Boston Scientific CRMV17311 K172, K173, K174, K175, K176, K177, K062, K063, K064, K065, K066, K067, K272, K 273, K274, K275, K276, K277, V272, V273, V172, V173, K278, K279 User Manual wrench rotation side
Boston Scientific Corporation K172, K173, K174, K175, K176, K177, K062, K063, K064, K065, K066, K067, K272, K 273, K274, K275, K276, K277, V272, V273, V172, V173, K278, K279 wrench rotation side
User Manual
PHYSICIAN’S TECHNICAL MANUAL
INGENIO™
PACEMAKER
Model K172, K173, K174
CAUTION: Federal law (USA)
restricts this device to sale by
or on the order of a physician
trained or experienced in
device implant and follow-up
procedures.


Table of Contents
Additional Technical Information................................................................................. 1
Device Description...................................................................................................... 1
Related Information .................................................................................................... 3
Indications and Usage ................................................................................................ 3
Contraindications........................................................................................................ 5
Warnings .................................................................................................................... 6
Precautions................................................................................................................. 8
Supplemental Precautionary Information ................................................................. 27
Post-Therapy Pulse Generator Follow Up........................................................ 27
Transcutaneous Electrical Nerve Stimulation (TENS)...................................... 29
Electrocautery and Radio Frequency (RF) Ablation......................................... 31
Ionizing Radiation............................................................................................. 33
Elevated Pressures .......................................................................................... 34
Potential Adverse Events ......................................................................................... 37
Mechanical Specifications ........................................................................................ 39
Items Included in Package ....................................................................................... 41
Symbols on Packaging ............................................................................................. 42
Characteristics as Shipped....................................................................................... 45
X-Ray Identifier......................................................................................................... 47
Federal Communications Commission (FCC) .......................................................... 48
Pulse Generator Longevity ....................................................................................... 49
Warranty Information ................................................................................................ 55

Product Reliability..................................................................................................... 55
Patient Counseling Information ................................................................................ 56
Patient Handbook............................................................................................. 57
Lead Connections..................................................................................................... 58
Implanting the Pulse Generator................................................................................ 59
Step A: Check Equipment.............................................................................. 60
Step B: Interrogate and Check the Pulse Generator ..................................... 60
Step C: Implant the Lead System .................................................................. 61
Step D: Take Baseline Measurements........................................................... 62
Step E: Form the Implantation Pocket ........................................................... 64
Step F: Connect the Leads to the Pulse Generator....................................... 66
Step G: Evaluate Lead Signals...................................................................... 71
Step H: Program the Pulse Generator ........................................................... 72
Step I: Implant the Pulse Generator .............................................................. 72
Step J: Complete and Return the Implantation Form .................................... 73
Bidirectional Torque Wrench..................................................................................... 74
Follow Up Testing ..................................................................................................... 76
Predischarge Follow Up ................................................................................... 77
Routine Follow Up ............................................................................................ 77
Explantation.............................................................................................................. 79

ADDITIONAL TECHNICAL INFORMATION
For additional technical reference guides, go to www.bostonscientific.com/ifu.
Boston Scientific Corporation acquired Guidant Corporation in April 2006. During
our transition period, you may see both the Boston Scientific and Guidant names on
product and patient material. As we work through the transition, we will continue to
offer doctors and their patients technologically advanced and high quality medical
devices and therapies.
DEVICE DESCRIPTION
This manual contains information about the INGENIO family of implantable
pacemakers, including the following types of pulse generators (specific models are
listed in "Mechanical Specifications" on page 39):
• SR—single chamber pacemaker providing ventricular or atrial pacing and sensing
• DR—dual-chamber pacemaker providing ventricular and atrial pacing and sensing
Therapies
These pulse generators provide bradycardia pacing and adaptive rate pacing to detect
and treat bradyarrhythmias.
1
Leads
The pulse generator has independently programmable outputs and accepts one or
more of the following leads, depending on the model:
•OneIS-1
1unipolar or bipolar atrial lead
• One IS-1 unipolar or bipolar right ventricular lead
NOTE: Single-chamber devices will accept either an IS-1 atrial or an IS-1
ventricular lead.
The pulse generator and the leads constitute the implantable portion of the pulse
generator system.
PRM System
These pulse generators can be used only with the ZOOM LATITUDE Programming
System, which is the external portion of the pulse generator system and includes:
• Model 3120 Programmer/Recorder/Monitor (PRM)
• Model 2869 ZOOMVIEW Software Application
• Model 6577 Accessory Telemetry Wand
1. IS-1 refers to the international standard ISO 5841-3:2000.
2

You can use the PRM system to do the following:
• Interrogate the pulse generator
• Program the pulse generator to provide a variety of therapy options
• Access the pulse generator’s diagnostic features
• Perform noninvasive diagnostic testing
• Access therapy history data
RELATED INFORMATION
Refer to the lead’s instruction manual for implant information, general warnings
and precautions, indications, contraindications, and technical specifications. Read
this material carefully for implant procedure instructions specific to the chosen lead
configurations.
Refer to the PRM system Operator’s Manual for specific information about the PRM
such as setup, maintenance, and handling.
INDICATIONS AND USAGE
Boston Scientific pacemakers are indicated for treatment of the following conditions:
• Symptomatic paroxysmal or permanent second- or third-degree AV block
• Symptomatic bilateral bundle branch block
3

• Symptomatic paroxysmal or transient sinus node dysfunction with or without
associated AV conduction disorders (i.e., sinus bradycardia, sinus arrest, sinoatrial
[SA] block
• Bradycardia-tachycardia syndrome, to prevent symptomatic bradycardia or some
forms of symptomatic tachyarrhythmias
• Neurovascular (vaso-vagal) syndromes or hypersensitive carotid sinus syndromes
Adaptive-rate pacing is indicated for patients exhibiting chronotropic incompetence and
who may benefit from increased pacing rates concurrent with increases in minute
ventilation and/or level of physical activity.
Dual-chamber and atrial tracking modes are also indicated for patients who may benefit
from maintenance of AV synchrony.
Dual chamber modes are specifically indicated for treatment of the following:
• Conduction disorders that require restoration of AV synchrony, including varying
degrees of AV block
• VVI intolerance (i.e., pacemaker syndrome) in the presence of persistent sinus
rhythm
• Low cardiac output or congestive heart failure secondary to bradycardia
4
CONTRAINDICATIONS
These Boston Scientific pacemakers are contraindicated in patients who have a
separate implanted cardioverter-defibrillator (ICD).
Use of certain pacing modes and/or features available in these Boston Scientific
pacemakers is contraindicated for the following patients under the circumstances listed:
• Minute ventilation in patients with both unipolar atrial and ventricular leads
• Single-chamber atrial pacing in patients with impaired AV nodal conduction
• Atrial tracking modes for patients with chronic refractory atrial tachyarrhythmias
(atrial fibrillation or flutter), which might trigger ventricular pacing
• Dual-chamber and single-chamber atrial pacing in patients with chronic refractory
atrial tachyarrhythmias
• Asynchronous pacing in the presence (or likelihood) of competition between
paced and intrinsic rhythms
5

WARNINGS
General
• Labeling knowledge. Read this manual thoroughly before implantation to avoid
damage to the pulse generator and/or lead. Such damage can result in patient
injury or death.
• For single patient use only. Do not reuse, reprocess, or resterilize. Reuse,
reprocessing, or resterilization may compromise the structural integrity of the
device and/or lead to device failure which, in turn, may result in patient injury,
illness, or death. Reuse, reprocessing, or resterilization may also create a risk
of contamination of the device and/or cause patient infection or cross-infection,
including, but not limited to, the transmission of infectious disease(s) from one
patient to another. Contamination of the device may lead to injury, illness, or
death of the patient.
• Backup defibrillation protection. Always have external defibrillation protection
available during implant and electrophysiologic testing. If not terminated in a timely
fashion, an induced ventricular tachyarrhythmia can result in the patient’s death.
• Separate pulse generator. Do not use this pulse generator with another pulse
generator. This combination could cause pulse generator interaction, resulting in
patient injury or a lack of therapy delivery.
6

• Safety Core operation. In response to applicable nonrecoverable or repeat fault
conditions, the pulse generator will switch irreversibly to Safety Core operation.
Safety Core pacing is unipolar, which is contraindicated for patients with an ICD.
Handling
• Do not kink leads. Do not kink, twist, or braid the lead with other leads as doing
so could cause lead insulation abrasion damage or conductor damage.
Programming and Device Operations
• Atrial tracking modes. Do not use atrial tracking modes in patients with chronic
refractory atrial tachyarrhythmias. Tracking of atrial arrhythmias could result in
ventricular tachyarrhythmias.
• Lead safety switch programmed to On. In devices with the lead safety switch
programmed to On, the lead polarity will switch to unipolar in the presence of a
lead impedance of ≤200 or ≥2000 Ω. Unipolar pacing is contraindicated for
patients with an ICD.
• Sensitivity settings and EMI. If programmed to a fixed atrial sensitivity value
of 0.15 mV, the pulse generator may be more susceptible to electromagnetic
interference. This increased susceptibility should be taken into consideration
when determining the follow-up schedule for patients requiring such a setting.
7

Post-Implant
• Protected environments. Advise patients to seek medical guidance before
entering environments that could adversely affect the operation of the active
implantable medical device, including areas protected by a warning notice that
prevents entry by patients who have a pulse generator.
• Magnetic Resonance Imaging (MRI) exposure. Do not expose a patient to MRI
scanning. Strong magnetic fields may damage the pulse generator and/or lead
system, possibly resulting in injury to or death of the patient.
• Diathermy. Do not subject a patient with an implanted pulse generator and/or lead
to diathermy since diathermy may cause fibrillation, burning of the myocardium,
and irreversible damage to the pulse generator because of induced currents.
PRECAUTIONS
Clinical Considerations
•STATPACE.STAT PACE will initiate unipolar pacing.
• Pacemaker-mediated tachycardia (PMT). Programming minimum PVARP less
than retrograde V–A conduction may increase the likelihood of a PMT.
• Automatic Capture. Automatic Capture is intended for ventricular use only. Do
not program Amplitude to Auto for single-chamber devices implanted in the atrium.
8

• MV sensor modes. The safety and efficacy of the MV sensor modes have not
been clinically established in patients with abdominal implant sites.
• MV sensor mode performance. MV sensor performance may be adversely
affected under transient conditions such as pneumothorax, pericardial effusion, or
pleural effusion. Consider programming the MV sensor Off until these conditions
are resolved.
9

• Adaptive-rate modes. Adaptive-rate modes based completely or in part on MV
might be inappropriate for patients who can achieve respiratory cycles shorter
than one second (greater than 60 breaths per minute). Higher respiration rates
attenuate the impedance signal, which diminishes the MV rate response (i.e., the
pacing rate will drop toward the programmed LRL).
Adaptive-rate modes based completely or in part on MV should not be used for
patients with:
•AnICD
• Unipolar leads—for MV detection, a bipolar lead is required in either the
atrium or ventricle
• Epicardial ventricular leads—MV measurement has only been tested with
a bipolar transvenous lead
• A mechanical ventilator—use of the ventilator might result in an inappropriate
MV sensor-driven rate
10

Sterilization and Storage
• If package is damaged. The blister trays and contents are sterilized with
ethylene oxide gas before final packaging. When the pulse generator and/or lead
is received, it is sterile provided the container is intact. If the packaging is wet,
punctured, opened, or otherwise damaged, return the pulse generator and/or
lead to Boston Scientific.
• Storage temperature and equilibration. Recommended storage temperatures
are 0°C–50°C (32°F–122°F). Allow the device to reach a proper temperature
before using telemetry communication capabilities, programming or implanting the
device because temperature extremes may affect initial device function.
• Device storage. Store the pulse generator in a clean area away from magnets,
kits containing magnets, and sources of EMI to avoid device damage.
•Usebydate.Implant the pulse generator and/or lead before or on the USE BY
date on the package label because this date reflects a validated shelf life. For
example, if the date is January 1, do not implant on or after January 2.
Implantation
• Expected benefits. Determine whether the expected device benefits provided by
programmable options outweigh the possibility of more rapid battery depletion.
11

• Evaluate patient for surgery. There may be additional factors regarding the
patient’s overall health and medical condition that, while not related to device
function or purpose, could render the patient a poor candidate for implantation of
this system. Cardiac health advocacy groups may have published guidelines that
may be helpful in conducting this evaluation.
• Lead compatibility. Prior to implantation, confirm the lead-to-pulse generator
compatibility. Using incompatible leads and pulse generators can damage the
connector and/or result in potential adverse consequences, such as undersensing
of cardiac activity or failure to deliver necessary therapy.
• Telemetry wand. Make sure a sterile telemetry wand is available should loss
of ZIP telemetry occur. Verify that the wand can easily be connected to the
programmer and is within reach of the pulse generator.
• Line-powered equipment. Exercise extreme caution if testing leads using
line-powered equipment because leakage current exceeding 10 µA can induce
ventricular fibrillation. Ensure that any line-powered equipment is within
specifications.
12

