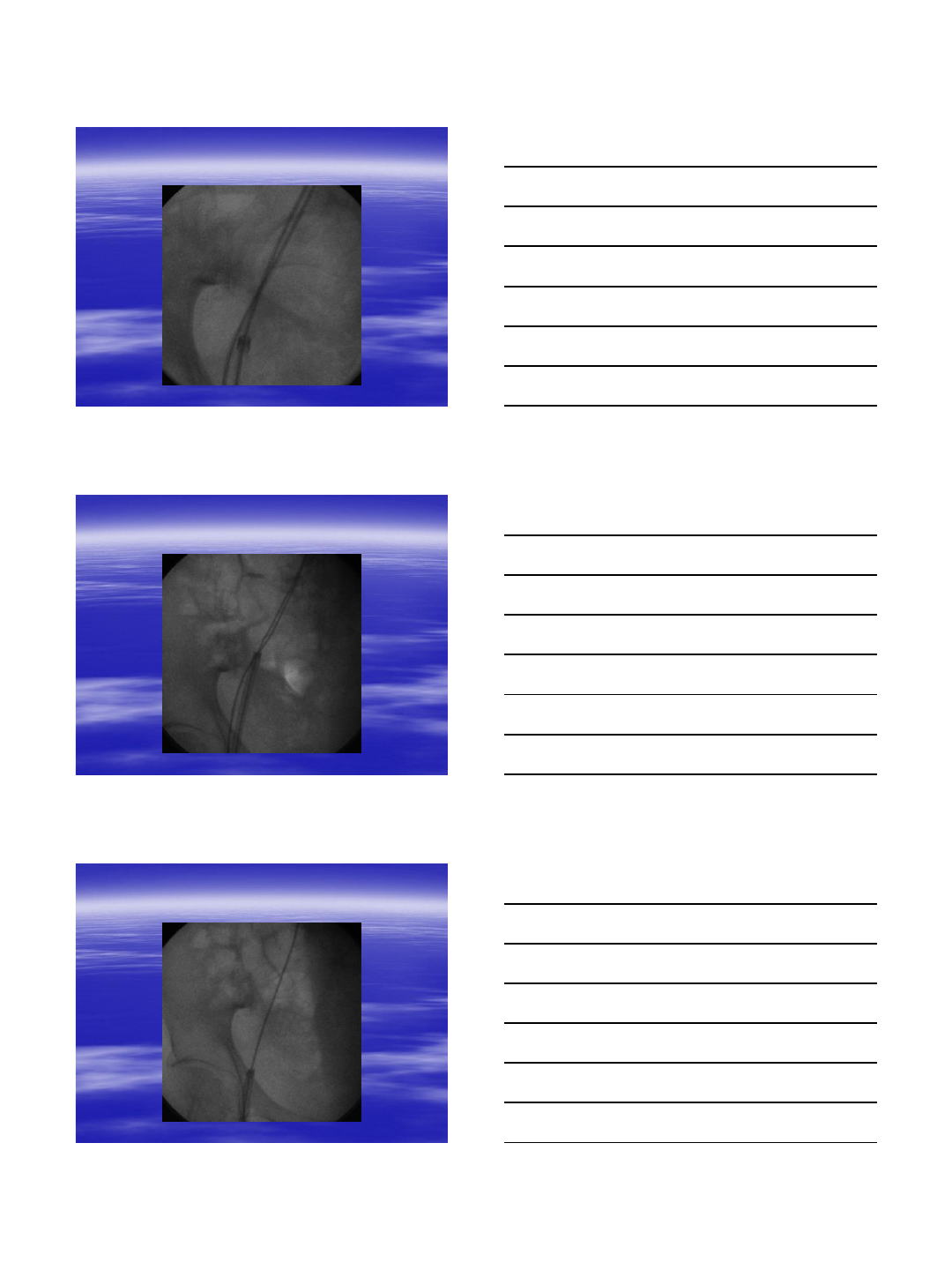
10
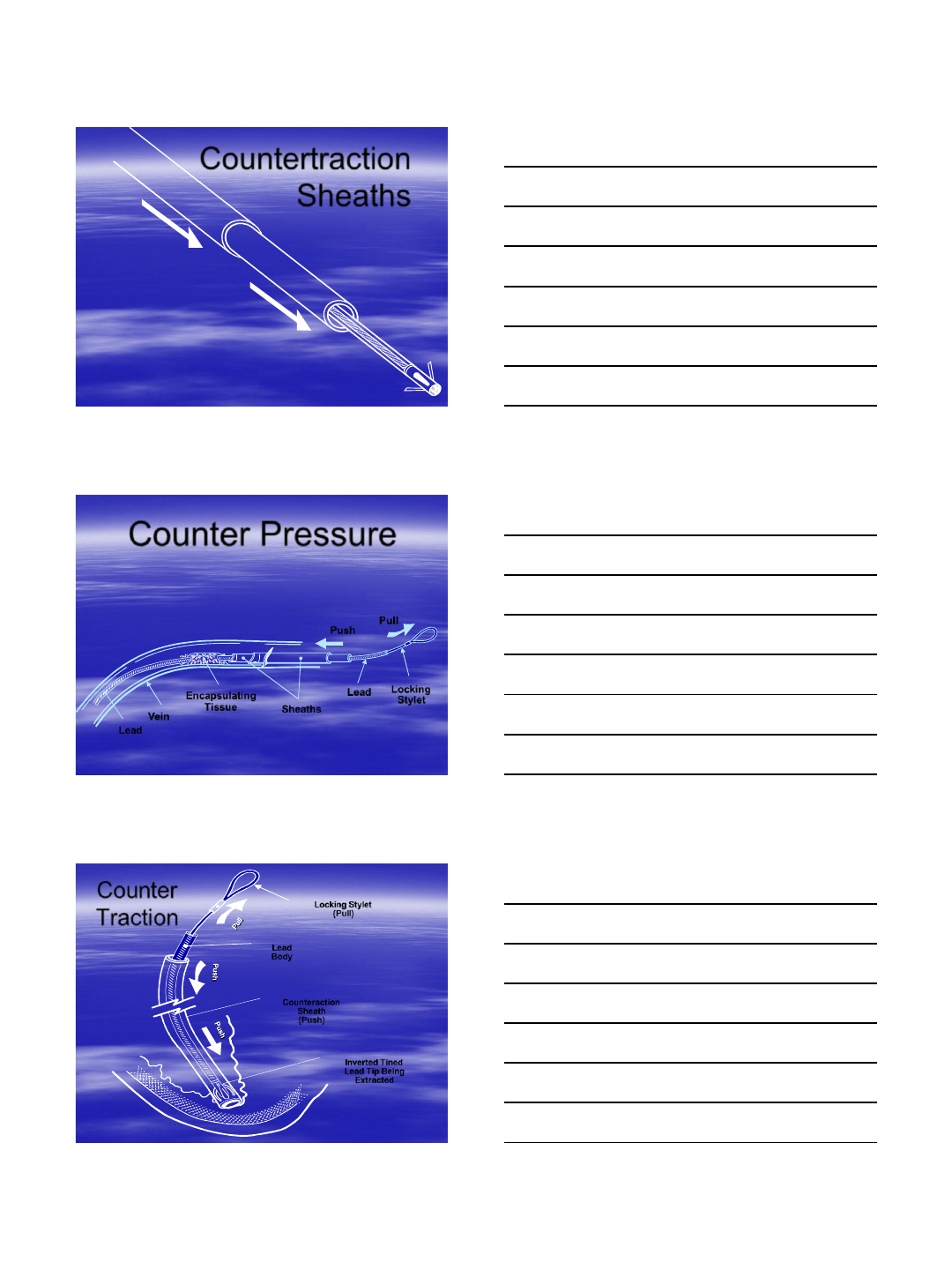
Countertraction
Sheaths
Push Pull
Locking
Stylet
Lead
Sheaths
Encapsulating
Tissue
Vein
Lead
Counter Pressure
Locking Stylet
(Pull)
Lead
Body
Counteraction
Sheath
(Push)
Inverted Tined
