Philips Medical Systems North America SRRBV1 Short Range Radio Module User Manual m81029001b
Philips Medical Systems North America Co. Short Range Radio Module m81029001b
Contents
User Manual MP2

Patient Monitoring
INSTRUCTIONS FOR USE
IntelliVue MP2
Patient Monitor
Release G.0 with Software Revision G.0x.xx
S
Printed in Germany 09/08
*M8102-9001B*
Part Number M8102-9001B
4512 610 28821
M8102-9001B
i
1Table Of Contents
1Installation 1
Installation Checklist 1
Unpacking and Checking the Shipment 2
Mounting the Monitor 3
Mounting the External Power Supply (M8023A) 3
Connecting the Monitor to AC Mains 3
Checking Out the Monitor 5
Operating the Monitor 6
Setting the Date and Time 7
Checking Country-Specific Default Settings 7
Handing Over the Monitor 7
2Basic Operation 9
Introducing the IntelliVue MP2 10
Controls, Indicators and Connectors 10
Extending Measurements 13
Operating and Navigating 16
Operating Modes 22
Understanding Screens 23
Using the XDS Remote Display 24
Using the Visitor Screen 24
Understanding Profiles 25
Understanding Settings 26
Changing Measurement Settings 27
Switching a Measurement On and Off 27
Adjusting a Measurement Wave 27
Using Labels 28
Changing Monitor Settings 30
Checking Your Monitor Revision 30
Getting Started 31
Disconnecting from AC Mains Power 32
Monitoring After a Power Failure 32
Networked Monitoring 32
Capturing Alarm Reports and Printing 33
3What’s New? 35
What’s New in Release G.0? 35
What’s New in Release F.0? 36
4Alarms 39
Visual Alarm Indicators 40
Audible Alarm Indicators 41
Acknowledging Alarms 42
ii
Pausing or Switching Off Alarms 43
Alarm Limits 45
Reviewing Alarms 49
Latching Alarms 50
Testing Alarms 51
Alarm Behavior at On/Off 51
Alarm Recordings 51
5Patient Alarms and INOPs 53
Patient Alarm Messages 53
Technical Alarm Messages (INOPs) 59
6Managing Patients 83
Admitting a Patient 83
Quick Admitting a Patient 85
Editing Patient Information 85
Discharging a Patient 85
Transferring Patients 86
7ECG, Arrhythmia, ST and QT Monitoring 89
Skin Preparation for Electrode Placement 89
Connecting ECG Cables 89
Selecting the Primary and Secondary ECG Leads 90
Checking Paced Status 90
Understanding the ECG Display 91
Monitoring Paced Patients 92
Changing the Size of the ECG Wave 93
Changing the Volume of the QRS Tone 94
Changing the ECG Filter Settings 94
Selecting Positions of Va and Vb Chest Leads (for 6-lead placement) 95
Choosing EASI or Standard Lead Placement 95
About ECG Leads 95
ECG Lead Fallback 96
ECG Lead Placements 96
Capture 12-Lead 100
EASI ECG Lead Placement 101
ECG and Arrhythmia Alarm Overview 102
Using ECG Alarms 103
ECG Safety Information 104
About Arrhythmia Monitoring 105
Switching Arrhythmia Analysis On and Off 106
Choosing an ECG Lead for Arrhythmia Monitoring 106
Understanding the Arrhythmia Display 107
Arrhythmia Relearning 110
Arrhythmia Alarms 111
About ST Monitoring 117
iii
Switching ST On and Off 117
Understanding the ST Display and Windows 118
Updating ST Baseline Snippets 119
About the ST Measurement Points 120
ST Alarms 122
Viewing ST Maps 122
About QT/QTc Interval Monitoring 127
QT Alarms 130
Switching QT Monitoring On and Off 131
8Monitoring Pulse Rate 133
Entering the Setup Pulse Menu 133
System Pulse Source 133
Switching Pulse On and Off 134
Using Pulse Alarms 134
9Monitoring Respiration Rate (Resp) 137
Lead Placement for Monitoring Resp 137
Understanding the Resp Display 138
Changing Resp Detection Modes 138
Changing the Size of the Respiration Wave 139
Changing the Speed of the Respiration Wave 140
Using Resp Alarms 140
Changing the Apnea Alarm Delay 140
Resp Safety Information 140
10 Monitoring SpO2143
SpO2 Sensors 143
Applying the Sensor 143
Connecting SpO2 Cables 144
Measuring SpO2144
SpO2 Signal Quality Indicator (Fast SpO2 only) 145
Assessing a Suspicious SpO2 Reading 145
Changing the Averaging Time 146
Setting the Measurement Mode 146
Understanding SpO2 Alarms 146
Pleth Wave 147
Perfusion Numeric 148
Perfusion Change Indicator 148
Setting SpO2/Pleth as Pulse Source 148
Setting Up Tone Modulation 148
Setting the QRS Volume 149
11 Monitoring NBP 151
Introducing the Oscillometric NBP Measurement 151
Preparing to Measure NBP 152
iv
Starting and Stopping Measurements 154
Enabling Automatic Mode and Setting Repetition Time 154
Enabling Sequence Mode and Setting Up The Sequence 154
Choosing the NBP Alarm Source 154
Switching Pulse from NBP On/Off 155
Assisting Venous Puncture 155
Calibrating NBP 156
12 Monitoring Temperature 157
Making a Temp Measurement 157
Calculating Temp Difference 158
13 Monitoring Invasive Pressure 159
Setting up the Pressure Measurement 159
Zeroing the Pressure Transducer 161
Adjusting the Calibration Factor 162
Displaying a Mean Pressure Value Only 162
Changing the Pressure Wave Scale 163
Optimizing the Waveform 163
Non-Physiological Artifact Suppression 163
Choosing the Pressure Alarm Source 163
Calibrating Reusable Transducer CPJ840J6 165
Calculating Cerebral Perfusion 166
14 Monitoring Carbon Dioxide 167
Measuring CO2 using the CO2 Option or M3014A 168
Measuring Mainstream CO2 using M3016A 171
Measuring Microstream CO2 using M3015A 173
Setting up all CO2 Measurements 174
15 Assigning Two Devices to One Patient 177
How Can You Combine Devices? 177
Functions Available When the Telemetry Data Window is Displayed 181
Functions Available For Devices Connected Via SRR 182
General Telemetry-related Functions 182
16 Enhancing Telemetry Monitoring with the Monitor 185
17 Tre n d s 187
Viewing Trends 187
Setting Up Trends 189
Documenting Trends 192
Trends Databases 192
Screen Trends 193
v
18 Recording 199
Starting and Stopping Recordings 199
Overview of Recording Types 200
Creating and Changing Recordings Templates 200
Recorder Status Messages 201
19 Printing Patient Reports 203
Starting Report Printouts 203
Stopping Reports Printouts 204
Setting Up Reports 204
Setting Up Individual Print Jobs 205
Checking Printer Settings 206
Printing a Test Report 206
Switching Printers On Or Off for Reports 206
Dashed Lines on Reports 207
Unavailable Printer: Re-routing Reports 207
Checking Report Status and Printing Manually 207
Printer Status Messages 208
Sample Report Printouts 209
20 Care and Cleaning 213
General Points 213
Cleaning the Monitor 214
Disinfecting the Monitor 214
Sterilizing the Monitor 214
Cleaning, Sterilizing and Disinfecting Monitoring Accessories 215
Cleaning Batteries and the Battery Compartment 215
21 Using Batteries 217
Battery Power Indicators 218
Checking Battery Charge 220
Replacing a Battery 220
Optimizing Battery Performance 221
Battery Safety Information 222
22 Maintenance and Troubleshooting 225
Inspecting the Equipment and Accessories 225
Inspecting the Cables and Cords 225
Maintenance Task and Test Schedule 226
Troubleshooting 227
Disposing of the Monitor 227
Disposing of Empty Calibration Gas Cylinders 227
23 Accessories 229
ECG/Resp Accessories 229
NBP Accessories 233
vi
Invasive Pressure Accessories 234
SpO2 Accessories 235
Temperature Accessories 239
Mainstream CO2 Accessories 239
Sidestream CO2 Accessories 240
Mainstream CO2 Accessories (for M3016A) 240
Microstream CO2 Accessories 240
Battery Accessories 241
24 Specifications 243
Intended Use 243
Manufacturer’s Information 244
Symbols 244
Installation Safety Information 246
Altitude Setting 246
Monitor Safety Specifications 246
EMC And Radio Regulatory Compliance 247
Out-Of-Hospital Transport - Standards Compliance 248
Monitor Performance Specifications 251
M4607A Battery Specifications 254
Measurement Specifications 255
Safety and Performance Tests 267
25 Default Settings Appendix 271
Country-Specific Default Settings 271
Alarm and Measurement Default Settings 277
Alarm Default Settings 277
ECG, Arrhythmia, ST and QT Default Settings 278
Pulse Default Settings 281
Respiration Default Settings 281
SpO2 Default Settings 282
NBP Default Settings 283
Temperature Default Settings 283
Invasive Pressure Default Settings 283
CO2 Default Settings 286
1
1
1Installation
Installation should be carried out by qualified service personnel, either by the hospital’s biomedical
department, or by Philips Support.
If you have purchased a “customer-installable bundle”, it is assumed that your own hospital personnel
will install and, if necessary, configure the monitor. You can contact Philips Support for assistance if
required; any assistance will be associated with additional costs.
For mechanical and electrical installation, you need technically qualified personnel with a knowledge of
english. Additionally, for monitor configuration, you need clinically qualified personnel with a
knowledge of the use environment. For further information on Installation, refer to the Service Guide.
WARNING • Monitor configuration settings must be specified by authorized hospital personnel.
• For installation of the device as part of a system, always refer to the Service Guide.
• As the first step in preparing the monitor for use, follow the installation instructions given in this
chapter.
Installation Checklist
Use this checklist to document your installation.
Step Task Check Box
when Task
Done
1 Perform initial inspection of delivery, unpack and check the shipment (see
“Unpacking and Checking the Shipment” on page 2).
❏
2 Mount the monitor as appropriate for your installation (see “Mounting the
Monitor” on page 3).
❏
3 Insert the battery into the battery compartment (the battery must always be
in the battery compartment during use). Connect the monitor to AC mains
via the external power supply using the supplied power cord (see “Connecting
the Monitor to AC Mains” on page 3).
❏
4 Perform Visual, Power On and Functional test blocks (see “Checking Out the
Monitor” on page 5).
❏
5 Perform Safety Tests, if required by local laws and regulations (see “Checking
Out the Monitor” on page 5).
❏
1 Installation Unpacking and Checking the Shipment
2
Unpacking and Checking the Shipment
The monitor and any supporting options ordered are supplied packed in protective shipping cartons.
Initial Inspection
Before unpacking, check the packaging and ensure that there are no signs of mishandling or damage.
Open the package carefully and remove the monitor and accessories.
Check that the contents are complete and that the correct options and accessories have been delivered.
Claims for Damage
If the shipping cartons are damaged, contact the carrier.
If any of the equipment is damaged, contact both the carrier and your local Philips service organization
for repair or replacement arrangements.
Repacking
Retain the original packing carton and material, in case you need to return equipment to Philips for
service. If you no longer have the original packing materials, Philips can advise you on alternatives.
6 Check/set the time and date (see “Setting the Date and Time” on page 7). ❏
7 Check that the country-specific default settings are appropriate (see
“Checking Country-Specific Default Settings” on page 7)
❏
8 Perform System Test as necessary (see the Service Guide)❏
Step Task Check Box
when Task
Done
System Components, Accessories and Supplies Comments
Monitor with options as ordered 1
ECG accessories optional
NBP accessories optional
SpO2 accessories optional
Pressure accessories optional
Temperature accessories optional
CO2 Accessories optional
External Power Supply including AC power cord and MSL cable 1
Rechargeable battery 1
Instructions for Use 1
Quick Guide 1
Documentation CD-ROM (includes Service Guide and Instructions
for Use)
1
Mounting the Monitor 1 Installation
3
Mounting the Monitor
The monitor can be rested on a flat, level surface, hung on the bed rail, or mounted on a wall or on a
rollstand. See the Service Guide for details.
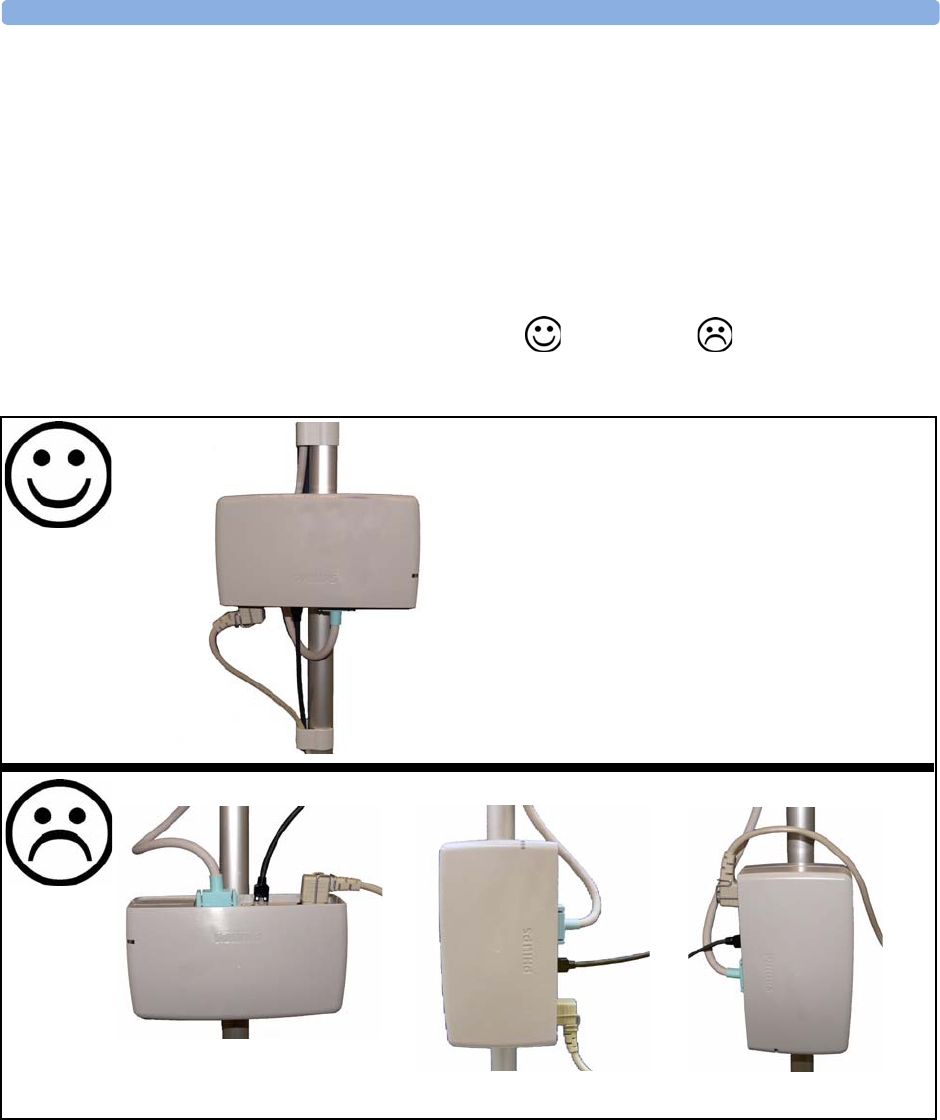
Mounting the External Power Supply (M8023A)
The external power supply (M8023A) can be rested on its rubber feet on a flat, level surface, or
mounted as described in the Service Guide.
The following pictures show examples of correct ( ) and incorrect ( ) ways to mount the
power supply.
Connecting the Monitor to AC Mains
The monitor is an electrical Class II device in which the protection against electric shock does not rely
on basic insulation and a protective earth conductor but on double and/or reinforced insulation.
1 Installation Connecting the Monitor to AC Mains
4
The monitor has a wide-range external power supply (M8023A) that allows you to operate the monitor
from an AC (alternating current) power source of 100 V to 240 V (± 10%) and 50/60 Hz (± 5%). The
external power supply also charges the monitor’s battery.
WARNING • Always use the supplied power cord with the earthed mains plug to connect the external power
supply (M8023A) to an earthed AC mains socket. Never adapt the mains plug from the power
supply to fit an unearthed AC mains socket.
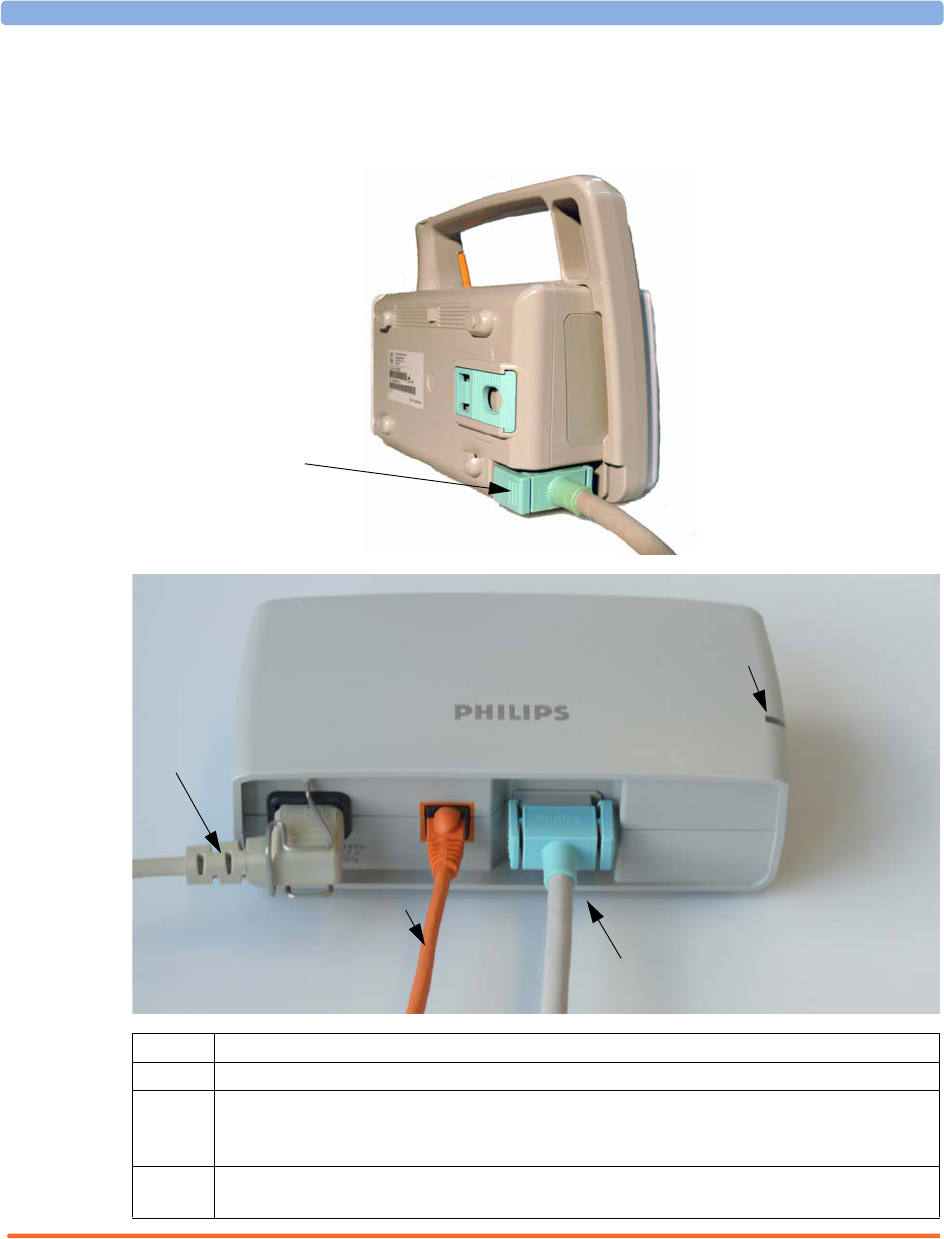
1 AC power cord. Connect to AC mains socket.
2 Connect LAN cable here. For connection to a PC or Information Center.
3 Measurement Link (MSL) cable. Supplies AC input power to the monitor for AC operation and
for battery charging. When there is a LAN connection to a PC or Information Center, the MSL
cable also carries this data to and from the monitor.
4 Power-on LED. The green light is on when the external power supply is connected to AC
mains.
MSL Cable
connects to power
supply (M8023A)
1
3
4
2
Checking Out the Monitor 1 Installation
5
• Do not use AC mains extension cords or multiple portable socket-outlets. If a multiple portable
socket-outlet without an approved isolation transformer is used, the interruption of its protective
earthing may result in enclosure leakage currents equal to the sum of the individual earth leakage
currents, so exceeding allowable limits.
• Do not connect any devices that are not supported as part of a system.
• Any non-medical device placed and operated in the patient’s vicinity must be powered via an
approved isolation transformer that ensures mechanical fixing of the power cords and covering of
any unused power outlets.
Checking Out the Monitor
The following table defines which tests and inspections need to be performed, and when they are
required.
For test and inspection information regarding repairs, upgrades and all other service events, refer to the
Service Guide.
Te st Test or Inspection to be Performed
Visual Inspect the monitor, measurement accessories and cables for any damage.
Are they free of damage?
Power On Power on the monitor. Does it start up successfully without errors? Do all alarm
lamps light up during power up?
After start up, the monitor sounds a tone, and you can see the monitoring main
screen (normally with measurement wave channels and numeric positions).
Functionality Test After power up, touch the battery status indicator in the bottom right of the
screen. The battery status window should open. Press the blue Main Screen key
to close the window and return to the main screen.
Safety Tests (1) to (4) Perform safety tests (1) to (4), as described in the Service Guide, for standalone
devices if required by local laws and regulations, and each time you combine
equipment to form a system, or exchange system components. Details of the
safety tests and procedures are described in the Service Guide. These safety
tests are derived from international standards but may not always be
sufficient to meet local requirements.
System Perform the system test according to IEC 60601-1-1, if applicable, after
combining equipment to form a system (see the Service Guide).
1 Installation Operating the Monitor
6
Operating the Monitor
To complete installation you will need to operate the monitor to check basic functionality. Here is a
quick introduction to the monitor.
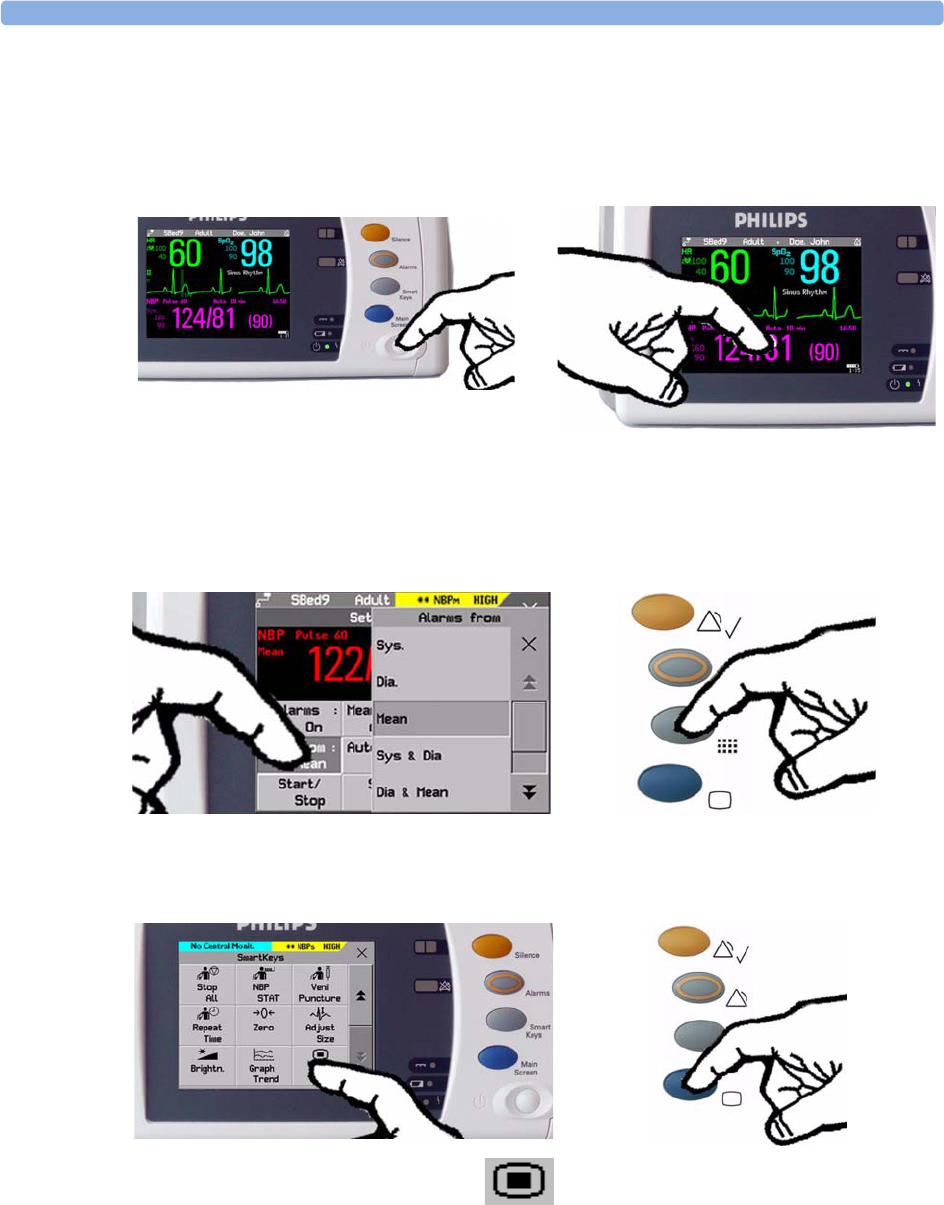
1Switch on the monitor. After start-up the
monitor display will become active. You operate
the monitor using the touch screen.
2Touch something on the screen (numerics,
waves, other screen items) to enter the
corresponding menu. Touching the NBP
numeric, for example, brings you to the
Setup NBP menu.
3Touch again to select an item on the menu and
work through the menu activities.
4To access SmartKeys, press the SmartKeys
key. Main Setup is one of the
SmartKeys.
5If you cannot find a menu by
touching the screen you can always
use the Main Setup SmartKey
which will get you to all menus on the monitor.
6Press the Main Screen key to close all open
menus/windows and return to the main
screen. Press again to enter the Change
Screen window, where you can choose
from a number of pre-configured screens.
Setting the Date and Time 1 Installation
7
Setting the Date and Time
To set the date and time:
1Press the SmartKeys key to enter the SmartKeys window.
2Select the Main Setup SmartKey to enter the Main Setup menu.
3Select the Date, Time screen element from the monitor’s info line to enter the Date, Time
menu.
4Select, in turn, the Year, Month, Day, Hour (in 24 hour format, only) and Minute as
necessary. Select the correct values from the pop-up list.
5Select Store Date, Time to change the date and time.
If your monitor is connected to an Information Center, the date and time are automatically taken from
this.
Once it is set, the internal clock retains the setting even when you switch off the monitor.
Checking Country-Specific Default Settings
Some settings are made in the factory to match the typical requirements in a specific country. Line
frequency, units for weight and height, and ECG cable colors (AAMI or IEC) have been set to
appropriate values. If you suspect that these settings may not match your institution’s requirements,
check the settings and change them if necessary as described in the Configuration Guide.
WARNING Before starting monitoring, check that the current configuration meets your requirements, especially
patient category, alarm limits and paced setting.
If you need to enter configuration mode:
1In the Main Setup menu, select Operating Modes.
2Select Config and enter the passcode.
The passcode for configuration mode is given in the monitor’s service documentation.
The monitor displays Config at the right hand side of the status line and in the center of the Screen
while you are in configuration mode.
Before you leave configuration mode, always be sure to store any changes you made. You must store
changes made to each Settings Block and to each Profile, individually. As it may be difficult to
remember whether the settings you changed belong to a Monitor Settings block or a Measurement
Settings block, we recommend that you store each block before you leave configuration mode.
To leave configuration mode:
♦In the Main Setup menu, select Operating Modes and then select Monitoring.
Handing Over the Monitor
If you are handing over the monitor to the end-users directly after configuration, make sure that it is in
Monitoring mode.

1 Installation Handing Over the Monitor
8
Users must be adequately trained to use the monitor before monitoring a patient. To achieve this, they
should have access to, and read, the following documentation delivered with the monitor:
• Instructions for Use (this book) - for full operating instructions
• Quick Guide - for quick reminders during use
Additionally, we recommend working through the Training Guide for self-training on the monitor
before use (not available in all languages). The part number is M8102-944XB, where X is a digit
dependent on the language. The English training guide is M8102-9441B.

9
2
2Basic Operation
These Instructions for Use are for clinical professionals using the IntelliVue MP2 (M8102A) patient
monitor.
This basic operation section gives you an overview of the device and its functions. It tells you how to
perform tasks that are common to all measurements (such as entering data, switching a measurement
on and off, setting up and adjusting wave speeds, working with profiles). The alarms section gives an
overview of alarms. The remaining sections tell you how to perform individual measurements, and how
to care for and maintain the equipment.
Familiarize yourself with all instructions including warnings and cautions before starting to monitor
patients. Read and keep the Instructions for Use that come with any accessories, as these contain
important information about care and cleaning that is not repeated here.
This guide describes all features and options. Your monitor may not have all of them; they are not all
available in all geographies. Your monitor is highly configurable. What you see on the screen, how the
menus appear and so forth, depends on the way it has been tailored for your hospital and may not be
exactly as shown here.
In this guide:
•A warning alerts you to a potential serious outcome, adverse event or safety hazard. Failure to
observe a warning may result in death or serious injury to the user or patient.
•A caution alerts you to where special care is necessary for the safe and effective use of the product.
Failure to observe a caution may result in minor or moderate personal injury or damage to the
product or other property, and possibly in a remote risk of more serious injury.
•Monitor refers to the entire patient monitor. Display refers to the physical display unit. Display
Screen and Screen refer to everything you see on monitor’s display, such as measurements, alarms,
patient data and so forth.
2 Basic Operation Introducing the IntelliVue MP2
10
Introducing the IntelliVue MP2
The Philips IntelliVue MP2 monitor provides a comprehensive set of basic physiological
measurements: ECG (including ST analysis and optional 10-lead ECG), NBP, SpO2, and optionally
invasive blood pressure, temperature and CO2. Through networking it provides information
integration, documentation and information access. The MP2 can be used with adult, pediatric and
neonatal patients in a hospital environment and during patient transport both inside and outside
hospitals.
The monitor stores data in trend databases. You can see tabular trends (vital signs) and document them
on a central printer. You can view measurement trend graphs, including horizon trends, to help you
identify changes in the patient’s physiological condition.
The monitor can be powered by a rechargeable battery, or from AC mains using the external power
supply (M8023A). For battery charging, care and status information, refer to the chapter “Using
Batteries” on page 217.
Controls, Indicators and Connectors
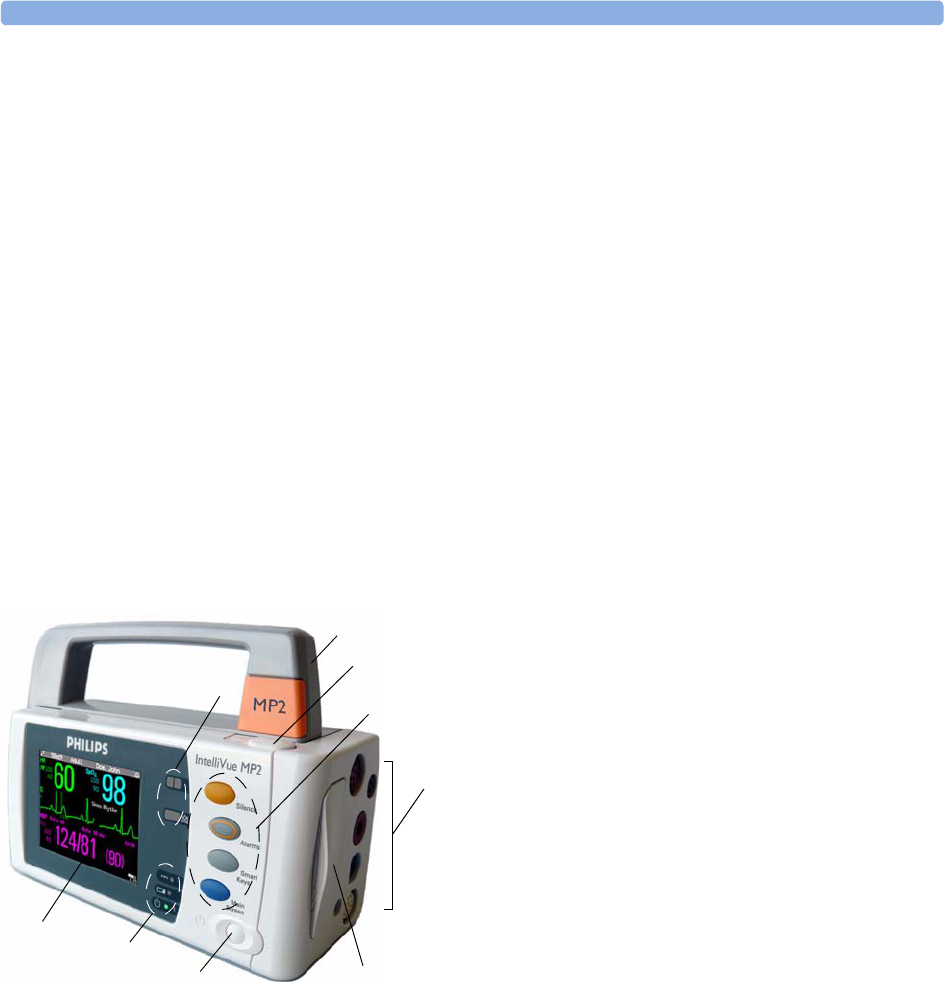
MP2 Overview
1On/Standby Switch
2Power and battery indicators (see “MP2
Controls and Indicators” on page 11)
33.5-inch TFT LCD touchscreen QVGA
display
4Alarm lamps (see “MP2 Controls and
Indicators” on page 11)
5Built-in carrying handle
6Battery eject button
7Keys (see “MP2 Controls and Indicators”
on page 11)
8Measurement connectors (see “MP2
Patient Connectors, Right Side” on
page 12)
9Battery
45
6
1
2
3
5
8
47
9
6
Controls, Indicators and Connectors 2 Basic Operation
11
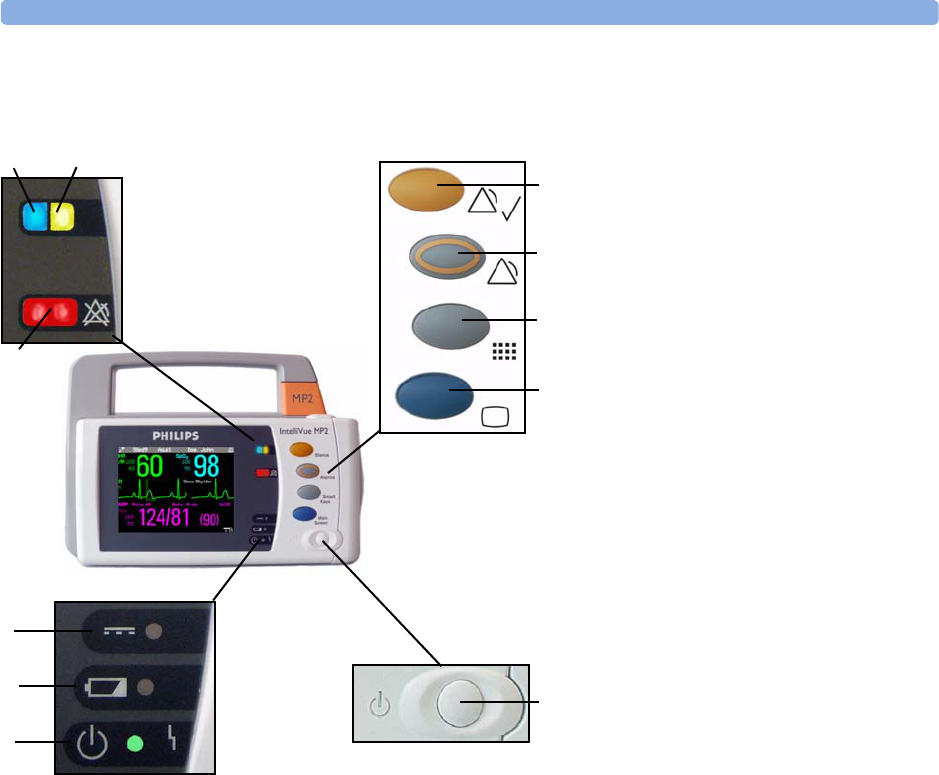
MP2 Controls and Indicators
1On/Standby switch
2On/Standby LED. Green when
monitor is on. Red indicates an error.
3Battery status LED. Yellow when
charging. Flashing red when battery is
empty, or a battery malfunction is
detected.
4External power LED. Green when
monitor is powered from an external
power source.
5Alarms off indicator. When alarms are
suspended, the lamp is red, and the
ALARMS OFF message appears on the
screen.
6Active INOP alarm lamp in light blue.
Stays lit until active INOP is
acknowledged.
7Active alarm lamp. Red or yellow,
depending on alarm level. Stays lit until
active alarm is acknowledged.
8Silence key
9Alarms key: turns alarms On/Off, or
pauses them
10 SmartKeys key: brings up SmartKeys
on the screen
11 Main Screen key: closes all open
menus/windows and returns to the
main screen, or selects current screen.
2
3
4
67
5
1
11
10
9
8
2 Basic Operation Controls, Indicators and Connectors
12
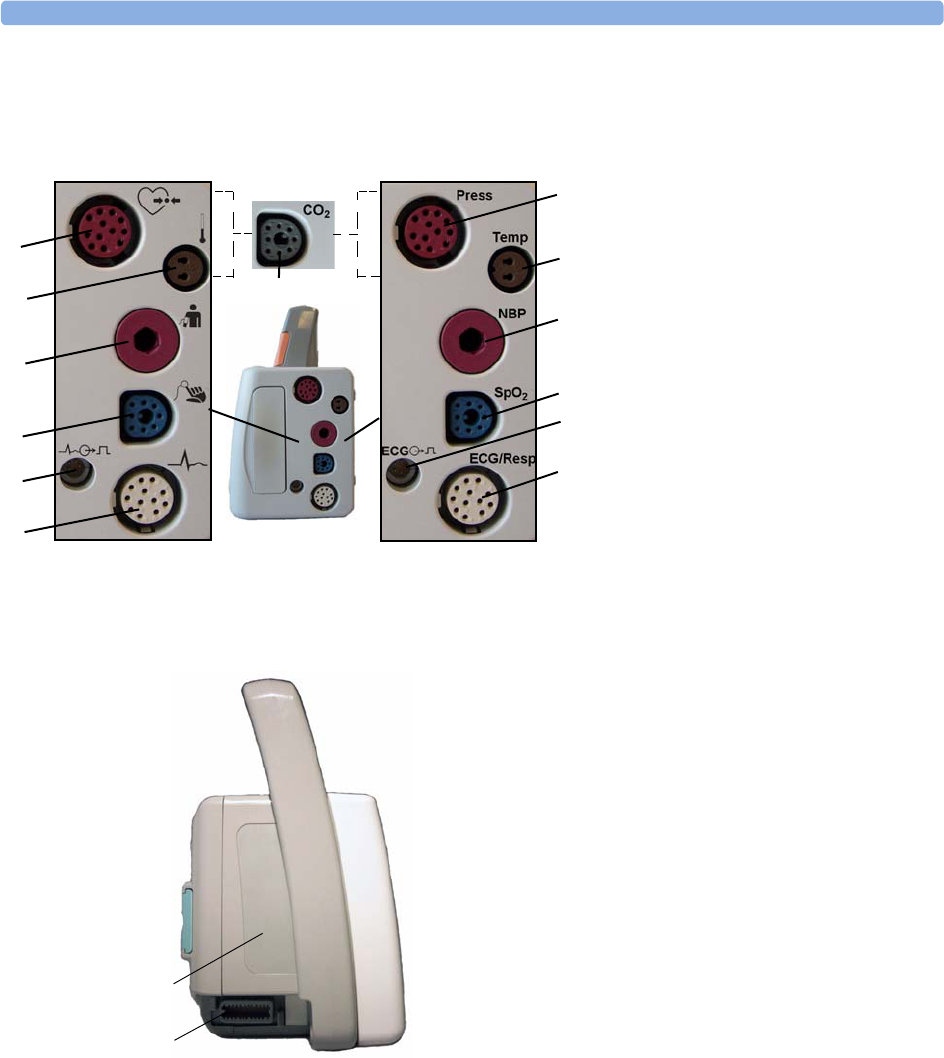
MP2 Patient Connectors, Right Side
1Pressure (option)
2Temperature (option)
3Noninvasive blood pressure
4SpO2
5ECG sync pulse output
(See page 252 for specifications)
6ECG/Respiration
7CO2 (option)
12
4
3
5
6
6
5
4
3
2
1
1
2
3
4
5
6
Symbols (International) Text (English versions only)
7
MP2 Left Side
1Loudspeaker
2MSL Connector. Connects to the
external power supply via the MSL
cable for AC mains operation,
battery charging, and
communication with a network.
2
1
Extending Measurements 2 Basic Operation
13
Extending Measurements
Your monitor is compatible with Philips measurement extensions for use with other IntelliVue patient
monitoring devices. These allow you to add specific measurements to those already integrated into
your monitor. These measurement extensions are referred to as MMS extensions.
The MMS extensions connect to the monitor and use the monitor’s settings and power. Trend data
and measurement settings from the measurements in the extensions are stored in the monitor.
WARNING • Measurements from a MMS extension are only available when the extension is connected to the
monitor, and the monitor is running on AC mains via the external power supply (M8023A).
Measurements from a MMS extension connected to the monitor are not available when the monitor
is running on battery power.
• Any measurements on a MMS extension that conflict with those in the monitor cannot be used. For
example, only one CO2 measurement is supported.
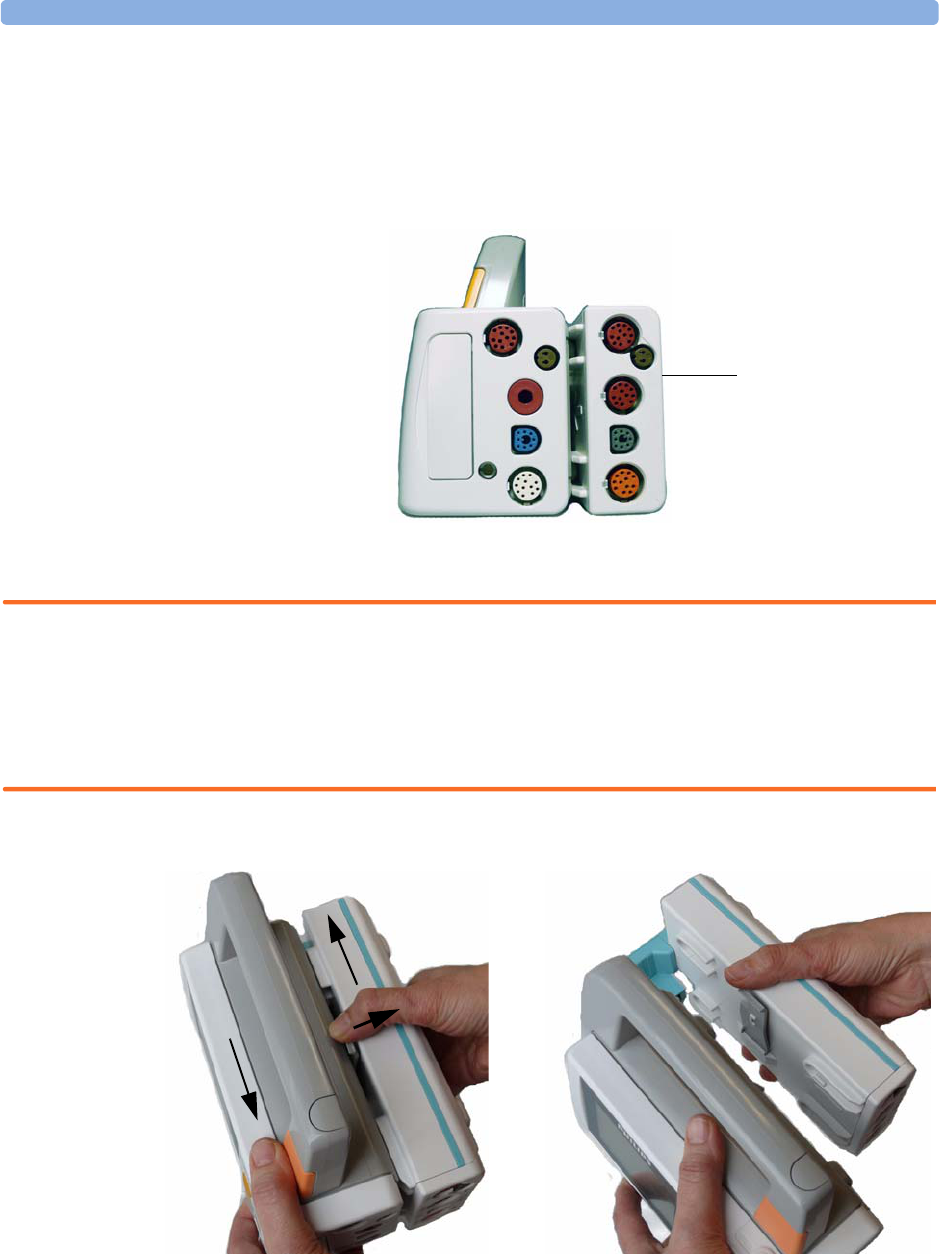
To separate an extension from the monitor, press the release lever and push the extension forward.
MMS Extension
M3014A attached to
the MP2

2 Basic Operation Extending Measurements
14
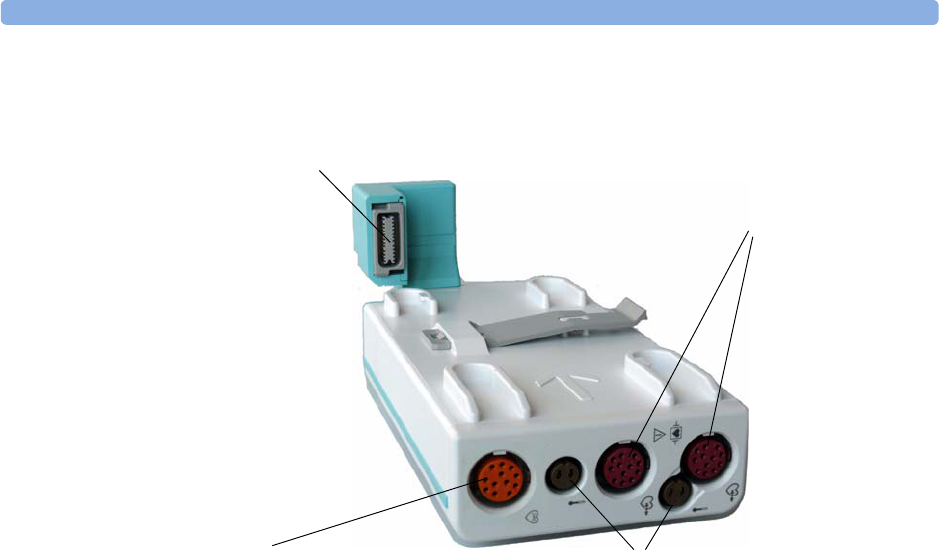
M3014A, M3015A and M3016A Measurement Extensions
The optional M3014A Capnography extension adds mainstream capnography, and optionally one
pressure plus either a pressure or a temperature to the monitor. Cardiac Output and Continuous
Cardiac Output are not available when used with the MP2.
The optional M3015A Microstream CO2 extension adds microstream capnography and optionally
either pressure or temperature to the monitor. The optional M3016A Mainstream CO2 extension adds
mainstream capnography and optionally either pressure or temperature to the monitor.
Only one CO2 measurement at a time is supported.
1Pressure connectors (red) 5Inlet
2Temperature connector (brown) 6Microstream connector CO2
3Mainstream/sidestream connector CO2
(optional)
7Gas sample outlet
4Cardiac Output connector
M3014A Capnography M3015A Microstream
1
2
6
1
3275
4
1
2
M3016A Mainstream
3
Extending Measurements 2 Basic Operation
15
M3012A Hemodynamic MMS Extension
When attached to the MP2 connected to the external power supply, the optional M3012A
Hemodynamic extension adds temperature, pressure, and an additional pressure or a temperature to
the monitor.
Cardiac Output and Continuous Cardiac Output are not available when used with the MP2.
Temperature connectors (brown)
Cardiac Output (orange; optional)
Pressure connectors
(red)
MSL Connector to MP2
2 Basic Operation Operating and Navigating
16
Operating and Navigating
The principle method of operating your monitor is via the touchscreen. Almost every element on the
screen is interactive. Screen elements include measurement numerics, information fields, alarms fields,
waveforms and menus.
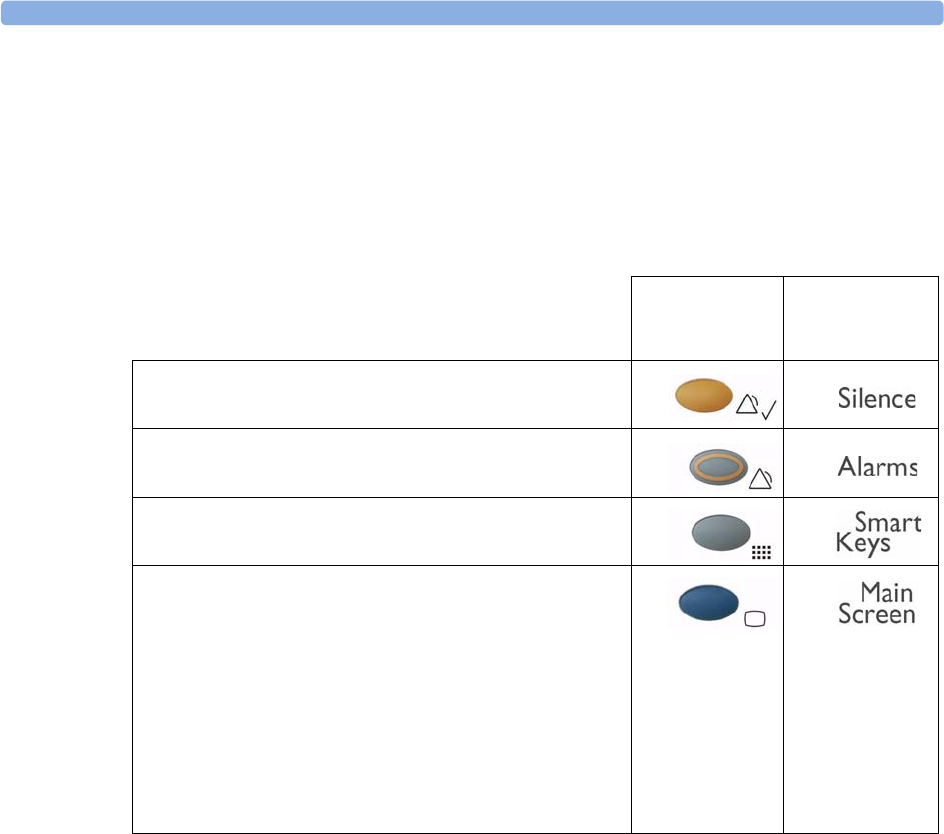
There are also four keys to the right of the screen (see also “MP2 Controls and Indicators” on page 11).
These let you: Key with symbol
(international)
Text replac e s
symbol (English
versions only)
• Silence alarms: the Silence key acknowledges all active
alarms by switching off audible alarm indicators and lamps.
• Switch alarms on or off, or pause alarms.
• Call up SmartKeys on the screen (see below).
• Close all open menus/windows and return to the main
screen.
• If you are already in the main screen (no additional menus/
windows are open), then pressing this key opens the
Change Screen window, where you can choose from a
number of pre-configured screens.
• To temporarily disable the touchscreen operation, press and
hold this key for 2 seconds. Press the key again to re-enable
the touchscreen operation.
Operating and Navigating 2 Basic Operation
17
A typical main screen looks like this:
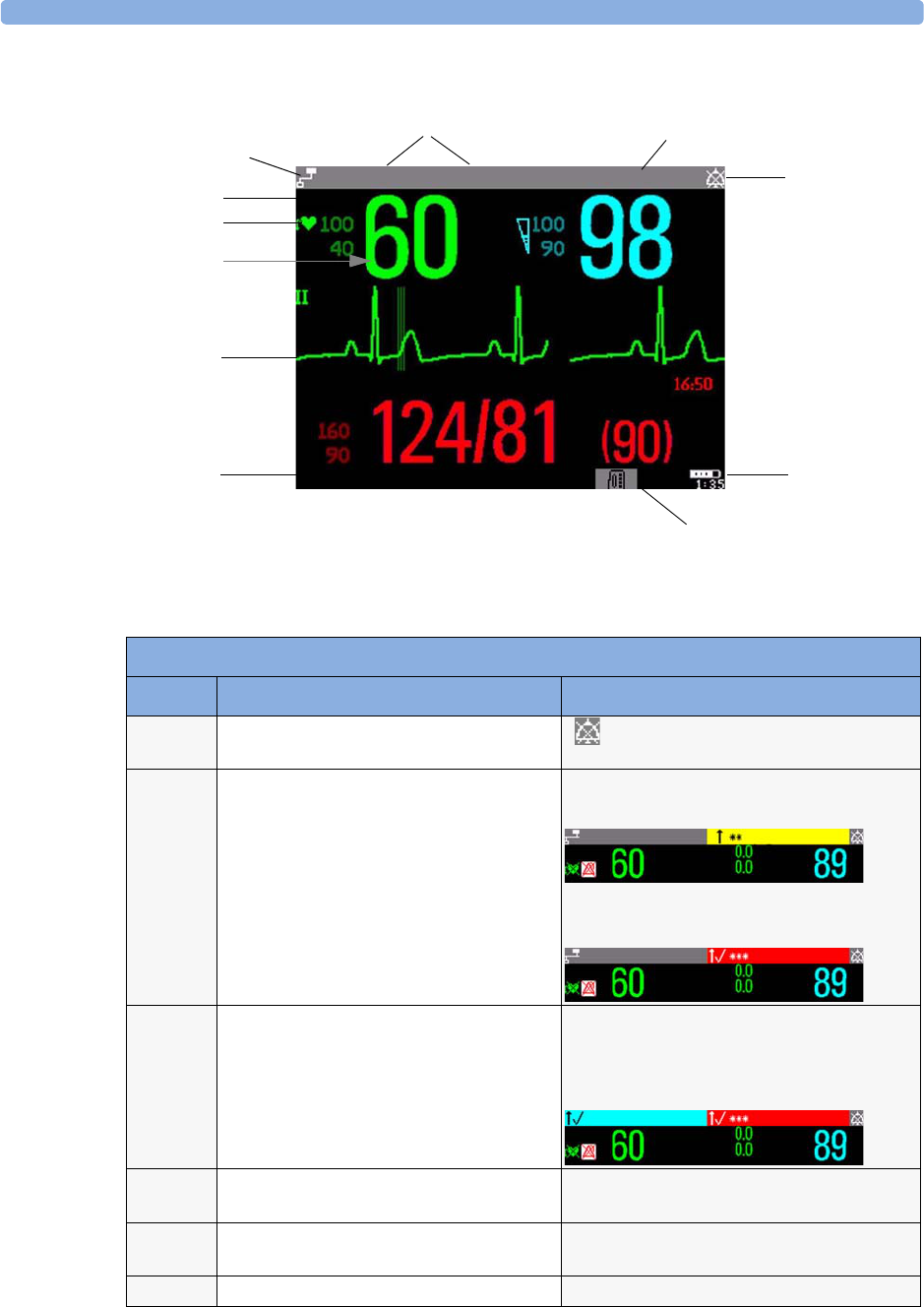
MP2 Screen Elements
Item Description Comments
1 Alarm volume off indicator is displayed when the alarm volume is set
to zero (0).
2 Patient name / alarm message field Patient name can be covered by alarm messages
or alarms On/Off/Paused message.
If red and yellow alarms are active at the same
time, they rotate in the alarm field.
3 Patient category and bed label / INOP
message field
Patient category and bed label can be covered
by INOP messages. If there are multiple red/
yellow/cyan INOPs active at the same time,
they rotate in the INOP field.
4 Network connection indicator Documented in Information Center
Instructions for Use.
5 Measurement label Touch the measurement to enter the
measurement setup menu.
6 Paced status Displayed below the HR label.
All Sett. reset Profile Adult
Sys.
M
1mV
HR SpO2
Doe, John
Sinus Rhythm
2
5
6
8
911
Adult 1
3
4
7
Bed9
NBP
10
Bed4
HR ST-I
ST-V6
SpO2
Adult SpO2 LOW
APNEA
HR ST-I
ST-V6
SpO2
Bed4 Adult
ALL ECG ALARMS OFF APNEA
HR ST-I
ST-V6
SpO2
2 Basic Operation Operating and Navigating
18
Using the Touchscreen
Touch a screen element to get to the actions linked to that element. For example, touch a measurement
numeric and the setup menu for that measurement opens. Touch a wave to enter the setup menu for
that wave.
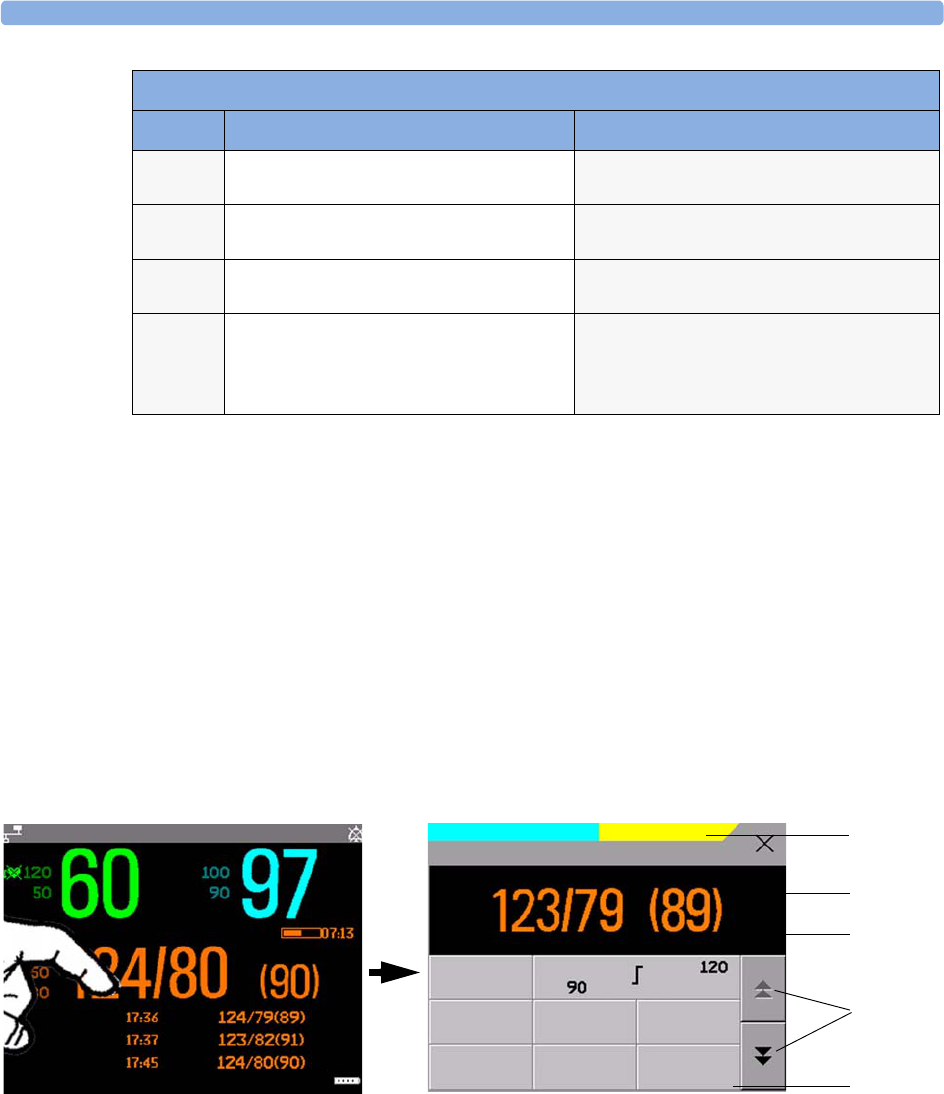
Measurement Setup Menus
Each measurement has a setup menu where you can perform operations or change settings. Typically,
the setup menu window covers the whole screen, with the exception of the INOP and alarm message
fields, which are always displayed at the top. The following picture is for illustration purposes, and may
not exactly represent what you see on the screen. We are using non invasive blood pressure as an
example, but all measurement setup windows are similar and share the same basic layout and
components.
Touch the measurement numeric on the screen to enter the setup menu.
7 Measurement numeric/values Touch the numeric to enter the measurement
setup menu.
8Measurement wave Touch the wave to enter the measurement
setup menu.
9 Status line Shows information and messages prompting
you for action.
10 Battery status indicator Gives information about remaining battery
charge, estimated operating time, maintenance
requirements and malfunctions. See the
chapter “Using Batteries” on page 217.
MP2 Screen Elements
Item Description Comments
HR SpO2
Pulse 60 Auto 15 min
Bed4 Doe, John
Adult No Central Monit. NBPs HIGH
**
Alarms :
On
Sys.
Al. from :
Sys
Mode :
Auto
Repeat:
15 min
Start/
Stop
Stop
All
NBP
STAT
NBP meas. + autom. cycle started
NBP 2
3
4
5
1
Main screen Measurement setup menu
Pulse 60 Auto 08:28
Setup NBP
Operating and Navigating 2 Basic Operation
19
Main Setup Menu
There is usually more than one way to enter a setup menu for a measurement, to change a setting or to
execute a task. Some routes are more direct than others. You can use whichever method you find most
convenient. Which routes are available to you, however, can vary depending on your monitor’s
configuration.
For this reason, this book generally describes entry to a measurement’s setup menu via the Main Setup
menu, as this route is always available and is not subject to configuration dependencies. You can get to
all setup windows from the Main Setup menu. You enter the Main Setup menu by pressing the
SmartKeys key, then selecting the Main Setup SmartKey.
SmartKeys
A SmartKey is a configurable graphical key on the screen allowing fast access to frequently used
functions. Press the SmartKeys hard key to call up a set of SmartKeys on the screen. Although the
selection of SmartKeys available on your monitor depends on the monitor configuration and on the
options purchased, the SmartKeys window generally looks like this:
Key to measurement setup menu:
Item Description Comment
1 INOP and alarm message field. These are always displayed at the top of the screen.
2 Wave/numerics window. The main measurement numeric and wave (if applicable) are shown in
this window so that you do not lose sight of the current measurement
while making changes in the menu.
3 Status/prompt message. Status/prompt messages related to the measurement menu are displayed
below the wave/numerics. General status/prompt messages on the main
screen are covered by the measurement setup menu.
4 Next page arrows. The menu may have more than one page, as shown here. Move to another
page by touching these arrows.
5 Measurement menu buttons. Each button has two lines of text. To perform an operation on a
measurement, press one of the buttons. Some buttons lead directly to a
task. For example, pressing the Start/Stop button for noninvasive
blood pressure starts a measurement. Other buttons open a pop-up
window, which can have more than one page, from which you make a
selection. Again, using noninvasive blood pressure as an example, pressing
the Repeat Time button for setting the repetition time opens a pop-
up window from which you pick a time, scrolling if necessary.
Main Setup menu
From here you can get to all setup
menus
2 Basic Operation Operating and Navigating
20
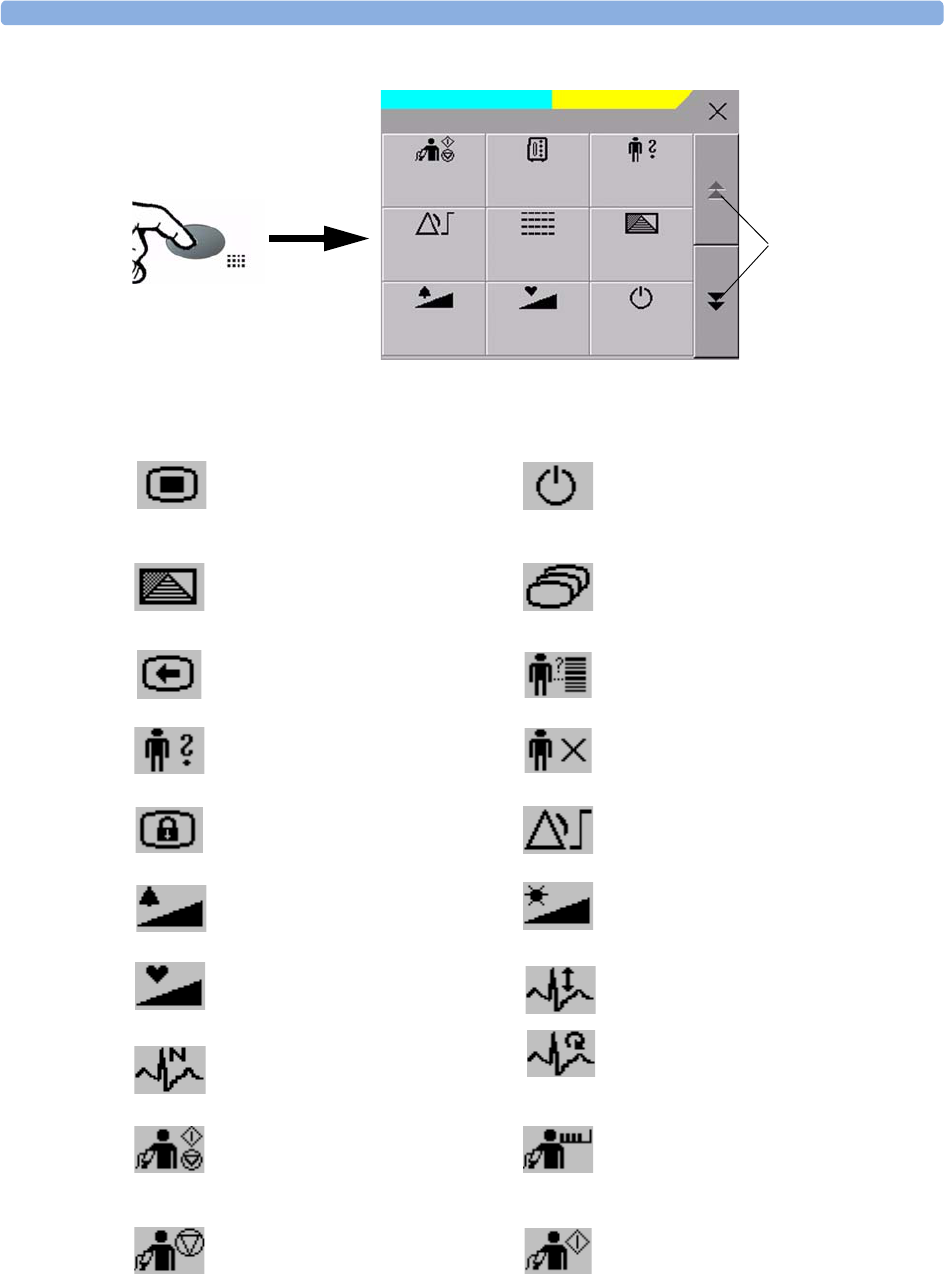
Main Setup is one of the SmartKeys.
enter Main Setup menu - you can get
to all setup windows using this key
enter standby mode - suspends patient
monitoring. All waves and numerics
disappear from the display. All settings
and patient data information are retained.
enter profile menu, or
revert to default profile
change Screen, or
revert to default screen
previous Screen quick admit a patient
enter patient identification menu to
admit/discharge/transfer end case to discharge a patient
lock touchscreen operation set alarm limits
change alarm volume change screen brightness (not for
independent displays)
change QRS volume change amplitude (size) of ECG wave
review beat labels (annotate
arrhythmia wave) re-learn arrhythmia
- start/stop manual NBP measurement
- start auto series
- stop current automatic measurement
within series
start NBP STAT measurement
stop automatic or STAT NBP
measurement and measurement series
start NBP measurement and
measurement series
Touch to view more
SmartKeys
No Central Monit. NBPs HIGH
**
Start/
Stop
Measmt.
Select.
Admit/
Dischrge
Alarm
Limits
Vitals
Trend Profiles
Alarm
Volume
QRS
Volume
Monitor
Standby
SmartKeys
Operating and Navigating 2 Basic Operation
21
Pop-Up Keys
Pop-up keys are task-related graphical keys that appear automatically on the monitor screen when
required. For example, the confirm pop-up key appears only when you need to confirm a change.
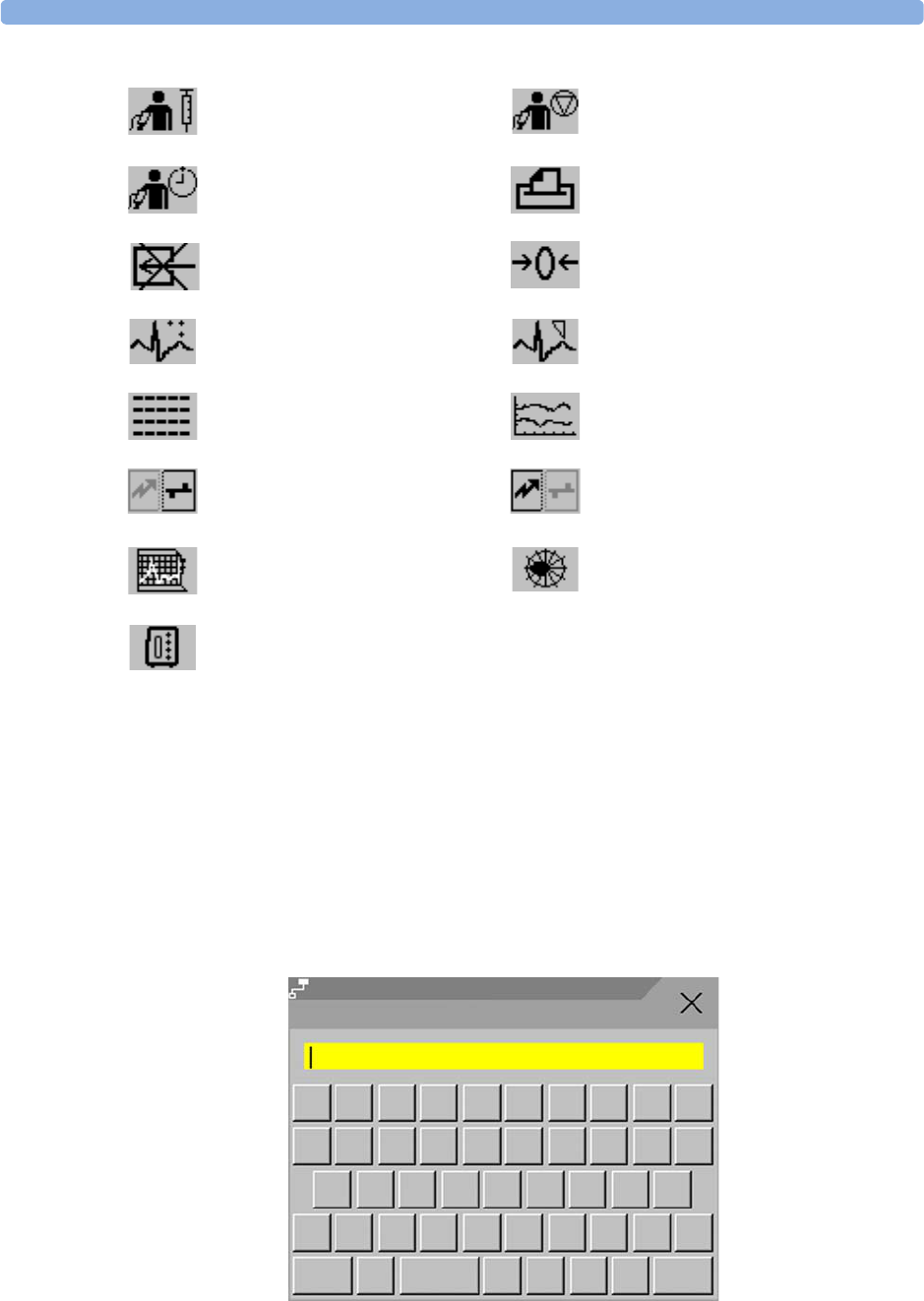
Using the On-Screen Keyboard
Use this as you would a conventional keyboard. Enter the information by selecting one character after
another. Use the Shift key to access uppercase letters. Use the Back key to delete single characters,
or use the Clr key to delete entire entries. Select Enter to confirm what you have entered and close
the on-screen keyboard.
start veni puncture (inflate cuff to
subdiastolic pressure)
stop current NBP measurement
set the NBP repeat time access patient reports
switch CO2 pump off zero invasive pressure transducer
new lead setup set standard or EASI lead placement
review vital signs trend review graph trend
unpair equipment and continue
central monitoring with the monitor
unpair equipment and continue central
monitoring with the telemetry device
start 12-Lead Capture (only available
if Information Center is connected) access ST Map application
select measurement device
Adult
Bed10 Not Admitted
@!#
$%^*()
QWETR
&
J
GH
F
DS
A
P
OI
U
Y
?Z
XV
C>
<M
N
B
KL
Alt <> Clr
Shift Back Enter
Last Name

2 Basic Operation Operating Modes
22
Operating Modes
When you switch the monitor on, it starts up in monitoring mode. To change to a different mode:
1Select the Main Setup menu.
2Select Operating Modes and choose the mode you require.
Your monitor has four operating modes. Some are passcode protected.
•Monitoring Mode: This is the normal, every day working mode that you use for monitoring
patients. You can change elements such as alarm limits, patient category and so forth. When you
discharge the patient, these elements return to their default values. Changes can be stored
permanently only in Configuration Mode. You may see items, such as some menu options or the
altitude setting, that are visible but ‘grayed out’ so that you can neither select nor change them.
These are for your information and can be changed only in Configuration Mode.
•Demonstration Mode: Passcode protected, this is for demonstration purposes only. You must not
change into Demonstration Mode during monitoring. In Demonstration Mode, all stored trend
information is deleted from the monitor’s memory.
•Configuration Mode: Passcode protected, this mode is for personnel trained in configuration tasks.
These tasks are described in the Configuration Guide. During installation the monitor is configured
for use in your environment. This configuration defines the default settings you work with when
you switch on, the number of waves you see and so forth.
•Service Mode: Passcode protected, this is for trained service personnel.
When the monitor is in Demonstration Mode, Configuration Mode, or
Service Mode, this is indicated by a box with the mode name in the center
of the Screen and a symbol in the bottom right-hand corner. Select this
field to change to a different mode.
Standby Mode
Standby mode can be used when you want to temporarily interrupt monitoring.
To enter Standby mode,
1Press the SmartKeys key .
2Either select the Monitor Standby SmartKey
Or select the Main Setup SmartKey, then select Monitor Standby.
The Standby screen looks like this:
Config

Understanding Screens 2 Basic Operation
23
The monitor enters Standby mode automatically after the End Case function is used to discharge a
patient. Standby suspends patient monitoring. All waves and numerics disappear from the display but
all settings and patient data information are retained. A special Standby screen is displayed.
If a patient location is entered at the Information Center, this will also be displayed on the Standby
screen (availability depends on Information Center revision).
To resume monitoring,
♦Select anything on the screen or press any key.
Understanding Screens
Your monitor comes with a set of pre-configured Screens, optimized for common monitoring
scenarios. A Screen defines the overall selection, size and position of waves and numerics on the
monitor screen when you switch on. You can easily switch between different Screens during
monitoring. Screens do NOT affect alarm settings, patient category and so forth.
Switching to a Different Screen
To switch to a different Screen:
1After closing any open menus or windows, press the Main Screen key to access the Change
Screens menu.
2Choose the new Screen from the Change Screens menu.
Changing a Screen’s Content
If you do not want to change the entire Screen content, but only some parts of it, you can substitute
individual waves, numerics, or trends. Be aware that these changes cannot be stored permanently in
Monitoring Mode.
To change the selection of elements on a Screen,
1Select the element you want to change. For example, touch the wave to enter the wave setup menu,
or touch the numeric to enter the numeric setup menu.
2From the menu that appears, select Change Wave or Change Numeric, and then select the
wave or numeric you want.
STANDBY
Press any key or select any field on the screen
to resume monitoring
2 Basic Operation Using the XDS Remote Display
24
In the Change Screen menu, the
changed Screen is shown linked to the
original Screen and marked with an
asterisk.
Up to three modified Screens can be
accessed via the Change Screen
menu.
To recall Screens, select the name of the
Screen in the Change Screen menu
After a patient discharge, the monitor’s
default Screen is shown. Modified Screens
are still available in the
Change Screen menu.
If the monitor is switched off and then on again, modified Screens are erased from the monitor’s
memory and cannot be recalled. If a modified Screen was the last active Screen when the monitor was
switched off, it is retained (unless Automat. Default is set to Yes in Configuration Mode).
Using the XDS Remote Display
Using the IntelliVue XDS solution it is possible to view an independent monitor screen on an external
display. The XDS solution consists of a medical grade PC-based hardware platform, XDS application
software and the XDS connectivity option on the monitor. Depending on the configuration you can
also operate the monitor from the external display. The XDS must be connected to the same Local
Area Network (LAN) as the monitor.
It is also possible to use an existing PC, connected to the same LAN, to host the XDS Application
software.
For more details, including limitations and restrictions, refer to the Instructions for Use for the XDS
Application.
Using the Visitor Screen
If a visitor Screen is configured for your monitor, you can use it to clear the screen of all waves and
numerics but continue to monitor the patient with active alarms and trend storage at the bedside and
Information Center. You can change the name of the visitor Screen in Configuration Mode.
To activate this Screen,
1Press the Main Screen key to open the Change Screen menu.
2Select the name of the visitor Screen configured for your monitor from the list of available Screens.
To select a Screen with waves and numerics again,
♦Touch the gray rectangle in the center of the screen showing the visitor Screen’s name, or press the
Main Screen key, to open the Change Screen menu and then select a Screen from the list.
1 Wave B
1 Big Wave
Vital Signs B
2 Waves A
2 Waves B
Change Screen
Understanding Profiles 2 Basic Operation
25
Understanding Profiles
Profiles are predefined monitor configurations. They let you change the configuration of the whole
monitor so you can adapt it to different monitoring situations. The changes that occur when you
change a complete profile are more far reaching than those made when you change a Screen. Screens
affect only what is shown on the display. Profiles affect all monitor and measurement settings.
The settings that are defined by Profiles are grouped into three categories. Each category offers a choice
of ‘settings blocks’ customized for specific monitoring situations. These categories are:
Display (screens)
– Each profile can have a choice of many different predefined screens. When you change the
profile, the screen selection configured for the new profile becomes active.
• Measurement Settings
– Each profile can have a choice of different predefined measurement settings. These relate directly
to individual measurements, for example, measurement on/off, measurement color, alarms limits,
NBP alarm source, NBP repeat time, temperature unit (oF or oC) pressure unit (mmHg or kPa).
• Monitor Settings
– Each profile can have a choice of different predefined monitor settings. These relate to the
monitor as a whole; for example, display brightness, alarms off/paused, alarm volume, QRS tone
volume, tone modulation, prompt tone volume, wave speed, resp wave speed, pulse source.
You can change from one complete profile to another or swap individual settings blocks (display
screen/monitor settings/measurement settings) to change a subset of a profile. Changes you make to
any element within the settings blocks are not saved when you discharge the patient, unless you save
them in Configuration Mode.
Depending on your monitor configuration, when you switch on or discharge a patient the monitor
either continues with the previous profile, or resets to the default profile configured for that monitor.
PAP ZERO+CHECK CAL Doe, John
Profile : Profile Adult
Patient Category : Adult
Paced : No
Display : Vital Signs
Profiles
Measmnt.Settings : Measmt. Adult
Measmnt. Adult
Measmnt. Pedi
Please Confirm
To activate the highlighted settings block
select Confirm
PAP ZERO+CHECK CAL Doe, John
Confirm Cancel
Profile
Patient
Profiles Menu, showing current settings Available choices in measurement menu. Confirm your
choice when prompted.
Please Confirm
2 Basic Operation Understanding Settings
26
WARNING If you switch to a different profile, the patient category and paced status normally change to the setting
specified in the new profile. However some profiles may be setup to leave the patient category and
paced status unchanged. Always check the patient category, paced status, and all alarms and settings,
when you change profiles.
When you leave Demonstration Mode, the monitor uses the default profile.
Swapping a Complete Profile
1Press the SmartKeys key and
–Either select Main Setup and then Profiles in the Setup menu.
–Or select the Profiles SmartKey .
2In the Profiles menu, select Profile.
3Chose a profile from the pop-up list.
4Confirm your selection.
Swapping a Settings Block
1Select the Main Setup SmartKey and then Profiles in the Main Setup menu, or
select the Profiles SmartKey.
2In the Profiles menu, select Display or Measmnt. Settings or
Monitor Settings to call up a list of the settings blocks in each category.
3Choose a settings block from the pop-up list.
4Confirm your selection.
Default Profile
Your monitor has a default profile that it uses when you leave Demonstration, or Service modes, or
when you discharge a patient. This profile is indicated by a diamond .
Locked Profiles
Some profiles are locked, so that you cannot change them, even in Configuration Mode. These are
indicated by this lock symbol.
Understanding Settings
Each aspect of how the monitor works and looks is defined by a setting. There are a number of
different categories of settings, including,
Screen Settings, to define the selection and appearance of elements on each individual Screen
Measurement settings, to define settings unique to each measurement, for example, high and low
alarm limits

Changing Measurement Settings 2 Basic Operation
27
Monitor settings, including settings that affect more than one measurement or Screen and define
general aspects of how the monitor works, for example, alarm volume, reports and recordings, and
display brightness.
You must be aware that, although many settings can be changed in Monitoring Mode, permanent
changes to settings can only be done in the monitor’s Configuration Mode. All settings are reset to the
stored defaults:
• when you discharge a patient
• when you load a Profile
• when the monitor is switched off for more than one minute (if Automat. Default is set to
Yes).
Changing Measurement Settings
Each measurement has a setup menu in which you can adjust all of its settings. You can enter a setup
menu:
• via the measurement numeric - select the measurement numeric to enter its setup menu. For
example, to enter the Setup ECG menu, select the HR (heart rate) numeric.
•via the Main Setup SmartKey - if you want to setup a measurement when the measurement is
switched off, use the Main Setup SmartKey and select Measurements. Then select the
measurement name from the popup list. With this permanent key you can access any setup menu in
the monitor.
• via the Measurement Selection key.
Switching a Measurement On and Off
When a measurement is off, its waves and numerics are removed from the monitor’s screen. The
monitor stops data acquisition and alarming for this measurement.
1Enter the measurement’s setup menu and select the measurement.
2Select the measurement name to toggle between on and off. The screen display indicates the active
setting.
Adjusting a Measurement Wave
To quickly adjust wave-related measurement settings (such as speed or size), select the measurement
wave itself. This displays the measurement Wave menu, which has only wave-related measurement
settings.
Changing Wave Speeds
Lowering the wave speed compresses the wave and lets you view a longer time period. Increasing the
speed expands the waveform, giving you a more detailed view.
The monitor distinguishes two groups of wave speed settings,
•RespiratorySpeed, for CO2 waves.
•Global Speed, for all waves not included in the other group.

2 Basic Operation Using Labels
28
Changing the Wave Group Speed
The wave speed group setting defines the speed of all the waves in the group.
To change the wave speed of a wave speed group,
1Select Main Setup -> User Interface
2Select Global Speed or RespiratorySpeed, as required
3Select a value from the list of available speeds.
Changing Wave Speed for a Channel
To change the wave speed of an individual wave channel,
1Enter the Wave menu for a measurement by selecting its wave.
2Select Change Speed.
3To set the speed to the wave group speed, select RespiratorySpeed or Global Speed.
To set an individual channel speed, select a numeric value from the list of available speeds. This
overrides the wave group speed setting and sets the speed for the individual wave channel on the
monitor Screen. The wave channel speed is independent of the wave (label) depicted in the
channel, if you change the wave, the new wave will retain the set channel speed.
Using Labels
You can measure up to three invasive pressures and temperatures simultaneously. The monitor uses
labels to distinguish between them. The default settings defined in the profile (such as measurement
color, wave scale, and alarm settings) are stored within each label. When you assign a label to a
measurement, the monitor automatically applies these default settings to the measurement. The labels
assigned are used throughout the monitor, in reports, recordings, and in trends.
Changing Measurement Labels (e.g. Pressure)
To change a measurement label of a measurement with multiple labels (invasive pressure or
temperature),
1Enter the Wave menu of the measurement.
2Select Label.
3Choose a label from the list.
The monitor automatically applies the scale, color, etc. settings stored in the Profile for the label you
select. You can change scale settings in Monitoring Mode, but color can only be changed in the
monitor’s Configuration Mode.
Any labels already being used in the monitor are shown “grayed-out” in the list and cannot be selected.
Resolving Label Conflicts
Each label must be unique, that is, it can only be assigned once. If you have a MMS Extension
equipped with a pressure measurement connected to the monitor, there is a potential conflict with, for
example, the ABP label. If you manually enter measurement values these may also conflict with existing
labels on the monitor.
Depending on your configuration, the monitor will either
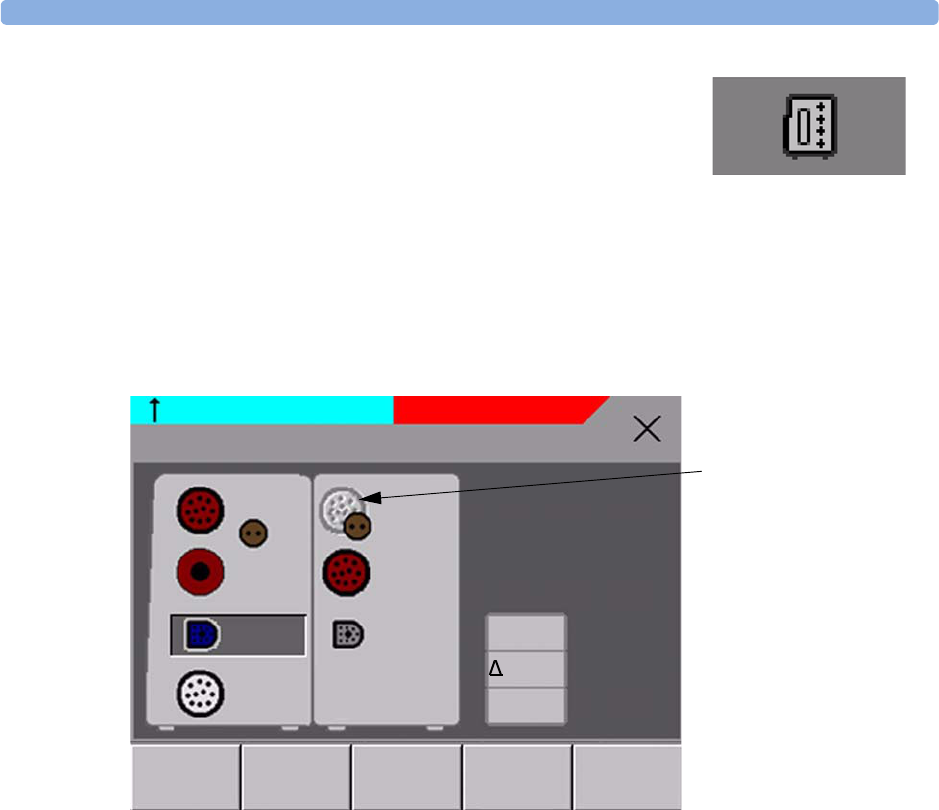
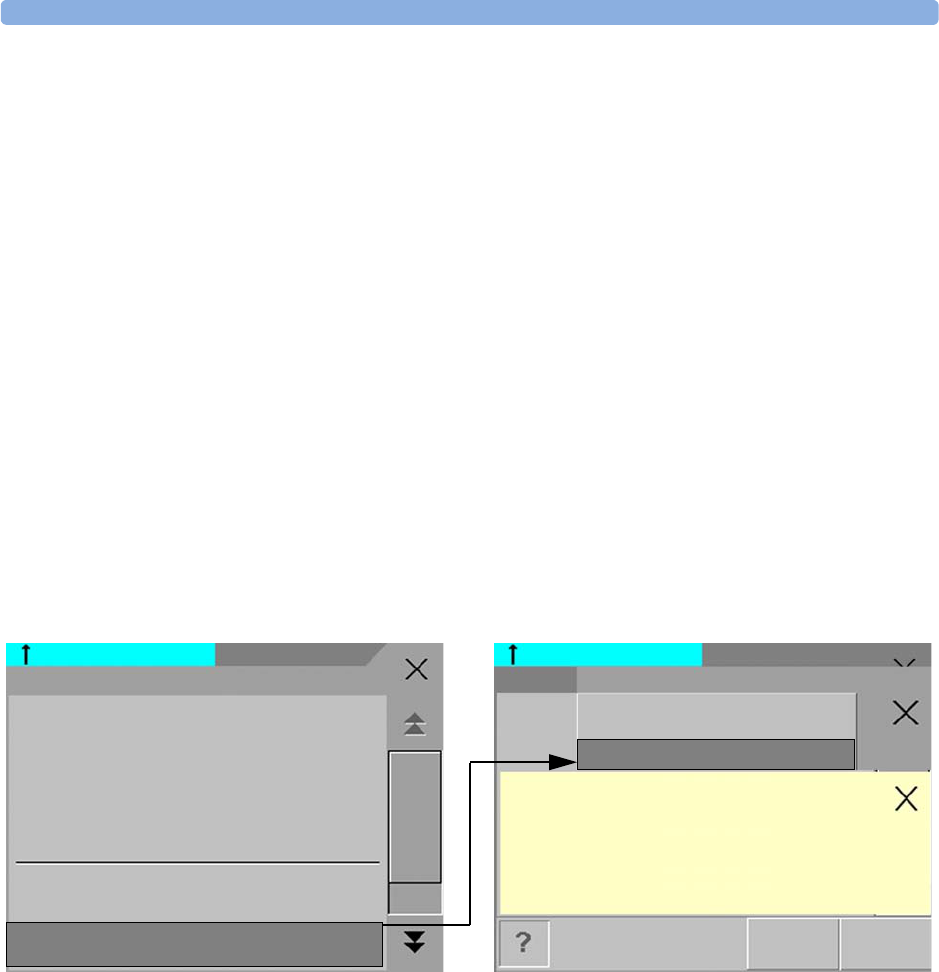
Using Labels 2 Basic Operation
29
• display the Measurement Selection window automatically
for you to resolve the conflict
• take no action, you must enter the Measurement Selection
window and resolve the conflict
All the currently available measurements are depicted in the
Measurement Selection window. Any measurement labels
causing a label conflict are shown in red. If a measurement is connected but currently unavailable, for
example, because it was deactivated due to a label conflict, that measurement is shown “grayed-out”. If
a MMS Extension is not available, for example if monitor is running on battery power and not an
external power source, the MMS Extension is not displayed.
A MMS Extension is only shown in the Measurement Selection window when the monitor is
connected to the external power supply (M8023A) and running on AC mains power, and not when
running on battery power.
To resolve a label conflict:
1Press the SmartKeys key and
–Either select Main Setup and then Meas. Selection
–Or select the Meas. Select. SmartKey
to display the Measurement Selection window.
2Select the label to be corrected.
3Use the measurement selection keys to resolve the conflict. Select either:
–Change Label: to assign a different label to the conflicting label.
–De-activate: to disable the conflicting measurement. It retains its label for future use but
becomes invisible to the monitor, as though it had been unplugged.
–Setup <Measurement label>: to enter the Setup menu for the measurement and change
the conflicting device’s label to a different label.
4Select the De-activate pop-up key to disable the conflicting measurement.
measurement selection key
PAP ZERO+CHECK CAL
ABP
Tcore
NBP
SpO2
ECG
Resp
Temp
PAP
CO2
Measurement Selection
*** APNEA
De-
Activate
Setup SpO2More
Change
Label
CPP
Temp
Unavailable measurements
are grayed-out
2 Basic Operation Changing Monitor Settings
30
Label Compatibility
When a new measurement is introduced, or new labels for an existing measurement, these labels will
not be shown on older Information Centers, and consequently not on the Overview screen sourced
from the Information Center.
When a patient is transferred from a monitor with these new labels to one with an older software
revision, the labels will be replaced with a generic label for that measurement. The settings for that
generic label will then be used.
If it is critical that the measurement labels are available at the Information Center and after transfers,
the older monitors and the Information Center must be upgraded to the appropriate software revision.
Changing Monitor Settings
To change monitor settings such as brightness, or QRS tone volume:
1Press the SmartKeys key .
2Either Enter the Main Setup menu by selecting the SmartKey . Select the setting you
want to change, or select User Interface to enter a submenu where you can change user
interface settings.
Or Select the appropriate SmartKey for the setting you want to change.
Adjusting the Screen Brightness
1Select the Brightness SmartKey.
2Select the appropriate setting for the screen brightness. 10 is the brightest, 1 is the least
bright. Optimum is suitable for most monitoring locations and optimizes power usage
for battery powered monitors.
Your monitor may be configured with a lower brightness for Standby mode and also for transport to
conserve battery power. These settings can only be changed in the monitor’s Configuration Mode.
Setting the Date and Time
If your monitor is connected to an Information Center, the date and time are automatically taken from
this.
Once it is set, the internal clock retains the setting even when you switch off the monitor.
1In the Main Setup menu, select Date, Time.
2Select, in turn, the Year, Month, Day, Hour (in 24 hour format, only) and Minute as
necessary. Select the correct values from the pop-up list.
3Select Store Date, Time to change the date and time.
Checking Your Monitor Revision
1Select Main Setup -> Revision to open the Monitor Revision menu.
2Select the correct device from the device pop-up keys.

Getting Started 2 Basic Operation
31
3From the Monitor Revision menu, select the monitor component for which you need
revision information.
Getting Started
Once you understand the basic operation principles, you can get ready for monitoring.
Inspecting the Monitor
WARNING If the monitor is mechanically damaged, or if it is not working properly, do not use it for any
monitoring procedure on a patient. Contact your service personnel.
1Before you start to make measurements, carry out the following checks on the monitor.
– Check for any mechanical damage.
– Check all the external cables, plug-ins and accessories.
2Always ensure that the battery is loaded in the battery compartment when monitoring a patient,
even when the monitor is running on external power.
3If you are using battery power, ensure that the battery has sufficient power for monitoring. Before
using a battery for the first time, you must charge it, following the instructions given in the section
on Charging Batteries.
4Measurements from measurement extensions attached to the monitor are only available when the
monitor is operating from AC mains power. The measurement extensions are not active when the
monitor is operating from battery power.
5Check all the functions of the instrument that you need to monitor the patient, and ensure that the
instrument is in good working order.
Switching On
Press the on/off switch on the monitor for one second. The monitor performs a self test and is then
ready to use. If you see a message such as CO2SENSOR WARMUP wait until it disappears before
starting to monitor that measurement.
Power On/Power Off Behavior
The general rules determining the behavior of the monitor when connected to, or disconnected from
power are as follows:
• A monitor that was switched on prior to a temporary power loss switches on again when power is
restored.
• A monitor that was switched off prior to a temporary power loss remains off when power is restored.
• When AC mains power is lost, a battery powered monitor continues to run without interruption on
battery power.
Setting up the Measurements
1Decide which measurements you want to make.
2 Basic Operation Disconnecting from AC Mains Power
32
2Connect the required patient cables and sensors. The connectors are color-coded to the patient
cables and sensors for easy identification.
WARNING When connecting devices for acquiring measurements, always position cables and tubing carefully to
avoid entanglement or potential strangulation.
Starting Monitoring
After you switch on the monitor,
1Admit your patient to the monitor.
2Check that the profile, alarm limits, alarm and QRS volumes, patient category and paced status
and so forth are appropriate for your patient. Change them if necessary.
3Refer to the appropriate measurement section for details of how to perform the measurements you
require.
Disconnecting from AC Mains Power
To disconnect the monitor from AC mains power, unplug the power cord for the external power
supply (M8023A) from the mains socket.
Monitoring After a Power Failure
If external power is disconnected or there is a power failure, the monitor continues to run on its
rechargeable battery.
If the monitor is without any power (no external power or the battery is empty) for less than one
minute, monitoring will resume with all active settings unchanged. If the monitor is without power for
more than one minute, the behavior depends on your configuration. If Automat. Default is set
to Yes, the default profile will be loaded when power is restored. If Automat. Default is set to
No, all active settings are retained, if power is restored within 48 hours. The Automat. Default
setting is made in Configuration Mode.
Networked Monitoring
You can connect your monitor to an Information Center on a network, using one of the optional
interfaces:
• Standard wired LAN
• Wireless LAN
• IntelliVue Instrument Telemetry System (IIT)
WARNING Do not connect patient monitors to the standard hospital network.

Capturing Alarm Reports and Printing 2 Basic Operation
33
If your monitor is connected to a network, a network symbol is displayed in the upper left corner next
to the bed label. To see details about the monitoring equipment and technical information about the
network, select the Main Setup SmartKey to enter the Setup menu, then select
Bed Information.
Be aware that some network-based functions may be limited for monitors on wireless networks in
comparison to those on wired networks.
Capturing Alarm Reports and Printing
You can print out standard reports, alarm reports and trends with the IntelliVue PC Printing Solution.
This is a software package which allows you to print to a standard, off-the-shelf printer or to an
electronic file such as PDF. You can download the IntelliVue PC Printing Solution free-of-charge from
the Internet and install it on an existing PC.
Capturing Alarm Reports
The monitor can be set up to automatically capture alarm reports, triggered by selected alarms. The
necessary settings must be made in Configuration mode.
When one of the selected alarms occurs, the monitor automatically captures the alarm and creates a
report which is stored in the database. As soon as the monitor is connected to a PC or network with the
IntelliVue PC Printing Solution software, it will automatically print the reports, or send them to a
patient-specific folder as an electronic file.

2 Basic Operation Capturing Alarm Reports and Printing
34

35
3
3What’s New?
This section lists the most important new features and improvements to the monitor and its user
interface introduced with each release. Further information is provided in other sections of this book.
You may not have all of these features, depending on the monitor configuration purchased by your
hospital.
What’s New in Release G.0?
Short Range Radio Interface for MP2
A short range radio interface is now available for the MP2 monitor. This allows a telemetry transceiver
with a short range radio adapter to be assigned to the monitor, resulting in a direct connection. The
measurement data from the telemetry transceiver appear directly on the monitor screen with a minimal
delay and are combined with the monitor data in one sector at the Information Center.
IntelliVue XDS Solution
Using the IntelliVue XDS solution it is possible to view an independent monitor screen on an external
display. The XDS solution consists of a medical grade PC-based hardware platform, XDS application
software and the XDS connectivity option on the monitor. Depending on the configuration you can
also operate the monitor from the external display. The XDS must be connected to the same Local
Area Network (LAN) as the monitor.
It is also possible to use an existing PC, connected to the same LAN, to host the XDS Application
software.
New Fields in the Admission Form
A Middle Name field is now available in the admission form - whether it appears is configurable. Two
additional ID fields, Lifetime Id and Encounter Id, can also be configured to appear and their names
can be customized to fit hospital requirements.
SpO2 Enhancements
•Additional SpO2 Labels - SpO2pr and SpO2po labels have been added.
•New manual measurement mode when telemetry devices are connected via a short range radio link.
• Signal Quality Indicator displayed with the SpO2 numerics.
ECG Enhancements
•New */**Afib yellow alarm when an atrial fibrillation waveform is detected.
•QT View window - shows current wave and baseline wave with Q and T points marked so that you
can verify that the QT algorithm detects correct Q and T points.

3What’s New? What’s New in Release F.0?
36
What’s New in Release F.0?
QT/QTc Interval Monitoring
QT interval monitoring is used to assist in the detection of prolonged QT interval syndrome. The QT
interval is measured and the heart-rate corrected QT value, QTc, is calculated. The monitor also
provides a 'QTc value which tracks variation in the QT interval in relation to a baseline value. High
alarm limits can be set for QTc and 'QTc enabling alarm notification.
Manual Data Entry
Measurement values (for example lab data or manually measured temperatures) can be entered
manually into the monitor and stored in the database. They can then be used for trends, reports and
also be displayed as a numeric on screen, if required.
Horizon Trend Enhancements
The trend indicator arrow indicates how the patient trend has developed in a set time period. This
period is now configurable and can be set to 10 minutes, 5 minutes or 2 minutes. The horizon (or
baseline) can now be set to a range or to a specific value.
Connecting an MP5 to a Monitor (Companion Mode is indicated)
The MP5 monitor can be connected to one of the MP20 to MP90 monitors (then called the host
monitor) and used like an MMS. This provides monitoring continuity in transport situations allowing
measurement data and patient demographics from the MP5 to be transferred to another monitor.
When the MP5 is connected to a host monitor, no alarms will be announced on the MP5.
NBP - Programmable Measurement Sequence
Up to four measurement cycles can be set up which will run consecutively. For each cycle you can set
the number of measurements and the interval between them. By setting the last cycle to run
continuously you can have regular measurements continue after the sequence has run.
New Printing Options For Reports
Reports can now also be printed via an external PC-based print server or to an internal print database,
when no printer is available (for example, during transport). As soon as a printer becomes available, the
reports stored in the database will print automatically.
Manual Pairing At Monitor
Previously, devices could only be manually paired at the Information Center. You can now pair devices
at the monitor as long as the monitor is already connected to the Information Center.
Moving Windows And Menus
Windows and menus can now be moved on the monitor screen. Using touch or a mouse you can select
the title of a window and then “drag” it across the screen. Some positions on the screen are not allowed,
such as ones overlapping the alarm field or the monitor info line.
Invasive Pressure Changes
Wave cursor - A cursor is now available on the realtime pressure wave to allow you to define a position
and store the corresponding value.
Reduced alarm limit steps in lower ranges - The alarm limits setting in 2 mmHg steps is now possible
in ranges up to 50 mmHg (previously up to 30 mmHg).

What’s New in Release F.0? 3What’s New?
37
New Patient Check
The monitor can be configured to ask you in certain situations: after a specified power-off period, after
a specified standby period and when no basic vitals (HR, RR, Pulse, SpO2, NBP) have been measured
for a specified period, whether a new patient is now being monitored. By selecting the Yes pop-up key
you can discharge the previous patient and reset settings.
New Smart Keys
A SmartKey is available for New Lead Setup when a new ECG lead set with fewer leads than
previously is being used.
Better Visibility Of Gridlines
The brightness of the gridlines on the realtime waves has been increased for better visibility.

