Radial Approach International Perspective Syllabus
Radial Approach International Perspective Syllabus Radial_Approach_International_Perspective_Syllabus Radial_Approach_International_Perspective_Syllabus 6 2013 pdfdoc 258413772373414384 3:
2013-06-03
: Pdf Radial Approach International Perspective Syllabus Radial_Approach_International_Perspective_Syllabus 6 2013 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 51
6/1/2013
1
Tejas M. Patel, MD, DM, FACC, FESC, FSCAI
Chairman & Chief Interventional Cardiologist, Apex Heart Institute,
Professor & Head, Department of Cardiology, Sheth V. S. General Hospital,
Ahmedabad, India.
Professor of Medicine (Cardiology), Department of Internal Medicine,
Virginia Commonwealth University Medical Center, Richmond, USA.
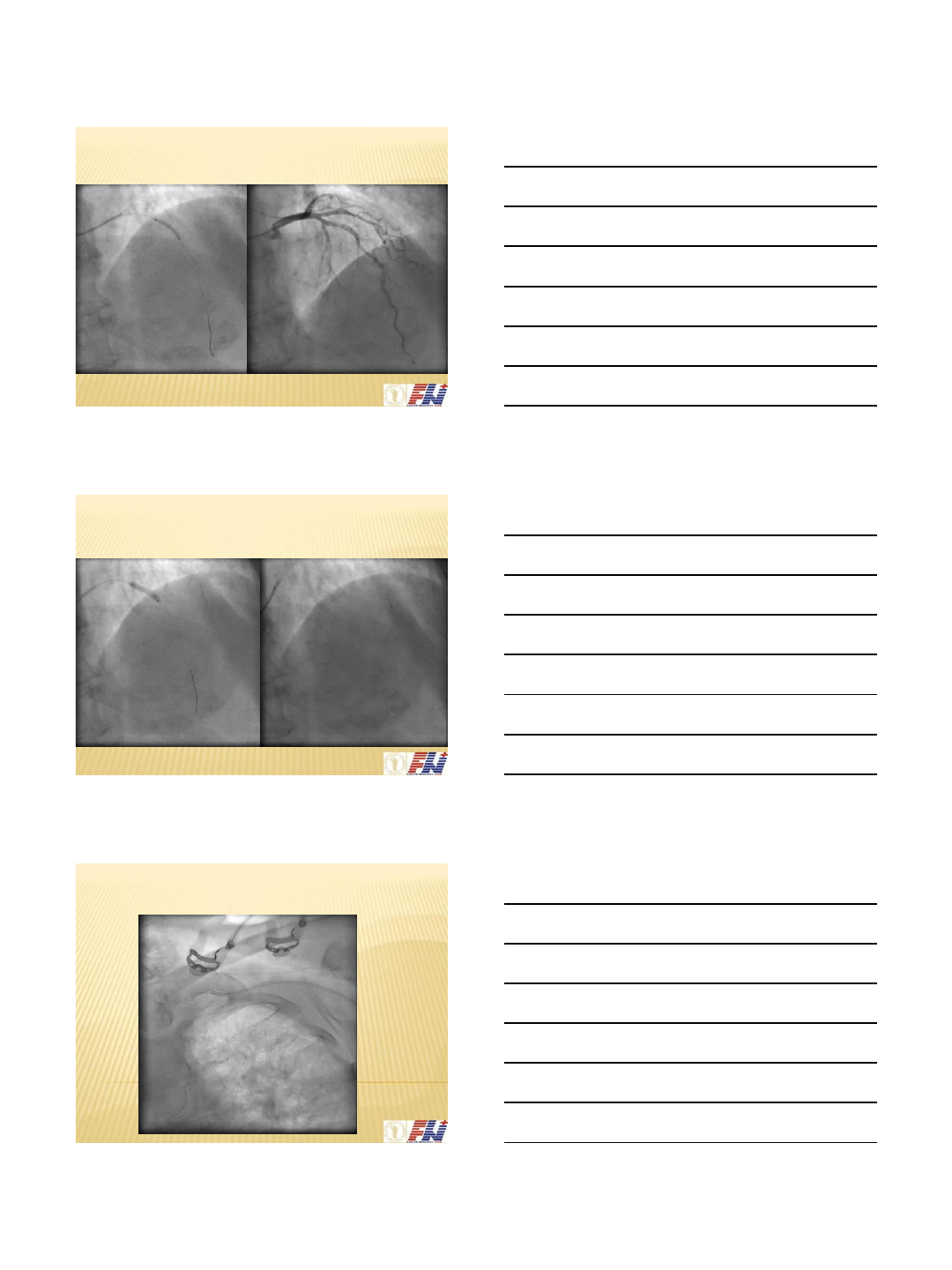
Balloon Assisted Tracking for Challenging
Anatomy
Disclosure
•I have no relevant disclosure
related to this presentation
