Renal Ablation Challenges And Clinical Changes Syllabus
2016-01-06
: Pdf Renal Ablation Challenges And Clinical Changes Syllabus Renal_Ablation_Challenges_and_Clinical_Changes_Syllabus 1 2016 pdf
Open the PDF directly: View PDF ![]() .
.
Page Count: 31
1/5/2016
1
NeuWave Microwave:
Overview of thermal ablation
Chris Brace Ph.D.
University of Wisconsin
DISCLAIMER
PLEASE NOTE: The Certus 140 2.45 GHz Ablation System is a tool, not a treatment for any disease or condition. It is
cleared for the ablation (coagulation) of soft tissue in percutaneous, open surgical and in conjunction with laparoscopic
surgical settings in patients who present themselves to a treating physician with a wide variety of diseases or
conditions..The Certus 140 2.45 GHz Ablation System is not indicated for use in cardiac procedures. The system is
designed for facility use and should only be used under the orders of a physician.
The information in these cases is not meant to convey recommendations from NeuWave Medical, Inc. regarding
appropriateness for a particular patient, power and time settings, final ablation zone size and shape or other procedure
guidance. NeuWave Medical makes no representations and assumes no liability regarding the accuracy of the
information provided herein or the effectiveness of any of the treatment or for any action or inaction you take based on
or made in reliance on the information. These are individual cases and your results may vary. When planning a case,
consider all unique aspects, including tissue type, lesion location, surrounding vasculature and proximity to critical
structures when determining probe type and power/time settings. Consult the product Instructions For Use for
information regarding expected ablation sizes
December 2015
Disclosure
•Co-founder of NeuWave Medical
December 2015
1/5/2016
2
SYLLABUS
•Physics of microwave
•Benefits of synchronous in-phase technology
•Clinical differentiators
•Probe placement
•Advanced Education Programs
•Clinical cases for development of best practices
Objectives of Presentation
December 2015
EVOLUTION OF ABLATION TECHNOLOGY
1960 1980 2000
‘02 ‘06 ‘ 07 ‘08 ‘0 9
Vivawave
Microsulis
Medwaves
Microthermx
HS Amica
MWA 510K Approvals
Evident
1970 1990
1980’s
1st Generation Microwave
Single-probe, uncooled
Late 2000’s
3rd Generation Microwave
Single-probe except MTX
1990’s
Single-Probe RF
Single-probe
Early 2000’s
2nd Generation Microwave
Single-Probe, Low Power
Multi-Probe RF
RF switching controller
1960’s
1st Generation Cryoablation
Liquid-cooled, open ablation
Late 1990’s
3rd Generation Cryoablation
Gas -cooled, smaller probes
2010
New Generation
Microwave
NeuWave
•Multi-Probe
•High Power, 2.45 GHz
•Real-Time Control
•Gas -Cooled
•Smaller Probes
•Large or Focal
Ablation Capable
‘10
Late 1980’s
2nd Generation
Cryoablation
Liquid-cooled,
percutaneous ablation
‘12
Precision Probe
‘15
ABLATION
CONFIRMATION
December 2015
2 MODES OF THERMAL ABLATION
Freezing and Heating
Cryoablation
Cell death by freezing
Radiofrequency ablation
Microwave ablation
Cell death by heating
When tissue is heated to ≥ 60° C, proteins
denature, lipids in the cell membrane melt
and cells are killed instantaneously
When tissue is cooled to ≤ -40° C,
intracellular ice formation ruptures cell
membrane and kills cells via a
freeze/thaw method
≤ -40° C ≥ 60° C
December 2015
1/5/2016
3
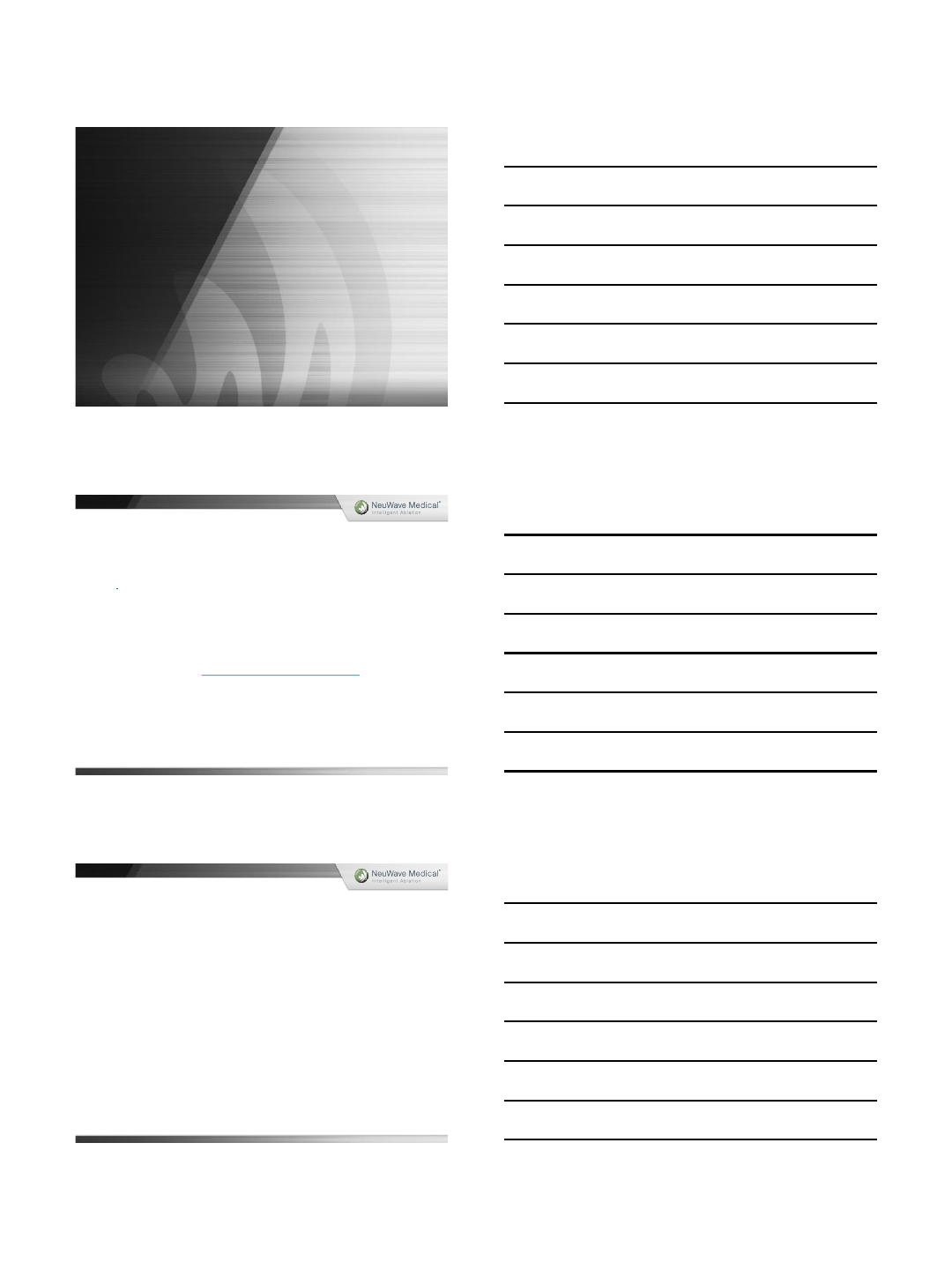
CRYOABLATION OVERVIEW
HOW CRYOABLATION WORKS:
•1 probe per 1 cm ablation zone
inserted into/near target2
•Cells are killed using a freeze/thaw
method
FREEZE: Cell dehydration
Membrane & essential constituents
are severely damaged and cells die
slowly
THAW: Cell Re-hydration
Thaw phase causes the cells to burst
from rapid rehydration. Ischemia is
caused by damage to vascular system
& membranes
December 2015
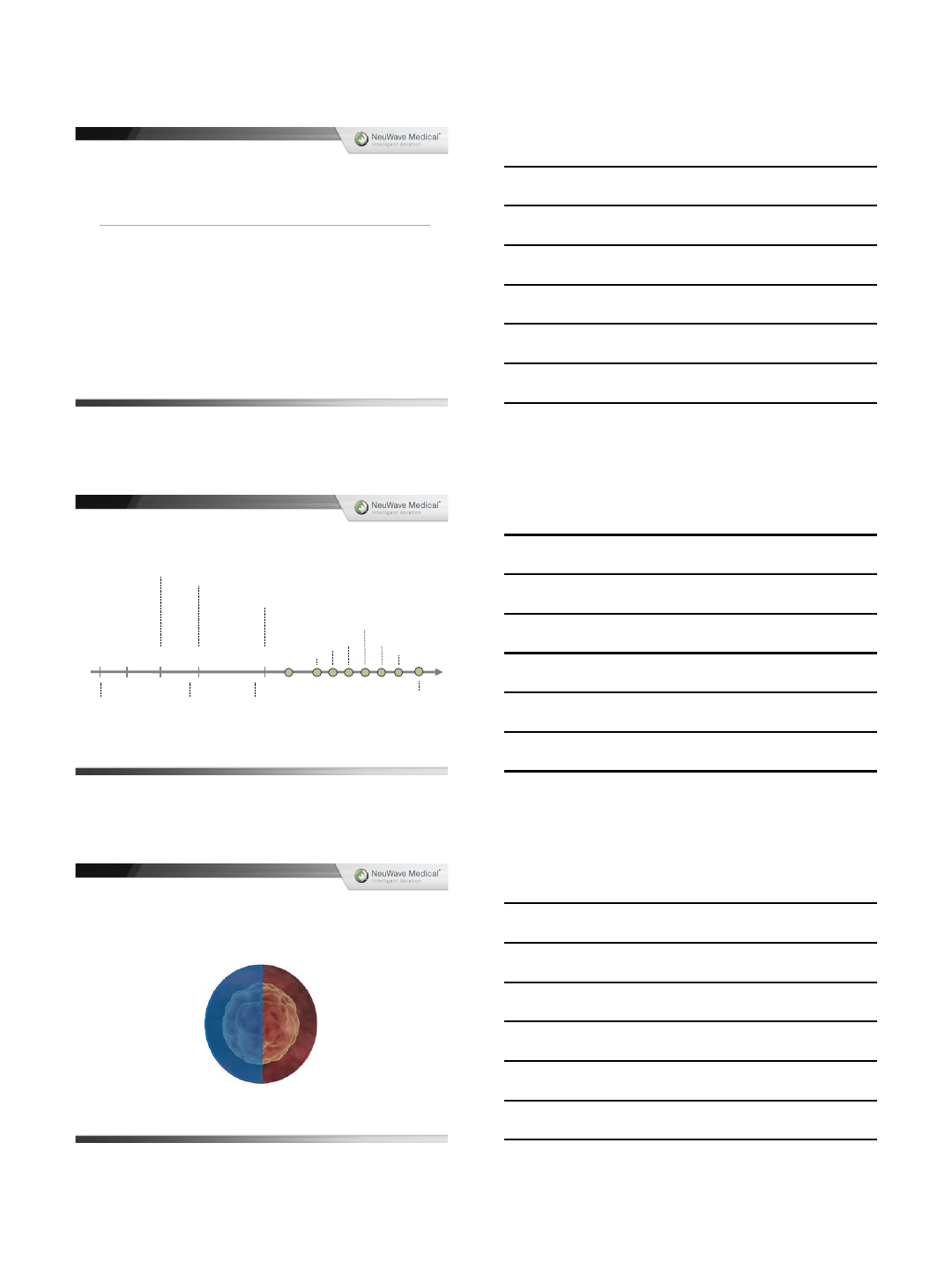
LOW PROCEDURAL PAIN3
PRESERVES ADJACENT
NORMAL CRITICAL
STRUCTURES & MINIMAL
SCARRING3
ICE BALL HIGHLY VISIBLE
ON CT/MRI/US3
REQUIRES MULTIPLE, OFTEN
LARGE (13 GAUGE) PROBES2
LENGTHY PROCEDURE
(APPROX. ≥ 30 MIN6)
POTENTIALLY HIGHER COST
DUE TO MULTIPLE PROBES &
EXPENSIVE GASES6
RISK OF SYSTEMIC EFFECTS
(CRYOSHOCK, LIVER
FRACTURE5)
VISIBLE ICE BALL IS NOT
TREATMENT ZONE4
NO ACTIVE PROCESSES –
COOLING IS PASSIVE BY
CONDUCTION
CRYOABLATION OVERVIEW
+ -
December 2015
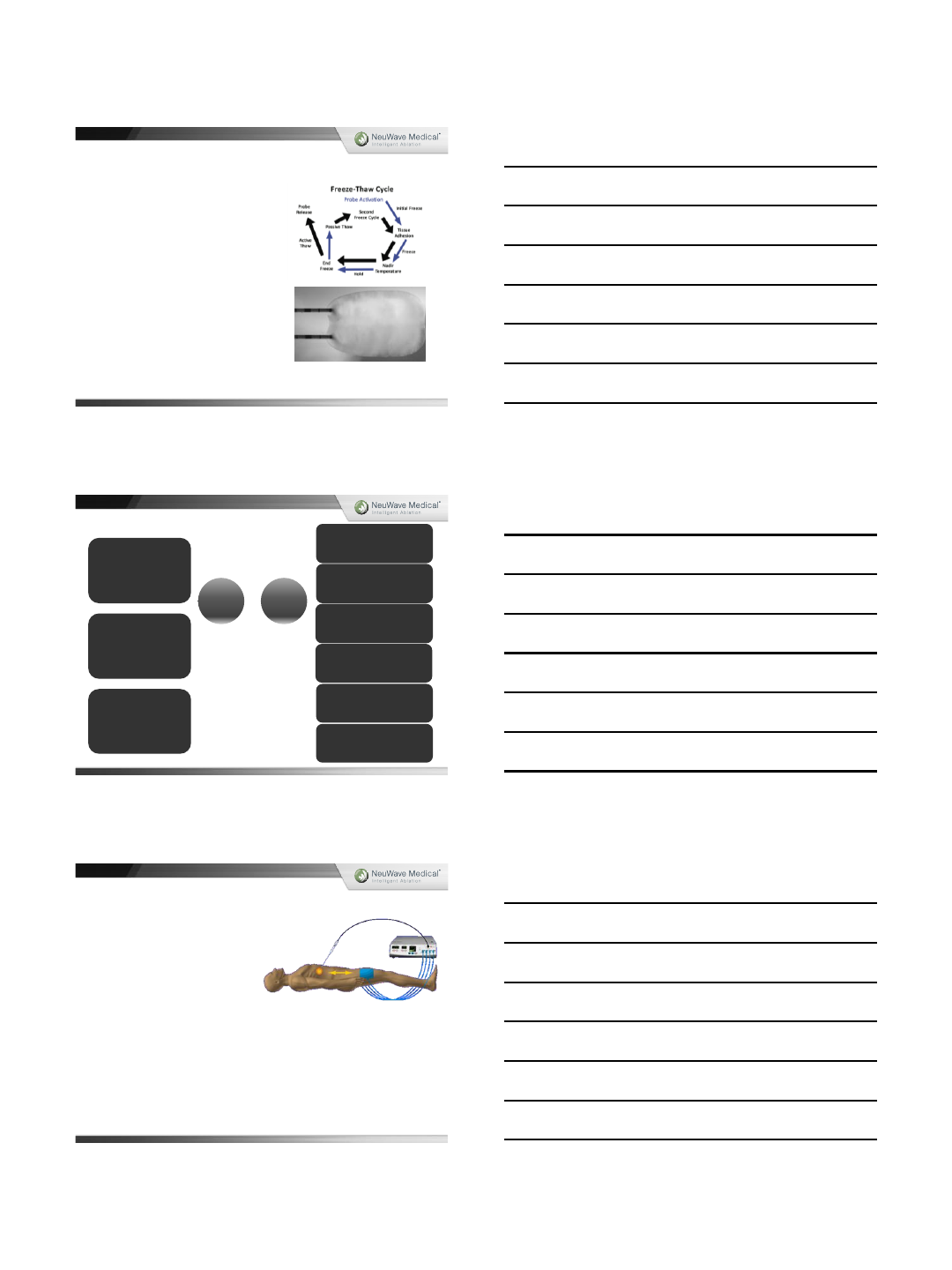
RADIOFREQUENCY OVERVIEW
HOW RADIOFREQUENCY ABLATION
WORKS:
•Heating is produced when an
electrical current agitates ions
•Grounding pads placed externally on
patient to complete the electrical
circuit
Tissue near electrode:
Active heating by ionic agitation
Tissue away from electrode:
Passive heating by thermal
conduction. Once tissue becomes
dehydrated/charred, the tissue acts
as an electrical insulator preventing
further current flow.
