Philips 89000 User Manual Rotational IVUS Image Interpretation Pocket Guide Revolution
User Manual: Philips 89000 Rotational IVUS image interpretation pocket guide Philips Volcano - Revolution 45 MHz rotational IVUS imaging catheter89000
Open the PDF directly: View PDF ![]() .
.
Page Count: 16
Catheter
Rotational IVUS
Image Interpretation Pocket Guide

4 5
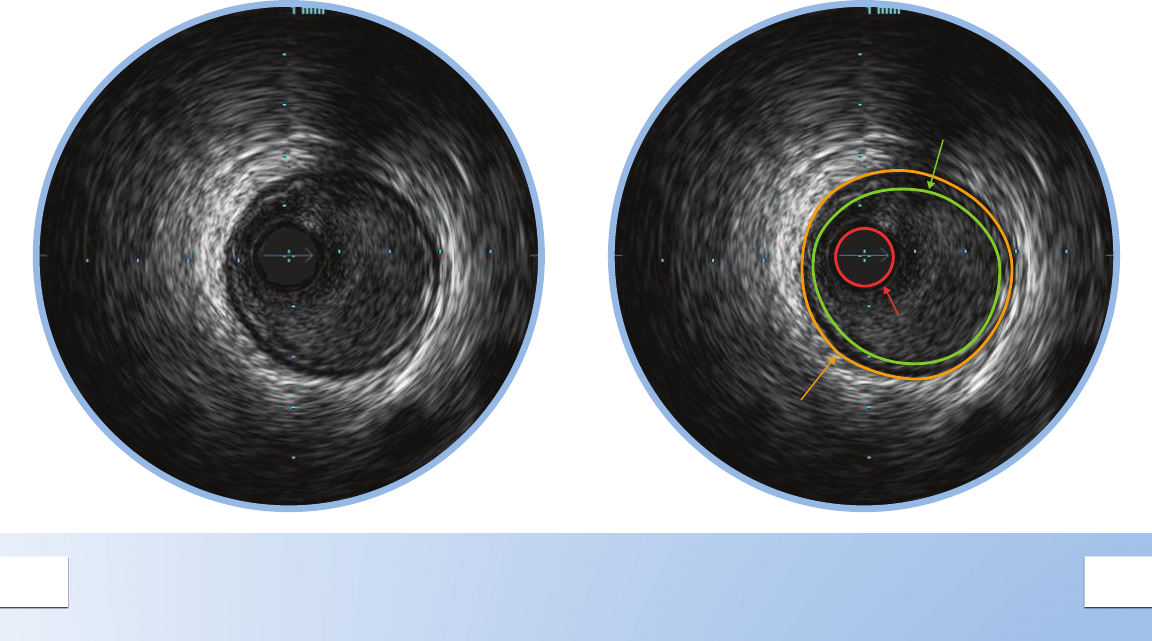
Vessel Border
Lumen Border
Catheter
Mask
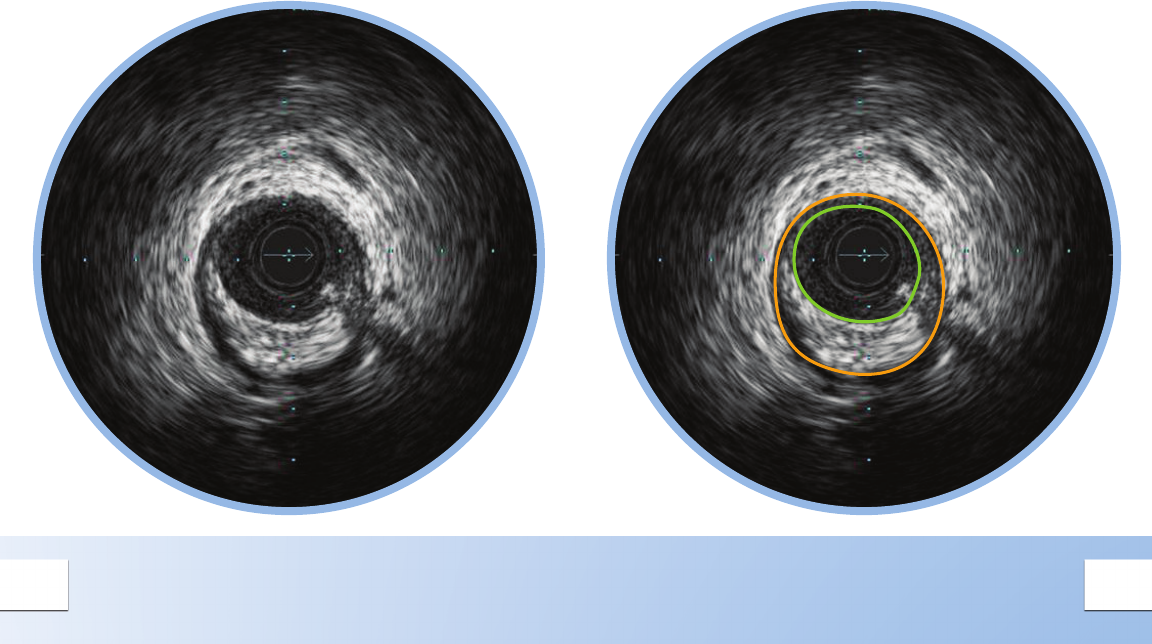
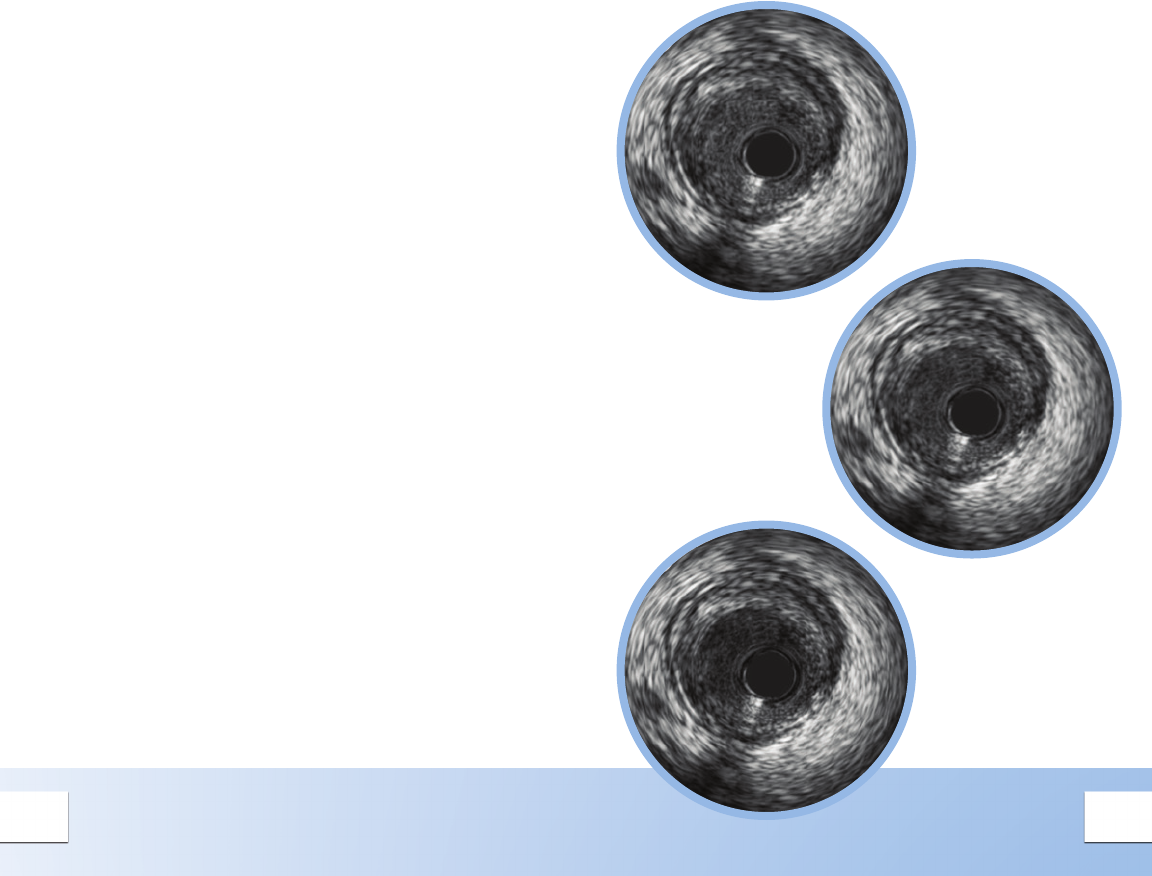
NORMAL VESSEL
In a normal vessel, the lumen border is almost
indistinguishable from the vessel border. While
