Boston Scientific Neuromodulation PSC5210W Precision SCS System Remote Control User Manual II Physicians Lead and Extension
Boston Scientific Neuromodulation Corporation Precision SCS System Remote Control II Physicians Lead and Extension
Contents
Lead manual
Physician Lead Manual
CAUTION:
Federal law restricts this device to sale, distribution and use by or on
the order of a physician.
MP9055183 Rev A
DRAFT

Physician Lead Manual
ii ©2004 by Advanced Bionics Corporation. All Rights Reserved.
Copyright
©2004 by Advanced Bionics Corporation. All Rights Reserved. Any
copying, reproduction or translation of all or part of the contents of
this document without the express written permission of Advanced
Bionics Corporation is strictly forbidden by the provisions of the law
of March 11th, 1957.
Guarantees
Advanced Bionics Corporation reserves the right to modify, without
prior notice, information relating to its products in order to improve
their reliability or operating capacity.
Registered Trademarks
Linear™, BionicNavigator™ and Precision™ are registered trademarks
of Advanced Bionics Corporation. Velcro® is a registered mark of
Velcro Industries, Manchester, New Hampshire. Other brands and
their products are trademarks or registered trademarks of their respec-
tive holders and should be noted as such.

Table of Contents
i
Table of Contents
Introduction ............................................... 1
Manual Overview ........................................................... 1
Product Description .......................................................... 1
Indications for Use ...........................................................3
Precision System Clinical Summary .....................................3
Contraindications ..........................................................10
Safety Information ................................... 11
Warnings .................................................................... 11
Precautions .................................................................. 12
Adverse Effects .............................................................14
Instructions for the Physician .............................................16
Package Contents .................................... 17
Lead Kit - Model SC-2108 ............................................. 17
Lead Extension Kit - Model SC-3108 ................................17
Sterilization and Handling ........................ 18
Sterilization ..................................................................18
Handling .....................................................................18
Storage .......................................................................19
Guidelines for Trial-phase Implantation .... 20
Pre-op Instructions ..........................................................20
Lead Placement ............................................................ 21
Connecting the OR Cable Assembly ................................. 23
Intraoperative Stimulation Testing ......................................26
OPTION A: Temporary Lead Trial .................................... 26
OPTION B: Permanent Lead Trial ..................................... 28

ii
Physician’s Lead and Extension Manual
Connecting to the Trial Stimulator ............. 36
Guidelines for Permanent Implantation .... 38
Percutaneous Lead/Extension Removal ..............................38
IPG Implantation ...................................... 40
Tool Assembly .............................................................. 41
Tunneling The Lead ........................................................ 41
Connecting To the IPG ...................................................45
Specifications and Technical Data ............. 48
Lead ..........................................................................48
Lead Extension ............................................................. 49
Registration Information .......................... 50
Technical Service ...................................... 51
Limited Warranty ..................................... 52

Introduction
1
Introduction
Manual Overview
This manual provides basic information for the implantation and use
of the Advanced Bionics® Lead Model SC-2108 and Lead Extension
Model SC-3108. These products are designed to be percutaneously or
surgically implanted for use with the PrecisionTM Spinal Cord Stimu-
lation (SCS) System to aid in the management of chronic intractable
pain. Information on other system components and their operation can
be found in the BionicNavigatorTM Software Guide.
General surgical guidelines are presented for temporary and perma-
nent implantation of leads and extensions.
Product Description
Lead
The lead functions as a component of the Precision system by deliver-
ing electrical stimulation to the nerve structures in the dorsal aspect of
the spinal cord, resulting in an inhibition of pain sensation.
Model SC-2108 has eight electrode contacts located near the distal
end. Each contact is 3 mm in length and is spaced 1 mm from the
adjacent contact. The lead body is made of medical grade polyure-
thane with a stiffer proximal end to aid insertion into the connector.
To aid in intraoperative testing and positioning, a curved stylet is pre-
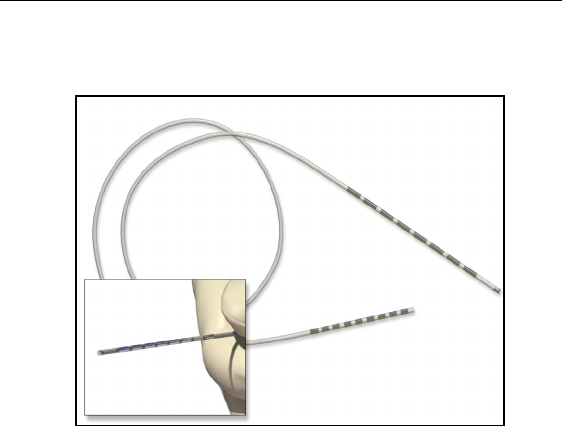
2
Physician Lead Manual
inserted into the lead. The lead can be connected to either an exten-
sion or directly to an implantable pulse generator (IPG).
Lead Extension
Lead Extension Model SC-3108 is designed to connect the Lead
Model SC-2108 to the Advanced Bionics Precision implantable pulse
generator for spinal cord stimulation. The extension may be added to
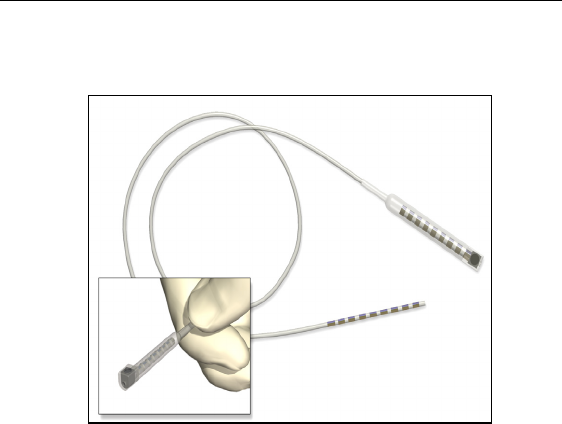
Introduction
3
a lead to externalize the lead for a trial phase or to extend a lead when
a permanent IPG is implanted.
Indications for Use
The Advanced Bionics Precision™ Spinal Cord Stimulator System
(Precision System) is indicated as an aid in the management of
chronic intractable pain of the trunk and/or limbs, including unilateral
or bilateral pain associated with the following: failed back surgery
syndrome, intractable low back pain and leg pain.
Precision System Clinical Summary
Determination of the safety and effectiveness of the PRECISION Sys-
tem was based on available published clinical studies for similar
implanted spinal cord stimulation systems. The PRECISION System
is similar to the SCS systems reported in published literature in
intended use, target patient population, technology, device design, and
output characteristics. Therefore, the clinical data from the published
literature described below represents evidence supporting the safety
and effectiveness of the PRECISION System for the treatment
chronic intractable pain of the trunk and/or limbs, including unilateral

4
Physician Lead Manual
or bilateral pain associated with the following: failed back surgery
syndrome, intractable low back and leg pain.
Efficacy Evaluation
Three (3) clinical literature studies were used to support the effective-
ness of the PRECISION System (Ohnmeiss et al. 1996, Villavincen-
cio et al. 2000, Hassenbach SJ et al. 1995). The studies included a
total of 116 patients that were implanted with an SCS system. A total
of approximately 3166 device months of experience was depicted
from the retrospective clinical evaluation. All three studies examined
the effectiveness of SCS on patients with chronic pain of the trunk
and/or limbs including unilateral or bilateral pain associated with the
following: failed back surgery syndrome or intractable low back and
leg pain. In all studies, a totally implantable spinal cord stimulator
was used in association with a percutaneous and/or surgical lead.
These studies provide the same diagnostic or therapeutic intervention
for the same disease/conditions and patient population as the PRECI-
SION System.
The prospective study by Ohnmeiss et al. 1996, examined the long-
term effectiveness of SCS in patients with intractable leg pain. Forty
patients were implanted with SCS systems and evaluated at 6 weeks,
12 months, and 24 months follow-up. Outcome measures included the
VAS, pain drawings, medication use, SIP (Sickness Impact Profile),
isometric lower extremity testing, and patient questionnaires. An
intent-to-treat analysis was performed. After patients had SCS for 24
months, leg pain, pain when walking, standing pain, pain’s effect on
overall lifestyle, and the total analog scale scores were significantly
improved from baseline. In this study, 25% of the implanted patients
had greater than 50% improvement in pain rating.
In addition, 3 patients from this study had their stimulators reposi-
tioned due to pain at the original location. Three patients had reopera-
tions to adjust lead position; 1 patient required 2 reoperations, 1
patient had the device removed due to infection and later to have a
new device implanted. A diabetic patient had skin problems which