December 2015
1/5/2016
4
PROVIDES
CAUTERIZATION5
MINIMAL # OF
ELECTRODES AND GASES
REQUIRED
DEHYDRATED/CHARRED
TISSUE (>100 °C) HIGH
IMPEDANCE, LIMITED
POWER5
PULSING OR SLOW HEATING
REQUIRED TO AVOID TISSUE
DEHYDRATION/CHAR5
GROUNDING PADS = RISK OF
SKIN BURNS8
HEAT SINK
LOBULATED ABLATIONS &
HIGHER RECURRENCE RATES7
SUBSTANTIAL PEER-
REVIEWED LITERATURE,
(OLDER TECHNOLOGY)
RADIOFREQUENCY OVERVIEW
+ -
December 2015
MW AND RF SIMILARITIES
Mechanism of cell kill is identical (indistinguishable under the microscope)
Microwave-penetrates all biologic tissues (including aerated lung, bone,
char)10
December 2015
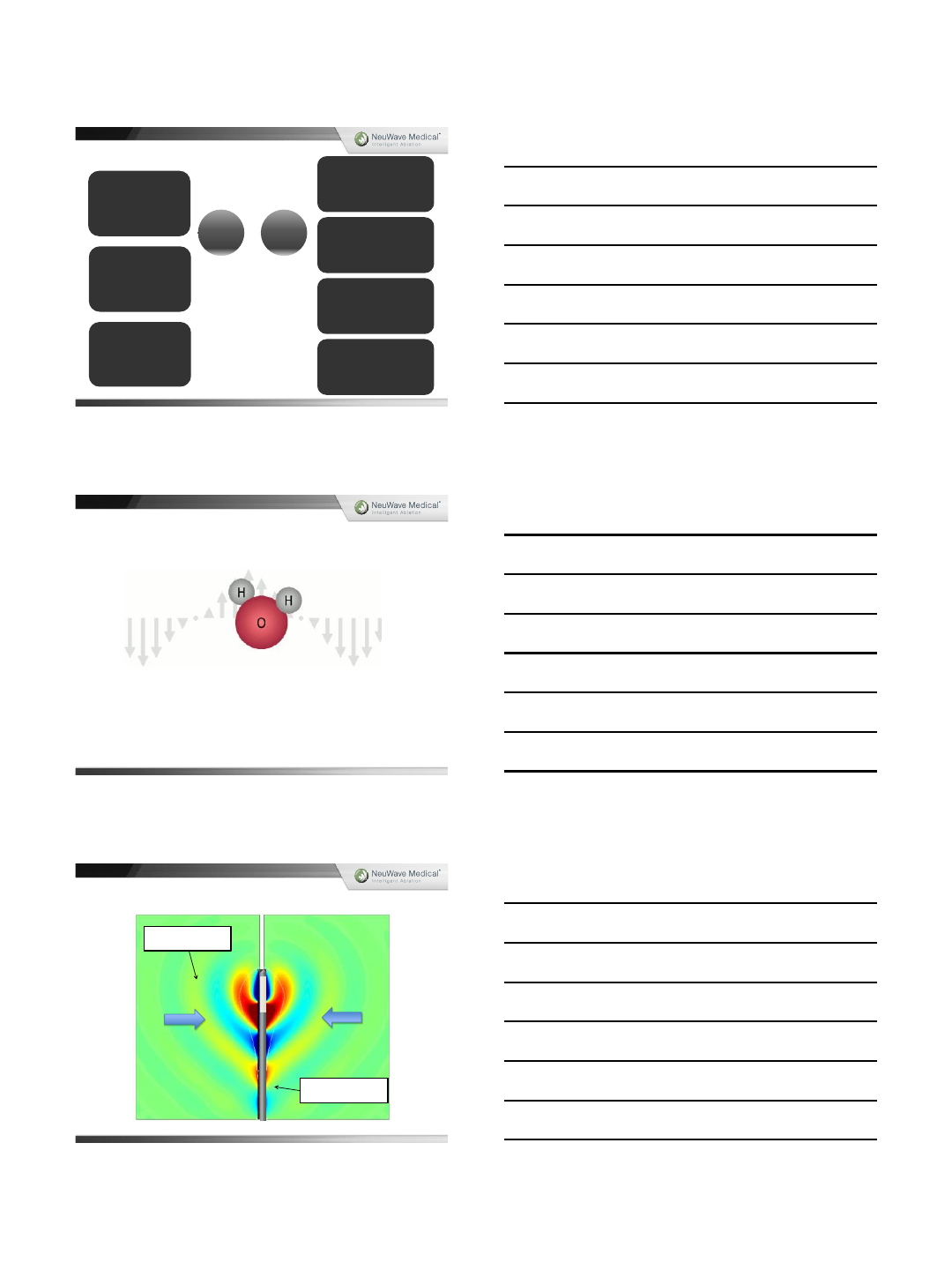
ANTENNA RADIATION
Energy converted to
heat
Energy flow along
antenna shaft
December 2015

1/5/2016
5
EARLY MICROWAVE SYSTEMS OVERVIEW
•EM field (915 MHz or 2.45 GHz)
•Rapidly oscillates water molecules to generate heat
•The EM field penetrates all biologic tissues including dehydrated/charred tissue created
during ablation
•No limit to temperature, power
Exhibi t 1: Because of the signi ficant s haft heating that occu rred with 1st gen
microwave, a robu st shaft cool ing mechanism was required to minimize thermal
damage to the subcutaneous tissues and the skin, especially with the development
of h igher power systems 9
10
December 2015
WAVE INTERFERENCE &
INEFFECTIVE COOLING
UNPREDICTABLE “HOT DOG”
SHAPED ABLATIONS11
NO SYNCHRONY WITH
MULTI-ANTENNA USE =
INCONSISTENT ABLATION
ZONES
ENERGY CAN BE APPLIED
CONTINUOUSLY DESPITE
CHANGES IN TISSUE
EFFECTIVE IN ALL SOFT
TISSUE TYPES7UNDER POWERED
IMPROVED
PERIVASCULAR
PERFORMANCE VS RF
(LESS HEAT SINK EFFECT7)
SOME TISSUE
CONTRACTION11
LARGE GAUGE ANTENNAS
EARLY MICROWAVE SYSTEMS OVERVIEW
+ -
December 2015
Segment II
NeuWave Medical –Certus 140
Technical Differences
December 2015
1/5/2016
6
NEUWAVE MICROWAVE SYSTEM OVERVIEW
NEUWAVE IMPROVEMENTS11:
2.45 GHz frequency
•Less electromagnetic interference during multiple
probe use for predictable, reproducible burns12
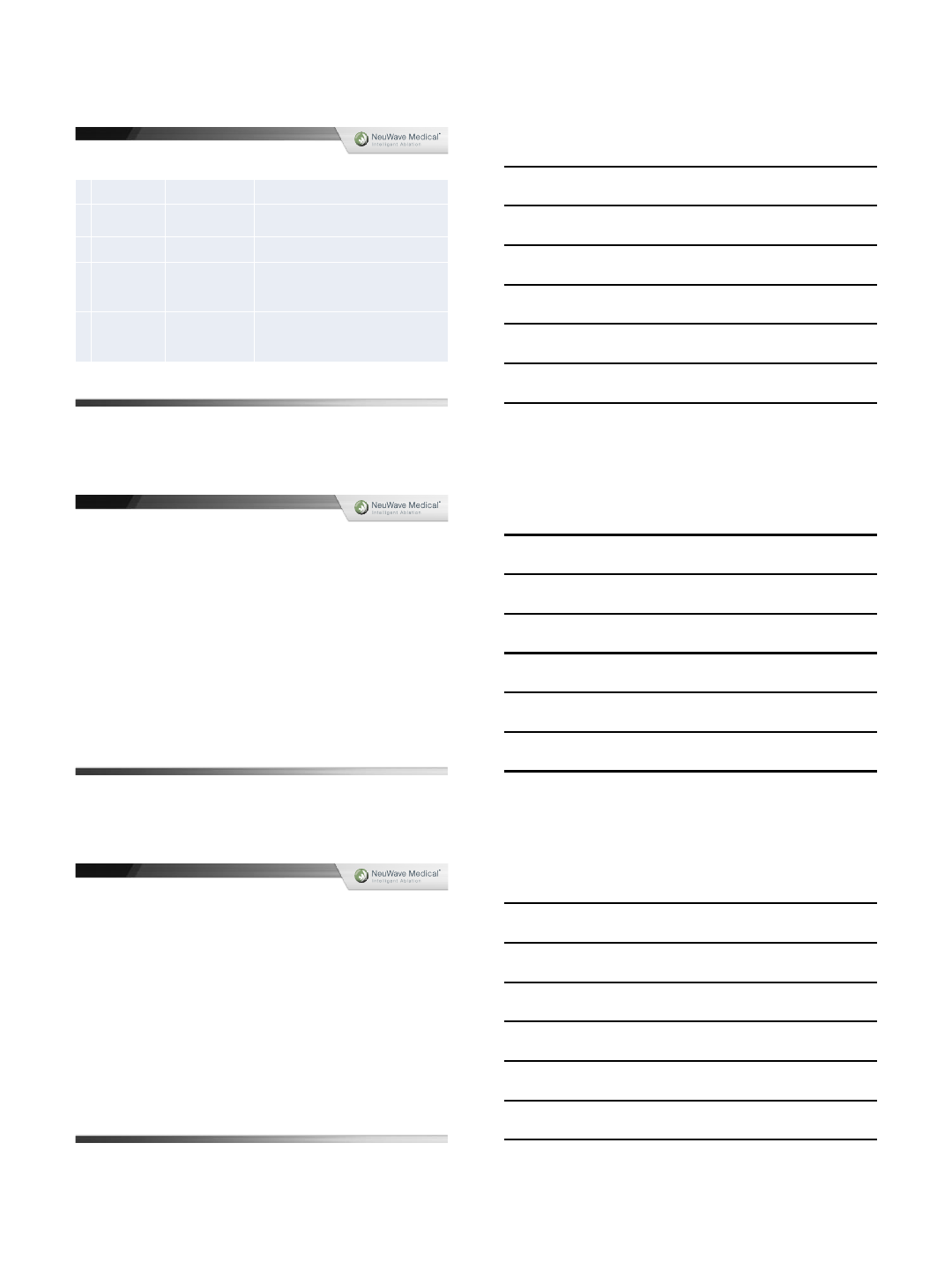
Triaxial antenna design
•High energy throughput
•Minimal backward heating
Multi-antenna wave synchrony
•Consistent, reproducible large burns
CO2cooling
•Eliminates heating along antenna shaft (no comet tail)
•Tissu-Loc™ for reducing antenna migration during
scanning and additional antenna placement
Tissu-Lociceball
December 2015
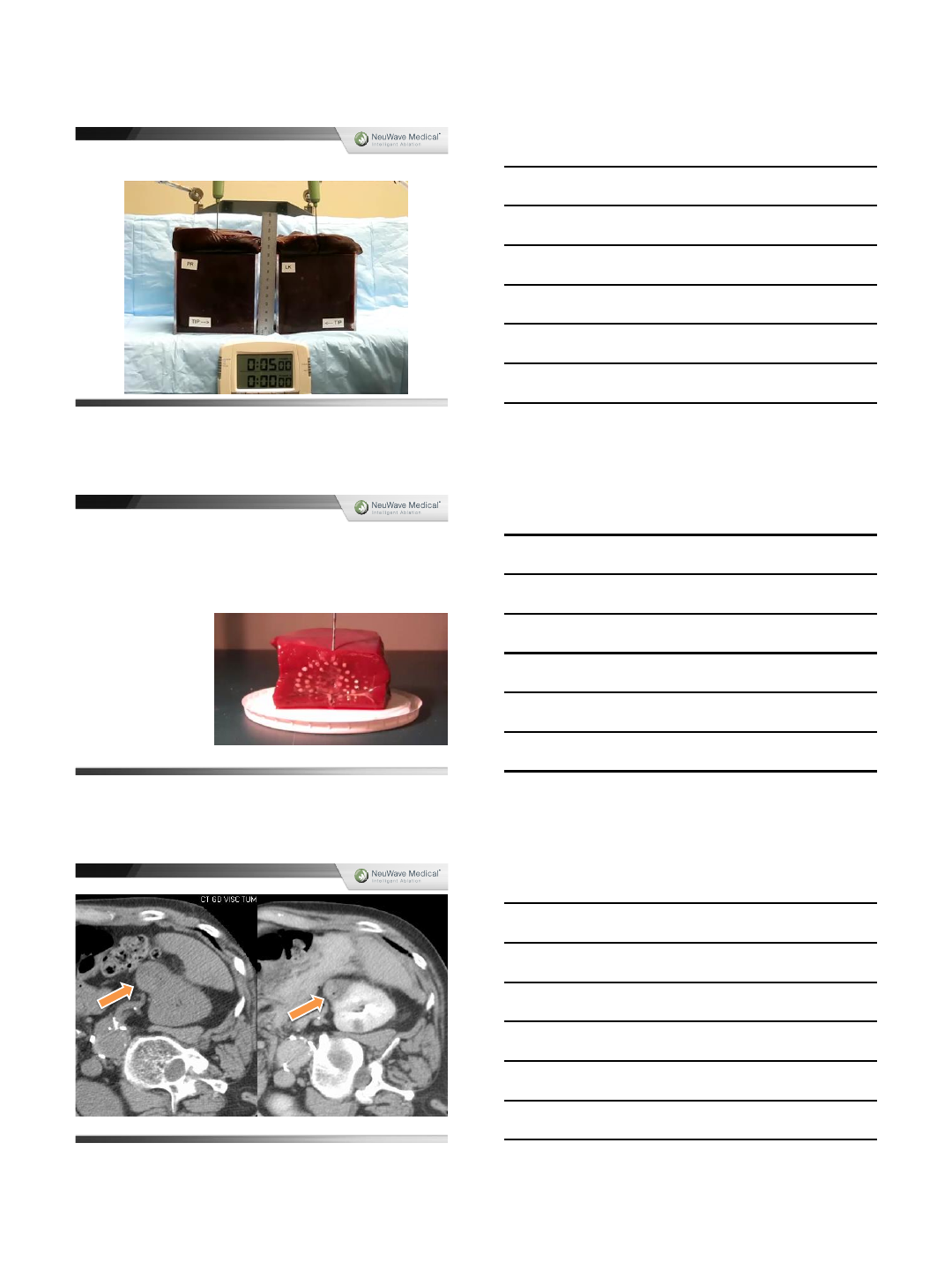
Power Distribution: 2.45GHz
Power Distribution: Cable Loss
12%
20%
21%
33%
0%
5%
10%
15%
20%
25%
30%
35%
915 MHz 2.45 GHz
Large Cable Small Cable
Delivered = Generated –Distribution Losses
The inherent loss of generated microwave energy due to smaller diameter cables led to
NeuWave creating the Power Distribution Module (PDM)
December 2015
1/5/2016
7
December 2015
Antenna Design
December 2015
1/5/2016
8
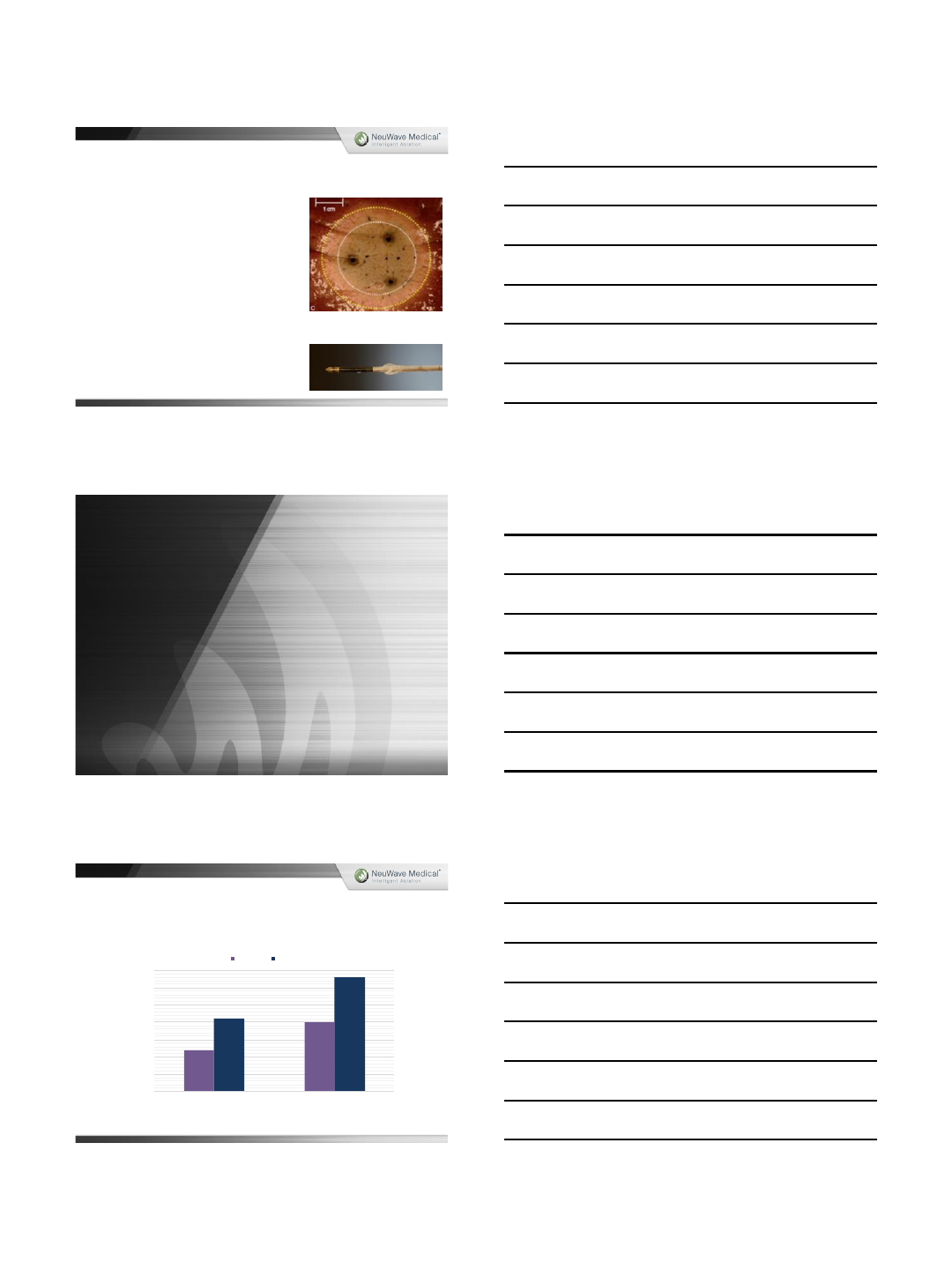
PR & LK ANTENNAS
TISSUE SHRINKAGE CAUSED BY MW
Marked tissue shrinkage with high power MW
devices
~30% liver/kidney
~50% lung16
December 2015
Pre-ablation After 3-minute ablation
D5 w/
contrast
December 2015
1/5/2016
9
ABLATION FOR RENAL SOFT TISSUE:
This material/information may include discussions of off-label use of our product, the Certus 140, for which we
cannot promote the product. We disseminate this information to you only to provide you with a fair
representation of the current published information
2014
A. Moreland, et al
UW paper
High
-
Powered Microwave Ablation of T1a Renal Cell Carcinoma:
Safety and Initial Clinical Evaluation
2012
J. Yu, et al
Radiology
US
-guided Percutaneous Microwave Ablation of Renal Cell
Carcinoma: Intermediate
-term Results
2014
Y. Lin, et al
Urology
Percutaneous Microwave Ablation of Renal Cell Carcinoma Is Safe
in Patients With a Solitary Kidney
2013
M. Cristescu, et al
WCIO abstract
Percutaneous Microwave Ablation for the Treatment of Renal
Angiomyolipoma
(APL): Initial Experience
2014
J. Horn , et al
J Vasc Interv Radiol
Percutaneous
Microwave Ablation of Renal Tumors Using a Gas-
Cooled 2.4
-GHz Probe: Technique and Initial Results
December 2015
REFERENCES
Disclosure: Dr. Christopher Brace is a shareholder and consultant for NeuWave Medical, Inc., and a co-inventor on patents related to thermal tumor ablation. Dr. Fred
Lee is the founder and shareholder for NeuWave Medical, Inc., and a co-inventor on patents related to thermal tumor ablation. . Dr. Paul Laeseke is a shareholder and
consultant for NeuWave Medical, Inc. and a co-inventor on patents related to thermal tumor ablation. Dr. J. Louis Hinshaw is a shareholder for NeuWave Medical Inc.
1. D. Dupuy & K. Chu, Biological mechanisms and advances in therapy. Nature Reviews Cancer 2014 14,199–208 doi:10.1038/nrc3672
2. H. Bang, et al. Percutaneous cryoablation of metastatic lesions from non-small cell lung carcinoma: Initial survival, local control, and cost observations. JV IR 2012.
3. Kurup, N, et al. Image-Guided Percutaneous Ablation of Bone and Soft Tissue Tumors. Semin Interv ent Radiol. 2010.
4. Georgiades, C, et al. Determination of the Nonlethal Margin Inside the Visible ‘‘Ice-Ball’’ During Percutaneous Cryoablation of Renal Tissue. Cardiovasc Intervent
Radiol (2013) 36:783–790
5. Knavel, E, et al. Tumor Ablation: Common Modalities and General Practices. Techniques in Vascular and Interventional Radiology 2013.
6. Mahnken, A, et al. CT- and MR-Guided Interventions in Radiology 2nd Edition 2013.