Balloon-assisted tracking of a guide catheter
through difficult radial anatomy: A technical
report
Patel T, Shah S, Pancholy S.
Catheter Cardiovasc Interv. 2013 Apr;81(5):E215-8.

6/1/2013
2
Balloon-assisted tracking: A must-known
technique to overcome difficult anatomy during
transradial approach
Patel T, Shah S, Pancholy S, Rao S, Bertrand OF, Kwan T.
Catheter Cardiovasc Interv. 2013 Apr 16. doi: 10.1002/ccd.24959. [press]
6/1/2013
3
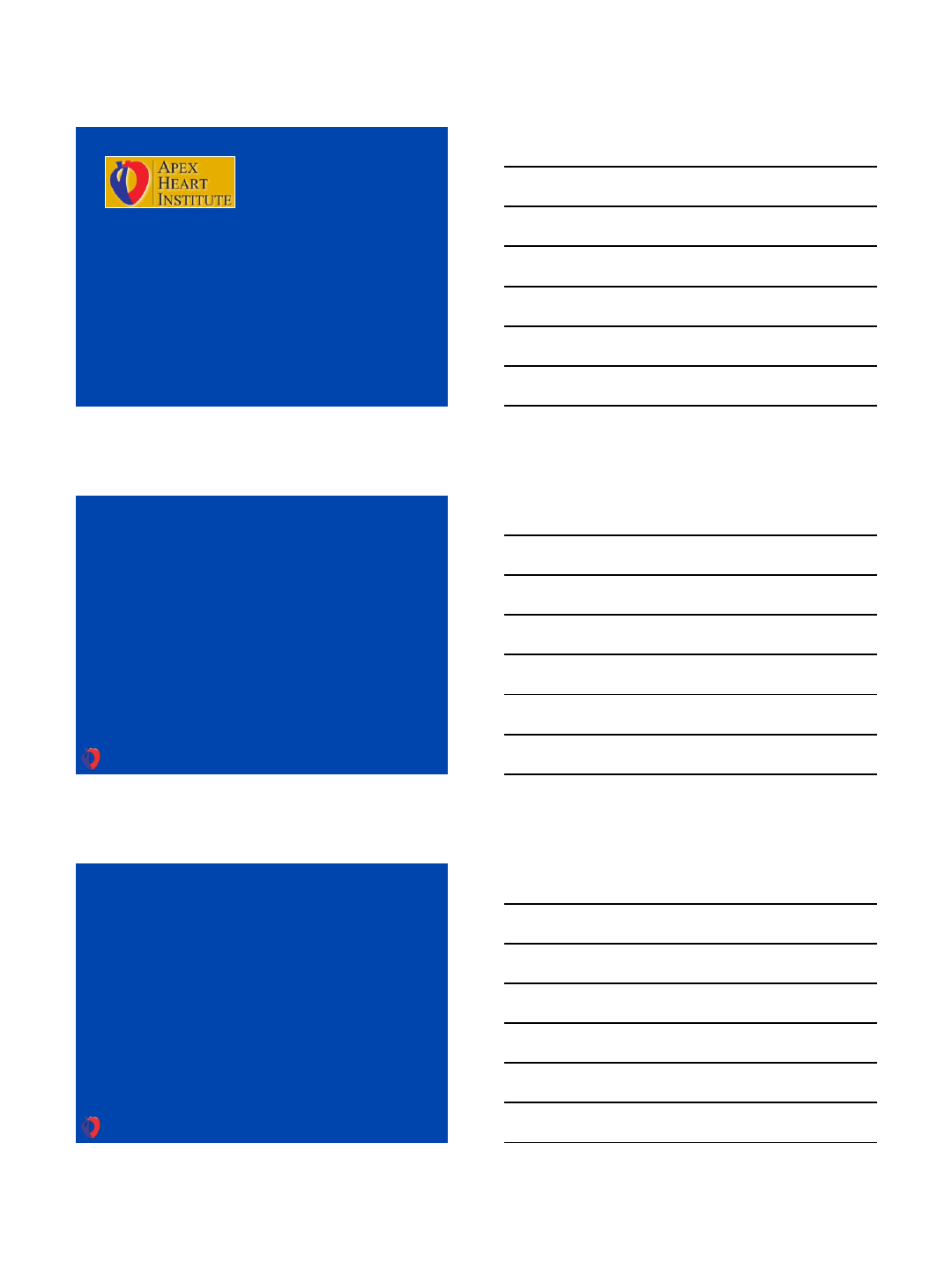
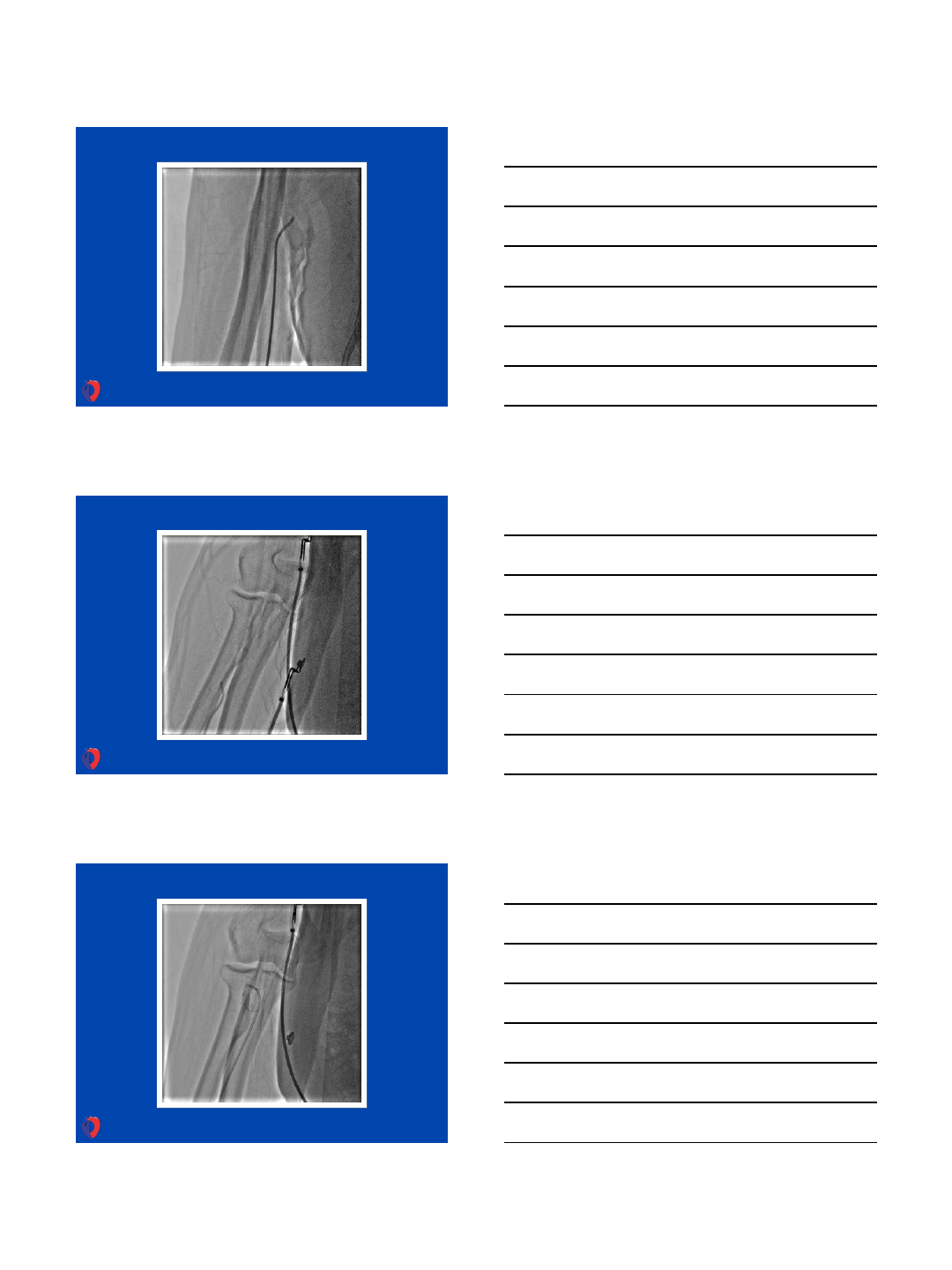
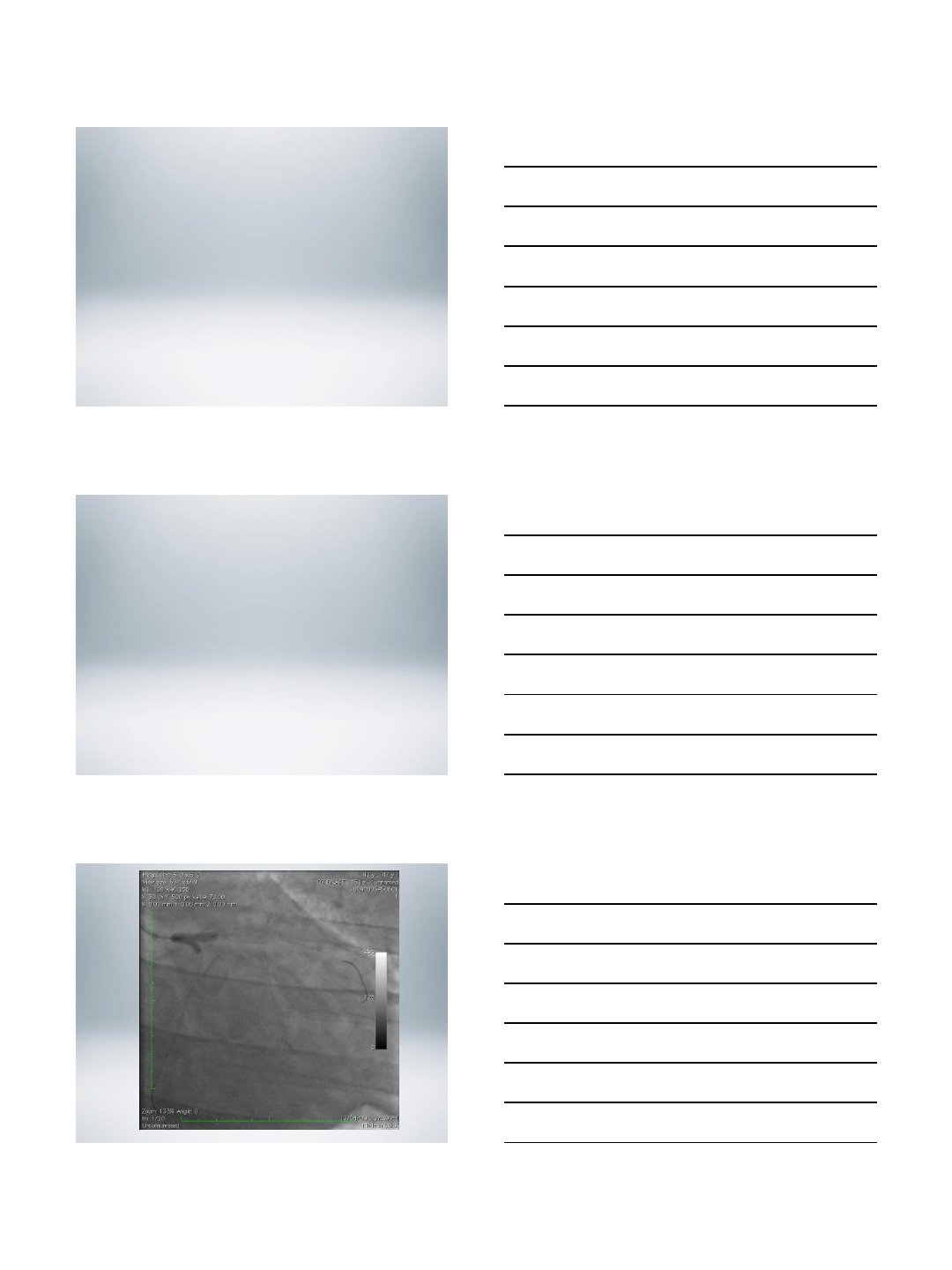
Working through small RA & 7F guide
6/1/2013
4
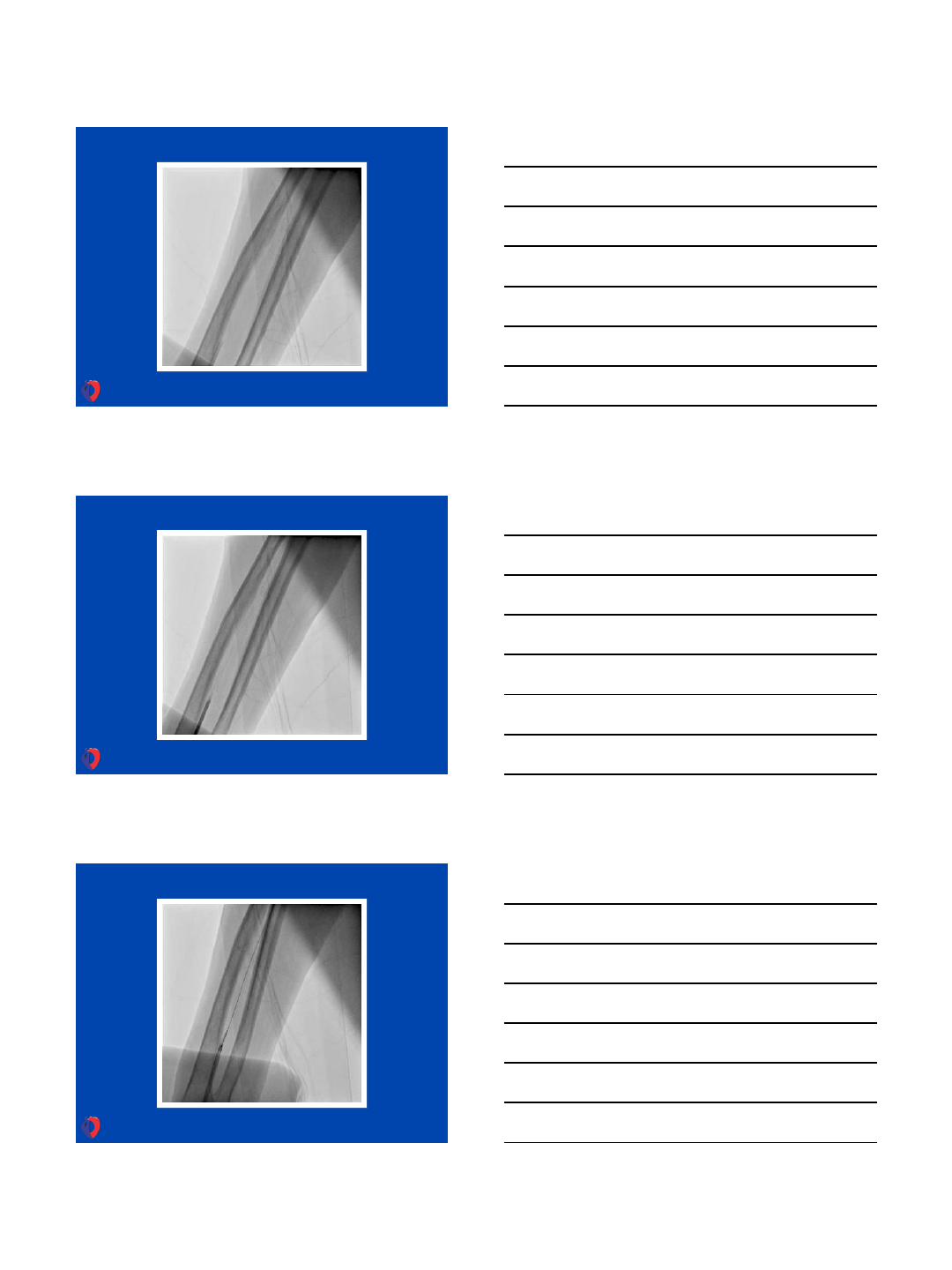
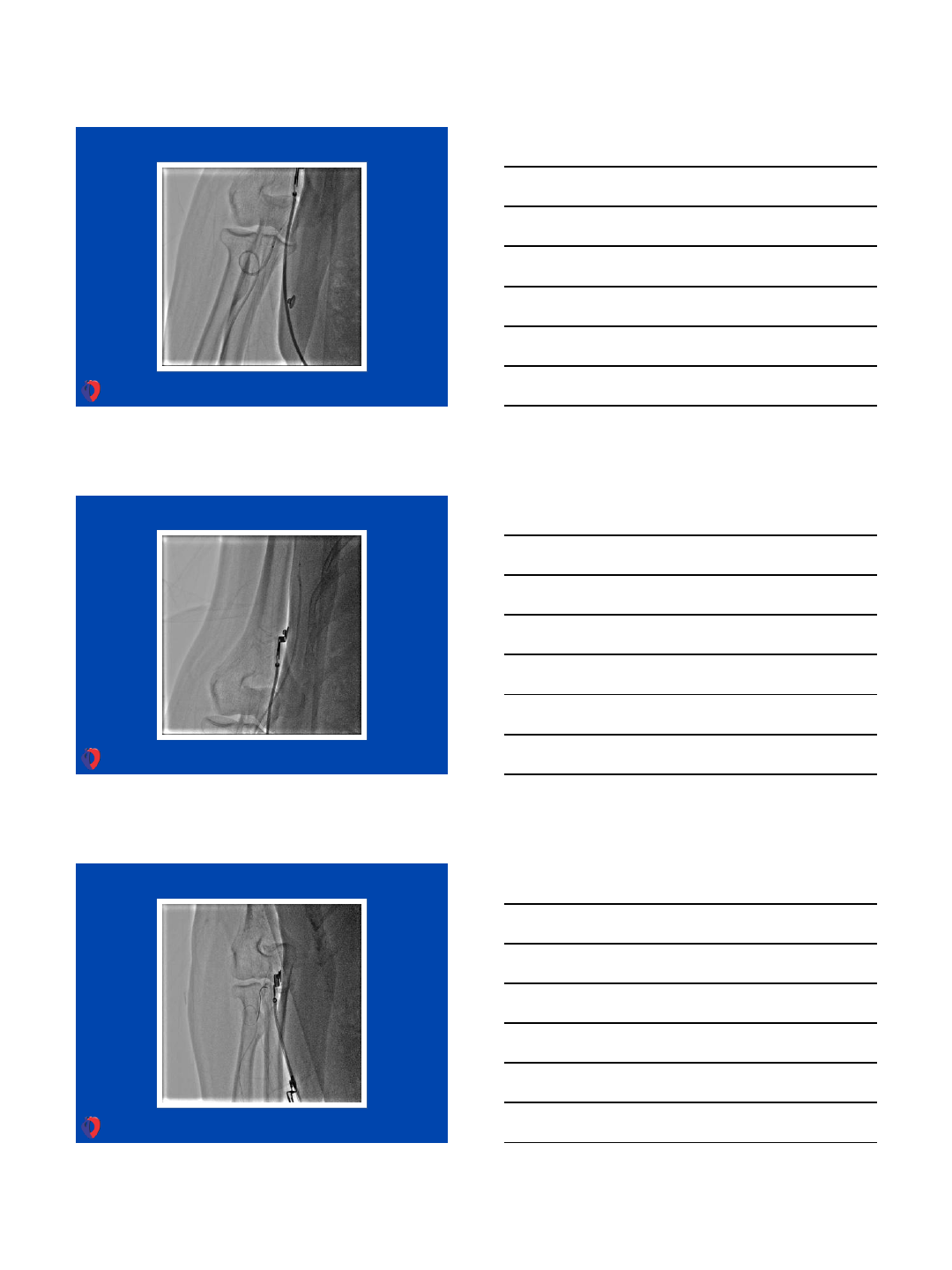
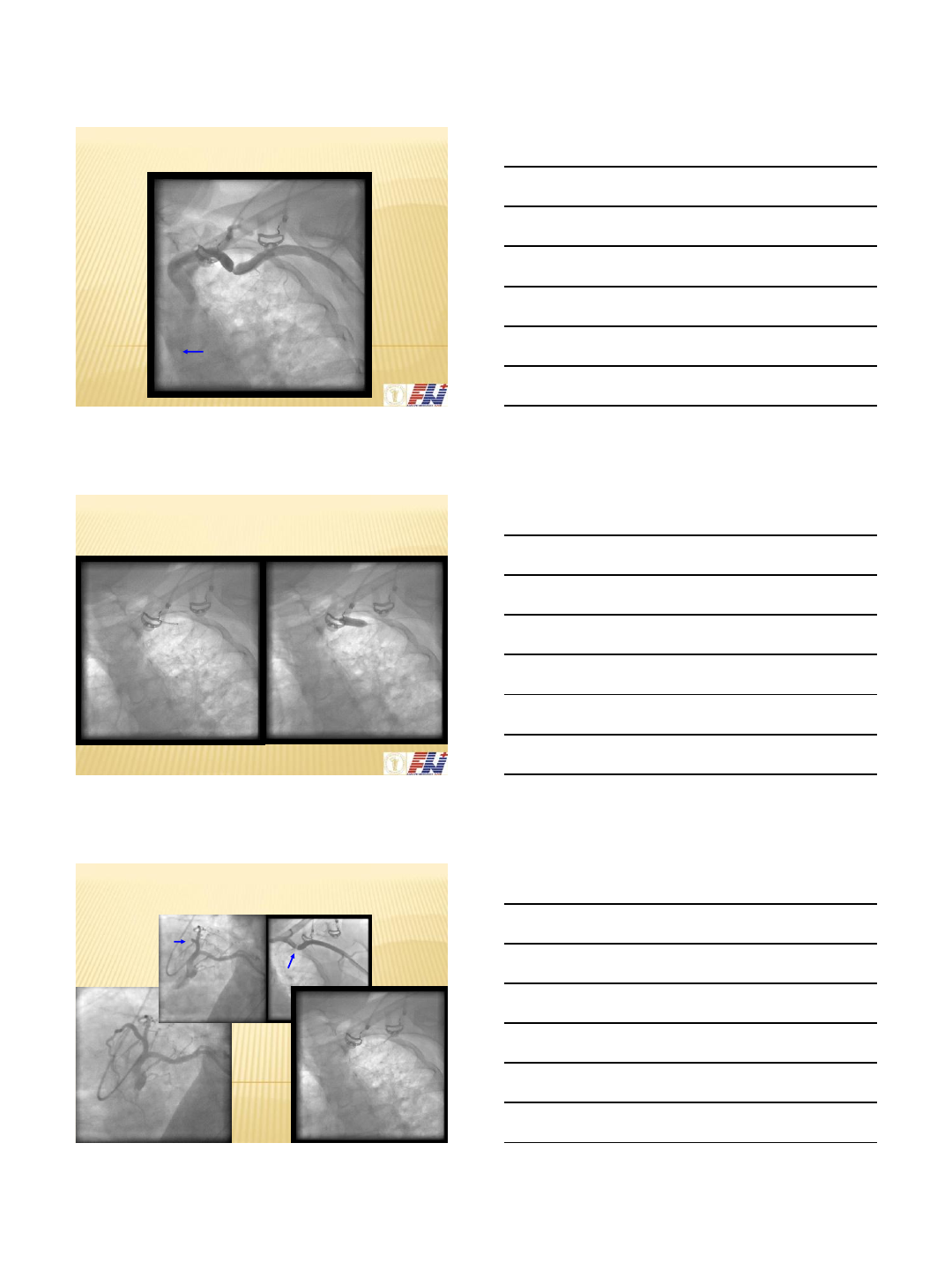
Working through complex tortuosity of RA
6/1/2013
5
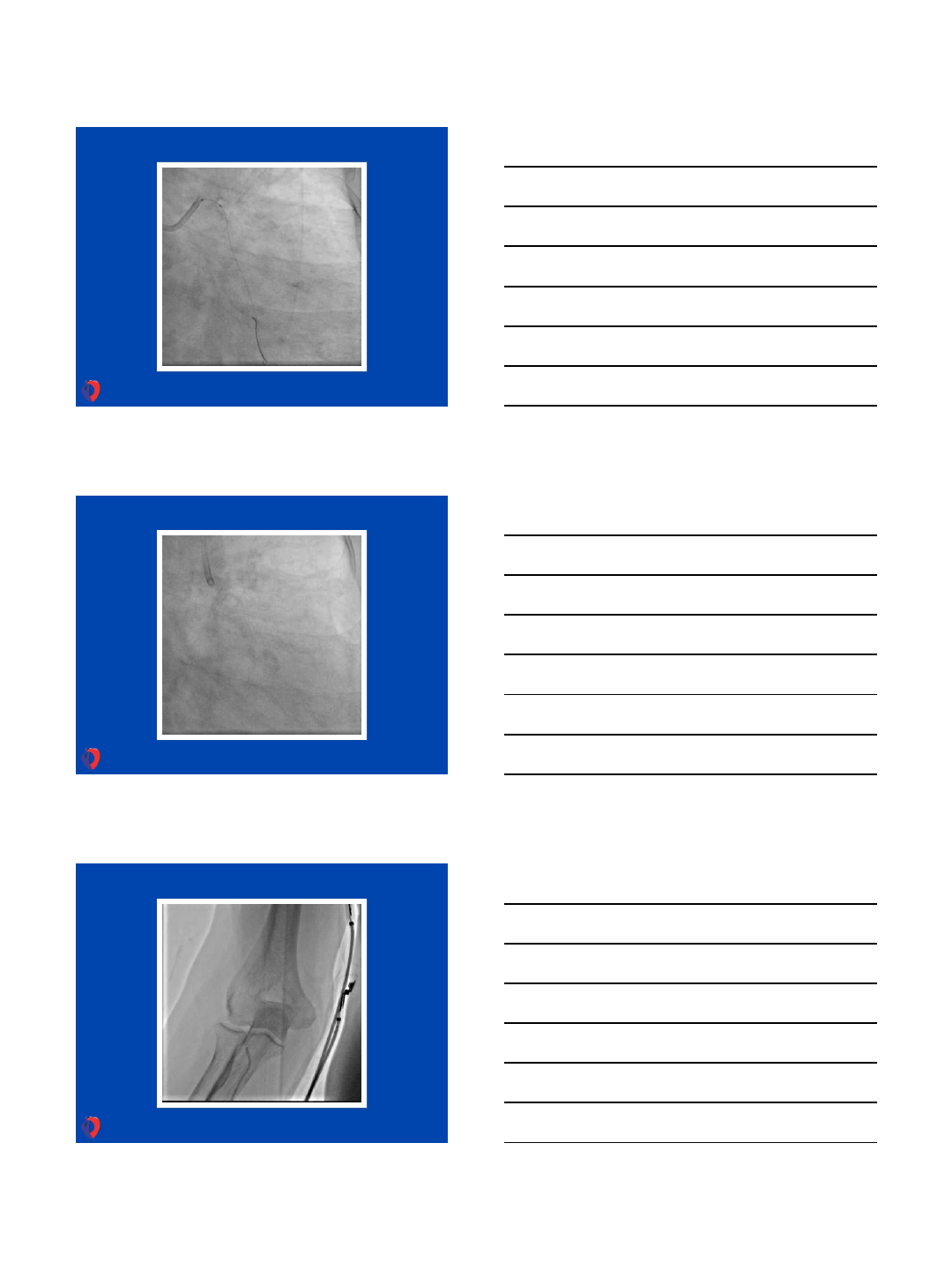
Another Example
6/1/2013
6
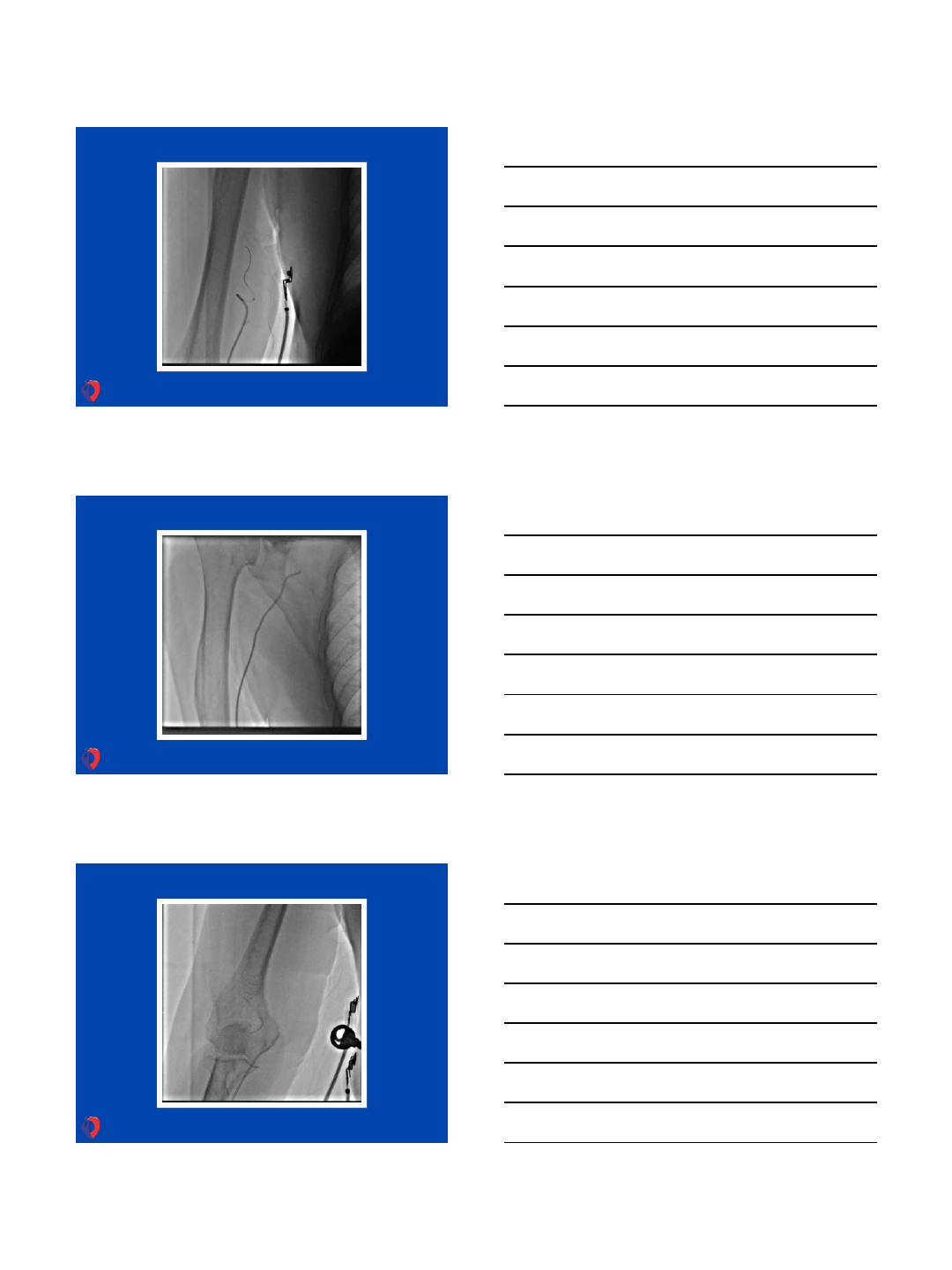
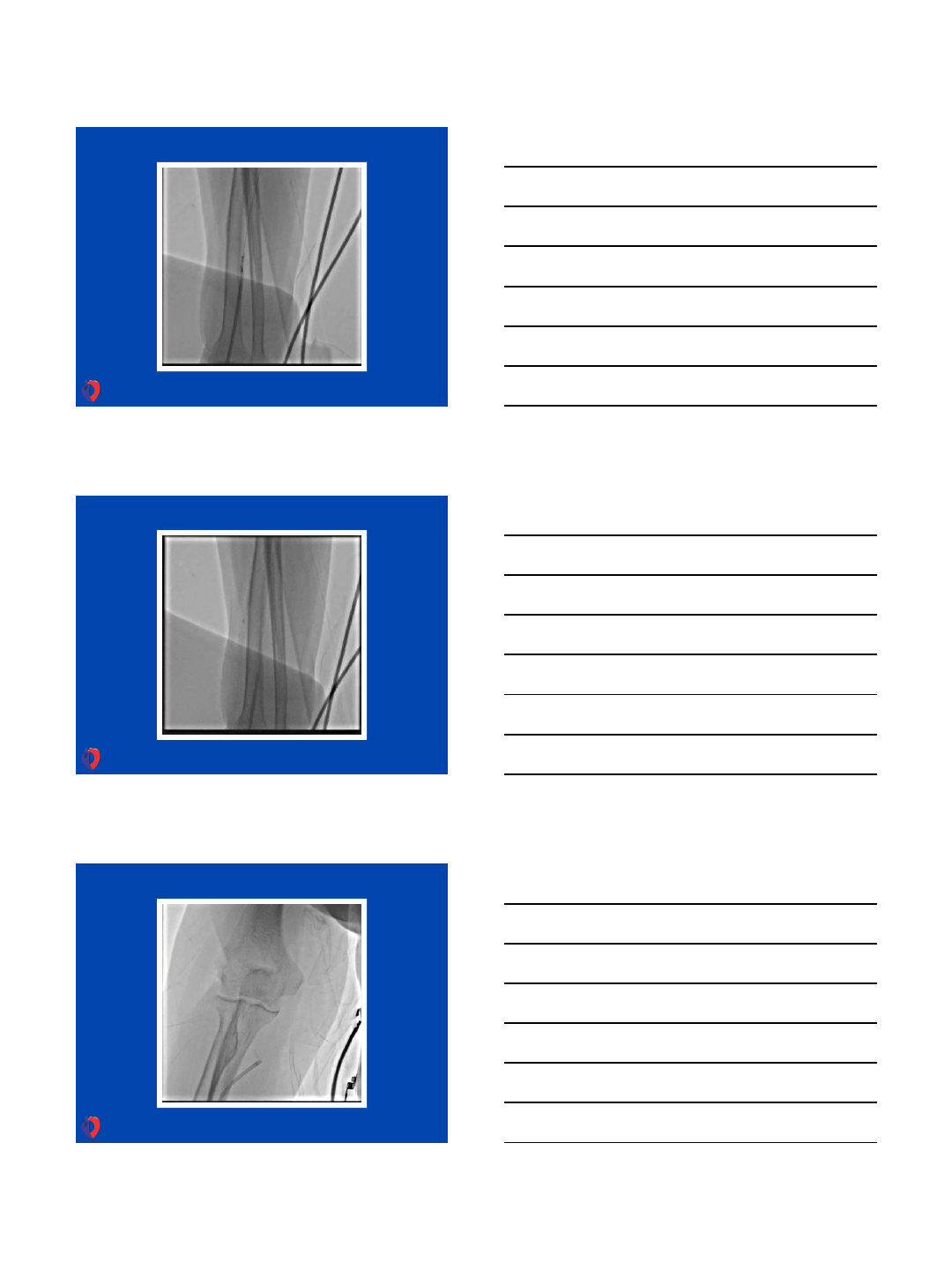