3What’s New? What’s New in Release F.0?
38

39
4
4Alarms
The alarm information here applies to all measurements. Measurement-specific alarm information is
discussed in the sections on individual measurements.
The monitor has two different types of alarm: patient alarms and INOPs.
Patient Alarms are red and yellow alarms. A red alarm indicates a high priority patient alarm such as a
potentially life threatening situation (for example, asystole). A yellow alarm indicates a lower priority
patient alarm (for example, a respiration alarm limit violation). Additionally there are short yellow
alarms, most of which are specific to arrhythmia-related patient conditions (for example, ventricular
bigeminy).
INOPs are technical alarms, they indicate that the monitor cannot measure or detect alarm conditions
reliably. If an INOP interrupts monitoring and alarm detection (for example, LEADS OFF), the
monitor places a question mark in place of the measurement numeric and an audible indicator tone
will be sounded. INOPs without this audible indicator indicate that there may a problem with the
reliability of the data, but that monitoring is not interrupted.
Most INOPs are light blue, however there are a small number of INOPS which are always yellow or
red to indicate a severity corresponding to red and yellow alarms. The following INOPs can also be
configured as red or yellow INOPs to provide a severity indication:
• ECG LEADS OFF
•ECG/ARRH ALARM OFF (yellow only, no red INOP)
• CUFF OVERPRESS
• CUFF NOT DEFLATED
• OCCLUSION
• TELE DISCONNECT.
• Replace TeleBatt
All monitors in a unit should have the same severity configured for these INOPs.
Alarms are indicated after the alarm delay time. This is made up of the system delay time plus the
trigger delay time for the individual measurement. See the specifications section for details.
If more than one alarm is active, the alarm messages are shown in the
alarm status area in succession. An arrow symbol next to the alarm
message informs you that more than one message is active.
n** HR HIGH
4Alarms Visual Alarm Indicators
40
The monitor sounds an audible indicator for the highest priority alarm. If more than one alarm
condition is active in the same measurement, the monitor announces the most severe. Your monitor
may be configured to increase alarm indicator volume automatically during the time when the alarm is
not acknowledged.
Visual Alarm Indicators
Alarm message: An alarm message text appears in the alarm status area at the top of the screen
indicating the source of the alarm. There is a field for INOPs (light blue, red or yellow) and a field for
patient alarms, which is shared for red and yellow alarms. If more than one measurement is in an alarm
condition, the message changes every two seconds, and has an arrow ( ) at the side. If both red and
yellow alarm conditions are active simultaneously, they alternate every two seconds in the patient
alarms field. The background color of the alarm message matches the alarm priority: red for red alarms,
yellow for yellow alarms, light blue for standard INOPs, red for red INOPs and yellow for yellow
INOPs. The asterisk symbols (*) beside the alarm message match the alarm priority: *** for red alarms,
** for yellow alarms, * for short yellow alarms. Standard INOPs do not have a symbol, red and yellow
INOPs have exclamation marks beside the alarm message: !!! for red INOPs and !! for yellow INOPs.
Depending on how your monitor is configured, it may display alarm limit violation messages
• in text form, for example “**SpO2 LOW” or
• in numeric form, for example “**SpO2 94<96”, where the first number shows the maximum
deviation from the alarm limit, and the second number shows the currently set limit.
Flashing numeric: The numeric of the measurement in alarm flashes.
Bright alarm limits: If the alarm was triggered by an alarm limit violation, the corresponding alarm
limit on the monitor screen is shown more brightly if Show AlarmLimits is enabled and there is
sufficient room on the screen.
Alarm lamp: A lamp on the monitor’s front panel flashes. The alarm lamp is divided into two
sections. The right one flashes for a patient alarm, except for short yellow alarms where the lamp will
light for approximately six seconds. The color is yellow or red corresponding to the highest priority
patient alarm currently present. The left one lights continuously for a light blue INOP and flashes for
yellow or red INOPs as follows:
If only patient alarms are present, and no INOPs, the patient alarms will use both left and right
sections to flash (for red and yellow alarms) or light for approximately six seconds (for short yellow
alarms). If only INOPs are present, and no patient alarms, red and yellow INOPs will use both left and
right sections to flash but light blue INOPs will always light continuously in the left section only.
INOP Lamp
Color
Modulation (how long the lamp is on or off while flashing)
On Off
Yellow 1.0 seconds 1.0 seconds
Red 0.25 seconds 0.25 seconds
Audible Alarm Indicators 4Alarms
41
Audible Alarm Indicators
The audible alarm indicators configured for your monitor depend on which alarm standard applies in
your hospital. Audible alarm indicator patterns are repeated until you acknowledge the alarm by
switching it off or pausing it, or until the alarm condition ceases (if audible alarm indication is set to
non-latching).
WARNING • Do not rely exclusively on the audible alarm system for patient monitoring. Adjustment of alarm
volume to a low level or off during patient monitoring may result in patient danger. Remember that
the most reliable method of patient monitoring combines close personal surveillance with correct
operation of monitoring equipment.
Alarm Tone Configuration
The audible alarm indicators of your monitor are configurable. In the monitor’s Configuration Mode,
you can:
• increase the alarm volume of unacknowledged alarms at regular intervals
• change the interval between alarm sounds (ISO/IEC Standard alarms only)
• change the base volume of the red and yellow alarm tones and the INOP tones
• change the alarm sound to suit the different alarm standards valid in different countries.
Traditional Audible Alarms (HP/Agilent/Philips/Carenet)
• Red alarms and red INOPs: A high pitched sound is repeated once a second.
• Two-star yellow alarms and yellow INOPs: A lower pitched sound is repeated every two seconds.
• One-star yellow alarms (short yellow alarms): The audible indicator is the same as for yellow alarms,
but of shorter duration.
• Standard INOPs: an INOP tone is repeated every two seconds.
ISO/IEC Standard Audible Alarms
• Red alarms and red INOPs: A high pitched tone is repeated five times, followed by a configurable
pause.
• Two-star yellow alarms and yellow INOPs: A lower pitched tone is repeated three times, followed by
a configurable pause.
• One-star yellow alarms (short yellow alarms): The audible indicator is the same as for yellow alarms,
but of shorter duration.
• Standard INOPs: a lower pitched tone is repeated twice, followed by a pause.
Changing the Alarm Tone Volume
4Alarms Acknowledging Alarms
42
♦If you want to see a numerical indication of the current alarm volume on a scale
from zero to 10, or change the setting, select the Alarm Volume SmartKey. The
volume scale pops up. The current setting is indented. To change the setting, select
the required number on the scale. Any settings that are inactive (“grayed out”) have
been disabled in the monitor’s Configuration Mode.
When the alarm volume is set to zero (off), the alarm volume symbol reflects this. If you
switch the alarm volume off, you will not get any audible indication of alarm conditions.
Minimum Volume for No Central Monitoring INOP
If your monitor is connected to an Information Center, and the connection is interrupted, the INOP
message No Central Monit. will appear within 30 seconds, accompanied by an INOP tone. To
help ensure that this INOP, and any other active alarm, is not overlooked, the INOP and alarm tones
may be configured to have a minimum volume. In this case, INOP and alarm tones will sound even if
the monitor alarm volume is set to zero.
Minimum Volume for Severe Yellow or Red INOPs
Severe yellow or red INOPs require action to ensure the well-being of the patient. Therefore the
minimum volume for the INOP tone is set to at least alarm volume 8, irrespective of the current alarm
volume setting. The INOP tone will sound even if the monitor alarm volume is set to zero.
The severe INOPs for which this applies are:
Cuff Not Deflated (configurable to yellow or red)
NBP Cuff Overpress (configurable to yellow or red)
Insert Battery (yellow)
Acknowledging Alarms
To acknowledge all active alarms and INOPs, press the Silence key. This switches
off the audible alarm indicators and alarm lamps.
A check mark beside the alarm message indicates that the alarm has been
acknowledged. If the monitor is configured to re-alarm, a dashed check mark will
be shown.
If the condition that triggered the alarm is still present
after the alarm has been acknowledged, the alarm message
stays on the screen with a check mark symbol beside it, except for NBP alarms. When an NBP alarm is
acknowledged the alarm message disappears.
If the alarm condition is no longer present, all alarm indicators stop and the alarm is reset.
Switching off the alarms for the measurement in alarm, or switching off the measurement itself, also
stops alarm indication.
Alarm
Volume
APNEA

Pausing or Switching Off Alarms 4Alarms
43
Acknowledging Disconnect INOPs
Acknowledging an INOP that results from a disconnected transducer switches off the associated
measurement. The only exception is ECG/Resp: acknowledging a disconnect INOP for ECG leads
does not switch off the ECG and Resp measurements. Acknowledging a disconnect INOP at the
Information Center switches off the audible INOP indicator but does not switch off the measurement.
Alarm Reminder (ReAlarm)
If Alarm Reminder is configured on for your monitor, you will get an audible reminder of alarm
conditions that remain active after you have acknowledged the alarm. This reminder may take the form
of a repetition of the alarm tone for a limited time, or an unlimited repetition of the alarm tone (this is
the same as a new alarm). Alarm reminder is not available for standard, light blue INOPs but for yellow
and red INOPs.
In Configuration Mode, you can set the interval between silencing the alarm and sounding the
reminder tone to one, two, or three minutes.
The alarm reminder behavior at the Information Center is different to that at the monitor. Refer to the
Information Center Instructions for Use for further information.
Pausing or Switching Off Alarms
If you want to temporarily prevent alarms from sounding, for example while you are moving a patient,
you can pause alarms. Depending on your monitor configuration, alarms are paused for one, two, or
three minutes, or infinitely.
To view the alarm pause setting chosen for your unit,
1Select Main Setup -> Alarms -> Alarm Settings
2Check the Alarms Off setting.
This setting can only be changed in Configuration Mode.
To Pause All Alarms
♦Press the Alarms key.
♦If your monitor is configured to infinite pause time, the lamp next to the
alarms off symbol is red, and pressing this key switches alarms off.
Depending on the configuration, you may need to select Confirm to complete the change.
To Switch All Alarms Off
You can only switch alarms off permanently if your monitor is configured to allow infinite alarms
pause.
Alarms
Off
4Alarms Pausing or Switching Off Alarms
44
♦Press the Alarms key.
Pausing alarms infinitely is the same as switching them off.
To Switch Individual Measurement Alarms On or Off
1Select the measurement numeric to enter its setup menu.
2Select Alarms to toggle between On and Off.
The alarms off symbol is shown beside the measurement numeric.
While Alarms are Paused or Off
• The red Alarms Paused lamp on the monitor front panel is lit.
•In the alarm field, the monitor displays the message
ALARMS PAUSED or ALARMS OFF, together with
the alarms paused symbol and the remaining pause
time in minutes and seconds, or alarms off symbol.
• No alarms are sounded and no alarm messages are
shown.
• INOP messages are shown but no INOP tones are
sounded.
The only exceptions are the INOPs CUFF NOT DEFLATED, CUFF OVERPRESS and INOPs
relating to empty, missing and malfunctioning batteries.
These INOPs switch the alarms on, and the INOP tones are sounded, even if alarms are paused or
off. You need to remove the INOP condition first before you can switch the alarm tones off again.
If a NO SENSOR or NO TRANSDUCER INOP is present and alarms are paused or switched off, the
measurement in question is switched off.
Restarting Paused Alarms
♦To manually switch on alarm indication again after a pause, press the Alarms key again.
Alarm indication starts again automatically after the pause period expires. If the monitor is configured
to stay paused infinitely, you must select ALARMS OFF again to restart alarm indication.
Resetting Arrhythmia Alarm Timeouts
♦To reset the arrhythmia alarm timeout period, press the Alarms key and then press it again.
Extending the Alarm Pause Time
If your monitor has extended alarm pause enabled, you can extend the alarm pause time. Use this to
prevent alarms being indicated, for example, while you are washing a patient or carrying out a
procedure. Only extend the alarm pause time when you are sure that clinical personnel are available to
monitor the patient’s condition closely.
To extend the alarm pause time to five or 10 minutes,
ALARMS PAUSED 1:28
ALARMS OFF
Alarm Limits 4Alarms
45
1Select one of the alarm fields. This calls up the Review Alarms window.
2Select either the pop-up key Pause Al. 5 min or the pop-up key Pause Al. 10 min.
Each time you select one of these pop-up keys, the Alarm Pause Time is reset to five (or 10)
minutes.
Alarm Limits
The alarm limits you set determine the conditions that trigger yellow and red limit alarms. For some
measurements (for example, SpO2), where the value ranges from 100 to 0, setting the high alarm limit
to 100 switches the high alarm off. In these cases, the alarms off symbol is not displayed.
WARNING Be aware that the monitors in your care area may each have different alarm settings, to suit different
patients. Always check that the alarm settings are appropriate for your patient before you start
monitoring.
Viewing Individual Alarm Limits
You can usually see the alarm limits set for each measurement next to the
measurement numeric on the main screen.
If your monitor is not configured to show the alarm limits next to the numeric,
you can see them in the appropriate measurement setup menu. Select the
measurement numeric to enter the menu and check the limits.
Viewing All Alarm Limits
The Alarm Limits overview window lists the currently set alarm limits for all measurements. If an
Apnea alarm delay time is set, this is also shown. The ALARMS OFF symbol is shown beside the
measurement label of any measurement whose alarm switched off.
To open the Alarm Limits window, either select one of the alarm fields then select the
Alarm Limits pop-up key, or select the Alarm Limits SmartKey, if configured.
85
120
50
HR
Alarm limits
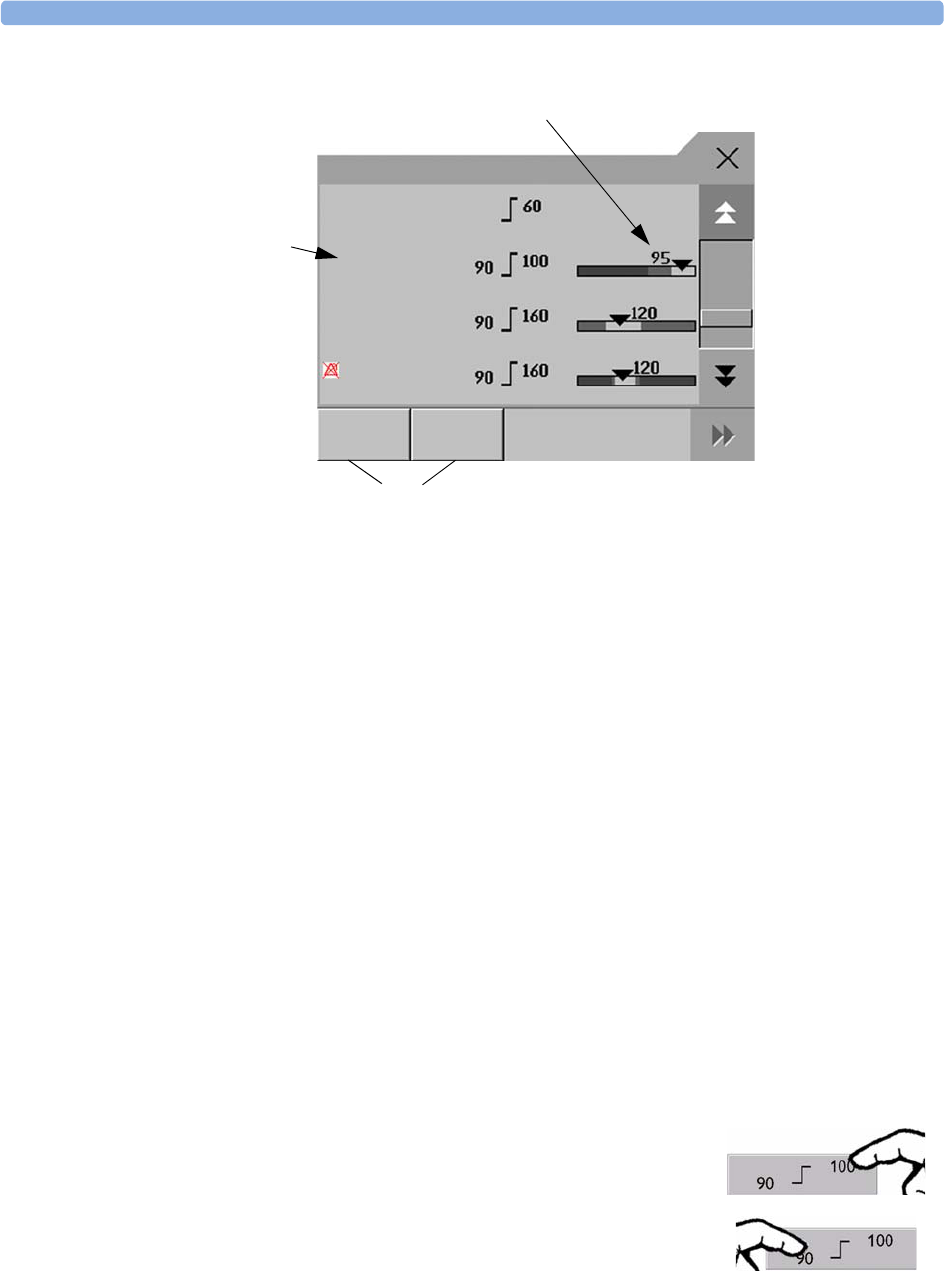
4Alarms Alarm Limits
46
♦Select Show ST Limits to expand the list of ST leads and view the currently set alarm limits.
Selecting Hide ST Limits hides the list again.
You can use the pop-up keys that open with the Alarm Limits window to perform common tasks:
–All Lim. Narrow/All Lim. Wide to set narrow or wide alarm AutoLimits for all
measurements.
These pop-up keys are not available in the window for changing individual alarm limits which you
access by selecting the measurement label in the Alarm Limits window.
Changing Alarm Limits
To change individual measurement alarm limits using the measurement’s Setup Menu,
1In the measurement’s setup menu, select the alarm limit you want to change. This calls up a list of
available values for the alarm limit.
2Select a value from the list to adjust the alarm limit.
For example, to change the alarm limits for SpO2:
1Graphic view of current yellow and red alarm limits and currently monitored measurement value
Off indicates the measurement is switched off
2Measurement labels, with alarms off symbol where appropriate
3Set narrow or wide alarm AutoLimits for all measurements
SpO2
NBPs
ABPs
Off
'QTc
All Lim.
Narrow
All Lim.
Wide
Alarm Limits
1
2
3
• Touch the high limit on the alarm limits menu button. Choose the
high alarm limit from the pop-up list that opens.
• Touch the low limit on the alarm limits menu button. Choose the
low alarm limit from the pop-up list that opens.
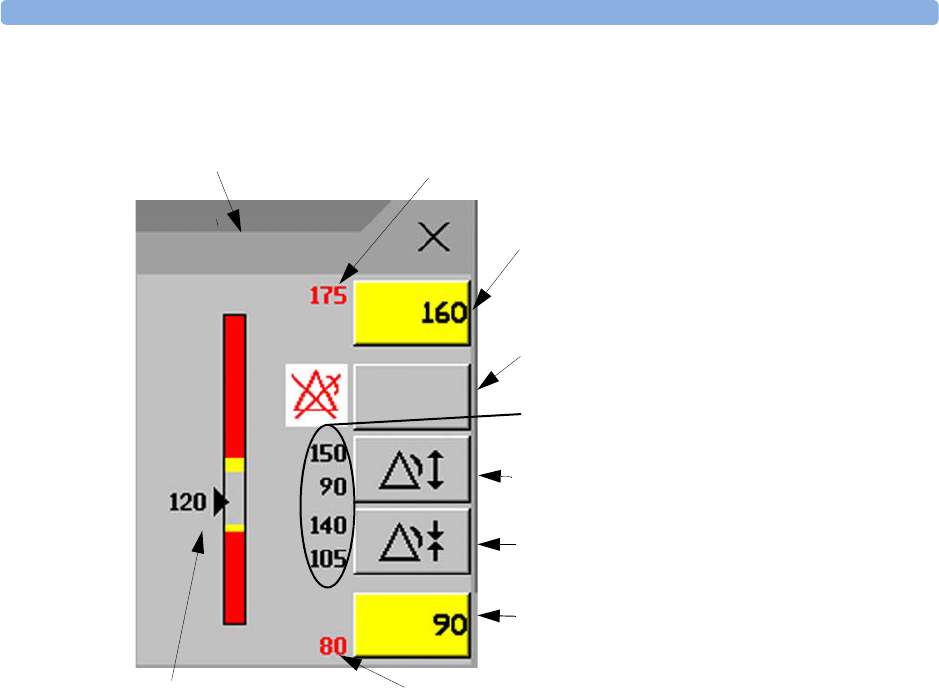
Alarm Limits 4Alarms
47
Alternatively, you can use the keys in the measurement Change Limits window, which you access by
selecting the measurement label in the Alarm Limits window.
To change alarm limits,
1Enter the Alarm Limits window.
2To set the high alarm limit, select the high yellow alarm field to open a pop-up list of high alarm
limits. Select a limit from the list. Repeat to set the low yellow alarm field.
If you set the yellow alarm limit outside the red alarm limit, the monitor will automatically set the red
alarm to the yellow alarm limit.
1Parameter label
2High red alarm (view only)
3High yellow alarm field
Select to open a pop-up list of high alarm limits
4Alarms On/Off key - select to toggle between alarms on or off
5Preview Alarm AutoLimits for a measurement before applying
6Select to apply wide AutoLimits
7Select to apply narrow AutoLimits
8Low yellow alarm field
Select to open a pop-up list of low alarm limits
9Low red alarm (view only)
10 Graphic view of alarm limits with currently measured value
4
5
8
2
3
9
10
Alarms
On/Off
ABPs
1
6
7
4Alarms Alarm Limits
48
When an ST measurement is in the Change Limits window there are also two pop-up keys available
labeled All ST Narrow/All ST Wide. With these keys you can set Auto Limits for all ST
Leads.
About Automatic Alarm Limits (AutoLimits)
The monitor can automatically set alarm limits suited to your individual patient, using the Automatic
Alarm Limits function. This tells the monitor to adapt the alarm limits of selected measurements to the
measured vital signs within a defined safe limit. The monitor calculates safe AutoLimits for each
patient based on the measured values from the last 12 seconds.
The wide and narrow limits have a fixed relationship to the measured value within the non-
pathological range. Outside of this range, no auto limits are calculated. To set values outside of the
non-pathological range, limits must be changed manually, based on the clinician’s judgement about the
specific patient.
Limits Narrow sets limits close to the currently measured values for situations where it is critical
for you to be informed about small changes in your patient’s vital signs.
Limits Wide sets limits further away from the currently measured values for situations where small
changes are not so critical.
♦Use the keys in the Change Limits window to apply AutoLimits for individual measurements.
These keys are not available if AutoLimits have been disabled for the measurement in the monitor’s
Configuration Mode.
AutoLimits are not available for all measurements. The list of measurements for which AutoLimits can
be used is defined in the monitor’s Configuration mode.
Use the Change Limits window to check AutoLimits before you apply them to ensure that they are
appropriate for your individual patient and their clinical condition. Once applied, AutoLimits are
shown on the monitor screen just like manually-set alarm limits. If the AutoLimits are not appropriate
for your patient, you must set alarm limits manually. The limits remain unchanged until you set them
again or change them manually.
1 Wide alarm limits
2 Narrow alarm limits
3Alarm Limits
4 Measurement value
1
2
2
1
4
3
Reviewing Alarms 4Alarms
49
Documenting Alarm Limits
To print a list of all current alarm limit settings on an available printer:
1Select the Main Setup SmartKey.
2Select Reports from the Main Setup menu.
3Select Alarm Limits.
Reviewing Alarms
You can see which alarms and INOPs are currently active in the respective alarms and INOPs fields at
the top of the screen.
To review the history of alarms and INOPs, select the alarms or INOPs field to open the Review
Alarms window.
All alarms and INOPs are erased from the Review Alarms window when you discharge a patient,
or if you change to Demonstration Mode.
Review Alarms Window
The Review Alarms window contains a list of the most recent alarms and INOPs with date and
time information.
If configured to do so, each alarm is shown with the alarm limit active when the alarm was triggered
and the maximum value measured beyond this limit. The Review Alarms window also shows
when the monitor was switched on (after being switched off for longer than 1 minute) and any changes
made to the Alarms On/Off, Standby, Silence or ECG source.
When you select an item from the list, you can get additional information about that item. If you select
a high or low limit alarm in the list, the Graphical Trends window will open to provide further
data. If you select an alert other than a high or low alarm, a help text window opens with more
information. Some items in the list are simply log items not related to a patient alert as such (for
example, Alarms On or Alarms Off). You cannot see any further information if you select one of these
items. When you close these windows you will return to the Review Alarms window.
The information in the Review Alarms window is deleted when a patient is discharged, and when you
leave Demonstration Mode.
Review Alarms
23 Apr 14:08:30 ***Apnea
23 Apr 14:08:30 Alarms Silenced
23 Apr 14:08:19 **AwRR LOW (14<15)
23 Apr 14:42:55 **SpO2 NON-PULSAT.
Alarm
Limits
PauseAl.
5 MIn
PauseAl.
10 MIn
4Alarms Latching Alarms
50
The Review Alarms window pop-up keys appear when the window is opened. If alarm pause
extension is disabled, the pause pop-up keys are inactive.
Latching Alarms
The alarm latching setting for your monitor defines how the alarm indicators behave when you do not
acknowledge them. When alarms are set to non-latching, their indicators end when the alarm
condition ends. Switching alarm latching on means that visual and/or audible alarm indications are still
displayed or announced by the monitor after the alarm condition ends. The indication lasts until you
acknowledge the alarm.
Viewing the Alarm Latching Settings
To see the alarm latching setting for your monitor
1In the monitor’s Main Setup menu, select Alarms.
2Select Alarm Settings, and see the Visual Latching and Audible Latching
settings.
This setting can only be changed in Configuration Mode. You should be aware of the settings chosen
for your unit. There are three possible choices each for visual and audible latching, Red, Red and
Yellow, and Off. These choices can be combined to give the following settings:
R = red alarms, Y = yellow alarms
Alarm Latching Behavior
All INOPs are non-latching. See “Yellow Arrhythmia Alarms” on page 112 for information on one-star
yellow alarms latching behavior.
Alarm
Limits
Pause Al.
5 Min.
Pause Al.
10 Min.
Visual Latching R&Y R&Y R&Y RROff
Audible latching R&Y ROffROffOff
Red and Yellow Measurement
Alarms
Non-latching
alarms
Visual and audible
latching
Visual latching,
audible non-latching
Alarm has not been
acknowledged.
Alarm condition
still present.
Alarm tone on. Alarm lamp on. Alarm message. Flashing numerics.
Alarm condition
no longer present.
All audible and visual
alarm indicators
automatically stop.
Alarm tone on.
Alarm lamp on.
Alarm message.
Flashing numerics.
Alarm message. Flashing
numerics.
Audible alarm indicators
automatically stop.
Alarm has been
acknowledged.
Alarm condition
still present.
Alarm tone off. Alarm lamp off. Alarm message. Flashing numerics. Audible
alarm reminder (if configured).
Alarm condition
no longer present.
Audible and visual alarm indicators automatically stop.

Testing Alarms 4Alarms
51
Te s t i n g A l a r m s
When you switch the monitor on, a selftest is started. You must check that the alarms lamps light, one
after the other, and that you hear a single tone. This indicates that the visible and audible alarm
indicators are functioning correctly. For further testing of individual measurement alarms, perform the
measurement on yourself (for example SpO2 or CO2) or use a simulator. Adjust alarm limits and check
that appropriate alarm behavior is observed.
Alarm Behavior at On/Off
When you switch alarms on, the settings defined in the currently active Profile are used.
If the monitor is switched off for longer than one minute and then switched on again, or after a loss of
power lasting longer than one minute, or when a patient is discharged, the monitor can be configured
to restore either the alarm settings from the monitor's configured default Profile, or the most recently
used alarm settings. After any of these situations, you should check that the alarm settings are
appropriate for your patient, and if necessary, select the correct Profile and patient category.
If power is lost for less than one minute, the alarm settings prior to the power loss are restored.
Alarm Recordings
You can set up your monitor so that it automatically triggers alarm recordings at the Information
Center, or if configured, to a printer as a realtime report.
1Press the Main Setup SmartKey.
2Select Alarms from the Main Setup menu.
3Select Alarm Recording from the Alarms menu to open the Alarm Recordings menu.
4Select a measurement from those listed for which you want to change the alarm condition that
triggers an alarm recording. This opens a pop-up list.
5For the desired measurement(s), choose the alarm condition to trigger an alarm recording:
Red Only: an alarm recording will automatically be triggered when the measurement enters a
red alarm condition.
Red&Yell: both yellow and red alarms will trigger an alarm recording.
Off: disables automatic alarm recording.
Refer to the chapter “Recording” for details of how to set up a recording.

4Alarms Alarm Recordings
52
53
5
5Patient Alarms and INOPs
This chapter lists patient alarms and technical alarms (INOPs) alphabetically, irrespective of their
priority. INOPs start on page 59. All alarms and INOPs are listed here; the ones which can appear on
your monitor will depend on the model and the individual options.
Patient Alarm Messages
The measurement labels and abbreviations for pressure, temperature, SpO2, and anesthetic agent
alarms are explained in the individual chapters.
Some alarms may be shown at the Information Center in shortened form, when transferred through
IntelliVue Instrument Telemetry. These shortened alarm texts are included in the list and identified
with the note “at Information Center”.
Note that yellow arrhythmia alarms may be shown with one or with two stars, depending on your
monitor configuration and the Information Center revision you are using.
Refer to your IntelliBridge Device Driver Instructions for Use for patient alarms from connected
external devices.
Alarm Message From Condition Indication
*/**AFIB ECG/
Arrhythmia
Atrial fibrillation waveform detected yellow alarm lamp, short
yellow audible alarm.
***APNEA or
***APNEA mm:ss sec
or
***APNEA >10min
CO2, Resp,
Spirometry
Respiration has stopped for longer than
the preset apnea time. “mm:ss” denotes
the Apnea duration in minutes and
seconds.
numeric flashes, red alarm
lamp, alarm tone.
***ASYSTOLE ECG No QRS detected for a period greater
than the asystole threshold (in the
absence of Vfib or chaotic ECG).
numeric flashes, red alarm
lamp, alarm tone.
**awRR HIGH CO2, Resp,
AGM
The airway respiration rate has
exceeded the high alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**awRR LOW CO2, Resp,
AGM
The airway respiration rate has dropped
below the low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
**BIS HIGH BIS The Bispectral Index value has
exceeded the high alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
5 Patient Alarms and INOPs Patient Alarm Messages
54
**BIS LOW BIS The Bispectral Index value has dropped
below the low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
***BRADY/P xxx<yyy
or
***BRADY xxx<yyy
Press, SpO2The heart rate from the Pulse signal has
fallen below the bradycardia limit. xxx
denotes the lowest measured value; yyy
is the bradycardia limit.
numeric flashes and alarm
limit is highlighted, red alarm
lamp, alarm tone.
**CCO/CCI HIGH CCO Continuous Cardiac Output or CC
Index is above the high alarm limit.
numeric flashes and high alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**CCO/CCI LOW CCO Continuous Cardiac Output or CC
Index is below the low alarm limit.
numeric flashes and low alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**CPP HIGH CPP The CPP value has exceeded the high
alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone
**CPP LOW CPP The CPP value has fallen below the low
alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
***DESAT or
***DESAT xxx<yyy
SpO2The SpO2 value has fallen below the
desaturation alarm limit. xxx denotes
the lowest measured value, and yyy is
the desaturation limit.
numeric flashes, red alarm
lamp, alarm tone.
**etCO2 HIGH CO2, Resp,
AGM
The end tidal CO2 high alarm limit has
been exceeded.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**etCO2 LOW CO2, Resp,
AGM
The end tidal CO2 value has fallen
below the low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
**etO2 HIGH O2, AGM The end tidal O2 high alarm limit has
been exceeded.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**etO2 LOW O2, AGM The end tidal O2 value has fallen below
the low alarm limit.
numeric flashes, and low limit
is highlighted, yellow alarm
lamp, alarm tone.
*/**/***
EVENT:<GRP>
Event
surveillance
An event has occurred and the event
notification is configured to alarm.
<GRP> is the event group
event group name flashes,
yellow or red alarm lamp and
alarm tone
*/**/*** EVENT
at Information center
Event
surveillance
An event has occurred and the event
notification is configured to alarm.
Check on the monitor for more details
on event group.
(on monitor) event group
name flashes, yellow or red
alarm lamp and alarm tone
***EXTREME BRADY ECG The bradycardia limit has been
exceeded.
numeric flashes and alarm
limit is highlighted, red alarm
lamp, alarm tone.
***EXTREME TACHY ECG The tachycardia limit has been
exceeded.
numeric flashes and alarm
limit is highlighted, red alarm
lamp, alarm tone.
Alarm Message From Condition Indication
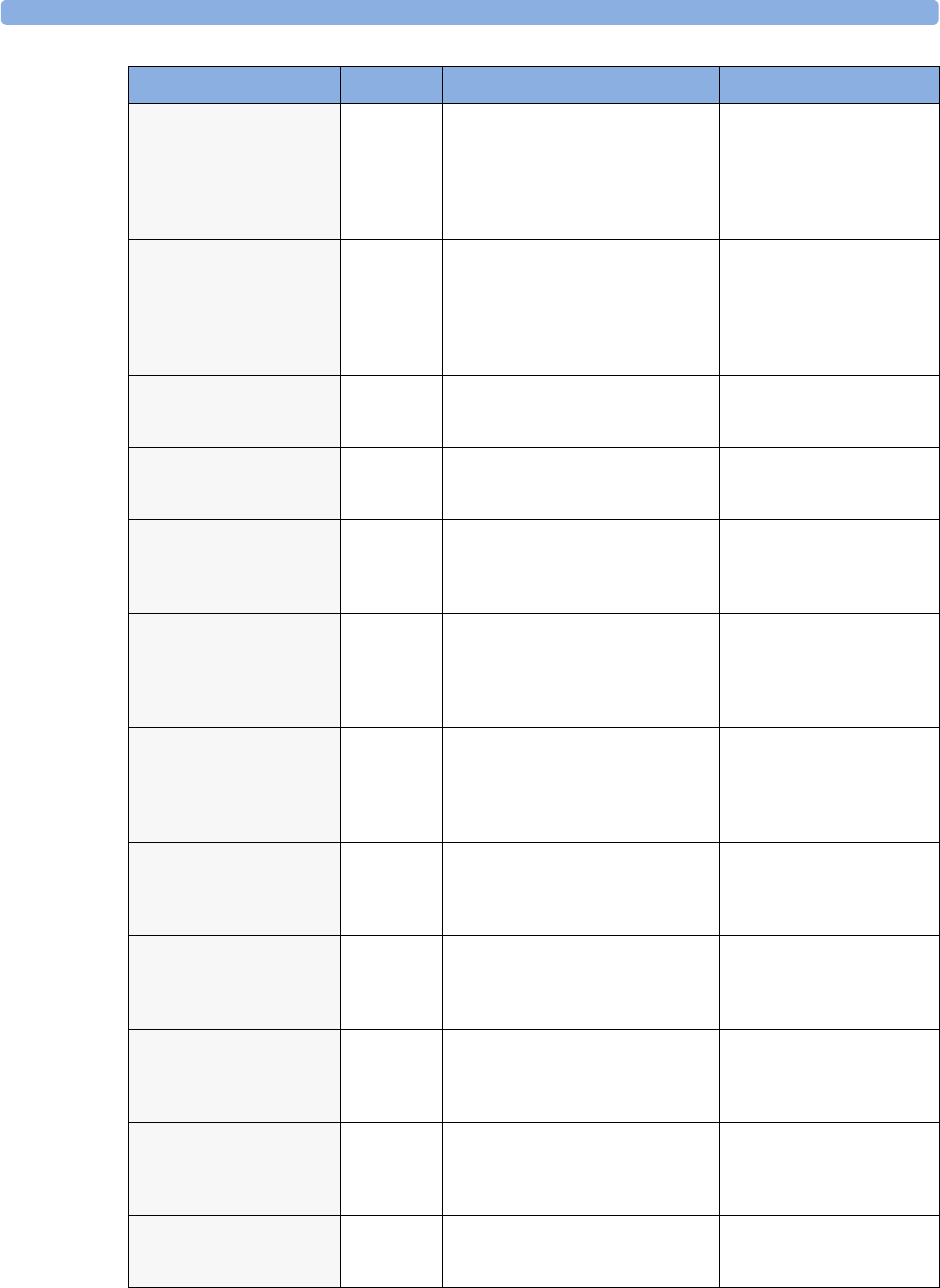
Patient Alarm Messages 5 Patient Alarms and INOPs
55
**HR HIGH ECG The heart rate high alarm limit has
been exceeded.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone. If configured
to short yellow, the sound
switches off after 5 seconds if
Arrhythmia is On.
**HR LOW ECG The heart rate has fallen below the low
alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone. If configured
to short yellow, the sound
switches off after 5 seconds if
Arrhythmia is On.
*/**IRREGULAR HR ECG/
Arrhythmia
Consistently irregular heart rhythm. numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**MISSED BEAT ECG/
Arrhythmia
No beat detected for 1.75*R-R interval,
or if HR>120bpm no beat detected for
one second (non-paced patients only).
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**MULTIFORM PVCs ECG/
Arrhythmia
Two differently shaped Vs detected,
each occurring at least twice within the
last 300 beats and at least once within
the last 60 beats.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
**NBP HIGH NBP The measured NBP value is above the
high alarm limit.
s, d, or m after the label indicates
whether the systolic, diastolic or mean
pressure has crossed the limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**NBP LOW NBP The measured NBP value is below the
low alarm limit.
s, d, or m after the label indicates
whether the systolic, diastolic or mean
pressure has crossed the limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
*/**NON-SUSTAIN VT ECG/
Arrhythmia
A run of Vs having a ventricular
HR>V-Tach HR limit, but lasting for
less than the V-Tach Run limit has been
detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**PACER NOT CAPT ECG/
Arrhythmia
(paced
patients only)
A missed beat with a pace pulse was
detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**PACER NT PACING ECG/
Arrhythmia
(paced
patients only)
A missed beat without a pace pulse was
detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**PAIR PVCs ECG/
Arrhythmia
A non-ventricular contraction, followed
by two ventricular contractions,
followed by a non-ventricular
contraction has been detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**PAUSE ECG/
Arrhythmia
No beat detected for a period greater
than the pause threshold.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
Alarm Message From Condition Indication
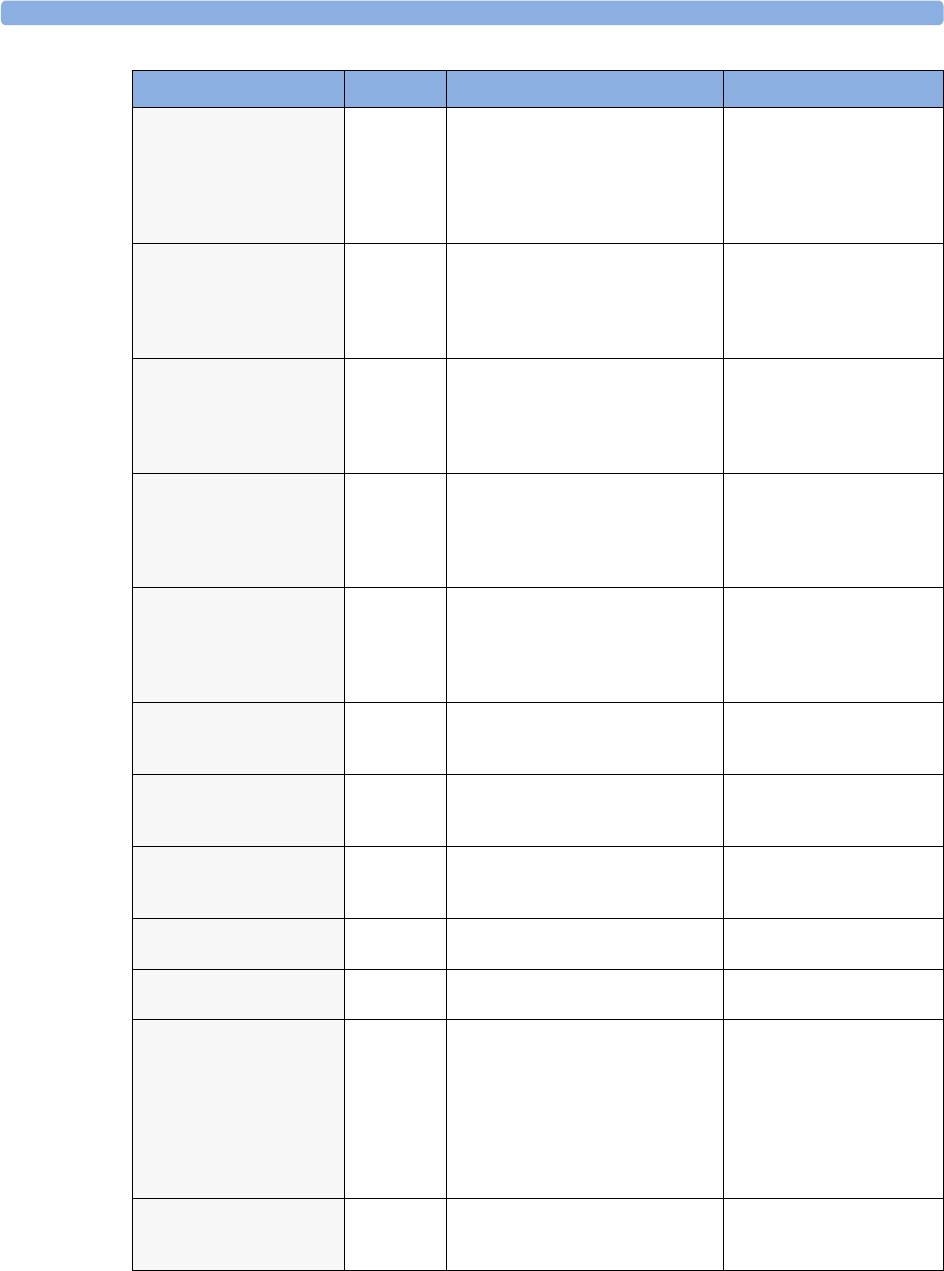
5 Patient Alarms and INOPs Patient Alarm Messages
56
***<Pressure>
DISCONNECT
PRESS The pressure is non-pulsatile and the
mean pressure is continuously less than
10mmHg (1.3kPa). This alarm occurs
only with arterial pressures (P, ABP,
ART, Ao, BAP, FAP, PAP, UAP, P1, P2,
P3, P4).
numeric flashes, red alarm
lamp, alarm tone.
***<Pressure> HIGH PRESS The measured pressure value is above
the extreme high alarm limit. s, d, or m
after the label indicates whether the
systolic, diastolic or mean pressure has
crossed the limit.
numeric flashes, high limit is
highlighted, red alarm lamp,
alarm tone.
**<Pressure> HIGH PRESS The measured pressure value is above
the high alarm limit. s, d, or m after the
label indicates whether the systolic,
diastolic or mean pressure has crossed
the limit.
numeric flashes, high limit is
highlighted, yellow alarm
lamp, alarm tone.
***<Pressure> LOW PRESS The measured pressure value is below
the extreme low alarm limit. s, d, or m
after the label indicates whether the
systolic, diastolic or mean pressure has
crossed the limit.
numeric flashes and low limit
is highlighted, red alarm lamp,
alarm tone.
**<Pressure> LOW PRESS The measured pressure value is below
the low alarm limit. s, d, or m after the
label indicates whether the systolic,
diastolic or mean pressure has crossed
the limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
**Pulse HIGH PRESS
SpO2
The pulse rate has exceeded the high
alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**Pulse LOW PRESS
SpO2
The pulse rate has dropped below the
low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
*/**PVCs/min HIGH ECG/
Arrhythmia
More premature ventricular
contractions have been detected in a
minute than the limit.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
**QTc HIGH ECG/QT QTc value has exceeded the QTc high
limit for more than 5 minutes
numeric flashes, yellow alarm
lamp, alarm tone.
**'QTc HIGH ECG/QT 'QTc value has exceeded the 'QTc
high limit for more than 5 minutes
numeric flashes, yellow alarm
lamp, alarm tone.
*/**R-ON-T PVCs ECG/
Arrhythmia
For HR <100, a PVC with R-R interval
< 1/3 the average interval followed by a
compensatory pause of 1.25 x average
R-R interval or two such Vs without
compensatory pause occurring within 5
minutes of each other. (When HR
>100, 1/3 R-R interval is too short for
detection.).
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
**RR HIGH RESP The respiration rate has exceeded the
high alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
Alarm Message From Condition Indication
Patient Alarm Messages 5 Patient Alarms and INOPs
57
**RR LOW RESP The respiration rate has dropped below
the low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
*/**RUN PVCs HIGH ECG/
Arrhythmia
A run of PVCs greater than 2 was
detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
**<SO2 label> HIGH SvO2/SO2The the measured intravascular oxygen
saturation has exceeded the high limit.
numeric flashes and high alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**<SO2 label> LOW SvO2/SO2The measured intravascular oxygen
saturation has fallen below the low
limit.
numeric flashes and low alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**<SpO2 label> HIGH SpO2The arterial oxygen saturation has
exceeded the high alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**<SpO2 label> LOW SpO2The arterial oxygen saturation has
fallen below the low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
**ST<n> HIGH ECG/ST The ST elevation in lead <n> is higher
than the limit.
numeric flashes and high alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**ST<n> LOW ECG/ST The ST depression in lead <n> is lower
than the limit.
numeric flashes and low alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**ST MULTI <n>,<n> ECG/ST The ST depression or elevation is
outside of the limit in two or more
leads <n> and <n>
numeric flashes, yellow alarm
lamp, alarm tone
**ST MULTI
at Information Center
ECG/ST The ST depression or elevation is
outside of the limit in two or more
leads. Check on the monitor for more
details about which leads are affected.
(on monitor) numeric flashes,
yellow alarm lamp, alarm tone
*/**SVT ECG/
Arrhythmia
A run of supraventricular beats greater
than the SVT run limit has been
detected and the HR has exceeded the
SVT HR limit.
numeric flashes, yellow alarm
lamp, alarm tone.
***TACHY/P xxx>yyy
or
***TACHY xxx>yyy
Press, SpO2The heart rate from the Pulse signal has
exceeded the tachycardia limit. xxx
denotes the highest measured value; yyy
is the tachycardia limit.
numeric flashes, alarm limit is
highlighted, red alarm lamp,
alarm tone.
**Tblood HIGH C.O. The blood temperature value has
exceeded the high alarm limit.
numeric flashes, high alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**Tblood LOW C.O. The blood temperature value has fallen
below the low alarm limit.
numeric flashes, low alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**tcpO2 HIGH/
**tcpCO2 HIGH
tcGas The tcpO2 or tcpCO2 value has
exceeded the high alarm limit.
numeric flashes, high alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
**tcpO2 LOW/
**tcpCO2 LOW
tcGas The tcpO2 or tcpCO2 value has fallen
below the low alarm limit.
numeric flashes, low alarm
limit is highlighted, yellow
alarm lamp, alarm tone.
Alarm Message From Condition Indication
5 Patient Alarms and INOPs Patient Alarm Messages
58
*/**/***TELE ALARM Telemetry This is a generic alarm from the
telemetry system. The specific alarm
cause is indicated in the alarm message
in the Telemetry Data Window.
yellow or red alarm lamp and
alarm tone
**<Temperature
label> HIGH
TEMP The temperature has exceeded the high
alarm limit.
numeric flashes and high limit
is highlighted, yellow alarm
lamp, alarm tone.
**<Temperature
label> LOW
TEMP The temperature has fallen below the
low alarm limit.
numeric flashes and low limit
is highlighted, yellow alarm
lamp, alarm tone.
*/**VENT BIGEMINY ECG/
Arrhythmia
A dominant rhythm of N, V, N, V (N =
supraventricular beat, V = ventricular
beat) was detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
***VENT FIB/TACH ECG A fibrillatory waveform for 4
consecutive seconds was detected.
numeric flashes, red alarm
lamp, alarm tone.
*/**VENT RHYTHM ECG/
Arrhythmia
A dominant rhythm of adjacent Vs >
vent rhythm limit and ventricular HR <
VTach HR limit was detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
*/**VENT TRIGEMINY ECG/
Arrhythmia
A dominant rhythm of N, N, V, N, N,
V (N = supraventricular beat, V =
ventricular beat) was detected.
numeric flashes, yellow alarm
lamp, short yellow audible
alarm.
***VTACH ECG,
Arrhythmia
Ventricular tachycardia has been
detected (Consecutive PVCs exceed V-
Tach Run limit and HR exceeds V-Tach
HR limit).
numeric flashes, red alarm
lamp, alarm tone.
**/***VueLink ALARM
at Information Center
VueLink A yellow (**) or red (***) patient alarm
is present on the VueLink module.
Check the monitor display for more
detailed alarm information.
(on monitor) yellow or red
alarm lamp, alarm tone
Alarm Message From Condition Indication
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
59
Technical Alarm Messages (INOPs)
If an INOP interrupts monitoring and alarm detection, the measurement numeric will be replaced
by -?-. If an INOP may lead to unreliable measurement values, a ?appears next to the numeric.
INOP Message, Indication Source What to do
ABP INOPS PRESS See <Pressure label> INOPS (under Pressure).
ALL ECG ALARMS OFF ECG/
Arrhythmia
All ECG alarms have been switched off, or the HR alarm
source is not ECG. To resume ECG alarm generation, switch
ECG alarms on or select ECG as the alarms source.
Ao INOPS PRESS See <Pressure label> INOPS (under Pressure).
ART INOPS PRESS See <Pressure label> INOPS (under Pressure).
AWF CHANGE SCALE Spirometry Airway flow signal exceeds range of selected scale. Adjust scale
to display complete wave.
AWP CHANGE SCALE Spirometry Airway pressure signal exceeds range of selected scale. Adjust
scale to display complete wave
AWV CHANGE SCALE Spirometry Airway volume signal exceeds range of selected scale. Adjust
scale to display complete wave.
Bad Serverlink
INOP tone
Monitor 1) An MMS with an incompatible software revision is
connected to the monitor. This combination does not allow
monitoring, OR
2) You cannot use this combination of monitor, MMS and
cable. Switch off the monitor and contact your service
personnel.
BAP INOPS PRESS See <Pressure label> INOPS (under Pressure).
BATT EMPTY
INOP tone, battery LED flashes
During this INOP, alarms cannot be
paused or switched off.
Battery The estimated remaining battery-powered operating time is less
than 10 minutes. Replace the battery immediately.
If the condition persists and the monitor is not connected to
mains power, this INOP is re-issued two minutes after you
acknowledge it.
BATT INCOMPAT
INOP tone
Battery The battery cannot be used with this monitor. Replace with the
correct battery (M4607A).
BATT LOW
INOP tone
Battery The estimated battery-powered operating time remaining is less
than 20 minutes.
BATT MALFUNCTION
INOP tone, battery LED flashes
During this INOP, alarms cannot be
paused or switched off unless the
monitor is connected to mains power.
Battery The monitor cannot determine the battery status. If this INOP
persists, replace the faulty battery. If the condition persists and
the monitor is not connected to mains power, this INOP is re-
issued two minutes after you acknowledge it.
Place the battery in a different monitor or in a battery charger.
If the same INOP is shown, contact your service personnel.
BATTERIES EMPTY or BATT 1/
BATT 2 EMPTY
INOP tone, battery LED flashes
During this INOP, alarms cannot be
paused or switched off.
Batteries The estimated remaining battery-powered operating time of
the indicated battery or batteries is less than 10 minutes.
Replace the batteries immediately.
If the condition persists and the monitor is not connected to
mains power, this INOP is re-issued two minutes after you
acknowledge it.
BATTERIES INCOMP or BATT 1/
BATT 2 INCOMPAT
INOP tone
Batteries The indicated battery or batteries cannot be used with this
monitor. Replace with the correct battery or batteries as
specified in this book.
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
60
BATTERIES LOW or BATT 1/
BATT 2 LOW
INOP tone
Batteries The estimated battery-powered operating time remaining is less
than 20 minutes.
BATTERIES MALFUNC. or
BATT 1/BATT 2/ BATTERY
MALFUNCT.
INOP tone, battery LED flashes
During this INOP, alarms cannot be
paused or switched off unless the
monitor is connected to mains power.
Batteries The monitor cannot determine the battery status. If this INOP
persists, replace the faulty battery or batteries. If the condition
persists and the monitor is not connected to mains power, this
INOP is re-issued two minutes after you acknowledge it.
Place the batteries in a different monitor or in a battery charger.
If the same INOP is shown, contact your service personnel.
BATTERY LOW T Telemetry The battery in the Telemetry device is low and must be
replaced soon.
BATT 1/BATT 2 MISSING
INOP tone.
During this INOP, alarms cannot be
paused or switched off.
Batteries The monitor requires two batteries but can detect only one
battery. Insert the missing battery immediately.
BIS CABLE INCOMPAT
INOP tone.
BIS The semi-reusable sensor cable connected is unknown or not
supported by your software revision. Replace it with a Philips-
supported sensor cable.
BIS CABLE USAGE
INOP tone.
BIS The semi-reusable sensor cable has exceeded the maximum
number of uses. Replace the cable.
BIS DSC DISCONN
INOP tone
BIS DSC is not properly connected OR either DSC or BIS engine
may be faulty.
Make sure that the DSC is properly connected to the BIS
Engine. If INOP persists, replace DSC with a known good one
of the same type.
If INOP persists replace BIS engine.
Silencing this INOP switches the measurement off.
BIS DSC INCOMPT
INOP tone
BIS DSC is not supported by the BIS engine or new DSC
connected to an old BIS engine. A software upgrade may be
required. Contact your service personnel.
BIS DSC MALFUNC BIS Electrocautery used during self-test OR malfunction in the
DSC hardware.
Make sure not to use electrocautery during the self-test
procedure. Disconnect and reconnect the DSC to the BIS
engine. If the INOP persists, replace the DSC or contact your
service personnel.
BIS DSC UPDATE
INOP tone
BIS DSC update currently being carried out. This INOP will
disappear when the DSC update is finished. Do not disconnect
the DSC during the update. No action is needed.
BIS ELECTR. DISC
INOP tone.
BIS One or more electrodes are not connected to the semi-reusable
sensor cable. Check all electrode connections.
BIS ENGINE DISCONN
INOP tone
BIS BIS engine not connected OR Module Cable defective.
Make sure that the Module Cable is properly connected. If
INOP persists, replace the Module Cable.
Silencing this INOP switches the measurement off.
BIS ENGINE INCOMPT
INOP tone
BIS BIS engine software is not supported. A software upgrade may
be required. Contact your service personnel.
MP20/30 - BIS engine not supported.
INOP Message, Indication Source What to do
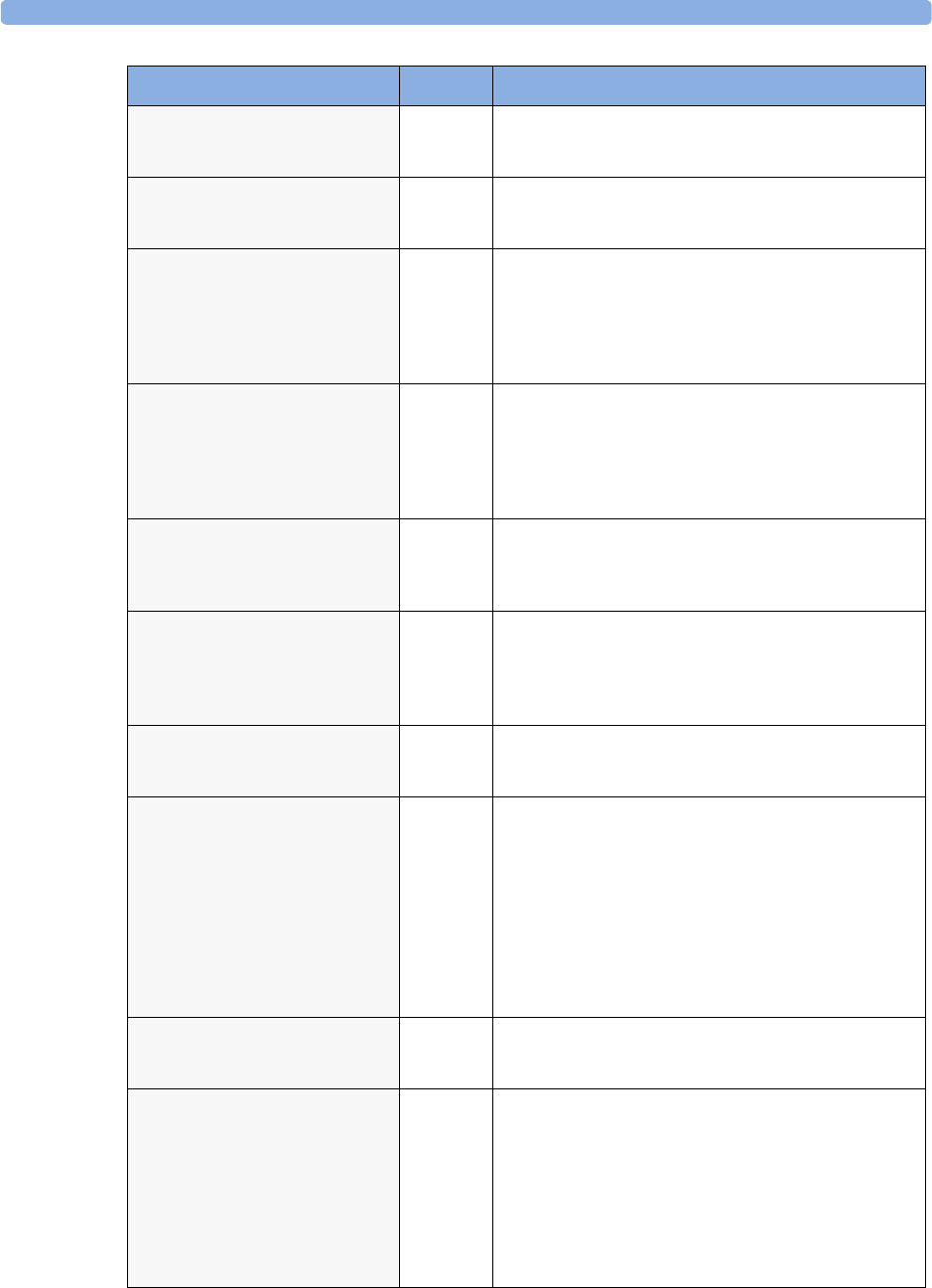
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
61
BIS ENGINE MALFUNC
INOP tone
BIS Malfunction in the BIS engine hardware. Disconnect and
reconnect the BIS engine. If the INOP persists, replace BIS
engine.
BIS EQUIP MALF
INOP tone
BIS There is a malfunction in the BIS hardware. Unplug and replug
the BIS module. If the INOP persists, contact your service
personnel.
BIS HIGH IMPEDANCE
INOP tone may sound
BIS Impedance of one or more electrode(s) is above the valid range,
most often caused by bad skin preparation. Check the sensor
montage and press the electrode pads firmly. If this INOP
persists, replace the sensor(s) in question using correct skin
preparation.
If INOP persists, contact your service personnel.
BIS IMPEDANCE CHCK
INOP tone may sound
BIS The Cyclic Impedance check is running. It will stop
automatically if all impedances are within the valid range. If
any electrodes do not pass the impedance test, check the sensor
montage and press the electrode pads firmly.
To manually stop the Cyclic Impedance Check, select
Cyclic Check off in the Setup BIS menu.
BIS ISOELECTRC EEG BIS No discernible EEG activity is detected for longer than one
minute.
Check the patient. Check that the electrodes are properly
connected.
BIS LEAD OFF
INOP tone may sound
BIS One or more electrodes have no skin contact and therefore
impedances cannot be measured. Check the sensor montage
and press the electrode pads firmly.
If this INOP persists, replace the sensor(s) in question, using
correct skin preparation.
BIS OVERCURRENT
INOP tone
BIS Unplug and replug the BIS module or, f or the MP20/MP30,
disconnect and reconnect the BISx from the Interface board. If
the INOP persists, contact your service personnel.
BIS SENSOR DISCONN
INOP tone
BIS The sensor is not properly connected to the patient interface
cable (PIC) and/or the PIC is not properly connected to the
DSC or BISx, or the sensor or PIC or DSC or BISx may be
faulty.
Check all the connections.
Disconnect and reconnect the sensor, PIC, DSC, BISx.
If the INOP persists, replace the sensor.
If the INOP persists, replace PIC. If INOP persists, contact
your service personnel.
Silencing this INOP switches the measurement off.
BIS SENSOR INCOMPT
INOP tone
BIS Unsupported sensor connected or sensor type unknown or not
supported by your software revision. Replace the sensor, using
only Philips supported sensors.
BIS SENSOR MALFUNC
INOP tone
BIS Malfunction in the sensor hardware, most often caused by
liquids permeating into the connectors OR patient interface
cable (PIC) or DSC or BISx may be faulty.
Replace the sensor. Manually initiate a Cyclic Impedance
Check. Make sure all electrodes pass the test. Make sure that
the both sides of the PIC connector (between PIC and sensor)
are dry. If you are not sure that the connector is dry, replace the
PIC until it has dried. If this INOP persists, contact your
service personnel.
INOP Message, Indication Source What to do
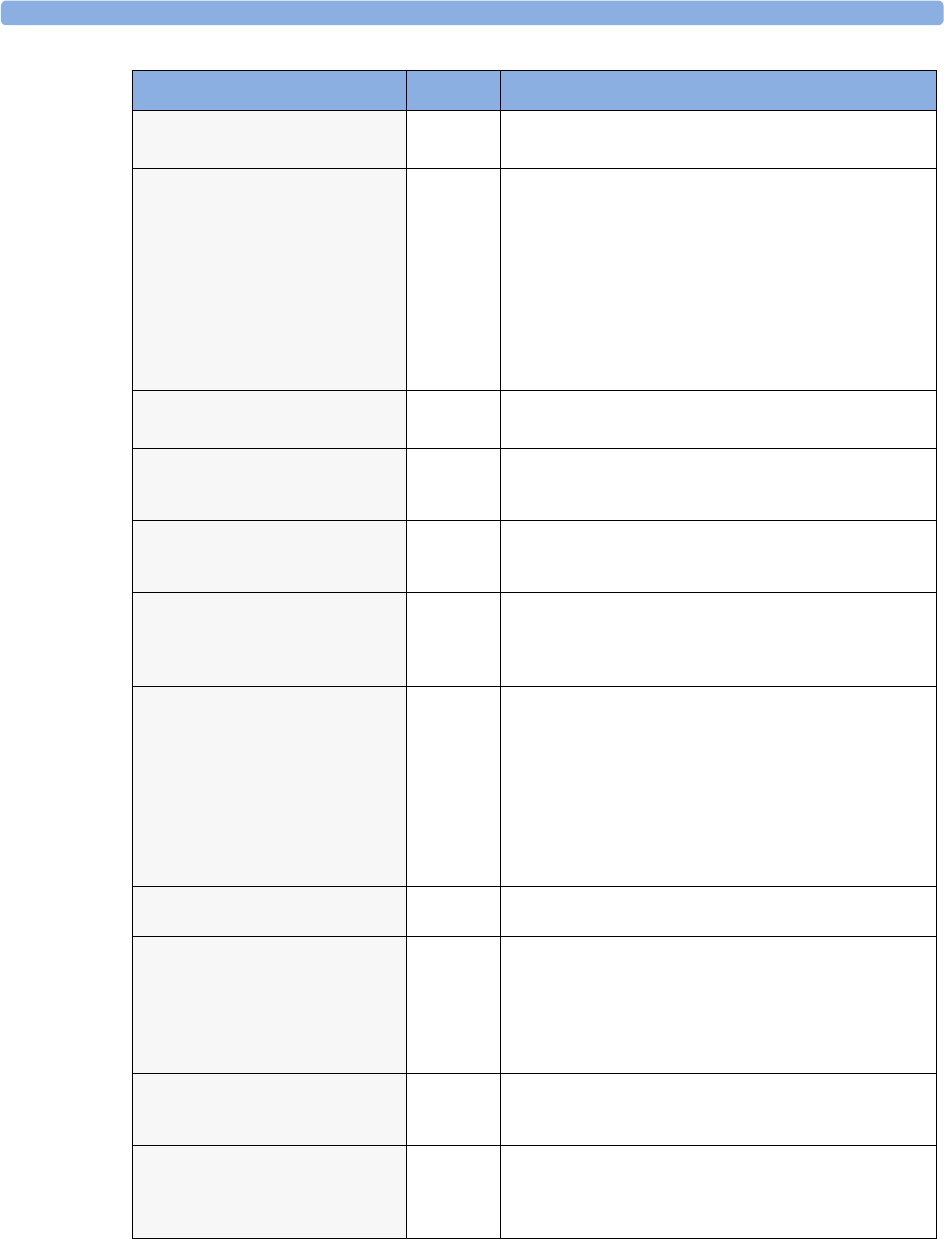
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
62
BIS SENSOR USAGE
INOP tone
BIS Excessive sensor usage. Replace sensor.
A Cyclic Impedance Check will start automatically.
BIS SQI < 15% (INOP tone)
OR
BIS SQI < 50% (no INOP tone)
BIS If the signal quality is below 50%, BIS numerics cannot be
reliably derived.
If the signal quality is below 15%, no BIS numerics can be
derived.
This may occur as a result of artifacts such as those generated
from motion or the presence of electrocautery devices. Make
sure the sensor is properly attached to the patient. Manually
initiate a Cyclic Impedance Check. Make sure all electrodes
pass the test. Make sure the patient is completely relaxed (even
small motions of the facial muscles affect the signal quality).
BIS UNPLUGGED
INOP tone
BIS Plug in the BIS module. Silencing this INOP switches off the
measurement.
BISx DISCONNECTED
INOP tone
BIS The BISx is not connected to the BIS module or the BIS
interface board. Silencing this INOP switches the measurement
off.
BISx INCOMPATIBLE
INOP tone
BIS The BISx software is not compatible with the BIS module or
with the MP20/MP30 monitor software. A software upgrade
may be required. Contact your service personnel.
BISx MALFUNCTION
INOP tone
BIS The BISx is faulty. Disconnect and reconnect it to the module
or BIS interface board. If the INOP persists, replace the BISx.
MP20/MP30 - Malfunction on interface board. If the INOP
persists, contact your service personnel.
CANNOT ANALYZE ECG ECG/
Arrhythmia
The arrhythmia algorithm cannot reliably analyze the ECG
data. Check the ECG signal quality of the selected primary and
secondary leads. If necessary, improve lead position or reduce
patient motion.
If you have arrhythmia analysis on, and you are not getting a
reliable HR because the signal is below a minimum amplitude,
unstable, or contains artifact, and you have tried to improve the
system performance by choosing another lead and changing
electrodes, you should consider turning arrhythmia analysis off.
CANNOT ANALYZE QT QT The QT algorithm cannot generate a valid QT value for more
than 10 minutes, or 1 minute in the initial phase.
CANNOT ANALYZE ST ST The ST algorithm cannot generate a valid ST value. Possible
causes are large variations in the measured ST values for
consecutive beats, or ventricular paced beats. Review the ECG
signal quality and the ST measurement points.
If the patient has a ventricular pacemaker, ST analysis is not
possible.
CCI NO BSA
CCI numeric unavailable
INOP tone
C.O. CCI cannot be calculated because the patient's body surface
area is unknown. Enter the patient weight and height to
provide the BSA for CCI calculation.
CCO BAD PRESS SIGN
numeric is replaced by -?-
INOP tone
C.O. The arterial pressure wave can currently not be used for pulse
contour calculation for CCO or CCI measurement. Possible
causes are air bubbles in the tubing or a physiological
condition, for example severe arrhythmia.
INOP Message, Indication Source What to do
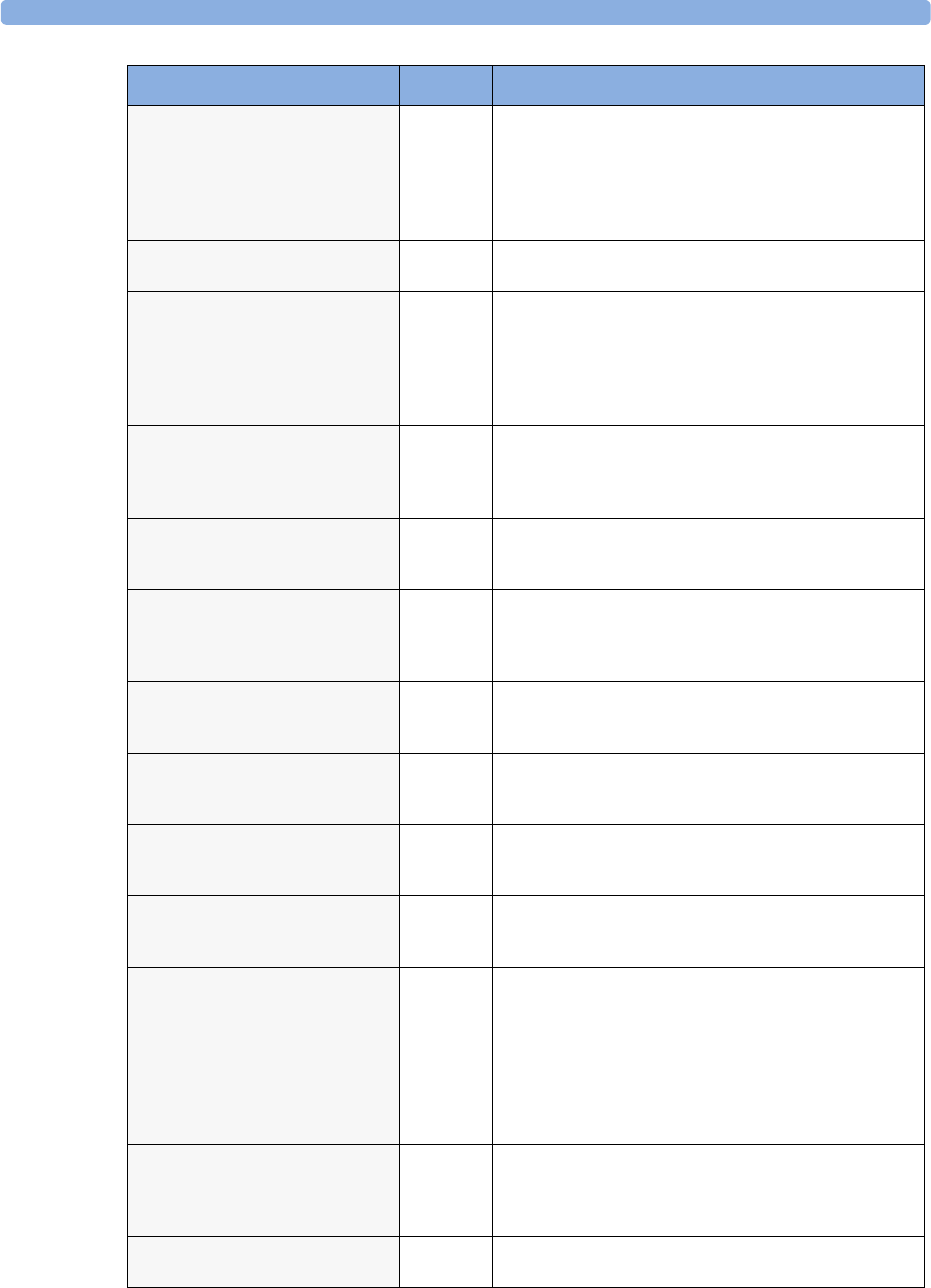
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
63
CCO NO <Pressure label>
numeric is replaced by -?-
INOP tone may sound
C.O. CCO/CCI cannot be calculated. Make sure that the pressure
chosen in the Setup CCO menu under CCO From
matches the pressure measured with the arterial catheter for
CCO measurement. A pressure from an external device cannot
be used. Select another pressure label, either ABP, Ao, ART,
B A P, FA P, o r U A P.
CCO NO CALIBRATION
numeric is replaced by -?-
C.O. The CCO measurement is currently not calibrated.
CCO NO PRESS
at Information Center
C.O. CCO/CCI cannot be calculated. Make sure that the pressure
chosen in the Setup CCO menu under CCO From
matches the pressure measured with the arterial catheter for
CCO measurement. A pressure from an external device cannot
be used. Select another pressure label, either ABP, Ao, ART,
B A P, FA P, o r U A P.
CCO NOT SUPPORTED
numeric is replaced by -?-
INOP tone
C.O. A catheter for transpulmonary C.O. measurements has been
unplugged and replaced with a Right Heart C.O. catheter, or
the measurement mode has been changed manually. Silencing
this INOP switches the measurement off.
CCO/CCI OVERRANGE
numeric is replaced by -?-
INOP tone
C.O. The measured CCO or CCI value is not within the specified
range for CCO/CCI measurement.
CCO <Pressure label>
INVALID
numeric is replaced by -?-
INOP tone may sound
C.O. The arterial pressure selected for pulse contour calculation for
CCO is available but currently invalid. Make sure the pressure
transducer is connected and the zero calibration is valid.
CCO PRESS INVALID
at Information Center
C.O. The arterial pressure selected for pulse contour calculation for
CCO is available but currently invalid. Make sure the pressure
transducer is connected and the zero calibration is valid.
CCO PRESS OVERRANG
numeric is replaced by -?-
INOP tone
C.O. The mean value of the arterial pressure values used for pulse
contour calculation for CCO is below 0 mmHg or above 300
mmHg.
CCO PULSE OVERRANG
numeric is replaced by -?-
INOP tone
C.O. The pulse rate of the pressure used for pulse contour
calculation for CCO is below 30 bpm or above 240 bpm.
CCO/Tbl NO TRANSD
Numeric is replaced by -?-
INOP tone
C.O. No transducer attached to the module or catheter
disconnected.
CCO RECALIBRATE
numeric is replaced by -?-
C.O. The most recent CCO or CCI calibration was made over 8
hours ago or the arterial pressure measurement used for CCO
calculation has been zeroed after the CCO calibration was
performed. You should recalibrate CCO or CCI with
transpulmonary C.O. measurements at least every 8 hours or
when the hemodynamic condition of the patient has changed.
The pressure measurement must be zeroed before a CCO
calibration.
CENTRAL:TELE ONLY
INOP tone
Monitor System connectivity via telemetry device is limited (No alarms,
only local numerics) when in companion mode and host
monitor does not have system connectivity. Only telemetry
device parameters can be displayed at central station.
Charge BATT1/BATT2 now
INOP tone
Batteries Battery must be charged. Connect the monitor to mains power
or exchange the battery.
INOP Message, Indication Source What to do
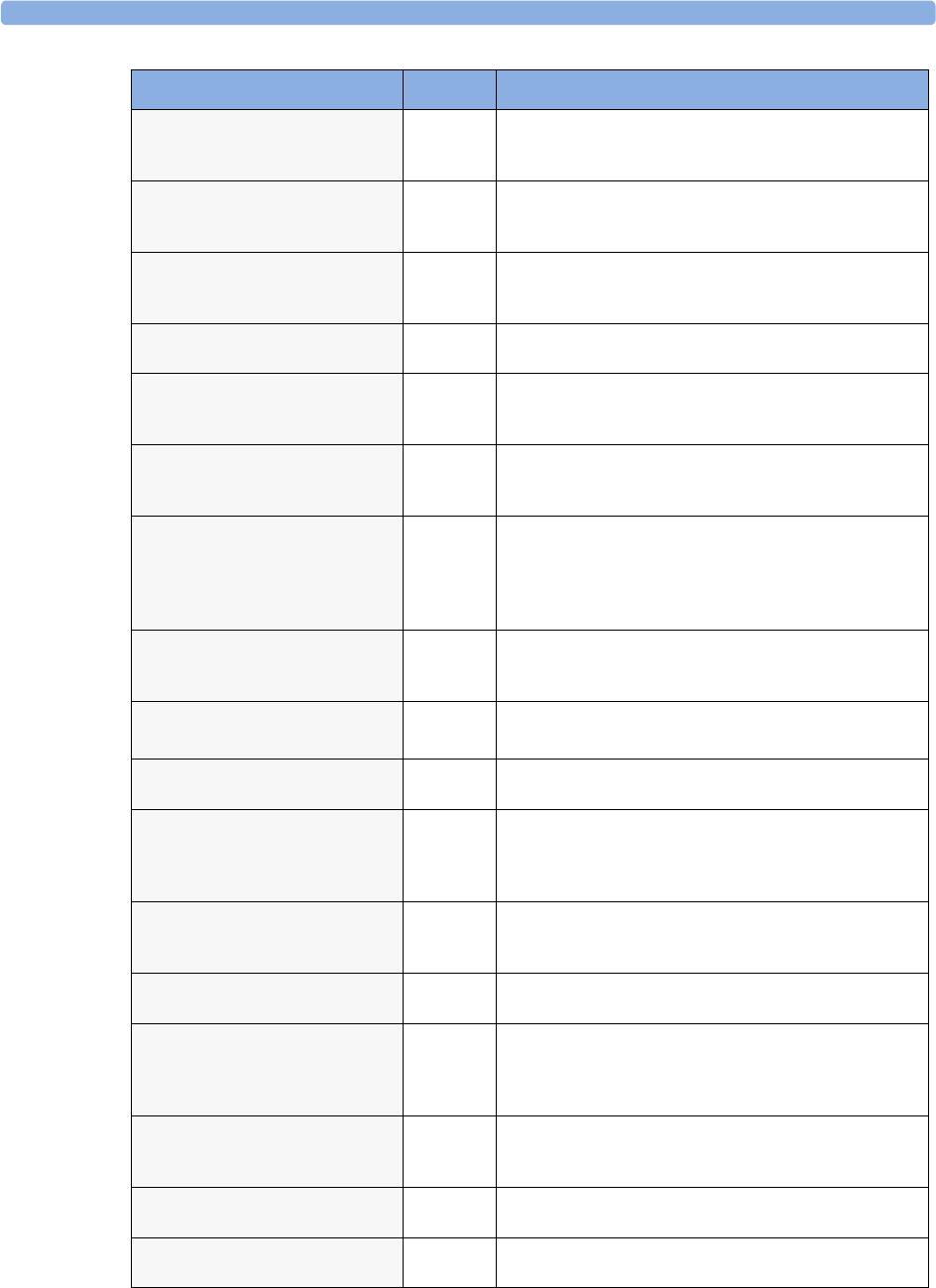
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
64
CHARGER MALFUNC
INOP tone, battery LED may flash
Batteries There is a problem with the battery charger in the monitor.
Connect the monitor to mains power and contact your service
personnel.
Check Alarm Lamps
INOP tone.
Monitor Perform a visual check of the alarm lamp to establish whether
there is a problem. Contact your service personnel to check the
internal connections to the alarm lamps.
CHECK BATT TEMP
INOP tone
Battery The temperature of one or both batteries is too high. Check
that ventilation openings (if applicable) are not blocked and
monitor is not exposed to heat.
Check DrugSettings
INOP tone
Monitor There was a problem loading the drug settings. Check that the
settings are complete and correct.
Check ECG Settings
INOP tone
Telemetry Synchronization of ECG settings between the monitor and
Information Center has failed. Check that the ECG settings in
use are appropriate.
!!CHECK ECG SOURCE
INOP tone
Monitor The telemetry device and the monitor both have valid ECG
signals. Unpair the telemetry device and the monitor if they are
no longer used for the same patient.
Check Flex Texts
INOP tone
Monitor Check the names of the monitor menus, for example the labels
for screens, profiles, event or trend group names, before you
resume monitoring. If they are unexpected, there may be a
problem with the monitor software. Contact your service
personnel.
CheckInternVoltage
at Information Center
Monitor Potential problem with alarm lamps, display or interfaces
detected. Contact your service personnel. This INOP will
appear on the monitor as Check Monitor Func.
Check Keyboard
INOP tone
Monitor Perform a visual and functional check of the keyboard. Contact
your service personnel.
Check Main Board 2
INOP tone.
Monitor There is a problem with the second main board in the monitor.
Contact your service personnel.
Check Monitor Func
INOP tone.
Monitor Potential problem with alarm lamps, display or interfaces
detected. Contact your service personnel. This INOP may
appear on the Information Center as
CheckInternVoltage.
Check Monitor Temp
INOP tone
Monitor The temperature inside the monitor is too high. Check that the
monitor ventilation is not obstructed. If the situation
continues, contact your service personnel.
Check Mouse Device
INOP tone.
Monitor Perform a visual and functional check of the mouse input
device. Contact your service personnel.
Check MSL Voltage
INOP tone
Monitor/
Multi-
Measuremt
Module
There is a problem with the voltage of the Measurement Link
(MSL). Contact your service personnel.
Check Network Conf
INOP tone
Monitor The monitor is receiving network topology information from
more than one source, e.g. the Database Server and an
Application Server. Contact your service personnel.
Check Nurse Relay
INOP tone
Monitor There is a problem with the connection to the nurse relay.
Contact your service personnel.
!!Check Pairing
INOP tone
Monitor There is a problem with device pairing. Check that the monitor
and telemetry device are correctly paired.
INOP Message, Indication Source What to do
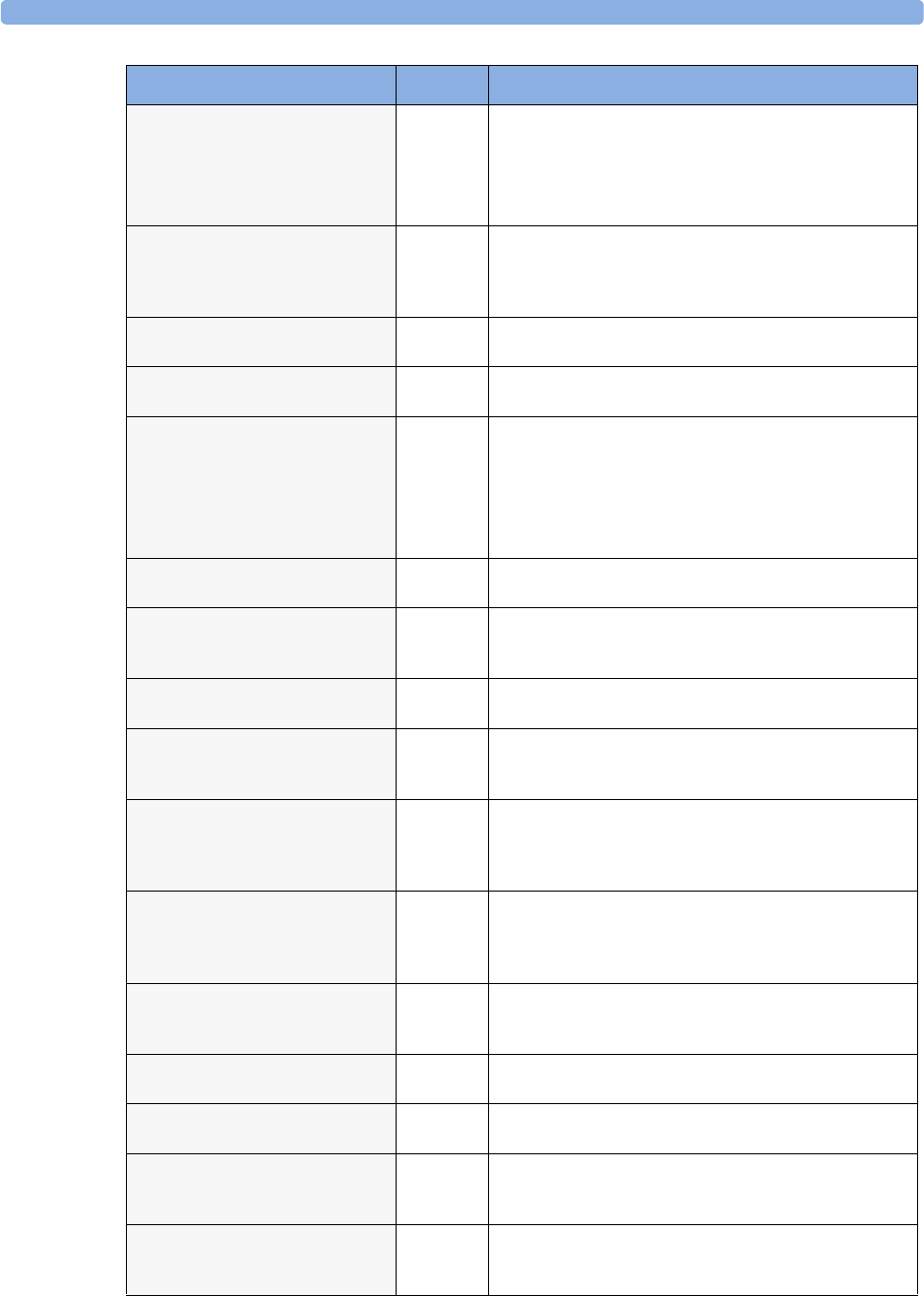
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
65
Check Screen Res
INOP tone
Monitor The Screen you have selected uses a resolution which is not
supported by the display. The monitor will show a generic
Screen instead until you select a different Screen.
Contact your service personnel if you want the Screen deleted
from the Profile(s) to avoid this in future.
Check Settings
INOP tone
Monitor If this INOP appears, check the monitor and patient settings
before you resume monitoring. If the settings are unexpected,
there may be a problem with the monitor software. Contact
your service personnel.
Check SpeedPoint
INOP tone.
Monitor Perform a visual and functional check of the SpeedPoint input
device. Contact your service personnel.
Check Touch Input
INOP tone
Monitor Perform a visual and functional check of the touch input
device. Contact your service personnel.
Check Waves
INOP tone
Monitor The options purchased with this monitor may not support the
number of waves required to show the selected Screen, so some
waves or high resolution trends are missing from the Screen.
Select a different Screen with fewer waves.
Contact your service personnel if you want the Screen deleted
from the Profile(s) to avoid this in future.
CHK ECG Sync Cable
INOP tone
Monitor The ECG Sync is detecting an invalid signal, or the ECG Sync
cable is disconnected.
Chk IndepDsp Cable Monitor The monitor cannot communicate with the D80 Intelligent
Display. Check the MSL coupling cable. The end with the grey
connector must be connected to the Intelligent Display.
CHK MSL Connection
INOP tone
Monitor Check that the MSL connector or cable are properly
connected. Check the cable and connector for damage.
Chk SpO2T Settings
INOP tone
Telemetry Synchronization of SpO2T settings between the monitor and
Information Center has failed. Check that the SpO2T settings
in use are appropriate.
C LEAD OFF
HR Numeric is replaced by -?- for 10
seconds. INOP tone.
ECG The C electrode (AAMI: V electrode) has become detached
from the patient or the lead set has been changed. Reattach the
electrode or select New Lead Setup in the Setup ECG
menu to confirm the new lead set.
CO2 AUTO ZERO
Numeric is replaced by a -?-
if the Autozero lasts >15 sec, INOP
tone sounds.
CO2The automatic zero calibration is in progress. This typically
takes 10 seconds. During this time the CO2 values may not be
updated, or they may be replaced by -?-. Wait until the zero
calibration is complete to resume monitoring.
CO2 CAL MODE
CO2 numeric displays current CO2
value for accuracy check
CO2Currently no calibration is running. Accuracy can be checked
by placing the transducer on the two cells of the calstick and
starting calibration. To start monitoring, leave Cal. Mode.
CO2 CAL RUNNING
Numeric is replaced by a -?-
CO2Wait until calibration is finished.
CO2 CHANGE SCALE CO2The CO2 wave is clipped. Select a more appropriate wave scale
to display the whole wave.
CO2 CHK ADAPTER
Numeric is replaced by a -?-
INOP tone.
CO2Check that the sensor is connected to the airway adapter, clean
the airway adapter, if necessary. Perform a zero calibration. If
the INOP persists, contact your service personnel.
CO2 CHECK CAL
Numeric is replaced by a -?-
INOP tone.
CO2The CO2 value is outside the measurement range. Perform an
accuracy check for both calstick cells and, if necessary,
recalibrate the transducer.
INOP Message, Indication Source What to do
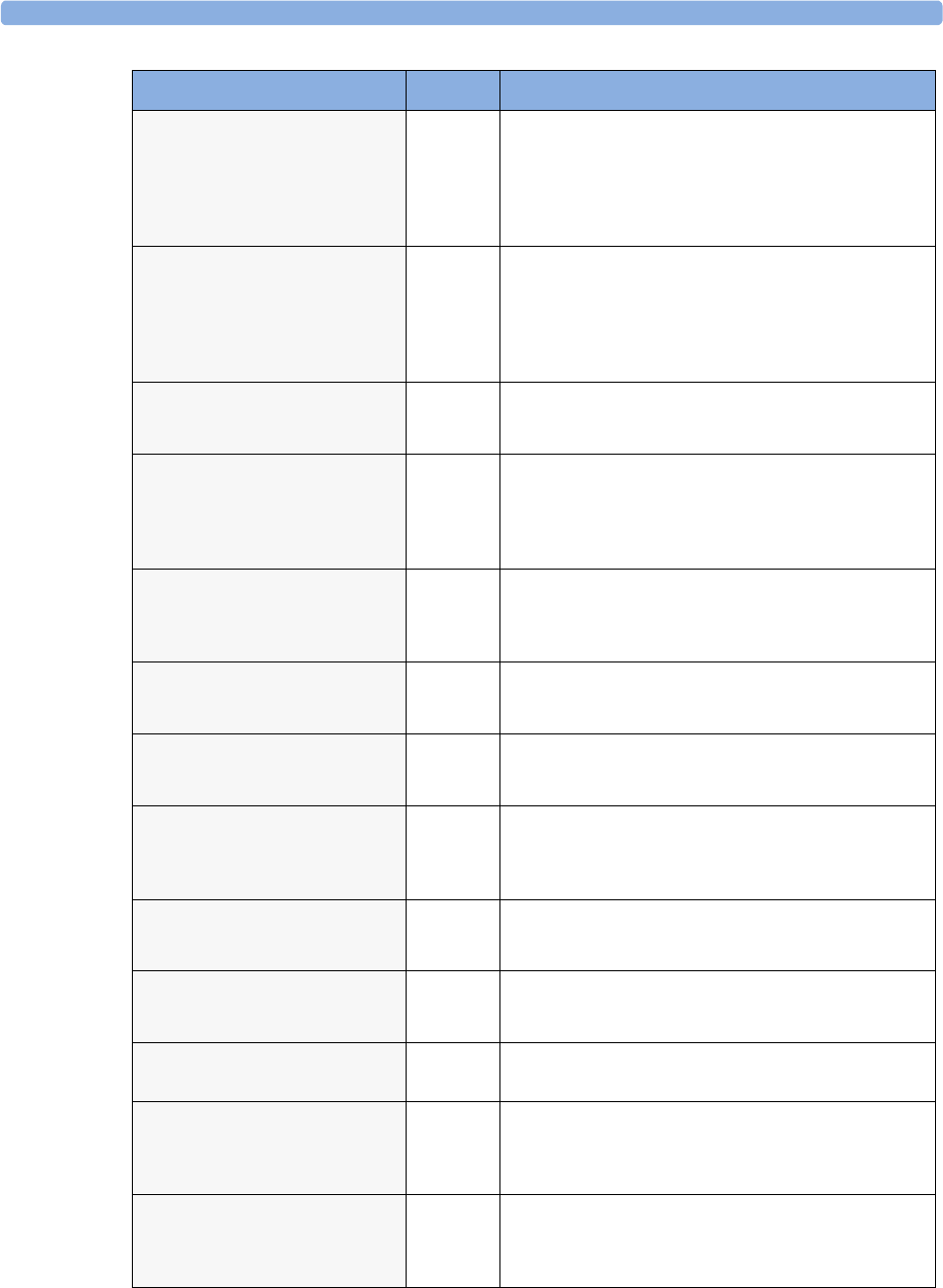
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
66
CO2 DEACTIVATED
INOP tone.
CO2The CO2 measurement label in the measurement device has
been deactivated by deactivating the label in the Measurement
Selection window. The measurement automatically disappears
from the display. To switch the measurement on again,
reactivate the measurement label in the Measurement Selection
window.
C.O. DEACTIVATED
INOP tone.
C.O. The Cardiac Output measurement label in the measurement
device has been deactivated by deactivating the label in the
Measurement Selection window. The measurement
automatically disappears from the display. To switch the
measurement on again, reactivate the measurement label in the
Measurement Selection window.
C.O. EQUIP MALF
Numeric is replaced by a -?-
INOP tone.
C.O. There is a problem with the C.O. hardware. Contact your
service personnel.
CO2 EQUIP MALF
Numeric is replaced by -?-
INOP tone.
CO2The Measurement Extension is faulty. Unplug and replug the
Multi-Measurement Module with Extension. If you are using
the mainstream method, unplug and replug the transducer or
try another transducer. If the INOP persists, contact your
service personnel.
CO2 FAILED CAL
Numeric is replaced by -?-
INOP tone.
CO2Make sure that the Cal cell was changed between CAL1 and
CAL2. Repeat the calibration. If the INOP reappears, try
another transducer. If the INOP persists, contact your service
personnel.
CO2 NO SENSOR
Numeric is replaced by -?-
INOP tone.
CO2There is no CO2 sensor connected. If you silence this INOP
the CO2 measurement will be switched off.
CO2 NO TRANSDUC
Numeric is replaced by -?-
INOP tone.
CO2There is no CO2 transducer connected. If you replace the
transducer, the new transducer must be calibrated. If you
silence this INOP the CO2 measurement will be switched off.
CO2 NO TUBING
Numeric is replaced by -?-
INOP tone.
CO2Either the sample line is disconnected, or an incorrect line is
attached. Check the connection. If necessary, connect another
sample line (Use only the approved accessories).
If you silence this INOP, the measurement will be switched off.
(!!/!!!)CO2 OCCLUSION
Numeric is replaced by a -?-
INOP tone.
CO2The sample line or exhaust tube is blocked. Check the tubing,
then disconnect and reconnect the sample line. If the INOP
persists, connect a new sample line.
CO2 OVERRANGE
Numeric is replaced by -?-
INOP tone.
CO2The CO2 value is higher than the measurement range. If you
suspect a false high value, contact your service personnel.
CO2 PUMP OFF
Numeric is replaced by a -?-.
CO2The pump has been switched off for fifteen minutes. To switch
it on again, select Pump On in the Setup CO2 menu.
CO2 PURGING
Numeric is replaced by a -?-
INOP tone.
CO2The Filterline is being purged to remove an occlusion in the
line or airway adapter. If the occlusion is removed, the INOP
will disappear. If not, the INOP CO2 OCCLUSION is
displayed.
CO2 SENS. WARMUP
Numeric is displayed with a -?-
Microstream CO2: INOP tone.
Mainstream CO2: no INOP tone
CO2Wait until the sensor reaches operating temperature and the
INOP disappears.
INOP Message, Indication Source What to do
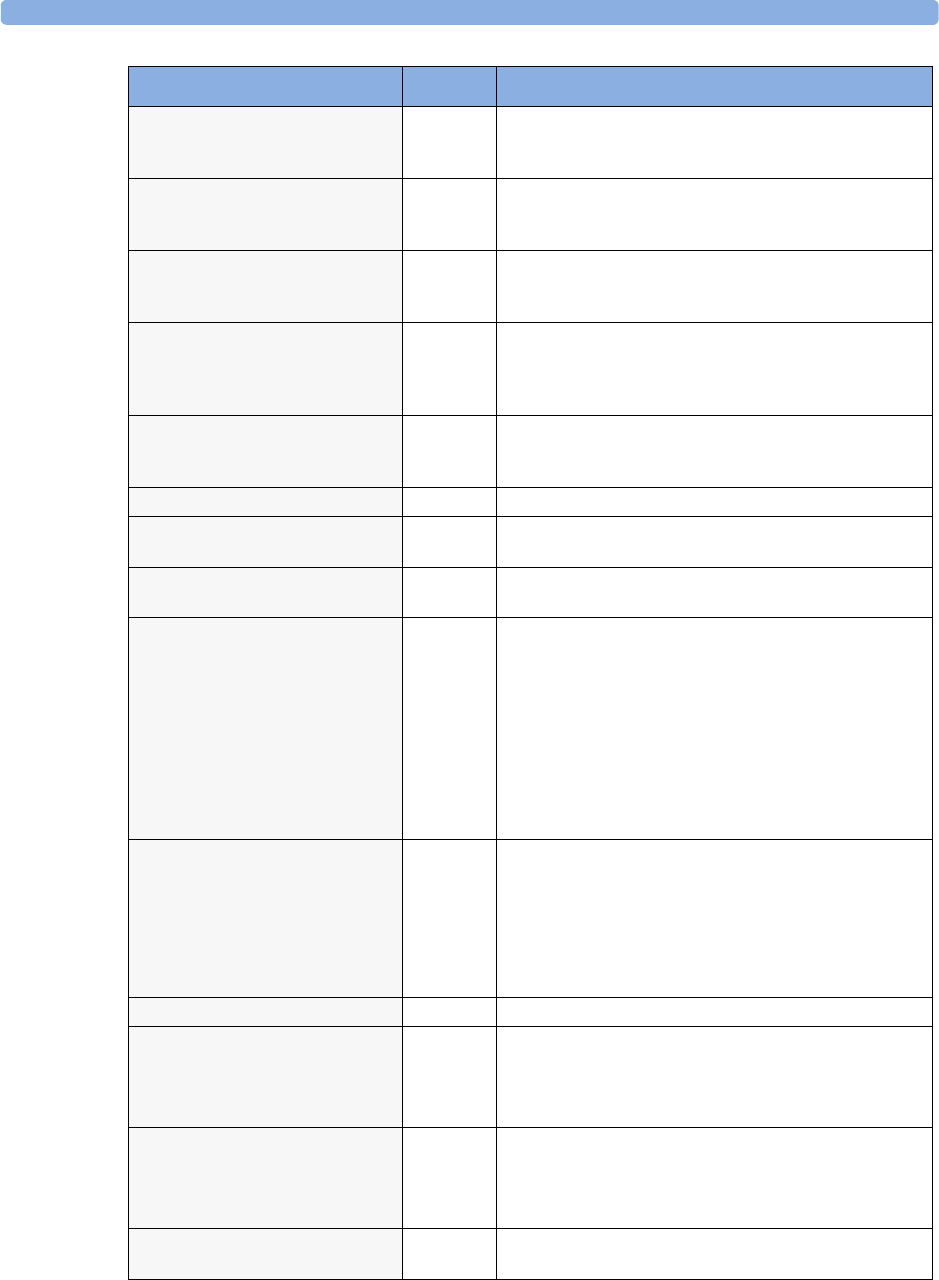
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
67
C.O. UNPLUGGED
numeric is replaced by -?-
INOP tone.
C.O. Plug in the C.O. module. Silencing this INOP switches off the
measurement.
CO2 UPDATE FW
Numeric is replaced by a -?-
INOP tone.
CO2The software in the Measurement Extension does not match
the software in the MMS. Contact your service personnel.
CO2 WAIT CAL2
Numeric is replaced by a -?-
CO2Calibration on the first calstick cell is complete. Place the
transducer on the other calstick cell and start the CAL2
calibration cycle.
CO2 ZERO FAILED
Numeric is replaced by a -?-
INOP tone.
CO2An error occurred during the last zero calibration. Check the
airway adapter and clean, if necessary. Perform another zero
calibration. If the INOP persists, contact your service
personnel.
CO2 ZERO REQU’D
Numeric is replaced by a -?-
INOP tone
CO2Perform zero calibration for the CO2 sensor. If the INOP
persists, contact your service personnel.
CO2 ZERO RUNNING CO2Wait until zero calibration is finished.
CPP CHK SOURCES
Numeric is replaced by a -?-
CPP Not all measurements or values required to perform the
calculation are available. Check the measurement sources.
CPP CHK UNITS
Numeric is replaced by a -?-
CPP The monitor has detected a conflict in the units used for this
calculation. Check the unit settings.
!!/!!!CUFF NOT DEFLAT
Numeric is displayed with a -?-
Severe yellow/red INOP tone.
During this INOP, alarms cannot be
paused or switched off.
NBP Remove the cuff from the patient. Make sure that the tubing is
not kinked or twisted and that the correct patient category is
selected. Try repeating the measurement.
You can silence the INOP, but the INOP message remains
visible until the next NBP measurement is started or the
Stop All SmartKey is selected.
[Adult or pediatric patients: The NBP cuff pressure has exceeded
15mmHg (2kPa) for more than 3 minutes.
Neonatal patients: The NBP cuff pressure has exceeded 5mmHg
(0.7kPa) for more than 90 seconds.]
!!/!!!CUFF OVERPRESS
Numeric displayed with -?- ;
Severe yellow/red INOP tone.
During this INOP, alarms cannot be
paused or switched off.
NBP The NBP cuff pressure exceeds the overpressure safety limits.
Remove the cuff from the patient. Make sure that the tubing is
not kinked or twisted and that the correct patient category is
selected. Try restarting the measurement.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the Stop
All SmartKey is selected.
CVP INOPS PRESS See <Pressure label> INOPS (under Pressure).
DEVICE CHECK SETUP
INOP tone.
IntelliBridge Device identification completed, but communication could
not be established due to timeout.
IntelliBridge INOP abbreviations may differ slightly depending
on the device category.
DEVICE CHECK CONF.
INOP tone.
IntelliBridge Device identification completed, but communication could
not be established due to error.
IntelliBridge INOP abbreviations may differ slightly depending
on the device category.
DEVICE DEMO DATA
INOP tone
IntelliBridge The device connected to the IntelliBridge module reports demo
data but the monitor is not in DEMO mode.
INOP Message, Indication Source What to do
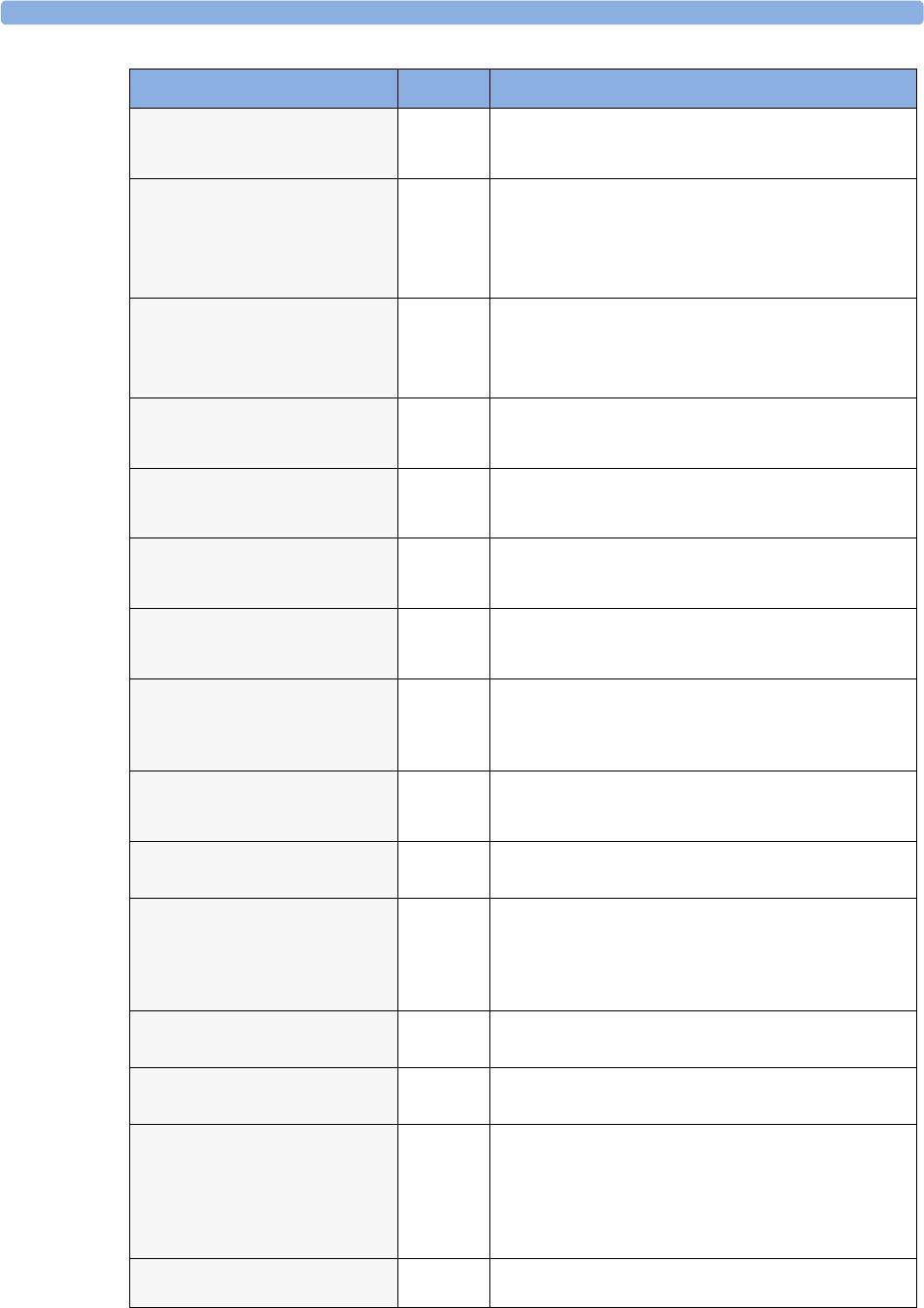
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
68
DEVICE REAL DATA
INOP tone
IntelliBridge The monitor is in DEMO mode but the device connected to
the IntelliBridge module reports data that are not flagged as
demo data.
<Device> UNPLUGGED
INOP tone.
IntelliBridge The IntelliBridge module has been unplugged from the rack, or
the whole rack has been disconnected. Silencing this INOP
switches off the measurement.
IntelliBridge INOP abbreviations may differ slightly depending
on the device category.
DEVICE UNSUPPORTED
INOP tone.
IntelliBridge Device identification completed, but no appropriate device
driver installed.
IntelliBridge INOP abbreviations may differ slightly depending
on the device category.
<EC10/EC40> EQUIP MALF
INOP tone.
IntelliBridge Malfunction in the IntelliBridge module. If this message
appears repeatedly, the module must be replaced. Contact your
service personnel.
ECG/ARRH ALARM OFF
!!ECG/AR ALARM OFF
ECG All ECG alarms have been switched off, or the HR alarm
source is not ECG. To resume ECG alarm generation, switch
ECG alarms on or select ECG as the alarm source.
ECG EQUIP MALF
Numeric is displayed with a -?-
INOP tone.
ECG Contact your service personnel.
The ECG hardware is faulty.
ECG EQUIP MALF T
Numeric is displayed with a -?-
INOP tone.
Monitor Contact your service personnel.
The ECG in the Telemetry device is faulty.
(!!/!!!)<ECG LEAD> LEAD
OFF
Numeric is displayed with a -?-
INOP tone.
ECG Not all the required leads for ECG monitoring are connected.
Check the ECG connections and make sure that the electrode
indicated by <ECG lead> [RA, LA, LL, RL, V or C] electrodes
is attached. In EASI mode, all 5 electrodes must be connected.
ECG EL. NOISY <ECG LEAD> ECG The ECG signal from the named ECG electrodes [RA, LA, LL,
RL, V (or C)] is noisy. Check the ECG connections and make
sure that the electrode indicated is attached.
(!!/!!!)ECG LEADS OFF ECG Check that all of the required ECG leads are attached, and that
none of the electrodes have been displaced.
ECG NOISY SIGNAL
INOP tone.
ECG The ECG signal is too noisy. Check that the electrodes are
properly placed and have not dried out. Remove any possible
sources of signal noise (such as power cords) from the area
around the cable and the patient.
The ECG signal may be saturated or overloaded.
EcgOut EQUIP MALF
INOP tone
ECG Check that the ECG out cable is securely connected. Contact
your service personnel.
EEG EQUIP MALF
INOP tone
EEG The EEG hardware is faulty. Contact your service personnel.
EEG IMPEDANCE HIGH or
EEG1 and/or EEG2 IMPED. HIGH
EEG The signal electrode in one or both channels exceeds the user-
selected impedance limit, or the impedance of a single electrode
exceeds the limit. Check the impedance. If the impedance is
too high, reconnect the electrodes according to the EEG
monitoring setup guidelines. If the INOP persists, contact your
service personnel.
EEG<X> LEAD OFF <n>
[X = channel, n = electrode]
EEG Reconnect specified electrode.
INOP Message, Indication Source What to do
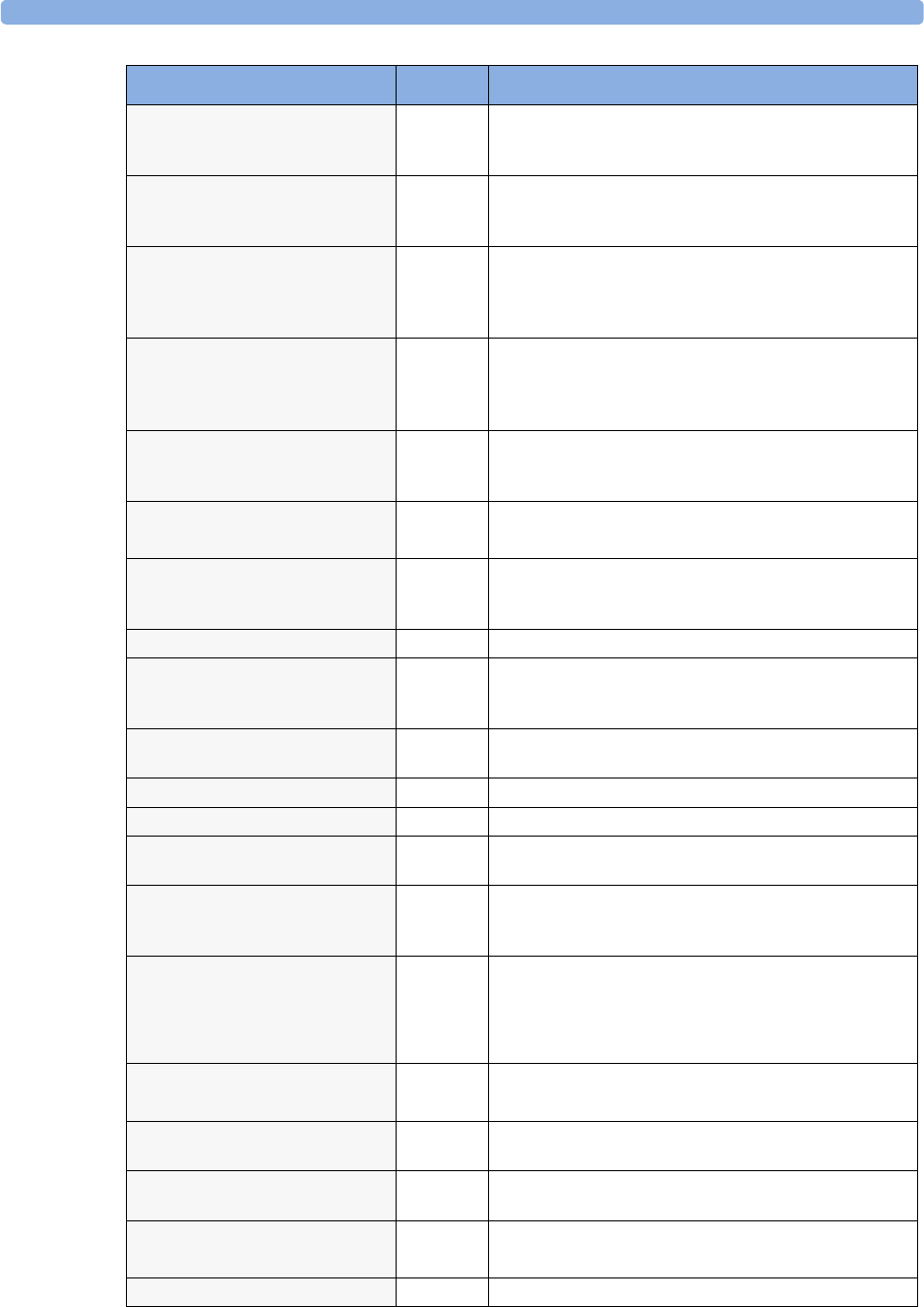
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
69
EEG<X> LEAD OFF
[X = channel]
at Information Center
EEG One or more electrodes are not connected. Check in the EEG
Impedance/Montage window on the monitor which
electrode(s) are affected and reconnect the electrodes.
EEG<X> LEADS OFF
[X = channel]
EEG Two or more electrodes are not connected. Check in the EEG
Impedance/Montage window which electrodes are
affected and reconnect the electrodes.
EEG LINE NOISE
EEG 1 or 2 LINE NOISE
EEG Excessive line noise has been detected in either channel EEG1
or EEG2, or in both EEG channels.
Keep all cables together and away from metallic bodies, other
cables & radiated fields.
EEG MUSCLE NOISE
EEG 1 or 2 MUSCLE NOISE
EEG Too much power above 30 Hz has been detected in channel
EEG1 or EEG2, or both.
Check the Electrode-to-Skin Impedance and reposition the
electrode away from possible muscle activity, if necessary.
EEG NO TRANSDUCER
INOP tone
EEG The trunk cable is disconnected from the EEG plug-in module.
Reconnect the trunk cable. Silencing this INOP switches the
measurement off.
EEG UNPLUGGED
INOP tone
EEG Plug in module. Silencing this INOP switches off the
measurement.
EEG OVERRANGE, or
EEG<X> OVERRANGE
EEG Input signal is too high in one or both channels. This is usually
caused by interfering signals such as line noise or electro-
surgery. X denotes the EEG channel.
FAP INOPS PRESS See <Pressure label> INOPS (under Pressure).
FMS UNPLUGGED
INOP tone.
FMS Make sure that the Flexible Module Rack is connected to the
monitor. All FMS measurements are off while the FMS is
unplugged.
FMS UNSUPPORTED
INOP tone.
FMS The Flexible Module Rack is not supported by your monitor.
Contact your service personnel.
IC1/IC2 INOPS PRESS See <Pressure label> INOPS (under Pressure).
ICP INOPs PRESS See <Pressure label> INOPS (under Pressure).
Indep.Dsp Malfunc. Display A problem has occurred with the second main display. Contact
your service personnel.
Indep.Dsp NotSupp. Display The monitor does not support a second main display. The
monitor software is incompatible. Contact your service
personnel.
!!INSERT BATTERY
Severe yellow INOP tone.
During this INOP, alarms cannot be
paused or switched off.
Battery X2/MP2 only: There is no battery in the battery compartment.
You cannot operate the monitor on AC mains while the battery
compartment is open (not sealed with a battery). Load a
battery immediately.
Intell.Dsp Malf.
INOP tone
Display There is a problem with the Intelligent Display. Check the
MSL coupling cable then contact your service personnel.
Intell.Dsp Missing Display The monitor has lost contact with the connected Intelligent
Display. Contact your service personnel.
Intell.Dsp Unsupp. Display The monitor does not support the connected Intelligent
Display. The monitor software is incompatible.
Internal.Comm.Malf
INOP tone
Monitor There is a problem with I2C Bus communication in the
monitor. Contact your service personnel.
INVALID LEADSET Telemetry
INOP Message, Indication Source What to do
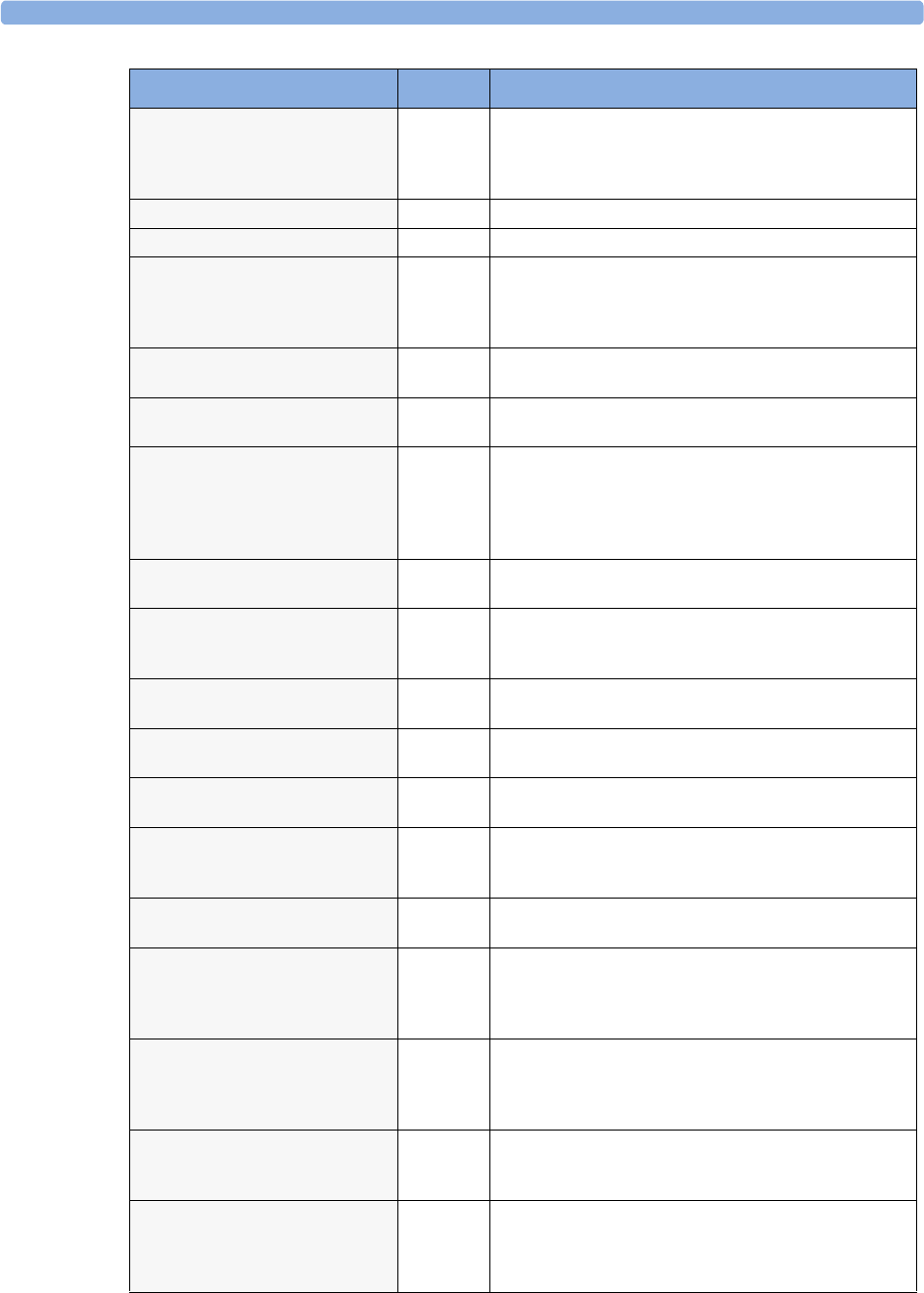
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
70
LA LEAD OFF
Numeric is replaced by -?- for 10
seconds; INOP tone.
ECG The LA electrode has become detached from the patient or the
lead set has been changed. Reattach the electrode or select New
Lead Setup in the Setup ECG menu to confirm the
new lead set.
LAP INOPs PRESS See <Pressure label> INOPS (under Pressure).
LEADSET UNPLUGGED Telemetry The leadset has been unplugged from the telemetry device.
LL LEAD OFF
Numeric is replaced by -?- for 10
seconds; INOP tone.
ECG The LL electrode has become detached from the patient or the
lead set has been changed. Reattach the electrode or select New
Lead Setup in the Setup ECG menu to confirm the
new lead set.
MCC Reversed
INOP tone
Monitor The MSL coupling cable is reversed. Connect the end with the
grey connector to the Intelligent Display.
MCC Unsupported
INOP tone
Monitor An MSL coupling cable has been connected to a device which
does not support MSL coupling.
Meas. DEACTIVATED An X2 or MP5 has been connected to a host monitor
(companion mode) and all derived measurements have been
deactivated and/or measurements with a label conflict. The
measurements can only be reactivated by disconnecting the
measurement device from the host monitor.
MEASSRV UNSUPPORTD
INOP tone
MMS The Multi-Measurement module is not supported by the
monitor. Contact your service personnel.
MMS Ext. EQUIP MALF
INOP tone
MMS
Extension
Loss of communication between the Multi-Measurement
Module and the MMS extension. Contact your service
personnel.
MMS Ext. UNPLUGGED
INOP tone
MMS
Extension
The MMS extension has been disconnected from the Multi-
Measurement Module.
MMS Ext. Unpowered
INOP tone
MMS
Extension
The MMS extension cannot operate while the Multi-
Measurement Module is running on battery power.
MMSExt.Unsupported
INOP tone
MMS
Extension
The MMS extensions not supported by your monitor. Contact
your service personnel.
MMS UNPLUGGED
INOP tone.
MMS Make sure that the Multi-Measurement Module is connected
to the monitor. All MMS measurements are off while the MMS
is unplugged.
MMS UNSUPPORTED
INOP tone.
MMS The Multi-measurement Module is not supported by your
monitor. Contact your service personnel.
!!/!!!MORE BED ALARMS
At Information Center
Monitor The monitor is associated with a telemetry device and is
sending data to the Information Center via the telemetry
device. There are currently more alarms at the bedside than can
be transmitted to the Information Center.
MSL Power High Monitor The power consumption of the devices connected to the
Measurement Link (MSL) cable is too high. If this situation
continues, the MSL will be switched off. Contact your service
personnel.
MSL Power Off
INOP tone.
Monitor The power consumption of the devices connected to the
Measurement Link (MSL) cable was too high for too long and
the MSL has been switched off. Contact your service personnel.
MSL Power Overload
INOP tone.
Monitor The power consumption of the devices connected to the
Measurement Link (MSL) cable is much too high or there has
been a short circuit. The MSL has been switched off. Contact
your service personnel.
INOP Message, Indication Source What to do
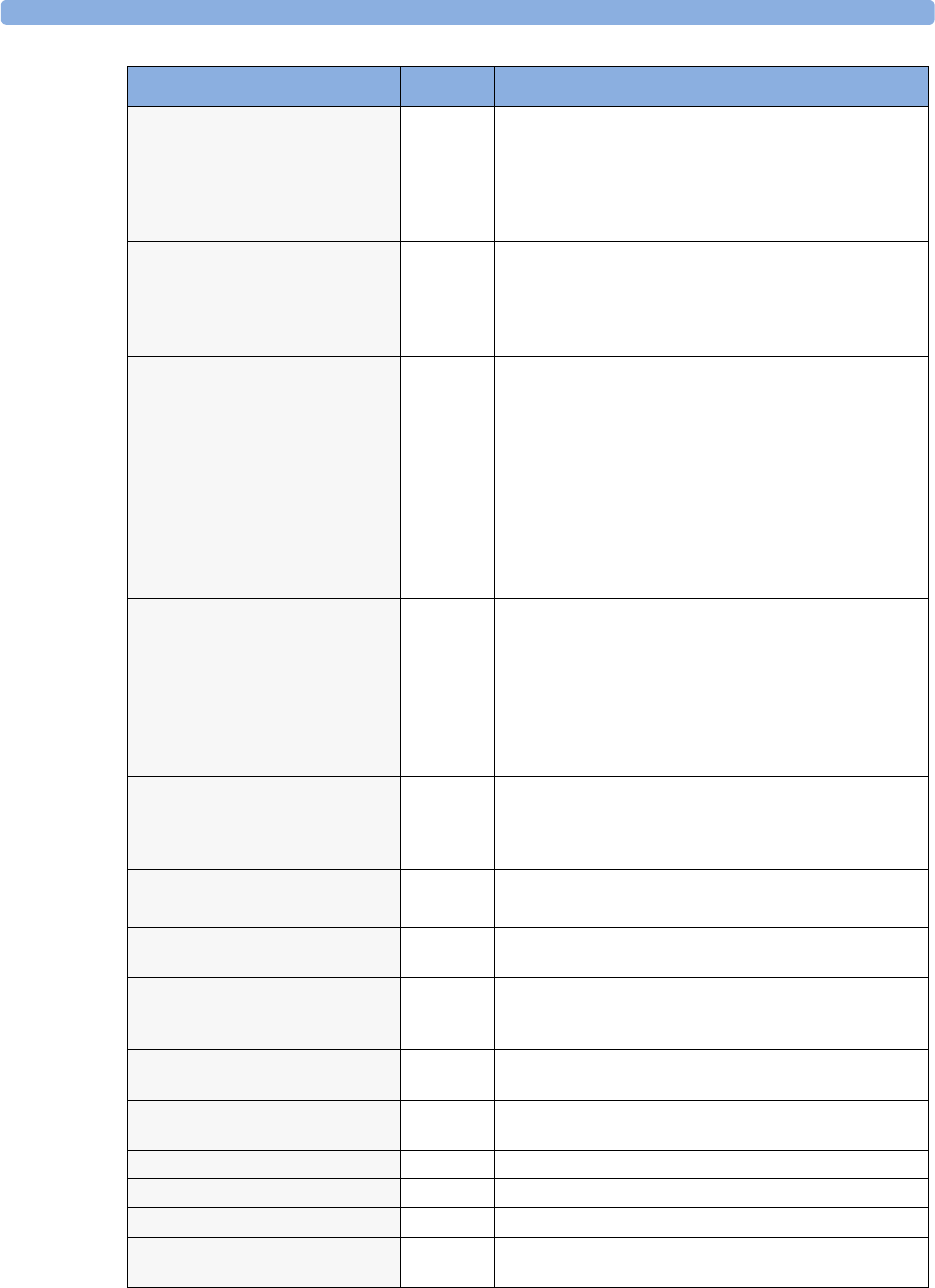
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
71
NBP Deactivated
INOP tone.
NBP The NBP measurement label in the measurement device has
been deactivated by deactivating the label in the Measurement
Selection window. The measurement automatically disappears
from the display. To switch the measurement on again,
reactivate the measurement label in the Measurement Selection
window.
NBP EQUIP MALF
Numeric is replaced by -?-
INOP tone.
NBP Remove the cuff from the patient. The NBP hardware is faulty.
Contact your service personnel.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the Stop
All SmartKey is selected.
NBP INTERRUPTED
Numeric is replaced by -?-
INOP tone.
NBP Check the tubing and cuff for leakages or kinks. Check that
you are using the correct cuff size and placement, and that the
correct patient category is selected. Try restarting the
measurement.
If the INOP occurs repeatedly, contact your service personnel.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the Stop
All SmartKey is selected.
This INOP arises when the measurement needed longer than
the maximum time for inflation, deflation or the total
measurement.
NBP MEASURE FAILED
Numeric may be displayed with a -?-
INOP tone.
NBP Check that you are using the correct cuff size and placement,
and that the correct patient category is selected. Try restarting
the measurement.
You can silence this INOP, but the INOP message remains
visible until the next measurement is started or the Stop
All SmartKey is selected.
Check the condition and suitability of the patient for NBP
monitoring. Use another cuff to continue measuring.
No Central Monit.
INOP tone
Monitor There is a problem with the communication to the network.
Central monitoring is currently not possible (no patient alarms
or information). Check the connection. Contact your service
personnel.
!!/!!! NO DEVICE DATA
NO DEVICE DATA
IntelliBridge Communication with connected device has been lost.
NO ECG AT CENTRAL Monitor The ECG measured with the monitor ECG is not being sent to
the Information Center via the telemetry device.
NO ECG SOURCE Telemetry A telemetry device is paired with the monitor but the
Information Center is not detecting a valid ECG signal from
either of them.
NO PPV FROM MeasSrv
at Information Center
MMS or
FMS
The measurement device does not supply a beat-to-beat arterial
pressure value. Contact your service personnel.
NO PPV FROM <Device> MMS or
FMS
The measurement device does not supply a beat-to-beat arterial
pressure value. Contact your service personnel.
OUT OF AREA Telemetry The telemetry device has left the access point coverage area.
P/P1/P2/P3/P4 INOPS PRESS See <Pressure label> INOPS (under Pressure).
PAP INOPS PRESS See <Pressure label> INOPS (under Pressure).
PPV BAD <Pressure Label>
SIGNAL
PPV The arterial pressure source selected for PPV is not providing a
pulsatile signal.
INOP Message, Indication Source What to do
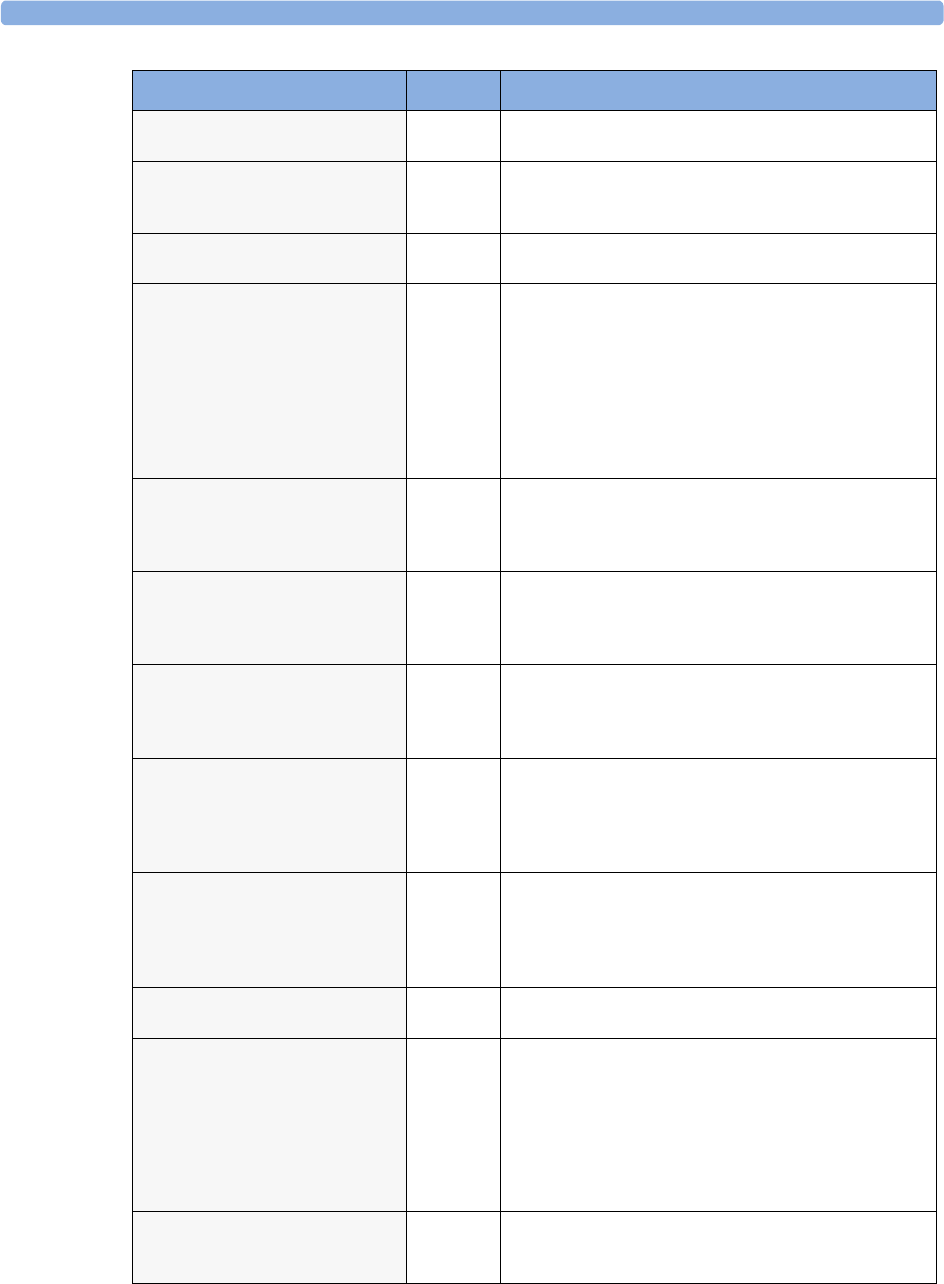
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
72
PPV BAD SIGNAL
at Information Center
PPV The arterial pressure source selected for PPV is not providing a
pulsatile signal.
PPV CHK SOURCES PPV The arterial pressure source selected for PPV is unplugged or
switched off. When this INOP has displayed for 1 minute PPV
will be switched off.
<Pressure label> ARTIFACT
Numeric questionable
PRESS A non-physiological event is detected (for example, a flush or
blood sample). A resulting high limit alarm will be suppressed.
<Pressure label>
DEACTIVATED
INOP tone
PRESS A Pressure measurement label in the measurement device or
extension has been deactivated, either by connecting a Temp
transducer in the shared Press/Temp socket, or by deactivating
the label in the Measurement Selection window.
The measurement automatically disappears from the display.
To switch the measurement on again, either reconnect a
Pressure transducer or reactivate the measurement label in the
Measurement Selection window.
<Pressure label> EQUIP
MALF
Numeric is replaced by -?-
INOP tone.
PRESS Contact your service personnel.
The pressure hardware is faulty.
<Pressure label> NO
TRANSDUCER
Numeric is replaced by -?-
INOP tone.
PRESS Make sure that the pressure transducer is connected to the
measurement device or module.
If you silence this INOP, the measurement will be switched off.
<Pressure label> NOISY
SIGNAL
Pulse numeric is replaced by -?-
INOP tone.
PRESS This INOP can only arise when a pressure is selected as the
pulse source. It occurs when the pulse detector finds a pulse
rate above 350bpm. This is usually caused by movement
artifact or electrical interference.
<Pressure label> NON-
PULSATILE
Pulse numeric is replaced by -?-
INOP tone.
PRESS This INOP can only arise when a pressure is selected as the
pulse source. It occurs when the pulse rate being measured is
less than 25 beats per minute or the amplitude is less than three
mmHg.
Check the catheter and connections to the patient.
<Pressure label>
OVERRANGE
Numeric is replaced by -?-
INOP tone.
PRESS Make sure that the measurement has been properly prepared
and zeroed, and that the transducer is level with the heart. If
this INOP persists, try another transducer.
Possible causes are a measured pressure outside the allowed
pressure range, or a broken wire to the transducer.
<Pressure label> REDUCE
SIZE
PRESS Increase the scale for the pressure wave.
<Pressure label>
UNPLUGGED
INOP tone.
PRESS A Pressure measurement label has been deactivated, either by
unplugging a module, or by deactivating the label in the
Measurement Selection window.
The measurement automatically disappears from the display.
To switch the measurement on again, either replug the module
or reactivate the measurement label in the Measurement
Selection window.
<Pressure label>
ZERO+CHECK CAL
Numeric is replaced by -?-
PRESS Perform a zero and check the calibration of the transducer.
INOP Message, Indication Source What to do
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
73
<pTemp label> CHECK PROBE
Numeric is replaced by -?-
INOP tone.
Predictive
Temp
Check that the probe holder is correctly installed and that a
compatible probe is in use. If the INOP does not clear, remove
the probe from the holder then replace it. If the INOP still does
not clear, disconnect and reconnect the probe.
<pTemp label> DEACTIVATED
INOP tone.
Predictive
Temp
The Predictive temperature has been deactivated.
<pTemp label> EQUIP MALF
Numeric is replaced by -?-
INOP tone.
Predictive
Temp
The Predictive Temperature hardware is defective. Contact
your service personnel.
<pTemp label> INCOMPAT. Predictive
Temp
The Predictive Temperature version is not supported by the
monitor.
<pTemp label> MEAS FAILED
Numeric is replaced by -?-
INOP tone.
Predictive
Temp
The ambient temperature is outside the specified range (10 to
40°C /50 to 104°F). Bring the temperature into range to
continue monitoring. If the INOP does not clear, disconnect
and reconnect the probe.
<pTemp label> NO PROBE
Numeric is replaced by -?-
INOP tone.
Predictive
Temp
Connect a probe to the Predictive temperature unit.
<pTemp label> OVERRANGE
Numeric is replaced by -?-
INOP tone.
Predictive
Temp
The temperature at the measurement site is out of range. Check
that the probe is correctly located. If the INOP does not clear,
disconnect and reconnect the probe.
<pTemp label> PROBE MALF
Numeric is replaced by -?-
INOP tone.
Predictive
Temp
The connected probe may be defective. Disconnect and
reconnect the probe. If the INOP does not clear, try another
probe.
pTaxil INOPS Predictive
Temp
See <pTemp label> INOPS
pToral INOPS Predictive
Temp
See <pTemp label> INOPS
pTrect INOPS Predictive
Temp
See <pTemp label> INOPS
(!!)PW:Action Required Protocol
Watch
The protocol currently running requires a user response. Check
which pop-up window is displayed and provide the appropriate
response.
PW:Check Settings Protocol
Watch
Contact your service personnel. Settings could not be loaded or
interpreted correctly
PW in conflict Protocol
Watch
There is a patient information mismatch which has not yet
been resolved (>15 minutes).
RA LEAD OFF
Numeric is replaced by -?-
INOP tone.
ECG The RA electrode has become detached from the patient or the
lead set has been changed. Reattach the electrode or select New
Lead Setup in the Setup ECG menu to confirm the
new lead set.
RAP INOPS PRESS See <Pressure label> INOPS (under Pressure).
Rem.Alarmdev.Malf
INOP tone
Monitor There is a problem with the connection to the remote alert
device. Contact your service personnel to check the remote
alert device and its connections.
Rem. Display Malf. Remote
display
There is a problem with an input device at the remote display.
Perform a visual and functional check of all input devices.
Contact your service personnel.
INOP Message, Indication Source What to do
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
74
!!/!!! REPLACE BATTERY T
Severe yellow/red INOP tone.
During this INOP, alarms cannot be
paused or switched off.
Telemetry The battery in the telemetry device is almost empty and must
be replaced.
RESP EQUIP MALF
Numeric is replaced by -?-
INOP tone.
RESP Contact your service personnel. The RESP hardware is faulty.
RESP ERRATIC
Numeric is replaced by -?-
RESP The monitor has detected too many artifacts in the measured
Resp signal. Check that the RA and LL electrodes are correctly
attached and have not dried out.
RESP LEADS OFF
Numeric is replaced by -?-
INOP tone.
RESP Not all the required leads for Resp monitoring are attached.
Make sure that the RA and LL leads are attached.
RL LEAD OFF
Numeric is replaced by -?- for 10
seconds; INOP tone.
ECG The RL electrode has become detached from the patient or the
lead set has been changed. Reattach the electrode or select New
Lead Setup in the Setup ECG menu to confirm the
new lead set.
Settings Malfunc.
INOP tone.
Monitor The monitor cannot use the predefined settings for
monitoring. Contact your service personnel.
<SO2 Label> CAL FAILED
Numeric is replaced by -?-
INOP tone.
SO2The calibration failed. Check the catheter-to-Optical-Module
connection. Manually restart the calibration. Try another
catheter and Optical Module. If the catheter is already inserted,
perform an in-vivo calibration.
<SO2 Label> CAL MODE
Numeric is replaced by -?-
INOP tone.
SO2Pre-insertion calibration is complete, but the catheter tip is still
inside the optical reference. The catheter is now ready for
insertion.
<SO2 Label>CAL REQUIRED
Numeric is replaced by -?-
INOP tone.
SO2There is no valid calibration data in the Optical Module.
Perform either a pre-insertion or an in-vivo calibration.
<SO2 Label> CANNOT MEAS
Numeric is replaced by -?-
INOP tone.
SO2The signal is out of the normal range, and no oxygen saturation
can be derived. Perform an in-vivo calibration. If the INOP
persists, try another Optical Module and catheter.
<SO2 Label>CONFIG ERROR
Numeric is replaced by -?-
INOP tone.
SO2The Optical Module has been configured to SaO2 Mode. Use
Change to Venous in the setup menu to reconfigure to venous
saturation mode.
<SO2 Label> CONN OPTMOD
Numeric is replaced by -?-
INOP tone.
SO2The Optical Module was disconnected during data storage.
Reconnect the Optical Module for at least 20 seconds.
<SO2 Label> EQUIP MALF
Numeric displays -?-.
INOP tone
SO2The SO2/SvO2 Module or Optical Module is faulty. Unplug
and replug the Optical Module and SO2/SvO2 module.
Exchange the modules. If the INOP persists, contact your
service personnel.
SO2 INCOMPATIBLE
INOP tone
SO2The SO2 Module or Optical Module is not supported. Contact
your service personnel.
<SO2 Label> IN-VIVO CAL SO2The in-vivo calibration is not yet complete. Lab values must be
stored to the Optical Module to complete the calibration.
Either continue with the next steps of the current calibration or
recall the previous calibration.
INOP Message, Indication Source What to do
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
75
<SO2 Label>LIGHT INTENS
Numeric is replaced by -?-
INOP tone.
SO2The intensity changed considerably since the last light intensity
calibration. This may indicate that the catheter tip is positioned
against a blood vessel wall or that there is low blood flow.
Reposition the catheter (and perform a Light Intensity
Calibration).
<SO2 Label> LOW LIGHT
Numeric is replaced by -?-
INOP tone.
SO2The optical signal levels are too low. Check that the catheter is
either in the optical reference or inserted into the patient.
Check the catheter-to-Optical Module connection. If INOP
persists, try another catheter and Optical Module.
<SO2 Label> NO OPTMOD
Numeric is replaced by -?-
INOP tone.
SO2Connect the Optical Module. If the INOP persists, try another
Optical Module. Silencing this INOP switches the
measurement off.
<SO2 Label> OPTMOD MALF SO2The Optical Module memory is faulty, and calibration data
cannot be stored for transport or during power failure. If this
capability is needed, use another Optical Module.
<SO2 Label> PRE-INS CAL
Numeric displays -?-
INOP tone
SO2The pre-insertion calibration is running. This typically takes
one minute. During this time alarms are switched off. Wait
until the calibration is complete.
<SO2 Label> UNPLUGGED
Numeric displays -?-.
INOP tone
SO2Measurement switched on and SO2/SvO2 module unplugged
from the rack.
SO2 UPGRADE
INOP tone
SO2The SO2 module is currently in upgrade mode.
Monitoring is not possible in this mode.
<SO2 Label> WARMUP
Numeric is displayed with ?
SO2The Optical Module has not yet reached the operating
temperature. Wait a few minutes until warm-up is finished.
SOME ECG ALRMS OFF Arrhythmia This message appears (if configured to do so) when the on/off
settings of the yellow arrhythmia alarms differ from the current
Profile.
Speaker Malfunct.
INOP tone
Monitor Contact your service personnel to check the speaker and the
connection to the speaker.
SPIRO MALFUNCTION Spirometry Module failure detected. Contact your service personnel.
SPIRO INCOMPATIBLE Spirometry Module revision not compatible with the host monitor
software revision. Contact your service personnel.
SPIRO UPGRADE Spirometry The module is running a firmware upgrade. Wait until upgrade
is completed before resuming monitoring.
SPIRO CANNOT MEAS Spirometry Measurement is at its limit, e.g. ambient pressure out of range.
SPIRO PURGE FAILED Spirometry The purge operation could not be completed successfully.
Check for kinked sensor tubings, hard occlusions and make
sure that the pump is running and all valves are switching.
SPIRO UNKN. SENSOR Spirometry An unknown sensor ID code was detected. Use only the sensors
listed in the Accessories chapter.
SPIRO ALARMS SUPPR Spirometry Alarming is suppressed for the spirometry module.
SPIRO PURGING Spirometry A purge operation is in progress - no data update on the screen.
Wait until purge is complete.
SPIRO NO SENSOR Spirometry No sensor detected. Make sure the correct sensor is attached to
the breathing circuit.
INOP Message, Indication Source What to do
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
76
SPIRO NO BREATH Spirometry No breath was detected for more than 25 seconds. Breath
derived numerics are not available.
SPIRO GAS COMPENS? Spirometry Gas compensation is set to “gas analyzer” but not all gases
necessary for compensation are measured by a gas monitor.
Some of the fall-back values provided by the user are used.
Measurement accuracy might be reduced.
SPIRO PATIENT CAT. Spirometry Mismatch of patient size configured in the host monitor and
sensor type plugged into the module. Check the instructions
on selecting the correct sensor in the Spirometry chapter.
'SpO2 CHK SOURCES
Numeric is replaced by -?-
SpO2
Difference
Not all measurements or values required to perform the
calculation are available. Check measurement sources.
'SpO2 CHK UNITS
Numeric is replaced by -?-
SpO2
Difference
The monitor has detected a conflict in the units used for this
calculation. Check the unit settings.
<SpO2 label> DEACTIVATED
INOP tone
SpO2The SpO2 measurement label in the measurement device has
been deactivated by deactivating the label in the Measurement
Selection window. The measurement automatically disappears
from the display. To switch the measurement on again,
reactivate the measurement label in the Measurement Selection
window.
<SpO2 label> EQUIP MALF
Numeric is replaced by -?-
INOP tone.
SpO2The MMS or module is faulty. Unplug and replug the MMS or
module. If the INOP persists, contact your service personnel.
<SpO2 label> ERRATIC
Numeric is replaced by -?-
INOP tone.
SpO2Check the sensor placement. Try another adapter cable and
sensor. If the INOP persists, contact your service personnel.
<SpO2 label> EXTD. UPDATE
Label is displayed with a -?-
(questionable numeric)
SpO2The update period of displayed values is extended due to an
NBP measurement on the same limb or an excessively noisy
signal.
<SpO2 label> INTERFERNCE
Numeric is replaced by -?-
INOP tone.
SpO2There is too much interference, caused by a high level of
ambient light and/or electrical interference. Cover the sensor to
minimize ambient light. If the INOP persists, make sure that
the sensor cable is not damaged or positioned too close to
power cables.
<SpO2 label> LOW PERF
Label is displayed with a -?-
(questionable numeric)
SpO2Accuracy may be compromised due to very low perfusion.
Stimulate circulation at sensor site. If INOP persists, change
the measurement site.
<SpO2 label> NOISY SIGN.
Numeric is replaced by -?-
INOP tone.
SpO2Excessive patient movement or electrical interference is causing
irregular pulse patterns. Try to reduce patient movement or to
relieve the cable strain on the sensor.
<SpO2 label> NON-PULSAT.
Numeric is replaced by -?-
INOP tone.
SpO2Check the perfusion at measurement site. If necessary,
stimulate circulation or change measurement site. If the INOP
is due to NBP measurement on the same limb, wait until the
NBP measurement is finished.
<SpO2 label> NO SENSOR
Numeric is replaced by -?-
INOP tone.
SpO2Make sure the SpO2 sensor is connected. If the INOP persists,
try another adapter cable and sensor. If you silence this INOP,
the measurement will be switched off.
<SpO2 LABEL> POOR SIGNAL
Label is displayed with a -?-
(questionable numeric)
SpO2The signal condition of the SpO2 measurement is poor and
measurement accuracy may be compromised.
INOP Message, Indication Source What to do
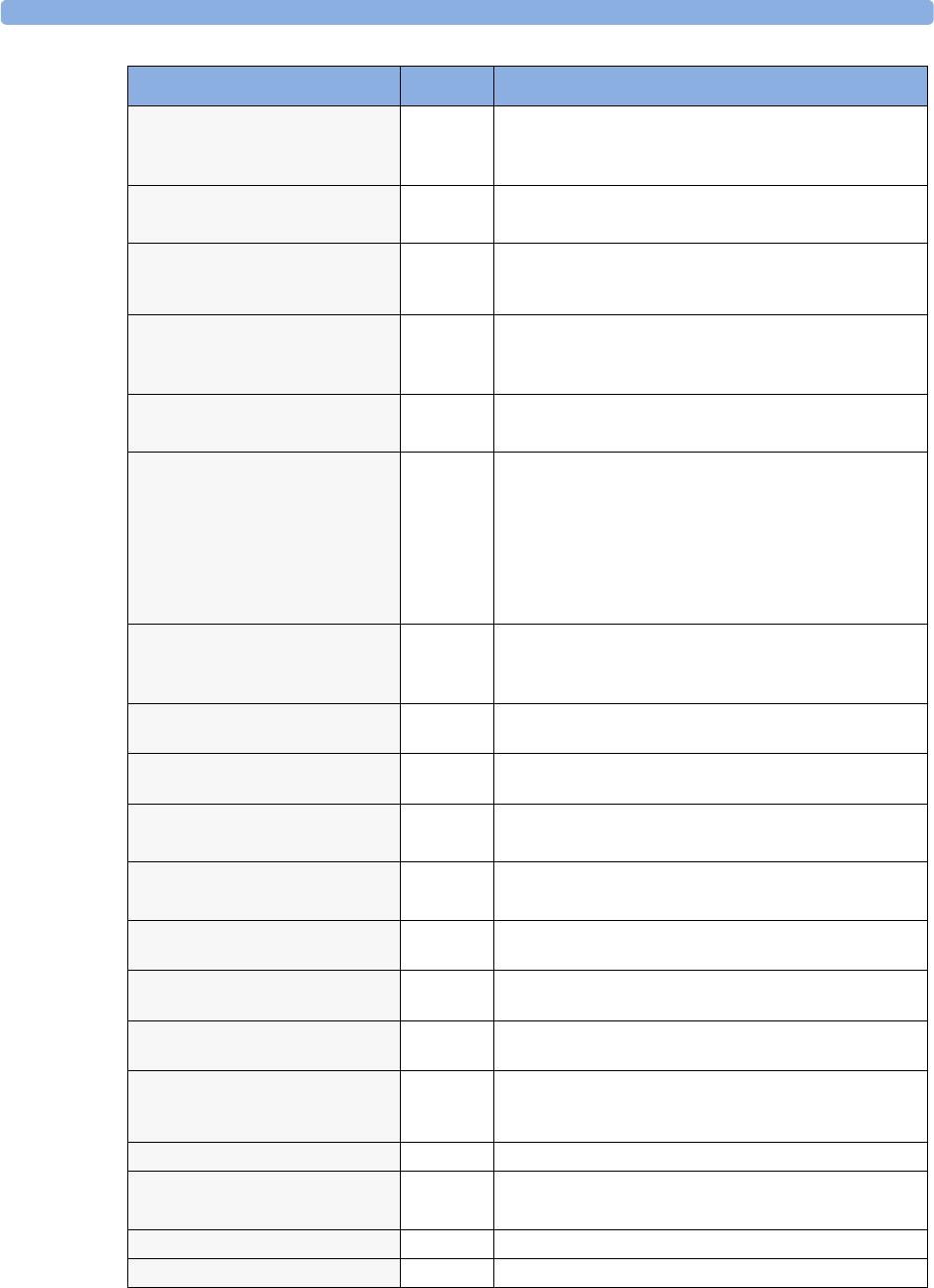
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
77
<SpO2 LABEL> PULSE?
Numeric is replaced by -?-
INOP tone
SpO2The detectable pulsations of the SpO2 signal are outside the
specified pulse rate range.
<SpO2 LABEL> SEARCHING
Numeric unavailable
SpO2SpO2 is analyzing the patient signal to derive Pulse, SpO2 and
Perf values. Please wait until the search analysis is complete.
<SpO2 label> SENSOR MALF
Numeric is replaced by -?-
INOP tone.
SpO2The SpO2 sensor or adapter cable is faulty. Try another adapter
cable and sensor. If the INOP persists, contact your service
personnel.
<SpO2 LABEL> SENSOR OFF
Numeric is replaced by -?-
INOP tone
SpO2The SpO2 sensor is not properly applied to the patient. Apply
the sensor following the instructions supplied by the
manufacturer.
<SpO2 LABEL> UNKN.SENSOR
Numeric is replaced by a -?-
SpO2The connected sensor or adapter cable is not supported by the
SpO2 measurement. Use only specified sensors and cables.
<SpO2 LABEL> UNPLUGGED
Numeric is replaced by -?-
INOP tone
SpO2An SpO2 measurement label has been deactivated, either by
unplugging a module, or by deactivating the label in the
Measurement Selection window.
The measurement automatically disappears from the display.
To switch the measurement on again, either replug the module
or reactivate the measurement label in the Measurement
Selection window.
<SpO2 LABEL> UPGRADE
Label is displayed with a -?-, numeric is
unavailable
SpO2The SpO2 measurement is currently in UPGRADE mode.
Monitoring is not possible in this mode.
Sp - vO2 CHK SOURCES
Numeric is replaced by -?-
Sp - vO2Not all measurements or values required to perform the
calculation are available. Check measurement sources.
Sp - vO2 CHK UNITS
Numeric is replaced by -?-
Sp - vO2The monitor has detected a conflict in the units used for this
calculation. Check the unit settings.
SRR INTERFERENCE
INOP tone
Monitor The short range radio connection has interference from
another device. Try using another channel.
SRR INVALID CHAN
INOP tone
Monitor The channel configuration of the Short Range Radio is invalid.
Check channel and channel mask configuration.
SRR MALFUNCTION Malfunction in the short range radio device. If the INOP
persists contact your service personnel.
SVR/SVRI CHK SOURCES
Numeric is replaced by -?-
SVR/SVRI Not all measurements or values required to perform the
calculation are available. Check measurement sources.
SVR/SVRI CHK UNITS
Numeric is replaced by -?-
SVR/SVRI The monitor has detected a conflict in the units used for this
calculation. Check the unit settings.
SVR/SVRI SET CVP USED
Numeric is replaced by -?-
SVR/SVRI A CVP value is required for this calculation, but is not
currently being measured. The monitor is using the CVP value
preset in the Setup SVR menu.
T/T1/T2/T3/T4 INOPs TEMP See <Temp label> INOPs (under Temp)
TAAP DISABLED
INOP tone
Monitor The currently selected telemetry configuration on the monitor
does not allow connection of telemetry devices to the monitor.
Tamb INOPs TEMP See <Temp label> INOPs (under Temp)
Tart INOPs TEMP See <Temp label> INOPs (under Temp)
INOP Message, Indication Source What to do
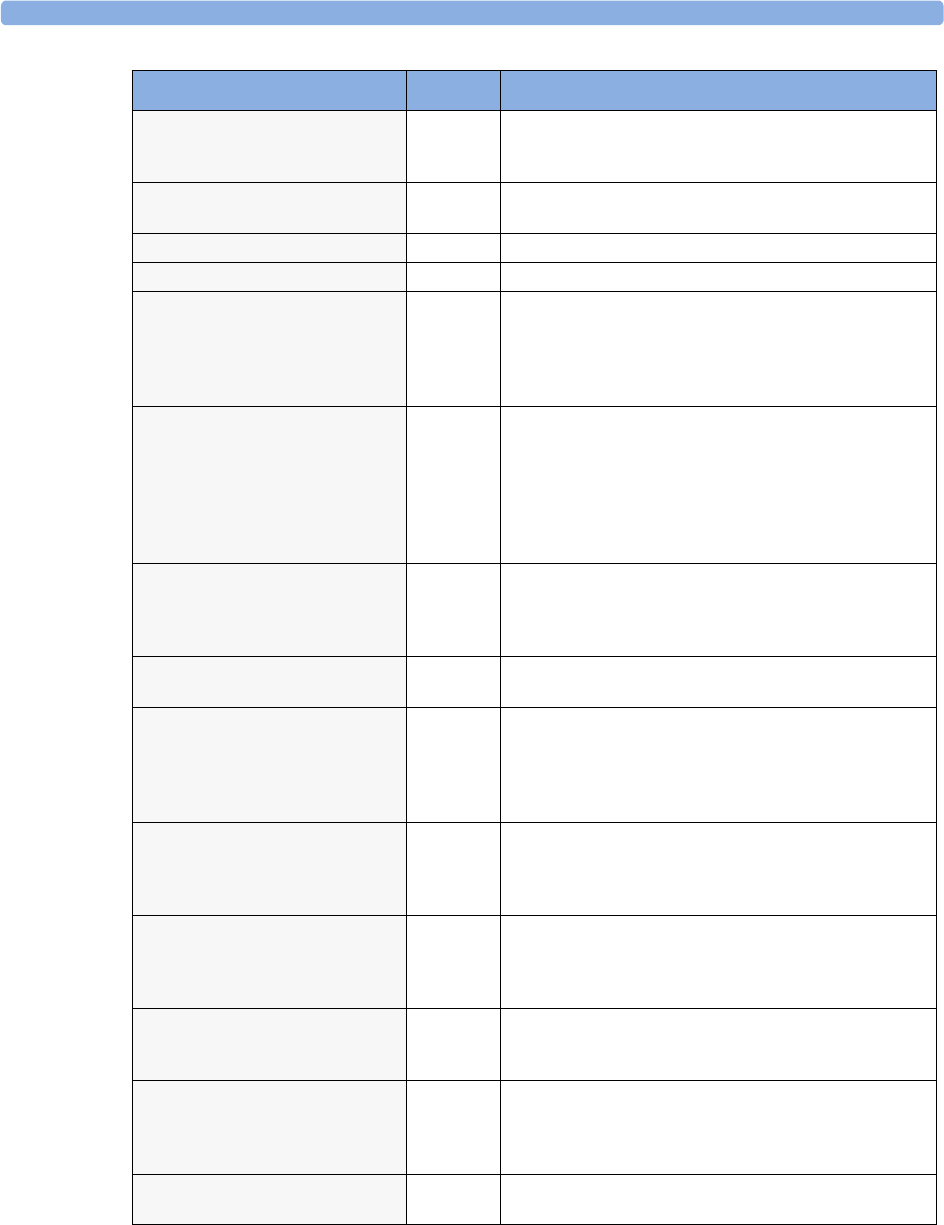
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
78
Tblood NO TRANSDUC
Numeric is replaced by -?-
INOP tone
C.O. No transducer attached to the module or catheter
disconnected.
Tblood OVERRANGE
Numeric is replaced by -?-
C.O. Tblood out of range 17°C - 43°C.
Tcereb INOPS TEMP See <Temp label> INOPs (under Temp)
Tcore INOPs TEMP See <Temp label> INOPs (under Temp).
tcpO2 (or tcpCO2 or tcGas)
CAL FAILED
Numeric is replaced by -?-
INOP tone.
tcGas A calibration failed. Check the calibration unit, gas pressure,
and tubing connections, then restart the calibration. If the
calibration has failed more than once, remembrane the
transducer and restart the calibration. If this INOP persists,
contact your service personnel.
tcpO2 (or tcpCO2 or tcGas)
CAL REQUIRD
Numeric is replaced by -?-
INOP tone.
tcGas Calibration is required before applying the transducer to the
patient.
Insert a membraned transducer into the calibration chamber on
the module, connect the calibration unit to the calibration
chamber, open the gas valve and start the calibration. If this
INOP occurs during a calibration, there may be a module or
transducer malfunction: contact your service personnel.
tcpO2 (or tcpCO2 or tcGas)
CAL RUNNING
Numeric displays first -?- , then
numeric is displayed with a ?
tcGas Wait until the tcpO2/tcpCO2 calibration is finished.
tcpO2 (or tcpCO2 or tcGas)
CHECK TIME
tcGas Site Timer due to time out in 15 minutes or less.
tcpO2 (or tcpCO2 or tcGas)
CHANGE SITE
If Heat Switch Off is configured to Yes,
numeric is replaced by -?-
INOP tone.
tcGas Site Timer has timed out. Change the application site to avoid
skin burns. To reset the Site Timer, either calibrate and change
the measurement site, or change the measurement site and reset
the Site Timer manually by selecting the appropriate site time
from the Setup TCGas menu.
tcpO2 (or tcpCO2 or tcGas)
EQUIP MALF
Numeric is replaced by -?-
INOP tone.
tcGas There is a malfunction in the transducer or module. Connect
another transducer. If this INOP persists, contact your service
personnel.
tcpO2 (or tcpCO2 or tcGas)
NO TRANSDUC
Numeric is replaced by -?-
INOP tone.
tcGas No transducer is connected to the tcpO2/tcpCO2 module.
Silencing the alarm switches off the measurement.
tcpO2 (or tcpCO2 or tcGas)
STABILIZING
Numeric is displayed with a ?
tcGas The transducer has not yet reached the selected temperature
and/or skin hyperemization is not yet finished. This INOP will
disappear within three minutes.
tcpO2 (or tcpCO2 or tcGas)
UNPLUGGED
Numeric is replaced by -?-
INOP tone.
tcGas The measurement is switched on but the module is unplugged.
The measurement automatically disappears from the display.
Silencing this INOP switches off the measurement.
TELE CONFIG UNSUPP
INOP tone
Monitor Telemetry device not supported (companion mode)
INOP Message, Indication Source What to do
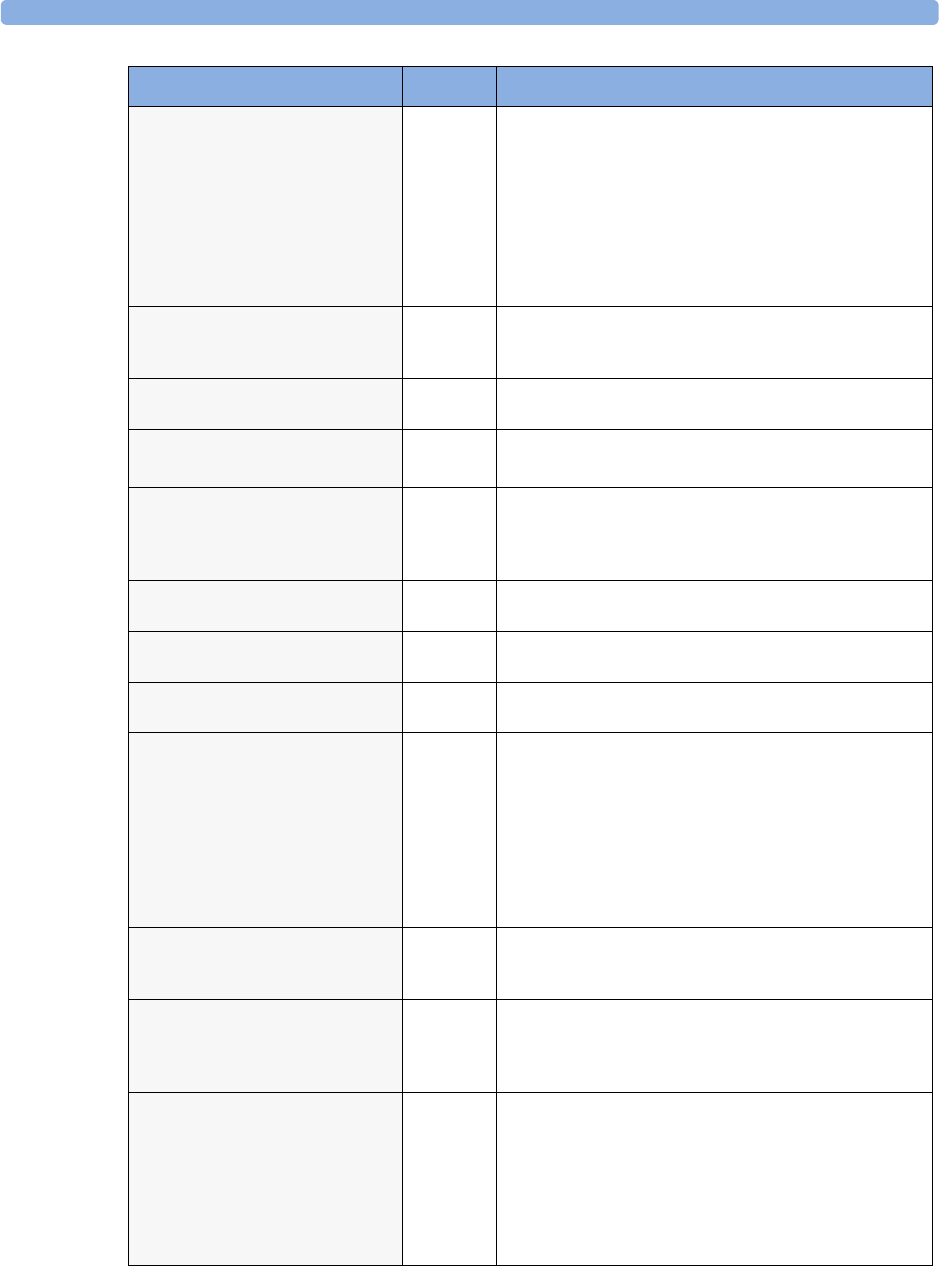
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
79
!!/!!!TELE DISCONNECT
INOP tone
Telemetry Telemetry transceiver was disconnected or short range radio
link was lost.
For cable connections; check Telemetry interface, cable
connection and setup.
For short range radio connections: if the telemetry transceiver
has not moved out-of-range, check for interference sources
close to the monitor (bluetooth devices, DECT phones,
cellular phones, microwaves, etc.) If this INOP persists, ask
your service personnel to survey the interference sources.
TELE EQUIP MALF
INOP tone
Monitor The telemetry device has a malfunction. Disconnect and
reconnect the telemetry device. If the INOP reappears, replace
the telemetry device.
TELE INCOMPATIBLE Monitor SRR-enabled telemetry device is not supported by this central
software revision. Please check configuration.
!!/!!! TELE INOP
Severe yellow/red INOP tone.
Telemetry Check for further details at the Information Center or in the
Telemetry Data window on the monitor.
Tele Sync Unsupp.
INOP tone
Telemetry The MMS in use does not support synchronization of ECG
and SpO2 settings between the monitor and central station
after a telemetry device has been paired. Use an MMS with
revision E.0 or above.
TELE UNSUPPORTED
INOP tone
Monitor This telemetry device is not supported for direct connection to
the monitor.
<'Temp> CHK SOURCES
Numeric is replaced by -?-
TEMP
Difference
Not all measurements or values required to perform the
calculation are available. Check measurement sources.
<'Temp> CHK UNITS
Numeric is replaced by -?-
TEMP
Difference
The monitor has detected a conflict in the units used for this
calculation. Check the unit settings.
<Temp label> DEACTIVATED
INOP tone
TEMP A Temp measurement label in the measurement device has
been deactivated, either by connecting a Pressure transducer in
the shared Press/Temp socket, or by deactivating the label in
the Measurement Selection window.
The measurement automatically disappears from the display.
To switch the measurement on again, either reconnect a Temp
transducer or reactivate the measurement label in the
Measurement Selection window.
<Temp label> EQUIP MALF
Numeric is replaced by -?-
INOP tone.
TEMP Contact your service personnel.
The temperature hardware is faulty.
<Temp label> NO
TRANSDUCER
Numeric is replaced by -?-
INOP tone.
TEMP Make sure the TEMP probe is connected to the MMS or
module.
If you silence this INOP, the measurement will be switched off.
<Temp label> UNPLUGGED
INOP tone
TEMP A Temp measurement label has been deactivated, either by
unplugging a module, or by deactivating the label in the
Measurement Selection window.
The measurement automatically disappears from the display.
To switch the measurement on again, either replug the module
or reactivate the measurement label in the Measurement
Selection window.
INOP Message, Indication Source What to do
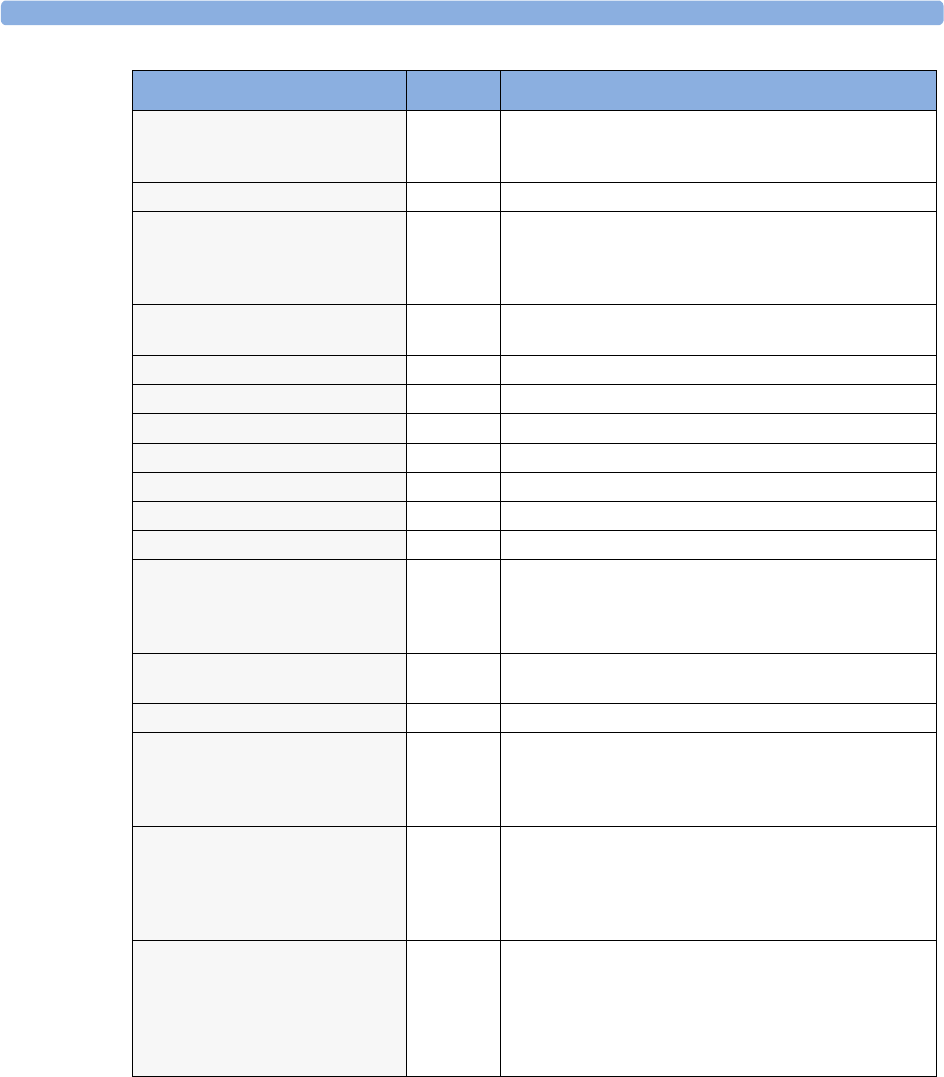
5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
80
<Temp label> OVERRANGE
Numeric is replaced by -?-
INOP tone.
TEMP Try changing the application site of the transducer.
[The temperature is less than -1qC, or greater than 45qC.]
Tesoph INOPS TEMP See <Temp label> INOPs (under Temp).
TEXT UPLOAD FAILED
INOP tone
IntelliBridge Incoming text from the IntelliBridge modules exceeds the
maximum limit. Try unplugging one of the IntelliBridge
modules. If the INOP occurs repeatedly contact your service
personnel; a software upgrade may be necessary.
TimeExpired:<timer label>
INOP tone
Monitor The time has expired for the timer indicated in the INOP text.
Clearing the timer clears the INOP.
Tnaso INOPS TEMP See <Temp label> INOPs (under Temp).
Trect INOPS TEMP See <Temp label> INOPs (under Temp).
Tskin INOPS TEMP See <Temp label> INOPs (under Temp).
Ttymp INOPS TEMP See <Temp label> INOPs (under Temp)
Tven INOPS TEMP See <Temp label> INOPs (under Temp).
Tvesic INOPS TEMP See <Temp label> INOPs (under Temp)
UAP INOPS PRESS See <Pressure label> INOPS (under Pressure).
Unsupported LAN
INOP tone
Monitor There is a problem with the communication to the network
and central monitoring is currently not possible. Check the
connection. If the INOP persists, switch off the monitor and
contact your service personnel.
User I/F Malfunct.
INOP tone.
Monitor Perform a visual and functional check of all the monitor input
devices. Contact your service personnel.
UVP INOPS PRESS See <Pressure label> INOPS (under Pressure).
V LEAD OFF
Numeric is replaced by -?- for 10
seconds; INOP tone.
ECG The V electrode (IEC: C electrode) has become detached from
the patient or the lead set has been changed. Reattach the
electrode or select New Lead Setup in the Setup ECG
menu to confirm the new lead set.
<VueLink option> CHK
CABLE
INOP tone.
VueLink No cable or the wrong cable connected to the VueLink module,
or incorrect device selected. Silencing this INOP switches the
measurement off.
VueLink INOP abbreviations may differ slightly depending on
the device category.
<VueLink option> CHK
CONF.
INOP tone.
VueLink The wrong external device has been selected on the VueLink
module, or the external device has not been correctly setup, or
the wrong cable has been used to connect the device to the
VueLink module.
VueLink INOP abbreviations may differ slightly depending on
the device category.
INOP Message, Indication Source What to do
Technical Alarm Messages (INOPs) 5 Patient Alarms and INOPs
81
<VueLink option> CHECK
SETUP
INOP tone.
VueLink No information was received from the external device. The
device may be switched off or disconnected.
VueLink INOP abbreviations may differ slightly depending on
the device category.
VueLnk EQUIP MALF
INOP tone.
VueLink Malfunction in the VueLink module. If this message appears
repeatedly, the module must be replaced. Contact your service
personnel.
VueLink INOP abbreviations may differ slightly depending on
the device category.
VueLnk NO CONFIG
INOP tone.
VueLink The VueLink module has not been configured during
installation. The installation process should be completed by
either your biomedical engineering department or the Philips
service engineer.
VueLink INOP abbreviations may differ slightly depending on
the device category.
VueLnk UNPLUGGED
INOP tone.
VueLink The VueLink module has been unplugged from the rack, or the
whole rack has been disconnected. The measurement
automatically disappears from the display. Silencing this INOP
switches off the measurement.
VueLink INOP abbreviations may differ slightly depending on
the device category.
INOP Message, Indication Source What to do