7. Lu. D, et al, Influence of Large Peritumoral Vessels on Outcome of Radiofrequency Ablation of Liver Tumors. JV IR 2003.
8. Huffman, S.D., et al. Radiofrequency Ablation Complicated by Skin Burn. Semin Intervent Radiol. 2011.
9. JVIR. Aug 2010; 21(8 Suppl): S192–S203. doi: 10.1016/j.jvir.2010.04.007
10. Brace C., et al. Microwave ablation technology: what ev ery user should know. Curr Probl Diagn Radiol. 2009;38(2):61–67.
11. Brace, C. Microwave Tissue Ablation: Biophysics, Technology and Applications. Critical Reviews in Biomedical Engineering 38(1):65-78, 2010.
12. Sun, et al. Comparison of temperature curve and ablation zone between 915-and 2450-MHz cooled-shaft microwave antenna: Results in ex vivo porcine livers.
European Journal of Radiology. 2011.
13. NeuWave Medical Time and Power Guide - ex-vivo bovine lung and liver.
14. Lubner, M. et al. Microwave Tumor Ablation: Mechanism of Action, Clinical Results and Devices. J Vasc Interv Radiol. 2010 Aug; 21(8 Suppl): S192–S203.
15. Yu, et al. JVIR 19:1084-1092, 2008. Bhardwaj, et al. Pathology 41:168-172, 2009.
16. Brace, C. et al. Radiofrequency and Microwave Ablation of the Liver, Lung, Kidney, and Bone: What Are the Differences? Curr Probl Diagn Radiol 2009.
17. Brace C. et. al. Pulmonary Thermal Ablation: Comparison of Radiofrequency and Microwave Devices by Using Gross Pathologic and CT Findings in a Swine Model.
Radiology: Volume 251: Number 3—June 2009.
18. Poggi, et al. Microwave Ablation of Hepatocellular Carcinoma Using a New Percutaneous Device: Preliminary Results. Anticancer Research. 33: 1221-1228 (2013).
19. Groeschl, et al. Abstract: Microwave ablation for hepatic malignancies: A multi -institutional analysis. 2013 Gastrointestinal Cancers Symposium. J Clin Oncol
30: 2012 (suppl34; abstr218).
20. Liu, et al. Percutaneous microwave ablation of larger hepatocellular carcinoma. Clinical Radiology 68 (2013) 21e26.
21. Groeschl, et al. Recurrence after microwave ablation of liver malignancies: a single institution experience. HPB (Oxford). 2013 May;15(5):365-71.
22. Liu, et al. Efficacy and safety of thermal ablation in patients with liver metastases. European Journal of Gastroenterology & Hepatology 2013, 25:442–446.
23. Liang, et al. Percutaneous cooled-tip microwave ablation under ultrasound guidance for primary liver cancer: a multi centre analysis of 1363 treatment-naive lesions
in 1007 patients in China. Gut 2012;61:1100-1101.
24. Lin-Feng, et al Large primary hepatocellular carcinoma: Transarterial chemoembolization monotherapy versus combined transarterial chemoembolization-
percutaneous microwave coagulation therapy. Journal of Gastroenterology and Hepatology 28 (2013) 456–463.
December 2015
25. Martin, et al. Safety and efficacy of microwave ablation of hepatic tumors: a prospective review of a 5-year experience. Ann Surg Oncol. 2010 Jan;17(1):171-8.
26. Livraghi, et al. Complications of Microwave Ablation for Liver Tumors: Results of a Multicenter Study. CVIR, August 2012, Volume 35,Issue 4, pp 868-874.
27. Lin, et al. Percutaneous Microwave Ablation of Renal Cell Carcinoma Is Safe in Patients With a Solitary Kidney. Urology. 2014 Feb;83(2):357-63.
28. Moreland, et al. Percutaneous Microwave Ablation of T1 Renal Cell Carcinoma: Multicenter Evaluation of Safety and Early Clinical Effi cacy. Journal Of
Endourology Sept. 2014; Volume 28, Number 9
29. Guan, et al. Microwave Ablation Versus Partial Nephrectomy for Small Renal Tumors: Intermediate-Term Results. Journal of Surgical Oncology 2012;106
30. Yu, et al. Us-guided Percutaneous Microwave ablation of renal cell carcinoma: Intermediate-term Results. Radiology: Volume 263: Number 3—June 2012.
31. Muto, et al. Laparoscopic Microwave Ablation and Enucleation of Small Renal Masses: Preliminary Experience. European Urology 60 (2011) 173-176.
32. Guan, et al. Retroperitoneoscopic Microwave Ablation of Renal Hamartoma: Middle-term Results . J HuazhongUnivSciTechnol[MedSci]30(5):2010."
33. Carrafiello, et al. Single-antenna microwave ablation under contrast-enhanced ultrasound guidance for treatment of small renal cell carcinoma: preliminary
experience. Cardiovasc Intervent Radiol. 2010 Apr;33(2):367-74.
34. Liang, et al. Ultrasound guided percutaneous microwave ablation for small renal cancer: initial experience. J Urol. 2008;180:844-848.
35. http://www.sirweb.org/patients/liver -cancer/ accessed on 2/17/15
36. National Lung Cancer Alliance accessed on 2/19/15
37. NCCN Guidelines
REFERENCES
December 2015
1/5/2016
1
Fred T. Lee Jr., MD
Department of Radiology
Microwave ablation for T1a RCC
Disclosures
•Founder, NeuWave Medical Inc. (Microwave)
•Inventor, patents: Certus 140TM
•Inventor, patents, royalties, Covidien Switching
ControllerTM (RF)
•NIH grants: R21RR018303
R01CA108869
R01CA118990
R01CA112192
0
10
20
30
40
50
60
02' 03' 04' 05' 06' 07' 08' 09' 10' 11' 12' 13' 14' 15'
Procedures performed
Year
U Wisconsin RCC Percutaneous Ablation
Procedures 2002-2015
MW
Cryo
RF
1/5/2016
2
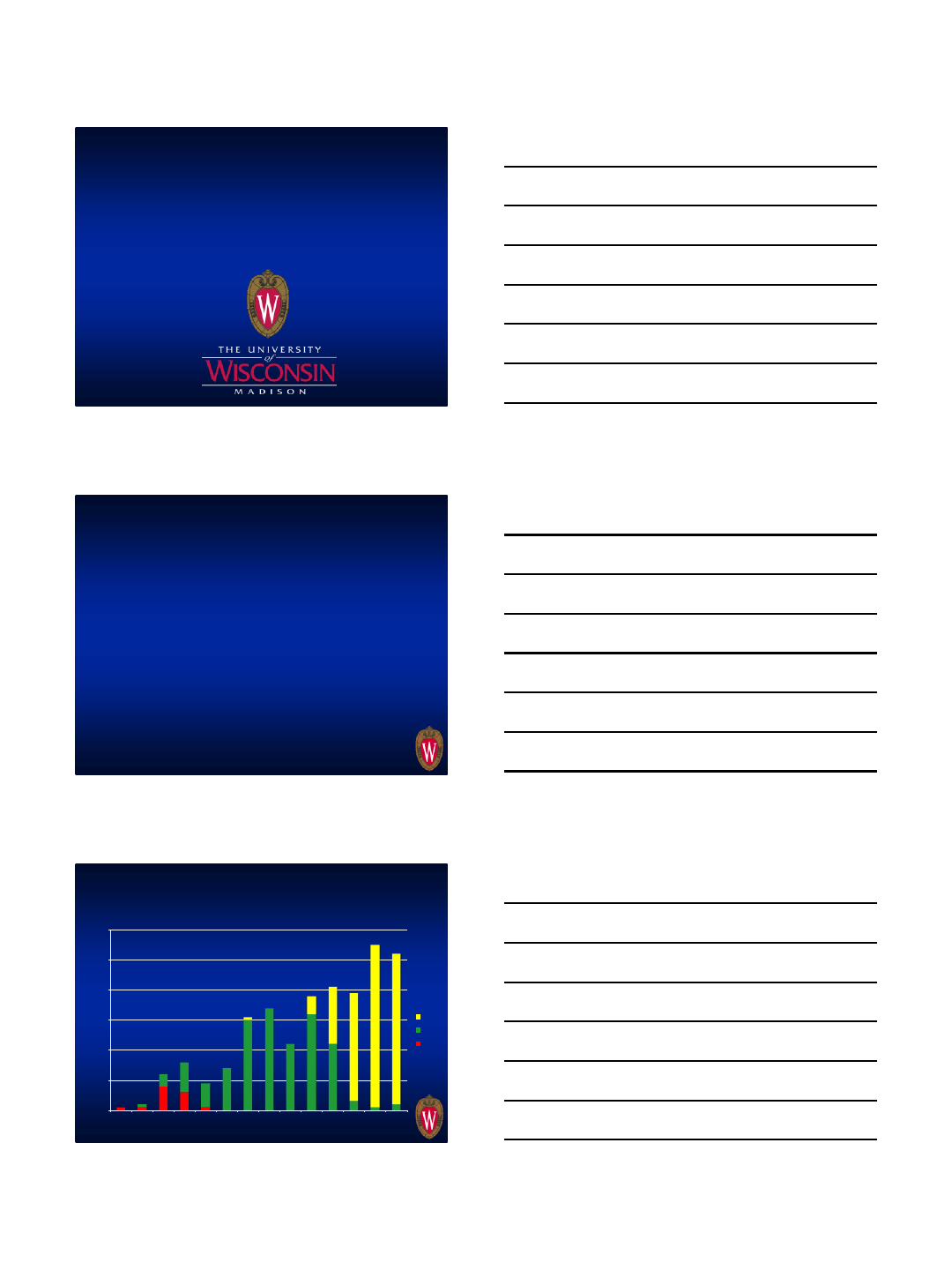
T1a RCC-anatomy is everything
•Defined as < 4cm in size
•Not all are created equal
•Anatomic position is probably more important than size
•Nephrometry (RENAL) score predicts LTP and complications
Reyes, et al. Urol
Onc 2013;31
Schmidt, et al. J
Urol 2013;189
www.nephrometry.