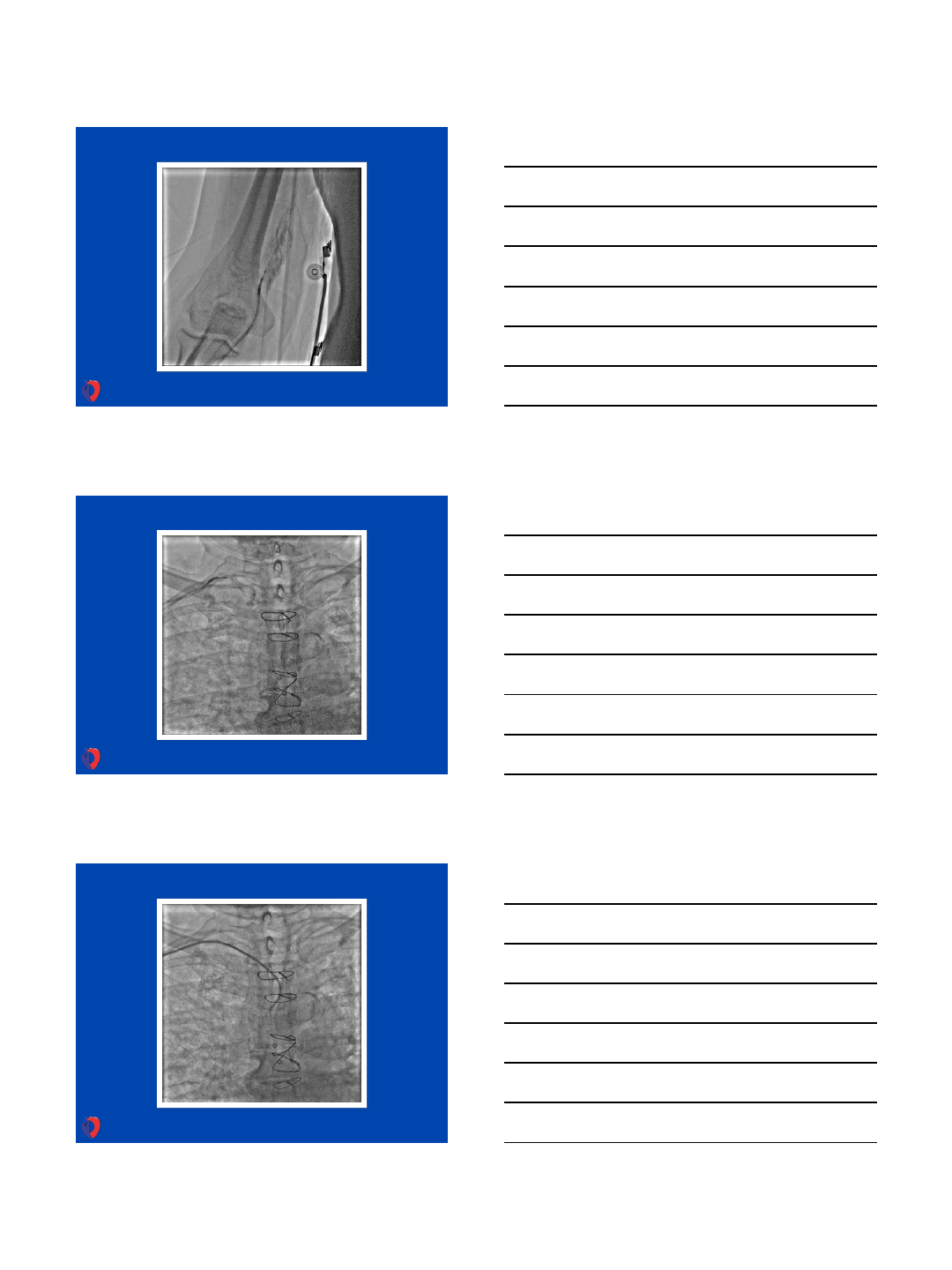
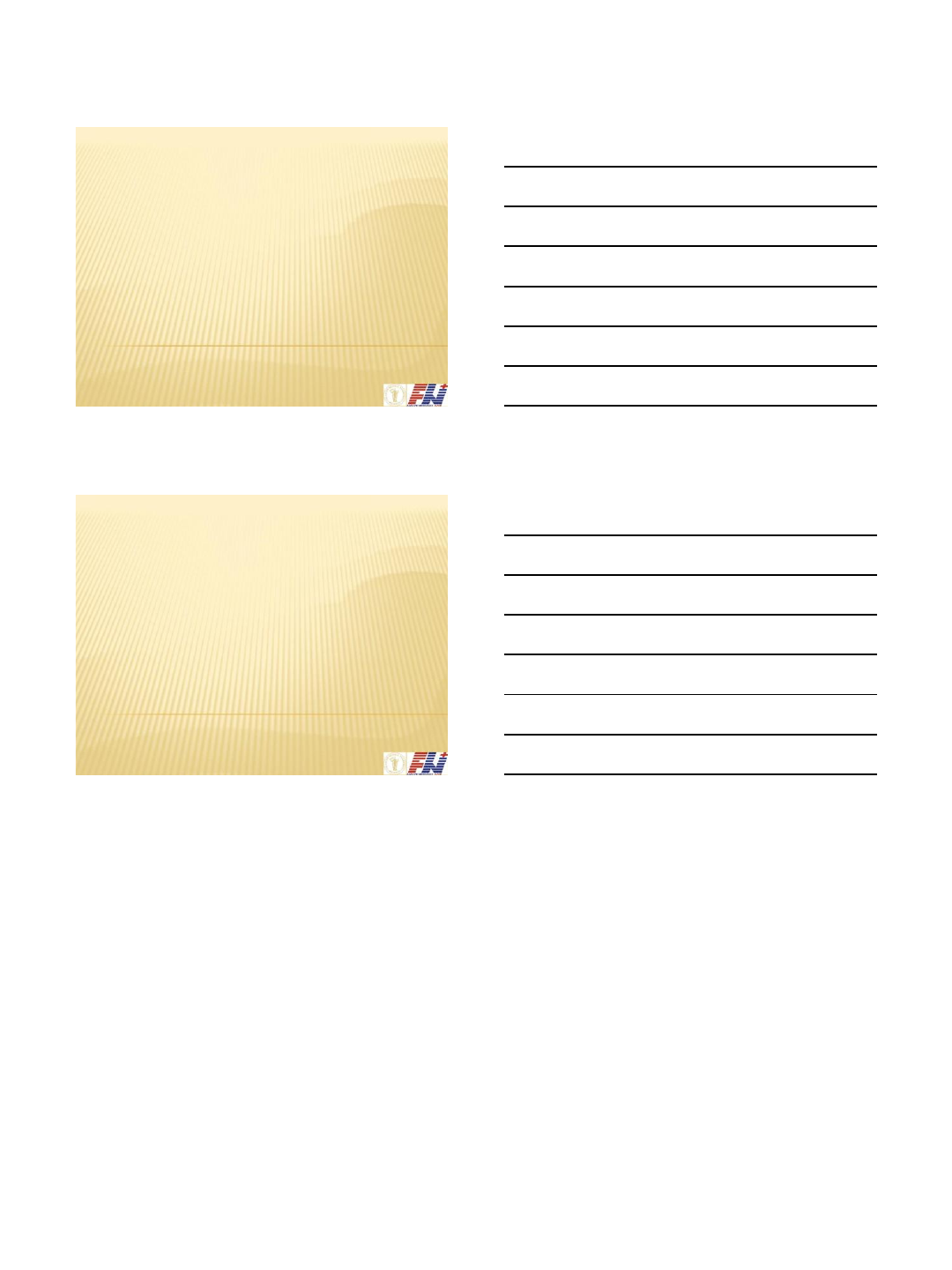
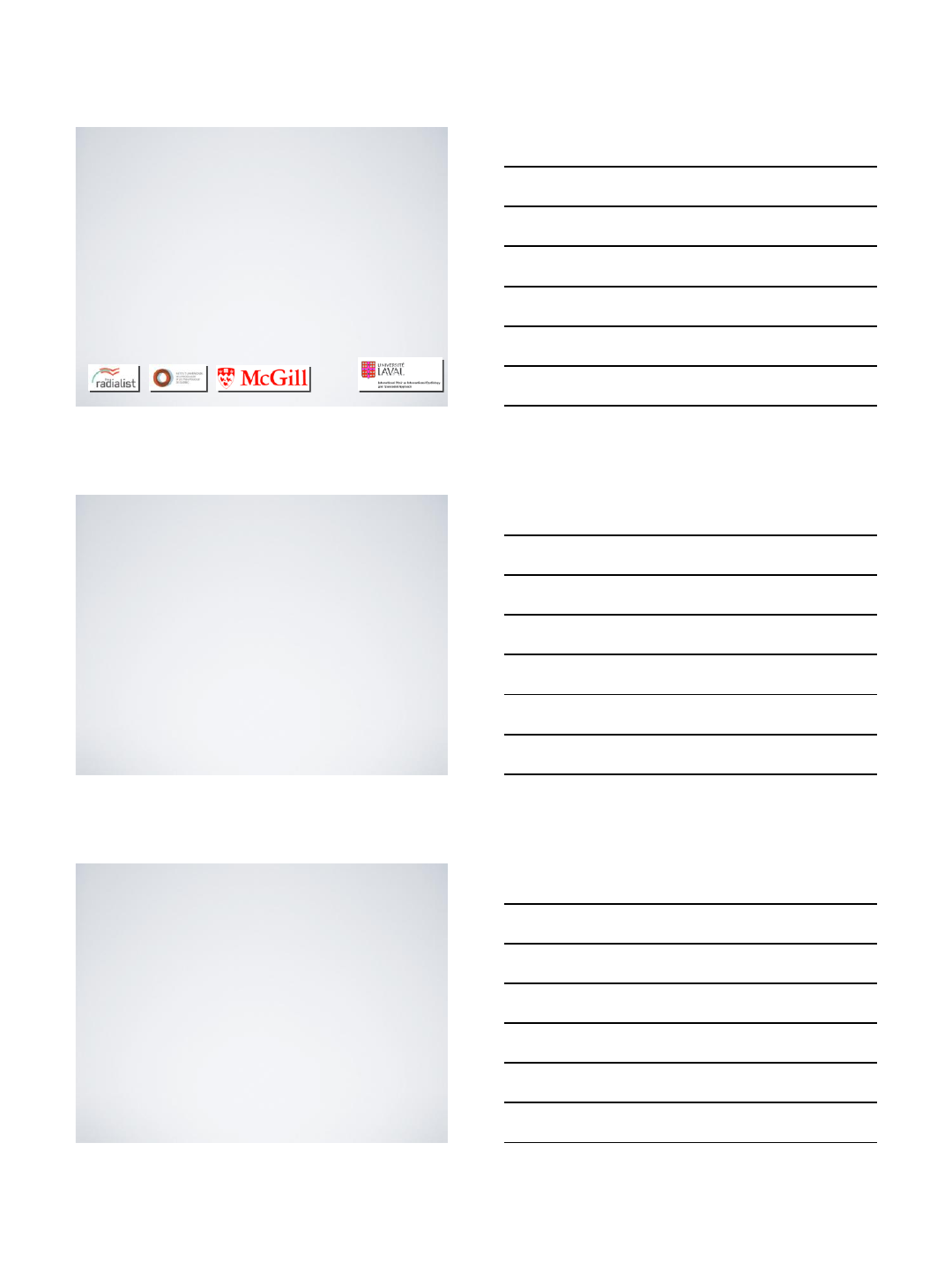
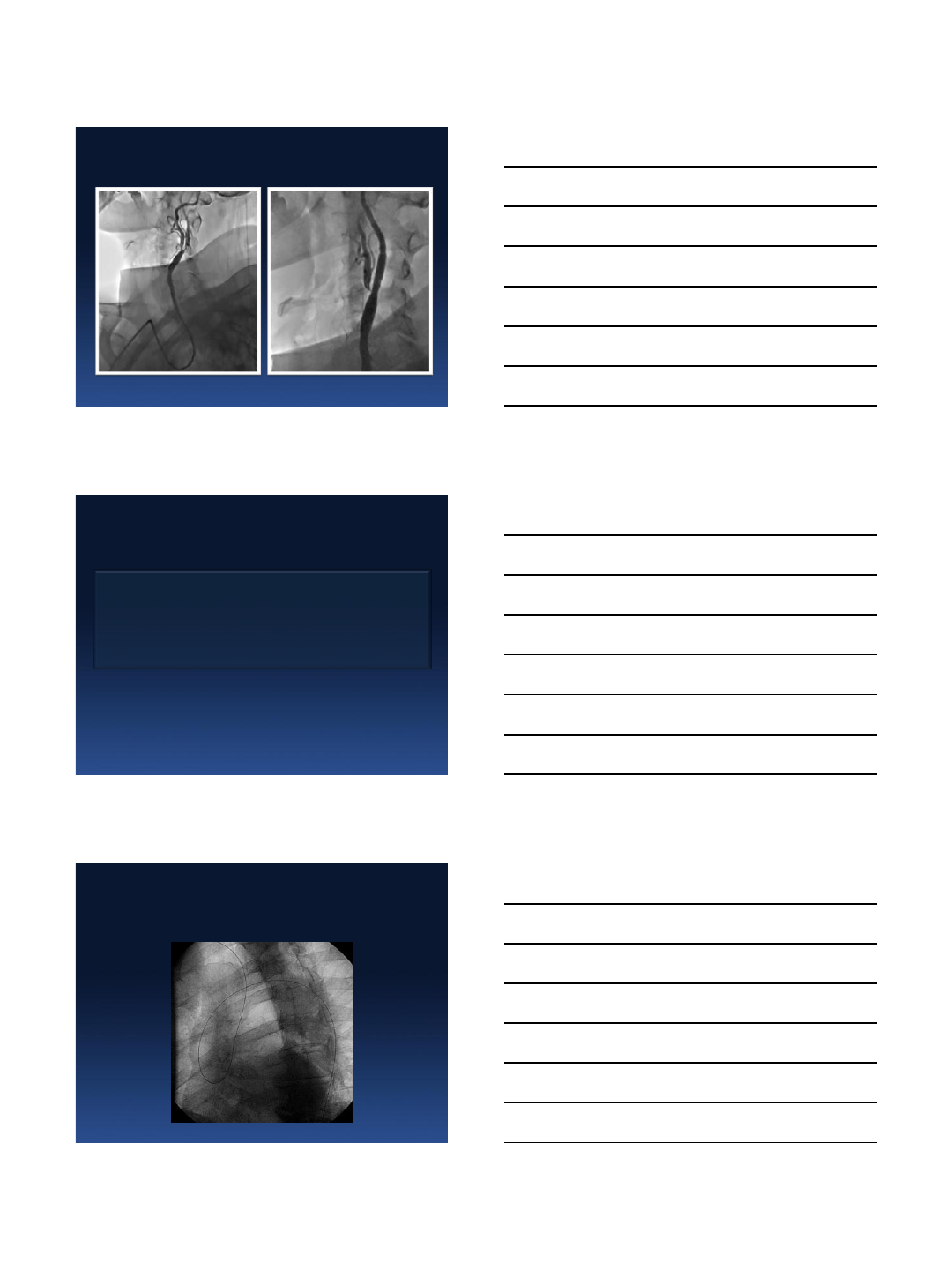
Perforation of RA & Subclavian tortuosity
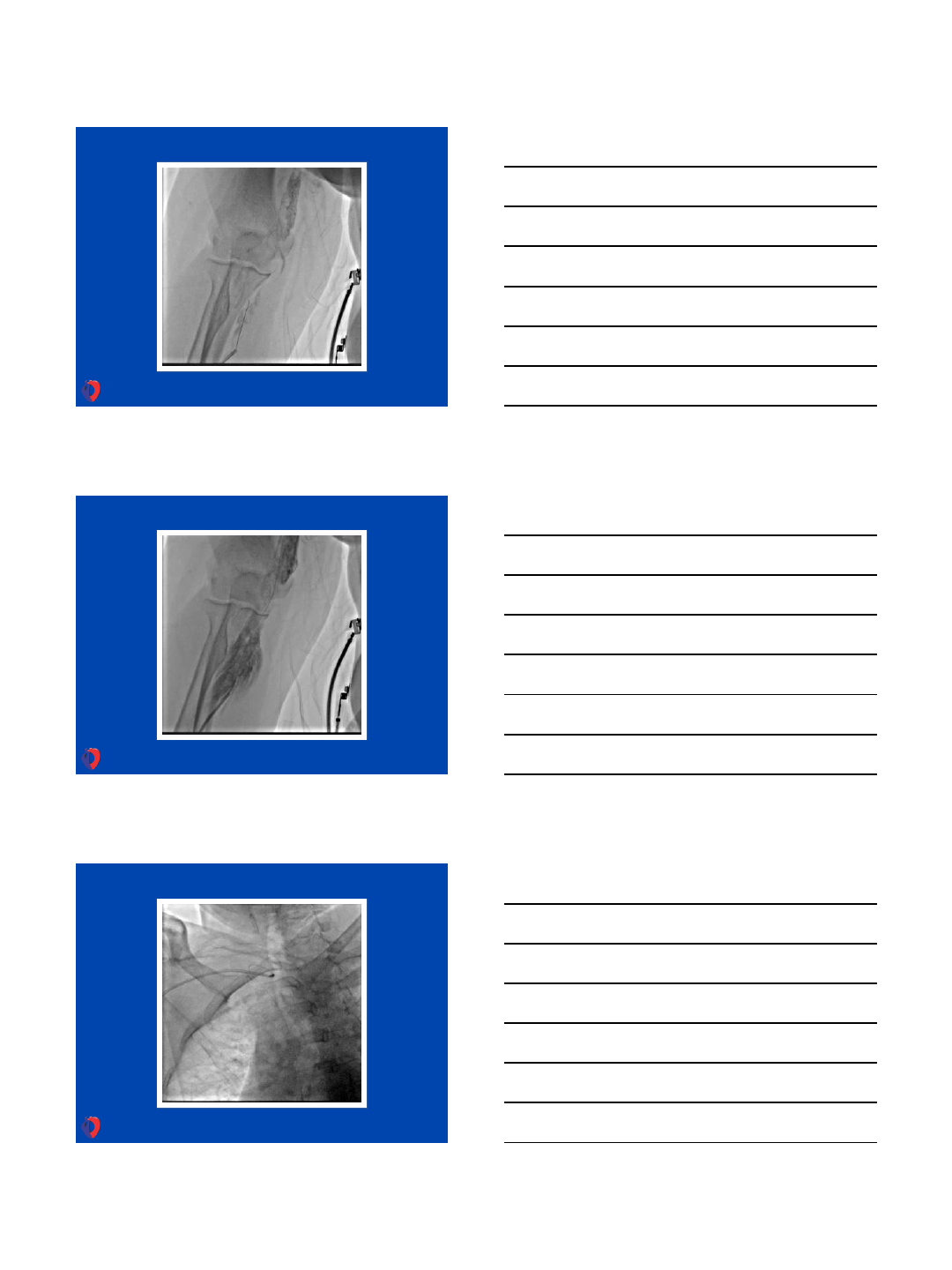
6/1/2013
7
6/1/2013
8
6/1/2013
9
Another Example
6/1/2013
10
6/1/2013
11
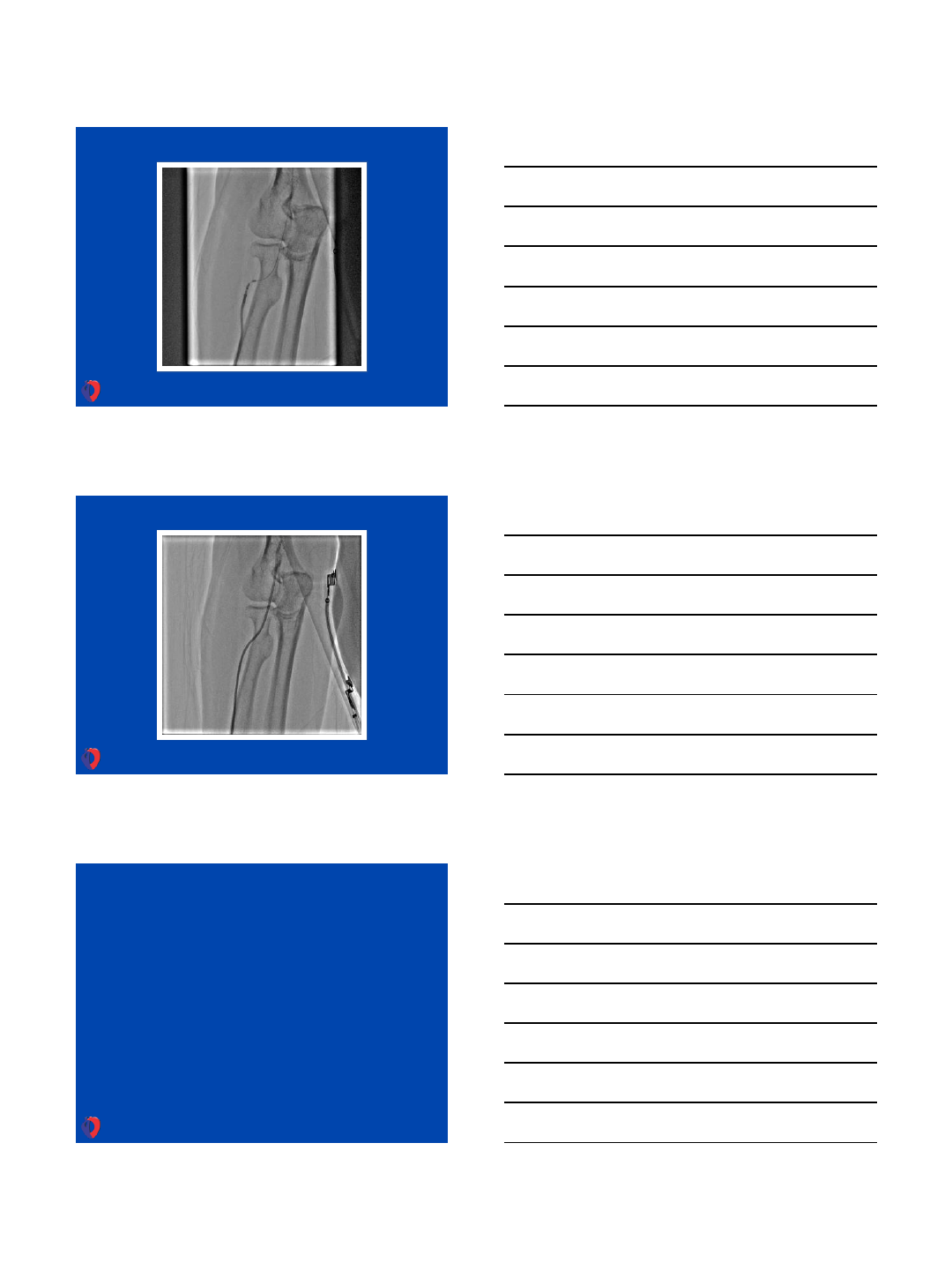
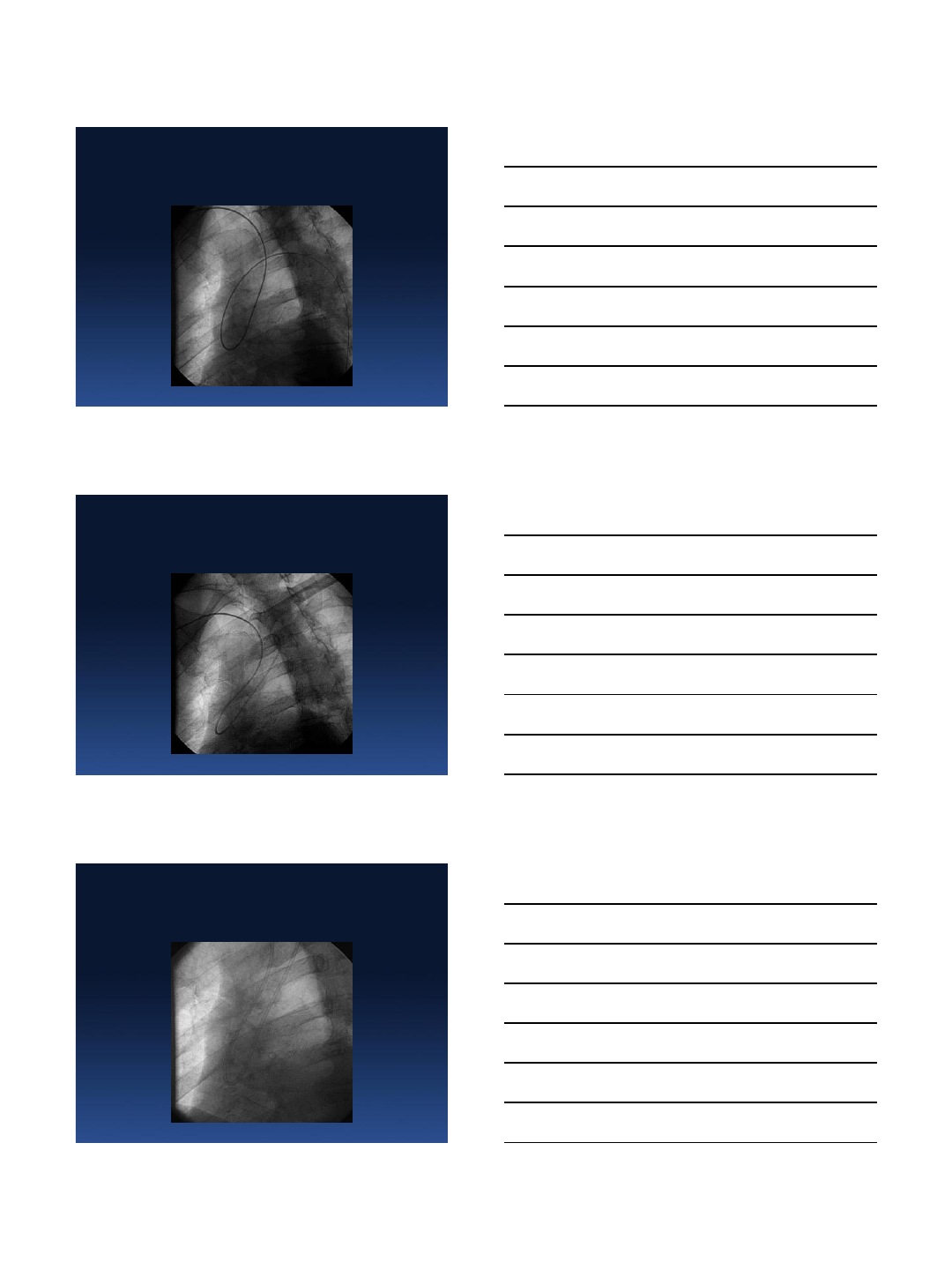
Working through 360 degree loop
6/1/2013
12
Another Example
6/1/2013
13
Thank You
www.transradialworld.com
31.5.2013
1
Radial access for STEMI -
Case
Ivo Bernat MD, Ph.D.
University Hospital and Faculty of Medicine Pilsen, Czech Republic
Disclosure Statement of Financial Interest
I, Ivo Bernat DO NOT have a financial
interest/arrangement or affiliation with one or
more organizations that could be perceived as a
real or apparent conflict of interest in the
context of the subject of this presentation.