5 Patient Alarms and INOPs Technical Alarm Messages (INOPs)
82
83
6
6Managing Patients
Use the Patient Demographics window and its associated pop-up keys to admit, discharge, and transfer
(ADT) patients.
All patient demographic and ADT information is shared between the patient monitor and the
Information Center, for example, patients admitted to the monitor are automatically admitted to a
connected Information Center.
Admitting a Patient
The monitor displays physiological data and stores it in the trends as soon as a patient is connected.
This lets you monitor a patient who is not yet admitted. It is however important to admit patients
properly so that you can identify your patient on recordings, reports, and networked devices.
During admission you enter data that the monitor needs for safe and accurate operation. For example,
the patient category setting determines the algorithm the monitor uses to process and calculate some
measurements, the safety limits that apply for some measurements, and the alarm limit ranges.
NOTE It is strongly recommended that the same patient data fields be configured to be mandatory at the
monitor and the Information Center.
To admit a patient,
1Select the patient name field or select the Admit/Dischrge SmartKey to open the
Patient Demographics window.
Adult
SBed10 Doe, John
Patient Demographics
Last Name : Doe
First Name : John
MRN : 12345678
Patient
Cat.
Tr a n s f e r
: Adult
Dischrge
Patient
End
Case
Admit
Patient
6 Managing Patients Admitting a Patient
84
2Clear any previous patient data by selecting the Dischrge Patient or End Case pop-up
key and then Confirm.
If you do not discharge the previous patient, you will not be able to distinguish data from the
previous and current patients, for example, in the trend database.
3Select Admit Patient.
4Enter the patient information: select each field and use the on-screen keyboard or choose from the
pop-up list of alternatives to input information.
–Last Name: Enter the patient’s last name (family name), for example Smith.
–First Name: Enter the patient’s first name, for example Joseph.
–Middle Name (if configured to appear): Enter the patient’s middle name.
–Lifetime Id, Encounter Id: Whether these fields appear and how they are labelled can
be configured for your hospital. One or both fields may be displayed and the labels may read:
MRN, Case Id, Visit Id, etc. Enter the appropriate data for the fields displayed.
–Patient Cat: Choose the patient category, either Adult, Pediatric, or Neonatal.
–Paced: Choose Yes or No (You must use “Yes” if your patient has a pacemaker).
–Height: Enter the patient’s height.
–Weight: Enter the patient’s weight.
–BSA: The monitor calculates the body surface area automatically.
–Date Of Birth: Enter the patient’s date of birth. Enter this in the form dd/mm/yyyy.
–Age: The monitor calculates the patient age automatically.
–Gender: Choose Male or Female.
–Notes: Enter any extra information about the patient or treatment.
5Select Confirm. The patient status changes to admitted.
Patient Category and Paced Status
The patient category setting determines the algorithm the monitor uses to process and calculate some
measurements, the safety limits that apply for some measurements, and the alarm limit ranges.
The paced setting determines whether the monitor shows pacemaker pulses or not. When Paced is
set to No, pace pulses are filtered and therefore do not show in the ECG wave.
WARNING Patient Category and Paced status will always contain a value, regardless of whether the
patient is fully admitted or not. If you do not specify settings for these fields, the monitor uses the
default settings from the current profile, which might not be correct for your patient.
Patient category Changing the patient category may change the arrhythmia and NBP alarm limits.
Always check alarm limits to make sure that they are appropriate for your patient.
Paced status For paced patients, you must set Paced to Yes. If it is incorrectly set to No, the
monitor could mistake a pace pulse for a QRS and fail to alarm during asystole.
Admitting a Centrally-Monitored Patient
You can admit a patient at either the bedside or the Information Center. When you admit a patient,
the patient’s name appears on the bedside monitor and the Information Center.
Quick Admitting a Patient 6 Managing Patients
85
If you do not fill in all patient information required by the Information Center, the Information
Center may reject the admission. Complete all the required fields and try again to admit the patient.
Quick Admitting a Patient
Use Quick Admit only if you do not have the time or information to fully admit a patient. Complete
the rest of the patient demographic details later.
1Select the Quick Admit SmartKey.
2Enter the required data (ID fields or Last Name depending on configuration) with the keyboard.
3Select Enter.
4In the confirmation window, select Confirm to discharge the previous patient (if confirmation is
configured).
5Check that patient category and paced status are correct for the new patient.
If the monitor is connected to an Information Center and only the ID field is entered, the patient
name is set to - - - at the Information Center. Complete the rest of the demographic details as soon as
possible to fully identify the patient on the network, on the monitor and on printed reports. To
complete the details, select Admit Patient again and complete all required fields.
Editing Patient Information
To edit the patient information after a patient has been admitted, select the patient name field on the
Main Screen to open the Patient Demographics window, and make the required changes.
Discharging a Patient
WARNING Always perform a discharge before starting monitoring for a new patient, even if your previous patient
was not admitted. Failure to do so can lead to data being attributed to the wrong patient.
A discharge:
– clears the information in the Patient Demographics window
– erases all patient data (including trend data) from the monitor and Information Center. This
ensures that data from a previous patient are not mixed with data from the new patient.
– resets patient category and paced settings to the settings defined in the default Profile
– resets all monitor and measurement settings as well as the active Screen to the settings defined in
the default Profile
– discharges the patient from the Information Center.
When a patient is discharged from the monitor or from an Information Center, all patient data is
deleted. Make sure that you have printed out any required reports before discharging. Check that a
functioning central printer is available before you use End Case.
To discharge a patient,
1Select the patient name field or select the Admit/Dischrge SmartKey to open the
Patient Demographics window and associated pop-up keys.

6 Managing Patients Transferring Patients
86
2Select the pop-up key for either:
–End Case - to print any configured end case reports or vital signs recording, discharge the
patient and clear the patient database, then enter standby mode. If an End Case SmartKey is
configured for your monitor, you can also select this instead and then confirm.
To see which end case reports are set up for your monitor, select Main Setup -> Reports ->
Auto Reports. For each auto report, if End Case Report is set to On, this report will
be printed when you select End Case. See the section on AutoReports for information on
setting up end case reports.
–Dischrge Patient - to discharge the patient without printing any reports.
New Patient Check
The monitor can be configured to ask you in certain situations:
• after a specified power-off period
• after a specified standby period
• when no basic vitals (HR, RR, Pulse, SpO2, NBP) have been measured for a specified period
whether a new patient is now being monitored. The pop-up window is entitled Is this a new
Patient?. The monitor offers a Yes key to discharge the previous patient and begin monitoring a
new patient and a No key to continue monitoring with the current patient data and settings.
The time periods for the three conditions can be configured independently.
Transferring Patients
To save you from having to enter the same patient data multiple times and enable patient transfer
without loss of data, patient demographic information is shared between patient monitors and
Information Centers.
Transferring a Centrally-Monitored Patient with the Monitor
Scenario: A centrally-monitored patient is moved with the monitor to another monitoring location on
the same Information Center database server without interrupting the collection of patient trend
information.
1Select the patient name field or select the Admit/Dischrge SmartKey to open the
Patient Demographics window, then select the Transfer pop-up key. If the patient is
not admitted or not monitored by an Information Center, the Transfer key is inactive
(“grayed-out”).
This step preserves the patient’s demographic data during the transfer.
2At the new location, connect the monitor to the network (only needed for wired networks). If the
monitor detects a patient mismatch, a window will open showing your patient’s data and asking
Complete transfer of this patient?.
3Select Yes to complete the transfer.
4Verify that the settings for patient category and paced mode are correct.
If you accidentally transfer a patient, use Re-Admit to restore this patient’s data to the Information
Center. If you are not connected to the network, select Clear Transfer to leave transfer mode.
The patient data remains in the monitor.
Transferring Patients 6 Managing Patients
87
Data Exchange Between Information Centers
You can transfer demographic data and trend data from one IIC to another by selecting Transfer
on the patient monitor. Trend data is not shared between Information Centers and monitors.
Resolving Patient Information Mismatch
When you connect together devices which store patient demographic data, for example:
• an MMS and a monitor,
• an X2 or MP5 and a host monitor,
• a monitor and an Information Center,
the system compares patient category, paced status, and unique patient identification in order to
synchronize this information. If configured to do so, the monitor indicates a mismatch if the
information is not identical.
WARNING 1When a monitor is connected to an Information Center by the wireless IntelliVue Instrument
Telemetry interface, the patient data will automatically be merged in the case of a transfer. This
means there is no patient discharge at the monitor and settings and trend data will be retained. You
will see a message on the monitor and the Patient Demographics window will automatically appear
so that you can check the data and change it if necessary.
2It is important to resolve the mismatches as soon as they are identified. Failure to do so could result
in using incorrect/confusing data to make clinical decisions. Certain settings, for example Paced
and Patient Category, may not match between the Information Center and the monitor. If the
Paced status is set incorrectly, the system could mistake a pace pulse for a QRS and fail to alarm in
the case of asystole. It is important that the Patient Category is set correctly so the ECG can be
analyzed correctly and initial arrhythmia alarm limits set.
In the case where an MP5 or X2 with an IntelliVue Instrument Telemetry interface is declared as a
“telemetry device” at the Information Center and is connected to a host monitor, it is important to
resolve an existing mismatch between the monitor and the Information Center before
disconnecting the MP5/X2. Failure to do so discharges the MP5/X2 and synchronizes the
demographics and settings to the Information Center.
Manually Resolving Patient Mismatch
The source of the patient mismatch is indicated by question marks (???) and displayed in the status line
at the bottom of the screen (Patient ???,Patient Category ??? or Paced ???).
The Select Patient window automatically opens so you can decide which patient data to use.
You do not have to resolve the mismatch immediately, but the indicators remain until you do.
For some common mismatch situations, the monitor will simplify the resolution by suggesting a
solution for the mismatch. For example, when a patient arrives after transport and the Transfer key
has been selected, the monitor will show this patient’s data and ask Complete transfer of
this patient?. You can then select Yes to complete the transfer. If you select No you will go to
the Select Patient window.
After you resolve the mismatch, the monitor displays a confirmation window that shows the patient
that has been selected and where data will be erased, if applicable. Confirm your choice. The monitor
automatically displays the Patient Demographics window after confirmation. Verify that the
settings shown are correct for the patient.
6 Managing Patients Transferring Patients
88
Gender, date of birth, height, weight, and nursing notes do not generate a mismatch. If these fields are
different on different devices, the monitor resolves them itself. For example, it may take date of birth
from the Information Center, whilst taking gender from the monitor. Always check the Patient
Demographics after combining patients, to ensure that you are satisfied with the results. Change them
if necessary.
WARNING After resolving a patient mismatch, check that the monitor settings (especially patient category, paced
status and alarm limits) are correct for the patient.
Patient Mismatch - If One Set of Patient Data is Correct
♦If there is a mismatch between an
Information Center and a monitor, choose
the data set you want to continue using for
this patient by selecting one of the sectors in
the Select Patient window.
After you resolve the mismatch, the monitor
displays a confirmation window that shows the
patient that has been selected and where data
will be erased, if applicable. Confirm your
choice. The monitor automatically displays the
Patient Demographics window after
confirmation. Verify that the settings shown are correct for the patient.
Patient Mismatch - If Neither Patient Data Set is Correct
A patient mismatch where neither set of patient data is correct might occur if you connect a new MMS
to a monitor in order to prepare for a new patient, before you actually start measuring.
♦Select New Patient if you are sure that none of the information is correct. This discharges all
patients, erases all data in both the monitor and MMS, resets all settings to the default Profile, and
lets you admit a new patient.
Patient Mismatch - If Both Patient Data Sets Are Correct
A patient mismatch where both sets of patient data are correct might occur if you admit a new patient
at the monitor (or Information Center) before the patient arrives at your unit and then connect the
MMS that was used during the patient transport to the monitor.
♦Select Same Patient if the patient information is different, but you are sure it is the same
patient. This merges the demographics and updates them in the Information Center, monitor, and
MMS, according to this table. Be aware that your monitor may be configured to merge trend data
from the MMS and the monitor, and to upload measurement settings from the MMS to the
monitor.
Select Patient
DOE, JOHN F
1234HG9556, 2008/00123
Adult Non-Paced
MILLER,
Adult Paced
Same Patient
New Patient

89
7
7ECG, Arrhythmia, ST and QT
Monitoring
The electrocardiogram (ECG) measures the electrical activity of the heart and displays it on the
monitor as a waveform and a numeric. This section also tells you about arrhythmia monitoring (see
page 105), ST monitoring (see page 117) and QT monitoring (see page 127).
Skin Preparation for Electrode Placement
Good electrode-to-skin contact is important for a good ECG signal, as the skin is a poor conductor of
electricity.
1Select sites with intact skin, without impairment of any kind.
2Clip or shave hair from sites as necessary.
3Wash sites thoroughly with soap and water, leaving no soap residue.
We do not recommend using ether or pure alcohol, because this dries the skin and increases the
resistance.
4Dry skin thoroughly.
5Gently abrade the skin using ECG skin preparation paper to remove dead skin cells to improve the
conductivity of the electrode site.
Connecting ECG Cables
1Attach the clips or snaps to the electrodes before placing them. If you are not using pre-gelled
electrodes, apply electrode gel to the electrodes before placement.
2Place the electrodes on the patient according to the lead placement you have chosen.
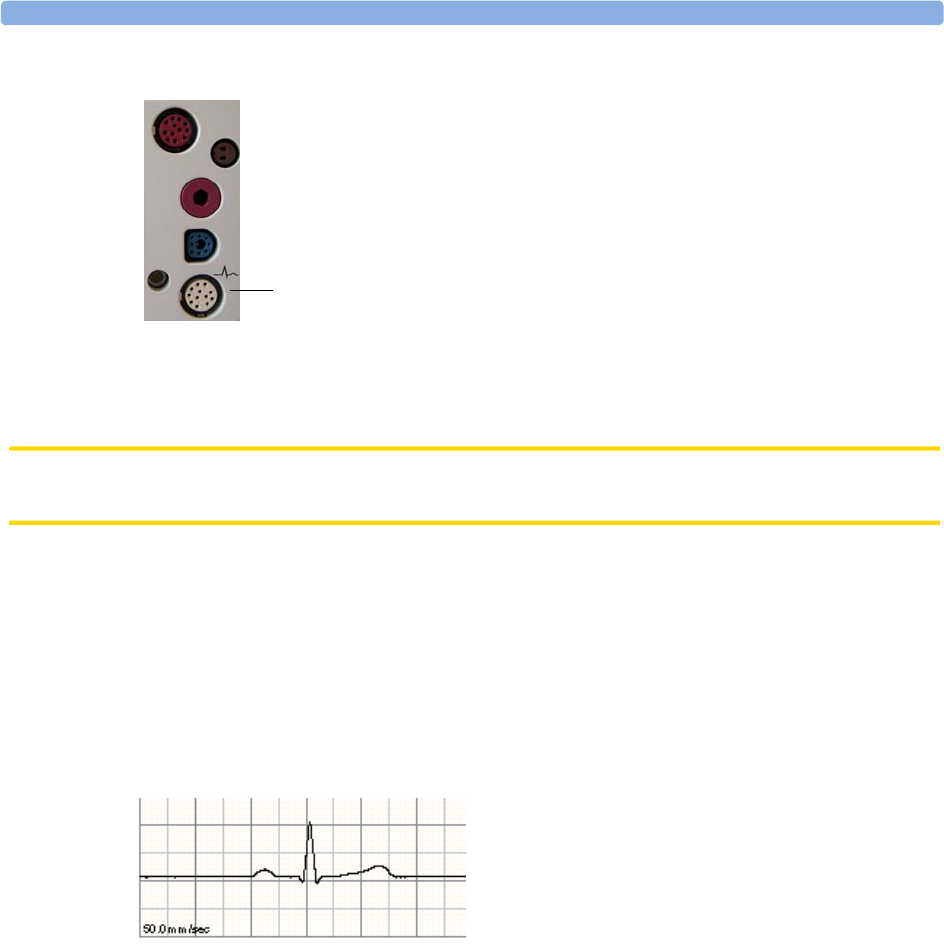
7 ECG, Arrhythmia, ST and QT Monitoring Selecting the Primary and Secondary ECG Leads
90
3Attach the electrode cable to the patient cable.
4Plug the patient cable into the white ECG connector on the monitor. An ECG waveform and
numeric appears on the monitor display.
CAUTION To protect the monitor from damage during defibrillation, for accurate ECG information and to
protect against noise and other interference, use only ECG electrodes and cables specified by Philips.
Selecting the Primary and Secondary ECG Leads
The monitor uses the primary and secondary lead to compute HR and to analyze and detect cardiac
arrhythmias. They are also available for recordings and for display on the Information Center.
The secondary lead is only used if your monitor is configured for multi-lead (instead of single-lead)
arrhythmia analysis.
To select a lead as primary or secondary lead:
♦In the Setup ECG menu, select Primary or Secondary, then select the appropriate lead.
You can assign any available lead whether it is currently displayed or not.
Checking Paced Status
It is important to set the paced status correctly when you start monitoring ECG.
♦To change the paced status in the Setup ECG menu, select Paced to toggle between Yes or
No.
1 - ECG Connector
1
You should choose a lead as primary or secondary lead that
has the following characteristics:
• the QRS complex should be either completely above or
below the baseline and it should not be biphasic
• the QRS complex should be tall and narrow
• the P-waves and T-waves should be less than 0.2 mV
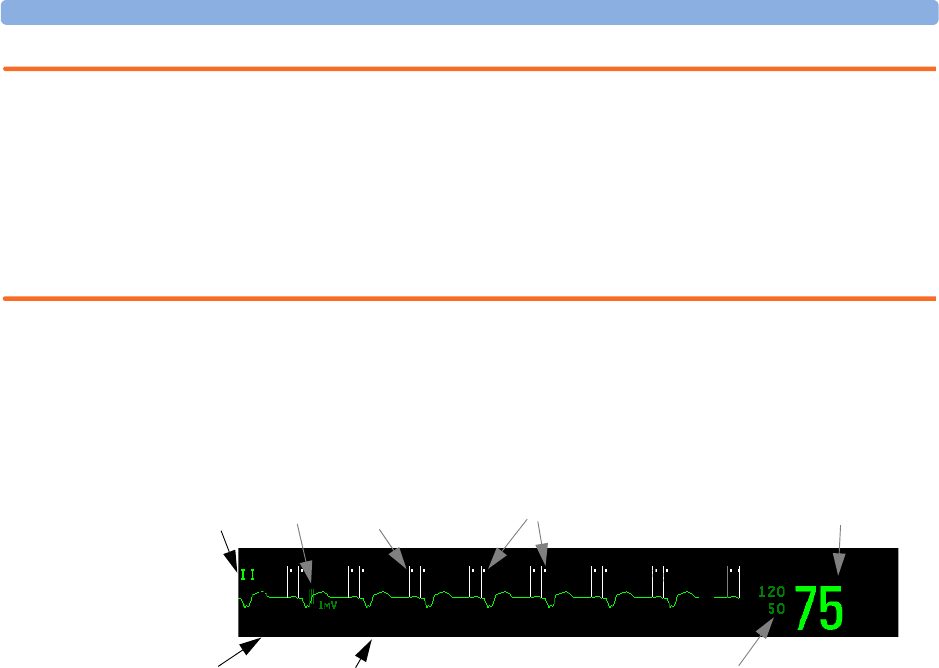
Understanding the ECG Display 7 ECG, Arrhythmia, ST and QT Monitoring
91
WARNING Pace pulse rejection must be switched on for paced patients by setting “Paced” to Yes. Switching pace
pulse rejection off for paced patients may result in pace pulses being counted as regular QRS
complexes, which could prevent an asystole event from being detected. When changing profiles, and at
admission/discharge, always check that paced status is correct for the patient.
Some pace pulses can be difficult to reject. When this happens, the pulses are counted as a QRS
complex, and could result in an incorrect HR and failure to detect cardiac arrest or some arrhythmias.
Make sure that pace pulses are detected correctly by checking the pace pulse markers on the display.
Keep pacemaker patients under close observation.
Understanding the ECG Display
Your display may be configured to look slightly different.
ECG HR numeric: This is the heart rate derived from the monitored ECG.
Pace pulse markers: These are shown if the Paced status has been set to Yes, the pacer spikes are not
configured to have a fixed size, and the patient has a paced signal.
Pacer Spikes: The pacer spikes are shown in white, unless the ECG wave is white, then they will be
green. If the pacer spikes have been configured to have a fixed size, they will be displayed in the
background as a dotted line.
1 Lead label of the displayed wave
2 1 mV calibration bar
3Pacer spikes
4 Pace pulse markers
5 Current heart rate
6 Current heart rate alarm limits
7 EASI lead placement label
8 ECG Filter label
EASI
M
HR bpm
4
8
1
6
5
7
3
Paced Rhythm
2
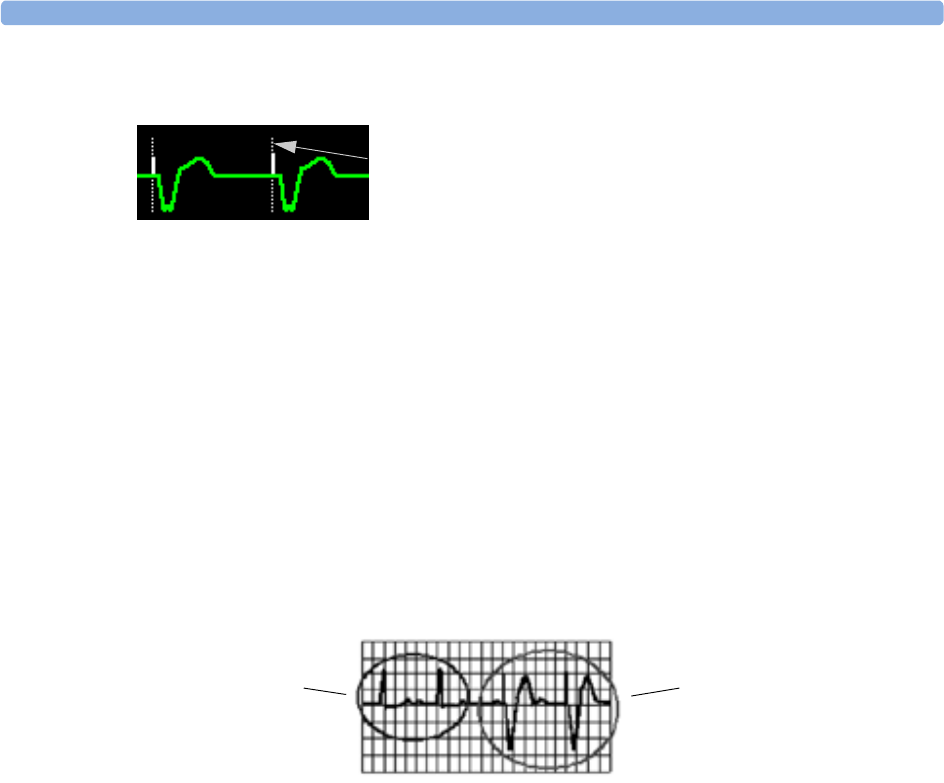
7 ECG, Arrhythmia, ST and QT Monitoring Monitoring Paced Patients
92
Defibrillator synchronization marks: If an HP/Agilent/Philips defibrillator is connected, the
synchronization marks (vertical lines on the ECG wave) are shown on the ECG wave. The
synchronization marks will be shown in yellow, unless the ECG wave is yellow, then they will be green.
If so configured, the monitor can supply its own synchronization marks; in this case the
synchronization marks from a defibrillator will not be shown.
ST numerics in ECG wave: ST numerics can be configured to show underneath the ECG wave on
the left side.
Monitoring Paced Patients
An ECG optimized for monitoring a paced patient should look like this:
You should choose a lead as primary or secondary lead that has these characteristics:
• the normal QRS complex should be either completely above or below the baseline and it should not
be biphasic. For paced patients, the QRS complexes should be at least twice the height of pace
pulses.
• the QRS complex should be tall and narrow
• the P-waves and the T-waves should be less than 0.2 mV.
For ease of identification on the screen, the pacer spikes can be configured to have a fixed size. They are
then shown in the background as a dotted lines. The length of the dotted line is fixed to the wave
channel height and is independent of the actual pacer amplitude.
1 Pacer spikes configured to have a fixed size
1
1Normal Beats
2 Pace Pulses/Beats
2
1
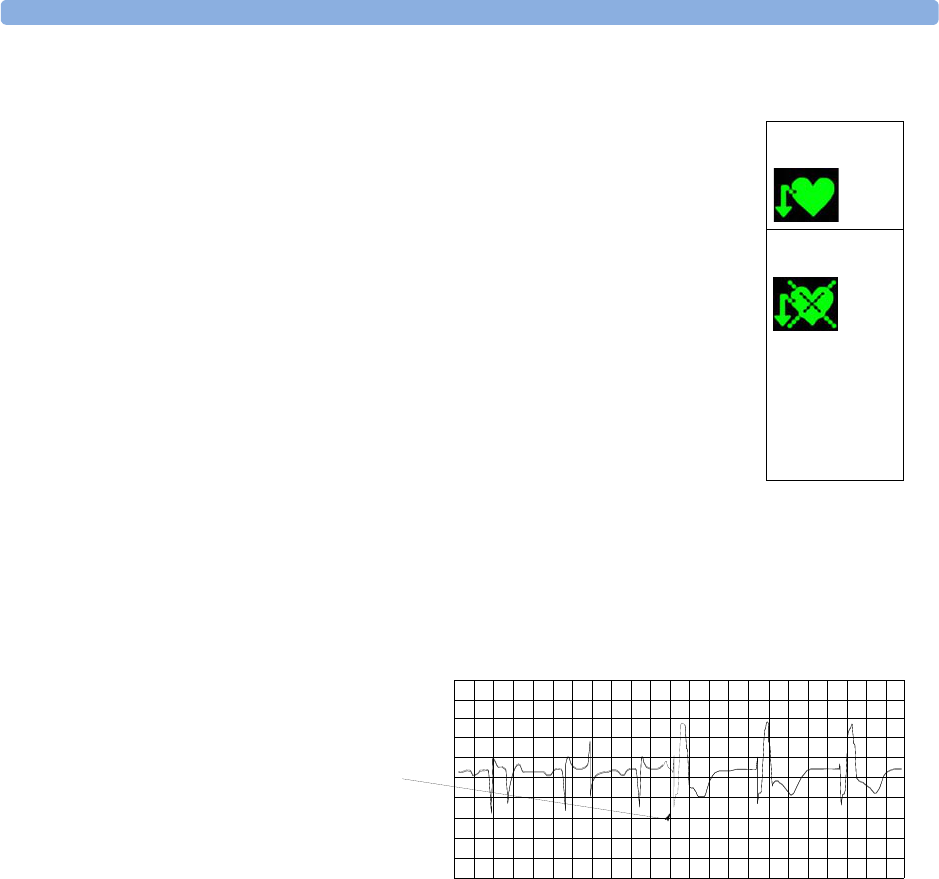
Changing the Size of the ECG Wave 7 ECG, Arrhythmia, ST and QT Monitoring
93
Setting the Paced Status (Pace Pulse Rejection)
Avoiding Pace Pulse Repolarization Tails
Some unipolar pacemakers display pace pulses with repolarization tails. These tails may be counted as
QRSs in the event of cardiac arrest or other arrhythmias.
If you note a visible repolarization tail, choose a lead that decreases the size of the repolarization tail.
Changing the Size of the ECG Wave
If any of the displayed ECG waves is too small or clipped, you can change the size of one or all of the
ECG waves on the screen.
Changing the adjustment factor only changes the visual appearance of the ECG wave on the screen. It
does not affect the ECG signal analyzed by the monitor.
Comparing the wave size to the 1 mV calibration bar on the ECG wave segment can help you to get an
idea of the true ECG signal strength. If you choose a fixed adjustment factor, the 1 mV calibration bar
will be the same size for all the displayed ECG waves. If you choose AutoSize, or an individual size
using the Size Up / Size Down keys, the calibration bar may be a different size for each wave.
To Change the Size of an Individual ECG Wave
1Select the wave segment you want to change. This calls up the lead menu for this segment.
♦In the Setup ECG menu, select Paced to toggle between Yes and No.
You can also change the paced status in the Patient Demographics window.
When Paced is set to Yes:
– Pace Pulse Rejection is switched on. This means that pacemaker pulses are
not counted as extra QRS complexes.
– pace pulse marks are shown on the ECG wave as a small dash (only when
the pacer spikes are not configured to have a fixed size)
– the paced symbol is displayed under the HR label.
When Paced is set to No, pacer spikes are not shown in the ECG wave. Be
aware that switching pace pulse rejection off for paced patients may result in
pace pulses being counted as regular QRS complexes, which could prevent an
asystole event from being detected.
Paced
Non-Paced
1 Repolarization tail
(note width)
1

7 ECG, Arrhythmia, ST and QT Monitoring Changing the Volume of the QRS Tone
94
2In the lead menu, select Size Up to increase wave size or Size Down to decrease the size.
Selecting AutoSize lets the monitor choose the optimal adjustment factor for all displayed ECG
waves.
To Change the Size of all the ECG Waves
To change the size of all the ECG waves on the screen by a fixed adjustment factor,
1In the Setup ECG menu, select Adjust Size.
2Select the required adjustment factor from the line of pop-up keys.
–Size x0.5 to halve the wave size
–Size x1 to display the wave without zoom
–Size x2 to double the wave size
–Size x4 to multiply the wave size by four
Changing the Volume of the QRS Tone
The QRS tone is derived from either the HR or Pulse, depending on which is currently selected as the
alarm source. The QRS volume can be set from 0 to 10 (0 means off).
♦To change the QRS volume, in the Setup ECG menu select QRS Volume and then select the
appropriate volume from the pop-up list.
Changing the ECG Filter Settings
The ECG filter setting defines how ECG waves are smoothed. An abbreviation indicating the filter
type is shown underneath the lead label on the monitor display. Filter settings do not affect ST
measurement.
♦To change the filter setting, in the Setup ECG menu, select Filter and then select the
appropriate setting.
–Monitor: Use under normal measurement conditions.
–Ext. Monitor: Use for pediatric and neonatal patients when diagnostic quality is required
but low frequency interference or a wandering baseline may be expected. The upper edge
frequency is the same as the Diag setting and the lower edge frequency is the same as the
Monitor setting.
–Filter: The filter reduces interference to the signal. It should be used if the signal is distorted
by high frequency or low frequency interference. High frequency interference usually results in
large amplitude spikes making the ECG signal look irregular. Low frequency interference usually
leads to a wandering or rough baseline. In the operating room, the Filter reduces artifacts and
interference from electro-surgical units. Under normal measurement conditions, selecting
Filter may suppress the QRS complexes too much and thus interfere with the clinical
evaluation of the ECG displayed on the monitor. This does not affect the ECG analysis
performed by the monitor.
If AutoFilter is set to On in Configuration Mode, the filter setting will automatically be set
to Filter if electromagnetic interference is detected.