com
1/5/2016
3
6.3 cm RCC: Pre-ablation scans
3 LK’s placed in top half of tumor
Ablated 140W each x 1 minute, then 65W for 5 minutes
1/5/2016
4
Pre 15 mo post
Pre 15 mo post
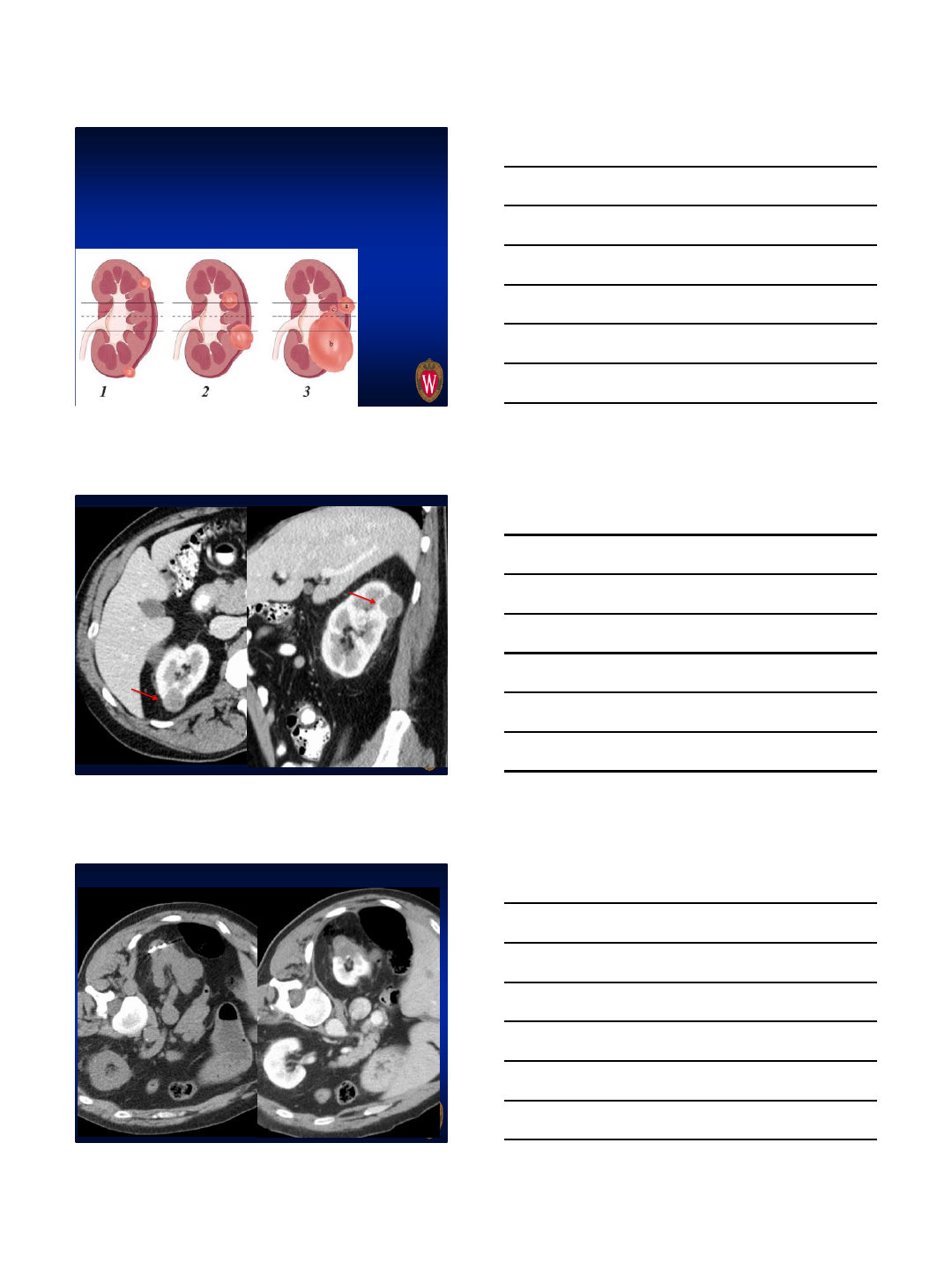
The one place ablation struggles
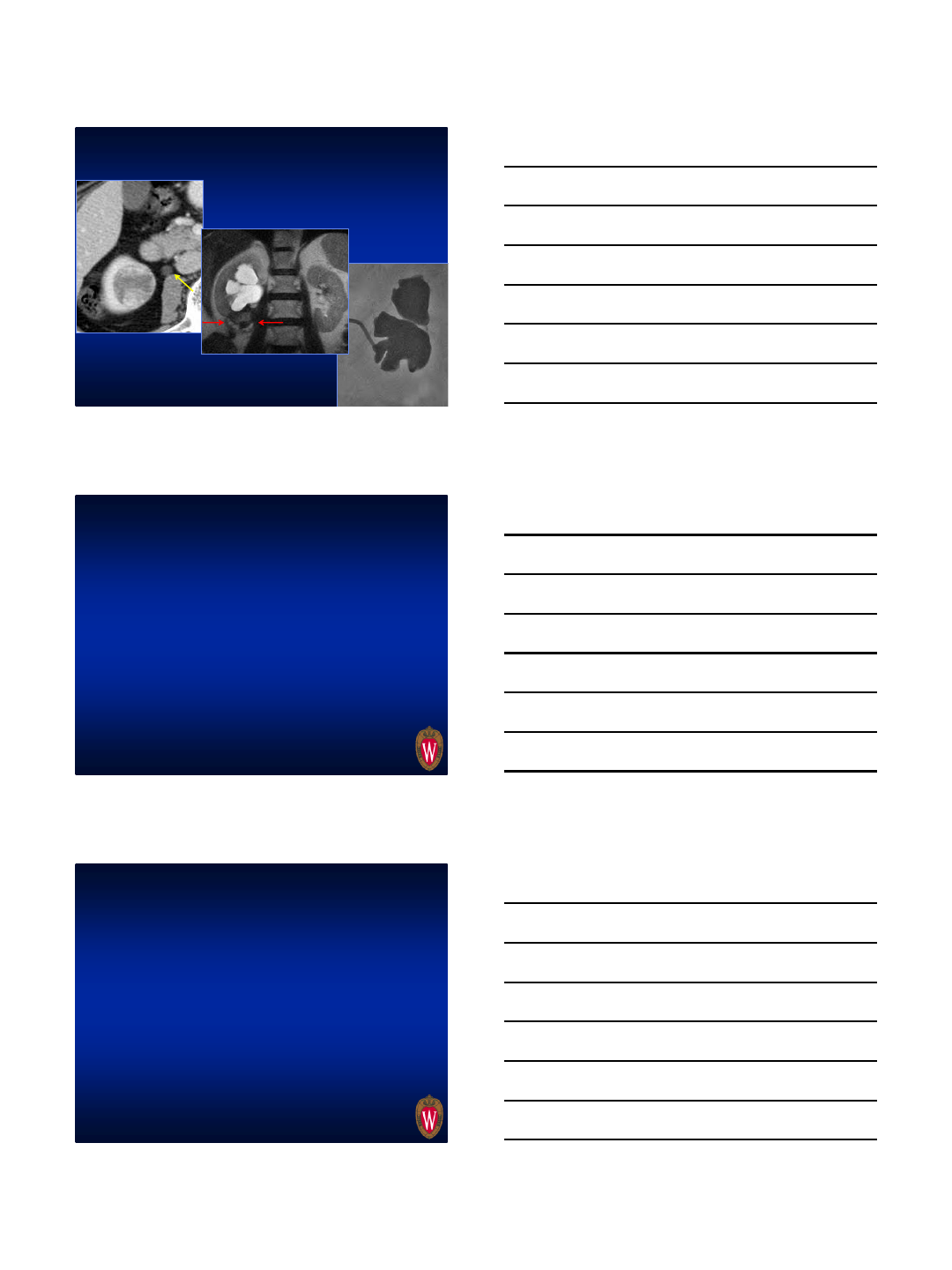
1/5/2016
5
Ureteral injury after cryo
Why we use mostly MW
• Tumor control (I’ll show you our data)
•Physics (esp tissue contraction)
•Speed
•Pain (?)
•Costs
•Hassle
•Visibility
MW and RF are closely related
•Mechanism of cell kill is identical (indistinguishable
under the microscope)
• “Microwave” is actually in the RF spectrum
•AMA and SIR coding guidelines for MW: Use RF
codes
•MW hotter (more likely to reach 60°C) , faster, no
ground pads, fewer probes, better against vessels
•Microwave-penetrates all biologic tissues (including
aerated lung, bone, char)
•Think of MW as an advanced RF system
1/5/2016
6
Why do you need such high temps?
•No resistant cells> 60
°
C
•Chemo, radiation, cryo all have resistant cells
(Tatsutani)
•Cancer stem cells are radio/chemo resistant,
?cold resistant
•Phospholipids in cell membranes melt between
45-55 °C
–Furuya, J Phys Soc Jn 1978
If you use heat: Hotter is better!