• Replacement device. Implanting a replacement device in a subcutaneous pocket
that previously housed a larger device may result in pocket air entrapment,
migration, erosion, or insufficient grounding between the device and tissue.
Irrigating the pocket with sterile saline solution decreases the possibility of pocket
air entrapment and insufficient grounding. Suturing the device in place reduces
the possibility of migration and erosion.
• Do not bend the lead near the lead-header interface. Insert the lead terminal
straight into the lead port. Do not bend the lead near the lead-header interface.
Improper insertion can cause insulation or connector damage.
• Absence of a lead. The absence of a lead or plug in a lead port may affect
device performance. If a lead is not used, be sure to properly insert a plug in the
unused port, and then tighten the setscrew onto the plug.
• Dual chamber device without a functional RV lead. If a dual-chamber
device is programmed to AAI(R), ensure that a functional RV lead is present.
In the absence of a functional RV lead, programming to AAI(R) may result in
undersensing or oversensing.
13

• Electrode connections. Do not insert a lead into the pulse generator connector
without taking the following precautions to ensure proper lead insertion:
• Insert the torque wrench into the preslit depression of the seal plug before
inserting the lead into the port, to release any trapped fluid or air.
• Visually verify that the setscrew is sufficiently retracted to allow insertion.
Use the torque wrench to loosen the setscrew if necessary.
• Fully insert each lead into its lead port and then tighten the setscrew onto
the terminal pin.
• Shunting energy. Do not allow any object that is electrically conductive to come
into contact with the lead or device during induction because it may shunt energy,
resulting in less energy getting to the patient, and may damage the implanted
system.
• Do not suture directly over lead. Do not suture directly over the lead body, as
this may cause structural damage. Use the suture sleeve to secure the lead
proximal to the venous entry site to prevent lead movement.
• MV Sensor. Do not program the MV sensor to On until after the pulse generator
has been implanted and system integrity has been tested and verified.
14

Device Programming
• Device communication. Use only the designated PRM and software application
to communicate with this pulse generator.
• STAT PACE settings. When a pulse generator is programmed to STAT PACE
settings, it will continue to pace at the high-energy STAT PACE values if it is not
reprogrammed. The use of STAT PACE parameters will likely decrease device
longevity.
• Pacing and sensing margins. Consider lead maturation in your choice of pacing
amplitude, pacing pulse width, and sensitivity settings.
• An acute pacing threshold greater than 1.5 V or a chronic pacing threshold
greater than 3 V can result in loss of capture because thresholds may
increase over time.
• An R-wave amplitude less than 5 mV or a P-wave amplitude less than 2 mV
can result in undersensing because the sensed amplitude may decrease
after implantation.
• Pacing lead impedance should be within the range of 200 Ωand 2000 Ω.
• Lead impedance values and Lead Safety Switch. If leads with measured
impedance values approaching 200 or 2000 Ωare used, consider programming
Lead Safety Switch Off.
15

• Proper programming of the lead configuration. If the Lead Configuration is
programmed to Bipolar when a unipolar lead is implanted, pacing will not occur.
• Programming for supraventricular tachyarrhythmias (SVTs). Determine if the
device and programmable options are appropriate for patients with SVTs because
SVTs can initiate unwanted device therapy.
• Adaptive-rate pacing. Rate adaptive pacing should be used with care in patients
who are unable to tolerate increased pacing rates.
• Ventricular refractory periods (VRPs) in adaptive-rate pacing. Adaptive-rate
pacing is not limited by refractory periods. A long refractory period programmed in
combination with a high MSR can result in asynchronous pacing during refractory
periods since the combination can cause a very small sensing window or none at
all. Use dynamic AV Delay or dynamic PVARP to optimize sensing windows. If
you are entering a fixed AV delay, consider the sensing outcomes.
• Atrial oversensing. Take care to ensure that artifacts from the ventricles are
not present on the atrial channel, or atrial oversensing may result. If ventricular
artifacts are present in the atrial channel, the atrial lead may need to be
repositioned to minimize its interaction.
16

• ATR entry count. Exercise care when programming the Entry Count to low
values in conjunction with a short ATR Duration. This combination allows mode
switching with very few fast atrial beats. For example, if the Entry Count was
programmed to 2 and the ATR Duration to 0, ATR mode switching could occur on
2 fast atrial intervals. In these instances, a short series of premature atrial events
could cause the device to mode switch.
• ATR exit count. Exercise care when programming the Exit Count to low values.
For example, if the Exit Count was programmed to 2, a few cycles of atrial
undersensing could cause termination of mode switching.
• Proper programming without an atrial lead. If an atrial lead is not implanted
(port is plugged instead), or an atrial lead is abandoned but remains connected
to the header, device programming should be consistent with the number and
type of leads actually in use.
• MV Recalibration. To obtain an accurate MV baseline, the MV sensor will be
calibrated automatically or can be calibrated manually. A new, manual calibration
should be performed if the pulse generator is removed from the pocket following
implant, such as during a lead repositioning procedure, or in cases where the
MV baseline may have been affected by factors such as lead maturation, air
entrapment in the pocket, pulse generator motion due to inadequate suturing,
external defibrillation or cardioversion, or other patient complications (e.g.,
pneumothorax).
17

• Sensing adjustment. Following any Sensitivity parameter adjustment or any
modification of the sensing lead, always verify appropriate sensing. Programming
Sensitivity to the highest value (lowest sensitivity) may result in undersensing of
cardiac activity. Likewise, programming to the lowest value (highest sensitivity)
may result in oversensing of non-cardiac signals.
• Sensitivity in unipolar lead configuraton. The amplitude and prevalence of
myopotential noise is increased in unipolar lead configurations, as compared
to bipolar lead configurations. For patients with a unipolar lead configuration
and myopotential oversensing during activity involving the pectoral muscles, the
programming of Fixed Sensitivity is recommended.
Environmental and Medical Therapy Hazards
• Avoid electromagnetic interference (EMI). Advise patients to avoid sources of
EMI. The pulse generator may inhibit pacing due to oversensing, or may switch
to asynchronous pacing at the programmed pacing rate or at the magnet rate in
thepresenceofEMI.
Moving away from the source of the EMI or turning off the source usually allows
the pulse generator to return to normal operation.
18

Examples of potential EMI sources are:
• Electrical power sources, arc welding or resistance welding equipment, and
robotic jacks
• High voltage power distribution lines
• Electrical smelting furnaces
• Large RF transmitters such as radar
• Radio transmitters, including those used to control toys
• Electronic surveillance (antitheft) devices
• An alternator on a car that is running
• Medical treatments and diagnostic tests in which an electrical
current is passed through the body, such as TENS, electrocautery,
electrolysis/thermolysis, electrodiagnostic testing, electromyography, or
nerve conduction studies
• Any externally applied device that uses an automatic lead detection alarm
system (e.g., an EKG machine)
19

Hospital and Medical Environments
• Mechanical ventilators.
Program the MV Sensor to Off during mechanical ventilation. Otherwise, the following
may occur:
• Inappropriate MV sensor-driven rate
• Misleading respiration-based trending
• Conducted electrical current. Any medical equipment, treatment, therapy, or
diagnostic test that introduces electrical current into the patient has the potential
to interfere with pulse generator function.
• External patient monitors (e.g., respiratory monitors, surface ECG
monitors, hemodynamic monitors) may interfere with the pulse generator’s
impedance-based diagnostics (e.g., Respiratory Rate trend). This
interference may also result in accelerated pacing, possibly up to the
maximum sensor-driven rate, when MV is programmed to On. To resolve
suspected interactions, deactivate the MV sensor either by programming it to
Off (no MV rate driving or MV sensor-based trending will occur), or Passive
(no MV rate driving will occur). Alternatively, program the Brady Mode to a
non-rate responsive mode (no MV rate driving will occur). If a PRM is not
available and the pulse generator is pacing at the sensor-driven rate, apply a
20
magnet to the pulse generator to initiate temporary asynchronous, non-rate
responsive pacing.
• Medical therapies, treatments, and diagnostic tests that use conducted
electrical current (e.g., TENS, electrocautery, electrolysis/thermolysis,
electrodiagnostic testing, electromyography, or nerve conduction studies)
may interfere with or damage the pulse generator. Program the device to
Electrocautery Mode prior to the treatment, and monitor device performance
during the treatment. After the treatment, verify pulse generator function
("Post-Therapy Pulse Generator Follow Up" on page 27).
• Internal defibrillation. Do not use internal defibrillation paddles or catheters
unless the pulse generator is disconnected from the leads because the leads
may shunt energy. This could result in injury to the patient and damage to the
implanted system.
21
• External defibrillation. It can take up to 15 seconds for sensing to recover
after an external shock is delivered. In non-emergency situations, for
pacemaker dependent patients, consider programming the pulse generator to
an asynchronous pacing mode prior to performing external cardioversion or
defibrillation.
External defibrillation or cardioversion can damage the pulse generator. To help
prevent damage to the pulse generator, consider the following:
• Avoid placing a pad (or paddle) directly over the pulse generator. Position
the pads (or paddles) as far from the pulse generator as possible.
• Position the pads (or paddles) in a posterior-anterior orientation when the
device is implanted in the right pectoral region or an anterior-apex orientation
when the device is implanted in the left pectoral region.
• Set energy output of external defibrillation equipment as low as clinically
acceptable.
• In non-emergency situations, prior to performing external cardioversion or
defibrillation, program the MV sensor to Off.
Following external cardioversion or defibrillation, verify pulse generator function
("Post-Therapy Pulse Generator Follow Up" on page 27).
22

•Lithotripsy.Extracorporeal shock wave lithotripsy (ESWL) may cause
electromagnetic interference with or damage to the pulse generator. If ESWL
is medically necessary, consider the following to minimize the potential for
encountering interaction:
• Focus the ESWL beam at least 15 cm (6 in) away from the pulse generator.
• Depending on the pacing needs of the patient, program the Brady Mode to a
non-rate-responsive VVI or VOO mode.
• Ultrasound energy. Therapeutic ultrasound (e.g., lithotripsy) energy may damage
the pulse generator. If therapeutic ultrasound energy must be used, avoid focusing
near the pulse generator site. Diagnostic ultrasound (e.g., echocardiography) is
not known to be harmful to the pulse generator.
• Electrical interference. Electrical interference or “noise” from devices such
as electrocautery and monitoring equipment may interfere with establishing or
maintaining telemetry for interrogating or programming the device. In the presence
of such interference, move the programmer away from electrical devices, and
ensure that the wand cord and cables are not crossing one another. If telemetry is
cancelled as a result of interference, the device should be re-interrogated prior to
evaluating information from pulse generator memory.
23

• Radio frequency (RF) interference. RF signals from devices that operate at
frequencies near that of the pulse generator may interrupt ZIP telemetry while
interrogating or programming the pulse generator. This RF interference can be
reduced by increasing the distance between the interfering device and the PRM
and pulse generator. Examples of devices that may cause interference include:
• Cordless phone handsets or base stations
• Certain patient monitoring systems
• Central line guidewire insertion. Use caution when inserting guidewires for
placement of other types of central venous catheter systems such as PIC lines or
Hickman catheters in locations where pulse generator leads may be encountered.
Insertion of such guidewires into veins containing leads could result in the leads
being damaged or dislodged.
Home and Occupational Environments
• Home appliances. Home appliances that are in good working order and properly
grounded do not usually produce enough EMI to interfere with pulse generator
operation. There have been reports of pulse generator disturbances caused
by electric hand tools or electric razors used directly over the pulse generator
implant site.
24
• Magnetic fields. Advise patients that extended exposure to strong (greater than
10 gauss or 1 mTesla) magnetic fields may trigger the magnet feature. Examples
of magnetic sources include:
• Industrial transformers and motors
• MRI scanners
• Large stereo speakers
• Telephone receivers if held within 1.27 cm (0.5 inches) of the pulse generator
• Magnetic wands such as those used for airport security and in the Bingo
game
• Electronic Article Surveillance (EAS). Advise patients to avoid lingering near
antitheft devices such as those found in the entrances and exits of department
stores and public libraries. Patients should walk through them at a normal pace
because such devices may cause inappropriate pulse generator operation.
• Cellular phones. Advise patients to hold cellular phones to the ear opposite the
side of the implanted device. Patients should not carry a cellular phone that is
turned on in a breast pocket or on a belt within 15 cm (6 inches) of the implanted
device since some cellular phones may cause the pulse generator to deliver
inappropriate therapy or inhibit appropriate therapy.
25