IVUS allows visualization of vessel and lumen,
angiograms only provide a shadow of the
lumen. In patients with diffuse disease, relying
on the angiogram alone can potentially lead to
underestimation of stenosis.
The lumen border is drawn inside the intima
or plaque.
The intimal layer is normally not seen unless it has
begun to thicken.
The catheter mask (red area) indicates the location
of the ultrasound transducer.
The media is the dark band between the adventitia
and the intima.
6 7
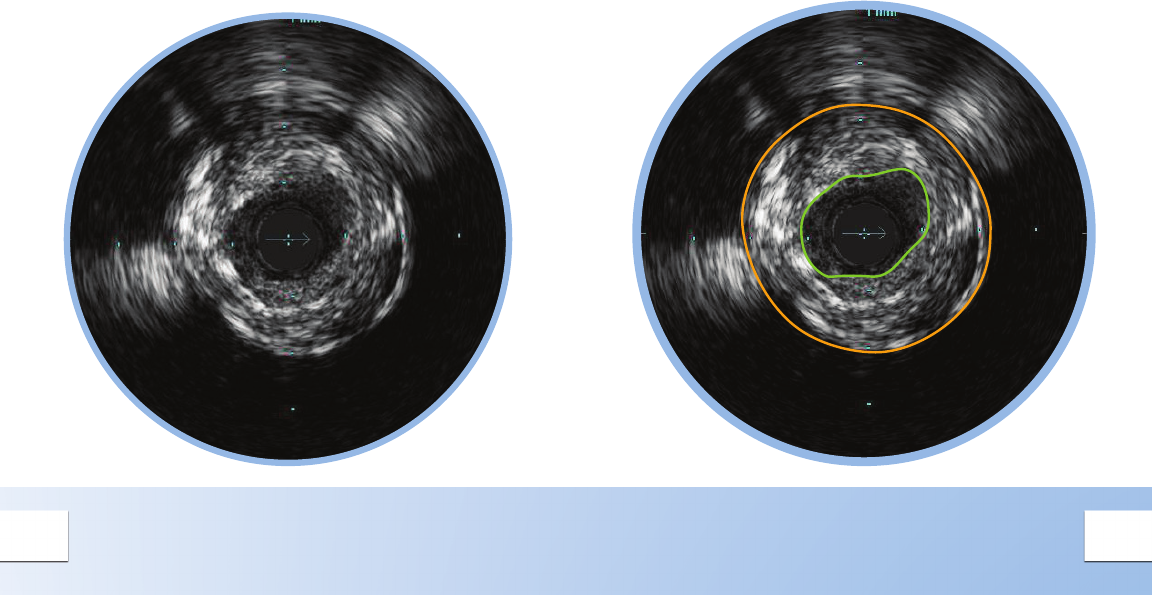
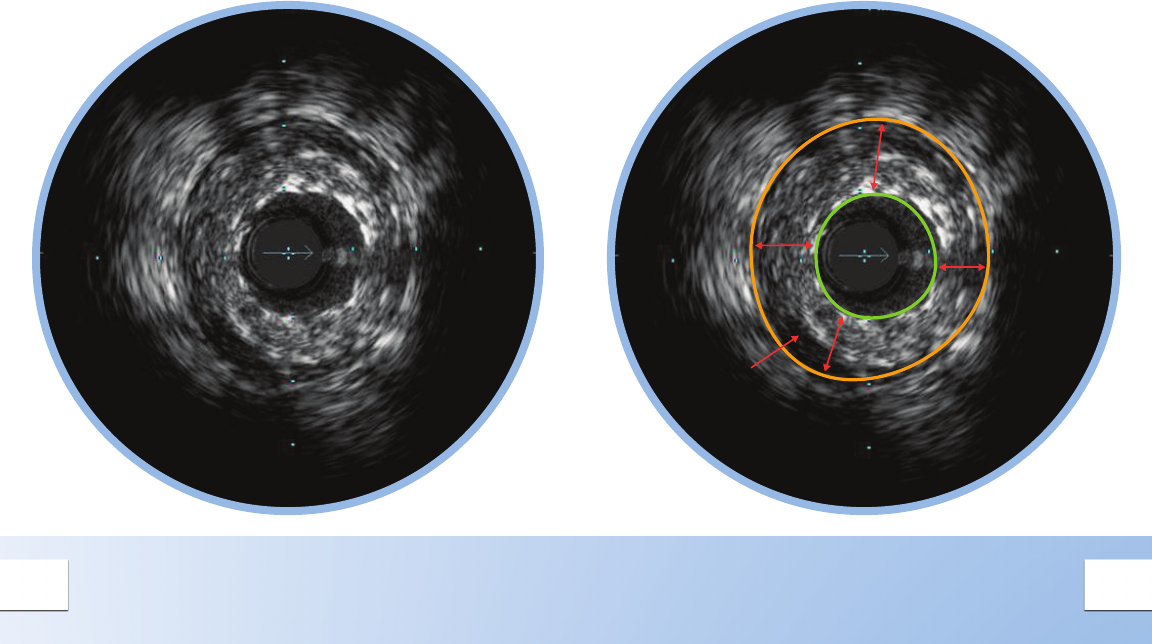
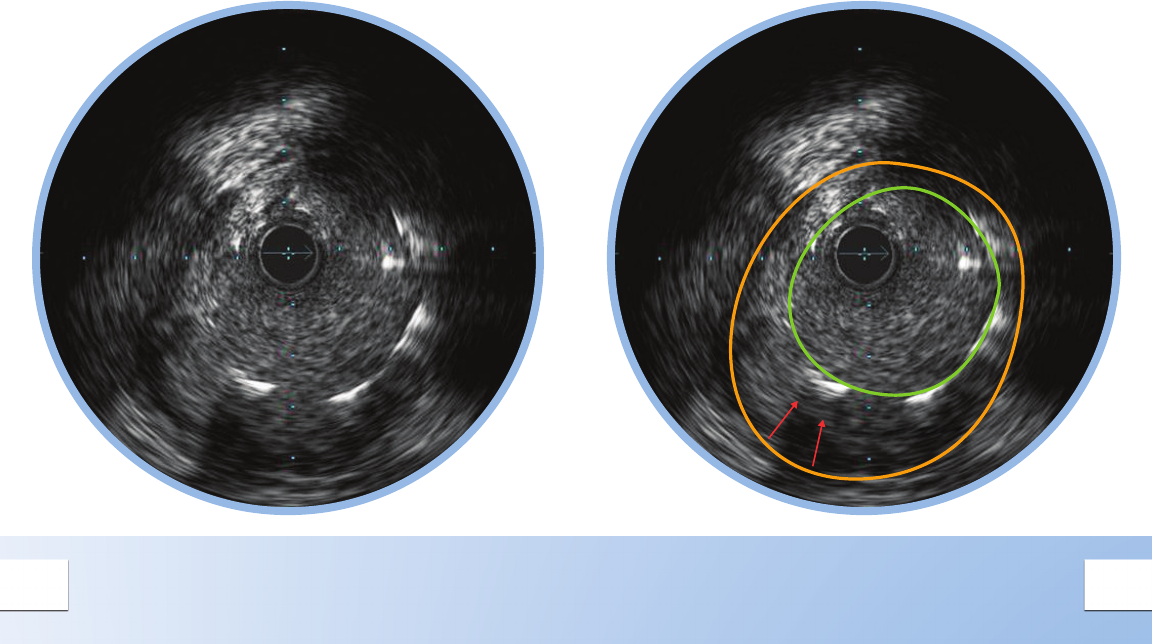
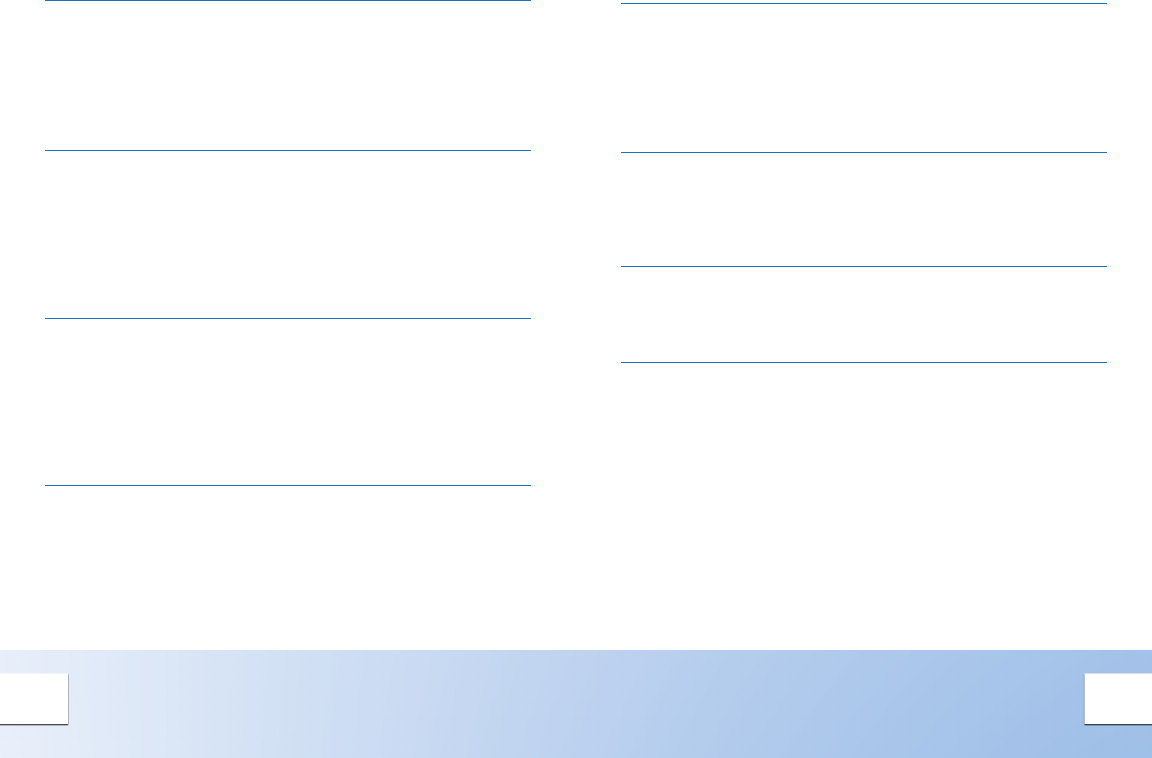
CONCENTRIC MIXED PLAQUE