Costs
•UW experience:
–Cryo 2.8 probes/procedure+gas
($113.65/tank)
–MW: 1.8 probes/procedure+gas ($5.24/tank)
–~150 cases, assume $1500/probe
–Cost savings= ~$271,270 + physician time +
room time
Hassle factor:
•No ground pads
•No heavy tanks
•No wrenches
•No heavy
cables/lines
•No water lines
•Fast
1/5/2016
7
Cryo Failures
2006
Preablation 1st Cryo 21 Months
Post 2nd Cryo 4 Years
Post MW 8/2013
Local tumor control: MW
9 mos post
2 probe
cryoablation
MW RCC-literature
•~700 patients reported, pace increasing
•All studies positive w/one exception (Castle, Urology
2011). 10 patients, LTP 38%
–Perc CT, 1st gen MW, cases done by urologists, no
radiology
•Yu, et al (Radiology 2012): n=49, LTP 7.7%, 20.1 mo f/u,
no severe complications
•Yu, et al (Radiology 2013): MW (n=65) vs. nephrectomy
(n=98). 5-yr survival (cancer specific)=97.1 MW vs. 97.6%
nephrectomy
•Martin, et al (Diagn Int Radiol 2013): Meta-analysis 1st gen
MW vs. Cryo, conclusion: no difference (but more studies
for cryo)
1/5/2016
8
•MW=105 (2.7 cm) vs. Nephrectomy=328 (2.8 cm)
•MW patients older, sicker, worse renal fxn
•Complications NSD, renal function better w/ MW
•Overall survival better w/ nephrectomy (p=0.0004)
•Tumor specific survival same (p=0.38)
UW data-T1a RCC
•N=100, dia=2.6 cm, f/u=17 mo (out to 48 mo)
•BMI 32.2, nephrometry score 7 (moderate
complexity)
•eGFR pre 71.8, post 68.7
•Hydrodissection 34%
•1.8 antennas, 65W, 5 min
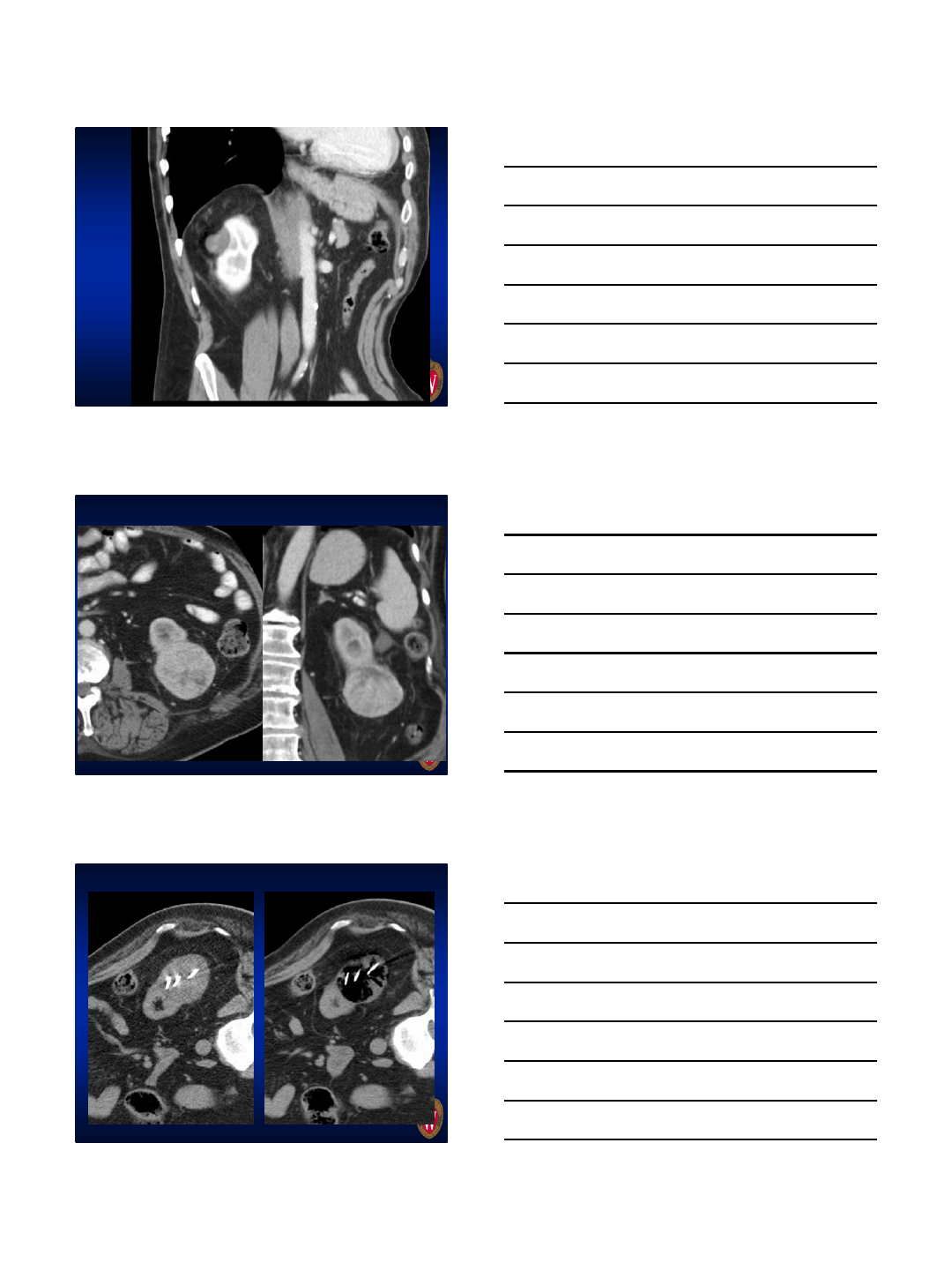
• We’ve done 3 RCC in renal transplants
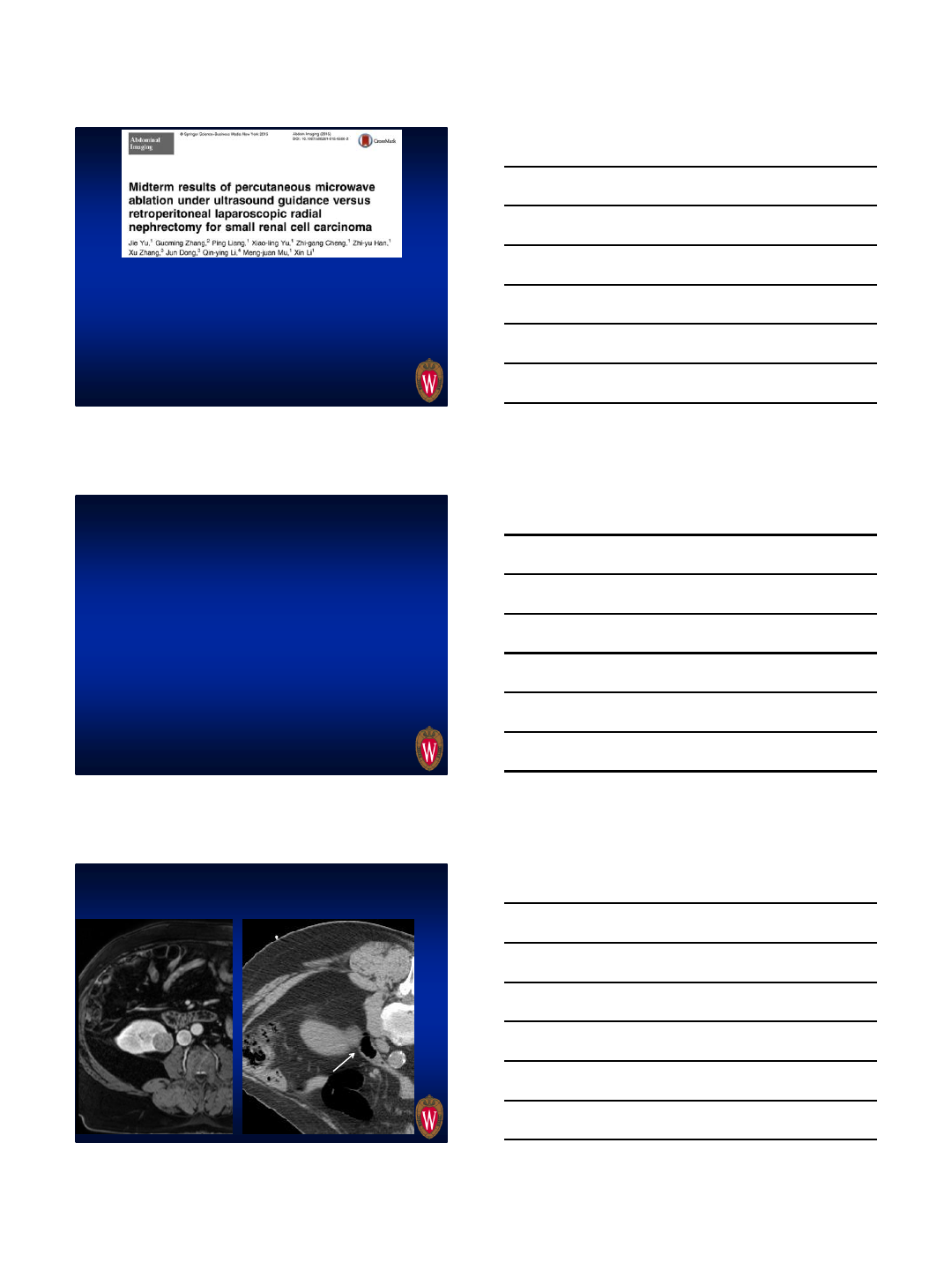
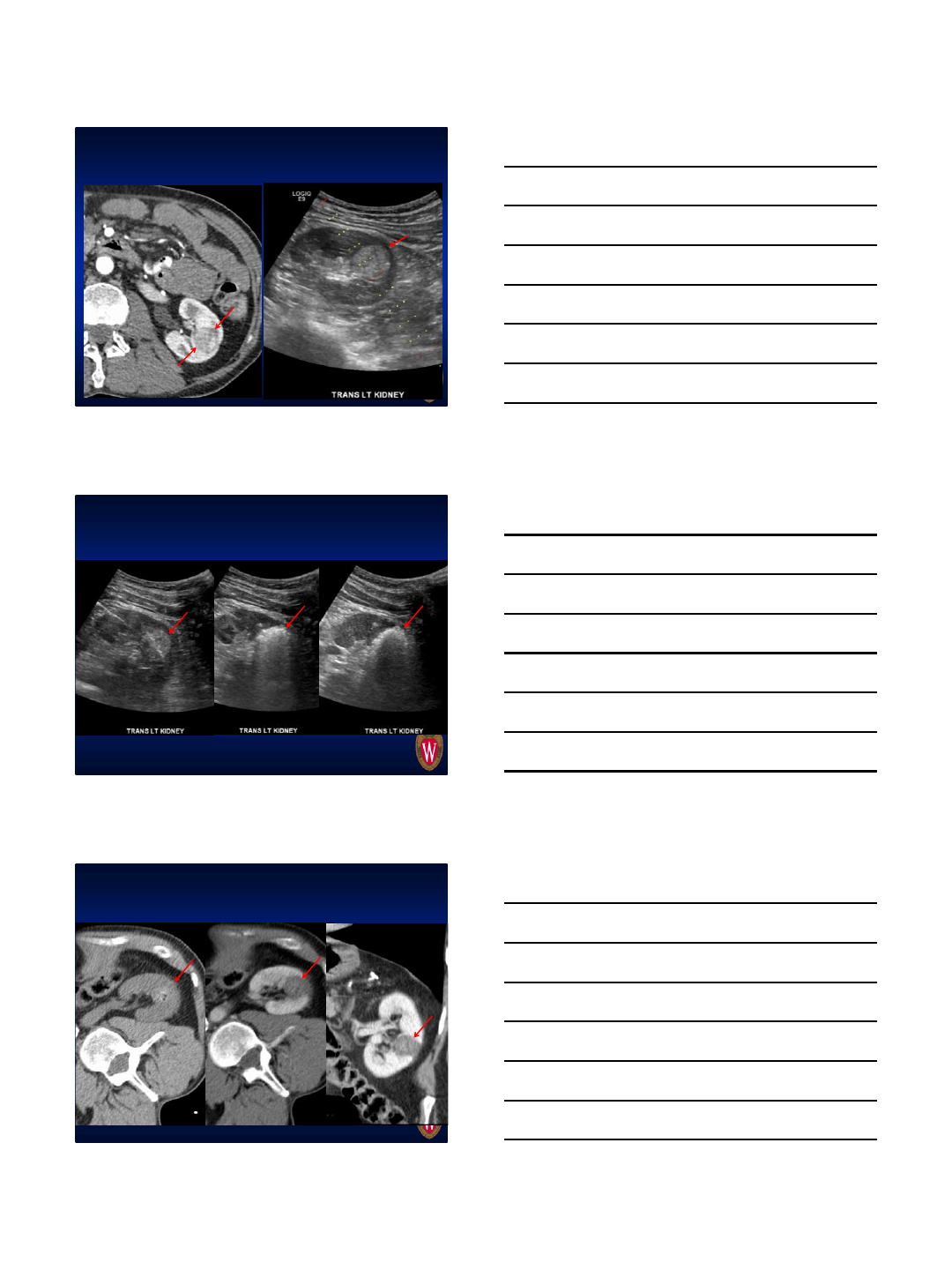
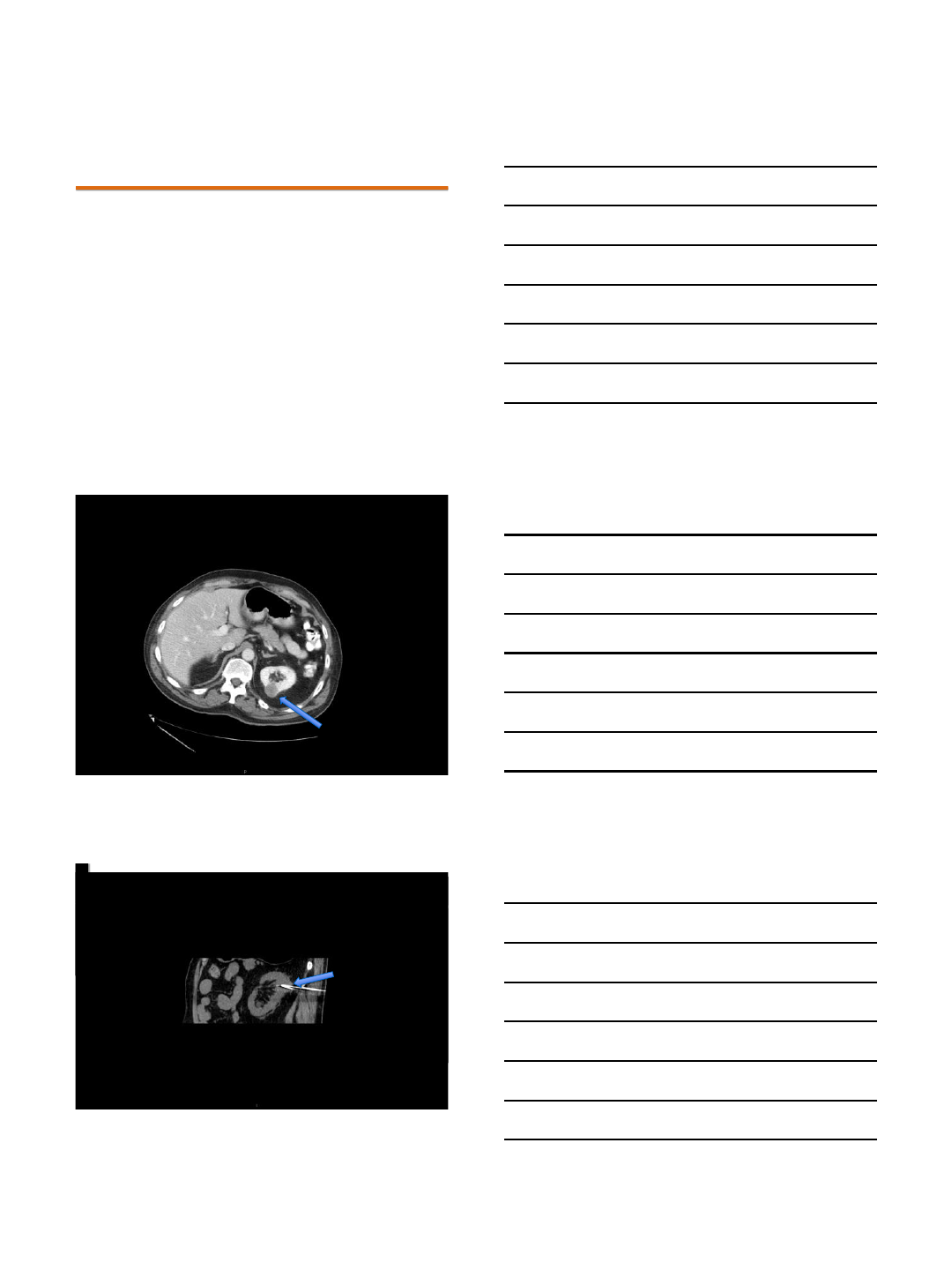
RCC in renal transplant
Duodenum
*
*
1/5/2016
9
RCC in renal transplant
D
D
D
*
*
*
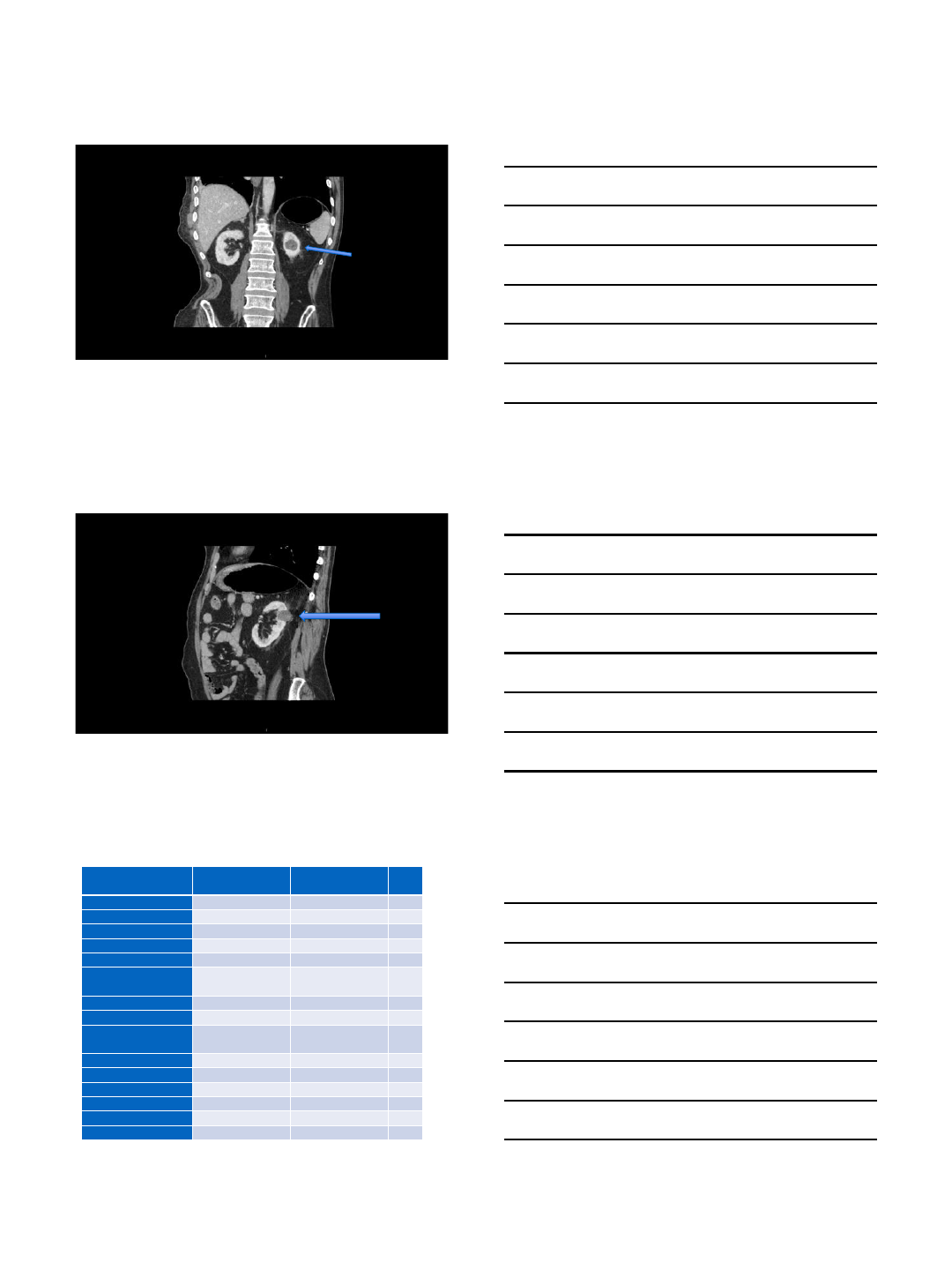
