Medtronic MiniMed 2007C Implantable Insulin Pump User Manual Dmp9196021 011 c
Medtronic MiniMed, Inc. Implantable Insulin Pump Dmp9196021 011 c
Contents
physician part2

85
Fill the Pump with insulin
1. Remove another refill syringe (IN2) from a refill kit package.
2. Firmly attach the two-way stopcock to the refill syringe and attach an
18 gauge needle to the stopcock. Label the syringe IN2.
3. Draw 20 mL of INSULIN (two vials) into the IN2 syringe.
4. Remove the 18 gauge needle and expel all air bubbles in the syringe.
5. Close the stopcock.
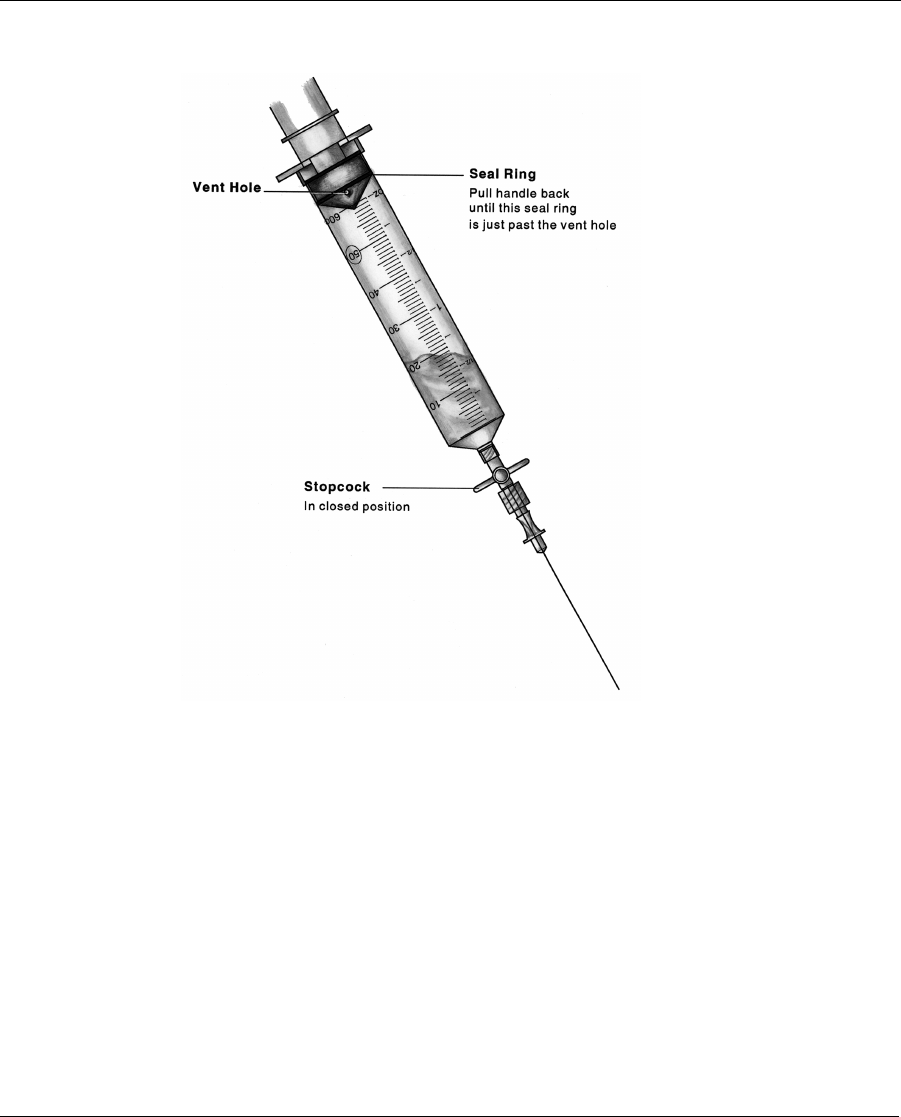
6. Retract the plunger until it locks into place. This should be no further
than 55 mL. Do not go beyond the vent hole. Press the lock into the
plunger groove to be sure it is firmly secured.
7. Shake vigorously for a minimum of 30 seconds to degas the INSU-
LIN.
8. Point the syringe tip upward and slowly open the stopcock to vent the
syringe.
9. Release the locking ring on the refill syringe.
10. Expel the air in the syringe and carefully observe it to ensure no air
bubbles remain in the syringe. If air bubbles are noted, repeat steps
5 - 10.
11. Fill the hub of the refill needle with INSULIN and attach it to the
stopcock.
12. Prime the needle and close the stopcock.
13. Place a sterile beaker or sterile barrier towel on the scale and tare it
(position balance at 0.)
14. Weigh the refill syringe and record the weight on the Implant Work-
sheet.
Dmp9196021-011_c.book Page 85 Wednesday, April 3, 2002 5:04 PM

86
15. Press the refill syringe into the Pump fill port, open the stopcock and
allow the Pump vacuum to draw INSULIN into the reservoir until the
fluid level stops moving. Close the stopcock.
16. Remove the IN2 syringe and prepare for aspiration without expelling
any fluid. Obtain a vacuum by pulling back on the plunger until it
locks. Press the lock into the plunger groove to be sure it is firmly
secured.
17. Reenter the Pump fill port with the stopcock closed.
18. Open the stopcock and withdraw 2 mL in order to activate the nega-
tive pressure safety feature of the Pump. Close the stopcock and
remove the syringe.
19. Weigh the IN2 syringe to calculate the Pump refill amount. Subtract
the weight after the fill and 2 mL withdrawal from the weight before
the fill and record the difference on the Implant Worksheet.
Measure stroke volume
1. Place the PPC in the sterile bag. Enter the Supervisor Mode. The
screen displays “PUMP REFILL”. Press ACT until the “SET
REFILL AMOUNT” screen appears. When filling the Pump for the
first time, set the “EXTRACTED AMOUNT” to zero. Otherwise,
enter the amount of insulin extracted. Then use the ▲
▲▲
▲ and ▼
▼▼
▼ buttons
to enter the refill amount from the Implant Worksheet. Program the
Pump.
2. Again, enter the Supervisor Mode and program “STOP PUMP”.
From the screen “PUMP STOPPED”, press SEL. “PUMP
STOPPED” will begin flashing. Press both the ▲
▲▲
▲ and ▼
▼▼
▼ buttons at
the same time, until the screen changes to the password screen. Reen-
ter the password and the screen will change to “PUMP REFILL.”
Press SEL to reach the “PRIMING” screen. “NO” will be flashing.
Use the ▲
▲▲
▲ and ▼
▼▼
▼ buttons to select “YES,” then press ACT. When the
word “CONFIRM” is highlighted, press ACT again. Place the PPC
near the Pump to complete the communication process. Record the
Dmp9196021-011_c.book Page 86 Wednesday, April 3, 2002 5:04 PM
87
time the priming bolus was initiated on the implant worksheet.
If you have removed the plastic tubing
placed on the Pump outlet, DO NOT TRY
TO REPLACE THE TUBING BACK ON
THE PUMP OUTLET. You can displace
or damage the “O” ring placed around the
outlet. To measure the stroke volume, you
need to use the procedure described in Appendix G, after
the Catheter has been attached.
3. Listen for five beeps and observe that fluid is being pumped from tub-
ing attached to the Pump outlet.