Lead Tip Being
Extracted
Counter
Traction
7/5/2013
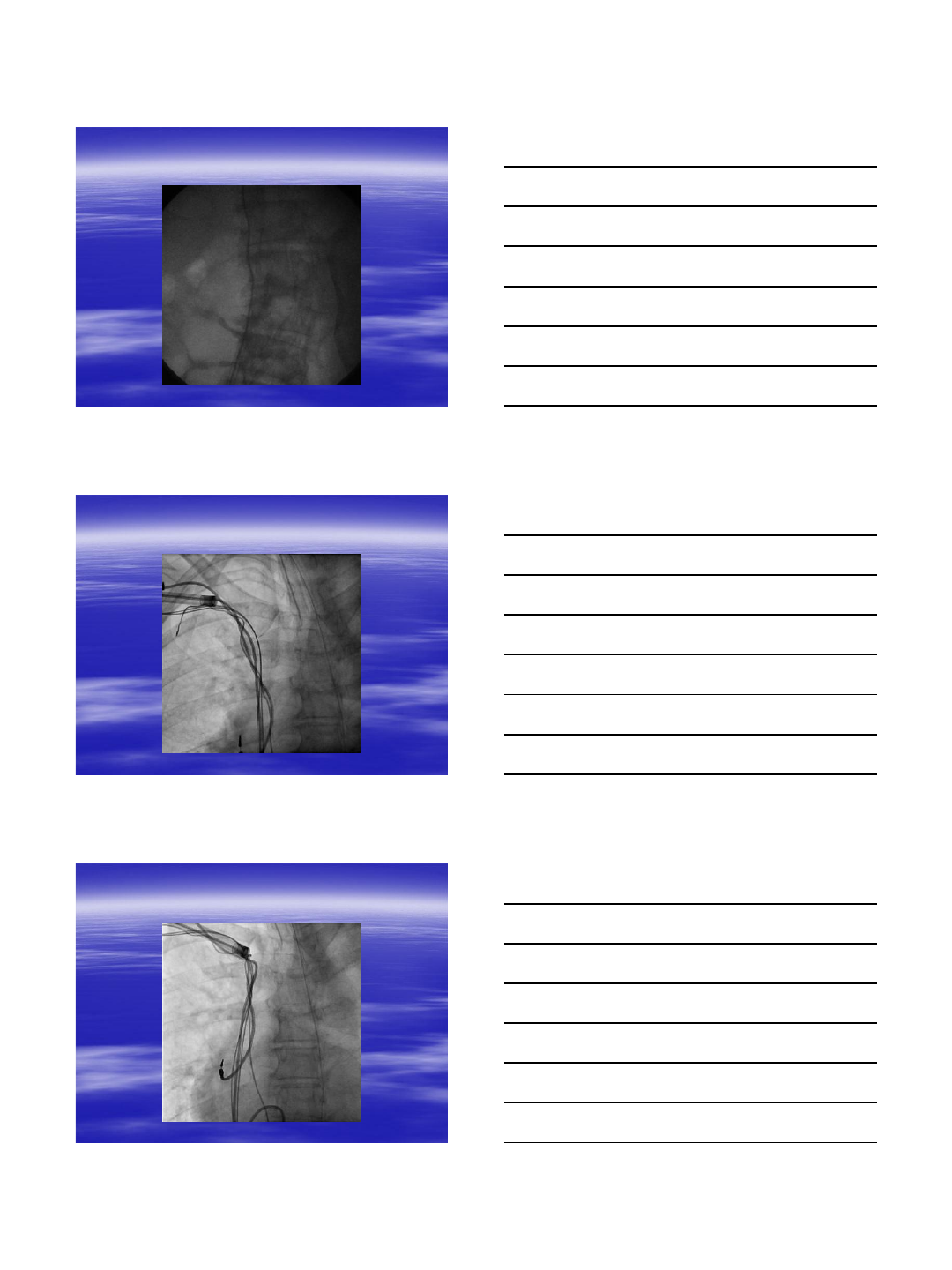
11
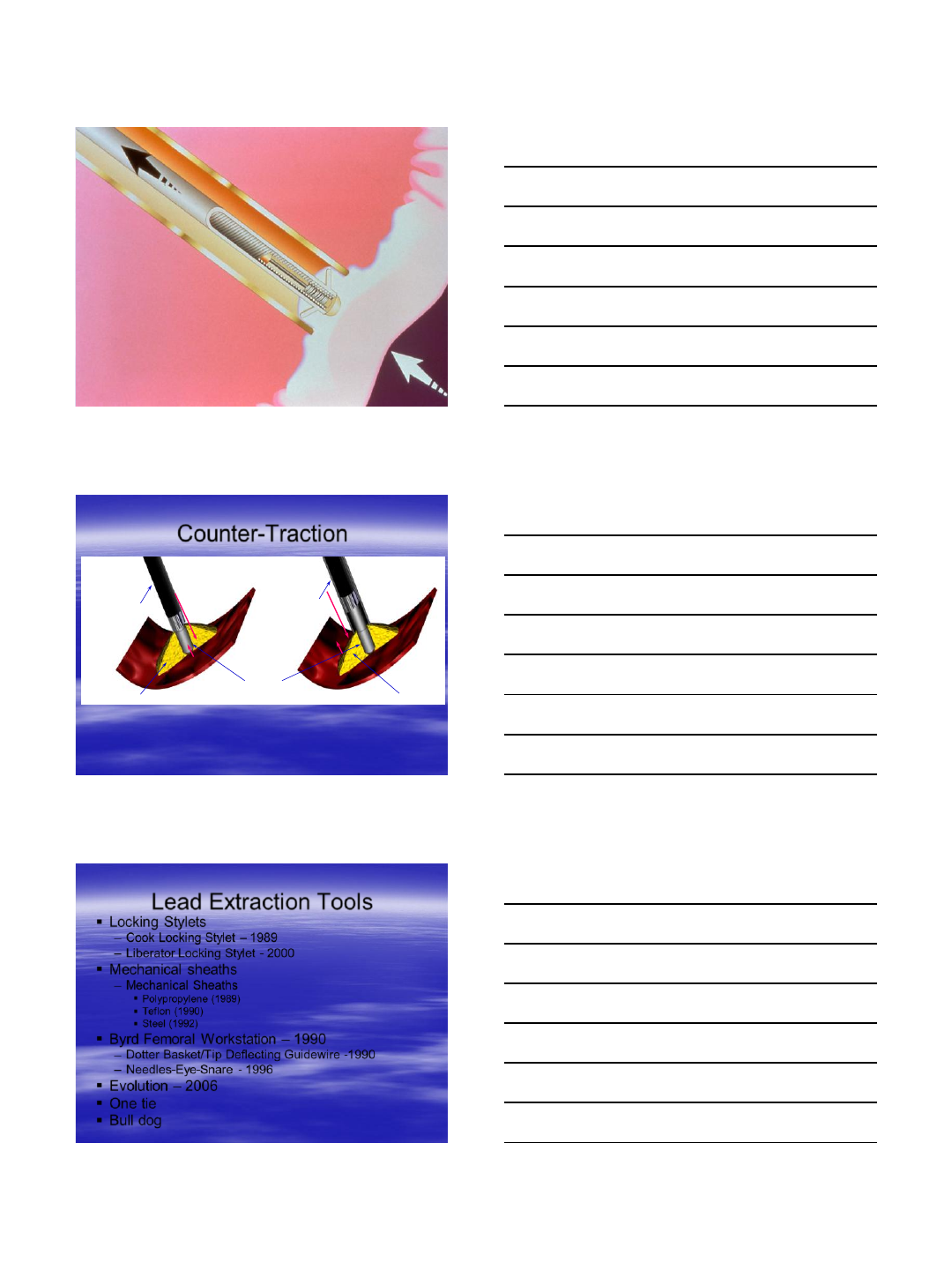
Using SLS II Alone Using the Outer Sheath
Target Lead
Outer Sheath SLS II
Scar Tissue Scar Tissue
Counter-Traction