Concentric plaques are distributed
circumferentially in the vessel.
Concentric plaques tend to occur in areas of
negative remodeling; use of angiography alone
could result in too large a stent diameter.
Mixed plaque is a combination of tissues of varying
echogenecity. The distribution of light and dark
may be distinct, or light and dark variations may be
intermingled as shown here.
Minimum Lumen Area (MLA) can dene a threshold
for a signicant stenosis to determine the need for
catheter-based or surgical intervention.
• MLA < 4 mm2 in LAD, LCX, and RCA vessels > 3
mm in diameter correlates with physiological
signicance1
• MLA < 6 mm2 in left main correlates with FFR <
0.75 indicating physiological signicance1,2,3
1. Jasti, et al. Correlations between fractional ow reserve and
intravascular ultrasound in patients with an ambiguous left main
coronary artery stenosis Circulation, 2004;110:2831-2836.
2. Jose M. de la Torre Hernandez et al. Prospective Application of
Pre-Dened Intravascular Ultrasound Criteria for Assessment of
Intermediate Left Main Coronary Artery Lesions: Results From the
Multicenter LITRO Study, J Am Coll Cardiol, 2011 58: 351-358.
3. Levine et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous
Coronary Intervention. J Am Coll Cardiol, 2011; 58:44-122.