Selecting Positions of Va and Vb Chest Leads (for 6-lead placement) 7 ECG, Arrhythmia, ST and QT
Monitoring
95
–Diag: Use when diagnostic quality is required. The unfiltered ECG wave is displayed so that
changes such as R-wave notching or discrete elevation or depression of the ST segments are
visible.
The setting Diag selects the highest available ECG bandwidth which is 0.05 to 150 Hz for the
Adult, Pedi and Neo patient category. The term “diagnostic” relates only to the ECG bandwidth
requirements for diagnostic electrocardiographic devices as outlined in the ANSI/AAMI standard
EC11-1991.
When you are using a telemetry transmitter connected via short range radio to the monitor, the
upper bandwidth for all filter settings is limited to 40 Hz.
Selecting Positions of Va and Vb Chest Leads (for 6-
lead placement)
The two chest leads for the 6-lead placement can be positioned at any two of the V1 to V6 positions.
Select the positions you have used in the Setup ECG menu, so that the chest leads will be correctly
labeled.
1In the Setup ECG menu, select Va Lead.
2Select the position used from the list.
3Select Vb Lead and select the position used from the list
Choosing EASI or Standard Lead Placement
You must enable either standard lead placement or EASI lead placement.
♦In the Setup ECG menu, select Placement and then Standard or EASI.
EASI is shown beside the 1mV calibration bar on the ECG wave on the display, and EASI is marked
on any printouts.
See the section on EASI ECG Lead Placement for electrode placement diagrams.
About ECG Leads
To make it possible to compare measured ECG signals, the electrodes (or lead sets) are placed in
standardized positions, forming so-called “leads”. To obtain ECG signals optimized for use in
diagnosis and patient management in different care environments, different lead sets in varying lead
placements can be used. You can use either standard lead placements or EASI lead placements with this
monitor.
When placing electrodes, choose a flat, non-muscular site where the signal will not be interfered with
by either movement or bones. Correct lead placement is always important for accurate diagnosis.
Especially in the precordial leads, which are close to the heart, QRS morphology can be greatly altered
if an electrode is moved away from its correct location.
7 ECG, Arrhythmia, ST and QT Monitoring ECG Lead Fallback
96
ECG Leads Monitored
Changing Lead Sets
To change the ECG lead set,
•When adding leads: place the additional electrodes as required - the monitor automatically
recognizes the new lead placement.
•When removing leads: there are two possibilities - removing the complete chest leads block or
removing individual leads. If you unplug the chest lead block from the trunk cable connector, the
monitor will automatically recognize the new lead placement. Remove individual leads by removing
the electrodes. The monitor will issue a Lead Off INOP message; select New Lead Setup in
the Setup ECG menu and the INOP message will disappear.
ECG Lead Fallback
If fallback is configured on and there is a leads off INOP in the primary lead (and in the secondary
lead, if you are using multi-lead monitoring) for longer than 10 seconds, and if another lead is
available, this available lead automatically becomes the primary lead. This is known as lead fallback.
When the Leads Off condition is corrected, the leads are automatically switched back.
This setting can only be changed in Configuration Mode.
ECG Lead Placements
The labels and colors of the ECG electrodes differ according to the standards that apply for your
hospital. The electrode placement illustrations in this chapter use the AAMI labels and colors.
If you are using these leads are available: Resp is measured
between electrodes:
a 3-electrode set I, II, III RA and LL
a 5-electrode set I, II, III, aVR, aVL, aVF, V and MCL RA and LL
a 6-electrode set I, II, III, aVR, aVL, aVF, Va, Vb RA and LL
a 10-electrode set I, II, III, aVR, aVL, aVF, V1, V2, V3, V4, V5, V6 RA and LL
an EASI 5-electrode set I, II, III, aVR, aVL, aVF, V1, V2, V3, V4, V5, V6 I and A
Electrode labels Electrode colors
AAMI EASI IEC AAMI IEC
RA I RWhite Red
LA S LBlack Yellow
LL A FRed Green
RL N N Green Black
V E CBrown White
V1 C1 Brown/Red White/Red
V2 C2 Brown/Yellow White/Yellow
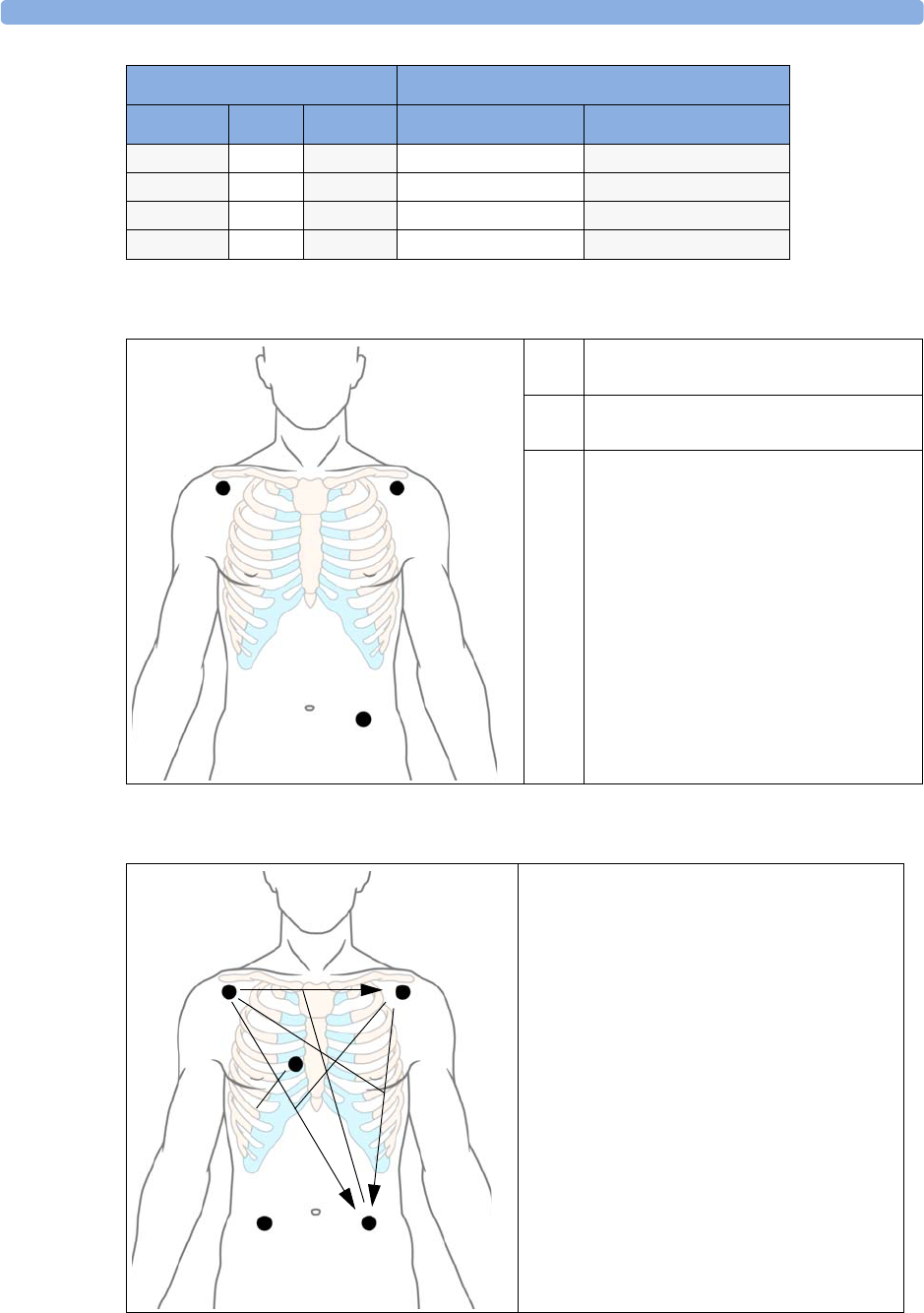
ECG Lead Placements 7 ECG, Arrhythmia, ST and QT Monitoring
97
Standard 3-Lead Placement
Standard 5-Lead Placement
V3 C3 Brown/Green White/Green
V4 C4 Brown/Blue White/Brown
V5 C5 Brown/Orange White/Black
V6 C6 Brown/Violet White/Violet
Electrode labels Electrode colors
AAMI EASI IEC AAMI IEC
1 RA placement: directly below the clavicle
and near the right shoulder
2 LA placement: directly below the
clavicle and near the left shoulder
3 LL placement: on the left lower
abdomen
12
3
RA placement: directly below the clavicle and
near the right shoulder
LA placement: directly below the clavicle and
near the left shoulder
RL placement: on the right lower abdomen
LL placement: on the left lower abdomen
V placement: on the chest, the position depends
on your required lead selection
2
4
1
V
3
I
III
II
aVR
aVL
aVF
5
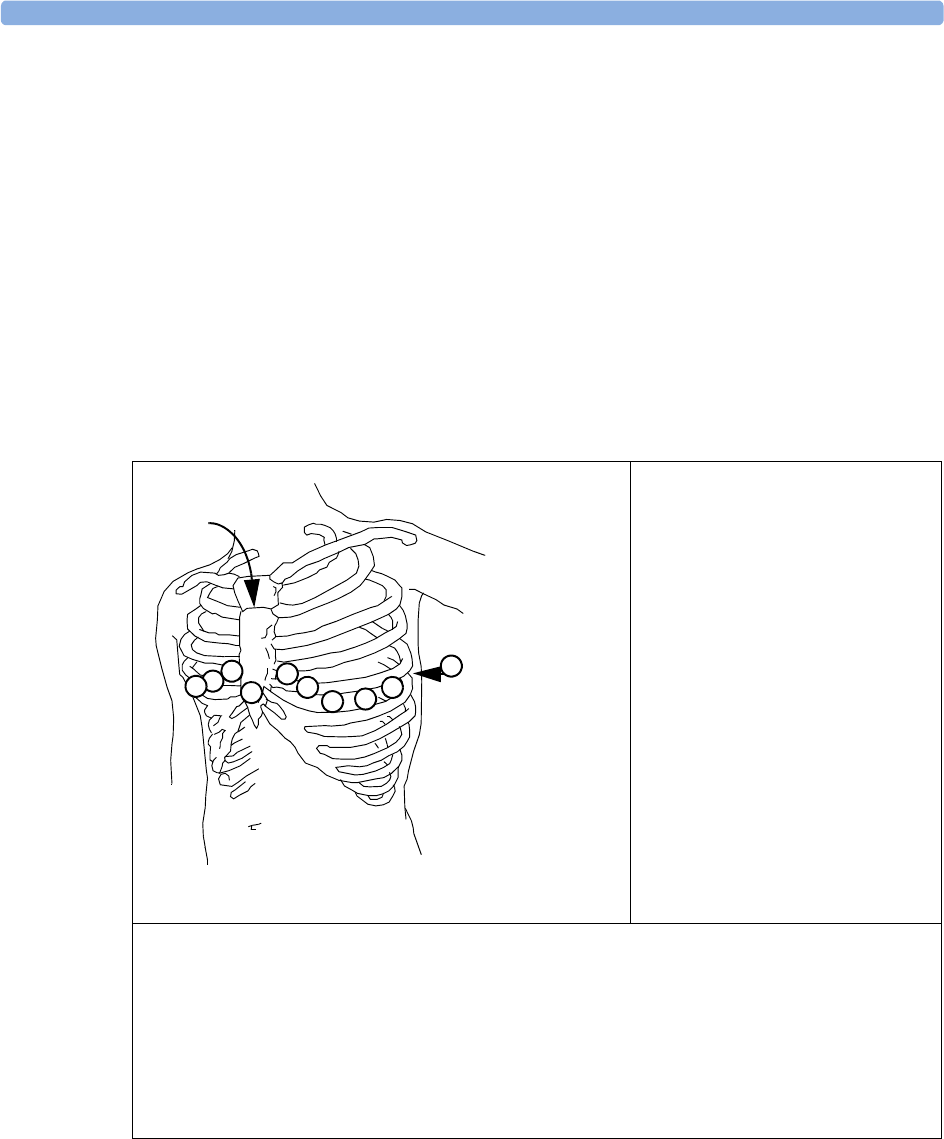
7 ECG, Arrhythmia, ST and QT Monitoring ECG Lead Placements
98
6-Lead Placement
For a 6-lead placement use the positions from the 5-lead diagram above but with two chest leads. The
two chest leads, Va and Vb, can be positioned at any two of the V1 to V6 positions shown in the chest
electrode diagram below. The Va and Vb lead positions chosen must be selected in the ECG Setup
Menu to ensure correct labeling.
Chest Electrode Placement
For accurate chest electrode placement and measurement, it is important to locate the fourth
intercostal space.
1Locate the second intercostal space by first palpating the Angle of Lewis (the little bony
protuberance where the body of the sternum joins the manubrium). This rise in the sternum is
where the second rib is attached, and the space just below this is the second intercostal space.
2Palpate and count down the chest until you locate the fourth intercostal space.
V1 placement: on the fourth
intercostal space at the right sternal
border
V2 placement: on the fourth
intercostal space at the left sternal
border
V3 placement: midway between the
V2 and V4 electrode positions
V4 placement: on the fifth
intercostal space at the left
midclavicular line
V5 placement: on the left anterior
axillary line, horizontal with the V4
electrode position
V6 placement: on the left midaxillary line, horizontal with the V4 electrode position
V3R to V6R placement: on the right side of the chest in positions corresponding to those on the left
VE placement: over the xiphoid process
V7 placement: on posterior chest at the left posterior axillary line in the fifth intercostal space
V7R placement: on posterior chest at the right posterior axillary line in the fifth intercostal space
VE
V1 V2
V3
V4 V5
V6
V7
V3R
V4R
2
3
4
Angle of
Lewis
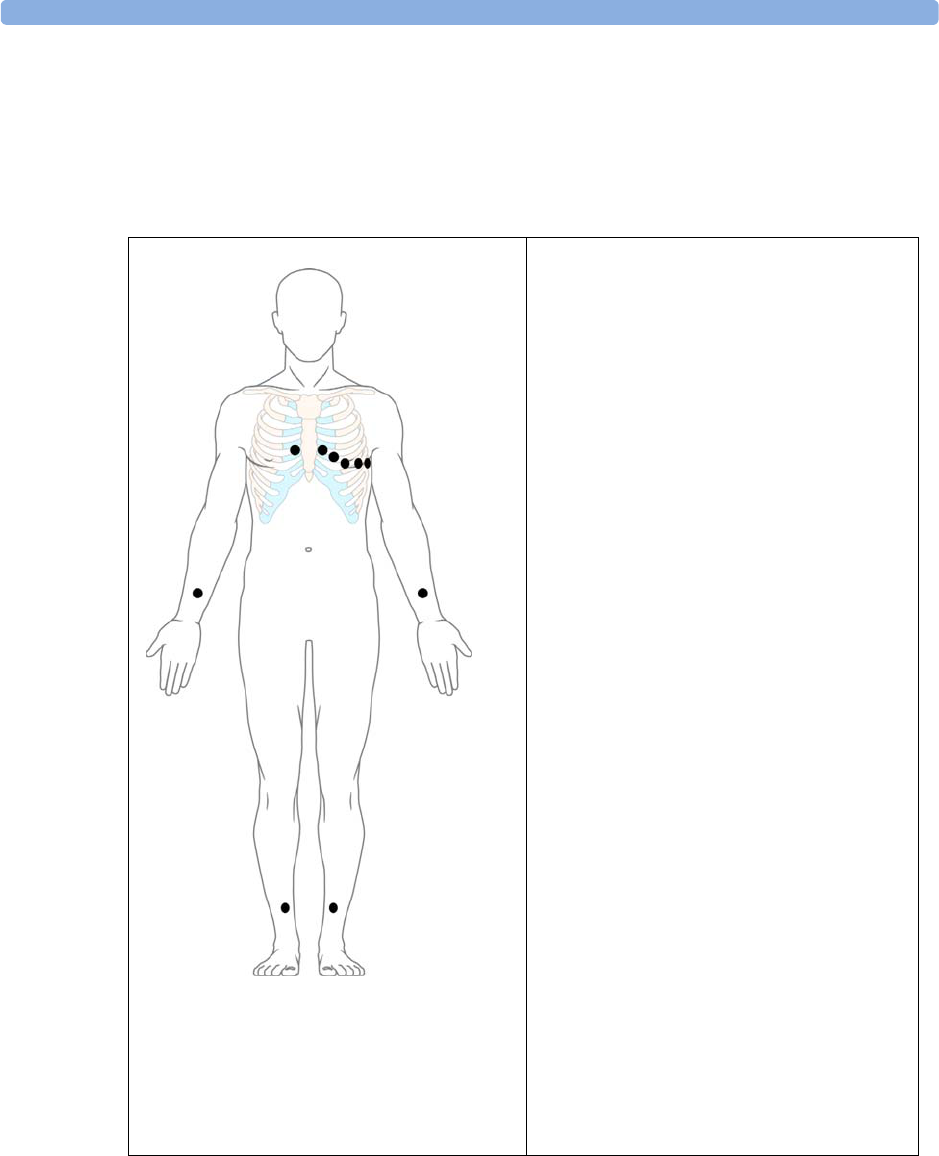
ECG Lead Placements 7 ECG, Arrhythmia, ST and QT Monitoring
99
10-Lead Placement
When monitoring 12-leads of ECG, using a 10-Electrode Lead Placement, it is important to correctly
place electrodes and to label all 12-lead ECG reports with the correct lead placement.
Conventional 12-Lead ECG
1 - V1 - V6
2 - LA
3 - LL
4 - RL
5 - RA
In conventional 12-Lead ECG using 10
electrodes, an electrode is placed on the right
arm, left arm, right leg, and left leg. Six V-
electrodes are placed on the chest. The right leg
electrode is the reference electrode.
Limb electrodes:
– Place arm electrodes on the inside of each
arm, between the wrist and the elbow.
– Place leg electrodes inside of each calf,
between the knee and the ankle.
Chest electrodes:
V1 - on the 4th intercostal space at the right
sternal border
V2 - on the 4th intercostal space at the left
sternal border
V3 - midway between the V2 and V4 electrode
positions
V4 - on the 5th intercostal space at the left
midclavicular line
V5 - on the left anterior axillary line, horizontal
with the V4 electrode position
V6 - on the left midaxillary line, horizontal with
the V4 electrode position
52
1
43
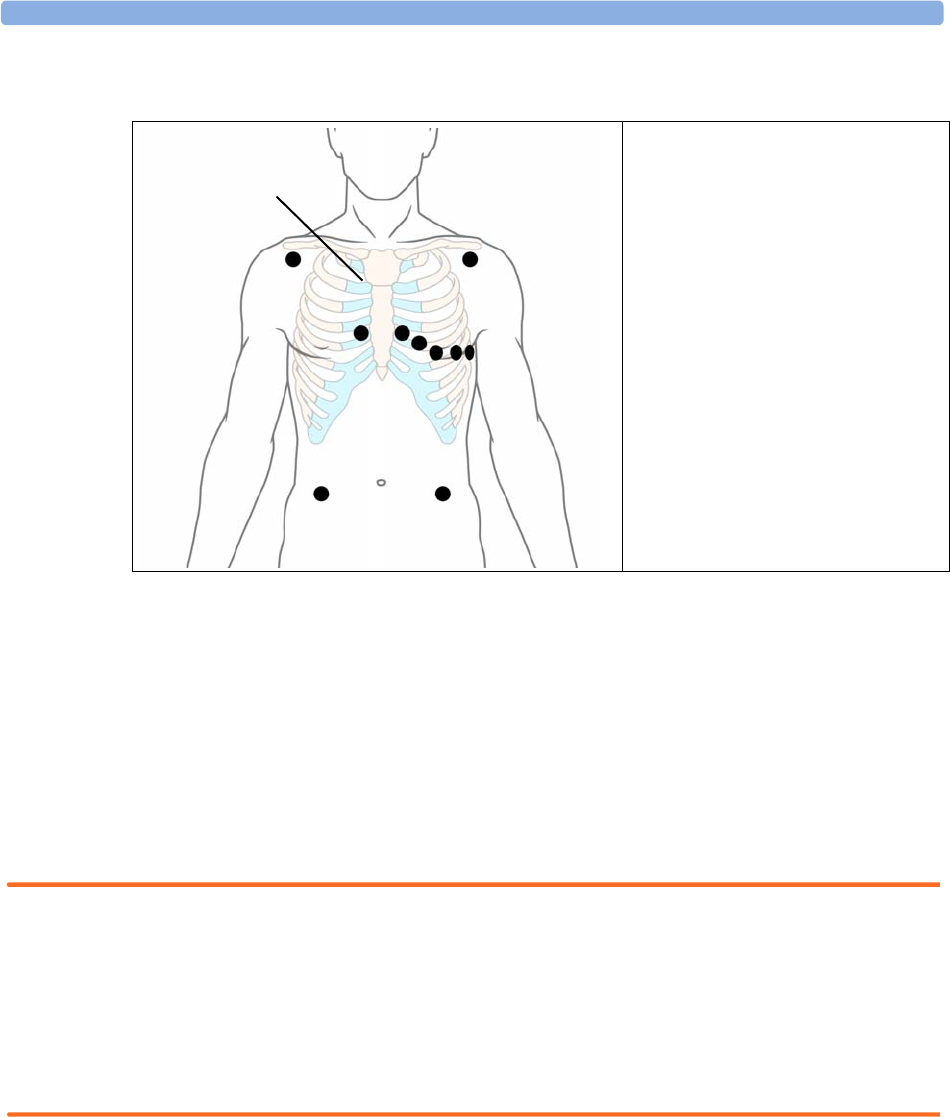
7 ECG, Arrhythmia, ST and QT Monitoring Capture 12-Lead
100
Modified 12-Lead ECG
Choosing Standard or Modified Electrode Placement
If your institution uses modified 10 Lead ECG electrode placement (the Mason-Likar Lead System),
you must switch ModLdPlcmt to On in the monitor. To do this,
♦in the Setup ECG menu, select ModLdPlcmt to toggle between On and Off.
–When ModLdPlcmt is set to On, 12 Lead ECG Reports will be labelled 12 Lead ECG
Report (Mason-Likar), and captured 12-lead ECGs will be labelled Mason-Likar to
the right of the bandwidth annotation at the Information Center.
–When ModLdPlcmt is set to Off, 12 Lead ECG Reports will be labelled 12 Lead ECG
Report, and captured 12-lead ECGs will not be annotated at the Information Center.
WARNING Do not use ECG analysis interpretation statements and measurements for 12-lead ECGs obtained
using the modified (Mason-Likar) limb electrode placement. This may lead to misdiagnosis since the
modified (Mason-Likar) limb electrode placement does not look the same as the conventional 12-lead
ECG and may mask inferior infarction due to calculated axis, R, P and T wave magnitudes shifts and
ST slope.
Do not export 12-lead ECGs obtained using the modified (Mason-Likar) limb electrode placement.
Captured 12-Lead ECGs using the modified (Mason-Likar) limb electrode placement exported from
the Information Center are not annotated with the Mason-Likar label.
Capture 12-Lead
If the monitor is connected to an Information Center via a wired network, the Capture 12-Lead
SmartKey may be configured. Selecting this exports 12-Lead ECG information to the Information
Center for analysis. For details see the Instructions for Use supplied with the Information Center.
1 - LA
2 - V1 - V6
3 - LL
4 - RL
5 - RA
6 - Angle of Lewis
If your institution uses modified 10
Lead ECG electrode placement (the
Mason-Likar Lead System), place the
four limb electrodes close to the
shoulders and lower abdomen.
The six V electrodes are placed on the
chest in the same position as the
conventional 12-lead placement.
1
3
5
4
6
2
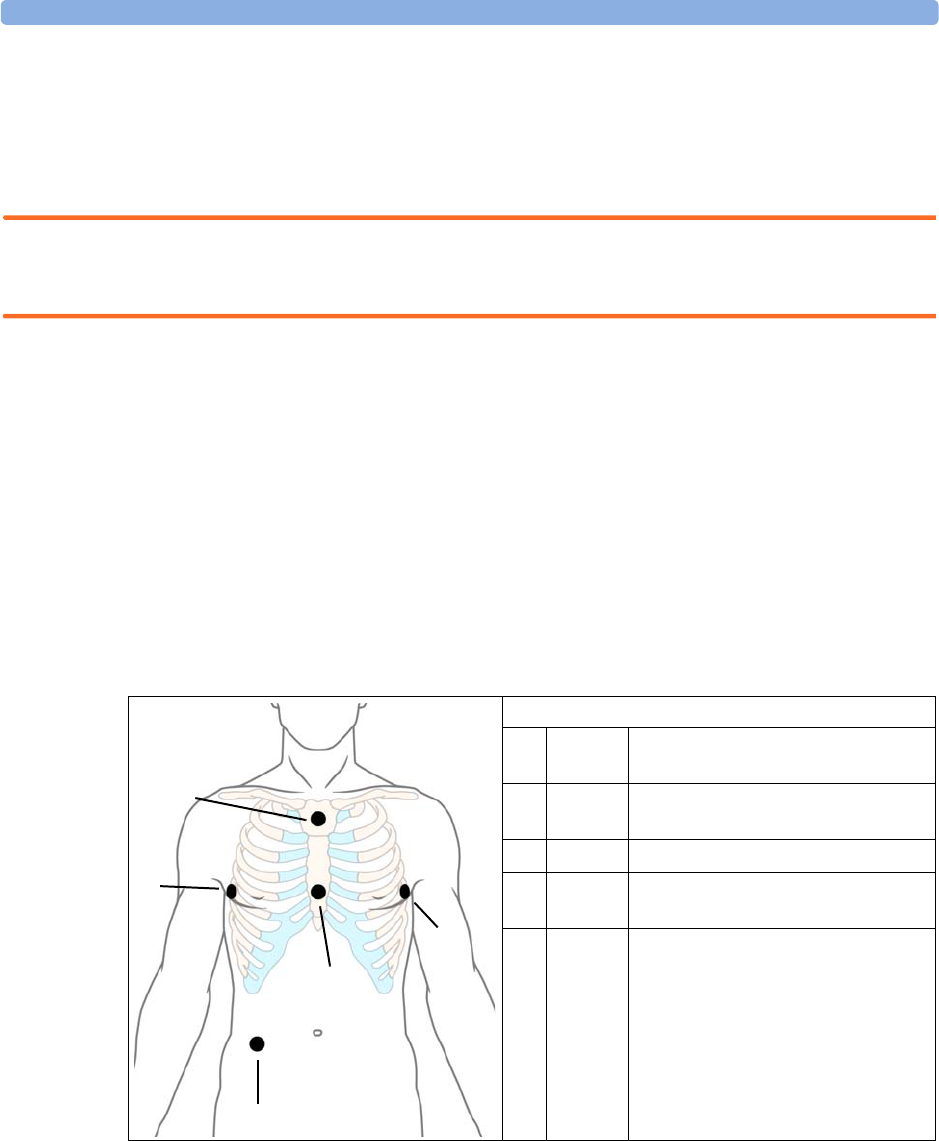
EASI ECG Lead Placement 7 ECG, Arrhythmia, ST and QT Monitoring
101
EASI ECG Lead Placement
Using a standard 5-electrode set in EASI lead placement you can monitor up to 12 standard ECG leads
simultaneously and continuously at the bedside. EASI provides a monitoring method for trending ST
segment changes that can provide an early indication of ischemia.
WARNING EASI-derived 12-lead ECGs and their measurements are approximations to conventional 12-lead
ECGs. As the 12-lead ECG derived with EASI is not exactly identical to the 12-lead conventional
ECG obtained from an electrocardiograph, it should not be used for diagnostic interpretations.
Respiratory monitoring is also possible with the EASI placement; respiration is measured between the I
and A electrodes.
Place the electrodes as accurately as possible to obtain the best quality EASI measurements.
When EASI lead placement is selected, EASI is shown beside the 1mV calibration bar on the ECG
wave on the display, and EASI is marked on any recorder strips and printouts.
When EASI lead placement is selected, EASI is shown beside the 1mV calibration bar on the ECG
wave on the display, and EASI is marked on any printouts.
EASI Monitoring During INOP Conditions If one of the derived EASI leads has an INOP
condition (for example, LEAD OFF), a flat line is displayed. After 10 seconds, the directly acquired
EASI AI, AS, or ES lead (depending on which is available) is displayed with the corresponding lead
label. This causes an arrhythmia relearn.
EASI Electrode Placement
1E (V) on the lower sternum at the level of
the fifth intercostal space
2A (LL) on the left midaxillary line at the
same level as the E electrode
3S (LA) on the upper sternum
4I (RA) on the right midaxillary line at the
same level as the E electrode
5Nreference electrode - can be anywhere,
usually below the sixth rib on the
right hip
1
2
3
4
5
7 ECG, Arrhythmia, ST and QT Monitoring ECG and Arrhythmia Alarm Overview
102
ECG and Arrhythmia Alarm Overview
The ECG and arrhythmia alarms available depend on which measurements are switched on, and the
arrhythmia option enabled for your monitor.
• Cardiotach alarms are available when HR is on and the active alarm source is ECG, but arrhythmia
is switched off
• Basic arrhythmia alarms are available when Arrhythmia is switched on
• Advanced arrhythmia alarms are available when Arrhythmia is switched on and the Advanced
Arrhythmia option has been enabled for your monitor
Cardiotach Alarms Additional Alarms with Basic
Arrhythmia Option
Additional Alarms with
Enhanced Arrhythmia
Option
***Asystole
***Ventricular Fibrillation/
Tachycardia
***Extreme Bradycardia
***Extreme Tachycardia
**High heart rate
**Low heart rate
***Ventricular Tachycardia
**Pacer Not Capture
**Pacer Not Pacing
**PVCs/min HIGH(PVC >
limit/min)
**Afib
**Supraventricular Tach
**Missed Beat
**Pause
**Irregular HR
**Ventricular Rhythm
**Run PVCs High
**Pair PVCs
**R-on-T PVCs
**Ventricular bigeminy
**Ventricular trigeminy
**Non-sustain VT
**Multiform PVCs
Using ECG Alarms 7 ECG, Arrhythmia, ST and QT Monitoring
103
Using ECG Alarms
ECG alarms can be switched on and off and the high and low alarm limits changed just like other
measurement alarms, as described in the Alarms section. Special alarm features which apply only to
ECG are described here.
Extreme Alarm Limits
The extreme rate alarms, Extreme Tachy and Extreme Brady, generated by the active alarm source,
either HR or Pulse, are set in Configuration Mode by adding a set value (the ' value) to the high and
low alarm limits.
You need to know which value has been configured for your monitor. Changing the high and low
alarm limits automatically changes the extreme alarm limits within the allowed range.
♦To see the extreme rate alarms set for your monitor, in the Setup ECG menu, see the menu items
'ExtrTachy and 'ExtrBrady.
ECG Alarms Off Disabled
Be aware that your hospital department may have decided to disable the setting ECG Alarms Off in
the monitor’s Configuration Mode. In this case, HR alarms cannot be switched off in Monitoring
Mode. If you try to switch off the HR alarms, you will see the message To activate enter
Config and enable Alarms Off.
HR Alarms When Arrhythmia Analysis is Switched Off
When arrhythmia analysis is switched off, only these HR-related alarms will be detected:
• the asystole alarm
• the ventricular fibrillation/tachycardia alarm
• the extreme tachycardia and extreme bradycardia alarms
• the high heart rate and low heart rate alarms.
Enhanced Asystole Detection
In order to improve alarming on asystole under certain conditions, you can set Asystole
Detect. in Configuration Mode to Enhanced. In enhanced mode an asystole alarm will be
suppressed for up to five seconds if a valid beat-to-beat Pulse is detected from a Pressure.
Extreme
Brady Limit Low
Limit
High
Limit
Extreme
Tachy Limit
' Extreme Brady ' Extreme Tachy
7 ECG, Arrhythmia, ST and QT Monitoring ECG Safety Information
104
ECG Safety Information
CAUTION Interference from instruments near the patient and ESU interference can cause problems with the
ECG wave. See the monitor specifications for more information.
WARNING Defibrillation and Electrosurgery: Do not touch the patient, or table, or instruments, during
defibrillation.
After defibrillation, the screen display recovers within 10 seconds if the correct electrodes are used and
applied in accordance with the manufacturers instructions.
ECG cables can be damaged when connected to a patient during defibrillation. Check cables for
functionality before using them again.
According to AAMI specifications the peak of the synchronized defibrillator discharge should be
delivered within 60 ms of the peak of the R wave. The signal at the ECG output on the IntelliVue
patient monitors is delayed by a maximum of 30 ms. Your biomedical engineer should verify that your
ECG/Defibrillator combination does not exceed the recommended maximum delay of 60 ms.
When using electrosurgical (ES) equipment, never place ECG electrodes near to the grounding plate of
the ES device, as this can cause a lot of interference on the ECG signal.
General: When you are connecting the electrodes or the patient cable, make sure that the connectors
never come into contact with other conductive parts, or with earth. In particular, make sure that all of
the ECG electrodes are attached to the patient, to prevent them from contacting conductive parts or
earth.
During surgery: Use the appropriate orange electrode ECG safety cable, or lead cable with an orange
connector, for measuring ECG in the operating room. These cables have extra circuitry to protect the
patient from burns during cautery, and they decrease electrical interference. This also reduces the
hazard of burns in case of a defective neutral electrode at the HF device. These cables cannot be used
for measuring respiration.
Pacemaker failure: During complete heart block or pacemaker failure to pace/capture, tall P-waves
(greater than 1/5 of the average R-wave height) may be erroneously counted by the monitor, resulting
in missed detection of cardiac arrest.
Patients exhibiting intrinsic rhythm: When monitoring paced patients who exhibit only intrinsic
rhythm, the monitor may erroneously count pace pulses as QRS complexes when the algorithm first
encounters them, resulting in missed detection of cardiac arrest.
The risk of missing cardiac arrest may be reduced by monitoring these patients with low heart rate limit
at or slightly above the basic/demand pacemaker rate. A low heart rate alarm alerts you when the
patient’s heart rate drops to a level where pacing is needed. Proper detection and classification of the
paced rhythm can then be determined.
Filtered ECG signal from external instruments: Instruments such as defibrillators or telemetry units
produce a filtered ECG signal. When this signal is used as an input to the bedside monitor, it is filtered
again. If this twice-filtered signal is passed to the arrhythmia algorithm, it may cause the algorithm to
fail to detect pace pulses, pacemaker non-capture, or asystole, thus compromising paced patient
monitoring performance.

About Arrhythmia Monitoring 7 ECG, Arrhythmia, ST and QT Monitoring
105
External pacing electrodes: When a pacemaker with external pacing electrodes is being used on a
patient, arrhythmia monitoring is severely compromised due to the high energy level in the pacer pulse.
This may result in the arrhythmia algorithm’s failure to detect pacemaker noncapture or asystole.
Fusion beat pacemakers: Pacemakers that create fusion beats (pace pulse on top of the QRS complex)
cannot be detected by the monitor’s QRS detector.
Rate adaptive pacemakers: Implanted pacemakers which can adapt to the Minute Ventilation rate
may occasionally react on the Impedance measurement used by patient monitors for the determination
of the Resp value and execute pacing with the maximum programmed rate. Switching off the Resp
measurement can prevent this.
About Arrhythmia Monitoring
Arrhythmia analysis provides information on your patient’s condition, including heart rate, PVC rate,
rhythm, and ectopics. The monitor uses the user-selected primary and secondary ECG leads for single-
lead or multi-lead arrhythmia analysis. During arrhythmia analysis, the monitor continuously
• optimizes ECG signal quality. This is important for arrhythmia analysis. The monitor continuously
filters the ECG signal to remove baseline wander, muscle artifact, and signal irregularities. Also, if
the Patient Paced status is set to Yes, pace pulses are filtered out to avoid processing them as QRS
beats.
• detects beats, for example, QRS complexes, identifying them for further analysis.
• measures signal features such as R-wave height, width, and timing.
• creates beat templates, and classifies and labels beats to aid in rhythm analysis and alarm detection.
• examines the ECG signal for ventricular fibrillation, asystole, and noise.
Arrhythmia Options
Your monitor has either the basic or the enhanced arrhythmia option. Both options provide rhythm
and ectopic status messages and beat labelling. The number of rhythms being classified, events being
detected, and alarms generated differs according to the option. The alarms available with the different
options are listed in the section “ECG and Arrhythmia Alarm Overview” on page 102, the rhythm and
ectopic messages detected are listed in “Arrhythmia Status Messages” on page 109.
Where Can I Find More Information?
See the Application Notes on ST and Arrhythmia supplied on your documentation DVD for detailed
information on the arrhythmia algorithm and its clinical application.

7 ECG, Arrhythmia, ST and QT Monitoring Switching Arrhythmia Analysis On and Off
106
Switching Arrhythmia Analysis On and Off
1In the Setup Arrhy menu, select Arrhythmia to toggle between On and Off.
2Select the Confirm pop-up key which appears at the bottom of the screen.
Be aware that when arrhythmia analysis is switched off,
–the message Arrhythmia Off appears beside the ECG wave, if configured to do so
– only the HR-related alarms are detected (the asystole alarm, the ventricular fibrillation/
tachycardia alarm, the extreme tachycardia and extreme bradycardia alarms, the high heart rate
and low heart rate alarms)
– HR High and HR Low alarms behave like normal yellow alarms, no timeout periods are active.
Choosing an ECG Lead for Arrhythmia Monitoring
It is important to select a suitable lead for arrhythmia monitoring.
Guidelines for non-paced patients are:
– QRS complex should be tall and narrow (recommended amplitude > 0.5 mV)
– R-Wave should be above or below the baseline (but not bi-phasic)
– T-wave should be smaller than 1/3 R-wave height
– the P-wave should be smaller than 1/5 R-wave height.
For paced patients, in addition to the above, the pace pulse should be:
– not wider than the normal QRS
– the QRS complexes should be at least twice the height of pace pulses
– large enough to be detected, with no re-polarization.
To prevent detection of P-waves or baseline noises as QRS complexes, the minimum detection level for
QRS complexes is set at 0.15 mV, according to AAMI-EC 13 specifications. Adjusting the ECG wave
size on the monitor display (gain adjustment) does not affect the ECG signal which is used for
arrhythmia analysis. If the ECG signal is too small, you may get false alarms for pause or asystole.
Aberrantly-Conducted Beats
As P-waves are not analyzed, it is difficult and sometimes impossible for the monitor to distinguish
between an aberrantly-conducted supraventricular beat and a ventricular beat. If the aberrant beat
resembles a ventricular beat, it is classified as ventricular. You should always select a lead where the
aberrantly-conducted beats have an R-wave that is as narrow as possible to minimize incorrect calls.
Ventricular beats should look different from these ‘normal beats’. Instead of trying to select two leads
with a narrow R-wave, it may be easier to just select one lead and use single lead arrhythmia
monitoring. Extra vigilance is required by the clinician for this type of patient.
Atrial Fibrillation Alarm
The monitor performs atrial fibrillation analysis using information about the RR irregularity, PR
interval variability and P wave variability.
In order to generate an Afib alarm the following criteria must be detected for 1 minute:
• normal beat RR intervals must be irregular

Understanding the Arrhythmia Display 7 ECG, Arrhythmia, ST and QT Monitoring
107
• PR interval deviation must be large
• P-wave region must not match well
Atrial fibrillation analysis is only available for adult patients and atrial fibrillation detection cannot be
performed on PVCs or Paced beats.
Since most atrial flutters have regular RR intervals, they cannot be detected by the atrial fibrillation
algorithm.
An Afib alarm can be falsely detected in the presence of:
• sinus arrhythmia,
• muscle noise, or
• electrode motion artifact.
If you also have monitors with earlier software revisions, the Afib alarm will not be generated after a
transfer to one of these monitors. Always leave the Irregular HR alarm switched on, so that this alarm
can be generated in such situations.
See the Application Note on Arrhythmia/ST supplied on your documentation DVD for detailed
information on the arrhythmia algorithm and ECG analysis.
Intermittent Bundle Branch Block
Bundle branch and the other fascicular blocks create a challenge for the arrhythmia algorithm. If the
QRS during the block changes considerably from the learned normal, the blocked beat may be
incorrectly classified as ventricular, causing false PVC alarms. You should always select a lead where the
bundle branch block beats have an R-wave that is as narrow as possible to minimize incorrect calls.
Ventricular beats should look different from these ‘normal beats’. Instead of trying to select two leads
with a narrow R-wave, it may be easier to just select one lead and use single lead arrhythmia
monitoring. Extra vigilance is required by the clinician for this type of patient.
Understanding the Arrhythmia Display
Your monitor screen may look slightly different from the illustration.
PP P
Delayed
1mV
II
M
45
7
13
Pair PVCs
6
Paced Rhythm
75
HR
2
PVC
2
1 Beat label
2 Pace pulse marks
3 Rhythm status message

7 ECG, Arrhythmia, ST and QT Monitoring Understanding the Arrhythmia Display
108
Viewing Arrhythmia Waves
♦To review arrhythmia beat labels, in the Setup Arrhy menu, select Annotate Arrhy.
The wave showing the primary ECG lead will be delayed by six seconds and shown on a grey
background. Beat labels will be annotated above the ECG wave and Delayed will be written
beside it.
♦To return to the normal ECG primary lead display, select Annotate Arrhy again.
Arrhythmia Beat Labels
Arrhythmia beat labels tell you how the monitor is classifying beats.
N = Normal
V = Ventricular Ectopic
S = Supra-ventricular Premature
P = Paced
' = Pacer spike
“ = Biventricular Pacer Spike
L = Learning patient's ECG
A = Artifact (noisy episode)
? = Insufficient information to classify beats
I = Inoperative condition (e.g., LEADS OFF)
M = Pause or missed beat
4PVC Numeric
5HR Numeric
6 Ectopic status message
7 Delayed arrhythmia wave
Understanding the Arrhythmia Display 7 ECG, Arrhythmia, ST and QT Monitoring
109
Arrhythmia Status Messages
The monitor displays two types of status messages:
• Rhythm Status Messages -- to indicate the patient’s rhythm.
• Ectopic Status Messages -- to indicate the presence of ectopic beats.
These status messages are shown on the right hand side of the primary ECG wave. They are updated
every second, with the exception of the Sinus and Supraventricular (SV) rhythm messages.
The Sinus and SV rhythm messages are updated based on the current heart rate, taking into account
the patient category (adult, pediatric, or neonatal). For the message to change from one rhythm status
to another, the HR must be in the new range for five beats.
If you have basic arrhythmia capability, you will get only messages for the alarms provided with this
level.
Rhythm Status Messages
The label B or E indicates basic (B) or enhanced (E) arrhythmia capability.
Rhythm Status Message Description B or E
ASYSTOLE No QRS for 4 consecutive seconds in absence of vent fib or chaotic
signal
B, E
VENT FIB/TACH A fibrillatory wave for 4 consecutive seconds B, E
V-TACH A dominant rhythm of adjacent Vs and a HR > the V-Tach Heart
Rate Limit
B, E
SUSTAINED V-TACH Ventricular tachycardia rhythm for more than 15 seconds E
VENT RHYTHM A dominant rhythm of adjacent PVCs and a HR dthe V-Tach HR
Limit
E
VENT BIGEMINY A dominant rhythm of N, V, N, V E
VENT TRIGEMINY A dominant rhythm of N, N, V, N, N, V E
PACED RHYTHM A dominant rhythm of paced beats B, E
IRREGULAR HR Consistently irregular rhythm E
SINUS BRADY
SINUS RHYTHM
SINUS TACHY
A dominant rhythm of SV beats preceded by P-waves B, E
SV BRADY
SV RHYTHM
SV TACHY
A dominant rhythm of SV beats not preceded by P-waves B, E
UNKNOWN ECG RHYTHM Rhythm cannot be determined B, E
LEARNING ECG Algorithm is learning the ECG beat morphology B, E
LEARNING RHYTHM Algorithm is learning the rhythm of the classified beats B, E
CANNOT ANALYZE ECG ECG signal is predominantly invalid and therefore cannot be
analyzed
B, E
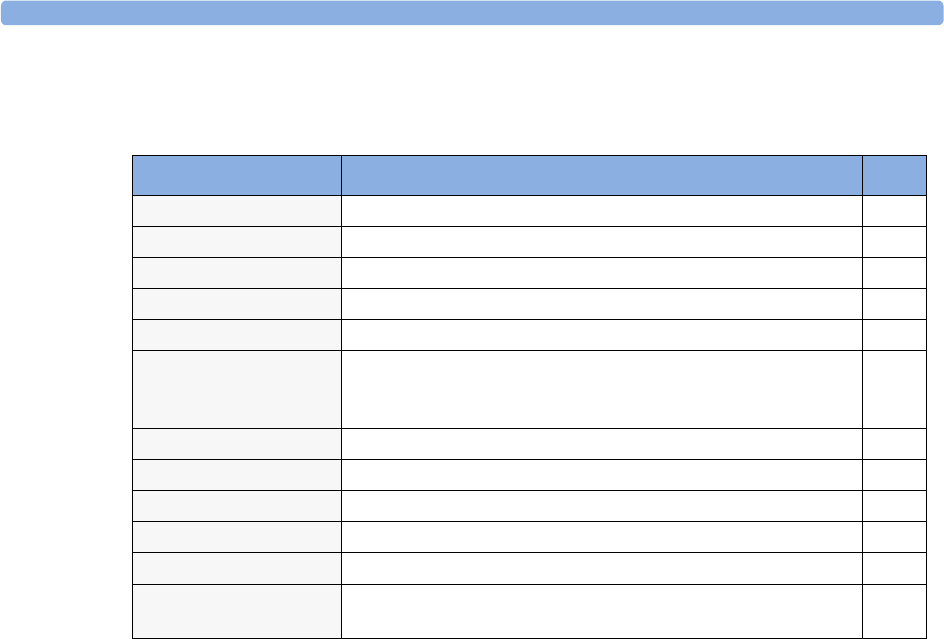
7 ECG, Arrhythmia, ST and QT Monitoring Arrhythmia Relearning
110
Ectopic Status Messages
The label B or E indicates basic (B) or enhanced (E) arrhythmia capability.
Arrhythmia Relearning
During a learning phase:
• Alarm timeout periods are cleared
• Stored arrhythmia templates are cleared
•Asystole, Vfib, and HR alarms (when there are enough beats to compute the HR) are active. No other
alarms are active.
Initiating Arrhythmia Relearning Manually
1To initiate relearning manually, in the Setup Arrhy menu, select Relearn Arrhy.
– While the monitor is learning, the delayed arrhythmia wave displays the beat label L and the
rhythm status message Learning ECG.
– Next, the monitor determines the dominant rhythm. The beats are labeled N, and the rhythm
status message changes to Learning Rhythm.
2After relearning is complete, you should check the delayed arrhythmia wave to ensure that the
algorithm is labeling the beats correctly.
3If beats are still not classified correctly, check that the ECG is optimized for arrhythmia
monitoring. You may need to select a different lead or change the electrodes or electrode positions
if there is excessive noise, unstable voltage, low amplitude, or large P- or T-waves.
Ectopic Status Message Explanation B or E
(No message displayed) No ectopic activity within the last minute
RUN PVCs More than 2 consecutive PVCs within the last minute E
PAIR PVCs Pair PVCs within the last minute E
PACER NOT CAPT Pause with pace pulse (paced patient only) within the last minute B, E
PACER NT PACING Pause without pace pulse (paced patient only) within the last minute B, E
PAUSE No beat detected for 1.75 x average R-R interval for HR <120, or
No beat for 1 second with HR >120 (non-paced patient only), or
No beat detected for more than the set pause threshold.
E
R-ON-T PVCs R-ON-T detected within the last minute E
MULTIFORM PVCs Multiform PVCs detected within the last minute E
FREQUENT SVPBs SVPB count within last minute is greater than 5 E
SVPBs 1-5 SVPBs in the last minute with a sinus rhythm and no Vs E
SV BEATS SV count within last minute and rhythm status is PACED B, E
PACED BEATS Paced beat count within last minute and rhythm status is NOT
PACED
B, E
Arrhythmia Alarms 7 ECG, Arrhythmia, ST and QT Monitoring
111
Automatic Arrhythmia Relearn
Arrhythmia relearning is initiated automatically whenever:
• ECG monitoring is switched on
• The ECG Lead or Lead Label of the primary/secondary lead is changed manually, or when fallback
occurs
•A Leads Off INOP condition (that has been active for > 60 seconds) ends.
If you are monitoring multi-lead arrhythmia and there is a change in one lead only, relearning happens
only in the affected lead. During this learning phase, the system will continue monitoring using the
other lead. Therefore, the delayed arrhythmia wave is not labeled L and there is no Learning ECG
rhythm status message. In addition, alarm timeout periods are maintained, stored arrhythmia
templates are maintained for the operative lead, and all alarms switched on are active.
Arrhythmia Relearn and Lead Fallback
Lead fallback triggers an automatic arrhythmia relearn.
WARNING If arrhythmia learning takes place during ventricular rhythm, the ectopics may be incorrectly learned as
the normal QRS complex. This may result in missed detection of subsequent events of V-Tach and V-
Fib.
For this reason you should:
• take care to initiate arrhythmia relearning only during periods of predominantly normal rhythm and
when the ECG signal is relatively noise-free
• be aware that arrhythmia relearning can happen automatically
• respond to any INOP messages (for example, if you are prompted to reconnect electrodes)
• be aware that a disconnected EASI electrode triggers an arrhythmia relearn on all leads
• always ensure that the arrhythmia algorithm is labeling beats correctly.
Arrhythmia Alarms
Arrhythmia alarms can be switched on and off and the alarm settings changed just like other
measurement alarms, as described in the Alarms section. Special alarm features which apply only to
arrhythmia are described here.
The different alarms detected and generated by the monitor depend on the level of arrhythmia analysis
that is enabled. For a complete list of arrhythmia alarms and INOPs, see the Alarms chapter.
The monitor detects arrhythmia alarm conditions by comparing ECG data to a set of pre-defined
criteria. An alarm can be triggered by a rate exceeding a threshold (for example, HR >xx), an abnormal
rhythm (for example, Ventricular Bigeminy), or an ectopic event (for example, Pair PVCs).
7 ECG, Arrhythmia, ST and QT Monitoring Arrhythmia Alarms
112
Yellow Arrhythmia Alarms
Yellow arrhythmia alarms are short yellow alarms specific to arrhythmia-related patient conditions.
Depending on your monitor and Information Center configuration, they may be shown with one or
two stars. The heart rate alarms (High HR and Low HR) can be configured as short yellow or standard
yellow alarms. When they are standard yellow alarms they exist independently of the other arrhythmia
alarms and no timeout periods apply.
WARNING When arrhythmia analysis is on, all yellow ECG and arrhythmia alarms are short yellow alarms (one-
star). This means that the yellow alarm lamp and the tones are active for six seconds only, after which
the blinking numeric and the alarm message remain for up to three minutes. The only exception to this
are the HR High and Low alarms which can be configured as standard yellow alarms. Red alarms
behave as usual.
Arrhythmia Alarms and Latching
When using arrhythmia analysis, Visual Latching and Audible Latching should be on
for red alarms, or at least Visual Latching should be on. Because of the transient nature of
arrhythmia alarms, many arrhythmia conditions may go unnoticed if alarm latching is off. This setting
can only be changed in Configuration Mode.
Switching Individual Arrhythmia Alarms On and Off
Some arrhythmia alarms can be individually switched on or off. They are:
Pacer not capture, Pacer not pace, Non-Sustain VT, Vent Rhythm, Run PVCs, Pair PVCs, R-on-T
PVCs, V.Bigeminy, V.Trigeminy, Multif.PVCs, Pause, SVT, Irregular HR, Missed Beat, PVCs/min
and Afib.
♦To switch individual alarms on or off, in the Setup Arrhythmia menu, select the alarm from
the list to toggle between On and Off. The monitor displays the INOP message SOME ECG
ALRMS OFF, if configured, when more alarms are switched off than configured in your active
profile.
Switching All Yellow Arrhythmia Alarms On or Off
All yellow arrhythmia alarms can be switched on and off together. To do this,
♦In the Setup Arrhythmia menu, select All Yellow Off or All Yellow On.
Adjusting the Arrhythmia Alarm Limits
Some arrhythmia alarms have limits which can be individually adjusted. They are:
Vtach HR, Vtach Run, PVCs/min, Vent Rhythm, SVT HR, SVT Run, Asystole Thresh., Pause
Threshold.
1To adjust alarm limits, in the Setup Arrhythmia menu, select the alarm to be adjusted.
2Select the appropriate setting from the pop-up list.
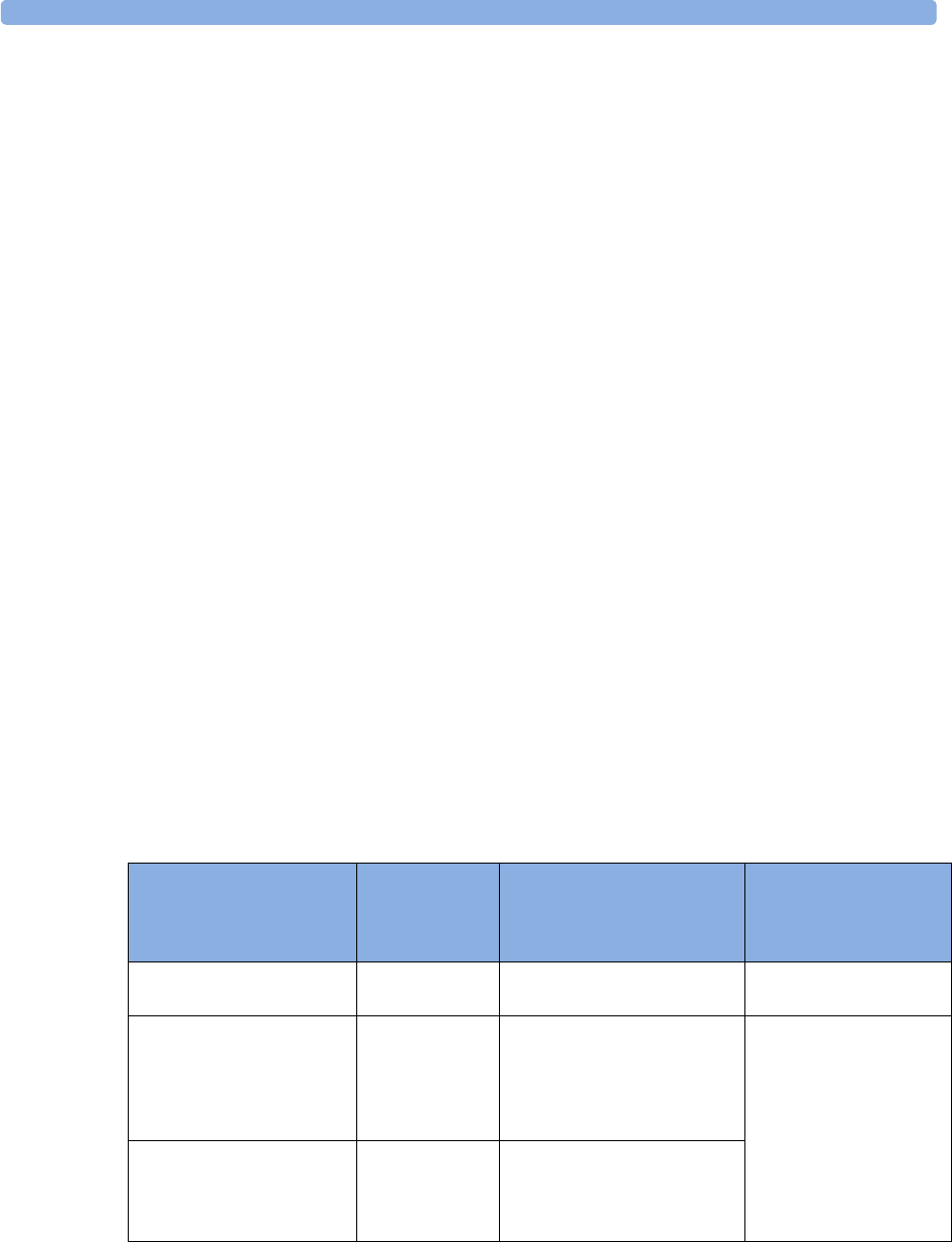
Arrhythmia Alarms 7 ECG, Arrhythmia, ST and QT Monitoring
113
Arrhythmia Alarm Timeout Periods
Normally, an arrhythmia alarm is announced when an alarm condition is detected. However, there are
certain situations that can inhibit the audible and visible indications of the alarm even though the
alarm condition was detected. These include:
• if a more serious alarm condition is active in the same chain
• if a timeout period is in effect for a particular alarm
• if a timeout period is in effect for a higher alarm in that chain.
See “Arrhythmia Alarm Chaining” on page 114 for more details on alarm chains.
What is a Timeout Period?
Timeout periods are automatically started when a yellow arrhythmia alarm is detected. During this
period, the same alarm condition will not generate another alarm. Alarm conditions further down the
same arrhythmia alarm chain will also not generate an alarm, but alarms further up the chain will: see
“Arrhythmia Alarm Chaining” on page 114).
This setting can only be changed in Configuration Mode.
♦To view the timeout period configured for your monitor, in the Setup Arrhythmia menu,
see the menu items TimeOut 1st and TimeOut 2nd.
Resetting the Timeout Period
♦To reset the timeout period, press the Alarms key and then reselect it.
How are Yellow Arrhythmia Alarms Indicated?
When a yellow arrhythmia alarm is generated, it triggers visual and audible indicators. Yellow
arrhythmia alarms are always set to latch visually for three minutes except HR High/Low alarms, if
configured to standard yellow. Depending on the alarm condition, audible and visual alarm indicators
will appear as follows:
Alarm Condition Example Audible Indicators
Short yellow alarm tone
sounds ...
Visual Indicators
Alarm message
displayed ...
Single alarm instance Non-sustained
V-tach
when alarm condition is
initially detected
for 3 minutes (latching
time)
Continuous alarm condition PVCs/min
HIGH
when alarm condition is
initially detected and - as an
alarm reminder - every time
the configured time out
period has expired
until the alarm condition
stops, plus a maximum of
three minutes latching
time
Same intermittent alarm
condition
Pair of PVCs each time the alarm condition
is detected, provided that the
configured timeout period has
expired

7 ECG, Arrhythmia, ST and QT Monitoring Arrhythmia Alarms
114
If you silence a yellow arrhythmia alarm and the alarm condition still exists, the visual indicators
continue until the condition stops. You will get an alarm reminder every time the configured timeout
period has expired.
If you silence a yellow arrhythmia alarm and the alarm condition has stopped, the visual indicators
are immediately cleared. Silencing an alarm does not reset its time out period, so you will not get a
realarm for the same condition or lower on the chain until the timeout expires.
Arrhythmia Alarm Chaining
When arrhythmia analysis is switched on, multiple alarm conditions may be present. Announcing all of
the detected alarm conditions would be confusing, and might hide a more serious condition. For this
reason, arrhythmia alarms are prioritized in three alarm “chains”: PVC Alarms; Beat Detection Alarms,
and Rate Alarms.
Only the highest priority alarm condition in each chain is announced. Lower priority alarms in the
same chain will not be announced while an alarm is active or during the configured timeout period. If
alarm conditions of equal severity from different chains are detected, the alarm condition that occurred
most recently is announced. The exception is Irregular HR, which only occurs if no other alarms are
occurring.
See “ECG and Arrhythmia Alarm Overview” on page 102 for information on which alarms are
included in the different arrhythmia options. See “Arrhythmia Alarm Timeout Periods” on page 113
for an explanation of how alarm timeouts work.
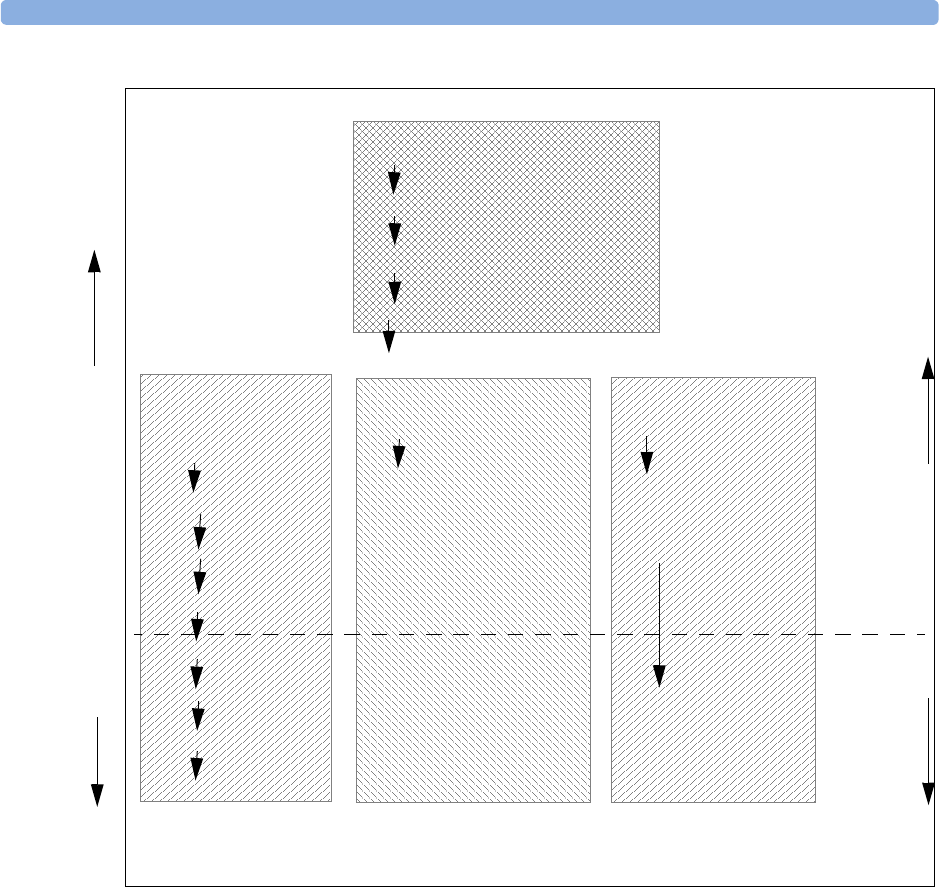
Arrhythmia Alarms 7 ECG, Arrhythmia, ST and QT Monitoring
115
– If there is an active Vent Bigeminy alarm, a PVCs > xx/min will not be triggered because it is
lower on the same chain. However, a high HR alarm will become active because it is on a
different chain.
– Higher priority alarms supersede previous alarms. For example, if a Vent Trigeminy alarm is active
and a Pair PVCs occurs, the Pair alarm will be activated.
Understanding PVC-Related Alarms
PVC-related alarms are detected on the basis of the current ventricular heart rate and the number of
consecutive PVCs counted (referred to as PVC Runs).
Example: This diagram illustrates the conditions under which PVC alarms would be generated if the
Vent Rhythm Run limit is set to 12, the V-Tach Run Limit is set to eight, and the V-Tach HR Limit
is set to 100.
Red Arrhythmia Alarms
Asystole
Vent Fib/Tach
V-Tach
Extreme Tachy/Extreme Brady
Yellow Arrhythmia Alarms
PVC Alarms Chain Beat Detection Alarms Chain Rate Alarms Chain
Pacer Not Captured/
Pacer Not Pacing/
Missed Beat
HR High/ HR Low*
PVCs > xx/min
Non-sustain VT/
Vent Rhythm
Run PVCs
R-on-T PVCs
Pause SVT
Multiform PVCs
Vent Bigeminy
Vent Trigeminy Irregular HR
(occurs only if no other
arrhythmia alarms are
present)
First level
timeout
period
(TimeOut
1st)
Second
level
timeout
period
(TimeOut
2nd)
Pair PVCs
lower priority higher priority
AFib
*If HR High/Low alarms are configured as standard yellow alarms,
they are independent of the arrhythmia alarms and are not in the Rate
alarms chain.
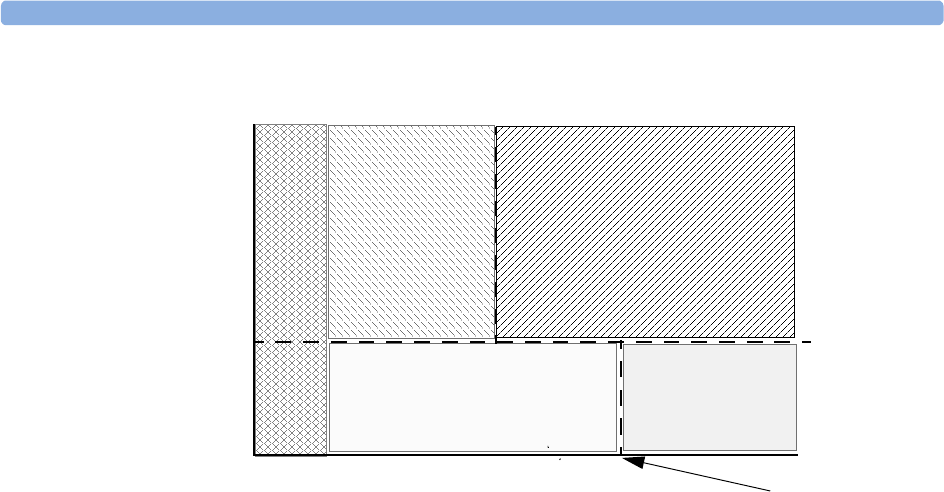
7 ECG, Arrhythmia, ST and QT Monitoring Arrhythmia Alarms
116
You will see that
• if both the V-Tach Heart Rate Limit and the V-Tach Run Limit are exceeded, a red V-Tach alarm is
generated
• if the ventricular heart rate exceeds the V-Tach Heart Rate Limit but not the V-Tach Run Limit, a
yellow Non-Sustain VT alarm is generated.
Ventricular Heart Rate
Number of Consecutive PVCs (PVC Run)
**Pair
PVCs
PVC =
2
** Non-Sustain VT
PVC Run < 8
HR > 100
***V-Tach
PVC Run t8
HR > 100
** Run PVCs
PVC Run > 2butd12
HR d 100
** Vent Rhythm
PVC Run > 12
HR d 100
V-Tach Heart
Rate Limit
V-Tach Run Limit
Ventricular Rhythm
Run Limit
1 2 3 4 5 6 7 8 9 10 11 12 14 15
100

About ST Monitoring 7 ECG, Arrhythmia, ST and QT Monitoring
117
About ST Monitoring
The monitor performs ST segment analysis on normal and atrially paced beats and calculates ST
segment elevations and depressions. This information can be displayed in the form of ST numerics and
snippets on the monitor.
All available leads can be monitored continuously. The ECG waveform does not need to be displayed
on the monitor for ST Segment analysis.
ST analysis is always performed using a dedicated filter which ensures diagnostic quality. If you are
monitoring ECG using an ECG filter mode other than Diagnostic, the ST segment of the ECG wave
may look different from the ST segment of the ST snippet for the same wave. For diagnostic evaluation
of the ST segment, always switch to Diagnostic filter mode or use the ST snippet.
WARNING Some clinical conditions may make it difficult to achieve reliable ST monitoring, for example:
• if you are unable to get a lead that is not noisy
• if arrhythmias such as atrial fib/flutter are present, which may cause an irregular baseline
• if the patient is continuously ventricularly paced
• if the patient has left bundle branch block.
You should consider switching ST monitoring off if these conditions are present.
This monitor provides ST level change information; the clinical significance of the ST level change
information should be determined by a physician.
ST segment monitoring is intended for use with adult patients only and is not clinically validated for
use with neonatal and pediatric patients. For this reason, the recommended - and default - setting for
ST monitoring in neonatal and pediatric modes is ST Analysis: Off.
Switching ST On and Off
♦To switch all ST monitoring on or off, in the Setup ST Analysis menu, select ST
Analysis to toggle between On and Off.
Selecting Leads for ST Analysis
You select which leads to use for ST analysis in the Setup ST Analysis menu.
To see the current list of leads selected for ST analysis:
1Enter the Setup ST Analysis menu.
2Select Setup ST Leads. This opens the Setup ST Leads pop-up window. Leads chosen
for ST monitoring are listed here. There are two pop-up keys at the bottom of the screen:
If all leads are already selected, the Add pop-up key is disabled.
To choose a lead for ST monitoring:
1Select the Add key at the bottom of the Setup ST Leads window. This opens the Choices
pop-up window.
Add Delete
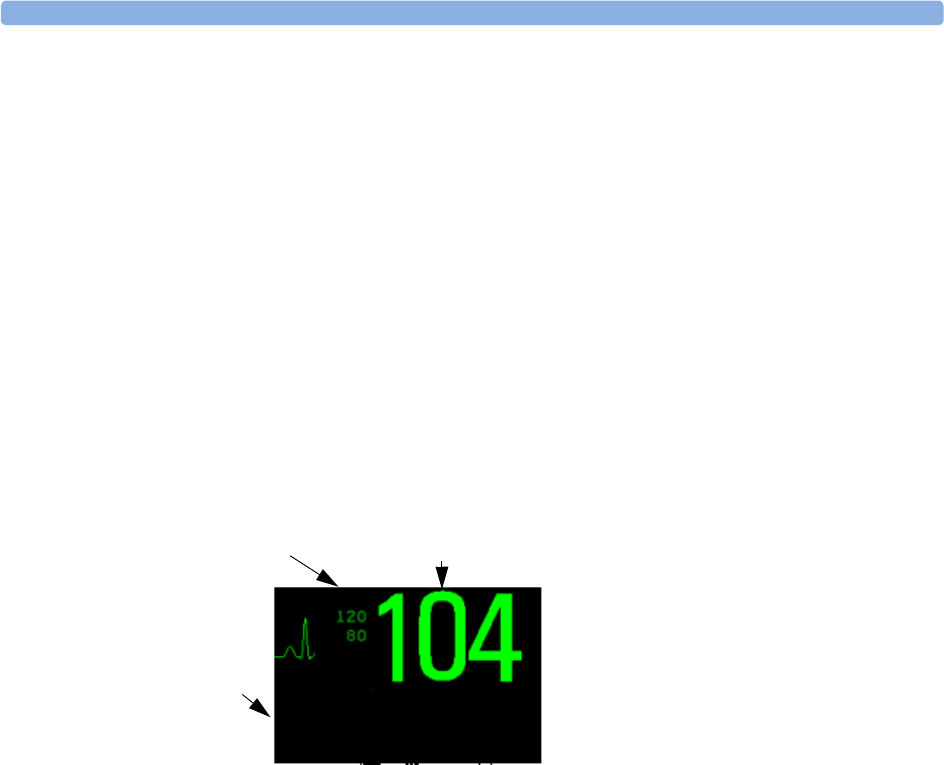
7 ECG, Arrhythmia, ST and QT Monitoring Understanding the ST Display and Windows
118
2Choose a lead from the list for ST monitoring. This closes the Choices window and adds the
selected lead to the list of chosen leads.
To disable ST monitoring for a lead:
1Choose a lead from the list in the Setup ST Leads window.
2Select the Delete key. This removes this lead from the list.
NOTE The order in which ST leads are listed in the Setup ST Leads menu determines the order in which ST
leads are displayed on the monitor screen.
To change the order in which ST leads are displayed,
1In the Setup ST Leads menu, choose a lead from the list.
2Select the Sort Up or Sort Down key to move the lead up or down in the list.
Understanding the ST Display and Windows
Your monitor screen may be configured to look slightly different from the illustrations.
ST Numerics Up to 12 ST numerics plus the ST index can be displayed on the monitor screen. They
can be configured to show beside the measurement numerics, beside the ECG wave, or beside the ST
snippet.
A positive ST value indicates ST segment elevation; a negative value indicates depression.
ST numerics are displayed in the order in which you select ST leads for analysis. If there is additional
space in the field assigned to ST numerics, the monitor will display extra numerics in the order in
which they appear in the Setup ST Analysis -> Setup ST Leads list. Any ST leads
switched on for analysis that do not fit in the assigned numerics field are shown in succession in place
of the last ST numeric.
ST Index The ST index numeric (STindx) is the sum of the absolute values for the ST leads V2, V5,
aVF. Because it is based on absolute values, it is always a positive number. If you haven’t selected one of
the leads V2, V5, and aVF for ST analysis, the STindx numeric will display a question mark “?”.
♦To switch the ST index numeric on or off for display, in the Setup ST Analysis menu,
select ST-Index to toggle between On and Off.
1ST numerics
2 Current HR alarm limits
3 Current heart rate
ST-II 1.2
ST-V 2.5
ST-aVR -3.0
3
1
2
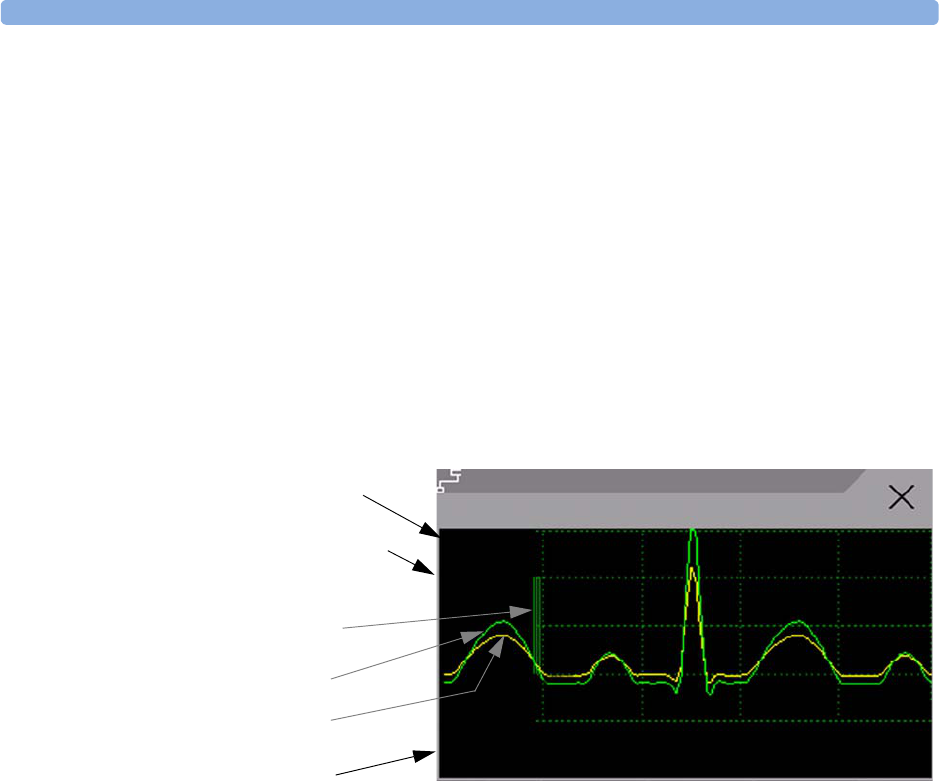
Updating ST Baseline Snippets 7 ECG, Arrhythmia, ST and QT Monitoring
119
ST Snippets ST snippets show a one second wave segment for each measured ST lead. The most
recent snippet is drawn in the same color as the ECG wave, usually green, superimposed over the
stored baseline snippet, drawn in a different color. The comparison shows any deviation in the
measurement since the baseline snippet was stored, for example as a result of a procedure carried out on
the patient.
The information is updated once per minute.
You can see ST snippets in the Adjust ST Points window or the ST Baseline window.
ST Baseline Window The ST Baseline Window shows an ST snippet drawn on a grid. The current
ST numeric and the ST numeric stored with the baseline are shown, as well as the difference between
these two numerics.
A “?” in front of the difference numeric indicates that the ST measurement points were adjusted since
the baseline snippet was stored.
♦To vie w th e ST Baseline window, select the ST numerics, then ST Baseline.
Updating ST Baseline Snippets
ST analysis requires valid samples to measure and store a snippet. ST Snippets and ST values are
updated every minute. If there is artifact in the signal, it may take longer for an ST snippet and an ST
value to appear.
The first baseline is stored automatically after ST monitoring is started, or when a new patient is
admitted. To update ST baselines,
1Select the ST numerics then ST Baseline to open the ST Baseline window.
2In the ST Baseline window, select Update Baseline to store all current snippets as
baselines. This deletes all previously-stored baselines.
1 ST label and numeric
2 Baseline ST numeric and difference since baseline was stored
3 1mV calibration bar
4Current snippet
5ST baseline
6 Timestamp of most recently stored baseline snippet
1
ST Baseline from 04 Apr 07 9:38
6
ST Baseline
3
4
5
2ST-II
-0.3
0.8
?-1.1
1mv 1sec
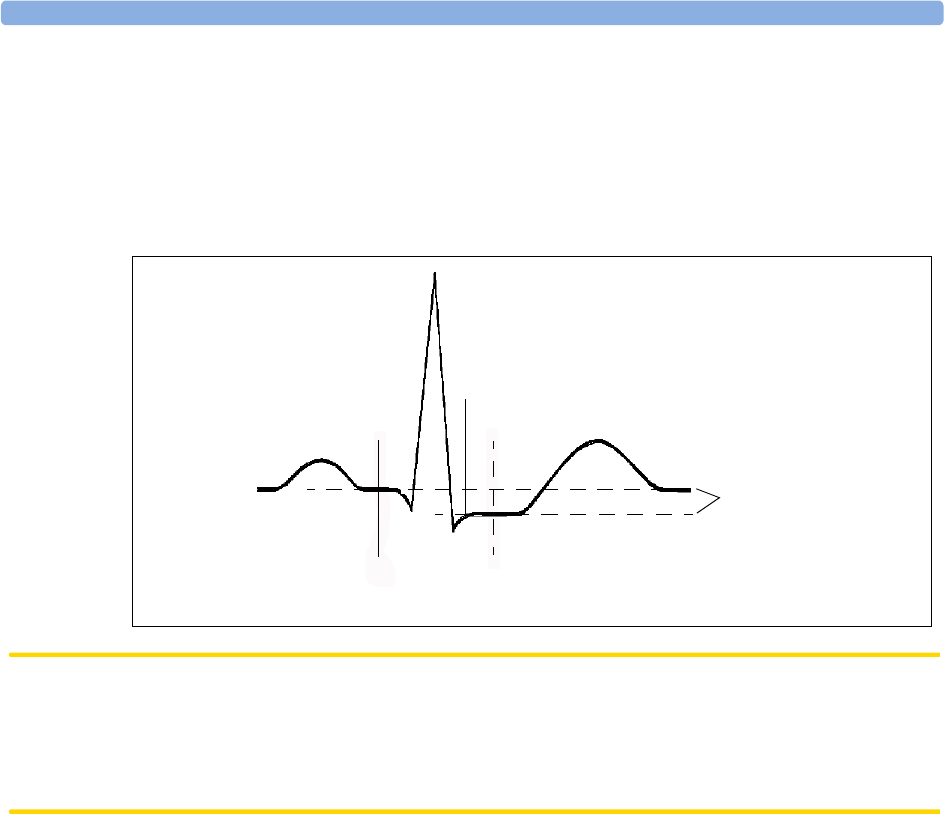
7 ECG, Arrhythmia, ST and QT Monitoring About the ST Measurement Points
120
About the ST Measurement Points
The ST value for each beat complex is the vertical difference between the ISO point and the ST point,
as shown in the diagram below. The isoelectric (ISO) point provides the baseline, the ST point is at the
midpoint of the ST segment. The J point is where the QRS complex changes its slope; as it is a fixed
distance away from the ST point, it can be useful to help you position the ST point correctly.
CAUTION The ST measurement points need to be adjusted when you start monitoring, and if the patient's heart
rate or ECG morphology changes significantly, as this may affect the size of the QT interval and thus
the placement of the ST point. Artifactual ST segment depression or elevation may occur if the
isoelectric point or the ST point is incorrectly set.
Always ensure that ST measurement points are appropriate for your patient.
Adjusting ST Measurement Points
Depending on your monitor’s configuration, the ST point can be positioned either
• relative to the J-point.
In the Adjust ST Points window, the pop-up keys ISO Point, J Point and ST Point are
visible and can be adjusted.
or
• directly by selecting a numeric value for the ST point.
In the Adjust ST Points window, you can adjust the ISO and ST point.
The ST Uses setting can only be changed in Configuration Mode.
To adjust the ST measurement points,
1In the Setup ST Analysis menu, select Adjust ST Points to open the Adjust ST
Points window. Alternatively, you can use the Adjust ST Points pop-up key in the ST
Baseline window.
2Select a suitable ECG lead for ST measurement, with a visible J-point and a visible P wave. Use the
up and down arrow keys to scroll through the ST snippets for the other ECG leads.
J point, for example, 48 msec
R-wave peak at 0 msec
Isoelectric point set to -80 msec
Difference = ST value
ST measurement point, for example, J + 60 msec
T
P
Q
S
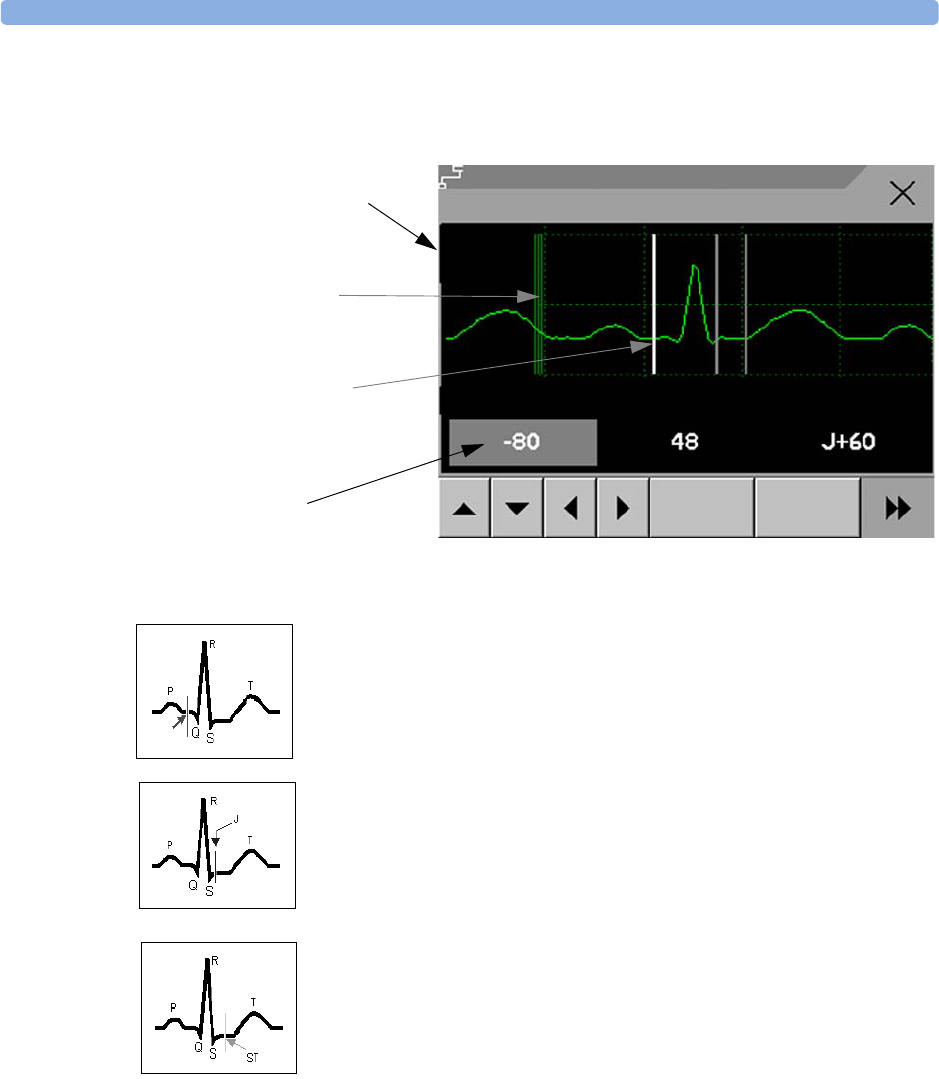
About the ST Measurement Points 7 ECG, Arrhythmia, ST and QT Monitoring
121
3Select the ST point you need to adjust by touching the appropriate point on the screen. The
current choice is highlighted (ISO point -80 in the screen example).
The ISO-point cursor positions the isoelectric point relative to the R-wave
peak. The relation is shown beside the ISO-point in milliseconds. Position the
ISO-point in the middle of the flattest part of the baseline (between the P and
Q waves or in front of the P wave).
The J-point cursor positions the J-point relative to the R-wave peak. It helps
you to correctly position the ST-point. Position the J-point at the end of the
QRS complex and the beginning of the ST segment.
The J-point cursor is not available if your monitor is configured to let you set
the ST point directly.
To position the ST-point relative to the J-point:
select either J+60 or J+80. Select J Point and use the arrow keys
to move the J-Point and position the ST-point at the midpoint of the ST
segment.
To position the ST-point directly:
select ST Point and use the left and right arrow keys to position the ST
point at the midpoint of the ST segment.
4Select the Apply Changes pop-up key to activate the new ST measurement points and
recalculate all ST values.
The most recent ST Points adjustment time is displayed in the Adjust ST Points window.
This information is cleared when a patient is discharged or when a new Profile is loaded into the
monitor.
1mV calibration bar
H
ighlighted ST point
ST label and the ST numeric
that would apply using the
current points
Cursors for adjusting ST
points
Adjust ST Points
ST-I
0.1
Update Apply
Changes
1mv 1sec
ST Points adjusted at 04 Apr 07 11:38
ISO

7 ECG, Arrhythmia, ST and QT Monitoring ST Alarms
122
5To update the ST snippet shown in the Adjust ST Points window, select the Update pop-
up key.
ST Alarms
ST alarms are yellow alarms. Each ST lead has its own alarm limit. ST alarms are triggered when an ST
value exceeds its alarm limit for more than one minute. Switching ST alarms off switches off alarms for
all ST leads.
If more than one ST measurement is in alarm, the monitor only displays the alarm message of the ST
lead which is currently furthest from its set alarm limits.
Single- or Multi-lead ST Alarming
Be aware that if multi-lead ST alarming is switched on, only alarms involving more than one ST lead
will be announced.
To choose individual or multi-lead ST alarming,
♦In the Setup ST Analysis menu, select ST Alarm Mode and select either Single ST
or Multi ST.
Changing ST Alarm Limits
The monitor can detect alarms on each ST lead separately, so you can set high and low ST alarm limits
individually for each ST lead. You can also set separate alarm limits for single-lead and multi-lead ST
monitoring. Set the high and low alarm limits based on your assessment of the patient's clinical
condition, unit protocols, physician orders or medication specified limits. A good guideline is + 1.0
mm or - 1.0 mm from the patients's ST, or follow your hospital protocol.
1In the Setup ST Analysis menu, select ST Alarm Mode and select Single ST or
Multi ST.
2Select the alarm to be adjusted.
3Select the appropriate setting.
Viewing ST Maps
The monitor can derive a multi-axis portrait (map) from the ST analysis to help you detect changes in
ST values. It displays two planes obtained from a multilead ECG in a multi-axis diagram, where each
axis represents a lead. The ST value at the J point is given. The position of the axes within the diagram
correspond to the placement of the ECG leads. Each ST value is assigned to either a limb lead, or to a
chest lead. Every axis shows the polarity of the lead it represents. By joining adjacent ST values, the
monitor obtains the ST map. The contour line, and the map shading, is shown in the same color as the
ECG parameter.
Current View
In current view, the monitor displays an ST map that corresponds to the current ST values. Three or
more leads per plane are necessary to display a map.
The left of the following diagram shows leads I, II, III, aVR, aVL, and aVF on the limb leads. On the
right, the V-leads (V1, V2, V3, V4, V5, and V6) are on the chest leads.
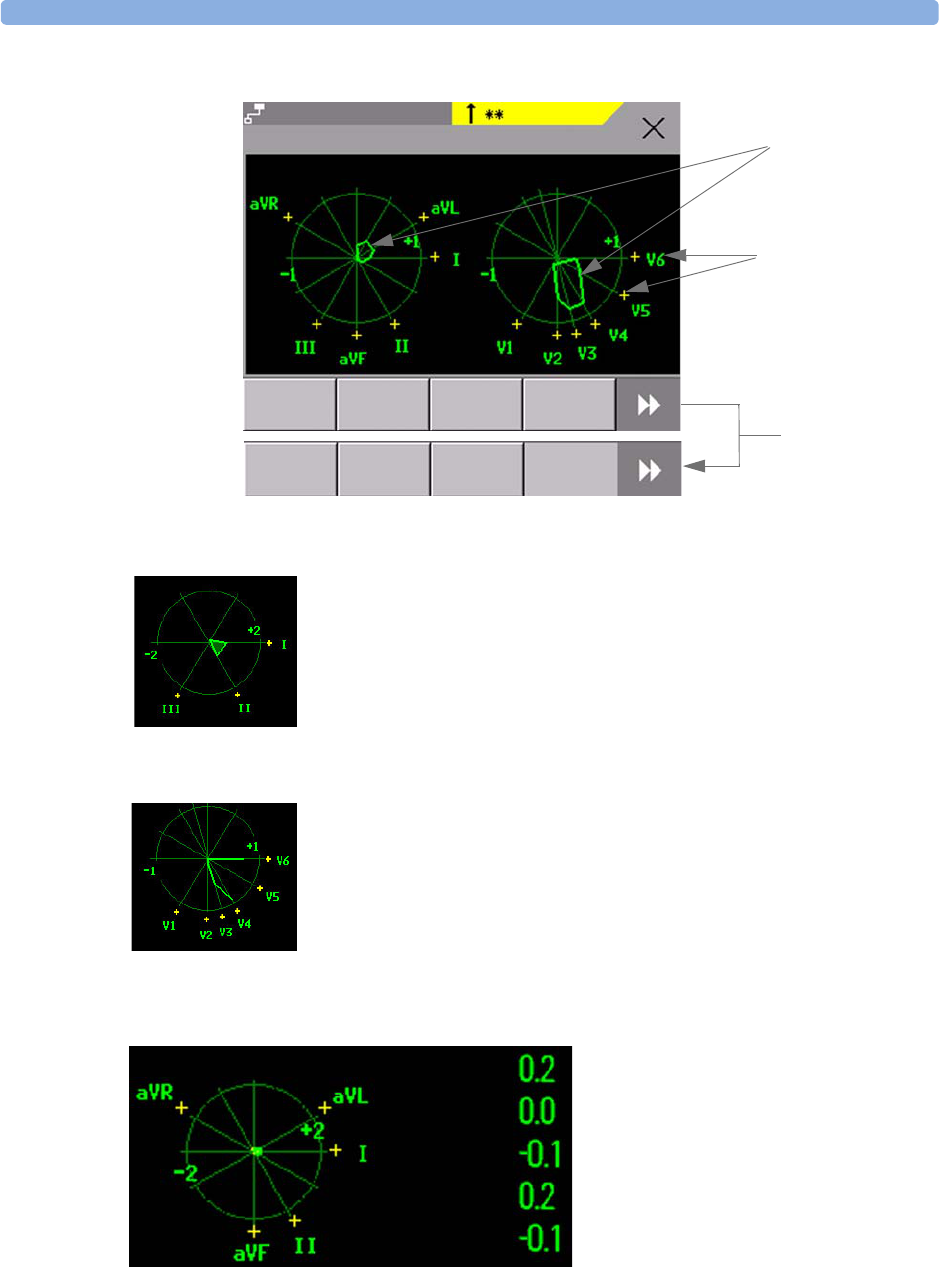
Viewing ST Maps 7 ECG, Arrhythmia, ST and QT Monitoring
123
If an ST lead is switched off, its axis is not shown in the map.
If a lead is in INOP (the value is being measured but is invalid or unavailable because, for example, the
corresponding ECG electrode is unplugged), the area formed by the remaining ST leads is left open.
If there is insufficient information (for example, there are less than three chest leads) for a second ST map to
be displayed, the currently available ST values are displayed in place of the second ST map.
ST label and polarity
of corresponding lead
ST map
Trend
View
Print
Size
Up
Size
Down
Show
Baseline Scroll to view
more pop-up keys
ST Map (Current)
Select
Interval
ST-II HIGH
Adult
SBed10
Limb Leads Chest Leads
Show
Values
ST-I
ST-II
ST-aVR
ST-aVL
ST-aVF
Limb Leads
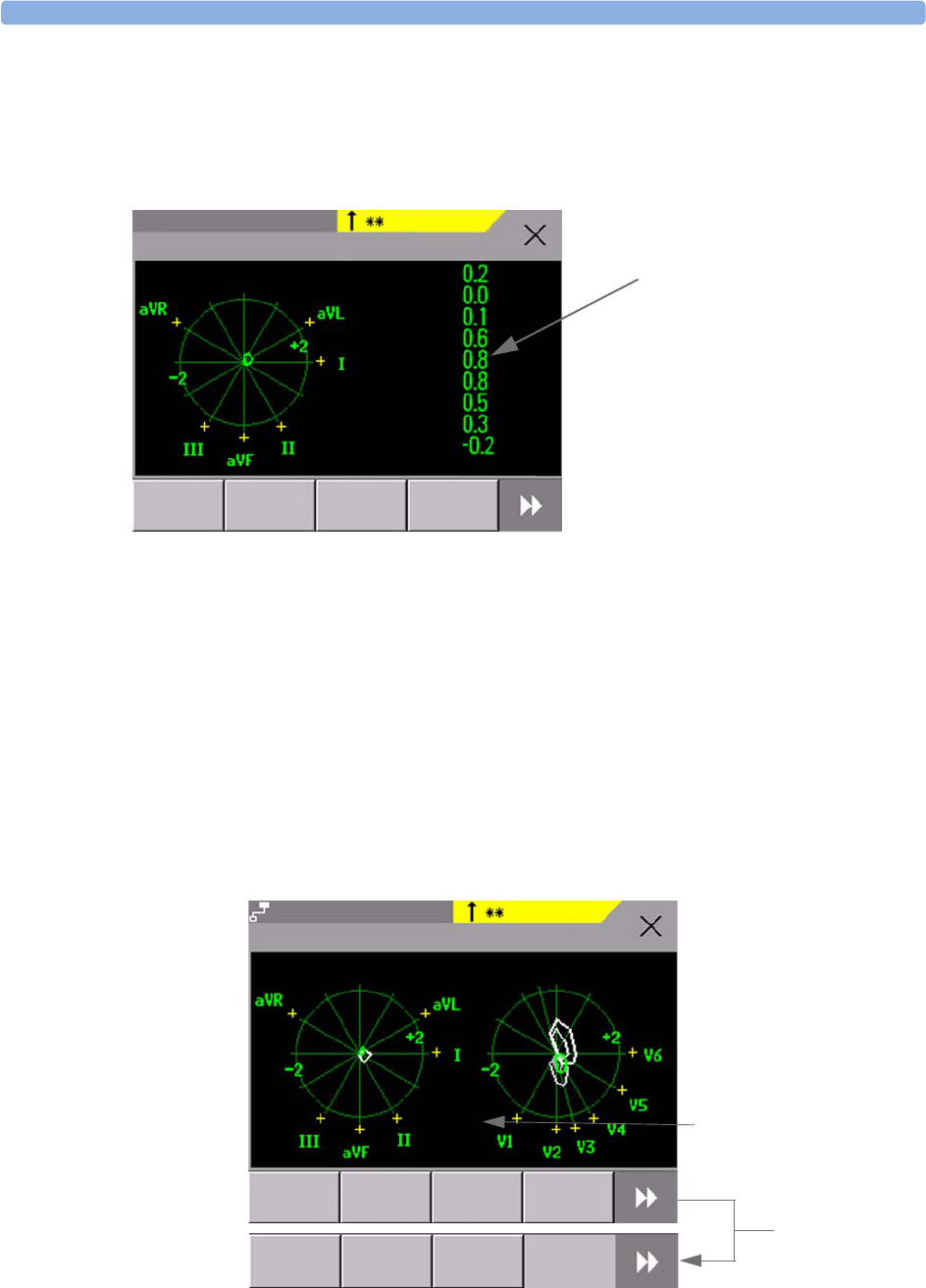
7 ECG, Arrhythmia, ST and QT Monitoring Viewing ST Maps
124
Additionally, when both ST maps are displayed, you can view the currently available ST values in the
ST Map window (Current or Trend) at any time. To do this, select the Show Values pop-up key.
The ST values are shown in place of the second ST map, and the pop-up key text changes to Hide
Values. Select the Hide Values pop-up key and the display shows both ST maps again.
Trend View
In trend view, you can see up to four trended ST maps, and the current ST map, simultaneously. You
can configure the time interval between trended samples. The most recent map is shown in the same
color as the parameter itself. Past values change from white through dark gray. In the diagram below,
the time interval between trends is 12 seconds. The first trended sample is white and is 12 seconds old.
The second trended sample corresponds to the ST values 24 seconds ago and so forth. The ST values
on the diagrams show the current ST values.
If a lead is turned off, its axis is no longer shown. This has no impact on the presentation of trended
values that were recorded while the lead was still on. In the diagram below, lead V4 was switched off 20
seconds ago. The current ST values and the first trended value reflect this change in the lead setup. All
other maps are displayed the way in which they were recorded.
ST-I
ST-II
ST-VI
ST-V2
ST-V3
ST-V4
ST-V5
ST-V6
ST-aVF
Size
Up
Size
Down
Show
Baseline
ST Map (Current)
ST-II HIGH
Adult
SBed10
Limb Leads
ST values are shown where the
STmap for the chest leads is
normally displayed.
Select the Show Values pop-up
key to see the current ST values.
Select Hide Values and the
display shows both ST maps again.
Hide
Values
Scroll to view
more pop-up
keys
Current
View
Select
Interval
Print
Size
Up
Size
Down
Show
Baseline
Show
Values
ST Map (Trend)
ST-II HIGH
Adult
SBed10
Limb Leads Chest Leads
5 min trending interval

Viewing ST Maps 7 ECG, Arrhythmia, ST and QT Monitoring
125
Viewing an ST Map
To display an ST map,
♦In the Setup ST Analysis menu, select ST Map.
Working in the ST Map Task Window
You may need to activate the ST map task window to see all the data, and to access the pop-up keys.
Select the map view on screen to activate its task window. Once you activate it, you can perform the
tasks detailed here.
Switching Between ST Map Views
To switch between views,
♦Select Current View or Trend View to toggle between views.
If your trend view is empty, you need to adjust the priority of this measurement in the trending
priority list. See “Trend Priority” on page 191.
Displaying an ST Reference Baseline
You can display an ST reference baseline for the current view, or for the trended view. The baseline is
shown in yellow. However, if the ECG color is yellow, the baseline is shown in green. Use this baseline
to detect ST changes. The baseline is derived automatically whenever the monitor relearns arrhythmia
and also on user request.
♦Select Show Baseline/Hide Baseline to toggle between baseline display on and off.
Updating an ST Map Reference Baseline
To update the baseline,
♦In the Setup ST Analysis menu, select ST Baseline -> Update baseline.
Changing the Scale of the ST Map
To change scale,
♦Select Size Up or Size Down to alter the size at which monitor displays the map.
In this diagram, V4 was either temporarily switched off, or in INOP,
for around 30 seconds. No data was recorded. Consequently, the
affected maps are not closed.

7 ECG, Arrhythmia, ST and QT Monitoring Viewing ST Maps
126
Changing the Trending Interval
To determine how frequently the monitor displays a trended sample,
1In Trend view, select Select Interval.
2Select the required interval from the menu. The interval ranges between 12 seconds to 30 minutes.
Printing an ST Map Report
To print the most recently viewed (current or trend) window,
1Select Main Setup - > Reports.
2Select ST Map.
3Press Print.
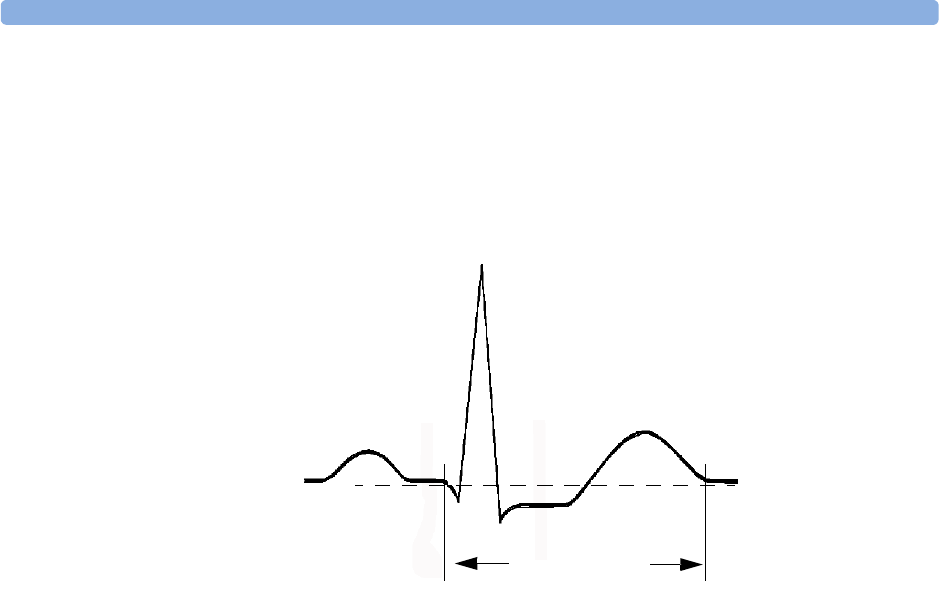
About QT/QTc Interval Monitoring 7 ECG, Arrhythmia, ST and QT Monitoring
127
About QT/QTc Interval Monitoring
The QT interval is defined as the time between the beginning of the Q-wave and the end of the
T-wave. It measures the total duration of the depolarization (QRS duration) and repolarization (ST-T)
phases of the ventricular action potential. QT interval monitoring can assist in the detection of
prolonged QT interval syndrome.
The QT interval has an inverse relationship to heart rate. Faster heart rates shorten the QT interval and
slower heart rates prolong the QT interval. Therefore there are several formulas used to correct the QT
interval for heart rate. The heart rate corrected QT interval is abbreviated as QTc. The monitor uses as
a default the Bazett correction formula and the alternative Fridericia formula can be selected in
Configuration Mode.
For QT interval monitoring to be effective, basic or enhanced arrhythmia monitoring should be turned
on.
QT Measurement Algorithm
The QT values are updated every five minutes except in the initial phase (first five minutes) where they
are updated once per minute. Normal or atrial paced beats and beats with a similar morphology are
averaged to form a representative waveform for further processing. Normal beats followed by a
premature QRS will be excluded from the measurements to prevent the premature beat from obscuring
the end of the T-wave. If the algorithm cannot form a representative waveform, for example because
the morphology of the beats is too varied, a CANNOT ANALYZE QT INOP will be generated after 10
minutes. This is also the case if normal beats have been falsely labelled so that the algorithm does not
have enough valid beats to make QT measurements. No QT value is calculated if the QT-HR is
>150 bpm (Adult) or >180 bpm (Pedi/Neo).
Because of the different algorithm approaches, a QT/QTc measurement from a diagnostic 12-lead
program may differ from the realtime measurement on the monitor.
Where Can I Find More Information?
See the Application Note on QT/QTc Interval Monitoring and the QT Interval Monitoring Quick
Guide supplied on your documentation DVD for detailed information on the QT algorithm and
performance.
T
QS
P
R
QT interval
7 ECG, Arrhythmia, ST and QT Monitoring About QT/QTc Interval Monitoring
128
Indications For Use Of QT Interval Monitoring
Of special concern for QT monitoring is the administration of QT prolonging drugs to patients
identified with risk factors for Torsade de Pointe. Females, older patients and patients with
bradycardia, impaired left ventricular function (ischemia, left ventricular hypertrophy), hypokalemia
and hypomagnesemia are in this increased risk category.
Limitations For Use Of QT Interval Monitoring
Some conditions may make it difficult to achieve reliable QT monitoring, for example:
• the T-wave is very flat
• T-waves are not well defined due to atrial flutter or atrial fibrillation
• the end of the T-wave is difficult to define because of the presence of U-waves
• a high heart rate causes the P-wave to encroach on the end of the previous T-wave
• noise or high QRS morphology variation
For these cases you should select a lead with a good T-wave amplitude and no visible flutter activity,
and without a predominant U-wave or P-wave.
Some conditions such as left or right bundle branch block or hypertrophy can lead to a widened QRS
complex. If a long QTc is observed you should verify it to ensure that it is not caused by QRS
widening.
Because normal beats followed by ventricular beats are not included in the analysis, no QT
measurement will be generated in the presence of a bigeminy rhythm.
If the heart rate is extremely high (over 150 bpm for adults and over 180 bpm for pediatrics and
neonates) QT will not be measured.
When the heart rate changes, it can take several minutes for the QT interval to stabilize. For reliable
QTc calculation it is important to avoid a region where the heart rate is changing.
WARNING QT/QTc measurements should always be verified by a qualified clinician.
Selecting The QT Leads
For QT Monitoring you can select one of the following three modes:
• All Leads mode - all available leads (I, II, III, V, MCL, V1 - V6) are used to produce a global QT
measurement. For EASI lead placement, directly acquired AI, AS and ES leads are used.
• Primary-Lead mode - the primary lead will be used for QT measurement. If the original primary
lead becomes unavailable or is changed, QT measurement will continue with the new primary lead.
• Single-Lead mode - a single lead selected from all available leads (except the augmented leads) will be
used for QT measurement. QT measurement will stop if the selected lead becomes unavailable.
To select the mode,
1Select the QT numeric to enter the Setup QT Analysis window.
2Select QT Lead and select All, Primary Lead or one of the available single leads.
When using the All Leads mode, make sure when you compare QT values that they are based on the
same set of leads.
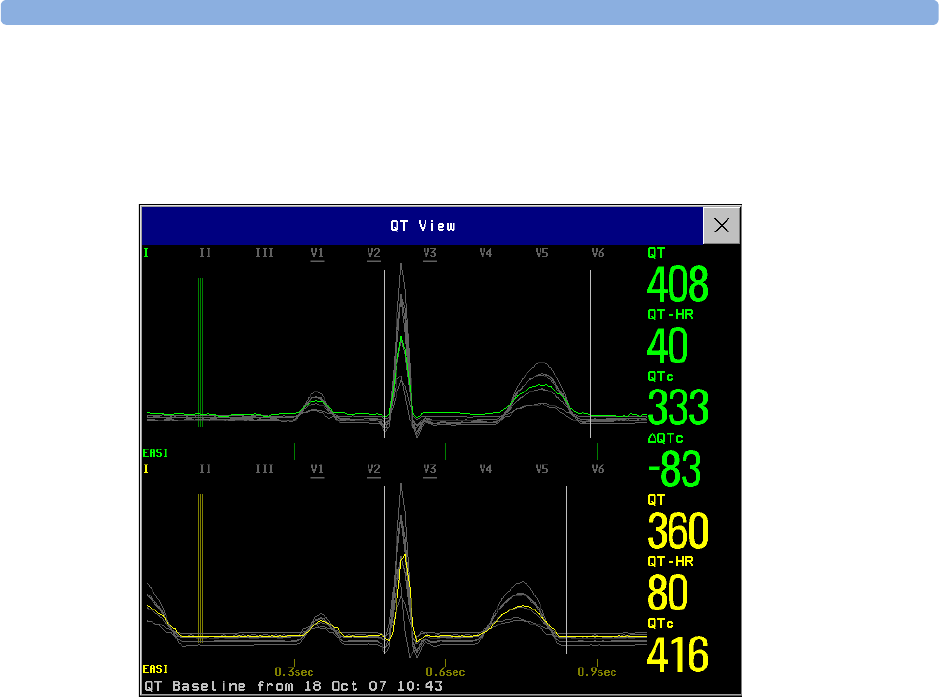
About QT/QTc Interval Monitoring 7 ECG, Arrhythmia, ST and QT Monitoring
129
Changing the lead(s) used for QT measurements will not cause the baseline to be reset.
QT View
In the QT View window you can verify that the QT algorithm detects correct Q and T points.
The current waves are shown in the upper half of the window and the baseline waves in a different
color below. The Q and T points are marked with a vertical line. By selecting one of the lead labels at
the top of the window you can highlight the corresponding wave; the other waves are shown in gray.
The underlined lead labels are the leads used for the QT calculation. By selecting the numeric area you
can highlight all underlined leads.
Changing The View To A Single Wave Set
To view one set of waves in a larger scale, you can cycle through the different views,
1Select Current view to see the set of current waves.
2Select Baseline view to see the set of baseline waves.
3Select Split view to return to the combined view with current and baseline waves.
Setting The QT Baseline
In order to quantify changes in the QTc value, you can set a QTc baseline. For example to assess the
effect of medication on the QT interval you can set the current value as the baseline before you begin
medication. This baseline will then be used to calculate the 'QTc value.
To set the baseline,
♦Select Set Baseline and set the value.
7 ECG, Arrhythmia, ST and QT Monitoring QT Alarms
130
If no baseline has been set for this patient, the first five minute value after the start of monitoring is
automatically set as baseline. If you set a new baseline the previous baseline is discarded. As the 'QTc
alarm is based on the difference between the baseline and the current value, setting an inappropriate
new baseline may prevent a 'QTc alarm from being generated. Discharging a patient clears the
baseline.
Printing The QT Waves
To start a printout,
♦Select Print QT.
Recording The QT Waves
To start a recording,
♦Select Record QT.
QT Alarms
There are two QT alarms, QTc high limit alarm and 'QTc high alarm. The QTc high limit alarm is
generated when the QTc value exceeds the set limit for more than 5 minutes. The 'QTc alarm is
generated when the difference between the current value and the baseline value exceeds the set limit for
more than 5 minutes.
The CANNOT ANALYZE QT INOP and the ?_will be displayed when no QT measurement could be
calculated for 10 minutes. Up to this time the previous valid value will be displayed. The following
additional messages on the cause of the invalid measurements may also be displayed.
Additional Message Cause of Invalid QT Measurement
QT Startup QT monitoring was just turned on or has been reset
Asystole or Leads Off 1Not all specified leads needed to perform QT analysis are
available, or
2Asystole condition is detected
Insufficient Valid
Leads
Not enough valid QRS complexes to generate a QT measurement
Invalid rhythm for QTc Not enough valid RR intervals to generate QT-HR, the averaged HR
used for QTc calculation
High QT-HR QT-HR exceeds the specified upper limit of 150 bpm (for adults) or 180
bpm (for neonates and pediatrics)
Small R Wave R-wave of the signal is too small
Small T Wave T-wave of the signal is too small
End of T Not detected End of the T-Wave cannot be accurately detected
QT Out Of Range QT measurement is outside the specified range of valid QT values (200-
800 msec)
QTc Out Of Range QTc measurement is outside the specified range of valid QTc values
(200-800 msec)
QTc Erratic QTc measurements are not stable

Switching QT Monitoring On and Off 7 ECG, Arrhythmia, ST and QT Monitoring
131
Switching Individual QTc Alarms On and Off
Each QTc alarm can be switched off individually.
♦To switch an alarm on or off, in the Setup QT Analysis menu, select QTc Alarm or
'QTc Alarm to toggle between On and Off.
Changing QTc Alarm Limits
Set the high alarm limits based on your assessment of the patient's clinical condition, unit protocols,
physician orders or medication specified limits.
1In the Setup QT Analysis menu, select High Limit.
2Select the appropriate setting.
3Select 'High Limit.
4Select the appropriate setting.
Switching QT Monitoring On and Off
♦To switch all QT monitoring on or off, in the Setup QT Analysis menu, select QT
Analys. to switch between On and Off.

7 ECG, Arrhythmia, ST and QT Monitoring Switching QT Monitoring On and Off
132

133
8
8Monitoring Pulse Rate
The pulse numeric counts the arterial pulsations that result from the mechanical activity of the heart in
beats per minute (bpm). You can display a pulse from any measured SpO2 signal (pleth wave), or any
arterial pressure (P, ABP, ART, Ao, PAP, UAP, FAP, BAP: see the pressure section for an explanation
of the pressure labels). The displayed pulse numeric is labeled and color-coded to match its source
wave. If the pulse numeric is not displayed, see the Setup Pulse menu to check whether it is
switched on.
Entering the Setup Pulse Menu
If a pulse numeric is displayed on the screen, select it to enter the Setup Pulse (Pulse
Source) menu. If no pulse numeric is visible, in the Setup SpO2 menu or a Setup arterial
pressure menu, select Pulse (Pulse Source).
System Pulse Source
The currently selected system pulse source is shown in the setup menus of the pulse source
measurements. The pulse rate chosen as system pulse:
• is monitored as system pulse and generates alarms when you select pulse as the active alarm source
• is sent via the network to the Information Center, if available
• is trended in the HighRes Trends and stored in the monitor’s databases.
To define which pulse rate is used as system pulse,
1In the Setup Pulse menu, select System Pulse.
2Select one of the SpO2 or arterial pressure labels from the pop-up list, or select Auto.
If you select Auto, the monitor automatically chooses a pulse rate to be used as system pulse. It
looks through the list from top to bottom and activates the first pulse rate that is switched on and
available.
If your selected pulse source measurement becomes unavailable or is switched off, the monitor will use
the next measurement from the list as system pulse until the selected pulse source measurement
becomes available again.

8 Monitoring Pulse Rate Switching Pulse On and Off
134
Switching Pulse On and Off
To switch a particular pulse numeric on or off, enter the Setup Pulse menu via the measurement
setup menu or wave menu of the pulse source. For example, to switch an SpO2 pulse numeric on or
off,
1Enter the Setup Pulse menu by selecting the Pulse numeric or by selecting Pulse in the
Setup SpO2 menu.
2In the Setup Pulse menu, select Pulse (Pulse Source) to toggle between On and
Off.
Using Pulse Alarms
You can change pulse rate alarm limits in the ECG/Pulse Alarms menu which can be accessed
from the Setup Pulse menu or the Setup ECG menu by selecting AlarmSrc (xxx) where
xxx is the current alarm source. Changing the alarm limits for a specific Pulse numeric changes the
alarm limits for all pulse rate alarms and heart rate alarms.
Pulse alarms are only generated when the active alarm source is set to Pulse, a pulse source is set as
system pulse and pulse alarms are switched on.
Selecting the Active Alarm Source: ECG or Pulse?
In most cases the HR and Pulse numerics are identical. In order to avoid simultaneous alarms on HR
and Pulse, the monitor uses either ECG or Pulse as its active alarm source. To change the alarm source,
select AlarmSrc in the ECG/Pulse Alarms menu, then select
•ECG: if you want the HR to be the alarm source for HR/Pulse.
•Pulse: If you select Pulse as the active alarm source, the monitor will prompt you to confirm your
choice. Be aware that if you select Pulse as the alarm source, all arrhythmia and ECG HR alarms are
switched off.
•Auto: If the AlarmSrc is set to Auto, the monitor will use the heart rate from the ECG
measurement as the alarm source whenever the ECG measurement is switched on and at least one
ECG lead can be measured without an INOP condition.
The monitor will automatically switch to Pulse as the alarm source if:
– a valid ECG lead can no longer be measured
and
– a Pulse source is switched on and available,
The monitor then uses the pulse rate from the measurement currently active as system pulse. While
Pulse is the alarm source, all arrhythmia and ECG HR alarms are switched off. If an ECG lead
becomes available again, the monitor automatically uses HR as alarm source.
Note: If ECG is switched off, the monitor will always change to Pulse as alarm source, if a Pulse is
available. One exception to this rule can arise when you have a telemetry device paired with your
monitor. The monitor ECG is then deactivated but the monitor may be configured to allow only ECG
as the active alarm source. In this case the monitor will not switch to Pulse as alarm source and Pulse
will not be available as a selection in the ECG/Pulse Alarms menu.
Using Pulse Alarms 8 Monitoring Pulse Rate
135
WARNING Selecting Pulse as the active alarm source for HR/Pulse switches off the arrhythmia alarms listed in the
section “ECG and Arrhythmia Alarm Overview” on page 102, including Asystole, Vfib and Vtach
alarms, and the heart rate alarms. This is indicated by the message ECG/ARRH ALARM OFF (unless
this has been configured off for your monitor), and the crossed-out alarm symbol beside the ECG heart
rate numeric. The message ECG/ARRH ALARM OFF can be configured off, or to switch to a yellow
(medium severity) INOP after a fixed number of hours.
High and low pulse rate and extreme bradycardia and extreme tachycardia alarms from pulse are active.
Alarm Source Selection Disabled
If Alarm Source Selection is disabled, you cannot change the alarm source. If you try to change the
source, the monitor displays the message To activate enter Config and enable
Alarm Source Selection. This setting can only be changed in Configuration Mode.
Changing HR/Pulse Alarm Limits
As Pulse and HR share the same high and low alarm limits, if you change the alarm limit in the
Setup Pulse menu, the high or low alarm limits for HR in the Setup ECG menu change
automatically, and vice versa. The only exceptions are caused by a low limit clamp for each
measurement: the lowest value for Pulse when derived from SpO2 is 30 bpm; for HR 15 bpm, and for
Pressure 25 bpm.
Extreme Alarm Limits
The extreme rate alarms, Extreme Tachy and Extreme Brady, generated by the active alarm source,
either HR or Pulse, are set in Configuration Mode by adding a set value to the high and low alarm
limits. You need to know what value has been configured for your monitor. Changing the high and
low alarm limits automatically changes the extreme alarm limits within the allowed range.
♦To see the values added to the high and low limit alarms to create the extreme rate alarms for your
monitor, in the Setup ECG menu, see the menu items Extr.Tachy and Extr.Brady.
QRS Tone
The active alarm source is also used as a source for the QRS tone. You can change the tone volume in
the Setup SpO2 and Setup ECG menus and the QRS tone modulation in the Setup SpO2
menu.
WARNING The audible QRS tone might be influenced by external interference and is not intended to be used as a
substitute for ECG based arrhythmia analysis.
If arrhythmia detection is needed, do not rely on the audible QRS tone.