Follow-up Testing
• Pacing threshold testing. If the patient’s condition or drug regimen has changed
or device parameters have been reprogrammed, consider performing a pacing
threshold test to confirm adequate margins for pace capture.
• Follow-up considerations for patients leaving the country. Pulse generator
follow-up considerations should be made in advance for patients who plan to
travel or relocate post-implant to a country other than the country in which their
device was implanted. Regulatory approval status for devices and associated
programmer software configurations varies by country; certain countries may not
have approval or capability to follow specific products.
Contact Boston Scientific, using the information on the back cover, for help in
determining feasibility of device follow-up in the patient’s destination country.
Explant and Disposal
• Incineration. Be sure that the pulse generator is removed before cremation.
Cremation and incineration temperatures might cause the pulse generator to
explode.
26

• Device handling. Before explanting, cleaning, or shipping the device, complete
the following actions to prevent overwriting of important therapy history data:
• Program the pulse generator Brady Mode to Off
• Program Ventricular Tachy EGM Storage to Off
Clean and disinfect the device using standard biohazard handling techniques.
• Explanted devices. Return all explanted pulse generators and leads to
Boston Scientific. Examination of explanted pulse generators and leads can
provide information for continued improvement in system reliability and warranty
considerations.
Do not implant an explanted pulse generator and/or lead in another patient as
sterility, functionality, and reliability cannot be ensured.
SUPPLEMENTAL PRECAUTIONARY INFORMATION
Post-Therapy Pulse Generator Follow Up
Following any surgery or medical procedure with the potential to affect pulse generator
function, you should perform a thorough follow-up, which may include the following:
• Interrogating the pulse generator with a programmer
• Reviewing clinical events and fault codes
27

• Reviewing the Arrhythmia Logbook, including stored electrograms (EGMs)
• Reviewing real-time EGMs
• Testing the leads (threshold, amplitude, and impedance)
• Reviewing MV sensor-based diagnostics, MV sensor performance, and
performing a manual MV sensor calibration if desired
• Verifying battery status
• Programming any permanent brady parameter to a new value and then
reprogramming it back to the desired value
• Saving all patient data
• Verifying the appropriate final programming prior to allowing the patient to leave
the clinic
28

Transcutaneous Electrical Nerve Stimulation (TENS)
CAUTION: TENS involves passing electrical current through the body, and may
interfere with pulse generator function. If TENS is medically necessary, evaluate
the TENS therapy settings for compatibility with the pulse generator. The following
guidelines may reduce the likelihood of interaction:
• Place the TENS electrodes as close together and as far away from the pulse
generator and leads as possible.
• Use the lowest clinically-appropriate TENS energy output.
• Consider cardiac monitoring during TENS use, especially for
pacemaker-dependent patients.
Additional steps can be taken to help reduce interference during in-clinic use of TENS:
• If interference is suspected during in-clinic use, turn off the TENS unit.
• If pacing inhibition is observed, use a magnet to pace asynchronously.
• Do not change TENS settings until you have verified that the new settings do not
interfere with pulse generator function.
29

If TENS is medically necessary outside the clinical setting (at-home use), provide
patients with the following instructions:
• Do not change the TENS settings or electrode positions unless instructed to do so.
• End each TENS session by turning off the unit before removing the electrodes.
• If the patient experiences symptoms of lightheadedness, dizziness, or loss of
consciousness during TENS use, they should turn off the TENS unit and contact
their physician.
Follow these steps to use the PRM to evaluate pulse generator function during TENS
use:
1. Observe real-time EGMs at prescribed TENS output settings, noting when
appropriate sensing or interference occurs.
NOTE: Patient triggered monitoring may be used as an additional method to confirm
device function during TENS use.
2. When finished, turn off the TENS unit.
You should also perform a thorough follow-up evaluation of the pulse generator
following TENS, to ensure that device function has not been compromised
("Post-Therapy Pulse Generator Follow Up" on page 27).
30

For additional information, contact Boston Scientific using the information on the back
cover.
Electrocautery and Radio Frequency (RF) Ablation
CAUTION: Electrocautery and RF ablation may induce ventricular arrhythmias
and/or fibrillation, and may cause asynchronous pacing, inhibition of pacing and/or a
reduction in pulse generator pacing output possibly leading to loss of capture. RF
ablation may also cause ventricular pacing up to the MTR and/or changes in pacing
thresholds. Additionally, exercise caution when performing any other type of cardiac
ablation procedure in patients with implanted devices.
If electrocautery or RF ablation is medically necessary, observe the following to
minimize risk to the patient and device:
• Depending on the pacing needs of the patient, enable the Electrocautery
Protection Mode, program to an asynchronous pacing mode, or use a magnet
to switch to asynchronous pacing. An option for patients with intrinsic rhythm
is to program the Brady Mode to VVI at a rate below the intrinsic rate to avoid
competitive pacing.
• Have temporary pacing and external defibrillation equipment available.
31

• Avoid direct contact between the electrocautery equipment or ablation catheters
and the pulse generator and leads. RF ablation close to the lead electrode may
damage the lead-tissue interface.
• Keep the path of the electrical current as far away as possible from the pulse
generator and leads.
• If RF ablation and/or electrocautery is performed on tissue near the device or
leads, monitor pre- and post-measurements for sensing and pacing thresholds
and impedances to determine the integrity and stability of the system.
• For electrocautery, use a bipolar electrocautery system where possible and use
short, intermittent, and irregular bursts at the lowest feasible energy levels.
• RF ablation equipment may cause telemetry interference between the pulse
generator and PRM. If device programming changes are necessary during an RF
ablation procedure, turn off the RF ablation equipment before interrogation.
When the procedure is finished, cancel the Electrocautery Protection Mode in order to
reactivate the previously programmed therapy modes.
32

Ionizing Radiation
CAUTION: It is not possible to specify a safe radiation dosage or guarantee proper
pulse generator function following exposure to ionizing radiation. Multiple factors
collectively determine the impact of radiation therapy on an implanted pulse generator,
including proximity of the pulse generator to the radiation beam, type and energy
level of the radiation beam, dose rate, total dose delivered over the life of the pulse
generator, and shielding of the pulse generator. The impact of ionizing radiation
will also vary from one pulse generator to another and may range from no changes
in function to a loss of pacing.
Sources of ionizing radiation vary significantly in their potential impact on an implanted
pulse generator. Several therapeutic radiation sources are capable of interfering with
or damaging an implanted pulse generator, including those used for the treatment
of cancer, such as radioactive cobalt, linear accelerators, radioactive seeds, and
betatrons.
Prior to a course of therapeutic radiation treatment, the patient’s radiation oncologist
and cardiologist or electrophysiologist should consider all patient management options,
including increased follow-up and device replacement. Other considerations include:
• Maximizing shielding of the pulse generator within the treatment field
• Determining the appropriate level of patient monitoring during treatment
33

Evaluate pulse generator operation during and following the course of radiation
treatment to exercise as much device functionality as possible ("Post-Therapy Pulse
Generator Follow Up" on page 27). The extent, timing, and frequency of this evaluation
relative to the radiation therapy regimen are dependent upon current patient health,
and therefore should be determined by the attending cardiologist or electrophysiologist.
Many pulse generator diagnostics are performed automatically once per hour, so pulse
generator evaluation should not be concluded until pulse generator diagnostics have
been updated and reviewed (at least one hour after radiation exposure). The effects
of radiation exposure on the implanted pulse generator may remain undetected until
some time following exposure. For this reason, continue to monitor pulse generator
function closely and use caution when programming a feature in the weeks or months
following radiation therapy.
Elevated Pressures
The International Standards Organization (ISO) has not approved a standardized
pressure test for implantable pulse generators that experience hyperbaric oxygen
therapy (HBOT) or SCUBA diving. However, Boston Scientific developed a test
protocol to evaluate device performance upon exposure to elevated atmospheric
pressures. The following summary of pressure testing should not be viewed as and is
not an endorsement of HBOT or SCUBA diving.
34
CAUTION: Elevated pressures due to HBOT or SCUBA diving may damage the
pulse generator. During laboratory testing, all pulse generators in the test sample
functioned as designed when exposed to more than 1000 cycles at a pressure up to 5.0
ATA. Laboratory testing did not characterize the impact of elevated pressure on pulse
generator performance or physiological response while implanted in a human body.
Pressure for each test cycle began at ambient/room pressure, increased to a high
pressure level, and then returned to ambient pressure. Although dwell time (the amount
of time under elevated pressure) may have an impact on human physiology, testing
indicated it did not impact pulse generator performance. Pressure value equivalencies
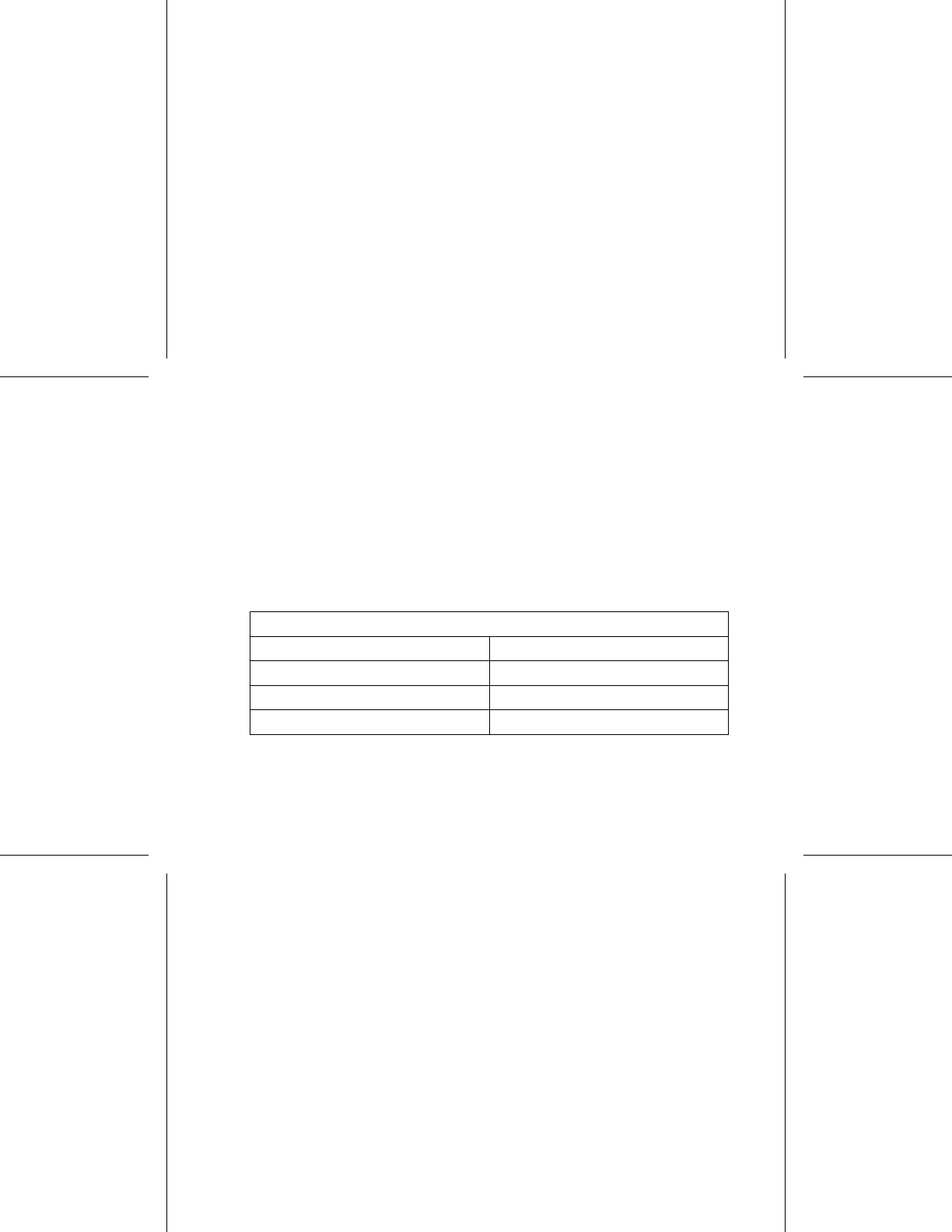
are provided below (Table 1 on page 35).
Table 1. Pressure Value Equivalencies
Pressure value equivalencies
Atmospheres Absolute 5.0 ATA
Sea water deptha40 m (130 ft)
Pressure, absolute 72.8 psia
Pressure, gaugeb58.8 psig
35

Table 1. Pressure Value Equivalencies (continued)
Pressure value equivalencies
Bar 5.0
kPa Absolute 500
a. All pressures were derived assuming sea water density of 1030 kg/m3.
b. Pressure as read on a gauge or dial (psia = psig + 14.7 psi).
Prior to SCUBA diving or starting an HBOT program, the patient’s attending
cardiologist or electrophysiologist should be consulted to fully understand the potential
consequences relative to the patient’s specific health condition. A Dive Medicine
Specialist may also be consulted prior to SCUBA diving.
More frequent device follow-up may be warranted in conjunction with HBOT or
SCUBA diving. Evaluate pulse generator operation following high pressure exposure
("Post-Therapy Pulse Generator Follow Up" on page 27). The extent, timing, and
frequency of this evaluation relative to the high pressure exposure are dependent
upon current patient health, and should be determined by the attending cardiologist or
electrophysiologist.
If you have additional questions, or would like more detail regarding the test protocol
or test results specific to HBOT or SCUBA diving, contact Boston Scientific using the
informationonthebackcover.
36