8 9
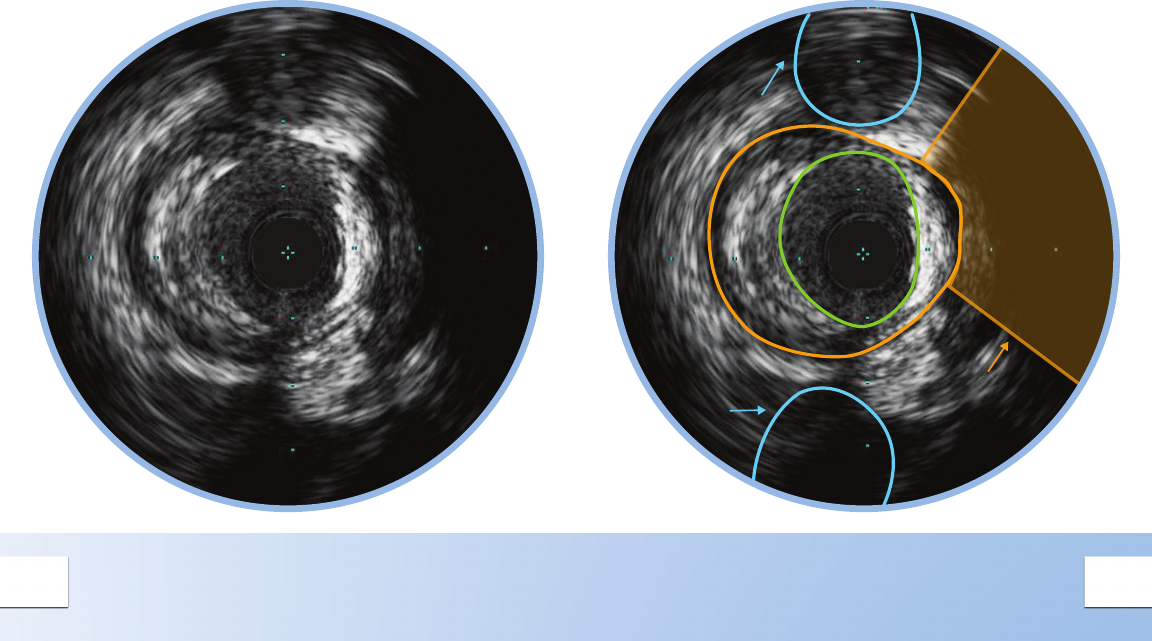
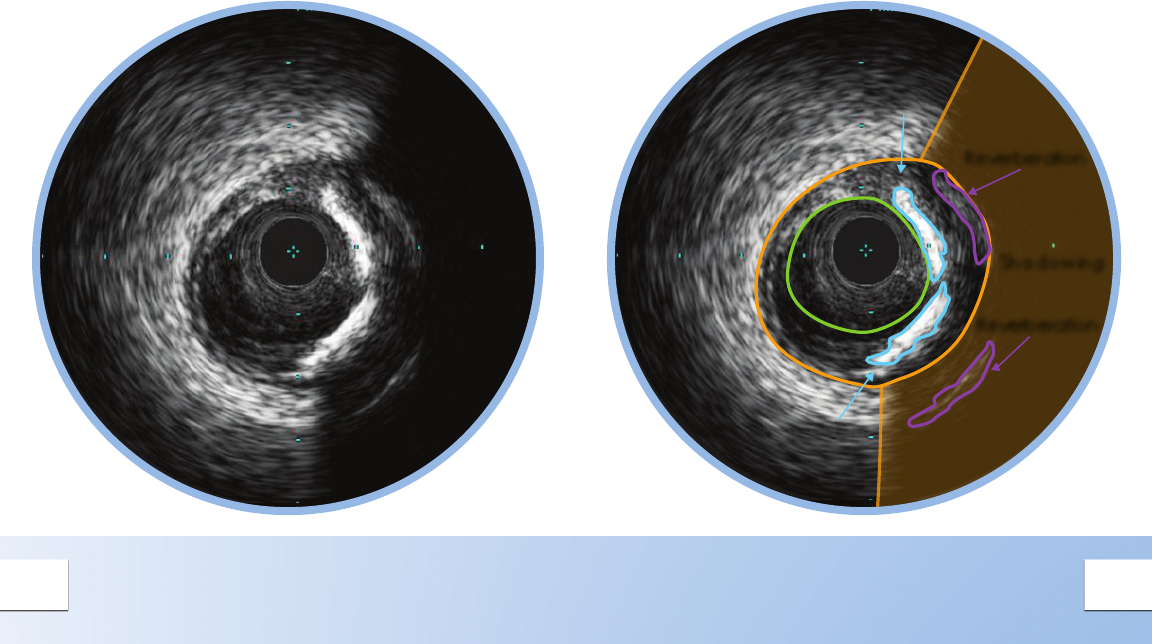
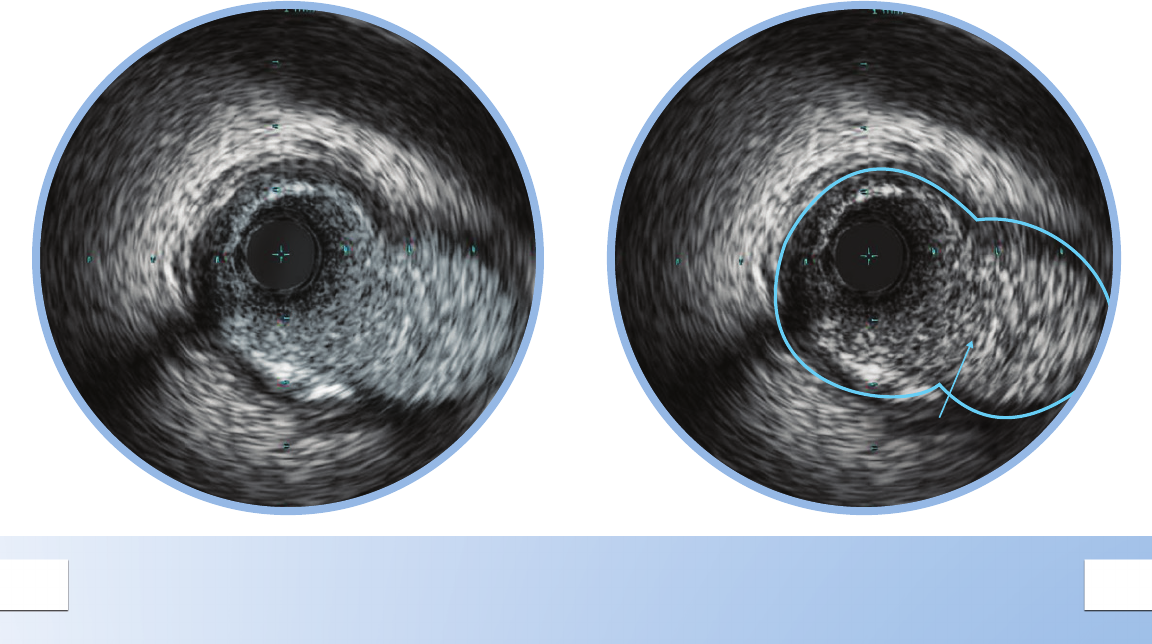
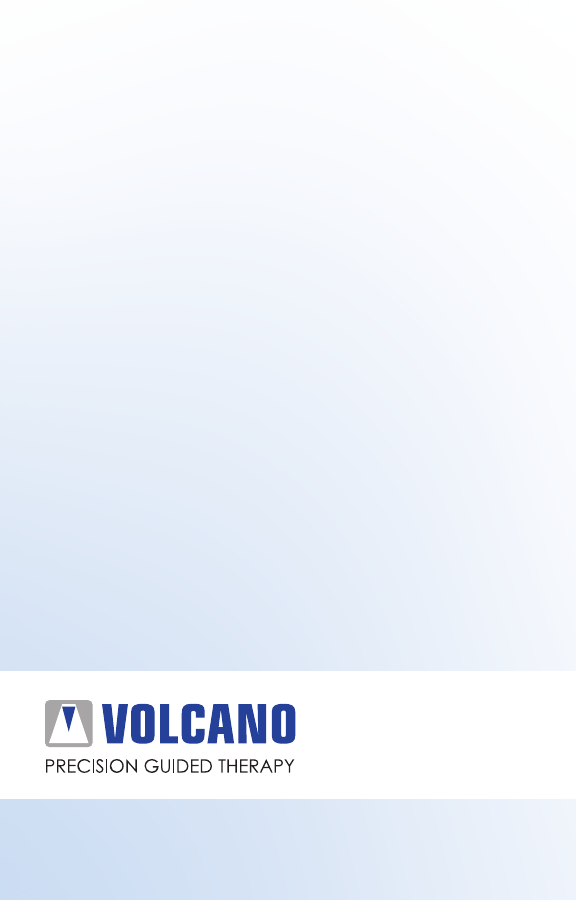
ECCENTRIC MIXED PLAQUE
Eccentric plaques are distributed non-
circumferentially in the vessel; this makes the
assessment of disease by angiography especially
prone to underestimation or overestimation
depending on the angle of view.
Side
Branch
Side
Branch Acoustic
Shadowing
Calcium is indicated by very bright areas with
acoustic shadowing that blocks out the image
behind. This shadowing occurs because the high
density of calcium dampens the ultrasound echo.
Nearby vessels on the periphery can be seen
moving in and out of the eld of view and can be
used as landmarks.
10 11
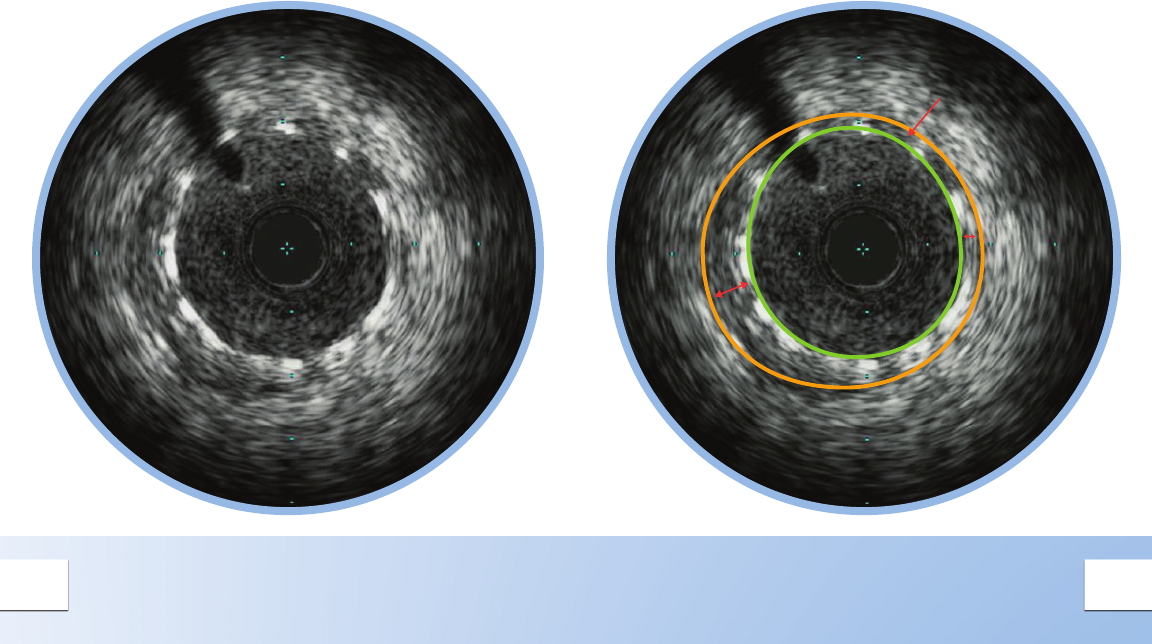
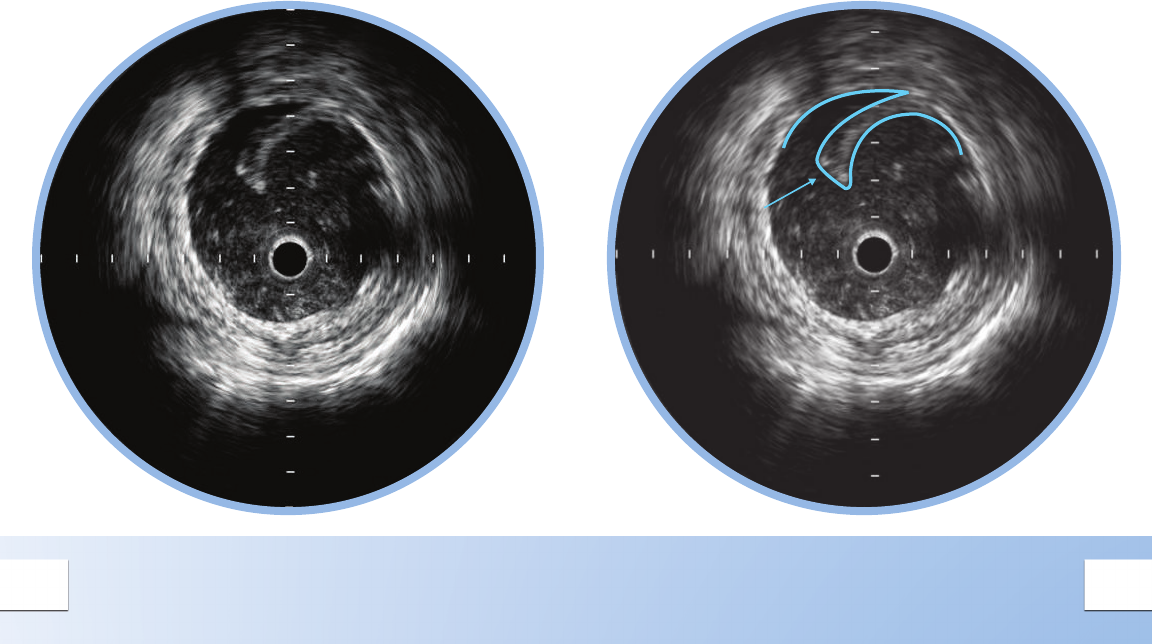
FIBROUS PLAQUE
These plaques have an intermediate echogenicity
between soft (echolucent) atheromas and highly
echogenic calcic plaques.
Fibrous plaques exhibit little or no
acoustic shadowing.
12 13
Calcium
Shadowing
Reverberation
Reverberation