Introduction
5
required device removal; a new device was later implanted. Two
patients had the device removed due to unsatisfactory pain relief.
The prospective study performed by Villavicencio et al. 2000
included 41 patients with pain of various etiologies. The majority of
the patients, 24 (59%), had Failed Back Surgery Syndrome (FBSS), 7
(17%) had Complex Regional Pain Syndrome (CRPS I and II), 4
(10%) had neuropathic pain syndrome, and 6 (15%) were diagnosed
as stroke or other. Patients underwent an initial trial period for SCS
with temporary leads. If the trial resulted in greater than 50% reduc-
tion in the patient’s pain, as measured by the VAS, the patient was
implanted with a SCS system. In this study, 27/41 patients, 66%, had
permanent implants. All patients were examined after 6 weeks. Pain
measurements were assessed at 3-6 month intervals for the first year
and annually thereafter. The median long-term follow-up was 34
months. A total of 24/27 (89%), reported greater than 50% reduction
in pain. Since the majority of the patients were treated for FBSS, this
article supports the use of SCS for the treatment of FBSS.
In this study, one patient required a revision because of electrode frac-
ture. One patient required removal of the system due to local infec-
tion. One patient required replacement of the IPG due to mechanical
failure. Overall, 16 of 27 (59%) patients required a total of 36 reposi-
tioning procedures.
A retrospective analysis performed by Hassenbusch SJ et al. 1995
included patients with chronic lower body pain, predominately neuro-
pathic pain and pain either midline lower back and/or unilateral or
bilateral leg pain treated over a 5 year period. The study was a com-
parison of SCS to spinal infusion of opiods. For patients with radicu-
lar pain involving one leg with or without unilateral buttock pain, a
trial of SCS was recommended first. For patients with midline back
pain and /or bilateral leg pain, a trial of long-term spinal infusion was
recommended first. If the patients failed screening with either of these
modalities, the other was then tested. If the treatment reduced the pain
by 50%, the systems were internalized. A retrospective analysis of
6
Physician Lead Manual
patients with unilateral leg and/or buttock pain treated initially with
SCS and bilateral leg or mainly low back pain treated initially with
spinal infusions of opioids was then done.
In this study, 42 patients were screened; 26 (62%) patients received
spinal stimulation; 16 (38%) received opioids via a spinal infusion
pump. Five patients did not receive adequate pain relief with SCS; 3
(7%) of these patients underwent trial spinal infusions and had effec-
tive pain relief. There were 4 (10%) patients who underwent a trial of
spinal infusion of opioid but did not receive adequate pain relief;
these patients were not tested with SCS. Pain severity was rated using
a verbal digital pain scale: “On a scale of 0 to 10 where 0 is no pain
and 10 is the worst pain you could ever imagine, what is your pain
now?” 16/26 patients (62%) had greater than 50% pain relief with
SCS. In this study, 2/16 (13%) had greater than 50% pain relief with
opioids. Mean follow-up was 2.1 + 0.3 years. This analysis supports
the use of SCS for intractable low back and leg pain.
In this study, 7 (17%) patients suffered complications after implanta-
tion of the device; 5 (12%) patients required repositioning of catheter
type electrodes and 2 patients required revision of the stimulator gen-
erator.
Safety Evaluation
Eleven studies were identified based on the detailed inclusion/exclu-
sion criteria to demonstrate the safety of the PRECISION System.
The studies included a total of 1056 patients that were trialed with
SCS systems and 880 patients that received implants. The table below
depicts the number of patients, the number of events, and the percent-
age of occurrences of each event compared to the total number of
patients. It should be noted that citations cover both IPG and RF Sys-
tems. The clinical experience reported in the literature on RF systems
is relevant to determining the safety of totally implantable IPG sys-
tems.
Introduction
7
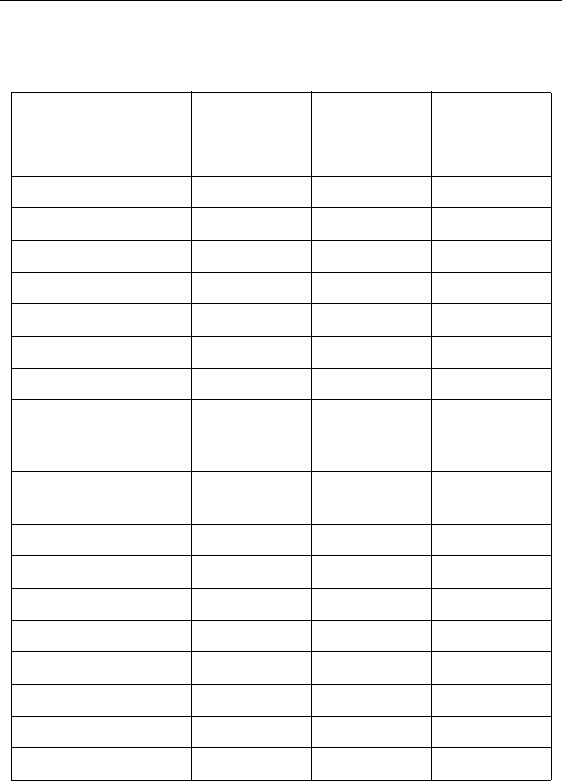
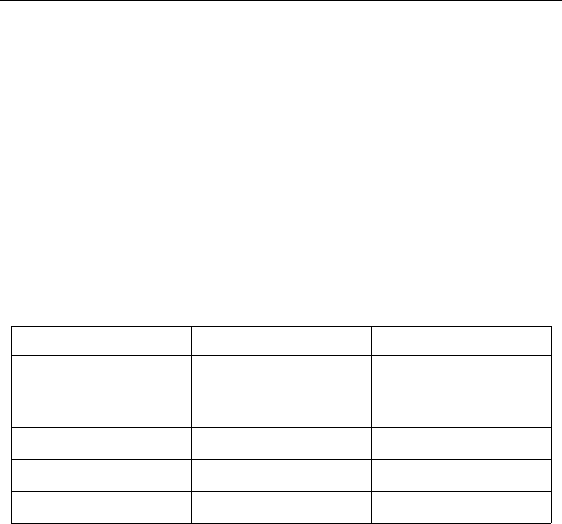
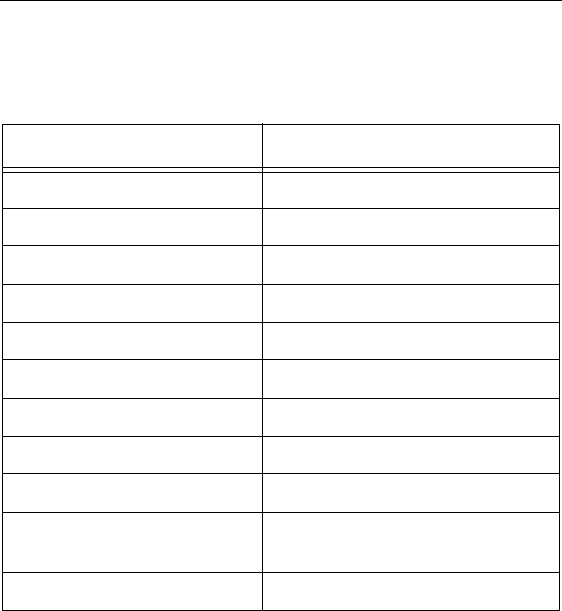
Table 1: Summary of Risks Identified in the Retrospective
Clinical Studies
Risks
# Patients
With
Adverse
Event
Intent-to-
Treat Basis
N = 1056
Implanted
Patient
Basis
N = 880
Lead Migration 175 16.6% 19.9%
Infection 39 3.7% 4.4%
Epidural Hemorrhage 0 0% 0%
Seroma 0 0% 0%
Hematoma 1 0.1% 0.1%
Paralysis 0 0% 0%
CSF Leak 5 0.5% 0.6%
Over/Under Stimula-
tion, Ineffective Pain
Control
46 4.4% 5.2%
Intermittent Stimula-
tion
00%0%
Pain Over Implant 16 1.5% 1.8%
Allergic Reaction 6 0.6% 0.7%
Skin Erosion 0 0% 0%
Lead Breakage 35 3.3% 4.0%
Hardware Malfunction 22 2.1% 2.5%
Loose Connection 0 0% 0%
Battery Failure 2 0.2% 0.2%
Other 45 4.3% 5.1%
8
Physician Lead Manual
Clinical Experience-Safety
Clinical data has been collected during a clinical study of the PRECI-
SION™ System. As of January 15, 2004, 35 subjects were enrolled in
the study at multiple sites and 26 subjects had a successful trial stimu-
lation period and were implanted with the PRECISION™ System.
The follow-up period for the 26 implanted patients ranged from two
weeks to six months. The following major adverse events were
reported.
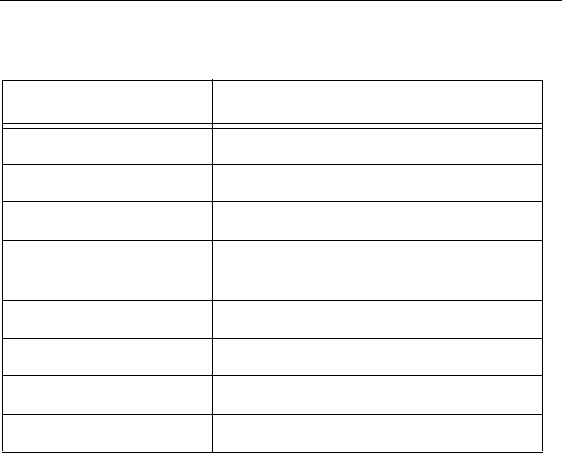
Table 2: Clinical Experience Safety
Other minor adverse events reported by at least one patient included:
receiver malfunction, skin irritation, unpleasant stimulation, CSF
leak, infection at implant site, lead migration, and OR cable malfunc-
tion. Two of the subjects reported multiple events.
References
Burchiel, K.J., V.C. Anderson, F.D. Brown, R.G. Fessler, W.A.
Friedman, S. Pelofsky, R.L. Weiner, J. Oakley,and D. Shatin.
“Prospective, Multicenter Study of Spinal Cord Stimulation for
Relief of Chronic Back and Extremity Pain.” Spine, 21:2786-
2793, 1996.
Type Number of Patients Resolution
Lead Migration 1 Lead repositioning
and subsequent
replacement
Output malfunction 1 Device replaced
Infection 1 Infection treated
Pain 1 Lead explanted

Introduction
9
Hassenbusch, S.J., M. Stanton-Hicks, E.C. Covington. “Spinal cord
stimulation verses spinal infusion for low back and leg pain”.
Acta Neurochirgica, 64:109-115, 1995.
Kemler, M.A., G.A.M. Barendse, M. Van Kleef, H.C.W. De Vet,
C.P.M. Rijks, C.A. Furnee and F.A.J.M. Van den Wilderberg.
“Spinal Cord Stimulation in Patients with Chronic Reflex
Sympathetic Dystrophy.” New England J of Medicine, 343:
618-24, 2000.
Kim S. H., R.R. Tasker, and M.Y. Oh. “Spinal Cord Stimulation for
Nonspecific Limb Pain versus Neuropathic Pain and
Spontaneous versus Evoked Pain.” Neurosurgery, 48(5): 1056-
1064, 2001.
Kumar, K., C. Toth, R. Nath, and P. Lang. “Epidural Spinal Cord
Stimulation for Treatment of Chronic Pain-Some Predictors of
Success. A 15 year experience.” Surg Neurol, 50: 110-120,
1998.
Lang, P. “The Treatment of Chronic Pain by Epidural Spinal Cord
Stimulation.” AXON, 18(4): 71-73, 1997.
Ohnmeiss, D., R. Rashbaum, M. Bogdanffy. Prospective Outcome
Evaluation of Spinal Cord Stimulation in Patients With
Intractable Leg Pain. Spine, 21:1344-1351, 1996.
Rainov, N.G., V. Heidecke, and W. Burkert. “Short Test-Period Spinal
Cord Stimulation for Failed Back Surgery Syndrome.” Minim
Invasive Neurosurg, 39(2):41-44, 1996.
Segal, R., B. Stacey, T. Rudy, S. Basser, J. Markham. “Spinal Cord
Stimulation Revisited.” Neurological Research, 20:391-396,
1998.