POTENTIAL ADVERSE EVENTS
Based on the literature and on pulse generator implant experience, the following
alphabetical list includes the possible adverse events associated with implantation of
a pulse generator and/or lead system:
•Airembolism
• Allergic reaction
• Bleeding
• Cardiac tamponade
• Chronic nerve damage
• Component failure
• Conductor coil fracture
• Death
• Elevated thresholds
•Erosion
• Excessive fibrotic tissue growth
• Extracardiac stimulation (muscle/nerve stimulation)
• Foreign body rejection phenomena
• Fluid accumulation
• Formation of hematomas or seromas
37

• Heart block
• Inability to pace
• Inappropriate pacing
• Incisional pain
• Incomplete lead connection with pulse generator
• Infection including endocarditis
• Lead dislodgment
•Leadfracture
• Lead insulation breakage or abrasion
• Lead perforation
• Lead tip deformation and/or breakage
• Local tissue reaction
• Myocardial infarction (MI)
• Myocardial necrosis
• Myocardial trauma (e.g., tissue damage, valve damage)
• Myopotential sensing
• Oversensing/undersensing
• Pacemaker-mediated tachycardia (PMT) (Applies to dual-chamber devices only.)
• Pericardial rub, effusion
38

• Pneumothorax
• Pulse generator migration
• Shunting current during defibrillation with internal or external paddles
• Tachyarrhythmias, which include acceleration of arrhythmias and early, recurrent
atrial fibrillation
• Thrombosis/thromboemboli
• Valve damage
• Venous occlusion
• Venous trauma (e.g., perforation, dissection, erosion)
• Worsening heart failure
Patients may develop psychological intolerance to a pulse generator system and may
experience the following:
• Dependency
• Depression
• Fear of premature battery depletion
• Fear of device malfunction
MECHANICAL SPECIFICATIONS
Mechanical and material specifications specific to each model are listed below.
39
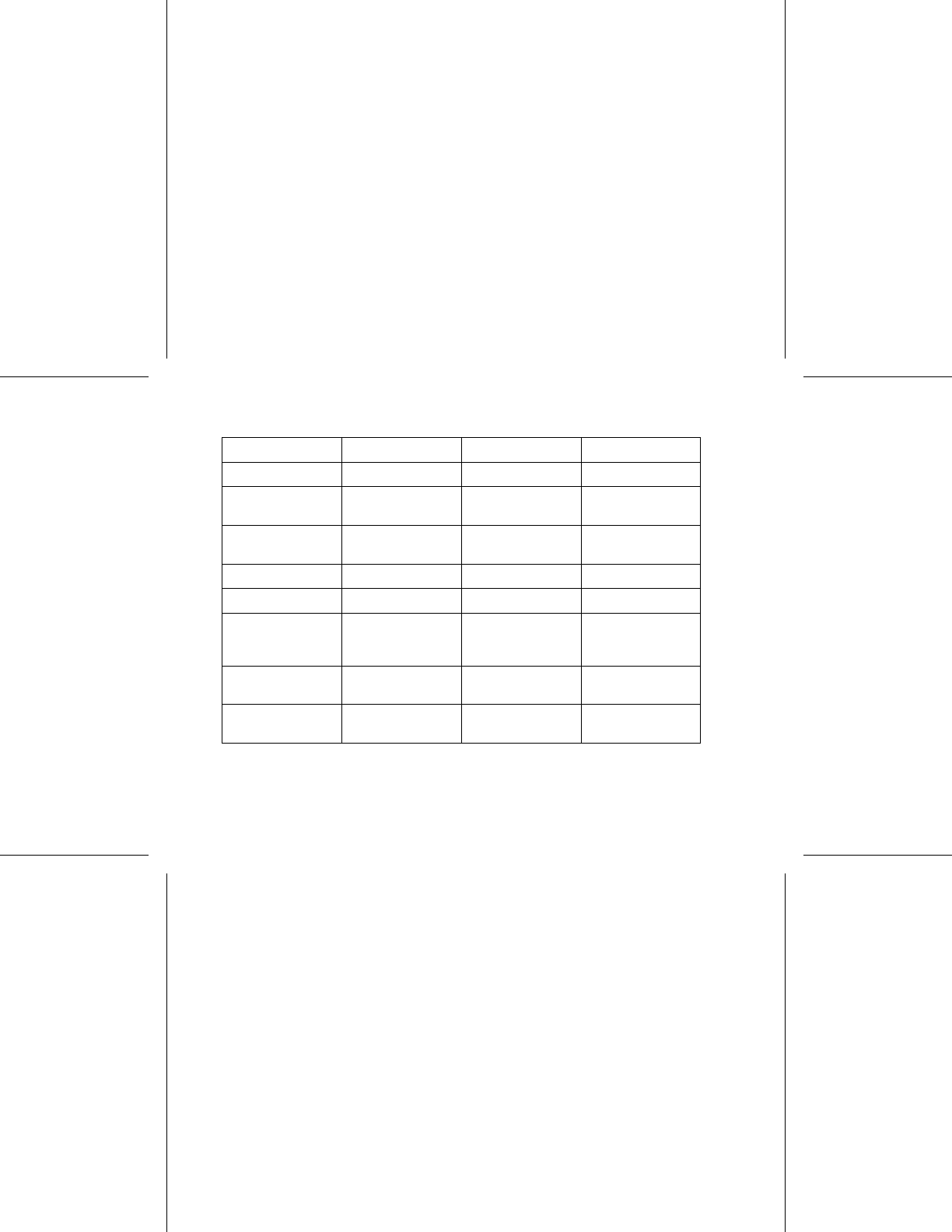
Table 2. Mechanical and Material Specifications
K172 K173 K174
Type SR DR DR
Connector RA/RV: IS-1 RA:IS-1
RV: IS-1
RA:IS-1
RV: IS-1
Dimensions
WxHxD(cm)
4.45 x 4.57 x 0.75 4.45 x 4.70 x 0.75 4.45 x 5.56 x 0.75
Volume (cm3)11.5 12.0 14.0
Mass (g) 23.5 24.5 32.0
Case Electrode
Surface Area
(cm2)
29.78 29.78 35.98
Case Material hermetically
sealed titanium
hermetically
sealed titanium
hermetically
sealed titanium
Header Material implantation-grade
polymer
implantation-grade
polymer
implantation-grade
polymer
40

Table 2. Mechanical and Material Specifications (continued)
K172 K173 K174
Power Supply Lithium-carbon
monofluoride-
silver vanadium
oxide cell
Greatbatch 2808
Lithium-carbon
monofluoride-
silver vanadium
oxide cell
Greatbatch 2808
Lithium-
manganese
dioxide cell
Boston Scientific
402125
Usable Battery
Capacity (Ah)
1.05 1.05 1.47
Residual Usable
Battery Capacity
at Explant (Ah)
0.06 0.08 0.08
Models include ZIP telemetry operating with a transmit frequency of 916.5 MHz.
ITEMS INCLUDED IN PACKAGE
The following items are included with the pulse generator:
• One torque wrench
• Product literature
41
NOTE: Accessories (e.g., wrenches) are intended for one-time use only. They should
not be resterilized or reused.
SYMBOLS ON PACKAGING
The following symbols may be used on packaging and labeling (Table 3 on page 42):
Table 3. Symbols on packaging
Symbol Description
Reference number
Package contents
Pulse generator
Torque wrench
42
Table 3. Symbols on packaging (continued)
Symbol Description
Literature enclosed
Serial number
Use by
Lot number
Date of manufacture
Non-ionizing electromagnetic radiation
Sterilized using ethylene oxide
43
Table 3. Symbols on packaging (continued)
Symbol Description
Do not resterilize
Do not reuse
Do not use if package is damaged
Consult instructions for use
Temperature limitation
44
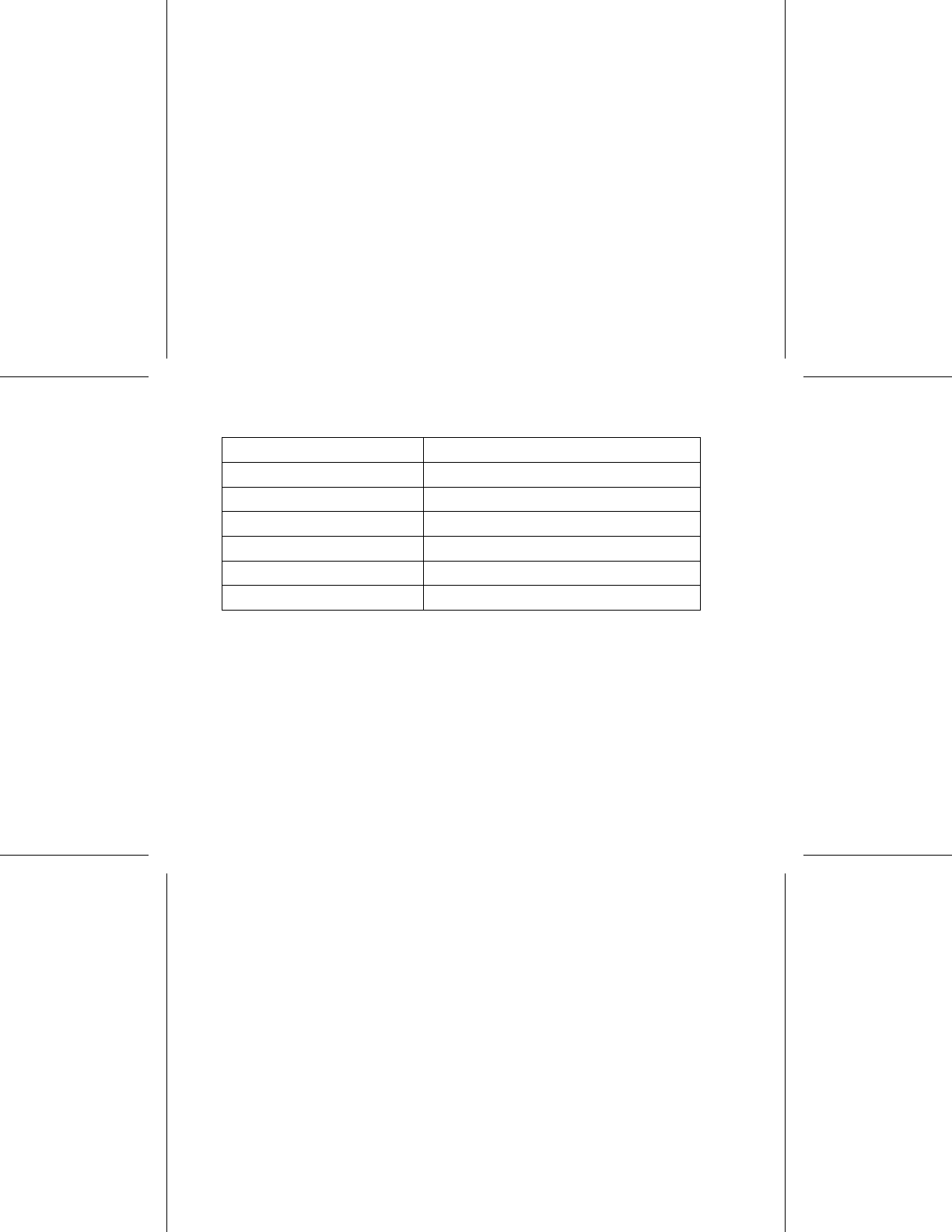
Table 4. Characteristics as shipped
Parameter Setting
Pacing Mode Storage
Pacing Therapy available DDDR (DR models) SSIR (SR models)
Sensor Blend (Accel and MV)
Pace/Sense Configuration RA: BI/BI (DR models)
Pace/Sense Configuration RV: BI/BI
Magnet Rate 100 ppm
The pulse generator is shipped in a power-saving Storage mode to extend its shelf life.
In Storage mode, all features are inactive except:
• Telemetry support, which allows interrogation and programming
• Real-time clock
• STAT PACE command
The device leaves Storage mode when one of the following actions occurs; however,
programming other parameters will not affect the Storage mode:
46