8 Monitoring Pulse Rate Using Pulse Alarms
136

137
9
9Monitoring Respiration Rate
(Resp)
For the respiratory measurement (Resp), the monitor measures the thoracic impedance between two
ECG electrodes on the patient’s chest. Changes in the impedance due to thoracic movement produce
the Resp waveform on the monitor screen. The monitor counts the waveform cycles to calculate the
respiration rate (RR).
Lead Placement for Monitoring Resp
Correct patient skin preparation techniques for electrode placement are important for Resp
measurement: you will find this information in the chapter on ECG.
The Resp measurement uses the standard ECG cable sets and lead placements. You can use any of the
different types of ECG cable sets - 3-lead, 5-lead, 6-lead or 10-lead, using either standard or EASI™
placement - to measure Resp, as long as you use ICU ECG cables.
The Resp signal is always measured between two of the ECG electrodes. If you are using standard ECG
electrode placement, Resp is measured between the RA and LL electrodes. If you are using EASI™
ECG electrode placement, Resp is measured between the I and A electrodes.
Optimizing Lead Placement for Resp
If you want to measure Resp and you are already measuring ECG, you may need to optimize
placement of the two electrodes between which Resp will be measured for some patients. Repositioning
ECG electrodes from standard positions, especially when you are using EASI™ ECG electrode
placement, results in changes in the ECG waveform and may influence ST and arrhythmia
interpretation.
Cardiac Overlay
Cardiac activity that affects the Resp waveform is called cardiac overlay. It happens when the Resp
electrodes pick up impedance changes caused by the rhythmic blood flow. Correct electrode placement
can help to reduce cardiac overlay: avoid the liver area and the ventricles of the heart in the line
between the respiratory electrodes. This is particularly important for neonates.
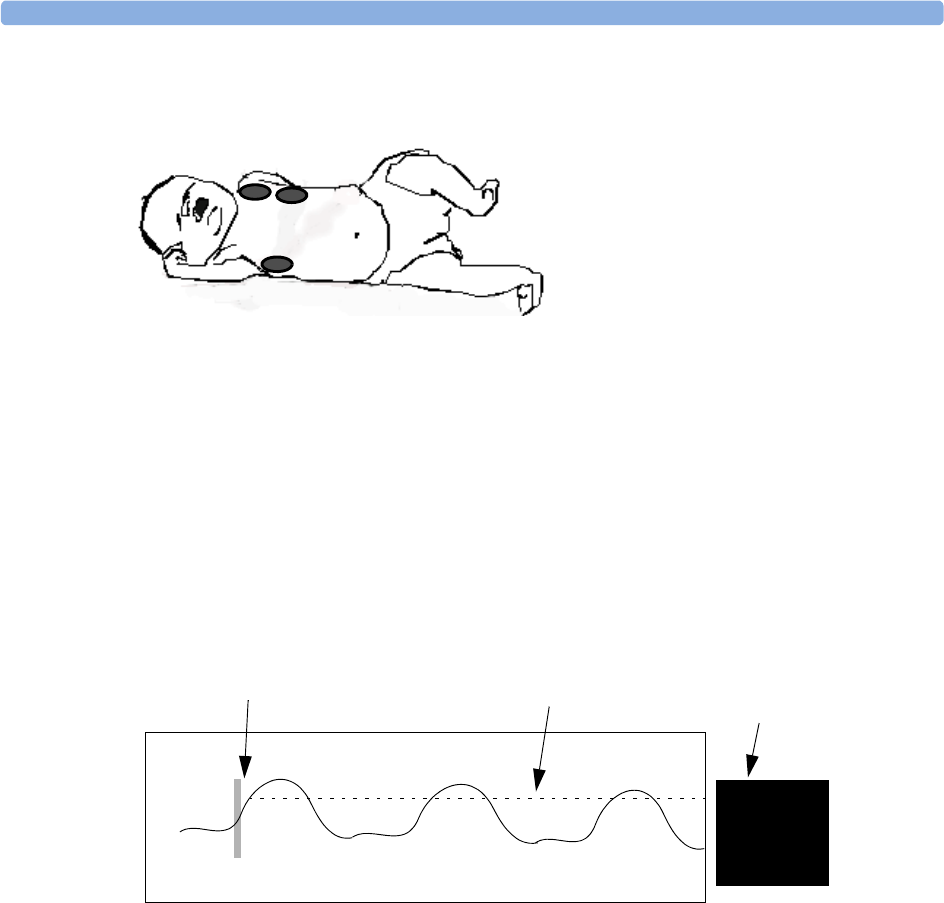
9 Monitoring Respiration Rate (Resp) Understanding the Resp Display
138
Lateral Chest Expansion
Abdominal Breathing
Some patients with restricted chest movement breathe mainly abdominally. In these cases, you may
need to place the left leg electrode on the left abdomen at the point of maximum abdominal expansion
to optimize the respiratory wave.
Understanding the Resp Display
The Resp measurement is displayed on the monitor as a continuous wave and a numeric respiration
rate. If the detected respiration rate is close to the heart rate, this is indicated by the text HR = RR
next to the respiration wave if you are in manual monitoring mode. Your monitor screen may look
slightly different from the illustration.
Changing Resp Detection Modes
The Resp detection level can be set either automatically or manually.
♦To change the resp detection mode, in the Setup Resp menu, select Detection to toggle
between the settings.
Auto Detection Mode
In Auto Detection Mode, the monitor adjusts the detection level automatically, depending on the wave
height and the presence of cardiac artifact. Note that in Auto Detection Mode,
• the detection level (a dotted line) is not displayed on the waveform,
Some patients, especially neonates, expand
their chests laterally. In these cases it is best
to place the two respiratory electrodes in the
right midaxillary and left lateral chest areas at
the patient’s maximum point of breathing
movement to optimize the respiratory wave.
Resp
1 Ohm
22
RR
Manually-set Resp detection level
1 Ohm calibration bar Resp numeric and
label

Changing the Size of the Respiration Wave 9 Monitoring Respiration Rate (Resp)
139
• the algorithm expects a heart rate and therefore needs at least 3 electrodes attached to the patient. If
you are monitoring respiration with only two electrodes, the detection algorithm becomes less
sensitive which may result in reduced breath detection performance.
Use Auto Detection Mode for situations where:
• the respiration rate is not close to the heart rate
• breathing is spontaneous, with or without continuous positive airway pressure (CPAP)
• patients are ventilated, except patients with Intermittent Mandatory Ventilation (IMV).
Manual Detection Mode
In Manual Detection Mode you must set the Resp detection level.
♦In the Setup Resp menu, select Manual Up or Manual Down. Use the dotted detection
level line in the Resp waveform to determine when the desired level is reached.
Once set, the detection level will not adapt automatically to different respiration depths. It is important
to remember that if the depth of breathing changes, you may need to change the detection level.
Use Manual Detection Mode for situations where:
• the respiration rate and the heart rate are close.
• patients have Intermittent Mandatory Ventilation.
• respiration is weak. Try repositioning the electrodes to improve the signal.
Resp Detection Modes and Cardiac Overlay
In Auto Detection Mode: If you are monitoring Resp and the ECG is switched off, the monitor
cannot compare the ECG and Resp rates to detect cardiac overlay. The respiration detection level is
automatically set higher to prevent the detection of cardiac overlay as respiration.
In Manual Detection Mode: Cardiac overlay can in certain situations trigger the respiration counter.
This may lead to a false indication of a high respiration rate or an undetected apnea condition. If you
suspect that cardiac overlay is being registered as breathing activity, raise the detection level above the
zone of cardiac overlay. If the Resp wave is so small that raising the detection level is not possible, you
may need to optimize the electrode placement as described in the section ”Lateral Chest Expansion”.
Changing the Size of the Respiration Wave
WARNING When monitoring in Manual Detection Mode, make sure to check the respiration detection level after
you have increased or decreased the size of the respiration wave.
♦In the Setup Resp menu, select Size Up to increase the size of the wave or Size Down to
decrease it.
9 Monitoring Respiration Rate (Resp) Changing the Speed of the Respiration Wave
140
Changing the Speed of the Respiration Wave
Resp waveforms are usually viewed at a slower speed than other waveforms. For this reason, the Resp
measurement has its own speed control and is not affected by the wave speed settings of the other
measurements.
♦Select the Resp wave to enter the Resp Wave menu, then select Change Speed. Choose the
required speed from the pop-up list. This defines the speed at which the wave is drawn across the
screen in millimeters per second (mm/s).
Using Resp Alarms
Resp alarms can be switched on and off and the high and low alarm limits can be changed just like
other measurement alarms, as described in the Alarms chapter.
Changing the Apnea Alarm Delay
The apnea alarm is a high priority red alarm used to detect apneas. The apnea alarm delay time defines
the time period between the point where the monitor cannot detect any respiration activity and the
indication of the apnea alarm.
1In the Setup Resp menu, select Apnea Time.
2Select the appropriate setting.
Resp Safety Information
WARNING Respiration detection level If you do not set the detection level for the respiration correctly in manual
detection mode, it may not be possible for the monitor to detect apnea. If you set the detection level
too low, the monitor is more likely to detect cardiac activity, and to falsely interpret cardiac activity as
respiratory activity in the case of apnea.
Apnea The respiration measurement does not recognize obstructive and mixed apneas — it only
indicates an alarm when a pre-adjusted time has elapsed since the last detected breath.
The safety and effectiveness of the respiration measurement method in the detection of apnea,
particularly the apnea of prematurity and apnea of infancy, has not been established.
Interference If operating under conditions according to the EMC Standard EN 60601-1-2 (Radiated
Immunity 3V/m), field strengths above 1V/m may cause erroneous measurements at various
frequencies. Therefore it is recommended to avoid the use of electrically radiating equipment in close
proximity to the respiration measurement unit.
Resp Accessories To monitor respiration, use only the non-OR ECG accessories listed in the Resp
section of the accessories chapter. You cannot measure respiration if you are using an orange OR ECG
cable set. This is because of the higher internal impedance of the OR cable set, required for use if
electro-surgery is being performed.

Resp Safety Information 9 Monitoring Respiration Rate (Resp)
141
Rate adaptive pacemakers: Implanted pacemakers which can adapt to the Minute Ventilation rate
may occasionally react on the Impedance measurement used by patient monitors for the determination
of the Resp value and execute pacing with the maximum programmed rate. Switching off the Resp
measurement can prevent this.

9 Monitoring Respiration Rate (Resp) Resp Safety Information
142
143
10
10Monitoring SpO2
Philips pulse oximetry uses a motion-tolerant signal processing algorithm, based on Fourier artefact
suppression technology (FAST). It provides four measurements:
• Oxygen saturation of arterial blood (SpO2) - percentage of oxygenated hemoglobin in relation to the
sum of oxyhemoglobin and deoxyhemoglobin (functional arterial oxygen saturation).
• Pleth waveform - visual indication of patient’s pulse.
• Pulse rate (derived from pleth wave) - detected pulsations per minute.
• Perfusion indicator - numerical value for the pulsatile portion of the measured signal caused by
arterial pulsation.
The monitors are also compatible with SpO2 technologies from other manufacturers. Please refer to the
instructions for use provided with these devices for further information.
SpO2 Sensors
Familiarize yourself with the instructions for use supplied with your sensor before using it. In
particular, check that the sensor being used is appropriate for your patient category and application
site.
CAUTION Do not use OxiCliq disposable sensors in a high humidity environment, such as in neonatal incubators
or in the presence of fluids, which may contaminate sensor and electrical connections causing
unreliable or intermittent measurements. Do not use disposable sensors on patients who have allergic
reactions to the adhesive.
Applying the Sensor
1Follow the SpO2 sensor’s instructions for use, adhering to all warnings and cautions.
2Remove colored nail polish from the application site.
3Apply the sensor to the patient. The application site should match the sensor size so that the sensor
can neither fall off, nor apply excessive pressure. When using the M1195A Infant Finger Sensor,
select a finger or toe with a diameter of between 7 and 8 mm (0.27” and 0.31”). When applying a
M1193A neonatal sensor do not overtighten the strap.
10 Monitoring SpO2Connecting SpO2 Cables
144
4Check that the light emitter and the photodetector are directly opposite each other. All light from
the emitter must pass through the patient’s tissue.
WARNING Loose Sensor: If a sensor is too loose, it might compromise the optical alignment or fall off. If it is too
tight, for example because the application site is too large or becomes too large due to edema, excessive
pressure may be applied. This can result in venous congestion distal from the application site, leading
to interstitial edema, hypoxemia and tissue malnutrition. Skin irritations or lacerations may occur as a
result of the sensor being attached to one location for too long. To avoid skin irritations and
lacerations, periodically inspect the sensor application site and change the application site at least every
four hours.
Venous Pulsation: Do not apply sensor too tightly as this results in venous pulsation which may
severely obstruct circulation and lead to inaccurate measurements.
Ambient Temperature: At elevated ambient temperatures be careful with measurement sites that are
not well perfused, because this can cause severe burns after prolonged application. All listed sensors
operate without risk of exceeding 41°C on the skin if the initial skin temperature does not exceed 35°C.
Extremities to Avoid: Avoid placing the sensor on extremities with an arterial catheter, or intravascular
venous infusion line.
Connecting SpO2 Cables
♦Connect the sensor cable to the color-coded socket on the monitor. You can connect some Philips
sensors directly to the monitor. For other sensors, use the corresponding adapter cable.
CAUTION Extension cables: Do not use more than one extension cable (M1941A). Do not use an extension cable
with Philips reusable sensors or adapter cables with part numbers ending in -L (indicates “long” cable
version).
Electrical Interference: Position the sensor cable and connector away from power cables, to avoid
electrical interference.
Humidity: For neonatal patients, make sure that all sensor connectors and adapter cable connectors are
outside the incubator. The humid atmosphere inside can cause inaccurate measurements.
Measuring SpO2
1Select the correct patient category setting (adult/pediatric and neonatal), as this is used to optimize
the calculation of the SpO2 and pulse numerics.
2During measurement, ensure that the application site:
– has a pulsatile flow, ideally with a perfusion indicator value above 1.0.
– has not changed in its thickness (for example, due to edema), causing an improper fit of the
sensor.
SpO2 Signal Quality Indicator (Fast SpO2 only) 10 Monitoring SpO2
145
WARNING Inspect the application site every two to three hours to ensure skin quality and correct optical
alignment. If the skin quality changes, move the sensor to another site. Change the application site at
least every four hours.
CAUTION • Injected dyes such as methylene blue, or intravascular dyshemoglobins such as methemoglobin and
carboxyhemoglobin may lead to inaccurate measurements.
• Interference can be caused by:
– High levels of ambient light or strobe lights or flashing lights (such as fire alarm lamps). (Hint:
cover application site with opaque material.)
– Electromagnetic interference.
– Excessive patient movement and vibration.
SpO2 Signal Quality Indicator (Fast SpO2 only)
The SpO2 numeric is displayed together with a signal quality indicator (if configured and enough space
is available) which gives an indication of the reliability of the current values.
The level to which the triangle is filled shows the quality of the signal; the indicator below shows a
medium signal quality, the signal quality is at a maximum when the triangle is completely filled.
Assessing a Suspicious SpO2 Reading
Traditionally, pulse rate from SpO2 was compared with heart rate from ECG to confirm the validity of
the SpO2 reading. With newer algorithms, such as FAST-SpO2, this is no longer a valid criteria
because the correct calculation of SpO2 is not directly linked to the correct detection of each pulse.
When pulse rate is very low, or strong arrhythmia is present, the SpO2/Pleth pulse rate may differ from
the heart rate calculated from ECG but this does not indicate an inaccurate SpO2 value.
If you doubt the measured SpO2, use the signal quality indicator (if available) or the pleth wave and
perfusion indicator instead to assess the signal quality.
NOTE With pulse oximetry, sensor movement, ambient light (especially strobe lights or flashing lights) or
electromagnetic interference can give unexpected intermittent readings when the sensor is not attached
to a patient. Especially bandage-type sensor designs are sensitive to minimal sensor movement that
might occur when the sensor is dangling.
SpO2
10 Monitoring SpO2Changing the Averaging Time
146
Changing the Averaging Time
Depending on the monitor configuration, you may be able to change the averaging time for the SpO2
values. The averaging time represents the approximate time period used for the calculation. The exact
averaging algorithm depends on the SpO2 technology (option) used and on the signal conditions. The
longer the averaging time, the longer the time needed until the SpO2 value reflects the physiological
event. Fast averaging is useful for situations where an extremely fast measurement is required or few
artifacts are expected. Use slow averaging where you expect the number of artifacts to be relatively high.
1In the SpO2 Setup, select Average.
2Select the required averaging time from the list.
Setting the Measurement Mode
When a telemetry device supplies SpO2T to the monitor via short range radio transmission, the
monitor will have a manual measurement mode available. This allows SpO2 measurements to be made
on request and not continuously, helping to save the telemetry device’s battery power.
To set the measurement mode,
1In the SpO2 Setup, select Mode.
2Select Continuous or Manual mode.
Making a Manual Measurement
When the measurement mode is set to manual,
♦In the SpO2 Setup, select Measure SpO2.
When manual measurements are made, there will be no continuous SpO2 monitoring or alarming.
The manual measurement value reflects a momentary status. The numerics from SpO2T
measurements made in manual mode, for example SpO2T, PerfT, PulseT, will remain for a time on
the main screen. They are annotated with the time that the measurement was made to distinguish them
from continuously measured values.
Understanding SpO2 Alarms
This refers to SpO2 specific alarms. See the Alarms section for general alarm information. SpO2 offers
high and low limit alarms, and a high priority desat alarm. You cannot set the low alarm limit below
the desat alarm limit.
Perf T
Pleth Wave 10 Monitoring SpO2
147
CAUTION If you measure SpO2 on a limb that has an inflated NBP cuff, a non-pulsatile SpO2 INOP can occur.
If the monitor is configured to suppress this alarm there may be a delay of up to 60 seconds in
indicating critical patient status, such as sudden pulse loss or hypoxia.
Alarm Delays
There is a delay between a physiological event at the measurement site and the corresponding alarm at
the monitor. This delay has two components:
• The time between the occurrence of the physiological event and when this event is represented by
the displayed numerical values. This delay depends on the algorithmic processing and the
configured averaging time. The longer the averaging time configured, the longer the time needed
until the numerical values reflect the physiological event.
• The time between the displayed numerical values crossing an alarm limit and the alarm indication
on the monitor. This delay is the combination of the configured alarm delay time plus the general
system delay time (see “Monitor Performance Specifications” on page 251).
Adjusting the Alarm Limits
In the Setup SpO2 menu:
• Touch the high limit on the alarm limits menu button. Choose the high alarm limit from the pop-
up list that opens.
• Touch the low limit on the alarm limits menu button. Choose the low alarm limit from the pop-up
list that opens.
WARNING High oxygen levels may predispose a premature infant to retrolental fibroplasia. If this is a
consideration do NOT set the high alarm limit to 100%, which is equivalent to switching the alarm
off.
Adjusting the Desat Limit Alarm
The Desat alarm is a high priority (red) alarm notifying you of potentially life threatening drops in
oxygen saturation.
1In the Setup SpO2 menu, select DesatLimit.
2Adjust the limit.
Pleth Wave
The Pleth wave is autoscaled to maximum display size. It decreases only when the signal quality
becomes marginal. It is NOT directly proportional to the pulse volume. If you need an indication of
change in pulse volume, use the perfusion indicator.
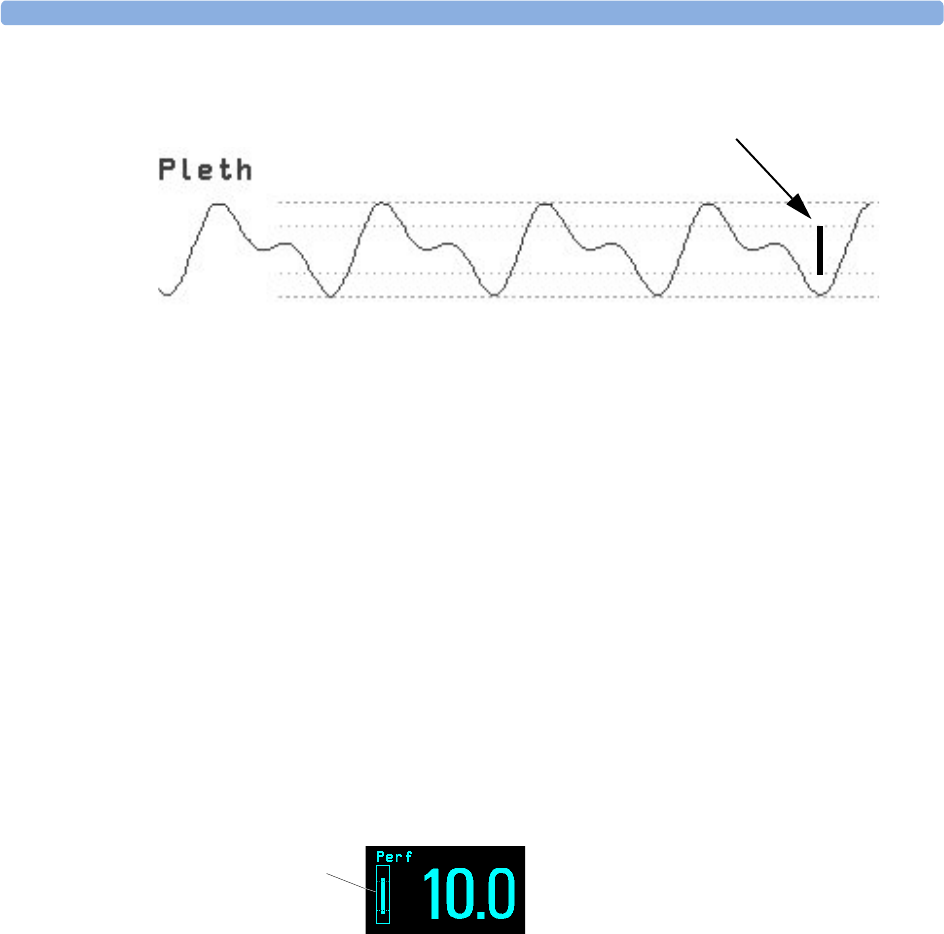
10 Monitoring SpO2Perfusion Numeric
148
Perfusion Numeric
The perfusion numeric (Perf) gives a value for the pulsatile portion of the measured signal caused by
the pulsating arterial blood flow.
As pulse oximetry is based on the pulsatile nature of the signal, you can also use the perfusion numeric
as a quality indicator for the SpO2 measurement. Above 1 is optimal, between 0.3-1 is acceptable.
Below 0.3 is marginal; reposition the sensor or find a better site.
Perfusion Change Indicator
The perfusion change indicator is a graphic symbol which shows the change in the perfusion value,
relative to a reference value which you can set.
To set the current perfusion value as the reference value:
♦In the Setup SpO2 menu, select Set Perf Ref..
When a reference value has been set, the perfusion change indicator is displayed next to the perfusion
numeric.
Setting SpO2/Pleth as Pulse Source
1In the Setup SpO2 menu, select Pulse (SpO2) to enter the Setup Pulse menu.
2In the Setup Pulse menu, select SystPulse and select SpO2 from the pop-up list.
Setting Up Tone Modulation
If tone modulation is on, the QRS tone pitch lowers when the SpO2 level drops. Remember, the QRS
tone is derived from either heart rate or pulse depending on which is currently selected as the active
alarm source.
♦In the Setup SpO2 menu, select Tone Mod. to toggle between Yes (for on) and No (for
off).
minimum size for reliable SpO2 value
Perfusion change
indicator

Setting the QRS Volume 10 Monitoring SpO2
149
Tone modulation is licensed under US patent US 4,653,498 from Nellcor Puritan Bennett
Incorporated.
Setting the QRS Volume
♦In the Setup SpO2 menu, select QRS Volume and set the appropriate QRS tone volume.

10 Monitoring SpO2Setting the QRS Volume
150

151
11
11Monitoring NBP
This monitor uses the oscillometric method for measuring NBP. In adult and pediatric mode, the
blood pressure measurements determined with this device comply with the American National
Standard for Electronic or Automated Sphygmomanometers (ANSI/AAMI SP10-1992) in relation to
mean error and standard deviation, when compared to intra-arterial or auscultatory measurements
(depending on the configuration) in a representative patient population. For the auscultatory reference,
the fifth Korotkoff sound was used to determine the diastolic pressure.
In neonatal mode, the blood pressure measurements determined with this device comply with the
American National Standard for Electronic or Automated Sphygmomanometers (ANSI/AAMI SP10-
1992) in relation to mean error and standard deviation, when compared to intra-arterial measurements
in a representative patient population.
The NBP measurement is suitable for use in the presence of electrosurgery and during the discharge of
a cardiac defibrillator according to IEC 601-2-30:1999/EN 60601-2-30:2000.
A physician must determine the clinical significance of the NBP information.
Introducing the Oscillometric NBP Measurement
Oscillometric devices measure the amplitude of pressure changes in the occluding cuff as the cuff
deflates from above systolic pressure. The amplitude suddenly increases as the pulse breaks through the
occlusion in the artery. As the cuff pressure decreases further, the pulsations increase in amplitude,
reach a maximum (which approximates to the mean pressure), and then diminish.
Studies show that, especially in critical cases (arrhythmia, vasoconstriction, hypertension, shock),
oscillometric devices are more accurate and consistent than devices using other noninvasive measuring
techniques.
WARNING Patient Category: Select the correct patient category setting for your patient. Do not apply the higher
adult inflation, overpressure limits and measurement duration to neonatal patients.
Intravenous infusion: Do not use the NBP cuff on a limb with an intravenous infusion or arterial
catheter in place. This could cause tissue damage around the catheter when the infusion is slowed or
blocked during cuff inflation.
Skin Damage: Do not measure NBP on patients with sickle-cell disease or any condition where skin
damage has occurred or is expected.
Unattended measurement: Use clinical judgement to decide whether to perform frequent unattended
blood pressure measurements on patients with severe blood clotting disorders because of the risk of
hematoma in the limb fitted with the cuff.

11 Monitoring NBP Preparing to Measure NBP
152
CAUTION If you spill liquid onto the equipment or accessories, particularly if there is a chance that it can get
inside the tubing or the measurement device, contact your service personnel.
Measurement Limitations
Measurements are impossible with heart rate extremes of less than 40 bpm or greater than 300 bpm, or
if the patient is on a heart-lung machine.
The measurement may be inaccurate or impossible:
• if a regular arterial pressure pulse is hard to detect
• with cardiac arrhythmias
• with excessive and continuous patient movement such as shivering or convulsions
• with rapid blood pressure changes
• with severe shock or hypothermia that reduces blood flow to the peripheries
• with obesity, where a thick layer of fat surrounding a limb dampens the oscillations coming from the
artery
• on an edematous extremity.
Measurement Methods
There are three methods of measuring NBP:
•Manual - measurement on demand.
•Auto - continually repeated measurements (between one and 120 minute adjustable interval).
•Sequence - up to four measurement cycles which will run consecutively, with number of
measurements and interval between them configurable for each cycle.
•STAT - rapid series of measurements over a five minute period, then the monitor returns to the
previous mode. Use only on supervised patients.
Reference Method
The NBP measurement reference method can be Auscultatory (manual cuff) or Invasive (intra-
arterial). For further information, see the Application Note on NBP supplied on the monitor
documentation CD-ROM.
In Adult and Pediatric mode to check the current setting, select Main Setup -> Measurements
-> NBP, and check whether the Reference setting is set to Auscult. or Invasive. This
setting can only be changed in Configuration Mode.
In Neonatal mode, to comply with safety standards, invasive is always used as the reference method.
This setting cannot be changed and is not visible in any operating mode.
Preparing to Measure NBP
1Connect the cuff to the air tubing.
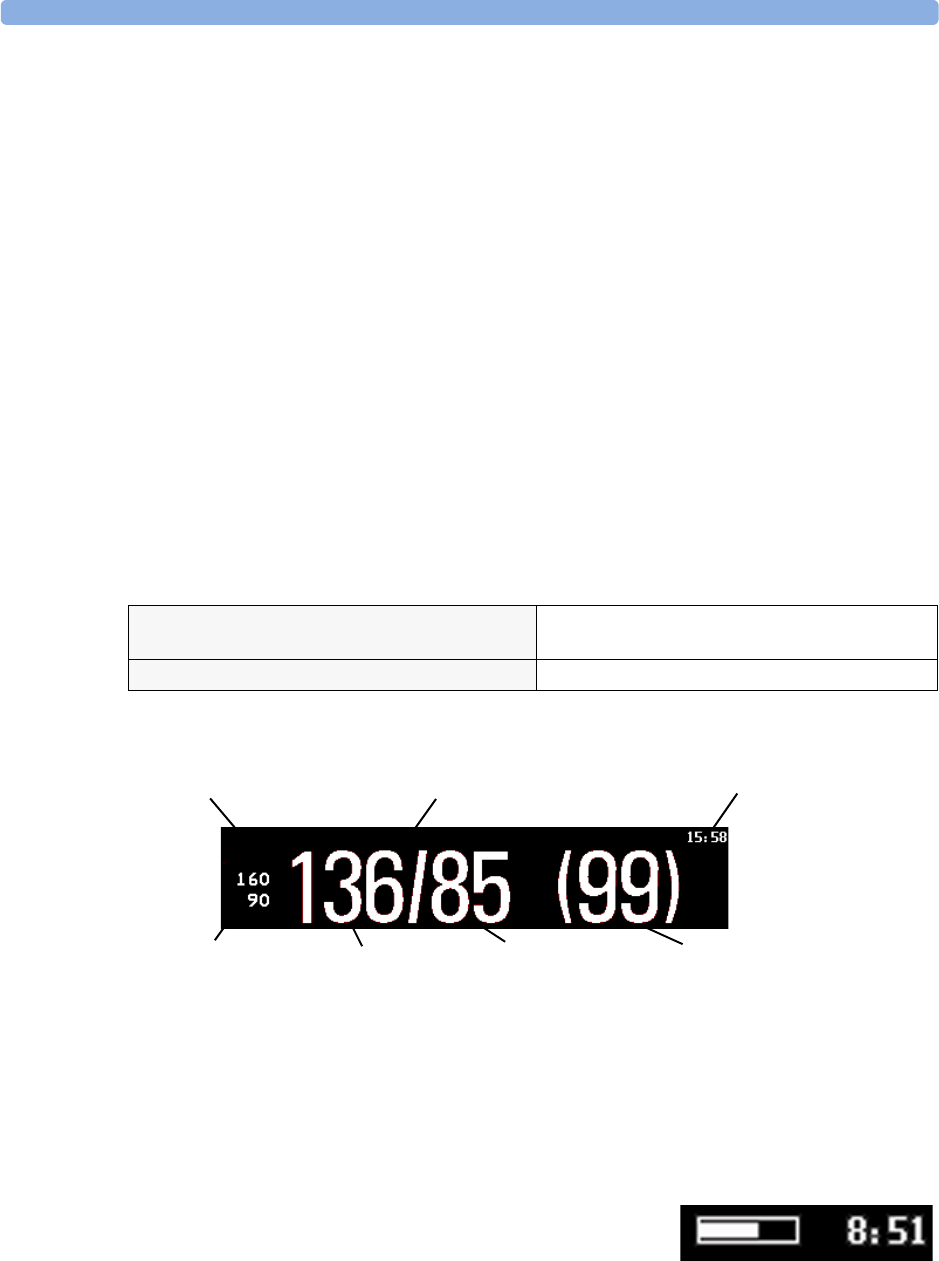
Preparing to Measure NBP 11 Monitoring NBP
153
2Plug the air tubing into the red NBP connector. Avoid compression or restriction of pressure tubes.
Air must pass unrestricted through the tubing.
3Make sure that you are using a Philips-approved correct sized cuff and that the bladder inside the
cover is not folded or twisted.
A wrong cuff size, and a folded or twisted bladder, can cause inaccurate measurements. The width
of the cuff should be in the range from 37% to 47% of the limb circumference. The inflatable part
of the cuff should be long enough to encircle at least 80% of the limb.
4Apply the cuff to a limb at the same level as the patient’s heart. If it is not, you must use the
measurement correction formula to correct the measurement.
The marking on the cuff must match the artery location. Do not wrap the cuff too tightly around
the limb. It may cause discoloration, and ischemia of the extremities. Inspect the application site
regularly to ensure skin quality and inspect the extremity of the cuffed limb for normal color,
warmth and sensitivity. If the skin quality changes, or if the extremity circulation is being affected,
move the cuff to another site or stop the blood pressure measurements immediately. Check more
frequently when making automatic or stat measurements.
Correcting the Measurement if Limb is not at Heart Level
To correct the measurement if the limb is not at heart level, to the displayed value
Understanding the NBP Numerics
Depending on the NBP numeric size, not all elements may be visible. Your monitor may be configured
to display only the systolic and diastolic values.
Alarm Sources if you have parallel alarm sources, the sources are displayed instead of the alarm limits.
NBP Timestamp depending on the configured NBP Time setting, the time shown beside the NBP
numeric can be:
–Meas Time: the time of the most recent NBP measurement, or
–Next Meas: the time until the next measurement in an
automatic series, displayed with a graphic representation of the
remaining time, as shown here.
add 0.75mmHg (0.10kPa) for each centimeter
higher or
deduct 0.75mmHg (0.10kPa) for each centimeter
lower or
add 1.9mmHg (0.25kPa) for each inch higher. deduct 1.9mmHg (0.25kPa) for each inch lower.
Auto
Sys.
Measurement Mode Timestamp/
Timer
Mean pressure
Diastolic
Alarm limits
Alarm source
Systolic
11 Monitoring NBP Starting and Stopping Measurements
154
During measurements the cuff pressure is displayed instead of the units and the repeat time. An early
systolic value gives you a preliminary indication of the systolic blood pressure during measurement.
Starting and Stopping Measurements
Use the Setup menu or SmartKeys to start and stop measurements.
CAUTION Use clinical judgement to decide whether to perform repeated series of STAT measurements because of
the risk of purpura, ischemia and neuropathy in the limb with the cuff.
Enabling Automatic Mode and Setting Repetition
Time
1In the Setup NBP menu, select Mode and select Auto from the pop-up menu.
2For an automatic measurement, select Repeat and set the time interval between two
measurements.
Enabling Sequence Mode and Setting Up The
Sequence
1In the Setup NBP menu, select Mode and select Sequence from the pop-up menu.
2Select Setup Sequence to open the Setup Sequence window.
Up to four measurement cycles can be setup which will run consecutively. For each cycle you can
set the number of measurements and the interval between them. If you want to run less than four
cycles in a sequence, you can set the number of measurements for one or more cycles to Off.
3Select each sequence in turn and select the number of measurements and the time interval between
the measurements.
4To have measurements continue after the sequence, set the number of measurements for your last
cycle to Continuous and this cycle will run indefinitely.
CAUTION Be aware that, if none of the cycles are set to Continuous, NBP monitoring will end after the last
measurement of the cycle.
When the NBP measurement mode is set to Sequence, the repetition time for Auto mode cannot
be changed.
Choosing the NBP Alarm Source
You can monitor for alarm conditions in systolic, diastolic and mean pressure, either singly or in
parallel. Only one alarm is given, with the priority of mean, systolic, diastolic.
In the Setup NBP menu, select Al. from and choose from:
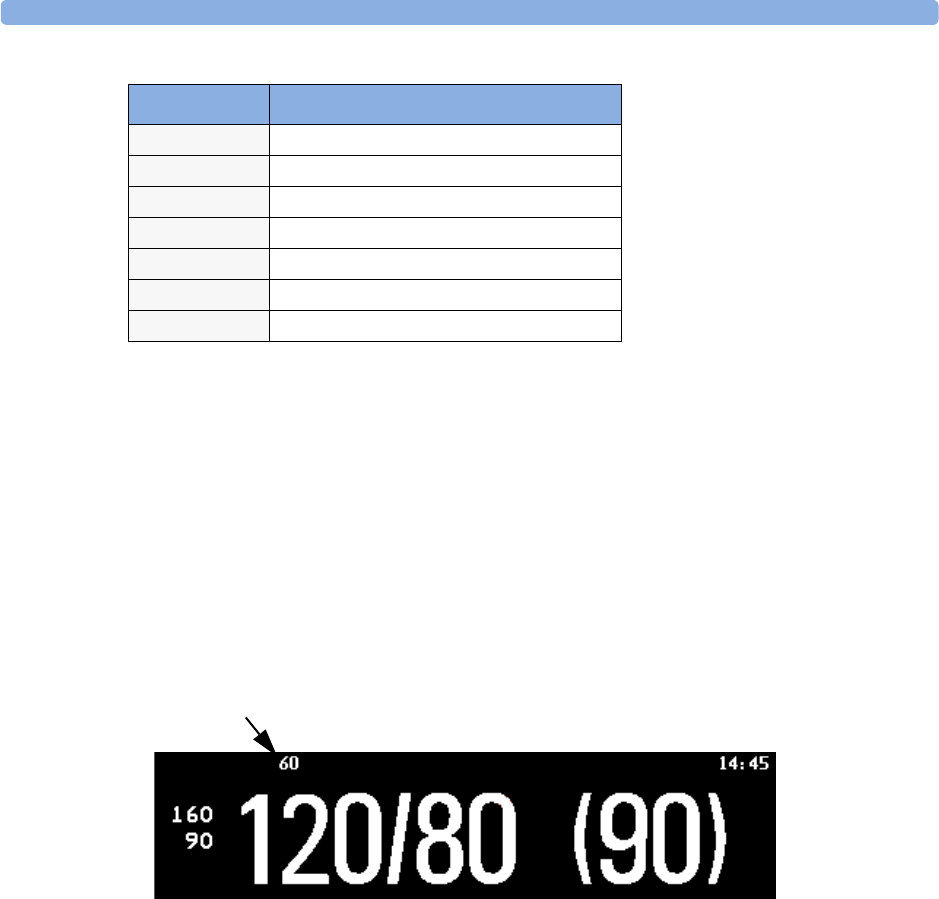
Switching Pulse from NBP On/Off 11 Monitoring NBP
155
If mean is not selected as alarm source (Sys, Dia, or Sys&Dia selected), but the monitor can only derive
a mean value, mean alarms will nevertheless be announced using the most recent mean alarm limits.
When no value can be derived an NBP MEASURE FAILED INOP will be displayed.
Switching Pulse from NBP On/Off
In the process of making the NBP measurement, a pulse value can be derived and displayed. The pulse
value is displayed together with the time the measurement was made. After one hour the value becomes
invalid. There are no alarms associated with pulse from NBP.
To switch the display of the pulse value on or off:
♦In the NBP Setup menu select Pulse (NBP).
Assisting Venous Puncture
You can use the NBP cuff to cause sub-diastolic pressure. The cuff deflates automatically after a set
time (adult/pediatric 170 seconds, neonatal 85 seconds) if you do not deflate it.
1In the NBP Setup menu select VeniPuncture.
2Puncture vein and draw blood sample.
3Reselect VeniPuncture to deflate the cuff.
During measurement, the NBP display shows the inflation pressure of the cuff and the remaining time
in venous puncture mode.
Menu option Pressure value monitored
Sys. systolic
Dia. diastolic
Mean mean
Sys&Dia systolic and diastolic in parallel
Dia&Mean diastolic and mean in parallel
Sys&Mean systolic and mean in parallel
Sys&Dia&Mean all three pressures in parallel
Pulse from NBP
NBP Auto
Sys.
Pulse
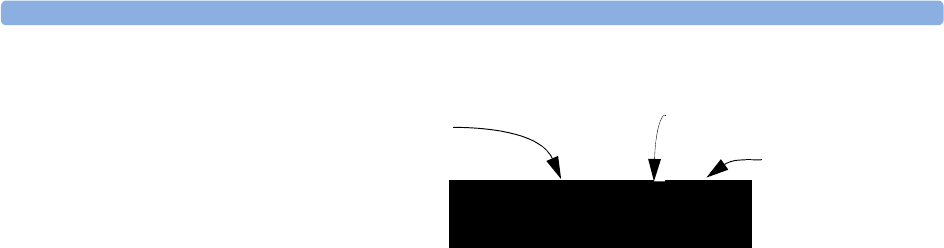
11 Monitoring NBP Calibrating NBP
156
Calibrating NBP
NBP is not user-calibrated. Cuff-pressure transducers must be verified and calibrated, if necessary, at
least once every two years by a qualified service professional. See the Service Guide for details.
(60)
Cuff pressure
Venous puncture measurement mode
VP
NBP 01:45
Time left in venous
puncture mode
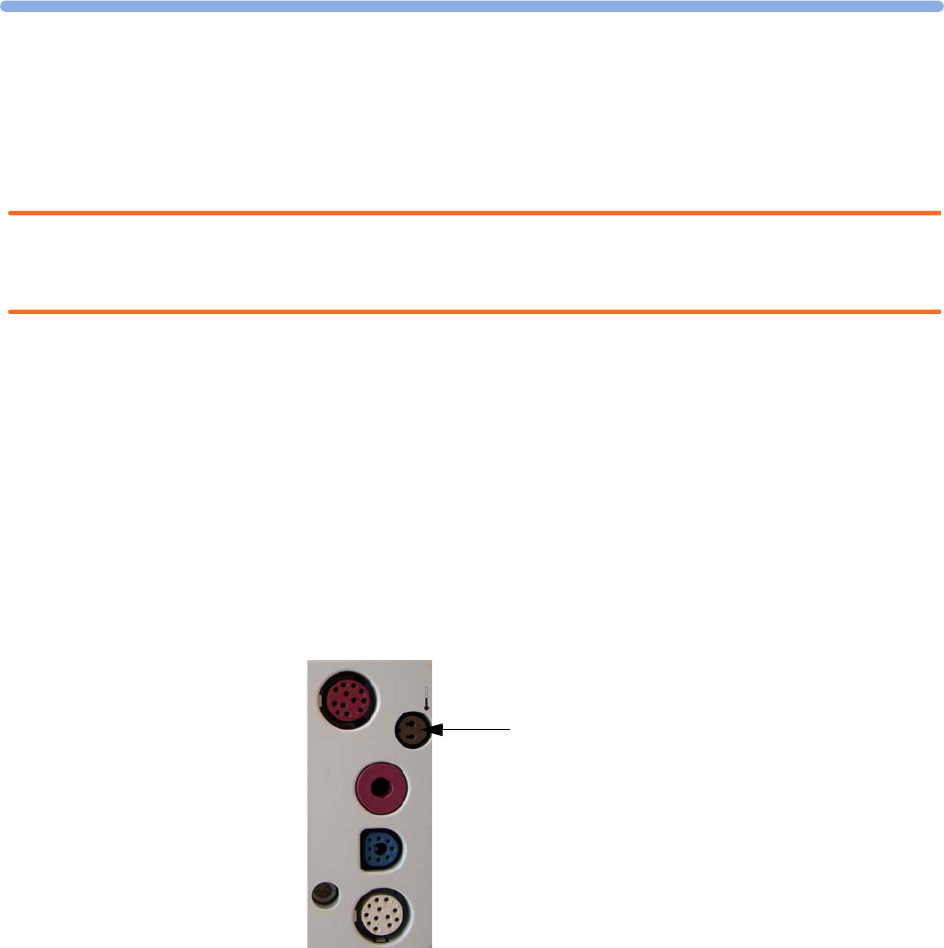
157
12
12Monitoring Temperature
WARNING Measurements from an MMS extension connected to the monitor are not available when the monitor
is running on battery power. They are only available when the monitor is powered by the external
power supply (M8023A).
You can measure temperature using the built-in temperature measurement (optional), or one of the
MMS extensions.
Temp measurement automatically switches on when you connect a probe. You can switch the
measurement off manually.
Making a Temp Measurement
1Select the correct type and size of probe for your patient.
2If you are using a disposable probe, connect the probe to the temperature cable.
3Plug the probe or temperature cable into the temperature connector socket.
4Apply the probe to the patient. You are advised to use a protective rubber cover on rectal probes.
5Select an appropriate temperature label.
6Check that the alarm settings (on or off, high and low limits) are appropriate for this patient and
this type of temperature measurement.
Temp connector socket
12 Monitoring Temperature Calculating Temp Difference
158
WARNING Make sure you set alarm limits for the correct label. The alarm limits you set are stored for that
particular label only. Changing the label may change the alarm limits.
Selecting a Temperature for Monitoring
Tell the monitor which temperature you want to monitor by selecting its temperature label. The label
is a unique identifier for each type of temperature. When you choose a label, the monitor uses that
label’s stored color and alarm settings.
1In the Setup <Temp> menu, select Label.
2Select the appropriate label from the list.
Extended Temperature Label Set
The following additional labels are available if Label Set is set to Full. This setting can only be
changed in Configuration Mode.
Note that if your monitor is connected to an Information Center, the additional labels in the extended
label set may not be correctly displayed. See the Configuration Guide for your monitor for more
information.
Calculating Temp Difference
The monitor can calculate and display the difference between two temperature values by subtracting
the second value from the first. The difference is labeled 'Temp.
1In the Main Setup menu, select Measurements.
2In the Setup 'Temp menu, select First Temp.
3Label the measurement source as appropriate.
4Select Second Temp.
5Label the measurement source as appropriate.
Temp non-specific temperature label. Trect rectal temperature
Tart arterial temperature Tskin skin temperature
Tcore core temperature Tven venous temperature
Tesoph esophageal temperature Tnaso nasopharyngeal temperature
T1, T2, T3, T4 Non-specific temperature labels
Tamb ambient temperature
Tcereb cerebral temperature
Ttymp tympanic temperature
Tvesic vesical temperature
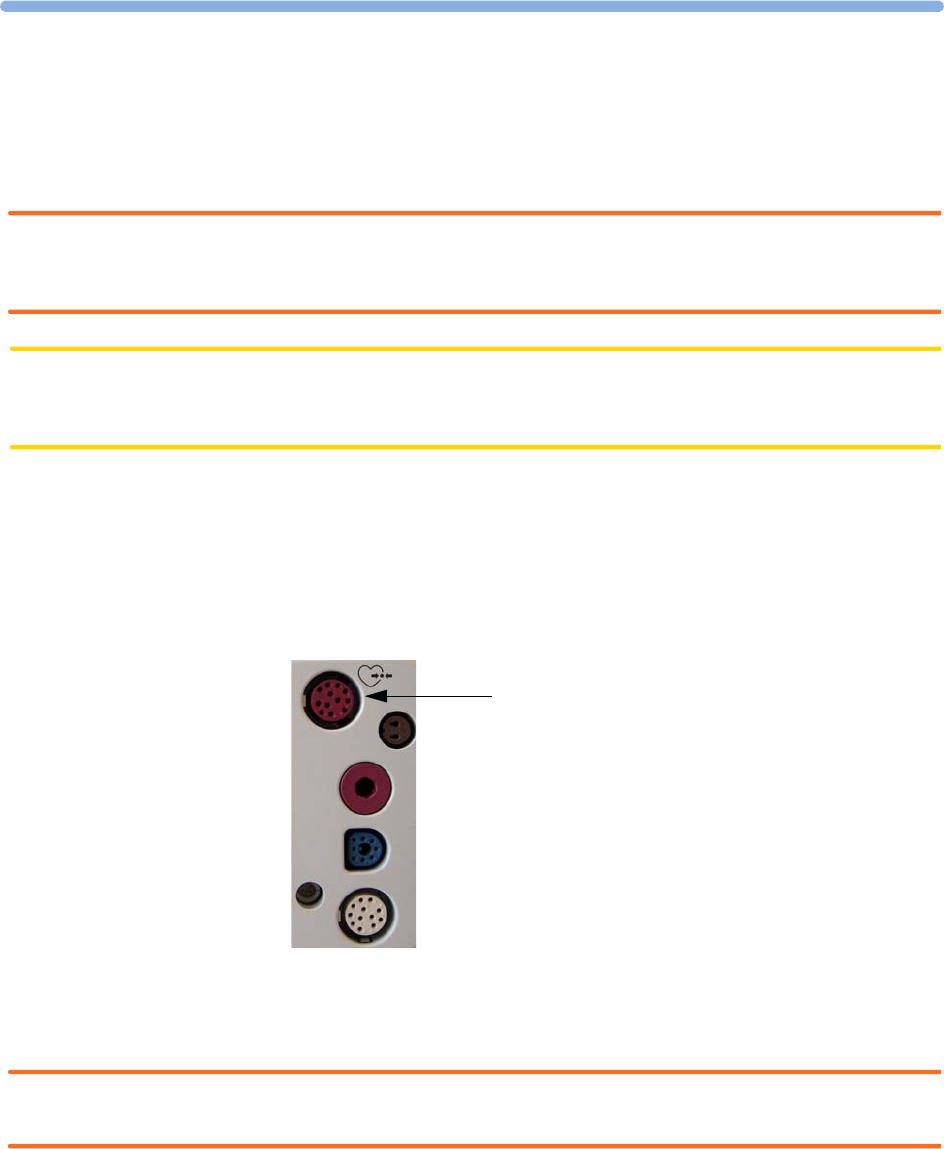
159
13
13Monitoring Invasive Pressure
WARNING Measurements from an MMS extension connected to the monitor are not available when the monitor
is running on battery power. They are only available when the monitor is powered by the external
power supply (M8023A).
CAUTION Do not use the MP2 in combination with other monitors using an M1006A pressure module and the
HP1290A pressure transducer. This may cause interference on the respiration or invasive pressure
signals.
You can measure pressure using the monitor’s built-in pressure measurement (optional), or one of the
MMS extensions.
Setting up the Pressure Measurement
1Plug in the pressure cable.
2Prepare the flush solution.
3Flush the system to exhaust all air from the tubing. Ensure that the transducer and stopcocks are
free of air bubbles.
WARNING If air bubbles appear in the tubing system, flush the system with the infusion solution again. Air
bubbles may lead to a wrong pressure reading.
Pressure connector
13 Monitoring Invasive Pressure Setting up the Pressure Measurement
160
4Connect the pressure line to the patient catheter.
5If you are using an infusion pressure cuff with the pressure line, attach the pressure cuff to the fluid
to be infused. Inflate it according to your standard hospital procedure, then start the infusion.
6Position the transducer so that it is level with the heart, approximately at the level of the
midaxillary line.
WARNING If measuring intracranial pressure (ICP, IC1 or IC2) with a sitting patient, level the transducer with the
top of the patient’s ear. Incorrect leveling may give incorrect values.
Selecting a Pressure for Monitoring
Tell the monitor which pressure you want to monitor by selecting its pressure label. The label is a
unique identifier for each type of pressure. When you choose a label, the monitor uses that label’s
stored settings, for example color, wave scale and alarm settings. The label also determines which
algorithm is used to process the pressure signal, so an incorrect label can lead to incorrect pressure
values.
1In the Setup <Press> menu, select Label.
2Select the appropriate label from the list.
Extended Pressure Label Set
The following additional labels are available if Label Set is set to Full. This setting can only be
changed in Configuration Mode.
Note that if your monitor is connected to an Information Center, the additional labels in the extended
label set may not be correctly displayed. See the Configuration Guide for your monitor for more
information.
Label Description Label Description
ABP Arterial blood pressure PNon-specific pressure label
ART Arterial blood pressure (alternative) PAP Pulmonary artery pressure
Ao Aortic pressure RAP Right atrial pressure
CVP Central venous pressure UAP Umbilical arterial pressure
ICP Intracranial pressure UVP Umbilical venous pressure
LAP Left atrial pressure
Label Description
BAP Brachial arterial pressure
FAP Femoral arterial pressure
IC1, IC2 Alternative intracranial pressures
P1, P2, P3, P4 Alternative non-specific pressure labels

Zeroing the Pressure Transducer 13 Monitoring Invasive Pressure
161
Zeroing the Pressure Transducer
To avoid inaccurate pressure readings, the monitor requires a valid zero. Zero the transducer in
accordance with your hospital policy (at least once per day). You must perform a zero:
• when you use a new transducer or tubing
• every time you reconnect the transducer cable to the monitor
• if you think the monitor’s pressure readings are not correct.
Zeroing ICP (or IC1/IC2)
Your hospital guidelines may require you to zero the ICP transducer less frequently than other
transducers, due to the need for aseptic conditions. When you zero an ICP transducer, the zero values
are automatically stored and you will not be prompted to repeat the zero procedure.
If you want to simultaneously zero all pressures except ICP, disconnect the ICP transducer from the
monitor while zeroing. Reconnecting the transducer recalls the stored values.
WARNING If you select the label ICP (or IC1/IC2), the measurement device uses the most recently stored zero.
Therefore, make sure you zeroed the transducer correctly in accordance with the transducer
manufacturer’s instructions and your hospital policy. When you use a transducer that you cannot
rezero after placement, ensure that you keep the measuring device with the patient so that you are
certain you have the correct zero data for this patient.
Determining a Pressure’s Most Recent Zero
The monitor displays the most recent zero on the status line. If this has “timed-out” after you have
performed a zero, redisplay the information in the status line by entering the pressure’s setup menu.
Zeroing a Pressure Measurement
WARNING Invasive pressure alarms (and pulse alarms, if derived from invasive pressure) are temporarily
suppressed until 30 seconds after the transducer finishes zeroing.
1Turn off the stopcock to the patient.
2Vent the transducer to atmospheric pressure, to compensate for the static and atmospheric pressure
exerted on the transducer.
3In the setup menu for the pressure, select Zero <Press>.
4When you see the message <Press> zero done at <date and time> on the status
line, (for example, ABP zero done at 13 Mar 02 23.35) close the stopcock to
atmospheric pressure, and open the stopcock to the patient.
CAUTION When using high frequency ventilation, ensure that the tubing from the ventilator does not touch the
arterial line, or connect with it indirectly, while zeroing the pressure. This could cause small pressure
variations which can interfere with the zero procedure.
13 Monitoring Invasive Pressure Adjusting the Calibration Factor
162
Zeroing All Pressures Simultaneously
WARNING Before zeroing all pressures, make sure that all pressure transducers are vented to atmospheric pressure.
If you are measuring pressures with more than one measuring device, using the Zero Press
SmartKey to initiate the zeroing calls up a list of all active pressures. Select the pressure you want to
zero or select All Press to zero all pressures simultaneously.
Troubleshooting the Zero
The status line lists the probable cause of an unsuccessful zero:
Adjusting the Calibration Factor
Each time you use a reusable transducer, compare the calibration factor written on your transducer
with the calibration factor shown on the monitor. To ensure accurate measurement, they must be the
same.
1In the Setup <Press> menu, select Cal. Factor.
If the value here does not match that on the transducer, select the corresponding value from the
list now in accordance with your hospital’s procedure.
2To confirm you want to use the new calibration factor, select the Confirm popup.
Displaying a Mean Pressure Value Only
Use this when you want to see only the mean pressure.
♦In the pressure’s setup menu, select Mean only. Toggle between On to display mean pressure
value only, and Off to display all pressure values (systolic, diastolic and mean).
Message Corrective Action
can’t zero;
equipment malf.
The hardware is faulty. Contact your service personnel.
can’t zero;
excessive offset
Make sure the transducer is vented to air and try again. If this fails, the hardware
may be faulty. Replace the adapter cable and try again. If it fails, replace the
transducer and try again. If it still fails, contact your service personnel.
can’t zero -
unstable signal
can’t zero - no
transducer
Make sure that the transducer is connected and try again. If this fails, exchange
the adapter cable and try again. If this fails, exchange the transducer.
can’t zero;
pulsat. pressure
Make sure that the transducer is vented to air, not to the patient, and try again.
unable to zero -
timed out
Try pressing the Zero key again. If this fails, replace the transducer and adapter
cable and contact your service personnel.
switch <Press> on
first
Pressure measurement is switched off. To switch it on, in the Setup Pressure
menu, select the pressure’s label.
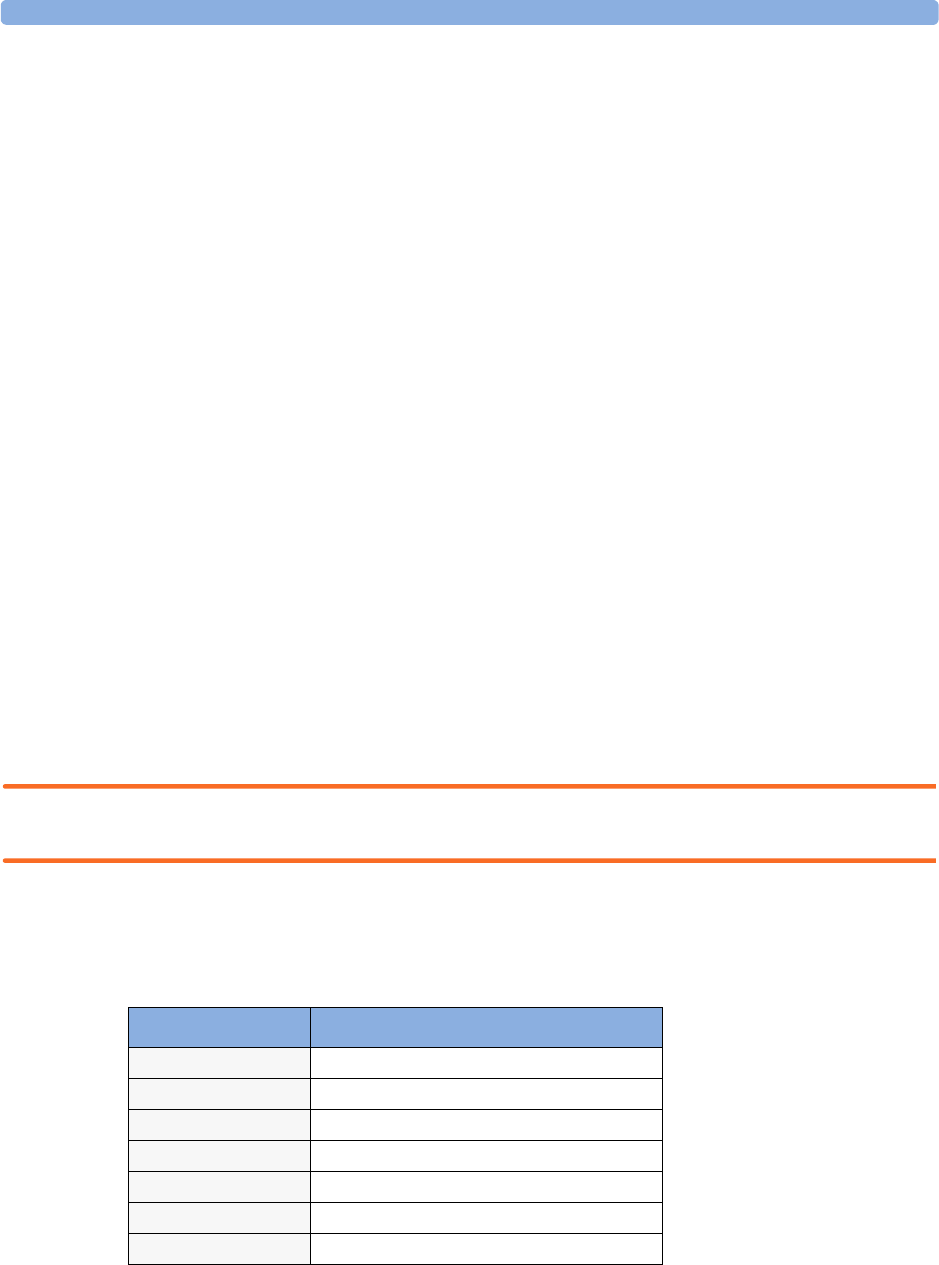
Changing the Pressure Wave Scale 13 Monitoring Invasive Pressure
163
Changing the Pressure Wave Scale
1Select the label of the pressure wave whose scale you want to set to enter the Setup menu.
2In the Setup <Press> menu, (for example ABP) select Scale.
3Select a value from the pop-up list:
– a positive value sets the top gridline. The bottom gridline is set at zero.
– a negative value sets the bottom gridline. The middle gridline is set at zero.
Optimizing the Waveform
♦In the Setup <Press> menu, select Optimum Scale to let the monitor select the best
minimum and maximum scales for the current wave.
Non-Physiological Artifact Suppression
Some clinical procedures may affect blood pressure, for example, a flush procedure or a blood sample.
Your monitor may be configured to suppress these non-physiological artifacts for a specified duration
(Artifact Suppression is configured to 30, 60, or 90 seconds). During artifact suppression,
the monitor shows the INOP message <Pressure label> ARTIFACT, and a question mark is
shown beside the pressure numerics. Pressure alarms and the Pulse NON-PULSATILE INOP are
suppressed during the configured period. The CPP high alarm is not suppressed.
Choosing the Pressure Alarm Source
WARNING Make sure you set alarm limits for the correct label. The alarm limits you set are stored for that
particular label only. Changing the label may change the alarm limits.
You can monitor for alarm conditions in systolic, diastolic and mean pressure, either singly or in
parallel. Only one alarm is given at a time, in this order of priority: mean, systolic, diastolic.
♦In the Setup <Press> menu, select Al. from and choose the source.
♦Select and set the High Limit and Low Limit for the pressure(s) you have selected.
Menu option Pressure value monitored
Sys. systolic
Dia. diastolic
Mean mean
Sys & Dia systolic and diastolic in parallel
Dia & Mean diastolic and mean in parallel
Sys & Mean systolic and mean in parallel
Sys&Dia&Mean all three pressures in parallel
13 Monitoring Invasive Pressure Choosing the Pressure Alarm Source
164
Extreme Alarm Limits
The extreme pressure alarms, Extreme High and Extreme Low, can be made available for your monitor
in Configuration Mode and are additional to the standard High and Low limit alarms. They are
generated by the active pressure alarm source, and are setup in Configuration Mode by adding a set
value (the ' value) to the high and low alarm limits. This value can be set for each pressure label
individually.
You need to know which values have been configured for your monitor. Changing the high and low
alarm limits automatically changes the extreme alarm limits within the allowed range.
♦To see the extreme pressure alarms set for your monitor, in the Setup <Press> menu, see the
menu items 'Extr. High and 'Extr. Low.
The extreme pressure alarms are high priority, red alarms, marked *** in the alarm message.
Low
Limit
High
Limit
Extreme
Low Limit
Extreme
High Limit
' Extreme Low ' Extreme High
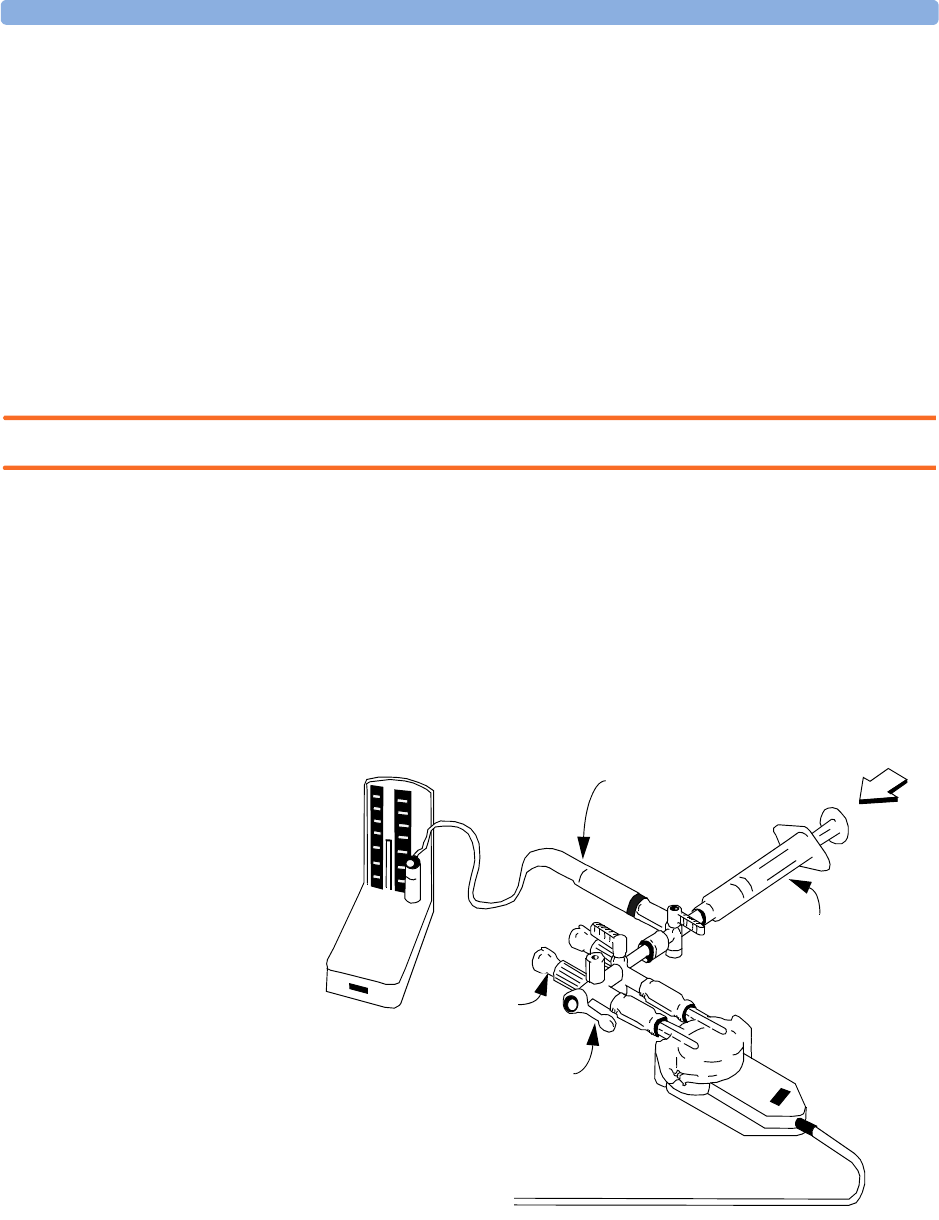
Calibrating Reusable Transducer CPJ840J6 13 Monitoring Invasive Pressure
165
Calibrating Reusable Transducer CPJ840J6
Depending on your monitor’s configuration, you may be able to perform a calibration in monitoring
mode. Perform a mercury calibration when you use a new transducer, and at regular intervals according
to your hospital policy. You require:
• standard sphygmomanometer.
• sterile 10cc syringe with heparinised solution.
• 3-way stopcock.
• approximately 25cm of tubing.
Making the Pressure Calibration
WARNING Never perform the invasive pressure calibration while a patient is being monitored.
1Zero the transducer.
2Connect the syringe and manometer.
a. Attach the tubing to the manometer.
b. Connect the 3-way stopcock to the stopcock that is not connected to the patient catheter when
you measure a patient.
c. Attach the syringe to one port and the manometer tubing to the other port.
d. Open the port to the manometer.
3Move the syringe barrel in and raise the mercury to 200mmHg (30kPa). 200mmHg is the
recommended calibration pressure.
4In the Setup Pressure menu, select Cal. Press.
M1006A
12
PIN
PRESS
PRESS
T
ZERO
tubing to manometer
Syringe with
heparinised solution
Off
Patient
connection
stoppered
Pressure connector on
monitor
13 Monitoring Invasive Pressure Calculating Cerebral Perfusion
166
5Select the calibration pressure from the list, for example 200 mmHg.
6Select Confirm to recalculate the calibration factor using the applied pressure.
7When the monitor displays <Press> calibration done at <date and time>,
remove the manometer tubing, syringe and extra stopcock. We recommend you replace the
transducer dome and tubing with sterile ones.
8Label the transducer with the calibration factor shown in the Cal. Factor field in the
pressure’s setup menu.
9Reconnect the patient and start measuring again.
Troubleshooting the Pressure Calibration
The status line lists the probable cause of an unsuccessful calibration.
Calculating Cerebral Perfusion
The monitor can calculate the difference between mean arterial pressure and the intracranial pressure.
The difference is labeled CPP.
1In the Main Setup menu, select Measurements.
2In the Setup CPP menu, select ABP, ART, Ao, BAP or FAP as the arterial pressure source.
Message Corrective Action
can’t calibr.; equipmt
malf.
Contact your service department. The pressure hardware is faulty.
can’t calibrate;out of
range
Make sure that you have selected the value for Cal. Press that
you are applying to the transducer, and repeat the calibration.
can’t calibr.; no
transd.
Make sure that the transducer is connected and try again.
can’t cal.; unstable
signal
Make sure there are no disturbances to the transducer, and repeat
the calibration.
can’t calibr.;do zero
first
No valid zero. Zero the transducer.
167
14
14Monitoring Carbon Dioxide
WARNING • Measurements from an MMS extension connected to the monitor are not available when the
monitor is running on battery power. They are only available when the monitor is powered by the
external power supply (M8023A).
•Only one CO
2 measurement at a time is supported.
Use the CO2 measurement to monitor the patient’s respiratory status and to control patient
ventilation.
There are two methods for measuring carbon dioxide in the patient’s airway:
• Mainstream measurement uses a CO2 sensor attached to an airway adapter directly inserted into the
patient’s breathing system. This method is available using the monitor’s built-in CO2 measurement
(optional), the M3014A Capnography Extension or the M3016A Mainstream Extension.
• Sidestream measurement takes a sample of the respiratory gas with a constant sample flow from the
patient’s airway and analyzes it with a remote CO2 sensor. You can measure sidestream CO2 using
the monitor’s built-in CO2 measurement (optional) or using the M3014A Capnography Extension,
or the M3015A Microstream CO2 Extension.
In both cases, the measurement principle is infrared transmission, where the intensity of infrared light
passing the respiratory gas is measured with a photo detector. As some of the infrared light is absorbed
by the CO2 molecules, the amount of light passing the gas probe depends on the concentration of the
measured CO2.
When using a wet ventilator circuit, monitor mainstream CO2 if available, in preference to sidestream
CO2.
The partial pressure is calculated from the gas concentration by multiplying the concentration value
with the ambient pressure.
The measurement provides:
•a CO
2 waveform.
• an end tidal CO2 (etCO2) value: the CO2 value measured at the end of the expiration phase.
• an inspired minimum CO2 (imCO2): the smallest value measured during inspiration.
• an airway respiration rate (awRR): the number of breaths per minute, calculated from the CO2
waveform.
14 Monitoring Carbon Dioxide Measuring CO2 using the CO2 Option or M3014A
168
Depending on the Max Hold setting configured for your monitor, the etCO2 numeric shows either
the highest CO2 value measured within the configured time period (Max Hold set to 10 sec or
20 sec) or the etCO2 numeric shows breath-to-breath value (Max Hold set to Off).
WARNING Correlation: The etCO2 readings do not always correlate closely with paCO2, especially in neonatal
patients and patients with pulmonary disease, pulmonary embolism or inappropriate ventilation.
Pharmaceuticals in aerosols: Do not measure CO2 in the presence of pharmaceuticals in aerosols.
Explosion Hazard: Do not use in the presence of flammable anesthetics or gases, such as a flammable
anesthetic mixture with air, oxygen or nitrous oxide. Use of the devices in such an environment may
present an explosion hazard.
Failure of operation: if the measurement or a sensor fails to respond as described, do not use it until
the situation has been corrected by qualified personnel.
Low etCO2 values: Leakages in the breathing system or sampling system may cause the displayed
etCO2 values to be significantly too low. Always connect all components securely and check for leaks
according to standard clinical procedures. Displacement of the nasal or combined nasal oral cannulas
can cause lower than actual etCO2 readings. Even with combined nasal oral cannulas, the etCO2
readings may be slightly lower than actual in patients breathing through the mouth only.
Measuring CO2 using the CO2 Option or M3014A
The monitor (with the CO2 option) or the M3014A Capnography Extension measures partial pressure
of carbon dioxide in a patient’s expired gas using the mainstream method or the sidestream method.
The mainstream CO2 measurement can be used, with appropriate accessories, with intubated adult,
pediatric and neonatal patients. The sidestream CO2 measurement can be used, with appropriate
accessories, with intubated and nonintubated adult, pediatric, infant and neonatal patients. With
intubated patients, a sample of the respiratory gas is drawn from the patient’s breathing circuit through
an airway adapter and a gas sampling tube. With non-intubated patients, the gas sample is drawn
through a nasal or oral-nasal cannula.
WARNING Altitude Setting: The monitor is not equipped with automatic barometric pressure compensation.
Before the CO2 measurement is used for the first time, the altitude must be set to the correct value. An
incorrect altitude setting will result in incorrect CO2 readings. The CO2 readings will typically deviate
5% for every 1000m difference.
Electrical Shock Hazard: Do not open the monitor or measurement device. Contact with exposed
electrical components may cause electrical shock. Always turn off and remove power before cleaning
the sensor, monitor or measurement device. Do not use a damaged sensor or one with exposed
electrical contacts. Refer servicing to qualified service personnel.
Preparing to Measure Mainstream CO2
You must perform a zero as described in this procedure each time you use a new airway adapter.
1Attach the sensor connector to the CO2 connector on the monitor (when the optional CO2
measurement is integrated) or on the extension.
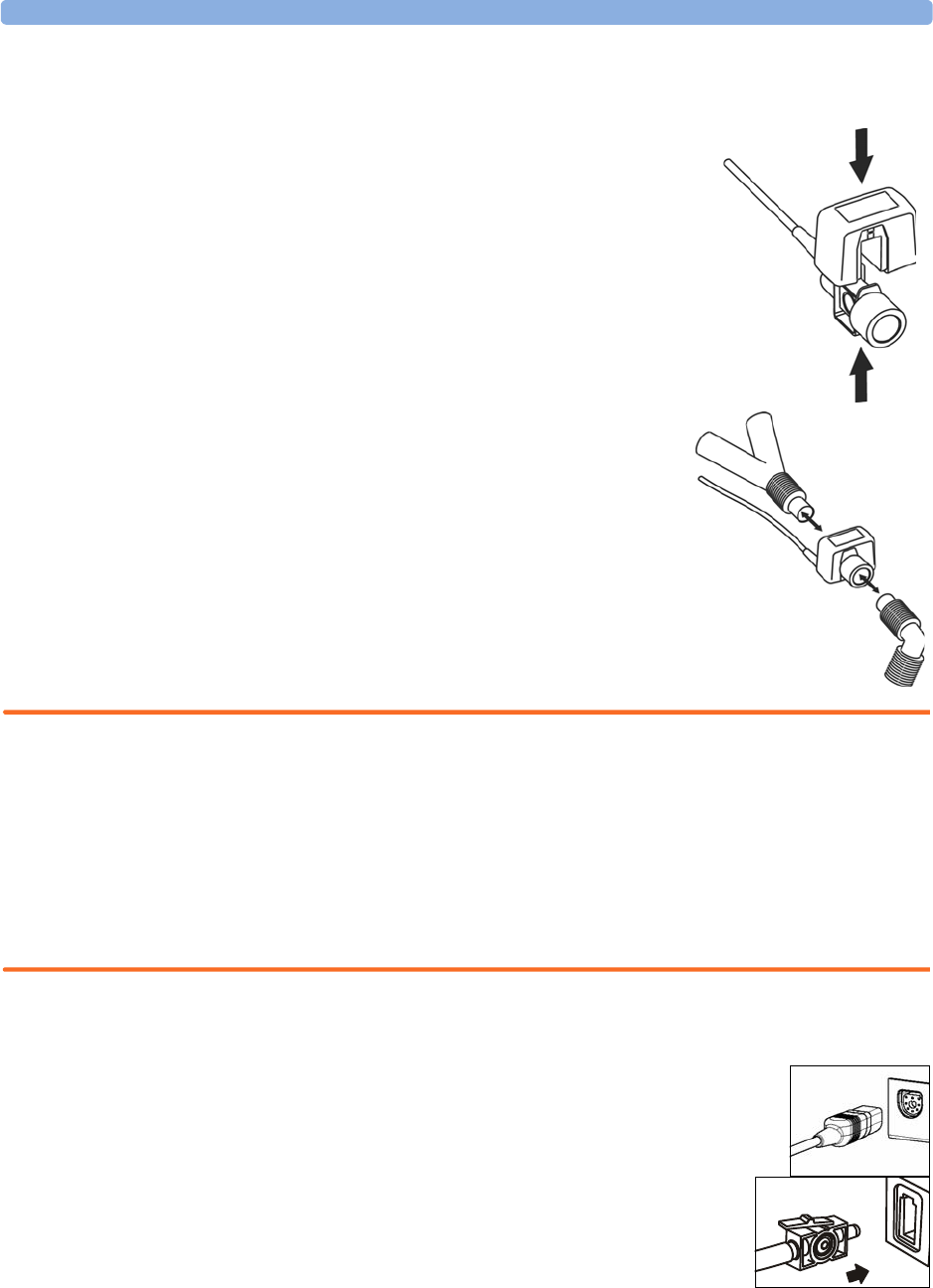
Measuring CO2 using the CO2 Option or M3014A 14 Monitoring Carbon Dioxide
169
2Wait 2 minutes, allowing the sensor to reach its operating temperature and a stable thermal
condition.
3Choose the appropriate airway adapter and connect it to the sensor
head. The airway adapter clicks into place when seated correctly.
4To zero the se nsor :
– expose the sensor to room air and keep it away from all sources of
CO2 including the ventilator, the patient’s breath and your own.
– in the setup menu for the CO2, select Start Zero Cal.
– When you see the message Zero done at <date and
time> on the status line, the zero calibration is finished and you
can begin monitoring.
5Install the airway adapter at the proximal end of the circuit
between the elbow and the ventilator Y-section.
WARNING To prevent stress on the endotrachial tube, support the sensor and airway adapter.
Position sensor cables and tubing carefully to avoid entanglement or potential strangulation. Do not
apply excessive tension to any cable.
Replace the airway adapter, if excessive moisture or secretions are observed in the tubing or if the CO2
waveform changes unexpectedly without a change in patient status.
To avoid infection, use only sterilized, disinfected or disposable airway adapters.
Inspect the airway adapters prior to use. Do not use if airway adapter appears to have been damaged or
broken. Observe airway adapter color coding for patient population.
Preparing to Measure Sidestream CO2
1Plug the sensor cable into the monitor’s CO2 input connector. Allow the sensor
two minutes warm up time
2Connect the cannula, airway adapter, or sample line as appropriate, to the
sensor. It will click into place when seated correctly.
3To zero the se nsor :
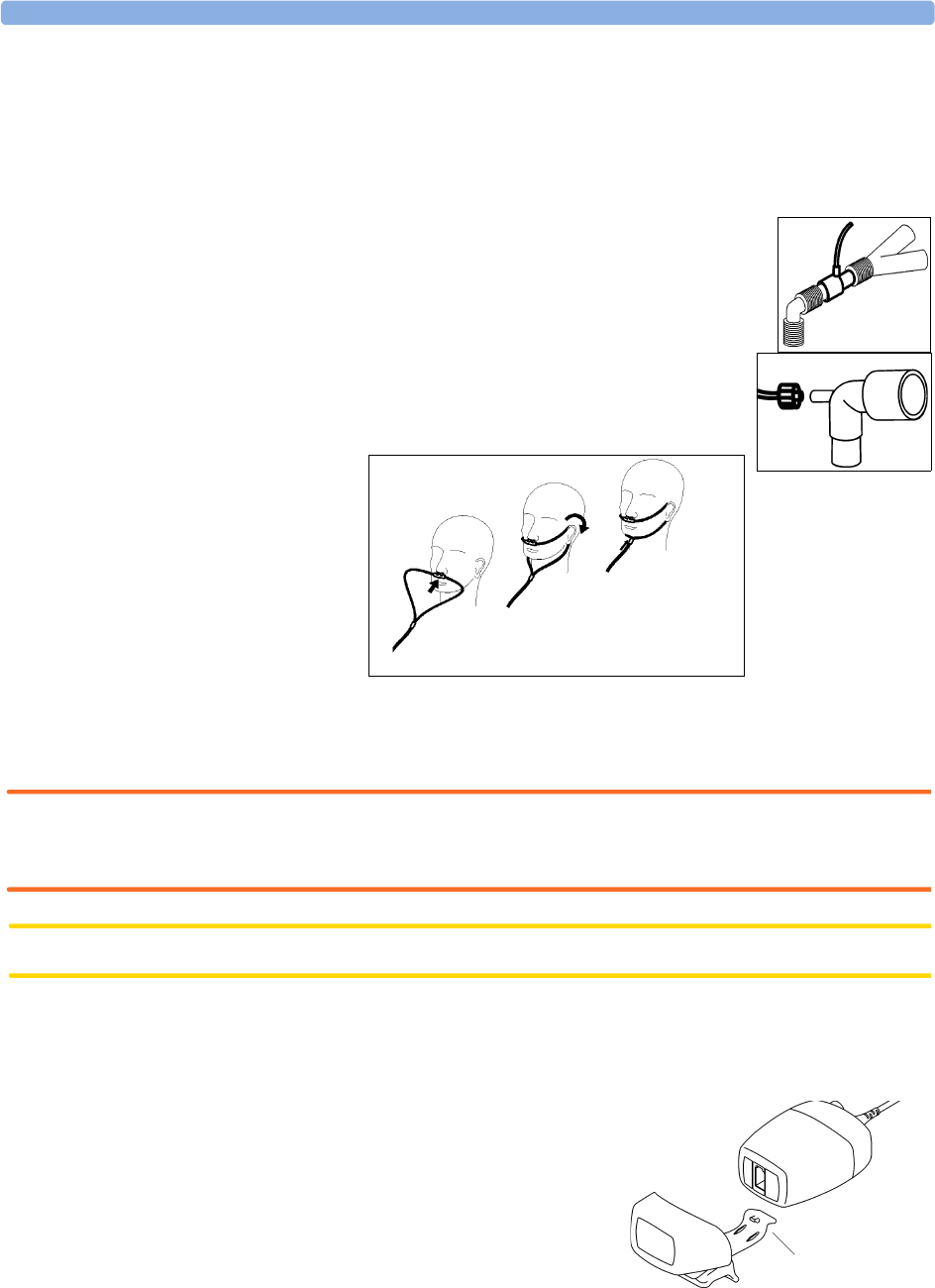
14 Monitoring Carbon Dioxide Measuring CO2 using the CO2 Option or M3014A
170
– expose the sensor to room air and keep it away from all sources of CO2 including the ventilator,
the patient’s breath and your own.
– In the setup menu for the CO2, select Start Zero Cal.
– When you see the message Zero done at <date and time> on the status line, the zero
calibration is finished and you can begin monitoring.
4For intubated patients requiring an airway adapter: Install the airway adapter at
the proximal end of the circuit between the elbow and the ventilator Y-
section.
For intubated patients with an integrated airway adapter in the breathing
circuit.: Connect the male luer connector on the straight sample line to the
female port on the airway adapter.
For non-intubated patients: Place the nasal cannula onto the patient.
For patients prone to mouth breathing use an oral-nasal cannula.
For nasal or oral-nasal cannulas with oxygen delivery, place the cannula on the patient as shown then
attach the oxygen supply tubing to the oxygen delivery system and set the prescribed oxygen flow.
WARNING Always connect the airway adapter to the sensor before inserting the airway adapter into the breathing
circuit. In reverse, always remove the airway adapter from the breathing circuit before removing the
sensor.
CAUTION Always disconnect the cannula, airway adapter or sample line from the sensor when not in use.
Using the Sidestream Sensor Holder
The holder delivered with the sensor can be used to clamp the sensor onto an IV pole or a shelf.
1Push the sensor into the holder until it clicks into
position.
2Clamp the holder onto an IV pole, a shelf or another
appropriate location.
To remove the sensor from the holder, release the clip and
pull the sensor out of the holder. clip
Measuring Mainstream CO2 using M3016A 14 Monitoring Carbon Dioxide
171
Removing Exhaust Gases from the System
WARNING Anesthetics: When using the sidestream CO2 measurement on patients who are receiving or have
recently received anesthetics, connect the outlet to a scavenging system, to avoid exposing medical staff
to anesthetics.
Use an exhaust tube to remove the sample gas to a scavenging system. Attach it to the sidestream sensor
at the outlet connector.
Measuring Mainstream CO2 using M3016A
The M3016A Mainstream CO2 Extension measures partial pressure of carbon dioxide in a patient’s
expired gas using the mainstream method. When using the appropriate accessories you can use the
mainstream CO2 measurement with ventilated adults, pediatric and neonatal patients.
WARNING Infra-red radiation: Do not expose the airway adapter or M1460A transducer to infra-red radiation
during use. This may cause incorrect readings.
Preparing to Measure Mainstream CO2
1Attach the transducer connector to the CO2 connector on the M3016A extension.
2Wait 20 minutes, allowing the transducer to reach its operating temperature and a stable thermal
condition.
3Perform an accuracy check and then, if necessary, calibrate the transducer.
Checking Transducer Accuracy
WARNING Check transducer accuracy at least once a week or if you doubt the CO2 readings.
1In Setup CO2 menu, select Cal. Mode to switch on calibration mode.
2Look at the calibration value displayed in the Setup CO2 menu next to Start CAL1. Is it the
same as the value on the calstick? If not, calibrate the transducer now.
3Place the transducer on the low cell of the calstick (labelled 0.0 mmHg or “ZERO”). The reading
on the screen should be zero within ±1 mmHg within one minute.
4Place the transducer on the high cell of the calstick. The reading on the screen should be within ±1
mmHg of the value on the calstick within one minute.
5If both readings are in range, you can leave calibration mode and begin monitoring. If either of the
readings is out of range, calibrate the transducer.
Calibrating the Transducer
1Check that the windows on the calstick are clean and clear.
2Place the transducer on one of the calstick cells and select Start CAL1.

14 Monitoring Carbon Dioxide Measuring Mainstream CO2 using M3016A
172
3Enter the calibration value printed on the calstick then press Confirm to start calibration.
4When the message CO2 CAL1 done;Start CAL2 cal appears, put the transducer on the
other cell and select Start CAL2 then press Confirm.
5When you see the message CO2 cal done;leave Cal. Mode, calibration is complete.
6Select Cal. Mode to switch calibration mode off. You cannot monitor in calibration mode.
Attaching and Removing the CO2 Transducer
1Open the latch and place the
transducer onto the airway adapter.
Place the airway adapter in the
patient’s breathing circuit between
the endotracheal tube and the Y-
piece. You may see the CO2
SENSOR WARMUP message until
the transducer reaches operating
temperature. Wait until this
disappears before starting the
measurement.
2To remove the transducer from the
airway adapter, open the latch and
pull out the airway adapter.
WARNING To prevent stress on the endotrachial tube, support the transducer and airway adapter.
To avoid infection, use only sterilized airway adapters.
Airway Adapter
CO2 Tra n s d u c e r

Measuring Microstream CO2 using M3015A 14 Monitoring Carbon Dioxide
173
Measuring Microstream CO2 using M3015A
The M3015A Microstream CO2 Extension measures the partial pressure of carbon dioxide in a
patient’s expired gas using Microstream technology.
The measurement is equipped with an automatic barometric pressure compensation.
Preparing to Measure Microstream CO2
Use appropriate accessories for:
• the patient type (adult, pediatric or neonatal),
• the ventilation situation (including humidification)
• the duration - short term use, up to 24 hours (typically OR), or long term use (typically ICU).
All accessories are for single patient use only.
Using Microstream Accessories
The Microstream measurement can be operated with the special Microstream accessories only. Refer to
the instructions for use provided with the accessory.
For intubated patient with non-humidified ventilation, you can use a Microstream FilterLine set. For
humidified ventilation, use a FilterLine H Set.
For non-intubated patients, the gas sample is taken through a Nasal FilterLine, or a Smart CapnoLine
(which is a combined oral-nasal FilterLine). In parallel to the measurement of the CO2, oxygen (O2)
may be delivered to the patient to support gas exchange. This is done by using an O2/CO2 FilterLine,
or a Smart CapnoLine O2 (a combined oral-nasal O2/CO2 FilterLine).
Using the FilterLine and Airway Adapter
1Attach the female Luer connector to the CO2 inlet connector on the extension by pushing the
socket cover down and screwing the connector into place.
2Check that the FilterLine is not kinked.
3Change the FilterLine if a CO2OCCLUSION INOP appears on the monitor or if the readings
become extremely erratic.
inlet connector cover
outlet connector
14 Monitoring Carbon Dioxide Setting up all CO2 Measurements
174
Disconnect the FilterLine during suctioning and nebulizing therapies.
Check the table in the Microstream CO2 Accessories section of the Accessories chapter for typical
usage times for the different Microstream accessories.
CO2 values for non-intubated patients using Microstream accessories will always tend to be lower than
for intubated patients. If values appear extremely low, check whether the patient is breathing through
the mouth or whether one nostril is blocked
Removing Exhaust Gases from the System
WARNING Anesthetics: When using the Microstream CO2 measurement on patients who are receiving or have
recently received anesthetics, connect the outlet to a scavenging system, or to the anesthesia machine/
ventilator, to avoid exposing medical staff to anesthetics.
Use an exhaust tube to remove the sample gas to a scavenging system. Attach it to the MMS Extension
at the outlet connector.
Suppressing Zero Calibration
To prevent an automatic zero calibration from being started in the next five minutes,
♦in the Setup CO2 menu, select No Zero For 5Min, or select the Suppress CO2Zero
SmartKey, if configured.
Selecting No Zero For 5Min or selecting the Suppress CO2Zero SmartKey again before
the timer has timed out resets the timer to five minutes, unless an AutoZero became due during the
previous suppression.
Setting up all CO2 Measurements
These tasks are common to all CO2 measurements except where otherwise noted.
Adjusting the CO2 Wave Scale
1In the CO2 Wave menu or the Setup CO2 menu, select Scale.
2Choose a suitable scale range from the pop-up list.
Setting up CO2 Corrections
Temperature, water vapor in the patient’s breath, barometric pressure, and the proportions of O2, N2O
and Helium in the mixture all influence CO2 absorption. If values seem inaccurately high or low,
check that the monitor is using the appropriate corrections.
Correction
Altitude
(M3014A
only)
Altitude is set during installation. The monitor automatically applies an appropriate
correction.
Setting up all CO2 Measurements 14 Monitoring Carbon Dioxide
175
Suppressing Sampling (not Mainstream CO2)
To temporarily stop sampling,
♦in the Setup CO2 menu, select Pump 15Min Off or use the CO2 Pump Off SmartKey if
available.
Selecting Pump 15Min Off again before fifteen minutes have passed resets the timer to fifteen
minutes.
To re-start the pump,
♦in the Setup CO2 menu, select Pump On.
Changing CO2 Alarms
This refers to CO2 specific alarms. See the Alarms section for general alarm information.
You change CO2 alarm settings in the Setup CO2 menu.
To switch etCO2 alarms on and off:
♦Select etCO2 Alarms and toggle between On and Off.
To change the etCO2 alarm limits:
• Touch the high limit on the alarm limits menu button. Choose the high alarm limit from the pop-
up list that opens.
• Touch the low limit on the alarm limits menu button. Choose the low alarm limit from the pop-up
list that opens.
O2
(M3014A
only)
In the Setup CO2 menu, select Oxy. Corr and select a value between 20% and
100%, the default value is 20%. If you are not measuring the expired O2, estimate it by
subtracting 5% from the inspired O2 then select the nearest value from the list.
Humidity At installation, the monitor is configured to automatically apply either Body Temperature
Pressure Saturated (BTPS) or Ambient Temperature Pressure Dry (ATPD). To see
which, go to the Setup CO2 menu, and scroll down to look at Hum. Corr or
HumidityCorr.
N2O
(M3016A
mainstream
and M3015A
microstream
only)
In the Setup CO2 menu, select N2O Corr. and turn on or off. If N2O is present
in the ventilation gas mixture, you must turn this on.
If the N2O correction is not available in the Setup CO2 menu, the CO2
measurement in your MMS Extension does not require N2O correction or it is setup
with Gas Corr. (see below).
Gas
(M3014A
only)
In the Setup CO2 menu, select Gas Corr. and select Helium, N2O or turn off.
If Helium or N2O is present in the ventilation gas mixture, you must make the
appropriate selection.
If the Gas correction is not available in the Setup CO2 menu, the CO2 measurement
in your MMS Extension does not require N2O or Helium correction or the N2O
correction is setup with N2O Corr. (see above).
Agent
(M3014A
only)
In the Setup CO2 menu, select Agt. Corr. and select the concentration of the
anesthetic agent (between 0.0% and 20.0%). If an anesthetic agent is present in the
ventilation gas mixture, you must select the appropriate concentration.
Correction
14 Monitoring Carbon Dioxide Setting up all CO2 Measurements
176
To change the imCO2 high limit:
♦Select imCO2 High and choose the high alarm limit from the pop-up list that opens.
Changing the Apnea Alarm Delay
This determines the time limit after which the monitor alarms if the patient stops breathing.
1In the Setup CO2 menu, select awRR.
2In Setup awRR menu, select Apnea.
3Choose the apnea alarm delay time.
WARNING Safety and effectiveness of the respiration measurement method in the detection of apnea, particularly
the apnea of prematurity and apnea of infancy, has not been established.
Prolonged delay: The selected apnea alarm delay may be prolonged by up to 17 seconds, if an apnea
occurs during the automatic zero process. This applies to the Microstream (M3015A) measurement
only.
Deriving Alarms From awRR
1In the Setup CO2 menu, select awRR.
2In the Setup awRR menu, select Alarms.
3Choose On to derive alarms from the airway respiration signal or Off to disable them.
Changing awRR Alarm Limits
1In the Setup CO2 menu, select awRR.
2Select High Limit to set the upper alarm limit.
Select Low Limit to set the lower alarm limit.
3Select the appropriate setting.

177
15
15Assigning Two Devices to One
Patient
It is possible to assign a monitor and a telemetry device to the same patient, resulting in the
information from both devices being combined in one sector at the Information Center. This is called
“pairing” and when a telemetry device and a monitor are paired, the measurement data from the
telemetry device will be displayed on the monitor screen.
A telemetry device can be:
• any Philips telemetry device (only for indirect connections, see below).
• a TRx+/TRx+ Intellivue Telemetry system transceiver.
How Can You Combine Devices?
•With an indirect connection, using standard telemetry transmission - the data are sent to the
monitor via the Information Center and arrive with a delay of several seconds at the monitor.
•With a direct connection to the monitor, via a short range radio link - the data arrive with a minimal
delay on the monitor screen.
Indirect Connection - Manual Pairing
The telemetry device can be paired with the monitor at the Information Center or at the monitor. For
detailed information regarding pairing and configuration at the Information Center, see the
Information Center Instructions for Use.
To pair the monitor with a telemetry device at the monitor:
1Select Main Setup then Measurements
2Select Telemetry
The Setup Telemetry menu will appear with only one entry Paired Equipment.
3Enter here the equipment label of the telemetry device to be paired.
Pairing at the monitor is only possible when the monitor already has a connection to the Information
Center and the Information Center software version allows pairing at the monitor.
Telemetry Data Window
The measurements from the telemetry device are shown in the telemetry data window on the monitor
when there is no direct connection via short range radio link.
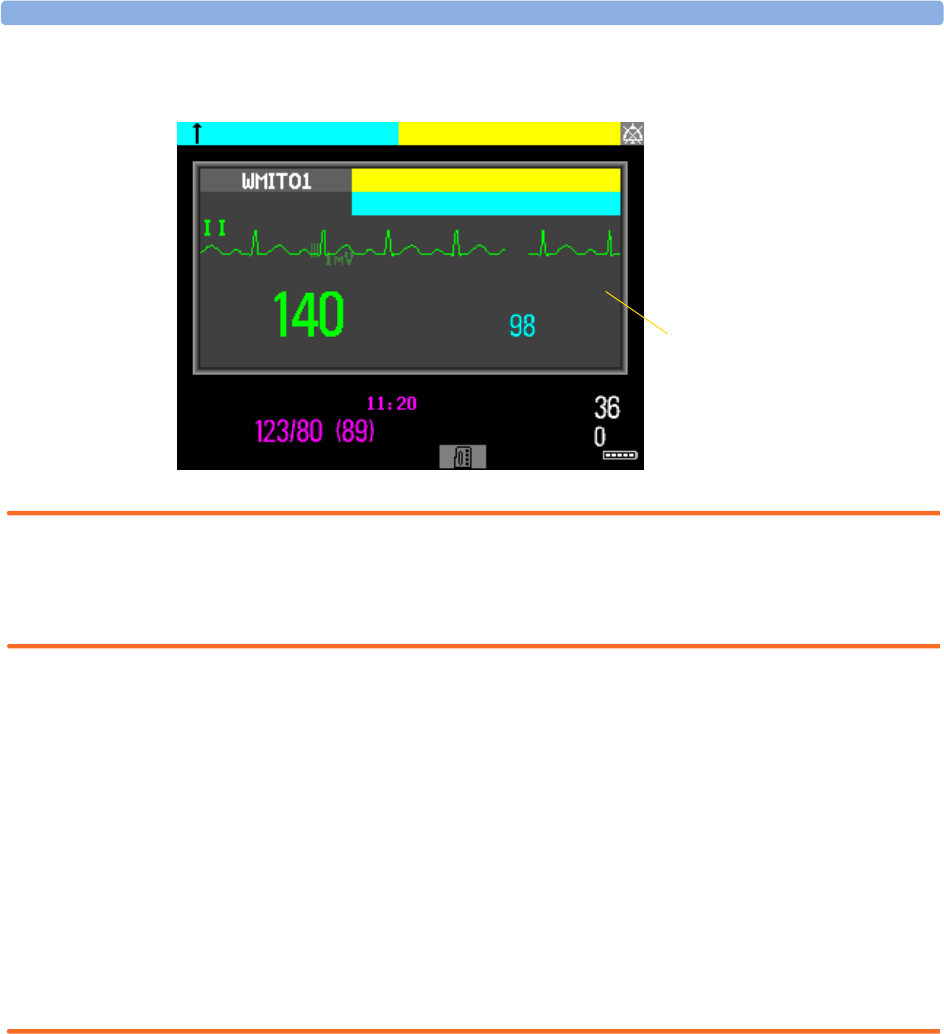
15 Assigning Two Devices to One Patient How Can You Combine Devices?
178
WARNING All data presented in the telemetry data window are delayed for several seconds.
If you need realtime data, for example for defibrillation, always use the monitor ECG instead of
telemetry. As long as the ECG is being measured with the telemetry device there will be no ECG signal
available at the ECG Sync Pulse output.
Direct Connection - Automatic Pairing
The following direct connections are possible:
• a TRx+4841A Intellivue Telemetry system transceiver connected via short range radio (SRR) link to
an MP2 with SRR capability.
If a telemetry device is assigned to a monitor via a direct short range radio link, the monitor and the
telemetry device are automatically paired at the Information Center (if configured).
The measured data from the telemetry device — ECG and, if available, SpO2T— will appear on the
monitor screen and will be sent through the monitor to the Information Center. The ECG waves and
numerics appear in place of the monitor’s own ECG, and SpO2T is displayed as an additional
measurement. When ECG is measured with the telemetry device there will be no Respiration
measurement derived.
WARNING • When ECG is being measured with a telemetry device directly connected to the monitor, there will
be no ECG signal available at the ECG analog output or ECG Sync Pulse output and no
synchronization marks on the ECG wave. A No ECG Out message will appear in the ECG wave
channel.
• When a telemetry device is connected to the monitor, arrhythmia relearning is initiated, and again
when the telemetry device is disconnected.
Telemetry data
window
NBP
Sys.
Auto 10 min etCO2
imCO2
* TELE ALARM
TELE INOP
Delayed
** HR 140>120
SOME ECG ALRMS OFF
HR %SpO2T
How Can You Combine Devices? 15 Assigning Two Devices to One Patient
179
• Controls on the Telemetry Device (e.g. nurse call) will be inactive when the device is directly
connected to the monitor except in the case when the monitor has no network connection and data
are transferred via the telemetry device. See the "Enhancing Telemetry Monitoring with the
Monitor" chapter.
Assigning a Telemetry Transceiver with an SRR Adapter to a Monitor
Monitors which have this capability have a short range radio symbol on the model label.
A telemetry device with a short range radio adapter can be assigned to a monitor directly. To assign a
telemetry device to a monitor:
1Press the Check button on the telemetry device.
The measurement selection key on the monitor will change to show the “assign telemetry” icon
2Select the assign telemetry icon.
3In the Assign Telemetry Device menu, select the correct equipment label for the
telemetry device.
4Check that the assignment is successful and that transmission has begun:
•A Tele Device assigned message appears on the monitor
• a tone sounds at the telemetry device and the Laeds Off indicators light
• the ECG wave appears on the monitor
To confirm that the correct telemetry device has been assigned, open the ECG Setup menu. The title
of the menu contains the equipment label of the telemetry device; check that this is the correct label.
If a monitor is already paired to another device, you cannot assign a telemetry device to that monitor.
If the telemetry device goes out-of-range or loses the short range radio connection, it will switch over to
standard telemetry transmission to the Information Center. In this case, the telemetry data is displayed
in the Telemetry Data Window as described above.
If a monitor is manually paired with a telemetry device with a short range radio adapter, the short range
radio assignment will be automatically made.
If a telemetry device disappears from the list in the Assign Telemetry Device menu, press the
Check button on the telemetry device again. If the monitor is not configured to be used with a
telemetry device, the “assign telemetry” icon will appear crossed out .
If the devices are unpaired, the short range radio connection will be ended.
WARNING Short range radio connections are subject to interruption due to interference from other radio sources
in the vicinity, including microwaves, bluetooth devices and DECT phones. Outside the operating
frequency band and 5% above and below, i.e. the exclusion band according IEC 60601-1-2, section
36.202.3a)4), the short range radio connection is immune up to 3V/m in the frequency range from 80
MHz to 2.0 GHz and up to 1V/m in the frequency range from 2.0 to 2.3 GHz. Depending on the
strength and duration of the interference, the interruption may occur for an extended period. A loss of
connection, due to moving out-of-range, interference, or for other reasons, is indicated with a
TELE DISCONNECT INOP.
15 Assigning Two Devices to One Patient How Can You Combine Devices?
180
Correct channel configuration is important, refer to the Configuration Guide for details.
If a TELE DISCONNECT INOP occurs when the telemetry device goes out-of-range, the INOP will
disappear (without being silenced) as soon as the ECG signal from the telemetry device is available at
the Information Center via standard telemetry transmission.
SpO2T Manual Mode
When a telemetry device with a short range radio connection supplies SpO2T to the monitor, the
monitor will have a manual measurement mode available. This allows SpO2 measurements to be made
on request and not continuously, helping to save battery power. To ensure there is no gap in SpO2
measurements when moving from standard telemetry transmission to short range radio transmission,
the measurement mode will always be set to continuous in this situation unless manual mode is set in
both the telemetry device and the monitor.
Unassigning a Telemetry Transceiver with SRR Adapter at the Monitor
If a monitor and a telemetry device are paired, the assignment and the short range radio connection
will be ended when the devices are unpaired (see “Unpairing the Monitor and Telemetry Device” on
page 180).
If the monitor does not have a connection to an Information Center, you must manually end the
assignment and the short range radio connection.
1Select the Measurement Selection key.
2In the Measurement Selection window, select the Tele pop-up key.
3In the Tele device window select Unassign Tele.
Refer also to “Use Models With Telemetry” on page 202 for further related use modes.
Unpairing the Monitor and Telemetry Device
If the patient will no longer be monitored with the telemetry device, or only with the telemetry device
and no longer with the monitor, you need to end the device pairing. After unpairing, the Information
Center will receive data exclusively from the monitor or from the telemetry device:
♦select the Unpair To Mon. SmartKey to end pairing and have the Information
Center receive the measurement data from the monitor
♦select the Unpair To Tele SmartKey to end pairing and have the Information
Center receive the measurement data from the telemetry device
or
♦use the Unpair function at the Information Center.
NOTE The Unpair SmartKeys and pop-up keys appear only on the monitor which is directly involved in
pairing.
Functions Available When the Telemetry Data Window is Displayed 15 Assigning Two Devices to One Patient
181
Functions Available When the Telemetry Data
Window is Displayed
Controlling the Telemetry Device from the Bedside
You can change settings for a paired telemetry device at the monitor:
1Select the telemetry data screen element
2Select the Setup Tele pop-up key
The Setup Telemetry menu will appear with the settings available for the telemetry device.
These will normally include: adjusting heart rate alarms, ECG size control, selecting primary/secondary
lead, relearning arrhythmia, and selecting the arrhythmia analysis mode. The Equipment label of the
paired device is also shown here.
Viewing and Silencing Telemetry Alarms at the Bedside
When a telemetry device is paired with the monitor, telemetry alarms will also be indicated on the
monitor, in addition to the main indication at the Information Center.
If configured, a generic Tele Alarm message will appear in the alarm status area with standard
alarm tones. The Tele Alarm message will have the color and * or !coding corresponding to the
severity of the alarm. The specific alarm message (for example *HR Low) will appear in the Telemetry
Data Window.
If configured, alarms generated from a paired telemetry device can be silenced at the bedside. Either the
monitor Silence key is configured to silence both monitor and telemetry alarms (must be
configured at the Information Center) or the Silence Bed pop-up key will be available:
1Select the telemetry screen element.
2Select the Silence Bed pop-up key.
Depending on your Information Center configuration, the Silence Bed key may silence both
telemetry alarms and bedside alarms.
WARNING Even when the telemetry data is not visible on the screen, you may be silencing telemetry and monitor
alarms, if the Information Center and monitor are so configured.
Suspending Telemetry Alarms
When you select Pause Alarms or Alarms Off at the monitor, the alarms are off or paused for
the bedside measurements. When you switch alarms off or pause alarms at the Information Center,
both telemetry and monitor alarms are affected.
Refer to the Information Center Instructions for Use for more details on the Suspend/Pause alarms
behavior of the Information Center and telemetry device.
Using Standby
When you select Standby mode at the monitor, the bedside goes into Standby mode but the telemetry
device will continue monitoring.
Refer to the Information Center Instructions for Use for details on the Standby behavior of the
Information Center and telemetry device.
15 Assigning Two Devices to One Patient Functions Available For Devices Connected Via SRR
182
Functions Available For Devices Connected Via
SRR
The Telemetry Device window can be opened from the Measurement Selection
window, by selecting the Tele pop-up key, or via Main Setup -> Telemetry Device.
The window shows the equipment label of the assigned telemetry device and, for monitors with SRR
capability, a battery status symbol and a symbol indicating the signal quality of the
SRR link .
If the monitor has a connection to an Information Center, the pop-up keys Unpair to Mon. and
Unpair to Tele let you end the device pairing. After unpairing, the Information Center will
receive data exclusively from the monitor or from the telemetry device.
If the monitor does not have a connection to an Information Center, or there is a pairing mismatch,
the Unassign Tele pop-up key lets you end the telemetry device assignment and close the SRR
link.
Temporarily Stopping the Short Range Radio Connection
To temporarily disable the SRR connection for this device, for example, in case of interference:
♦Select the Stop SRR pop-up key.
This closes the SRR link and the telemetry device switches over to standard telemetry transmission.
The battery status symbol will no longer be shown and the SRR quality indicator symbol will be
crossed out.
To return to SRR use:
♦Select the Start SRR pop-up key and press the Check button on the telemetry transceiver.
Setting Up Measurements
The Setup ECG and Setup SpO2T pop-up keys give you access to the measurement setup menus.
The Measmt. Select. pop-up key takes you directly to the Measurement Selection window where
all connected measurement devices are shown.
General Telemetry-related Functions
The following functions are valid for directly and indirectly connected telemetry devices.
Telemetry Device
Tele 1
General Telemetry-related Functions 15 Assigning Two Devices to One Patient
183
ECG Source Tracking at the Information Center
The Information Center continuously checks whether a valid ECG signal is coming from the monitor
or the telemetry device. If you unplug the ECG patient cable from the monitor and plug it into the
telemetry device, the Information Center will automatically switch to monitoring the ECG from the
telemetry device. At the monitor, its own ECG measurement will be deactivated — the ECG Setup
menu will no longer be accessible.
When you unplug the patient cable from the telemetry device and plug it back into the monitor again,
the Information Center will switch back to monitoring the ECG from the monitor. The ECG
measurement will be activated again at the monitor. Note that in this case, as the screen switches back
to the monitor’s own measurements, the SpO2T measurement (if present) will no longer be displayed.
In the same way the source is tracked when a telemetry device is directly connected to a monitor, then
disconnected and vice versa.
In case of ambiguity, a yellow INOP message !!CHECK ECG SOURCE indicates that more than one
valid ECG source is active.
Synchronized Settings
If ECG is measured at the monitor, and then the patient is connected to a telemetry device for
monitoring, the Information Center will use the monitor settings for the telemetry device. In general,
the following settings will be synchronized:
WARNING • Not all settings are synchronized; after changing the ECG source, always check that the settings are
appropriate.
• Va and Vb leads are reset to default (V2, V5) if the configured Va or Vb lead for the telemetry device
is not one of V1 through V6
Heart Rate HR/Pulse Alarm On/Off, Heart Rate High/Low Limit,
ECG Primary Lead, Secondary Lead, Va Lead1, Vb Lead1, Lead Placement
1.Va and Vb leads are reset to default (V2, V5) if the configured Va or Vb lead for the telemetry device is not
one of V1 through V6.
Arrhythmia Analysis Mode, Asystole Threshold, Pause Threshold, VTach HR,
VTach Run, PVCs/min, Vent. Rhythm, SVT HR, SVT Run, PVCs/
min On/Off, Pacer not capture On/Off, Pacer not pace On/Off, Non-
Sustain On/Off, Vent. Rhythm On/Off, Run PVCs On/Off, Pair
PVCs On/Off, Missed Beat On/Off, Pause On/Off, R-on-T On/Off,
Vent. Bigeminy On/Off, Vent. Trigeminy On/Off, Multiform PVCs
On/Off, Irregular HR On/Off, SVT On/Off, Afib On/Off
ST ST Analysis On/Off, ST Alarm On/Off, ISO Point, J point, ST point,
ST Priority List, Single ST Alarm Limit, Multi ST Alarm Limit
QT QT analysis On/Off, QT Lead, QTc High Alarm On/Off, 'QTc
Alarm On/Off, QTc High Limit, 'QTc High Limit, QTc Formula2,
QT Baseline
2.These setting will only be synchronized when the Information Center supports QT Analysis for Telemetry.
SpO2TSpO
2 Alarms on/off, SpO2 Alarm limits
NBP Alarm Suppression On/Off, Pulse(SpO2) On/Off

15 Assigning Two Devices to One Patient General Telemetry-related Functions
184
If later the patient is disconnected from the telemetry device, and reconnected to the monitor again,
any changes in the settings made in the meantime will be passed on to the monitor. In this way,
settings continuity is preserved when the ECG source changes.
Settings synchronization can only take place when there is no patient information mismatch between
the monitor and the Information Center. If a Check ECG Settings or CHECK PAIRING
INOP appears always check that the ECG settings, especially the paced setting, are appropriate for
your patient.