10
Physician Lead Manual
Spieglemann, R. and W.A. Friedman. “Spinal Cord Stimulation: A
Contemporary Series.” Neurosurg 28:65-71, 1991.
Villavicencio, A.T., J.C. Leveque, L. Rubin, K. Bulsara, and J.P.
Gorecki. “Laminectomy versus percutaneous electrode
placement for spinal cord stimulation.” Neurosurgery, 46:399-
406, 2000.
Contraindications
Patients contraindicated for permanent SCS therapy are those who:
• are unable to operate the SCS system
• have failed trial stimulation by failing to receive effec-
tive pain relief
• are poor surgical risks
• are pregnant

Safety Information
11
Safety Information
Warnings
Magnetic Resonance Image (MRI). Patients implanted with the
Precision SCS system should not be subjected to MRI. MRI exposure
may result in dislodgement of implanted components, heating of the
neurostimulator, damage to the device electronics and/or voltage
induction through the leads and stimulator causing an uncomfortable
or “jolting” sensation.
Pediatric Use. The safety and effectiveness of spinal cord stimula-
tion has not been established for pediatric use.
Diathermy. Shortwave, microwave and/or therapeutic ultrasound
diathermy should not be used on SCS patients. The energy generated
by diathermy can be transferred through the stimulator system, caus-
ing tissue damage at the lead site which may result in severe injury or
death. The IPG, whether it is turned on or off, may be damaged.
Implanted Stimulation Devices. Spinal cord stimulators may
interfere with the operation of implanted sensing stimulators such as
pacemakers or cardioverter defibrillators. The effects of implanted
stimulation devices on neurostimulators is unknown.
Implant Damage. Burns may result if the pulse generator case is
ruptured or pierced and patient tissue is exposed to battery chemicals.
Do not implant the device if the case is damaged.
Postural Changes. Patients should be advised that changes in pos-
ture or abrupt movements may cause decreases, or uncomfortable or
painful increases in the perceived stimulation level. Patients should be
advised to turn down the amplitude or turn off the IPG before making
posture changes. If unpleasant sensations occur, the IPG should be
turned off immediately.

12
Physician Lead Manual
Electromagnetic Interference. Strong electromagnetic fields can
potentially turn the stimulator off, or cause uncomfortable or jolting
stimulation. Patients should be counseled to avoid or exercise care
around:
• Theft detectors or security screeners
• Power lines or power generators
• Electric steel furnaces and arc welders
• Large, magnetized stereo speakers
Precautions
Physician training is required.
Medical Devices/Therapies. The following medical therapies or
procedures may turn stimulation off or may cause permanent damage
to the implant, particularly if used in close proximity to the device:
• lithotripsy
• electrocautery: Do not use monopolar cautery.
• external defibrillation
• radiation therapy
• ultrasonic scanning
• high-output ultrasound
If any of the above is required by medical necessity, refer to “Instruc-
tions for the Physician” on page 16. Ultimately, however, the device
may need to be explanted as a result of associated failure.
Automobiles and Other Equipment. Patients should not operate
automobiles, other motorized vehicles, or potentially dangerous
machinery/equipment with therapeutic stimulation turned on. Stimu-
lation must be turned off first. Sudden stimulation changes, if they
occur, may distract patients from attentive operation of the vehicle or
equipment.

Safety Information
13
Cell Phones. While we don’t anticipate any interference with cell
phones, the full effects of interaction with cell phones are unknown at
this time.
Post Operative. During the two weeks following surgery, it is
important to use extreme care so that appropriate healing will secure
the implanted components and close the surgical incisions:
Do not exercise or attempt to move heavy objects, and avoid deep
bending and stretching. Temporarily, there may be some pain in the
area of the implant as the incisions heal. If discomfort continues
beyond two weeks, contact your physician.
If you notice excessive redness around the wound areas during this
time, contact your physician to check for infection and administer
proper treatment. In rare cases, adverse tissue reaction to implanted
materials can occur during this period.
Implant Location. Never attempt to change the orientation or “flip”
the implant. Do not “finger” or play with the implant. If the implant
flips over in your body it cannot be charged. If you know that the
device has turned, or if stimulation cannot be turned on after charging,
contact your physician to arrange an evaluation of the system.
In some cases, the skin over your implant may become very thin over
time. If this occurs, contact your physician.
Lead Location. In some instances a lead can move from its original
location, and stimulation at the intended pain site can be lost. If this
occurs, consult your physician who may able to restore stimulation by
reprogramming the implant in the clinic or repositioning the lead
during another operation.
Device Failure. Implants can fail at any time due to random
component failure, loss of battery functionality, or lead breakage. If
the device stops working even after complete charging (up to four
hours), turn off the implant and contact your physician so that the
system can be evaluated.

14
Physician Lead Manual
Storage. Do not expose the Remote Control or Charging System
components to excessively hot or cold conditions. Do not leave the
devices in your car or outdoors for extended periods of time. The
sensitive electronics can be damaged by temperature extremes,
particularly high heat. If the Remote Control or the Charging System
is to be stored for a period of time, be careful that the storage
temperature does not exceed -20–60 °C (-4–140 °F).
Handling. Handle the system components and accessories with care.
Do not drop them or submerge them in water. Although reliability
testing has been performed to ensure quality manufacturing and
performance, dropping the devices on hard surfaces or in water, or
other rough handling, can permanently damage the components. (See
“Limited Warranty” on page 52.)
Component Disposal. Do not dispose of the Remote Control or
Charger in fire. The battery in these devices can explode in fire.
Dispose of used batteries in accordance with local regulations. The
IPG should be explanted in the case of cremation, and returned to
Advanced Bionics.
Remote Control, Charging System Cleaning. The components
can be cleaned using alcohol or a mild detergent applied with a cloth
or tissue. Residue from soapy detergents should be removed with a
damp cloth. Do not use abrasive cleansers for cleaning.
Adverse Effects
Potential risks are involved with any surgery. In addition to those typ-
ically associated with surgery, possible risks of stimulation system
implantation include:
• Lead migration, resulting in undesirable changes in
stimulation and subsequent reduction in pain relief.
• System failure, which can occur at any time due to ran-
dom failure(s) of the components or the battery. These
events, which may include battery leakage, device fail-

Safety Information
15
ure, lead breakage, hardware malfunctions, loose con-
nections, electrical shorts or open circuits and lead
insulation breaches, can result in ineffective pain con-
trol.
• Tissue reaction to implanted materials can occur.
• Skin erosion or seroma at the IPG site can occur over
time.
• Possible surgical procedural risks are: temporary pain at
the implant site, infection, spinal cord compression,
cerebrospinal fluid (CSF) leakage and, although rare,
epidural hemorrhage, seroma, hematoma and paralysis.
• External sources of electromagnetic interference may
cause the device to malfunction and affect stimulation.
• Exposure to MRI can result in heating of tissue, image
artifacts, induced voltages in the neurostimulator and/or
leads, lead dislodgement.
• Undesirable stimulation may occur over time due to cel-
lular changes in tissue around the electrodes, changes in
electrode position, loose electrical connections and/or
lead failure.
• The patient may experience painful electrical stimula-
tion of the chest wall as a result of stimulation of certain
nerve roots several weeks after surgery.
• Over time, the implant may move from its original posi-
tion.
• Weakness, clumsiness, numbness or pain below the
level of implantation.
• Persistent pain at the IPG or lead site.

16
Physician Lead Manual
Instructions for the Physician
Implanted Stimulation Devices. If other implanted devices are
indicated for the patient, careful screening is required to determine if
safe results can be achieved before permanently implementing con-
current electrical therapies.
Postural Changes. Depending on the activity level of the patient,
postural changes may affect stimulation intensity. Instruct patients to
keep the Remote Control at hand at all times, and ensure that they
understand how to adjust stimulation levels.
Medical Devices/Therapies. If the patient is required to undergo
lithotripsy, electrocautery, external defibrillation, radiation therapy,
ultrasonic scanning, or high-output ultrasound:
• Turn off stimulation at least five minutes before the pro-
cedure or application.
• All equipment, including ground plates and paddles,
must be used as far away from the IPG as possible.
• Bipolar electrocautery is recommended: Do not use
monopolar electrocautery.
• Every effort should be taken to keep fields, including
current, radiation, or high-output ultrasonic beams,
away from the IPG.
• Equipment should be set to the lowest energy setting
clinically indicated.
• Instruct patients to confirm IPG functionality following
treatment by turning on the IPG and gradually increas-
ing stimulation to the desired level.