4. Attach the 18 gauge needle (from the 3 ml syringe filled with RINSE
BUFFER) to the plastic tubing from the Pump outlet.
5. Remove the 3 ml syringe and fill the needle hub.
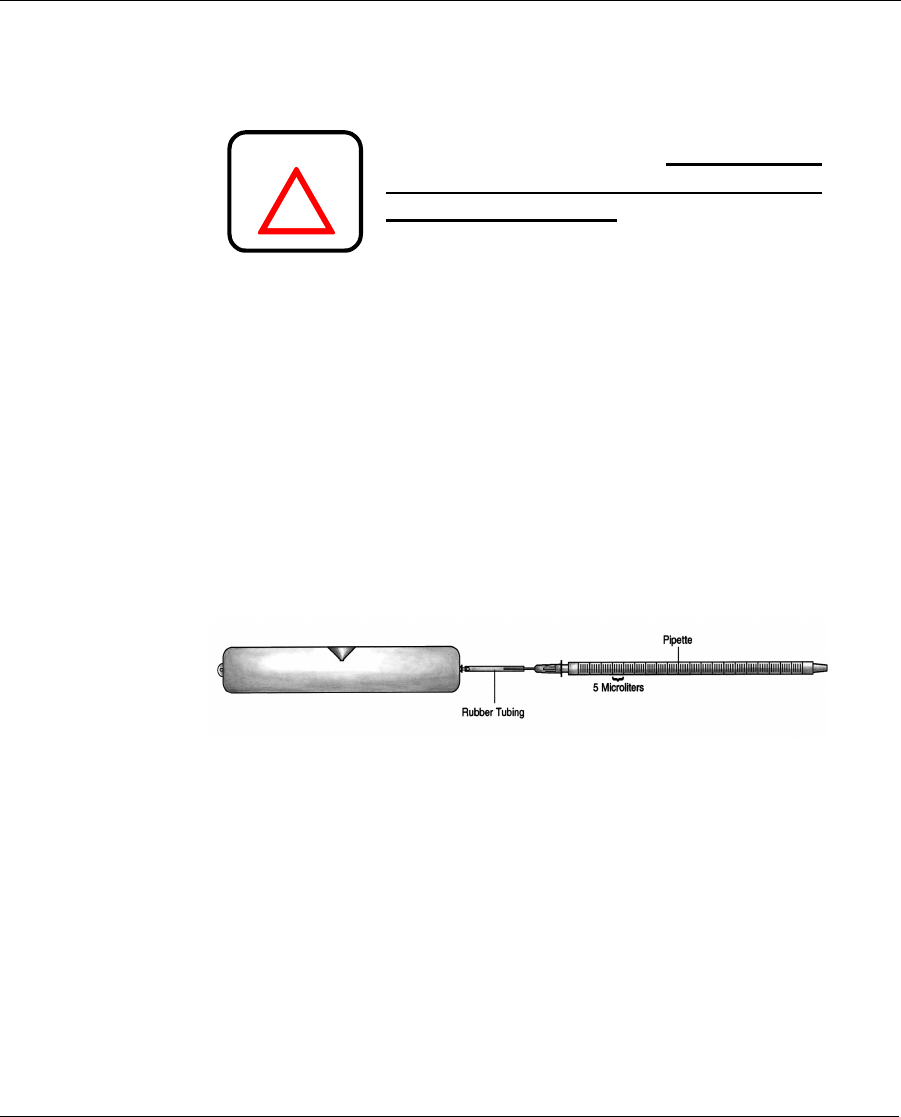
6. Insert the pipette into the hub. A meniscus of fluid will be present in
the pipette. This should be done on a flat surface with the pipette/tub-
ing assembly horizontal. (see Figure 8).
Figure 8: Testing Pump Stroke Volume with a Pipette
7. Note the exact location of the fluid meniscus in the pipette.
8. Measure the stroke volume by noting the volume displaced by a mini-
mum of 10 pulses. Record the total volume delivered and the number
of pulses on the Implant Worksheet. Divide the total volume deliv-
ered by the total number of pulses used to deliver that volume. The
volume per stroke must be between 0.40 and 0.60 µL. Record this
value on the Implant Worksheet.
!
WARNING
Dmp9196021-011_c.book Page 87 Wednesday, April 3, 2002 5:04 PM
88
Prepare the Side Port Catheter
The Side Port Catheter (“Catheter”) is attached to the Pump before
implantation; however, it must be primed with INSULIN and
inspected before being attached to the Pump.
Never insert a needle into the connector end
of the Catheter for priming or for testing.
there may be a precision sealing surface in
the connector that will be damaged by the
insertion of any needle.
1. Keep the Catheter in its package until the Pump is prepared and stroke
volume has been verified. Remove the Catheter from its sterile pack-
age and document the serial number on the Implant Worksheet.
2. Using the last insulin syringe (IN2) from the Pump preparation proce-
dure, enter the Catheter port cone and push a small volume of insulin
out of the connector end of the Catheter. This primes the proximal
portion of the Catheter and cleans any debris from the connector out-
let. Remove the syringe.