Calcium
PLAQUE WITH CALCIUM
There are two large bands of calcium in this plaque
with acoustic shadowing arcs behind them.
Calcium is indicated by very bright areas with acoustic
shadowing that blocks out the image behind it.
Reverberations may also been seen. This shadowing
occurs because the high density of calcium prevents the
ultrasound from passing through.
Detection of calcium is a critical factor in
determining the optimal PCI strategy.
Study data comparing IVUS and angiographic
based assessments of calcium reported that IVUS
detected calcium signicantly more often.*
*Mintz et al. Patterns of calcication in coronary artery disease.
Circulation 1995; 91:1959-1965.
14 15
Area of
Under Expansion
UNDER EXPANDED STENT
Stent struts appear as bright marks spaced around
the lumen (eleven struts seen here).
Large presence of plaque behind stent struts may
indicate under-expansion.
Device size is an independent predictor of
stent thrombosis*
* Witzenbichler et al. Relationship Between Intravascular Ultrasound
Guidance and Clinical Outcomes After Drug-Eluting Stents: The
ADAPT-DES Study. Circulation. Published online November 26, 2013.
16 17
Area of
Complete
Apposition
STENT WITH COMPLETE
APPOSITION
Complete apposition is indicated by consistent
stent strut contact with tissue.
Complete apposition does not guarantee that a
stent is not under-sized or under-expanded.
18 19
Area of
Malapposition
STENT WITH MALAPPOSITION
Malapposition is indicated by blood visible
behind stent struts.
Blood may appear as a very faint speckle or
black on grayscale IVUS.
Stents may be completely or only partially
malapposed depending on how much of the
stent is in contact with the lumen wall.
20 21
Side Branches
Merging
VESSEL BRANCHES MERGING
Nearby side branches can act as landmarks.
Side branches can be used to determine where
or where not to stent within a vessel.
22 23
Dissection
Area
VEIN GRAFT DISSECTION
A dissection, or tear in the vessel wall can be
seen as a ap with blood ow behind it.
Only the intimal layer is dissected.
When detecting a dissection, the catheter may be
ushed with contrast to reduce the blood speckle.