• STAT PACE is commanded
• The pulse generator automatically detects lead insertion (refer to "Implanting the
Pulse Generator" on page 59)
• Device Mode is programmed to Exit Storage
Once you have programmed the pulse generator out of Storage mode, the device
cannot be reprogrammed to that mode.
X-RAY IDENTIFIER
The pulse generator has an identifier that is visible on x-ray film or under fluoroscopy.
This identifier provides noninvasive confirmation of the manufacturer and consists of
the following:
• The letters, BSC, to identify Boston Scientific as the manufacturer
• The number, 011, to identify the Model 2869 PRM software application needed to
communicate with the pulse generator
The x-ray identifier is embedded in the header of the device at the approximate location
shown (Figure 1 on page 48).
47
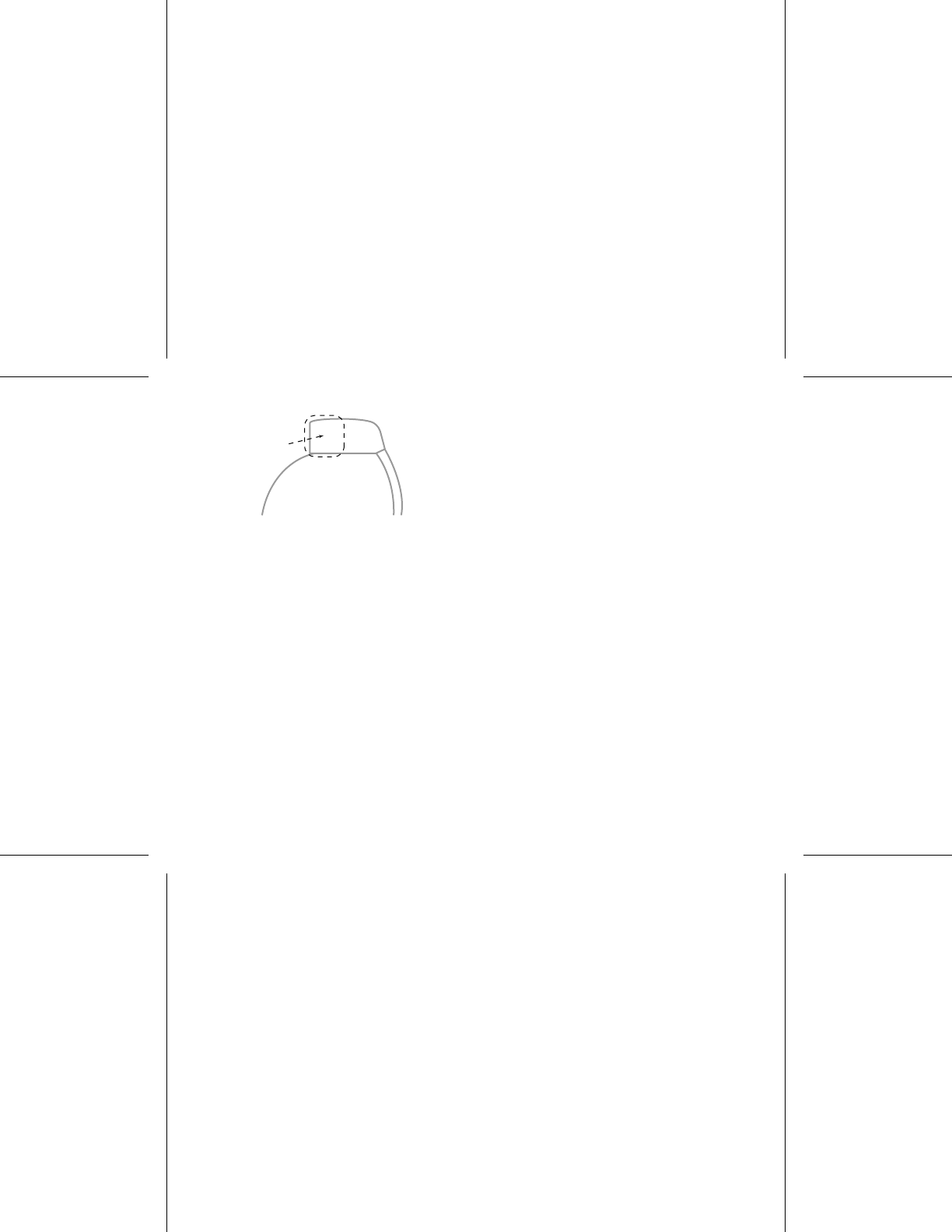
Header
Pulse Generator Case
X-Ray Identifier
Figure 1. X-ray identifier
For information on identifying the device via the PRM, refer to the PRM Operator’s
Manual.
The pulse generator model number is stored in device memory and is shown on the
PRM summary screen once the pulse generator is interrogated.
FEDERAL COMMUNICATIONS COMMISSION (FCC)
This device complies with Title 47, Part 15 of the FCC rules. Operation is subject
to the following two conditions:
• This device may not cause harmful interference, and
• This device must accept any interference received, including interference that
may cause undesired operation.
48

CAUTION: Changes or modifications not expressly approved by Boston Scientific
could void the user’s authority to operate the equipment.
PULSE GENERATOR LONGEVITY
Based on simulated studies, it is anticipated that these pulse generators have average
longevity to explant as shown below.
The longevity expectations, which account for the energy used during manufacture and
storage, apply at the conditions shown in the table along with the following:
• Assumes 60 ppm LRL, ventricular and atrial settings of 0.4 ms pacing pulse width;
sensors On.
• These calculations also assume EGM Onset is set to On.
Table 5. INGENIO Longevity Projections (Years)
Amplitude and
Pacing
Modelsa
K172 SR K173 DR K174 DR EL
A and V Amplitudes 3.5 V
100% Paced
49
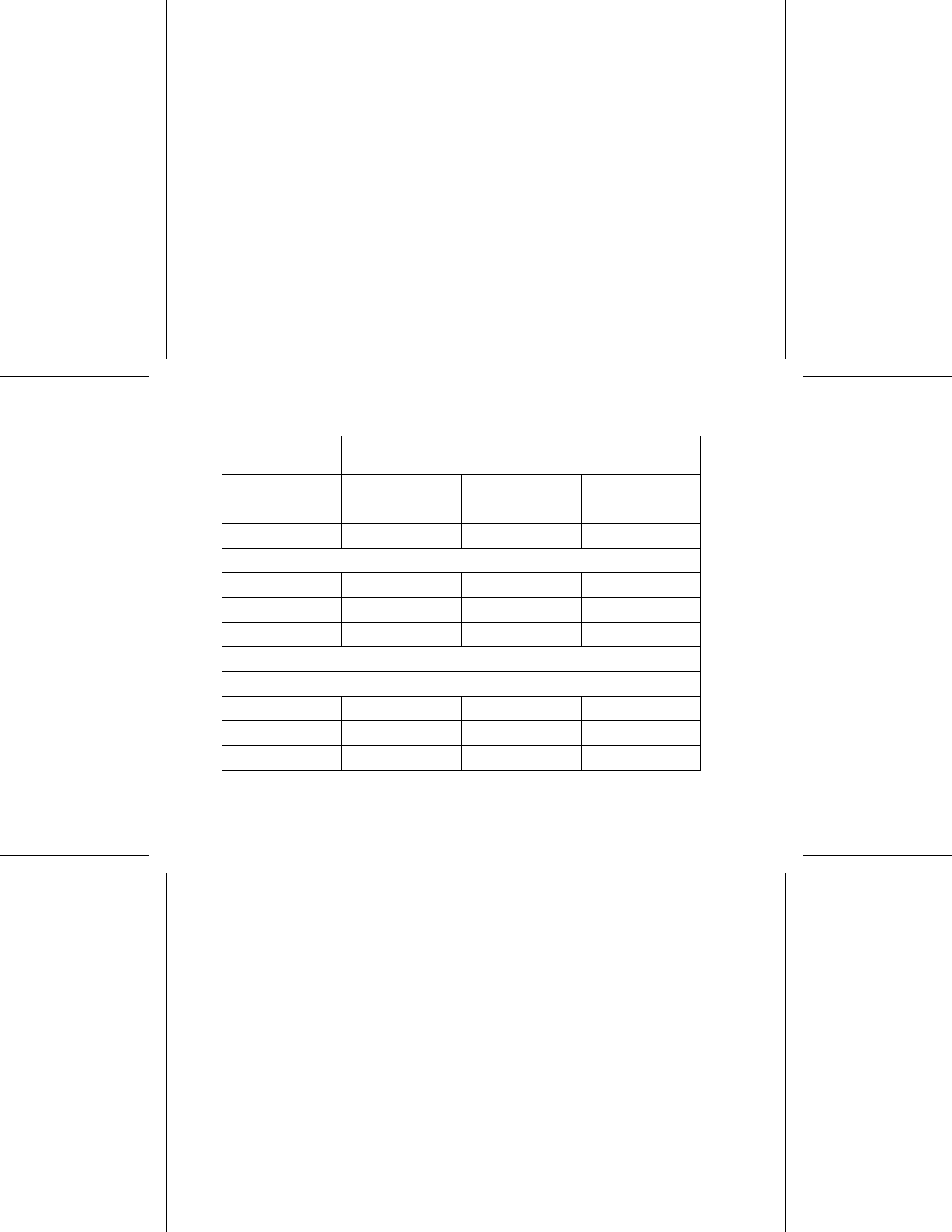

Table 5. INGENIO Longevity Projections (Years) (continued)
Amplitude and
Pacing
Modelsa
50% Paced
500 Ω9.3 7.9 11.3
750 Ω9.5 8.4 11.8
1000 Ω9.6 8.6 12.1
a. Assumes ZIP telemetry use for 1 hour at implant and for 20 minutes during each quarterly
follow-up.
Table 6. INGENIO Longevity Projections (Years) with Right Ventricular
Automatic Capture
Amplitude and
Pacing
Modelsa
K172 SR K173 DR K174 DR EL
Automatic Capture On (A = 3.5 Vb, V = 1.0 V [assuming a threshold of 0.5])
100% Paced
51
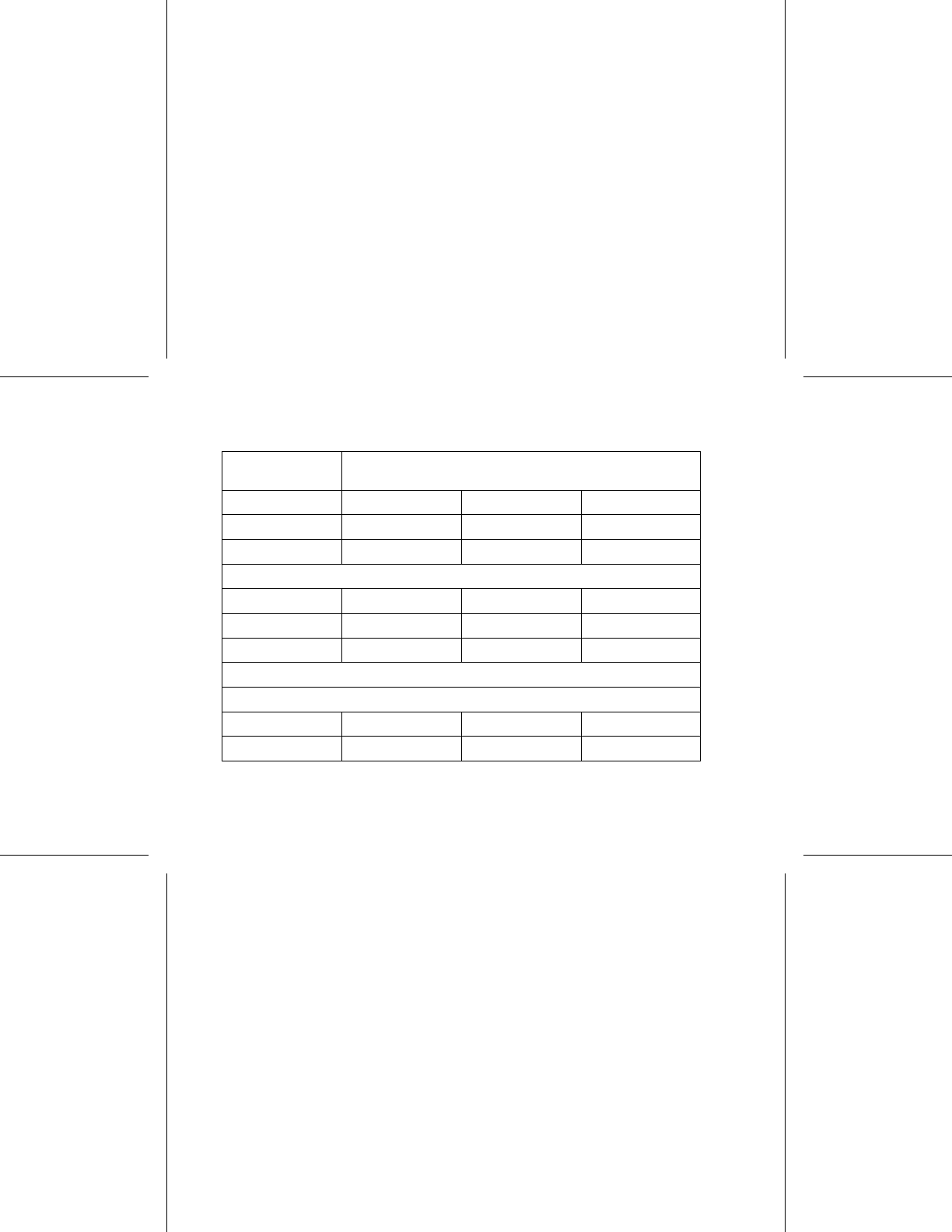
Table 6. INGENIO Longevity Projections (Years) with Right Ventricular
Automatic Capture (continued)
Amplitude and
Pacing
Modelsa
500 Ω9.7 6.8 9.6
750 Ω9.8 7.3 10.5
1000 Ω9.8 7.8 11.0
50% Paced
500 Ω9.9 7.9 11.2
750 Ω9.9 8.3 11.6
1000 Ω9.9 8.5 11.9
Automatic Capture On (A = 2.5 Vb, V = 1.0 V [assuming a threshold of 0.5])
100% Paced
500 Ω9.7 7.8 11.0
750 Ω9.8 8.2 11.5
52
Table 6. INGENIO Longevity Projections (Years) with Right Ventricular
Automatic Capture (continued)
Amplitude and
Pacing
Modelsa
1000 Ω9.8 8.4 11.8
50% Paced
500 Ω9.9 8.5 12.0
750 Ω9.9 8.8 12.3
1000 Ω9.9 8.9 12.4
a. Assumes ZIP telemetry use for 1 hour at implant and for 20 minutes during each quarterly
follow-up.
b. This value is not applicable in single chamber devices programmed to VVI(R).
Longevities at “worst case” settings of 5.0 V, 500 Ω, 1.0 ms are: 3.2 years for K172;
1.7 years for K173; 2.7 years for K174 at 70 ppm, and 2.4 years for K172; 1.1 years
for K173; 1.9 years for K174 at 100 ppm.
Longevities at an LRL of 70 ppm, 500 Ω, 0.5 ms, 100% paced, sensors On, and pacing
mode most comprehensive are: K172 at 2.5 V = 7.9 years, at 5.0 V = 4.7 years; K173 at
2.5 V = 6.3 years, at 5.0 V = 2.9 years; K174 at 2.5 V = 8.9 years, at 5.0 V = 4.3 years.
53