Package Contents
17
Package Contents
Lead Kit - Model SC-2108
(1) Lead
(1) Curved Stylet (pre-loaded in Lead)
(1) Straight Stylet
(2) Suture Sleeves
(1) Insertion Needle
(1) Lead Blank
(1) OR Cable Assembly
(2) Lead Position Labels—left and right (non-sterile)
(1) Manual
(1) Product Registration Form
(1) Temporary Patient Identification Card
Lead Extension Kit - Model SC-3108
(1) Lead Extension
(1) Skin Marker
(1) Hex Torque Wrench
(1) Tunneling Tool Assembly
(1) Manual
(1) Product Registration Form
(1) Temporary Patient Identification Card

18
Physician Lead Manual
Sterilization and Handling
Sterilization
The Advanced Bionics Lead Model SC-2108 and Lead Extension
Model SC-3108 and accessories (except for the Lead Position Labels)
were sterilized with ethylene oxide prior to shipment. Red lines on the
green tape located near the bottom of the inner tray cover indicate
exposure to the sterilization process.
Inspect the condition of the sterilization indicator and the sterile pack-
age before opening the package and using the contents. Do not use the
contents if the indicator lines are not red, if the package is broken or
torn, or if contamination is suspected because of a defective sterile
package seal.
• Do not use any component that shows signs of damage.
• Do not resterilize the package or the contents. Obtain a
sterile package from Advanced Bionics.
• Do not use if “Use Before” date has expired.
Note: The lead, lead extension and accessories are intended for
single use only.
Handling
The lead is designed to perform in the hostile environment of the
human body. Care must be taken to avoid damaging the lead with
sharp instruments or excessive force during surgery. The following
guidelines will help to ensure the longevity of components:
• Do not sharply bend or kink the lead or extension.
• Do not tie suture(s) directly to the lead or extension
body; use the provided suture sleeves.
• Avoid forcing the lead into the epidural space by care-
fully clearing a path using the lead blank.

Sterilization and Handling
19
• Avoid pulling an implanted lead taut; provide a stress
relief loop at the insertion site to minimize tension on
the lead.
• Avoid handling the lead with sharp instruments; use
only rubber-tipped forceps.
• Take care when using sharp instruments such as hemo-
stats or scalpels to prevent damaging the lead.
• Wipe off any body fluids from the lead connector end
before connecting it to any other component. Fluid con-
tamination of these connections could compromise the
integrity of the stimulation circuit.
• Wipe off any body fluids from the stylet before inserting
or reinserting it into the lead.
Storage
Store components between 5 °C and 40 °C (41 °F–104 °F) in an area
where they are not exposed to liquids or excessive moisture. Temper-
atures outside of the stated range can cause damage.
20
Physician Lead Manual
Guidelines for Trial-phase Implantation
This section details the recommended procedures for trial-phase tem-
porary implantation of the lead.
Pre-op Instructions
• Check that the sterile package is intact. (See “Steriliza-
tion” on page 18.)
• Ensure that a Trial Stimulator and Patient Trial Kit are
available for use following lead placement. Install a new
6 volt battery (included in the Patient Trial Kit) in the
Trial Stimulator.
• Be sure the Trial Stimulator and Remote Control stimu-
lation settings have been reset. Refer to the IPG manual
for links and resets.
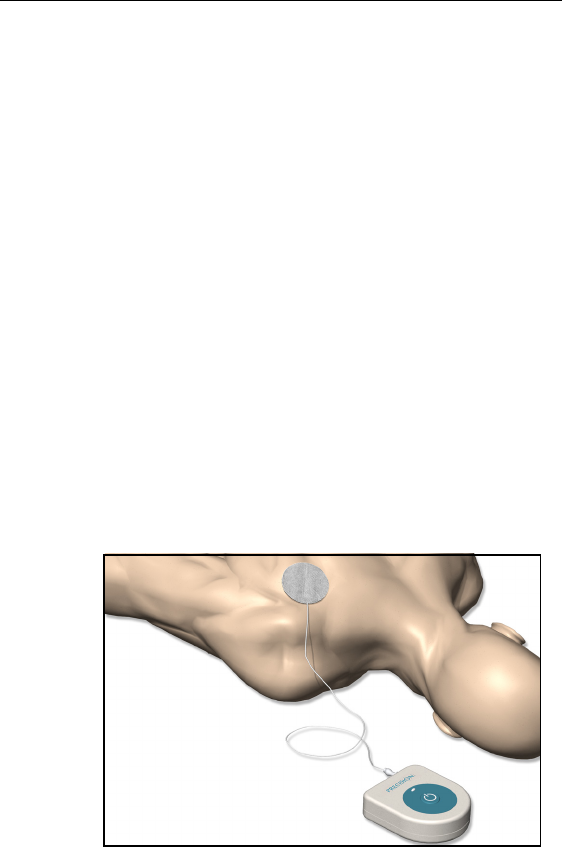
• If monopolar testing is anticipated, place the monopolar/
indifferent electrode (available separately) on the
patient’s shoulder or leg and run the cable to the Trial
Stimulator testing site before the patient is prepped and
draped.
Guidelines for Trial-phase Implantation
21
Lead Placement
Note: Fluoroscopic evaluation of the lead position during this
procedure will aid the physician in achieving an optimum pain
coverage location, and is recommended.
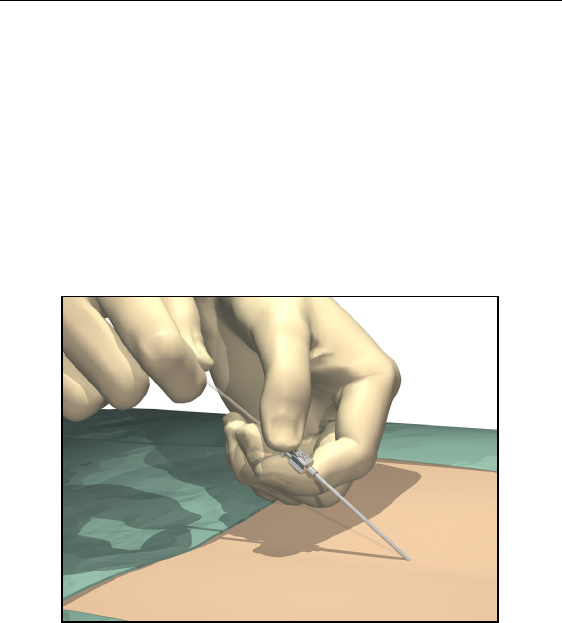
1. Position, prep and drape the patient in the usual accepted manner.
Inject a local anesthetic at the needle insertion site.
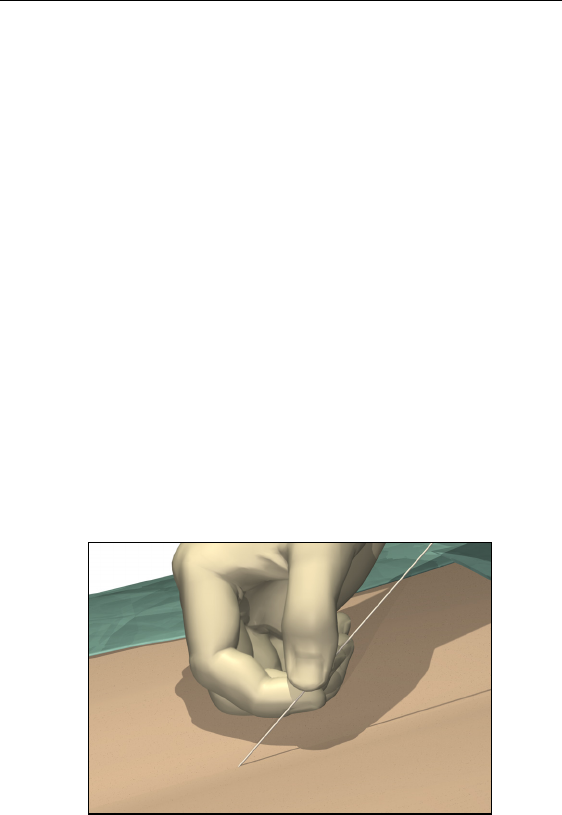
2. Insert the needle into the epidural space with the opening facing
up using an angle of 45° or less.
CAUTION: Use only the insertion needle provided in the
Lead Kit. Other needles may damage the lead. The stamped
number on the needle hub corresponds to the orientation of
the bevel, which must face up. Turning the bevel ventral
(down) may result in lead damage. An angle of more than
45º increases the risk of lead damage.
3. Remove the needle stylet and verify entry into the epidural space
using the standard technique.
22
Physician Lead Manual
4. OPTIONAL. Under fluoroscopic guidance, insert the lead blank
through the needle and into the epidural space. Advance the lead
blank to the target location, then withdraw the blank.
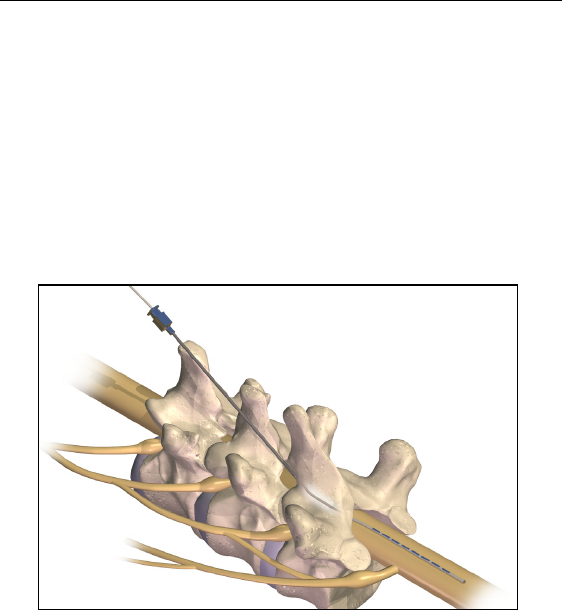
5. Slowly insert the lead, with stylet, through the needle (lead stylet
should extend completely to the tip of the lead).
6. Advance the lead to the appropriate vertebral level using fluoro-
scopic guidance. A sufficient length of lead (i.e., at least 10 cm,
or approximately three vertebrae) should reside in the epidural
space and aids in lead stabilization.
To facilitate advancement and placement, the lead body may be
rotated.