Hydrodissection
RCC in renal transplant
*
Ablation
82 yo with 48 mo f/u
Pre MW 44 mo post MW
1/5/2016
10
82 yo with 48 mo f/u
Pre MW 44 mo post MW
65 yo with 35 mo f/u
•1 LTP (1%), Furhman Gr 4, at 25 mo
•No RCC deaths, no mets
•3 deaths: MI (5 mo), lymphoma (9 mo), GI
bleed (39 mo)
•PFS=99%, CSS=100%, OS=97%
• Tumor complexity, BMI didn’t effect results
•11 complications, most minor, 3 related to
procedure (RP bleed, hematuria x 2)
•6 urinomas on delayed imaging
UW data-T1a RCC
1/5/2016
11
Retroperitoneal hematoma Day 10
Pre MW
Pre MW
During MW
Retroperitoneal hematoma Day 10
Retroperitoneal hematoma, POD#10
Coinciding w/ restarting heparin + warfarin 28 mo post
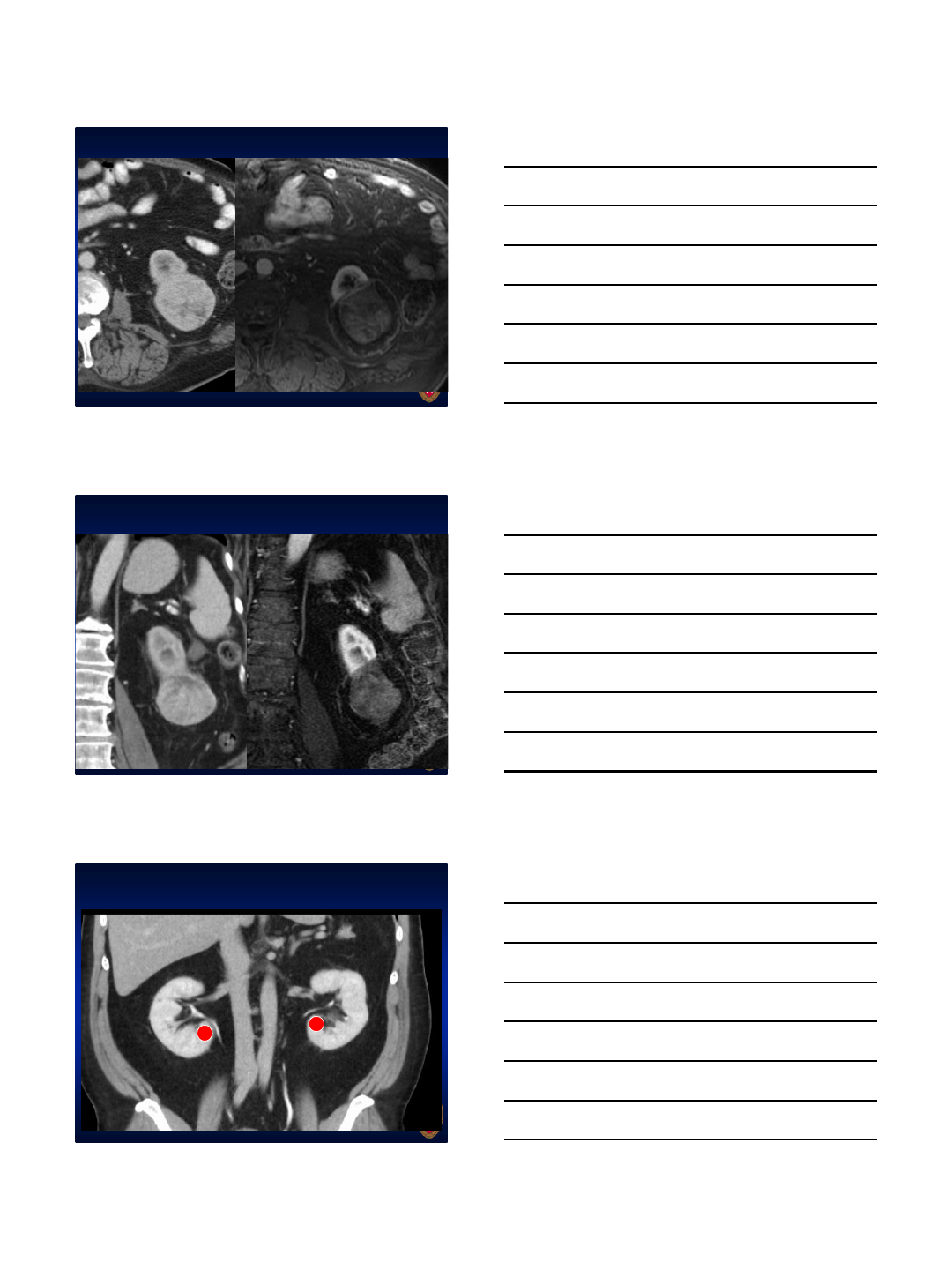
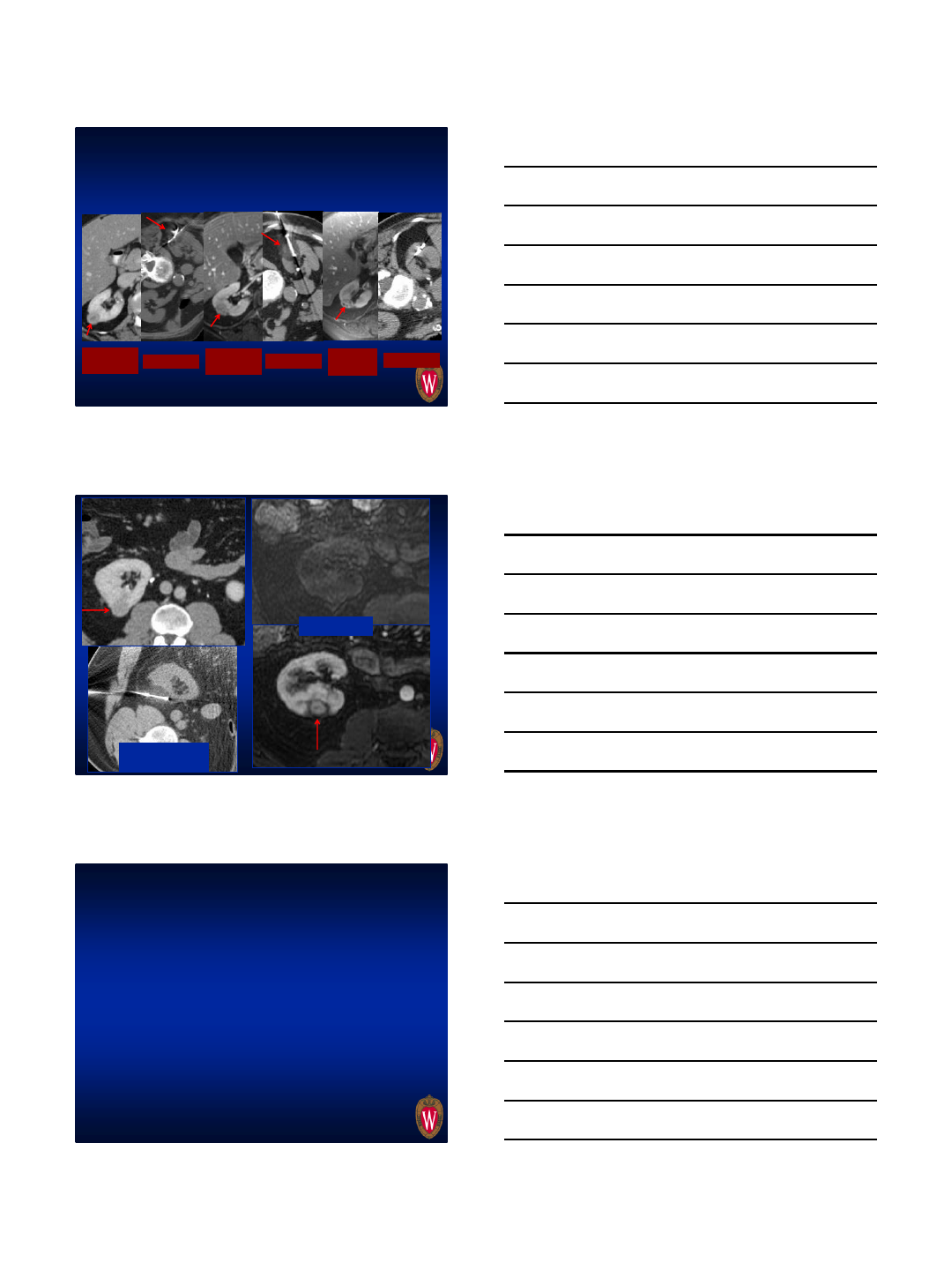
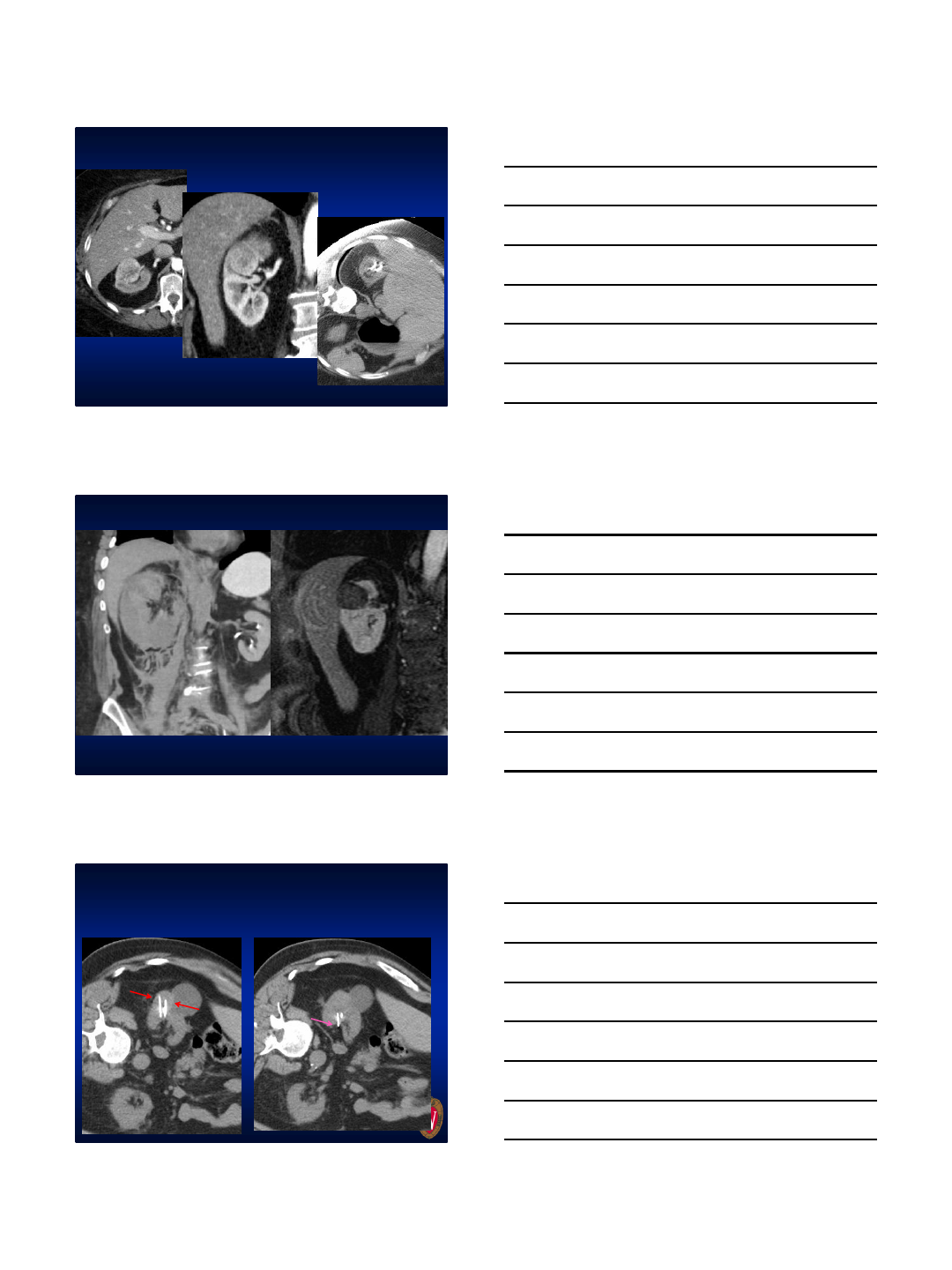
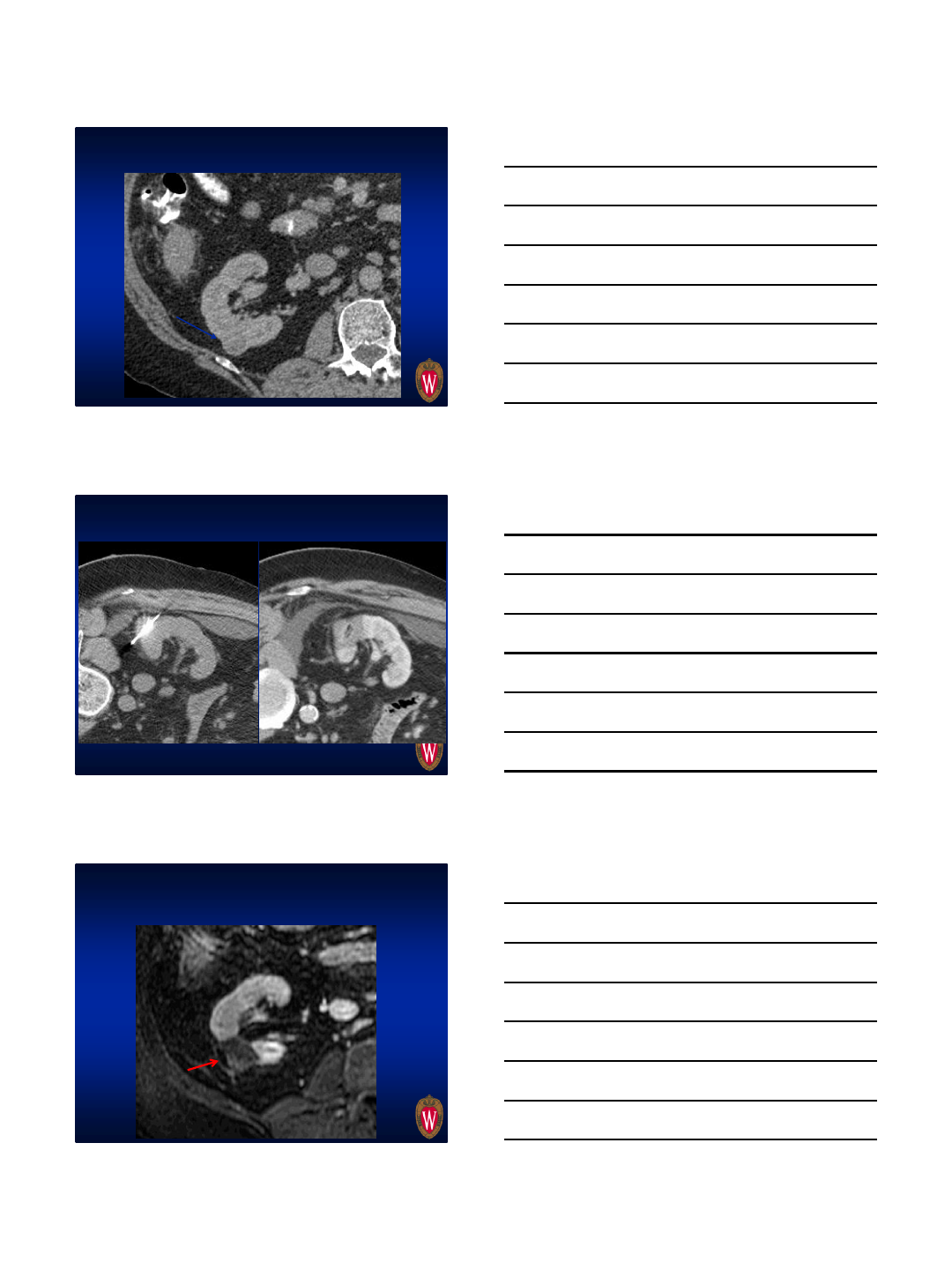
Urinomas, most detected late
Probe tip too deep
In collecting system
1/5/2016
12
Urinomas, most detected late
Track
Immed
post T2WI 24 mo
post T1WI+C 24 mo
post
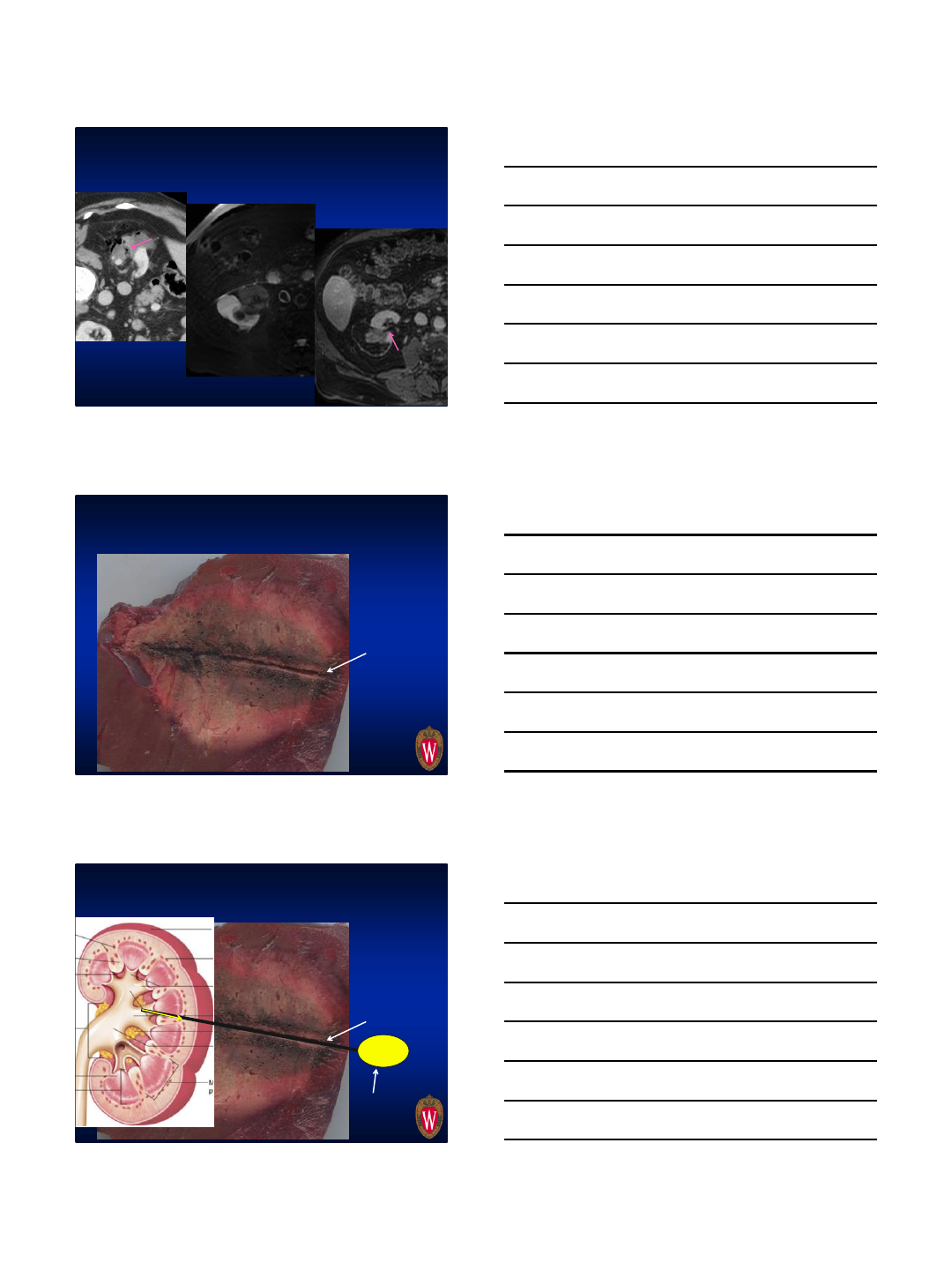
Urinomas, mechanism
Probe track
Urinomas, mechanism
Probe track
www.studyblue.com
Urinoma
1/5/2016
13
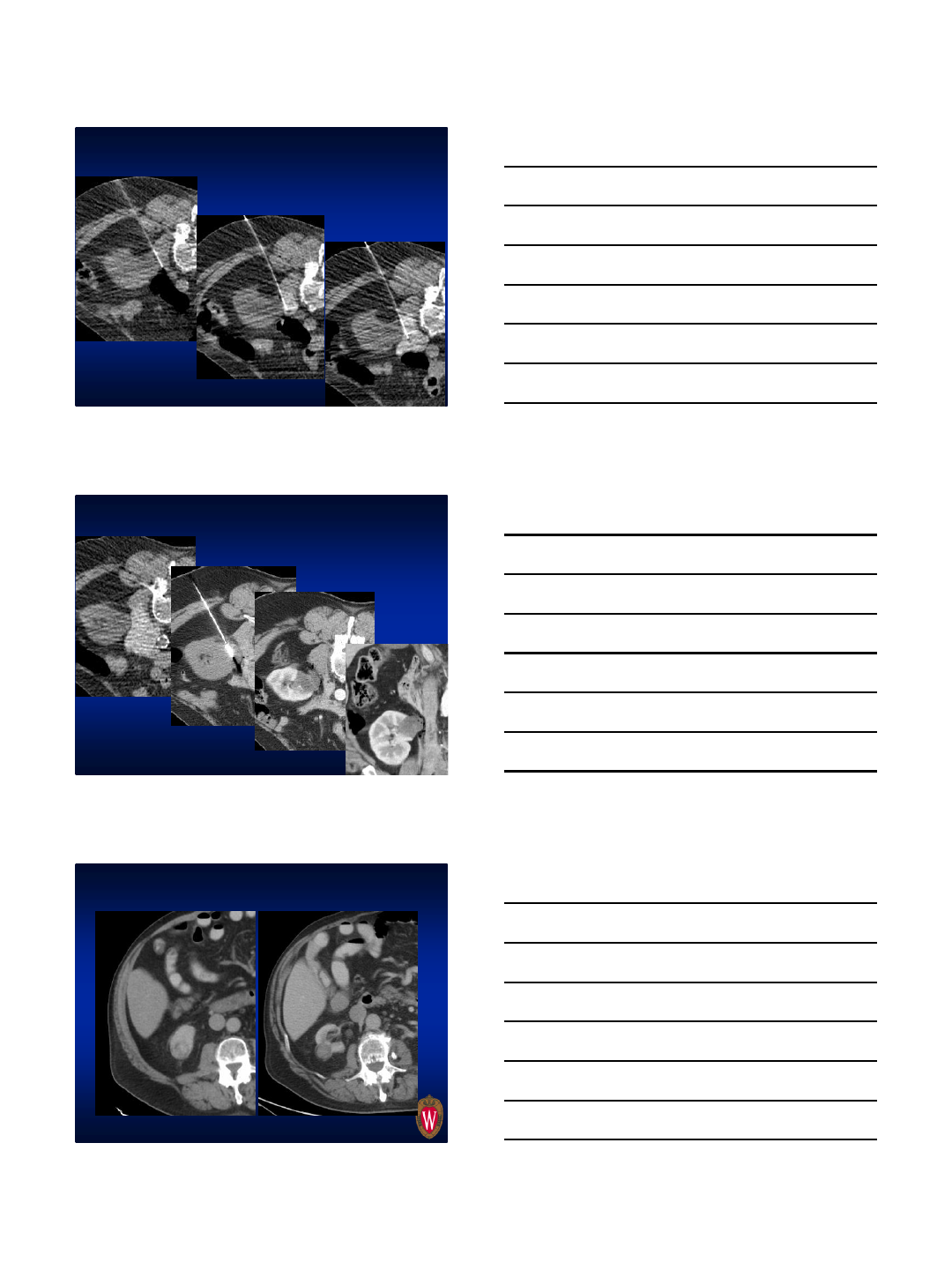
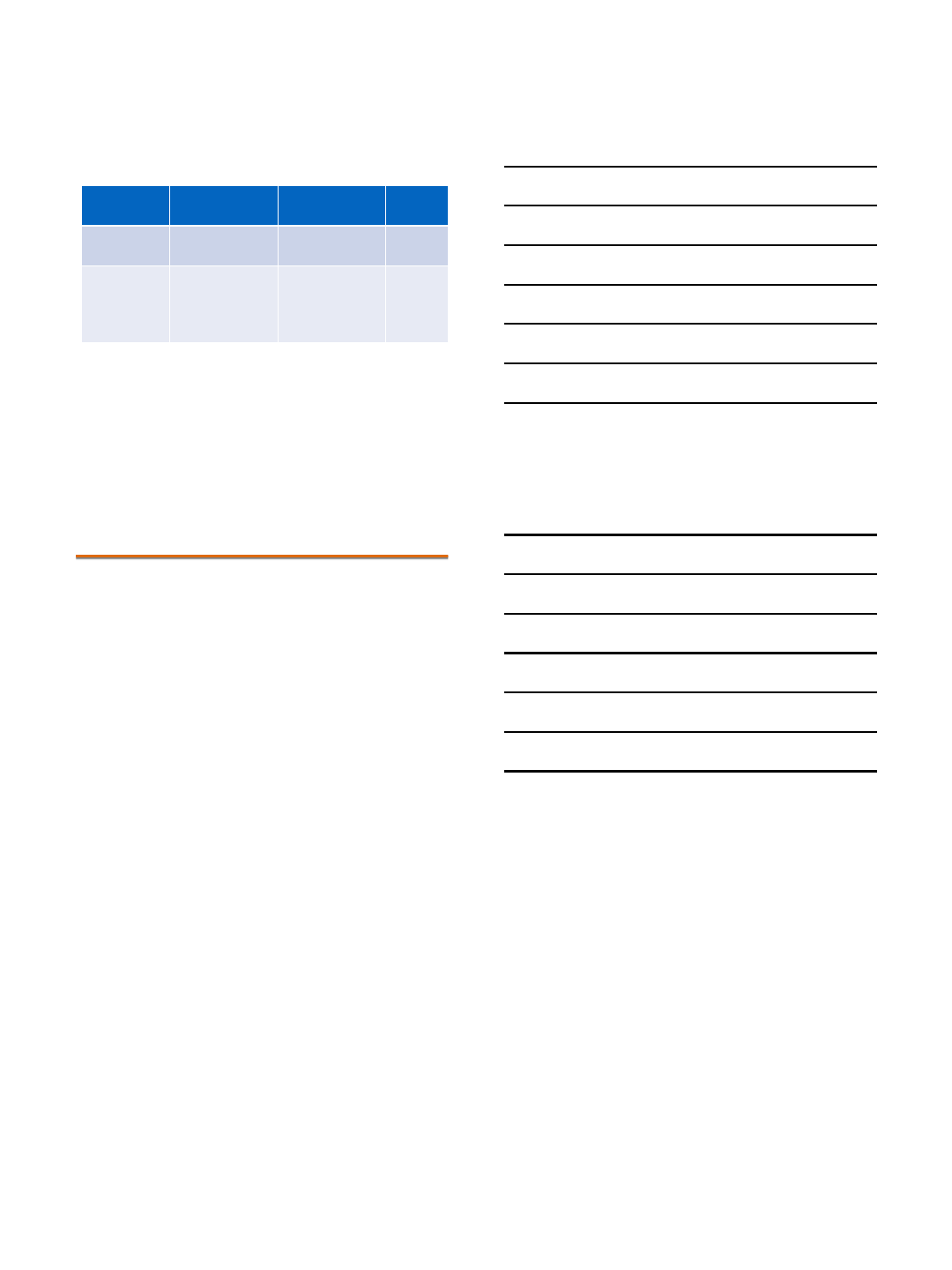
How we place probes now
2.2 cm endophytic RCC
2PR’s, 65W for 3 minutes, then 40W for 2
minutes
During ablation (bubbles highly visible)
Post ablation CT
1/5/2016
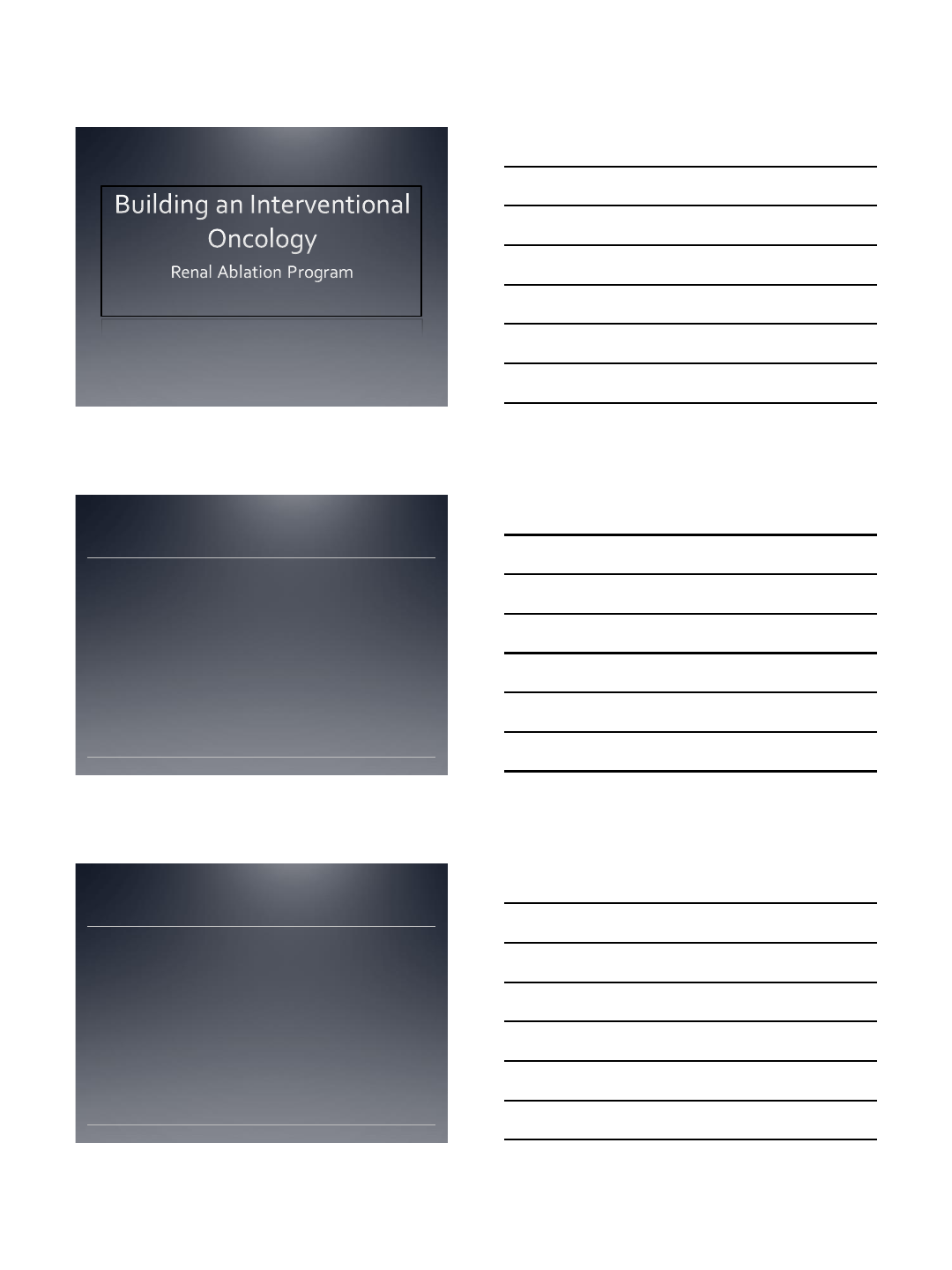
14
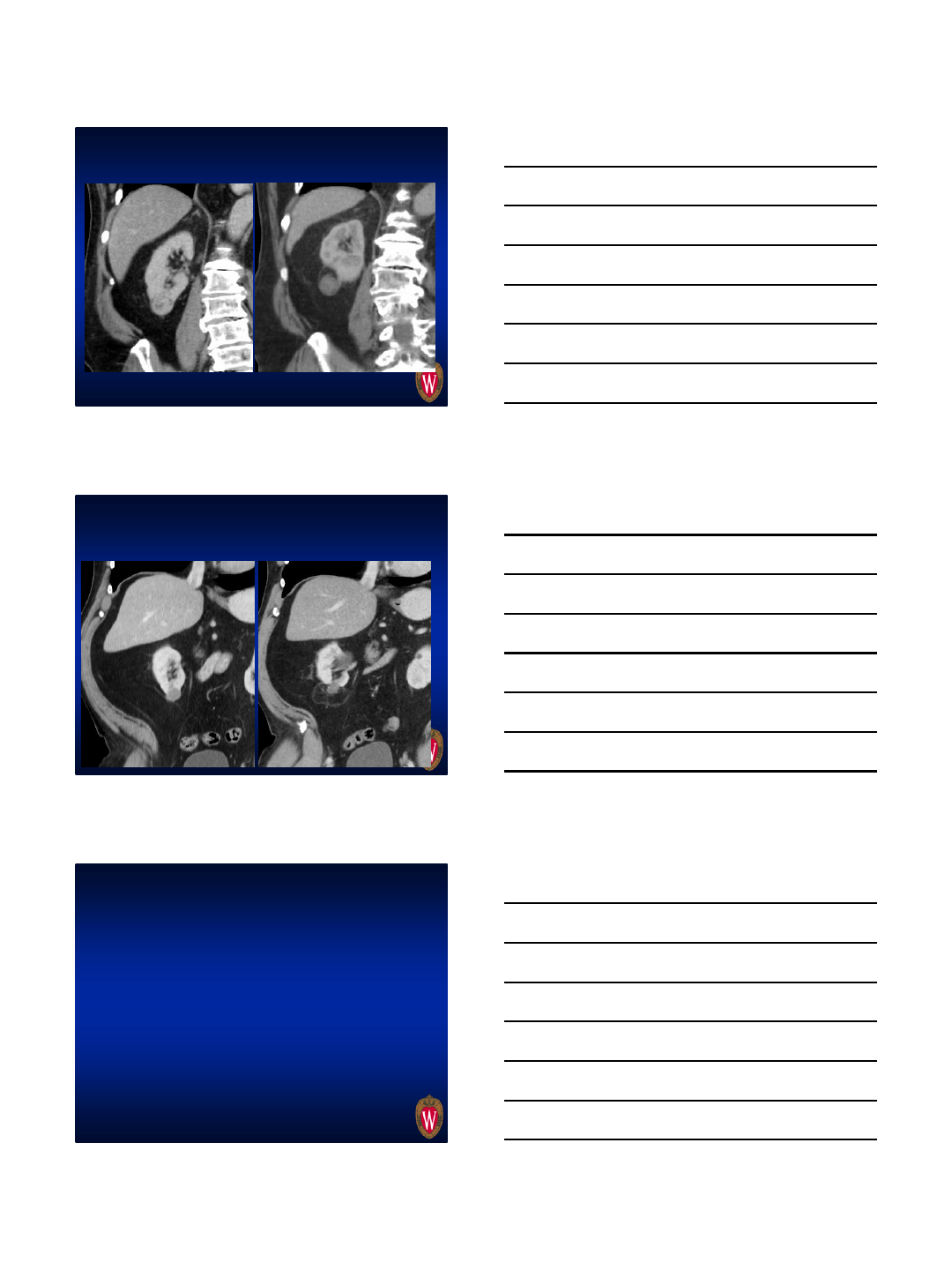
Tangential approach to avoid collecting
system
2.9 cm
Immediate Pre Immediate Post ablation
7 months post ablation
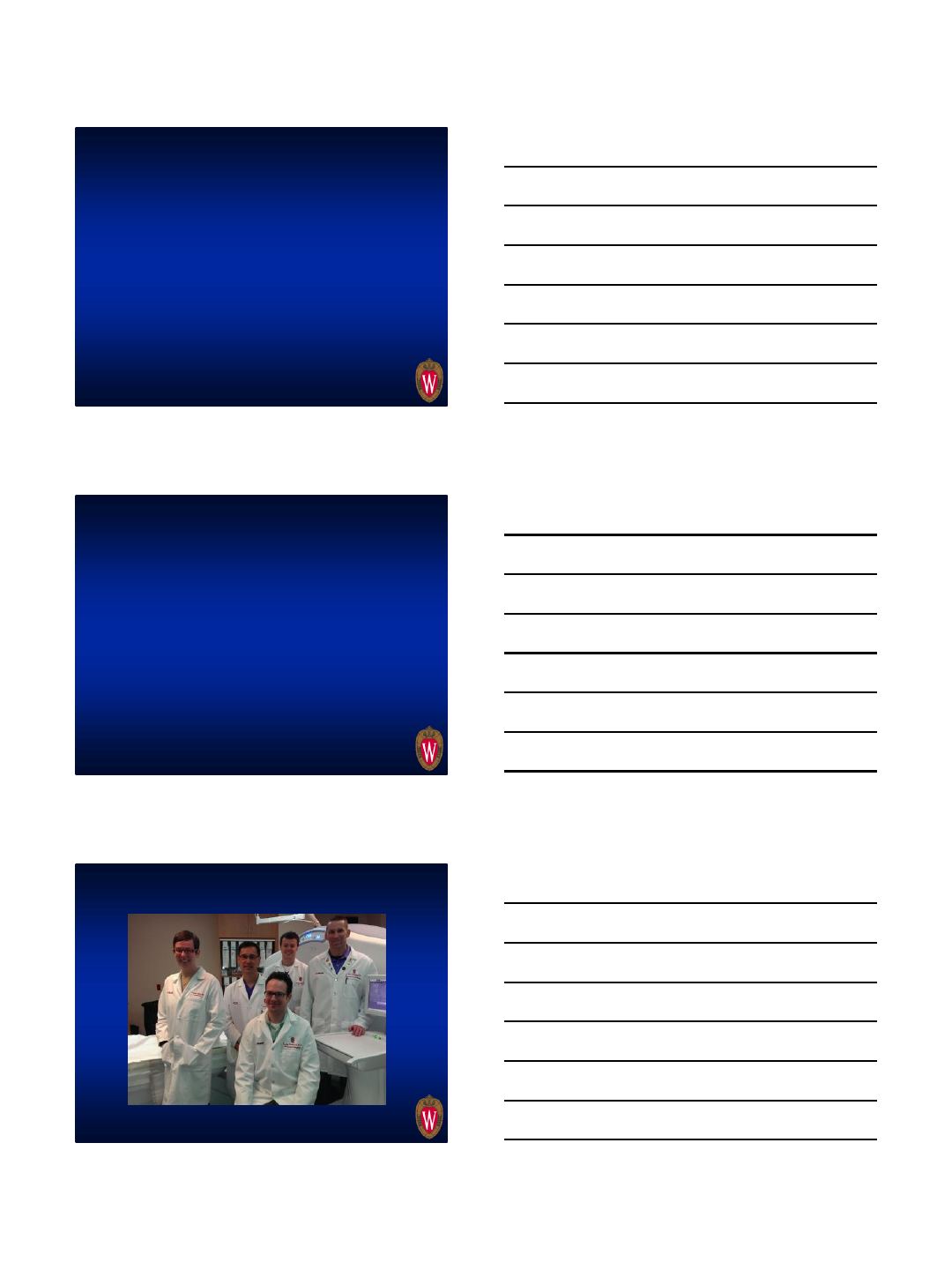
1/5/2016
15
Preventing urinomas: Don’t puncture
collecting system!
•Before tangential approach=29 endophytic RCC