NOTE: The energy consumption in the longevity table is based upon theoretical
electrical principles and verified via bench testing only.
The pulse generator longevity may increase with a decrease in any of the following:
•Pacingrate
• Pacing pulse amplitude(s)
• Pacing pulse width(s)
• Percentage of paced to sensed events
Longevity is also reduced in the following circumstances:
• With a decrease in pacing impedance
• When Patient Triggered Monitor is programmed to On for 60 days, longevity is
reduced by approximately 5 days
• One hour of additional ZIP wandless telemetry reduces longevity by approximately
9 days.
Device longevity may also be affected by:
• Tolerances of electronic components
• Variations in programmed parameters
• Variations in usage as a result of patient condition
54

Refer to the PRM Summary and Battery Detail Summary screens for an estimate of
pulse generator longevity specific to the implanted device.
WARRANTY INFORMATION
A limited warranty certificate for the pulse generator is packaged with the device. For
additional copies, contact Boston Scientific using the information on the back cover.
PRODUCT RELIABILITY
It is Boston Scientific’s intent to provide implantable devices of high quality and
reliability. However, these devices may exhibit malfunctions that may result in lost or
compromised ability to deliver therapy. These malfunctions may include the following:
• Premature battery depletion
• Sensing or pacing issues
• Error codes
• Loss of telemetry
Refer to Boston Scientific’s CRM Product Performance Report on
www.bostonscientific.com for more information about device performance, including
the types and rates of malfunctions that these devices have experienced historically.
While historical data may not be predictive of future device performance, such data
can provide important context for understanding the overall reliability of these types of
products.
55

Sometimes device malfunctions result in the issuance of product advisories. Boston
Scientific determines the need to issue product advisories based on the estimated
malfunction rate and the clinical implication of the malfunction. When Boston Scientific
communicates product advisory information, the decision whether to replace a device
should take into account the risks of the malfunction, the risks of the replacement
procedure, and the performance to date of the replacement device.
PATIENT COUNSELING INFORMATION
The following topics should be discussed with the patient prior to discharge.
• External defibrillation—the patient should contact their physician to have their
pulse generator system evaluated if they receive external defibrillation
• Signs and symptoms of infection
• Symptoms that should be reported (e.g., sustained high-rate pacing requiring
reprogramming)
• Protected environments—the patient should seek medical guidance before
entering areas protected by a warning notice that prevents entry by patients who
have a pulse generator
• Avoiding potential sources of EMI in home, work, and medical environments
• Reliability of their pulse generator ("Product Reliability" on page 55)
56

• Activity restrictions (if applicable)
• Minimum heart rate (lower rate limit of the pulse generator)
• Frequency of follow up
• Travel or relocation—Follow-up arrangements should be made in advance if the
patient is leaving the country of implant
• Patient ID card—the patient should be advised to carry their patient ID card at all
times (a temporary patient ID card is provided with the device, and a permanent
ID card will be sent to the patient 4 to 6 weeks after the implant form is received
by Boston Scientific)
Patient Handbook
The Patient Handbook is provided for each device.
It is recommended that you discuss the information in the Patient Handbook with
concerned individuals both before and after implantation so they are fully familiar with
pulse generator operation.
For additional copies, contact Boston Scientific using the information on the back cover.
57
LEAD CONNECTIONS
Lead connections are illustrated below.
CAUTION: Prior to implantation, confirm the lead-to-pulse generator compatibility.
Using incompatible leads and pulse generators can damage the connector and/or
result in potential adverse consequences, such as undersensing of cardiac activity
or failure to deliver necessary therapy.
CAUTION: If the Lead Configuration is programmed to Bipolar when a unipolar lead
is implanted, pacing will not occur.
IS-1
UNI/BI
[1] RA/RV [2] Suture Hole
Figure 2. Lead connections and setscrew locations, RA/RV: IS1
58
RA
RV
IS-1
UNI/BI
IS-1
UNI/BI
[1] RA [2] RV [3] Suture Hole
Figure 3. Lead connections and setscrew locations, RA: IS-1, RV: IS-1
NOTE: The pulse generator case is used as a pace electrode when the pulse
generator has been programmed to a unipolar lead setting.
IMPLANTING THE PULSE GENERATOR
Implant the pulse generator by performing the following steps in the sequence provided.
Some patients may require pacing therapies immediately upon connecting the leads
to the pulse generator. If modifications to the nominal settings are needed, consider
programming the pulse generator before or in parallel with implanting the lead system
and forming the implantation pocket.
59

Step A: Check Equipment
It is recommended that instrumentation for cardiac monitoring, defibrillation, and lead
signal measurement should be available during the implant procedure. This includes
the PRM system with its related accessories and the software application. Before
beginning the implantation procedure, become completely familiar with the operation of
all the equipment and the information in the respective operator’s and user’s manuals.
Verify the operational status of all equipment that may be used during the procedure. In
case of accidental damage or contamination, the following should be available:
• Sterile duplicates of all implantable items
• Sterile wand
•SterilePSAcables
• Torque and non-torque wrenches
• External defibrillation equipment
Step B: Interrogate and Check the Pulse Generator
To maintain sterility, test the pulse generator as described below before opening the
sterile blister tray. The pulse generator should be at room temperature to ensure
accurately measured parameters.
60

1. Interrogate the pulse generator using the PRM. Verify that the pulse generator’s
device mode is programmed to Storage. If otherwise, contact Boston Scientific
using the information on the back cover.
2. Review the pulse generator’s current battery status. Counters should be at zero.
If the pulse generator battery status is not at full capacity, do not implant the pulse
generator. Contact Boston Scientific using the information on the back cover.
3. If a unipolar pacing configuration is required at implant, program the lead
configuration to unipolar before implant.
Step C: Implant the Lead System
The pulse generator requires a lead system for pacing and sensing.
Selection of lead configuration and specific surgical procedures is a matter of
professional judgment. The following leads are available for use with the pulse
generator depending on the device model.
• Unipolar or bipolar atrial lead
• Unipolar or bipolar right ventricular lead.
NOTE: Single-chamber devices can be used with either an atrial or a ventricular lead.
NOTE: Using bipolar pacing leads will reduce the chance of myopotential sensing.
61

CAUTION: The absence of a lead or plug in a lead port may affect device
performance. If a lead is not used, be sure to properly insert a plug in the unused port,
and then tighten the setscrew onto the plug.
CAUTION: If a dual-chamber device is programmed to AAI(R), ensure that a
functional RV lead is present. In the absence of a functional RV lead, programming
to AAI(R) may result in undersensing or oversensing.
CAUTION: Do not suture directly over the lead body, as this may cause structural
damage. Use the lead stabilizer to secure the lead proximal to the venous entry site to
prevent lead movement.
Implant the leads via the surgical approach chosen.
When replacing a previously implanted pulse generator, it may be necessary to use an
adapter to enable the new pulse generator to be connected to the existing leads. When
using an adapter, follow the connection procedure described in the applicable adapter
product data sheet. Always connect the adapter to the lead and repeat threshold and
sensing measurements before connecting the adapter to the pulse generator.
Step D: Take Baseline Measurements
Once the leads are implanted, take baseline measurements. Evaluate the lead
signals. If performing a pulse generator replacement procedure, existing leads should
be reevaluated, (e.g., signal amplitudes, pacing thresholds, and impedance). The
62
use of radiography may help ensure lead position and integrity. If testing results are
unsatisfactory, lead system repositioning or replacement may be required.
• Connect the pace/sense lead(s) to a pacing system analyzer (PSA).
• Pace/sense lead measurements, measured approximately 10 minutes after
placement, are listed below. Note that the pulse generator measurements may
not exactly correlate to the PSA measurements due to signal filtering.
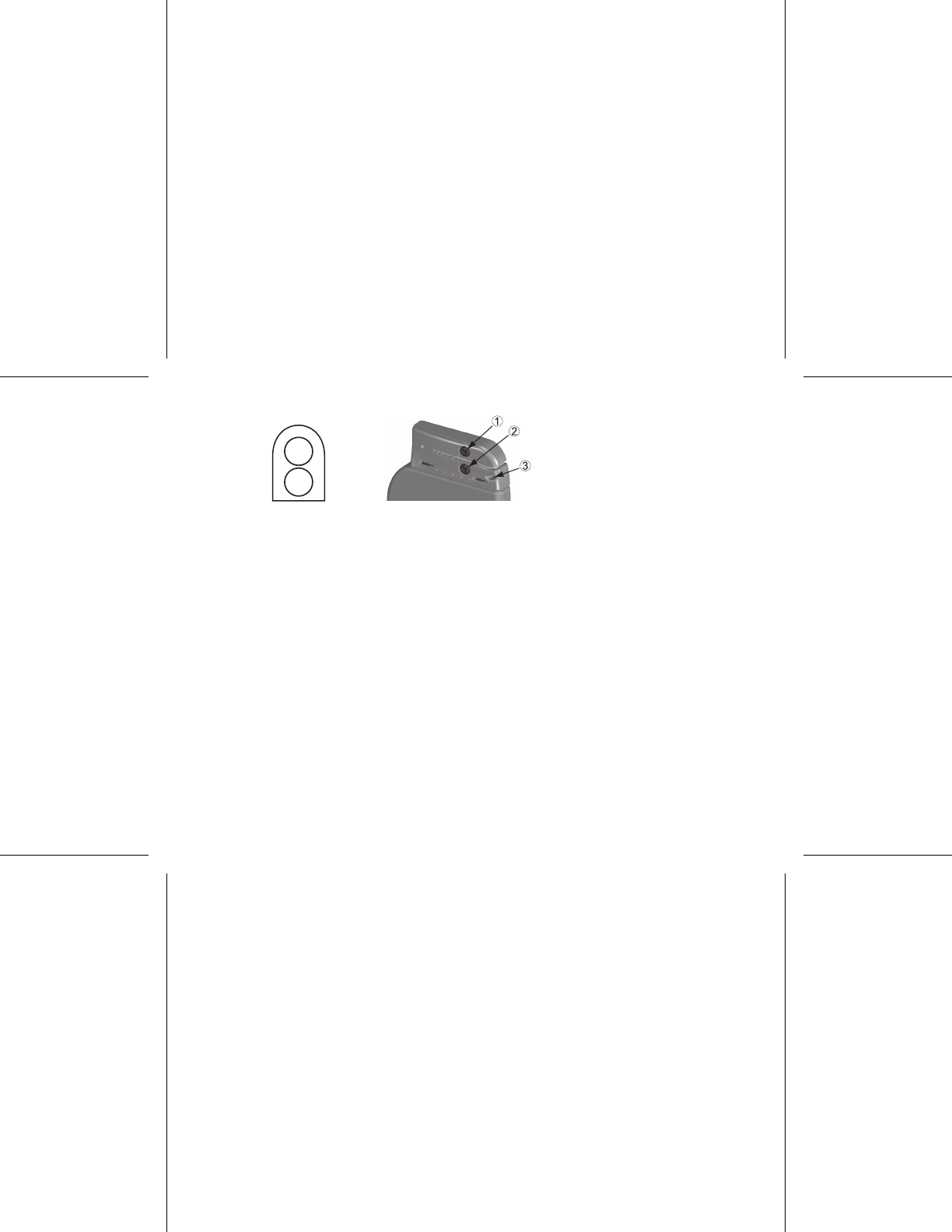
Table 7. Lead measurements
Pace/ sense lead (acute) Pace/ sense lead
(chronic)
R-wave amplitudeab >5mV >5mV
P-wave amplitudeab > 1.5 mV > 1.5 mV
R-wave durationbcd < 100 ms < 100 ms
Pacing threshold (right
ventricle)
< 1.5 V endocardial
< 2.0 V epicardial
< 3.0 V endocardial
<3.5Vepicardial
Pacing threshold (atrium) < 1.5 V endocardial < 3.0 V endocardial
63
Table 7. Lead measurements (continued)
Pace/ sense lead (acute) Pace/ sense lead
(chronic)
Lead impedance (at 5.0
V and 0.5 ms atrium and
right ventricle)
200–2000 Ω200–2000 Ω
a. Amplitudes less than 2 mV cause inaccurate rate counting in the chronic state, and result in
inability to sense a tachyarrhythmia or the misinterpretation of a normal rhythm as abnormal.
b. Lower R-wave amplitudes and longer duration may be associated with placement in ischemic
or scarred tissues. Since signal quality may deteriorate chronically, efforts should be made to
meet the above criteria by repositioning the leads to obtain signals with the largest possible
amplitude and shortest duration.
c. Durations longer than 135 ms (the pulse generator’s refractory period) may result in inaccurate
cardiac rate determination, inability to sense a tachyarrhythmia, or in the misinterpretation
of a normal rhythm as abnormal.
d. This measurement is not inclusive of current of injury.
Step E: Form the Implantation Pocket
Using standard operating procedures to prepare an implantation pocket, choose the
position of the pocket based on the implanted lead configuration and the patient’s
body habitus. Giving consideration to patient anatomy and pulse generator size and
motion, gently coil any excess lead and place adjacent to the pulse generator. It is
64