Primary PCI in Europe
Widimsky et al. Eur Heart J 2010; 31,943-957
Primary 22
PCI Centers - no thrombolysis in CZ …
31.5.2013
2
All Czech PCI centers (n=22) - 24/7 service for AMI since 2002
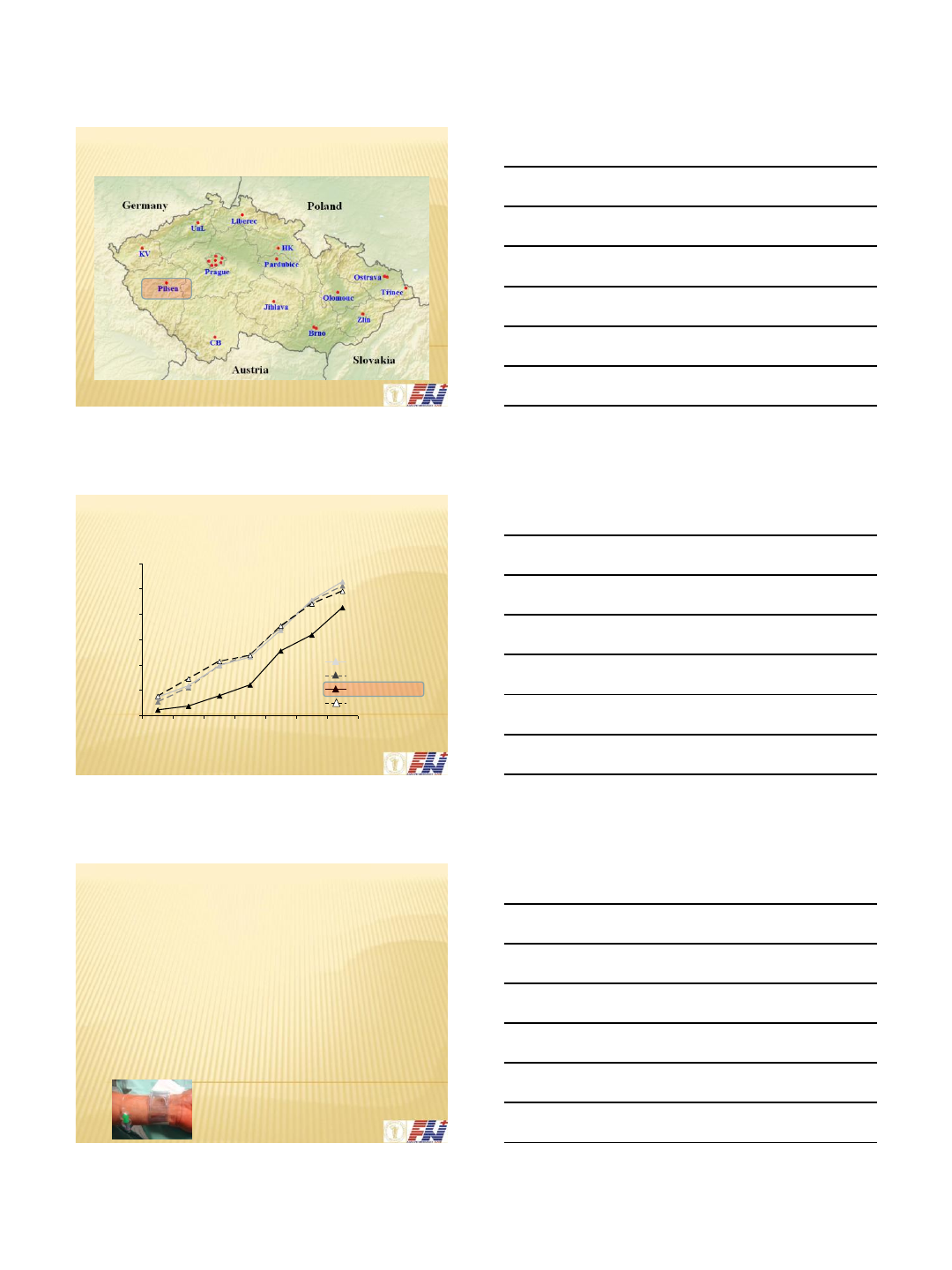
Trend in the use of radial approach in CZ (PCI)
0%
10%
20%
30%
40%
50%
60%
2005
2006
2007
2008
2009
2010
6/2011
ACS –Non-STE
ACS –STEMI
Stable CAD
Others
% of radial approach
Total : 5%......10%....17%.....21%.....32%.....42%....50%...2012 >50%
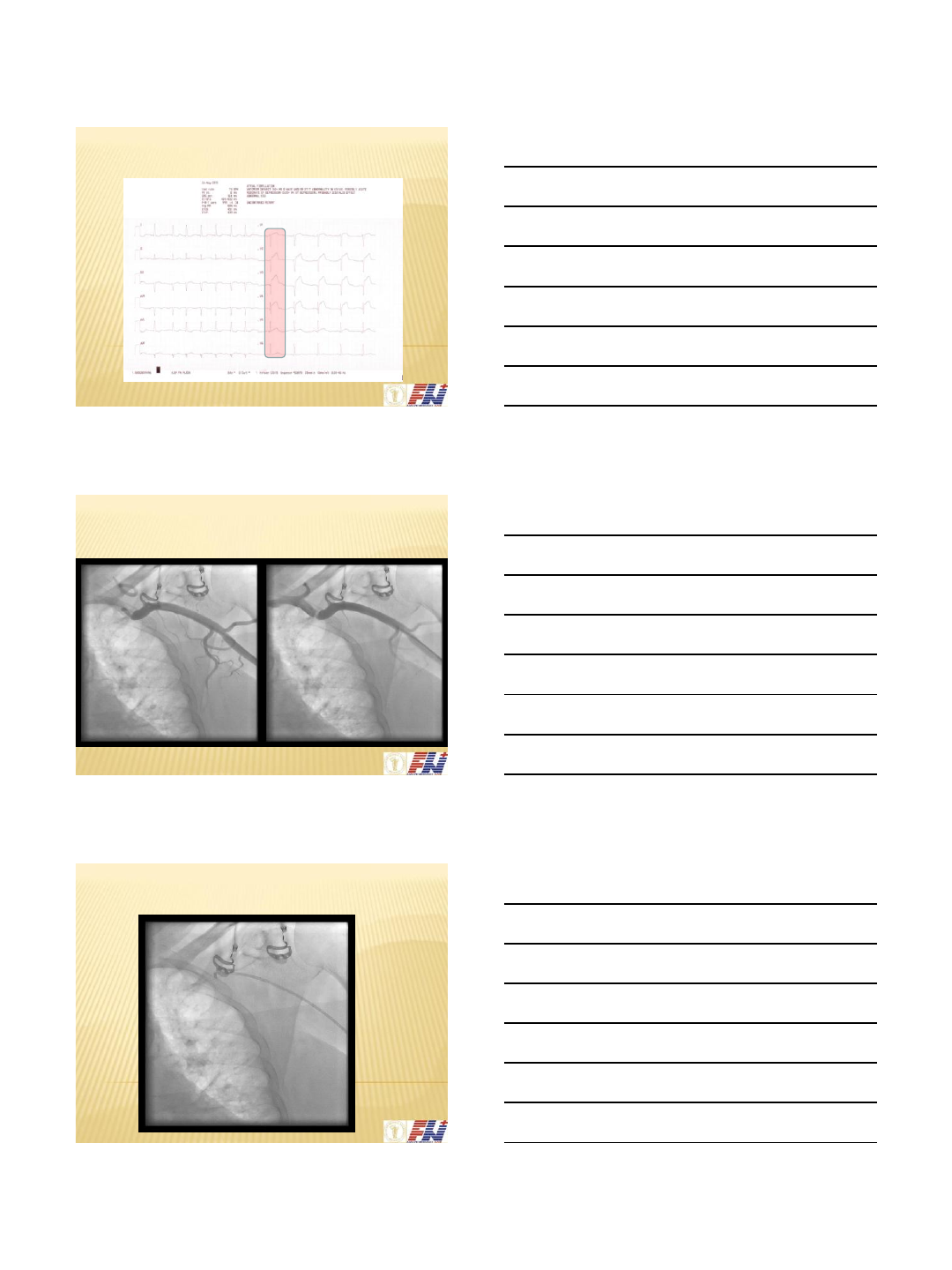
Case from Sunday evening - May 26, 2013
•woman - 76 y.
•treated hypertension - betabl. + ACEI
•2 hours of chest pain
•anterior STEMI
•EMS: UFH 5000 IU i.v., clopidogrel 600 mg p.o., Aspegic
250 mg i.v.
•direct transport to our cathlab
•Our PCI center : 95% TRA incl. STEMI - 90% from the left
31.5.2013
3
ECG before pPCI
Left radial approach - 80% AS l.sin. stenosis
Question - go on from the left ?
31.5.2013
4
Angled hydrophilic wire 0.035 ….
CAG with 5F dg. Tiger catheter
Next step - 5F guiding XB 3,5, bolus GPI, coronary wire…
31.5.2013
5
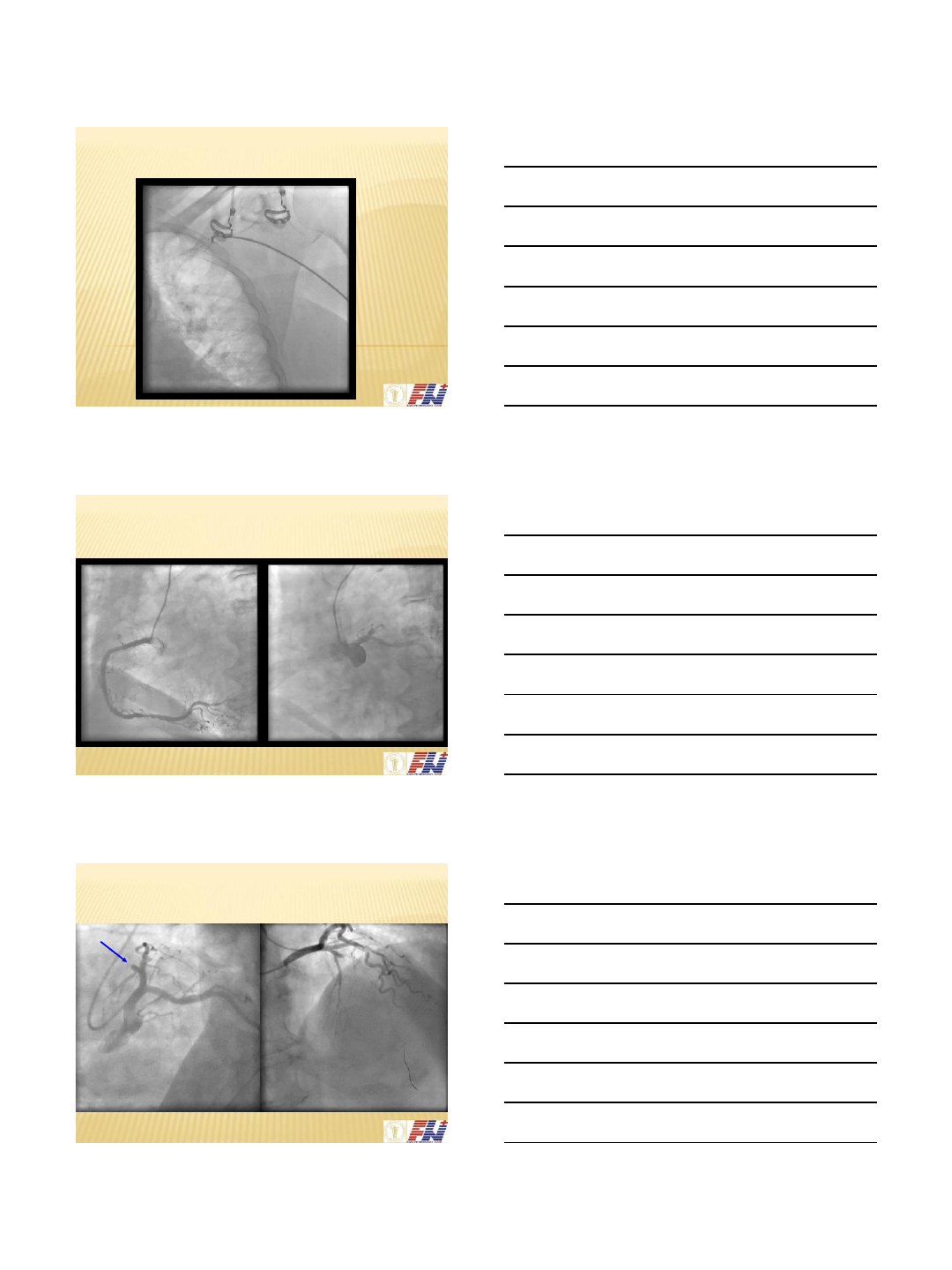
… minimal predilatation (2,0/20mm with 4atm)
DES 3.0/16 implantation - 18 atm
After primary PCI …
31.5.2013
6
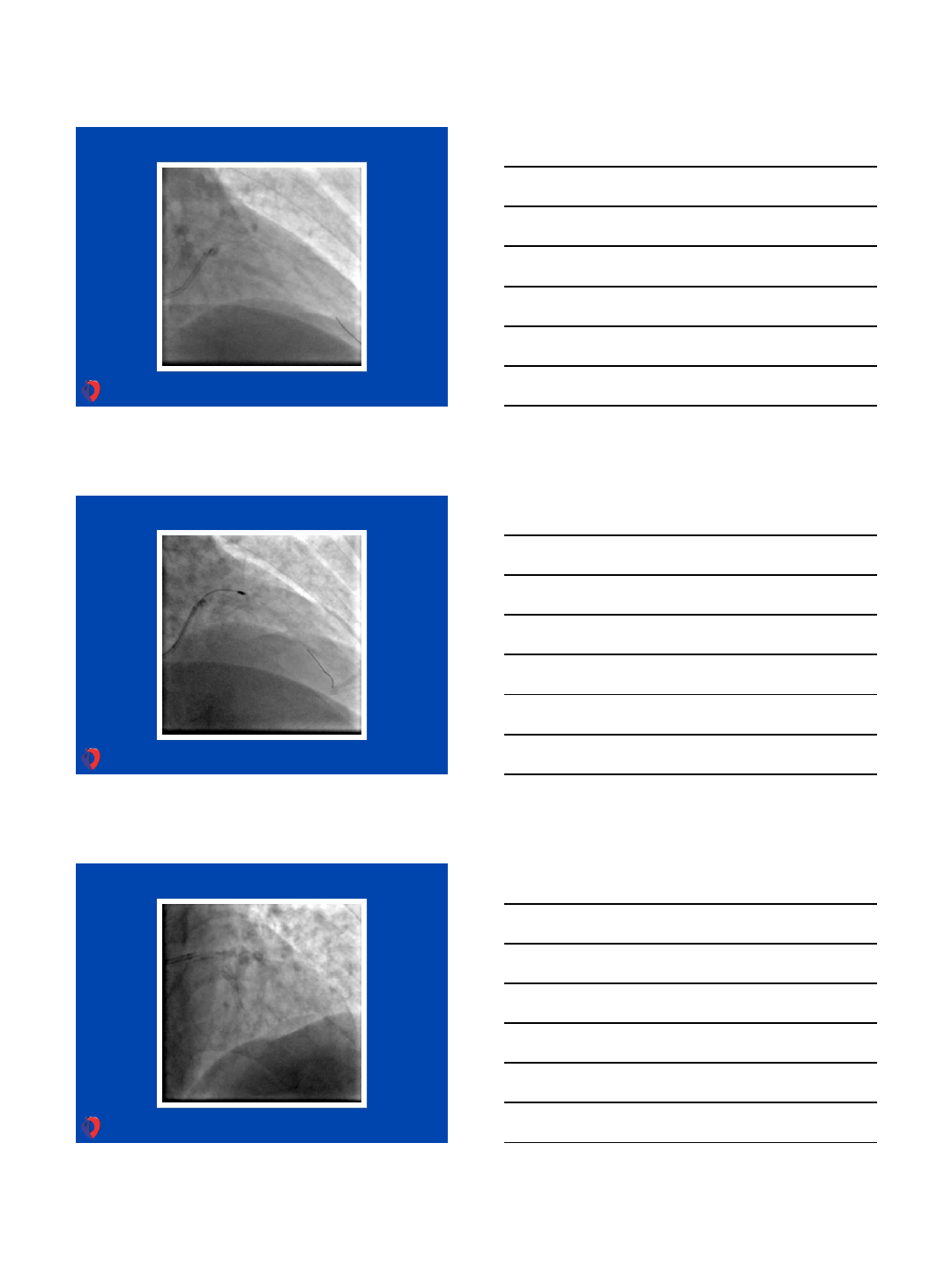
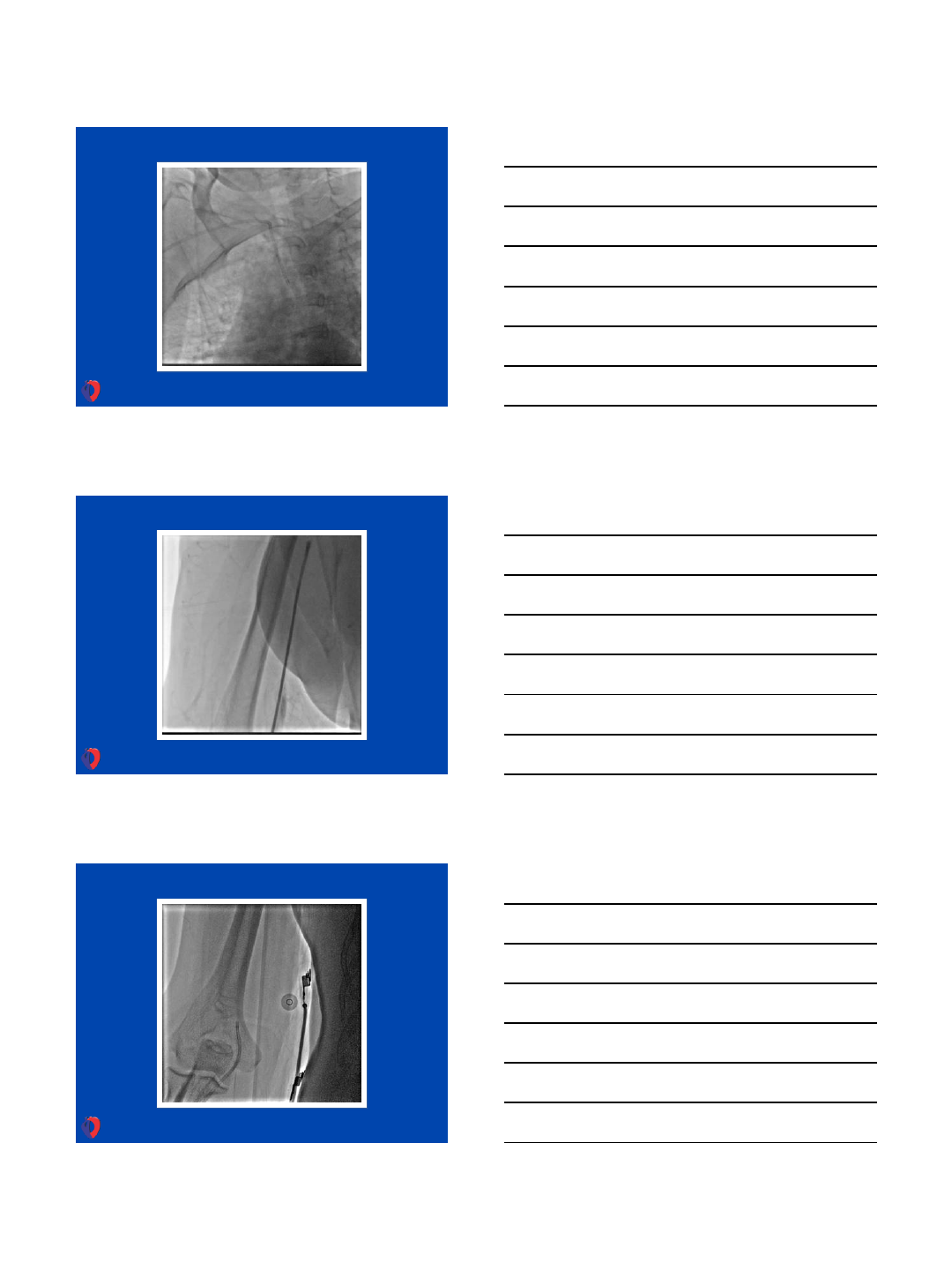
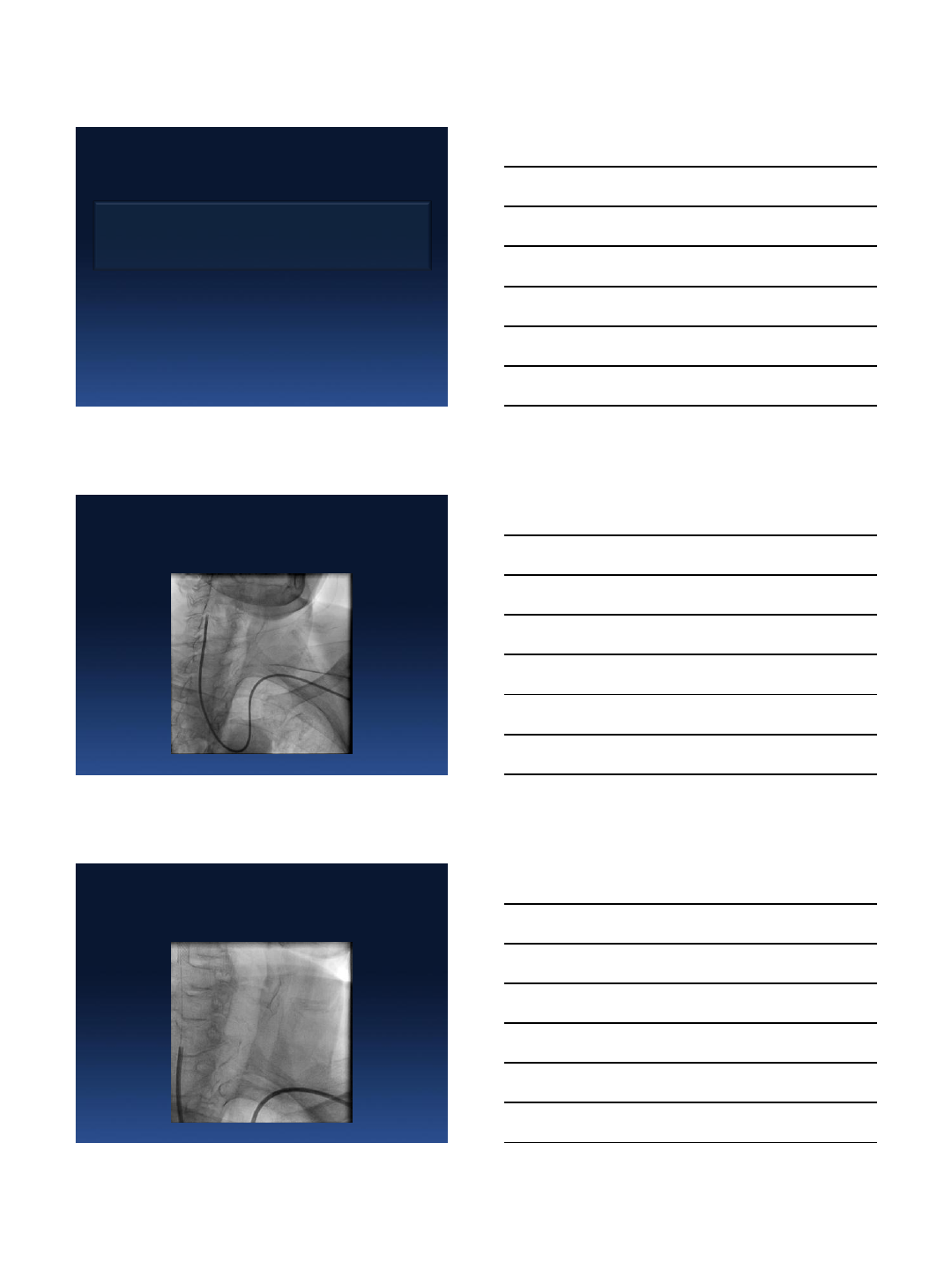
Next step - tight subclavian stenosis - to treat or not to treat
…..???