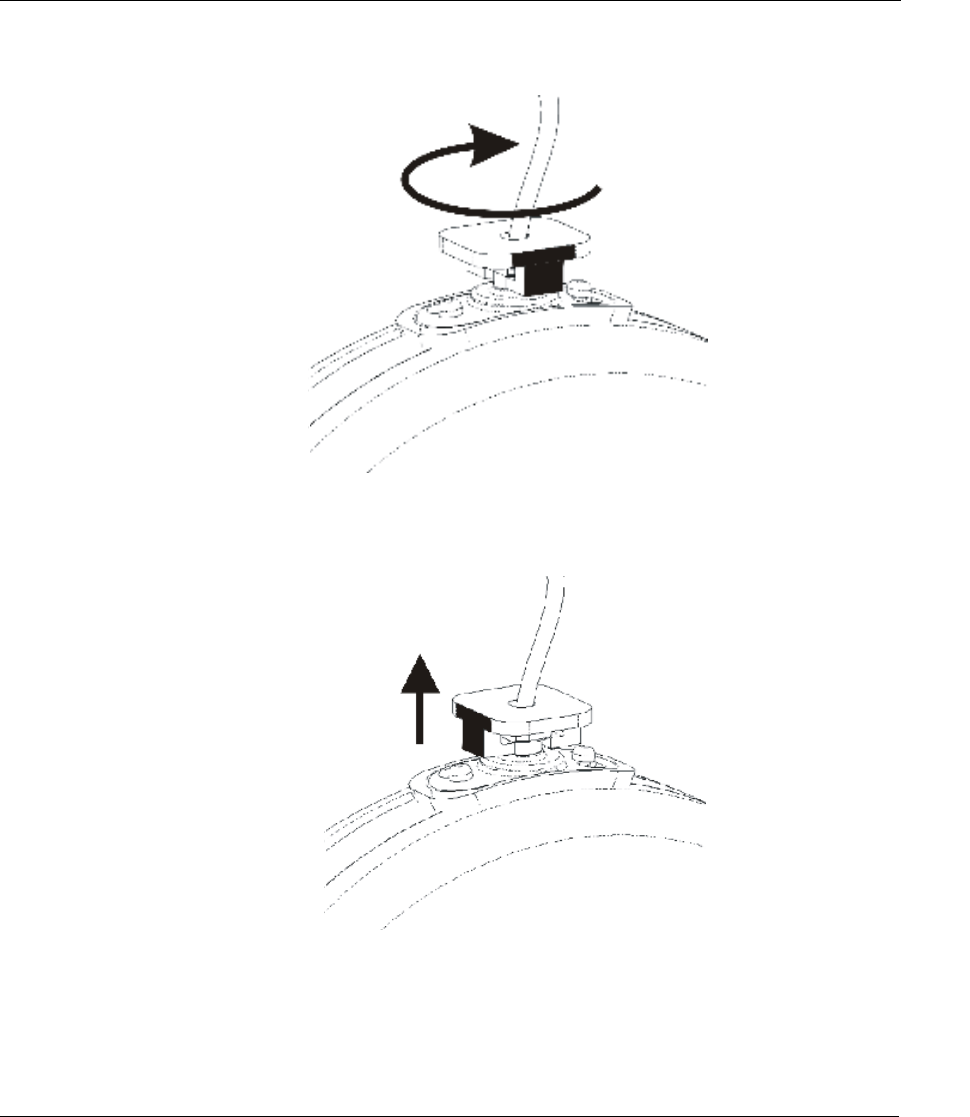
3. Remove the plastic tubing and tubing retainer from the Pump outlet.
Remove the tubing retainer, by rotating it one-quarter turn clockwise
to disengage it from the connector flange.Then lift and remove the
tubing and retainer together from the Pump outlet.Dispose of the tub-
ing and retainer.
!
WARNING
Dmp9196021-011_c.book Page 88 Wednesday, April 3, 2002 5:04 PM
89
Figure 9: Rotate Tubing Retainer
Figure 9-2: Pull Tubing Retainer off Pump.
Dmp9196021-011_c.book Page 89 Wednesday, April 3, 2002 5:04 PM
90
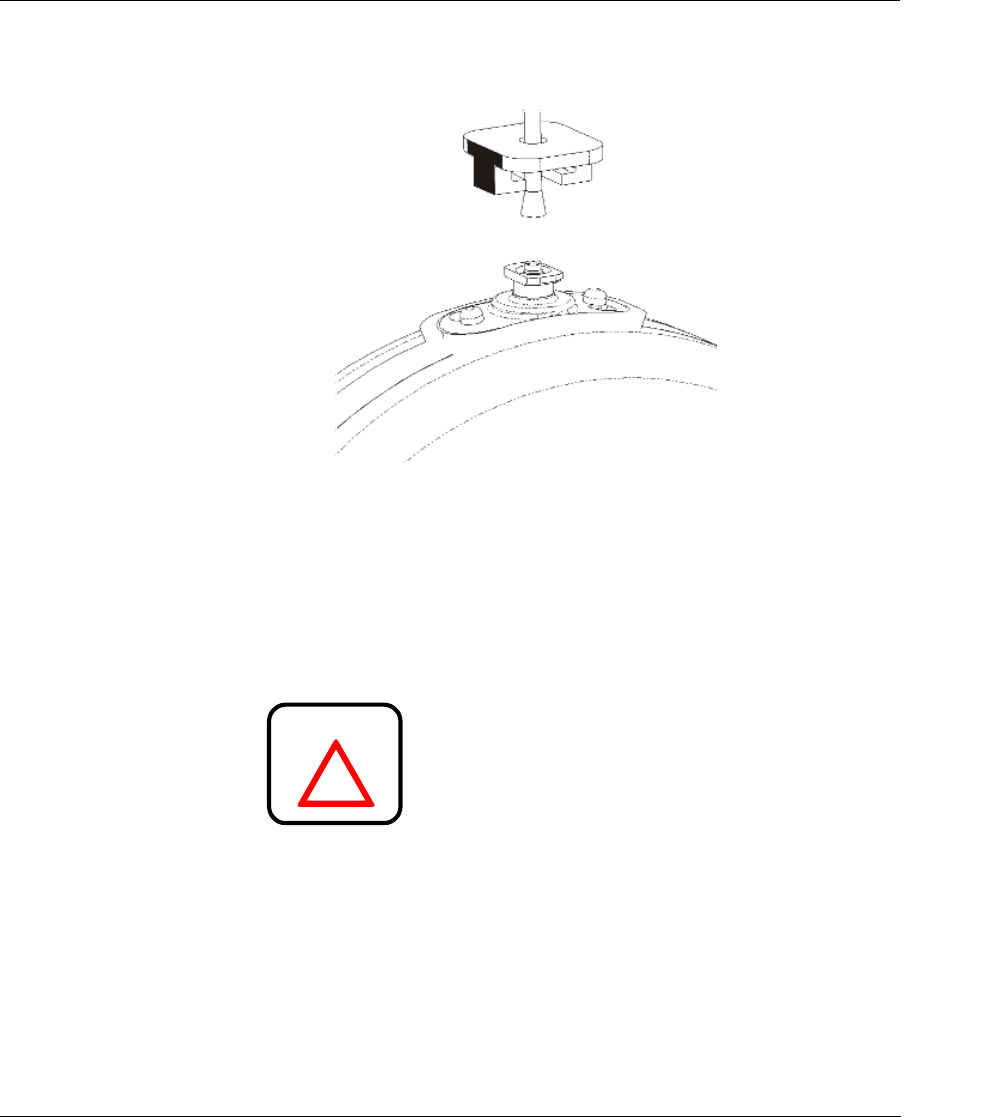
Figure 9-3: Tubing and Retainer Removed.
Step 4 Inspect the outlet of the Pump for debris. Debris, espe-
cially fibers, left in the fluid path will compromise the
function of the Catheter check valve. Rinse the outlet
tube of the Pump with water from a syringe, if necessary.
Avoid wiping the Pump with gauze or drapes that will
leave fibrous debris.
Use caution when removing debris from
the outlet of the Pump. There is a precision
rubber seal on the outlet that will be dam-
aged by handling with surgical instru-
ments.