important to place the lead into the pocket in a manner that minimizes lead tension,
twisting, sharp angles, and/or pressure. Pulse generators are typically implanted
subcutaneously in order to minimize tissue trauma and facilitate explant. However,
deeper implantation (e.g., subpectoral) may help avoid erosion or extrusion in some
patients. Verify magnet function and wanded telemetry to ensure the pulse generator is
within acceptable range.
If an abdominal implant is suitable, it is recommended that implantation occur on the
left abdominal side.
If it is necessary to tunnel the lead, consider the following:
• If a Guidant tunneler is not used, cap the lead terminal pins. A Penrose drain,
large chest tube, or tunneling tool may be used to tunnel the leads.
• Gently tunnel the leads subcutaneously to the implantation pocket, if necessary.
• Reevaluate all lead signals to determine if any of the leads have been damaged
during the tunneling procedure.
If the leads are not connected to a pulse generator at the time of lead implantation,
they must be capped before closing the incision.
65

Step F: Connect the Leads to the Pulse Generator
To connect leads to the pulse generator, use only the tools provided in the pulse
generator sterile tray or accessory kit. Failure to use the supplied torque wrench may
result in damage to the setscrews, seal plugs, or connector threads. Do not implant
the pulse generator if the seal plugs appear to be damaged. Retain the tools until all
testing procedures are complete and the pulse generator is implanted.
Automatic Lead Detection
Until a right ventricular lead is detected (or any appropriate lead in a single chamber
device), the lead impedance is measured in both unipolar and bipolar configurations.
Upon insertion of the lead into the header the impedance measurement circuit will
detect an impedance which indicates that the device is implanted (automatic lead
detection). If the impedance is in range (200 – 2000 Ω, inclusive) the pulse generator
will automatically switch to the nominal parameters and start sensing and delivering
therapy. The pulse generator can also be programmed out of the Storage mode prior to
implant using the PRM.
NOTE: If the lead being used for automatic lead detection is unipolar, an in-range
impedance will not be obtained until the pulse generator is in stable contact with the
subcutaneous tissue of the pocket.
66

NOTE: Arrhythmia Logbook and stored EGM data will not be stored for the first two
hours after the lead is detected except for PaceSafe and patient triggered episodes.
If the device is programmed out of Storage, asynchronous pacing spikes could be
observed on intracardiac EGMs before bipolar RV lead insertion or before placing the
pulse generator into the subcutaneous pocket if a unipolar RV lead is present. These
subthreshold spikes will not occur once a bipolar RV lead is detected in the header or
when contact between the pacemaker case and subcutaneous tissue completes the
normal pacing circuit for a unipolar RV lead. If the device exits Storage as the result of
automatic lead detection, the pulse generator may take up to 2 seconds plus one LRL
interval before pacing begins as a result of lead detection.
Leads should be connected to the pulse generator in the following sequence (for pulse
generator header and setscrew location illustrations, refer to "Lead Connections" on
page 58):
NOTE: For single-chamber devices, use an RA or RV lead as appropriate.
a. Right ventricle. Connect the RV lead first because it is required to establish
RV-based timing cycles that yield appropriate sensing and pacing in all chambers,
regardless of the programmed configuration.
NOTE: Tightening the RV setscrew is not required for automatic lead detection
to occur but should be done to ensure full electrical contact.
67

• In models with an IS-1 RV lead port, insert and secure the terminal pin of
an IS-1 RV pace/sense lead.
b. Right atrium.
• In models with an IS-1 RA lead port, insert and secure the terminal pin of an
IS-1 atrial pace/sense lead.
Connect each lead to the pulse generator by following these steps (for additional
information about the torque wrench, refer to "Bidirectional Torque Wrench" on page
74):
a. Check for the presence of any blood or other body fluids in the lead ports on
the pulse generator header. If fluid inadvertently enters the ports, clean them
thoroughly with sterile water.
b. If applicable, remove and discard the tip protection before using the torque wrench.
c. Gently insert the torque wrench blade into the setscrew by passing it through the
preslit, center depression of the seal plug at a 90° angle (Figure 4 on page 69).
This will open up the seal plug, relieving any potential pressure build-up from the
lead port by providing a pathway to release trapped fluid or air.
NOTE: Failure to properly insert the torque wrench in the preslit depression of
the seal plug may result in damage to the plug and its sealing properties.
68
CAUTION: Do not insert a lead into the pulse generator connector without taking
the following precautions to ensure proper lead insertion:
• Insert the torque wrench into the preslit depression of the seal plug before
inserting the lead into the port, to release any trapped fluid or air.
• Visually verify that the setscrew is sufficiently retracted to allow insertion.
Use the torque wrench to loosen the setscrew if necessary.
• Fully insert each lead into its lead port and then tighten the setscrew onto
the terminal pin.
Figure 4. Inserting the torque wrench
69

d. With the torque wrench in place, fully insert the lead terminal into the lead port.
The lead terminal pin should be clearly visible beyond the connector block when
viewed through the side of the pulse generator header. Place pressure on the lead
to maintain its position and ensure that it remains fully inserted in the lead port.
CAUTION: Insert the lead terminal straight into the lead port. Do not bend the
lead near the lead-header interface. Improper insertion can cause insulation
or connector damage.
NOTE: If necessary, lubricate the lead connectors sparingly with sterile water to
make insertion easier.
NOTE: For IS-1 leads, be certain that the terminal pin visibly extends beyond
the connector block at least 1 mm.
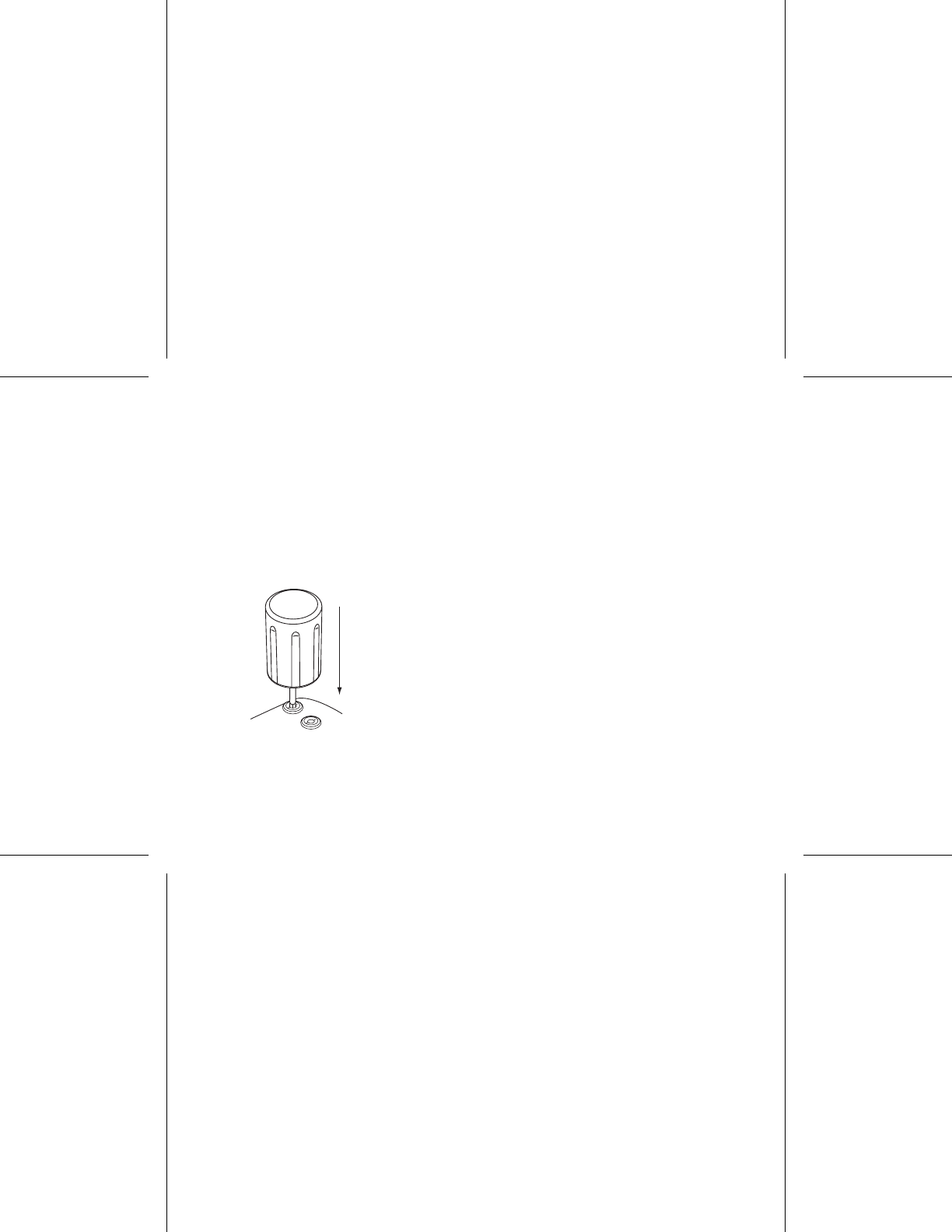
e. Apply gentle downward pressure on the torque wrench until the blade is fully
engaged within the setscrew cavity, taking care to avoid damage to the seal
plug. Tighten the setscrew by slowly turning the torque wrench clockwise, until it
ratchets once. The torque wrench is preset to apply the proper amount of force to
the captive setscrew; additional rotation and force is unnecessary.
f. Remove the torque wrench.
g. Apply gentle traction to the lead to ensure a secure connection.
70

h. If the lead terminal is not secure, attempt to reseat the setscrew. Reinsert the
torque wrench as described above, and loosen the setscrew by slowly turning the
wrench counterclockwise, until the lead is loose. Then repeat the sequence above.
i. If a lead port is not used, insert a plug into the unused port and tighten the
setscrew.
CAUTION: The absence of a lead or plug in a lead port may affect device
performance. If a lead is not used, be sure to properly insert a plug in the unused
port, and then tighten the setscrew onto the plug.
Step G: Evaluate Lead Signals
1. Evaluate the pace/sense lead signals by viewing the real-time EGMs and markers.
Lead measurements should reflect those above (Table 7 on page 63)
Depending on the patient’s intrinsic rhythm, it may be necessary to temporarily
adjust pacing parameters to allow assessment of pacing and sensing. If proper
pacing and/or sensing are not demonstrated, disconnect the lead from the pulse
generator and visually inspect the connector and leads. If necessary, retest the
lead.
CAUTION: Take care to ensure that artifacts from the ventricles are not present on
the atrial channel, or atrial oversensing may result. If ventricular artifacts are present in
the atrial channel, the atrial lead may need to be repositioned to minimize its interaction.
71