Stent 6,0/14mm (18 atm = 6,99mm) without
guiding catheter …
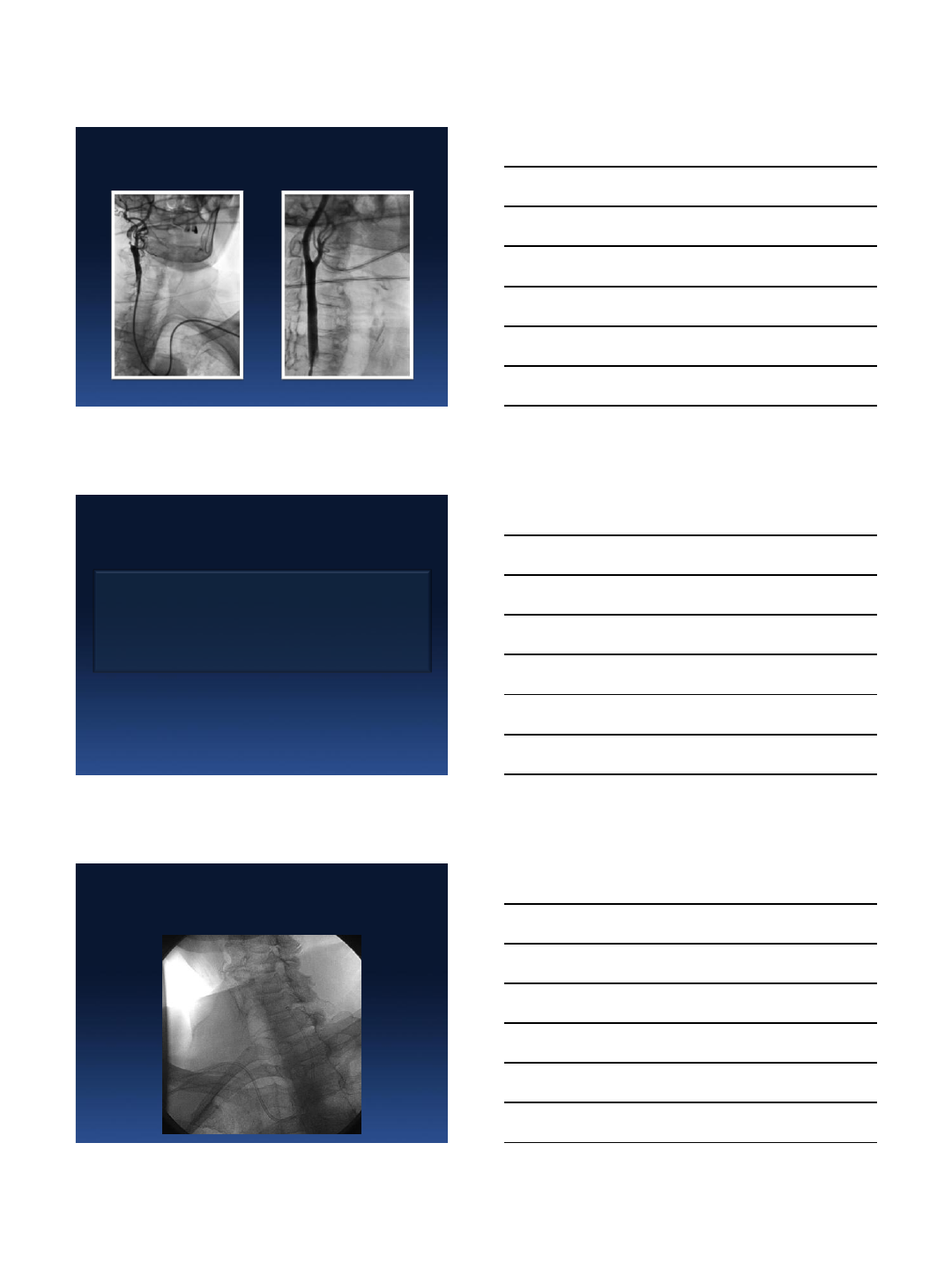
Final result of pPCI and subclavian stenting
31.5.2013
7
After primary PCI and subclavian stenting
(contrast 150 ml, skia 9.8 min)
•radial artery compression time - 100 min
•complications - 0
•echo next day - LVEF 45%
•ICU stay - 32 hours (Sunday midnight - Tuesday morning)
Conclusion
•Transradial primary PCI (in experience radial center) is the best way how to :
•- minimize local bleeding
•- increase patient comfort with soon mobilisation and earlier discharge
•- reduce the cost
•- also reduce mortality
Additional non coronary intervention in our case was safe and easy.
6/2/2013
1
Complex transradial LEFT MAIN PCI in
CARDiogenic shock
QuickTime™ and a
YUV420 codec decompres sor
are needed to see this picture.
Olivier F. Bertrand, MD, PhD
Associate-Professor of Medicine, Laval University
Adjunct-Professor, Department of Mechanical Engineering,
McGill University
International Chair on Interventional
Cardiology and Transradial Approach
Quebec Heart-Lung Institute
VuMedi-June 3, 2013
Disclosures
•Consultant: OPSENS
Case Scenario
•57 y old man, crushing chest pain while working on his
roof
•RF: Smoker
•ECG in ambulance: Antero-Lateral STEMI
•VF 2 episodes during transfert. Cardiogenic shock
upon arrival in cath lab
6/2/2013
2
QuickTime™ and a
decompressor
are needed to see this picture.
QuickTime™ and a
decompressor
are needed to see this picture.
6/2/2013
3
QuickTime™ and a
decompressor
are needed to see this picture.
QuickTime™ and a
decompressor
are needed to see this picture.
Key points
•Radial access permits complex LM PCI
•Having the groins prep during cardiogenic shock allows
quick access for LV support (BIA, ECMO, LVAD,
Impella) and PCMK
•Biggest challenge remains to get the radial access
when faint/no pulse. Role for ultrasound guidance ?
01.06.2013
1
Sasko Kedev MD, PhD, FESC, FACC
University Clinic of Cardiology
Skopje, Macedonia
skedev@gmail.com
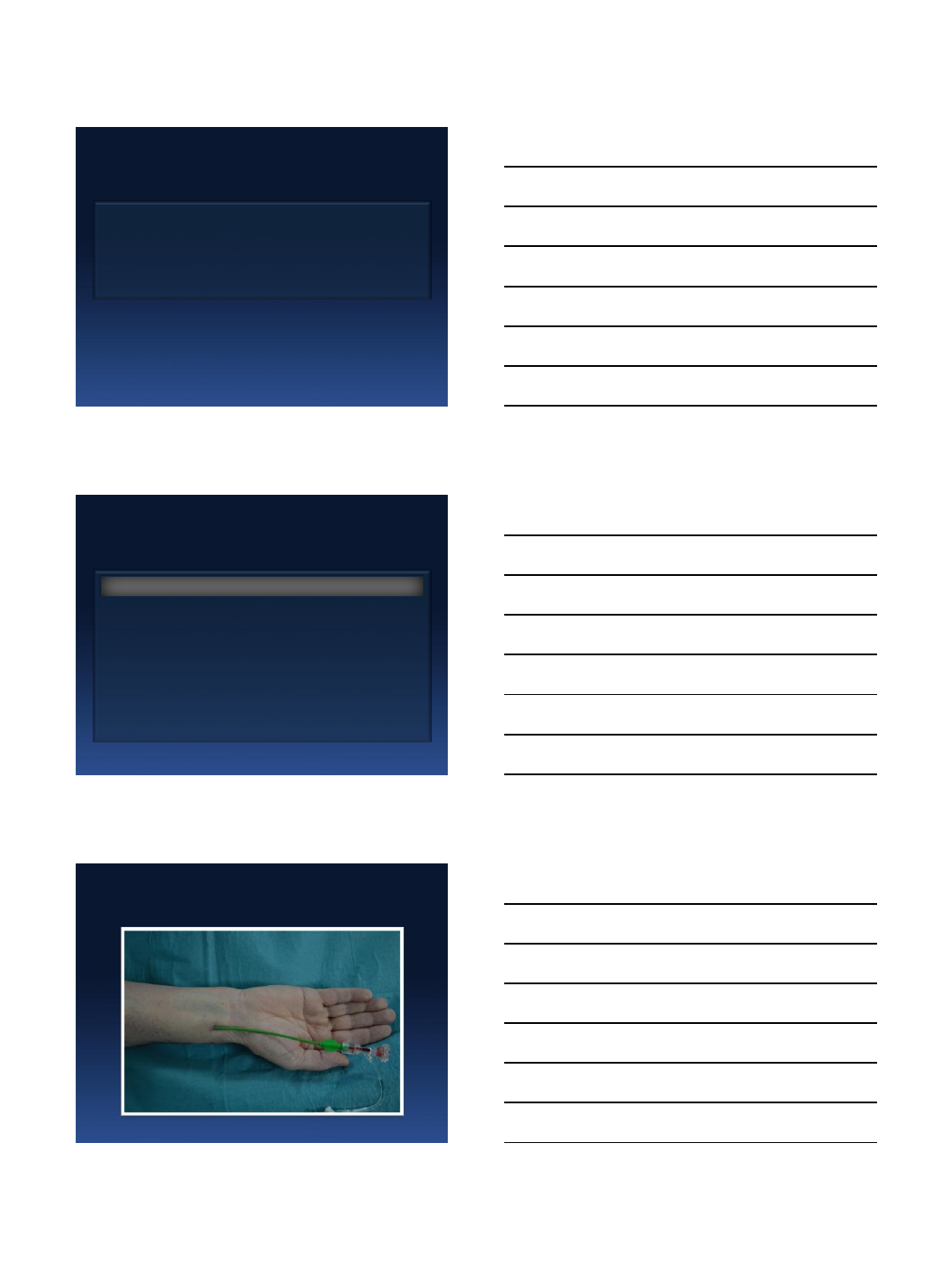
Radial Access for
Carotid Interventions
DISCLOSURE
Nothing to disclose
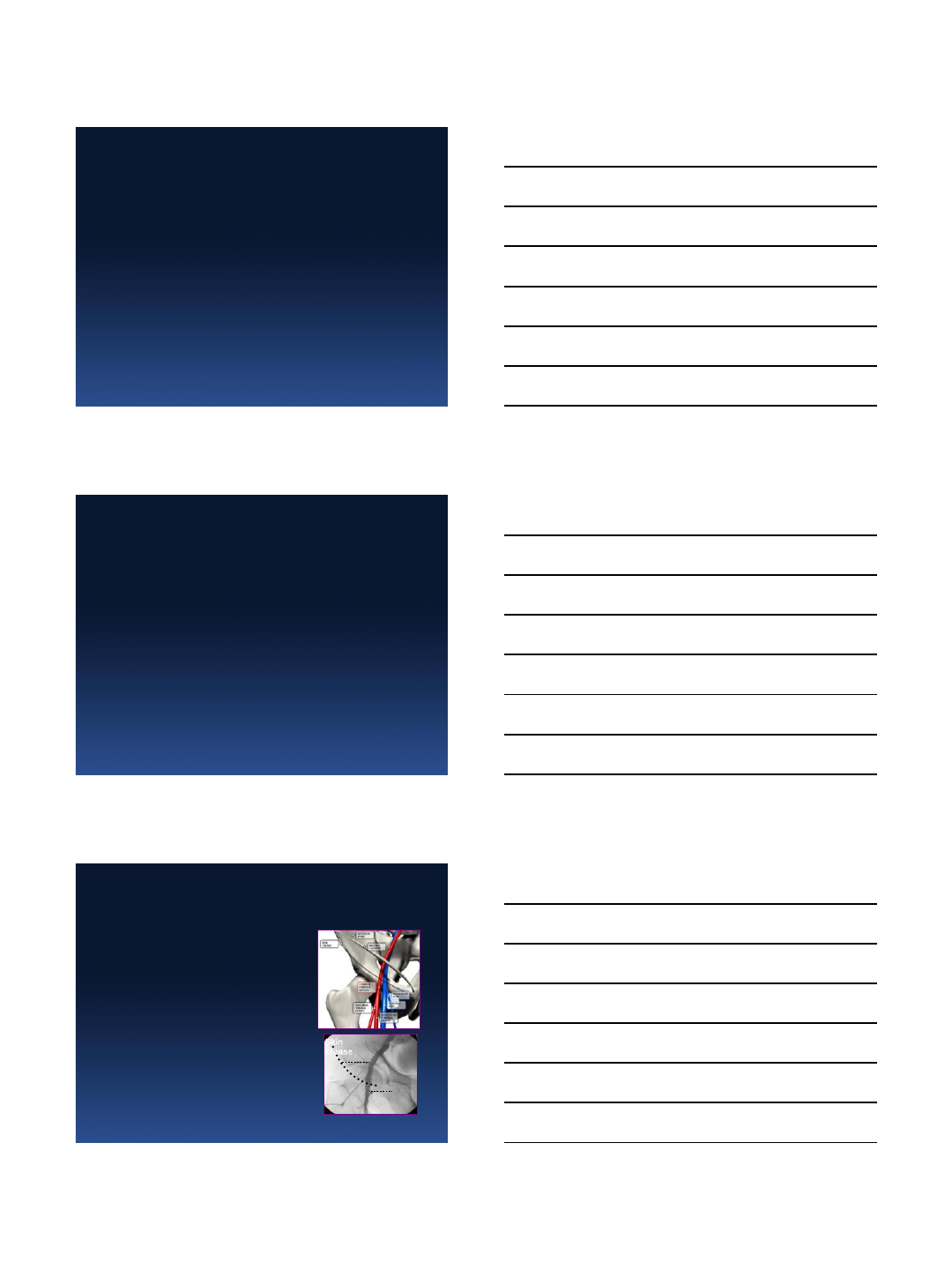
Skin
crease
CFA
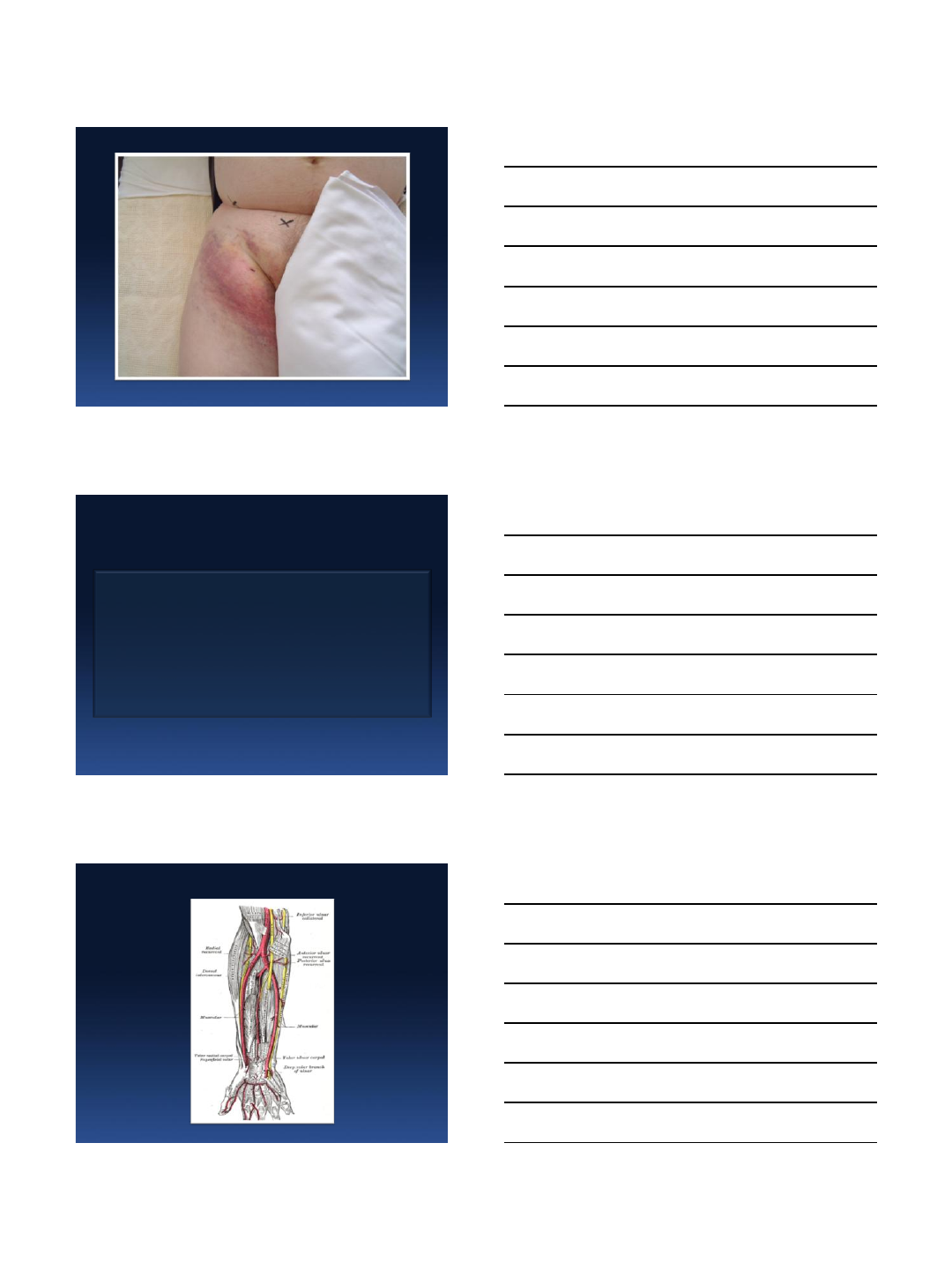
Potential Vascular Complication
Femoral Approach
Hematoma-bleeding
Pseudoaneurysm
RetroPeritoneal Hemorrhage
AV fistula
Ischemia-Thrombosis-Emboli
Infection
Neuropathy
01.06.2013
2
ACCESS SITE COMPLICATIONS
Vascular access is 1st reason of bleeding
complications & MACE after PCI
BLEEDING INCREASES MORTALITY ! ! !
Radial Artery Access
01.06.2013
3
FEMORAL APPROACH LIMITATIONS
for CAS
Aorto-iliac disease or occlusion
Previous surgical bypass at this level
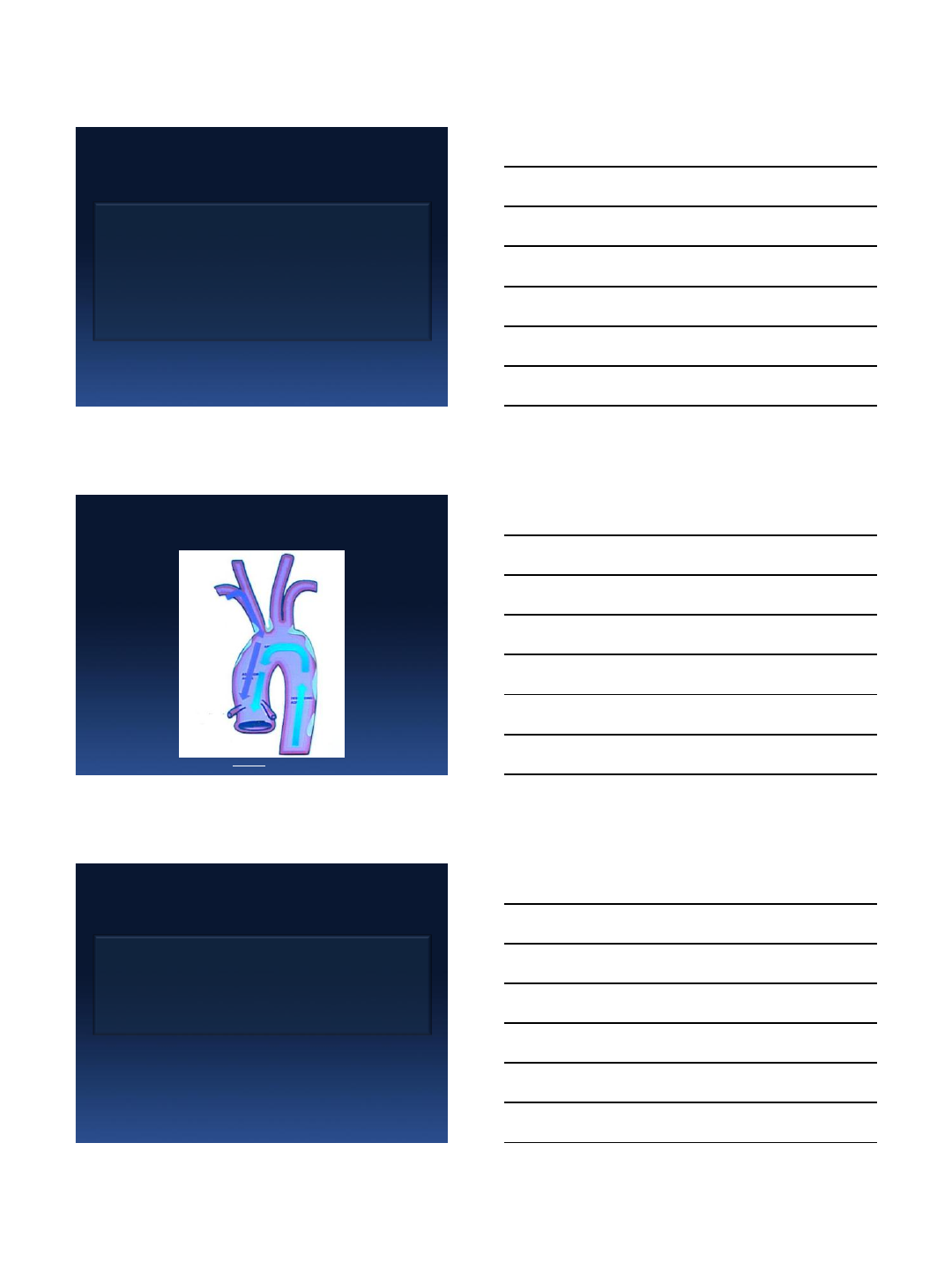
Diseased and Complex aortic arch with
Tortuous SAA originating from elongated,
or type II, III, or bovine aortic arch
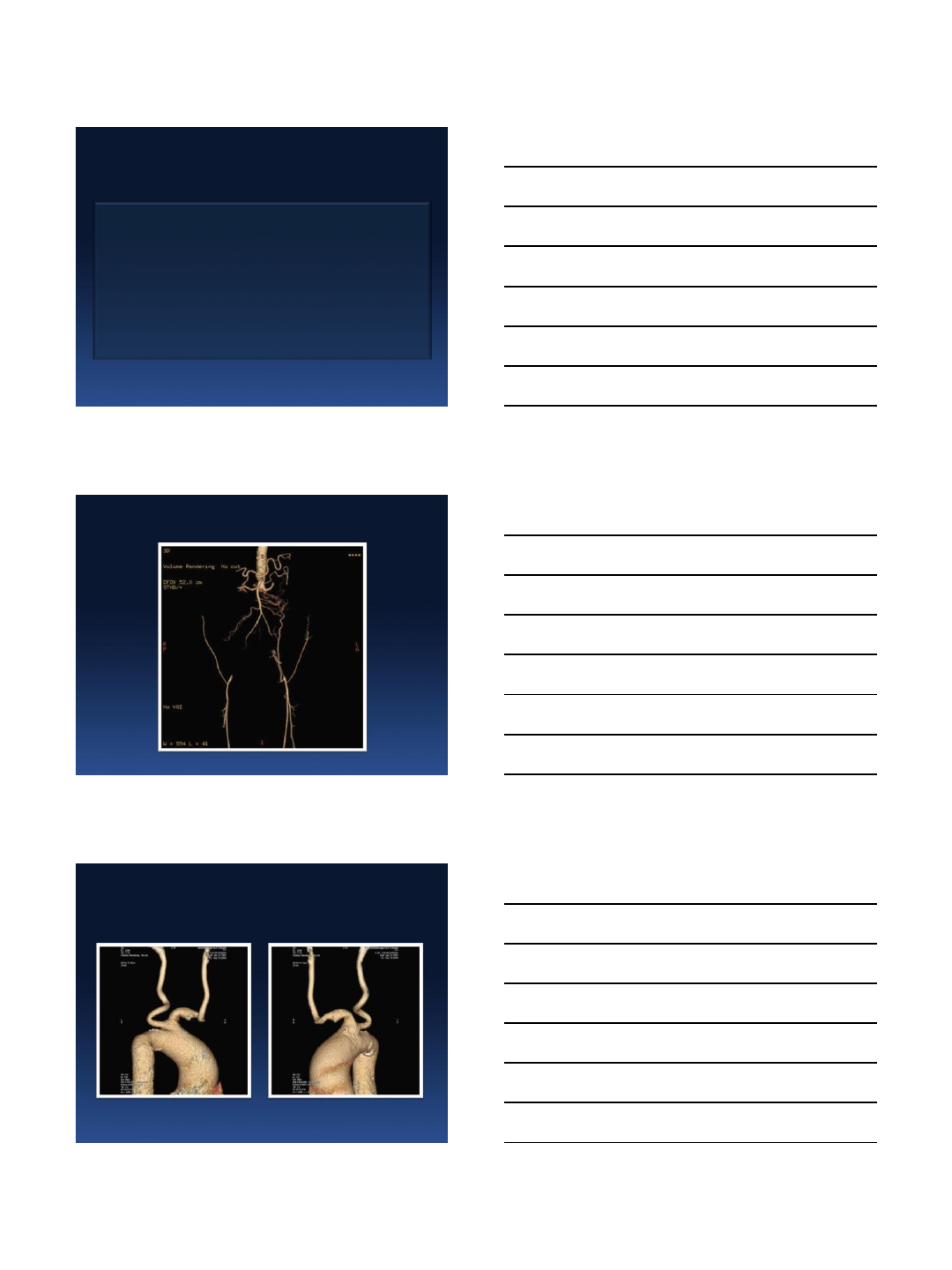
Aorto-iliac Disease or Occlusion
Tortuous SAA Originating from Elongated or
Bovine Aortic Arch
01.06.2013
4
ACCESS SITE COMPLICATIONS
The most common adverse event after CAS
from the femoral approach
MOST TECHNICAL FAILURES ARE
RELATED TO A COMPLEX ARCH
Risk of catheter-related emboli in patients with
atherosclerotic debris in the thoracic aorta
Karalis DG et al. Am Heart J. 1996 Jun;131(6):1149-55.