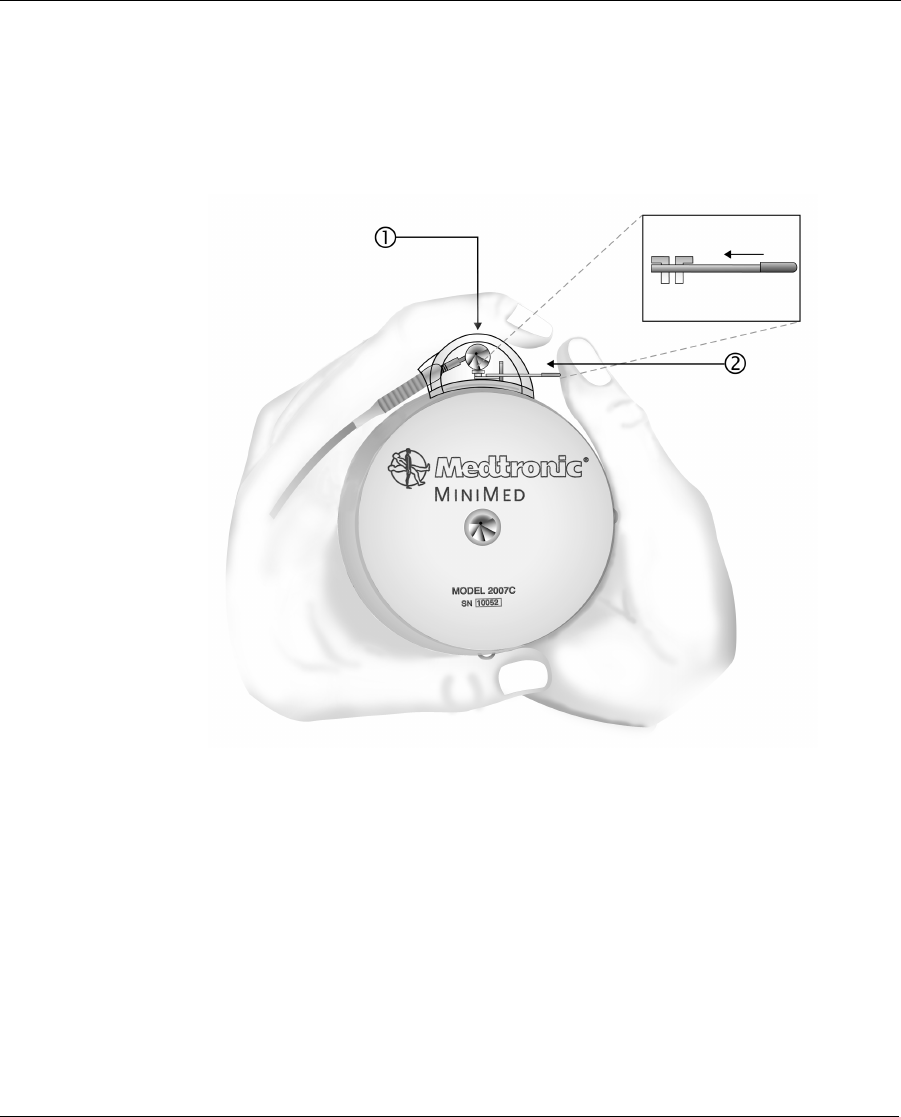
Step 5 Pull the locking bar out and gently push the Catheter
straight down onto the Pump outlet. Never twist the
connector.
!
WARNING
Dmp9196021-011_c.book Page 90 Wednesday, April 3, 2002 5:04 PM
91
Step 6 Only after the Catheter is seated, squeeze the connector,
1, firmly against the Pump between the thumb and fore-
finger of one hand. Then push the locking bar, 2, into
place with the thumb of the other hand.
Figure 10: Proper Attachment of the Side Port Catheter to Pump
Dmp9196021-011_c.book Page 91 Wednesday, April 3, 2002 5:04 PM
92
Step 7 Verify the Catheter is securely attached to the Pump.
Look into the connector and observe the position of the
locking bar with respect to the Pump connector outlet.
Check the side port connector hub for abnormalities
(e.g., cracks, misalignment.)
Step 8 Using the IN2 refill syringe, enter the Catheter side port
cone and push a small amount of INSULIN out the Cath-
eter tip. Verify that no insulin flow is observed at Pump/
Catheter interface. Remove and reseat Catheter if flow is
noted. Remove the syringe.
Step 9 Confirm insulin delivery from the tip of the Catheter and
note it on the Implant Worksheet. The INSULIN will
form a dome on the tip of the Catheter. Pulsatile delivery
will not be obvious. If the priming bolus has already
ended, program an immediate bolus (about 20 units) to
confirm delivery. (This bolus may be canceled after
delivery is verified.)
Step 10 At the end of the bolus, rinse the outside of the Pump
thoroughly with sterile water to remove traces of
INSULIN. The Catheter tip should not be placed in the
water. Protect the Pump with sterile drapes until the sur-
geon is ready to implant it. Verify that the priming bolus
is finished or canceled prior to the implantation.
The Pump and Catheter are now ready for implantation.
Dmp9196021-011_c.book Page 92 Wednesday, April 3, 2002 5:04 PM

93
Performing the surgical procedure
Pre-operative evaluation
The Pump implant depth should not exceed 5 cm (2 inches) beneath the
surface of the skin. If the Pump is implanted too deeply in the subcutane-
ous tissue it may be difficult to access the refill port.
Formation of the pump pocket
Pump implantation can be performed either under local or general anes-
thesia. After satisfactory anesthesia, a pre-selected abdominal site is
prepped and draped in the customary surgical method.
A transverse or longitudinal incision is made and deepened through the
skin and subcutaneous tissue. Care should be taken in choosing the loca-
tion of the incision so the suture line is next to but not over the Pump inlet
fill port or the Catheter side port. A subcutaneous blunt dissection is per-
formed to create a pocket large enough to accommodate the Pump.
Meticulous hemostasis should be established with electrocautery.
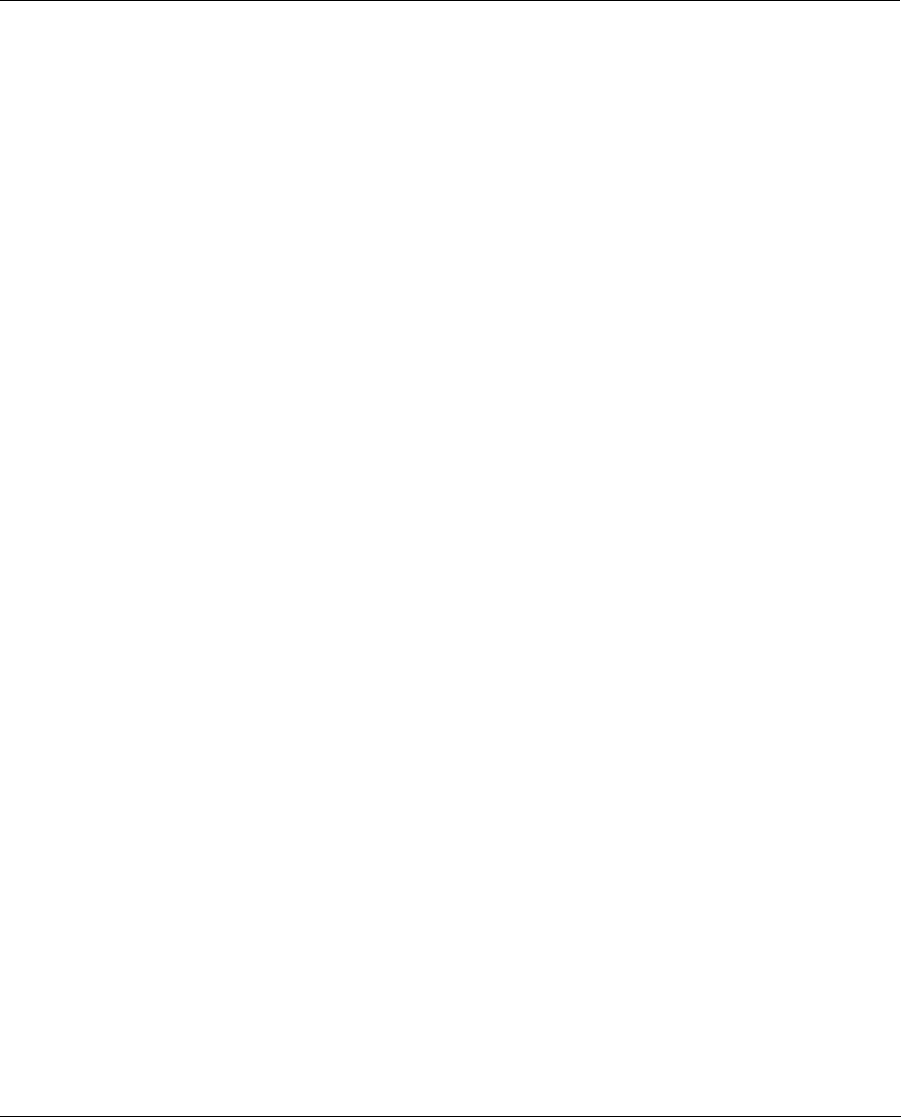
Figure 11 indicates a possible Pump placement and corresponding inci-
sion sites.