Guidelines for Trial-phase Implantation
23
Connecting the OR Cable Assembly
The OR cable extension is designed for temporary connection to the
OR cable to facilitate stimulation testing outside of the sterile field.
After stimulation testing, the cable extension is typically removed and
the OR cable is connected directly to the Trial Stimulator for use dur-
ing the trial phase.
CAUTION: Do not immerse the OR cable connector or plug
in water or other liquids. The OR Cable Assembly is intended
for one-time only use; do not resterilize.
1. If two leads are being implanted, wrap the non-sterile 1-L and 2-
R labels around the cables at the Trial Stimulator to identify lead
connections.
2. Verify that the Trial Stimulator is off.
CAUTION: Always turn the Trial Stimulator off before
connecting or disconnecting the Cable Assemblies.
3. Check that the locking lever on the OR cable connector is in the
open position (0).
4. Slide the proximal end of the lead, with stylet, into the open port
on the OR cable connector.
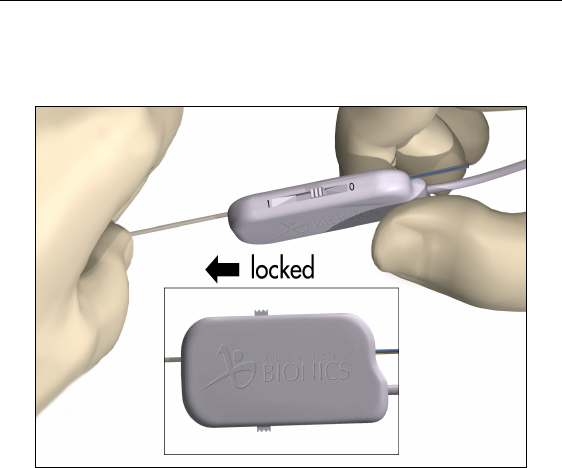
24
Physician Lead Manual
5. Push the end of the lead into the port until it stops. Hold the lead
in place while sliding the locking lever to the “1” (locked) posi-
tion.
Note: Once the lead is secured in the connector, the stylet can be
manipulated in, but not removed from, the lead.
Guidelines for Trial-phase Implantation
25
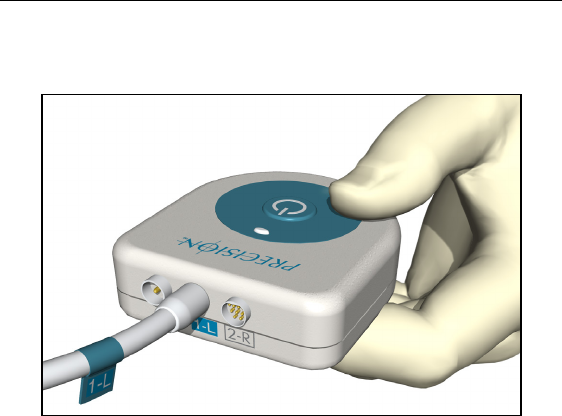
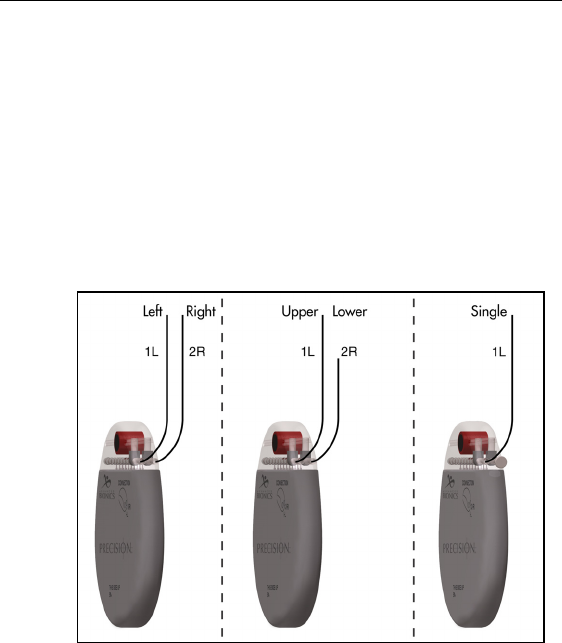
6. Plug the OR Cable Assembly into the Trial Stimulator socket(s)
labeled 1-L (left) and 2-R (right).
Superior (upper or left) leads connect to socket 1-L. Inferior
(lower or right) leads connect to socket 2-R. If only a single lead
is being used, connect it to 1-L.