Brachial
Radial / Ulnar
Direct puncture
Alternatives to FA
01.06.2013
5
Radial Access - Alternatives
Right Radial Artery is
1st choice !
Right Ulnar Artery
Left Radial Artery
Left Ulnar Artery
TRANSRADIAL CAS
Patient comfort and satisfaction
Reduced nursing cost
Reduced vagal reaction
Reduced hypotensive response
Reduced bleeding complications
IMPORTANCE OF EARLY AMBULATION
01.06.2013
6
TRANSRADIAL CAS
Anchoring technique
Telescopic approach
TRANSRADIAL CAS
SIM 1-3 in CCA
Long hydrophilic GW in ECA
Exchange with transfer catheter
Exchange with extra stiff GW in ECA
Advance 6F GS in CCA
Anchoring Technique
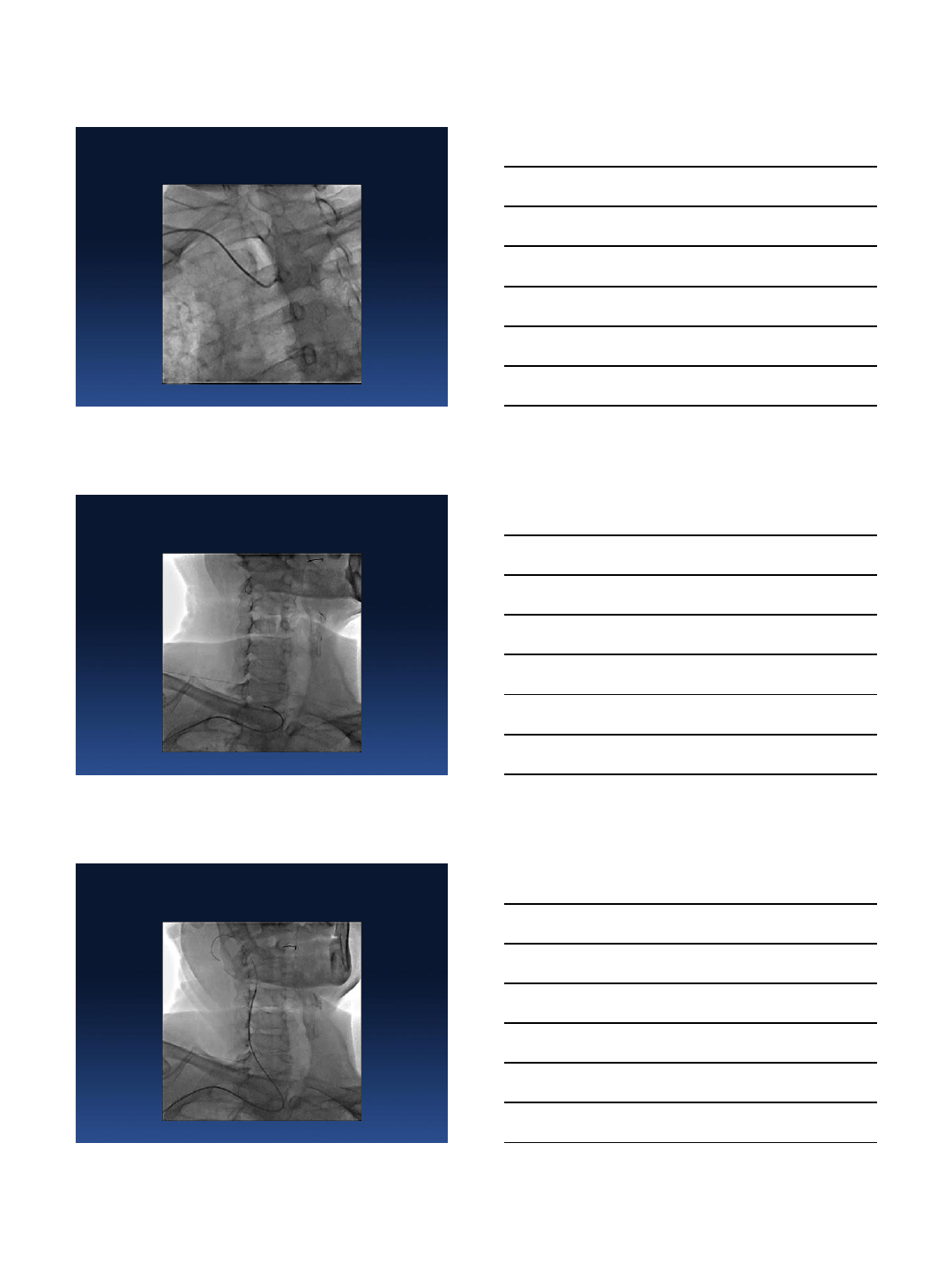
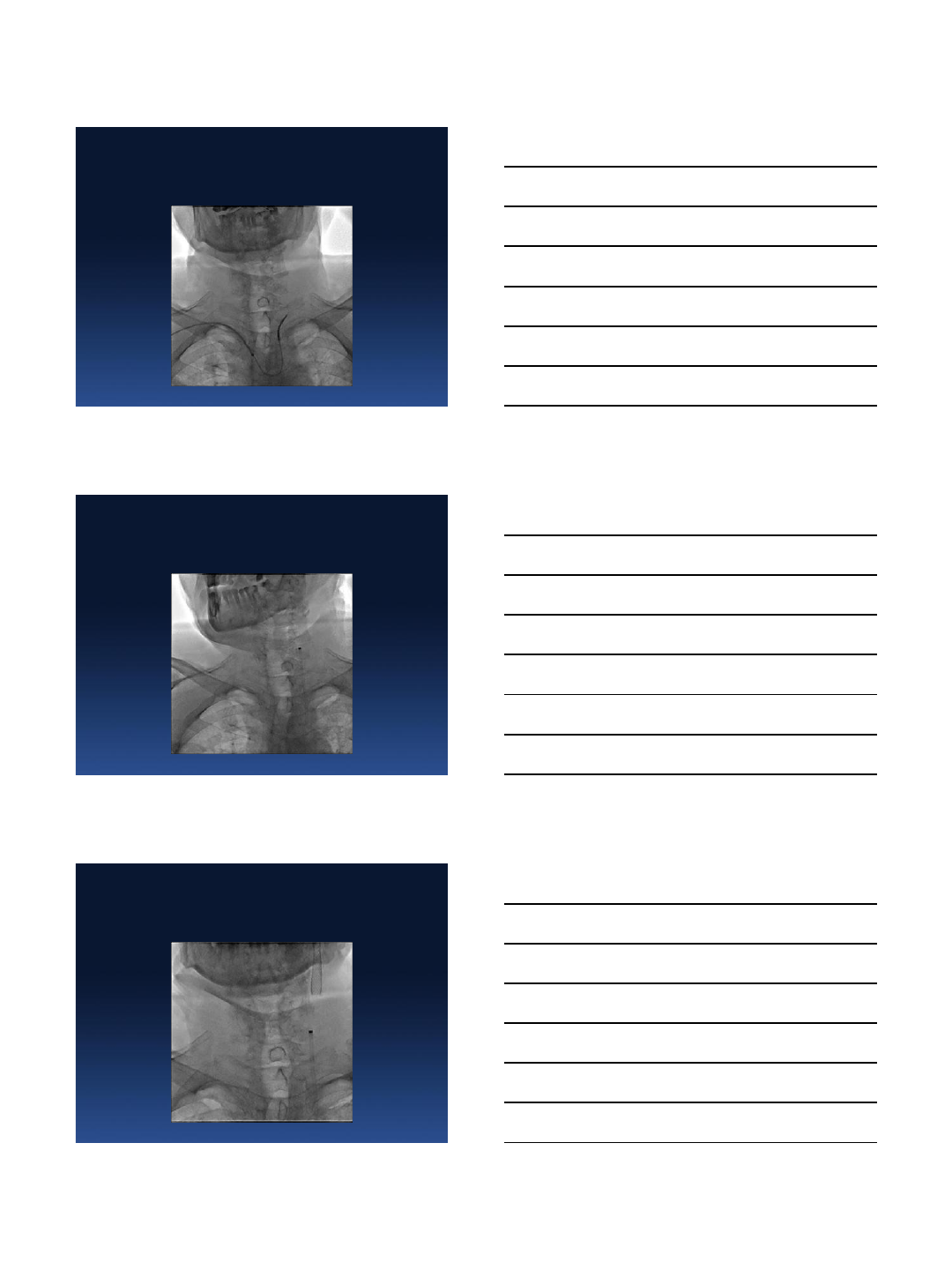
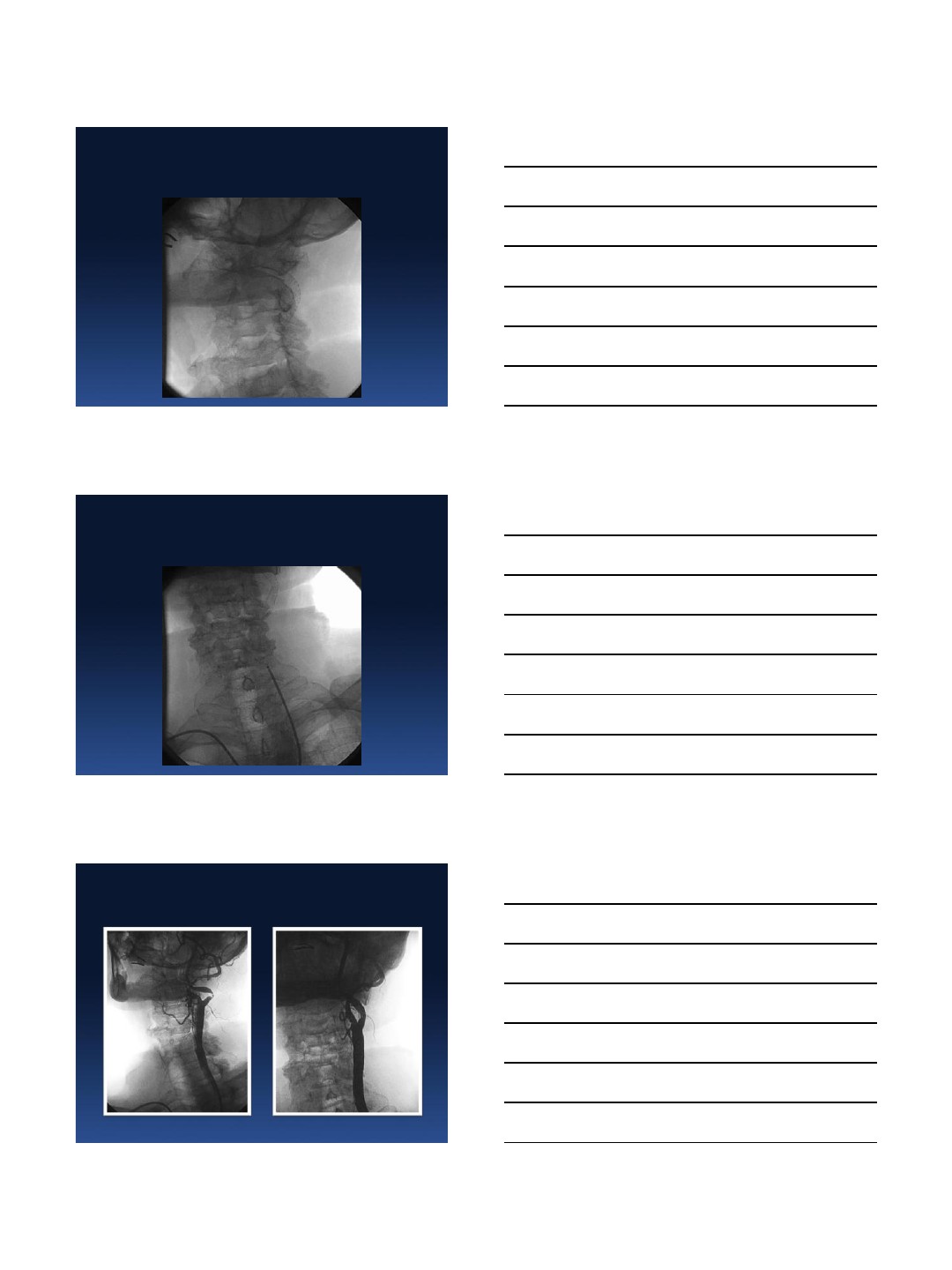
TRA CAS of RICA in a patient with
Acute Carotid Syndrome
01.06.2013
7
Left ACC 100%
Case 1.
RICA
Terumo advantage wire in RECA
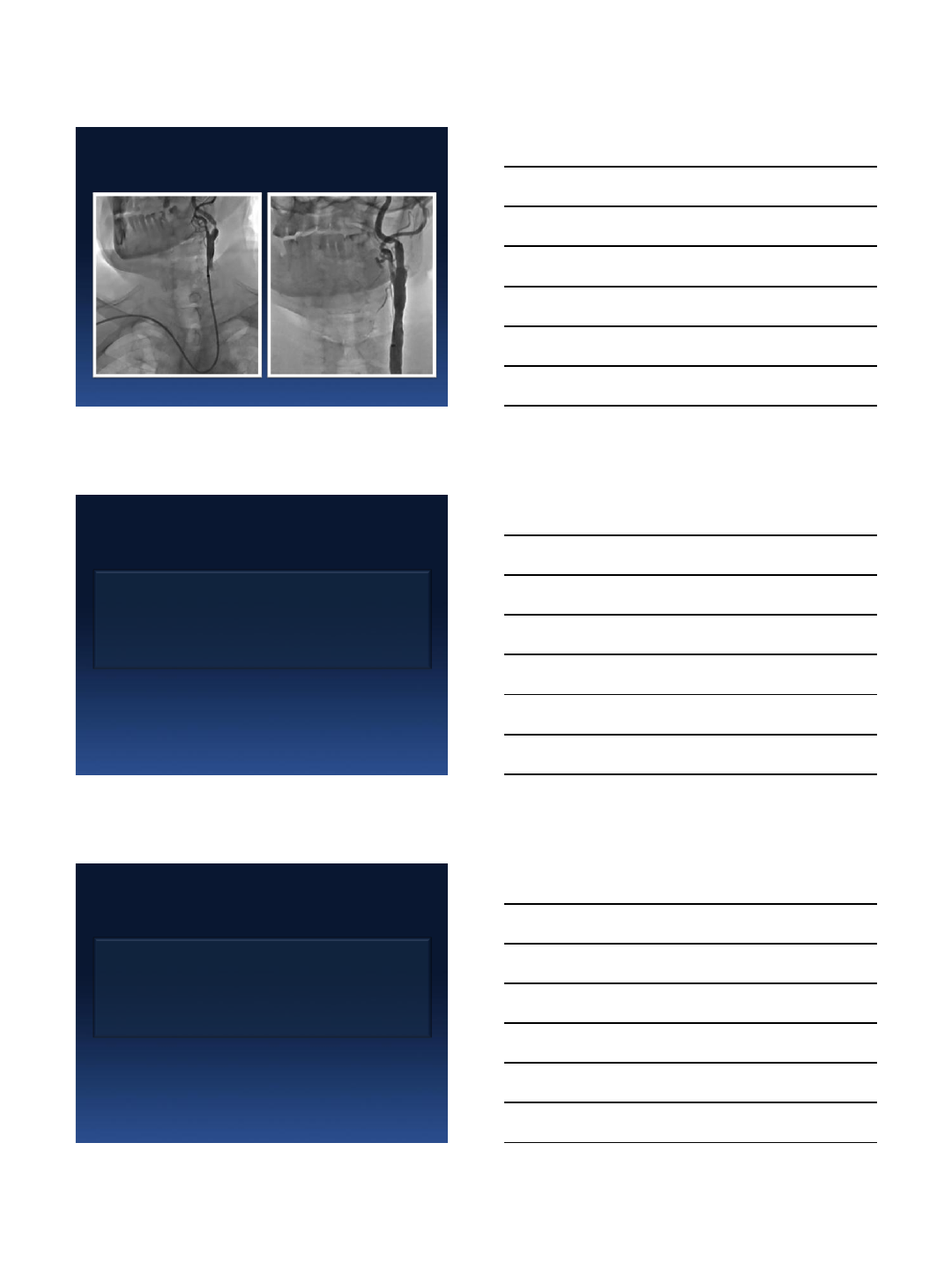
01.06.2013
8
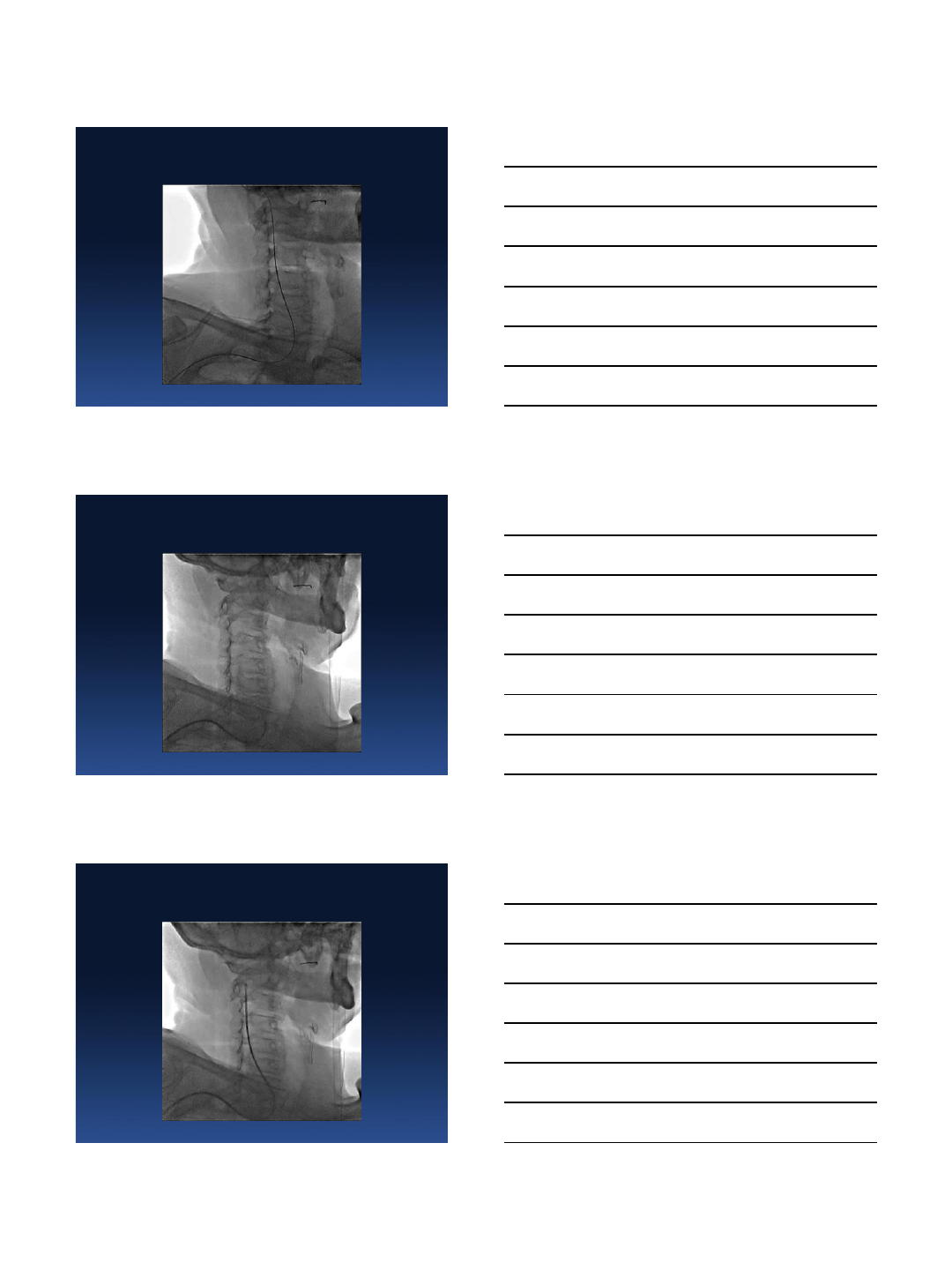
Amplatz Stiff wire in RECA
Destination sheath 6Fr
Xact 8-6/40mm
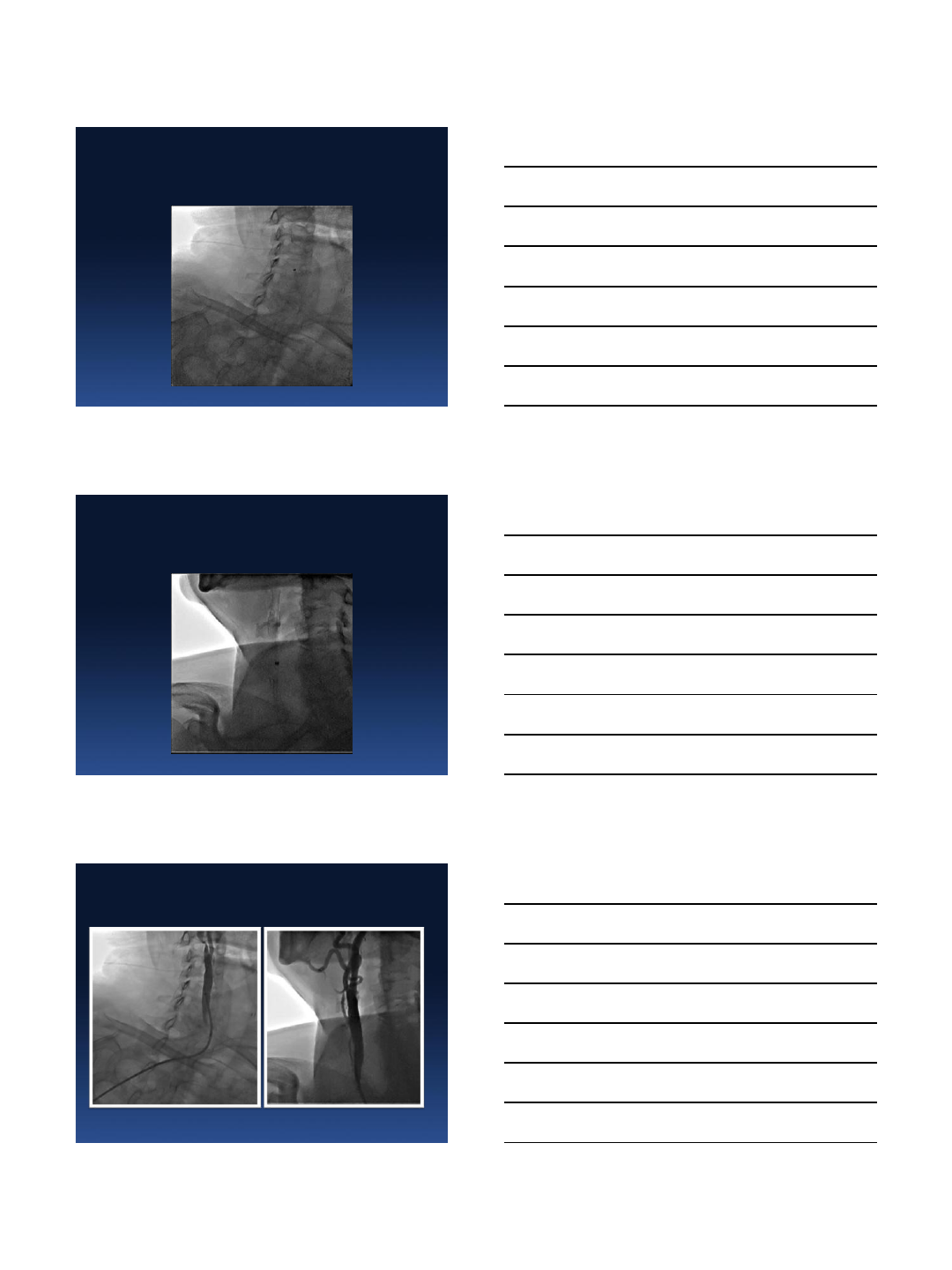
01.06.2013
9
Final result
TRANSRADIAL CAS
Anchoring technique
Telescopic approach
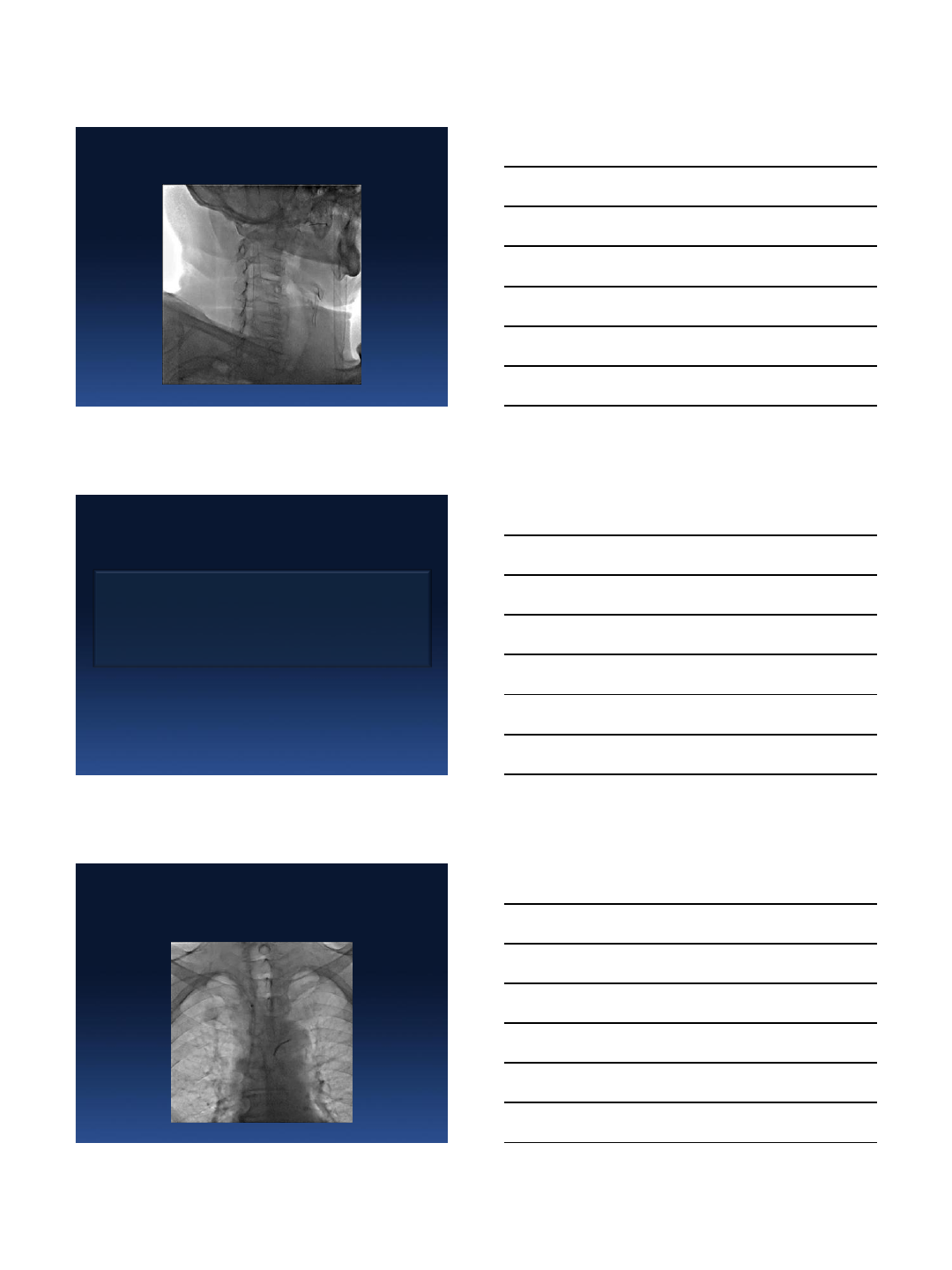
SIM 2 Cook into Shuttle Sheath
Case 2.
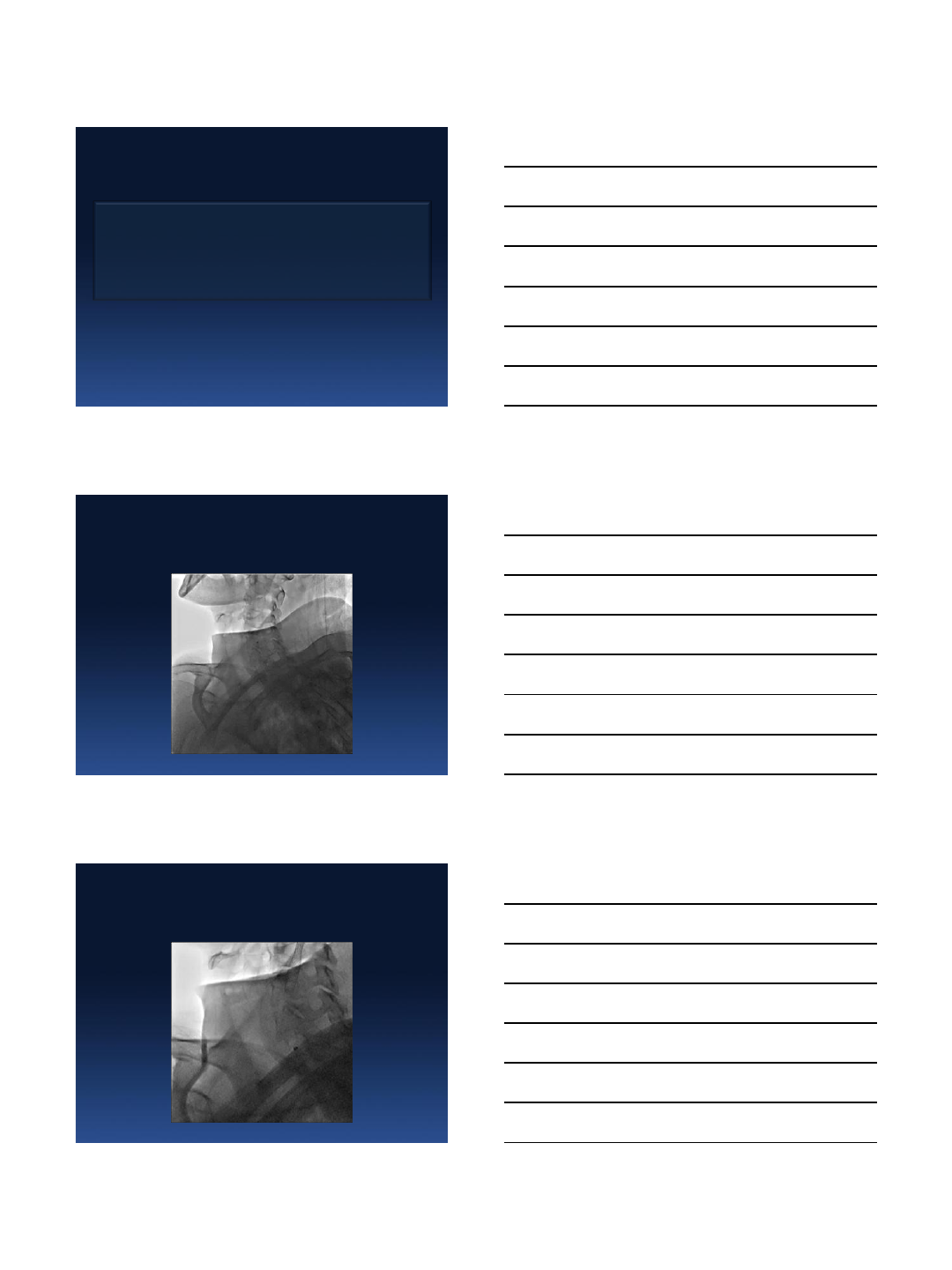
01.06.2013
10
Shuttle Sheath Positioning
LICA 95 %
Final Result
01.06.2013
11
Before / After
TRANSRADIAL CAS
Direct Cannulation