24 25
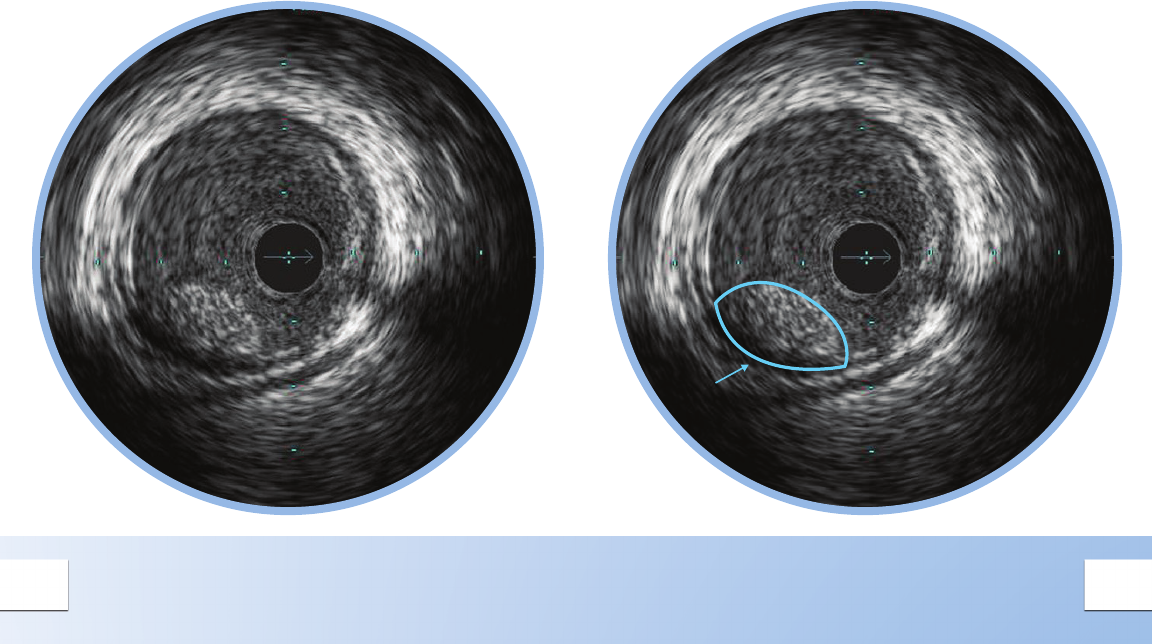
Thrombus
INTRA LUMINAL THROMBUS
Thrombus is usually circular in appearance and
non-stationary.
When viewed during a pullback, thrombus rst
appears small in size becoming larger and then
smaller again.
When detecting a thrombus, the catheter may be
ushed with contrast to highlight the contours.
26 27
HI-Q™ IMAGING OPTIONS
Hi-Q™ Imaging1 Allows You to
Customize Your Image to Better
Identify Lumen Features
Choose from three high quality2, optimized imaging
modes with different levels of darkness and neness of
blood speckle:
May help differentiate between tissue and blood
along the lumen border
May help identify stent struts, dissection, or other
lumen features
1. Available on all Revolution® catheters when using
v3.3 software or higher.
2. Catheter must be plugged in with Image On;
Selection accessible via the Adjust Image Menu.
Hi-Q OFF
Imaging
equivalent to
systems with
software versions
prior to v.3.3.
Hi-Q LEVEL 2
Imaging with an
even darker and
ner blood speckle
appearance than in
the Level 1 mode.
Hi-Q LEVEL 1
Imaging with a darker
and ner blood
speckle appearance
than in the Off mode.
Level is also the default
mode1 for new systems.
28 29
Calcium
Angiography
Less sensitive than IVUS for
detecting calcium1
IVUS
Makes the presence of
calcium clear, helping to
identify lesions that need
pre-treatment.
Dissection
Angiography
Cannot determine where
the dissection begins.
IVUS
Can be determined.
Thrombus
Angiography
Difcult to determine.
IVUS
Can be determined.
Side Branches Merging
Angiography
Cannot tell how diseased
the vessels are.
IVUS
Helps to determine where to
place or not place a stent as
well as providing information
on the disease state in the
ostium and side branch.
1. Reference vessels are diseased 93% of the time.
Mintz et al. Patterns of Calcication in Coronary Artery Disease A
Statistical Analysis of Intravascular Ultrasound and Coronary Angi-
ography in 1155 Lesions JACC 25; 7:1479-85, June 1995.
See What You’ve Been
Missing With IVUS
Stent Sizing
Angiography
Must rely on “eyeball”
estimate.
IVUS
Enables you to make
lumen and reference vessel
measurements that can be
used when selecting stent size.
Stent Expansion and Apposition
Angiography
Cannot see the vessel wall to
verify optimal placement.
IVUS
User-dened cross-sectional
area measurements and
views allow verication and
documentation of stent
placement.
Normal Vessels vs. Diffuse Disease
Angiography
Tends to underestimate
degree of stenosis in diffuse
disease1 or with positive
remodeling.
IVUS
Helps you distinguish normal
from abnormal vessels and
nd the location of disease
in patients with a normal
angiogram.
Concentric and Eccentric Plaques
Angiography
Must rely on “eyeball”
estimate. Assessment of
eccentric plaque lesion size
especially prone to error
based on angle of view.
IVUS
Helps you get an accurate
lumen area to determine
lesion signicance and
stent size.
Volcano Corporation
Corporate Headquarters
3721 Valley Centre Drive, Suite 500
San Diego, CA 92130 USA
Phone: 800-228-4728
Fax: 858-720-0325
Volcano Corporation
Manufacturing Headquarters
2870 Kilgore Road
Rancho Cordova, CA 95670 USA
Phone: 800-228-4728
Fax: 916-638-8812
Volcano Europe SPRL/BVBA
Europe Headquarters
Excelsiorlaan 41
B-1930 Zaventem Belgium
Phone: +32-2-679-1076
Fax: +32-2-679-1079
Volcano Japan Co., Ltd
Japan Headquarters
Hamamatsucho Square 6F
1-30-5, Hamamatsucho,
Minato-ku, Tokyo 105-0013, Japan
Phone: +81-3-6430-9400
Fax: +81-3-6430-9401
600-0000.01/002
Volcano, the Volcano logo, and Revolution are registered
trademarks of Volcano Corporation. Hi-Q is a trademark
of Volcano Corporation.