The Pump is secured to the fascia of the abdominal musculature using the
three suture tabs provided. Securing the Pump with all three suture tabs is
recommended, as it will prevent migration, rotation or inversion in the
pocket and possible dislodgment of the Catheter.
Dmp9196021-011_c.book Page 93 Wednesday, April 3, 2002 5:04 PM
94
Figure 11: Example of Pump Placement
Dmp9196021-011_c.book Page 94 Wednesday, April 3, 2002 5:04 PM
95
Catheter placement
The Catheter is not designed to be tunneled subcutaneously. The Catheter
insertion should be at the extreme edges of the Pump pocket.
At a site not directly beneath the Pump, the layers of abdominal muscula-
ture are divided to expose the peritoneum. Concentric purse string sutures
are placed and the peritoneum is exposed with a 1 cm incision. The distal
tip of the Catheter is placed in the peritoneal space. The flange of the
Catheter is sutured firmly to the fascia of the abdominal musculature.
Sutures should only be placed on the reinforced flange of the Catheter.
Sutures must not be placed directly on the Catheter itself.
Never trim or cut the tip of the Catheter.
The implant site should be irrigated with an antibiotic solution. Inter-
rupted absorbable sutures should be used to approximate the subcutane-
ous tissues and the skin closed with a running subcuticular absorbable
suture. The wound is dressed using standard surgical technique. At the
end of the surgery, place an abdominal binder over the implant site. This
binder must be worn until the capsule has formed (about 1 month.) The
binder is recommended because it will obtain a better cosmetic result and
minimize the post operative swelling.
Post-operative management
Post-operative hospitalization
After implantation, the surgical incision should be inspected for any signs
of unusual swelling, tenderness, pain, or drainage. Potential post-opera-
tive complications include Pump pocket seroma, wound dehiscence,
wound infection, and catheter dislodgment.
Length of post-operative hospitalization depends upon how rapidly the
patient adjusts to the Pump and how quickly blood glucose levels
!
WARNING
Dmp9196021-011_c.book Page 95 Wednesday, April 3, 2002 5:04 PM

96
stabilize. During post-operative hospitalization, the Pump can be repro-
grammed to accommodate the needs of the patient. As post-operative
stress decreases, insulin requirements may decline. It may be necessary
to make several changes in insulin delivery rates during the first few days
following implantation.
Patients must be thoroughly educated in all aspects of follow-up care with
the Pump. The MiniMed Patient Manual should be used to supplement
patient education. Prior to discharge, patients should:
• Fully understand how to use their PPC;
• Know what to do in the event of Pump or PPC difficulties;
• Have scheduled their first refill appointment;
• Have set an appointment for their first follow-up visit;
Post-operative x-rays
The Catheter has been designed with a radio-opaque stripe for identifica-
tion after implantation. A lateral and anterior X-ray is recommended after
implantation to locate and document the position of the Catheter. This
radiograph should be kept with the patient’s records for future reference.
Dmp9196021-011_c.book Page 96 Wednesday, April 3, 2002 5:04 PM
97
CHAPTER 5 Pump Refill Procedure
Introduction
Initial appointments for Pump Refills should be made with patients at the
time of implantation. Subsequent appointments should be made in
advance, normally during each refill procedure. The Pump stores approx-
imately 6,000 units of insulin medication and typically requires a refill
every two to three months. In order to maintain the physical stability of
the insulin, the Pump must be refilled at a maximum interval of no more
than 90 days. The PPC will display warning messages to alert the patient
of calculated low or emptied reservoir volumes.
The low reservoir message will appear when the PPC calculates that 800
(2 ml) or fewer units of insulin medication remain in the Pump. The
empty reservoir message will appear when the PPC calculates that 400 or
fewer units (1 ml) of insulin remain. The time to medication depletion
depends upon the delivery rate of the Pump.
The Pump refill procedure should always be
scheduled in advance of PPC “low reservoir” or
“empty reservoir” messages.
!
WARNING
Dmp9196021-011_c.book Page 97 Wednesday, April 3, 2002 5:04 PM
Pump Refill Procedure
98
Supplies and solutions
The refill kit (MMT-4105) is intended exclusively for use with the
Medtronic MiniMed 2007C Implantable Insulin Pump System. The refill
kit consists of a specially designed syringe and stopcock for removing flu-
ids from and placing fluids into the Pump. Use only refill needles (MMT-
4102) available from MiniMed to perform all Pump refill procedures.
This 22 gauge needle, featuring a rounded, lubricated tip and a beveled
side hole, has been specially developed to mate with the Pump fill port.
Use of other needles may result in damage
to the Pump septum in the fill port, and
may allow body fluids to enter the Pump.
Below is a list of the supplies and solutions necessary to perform the refill
procedure:
Supplies:
• Steri-Strips® and Markers
• The Patient’s PPC
• Glucose Monitoring Equipment
•Drapes
• One (1) Scale (0.01 gram resolution)
• One (1) 250 ml Sterile Beaker
• One (1) Port Locating Template - MMT-4106
• Two (2) Refill Kits - MMT-4105
• Three (3) MiniMed MMT-4102 Refill Needles (Extra needles
should be available for use.)
• Four (4) Sharp 18 Gauge Regular Bevel Needles
Solutions:
• One (1) 10 ml Vial, Aventis Rinse Buffer Solution
• Two (2) 10 ml Vials, Aventis HOE 21 PH, U-400 Insulin
!
WARNING
Dmp9196021-011_c.book Page 98 Wednesday, April 3, 2002 5:04 PM
Introduction 99
Prepare for pump refill
NOTE: Before beginning any refill, rinse, flush, or pres-
sure measurement procedure, carefully read
Appendix D, Precautions and General Proce-
dures.
Never push on the refill syringe plunger to
fill the Pump. When the refill needle is
properly seated in the Pump fill port, the
vacuum in the Pump reservoir will draw the
insulin from the syringe into the reservoir.
To prepare for emptying and refilling the Pump, perform the following
steps:
• Use the “HISTORY” feature of the PPC to determine the amount
of insulin medication remaining in the Pump. Make sure that
ACT is pressed on the “READ PUMP DATA” screen to update
PPC history from the Pump. Record this value on the refill work-
sheet (Appendix C).
• Prepare a sterile field. The physician should scrub, mask and
glove for the refill procedure. Refilling the Pump is an aseptic
procedure.
• (See Appendix D, Precautions and General Procedures.)
• Aseptic skin preparation of the patient’s Pump refill site should
be performed using your institution’s standard operating proce-
dures.
!
WARNING
Dmp9196021-011_c.book Page 99 Wednesday, April 3, 2002 5:04 PM

Pump Refill Procedure
100
Perform the refill procedure
Fill out the refill form
Fill out the top part of the Refill Form (Appendix C) with the patient’s
I.D., refill date, insulin lot number, previous refill volumes, insulin medi-
cation remaining, and the name of the person performing the refill proce-
dure. This information can be helpful for diagnostic purposes.
Label syringes
Use a sterile marker and Steri-Strips® to label one refill syringe “RB”
(rinse buffer syringe) and the other “IN” (insulin syringe).