Simple Loop Cannulation
Deep Loop Retrograde Cannulation
TRANSRADIAL CAS
Direct Cannulation
Simple Loop Cannulation
Deep Loop Retrograde Cannulation
01.06.2013
12
CAS of RICA – Direct cannulation
Case 3.
CAS of RICA – Final Result
Before / After
01.06.2013
13
TRANSRADIAL CAS
Direct Cannulation
Simple Loop Cannulation
Deep Loop Retrograde Cannulation
CAS of LICA – Simple Loop Cannulation
Case 4.
CAS of LICA - Final Result
01.06.2013
14
Before / After
TRANSRADIAL CAS
Direct Cannulation
Simple Loop Cannulation
Deep Loop Retrograde Cannulation
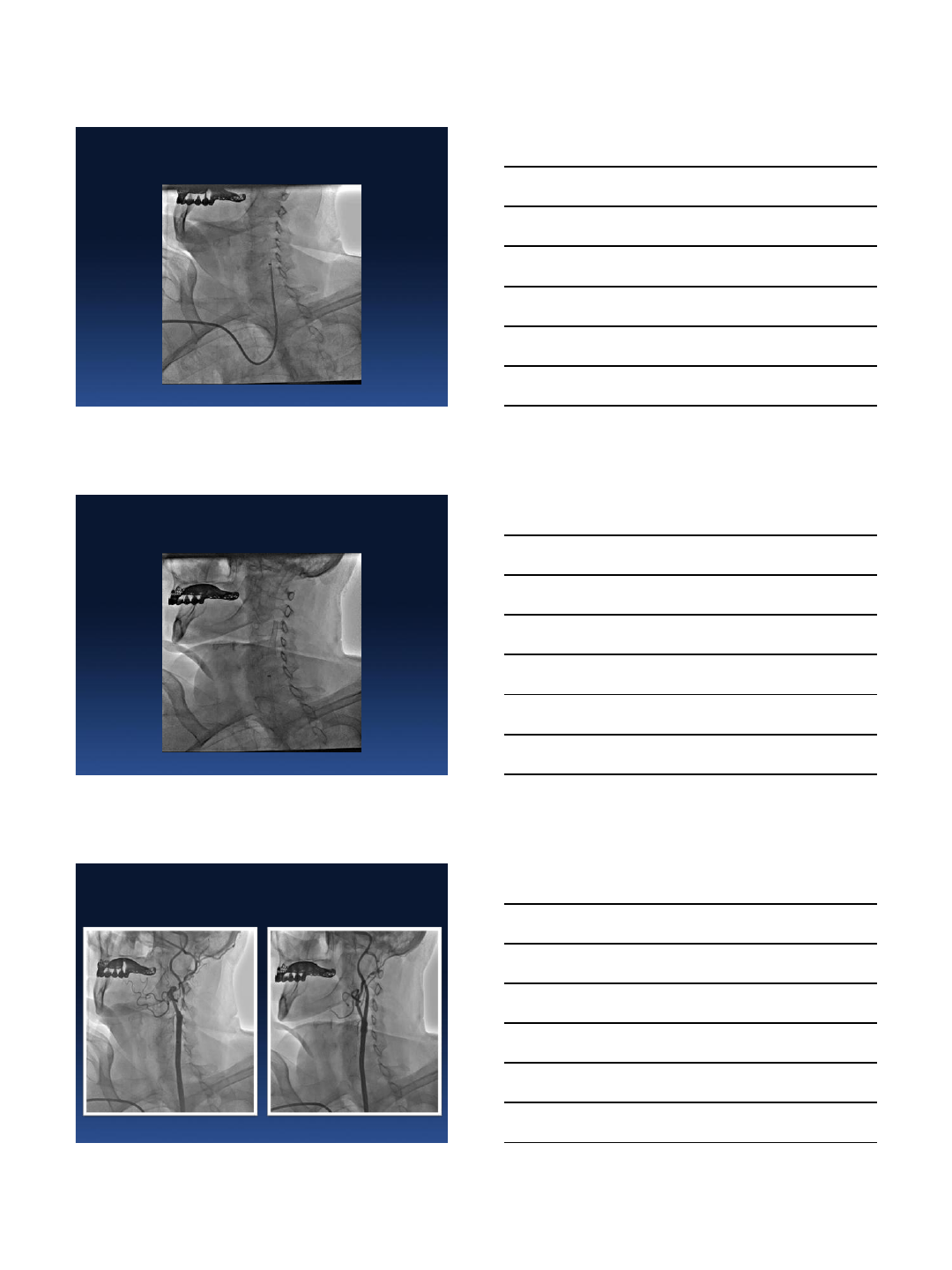
TRA CAS of LICA – DLRC – Transfer
Catheter
Case 5.
01.06.2013
15
TRA CAS of LICA – DLRC – Transfer
Catheter
TRA CAS of LICA – DLRC – 5F JR GC
TRA CAS of LICA – DLRC – 7F MP GC
01.06.2013
16
TRANSRADIAL CAS
Right Wrist Access
Left Wrist Access
Left TRA CAS of RICA – Simple Loop
Cannulation
Case 6.
Left TRA CAS of RICA – Final Result
01.06.2013
17
Before / After
TRANSRADIAL CAS
Tortuous Internal Carotid Artery
String Sign
Contralateral Occlusion
Tortuous LICA Subocclusion in Octogenarian
Case 7.
01.06.2013
18
Stent: Precise 7.0/40mm
Final Result
Before / After
01.06.2013
19
LICA: String sign
Case 8.
Final result
Before / After
01.06.2013
20
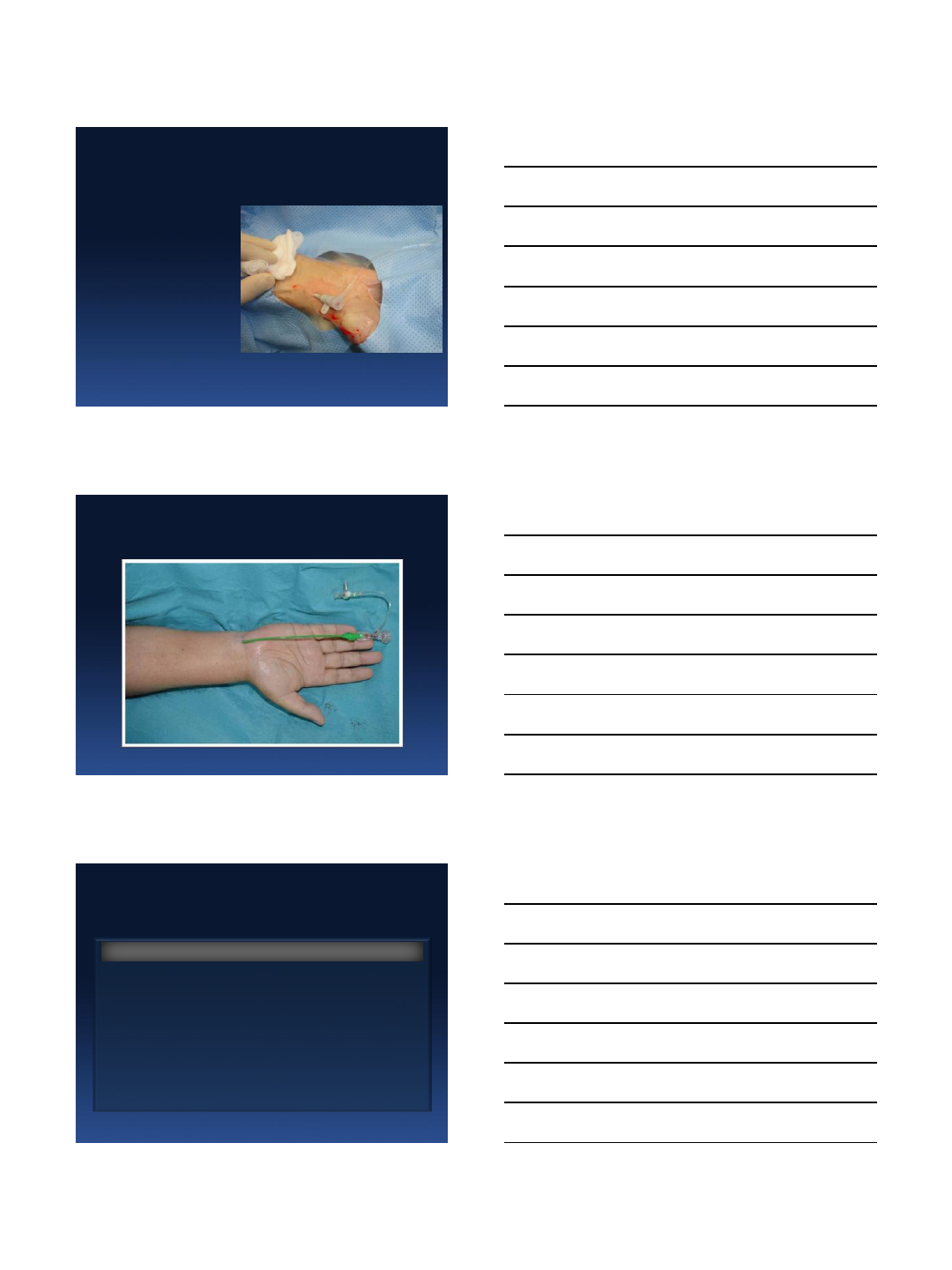
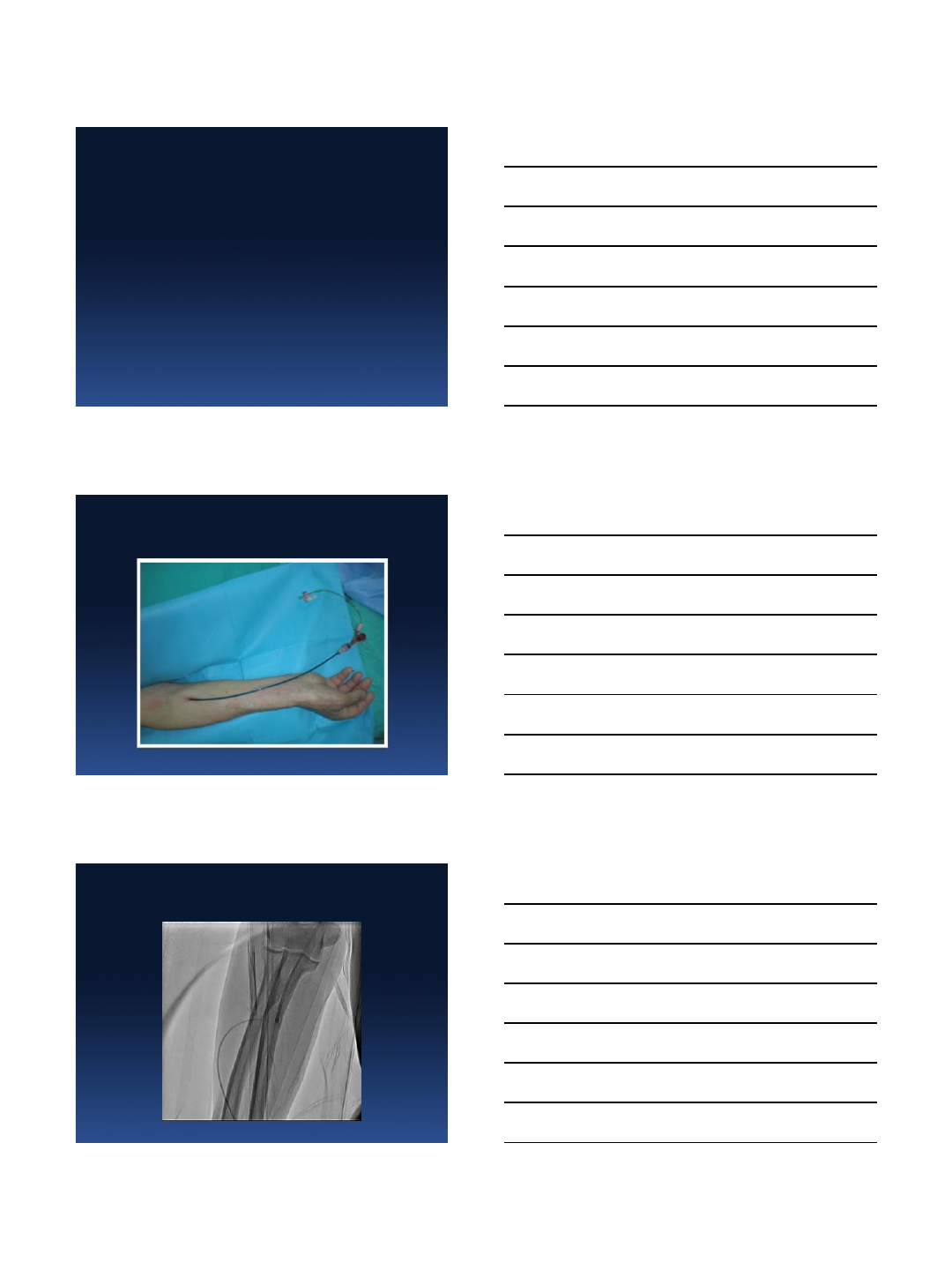
TUA for CAS of LICA with
contralateral occlusion
Male
J. A.
66 y.o.