2. Evaluate all lead impedances.
Step H: Program the Pulse Generator
1. Check the programmer clock and set and synchronize the pulse generator as
necessary so that the proper time appears on printed reports and PRM strip
chart recordings.
2. Program the pulse generator appropriately if a lead port(s) is not used.
Step I: Implant the Pulse Generator
1. Ensure that the pulse generator has good contact with surrounding tissue of the
implantation pocket, and then suture it in place to minimize device migration (for
suture hole location illustrations, refer to "Lead Connections" on page 58). Gently
coil excess lead and place adjacent to the pulse generator. Flush the pocket with
saline solution, if necessary, to avoid a dry pocket.
WARNING: Do not kink, twist, or braid the lead with other leads as doing so
could cause lead insulation abrasion damage or conductor damage.
2. Close the implantation pocket. Consideration should be given to place the leads
in a manner to prevent contact with suture materials. It is recommended that
absorbable sutures be used for closure of tissue layers.
72

3. If Electrocautery mode was used during the implant procedure, cancel it when
done.
4. Confirm final programmed parameters.
CAUTION: Following any Sensitivity parameter adjustment or any modification
of the sensing lead, always verify appropriate sensing. Programming Sensitivity
to the highest value (lowest sensitivity) may result in undersensing of cardiac
activity. Likewise, programming to the lowest value (highest sensitivity) may result
in oversensing of non-cardiac signals.
5. Use the PRM to print out parameter reports and save all patient data.
Step J: Complete and Return the Implantation Form
Within ten days of implantation, complete the Warranty Validation and Lead Registration
form and return the original to Boston Scientific along with a copy of the patient data
saved from the PRM. This information enables Boston Scientific to register each
implanted pulse generator and set of leads, initiate the warranty period, and provide
clinical data on the performance of the implanted system. Keep a copy of the Warranty
Validation and Lead Registration form and programmer printouts, and the original
patient data for the patient’s file.
73

Complete the temporary patient identification card and give it to the patient. After
receiving the validation form, Boston Scientific sends the patient a permanent
identification card.
NOTE: A registration form is packaged with each pulse generator lead. If completing
the pulse generator Warranty Validation and Lead Registration form for the pulse
generator, completing separate validation forms for each lead is not necessary.
BIDIRECTIONAL TORQUE WRENCH
A torque wrench (model 6628) is included in the sterile tray with the pulse generator,
and is designed for tightening and loosening #2-56 setscrews, captured setscrews, and
setscrews on this and other Boston Scientific pulse generators and lead accessories
that have setscrews that spin freely when fully retracted (these setscrews typically
have white seal plugs).
This torque wrench is bidirectional, and is preset to apply adequate torque to the
setscrew and will ratchet when the setscrew is secure. The ratchet release mechanism
prevents overtightening that could result in device damage. To facilitate the loosening
of tight extended setscrews, this wrench applies more torque in the counterclockwise
direction than in the clockwise direction.
NOTE: As an additional safeguard, the tip of the torque wrench is designed to break
off if used to overtighten beyond preset torque levels. If this occurs, the broken tip must
be extracted from the setscrew using forceps.
74

This torque wrench may also be used for loosening setscrews on other Boston
Scientific pulse generators and lead accessories that have setscrews that tighten
against a stop when fully retracted (these setscrews typically have clear seal plugs).
However, when retracting these setscrews, stop turning the torque wrench when the
setscrew has come in contact with the stop. The additional counterclockwise torque of
this wrench may cause these setscrews to become stuck if tightened against the stop.
Loosening Stuck Setscrews
Follow these steps to loosen stuck setscrews:
1. From a perpendicular position, tilt the torque wrench to the side 20º to 30º from
the vertical center axis of the setscrew (Figure 5 on page 76).
2. Rotate the wrench clockwise (for retracted setscrew) or counterclockwise (for
extended setscrew) around the axis three times, such that the handle of the
wrench orbits the centerline of the screw (Figure 5 on page 76). The torque
wrench handle should not turn or twist during this rotation.
3. As needed, you may attempt this up to four times with slightly more angle each
time. If you cannot fully loosen the setscrew, use the #2 torque wrench from
Wrench Kit Model 6501.
4. Once the setscrew has been freed, it may be extended or retracted as appropriate.
5. Discard the torque wrench upon completion of this procedure.
75
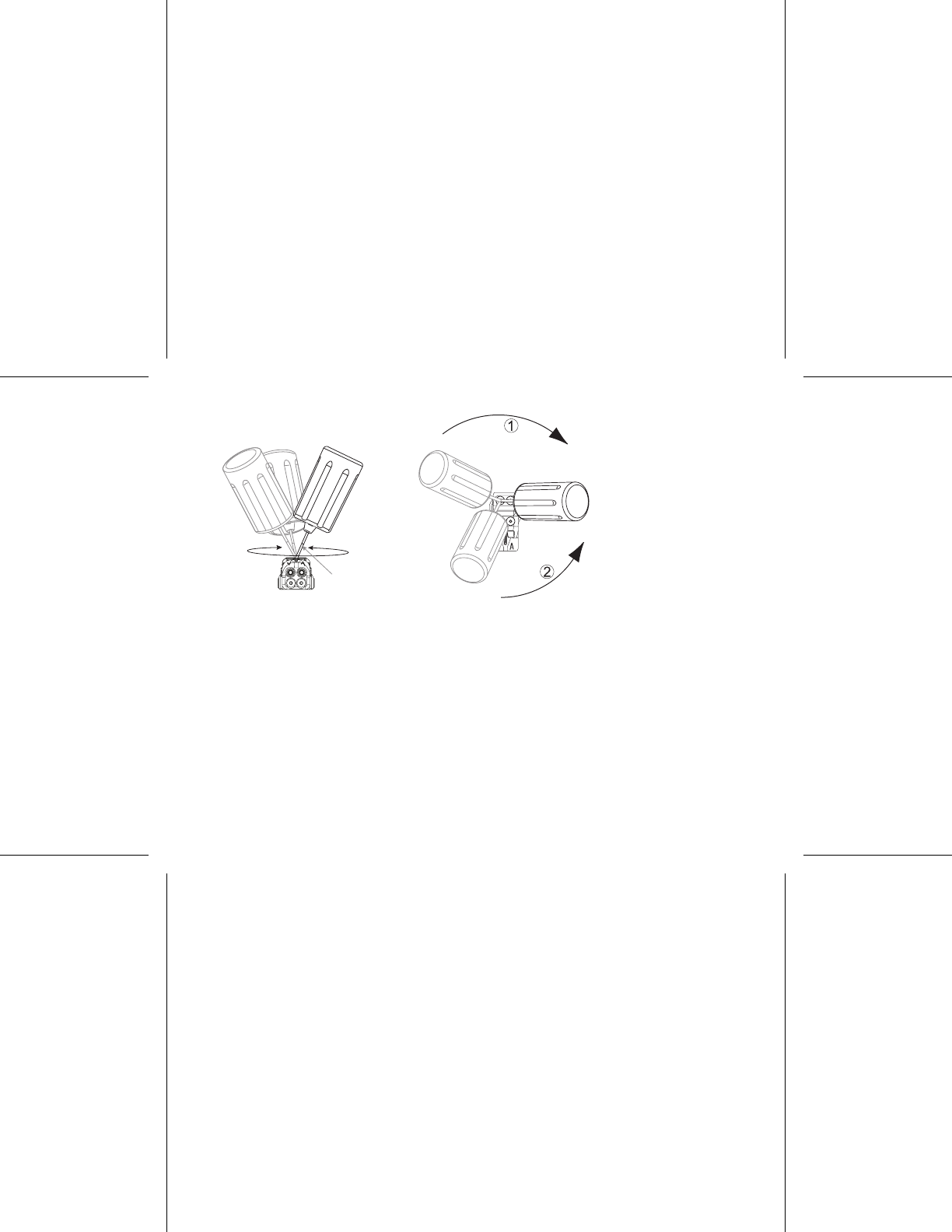
20°–30°
[1] Clockwise rotation to free setscrews stuck in the retracted position [2]
Counterclockwise rotation to free setscrews stuck in the extended position
Figure 5. Rotating the torque wrench to loosen a stuck setscrew
FOLLOW UP TESTING
It is recommended that device functions be evaluated with periodic follow-up testing by
trained personnel. Follow up guidance below will enable thorough review of device
performance and associated patient health status throughout the life of the device.
76

Predischarge Follow Up
The following procedures are typically performed during the predischarge follow up
test using PRM telemetry:
1. Interrogate the pulse generator and review the Summary screen.
2. Verify pacing thresholds, lead impedance, and amplitude of intrinsic signals.
3. Review counters and histograms.
4. When all testing is complete, perform a final interrogation and save all the patient
data.
5. Print the Quick Notes and Patient Data reports to retain in your files for future
reference.
6. Clear the counters and histograms so that the most recent data will be displayed
at the next follow up session. Counters and histograms can be cleared by
pressing Reset on the Histogram screen, Tachy Counters screen, or Brady
Counters screen.
Routine Follow Up
During early and middle life of the device, monitor performance by routine follow up
one month after the predischarge check and at least annually thereafter. Office visits
77
may be supplemented by remote monitoring where available. As always, the physician
should evaluate the patient’s current health status, device status and parameter values,
and local medical guidelines to determine the most appropriate follow up schedule.
When the device reaches One Year Remaining status and/or a magnet rate of 90 ppm
is observed, follow up at least every three months to facilitate timely detection of
replacement indicators.
NOTE: Because the duration of the device replacement timer is three months (starting
when Explant status is reached), three month follow up frequency is particularly
important after the One Year Remaining status is reached.
Consider performing the following procedures during a routine follow-up test:
1. Interrogate the pulse generator and review the Summary screen.
2. Verify pacing thresholds, lead impedance, and amplitude of intrinsic signals.
3. Print the Quick Notes and Patient Data reports to retain in your files for future
reference.
4. Review the Arrhythmia Logbook screen and for episodes of interest, print episode
details and stored electrogram information.
5. Clear the counters and histograms so that the most recent episode data will be
displayed at the next follow-up session.
78

6. Verify that important programmed parameter values (e.g., lower rate limit, AV
Delay, rate adaptive pacing, output amplitude, pulse width, sensitivity) are optimal
for current patient status.
NOTE: Echo-Doppler studies may be used to non-invasively evaluate AV Delay and
other programming options post-implant.
EXPLANTATION
NOTE: Return all explanted pulse generators and leads to Boston Scientific.
Examination of explanted pulse generators and leads can provide information for
continued improvement in system reliability and warranty considerations.
WARNING: Do not reuse, reprocess, or resterilize. Reuse, reprocessing, or
resterilization may compromise the structural integrity of the device and/or lead to
device failure which, in turn, may result in patient injury, illness, or death. Reuse,
reprocessing, or resterilization may also create a risk of contamination of the device
and/or cause patient infection or cross-infection, including, but not limited to, the
transmission of infectious disease(s) from one patient to another. Contamination of the
device may lead to injury, illness, or death of the patient.
Complete and send an Observation/Complication/Out-of-Service Reporting form to
Boston Scientific when any of the following occur:
• When a product is removed from service.
79

• In the event of patient death (regardless of cause), along with an autopsy report,
if performed.
• For other observation or complications reasons.
NOTE: Disposal of explanted pulse generators and/or leads is subject to applicable
laws and regulations. For a Returned Product Kit, contact Boston Scientific using the
informationonthebackcover.
NOTE: Discoloration of the pulse generator may have occurred due to a normal
process of anodization, and has no effect on the pulse generator function.
CAUTION: Be sure that the pulse generator is removed before cremation. Cremation
and incineration temperatures might cause the pulse generator to explode.
CAUTION: Before explanting, cleaning, or shipping the device, complete the following
actions to prevent overwriting of important therapy history data:
• Program the pulse generator Brady Mode to Off
• Program Ventricular Tachy EGM Storage to Off
Clean and disinfect the device using standard biohazard handling techniques.
Consider the following items when explanting and returning the pulse generator and/or
lead:
80

• Interrogate the pulse generator and print a Combined Follow-up report.
• Deactivate the pulse generator before explantation.
• Disconnect the leads from the pulse generator.
• If leads are explanted, attempt to remove them intact, and return them regardless
of condition. Do not remove leads with hemostats or any other clamping tool
that may damage the leads. Resort to tools only if manual manipulation cannot
free the lead.
• Wash, but do not submerge, the pulse generator and leads to remove body fluids
and debris using a disinfectant solution. Do not allow fluids to enter the pulse
generator’s lead ports.
• UseaBostonScientific Returned Product Kit to properly package the pulse
generator and send it to Boston Scientific.
81

82

For additional technical reference guides, go to
www.bostonscientific.com/ifu.
Boston Scientific
4100 Hamline Avenue North
St. Paul, MN 55112–5798 USA
www.bostonscientific.com
1.800.CARDIAC (227.3422)
+1.651.582.4000
© 2011 Boston Scientificoritsaffiliates.
All rights reserved.
358566-004 EN US 6/11
FCC ID: ESCCRMV17311 *358566-004*