Prepare the refill syringe for emptying the Pump
1. Firmly attach the stopcock to the RB refill
syringe and attach the 18 gauge needle to
the stopcock. Check connections to
ensure they are secure. Draw 5 ml of
Rinse Buffer into the RB refill syringe.
2. Expel all air bubbles from the refill
syringe. Remove the 18 gauge needle
from the stopcock.
3. Fill the hub of the refill needle with Rinse
Buffer from the RB refill syringe and
attach it to the stopcock. Prime the refill
needle completely. Close the stopcock.
4. Obtain the weight and record it on the
Refill Form. Set the syringe aside.
Figure 12: Filling the Hub of the Refill Needle
Dmp9196021-011_c.book Page 100 Wednesday, April 3, 2002 5:04 PM

Perform the refill procedure 101
Prepare the refill syringe for filling the Pump
1. Firmly attach the stopcock to the IN refill syringe and attach an 18
gauge needle to the stopcock. Draw 20 ml of Aventis HOE PH U-400
insulin into the syringe.
2. Expel all air from the refill syringe. Close the stopcock and remove
the 18 gauge needle.
3. Retract the plunger until it locks into place. This should be no further
than 55 ml - do not go beyond the vent hole. Press the lock into the
plunger groove to be sure it is firmly secured.
4. Shake vigorously for a minimum of 30 seconds.
5. Point the syringe tip upward and slowly open the stopcock to allow air
to enter the syringe.
6. Release the locking ring on the refill syringe. With the syringe pointed
upward, push on the plunger to expel the air and prime the stopcock.
7. Open the stopcock and prime the refill needle. Attach the refill needle
to the stopcock. Close the stopcock.
8. Inspect the syringe to ensure there are no air bubbles. If air bubbles
are noted, remove the refill needle and repeat steps 2 - 7.
9. Weigh the refill syringe and record on the refill form.
10. Set the syringe aside.
Dmp9196021-011_c.book Page 101 Wednesday, April 3, 2002 5:04 PM

Pump Refill Procedure
102
Empty the Pump
1. Obtain a vacuum in the RB syringe by pulling back on the plunger
until it locks. Press the lock into the plunger groove and be sure it is
firmly secured.
2. Locate the fill port by centering the template over the Pump. The cen-
ter hole in the template should be directly over the Pump fill port.
Insert the 18 gauge guide needle into the Pump fill port. Local anes-
thesia may be used prior to insertion of the 18 gauge needle.
3. Press the primed refill needle (attached to the RB syringe) into the
Pump fill port, by sliding it through the 18 gauge guide needle. Pull
back slightly (approximately 2 mm) on the guide needle to allow the
refill needle to enter the Pump fill port and actuate the inlet valve.
4. Actuate the valve by applying a gentle downward force on the refill
needle. This depresses the valve approximately 0.5 mm.
5. Open the stopcock and allow residual insulin from the Pump to be
drawn into the RB refill syringe. Maintain a downward pressure on
the syringe to ensure that the inlet valve in the Pump remains open.
Wait 30 additional seconds after the insulin level appears to have
stopped rising in the RB refill syringe to ensure the Pump is com-
pletely emptied.
6. When all residual insulin is withdrawn from the Pump, close the stop-
cock. Remove the RB refill syringe.
NOTE: Do not remove the 18 gauge guide needle.
7. Weigh the RB syringe and record on the refill form.
Dmp9196021-011_c.book Page 102 Wednesday, April 3, 2002 5:04 PM
Perform the refill procedure 103
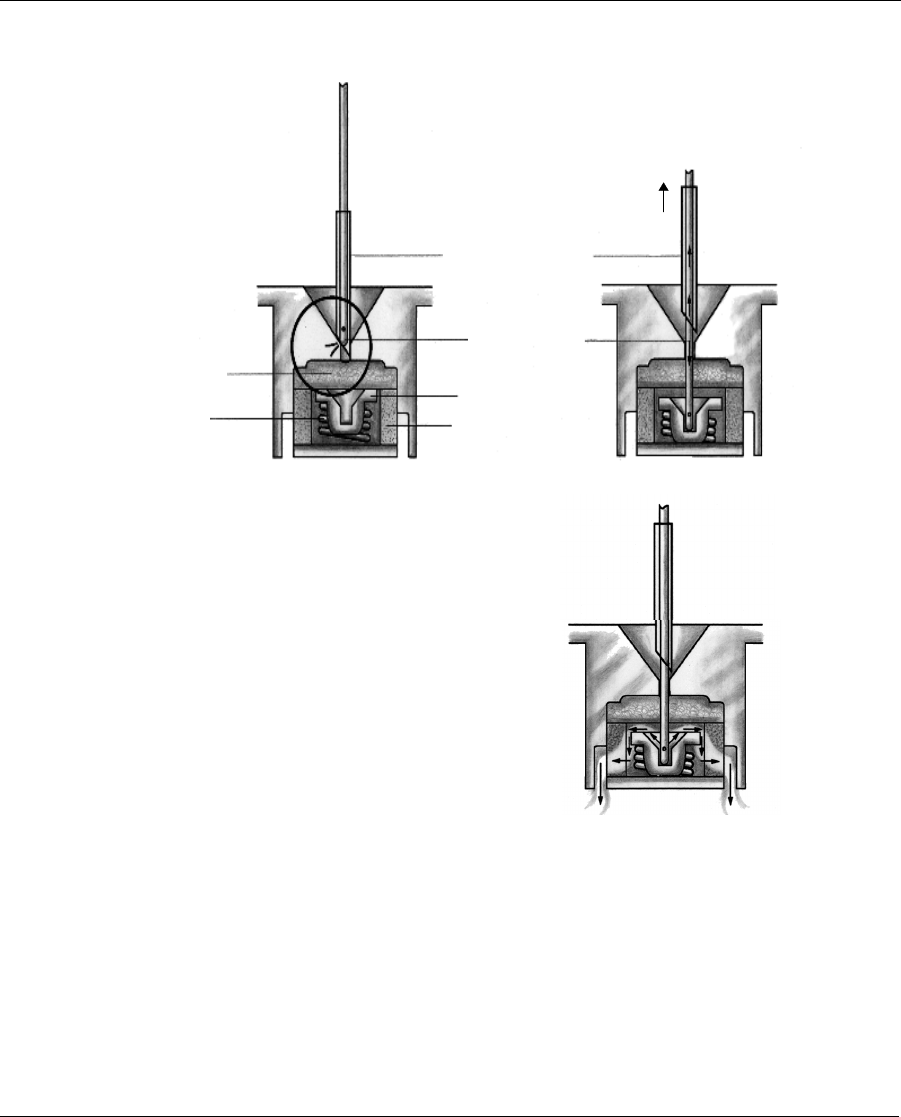
Figure 13: Operation of the Pump Inlet Valve
18G Guide Needle
Refill Needle
Valve
Filter
Septu
m
Spring
2mm
St e p 3 C: A pp ly fi r m pr e s su re t o m o ve t h e va lv e
back and allow the insulin to pass above the valve
through the filter and into the reservoir.
Step 3A: Locate the port using the 18Ga guide needle
slide the refill needle down the guide needle.
Step 3B: Pull back approxiamately 2mm on the guide
needle to enter the Pump.