185
16
16Enhancing Telemetry
Monitoring with the Monitor
You can use a monitor without a network connection to view measurement data from a telemetry
transceiver at the bedside. You can also use the monitor to make additional measurements and send
this measurement data to the Information Center via the telemetry transceiver. The monitor can so be
used as a mobile viewer and measurement device, and is set up to simplify the assign/unassign
procedures when used with short range radio.
Monitor and Telemetry Transceiver Requirements
The monitor and the telemetry transceiver need a direct connection via a short range radio link. Not all
revisions of the telemetry transceiver can be used directly with the monitor, if you connect a device that
cannot be used you will see a TELE UNSUPPORTED INOP.
Data Sent to the Information Center
The data sent to the Information Center includes numerics from NBP, SpO2, Pulse from SpO2 and
predictive temperature. INOPs from these measurements, battery INOPs and a general INOP
generated by alarms from any other measurement (MORE BED ALARMS) will also be transmitted.
NOTE The monitor must be configured appropriately to support direct connection to a telemetry transceiver;
refer to the Configuration Guide for details.
Changing Assignment to a New Telemetry Transceiver
1Assign the telemetry transceiver to the monitor; see “Assigning a Telemetry Transceiver with an
SRR Adapter to a Monitor” on page 179.
2Make the required measurements; the data will be automatically sent to the Information Center via
the telemetry transceiver.
It is not necessary to unassign the telemetry transceiver. This will happen automatically when the
next telemetry transceiver is assigned. The patient is also discharged (if configured), ensuring that
the measurement data is erased before data from the next patient appears. Always assign the
telemetry transceiver before you start making measurements.

16 Enhancing Telemetry Monitoring with the Monitor
186

187
17
17Trends
Trends are patient data collected over time and displayed in graphic or tabular form to give you a
picture of how your patient’s condition is developing. Trend information is stored in the trends
database for continuously-monitored measurements, such as ECG, as well as for aperiodically-
measured parameters, such as Cardiac Output.
Viewing Trends
Trend information can be viewed embedded as a screen element on specially-designed Screens, or you
can open a trend window over the current Screen.
♦To view trends embedded as a screen element, enter the Change Screen window, then select a
Screen designed to show an embedded trend window.
♦To open the tabular trends window, select Main Setup > Trends >
Vitals Trend, or select the Vitals Trend SmartKey.
♦To open the graphic trends window over the current Screen, select Main
Setup > Trends > Graph Trend, or select the Graph Trend
SmartKey.
The trend windows open displaying the most recent data and are updated as new
data is stored. A timescale along the bottom of the screen shows you where you
are in the trends database. The preview column on the right-hand side shows the latest available
measurement value. The preview column is updated every five minutes or whenever an NBP or other
aperiodic measurement is completed.
A question mark (?) beside a value means that the data may not be reliable, due perhaps to an INOP
condition in the measurement.
Your monitor screen may look slightly different to the examples shown in this chapter.
Trends Pop-Up Keys
When you open the graphic or tabular trends window, a selection of pop-up keys appears to let you
navigate through the stored trend data and carry out trends-related tasks.
Vitals
Trend
Graph
Trend
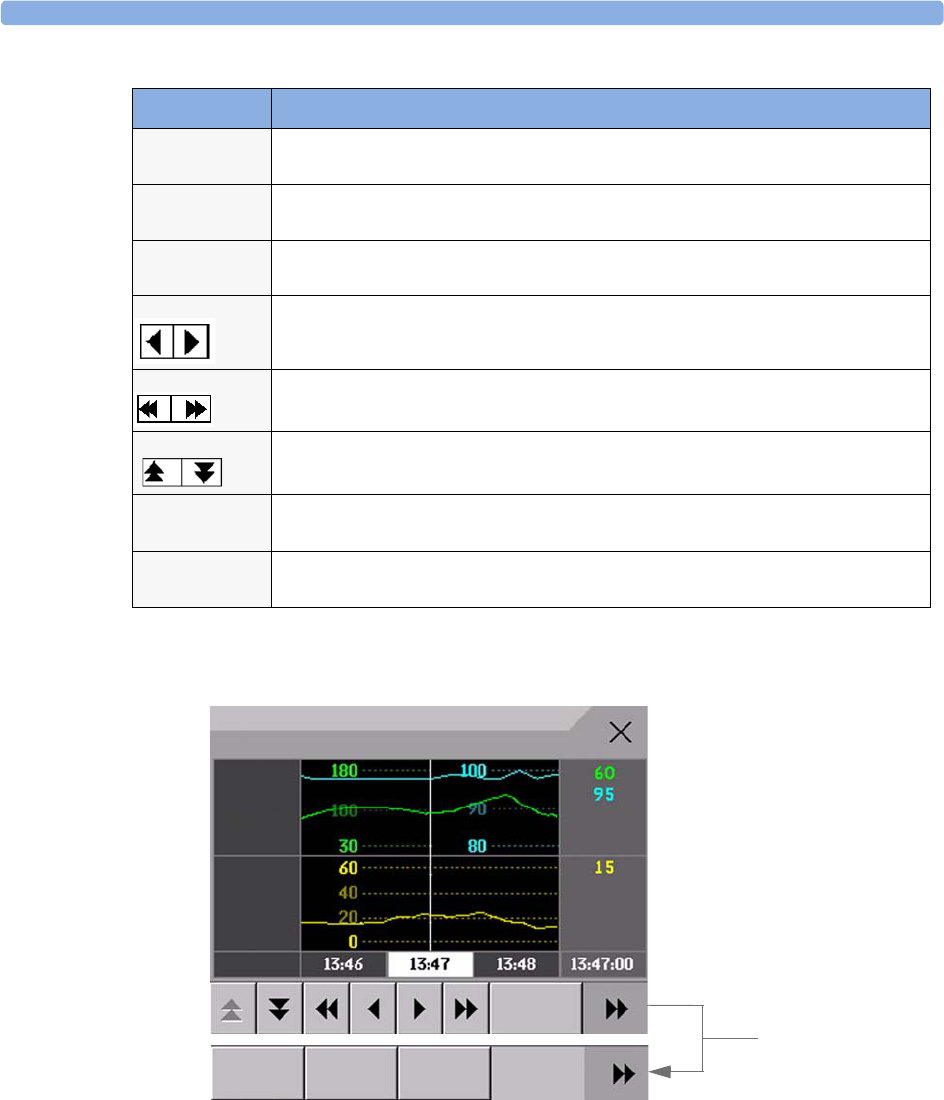
17 Trends Viewing Trends
188
Viewing Graphic Trends
A cursor spanning all measurements in the trend group helps you to navigate through the trends
database and shows you your current position in the database. When the cursor is moved across the
time line, the values measured at the cursor time are shown in the right hand column.
In graphical trends, aperiodic measurement trends are shown as an asterisk, NBP has a special symbol.
To use the trend cursor to navigate in time through the trends database,
1Select the graphical trend or the arrow pop-up keys to activate the cursor.
2Use the arrow pop-up keys to move the trend cursor backwards and forwards in time, or
Pop-Up Keys Selecting this pop-up key lets you....
Select
Group
see a pop-up list of trend groups and select a group for viewing.
Select
Interval
see a pop-up list of available data resolution settings and select the level of detail shown
in the trend view.
Print print a graphic trends report of the data in the current window. The report will use the
current trend interval settings.
move the cursor one step to the left or right to navigate through the trends database
timeline.
move the cursor one page to the left or right to navigate through the trends database
timeline.
scroll up and down the screen to see measurement trends that do not fit in the current
view.
Vital
Signs
open the current trend view in tabular form. The displayed time period and resolution
stay the same.
Graph
Trend
open the current trend view in graphic form. The displayed time period and resolution
stay the same.
Graphical Trends: Standard
HR
SpO2
RR
4 Apr
Select
Interval Scroll to view more
pop-up keys
Select
Group
Vital
Signs
Print
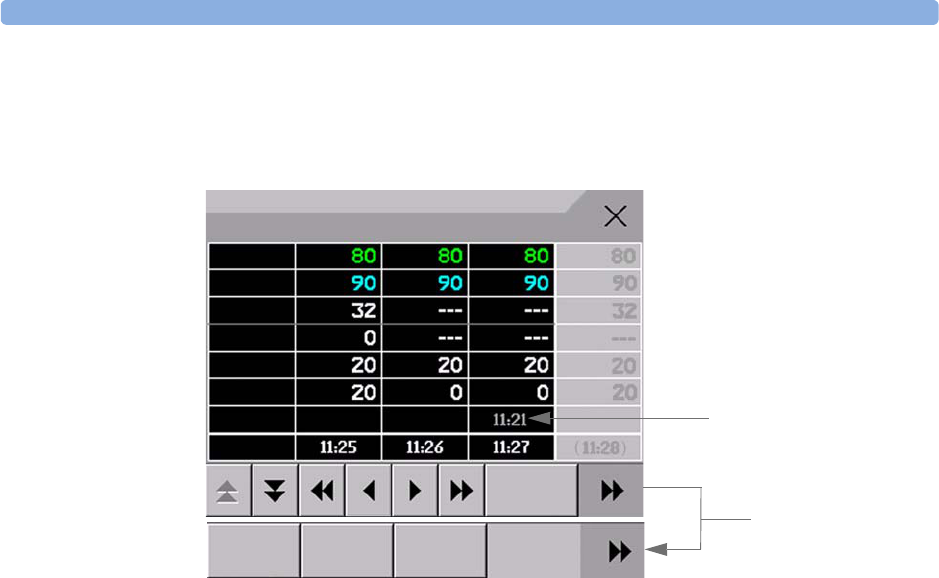
Setting Up Trends 17 Trends
189
3Place the cursor at a specific time by touching the graph.
Viewing Vital Signs Trends
The currently-selected column is highlighted. The values can be configured to display in the same
colors as the waves and numerics on the realtime display.
Any values available for display before the next scheduled update are shown in the right hand column,
with a timestamp in brackets.
If more than one value is available for an aperiodic trend for a certain trend period, all measured values
are stored in the database and the value closest to the timestamp is shown in the Vital Signs display
marked with an arrow.
Setting Up Trends
Trends are set up in Configuration Mode. You can make temporary changes to trends settings such as
trend groups, priorities, or scales in Monitoring Mode. The general settings for all Trends are under
Main Setup -> Trends.
Settings for a single segment in graphical trends or for the corresponding trend group can be made
more easily in that segment menu.
Making Segment Settings
The Graphical Trends window is divided into measurement segments, each of which has its
own settings.
To enter the segment menu,
♦select the left hand column of the segment, where the measurement label is displayed.
Expanded View
To expand the segment to fill the Graphical Trends window,
♦in the Segment menu, select Expand to have that segment enlarged to fill the window.
Vital Signs: Standard
HR
SpO2
etCO2
Aperiodic values are shown
with a timestamp
imCO2
RR
awRR
Select
Group
Graph
Trend
Print
Select
Interval Scroll to view more
pop-up keys

17 Trends Setting Up Trends
190
In the expanded view, you can also highlight a measurement to make it more easily visible (for example
when multiple ST trends are in one segment). To highlight a measurement,
♦in the Segment menu, select Highlight repeatedly until the highlight is on the required
measurement.
To return the segment to its original size,
♦in the Segment menu, select Expand again.
Trend Scales for Segment Measurements
To change the trend scales for a measurement in the current segment:
1In the segment menu, select the measurement label
2Select Upper to change the upper limit of the scale or Lower to change the lower limit of the
scale.
Optimum Scale
To have the monitor automatically select an optimum scale for viewing, based on current values,
♦in the Segment menu, select Optimum Scale.
This scale change is temporary. When the graphical trend window is closed the scale reverts back to the
setting in Parameter Scales.
To switch off automatic optimum scaling,
♦in the Segment menu, select Optimum Scale again.
Trend Group
To add or remove measurements for this trend group or change the order of the existing
measurements:
1In the Segment menu, select Change Group
2Use the Add, Change, Sort Up and Sort Down popup keys to change or re-order the group
as required.
No. of Segments
In an embedded graphical trend window, you can select the number of segments to be displayed in the
Segment menu:
♦In the Segment menu, select No. of Segments
Trend Groups
The measurements grouped in trend groups define the trends displayed together in the Vital Signs or
Graphics Trends windows and printed in trends reports and recordings. The sequence of the
measurements in the group defines the order in which they are displayed. Measurements listed between
dotted line separators are displayed overlapping. The trend group All contains all available
measurements, you cannot change the order or selection of this group.
To change the selection of measurements in a trend group, either use the Change Group setting in
the Segment menu or:

Setting Up Trends 17 Trends
191
1Select Main Setup -> Trends -> Trend Groups
2Select the Trend Group you want to change and use the pop-up keys to Add, Change, or
Delete the selection of measurements trended.
To temporarily change the order in which the measurements are displayed in a group,
1Select Main Setup -> Trends -> Trend Groups
2Select the Trend Group and then the measurement you want to move and use the Sort Up/
Sort Down pop-up keys.
Trend Interval
The trend interval defines the resolution of trend data shown on the Screen.
To set the trend resolution, in the Vital Signs or Graphical Trends window,
♦Select the Select Interval pop-up key and then select the required interval from the list.
Trend Priority
The monitor stores trend information for all monitored measurements, if configured to do so. If your
configuration restricts the number of measurements trended, you must choose which measurements
will be included. A priority list is used to select the trended measurements.
To see the measurement priority list for trending,
1In the Main Setup menu, select Trends.
2Select Trend Priority.
To add measurements to the priority list,
1Select the pop-up key Add and choose from the pop-up list of available measurements.
2Use the Sort Up and Sort Down pop-up keys to change the priority order.
Trend Parameter Scales
Parameter scales define how the trend waveform will appear on the screen and in trend reports.
Separate scales can be set for adult, pediatric, and neonatal patient trends.
To change the trend parameter scales settings, either use the Scale setting in the Segment menu or:
1In the Main Setup menu, select Trends.
2Select Parameter Scales.
3Select the measurement or parameter you want to change from the list.
4Select the pop-up key Change to call up the Scale menu.
5In the Scale menu, select the parameter label you want to define settings for. Select Adult,
Pedi, and Neo and use the pop-up keypad to enter new upper and lower scale definitions.
Graphical Trend Presentation
Graphical trends and screen trends for measurements with compound values (for example ABP or
CO2) can be viewed in line or band form.
To change the presentation style,
1Select Main Setup -> Trends
17 Trends Documenting Trends
192
2Select Global Style and choose
•Line to display the trends as a continuous line
•Band to fill the area between the trend lines, for example, between the systolic and diastolic
pressures, with color.
This sample ABP
trend shows the
continuously-
measured values for
the systolic, diastolic
and mean pressures
displayed in band
form.
Documenting Trends
To print a Vital Signs or Graphical Trends report,
♦in the Vital Signs or Graph Trends window, select the pop-up key Print to print a
report for the trend group currently on the monitor screen.
Reports include the most recent information in the trends database and extend backwards in time
according to the selected trend interval and your monitor’s configuration. Trends reports can be
printed on central or local printers.
Trends Databases
The trend databases store information for up to 16 measurements for up to 48 hours.
The values in the trends database are stored as measured by the monitor, they are not averaged values.
The trend resolution defines how often a value is stored. In general, if more than one value is available
for storage in the trends database, the most recent value is used. Some values in the trends are marked
with arrows. This indicates that for this time period, more values were available and the most recent
one is shown.
Example database configuration In this example, we see that the monitor stores the most recent data
at the highest resolution, older data are stored at a lower resolution.
“4 hours @ 12 second resolution” means that the monitor stores trend data every 12 seconds, for the
most recent four hours.
ABP
240
50
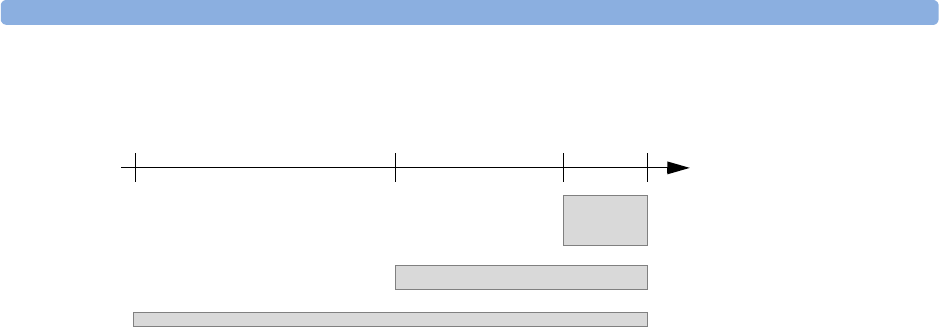
Screen Trends 17 Trends
193
Aperiodic Trends Database
Aperiodic trends do not count toward the maximum number of trends allowed by the trend
configuration. Trend data for aperiodic measurements is stored in a separate database and timestamped
with the measurement time.
Trending Multiple-Value Measurements
Some measurements generate multiple values, for example invasive pressure measurements can provide
systolic, diastolic, and mean values. These values are trended as separate measurements.
Screen Trends
Trends configured to display permanently on special monitor Screens are called screen trends. The
selection and number of measurement waves in the Screen Trend segment depends on your monitor
configuration. Screen trends are color-coded to match the measurement wave and numerics, and they
can be viewed in graphical, tabular, histogram or horizon format.
If you do not see screen trends on the monitor Screen, select a different Screen, one that is configured
to show screen trends. Screen trends are only available on specially designed Screens.
Screen Trend information is taken from the Trends database. If you do not see a Screen Trend for a
particular measurement on the Screen, check the trend priority list to ensure that this measurement is
being trended.
- 48
hours
- 24
hours
- 4
hours now
time
4 hours @12 second resolution
24 hours @ 1 minute resolution
48 hours @ 5 minute resolution
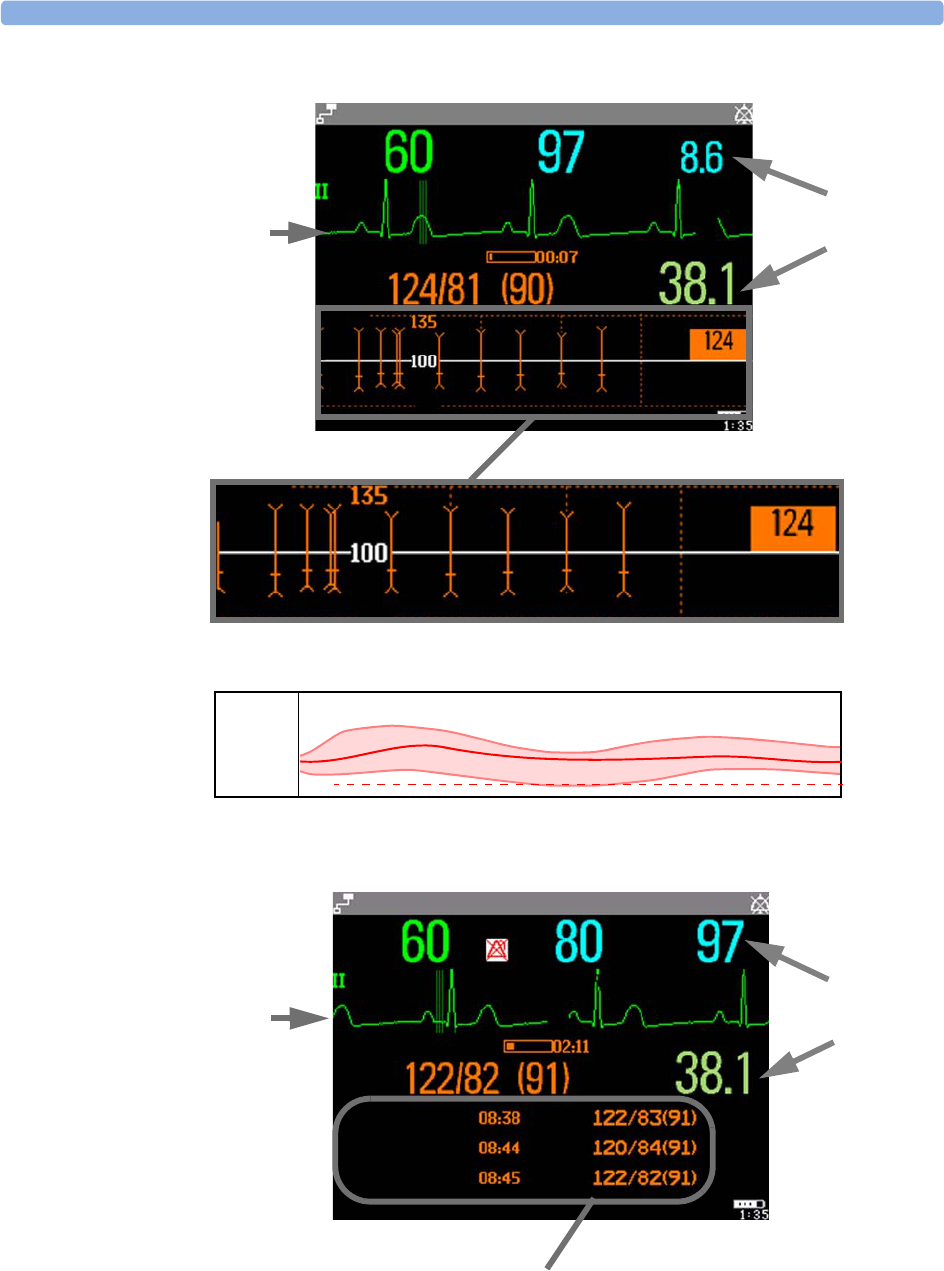
17 Trends Screen Trends
194
NBPs
NBP
M
1mV
HR Perf
Temp
ALARMS OFF
Arrhythmia Off
SBed9 Adult
SpO2
Auto 15 min
-60min -30min
Sys.
ABP
240
50
NBP graphical screen trend
Example of other graphical screen trends: ABP
Measurement
wave
Measurement
numerics
65
NBPs
-60min -30min
65
NBP
NBP
Sys.
M
1mV
HR SpO2
Temp
ALARMS OFF
Arrhythmia Off
Measurement
wave
SBed9 Adult
Pulse
Auto 15 min
Measurement
numerics
Tabular screen trend

Screen Trends 17 Trends
195
Setting the Screen Trend Time
To set the ScreenTrend Time for all graphical, histogram and horizon screen trends (“global”
trend time),
1Select a screen trend then select Setup Trend, or select Main Setup -> Trends.
2Select ScreenTrend Time and select the required time: 30 minutes, one, two, four, eight, or
twelve hours.
This is now the Global screen trend time and defines the period of trend information shown for all
screen trends.
To set a different ScreenTrend Time for a screen trend or a group of aligned screen trends,
1Select a screen trend
2Select Change TrendTime
3Select the required trend time.
Selecting Global leaves the trend time set to the global screen trend time.
Changing the Selection of Screen Trends Displayed
1Select the screen trend.
2Select Change Trend and select the required trend from the list of available trends.
Select Blank to remove the selected trend from the Screen.
If you do not see Change Trend in the screen trend menu, the trend is aligned to display with
the measurement wave. Changing the wave automatically changes the trend.
To display two or more screen trends overlapping,
1Select the screen trend to open the screen trend menu,
2Select Change Trend -> Add Trend and select a screen trend from the pop-up list.
Activating the Cursor for Screen Trends
To activate the cursor for Screen Trends:
1Select the screen trend.
2Select Activate Cursor
You can now use the arrow keys to move the cursor across the time line. The values measured at the
cursor time are shown next to the cursor.
To de-activate the cursor,
♦Press the Main Screen key.
Changing the Screen Trend View
♦To switch between tabular, graphic, histogram and horizon views, select the screen trend then select
Change View and select the required view.
Tabular View
Aperiodic measurements such as NBP, can be viewed as a screen trend in tabular form. The measured
values and their timestamps are shown, with the measurement label.
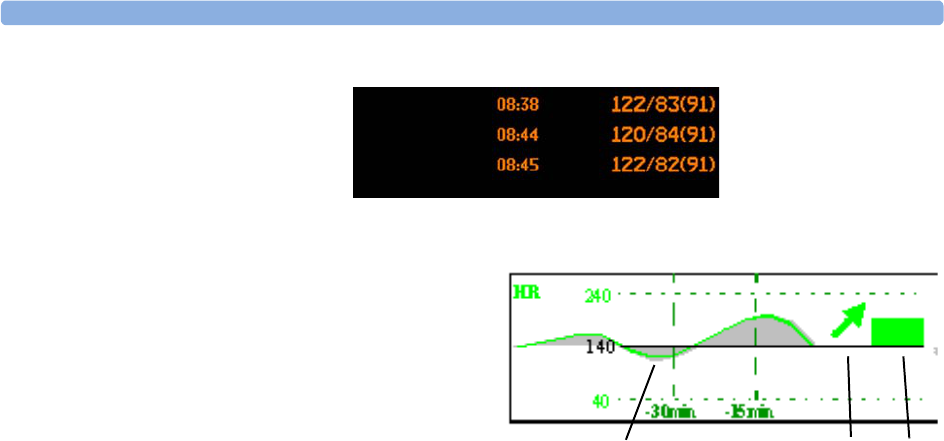
17 Trends Screen Trends
196
Horizon View
The horizon view presents trend information
superimposed over a defined baseline or base
range. This helps you visualize changes in
your patient’s condition since the baseline
was set.
The horizon view is made up of:
• a horizon, drawn in white, as a reference
point or baseline to help you visualize
changes in your patient’s condition. The horizon can be set to represent your patient’s current
condition, or a target condition and can be a single value or a range.
• a graphical trend, displaying patient data for the set TrendTime (1).
• a trend indicator arrow, indicating how the patient trend has developed in the set time period
(10 minutes, 5 minutes or 2 minutes) (2).
• a deviation bar, showing how the currently measured value deviates from the set horizon (3). The
height of the deviation bar is an indication of the extent of the change in your patient’s condition
relative to the (horizon) baseline.
Your monitor may not be configured to show all elements of the screen trend horizon view.
Setting the Horizon
The horizon is the reference value to which deviations in the measurements are compared.
1To set the horizon, select the horizon trend
2Select
–Set High Horizon to select the upper horizon value. If the high and low horizon values are
the same, the horizon is a baseline - if the values are different the horizon is a range.
–Set Low Horizon to select the lower horizon value.
–Auto Horizon to set the horizon for the selected horizon trend to the currently-measured
value
–Auto All to reset the horizon for all horizon screen trends to the currently-measured values
–Set Horizon to set the horizon to a specific value from a pop-up list.
Setting the Horizon Trend Scale
The horizon trend scale is defined with respect to the horizon. If your horizon is set to 100 and you
select 20 as the horizon scale delta, the upper limit of the horizon scale will be 120 and lower limit 80.
To set the horizon trend scale delta,
1Select the horizon trend.
NBP
Sys.
123

Screen Trends 17 Trends
197
2Select Set Scale Delta and select a value to define the distance between the horizon and the
upper and lower scale limits.
Be aware that changing the horizon trend scale can change the angle of the trend indicator, without the
patient’s condition having changed.
If a measurement exceeds the outer limits of the scale, the wave will be clipped and you must either
reset the horizon or the horizon trend scale to display the values outside the scale limits.
Setting the Time Period for the Trend Indicator Arrow
The time period for which the trend indicator arrow can be set in the Trends window.
1Select Main Setup > Trends
2Select HorizonArrowTime.
3Select 10, 5 or 2 minutes.

17 Trends Screen Trends
198
199
18
18 Recording
Central
Recording
For central recording from the bedside, your monitor must be connected via a network to an
Information Center. You can use either the M1116B 2-Channel Recorder or the standalone M3160A
4-Channel Recorder. See the documentation supplied with the Information Center for information on
the 4-Channel Recorder.
Starting and Stopping Recordings
The recordings pop-up keys let you start and stop recordings. Select the Main Setup SmartKey then
select Recordings to call up the line of pop-up keys. Scroll right or left to see any pop-up keys not
displayed.
Recording Without a Template
To record without a preconfigured template, selecting the waves you require,
1Select the Main Setup SmartKey then select Recordings.
2Select the pop-up key Select Waves,
3Use the pop-up keys to choose up to three measurement waves to be printed on the recording. If
you want fewer than three waves on the recording, select the waves you want then select the
Continue pop-up key.
4Select one of the recording speed pop-up keys to set the required recording speed.
5Select the Start pop-up key to start the recording.
Select Waves recordings use default values for any recorder settings not defined: runtime is
continuous, overlapping is set to non-overlapping.
Delayed
Recordng
RT A
Recordng
RT B
Recordng
Select
Waves
Setup
Recordng
Stop all
Recordng
18 Recording Overview of Recording Types
200
Overview of Recording Types
Creating and Changing Recordings Templates
To save you defining recording settings each time you start a recording, you can create templates for
commonly-used types of recordings in the Setup Recording menu. You can create templates for
one delayed recording, one alarm recording and two realtime recordings (Realtime A and
Realtime B).
Changing recordings templates changes the settings that will be used each time a recording of this
name is triggered.
1Select the Main Setup SmartKey to call up the Main Setup menu.
2Select Recordings.
3Select the Setup Recording pop-up key to enter the Setup Recordings menu.
4Select the name of the template you want to create or change. Each recording name is linked to a
recording type: delayed, alarm, and realtime. Recording names can be changed in the monitor’s
Configuration Mode.
5Design the template by selecting each menu item and entering the information for the template.
•Recorder: choose which recorder the recording will print to (Central 2-Ch. or Central 4-
Ch. recorder, or a printer (for realtime reports in alarm recording only)).
•Channels 1 - 4: choose which waveform to record in each channel.
In addition to the currently available waves, you can choose from several other settings which make
an automatic allocation when the recording starts:
–Alarm Par will always record the measurement in alarm in the chosen recorder channel
–Primary Lead will always record the current primary lead in the chosen recorder channel
Delayed Alarm Realtime (RT)
Type of recording manual automatic, triggered by defined alarm
conditions
manual
Recording
Destination
central central printer central
Information
recorded
from the start trigger
minus the delay time
from the start trigger
minus the delay time
N/A from the start trigger
Number of waves up to 2 up to 2 N/A up to 2
Speed 50, 25, 6.25 mm/sec 25 mm/sec N/A 50, 25, 6.25 mm/sec
Runtime N/A N/A N/A continuously
Stops automatically automatically N/A manually
Delay Time 10, 15 seconds 10, 15 seconds N/A none
Overlap Off
On (up to 2 waves)
Off
On (up to 2 waves)
N/A Off
On (up to 2 waves)
N/A = not applicable
Recorder Status Messages 18 Recording
201
–Secondary Lead will always record the current secondary lead in the chosen recorder
channel
•Overlap: define whether the recorded waveforms will be printed overlapping or beside each other.
•Speed: choose the recording print speed.
•Delay Time: Delayed recordings start documenting on the recorder strip from a pre-set time
before the recording is started. This interval is called the “Delay Time” and can be set as specified in
the table on page 200. This setting can only be changed in Configuration Mode.
•Runtime: see how long this type of recording is configured to run. This setting can only be
changed in Configuration Mode. Continuous recordings run indefinitely.
•Central Config - if available in the General menu, select this setting to use the recording
settings made for the centrally-connected recorder.
Maintaining Recording Strips
Recording ink sometimes fades when covered with transparent tape. Avoid covering any part of a
recording that is clinically relevant (annotation or waveforms) when taping a recording strip to a
patient record or other patient documentation.
Recorder Status Messages
CAUTION If no central recorder is available, alarm recordings may be lost. The message No alarm
recording available will be displayed. This message is not shown if Printer is configured
as the alarm recording destination.
Recorder Status Messages Explanation
<Recording name> running The named recording is currently running.
No alarm recording available No recorder available. Alarm recordings will be lost.
Try configuring Printer as the alarm recording
destination.
Central Recorder out of
paper
The named recorder is out of paper.
Central Recorder door open The door of the specified recorder is open.

18 Recording Recorder Status Messages
202
203
19
19Printing Patient Reports
Starting Report Printouts
Most patient reports can be printed by selecting Main Setup - > Reports (or the Reports
SmartKey) and then selecting the report name in the top half of the Reports menu. Report names
are shown only for reports that have been correctly set up.
Data from the time of the print request is printed, even if the print job is delayed in the printer queue.
Your monitor can also be set up to automatically print all reports when a matching printer is available.
To set this up
1Select Main Setup - > Reports
2Select Auto Print Dbs.
–Always will print all reports when a matching printer is available.
–Host only will print the reports stored on the host monitor when a matching printer is
available. Reports stored in the companion database (shown in grey on the Reports Job List) must
be manually sent to the printer. See “Checking Report Status and Printing Manually” on
page 207.
–Never will print no reports automatically; all reports stored in the host or companion database
must be manually sent to the printer. See “Checking Report Status and Printing Manually” on
page 207.
Depending on availability, reports can be printed on printers connected to the Information Center, an
external PC-based print server or into the print database. Print jobs stored in the database are
automatically printed when a print device with a matching paper size becomes available.
Print jobs in the print database are not deleted after a patient discharge. A new patient can be admitted
and their reports are saved in addition to the previous reports. Always admit your patient so that
reports can be clearly assigned to a patient.
Report types Report contents How to start printing reports
Vital Signs Report depends on selected trend group, data
resolution, and period.
In the Vital Signs window, select Print
Graphic Trends Report In the Graphic Trends window, select Print
ECG Reports Depends on format selected Select the ECG Report SmartKeys, if configured
ST Map Report ST data in a transversal and/or horizontal
multiaxis diagram,
In the ST Map window, select Print.
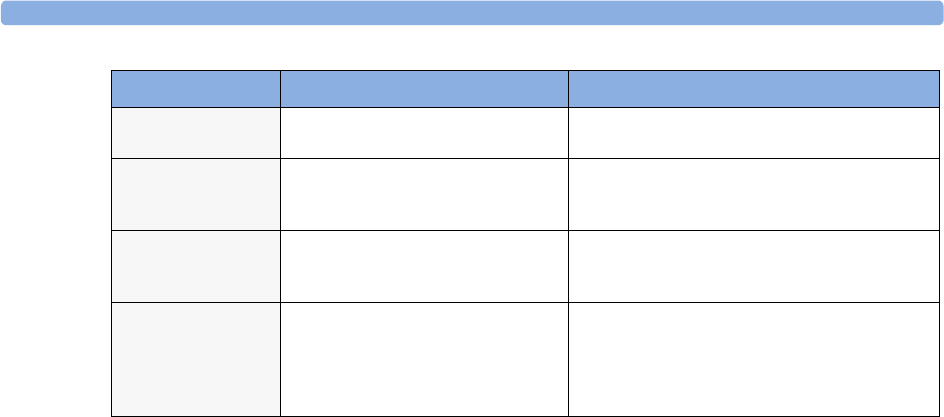
19 Printing Patient Reports Stopping Reports Printouts
204
Stopping Reports Printouts
♦To stop Reports printing, in the Reports menu, select
–Delete Report to stop the current print job
–Delete All Repts to cancel all queued report printouts
–Scheduled Rep. to toggle to Off and switch off scheduled reports.
Setting Up Reports
ECG report layout and Auto Reports settings must be defined in Configuration Mode.
The content you define in the individual Setup Reports menus will be used in all reports of this
type: for example, if you set a print speed of 50 mm/sec in the ECG Reports menu, every ECG
report will be printed at this speed, irrespective of format.
Setting Up ECG Reports
The settings you choose in the ECG Reports menu apply for all ECG reports printed. To set up
ECG Reports,
1Select Main Setup -> Reports -> ECG Reports. Note the report layout configured for
your monitor, either Internat. or Cabrera. This setting is inactive (“grayed-out”) in Monitoring Mode
and can only be changed in Configuration Mode.
2Select ECG Gain and set the required ECG Gain to define how ECG waves will appear on the
ECG report printouts.
3Select Speed and select the report print speed.
4Select Annotation and toggle to On if the printed ECG wave should be annotated with beat
labels or not. See the chapter on ECG for a list of beat labels. Pace pulse marks are automatically
printed beside the wave for paced patients.
Setting Up Vital Signs and Graphic Trend Reports
The settings you choose in the Vital Signs Report and Graphical Trend Report
menus apply for all Vital Signs and Graphic Trend reports printed.
Alarm Limits Report Graphic and numeric report of all
current alarm limits
In the Alarm Limits window, select Print
Limits
Realtime Reports Patient data and numerics, and either:
all displayed waves OR all measured
waves OR all measured RT waves
Select the Realtime Reports SmartKey, if
configured
Battery Report Battery serial number, information on
the currently-measured and potential
charge status of the battery
In the Battery Status window, select
Print Status.
Central Report A/B/C These are reports configured at the
Information Center. Monitors connected
via the IntelliVue Instrument Telemetry
wireless network can have these reports
available.
In the Main Setup select Reports then
Central Report A, B or C.
Report types Report contents How to start printing reports

Setting Up Individual Print Jobs 19 Printing Patient Reports
205
To set up Vital Signs and Graphic Trend reports,
1Select Main Setup -> Reports -> Vital Signs Rep. or Graph Trend Rep.
2Select Trend Group and select the group you want to print on the report. The groups available
depend on your monitor’s trend configuration.
3Select Period and select the period of time for which trend data should be printed on the report. If
Automatic Period is configured to On, all trend data for the current patient will be printed,
irrespective which trend period is selected.
4Select Interval (Vital Signs Reports only) and select the resolution of the trend data printed on the
report,
Setting Up Auto Reports
Auto Reports print automatically when a specified trigger occurs. There are two types of Auto Reports:
Scheduled Reports, which print at predefined intervals, and End Case Reports, which print when a
patient is discharged using the End Case function. An Auto Report can be both a Scheduled Report
and an End Case report.
To set up Auto Reports,
1Select Main Setup -> Reports -> Auto Reports and select the Auto Report you want to set up (A, B,
C, or D).
2Select Report and assign a report type to the Auto Report.
3Select End Case Report and toggle to On if you want the selected report to print
automatically when you select End Case to discharge a patient.
Toggle End Case Report to Off if the report is a Scheduled Report only.
4Select Scheduled Rep. and toggle to On if you want the selected report to print at predefined
intervals, starting at a predefined time of day. The start time you set applies for every following day.
For example, if you set a start time of 07:00 and a repeat time of six hours, the first report will print
at 07:00 every day, the next at 13:00 and so on.
– To set the time of day at which you want the report to print every day: select Start Hour and
Start Minute and select the required time from the pop-up list
– To set the time interval in minutes between two scheduled reports: select Rep. Freq.(Hr)
and Rep. Freq.(Min) and select the time interval from the pop-up list.
If you are setting up an end case report, these settings will be inactive (“grayed-out”).
Toggle Scheduled Rep. to Off if the report is an End Case Report only.
5Repeat the procedure for all Auto Reports you want to set up.
All Auto Reports or Scheduled Reports set to On print automatically at the predefined trigger.
Be aware that the monitor’s memory for reports is limited. If the memory is full, Auto Reports cannot
be printed and the information may be lost.
Setting Up Individual Print Jobs
To adjust the appearance of individual print jobs, in the Reports menu,
1Select Main Setup -> Reports -> Setup Reports to enter the Setup Reports
menu.

19 Printing Patient Reports Checking Printer Settings
206
2Select Report and then select the report you want to set up.
3Select Report Type and then select the reports template you want the report selected in Step 2
to use. The selection of templates listed depends on the report type selected.
Each template includes patient demographic data, and each Realtime Report also includes alarm
and INOP information. In addition, the templates include:
VisibleWaves: all waves currently visible, in the order they appear on the screen.
All Waves: all measured waves,
RT Waves: all currently measured realtime waves, according to the monitor’s priority list.
Vital Signs: trend information in tabular form.
Graph Trend: trend information in graphic form.
ECG3X4, ECG6X2, ECG12X1, ECG4X2, ECG8X1, ECG12X1(2P): ECG reports.
Alarm Limits: a list of all currently set alarm limits.
4Select Report Size to set the paper size to be used for the report: Unspecified to use the
default size for the template chosen, Universal, A4, Letter, LrgUniversal, A3, or
Ledger. The list of available sizes depends on the report type selected.
5Select Orientation to set the orientation of the report printout: Unspecified to use the
default size for the template chosen, Landscape or Portrait.
6Select Target Device and choose which printer the print job will be sent to: Unspec. to use
the default printer, or choose from the list of printer names defined at the Information Center or in
the monitor’s Configuration Mode (for example, Remote 1 or Database).
Some settings may be inactive (“grayed-out”) in this menu for reports that can only be started in a
special window.
Checking Printer Settings
The printer settings for your monitor are defined in Configuration Mode. The printer settings Paper
Size, Resolution, Color Support, and Duplex Option for the active printer are visible
but inactive (“grayed-out”) in the Setup Printers menu. When Print Database is selected
as active printer only the Paper Size setting will be shown.
♦To enter the Setup Printers menu, in the Reports menu, select Setup Printers.
Printing a Test Report
A test report can be printed in Configuration mode, refer to the Service Guide for details.
Switching Printers On Or Off for Reports
You can enable or disable printer status to switch individual printers on or off for report printouts.
1In the Setup Printers menu, select Printer and then select the name of the device you
want to switch on or off for Reports printing from the pop-up list.
Dashed Lines on Reports 19 Printing Patient Reports
207
2Select Printer Status to toggle between the settings Enabled and Disabled. If you set
this to Disabled, no reports will be printed to the named printer.
If the monitor detects that no printer of a particular type is available, the Enabled/Disabled
setting will automatically be set to Disabled and “grayed out”.
Dashed Lines on Reports
If a section of a wave on a report is drawn with dashed lines, this tells
you that a setting that affects the appearance of the wave on the
screen was changed while the report was printing.
For example, if you change the wave scale while a report is printing,
the wave scale and wave size are changed immediately on the
monitor screen and on the report. To indicate that the scale
information printed at the beginning of the report no longer matches the currently used scale, the wave
will be printed using dashed lines, starting from the moment the change took place.
Some examples of settings that cause dashed lines in reports if changed during printing are: Filter
mode, ECG lead placement, wave scale, measurement unit, paced/non-paced setting, and
measurement mode. Note that as ECG waves are drawn with a fixed gain on reports (either 10 mm/
mV or 20 mm/mV), changing the ECG wave scale will not cause dashed-line reports.
To avoid dashed lines on reports, wait 15 seconds after changing a setting before you trigger a report.
Unavailable Printer: Re-routing Reports
If you send a report to be printed on a printer that is not available, for example, because it has run out
of paper, this print job is suspended and stored in the monitor’s memory.
If the target device of this print job was set to Unspecified, the monitor will periodically try to
resend the print job to the first printer listed in the Setup Printers menu under Printer that
is set to Enabled and that has paper of the correct size.
To allow the report to print, you must either solve the problem with the target printer, or re-route the
print job to another printer with paper of the correct size. To re-route a print job,
♦Enable the new target printer by selecting it in the Setup Printers menu and toggling to
Enabled. As the monitor tries to send the report to the printers in the order they are listed, you
must make sure that all the printers above the new target printer are disabled.
If the target device of the print job was set to a specific printer, re-routing is not possible.
Checking Report Status and Printing Manually
A list of all print requests which are waiting, printing or stored can be viewed in the Reports Job List.
To view the list,
♦in the Reports menu, select Reports Job List.
The following information is displayed for each print request:
• Report title
• Patient name (except for system reports such as the battery status report)
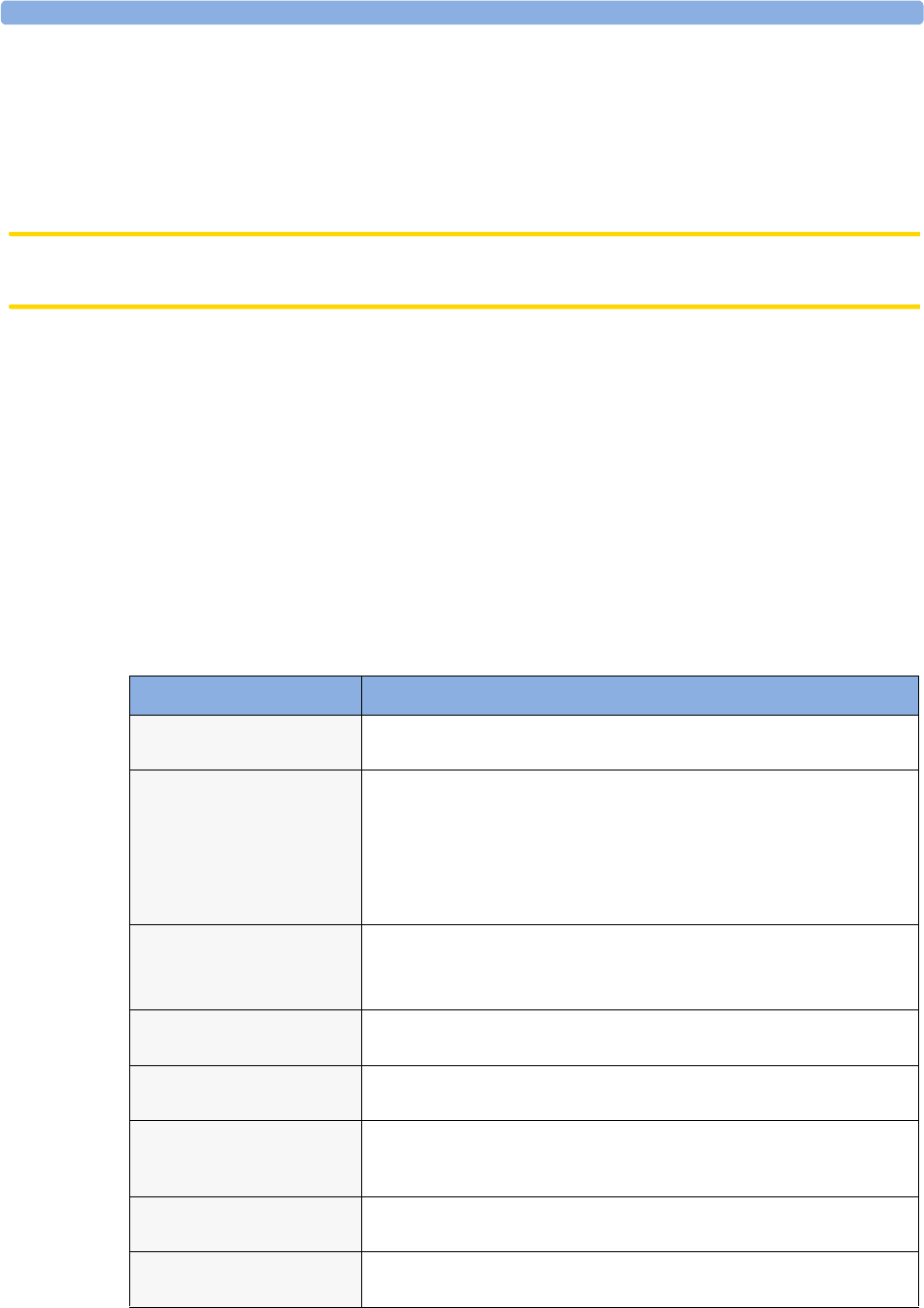
19 Printing Patient Reports Printer Status Messages
208
• Request date and time
• Report paper format
• Job status: Preparing, Printing, Waiting, In Database, In Companion, Retry, Cancelling, Error
Individual reports can be deleted from the list with the Delete Report key, and all reports with
the Delete All Reps key.
CAUTION The reports job list includes privacy information, in the form of the patient name with the related
report title and date. It is advisable to provide controlled access to this data to ensure confidentiality.
Printing Manually
Those jobs shown in black will be printed automatically when a matching printer is available. If the
Auto Print Dbs setting is Host only or Never, some or all reports will not be printed
automatically and will be shown in grey. Any jobs shown in grey must be printed manually; to do this,
1In the Reports Job List, select the required report
2Select Print Report.
Selecting Print All Reps. will send all reports to the printer.
Printer Status Messages
Printer Status Message Possible causes and suggested action
Print job queued
<Printer name>
The report has been placed in the queue for the named printer.
Print job can’t
queue;queue full
The printer queue is full and the monitor cannot accept another report
request. Wait until some more reports have been printed, then try again,
OR
A report has been triggered that uses a paper size unavailable with the
target printer. Try another printer, if available, or change the paper size of
the print request.
Cancelling all
print jobs
Stop All Reports has been selected in the Report menu, OR
The Operating Mode has been changed from Monitoring Mode to
Demonstration or Service Mode.
Cancelling the
active print job
The current report is being cancelled as the result of a user request.
Deleted N print
jobs;discharge
When a patient is discharged, all queued reports are cancelled except those
stored in the print database. “N” is the number of reports cancelled.
Deleted N print
jobs; hotstart
The monitor has restarted and all report requests have been cancelled
except those stored in the print database. “N” is the number of reports
cancelled.
Print failed;No
report configurd
A report has been triggered which has not been correctly set up. Enter the
setup menu for the report type to set up the report.
Printing on
<Printer name>
A report is in progress, or the monitor is waiting for the central printer to
accept the print job.
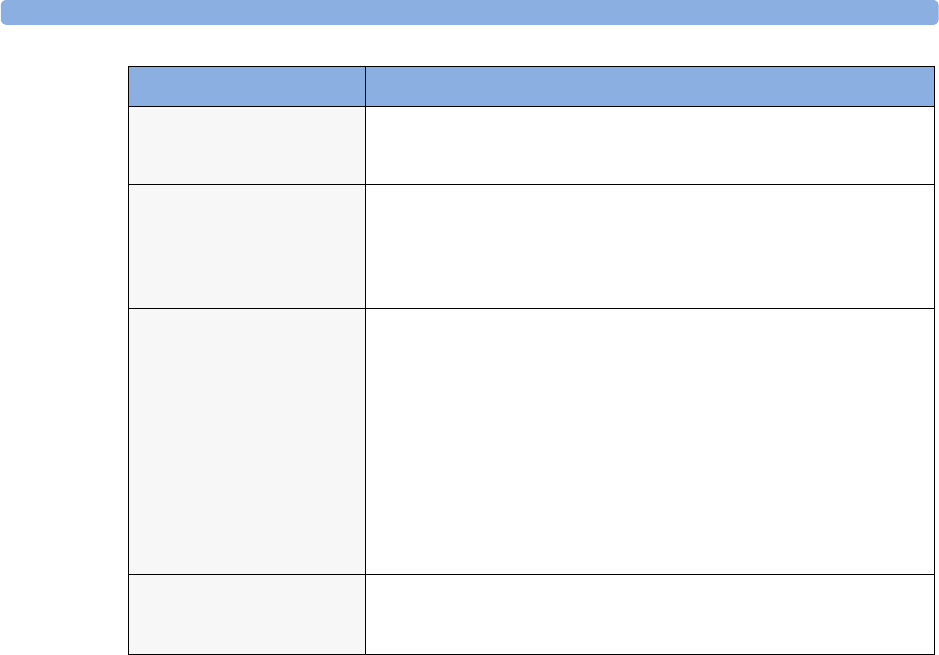
Sample Report Printouts 19 Printing Patient Reports
209
Sample Report Printouts
Each report header contains the patient’s bed label, last name and first name, middle name (if there is
enough space) the patient ID, the date and time, and the name of the report. The report footer
contains the hospital label and page number, and the last page contains a note to mark the report end.
The monitor may be configured to leave a space on the top left or right of the report printout to enable
you to stick a patient address label on it. This setting is called the Addressograph and it can only be
changed in the monitor’s Configuration Mode.
NoPrinter <Printer
name>;job susp
The chosen device is unavailable. Check that the printer is properly
connected and that paper is available. The requested report will start
printing when the printer becomes available.
Print Database
full->job suspnd.
The requested report does not fit into the print database. You can select
another printer to print the report (see “Unavailable Printer: Re-routing
Reports” on page 207). Alternatively you can delete another report from
the Reports Job List (using the Stop report key) to create space for your
report.
Job <Printer name>
fail;
A report cannot be started on the requested printer.
One of three reasons will also be shown in the status message:
• data requisition error (data error) - an internal error has caused
data required for the report to be unavailable, try starting the report
again.
• printer unavailable (no printer)- make sure the printer is
plugged in, switched on, and has paper loaded.
• data unavailable (no data) - the connected X2 or MP5 has been
removed before the data for the report was transferred.
Print job on
<Printer name>
done
The report has been printed.
Printer Status Message Possible causes and suggested action
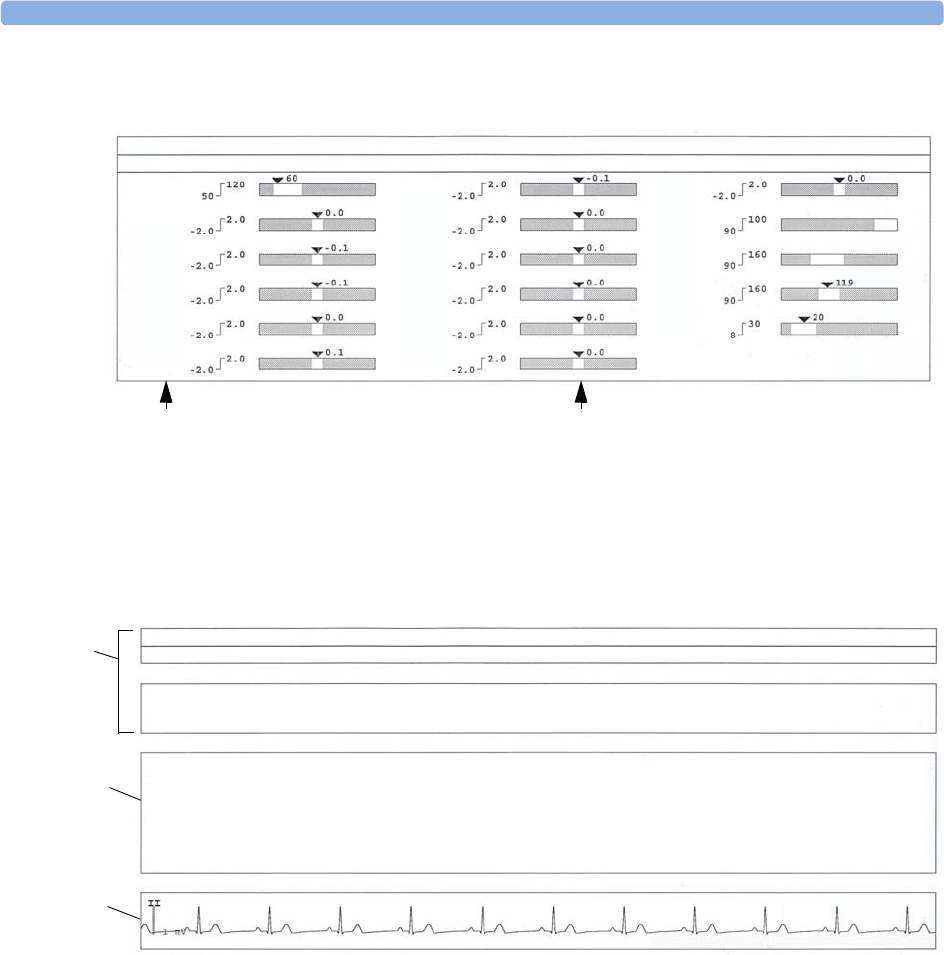
19 Printing Patient Reports Sample Report Printouts
210
Alarm Limits Report
Realtime Report
NBed6 Doe, John 123456789-P1
Alarm Limits 19 Apr 07 15:59:37
HR
ST-I
ST-II
ST-III
ST-aVR
ST-aVL
ST-aVF
ST-V1
ST-V2
ST-V3
ST-V4
ST-V5
ST-V6
SpO2
NBPs
ABPs
RR
Apnea Time 20 sec
Measurement labels, with alarms off symbol where
alarms are switched off
Graphic view of current alarm limits in relation to
currently monitored measurement value
NBed6 Doe, John 123456789-P1
Realtime Report 19 Apr 07 15:59:54
Patient Cat.: Adult
Paced: No
Gender: Male
Date of Birth: 19 Nov 1963
Age: 43 years
Height: 69 in
Patient Cat.: Adult
Paced: No
ST-aVR 0.0 mm
ST-aVL 0.0 mm
ST-aVF 0.0 mm
ST-V1 0.0 mm
ST-V2 0.0 mm
ST-V3 0.0 mm
ST-V4 -0.1 mm
ST-V5 0.0 mm
HR 60 bpm
PVC 0 /m
ST-I 0.0 mm
ST-II 0.0 mm
ST-III 0.0 mm
ST-V6 0.0 mm
SpO2 -?- %
Pulse -?- bpm
Perf -?-
NBP
Pulse
ABP 119/81 (93) mmHg
ST-V5 0.0 mm
**ABPs HIGH
SpO2 NON-PULSAT.
Bandwidth 0.5-40 Hz Non-Paced 10mm/mV 25mm/sec
Patient
demographic
information,
time stamp
Active Alarms
and INOPs,
followed by vital
signs
Measurement
waves section
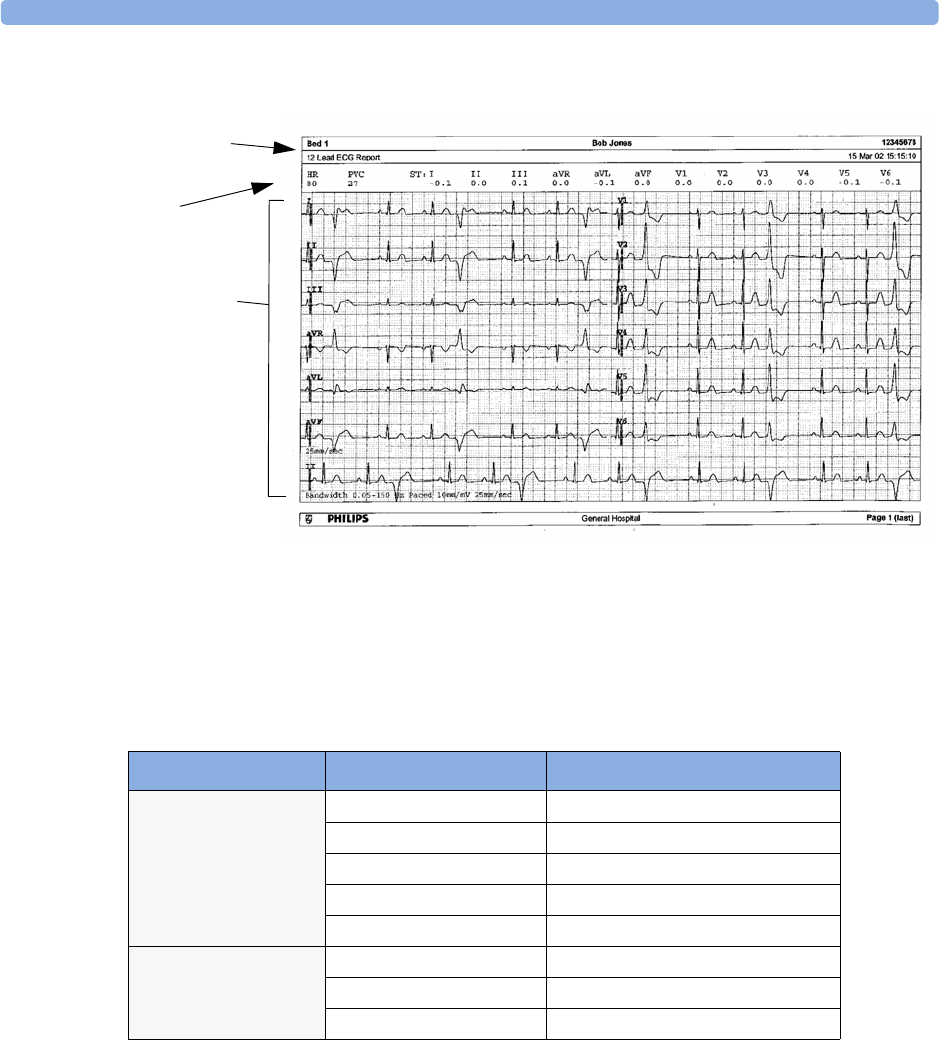
Sample Report Printouts 19 Printing Patient Reports
211
ECG Reports
Below the header on ECG Reports, the numeric block shows the current HR, PVC, and ST values.
The wave area shows the printed waves for all available ECG leads. A 1 mV calibration bar is printed at
the beginning of each wave. With the 3X4, 6X2, and 2X4 formats, a rhythm stripe prints a longer
section of the ECG wave from the primary ECG lead for ECG rhythm evaluation. The ECG signal
bandwidth, the patient’s paced status, the ECG gain, and the print speed are printed at the bottom of
the wave area. Pace pulse marks are automatically printed beside the wave for paced patients. Beat
labels can be set to print on the rhythm stripe. The 12X1 (2P) format prints the report over two pages.
Other Reports
See the sections on Trends for other example reports.
ECG Report type Available Formats Available Paper Sizes
12-Lead ECG 3X4 landscape A4, letter, A3, ledger
6X2 landscape A4, letter, A3, ledger
12X1 portrait A4 and letter only
12X1 landscape A4, letter, A3, ledger
12X1 (2P) landscape A4, letter (2 pages)
Multi-lead ECG 2X4 landscape A4, letter, A3, ledger
8X1 portrait A4 and letter only
8X1 landscape A4, letter, A3, ledger
Patient
information
Numeric block
Wave area

19 Printing Patient Reports Sample Report Printouts
212

213
20
20Care and Cleaning
Use only the Philips-approved substances and methods listed in this chapter to clean or disinfect your
equipment. Warranty does not cover damage caused by using unapproved substances or methods.
Philips makes no claims regarding the efficacy of the listed chemicals or methods as a means for
controlling infection. Consult your hospital’s Infection Control Officer or Epidemiologist. For
comprehensive details on cleaning agents and their efficacy refer to “Guidelines for Prevention of
Transmission of Human Immunodeficiency Virus and Hepatitis B Virus to Health Care and Public-
Safety Workers” issued by the U.S. Department of Health and Human Services, Public Health Service,
Centers for Disease Control, Atlanta, Georgia, February 1989. See also any local policies that apply
within your hospital, and country.
General Points
Keep your monitor, cables and accessories free of dust and dirt. After cleaning and disinfection, check
the equipment carefully. Do not use if you see signs of deterioration or damage. If you need to return
any equipment to Philips, decontaminate it first.
Observe the following general precautions:
• Always dilute according to the manufacturer’s instructions or use lowest possible concentration.
• Do not allow liquid to enter the case.
• Do not immerse any part of the equipment or any accessories in liquid.
• Do not pour liquid onto the system.
• Never use abrasive material (such as steel wool or silver polish).
• Never use bleach.
WARNING If you spill liquid on the equipment, battery, or accessories, or they are accidentally immersed in liquid,
contact your service personnel or Philips service engineer. Do not operate the equipment before it has
been tested and approved for further use.
20 Care and Cleaning Cleaning the Monitor
214
Cleaning the Monitor
Clean with a lint-free cloth, moistened with warm water (40°C/104°F maximum) and soap, a diluted
non-caustic detergent, tenside, ammonia- or alcohol-based cleaning agent. Do not use strong solvents
such as acetone or trichloroethylene.
Take extra care when cleaning the screen of the monitor because it is more sensitive to rough cleaning
methods than the housing. Do not permit any liquid to enter the monitor case and avoid pouring it on
the monitor while cleaning. Do not allow water or cleaning solution to enter the measurement
connectors. Wipe around, not over, connector sockets.
CAUTION To clean the touch-enabled display, disable the touch operation by switching off the monitor during
the cleaning procedure, or by pressing and holding the Main Screen key for two seconds. Press the
Main Screen key again to re-enable touch operation.
Recommended cleaning agents are:
Disinfecting the Monitor
CAUTION Solutions: Do not mix disinfecting solutions (such as bleach and ammonia) as hazardous gases may
result.
Hospital policy: Disinfect the product as determined by your hospital’s policy, to avoid long term
damage to the product.
Clean equipment before disinfecting. Recommended types of disinfecting agents are:
Sterilizing the Monitor
Sterilization is not recommended for this monitor, related products, accessories or supplies unless
otherwise indicated in the Instructions for Use that accompany the accessories and supplies.
Tensides (dishwasher detergents) Edisonite Schnellreiniger£, Alconox£
Ammonias Dilution of Ammonia <3%, Window cleaner
Alcohol Ethanol 70%, Isopropanol 70%, Window cleaner
Base Approved Agents
Alcohol Ethanol up to 70%
1- and 2- Propanol up to 70%
Aldehyde Glutaraldehyde up to 3.6%

Cleaning, Sterilizing and Disinfecting Monitoring Accessories 20 Care and Cleaning
215
Cleaning, Sterilizing and Disinfecting Monitoring
Accessories
To clean, disinfect and sterilize reusable transducers, sensors, cables, leads, and so forth, refer to the
instructions delivered with the accessory.
Cleaning Batteries and the Battery Compartment
Wipe with a lint-free cloth, moistened with warm water (40°C/104°F maximum) and soap. Do not use
strong solvents. Do not soak the battery.

20 Care and Cleaning Cleaning Batteries and the Battery Compartment
216
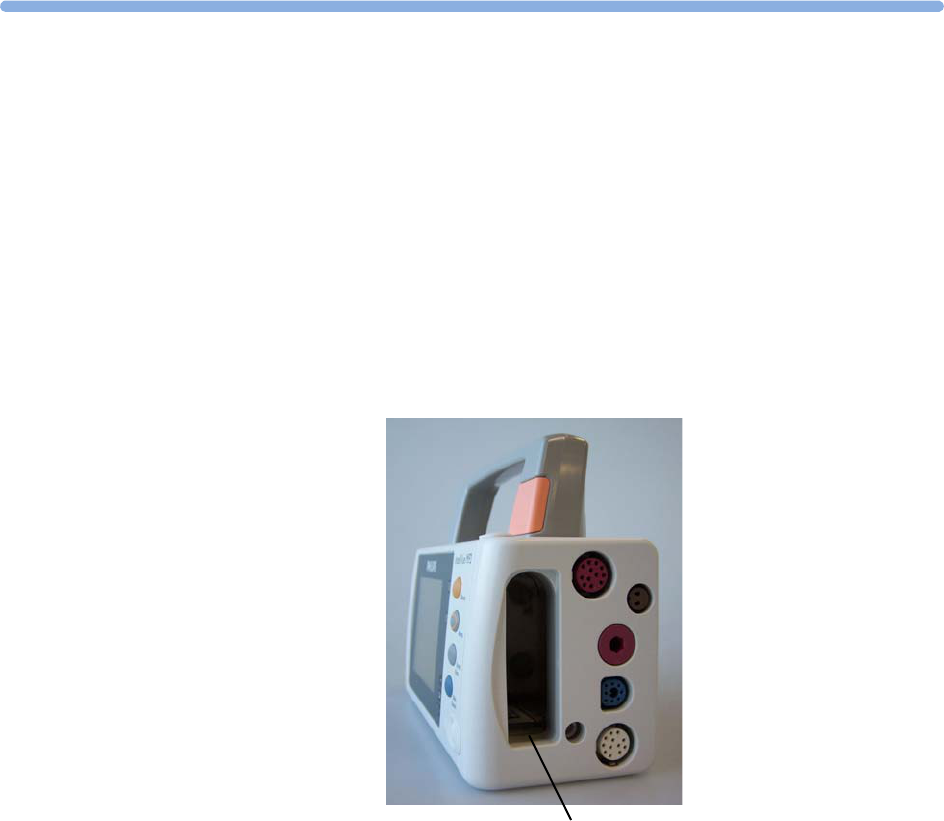
217
21
21Using Batteries
When monitoring a patient, one Philips M4607A rechargeable Lithium Ion battery must always be
inserted into the battery compartment on the right side of the monitor. This applies even when you are
running the monitor from the external power supply. The battery seals the battery compartment,
thereby preventing the ingress of fluids or foreign bodies. A severe yellow INOP (!!INSERT
BATTERY) will be issued if the monitor is connected to AC mains without a battery fully inserted in
the battery compartment. This INOP will persist until a battery is loaded.
To use the monitor with battery power, disconnect the MSL cable (connecting the external power
supply) from the monitor.
You can switch between battery-powered and mains-powered (AC) operation without interrupting
monitoring.
The battery recharges automatically when the monitor is connected to the external power supply
(M8023A).
Battery compartment
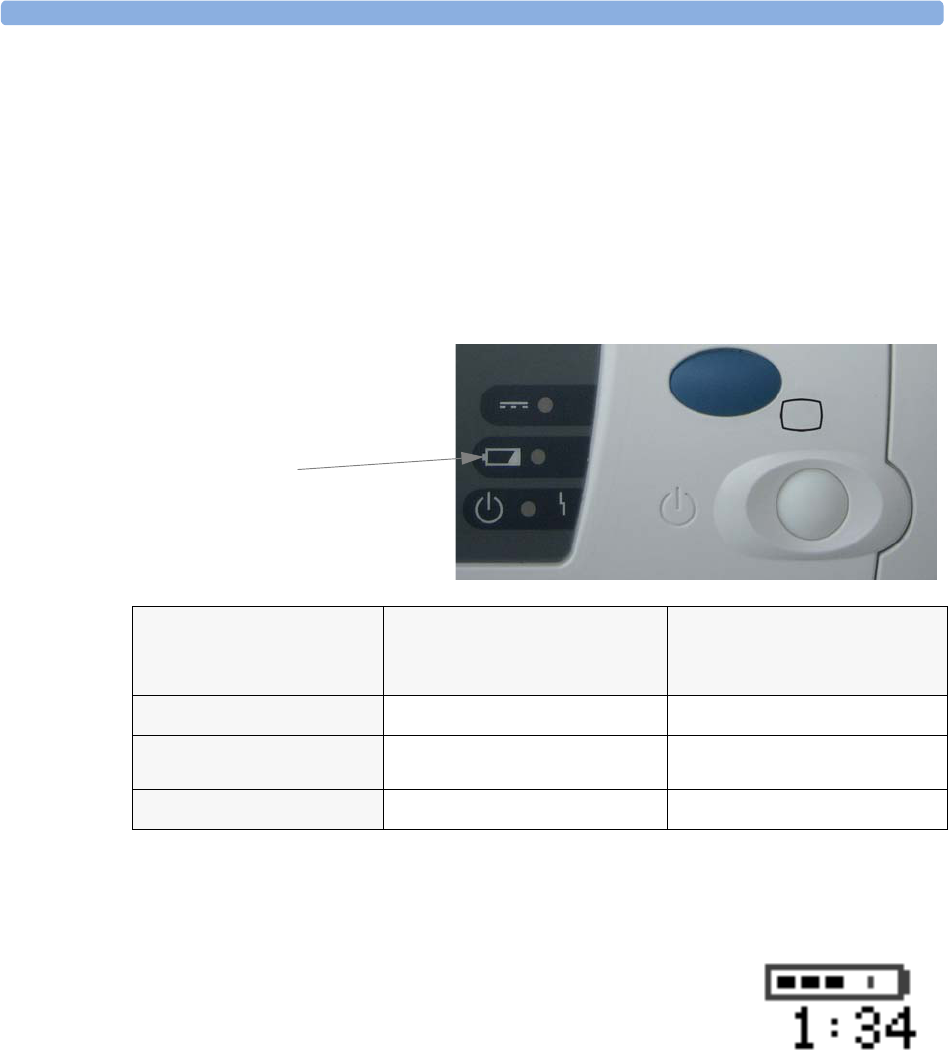
21 Using Batteries Battery Power Indicators
218
Battery Power Indicators
The battery LED and battery status information on the Main Screen, in combination with INOP
messages and prompts, help you keep track of the battery power status. The indicators always show the
remaining capacity in relation to the battery’s actual maximum capacity, which may lessen as the
battery ages. You can see the actual capacity in the Battery Status window.
Battery LED
The battery LED on the front panel of the monitor is indicated by a battery symbol.
The battery LED is yellow during charging and switches off when the battery is charged.
Battery Status on the Main Screen
Battery status information can be configured to display permanently on all
Screens. It shows the status of the battery, with the battery power
remaining and, when the battery is not charging, an estimate of the
monitoring time this represents.
Battery power gauge: This shows the remaining battery power. It is
divided into sections, each representing 20% of the total power. If three sections are filled, as in this
example, this indicates that 60% battery power remains. If no battery is detected, a blank battery gauge
marked with a flashing red X is displayed. If no data is available from the battery, a question mark is
shown in the gauge.
Battery LED Colors If the monitor is connected to
the external power supply
(M8023A), this means
If the monitor is running on
battery power, this means
Yellow battery charging
Red, flashing less than 10 minutes power
remaining
Red, flashes intermittently battery or charger malfunction battery malfunction
Battery LED
Battery Power Indicators 21 Using Batteries
219
Battery status/malfunction indicator: Normal battery function is indicated by the battery power
gauge, together with the remaining operating time, on the Main Screen. You are informed of problems
or changes in the status of the battery by the battery status/malfunction indicator. This consists of a
blank battery gauge containing a symbol. If the symbol is red, this indicates a critical situation. You can
check the specific cause of the problem by looking at the symbol(s) displayed in the Battery
Status window (see page 219).
Monitoring Time Available: While the monitor is running on battery power, a time is displayed
below the battery power gauge. No time is displayed when the monitor is running on AC mains power
via the external power supply (M8023A). This is the estimated monitoring time available with the
current battery power. Note that this time fluctuates depending on the system load (the display
brightness and how many measurements you carry out), the age of the battery, and the remaining
capacity of the battery.
Battery Status Window
♦To access the Battery Status window and its associated pop-up keys, select the battery status
information on the Screen, or select Main Setup -> Battery.
Capacity, remaining tells you how much power is left in the battery.
Capacity, fullCharge tells you how much power the battery can hold when fully charged.
Battery status indicator Battery malfunction indicator
Alternates with the battery gauge on the
Main Screen.
Check in the Battery Status
window to see which status symbol is
displayed to identify the cause.
The red ! flashes. Critical battery
situation or malfunction. Check
in the Battery Status
window to see which malfunction
indicator is displayed, or refer to
the INOP, to identify the cause.
Indicator for missing battery
(flashing red X). An INOP is
issued when the battery
compartment is empty, and the
monitor is connected to AC
mains via the external power
supply. This !!INSERT
BATTERY INOP is suppressed
for 15 seconds while the monitor
is connected to AC mains power,
allowing you sufficient time to
load a new battery. After
silencing, the INOP cycles every
10 seconds until a battery is
loaded.
!
!
X
Battery Status
TimeToEmpty:
Capacity
remaining
fullCharge
[mAh]
[mAh]
2:33 hrs
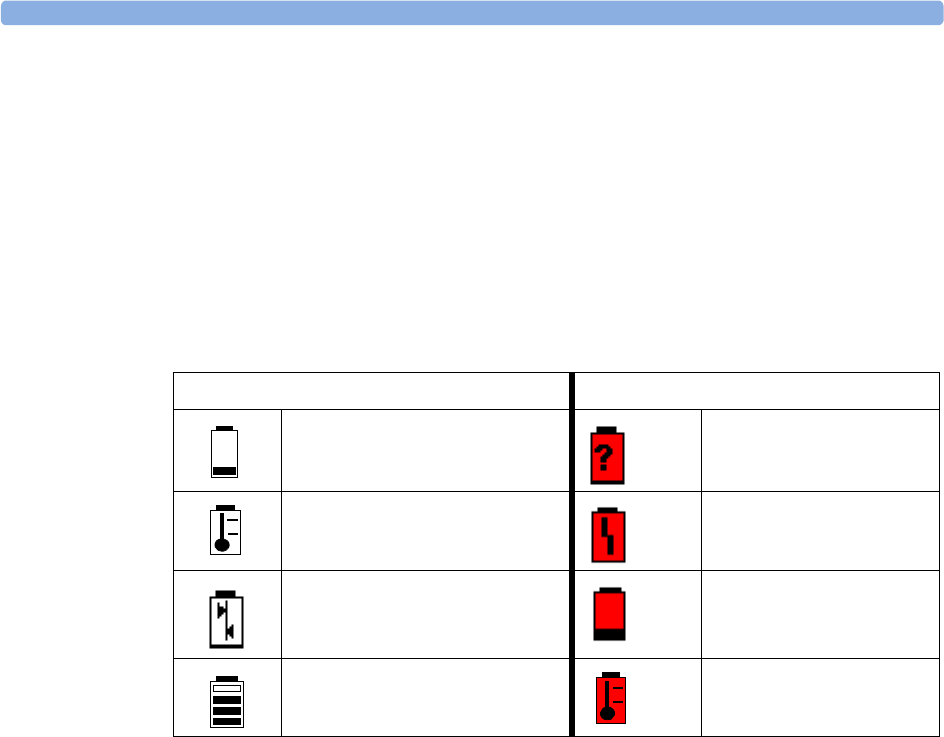
21 Using Batteries Checking Battery Charge
220
TimeToEmpty tells you approximately how long you can continue to use the monitor with this
battery. Note that this time fluctuates depending on the system load (the display brightness and how
many measurements you carry out), the age of the battery, and the remaining capacity of the battery.
TimeToFull is shown in place of TimeToEmpty if the monitor is connected to mains power via
the M8023A external power supply, and tells you how much time is left until the battery is charged to
90%. You can use the M8043A Smart Battery Charger to charge the batteries externally.
Battery status/malfunction symbols: If a problem is detected with the battery, an INOP may be
issued, and the following symbols are displayed in the Battery Status window, where they may
be accompanied by a battery status message providing more details. Messages appear in the line where
TimeToFull/TimetoEmpty is shown. Symbols indicating critical situations are colored red.
Printing Battery Reports
To print the information in the Battery Status window on a connected printer,
1Select the battery status information on the Screen to open the Battery Status window
2Select the Print Status pop-up key.
Checking Battery Charge
♦To check the charge status of a battery in a monitor, see the battery power gauge on the Screen or
select Main Setup -> Battery to enter the Battery Status window.
♦To check the charge status of a battery that is not connected to a monitor or battery charger, press
the black dot marked “PUSH” on the labeled side of the battery. The remaining charge is indicated
by four LEDs on the electronic fuel gauge directly above the dot. Each LED represents 25% of
charge. If all LEDs are lit, the battery is fully charged, if only one LED is lit, 25% or less charge is
left.
Replacing a Battery
To replace the battery,
1Press the battery eject button. This releases the battery.
Battery status symbols Battery malfunction symbols
battery is empty (red) incompatible battery
battery not charging as the temperature is
above or below the specified range
(red) battery malfunction
battery requires maintenance (red) battery has no power left
charging stopped to protect the battery (red) battery temperature too
high

Optimizing Battery Performance 21 Using Batteries
221
The INOP !!INSERT BATTERY is suppressed for 15 seconds, allowing you sufficient time to
load a new battery.
2Remove the battery from the compartment.
3Slide the new battery into position with the contacts facing downwards. It should ‘click’ into
position when it is fully inserted.
Optimizing Battery Performance
The performance of rechargeable batteries may deteriorate over time. Battery maintenance as
recommended here can help to slow down this process.
Display Brightness Setting
♦In the Main Setup menu, select User Interface -> Brightness - > Optimum. This
selects a level of brightness suitable for most monitoring locations that uses less battery power than
brighter settings.
Satisfy yourself that this level of brightness is suitable for your monitoring location.
Note that your monitor may be configured to dim or brighten the display brightness automatically
when you disconnect from power, to suit the most common transport scenario
(“TransportBrightn” setting).
Battery eject button
Click!
21 Using Batteries Battery Safety Information
222
Charging a Battery
A battery can be charged in a monitor during monitoring. You can also use the M8043A Smart Battery
Charger to charge batteries.
1Insert the battery into a monitor connected to the external power supply (M8023A).
2Charge the battery until it is full, the battery LED goes out, and the battery power gauge is filled.
In certain situations, internal temperature conditions may mean that the battery will not charge. This is
sometimes necessary to protect the battery from damage, and does not indicate a malfunction. In this
case you must use the M8043A Smart Battery Charger to charge the battery.
Conditioning a Battery
You must condition a battery when its “battery requires maintenance” symbol shows on the Screen. Do
not interrupt the charge or discharge cycle during conditioning.
CAUTION Do not use a monitor being used to monitor patients to condition batteries. The monitor switches off
automatically when there is no battery power left.
You can also use the M8043A Smart Battery Charger for external battery conditioning (requires
adapter, order number 4512 610 17451). For details please see the Instructions for Use for the Smart
Battery Charger. Do not use any other battery chargers or conditioners.
To condition a battery using a monitor,
1Insert the battery into a monitor connected to the external power supply.
2Charge the battery until it is completely full. Open the Battery Status window and check
that the Batt Fully Charged message is displayed.
3Disconnect the monitor from mains power, and let the monitor run until there is no battery power
left and the monitor switches itself off.
4Reconnect the monitor to mains power and charge the battery until it is full for use or charge to
50% for storage.
Storing a Battery
A battery should not remain inside the monitor if it is not used for a longer period of time. Batteries
should be charged to a maximum of 50% for storage.
NOTE The battery will discharge over time if it is stored inside the monitor when not connected to AC power
via the external power supply (M8023A). The reported values for “remaining capacity” and “runtime”
will become less accurate when the battery is stored in this way for a longer period of time (that is,
several weeks).
Battery Safety Information
WARNING Use only Philips batteries part number M4607A. Use of a different battery may present a risk of fire or
explosion.
Do not open batteries, or dispose of them in fire, or cause them to short circuit. They may ignite,
explode, leak or heat up, causing personal injury.
Battery Safety Information 21 Using Batteries
223
Dispose of used batteries promptly and in an environmentally-responsible manner. Do not dispose of
the battery in normal waste containers. Consult your hospital administrator to find out about local
arrangements.
CAUTION Do not disassemble, heat above 100°C (212°F) or incinerate the batteries, to avoid the risk of fire and
burns. Keep batteries out of the reach of children and in their original package until you are ready to
use them.
If battery leakage should occur, use caution in removing the battery. Avoid contact with skin. Refer to
qualified service personnel.

21 Using Batteries Battery Safety Information
224
225
22
22Maintenance and
Troubleshooting
WARNING Schedule: Failure on the part of the responsible individual hospital or institution employing the use of
this equipment to implement a satisfactory maintenance schedule may cause undue equipment failure
and possible health hazards.
Contact: If you discover a problem with any of the equipment, contact your service personnel, Philips,
or your authorized supplier.
Inspecting the Equipment and Accessories
You should perform a visual inspection before every use, and in accordance with your hospital’s policy.
With the monitor switched off:
1Examine unit exteriors for cleanliness and general physical condition. Make sure that the housings
are not cracked or broken, that everything is present, that there are no spilled liquids and that there
are no signs of abuse.
2Inspect all accessories (cables, transducers, sensors and so forth). If any show signs of damage, do
not use.
3Switch the monitor on and make sure the backlight is bright enough. Check that screen is at its full
brightness. If the brightness is not adequate, contact your service personnel or your supplier.
Inspecting the Cables and Cords
1Examine all system cables, the power plug and cord for damage. Make sure that the prongs of the
plug do not move in the casing. If damaged, replace it with an appropriate Philips power cord.
2Inspect the patient cables, leads and their strain reliefs for general condition. Make sure there are
no breaks in the insulation. Make sure that the connectors are properly engaged at each end to
prevent rotation or other strain.
3Apply the transducer or electrodes to the patient, and with the monitor switched on, flex the
patient cables near each end to make sure that there are no intermittent faults.
22 Maintenance and Troubleshooting Maintenance Task and Test Schedule
226
Maintenance Task and Test Schedule
The following tasks are for Philips-qualified service professionals only. All maintenance tasks and
performance tests are documented in detail in the service documentation supplied on the monitor
documentation CD.
Ensure that these tasks are carried out as indicated by the monitor’s maintenance schedule, or as
specified by local laws. Contact a Philips-qualified service provider if your monitor needs a safety or
performance test. Clean and disinfect equipment to decontaminate it before testing or maintaining it.
Maintenance and Test Schedule Frequency
Monitor Tests
Safety checks. Selected tests on the basis
of IEC 60601-1
At least once every two years, or as needed, after any repairs
where the power supply is removed or replaced, or if the
monitor has been dropped.
Monitor Maintenance
Check ECG synchronization of the
monitor and defibrillator (only if
hospital protocol requires use of
monitor during defibrillation)
At least once every two years, or as needed.
Measurement Tests
Performance assurance for all
measurements not listed below.
At least once every two years, or if you suspect the measurement
values are incorrect.
Measurement Maintenance
NBP calibration At least once every two years, or as specified by local laws.
Microstream CO2 calibration and
performance test
At least once a year or after 4000 operating hours.
Mainstream and sidestream CO2
calibration check
At least once a year, or if you suspect the measurement values are
incorrect.
Battery Maintenance
Battery See the section on Maintaining Batteries
Troubleshooting 22 Maintenance and Troubleshooting
227
Troubleshooting
If you suspect a problem with an individual measurement, read the Instructions for Use and
doublecheck that you have set up the measurement correctly.
If you suspect an intermittent, system-wide problem call your service personnel. You may be asked for
information from the status log. To view the status log,
1In the Main Setup menu, select Revision.
2View the status log by selecting Status Log from the Monitor Revision window.
Disposing of the Monitor
WARNING To avoid contaminating or infecting personnel, the environment or other equipment, make sure you
disinfect and decontaminate the monitor appropriately before disposing of it in accordance with your
country’s laws for equipment containing electrical and electronic parts. For disposal of parts and
accessories such as thermometers, where not otherwise specified, follow local regulations regarding
disposal of hospital waste.
You can disassemble the monitor as described in the Service Guide.
You will find detailed disposal information on the following web page:
http://www.medical.philips.com/main/company/sustainability/recycling/patient_monitoring/
The Recycling Passports located there contain information on the material content of the equipment,
including potentially dangerous materials which must be removed before recycling (for example,
batteries and parts containing mercury or magnesium).
Do not dispose of waste electrical and electronic equipment as unsorted municipal waste.
Collect it separately, so that it can be safely and properly reused, treated, recycled, or
recovered.
Disposing of Empty Calibration Gas Cylinders
1Empty the cylinder completely by pushing in the pin of the regulator valve or by pulling out the
pin of the fill valve using a tire valve stem wrench or a pair of needle nose pliers.
2When the cylinder is empty, either remove the valve stem from the fill (or regulator) hole, or drill a
hole in the cylinder.
3Write “Empty” on the cylinder and dispose of it appropriately for scrap metal.
WARNING Ensure that the cylinder is completely empty before trying to remove the valve stem or drill a hole in
the cylinder.