26
Physician Lead Manual
Intraoperative Stimulation Testing
Note: The following steps are for procedural reference only. Please
refer to the BionicNavigator Software Guide for detailed
stimulation testing procedures and guidelines.
1. Test various electrode configurations to obtain paresthesia.
Note: If lead repositioning is necessary, turn stimulation off before
proceeding.
2. When the desired paresthesia is achieved:
• turn the Trial Stimulator off
• unlock each OR cable connector and disconnect from
the lead(s)
• slowly withdraw the stylet(s)
3. Record the lead position by capturing a fluoroscopic image to be
sure the leads have not moved. Retest if necessary. The image
can also be used for a position comparison at closure to ensure
that the leads did not move.
OPTION A: Temporary Lead Trial
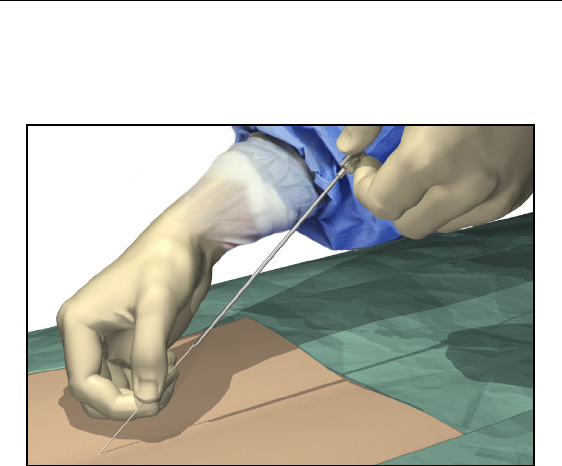
1. Hold the lead distal to the needle hub to maintain lead position
during needle removal.
2. Carefully withdraw the insertion needle from the epidural space
by slowly pulling the needle up towards the proximal end of the
lead.
3. Continue to pull the needle back approximately one centimeter at
a time until the needle tip is exposed.
Guidelines for Trial-phase Implantation
27
4. Once the needle tip is exposed, hold the lead as close to the per-
cutaneous exit site as possible, then carefully pull the needle
completely from the lead.
5. If desired, a small suture may be used to close the wound and sta-
bilize the lead. Place and tape a stress relief loop and dress the
wound.
6. Continue with “Connecting to the Trial Stimulator” on page 36.
28
Physician Lead Manual
OPTION B: Permanent Lead Trial
Removing the Needle
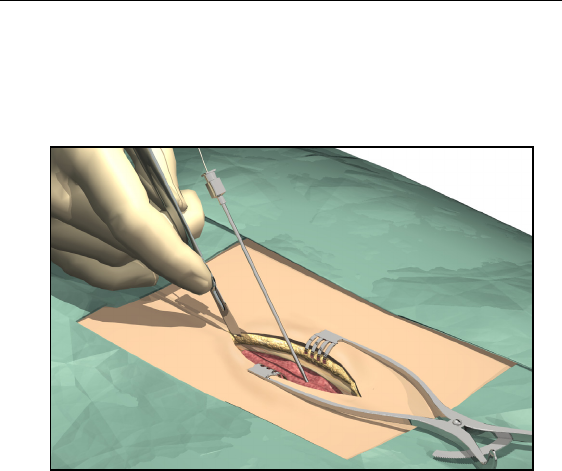
1. Cut down around the needle to access the supraspinous ligament.
2. Hold the lead distal to the needle hub to maintain lead position
during needle removal.
3. Carefully withdraw the insertion needle from the epidural space
by slowly pulling the needle up towards the proximal end of the
lead.
4. Continue to pull the needle back approximately one centimeter at
a time until the needle tip is exposed.
Guidelines for Trial-phase Implantation
29
5. Once the needle tip is exposed, hold the lead as close to the tip as
possible, then carefully pull the needle completely from the lead.
Anchoring the Lead
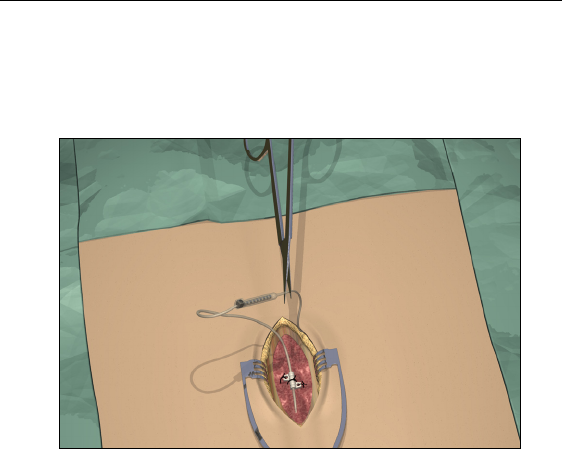
1. Place a suture through the supraspinous ligament or deep fascial
tissue.
2. Slide a suture sleeve over the lead and down to the supraspinous
ligament.
3. Ligate the sleeve onto the lead by tying a 2-0 silk or other nonab-
sorbable suture around the center groove of the sleeve to prevent
sliding.
CAUTION: Do not use polypropylene sutures as they may
damage the suture sleeve. Do not suture directly onto the
lead or use a hemostat on the lead body. This may damage
the lead insulation.
30
Physician Lead Manual
4. Suture the sleeve to the supraspinous ligament or deep fascia
through the suture sleeve holes.
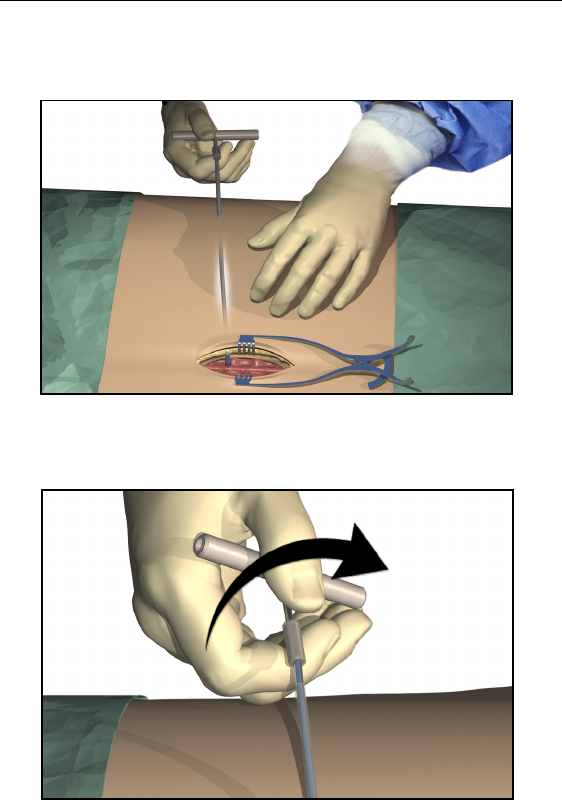
Tunneling And Connecting Extension
A tunneling tool and straw are provided with the Lead Extension Kit
to facilitate percutaneous tunneling of the lead or extension.
• Attach the tunneling tool handle to the shaft by turning
the locking mechanism clockwise.
Guidelines for Trial-phase Implantation
31
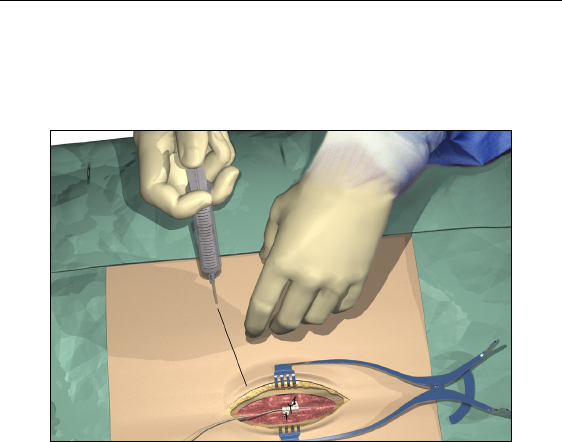
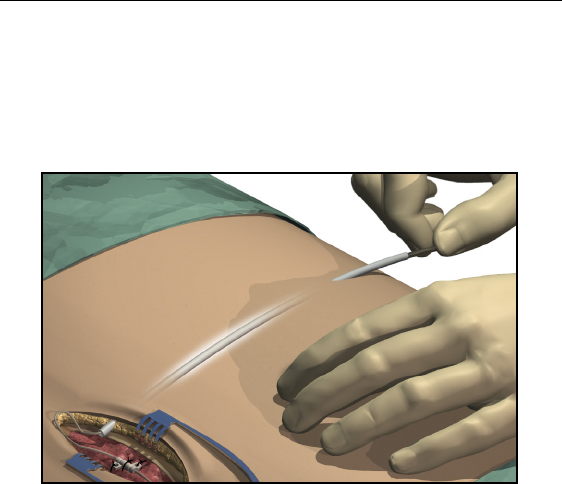
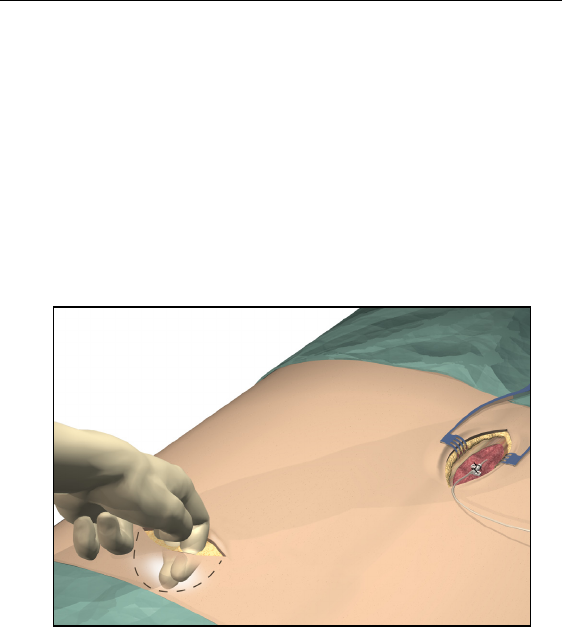
1. Mark the desired route of the tunnel.
2. Administer the appropriate local anesthetic along the tunneling
path.
3. Make a small incision at the desired exit site.
32
Physician Lead Manual
4. Create a subcutaneous tunnel from the exit site to the midline
incision until the straw is visible and accessible at the exit point.
5. Unscrew and remove the tool handle.
Guidelines for Trial-phase Implantation
33
6. Grasp the tip of the tool with one hand while holding the straw in
place with the other hand. Pull the tunneling tool shaft out
through the straw.
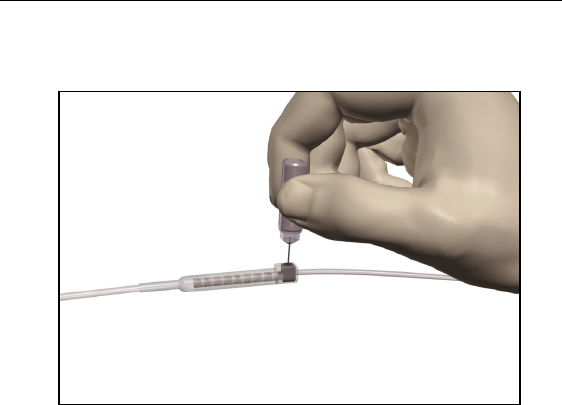
7. Push the lead or extension proximal ends through the straw, then
withdraw the straw.
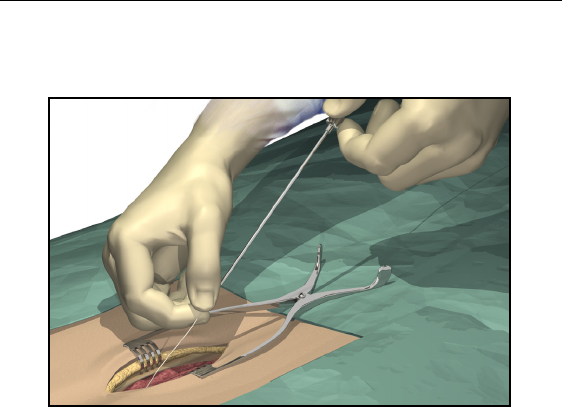
8. Wipe clean the proximal end of the lead, then insert the proximal
end into the extension connector until it stops and the retention
ring (long ring) is under the setscrew.
Note: • If there appears to be an obstruction, use the torque wrench
to loosen (counterclockwise) the setscrew and/or gently
rotate the lead to help advance the proximal end.
•Ensure that the lead is fully inserted before tightening the
setscrew to prevent lead damage.
34
Physician Lead Manual
9. Using the torque wrench supplied, turn the extension connector
setscrew clockwise until it clicks, indicating lock.
Note: • Ensure that the wrench is fully seated in the setscrew before
tightening.
•The wrench is torque-limited and cannot be overtightened.
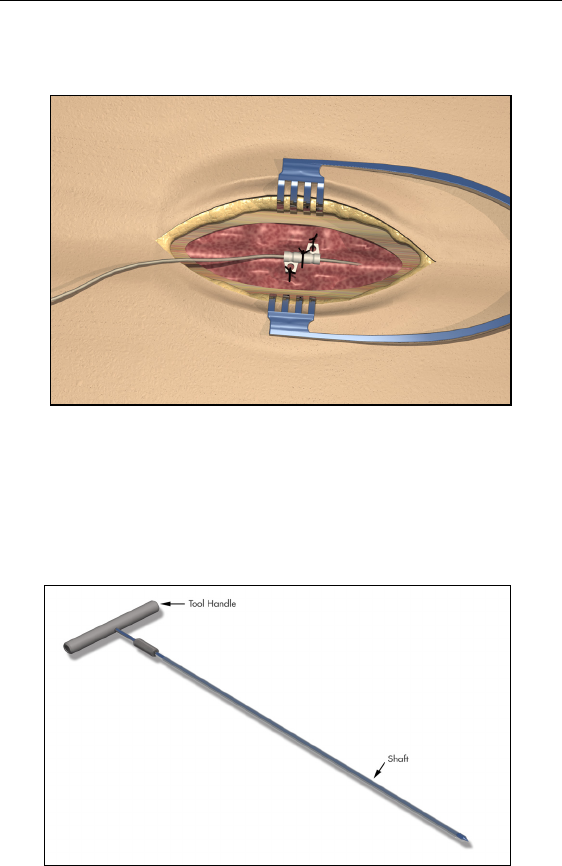
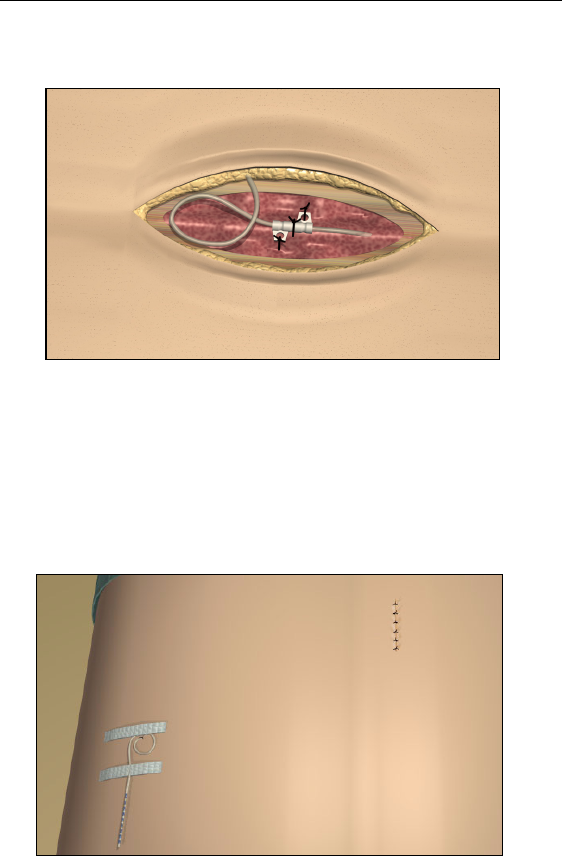
10. Form an appropriately-sized pocket using blunt dissection on
either side of midline for coiled excess lead and extension con-
nectors.
11. Place a small loop at the lead for slack. If necessary, loosely tie a
suture around the lead-loop, but do not tighten onto the lead.
Guidelines for Trial-phase Implantation
35
CAUTION: Tightening sutures directly on the lead can
damage the lead.
12. Carefully remove excess slack by gently pulling the extensions
from the exit wound.
13. Close the midline incision.
14. If desired, a small suture may be used to close the exit wound of
the extension. Place and tape a stress relief loop and dress the
wound.
36
Physician Lead Manual
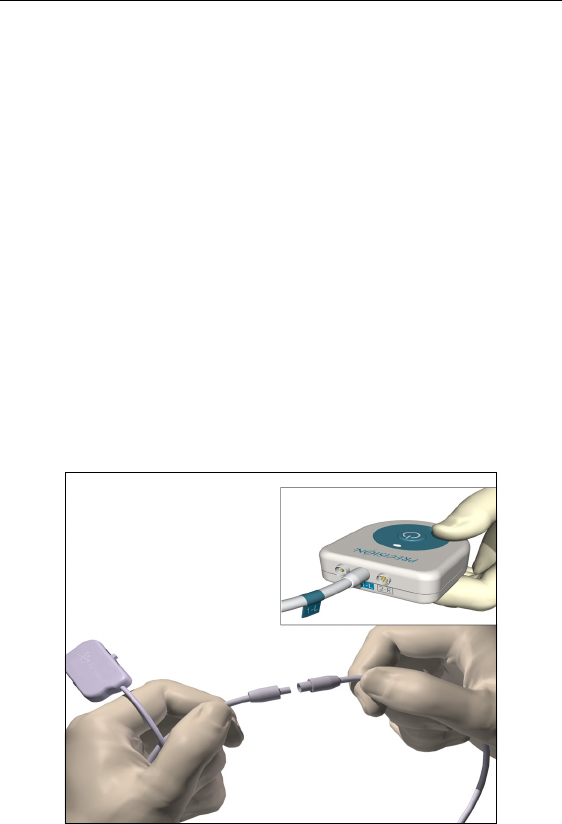
Connecting to the Trial Stimulator
1. Wipe fluids off the exposed lead connections.
2. Disconnect and discard the OR cable extension, unless extra
length is needed for trial use.
3. Connect the OR cable(s) to the lead(s) or lead extensions: Slide
the locking lever to “0,” fully insert the end of the extension into
the port, slide the locking lever to “1.”
4. If two leads are used, connect the cable labeled 1-L to the upper
or left lead, and the cable labeled 2-R to the lower or right lead.
Labels are provided.
5. Next, connect the right and left-sided OR cables to the Trial Stim-
ulator, referencing the position labels previously fixed to the
cables.
If only one lead is used, connect the OR cable to 1-L on the Trial
Stimulator.
Connecting to the Trial Stimulator
37
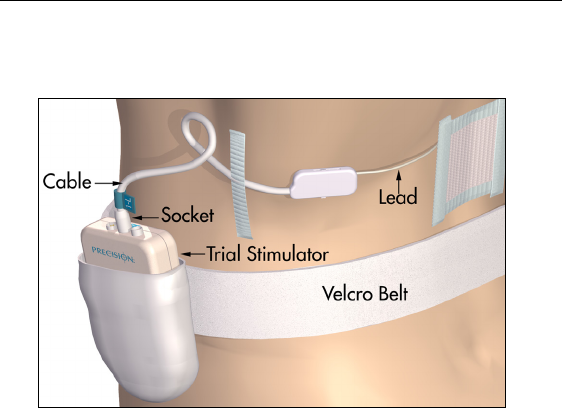
6. Fit the Velcro® belt to the patient, cut off the excess length, and
place the Trial Stimulator in the belt pocket.
38
Physician Lead Manual
Guidelines for Permanent Implantation
This section details the procedures for
• tunneling the lead/extension as part of an IPG implant
• connection of lead/extension to the IPG
The Tunneling Tool Assembly used in this procedure is provided with
the Precision device as part of the IPG Kit.
Percutaneous Lead/Extension Removal
Before revising a trial system for chronic stimulation, the exposed
portion of the lead or extension must be removed. The method chosen
from the choices below will depend upon how the patient was pre-
pared for the trial phase.
Remove bandages and properly cleanse the exit site.
Option A. Temporary Lead Removal
1. Clip sutures if used to secure the trial lead(s) in place.
2. Remove the lead(s) completely and discard.
Guidelines for Permanent Implantation
39
Option B. Extension Removal
1. Open the midline incision to expose the lead and connector.
2. Cut the lead extension at the connector.
3. Pull the lead extension through the tunnel and away from body at
the externalized site.
4. Loosen the connector setscrew using the torque wrench provided.
Disconnect and remove the connector.
Note: Connect a new lead extension, if necessary, to reach the
selected IPG site.
40
Physician Lead Manual
IPG Implantation
1. Ensure that the area surrounding the lead entry site is incised to a
dimension that will accommodate the tunneling tool. Check that
the lead is securely sutured with the suture sleeve.
2. Select and mark the intended IPG site several inches away from
the previously externalized leads, and create an incision at the top
of the site.
3. Create a subcutaneous pocket no larger than the IPG outline at a
depth of up to 3/4 inch (2.0 cm) from the surface.
Note: • Using the template will help guide the correct pocket sizing.
It is important to keep the pocket small to reduce the
chances of patient manipulation and IPG flipping.
•Implant charging could become ineffective at depths greater
than 3/4 inch (2.0 cm).
IPG Implantation
41
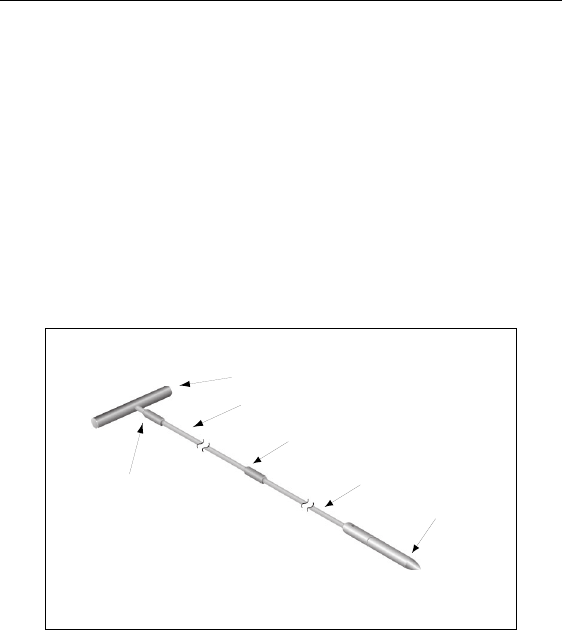
Tool Assembly
The tunneling tool provided with the IPG includes a shaft extender to
be used for up to two leads (with or without extensions).
1. Attach the handle to the tunneling tool shaft by turning the lock-
ing mechanism clockwise.
Note: For more length, attach the shaft extension to the handle, and
then attach the carrier shaft.
2. Thread the tip cover onto the tunneling tool and tighten by turn-
ing clockwise.
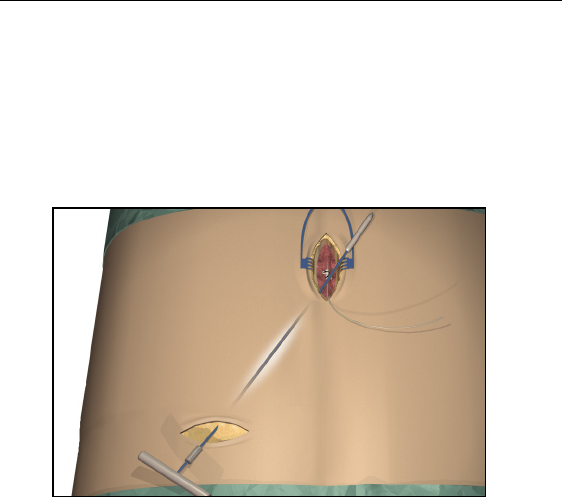
Tunneling The Lead
1. Mark the desired route of the tunnel.
2. Administer the appropriate local anesthetic along the tunneling
path.
Note: Check that the tunneling tool tip is securely threaded onto the
carrier.
Tool Handle
Locking Mechanism
Locking Mechanism
Shaft Extension
Shaft
Carrier Tip Cover
42
Physician Lead Manual
3. OPTIONAL. If necessary, bend the tool shaft to conform to the
patient’s body.
CAUTION: Do not bend locking joints.
4. Create a subcutaneous tunnel from the IPG site to the midline
incision.
Note: Deep tunneling is not recommended.
IPG Implantation
43
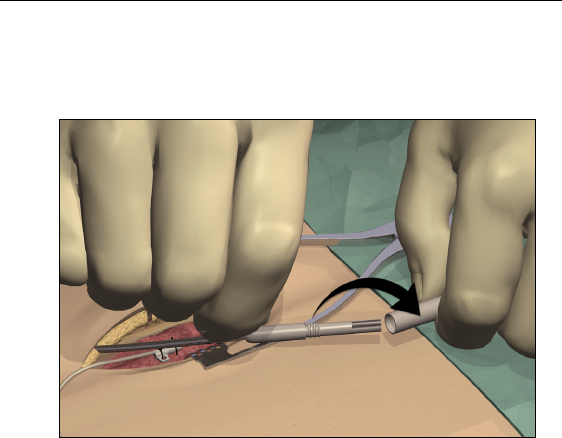
5. Once the tunneling tip is completely exposed at midline, press it
toward the shaft and turn it counterclockwise to remove it for
access to the carrier.
Note: You may feel the tip slide back before the cover begins to
unscrew.
44
Physician Lead Manual
6. Carefully position each lead or extension into the carrier shaft
and press the lead/extension into the groove.
Note: If necessary, swivel the carrier by pulling it away from the
handle and turning it to get better access to the cavities.
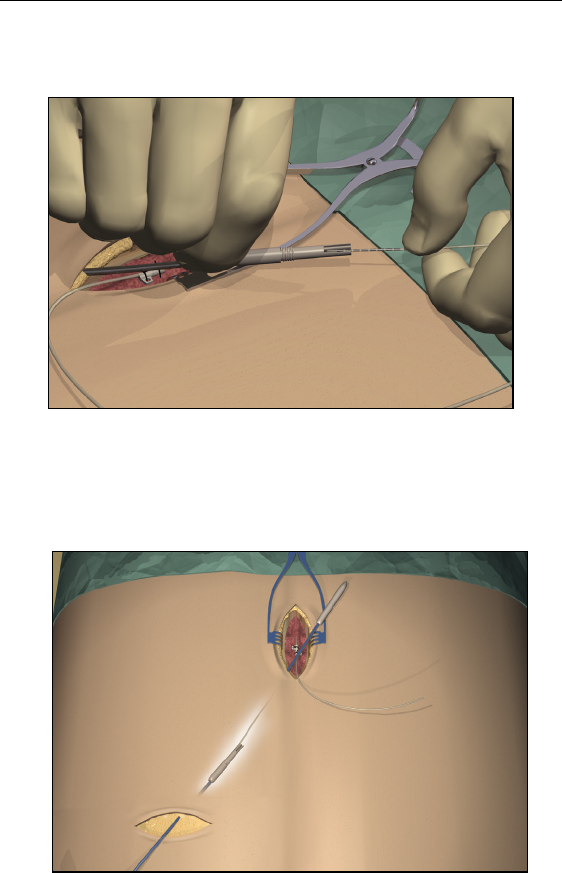
7. Gently pull the tunneling tool back through the tunnel.
IPG Implantation
45
8. Gently lift the lead(s) out of the locking groove(s).
9. Wipe off any fluids from the proximal end of the lead(s).
Connecting To the IPG
Before implanting the IPG, refer to the IPG Implant Manual.
Dual Lead Connection
• Superior (upper or left) leads connect to IPG port 1-L.
• Inferior (lower or right) leads connect to IPG port 2-R.
Single Lead Connection
• Connect a single lead to IPG port 1-L.
• Plug port 2-R with the connector plug supplied in the
IPG Kit.
46
Physician Lead Manual
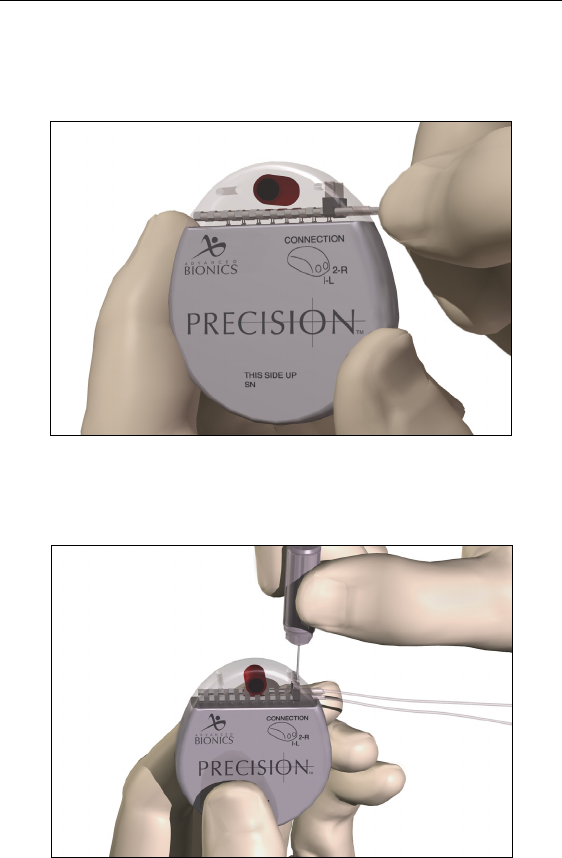
1. Fully insert the lead(s) into the IPG port(s). When the lead is
properly inserted, the lead will stop and the retention ring will be
located under the setscrew.
2. Pass the torque wrench through the slit in the septum located on
the top of the IPG header and tighten both set screws, one at a
time, until the torque wrench “clicks,” indicating lock.