•Median RENAL score of 8.5
•6 urinomas
•With tangential approach=35 endophytic RCC
•Median RENAL score of 8.5
•0 urinomas
Summary
•MW highly effective for local control T1a RCC
• Is MW “better” than other modalities? You be
the judge
•We favor MW due to effectiveness, speed,
costs, decreased hassle
•Watch out for inferior medial pole tumors with
any modality
•Urinomas associated with puncture of collecting
system, ergo, don’t do it…
Thank you for your attention!
flee@uwhealth.org
UW Tumor Ablation Team: Meg Lubner, Fred Lee,
Tim Ziemlewicz, Shane Wells, Louis Hinshaw
1/5/2016
1
Percutaneous Microwave Ablation
Noah S. Schenkman, MD
University of Virginia Health System
Disclosures
Paid physician consultant by NeuWave for my time
to present my experience in this presentation.
Multi-Disciplinary: Radiology and Urology
Combined Decision-making
Small Renal Mass Conference
Active surveillance consideration
Timing of biopsy
US and CT
Immediate imaging
6 month imaging
Intraoperative uses?
Virginia Approach: Small Renal Mass
1/5/2016
2
Case
70 year old man incidentally found 1.5 cm renal
mass
Follow up CT 2 yrs later: 2.5 cm
Biopsy: Papillary Renal Cell Carcinoma
HTN, DM, paraplegia
Serum Cr 0.9, eGFR= 97
Preoperative CT
Needle Placement
1/5/2016
3
stPost-Procedure
Post-Procedure
Cryoablation
(n=21)
Microwave Ablation
(n=38)
p-
value
Gender
0.56
Male
13 (62%) 27 (71%)
Female
8 (38%) 11 (29%)
Age -
years (range)
67.0 (44-88) 67.2 (40-87)
0.96
BMI - cm2
/kg (95%CI)
29.3 (27.1-31.5) 29.9 (28.0-31.8)
0.69
Charlson Comorbidity
Score
Nephrometry Score
Numerical (95%CI)
6.6 (5.6-7.6) 6.7 (6.0-7.4)
0.93
Posterior location –
N
(%)
12 (57.1%) 26 (78.8%)
0.23
Volume –mm3
(95%CI)
12.5 (6.7-18.2) 15.3 (8.7-22.0)
0.50
Pathology
0.06
Clear Cell RCC