Lead Extraction Tools
Locking Stylets
–Cook Locking Stylet – 1989
–Liberator Locking Stylet - 2000
Mechanical sheaths
–Mechanical Sheaths
Polypropylene (1989)
Teflon (1990)
Steel (1992)
Byrd Femoral Workstation – 1990
–Dotter Basket/Tip Deflecting Guidewire -1990
–Needles-Eye-Snare - 1996
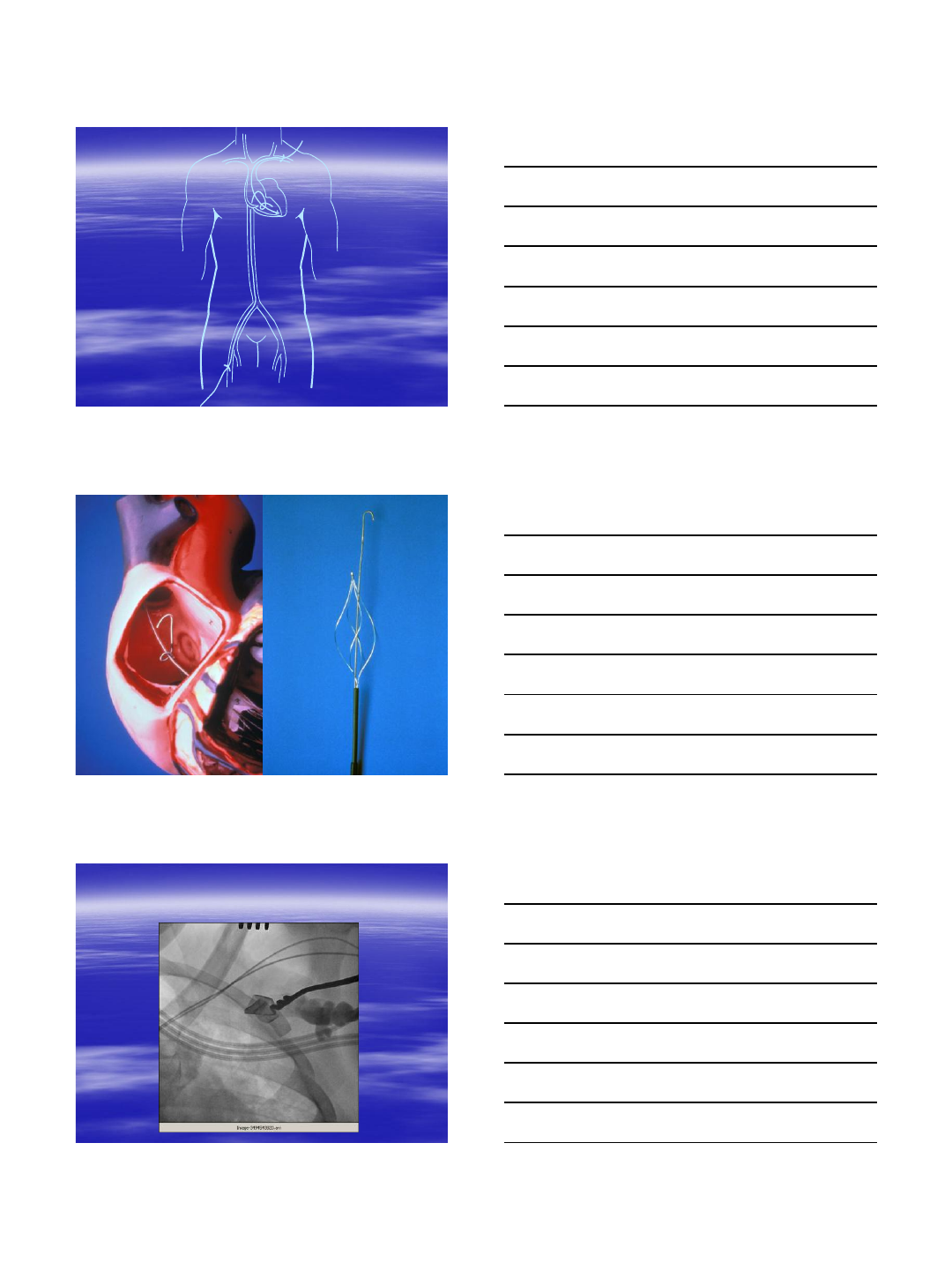
Evolution – 2006
One tie
Bull dog

7/5/2013
12
Powered Lead Removal
Technologies
12F - Excimer Laser – 1994 (Clinical Trial)
12F – Excimer Laser – 1997 (FDA approval)
Lead Locking Device (LLD™) –1999