IPG Implantation
47
Note: • Ensure that the lead is fully inserted before tightening the
setscrew to prevent lead damage.
•If the connector plug is used in port 2-R, it is still necessary
to tighten the setscrew as described.
•The wrench is torque-limited and cannot be overtightened.
3. Place the IPG in the subcutaneous pocket with “This Side Up”
facing towards the skin.
4. Coil excess lead or extension under the IPG.
Note: To confirm good connections, check impedances before
tightening the setscrew.
5. Secure the IPG in the pocket by suturing through the holes in the
connector.
6. Close and dress the wound(s).
48
Physician Lead Manual
Specifications and Technical Data
Lead
Part Specifications
Model Number SC-2108
Lead Lengths 30, 50, 70 cm
Lead Shape In-line
Lead Diameter 1.3 mm
Number of Electrode Contacts 8
Electrode Length 3 mm
Electrode Spacing 1 mm
Contact Material Platinum/Iridium
Insulation Material Polyurethane
Conductor Material Shell: MP35N
Core: MP-DFT (28% Ag)
Conductor Resistance < 7 Ohms
Specifications and Technical Data
49
Lead Extension
Part Specifications
Model Number SC-3108
Extension Lengths 15, 25, 35 cm
Extension Diameter 1.3 mm
Number of Electrode
Contacts
8
Contact Material Platinum/Iridium, MP35N, Stainless Steel
Insulation Material Polyurethane, Silicone
Conductor Material MP35N
Conductor Resistance < 10 Ohms