22 Maintenance and Troubleshooting Disposing of Empty Calibration Gas Cylinders
228
229
23
23Accessories
You can order parts and accessories from Philips supplies at www.medical.philips.com or consult your
local Philips representative for details.
WARNING Reuse: Never reuse disposable transducers, sensors, accessories and so forth that are intended for single
use, or single patient use only. Reuse may compromise device functionality and system performance
and cause a potential hazard.
Philips’ approval: Use only Philips-approved accessories. Using non-Philips-approved accessories may
compromise device functionality and system performance and cause a potential hazard.
Packaging: Do not use a sterilized accessory if its packaging is damaged.
ECG/Resp Accessories
This symbol indicates that the cables and accessories are designed to have special
protection against electric shocks (particularly regarding allowable leakage currents),
and are defibrillator proof.
The following cables may not all be available in all countries. Please check availability with your local
Philips supplier.
Recommended Cables
Trunk Cables
3-Electrode
Cable Set
5-Electrode
Cable Set
6-Electrode
Cable Set
10-Electrode
Cable set
(5+5)
10-Electrode
Cable set
(6+4)
Part No. M1669A M1668A M1667A M1663A M1665A
Length 2.7m 2.7m 2.7m 2.0m 2.7m
23 Accessories ECG/Resp Accessories
230
3-Electrode Cable Sets
5-Electrode Cable Sets
6-Electrode Cable Sets
10-Electrode (5+5)Cable Sets
10-Electrode (6+4)Cable Sets
Description Length AAMI Part No. IEC Part No.
OR Grabber shielded 1.0m M1675A M1678A
ICU Grabber shielded 1.0m M1671A M1672A
ICU snap shielded 1.0m M1673A M1674A
ICU Clip non-shielded 0.45m M1622A --
ICU Clip non-shielded 0.7m M1624A M1626A
Description Length AAMI Part No. IEC Part No.
OR Grabber shielded 1.0m/1.6m M1973A M1974A
ICU Grabber shielded 1.0m/1.6m M1968A M1971A
ICU Snap shielded 1.0m/1.6m M1644A M1645A
ICU Miniclip non-shielded 0.7m/1.3m M1647A M1648A
Description Length AAMI Part No. IEC Part No.
OR Grabber 1.0m/1.6m M1684A M1685A
ICU Grabber 1.0m/1.6m M1680A M1681A
ICU Snap 1.0m/1.6m M1682A M1683A
Description Length AAMI Part No. IEC Part No.
ICU Grabber, chest, shielded 1.0m M1976A M1978A
ICU Snap, chest, shielded 1.0m M1602A M1604A
OR Grabber, chest, shielded 1.0m M1979A M1984A
For Limb Leads see 5-electrode cable sets
Description Length AAMI Part No. IEC Part No.
ICU Grabber, chest, shielded 1.0m M1532A M1533A
ICU Snap, chest, shielded 1.0m M1537A M1538A
OR Grabber, chest, shielded 1.0m M1557A M1558A
For Limb Leads see 6-electrode cable sets
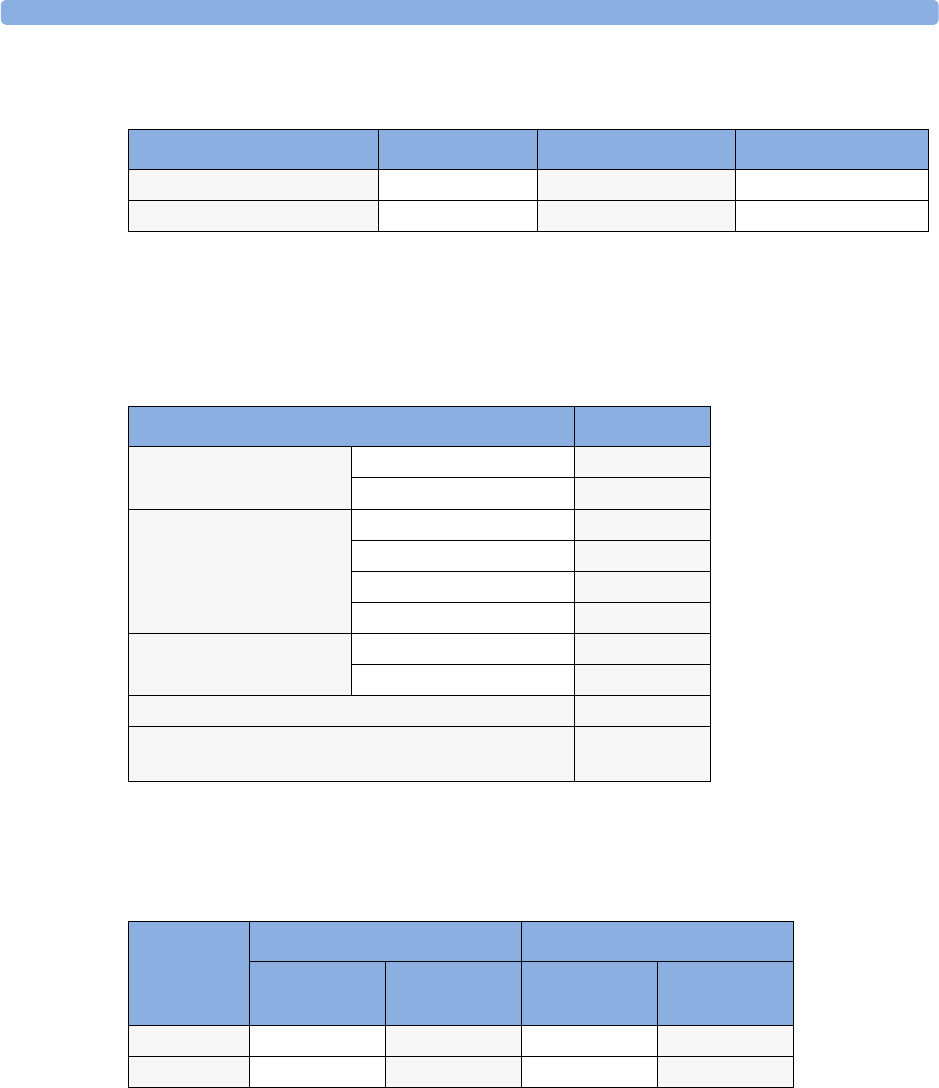
ECG/Resp Accessories 23 Accessories
231
One-piece Cables
Radio-translucent Cables
Pack of five single wires, radio-translucent, 0.9m, M1649A
Set Combiners and Organizers
Supported Cables
Trunk Cables
Description Length AAMI Part No. IEC Part No.
3-lead Grabber, ICU 1.0m 989803143181 989803143171
5-lead Grabber, ICU 1.0m 989803143201 989803143191
Set combiners and organizers Part No.
Set combiner 3-electrode M1501A
5-electrode M1502A
Set organizer for shielded
leadsets - grabber and snap
3-electrode M1503A
4-electrode M1664A
5-electrode M1504A
6-electrode M1679A
Set organizer for non-
shielded lead sets - miniclip
3-electrode M1636A
5-electrode M1638A
Bedsheet clip M1509A
Replacement red cover for trunk cable (for 5-electrode
cable sets)
989808148861
Length 3-Electrode Cable Set 5-Electrode Cable Set
AAMI
Part No.
IEC
Part No.
AAMI
Part No.
IEC
Part No.
0.9m M1540C M1550C M1560C M1570C
2.7m M1500A M1510A M1520A M1530A
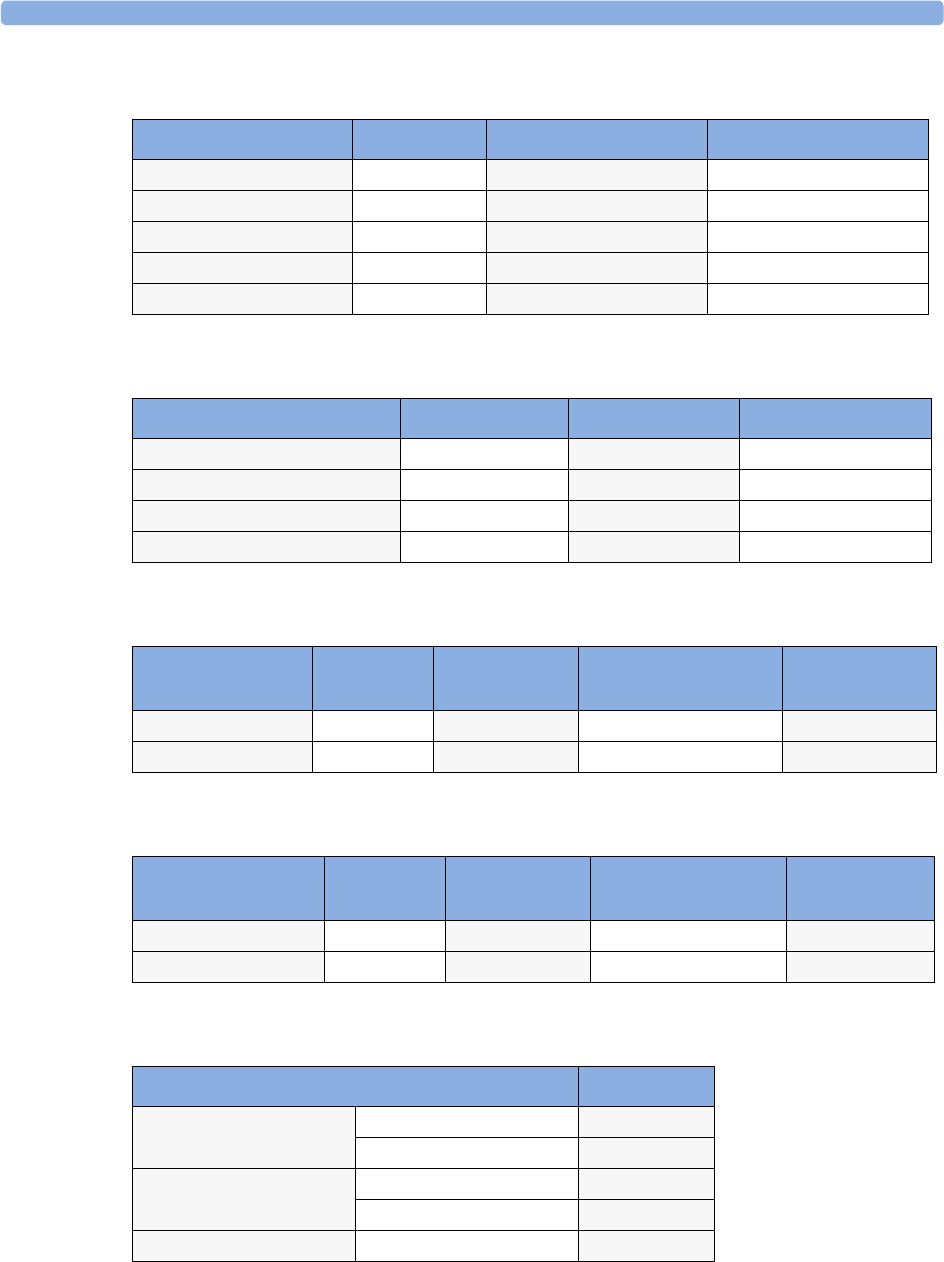
23 Accessories ECG/Resp Accessories
232
3-Electrode Cable Sets
5-Electrode Cable Sets
3-Electrode One Piece Cables
5-Electrode One Piece Cables
Set Combiners and Organizers
Description Length AAMI Part No. IEC Part No.
OR 1.0m M1601A M1611A
ICU Grabber shielded 1.0m M1603A M1613A
ICU snap shielded 1.0m M1605A M1615A
ICU Clip non-shielded 0.45m M1608A M1618A
ICU Clip non-shielded 0.7m M1609A M1619A
Description Length AAMI Part No. IEC Part No.
OR Grabber shielded 1.0m/1.6m M1621A M1631A
ICU Grabber shielded 1.0m/1.6m M1623A M1633A
ICU Snap shielded 1.0m/1.6m M1625A M1635A
ICU Clip non-shielded 0.7m/1.3m M1629A M1639A
AAMI 3-Electrode
One Piece Cables
Length AAMI
Part No.
IEC 3-electrode One
Piece Cables
IEC
Part No.
OR Grabber 1.9m M1970A OR Grabber M1980A
ICU Snap 1.9m M1972A ICU Grabber M1981A
AAMI 5-electrode
One Piece Cables
Length AAMI
Part No.
IEC 5-electrode One
Piece Cables
IEC
Part No.
OR Grabber 2.5m M1975A OR Grabber M1985A
ICU Snap 2.5m M1977A ICU Grabber M1986A
Set combiners and organizers Part No.
Set combiner 3-electrode M1501A
5-electrode M1502A
Set organizer Shielded 3-electrode M1503A
Shielded 5-electrode M1504A
Bedsheet clip M1509A
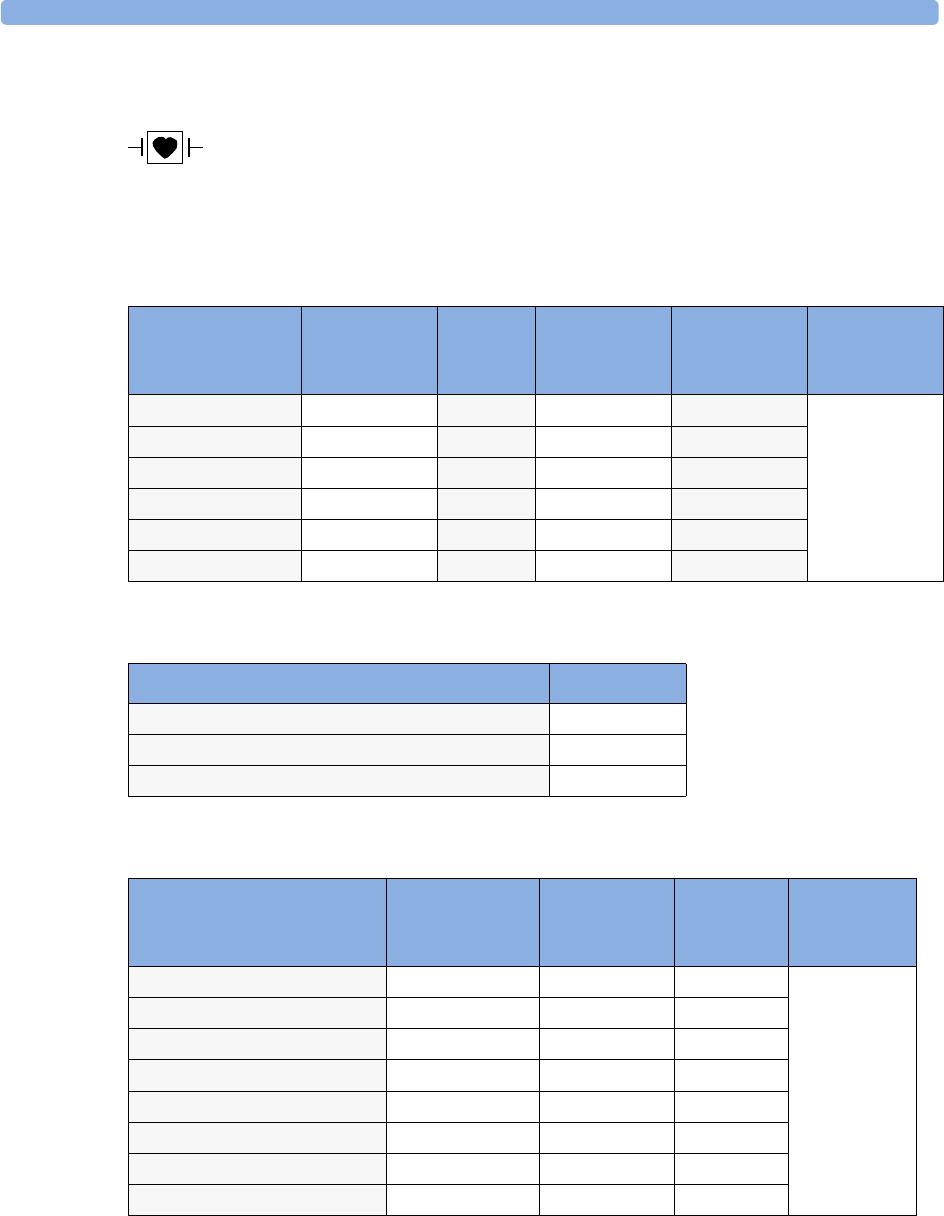
NBP Accessories 23 Accessories
233
NBP Accessories
These cuffs and tubings are designed to have special protection against electric shocks
(particularly regarding allowable leakage currents), and are defibrillator proof. You can
use them during electrosurgery.
Adult/Pediatric Multi-Patient Comfort Cuffs and Disposable Cuffs
Reusable Cuff Kits
Adult/Pediatric Antimicrobial Coated Reusable cuffs
Patient Category Limb
Circumference
Bladder
Width
Disposable
cuff
Part No.
Reusable cuff
Part No.
Tu b i n g
Adult (Thigh) 42 to 54 cm 20 cm M1879A M1576A M1598B (1.5m)
or
M1599B (3m)
Large Adult 34 to 43 cm 16 cm M1878A M1575A
Adult 27 to 35 cm 13 cm M1877A M1574A
Small Adult 20.5 to 28 cm 10.5 cm M1876A M1573A
Pediatric 14 to 21.5 cm 8 cm M1875A M1572A
Infant 10 to 15 cm 5.5 cm M1874A M1571A
Cuff Kits Part No.
Infant, pediatric, small adult, adult M1577A
Small adult, adult, large adult, thigh M1578A
Infant, pediatric, small adult, adult, large adult, thigh M1579A
Patient Category (color) Limb
Circumference
(cm)
Bladder Width Part No. Tu b i n g
Adult Thigh (grey) 45 - 56.5 21.0 cm M4559A M1598B
(1.5m) or
M1599B (3m)
Large Adult X-Long (burgundy) 35.5 - 46.0 17.0 cm M4558A
Large Adult (burgundy) 35.5 - 46.0 17.0 cm M4557A
Adult X-Long (navy blue) 27.5 - 36.5 13.5 cm M4556A
Adult (navy blue) 27.5 - 36.5 13.5 cm M4555A
Small Adult (royal blue) 20.5 - 28.5 10.6 cm M4554A
Pediatric (green) 13.8 - 21.5 8.0 cm M4553A
Infant (orange) 9 - 14.8 5.4 cm M4552A
23 Accessories Invasive Pressure Accessories
234
Adult/Pediatric Soft Single Patient Single-Hose Disposable Cuffs
Neonatal/Infant Cuffs (Disposable, non-sterile)
Invasive Pressure Accessories
These transducers and accessories are designed to have special protection against electric
shocks (particularly regarding allowable leakage currents), and are defibrillator proof.
Patient Category Limb Circumference
(cm)
Bladder
Width
Part No. Tu b i n g
Adult (Thigh) 45 - 56.5 cm 20.4 cm M4579A M1598B (1.5m)
or
M1599B (3m)
Large Adult X-Long 35.5 - 46 cm 16.4 cm M4578A
Large Adult 35.5 - 46 cm 16.4 cm M4577A
Adult X-Long 27.5 - 36.5 13.1 cm M4576A
Adult 27.5 - 36.5 cm 13.1 cm M4575A
Small Adult 20.5 - 28.5 cm 10.4 cm M4574A
Pediatric 15.0 - 21.5 cm 8.0 cm M4573A
Infant 9 - 15 cm 5.6 cm M4572A
Cuffs Limb Circumference
(cm)
Bladder Width Part No. Tu b i n g
Size 1 3.1 to 5.7 cm 2.2 cm M1866A M1596B (1.5m)
or
M1597B (3m)
Size 2 4.3 to 8.0 cm 2.8 cm M1868A
Size 3 5.8 to 10.9 cm 3.9 cm M1870A
Size 4 7.1 to 13.1 cm 4.7 cm M1872A
Transducer, accessories, sensor kits Part No
Reusable pressure transducer 5 PV/.V/mmHg sensitivity CPJ840J6
Sterile disposable pressure domes for CPJ840J6 (pack of 50) CPJ84022
Transducer holder for CPJ840J6 (pack of 4) CPJ84046
IV pole mount for CPJ840J6 CPJ84447
Single channel disposable sensor kit (20) - (EU/EFTA only) M1567A
Dual channel disposable sensor kit (20) (EU/EFTA only) M1568A
Transducer holder for M1567/8A (EU/EFTA only) M2271A
IV pole mount for M1567/8A (EU/EFTA only) M2272C
Adapter cable for disposable sensor kit 3,0m for M1567/8A M1634A
Monitoring Line Set CPJ84026
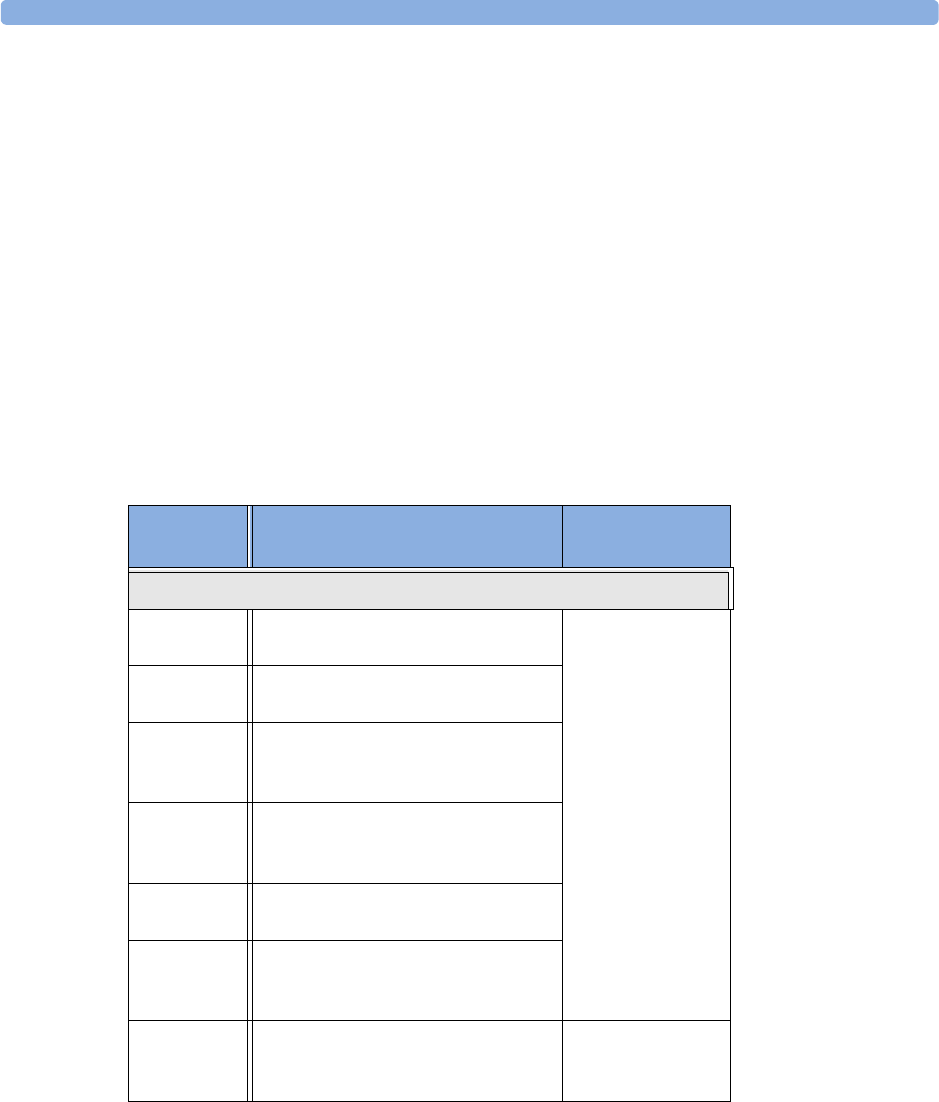
SpO2 Accessories 23 Accessories
235
SpO2 Accessories
Some Nellcor sensors contain natural rubber latex which may cause allergic reactions. See the
Instructions for Use supplied with the sensors for more information. M1901B, M1902B, M1903B
and M1904B disposable sensors are not available in USA from Philips. Purchase Nellcor sensors and
adapter cables directly from Tyco Healthcare.
Do not use more than one extension cable with any sensors or adapter cables. Do not use an extension
cable with:
• Masimo adapter cables,
• Philips reusable sensors or adapter cables with part numbers ending in -L (indicates “Long” version).
All listed sensors operate without risk of exceeding 41°C on the skin, if the initial skin temperature
does not exceed 35°C.
Make sure that you use only the accessories that are specified for use with this device, otherwise patient
injury can result.
Product
Number
Description Comments
Philips reusable sensors.
M1191A/B Adult sensor (2m cable), for patients
over 50 kg. Any finger, except thumb.
No adapter cable
required.
M1191AL/
BL
M1191A/B with longer cable (3 m)
M1192A Small adult, pediatric sensor (1.5m
cable) for patients between 15 kg and
50 kg. Any finger except thumb.
M1193A Neonatal sensor (1.5m cable) for
patients between 1kg and 4 kg. Hand
or foot.
M1194A Ear sensor (1.5m cable) for patients
more than 40 kg.
M1195A Infant sensor (1.5m cable) for patients
between 4kg and 15 kg. Any finger
except thumb.
M1196A Adult clip sensor (3m cable) for
patients over 40 kg. Any finger except
thumb.
No adapter cable
required.
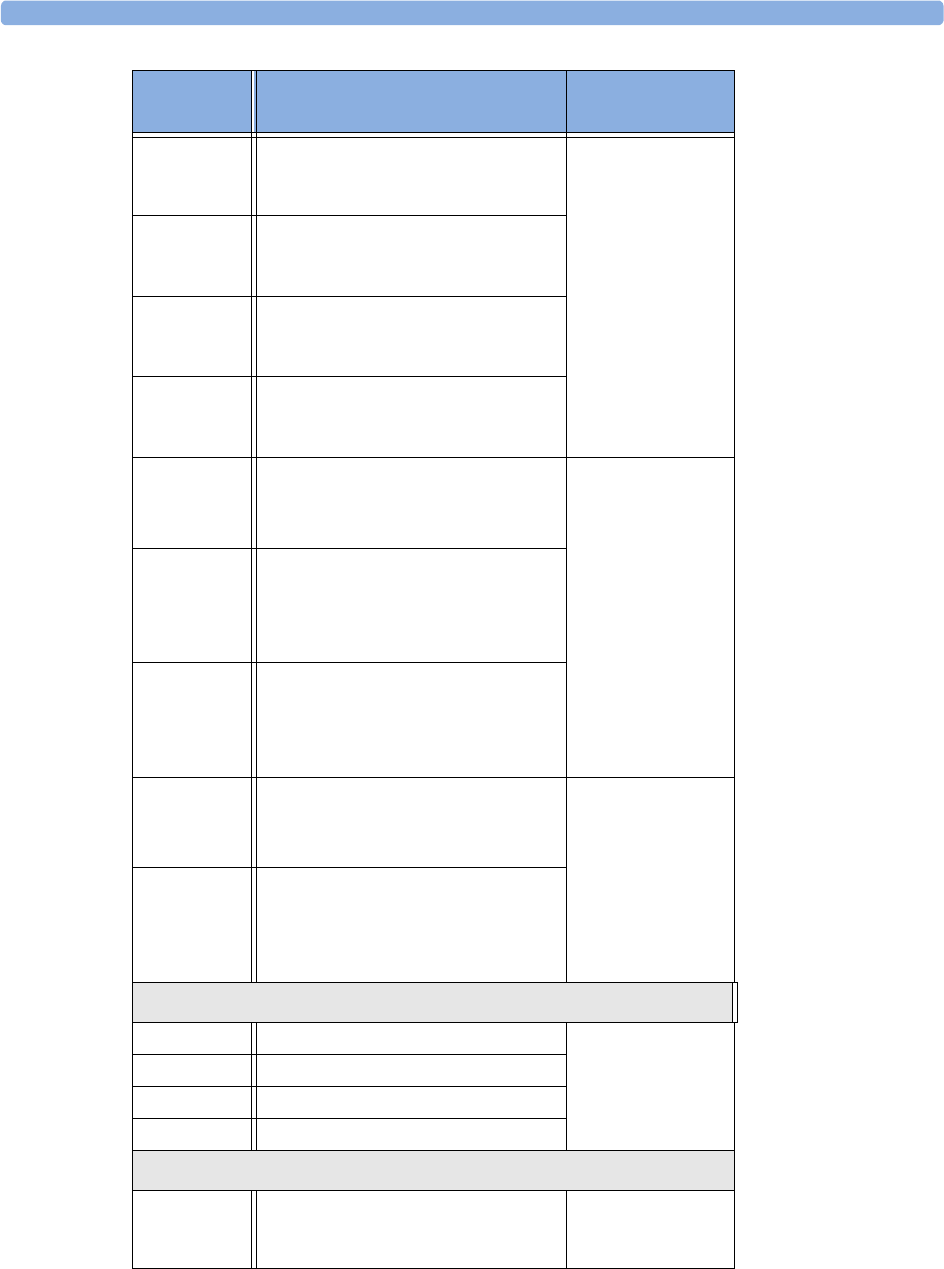
23 Accessories SpO2 Accessories
236
M1191T Adult sensor (0.45m cable), for
patients over 50 kg. Any finger, except
thumb.
Requires M1943
(1 m) or M1943AL
(3 m) adapter cable
M1192T Small adult, pediatric sensor (0.45m
cable) for patients between 15 kg and
50 kg. Any finger except thumb.
M1193T Neonatal sensor (0.9m cable) for
patients between 1kg and 4 kg. Hand
or foot.
M1196T Adult clip sensor (0.9m cable) for
patients over 40 kg. Any finger except
thumb.
M1191ANL Special Edition (SE)
Adult sensor (3m cable), for patients
over 50 kg. Any finger, except thumb.
No adapter cable
required.
M1192AN Special Edition (SE)
Small adult, pediatric sensor (1.5m
cable) for patients between 15 kg and
50 kg. Any finger except thumb.
M1193AN Special Edition (SE)
Neonatal sensor (1.5m cable) for
patients between 1kg and 4 kg. Hand
or foot.
M1194AN Special Edition (SE)
Ear sensor (1.5m cable) for patients
more than 40 kg.
No adapter cable
required.
M1195AN Special Edition (SE)
Infant sensor (1.5m cable) for patients
between 4 kg and 15 kg. Any finger
except thumb.
Philips disposable sensors. Not available in the USA and Canada.
M1904B Identical to OxiMax MAX-A Use adapter cable
M1943A or
M1943AL.
M1903B Identical to OxiMax MAX-P
M1902B Identical to OxiMax MAX-I
M1901B Identical to OxiMax MAX-N
Philips disposable sensors. Available worldwide.
M1131A Adult/Pediatric finger sensor, 0.45m
cable (patient size >20 kg)
Use adapter cable
M1943A or
M1943AL.
Product
Number
Description Comments
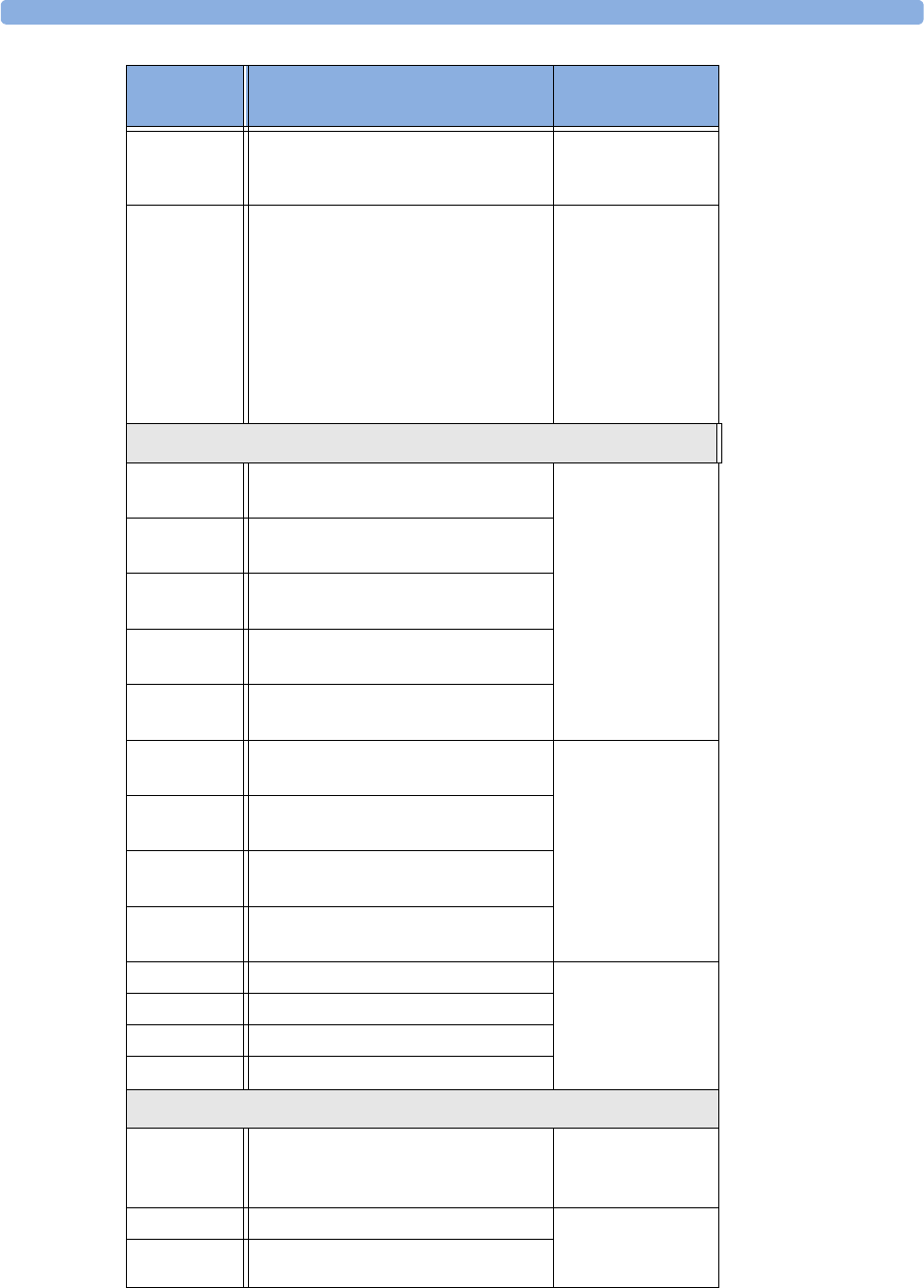
SpO2 Accessories 23 Accessories
237
M1132A Infant finger or toe sensor, 0.9m cable
(patient size 3 - 10 kg)
Use adapter cable
M1943A or
M1943AL.
M1133A Adult/Infant/Neonatal, 0.9m cable
Foot or hand for neonates < 3 kg
Big toe or thumb for patients between
10kg and 20kg
Any finger except thumb for patients
> 40kg
Use adapter cable
M1943A or
M1943AL.
NELLCOR disposable sensors (must be ordered from Nellcor)
OxiMax
MAX-A
Adult finger sensor (patient size >30
kg)
Use adapter cable
M1943A or
M1943AL.
OxiMax
MAX-AL
OxiMax MAX-A with long cable
OxiMax
MAX-P
Pediatric foot/hand sensor (patient
size 10-50 kg)
OxiMax
MAX-I
Infant foot/hand sensor (patient size
3-20 kg)
OxiMax
MAX-N
Adult finger or neonatal foot/hand
sensor (patient size >40 kg or <3 kg)
Oxisensor II
D-25
Adult sensor (patient size >30kg) Use adapter cable
M1943A or
M1943AL
Oxisensor II
D-20
Pediatric sensor (patient size 10-50 kg)
Oxisensor II
I-20
Infant sensor (patient size 3-20 kg)
Oxisensor II
N-25
Neonatal sensor (patient size <3 kg or
>40 kg)
OxiCliq A See OxiMax MAX-A Use adapter cable
M1943A or
M1943AL together
with OC-3 adapter
cable.
OxiCliq P See OxiMax MAX-P
OxiCliq I See OxiMax MAX-I
OxiCliq N See OxiMax MAX-N
Extension / Adapter Cables for Philips and Nellcor Sensors
M1941A Extension cable (2 m) For use with Philips
reusable sensors and
adapter cables.
M1943A Adapter cable (1.1 m cable) Adapter cable for
Philips/Nellcor
disposable sensors.
M1943AL Adapter cable (3 m cable)
Product
Number
Description Comments
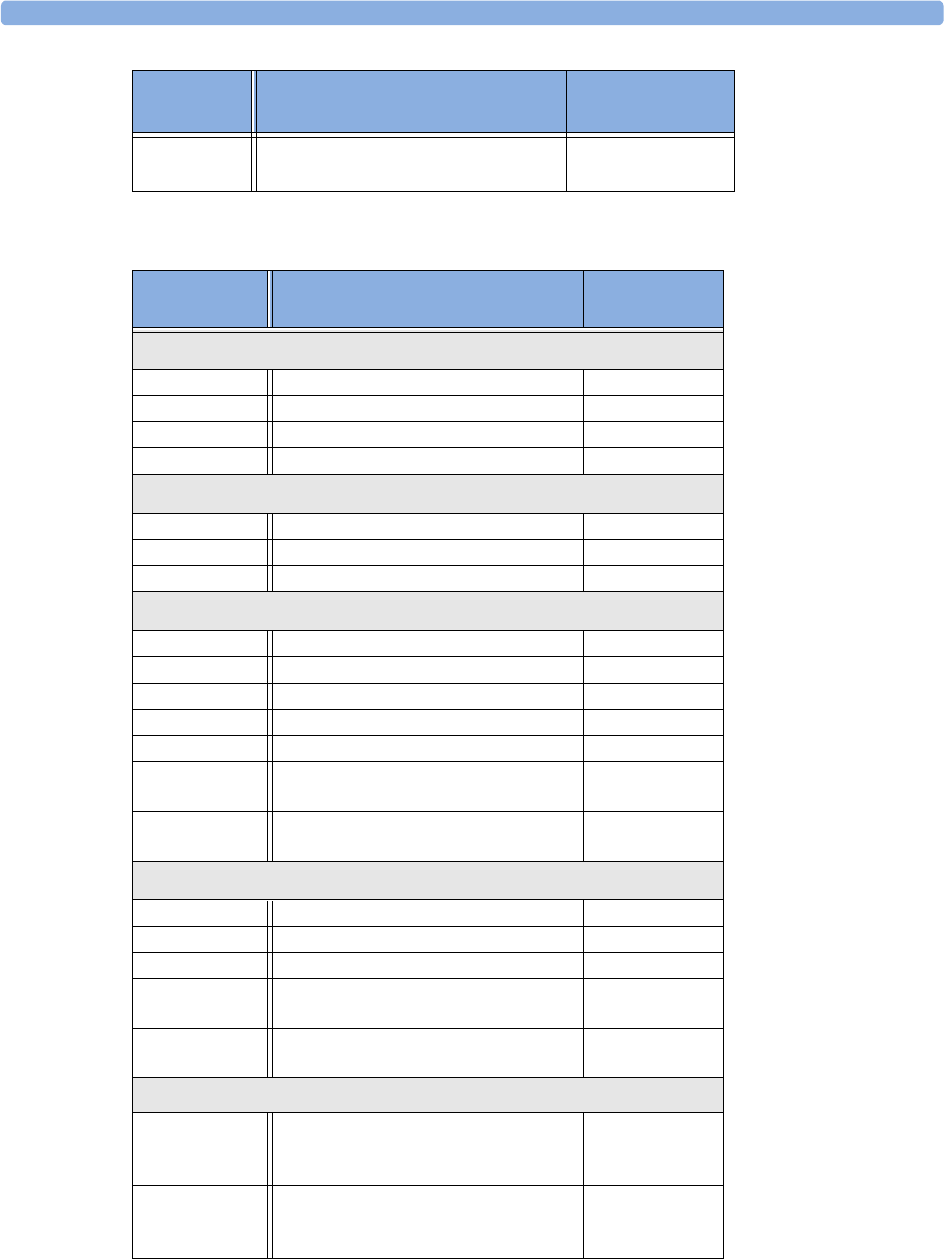
23 Accessories SpO2 Accessories
238
OC-3 Adapter Cable for OxiCliq sensors Available from
Nellcor only.
Product
Number Description Philips Part
Number
MASIMO LNOP reusable sensors.
LNOP DC-I Adult Finger Sensor (> 30 kg) 989803140321
LNOP DC-IP Pediatric Finger Sensor (10 - 50 kg) 989803140331
LNOP YI Multi-site Sensor (> 1 kg) n/a
LNOP TC-I Ear Sensor (> 30 kg) 989803140341
MASIMO LNCS reusable sensors.
LNCS DC-I Adult reusable Sensor (> 30 kg) 989803148281
LNCS DC-IP Pediatric reusable Sensor (10 - 50 kg) 989803148291
LNCS TC-I Reusable ear Sensor (> 30 kg) 989803148301
MASIMO LNOP disposable adhesive sensors.
LNOP Adt Adult Sensor (> 30 kg) 989803140231
LNOP Adtx Adult Sensor (> 30 kg) n/a
LNOP Pdt Pediatric Sensor (10 - 50 kg) 989803140261
LNOP Pdtx Pediatric Sensor (10 - 50 kg) n/a
LNOP Inf-L Infant Toe Sensor (3 - 20 kg) 989803140311
LNOP Neo-L Neonatal Sensor (<3kg)
or Adult adhesive Sensor (> 40 kg)
989803140291
LNOP NeoPt-L Neonatal Pre-Term Sensitive Skin
Sensors (<1kg)
989803140301
MASIMO LNCS disposable adhesive sensors.
LNCS Adtx Adult Finger Sensor (> 30 kg) 989803148231
LNCS Pdtx Pediatric Finger Sensor (10 - 50 kg) 989803148241
LNCS Inf-L Infant Toe Sensor (3 - 20 kg) 989803148251
LNCS Neo-L Neonatal Foot Sensor (< 3 kg)
or Adult Finger Sensor (> 40 kg)
989803148271
LNCS NeoPt-L Neonatal pre-term sensitive skin Sensor
(< 1 kg)
989803148261
Adapter Cable for MASIMO sensors.
LNOP MP12 LNOP MP Series Patient Cable (3.6 m)
Adapter Cable for Masimo LNOP
Sensors
451261000761
LNC MP10 LNCS MP Series Patient Cable (3.0 m)
Adapter Cable for Masimo LNCS
Sensors
989803148221
Product
Number
Description Comments
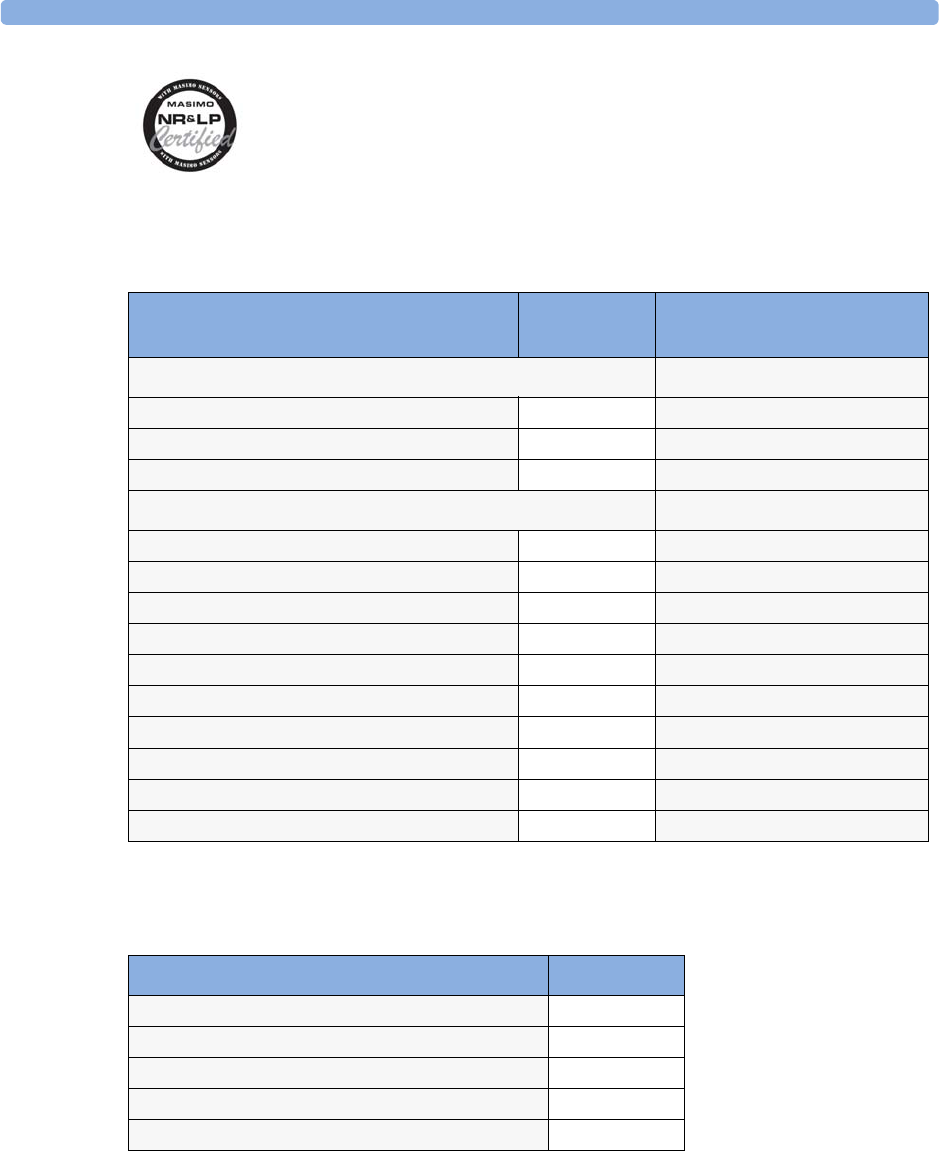
Temperature Accessories 23 Accessories
239
The monitor uses Masimo certified pulse oximetry for reduced noise and low
perfusion performance with Masimo Sensors under the Masimo NR&LP protocol
available from Masimo
Temperature Accessories
Mainstream CO2 Accessories
Temperature Probes Part No. Minimum measurement time
for accurate readings
Reusable
General purpose probe 21075A 90 sec
Small flexible vinyl probe (Infant/Pediatric) 21076A 60 sec
Attachable surface probe 21078A 60 sec
Disposable
General purpose probe M1837A 90 sec
Skin probe 21091A 60 sec
Esophageal/Stethoscope Probe (12 French) 21093A 180 sec
Esophageal/Stethoscope Probe (French 18) 21094A 210 sec
Esophageal/Stethoscope Probe (French 24) 21095A 310 sec
Foley Catheter Probe (12 French) M2255A 180 sec
Foley Catheter Probe (16 French) 21096A 180 sec
Foley Catheter Probe (18 French) 21097A 180 sec
Adapter cable 1.5m 21082B
Adapter cable 3.0m 21082A
Description Part No.
CO2 Sensor M2501A
Adult/Pediatric Airway Adapter (reusable) M2513A
Infant Airway Adapter (reusable) M2516A
Adult Airway Adapter (single-patient use) M2533A
Infant Airway Adapter (single-patient use) M2536A
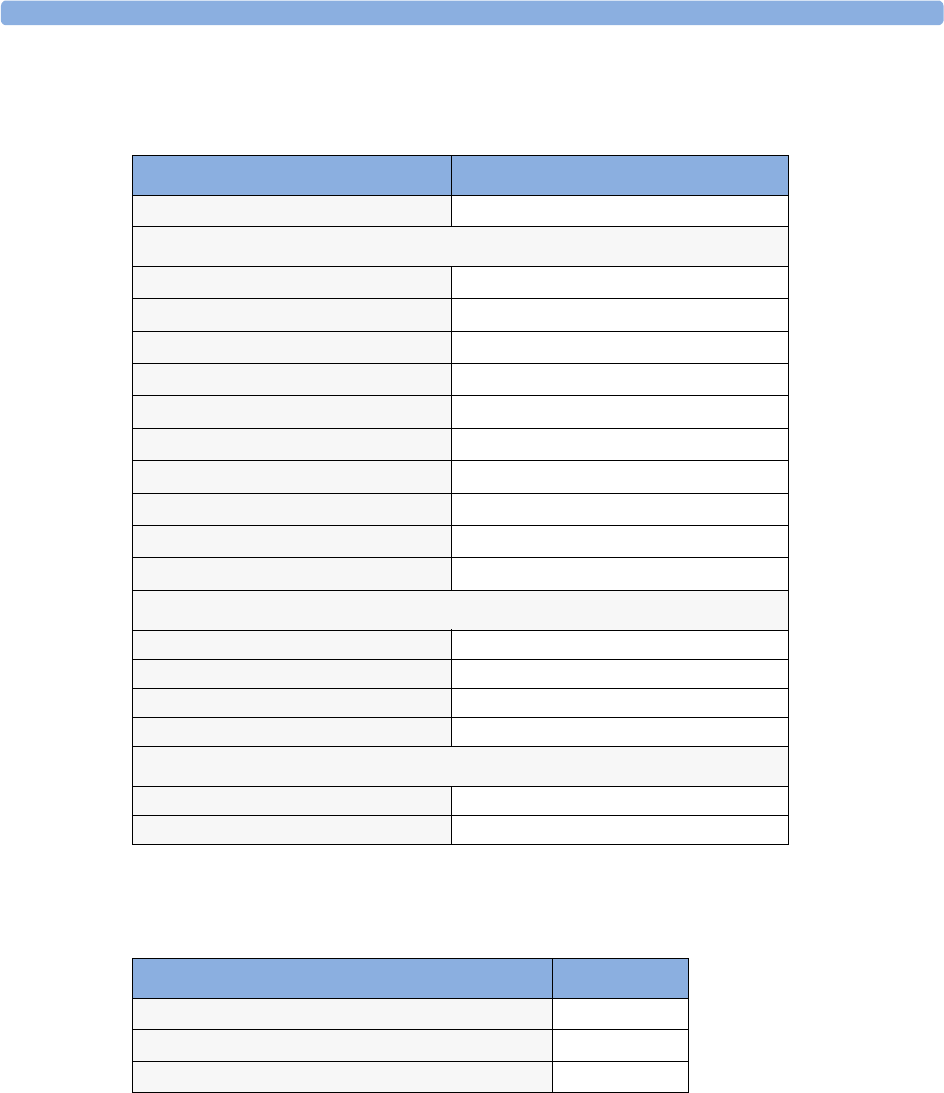
23 Accessories Sidestream CO2 Accessories
240
Sidestream CO2 Accessories
Mainstream CO2 Accessories (for M3016A)
Microstream CO2 Accessories
• “FilterLine Set” is a combination of a FilterLine with an Airway Adapter.
• “H” in the accessory name indicates suitability for humidified ventilation and longer usage due to
the active removal of humidity from the sample line.
• “Smart CapnoLine” is a combined oral-nasal FilterLine.
Description Part No.
CO2 Sensor M2741A
Nasal and Oral-Nasal Cannulas
CO2 Nasal Cannula, Adult M2744A
CO2 Nasal Cannula, Pediatric M2745A
CO2 Nasal Cannula, Infant M2746A
CO2 / O2 Nasal Cannula, Adult M2750A
CO2 / O2 Nasal Cannula, Pediatric M2751A
CO2 / O2 Nasal Cannula, Infant 989803144471
CO2 Oral-Nasal Cannula, Adult M2756A
CO2 Oral-Nasal Cannula, Pediatric M2757A
CO2 / O2 Oral-Nasal Cannula, Adult M2760A
CO2 / O2 Oral-Nasal Cannula, Pediatric M2761A
Airway Adapters
Airway Adapter Set, ET > 4.0 mm M2768A
Airway Adapter Set, ET =< 4.0 mm 989803144531
Airway Adapter Set H, ET > 4.0 mm M2772A
Airway Adapter Set H, ET =< 4.0 mm M2773A
Straight Sample Lines
Straight Sample Line M2776A
Straight Sample Line H M2777A
Description Part No.
CO2 Sensor M1460A
Standard Airway Adapter (reusable) M1465A
Small Airway Adapter (reusable) 14363A
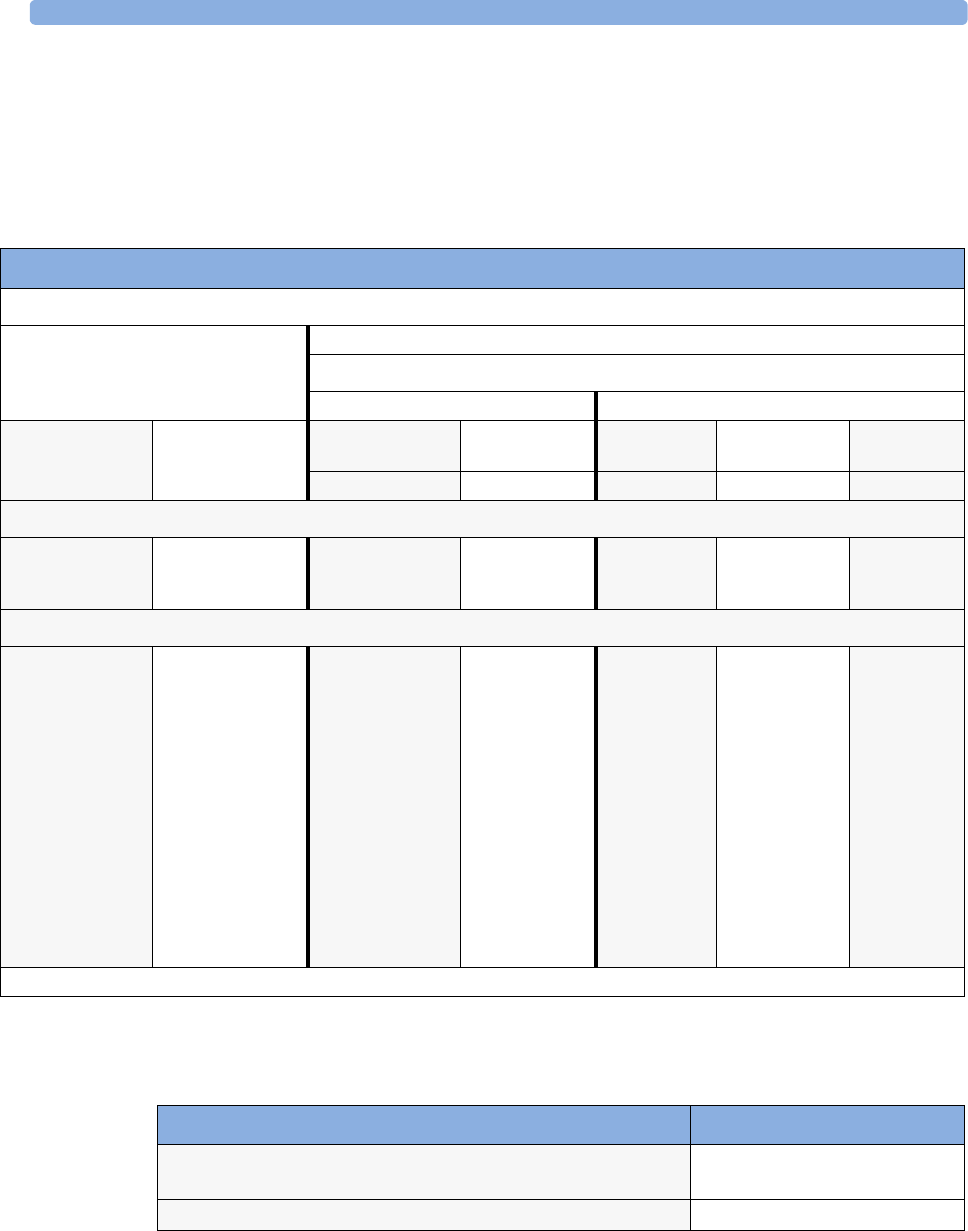
Battery Accessories 23 Accessories
241
• “Smart CapnoLine O2” is a combined oral-nasal-O2-CO2 FilterLine.
• “NIV Line” is a nasal FilterLine suitable for mask ventilation (for example, C-PAP).
•“Single purpose” means CO
2 measurement only, “dual purpose” means CO2 measurement and O2
delivery.
• The accessories are supplied in packs of 25.
Battery Accessories
Microstream accessory selection flowchart
Is the patient intubated?
Yes No
Does the patient need oxygen?
Yes No
Short-term
(up to 6 hours)
Long-term
(up to 72 hours)
Short term
(up to 8 hours)
Long term
(up to 24 hours)
Long-term
(up to 24 hours)
Short term
(up to 8 hours)
Short term
(up to 8 hours)
Oral/Nasal Nasal Nasal Oral/Nasal Nasal
Key Applications
Critical Care OR, EMS, ED Procedural Sedation,
Critical Care, EMS,
ED
Critical Care, Sleep
Lab, Long-term
Pain Management
Critical Care,
Sleep Lab
Procedural
Sedation, Critical
Care, EMS, ED
EMS, ED
Philips part numbers (A = Adult, P= Pediatric, I = Infant, N = Neonate)
FilterLine Set:
A/P: M1920A
FilterLine Set Long:
A/P:989803160241*
FilterLine:
M1925A*
FilterLine H Set:
A/P: M1921A
I/N: M1923A
FilterLine H Set Long
A/P:989803160251*
I/N:989803160261*
VitaLine H Set:
A/P:989803159571*
I/N: 989803159581*
FilterLine H:
M1926A*
Smart CapnoLine
O2:
A: M2522A
P: M2520A
Smart CapnoLine O2
Long
A:989803160281*
P:989803160271*
CapnoLine HO2:
A: M4680A
P: M4681A
CapnoLine H:
A: M4689A
P: M4690A
I/N: M4691A
Smart CapnoLine:
A: M2526A
P: M2524A
Smart CapnoLine
Plus Long
A:989803160301*
NIV Line:
A: 4686A
P: M4687A
*Not available in all geographies.
Description Part No.
Battery Charger and Conditioner (requires size adapter 4512 610
17451 to charge M4607A battery)
M8043A
Size adapter for M4607A battery 4512 610 17451

23 Accessories Battery Accessories
242

243
24
24Specifications
Intended Use
The monitor is intended to be used for monitoring and recording of, and to generate alarms for,
multiple physiological parameters of adults, pediatrics, and neonates in a hospital environment and
during patient transport inside and outside of the hospital environment. The monitor is intended for
use by health care professionals.
The monitor is only for use on one patient at a time. It is not intended for home use. Not a therapeutic
device.
Rx only: U.S. Federal Law restricts this device to sale by or on the order of a physician.
ST segment monitoring is intended for use with adult patients only and is not clinically validated for
use with neonatal and pediatric patients.
The ECG measurement is intended to be used for diagnostic recording of rhythm and detailed
morphology of complex cardiac complexes (according to AAMI EC 11).
NOTE1 Hospital Environment
The monitor is suitable for use in all medically used rooms which fulfil the requirements regarding
electrical installation according to IEC60364-7-710 “Requirements for special installations or locations
- Medical locations”, or corresponding local regulations.
NOTE2 EMC Environment
All measurements (except the sidestream CO2 measurement with M2741A sensor) and system
interfaces (except short range radio and wireless LAN) are, in addition, suitable for use in
establishments directly connected to the public low-voltage supply network that supplies buildings
used for domestic purposes (see table in “Electromagnetic Emissions” on page 267).
The monitor is indicated for use by health care professionals whenever there is a need for monitoring
the physiological parameters of patients.
WARNING The monitors are not intended for use in an MRI environment or in an oxygen-enriched environment
(for example, hyperbaric chambers.
Manufacturer’s Information
You can write to Philips at this address
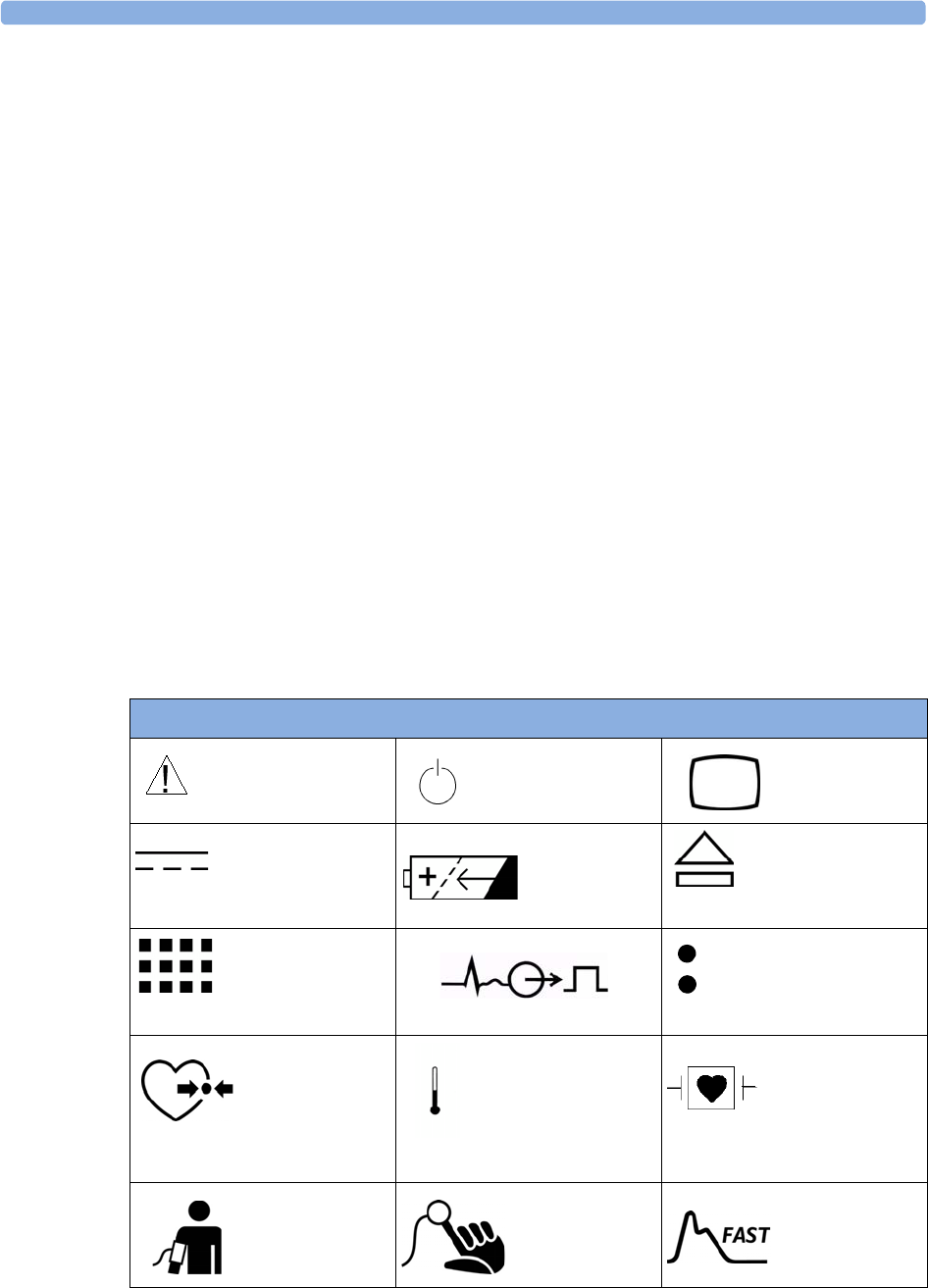
24 Specifications Symbols
244
Philips Medizin Systeme Boeblingen GmbH
Hewlett-Packard-Str. 2
71034 Boeblingen
Germany
Visit our website at: www.philips.com.
© Copyright 2002 - 2008. Koninklijke Philips Electronics N.V. All Rights Reserved.
Trademark Acknowledgement
The following are trademarks of Nellcor Puritan Bennett Incorporated: Nellcor®, Durasensor®, Dura-
Y®, Oxiband®, Oxicliq®, OxiMax®. MAX-FAST® is a trademark of Mallinckrodt Inc.
Microstream, FilterLine, and Smart CapnoLine are trademarks or registered trademarks of Oridion
Systems Ltd.
Masimo, Masimo SET, and LNOP are federally registered trademarks of the Masimo Corporation.
Other product and company names mentioned in this book may be trademarks of their respective
owners.
Symbols
These symbols can appear on the monitor and its associated equipment.
‘These symbols can appear on the monitor and its associated equipment (depending on options).
Symbols
Refer to accompanying
documents
On/Off/Standby Main Screen
DC power source Battery symbol Battery Eject
SmartKeys
ECG Sync Pulse Output indicator
Connection direction
indicator
Pressure connector Temperature connector Connector has
special protection
against electric
shocks and is
defibrillator proof
NBP connector SpO2 connector Uses FAST SpO2
algorithm
Installation Safety Information 24 Specifications
245
Installation Safety Information
WARNING If multiple instruments are connected to a patient, the sum of the leakage currents may exceed the
limits given in IEC/EN60601-1, IEC60601-1-1, UL60601-1. Consult your service personnel.
Connectors
The actual placement of boards and configuration of connections for your monitor depends on how
your hardware has been configured. See the symbols table on page 244 to see which symbols are used
to mark the connections.
WARNING • Connect only medical devices to the ECG output connector socket.
• Connecting the ECG sync out to external equipment should only be done by a qualified user. Do
not touch the patient when you have contact to the ECG output connector socket.
Silence Alarms Alarms Alarms Off
ECG connector Error LED Identifies year
and month of
manufacture
LAN connection
indicator for
connection to a wired
network
IntelliVue
Instrument
Telemetry wireless
network
Always use separate
collection for waste
electrical and
electronic equipment (WEEE)
Monitor supports 12-
lead ECG
built-in short
range radio
interface
built-in wireless
network
Symbols
2002-
06
Earthing The monitor must be earthed during operation. The earthing is for functional purposes
and does not provide protection against electric shock. The protection against electric
shock in this device is provided by double and/or reinforced insulation. If a three-wire
receptacle is not available, consult the hospital electrician. Never use a three-wire to two-
wire adapter.
Combining equipment Combinations of medical equipment with non-medical equipment must comply with
IEC 60601-1-1. Never use a multiple portable socket-outlet or extension cord when
combining equipment unless the socket outlet is supplied specifically for use with that
equipment.
Network Cables All network cables must be unshielded.
24 Specifications Altitude Setting
246
• Always connect the ECG sync cable first to the external device and then to the monitor. Wherever
possible, pre-install the cable before the patient is brought into the vicinity of the equipment.
Altitude Setting
Altitude affects CO2 measurements. The monitor must be configured at installation to the correct
altitude.
Monitor Safety Specifications
The monitor complies with the Medical Device Directive 93/42/EEC.
In addition, the product complies with:
IEC 60601-1:1988 + A1:1991 + A2:1995; EN60601-1:1990 + A1:1993 + A2:1995; UL 60601-
1:2003; CAN/CSA C22.2#601.1-M90; JIS T 0601-1:1999; IEC 60601-1-1:2001; EN 60601-1-
1:2001; IEC 60601-1-2:2001; EN 60601-1-2:2001.
Classification (according to IEC 60601-1): Class II, Type CF, Continuous Operation.
The possibility of hazards arising from software errors was minimized in compliance with ISO
14971:2000, EN60601-1-4:1996 + A1:1999 and IEC 60601-1-4:1996 + A1:1999.
EMC And Radio Regulatory Compliance
This ISM device complies with Canadian ICES-001. Cet appareil ISM est conforme a la norme NMB-
001 du Canada.
The MP2 including IntelliVue Instrument Telemetry WMTS (US only) complies with part 15 of the
FCC Rules. Operation is subject to the condition that this device does not cause harmful interference.
Operation of this equipment requires the prior coordination with a frequency coordinator designated
by the FCC for the Wireless Medical Telemetry Service.
The MP2 including IntelliVue Instrument Telemetry ISM (2.4 GHz) - FCC and Industry Canada
Radio Compliance: This device complies with Part 15 of the FCC Rules and RSS-210 of Industry
Canada. Operation is subject to the following two conditions: (1) this device may not cause harmful
interference, and (2) this device must accept any interference received, including interference that may
cause undesired operation. Any changes or modifications to this equipment not expressly approved by
Philips Medical Systems may cause harmful radio frequency interference and void your authority to
operate this equipment.
The radio device used in this product is in compliance with the essential requirements and
other relevant provisions of Directive 1999/5/EC (Radio Equipment and
Telecommunications Terminal Equipment Directive). Class 2 radio equipment. Member
states may apply restrictions on putting this device into service or placing it on the market.
This product is intended to be connected to the Publicly Available Interfaces (PAI) and used
throughout the EEA.
0366
Out-Of-Hospital Transport - Standards Compliance 24 Specifications
247
The MP2 including the Wireless IntelliVue Adapter - FCC and Industry Canada Radio Compliance:
This device complies with Part 15 of the FCC Rules and RSS-210 of Industry Canada. Operation is
subject to the following two conditions: (1) this device may not cause harmful interference, and (2) this
device must accept any interference received, including interference that may cause undesired
operation. Any changes or modifications to this equipment not expressly approved by Philips Medical
Systems may cause harmful radio frequency interference and void your authority to operate this
equipment.
The maximum antenna gain permitted (for devices in the 5250-5350 MHz and 5470-5725 MHz
bands) complies with the e.i.r.p. limits as stated in RSS-210.
The maximum antenna gain permitted (for devices in the 5725-5825 MHz band) complies with the
e.i.r.p. limits specified for point-to-point operation, as stated in RSS-210.
The device for the band 5150-5250 MHz is only for indoor usage to reduce potential for harmful
interference to co-channel mobile satellite systems.
CAUTION High power radars are allocated as primary users (meaning they have priority) of 5250-5350 MHz and
5650-5850 MHz and these radars could cause interference and /or damage to LE-LAN devices.
The radio device used in this product is in compliance with the essential requirements and other
relevant provisions of Directive 1999/5/EC. This product is intended to be connected to the Publicly
Available Interfaces (PAI) and used throughout the EEA.
The radio component contained in this device is compliant to Council Directive 1999/5/
EC (Radio Equipment and Telecommunications Terminal Equipment Directive)
In addition the product complies with: ETSI EN 300 328; ETSI EN 301 893; AS/NZS 4771+A1;
ARIB STD-T66.
The MP2 including the short range radio interface - FCC and Industry Canada Radio Compliance:
This device complies with Part 15 of the FCC Rules and RSS-210 of Industry Canada. Operation is
subject to the following two conditions: (1) this device may not cause harmful interference, and (2) this
device must accept any interference received, including interference that may cause undesired
operation. Any changes or modifications to this equipment not expressly approved by Philips Medical
Systems may cause harmful radio frequency interference and void your authority to operate this
equipment.
The radio device used in this product is in compliance with the essential requirements and
other relevant provisions of Directive 1999/5/EC (Radio Equipment and
Telecommunications Terminal Equipment Directive). Class 1 radio equipment.
In addition the product complies with: ETSI EN 300 328; AS/NZS 4771+A1; ARIB STD-T66.
Out-Of-Hospital Transport - Standards Compliance
The MP2 patient monitor with measurements and interfaces other than those listed below cannot be
used for patient transport outside of the hospital environment.
The MP2 patient monitor, with the following measurements and interfaces:
–ECG/Respiration, NBP, SpO
2, Pressure, Temperature, CO2 (only Mainstream Sensor M2501A)
– LAN, Battery
24 Specifications Out-Of-Hospital Transport - Standards Compliance
248
can be used in a transport environment such as a road ambulance, airplane or helicopter. For this
purpose the monitor fulfils the following additional mechanical, EMC and environmental
requirements:
•Shock Tests according to IEC TR 60721-4-7, Class 7M3. Test procedure according to IEC/EN
60068-2-27 (peak acceleration up to 100 g).
•Random Vibration according to IEC TR 60721-4-7, Class 7M3. Test procedure according to IEC/
EN 60068-2-64 (RMS acceleration 5 g).
•Sinusoidal Vibration according to IEC TR 60721-4-7, Class 7M3. Test procedure according to
IEC/EN 60068-2-6 (acceleration up to amplitude 2 g).
•Bump Test according to IEC/EN60068-2-29 (peak acceleration 15 g, 1000 bumps).
•Free Fall Test according to EN1789 (covers also IEC TR 60721-4-7 and Class 7M3). Test
procedure according to EN 60068-2-32 (height 0.75 m).
• Specification for degrees of protection provided by enclosures according to IEC/EN 60529: IP 32
•EN 1789 +A1:2003 Medical vehicles and their equipment - Road ambulances (chapter 6 - Medical
Devices).
•Radiated susceptibility 20 V/m according to EN ISO 9919 (SpO2) and EN ISO 21647 (CO2).
•Altitude Range from -500 to 3000 m operating and -500 to 4600 m storage and transportation.
•Extended radiated susceptibility tests
The MP2 patient monitor with its out-of-hospital parameter set provides a general immunity level of
20 V/m with only few restrictions. Details are as listed below:
– GSM 900: Immunity at 900 MHz (uplink mobile phone), 20 V/m (ECG:10V/m), duty cycle
1:8
– GSM 1800: Immunity at 1800 MHz (uplink mobile phone), 20 V/m, duty cycle 1:8.
– DECT: Immunity at 1800 MHz (digital cordless phone), 20 V/m, duty cycle 1:24
– AM: 1 kHz Immunity from 80 MHz to 1.0 GHz (any radio communication unit, broadcasting
and TV transmitter), 20 V/m, modulation factor 80%. (ECG: 20 V/m except 600-950 MHz
where it is 10 V/m and Temperature which holds 3 V/m over the full range).
CAUTION Temperature measurement accuracy may be compromised in the presence of strong electromagnetic
fields (>3 V/m) in certain small frequency bands.
•Magnetic Field emission according to MIL STD 461E, Chapter RE101: Radiated emissions,
magnetic field, 30 Hz to 100 kHz. Limit class: Army.
•Magnetic Field susceptibility: Radiated susceptibility, magnetic field, 50, 60 and 400 Hz,
18 μT(15 A/m)
•Operating ambient temperature testing over the range from 0 to 40°C (32 to 100°F).
•Operating ambient humidity testing up to 95% RH at 40°C (100°F), non condensing.
NOTE Additional requirements can be necessary for transport situations in air, on water or in difficult terrain
in certain countries, e.g. EU.
Out-Of-Hospital Transport - Standards Compliance 24 Specifications
249
Physical Specifications
Environmental Specifications
The monitor may not meet the performance specifications given here if stored or used outside the
specified temperature and humidity ranges.
The monitor is protected against ingress of objects and fluids according to IEC 60529 IP32 (applies to
all options intended for out-of-hospital use). However, do not expose the monitor directly to heavy
rain.
When the monitor and related products have differing environmental specifications, the effective range
for the combined products is that range which is common to the specifications for all products.
Specification Comments
Maximum Weight
1.25 kg
(2.8 lb)
including battery, without options
Size (W x H x D)
188 x 99 x 86 mm
7.4 x 3.9 x 3.4 in
without handle and options
M8023A External Power Supply Weight and Dimensions
Maximum Weight
700 g ±10%
(1.5 lb ±10%)
Size (W x H x D)
207 x 70 x 113 mm
8.1 x 2.8 x 4.4 in
Item Condition Range
Temperature Range Operating 0 to 40°C (32 to 104°F)
Storage including
transportation
-20 to 60°C (-4 to 140°F)
Temperature Range with
the Wireless IntelliVue
Adapter or IntelliVue
Instrument Telemetry
Wireless Network or
when charging the battery
Operating 0 to 35°C (32 to 95°F)
Humidity Range Operating 15% to 95% Relative Humidity (RH)
Storage including
transportation
5% to 95% Relative Humidity (RH)
24 Specifications Monitor Performance Specifications
250
Monitor Performance Specifications
Altitude Range Operating -500 m to 3000 m (10000 ft)
Storage including
transportation
-500 m to 4600 m1 (15000 ft)
Ingress Protection Monitor IP32 (protected against ingress of water when the water is
dripping vertically and the monitor is tilted up to 15°)
External Power Supply
(M8023A)
IP31(protected against the ingress of solid foreign objects 2.5 mm
in diameter or larger, and the ingress of water when the water is
dripping vertically) when rested on its rubber feet on a flat, level
surface.
IP32 when mounted as shown in the section ““Mounting the
External Power Supply (M8023A)” on page 3 of the Installation
chapter and as described in the Service Guide.
1.Sufficient for flight altitudes up to 12,000 m with pressurized cabins.
Item Condition Range
Performance Specifications
Power Specifications Power consumption <12 W average
<30 W while battery is loading
Operating Voltage 36 to 60 V DC floating
Battery Specifications Operating Time
(with new, fully
charged battery at
25°C)
Basic monitoring configuration: 2.5 hours
(Brightness set to Optimum, ECG/Resp, SpO2
measurements in use, NBP measurement every 15 minutes)
Charge Time When monitor is off: 2 hours
When monitor is in use, and connected to the external power
supply (M8023A), without MMS extensions: 12 hours
approx.
Indicators Alarms Off red (crossed-out alarm symbol) LED
Alarms red/yellow/light blue (cyan) LED
On/Standby / Error green / red LED
AC Power green LED
Battery yellow (charging)/red blinking (empty) LED
External Power green LED
Sounds Audible feedback for user input
Prompt tone
QRS tone, or SpO2 modulation tone
4 different alarm sounds
Trends Resolution 12 or 16 numerics @ 12 sec, 1 minute, 5 minute resolution.
Information Multiple choices of number of numerics, resolution and
duration depending on trend option and application area.
For example:
For neonatal, you can choose between 12 and 16 numerics.
Monitor Performance Specifications 24 Specifications
251
Alarm signal System delay less than 3 seconds
Pause duration 1,2,3 minutes or infinite, depending on configuration
Extended alarm pause 5 or 10 minutes
Review Alarms Information all alarms / inops, main alarms on/off, alarm silence and time
of occurrence
Capacity 300 items
Real Time Clock Range from: January 1, 1997, 00:00 to: December 31, 2080, 23:59
Accuracy <4 seconds per day (typically)
Hold Time infinite if powered by external power supply; otherwise at least
48 hours
Buffered Memory Hold Time if powered by external power supply: infinite
without power: at least 48 hours
Contents Active settings, trends, patient data, realtime reports, review
alarms
M8023A External Power Supply Performance Specifications
Power Specifications Power consumption <12 W average
<30 W peak
Line Voltage 100 to 240 V ~
Current 1.3 to 0.7 A
Frequency 50/60 Hz ~
Indicators AC Power green LED
Monitor Interface Specifications
Measurement Link
(MSL)
Connectors Female ODU (Proprietary)
Power 30 V to 60 V input
Power Sync. RS-422 compliant input 78.125k Hz (typical)
LAN signals IEEE 802.3 10-Base-T compliant
Serial signals RS-422 compliant
Local signals Provided for connecting measurement extensions
ECG Sync Pulse
Output
(See “Connectors” on
page 246 for safety-
related information)
Cable detection Yes
Marker In No
Wave Output No
Connector Binder Series 709/719
Output levels Output low <0.8 V @ I = -4 mA
Output high >2.4 V @ I = 4 mA
Isolation None
Pulse Width 100 +/-10 ms (high)
Delay from R-wave
peak to start of pulse
20 ms maximum per AAMI EC13
Minimum required R-
wave amplitude
0.5 V
Performance Specifications
24 Specifications Monitor Performance Specifications
252
Wireless Network
Device Interface
(integrated, for
compatible network
options see below)
Signals RD+/-, TD+/-: IEEE 802.3 10Base-T, PWR, GND
12.5 V ±20%, 3.5 W continuous
Frequency Band USA: 2.400 – 2.483GHz, 5.15 ~ 5.35Ghz, 5.725 ~ 5.825Ghz
Europe: 2.400 – 2.483GHz, 5.15~ 5.35Ghz, 5.47 ~ 5.725Ghz
Japan: 2.400 – 2.483GHz, 4.90 – 5.091GHz, 5.15 – 5.25GHz
China: 2.400 – 2.483GHz, 5.725 ~5.85Ghz
Modulation Technique 802.11b/g
DSSS (DBPSK, DQPSK, CCK)
OFDM (BPSK,QPSK, 16-QAM, 64-QAM)
802.11a
OFDM (BPSK,QPSK, 16-QAM, 64-QAM)
Effective radiated
power
2.4 GHz
FCC: max 18 dBm
ETSI: max 18 dBm
5GHz
FCC: max 24 dBm
ETSI: max 18 dBm
Short Range Radio
Interface1Typ e Internal SRR interface
Tech nology IEEE 802.15.4
Frequency Band 2.4 GHz ISM (2.400 - 2.483 GHz)
Modulation Technique DSSS (O -QPSK)
Effective radiated
power
max. 0 dBm (1 mW)
1.The short range radio interface is compatible with the following telemetry devices: TRx4841A/TRx4851A IntelliVue
Telemetry System Transceiver.
M8023A External Power Supply Interface Specifications
Measurement Link
(MSL)
Connectors Male ODU (Proprietary)
Power 48 V output
Power Sync. RS-422 compliant output 78.125 kHz (typical)
LAN signals IEEE 802.3 10-Base-T compliant
Serial signals RS-422 compliant output 78.125 kHz (typical)
Local signals Not connected
Display Specifications
Integrated QVGA
Display
Sweep Speeds 6.25, 12.5, 25 and 50 mm/s;
Resolution 320 x 240
Refresh frequency 60 Hz
Useful screen 72 x 54 mm (2.8 x 2.1 in)
Pixel size 0.22 x 0.22 mm
Monitor Interface Specifications
M4607A Battery Specifications 24 Specifications
253
M4607A Battery Specifications
One battery is required for battery operation of the monitor.
Compatible Devices
IntelliVue Instrument Telemetry Wireless Network (USA only)
Internal WMTS Adapter Technology compatible with Philips Cellular Telemetry System
(CTS), cellular infrastructure
Frequency Band WMTS, 1395-1400 MHz and 1427-1432 MHz
IntelliVue Instrument Telemetry Wireless Network (except USA)
Internal ISM Adapter Technology compatible with Philips Cellular Telemetry System
(CTS), cellular infrastructure
Frequency Band 2.4 GHz ISM
IntelliVue 802.11 Bedside Adapter (Wireless Network Adapter)
Internal Wireless Adapter Technology IEEE 802.11a/b/g
Frequency Band 2.4 GHz and 5 GHz ISM Band
M4607A Battery Specifications
Physical Specifications
W x D x H 66 mm (2.36 in) x 80 mm (3.15 in) x 20 mm (0.79 in)
Weight 160 g ±5%
Performance Specifications
Nominal Voltage 10.8 Volt
Rated Capacity at discharge C/5 1000 mAh (typical)
Environmental Specifications
Temperature Range Discharge 0 to 60qC (32 to 122qF)
Charge 0 to 60qC (32 to 122qF)
Storage and Transportation: -20 to 65qC (-4 to 140qF)
Humidity Range Operating: 15% to 95% Relative Humidity (RH)
Storage and Transportation: 5% to 95% Relative Humidity (RH)
Battery Type Lithium Ion Mangan, 10.8 V, 1000 mAh,
Safety complies with UL 2054
Electromagnetic Compatibility (EMC) complies with the requirements for FCC Type B computing Device,
and EN 61000-4-2 and EN 61000-3-2
Communication Standard complies with the SMBus specification v1.1
24 Specifications Measurement Specifications
254
Measurement Specifications
See the Appendix on Default Settings for a list of the settings the monitor is initially shipped with.
ECG/Arrhythmia/ST/QT
Complies with IEC 60601-2-25:1993 + A1:1999 /EN60601-2-25:1995 + A1:1999, IEC 60601-2-
27:2005/EN60601-2-27:2006, IEC 60601-2-51:2003 /EN 60601-2-51:2003 and AAMI EC11/
EC13:1991/2002.
ECG/Arrhythmia/ST Performance Specifications
Cardiotach Range Adult/pedi: 15 to 300 bpm
Neo range: 15 to 350 bpm
Accuracy ±1% of range
Resolution 1bpm
Sensitivity t200 μVpeak
PVC Rate Range 0 to 300 bpm
Resolution 1bpm
ST Numeric Range -20 to +20 mm
Accuracy ±0.5 mm or 15%, whichever is greater
Resolution 0.1 mm
QT Numeric Range 200 to 800 ms
Accuracy ±30 ms
Resolution 8ms
QTc Numeric Range 200 to 800 ms
Resolution 1ms
'QTc Numeric Range -600 to +600 ms
Resolution 1ms
QT-HR Numeric Range - adult 15 to 300 bpm
Range - pediatric
and neonatal
15 to 350 bpm
Sinus and SV Rhythm
Ranges
Brady Adult: 15 to 59 bpm
Pedi: 15 to 79 bpm
Neo: 15 to 89 bpm
Normal Adult: 60 to 100 bpm
Pedi: 80 to 160 bpm
Neo: 90 to 180 bpm
Tachy Adult: >100 bpm
Pedi: >160 bpm
Neo: >180 bpm
Bandwidth Diagnostic Mode Adult/neo/pedi: 0.05 to 150 Hz
Extended
Monitoring Mode
Neo/pedi: 0.5 to 150 Hz
Monitoring Mode Adult: 0.5 to 40 Hz
Neo/pedi: 0.5 to 55 Hz
Filter Mode Adult/neo/pedi: 0.5 to 20 Hz
Measurement Specifications 24 Specifications
255
Bandwidth
when the ECG is
transmitted from a
telemetry device via short
range radio
Diagnostic Mode Adult/neo/pedi: 0.05 to 40 Hz
Extended
Monitoring Mode
Neo/pedi: 0.5 to 40 Hz
Monitoring Mode Adult: 0.5 to 40 Hz
Neo/pedi: 0.5 to 40 Hz
Filter Mode Adult/neo/pedi: 0.5 to 20 Hz
Differential Input Impedance >2 M: RA-LL leads (Resp)
>5 M: at all other leads (at 10 Hz including patient cable)
Common Mode Rejection Ratio Diagnostic mode: >86 dB (with a 51 k:/47 nF imbalance).
Filter mode: >106 dB (with a 51 k:/47 nF imbalance).
Electrode Offset Potential Tolerance ±500 mV
Auxiliary Current
(Leads off Detection)
Active electrode: <100 nA
Reference electrode: <900 nA
Input Signal Range ±5 mV
ECG/Arrhythmia/ST/QT
Alarm Specifications Range Adjustment
HR 15 to 300 bpm
maximum delay: 10 seconds according
to AAMI EC 13-1992 standard
Adult:1 bpm steps (15 to 40 bpm)
5 bpm steps (40 to 300 bpm)
Pedi/Neo:1 bpm steps (15 to 50 bpm)
5 bpm steps (50 to 300 bpm)
Extreme Tachy Difference to high limit 0 to 50 bpm 5 bpm steps
Clamping at 150 to 300 bpm 5 bpm steps
Extreme Brady Difference to low limit 0 to 50 bpm 5 bpm steps
Clamping at 15 to 100 bpm 5 bpm steps
Run PVCs 2 PVCs Not adjustable by user
PVCs Rate 1 to 99 PVCs/minute 1PVC
Ven t Tach HR 20 to 300 bpm 5bpm
Ven t Tach Ru n 3 to 99 PVCs/minute 1PVC
Ven t Rhythm Run 3 to 99 PVCs/minute 1PVC
SVT HR 120 to 300 bpm 5bpm
SVT Run 3 to 99 SV beats 1SV beat
ST High -19.8 to +20 mm 0.2 mm
ST Low -20 to +19.8 mm 0.2 mm
QTc High 200 ms to 800 ms 10 ms steps
'QTc High 30 ms to 200 ms 10 ms steps
ECG/Arrhythmia/ST Supplemental Information as required by AAMI EC11/13
Respiration Excitation Waveform Sinusoidal signal, 260 PA, 40.5 kHz
Noise Suppression RL drive gain 44 dB max., max. voltage 1.8 Vrms
ECG/Arrhythmia/ST Performance Specifications
24 Specifications Measurement Specifications
256
Respiration
Time to Alarm for
Tachycardia
Vent Tachycardia
1mV
pp,206 bpm
Gain 0.5, Range 6.5 to 8.4 seconds, Average 7.2 seconds
Gain 1.0 Range 6.1 to 6.9 seconds, Average 6.5 seconds
Gain 2.0, Range 5.9 to 6.7 seconds, Average 6.3 seconds
Vent Tachycardia
2mV
pp,195 bpm
Gain 0.5, Range 5.4 to 6.2 seconds, Average 5.8 seconds
Gain 1.0, Range 5.7 to 6.5 seconds, Average 6.1 seconds
Gain 2.0, Range 5.3 to 6.1 seconds, Average 5.7 seconds
Tall T-Wave Rejection Capability Exceeds ANSI/AAMI EC 13 Sect. 3.1.2.1(c) minimum
recommended 1.2 mV T-Wave amplitude
Heart Rate Averaging Method Three different methods are used:
Normally, heart rate is computed by averaging the 12 most
recent RR intervals.
For runs of PVCs, up to 8 RR intervals are averaged to compute
the HR.
If each of 3 consecutive RR intervals is greater than 1200 ms
(that is, rate less than 50 bpm), then the 4 most recent RR
intervals are averaged to compute the HR.
Response Time of Heart Rate Meter to Change in
Heart Rate
HR change from 80 to 120 bpm:
Range: [6.4 to 7.2 seconds] Average: 6.8 seconds
HR change from 80 to 40 bpm:
Range: [5.6 to 6.4 sec] Average: 6.0 seconds
Heart Rate Meter Accuracy and Response to
Irregular Rhythm
Ventricular bigeminy: 80 bpm
Slow alternating ventricular bigeminy: 60 bpm
Rapid alternating ventricular bigeminy: 120 bpm
Bidirectional systoles: 90 bpm
Accuracy of Input Signal Reproduction Methods A and D were used to establish overall system error
and frequency response.
Pacemaker Pulse Rejection Performance Rejection of pacemaker pulses with amplitudes from ±2 mV to
±700 mV and widths from 0.1 ms to 2.0 ms (Method A)
ECG/Arrhythmia/ST Supplemental Information as required by AAMI EC11/13
Respiration Performance Specifications
Respiration Rate Range Adult/pedi: 0 to 120 rpm
Neo: 0 to 170 rpm
Accuracy at 0 to 120 rpm ±1 rpm
at 120 to 170 rpm ±2 rpm
Resolution 1rpm
Bandwidth 0.3 to 2.5 Hz (–6 dB)
Noise Less than 25 m:(rms) referred to the input
Measurement Specifications 24 Specifications
257
Respiration Alarm
Specifications Range Adjustment Delay
High Adult/pedi: 10 to 100 rpm
Neo: 30 to 150 rpm
under 20 rpm: 1 rpm steps
over 20 rpm: 5 rpm steps
max. 14 seconds
Low Adult/pedi: 0 to 95 rpm
Neo: 0 to 145 rpm
under 20 rpm: 1 rpm steps
over 20 rpm: 5 rpm steps
for limits from 0 to 20 rpm:
max. 4 seconds
for limits above 20 rpm: max.
14 seconds
Apnea Alarm 10 to 40 seconds 5 second steps
24 Specifications Measurement Specifications
258
SpO2
Complies with EN ISO 9919:2005 (except alarm system; alarm system complies with IEC 60601-2-
49:2001).
Measurement Validation: The SpO2 accuracy has been validated in human studies against arterial
blood sample reference measured with a CO-oximeter. Pulse oximeter measurements are statistically
distributed, only about two-thirds of the measurements can be expected to fall within the specified
accuracy compared to CO-oximeter measurements. Display Update Period: Typical: 2 seconds,
Maximum: 30 seconds. Maximum with NBP INOP suppression on60 seconds.
SpO2 Performance Specifications
SpO2
The specified accuracy
is the root-mean-
square (RMS)
difference between the
measured values and
the reference values
Range 0 to 100%
Accuracy Philips Reusable Sensors:
M1191A, M1191AL, M1191ANL, M1191B, M1191BL, M1192A,
M1192AN = 2% (70% to 100%)
M1193A, M1193AN, M1194A, M1194AN, M1195A, M1195AN,
M1196A = 3% (70% to 100%)
M1191T, M1192T, M1193T (Adult), M1196T = 3% (70% to 100%)
M1193T (Neonate) = 4% (70% to 100%)
Philips Disposable Sensors with M1943A(L):
M1132A, M1133A (adult/infant) = 2%
M1901B, M1902B, M1903B, M1904B, M1131A, M1133A (neonate)
= 3% (70% to 100%)
NellcorPB® Sensors with M1943A(L):
MAX-A, MAX-AL, MAX-P, MAX-I, MAX-N, D-25, D-20, I-20, N-
25, OxiCliq A, P, I, N = 3% (70% to 100%)
Masimo Reusable Sensors® with LNOP MP12 or LNC MP10:
LNOP DC-I, LNOP DC-IP, LNOP YI, LNCS DC-1, LNCS DC-IP:
2% (70% to 100%)
LNOP TC-I, LNCS TC-I: 3.5% (70% to 100%)
Masimo Disposable Sensors® with LNOP MP12 or LNC MP10:
LNOP Adt, LNOP Adtx, LNOP Pdt, LNOP Pdtx, LNOP Inf-L,
LNCS Adtx, LNCS Pdtx, LNCS Inf-L: 2% (70% to 100%)
LNOP Neo-L, LNOP NeoPt-L, LNCS Neo-L, LNCS NeoPt-L: 3%
(70% to 100%)
Resolution 1%
Pulse Range 30 to 300 bpm
Accuracy ±2% or 1 bpm, whichever is greater
Resolution 1bpm
Sensors Wavelength range: 500 to 1000 nm
Emitted Light Energy: d15 mW
Information about the wavelength range can be especially useful to
clinicians (for instance, when photodynamic therapy is performed)
Pulse Oximeter Calibration Range 70% to 100%
Measurement Specifications 24 Specifications
259
NBP
Complies with IEC 60601-2-30:1999/EN60601-2-30:2000.
SpO2 Alarm
Specifications Range Adjustment Delay
SpO2Adult: 50 to 100%
Pedi/Neo: 30 to 100%
1% steps (0, 1, 2, 3,... 30)
+4 seconds
Desat Adult: 50 to Low alarm limit
Pedi/Neo: 30 to Low alarm limit
1% steps
Pulse 30 to 300 bpm Adult:
1 bpm steps (30 to 40 bpm)
5 bpm steps (40 to 300 bpm)
Pedi/Neo:
1 bpm steps (30 to 50 bpm)
5 bpm steps (50 to 300 bpm)
max. 14 seconds
Tachycardia Difference to high limit 0 to 50 bpm 5 bpm steps max. 14 seconds
Clamping at 150 to 300 bpm 5 bpm steps
Bradycardia Difference to low limit 0 to 50 bpm 5 bpm steps max. 14 seconds
Clamping at 30 to 100 bpm 5 bpm steps
NBP Performance Specifications
Measurement Ranges Systolic Adult: 30 to 270 mmHg (4 to 36 kPa)
Pedi: 30 to 180 mmHg (4 to 24 kPa)
Neo: 30 to 130 mmHg (4 to 17 kPa)
Diastolic Adult: 10 to 245 mmHg (1.5 to 32 kPa)
Pedi: 10 to 150 mmHg (1.5 to 20 kPa)
Neo: 10 to 100 mmHg (1.5 to 13 kPa)
Mean Adult: 20 to 255 mmHg (2.5 to 34 kPa)
Pedi: 20 to 160 mmHg (2.5 to 21 kPa)
Neo: 20 to 120 mmHg (2.5 to 16 kPa)
Pulse Rate Adult: 40 to 300
Pedi: 40 to 300
Neo: 40 to 300
Accuracy Max. Std. Deviation: 8 mmHg (1.1 kPa)
Max. Mean Error: ±5 mmHg (±0.7 kPa)
Pulse Rate Measurement Accuracy 40 to 100 bpm: ±5bpm
101 to 200 bpm: ±5% of reading
201 to 300 bpm: ±10% of reading
(average over NBP measurement cycle)
Pulse Rate Range 40 to 300 bpm
Measurement Time Typical at HR >60 bpm
Auto/manual/sequence: 30 seconds (adult)
25 seconds (neonatal)
Stat: 20 seconds
Maximum time: 180 seconds (adult/pediatric)
90 seconds (neonates)
24 Specifications Measurement Specifications
260
Measurement Validation: In adult and pediatric mode, the blood pressure measurements determined
with this device comply with the American National Standard for Electronic or Automated
Sphygmomanometers (ANSI/AAMI SP10 - 1992) in relation to mean error and standard deviation,
when compared to intra-arterial or auscultatory measurements (depending on the configuration) in a
representative patient population. For the auscultatory reference the 5th Korotkoff sound was used to
determine the diastolic pressure.
In neonatal mode, the blood pressure measurements determined with this device comply with the
American National Standard for Electronic or Automated Sphygmomanometers (ANSI/AAMI SP10 -
1992 and AAMI/ANSI SP10A -1996) in relation to mean error and standard deviation, when
compared to intra-arterial measurements in a representative patient population.
Cuff Inflation Time Typical for normal adult cuff: Less than 10 seconds
Typical for neonatal cuff: Less than 2 seconds
Initial Cuff Inflation Pressure Adult: 165 ±15 mmHg
Pedi: 130 ±15 mmHg
Neo: 100 ±15 mmHg
Auto Mode Repetition Times 1, 2, 2.5, 3, 5, 10, 15, 20, 30, 45, 60 or 120 minutes
STAT Mode Cycle Time 5minutes
Venipuncture Mode Inflation
Inflation Pressure Adult 20 to 120 mmHg (3 to 16 kPa)
Pediatric 20 to 80 mmHg (3 to 11 kPa)
Neonatal 20 to 50 mmHg (3 to 7 kPa)
Automatic deflation
after
Adult/pediatric 170 seconds
Neonatal 85 seconds
NBP Alarm Specifications Range Adjustment
Systolic Adult: 30 to 270 mmHg (4 to 36 kPa) 10 to 30 mmHg: 2 mmHg (0.5 kPa)
>30 mmHg: 5 mmHg (1 kPa)
Pedi: 30 to 180 mmHg (4 to 24 kPa)
Neo: 30 to 130 mmHg (4 to 17 kPa)
Diastolic Adult: 10 to 245 mmHg (1.5 to 32 kPa)
Pedi: 10 to 150 mmHg (1.5 to 20 kPa)
Neo: 10 to 100 mmHg (1.5 to 13 kPa)
Mean Adult: 20 to 255 mmHg (2.5 to 34 kPa)
Pedi: 20 to 160 mmHg (2.5 to 21 kPa)
Neo: 20 to 120 mmHg (2.5 to 16 kPa)
NBP Overpressure Settings
Adult >300 mmHg (40 kPa) >2 sec not user adjustable
Pedi >300 mmHg (40 kPa) >2 sec
Neo >150 mmHg (20 kPa) >2 sec
NBP Performance Specifications
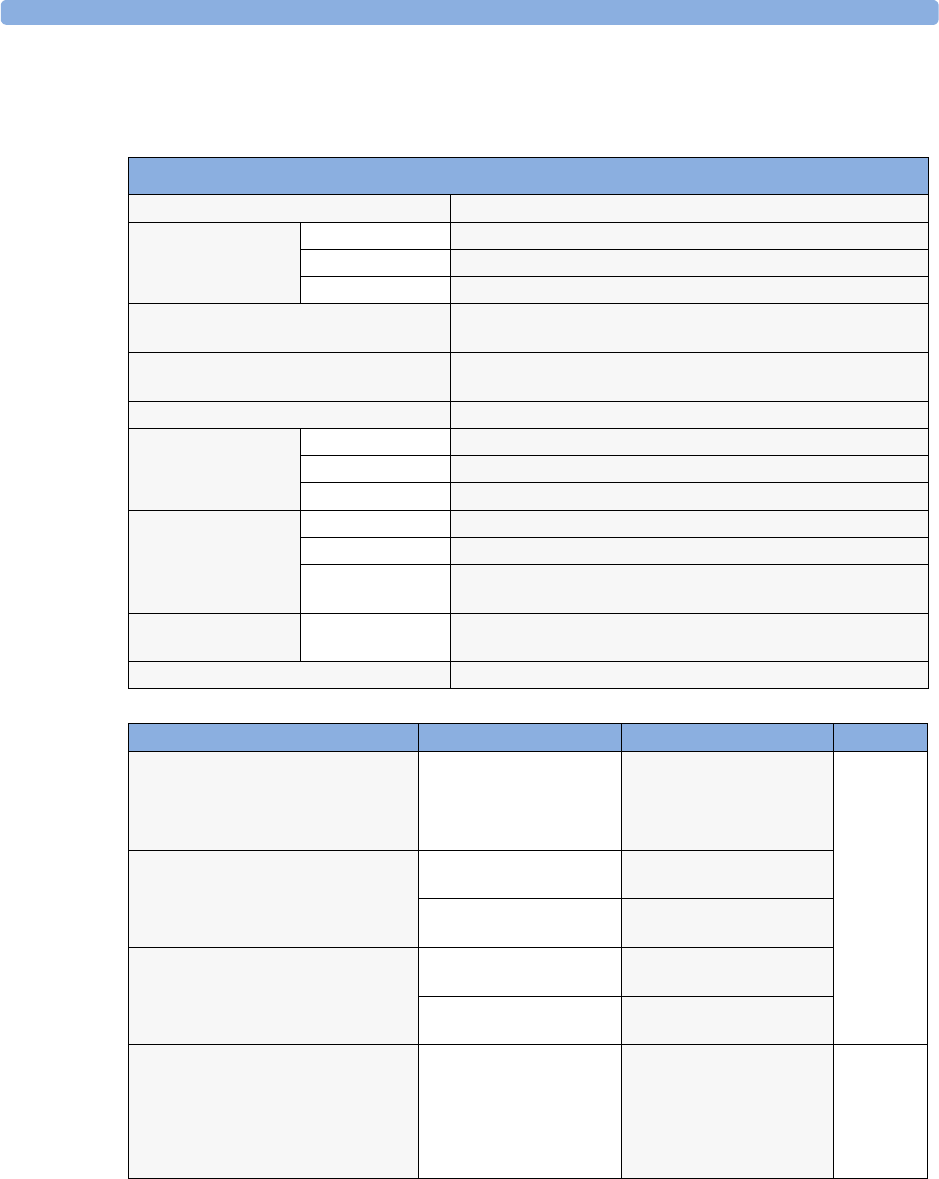
Measurement Specifications 24 Specifications
261
Invasive Pressure and Pulse
Complies with IEC 60601-2-34:2000/EN60601-2-34:2000.
Invasive Pressure Performance Specifications
Measurement Range –40 to 360 mmHg
Pulse Rate Range 25 to 350 bpm
Accuracy ±1% Full Range
Resolution 1bpm
Input Sensitivity Sensitivity:5 μV/V/mmHg (37.5 μV/V/kPa)
Adjustment range:±10%
Tr a n s d u c e r Load Impedance:200 to 2000 : (resistive)
Output Impedance:d3000 : (resistive)
Frequency Response dc to 12.5 Hz or 40 Hz
Zero Adjustment Range: ±200 mmHg (±26 kPa)
Accuracy ±1 mmHg (±0.1 kPa)
Drift Less than 0.1 mmHg/°C (0.013 kPa/°C)
Gain Accuracy Accuracy ±1%
Drift Less than 0.05%/°C
Non linearity
and Hysteresis
Error of d0.4% FS (@CAL 200 mmHg)
Overall Accuracy (including
transducer)
±4% of reading or ±4 mmHg (±0.5 kPa), whichever is greater
Volume displacement of CPJ840J6 0.1 mm3 /100 mmHg
Invasive Pressure Alarm Specifications Range Adjustment Delay
Pressure –40 to 360 mmHg
(–5.0 to 48 kPa)
-40 to 50 mmHg
2 mmHg (0.5 kPa)
>50 mmHg
5 mmHg (1 kPa)
max.
12 seconds
Extreme High Difference to high limit 0 to
25 mmHg
5 mmHg steps (0.5 kPa)
Clamping at -40 to
360 mmHg
5 mmHg steps (1.0 kPa)
Extreme Low Difference to low limit 0 to
25 mmHg
5 mmHg steps (0.5 kPa)
Clamping at -40 to
360 mmHg
5 mmHg steps (1.0 kPa)
Pulse 25 to 300 bpm Adult:
1 bpm steps (25 to 40 bpm)
5 bpm steps (40 to 300 bpm)
Pedi/Neo:
1 bpm steps (25 to 50 bpm)
5 bpm steps (50 to 300 bpm)
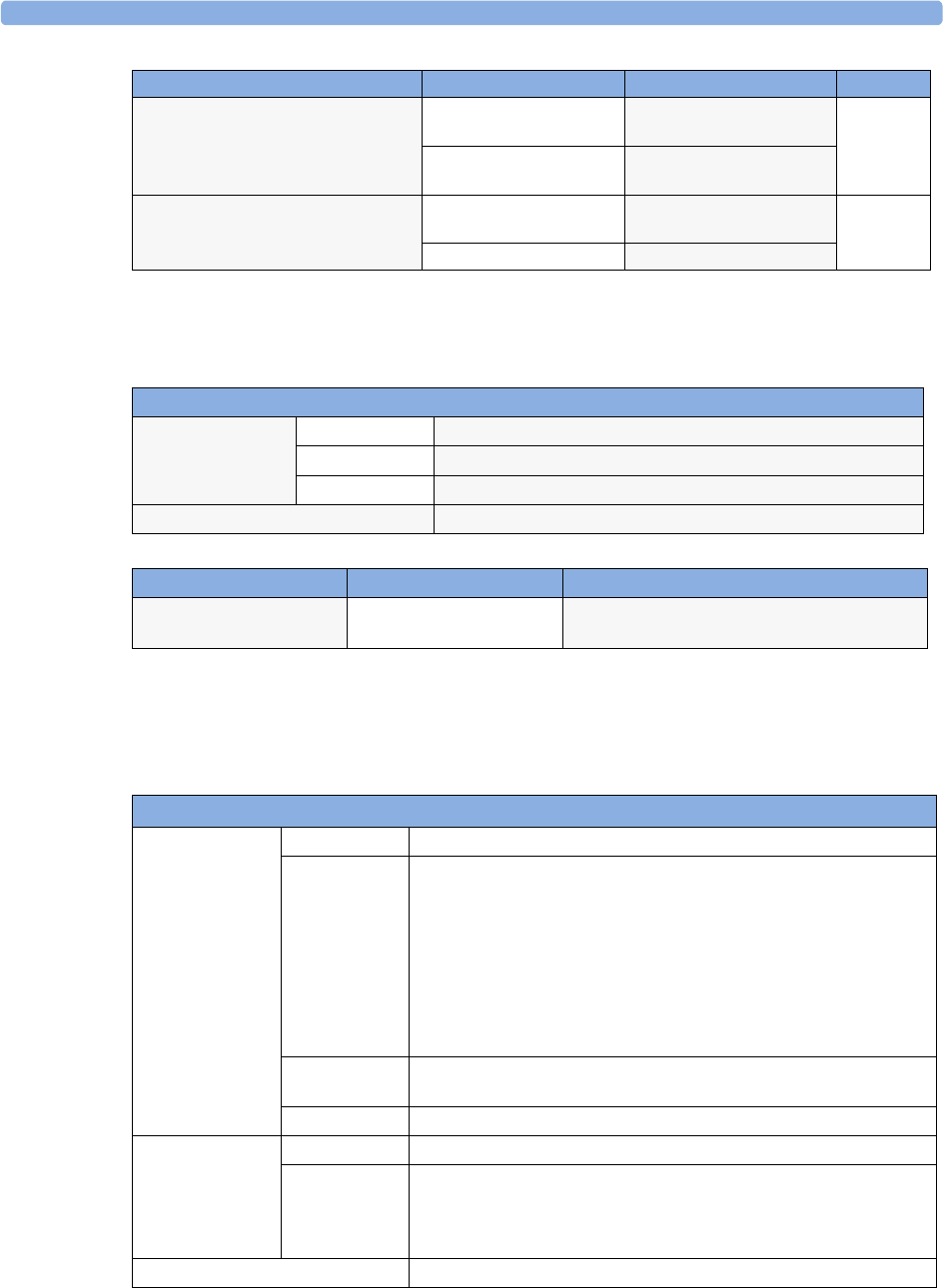
24 Specifications Measurement Specifications
262
Te m p
Complies with EN 12470-4:2000. Specified without transducer.
CO2
The CO2 measurement in the monitor, M3014A and M3015A complies with EN ISO 21647:2004 +
Cor.1:2005 (except alarm system; alarm system complies with IEC 60601-2-49:2001).
Tachycardia Difference to high limit 0 to
50 bpm
5 bpm steps max.
14 seconds
Clamping at 150 to
300 bpm
5 bpm steps
Bradycardia Difference to low limit 0 to
50 bpm
5 bpm steps max.
14 seconds
Clamping at 25 to 100 bpm 5 bpm steps
Invasive Pressure Alarm Specifications Range Adjustment Delay
Temp Performance Specifications
Te m p Range –1 to 45qC (30 to 113qF)
Resolution 0.1qC (0.2qF)
Accuracy ±0.1qC (±0.2qF)
Average Time Constant Less than 10 seconds
Temp Alarm Specifications Range Adjustment
Tem p Hi g h/ Low A la rms –1 to 45qC (30 to 113qF) -1 to 35qC (30 to 95qF), 0.5qC (1.0qF) steps
35 to 45qC (95 to 113qF), 0.1qC (0.2qF) steps
M3015A Microstream CO2 Performance Specifications
CO2Range 0 to 150 mmHg (0 to 20 kPa), or 20% CO2, whichever is lower
Accuracy Up to 5 minutes during warmup: ±4 mmHg or 12%, whichever is greater
After 5 minutes warmup:
0 to 40 mmHg (0 to 5.3 kPa):±2.2 mmHg (±0.3 kPa)
Above 40 mmHg (5.3 kPa):±(5.5% + (0.08%/mmHg above 40 mmHg)) of
reading
These specifications are valid for 21% O2 and N2 balance, up to 35qC
ambient temperature, up to 60 rpm in adult mode and 100 rpm in neonatal
mode. Outside of these conditions the accuracy reaches at a minimum
±4 mmHg or ±12% of the reading, whichever is greater.
Resolution Numeric: 1.0 mmHg (0.1 kPa)
Wave: 0.1 mmHg (0.01 kPa)
Stability Included in Accuracy specifications
awRR Range 0 to 150 rpm
Accuracy 0 to 40 rpm: ±1 rpm
41 to 70 rpm: ±2 rpm
71 to 100 rpm: ±3 rpm
>100 rpm: ±5% of reading
Warm-up Tim e 5 minutes for full accuracy specification
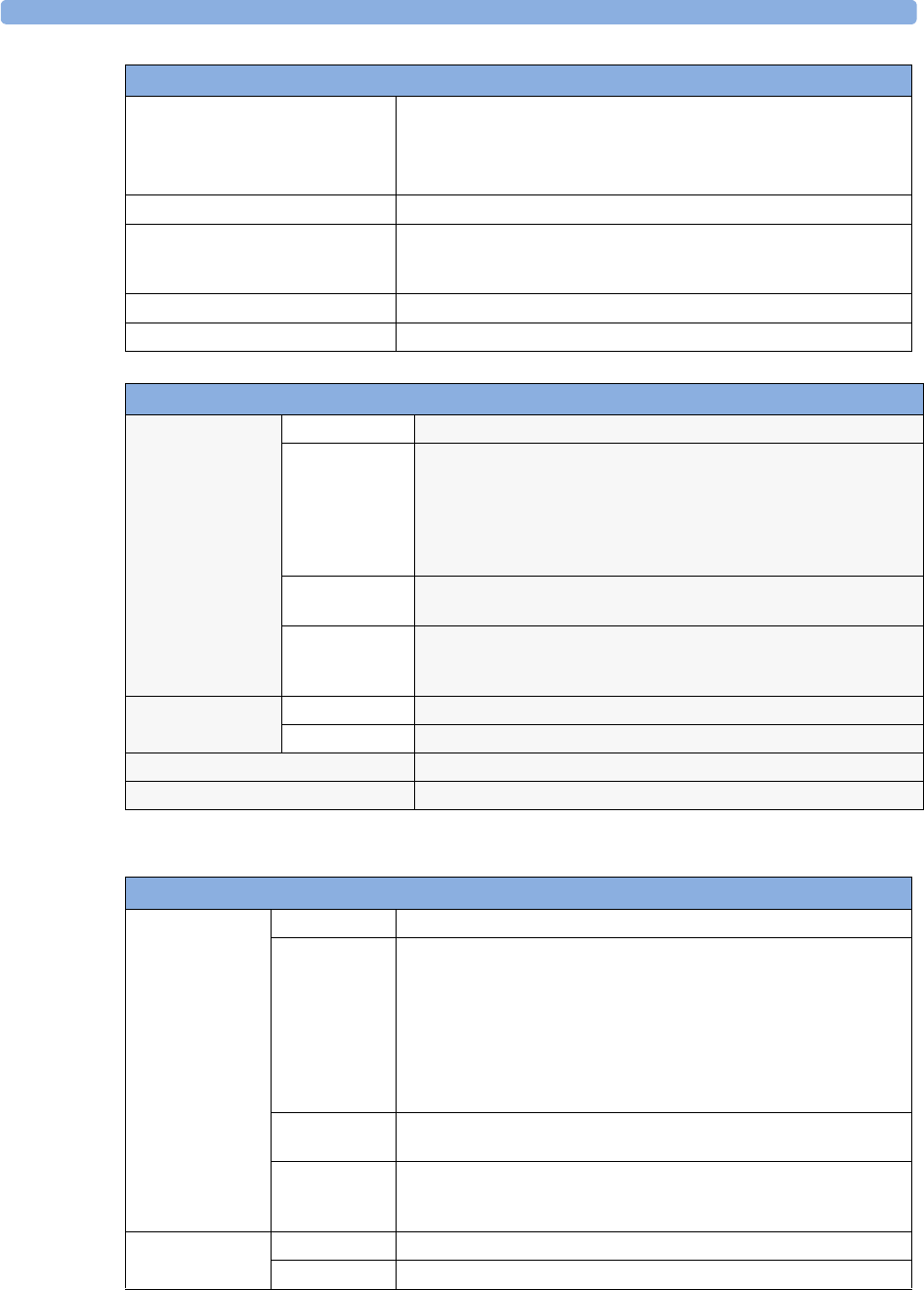
Measurement Specifications 24 Specifications
263
Rise Time 190 ms for neonatal mode
(measured with FilterLine H for neonatal)
240 ms for adult mode
(measured with FilterLine H for adult)
Sample Flow Rate 50 + 15/-7.5 ml/minute
Gas Sampling Delay Time Maximum:
3 seconds (2m sample lines)
6 seconds (4m sample lines)
Sound Pressure Acoustic noise: <45 dBA
Total System Response Time The total system response time is the sum of the delay time and the rise time.
M3014A Mainstream CO2 Performance Specifications
CO2Range 0 to 150 mmHg (0 to 20.0 kPa)
Accuracy after 2 minutes warmup:
For values between 0 and 40 mmHg: ±2.0 mmHg (±0.29 kPa)
For values from 41 to 70 mmHg: ±5% of reading
For values from 71 to 100 mmHg: ±8% of reading
The specifications are valid for standard gas mixtures, balance air, fully
hydrated at 35°C, Pabs = 760 mmHg, flow rate = 2 l/min.
Resolution Numeric: 1.0 mmHg (0.1 kPa)
Wave: 0.1 mmHg (0.01 kPa)
Stability:
Short term drift
Long term drift
±0.8 mmHg over four hours
Accuracy specification will be maintained over a 120 hour period
awRR Range 2 to 150 rpm
Accuracy ±1 rpm
Warm-up Tim e 2 minutes with CO2 transducer attached for full accuracy specification
Response Time Less than 60 ms (with adult or infant reusable or disposable adapter)
M3014A Sidestream CO2 Performance Specifications
CO2Range 0 to 150 mmHg (0 to 20.0 kPa)
Accuracy after 2 minutes warmup:
For values between 0 and 40 mmHg: ±2.0 mmHg (±0.29 kPa)
For values from 41 to 70 mmHg: ±5% of reading
For values from 71 to 100 mmHg: ±8% of reading
For values from 101 to 150 mmHg: ±10% of reading
At respiration rates above 80 rpm, all ranges are ±12% of actual. The
specifications are valid for gas mixtures of CO2, balance N2, dry gas at
760 mmHg within specified operating temperature range.
Resolution Numeric: 1.0 mmHg (0.1 kPa)
Wave: 0.1 mmHg (0.01 kPa)
Stability:
Short term drift
Long term drift
±0.8 mmHg over four hours
Accuracy specification will be maintained over a 120 hour period
awRR Range 2 to 150 rpm
Accuracy ±1 rpm
M3015A Microstream CO2 Performance Specifications
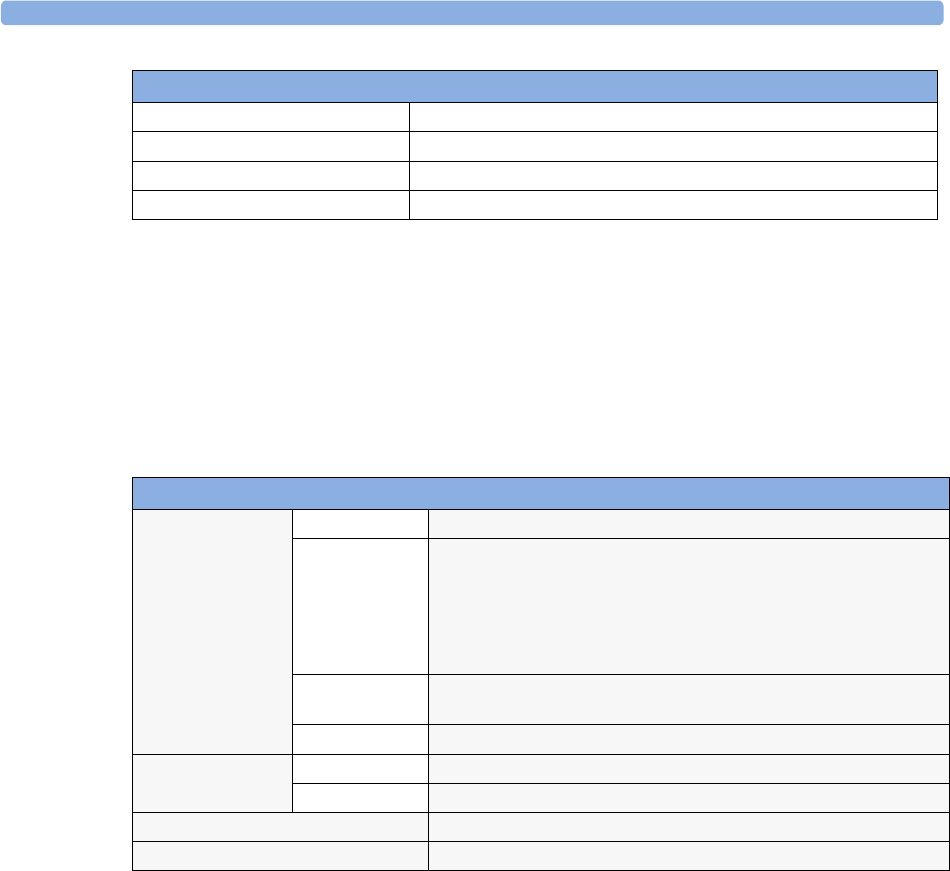
24 Specifications Measurement Specifications
264
M8102A/M3014A Mainstream and Sidestream CO2 Humidity Correction Factor
Either BTPS or ATPD can be selected as the humidity correction factor for the CO2 readings. The
formula for the correction calculation is:
Where p = partial pressure, Pabs = absolute pressure, and PH2O = 42 mmHg @35°C and 100% RH.
Mainstream CO2 Humidity Correction Factor
Either BTPS or ATPD can be selected as the humidity correction factor for the Mainstream CO2
readings. The formula for the correction calculation is:
Where p = partial pressure, Pabs = absolute pressure, and PH2O = 47 mmHg @37qC and 100% RH.
Warm-up Tim e 2 minutes with CO2 sensor attached for full accuracy specification
Sample Flow Rate 50 ±10 ml/minute
Total System Response Time 3seconds
Operating Temperature 0 to 40°C (32 to 100°F)
M3016A Mainstream CO2 Performance Specifications
CO2Range –4 to 150 mmHg (-0.5 to 20.0 kPa)
Accuracy after 20 minutes warmup and calibration:
For values between 0 and 40 mmHg: ±2.2 mmHg (±0.29 kPa)
For values between 40 and 76 mmHg: ±5.5% of reading
The specifications are valid for 45% O2 and N2 or N2O balance. Outside
these conditions the accuracy reaches at a minimum the requirements of
EN864/ISO9918.
Resolution Numeric: 1.0 mmHg (0.1 kPa)
Wave: 0.1 mmHg (0.01 kPa)
Stability ±1.0 mmHg over a 7 day period
awRR Range 0 to 150 rpm
Accuracy ±2 rpm
Warm-up Tim e 20 minutes with CO2 transducer attached for full accuracy specification
Response Time Less than 125 ms (for step from 10% to 90%)
M3014A Sidestream CO2 Performance Specifications
PATPD PBTPS
=Pabs
Pabs PH2O
–
-----------------------------
PATPD PBTPS
=Pabs
Pabs PH2O
–
-----------------------------
Measurement Specifications 24 Specifications
265
Interfering Gas and Vapor Effects On CO2 Measurement Values
The specified deviations for M8102A/M3014A are valid when the appropriate corrections are switched
on and set correctly.
CO2 Alarm
Specifications Range Adjustment Delay
etCO2 High 20 to 95 mmHg (2 to 13 kPa) 1 mmHg (0.1 kPa) M8102A/M3014A/M3016A: less than
14 seconds
M3015A: less than18 seconds.
etCO2 Low 10 to 90 mHg (1 to 12 kPa)
imCO2 High 2 to 20 mmHg
(0.3 to 3.0 kPa)
steps of 1 mmHg
(0.1 kPa)
M8102A/M3014A/M3016A: less than
14 seconds
M3015A: less than18 seconds.
awRR High Adult/pedi: 10 to 100 rpm
Neo: 30 to 150 rpm
under 20 rpm: 1 rpm
steps
over 20 rpm:5 rpm
steps
M8102A/M3014A/M3016A: less than
14 seconds
M3015A: less than18 seconds.
awRR Low Adult/pedi: 0 to 95 rpm
Neo: 0 to 145 rpm
M3015A:
settings <20 rpm: less than 8 seconds
>20 rpm: less than 18 seconds
M8102A/M3014A/M3016A
settings <20 rpm: less than 4 seconds
>20 rpm: less than 14 seconds
Apnea delay 10 to 40 seconds 5 second steps set apnea delay time +4 seconds
(M8102A/M3014A/M3016A) or
8 seconds (M3015A)
Gas or Vapor
Gas Level
(% volume fraction)
M8102A/M3014A M3015A
Additional deviation due to gas interfence, measured at
0 - 40 mmHg CO2
Nitrous Oxide 60 ±1 mmHg ±5%
Halothane 4 ±2 mmHg ±5%
Enflurane 5 ±2 mmHg ±5%
Isoflurane 5 ±2 mmHg ±5%
Sevoflurane 5 ±2 mmHg ±5%
Xenon 80 -5 mmHg ±5%
Helium 50 ±1 mmHg ±5%
Metered dose inhaler
propellants
- not specified for use
Desflurane 15 +5 mmHg ±5%
Ethanol 0.1 ±1 mmHg ±5%
Isopropanol 0.1 ±1 mmHg ±5%
Acetone 0.1 ±1 mmHg ±5%
Methane 1.0 ±1 mmHg ±5%
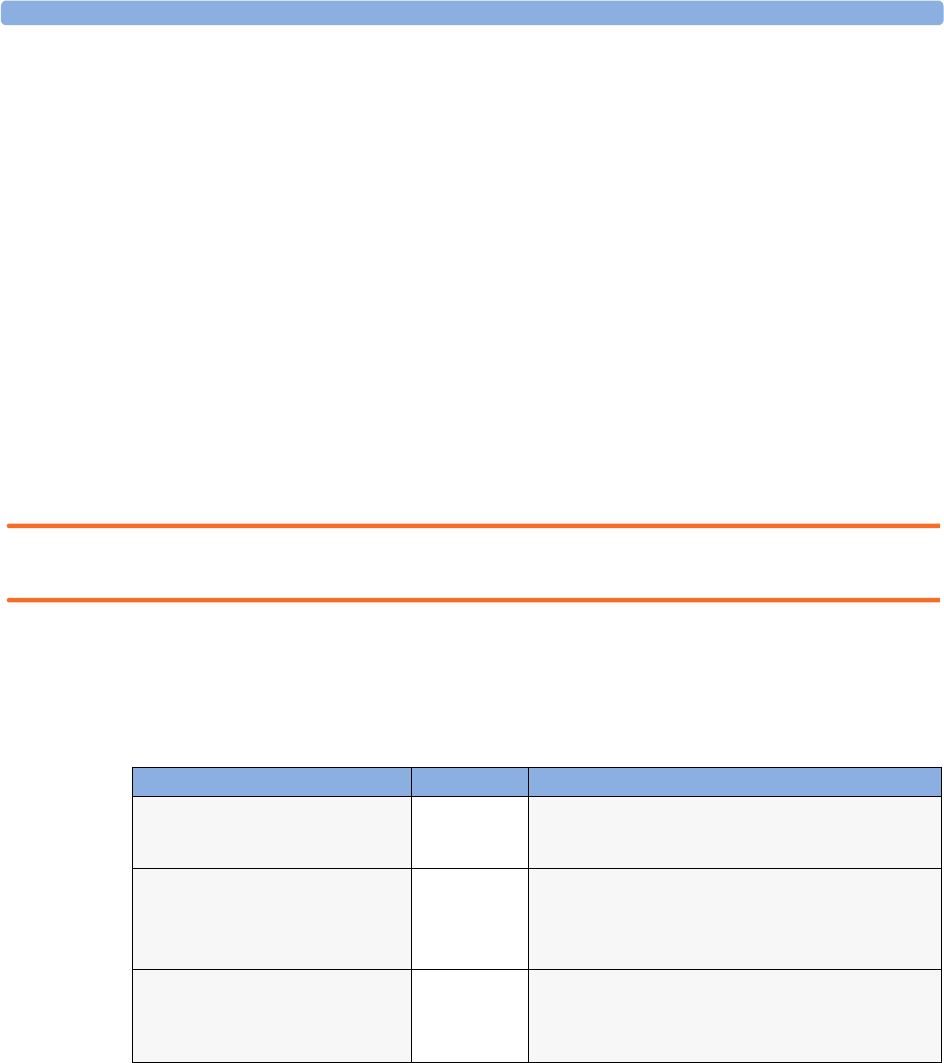
24 Specifications Safety and Performance Tests
266
Safety and Performance Tests
You must observe any national regulations on the qualification of the testing personnel and suitable
measuring and testing facilities. See the maintenance section for a list of required tests. Safety and
performance tests, and what to do if the instrument does not meet these specifications are described in
the Installation and Service guide.
Electromagnetic Compatibility (EMC) Specifications
Take special precautions regarding electromagnetic compatibility (EMC) when using medical electrical
equipment. You must operate your monitoring equipment according to the EMC information
provided in this book. Portable and mobile radio frequency (RF) communications equipment can
affect medical electrical equipment.
Accessories Compliant with EMC Standards
All accessories listed in the accessories section comply, in combination with the monitor, with the
requirements of IEC 60601-1-2:2001 + A1:2004.
WARNING Using accessories other than those specified may result in increased electromagnetic emission or
decreased electromagnetic immunity of the monitoring equipment.
Electromagnetic Emissions
The monitor is suitable for use in the electromagnetic environment specified in the table below. You
must ensure that it is used in such an environment
Avoiding Electromagnetic Interference (Resp)
The respiration (Resp) measurement is a very sensitive measurement that measures a very small signal.
Technological limitations do not allow higher immunity levels than 1 V/m for radiated RF
electromagnetic fields and 1 Vrms for conducted disturbances induced by RF fields. Electromagnetic
fields with field strengths above 1 V/m and conducted disturbances above 1 Vrms may cause erroneous
measurements. Therefore Philips recommends that you avoid using electrically radiating equipment in
the close proximity of this measurement.
Emissions test Compliance Avoiding Electromagnetic Interference
Radio Frequency (RF) emissions Group 1 The monitor uses RF energy only for its internal function.
Therefore, its RF emissions are very low and are not likely
to cause any interference in nearby electronic equipment
RF emissions CISPR 11
for the MP2 or X2 with all accessories
except the M2741A Sidestream CO2
sensor
Class B The monitor is suitable for use in all establishments,
including domestic establishments and those directly
connected to the public low-voltage supply network that
supplies buildings used for domestic purposes.
RF emissions CISPR 11
for the MP2 or X2 whenever used with
the M2741A Sidestream CO2 sensor
Class A The monitor is suitable for use in all establishments other
than those directly connected to the public low-voltage
power supply network that supplies buildings used for
domestic purposes.
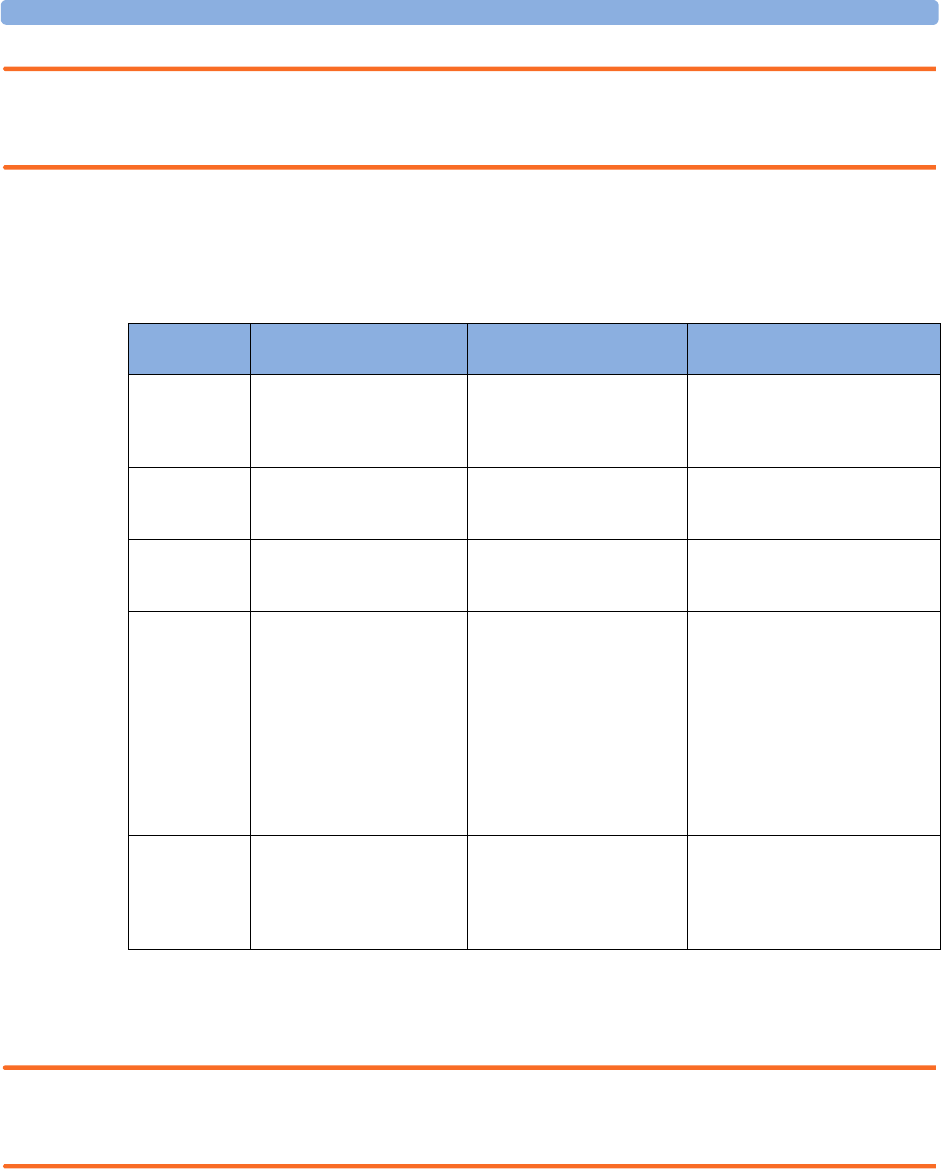
Safety and Performance Tests 24 Specifications
267
WARNING The monitor should not be used next to or stacked with other equipment. If you must stack the
monitor, you must check that normal operation is possible in the necessary configuration before you
start monitoring patients.
Electromagnetic Immunity
The monitor is suitable for use in the specified electromagnetic environment. The user must ensure
that it is used in the appropriate environment as described below.
In this table, UT is the a.c. mains voltage prior to application of the test level.
Recommended Separation Distance
WARNING The monitor, equipped with a wireless network interface, intentionally receives RF electromagnetic
energy for the purpose of its operation. Therefore, other equipment may cause interference, even if that
other equipment complies with CISPR emission requirements.
In the following table, P is the maximum output power rating of the transmitter in watts (W)
according to the transmitter manufacturer and d is the recommended separation distance in metres
(m). The values given in brackets are for respiration.
Immunity test
IEC 60601-1-2
test level Compliance level
Electromagnetic environment
guidance
Electrostatic
discharge (ESD)
IEC 61000-4-2
±6 kV contact
±8 kV air
±6 kV contact
±8 kV air
Floors should be wood, concrete, or
ceramic tile. If floors are covered
with synthetic material, the relative
humidity should be at least 30%.
Electrical fast
transient/burst
IEC 61000-4-4
±2 kV for power supply lines
±1 kV for input/output lines
±2 kV for power supply lines
±1 kV for input/output lines
Mains power quality should be that
of a typical commercial and/or
hospital environment
Surge
IEC 61000-4-5
±1 kV differential mode
±2 kV common mode
±1 kV differential mode
±2 kV common mode
Mains power quality should be that
of a typical commercial and/or
hospital environment
Voltage dips,
short
interruptions
and voltage
variations on
power supply
input lines
IEC 61000-4-
11
<5% UT
(>95% dip in UT) for
0.5 cycles
40% UT
(60% dip in UT) for 5 cycles
70% UT
(30% dip in UT) for 25 cycles
<5% UT
(>95% dip in UT) for 5 sec
<5% UT
(>95% dip in UT) for
0.5 cycles
40% UT
(60% dip in UT) for 5 cycles
70% UT
(30% dip in UT) for 25 cycles
<5% UT
(>95% dip in UT) for 5 sec
Mains power quality should be that
of a typical commercial and/or
hospital environment. If the user of
the monitor requires continued
operation during power mains
interruptions, it is recommended
that the monitor is equipped with
an internal battery or is powered
from an uninterruptible power
supply.
Power frequency
(50/60 Hz)
magnetic field
IEC 61000-4-8
3 A/m 3 A/m Power frequency magnetic fields
should be a t levels characteristic of
a typical location in a typical
commercial and/or hospital
environment
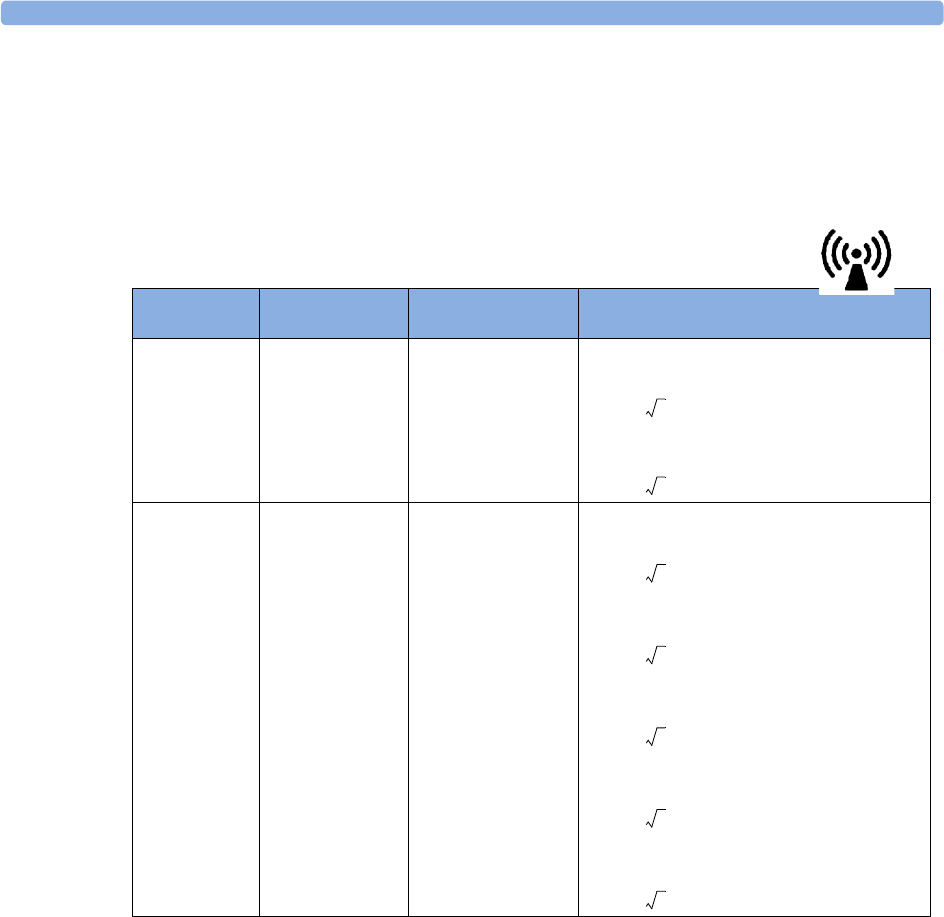
24 Specifications Safety and Performance Tests
268
Portable and mobile RF communications equipment should be used no closer to any part of the
monitor, including cables, than the recommended separation distance calculated from the equation
appropriate for the frequency of the transmitter.
Field strengths from fixed RF transmitters, as determined by an electromagnetic site survey, should be
less than the compliance level in each frequency range.
Interference may occur in the vicinity of equipment marked with this symbol:
Field strengths from fixed transmitters, such as base stations for radio (cellular, cordless) telephones and
land mobile radios, amateur radio, AM and FM radio broadcast and TV broadcast cannot be predicted
theoretically with accuracy. To assess the electromagnetic environment due to fixed RF transmitters, an
electromagnetic site survey should be considered. If the measured field strength in the location in
which the monitor is used exceeds the applicable RF compliance level above, the monitor should be
observed to verify normal operation. If abnormal performance is observed, additional measures may be
necessary, such as reorienting or relocating the monitor.
These guidelines may not apply in all situations. Electromagnetic propagation is affected by absorption
and reflection from structures, objects, and people.
Immunity test
IEC 60601-1-2
test level Compliance level Electromagnetic environment guidance
Conducted RF
IEC 61000-4-6
3V
RMS
150 kHz to
80 MHz
3V
RMS
(1 VRMS for
respiration)
Recommended separation distance:
:
for respiration:
:
Radiated RF
IEC 61000-4-3
3V/m
80 MHz to
2.5 GHz
3V/m
(1 V/m for respiration)
For short range radio,
see note1.
1.If ECG/SpO2 signals are acquired from a telemetry device via short range radio the compliance level is 3V/m except in
the range 2.0 to 2.3 GHz where it is 1 V/m.
Recommended separation distance:
80 MHz to 800 MHz
80 MHz to 800 MHz for respiration
:
800 MHz to 2,5 GHz
800 MHz to 2,5 GHz for respiration
2.0 to 2,3 GHz for short range radio
d1,2P=
d3,5P=
d1,2P=
d3,5P=
d2,3P=
d7,0P=
d7,0P=
Safety and Performance Tests 24 Specifications
269
Recommended separation distances from portable and mobile RF
communication equipment
The monitor is intended for use in an electromagnetic environment in which radiated RF disturbances
are controlled. The customer or user of the monitor can help prevent electromagnetic interference by
maintaining a minimum distance between portable and mobile RF communications equipment and
the monitor as recommended below, according to the maximum output power of the communications
equipment.
In the following table, P is the maximum output power rating of the transmitter in watts (W)
according to the transmitter manufacturer and d is the recommended separation distance in metres
(m). The values given in brackets are for those measurements which do not use the general formula.
Electrosurgery Interference/Defibrillation/Electrostatic Discharge
The equipment returns to the previous operating mode within 10 seconds without loss of any stored
data. Measurement accuracy may be temporarily decreased while performing electro-surgery or
defibrillation. This does not affect patient or equipment safety. Do not expose the equipment to x-ray
or strong magnetic fields (MRI).
Fast Transients/Bursts
The equipment will return to the previous operating mode within 10 seconds without loss of any
stored data. If any user interaction is required, the monitor indicates with a technical alarm (INOP).
Restart time
After power interruption, an ECG wave will be shown on the display after 30 seconds maximum.
Frequency of transmitter 150 kHz to 80 MHz 80 MHz to 800 MHz 800 MHz to 2,5 GHz
Equation
for respiration: for respiration: for respiration:
for short range radio in
the range 2.0 to 2.3 GHz:
Rated max. output power
of transmitter (W) Separation distance (m) Separation distance (m) Separation distance (m)
0.01 0.1 (0.4) 0.1 (0.4) 0.2 (0.7)
0.1 0.4 (1.1) 0.4 (1.1) 0.7 (2.2)
1 1.3 (3.5) 1.3 (3.5) 2.3 (7.0)
10 3.8 (11.1) 3.8 (11.1) 7.3 (22.1)
100 12.0 (35.0) 12.0 (35.0) 23.0 (70.0)
d1,2P=
d3,5p=
d1,2P=
d3,5P=
d2,3P=
d7,0P=
d7,0P=