Case 9.
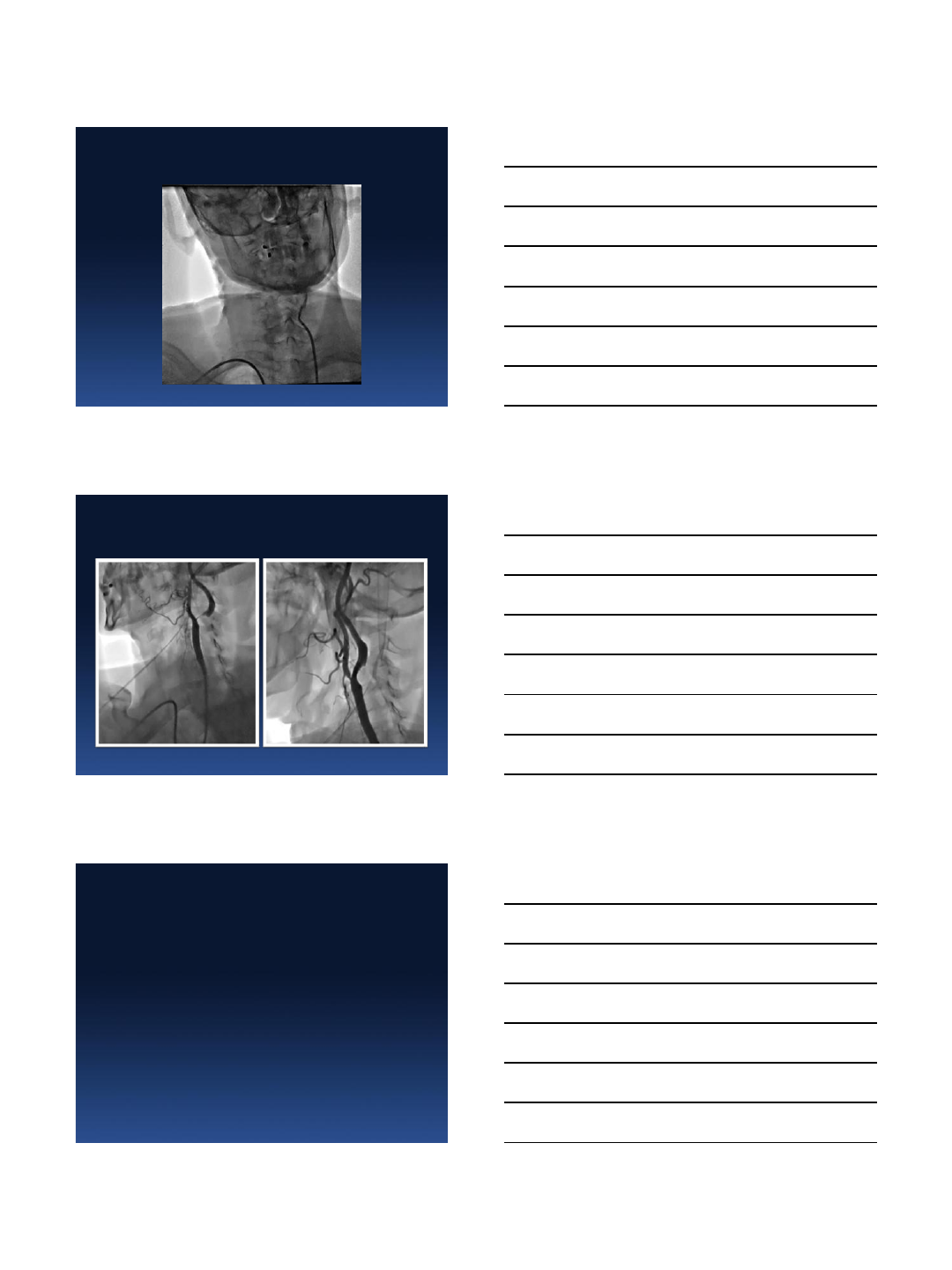
High Puncture of Ulnar Artery
High Puncture of Ulnar Artery:
High Take-off of Radial Artery
01.06.2013
21
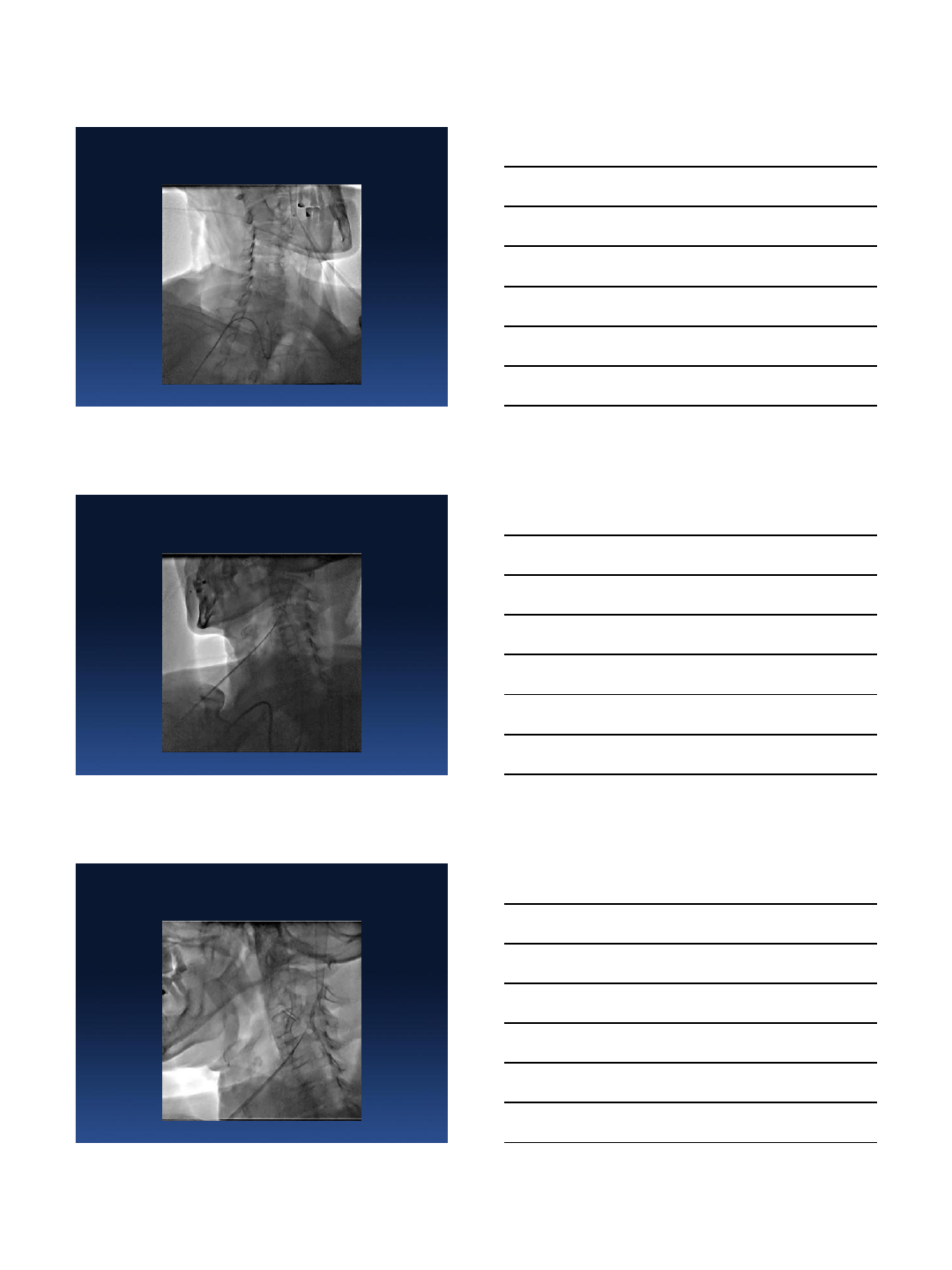
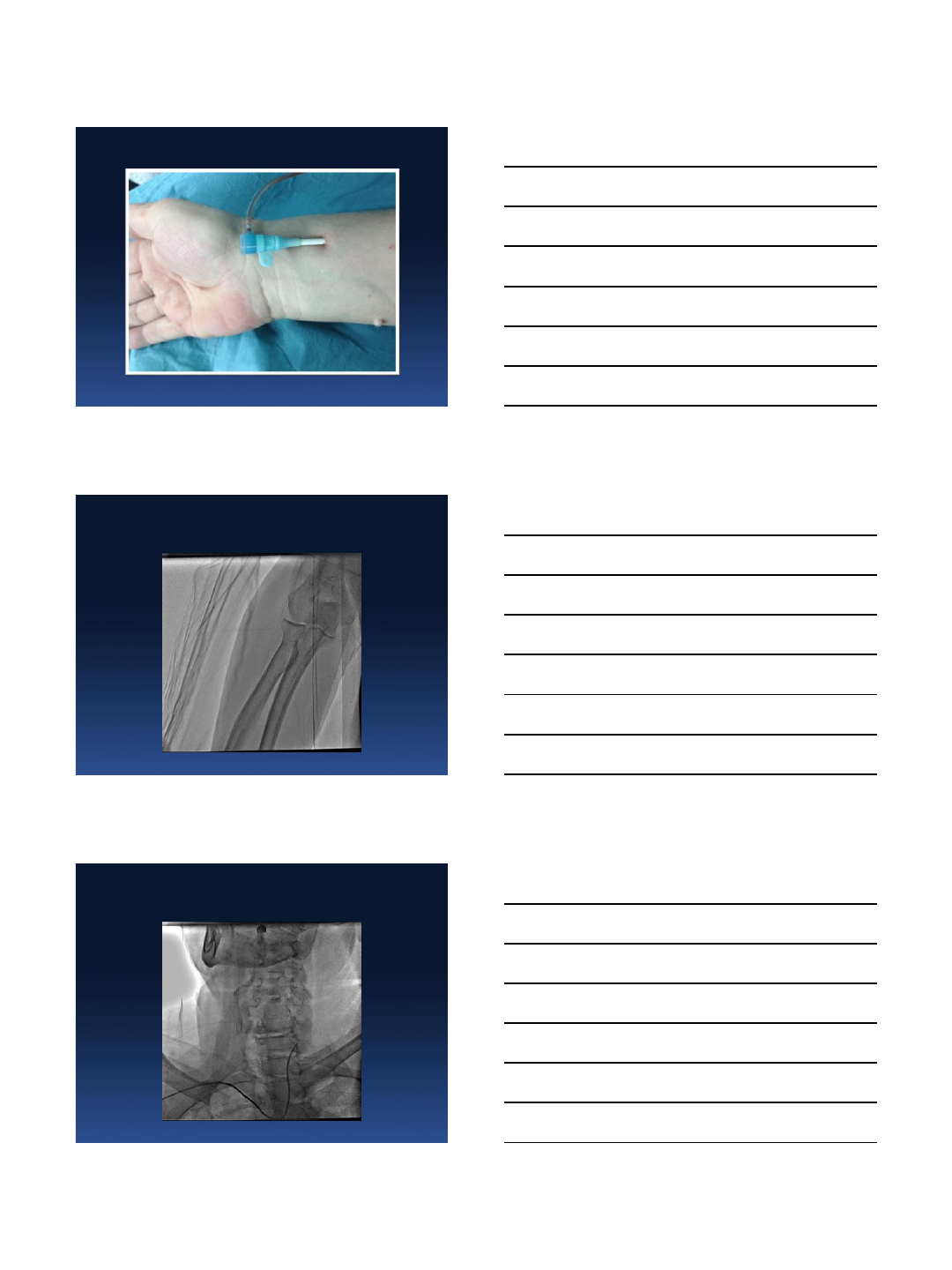
RICA 100%
Destination sheath 6Fr
Final Result
01.06.2013
22
Final Result
Before / After
Male
M. D.
66 y.o.
TRA CAS of LICA with
MoMa proximal protection
Case 10.
01.06.2013
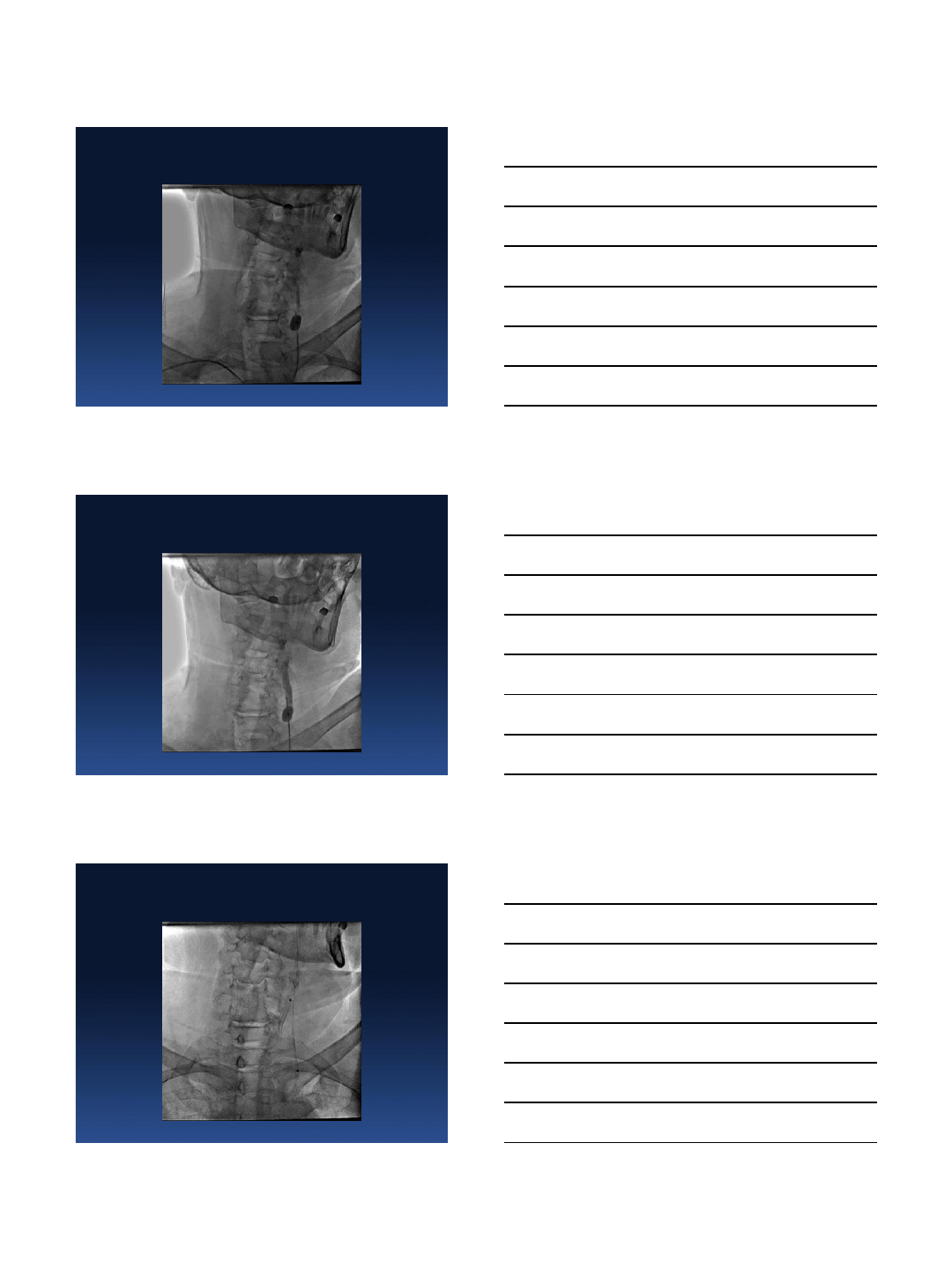
23
TRA
LICA 90%
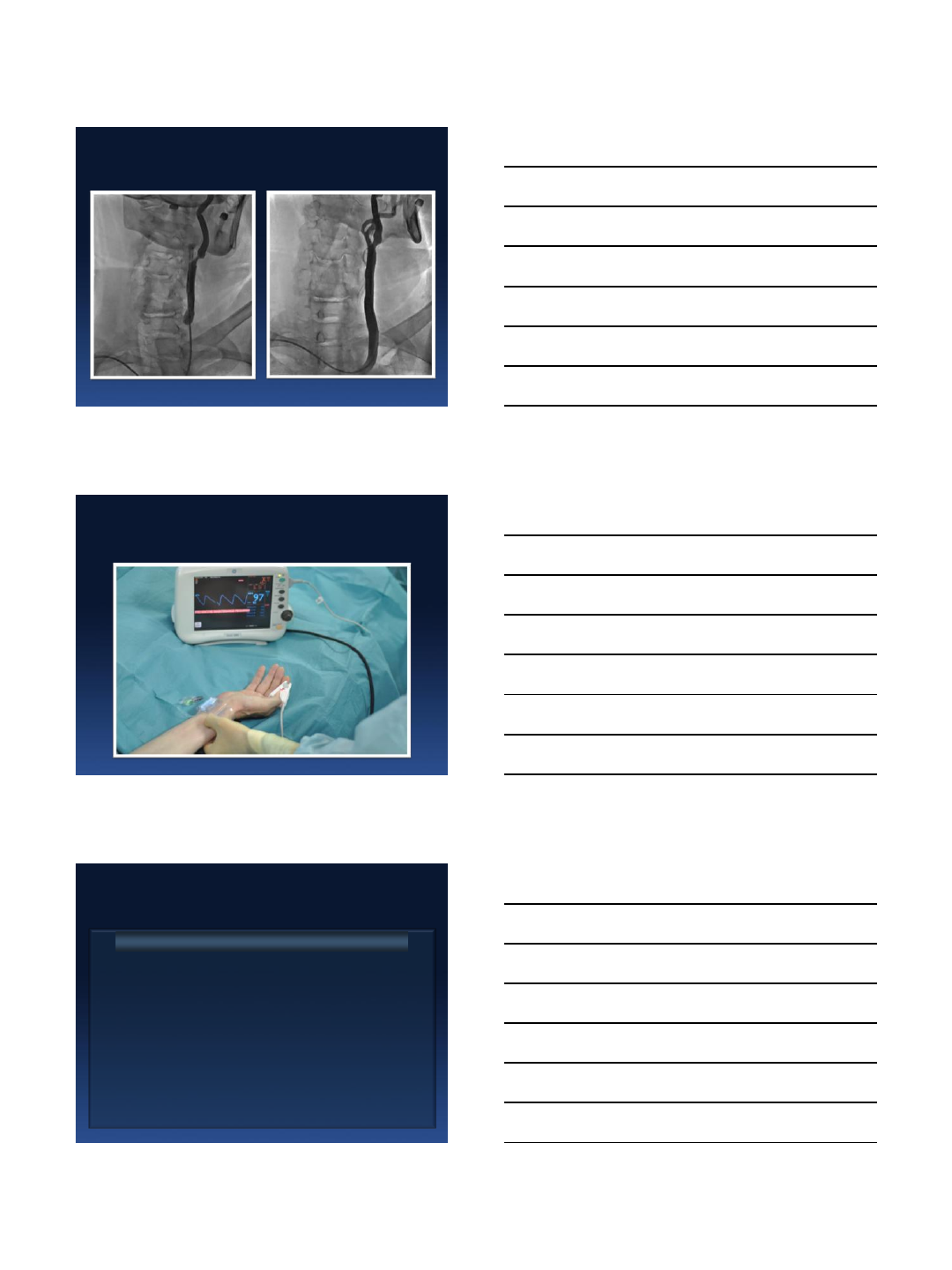
01.06.2013
24
MOMA proximal protection device
Stent: Precise RX 8.0/30mm
Final result
01.06.2013
25
Before / After
Radial Approach - Hemostasis
Transradial CAS
Easy access in otherwise very complex aortic arcs
Immediate patient mobilisation
Reduced hypotensive response
No bleeding
Anticoagulation is not an issue
Reduced nursing cost
Outpatient performance in selected cases
ADVANTAGE
01.06.2013
26
Significant learning curve for new TRA operators
Sometimes longer procedure for “easy case”
with type I aortic arch
Proximal PD and larger devices could not
be used freely in all cases
Radial artery occlusion ≈ 10 %
DISADVANTAGE
Transradial CAS
MISTAKE
Perform TRA only when FA is not possible !!!
Transradial CAS
Conclusions I
TRA & TUA CAS is feasible and safe when
performed by experienced TRA operator
Easy access in difficult anatomies (bovine arch
LCCA)and most of the innominate artery take offs
Severe angulations at the origin might be
negotiated safely and efficiently with DLRC as
alternative of Direct and Simple Loop
cannulation for CAS

01.06.2013
27
Conclusions II
Allows early patient mobilization
Eliminates bleeding complications
Further studies are needed before
recommending wrist access (TRA or TUA) for
CAS as primary approach over femoral access