50
Physician Lead Manual
Registration Information
In accordance with international practice and regulatory legislation in
some countries, a registration form is packed with each Advanced
Bionics Corporation lead/lead extension.
The purpose of this form is to maintain traceability of all products and
to secure warranty rights. It also allows the institution involved in the
evaluation or replacement of a specific implanted lead, accessory or
device to gain quick access to pertinent data from the manufacturer.
Fill out the registration form included in the package contents. Return
one copy to Advanced Bionics, keep one copy for patient records, and
provide one copy to the patient and physician.
Advanced Bionics Corporation
25129 Rye Canyon Loop
Valencia, California 91355
Attention: Customer Service Department

Technical Service
51
Technical Service
Advanced Bionics Corporation has highly trained service profession-
als located worldwide to assist you. The Technical Service Depart-
ment is available to provide technical consultation 24 hours a day.
In North America please call (866) 566-8913 to speak to a representa-
tive.

52
Physician Lead Manual
Limited Warranty
Advanced Bionics® Corporation warrants to the patient that the Lin-
ear Lead, Model SC-2108, and Extension, Model SC-3108, are free
from defects in workmanship and materials for a period of one (1)
year from the date of implantation.
A Lead or Extension that fails to function within normal tolerances
within (1) year from the date of surgery is covered under this Limited
Warranty. The liability of Advanced Bionics® under this warranty
shall be limited to: (a) replacement with a functionally equivalent
Lead or Extension; or (b) full credit equal to the original purchase
price to be applied towards the purchase of a new Lead or Extension.
Product claims under Advanced Bionics® Limited Warranty are sub-
ject to the following conditions and limitations:
1. The product registration card must be completed and returned to
Advanced Bionics® within 30 days of surgery in order to obtain
warranty rights.
2. The Lead or Extension must be returned to Advanced Bionics®
(or authorized agent) within 30 days of malfunction or discovery
of defect, and shall be the property of Advanced Bionics®.
3. The Lead or Extension must be implanted prior to the “use
before” date.
4. Failure of the Lead or Extension must be confirmed by Advanced
Bionics®. This warranty specifically excludes defects or malfunc-
tions caused by: (a) fire, floods, lightning, natural disasters, water
damage and other calamities commonly defined as “Acts of
God”; (b) accident, misuse, abuse, negligence, or the customer’s
failure to operate the Lead or Extension in accordance with man-
ufacturer's instructions; (c) unauthorized attempts to repair, main-
tain, or modify the equipment by the customer or any
unauthorized third party; or (d) attachment of any equipment not
supplied by Advanced Bionics® without prior approval.

Limited Warranty
53
a. This warranty does not include surgical accessories used
with the Linear Lead or Extension.
5. The decision as to product replacement or credit shall be made
solely at the discretion of Advanced Bionics®. For a replacement
Lead or Extension, the warranty will run only to the end of the
warranty period for the original Lead or Extension that was
replaced.
This warranty is in lieu of any other warranty, expressed or implied,
including any warranty of merchantability or fitness for intended use.
Except as expressly provided by this Limited Warranty, Advanced
Bionics® shall not be responsible or liable for any direct, consequen-
tial or incidental damages caused by device malfunction, failure or
defect, whether the claim is based on warranty, contract, tort or other-
wise.

54
Physician Lead Manual
The following is federal government communications regulation
information about the Precision™ System.
This device complies with part 15 of the FCC Rules. Operation is sub-
ject to the following two conditions: (1) This device may not cause
harmful interference, and (2) This device must accept any interfer-
ence received including interference that may cause undesired opera-
tion.
The Precision™ System components should only be serviced by
Advanced Bionics. Do not attempt to open or repair any of the com-
ponents. Unauthorized opening of or attempts to repair the compo-
nents will void the warranty.
Changes of modifications to this product not authorized by Advanced
Bionics Corporation could void the FCC Certification and negate
your authority to operate this product.