24 Specifications Safety and Performance Tests
270
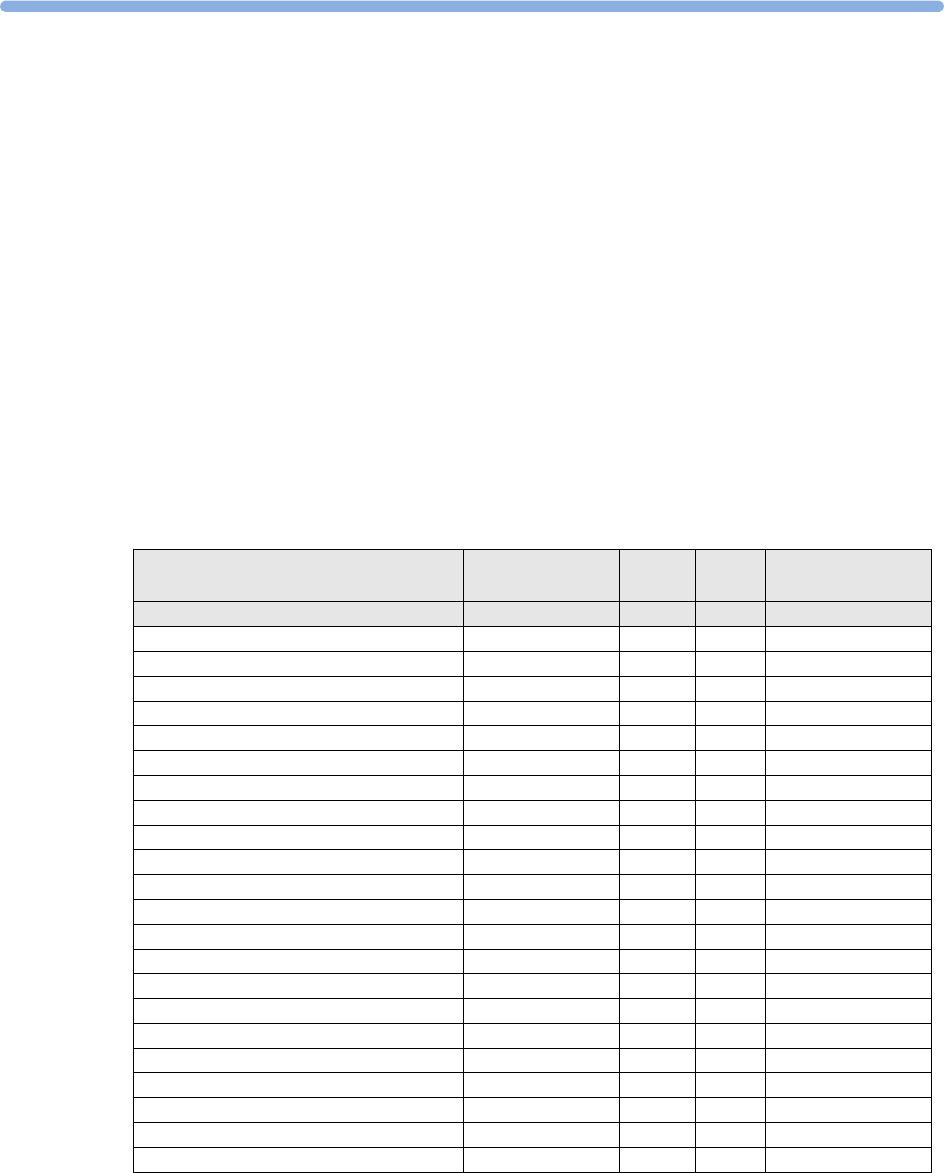
271
25
25Default Settings Appendix
This appendix documents the most important default settings of your monitor as it is delivered from
the factory. For a comprehensive list and explanation of default settings, see the Configuration Guide
supplied with your monitor. The monitor’s default settings can be permanently changed in
Configuration Mode.
Note: If your monitor has been ordered preconfigured to your requirements, the settings at delivery
will be different from those listed here.
Country-Specific Default Settings
Certain default settings are specific to a particular country. These are listed here for all countries
alphabetically.
Country-Description Line Frequency Units
Weight
Units
Height
ECG Cable Color
50/60 [Hz] kg, lb in, cm IEC, AAMI
Afghanistan 50 kg cm AAMI
Åland Islands 50 kg cm IEC
Albania 50 kg cm IEC
Algeria 50 kg cm IEC
American Samoa 60 lb in AAMI
Andorra 60 lb in AAMI
Angola 50 kg cm IEC
Anguilla 60 lb in AAMI
Antarctica 60 lb in AAMI
Antigua and Barbuda 50 kg cm AAMI
Argentina 50 kg cm AAMI
Armenia 50 kg cm IEC
Aruba 60 kg cm AAMI
Australia 50 kg cm AAMI
Austria 50 kg cm IEC
Azerbaijan 50 kg cm IEC
Bahamas, The 60 kg cm AAMI
Bahrain 50 kg cm AAMI
Bangladesh 60 lb in AAMI
Barbados 50 kg cm AAMI
Belarus 50 kg cm IEC
Belgium 50 kg cm IEC
25 Default Settings Appendix Country-Specific Default Settings
272
Belize 60 lb in AAMI
Benin 60 lb in AAMI
Bermuda 60 kg cm AAMI
Bhutan 60 lb in AAMI
Bolivia 50 kg cm AAMI
Bosnia and Herzegovina 50 kg cm IEC
Botswana 50 kg cm IEC
Bouvet Island 60 lb in AAMI
Brazil 60 kg cm AAMI
British Indian Ocean Territory 60 lb in AAMI
Brunei Darussalam 50 kg cm AAMI
Brunei 50 kg cm IEC
Bulgaria 50 kg cm IEC
Burkina Faso 50 kg cm IEC
Burundi 50 kg cm IEC
Cambodia 50 kg cm IEC
Cameroon 50 kg cm IEC
Canada 60 kg cm AAMI
Cape Verde 60 lb in AAMI
Cayman Islands 60 kg cm AAMI
Central African Republic 50 kg cm IEC
Chad 60 lb in AAMI
Chile 50 kg cm AAMI
China 50 kg cm IEC
Christmas Islands 60 lb in AAMI
Cocos Keeling Islands 60 lb in AAMI
Colombia 60 kg cm AAMI
Comoros 60 lb in AAMI
Congo 50 kg cm IEC
Congo, Democratic Republic of the 50 kg cm IEC
Cook Islands 60 lb in AAMI
Costa Rica 60 kg cm AAMI
Côte d'Ivoire 50 kg cm IEC
Croatia 50 kg cm IEC
Cuba 60 kg cm IEC
Cyprus 50 kg cm IEC
Czech Republic 50 kg cm IEC
Denmark 60 lb in AAMI
Djibouti 50 kg cm IEC
Dominica 50 kg cm AAMI
Dominican Republic 60 kg cm AAMI
Ecuador 60 kg cm AAMI
Egypt 50 kg cm IEC
El Salvador 60 kg cm AAMI
Equatorial Guinea 50 kg cm IEC
Eritrea 50 kg cm IEC
Estonia 50 kg cm IEC
Ethiopia 50 kg cm IEC
Falkland Islands, Malvinas 60 lb in AAMI
Faroe Islands 60 lb in AAMI
Fiji 60 lb in AAMI
Country-Specific Default Settings 25 Default Settings Appendix
273
Finland 50 kg cm IEC
France 50 kg cm IEC
French Guiana 50 kg cm IEC
French Polynesia 60 lb in AAMI
French Southern Territories 60 lb in AAMI
Gabon 50 kg cm IEC
Gambia, The 50 kg cm IEC
Georgia 60 lb in AAMI
Germany 50 kg cm IEC
Ghana 50 kg cm IEC
Gibraltar 60 lb in AAMI
Greece 50 kg cm IEC
Greenland 60 lb in AAMI
Grenada 50 kg cm AAMI
Guadeloupe 50 kg cm IEC
Guam 60 lb in AAMI
Guatemala 60 kg cm AAMI
Guernsey 50 kg cm IEC
Guinea 60 lb in AAMI
Guinea-Bissau 60 lb in AAMI
Guyana 60 kg cm AAMI
Haiti 60 kg cm AAMI
Heard Island and McDonald Islands 60 lb in AAMI
Holy See, Vatican City State 60 lb in AAMI
Honduras 60 kg cm AAMI
Hong Kong 50 kg cm IEC
Hungary 50 kg cm IEC
Iceland 50 kg cm IEC
India 50 kg cm IEC
Indonesia 50 kg cm IEC
Iran, Islamic Republic of 50 kg cm AAMI
Iraq 50 kg cm AAMI
Ireland 50 kg cm IEC
Isle of Man 50 kg cm IEC
Israel 50 kg cm IEC
Italy 50 kg cm IEC
Jamaica 50 kg cm AAMI
Japan 60 kg cm IEC
Jersey 50 kg cm IEC
Jordan 50 kg cm AAMI
Kazakhstan 50 kg cm IEC
Kenya 50 kg cm IEC
Kiribati 60 lb in AAMI
Korea, Democratic People’s Republic of 60 lb in AAMI
Korea, Republic of 60 kg cm AAMI
Kuweit 50 kg cm AAMI
Kyrgyzstan 60 lb in AAMI
Lao People’s Democratic Republics 50 kg cm IEC
Latvia 50 kg cm IEC
Lebanon 50 kg cm AAMI
Lesotho 50 kg cm IEC
25 Default Settings Appendix Country-Specific Default Settings
274
Liberia 50 kg cm IEC
Libyan Arab. Jamahiriya 60 lb in AAMI
Liechtenstein 60 lb in AAMI
Lithuania 50 kg cm IEC
Luxembourg 50 kg cm IEC
Macao 60 lb in AAMI
Macedonia, The former Yugoslavian
Republic of
50 kg cm IEC
Madagascar 50 kg cm IEC
Malawi 50 kg cm IEC
Malaysia 50 kg cm IEC
Maldives 60 lb in AAMI
Mali 50 kg cm IEC
Malta 50 kg cm IEC
Marshall Islands 60 lb in AAMI
Martinique 60 kg cm IEC
Mauritania 50 kg cm IEC
Mauritius 60 lb in AAMI
Mayotte 60 lb in AAMI
Mexico 60 kg cm AAMI
Micronesia, Federal States of 60 lb in AAMI
Moldova, Republic of 60 lb in AAMI
Monaco 60 lb in AAMI
Mongolia 60 lb in AAMI
Montenegro 50 kg cm IEC
Montserrat 50 kg cm AAMI
Morocco 50 kg cm IEC
Mozambique 50 kg cm IEC
Myanmar 60 lb in AAMI
Namibia 50 kg cm IEC
Nauru 60 lb in AAMI
Nepal 60 lb in AAMI
Netherlands 50 kg cm IEC
Netherlands Antilles 50 kg cm AAMI
New Caledonia 60 lb in AAMI
New Zealand 50 kg cm AAMI
Nicaragua 60 kg in AAMI
Niger 50 kg cm IEC
Nigeria 50 kg cm IEC
Niue 60 lb in AAMI
Norfolk Islands 60 lb in AAMI
Northern Mariana Islands 60 lb in AAMI
Norway 50 kg cm IEC
Oman 50 kg cm AAMI
Pakistan 50 kg cm IEC
Palau 60 lb in AAMI
Palestinian Territory 50 kg cm AAMI
Panama 60 lb in AAMI
Papua New Guinea 60 lb in AAMI
Paraguay 50 kg cm AAMI
Peru 60 kg cm AAMI
Country-Specific Default Settings 25 Default Settings Appendix
275
Philippines 60 kg cm AAMI
Pitcairn 60 lb in AAMI
Poland 50 kg cm IEC
Portugal 50 kg cm IEC
Puerto Rico 60 lb in AAMI
Qatar 50 kg cm AAMI
Reunion 60 lb in AAMI
Romania 50 kg cm IEC
Russian Federation 50 kg cm IEC
Rwanda 50 kg cm IEC
Saint Helena 60 lb in AAMI
Saint Kitts and Nevis 60 kg cm AAMI
Saint Lucia 50 kg cm AAMI
Saint Pierre and Miquelon 60 lb in AAMI
Saint Vincent and the Grenadines 50 kg cm AAMI
Samoa 60 lb in AAMI
San Marino 60 lb in AAMI
Sao Tome and Principe 60 lb in AAMI
Saudi Arabia 50 kg cm AAMI
Senegal 50 kg cm IEC
Serbia 50 kg cm IEC
Serbia & Montenegro 50 kg cm IEC
Seychelles 60 lb in AAMI
Sierra Leone 50 kg cm IEC
Singapore 50 kg cm IEC
Slovakia 50 kg cm IEC
Slovenia 50 kg cm IEC
Solomon Islands 60 lb in AAMI
Somalia 50 kg cm IEC
South Africa 60 lb in AAMI
South Georgia and the South Sandwich
Islands
60 lb in AAMI
Spain 50 kg cm IEC
Sri Lanka 60 lb in AAMI
Sudan 50 kg cm IEC
Suriname 60 kg cm AAMI
Svalbard and Jan Mayen 60 lb in AAMI
Swaziland 60 lb in AAMI
Sweden 50 kg cm IEC
Switzerland 50 kg cm IEC
Syrian Arab Rep 50 kg cm AAMI
Taiwan, Province of China 60 kg cm AAMI
Tajikistan 60 lb in AAMI
Tanzania, United Republic of 60 lb in AAMI
Thailand 50 kg cm AAMI
Timor-Leste 60 lb in AAMI
Togo 60 lb in AAMI
Tokelau 60 lb in AAMI
Tonga 60 lb in AAMI
Trinidad and Tobago 60 lb in AAMI
Tu n i s i a 5 0 k g c m I E C
25 Default Settings Appendix Country-Specific Default Settings
276
Turkey 50 kg cm IEC
Turkmenistan 60 lb in AAMI
Turks and Caicos Islands 60 kg cm AAMI
Tuvalu 60 lb in AAMI
Uganda 60 lb in AAMI
Ukraine 60 lb in AAMI
UK 50 kg cm IEC
United Arab Emirates 50 kg cm AAMI
United Kingdom 50 kg cm IEC
United States 60 lb in AAMI
United States Minor Outlying Islands 60 lb in AAMI
Uruguay 50 kg cm AAMI
Uzbekistan 60 lb in AAMI
Vanuatu 60 lb in AAMI
Venezuela 60 lb in AAMI
Viet Nam 50 kg cm IEC
Virgin Islands (British) 50 kg cm AAMI
Virgin Islands (US) 60 lb in AAMI
Wallis and Futuna Islands 60 lb in AAMI
Western Sahara 50 kg cm IEC
Yemen 50 kg cm AAMI
Zambia 60 lb in AAMI
Zimbabwe 60 lb in AAMI
Alarm and Measurement Default Settings 25 Default Settings Appendix
277
Alarm and Measurement Default Settings
Settings are only entered once per table row if they are the same for all patient categories1.
Alarm Default Settings
1.A profile “Outdoor” exists for use in typical outdoor conditions (bright sunlight, higher ambient noise). See the Configuration
Guide for details.
Alarm Settings Factory Default
Alarm Volume 5
Alarms Off 2 min.
Pause Al. 5min Enabled
Pause Al. 10min Enabled
Auto Alarms Off Off
Alarm Off Reminder Off
Visual Latching Red & Yell
Audible Latching Red & Yell
Alarm Reminder On
Reminder Time 3 min
Alarm Sounds Traditional
Red Alarm Interval 10 sec
Yel. Al. Interval 20 sec
Alarm Low 4
Red Alarm Volume AlarmVol +2
Yell. Alarm Volume AlarmVol +0
Inop Volume AlarmVol +0
Auto Increase Vol. 2 Steps
Increase Vol Delay 20 sec
Keep Blinking No
Relay 1 Sensitiv. R & Y & I
Relay 2 Sensitiv. Red & Yell
Relay 3 Sensitiv. Red
Inop Relay Latency 5 sec
Yel. Relay Latency 2 sec
Alarm Text Standard
No Centr Mon Min Vol 4
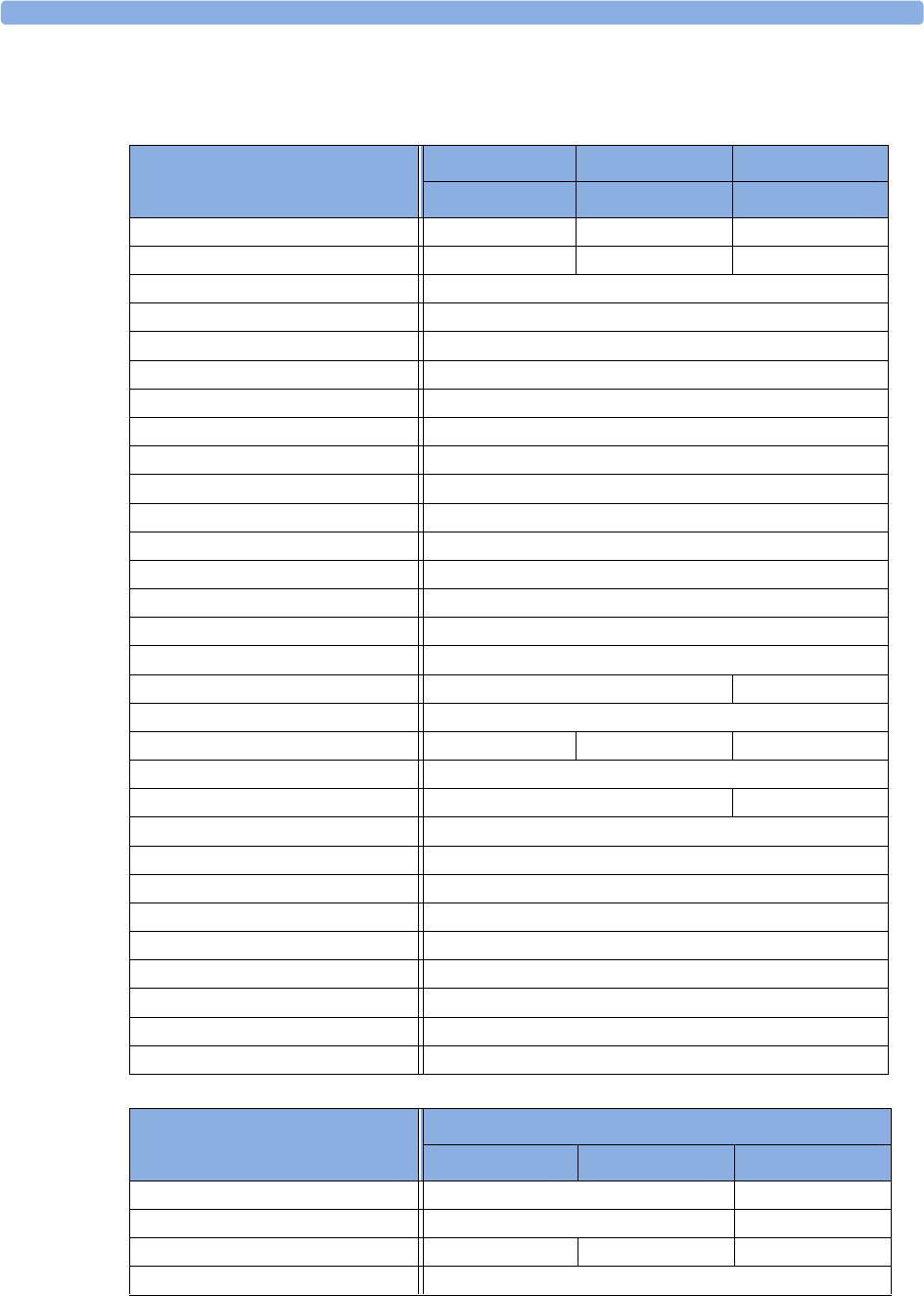
25 Default Settings Appendix ECG, Arrhythmia, ST and QT Default Settings
278
ECG, Arrhythmia, ST and QT Default Settings
ECG Settings
Factory Defaults
Adult Pedi Neo
High Limit 120 bpm 160 bpm 200 bpm
Low Limit 50 bpm 75 bpm 100 bpm
Alarms On
Alarm Source Auto
ECG On
QRS Volume 1
Primary Lead II
Secondary Lead V
Analysis Mode Multi-lead
Lead Placement Standard
Mod. Lead Placment Off
Filter Monitor
Speed 25 mm/s
Auto Filter Off
Default ECG Size x1
Color Green
Asystole Thresh 4.0 sec 3.0 sec
'ExtrTachy 20 bpm
Tachy Clamp 200 bpm 220 bpm 240 bpm
'ExtrBrady 20 bpm
Brady Clamp 40 bpm 50 bpm
ALL ECG IN. On
Fallback On
Alarms Off Enabled
Alarm Source Sel. Enabled
Va Lead V2
Vb Lead V5
SyncPulse sensit Medium
SyncPulse Marker On
Fallback ECGTele Enabled
Arrhythmia Settings
Factory Defaults
Adult Pedi Neo
Arrhythmia On Off
Pause Threshold 2.0 sec 1.5 sec
VTach HR 100 120 150
VTach Run 5
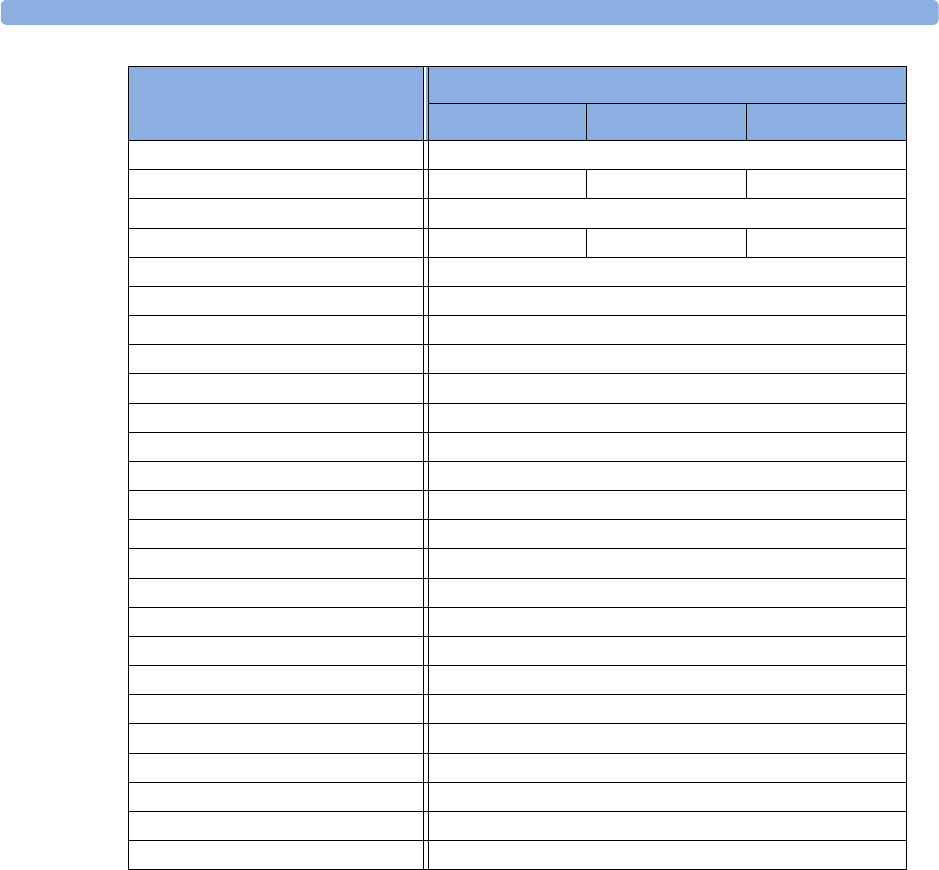
ECG, Arrhythmia, ST and QT Default Settings 25 Default Settings Appendix
279
Vent Rhythm 14
SVT HR 180 200 210
SVT Run 5
PVCs/min 10 5 5
Non-Sustain On
Vent Rhythm On
Run PVCs On
Pair PVCs On
R-On-T PVCs On
V.Bi gem in y On
V.Trig em iny On
PVCs/min On
Multif. PVCs On
Pacer N. Cap On
Pacer N. Pac On
Pause On
Missed Beat On
SVT On
Afib On
IrregularHR On
HR Alarms Short Yell
TimeOut 1st 3 min
TimeOut 2nd 10 min
Arrhy Off Message Yes
SOME ECG IN On
Arrhythmia Settings
Factory Defaults
Adult Pedi Neo
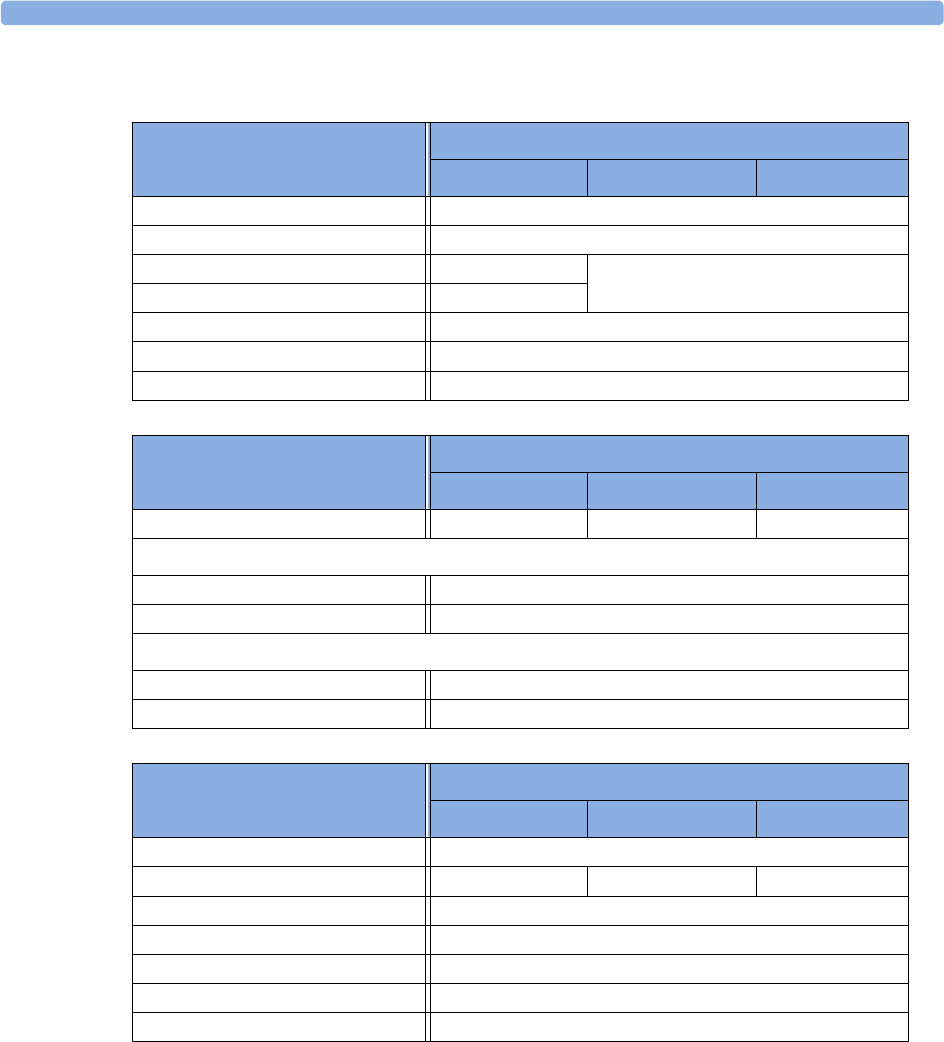
25 Default Settings Appendix ECG, Arrhythmia, ST and QT Default Settings
280
Lead-independent ST Settings
Factory Defaults
Adult Pedi Neo
ST Alarm Mode Single ST
Alarms On
ST Analysis On Off
ST-Index On
ISO Point -80 ms
J Point 48 ms
ST Point J+60
Lead I, II, III, V, aVR, aVL, aVF, V1-6,
MCL Settings
Factory Defaults
Factory Adult Factory Pedi Factory Neo
ST(Label) On Off
For Alarm Mode = Single-ST
ST(Label) High +2.0 mm
ST(Label) Low -2.0 mm
For Alarm Mode = Multi-ST
ST(Label) High +1.0 mm
ST(Label) Low -1.0 mm
QT Settings
Factory Defaults
Factory Adult Factory Pedi Factory Neo
QT Lead All
QTc High Limit 500 ms 480 ms 460 ms
'QTc Limit 60 ms
QTc High Alarm On/Off On
'QTc High Alarm On/Off On
QT Analysis Off
QTc Formula Bazett
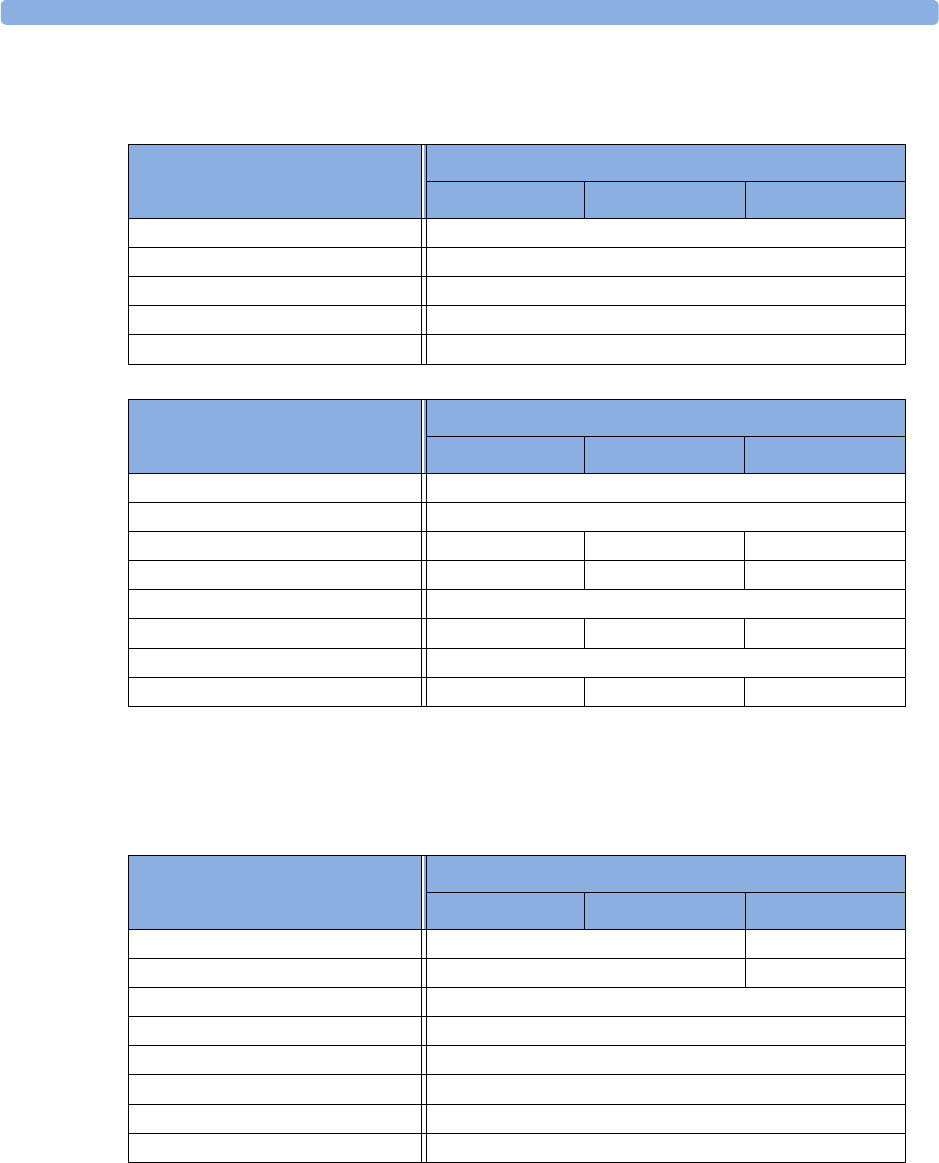
Pulse Default Settings 25 Default Settings Appendix
281
Pulse Default Settings
Pulse alarms use the settings of the currently selected Pulse alarm source.
Respiration Default Settings
Pulse Settings
Factory Defaults
Adult Pedi Neo
Alarms Source Auto
Pulse (Label) On
System Pulse SpO2
Alarms Off Enabled
Alarm Source Sel. Enabled
Pulse Alarm Settings
Factory Defaults
Adult Pedi Neo
Pulse (SpO2) On
Pulse Alarms Off
High Limit 120 bpm 160 bpm 200 bpm
Low Limit 50 bpm 75 bpm 100 bpm
' Extr Brady 20 bpm
Brady Clamp 40 bpm 40 bpm 50 bpm
' Extr Tachy 20 bpm
Tachy Clamp 200 bpm 220 bpm 240 bpm
Respiration Settings
Factory Defaults
Adult Pedi Neo
High Limit 30 rpm 100 rpm
Low Limit 8 rpm 30 rpm
Apnea Time 20 sec
Alarms On
Resp On
Auto/Manual Auto (Trigger Mode)
Resp Speed 6.25 mm/s
Color Yellow
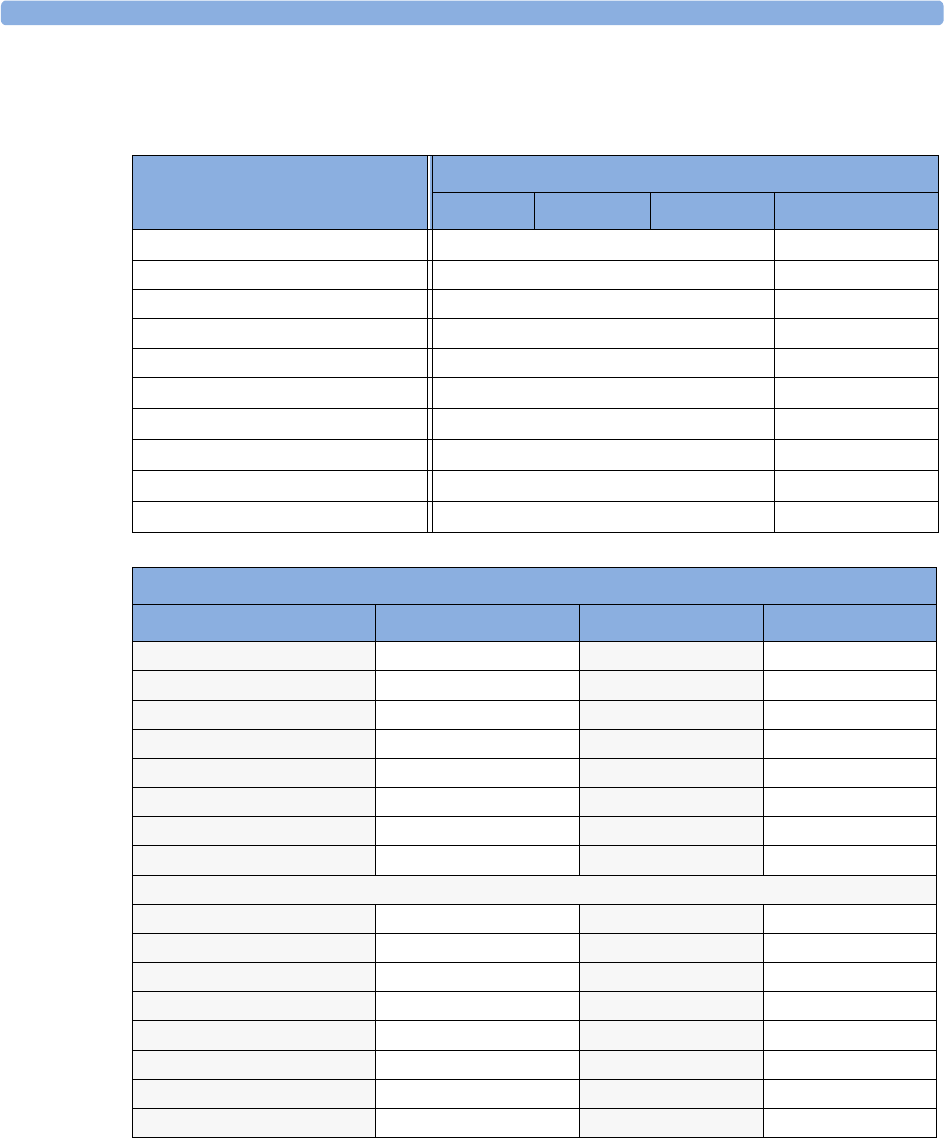
25 Default Settings Appendix SpO2 Default Settings
282
SpO2 Default Settings
SpO2 Settings
Factory Defaults
Adult Pedi Neo
Alarms On
QRS Volume 1
Tone Modulation Yes
Tone Mod. Type Enhanced
Speed 25 mm/s
Perfusion On
Average 10 sec
NBP Alarm Suppr. On
Extd. Auto OnOff Disabled
Color light blue (cyan)
SpO2 Alarm Default Settings
Setting Adult Pediatric Neonatal
Desat Limit 80 80 80
Low Limit 90 90 85
High Limit 100 100 95
Desat delay 20 sec 20 sec 20 sec
High Alarm delay 10 sec 10 sec 10 sec
Low Alarm delay 10 sec 10 sec 10 sec
Parameter Alarms On/Off on on on
Label SpO2SpO2SpO2
Pulse Settings
Pulse (SpO2) On/Off on on on
Pulse Alarms On/Off on on on
Pulse High Limit 120 bpm 160 bpm 200 bpm
Pulse Low Limit 50 bpm 75 bpm 100 bpm
'Extr Brady 20 bpm 20 bpm 20 bpm
Brady Clamp 40 bpm 40 bpm 50 bpm
' ExtrTachy 20 bpm 20 bpm 20 bpm
Tachy Clamp 200 bpm 220 bpm 240 bpm
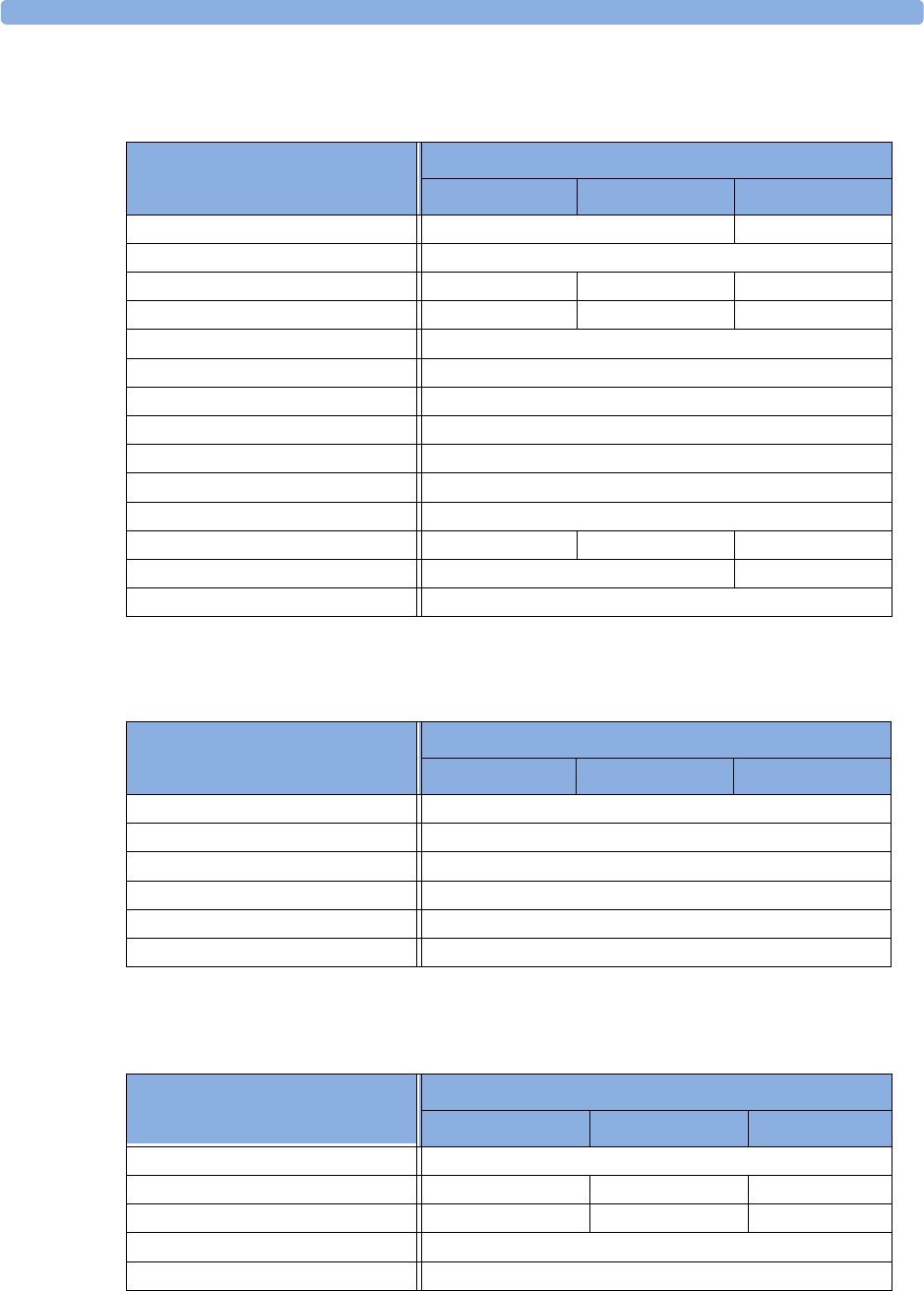
NBP Default Settings 25 Default Settings Appendix
283
NBP Default Settings
Temperature Default Settings
Invasive Pressure Default Settings
NBP Settings
Factory Defaults
Adult Pedi Neo
Mode Auto Manual
Alarms from Sys.
High Alarm Limit 160/90 (110) 120/70 (90) 90/60 (70)
Low Alarm Limit 90/50 (60) 70/40 (50) 40/20 (24)
Alarms On
NBP On
Repetition Time 10 min
Pulse (NBP) On
Unit mmHg
Done Tone Off
Start Time Synchronized
VP Pressure 60 mmHg 40 mmHg 30 mmHg
Reference Auscultatory Invasive
Color Red
Temp Settings
Factory Defaults
Adult Pedi Neo
Low Limit 36
High Limit 39
Alarms On
Unit qC
Range 35...43
Color Green
ABP, ART, Ao, BAP, FAP, P, P1, P2, P3,
P4, UAP Settings
Factory Defaults
Adult Pedi Neo
Alarms from Sys.
High Limit 160/90 (110) 120/70 (90) 90/60 (70)
Low Limit 90/50 (70) 70/40 (50) 55/20 (36)
Alarms On
Extreme Alarms Disabled
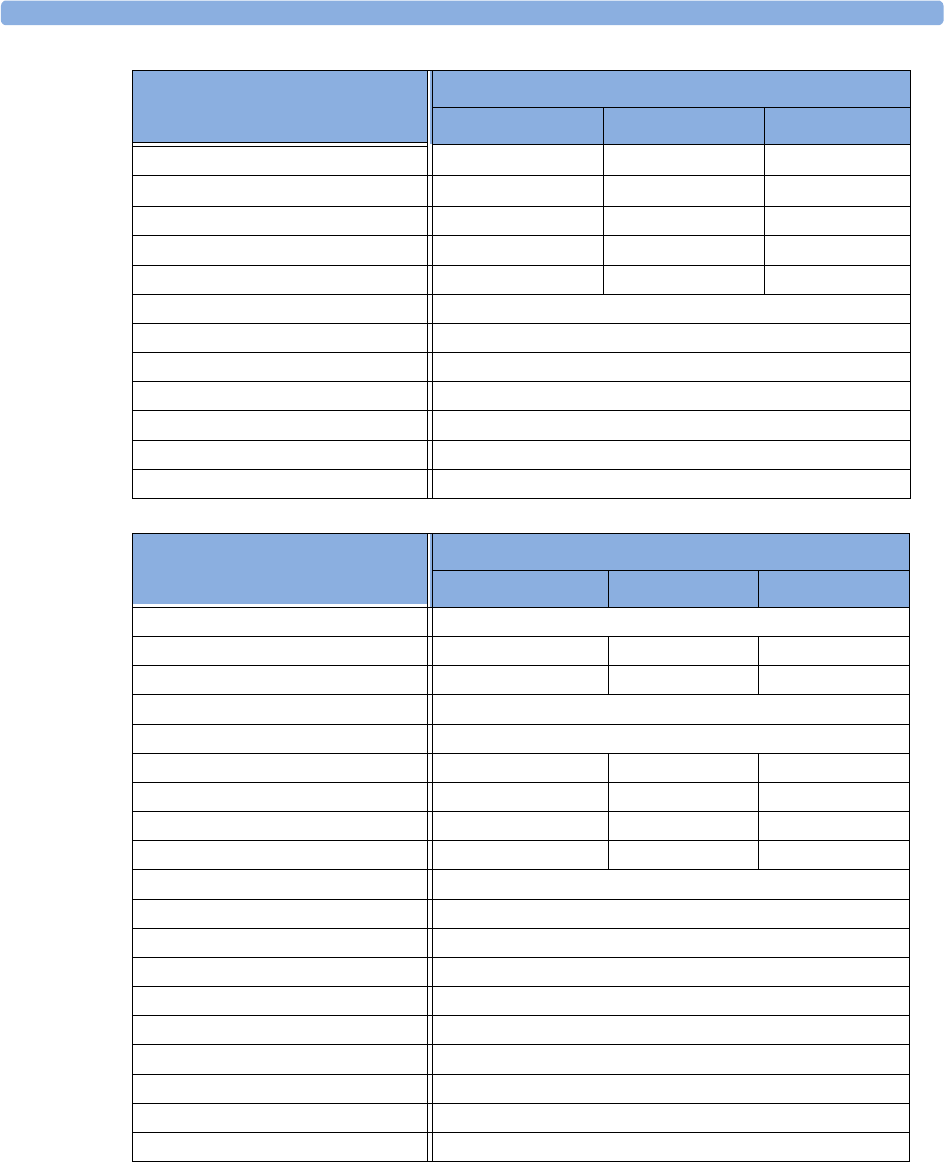
25 Default Settings Appendix Invasive Pressure Default Settings
284
'Extreme High 15 10 5
'Extreme Low 15 10 5
High Clamp 190/100 (125) 140/80 (100) 105/75 (75)
Low Clamp 80/45 (65) 60/35 (45) 45/15 (30)
Scale 150 100 100
Speed 25 mm/s
Mean Only No
Filter 12 Hz
Mercury Cal. Yes
Artifact Suppr. 60 sec
Unit mmHg
Color Red
C V P, R A P, L A P, U V P S e t t i n g s
Factory Defaults
Adult Pedi Neo
Alarms from Mean
High Limit 14/6 (10) 10/2 (4) 10/2 (4)
Low Limit 6/-4 (0) 2/-4 (0) 2/-4 (0)
Alarms On
Extreme Alarms Enabled
'Extreme High 5 5 5
'Extreme Low 5 5 5
High Clamp 20/10 (15) 15/5 (10) 15/5 (10)
Low Clamp 0/-5 (-5) 0/-5 (-5) 0/-5 (-5)
Scale 30
Speed 25 mm/s
Mean Only Yes
Filter 12 Hz
Mercury Cal. Yes
Artifact Suppr. 60 sec
Unit mmHg
Color light blue (cyan)
Average in Mon. No
Signal Quality On
ABP, ART, Ao, BAP, FAP, P, P1, P2, P3,
P4, UAP Settings
Factory Defaults
Adult Pedi Neo
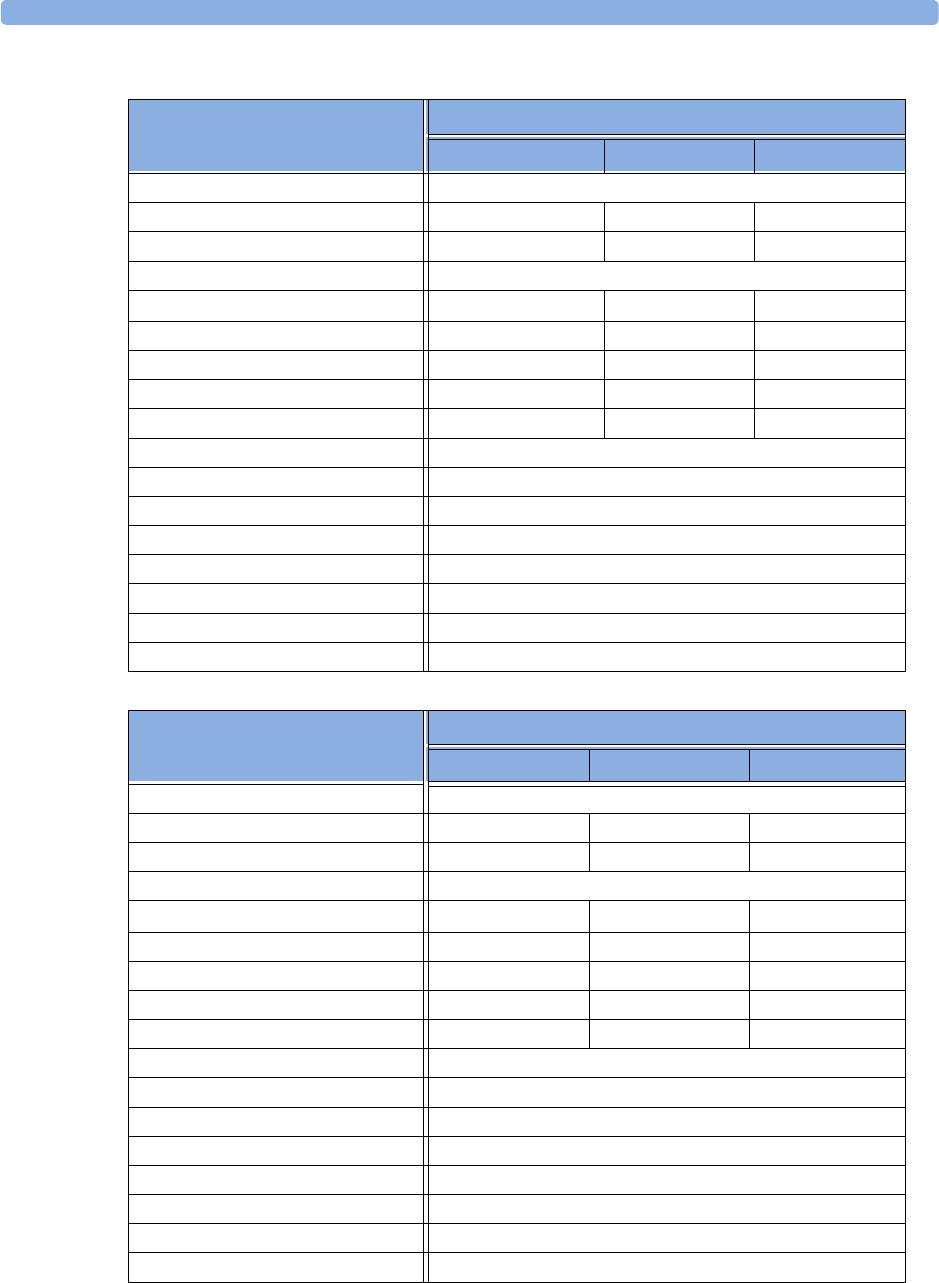
Invasive Pressure Default Settings 25 Default Settings Appendix
285
PAP Settings Factory Defaults
Adult Pedi Neo
Alarms from Dia.
High Limit 34/16 (20) 60/4 (26) 60/4 (26)
Low Limit 10/0 (0) 24/-4 (12) 24/-4 (12)
Alarms On
Extreme Alarms Enabled Enabled Enabled
'Extreme High 5 5 5
'Extreme Low 5 5 5
High Clamp 45/20 (25) 65/5 (35) 65/5 (35)
Low Clamp 5/-5 (-5) 15/-5 (5) 15/-5 (5)
Scale 30
Speed 25 mm/s
Mean Only No
Filter 12 Hz
Mercury Cal. Yes
Artifact Suppr. 60 sec
Unit mmHg
Color Yellow
ICP, IC1, IC2 Settings Factory Defaults
Adult Pedi Neo
Alarms from Mean
High Limit 14/6 (10) 10/2 (4) 10/2 (4)
Low Limit 6/-4 (0) 2/-4 (0) 2/-4 (0)
Alarms On
Extreme Alarms Enabled Enabled Enabled
'Extreme High 10 10 10
'Extreme Low 10 10 10
Low Clamp 20/10 (-5) 15/5 (-5) 15/5 (-5)
High Clamp 0/-5 (0) 0/-5 (0) 0/-5 (0)
Scale 30
Speed 25 mm/s
Mean Only Yes
Filter 12 Hz
Mercury Cal. Yes
Artifact Suppr. 60 sec
Unit mmHg
Color Magenta
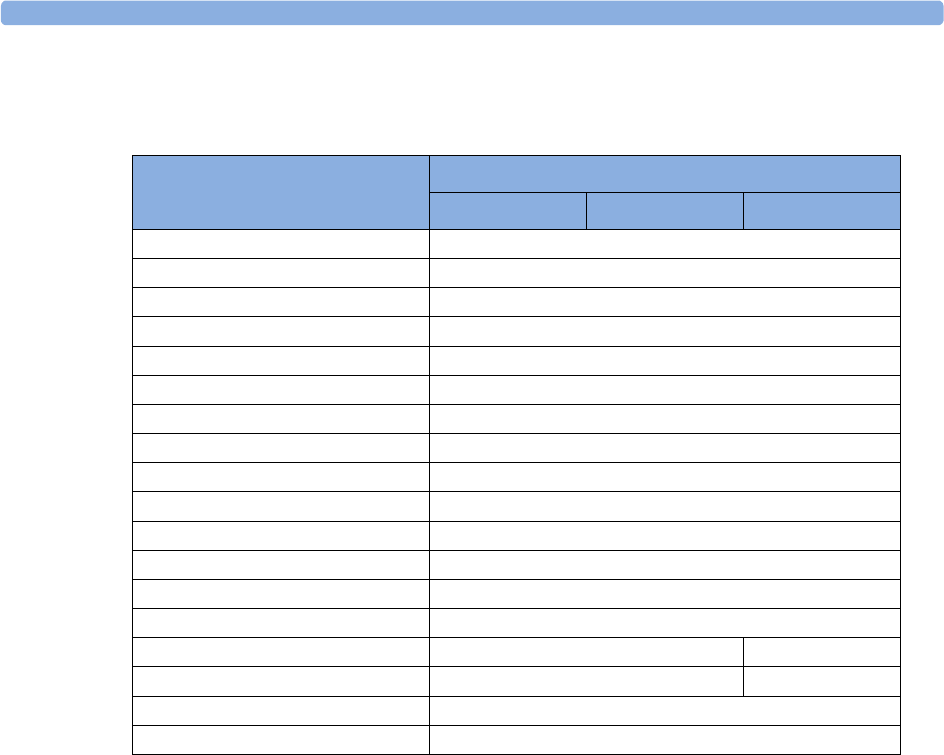
25 Default Settings Appendix CO2 Default Settings
286
CO2 Default Settings
CO2 Settings
Factory Defaults
Adult Pedi Neo
etCO2 low 30
etCO2 high 50
imCO2 high 4
CO2 Alarms on
Unit mmHg
Scale 40 mmHg
ImCO2on
N2O Corr (only M3015A/M3016A) Off
Oxygen Corr (only M3014A) 16%
Gas Corr (only M3014A) Off
Humidity Corr BTPS
Max Hold Off
AwRR On
AwRR Alarms On
AwRR high limit 30 100
AwRR low limit 8 30
Apnea time 20 secs
Color Yellow
i
1Index
#
10-lead placement (ECG) 99
12-lead placement (ECG) 99
3-lead placement (ECG) 97
5-lead placement (ECG) 97
A
AAMI ECG lead labels 96
abdominal breathing
and Resp electrode placement 138
aberrantly conducted beats 106
accessories
10-electrode cable sets 230
3-electrode cable sets 230, 232
5-electrode cable sets 230, 232
5-electrode one piece cables 232
6-electrode cable sets 230
CO2 173
CO2 (mainstream) 239, 240
CO2 (microstream) 240
ECG 229
NBP
adult cuffs 234
comfort cuffs 233
disposable cuffs 233
multi-patient comfort cuff kits 233
neonatal/infant cuffs
(disposable) 234
reusable cuffs 233
single-hose disposable cuffs 234
Nellcor 235
pressure 234
Pulsion 234
resp 229
set combiners and organizers 231, 232
SpO2 235
Nellcor adhesive sensors
(disposable) 235
Philips sensors (disposable) 235
Philips sensors (reusable) 235
temperature 239
trunk cables 229, 231
active alarms 39
address, Philips 244
addressograph (printer configuration
setting) 209
adjusting ST measurement points 120
adjusting wave scale (pressure) 163
adjusting wave size (CO2) 174
admit
editing information 85
quick admit 85
admitting a patient 83
airway adapter
CO2, microstream accessory 173
alarm latching 50, 112
alarm limits
changing 46
checking 45
manually adjusting 46
narrow 48
report 210
ST 122
switching auto limits on/off 48
using automatic limits 48
wide 48
window 45
alarm recording
choosing recorded measurements 200
alarm source selection, disabled 135
alarms
acknowledging 42
active 39
active SpO2 source 148
alphabetical listing 53
apnea delay 176
apnea delay time (Resp) 140
arrhythmia 39
audible indicators 41
awrr limits 176
chaining 114
CO2 specific 175
CO2, apnea delay 176
CO2, awRR 176
desat, SpO2 147
effect on pressure alarms during
zero 161
extending pause time 44
high priority 39
INOP 39
ISO/IEC standard 41
key 16
limit, SpO2 260
message field 17
NBP source 154
off indicator 17
patient messages 53
pausing 43
physiological 53
pleth as source 148
recordings 51
red 39
reminder 43
restarting 44
reviewing window 49
selftest 51
silencing 42
SpO2 high and low limits 147
SpO2 specific 146
ST 122
suspended symbol 44
switching on and off 44
temperature 157
testing 51
tone configuration 41
traditional 41
visual indicators 40
volume, changing 41
yellow 39
alarms key 16
alphabetical listing of alarms 53
analog output
ECG 246
apnea alarm delay
CO2 176
apnea alarm delay time (RESP) 140
apnea alarms
and Resp detection modes 140
arrhythmia
aberrantly conducted beats 106
analysis, how it works 105
atrial fibrillation and flutter 106
beat labels 108
initiating learning 110, 111
intermittent bundle branch block 107
learning during ventricular rhythm 111
levels of analysis 102, 105
monitoring non-paced patients 106
monitoring paced patients 106
options 105
relearning 110
relearning and lead fallback 111
status messages 109
switching on/off 106
understanding the display 107
arrhythmia alarms 39, 111
adjusting alarm limits 112
all yellow on/off 112

ii
chaining 114
latching 112
multiple 114
pvc-related alarms 115
sinus and SV rhythm ranges 257, 260
switching on/off 112
timeout periods 113
arrhythmia monitoring
and defibrillation 104
arrhythmia options 102
arrhythmia relearning
with EASI INOP 101
arterial pressure source 166
arterial pulsation 143
artifact suppression (pressure) 163
atrial fibrillation and flutter 106
audlatching (arrhythmia alarms) 112
auto alarm limits
switching on/off 48
using 48
auto detection mode (Resp) 138
autofilter 94
automatic arrhythmia relearn 111
automatic default setting 27
automatic NBP
repeat time 154
autosize
ECG wave 94
awRR alarm
limits 176
awRR alarms
CO2 176
B
baseline
ST map, updating 125
ST, updating 119
basic arrhythmia option 102, 105
battery
and display brightness 221
battery reports 220
battery status window 219
charge status 220
compartment 217
conditioning 222
conserving power 221
indicators 218
LED 218
malfunction indicator 219
malfunction symbols 218
monitoring time 219
power gauge 218
recharging 217
replacing 220
safety information 222
status indicator 18, 219
symbol 245
time to empty 220
time to full 220
battery eject symbol 245
battery performance
optimizing 221
battery status indicator 18
beat labels
arrhythmia 108
bed information 33
blood pressure. See also NBP (non-invasive)
or PRESS (invasive)
Brightness SmartKey 30
brightness, adjusting 30
C
calculating cerebral perfusion 166
calculating temperature difference 158
calibrating
CO2 transducer 171
calibration
interval, NBP 226
NBP 156
pressure 165
pressure transducer 165
capnography
mainstream 14
Microstream 14
carbon dioxide, see CO2 167
cardiac overlay
and Resp detection modes 139
when measuring Resp 137
cardiotach alarms 102
cautions 9
central recorder
choosing 200
cerebral perfusion 166
chaining 114
change screen menu 23
change screen window 16, 24
Changing 23
changing ECG lead sets 96
changing Resp detection mode 138
changing Resp wave size 139
changing Resp wave speed 140
changing screen content 23
channels
recorder 200
checking battery charge 220
checking paced status 90
checklist
delivery 2
installation 1
cleaning
infection control 213
method 214
monitoring accessories 215
recommended substances 214
CO2
airway adapter 173
alarms, apnea delay 176
alarms, awRR 176
alarms, specific 175
awRR alarm limits 176
checking transducer accuracy 171
correction, humidity 175
correction, N2O 175
corrections 174
FilterLine 173
measuring mainstream 168, 171
measuring microstream 173
method, mainstream 167
method, microstream 167
method, sidestream 167
microstream accessories 173
microstream extension 173
removing exhaust gases 171, 174
transducer, calibrating 171
transducer, using 172
troubleshooting 174
wave scale, adjusting 174
CO2 (mainstream).
accessories 239, 240
CO2 (microstream).
accessories 240
conditioning batteries 222
configuration mode 22
entering 7
conflict
label 28
connecting power 4
connecting temperature probe 157
connection direction symbol 245
connectors 246
temp 157
conventional 12-lead ECG 99
correcting the NBP measurement 153
CPAP (RESP) 139
cuff
pressure, NBP 154
selection, NBP 153
current view
ST map 122
D
damage
mechanical 31
iii
damage claims 2
date, setting 7, 30
DC power symbol 245
default profile 26
default settings 271
checking country-specific 7
defibrillation
and arrhythmia monitoring 104
and ECG monitoring 104
synchronization marks 91
defibrillator proof symbol 245
defibrillator synch
maintenance interval 226
delay time
recording 201
demonstration mode 22
desat alarm, SpO2 147
detection modes (Resp) 138
diagnostic (ECG filter setting) 95
discharging a patient 85
disconnect INOPs
silencing 43
disinfecting
infection control 213
recommended substances 214
display
arrhythmia 107
ECG 91
NBP 153
Resp 138
ST 118
display brightness 221
display settings 25
disposal
gas cylinder 227
parts and accessories 227
dual Temp measurement 158
dyshemoglobins
intravascular (SpO2) 145
E
early systolic blood pressure, NBP 154
EASI
activating 95
ECG monitoring 101
lead placement 101
EASI ECG lead labels 96
ECG 89
accessories 229
alarms off (Config Mode) 103
changing lead sets 96
choosing electrode sites 95
conventional 12-lead 99
external pacing electrodes 105
filter settings 94
fusion beat pacemakers 105
intrinsic rhythm 104
modified 12-lead 99
New Lead Setup 96
pacemaker failure 104
rate adaptive pacemakers 105
unfiltered 95
wave size 93
ECG analog output 246
ECG cable
for operating room 104
ECG cables, connecting 90
ECG connector 90
ECG display 91
ECG electrode colors 96
ECG electrode placement
during electro-surgery 104
ECG gain
in reports 204
ECG lead labels 96
ECG lead placement
choosing EASI/Standard 95
ECG leads monitored 96
ECG report 211
lead layout 204
ECG safety information 104
ECG source tracking 183
ECG wave
autosize 94
calibration bar 94
ectopic status messages (arrhythmia
monitoring) 110
electrical output symbol 245
electrode placement (ECG) 89
conventional 12-lead 99
modified 12-lead 99
electrode placement (Resp) 137
with abdominal breathing 138
with lateral chest expansion 138
electro-surgery
and ECG 104
EMC interference
Resp 140
EMI filter for ECG 94
end case
discharging a patient 85
report, printing 85
end case reports
setup 205
enhanced arrhythmia option 102, 105
exclamation mark symbol 245
exhaust gases, removing 171, 174
extension cable for SpO2 144
external pacing electrodes
and ECG monitoring 105
extreme bradycardia alarm 103, 135
extreme pressure alarms 164
extreme rate alarms 103, 135
extreme tachycardia alarm 103, 135
F
fallback (ECG) 96
FAST
Fourier artefact suppression
technology 143
filter (ECG filter setting) 94
filter (ECG) 94
FilterLine
CO2, microstream accessory 173
flushing invasive pressure accessories 159
functional arterial oxygen saturation 143
fusion beat pacemakers
and ECG monitoring 105
G
gas cylinder
empty, disposing of 227
getting started 31
global trend time 195
graphic trends 188
graphic trends report 192
H
hemodynamic measurement extension 15
hemodynamic MMS extension 15
horizon trend
trend time 195
HR = RR (Resp) 138
HR alarms
when arrhythmia off 103
HR alarms off (Config Mode) 103
HR and pulse alarm source selection 135
HR from (heart rate source) 134
humidity correction
CO2 175
I
IEC ECG lead labels 96
If 183
IIT 32
IMV (Resp) 139
indicators
battery malfunction 219
battery status 18, 219
infection control
iv
cleaning 213
disinfecting 213
sterilizing 213
Information Center
central recording 199
transferring patients 86
INOPs
indicators 39
message field 17
silencing 43
installation
checklist 1
connectors 246
personnel 1
Instructions for Use
intended audience 9
IntelliVue Instrument Telemetry System
(IIT) 32
intermittent bundle branch block 107
intermittent mandatory ventilation
(Resp) 139
interruption symbol 245
intravascular dyshemoglobins (SpO2) 145
intrinsic rhythm 104
ISO point (ST) 120
J
J point (ST) 120
K
keyboard, on screen 21
keys
alarms 16
main screen 16
pop-up 21
silence 16
SmartKeys 16
L
label conflict resolution 28
label conflicts,resolving 28
labels 28
changing 28
LAN connection 4
latching
alarms 50
alarms, behavior 50
latching arrhythmia alarms 112
lateral chest expansion (neonates)
monitoring Resp 138
lead fallback
and arrhythmia relearning 111
lead fallback (ECG) 96
lead labels (ECG) 96
lead placement
activating EASI/Standard 95
for Resp measurement 137
leads monitored (ECG) 96
Leads Off INOP (ECG) 96
levels of arrhythmia analysis 105
M
main screen key 16
main setup 19
mains power
connecting to 3
mainstream
capnography 14
mainstream CO2
measuring 168, 171
maintenance
cables 225
cords 225
measurements, schedule 226
microstream CO2, calibration 226
schedule 225
visual inspection 225
malfunction symbols
battery 218
manual detection mode (Resp) 139
and apnea alarms 140
manufacture date symbol 245
manufacturer’s information 244
map
ST 122
Mason-Likar lead system 99
max hold setting (CO2) 168
measurement
adjusting a wave 27
preparation 31
setting up 27
wave speed, changing 27
measurement extension
M3012A 15
M3015A 14
M3016A 14
measurement label 17
measurement labels 28
changing 28
measurement points, ST 120
measurement server
ECG connector 90
measurement settings 25
measurement setup menu 18
measurements
setting up 31
switching on and off 27
mechanical damage 31
menu
main setup 19
measurement setup 18
merging patient data 88
messages
alarm 17
INOP 17
status and prompt 18
methemoglobin (SpO2) 145
Microstream capnography 14
microstream CO2 173
accessories 173
maintenance, calibration 226
measuring 173
mismatch
patient data, resolving 87
MMS extensions 14
modified 12-lead ECG 99
modifying
screens 23
monitor
inspecting before use 31
quick operating giude 6
starting monitoring 32
switching on 31
monitor (ECG filter setting) 94
monitor defaults 271
monitor revision
how to find 30
monitor settings 25
changing 30
monitoring
preparation 31
starting 31
monitoring mode 22
mounting
power supply 3
mounting information 3
MSL cable 4
multi-lead ST alarming 122
N
N2O correction
CO2 175
narrow alarm limits 48
NBP
adult cuffs 234
alarm source 154
ANSI/AAMI SP10-1992 151
automatic mode, enabling 154
calibrating 156
calibration interval 226
comfort cuff kits 233
comfort cuffs 233

v
cuff pressure 154
cuff, applying 153
cuff, selecting 153
cuff, tightness 153
disposable cuffs 233
how the measurement works 151
measurement correction 153
measurement limitations 152
measurement methods, auto 152
measurement methods, manual 152
measurement methods, sequence 152
measurement methods, stat 152
measurement, starting 154
measurement, stopping 154
neonatal cuffs (disposable) 234
numerics 153
oscillometric method 151
pediatric cuffs 234
preparing to measure 152
repeat time 153
repeat time for automatic 154
repetition time, setting 154
reusable cuffs 233
single-hose disposable cuffs 234
site inspection 153
time of last measurement 153
units 153
venous puncture 155
neonates
Resp electrode placement 138
network connection indicator 17
networked monitoring 33
new features 35
non-invasive blood pressure. See NBP
non-paced patients
arrhythmia monitoring 106
numerics
explanation of NBP display 153
O
on-screen keyboard 21
operating modes 22
configuration 22
demonstration 22
monitoring 22
passcode protection 22
service 22
operating room ECG cable 104
orange ECG cable 104
organizers 231, 232
Oridion Systems Ltd 244
oscillometric NBP measurement
method 151
overlap
in recordings 201
overlapping screen trends 195
P
pace pulse rejection (ECG)
about 91
switching on/off 93
paced patients
arrhythmia monitoring 106
repolarization tails 93
safety information 104
setting status 104
paced status 17
checking 90
pacemaker failure 104
paper size
for reports 206
parameter scales
trends 191
passcode protection 22
patient
admit 83
category, NBP 151
discharge 85
end case 85
patient alarm messages 53
patient category field 17
patient demographics window 83
patient mismatch 87
patient name field 17
patient reports
contents 209
patient trends
viewing 187
paused alarms 43
extending time 44
restarting 44
performance specifications
pressure 255, 262
performance test 267
perfusion indicator 143, 144, 148
Philips contact information 244
physiological alarms 39
pleth alarm source 148
pleth wave 147
pleth waveform 143
Pop 21
pop-up keys 21
power
connecting 4
connection 3
disconnecting from
mains power
disconnecting from 32
power supply 4
mounting 3
power-on LED 4
preparing skin
for ECG 89
pressure
alarms during zero 161
arterial source 166
calibration pressure 165
cerebral perfusion, calculating 166
performance specifications 255, 262
wave scale 163
wave size 163
zeroing the transducer 161
pressure accessories 234
pressure artifact suppression 163
pressure of NBP cuff 154
pressure transducer
calibration 165
zeroing 161
primary lead (ECG)
selecting 90
print job
suspended 207
printer
disabling 206
settings 206
status messages 208
unavailable 207
printing
ST map reports 126
status log 227
trends reports 192
priority list for trends 191
probes
disposable temperature 157
profiles 25
default profile 26
patient category 26
swapping a complete profile 26
swapping setting block 26
prompts 18
pulse
alarms 134
system pulse source 133
pulse numerics for SpO2 144
PVC-related alarms 115
Q
QRS tone 135
changing volume 30
QRS tone pitch, SpO2 148
QRS volume, changing 94
QT alarms 130
QT baseline 129
QT measurement algorithm 127
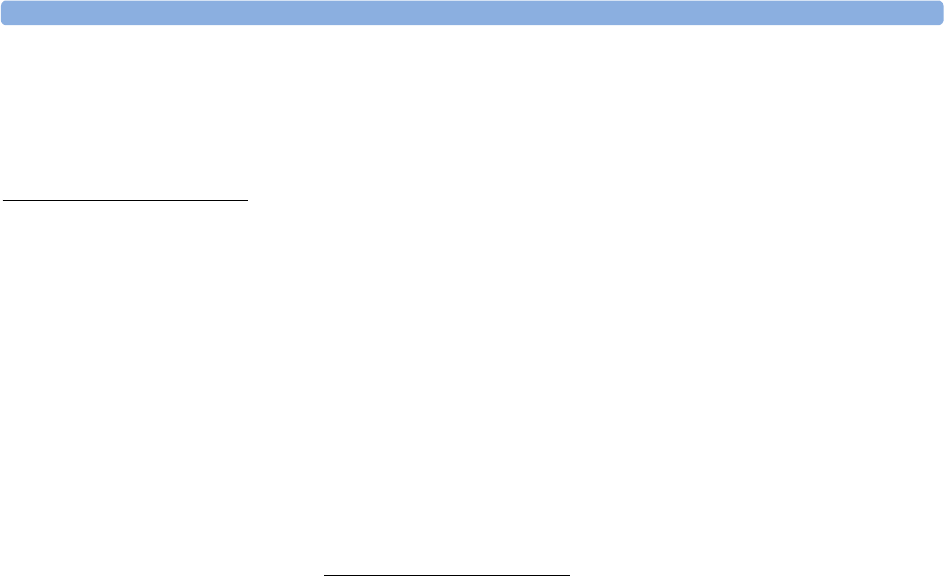
vi
QT monitoring
limitations 128
QT/QTc monitoring 127
quick admit 85
R
radiated field immunity
Resp 140
rate adaptive pacemakers
and ECG monitoring 105
realtime report 210
realtime reports
content 206
recorder status messages 201
recording
central 199
changing recording type 200
channels 200
choosing central recorder 200
choosing recording speed 201
creating templates 200
preventing fading ink 201
runtime 201
setting the runtime 201
setup menu 200
starting and stopping 199
wave overlap 201
recording alarms 51
recording delay time 201
recycling 227
rejecting pace pulses 91
relearning arrhythmia 110
reminder, alarm 43
replacing batteries 220
repolarization tails 93
reports
alarm limits 210
battery reports 220
choosing paper size 206
contents 209
ECG 211
end case 205
patient trends 192
realtime report 210
re-routing 207
scheduled 205
setting up 204
ST map 126
stopping printouts 204
re-routing reports 207
resolution
trends 191
resolving patient mismatch 87
resp accessories 229
Resp alarms
apnea alarm delay time 140
Resp detection level
and apnea detection 140
Resp detection modes
and cardiac overlay 139
changing 138
Resp display 138
Resp monitoring
and cardiac overlay 137
Resp safety information 140
Resp wave
changing size 139
changing speed 140
restarting paused alarms 44
retrolental fibroplasia (SpO2) 147
reviewing alarms window 49
rhythm status messages (arrhythmia
monitoring) 109
runtime
setting recording runtime 201
S
safety
maintenance interval 226
monitor 246
safety information
batteries 222
ECG 104
Resp 140
safety test 267
safety tests
performance tests 5
power on test 5
system 5
visual inspection 5
same patient data merge 88
scale
ECG wave 93
Resp wave 139
scales
for trends waveforms 191
scheduled reports 205
screen
adjusting brightness 30
screen trend
trend time 195
screen trends 193
screens
changing content 23
switching 23
understanding 23
visitor screen 24
secondary lead (ECG)
selecting 90
selecting the primary lead (ECG) 90
selecting the secondary lead (ECG) 90
selftest
alarms 51
sensor
disposable SpO2 143
sequence mode 154
service mode 22
set combiners 231, 232
setting up
trends 189
setting up reports 204
setting up the sepuence 154
settings 26
about 26
default 271
measurement settings 26
monitor settings 26
screen settings 26
synchronized telemetry and
monitor 183
settings blocks 25
Setup Recording menu 200
short yellow alarms on/off 112
signal quality of SpO2 145
silence key 16
sinus and SV rhythm ranges 257, 260
skin preparation
ECG 89
SmartKeys 19
key 16
SmartKeys key 16
SmartKeys symbol 245
source tracking
ECG 183
specifications 243
arrhythmia 255
speed
recording 201
wave speed, changing 27
SpO2
accessories 235
active alarm source 148
alarms specific to 146
arterial pulsation 143
assessing suspicious reading 145
connecting the cables 144
disposable sensors 143
extension cable 144
FAST technology 143
Nellcor adhesive sensors
(disposable) 235
perfusion indicator 143, 144, 148
Philips sensors (disposable) 235
Philips sensors (reusable) 235
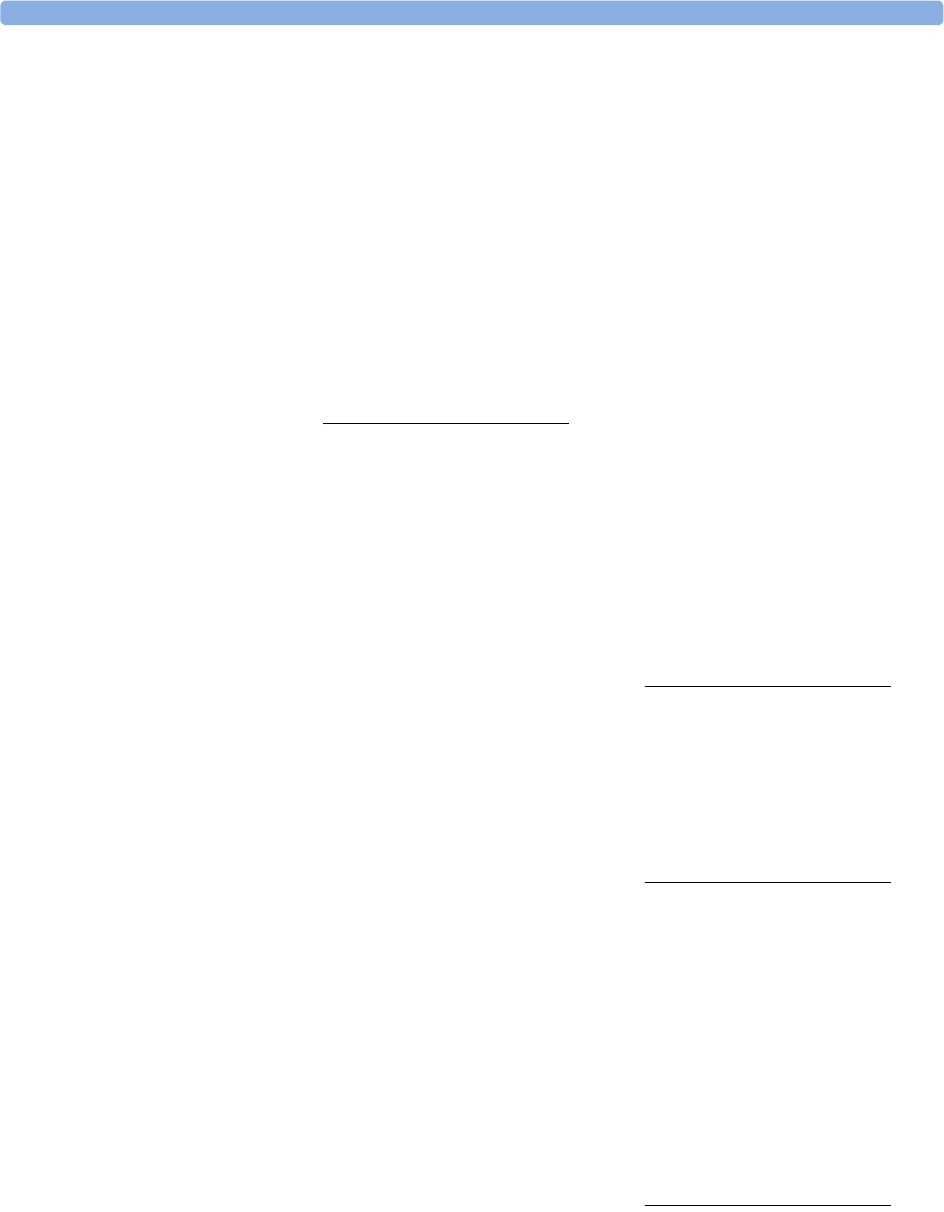
vii
pleth as alarm source 148
pleth wave 147
pleth waveform 143
pulse numerics 144
QRS tone 148
signal quality 145
site inspection 145
site selection 143
tone modulation 148
SpO2 desat alarm 147
SpO2 limit alarms 147
ST
adjusting alarm limits 122
alarms 102, 122
baseline, updating 119
ensuring diagnostic quality 117
filtering 117
measurement points, adjusting
adjusting 120
multi-lead alarms 122
numerics in ECG wave 92
snippets 119
ST display 118
ST map
baseline, updating 125
current view 122
report, printing
printing
ST map report 126
scale, changing
scale
ST map 125
task window 125
trend view 124
trending interval, changing 126
trending priority 125
ST maps 122
ST point 120
standard 10-lead placement 99
standard 3-lead placement 97
standard 5-lead placement (ECG) 97
standby mode 22
Standby screen 22
standby symbol 245
starting monitoring 32
status line 18
status log
printing 227
status messages
printer 208
recorder 201
status messages (arrhythmia) 109
ectopic 110
rhythm 109
sterilizing
infection control 213
stopping reports printouts 204
surgical ECG cable 104
suspended alarm 44
suspicious SpO2 reading 145
switching on
monitor 31
switching screens 23
symbols 244
battery 218
synchronization marks (defibrillator) 91
system pulse 133
systolic blood pressure, NBP, early 154
T
tabular trends 189
Tamb 158
task window for ST map 125
Tcereb 158
telemetry alarms 181
suspending at bedside 181
telemetry device
controlling from bedside 181
silencing alarms at bedside 181
unpairing 180
temperature 157
accessories 239
alarm settings 157
connecting probe to monitor 157
difference, calculating 158
dual Temp measurement 158
extended label set 158
first 158
label 158
making a measurement 157
probe, disposable 157
probe, selecting 157
second 158
temperature probe
connecting 157
templates
creating for recordings 200
test blocks, how to perform 5
testing alarms 51
time, setting 7, 30
tone configuration, alarm 41
tone mod (SpO2) 148
tone modulation 148
touchscreen
disable/re-enable 16
using 18
transducer
CO2, accuracy 171
CO2, calibrating 171
pressure, zeroing 161
transferring centrally-monitored
patients 86
transport brightness setting 221
trend time 195
global 195
trend view
ST map 124
trending interval
ST map 126
trends
resolution 191
screen trends 193
setting parameter scales 191
setup 189
viewing 187
trends pop-up keys 187
trends priority list 191
ST map 125
troubleshooting
CO2 174
trunk cables
accessories 229, 231
Ttymp 158
Tvesic 158
U
Understanding 25
unfiltered ECG signal 95
unpacking 2
unpairing 180
user interface settings
changing 30
V
V electrode placement (ECG) 98
venous puncture 155
viewing arrhythmia waves 108
viewing trends 187
visible waves report 206
visitor screen 24
vislatching (arrhythmia alarms) 112
vital signs report 192
voltage setting 4
volume
alarm 41
W
warnings 9
wave
adjusting 27
changing speed 27
scale (CO2) 174
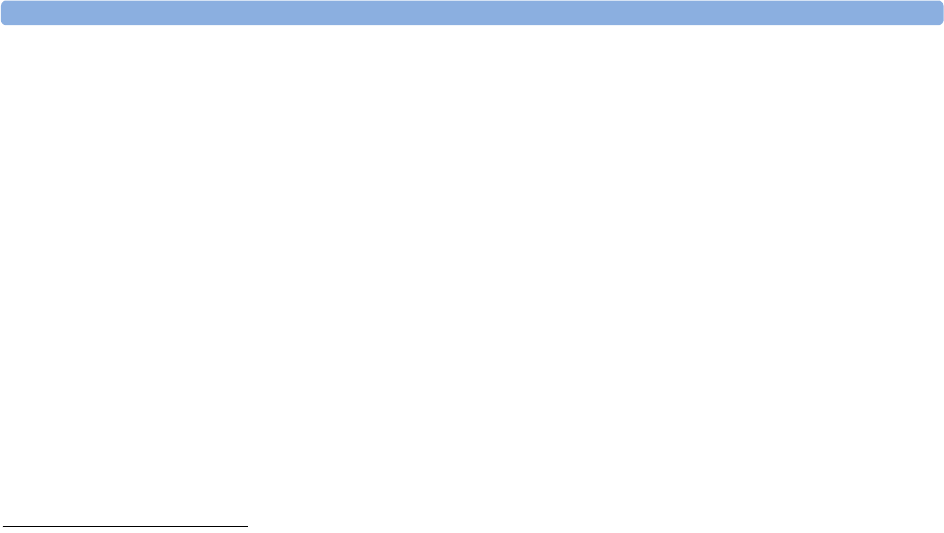
viii
scale (pressure) 163
size (CO2) 174
size (pressure) 163
wave channel speed 28
wave group speed 28
wave size
Resp 139
wave size (ECG)
changing 93
wave speed
eeg speed
wave speed
global speed 27
respiratory speed 27
wave speed (Resp) 140
what’s new 35
wide alarms limits 48
wired network connection symbol 245
Z
zero
effect on pressure alarms 161
zeroing
pressure transducer 161