Step3A
Step3B
Step3C
Dmp9196021-011_c.book Page 103 Wednesday, April 3, 2002 5:04 PM

Pump Refill Procedure
104
Refill the Pump
1. Use the IN refill syringe containing 20 ml of degassed insulin.
2. Enter the Pump by passing the refill needle with the attached IN refill
syringe through the 18 gauge guide needle. Pull back slightly
(approximately 2 mm) on the 18 gauge needle to allow the refill nee-
dle to enter the Pump and actuate the inlet valve (see Figure 13).
3. Open the stopcock. Maintain downward pressure on the IN refill
syringe to ensure the inlet valve in the Pump remains open. Allow the
Pump to draw in insulin until the fluid level stops moving. Close the
stopcock.
4. Remove the IN syringe and prepare for aspiration without expelling
any fluid by pulling back on the plunger until it locks. Re-enter the
Pump, open the stopcock and withdraw 2 ml in order to activate the
negative pressure safety feature of the Pump.
Dmp9196021-011_c.book Page 104 Wednesday, April 3, 2002 5:04 PM
Perform the refill procedure 105
OPTIONAL
Use this step only
if the plunger is
not moving dur-
ing the fill of the
reservoir.
With the refill nee-
dle pointing down,
vent the syringe
head space by pull-
ing back firmly on
the plunge until the
second sealing ring
on the black rubber
cap passes beyond
the vent hole
(see Figure 14).
Figure 14: Venting the MiniMed Refill Syringe
5. Remove the IN syringe. Remove the 18 gauge needle and apply pres-
sure to the insertion site.
6. Weigh the IN syringe and record on the Refill Form.
Dmp9196021-011_c.book Page 105 Wednesday, April 3, 2002 5:04 PM

Pump Refill Procedure
106
Calculate extracted and refill amounts
1. Calculate the extracted amount by using the calculation section of the
refill form.
2. Calculate the refill amount by using the calculation section of the
refill form.
3. Enter the extracted amount (amount withdrawn as calculated on the
refill worksheet at line E) and the refill amount (as calculated on the
refill worksheet at line G) into the PPC (see Chapter 3).
Calculate refill accuracy
The PPC automatically calculates the refill accuracy following the PPC
refill programming. You can also follow the calculation section of the
refill form to calculate the refill accuracy.
Enter the refill accuracy value (IN %) on the line provided on the refill
form. It is important to record this value to evaluate the functioning of the
Pump system.
Dmp9196021-011_c.book Page 106 Wednesday, April 3, 2002 5:04 PM
107
CHAPTER 6 Explanting the Pump
System
Explant considerations
When the battery in the Pump is depleted or if acceptable glycemic con-
trol cannot be achieved, it may become necessary to explant the Pump
system.
Prior to explantation, it may be possible to perform interventions that
could correct certain conditions. These procedures are described in
Appendices E and F.
If all appropriate interventions have been exhausted without an acceptable
outcome, please contact MiniMed prior to scheduling a Pump explanta-
tion.
Returning devices/components to MiniMed
Explanted Pumps and Catheters or other components should be returned
to MiniMed for evaluation. Please call MiniMed and obtain a Returned
Materials Authorization (RMA) number prior to each return.
Explanted devices must be sealed in an appropriate biohazard container
and packed with a gauze pad soaked with sterile saline. The shipping con-
tainer should be water tight. Chemical and reliability analysis require that
the device not dry out during transportation.
Dmp9196021-011_c.book Page 107 Wednesday, April 3, 2002 5:04 PM

Explanting the Pump System
108
Be certain to include required patient information as well as the RMA
number, date, and reason for the explant and place all pertinent documen-
tation in a water tight document package. Put the RMA number on the
shipping label.
Please take the necessary precautions when shipping the Pump System
via commercial carrier to avoid damage to the Pump. Please return
explanted Pump Systems to:
United States:
MiniMed Inc.
18000 Devonshire Street
Northridge, CA 91325
Telephone: 1-818-578-6700
or
Europe:
MiniMed S.A.
30, Boulevard Vital Bouhot
92200 Neuilly-sur-Seine, France
Telephone: 33 (1) 46 43 16 16
Dmp9196021-011_c.book Page 108 Wednesday, April 3, 2002 5:04 PM
109
CHAPTER 7 Warnings And Precautions
Warnings
The Physician should be completely familiar with the function of the
Pump, Catheter, and PPC prior to use. Patients should be provided a com-
plete copy of the Patient Manual and have demonstrated the ability to pro-
gram the PPC, recognize and respond to safety alarms, and take care of
the device prior to discharge.
The Implantable Insulin Pump can only be used with MMT-4027A and
4024A Side Port Catheters.
Only Aventis HOE 21 PH U-400 insulin may be used in the Medtronic
MiniMed 2007C Implantable Insulin Pump System. Use of other insulin
types may cause damage to the Pump mechanism resulting in impaired
insulin delivery or Pump failure.
Any unauthorized changes or modifications made to any component of
the Medtronic MiniMed 2007C Implantable Insulin Pump System may
prevent effective use of that and other components.
Electrotherapy
The Medtronic MiniMed 2007C Implantable Insulin Pump System has
been tested in close proximity with electrosurgical, electrocoagulation,
and cardiac defibrillation medical equipment. Typical use of this type of
device has not affected the Pump. However, patients should be instructed
Dmp9196021-011_c.book Page 109 Wednesday, April 3, 2002 5:04 PM

Warnings And Precautions
110
to test Pump function (e.g., program a bolus and then cancel the bolus)
after such procedures, to determine that the Pump and PPC are operating
properly. If the system is not performing correctly, contact MiniMed.
Diagnostic ultrasound
The Medtronic MiniMed 2007C Implantable Insulin Pump System has
been tested during diagnostic ultrasound procedures. These procedures
have no effect on Pump performance. However, patients should be
instructed to test the Pump function (e.g., program a bolus and then cancel
the bolus) after such procedures, to determine that the Pump and PPC are
operating properly. If the system is not performing correctly, contact
MiniMed.
Ultrasound therapy
The Medtronic MiniMed 2007C Implantable Insulin Pump System should
not be exposed to therapeutic ultrasound procedures, such as lithotripsy.
Exposure to ultrasound therapy may damage the Pump, and not be imme-
diately apparent.
Diagnostic radiation
The Medtronic MiniMed 2007C Implantable Insulin Pump System has
been tested during diagnostic radiation procedures, such as Computed
Tomography and X-ray. These procedures have no effect on Pump perfor-
mance. However, patients should be instructed to test the Pump function
(e.g., program a bolus and then cancel the bolus) after such procedures, to
determine that the Pump and PPC are operating properly. If the system is
not performing correctly, contact MiniMed.
Therapeutic radiation
The MiniMed 2007 Implantable Insulin Pump has been tested during
therapeutic radiation procedures. These procedures have no effect on
Pump performance. However, patients should be instructed to test the
Pump function (e.g., program a bolus and then cancel the bolus) after
such procedures, to determine that the Pump and PPC are operating prop-
erly. If the system is not performing correctly, contact MiniMed.
Dmp9196021-011_c.book Page 110 Wednesday, April 3, 2002 5:04 PM

Warnings 111
Elevated anti-insulin antibodies
The result of clinical investigations suggest a small population of patients
may develop anti-insulin antibodies when using the MiniMed 2007
Implantable Pump System and HOE 21 PH U-400 insulin. Patients with
multiple autoimmune disorders may be more susceptible to developing
high titers of anti-insulin antibodies, which in turn may cause symptoms.