14F & 16F Excimer Laser -
Electrosurgical Dissection Sheaths - 2001
SLSII – 12F, 14F, 16F – 2003
Locking Stylet™ by COOK®
CVX-300® Excimer Laser
Generates light at 308 nm
wavelength in the
ultraviolet spectrum
Excimer laser enables
photoablation of lipids and
proteins
Laser Medium = XeCI gas
7/5/2013
13
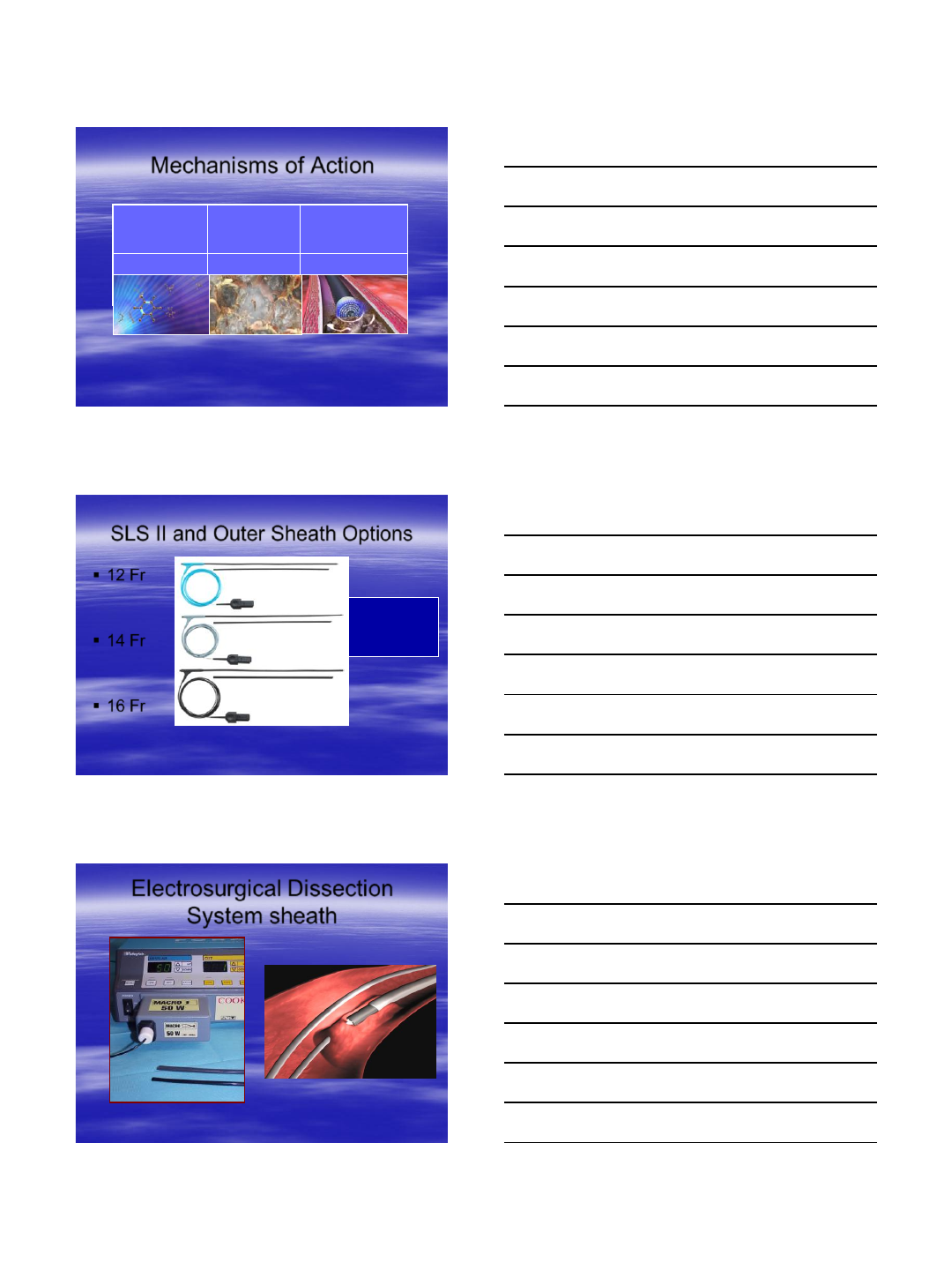
Photochemica
l
Photothermal
Photomechanica
l
Dissolving
molecular bonds Produces photo-
thermal energy Creating
kinetic energy
Mechanisms of Action
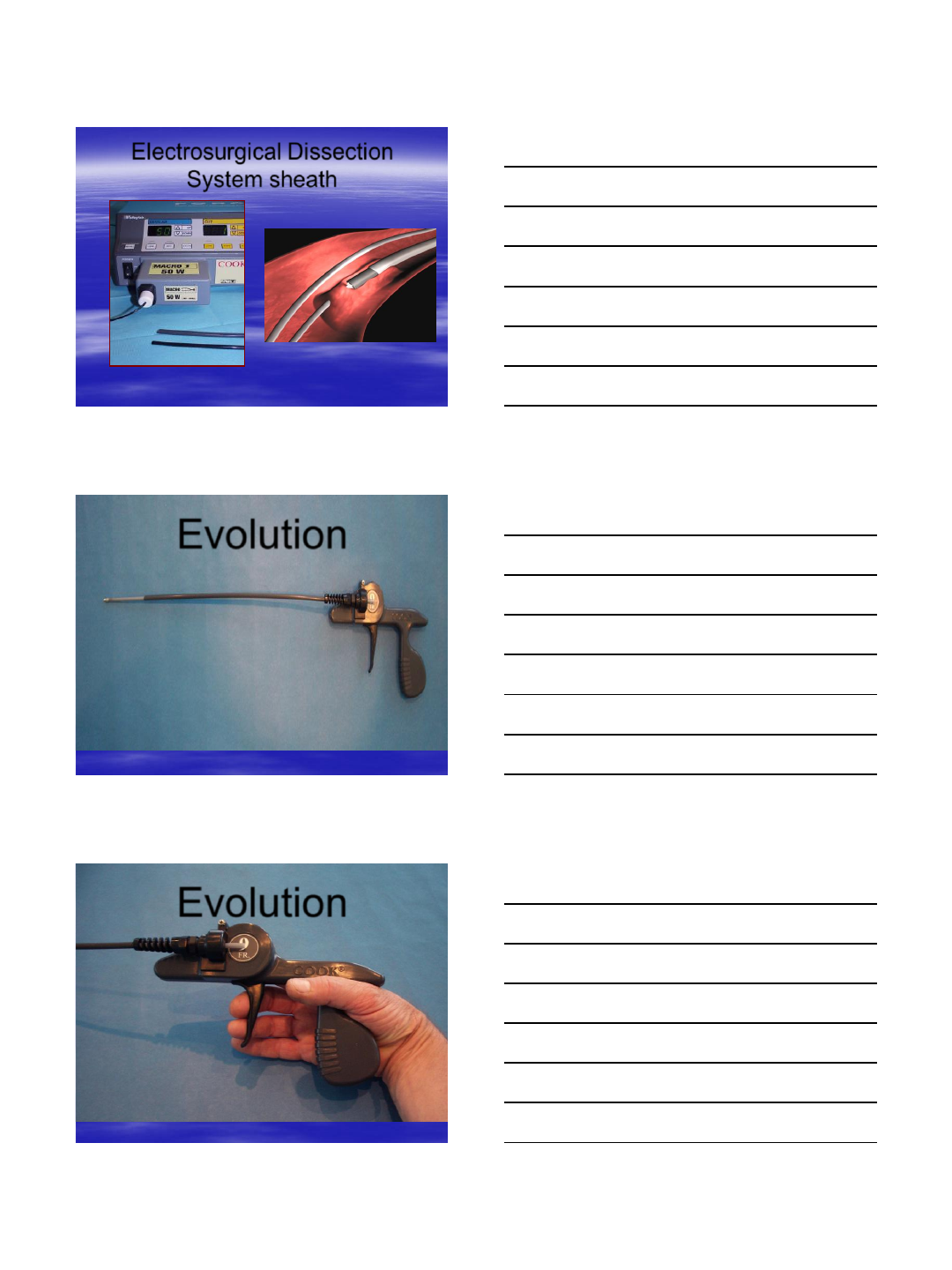