10 (47.6%) 17 (56.7%)
Papillary RCC
4 (19.0%) 11 (36.7%)
Chromophobe RCC
1 (4.8%) 1 (3.3%)
NOS
6 (28.6) 1 (3.3%)
1/5/2016
4
Cryoablation
Microwave
Ablation
P
-
value
Recurrence
4 (19%) 1 (3.0%) 0.05
Average
Cost
(U.S. Dollars)
6354.1 (4777.1-
7931.0)
4121.9 (3269.0-
4974.8)
0.02
Complications
Cryoablation
Non-ST Elevation Myocardial Infarction
Pulmonary Embolus
Hematoma Requiring Transfusion
Microwave
Pneumonia
UTI
1/5/2016
1
Dr Roger Williams
Interventional Oncology
Interventional Radiology
Quantum Radiology
Marietta, GA
Disclosure:
Paid clinical education consultant for NeuWave Medical
Overview
The principle of moving to a new country.
Securing Employment (Service line)
Establish Housing (Clinic)
Developing Friendships (Referrals)
Understanding Landscape of Tumor Board
(Bureaucracy )
Partnering in Multidisciplinary Tumor Board
(Currency)
1/5/2016
2
Service Line
Interventional oncologist
= Clinician, administrator,
scheduler, **advocate
for patient, cache
Become educated on the
pertinent literature (BPO)
Develop technical skills
to become successful
Develop skill set
through challenging
cases
Clinic
Establish a dedicated
space, time and contact
numbers
Establish a streamline
EASY means for referrals
Lab and Imaging review
Lend Imaging expertise
to patient
Referrals
Simplify process for
referrals
Not all Urologist are the
same (Prostate v. Kidney)
Discuss criteria:
Operative/ Non
Operative
Ablation under
conscious sedation
Partial nephrectomy
TNM Staging
1/5/2016
3
Bureaucracy
Urologist thoughts on
Ablation
Prior experience:
In training
At facility
Cryo v. RFA v. Microwave
Complications
Management
Currency
Procedural control
Partial nephrectomy
Ablation
Procedural control
(Ablation)
Urology
Radiology
Follow up
Urology
Radiology