There was no correlation between length of exposure to the study drug
and the resultant titer of anti-insulin antibodies. Elevated levels of anti-
insulin antibodies alone have been proven not to interfere with diabetes
management using continuous intraperitoneal insulin infusion with this
system.
Environmental conditions
The Medtronic MiniMed 2007C Implantable Insulin Pump System should
not be exposed to extreme electrical or magnetic fields. Although it is not
possible to include every environmental condition that may affect the
Pump, most are listed below. Please contact MiniMed when in doubt if
certain environmental exposure will affect the pump.
DO NOT EXPOSE THE MINIMED 2007 IMPLANTABLE
INSULIN PUMP SYSTEM TO ANY OF THE FOLLOWING
CONDITIONS
• Magnetic Resonance Imaging (MRI) Procedures.
• Lithotripsy Treatment.
• Large Rotating Magnetic Fields -
- -
- Refers to large industrial rotat-
ing magnetic fields, such as those found in Industrial Power
Plants.
• Magnets Held Directly Over the Pump.
• High Power Radio or Satellite Transmitting Towers.
• Altitudes Above 2,400 meters (8,000 feet).
The Medtronic MiniMed 2007C Implantable Insulin Pump System is not
designed for use at elevations above 2,400 meters (8,000 feet). Use of the
Pump System at higher elevations may result in insulin over delivery,
which may cause personal injury or death. Therefore, patients who live at
Dmp9196021-011_c.book Page 111 Wednesday, April 3, 2002 5:04 PM

Warnings And Precautions
112
elevations above 8,000 feet or 2,400 meters should not use the Pump.
Patients who use the Pump and who plan to travel to an elevation above
2,400 meters (8,000 feet) should first have their Pump reservoir emptied
of insulin, and they must self-administer insulin by other means for the
duration of the trip and until their Pump reservoir is refilled again.
• This warning does not apply to travel on commercial aircraft
because normal cabin pressurization is adequate to ensure proper
operation of the Pump.
• Diving Below 7.6 Meters (25 Feet).
• Physical Damage to the Pump or Pump Pocket.
Physicians should instruct patients to avoid any sharp blows or pressure
directly at the Pump location. A direct hit by an object such as a baseball
may damage the Pump and/or injure the Pump pocket. Extreme pressure
on the Pump may cause the sutures and the tissue pocket to be damaged.
As a result, the Pump may move from its pocket and possibly dislodge
from the Catheter.
If the Pump has been damaged by such a blow, the patient should be
instructed to contact their physician. Physicians may order a pressure ban-
dage or a reduction in the patient’s physical activity until the pump pocket
reheals completely.
• Exposure to Extreme Body Temperatures
Exposure to elevated body temperature in excess of 104°F (40°C) will
compromise the negative pressure reservoir safety feature of the MiniMed
2007 Implantable Pump. Glucose levels should be monitored closely if
this occurs.
Sterilization
The Pump, Catheter and the refill kit are sterilized with ethylene oxide
(EtO).
The Pump System is NOT Reusable.
If the sterile package has been opened, damaged or tampered with DO
NOT USE the packaged device.
Dmp9196021-011_c.book Page 112 Wednesday, April 3, 2002 5:04 PM
Precautions 113
NOTE: Do Not Re-Sterilize the Implantable Insulin Pump
NOTE: Do Not Re-Sterilize the Side Port Catheter
NOTE: Do Not Re-Sterilize Components of the Refill Kit.
The Pipette (MMT -4104), may be resterilized using autoclave or EtO.
The Template MMT-4106 may be resterilized using steam autoclave or
EtO. This template is made from polycarbonate plastic and will have a
limited life in steam autoclave cycle. The template will not withstand dry
heat autoclave cycles.
Precautions
Emergencies and the use of conventional insulin supplies
Physicians should advise patients who wear the Medtronic MiniMed
2007C Implantable Insulin Pump System how to deal with emergency
conditions such as hyperglycemia. Patients should always carry conven-
tional insulin supplies with them, including insulin and a means to inject
it, in the event of impaired insulin delivery by the Pump System. Delivery
of insulin can become impaired due to a failure of a Pump and/or PPC, or
a Catheter occlusion. Replacement of the Pump, PPC or Catheter may be
required. Physicians should review the Pump replacement and Catheter
clearing procedures in this Physicians Manual
PPC reliability requirements
The PPC is a sensitive electronic device, and can incur physical damage.
If the PPC is dropped or receives an impact, immediately perform a SELF
TEST to check the displays for proper operation. If the PPC does not dis-
play correctly, a replacement PPC is required. Patients should initiate
alternative diabetes management until a replacement PPC is received.
The PPC housing is not watertight and it may malfunction if immersed in
water. “Condensing humidity” conditions such as steam rooms should
also be avoided, because condensation can also damage the PPC’s micro-
Dmp9196021-011_c.book Page 113 Wednesday, April 3, 2002 5:04 PM

Warnings And Precautions
114
electronics. If either situation occurs, contact MiniMed immediately and
arrange for the repair or replacement of the PPC. If the PPC is acciden-
tally splashed, sprayed or immersed, remove excess moisture with a soft
towel and then place the PPC in a warm place to thoroughly dry. When
dry, perform a “SELF TEST.” If the PPC does not display correctly, call
MiniMed to replace the device.
Maximum dosages
The physician can program specific limitations to insulin Basal Rates and
Bolus amounts, as well as total daily insulin usage. These limitations pro-
vide some control of patients’ ability to program their insulin regimens,
and to avoid overdosing.
Electrical and magnetic fields
Common electrical and magnetic fields that do not affect the Pump
include microwave ovens, satellite receiving dishes, common household
appliances, security devices found in department stores and airports, stan-
dard medical X-rays, cellular phone, and radiowaves.
Dmp9196021-011_c.book Page 114 Wednesday, April 3, 2002 5:04 PM
115
CHAPTER 8 Adverse Reactions
Adverse reactions
In clinical studies, adverse reactions associated with the Medtronic Min-
iMed 2007C Implantable Pump included hypoglycemia, diabetic ketoaci-
dosis, hyperglycemia, skin erosion, infection, abnormal healing, elevated
anti-insulin antibodies, intestinal obstruction, post-operative discomfort
and pain, and corrective surgery for Pump and Catheter malfunctions.
Pump System malfunctions in order of frequency and seriousness include
insulin aggregation resulting in Pump under-delivery, Catheter occlusion
or tissue overgrowth, premature depletion of the Pump battery, and failure
of Pump electronics. Adverse events associated with the use of Aventis
HOE 21 PH U-400 insulin are described in the package insert accompa-
nying the insulin medication.
Dmp9196021-011_c.book Page 115 Wednesday, April 3, 2002 5:04 PM
Adverse Reactions
116
Prevention
The majority of adverse reactions in patients using the Medtronic
MiniMed 2007C Implantable Pump System can be prevented by teaching
patients dependable blood glucose monitoring. The patient plays a signif-
icant role in diagnosing and correcting Pump System performance prob-
lems. Should Pump performance change, the patient would be able to
detect a change in blood glucose levels.
Patients should be instructed to contact
their physician’s office, if they experience
unresolvable difficulties with the Pump
System. Emergency patient visits and
diagnostic procedures may be necessary
to correct adverse conditions.
!
WARNING
Dmp9196021-011_c.book Page 116 Wednesday, April 3, 2002 5:04 PM