SLS II and Outer Sheath Options
12 Fr
14 Fr
16 Fr
Teflon outer
sheath offers
blunt and
beveled ends
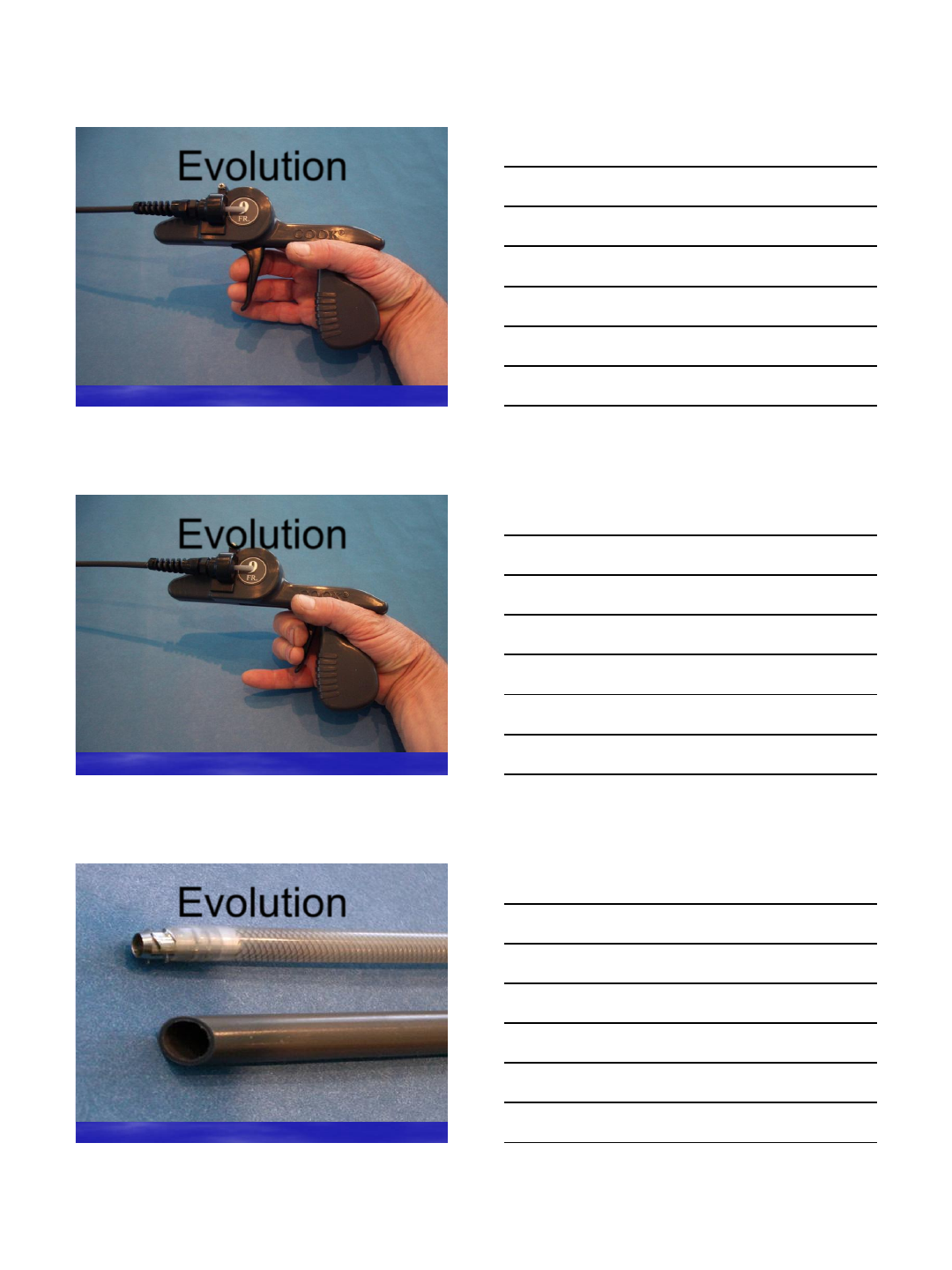
Electrosurgical Dissection
System sheath
7/5/2013
14
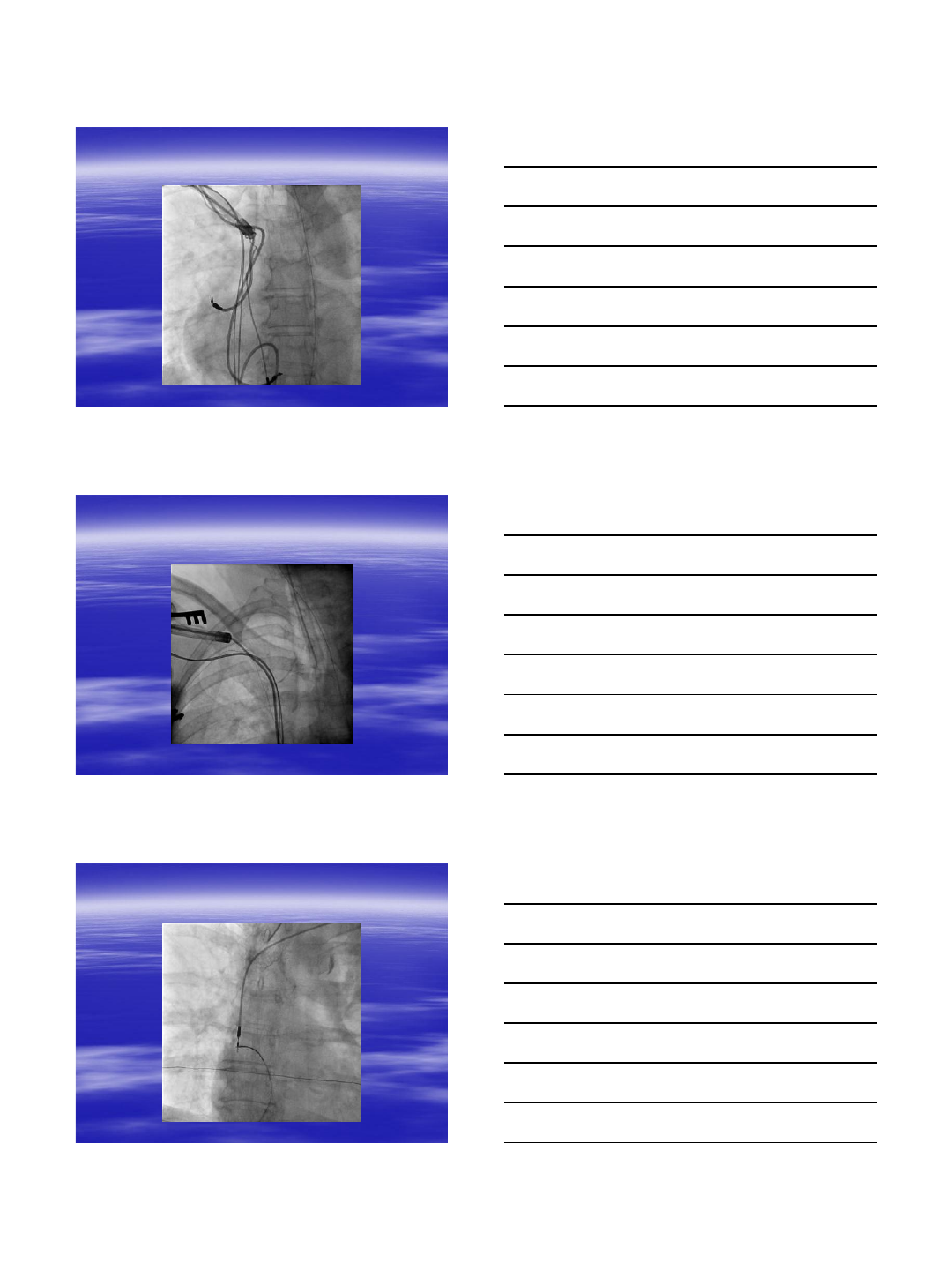
Electrosurgical Dissection
System sheath
Evolution
Evolution
7/5/2013
15
Evolution
Evolution
Evolution
7/5/2013
16
7/5/2013
17
7/5/2013
18
7/5/2013
19
7/5/2013
20
7/5/2013
21
7/5/2013
22
Conclusion
In the right patients if you know what you
are doing extraction is useful and safe
